User login
Tinzaparin is a safe, effective anticoagulant in patients on dialysis
CHICAGO – Tinzaparin was safe and effective as an anticoagulant for hemodialysis patients based on results from the Intermittent Hemodialysis Anticoagulation with Tinzaparin (HEMO-TIN) trial presented at the annual meeting sponsored by the American Society for Nephrology.
In the multicenter randomized controlled trial of 192 adults on hemodialysis, tinzaparin, a low molecular weight heparin with antithrombotic properties, was compared with unfractionated heparin. Tinzaparin has been considered for hemodialysis patients because it is thought to be less dependent on renal clearance than are other low molecular weight heparins, Christine Ribic, MD, MSc, of McMaster University, Hamilton, Ont., said in reporting the results.

After 3 months, the 78 patients remaining in the tinzaparin group crossed over to receive unfractionated heparin for 3 months. The 79 patients remaining in the unfractionated heparin group crossed over to receive tinzaparin for 3 months. Of these 156 patients, 125 completed the 3-month crossover phase.
There were 421 bleeding events in the 12,125 hemodialysis sessions studied. They were evenly distributed in the groups, with 212 (50.4%) in those receiving unfractionated heparin and 209 (49.6%) in those receiving tinzaparin. The prevalence of major bleeds (2.1 vs 1.6%), clinically important nonmajor bleeds (1.2% vs 0.2%), and minor bleeds (47.0% vs 47.7%) was also similar between the unfractionated heparin and tinzaparin groups.
Anti-Xa heparin levels were used as a surrogate measure of low molecular weight heparin activity levels and bleeding risk due to bioaccumulation. In tinzaparin-treated patients, anti-Xa heparin levels never exceeded a value of 0.2 either before or after dialysis. This value was considered the threshold between safety and increased risk for bleeding. This threshold level was routinely exceeded pre- and post-dialysis in patients receiving unfractionated heparin at baseline and both before and after crossover.
Grade 4 clotting was similar for tinzaparin and unfractionated heparin, occurring in 23 of 6,095 (0.4%) unfractionated heparin hemodialysis sessions and 41 of 6030 (0.7%) tinzaparin hemodialysis sessions. Mean dialyzer clotting scores and mean air trap clotting scores were also comparable.
The trial was supported by Leo Pharma, the maker of tinzaparin (innohep), in collaboration with McMaster University. Dr. Ribic is the sponsor of the trial.
CHICAGO – Tinzaparin was safe and effective as an anticoagulant for hemodialysis patients based on results from the Intermittent Hemodialysis Anticoagulation with Tinzaparin (HEMO-TIN) trial presented at the annual meeting sponsored by the American Society for Nephrology.
In the multicenter randomized controlled trial of 192 adults on hemodialysis, tinzaparin, a low molecular weight heparin with antithrombotic properties, was compared with unfractionated heparin. Tinzaparin has been considered for hemodialysis patients because it is thought to be less dependent on renal clearance than are other low molecular weight heparins, Christine Ribic, MD, MSc, of McMaster University, Hamilton, Ont., said in reporting the results.
After 3 months, the 78 patients remaining in the tinzaparin group crossed over to receive unfractionated heparin for 3 months. The 79 patients remaining in the unfractionated heparin group crossed over to receive tinzaparin for 3 months. Of these 156 patients, 125 completed the 3-month crossover phase.
There were 421 bleeding events in the 12,125 hemodialysis sessions studied. They were evenly distributed in the groups, with 212 (50.4%) in those receiving unfractionated heparin and 209 (49.6%) in those receiving tinzaparin. The prevalence of major bleeds (2.1 vs 1.6%), clinically important nonmajor bleeds (1.2% vs 0.2%), and minor bleeds (47.0% vs 47.7%) was also similar between the unfractionated heparin and tinzaparin groups.
Anti-Xa heparin levels were used as a surrogate measure of low molecular weight heparin activity levels and bleeding risk due to bioaccumulation. In tinzaparin-treated patients, anti-Xa heparin levels never exceeded a value of 0.2 either before or after dialysis. This value was considered the threshold between safety and increased risk for bleeding. This threshold level was routinely exceeded pre- and post-dialysis in patients receiving unfractionated heparin at baseline and both before and after crossover.
Grade 4 clotting was similar for tinzaparin and unfractionated heparin, occurring in 23 of 6,095 (0.4%) unfractionated heparin hemodialysis sessions and 41 of 6030 (0.7%) tinzaparin hemodialysis sessions. Mean dialyzer clotting scores and mean air trap clotting scores were also comparable.
The trial was supported by Leo Pharma, the maker of tinzaparin (innohep), in collaboration with McMaster University. Dr. Ribic is the sponsor of the trial.
CHICAGO – Tinzaparin was safe and effective as an anticoagulant for hemodialysis patients based on results from the Intermittent Hemodialysis Anticoagulation with Tinzaparin (HEMO-TIN) trial presented at the annual meeting sponsored by the American Society for Nephrology.
In the multicenter randomized controlled trial of 192 adults on hemodialysis, tinzaparin, a low molecular weight heparin with antithrombotic properties, was compared with unfractionated heparin. Tinzaparin has been considered for hemodialysis patients because it is thought to be less dependent on renal clearance than are other low molecular weight heparins, Christine Ribic, MD, MSc, of McMaster University, Hamilton, Ont., said in reporting the results.
After 3 months, the 78 patients remaining in the tinzaparin group crossed over to receive unfractionated heparin for 3 months. The 79 patients remaining in the unfractionated heparin group crossed over to receive tinzaparin for 3 months. Of these 156 patients, 125 completed the 3-month crossover phase.
There were 421 bleeding events in the 12,125 hemodialysis sessions studied. They were evenly distributed in the groups, with 212 (50.4%) in those receiving unfractionated heparin and 209 (49.6%) in those receiving tinzaparin. The prevalence of major bleeds (2.1 vs 1.6%), clinically important nonmajor bleeds (1.2% vs 0.2%), and minor bleeds (47.0% vs 47.7%) was also similar between the unfractionated heparin and tinzaparin groups.
Anti-Xa heparin levels were used as a surrogate measure of low molecular weight heparin activity levels and bleeding risk due to bioaccumulation. In tinzaparin-treated patients, anti-Xa heparin levels never exceeded a value of 0.2 either before or after dialysis. This value was considered the threshold between safety and increased risk for bleeding. This threshold level was routinely exceeded pre- and post-dialysis in patients receiving unfractionated heparin at baseline and both before and after crossover.
Grade 4 clotting was similar for tinzaparin and unfractionated heparin, occurring in 23 of 6,095 (0.4%) unfractionated heparin hemodialysis sessions and 41 of 6030 (0.7%) tinzaparin hemodialysis sessions. Mean dialyzer clotting scores and mean air trap clotting scores were also comparable.
The trial was supported by Leo Pharma, the maker of tinzaparin (innohep), in collaboration with McMaster University. Dr. Ribic is the sponsor of the trial.
AT KIDNEY WEEK 2016
Key clinical point: Tinzaparin outcomes compare to those with low molecular weight heparin, and tinzaparin may be safer because it is less dependent on renal clearance than are low molecular weight heparins.
Major finding: Mean anti-Xa levels post-hemodialysis did not exceed 0.2 for tinzaparin, indicating no residual anticoagulant effect.
Data source: Randomized, double-dummy, blinded crossover controlled trial involving 192 patients.
Disclosures: Study sponsor was McMaster University, Hamilton, Ont. The study was funded by Leo Pharma. Dr. Ribic reported having no financial disclosures.
Factor VIII microcapsules eyed for eluding neutralizing antibodies
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
Using platelet microcapsules to deliver factor VIII, a process that is expected to increase factor VIII efficacy and avoid the development of neutralizing antibodies, is being examined via in vitro testing, according to an abstract to be featured during a press conference at the annual meeting of the American Society of Hematology.
Caroline E. Hansen of the Georgia Institute of Technology, Atlanta, and her colleagues performed in vitro experiments that show this technology has the potential to increase factor VIII efficacy for hemophilia A patients with inhibitors.
“Current work evaluating localized thrombin generation due to the factor VIII–loaded microcapsules and the effect of platelet contraction force via pharmacologic agents, such as blebbistatin, ROCK, and myosin inhibitors, [is] ongoing,” the researchers wrote in their abstract.
They fabricated polyelectrolyte layers onto calcium carbonate cores and incorporated fibrinogen into the final layer to facilitate binding with platelets. The microcapsule’s inner core contains factor VIII separated from the polyelectrolyte layers by a dextran core.
In the in vitro model, platelets adhered to the microcapsules, which were incorporated into fibrin networks upon platelet activation. During clot contraction, the microcapsules ruptured only in the vicinity of contracting platelets, ensuring drug delivery was targeted at sites of active clot formation.
The researchers perfused recalcified whole blood and platelet poor plasma into in vitro microfluidic models of vascular injury, which consisted of a collagen/tissue factor patch. The efficacy of systemic and microcapsular factor VIII was quantitatively evaluated by comparing fibrin fluorescence intensity on the patch, which was normalized to platelet number.
Fibrin formation was comparable using microcapsules without dextran, fibrinogen, and loaded factor VIII. Compared with standard systemic infusion of 0.05 U/mL factor VIII, however, microcapsules loaded with 0.01 U/mL factor VIII produced four times as much fibrin.
To mimic hemophilia A blood with inhibitors, a factor VIII inhibitory antibody was introduced into healthy blood samples. Again, significantly more fibrin was produced in samples with microcapsules loaded with 0.01 U/mL factor VIII than with systemic factor VIII infusions at clinically relevant high and low dosages of 0.05 and 0.5 U/mL (P less than .05).
This increased efficacy is likely due to the microcapsule shielding effect on factor VIII, preventing exposure to inhibitory antibodies, the researchers reported.
Ms. Hansen had no relevant financial disclosures. One of her colleagues, Shannon L. Meeks, MD, disclosed adviser relationships with Biogen, Genentech, Bayer Healthcare, Grifols, CSL Behring, and Shire. Another, Wilbur A Lam, MD, PhD, disclosed equity ownership in Sanguina.
Abstract 81: Leveraging the Contractile Force of Platelets for Targeted Factor VIII Delivery in Hemophilia With Inhibitors.
[email protected]
On Twitter @maryjodales
ASH 2016 PREVIEW
Age of blood did not affect mortality in transfused patients
In-hospital mortality did not vary for patients who received transfusions of blood that had been stored for 2 weeks and for patients who got blood that had been stored for 4 weeks, based on results from 20,858 hospitalized patients in the randomized, controlled INFORM (Informing Fresh versus Old Red Cell Management) trial conducted at six hospitals in four countries.
While previous trials have concluded that the storage time of blood did not affect patient mortality, those studies largely included high-risk patients and were not statistically powered to detect small mortality differences, Nancy M. Heddle, professor of medicine and director of the McMaster (University) transfusion research program, Hamilton, Ont., and colleagues reported in an article published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1609014). Standard practice is to transfuse with the oldest available blood, which can be stored up to 42 days.
Their study included general hospitalized patients who required a red cell transfusion. From April 2012 through October 2015, patients were randomly assigned in a 1:2 ratio patients to receive blood that had been stored for the shortest duration (mean duration 13 days, 6,936 patients) or the longest duration (mean duration 23.6 days, 13,922 patients).
Only patients with type A or O blood were included in the study’s primary analysis, because of the difficulty of achieving a difference of at least 10 days in the mean duration of blood storage with other blood types.
There were 634 deaths (9.1% mortality) among patients in the short-term blood storage group and 1,213 deaths (8.7% mortality) in the long-term blood storage group. The difference was not statistically significant. Similar results were seen when the analysis was expanded to include all 24,736 patients with any blood type; the mortality rates were 9.1% and 8.8%, respectively.
An additional analysis found similar results in three prespecified high-risk subgroups – patients undergoing cardiovascular surgery, those admitted to intensive care, and those with cancer.
INFORM, Current Controlled Trials number ISRCTN08118744, was funded by the Canadian Institutes of Health Research, Canadian Blood Services, and Health Canada. Ms. Heddle had no relevant financial disclosures.
[email protected]
On Twitter @maryjodales
The results of the INFORM trial should end the debate regarding whether short-term or long-term storage of blood is advantageous. However, questions remain about whether red cells transfused during the last allowed week of storage (35-42 days) pose more risk. Observational studies continue to raise concerns about the use of the oldest blood.
The INFORM trial, with its large numbers of patients, should permit researchers to analyze enough data to address this remaining issue. The transfusion medicine community needs to know whether the storage period should be reduced to less than 35 and whether new preservative solutions should be sought.
Aaron A.R. Tobian, MD, PhD, and Paul M. Ness, MD, are with the division of transfusion medicine, department of pathology, Johns Hopkins University, Baltimore. They had no relevant financial conflicts of interest and made their remarks in an editorial (10.1056/NEJMe1612444) that accompanied the published study.
The results of the INFORM trial should end the debate regarding whether short-term or long-term storage of blood is advantageous. However, questions remain about whether red cells transfused during the last allowed week of storage (35-42 days) pose more risk. Observational studies continue to raise concerns about the use of the oldest blood.
The INFORM trial, with its large numbers of patients, should permit researchers to analyze enough data to address this remaining issue. The transfusion medicine community needs to know whether the storage period should be reduced to less than 35 and whether new preservative solutions should be sought.
Aaron A.R. Tobian, MD, PhD, and Paul M. Ness, MD, are with the division of transfusion medicine, department of pathology, Johns Hopkins University, Baltimore. They had no relevant financial conflicts of interest and made their remarks in an editorial (10.1056/NEJMe1612444) that accompanied the published study.
The results of the INFORM trial should end the debate regarding whether short-term or long-term storage of blood is advantageous. However, questions remain about whether red cells transfused during the last allowed week of storage (35-42 days) pose more risk. Observational studies continue to raise concerns about the use of the oldest blood.
The INFORM trial, with its large numbers of patients, should permit researchers to analyze enough data to address this remaining issue. The transfusion medicine community needs to know whether the storage period should be reduced to less than 35 and whether new preservative solutions should be sought.
Aaron A.R. Tobian, MD, PhD, and Paul M. Ness, MD, are with the division of transfusion medicine, department of pathology, Johns Hopkins University, Baltimore. They had no relevant financial conflicts of interest and made their remarks in an editorial (10.1056/NEJMe1612444) that accompanied the published study.
In-hospital mortality did not vary for patients who received transfusions of blood that had been stored for 2 weeks and for patients who got blood that had been stored for 4 weeks, based on results from 20,858 hospitalized patients in the randomized, controlled INFORM (Informing Fresh versus Old Red Cell Management) trial conducted at six hospitals in four countries.
While previous trials have concluded that the storage time of blood did not affect patient mortality, those studies largely included high-risk patients and were not statistically powered to detect small mortality differences, Nancy M. Heddle, professor of medicine and director of the McMaster (University) transfusion research program, Hamilton, Ont., and colleagues reported in an article published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1609014). Standard practice is to transfuse with the oldest available blood, which can be stored up to 42 days.
Their study included general hospitalized patients who required a red cell transfusion. From April 2012 through October 2015, patients were randomly assigned in a 1:2 ratio patients to receive blood that had been stored for the shortest duration (mean duration 13 days, 6,936 patients) or the longest duration (mean duration 23.6 days, 13,922 patients).
Only patients with type A or O blood were included in the study’s primary analysis, because of the difficulty of achieving a difference of at least 10 days in the mean duration of blood storage with other blood types.
There were 634 deaths (9.1% mortality) among patients in the short-term blood storage group and 1,213 deaths (8.7% mortality) in the long-term blood storage group. The difference was not statistically significant. Similar results were seen when the analysis was expanded to include all 24,736 patients with any blood type; the mortality rates were 9.1% and 8.8%, respectively.
An additional analysis found similar results in three prespecified high-risk subgroups – patients undergoing cardiovascular surgery, those admitted to intensive care, and those with cancer.
INFORM, Current Controlled Trials number ISRCTN08118744, was funded by the Canadian Institutes of Health Research, Canadian Blood Services, and Health Canada. Ms. Heddle had no relevant financial disclosures.
[email protected]
On Twitter @maryjodales
In-hospital mortality did not vary for patients who received transfusions of blood that had been stored for 2 weeks and for patients who got blood that had been stored for 4 weeks, based on results from 20,858 hospitalized patients in the randomized, controlled INFORM (Informing Fresh versus Old Red Cell Management) trial conducted at six hospitals in four countries.
While previous trials have concluded that the storage time of blood did not affect patient mortality, those studies largely included high-risk patients and were not statistically powered to detect small mortality differences, Nancy M. Heddle, professor of medicine and director of the McMaster (University) transfusion research program, Hamilton, Ont., and colleagues reported in an article published online in the New England Journal of Medicine (doi: 10.1056/NEJMoa1609014). Standard practice is to transfuse with the oldest available blood, which can be stored up to 42 days.
Their study included general hospitalized patients who required a red cell transfusion. From April 2012 through October 2015, patients were randomly assigned in a 1:2 ratio patients to receive blood that had been stored for the shortest duration (mean duration 13 days, 6,936 patients) or the longest duration (mean duration 23.6 days, 13,922 patients).
Only patients with type A or O blood were included in the study’s primary analysis, because of the difficulty of achieving a difference of at least 10 days in the mean duration of blood storage with other blood types.
There were 634 deaths (9.1% mortality) among patients in the short-term blood storage group and 1,213 deaths (8.7% mortality) in the long-term blood storage group. The difference was not statistically significant. Similar results were seen when the analysis was expanded to include all 24,736 patients with any blood type; the mortality rates were 9.1% and 8.8%, respectively.
An additional analysis found similar results in three prespecified high-risk subgroups – patients undergoing cardiovascular surgery, those admitted to intensive care, and those with cancer.
INFORM, Current Controlled Trials number ISRCTN08118744, was funded by the Canadian Institutes of Health Research, Canadian Blood Services, and Health Canada. Ms. Heddle had no relevant financial disclosures.
[email protected]
On Twitter @maryjodales
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: There were 634 deaths (9.1% mortality) among patients in the short-term blood storage group and 1,213 deaths (8.7% mortality) in the long-term blood storage group.
Data source: The randomized, controlled INFORM (Informing Fresh versus Old Red Cell Management) trial.
Disclosures: INFORM, Current Controlled Trials number ISRCTN08118744, was funded by the Canadian Institutes of Health Research, Canadian Blood Services, and Health Canada. Ms. Heddle had no relevant financial disclosures.
Calcium channel blocker reduces cardiac iron loading in thalassemia major
The calcium channel blocker amlodipine, added to iron chelation therapy, significantly reduced excess myocardial iron concentration in patients with thalassemia major, compared with chelation alone, according to results from a randomized trial.
The findings (Blood. 2016;128[12]:1555-61) suggest that amlodipine, a cheap, widely available drug with a well-established safety profile, may serve as an adjunct to standard treatment for people with thalassemia major and cardiac siderosis. Cardiovascular disease caused by excess myocardial iron remains a major cause of morbidity and mortality in thalassemia major.
Juliano L. Fernandes, MD, PhD, of the Jose Michel Kalaf Research Institute in Campinas, Brazil, led the study, which randomized 62 patients already receiving chelation treatment for thalassemia major to 1 year of chelation plus placebo (n = 31) or chelation plus 5 mg daily amlodipine (n = 31).
Patients in each arm were subdivided into two subgroups: those whose baseline myocardial iron concentration was within normal thresholds, and those with excess myocardial iron concentration as measured by magnetic resonance imaging (above 0.59 mg/g dry weight or with a cardiac T2* below 35 milliseconds).
In the amlodipine arm, patients with excess cardiac iron at baseline (n = 15) saw significant reductions in myocardial iron concentrations at 1 year, compared with those randomized to placebo (n = 15). The former had a median reduction of –0.26 mg/g (95% confidence interval, –1.02 to –0.01) while the placebo group saw an increase of 0.01 mg/g (95% CI, 20.13 to 20.23; P = .02).
The investigators acknowledged that some of the findings were limited by the study’s short observation period.
Patients without excess myocardial iron concentration at baseline did not see significant changes associated with amlodipine. While Dr. Fernandes and his colleagues could not conclude that the drug prevented excess cardiac iron from accumulating, “our data cannot rule out the possibility that extended use of amlodipine might prevent myocardial iron accumulation with a longer observation period.”
Secondary endpoints of the study included measurements of iron storage in the liver and of serum ferritin, neither of which appeared to be affected by amlodipine treatment, which the investigators said was consistent with the drug’s known mechanism of action. No serious adverse effects were reported related to amlodipine treatment.
Dr. Fernandes and his colleagues also did not find improvements in left ventricular ejection fraction associated with amlodipine use at 12 months. This may be due, they wrote in their analysis, to a “relatively low prevalence of reduced ejection fraction or severe myocardial siderosis upon trial enrollment, limiting the power of the study to assess these outcomes.”
The government of Brazil and the Sultan Bin Khalifa Translational Research Scholarship sponsored the study. Dr. Fernandes reported receiving fees from Novartis and Sanofi. The remaining 12 authors disclosed no conflicts of interest.
Why is this small clinical trial of such pivotal importance in this day and age of massive multicenter prospective randomized studies? The answer is that it tells us that iron entry into the heart through L-type calcium channels, a mechanism that has been clearly demonstrated in vitro, seems to be actually occurring in humans. As an added bonus, we have a possible new adjunctive treatment of iron cardiomyopathy. More clinical studies are needed, and certainly biochemical studies need to continue because all calcium channel blockers do not have the same effect in vitro, but at least the “channels” for more progress on both clinical and biochemical fronts are now open.
Thomas D. Coates, MD, is with Children’s Hospital of Los Angeles and University of Southern California, Los Angeles. He made his remarks in an editorial that accompanied the published study.
Why is this small clinical trial of such pivotal importance in this day and age of massive multicenter prospective randomized studies? The answer is that it tells us that iron entry into the heart through L-type calcium channels, a mechanism that has been clearly demonstrated in vitro, seems to be actually occurring in humans. As an added bonus, we have a possible new adjunctive treatment of iron cardiomyopathy. More clinical studies are needed, and certainly biochemical studies need to continue because all calcium channel blockers do not have the same effect in vitro, but at least the “channels” for more progress on both clinical and biochemical fronts are now open.
Thomas D. Coates, MD, is with Children’s Hospital of Los Angeles and University of Southern California, Los Angeles. He made his remarks in an editorial that accompanied the published study.
Why is this small clinical trial of such pivotal importance in this day and age of massive multicenter prospective randomized studies? The answer is that it tells us that iron entry into the heart through L-type calcium channels, a mechanism that has been clearly demonstrated in vitro, seems to be actually occurring in humans. As an added bonus, we have a possible new adjunctive treatment of iron cardiomyopathy. More clinical studies are needed, and certainly biochemical studies need to continue because all calcium channel blockers do not have the same effect in vitro, but at least the “channels” for more progress on both clinical and biochemical fronts are now open.
Thomas D. Coates, MD, is with Children’s Hospital of Los Angeles and University of Southern California, Los Angeles. He made his remarks in an editorial that accompanied the published study.
The calcium channel blocker amlodipine, added to iron chelation therapy, significantly reduced excess myocardial iron concentration in patients with thalassemia major, compared with chelation alone, according to results from a randomized trial.
The findings (Blood. 2016;128[12]:1555-61) suggest that amlodipine, a cheap, widely available drug with a well-established safety profile, may serve as an adjunct to standard treatment for people with thalassemia major and cardiac siderosis. Cardiovascular disease caused by excess myocardial iron remains a major cause of morbidity and mortality in thalassemia major.
Juliano L. Fernandes, MD, PhD, of the Jose Michel Kalaf Research Institute in Campinas, Brazil, led the study, which randomized 62 patients already receiving chelation treatment for thalassemia major to 1 year of chelation plus placebo (n = 31) or chelation plus 5 mg daily amlodipine (n = 31).
Patients in each arm were subdivided into two subgroups: those whose baseline myocardial iron concentration was within normal thresholds, and those with excess myocardial iron concentration as measured by magnetic resonance imaging (above 0.59 mg/g dry weight or with a cardiac T2* below 35 milliseconds).
In the amlodipine arm, patients with excess cardiac iron at baseline (n = 15) saw significant reductions in myocardial iron concentrations at 1 year, compared with those randomized to placebo (n = 15). The former had a median reduction of –0.26 mg/g (95% confidence interval, –1.02 to –0.01) while the placebo group saw an increase of 0.01 mg/g (95% CI, 20.13 to 20.23; P = .02).
The investigators acknowledged that some of the findings were limited by the study’s short observation period.
Patients without excess myocardial iron concentration at baseline did not see significant changes associated with amlodipine. While Dr. Fernandes and his colleagues could not conclude that the drug prevented excess cardiac iron from accumulating, “our data cannot rule out the possibility that extended use of amlodipine might prevent myocardial iron accumulation with a longer observation period.”
Secondary endpoints of the study included measurements of iron storage in the liver and of serum ferritin, neither of which appeared to be affected by amlodipine treatment, which the investigators said was consistent with the drug’s known mechanism of action. No serious adverse effects were reported related to amlodipine treatment.
Dr. Fernandes and his colleagues also did not find improvements in left ventricular ejection fraction associated with amlodipine use at 12 months. This may be due, they wrote in their analysis, to a “relatively low prevalence of reduced ejection fraction or severe myocardial siderosis upon trial enrollment, limiting the power of the study to assess these outcomes.”
The government of Brazil and the Sultan Bin Khalifa Translational Research Scholarship sponsored the study. Dr. Fernandes reported receiving fees from Novartis and Sanofi. The remaining 12 authors disclosed no conflicts of interest.
The calcium channel blocker amlodipine, added to iron chelation therapy, significantly reduced excess myocardial iron concentration in patients with thalassemia major, compared with chelation alone, according to results from a randomized trial.
The findings (Blood. 2016;128[12]:1555-61) suggest that amlodipine, a cheap, widely available drug with a well-established safety profile, may serve as an adjunct to standard treatment for people with thalassemia major and cardiac siderosis. Cardiovascular disease caused by excess myocardial iron remains a major cause of morbidity and mortality in thalassemia major.
Juliano L. Fernandes, MD, PhD, of the Jose Michel Kalaf Research Institute in Campinas, Brazil, led the study, which randomized 62 patients already receiving chelation treatment for thalassemia major to 1 year of chelation plus placebo (n = 31) or chelation plus 5 mg daily amlodipine (n = 31).
Patients in each arm were subdivided into two subgroups: those whose baseline myocardial iron concentration was within normal thresholds, and those with excess myocardial iron concentration as measured by magnetic resonance imaging (above 0.59 mg/g dry weight or with a cardiac T2* below 35 milliseconds).
In the amlodipine arm, patients with excess cardiac iron at baseline (n = 15) saw significant reductions in myocardial iron concentrations at 1 year, compared with those randomized to placebo (n = 15). The former had a median reduction of –0.26 mg/g (95% confidence interval, –1.02 to –0.01) while the placebo group saw an increase of 0.01 mg/g (95% CI, 20.13 to 20.23; P = .02).
The investigators acknowledged that some of the findings were limited by the study’s short observation period.
Patients without excess myocardial iron concentration at baseline did not see significant changes associated with amlodipine. While Dr. Fernandes and his colleagues could not conclude that the drug prevented excess cardiac iron from accumulating, “our data cannot rule out the possibility that extended use of amlodipine might prevent myocardial iron accumulation with a longer observation period.”
Secondary endpoints of the study included measurements of iron storage in the liver and of serum ferritin, neither of which appeared to be affected by amlodipine treatment, which the investigators said was consistent with the drug’s known mechanism of action. No serious adverse effects were reported related to amlodipine treatment.
Dr. Fernandes and his colleagues also did not find improvements in left ventricular ejection fraction associated with amlodipine use at 12 months. This may be due, they wrote in their analysis, to a “relatively low prevalence of reduced ejection fraction or severe myocardial siderosis upon trial enrollment, limiting the power of the study to assess these outcomes.”
The government of Brazil and the Sultan Bin Khalifa Translational Research Scholarship sponsored the study. Dr. Fernandes reported receiving fees from Novartis and Sanofi. The remaining 12 authors disclosed no conflicts of interest.
FROM BLOOD
Key clinical point: Amlodipine added to standard chelation therapy significantly reduced cardiac iron in thalassemia major patients with cardiac siderosis.
Major finding: At 12 months, cardiac iron was a median 0.26 mg/g lower in subjects with myocardial iron overload treated with 5 mg daily amlodipine plus chelation, while patients treated with chelation alone saw a 0.01 mg/g increase (P = .02).
Data source: A randomized, double-blind, placebo-controlled trial enrolling from 62 patients with TM from six centers in Brazil, about half with cardiac siderosis at baseline.
Disclosures: The Brazil government and the Sultan Bin Khalifa Translational Research Scholarship sponsored the investigation. Its lead author reported receiving fees from Novartis and Sanofi. Other study investigators and the author of a linked editorial declared no conflicts of interest.
Extended half-life clotting factors are safe, effective, and pricey
ORLANDO – Early experience with extended half-life clotting factor concentrates suggests these products are generally safe and effective, at least in the short term, according to hemophilia experts.
“In adolescent and adult patients, the extended half-life clotting factor concentrates demonstrate efficacy and safety in a variety of clinical settings, including prophylaxis, treatment of bleeds, and perisurgical hemostasis,” said Johnny Mahlangu, MD, director of the Haemophilia Comprehensive Care Centre in Johannesburg, South Africa.

Barriers to prophylaxis include “the need to inject the clotting factor concentrate at least two or three times a week, poor venous access, and, of course, poor adherence and compliance from our patients. Essentially, the extended half-life products were developed to mitigate these limitations,” he said.
Dr. Mahlangu and Guy Young, MD, a pediatric hematologist at Children’s Hospital Los Angeles, discussed results from published clinical trials of EHL products in children and adults.
The X factor
Extended half-life products currently available or in development include those created through fusion technology, including factor VIII products for treatment of hemophilia A, factor IX for treating hemophilia B, and factor VII products for treating factor VII deficiency (Alexander’s Disease).
More recent products created through pegylation technology include recombinant FVIII products.
Factor IX EHL CFCs
The three recombinant factor IX (rFIX) products that have completed phase III clinical trials are: nonacog beta pegol (N9-GP), rFIXFc (Alprolix), and rFIX-FP (Idelvion). The latter two are approved by the U.S. Food and Drug Administration; the former is waiting European and U.S. approval.
In clinical trials in adolescents and adults, these agents were associated with low median annualized bleeding rates, as follows:
• rFIXFc: 3.0 for a 50 IU/kg dose given every 7 days, and 1.4 for a 100 IU/kg dose given every 10 days
• rFIX-FP: 0.0 for a 40 IU/kg dose given every 7 days, and 1.08 for a 75 IU/kg dose given every 14 days
• Nonacog beta pegol: 2.93 for a 10 IU/kg dose and 1.0 for a 40 IU/kg dose, each given every 7 days.
All of these agents effectively treated bleeding episodes after one or two doses, Dr. Mahlangu said. The respective overall hemostatic efficacy rates were 97.2%, 96.7%, and 97.1%.
Safety analyses from published studies showed that no patients exposed to any of these agents developed inhibiting antibodies, although three patients treated with rFIXFc and nonacog beta pegol each developed noninhibitory antibodies.
There were no deaths from thromboembolic episodes and no drug-related serious adverse events.
Data are more limited for children treated with rFIX products, Dr. Young noted. In studies thus far, no children developed inhibitors, although this population had been heavily pretreated, he noted. Median annualized bleeding rates ranged from 1 to 3 and did not differ significantly between the products.
Factor VIII EHL CFCs
Four factor VIII EHL products are available or in development: rFVIIIFc (Eloctate); antihemophilic factor, pegylated (Adynovate); turoctocog alfa pegol (N8-GP); and BAY 94-9027. The former two agents are approved in the United States.
In adults and adolescents, these products have half-lives comparatively shorter than those seen with Factor IX products, the researchers noted.
Annualized bleeding rates for patients on prophylaxis with these agents were less than 4 bleeds per year, ranging from 1.3 to 3.6. In all, 96% of bleeds that did occur could be resolved with one or two injections of the extended half-life rFVIII products.
All patients had at least 50 exposures to these products, and none have developed inhibitors to date.
Only one study has been published to date of factor VIII products in children, comparing a standard half-life product with rFVIIIFc, Dr. Young said.
In this study, the patients were treated with a twice weekly, split-dose regimen. No patients developed inhibitors, and the mean annualized bleeding rate was a low 1.96.
Dr. Mahlangu disclosed research grants from Bayer, Biogen, CSL Behring, Novo Nordisk, and Roche, and speakers bureau participation for Amgen, Biotest, Biogen, CSL Behring, Novo Nordisk, and Sobi. Dr. Young disclosed honoraria and consulting fees from Baxalta, Bayer, Biogen, CSL Behring, and Novo Nordisk. Ellis J. Neufeld, MD, PhD, the invited discussant of the presentation, disclosed institutional grants from Baxalta, Novo Nordisk, and Octapharma, consulting/advising for those companies and for CSL Behring, Genentech, Hema Biologics, and Pfizer.
Improvements in half-life are incremental with the factor VIII products, but ground breaking with the factor IX products, allowing treatment intervals to be substantially prolonged. Pivotal trials of the several longer-acting products have been positive and generally convincing.
However, the pricing of these extended half-life products seems to reflect the so called “value proposition,” a concept from Big Pharma that puts a premium on convenience or novelty when determining the marketing price for a new drug. But the price may not always be commensurate with the clinical benefits patients derive from these newer agents.

How trials translate into treatment recommendations is complicated, and as Dr. Young and Dr. Mahlangu both made very clear, you need to consider that factor VIII and factor IX prolongation is entirely separate, even when the same technology is used, because the consequences are very different.
Ellis J. Neufeld, MD, PhD, is the associate chief of hematology/oncology at Boston Children’s Hospital, and was the invited discussant of the presentation.
Improvements in half-life are incremental with the factor VIII products, but ground breaking with the factor IX products, allowing treatment intervals to be substantially prolonged. Pivotal trials of the several longer-acting products have been positive and generally convincing.
However, the pricing of these extended half-life products seems to reflect the so called “value proposition,” a concept from Big Pharma that puts a premium on convenience or novelty when determining the marketing price for a new drug. But the price may not always be commensurate with the clinical benefits patients derive from these newer agents.
How trials translate into treatment recommendations is complicated, and as Dr. Young and Dr. Mahlangu both made very clear, you need to consider that factor VIII and factor IX prolongation is entirely separate, even when the same technology is used, because the consequences are very different.
Ellis J. Neufeld, MD, PhD, is the associate chief of hematology/oncology at Boston Children’s Hospital, and was the invited discussant of the presentation.
Improvements in half-life are incremental with the factor VIII products, but ground breaking with the factor IX products, allowing treatment intervals to be substantially prolonged. Pivotal trials of the several longer-acting products have been positive and generally convincing.
However, the pricing of these extended half-life products seems to reflect the so called “value proposition,” a concept from Big Pharma that puts a premium on convenience or novelty when determining the marketing price for a new drug. But the price may not always be commensurate with the clinical benefits patients derive from these newer agents.
How trials translate into treatment recommendations is complicated, and as Dr. Young and Dr. Mahlangu both made very clear, you need to consider that factor VIII and factor IX prolongation is entirely separate, even when the same technology is used, because the consequences are very different.
Ellis J. Neufeld, MD, PhD, is the associate chief of hematology/oncology at Boston Children’s Hospital, and was the invited discussant of the presentation.
ORLANDO – Early experience with extended half-life clotting factor concentrates suggests these products are generally safe and effective, at least in the short term, according to hemophilia experts.
“In adolescent and adult patients, the extended half-life clotting factor concentrates demonstrate efficacy and safety in a variety of clinical settings, including prophylaxis, treatment of bleeds, and perisurgical hemostasis,” said Johnny Mahlangu, MD, director of the Haemophilia Comprehensive Care Centre in Johannesburg, South Africa.
Barriers to prophylaxis include “the need to inject the clotting factor concentrate at least two or three times a week, poor venous access, and, of course, poor adherence and compliance from our patients. Essentially, the extended half-life products were developed to mitigate these limitations,” he said.
Dr. Mahlangu and Guy Young, MD, a pediatric hematologist at Children’s Hospital Los Angeles, discussed results from published clinical trials of EHL products in children and adults.
The X factor
Extended half-life products currently available or in development include those created through fusion technology, including factor VIII products for treatment of hemophilia A, factor IX for treating hemophilia B, and factor VII products for treating factor VII deficiency (Alexander’s Disease).
More recent products created through pegylation technology include recombinant FVIII products.
Factor IX EHL CFCs
The three recombinant factor IX (rFIX) products that have completed phase III clinical trials are: nonacog beta pegol (N9-GP), rFIXFc (Alprolix), and rFIX-FP (Idelvion). The latter two are approved by the U.S. Food and Drug Administration; the former is waiting European and U.S. approval.
In clinical trials in adolescents and adults, these agents were associated with low median annualized bleeding rates, as follows:
• rFIXFc: 3.0 for a 50 IU/kg dose given every 7 days, and 1.4 for a 100 IU/kg dose given every 10 days
• rFIX-FP: 0.0 for a 40 IU/kg dose given every 7 days, and 1.08 for a 75 IU/kg dose given every 14 days
• Nonacog beta pegol: 2.93 for a 10 IU/kg dose and 1.0 for a 40 IU/kg dose, each given every 7 days.
All of these agents effectively treated bleeding episodes after one or two doses, Dr. Mahlangu said. The respective overall hemostatic efficacy rates were 97.2%, 96.7%, and 97.1%.
Safety analyses from published studies showed that no patients exposed to any of these agents developed inhibiting antibodies, although three patients treated with rFIXFc and nonacog beta pegol each developed noninhibitory antibodies.
There were no deaths from thromboembolic episodes and no drug-related serious adverse events.
Data are more limited for children treated with rFIX products, Dr. Young noted. In studies thus far, no children developed inhibitors, although this population had been heavily pretreated, he noted. Median annualized bleeding rates ranged from 1 to 3 and did not differ significantly between the products.
Factor VIII EHL CFCs
Four factor VIII EHL products are available or in development: rFVIIIFc (Eloctate); antihemophilic factor, pegylated (Adynovate); turoctocog alfa pegol (N8-GP); and BAY 94-9027. The former two agents are approved in the United States.
In adults and adolescents, these products have half-lives comparatively shorter than those seen with Factor IX products, the researchers noted.
Annualized bleeding rates for patients on prophylaxis with these agents were less than 4 bleeds per year, ranging from 1.3 to 3.6. In all, 96% of bleeds that did occur could be resolved with one or two injections of the extended half-life rFVIII products.
All patients had at least 50 exposures to these products, and none have developed inhibitors to date.
Only one study has been published to date of factor VIII products in children, comparing a standard half-life product with rFVIIIFc, Dr. Young said.
In this study, the patients were treated with a twice weekly, split-dose regimen. No patients developed inhibitors, and the mean annualized bleeding rate was a low 1.96.
Dr. Mahlangu disclosed research grants from Bayer, Biogen, CSL Behring, Novo Nordisk, and Roche, and speakers bureau participation for Amgen, Biotest, Biogen, CSL Behring, Novo Nordisk, and Sobi. Dr. Young disclosed honoraria and consulting fees from Baxalta, Bayer, Biogen, CSL Behring, and Novo Nordisk. Ellis J. Neufeld, MD, PhD, the invited discussant of the presentation, disclosed institutional grants from Baxalta, Novo Nordisk, and Octapharma, consulting/advising for those companies and for CSL Behring, Genentech, Hema Biologics, and Pfizer.
ORLANDO – Early experience with extended half-life clotting factor concentrates suggests these products are generally safe and effective, at least in the short term, according to hemophilia experts.
“In adolescent and adult patients, the extended half-life clotting factor concentrates demonstrate efficacy and safety in a variety of clinical settings, including prophylaxis, treatment of bleeds, and perisurgical hemostasis,” said Johnny Mahlangu, MD, director of the Haemophilia Comprehensive Care Centre in Johannesburg, South Africa.
Barriers to prophylaxis include “the need to inject the clotting factor concentrate at least two or three times a week, poor venous access, and, of course, poor adherence and compliance from our patients. Essentially, the extended half-life products were developed to mitigate these limitations,” he said.
Dr. Mahlangu and Guy Young, MD, a pediatric hematologist at Children’s Hospital Los Angeles, discussed results from published clinical trials of EHL products in children and adults.
The X factor
Extended half-life products currently available or in development include those created through fusion technology, including factor VIII products for treatment of hemophilia A, factor IX for treating hemophilia B, and factor VII products for treating factor VII deficiency (Alexander’s Disease).
More recent products created through pegylation technology include recombinant FVIII products.
Factor IX EHL CFCs
The three recombinant factor IX (rFIX) products that have completed phase III clinical trials are: nonacog beta pegol (N9-GP), rFIXFc (Alprolix), and rFIX-FP (Idelvion). The latter two are approved by the U.S. Food and Drug Administration; the former is waiting European and U.S. approval.
In clinical trials in adolescents and adults, these agents were associated with low median annualized bleeding rates, as follows:
• rFIXFc: 3.0 for a 50 IU/kg dose given every 7 days, and 1.4 for a 100 IU/kg dose given every 10 days
• rFIX-FP: 0.0 for a 40 IU/kg dose given every 7 days, and 1.08 for a 75 IU/kg dose given every 14 days
• Nonacog beta pegol: 2.93 for a 10 IU/kg dose and 1.0 for a 40 IU/kg dose, each given every 7 days.
All of these agents effectively treated bleeding episodes after one or two doses, Dr. Mahlangu said. The respective overall hemostatic efficacy rates were 97.2%, 96.7%, and 97.1%.
Safety analyses from published studies showed that no patients exposed to any of these agents developed inhibiting antibodies, although three patients treated with rFIXFc and nonacog beta pegol each developed noninhibitory antibodies.
There were no deaths from thromboembolic episodes and no drug-related serious adverse events.
Data are more limited for children treated with rFIX products, Dr. Young noted. In studies thus far, no children developed inhibitors, although this population had been heavily pretreated, he noted. Median annualized bleeding rates ranged from 1 to 3 and did not differ significantly between the products.
Factor VIII EHL CFCs
Four factor VIII EHL products are available or in development: rFVIIIFc (Eloctate); antihemophilic factor, pegylated (Adynovate); turoctocog alfa pegol (N8-GP); and BAY 94-9027. The former two agents are approved in the United States.
In adults and adolescents, these products have half-lives comparatively shorter than those seen with Factor IX products, the researchers noted.
Annualized bleeding rates for patients on prophylaxis with these agents were less than 4 bleeds per year, ranging from 1.3 to 3.6. In all, 96% of bleeds that did occur could be resolved with one or two injections of the extended half-life rFVIII products.
All patients had at least 50 exposures to these products, and none have developed inhibitors to date.
Only one study has been published to date of factor VIII products in children, comparing a standard half-life product with rFVIIIFc, Dr. Young said.
In this study, the patients were treated with a twice weekly, split-dose regimen. No patients developed inhibitors, and the mean annualized bleeding rate was a low 1.96.
Dr. Mahlangu disclosed research grants from Bayer, Biogen, CSL Behring, Novo Nordisk, and Roche, and speakers bureau participation for Amgen, Biotest, Biogen, CSL Behring, Novo Nordisk, and Sobi. Dr. Young disclosed honoraria and consulting fees from Baxalta, Bayer, Biogen, CSL Behring, and Novo Nordisk. Ellis J. Neufeld, MD, PhD, the invited discussant of the presentation, disclosed institutional grants from Baxalta, Novo Nordisk, and Octapharma, consulting/advising for those companies and for CSL Behring, Genentech, Hema Biologics, and Pfizer.
AT WFH 2016 WORLD CONGRESS

Rivaroxaban linked to more bleeding compared with dabigatran in elderly patients with nonvalvular AF
Rivaroxaban is associated with significantly more intra- and extracranial bleeding than is dabigatran in older patients who have nonvalvular atrial fibrillation, according to a report published online Oct. 3 in JAMA Internal Medicine.
This is the principal finding of a retrospective cohort study – the only study to directly compare the two oral non–vitamin-K-antagonists – that involved more than 118,000 patients who initiated anticoagulation treatment during a 2.5-year period. The Centers for Medicare & Medicaid Services and the Food and Drug Administration jointly conducted the study.
During the study period, rivaroxaban was used 2-3 times more often than was dabigatran in AF patients in the United States, “perhaps partly because of prescriber misperceptions about bleeding risks with dabigatran, arising from FDA receipt of a large number of postmarketing case reports following its approval. Ironically, we [now find] substantially higher bleeding risks with use of rivaroxaban than dabigatran,” said David J. Graham, MD, of the Office of Surveillance and Epidemiology, Center for Drug Evaluation and Research, FDA, Silver Spring, Md., and his associates.
The researchers assessed Medicare beneficiaries who initiated standard oral doses of rivaroxaban (66,651 patients) or dabigatran (52,240 patients) and were followed for a mean of 110 days.
The primary outcome measure – a composite of thromboembolic stroke, intracranial hemorrhage, major extracranial bleeding events including GI bleeding, and mortality – occurred in significantly more patients taking rivaroxaban than in those taking dabigatran. When the individual components of this composite outcome were considered, rivaroxaban was associated with significant increases in intracranial hemorrhage (HR, 1.65), major extracranial bleeding (HR, 1.48), and major GI bleeding (HR, 1.40); a nonsignificant decrease in thromboembolic stroke (HR, 0.81); and a nonsignificant increase in mortality (HR, 1.15).
In a further analysis of the data, rivaroxaban was linked to 2.3 excess cases of intracranial hemorrhage, 13 excess cases of major extracranial bleeding, 9.4 excess cases of major GI bleeding, and 3.1 excess deaths per 1,000 person-years of treatment. In addition, rivaroxaban was associated with a significantly increased risk of death in two subgroups of patients: those aged 75 and older and those whose CHADS-2 scores indicated higher bleeding risk, Dr. Graham and his associates said (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5954).
Of note, “the net increase in intracranial hemorrhage, the outcome with the highest case fatality rate, exceeded the net reduction in thromboembolic stroke” with rivaroxaban treatment, they added.
This “milestone” study offers real-world data for a large number of older patients with multiple comorbidities who constitute the rising tide of the AF population.
The findings should lead physicians to prescribe dabigatran over rivaroxaban in most patients with AF. Even though this was a retrospective cohort study, there are no prospective randomized trials directly comparing the two non–vitamin-K oral anticoagulants, and the few indirect comparisons derived from clinical trial data are very limited.
Anna L. Parks, MD, is at the University of California, San Francisco. Rita F. Redberg, M.D., is the editor of JAMA Internal Medicine and professor of cardiology at UCSF. Dr. Parks and Dr. Redberg made these remarks in an Editor’s Note accompanying Dr. Graham’s report (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.6429).
This “milestone” study offers real-world data for a large number of older patients with multiple comorbidities who constitute the rising tide of the AF population.
The findings should lead physicians to prescribe dabigatran over rivaroxaban in most patients with AF. Even though this was a retrospective cohort study, there are no prospective randomized trials directly comparing the two non–vitamin-K oral anticoagulants, and the few indirect comparisons derived from clinical trial data are very limited.
Anna L. Parks, MD, is at the University of California, San Francisco. Rita F. Redberg, M.D., is the editor of JAMA Internal Medicine and professor of cardiology at UCSF. Dr. Parks and Dr. Redberg made these remarks in an Editor’s Note accompanying Dr. Graham’s report (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.6429).
This “milestone” study offers real-world data for a large number of older patients with multiple comorbidities who constitute the rising tide of the AF population.
The findings should lead physicians to prescribe dabigatran over rivaroxaban in most patients with AF. Even though this was a retrospective cohort study, there are no prospective randomized trials directly comparing the two non–vitamin-K oral anticoagulants, and the few indirect comparisons derived from clinical trial data are very limited.
Anna L. Parks, MD, is at the University of California, San Francisco. Rita F. Redberg, M.D., is the editor of JAMA Internal Medicine and professor of cardiology at UCSF. Dr. Parks and Dr. Redberg made these remarks in an Editor’s Note accompanying Dr. Graham’s report (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.6429).
Rivaroxaban is associated with significantly more intra- and extracranial bleeding than is dabigatran in older patients who have nonvalvular atrial fibrillation, according to a report published online Oct. 3 in JAMA Internal Medicine.
This is the principal finding of a retrospective cohort study – the only study to directly compare the two oral non–vitamin-K-antagonists – that involved more than 118,000 patients who initiated anticoagulation treatment during a 2.5-year period. The Centers for Medicare & Medicaid Services and the Food and Drug Administration jointly conducted the study.
During the study period, rivaroxaban was used 2-3 times more often than was dabigatran in AF patients in the United States, “perhaps partly because of prescriber misperceptions about bleeding risks with dabigatran, arising from FDA receipt of a large number of postmarketing case reports following its approval. Ironically, we [now find] substantially higher bleeding risks with use of rivaroxaban than dabigatran,” said David J. Graham, MD, of the Office of Surveillance and Epidemiology, Center for Drug Evaluation and Research, FDA, Silver Spring, Md., and his associates.
The researchers assessed Medicare beneficiaries who initiated standard oral doses of rivaroxaban (66,651 patients) or dabigatran (52,240 patients) and were followed for a mean of 110 days.
The primary outcome measure – a composite of thromboembolic stroke, intracranial hemorrhage, major extracranial bleeding events including GI bleeding, and mortality – occurred in significantly more patients taking rivaroxaban than in those taking dabigatran. When the individual components of this composite outcome were considered, rivaroxaban was associated with significant increases in intracranial hemorrhage (HR, 1.65), major extracranial bleeding (HR, 1.48), and major GI bleeding (HR, 1.40); a nonsignificant decrease in thromboembolic stroke (HR, 0.81); and a nonsignificant increase in mortality (HR, 1.15).
In a further analysis of the data, rivaroxaban was linked to 2.3 excess cases of intracranial hemorrhage, 13 excess cases of major extracranial bleeding, 9.4 excess cases of major GI bleeding, and 3.1 excess deaths per 1,000 person-years of treatment. In addition, rivaroxaban was associated with a significantly increased risk of death in two subgroups of patients: those aged 75 and older and those whose CHADS-2 scores indicated higher bleeding risk, Dr. Graham and his associates said (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5954).
Of note, “the net increase in intracranial hemorrhage, the outcome with the highest case fatality rate, exceeded the net reduction in thromboembolic stroke” with rivaroxaban treatment, they added.
Rivaroxaban is associated with significantly more intra- and extracranial bleeding than is dabigatran in older patients who have nonvalvular atrial fibrillation, according to a report published online Oct. 3 in JAMA Internal Medicine.
This is the principal finding of a retrospective cohort study – the only study to directly compare the two oral non–vitamin-K-antagonists – that involved more than 118,000 patients who initiated anticoagulation treatment during a 2.5-year period. The Centers for Medicare & Medicaid Services and the Food and Drug Administration jointly conducted the study.
During the study period, rivaroxaban was used 2-3 times more often than was dabigatran in AF patients in the United States, “perhaps partly because of prescriber misperceptions about bleeding risks with dabigatran, arising from FDA receipt of a large number of postmarketing case reports following its approval. Ironically, we [now find] substantially higher bleeding risks with use of rivaroxaban than dabigatran,” said David J. Graham, MD, of the Office of Surveillance and Epidemiology, Center for Drug Evaluation and Research, FDA, Silver Spring, Md., and his associates.
The researchers assessed Medicare beneficiaries who initiated standard oral doses of rivaroxaban (66,651 patients) or dabigatran (52,240 patients) and were followed for a mean of 110 days.
The primary outcome measure – a composite of thromboembolic stroke, intracranial hemorrhage, major extracranial bleeding events including GI bleeding, and mortality – occurred in significantly more patients taking rivaroxaban than in those taking dabigatran. When the individual components of this composite outcome were considered, rivaroxaban was associated with significant increases in intracranial hemorrhage (HR, 1.65), major extracranial bleeding (HR, 1.48), and major GI bleeding (HR, 1.40); a nonsignificant decrease in thromboembolic stroke (HR, 0.81); and a nonsignificant increase in mortality (HR, 1.15).
In a further analysis of the data, rivaroxaban was linked to 2.3 excess cases of intracranial hemorrhage, 13 excess cases of major extracranial bleeding, 9.4 excess cases of major GI bleeding, and 3.1 excess deaths per 1,000 person-years of treatment. In addition, rivaroxaban was associated with a significantly increased risk of death in two subgroups of patients: those aged 75 and older and those whose CHADS-2 scores indicated higher bleeding risk, Dr. Graham and his associates said (JAMA Intern. Med. 2016 Oct 3. doi: 10.1001/jamainternmed.2016.5954).
Of note, “the net increase in intracranial hemorrhage, the outcome with the highest case fatality rate, exceeded the net reduction in thromboembolic stroke” with rivaroxaban treatment, they added.
Key clinical point: Rivaroxaban is associated with significantly more intra- and extracranial bleeding than dabigatran in patients aged 75 and older with nonvalvular atrial fibrillation.
Major finding: Rivaroxaban was linked to 2.3 excess cases of intracranial hemorrhage, 13 excess cases of major extracranial bleeding, 9.4 excess cases of major GI bleeding, and 3.1 excess deaths per 1,000 person-years of treatment.
Data source: A retrospective cohort study of 118,891 patients aged 65 and older who initiated anticoagulation therapy for AF during a 2.5-year period.
Disclosures: This study was conducted by employees or contractors of the Centers for Medicare & Medicaid Services and the Food and Drug Administration. Dr. Graham and his associates reported having no relevant financial disclosures.
Planning, education smooth transition to longer-acting clotting factors
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.

Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.
Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
ORLANDO – Transitioning patients with hemophilia from standard clotting factor concentrates to newer extended half-life products takes planning, education, and a little patience, but the payoff can be better hemostasis, a hemophilia treatment specialist said.
“Real-world experience shows us that you can maintain effective protection with less infusion with these new products, but we also know that each person should be evaluated individually when determining what their specific optimal treatment is,” said Jennifer Maahs, a hemophilia nurse practitioner at the Indiana Hemophilia and Thrombosis Center in Indianapolis.
Staff and patient education about the proper use of newer extended half-life (EHL) products is the key to success, she added in an oral session at the World Federation of Hemophilia World Congress.
The new EHL products allow for longer intervals between doses, especially with EHL recombinant factor IX used to treat hemophilia B. Prophylaxis with standard factor IX concentrates requires doses of 25-40 IU/kg twice weekly; in contrasts, EHL products can be given in various doses based on patient responses of either 50 IU/kg every 7 days, 100 IU/kg every 10 days, 25-40 IU/kg every 7 days, or 50-75 IU/kg every 14 days.
In general, the longer intervals between dosing occur in adults; young children tend to require more frequent dosing and have lower levels of factor recovery, she noted.
Extended Experience
Her center currently has more than 100 patients maintained on prolonged half-life factor VIII and factor IX products.
“We have really learned a lot of lessons along the way, and we have had to modify our approach based on these lessons,” she said. “Each patient situation is unique, and everything needs to be individualized.”
Staff review the published literature to educate themselves on the EHL products and prepare answers to expected questions from patients. Ms. Maahs suggested identifying key staff who are best equipped to answer specific questions.
“From a patient standpoint, we’ve developed a patient notification letter, so for any new product that comes out – for example a new factor VIII product – the notification gets sent out factor VIII patients, and we do that for every new product that comes out,” she said.
PK OK
Pharmacokinetic (PK) analyses may also be helpful in transitioning patients to EHL products.
To test patient responses to new products, her center tests patients for recovery from 15 minutes to 1 hour post-infusion, which will provide information about how the patient may respond to the product during a bleeding episode.
If the patient is on prophylaxis they will evaluate trough effectiveness to determine that patient’s responsiveness at the lowest level prior to the next infusion. Testing at other time points may be required based on the patient’s individual clinical history.
Center staff talk with each patient to discuss his needs and capabilities. If the patient is currently being managed with on-demand therapy, the talk may center on obstacles to utilization of prophylaxis and the patient’s desired infusion interval.
For patients currently on prophylaxis, they discuss the current regimen frequency and dose and assess how well it’s working. Staff members also provide information about alternative approaches to therapy, and ask patients specifically about their activity levels and dates of activity, compared with currently scheduled infusion days.
Patients are also educated about the reconstitution requirements for the new product, and are told to use up any remaining concentrates before switching over to the new product.
“As we move forward, within 2 to 4 weeks of starting a new therapy, we like to obtain a trough to see how their prophylaxis is working. At that time we ask how have you been doing on the new product, are you having any breakthrough bleeding, and how are you feeling about it,” Ms. Maahs said.
Weekly phone calls to the patient during the first month are also very helpful for reinforcing information about dosing regimens for bleeding episodes, reminding patients to call in if they experience a lead, and encouraging them to keep a treatment log. The phone call can also be helpful in identifying potential product-related reactions or other issues, she said.
‘Big impact’
“What’s the impact that we’ve seen? With factor IX, it has been really big. Previous on-demand patients have agreed that, ‘gosh, I’m infusing a couple of times a month anyway,’ so starting an every 14-day prophylactic regimen seems pretty reasonable,” she said.
“We’ve had infusion schedules in children change from twice weekly to once weekly and that has really decreased the burden of disease,” she added.
A few adults, however, have gone back to standard half-life products because of concerns that they would not be able to infuse when they thought they needed treatment, she noted.
The impact of the EHL factor VIII products has been smaller, although it has allowed slight increases in the dosing intervals (from every other day to every third day in children, for example), and has overall decreased the average number of monthly infusions from about 15 to about 10.
Some adolescents and young adults, who often have been on prophylaxis for all of their lives, have experienced absent or only minimal joint disease, and some have been able to extend their dosing intervals from every 4 to every 5 to 7 days, she said.
Ms. Maahs disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.
EXPERT ANALYSIS AT WFH 2016 WORLD CONGRESS
Key clinical point: Transitioning patients to extended half-life clotting factor concentrates requires tailoring treatment to individual patients.
Major finding: Many patients can transition from on-demand dosing with factor IX to prophylaxis infusions once every 2 weeks.
Data source: Review of a hemophilia treatment center experience transitioning patients to extended half-life products.
Disclosures: Jennifer Maahs, RN-BC, disclosed serving on advisory committees to Baxalta, Novo Nordisk, Biogen, Genentech, and CSL, and receiving honoraria related to those activities.

IVIg, corticosteroids appear comparable for ITP in pregnancy
Most pregnant women with a history of immune thrombocytopenia purpura need no treatment. Of those who do, neonatal outcomes were comparable for mothers who received treatment with intravenous immunoglobulin and for those who received corticosteroids, results of an observational study indicate.
Though limited by its retrospective design and low event rates that limit inferences about treatment effects, this observational study – the first to compare the effectiveness of treatment with IVIg to treatment with corticosteroids for immune thrombocytopenia purpura (ITP) in pregnancy – shows that outcomes did not significantly differ with the two regimens. The findings also highlight the need for ongoing neonatal platelet count monitoring throughout the first week of life, regardless of the maternal platelet count, the investigators said.

A review of medical records at two tertiary care centers identified 235 pregnancies in 195 women with a history of ITP. No treatment was required in 137 pregnancies. Of the remaining 98 pregnancies in 91 women, 47 (48%) were treated initially with intravenous immunoglobulin (IVIg) and 51 were treated initially with corticosteroids, reported Dongmei Sun, MD, of University of Western Ontario, London, and colleagues (Blood. 2016;128[10]:1329-35).
The two treatment groups had similar mean maternal platelet counts at birth (68.7 x 109/L and 77.3 x 109/L for IVIg and corticosteroids, respectively). The proportion of mothers who achieved a platelet count response did not significantly differ (38% vs. 39%), the researchers reported.
“The sole difference between treatments was a higher maternal composite outcome noted in the IVIg group,” they wrote, referring to a secondary composite outcome of postpartum hemorrhage, predelivery platelet transfusion, peripartum transfusion of any blood product, or postpartum reduction in the hemoglobin concentration of 30 g/L or more. That composite outcome occurred in 46.8% of pregnancies in the IVIg group and 23.5% in the corticosteroid group.
Adverse events were reported in 13% of cases in each group, and included hemolytic anemia, headache, and “other” in those treated with IVIg, and hyperglycemia requiring treatment, hyperglycemia with neonatal hypoglycemia, infection, and “other” in those receiving corticosteroids.
No severe or fatal maternal, fetal, or neonatal hemorrhages occurred, but two newborns did experience intracranial hemorrhage. No maternal or neonatal deaths occurred, the investigators said.
In 203 neonates for whom platelet counts were available, 56 (28%) had a count of less than 150 x 109/L and 18 (9%) had a count of less than 50 x 109/L.
Nadir platelet counts occurred at birth for 30% of neonates. In two cases, the nadir occurred as late as day 6 postnatally. Of note, a drop in platelets to below 150 x 109/L was found in 9 (11%) of 129 neonates who had a normal cord platelet count and had a repeat count.
ITP occurs in 1 to 10 of every 10,000 pregnancies, and about one-third of cases require intervention. IVIg and corticosteroids are acceptable treatments, but most data on their effectiveness are extrapolated from nonpregnant patients and the treatments have not been adequately assessed in pregnancy, the investigators said. The current study was designed to compare the efficacy of the two treatments for maternal ITP.
Study subjects were women with singleton pregnancies with an ITP diagnosis either before or during pregnancy.
At less than 40% in both groups, the response to ITP therapies was lower than has been reported for nonpregnant patients, the investigators noted.
“Our observation of a relative resistance to ITP treatment during pregnancy requires further validation in prospective studies. We speculate that increased potency of antiplatelet antibodies during pregnancy, pregnancy-associated changes in platelet turnover, or altered drug metabolism may contribute to the lower response rates we observed,” they wrote.
With respect to corticosteroids, this “may warrant consideration of starting therapy earlier in the third trimester to maximize the likelihood of reaching target platelet counts in time for delivery and raises the possibility that lower corticosteroid doses are ineffective in this setting,” they added.
“Also of significance is the finding that 9 neonates (11%) with normal cord platelet counts were found to have a reduction in their platelet count on repeat measurement. These findings highlight the need for determination of cord platelet counts in all neonates born to mothers with active or previous ITP and the need for continued monitoring of the neonatal platelet count during the first week of life, despite normal cord platelet counts,” they wrote.
“Prospective studies are needed to better characterize the safety of these regimens, to determine the optimal dose of corticosteroids, to identify risk factors for neonatal thrombocytopenia, and to explore new therapeutic options,” they concluded.
Among the options worth exploring are rituximab, a monoclonal antibody against B-cell surface antigen CD20, for which “pregnancy data are accumulating,” and romiplostim, a thrombopoietin receptor agonist, which has been used in a few cases without reported fetal complications, they noted.
This study was supported by Canadian Blood Services Small Projects Fund and Canadian Institute of Health Research/Canadian Blood Services New Investigator Award. Individual authors reported receiving support from the Canadian Institutes of Health Research and McMaster University. The authors reported having no other disclosures.
Most pregnant women with a history of immune thrombocytopenia purpura need no treatment. Of those who do, neonatal outcomes were comparable for mothers who received treatment with intravenous immunoglobulin and for those who received corticosteroids, results of an observational study indicate.
Though limited by its retrospective design and low event rates that limit inferences about treatment effects, this observational study – the first to compare the effectiveness of treatment with IVIg to treatment with corticosteroids for immune thrombocytopenia purpura (ITP) in pregnancy – shows that outcomes did not significantly differ with the two regimens. The findings also highlight the need for ongoing neonatal platelet count monitoring throughout the first week of life, regardless of the maternal platelet count, the investigators said.
A review of medical records at two tertiary care centers identified 235 pregnancies in 195 women with a history of ITP. No treatment was required in 137 pregnancies. Of the remaining 98 pregnancies in 91 women, 47 (48%) were treated initially with intravenous immunoglobulin (IVIg) and 51 were treated initially with corticosteroids, reported Dongmei Sun, MD, of University of Western Ontario, London, and colleagues (Blood. 2016;128[10]:1329-35).
The two treatment groups had similar mean maternal platelet counts at birth (68.7 x 109/L and 77.3 x 109/L for IVIg and corticosteroids, respectively). The proportion of mothers who achieved a platelet count response did not significantly differ (38% vs. 39%), the researchers reported.
“The sole difference between treatments was a higher maternal composite outcome noted in the IVIg group,” they wrote, referring to a secondary composite outcome of postpartum hemorrhage, predelivery platelet transfusion, peripartum transfusion of any blood product, or postpartum reduction in the hemoglobin concentration of 30 g/L or more. That composite outcome occurred in 46.8% of pregnancies in the IVIg group and 23.5% in the corticosteroid group.
Adverse events were reported in 13% of cases in each group, and included hemolytic anemia, headache, and “other” in those treated with IVIg, and hyperglycemia requiring treatment, hyperglycemia with neonatal hypoglycemia, infection, and “other” in those receiving corticosteroids.
No severe or fatal maternal, fetal, or neonatal hemorrhages occurred, but two newborns did experience intracranial hemorrhage. No maternal or neonatal deaths occurred, the investigators said.
In 203 neonates for whom platelet counts were available, 56 (28%) had a count of less than 150 x 109/L and 18 (9%) had a count of less than 50 x 109/L.
Nadir platelet counts occurred at birth for 30% of neonates. In two cases, the nadir occurred as late as day 6 postnatally. Of note, a drop in platelets to below 150 x 109/L was found in 9 (11%) of 129 neonates who had a normal cord platelet count and had a repeat count.
ITP occurs in 1 to 10 of every 10,000 pregnancies, and about one-third of cases require intervention. IVIg and corticosteroids are acceptable treatments, but most data on their effectiveness are extrapolated from nonpregnant patients and the treatments have not been adequately assessed in pregnancy, the investigators said. The current study was designed to compare the efficacy of the two treatments for maternal ITP.
Study subjects were women with singleton pregnancies with an ITP diagnosis either before or during pregnancy.
At less than 40% in both groups, the response to ITP therapies was lower than has been reported for nonpregnant patients, the investigators noted.
“Our observation of a relative resistance to ITP treatment during pregnancy requires further validation in prospective studies. We speculate that increased potency of antiplatelet antibodies during pregnancy, pregnancy-associated changes in platelet turnover, or altered drug metabolism may contribute to the lower response rates we observed,” they wrote.
With respect to corticosteroids, this “may warrant consideration of starting therapy earlier in the third trimester to maximize the likelihood of reaching target platelet counts in time for delivery and raises the possibility that lower corticosteroid doses are ineffective in this setting,” they added.
“Also of significance is the finding that 9 neonates (11%) with normal cord platelet counts were found to have a reduction in their platelet count on repeat measurement. These findings highlight the need for determination of cord platelet counts in all neonates born to mothers with active or previous ITP and the need for continued monitoring of the neonatal platelet count during the first week of life, despite normal cord platelet counts,” they wrote.
“Prospective studies are needed to better characterize the safety of these regimens, to determine the optimal dose of corticosteroids, to identify risk factors for neonatal thrombocytopenia, and to explore new therapeutic options,” they concluded.
Among the options worth exploring are rituximab, a monoclonal antibody against B-cell surface antigen CD20, for which “pregnancy data are accumulating,” and romiplostim, a thrombopoietin receptor agonist, which has been used in a few cases without reported fetal complications, they noted.
This study was supported by Canadian Blood Services Small Projects Fund and Canadian Institute of Health Research/Canadian Blood Services New Investigator Award. Individual authors reported receiving support from the Canadian Institutes of Health Research and McMaster University. The authors reported having no other disclosures.
Most pregnant women with a history of immune thrombocytopenia purpura need no treatment. Of those who do, neonatal outcomes were comparable for mothers who received treatment with intravenous immunoglobulin and for those who received corticosteroids, results of an observational study indicate.
Though limited by its retrospective design and low event rates that limit inferences about treatment effects, this observational study – the first to compare the effectiveness of treatment with IVIg to treatment with corticosteroids for immune thrombocytopenia purpura (ITP) in pregnancy – shows that outcomes did not significantly differ with the two regimens. The findings also highlight the need for ongoing neonatal platelet count monitoring throughout the first week of life, regardless of the maternal platelet count, the investigators said.
A review of medical records at two tertiary care centers identified 235 pregnancies in 195 women with a history of ITP. No treatment was required in 137 pregnancies. Of the remaining 98 pregnancies in 91 women, 47 (48%) were treated initially with intravenous immunoglobulin (IVIg) and 51 were treated initially with corticosteroids, reported Dongmei Sun, MD, of University of Western Ontario, London, and colleagues (Blood. 2016;128[10]:1329-35).
The two treatment groups had similar mean maternal platelet counts at birth (68.7 x 109/L and 77.3 x 109/L for IVIg and corticosteroids, respectively). The proportion of mothers who achieved a platelet count response did not significantly differ (38% vs. 39%), the researchers reported.
“The sole difference between treatments was a higher maternal composite outcome noted in the IVIg group,” they wrote, referring to a secondary composite outcome of postpartum hemorrhage, predelivery platelet transfusion, peripartum transfusion of any blood product, or postpartum reduction in the hemoglobin concentration of 30 g/L or more. That composite outcome occurred in 46.8% of pregnancies in the IVIg group and 23.5% in the corticosteroid group.
Adverse events were reported in 13% of cases in each group, and included hemolytic anemia, headache, and “other” in those treated with IVIg, and hyperglycemia requiring treatment, hyperglycemia with neonatal hypoglycemia, infection, and “other” in those receiving corticosteroids.
No severe or fatal maternal, fetal, or neonatal hemorrhages occurred, but two newborns did experience intracranial hemorrhage. No maternal or neonatal deaths occurred, the investigators said.
In 203 neonates for whom platelet counts were available, 56 (28%) had a count of less than 150 x 109/L and 18 (9%) had a count of less than 50 x 109/L.
Nadir platelet counts occurred at birth for 30% of neonates. In two cases, the nadir occurred as late as day 6 postnatally. Of note, a drop in platelets to below 150 x 109/L was found in 9 (11%) of 129 neonates who had a normal cord platelet count and had a repeat count.
ITP occurs in 1 to 10 of every 10,000 pregnancies, and about one-third of cases require intervention. IVIg and corticosteroids are acceptable treatments, but most data on their effectiveness are extrapolated from nonpregnant patients and the treatments have not been adequately assessed in pregnancy, the investigators said. The current study was designed to compare the efficacy of the two treatments for maternal ITP.
Study subjects were women with singleton pregnancies with an ITP diagnosis either before or during pregnancy.
At less than 40% in both groups, the response to ITP therapies was lower than has been reported for nonpregnant patients, the investigators noted.
“Our observation of a relative resistance to ITP treatment during pregnancy requires further validation in prospective studies. We speculate that increased potency of antiplatelet antibodies during pregnancy, pregnancy-associated changes in platelet turnover, or altered drug metabolism may contribute to the lower response rates we observed,” they wrote.
With respect to corticosteroids, this “may warrant consideration of starting therapy earlier in the third trimester to maximize the likelihood of reaching target platelet counts in time for delivery and raises the possibility that lower corticosteroid doses are ineffective in this setting,” they added.
“Also of significance is the finding that 9 neonates (11%) with normal cord platelet counts were found to have a reduction in their platelet count on repeat measurement. These findings highlight the need for determination of cord platelet counts in all neonates born to mothers with active or previous ITP and the need for continued monitoring of the neonatal platelet count during the first week of life, despite normal cord platelet counts,” they wrote.
“Prospective studies are needed to better characterize the safety of these regimens, to determine the optimal dose of corticosteroids, to identify risk factors for neonatal thrombocytopenia, and to explore new therapeutic options,” they concluded.
Among the options worth exploring are rituximab, a monoclonal antibody against B-cell surface antigen CD20, for which “pregnancy data are accumulating,” and romiplostim, a thrombopoietin receptor agonist, which has been used in a few cases without reported fetal complications, they noted.
This study was supported by Canadian Blood Services Small Projects Fund and Canadian Institute of Health Research/Canadian Blood Services New Investigator Award. Individual authors reported receiving support from the Canadian Institutes of Health Research and McMaster University. The authors reported having no other disclosures.
FROM BLOOD
Key clinical point: Most pregnant women with a history of immune thrombocytopenia purpura in an observational study needed no treatment, but neonatal outcomes were comparable for mothers who received treatment with intravenous immunoglobulin and those who received corticosteroids.
Major finding: Groups given IVIg or corticosteroids had similar mean maternal platelet counts at birth (68.7 x 109/L and 77.3 x 109/L for IVIg and corticosteroids, respectively), and no difference was seen in the proportion of mothers who achieved a platelet count response (38% and 39%, respectively).
Data source: A retrospective observational study of 235 pregnancies.
Disclosures: This study was supported by Canadian Blood Services Small Projects Fund and Canadian Institute of Health Research/Canadian Blood Services New Investigator Award. Individual authors reported receiving support from the Canadian Institutes of Health Research and McMaster University. The authors reported having no other disclosures.

Early intensive prophylaxis provides better QoL in hemophilia
ORLANDO – Boys with hemophilia have a better quality of life when they are managed with intensive bleeding prophylaxis with clotting factor concentrates rather than on-demand therapy, results of an international study suggest.
An analysis of pooled data from six studies conducted in eight countries showed that boys with severe hemophilia who received limited on-demand factor replacement had significantly lower health-related quality of life (HRQoL) scores than did boys treated prophylactically, reported Victoria Price, MB, of Dalhousie University, Halifax, N.S., and colleagues.

“Early initiation of intensive prophylaxis has the greatest impact on HRQoL in boys with severe hemophilia. HRQoL in boys with severe hemophilia exposed to early initiation of intensive prophylaxis is comparable to boys with mild hemophilia receiving on-demand therapy,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
In countries where patients have access to safe clotting factor concentrates, prophylaxis has become the standard of care for management of hemophilia A and B, because it has been shown to reduce the frequency of bleeds. But because of the small sample sizes in most studies of hemophilia, it has been difficult to determine whether prophylaxis actually has a significant effect on HRQoL, the investigators noted.
To get an answer to that question, they looked at data from six studies in boys younger than 18 that measured HRQoL using the same standard instrument, the Canadian Haemophilia Outcomes–Kids’ Life Assessment Tool (CHO-KLAT). The studies were conducted in Brazil, Canada, China, France, Germany, the Netherlands, Spain, and the United Kingdom.
Patients in the studies were grouped into one of five categories:
• Early initiation with intensive prophylaxis (Germany, the Netherlands, Spain, UK)
• Gradual initiation with intensive prophylaxis (Canada, France)
• Late initiation with limited prophylaxis (Brazil, China)
• On-demand with good access to factor (Canada and European nations)
• On-demand with variable or limited access to factor (Brazil and China).
Data on a total of 254 boys with severe hemophilia were analyzed and compared with estimated scores from boys with mild hemophilia in the pooled dataset.
Of the boys with severe hemophilia, 220 (86.6% had hemophilia A, and 34 (13.4%) had hemophilia B. They ranged in age from 4.4 to 17.9 years; 21 of the boys were younger than 7 years.
The investigators found that in a linear regression model, patients with early initiation and intensive prophylaxis had the highest CHO-KLAT scores, followed by those who had gradual initiation with intensive prophylaxis (P = .003), late initiation/limited prophylaxis (P = .005), on-demand with good access (P = .008) and, lastly, on-demand with limited access to factor (P less than .001)
The authors noted that the differences by treatment group in the analysis were defined by expert consensus, and may not reflect changes in treatment protocols over the last 10 years. The studies were published between 2006 and 2016.
“Despite this limitation, important differences were observed between groups,” they wrote.
The studies were supported by grants from the Canadian Haemophilia Society and the Society of Haemophilia Clinic Directors of Canada, Bayer, Baxalta, and CSL Behring. The authors did not report conflict of interest disclosures.
ORLANDO – Boys with hemophilia have a better quality of life when they are managed with intensive bleeding prophylaxis with clotting factor concentrates rather than on-demand therapy, results of an international study suggest.
An analysis of pooled data from six studies conducted in eight countries showed that boys with severe hemophilia who received limited on-demand factor replacement had significantly lower health-related quality of life (HRQoL) scores than did boys treated prophylactically, reported Victoria Price, MB, of Dalhousie University, Halifax, N.S., and colleagues.
“Early initiation of intensive prophylaxis has the greatest impact on HRQoL in boys with severe hemophilia. HRQoL in boys with severe hemophilia exposed to early initiation of intensive prophylaxis is comparable to boys with mild hemophilia receiving on-demand therapy,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
In countries where patients have access to safe clotting factor concentrates, prophylaxis has become the standard of care for management of hemophilia A and B, because it has been shown to reduce the frequency of bleeds. But because of the small sample sizes in most studies of hemophilia, it has been difficult to determine whether prophylaxis actually has a significant effect on HRQoL, the investigators noted.
To get an answer to that question, they looked at data from six studies in boys younger than 18 that measured HRQoL using the same standard instrument, the Canadian Haemophilia Outcomes–Kids’ Life Assessment Tool (CHO-KLAT). The studies were conducted in Brazil, Canada, China, France, Germany, the Netherlands, Spain, and the United Kingdom.
Patients in the studies were grouped into one of five categories:
• Early initiation with intensive prophylaxis (Germany, the Netherlands, Spain, UK)
• Gradual initiation with intensive prophylaxis (Canada, France)
• Late initiation with limited prophylaxis (Brazil, China)
• On-demand with good access to factor (Canada and European nations)
• On-demand with variable or limited access to factor (Brazil and China).
Data on a total of 254 boys with severe hemophilia were analyzed and compared with estimated scores from boys with mild hemophilia in the pooled dataset.
Of the boys with severe hemophilia, 220 (86.6% had hemophilia A, and 34 (13.4%) had hemophilia B. They ranged in age from 4.4 to 17.9 years; 21 of the boys were younger than 7 years.
The investigators found that in a linear regression model, patients with early initiation and intensive prophylaxis had the highest CHO-KLAT scores, followed by those who had gradual initiation with intensive prophylaxis (P = .003), late initiation/limited prophylaxis (P = .005), on-demand with good access (P = .008) and, lastly, on-demand with limited access to factor (P less than .001)
The authors noted that the differences by treatment group in the analysis were defined by expert consensus, and may not reflect changes in treatment protocols over the last 10 years. The studies were published between 2006 and 2016.
“Despite this limitation, important differences were observed between groups,” they wrote.
The studies were supported by grants from the Canadian Haemophilia Society and the Society of Haemophilia Clinic Directors of Canada, Bayer, Baxalta, and CSL Behring. The authors did not report conflict of interest disclosures.
ORLANDO – Boys with hemophilia have a better quality of life when they are managed with intensive bleeding prophylaxis with clotting factor concentrates rather than on-demand therapy, results of an international study suggest.
An analysis of pooled data from six studies conducted in eight countries showed that boys with severe hemophilia who received limited on-demand factor replacement had significantly lower health-related quality of life (HRQoL) scores than did boys treated prophylactically, reported Victoria Price, MB, of Dalhousie University, Halifax, N.S., and colleagues.
“Early initiation of intensive prophylaxis has the greatest impact on HRQoL in boys with severe hemophilia. HRQoL in boys with severe hemophilia exposed to early initiation of intensive prophylaxis is comparable to boys with mild hemophilia receiving on-demand therapy,” they wrote in a scientific poster presented at the World Federation of Hemophilia World Congress.
In countries where patients have access to safe clotting factor concentrates, prophylaxis has become the standard of care for management of hemophilia A and B, because it has been shown to reduce the frequency of bleeds. But because of the small sample sizes in most studies of hemophilia, it has been difficult to determine whether prophylaxis actually has a significant effect on HRQoL, the investigators noted.
To get an answer to that question, they looked at data from six studies in boys younger than 18 that measured HRQoL using the same standard instrument, the Canadian Haemophilia Outcomes–Kids’ Life Assessment Tool (CHO-KLAT). The studies were conducted in Brazil, Canada, China, France, Germany, the Netherlands, Spain, and the United Kingdom.
Patients in the studies were grouped into one of five categories:
• Early initiation with intensive prophylaxis (Germany, the Netherlands, Spain, UK)
• Gradual initiation with intensive prophylaxis (Canada, France)
• Late initiation with limited prophylaxis (Brazil, China)
• On-demand with good access to factor (Canada and European nations)
• On-demand with variable or limited access to factor (Brazil and China).
Data on a total of 254 boys with severe hemophilia were analyzed and compared with estimated scores from boys with mild hemophilia in the pooled dataset.
Of the boys with severe hemophilia, 220 (86.6% had hemophilia A, and 34 (13.4%) had hemophilia B. They ranged in age from 4.4 to 17.9 years; 21 of the boys were younger than 7 years.
The investigators found that in a linear regression model, patients with early initiation and intensive prophylaxis had the highest CHO-KLAT scores, followed by those who had gradual initiation with intensive prophylaxis (P = .003), late initiation/limited prophylaxis (P = .005), on-demand with good access (P = .008) and, lastly, on-demand with limited access to factor (P less than .001)
The authors noted that the differences by treatment group in the analysis were defined by expert consensus, and may not reflect changes in treatment protocols over the last 10 years. The studies were published between 2006 and 2016.
“Despite this limitation, important differences were observed between groups,” they wrote.
The studies were supported by grants from the Canadian Haemophilia Society and the Society of Haemophilia Clinic Directors of Canada, Bayer, Baxalta, and CSL Behring. The authors did not report conflict of interest disclosures.
AT WFH 2016 WORLD CONGRESS
Key clinical point: Early initiation of intensive bleeding prophylaxis was associated with significantly better health-related quality of life (HRQoL).
Major finding: Boys with severe hemophilia started early on intensive prophylaxis had HRQoL comparable to that of boys with mild hemophilia with good access to factor.
Data source: Pooled analysis of six studies comprising 254 boys with severe hemophilia.
Disclosures: The studies were supported by grants from the Canadian Haemophilia Society and the Society of Haemophilia Clinic Directors of Canada, Bayer, Baxalta, and CSL Behring. The authors did not report conflict of interest disclosures.

Decision rule identifies unprovoked VTE patients who can halt anticoagulation
ROME – Half of all women who experience a first unprovoked venous thromboembolism (VTE) can safely be spared lifelong anticoagulation through application of the newly validated HERDOO2 decision rule, Marc A. Rodger, MD, reported at the annual congress of the European Society of Cardiology.
“We’ve validated that a simple, memorable decision rule on anticoagulation applied at the clinically relevant time point works. And it is the only clinical decision rule that has now been prospectively validated,” said Dr. Rodger, professor of medicine, chief and chair of the division of hematology, and head of the thrombosis program at the University of Ottawa.

He presented the results of the validation study, known as the REVERSE II study, which included 2,779 patients with a first unprovoked VTE at 44 centers in seven countries. The full name of the decision rule is “Men Continue and HERDOO2,” a name that says it all: the rule posits that all men as well as those women with a HERDOO2 (Hyperpigmentation, Edema, Redness, d-dimer, Obesity, Older age, 2 or more points) score of at least 2 out of a possible 4 points need to stay on anticoagulation indefinitely because their risk of a recurrent VTE off-therapy clearly exceeds that of a bleeding event on-therapy. In contrast, women with a HERDOO2 score of 0 or 1 can safely stop anticoagulation after the standard 3-6 months of acute short-term therapy.
“Sorry, gentlemen, but we could find no low-risk group of men. They were all high risk,” he said. “But 50% of women with unprovoked vein blood clots can be spared the burdens, costs, and risks of lifelong blood thinners.”
Dr. Rodger and coinvestigators began work on developing a multivariate clinical decision rule in 2001. They examined 69 risk predictors, eventually winnowing down to a manageable four potent risk predictors identified by the acronym HERDOO2.
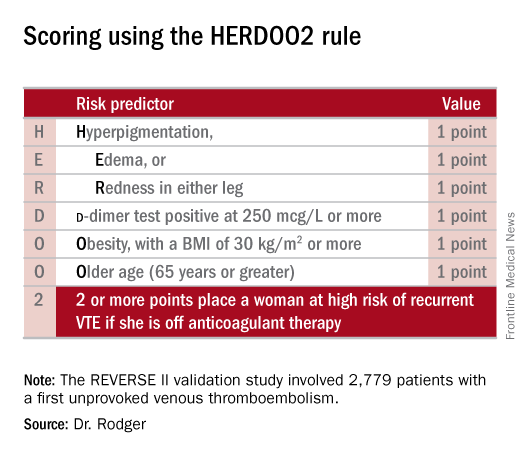
The derivation study was published 8 years ago (CMAJ. 2008;Aug 26;179[5]:417-26). It showed that women with a HERDOO2 score of 2 or more as well as all men had roughly a 14% rate of recurrent VTE in the first year after stopping anticoagulation, while women with a score of 0 or 1 had about a 1.6% risk. The International Society on Thrombosis and Haemostasis suggests that it’s safe to discontinue anticoagulants if the risk of recurrent thrombosis at 1 year off-therapy is less than 5%, given the significant risk of serious bleeding on-therapy and the fact that a serious bleed event is two to three times more likely than a VTE to be fatal.
Dr. Rodger and coinvestigators recognized that a clinical decision rule needs to be externally validated before it’s ready for prime-time use in clinical practice. Thus, they conducted the REVERSE II study, in which the decision rule was applied after the 2,799 participants had been on anticoagulation for 5-12 months. All had a first proximal deep vein thrombosis and/or a segmental or greater pulmonary embolism. Patients were still on anticoagulation at the time the rule was applied, which is why the cut point for a positive d-dimer test in HERDOO2 is 250 mcg/L, half of the threshold value for a positive test in patients not on anticoagulation.
They identified 631 women as low risk, with a HERDOO2 score of 0 or 1. They and their physicians were instructed to stop anticoagulation at that time. The 2,148 high-risk subjects – that is, all of the men and the high-risk women – were advised to remain on anticoagulation. The primary study endpoint was the rate of recurrent VTE in the 12 months following testing and patient guidance. The lost-to-follow-up rate was 2.2%.
The recurrent VTE rate was 3% in the 591 low-risk women who discontinued anticoagulants and zero in 31 others who elected to stay on medication. In the high-risk group identified by the HERDOO2 rule, the recurrent VTE rate at 12 months was 8.1% in the 323 who opted to discontinue anticoagulants and just 1.6% in 1,802 who continued on therapy as advised, a finding that underscores the effectiveness of selectively applied long-term anticoagulation therapy, he continued.
The recurrent VTE rate among the 291 women with a HERDOO2 score of 0 or 1 who were on exogenous estrogen was 1.4%, while in high-risk women taking estrogen the rate was more than doubled at 3.1%. But in women aged 50-64 identified by the HERDOO2 rule as being low risk, the actual recurrent VTE rate was 5.7%, a finding that raised a red flag for the investigators.
“There may be an evolution of the HERDOO2 decision rule to a lower age cut point. But that’s something that requires further study in postmenopausal women,” according to Dr. Rodger.
The investigators defined a first unprovoked VTE as one occurring in the absence during the previous 90 days of major surgery, a fracture or cast, more than 3 days of immobilization, or malignancy within the last 5 years.
Venous thromboembolism is the second most common cardiovascular disorder and the third most common cause of cardiovascular death. Unprovoked VTEs account for half of all VTEs. Their management has been a controversial subject. Both the American College of Chest Physicians and the European Society of Cardiology recommend continuing anticoagulation indefinitely in patients who aren’t at high bleeding risk.
“But this is a relatively weak 2B recommendation because of the tightly balanced competing risks of recurrent thrombosis off anticoagulation and major bleeding on anticoagulation,” Dr. Rodger said. He added that he considers REVERSE II to be practice changing, and predicted that once the results are published the guidelines will be revised.
Discussant Giancarlo Agnelli, MD, was a tough critic who gave fair warning.
“I am friends with many of the authors of this paper, and in this country we are usually gentle with enemies and nasty with friends,” declared Dr. Agnelli, professor of internal medicine and director of internal and cardiovascular medicine and the stroke unit at the University of Perugia, Italy.
He didn’t find the REVERSE II study or the HERDOO2 rule persuasive. On the plus side, he said, the HERDOO2 rule has now been validated, unlike the proposed DASH and Vienna rules. And it was tested in a diverse multinational patient population. But the fact that the HERDOO2 rule is only applicable in women is a major limitation. And REVERSE II was not a randomized trial, Dr. Agnelli noted.
Moreover, 1 year of follow-up seems insufficient, he continued. He cited a French multicenter trial in which patients with a first unprovoked VTE received 6 months of anticoagulants and were then randomized to another 18 months of anticoagulation or placebo. During that 18 months, the group on anticoagulants had a significantly lower rate of the composite endpoint comprised of recurrent VTE or major bleeding, but once that period was over they experienced catchup. By the time the study ended at 42 months, the two study arms didn’t differ significantly in the composite endpoint (JAMA. 2015 Jul 7;314[1]:31-40).
More broadly, Dr. Agnelli also questioned the need for an anticoagulation discontinuation rule in the contemporary era of new oral anticoagulants (NOACs). He was lead investigator in the AMPLIFY study, a major randomized trial of fixed-dose apixaban (Eliquis) versus conventional therapy with subcutaneous enoxaparin (Lovenox) bridging to warfarin in 5,395 patients with acute VTE. The NOAC was associated with a 69% reduction in the relative risk of bleeding and was noninferior to standard therapy in the risk of recurrent VTE (N Engl J Med. 2013 Aug 29;369[9]:799-808).
“Why should we think about withholding anticoagulation in some patients when we now have such a safe approach?” he asked.
Dr. Rodger reported receiving research grants from the French government as well as from Biomerieux, which funded the REVERSE II study. Dr. Agnelli reported having no financial conflicts.
ROME – Half of all women who experience a first unprovoked venous thromboembolism (VTE) can safely be spared lifelong anticoagulation through application of the newly validated HERDOO2 decision rule, Marc A. Rodger, MD, reported at the annual congress of the European Society of Cardiology.
“We’ve validated that a simple, memorable decision rule on anticoagulation applied at the clinically relevant time point works. And it is the only clinical decision rule that has now been prospectively validated,” said Dr. Rodger, professor of medicine, chief and chair of the division of hematology, and head of the thrombosis program at the University of Ottawa.
He presented the results of the validation study, known as the REVERSE II study, which included 2,779 patients with a first unprovoked VTE at 44 centers in seven countries. The full name of the decision rule is “Men Continue and HERDOO2,” a name that says it all: the rule posits that all men as well as those women with a HERDOO2 (Hyperpigmentation, Edema, Redness, d-dimer, Obesity, Older age, 2 or more points) score of at least 2 out of a possible 4 points need to stay on anticoagulation indefinitely because their risk of a recurrent VTE off-therapy clearly exceeds that of a bleeding event on-therapy. In contrast, women with a HERDOO2 score of 0 or 1 can safely stop anticoagulation after the standard 3-6 months of acute short-term therapy.
“Sorry, gentlemen, but we could find no low-risk group of men. They were all high risk,” he said. “But 50% of women with unprovoked vein blood clots can be spared the burdens, costs, and risks of lifelong blood thinners.”
Dr. Rodger and coinvestigators began work on developing a multivariate clinical decision rule in 2001. They examined 69 risk predictors, eventually winnowing down to a manageable four potent risk predictors identified by the acronym HERDOO2.
The derivation study was published 8 years ago (CMAJ. 2008;Aug 26;179[5]:417-26). It showed that women with a HERDOO2 score of 2 or more as well as all men had roughly a 14% rate of recurrent VTE in the first year after stopping anticoagulation, while women with a score of 0 or 1 had about a 1.6% risk. The International Society on Thrombosis and Haemostasis suggests that it’s safe to discontinue anticoagulants if the risk of recurrent thrombosis at 1 year off-therapy is less than 5%, given the significant risk of serious bleeding on-therapy and the fact that a serious bleed event is two to three times more likely than a VTE to be fatal.
Dr. Rodger and coinvestigators recognized that a clinical decision rule needs to be externally validated before it’s ready for prime-time use in clinical practice. Thus, they conducted the REVERSE II study, in which the decision rule was applied after the 2,799 participants had been on anticoagulation for 5-12 months. All had a first proximal deep vein thrombosis and/or a segmental or greater pulmonary embolism. Patients were still on anticoagulation at the time the rule was applied, which is why the cut point for a positive d-dimer test in HERDOO2 is 250 mcg/L, half of the threshold value for a positive test in patients not on anticoagulation.
They identified 631 women as low risk, with a HERDOO2 score of 0 or 1. They and their physicians were instructed to stop anticoagulation at that time. The 2,148 high-risk subjects – that is, all of the men and the high-risk women – were advised to remain on anticoagulation. The primary study endpoint was the rate of recurrent VTE in the 12 months following testing and patient guidance. The lost-to-follow-up rate was 2.2%.
The recurrent VTE rate was 3% in the 591 low-risk women who discontinued anticoagulants and zero in 31 others who elected to stay on medication. In the high-risk group identified by the HERDOO2 rule, the recurrent VTE rate at 12 months was 8.1% in the 323 who opted to discontinue anticoagulants and just 1.6% in 1,802 who continued on therapy as advised, a finding that underscores the effectiveness of selectively applied long-term anticoagulation therapy, he continued.
The recurrent VTE rate among the 291 women with a HERDOO2 score of 0 or 1 who were on exogenous estrogen was 1.4%, while in high-risk women taking estrogen the rate was more than doubled at 3.1%. But in women aged 50-64 identified by the HERDOO2 rule as being low risk, the actual recurrent VTE rate was 5.7%, a finding that raised a red flag for the investigators.
“There may be an evolution of the HERDOO2 decision rule to a lower age cut point. But that’s something that requires further study in postmenopausal women,” according to Dr. Rodger.
The investigators defined a first unprovoked VTE as one occurring in the absence during the previous 90 days of major surgery, a fracture or cast, more than 3 days of immobilization, or malignancy within the last 5 years.
Venous thromboembolism is the second most common cardiovascular disorder and the third most common cause of cardiovascular death. Unprovoked VTEs account for half of all VTEs. Their management has been a controversial subject. Both the American College of Chest Physicians and the European Society of Cardiology recommend continuing anticoagulation indefinitely in patients who aren’t at high bleeding risk.
“But this is a relatively weak 2B recommendation because of the tightly balanced competing risks of recurrent thrombosis off anticoagulation and major bleeding on anticoagulation,” Dr. Rodger said. He added that he considers REVERSE II to be practice changing, and predicted that once the results are published the guidelines will be revised.
Discussant Giancarlo Agnelli, MD, was a tough critic who gave fair warning.
“I am friends with many of the authors of this paper, and in this country we are usually gentle with enemies and nasty with friends,” declared Dr. Agnelli, professor of internal medicine and director of internal and cardiovascular medicine and the stroke unit at the University of Perugia, Italy.
He didn’t find the REVERSE II study or the HERDOO2 rule persuasive. On the plus side, he said, the HERDOO2 rule has now been validated, unlike the proposed DASH and Vienna rules. And it was tested in a diverse multinational patient population. But the fact that the HERDOO2 rule is only applicable in women is a major limitation. And REVERSE II was not a randomized trial, Dr. Agnelli noted.
Moreover, 1 year of follow-up seems insufficient, he continued. He cited a French multicenter trial in which patients with a first unprovoked VTE received 6 months of anticoagulants and were then randomized to another 18 months of anticoagulation or placebo. During that 18 months, the group on anticoagulants had a significantly lower rate of the composite endpoint comprised of recurrent VTE or major bleeding, but once that period was over they experienced catchup. By the time the study ended at 42 months, the two study arms didn’t differ significantly in the composite endpoint (JAMA. 2015 Jul 7;314[1]:31-40).
More broadly, Dr. Agnelli also questioned the need for an anticoagulation discontinuation rule in the contemporary era of new oral anticoagulants (NOACs). He was lead investigator in the AMPLIFY study, a major randomized trial of fixed-dose apixaban (Eliquis) versus conventional therapy with subcutaneous enoxaparin (Lovenox) bridging to warfarin in 5,395 patients with acute VTE. The NOAC was associated with a 69% reduction in the relative risk of bleeding and was noninferior to standard therapy in the risk of recurrent VTE (N Engl J Med. 2013 Aug 29;369[9]:799-808).
“Why should we think about withholding anticoagulation in some patients when we now have such a safe approach?” he asked.
Dr. Rodger reported receiving research grants from the French government as well as from Biomerieux, which funded the REVERSE II study. Dr. Agnelli reported having no financial conflicts.
ROME – Half of all women who experience a first unprovoked venous thromboembolism (VTE) can safely be spared lifelong anticoagulation through application of the newly validated HERDOO2 decision rule, Marc A. Rodger, MD, reported at the annual congress of the European Society of Cardiology.
“We’ve validated that a simple, memorable decision rule on anticoagulation applied at the clinically relevant time point works. And it is the only clinical decision rule that has now been prospectively validated,” said Dr. Rodger, professor of medicine, chief and chair of the division of hematology, and head of the thrombosis program at the University of Ottawa.
He presented the results of the validation study, known as the REVERSE II study, which included 2,779 patients with a first unprovoked VTE at 44 centers in seven countries. The full name of the decision rule is “Men Continue and HERDOO2,” a name that says it all: the rule posits that all men as well as those women with a HERDOO2 (Hyperpigmentation, Edema, Redness, d-dimer, Obesity, Older age, 2 or more points) score of at least 2 out of a possible 4 points need to stay on anticoagulation indefinitely because their risk of a recurrent VTE off-therapy clearly exceeds that of a bleeding event on-therapy. In contrast, women with a HERDOO2 score of 0 or 1 can safely stop anticoagulation after the standard 3-6 months of acute short-term therapy.
“Sorry, gentlemen, but we could find no low-risk group of men. They were all high risk,” he said. “But 50% of women with unprovoked vein blood clots can be spared the burdens, costs, and risks of lifelong blood thinners.”
Dr. Rodger and coinvestigators began work on developing a multivariate clinical decision rule in 2001. They examined 69 risk predictors, eventually winnowing down to a manageable four potent risk predictors identified by the acronym HERDOO2.
The derivation study was published 8 years ago (CMAJ. 2008;Aug 26;179[5]:417-26). It showed that women with a HERDOO2 score of 2 or more as well as all men had roughly a 14% rate of recurrent VTE in the first year after stopping anticoagulation, while women with a score of 0 or 1 had about a 1.6% risk. The International Society on Thrombosis and Haemostasis suggests that it’s safe to discontinue anticoagulants if the risk of recurrent thrombosis at 1 year off-therapy is less than 5%, given the significant risk of serious bleeding on-therapy and the fact that a serious bleed event is two to three times more likely than a VTE to be fatal.
Dr. Rodger and coinvestigators recognized that a clinical decision rule needs to be externally validated before it’s ready for prime-time use in clinical practice. Thus, they conducted the REVERSE II study, in which the decision rule was applied after the 2,799 participants had been on anticoagulation for 5-12 months. All had a first proximal deep vein thrombosis and/or a segmental or greater pulmonary embolism. Patients were still on anticoagulation at the time the rule was applied, which is why the cut point for a positive d-dimer test in HERDOO2 is 250 mcg/L, half of the threshold value for a positive test in patients not on anticoagulation.
They identified 631 women as low risk, with a HERDOO2 score of 0 or 1. They and their physicians were instructed to stop anticoagulation at that time. The 2,148 high-risk subjects – that is, all of the men and the high-risk women – were advised to remain on anticoagulation. The primary study endpoint was the rate of recurrent VTE in the 12 months following testing and patient guidance. The lost-to-follow-up rate was 2.2%.
The recurrent VTE rate was 3% in the 591 low-risk women who discontinued anticoagulants and zero in 31 others who elected to stay on medication. In the high-risk group identified by the HERDOO2 rule, the recurrent VTE rate at 12 months was 8.1% in the 323 who opted to discontinue anticoagulants and just 1.6% in 1,802 who continued on therapy as advised, a finding that underscores the effectiveness of selectively applied long-term anticoagulation therapy, he continued.
The recurrent VTE rate among the 291 women with a HERDOO2 score of 0 or 1 who were on exogenous estrogen was 1.4%, while in high-risk women taking estrogen the rate was more than doubled at 3.1%. But in women aged 50-64 identified by the HERDOO2 rule as being low risk, the actual recurrent VTE rate was 5.7%, a finding that raised a red flag for the investigators.
“There may be an evolution of the HERDOO2 decision rule to a lower age cut point. But that’s something that requires further study in postmenopausal women,” according to Dr. Rodger.
The investigators defined a first unprovoked VTE as one occurring in the absence during the previous 90 days of major surgery, a fracture or cast, more than 3 days of immobilization, or malignancy within the last 5 years.
Venous thromboembolism is the second most common cardiovascular disorder and the third most common cause of cardiovascular death. Unprovoked VTEs account for half of all VTEs. Their management has been a controversial subject. Both the American College of Chest Physicians and the European Society of Cardiology recommend continuing anticoagulation indefinitely in patients who aren’t at high bleeding risk.
“But this is a relatively weak 2B recommendation because of the tightly balanced competing risks of recurrent thrombosis off anticoagulation and major bleeding on anticoagulation,” Dr. Rodger said. He added that he considers REVERSE II to be practice changing, and predicted that once the results are published the guidelines will be revised.
Discussant Giancarlo Agnelli, MD, was a tough critic who gave fair warning.
“I am friends with many of the authors of this paper, and in this country we are usually gentle with enemies and nasty with friends,” declared Dr. Agnelli, professor of internal medicine and director of internal and cardiovascular medicine and the stroke unit at the University of Perugia, Italy.
He didn’t find the REVERSE II study or the HERDOO2 rule persuasive. On the plus side, he said, the HERDOO2 rule has now been validated, unlike the proposed DASH and Vienna rules. And it was tested in a diverse multinational patient population. But the fact that the HERDOO2 rule is only applicable in women is a major limitation. And REVERSE II was not a randomized trial, Dr. Agnelli noted.
Moreover, 1 year of follow-up seems insufficient, he continued. He cited a French multicenter trial in which patients with a first unprovoked VTE received 6 months of anticoagulants and were then randomized to another 18 months of anticoagulation or placebo. During that 18 months, the group on anticoagulants had a significantly lower rate of the composite endpoint comprised of recurrent VTE or major bleeding, but once that period was over they experienced catchup. By the time the study ended at 42 months, the two study arms didn’t differ significantly in the composite endpoint (JAMA. 2015 Jul 7;314[1]:31-40).
More broadly, Dr. Agnelli also questioned the need for an anticoagulation discontinuation rule in the contemporary era of new oral anticoagulants (NOACs). He was lead investigator in the AMPLIFY study, a major randomized trial of fixed-dose apixaban (Eliquis) versus conventional therapy with subcutaneous enoxaparin (Lovenox) bridging to warfarin in 5,395 patients with acute VTE. The NOAC was associated with a 69% reduction in the relative risk of bleeding and was noninferior to standard therapy in the risk of recurrent VTE (N Engl J Med. 2013 Aug 29;369[9]:799-808).
“Why should we think about withholding anticoagulation in some patients when we now have such a safe approach?” he asked.
Dr. Rodger reported receiving research grants from the French government as well as from Biomerieux, which funded the REVERSE II study. Dr. Agnelli reported having no financial conflicts.
AT THE ESC CONGRESS 2016
Key clinical point: Half of women who have a first unprovoked venous thromboembolism can safely be spared lifelong anticoagulation through application of the newly validated HERDOO2 decision rule.
Major finding: Women with a first unprovoked venous thromboembolism identified as being at low risk of recurrence on the basis of the HERDOO2 decision rule had a 3% recurrence rate in the year after stopping anticoagulation therapy, while those identified as high risk had an 8.1% recurrence rate if they discontinued anticoagulants.
Data source: This was a prospective, multinational, observational study involving 2,779 patients with a first unprovoked venous thromboembolism.
Disclosures: The presenter reported receiving research grants from the French government as well as from Biomerieux, which funded the REVERSE II study.
