User login
Why our brains wear out at the end of the day
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”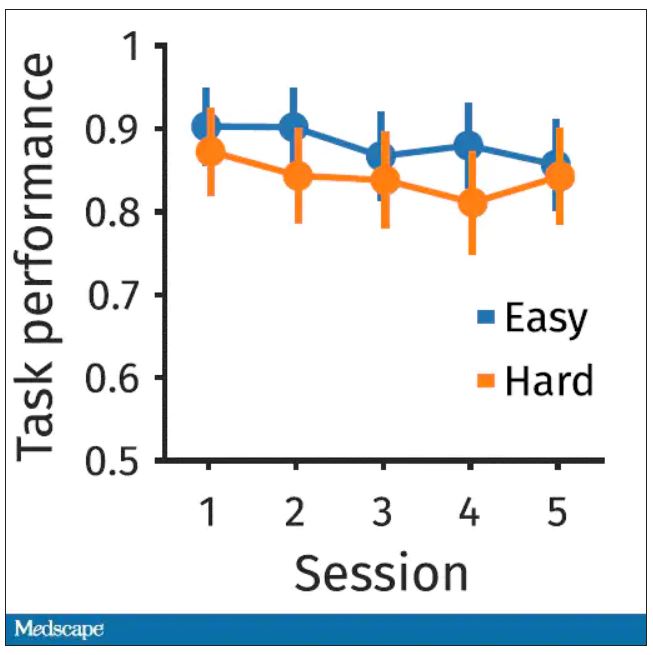
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.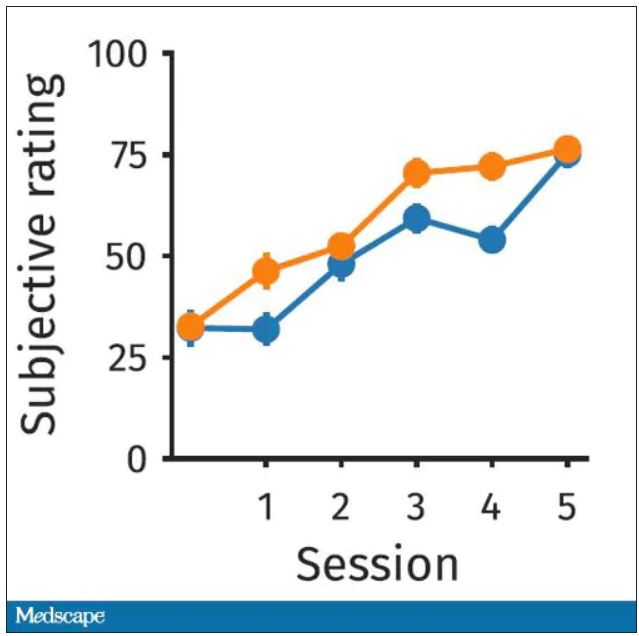
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”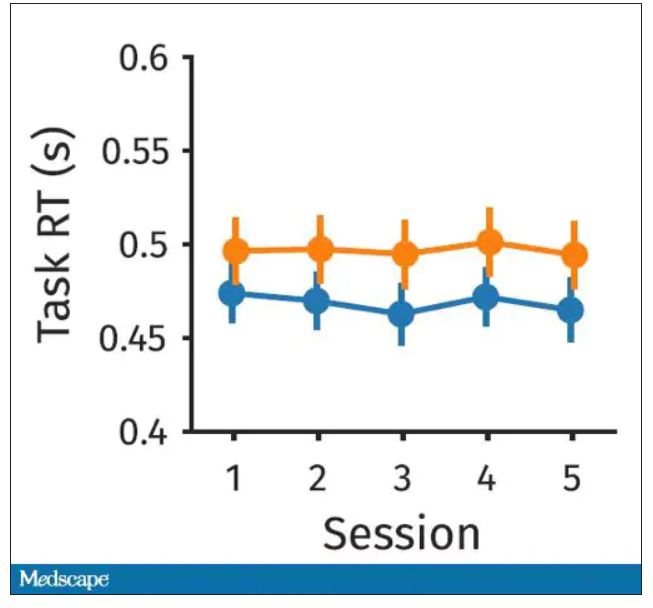
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.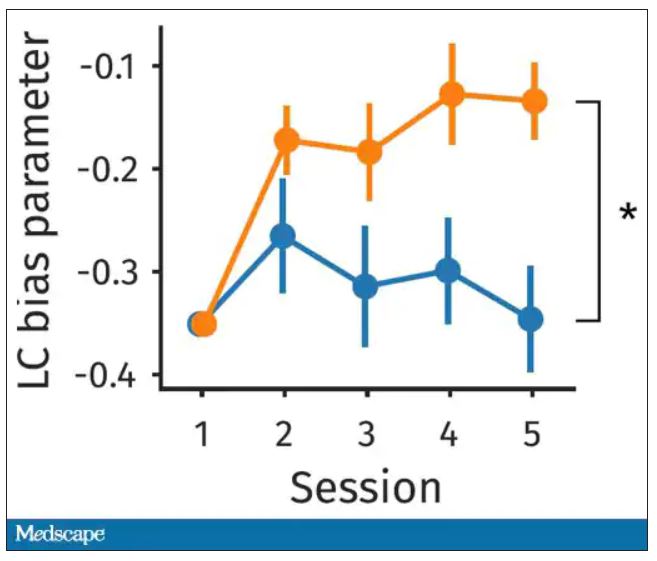
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.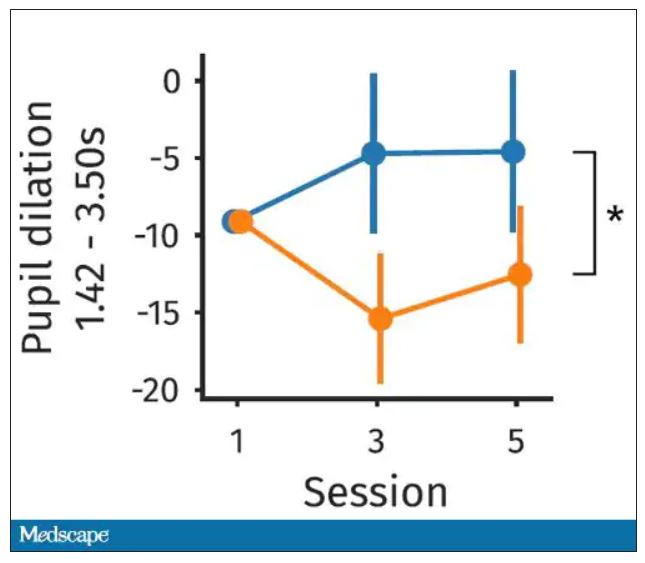
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.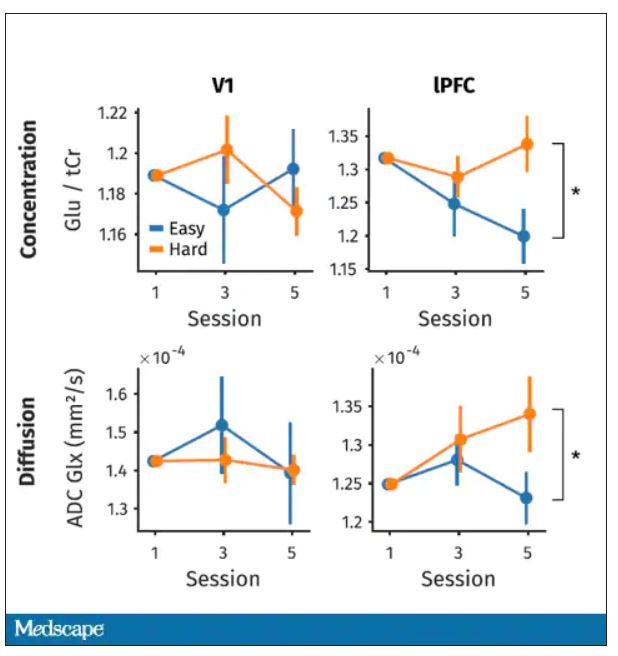
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Alzheimer’s disease: Alternative mechanisms make clinical progress
SAN DIEGO – In 1906, a neuroanatomist and psychiatrist named Alois Alzheimer examined the brain of a 50-year-old woman whom he had treated for paranoia, sleep and memory problems, aggression, and confusion. His autopsy revealed plaques and tangles in her brain. The most common components of these tangles are beta-amyloid peptide (A-beta) and the microtubule binding protein tau. Over the past few decades, that finding has launched many clinical development programs and dozens of clinical trials.
To date, all but one program has failed. In 2021, amidst much controversy, FDA granted accelerated approval to Biogen’s Aduhelm, which effectively clears A-beta and tau deposits from patients’ brains. The problem is that the clinical benefit is small, and uptake has been so low that the company was forced to abandon a planned postmarketing observational trial.
Chasing the wrong target?
At a session at the 2022 Alzheimer’s Association International Conference, Raymond J. Tesi, MD, rather forcefully refuted that approach. “Amyloid and tau therapies have had 20 years to prove themselves. We have multiple cases where we’ve been able to decrease amyloid, maybe not so much tau, but certainly amyloid, and the benefits are mild at best. So I think that the Alzheimer’s drug development community, whether you look at the NIH, whether you look at academia, whether you look at biopharma, has focused on a target that has not proven itself, and it’s time to move on,” said Dr. Tesi, who is president, CEO, and chief medical officer at INmune Bio.
Later in the session,
One audience member defended the potential importance of A-beta and tau, especially in astrogliosis, which is a reaction to stress by astrocytes that attempts to limit tissue damage. The questioner suggested that it was still important to measure the effect of a novel drug on A-beta and tau. “What would be the cause of the reactive astrogliosis and microglia activation, if we are not giving a damn about amyloid and tau?” he asked.
After a bit of back and forth, Dr. Tesi replied: “We both have a religious belief here, and sooner or later we’ll get the answer.”
A diverse clinical pipeline
The session itself focused on four companies, including Dr. Tesi’s INmune Bio, which have drugs with alternative mechanisms entering the advanced stages of clinical development. That’s good news, according to Heather Snyder, PhD, who is vice president of Medical & Scientific Relations at the Alzheimer’s Association. “One of the things that I think is really important is the diversity of what’s in the clinical pipeline, and it’s not just in the very beginning anymore. We’re seeing [companies] now reporting phase 2 [studies] and planning their next stage. That’s something that as a field we should be excited about. As we understand more and more about the biology, we’re now seeing that translating into clinical trials and we’re seeing that translate through the clinical pipeline of development,” said Dr. Snyder in an interview.
Targeting neuroinflammation
Dr. Tesi kicked off the session describing INmune Bio’s focus on neuroinflammation. The company’s drug candidate targets soluble tumor necrosis factor (TNF), which the company believes is a direct cause of Alzheimer’s disease through promotion of inflammation. He noted that TNF is a primary mediator of inflammation in rheumatoid arthritis, and patients with RA have an eightfold increased risk of developing Alzheimer’s disease, compared with the general population, while patients with RA who are taking anti-TNF medication have a 60% lower risk than the general population.
The company’s TNF inhibitor XPro is also unique in that it induces remyelination in mice, while other TNF inhibitors potentially “abuse” the brain by causing demyelination. Earlier research showed that it reduces neuroinflammation, improves nerve cell survival, and improves synaptic function. The company is conducting two phase 2 clinical trials, one in patients with mild cognitive impairment (MCI) and one in mild Alzheimer’s disease. They also use the MCI Alzheimer’s Cognitive Composite (EMACC) tool for assessing outcomes rather than the more commonly used Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-Cog). “ADAS-Cog is like trying to make sushi with an axe. It is designed for moderate to severe disease, and trying to use it for mild (Alzheimer’s disease) or MCI is a mistake. EMACC is purpose built for mild [AD] and MCI patients,” said Dr. Tesi.
Maintaining homeostatis
Next, Hans Moebius, MD, PhD, chief medical officer of Athira Pharma, described his company’s focus on the hepatocyte growth factor (HGF) receptor, also known as tyrosine kinase MET (HGF/MET). It plays an important role in brain development and homeostasis, and it is expressed at lower levels in the frontal cortex and hippocampus of patients with Alzheimer’s disease. The company’s small-molecule drug candidate boosts the HGF/MET pathway, leading to downstream neuroprotection and neurotrophic effects. It also promotes formation of new synapses.
Dr. Moebius presented the results of a phase 2 trial showing that the drug, called fosgonimeton, led to significant cognitive improvement compared with placebo. The company is conducting a phase 3 clinical trial.
Type 3 diabetes?
In his talk, John Didsbury, PhD, founder and CEO of T3D Therapeutics, framed Alzheimer’s disease as a disease of metabolic dysfunction. He believes alterations to glucose and lipids in the brain cause structural changes that lead to symptoms. He pointed out that the strongest genetic Alzheimer’s disease risk factor is a mutant form of the lipid transport protein APOE4.
“What we have is dysregulated glucose energy metabolism and lipid metabolism that really cause, in our mind, the structural event changes and the stress event changes – plaques, tangles, inflammation, etc. – but these events perpetuate the dysregulated metabolism. It’s a massive positive feedback loop that many have called type 3 diabetes – a brain-specific form of diabetes,” said Dr. Didsbury.
The company’s approach is to use systems biology to identify a drug target that can bypass multiple aberrant insulin signaling pathways. Its drug candidate regulates the expression of multiple genes involved in glucose metabolism. Dr. Didsbury presented interim results from a phase 2 study showing improvement over placebo.
Focusing on neurotoxic proteins
The final presentation of the session was by Maria Maccecchini, PhD, founder, president, and CEO of Annovis Bio. The company’s drug, buntanetap, reduces expression of a range of neurotoxic proteins. The downstream effects include restoration of axonal transport, reduction of inflammation, and protection of nerve cells. The company believes that Alzheimer’s disease results from acute and chronic stress events that lead to high levels of neurotoxic proteins, which include A-beta, tau, alpha-synuclein, and TDP43. The proteins aren’t just players in Alzheimer’s disease – they are present in abnormal levels in Parkinson’s disease and a range of other brain pathologies.
“In the brain of an Alzheimer’s and of a Parkinson’s [patient], you’re going to find all four proteins. You’ll find them in different concentrations, at different time points, in different brain areas. If you just remove one, you still have the other three that cause impairment in axonal transport, and that leads to inflammation that leads to neurodegeneration,” said Dr. Maccecchini.
The company’s drug manages to reduce levels of all four proteins by binding to a segment of messenger RNA (mRNA) shared by all of them. mRNA serves as a template for protein synthesis. Under normal conditions, the neurotoxic protein concentrations are kept low because the mRNA segment remains bound to a regulatory protein that prevents synthesis from occurring. However, when stress leads to high levels of iron, this regulatory binding protein releases the mRNA segment (along with the rest of the mRNA). The freed mRNA becomes available to the cell’s protein synthesis machinery, which starts producing high levels of neurotoxic proteins. Annovis Bio’s drug improves the ability of the regulatory protein to bind to the mRNA segment, preventing protein expression even in high-iron conditions. It works on all four neurotoxic proteins because they all have the regulatory segment in their mRNA.
The drug led to improvements in phase 2 studies of Alzheimer’s disease and Parkinson’s disease, and the company is currently recruiting for a phase 3 study in Parkinson’s disease and a phase 2/3 dose-response study in Alzheimer’s disease.
Combination treatments for a complex disease
Taken together, the presentations provided a snapshot of the post–A-beta/tau Alzheimer’s development world, and the future could be messy. Alzheimer’s disease and other dementias are likely to require combination treatments, according to Dr. Snyder. “This is a complex disease, not just Alzheimer’s but other dementias. It’s not going to be a single drug, a single target. It’s going to require some type of combinatorial approach, whether that be with medication and lifestyle interventions, or risk reduction, and different medications,” she said.
The latest results are good news for that approach: “We’re seeing that maturation of the science in these trials,” said Dr. Snyder.
Cheng Fang, PhD, senior vice president of research and development at Annovis Bio, agreed with that sentiment. “I believe [Alzheimer’s disease and dementia] is a very complicated disease. I always call them diseases instead of a disease because it’s a spectrum. I don’t believe one drug can cure them all, as much as I am confident in our drug. I think it’s extremely important to encourage this kind of diverse thinking,” said Dr. Fang.
Dr. Snyder has no relevant financial disclosures. Dr. Tesi, Dr. Moebius, Dr. Didsbury, Dr. Maccecchini, and Dr. Fang are employees and in some cases stockholders of their respective companies.
SAN DIEGO – In 1906, a neuroanatomist and psychiatrist named Alois Alzheimer examined the brain of a 50-year-old woman whom he had treated for paranoia, sleep and memory problems, aggression, and confusion. His autopsy revealed plaques and tangles in her brain. The most common components of these tangles are beta-amyloid peptide (A-beta) and the microtubule binding protein tau. Over the past few decades, that finding has launched many clinical development programs and dozens of clinical trials.
To date, all but one program has failed. In 2021, amidst much controversy, FDA granted accelerated approval to Biogen’s Aduhelm, which effectively clears A-beta and tau deposits from patients’ brains. The problem is that the clinical benefit is small, and uptake has been so low that the company was forced to abandon a planned postmarketing observational trial.
Chasing the wrong target?
At a session at the 2022 Alzheimer’s Association International Conference, Raymond J. Tesi, MD, rather forcefully refuted that approach. “Amyloid and tau therapies have had 20 years to prove themselves. We have multiple cases where we’ve been able to decrease amyloid, maybe not so much tau, but certainly amyloid, and the benefits are mild at best. So I think that the Alzheimer’s drug development community, whether you look at the NIH, whether you look at academia, whether you look at biopharma, has focused on a target that has not proven itself, and it’s time to move on,” said Dr. Tesi, who is president, CEO, and chief medical officer at INmune Bio.
Later in the session,
One audience member defended the potential importance of A-beta and tau, especially in astrogliosis, which is a reaction to stress by astrocytes that attempts to limit tissue damage. The questioner suggested that it was still important to measure the effect of a novel drug on A-beta and tau. “What would be the cause of the reactive astrogliosis and microglia activation, if we are not giving a damn about amyloid and tau?” he asked.
After a bit of back and forth, Dr. Tesi replied: “We both have a religious belief here, and sooner or later we’ll get the answer.”
A diverse clinical pipeline
The session itself focused on four companies, including Dr. Tesi’s INmune Bio, which have drugs with alternative mechanisms entering the advanced stages of clinical development. That’s good news, according to Heather Snyder, PhD, who is vice president of Medical & Scientific Relations at the Alzheimer’s Association. “One of the things that I think is really important is the diversity of what’s in the clinical pipeline, and it’s not just in the very beginning anymore. We’re seeing [companies] now reporting phase 2 [studies] and planning their next stage. That’s something that as a field we should be excited about. As we understand more and more about the biology, we’re now seeing that translating into clinical trials and we’re seeing that translate through the clinical pipeline of development,” said Dr. Snyder in an interview.
Targeting neuroinflammation
Dr. Tesi kicked off the session describing INmune Bio’s focus on neuroinflammation. The company’s drug candidate targets soluble tumor necrosis factor (TNF), which the company believes is a direct cause of Alzheimer’s disease through promotion of inflammation. He noted that TNF is a primary mediator of inflammation in rheumatoid arthritis, and patients with RA have an eightfold increased risk of developing Alzheimer’s disease, compared with the general population, while patients with RA who are taking anti-TNF medication have a 60% lower risk than the general population.
The company’s TNF inhibitor XPro is also unique in that it induces remyelination in mice, while other TNF inhibitors potentially “abuse” the brain by causing demyelination. Earlier research showed that it reduces neuroinflammation, improves nerve cell survival, and improves synaptic function. The company is conducting two phase 2 clinical trials, one in patients with mild cognitive impairment (MCI) and one in mild Alzheimer’s disease. They also use the MCI Alzheimer’s Cognitive Composite (EMACC) tool for assessing outcomes rather than the more commonly used Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-Cog). “ADAS-Cog is like trying to make sushi with an axe. It is designed for moderate to severe disease, and trying to use it for mild (Alzheimer’s disease) or MCI is a mistake. EMACC is purpose built for mild [AD] and MCI patients,” said Dr. Tesi.
Maintaining homeostatis
Next, Hans Moebius, MD, PhD, chief medical officer of Athira Pharma, described his company’s focus on the hepatocyte growth factor (HGF) receptor, also known as tyrosine kinase MET (HGF/MET). It plays an important role in brain development and homeostasis, and it is expressed at lower levels in the frontal cortex and hippocampus of patients with Alzheimer’s disease. The company’s small-molecule drug candidate boosts the HGF/MET pathway, leading to downstream neuroprotection and neurotrophic effects. It also promotes formation of new synapses.
Dr. Moebius presented the results of a phase 2 trial showing that the drug, called fosgonimeton, led to significant cognitive improvement compared with placebo. The company is conducting a phase 3 clinical trial.
Type 3 diabetes?
In his talk, John Didsbury, PhD, founder and CEO of T3D Therapeutics, framed Alzheimer’s disease as a disease of metabolic dysfunction. He believes alterations to glucose and lipids in the brain cause structural changes that lead to symptoms. He pointed out that the strongest genetic Alzheimer’s disease risk factor is a mutant form of the lipid transport protein APOE4.
“What we have is dysregulated glucose energy metabolism and lipid metabolism that really cause, in our mind, the structural event changes and the stress event changes – plaques, tangles, inflammation, etc. – but these events perpetuate the dysregulated metabolism. It’s a massive positive feedback loop that many have called type 3 diabetes – a brain-specific form of diabetes,” said Dr. Didsbury.
The company’s approach is to use systems biology to identify a drug target that can bypass multiple aberrant insulin signaling pathways. Its drug candidate regulates the expression of multiple genes involved in glucose metabolism. Dr. Didsbury presented interim results from a phase 2 study showing improvement over placebo.
Focusing on neurotoxic proteins
The final presentation of the session was by Maria Maccecchini, PhD, founder, president, and CEO of Annovis Bio. The company’s drug, buntanetap, reduces expression of a range of neurotoxic proteins. The downstream effects include restoration of axonal transport, reduction of inflammation, and protection of nerve cells. The company believes that Alzheimer’s disease results from acute and chronic stress events that lead to high levels of neurotoxic proteins, which include A-beta, tau, alpha-synuclein, and TDP43. The proteins aren’t just players in Alzheimer’s disease – they are present in abnormal levels in Parkinson’s disease and a range of other brain pathologies.
“In the brain of an Alzheimer’s and of a Parkinson’s [patient], you’re going to find all four proteins. You’ll find them in different concentrations, at different time points, in different brain areas. If you just remove one, you still have the other three that cause impairment in axonal transport, and that leads to inflammation that leads to neurodegeneration,” said Dr. Maccecchini.
The company’s drug manages to reduce levels of all four proteins by binding to a segment of messenger RNA (mRNA) shared by all of them. mRNA serves as a template for protein synthesis. Under normal conditions, the neurotoxic protein concentrations are kept low because the mRNA segment remains bound to a regulatory protein that prevents synthesis from occurring. However, when stress leads to high levels of iron, this regulatory binding protein releases the mRNA segment (along with the rest of the mRNA). The freed mRNA becomes available to the cell’s protein synthesis machinery, which starts producing high levels of neurotoxic proteins. Annovis Bio’s drug improves the ability of the regulatory protein to bind to the mRNA segment, preventing protein expression even in high-iron conditions. It works on all four neurotoxic proteins because they all have the regulatory segment in their mRNA.
The drug led to improvements in phase 2 studies of Alzheimer’s disease and Parkinson’s disease, and the company is currently recruiting for a phase 3 study in Parkinson’s disease and a phase 2/3 dose-response study in Alzheimer’s disease.
Combination treatments for a complex disease
Taken together, the presentations provided a snapshot of the post–A-beta/tau Alzheimer’s development world, and the future could be messy. Alzheimer’s disease and other dementias are likely to require combination treatments, according to Dr. Snyder. “This is a complex disease, not just Alzheimer’s but other dementias. It’s not going to be a single drug, a single target. It’s going to require some type of combinatorial approach, whether that be with medication and lifestyle interventions, or risk reduction, and different medications,” she said.
The latest results are good news for that approach: “We’re seeing that maturation of the science in these trials,” said Dr. Snyder.
Cheng Fang, PhD, senior vice president of research and development at Annovis Bio, agreed with that sentiment. “I believe [Alzheimer’s disease and dementia] is a very complicated disease. I always call them diseases instead of a disease because it’s a spectrum. I don’t believe one drug can cure them all, as much as I am confident in our drug. I think it’s extremely important to encourage this kind of diverse thinking,” said Dr. Fang.
Dr. Snyder has no relevant financial disclosures. Dr. Tesi, Dr. Moebius, Dr. Didsbury, Dr. Maccecchini, and Dr. Fang are employees and in some cases stockholders of their respective companies.
SAN DIEGO – In 1906, a neuroanatomist and psychiatrist named Alois Alzheimer examined the brain of a 50-year-old woman whom he had treated for paranoia, sleep and memory problems, aggression, and confusion. His autopsy revealed plaques and tangles in her brain. The most common components of these tangles are beta-amyloid peptide (A-beta) and the microtubule binding protein tau. Over the past few decades, that finding has launched many clinical development programs and dozens of clinical trials.
To date, all but one program has failed. In 2021, amidst much controversy, FDA granted accelerated approval to Biogen’s Aduhelm, which effectively clears A-beta and tau deposits from patients’ brains. The problem is that the clinical benefit is small, and uptake has been so low that the company was forced to abandon a planned postmarketing observational trial.
Chasing the wrong target?
At a session at the 2022 Alzheimer’s Association International Conference, Raymond J. Tesi, MD, rather forcefully refuted that approach. “Amyloid and tau therapies have had 20 years to prove themselves. We have multiple cases where we’ve been able to decrease amyloid, maybe not so much tau, but certainly amyloid, and the benefits are mild at best. So I think that the Alzheimer’s drug development community, whether you look at the NIH, whether you look at academia, whether you look at biopharma, has focused on a target that has not proven itself, and it’s time to move on,” said Dr. Tesi, who is president, CEO, and chief medical officer at INmune Bio.
Later in the session,
One audience member defended the potential importance of A-beta and tau, especially in astrogliosis, which is a reaction to stress by astrocytes that attempts to limit tissue damage. The questioner suggested that it was still important to measure the effect of a novel drug on A-beta and tau. “What would be the cause of the reactive astrogliosis and microglia activation, if we are not giving a damn about amyloid and tau?” he asked.
After a bit of back and forth, Dr. Tesi replied: “We both have a religious belief here, and sooner or later we’ll get the answer.”
A diverse clinical pipeline
The session itself focused on four companies, including Dr. Tesi’s INmune Bio, which have drugs with alternative mechanisms entering the advanced stages of clinical development. That’s good news, according to Heather Snyder, PhD, who is vice president of Medical & Scientific Relations at the Alzheimer’s Association. “One of the things that I think is really important is the diversity of what’s in the clinical pipeline, and it’s not just in the very beginning anymore. We’re seeing [companies] now reporting phase 2 [studies] and planning their next stage. That’s something that as a field we should be excited about. As we understand more and more about the biology, we’re now seeing that translating into clinical trials and we’re seeing that translate through the clinical pipeline of development,” said Dr. Snyder in an interview.
Targeting neuroinflammation
Dr. Tesi kicked off the session describing INmune Bio’s focus on neuroinflammation. The company’s drug candidate targets soluble tumor necrosis factor (TNF), which the company believes is a direct cause of Alzheimer’s disease through promotion of inflammation. He noted that TNF is a primary mediator of inflammation in rheumatoid arthritis, and patients with RA have an eightfold increased risk of developing Alzheimer’s disease, compared with the general population, while patients with RA who are taking anti-TNF medication have a 60% lower risk than the general population.
The company’s TNF inhibitor XPro is also unique in that it induces remyelination in mice, while other TNF inhibitors potentially “abuse” the brain by causing demyelination. Earlier research showed that it reduces neuroinflammation, improves nerve cell survival, and improves synaptic function. The company is conducting two phase 2 clinical trials, one in patients with mild cognitive impairment (MCI) and one in mild Alzheimer’s disease. They also use the MCI Alzheimer’s Cognitive Composite (EMACC) tool for assessing outcomes rather than the more commonly used Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-Cog). “ADAS-Cog is like trying to make sushi with an axe. It is designed for moderate to severe disease, and trying to use it for mild (Alzheimer’s disease) or MCI is a mistake. EMACC is purpose built for mild [AD] and MCI patients,” said Dr. Tesi.
Maintaining homeostatis
Next, Hans Moebius, MD, PhD, chief medical officer of Athira Pharma, described his company’s focus on the hepatocyte growth factor (HGF) receptor, also known as tyrosine kinase MET (HGF/MET). It plays an important role in brain development and homeostasis, and it is expressed at lower levels in the frontal cortex and hippocampus of patients with Alzheimer’s disease. The company’s small-molecule drug candidate boosts the HGF/MET pathway, leading to downstream neuroprotection and neurotrophic effects. It also promotes formation of new synapses.
Dr. Moebius presented the results of a phase 2 trial showing that the drug, called fosgonimeton, led to significant cognitive improvement compared with placebo. The company is conducting a phase 3 clinical trial.
Type 3 diabetes?
In his talk, John Didsbury, PhD, founder and CEO of T3D Therapeutics, framed Alzheimer’s disease as a disease of metabolic dysfunction. He believes alterations to glucose and lipids in the brain cause structural changes that lead to symptoms. He pointed out that the strongest genetic Alzheimer’s disease risk factor is a mutant form of the lipid transport protein APOE4.
“What we have is dysregulated glucose energy metabolism and lipid metabolism that really cause, in our mind, the structural event changes and the stress event changes – plaques, tangles, inflammation, etc. – but these events perpetuate the dysregulated metabolism. It’s a massive positive feedback loop that many have called type 3 diabetes – a brain-specific form of diabetes,” said Dr. Didsbury.
The company’s approach is to use systems biology to identify a drug target that can bypass multiple aberrant insulin signaling pathways. Its drug candidate regulates the expression of multiple genes involved in glucose metabolism. Dr. Didsbury presented interim results from a phase 2 study showing improvement over placebo.
Focusing on neurotoxic proteins
The final presentation of the session was by Maria Maccecchini, PhD, founder, president, and CEO of Annovis Bio. The company’s drug, buntanetap, reduces expression of a range of neurotoxic proteins. The downstream effects include restoration of axonal transport, reduction of inflammation, and protection of nerve cells. The company believes that Alzheimer’s disease results from acute and chronic stress events that lead to high levels of neurotoxic proteins, which include A-beta, tau, alpha-synuclein, and TDP43. The proteins aren’t just players in Alzheimer’s disease – they are present in abnormal levels in Parkinson’s disease and a range of other brain pathologies.
“In the brain of an Alzheimer’s and of a Parkinson’s [patient], you’re going to find all four proteins. You’ll find them in different concentrations, at different time points, in different brain areas. If you just remove one, you still have the other three that cause impairment in axonal transport, and that leads to inflammation that leads to neurodegeneration,” said Dr. Maccecchini.
The company’s drug manages to reduce levels of all four proteins by binding to a segment of messenger RNA (mRNA) shared by all of them. mRNA serves as a template for protein synthesis. Under normal conditions, the neurotoxic protein concentrations are kept low because the mRNA segment remains bound to a regulatory protein that prevents synthesis from occurring. However, when stress leads to high levels of iron, this regulatory binding protein releases the mRNA segment (along with the rest of the mRNA). The freed mRNA becomes available to the cell’s protein synthesis machinery, which starts producing high levels of neurotoxic proteins. Annovis Bio’s drug improves the ability of the regulatory protein to bind to the mRNA segment, preventing protein expression even in high-iron conditions. It works on all four neurotoxic proteins because they all have the regulatory segment in their mRNA.
The drug led to improvements in phase 2 studies of Alzheimer’s disease and Parkinson’s disease, and the company is currently recruiting for a phase 3 study in Parkinson’s disease and a phase 2/3 dose-response study in Alzheimer’s disease.
Combination treatments for a complex disease
Taken together, the presentations provided a snapshot of the post–A-beta/tau Alzheimer’s development world, and the future could be messy. Alzheimer’s disease and other dementias are likely to require combination treatments, according to Dr. Snyder. “This is a complex disease, not just Alzheimer’s but other dementias. It’s not going to be a single drug, a single target. It’s going to require some type of combinatorial approach, whether that be with medication and lifestyle interventions, or risk reduction, and different medications,” she said.
The latest results are good news for that approach: “We’re seeing that maturation of the science in these trials,” said Dr. Snyder.
Cheng Fang, PhD, senior vice president of research and development at Annovis Bio, agreed with that sentiment. “I believe [Alzheimer’s disease and dementia] is a very complicated disease. I always call them diseases instead of a disease because it’s a spectrum. I don’t believe one drug can cure them all, as much as I am confident in our drug. I think it’s extremely important to encourage this kind of diverse thinking,” said Dr. Fang.
Dr. Snyder has no relevant financial disclosures. Dr. Tesi, Dr. Moebius, Dr. Didsbury, Dr. Maccecchini, and Dr. Fang are employees and in some cases stockholders of their respective companies.
AT AAIC 2022
Plasma biomarkers predict COVID’s neurological sequelae
SAN DIEGO – Even after recovery of an acute COVID-19 infection, some patients experience extended or even long-term symptoms that can range from mild to debilitating. Some of these symptoms are neurological: headaches, brain fog, cognitive impairment, loss of taste or smell, and even cerebrovascular complications such stroke. There are even hints that COVID-19 infection could lead to future neurodegeneration.
Those issues have prompted efforts to identify biomarkers that can help track and monitor neurological complications of COVID-19. “Throughout the course of the pandemic, it has become apparent that COVID-19 can cause various neurological symptoms. Because of this, ,” Jennifer Cooper said during a lecture at the Alzheimer’s Association International Conference. She presented new research suggesting that neurofilament light (NfL) and glial fibrillary acidic protein (GFAP) may prove useful.
Ms. Cooper is a master’s degree student at the University of British Columbia and Canada.
Looking for sensitivity and specificity in plasma biomarkers
The researchers turned to plasma-based markers because they can reflect underlying pathology in the central nervous system. They focused on NfL, which reflects axonal damage, and GFAP, which is a marker of astrocyte activation.
The researchers analyzed data from 209 patients with COVID-19 who were admitted to the Vancouver (B.C.) General Hospital intensive care unit. Sixty-four percent were male, and the median age was 61 years. Sixty percent were ventilated, and 17% died.
The researchers determined if an individual patient’s biomarker level at hospital admission fell within a normal biomarker reference interval. A total of 53% had NfL levels outside the normal range, and 42% had GFAP levels outside the normal range. In addition, 31% of patients had both GFAP and NfL levels outside of the normal range.
Among all patients, 12% experienced ischemia, 4% hemorrhage, 2% seizures, and 10% degeneration.
At admission, NfL predicted a neurological complication with an area under the curve (AUC) of 0.702. GFAP had an AUC of 0.722. In combination, they had an AUC of 0.743. At 1 week, NfL had an AUC of 0.802, GFAP an AUC of 0.733, and the combination an AUC of 0.812.
Using age-specific cutoff values, the researchers found increased risks for neurological complications at admission (NfL odds ratio [OR], 2.9; GFAP OR, 1.6; combined OR, 2.1) and at 1 week (NfL OR, not significant; GFAP OR, 4.8; combined OR, 6.6). “We can see that both NFL and GFAP have utility in detecting neurological complications. And combining both of our markers improves detection at both time points. NfL is a marker that provides more sensitivity, where in this cohort GFAP is a marker that provides a little bit more specificity,” said Ms. Cooper.
Will additional biomarkers help?
The researchers are continuing to follow up patients at 6 months and 18 months post diagnosis, using neuropsychiatric tests and additional biomarker analysis, as well as PET and MRI scans. The patient sample is being expanded to those in the general hospital ward and some who were not hospitalized.
During the Q&A session, Ms. Cooper was asked if the group had collected reference data from patients who were admitted to the ICU with non-COVID disease. She responded that the group has some of that data, but as the pandemic went on they had difficulty finding patients who had never been infected with COVID to serve as reliable controls. To date, they have identified 33 controls who had a respiratory condition when admitted to the ICU. “What we see is the neurological biomarker levels in COVID are slightly lower than those with another respiratory condition in the ICU. But the data has a massive spread and the significance is very small between the two groups,” said Ms. Cooper.
Unanswered questions
The study is interesting, but leaves a lot of unanswered questions, according to Wiesje van der Flier, PhD, who moderated the session where the study was presented. “There are a lot of unknowns still: Will [the biomarkers] become normal again, once the COVID is over? Also, there was an increased risk, but it was not a one-to-one correspondence, so you can also have the increased markers but not have the neurological signs or symptoms. So I thought there were lots of questions as well,” said Dr. van der Flier, professor of neurology at Amsterdam University Medical Center.
She noted that researchers at her institution in Amsterdam have observed similar relationships, and that the associations between neurological complications and plasma biomarkers over time will be an important topic of study.
The work could provide more information on neurological manifestations of long COVID, such as long-haul fatigue. “You might also think that’s some response in their brain. It would be great if we could actually capture that [using biomarkers],” said Dr. van der Flier.
Ms. Cooper and Dr. van der Flier have no relevant financial disclosures.
SAN DIEGO – Even after recovery of an acute COVID-19 infection, some patients experience extended or even long-term symptoms that can range from mild to debilitating. Some of these symptoms are neurological: headaches, brain fog, cognitive impairment, loss of taste or smell, and even cerebrovascular complications such stroke. There are even hints that COVID-19 infection could lead to future neurodegeneration.
Those issues have prompted efforts to identify biomarkers that can help track and monitor neurological complications of COVID-19. “Throughout the course of the pandemic, it has become apparent that COVID-19 can cause various neurological symptoms. Because of this, ,” Jennifer Cooper said during a lecture at the Alzheimer’s Association International Conference. She presented new research suggesting that neurofilament light (NfL) and glial fibrillary acidic protein (GFAP) may prove useful.
Ms. Cooper is a master’s degree student at the University of British Columbia and Canada.
Looking for sensitivity and specificity in plasma biomarkers
The researchers turned to plasma-based markers because they can reflect underlying pathology in the central nervous system. They focused on NfL, which reflects axonal damage, and GFAP, which is a marker of astrocyte activation.
The researchers analyzed data from 209 patients with COVID-19 who were admitted to the Vancouver (B.C.) General Hospital intensive care unit. Sixty-four percent were male, and the median age was 61 years. Sixty percent were ventilated, and 17% died.
The researchers determined if an individual patient’s biomarker level at hospital admission fell within a normal biomarker reference interval. A total of 53% had NfL levels outside the normal range, and 42% had GFAP levels outside the normal range. In addition, 31% of patients had both GFAP and NfL levels outside of the normal range.
Among all patients, 12% experienced ischemia, 4% hemorrhage, 2% seizures, and 10% degeneration.
At admission, NfL predicted a neurological complication with an area under the curve (AUC) of 0.702. GFAP had an AUC of 0.722. In combination, they had an AUC of 0.743. At 1 week, NfL had an AUC of 0.802, GFAP an AUC of 0.733, and the combination an AUC of 0.812.
Using age-specific cutoff values, the researchers found increased risks for neurological complications at admission (NfL odds ratio [OR], 2.9; GFAP OR, 1.6; combined OR, 2.1) and at 1 week (NfL OR, not significant; GFAP OR, 4.8; combined OR, 6.6). “We can see that both NFL and GFAP have utility in detecting neurological complications. And combining both of our markers improves detection at both time points. NfL is a marker that provides more sensitivity, where in this cohort GFAP is a marker that provides a little bit more specificity,” said Ms. Cooper.
Will additional biomarkers help?
The researchers are continuing to follow up patients at 6 months and 18 months post diagnosis, using neuropsychiatric tests and additional biomarker analysis, as well as PET and MRI scans. The patient sample is being expanded to those in the general hospital ward and some who were not hospitalized.
During the Q&A session, Ms. Cooper was asked if the group had collected reference data from patients who were admitted to the ICU with non-COVID disease. She responded that the group has some of that data, but as the pandemic went on they had difficulty finding patients who had never been infected with COVID to serve as reliable controls. To date, they have identified 33 controls who had a respiratory condition when admitted to the ICU. “What we see is the neurological biomarker levels in COVID are slightly lower than those with another respiratory condition in the ICU. But the data has a massive spread and the significance is very small between the two groups,” said Ms. Cooper.
Unanswered questions
The study is interesting, but leaves a lot of unanswered questions, according to Wiesje van der Flier, PhD, who moderated the session where the study was presented. “There are a lot of unknowns still: Will [the biomarkers] become normal again, once the COVID is over? Also, there was an increased risk, but it was not a one-to-one correspondence, so you can also have the increased markers but not have the neurological signs or symptoms. So I thought there were lots of questions as well,” said Dr. van der Flier, professor of neurology at Amsterdam University Medical Center.
She noted that researchers at her institution in Amsterdam have observed similar relationships, and that the associations between neurological complications and plasma biomarkers over time will be an important topic of study.
The work could provide more information on neurological manifestations of long COVID, such as long-haul fatigue. “You might also think that’s some response in their brain. It would be great if we could actually capture that [using biomarkers],” said Dr. van der Flier.
Ms. Cooper and Dr. van der Flier have no relevant financial disclosures.
SAN DIEGO – Even after recovery of an acute COVID-19 infection, some patients experience extended or even long-term symptoms that can range from mild to debilitating. Some of these symptoms are neurological: headaches, brain fog, cognitive impairment, loss of taste or smell, and even cerebrovascular complications such stroke. There are even hints that COVID-19 infection could lead to future neurodegeneration.
Those issues have prompted efforts to identify biomarkers that can help track and monitor neurological complications of COVID-19. “Throughout the course of the pandemic, it has become apparent that COVID-19 can cause various neurological symptoms. Because of this, ,” Jennifer Cooper said during a lecture at the Alzheimer’s Association International Conference. She presented new research suggesting that neurofilament light (NfL) and glial fibrillary acidic protein (GFAP) may prove useful.
Ms. Cooper is a master’s degree student at the University of British Columbia and Canada.
Looking for sensitivity and specificity in plasma biomarkers
The researchers turned to plasma-based markers because they can reflect underlying pathology in the central nervous system. They focused on NfL, which reflects axonal damage, and GFAP, which is a marker of astrocyte activation.
The researchers analyzed data from 209 patients with COVID-19 who were admitted to the Vancouver (B.C.) General Hospital intensive care unit. Sixty-four percent were male, and the median age was 61 years. Sixty percent were ventilated, and 17% died.
The researchers determined if an individual patient’s biomarker level at hospital admission fell within a normal biomarker reference interval. A total of 53% had NfL levels outside the normal range, and 42% had GFAP levels outside the normal range. In addition, 31% of patients had both GFAP and NfL levels outside of the normal range.
Among all patients, 12% experienced ischemia, 4% hemorrhage, 2% seizures, and 10% degeneration.
At admission, NfL predicted a neurological complication with an area under the curve (AUC) of 0.702. GFAP had an AUC of 0.722. In combination, they had an AUC of 0.743. At 1 week, NfL had an AUC of 0.802, GFAP an AUC of 0.733, and the combination an AUC of 0.812.
Using age-specific cutoff values, the researchers found increased risks for neurological complications at admission (NfL odds ratio [OR], 2.9; GFAP OR, 1.6; combined OR, 2.1) and at 1 week (NfL OR, not significant; GFAP OR, 4.8; combined OR, 6.6). “We can see that both NFL and GFAP have utility in detecting neurological complications. And combining both of our markers improves detection at both time points. NfL is a marker that provides more sensitivity, where in this cohort GFAP is a marker that provides a little bit more specificity,” said Ms. Cooper.
Will additional biomarkers help?
The researchers are continuing to follow up patients at 6 months and 18 months post diagnosis, using neuropsychiatric tests and additional biomarker analysis, as well as PET and MRI scans. The patient sample is being expanded to those in the general hospital ward and some who were not hospitalized.
During the Q&A session, Ms. Cooper was asked if the group had collected reference data from patients who were admitted to the ICU with non-COVID disease. She responded that the group has some of that data, but as the pandemic went on they had difficulty finding patients who had never been infected with COVID to serve as reliable controls. To date, they have identified 33 controls who had a respiratory condition when admitted to the ICU. “What we see is the neurological biomarker levels in COVID are slightly lower than those with another respiratory condition in the ICU. But the data has a massive spread and the significance is very small between the two groups,” said Ms. Cooper.
Unanswered questions
The study is interesting, but leaves a lot of unanswered questions, according to Wiesje van der Flier, PhD, who moderated the session where the study was presented. “There are a lot of unknowns still: Will [the biomarkers] become normal again, once the COVID is over? Also, there was an increased risk, but it was not a one-to-one correspondence, so you can also have the increased markers but not have the neurological signs or symptoms. So I thought there were lots of questions as well,” said Dr. van der Flier, professor of neurology at Amsterdam University Medical Center.
She noted that researchers at her institution in Amsterdam have observed similar relationships, and that the associations between neurological complications and plasma biomarkers over time will be an important topic of study.
The work could provide more information on neurological manifestations of long COVID, such as long-haul fatigue. “You might also think that’s some response in their brain. It would be great if we could actually capture that [using biomarkers],” said Dr. van der Flier.
Ms. Cooper and Dr. van der Flier have no relevant financial disclosures.
AT AAIC 2022
In MCI, combo training boosts effect
SAN DIEGO – The findings were drawn from an unusual study design that split patients into five groups, one of which included both interventions.
After the study was completed, researchers collapsed the groups into a single analysis to compare the different regimens, according to Manuel Montero-Odasso, MD, PhD, who presented the work at the Alzheimer’s Association International Conference. He is a geriatrician at Parkwood Institute, London, Ont.
Two previous trials looked at whether the combination of exercise plus cognitive training could outperform either intervention alone. In both, the combination improved cognition but not as much as either intervention alone. “So it seemed that when they combine it, they didn’t do as well,” said Dr. Montero-Odasso. Those findings left doubt about whether or not there is synergism between the two approaches.
Sequential, not simultaneous
A possible explanation for the finding is that patients who are doing both cognitive training and physical exercise simultaneously might not be able to focus enough on either task to do get the maximum benefit. “When we try to combine concurrently, participants or patients cannot focus and do enough progression in both at the same time. That’s the reason we designed the trial in a way that the interventions were sequential. You got a very good quality (cognitive) training, and later you got the exercise,” said Dr. Montero-Odasso.
In the new study, patients receiving both interventions conducted the cognitive training first, then did physical exercises 30 minutes later. “The practical message is that you should follow a program. Something I see in my patients, when they do the two things at the same time, they don’t pay enough attention,” said Dr. Montero-Odasso.
The researchers added vitamin D to the regimen as there have been small studies reporting that vitamin D supplementation can lead to greater muscle mass resulting from exercise.
The study included 176 patients aged 60-85 with MCI. The researchers excluded patients already participating in an active exercise program with a personal trainer, as well as those taking vitamin D at doses higher than 1,000 IU/day.
Over 20 weeks, the randomized groups included combination exercise and cognitive training with vitamin D (10,000 IU three times per week), exercise and cognitive training with placebo, exercise with a cognitive control and vitamin D, exercise with a cognitive control and placebo, and an exercise control (balance and toning) with cognitive control and placebo.
The interventions were completed three times per week. Cognitive training employed a tablet with multifunctional tasks and memory components. It was adaptive, becoming more difficult as patients improved or simplifying the task if a patient struggled. The exercise component included 40 minutes of progressive, supervised resistance training, followed by 20 minutes of aerobic exercise.
Compared with the double-placebo group, the double-intervention group had significant improvement in cognitive performance. “Exercise alone without cognitive training shows an effect, but that effect was lower than a combination with cognitive training,” said Dr. Montero-Odasso.
The combined groups had medium effect sizes on cognition when combined with vitamin D (Cohen’s d, 0.65; P = .003) and with vitamin D placebo (Cohen’s d, 0.58; P = .013). There were nonsignificant improvements in the exercise and vitamin D group (Cohen’s d, 0.30; P = .241) and the exercise plus placebo group (Cohen’s d, 0.42; P = .139)
After collapsing the arms, the researchers found that the exercise plus cognitive training regimen had an effect size of 0.62 (P = .002), while exercise alone only trended toward improvement and with a small effect size (Cohen’s d, 0.36; P = .13). There was no apparent effect of vitamin D supplementation, though Dr. Montero-Odasso pointed out that most participants were taking vitamin D supplements before study entry and had normal to high serum levels of vitamin D.
‘Optimistic’ results
The study was limited by an inability to retain patients due to the COVID-19 pandemic, leading to a dropout rate of 17%.
“I think the idea of combining risk reduction strategies together in a population and individuals with MCI is really exciting. These are optimistic results. You certainly need to look into a larger and more diverse population as it goes forward,” said Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, who was asked to comment on the study.
She noted that the study looked at all-cause cognitive impairment. It would be interesting, Dr. Snyder said, to see how individuals with different underlying conditions handle the combination intervention.
The researchers are now in the planning stage of the Synergic 2 trial, which will incorporate exercise and cognitive training, plus diet and sleep counseling. It will be conducted virtually, involving one-to-one interactions with coaches.
Dr. Montero-Odasso and Dr. Snyder have no relevant financial disclosures.
SAN DIEGO – The findings were drawn from an unusual study design that split patients into five groups, one of which included both interventions.
After the study was completed, researchers collapsed the groups into a single analysis to compare the different regimens, according to Manuel Montero-Odasso, MD, PhD, who presented the work at the Alzheimer’s Association International Conference. He is a geriatrician at Parkwood Institute, London, Ont.
Two previous trials looked at whether the combination of exercise plus cognitive training could outperform either intervention alone. In both, the combination improved cognition but not as much as either intervention alone. “So it seemed that when they combine it, they didn’t do as well,” said Dr. Montero-Odasso. Those findings left doubt about whether or not there is synergism between the two approaches.
Sequential, not simultaneous
A possible explanation for the finding is that patients who are doing both cognitive training and physical exercise simultaneously might not be able to focus enough on either task to do get the maximum benefit. “When we try to combine concurrently, participants or patients cannot focus and do enough progression in both at the same time. That’s the reason we designed the trial in a way that the interventions were sequential. You got a very good quality (cognitive) training, and later you got the exercise,” said Dr. Montero-Odasso.
In the new study, patients receiving both interventions conducted the cognitive training first, then did physical exercises 30 minutes later. “The practical message is that you should follow a program. Something I see in my patients, when they do the two things at the same time, they don’t pay enough attention,” said Dr. Montero-Odasso.
The researchers added vitamin D to the regimen as there have been small studies reporting that vitamin D supplementation can lead to greater muscle mass resulting from exercise.
The study included 176 patients aged 60-85 with MCI. The researchers excluded patients already participating in an active exercise program with a personal trainer, as well as those taking vitamin D at doses higher than 1,000 IU/day.
Over 20 weeks, the randomized groups included combination exercise and cognitive training with vitamin D (10,000 IU three times per week), exercise and cognitive training with placebo, exercise with a cognitive control and vitamin D, exercise with a cognitive control and placebo, and an exercise control (balance and toning) with cognitive control and placebo.
The interventions were completed three times per week. Cognitive training employed a tablet with multifunctional tasks and memory components. It was adaptive, becoming more difficult as patients improved or simplifying the task if a patient struggled. The exercise component included 40 minutes of progressive, supervised resistance training, followed by 20 minutes of aerobic exercise.
Compared with the double-placebo group, the double-intervention group had significant improvement in cognitive performance. “Exercise alone without cognitive training shows an effect, but that effect was lower than a combination with cognitive training,” said Dr. Montero-Odasso.
The combined groups had medium effect sizes on cognition when combined with vitamin D (Cohen’s d, 0.65; P = .003) and with vitamin D placebo (Cohen’s d, 0.58; P = .013). There were nonsignificant improvements in the exercise and vitamin D group (Cohen’s d, 0.30; P = .241) and the exercise plus placebo group (Cohen’s d, 0.42; P = .139)
After collapsing the arms, the researchers found that the exercise plus cognitive training regimen had an effect size of 0.62 (P = .002), while exercise alone only trended toward improvement and with a small effect size (Cohen’s d, 0.36; P = .13). There was no apparent effect of vitamin D supplementation, though Dr. Montero-Odasso pointed out that most participants were taking vitamin D supplements before study entry and had normal to high serum levels of vitamin D.
‘Optimistic’ results
The study was limited by an inability to retain patients due to the COVID-19 pandemic, leading to a dropout rate of 17%.
“I think the idea of combining risk reduction strategies together in a population and individuals with MCI is really exciting. These are optimistic results. You certainly need to look into a larger and more diverse population as it goes forward,” said Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, who was asked to comment on the study.
She noted that the study looked at all-cause cognitive impairment. It would be interesting, Dr. Snyder said, to see how individuals with different underlying conditions handle the combination intervention.
The researchers are now in the planning stage of the Synergic 2 trial, which will incorporate exercise and cognitive training, plus diet and sleep counseling. It will be conducted virtually, involving one-to-one interactions with coaches.
Dr. Montero-Odasso and Dr. Snyder have no relevant financial disclosures.
SAN DIEGO – The findings were drawn from an unusual study design that split patients into five groups, one of which included both interventions.
After the study was completed, researchers collapsed the groups into a single analysis to compare the different regimens, according to Manuel Montero-Odasso, MD, PhD, who presented the work at the Alzheimer’s Association International Conference. He is a geriatrician at Parkwood Institute, London, Ont.
Two previous trials looked at whether the combination of exercise plus cognitive training could outperform either intervention alone. In both, the combination improved cognition but not as much as either intervention alone. “So it seemed that when they combine it, they didn’t do as well,” said Dr. Montero-Odasso. Those findings left doubt about whether or not there is synergism between the two approaches.
Sequential, not simultaneous
A possible explanation for the finding is that patients who are doing both cognitive training and physical exercise simultaneously might not be able to focus enough on either task to do get the maximum benefit. “When we try to combine concurrently, participants or patients cannot focus and do enough progression in both at the same time. That’s the reason we designed the trial in a way that the interventions were sequential. You got a very good quality (cognitive) training, and later you got the exercise,” said Dr. Montero-Odasso.
In the new study, patients receiving both interventions conducted the cognitive training first, then did physical exercises 30 minutes later. “The practical message is that you should follow a program. Something I see in my patients, when they do the two things at the same time, they don’t pay enough attention,” said Dr. Montero-Odasso.
The researchers added vitamin D to the regimen as there have been small studies reporting that vitamin D supplementation can lead to greater muscle mass resulting from exercise.
The study included 176 patients aged 60-85 with MCI. The researchers excluded patients already participating in an active exercise program with a personal trainer, as well as those taking vitamin D at doses higher than 1,000 IU/day.
Over 20 weeks, the randomized groups included combination exercise and cognitive training with vitamin D (10,000 IU three times per week), exercise and cognitive training with placebo, exercise with a cognitive control and vitamin D, exercise with a cognitive control and placebo, and an exercise control (balance and toning) with cognitive control and placebo.
The interventions were completed three times per week. Cognitive training employed a tablet with multifunctional tasks and memory components. It was adaptive, becoming more difficult as patients improved or simplifying the task if a patient struggled. The exercise component included 40 minutes of progressive, supervised resistance training, followed by 20 minutes of aerobic exercise.
Compared with the double-placebo group, the double-intervention group had significant improvement in cognitive performance. “Exercise alone without cognitive training shows an effect, but that effect was lower than a combination with cognitive training,” said Dr. Montero-Odasso.
The combined groups had medium effect sizes on cognition when combined with vitamin D (Cohen’s d, 0.65; P = .003) and with vitamin D placebo (Cohen’s d, 0.58; P = .013). There were nonsignificant improvements in the exercise and vitamin D group (Cohen’s d, 0.30; P = .241) and the exercise plus placebo group (Cohen’s d, 0.42; P = .139)
After collapsing the arms, the researchers found that the exercise plus cognitive training regimen had an effect size of 0.62 (P = .002), while exercise alone only trended toward improvement and with a small effect size (Cohen’s d, 0.36; P = .13). There was no apparent effect of vitamin D supplementation, though Dr. Montero-Odasso pointed out that most participants were taking vitamin D supplements before study entry and had normal to high serum levels of vitamin D.
‘Optimistic’ results
The study was limited by an inability to retain patients due to the COVID-19 pandemic, leading to a dropout rate of 17%.
“I think the idea of combining risk reduction strategies together in a population and individuals with MCI is really exciting. These are optimistic results. You certainly need to look into a larger and more diverse population as it goes forward,” said Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, who was asked to comment on the study.
She noted that the study looked at all-cause cognitive impairment. It would be interesting, Dr. Snyder said, to see how individuals with different underlying conditions handle the combination intervention.
The researchers are now in the planning stage of the Synergic 2 trial, which will incorporate exercise and cognitive training, plus diet and sleep counseling. It will be conducted virtually, involving one-to-one interactions with coaches.
Dr. Montero-Odasso and Dr. Snyder have no relevant financial disclosures.
AT AAIC 2022
Concerns that low LDL-C alters cognitive function challenged in novel analysis
PCSK9 inhibitors, which are among the most effective therapies for reducing LDL cholesterol (LDL-C), are associated with a neutral effect on cognitive function, according to a genetics-based Mendelian randomization study intended to sort out through the complexity of confounders.
The same study linked HMG-Co A reductase inhibitors (statins) with the potential for modest adverse neurocognitive effects, although these are likely to be outweighed by cardiovascular benefits, according to a collaborating team of investigators from the U.S. National Institutes of Health and the University of Oxford (England).
For clinicians and patients who continue to harbor concerns that cognitive function is threatened by very low LDL-C, this novel approach to evaluating risk is “reassuring,” according to the authors.
Early in clinical testing of PCSK9 inhibitors, a potential signal for adverse effects on cognitive function was reported but unconfirmed. This signal raised concern that extremely low levels of LDL-C, such as < 25 mg/dL, achieved with PCSK9 inhibitors might pose a risk to neurocognitive function.
Of several factors that provided a basis for concern, the PCSK9 enzyme is known to participate in brain development, according to the authors of this newly published study.
Mendelian randomization addresses complex issue
The objective of this Mendelian randomization analysis was to evaluate the relationship of PCSK9 inhibitors and statins on long-term neurocognitive function. Used previously to address other clinical issues, a drug-effect Mendelian randomization analysis evaluates genetic variants to determine whether there is a causal relationship between a risk, which in this case was lipid-lowering drugs, to a specific outcome, which was cognitive performance.
By looking directly at genetic variants that simulate the pharmacological inhibition of drug gene targets, the bias of confounders of clinical effects, such as baseline cognitive function, are avoided, according to the authors.
The message from this drug-effect Mendelian analysis was simple, according to the senior author of the study, Falk W. Lohoff, MD, chief of the section on clinical genomics and experimental therapeutics, National Institute of Alcohol Abuse and Alcoholism.
“Based on our data, we do not see a significant cognitive risk profile with PCSK9 inhibition associated with low LDL-C,” Dr. Lohoff said in an interview. He cautioned that “future long-term clinical studies are needed to confirm the absence of this effect,” but he and his coauthors noted that these data concur with the clinical studies.
From genome-wide association studies, single-nucleotide polymorphisms in PCSK9 and HMG-Co A reductase were extracted from a sample of more than 700,000 individuals of predominantly European ancestry. In the analysis, the investigators evaluated whether inhibition of PCSK9 or HMG-Co A reductase had an effect on seven clinical outcomes that relate to neurocognitive function, including memory, verbal intelligence, and reaction time, as well as biomarkers of cognitive function, such as cortical surface area.
The genetic effect of PCSK9 inhibition was “null for every cognitive-related outcome evaluated,” the investigators reported. The genetic effect of HMG-Co A reductase inhibition had a statistically significant but modest effect on cognitive performance (P = .03) and cortical surface area (P = .03). While the impact of HMG-Co A reductase inhibition on reaction time was stronger on a statistical basis (P = .0002), the investigators reported that it translated into a decrease of only 0.067 milliseconds per 38.7 mg/dL. They characterized this as a “small impact” unlikely to outweigh clinical benefits.
In an editorial that accompanied publication of this study, Brian A. Ference, MD, MPhil, provided context for the suitability of a Mendelian randomization analysis to address this or other questions regarding the impact of lipid-lowering therapies on clinical outcomes, and he ultimately concurred with the major conclusions

Ultimately, this analysis is consistent with other evidence that PCSK9 inhibition does not pose a risk of impaired cognitive function, he wrote. For statins, he concluded that this study “does not provide compelling evidence” to challenge their current clinical use.
Data do not support low LDL-C as cognitive risk factor
Moreover, this study – as well as other evidence – argues strongly against very low levels of LDL-C, regardless of how they are achieved, as a risk factor for diminished cognitive function, Dr. Ference, director of research in the division of translational therapeutics, University of Cambridge (England), said in an interview.
“There is no evidence from Mendelian randomization studies that lifelong exposure to lower LDL-C increases the risk of cognitive impairment,” he said. “This is true when evaluating lifelong exposure to lower LDL-C due to genetic variants in a wide variety of different genes or the genes that encode the target PCKS9 inhibitors, statins, or other lipid-lowering therapies.”
In other words, this study “adds to the accumulating evidence” that LDL-C lowering by itself does not contribute to an adverse impact on cognitive function despite persistent concern. This should not be surprising. Dr. Ference emphasized that there has never been strong evidence for an association.
“As I point out in the editorial, there is no biologically plausible mechanism by which reducing peripheral LDL-C should impact neurological function in any way, because the therapies do not cross the blood brain barrier, and because the nervous system produces its own cholesterol to maintain the integrity of membranes in nervous system cells,” he explained.
Dr. Lohoff reports no potential conflicts of interest. Dr. Ference has financial relationships with numerous pharmaceutical companies including those that make lipid-lowering therapies.
PCSK9 inhibitors, which are among the most effective therapies for reducing LDL cholesterol (LDL-C), are associated with a neutral effect on cognitive function, according to a genetics-based Mendelian randomization study intended to sort out through the complexity of confounders.
The same study linked HMG-Co A reductase inhibitors (statins) with the potential for modest adverse neurocognitive effects, although these are likely to be outweighed by cardiovascular benefits, according to a collaborating team of investigators from the U.S. National Institutes of Health and the University of Oxford (England).
For clinicians and patients who continue to harbor concerns that cognitive function is threatened by very low LDL-C, this novel approach to evaluating risk is “reassuring,” according to the authors.
Early in clinical testing of PCSK9 inhibitors, a potential signal for adverse effects on cognitive function was reported but unconfirmed. This signal raised concern that extremely low levels of LDL-C, such as < 25 mg/dL, achieved with PCSK9 inhibitors might pose a risk to neurocognitive function.
Of several factors that provided a basis for concern, the PCSK9 enzyme is known to participate in brain development, according to the authors of this newly published study.
Mendelian randomization addresses complex issue
The objective of this Mendelian randomization analysis was to evaluate the relationship of PCSK9 inhibitors and statins on long-term neurocognitive function. Used previously to address other clinical issues, a drug-effect Mendelian randomization analysis evaluates genetic variants to determine whether there is a causal relationship between a risk, which in this case was lipid-lowering drugs, to a specific outcome, which was cognitive performance.
By looking directly at genetic variants that simulate the pharmacological inhibition of drug gene targets, the bias of confounders of clinical effects, such as baseline cognitive function, are avoided, according to the authors.
The message from this drug-effect Mendelian analysis was simple, according to the senior author of the study, Falk W. Lohoff, MD, chief of the section on clinical genomics and experimental therapeutics, National Institute of Alcohol Abuse and Alcoholism.
“Based on our data, we do not see a significant cognitive risk profile with PCSK9 inhibition associated with low LDL-C,” Dr. Lohoff said in an interview. He cautioned that “future long-term clinical studies are needed to confirm the absence of this effect,” but he and his coauthors noted that these data concur with the clinical studies.
From genome-wide association studies, single-nucleotide polymorphisms in PCSK9 and HMG-Co A reductase were extracted from a sample of more than 700,000 individuals of predominantly European ancestry. In the analysis, the investigators evaluated whether inhibition of PCSK9 or HMG-Co A reductase had an effect on seven clinical outcomes that relate to neurocognitive function, including memory, verbal intelligence, and reaction time, as well as biomarkers of cognitive function, such as cortical surface area.
The genetic effect of PCSK9 inhibition was “null for every cognitive-related outcome evaluated,” the investigators reported. The genetic effect of HMG-Co A reductase inhibition had a statistically significant but modest effect on cognitive performance (P = .03) and cortical surface area (P = .03). While the impact of HMG-Co A reductase inhibition on reaction time was stronger on a statistical basis (P = .0002), the investigators reported that it translated into a decrease of only 0.067 milliseconds per 38.7 mg/dL. They characterized this as a “small impact” unlikely to outweigh clinical benefits.
In an editorial that accompanied publication of this study, Brian A. Ference, MD, MPhil, provided context for the suitability of a Mendelian randomization analysis to address this or other questions regarding the impact of lipid-lowering therapies on clinical outcomes, and he ultimately concurred with the major conclusions
Ultimately, this analysis is consistent with other evidence that PCSK9 inhibition does not pose a risk of impaired cognitive function, he wrote. For statins, he concluded that this study “does not provide compelling evidence” to challenge their current clinical use.
Data do not support low LDL-C as cognitive risk factor
Moreover, this study – as well as other evidence – argues strongly against very low levels of LDL-C, regardless of how they are achieved, as a risk factor for diminished cognitive function, Dr. Ference, director of research in the division of translational therapeutics, University of Cambridge (England), said in an interview.
“There is no evidence from Mendelian randomization studies that lifelong exposure to lower LDL-C increases the risk of cognitive impairment,” he said. “This is true when evaluating lifelong exposure to lower LDL-C due to genetic variants in a wide variety of different genes or the genes that encode the target PCKS9 inhibitors, statins, or other lipid-lowering therapies.”
In other words, this study “adds to the accumulating evidence” that LDL-C lowering by itself does not contribute to an adverse impact on cognitive function despite persistent concern. This should not be surprising. Dr. Ference emphasized that there has never been strong evidence for an association.
“As I point out in the editorial, there is no biologically plausible mechanism by which reducing peripheral LDL-C should impact neurological function in any way, because the therapies do not cross the blood brain barrier, and because the nervous system produces its own cholesterol to maintain the integrity of membranes in nervous system cells,” he explained.
Dr. Lohoff reports no potential conflicts of interest. Dr. Ference has financial relationships with numerous pharmaceutical companies including those that make lipid-lowering therapies.
PCSK9 inhibitors, which are among the most effective therapies for reducing LDL cholesterol (LDL-C), are associated with a neutral effect on cognitive function, according to a genetics-based Mendelian randomization study intended to sort out through the complexity of confounders.
The same study linked HMG-Co A reductase inhibitors (statins) with the potential for modest adverse neurocognitive effects, although these are likely to be outweighed by cardiovascular benefits, according to a collaborating team of investigators from the U.S. National Institutes of Health and the University of Oxford (England).
For clinicians and patients who continue to harbor concerns that cognitive function is threatened by very low LDL-C, this novel approach to evaluating risk is “reassuring,” according to the authors.
Early in clinical testing of PCSK9 inhibitors, a potential signal for adverse effects on cognitive function was reported but unconfirmed. This signal raised concern that extremely low levels of LDL-C, such as < 25 mg/dL, achieved with PCSK9 inhibitors might pose a risk to neurocognitive function.
Of several factors that provided a basis for concern, the PCSK9 enzyme is known to participate in brain development, according to the authors of this newly published study.
Mendelian randomization addresses complex issue
The objective of this Mendelian randomization analysis was to evaluate the relationship of PCSK9 inhibitors and statins on long-term neurocognitive function. Used previously to address other clinical issues, a drug-effect Mendelian randomization analysis evaluates genetic variants to determine whether there is a causal relationship between a risk, which in this case was lipid-lowering drugs, to a specific outcome, which was cognitive performance.
By looking directly at genetic variants that simulate the pharmacological inhibition of drug gene targets, the bias of confounders of clinical effects, such as baseline cognitive function, are avoided, according to the authors.
The message from this drug-effect Mendelian analysis was simple, according to the senior author of the study, Falk W. Lohoff, MD, chief of the section on clinical genomics and experimental therapeutics, National Institute of Alcohol Abuse and Alcoholism.
“Based on our data, we do not see a significant cognitive risk profile with PCSK9 inhibition associated with low LDL-C,” Dr. Lohoff said in an interview. He cautioned that “future long-term clinical studies are needed to confirm the absence of this effect,” but he and his coauthors noted that these data concur with the clinical studies.
From genome-wide association studies, single-nucleotide polymorphisms in PCSK9 and HMG-Co A reductase were extracted from a sample of more than 700,000 individuals of predominantly European ancestry. In the analysis, the investigators evaluated whether inhibition of PCSK9 or HMG-Co A reductase had an effect on seven clinical outcomes that relate to neurocognitive function, including memory, verbal intelligence, and reaction time, as well as biomarkers of cognitive function, such as cortical surface area.
The genetic effect of PCSK9 inhibition was “null for every cognitive-related outcome evaluated,” the investigators reported. The genetic effect of HMG-Co A reductase inhibition had a statistically significant but modest effect on cognitive performance (P = .03) and cortical surface area (P = .03). While the impact of HMG-Co A reductase inhibition on reaction time was stronger on a statistical basis (P = .0002), the investigators reported that it translated into a decrease of only 0.067 milliseconds per 38.7 mg/dL. They characterized this as a “small impact” unlikely to outweigh clinical benefits.
In an editorial that accompanied publication of this study, Brian A. Ference, MD, MPhil, provided context for the suitability of a Mendelian randomization analysis to address this or other questions regarding the impact of lipid-lowering therapies on clinical outcomes, and he ultimately concurred with the major conclusions
Ultimately, this analysis is consistent with other evidence that PCSK9 inhibition does not pose a risk of impaired cognitive function, he wrote. For statins, he concluded that this study “does not provide compelling evidence” to challenge their current clinical use.
Data do not support low LDL-C as cognitive risk factor
Moreover, this study – as well as other evidence – argues strongly against very low levels of LDL-C, regardless of how they are achieved, as a risk factor for diminished cognitive function, Dr. Ference, director of research in the division of translational therapeutics, University of Cambridge (England), said in an interview.
“There is no evidence from Mendelian randomization studies that lifelong exposure to lower LDL-C increases the risk of cognitive impairment,” he said. “This is true when evaluating lifelong exposure to lower LDL-C due to genetic variants in a wide variety of different genes or the genes that encode the target PCKS9 inhibitors, statins, or other lipid-lowering therapies.”
In other words, this study “adds to the accumulating evidence” that LDL-C lowering by itself does not contribute to an adverse impact on cognitive function despite persistent concern. This should not be surprising. Dr. Ference emphasized that there has never been strong evidence for an association.
“As I point out in the editorial, there is no biologically plausible mechanism by which reducing peripheral LDL-C should impact neurological function in any way, because the therapies do not cross the blood brain barrier, and because the nervous system produces its own cholesterol to maintain the integrity of membranes in nervous system cells,” he explained.
Dr. Lohoff reports no potential conflicts of interest. Dr. Ference has financial relationships with numerous pharmaceutical companies including those that make lipid-lowering therapies.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Regular exercise appears to slow cognitive decline in MCI
(MCI), new research from the largest study of its kind suggests. Topline results from the EXERT trial showed patients with MCI who participated regularly in either aerobic exercise or stretching/balance/range-of-motion exercises maintained stable global cognitive function over 12 months of follow-up – with no differences between the two types of exercise.
“We’re excited about these findings, because these types of exercises that we’re seeing can protect against cognitive decline are accessible to everyone and therefore scalable to the public,” study investigator Laura Baker, PhD, Wake Forest University School of Medicine, Winston-Salem, N.C., said at a press briefing.
The topline results were presented at the 2022 Alzheimer’s Association International Conference.
No decline
The 18-month EXERT trial was designed to be the definitive study to answer the question about whether exercise can slow cognitive decline in older adults with amnestic MCI, Dr. Baker reported. Investigators enrolled 296 sedentary men and women with MCI (mean age, about 75 years). All were randomly allocated to either an aerobic exercise group (maintaining a heart rate at about 70%-85%) or a stretching and balance group (maintaining heart rate less than 35%).
Both groups exercised four times per week for about 30-40 minutes. In the first 12 months they were supervised by a trainer at the YMCA and then they exercised independently for the final 6 months.
Participants were assessed at baseline and every 6 months. The primary endpoint was change from baseline on the ADAS-Cog-Exec, a validated measure of global cognitive function, at the end of the 12 months of supervised exercise.
During the first 12 months, participants completed over 31,000 sessions of exercise, which is “quite impressive,” Dr. Baker said.
Over the first 12 months, neither the aerobic group nor the stretch/balance group showed a decline on the ADAS-Cog-Exec.
“We saw no group differences, and importantly, no decline after 12 months,” Dr. Baker reported.
Supported exercise is ‘crucial’
To help “make sense” of these findings, Dr. Baker noted that 12-month changes in the ADAS-Cog-Exec for the EXERT intervention groups were also compared with a “usual care” cohort of adults matched for age, sex, education, baseline cognitive status, and APOE4 genotype.
In this “apples-to-apples” comparison, the usual care cohort showed the expected decline or worsening of cognitive function over 12 months on the ADAS-Cog-Exec, but the EXERT exercise groups did not.
Dr. Baker noted that both exercise groups received equal amounts of weekly socialization, which may have contributed to the apparent protective effects on the brain.
A greater volume of exercise in EXERT, compared with other trials, may also be a factor. Each individual participant in EXERT completed more than 100 hours of exercise.
“The take-home message is that an increased amount of either low-intensity or high-intensity exercise for 120-150 minutes per week for 12 months may slow cognitive decline in sedentary older adults with MCI,” Dr. Baker said.
“What’s critical is that this regular exercise must be supported in these older [patients] with MCI. It must be supervised. There has to be some social component,” she added.
In her view, 120 minutes of regular supported exercise for sedentary individuals with MCI “needs to be part of the recommendation for risk reduction.”
Important study
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that several studies over the years have suggested that different types of exercise can have benefits on the brain.
“What’s important about this study is that it’s in a population of people that have MCI and are already experiencing memory changes,” Dr. Snyder said.
“The results suggest that engaging in both of these types of exercise may be beneficial for our brain. And given that this is the largest study of its kind in a population of people with MCI, it suggests it’s ‘never too late’ to start exercising,” she added.
Dr. Snyder noted the importance of continuing this work and to continue following these individuals “over time as well.”
The study was funded by the National Institutes of Health, National Institute on Aging. Dr. Baker and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(MCI), new research from the largest study of its kind suggests. Topline results from the EXERT trial showed patients with MCI who participated regularly in either aerobic exercise or stretching/balance/range-of-motion exercises maintained stable global cognitive function over 12 months of follow-up – with no differences between the two types of exercise.
“We’re excited about these findings, because these types of exercises that we’re seeing can protect against cognitive decline are accessible to everyone and therefore scalable to the public,” study investigator Laura Baker, PhD, Wake Forest University School of Medicine, Winston-Salem, N.C., said at a press briefing.
The topline results were presented at the 2022 Alzheimer’s Association International Conference.
No decline
The 18-month EXERT trial was designed to be the definitive study to answer the question about whether exercise can slow cognitive decline in older adults with amnestic MCI, Dr. Baker reported. Investigators enrolled 296 sedentary men and women with MCI (mean age, about 75 years). All were randomly allocated to either an aerobic exercise group (maintaining a heart rate at about 70%-85%) or a stretching and balance group (maintaining heart rate less than 35%).
Both groups exercised four times per week for about 30-40 minutes. In the first 12 months they were supervised by a trainer at the YMCA and then they exercised independently for the final 6 months.
Participants were assessed at baseline and every 6 months. The primary endpoint was change from baseline on the ADAS-Cog-Exec, a validated measure of global cognitive function, at the end of the 12 months of supervised exercise.
During the first 12 months, participants completed over 31,000 sessions of exercise, which is “quite impressive,” Dr. Baker said.
Over the first 12 months, neither the aerobic group nor the stretch/balance group showed a decline on the ADAS-Cog-Exec.
“We saw no group differences, and importantly, no decline after 12 months,” Dr. Baker reported.
Supported exercise is ‘crucial’
To help “make sense” of these findings, Dr. Baker noted that 12-month changes in the ADAS-Cog-Exec for the EXERT intervention groups were also compared with a “usual care” cohort of adults matched for age, sex, education, baseline cognitive status, and APOE4 genotype.
In this “apples-to-apples” comparison, the usual care cohort showed the expected decline or worsening of cognitive function over 12 months on the ADAS-Cog-Exec, but the EXERT exercise groups did not.
Dr. Baker noted that both exercise groups received equal amounts of weekly socialization, which may have contributed to the apparent protective effects on the brain.
A greater volume of exercise in EXERT, compared with other trials, may also be a factor. Each individual participant in EXERT completed more than 100 hours of exercise.
“The take-home message is that an increased amount of either low-intensity or high-intensity exercise for 120-150 minutes per week for 12 months may slow cognitive decline in sedentary older adults with MCI,” Dr. Baker said.
“What’s critical is that this regular exercise must be supported in these older [patients] with MCI. It must be supervised. There has to be some social component,” she added.
In her view, 120 minutes of regular supported exercise for sedentary individuals with MCI “needs to be part of the recommendation for risk reduction.”
Important study
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that several studies over the years have suggested that different types of exercise can have benefits on the brain.
“What’s important about this study is that it’s in a population of people that have MCI and are already experiencing memory changes,” Dr. Snyder said.
“The results suggest that engaging in both of these types of exercise may be beneficial for our brain. And given that this is the largest study of its kind in a population of people with MCI, it suggests it’s ‘never too late’ to start exercising,” she added.
Dr. Snyder noted the importance of continuing this work and to continue following these individuals “over time as well.”
The study was funded by the National Institutes of Health, National Institute on Aging. Dr. Baker and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
(MCI), new research from the largest study of its kind suggests. Topline results from the EXERT trial showed patients with MCI who participated regularly in either aerobic exercise or stretching/balance/range-of-motion exercises maintained stable global cognitive function over 12 months of follow-up – with no differences between the two types of exercise.
“We’re excited about these findings, because these types of exercises that we’re seeing can protect against cognitive decline are accessible to everyone and therefore scalable to the public,” study investigator Laura Baker, PhD, Wake Forest University School of Medicine, Winston-Salem, N.C., said at a press briefing.
The topline results were presented at the 2022 Alzheimer’s Association International Conference.
No decline
The 18-month EXERT trial was designed to be the definitive study to answer the question about whether exercise can slow cognitive decline in older adults with amnestic MCI, Dr. Baker reported. Investigators enrolled 296 sedentary men and women with MCI (mean age, about 75 years). All were randomly allocated to either an aerobic exercise group (maintaining a heart rate at about 70%-85%) or a stretching and balance group (maintaining heart rate less than 35%).
Both groups exercised four times per week for about 30-40 minutes. In the first 12 months they were supervised by a trainer at the YMCA and then they exercised independently for the final 6 months.
Participants were assessed at baseline and every 6 months. The primary endpoint was change from baseline on the ADAS-Cog-Exec, a validated measure of global cognitive function, at the end of the 12 months of supervised exercise.
During the first 12 months, participants completed over 31,000 sessions of exercise, which is “quite impressive,” Dr. Baker said.
Over the first 12 months, neither the aerobic group nor the stretch/balance group showed a decline on the ADAS-Cog-Exec.
“We saw no group differences, and importantly, no decline after 12 months,” Dr. Baker reported.
Supported exercise is ‘crucial’
To help “make sense” of these findings, Dr. Baker noted that 12-month changes in the ADAS-Cog-Exec for the EXERT intervention groups were also compared with a “usual care” cohort of adults matched for age, sex, education, baseline cognitive status, and APOE4 genotype.
In this “apples-to-apples” comparison, the usual care cohort showed the expected decline or worsening of cognitive function over 12 months on the ADAS-Cog-Exec, but the EXERT exercise groups did not.
Dr. Baker noted that both exercise groups received equal amounts of weekly socialization, which may have contributed to the apparent protective effects on the brain.
A greater volume of exercise in EXERT, compared with other trials, may also be a factor. Each individual participant in EXERT completed more than 100 hours of exercise.
“The take-home message is that an increased amount of either low-intensity or high-intensity exercise for 120-150 minutes per week for 12 months may slow cognitive decline in sedentary older adults with MCI,” Dr. Baker said.
“What’s critical is that this regular exercise must be supported in these older [patients] with MCI. It must be supervised. There has to be some social component,” she added.
In her view, 120 minutes of regular supported exercise for sedentary individuals with MCI “needs to be part of the recommendation for risk reduction.”
Important study
Commenting on the findings, Heather Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, noted that several studies over the years have suggested that different types of exercise can have benefits on the brain.
“What’s important about this study is that it’s in a population of people that have MCI and are already experiencing memory changes,” Dr. Snyder said.
“The results suggest that engaging in both of these types of exercise may be beneficial for our brain. And given that this is the largest study of its kind in a population of people with MCI, it suggests it’s ‘never too late’ to start exercising,” she added.
Dr. Snyder noted the importance of continuing this work and to continue following these individuals “over time as well.”
The study was funded by the National Institutes of Health, National Institute on Aging. Dr. Baker and Dr. Snyder have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From AAIC 2022
Chronically low wages linked to subsequent memory decline
, new research suggests. In a new analysis of more than 3,000 participants in the Health and Retirement Study, those who sustained low wages in midlife showed significantly faster memory decline than their peers who never earned low wages.
The findings could have implications for future public policy and research initiatives, the investigators noted.
“Our findings, which suggest a pattern of sustained low-wage earning is harmful for cognitive health, [are] broadly applicable to researchers across numerous health disciplines,” said co-investigator Katrina Kezios, PhD, postdoctoral researcher, department of epidemiology, Mailman School of Public Health, Columbia University, New York.
The findings were presented at the 2022 Alzheimer’s Association International Conference.
Growing number of low-wage workers
Low-wage workers make up a growing share of the U.S. labor market. Yet little research has examined the long-term relationship between earning low wages and memory decline.
The current investigators assessed 1992-2016 data from the Health and Retirement Study, a longitudinal survey of nationally representative samples of Americans aged 50 years and older. Study participants are interviewed every 2 years and provide, among other things, information on work-related factors, including hourly wages.
Memory function was measured at each visit from 2004 to 2016 using a memory composite score. The score included immediate and delayed word recall memory assessments. For those who became too impaired to complete cognitive assessment, memory tests by proxy informants were utilized.
On average, participants completed 4.8 memory assessments over the course of the study.
Researchers defined “low wage” as an hourly wage lower than two-thirds of the federal median wage for the corresponding year. They categorized low-wage exposure history as “never” or “intermittent” or “sustained” on the basis of wages earned from 1992 to 2004.
The current analysis included 3,803 participants, 1,913 of whom were men. All participants were born from 1936 to 1941. In 2004, the average age was 65 years, and the mean memory score was 1.15 standard units.
The investigators adjusted for factors that could confound the relationship between wages and cognition, including the participant’s education, parental education, household wealth, and marital status. Later, whether the participants’ occupation type was of low skill or not was also included.
Cognitive harm
The confounder-adjusted annual rate of memory decline among workers who never earned low wages was –0.12 standard units (95% confidence interval, –0.14 to –0.10).
Compared with these workers, memory decline was significantly faster among participants with sustained low wage–earning during midlife (beta for interaction between time and exposure group, –0.012; 95% CI, –0.02 to 0.01), corresponding to an annual rate of –0.13 standard units.
Put another way, the cognitive aging experienced by workers earning low wages over a 10-year period was equivalent to what workers who never earned low wages would experience over 11 years.
Although similar associations were found for men and women, it was stronger in magnitude for men – a finding Dr. Kezios said was somewhat surprising. She noted that women are commonly more at risk for dementia than men.
However, she advises caution in interpreting this finding, as there were so few men in the sustained low-wage group. “Women disproportionately make up the group of workers earning low wages,” she said.
The negative low coefficient found for those who persistently earned low wages was also observed for those who intermittently earned low wages, but this was not statistically significant.
“We can speculate or hypothesize the cumulative effect of earning low wages at each exposure interval produces more cognitive harm than maybe earning low wages at some time points over that exposure period,” said Dr. Kezios.
A sensitivity analysis that examined wage earning at the same ages but in two different birth cohorts showed similar results for the two groups. When researchers removed self-employed workers from the study sample, the same association between sustained low wages and memory decline was found.
“Our findings held up, which gave us a little more reassurance that what we were seeing is at least signaling there might be something there,” said Dr. Kezios.
She described the study as a “first pass” for documenting the harmful cognitive effects of consistently earning low wages.
It would be interesting, she said, to now determine whether there’s a “dose effect” for having a low salary. However, other studies with different designs would be needed to determine at what income level cognitive health starts to be protected and the impact of raising the minimum wage, she added.
Unique study
Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, said the study was unique. “I don’t think we have seen anything like this before,” said Dr. Snyder.
The study, which links sustained low-wage earning in midlife to later memory decline, “is looking beyond some of the other measures we’ve seen when we looked at socioeconomic status,” she noted.
The results “beg the question” of whether people who earn low wages have less access to health care, she added.
“We should think about how to ensure access and equity around health care and around potential ways that may address components of risk individuals have during their life course,” Dr. Snyder said.
She noted that the study provides a “start” at considering potential policies to address the impact of sustained low wages on overall health, particularly cognitive health, throughout life.
The study had no outside funding. Dr. Kezios has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a new analysis of more than 3,000 participants in the Health and Retirement Study, those who sustained low wages in midlife showed significantly faster memory decline than their peers who never earned low wages.
The findings could have implications for future public policy and research initiatives, the investigators noted.
“Our findings, which suggest a pattern of sustained low-wage earning is harmful for cognitive health, [are] broadly applicable to researchers across numerous health disciplines,” said co-investigator Katrina Kezios, PhD, postdoctoral researcher, department of epidemiology, Mailman School of Public Health, Columbia University, New York.
The findings were presented at the 2022 Alzheimer’s Association International Conference.
Growing number of low-wage workers
Low-wage workers make up a growing share of the U.S. labor market. Yet little research has examined the long-term relationship between earning low wages and memory decline.
The current investigators assessed 1992-2016 data from the Health and Retirement Study, a longitudinal survey of nationally representative samples of Americans aged 50 years and older. Study participants are interviewed every 2 years and provide, among other things, information on work-related factors, including hourly wages.
Memory function was measured at each visit from 2004 to 2016 using a memory composite score. The score included immediate and delayed word recall memory assessments. For those who became too impaired to complete cognitive assessment, memory tests by proxy informants were utilized.
On average, participants completed 4.8 memory assessments over the course of the study.
Researchers defined “low wage” as an hourly wage lower than two-thirds of the federal median wage for the corresponding year. They categorized low-wage exposure history as “never” or “intermittent” or “sustained” on the basis of wages earned from 1992 to 2004.
The current analysis included 3,803 participants, 1,913 of whom were men. All participants were born from 1936 to 1941. In 2004, the average age was 65 years, and the mean memory score was 1.15 standard units.
The investigators adjusted for factors that could confound the relationship between wages and cognition, including the participant’s education, parental education, household wealth, and marital status. Later, whether the participants’ occupation type was of low skill or not was also included.
Cognitive harm
The confounder-adjusted annual rate of memory decline among workers who never earned low wages was –0.12 standard units (95% confidence interval, –0.14 to –0.10).
Compared with these workers, memory decline was significantly faster among participants with sustained low wage–earning during midlife (beta for interaction between time and exposure group, –0.012; 95% CI, –0.02 to 0.01), corresponding to an annual rate of –0.13 standard units.
Put another way, the cognitive aging experienced by workers earning low wages over a 10-year period was equivalent to what workers who never earned low wages would experience over 11 years.
Although similar associations were found for men and women, it was stronger in magnitude for men – a finding Dr. Kezios said was somewhat surprising. She noted that women are commonly more at risk for dementia than men.
However, she advises caution in interpreting this finding, as there were so few men in the sustained low-wage group. “Women disproportionately make up the group of workers earning low wages,” she said.
The negative low coefficient found for those who persistently earned low wages was also observed for those who intermittently earned low wages, but this was not statistically significant.
“We can speculate or hypothesize the cumulative effect of earning low wages at each exposure interval produces more cognitive harm than maybe earning low wages at some time points over that exposure period,” said Dr. Kezios.
A sensitivity analysis that examined wage earning at the same ages but in two different birth cohorts showed similar results for the two groups. When researchers removed self-employed workers from the study sample, the same association between sustained low wages and memory decline was found.
“Our findings held up, which gave us a little more reassurance that what we were seeing is at least signaling there might be something there,” said Dr. Kezios.
She described the study as a “first pass” for documenting the harmful cognitive effects of consistently earning low wages.
It would be interesting, she said, to now determine whether there’s a “dose effect” for having a low salary. However, other studies with different designs would be needed to determine at what income level cognitive health starts to be protected and the impact of raising the minimum wage, she added.
Unique study
Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, said the study was unique. “I don’t think we have seen anything like this before,” said Dr. Snyder.
The study, which links sustained low-wage earning in midlife to later memory decline, “is looking beyond some of the other measures we’ve seen when we looked at socioeconomic status,” she noted.
The results “beg the question” of whether people who earn low wages have less access to health care, she added.
“We should think about how to ensure access and equity around health care and around potential ways that may address components of risk individuals have during their life course,” Dr. Snyder said.
She noted that the study provides a “start” at considering potential policies to address the impact of sustained low wages on overall health, particularly cognitive health, throughout life.
The study had no outside funding. Dr. Kezios has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. In a new analysis of more than 3,000 participants in the Health and Retirement Study, those who sustained low wages in midlife showed significantly faster memory decline than their peers who never earned low wages.
The findings could have implications for future public policy and research initiatives, the investigators noted.
“Our findings, which suggest a pattern of sustained low-wage earning is harmful for cognitive health, [are] broadly applicable to researchers across numerous health disciplines,” said co-investigator Katrina Kezios, PhD, postdoctoral researcher, department of epidemiology, Mailman School of Public Health, Columbia University, New York.
The findings were presented at the 2022 Alzheimer’s Association International Conference.
Growing number of low-wage workers
Low-wage workers make up a growing share of the U.S. labor market. Yet little research has examined the long-term relationship between earning low wages and memory decline.
The current investigators assessed 1992-2016 data from the Health and Retirement Study, a longitudinal survey of nationally representative samples of Americans aged 50 years and older. Study participants are interviewed every 2 years and provide, among other things, information on work-related factors, including hourly wages.
Memory function was measured at each visit from 2004 to 2016 using a memory composite score. The score included immediate and delayed word recall memory assessments. For those who became too impaired to complete cognitive assessment, memory tests by proxy informants were utilized.
On average, participants completed 4.8 memory assessments over the course of the study.
Researchers defined “low wage” as an hourly wage lower than two-thirds of the federal median wage for the corresponding year. They categorized low-wage exposure history as “never” or “intermittent” or “sustained” on the basis of wages earned from 1992 to 2004.
The current analysis included 3,803 participants, 1,913 of whom were men. All participants were born from 1936 to 1941. In 2004, the average age was 65 years, and the mean memory score was 1.15 standard units.
The investigators adjusted for factors that could confound the relationship between wages and cognition, including the participant’s education, parental education, household wealth, and marital status. Later, whether the participants’ occupation type was of low skill or not was also included.
Cognitive harm
The confounder-adjusted annual rate of memory decline among workers who never earned low wages was –0.12 standard units (95% confidence interval, –0.14 to –0.10).
Compared with these workers, memory decline was significantly faster among participants with sustained low wage–earning during midlife (beta for interaction between time and exposure group, –0.012; 95% CI, –0.02 to 0.01), corresponding to an annual rate of –0.13 standard units.
Put another way, the cognitive aging experienced by workers earning low wages over a 10-year period was equivalent to what workers who never earned low wages would experience over 11 years.
Although similar associations were found for men and women, it was stronger in magnitude for men – a finding Dr. Kezios said was somewhat surprising. She noted that women are commonly more at risk for dementia than men.
However, she advises caution in interpreting this finding, as there were so few men in the sustained low-wage group. “Women disproportionately make up the group of workers earning low wages,” she said.
The negative low coefficient found for those who persistently earned low wages was also observed for those who intermittently earned low wages, but this was not statistically significant.
“We can speculate or hypothesize the cumulative effect of earning low wages at each exposure interval produces more cognitive harm than maybe earning low wages at some time points over that exposure period,” said Dr. Kezios.
A sensitivity analysis that examined wage earning at the same ages but in two different birth cohorts showed similar results for the two groups. When researchers removed self-employed workers from the study sample, the same association between sustained low wages and memory decline was found.
“Our findings held up, which gave us a little more reassurance that what we were seeing is at least signaling there might be something there,” said Dr. Kezios.
She described the study as a “first pass” for documenting the harmful cognitive effects of consistently earning low wages.
It would be interesting, she said, to now determine whether there’s a “dose effect” for having a low salary. However, other studies with different designs would be needed to determine at what income level cognitive health starts to be protected and the impact of raising the minimum wage, she added.
Unique study
Heather Snyder, PhD, vice president of medical and scientific relations, Alzheimer’s Association, said the study was unique. “I don’t think we have seen anything like this before,” said Dr. Snyder.
The study, which links sustained low-wage earning in midlife to later memory decline, “is looking beyond some of the other measures we’ve seen when we looked at socioeconomic status,” she noted.
The results “beg the question” of whether people who earn low wages have less access to health care, she added.
“We should think about how to ensure access and equity around health care and around potential ways that may address components of risk individuals have during their life course,” Dr. Snyder said.
She noted that the study provides a “start” at considering potential policies to address the impact of sustained low wages on overall health, particularly cognitive health, throughout life.
The study had no outside funding. Dr. Kezios has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From AAIC 2022
Individualized sensory care for older patients with dementia
Everyone gets by using environmental cues: For example, if you have to go to use the toilet in public, a bathroom sign prompts an immediate response. However, patients with dementia often struggle with environmental cues, which can complicate the already difficult task faced by their caregivers.
Individuals with dementia can lose awareness of such signs, and even colors, making it harder for them to interpret environmental cues.
The study, presented at the Alzheimer’s Association International Conference, recruited 30 pairs of patients and their caregivers. The approach is based on the Dunn model of sensory processing, which focuses on altering environments to maximize chances of success. It “explains that sensory processing is the information coming in, and then our ability to regulate and habituate to those sensations (creates) behavior,” Elizabeth Rhodus, MD, PhD, said during her talk. Dr. Rhodus is assistant professor of medicine at the University of Kentucky, Lexington.
Sensory-based interventions are not uncommon, but most are applied to pediatric populations and tend to focus on sensory processing disorders and autism spectrum disorder. The few programs that do focus on adults have varying methods and produce mixed results. Dr. Rhodus thinks that the key to success is individualization of therapy. “You’re going to like a certain sensation, and I might not like it. You can’t put us in the same room and expect the same results. We have to identify the preferences of how people interact with their environment, and what their brain does at a neuroscience level with that information,” she said.
Caregiving hacks
The program employs telehealth to work with caregivers so they can also create sensory environments within the home, using environment to trigger behavior.
For example, although individuals with dementia may have reduced response to color, the color red is unique. “Red is a cortical trigger. Red always stands out to people, so in our package that we send out as part of this intervention, we send out a roll of red duct tape,” said Dr. Rhodus.
An example of the use of red was a patient with dementia who had stopped drinking on his own, causing his caregiver daughter to be concerned that he would soon have to enter a nursing home. Examining the room, the occupational therapist realized that the water was kept out of sight, and suggested that the water glass be placed within the patient’s view, atop a square created with the red duct tape.
“These are just some of the simple concepts. They kind of seem easy. Some of my participants call them caregiving hacks, but it’s things that are grounded in neuroscience – how the brain processes the environment, and then how can we plug in supports and cues in whatever area is missing,” said Dr. Rhodus.
In the program, the caregiver fills out several online surveys, and an occupational therapist conducts an interview to identify specific challenges, such as bathing, or using the toilet, or going to church. Then an adult sensory profile reveals how the patient perceives his or her environment. “It’s taking those individual pieces, and then boiling it down to these mechanisms at the behavioral and neuroscience level,” said Dr. Rhodus. She said the entire setup process takes about an hour.
Impactful care
The individualized approach of the HARMONY (Helping Older Adults Create and Manage Occupations Successfully) method is promising, according to Monika Gross, executive director of the Poise Project, which uses the Alexander Technique to help people with chronic conditions such as Parkinson’s disease.
“Although it’s always a very simple idea that human beings need sensory processing aspects in their lives, from the time they’re infants through to the end of life, we don’t really focus on the end of life in a way that can bring meaning between the care partner and the person living with dementia. The other thing that was impressive is that this is in a rural community, where there often aren’t a lot of resources available, (such as) classes that the care partner can take their loved one to. So having something where the care partner has some confidence that they can really make an impact in that person that they are seeing decline, that they can see their behavior change [is good],” said Ms. Gross.
Empowering caregivers
The study included 30 pairs of patients and caregivers who were randomized to the individualized care (I), standardized care, or a control group. Adherence to weekly visits was high (I, 88%; S, 100%; C, 60%; P = .061). Retention was strong (I, 80%; S, 60%; C, 50%).
“It was feasible ... and at the end, we found a significant improvement in care partner satisfaction. We actually empowered these people to care for their loved ones, and in doing that, and helping them set up environmental cues, it allowed that person to perform at a more independent level,” said Dr. Rhodus.
The trial was only a proof of concept, so although the researchers saw signs of efficacy, it wasn’t powered to show that. They are currently enrolling additional patients and caregivers for larger studies to further test the approach.
Dr. Rhodus and Ms. Gross have no relevant financial disclosures.
Everyone gets by using environmental cues: For example, if you have to go to use the toilet in public, a bathroom sign prompts an immediate response. However, patients with dementia often struggle with environmental cues, which can complicate the already difficult task faced by their caregivers.
Individuals with dementia can lose awareness of such signs, and even colors, making it harder for them to interpret environmental cues.
The study, presented at the Alzheimer’s Association International Conference, recruited 30 pairs of patients and their caregivers. The approach is based on the Dunn model of sensory processing, which focuses on altering environments to maximize chances of success. It “explains that sensory processing is the information coming in, and then our ability to regulate and habituate to those sensations (creates) behavior,” Elizabeth Rhodus, MD, PhD, said during her talk. Dr. Rhodus is assistant professor of medicine at the University of Kentucky, Lexington.
Sensory-based interventions are not uncommon, but most are applied to pediatric populations and tend to focus on sensory processing disorders and autism spectrum disorder. The few programs that do focus on adults have varying methods and produce mixed results. Dr. Rhodus thinks that the key to success is individualization of therapy. “You’re going to like a certain sensation, and I might not like it. You can’t put us in the same room and expect the same results. We have to identify the preferences of how people interact with their environment, and what their brain does at a neuroscience level with that information,” she said.
Caregiving hacks
The program employs telehealth to work with caregivers so they can also create sensory environments within the home, using environment to trigger behavior.
For example, although individuals with dementia may have reduced response to color, the color red is unique. “Red is a cortical trigger. Red always stands out to people, so in our package that we send out as part of this intervention, we send out a roll of red duct tape,” said Dr. Rhodus.
An example of the use of red was a patient with dementia who had stopped drinking on his own, causing his caregiver daughter to be concerned that he would soon have to enter a nursing home. Examining the room, the occupational therapist realized that the water was kept out of sight, and suggested that the water glass be placed within the patient’s view, atop a square created with the red duct tape.
“These are just some of the simple concepts. They kind of seem easy. Some of my participants call them caregiving hacks, but it’s things that are grounded in neuroscience – how the brain processes the environment, and then how can we plug in supports and cues in whatever area is missing,” said Dr. Rhodus.
In the program, the caregiver fills out several online surveys, and an occupational therapist conducts an interview to identify specific challenges, such as bathing, or using the toilet, or going to church. Then an adult sensory profile reveals how the patient perceives his or her environment. “It’s taking those individual pieces, and then boiling it down to these mechanisms at the behavioral and neuroscience level,” said Dr. Rhodus. She said the entire setup process takes about an hour.
Impactful care
The individualized approach of the HARMONY (Helping Older Adults Create and Manage Occupations Successfully) method is promising, according to Monika Gross, executive director of the Poise Project, which uses the Alexander Technique to help people with chronic conditions such as Parkinson’s disease.
“Although it’s always a very simple idea that human beings need sensory processing aspects in their lives, from the time they’re infants through to the end of life, we don’t really focus on the end of life in a way that can bring meaning between the care partner and the person living with dementia. The other thing that was impressive is that this is in a rural community, where there often aren’t a lot of resources available, (such as) classes that the care partner can take their loved one to. So having something where the care partner has some confidence that they can really make an impact in that person that they are seeing decline, that they can see their behavior change [is good],” said Ms. Gross.
Empowering caregivers
The study included 30 pairs of patients and caregivers who were randomized to the individualized care (I), standardized care, or a control group. Adherence to weekly visits was high (I, 88%; S, 100%; C, 60%; P = .061). Retention was strong (I, 80%; S, 60%; C, 50%).
“It was feasible ... and at the end, we found a significant improvement in care partner satisfaction. We actually empowered these people to care for their loved ones, and in doing that, and helping them set up environmental cues, it allowed that person to perform at a more independent level,” said Dr. Rhodus.
The trial was only a proof of concept, so although the researchers saw signs of efficacy, it wasn’t powered to show that. They are currently enrolling additional patients and caregivers for larger studies to further test the approach.
Dr. Rhodus and Ms. Gross have no relevant financial disclosures.
Everyone gets by using environmental cues: For example, if you have to go to use the toilet in public, a bathroom sign prompts an immediate response. However, patients with dementia often struggle with environmental cues, which can complicate the already difficult task faced by their caregivers.
Individuals with dementia can lose awareness of such signs, and even colors, making it harder for them to interpret environmental cues.
The study, presented at the Alzheimer’s Association International Conference, recruited 30 pairs of patients and their caregivers. The approach is based on the Dunn model of sensory processing, which focuses on altering environments to maximize chances of success. It “explains that sensory processing is the information coming in, and then our ability to regulate and habituate to those sensations (creates) behavior,” Elizabeth Rhodus, MD, PhD, said during her talk. Dr. Rhodus is assistant professor of medicine at the University of Kentucky, Lexington.
Sensory-based interventions are not uncommon, but most are applied to pediatric populations and tend to focus on sensory processing disorders and autism spectrum disorder. The few programs that do focus on adults have varying methods and produce mixed results. Dr. Rhodus thinks that the key to success is individualization of therapy. “You’re going to like a certain sensation, and I might not like it. You can’t put us in the same room and expect the same results. We have to identify the preferences of how people interact with their environment, and what their brain does at a neuroscience level with that information,” she said.
Caregiving hacks
The program employs telehealth to work with caregivers so they can also create sensory environments within the home, using environment to trigger behavior.
For example, although individuals with dementia may have reduced response to color, the color red is unique. “Red is a cortical trigger. Red always stands out to people, so in our package that we send out as part of this intervention, we send out a roll of red duct tape,” said Dr. Rhodus.
An example of the use of red was a patient with dementia who had stopped drinking on his own, causing his caregiver daughter to be concerned that he would soon have to enter a nursing home. Examining the room, the occupational therapist realized that the water was kept out of sight, and suggested that the water glass be placed within the patient’s view, atop a square created with the red duct tape.
“These are just some of the simple concepts. They kind of seem easy. Some of my participants call them caregiving hacks, but it’s things that are grounded in neuroscience – how the brain processes the environment, and then how can we plug in supports and cues in whatever area is missing,” said Dr. Rhodus.
In the program, the caregiver fills out several online surveys, and an occupational therapist conducts an interview to identify specific challenges, such as bathing, or using the toilet, or going to church. Then an adult sensory profile reveals how the patient perceives his or her environment. “It’s taking those individual pieces, and then boiling it down to these mechanisms at the behavioral and neuroscience level,” said Dr. Rhodus. She said the entire setup process takes about an hour.
Impactful care
The individualized approach of the HARMONY (Helping Older Adults Create and Manage Occupations Successfully) method is promising, according to Monika Gross, executive director of the Poise Project, which uses the Alexander Technique to help people with chronic conditions such as Parkinson’s disease.
“Although it’s always a very simple idea that human beings need sensory processing aspects in their lives, from the time they’re infants through to the end of life, we don’t really focus on the end of life in a way that can bring meaning between the care partner and the person living with dementia. The other thing that was impressive is that this is in a rural community, where there often aren’t a lot of resources available, (such as) classes that the care partner can take their loved one to. So having something where the care partner has some confidence that they can really make an impact in that person that they are seeing decline, that they can see their behavior change [is good],” said Ms. Gross.
Empowering caregivers
The study included 30 pairs of patients and caregivers who were randomized to the individualized care (I), standardized care, or a control group. Adherence to weekly visits was high (I, 88%; S, 100%; C, 60%; P = .061). Retention was strong (I, 80%; S, 60%; C, 50%).
“It was feasible ... and at the end, we found a significant improvement in care partner satisfaction. We actually empowered these people to care for their loved ones, and in doing that, and helping them set up environmental cues, it allowed that person to perform at a more independent level,” said Dr. Rhodus.
The trial was only a proof of concept, so although the researchers saw signs of efficacy, it wasn’t powered to show that. They are currently enrolling additional patients and caregivers for larger studies to further test the approach.
Dr. Rhodus and Ms. Gross have no relevant financial disclosures.
FROM AAIC 2022
The gut microbes have spoken: All fiber is good fiber
Finding a fiber of good moral fiber
If you’ve ever wandered into the supplement aisle at your local grocery store, you’ve probably noticed an overabundance of fiber supplements that claim to do this for you and benefit that. Since there’s no Food and Drug Administration regulation on fiber supplements, manufacturers are free to (and do) make whatever wild claims they like. And much like choosing which of 500 shows to watch on Netflix, when you’re spoiled for choice, it can be difficult to pick.

Enter a team of molecular geneticists and microbiologists from Duke University. They can’t tell you what show to watch next, but they can tell you which fiber to choose, thanks to their new study. And the answer? Yes.
Well that’s not very helpful, but let us explain. For their study, a group of 28 received three of the main fiber supplements (inulin, dextrin, and galactooligosaccharides) for a week each, followed by a week off of fibers for their gut to return to baseline until they’d received all three. Those who consumed the least fiber at baseline saw the greatest benefit from fiber supplementation, with no appreciable difference between the three types. It was the same story for study participants who already consumed enough fiber; because their guts already hosted a more-optimal microbiome, the type of supplement didn’t matter. The benefits were the same across the board.
In an additional study, the Duke researchers found that gut microbiomes reacted to new fiber within a day, being primed to consume fiber on the first dose and digesting it more quickly on the second fiber dose.
The results, the researchers pointed out, make sense, since the average American only consumes 20%-40% of their daily recommended supply of fiber. Our digestive systems aren’t picky; they just want more, so go out there and choose whatever fiber you’d like. Do that, and then feel free to eat as many double bacon cheeseburgers as you’d like. That is the pinnacle of diet right there. Dietitians literally could not complain about it.
Jarlsberg vs. Camembert: This time it’s skeletal
Fiber is fabulous, of course, but the road to dietary health and wellness fulfillment takes us to many other, equally wondrous places. Hey, look! This next exit is covered with cheese.

All the cheeses are here, from Abbaye de Belloc to Zwitser, and there, right between the jalapeno cheddar and the Jermi tortes you’ll find Jarlsberg, a mild, semisoft, nutty-flavored cheese that comes from Jarlsberg in eastern Norway. A recent study also suggests that Jarlsberg may help to prevent osteopenia and osteoporosis.
A group of Norwegian investigators gathered together 66 healthy women and gave them a daily portion of either Jarlsberg or Camembert for 6 weeks, at which point the Camembert group was switched to Jarlsberg for another 6 weeks.
The research team choose Camembert because of its similarity to Jarlsberg in fat and protein content. Jarlsberg, however, also is rich in vitamin K2, which is important for bone health, and a substance known as DHNA, which “might combat bone thinning and increase bone tissue formation,” they said in a Eurekalert release.
After the first 6 weeks, blood levels of osteocalcin; vitamin K2; and PINP, a peptide involved in bone turnover, were significantly higher in the Jarlsberg group only. All those measures rose significantly after the switch from Camembert to Jarlsberg, while levels of total and LDL cholesterol “fell significantly in the Camembert group after they switched to Jarlsberg,” the team added.
But wait! There’s more! HbA1c fell significantly among those initially eating the Jarlsberg but rose sharply in those eating Camembert. Do you see where this is going? After the Camembert group made the switch to Jarlsberg, their HbA1c levels fell significantly as well.
So it’s not just a cheese thing: The effects are specific to Jarlsberg. Can you guess what we’re having for lunch? Double bacon and fiber Jarlsbergers. Mmm, Jarlsburgers.
Luck be a lady: The mother of twins
It’s widely believed that women who have twins must be more fertile, giving birth to more than one child at a time. Some studies have supported the idea, but more recent work is refuting that claim. In actuality, it might just be more statistics and luck than fertility after all.

Those earlier studies supporting fertility didn’t specify whether the chances of twin births were based on the ability to produce more than one egg at a time or on the number of births that women had overall. Looking at 100,000 preindustrial European births, before contraception was available, researchers from Norway, Germany, France, and the United Kingdom found that the number of total births, twins included, makes all the difference.
“When a woman gives birth several times, the chances increase that at least one of these births will be a twin birth,” investigator Gine Roll Skjærvø of the Norwegian University of Science and Technology said in a written statement.
Since twins occur in 1%-3% of all births, the more births that a woman has, the better her chances of giving birth to twins. The researchers compared it to playing the lottery. You buy enough tickets, eventually your numbers are going to come up. Despite that, however, they found that women who give birth to twins give birth less often than those who don’t have twins. Which raises the idea of sheer luck.
The researchers said that there’s still a lot to uncover in twin births, noting that “uncritically comparing groups of women with and without twins can trick us into believing the opposite of what is really true. These groupings may either hide the effects of twinning and fertility genes where they exist, or vice versa, create the illusion of these if they do not exist.”
For now, this new research claims that it’s basically a lottery. And women who give birth to twins hit the jackpot.
Those with low wages may be earning future memory loss
Not only are low wages detrimental to our souls, hopes, and dreams, but a new study shows that low wages also are linked to quicker memory decline later in life. Sustained low wages not only cause stress and food insecurity in the lives of many, but they also can cause diseases such as depression, obesity, and high blood pressure, which are risk factors for cognitive aging.
![]()
The study was conducted using records from the Health and Retirement Study for the years 1992-2016 and focused on 2,879 adults born between 1936 and 1941. The participants were divided into three groups: those who never earned low wages, those who sometimes did, and those who always did.
The investigators found that workers who earned sustained low wages – defined as an hourly wage lower than two-thirds of the federal median wage for the corresponding year – “experienced significantly faster memory decline in older age” than did those who never earned low wages.
There are signs of inflation everywhere we look these days, but many people are not earning higher wages to compensate for the extra expenses. “Increasing the federal minimum wage, for example to $15 per hour, remains a gridlock issue in Congress,” lead author Katrina Kezios of the Columbia University Mailman School of Public Health, said in a statement released by the university.
If only salaries would rise instead of prices for once.
Finding a fiber of good moral fiber
If you’ve ever wandered into the supplement aisle at your local grocery store, you’ve probably noticed an overabundance of fiber supplements that claim to do this for you and benefit that. Since there’s no Food and Drug Administration regulation on fiber supplements, manufacturers are free to (and do) make whatever wild claims they like. And much like choosing which of 500 shows to watch on Netflix, when you’re spoiled for choice, it can be difficult to pick.
Enter a team of molecular geneticists and microbiologists from Duke University. They can’t tell you what show to watch next, but they can tell you which fiber to choose, thanks to their new study. And the answer? Yes.
Well that’s not very helpful, but let us explain. For their study, a group of 28 received three of the main fiber supplements (inulin, dextrin, and galactooligosaccharides) for a week each, followed by a week off of fibers for their gut to return to baseline until they’d received all three. Those who consumed the least fiber at baseline saw the greatest benefit from fiber supplementation, with no appreciable difference between the three types. It was the same story for study participants who already consumed enough fiber; because their guts already hosted a more-optimal microbiome, the type of supplement didn’t matter. The benefits were the same across the board.
In an additional study, the Duke researchers found that gut microbiomes reacted to new fiber within a day, being primed to consume fiber on the first dose and digesting it more quickly on the second fiber dose.
The results, the researchers pointed out, make sense, since the average American only consumes 20%-40% of their daily recommended supply of fiber. Our digestive systems aren’t picky; they just want more, so go out there and choose whatever fiber you’d like. Do that, and then feel free to eat as many double bacon cheeseburgers as you’d like. That is the pinnacle of diet right there. Dietitians literally could not complain about it.
Jarlsberg vs. Camembert: This time it’s skeletal
Fiber is fabulous, of course, but the road to dietary health and wellness fulfillment takes us to many other, equally wondrous places. Hey, look! This next exit is covered with cheese.
All the cheeses are here, from Abbaye de Belloc to Zwitser, and there, right between the jalapeno cheddar and the Jermi tortes you’ll find Jarlsberg, a mild, semisoft, nutty-flavored cheese that comes from Jarlsberg in eastern Norway. A recent study also suggests that Jarlsberg may help to prevent osteopenia and osteoporosis.
A group of Norwegian investigators gathered together 66 healthy women and gave them a daily portion of either Jarlsberg or Camembert for 6 weeks, at which point the Camembert group was switched to Jarlsberg for another 6 weeks.
The research team choose Camembert because of its similarity to Jarlsberg in fat and protein content. Jarlsberg, however, also is rich in vitamin K2, which is important for bone health, and a substance known as DHNA, which “might combat bone thinning and increase bone tissue formation,” they said in a Eurekalert release.
After the first 6 weeks, blood levels of osteocalcin; vitamin K2; and PINP, a peptide involved in bone turnover, were significantly higher in the Jarlsberg group only. All those measures rose significantly after the switch from Camembert to Jarlsberg, while levels of total and LDL cholesterol “fell significantly in the Camembert group after they switched to Jarlsberg,” the team added.
But wait! There’s more! HbA1c fell significantly among those initially eating the Jarlsberg but rose sharply in those eating Camembert. Do you see where this is going? After the Camembert group made the switch to Jarlsberg, their HbA1c levels fell significantly as well.
So it’s not just a cheese thing: The effects are specific to Jarlsberg. Can you guess what we’re having for lunch? Double bacon and fiber Jarlsbergers. Mmm, Jarlsburgers.
Luck be a lady: The mother of twins
It’s widely believed that women who have twins must be more fertile, giving birth to more than one child at a time. Some studies have supported the idea, but more recent work is refuting that claim. In actuality, it might just be more statistics and luck than fertility after all.
Those earlier studies supporting fertility didn’t specify whether the chances of twin births were based on the ability to produce more than one egg at a time or on the number of births that women had overall. Looking at 100,000 preindustrial European births, before contraception was available, researchers from Norway, Germany, France, and the United Kingdom found that the number of total births, twins included, makes all the difference.
“When a woman gives birth several times, the chances increase that at least one of these births will be a twin birth,” investigator Gine Roll Skjærvø of the Norwegian University of Science and Technology said in a written statement.
Since twins occur in 1%-3% of all births, the more births that a woman has, the better her chances of giving birth to twins. The researchers compared it to playing the lottery. You buy enough tickets, eventually your numbers are going to come up. Despite that, however, they found that women who give birth to twins give birth less often than those who don’t have twins. Which raises the idea of sheer luck.
The researchers said that there’s still a lot to uncover in twin births, noting that “uncritically comparing groups of women with and without twins can trick us into believing the opposite of what is really true. These groupings may either hide the effects of twinning and fertility genes where they exist, or vice versa, create the illusion of these if they do not exist.”
For now, this new research claims that it’s basically a lottery. And women who give birth to twins hit the jackpot.
Those with low wages may be earning future memory loss
Not only are low wages detrimental to our souls, hopes, and dreams, but a new study shows that low wages also are linked to quicker memory decline later in life. Sustained low wages not only cause stress and food insecurity in the lives of many, but they also can cause diseases such as depression, obesity, and high blood pressure, which are risk factors for cognitive aging.
![]()
The study was conducted using records from the Health and Retirement Study for the years 1992-2016 and focused on 2,879 adults born between 1936 and 1941. The participants were divided into three groups: those who never earned low wages, those who sometimes did, and those who always did.
The investigators found that workers who earned sustained low wages – defined as an hourly wage lower than two-thirds of the federal median wage for the corresponding year – “experienced significantly faster memory decline in older age” than did those who never earned low wages.
There are signs of inflation everywhere we look these days, but many people are not earning higher wages to compensate for the extra expenses. “Increasing the federal minimum wage, for example to $15 per hour, remains a gridlock issue in Congress,” lead author Katrina Kezios of the Columbia University Mailman School of Public Health, said in a statement released by the university.
If only salaries would rise instead of prices for once.
Finding a fiber of good moral fiber
If you’ve ever wandered into the supplement aisle at your local grocery store, you’ve probably noticed an overabundance of fiber supplements that claim to do this for you and benefit that. Since there’s no Food and Drug Administration regulation on fiber supplements, manufacturers are free to (and do) make whatever wild claims they like. And much like choosing which of 500 shows to watch on Netflix, when you’re spoiled for choice, it can be difficult to pick.
Enter a team of molecular geneticists and microbiologists from Duke University. They can’t tell you what show to watch next, but they can tell you which fiber to choose, thanks to their new study. And the answer? Yes.
Well that’s not very helpful, but let us explain. For their study, a group of 28 received three of the main fiber supplements (inulin, dextrin, and galactooligosaccharides) for a week each, followed by a week off of fibers for their gut to return to baseline until they’d received all three. Those who consumed the least fiber at baseline saw the greatest benefit from fiber supplementation, with no appreciable difference between the three types. It was the same story for study participants who already consumed enough fiber; because their guts already hosted a more-optimal microbiome, the type of supplement didn’t matter. The benefits were the same across the board.
In an additional study, the Duke researchers found that gut microbiomes reacted to new fiber within a day, being primed to consume fiber on the first dose and digesting it more quickly on the second fiber dose.
The results, the researchers pointed out, make sense, since the average American only consumes 20%-40% of their daily recommended supply of fiber. Our digestive systems aren’t picky; they just want more, so go out there and choose whatever fiber you’d like. Do that, and then feel free to eat as many double bacon cheeseburgers as you’d like. That is the pinnacle of diet right there. Dietitians literally could not complain about it.
Jarlsberg vs. Camembert: This time it’s skeletal
Fiber is fabulous, of course, but the road to dietary health and wellness fulfillment takes us to many other, equally wondrous places. Hey, look! This next exit is covered with cheese.
All the cheeses are here, from Abbaye de Belloc to Zwitser, and there, right between the jalapeno cheddar and the Jermi tortes you’ll find Jarlsberg, a mild, semisoft, nutty-flavored cheese that comes from Jarlsberg in eastern Norway. A recent study also suggests that Jarlsberg may help to prevent osteopenia and osteoporosis.
A group of Norwegian investigators gathered together 66 healthy women and gave them a daily portion of either Jarlsberg or Camembert for 6 weeks, at which point the Camembert group was switched to Jarlsberg for another 6 weeks.
The research team choose Camembert because of its similarity to Jarlsberg in fat and protein content. Jarlsberg, however, also is rich in vitamin K2, which is important for bone health, and a substance known as DHNA, which “might combat bone thinning and increase bone tissue formation,” they said in a Eurekalert release.
After the first 6 weeks, blood levels of osteocalcin; vitamin K2; and PINP, a peptide involved in bone turnover, were significantly higher in the Jarlsberg group only. All those measures rose significantly after the switch from Camembert to Jarlsberg, while levels of total and LDL cholesterol “fell significantly in the Camembert group after they switched to Jarlsberg,” the team added.
But wait! There’s more! HbA1c fell significantly among those initially eating the Jarlsberg but rose sharply in those eating Camembert. Do you see where this is going? After the Camembert group made the switch to Jarlsberg, their HbA1c levels fell significantly as well.
So it’s not just a cheese thing: The effects are specific to Jarlsberg. Can you guess what we’re having for lunch? Double bacon and fiber Jarlsbergers. Mmm, Jarlsburgers.
Luck be a lady: The mother of twins
It’s widely believed that women who have twins must be more fertile, giving birth to more than one child at a time. Some studies have supported the idea, but more recent work is refuting that claim. In actuality, it might just be more statistics and luck than fertility after all.
Those earlier studies supporting fertility didn’t specify whether the chances of twin births were based on the ability to produce more than one egg at a time or on the number of births that women had overall. Looking at 100,000 preindustrial European births, before contraception was available, researchers from Norway, Germany, France, and the United Kingdom found that the number of total births, twins included, makes all the difference.
“When a woman gives birth several times, the chances increase that at least one of these births will be a twin birth,” investigator Gine Roll Skjærvø of the Norwegian University of Science and Technology said in a written statement.
Since twins occur in 1%-3% of all births, the more births that a woman has, the better her chances of giving birth to twins. The researchers compared it to playing the lottery. You buy enough tickets, eventually your numbers are going to come up. Despite that, however, they found that women who give birth to twins give birth less often than those who don’t have twins. Which raises the idea of sheer luck.
The researchers said that there’s still a lot to uncover in twin births, noting that “uncritically comparing groups of women with and without twins can trick us into believing the opposite of what is really true. These groupings may either hide the effects of twinning and fertility genes where they exist, or vice versa, create the illusion of these if they do not exist.”
For now, this new research claims that it’s basically a lottery. And women who give birth to twins hit the jackpot.
Those with low wages may be earning future memory loss
Not only are low wages detrimental to our souls, hopes, and dreams, but a new study shows that low wages also are linked to quicker memory decline later in life. Sustained low wages not only cause stress and food insecurity in the lives of many, but they also can cause diseases such as depression, obesity, and high blood pressure, which are risk factors for cognitive aging.
![]()
The study was conducted using records from the Health and Retirement Study for the years 1992-2016 and focused on 2,879 adults born between 1936 and 1941. The participants were divided into three groups: those who never earned low wages, those who sometimes did, and those who always did.
The investigators found that workers who earned sustained low wages – defined as an hourly wage lower than two-thirds of the federal median wage for the corresponding year – “experienced significantly faster memory decline in older age” than did those who never earned low wages.
There are signs of inflation everywhere we look these days, but many people are not earning higher wages to compensate for the extra expenses. “Increasing the federal minimum wage, for example to $15 per hour, remains a gridlock issue in Congress,” lead author Katrina Kezios of the Columbia University Mailman School of Public Health, said in a statement released by the university.
If only salaries would rise instead of prices for once.
Fraud
News reports this week indicate that the U.S. Department of Justice is investigating Cassava Sciences over the investigational Alzheimer’s disease agent simufilam. An article in Science alleged that the company’s research included altered or duplicated brain images.
Cassava, not surprisingly, denies this. And I’m not going to take sides. Maybe they’ll be exonerated, maybe not.

But the bigger point here is the importance of checking such things. Alzheimer’s disease, beyond being a horrible neurological disease, is also big money. REALLY big money. If a company were to develop a truly effective treatment for it, they’d be poised to reap a worldwide financial windfall.
I’m not criticizing that, either. If such a drug were to be developed, with all of the time and money that goes into such things, they’d have earned every penny.
But the financial incentives certainly do increase the risk of less-than-ethical behavior. This isn’t just in Alzheimer’s disease, but across the board in medicine. The main plot line of the 1993 Harrison Ford flick “The Fugitive” was based on a drug company using falsified data, bribes, and other criminal activities (like murder) to bring a potentially dangerous (but high-profit) drug to market.
Less-than-ethical behavior is not new in research either. In 1926 Paul Kammerer’s attempt to prove Lamarckian evolution was shown to be a fraud. Cover-ups of potentially dangerous drugs have also occurred, or been alleged, and resulted in some being withdrawn from the market.
I’m not sure this is any worse than the multitude of over-the-counter products I see in the store saying they promote brain health, joint health, immune health, whatever ... then, in tiny letters, adding “these statements have not been authorized by the FDA. This drug is not intended to cure, prevent, or treat any disease.” This is no different than guys selling snake oil and other worthless elixirs out of a horse-drawn wagon. Why they aren’t regulated in the same way Pfizer or Lilly are is beyond me.
Even beyond the old method of making up figures, data can still be iffy. We use the phrase “numbers don’t lie” – and generally they don’t – but the ability to “spin” them to suit any narrative has become an art form. If you can’t change the data, make them fit into a better scenario. Somehow.
Which brings me back to why it’s critically important that such studies be open to review by people who don’t have a conflict of interest in the success or failure of the drugs. And there are many: from shareholders, from executives, even from the knowledge that a bad outcome may mean they’re out of a job.
Fraud is nothing new in medicine. I also don’t see it going away anytime in the future. It’s not the nature of medicine, but it is the nature of some people. And a few of them increase the need for legitimacy in everyone else.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
News reports this week indicate that the U.S. Department of Justice is investigating Cassava Sciences over the investigational Alzheimer’s disease agent simufilam. An article in Science alleged that the company’s research included altered or duplicated brain images.
Cassava, not surprisingly, denies this. And I’m not going to take sides. Maybe they’ll be exonerated, maybe not.
But the bigger point here is the importance of checking such things. Alzheimer’s disease, beyond being a horrible neurological disease, is also big money. REALLY big money. If a company were to develop a truly effective treatment for it, they’d be poised to reap a worldwide financial windfall.
I’m not criticizing that, either. If such a drug were to be developed, with all of the time and money that goes into such things, they’d have earned every penny.
But the financial incentives certainly do increase the risk of less-than-ethical behavior. This isn’t just in Alzheimer’s disease, but across the board in medicine. The main plot line of the 1993 Harrison Ford flick “The Fugitive” was based on a drug company using falsified data, bribes, and other criminal activities (like murder) to bring a potentially dangerous (but high-profit) drug to market.
Less-than-ethical behavior is not new in research either. In 1926 Paul Kammerer’s attempt to prove Lamarckian evolution was shown to be a fraud. Cover-ups of potentially dangerous drugs have also occurred, or been alleged, and resulted in some being withdrawn from the market.
I’m not sure this is any worse than the multitude of over-the-counter products I see in the store saying they promote brain health, joint health, immune health, whatever ... then, in tiny letters, adding “these statements have not been authorized by the FDA. This drug is not intended to cure, prevent, or treat any disease.” This is no different than guys selling snake oil and other worthless elixirs out of a horse-drawn wagon. Why they aren’t regulated in the same way Pfizer or Lilly are is beyond me.
Even beyond the old method of making up figures, data can still be iffy. We use the phrase “numbers don’t lie” – and generally they don’t – but the ability to “spin” them to suit any narrative has become an art form. If you can’t change the data, make them fit into a better scenario. Somehow.
Which brings me back to why it’s critically important that such studies be open to review by people who don’t have a conflict of interest in the success or failure of the drugs. And there are many: from shareholders, from executives, even from the knowledge that a bad outcome may mean they’re out of a job.
Fraud is nothing new in medicine. I also don’t see it going away anytime in the future. It’s not the nature of medicine, but it is the nature of some people. And a few of them increase the need for legitimacy in everyone else.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
News reports this week indicate that the U.S. Department of Justice is investigating Cassava Sciences over the investigational Alzheimer’s disease agent simufilam. An article in Science alleged that the company’s research included altered or duplicated brain images.
Cassava, not surprisingly, denies this. And I’m not going to take sides. Maybe they’ll be exonerated, maybe not.
But the bigger point here is the importance of checking such things. Alzheimer’s disease, beyond being a horrible neurological disease, is also big money. REALLY big money. If a company were to develop a truly effective treatment for it, they’d be poised to reap a worldwide financial windfall.
I’m not criticizing that, either. If such a drug were to be developed, with all of the time and money that goes into such things, they’d have earned every penny.
But the financial incentives certainly do increase the risk of less-than-ethical behavior. This isn’t just in Alzheimer’s disease, but across the board in medicine. The main plot line of the 1993 Harrison Ford flick “The Fugitive” was based on a drug company using falsified data, bribes, and other criminal activities (like murder) to bring a potentially dangerous (but high-profit) drug to market.
Less-than-ethical behavior is not new in research either. In 1926 Paul Kammerer’s attempt to prove Lamarckian evolution was shown to be a fraud. Cover-ups of potentially dangerous drugs have also occurred, or been alleged, and resulted in some being withdrawn from the market.
I’m not sure this is any worse than the multitude of over-the-counter products I see in the store saying they promote brain health, joint health, immune health, whatever ... then, in tiny letters, adding “these statements have not been authorized by the FDA. This drug is not intended to cure, prevent, or treat any disease.” This is no different than guys selling snake oil and other worthless elixirs out of a horse-drawn wagon. Why they aren’t regulated in the same way Pfizer or Lilly are is beyond me.
Even beyond the old method of making up figures, data can still be iffy. We use the phrase “numbers don’t lie” – and generally they don’t – but the ability to “spin” them to suit any narrative has become an art form. If you can’t change the data, make them fit into a better scenario. Somehow.
Which brings me back to why it’s critically important that such studies be open to review by people who don’t have a conflict of interest in the success or failure of the drugs. And there are many: from shareholders, from executives, even from the knowledge that a bad outcome may mean they’re out of a job.
Fraud is nothing new in medicine. I also don’t see it going away anytime in the future. It’s not the nature of medicine, but it is the nature of some people. And a few of them increase the need for legitimacy in everyone else.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.