User login
Beyond semaglutide, a coming pipeline of new antiobesity meds
“We are at a watershed [moment] brought on by the recent introduction of highly effective antiobesity medications,” Ania M. Jastreboff, MD, PhD, said in a lecture at the annual meeting of the Obesity Society.
Dr. Jastreboff, of Yale University and the Yale Center for Weight Management, New Haven, Conn., provided an overview of the many nutrient-stimulated hormone-based antiobesity therapies in late phases of development – including dual and triple therapies with glucagon-like peptide 1 receptor agonists (GLP-1 RAs), glucose-dependent insulinotropic polypeptide (GIP) agonists, glucagon, and amylin.
“I’ve shown you all of these agents that clearly produce substantial weight reduction,” she said. “The fact that these nutrient-stimulated, hormone-based therapies are not all the same is a good thing,” she stressed, because “it’s not likely that everyone will respond to each of these, and they are likely to respond differently.”
She then briefly touched on activin receptor inhibitors –”the next [medication] class that I think will be up and coming,” she speculated.
“Beyond (just) weight reduction,” Dr. Jastreboff concluded, clinicians “need to focus on optimizing health as we are treating obesity.” Clinicians need to consider the patient’s severity of obesity, overall health, and metabolic profile, and match the obesity treatment to the patient. They also need to consider the rate of weight reduction, potential bone loss, vitamin deficiencies, muscle loss and function, and side effects, and be mindful of affordability, bias, and stigma.
Looking forward to multiple options
W. Timothy Garvey, MD, of the University of Alabama at Birmingham, told this news organization that clinicians treating patients with obesity are looking forward to the decision from the Food and Drug Administration about tirzepatide (Mounjaro), expected by year’s end. Tirzepatide “is really the best medicine that we have for diabetes in terms of A1c control without much hypoglycemia,” he said, “and also the best medicine for treating obesity in patients with diabetes.”
A recent study found that people with type 2 diabetes who adhered to their tirzepatide regimen achieved a 15% weight loss from their baseline after 40-42 weeks.
Dr. Garvey added that he is looking forward to drugs in development such as survodutide (a GLP-1/glucagon agonist) and orforglipron (a small oral daily nonpeptide GLP-1 RA). “Orforglipron wouldn’t have to be refrigerated,” he noted, and it “could be cheaper to manufacture, might be preferred over subcutaneous medication by some people, and it showed pretty good efficacy in early studies.”
Retatrutide, a triple agonist (GLP-1/GIP/glucagon) and CagriSema (cagrilintide plus semaglutide) showed “pretty impressive weight loss in early studies,” Dr. Garvey said. “We’re optimistic.”
Also invited to comment, Sean Wharton, MD, PharmD, Wharton Medical Clinic and York University, Toronto, said that the recent developments in antiobesity medications are “so exciting that it’s difficult to make direct comments,” since “maybe there will be something bigger, or maybe something will go wrong with these molecules and we’ll have to back-step.”
Further studies are needed, he added, to determine outcomes in patients who reduce their intake to half or three-quarters of a dose, or who transition to intermittent therapy.
Nutrient-stimulated, hormone-based antiobesity medications
Here’s a status overview of the nutrient-stimulated hormone-based medications already approved and on the horizon:
Semaglutide. The GLP-1 RA semaglutide (Ozempic), was approved by the FDA for type 2 diabetes in 2017. In June 2021, the FDA approved the use of semaglutide (Wegovy) for obesity.
Topline results from the Semaglutide Effects on Heart Disease and Stroke in Patients with Overweight or Obesity (SELECT) cardiovascular outcome trial showed that in individuals with obesity without type 2 diabetes, semaglutide led to a 20% reduction in major cardiovascular events, Dr. Jastreboff noted, adding that full results will be presented at the American Heart Association meeting on Nov. 11.
Tirzepatide. In May 2022, the FDA approved tirzepatide (Mounjaro), a GIP/GLP-1RA, for type 2 diabetes, and a decision about the use of tirzepatide for obesity is expected by year’s end.
The full results of the phase 3 SURMOUNT-3 trial were presented at ObesityWeek (just after this session), as reported by this news organization.
And the full results of the phase 3 SURMOUNT-4 trial of tirzepatide for obesity were presented at the European Association for the Study of Diabetes meeting, Dr. Jastreboff noted. At 88 weeks, in the continued tirzepatide group, average weight reduction was 26%, absolute weight reduction was 62 pounds (28.1 kg), and > 50% of individuals achieved ≥ 25% weight loss.
The phase 3 SURMOUNT MMO trial of morbidity and mortality with tirzepatide in obesity is estimated to be completed in 2027.
Cagrilintide. In a phase 2 trial of the amylin analog cagrilintide in patients with obesity, more than half of participants lost at least 10% of their weight at 26 weeks.
CagriSema. In a phase 1b trial of the amylin analog/GLP-1 RA combination of cagrilintide/semaglutide (CagriSema), average weight reduction at 20 weeks was 17.1%. The estimated primary completion dates of phase 3 trials of CagriSema, REDEFINE 1 (obesity), REDEFINE 2 (obesity and type 2 diabetes), and REDEFINE 3 (obesity and established cardiovascular disease), are 2025, 2024, and 2027, respectively.
Survodutide. Findings from a phase 2 trial of the glucagon/GLP-1 RA survodutide were presented at the American Diabetes Association (ADA) meeting in June. With 46 weeks of treatment, the average weight reduction was 18.7%, and up to 40% of participants lost at least 20% of their body weight.
Survodutide is being studied in the phase 3 SYNCHRONIZE trials.
Retatrutide. Phase 2 findings of 12-mg weekly of the GIP/GLP-1/glucagon triple hormone receptor agonist retatrutide were also presented at ADA. On average, at 48 weeks, the placebo group lost 2.1% of their weight and the retatrutide group lost 24.2% of their weight, with an average absolute reduction of 58 pounds (26.3 kg). At the highest dose (12 mg), 9 out of 10 individuals lost ≥ 10%, nearly two-thirds lost ≥ 20%, and a quarter lost ≥ 30% of their weight, at 48 weeks.
With the two highest doses of retatrutide, 100% of participants lost ≥ 5% of weight, Dr. Jastreboff reported, adding, “I’m not sure how many other times I will ever be able to say ‘100%’ in any scientific presentation.”
TRIUMPH phase 3 studies of retatrutide are ongoing.
“All the agents I’ve spoken about thus far are once-weekly injectable,” Dr. Jastreboff said, turning her attention to oral drugs.
Oral semaglutide (Rybelsus) is already FDA-approved for type 2 diabetes. The phase 2 OASIS trial results presented at ADA showed that participants with obesity who received 50 mg daily of the oral medication had an average weight reduction of 17.4% at 68 weeks, which is comparable to the 16.9% weight reduction with subcutaneous semaglutide 2.4 once weekly. More than a third of patients receiving the treatment lost ≥ 20% weight at 68 weeks.
The phase 3 OASIS study of oral semaglutide in obesity is ongoing.
Orforglipron. Phase 2 data of the small molecule oral GLP-1 RA orforglipron presented at ADA showed that participants with obesity had up to a 14.7% body weight reduction at 36 weeks. Nearly half of participants lost ≥ 15% of their body weight at 36 weeks.
The phase 3 ATTAIN study of orforglipron in obesity is ongoing.
AMG133. In a phase 2 trial, participants with obesity who received the monthly GIP receptor antagonist/ GLP-1 receptor agonist AMG133 (Amgen) had an average weight reduction of 14.5% at just 12 weeks.
Activin receptor inhibitors
Bimagrumab. This drug is a monoclonal antibody activin receptor inhibitor that binds to activin type II receptors. In a phase 2 study of 58 individuals with type 2 diabetes and obesity who received monthly medication or placebo, participants receiving bimagrumab lost 20.5% of fat mass and gained 3.6% of lean mass at 48 weeks, and the most common adverse events were mild diarrhea and muscle spasm.
Bimagrumab and semaglutide for obesity are being studied in BELIEVE, an ongoing phase 2b study. Topline results are anticipated by the end of 2024.
Taldefgrobep. The fusion protein taldefgrobep binds active myostatin. A phase 2 study of taldefgrobep for obesity is planned to start in 2024.
Dr. Jastreboff is on the scientific advisory board for Amgen, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk, and has received research support form Novo Nordisk, Eli Lilly, Rhythm, and NIH/NIDDK.
A version of this article first appeared on Medscape.com.
“We are at a watershed [moment] brought on by the recent introduction of highly effective antiobesity medications,” Ania M. Jastreboff, MD, PhD, said in a lecture at the annual meeting of the Obesity Society.
Dr. Jastreboff, of Yale University and the Yale Center for Weight Management, New Haven, Conn., provided an overview of the many nutrient-stimulated hormone-based antiobesity therapies in late phases of development – including dual and triple therapies with glucagon-like peptide 1 receptor agonists (GLP-1 RAs), glucose-dependent insulinotropic polypeptide (GIP) agonists, glucagon, and amylin.
“I’ve shown you all of these agents that clearly produce substantial weight reduction,” she said. “The fact that these nutrient-stimulated, hormone-based therapies are not all the same is a good thing,” she stressed, because “it’s not likely that everyone will respond to each of these, and they are likely to respond differently.”
She then briefly touched on activin receptor inhibitors –”the next [medication] class that I think will be up and coming,” she speculated.
“Beyond (just) weight reduction,” Dr. Jastreboff concluded, clinicians “need to focus on optimizing health as we are treating obesity.” Clinicians need to consider the patient’s severity of obesity, overall health, and metabolic profile, and match the obesity treatment to the patient. They also need to consider the rate of weight reduction, potential bone loss, vitamin deficiencies, muscle loss and function, and side effects, and be mindful of affordability, bias, and stigma.
Looking forward to multiple options
W. Timothy Garvey, MD, of the University of Alabama at Birmingham, told this news organization that clinicians treating patients with obesity are looking forward to the decision from the Food and Drug Administration about tirzepatide (Mounjaro), expected by year’s end. Tirzepatide “is really the best medicine that we have for diabetes in terms of A1c control without much hypoglycemia,” he said, “and also the best medicine for treating obesity in patients with diabetes.”
A recent study found that people with type 2 diabetes who adhered to their tirzepatide regimen achieved a 15% weight loss from their baseline after 40-42 weeks.
Dr. Garvey added that he is looking forward to drugs in development such as survodutide (a GLP-1/glucagon agonist) and orforglipron (a small oral daily nonpeptide GLP-1 RA). “Orforglipron wouldn’t have to be refrigerated,” he noted, and it “could be cheaper to manufacture, might be preferred over subcutaneous medication by some people, and it showed pretty good efficacy in early studies.”
Retatrutide, a triple agonist (GLP-1/GIP/glucagon) and CagriSema (cagrilintide plus semaglutide) showed “pretty impressive weight loss in early studies,” Dr. Garvey said. “We’re optimistic.”
Also invited to comment, Sean Wharton, MD, PharmD, Wharton Medical Clinic and York University, Toronto, said that the recent developments in antiobesity medications are “so exciting that it’s difficult to make direct comments,” since “maybe there will be something bigger, or maybe something will go wrong with these molecules and we’ll have to back-step.”
Further studies are needed, he added, to determine outcomes in patients who reduce their intake to half or three-quarters of a dose, or who transition to intermittent therapy.
Nutrient-stimulated, hormone-based antiobesity medications
Here’s a status overview of the nutrient-stimulated hormone-based medications already approved and on the horizon:
Semaglutide. The GLP-1 RA semaglutide (Ozempic), was approved by the FDA for type 2 diabetes in 2017. In June 2021, the FDA approved the use of semaglutide (Wegovy) for obesity.
Topline results from the Semaglutide Effects on Heart Disease and Stroke in Patients with Overweight or Obesity (SELECT) cardiovascular outcome trial showed that in individuals with obesity without type 2 diabetes, semaglutide led to a 20% reduction in major cardiovascular events, Dr. Jastreboff noted, adding that full results will be presented at the American Heart Association meeting on Nov. 11.
Tirzepatide. In May 2022, the FDA approved tirzepatide (Mounjaro), a GIP/GLP-1RA, for type 2 diabetes, and a decision about the use of tirzepatide for obesity is expected by year’s end.
The full results of the phase 3 SURMOUNT-3 trial were presented at ObesityWeek (just after this session), as reported by this news organization.
And the full results of the phase 3 SURMOUNT-4 trial of tirzepatide for obesity were presented at the European Association for the Study of Diabetes meeting, Dr. Jastreboff noted. At 88 weeks, in the continued tirzepatide group, average weight reduction was 26%, absolute weight reduction was 62 pounds (28.1 kg), and > 50% of individuals achieved ≥ 25% weight loss.
The phase 3 SURMOUNT MMO trial of morbidity and mortality with tirzepatide in obesity is estimated to be completed in 2027.
Cagrilintide. In a phase 2 trial of the amylin analog cagrilintide in patients with obesity, more than half of participants lost at least 10% of their weight at 26 weeks.
CagriSema. In a phase 1b trial of the amylin analog/GLP-1 RA combination of cagrilintide/semaglutide (CagriSema), average weight reduction at 20 weeks was 17.1%. The estimated primary completion dates of phase 3 trials of CagriSema, REDEFINE 1 (obesity), REDEFINE 2 (obesity and type 2 diabetes), and REDEFINE 3 (obesity and established cardiovascular disease), are 2025, 2024, and 2027, respectively.
Survodutide. Findings from a phase 2 trial of the glucagon/GLP-1 RA survodutide were presented at the American Diabetes Association (ADA) meeting in June. With 46 weeks of treatment, the average weight reduction was 18.7%, and up to 40% of participants lost at least 20% of their body weight.
Survodutide is being studied in the phase 3 SYNCHRONIZE trials.
Retatrutide. Phase 2 findings of 12-mg weekly of the GIP/GLP-1/glucagon triple hormone receptor agonist retatrutide were also presented at ADA. On average, at 48 weeks, the placebo group lost 2.1% of their weight and the retatrutide group lost 24.2% of their weight, with an average absolute reduction of 58 pounds (26.3 kg). At the highest dose (12 mg), 9 out of 10 individuals lost ≥ 10%, nearly two-thirds lost ≥ 20%, and a quarter lost ≥ 30% of their weight, at 48 weeks.
With the two highest doses of retatrutide, 100% of participants lost ≥ 5% of weight, Dr. Jastreboff reported, adding, “I’m not sure how many other times I will ever be able to say ‘100%’ in any scientific presentation.”
TRIUMPH phase 3 studies of retatrutide are ongoing.
“All the agents I’ve spoken about thus far are once-weekly injectable,” Dr. Jastreboff said, turning her attention to oral drugs.
Oral semaglutide (Rybelsus) is already FDA-approved for type 2 diabetes. The phase 2 OASIS trial results presented at ADA showed that participants with obesity who received 50 mg daily of the oral medication had an average weight reduction of 17.4% at 68 weeks, which is comparable to the 16.9% weight reduction with subcutaneous semaglutide 2.4 once weekly. More than a third of patients receiving the treatment lost ≥ 20% weight at 68 weeks.
The phase 3 OASIS study of oral semaglutide in obesity is ongoing.
Orforglipron. Phase 2 data of the small molecule oral GLP-1 RA orforglipron presented at ADA showed that participants with obesity had up to a 14.7% body weight reduction at 36 weeks. Nearly half of participants lost ≥ 15% of their body weight at 36 weeks.
The phase 3 ATTAIN study of orforglipron in obesity is ongoing.
AMG133. In a phase 2 trial, participants with obesity who received the monthly GIP receptor antagonist/ GLP-1 receptor agonist AMG133 (Amgen) had an average weight reduction of 14.5% at just 12 weeks.
Activin receptor inhibitors
Bimagrumab. This drug is a monoclonal antibody activin receptor inhibitor that binds to activin type II receptors. In a phase 2 study of 58 individuals with type 2 diabetes and obesity who received monthly medication or placebo, participants receiving bimagrumab lost 20.5% of fat mass and gained 3.6% of lean mass at 48 weeks, and the most common adverse events were mild diarrhea and muscle spasm.
Bimagrumab and semaglutide for obesity are being studied in BELIEVE, an ongoing phase 2b study. Topline results are anticipated by the end of 2024.
Taldefgrobep. The fusion protein taldefgrobep binds active myostatin. A phase 2 study of taldefgrobep for obesity is planned to start in 2024.
Dr. Jastreboff is on the scientific advisory board for Amgen, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk, and has received research support form Novo Nordisk, Eli Lilly, Rhythm, and NIH/NIDDK.
A version of this article first appeared on Medscape.com.
“We are at a watershed [moment] brought on by the recent introduction of highly effective antiobesity medications,” Ania M. Jastreboff, MD, PhD, said in a lecture at the annual meeting of the Obesity Society.
Dr. Jastreboff, of Yale University and the Yale Center for Weight Management, New Haven, Conn., provided an overview of the many nutrient-stimulated hormone-based antiobesity therapies in late phases of development – including dual and triple therapies with glucagon-like peptide 1 receptor agonists (GLP-1 RAs), glucose-dependent insulinotropic polypeptide (GIP) agonists, glucagon, and amylin.
“I’ve shown you all of these agents that clearly produce substantial weight reduction,” she said. “The fact that these nutrient-stimulated, hormone-based therapies are not all the same is a good thing,” she stressed, because “it’s not likely that everyone will respond to each of these, and they are likely to respond differently.”
She then briefly touched on activin receptor inhibitors –”the next [medication] class that I think will be up and coming,” she speculated.
“Beyond (just) weight reduction,” Dr. Jastreboff concluded, clinicians “need to focus on optimizing health as we are treating obesity.” Clinicians need to consider the patient’s severity of obesity, overall health, and metabolic profile, and match the obesity treatment to the patient. They also need to consider the rate of weight reduction, potential bone loss, vitamin deficiencies, muscle loss and function, and side effects, and be mindful of affordability, bias, and stigma.
Looking forward to multiple options
W. Timothy Garvey, MD, of the University of Alabama at Birmingham, told this news organization that clinicians treating patients with obesity are looking forward to the decision from the Food and Drug Administration about tirzepatide (Mounjaro), expected by year’s end. Tirzepatide “is really the best medicine that we have for diabetes in terms of A1c control without much hypoglycemia,” he said, “and also the best medicine for treating obesity in patients with diabetes.”
A recent study found that people with type 2 diabetes who adhered to their tirzepatide regimen achieved a 15% weight loss from their baseline after 40-42 weeks.
Dr. Garvey added that he is looking forward to drugs in development such as survodutide (a GLP-1/glucagon agonist) and orforglipron (a small oral daily nonpeptide GLP-1 RA). “Orforglipron wouldn’t have to be refrigerated,” he noted, and it “could be cheaper to manufacture, might be preferred over subcutaneous medication by some people, and it showed pretty good efficacy in early studies.”
Retatrutide, a triple agonist (GLP-1/GIP/glucagon) and CagriSema (cagrilintide plus semaglutide) showed “pretty impressive weight loss in early studies,” Dr. Garvey said. “We’re optimistic.”
Also invited to comment, Sean Wharton, MD, PharmD, Wharton Medical Clinic and York University, Toronto, said that the recent developments in antiobesity medications are “so exciting that it’s difficult to make direct comments,” since “maybe there will be something bigger, or maybe something will go wrong with these molecules and we’ll have to back-step.”
Further studies are needed, he added, to determine outcomes in patients who reduce their intake to half or three-quarters of a dose, or who transition to intermittent therapy.
Nutrient-stimulated, hormone-based antiobesity medications
Here’s a status overview of the nutrient-stimulated hormone-based medications already approved and on the horizon:
Semaglutide. The GLP-1 RA semaglutide (Ozempic), was approved by the FDA for type 2 diabetes in 2017. In June 2021, the FDA approved the use of semaglutide (Wegovy) for obesity.
Topline results from the Semaglutide Effects on Heart Disease and Stroke in Patients with Overweight or Obesity (SELECT) cardiovascular outcome trial showed that in individuals with obesity without type 2 diabetes, semaglutide led to a 20% reduction in major cardiovascular events, Dr. Jastreboff noted, adding that full results will be presented at the American Heart Association meeting on Nov. 11.
Tirzepatide. In May 2022, the FDA approved tirzepatide (Mounjaro), a GIP/GLP-1RA, for type 2 diabetes, and a decision about the use of tirzepatide for obesity is expected by year’s end.
The full results of the phase 3 SURMOUNT-3 trial were presented at ObesityWeek (just after this session), as reported by this news organization.
And the full results of the phase 3 SURMOUNT-4 trial of tirzepatide for obesity were presented at the European Association for the Study of Diabetes meeting, Dr. Jastreboff noted. At 88 weeks, in the continued tirzepatide group, average weight reduction was 26%, absolute weight reduction was 62 pounds (28.1 kg), and > 50% of individuals achieved ≥ 25% weight loss.
The phase 3 SURMOUNT MMO trial of morbidity and mortality with tirzepatide in obesity is estimated to be completed in 2027.
Cagrilintide. In a phase 2 trial of the amylin analog cagrilintide in patients with obesity, more than half of participants lost at least 10% of their weight at 26 weeks.
CagriSema. In a phase 1b trial of the amylin analog/GLP-1 RA combination of cagrilintide/semaglutide (CagriSema), average weight reduction at 20 weeks was 17.1%. The estimated primary completion dates of phase 3 trials of CagriSema, REDEFINE 1 (obesity), REDEFINE 2 (obesity and type 2 diabetes), and REDEFINE 3 (obesity and established cardiovascular disease), are 2025, 2024, and 2027, respectively.
Survodutide. Findings from a phase 2 trial of the glucagon/GLP-1 RA survodutide were presented at the American Diabetes Association (ADA) meeting in June. With 46 weeks of treatment, the average weight reduction was 18.7%, and up to 40% of participants lost at least 20% of their body weight.
Survodutide is being studied in the phase 3 SYNCHRONIZE trials.
Retatrutide. Phase 2 findings of 12-mg weekly of the GIP/GLP-1/glucagon triple hormone receptor agonist retatrutide were also presented at ADA. On average, at 48 weeks, the placebo group lost 2.1% of their weight and the retatrutide group lost 24.2% of their weight, with an average absolute reduction of 58 pounds (26.3 kg). At the highest dose (12 mg), 9 out of 10 individuals lost ≥ 10%, nearly two-thirds lost ≥ 20%, and a quarter lost ≥ 30% of their weight, at 48 weeks.
With the two highest doses of retatrutide, 100% of participants lost ≥ 5% of weight, Dr. Jastreboff reported, adding, “I’m not sure how many other times I will ever be able to say ‘100%’ in any scientific presentation.”
TRIUMPH phase 3 studies of retatrutide are ongoing.
“All the agents I’ve spoken about thus far are once-weekly injectable,” Dr. Jastreboff said, turning her attention to oral drugs.
Oral semaglutide (Rybelsus) is already FDA-approved for type 2 diabetes. The phase 2 OASIS trial results presented at ADA showed that participants with obesity who received 50 mg daily of the oral medication had an average weight reduction of 17.4% at 68 weeks, which is comparable to the 16.9% weight reduction with subcutaneous semaglutide 2.4 once weekly. More than a third of patients receiving the treatment lost ≥ 20% weight at 68 weeks.
The phase 3 OASIS study of oral semaglutide in obesity is ongoing.
Orforglipron. Phase 2 data of the small molecule oral GLP-1 RA orforglipron presented at ADA showed that participants with obesity had up to a 14.7% body weight reduction at 36 weeks. Nearly half of participants lost ≥ 15% of their body weight at 36 weeks.
The phase 3 ATTAIN study of orforglipron in obesity is ongoing.
AMG133. In a phase 2 trial, participants with obesity who received the monthly GIP receptor antagonist/ GLP-1 receptor agonist AMG133 (Amgen) had an average weight reduction of 14.5% at just 12 weeks.
Activin receptor inhibitors
Bimagrumab. This drug is a monoclonal antibody activin receptor inhibitor that binds to activin type II receptors. In a phase 2 study of 58 individuals with type 2 diabetes and obesity who received monthly medication or placebo, participants receiving bimagrumab lost 20.5% of fat mass and gained 3.6% of lean mass at 48 weeks, and the most common adverse events were mild diarrhea and muscle spasm.
Bimagrumab and semaglutide for obesity are being studied in BELIEVE, an ongoing phase 2b study. Topline results are anticipated by the end of 2024.
Taldefgrobep. The fusion protein taldefgrobep binds active myostatin. A phase 2 study of taldefgrobep for obesity is planned to start in 2024.
Dr. Jastreboff is on the scientific advisory board for Amgen, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk, and has received research support form Novo Nordisk, Eli Lilly, Rhythm, and NIH/NIDDK.
A version of this article first appeared on Medscape.com.
FROM OBESITYWEEK® 2023
Another study ties statins to T2D: Should practice change?
Studies have shown links between statin use and type 2 diabetes (T2D) for more than a decade. A U.S. Food and Drug Administration label change for the drugs warned in 2012 about reports of increased risks of high blood glucose and glycosylated hemoglobin (A1c) levels. However, in the same warning, the FDA said it “continues to believe that the cardiovascular benefits of statins outweigh these small increased risks.”
Indeed, although the warning triggered much discussion at the time and a number of meta-analyses and other observational studies in more recent years, that conclusion seems to hold among clinicians and society guidelines.
For example, in a recent practice pointer on the risk of diabetes with statins published in the BMJ, Ishak Mansi, MD, of the Orlando VA Health Care System, and colleagues write, “This potential adverse effect of diabetes with statin use should not be a barrier to starting statin treatment when indicated.”
They also called for further research to answer such questions as, “Is statin-associated diabetes reversible upon statin discontinuation? Would intermittent use minimize this risk while maintaining cardiovascular benefits?”
An earlier study among individuals at high risk for diabetes found significantly higher rates of incident diabetes at 10 years among patients on placebo, metformin, or lifestyle intervention who also initiated statin therapy. Jill Crandall, MD, Albert Einstein College of Medicine, New York, and colleagues conclude, “For individual patients, a potential modest increase in diabetes risk clearly needs to be balanced against the consistent and highly significant reductions in myocardial infarction, stroke, and cardiovascular death associated with statin treatment.”
In the same vein, a recent review by Byron Hoogwerf, MD, Emeritus, department of endocrinology, diabetes, and metabolism, Cleveland Clinic, is titled, “Statins may increase diabetes, but benefit still outweighs risk.”
Rosuvastatin versus Atorvastatin
The latest study in this arena is an analysis of the LODESTAR randomized controlled trial of 4,400 patients with coronary artery disease in 12 hospitals in Korea which compares the risks associated with individual statins.
Senior author Myeong-Ki Hong, MD, PhD, Yonsei University College of Medicine, Severance Cardiovascular Hospital, Seoul, South Korea, said in an interview that the study was prompted by the “limited” studies evaluating clinical outcomes, including diabetes risk, according to statin type.
Dr. Hong and colleagues compared the risk of developing diabetes among those taking rosuvastatin (mean daily dose, 17.1 mg) or atorvastatin (mean daily dose 36 mg) for 3 years. While both statins effectively prevented myocardial infarction, stroke, and death, (2.5% vs. 1.5%; HR, 1.66).
Overall, the HR of new-onset T2D was 1.29 (95% confidence interval, 1.01-1.63; P = .04).
“The percentages of new-onset diabetes and cataract are in line with previous studies regarding statin therapy in patients with atherosclerotic cardiovascular disease,” Dr. Hong said. “Additional research specifically focusing on these outcomes is required, with more frequent measurement of glucose and A1c levels to detect new-onset diabetes and regular ophthalmologic examinations to detect cataracts.”
“However,” he added, “when using rosuvastatin over atorvastatin, we ... emphasize the importance of meticulous monitoring and appropriate lifestyle interventions to mitigate the risk of new-onset diabetes or cataracts.”
Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute, was not convinced, and said the study “does not provide useful insights into the use of these drugs.”
The investigators used whatever dose they wanted, “and the authors report only the median dose after 3 years,” he said in an interview. “Because there was a slightly greater reduction in low-density lipoprotein (LDL) cholesterol with rosuvastatin, the relative dose was actually higher.”
“We know that new-onset diabetes with statins is dose-dependent,” he said. “The P-values for diabetes incidence were marginal (very close to P = .05). Accordingly, the diabetes data are unconvincing. ... The similar efficacy is not surprising given the open-label dosing with relatively similar effects on lipids.”
Seth Shay Martin, MD, MHS, director of the Advanced Lipid Disorders Program and Digital Health Lab, Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins Medicine, Baltimore, also commented on the results. The findings are “in line with existing knowledge and current guidelines,” he said. “Therefore, the study should not influence prescribing.”
“Although the study suggests that rosuvastatin was associated with a higher risk of new-onset diabetes mellitus requiring antidiabetics and cataract surgery, compared with atorvastatin, these findings should be interpreted with caution given the open-label nature of the study and require further investigation,” he said.
“The mean daily doses of statins were somewhat below target for secondary prevention,” he noted. “Ideally, patients with coronary artery disease (CAD) take 20-40 mg daily of rosuvastatin or 40-80 mg daily of atorvastatin.”
“Furthermore, the LDL cholesterol levels were not optimized in the patients,” he said. “The mean LDL-C was 1.8-1.9 mmol/L, which is equivalent to 70-73 mg/dL. In the current treatment era, we generally treat to LDL-C levels less than 70 mg/dL and often less than 55 mg/dL in CAD patients.”
“The cataracts finding is particularly odd,” he added. “There was historic concern for cataracts with statin therapy, initially because of studies in beagle dogs. However, high-quality evidence from statin trials has not shown a risk for cataracts.”
So which statin has the lowest risk of triggering new-onset diabetes? As Dr. Hong noted, the literature is sparse when it comes to comparing the risk among specific statins. Some studies suggest that the risk may depend on the individual and their specific risk factors, as well as the dose and intensity of the prescribed statin.
One recent study suggests that while the overall chance of developing diabetes is small, when looking at risk by years of exposure, atorvastatin, rosuvastatin, and lovastatin carried the largest risk, whereas the risk was lower with pravastatin and simvastatin.
Risks also seemed lower with fluvastatin and pitavastatin, but there were too few study patients taking those drugs long-term to include in the subanalysis.
With input from the latest guidelines from the American Heart Association and the American Diabetes Association, as well as findings from a clinical guide on statin-associated diabetes, Dr. Hoogwerf suggests in his review that shared decision-making before starting statin therapy of any type include the following considerations/discussion points:
- For all patients: Screening to determine baseline glycemic status; nonstatin therapies to lower cholesterol; and variables associated with an increased risk of diabetes, including antihypertensive drugs.
- For patients without T2D: The possibility of developing T2D, types and doses of statins, and the fact that statin benefits “generally far outweigh” risks of developing diabetes.
- For patients with T2D: Possible small adverse effects on glycemic control; statin benefits in reducing risk for atherosclerotic cardiovascular disease, which “significantly outweigh” the small increase in A1c; and mitigation of adverse glycemic effects of statins with glucose-lowering therapies.
It’s worth noting that the AHA and ADA guidelines, among others, also emphasize that such discussions should include the importance of weight loss, regular exercise, and adhering to a healthy lifestyle to mitigate risks of both diabetes and heart disease, with or without statins.
Dr. Hong, Dr. Nissen, and Dr. Martin report no relevant financial relationships. Dr. Hoogwerf has disclosed ownership interest in Eli Lilly and consulting for MannKind and Zealand Pharmaceuticals.
A version of this article appeared on Medscape.com.
Studies have shown links between statin use and type 2 diabetes (T2D) for more than a decade. A U.S. Food and Drug Administration label change for the drugs warned in 2012 about reports of increased risks of high blood glucose and glycosylated hemoglobin (A1c) levels. However, in the same warning, the FDA said it “continues to believe that the cardiovascular benefits of statins outweigh these small increased risks.”
Indeed, although the warning triggered much discussion at the time and a number of meta-analyses and other observational studies in more recent years, that conclusion seems to hold among clinicians and society guidelines.
For example, in a recent practice pointer on the risk of diabetes with statins published in the BMJ, Ishak Mansi, MD, of the Orlando VA Health Care System, and colleagues write, “This potential adverse effect of diabetes with statin use should not be a barrier to starting statin treatment when indicated.”
They also called for further research to answer such questions as, “Is statin-associated diabetes reversible upon statin discontinuation? Would intermittent use minimize this risk while maintaining cardiovascular benefits?”
An earlier study among individuals at high risk for diabetes found significantly higher rates of incident diabetes at 10 years among patients on placebo, metformin, or lifestyle intervention who also initiated statin therapy. Jill Crandall, MD, Albert Einstein College of Medicine, New York, and colleagues conclude, “For individual patients, a potential modest increase in diabetes risk clearly needs to be balanced against the consistent and highly significant reductions in myocardial infarction, stroke, and cardiovascular death associated with statin treatment.”
In the same vein, a recent review by Byron Hoogwerf, MD, Emeritus, department of endocrinology, diabetes, and metabolism, Cleveland Clinic, is titled, “Statins may increase diabetes, but benefit still outweighs risk.”
Rosuvastatin versus Atorvastatin
The latest study in this arena is an analysis of the LODESTAR randomized controlled trial of 4,400 patients with coronary artery disease in 12 hospitals in Korea which compares the risks associated with individual statins.
Senior author Myeong-Ki Hong, MD, PhD, Yonsei University College of Medicine, Severance Cardiovascular Hospital, Seoul, South Korea, said in an interview that the study was prompted by the “limited” studies evaluating clinical outcomes, including diabetes risk, according to statin type.
Dr. Hong and colleagues compared the risk of developing diabetes among those taking rosuvastatin (mean daily dose, 17.1 mg) or atorvastatin (mean daily dose 36 mg) for 3 years. While both statins effectively prevented myocardial infarction, stroke, and death, (2.5% vs. 1.5%; HR, 1.66).
Overall, the HR of new-onset T2D was 1.29 (95% confidence interval, 1.01-1.63; P = .04).
“The percentages of new-onset diabetes and cataract are in line with previous studies regarding statin therapy in patients with atherosclerotic cardiovascular disease,” Dr. Hong said. “Additional research specifically focusing on these outcomes is required, with more frequent measurement of glucose and A1c levels to detect new-onset diabetes and regular ophthalmologic examinations to detect cataracts.”
“However,” he added, “when using rosuvastatin over atorvastatin, we ... emphasize the importance of meticulous monitoring and appropriate lifestyle interventions to mitigate the risk of new-onset diabetes or cataracts.”
Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute, was not convinced, and said the study “does not provide useful insights into the use of these drugs.”
The investigators used whatever dose they wanted, “and the authors report only the median dose after 3 years,” he said in an interview. “Because there was a slightly greater reduction in low-density lipoprotein (LDL) cholesterol with rosuvastatin, the relative dose was actually higher.”
“We know that new-onset diabetes with statins is dose-dependent,” he said. “The P-values for diabetes incidence were marginal (very close to P = .05). Accordingly, the diabetes data are unconvincing. ... The similar efficacy is not surprising given the open-label dosing with relatively similar effects on lipids.”
Seth Shay Martin, MD, MHS, director of the Advanced Lipid Disorders Program and Digital Health Lab, Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins Medicine, Baltimore, also commented on the results. The findings are “in line with existing knowledge and current guidelines,” he said. “Therefore, the study should not influence prescribing.”
“Although the study suggests that rosuvastatin was associated with a higher risk of new-onset diabetes mellitus requiring antidiabetics and cataract surgery, compared with atorvastatin, these findings should be interpreted with caution given the open-label nature of the study and require further investigation,” he said.
“The mean daily doses of statins were somewhat below target for secondary prevention,” he noted. “Ideally, patients with coronary artery disease (CAD) take 20-40 mg daily of rosuvastatin or 40-80 mg daily of atorvastatin.”
“Furthermore, the LDL cholesterol levels were not optimized in the patients,” he said. “The mean LDL-C was 1.8-1.9 mmol/L, which is equivalent to 70-73 mg/dL. In the current treatment era, we generally treat to LDL-C levels less than 70 mg/dL and often less than 55 mg/dL in CAD patients.”
“The cataracts finding is particularly odd,” he added. “There was historic concern for cataracts with statin therapy, initially because of studies in beagle dogs. However, high-quality evidence from statin trials has not shown a risk for cataracts.”
So which statin has the lowest risk of triggering new-onset diabetes? As Dr. Hong noted, the literature is sparse when it comes to comparing the risk among specific statins. Some studies suggest that the risk may depend on the individual and their specific risk factors, as well as the dose and intensity of the prescribed statin.
One recent study suggests that while the overall chance of developing diabetes is small, when looking at risk by years of exposure, atorvastatin, rosuvastatin, and lovastatin carried the largest risk, whereas the risk was lower with pravastatin and simvastatin.
Risks also seemed lower with fluvastatin and pitavastatin, but there were too few study patients taking those drugs long-term to include in the subanalysis.
With input from the latest guidelines from the American Heart Association and the American Diabetes Association, as well as findings from a clinical guide on statin-associated diabetes, Dr. Hoogwerf suggests in his review that shared decision-making before starting statin therapy of any type include the following considerations/discussion points:
- For all patients: Screening to determine baseline glycemic status; nonstatin therapies to lower cholesterol; and variables associated with an increased risk of diabetes, including antihypertensive drugs.
- For patients without T2D: The possibility of developing T2D, types and doses of statins, and the fact that statin benefits “generally far outweigh” risks of developing diabetes.
- For patients with T2D: Possible small adverse effects on glycemic control; statin benefits in reducing risk for atherosclerotic cardiovascular disease, which “significantly outweigh” the small increase in A1c; and mitigation of adverse glycemic effects of statins with glucose-lowering therapies.
It’s worth noting that the AHA and ADA guidelines, among others, also emphasize that such discussions should include the importance of weight loss, regular exercise, and adhering to a healthy lifestyle to mitigate risks of both diabetes and heart disease, with or without statins.
Dr. Hong, Dr. Nissen, and Dr. Martin report no relevant financial relationships. Dr. Hoogwerf has disclosed ownership interest in Eli Lilly and consulting for MannKind and Zealand Pharmaceuticals.
A version of this article appeared on Medscape.com.
Studies have shown links between statin use and type 2 diabetes (T2D) for more than a decade. A U.S. Food and Drug Administration label change for the drugs warned in 2012 about reports of increased risks of high blood glucose and glycosylated hemoglobin (A1c) levels. However, in the same warning, the FDA said it “continues to believe that the cardiovascular benefits of statins outweigh these small increased risks.”
Indeed, although the warning triggered much discussion at the time and a number of meta-analyses and other observational studies in more recent years, that conclusion seems to hold among clinicians and society guidelines.
For example, in a recent practice pointer on the risk of diabetes with statins published in the BMJ, Ishak Mansi, MD, of the Orlando VA Health Care System, and colleagues write, “This potential adverse effect of diabetes with statin use should not be a barrier to starting statin treatment when indicated.”
They also called for further research to answer such questions as, “Is statin-associated diabetes reversible upon statin discontinuation? Would intermittent use minimize this risk while maintaining cardiovascular benefits?”
An earlier study among individuals at high risk for diabetes found significantly higher rates of incident diabetes at 10 years among patients on placebo, metformin, or lifestyle intervention who also initiated statin therapy. Jill Crandall, MD, Albert Einstein College of Medicine, New York, and colleagues conclude, “For individual patients, a potential modest increase in diabetes risk clearly needs to be balanced against the consistent and highly significant reductions in myocardial infarction, stroke, and cardiovascular death associated with statin treatment.”
In the same vein, a recent review by Byron Hoogwerf, MD, Emeritus, department of endocrinology, diabetes, and metabolism, Cleveland Clinic, is titled, “Statins may increase diabetes, but benefit still outweighs risk.”
Rosuvastatin versus Atorvastatin
The latest study in this arena is an analysis of the LODESTAR randomized controlled trial of 4,400 patients with coronary artery disease in 12 hospitals in Korea which compares the risks associated with individual statins.
Senior author Myeong-Ki Hong, MD, PhD, Yonsei University College of Medicine, Severance Cardiovascular Hospital, Seoul, South Korea, said in an interview that the study was prompted by the “limited” studies evaluating clinical outcomes, including diabetes risk, according to statin type.
Dr. Hong and colleagues compared the risk of developing diabetes among those taking rosuvastatin (mean daily dose, 17.1 mg) or atorvastatin (mean daily dose 36 mg) for 3 years. While both statins effectively prevented myocardial infarction, stroke, and death, (2.5% vs. 1.5%; HR, 1.66).
Overall, the HR of new-onset T2D was 1.29 (95% confidence interval, 1.01-1.63; P = .04).
“The percentages of new-onset diabetes and cataract are in line with previous studies regarding statin therapy in patients with atherosclerotic cardiovascular disease,” Dr. Hong said. “Additional research specifically focusing on these outcomes is required, with more frequent measurement of glucose and A1c levels to detect new-onset diabetes and regular ophthalmologic examinations to detect cataracts.”
“However,” he added, “when using rosuvastatin over atorvastatin, we ... emphasize the importance of meticulous monitoring and appropriate lifestyle interventions to mitigate the risk of new-onset diabetes or cataracts.”
Steven Nissen, MD, chief academic officer of Cleveland Clinic’s Heart and Vascular Institute, was not convinced, and said the study “does not provide useful insights into the use of these drugs.”
The investigators used whatever dose they wanted, “and the authors report only the median dose after 3 years,” he said in an interview. “Because there was a slightly greater reduction in low-density lipoprotein (LDL) cholesterol with rosuvastatin, the relative dose was actually higher.”
“We know that new-onset diabetes with statins is dose-dependent,” he said. “The P-values for diabetes incidence were marginal (very close to P = .05). Accordingly, the diabetes data are unconvincing. ... The similar efficacy is not surprising given the open-label dosing with relatively similar effects on lipids.”
Seth Shay Martin, MD, MHS, director of the Advanced Lipid Disorders Program and Digital Health Lab, Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins Medicine, Baltimore, also commented on the results. The findings are “in line with existing knowledge and current guidelines,” he said. “Therefore, the study should not influence prescribing.”
“Although the study suggests that rosuvastatin was associated with a higher risk of new-onset diabetes mellitus requiring antidiabetics and cataract surgery, compared with atorvastatin, these findings should be interpreted with caution given the open-label nature of the study and require further investigation,” he said.
“The mean daily doses of statins were somewhat below target for secondary prevention,” he noted. “Ideally, patients with coronary artery disease (CAD) take 20-40 mg daily of rosuvastatin or 40-80 mg daily of atorvastatin.”
“Furthermore, the LDL cholesterol levels were not optimized in the patients,” he said. “The mean LDL-C was 1.8-1.9 mmol/L, which is equivalent to 70-73 mg/dL. In the current treatment era, we generally treat to LDL-C levels less than 70 mg/dL and often less than 55 mg/dL in CAD patients.”
“The cataracts finding is particularly odd,” he added. “There was historic concern for cataracts with statin therapy, initially because of studies in beagle dogs. However, high-quality evidence from statin trials has not shown a risk for cataracts.”
So which statin has the lowest risk of triggering new-onset diabetes? As Dr. Hong noted, the literature is sparse when it comes to comparing the risk among specific statins. Some studies suggest that the risk may depend on the individual and their specific risk factors, as well as the dose and intensity of the prescribed statin.
One recent study suggests that while the overall chance of developing diabetes is small, when looking at risk by years of exposure, atorvastatin, rosuvastatin, and lovastatin carried the largest risk, whereas the risk was lower with pravastatin and simvastatin.
Risks also seemed lower with fluvastatin and pitavastatin, but there were too few study patients taking those drugs long-term to include in the subanalysis.
With input from the latest guidelines from the American Heart Association and the American Diabetes Association, as well as findings from a clinical guide on statin-associated diabetes, Dr. Hoogwerf suggests in his review that shared decision-making before starting statin therapy of any type include the following considerations/discussion points:
- For all patients: Screening to determine baseline glycemic status; nonstatin therapies to lower cholesterol; and variables associated with an increased risk of diabetes, including antihypertensive drugs.
- For patients without T2D: The possibility of developing T2D, types and doses of statins, and the fact that statin benefits “generally far outweigh” risks of developing diabetes.
- For patients with T2D: Possible small adverse effects on glycemic control; statin benefits in reducing risk for atherosclerotic cardiovascular disease, which “significantly outweigh” the small increase in A1c; and mitigation of adverse glycemic effects of statins with glucose-lowering therapies.
It’s worth noting that the AHA and ADA guidelines, among others, also emphasize that such discussions should include the importance of weight loss, regular exercise, and adhering to a healthy lifestyle to mitigate risks of both diabetes and heart disease, with or without statins.
Dr. Hong, Dr. Nissen, and Dr. Martin report no relevant financial relationships. Dr. Hoogwerf has disclosed ownership interest in Eli Lilly and consulting for MannKind and Zealand Pharmaceuticals.
A version of this article appeared on Medscape.com.
More weight loss with time-restricted eating
TOPLINE:
, compared with calorie restriction, while hemoglobin A1c levels dropped with both approaches, compared with no intervention.
METHODOLOGY:
- Six-month clinical trial of 75 adult participants with type 2 diabetes and obesity, randomly assigned to either 8-hour TRE (noon to 8 p.m. only) without calorie counting, a 25% daily calorie restriction, or control.
TAKEAWAY:
- The primary outcome, change in body weight at month 6, was –3.56% (P = .004) with TRE vs. –1.78% with calorie restriction (P = .06), compared with controls.
- The mean calorie deficit over the 6 months was –313 kcal/day with TRE, –197 kcal/day with calorie restriction, and –16 kcal/day for controls.
- Self-reported adherence to the regimens was 87% of days with 8-hour TRE vs. 68% reporting adherence with calorie goals over the 6 months.
- A1c levels were reduced significantly by 0.91% in the TRE group and 0.94% in the calorie-restriction group, relative to controls, with no differences between the two intervention groups.
- No serious adverse events were reported.
- Hypoglycemia and hyperglycemia occurrences didn’t differ between groups.
IN PRACTICE:
“Our findings ... show that TRE is safe in patients who are using either diet alone or medications to control their [type 2 diabetes]. However, for people using sulfonylureas and/or insulin, adopting a TRE regimen will require medication changes and regular monitoring, particularly in the initial stages of the diet.”
SOURCE:
The study was conducted by Vasiliki Pavlou, MS, RD, of the department of kinesiology and nutrition, University of Illinois at Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
- Relatively short trial duration.
- Lack of blinding.
- A higher proportion in the TRE group were using newer type 2 diabetes medications at baseline.
- Self-reported dietary intake.
DISCLOSURES:
The study was supported by the University of Illinois at Chicago, and by grants from the National Institutes of Health. Ms. Pavlou reports no relevant financial relationships. Several authors reported relationships with industry. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
, compared with calorie restriction, while hemoglobin A1c levels dropped with both approaches, compared with no intervention.
METHODOLOGY:
- Six-month clinical trial of 75 adult participants with type 2 diabetes and obesity, randomly assigned to either 8-hour TRE (noon to 8 p.m. only) without calorie counting, a 25% daily calorie restriction, or control.
TAKEAWAY:
- The primary outcome, change in body weight at month 6, was –3.56% (P = .004) with TRE vs. –1.78% with calorie restriction (P = .06), compared with controls.
- The mean calorie deficit over the 6 months was –313 kcal/day with TRE, –197 kcal/day with calorie restriction, and –16 kcal/day for controls.
- Self-reported adherence to the regimens was 87% of days with 8-hour TRE vs. 68% reporting adherence with calorie goals over the 6 months.
- A1c levels were reduced significantly by 0.91% in the TRE group and 0.94% in the calorie-restriction group, relative to controls, with no differences between the two intervention groups.
- No serious adverse events were reported.
- Hypoglycemia and hyperglycemia occurrences didn’t differ between groups.
IN PRACTICE:
“Our findings ... show that TRE is safe in patients who are using either diet alone or medications to control their [type 2 diabetes]. However, for people using sulfonylureas and/or insulin, adopting a TRE regimen will require medication changes and regular monitoring, particularly in the initial stages of the diet.”
SOURCE:
The study was conducted by Vasiliki Pavlou, MS, RD, of the department of kinesiology and nutrition, University of Illinois at Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
- Relatively short trial duration.
- Lack of blinding.
- A higher proportion in the TRE group were using newer type 2 diabetes medications at baseline.
- Self-reported dietary intake.
DISCLOSURES:
The study was supported by the University of Illinois at Chicago, and by grants from the National Institutes of Health. Ms. Pavlou reports no relevant financial relationships. Several authors reported relationships with industry. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
, compared with calorie restriction, while hemoglobin A1c levels dropped with both approaches, compared with no intervention.
METHODOLOGY:
- Six-month clinical trial of 75 adult participants with type 2 diabetes and obesity, randomly assigned to either 8-hour TRE (noon to 8 p.m. only) without calorie counting, a 25% daily calorie restriction, or control.
TAKEAWAY:
- The primary outcome, change in body weight at month 6, was –3.56% (P = .004) with TRE vs. –1.78% with calorie restriction (P = .06), compared with controls.
- The mean calorie deficit over the 6 months was –313 kcal/day with TRE, –197 kcal/day with calorie restriction, and –16 kcal/day for controls.
- Self-reported adherence to the regimens was 87% of days with 8-hour TRE vs. 68% reporting adherence with calorie goals over the 6 months.
- A1c levels were reduced significantly by 0.91% in the TRE group and 0.94% in the calorie-restriction group, relative to controls, with no differences between the two intervention groups.
- No serious adverse events were reported.
- Hypoglycemia and hyperglycemia occurrences didn’t differ between groups.
IN PRACTICE:
“Our findings ... show that TRE is safe in patients who are using either diet alone or medications to control their [type 2 diabetes]. However, for people using sulfonylureas and/or insulin, adopting a TRE regimen will require medication changes and regular monitoring, particularly in the initial stages of the diet.”
SOURCE:
The study was conducted by Vasiliki Pavlou, MS, RD, of the department of kinesiology and nutrition, University of Illinois at Chicago, and colleagues. It was published online in JAMA Network Open.
LIMITATIONS:
- Relatively short trial duration.
- Lack of blinding.
- A higher proportion in the TRE group were using newer type 2 diabetes medications at baseline.
- Self-reported dietary intake.
DISCLOSURES:
The study was supported by the University of Illinois at Chicago, and by grants from the National Institutes of Health. Ms. Pavlou reports no relevant financial relationships. Several authors reported relationships with industry. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
Obesity boosts gestational diabetes risk in women with PCOS
In a population-based cohort study that included more than 1.2 million hospital live births, PCOS was associated with a 5% increase in risk for gestational diabetes. Almost 90% of this association was mediated by obesity.
“Women with PCOS are at higher risk, but it’s only 5% higher than the general population. However, that risk rises substantially with obesity,” senior author Maria P. Velez, MD, PhD, clinician-scientist and associate professor of obstetrics and gynecology at Queen’s University, Kingston, Ont., said in an interview. “Our study highlights the need for counseling our patients about the importance of weight optimization, ideally starting with lifestyle changes like diet and exercise.”The findings were published in the Journal of Obstetrics and Gynaecology Canada.
Major mediator
The estimated prevalence of PCOS is 8%-13%, and affected patients often present with anovulation, hyperandrogenism, obesity, metabolic syndrome, and infertility. Prepregnancy insulin resistance is common among women with PCOS and may play a major part in the pathogenesis of gestational diabetes. In addition, PCOS is often accompanied by excess weight gain; about 60% of women with PCOS are overweight or obese.
Previous research has shown that PCOS is a risk factor for gestational diabetes independent of obesity, while other research has shown that obesity has an important effect on this risk.
For the current study, the researchers used causal mediation analysis to elucidate more clearly the effect of obesity on the development of gestational diabetes among patients with PCOS. No previous study has used causal mediation analysis to examine this relationship.
Using data from linked universal health databases in Ontario, the researchers analyzed data on 1,268,901 births between 2006 and 2018. Of these births, 386,748 were associated with maternal PCOS.
The rate of gestational diabetes was higher among women with PCOS (60.2 per 1000 births), compared with women without PCOS (48.6 per 1,000 births). The finding resulted in an adjusted relative risk of 1.05. Obesity mediated 89.7% of this association.
“We hope that these data will inform preconception counseling and gestational diabetes screening in pregnant women with PCOS,” said Dr. Velez. “We have the data now to counsel our patients on the importance of weight management before pregnancy. But we need more resources, such as specialized clinics, to help these patients cope with managing their weight. We can tell our patients to work on their weight management, but they need much more support from the health care system.”
Results ‘not surprising’
Commenting on the study, Francine Hippolyte, MD, vice chair of obstetrics and gynecology at Long Island Jewish Medical Center, Katz Women’s Hospital, New Hyde Park, N.Y., said that the results are “not at all surprising.” Dr. Hippolyte was not involved in the research.
“We do know that PCOS is and should be treated as a metabolic syndrome. It’s a lot more than just infertility or changes or abnormalities with one’s menstrual cycle. It impacts a woman’s risk for diabetes, prediabetes, and abnormal lipid profile, regardless of whether or not she is obese,” said Dr. Hippolyte.
She agrees with the need for specialized clinics to help such vulnerable patients manage their weight.
“It would be great if insurances would cover things like nutritional counseling or have nutritionists on their roster so that patients can easily access that service. Many patients want to do right, especially preconceptually, but it is difficult without having access to resources. Unfortunately, as clinicians, we’re not as well versed in nutrition as we would like to be or should be, so we need a multidisciplinary approach. We need nutrition and weight loss clinics and proper services to really help these patients.”
The study was supported by the Canadian Institute of Health Research and ICES. Dr. Velez and Dr. Hippolyte reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a population-based cohort study that included more than 1.2 million hospital live births, PCOS was associated with a 5% increase in risk for gestational diabetes. Almost 90% of this association was mediated by obesity.
“Women with PCOS are at higher risk, but it’s only 5% higher than the general population. However, that risk rises substantially with obesity,” senior author Maria P. Velez, MD, PhD, clinician-scientist and associate professor of obstetrics and gynecology at Queen’s University, Kingston, Ont., said in an interview. “Our study highlights the need for counseling our patients about the importance of weight optimization, ideally starting with lifestyle changes like diet and exercise.”The findings were published in the Journal of Obstetrics and Gynaecology Canada.
Major mediator
The estimated prevalence of PCOS is 8%-13%, and affected patients often present with anovulation, hyperandrogenism, obesity, metabolic syndrome, and infertility. Prepregnancy insulin resistance is common among women with PCOS and may play a major part in the pathogenesis of gestational diabetes. In addition, PCOS is often accompanied by excess weight gain; about 60% of women with PCOS are overweight or obese.
Previous research has shown that PCOS is a risk factor for gestational diabetes independent of obesity, while other research has shown that obesity has an important effect on this risk.
For the current study, the researchers used causal mediation analysis to elucidate more clearly the effect of obesity on the development of gestational diabetes among patients with PCOS. No previous study has used causal mediation analysis to examine this relationship.
Using data from linked universal health databases in Ontario, the researchers analyzed data on 1,268,901 births between 2006 and 2018. Of these births, 386,748 were associated with maternal PCOS.
The rate of gestational diabetes was higher among women with PCOS (60.2 per 1000 births), compared with women without PCOS (48.6 per 1,000 births). The finding resulted in an adjusted relative risk of 1.05. Obesity mediated 89.7% of this association.
“We hope that these data will inform preconception counseling and gestational diabetes screening in pregnant women with PCOS,” said Dr. Velez. “We have the data now to counsel our patients on the importance of weight management before pregnancy. But we need more resources, such as specialized clinics, to help these patients cope with managing their weight. We can tell our patients to work on their weight management, but they need much more support from the health care system.”
Results ‘not surprising’
Commenting on the study, Francine Hippolyte, MD, vice chair of obstetrics and gynecology at Long Island Jewish Medical Center, Katz Women’s Hospital, New Hyde Park, N.Y., said that the results are “not at all surprising.” Dr. Hippolyte was not involved in the research.
“We do know that PCOS is and should be treated as a metabolic syndrome. It’s a lot more than just infertility or changes or abnormalities with one’s menstrual cycle. It impacts a woman’s risk for diabetes, prediabetes, and abnormal lipid profile, regardless of whether or not she is obese,” said Dr. Hippolyte.
She agrees with the need for specialized clinics to help such vulnerable patients manage their weight.
“It would be great if insurances would cover things like nutritional counseling or have nutritionists on their roster so that patients can easily access that service. Many patients want to do right, especially preconceptually, but it is difficult without having access to resources. Unfortunately, as clinicians, we’re not as well versed in nutrition as we would like to be or should be, so we need a multidisciplinary approach. We need nutrition and weight loss clinics and proper services to really help these patients.”
The study was supported by the Canadian Institute of Health Research and ICES. Dr. Velez and Dr. Hippolyte reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a population-based cohort study that included more than 1.2 million hospital live births, PCOS was associated with a 5% increase in risk for gestational diabetes. Almost 90% of this association was mediated by obesity.
“Women with PCOS are at higher risk, but it’s only 5% higher than the general population. However, that risk rises substantially with obesity,” senior author Maria P. Velez, MD, PhD, clinician-scientist and associate professor of obstetrics and gynecology at Queen’s University, Kingston, Ont., said in an interview. “Our study highlights the need for counseling our patients about the importance of weight optimization, ideally starting with lifestyle changes like diet and exercise.”The findings were published in the Journal of Obstetrics and Gynaecology Canada.
Major mediator
The estimated prevalence of PCOS is 8%-13%, and affected patients often present with anovulation, hyperandrogenism, obesity, metabolic syndrome, and infertility. Prepregnancy insulin resistance is common among women with PCOS and may play a major part in the pathogenesis of gestational diabetes. In addition, PCOS is often accompanied by excess weight gain; about 60% of women with PCOS are overweight or obese.
Previous research has shown that PCOS is a risk factor for gestational diabetes independent of obesity, while other research has shown that obesity has an important effect on this risk.
For the current study, the researchers used causal mediation analysis to elucidate more clearly the effect of obesity on the development of gestational diabetes among patients with PCOS. No previous study has used causal mediation analysis to examine this relationship.
Using data from linked universal health databases in Ontario, the researchers analyzed data on 1,268,901 births between 2006 and 2018. Of these births, 386,748 were associated with maternal PCOS.
The rate of gestational diabetes was higher among women with PCOS (60.2 per 1000 births), compared with women without PCOS (48.6 per 1,000 births). The finding resulted in an adjusted relative risk of 1.05. Obesity mediated 89.7% of this association.
“We hope that these data will inform preconception counseling and gestational diabetes screening in pregnant women with PCOS,” said Dr. Velez. “We have the data now to counsel our patients on the importance of weight management before pregnancy. But we need more resources, such as specialized clinics, to help these patients cope with managing their weight. We can tell our patients to work on their weight management, but they need much more support from the health care system.”
Results ‘not surprising’
Commenting on the study, Francine Hippolyte, MD, vice chair of obstetrics and gynecology at Long Island Jewish Medical Center, Katz Women’s Hospital, New Hyde Park, N.Y., said that the results are “not at all surprising.” Dr. Hippolyte was not involved in the research.
“We do know that PCOS is and should be treated as a metabolic syndrome. It’s a lot more than just infertility or changes or abnormalities with one’s menstrual cycle. It impacts a woman’s risk for diabetes, prediabetes, and abnormal lipid profile, regardless of whether or not she is obese,” said Dr. Hippolyte.
She agrees with the need for specialized clinics to help such vulnerable patients manage their weight.
“It would be great if insurances would cover things like nutritional counseling or have nutritionists on their roster so that patients can easily access that service. Many patients want to do right, especially preconceptually, but it is difficult without having access to resources. Unfortunately, as clinicians, we’re not as well versed in nutrition as we would like to be or should be, so we need a multidisciplinary approach. We need nutrition and weight loss clinics and proper services to really help these patients.”
The study was supported by the Canadian Institute of Health Research and ICES. Dr. Velez and Dr. Hippolyte reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF OBSTETRICS AND GYNAECOLOGY CANADA
SGLT2 inhibitors in type 2 diabetes linked to lower risk of developing GI cancers
VANCOUVER –
The SGLT2 inhibitors emerged superior to DPP4 inhibitors for reducing risk of colorectal, hepatic, esophageal, and other GI cancers except pancreatic cancer, said study investigator Shu-Yen Emily Chan, MD, a gastroenterologist in the departments of medicine and epidemiology at Weiss Memorial Hospital, Chicago.
On the basis of the findings, physicians could consider the SGLT2s canagliflozin, dapagliflozin, and empagliflozin or a GLP-1 as first-line therapy, particularly for people with T2D who are at elevated risk for GI cancers, Dr. Chan said in an interview at the American College of Gastroenterology (ACG): 2023 Annual Scientific Meeting.
Previous research focused on potential cardiovascular or renal benefits associated with SGLT2s, “but there are few looking at GI cancer risk and these medications,” she added. Most earlier studies in cancer have been preclinical and observational studies on colorectal cancer or hepatocellular carcinoma.
Using the TriNetX database of millions of medical claims from 92 hospitals across the United States, Dr. Chan and colleagues identified 706,390 adults who began first-line SGLT2 inhibitor therapy. They used propensity matching to link these patients with 706,390 other adults who began taking a DDP4 inhibitor (sitagliptin, saxagliptin, linagliptin, or alogliptin).
All participants had been diagnosed with type 2 diabetes. Patients were prescribed an SGLT2 inhibitor at least three times, and any cancer diagnosis that occurred at least 6 months after starting therapy was noted. Anyone with a history of cancer, cancer recurrence, or metastatic disease was excluded from the population-based cohort study.
In addition to evaluating a large number of patients, the study is notable for including people with ulcerative colitis and Crohn’s disease and for evaluating every GI cancer – esophageal, gastric, small intestinal, colorectal, rectal, anal, hepatic, biliary, and gallbladder malignancies.
Key findings
Among adults who received an SGLT2 inhibitor, there was a 15% decrease in overall risk of developing any GI cancer, compared with those who received a DPP4 inhibitor (hazard ratio, 0.85; 95% confidence interval, 0.82-0.88).
Colon cancer was the most common malignancy in the study. Dr. Chan and colleagues identified colon cancer among 1,789 people, or 0.25% of those taking an SGLT2 inhibitor, compared with 3,283 people, or 0.46%, of those taking a DPP4 inhibitor.
SGLT2 inhibitors were associated with a 16% decrease in risk of gastric cancer (HR, 0.84; 95% CI; 0.74-0.945; P = .005), a 13% decrease in risk of liver and intrahepatic bile duct cancer (HR, 0.87; 95% CI, 0.81-0.95), and a 22% decrease in risk of colon cancer (HR, 0.781; 95% CI, 0.74-0.83; P < .001), compared with the DPP4 medications.
The only cancer more likely in the SGLT2 inhibitor group than in the DPP4 inhibitor group was pancreatic cancer (HR, 1.035; 95% CI, 0.964-1.111; P = .340).
The SLGT2 inhibitor class also was superior to metformin for reducing risk of GI cancers.
Asked whether the study findings should alter current practice, Dr. Chan said that the study is new and hasn’t yet been published. “More studies will be needed and included in official guidelines before the findings become practice-changing,” she said.
Limitations of the study include residual confounding, absence of family cancer history, and information bias. Strengths include the large, national database and propensity score matching.
‘Eye-opening’ study
“It is a good study, and eye-opening because it shows that one class of diabetes medications is better than another one,” said session co-moderator Kenneth J. Vega, MD, professor of medicine and chief of the division of gastroenterology and hepatology at Augusta University–Medical College of Georgia.
Dr. Vega shared his theory on why diabetes medications could reduce risk of GI cancers. “I would think reducing diabetes means you can control inflammation ... and better controlling inflammation leads you to have less cancers.”
He added, “I think we need more long-term studies.”
The study was independently supported. Dr. Chan and Dr. Vega report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER –
The SGLT2 inhibitors emerged superior to DPP4 inhibitors for reducing risk of colorectal, hepatic, esophageal, and other GI cancers except pancreatic cancer, said study investigator Shu-Yen Emily Chan, MD, a gastroenterologist in the departments of medicine and epidemiology at Weiss Memorial Hospital, Chicago.
On the basis of the findings, physicians could consider the SGLT2s canagliflozin, dapagliflozin, and empagliflozin or a GLP-1 as first-line therapy, particularly for people with T2D who are at elevated risk for GI cancers, Dr. Chan said in an interview at the American College of Gastroenterology (ACG): 2023 Annual Scientific Meeting.
Previous research focused on potential cardiovascular or renal benefits associated with SGLT2s, “but there are few looking at GI cancer risk and these medications,” she added. Most earlier studies in cancer have been preclinical and observational studies on colorectal cancer or hepatocellular carcinoma.
Using the TriNetX database of millions of medical claims from 92 hospitals across the United States, Dr. Chan and colleagues identified 706,390 adults who began first-line SGLT2 inhibitor therapy. They used propensity matching to link these patients with 706,390 other adults who began taking a DDP4 inhibitor (sitagliptin, saxagliptin, linagliptin, or alogliptin).
All participants had been diagnosed with type 2 diabetes. Patients were prescribed an SGLT2 inhibitor at least three times, and any cancer diagnosis that occurred at least 6 months after starting therapy was noted. Anyone with a history of cancer, cancer recurrence, or metastatic disease was excluded from the population-based cohort study.
In addition to evaluating a large number of patients, the study is notable for including people with ulcerative colitis and Crohn’s disease and for evaluating every GI cancer – esophageal, gastric, small intestinal, colorectal, rectal, anal, hepatic, biliary, and gallbladder malignancies.
Key findings
Among adults who received an SGLT2 inhibitor, there was a 15% decrease in overall risk of developing any GI cancer, compared with those who received a DPP4 inhibitor (hazard ratio, 0.85; 95% confidence interval, 0.82-0.88).
Colon cancer was the most common malignancy in the study. Dr. Chan and colleagues identified colon cancer among 1,789 people, or 0.25% of those taking an SGLT2 inhibitor, compared with 3,283 people, or 0.46%, of those taking a DPP4 inhibitor.
SGLT2 inhibitors were associated with a 16% decrease in risk of gastric cancer (HR, 0.84; 95% CI; 0.74-0.945; P = .005), a 13% decrease in risk of liver and intrahepatic bile duct cancer (HR, 0.87; 95% CI, 0.81-0.95), and a 22% decrease in risk of colon cancer (HR, 0.781; 95% CI, 0.74-0.83; P < .001), compared with the DPP4 medications.
The only cancer more likely in the SGLT2 inhibitor group than in the DPP4 inhibitor group was pancreatic cancer (HR, 1.035; 95% CI, 0.964-1.111; P = .340).
The SLGT2 inhibitor class also was superior to metformin for reducing risk of GI cancers.
Asked whether the study findings should alter current practice, Dr. Chan said that the study is new and hasn’t yet been published. “More studies will be needed and included in official guidelines before the findings become practice-changing,” she said.
Limitations of the study include residual confounding, absence of family cancer history, and information bias. Strengths include the large, national database and propensity score matching.
‘Eye-opening’ study
“It is a good study, and eye-opening because it shows that one class of diabetes medications is better than another one,” said session co-moderator Kenneth J. Vega, MD, professor of medicine and chief of the division of gastroenterology and hepatology at Augusta University–Medical College of Georgia.
Dr. Vega shared his theory on why diabetes medications could reduce risk of GI cancers. “I would think reducing diabetes means you can control inflammation ... and better controlling inflammation leads you to have less cancers.”
He added, “I think we need more long-term studies.”
The study was independently supported. Dr. Chan and Dr. Vega report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER –
The SGLT2 inhibitors emerged superior to DPP4 inhibitors for reducing risk of colorectal, hepatic, esophageal, and other GI cancers except pancreatic cancer, said study investigator Shu-Yen Emily Chan, MD, a gastroenterologist in the departments of medicine and epidemiology at Weiss Memorial Hospital, Chicago.
On the basis of the findings, physicians could consider the SGLT2s canagliflozin, dapagliflozin, and empagliflozin or a GLP-1 as first-line therapy, particularly for people with T2D who are at elevated risk for GI cancers, Dr. Chan said in an interview at the American College of Gastroenterology (ACG): 2023 Annual Scientific Meeting.
Previous research focused on potential cardiovascular or renal benefits associated with SGLT2s, “but there are few looking at GI cancer risk and these medications,” she added. Most earlier studies in cancer have been preclinical and observational studies on colorectal cancer or hepatocellular carcinoma.
Using the TriNetX database of millions of medical claims from 92 hospitals across the United States, Dr. Chan and colleagues identified 706,390 adults who began first-line SGLT2 inhibitor therapy. They used propensity matching to link these patients with 706,390 other adults who began taking a DDP4 inhibitor (sitagliptin, saxagliptin, linagliptin, or alogliptin).
All participants had been diagnosed with type 2 diabetes. Patients were prescribed an SGLT2 inhibitor at least three times, and any cancer diagnosis that occurred at least 6 months after starting therapy was noted. Anyone with a history of cancer, cancer recurrence, or metastatic disease was excluded from the population-based cohort study.
In addition to evaluating a large number of patients, the study is notable for including people with ulcerative colitis and Crohn’s disease and for evaluating every GI cancer – esophageal, gastric, small intestinal, colorectal, rectal, anal, hepatic, biliary, and gallbladder malignancies.
Key findings
Among adults who received an SGLT2 inhibitor, there was a 15% decrease in overall risk of developing any GI cancer, compared with those who received a DPP4 inhibitor (hazard ratio, 0.85; 95% confidence interval, 0.82-0.88).
Colon cancer was the most common malignancy in the study. Dr. Chan and colleagues identified colon cancer among 1,789 people, or 0.25% of those taking an SGLT2 inhibitor, compared with 3,283 people, or 0.46%, of those taking a DPP4 inhibitor.
SGLT2 inhibitors were associated with a 16% decrease in risk of gastric cancer (HR, 0.84; 95% CI; 0.74-0.945; P = .005), a 13% decrease in risk of liver and intrahepatic bile duct cancer (HR, 0.87; 95% CI, 0.81-0.95), and a 22% decrease in risk of colon cancer (HR, 0.781; 95% CI, 0.74-0.83; P < .001), compared with the DPP4 medications.
The only cancer more likely in the SGLT2 inhibitor group than in the DPP4 inhibitor group was pancreatic cancer (HR, 1.035; 95% CI, 0.964-1.111; P = .340).
The SLGT2 inhibitor class also was superior to metformin for reducing risk of GI cancers.
Asked whether the study findings should alter current practice, Dr. Chan said that the study is new and hasn’t yet been published. “More studies will be needed and included in official guidelines before the findings become practice-changing,” she said.
Limitations of the study include residual confounding, absence of family cancer history, and information bias. Strengths include the large, national database and propensity score matching.
‘Eye-opening’ study
“It is a good study, and eye-opening because it shows that one class of diabetes medications is better than another one,” said session co-moderator Kenneth J. Vega, MD, professor of medicine and chief of the division of gastroenterology and hepatology at Augusta University–Medical College of Georgia.
Dr. Vega shared his theory on why diabetes medications could reduce risk of GI cancers. “I would think reducing diabetes means you can control inflammation ... and better controlling inflammation leads you to have less cancers.”
He added, “I think we need more long-term studies.”
The study was independently supported. Dr. Chan and Dr. Vega report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ACG 2023
Higher weight loss on tirzepatide links to seven factors
TOPLINE:
Among the 3,188 people with type 2 diabetes who were adherent to their tirzepatide (Mounjaro, Lilly) regimen in four pivotal trials of the agent, a quarter achieved at least a 15% cut from their baseline body weight after 40-42 weeks of treatment, and researchers found seven baseline variables that were significantly linked with a higher incidence of this level of weight loss.
say the authors.
METHODOLOGY:
- Investigators conducted a post hoc analysis of data collected from a total of 3,188 people with type 2 diabetes who had been adherent to their assigned tirzepatide regimen for 40-42 weeks in any one of four pivotal trials of the agent.
- The researchers aimed to identify predictors of a reduction in body weight of at least 15% with tirzepatide treatment at any of the three tested doses – 5 mg, 10 mg, or 15 mg – which were administered by subcutaneous injection once a week.
- All four trials that provided data prohibited concurrent therapy that would promote weight loss, and the people included in the analysis did not receive any rescue medications for controlling glycemia.
- The primary efficacy measure in all four studies was the ability of tirzepatide to improve glycemic control (measured by A1c level), compared with placebo, semaglutide (Ozempic) 1 mg SC once weekly, insulin degludec (Tresiba, Novo Nordisk), or insulin glargine (Basaglar, Lilly).
TAKEAWAY:
- Among the 3,188 people who remained adherent to their tirzepatide regimen for 40-42 weeks, 792 (25%) experienced a weight reduction of at least 15% from baseline.
- Multivariate analysis of baseline covariates showed that these seven factors were significantly linked with greater than or equal to 15% weight loss: higher tirzepatide dose, being female, being of White or Asian race, being of younger age, undergoing treatment with metformin, having better glycemic control (based on lower A1c and lower fasting serum glucose), and having lower non–high-density lipoprotein cholesterol level.
- During follow-up, achievement of at least a 15% cut in baseline body weight was significantly associated with greater reductions in A1c, fasting serum glucose level, waist circumference, blood pressure, serum triglyceride level, and serum level of the liver enzyme alanine transaminase.
IN PRACTICE:
“These findings may provide valuable information to clinicians and people with type 2 diabetes regarding the likelihood of achieving substantial body weight reduction with tirzepatide and also help to signal likely improvements to be seen in a range of cardiometabolic risk parameters with tirzepatide-induced weight loss,” the authors concluded in their report.
SOURCE:
The study was largely run by researchers who are employees of Lilly, the company that markets tirzepatide (Mounjaro). It was published in Diabetes Care.
LIMITATIONS:
- The analysis was post hoc.
- The follow-up was limited.
- The analysis focused entirely on baseline parameters as potential predictors of weight loss magnitude.
DISCLOSURES:
The study was funded by Eli Lilly, the company that markets tirzepatide (Mounjaro) and that sponsored the SURPASS trials. Six authors are employees of Lilly, one is a contractor for Lilly, and the two remaining authors have had financial relationships with Lilly and with several other companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among the 3,188 people with type 2 diabetes who were adherent to their tirzepatide (Mounjaro, Lilly) regimen in four pivotal trials of the agent, a quarter achieved at least a 15% cut from their baseline body weight after 40-42 weeks of treatment, and researchers found seven baseline variables that were significantly linked with a higher incidence of this level of weight loss.
say the authors.
METHODOLOGY:
- Investigators conducted a post hoc analysis of data collected from a total of 3,188 people with type 2 diabetes who had been adherent to their assigned tirzepatide regimen for 40-42 weeks in any one of four pivotal trials of the agent.
- The researchers aimed to identify predictors of a reduction in body weight of at least 15% with tirzepatide treatment at any of the three tested doses – 5 mg, 10 mg, or 15 mg – which were administered by subcutaneous injection once a week.
- All four trials that provided data prohibited concurrent therapy that would promote weight loss, and the people included in the analysis did not receive any rescue medications for controlling glycemia.
- The primary efficacy measure in all four studies was the ability of tirzepatide to improve glycemic control (measured by A1c level), compared with placebo, semaglutide (Ozempic) 1 mg SC once weekly, insulin degludec (Tresiba, Novo Nordisk), or insulin glargine (Basaglar, Lilly).
TAKEAWAY:
- Among the 3,188 people who remained adherent to their tirzepatide regimen for 40-42 weeks, 792 (25%) experienced a weight reduction of at least 15% from baseline.
- Multivariate analysis of baseline covariates showed that these seven factors were significantly linked with greater than or equal to 15% weight loss: higher tirzepatide dose, being female, being of White or Asian race, being of younger age, undergoing treatment with metformin, having better glycemic control (based on lower A1c and lower fasting serum glucose), and having lower non–high-density lipoprotein cholesterol level.
- During follow-up, achievement of at least a 15% cut in baseline body weight was significantly associated with greater reductions in A1c, fasting serum glucose level, waist circumference, blood pressure, serum triglyceride level, and serum level of the liver enzyme alanine transaminase.
IN PRACTICE:
“These findings may provide valuable information to clinicians and people with type 2 diabetes regarding the likelihood of achieving substantial body weight reduction with tirzepatide and also help to signal likely improvements to be seen in a range of cardiometabolic risk parameters with tirzepatide-induced weight loss,” the authors concluded in their report.
SOURCE:
The study was largely run by researchers who are employees of Lilly, the company that markets tirzepatide (Mounjaro). It was published in Diabetes Care.
LIMITATIONS:
- The analysis was post hoc.
- The follow-up was limited.
- The analysis focused entirely on baseline parameters as potential predictors of weight loss magnitude.
DISCLOSURES:
The study was funded by Eli Lilly, the company that markets tirzepatide (Mounjaro) and that sponsored the SURPASS trials. Six authors are employees of Lilly, one is a contractor for Lilly, and the two remaining authors have had financial relationships with Lilly and with several other companies.
A version of this article first appeared on Medscape.com.
TOPLINE:
Among the 3,188 people with type 2 diabetes who were adherent to their tirzepatide (Mounjaro, Lilly) regimen in four pivotal trials of the agent, a quarter achieved at least a 15% cut from their baseline body weight after 40-42 weeks of treatment, and researchers found seven baseline variables that were significantly linked with a higher incidence of this level of weight loss.
say the authors.
METHODOLOGY:
- Investigators conducted a post hoc analysis of data collected from a total of 3,188 people with type 2 diabetes who had been adherent to their assigned tirzepatide regimen for 40-42 weeks in any one of four pivotal trials of the agent.
- The researchers aimed to identify predictors of a reduction in body weight of at least 15% with tirzepatide treatment at any of the three tested doses – 5 mg, 10 mg, or 15 mg – which were administered by subcutaneous injection once a week.
- All four trials that provided data prohibited concurrent therapy that would promote weight loss, and the people included in the analysis did not receive any rescue medications for controlling glycemia.
- The primary efficacy measure in all four studies was the ability of tirzepatide to improve glycemic control (measured by A1c level), compared with placebo, semaglutide (Ozempic) 1 mg SC once weekly, insulin degludec (Tresiba, Novo Nordisk), or insulin glargine (Basaglar, Lilly).
TAKEAWAY:
- Among the 3,188 people who remained adherent to their tirzepatide regimen for 40-42 weeks, 792 (25%) experienced a weight reduction of at least 15% from baseline.
- Multivariate analysis of baseline covariates showed that these seven factors were significantly linked with greater than or equal to 15% weight loss: higher tirzepatide dose, being female, being of White or Asian race, being of younger age, undergoing treatment with metformin, having better glycemic control (based on lower A1c and lower fasting serum glucose), and having lower non–high-density lipoprotein cholesterol level.
- During follow-up, achievement of at least a 15% cut in baseline body weight was significantly associated with greater reductions in A1c, fasting serum glucose level, waist circumference, blood pressure, serum triglyceride level, and serum level of the liver enzyme alanine transaminase.
IN PRACTICE:
“These findings may provide valuable information to clinicians and people with type 2 diabetes regarding the likelihood of achieving substantial body weight reduction with tirzepatide and also help to signal likely improvements to be seen in a range of cardiometabolic risk parameters with tirzepatide-induced weight loss,” the authors concluded in their report.
SOURCE:
The study was largely run by researchers who are employees of Lilly, the company that markets tirzepatide (Mounjaro). It was published in Diabetes Care.
LIMITATIONS:
- The analysis was post hoc.
- The follow-up was limited.
- The analysis focused entirely on baseline parameters as potential predictors of weight loss magnitude.
DISCLOSURES:
The study was funded by Eli Lilly, the company that markets tirzepatide (Mounjaro) and that sponsored the SURPASS trials. Six authors are employees of Lilly, one is a contractor for Lilly, and the two remaining authors have had financial relationships with Lilly and with several other companies.
A version of this article first appeared on Medscape.com.
Tricyclics may raise fracture risk in type 2 diabetes
VANCOUVER – , independent of any prevalent neuropathy, according to findings from an analysis of a large, randomized clinical trial.
Although the findings are suggestive, they don’t definitively pin blame on TCAs, said Rachel Elam, MD, who presented the study at the annual meeting of the American Society for Bone and Mineral Research. “I think that there’s not enough information to conclude that tricyclic antidepressants directly lead to fractures, but I think it opens the door [to] something we should look into more. Is it being mediated by a better predictor, or is it the medication itself? I think it’s more hypothesis generating,” said Dr. Elam, an assistant professor of medicine in the division of rheumatology at the Medical College of Georgia, Augusta.
Patients with type 2 diabetes are known to be at increased risk of fracture, but prediction tools tend to underestimate this risk, Dr. Elam said. “Type 2 diabetes–specific clinical risk factors may be helpful for finding out fracture risk in this population,” Dr. Elam said during her talk.
Glycemic control is one candidate risk factor because advanced glycation end products are linked to reduced bone strength. Other factors include antidiabetic medication use, neuropathy, and microvascular disease, which has been linked to increased cortical porosity.
The study examined a somewhat younger population than previous surveys, having drawn from the Look AHEAD-C clinical trial, which examined the effects of an intensive lifestyle intervention on type 2 diabetes. Look AHEAD-C included 4,697 participants aged 45-75 from 16 U.S. clinical sites. Participants had a body mass index of 25.0 kg/m2 or higher and hemoglobin A1c levels of 11% or below.
Dr. Elam cited the database’s inclusion of factors like A1c levels, renal parameters, and diabetic neuropathy. “It gave us a really good population to look at those risk factors” in a large group of people with type 2 diabetes, she said.
Over a median follow-up of 16.6 years, there were 649 participants with incident first clinical fracture(s). Statistically significant factors predicting fracture risk included TCA use (hazard ratio, 2.24; 95% confidence interval, 1.14-4.43), female gender (HR, 2.20; 95% CI, 1.83-2.66), insulin use (HR, 1.26; 95% CI, 1.02-1.57), increases in A1c level (per 1% increase: HR, 1.12; 95% CI, 1.04-1.20), age (HR, 1.02; 95% CI, 1.01-1.04), other or mixed race/ethnicity (HR, 0.68; 95% CI, 0.52-0.87), Hispanic White race/ethnicity (HR, 0.60; 95% CI, 0.39-0.91), non-Hispanic Black race/ethnicity (HR, 0.35; 95% CI, 0.26-0.47), and estrogen use (HR, 0.65; 95% CI, 0.44-0.98).
During the Q&A session following the presentation, Elsa Strotmeyer, PhD, commented that TCAs have been linked to central nervous system pathways in falls in other populations. “It’s a very nice study. It’s important to look at the diabetes complications related to the fracture risk, but I thought that they should have emphasized some more of the diabetes complications being related to fracture rather than these tricyclic antidepressants, because that is not a unique factor to that population,” said Dr. Strotmeyer, who is an associate professor of epidemiology at the University of Pittsburgh.
Instead, she noted a different strength of the study. “The study population is important because they’re a relatively young population with type 2 diabetes, compared to many studies [that] have been published in older populations. Showing similar things that we found in older populations was the unique piece and the important piece of this study,” Dr. Strotmeyer said.
Ultimately, the model wasn’t sufficient to be used as a fall risk predictor, but it should inform future work, according to Dr. Elam. “I think it does lay some new groundwork that when we’re looking forward, it may [help in building] other models to better predict fracture risk in type 2 diabetes. Things that would be important to include [in future models] would be medication use, such as tricyclic antidepressants,” and to make sure we include glycemic control, A1c, and insulin medication.
The study was independently funded. Dr. Elam and Dr. Strotmeyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER – , independent of any prevalent neuropathy, according to findings from an analysis of a large, randomized clinical trial.
Although the findings are suggestive, they don’t definitively pin blame on TCAs, said Rachel Elam, MD, who presented the study at the annual meeting of the American Society for Bone and Mineral Research. “I think that there’s not enough information to conclude that tricyclic antidepressants directly lead to fractures, but I think it opens the door [to] something we should look into more. Is it being mediated by a better predictor, or is it the medication itself? I think it’s more hypothesis generating,” said Dr. Elam, an assistant professor of medicine in the division of rheumatology at the Medical College of Georgia, Augusta.
Patients with type 2 diabetes are known to be at increased risk of fracture, but prediction tools tend to underestimate this risk, Dr. Elam said. “Type 2 diabetes–specific clinical risk factors may be helpful for finding out fracture risk in this population,” Dr. Elam said during her talk.
Glycemic control is one candidate risk factor because advanced glycation end products are linked to reduced bone strength. Other factors include antidiabetic medication use, neuropathy, and microvascular disease, which has been linked to increased cortical porosity.
The study examined a somewhat younger population than previous surveys, having drawn from the Look AHEAD-C clinical trial, which examined the effects of an intensive lifestyle intervention on type 2 diabetes. Look AHEAD-C included 4,697 participants aged 45-75 from 16 U.S. clinical sites. Participants had a body mass index of 25.0 kg/m2 or higher and hemoglobin A1c levels of 11% or below.
Dr. Elam cited the database’s inclusion of factors like A1c levels, renal parameters, and diabetic neuropathy. “It gave us a really good population to look at those risk factors” in a large group of people with type 2 diabetes, she said.
Over a median follow-up of 16.6 years, there were 649 participants with incident first clinical fracture(s). Statistically significant factors predicting fracture risk included TCA use (hazard ratio, 2.24; 95% confidence interval, 1.14-4.43), female gender (HR, 2.20; 95% CI, 1.83-2.66), insulin use (HR, 1.26; 95% CI, 1.02-1.57), increases in A1c level (per 1% increase: HR, 1.12; 95% CI, 1.04-1.20), age (HR, 1.02; 95% CI, 1.01-1.04), other or mixed race/ethnicity (HR, 0.68; 95% CI, 0.52-0.87), Hispanic White race/ethnicity (HR, 0.60; 95% CI, 0.39-0.91), non-Hispanic Black race/ethnicity (HR, 0.35; 95% CI, 0.26-0.47), and estrogen use (HR, 0.65; 95% CI, 0.44-0.98).
During the Q&A session following the presentation, Elsa Strotmeyer, PhD, commented that TCAs have been linked to central nervous system pathways in falls in other populations. “It’s a very nice study. It’s important to look at the diabetes complications related to the fracture risk, but I thought that they should have emphasized some more of the diabetes complications being related to fracture rather than these tricyclic antidepressants, because that is not a unique factor to that population,” said Dr. Strotmeyer, who is an associate professor of epidemiology at the University of Pittsburgh.
Instead, she noted a different strength of the study. “The study population is important because they’re a relatively young population with type 2 diabetes, compared to many studies [that] have been published in older populations. Showing similar things that we found in older populations was the unique piece and the important piece of this study,” Dr. Strotmeyer said.
Ultimately, the model wasn’t sufficient to be used as a fall risk predictor, but it should inform future work, according to Dr. Elam. “I think it does lay some new groundwork that when we’re looking forward, it may [help in building] other models to better predict fracture risk in type 2 diabetes. Things that would be important to include [in future models] would be medication use, such as tricyclic antidepressants,” and to make sure we include glycemic control, A1c, and insulin medication.
The study was independently funded. Dr. Elam and Dr. Strotmeyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VANCOUVER – , independent of any prevalent neuropathy, according to findings from an analysis of a large, randomized clinical trial.
Although the findings are suggestive, they don’t definitively pin blame on TCAs, said Rachel Elam, MD, who presented the study at the annual meeting of the American Society for Bone and Mineral Research. “I think that there’s not enough information to conclude that tricyclic antidepressants directly lead to fractures, but I think it opens the door [to] something we should look into more. Is it being mediated by a better predictor, or is it the medication itself? I think it’s more hypothesis generating,” said Dr. Elam, an assistant professor of medicine in the division of rheumatology at the Medical College of Georgia, Augusta.
Patients with type 2 diabetes are known to be at increased risk of fracture, but prediction tools tend to underestimate this risk, Dr. Elam said. “Type 2 diabetes–specific clinical risk factors may be helpful for finding out fracture risk in this population,” Dr. Elam said during her talk.
Glycemic control is one candidate risk factor because advanced glycation end products are linked to reduced bone strength. Other factors include antidiabetic medication use, neuropathy, and microvascular disease, which has been linked to increased cortical porosity.
The study examined a somewhat younger population than previous surveys, having drawn from the Look AHEAD-C clinical trial, which examined the effects of an intensive lifestyle intervention on type 2 diabetes. Look AHEAD-C included 4,697 participants aged 45-75 from 16 U.S. clinical sites. Participants had a body mass index of 25.0 kg/m2 or higher and hemoglobin A1c levels of 11% or below.
Dr. Elam cited the database’s inclusion of factors like A1c levels, renal parameters, and diabetic neuropathy. “It gave us a really good population to look at those risk factors” in a large group of people with type 2 diabetes, she said.
Over a median follow-up of 16.6 years, there were 649 participants with incident first clinical fracture(s). Statistically significant factors predicting fracture risk included TCA use (hazard ratio, 2.24; 95% confidence interval, 1.14-4.43), female gender (HR, 2.20; 95% CI, 1.83-2.66), insulin use (HR, 1.26; 95% CI, 1.02-1.57), increases in A1c level (per 1% increase: HR, 1.12; 95% CI, 1.04-1.20), age (HR, 1.02; 95% CI, 1.01-1.04), other or mixed race/ethnicity (HR, 0.68; 95% CI, 0.52-0.87), Hispanic White race/ethnicity (HR, 0.60; 95% CI, 0.39-0.91), non-Hispanic Black race/ethnicity (HR, 0.35; 95% CI, 0.26-0.47), and estrogen use (HR, 0.65; 95% CI, 0.44-0.98).
During the Q&A session following the presentation, Elsa Strotmeyer, PhD, commented that TCAs have been linked to central nervous system pathways in falls in other populations. “It’s a very nice study. It’s important to look at the diabetes complications related to the fracture risk, but I thought that they should have emphasized some more of the diabetes complications being related to fracture rather than these tricyclic antidepressants, because that is not a unique factor to that population,” said Dr. Strotmeyer, who is an associate professor of epidemiology at the University of Pittsburgh.
Instead, she noted a different strength of the study. “The study population is important because they’re a relatively young population with type 2 diabetes, compared to many studies [that] have been published in older populations. Showing similar things that we found in older populations was the unique piece and the important piece of this study,” Dr. Strotmeyer said.
Ultimately, the model wasn’t sufficient to be used as a fall risk predictor, but it should inform future work, according to Dr. Elam. “I think it does lay some new groundwork that when we’re looking forward, it may [help in building] other models to better predict fracture risk in type 2 diabetes. Things that would be important to include [in future models] would be medication use, such as tricyclic antidepressants,” and to make sure we include glycemic control, A1c, and insulin medication.
The study was independently funded. Dr. Elam and Dr. Strotmeyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ASBMR 2023
Common meds link to sudden cardiac arrest in type 2 diabetes
HAMBURG, Germany – , shows the first such analysis of real-world, primary care data.
People with type 2 diabetes who do not have a history of CVD have almost three times the risk of SCA if they take antipsychotic medications and nearly double the risk if they take certain antibiotics that prolong the QT interval, notably, macrolides and fluoroquinolones.
“These data show that commonly prescribed drugs - antipsychotic medications, used by about 3% of people with type 2 diabetes, and antibiotics, taken by 5% to 10%, convey an increased risk of sudden cardiac arrest in those without a history of cardiovascular disease,” said Peter Harms, MSc, who presented the study at the annual meeting of the European Association for the Study of Diabetes. Another drug associated with an increase in SCA among patients with diabetes was domperidone, an antinausea medication.
“Perhaps these drugs could be avoided in some cases, and GPs should be more aware of the possible consequences of their use,” he added. “If the patient has type 2 diabetes, then maybe it’s better to avoid some of these medications and try and cope without them, or at least find an alternative antibiotic.”
Mr. Harms, an epidemiologist from Amsterdam University Medical Centers, highlighted that their study was unique because the investigators drew upon primary care data. “These data are extensive, and we find a lot of associations which are very real.”
SCA is associated with 50% of all cardiac deaths and accounts for 20% of all mortality in high-income countries. Of those people who experience SCA, 80% of cases prove fatal.
“As the name suggests, it is difficult to predict because it is sudden, especially in people without a cardiovascular disease history,” Mr. Harms pointed out in an interview with this news organization. He highlighted that “around half of those who experience SCA, often between the ages of 40 and 60 years, have never seen a cardiologist, but many do have type 2 diabetes.
“We need to better understand how to recognize people at risk of SCA, know who to watch and how to prevent these events,” he emphasized.
Vladimira Fejfarova, MD, comoderated the session and commented on the study. “From the clinical point of view, it’s necessary to evaluate risk factors that can contribute to sudden cardiac arrest.”
Overall, the researchers found that, among people with type 2 diabetes who do not have a history of CVD, hypoglycemia, severe hypertension, dyslipidemia, and use of QTc-prolonging medications are associated with SCA risk. Among people with type 2 diabetes and CVD, albuminuria and heart failure are associated with SCA risk.
Dr. Fejfarova added: “With type 2 diabetes and also type 1, we need to look more at adverse events, especially when treating infections with macrolides, but also mycotic infections, because antimycotic drugs are known to influence QT intervals that could contribute to sudden cardiac arrest.
“We need to be more cautious with prescribing certain antibiotics that have these side effects in our patients with diabetes,” asserted Dr. Fejfarova, from the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague.
Type 2 diabetes doubles the risk of SCA
The researcher decided to investigate the population of people with type 2 diabetes because their risk of SCD is around twice that of those without type 2 diabetes. Because these patients have relatively frequent checkups with general practitioners, Mr. Harms turned to primary care databases that contained comprehensive and relatively routine information on risk indicators.
Longitudinal associations between clinical characteristics of 3,919 patients with type 2 diabetes – both those with and those without a history of CVD – and SCA (a total of 689 patients) were determined.
Cases were found in the AmsteRdam REsuscitation STtudies (ARREST) registry of out-of-hospital resuscitation attempts by emergency medical services in the Dutch region of Noord-Holland from 2010 to 2019. Case patients were matched with up to five control patients. The control group comprised people with type 2 diabetes who had not experienced an SCA. Control patients were sourced from the same primary care practices who were of similar age and sex. Clinical measurements, including blood pressure and blood glucose readings, medication use, and medical history for the 5 years leading up to an SCA, were obtained from general practice records. A multivariable analysis was performed, and results were stratified for people with and for those without a history of CVD.
Of particular interest were drugs that interfere with cardiac function, including some prokinetic, antibiotic, and antipsychotic medications. All of the drugs are known to be associated with a change in QTc prolongation. Examples include domperidone (QTc-prolonging prokinetic), macrolides and fluoroquinolones (QTc-prolonging antibiotics), and haloperidol (a QTc-prolonging antipsychotic).
Antibiotic and antipsychotic use might contribute to SCA in T2D
Case patients and control patients were similar in age, hemoglobin A1c level, and other characteristics with the exception that more patients with SCA had a history of CVD (40.0% vs. 29.4%).
“Looking at the associations in the overall population, insulin use was strongly associated with SCA risk [hazard ratio, 2.38] and perhaps this was an indicator of severity of type 2 diabetes,” remarked Mr. Harms. “Also, unsurprisingly, a history of arrhythmia [HR, 1.68] and, more surprisingly, prokinetic drug use [HR, 1.66; 95% confidence interval, 1.20-2.31], specifically those known for QTc-prolongation, were associated with SCA.”
Among people who had experienced an SCA and who did not have a history of CVD (337 case patients/2,023 control patients), QTc-prolonging antipsychotic medication use was associated with SCA at an HR of 2.87, and antibiotic medication use was associated with SCA at an HR of 1.66. A low fasting glucose level (< 4.5 mmol/mol) was associated with SCA at an HR of 2.5; severely high systolic blood pressure (> 180 mm Hg) was associated with SCA at an HR of 2.21; low HDL cholesterol level, with an HR of 1.35; and high LDL cholesterol level (> 2.6 mmol/L), with an HR of 1.64.
Among people with a history of CVD (352 case patients/1,207 control patients), associations between albuminuria and SCA were moderate (HR, 1.54) and severe (HR, 1.55); heart failure was associated with SCA at an HR of 1.85 (95% CI, 1.50-2.29).
Comoderator Dr. Fejfarova added that, in addition to the findings from Dr. Harms’ study, other research presented in the same session highlighted the importance of checking patients for the presence of arrhythmias that could lead to the development of atrioventricular blocks, sinus node diseases, and SCA.
Mr. Harms and Dr. Fejfarova have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HAMBURG, Germany – , shows the first such analysis of real-world, primary care data.
People with type 2 diabetes who do not have a history of CVD have almost three times the risk of SCA if they take antipsychotic medications and nearly double the risk if they take certain antibiotics that prolong the QT interval, notably, macrolides and fluoroquinolones.
“These data show that commonly prescribed drugs - antipsychotic medications, used by about 3% of people with type 2 diabetes, and antibiotics, taken by 5% to 10%, convey an increased risk of sudden cardiac arrest in those without a history of cardiovascular disease,” said Peter Harms, MSc, who presented the study at the annual meeting of the European Association for the Study of Diabetes. Another drug associated with an increase in SCA among patients with diabetes was domperidone, an antinausea medication.
“Perhaps these drugs could be avoided in some cases, and GPs should be more aware of the possible consequences of their use,” he added. “If the patient has type 2 diabetes, then maybe it’s better to avoid some of these medications and try and cope without them, or at least find an alternative antibiotic.”
Mr. Harms, an epidemiologist from Amsterdam University Medical Centers, highlighted that their study was unique because the investigators drew upon primary care data. “These data are extensive, and we find a lot of associations which are very real.”
SCA is associated with 50% of all cardiac deaths and accounts for 20% of all mortality in high-income countries. Of those people who experience SCA, 80% of cases prove fatal.
“As the name suggests, it is difficult to predict because it is sudden, especially in people without a cardiovascular disease history,” Mr. Harms pointed out in an interview with this news organization. He highlighted that “around half of those who experience SCA, often between the ages of 40 and 60 years, have never seen a cardiologist, but many do have type 2 diabetes.
“We need to better understand how to recognize people at risk of SCA, know who to watch and how to prevent these events,” he emphasized.
Vladimira Fejfarova, MD, comoderated the session and commented on the study. “From the clinical point of view, it’s necessary to evaluate risk factors that can contribute to sudden cardiac arrest.”
Overall, the researchers found that, among people with type 2 diabetes who do not have a history of CVD, hypoglycemia, severe hypertension, dyslipidemia, and use of QTc-prolonging medications are associated with SCA risk. Among people with type 2 diabetes and CVD, albuminuria and heart failure are associated with SCA risk.
Dr. Fejfarova added: “With type 2 diabetes and also type 1, we need to look more at adverse events, especially when treating infections with macrolides, but also mycotic infections, because antimycotic drugs are known to influence QT intervals that could contribute to sudden cardiac arrest.
“We need to be more cautious with prescribing certain antibiotics that have these side effects in our patients with diabetes,” asserted Dr. Fejfarova, from the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague.
Type 2 diabetes doubles the risk of SCA
The researcher decided to investigate the population of people with type 2 diabetes because their risk of SCD is around twice that of those without type 2 diabetes. Because these patients have relatively frequent checkups with general practitioners, Mr. Harms turned to primary care databases that contained comprehensive and relatively routine information on risk indicators.
Longitudinal associations between clinical characteristics of 3,919 patients with type 2 diabetes – both those with and those without a history of CVD – and SCA (a total of 689 patients) were determined.
Cases were found in the AmsteRdam REsuscitation STtudies (ARREST) registry of out-of-hospital resuscitation attempts by emergency medical services in the Dutch region of Noord-Holland from 2010 to 2019. Case patients were matched with up to five control patients. The control group comprised people with type 2 diabetes who had not experienced an SCA. Control patients were sourced from the same primary care practices who were of similar age and sex. Clinical measurements, including blood pressure and blood glucose readings, medication use, and medical history for the 5 years leading up to an SCA, were obtained from general practice records. A multivariable analysis was performed, and results were stratified for people with and for those without a history of CVD.
Of particular interest were drugs that interfere with cardiac function, including some prokinetic, antibiotic, and antipsychotic medications. All of the drugs are known to be associated with a change in QTc prolongation. Examples include domperidone (QTc-prolonging prokinetic), macrolides and fluoroquinolones (QTc-prolonging antibiotics), and haloperidol (a QTc-prolonging antipsychotic).
Antibiotic and antipsychotic use might contribute to SCA in T2D
Case patients and control patients were similar in age, hemoglobin A1c level, and other characteristics with the exception that more patients with SCA had a history of CVD (40.0% vs. 29.4%).
“Looking at the associations in the overall population, insulin use was strongly associated with SCA risk [hazard ratio, 2.38] and perhaps this was an indicator of severity of type 2 diabetes,” remarked Mr. Harms. “Also, unsurprisingly, a history of arrhythmia [HR, 1.68] and, more surprisingly, prokinetic drug use [HR, 1.66; 95% confidence interval, 1.20-2.31], specifically those known for QTc-prolongation, were associated with SCA.”
Among people who had experienced an SCA and who did not have a history of CVD (337 case patients/2,023 control patients), QTc-prolonging antipsychotic medication use was associated with SCA at an HR of 2.87, and antibiotic medication use was associated with SCA at an HR of 1.66. A low fasting glucose level (< 4.5 mmol/mol) was associated with SCA at an HR of 2.5; severely high systolic blood pressure (> 180 mm Hg) was associated with SCA at an HR of 2.21; low HDL cholesterol level, with an HR of 1.35; and high LDL cholesterol level (> 2.6 mmol/L), with an HR of 1.64.
Among people with a history of CVD (352 case patients/1,207 control patients), associations between albuminuria and SCA were moderate (HR, 1.54) and severe (HR, 1.55); heart failure was associated with SCA at an HR of 1.85 (95% CI, 1.50-2.29).
Comoderator Dr. Fejfarova added that, in addition to the findings from Dr. Harms’ study, other research presented in the same session highlighted the importance of checking patients for the presence of arrhythmias that could lead to the development of atrioventricular blocks, sinus node diseases, and SCA.
Mr. Harms and Dr. Fejfarova have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HAMBURG, Germany – , shows the first such analysis of real-world, primary care data.
People with type 2 diabetes who do not have a history of CVD have almost three times the risk of SCA if they take antipsychotic medications and nearly double the risk if they take certain antibiotics that prolong the QT interval, notably, macrolides and fluoroquinolones.
“These data show that commonly prescribed drugs - antipsychotic medications, used by about 3% of people with type 2 diabetes, and antibiotics, taken by 5% to 10%, convey an increased risk of sudden cardiac arrest in those without a history of cardiovascular disease,” said Peter Harms, MSc, who presented the study at the annual meeting of the European Association for the Study of Diabetes. Another drug associated with an increase in SCA among patients with diabetes was domperidone, an antinausea medication.
“Perhaps these drugs could be avoided in some cases, and GPs should be more aware of the possible consequences of their use,” he added. “If the patient has type 2 diabetes, then maybe it’s better to avoid some of these medications and try and cope without them, or at least find an alternative antibiotic.”
Mr. Harms, an epidemiologist from Amsterdam University Medical Centers, highlighted that their study was unique because the investigators drew upon primary care data. “These data are extensive, and we find a lot of associations which are very real.”
SCA is associated with 50% of all cardiac deaths and accounts for 20% of all mortality in high-income countries. Of those people who experience SCA, 80% of cases prove fatal.
“As the name suggests, it is difficult to predict because it is sudden, especially in people without a cardiovascular disease history,” Mr. Harms pointed out in an interview with this news organization. He highlighted that “around half of those who experience SCA, often between the ages of 40 and 60 years, have never seen a cardiologist, but many do have type 2 diabetes.
“We need to better understand how to recognize people at risk of SCA, know who to watch and how to prevent these events,” he emphasized.
Vladimira Fejfarova, MD, comoderated the session and commented on the study. “From the clinical point of view, it’s necessary to evaluate risk factors that can contribute to sudden cardiac arrest.”
Overall, the researchers found that, among people with type 2 diabetes who do not have a history of CVD, hypoglycemia, severe hypertension, dyslipidemia, and use of QTc-prolonging medications are associated with SCA risk. Among people with type 2 diabetes and CVD, albuminuria and heart failure are associated with SCA risk.
Dr. Fejfarova added: “With type 2 diabetes and also type 1, we need to look more at adverse events, especially when treating infections with macrolides, but also mycotic infections, because antimycotic drugs are known to influence QT intervals that could contribute to sudden cardiac arrest.
“We need to be more cautious with prescribing certain antibiotics that have these side effects in our patients with diabetes,” asserted Dr. Fejfarova, from the Diabetes Centre, Institute for Clinical and Experimental Medicine, Prague.
Type 2 diabetes doubles the risk of SCA
The researcher decided to investigate the population of people with type 2 diabetes because their risk of SCD is around twice that of those without type 2 diabetes. Because these patients have relatively frequent checkups with general practitioners, Mr. Harms turned to primary care databases that contained comprehensive and relatively routine information on risk indicators.
Longitudinal associations between clinical characteristics of 3,919 patients with type 2 diabetes – both those with and those without a history of CVD – and SCA (a total of 689 patients) were determined.
Cases were found in the AmsteRdam REsuscitation STtudies (ARREST) registry of out-of-hospital resuscitation attempts by emergency medical services in the Dutch region of Noord-Holland from 2010 to 2019. Case patients were matched with up to five control patients. The control group comprised people with type 2 diabetes who had not experienced an SCA. Control patients were sourced from the same primary care practices who were of similar age and sex. Clinical measurements, including blood pressure and blood glucose readings, medication use, and medical history for the 5 years leading up to an SCA, were obtained from general practice records. A multivariable analysis was performed, and results were stratified for people with and for those without a history of CVD.
Of particular interest were drugs that interfere with cardiac function, including some prokinetic, antibiotic, and antipsychotic medications. All of the drugs are known to be associated with a change in QTc prolongation. Examples include domperidone (QTc-prolonging prokinetic), macrolides and fluoroquinolones (QTc-prolonging antibiotics), and haloperidol (a QTc-prolonging antipsychotic).
Antibiotic and antipsychotic use might contribute to SCA in T2D
Case patients and control patients were similar in age, hemoglobin A1c level, and other characteristics with the exception that more patients with SCA had a history of CVD (40.0% vs. 29.4%).
“Looking at the associations in the overall population, insulin use was strongly associated with SCA risk [hazard ratio, 2.38] and perhaps this was an indicator of severity of type 2 diabetes,” remarked Mr. Harms. “Also, unsurprisingly, a history of arrhythmia [HR, 1.68] and, more surprisingly, prokinetic drug use [HR, 1.66; 95% confidence interval, 1.20-2.31], specifically those known for QTc-prolongation, were associated with SCA.”
Among people who had experienced an SCA and who did not have a history of CVD (337 case patients/2,023 control patients), QTc-prolonging antipsychotic medication use was associated with SCA at an HR of 2.87, and antibiotic medication use was associated with SCA at an HR of 1.66. A low fasting glucose level (< 4.5 mmol/mol) was associated with SCA at an HR of 2.5; severely high systolic blood pressure (> 180 mm Hg) was associated with SCA at an HR of 2.21; low HDL cholesterol level, with an HR of 1.35; and high LDL cholesterol level (> 2.6 mmol/L), with an HR of 1.64.
Among people with a history of CVD (352 case patients/1,207 control patients), associations between albuminuria and SCA were moderate (HR, 1.54) and severe (HR, 1.55); heart failure was associated with SCA at an HR of 1.85 (95% CI, 1.50-2.29).
Comoderator Dr. Fejfarova added that, in addition to the findings from Dr. Harms’ study, other research presented in the same session highlighted the importance of checking patients for the presence of arrhythmias that could lead to the development of atrioventricular blocks, sinus node diseases, and SCA.
Mr. Harms and Dr. Fejfarova have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT EASD 2023
Higher fracture risk not seen with SGLT2 inhibitors
VANCOUVER – In patients with type 2 diabetes, sodium-glucose cotransporter 2 (SGLT2) inhibitors as an adjunct to metformin were not associated with an increase in fracture risk, according to a new real-world study.
There have been some reports of an increase in fracture risk associated with SGLT2 inhibitors, and it was observed in the phase 3 CANVAS trial of canagliflozin (Invokana), which led to a Food and Drug Administration warning of fracture risks associated with canagliflozin use. Some ensuing studies did not show an increased risk, but these studies were generally less than a year in duration and may have missed longer-term risk, according to Veerle van Hulten, MSc.
“Fracture risk is something that takes a long time to develop, so we wanted to have a longer follow-up. We looked into the CPRD [Clinical Practice Research Datalink], which is a beautiful database containing real-world data from primary care practices,” said Ms. van Hulten, a PhD student at Maastricht (the Netherlands) University, who presented the study at the annual meeting of the American Society for Bone and Mineral Research.
Ms. van Hulten and colleagues compared SGLT2 inhibitors with dipeptidyl peptidase–4 (DPP-4) inhibitors because the latter are used in similar populations and have been shown to have no effect on fracture risk.
“What we found is that SGLT2 inhibitors are not associated with an increased fracture risk. Even with a duration of use of over 811 days, we did not observe an increased hazard ratio for fractures when compared DPP-4 inhibitor users,” Ms. van Hulten said.
SGLT2 inhibitors reduce blood sugar by increasing elimination of sugar in the urine. They also increase phosphate, reduce calcium, and increase parathyroid hormone, which could in turn negatively affect bone turnover, according to Ms. van Hulten.
In the new study, conducted between January 2013 and June 2020, the researchers used propensity score matching to compare adult patients, including 13,807 who were prescribed SGLT2 inhibitors and 28,524 who were prescribed DPP-4 inhibitors for the first time. They matched patients based on demographics, comorbidities, comedication, and lifestyle factors.
There was no association between SGLT2 inhibitor use and overall fracture risk or major osteoporotic, hip, vertebral, humerus, radius, or ulna fractures. There was no difference in risk for any duration of use, even with the longest duration of use of 811 days (adjusted hazard ratio, 1.0). There were no differences among specific SGLT2 inhibitors, including canagliflozin (aHR, 1.12; 95% confidence interval, 0.73-1.72). Analyses by sex and age also revealed no statistically significant differences between the two drug classes.
During the Q&A session after the presentation, Sarah Berry, MD, MPH, an associate professor of medicine at Harvard Medical School and a clinical researcher at the Marcus Institute for Aging Research, both in Boston, noted the trend toward an increase in fracture risk in the first 90 days. “It looked like there was something going on in the first 90 days, and then after that the results were much closer to the null. I would put out maybe another potential mechanism whereby the SGLT2 inhibitors might cause fracture, and that’s falls. They cause polyuria, and any drug you give that causes women to rush to the bathroom may well cause fractures, particularly in the short term,” Dr. Berry said.
Ms. van Hulten agreed, and also brought up that the drugs can cause osmotic diuresis. That can lead to hypovolemia, the symptoms of which include weakness, fatigue, and dizziness. “And increased falls, of course, increases fracture risk. We do not expect anything to happen to bone metabolism in the first 90 days. I think we can agree that there would be more time needed to alter the bone enough to increase fracture risk, so we expect that this trend toward an increased risk might be attributable to that increased fall risk that might occur with SGLT2 inhibitor use,” she said.
It’s possible that such a mechanism explains increased fracture risk seen in some earlier short-term studies, she added.
Overall, Ms. van Hulten said that the results should provide some confidence in SGLT2 inhibitors, though more work needs to be done. “I think we provide reassurance that SGLT2 inhibitors are safe to use. However, we still only have a median follow-up of 1.6 years. It’s not as long as we maybe would like, but it’s the best we can do with the data available, since the SGLT2 inhibitors have only been used since 2013. So maybe it’s best to prescribe it and keep [fall risk] in mind and look into the effects later on again, but it seems to be safe to use.”
The study received funding from the Novo Nordisk Foundation. Ms. van Hulten and Dr. Berry reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VANCOUVER – In patients with type 2 diabetes, sodium-glucose cotransporter 2 (SGLT2) inhibitors as an adjunct to metformin were not associated with an increase in fracture risk, according to a new real-world study.
There have been some reports of an increase in fracture risk associated with SGLT2 inhibitors, and it was observed in the phase 3 CANVAS trial of canagliflozin (Invokana), which led to a Food and Drug Administration warning of fracture risks associated with canagliflozin use. Some ensuing studies did not show an increased risk, but these studies were generally less than a year in duration and may have missed longer-term risk, according to Veerle van Hulten, MSc.
“Fracture risk is something that takes a long time to develop, so we wanted to have a longer follow-up. We looked into the CPRD [Clinical Practice Research Datalink], which is a beautiful database containing real-world data from primary care practices,” said Ms. van Hulten, a PhD student at Maastricht (the Netherlands) University, who presented the study at the annual meeting of the American Society for Bone and Mineral Research.
Ms. van Hulten and colleagues compared SGLT2 inhibitors with dipeptidyl peptidase–4 (DPP-4) inhibitors because the latter are used in similar populations and have been shown to have no effect on fracture risk.
“What we found is that SGLT2 inhibitors are not associated with an increased fracture risk. Even with a duration of use of over 811 days, we did not observe an increased hazard ratio for fractures when compared DPP-4 inhibitor users,” Ms. van Hulten said.
SGLT2 inhibitors reduce blood sugar by increasing elimination of sugar in the urine. They also increase phosphate, reduce calcium, and increase parathyroid hormone, which could in turn negatively affect bone turnover, according to Ms. van Hulten.
In the new study, conducted between January 2013 and June 2020, the researchers used propensity score matching to compare adult patients, including 13,807 who were prescribed SGLT2 inhibitors and 28,524 who were prescribed DPP-4 inhibitors for the first time. They matched patients based on demographics, comorbidities, comedication, and lifestyle factors.
There was no association between SGLT2 inhibitor use and overall fracture risk or major osteoporotic, hip, vertebral, humerus, radius, or ulna fractures. There was no difference in risk for any duration of use, even with the longest duration of use of 811 days (adjusted hazard ratio, 1.0). There were no differences among specific SGLT2 inhibitors, including canagliflozin (aHR, 1.12; 95% confidence interval, 0.73-1.72). Analyses by sex and age also revealed no statistically significant differences between the two drug classes.
During the Q&A session after the presentation, Sarah Berry, MD, MPH, an associate professor of medicine at Harvard Medical School and a clinical researcher at the Marcus Institute for Aging Research, both in Boston, noted the trend toward an increase in fracture risk in the first 90 days. “It looked like there was something going on in the first 90 days, and then after that the results were much closer to the null. I would put out maybe another potential mechanism whereby the SGLT2 inhibitors might cause fracture, and that’s falls. They cause polyuria, and any drug you give that causes women to rush to the bathroom may well cause fractures, particularly in the short term,” Dr. Berry said.
Ms. van Hulten agreed, and also brought up that the drugs can cause osmotic diuresis. That can lead to hypovolemia, the symptoms of which include weakness, fatigue, and dizziness. “And increased falls, of course, increases fracture risk. We do not expect anything to happen to bone metabolism in the first 90 days. I think we can agree that there would be more time needed to alter the bone enough to increase fracture risk, so we expect that this trend toward an increased risk might be attributable to that increased fall risk that might occur with SGLT2 inhibitor use,” she said.
It’s possible that such a mechanism explains increased fracture risk seen in some earlier short-term studies, she added.
Overall, Ms. van Hulten said that the results should provide some confidence in SGLT2 inhibitors, though more work needs to be done. “I think we provide reassurance that SGLT2 inhibitors are safe to use. However, we still only have a median follow-up of 1.6 years. It’s not as long as we maybe would like, but it’s the best we can do with the data available, since the SGLT2 inhibitors have only been used since 2013. So maybe it’s best to prescribe it and keep [fall risk] in mind and look into the effects later on again, but it seems to be safe to use.”
The study received funding from the Novo Nordisk Foundation. Ms. van Hulten and Dr. Berry reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
VANCOUVER – In patients with type 2 diabetes, sodium-glucose cotransporter 2 (SGLT2) inhibitors as an adjunct to metformin were not associated with an increase in fracture risk, according to a new real-world study.
There have been some reports of an increase in fracture risk associated with SGLT2 inhibitors, and it was observed in the phase 3 CANVAS trial of canagliflozin (Invokana), which led to a Food and Drug Administration warning of fracture risks associated with canagliflozin use. Some ensuing studies did not show an increased risk, but these studies were generally less than a year in duration and may have missed longer-term risk, according to Veerle van Hulten, MSc.
“Fracture risk is something that takes a long time to develop, so we wanted to have a longer follow-up. We looked into the CPRD [Clinical Practice Research Datalink], which is a beautiful database containing real-world data from primary care practices,” said Ms. van Hulten, a PhD student at Maastricht (the Netherlands) University, who presented the study at the annual meeting of the American Society for Bone and Mineral Research.
Ms. van Hulten and colleagues compared SGLT2 inhibitors with dipeptidyl peptidase–4 (DPP-4) inhibitors because the latter are used in similar populations and have been shown to have no effect on fracture risk.
“What we found is that SGLT2 inhibitors are not associated with an increased fracture risk. Even with a duration of use of over 811 days, we did not observe an increased hazard ratio for fractures when compared DPP-4 inhibitor users,” Ms. van Hulten said.
SGLT2 inhibitors reduce blood sugar by increasing elimination of sugar in the urine. They also increase phosphate, reduce calcium, and increase parathyroid hormone, which could in turn negatively affect bone turnover, according to Ms. van Hulten.
In the new study, conducted between January 2013 and June 2020, the researchers used propensity score matching to compare adult patients, including 13,807 who were prescribed SGLT2 inhibitors and 28,524 who were prescribed DPP-4 inhibitors for the first time. They matched patients based on demographics, comorbidities, comedication, and lifestyle factors.
There was no association between SGLT2 inhibitor use and overall fracture risk or major osteoporotic, hip, vertebral, humerus, radius, or ulna fractures. There was no difference in risk for any duration of use, even with the longest duration of use of 811 days (adjusted hazard ratio, 1.0). There were no differences among specific SGLT2 inhibitors, including canagliflozin (aHR, 1.12; 95% confidence interval, 0.73-1.72). Analyses by sex and age also revealed no statistically significant differences between the two drug classes.
During the Q&A session after the presentation, Sarah Berry, MD, MPH, an associate professor of medicine at Harvard Medical School and a clinical researcher at the Marcus Institute for Aging Research, both in Boston, noted the trend toward an increase in fracture risk in the first 90 days. “It looked like there was something going on in the first 90 days, and then after that the results were much closer to the null. I would put out maybe another potential mechanism whereby the SGLT2 inhibitors might cause fracture, and that’s falls. They cause polyuria, and any drug you give that causes women to rush to the bathroom may well cause fractures, particularly in the short term,” Dr. Berry said.
Ms. van Hulten agreed, and also brought up that the drugs can cause osmotic diuresis. That can lead to hypovolemia, the symptoms of which include weakness, fatigue, and dizziness. “And increased falls, of course, increases fracture risk. We do not expect anything to happen to bone metabolism in the first 90 days. I think we can agree that there would be more time needed to alter the bone enough to increase fracture risk, so we expect that this trend toward an increased risk might be attributable to that increased fall risk that might occur with SGLT2 inhibitor use,” she said.
It’s possible that such a mechanism explains increased fracture risk seen in some earlier short-term studies, she added.
Overall, Ms. van Hulten said that the results should provide some confidence in SGLT2 inhibitors, though more work needs to be done. “I think we provide reassurance that SGLT2 inhibitors are safe to use. However, we still only have a median follow-up of 1.6 years. It’s not as long as we maybe would like, but it’s the best we can do with the data available, since the SGLT2 inhibitors have only been used since 2013. So maybe it’s best to prescribe it and keep [fall risk] in mind and look into the effects later on again, but it seems to be safe to use.”
The study received funding from the Novo Nordisk Foundation. Ms. van Hulten and Dr. Berry reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT ASBMR 2023
A focus on women with diabetes and their offspring
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.

We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2). 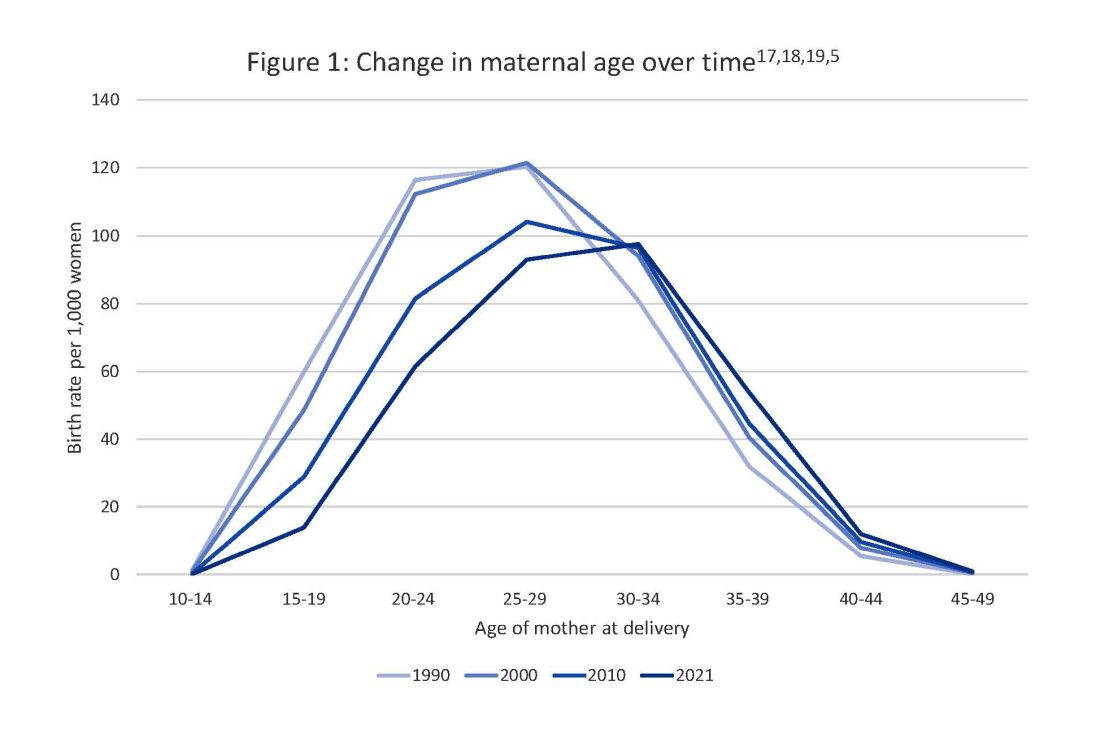
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy. 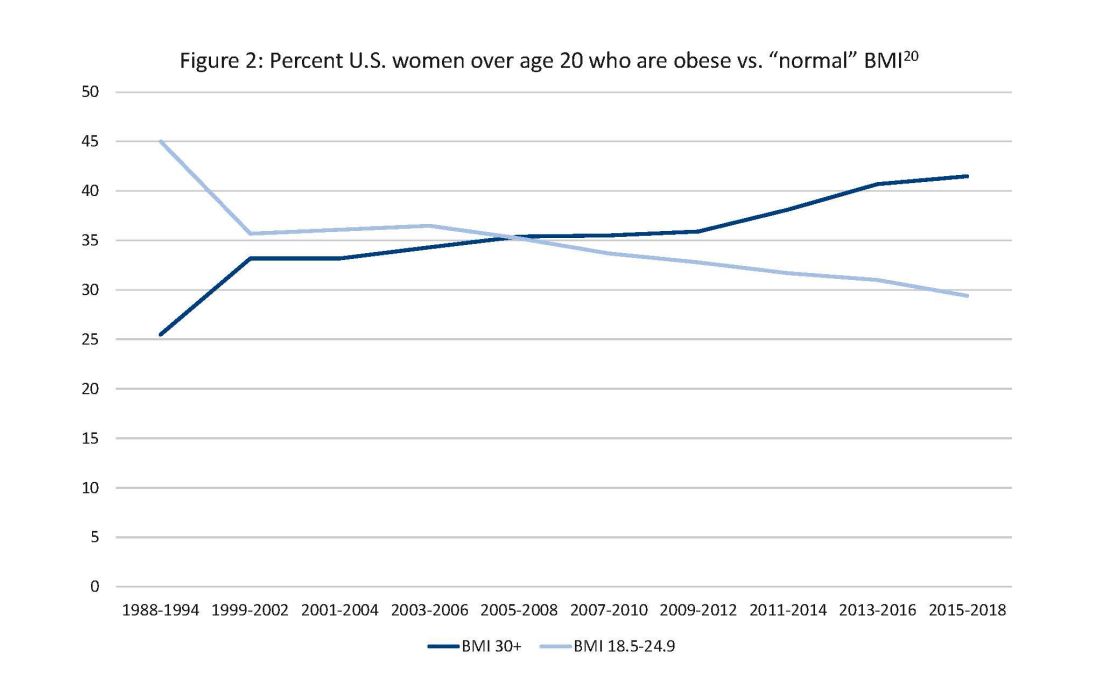
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.
In 2021, diabetes and related complications was the 8th leading cause of death in the United States.1 As of 2022, more than 11% of the U.S. population had diabetes and 38% of the adult U.S. population had prediabetes.2 Diabetes is the most expensive chronic condition in the United States, where $1 of every $4 in health care costs is spent on care.3
Where this is most concerning is diabetes in pregnancy. While childbirth rates in the United States have decreased since the 2007 high of 4.32 million births4 to 3.66 million in 2021,5 the incidence of diabetes in pregnancy – both pregestational and gestational – has increased. The rate of pregestational diabetes in 2021 was 10.9 per 1,000 births, a 27% increase from 2016 (8.6 per 1,000).6 The percentage of those giving birth who also were diagnosed with gestational diabetes mellitus (GDM) was 8.3% in 2021, up from 6.0% in 2016.7
Adverse outcomes for an infant born to a mother with diabetes include a higher risk of obesity and diabetes as adults, potentially leading to a forward-feeding cycle.
We and our colleagues established the Diabetes in Pregnancy Study Group of North America in 1997 because we had witnessed too frequently the devastating diabetes-induced pregnancy complications in our patients. The mission we set forth was to provide a forum for dialogue among maternal-fetal medicine subspecialists. The three main goals we set forth to support this mission were to provide a catalyst for research, contribute to the creation and refinement of medical policies, and influence professional practices in diabetes in pregnancy.8
In the last quarter century, DPSG-NA, through its annual and biennial meetings, has brought together several hundred practitioners that include physicians, nurses, statisticians, researchers, nutritionists, and allied health professionals, among others. As a group, it has improved the detection and management of diabetes in pregnant women and their offspring through knowledge sharing and influencing policies on GDM screening, diagnosis, management, and treatment. Our members have shown that preconceptional counseling for women with diabetes can significantly reduce congenital malformation and perinatal mortality compared with those women with pregestational diabetes who receive no counseling.9,10
We have addressed a wide variety of topics including the paucity of data in determining the timing of delivery for women with diabetes and the Institute of Medicine/National Academy of Medicine recommendations of gestational weight gain and risks of not adhering to them. We have learned about new scientific discoveries that reveal underlying mechanisms to diabetes-related birth defects and potential therapeutic targets; and we have discussed the health literacy requirements, ethics, and opportunities for lifestyle intervention.11-16
But we need to do more.
Two risk factors are at play: Women continue to choose to have babies at later ages and their pregnancies continue to be complicated by the rising incidence of obesity (see Figure 1 and Figure 2).
The global obesity epidemic has become a significant concern for all aspects of health and particularly for diabetes in pregnancy.
In 1990, 24.9% of women in the United States were obese; in 2010, 35.8%; and now more than 41%. Some experts project that by 2030 more than 80% of women in the United States will be overweight or obese.21
If we are to stop this cycle of diabetes begets more diabetes, now more than ever we need to come together and accelerate the research and education around the diabetes in pregnancy. Join us at this year’s DPSG-NA meeting Oct. 26-28 to take part in the knowledge sharing, discussions, and planning. More information can be found online at https://events.dpsg-na.com/home.
Dr. Miodovnik is adjunct professor of obstetrics, gynecology, and reproductive sciences at University of Maryland School of Medicine. Dr. Reece is professor of obstetrics, gynecology, and reproductive sciences and senior scientist at the Center for Birth Defects Research at University of Maryland School of Medicine.
References
1. Xu J et al. Mortality in the United States, 2021. NCHS Data Brief. 2022 Dec;(456):1-8. PMID: 36598387.
2. Centers for Disease Control and Prevention, diabetes data and statistics.
3. American Diabetes Association. The Cost of Diabetes.
4. Martin JA et al. Births: Final data for 2007. Natl Vital Stat Rep. 2010 Aug 9;58(24):1-85. PMID: 21254725.
5. Osterman MJK et al. Births: Final data for 2021. Natl Vital Stat Rep. 2023 Jan;72(1):1-53. PMID: 36723449.
6. Gregory ECW and Ely DM. Trends and characteristics in prepregnancy diabetes: United States, 2016-2021. Natl Vital Stat Rep. 2023 May;72(6):1-13. PMID: 37256333.
7. QuickStats: Percentage of mothers with gestational diabetes, by maternal age – National Vital Statistics System, United States, 2016 and 2021. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):16. doi: 10.15585/mmwr.mm7201a4.
8. Langer O et al. The Diabetes in Pregnancy Study Group of North America – Introduction and summary statement. Prenat Neonat Med. 1998;3(6):514-6.
9. Willhoite MB et al. The impact of preconception counseling on pregnancy outcomes. The experience of the Maine Diabetes in Pregnancy Program. Diabetes Care. 1993 Feb;16(2):450-5. doi: 10.2337/diacare.16.2.450.
10. McElvy SS et al. A focused preconceptional and early pregnancy program in women with type 1 diabetes reduces perinatal mortality and malformation rates to general population levels. J Matern Fetal Med. 2000 Jan-Feb;9(1):14-20. doi: 10.1002/(SICI)1520-6661(200001/02)9:1<14::AID-MFM5>3.0.CO;2-K.
11. Rosen JA et al. The history and contributions of the Diabetes in Pregnancy Study Group of North America (1997-2015). Am J Perinatol. 2016 Nov;33(13):1223-6. doi: 10.1055/s-0036-1585082.
12. Driggers RW and Baschat A. The 12th meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA): Introduction and overview. J Matern Fetal Neonatal Med. 2012 Jan;25(1):3-4. doi: 10.3109/14767058.2012.626917.
13. Langer O et al. The proceedings of the Diabetes in Pregnancy Study Group of North America 2009 conference. J Matern Fetal Neonatal Med. 2010 Mar;23(3):196-8. doi: 10.3109/14767050903550634.
14. Reece EA et al. A consensus report of the Diabetes in Pregnancy Study Group of North America Conference, Little Rock, Ark., May 2002. J Matern Fetal Neonatal Med. 2002 Dec;12(6):362-4. doi: 10.1080/jmf.12.6.362.364.
15. Reece EA and Maulik D. A consensus conference of the Diabetes in Pregnancy Study Group of North America. J Matern Fetal Neonatal Med. 2002 Dec;12(6):361. doi: 10.1080/jmf.12.6.361.361.
16. Gabbe SG. Summation of the second meeting of the Diabetes in Pregnancy Study Group of North America (DPSG-NA). J Matern Fetal Med. 2000 Jan-Feb;9(1):3-9.
17. Vital Statistics of the United States 1990: Volume I – Natality.
18. Martin JA et al. Births: final data for 2000. Natl Vital Stat Rep. 2002 Feb 12;50(5):1-101. PMID: 11876093.
19. Martin JA et al. Births: final data for 2010. Natl Vital Stat Rep. 2012 Aug 28;61(1):1-72. PMID: 24974589.
20. CDC Website. Normal weight, overweight, and obesity among adults aged 20 and over, by selected characteristics: United States.
21. Wang Y et al. Has the prevalence of overweight, obesity, and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int J Epidemiol. 2020 Jun 1;49(3):810-23. doi: 10.1093/ije/dyz273.