User login
Early treatment may delay atherosclerosis in familial hypercholesterolemia
Patients with familial hypercholesterolemia (FH) who start lipid-lowering treatment earlier in life may reduce their cardiovascular risk, compared with those who don’t begin treatment early, according to results of a recent meta-analysis.
They showed a difference in the carotid intima-media thickness (IMT) between patients with and without FH that increased with age, but there was also a difference in IMT seen among patients with FH who started treatment early, compared with untreated patients with FH, Kika van Bergen en Henegouwen, of the departments of pediatrics and epidemiology and data science at Amsterdam University Medical Center, and colleagues wrote in their report, published in the Journal of Clinical Lipidology.
“The fact that the difference in IMT increases with age between FH patients and unaffected controls, and is more pronounced in studies with untreated FH patients than in studies with treated patients, suggests that starting treatment already at a young age in patients with FH is preferred,” the researchers wrote. “However, despite treatment, IMT in treated FH patients is still thicker in comparison to subjects without FH.”
The researchers identified 42 studies with among patients with FH and healthy control groups across the MEDLINE, EMBASE and Trials.gov databases up to a cutoff date of April 2020, with 39 studies specifically examining carotid IMT, 2 studies evaluating carotid and femoral IMT, and 1 study evaluating femoral IMT alone. Overall, the researchers examined IMT measurements in 3,796 patients with FH and 2,363 control group participants.
Although data on age and gender for FH and control groups were not available in 6 studies, the mean age ranged from 9 to 57 years for patients with FH and from 8 to 61 years in the control group. Men comprised just under half of both the FH and control groups.
The mean between-group difference in carotid IMT in 34 studies was 0.11 mm (95% confidence interval, 0.06-0.15 mm; P < .001) for patients with FH, compared with the control group, while the mean difference in femoral IMT in three studies was 0.47 mm (95% CI, 0.19-0.74 mm; P < .001) between FH and control groups.
In 13 studies in which data on differences between partly treated and untreated FH were available, there was a significant between-group difference in carotid IMT with partly treated patients with FH, compared with the control group (0.05 mm; 95% CI, 0.03-0.08 mm; P < .001), but a larger mean between-group difference in carotid IMT among untreated patients with FH, compared with a control group (0.12 mm; 95% CI, 0.03-0.21 mm; P = .009).
The researchers also analyzed how age impacts carotid IMT, and they found patients with FH had a mean increase of 0.0018 mm (95% CI, –0.0007 to 0.0042 mm) over a control group in 34 studies. For patients with partly treated FH, compared with patients with untreated FH, the mean between-group increase per year was smaller (0.0023 mm; 95% CI, 0.0021-0.0025 mm), compared with the control group (0.0104 mm; 95% CI, 0.0100-0.0108 mm).
“This sign of residual risk might suggest that more robust cholesterol-lowering treatment and achieving treatment targets, or earlier treatment initiation, is needed to reduce IMT progression to non-FH conditions,” the researchers said. “Therefore, we must find and diagnose these patients, and treat them according to current guidelines.”
Limitations of the authors’ meta-analyses include heterogeneity among studies, differences in IMT measurement protocols, and inclusion of studies with an open-label design. Although randomized clinical trials would be preferable to compare treatment effect, “since statin therapy is indicated in FH patients to reduce [cardiovascular disease], it would be unethical to have a placebo group,” they said.
The authors reported no relevant financial disclosures.
Patients with familial hypercholesterolemia (FH) who start lipid-lowering treatment earlier in life may reduce their cardiovascular risk, compared with those who don’t begin treatment early, according to results of a recent meta-analysis.
They showed a difference in the carotid intima-media thickness (IMT) between patients with and without FH that increased with age, but there was also a difference in IMT seen among patients with FH who started treatment early, compared with untreated patients with FH, Kika van Bergen en Henegouwen, of the departments of pediatrics and epidemiology and data science at Amsterdam University Medical Center, and colleagues wrote in their report, published in the Journal of Clinical Lipidology.
“The fact that the difference in IMT increases with age between FH patients and unaffected controls, and is more pronounced in studies with untreated FH patients than in studies with treated patients, suggests that starting treatment already at a young age in patients with FH is preferred,” the researchers wrote. “However, despite treatment, IMT in treated FH patients is still thicker in comparison to subjects without FH.”
The researchers identified 42 studies with among patients with FH and healthy control groups across the MEDLINE, EMBASE and Trials.gov databases up to a cutoff date of April 2020, with 39 studies specifically examining carotid IMT, 2 studies evaluating carotid and femoral IMT, and 1 study evaluating femoral IMT alone. Overall, the researchers examined IMT measurements in 3,796 patients with FH and 2,363 control group participants.
Although data on age and gender for FH and control groups were not available in 6 studies, the mean age ranged from 9 to 57 years for patients with FH and from 8 to 61 years in the control group. Men comprised just under half of both the FH and control groups.
The mean between-group difference in carotid IMT in 34 studies was 0.11 mm (95% confidence interval, 0.06-0.15 mm; P < .001) for patients with FH, compared with the control group, while the mean difference in femoral IMT in three studies was 0.47 mm (95% CI, 0.19-0.74 mm; P < .001) between FH and control groups.
In 13 studies in which data on differences between partly treated and untreated FH were available, there was a significant between-group difference in carotid IMT with partly treated patients with FH, compared with the control group (0.05 mm; 95% CI, 0.03-0.08 mm; P < .001), but a larger mean between-group difference in carotid IMT among untreated patients with FH, compared with a control group (0.12 mm; 95% CI, 0.03-0.21 mm; P = .009).
The researchers also analyzed how age impacts carotid IMT, and they found patients with FH had a mean increase of 0.0018 mm (95% CI, –0.0007 to 0.0042 mm) over a control group in 34 studies. For patients with partly treated FH, compared with patients with untreated FH, the mean between-group increase per year was smaller (0.0023 mm; 95% CI, 0.0021-0.0025 mm), compared with the control group (0.0104 mm; 95% CI, 0.0100-0.0108 mm).
“This sign of residual risk might suggest that more robust cholesterol-lowering treatment and achieving treatment targets, or earlier treatment initiation, is needed to reduce IMT progression to non-FH conditions,” the researchers said. “Therefore, we must find and diagnose these patients, and treat them according to current guidelines.”
Limitations of the authors’ meta-analyses include heterogeneity among studies, differences in IMT measurement protocols, and inclusion of studies with an open-label design. Although randomized clinical trials would be preferable to compare treatment effect, “since statin therapy is indicated in FH patients to reduce [cardiovascular disease], it would be unethical to have a placebo group,” they said.
The authors reported no relevant financial disclosures.
Patients with familial hypercholesterolemia (FH) who start lipid-lowering treatment earlier in life may reduce their cardiovascular risk, compared with those who don’t begin treatment early, according to results of a recent meta-analysis.
They showed a difference in the carotid intima-media thickness (IMT) between patients with and without FH that increased with age, but there was also a difference in IMT seen among patients with FH who started treatment early, compared with untreated patients with FH, Kika van Bergen en Henegouwen, of the departments of pediatrics and epidemiology and data science at Amsterdam University Medical Center, and colleagues wrote in their report, published in the Journal of Clinical Lipidology.
“The fact that the difference in IMT increases with age between FH patients and unaffected controls, and is more pronounced in studies with untreated FH patients than in studies with treated patients, suggests that starting treatment already at a young age in patients with FH is preferred,” the researchers wrote. “However, despite treatment, IMT in treated FH patients is still thicker in comparison to subjects without FH.”
The researchers identified 42 studies with among patients with FH and healthy control groups across the MEDLINE, EMBASE and Trials.gov databases up to a cutoff date of April 2020, with 39 studies specifically examining carotid IMT, 2 studies evaluating carotid and femoral IMT, and 1 study evaluating femoral IMT alone. Overall, the researchers examined IMT measurements in 3,796 patients with FH and 2,363 control group participants.
Although data on age and gender for FH and control groups were not available in 6 studies, the mean age ranged from 9 to 57 years for patients with FH and from 8 to 61 years in the control group. Men comprised just under half of both the FH and control groups.
The mean between-group difference in carotid IMT in 34 studies was 0.11 mm (95% confidence interval, 0.06-0.15 mm; P < .001) for patients with FH, compared with the control group, while the mean difference in femoral IMT in three studies was 0.47 mm (95% CI, 0.19-0.74 mm; P < .001) between FH and control groups.
In 13 studies in which data on differences between partly treated and untreated FH were available, there was a significant between-group difference in carotid IMT with partly treated patients with FH, compared with the control group (0.05 mm; 95% CI, 0.03-0.08 mm; P < .001), but a larger mean between-group difference in carotid IMT among untreated patients with FH, compared with a control group (0.12 mm; 95% CI, 0.03-0.21 mm; P = .009).
The researchers also analyzed how age impacts carotid IMT, and they found patients with FH had a mean increase of 0.0018 mm (95% CI, –0.0007 to 0.0042 mm) over a control group in 34 studies. For patients with partly treated FH, compared with patients with untreated FH, the mean between-group increase per year was smaller (0.0023 mm; 95% CI, 0.0021-0.0025 mm), compared with the control group (0.0104 mm; 95% CI, 0.0100-0.0108 mm).
“This sign of residual risk might suggest that more robust cholesterol-lowering treatment and achieving treatment targets, or earlier treatment initiation, is needed to reduce IMT progression to non-FH conditions,” the researchers said. “Therefore, we must find and diagnose these patients, and treat them according to current guidelines.”
Limitations of the authors’ meta-analyses include heterogeneity among studies, differences in IMT measurement protocols, and inclusion of studies with an open-label design. Although randomized clinical trials would be preferable to compare treatment effect, “since statin therapy is indicated in FH patients to reduce [cardiovascular disease], it would be unethical to have a placebo group,” they said.
The authors reported no relevant financial disclosures.
FROM THE JOURNAL OF CLINICAL LIPIDOLOGY
How Lp(a) can help improve ASCVD risk assessment
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).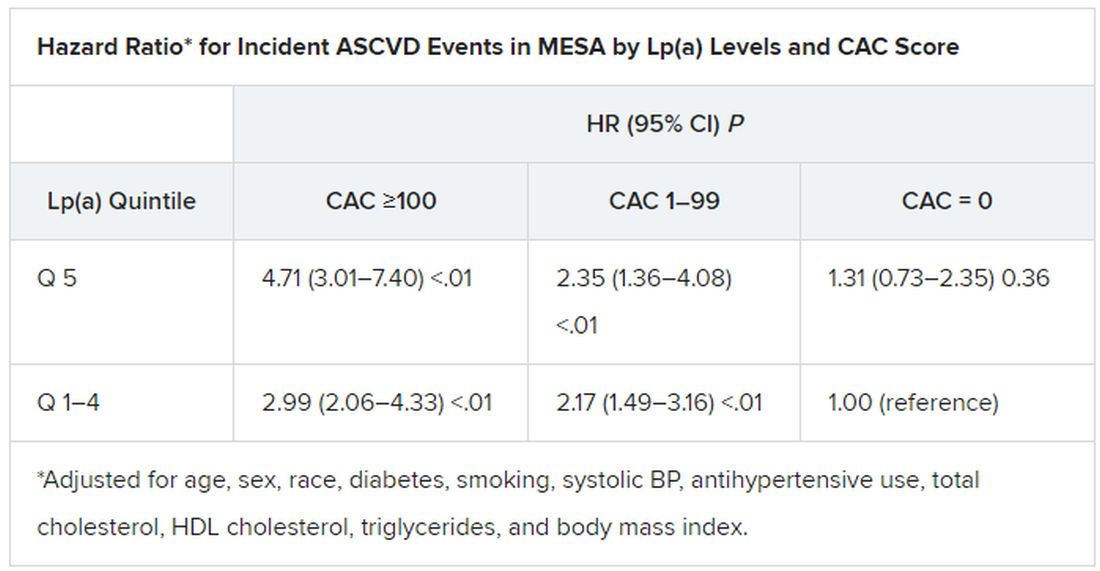
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).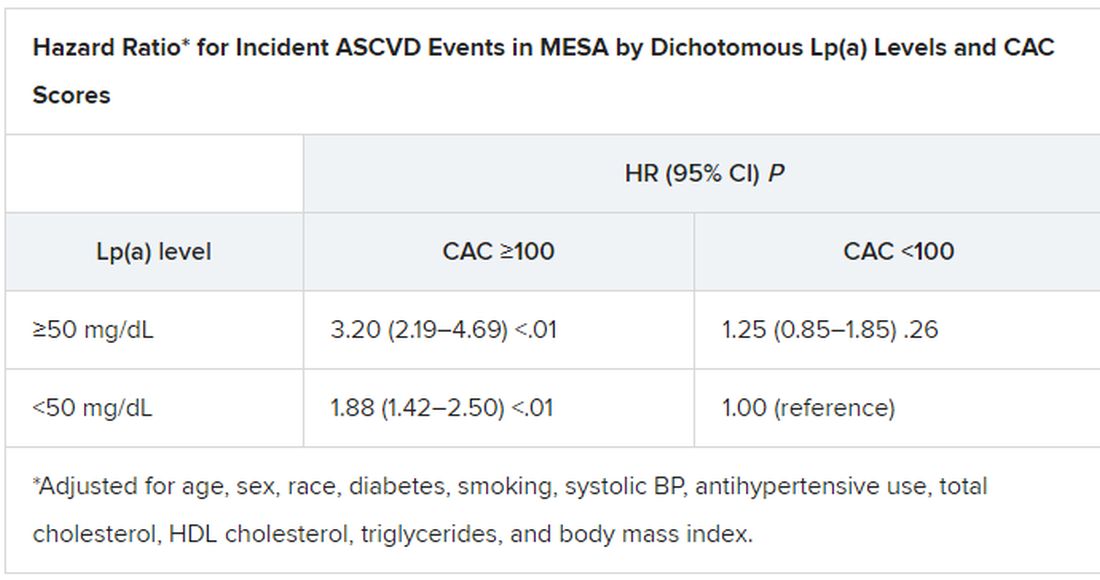
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
A look back at a pair of large cohort studies suggests a telling relation between two distinct predictors of atherosclerotic cardiovascular disease (ASCVD) risk and may offer guidance on how to interpret them together.
Elevated levels of lipoprotein(a), or Lp(a), and high coronary artery calcium (CAC) scores were both predictive of ASCVD risk over 10 years, but independent of each other and a host of more traditional cardiovascular risk factors, for example, in the analysis of data from the MESA (Multi-Ethnic Study of Atherosclerosis) and DHS (Dallas Heart Study) longitudinal cohorts.
Notably, the risk when both Lp(a) and CAC scores were high far exceeded that associated with either marker alone. But when CAC scores were less than 100 Agatston units, predicted ASCVD risk wasn’t influenced by levels of Lp(a). Indeed, a CAC score of 0 predicted the lowest levels of ASCVD risk, even with elevated Lp(a).
That is, the findings suggest, the addition of Lp(a) makes a difference to the risk assessment only when CAC scores are high, at least 100 units, and elevated Lp(a) doesn’t mean increased ASCVD risk in the absence of coronary calcium.
“Our novel findings indicate that elevated Lp(a) drives ASCVD risk independent of the subclinical coronary atherosclerosis burden captured by CAC score,” concluded a report on the analysis, published in the Journal of the American College of Cardiology, with lead author Anurag Mehta, MD, Emory University, Atlanta.
There are no formal recommendations on how to interpret Lp(a) and CAC scores together, but the current findings “provide impetus for measuring Lp(a) in more individuals as part of the shared decision-making process,” the authors contended.
“Really, the calcium score carries the majority of the information in terms of risk, except in the highest CAC score group. That is, if you have a high Lp(a) and a high burden of calcium, your risk is significantly higher than if you just have the high calcium score and the normal Lp(a),” senior author Parag H. Joshi, MD, MHS, said in an interview.
“We thought we would see that the group with higher Lp(a) would have more events over 10 years, even among those who didn’t have coronary calcium,” said Dr. Joshi, of the University of Texas Southwestern Medical Center, Dallas. “But we really don’t see that, at least in a statistically significant way.”
A CAC score of 0 would at least support a more conservative approach in a patient with elevated Lp(a) “who is hesitant to be on a statin or to be more aggressive managing their risk,” Dr. Joshi said.
“This study should be very reassuring for a patient like that,” Ron Blankstein, MD, director of cardiac computed tomography at Brigham and Women’s Hospital, Boston, said in an interview.
“If you have a high Lp(a) and you’re concerned, I think this study really supports the role of calcium scoring for further risk assessment,” said Dr. Blankstein, who is not associated with the new report. “We often check Lp(a) in individuals who perhaps have a family history or who come to see us in a preventive cardiology clinic. If it is high and there is concern, a calcium score can be very helpful. If it’s zero, that really means a very low risk of events. And if it’s elevated, I think we’re going to be more concerned about that patient.”
The current analysis suggests “that, when a patient without clinical cardiovascular disease is identified with either CAC ≥100 or Lp(a) >50 mg/dL, the next step in the risk evaluation should be to measure either Lp(a) or CAC, respectively – if not already performed – to identify the patients at highest risk,” Sotirios Tsimikas, MD, director of vascular medicine at University of California, San Diego, wrote in an accompanying editorial.
“Both Lp(a) and CAC should be more broadly applied in clinical care settings in patients without prior ASCVD to identify those that most likely will benefit from more aggressive therapy and, in the future, from Lp(a)-lowering therapies,” he wrote.
The analyses were conducted separately on data from 4,512 initially asymptomatic patients in MESA and 2,078 from the DHS cohort, who were followed for ASCVD events an average of 13 years and 11 years, respectively. Such events included coronary heart disease–related death, nonfatal MI, and fatal or nonfatal stroke.
In the MESA cohort – 52% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese – elevated Lp(a) (quintile 5 vs. quintiles 1-4) and CAC scores of 1-99 and above 100 (both compared with 0) were each independently associated with increased risk for ASCVD events. The hazard ratio was 1.29 (P = .02) for elevated Lp(a), 1.68 (P < .01) for a CAC score of 1-99, and 2.66 (P < .01) for a CAC score of at least 100.
The corresponding HRs in the DHS cohort were 1.54 (P = .07) for Lp(a), 3.32 (P < .01) for a CAC score of 1-99, and 5.21 (P < .01) for a CAC score of at least 100.
Of note, the authors wrote, ASCVD risk among MESA participants with a CAC score of 0 was not significantly different in those with normal and elevated Lp(a).
The findings were similar in the corresponding DHS analysis, the authors noted.
When both Lp(a) and CAC scores are considered as dichotomous variables, the highest 10-year ASCVD incidence in MESA was in participants with both elevated Lp(a) (≥50 mg/dL) and a high CAC score (≥100). The lowest risk was seen when Lp(a) was normal (<50 mg/dL) and the CAC score was no more than moderately high (<100).
The results in the corresponding DHS analysis, according to the report, again mirrored those from MESA.
“This study has important implications for our patients and also potentially for future clinical trial design,” Dr. Blankstein noted. “A big part of developing a trial in this space is identifying the patients who are at higher risk,” and the current analysis supports CAC scores for identifying the highest-risk patient among those with elevated Lp(a).
Current wisdom is that, for the most part, Lp(a) levels are genetically mediated and are mostly unaffected by interventions such as diet management or exercise. It’s unknown whether reducing elevated Lp(a) levels pharmacologically will cut ASCVD risk, but there are a number of clinical trial programs currently aimed at learning just that. They include the Novartis-sponsored phase 3 HORIZON trial of the antisense agent pelacarsen (TQJ230), with an estimated enrollment of almost 7,700; a randomized, controlled dose-finding study of the small interfering RNA agent olpasiran (AMG890), with 290 patients and funded by Amgen; and an 88-patient phase 1 study of another siRNA agent, SLN360, supported by Silence Therapeutics.
Dr. Mehta reported no relevant relationships. Dr. Joshi has received grant support from Novo Nordisk and consulting income from Bayer and Regeneron; holds equity in G3 Therapeutics; and has served as site investigator for GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. Dr. Blankstein reported serving as a consultant to Amgen, Novartis, and Silence Therapeutics.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
New data explore risk of magnetic interference with implantable devices
Building on several previous reports that the newest models of mobile telephones and other electronics that use magnets pose a threat to the function of defibrillators and other implantable cardiovascular devices, a new study implicates any device that emits a 10-gauss (G) magnetic field more than a couple of inches.
“Beside the devices described in our manuscript, this can be any portable consumer product [with magnets] like electric cigarettes or smart watches,” explained study author Sven Knecht, DSc, a research electrophysiologist associated with the department of cardiology, University Hospital Basel (Switzerland).

In the newly published article, the investigators evaluated earphones, earphone charging cases, and two electronic pens used to draw on electronic tablets. These particular devices are of interest because, like mobile phones, they are of a size and shape to fit in a breast pocket adjacent to where many cardiovascular devices are implanted.
The study joins several previous studies that have shown the same risk, but this study used three-dimensional (3D) mapping of the magnetic field rather than a one-axis sensor, which is a standard adopted by the U.S. Food and Drug Administration, according to the investigators.
3D mapping assessment used
Because of the 3D nature of magnetic fields, 3D mapping serves as a better tool to assess the risk of the magnetic force as the intensity gradient diminishes with distance from the source, the authors contended. The 3D maps used in this study have a resolution to 2 mm.
The ex vivo measurements of the magnetic field, which could be displayed in a configurable 3D volume in relation to the electronic products were performed on five different explanted cardioverter defibrillators from two manufacturers.
In the ex vivo setting, the ability of the earphones, earphone charging cases, and electronic pens to interfere with defibrillator function was compared to that of the Apple iPhone 12 Max, which was the subject of a small in vivo study published in 2021. When the iPhone 12 Max was placed on the skin over a cardiac implantable device in that study, clinically identifiable interference could be detected in all 3 patients evaluated.
Based on previous work, the International Organization for Standardization has established that a minimal field strength of 10 G is needed to interfere with an implantable device, but the actual risk from any specific device is determined by the distance at which this strength of magnetic field is projected.
In the 3D analysis, the 10-G intensity was found to project 20 mm from the surface of the ear phones, ear phone charging case, and one of the electronic pens and to project 29 mm from the other electronic pen. When tested against the five defibrillators, magnetic reversion mode was triggered by the portable electronics at distances ranging from 8 to 18 mm.
In an interview, Dr. Knecht explained that this study adds more devices to the list of those associated with potential for interfering with implantable cardiovascular devices, but added that the more important point is that any device that contains magnets emitting a force of 10 G or greater for more than a few inches can be expected to be associated with clinically meaningful interference. The devices tested in this study were produced by Apple and Microsoft, but a focus on specific devices obscures the main message.
“All portable electronics with an embedded permanent magnet creating a 10-G magnetic field have a theoretical capability of triggering implantable devices,” he said.
For pacemakers, the interference is likely to trigger constant pacing, which would not be expected to pose a significant health threat if detected with a reasonable period, according to Dr. Knecht. Interference is potentially more serious for defibrillators, which might fail during magnetic interference to provide the shock needed to terminate a serious arrhythmia.
The combination of events – interference at the time of an arrhythmia – make this risk “very low,” but Dr. Knecht said it is sufficient to mean that patients receiving an implantable cardiovascular device should be made aware of the risk and the need to avoid placing portable electronic products near the implanted device.
When in vivo evidence of a disturbance with the iPhone 12 was reported in 2021, it amplified existing concern. The American Heart Association maintains a list of electronic products with the potential to interfere with implantable devices on its website. But, again, understanding the potential for risk and the need to keep electronic products with magnets at a safe distance from cardiovascular implantable devices is more important than trying to memorize the ever-growing list of devices with this capability.
“Prudent education of patients receiving an implantable device is important,” said N.A. Mark Estes III, MD, professor of medicine in the division of cardiology at the University of Pittsburgh. However, in an interview, he warned that the growing list of implicated devices makes a complete survey impractical, and, even if achievable, likely to leave patients “feeling overwhelmed.”
In Dr. Estes’s practice, he does provide printed information about the risks of electronics to interfere with implantable devices as well as a list of dos and don’ts. He agreed that the absolute risk of interference from a device causing significant clinical complications is low, but the goal is to “bring it as close to zero as possible.”
“No clinical case of a meaningful interaction of an electronic product and dysfunction of an implantable device has ever been documented,” he said. Given the widespread use of the new generation of cellphones that contain magnets powerful enough to induce dysfunction in an implantable device, “this speaks to the fact that the risk continues to be very low.”
Dr. Knecht and coinvestigators, along with Dr. Estes, reported no potential conflicts of interest.
Building on several previous reports that the newest models of mobile telephones and other electronics that use magnets pose a threat to the function of defibrillators and other implantable cardiovascular devices, a new study implicates any device that emits a 10-gauss (G) magnetic field more than a couple of inches.
“Beside the devices described in our manuscript, this can be any portable consumer product [with magnets] like electric cigarettes or smart watches,” explained study author Sven Knecht, DSc, a research electrophysiologist associated with the department of cardiology, University Hospital Basel (Switzerland).
In the newly published article, the investigators evaluated earphones, earphone charging cases, and two electronic pens used to draw on electronic tablets. These particular devices are of interest because, like mobile phones, they are of a size and shape to fit in a breast pocket adjacent to where many cardiovascular devices are implanted.
The study joins several previous studies that have shown the same risk, but this study used three-dimensional (3D) mapping of the magnetic field rather than a one-axis sensor, which is a standard adopted by the U.S. Food and Drug Administration, according to the investigators.
3D mapping assessment used
Because of the 3D nature of magnetic fields, 3D mapping serves as a better tool to assess the risk of the magnetic force as the intensity gradient diminishes with distance from the source, the authors contended. The 3D maps used in this study have a resolution to 2 mm.
The ex vivo measurements of the magnetic field, which could be displayed in a configurable 3D volume in relation to the electronic products were performed on five different explanted cardioverter defibrillators from two manufacturers.
In the ex vivo setting, the ability of the earphones, earphone charging cases, and electronic pens to interfere with defibrillator function was compared to that of the Apple iPhone 12 Max, which was the subject of a small in vivo study published in 2021. When the iPhone 12 Max was placed on the skin over a cardiac implantable device in that study, clinically identifiable interference could be detected in all 3 patients evaluated.
Based on previous work, the International Organization for Standardization has established that a minimal field strength of 10 G is needed to interfere with an implantable device, but the actual risk from any specific device is determined by the distance at which this strength of magnetic field is projected.
In the 3D analysis, the 10-G intensity was found to project 20 mm from the surface of the ear phones, ear phone charging case, and one of the electronic pens and to project 29 mm from the other electronic pen. When tested against the five defibrillators, magnetic reversion mode was triggered by the portable electronics at distances ranging from 8 to 18 mm.
In an interview, Dr. Knecht explained that this study adds more devices to the list of those associated with potential for interfering with implantable cardiovascular devices, but added that the more important point is that any device that contains magnets emitting a force of 10 G or greater for more than a few inches can be expected to be associated with clinically meaningful interference. The devices tested in this study were produced by Apple and Microsoft, but a focus on specific devices obscures the main message.
“All portable electronics with an embedded permanent magnet creating a 10-G magnetic field have a theoretical capability of triggering implantable devices,” he said.
For pacemakers, the interference is likely to trigger constant pacing, which would not be expected to pose a significant health threat if detected with a reasonable period, according to Dr. Knecht. Interference is potentially more serious for defibrillators, which might fail during magnetic interference to provide the shock needed to terminate a serious arrhythmia.
The combination of events – interference at the time of an arrhythmia – make this risk “very low,” but Dr. Knecht said it is sufficient to mean that patients receiving an implantable cardiovascular device should be made aware of the risk and the need to avoid placing portable electronic products near the implanted device.
When in vivo evidence of a disturbance with the iPhone 12 was reported in 2021, it amplified existing concern. The American Heart Association maintains a list of electronic products with the potential to interfere with implantable devices on its website. But, again, understanding the potential for risk and the need to keep electronic products with magnets at a safe distance from cardiovascular implantable devices is more important than trying to memorize the ever-growing list of devices with this capability.
“Prudent education of patients receiving an implantable device is important,” said N.A. Mark Estes III, MD, professor of medicine in the division of cardiology at the University of Pittsburgh. However, in an interview, he warned that the growing list of implicated devices makes a complete survey impractical, and, even if achievable, likely to leave patients “feeling overwhelmed.”
In Dr. Estes’s practice, he does provide printed information about the risks of electronics to interfere with implantable devices as well as a list of dos and don’ts. He agreed that the absolute risk of interference from a device causing significant clinical complications is low, but the goal is to “bring it as close to zero as possible.”
“No clinical case of a meaningful interaction of an electronic product and dysfunction of an implantable device has ever been documented,” he said. Given the widespread use of the new generation of cellphones that contain magnets powerful enough to induce dysfunction in an implantable device, “this speaks to the fact that the risk continues to be very low.”
Dr. Knecht and coinvestigators, along with Dr. Estes, reported no potential conflicts of interest.
Building on several previous reports that the newest models of mobile telephones and other electronics that use magnets pose a threat to the function of defibrillators and other implantable cardiovascular devices, a new study implicates any device that emits a 10-gauss (G) magnetic field more than a couple of inches.
“Beside the devices described in our manuscript, this can be any portable consumer product [with magnets] like electric cigarettes or smart watches,” explained study author Sven Knecht, DSc, a research electrophysiologist associated with the department of cardiology, University Hospital Basel (Switzerland).
In the newly published article, the investigators evaluated earphones, earphone charging cases, and two electronic pens used to draw on electronic tablets. These particular devices are of interest because, like mobile phones, they are of a size and shape to fit in a breast pocket adjacent to where many cardiovascular devices are implanted.
The study joins several previous studies that have shown the same risk, but this study used three-dimensional (3D) mapping of the magnetic field rather than a one-axis sensor, which is a standard adopted by the U.S. Food and Drug Administration, according to the investigators.
3D mapping assessment used
Because of the 3D nature of magnetic fields, 3D mapping serves as a better tool to assess the risk of the magnetic force as the intensity gradient diminishes with distance from the source, the authors contended. The 3D maps used in this study have a resolution to 2 mm.
The ex vivo measurements of the magnetic field, which could be displayed in a configurable 3D volume in relation to the electronic products were performed on five different explanted cardioverter defibrillators from two manufacturers.
In the ex vivo setting, the ability of the earphones, earphone charging cases, and electronic pens to interfere with defibrillator function was compared to that of the Apple iPhone 12 Max, which was the subject of a small in vivo study published in 2021. When the iPhone 12 Max was placed on the skin over a cardiac implantable device in that study, clinically identifiable interference could be detected in all 3 patients evaluated.
Based on previous work, the International Organization for Standardization has established that a minimal field strength of 10 G is needed to interfere with an implantable device, but the actual risk from any specific device is determined by the distance at which this strength of magnetic field is projected.
In the 3D analysis, the 10-G intensity was found to project 20 mm from the surface of the ear phones, ear phone charging case, and one of the electronic pens and to project 29 mm from the other electronic pen. When tested against the five defibrillators, magnetic reversion mode was triggered by the portable electronics at distances ranging from 8 to 18 mm.
In an interview, Dr. Knecht explained that this study adds more devices to the list of those associated with potential for interfering with implantable cardiovascular devices, but added that the more important point is that any device that contains magnets emitting a force of 10 G or greater for more than a few inches can be expected to be associated with clinically meaningful interference. The devices tested in this study were produced by Apple and Microsoft, but a focus on specific devices obscures the main message.
“All portable electronics with an embedded permanent magnet creating a 10-G magnetic field have a theoretical capability of triggering implantable devices,” he said.
For pacemakers, the interference is likely to trigger constant pacing, which would not be expected to pose a significant health threat if detected with a reasonable period, according to Dr. Knecht. Interference is potentially more serious for defibrillators, which might fail during magnetic interference to provide the shock needed to terminate a serious arrhythmia.
The combination of events – interference at the time of an arrhythmia – make this risk “very low,” but Dr. Knecht said it is sufficient to mean that patients receiving an implantable cardiovascular device should be made aware of the risk and the need to avoid placing portable electronic products near the implanted device.
When in vivo evidence of a disturbance with the iPhone 12 was reported in 2021, it amplified existing concern. The American Heart Association maintains a list of electronic products with the potential to interfere with implantable devices on its website. But, again, understanding the potential for risk and the need to keep electronic products with magnets at a safe distance from cardiovascular implantable devices is more important than trying to memorize the ever-growing list of devices with this capability.
“Prudent education of patients receiving an implantable device is important,” said N.A. Mark Estes III, MD, professor of medicine in the division of cardiology at the University of Pittsburgh. However, in an interview, he warned that the growing list of implicated devices makes a complete survey impractical, and, even if achievable, likely to leave patients “feeling overwhelmed.”
In Dr. Estes’s practice, he does provide printed information about the risks of electronics to interfere with implantable devices as well as a list of dos and don’ts. He agreed that the absolute risk of interference from a device causing significant clinical complications is low, but the goal is to “bring it as close to zero as possible.”
“No clinical case of a meaningful interaction of an electronic product and dysfunction of an implantable device has ever been documented,” he said. Given the widespread use of the new generation of cellphones that contain magnets powerful enough to induce dysfunction in an implantable device, “this speaks to the fact that the risk continues to be very low.”
Dr. Knecht and coinvestigators, along with Dr. Estes, reported no potential conflicts of interest.
FROM CIRCULATION: ARRHYTHMIAS & ELECTROPHYSIOLOGY
More than half of U.S. women enter pregnancy at higher CVD risk
Less than half of women in the United States enter pregnancy in favorable cardiovascular health, new research suggests.
In 2019, among women aged 20 to 44 years with live births in the United States, only 40.2% were in favorable cardiovascular health prior to pregnancy, defined as normal weight, no diabetes, and no hypertension.
Although all regions and states showed a decline in prepregnancy favorable cardiometabolic health, there were significant differences among geographic regions in the country, the authors report. “These data reveal critical deficiencies and geographic disparities in prepregnancy cardiometabolic health,” they conclude.
“One of the things that we know in the U.S. is that the maternal mortality rate has been increasing, and there are significant differences at the state level in both adverse maternal outcomes, such as maternal mortality, as well as adverse pregnancy outcomes,” corresponding author Sadiya S. Khan, MD, MS, FACC, Northwestern University Feinberg School of Medicine, Chicago, told this news organization.
“These outcomes are often related to health factors that predate pregnancy,” Dr. Khan explained, “and the processes that begin at the very, very beginning of conception are informed by health factors prior to pregnancy, in particular cardiometabolic factors like body mass index or obesity, high blood pressure, and diabetes.”
The results were published online on Feb. 14 in a special “Go Red for Women” spotlight issue of Circulation.
Cardiometabolic health factors
Using maternal birth records from live births in the Centers for Disease Control and Prevention Natality Database between 2016 and 2019, the authors analyzed data on 14,174,625 women with live births aged 20 to 44 years. The majority (81.4%) were 20 to 34 years of age, 22.7% were Hispanic or Latina, and 52.7% were non-Hispanic White.
Favorable cardiometabolic health was defined as a BMI of 18 to 24.9 kg/m2, absence of diabetes, and absence of hypertension.
Although all regions and states experienced a decline in favorable cardiometabolic health during the study period of 2016 to 2019, with a drop overall of 3.2% – from 43.5 to 40.2 per 100 live births – it was especially true of the South and Midwest regions.
In 2019, favorable prepregnancy cardiometabolic health was lowest in the South (38.1%) and Midwest (38.8%) and highest in the West (42.2%) and Northeast (43.6%).
State by state, the lowest prevalence of favorable cardiometabolic health was found in Mississippi, at 31.2%, and highest in Utah, at 47.2%.
They also found a correlation between favorable cardiometabolic health and state-level percentages of high-school education or less and enrollment in Medicaid in 2019.
Similar to what has been seen with cardiovascular disease, “we observe that the states with the lowest prevalence of favorable cardiometabolic health were in the Southeast United States,” said Dr. Khan, “and similar geographic variation was observed with some more patterns in education and Medicaid coverage for birth, and these were used as proxies for socioeconomic status in those areas.”
Although Dr. Khan notes that the relationships cannot be determined to be causal from this analysis, she said that “it does suggest that upstream social determinants of health are important determinants of cardiometabolic health.”
Socioeconomic intervention
Dr. Khan noted that policies at the federal and state level can identify ways to “ensure that individuals who are thinking about pregnancy have access to health care and have access to resources, too, from a broad range of health determinants, including housing stability, food security, as well as access to health care be optimized prior to pregnancy.”
The authors note that this analysis may actually overestimate the prevalence of favorable cardiometabolic health, and data on cholesterol, diet, a distinction between type 1 and type 2 diabetes, and physical activity were not available.
Only individuals with live births were included, which could result in the elimination of a potentially high-risk group; however, late pregnancy losses represent less than 0.3% of all pregnancies, they say.
The authors conclude that “future research is needed to equitably improve health prior to pregnancy and quantify the potential benefits in cardiovascular disease outcomes for birthing individuals and their offspring.”
This work was supported by grants from the National Heart, Lung, and Blood Institute and American Heart Association Transformational Project Award awarded to Sadiya S. Khan.
A version of this article first appeared on Medscape.com.
Less than half of women in the United States enter pregnancy in favorable cardiovascular health, new research suggests.
In 2019, among women aged 20 to 44 years with live births in the United States, only 40.2% were in favorable cardiovascular health prior to pregnancy, defined as normal weight, no diabetes, and no hypertension.
Although all regions and states showed a decline in prepregnancy favorable cardiometabolic health, there were significant differences among geographic regions in the country, the authors report. “These data reveal critical deficiencies and geographic disparities in prepregnancy cardiometabolic health,” they conclude.
“One of the things that we know in the U.S. is that the maternal mortality rate has been increasing, and there are significant differences at the state level in both adverse maternal outcomes, such as maternal mortality, as well as adverse pregnancy outcomes,” corresponding author Sadiya S. Khan, MD, MS, FACC, Northwestern University Feinberg School of Medicine, Chicago, told this news organization.
“These outcomes are often related to health factors that predate pregnancy,” Dr. Khan explained, “and the processes that begin at the very, very beginning of conception are informed by health factors prior to pregnancy, in particular cardiometabolic factors like body mass index or obesity, high blood pressure, and diabetes.”
The results were published online on Feb. 14 in a special “Go Red for Women” spotlight issue of Circulation.
Cardiometabolic health factors
Using maternal birth records from live births in the Centers for Disease Control and Prevention Natality Database between 2016 and 2019, the authors analyzed data on 14,174,625 women with live births aged 20 to 44 years. The majority (81.4%) were 20 to 34 years of age, 22.7% were Hispanic or Latina, and 52.7% were non-Hispanic White.
Favorable cardiometabolic health was defined as a BMI of 18 to 24.9 kg/m2, absence of diabetes, and absence of hypertension.
Although all regions and states experienced a decline in favorable cardiometabolic health during the study period of 2016 to 2019, with a drop overall of 3.2% – from 43.5 to 40.2 per 100 live births – it was especially true of the South and Midwest regions.
In 2019, favorable prepregnancy cardiometabolic health was lowest in the South (38.1%) and Midwest (38.8%) and highest in the West (42.2%) and Northeast (43.6%).
State by state, the lowest prevalence of favorable cardiometabolic health was found in Mississippi, at 31.2%, and highest in Utah, at 47.2%.
They also found a correlation between favorable cardiometabolic health and state-level percentages of high-school education or less and enrollment in Medicaid in 2019.
Similar to what has been seen with cardiovascular disease, “we observe that the states with the lowest prevalence of favorable cardiometabolic health were in the Southeast United States,” said Dr. Khan, “and similar geographic variation was observed with some more patterns in education and Medicaid coverage for birth, and these were used as proxies for socioeconomic status in those areas.”
Although Dr. Khan notes that the relationships cannot be determined to be causal from this analysis, she said that “it does suggest that upstream social determinants of health are important determinants of cardiometabolic health.”
Socioeconomic intervention
Dr. Khan noted that policies at the federal and state level can identify ways to “ensure that individuals who are thinking about pregnancy have access to health care and have access to resources, too, from a broad range of health determinants, including housing stability, food security, as well as access to health care be optimized prior to pregnancy.”
The authors note that this analysis may actually overestimate the prevalence of favorable cardiometabolic health, and data on cholesterol, diet, a distinction between type 1 and type 2 diabetes, and physical activity were not available.
Only individuals with live births were included, which could result in the elimination of a potentially high-risk group; however, late pregnancy losses represent less than 0.3% of all pregnancies, they say.
The authors conclude that “future research is needed to equitably improve health prior to pregnancy and quantify the potential benefits in cardiovascular disease outcomes for birthing individuals and their offspring.”
This work was supported by grants from the National Heart, Lung, and Blood Institute and American Heart Association Transformational Project Award awarded to Sadiya S. Khan.
A version of this article first appeared on Medscape.com.
Less than half of women in the United States enter pregnancy in favorable cardiovascular health, new research suggests.
In 2019, among women aged 20 to 44 years with live births in the United States, only 40.2% were in favorable cardiovascular health prior to pregnancy, defined as normal weight, no diabetes, and no hypertension.
Although all regions and states showed a decline in prepregnancy favorable cardiometabolic health, there were significant differences among geographic regions in the country, the authors report. “These data reveal critical deficiencies and geographic disparities in prepregnancy cardiometabolic health,” they conclude.
“One of the things that we know in the U.S. is that the maternal mortality rate has been increasing, and there are significant differences at the state level in both adverse maternal outcomes, such as maternal mortality, as well as adverse pregnancy outcomes,” corresponding author Sadiya S. Khan, MD, MS, FACC, Northwestern University Feinberg School of Medicine, Chicago, told this news organization.
“These outcomes are often related to health factors that predate pregnancy,” Dr. Khan explained, “and the processes that begin at the very, very beginning of conception are informed by health factors prior to pregnancy, in particular cardiometabolic factors like body mass index or obesity, high blood pressure, and diabetes.”
The results were published online on Feb. 14 in a special “Go Red for Women” spotlight issue of Circulation.
Cardiometabolic health factors
Using maternal birth records from live births in the Centers for Disease Control and Prevention Natality Database between 2016 and 2019, the authors analyzed data on 14,174,625 women with live births aged 20 to 44 years. The majority (81.4%) were 20 to 34 years of age, 22.7% were Hispanic or Latina, and 52.7% were non-Hispanic White.
Favorable cardiometabolic health was defined as a BMI of 18 to 24.9 kg/m2, absence of diabetes, and absence of hypertension.
Although all regions and states experienced a decline in favorable cardiometabolic health during the study period of 2016 to 2019, with a drop overall of 3.2% – from 43.5 to 40.2 per 100 live births – it was especially true of the South and Midwest regions.
In 2019, favorable prepregnancy cardiometabolic health was lowest in the South (38.1%) and Midwest (38.8%) and highest in the West (42.2%) and Northeast (43.6%).
State by state, the lowest prevalence of favorable cardiometabolic health was found in Mississippi, at 31.2%, and highest in Utah, at 47.2%.
They also found a correlation between favorable cardiometabolic health and state-level percentages of high-school education or less and enrollment in Medicaid in 2019.
Similar to what has been seen with cardiovascular disease, “we observe that the states with the lowest prevalence of favorable cardiometabolic health were in the Southeast United States,” said Dr. Khan, “and similar geographic variation was observed with some more patterns in education and Medicaid coverage for birth, and these were used as proxies for socioeconomic status in those areas.”
Although Dr. Khan notes that the relationships cannot be determined to be causal from this analysis, she said that “it does suggest that upstream social determinants of health are important determinants of cardiometabolic health.”
Socioeconomic intervention
Dr. Khan noted that policies at the federal and state level can identify ways to “ensure that individuals who are thinking about pregnancy have access to health care and have access to resources, too, from a broad range of health determinants, including housing stability, food security, as well as access to health care be optimized prior to pregnancy.”
The authors note that this analysis may actually overestimate the prevalence of favorable cardiometabolic health, and data on cholesterol, diet, a distinction between type 1 and type 2 diabetes, and physical activity were not available.
Only individuals with live births were included, which could result in the elimination of a potentially high-risk group; however, late pregnancy losses represent less than 0.3% of all pregnancies, they say.
The authors conclude that “future research is needed to equitably improve health prior to pregnancy and quantify the potential benefits in cardiovascular disease outcomes for birthing individuals and their offspring.”
This work was supported by grants from the National Heart, Lung, and Blood Institute and American Heart Association Transformational Project Award awarded to Sadiya S. Khan.
A version of this article first appeared on Medscape.com.
Excess sodium in soluble acetaminophen tied to CVD risk, death
a large observational study of more than 300,000 adults suggests.
“Numerous studies have reported that high sodium intake is associated with increased risks of cardiovascular disease,” Yuqing Zhang, DSc, with Massachusetts General Hospital and Harvard Medical School, Boston, told this news organization. “Given that the pain relief effect of non–sodium-containing acetaminophen is similar to that of sodium-containing acetaminophen, clinicians may prescribe non–sodium-containing acetaminophen to their patients to minimize the risk of CVD and mortality,” Dr. Zhang said.
The study was published online Feb. 24 in the European Heart Journal.
‘Compelling results’
Dr. Zhang and colleagues note that the effervescent and soluble formulations of 0.5 g acetaminophen contain 0.44 and 0.39 g of sodium, respectively.
Therefore, the intake of maximum daily dose (4 g/day) of sodium-containing acetaminophen corresponds to the ingestion of more than 3 g of sodium, a dose that alone exceeds the recommended total daily sodium intake allowance of the World Health Organization (2 g/day).
“This hidden extra sodium intake is often overlooked,” Dr. Zhang told this news organization.
Using data from the Health Improvement Network, a U.K. primary care database, the researchers examined 4,532 patients with hypertension taking sodium-containing acetaminophen and compared them with 146,866 patients with hypertension taking non–sodium-containing acetaminophen (tablet, capsule, or oral suspension formulations).
After 1 year, the risk of incident CVD (myocardial infarction, stroke, and heart failure) was 5.6% in those taking sodium-containing acetaminophen, compared with 4.6% in those taking non–sodium-containing acetaminophen (average weighted hazard ratio, 1.59; 95% confidence interval, 1.32-1.92).
A separate analysis of normotensive patients taking sodium-containing acetaminophen (n = 5,351) or non–sodium-containing acetaminophen (n = 141,948) gave similar results.
The 1-year risk of incident CVD was 4.4% in those taking sodium-containing acetaminophen vs. 3.7% among those taking non–sodium-containing acetaminophen (average weighted HR, 1.45; 95% CI, 1.18-1.79).
There was also evidence of a dose-response relationship.
In those with hypertension, CVD risk increased by roughly one-quarter (odds ratio, 1.26) for those with one prescription of sodium-containing acetaminophen and by nearly one half (OR, 1.45) for those with five or more prescriptions of sodium-containing acetaminophen. Similar findings were observed among adults without hypertension.
Mortality at 1 year was also higher in those taking sodium-containing acetaminophen than non–sodium-containing acetaminophen, in patients with hypertension (7.6% vs. 6.1%) and without hypertension (7.3% vs. 5.9%).
“The results are compelling,” write the authors of an editorial published with the study.
“The direct message from this study is clear – there are likely to be millions of people worldwide taking paracetamol on a daily basis in a ‘fast-acting’ effervescent or soluble formulation who are increasing their risks of cardiovascular disease and premature death,” say Aletta Schutte, PhD, and Bruce Neal, MBChB, PhD, of the George Institute for Global Health, Sydney.
“The weight of the evidence makes ongoing inaction on sodium-containing medications untenable. The widespread use of effervescent medication in the general population, and the enormous doses of sodium that can be consumed inadvertently by unsuspecting consumers requires urgent action,” Dr. Schutte and Dr. Neal say.
The study was supported by the National Natural Science Foundation of China, the National Key Research and Development Project, the Project Program of National Clinical Research Center for Geriatric Disorders, the Key Research and Development Program of Hunan Province, and the Science and Technology Program of Hunan Province. Dr. Zhang, Dr. Schutte, and Dr. Neal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a large observational study of more than 300,000 adults suggests.
“Numerous studies have reported that high sodium intake is associated with increased risks of cardiovascular disease,” Yuqing Zhang, DSc, with Massachusetts General Hospital and Harvard Medical School, Boston, told this news organization. “Given that the pain relief effect of non–sodium-containing acetaminophen is similar to that of sodium-containing acetaminophen, clinicians may prescribe non–sodium-containing acetaminophen to their patients to minimize the risk of CVD and mortality,” Dr. Zhang said.
The study was published online Feb. 24 in the European Heart Journal.
‘Compelling results’
Dr. Zhang and colleagues note that the effervescent and soluble formulations of 0.5 g acetaminophen contain 0.44 and 0.39 g of sodium, respectively.
Therefore, the intake of maximum daily dose (4 g/day) of sodium-containing acetaminophen corresponds to the ingestion of more than 3 g of sodium, a dose that alone exceeds the recommended total daily sodium intake allowance of the World Health Organization (2 g/day).
“This hidden extra sodium intake is often overlooked,” Dr. Zhang told this news organization.
Using data from the Health Improvement Network, a U.K. primary care database, the researchers examined 4,532 patients with hypertension taking sodium-containing acetaminophen and compared them with 146,866 patients with hypertension taking non–sodium-containing acetaminophen (tablet, capsule, or oral suspension formulations).
After 1 year, the risk of incident CVD (myocardial infarction, stroke, and heart failure) was 5.6% in those taking sodium-containing acetaminophen, compared with 4.6% in those taking non–sodium-containing acetaminophen (average weighted hazard ratio, 1.59; 95% confidence interval, 1.32-1.92).
A separate analysis of normotensive patients taking sodium-containing acetaminophen (n = 5,351) or non–sodium-containing acetaminophen (n = 141,948) gave similar results.
The 1-year risk of incident CVD was 4.4% in those taking sodium-containing acetaminophen vs. 3.7% among those taking non–sodium-containing acetaminophen (average weighted HR, 1.45; 95% CI, 1.18-1.79).
There was also evidence of a dose-response relationship.
In those with hypertension, CVD risk increased by roughly one-quarter (odds ratio, 1.26) for those with one prescription of sodium-containing acetaminophen and by nearly one half (OR, 1.45) for those with five or more prescriptions of sodium-containing acetaminophen. Similar findings were observed among adults without hypertension.
Mortality at 1 year was also higher in those taking sodium-containing acetaminophen than non–sodium-containing acetaminophen, in patients with hypertension (7.6% vs. 6.1%) and without hypertension (7.3% vs. 5.9%).
“The results are compelling,” write the authors of an editorial published with the study.
“The direct message from this study is clear – there are likely to be millions of people worldwide taking paracetamol on a daily basis in a ‘fast-acting’ effervescent or soluble formulation who are increasing their risks of cardiovascular disease and premature death,” say Aletta Schutte, PhD, and Bruce Neal, MBChB, PhD, of the George Institute for Global Health, Sydney.
“The weight of the evidence makes ongoing inaction on sodium-containing medications untenable. The widespread use of effervescent medication in the general population, and the enormous doses of sodium that can be consumed inadvertently by unsuspecting consumers requires urgent action,” Dr. Schutte and Dr. Neal say.
The study was supported by the National Natural Science Foundation of China, the National Key Research and Development Project, the Project Program of National Clinical Research Center for Geriatric Disorders, the Key Research and Development Program of Hunan Province, and the Science and Technology Program of Hunan Province. Dr. Zhang, Dr. Schutte, and Dr. Neal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a large observational study of more than 300,000 adults suggests.
“Numerous studies have reported that high sodium intake is associated with increased risks of cardiovascular disease,” Yuqing Zhang, DSc, with Massachusetts General Hospital and Harvard Medical School, Boston, told this news organization. “Given that the pain relief effect of non–sodium-containing acetaminophen is similar to that of sodium-containing acetaminophen, clinicians may prescribe non–sodium-containing acetaminophen to their patients to minimize the risk of CVD and mortality,” Dr. Zhang said.
The study was published online Feb. 24 in the European Heart Journal.
‘Compelling results’
Dr. Zhang and colleagues note that the effervescent and soluble formulations of 0.5 g acetaminophen contain 0.44 and 0.39 g of sodium, respectively.
Therefore, the intake of maximum daily dose (4 g/day) of sodium-containing acetaminophen corresponds to the ingestion of more than 3 g of sodium, a dose that alone exceeds the recommended total daily sodium intake allowance of the World Health Organization (2 g/day).
“This hidden extra sodium intake is often overlooked,” Dr. Zhang told this news organization.
Using data from the Health Improvement Network, a U.K. primary care database, the researchers examined 4,532 patients with hypertension taking sodium-containing acetaminophen and compared them with 146,866 patients with hypertension taking non–sodium-containing acetaminophen (tablet, capsule, or oral suspension formulations).
After 1 year, the risk of incident CVD (myocardial infarction, stroke, and heart failure) was 5.6% in those taking sodium-containing acetaminophen, compared with 4.6% in those taking non–sodium-containing acetaminophen (average weighted hazard ratio, 1.59; 95% confidence interval, 1.32-1.92).
A separate analysis of normotensive patients taking sodium-containing acetaminophen (n = 5,351) or non–sodium-containing acetaminophen (n = 141,948) gave similar results.
The 1-year risk of incident CVD was 4.4% in those taking sodium-containing acetaminophen vs. 3.7% among those taking non–sodium-containing acetaminophen (average weighted HR, 1.45; 95% CI, 1.18-1.79).
There was also evidence of a dose-response relationship.
In those with hypertension, CVD risk increased by roughly one-quarter (odds ratio, 1.26) for those with one prescription of sodium-containing acetaminophen and by nearly one half (OR, 1.45) for those with five or more prescriptions of sodium-containing acetaminophen. Similar findings were observed among adults without hypertension.
Mortality at 1 year was also higher in those taking sodium-containing acetaminophen than non–sodium-containing acetaminophen, in patients with hypertension (7.6% vs. 6.1%) and without hypertension (7.3% vs. 5.9%).
“The results are compelling,” write the authors of an editorial published with the study.
“The direct message from this study is clear – there are likely to be millions of people worldwide taking paracetamol on a daily basis in a ‘fast-acting’ effervescent or soluble formulation who are increasing their risks of cardiovascular disease and premature death,” say Aletta Schutte, PhD, and Bruce Neal, MBChB, PhD, of the George Institute for Global Health, Sydney.
“The weight of the evidence makes ongoing inaction on sodium-containing medications untenable. The widespread use of effervescent medication in the general population, and the enormous doses of sodium that can be consumed inadvertently by unsuspecting consumers requires urgent action,” Dr. Schutte and Dr. Neal say.
The study was supported by the National Natural Science Foundation of China, the National Key Research and Development Project, the Project Program of National Clinical Research Center for Geriatric Disorders, the Key Research and Development Program of Hunan Province, and the Science and Technology Program of Hunan Province. Dr. Zhang, Dr. Schutte, and Dr. Neal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE EUROPEAN HEART JOURNAL
AHA targets ‘low-value’ heart care in new scientific statement
Low-value health care services that provide little or no benefit to patients are “common, potentially harmful, and costly,” and there is a critical need to reduce this kind of care, the American Heart Association said in a newly released scientific statement.
Each year, nearly half of patients in the United States will receive at least one low-value test or procedure, with the attendant risk of avoidable complications from cascades of care and excess costs to individuals and society, the authors noted. Reducing low-value care is particularly important in cardiology, given the high prevalence and costs of cardiovascular disease in the United States.
The statement was published online Feb. 22, 2022, in Circulation: Cardiovascular Quality and Outcomes.
High burden with uncertain benefit
“Cardiovascular disease is common and can present suddenly, such as a heart attack or abnormal heart rhythm,” Vinay Kini, MD, chair of the statement writing group and assistant professor of medicine at Weill Cornell Medicine, New York, said in a news release.
“Our desire to be vigilant about treating and preventing cardiovascular disease may sometimes lead to use of tests and procedures where the benefits to patients may be uncertain,” Dr. Kini said. “This may impose burdens on patients, in the form of increased risk of physical harm from the low-value procedure or potential complications, as well as follow-up care and out-of-pocket financial costs.”
For example, studies have shown that up to one in five echocardiograms and up to half of all stress tests performed in the United States may be rated as rarely appropriate, based on established guidelines for their use.
In addition, up to 15% of percutaneous coronary interventions (PCIs) are classified as rarely appropriate, the writing group said.
Annually, among Medicare fee-for-service beneficiaries, low-value stress testing in patients with stable coronary artery disease is estimated to cost between $212 million and $2.1 billion, while costs of PCI for stable CAD range from $212 million to $2.8 billion, the writing group noted.
“At best, spending on low-value care potentially diverts resources from higher-value services that would benefit patients more effectively at the same or reduced cost. At worst, low-value care results in physical harm in the form of preventable morbidity and mortality,” they said.
“Thus, reducing low-value care is one of the few patient-centered solutions that directly address both the need to control health care spending and the societal imperative to devote its limited resources to beneficial health care services that improve health,” they added.
The group outlines several ways to reduce low-value cardiovascular care targeting patients, providers, and payers/policymakers.
For patients, education and shared decision-making may help reduce low-value care and dispel misconceptions about the intended purpose of test or treatment, they suggested.
For clinicians, a “layered” approach to reducing low-value care may be most effective, such as through education, audit and feedback, and behavioral science tools (“nudges”) to shift behaviors and practices, they said.
For payers and policy leaders, interventions to reduce low-value care include national insurance coverage determinations; prior authorization; alternative payment models that reward lower costs and higher-quality health care; value-based insurance designs that financially penalize low-value care; and medical liability reform to reduce defensive medical practices.
Low-value cardiovascular care is a complex problem, the writing group acknowledged, and achieving meaningful reductions in low-value cardiovascular care will require a multidisciplinary approach that includes continuous research, implementation, evaluation, and adjustment while ensuring equitable access to care.
“Each approach has benefits and drawbacks,” Dr. Kini said. “For example, prior authorization imposes a large burden on health care professionals to obtain insurance approval for tests and treatments. Prior authorization and some value-based payment models may unintentionally worsen existing racial and ethnic health care disparities.
“A one-size-fits-all approach to reducing low-value care is unlikely to succeed; rather, acting through multiple perspectives and frequently measuring impacts and potential unintended consequences is critical,” he concluded.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Council on Quality of Care and Outcomes Research.
The research had no commercial funding. Dr. Kini disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Low-value health care services that provide little or no benefit to patients are “common, potentially harmful, and costly,” and there is a critical need to reduce this kind of care, the American Heart Association said in a newly released scientific statement.
Each year, nearly half of patients in the United States will receive at least one low-value test or procedure, with the attendant risk of avoidable complications from cascades of care and excess costs to individuals and society, the authors noted. Reducing low-value care is particularly important in cardiology, given the high prevalence and costs of cardiovascular disease in the United States.
The statement was published online Feb. 22, 2022, in Circulation: Cardiovascular Quality and Outcomes.
High burden with uncertain benefit
“Cardiovascular disease is common and can present suddenly, such as a heart attack or abnormal heart rhythm,” Vinay Kini, MD, chair of the statement writing group and assistant professor of medicine at Weill Cornell Medicine, New York, said in a news release.
“Our desire to be vigilant about treating and preventing cardiovascular disease may sometimes lead to use of tests and procedures where the benefits to patients may be uncertain,” Dr. Kini said. “This may impose burdens on patients, in the form of increased risk of physical harm from the low-value procedure or potential complications, as well as follow-up care and out-of-pocket financial costs.”
For example, studies have shown that up to one in five echocardiograms and up to half of all stress tests performed in the United States may be rated as rarely appropriate, based on established guidelines for their use.
In addition, up to 15% of percutaneous coronary interventions (PCIs) are classified as rarely appropriate, the writing group said.
Annually, among Medicare fee-for-service beneficiaries, low-value stress testing in patients with stable coronary artery disease is estimated to cost between $212 million and $2.1 billion, while costs of PCI for stable CAD range from $212 million to $2.8 billion, the writing group noted.
“At best, spending on low-value care potentially diverts resources from higher-value services that would benefit patients more effectively at the same or reduced cost. At worst, low-value care results in physical harm in the form of preventable morbidity and mortality,” they said.
“Thus, reducing low-value care is one of the few patient-centered solutions that directly address both the need to control health care spending and the societal imperative to devote its limited resources to beneficial health care services that improve health,” they added.
The group outlines several ways to reduce low-value cardiovascular care targeting patients, providers, and payers/policymakers.
For patients, education and shared decision-making may help reduce low-value care and dispel misconceptions about the intended purpose of test or treatment, they suggested.
For clinicians, a “layered” approach to reducing low-value care may be most effective, such as through education, audit and feedback, and behavioral science tools (“nudges”) to shift behaviors and practices, they said.
For payers and policy leaders, interventions to reduce low-value care include national insurance coverage determinations; prior authorization; alternative payment models that reward lower costs and higher-quality health care; value-based insurance designs that financially penalize low-value care; and medical liability reform to reduce defensive medical practices.
Low-value cardiovascular care is a complex problem, the writing group acknowledged, and achieving meaningful reductions in low-value cardiovascular care will require a multidisciplinary approach that includes continuous research, implementation, evaluation, and adjustment while ensuring equitable access to care.
“Each approach has benefits and drawbacks,” Dr. Kini said. “For example, prior authorization imposes a large burden on health care professionals to obtain insurance approval for tests and treatments. Prior authorization and some value-based payment models may unintentionally worsen existing racial and ethnic health care disparities.
“A one-size-fits-all approach to reducing low-value care is unlikely to succeed; rather, acting through multiple perspectives and frequently measuring impacts and potential unintended consequences is critical,” he concluded.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Council on Quality of Care and Outcomes Research.
The research had no commercial funding. Dr. Kini disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Low-value health care services that provide little or no benefit to patients are “common, potentially harmful, and costly,” and there is a critical need to reduce this kind of care, the American Heart Association said in a newly released scientific statement.
Each year, nearly half of patients in the United States will receive at least one low-value test or procedure, with the attendant risk of avoidable complications from cascades of care and excess costs to individuals and society, the authors noted. Reducing low-value care is particularly important in cardiology, given the high prevalence and costs of cardiovascular disease in the United States.
The statement was published online Feb. 22, 2022, in Circulation: Cardiovascular Quality and Outcomes.
High burden with uncertain benefit
“Cardiovascular disease is common and can present suddenly, such as a heart attack or abnormal heart rhythm,” Vinay Kini, MD, chair of the statement writing group and assistant professor of medicine at Weill Cornell Medicine, New York, said in a news release.
“Our desire to be vigilant about treating and preventing cardiovascular disease may sometimes lead to use of tests and procedures where the benefits to patients may be uncertain,” Dr. Kini said. “This may impose burdens on patients, in the form of increased risk of physical harm from the low-value procedure or potential complications, as well as follow-up care and out-of-pocket financial costs.”
For example, studies have shown that up to one in five echocardiograms and up to half of all stress tests performed in the United States may be rated as rarely appropriate, based on established guidelines for their use.
In addition, up to 15% of percutaneous coronary interventions (PCIs) are classified as rarely appropriate, the writing group said.
Annually, among Medicare fee-for-service beneficiaries, low-value stress testing in patients with stable coronary artery disease is estimated to cost between $212 million and $2.1 billion, while costs of PCI for stable CAD range from $212 million to $2.8 billion, the writing group noted.
“At best, spending on low-value care potentially diverts resources from higher-value services that would benefit patients more effectively at the same or reduced cost. At worst, low-value care results in physical harm in the form of preventable morbidity and mortality,” they said.
“Thus, reducing low-value care is one of the few patient-centered solutions that directly address both the need to control health care spending and the societal imperative to devote its limited resources to beneficial health care services that improve health,” they added.
The group outlines several ways to reduce low-value cardiovascular care targeting patients, providers, and payers/policymakers.
For patients, education and shared decision-making may help reduce low-value care and dispel misconceptions about the intended purpose of test or treatment, they suggested.
For clinicians, a “layered” approach to reducing low-value care may be most effective, such as through education, audit and feedback, and behavioral science tools (“nudges”) to shift behaviors and practices, they said.
For payers and policy leaders, interventions to reduce low-value care include national insurance coverage determinations; prior authorization; alternative payment models that reward lower costs and higher-quality health care; value-based insurance designs that financially penalize low-value care; and medical liability reform to reduce defensive medical practices.
Low-value cardiovascular care is a complex problem, the writing group acknowledged, and achieving meaningful reductions in low-value cardiovascular care will require a multidisciplinary approach that includes continuous research, implementation, evaluation, and adjustment while ensuring equitable access to care.
“Each approach has benefits and drawbacks,” Dr. Kini said. “For example, prior authorization imposes a large burden on health care professionals to obtain insurance approval for tests and treatments. Prior authorization and some value-based payment models may unintentionally worsen existing racial and ethnic health care disparities.
“A one-size-fits-all approach to reducing low-value care is unlikely to succeed; rather, acting through multiple perspectives and frequently measuring impacts and potential unintended consequences is critical,” he concluded.
The scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Council on Quality of Care and Outcomes Research.
The research had no commercial funding. Dr. Kini disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
EULAR CVD management guidance focuses on gout, lupus, vasculitis
New recommendations from the European Alliance of Associations for Rheumatology provide both broad and detailed advice for cardiovascular risk management in various rheumatic and musculoskeletal diseases (RMDs), many of which can lead to an increased possibility of cardiovascular disease (CVD).
“The panel believes that these recommendations will enable health care providers and patients to mutually engage in a long-term care pathway tailored to patients’ needs and expectations for improving cardiovascular health in RMDs,” write George C. Drosos, National and Kapodistrian University of Athens, and colleagues. The recommendations were published in February in Annals of the Rheumatic Diseases).

EULAR assembled a task force to generate best practices for preventing CVD in patients with gout, vasculitis, systemic sclerosis (SSc), myositis, mixed connective tissue disease (MCTD), Sjögren syndrome (SS), systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS).
The cardiovascular risk management of patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis was covered in prior EULAR recommendations.
The task force included 20 members from 11 European countries, including 12 rheumatologists, 2 cardiologists, 1 metabolic medicine physician, 1 health care professional, 2 patient representatives, and 2 EMEUNET (Emerging EULAR Network) members. One group of task force members conducted a systematic literature review of 105 articles about gout, vasculitis, SSc, myositis, MCTD, and SS, and another group evaluated 75 articles about SLE and APS. Together, they decided on four overarching principles:
Clinicians need to be aware of increased cardiovascular risk in patients with RMDs, with disease reduction likely decreasing risk.
Rheumatologists – in tandem with other health care providers – are responsible for their patients’ cardiovascular risk assessment and management.
Screening for cardiovascular risk should be performed regularly in all patients with RMDs, with an emphasis on factors like smoking and blood pressure management.
Patient education and counseling on cardiovascular risk, including important lifestyle modifications, is key for RMD patients.
Specific recommendations from the gout, vasculitis, SSc, myositis, MCTD, and SS group include deploying existing cardiovascular prediction tools as they are used in the general population, with the European Vasculitis Society model suggesting to supplement the Framingham Risk Score for patients with antineutrophil cytoplasmic antibody–associated vasculitis. They also recommended avoiding diuretics in patients with gout and beta-blockers in patients with SSc, as well as following the same blood pressure and lipid management strategies that are used among the general population.
Recommendations from the SLE and APS group include thoroughly assessing traditional cardiovascular risk factors in all patients, following typical blood pressure management strategies in patients with APS, and setting a blood pressure target of less than 130/80 mm Hg in patients with SLE. They also recommended administering the lowest possible glucocorticoid dose in patients with SLE, along with treatment with hydroxychloroquine – unless contraindicated – and even common preventive strategies like low-dose aspirin if it suits their cardiovascular risk profile.
As for next steps, the task force noted several areas where additional focus is needed, such as identifying patient subgroups with increased cardiovascular risk. This could include patients with a longer disease duration or more flare-ups, older patients, and those with certain disease characteristics like antiphospholipid positivity in SLE.
Can EULAR’s recommendations be implemented in U.S. rheumatology practices?
“We have been hearing for years that patients with rheumatic diseases have an increased risk of cardiovascular disease,” Ali A. Duarte Garcia, MD, a rheumatologist at the Mayo Clinic in Rochester, Minn., told this news organization. “That has been consistently published for more than a decade now. But any further guidance about it has not been issued. I think there was a void there.”

“Certainly, cardiovascular disease risk in rheumatoid and psoriatic arthritis has been front of mind for the last decade or so,” Christie M. Bartels, MD, chief of the division of rheumatology at the University of Wisconsin, Madison, said when asked to comment on the recommendations. “But in some of these other conditions, it hasn’t been.”
When asked if rheumatologists would be ready and willing to implement these recommendations, Dr. Duarte Garcia acknowledged that it could be challenging for some.
“It’s a different workflow,” he said. “You’ve been trained traditionally to assess inflammation, to keep the disease under control, which is something they recommend, by the way. If you control the disease, patients do better. But I think lipid screening, for example, and testing for cholesterol, smoking cessation, those well-established programs are harder to bring to a rheumatology clinic. It’s doable, but it’s something that needs to be implemented within the current workflows and could take a few years to take hold.”
Dr. Bartels, however, noted that her group has done extensive work over the last 5 years incorporating certain interventions into practice, including sending patients with high blood pressure back to primary care.
“It’s a sustainable intervention in our clinic that basically our medical assistants and nurses do as a routine operation,” she said. “Our primary care providers are grateful to get these patients back. Our patients are grateful because otherwise when they come to the rheumatologist, get their blood pressure measured, and don’t get feedback, they assume they’re OK. So, we’re giving them a false signal.
“We have a similar intervention with smoking,” she added. “Often our patients aren’t even aware that they’re at increased risk of cardiovascular disease or that smoking might make their rheumatic disease and their cardiovascular outcomes worse. No one has had that conversation with them. They really welcome engaging in those discussions.
“Our tobacco intervention takes 90 seconds at point of care. Our blood pressure intervention at point of care, we’ve timed it, takes 3 minutes. There are ways that we can hardwire this into care.”
Along those lines, Dr. Duarte Garcia stated that the recommendations – although released by EULAR – are largely intuitive and should be very adaptable to an American health care context. He also recognized this moment as an opportunity for rheumatologists to consider patient outcomes beyond what they usually encounter firsthand.
“I don’t think we have many rheumatologists with patients who get a stroke or heart attack because if that happens, it’s in a hospital context or they go see a cardiologist,” he said. “You may see it once it happens if they survive and come and see you – or perhaps if you’re in a more integrated practice – but I don’t think it’s as apparent in our clinics because it is a predominantly outpatient practice and many times those are emergencies or inpatient complications.
“The bottom line,” he added, “is these are practical guidelines. It’s a push in the right direction, but there is still work to be done. And hopefully some of the recommendations, like measuring high blood pressure and addressing it just as in the general population, are something we can start to implement.”
Dr. Duarte Garcia reported receiving grant funding from the Rheumatology Research Foundation and the Centers for Disease Control and Prevention. Dr. Bartels reported that her group’s tobacco cessation work is funded by Pfizer’s Independent Grants for Learning and Change.
A version of this article first appeared on Medscape.com.
New recommendations from the European Alliance of Associations for Rheumatology provide both broad and detailed advice for cardiovascular risk management in various rheumatic and musculoskeletal diseases (RMDs), many of which can lead to an increased possibility of cardiovascular disease (CVD).
“The panel believes that these recommendations will enable health care providers and patients to mutually engage in a long-term care pathway tailored to patients’ needs and expectations for improving cardiovascular health in RMDs,” write George C. Drosos, National and Kapodistrian University of Athens, and colleagues. The recommendations were published in February in Annals of the Rheumatic Diseases).
EULAR assembled a task force to generate best practices for preventing CVD in patients with gout, vasculitis, systemic sclerosis (SSc), myositis, mixed connective tissue disease (MCTD), Sjögren syndrome (SS), systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS).
The cardiovascular risk management of patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis was covered in prior EULAR recommendations.
The task force included 20 members from 11 European countries, including 12 rheumatologists, 2 cardiologists, 1 metabolic medicine physician, 1 health care professional, 2 patient representatives, and 2 EMEUNET (Emerging EULAR Network) members. One group of task force members conducted a systematic literature review of 105 articles about gout, vasculitis, SSc, myositis, MCTD, and SS, and another group evaluated 75 articles about SLE and APS. Together, they decided on four overarching principles:
Clinicians need to be aware of increased cardiovascular risk in patients with RMDs, with disease reduction likely decreasing risk.
Rheumatologists – in tandem with other health care providers – are responsible for their patients’ cardiovascular risk assessment and management.
Screening for cardiovascular risk should be performed regularly in all patients with RMDs, with an emphasis on factors like smoking and blood pressure management.
Patient education and counseling on cardiovascular risk, including important lifestyle modifications, is key for RMD patients.
Specific recommendations from the gout, vasculitis, SSc, myositis, MCTD, and SS group include deploying existing cardiovascular prediction tools as they are used in the general population, with the European Vasculitis Society model suggesting to supplement the Framingham Risk Score for patients with antineutrophil cytoplasmic antibody–associated vasculitis. They also recommended avoiding diuretics in patients with gout and beta-blockers in patients with SSc, as well as following the same blood pressure and lipid management strategies that are used among the general population.
Recommendations from the SLE and APS group include thoroughly assessing traditional cardiovascular risk factors in all patients, following typical blood pressure management strategies in patients with APS, and setting a blood pressure target of less than 130/80 mm Hg in patients with SLE. They also recommended administering the lowest possible glucocorticoid dose in patients with SLE, along with treatment with hydroxychloroquine – unless contraindicated – and even common preventive strategies like low-dose aspirin if it suits their cardiovascular risk profile.
As for next steps, the task force noted several areas where additional focus is needed, such as identifying patient subgroups with increased cardiovascular risk. This could include patients with a longer disease duration or more flare-ups, older patients, and those with certain disease characteristics like antiphospholipid positivity in SLE.
Can EULAR’s recommendations be implemented in U.S. rheumatology practices?
“We have been hearing for years that patients with rheumatic diseases have an increased risk of cardiovascular disease,” Ali A. Duarte Garcia, MD, a rheumatologist at the Mayo Clinic in Rochester, Minn., told this news organization. “That has been consistently published for more than a decade now. But any further guidance about it has not been issued. I think there was a void there.”
“Certainly, cardiovascular disease risk in rheumatoid and psoriatic arthritis has been front of mind for the last decade or so,” Christie M. Bartels, MD, chief of the division of rheumatology at the University of Wisconsin, Madison, said when asked to comment on the recommendations. “But in some of these other conditions, it hasn’t been.”
When asked if rheumatologists would be ready and willing to implement these recommendations, Dr. Duarte Garcia acknowledged that it could be challenging for some.
“It’s a different workflow,” he said. “You’ve been trained traditionally to assess inflammation, to keep the disease under control, which is something they recommend, by the way. If you control the disease, patients do better. But I think lipid screening, for example, and testing for cholesterol, smoking cessation, those well-established programs are harder to bring to a rheumatology clinic. It’s doable, but it’s something that needs to be implemented within the current workflows and could take a few years to take hold.”
Dr. Bartels, however, noted that her group has done extensive work over the last 5 years incorporating certain interventions into practice, including sending patients with high blood pressure back to primary care.
“It’s a sustainable intervention in our clinic that basically our medical assistants and nurses do as a routine operation,” she said. “Our primary care providers are grateful to get these patients back. Our patients are grateful because otherwise when they come to the rheumatologist, get their blood pressure measured, and don’t get feedback, they assume they’re OK. So, we’re giving them a false signal.
“We have a similar intervention with smoking,” she added. “Often our patients aren’t even aware that they’re at increased risk of cardiovascular disease or that smoking might make their rheumatic disease and their cardiovascular outcomes worse. No one has had that conversation with them. They really welcome engaging in those discussions.
“Our tobacco intervention takes 90 seconds at point of care. Our blood pressure intervention at point of care, we’ve timed it, takes 3 minutes. There are ways that we can hardwire this into care.”
Along those lines, Dr. Duarte Garcia stated that the recommendations – although released by EULAR – are largely intuitive and should be very adaptable to an American health care context. He also recognized this moment as an opportunity for rheumatologists to consider patient outcomes beyond what they usually encounter firsthand.
“I don’t think we have many rheumatologists with patients who get a stroke or heart attack because if that happens, it’s in a hospital context or they go see a cardiologist,” he said. “You may see it once it happens if they survive and come and see you – or perhaps if you’re in a more integrated practice – but I don’t think it’s as apparent in our clinics because it is a predominantly outpatient practice and many times those are emergencies or inpatient complications.
“The bottom line,” he added, “is these are practical guidelines. It’s a push in the right direction, but there is still work to be done. And hopefully some of the recommendations, like measuring high blood pressure and addressing it just as in the general population, are something we can start to implement.”
Dr. Duarte Garcia reported receiving grant funding from the Rheumatology Research Foundation and the Centers for Disease Control and Prevention. Dr. Bartels reported that her group’s tobacco cessation work is funded by Pfizer’s Independent Grants for Learning and Change.
A version of this article first appeared on Medscape.com.
New recommendations from the European Alliance of Associations for Rheumatology provide both broad and detailed advice for cardiovascular risk management in various rheumatic and musculoskeletal diseases (RMDs), many of which can lead to an increased possibility of cardiovascular disease (CVD).
“The panel believes that these recommendations will enable health care providers and patients to mutually engage in a long-term care pathway tailored to patients’ needs and expectations for improving cardiovascular health in RMDs,” write George C. Drosos, National and Kapodistrian University of Athens, and colleagues. The recommendations were published in February in Annals of the Rheumatic Diseases).
EULAR assembled a task force to generate best practices for preventing CVD in patients with gout, vasculitis, systemic sclerosis (SSc), myositis, mixed connective tissue disease (MCTD), Sjögren syndrome (SS), systemic lupus erythematosus (SLE), and antiphospholipid syndrome (APS).
The cardiovascular risk management of patients with rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis was covered in prior EULAR recommendations.
The task force included 20 members from 11 European countries, including 12 rheumatologists, 2 cardiologists, 1 metabolic medicine physician, 1 health care professional, 2 patient representatives, and 2 EMEUNET (Emerging EULAR Network) members. One group of task force members conducted a systematic literature review of 105 articles about gout, vasculitis, SSc, myositis, MCTD, and SS, and another group evaluated 75 articles about SLE and APS. Together, they decided on four overarching principles:
Clinicians need to be aware of increased cardiovascular risk in patients with RMDs, with disease reduction likely decreasing risk.
Rheumatologists – in tandem with other health care providers – are responsible for their patients’ cardiovascular risk assessment and management.
Screening for cardiovascular risk should be performed regularly in all patients with RMDs, with an emphasis on factors like smoking and blood pressure management.
Patient education and counseling on cardiovascular risk, including important lifestyle modifications, is key for RMD patients.
Specific recommendations from the gout, vasculitis, SSc, myositis, MCTD, and SS group include deploying existing cardiovascular prediction tools as they are used in the general population, with the European Vasculitis Society model suggesting to supplement the Framingham Risk Score for patients with antineutrophil cytoplasmic antibody–associated vasculitis. They also recommended avoiding diuretics in patients with gout and beta-blockers in patients with SSc, as well as following the same blood pressure and lipid management strategies that are used among the general population.
Recommendations from the SLE and APS group include thoroughly assessing traditional cardiovascular risk factors in all patients, following typical blood pressure management strategies in patients with APS, and setting a blood pressure target of less than 130/80 mm Hg in patients with SLE. They also recommended administering the lowest possible glucocorticoid dose in patients with SLE, along with treatment with hydroxychloroquine – unless contraindicated – and even common preventive strategies like low-dose aspirin if it suits their cardiovascular risk profile.
As for next steps, the task force noted several areas where additional focus is needed, such as identifying patient subgroups with increased cardiovascular risk. This could include patients with a longer disease duration or more flare-ups, older patients, and those with certain disease characteristics like antiphospholipid positivity in SLE.
Can EULAR’s recommendations be implemented in U.S. rheumatology practices?
“We have been hearing for years that patients with rheumatic diseases have an increased risk of cardiovascular disease,” Ali A. Duarte Garcia, MD, a rheumatologist at the Mayo Clinic in Rochester, Minn., told this news organization. “That has been consistently published for more than a decade now. But any further guidance about it has not been issued. I think there was a void there.”
“Certainly, cardiovascular disease risk in rheumatoid and psoriatic arthritis has been front of mind for the last decade or so,” Christie M. Bartels, MD, chief of the division of rheumatology at the University of Wisconsin, Madison, said when asked to comment on the recommendations. “But in some of these other conditions, it hasn’t been.”
When asked if rheumatologists would be ready and willing to implement these recommendations, Dr. Duarte Garcia acknowledged that it could be challenging for some.
“It’s a different workflow,” he said. “You’ve been trained traditionally to assess inflammation, to keep the disease under control, which is something they recommend, by the way. If you control the disease, patients do better. But I think lipid screening, for example, and testing for cholesterol, smoking cessation, those well-established programs are harder to bring to a rheumatology clinic. It’s doable, but it’s something that needs to be implemented within the current workflows and could take a few years to take hold.”
Dr. Bartels, however, noted that her group has done extensive work over the last 5 years incorporating certain interventions into practice, including sending patients with high blood pressure back to primary care.
“It’s a sustainable intervention in our clinic that basically our medical assistants and nurses do as a routine operation,” she said. “Our primary care providers are grateful to get these patients back. Our patients are grateful because otherwise when they come to the rheumatologist, get their blood pressure measured, and don’t get feedback, they assume they’re OK. So, we’re giving them a false signal.
“We have a similar intervention with smoking,” she added. “Often our patients aren’t even aware that they’re at increased risk of cardiovascular disease or that smoking might make their rheumatic disease and their cardiovascular outcomes worse. No one has had that conversation with them. They really welcome engaging in those discussions.
“Our tobacco intervention takes 90 seconds at point of care. Our blood pressure intervention at point of care, we’ve timed it, takes 3 minutes. There are ways that we can hardwire this into care.”
Along those lines, Dr. Duarte Garcia stated that the recommendations – although released by EULAR – are largely intuitive and should be very adaptable to an American health care context. He also recognized this moment as an opportunity for rheumatologists to consider patient outcomes beyond what they usually encounter firsthand.
“I don’t think we have many rheumatologists with patients who get a stroke or heart attack because if that happens, it’s in a hospital context or they go see a cardiologist,” he said. “You may see it once it happens if they survive and come and see you – or perhaps if you’re in a more integrated practice – but I don’t think it’s as apparent in our clinics because it is a predominantly outpatient practice and many times those are emergencies or inpatient complications.
“The bottom line,” he added, “is these are practical guidelines. It’s a push in the right direction, but there is still work to be done. And hopefully some of the recommendations, like measuring high blood pressure and addressing it just as in the general population, are something we can start to implement.”
Dr. Duarte Garcia reported receiving grant funding from the Rheumatology Research Foundation and the Centers for Disease Control and Prevention. Dr. Bartels reported that her group’s tobacco cessation work is funded by Pfizer’s Independent Grants for Learning and Change.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF THE RHEUMATIC DISEASES
Could the protective effect on heart disease of eating more veg be exaggerated?
Eating sufficient amounts of vegetables might be good for overall health, but surprising results from a study suggested that their inclusion in the diet might have little or no effect on the risk of developing cardiovascular disease (CVD).
An investigation, led by the Nuffield department of population health at the University of Oxford, found that They said their findings, published in the journal Frontiers in Nutrition might mean that advice on vegetable intake and heart disease in high-income countries should be reappraised.
However, leading experts commented that the findings confirmed that higher overall vegetable consumption did lower the risk of cardiovascular disease.
UK Biobank data
Boosting health through a diet rich in vegetables has been backed by a large body of evidence, with guidelines consistently recommending them as a valuable source of macronutrients and micronutrients, such as dietary fiber, vitamins, and phytochemicals. However, the research team, which included the Chinese University of Hong Kong and the University of Bristol, set out to probe the independent effects of cooked and raw vegetables on health outcomes. Previous epidemiological studies had demonstrated inconsistent findings, they said.
They based their research on 399,586 people with no history of angina, stroke, and myocardial infarction, who enrolled in the UK Biobank. Of those, 55.4% were women, and 90.9% were of White ethnicity. The average body mass index was 27.3.
Raw and cooked vegetables
From their enrollment questionnaire, the mean intake of vegetables was found to be 2.3 heaped tablespoons per day of raw vegetables, and 2.8 of cooked vegetables. During an average follow-up of 12.1 years, 4.5% of the participants went on to develop CVD.
There was an inverse association between incident CVD and total and raw vegetable intake, but not cooked vegetable intake. Those who ate the most vegetables – both cooked and raw – had a 10% lower incidence of CVD, compared with those who ate the least. However, whereas raw vegetable intake was associated with an 11% reduction in CVD for those who ate the most, compared with the least, no reduction was seen for cooked vegetables.
Consuming two or more heaped tablespoons each day of cooked and raw vegetables was associated with a lower risk of dying from CVD, but little evidence was seen that a higher intake increased protection further. Similarly, there was evidence of an inverse association of CVD mortality with raw vegetable intake.
Researcher Qi Feng, from the Nuffield department of population health, said: “Our large study did not find evidence for a protective effect of vegetable intake on the occurrence of CVD. Instead, our analyses show that the seemingly protective effect of vegetable intake against CVD risk is very likely to be accounted for by bias from residual confounding factors, related to differences in socioeconomic situation and lifestyle.”
Expert opinions
Some clinical specialists took issue with the interpretation of the findings.
Dr. Dipender Gill, BMBCh, PhD, National Institute for Health Research clinical lecturer at St George’s, University of London, told the Science Media Centre that: “Many of the considered confounders that were adjusted for may actually represent mediating mechanisms. For example, vegetable consumption may reduce cardiovascular risk by lowering blood pressure and bodyweight, and improving glycaemic control.
“By adjusting for such traits, the authors may inadvertently be negating some of the mechanisms by which vegetable consumption is exerting beneficial effects.”
Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics at King’s College London, said: “The conclusion that cooked vegetables may not be effective in reducing risk of cardiovascular disease may not be justified, especially as the group consuming the highest levels of vegetables were more likely to be receiving medication for high blood cholesterol and high blood pressure (i.e. this group was at higher risk of CVD), compared with those consuming the lowest intake.” He added: “These findings should not be taken to indicate that eating more vegetables has no benefit to health, especially cardiovascular health.”
Naveed Sattar, FMedSci, FRCPath, FRCPGlas, professor of metabolic medicine at the University of Glasgow, agreed. “In short, this paper should in no way change advice to eat at least five portions of fruit and vegetables a day,” he said. “Many living in the U.K. fall well short of this, sadly, and more needs to be done to encourage better intake of vegetables.
“In fact, I suspect we may have underestimated the importance of a healthy diet on health and disease in general.”
A version of this article first appeared on Medscape.com.
Eating sufficient amounts of vegetables might be good for overall health, but surprising results from a study suggested that their inclusion in the diet might have little or no effect on the risk of developing cardiovascular disease (CVD).
An investigation, led by the Nuffield department of population health at the University of Oxford, found that They said their findings, published in the journal Frontiers in Nutrition might mean that advice on vegetable intake and heart disease in high-income countries should be reappraised.
However, leading experts commented that the findings confirmed that higher overall vegetable consumption did lower the risk of cardiovascular disease.
UK Biobank data
Boosting health through a diet rich in vegetables has been backed by a large body of evidence, with guidelines consistently recommending them as a valuable source of macronutrients and micronutrients, such as dietary fiber, vitamins, and phytochemicals. However, the research team, which included the Chinese University of Hong Kong and the University of Bristol, set out to probe the independent effects of cooked and raw vegetables on health outcomes. Previous epidemiological studies had demonstrated inconsistent findings, they said.
They based their research on 399,586 people with no history of angina, stroke, and myocardial infarction, who enrolled in the UK Biobank. Of those, 55.4% were women, and 90.9% were of White ethnicity. The average body mass index was 27.3.
Raw and cooked vegetables
From their enrollment questionnaire, the mean intake of vegetables was found to be 2.3 heaped tablespoons per day of raw vegetables, and 2.8 of cooked vegetables. During an average follow-up of 12.1 years, 4.5% of the participants went on to develop CVD.
There was an inverse association between incident CVD and total and raw vegetable intake, but not cooked vegetable intake. Those who ate the most vegetables – both cooked and raw – had a 10% lower incidence of CVD, compared with those who ate the least. However, whereas raw vegetable intake was associated with an 11% reduction in CVD for those who ate the most, compared with the least, no reduction was seen for cooked vegetables.
Consuming two or more heaped tablespoons each day of cooked and raw vegetables was associated with a lower risk of dying from CVD, but little evidence was seen that a higher intake increased protection further. Similarly, there was evidence of an inverse association of CVD mortality with raw vegetable intake.
Researcher Qi Feng, from the Nuffield department of population health, said: “Our large study did not find evidence for a protective effect of vegetable intake on the occurrence of CVD. Instead, our analyses show that the seemingly protective effect of vegetable intake against CVD risk is very likely to be accounted for by bias from residual confounding factors, related to differences in socioeconomic situation and lifestyle.”
Expert opinions
Some clinical specialists took issue with the interpretation of the findings.
Dr. Dipender Gill, BMBCh, PhD, National Institute for Health Research clinical lecturer at St George’s, University of London, told the Science Media Centre that: “Many of the considered confounders that were adjusted for may actually represent mediating mechanisms. For example, vegetable consumption may reduce cardiovascular risk by lowering blood pressure and bodyweight, and improving glycaemic control.
“By adjusting for such traits, the authors may inadvertently be negating some of the mechanisms by which vegetable consumption is exerting beneficial effects.”
Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics at King’s College London, said: “The conclusion that cooked vegetables may not be effective in reducing risk of cardiovascular disease may not be justified, especially as the group consuming the highest levels of vegetables were more likely to be receiving medication for high blood cholesterol and high blood pressure (i.e. this group was at higher risk of CVD), compared with those consuming the lowest intake.” He added: “These findings should not be taken to indicate that eating more vegetables has no benefit to health, especially cardiovascular health.”
Naveed Sattar, FMedSci, FRCPath, FRCPGlas, professor of metabolic medicine at the University of Glasgow, agreed. “In short, this paper should in no way change advice to eat at least five portions of fruit and vegetables a day,” he said. “Many living in the U.K. fall well short of this, sadly, and more needs to be done to encourage better intake of vegetables.
“In fact, I suspect we may have underestimated the importance of a healthy diet on health and disease in general.”
A version of this article first appeared on Medscape.com.
Eating sufficient amounts of vegetables might be good for overall health, but surprising results from a study suggested that their inclusion in the diet might have little or no effect on the risk of developing cardiovascular disease (CVD).
An investigation, led by the Nuffield department of population health at the University of Oxford, found that They said their findings, published in the journal Frontiers in Nutrition might mean that advice on vegetable intake and heart disease in high-income countries should be reappraised.
However, leading experts commented that the findings confirmed that higher overall vegetable consumption did lower the risk of cardiovascular disease.
UK Biobank data
Boosting health through a diet rich in vegetables has been backed by a large body of evidence, with guidelines consistently recommending them as a valuable source of macronutrients and micronutrients, such as dietary fiber, vitamins, and phytochemicals. However, the research team, which included the Chinese University of Hong Kong and the University of Bristol, set out to probe the independent effects of cooked and raw vegetables on health outcomes. Previous epidemiological studies had demonstrated inconsistent findings, they said.
They based their research on 399,586 people with no history of angina, stroke, and myocardial infarction, who enrolled in the UK Biobank. Of those, 55.4% were women, and 90.9% were of White ethnicity. The average body mass index was 27.3.
Raw and cooked vegetables
From their enrollment questionnaire, the mean intake of vegetables was found to be 2.3 heaped tablespoons per day of raw vegetables, and 2.8 of cooked vegetables. During an average follow-up of 12.1 years, 4.5% of the participants went on to develop CVD.
There was an inverse association between incident CVD and total and raw vegetable intake, but not cooked vegetable intake. Those who ate the most vegetables – both cooked and raw – had a 10% lower incidence of CVD, compared with those who ate the least. However, whereas raw vegetable intake was associated with an 11% reduction in CVD for those who ate the most, compared with the least, no reduction was seen for cooked vegetables.
Consuming two or more heaped tablespoons each day of cooked and raw vegetables was associated with a lower risk of dying from CVD, but little evidence was seen that a higher intake increased protection further. Similarly, there was evidence of an inverse association of CVD mortality with raw vegetable intake.
Researcher Qi Feng, from the Nuffield department of population health, said: “Our large study did not find evidence for a protective effect of vegetable intake on the occurrence of CVD. Instead, our analyses show that the seemingly protective effect of vegetable intake against CVD risk is very likely to be accounted for by bias from residual confounding factors, related to differences in socioeconomic situation and lifestyle.”
Expert opinions
Some clinical specialists took issue with the interpretation of the findings.
Dr. Dipender Gill, BMBCh, PhD, National Institute for Health Research clinical lecturer at St George’s, University of London, told the Science Media Centre that: “Many of the considered confounders that were adjusted for may actually represent mediating mechanisms. For example, vegetable consumption may reduce cardiovascular risk by lowering blood pressure and bodyweight, and improving glycaemic control.
“By adjusting for such traits, the authors may inadvertently be negating some of the mechanisms by which vegetable consumption is exerting beneficial effects.”
Tom Sanders, DSc, PhD, professor emeritus of nutrition and dietetics at King’s College London, said: “The conclusion that cooked vegetables may not be effective in reducing risk of cardiovascular disease may not be justified, especially as the group consuming the highest levels of vegetables were more likely to be receiving medication for high blood cholesterol and high blood pressure (i.e. this group was at higher risk of CVD), compared with those consuming the lowest intake.” He added: “These findings should not be taken to indicate that eating more vegetables has no benefit to health, especially cardiovascular health.”
Naveed Sattar, FMedSci, FRCPath, FRCPGlas, professor of metabolic medicine at the University of Glasgow, agreed. “In short, this paper should in no way change advice to eat at least five portions of fruit and vegetables a day,” he said. “Many living in the U.K. fall well short of this, sadly, and more needs to be done to encourage better intake of vegetables.
“In fact, I suspect we may have underestimated the importance of a healthy diet on health and disease in general.”
A version of this article first appeared on Medscape.com.
FROM FRONTIERS IN NUTRITION
Full-press therapy rare in diabetes with ASCVD
A high percentage of people with type 2 diabetes also have atherosclerotic cardiovascular disease (ASCVD), but fewer than 1 in 20 get the triumvirate of evidence-based medications – drugs to lower cholesterol, blood pressure, and glucose levels – that can mitigate the dominant health risks they face, a large multicenter cohort study reported.
The cohort consisted of 324,706 patients with diabetes and ASCVD in the National Patient-Centered Clinical Research Network in 2018.

Senior study author Christopher B. Granger, MD, said in an interview that the findings represent “a shocking underuse of treatments proven to improve outcomes in this high-risk population.” For example, he noted that high-intensity statins are “inexpensive, well tolerated, and highly effective, but the fact that they’re only used in 26.8% of this population is really an indictment and embarrassment for our health-care system.”
The study analyzed prescriptions of high-intensity statins to lower cholesterol, ACE inhibitors or angiotensin-receptor blockers (ARBs) for blood pressure, and SGLT2 inhibitors or GLP-1 receptor agonists for hyperglycemia in a population with both diabetes and ASCVD.
This study amplifies the perceived treatment gap in cardiovascular risk reduction in persons with diabetes,” Paul S. Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “The unfortunate treatment deficiency documented among 325,000 patients in 12 health systems is carefully quantitated and the message is loud, clear, and simple: There is gross underutilization of agents – ACE inhibitors and ARBs, SGLT-2 inhibitors, GLP-1 receptor agonists, and high-intensity statins – with definitively proven ASCVD benefit.”
In the cohort population, 44% were women and 56% were men; 18.2% were black and 12.8% were Latinx. In terms of care patterns for the 205,885 patients who had specialized visit data from the year before the study, the most (74.8%) saw a primary care physician, while only 8.7% visited an endocrinologist and 26.4% saw a cardiologist.
In terms of the prescriptions they received, 58.6% were on a statin, with less than half on a high-intensity statin; 45.5% were on either an ACE inhibitor or ARB, 3.9% received a GLP-1 receptor agonist, and 2.8% were taking a SGLT2 inhibitor.
The investigators pointed out that figure of 58.6% for patients who got a statin was significantly lower than the 74.6% reported in a study of a database of commercially insured patients, but was more in line with findings a 2018 study of patients with diabetes and ASCVD.
Only 4.8% of patients got all three types of therapies, and a high percentage (42.6%) didn’t get any prescription for the three major risk factors.
Overcoming barriers to prescriptions
The study noted that more work needs to be done to overcome the barriers to more widespread use of these therapies in patients with both diabetes and ASCVD.
Specifically with SGLT2 inhibitors and GLP-1 receptor agonists, cost was more likely to be a barrier than with the other drug groups, but that didn’t explain the low levels of high-intensity statin prescriptions, said Dr. Granger of Duke University, Durham, N.C.
The first barrier he mentioned is what he called “clinical inertia.” He said: “I’m a cardiologist who cares for these patients in my clinic each week, and there are so many different things that we need to be trying to achieve with the brief time we have with each patient in our clinic setting that people tend to miss the opportunity.”
The cost barrier, especially with the glucose-lowering therapies, can be overcome with clinic and health care system programs that aid patients in getting discounted drugs, he noted.
Other barriers Dr. Granger pointed out are lack of education – “So many people think that people with previous muscle aches can’t take a high-intensity statin, and we know that’s not true” – and misinformation, which he called “the more nefarious issue.”
He said, “Part of the problem is that misinformation travels much faster than accurate information. There’s so much out there about statins being toxic, which is just not true.”
Fragmentation of the U.S. health care system and the lack of feedback on quality measures, and physicians deferring decisions on glucose-lowering therapy to endocrinologists also pose barriers to more widespread use of evidence-based therapies in patients with diabetes and ASCVD, Dr. Granger said.
“This is a call to action,” Dr. Granger said. “By clearly describing these gaps, we hope that people will see this as an important opportunity to improve care not only at the level of individual providers, but even more importantly at the level of health systems.”
Dr. Jellinger said the “dismal results” of the study serve as a “wake-up call,” adding that “my own perception among my colleagues, along with the data referred to in this article, point to definitely higher usage among commercially insured patients. However, even in more enriched populations the message is not having its full impact. We have remarkable agents for our patients with diabetes that can make a real impact in diabetes-related morbidity and mortality. Our twofold goal should be to aggressively educate a broad slate of health care professionals and, of course, make patient access easy and affordable without ‘prior authorization.’ ”
The study noted the need to bring the prescribing patterns for patients with both diabetes and ASCVD more in line with evidence-based guidelines. To that end, said Dr. Granger, the researchers are moving ahead on a randomized study of a quality improvement project involving about 45 U.S. cardiology clinics using a feedback loop to apply more consistent prescribing patterns for the three therapy groups. “Hopefully a year from now we’ll have a lot more information about this problem,” Dr. Granger added.
Boehringer Ingelheim and Lilly funded the study. Dr. Granger reported financial relationships with Boehringer Ingelheim, Bristol-Myers Squibb, Janssen, Pfizer, Medtronic, Akros Pharma, Apple, AstraZeneca, Daichi-Sankyo, Novartis, AbbVie, Bayer, Boston Scientific, CeleCor, Correvio, Espero, Merck, Novo Nordisk, Rhoshan Pharmaceuticals, and Roche Diagnostics. Dr. Jellinger is on speaker’s bureaus for Esperion and Amgen.
A high percentage of people with type 2 diabetes also have atherosclerotic cardiovascular disease (ASCVD), but fewer than 1 in 20 get the triumvirate of evidence-based medications – drugs to lower cholesterol, blood pressure, and glucose levels – that can mitigate the dominant health risks they face, a large multicenter cohort study reported.
The cohort consisted of 324,706 patients with diabetes and ASCVD in the National Patient-Centered Clinical Research Network in 2018.
Senior study author Christopher B. Granger, MD, said in an interview that the findings represent “a shocking underuse of treatments proven to improve outcomes in this high-risk population.” For example, he noted that high-intensity statins are “inexpensive, well tolerated, and highly effective, but the fact that they’re only used in 26.8% of this population is really an indictment and embarrassment for our health-care system.”
The study analyzed prescriptions of high-intensity statins to lower cholesterol, ACE inhibitors or angiotensin-receptor blockers (ARBs) for blood pressure, and SGLT2 inhibitors or GLP-1 receptor agonists for hyperglycemia in a population with both diabetes and ASCVD.
This study amplifies the perceived treatment gap in cardiovascular risk reduction in persons with diabetes,” Paul S. Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “The unfortunate treatment deficiency documented among 325,000 patients in 12 health systems is carefully quantitated and the message is loud, clear, and simple: There is gross underutilization of agents – ACE inhibitors and ARBs, SGLT-2 inhibitors, GLP-1 receptor agonists, and high-intensity statins – with definitively proven ASCVD benefit.”
In the cohort population, 44% were women and 56% were men; 18.2% were black and 12.8% were Latinx. In terms of care patterns for the 205,885 patients who had specialized visit data from the year before the study, the most (74.8%) saw a primary care physician, while only 8.7% visited an endocrinologist and 26.4% saw a cardiologist.
In terms of the prescriptions they received, 58.6% were on a statin, with less than half on a high-intensity statin; 45.5% were on either an ACE inhibitor or ARB, 3.9% received a GLP-1 receptor agonist, and 2.8% were taking a SGLT2 inhibitor.
The investigators pointed out that figure of 58.6% for patients who got a statin was significantly lower than the 74.6% reported in a study of a database of commercially insured patients, but was more in line with findings a 2018 study of patients with diabetes and ASCVD.
Only 4.8% of patients got all three types of therapies, and a high percentage (42.6%) didn’t get any prescription for the three major risk factors.
Overcoming barriers to prescriptions
The study noted that more work needs to be done to overcome the barriers to more widespread use of these therapies in patients with both diabetes and ASCVD.
Specifically with SGLT2 inhibitors and GLP-1 receptor agonists, cost was more likely to be a barrier than with the other drug groups, but that didn’t explain the low levels of high-intensity statin prescriptions, said Dr. Granger of Duke University, Durham, N.C.
The first barrier he mentioned is what he called “clinical inertia.” He said: “I’m a cardiologist who cares for these patients in my clinic each week, and there are so many different things that we need to be trying to achieve with the brief time we have with each patient in our clinic setting that people tend to miss the opportunity.”
The cost barrier, especially with the glucose-lowering therapies, can be overcome with clinic and health care system programs that aid patients in getting discounted drugs, he noted.
Other barriers Dr. Granger pointed out are lack of education – “So many people think that people with previous muscle aches can’t take a high-intensity statin, and we know that’s not true” – and misinformation, which he called “the more nefarious issue.”
He said, “Part of the problem is that misinformation travels much faster than accurate information. There’s so much out there about statins being toxic, which is just not true.”
Fragmentation of the U.S. health care system and the lack of feedback on quality measures, and physicians deferring decisions on glucose-lowering therapy to endocrinologists also pose barriers to more widespread use of evidence-based therapies in patients with diabetes and ASCVD, Dr. Granger said.
“This is a call to action,” Dr. Granger said. “By clearly describing these gaps, we hope that people will see this as an important opportunity to improve care not only at the level of individual providers, but even more importantly at the level of health systems.”
Dr. Jellinger said the “dismal results” of the study serve as a “wake-up call,” adding that “my own perception among my colleagues, along with the data referred to in this article, point to definitely higher usage among commercially insured patients. However, even in more enriched populations the message is not having its full impact. We have remarkable agents for our patients with diabetes that can make a real impact in diabetes-related morbidity and mortality. Our twofold goal should be to aggressively educate a broad slate of health care professionals and, of course, make patient access easy and affordable without ‘prior authorization.’ ”
The study noted the need to bring the prescribing patterns for patients with both diabetes and ASCVD more in line with evidence-based guidelines. To that end, said Dr. Granger, the researchers are moving ahead on a randomized study of a quality improvement project involving about 45 U.S. cardiology clinics using a feedback loop to apply more consistent prescribing patterns for the three therapy groups. “Hopefully a year from now we’ll have a lot more information about this problem,” Dr. Granger added.
Boehringer Ingelheim and Lilly funded the study. Dr. Granger reported financial relationships with Boehringer Ingelheim, Bristol-Myers Squibb, Janssen, Pfizer, Medtronic, Akros Pharma, Apple, AstraZeneca, Daichi-Sankyo, Novartis, AbbVie, Bayer, Boston Scientific, CeleCor, Correvio, Espero, Merck, Novo Nordisk, Rhoshan Pharmaceuticals, and Roche Diagnostics. Dr. Jellinger is on speaker’s bureaus for Esperion and Amgen.
A high percentage of people with type 2 diabetes also have atherosclerotic cardiovascular disease (ASCVD), but fewer than 1 in 20 get the triumvirate of evidence-based medications – drugs to lower cholesterol, blood pressure, and glucose levels – that can mitigate the dominant health risks they face, a large multicenter cohort study reported.
The cohort consisted of 324,706 patients with diabetes and ASCVD in the National Patient-Centered Clinical Research Network in 2018.
Senior study author Christopher B. Granger, MD, said in an interview that the findings represent “a shocking underuse of treatments proven to improve outcomes in this high-risk population.” For example, he noted that high-intensity statins are “inexpensive, well tolerated, and highly effective, but the fact that they’re only used in 26.8% of this population is really an indictment and embarrassment for our health-care system.”
The study analyzed prescriptions of high-intensity statins to lower cholesterol, ACE inhibitors or angiotensin-receptor blockers (ARBs) for blood pressure, and SGLT2 inhibitors or GLP-1 receptor agonists for hyperglycemia in a population with both diabetes and ASCVD.
This study amplifies the perceived treatment gap in cardiovascular risk reduction in persons with diabetes,” Paul S. Jellinger, MD, of the Center for Diabetes and Endocrine Care in Hollywood, Fla., said in an interview. “The unfortunate treatment deficiency documented among 325,000 patients in 12 health systems is carefully quantitated and the message is loud, clear, and simple: There is gross underutilization of agents – ACE inhibitors and ARBs, SGLT-2 inhibitors, GLP-1 receptor agonists, and high-intensity statins – with definitively proven ASCVD benefit.”
In the cohort population, 44% were women and 56% were men; 18.2% were black and 12.8% were Latinx. In terms of care patterns for the 205,885 patients who had specialized visit data from the year before the study, the most (74.8%) saw a primary care physician, while only 8.7% visited an endocrinologist and 26.4% saw a cardiologist.
In terms of the prescriptions they received, 58.6% were on a statin, with less than half on a high-intensity statin; 45.5% were on either an ACE inhibitor or ARB, 3.9% received a GLP-1 receptor agonist, and 2.8% were taking a SGLT2 inhibitor.
The investigators pointed out that figure of 58.6% for patients who got a statin was significantly lower than the 74.6% reported in a study of a database of commercially insured patients, but was more in line with findings a 2018 study of patients with diabetes and ASCVD.
Only 4.8% of patients got all three types of therapies, and a high percentage (42.6%) didn’t get any prescription for the three major risk factors.
Overcoming barriers to prescriptions
The study noted that more work needs to be done to overcome the barriers to more widespread use of these therapies in patients with both diabetes and ASCVD.
Specifically with SGLT2 inhibitors and GLP-1 receptor agonists, cost was more likely to be a barrier than with the other drug groups, but that didn’t explain the low levels of high-intensity statin prescriptions, said Dr. Granger of Duke University, Durham, N.C.
The first barrier he mentioned is what he called “clinical inertia.” He said: “I’m a cardiologist who cares for these patients in my clinic each week, and there are so many different things that we need to be trying to achieve with the brief time we have with each patient in our clinic setting that people tend to miss the opportunity.”
The cost barrier, especially with the glucose-lowering therapies, can be overcome with clinic and health care system programs that aid patients in getting discounted drugs, he noted.
Other barriers Dr. Granger pointed out are lack of education – “So many people think that people with previous muscle aches can’t take a high-intensity statin, and we know that’s not true” – and misinformation, which he called “the more nefarious issue.”
He said, “Part of the problem is that misinformation travels much faster than accurate information. There’s so much out there about statins being toxic, which is just not true.”
Fragmentation of the U.S. health care system and the lack of feedback on quality measures, and physicians deferring decisions on glucose-lowering therapy to endocrinologists also pose barriers to more widespread use of evidence-based therapies in patients with diabetes and ASCVD, Dr. Granger said.
“This is a call to action,” Dr. Granger said. “By clearly describing these gaps, we hope that people will see this as an important opportunity to improve care not only at the level of individual providers, but even more importantly at the level of health systems.”
Dr. Jellinger said the “dismal results” of the study serve as a “wake-up call,” adding that “my own perception among my colleagues, along with the data referred to in this article, point to definitely higher usage among commercially insured patients. However, even in more enriched populations the message is not having its full impact. We have remarkable agents for our patients with diabetes that can make a real impact in diabetes-related morbidity and mortality. Our twofold goal should be to aggressively educate a broad slate of health care professionals and, of course, make patient access easy and affordable without ‘prior authorization.’ ”
The study noted the need to bring the prescribing patterns for patients with both diabetes and ASCVD more in line with evidence-based guidelines. To that end, said Dr. Granger, the researchers are moving ahead on a randomized study of a quality improvement project involving about 45 U.S. cardiology clinics using a feedback loop to apply more consistent prescribing patterns for the three therapy groups. “Hopefully a year from now we’ll have a lot more information about this problem,” Dr. Granger added.
Boehringer Ingelheim and Lilly funded the study. Dr. Granger reported financial relationships with Boehringer Ingelheim, Bristol-Myers Squibb, Janssen, Pfizer, Medtronic, Akros Pharma, Apple, AstraZeneca, Daichi-Sankyo, Novartis, AbbVie, Bayer, Boston Scientific, CeleCor, Correvio, Espero, Merck, Novo Nordisk, Rhoshan Pharmaceuticals, and Roche Diagnostics. Dr. Jellinger is on speaker’s bureaus for Esperion and Amgen.
FROM JAMA OPEN NETWORK
Biden’s FDA chief nominee narrowly wins Senate confirmation
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.

The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.
The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.
The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.