User login
Intranasal DHE shows promise in migraine
, according to results from a phase 3 clinical trial. In development by Impel NeuroPharma, the new formulation could offer patients an at-home alternative to intramuscular infusions or intravenous injections currently used to deliver DHE.
“Our analysis of the data suggests that nothing new or untoward seemed to be happening as a result of delivering DHE to the upper nasal space,” Stephen Shrewsbury, MD, chief medical officer of Impel NeuroPharma, said in an interview. The company released key results from its phase 3 clinical trial, while a poster examining patient satisfaction was presented by Dr. Shrewsbury at the virtual annual meeting of the American Headache Society.
An improved intranasal formulation
The product isn’t the first effort to develop an inhaled form of DHE. An inhaled version called Migranal, marketed by Bausch Health, delivers DHE to the front part of the nose, where it may be lost to the upper lip or down the throat, according to Dr. Shrewsbury. Impel’s formulation (INP104) delivers the drug to the upper nasal space, where an earlier phase 1 trial demonstrated it could achieve higher serum concentrations compared with Migranal.
In 2018, MAP Pharmaceuticals came close to a product, but it was ultimately rejected by the Food and Drug Administration because DHE was not stable in the propellant used in the formulation. This time is different, said Dr. Shrewsbury, who was chief medical officer at MAP before joining Impel. The new device holds DHE and the propellant in separate compartments until they are combined right before use, which should circumvent stability problems.
Dr. Shrewsbury believes that patients will welcome an inhaled version of DHE. “People with migraines don’t want to have to go into hospital or even an infusion center if they can help it,” he said.
The study was one of a number of presentations at the AHS meeting that focused on novel delivery methods for established drugs. “The idea of taking things that we know work and improving upon them, both in terms of formulation and then delivery, that’s a common theme. My impression is that this will be an interesting arrow to have in our sling,” said Andrew Charles, MD, professor of neurology and director of the UCLA Goldberg Migraine Program, who was not involved in the study.
Open-label trial results
The STOP 301 phase 3 open-label safety and tolerability trial treated over 5,650 migraine attacks in 354 patients who self-administered INP104 for up to 52 weeks. They were provided up to three doses per week (1.45 mg in a dose of two puffs, one per nostril). Maximum doses included two per day and three per week.
There were no new safety signals or concern trends in nasal safety findings. 15.0% of patients experienced nasal congestion, 6.8% nausea, 5.1% nasal discomfort, and 5.1% unpleasant taste.
A total of 66.3% of participants reported pain relief by 2 hours (severe or moderate pain reduced to mild or none, or mild pain reduced to none) following a dose, and 38% had freedom from pain. 16.3% reported pain relief onset at 15 minutes, with continued improvement over time. During weeks 21-24 of the study, 98.4% and 95% of patients reporting no recurrence of their migraine or use of rescue medications during the 24- and 48-hour periods after using INP104. “Once they got rid of the pain, it didn’t come back, and that’s been one of the shortcomings of many of the available oral therapies – although some of them can be quite effective, that effect can wear off and people can find their migraine comes back within a 24- or 48-hour period,” said Dr. Shrewsbury.
The drug was also rated as convenient, with 83.6% of participants strongly agreeing (50%) or agreeing (33.6%) that it is easy to use.
“It certainly looks like compliance will be good. The possibility is that this will be quite useful,” said Dr. Charles, who is also enthusiastic about some of the other drug formulations announced at the meeting. “It really is just fun times for us as clinicians to be able to have so many different options for patients,” he said.
Dr. Shrewsbury is an employee of Impel NeuroPharma, which funded the study.* Dr. Charles consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
SOURCE: Shrewsbury S, et al. AHS 2020. Abstract 832509.
*Correction, 6/19/20: An earlier version of this article misstated the name of Impel NeuroPharma.
, according to results from a phase 3 clinical trial. In development by Impel NeuroPharma, the new formulation could offer patients an at-home alternative to intramuscular infusions or intravenous injections currently used to deliver DHE.
“Our analysis of the data suggests that nothing new or untoward seemed to be happening as a result of delivering DHE to the upper nasal space,” Stephen Shrewsbury, MD, chief medical officer of Impel NeuroPharma, said in an interview. The company released key results from its phase 3 clinical trial, while a poster examining patient satisfaction was presented by Dr. Shrewsbury at the virtual annual meeting of the American Headache Society.
An improved intranasal formulation
The product isn’t the first effort to develop an inhaled form of DHE. An inhaled version called Migranal, marketed by Bausch Health, delivers DHE to the front part of the nose, where it may be lost to the upper lip or down the throat, according to Dr. Shrewsbury. Impel’s formulation (INP104) delivers the drug to the upper nasal space, where an earlier phase 1 trial demonstrated it could achieve higher serum concentrations compared with Migranal.
In 2018, MAP Pharmaceuticals came close to a product, but it was ultimately rejected by the Food and Drug Administration because DHE was not stable in the propellant used in the formulation. This time is different, said Dr. Shrewsbury, who was chief medical officer at MAP before joining Impel. The new device holds DHE and the propellant in separate compartments until they are combined right before use, which should circumvent stability problems.
Dr. Shrewsbury believes that patients will welcome an inhaled version of DHE. “People with migraines don’t want to have to go into hospital or even an infusion center if they can help it,” he said.
The study was one of a number of presentations at the AHS meeting that focused on novel delivery methods for established drugs. “The idea of taking things that we know work and improving upon them, both in terms of formulation and then delivery, that’s a common theme. My impression is that this will be an interesting arrow to have in our sling,” said Andrew Charles, MD, professor of neurology and director of the UCLA Goldberg Migraine Program, who was not involved in the study.
Open-label trial results
The STOP 301 phase 3 open-label safety and tolerability trial treated over 5,650 migraine attacks in 354 patients who self-administered INP104 for up to 52 weeks. They were provided up to three doses per week (1.45 mg in a dose of two puffs, one per nostril). Maximum doses included two per day and three per week.
There were no new safety signals or concern trends in nasal safety findings. 15.0% of patients experienced nasal congestion, 6.8% nausea, 5.1% nasal discomfort, and 5.1% unpleasant taste.
A total of 66.3% of participants reported pain relief by 2 hours (severe or moderate pain reduced to mild or none, or mild pain reduced to none) following a dose, and 38% had freedom from pain. 16.3% reported pain relief onset at 15 minutes, with continued improvement over time. During weeks 21-24 of the study, 98.4% and 95% of patients reporting no recurrence of their migraine or use of rescue medications during the 24- and 48-hour periods after using INP104. “Once they got rid of the pain, it didn’t come back, and that’s been one of the shortcomings of many of the available oral therapies – although some of them can be quite effective, that effect can wear off and people can find their migraine comes back within a 24- or 48-hour period,” said Dr. Shrewsbury.
The drug was also rated as convenient, with 83.6% of participants strongly agreeing (50%) or agreeing (33.6%) that it is easy to use.
“It certainly looks like compliance will be good. The possibility is that this will be quite useful,” said Dr. Charles, who is also enthusiastic about some of the other drug formulations announced at the meeting. “It really is just fun times for us as clinicians to be able to have so many different options for patients,” he said.
Dr. Shrewsbury is an employee of Impel NeuroPharma, which funded the study.* Dr. Charles consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
SOURCE: Shrewsbury S, et al. AHS 2020. Abstract 832509.
*Correction, 6/19/20: An earlier version of this article misstated the name of Impel NeuroPharma.
, according to results from a phase 3 clinical trial. In development by Impel NeuroPharma, the new formulation could offer patients an at-home alternative to intramuscular infusions or intravenous injections currently used to deliver DHE.
“Our analysis of the data suggests that nothing new or untoward seemed to be happening as a result of delivering DHE to the upper nasal space,” Stephen Shrewsbury, MD, chief medical officer of Impel NeuroPharma, said in an interview. The company released key results from its phase 3 clinical trial, while a poster examining patient satisfaction was presented by Dr. Shrewsbury at the virtual annual meeting of the American Headache Society.
An improved intranasal formulation
The product isn’t the first effort to develop an inhaled form of DHE. An inhaled version called Migranal, marketed by Bausch Health, delivers DHE to the front part of the nose, where it may be lost to the upper lip or down the throat, according to Dr. Shrewsbury. Impel’s formulation (INP104) delivers the drug to the upper nasal space, where an earlier phase 1 trial demonstrated it could achieve higher serum concentrations compared with Migranal.
In 2018, MAP Pharmaceuticals came close to a product, but it was ultimately rejected by the Food and Drug Administration because DHE was not stable in the propellant used in the formulation. This time is different, said Dr. Shrewsbury, who was chief medical officer at MAP before joining Impel. The new device holds DHE and the propellant in separate compartments until they are combined right before use, which should circumvent stability problems.
Dr. Shrewsbury believes that patients will welcome an inhaled version of DHE. “People with migraines don’t want to have to go into hospital or even an infusion center if they can help it,” he said.
The study was one of a number of presentations at the AHS meeting that focused on novel delivery methods for established drugs. “The idea of taking things that we know work and improving upon them, both in terms of formulation and then delivery, that’s a common theme. My impression is that this will be an interesting arrow to have in our sling,” said Andrew Charles, MD, professor of neurology and director of the UCLA Goldberg Migraine Program, who was not involved in the study.
Open-label trial results
The STOP 301 phase 3 open-label safety and tolerability trial treated over 5,650 migraine attacks in 354 patients who self-administered INP104 for up to 52 weeks. They were provided up to three doses per week (1.45 mg in a dose of two puffs, one per nostril). Maximum doses included two per day and three per week.
There were no new safety signals or concern trends in nasal safety findings. 15.0% of patients experienced nasal congestion, 6.8% nausea, 5.1% nasal discomfort, and 5.1% unpleasant taste.
A total of 66.3% of participants reported pain relief by 2 hours (severe or moderate pain reduced to mild or none, or mild pain reduced to none) following a dose, and 38% had freedom from pain. 16.3% reported pain relief onset at 15 minutes, with continued improvement over time. During weeks 21-24 of the study, 98.4% and 95% of patients reporting no recurrence of their migraine or use of rescue medications during the 24- and 48-hour periods after using INP104. “Once they got rid of the pain, it didn’t come back, and that’s been one of the shortcomings of many of the available oral therapies – although some of them can be quite effective, that effect can wear off and people can find their migraine comes back within a 24- or 48-hour period,” said Dr. Shrewsbury.
The drug was also rated as convenient, with 83.6% of participants strongly agreeing (50%) or agreeing (33.6%) that it is easy to use.
“It certainly looks like compliance will be good. The possibility is that this will be quite useful,” said Dr. Charles, who is also enthusiastic about some of the other drug formulations announced at the meeting. “It really is just fun times for us as clinicians to be able to have so many different options for patients,” he said.
Dr. Shrewsbury is an employee of Impel NeuroPharma, which funded the study.* Dr. Charles consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
SOURCE: Shrewsbury S, et al. AHS 2020. Abstract 832509.
*Correction, 6/19/20: An earlier version of this article misstated the name of Impel NeuroPharma.
FROM AHS 2020
Daily Recap 6/17
Here are the stories our MDedge editors across specialties think you need to know about today:
Comorbidities increase COVID-19 deaths by factor of 12
COVID-19 patients with an underlying condition are 6 times as likely to be hospitalized and 12 times as likely to die, compared with those who have no such condition, according to the CDC.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females.
The pandemic “continues to affect all populations and result in severe outcomes including death,” noted the CDC, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.” Read more.
Preventive services coalition recommends routine anxiety screening for women
Women and girls aged 13 years and older with no current diagnosis of anxiety should be screened routinely for anxiety, according to a new recommendation from the Women’s Preventive Services Initiative.
The lifetime prevalence of anxiety disorders in women in the United States is 40%, approximately twice that of men, and anxiety can be a manifestation of underlying issues including posttraumatic stress, sexual harassment, and assault.
“The WPSI based its rationale for anxiety screening on several considerations,” the researchers noted. “Anxiety disorders are the most prevalent mental health disorders in women, and the problems created by untreated anxiety can impair function in all areas of a woman’s life.” Read more.
High-fat, high-sugar diet may promote adult acne
A diet higher in fat, sugar, and milk was associated with having acne in a cross-sectional study of approximately 24,000 adults in France.
Although acne patients may believe that eating certain foods exacerbates acne, data on the effects of nutrition on acne, including associations between acne and a high-glycemic diet, are limited and have produced conflicting results, noted investigators.
“The results of our study appear to support the hypothesis that the Western diet (rich in animal products and fatty and sugary foods) is associated with the presence of acne in adulthood,” the researchers concluded.
Population study supports migraine-dementia link
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that migraine with aura and frequent hospital contacts significantly increased dementia risk after age 60 years, according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Sabrina Islamoska said.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Comorbidities increase COVID-19 deaths by factor of 12
COVID-19 patients with an underlying condition are 6 times as likely to be hospitalized and 12 times as likely to die, compared with those who have no such condition, according to the CDC.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females.
The pandemic “continues to affect all populations and result in severe outcomes including death,” noted the CDC, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.” Read more.
Preventive services coalition recommends routine anxiety screening for women
Women and girls aged 13 years and older with no current diagnosis of anxiety should be screened routinely for anxiety, according to a new recommendation from the Women’s Preventive Services Initiative.
The lifetime prevalence of anxiety disorders in women in the United States is 40%, approximately twice that of men, and anxiety can be a manifestation of underlying issues including posttraumatic stress, sexual harassment, and assault.
“The WPSI based its rationale for anxiety screening on several considerations,” the researchers noted. “Anxiety disorders are the most prevalent mental health disorders in women, and the problems created by untreated anxiety can impair function in all areas of a woman’s life.” Read more.
High-fat, high-sugar diet may promote adult acne
A diet higher in fat, sugar, and milk was associated with having acne in a cross-sectional study of approximately 24,000 adults in France.
Although acne patients may believe that eating certain foods exacerbates acne, data on the effects of nutrition on acne, including associations between acne and a high-glycemic diet, are limited and have produced conflicting results, noted investigators.
“The results of our study appear to support the hypothesis that the Western diet (rich in animal products and fatty and sugary foods) is associated with the presence of acne in adulthood,” the researchers concluded.
Population study supports migraine-dementia link
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that migraine with aura and frequent hospital contacts significantly increased dementia risk after age 60 years, according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Sabrina Islamoska said.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
Comorbidities increase COVID-19 deaths by factor of 12
COVID-19 patients with an underlying condition are 6 times as likely to be hospitalized and 12 times as likely to die, compared with those who have no such condition, according to the CDC.
The most frequently reported underlying conditions were cardiovascular disease (32%), diabetes (30%), chronic lung disease (18%), and renal disease (7.6%), and there were no significant differences between males and females.
The pandemic “continues to affect all populations and result in severe outcomes including death,” noted the CDC, emphasizing “the continued need for community mitigation strategies, especially for vulnerable populations, to slow COVID-19 transmission.” Read more.
Preventive services coalition recommends routine anxiety screening for women
Women and girls aged 13 years and older with no current diagnosis of anxiety should be screened routinely for anxiety, according to a new recommendation from the Women’s Preventive Services Initiative.
The lifetime prevalence of anxiety disorders in women in the United States is 40%, approximately twice that of men, and anxiety can be a manifestation of underlying issues including posttraumatic stress, sexual harassment, and assault.
“The WPSI based its rationale for anxiety screening on several considerations,” the researchers noted. “Anxiety disorders are the most prevalent mental health disorders in women, and the problems created by untreated anxiety can impair function in all areas of a woman’s life.” Read more.
High-fat, high-sugar diet may promote adult acne
A diet higher in fat, sugar, and milk was associated with having acne in a cross-sectional study of approximately 24,000 adults in France.
Although acne patients may believe that eating certain foods exacerbates acne, data on the effects of nutrition on acne, including associations between acne and a high-glycemic diet, are limited and have produced conflicting results, noted investigators.
“The results of our study appear to support the hypothesis that the Western diet (rich in animal products and fatty and sugary foods) is associated with the presence of acne in adulthood,” the researchers concluded.
Population study supports migraine-dementia link
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that migraine with aura and frequent hospital contacts significantly increased dementia risk after age 60 years, according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Sabrina Islamoska said.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Persistent posttraumatic headache risk factors confirmed
It also revealed a surprisingly high frequency of misdiagnosis. The original sample included 500 patients drawn from the Stanford Research Repository Cohort Discovery Tool, but a review found 200 records that were misdiagnosed and had to be excluded.
“It’s very easy to label someone who suffered a head injury and say this is the reason why they have this (headache),” said lead author Tommy Chan, MBBS, a headache fellow in the department of neurology at Stanford (Calif.) University, in an interview. Such patients are often seen by ED or primary care physicians who do not have a lot of experience with posttraumatic headache, and that can lead to negative consequences if a low-pressure headache is mistaken as stemming from a skull fracture. “It’s a very different treatment plan for one versus the other,” said Dr. Chan in an interview.
He noted that it can help to take a patient history that includes the preaccident headache frequency and determine if there was a change in frequency post injury.
Dr. Chan presented the results at the virtual annual meeting of the American Headache Society.
“The results are what one might expect, although we haven’t studied it enough to really know. We haven’t systematically characterized these risk factors for chronic posttraumatic headache very well, [so] it’s useful to have this information,” said Andrew Charles, MD, professor neurology at the University of California, Los Angeles, and director of the UCLA Goldberg Migraine Program, who was not involved in the study. However, Dr. Charles emphasized the need to confirm the results prospectively.
Defining risk factors
The analysis found that a history of migraines, medication overuse, psychological disorders, and new posttraumatic headache–associated comorbidities were all associated with a greater risk for persistent posttraumatic headache. None of those came as a surprise, “but we live in a world where medicine is practiced based on evidence, and providers want to see data to support that. I think that this will help with resource allocation. It’s important to address [a patient’s] overuse of medications, or if they’re having psychological symptoms,” said Dr. Chan.
A total of 150 patients in the analysis had acute posttraumatic headache (mean duration, 0.7 months) while 150 had persistent posttraumatic headache (mean duration, 24 months; P < .00001). Clinical factors associated with risk of persistent headache included a history migraine (relative risk, 2.4; P < .0001), a previous head injury (odds ratio, 5.8; P < .0001), medication overuse (RR, 2.6; P < .0001), preexisting psychological history (OR, 5; P < .0001), and new posttraumatic headache–associated comorbidities, such as vertigo or posttraumatic stress disorder (RR, 9.8; P < .0001).
Identifying patient subgroups
The researchers also identified four subcategories of patients with persistent posttraumatic headache, each with differing risk factors and clinical characteristics. It’s too soon to use these identifiers to make clinical recommendations, but Dr. Chan hopes that further study of these groups will be informative. “It might point us toward (the idea) that each patient population is actually different, even within the chronic persistent posttraumatic headache population, we can’t group them all under the same umbrella term. If we can tease out that a patient has truly had a head injury, but no history of migraine, no overuse of medication, no psychological history, and no other associated symptoms, this would be a very interesting population to study because they would help us understand the pathophysiology [of persistent posttraumatic headache].”
Although the study was conducted by defining persistent posttraumatic headache as lasting at least 3 months, Dr. Chan took issue with that commonly held definition. That choice is arbitrary, with no pathophysiological basis or data to support it, and is based more on clinical trials testing preventative treatments. But when it is used in clinical practice, it can muddy communication with patients. “When this timeline is told to a patient, and when it’s not achieved, they might become disappointed. We should not put too much emphasis on time. Everybody is different,” he said.
The study did not receive any funding. Dr. Chan had no relevant financial disclosures. Dr. Charles consults for consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
It also revealed a surprisingly high frequency of misdiagnosis. The original sample included 500 patients drawn from the Stanford Research Repository Cohort Discovery Tool, but a review found 200 records that were misdiagnosed and had to be excluded.
“It’s very easy to label someone who suffered a head injury and say this is the reason why they have this (headache),” said lead author Tommy Chan, MBBS, a headache fellow in the department of neurology at Stanford (Calif.) University, in an interview. Such patients are often seen by ED or primary care physicians who do not have a lot of experience with posttraumatic headache, and that can lead to negative consequences if a low-pressure headache is mistaken as stemming from a skull fracture. “It’s a very different treatment plan for one versus the other,” said Dr. Chan in an interview.
He noted that it can help to take a patient history that includes the preaccident headache frequency and determine if there was a change in frequency post injury.
Dr. Chan presented the results at the virtual annual meeting of the American Headache Society.
“The results are what one might expect, although we haven’t studied it enough to really know. We haven’t systematically characterized these risk factors for chronic posttraumatic headache very well, [so] it’s useful to have this information,” said Andrew Charles, MD, professor neurology at the University of California, Los Angeles, and director of the UCLA Goldberg Migraine Program, who was not involved in the study. However, Dr. Charles emphasized the need to confirm the results prospectively.
Defining risk factors
The analysis found that a history of migraines, medication overuse, psychological disorders, and new posttraumatic headache–associated comorbidities were all associated with a greater risk for persistent posttraumatic headache. None of those came as a surprise, “but we live in a world where medicine is practiced based on evidence, and providers want to see data to support that. I think that this will help with resource allocation. It’s important to address [a patient’s] overuse of medications, or if they’re having psychological symptoms,” said Dr. Chan.
A total of 150 patients in the analysis had acute posttraumatic headache (mean duration, 0.7 months) while 150 had persistent posttraumatic headache (mean duration, 24 months; P < .00001). Clinical factors associated with risk of persistent headache included a history migraine (relative risk, 2.4; P < .0001), a previous head injury (odds ratio, 5.8; P < .0001), medication overuse (RR, 2.6; P < .0001), preexisting psychological history (OR, 5; P < .0001), and new posttraumatic headache–associated comorbidities, such as vertigo or posttraumatic stress disorder (RR, 9.8; P < .0001).
Identifying patient subgroups
The researchers also identified four subcategories of patients with persistent posttraumatic headache, each with differing risk factors and clinical characteristics. It’s too soon to use these identifiers to make clinical recommendations, but Dr. Chan hopes that further study of these groups will be informative. “It might point us toward (the idea) that each patient population is actually different, even within the chronic persistent posttraumatic headache population, we can’t group them all under the same umbrella term. If we can tease out that a patient has truly had a head injury, but no history of migraine, no overuse of medication, no psychological history, and no other associated symptoms, this would be a very interesting population to study because they would help us understand the pathophysiology [of persistent posttraumatic headache].”
Although the study was conducted by defining persistent posttraumatic headache as lasting at least 3 months, Dr. Chan took issue with that commonly held definition. That choice is arbitrary, with no pathophysiological basis or data to support it, and is based more on clinical trials testing preventative treatments. But when it is used in clinical practice, it can muddy communication with patients. “When this timeline is told to a patient, and when it’s not achieved, they might become disappointed. We should not put too much emphasis on time. Everybody is different,” he said.
The study did not receive any funding. Dr. Chan had no relevant financial disclosures. Dr. Charles consults for consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
It also revealed a surprisingly high frequency of misdiagnosis. The original sample included 500 patients drawn from the Stanford Research Repository Cohort Discovery Tool, but a review found 200 records that were misdiagnosed and had to be excluded.
“It’s very easy to label someone who suffered a head injury and say this is the reason why they have this (headache),” said lead author Tommy Chan, MBBS, a headache fellow in the department of neurology at Stanford (Calif.) University, in an interview. Such patients are often seen by ED or primary care physicians who do not have a lot of experience with posttraumatic headache, and that can lead to negative consequences if a low-pressure headache is mistaken as stemming from a skull fracture. “It’s a very different treatment plan for one versus the other,” said Dr. Chan in an interview.
He noted that it can help to take a patient history that includes the preaccident headache frequency and determine if there was a change in frequency post injury.
Dr. Chan presented the results at the virtual annual meeting of the American Headache Society.
“The results are what one might expect, although we haven’t studied it enough to really know. We haven’t systematically characterized these risk factors for chronic posttraumatic headache very well, [so] it’s useful to have this information,” said Andrew Charles, MD, professor neurology at the University of California, Los Angeles, and director of the UCLA Goldberg Migraine Program, who was not involved in the study. However, Dr. Charles emphasized the need to confirm the results prospectively.
Defining risk factors
The analysis found that a history of migraines, medication overuse, psychological disorders, and new posttraumatic headache–associated comorbidities were all associated with a greater risk for persistent posttraumatic headache. None of those came as a surprise, “but we live in a world where medicine is practiced based on evidence, and providers want to see data to support that. I think that this will help with resource allocation. It’s important to address [a patient’s] overuse of medications, or if they’re having psychological symptoms,” said Dr. Chan.
A total of 150 patients in the analysis had acute posttraumatic headache (mean duration, 0.7 months) while 150 had persistent posttraumatic headache (mean duration, 24 months; P < .00001). Clinical factors associated with risk of persistent headache included a history migraine (relative risk, 2.4; P < .0001), a previous head injury (odds ratio, 5.8; P < .0001), medication overuse (RR, 2.6; P < .0001), preexisting psychological history (OR, 5; P < .0001), and new posttraumatic headache–associated comorbidities, such as vertigo or posttraumatic stress disorder (RR, 9.8; P < .0001).
Identifying patient subgroups
The researchers also identified four subcategories of patients with persistent posttraumatic headache, each with differing risk factors and clinical characteristics. It’s too soon to use these identifiers to make clinical recommendations, but Dr. Chan hopes that further study of these groups will be informative. “It might point us toward (the idea) that each patient population is actually different, even within the chronic persistent posttraumatic headache population, we can’t group them all under the same umbrella term. If we can tease out that a patient has truly had a head injury, but no history of migraine, no overuse of medication, no psychological history, and no other associated symptoms, this would be a very interesting population to study because they would help us understand the pathophysiology [of persistent posttraumatic headache].”
Although the study was conducted by defining persistent posttraumatic headache as lasting at least 3 months, Dr. Chan took issue with that commonly held definition. That choice is arbitrary, with no pathophysiological basis or data to support it, and is based more on clinical trials testing preventative treatments. But when it is used in clinical practice, it can muddy communication with patients. “When this timeline is told to a patient, and when it’s not achieved, they might become disappointed. We should not put too much emphasis on time. Everybody is different,” he said.
The study did not receive any funding. Dr. Chan had no relevant financial disclosures. Dr. Charles consults for consults for Amgen, BioHaven, Eli Lilly, Novartis, and Lundbeck.
FROM AHS 2020
Few patients with migraine clear barriers to optimal care
, new research shows.
Results from a survey study showed less than 8% of patients with episodic migraine and less than 2% of patients with chronic migraine were able to overcome four key treatment barriers associated with optimal migraine management. These included current medical consultation, appropriate diagnosis, minimally adequate acute and preventive pharmacologic treatment (if indicated), and absence of acute medication overdose.
The researchers also evaluated any potential impact of race, ethnicity, and sociodemographic factors on these barriers.
“While chronic migraine was associated with higher rates of consulting, only 1.8% of respondents with chronic migraine traversed all four barriers compared with 8.5% of those with episodic migraine,” the investigators, led by Dawn C. Buse, PhD, clinical professor of neurology at Albert Einstein College of Medicine of Yeshiva University in New York City, noted.
The study was presented at the virtual annual meeting of the American Headache Society.
Ongoing challenges
Migraineurs’ challenges include receiving an appropriate diagnosis and finding effective acute and preventive treatments, the researchers noted. Many patients do not receive optimal care. Previous research by Dr. Buse and colleagues showed that general clinicians were less likely to provide an appropriate diagnosis of migraine compared with headache specialists.
Among patients with chronic migraine who consulted headache specialists, most did not receive an accurate diagnosis of chronic migraine. Data also indicate that a minority, approximately 34%, of patients with chronic migraine used preventive pharmacologic treatments.
The investigators analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study to determine the proportion of patients who overcame four prespecified barriers to good outcomes.
Eligible participants met modified International Classification of Headache Disorders (3rd edition) criteria for migraine, had Migraine Disability Assessment Scores (MIDAS) of grade II or higher, and provided data on health insurance status. In addition, all eligible participants had to be receiving appropriate treatment for either episodic or chronic migraine.
In all, 16,789 participants met criteria for migraine. Of this group, 9,184 patients had a MIDAS score of grade II or higher and reported health insurance status. In this subgroup, 7,930 (86.3%) patients had episodic migraine and 1,254 (13.7%) had chronic migraine.
A total of 2,187 (27.6%) patients with episodic migraine and 512 (40.8%) patients with chronic migraine were under the care of a healthcare professional. Of this group, 1,655 patients with episodic migraine (75.7%) and 168 with chronic migraine (32.8%) reported receiving an appropriate diagnosis.
Of participants who successfully overcame the first two optimal management barriers—a consultation with a healthcare professional and an appropriate diagnosis—1,133 (68.5%) episodic migraineurs and 113 (67.3%) chronic migraineurs reported receiving minimally adequate acute treatment.
Furthermore, 1,430 (86.4%) episodic migraineurs and 127 (75.6%) chronic migraineurs reported receiving minimally adequate preventive medication treatment. In addition, 982 (59.3%) episodic migraineurs and 88 (52.4%) chronic migraineurs received minimally adequate acute and preventive treatment.
Acute medication overuse was relatively common, the investigators reported. A total of 310 (31.6%) patients with episodic migraine and 66 (75%) patients with chronic migraine met criteria for acute medication overuse.
“Overuse of acute medication for migraine in people with chronic migraine is a serious concern and is associated with increased risks of migraine progression, headache-related disability, and anxiety and depression. Active patient management and education is important to reduce the likelihood of medication overuse,” said Dr. Buse.
Among all eligible respondents, only 672 (8.5%) patients with episodic migraine and 22 (1.8%) with chronic migraine overcame all four barriers to optimal care.
The researchers found no significant effect of ethnicity or race on the likelihood of overcoming any barrier, but they acknowledged that participation bias might have contributed to this lack of difference. Higher annual household income was significantly associated with high likelihood of surmounting all four barriers.
“The analysis of sociodemographics revealed that female sex and higher annual household income showed a strong relationship with likelihood of obtaining an accurate episodic migraine or chronic migraine diagnosis,” said Dr. Buse.
“Although the reasons for this are not clear, it may be that women are more likely to convey the full scope of their symptoms during consultation. Additionally, the known prevalence of migraine in women may influence healthcare providers by reducing suspicion of chronic migraine in men,” she added.
The CaMEO Study was funded by Allergan (now AbbVie). Dr. Buse reports receiving grant support and honoraria from Allergan, Amgen, Biohaven, Eli Lilly and Co, and Promius. She also receives compensation for work on the editorial board of Current Pain and Headache Reports.
This article first appeared on Medscape.com.
, new research shows.
Results from a survey study showed less than 8% of patients with episodic migraine and less than 2% of patients with chronic migraine were able to overcome four key treatment barriers associated with optimal migraine management. These included current medical consultation, appropriate diagnosis, minimally adequate acute and preventive pharmacologic treatment (if indicated), and absence of acute medication overdose.
The researchers also evaluated any potential impact of race, ethnicity, and sociodemographic factors on these barriers.
“While chronic migraine was associated with higher rates of consulting, only 1.8% of respondents with chronic migraine traversed all four barriers compared with 8.5% of those with episodic migraine,” the investigators, led by Dawn C. Buse, PhD, clinical professor of neurology at Albert Einstein College of Medicine of Yeshiva University in New York City, noted.
The study was presented at the virtual annual meeting of the American Headache Society.
Ongoing challenges
Migraineurs’ challenges include receiving an appropriate diagnosis and finding effective acute and preventive treatments, the researchers noted. Many patients do not receive optimal care. Previous research by Dr. Buse and colleagues showed that general clinicians were less likely to provide an appropriate diagnosis of migraine compared with headache specialists.
Among patients with chronic migraine who consulted headache specialists, most did not receive an accurate diagnosis of chronic migraine. Data also indicate that a minority, approximately 34%, of patients with chronic migraine used preventive pharmacologic treatments.
The investigators analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study to determine the proportion of patients who overcame four prespecified barriers to good outcomes.
Eligible participants met modified International Classification of Headache Disorders (3rd edition) criteria for migraine, had Migraine Disability Assessment Scores (MIDAS) of grade II or higher, and provided data on health insurance status. In addition, all eligible participants had to be receiving appropriate treatment for either episodic or chronic migraine.
In all, 16,789 participants met criteria for migraine. Of this group, 9,184 patients had a MIDAS score of grade II or higher and reported health insurance status. In this subgroup, 7,930 (86.3%) patients had episodic migraine and 1,254 (13.7%) had chronic migraine.
A total of 2,187 (27.6%) patients with episodic migraine and 512 (40.8%) patients with chronic migraine were under the care of a healthcare professional. Of this group, 1,655 patients with episodic migraine (75.7%) and 168 with chronic migraine (32.8%) reported receiving an appropriate diagnosis.
Of participants who successfully overcame the first two optimal management barriers—a consultation with a healthcare professional and an appropriate diagnosis—1,133 (68.5%) episodic migraineurs and 113 (67.3%) chronic migraineurs reported receiving minimally adequate acute treatment.
Furthermore, 1,430 (86.4%) episodic migraineurs and 127 (75.6%) chronic migraineurs reported receiving minimally adequate preventive medication treatment. In addition, 982 (59.3%) episodic migraineurs and 88 (52.4%) chronic migraineurs received minimally adequate acute and preventive treatment.
Acute medication overuse was relatively common, the investigators reported. A total of 310 (31.6%) patients with episodic migraine and 66 (75%) patients with chronic migraine met criteria for acute medication overuse.
“Overuse of acute medication for migraine in people with chronic migraine is a serious concern and is associated with increased risks of migraine progression, headache-related disability, and anxiety and depression. Active patient management and education is important to reduce the likelihood of medication overuse,” said Dr. Buse.
Among all eligible respondents, only 672 (8.5%) patients with episodic migraine and 22 (1.8%) with chronic migraine overcame all four barriers to optimal care.
The researchers found no significant effect of ethnicity or race on the likelihood of overcoming any barrier, but they acknowledged that participation bias might have contributed to this lack of difference. Higher annual household income was significantly associated with high likelihood of surmounting all four barriers.
“The analysis of sociodemographics revealed that female sex and higher annual household income showed a strong relationship with likelihood of obtaining an accurate episodic migraine or chronic migraine diagnosis,” said Dr. Buse.
“Although the reasons for this are not clear, it may be that women are more likely to convey the full scope of their symptoms during consultation. Additionally, the known prevalence of migraine in women may influence healthcare providers by reducing suspicion of chronic migraine in men,” she added.
The CaMEO Study was funded by Allergan (now AbbVie). Dr. Buse reports receiving grant support and honoraria from Allergan, Amgen, Biohaven, Eli Lilly and Co, and Promius. She also receives compensation for work on the editorial board of Current Pain and Headache Reports.
This article first appeared on Medscape.com.
, new research shows.
Results from a survey study showed less than 8% of patients with episodic migraine and less than 2% of patients with chronic migraine were able to overcome four key treatment barriers associated with optimal migraine management. These included current medical consultation, appropriate diagnosis, minimally adequate acute and preventive pharmacologic treatment (if indicated), and absence of acute medication overdose.
The researchers also evaluated any potential impact of race, ethnicity, and sociodemographic factors on these barriers.
“While chronic migraine was associated with higher rates of consulting, only 1.8% of respondents with chronic migraine traversed all four barriers compared with 8.5% of those with episodic migraine,” the investigators, led by Dawn C. Buse, PhD, clinical professor of neurology at Albert Einstein College of Medicine of Yeshiva University in New York City, noted.
The study was presented at the virtual annual meeting of the American Headache Society.
Ongoing challenges
Migraineurs’ challenges include receiving an appropriate diagnosis and finding effective acute and preventive treatments, the researchers noted. Many patients do not receive optimal care. Previous research by Dr. Buse and colleagues showed that general clinicians were less likely to provide an appropriate diagnosis of migraine compared with headache specialists.
Among patients with chronic migraine who consulted headache specialists, most did not receive an accurate diagnosis of chronic migraine. Data also indicate that a minority, approximately 34%, of patients with chronic migraine used preventive pharmacologic treatments.
The investigators analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study to determine the proportion of patients who overcame four prespecified barriers to good outcomes.
Eligible participants met modified International Classification of Headache Disorders (3rd edition) criteria for migraine, had Migraine Disability Assessment Scores (MIDAS) of grade II or higher, and provided data on health insurance status. In addition, all eligible participants had to be receiving appropriate treatment for either episodic or chronic migraine.
In all, 16,789 participants met criteria for migraine. Of this group, 9,184 patients had a MIDAS score of grade II or higher and reported health insurance status. In this subgroup, 7,930 (86.3%) patients had episodic migraine and 1,254 (13.7%) had chronic migraine.
A total of 2,187 (27.6%) patients with episodic migraine and 512 (40.8%) patients with chronic migraine were under the care of a healthcare professional. Of this group, 1,655 patients with episodic migraine (75.7%) and 168 with chronic migraine (32.8%) reported receiving an appropriate diagnosis.
Of participants who successfully overcame the first two optimal management barriers—a consultation with a healthcare professional and an appropriate diagnosis—1,133 (68.5%) episodic migraineurs and 113 (67.3%) chronic migraineurs reported receiving minimally adequate acute treatment.
Furthermore, 1,430 (86.4%) episodic migraineurs and 127 (75.6%) chronic migraineurs reported receiving minimally adequate preventive medication treatment. In addition, 982 (59.3%) episodic migraineurs and 88 (52.4%) chronic migraineurs received minimally adequate acute and preventive treatment.
Acute medication overuse was relatively common, the investigators reported. A total of 310 (31.6%) patients with episodic migraine and 66 (75%) patients with chronic migraine met criteria for acute medication overuse.
“Overuse of acute medication for migraine in people with chronic migraine is a serious concern and is associated with increased risks of migraine progression, headache-related disability, and anxiety and depression. Active patient management and education is important to reduce the likelihood of medication overuse,” said Dr. Buse.
Among all eligible respondents, only 672 (8.5%) patients with episodic migraine and 22 (1.8%) with chronic migraine overcame all four barriers to optimal care.
The researchers found no significant effect of ethnicity or race on the likelihood of overcoming any barrier, but they acknowledged that participation bias might have contributed to this lack of difference. Higher annual household income was significantly associated with high likelihood of surmounting all four barriers.
“The analysis of sociodemographics revealed that female sex and higher annual household income showed a strong relationship with likelihood of obtaining an accurate episodic migraine or chronic migraine diagnosis,” said Dr. Buse.
“Although the reasons for this are not clear, it may be that women are more likely to convey the full scope of their symptoms during consultation. Additionally, the known prevalence of migraine in women may influence healthcare providers by reducing suspicion of chronic migraine in men,” she added.
The CaMEO Study was funded by Allergan (now AbbVie). Dr. Buse reports receiving grant support and honoraria from Allergan, Amgen, Biohaven, Eli Lilly and Co, and Promius. She also receives compensation for work on the editorial board of Current Pain and Headache Reports.
This article first appeared on Medscape.com.
From AHS 2020
Population study supports migraine–dementia link
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.

“The findings of this study emphasize the need for studies in the migraine-dementia pathophysiology, in particular in migraine cases with aura,” said Sabrina Islamoska, MSc, PhD, a postdoctoral researcher in the department of public health at the University of Copenhagen. “This study highlights the importance of monitoring severe migraine to potentially prevent dementia.”
A national register-based study
The study used Danish national register–based data from 1988 to 2017 of 1.66 million individuals born between 1935 and 1956, retrieving exposure information until age 59 years and following individuals for dementia after age 60. The matched analysis included 18,135 people registered with migraine before age 59 and 1.38 million without migraine. The matched study population was 62,578.
A diagnosis of dementia or use of dementia medications after age 60 years was the main outcome. Covariates included socioeconomic factors, psychiatric comorbidities and other headache diagnoses.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Islamoska said.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“We also found a 20% higher but nonsignificant dementia rate in individuals who had migraine without aura,” she said. However, when the migraine-with-aura population was evaluated, it was found to have a dementia rate two times higher than people with no migraine. “The dementia rate was higher if individuals had more frequent hospital contacts with migraine.”
The findings support the hypothesis that migraine is a midlife risk factor for dementia later in life, she said.
“The findings underline the value of investigating the effect of migraine medications in dementia risk to assess the impact of mild to moderate migraines,” Dr. Islamoska said. “Therefore, the next step is to investigate the risk of dementia among users of migraine medications who are not diagnosed with migraines at hospitals.”
Strengths of the study, Dr. Islamoska noted, were its size and national nature of its population, that it included all migraine diagnoses at hospitals over a 29-year period, that it made adjustments for confounding of well-established dementia risk factors, and that it validated dementia diagnoses after age 60 years.
One limitation was that the study only included hospital-based diagnoses of dementia while 60% of cases in Denmark are undiagnosed, “thus our results only apply to migraine that is severe enough to require a hospital contact,” Dr. Islamoska said, while most migraine cases are treated in the primary care setting.
Also, the young study population may have a lower dementia risk. “We also know that age of migraine registration may not corresponded with the actual onset, since migraine is a complex disorder with individual variation in patient’s burden and course of disease,” Dr. Islamoska said.
“Future studies are needed to understand the pathological mechanisms underlying the relationship between migraine and dementia and to investigate whether proper prophylactic treatment of migraine can potentially prevent dementia,” Dr. Islamoska said. “In addition, when investigating the association between these two prevalent neurological disorders, the timing of migraine diagnosis and dementia onset is important to ensure temporality. We took this into account in our study to strengthen the validity of our results.”
‘Surprising’ findings
Andrew Charles, MD, director of the Goldberg Migraine Program at the University of California, Los Angeles, said the Danish study makes an important contribution to the literature on dementia risk factors. “Vanishingly small amounts of attention have been paid to migraine as a potential risk factor,” he said. However, he called the results “surprising” based on his own clinical experience. “I actually had a sense that migraine was somehow protective against Alzheimer’s or other kinds of dementias.”
He questioned if the migraine-dementia link could be a “reporting artifact” of migraine sufferers merely going to the neurologist, raising the likelihood of a positive migraine diagnosis. Nonetheless, the results are “intriguing” and raise important questions about migraine therapy and dementia risk.
“If it holds up, it really is something that behooves us to understand whether intervening in terms of therapy for migraine has even more consequences beyond just the immediate relief of symptoms,” Dr. Charles said. “It’s something we should be thinking about in terms of preventing longer-term consequences of this disorder.”
Dr. Islamoska disclosed that Veluxfondent funded the study as part of her PhD project. Dr. Charles disclosed he is a consultant to Amgen, Biohaven Pharmaceuticals, Eli Lilly, Lundbeck, and Novartis.
SOURCE: Islamoska S et al. AHS 2020, Submission 846214.
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.
“The findings of this study emphasize the need for studies in the migraine-dementia pathophysiology, in particular in migraine cases with aura,” said Sabrina Islamoska, MSc, PhD, a postdoctoral researcher in the department of public health at the University of Copenhagen. “This study highlights the importance of monitoring severe migraine to potentially prevent dementia.”
A national register-based study
The study used Danish national register–based data from 1988 to 2017 of 1.66 million individuals born between 1935 and 1956, retrieving exposure information until age 59 years and following individuals for dementia after age 60. The matched analysis included 18,135 people registered with migraine before age 59 and 1.38 million without migraine. The matched study population was 62,578.
A diagnosis of dementia or use of dementia medications after age 60 years was the main outcome. Covariates included socioeconomic factors, psychiatric comorbidities and other headache diagnoses.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Islamoska said.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“We also found a 20% higher but nonsignificant dementia rate in individuals who had migraine without aura,” she said. However, when the migraine-with-aura population was evaluated, it was found to have a dementia rate two times higher than people with no migraine. “The dementia rate was higher if individuals had more frequent hospital contacts with migraine.”
The findings support the hypothesis that migraine is a midlife risk factor for dementia later in life, she said.
“The findings underline the value of investigating the effect of migraine medications in dementia risk to assess the impact of mild to moderate migraines,” Dr. Islamoska said. “Therefore, the next step is to investigate the risk of dementia among users of migraine medications who are not diagnosed with migraines at hospitals.”
Strengths of the study, Dr. Islamoska noted, were its size and national nature of its population, that it included all migraine diagnoses at hospitals over a 29-year period, that it made adjustments for confounding of well-established dementia risk factors, and that it validated dementia diagnoses after age 60 years.
One limitation was that the study only included hospital-based diagnoses of dementia while 60% of cases in Denmark are undiagnosed, “thus our results only apply to migraine that is severe enough to require a hospital contact,” Dr. Islamoska said, while most migraine cases are treated in the primary care setting.
Also, the young study population may have a lower dementia risk. “We also know that age of migraine registration may not corresponded with the actual onset, since migraine is a complex disorder with individual variation in patient’s burden and course of disease,” Dr. Islamoska said.
“Future studies are needed to understand the pathological mechanisms underlying the relationship between migraine and dementia and to investigate whether proper prophylactic treatment of migraine can potentially prevent dementia,” Dr. Islamoska said. “In addition, when investigating the association between these two prevalent neurological disorders, the timing of migraine diagnosis and dementia onset is important to ensure temporality. We took this into account in our study to strengthen the validity of our results.”
‘Surprising’ findings
Andrew Charles, MD, director of the Goldberg Migraine Program at the University of California, Los Angeles, said the Danish study makes an important contribution to the literature on dementia risk factors. “Vanishingly small amounts of attention have been paid to migraine as a potential risk factor,” he said. However, he called the results “surprising” based on his own clinical experience. “I actually had a sense that migraine was somehow protective against Alzheimer’s or other kinds of dementias.”
He questioned if the migraine-dementia link could be a “reporting artifact” of migraine sufferers merely going to the neurologist, raising the likelihood of a positive migraine diagnosis. Nonetheless, the results are “intriguing” and raise important questions about migraine therapy and dementia risk.
“If it holds up, it really is something that behooves us to understand whether intervening in terms of therapy for migraine has even more consequences beyond just the immediate relief of symptoms,” Dr. Charles said. “It’s something we should be thinking about in terms of preventing longer-term consequences of this disorder.”
Dr. Islamoska disclosed that Veluxfondent funded the study as part of her PhD project. Dr. Charles disclosed he is a consultant to Amgen, Biohaven Pharmaceuticals, Eli Lilly, Lundbeck, and Novartis.
SOURCE: Islamoska S et al. AHS 2020, Submission 846214.
Preliminary results from a population-based cohort study support previous reports that migraine is a midlife risk factor for dementia later in life, but further determined that according to results from a Danish registry presented at the virtual annual meeting of the American Headache Society.
“The findings of this study emphasize the need for studies in the migraine-dementia pathophysiology, in particular in migraine cases with aura,” said Sabrina Islamoska, MSc, PhD, a postdoctoral researcher in the department of public health at the University of Copenhagen. “This study highlights the importance of monitoring severe migraine to potentially prevent dementia.”
A national register-based study
The study used Danish national register–based data from 1988 to 2017 of 1.66 million individuals born between 1935 and 1956, retrieving exposure information until age 59 years and following individuals for dementia after age 60. The matched analysis included 18,135 people registered with migraine before age 59 and 1.38 million without migraine. The matched study population was 62,578.
A diagnosis of dementia or use of dementia medications after age 60 years was the main outcome. Covariates included socioeconomic factors, psychiatric comorbidities and other headache diagnoses.
“To the best of our knowledge, no previous national register–based studies have investigated the risk of dementia among individuals who suffer from migraine with aura,” Dr. Islamoska said.
The preliminary findings revealed that the median age at diagnosis was 49 years and about 70% of the migraine population were women. “There was a 50% higher dementia rate in individuals who had any migraine diagnosis,” Dr. Islamoska said.
“We also found a 20% higher but nonsignificant dementia rate in individuals who had migraine without aura,” she said. However, when the migraine-with-aura population was evaluated, it was found to have a dementia rate two times higher than people with no migraine. “The dementia rate was higher if individuals had more frequent hospital contacts with migraine.”
The findings support the hypothesis that migraine is a midlife risk factor for dementia later in life, she said.
“The findings underline the value of investigating the effect of migraine medications in dementia risk to assess the impact of mild to moderate migraines,” Dr. Islamoska said. “Therefore, the next step is to investigate the risk of dementia among users of migraine medications who are not diagnosed with migraines at hospitals.”
Strengths of the study, Dr. Islamoska noted, were its size and national nature of its population, that it included all migraine diagnoses at hospitals over a 29-year period, that it made adjustments for confounding of well-established dementia risk factors, and that it validated dementia diagnoses after age 60 years.
One limitation was that the study only included hospital-based diagnoses of dementia while 60% of cases in Denmark are undiagnosed, “thus our results only apply to migraine that is severe enough to require a hospital contact,” Dr. Islamoska said, while most migraine cases are treated in the primary care setting.
Also, the young study population may have a lower dementia risk. “We also know that age of migraine registration may not corresponded with the actual onset, since migraine is a complex disorder with individual variation in patient’s burden and course of disease,” Dr. Islamoska said.
“Future studies are needed to understand the pathological mechanisms underlying the relationship between migraine and dementia and to investigate whether proper prophylactic treatment of migraine can potentially prevent dementia,” Dr. Islamoska said. “In addition, when investigating the association between these two prevalent neurological disorders, the timing of migraine diagnosis and dementia onset is important to ensure temporality. We took this into account in our study to strengthen the validity of our results.”
‘Surprising’ findings
Andrew Charles, MD, director of the Goldberg Migraine Program at the University of California, Los Angeles, said the Danish study makes an important contribution to the literature on dementia risk factors. “Vanishingly small amounts of attention have been paid to migraine as a potential risk factor,” he said. However, he called the results “surprising” based on his own clinical experience. “I actually had a sense that migraine was somehow protective against Alzheimer’s or other kinds of dementias.”
He questioned if the migraine-dementia link could be a “reporting artifact” of migraine sufferers merely going to the neurologist, raising the likelihood of a positive migraine diagnosis. Nonetheless, the results are “intriguing” and raise important questions about migraine therapy and dementia risk.
“If it holds up, it really is something that behooves us to understand whether intervening in terms of therapy for migraine has even more consequences beyond just the immediate relief of symptoms,” Dr. Charles said. “It’s something we should be thinking about in terms of preventing longer-term consequences of this disorder.”
Dr. Islamoska disclosed that Veluxfondent funded the study as part of her PhD project. Dr. Charles disclosed he is a consultant to Amgen, Biohaven Pharmaceuticals, Eli Lilly, Lundbeck, and Novartis.
SOURCE: Islamoska S et al. AHS 2020, Submission 846214.
FROM AHS 2020
Galcanezumab looks promising for treatment-resistant migraine
“The patients included in our study had previously tried multiple migraine preventive treatments that didn’t work for them. These patients are left with limited treatment options to help with the debilitating pain of migraine,” said lead author Holland C. Detke, PhD, senior clinical research advisor at Eli Lilly and Company Biomedicines.
Participants who took the drug experienced “a rapid reduction in migraine days starting as early as month 1, and continuing through the 6 months of the study,” Dr. Detke said.
The treatment group reported an average 4.0 fewer monthly migraine days at 3 months, for example, compared with a baseline of 13.4 days, whereas the placebo group decreased an average 1.29 days from a similar baseline of 13.0 migraine days.
Dr. Detke presented these and other results of the open-label phase of the CONQUER phase 3 trial online as part of the 2020 American Academy of Neurology Science Highlights.
The investigators enrolled 462 adults with episodic or chronic migraine. All participants previously failed two to four migraine treatments because of insufficient efficacy or issues around tolerability or safety. At month 0, 232 people were randomly assigned to galcanezumab and another 230 to placebo injections. At 3 months, 449 participants received a galcanezumab injection as part of the open-label treatment phase.
Participants were an average 48 years old, approximately 86% were women, and 82% were white. At baseline, mean Migraine Specific Quality of Life Role Function Restrictive (MSQ RFR) domain score was 45, “indicating significant impairment in functioning,” Dr. Detke said. At the same time, mean Migraine Disability Assessment Test (MIDAS) total score was 51, “indicating quite severe disability.”
Significant outcomes
The decrease in migraine days at 3 months – 4.0 days with treatment versus 1.29 with placebo – was statistically significant (P < .0001). During the open-label phase, participants who switched from placebo “essentially catch up to where the previously treated people were,” Dr. Detke said. At 6 months, the decrease in average monthly headache days was 5.60 in the initial galcanezumab group versus 5.24 in the initial placebo group.
Significant differences at 3 months versus baseline were observed in participants who received galcanezumab when investigators assessed reduction in 50% or more, 75% or more, or 100% of mean monthly migraine days. No such significant decreases were seen in the placebo group.
Treatment-emergent adverse events reported in the open-label phase included nasopharyngitis in 4.2%, injection site pain in 3.8%, and injection site erythema in 2.7%. Five participants discontinued during the open-label phase because of adverse events.
The results of the study suggest galcanezumab “should be considered as a treatment option for patients who have not had success with previous treatments,” Dr. Detke said.
Multiple strengths of study
“It is encouraging that galcanezumab works in patients who have failed prior reduction strategies,” A. Laine Green, MD, a neurologist at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., said when asked to comment.
This study did not look at patients who have failed more than four previous reduction strategies, he added. “Clinically we see many of these patients. To be fair, no one has studied this group using the monoclonal antibodies.”
Dr. Green noted several strengths of the study. The groups were similar, there were few dropouts during the open-label extension, and there were no unexpected side effects or adverse events. “Those who got placebo caught up to those who received active treatment in the double-blind phase,” he said. “It is also nice to see patient reported outcomes improved as headaches improve. This adds consistency to the results.”
One caveat, Dr. Green noted, is “with open-label extensions, there is always the potential for bias because patients know what treatment they are receiving.”
Overall [the study] gives hope that patients who have failed previous reduction strategies may respond to the newer monoclonal antibodies.”
Aligns with previous findings
The results are “the same as any other long-term extension study of a drug for migraine,” Stephen Silberstein, MD, said when asked to comment. “The longer one takes it, the better you get.”
The research also confirms that if you switch patients taking placebo to an active treatment, they get better, added Dr. Silberstein, director of the Headache Center at Jefferson Health in Philadelphia.
Because they are injections, agents such as galcanezumab, other monoclonal antibodies, and botulinum toxin offer better compliance for headache compared with small molecule medications that require daily oral dosing, he added.
Eli Lilly and Company funded the study. Dr. Holland Detke is a Lilly employee. Dr. Green collaborated with Lilly on a poster for the AHS scientific meeting on a similar topic but did not receive compensation. Up until August 2019, he served as a consultant for Lilly, Novartis, Teva and Allergan. Dr. Green is also a member of the Medscape and American Headache Society Migraine Steering Committee. Dr. Silberstein is a member of the advisory board and consultant for Lilly.
Source: Detke HC et al. AAN 2020. Abstract 43625.
“The patients included in our study had previously tried multiple migraine preventive treatments that didn’t work for them. These patients are left with limited treatment options to help with the debilitating pain of migraine,” said lead author Holland C. Detke, PhD, senior clinical research advisor at Eli Lilly and Company Biomedicines.
Participants who took the drug experienced “a rapid reduction in migraine days starting as early as month 1, and continuing through the 6 months of the study,” Dr. Detke said.
The treatment group reported an average 4.0 fewer monthly migraine days at 3 months, for example, compared with a baseline of 13.4 days, whereas the placebo group decreased an average 1.29 days from a similar baseline of 13.0 migraine days.
Dr. Detke presented these and other results of the open-label phase of the CONQUER phase 3 trial online as part of the 2020 American Academy of Neurology Science Highlights.
The investigators enrolled 462 adults with episodic or chronic migraine. All participants previously failed two to four migraine treatments because of insufficient efficacy or issues around tolerability or safety. At month 0, 232 people were randomly assigned to galcanezumab and another 230 to placebo injections. At 3 months, 449 participants received a galcanezumab injection as part of the open-label treatment phase.
Participants were an average 48 years old, approximately 86% were women, and 82% were white. At baseline, mean Migraine Specific Quality of Life Role Function Restrictive (MSQ RFR) domain score was 45, “indicating significant impairment in functioning,” Dr. Detke said. At the same time, mean Migraine Disability Assessment Test (MIDAS) total score was 51, “indicating quite severe disability.”
Significant outcomes
The decrease in migraine days at 3 months – 4.0 days with treatment versus 1.29 with placebo – was statistically significant (P < .0001). During the open-label phase, participants who switched from placebo “essentially catch up to where the previously treated people were,” Dr. Detke said. At 6 months, the decrease in average monthly headache days was 5.60 in the initial galcanezumab group versus 5.24 in the initial placebo group.
Significant differences at 3 months versus baseline were observed in participants who received galcanezumab when investigators assessed reduction in 50% or more, 75% or more, or 100% of mean monthly migraine days. No such significant decreases were seen in the placebo group.
Treatment-emergent adverse events reported in the open-label phase included nasopharyngitis in 4.2%, injection site pain in 3.8%, and injection site erythema in 2.7%. Five participants discontinued during the open-label phase because of adverse events.
The results of the study suggest galcanezumab “should be considered as a treatment option for patients who have not had success with previous treatments,” Dr. Detke said.
Multiple strengths of study
“It is encouraging that galcanezumab works in patients who have failed prior reduction strategies,” A. Laine Green, MD, a neurologist at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., said when asked to comment.
This study did not look at patients who have failed more than four previous reduction strategies, he added. “Clinically we see many of these patients. To be fair, no one has studied this group using the monoclonal antibodies.”
Dr. Green noted several strengths of the study. The groups were similar, there were few dropouts during the open-label extension, and there were no unexpected side effects or adverse events. “Those who got placebo caught up to those who received active treatment in the double-blind phase,” he said. “It is also nice to see patient reported outcomes improved as headaches improve. This adds consistency to the results.”
One caveat, Dr. Green noted, is “with open-label extensions, there is always the potential for bias because patients know what treatment they are receiving.”
Overall [the study] gives hope that patients who have failed previous reduction strategies may respond to the newer monoclonal antibodies.”
Aligns with previous findings
The results are “the same as any other long-term extension study of a drug for migraine,” Stephen Silberstein, MD, said when asked to comment. “The longer one takes it, the better you get.”
The research also confirms that if you switch patients taking placebo to an active treatment, they get better, added Dr. Silberstein, director of the Headache Center at Jefferson Health in Philadelphia.
Because they are injections, agents such as galcanezumab, other monoclonal antibodies, and botulinum toxin offer better compliance for headache compared with small molecule medications that require daily oral dosing, he added.
Eli Lilly and Company funded the study. Dr. Holland Detke is a Lilly employee. Dr. Green collaborated with Lilly on a poster for the AHS scientific meeting on a similar topic but did not receive compensation. Up until August 2019, he served as a consultant for Lilly, Novartis, Teva and Allergan. Dr. Green is also a member of the Medscape and American Headache Society Migraine Steering Committee. Dr. Silberstein is a member of the advisory board and consultant for Lilly.
Source: Detke HC et al. AAN 2020. Abstract 43625.
“The patients included in our study had previously tried multiple migraine preventive treatments that didn’t work for them. These patients are left with limited treatment options to help with the debilitating pain of migraine,” said lead author Holland C. Detke, PhD, senior clinical research advisor at Eli Lilly and Company Biomedicines.
Participants who took the drug experienced “a rapid reduction in migraine days starting as early as month 1, and continuing through the 6 months of the study,” Dr. Detke said.
The treatment group reported an average 4.0 fewer monthly migraine days at 3 months, for example, compared with a baseline of 13.4 days, whereas the placebo group decreased an average 1.29 days from a similar baseline of 13.0 migraine days.
Dr. Detke presented these and other results of the open-label phase of the CONQUER phase 3 trial online as part of the 2020 American Academy of Neurology Science Highlights.
The investigators enrolled 462 adults with episodic or chronic migraine. All participants previously failed two to four migraine treatments because of insufficient efficacy or issues around tolerability or safety. At month 0, 232 people were randomly assigned to galcanezumab and another 230 to placebo injections. At 3 months, 449 participants received a galcanezumab injection as part of the open-label treatment phase.
Participants were an average 48 years old, approximately 86% were women, and 82% were white. At baseline, mean Migraine Specific Quality of Life Role Function Restrictive (MSQ RFR) domain score was 45, “indicating significant impairment in functioning,” Dr. Detke said. At the same time, mean Migraine Disability Assessment Test (MIDAS) total score was 51, “indicating quite severe disability.”
Significant outcomes
The decrease in migraine days at 3 months – 4.0 days with treatment versus 1.29 with placebo – was statistically significant (P < .0001). During the open-label phase, participants who switched from placebo “essentially catch up to where the previously treated people were,” Dr. Detke said. At 6 months, the decrease in average monthly headache days was 5.60 in the initial galcanezumab group versus 5.24 in the initial placebo group.
Significant differences at 3 months versus baseline were observed in participants who received galcanezumab when investigators assessed reduction in 50% or more, 75% or more, or 100% of mean monthly migraine days. No such significant decreases were seen in the placebo group.
Treatment-emergent adverse events reported in the open-label phase included nasopharyngitis in 4.2%, injection site pain in 3.8%, and injection site erythema in 2.7%. Five participants discontinued during the open-label phase because of adverse events.
The results of the study suggest galcanezumab “should be considered as a treatment option for patients who have not had success with previous treatments,” Dr. Detke said.
Multiple strengths of study
“It is encouraging that galcanezumab works in patients who have failed prior reduction strategies,” A. Laine Green, MD, a neurologist at Dartmouth-Hitchcock Medical Center in Lebanon, N.H., said when asked to comment.
This study did not look at patients who have failed more than four previous reduction strategies, he added. “Clinically we see many of these patients. To be fair, no one has studied this group using the monoclonal antibodies.”
Dr. Green noted several strengths of the study. The groups were similar, there were few dropouts during the open-label extension, and there were no unexpected side effects or adverse events. “Those who got placebo caught up to those who received active treatment in the double-blind phase,” he said. “It is also nice to see patient reported outcomes improved as headaches improve. This adds consistency to the results.”
One caveat, Dr. Green noted, is “with open-label extensions, there is always the potential for bias because patients know what treatment they are receiving.”
Overall [the study] gives hope that patients who have failed previous reduction strategies may respond to the newer monoclonal antibodies.”
Aligns with previous findings
The results are “the same as any other long-term extension study of a drug for migraine,” Stephen Silberstein, MD, said when asked to comment. “The longer one takes it, the better you get.”
The research also confirms that if you switch patients taking placebo to an active treatment, they get better, added Dr. Silberstein, director of the Headache Center at Jefferson Health in Philadelphia.
Because they are injections, agents such as galcanezumab, other monoclonal antibodies, and botulinum toxin offer better compliance for headache compared with small molecule medications that require daily oral dosing, he added.
Eli Lilly and Company funded the study. Dr. Holland Detke is a Lilly employee. Dr. Green collaborated with Lilly on a poster for the AHS scientific meeting on a similar topic but did not receive compensation. Up until August 2019, he served as a consultant for Lilly, Novartis, Teva and Allergan. Dr. Green is also a member of the Medscape and American Headache Society Migraine Steering Committee. Dr. Silberstein is a member of the advisory board and consultant for Lilly.
Source: Detke HC et al. AAN 2020. Abstract 43625.
FROM AAN 2020
Chronic migraine is associated with changes in the amygdala
, according to researchers. This increased connectivity is associated with clinical and affective measures. The data suggest that changes in the amygdala’s structure and function may play a role in the transformation to chronic migraine, according to the researchers. The study was presented online as part of the American Academy of Neurology’s 2020 Science Highlights.
Approximately 3% of patients with episodic migraine progress to chronic migraine each year. Chronic migraine is associated with increased headache frequency, greater disability, and increased psychiatric comorbidities. The pathophysiological mechanisms of the transformation from episodic to chronic migraine are not completely understood.
Danielle D. DeSouza, PhD, instructor in neurology at Stanford (Calif.) University, and colleagues sought to investigate the role of the amygdala in the transformation of migraine. The amygdala is involved in nociceptive processing, emotional responses, and affective states such as depression and anxiety. Researchers have suggested that alterations in the structure or function of the amygdala might contribute to the worsening of pain and mood that coincides with the transformation of migraine.
Dr. DeSouza and colleagues enrolled 88 patients with migraine, diagnosed according to International Classification of Headache Disorders–3 criteria, in their study. Forty-four patients (36 women; mean age, 37.8 years) had chronic migraine, and 44 patients (36 women; mean age, 37.5 years) had episodic migraine. Participants underwent 3T MRI scanning during which investigators acquired T1-weighted structural and resting-state images of the brain. Participants also completed self-report questionnaires to evaluate depression and somatization (Patient Health Questionnaire), anxiety (Generalized Anxiety Disorder 7-item scale), pain catastrophizing (Pain Catastrophizing Scale), headache frequency, and headache intensity.
The investigators examined resting-state functional connectivity between the amygdala and the following three brain networks: DMN, salience network (SN), and central executive network (CEN). They assessed amygdala volume with voxel-based morphometry.
Analyses indicated that connectivity between the left amygdala and the DMN (i.e., the medial prefrontal cortex and the precuneus/posterior cingulate cortex) was increased in patients with chronic migraine, compared with those with episodic migraine. In all patients, resting-state functional connectivity between the amygdala and the DMN was positively associated with headache frequency. Connectivity between the left amygdala and the SN was positively associated with headache intensity, and connectivity between the right amygdala and the CEN was positively associated with pain catastrophizing. Both of these findings held in all patients.
In addition, Dr. DeSouza and colleagues found that bilateral amygdala volumes, including the basolateral and superficial/corticoid nuclei, were increased in patients with chronic migraine, compared with those with episodic migraine. Headache intensity and depression predicted differences in right amygdala volume, and depression alone predicted differences in left amygdala volume.
Dr. DeSouza reported no disclosures. One of the investigators acts as an adviser to Alder, Allergan, Amgen, Biohaven, Curex, Teva, and Xoc about matters unrelated to this study.
SOURCE: DeSouza DD et al. AAN 2020, Abstract 46914.
, according to researchers. This increased connectivity is associated with clinical and affective measures. The data suggest that changes in the amygdala’s structure and function may play a role in the transformation to chronic migraine, according to the researchers. The study was presented online as part of the American Academy of Neurology’s 2020 Science Highlights.
Approximately 3% of patients with episodic migraine progress to chronic migraine each year. Chronic migraine is associated with increased headache frequency, greater disability, and increased psychiatric comorbidities. The pathophysiological mechanisms of the transformation from episodic to chronic migraine are not completely understood.
Danielle D. DeSouza, PhD, instructor in neurology at Stanford (Calif.) University, and colleagues sought to investigate the role of the amygdala in the transformation of migraine. The amygdala is involved in nociceptive processing, emotional responses, and affective states such as depression and anxiety. Researchers have suggested that alterations in the structure or function of the amygdala might contribute to the worsening of pain and mood that coincides with the transformation of migraine.
Dr. DeSouza and colleagues enrolled 88 patients with migraine, diagnosed according to International Classification of Headache Disorders–3 criteria, in their study. Forty-four patients (36 women; mean age, 37.8 years) had chronic migraine, and 44 patients (36 women; mean age, 37.5 years) had episodic migraine. Participants underwent 3T MRI scanning during which investigators acquired T1-weighted structural and resting-state images of the brain. Participants also completed self-report questionnaires to evaluate depression and somatization (Patient Health Questionnaire), anxiety (Generalized Anxiety Disorder 7-item scale), pain catastrophizing (Pain Catastrophizing Scale), headache frequency, and headache intensity.
The investigators examined resting-state functional connectivity between the amygdala and the following three brain networks: DMN, salience network (SN), and central executive network (CEN). They assessed amygdala volume with voxel-based morphometry.
Analyses indicated that connectivity between the left amygdala and the DMN (i.e., the medial prefrontal cortex and the precuneus/posterior cingulate cortex) was increased in patients with chronic migraine, compared with those with episodic migraine. In all patients, resting-state functional connectivity between the amygdala and the DMN was positively associated with headache frequency. Connectivity between the left amygdala and the SN was positively associated with headache intensity, and connectivity between the right amygdala and the CEN was positively associated with pain catastrophizing. Both of these findings held in all patients.
In addition, Dr. DeSouza and colleagues found that bilateral amygdala volumes, including the basolateral and superficial/corticoid nuclei, were increased in patients with chronic migraine, compared with those with episodic migraine. Headache intensity and depression predicted differences in right amygdala volume, and depression alone predicted differences in left amygdala volume.
Dr. DeSouza reported no disclosures. One of the investigators acts as an adviser to Alder, Allergan, Amgen, Biohaven, Curex, Teva, and Xoc about matters unrelated to this study.
SOURCE: DeSouza DD et al. AAN 2020, Abstract 46914.
, according to researchers. This increased connectivity is associated with clinical and affective measures. The data suggest that changes in the amygdala’s structure and function may play a role in the transformation to chronic migraine, according to the researchers. The study was presented online as part of the American Academy of Neurology’s 2020 Science Highlights.
Approximately 3% of patients with episodic migraine progress to chronic migraine each year. Chronic migraine is associated with increased headache frequency, greater disability, and increased psychiatric comorbidities. The pathophysiological mechanisms of the transformation from episodic to chronic migraine are not completely understood.
Danielle D. DeSouza, PhD, instructor in neurology at Stanford (Calif.) University, and colleagues sought to investigate the role of the amygdala in the transformation of migraine. The amygdala is involved in nociceptive processing, emotional responses, and affective states such as depression and anxiety. Researchers have suggested that alterations in the structure or function of the amygdala might contribute to the worsening of pain and mood that coincides with the transformation of migraine.
Dr. DeSouza and colleagues enrolled 88 patients with migraine, diagnosed according to International Classification of Headache Disorders–3 criteria, in their study. Forty-four patients (36 women; mean age, 37.8 years) had chronic migraine, and 44 patients (36 women; mean age, 37.5 years) had episodic migraine. Participants underwent 3T MRI scanning during which investigators acquired T1-weighted structural and resting-state images of the brain. Participants also completed self-report questionnaires to evaluate depression and somatization (Patient Health Questionnaire), anxiety (Generalized Anxiety Disorder 7-item scale), pain catastrophizing (Pain Catastrophizing Scale), headache frequency, and headache intensity.
The investigators examined resting-state functional connectivity between the amygdala and the following three brain networks: DMN, salience network (SN), and central executive network (CEN). They assessed amygdala volume with voxel-based morphometry.
Analyses indicated that connectivity between the left amygdala and the DMN (i.e., the medial prefrontal cortex and the precuneus/posterior cingulate cortex) was increased in patients with chronic migraine, compared with those with episodic migraine. In all patients, resting-state functional connectivity between the amygdala and the DMN was positively associated with headache frequency. Connectivity between the left amygdala and the SN was positively associated with headache intensity, and connectivity between the right amygdala and the CEN was positively associated with pain catastrophizing. Both of these findings held in all patients.
In addition, Dr. DeSouza and colleagues found that bilateral amygdala volumes, including the basolateral and superficial/corticoid nuclei, were increased in patients with chronic migraine, compared with those with episodic migraine. Headache intensity and depression predicted differences in right amygdala volume, and depression alone predicted differences in left amygdala volume.
Dr. DeSouza reported no disclosures. One of the investigators acts as an adviser to Alder, Allergan, Amgen, Biohaven, Curex, Teva, and Xoc about matters unrelated to this study.
SOURCE: DeSouza DD et al. AAN 2020, Abstract 46914.
FROM AAN 2020
Yoga is a good adjunct to migraine therapy
in Neurology.
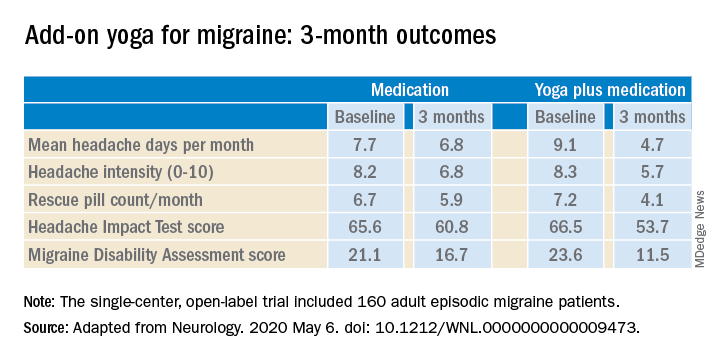
The structured yoga program resulted in “remarkably improved” outcomes at 3 months of follow-up in CONTAIN, with both headache frequency and use of medications cut in half, compared with baseline, according to the investigators.
Compared with the control group on standard antimigraine medications alone, the yoga group demonstrated significantly greater reductions in pain intensity, headache frequency, pill counts, and validated measures of disability and headache impact on daily life (see graphic).
“The good news is that practicing something as simple and accessible as yoga may help much more than medications alone. And all you need is a mat,” observed Dr. Bhatia, professor of neurology at the All India Institute of Medical Sciences in New Delhi.
The single-center, open-label, blinded-assessment CONTAIN trial included 160 adult episodic migraine patients ages 18-50 years experiencing 4-14 headaches per month. They were randomized to prophylactic and acute rescue medications alone or in combination with yoga instruction by a qualified yoga therapist in a class that met at the medical center 3 days per week for 1 month. This was followed by practice of the hour-long yoga program at home 5 days per week for the next 2 months, with twice-monthly telephone calls from the yoga center to encourage adherence and encouragement to call if questions arose. Both groups received counseling about the importance of lifestyle changes that may help with migraine, including diet, physical activity, adequate sleep, and stress reduction. Outcomes were assessed in an intent-to-treat analysis.
The yoga program included specific relaxation exercises, breathing techniques, meditation, and yoga postures, or asanas. The migraine-tailored program was vetted by yoga experts at five renowned Indian yoga centers.
No safety issues arose with the yoga program.
The investigators noted that the 47% reduction in migraine medication pill count and 49% decrease in headache frequency over the course of 3 months in the adjunctive yoga group have important implications, not only in a limited-resource country such as India, but also in the United States, where Americans spend an estimated $3.2 billion annually on prescription and over the counter headache medications, and the indirect cost associated with lost productivity due to migraine has been put at $13 billion per year.
Dr. Bhatia and colleagues speculated that the observed benefits of add-on yoga in migraineurs may involve previously described improved vagal tone and parasympathetic drive coupled with decreased sympathetic tone, increased nitric oxide levels, and loosening of stiff muscles, which can trigger headaches.
Real-life goals
Commenting on the research, neurologist Holly Yancy, DO, a headache specialist at the Banner Health - University Medicine Neuroscience Institute in Phoenix, said she was impressed by the high quality of this well-designed, adequately powered study of a complementary and alternative therapy.
“The primary and secondary endpoints were real-life goals of migraine treatment that we strive to achieve in clinical practice – and they were met in the study,” she observed. “To start with a month of in-house yoga classes to instill a baseline competence in yoga prior to transitioning to home practice and to provide resources for ongoing assistance for questions were nice touches.”
She noted that the control group also experienced reductions in migraine frequency, severity, and disability scores, albeit of significantly lesser magnitude than in the yoga group. This underscores how important it is in clinical practice to spend time counseling migraine patients on lifestyle choices.
“A trial such as this provides neurologists and other health care providers with an accessible, evidence-based treatment for migraines that can be used with other preventive treatments to decrease the frequency and the amount of medication their patients are taking. In addition, it is a behavioral therapy that can decrease triggers and potentially help patients cope with pain,” Dr. Yancy said.
“I suspect I’ll not hesitate to recommend yoga as an adjunctive treatment for patients in my clinic that are physically capable. I think it would be logical to try to extrapolate the concept to a chronic migraine population as well, though it would be ideal to base that recommendation on another study conducted with a chronic migraine population.”
Dr. Bhatia and his coinvestigators reported having no financial conflicts regarding their study, funded by the Government of India and the All India Institute of Medical Sciences.
SOURCE: Kumar A et al. Neurology. 2020 May 6. doi: 10.1212/WNL.0000000000009473.
in Neurology.
The structured yoga program resulted in “remarkably improved” outcomes at 3 months of follow-up in CONTAIN, with both headache frequency and use of medications cut in half, compared with baseline, according to the investigators.
Compared with the control group on standard antimigraine medications alone, the yoga group demonstrated significantly greater reductions in pain intensity, headache frequency, pill counts, and validated measures of disability and headache impact on daily life (see graphic).
“The good news is that practicing something as simple and accessible as yoga may help much more than medications alone. And all you need is a mat,” observed Dr. Bhatia, professor of neurology at the All India Institute of Medical Sciences in New Delhi.
The single-center, open-label, blinded-assessment CONTAIN trial included 160 adult episodic migraine patients ages 18-50 years experiencing 4-14 headaches per month. They were randomized to prophylactic and acute rescue medications alone or in combination with yoga instruction by a qualified yoga therapist in a class that met at the medical center 3 days per week for 1 month. This was followed by practice of the hour-long yoga program at home 5 days per week for the next 2 months, with twice-monthly telephone calls from the yoga center to encourage adherence and encouragement to call if questions arose. Both groups received counseling about the importance of lifestyle changes that may help with migraine, including diet, physical activity, adequate sleep, and stress reduction. Outcomes were assessed in an intent-to-treat analysis.
The yoga program included specific relaxation exercises, breathing techniques, meditation, and yoga postures, or asanas. The migraine-tailored program was vetted by yoga experts at five renowned Indian yoga centers.
No safety issues arose with the yoga program.
The investigators noted that the 47% reduction in migraine medication pill count and 49% decrease in headache frequency over the course of 3 months in the adjunctive yoga group have important implications, not only in a limited-resource country such as India, but also in the United States, where Americans spend an estimated $3.2 billion annually on prescription and over the counter headache medications, and the indirect cost associated with lost productivity due to migraine has been put at $13 billion per year.
Dr. Bhatia and colleagues speculated that the observed benefits of add-on yoga in migraineurs may involve previously described improved vagal tone and parasympathetic drive coupled with decreased sympathetic tone, increased nitric oxide levels, and loosening of stiff muscles, which can trigger headaches.
Real-life goals
Commenting on the research, neurologist Holly Yancy, DO, a headache specialist at the Banner Health - University Medicine Neuroscience Institute in Phoenix, said she was impressed by the high quality of this well-designed, adequately powered study of a complementary and alternative therapy.
“The primary and secondary endpoints were real-life goals of migraine treatment that we strive to achieve in clinical practice – and they were met in the study,” she observed. “To start with a month of in-house yoga classes to instill a baseline competence in yoga prior to transitioning to home practice and to provide resources for ongoing assistance for questions were nice touches.”
She noted that the control group also experienced reductions in migraine frequency, severity, and disability scores, albeit of significantly lesser magnitude than in the yoga group. This underscores how important it is in clinical practice to spend time counseling migraine patients on lifestyle choices.
“A trial such as this provides neurologists and other health care providers with an accessible, evidence-based treatment for migraines that can be used with other preventive treatments to decrease the frequency and the amount of medication their patients are taking. In addition, it is a behavioral therapy that can decrease triggers and potentially help patients cope with pain,” Dr. Yancy said.
“I suspect I’ll not hesitate to recommend yoga as an adjunctive treatment for patients in my clinic that are physically capable. I think it would be logical to try to extrapolate the concept to a chronic migraine population as well, though it would be ideal to base that recommendation on another study conducted with a chronic migraine population.”
Dr. Bhatia and his coinvestigators reported having no financial conflicts regarding their study, funded by the Government of India and the All India Institute of Medical Sciences.
SOURCE: Kumar A et al. Neurology. 2020 May 6. doi: 10.1212/WNL.0000000000009473.
in Neurology.
The structured yoga program resulted in “remarkably improved” outcomes at 3 months of follow-up in CONTAIN, with both headache frequency and use of medications cut in half, compared with baseline, according to the investigators.
Compared with the control group on standard antimigraine medications alone, the yoga group demonstrated significantly greater reductions in pain intensity, headache frequency, pill counts, and validated measures of disability and headache impact on daily life (see graphic).
“The good news is that practicing something as simple and accessible as yoga may help much more than medications alone. And all you need is a mat,” observed Dr. Bhatia, professor of neurology at the All India Institute of Medical Sciences in New Delhi.
The single-center, open-label, blinded-assessment CONTAIN trial included 160 adult episodic migraine patients ages 18-50 years experiencing 4-14 headaches per month. They were randomized to prophylactic and acute rescue medications alone or in combination with yoga instruction by a qualified yoga therapist in a class that met at the medical center 3 days per week for 1 month. This was followed by practice of the hour-long yoga program at home 5 days per week for the next 2 months, with twice-monthly telephone calls from the yoga center to encourage adherence and encouragement to call if questions arose. Both groups received counseling about the importance of lifestyle changes that may help with migraine, including diet, physical activity, adequate sleep, and stress reduction. Outcomes were assessed in an intent-to-treat analysis.
The yoga program included specific relaxation exercises, breathing techniques, meditation, and yoga postures, or asanas. The migraine-tailored program was vetted by yoga experts at five renowned Indian yoga centers.
No safety issues arose with the yoga program.
The investigators noted that the 47% reduction in migraine medication pill count and 49% decrease in headache frequency over the course of 3 months in the adjunctive yoga group have important implications, not only in a limited-resource country such as India, but also in the United States, where Americans spend an estimated $3.2 billion annually on prescription and over the counter headache medications, and the indirect cost associated with lost productivity due to migraine has been put at $13 billion per year.
Dr. Bhatia and colleagues speculated that the observed benefits of add-on yoga in migraineurs may involve previously described improved vagal tone and parasympathetic drive coupled with decreased sympathetic tone, increased nitric oxide levels, and loosening of stiff muscles, which can trigger headaches.
Real-life goals
Commenting on the research, neurologist Holly Yancy, DO, a headache specialist at the Banner Health - University Medicine Neuroscience Institute in Phoenix, said she was impressed by the high quality of this well-designed, adequately powered study of a complementary and alternative therapy.
“The primary and secondary endpoints were real-life goals of migraine treatment that we strive to achieve in clinical practice – and they were met in the study,” she observed. “To start with a month of in-house yoga classes to instill a baseline competence in yoga prior to transitioning to home practice and to provide resources for ongoing assistance for questions were nice touches.”
She noted that the control group also experienced reductions in migraine frequency, severity, and disability scores, albeit of significantly lesser magnitude than in the yoga group. This underscores how important it is in clinical practice to spend time counseling migraine patients on lifestyle choices.
“A trial such as this provides neurologists and other health care providers with an accessible, evidence-based treatment for migraines that can be used with other preventive treatments to decrease the frequency and the amount of medication their patients are taking. In addition, it is a behavioral therapy that can decrease triggers and potentially help patients cope with pain,” Dr. Yancy said.
“I suspect I’ll not hesitate to recommend yoga as an adjunctive treatment for patients in my clinic that are physically capable. I think it would be logical to try to extrapolate the concept to a chronic migraine population as well, though it would be ideal to base that recommendation on another study conducted with a chronic migraine population.”
Dr. Bhatia and his coinvestigators reported having no financial conflicts regarding their study, funded by the Government of India and the All India Institute of Medical Sciences.
SOURCE: Kumar A et al. Neurology. 2020 May 6. doi: 10.1212/WNL.0000000000009473.
FROM NEUROLOGY
Economic burden of migraine increases with the number of treatment failures
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.

Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
From AAN 2020

CGRP inhibitors receive reassuring real-world safety report
Stephen D. Silberstein, MD, reported online as part of the 2020 American Academy of Neurology Science Highlights.

He presented a retrospective analysis of spontaneous postmarketing reports to the Food and Drug Administration Adverse Events Reporting System (FAERS) for Aimovig (erenumab-aooe), Ajovy (fremanezumab-vfrm), and Emgality (galcanezumab-gnlm).
The top-10 lists of adverse events for all three monoclonal antibodies targeting CGRP were skewed heavily towards injection-site reactions, such as injection-site pain, itching, swelling, and erythema. The rates were relatively low. For example, injection-site pain was reported at a rate of 2.94 cases per 1,000 patients exposed to erenumab, 0.8/1,000 for fremanezumab, and 4.9/1,000 for galcanezumab, according to Dr. Silberstein, professor of neurology and director of the headache center at Sidney Kimmel Medical College, Philadelphia.
Migraine, headache, and drug ineffectiveness were in the top 10 for all three medications, as is typical in FAERS reports, since no drug is effective in everyone. These events were reported at rates of 1-5/1,000 exposed patients. Constipation was reported in association with the use of erenumab at a rate of 4.9 cases/1,000 patients, but did not reach the top-10 lists for the other two CGRP antagonists.
Notably, cardiovascular events were not among the top-10 adverse events reported for any of the novel preventive agents.
“These results will be practice changing, since some physicians have been holding back from prescribing these drugs pending the results of this sort of longer-term safety data,” Dr. Silberstein predicted in an interview.
Asked to comment on the FAERS study, neurologist Holly Yancy, DO, said that she found the findings unsurprising because the adverse effects were essentially as expected based upon the earlier favorable clinical trials experience.
“These medications are living up to the expectations for good tolerability that were in place when they were initially approved by the FDA just under 2 years ago,” said Dr. Yancy, a headache specialist at the Banner–University Medicine Neuroscience Institute in Phoenix.
“Injection-site reactions were anticipated. Clinically, I’ve found that if the medications reduce migraine days and severity, patients find the risk of temporary pain, redness, or itching at the injection site is an easy trade off,” she added.
CGRP is a vasoactive peptide. There has been a theoretic concern that its pharmacologic inhibition for prevention of migraine could lead to an increased risk of adverse cardiovascular events, especially in individuals with coronary disease or a history of stroke. The absence of any such signal during the first 6 months of widespread clinical use of the CGRP inhibitors is highly encouraging, although this is an issue that warrants longer-term study, Dr. Yancy continued.
These drugs, which were expressly designed for migraine prevention, are a considerable advance over what was previously available in her view. They’re equally or more effective and considerably better tolerated than the preventive medications physicians had long been using off label, including antidepressants, antiepileptics, and cardiac drugs.
Dr. Silberstein reported financial relationships with close to two dozen pharmaceutical companies. Dr. Yancy reported serving on speakers’ bureaus for Amgen and Novartis.
SOURCE: Silverstein SD et al. AAN 2020, Abstract S58.008.
Stephen D. Silberstein, MD, reported online as part of the 2020 American Academy of Neurology Science Highlights.
He presented a retrospective analysis of spontaneous postmarketing reports to the Food and Drug Administration Adverse Events Reporting System (FAERS) for Aimovig (erenumab-aooe), Ajovy (fremanezumab-vfrm), and Emgality (galcanezumab-gnlm).
The top-10 lists of adverse events for all three monoclonal antibodies targeting CGRP were skewed heavily towards injection-site reactions, such as injection-site pain, itching, swelling, and erythema. The rates were relatively low. For example, injection-site pain was reported at a rate of 2.94 cases per 1,000 patients exposed to erenumab, 0.8/1,000 for fremanezumab, and 4.9/1,000 for galcanezumab, according to Dr. Silberstein, professor of neurology and director of the headache center at Sidney Kimmel Medical College, Philadelphia.
Migraine, headache, and drug ineffectiveness were in the top 10 for all three medications, as is typical in FAERS reports, since no drug is effective in everyone. These events were reported at rates of 1-5/1,000 exposed patients. Constipation was reported in association with the use of erenumab at a rate of 4.9 cases/1,000 patients, but did not reach the top-10 lists for the other two CGRP antagonists.
Notably, cardiovascular events were not among the top-10 adverse events reported for any of the novel preventive agents.
“These results will be practice changing, since some physicians have been holding back from prescribing these drugs pending the results of this sort of longer-term safety data,” Dr. Silberstein predicted in an interview.
Asked to comment on the FAERS study, neurologist Holly Yancy, DO, said that she found the findings unsurprising because the adverse effects were essentially as expected based upon the earlier favorable clinical trials experience.
“These medications are living up to the expectations for good tolerability that were in place when they were initially approved by the FDA just under 2 years ago,” said Dr. Yancy, a headache specialist at the Banner–University Medicine Neuroscience Institute in Phoenix.
“Injection-site reactions were anticipated. Clinically, I’ve found that if the medications reduce migraine days and severity, patients find the risk of temporary pain, redness, or itching at the injection site is an easy trade off,” she added.
CGRP is a vasoactive peptide. There has been a theoretic concern that its pharmacologic inhibition for prevention of migraine could lead to an increased risk of adverse cardiovascular events, especially in individuals with coronary disease or a history of stroke. The absence of any such signal during the first 6 months of widespread clinical use of the CGRP inhibitors is highly encouraging, although this is an issue that warrants longer-term study, Dr. Yancy continued.
These drugs, which were expressly designed for migraine prevention, are a considerable advance over what was previously available in her view. They’re equally or more effective and considerably better tolerated than the preventive medications physicians had long been using off label, including antidepressants, antiepileptics, and cardiac drugs.
Dr. Silberstein reported financial relationships with close to two dozen pharmaceutical companies. Dr. Yancy reported serving on speakers’ bureaus for Amgen and Novartis.
SOURCE: Silverstein SD et al. AAN 2020, Abstract S58.008.
Stephen D. Silberstein, MD, reported online as part of the 2020 American Academy of Neurology Science Highlights.
He presented a retrospective analysis of spontaneous postmarketing reports to the Food and Drug Administration Adverse Events Reporting System (FAERS) for Aimovig (erenumab-aooe), Ajovy (fremanezumab-vfrm), and Emgality (galcanezumab-gnlm).
The top-10 lists of adverse events for all three monoclonal antibodies targeting CGRP were skewed heavily towards injection-site reactions, such as injection-site pain, itching, swelling, and erythema. The rates were relatively low. For example, injection-site pain was reported at a rate of 2.94 cases per 1,000 patients exposed to erenumab, 0.8/1,000 for fremanezumab, and 4.9/1,000 for galcanezumab, according to Dr. Silberstein, professor of neurology and director of the headache center at Sidney Kimmel Medical College, Philadelphia.
Migraine, headache, and drug ineffectiveness were in the top 10 for all three medications, as is typical in FAERS reports, since no drug is effective in everyone. These events were reported at rates of 1-5/1,000 exposed patients. Constipation was reported in association with the use of erenumab at a rate of 4.9 cases/1,000 patients, but did not reach the top-10 lists for the other two CGRP antagonists.
Notably, cardiovascular events were not among the top-10 adverse events reported for any of the novel preventive agents.
“These results will be practice changing, since some physicians have been holding back from prescribing these drugs pending the results of this sort of longer-term safety data,” Dr. Silberstein predicted in an interview.
Asked to comment on the FAERS study, neurologist Holly Yancy, DO, said that she found the findings unsurprising because the adverse effects were essentially as expected based upon the earlier favorable clinical trials experience.
“These medications are living up to the expectations for good tolerability that were in place when they were initially approved by the FDA just under 2 years ago,” said Dr. Yancy, a headache specialist at the Banner–University Medicine Neuroscience Institute in Phoenix.
“Injection-site reactions were anticipated. Clinically, I’ve found that if the medications reduce migraine days and severity, patients find the risk of temporary pain, redness, or itching at the injection site is an easy trade off,” she added.
CGRP is a vasoactive peptide. There has been a theoretic concern that its pharmacologic inhibition for prevention of migraine could lead to an increased risk of adverse cardiovascular events, especially in individuals with coronary disease or a history of stroke. The absence of any such signal during the first 6 months of widespread clinical use of the CGRP inhibitors is highly encouraging, although this is an issue that warrants longer-term study, Dr. Yancy continued.
These drugs, which were expressly designed for migraine prevention, are a considerable advance over what was previously available in her view. They’re equally or more effective and considerably better tolerated than the preventive medications physicians had long been using off label, including antidepressants, antiepileptics, and cardiac drugs.
Dr. Silberstein reported financial relationships with close to two dozen pharmaceutical companies. Dr. Yancy reported serving on speakers’ bureaus for Amgen and Novartis.
SOURCE: Silverstein SD et al. AAN 2020, Abstract S58.008.
FROM AAN 2020