User login
Forgetfulness and mood fluctuations
This patient's symptoms go beyond just memory problems: She has difficulty with daily tasks, shows behavioral changes, and has significant communication difficulties — symptoms not found in mild cognitive impairment. While the patient has some behavioral changes, she does not exhibit the pronounced personality changes typical of frontotemporal dementia. Finally, the patient's cognitive decline is gradual and consistent without the stepwise progression typical of vascular dementia. Given the comprehensive presentation of the patient's symptoms and the results of her clinical investigations, middle-stage Alzheimer's disease is the most fitting diagnosis.
Alzheimer's disease is a progressive and irreversible brain disorder that affects memory, behavior, and cognitive skills. This condition causes the degeneration and death of brain cells, leading to various cognitive issues. Alzheimer's disease is the most common cause of dementia and accounts for 60%-80% of dementia cases. Although the exact cause is unknown, it is believed to result from genetic, lifestyle, and environmental factors. Alzheimer's disease progresses through stages — mild (early stage), moderate (middle stage), and severe (late stage) — and each stage has different signs and symptoms.
Alzheimer's disease is commonly observed in individuals 65 years or older, as age is the most significant risk factor. Another risk factor for Alzheimer's disease is family history; individuals who have parents or siblings with Alzheimer's disease are more likely to develop the disease. The risk increases with the number of family members diagnosed with the disease. Genetics also contribute to the development of Alzheimer's disease. Genes for developing Alzheimer's disease have been classified as deterministic and risk genes, which imply that they can cause the disease or increase the risk of developing it; however, the deterministic gene, which almost guarantees the occurrence of Alzheimer's, is rare and is found in less than 1% of cases. Experiencing a head injury is also a possible risk factor for Alzheimer's disease.
Accurate diagnosis of Alzheimer's disease requires a thorough history and physical examination. Gathering information from the patient's family and caregivers is important because some patients may not be aware of their condition. It is common for Alzheimer's disease patients to experience "sundowning," which causes confusion, agitation, and behavioral issues in the evening. A comprehensive physical examination, including a detailed neurologic and mental status exam, is necessary to determine the stage of the disease and rule out other conditions. Typically, the neurologic exam of Alzheimer's disease patients is normal.
Volumetric MRI is a recent technique that allows precise measurement of changes in brain volume. In Alzheimer's disease, shrinkage in the medial temporal lobe is visible through volumetric MRI. However, hippocampal atrophy is also a normal part of age-related memory decline, which raises doubts about the appropriateness of using volumetric MRI for early detection of Alzheimer's disease. The full potential of volumetric MRI in aiding the diagnosis of Alzheimer's disease is yet to be fully established.
Alzheimer's disease has no known cure, and treatment options are limited to addressing symptoms. Currently, three types of drugs are approved for treating the moderate or severe stages of the disease: cholinesterase inhibitors, partial N-methyl D-aspartate (NMDA) antagonists, and amyloid-directed antibodies. Cholinesterase inhibitors increase acetylcholine levels, a chemical crucial for cognitive functions such as memory and learning. NMDA antagonists (memantine) blocks NMDA receptors whose overactivation is implicated in Alzheimer's disease and related to synaptic dysfunction. Antiamyloid monoclonal antibodies bind to and promote the clearance of amyloid-beta peptides, thereby reducing amyloid plaques in the brain, which are associated with Alzheimer's disease.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's symptoms go beyond just memory problems: She has difficulty with daily tasks, shows behavioral changes, and has significant communication difficulties — symptoms not found in mild cognitive impairment. While the patient has some behavioral changes, she does not exhibit the pronounced personality changes typical of frontotemporal dementia. Finally, the patient's cognitive decline is gradual and consistent without the stepwise progression typical of vascular dementia. Given the comprehensive presentation of the patient's symptoms and the results of her clinical investigations, middle-stage Alzheimer's disease is the most fitting diagnosis.
Alzheimer's disease is a progressive and irreversible brain disorder that affects memory, behavior, and cognitive skills. This condition causes the degeneration and death of brain cells, leading to various cognitive issues. Alzheimer's disease is the most common cause of dementia and accounts for 60%-80% of dementia cases. Although the exact cause is unknown, it is believed to result from genetic, lifestyle, and environmental factors. Alzheimer's disease progresses through stages — mild (early stage), moderate (middle stage), and severe (late stage) — and each stage has different signs and symptoms.
Alzheimer's disease is commonly observed in individuals 65 years or older, as age is the most significant risk factor. Another risk factor for Alzheimer's disease is family history; individuals who have parents or siblings with Alzheimer's disease are more likely to develop the disease. The risk increases with the number of family members diagnosed with the disease. Genetics also contribute to the development of Alzheimer's disease. Genes for developing Alzheimer's disease have been classified as deterministic and risk genes, which imply that they can cause the disease or increase the risk of developing it; however, the deterministic gene, which almost guarantees the occurrence of Alzheimer's, is rare and is found in less than 1% of cases. Experiencing a head injury is also a possible risk factor for Alzheimer's disease.
Accurate diagnosis of Alzheimer's disease requires a thorough history and physical examination. Gathering information from the patient's family and caregivers is important because some patients may not be aware of their condition. It is common for Alzheimer's disease patients to experience "sundowning," which causes confusion, agitation, and behavioral issues in the evening. A comprehensive physical examination, including a detailed neurologic and mental status exam, is necessary to determine the stage of the disease and rule out other conditions. Typically, the neurologic exam of Alzheimer's disease patients is normal.
Volumetric MRI is a recent technique that allows precise measurement of changes in brain volume. In Alzheimer's disease, shrinkage in the medial temporal lobe is visible through volumetric MRI. However, hippocampal atrophy is also a normal part of age-related memory decline, which raises doubts about the appropriateness of using volumetric MRI for early detection of Alzheimer's disease. The full potential of volumetric MRI in aiding the diagnosis of Alzheimer's disease is yet to be fully established.
Alzheimer's disease has no known cure, and treatment options are limited to addressing symptoms. Currently, three types of drugs are approved for treating the moderate or severe stages of the disease: cholinesterase inhibitors, partial N-methyl D-aspartate (NMDA) antagonists, and amyloid-directed antibodies. Cholinesterase inhibitors increase acetylcholine levels, a chemical crucial for cognitive functions such as memory and learning. NMDA antagonists (memantine) blocks NMDA receptors whose overactivation is implicated in Alzheimer's disease and related to synaptic dysfunction. Antiamyloid monoclonal antibodies bind to and promote the clearance of amyloid-beta peptides, thereby reducing amyloid plaques in the brain, which are associated with Alzheimer's disease.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's symptoms go beyond just memory problems: She has difficulty with daily tasks, shows behavioral changes, and has significant communication difficulties — symptoms not found in mild cognitive impairment. While the patient has some behavioral changes, she does not exhibit the pronounced personality changes typical of frontotemporal dementia. Finally, the patient's cognitive decline is gradual and consistent without the stepwise progression typical of vascular dementia. Given the comprehensive presentation of the patient's symptoms and the results of her clinical investigations, middle-stage Alzheimer's disease is the most fitting diagnosis.
Alzheimer's disease is a progressive and irreversible brain disorder that affects memory, behavior, and cognitive skills. This condition causes the degeneration and death of brain cells, leading to various cognitive issues. Alzheimer's disease is the most common cause of dementia and accounts for 60%-80% of dementia cases. Although the exact cause is unknown, it is believed to result from genetic, lifestyle, and environmental factors. Alzheimer's disease progresses through stages — mild (early stage), moderate (middle stage), and severe (late stage) — and each stage has different signs and symptoms.
Alzheimer's disease is commonly observed in individuals 65 years or older, as age is the most significant risk factor. Another risk factor for Alzheimer's disease is family history; individuals who have parents or siblings with Alzheimer's disease are more likely to develop the disease. The risk increases with the number of family members diagnosed with the disease. Genetics also contribute to the development of Alzheimer's disease. Genes for developing Alzheimer's disease have been classified as deterministic and risk genes, which imply that they can cause the disease or increase the risk of developing it; however, the deterministic gene, which almost guarantees the occurrence of Alzheimer's, is rare and is found in less than 1% of cases. Experiencing a head injury is also a possible risk factor for Alzheimer's disease.
Accurate diagnosis of Alzheimer's disease requires a thorough history and physical examination. Gathering information from the patient's family and caregivers is important because some patients may not be aware of their condition. It is common for Alzheimer's disease patients to experience "sundowning," which causes confusion, agitation, and behavioral issues in the evening. A comprehensive physical examination, including a detailed neurologic and mental status exam, is necessary to determine the stage of the disease and rule out other conditions. Typically, the neurologic exam of Alzheimer's disease patients is normal.
Volumetric MRI is a recent technique that allows precise measurement of changes in brain volume. In Alzheimer's disease, shrinkage in the medial temporal lobe is visible through volumetric MRI. However, hippocampal atrophy is also a normal part of age-related memory decline, which raises doubts about the appropriateness of using volumetric MRI for early detection of Alzheimer's disease. The full potential of volumetric MRI in aiding the diagnosis of Alzheimer's disease is yet to be fully established.
Alzheimer's disease has no known cure, and treatment options are limited to addressing symptoms. Currently, three types of drugs are approved for treating the moderate or severe stages of the disease: cholinesterase inhibitors, partial N-methyl D-aspartate (NMDA) antagonists, and amyloid-directed antibodies. Cholinesterase inhibitors increase acetylcholine levels, a chemical crucial for cognitive functions such as memory and learning. NMDA antagonists (memantine) blocks NMDA receptors whose overactivation is implicated in Alzheimer's disease and related to synaptic dysfunction. Antiamyloid monoclonal antibodies bind to and promote the clearance of amyloid-beta peptides, thereby reducing amyloid plaques in the brain, which are associated with Alzheimer's disease.
Jasvinder Chawla, MD, Professor of Neurology, Loyola University Medical Center, Maywood; Director, Clinical Neurophysiology Lab, Department of Neurology, Hines VA Hospital, Hines, IL.
Jasvinder Chawla, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
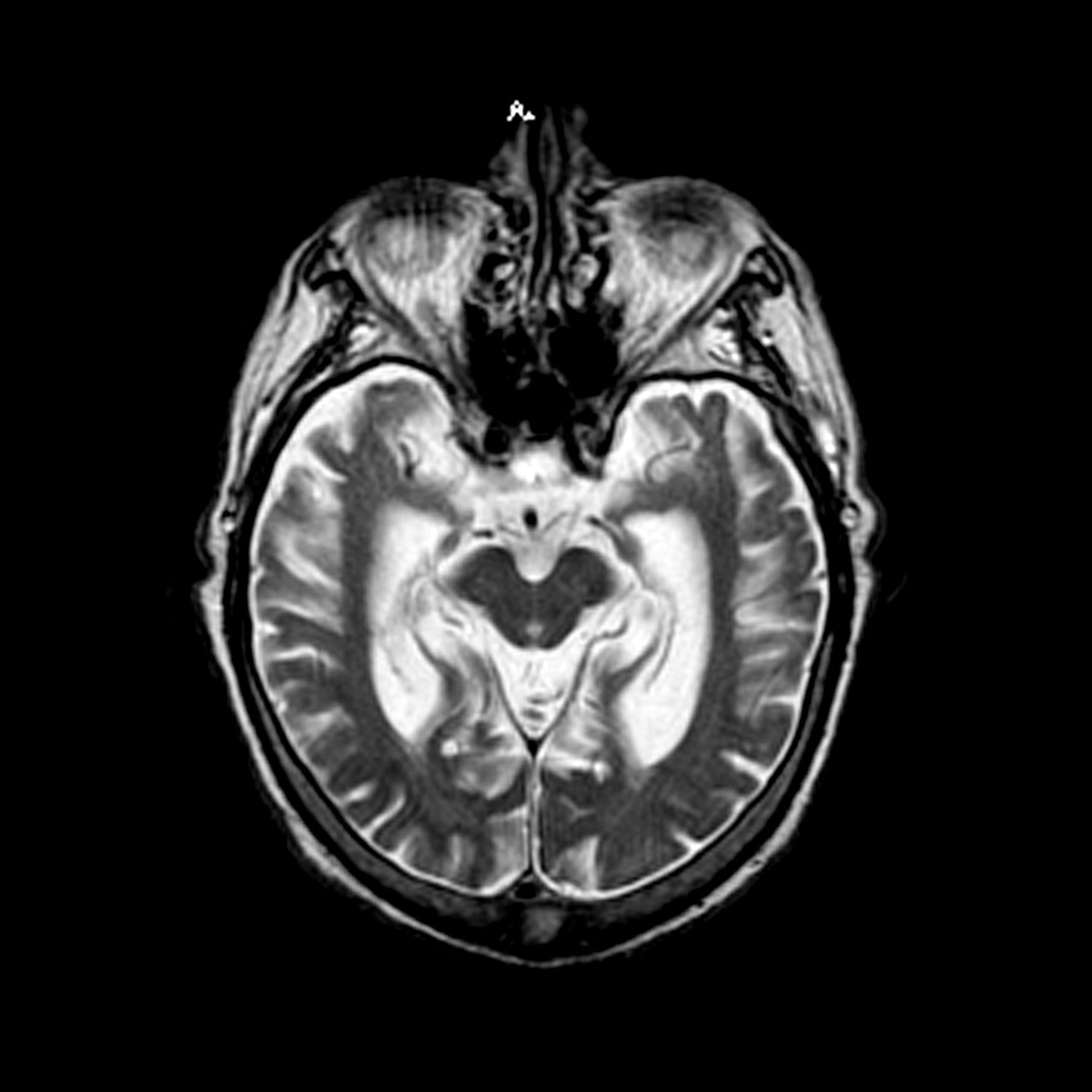
The patient is a 72-year-old retired schoolteacher accompanied by her daughter. Over the past year, her family has become increasingly concerned about her forgetfulness, mood fluctuations, and challenges in performing daily activities. The patient often forgets her grandchildren's names and struggles to recall significant recent events. She frequently misplaces household items and has missed several appointments. During her consultation, she has difficulty finding the right words, often repeats herself, and seems to lose track of the conversation. Her daughter shared concerning incidents, such as the patient wearing heavy sweaters during hot summer days and falling victim to a phone scam, which was uncharacteristic of her previous discerning nature. Additionally, the patient has become more reclusive, avoiding the social gatherings she once loved. She occasionally exhibits signs of agitation, especially in the evening. She has also stopped cooking as a result of instances of forgetting to turn off the stove and has had challenges managing her finances, leading to unpaid bills. A thorough neurologic exam is performed and is normal. Coronal T1-weighted MRI reveals hippocampal atrophy, particularly on the right side.

Enhanced natural killer cell therapy shows promise in Alzheimer’s
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
BOSTON – .
SNK01, being developed by NKGen Biotech, is an autologous, nongenetically modified NK cell product that has enhanced cytotoxicity and activating receptor expression.
“When we give these enhanced natural killer cells intravenously, not only do they get into the brain, but we’ve shown, through CSF biomarker data, that they reduce both amyloid and tau proteins, dramatically reducing the neuroinflammation,” said Paul Song, MD, chief executive officer of NKGen Biotech.
“Remarkably,” in the first 6 months, 90% of patients with Alzheimer’s disease demonstrated improvement or maintained stable cognitive function, based on the Alzheimer’s Disease Composite Score (ADCOMS), suggesting that SNK01 may do more than simply slow disease progression, Dr. Song said.
The findings were presented at the 16th Clinical Trials on Alzheimer’s Disease (CTAD) conference.
Sound rationale
NK cells are an essential part of the innate immune system that can shape the adaptive response by eliminating activated (not resting) autologous CD4+ T cells. Weak or deficient NK cells have been found to correlate with various diseases, including autoimmune diseases, and emerging data suggest an autoimmune component to Alzheimer’s disease.
The phase 1 study evaluated the safety, tolerability, and exploratory efficacy of SNK01 given intravenously in escalating doses every 3 weeks (four treatments in total).
Participants included 10 patients with Alzheimer’s disease confirmed by imaging. Five had mild Alzheimer’s disease, three had moderate Alzheimer’s disease, and two had advanced Alzheimer’s disease, based on baseline Clinical Dementia Rating–Sum of Boxes (CDR-SB) scores. Median baseline CDR-SB score was 9 (range, 4-18).
Cognitive assessments included CDR-SB, Mini-Mental State Examination (MMSE), Alzheimer’s disease Assessment Scale-Cognitive Subscale (ADAS-Cog) and ADCOMS. CSF biomarker analyses were performed at baseline and at 1 and 12 weeks after the final dose (weeks 11 and 22, respectively).
NK cells were successfully activated and expanded in all 10 patients and no treatment-related adverse events were observed.
Based on the CSF biomarker data, SNK01 crossed the blood–brain barrier and reduced CSF amyloid-beta 42/40 and pTau181 levels and neuroinflammation, as measured by glial fibrillary acid protein (GFAP), and the effects appeared to persist 12 weeks after the final dose.
The exploratory efficacy data show that, 1 week after final dose (week 11), compared with baseline, 30% of patients showed clinical improvement on the composite ADCOMS and 60% had a stable ADCOMS score; 50%-70% of patients were stable or improved on the CDR-SB, ADAS-Cog and/or MMSE.
“One patient went from a MMSE score of 14, which is moderate dementia, to 22, which is mild cognitive impairment,” said Dr. Song.
At 12 weeks after the final dose (week 22), 44%-89% of patients remained stable or improved in all cognitive scores compared with week 11; and 50% of the patients with stable ADCOMS scores at week 11 remained stable.
Based on the positive phase 1 data, the Food and Drug Administration has approved a phase 1/2a study in patients with moderate Alzheimer’s disease. “The trial will use a much higher dose and a prolonged dosing regimen and we think we’ll see even more dramatic results with more sustained higher dosing,” Dr. Song said.
Down the road, it will be interesting to see how NK cell therapy could “complement” anti-amyloid and anti-tau therapies, he added.
Ideal treatment approach
Commenting on this research, Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, said NK cells have “natural abilities that could make them an ideal treatment approach for Alzheimer’s and similar neurodegenerative diseases.
“NK cells have properties that allow them to recognize and destroy diseased brain cells while leaving healthy cells intact, without causing excessive inflammation or autoimmune issues. It has historically been difficult to get immune cells to access the privileged immunological environment of the brain,” Dr. Lakhan explained.
“However, this line of early research shows that NK cells safely crosses the blood–brain barrier, infiltrates brain tissue, and may stave off Alzheimer’s disease as measured by biomarkers and clinical symptoms,” he noted.
“This emerging cell-based immunotherapy is highly-specific to the cells responsible for Alzheimer’s, avoids drug resistance, has long-lasting results, and has fewer side effects than drug counterparts,” Dr. Lakhan said.
The trial was sponsored by NKGen Biotech. Dr. Song and six coauthors are employees and shareholders in the company. Dr. Lakhan reports no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM CTAD 2023
AF tied to 45% increase in mild cognitive impairment
TOPLINE:
results of a new study suggest.
METHODOLOGY:
- From over 4.3 million people in the UK primary electronic health record (EHR) database, researchers identified 233,833 (5.4%) with AF (mean age, 74.2 years) and randomly selected one age- and sex-matched control person without AF for each AF case patient.
- The primary outcome was incidence of mild cognitive impairment (MCI).
- The authors adjusted for age, sex, year at study entry, socioeconomic status, smoking, and a number of comorbid conditions.
- During a median of 5.3 years of follow-up, there were 4,269 incident MCI cases among both AF and non-AF patients.
TAKEAWAY:
- Individuals with AF had a higher risk of MCI than that of those without AF (adjusted hazard ratio [aHR], 1.45; 95% confidence interval [CI], 1.35-1.56).
- Besides AF, older age (risk ratio [RR], 1.08) and history of depression (RR, 1.44) were associated with greater risk of MCI, as were female sex, greater socioeconomic deprivation, stroke, and multimorbidity, including, for example, diabetes, hypercholesterolemia, and peripheral artery disease (all P < .001).
- Individuals with AF who received oral anticoagulants or amiodarone were not at increased risk of MCI, as was the case for those treated with digoxin.
- Individuals with AF and MCI were at greater risk of dementia (aHR, 1.25; 95% CI, 1.09-1.42). Sex, smoking, chronic kidney disease, and multi-comorbidity were among factors linked to elevated dementia risk.
IN PRACTICE:
The findings emphasize the association of multi-comorbidity and cardiovascular risk factors with development of MCI and progression to dementia in AF patients, the authors wrote. They noted that the data suggest combining anticoagulation and symptom and comorbidity management may prevent cognitive deterioration.
SOURCE:
The study was conducted by Sheng-Chia Chung, PhD, Institute of Health informatics Research, University College London, and colleagues. It was published online Oct. 25, 2023, as a research letter in the Journal of the American College of Cardiology (JACC): Advances.
LIMITATIONS:
The EHR dataset may have lacked granularity and detail, and some risk factors or comorbidities may not have been measured. While those with AF receiving digoxin or amiodarone treatment had no higher risk of MCI than their non-AF peers, the study’s observational design and very wide confidence intervals for these subgroups prevent making solid inferences about causality or a potential protective role of these drugs.
DISCLOSURES:
Dr. Chung is supported by the National Institute of Health and Care Research (NIHR) Author Rui Providencia, MD, PhD, of the Institute of Health informatics Research, University College London, is supported by the University College London British Heart Foundation and NIHR. All other authors report no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
results of a new study suggest.
METHODOLOGY:
- From over 4.3 million people in the UK primary electronic health record (EHR) database, researchers identified 233,833 (5.4%) with AF (mean age, 74.2 years) and randomly selected one age- and sex-matched control person without AF for each AF case patient.
- The primary outcome was incidence of mild cognitive impairment (MCI).
- The authors adjusted for age, sex, year at study entry, socioeconomic status, smoking, and a number of comorbid conditions.
- During a median of 5.3 years of follow-up, there were 4,269 incident MCI cases among both AF and non-AF patients.
TAKEAWAY:
- Individuals with AF had a higher risk of MCI than that of those without AF (adjusted hazard ratio [aHR], 1.45; 95% confidence interval [CI], 1.35-1.56).
- Besides AF, older age (risk ratio [RR], 1.08) and history of depression (RR, 1.44) were associated with greater risk of MCI, as were female sex, greater socioeconomic deprivation, stroke, and multimorbidity, including, for example, diabetes, hypercholesterolemia, and peripheral artery disease (all P < .001).
- Individuals with AF who received oral anticoagulants or amiodarone were not at increased risk of MCI, as was the case for those treated with digoxin.
- Individuals with AF and MCI were at greater risk of dementia (aHR, 1.25; 95% CI, 1.09-1.42). Sex, smoking, chronic kidney disease, and multi-comorbidity were among factors linked to elevated dementia risk.
IN PRACTICE:
The findings emphasize the association of multi-comorbidity and cardiovascular risk factors with development of MCI and progression to dementia in AF patients, the authors wrote. They noted that the data suggest combining anticoagulation and symptom and comorbidity management may prevent cognitive deterioration.
SOURCE:
The study was conducted by Sheng-Chia Chung, PhD, Institute of Health informatics Research, University College London, and colleagues. It was published online Oct. 25, 2023, as a research letter in the Journal of the American College of Cardiology (JACC): Advances.
LIMITATIONS:
The EHR dataset may have lacked granularity and detail, and some risk factors or comorbidities may not have been measured. While those with AF receiving digoxin or amiodarone treatment had no higher risk of MCI than their non-AF peers, the study’s observational design and very wide confidence intervals for these subgroups prevent making solid inferences about causality or a potential protective role of these drugs.
DISCLOSURES:
Dr. Chung is supported by the National Institute of Health and Care Research (NIHR) Author Rui Providencia, MD, PhD, of the Institute of Health informatics Research, University College London, is supported by the University College London British Heart Foundation and NIHR. All other authors report no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
results of a new study suggest.
METHODOLOGY:
- From over 4.3 million people in the UK primary electronic health record (EHR) database, researchers identified 233,833 (5.4%) with AF (mean age, 74.2 years) and randomly selected one age- and sex-matched control person without AF for each AF case patient.
- The primary outcome was incidence of mild cognitive impairment (MCI).
- The authors adjusted for age, sex, year at study entry, socioeconomic status, smoking, and a number of comorbid conditions.
- During a median of 5.3 years of follow-up, there were 4,269 incident MCI cases among both AF and non-AF patients.
TAKEAWAY:
- Individuals with AF had a higher risk of MCI than that of those without AF (adjusted hazard ratio [aHR], 1.45; 95% confidence interval [CI], 1.35-1.56).
- Besides AF, older age (risk ratio [RR], 1.08) and history of depression (RR, 1.44) were associated with greater risk of MCI, as were female sex, greater socioeconomic deprivation, stroke, and multimorbidity, including, for example, diabetes, hypercholesterolemia, and peripheral artery disease (all P < .001).
- Individuals with AF who received oral anticoagulants or amiodarone were not at increased risk of MCI, as was the case for those treated with digoxin.
- Individuals with AF and MCI were at greater risk of dementia (aHR, 1.25; 95% CI, 1.09-1.42). Sex, smoking, chronic kidney disease, and multi-comorbidity were among factors linked to elevated dementia risk.
IN PRACTICE:
The findings emphasize the association of multi-comorbidity and cardiovascular risk factors with development of MCI and progression to dementia in AF patients, the authors wrote. They noted that the data suggest combining anticoagulation and symptom and comorbidity management may prevent cognitive deterioration.
SOURCE:
The study was conducted by Sheng-Chia Chung, PhD, Institute of Health informatics Research, University College London, and colleagues. It was published online Oct. 25, 2023, as a research letter in the Journal of the American College of Cardiology (JACC): Advances.
LIMITATIONS:
The EHR dataset may have lacked granularity and detail, and some risk factors or comorbidities may not have been measured. While those with AF receiving digoxin or amiodarone treatment had no higher risk of MCI than their non-AF peers, the study’s observational design and very wide confidence intervals for these subgroups prevent making solid inferences about causality or a potential protective role of these drugs.
DISCLOSURES:
Dr. Chung is supported by the National Institute of Health and Care Research (NIHR) Author Rui Providencia, MD, PhD, of the Institute of Health informatics Research, University College London, is supported by the University College London British Heart Foundation and NIHR. All other authors report no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
Be advised: Thyroid hormones may increase risk of cognitive disorders in older adults
published in JAMA Internal Medicine.
The study found that these patients with thyrotoxicosis had a higher likelihood of incident cognitive disorder (adjusted hazard ratio, 1.39; 95% confidence interval, 1.18-1.64; P < .001). Broken down between internal and external causes of thyrotoxicosis, exogenous thyrotoxicosis continued to be a significant risk factor (aHR, 1.34: 95% CI, 1.10-1.63; P = .003), while endogenous thyrotoxicosis did not show a statistically significant risk estimates (aHR, 1.38; 95% CI, 0.96-1.98; P = .08).
The study also found that women were more likely to have low levels of thyrotropin (thyroid-stimulating hormone/TSH) than men and were more likely to be overtreated.
Previous studies looking at the correlation between hyperthyroidism and cognitive disorders often did not include participants who were already taking thyroid hormones, according to Jennifer S. Mammen, MD, PhD, assistant professor of medicine at the Asthma and Allergy Center at John Hopkins University, Baltimore, and the senior author of the study.
“The fact that we see the signal both in people who are being overtreated with thyroid hormone and in people who have endogenous hyperthyroidism is one way that we think that this supports the fact that it’s not just confounding, it’s not just bias,” Dr. Mammen said. “There’s two different sources of hyperthyroidism, and they’re both showing the same relationship.”
In the study, Dr. Mammen and colleagues analyzed electronic health records for patients aged 65 years and older who received primary care in the Johns Hopkins Community Physicians Network over a 10-year period starting in 2014. Patients had to have a minimum of two visits 30 days apart. None had a history of low TSH levels or cognitive disorder diagnoses within 6 months of their first doctor visit.
More than 65,000 patients were included in the study. Slightly more than half (56%) were female, almost 70% were White, 19.3% were Black, 4.6% were Asian, and 0.4% were American Indian. Almost 25,000 low TSH measurements among 2,710 patients were recorded during the study period. The majority of low TSH measurements were exogenous (14,875), followed by origins of unknown cause (5,833), and endogenous (4,159).
During the follow-up period, 7.2% (4,779) patients received a new cognitive disorder diagnosis, which was dementia in 77% of cases.
Dr. Mammen said primary care physicians should carefully consider whether thyroid hormone therapy is necessary for older patients, and, if so, great care should be taken to avoid overtreatment.
“This is yet another reason for us to be vigilant about not overtreating people with thyroid hormone, especially in older adults,” Dr. Mammen said. “We already know that atrial fibrillation rates are increased in people who are hyperthyroid. We know that fracture and osteoporosis is affected by hyperthyroidism. And now we also have an association with higher rates of cognitive disorders.”
Taking a cautious approach to prescribing thyroid hormone therapy for older patients is paramount, according to Jean Chen, MD, partner at Texas Diabetes & Endocrinology, who was not affiliated with the study.
“All medical providers need to be aware that the 65 and older population does not need to be treated as aggressively with their thyroid hormone,” Dr. Chen said. “We are finding more and more complications from overtreatment rather than benefit in this population.”
Often, older patients may complain of symptoms such as constipation, feeling cold, or tiredness, which can be symptoms of hypothyroidism. But these symptoms could also be from anemia, vitamin deficiencies, depression, perimenopause, menopause, insulin resistance, and sleep apnea. If necessary, Dr. Chen recommended primary care physicians consult with an endocrinologist regarding a possible treatment plan and making a differential diagnosis.
In addition, Dr. Chen said other studies have shown that treating patients with thyroid hormone either did not resolve the condition or negatively impacted anxiety, muscle strength, and bone density, or it increased the risk for arrhythmia. Therefore, it’s important to weight the risks versus the benefits.
“There’s so much gray zone here,” Dr. Chen said.
The study was supported by the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease, the Richman Family Foundation, the Rick Sharp Alzheimer’s Foundation, the Sharp Family Foundation, among others. The work was also supported by grants from the National Institutes of Health. One coauthor reported personal fees from Karuna, MapLight Therapeutics, Axsome Therapeutics, GIA, GW Research Limited, Merck, EXCIVA, Otsuka, IntraCellular Therapies, and Medesis Pharma for consulting for treatment development in Alzheimer’s disease outside the submitted work. No other disclosures were reported.
A version of this article appeared on Medscape.com.
published in JAMA Internal Medicine.
The study found that these patients with thyrotoxicosis had a higher likelihood of incident cognitive disorder (adjusted hazard ratio, 1.39; 95% confidence interval, 1.18-1.64; P < .001). Broken down between internal and external causes of thyrotoxicosis, exogenous thyrotoxicosis continued to be a significant risk factor (aHR, 1.34: 95% CI, 1.10-1.63; P = .003), while endogenous thyrotoxicosis did not show a statistically significant risk estimates (aHR, 1.38; 95% CI, 0.96-1.98; P = .08).
The study also found that women were more likely to have low levels of thyrotropin (thyroid-stimulating hormone/TSH) than men and were more likely to be overtreated.
Previous studies looking at the correlation between hyperthyroidism and cognitive disorders often did not include participants who were already taking thyroid hormones, according to Jennifer S. Mammen, MD, PhD, assistant professor of medicine at the Asthma and Allergy Center at John Hopkins University, Baltimore, and the senior author of the study.
“The fact that we see the signal both in people who are being overtreated with thyroid hormone and in people who have endogenous hyperthyroidism is one way that we think that this supports the fact that it’s not just confounding, it’s not just bias,” Dr. Mammen said. “There’s two different sources of hyperthyroidism, and they’re both showing the same relationship.”
In the study, Dr. Mammen and colleagues analyzed electronic health records for patients aged 65 years and older who received primary care in the Johns Hopkins Community Physicians Network over a 10-year period starting in 2014. Patients had to have a minimum of two visits 30 days apart. None had a history of low TSH levels or cognitive disorder diagnoses within 6 months of their first doctor visit.
More than 65,000 patients were included in the study. Slightly more than half (56%) were female, almost 70% were White, 19.3% were Black, 4.6% were Asian, and 0.4% were American Indian. Almost 25,000 low TSH measurements among 2,710 patients were recorded during the study period. The majority of low TSH measurements were exogenous (14,875), followed by origins of unknown cause (5,833), and endogenous (4,159).
During the follow-up period, 7.2% (4,779) patients received a new cognitive disorder diagnosis, which was dementia in 77% of cases.
Dr. Mammen said primary care physicians should carefully consider whether thyroid hormone therapy is necessary for older patients, and, if so, great care should be taken to avoid overtreatment.
“This is yet another reason for us to be vigilant about not overtreating people with thyroid hormone, especially in older adults,” Dr. Mammen said. “We already know that atrial fibrillation rates are increased in people who are hyperthyroid. We know that fracture and osteoporosis is affected by hyperthyroidism. And now we also have an association with higher rates of cognitive disorders.”
Taking a cautious approach to prescribing thyroid hormone therapy for older patients is paramount, according to Jean Chen, MD, partner at Texas Diabetes & Endocrinology, who was not affiliated with the study.
“All medical providers need to be aware that the 65 and older population does not need to be treated as aggressively with their thyroid hormone,” Dr. Chen said. “We are finding more and more complications from overtreatment rather than benefit in this population.”
Often, older patients may complain of symptoms such as constipation, feeling cold, or tiredness, which can be symptoms of hypothyroidism. But these symptoms could also be from anemia, vitamin deficiencies, depression, perimenopause, menopause, insulin resistance, and sleep apnea. If necessary, Dr. Chen recommended primary care physicians consult with an endocrinologist regarding a possible treatment plan and making a differential diagnosis.
In addition, Dr. Chen said other studies have shown that treating patients with thyroid hormone either did not resolve the condition or negatively impacted anxiety, muscle strength, and bone density, or it increased the risk for arrhythmia. Therefore, it’s important to weight the risks versus the benefits.
“There’s so much gray zone here,” Dr. Chen said.
The study was supported by the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease, the Richman Family Foundation, the Rick Sharp Alzheimer’s Foundation, the Sharp Family Foundation, among others. The work was also supported by grants from the National Institutes of Health. One coauthor reported personal fees from Karuna, MapLight Therapeutics, Axsome Therapeutics, GIA, GW Research Limited, Merck, EXCIVA, Otsuka, IntraCellular Therapies, and Medesis Pharma for consulting for treatment development in Alzheimer’s disease outside the submitted work. No other disclosures were reported.
A version of this article appeared on Medscape.com.
published in JAMA Internal Medicine.
The study found that these patients with thyrotoxicosis had a higher likelihood of incident cognitive disorder (adjusted hazard ratio, 1.39; 95% confidence interval, 1.18-1.64; P < .001). Broken down between internal and external causes of thyrotoxicosis, exogenous thyrotoxicosis continued to be a significant risk factor (aHR, 1.34: 95% CI, 1.10-1.63; P = .003), while endogenous thyrotoxicosis did not show a statistically significant risk estimates (aHR, 1.38; 95% CI, 0.96-1.98; P = .08).
The study also found that women were more likely to have low levels of thyrotropin (thyroid-stimulating hormone/TSH) than men and were more likely to be overtreated.
Previous studies looking at the correlation between hyperthyroidism and cognitive disorders often did not include participants who were already taking thyroid hormones, according to Jennifer S. Mammen, MD, PhD, assistant professor of medicine at the Asthma and Allergy Center at John Hopkins University, Baltimore, and the senior author of the study.
“The fact that we see the signal both in people who are being overtreated with thyroid hormone and in people who have endogenous hyperthyroidism is one way that we think that this supports the fact that it’s not just confounding, it’s not just bias,” Dr. Mammen said. “There’s two different sources of hyperthyroidism, and they’re both showing the same relationship.”
In the study, Dr. Mammen and colleagues analyzed electronic health records for patients aged 65 years and older who received primary care in the Johns Hopkins Community Physicians Network over a 10-year period starting in 2014. Patients had to have a minimum of two visits 30 days apart. None had a history of low TSH levels or cognitive disorder diagnoses within 6 months of their first doctor visit.
More than 65,000 patients were included in the study. Slightly more than half (56%) were female, almost 70% were White, 19.3% were Black, 4.6% were Asian, and 0.4% were American Indian. Almost 25,000 low TSH measurements among 2,710 patients were recorded during the study period. The majority of low TSH measurements were exogenous (14,875), followed by origins of unknown cause (5,833), and endogenous (4,159).
During the follow-up period, 7.2% (4,779) patients received a new cognitive disorder diagnosis, which was dementia in 77% of cases.
Dr. Mammen said primary care physicians should carefully consider whether thyroid hormone therapy is necessary for older patients, and, if so, great care should be taken to avoid overtreatment.
“This is yet another reason for us to be vigilant about not overtreating people with thyroid hormone, especially in older adults,” Dr. Mammen said. “We already know that atrial fibrillation rates are increased in people who are hyperthyroid. We know that fracture and osteoporosis is affected by hyperthyroidism. And now we also have an association with higher rates of cognitive disorders.”
Taking a cautious approach to prescribing thyroid hormone therapy for older patients is paramount, according to Jean Chen, MD, partner at Texas Diabetes & Endocrinology, who was not affiliated with the study.
“All medical providers need to be aware that the 65 and older population does not need to be treated as aggressively with their thyroid hormone,” Dr. Chen said. “We are finding more and more complications from overtreatment rather than benefit in this population.”
Often, older patients may complain of symptoms such as constipation, feeling cold, or tiredness, which can be symptoms of hypothyroidism. But these symptoms could also be from anemia, vitamin deficiencies, depression, perimenopause, menopause, insulin resistance, and sleep apnea. If necessary, Dr. Chen recommended primary care physicians consult with an endocrinologist regarding a possible treatment plan and making a differential diagnosis.
In addition, Dr. Chen said other studies have shown that treating patients with thyroid hormone either did not resolve the condition or negatively impacted anxiety, muscle strength, and bone density, or it increased the risk for arrhythmia. Therefore, it’s important to weight the risks versus the benefits.
“There’s so much gray zone here,” Dr. Chen said.
The study was supported by the Richman Family Precision Medicine Center of Excellence in Alzheimer’s Disease, the Richman Family Foundation, the Rick Sharp Alzheimer’s Foundation, the Sharp Family Foundation, among others. The work was also supported by grants from the National Institutes of Health. One coauthor reported personal fees from Karuna, MapLight Therapeutics, Axsome Therapeutics, GIA, GW Research Limited, Merck, EXCIVA, Otsuka, IntraCellular Therapies, and Medesis Pharma for consulting for treatment development in Alzheimer’s disease outside the submitted work. No other disclosures were reported.
A version of this article appeared on Medscape.com.
FROM JAMA INTERNAL MEDICINE
More evidence metformin may be neuroprotective
TOPLINE:
New research suggests terminating metformin may raise the risk for dementia in older adults with type 2 diabetes, providing more evidence of metformin’s potential neuroprotective effects.
METHODOLOGY:
- Researchers evaluated the association between discontinuing metformin for reasons unrelated to kidney dysfunction and dementia incidence.
- The cohort included 12,220 Kaiser Permanente Northern California members who stopped metformin early (with normal kidney function) and 29,126 routine metformin users.
- The cohort of early terminators was 46% women with an average age of 59 years at the start of metformin prescription. The cohort continuing metformin was 47% women, with a start age of 61 years.
TAKEAWAY:
- Adults who stopped metformin early were 21% more likely to be diagnosed with dementia during follow up (hazard ratio, 1.21; 95% confidence interval, 1.12-1.30), compared with routine metformin users.
- This association was largely independent of changes in A1c level and insulin usage.
IN PRACTICE:
The findings “corroborate the largely consistent evidence from other observational studies showing an association between metformin use and lower dementia incidence [and] may have important implications for clinical treatment of adults with diabetes,” the authors write.
SOURCE:
The study, with first author Scott Zimmerman, MPH, University of California, San Francisco, was published online in JAMA Network Open.
LIMITATIONS:
Dementia diagnosis was obtained based on medical records. Factors such as race, ethnicity, or time on metformin were not evaluated. Information on the exact reason for stopping metformin was not available.
DISCLOSURES:
The study was funded by grants from the National Institutes of Health, National Institute on Aging. Mr. Zimmerman owns stock in AbbVie, Gilead Sciences, CRISPR Therapeutics, and Abbott Laboratories. Disclosure for the other study authors can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
New research suggests terminating metformin may raise the risk for dementia in older adults with type 2 diabetes, providing more evidence of metformin’s potential neuroprotective effects.
METHODOLOGY:
- Researchers evaluated the association between discontinuing metformin for reasons unrelated to kidney dysfunction and dementia incidence.
- The cohort included 12,220 Kaiser Permanente Northern California members who stopped metformin early (with normal kidney function) and 29,126 routine metformin users.
- The cohort of early terminators was 46% women with an average age of 59 years at the start of metformin prescription. The cohort continuing metformin was 47% women, with a start age of 61 years.
TAKEAWAY:
- Adults who stopped metformin early were 21% more likely to be diagnosed with dementia during follow up (hazard ratio, 1.21; 95% confidence interval, 1.12-1.30), compared with routine metformin users.
- This association was largely independent of changes in A1c level and insulin usage.
IN PRACTICE:
The findings “corroborate the largely consistent evidence from other observational studies showing an association between metformin use and lower dementia incidence [and] may have important implications for clinical treatment of adults with diabetes,” the authors write.
SOURCE:
The study, with first author Scott Zimmerman, MPH, University of California, San Francisco, was published online in JAMA Network Open.
LIMITATIONS:
Dementia diagnosis was obtained based on medical records. Factors such as race, ethnicity, or time on metformin were not evaluated. Information on the exact reason for stopping metformin was not available.
DISCLOSURES:
The study was funded by grants from the National Institutes of Health, National Institute on Aging. Mr. Zimmerman owns stock in AbbVie, Gilead Sciences, CRISPR Therapeutics, and Abbott Laboratories. Disclosure for the other study authors can be found with the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
New research suggests terminating metformin may raise the risk for dementia in older adults with type 2 diabetes, providing more evidence of metformin’s potential neuroprotective effects.
METHODOLOGY:
- Researchers evaluated the association between discontinuing metformin for reasons unrelated to kidney dysfunction and dementia incidence.
- The cohort included 12,220 Kaiser Permanente Northern California members who stopped metformin early (with normal kidney function) and 29,126 routine metformin users.
- The cohort of early terminators was 46% women with an average age of 59 years at the start of metformin prescription. The cohort continuing metformin was 47% women, with a start age of 61 years.
TAKEAWAY:
- Adults who stopped metformin early were 21% more likely to be diagnosed with dementia during follow up (hazard ratio, 1.21; 95% confidence interval, 1.12-1.30), compared with routine metformin users.
- This association was largely independent of changes in A1c level and insulin usage.
IN PRACTICE:
The findings “corroborate the largely consistent evidence from other observational studies showing an association between metformin use and lower dementia incidence [and] may have important implications for clinical treatment of adults with diabetes,” the authors write.
SOURCE:
The study, with first author Scott Zimmerman, MPH, University of California, San Francisco, was published online in JAMA Network Open.
LIMITATIONS:
Dementia diagnosis was obtained based on medical records. Factors such as race, ethnicity, or time on metformin were not evaluated. Information on the exact reason for stopping metformin was not available.
DISCLOSURES:
The study was funded by grants from the National Institutes of Health, National Institute on Aging. Mr. Zimmerman owns stock in AbbVie, Gilead Sciences, CRISPR Therapeutics, and Abbott Laboratories. Disclosure for the other study authors can be found with the original article.
A version of this article first appeared on Medscape.com.
84-year-old MD contests employer’s mandatory cognitive tests for older docs
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Lylas G. Mogk, MD, recently sued Henry Ford Health and Henry Ford Medical Group in federal court, alleging that the mandatory cognitive test violates the Americans with Disabilities Act, the Age Discrimination in Employment Act, and two Michigan laws.
Dr. Mogk’s lawsuit follows a widely watched 2020 case in which the U.S. Equal Employment Opportunity Commission sued Yale New Haven Hospital, the teaching hospital of Yale University, for age discrimination. According to the lawsuit, the hospital illegally required neuropsychological and eye examinations of physicians aged 70 or older who sought to gain or renew staff privileges.
According to the lawsuit, Dr. Mogk is a member of Henry Ford Medical Group, which in 2017 required all members aged 70 and older to undergo cognitive screening tests. The tests would be repeated every 5 years thereafter, the lawsuit said, and anyone who refused would have to resign or be fired.
Dr. Mogk completed the screening, although no information about the results or outcome was mentioned in the lawsuit. It’s not clear whether Henry Ford’s cognitive test mandate remains in place; a spokesperson for Henry Ford Health and attorneys for Dr. Mogk declined to comment.
The number of practicing physicians in their 70s and beyond is rising. A 2021 report found that 12% of U.S. licensed physicians in 2020 were least 70 years old, up from 9% in 2010 and an increase from 75,627 to 120,510. The percentage of doctors aged 60-69 grew to 19% from 16% in 2010.
The number of health systems requiring testing of older physicians isn’t known, although various reports suggest at least a dozen have had mandates.
The University of California, San Diego, offers a physical and mental screening program that health organizations can use to evaluate “late-career physicians,” and a 2021 report noted that “Nebraska’s Children’s Hospital requires physicians aged 70 years and older to undergo an assessment by several peers, a complete physical, and unspecified cognitive screening.” Another system, Hartford HealthCare, mandated an annual reappointment process for clinicians aged 70 or older, requiring them to undergo various exams.
There’s evidence that physician performance declines with age. However, age-based cognitive testing can run afoul of federal and state laws against age discrimination, said Sharona Hoffman, JD, professor of law and bioethics at Case Western Reserve University, Cleveland, in an interview.
Federal law prohibits age-related restrictions on employment but allows exceptions in areas like public safety, said Ms. Hoffman, who’s written about age discrimination and testing requirements. Pilots, law enforcement officers, firefighters, and air controllers, for example, can be forced to retire at specific ages.
It’s not clear how many physicians took the cognitive tests required by Henry Ford Medical Group.
However, details are available about the policy at Yale New Haven Hospital: According to the EEOC lawsuit, from 2016 to 2019, 145 physicians aged 70 or older took the mandatory test. Of those, seven individuals failed either or both of the exams, 14 were listed as “borderline deficient,” and one was listed as “deficient.” Another five refused testing and either resigned or changed their status. The EEOC case against the hospital is still pending.
“You can make an argument that health care is like a public safety job because people put their lives in the hands of doctors,” Ms. Hoffman said.
In defending mandatory cognitive tests, she said, health care systems could say, “it’s not really discrimination; we’re not forcing them to retire, we’re not limiting their work in any way. We’re just doing testing to make sure they perform competently, and the ADA allows us to conduct testing that is job-related.”
Indeed, a Yale New Haven Hospital spokesman made an argument along these lines in a statement regarding the 2020 lawsuit: The “policy is designed to protect our patients from potential harm while including safeguards to ensure that our physicians are treated fairly. The policy is modeled on similar standards in other industries, and we are confident that no discrimination has occurred and will vigorously defend ourselves in this matter.”
However, Ms. Hoffman herself doesn’t buy these arguments. Requiring tests only for older physicians does appear to be discrimination based on age, she said. As an alternative, “employers can do close supervision of people. As soon as there are performance problems or patient complaints, you need to see a doctor or get testing done.”
Another option is to mandate tests at specific ages via licensing boards. “I don’t think that would be legally problematic,” Ms. Hoffman said.
What else can be done to protect patients from clinicians whose skills have significantly declined as they’ve aged? The 2021 report in Neurology Clinical Practice notes that there are disadvantages to several strategies.
One common approach, waiting to evaluate a clinician until an error occurs, can lead to patient harm, the report’s authors wrote. Relying on reporting by peers is problematic because “physicians have been very resistant to reporting colleagues who are impaired” and the “medical apprenticeship model discourages physicians from reporting on senior colleagues.”
Physician self-assessment is yet another option, but “loss of insight may be a component of an individual’s impairment,” the authors wrote.
So what’s the best solution? The authors recommended “a relatively brief cognitive screening followed by more extensive testing for the most impaired individuals.” This approach “appears most reliable in confidentially identifying truly impaired physicians while minimizing the chance of a falsely flagging unimpaired individuals. This strategy allows aging physicians to continue working while safeguarding both their reputations and their patients’ health.”
Ms. Hoffman has no disclosures.
A version of this article first appeared on Medscape.com.
Higher triglycerides linked to lower dementia risk
TOPLINE:
a large study of community-dwelling older adults suggests.
METHODOLOGY:
- The analysis included 18,294 participants, median age 75 years and median triglyceride level 106 mg/dL, from the Aspirin in Reducing Events in the Elderly (ASPREE) study, a placebo-controlled, randomized trial of daily low-dose aspirin in older people without dementia or history of cardiovascular disease (CVD) at recruitment.
- Researchers repeated their main analyses in a sub-cohort of 13,976 subjects with APOE epsilon-4 genetic data, and an external cohort of 68,200 participants, mean age 66.9 years and a median nonfasting triglyceride of 139 mg/dL, from the UK biobank, followed for a median of 12.5 years.
- The main outcome was incident dementia over 6.4 years and secondary outcomes included changes in composite cognitive function and domain-specific cognition.
- Researchers controlled for a number of potential confounders, including age, sex, race, smoking, alcohol consumption, education, family history of dementia, diabetes, hypertension, and statin use.
TAKEAWAY:
- Every doubling of baseline triglycerides was associated with an 18% lower risk of incident dementia across the entire study cohort (adjusted hazard ratio, 0.82) and in participants with genotypic data (aHR, 0.82) and a 17% lower risk in the external UK Biobank cohort (aHR, 0.83) (P ≤ .01 for all).
- In the entire cohort, the risk for dementia was 15% lower in those with triglyceride levels at 63-106 mg/dL (aHR, 0.85); 24% lower in those at 107-186 mg/dL (aHR, 0.76); and 36% lower for those with levels higher than 187 mg/dL (aHR, 0.64), compared with individuals with levels below 62 mg/dL (P for trend <.001).
- The direction and magnitude of the inverse association between triglycerides and dementia risk were not modified by age, sex, or risk factors related to triglycerides or dementia.
- In the entire study cohort, higher triglyceride levels were significantly associated with slower decline in global cognition (P = .02), composite cognition (P = .03), and a borderline significantly slower decline in episodic memory (P = .05).
IN PRACTICE:
“Triglyceride levels may serve as a useful predictor for dementia risk and cognitive decline in older populations,” the investigators write. Higher triglyceride levels may reflect better overall health and/or lifestyle behaviors that protect against dementia.
SOURCE:
The study was led by Zhen Zhou, of Monash University, Melbourne. It was published online in Neurology.
LIMITATIONS:
The study can’t establish a causal relationship between triglyceride levels and dementia or fully exclude reverse causality. As most ASPREE participants had normal to high-normal triglyceride levels, the results can’t be generalized to those with severe hypertriglyceridemia. The findings are unique to older people without CVD and may not be generalizable to other populations.
DISCLOSURES:
The study received support from the Royal Australian College of General Practitioners (RACGP)/HCF Research Foundation. Dr. Zhou reported receiving salary from the RACGP/HCF Research Foundation.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large study of community-dwelling older adults suggests.
METHODOLOGY:
- The analysis included 18,294 participants, median age 75 years and median triglyceride level 106 mg/dL, from the Aspirin in Reducing Events in the Elderly (ASPREE) study, a placebo-controlled, randomized trial of daily low-dose aspirin in older people without dementia or history of cardiovascular disease (CVD) at recruitment.
- Researchers repeated their main analyses in a sub-cohort of 13,976 subjects with APOE epsilon-4 genetic data, and an external cohort of 68,200 participants, mean age 66.9 years and a median nonfasting triglyceride of 139 mg/dL, from the UK biobank, followed for a median of 12.5 years.
- The main outcome was incident dementia over 6.4 years and secondary outcomes included changes in composite cognitive function and domain-specific cognition.
- Researchers controlled for a number of potential confounders, including age, sex, race, smoking, alcohol consumption, education, family history of dementia, diabetes, hypertension, and statin use.
TAKEAWAY:
- Every doubling of baseline triglycerides was associated with an 18% lower risk of incident dementia across the entire study cohort (adjusted hazard ratio, 0.82) and in participants with genotypic data (aHR, 0.82) and a 17% lower risk in the external UK Biobank cohort (aHR, 0.83) (P ≤ .01 for all).
- In the entire cohort, the risk for dementia was 15% lower in those with triglyceride levels at 63-106 mg/dL (aHR, 0.85); 24% lower in those at 107-186 mg/dL (aHR, 0.76); and 36% lower for those with levels higher than 187 mg/dL (aHR, 0.64), compared with individuals with levels below 62 mg/dL (P for trend <.001).
- The direction and magnitude of the inverse association between triglycerides and dementia risk were not modified by age, sex, or risk factors related to triglycerides or dementia.
- In the entire study cohort, higher triglyceride levels were significantly associated with slower decline in global cognition (P = .02), composite cognition (P = .03), and a borderline significantly slower decline in episodic memory (P = .05).
IN PRACTICE:
“Triglyceride levels may serve as a useful predictor for dementia risk and cognitive decline in older populations,” the investigators write. Higher triglyceride levels may reflect better overall health and/or lifestyle behaviors that protect against dementia.
SOURCE:
The study was led by Zhen Zhou, of Monash University, Melbourne. It was published online in Neurology.
LIMITATIONS:
The study can’t establish a causal relationship between triglyceride levels and dementia or fully exclude reverse causality. As most ASPREE participants had normal to high-normal triglyceride levels, the results can’t be generalized to those with severe hypertriglyceridemia. The findings are unique to older people without CVD and may not be generalizable to other populations.
DISCLOSURES:
The study received support from the Royal Australian College of General Practitioners (RACGP)/HCF Research Foundation. Dr. Zhou reported receiving salary from the RACGP/HCF Research Foundation.
A version of this article first appeared on Medscape.com.
TOPLINE:
a large study of community-dwelling older adults suggests.
METHODOLOGY:
- The analysis included 18,294 participants, median age 75 years and median triglyceride level 106 mg/dL, from the Aspirin in Reducing Events in the Elderly (ASPREE) study, a placebo-controlled, randomized trial of daily low-dose aspirin in older people without dementia or history of cardiovascular disease (CVD) at recruitment.
- Researchers repeated their main analyses in a sub-cohort of 13,976 subjects with APOE epsilon-4 genetic data, and an external cohort of 68,200 participants, mean age 66.9 years and a median nonfasting triglyceride of 139 mg/dL, from the UK biobank, followed for a median of 12.5 years.
- The main outcome was incident dementia over 6.4 years and secondary outcomes included changes in composite cognitive function and domain-specific cognition.
- Researchers controlled for a number of potential confounders, including age, sex, race, smoking, alcohol consumption, education, family history of dementia, diabetes, hypertension, and statin use.
TAKEAWAY:
- Every doubling of baseline triglycerides was associated with an 18% lower risk of incident dementia across the entire study cohort (adjusted hazard ratio, 0.82) and in participants with genotypic data (aHR, 0.82) and a 17% lower risk in the external UK Biobank cohort (aHR, 0.83) (P ≤ .01 for all).
- In the entire cohort, the risk for dementia was 15% lower in those with triglyceride levels at 63-106 mg/dL (aHR, 0.85); 24% lower in those at 107-186 mg/dL (aHR, 0.76); and 36% lower for those with levels higher than 187 mg/dL (aHR, 0.64), compared with individuals with levels below 62 mg/dL (P for trend <.001).
- The direction and magnitude of the inverse association between triglycerides and dementia risk were not modified by age, sex, or risk factors related to triglycerides or dementia.
- In the entire study cohort, higher triglyceride levels were significantly associated with slower decline in global cognition (P = .02), composite cognition (P = .03), and a borderline significantly slower decline in episodic memory (P = .05).
IN PRACTICE:
“Triglyceride levels may serve as a useful predictor for dementia risk and cognitive decline in older populations,” the investigators write. Higher triglyceride levels may reflect better overall health and/or lifestyle behaviors that protect against dementia.
SOURCE:
The study was led by Zhen Zhou, of Monash University, Melbourne. It was published online in Neurology.
LIMITATIONS:
The study can’t establish a causal relationship between triglyceride levels and dementia or fully exclude reverse causality. As most ASPREE participants had normal to high-normal triglyceride levels, the results can’t be generalized to those with severe hypertriglyceridemia. The findings are unique to older people without CVD and may not be generalizable to other populations.
DISCLOSURES:
The study received support from the Royal Australian College of General Practitioners (RACGP)/HCF Research Foundation. Dr. Zhou reported receiving salary from the RACGP/HCF Research Foundation.
A version of this article first appeared on Medscape.com.
Urgent need to improve early detection of mild cognitive impairment in primary care
TOPLINE:
Detection rates of mild cognitive impairment (MCI) in primary care are extremely low, with only about 8% of expected cases diagnosed on average, a finding that points to an urgent need to improve early detection in primary care.
METHODOLOGY:
- Researchers estimated MCI detection rates among 226,756 primary care clinicians and 54,597 practices that had at least 25 patients enrolled in Medicare between 2017 and 2019.
- They compared the expected number of MCI cases, based on a predictive model, to actual diagnosed cases as documented in claims and encounter data.
- They accounted for uncertainty in these estimates to determine whether detection rates are within the expected range or significantly higher or lower.
TAKEAWAY:
- More than 25% of clinicians and practices did not have a single patient with diagnosed MCI; the average detection rate was 0.01 for both clinicians and practices.
- The modeled expected MCI detection rate, however, was much higher (average 0.19 for clinicians and 0.20 for practices).
- Average detection rates for clinicians and practices was 0.08, with more than 99% of clinicians and practices underdiagnosing MCI; clinicians practicing geriatric medicine had higher detection rates than others.
IN PRACTICE:
The findings are “concerning not only because patients might not get identified for a disease-modifying AD treatment in time, but also because numerous causes of MCI – such as hypothyroidism and medication side effects – are reversible, and the condition itself can be stabilized by lifestyle modification interventions,” the authors write.
SOURCE:
The study was published online in the Journal of Prevention of Alzheimer’s Disease. The first author was Ying Liu, PhD, of the University of Southern California, Los Angeles.
LIMITATIONS:
The predictive model based on demographic information has only moderate accuracy. Expected prevalence of MCI was based on cognitive test scores, which is not the same as a true clinical diagnosis.
DISCLOSURES:
The study was partially funded by a contract from Genentech to the University of Southern California. Coauthors Soeren Mattke and Christopher Wallick have disclosed relationships with Genentech.
A version of this article appeared on Medscape.com.
TOPLINE:
Detection rates of mild cognitive impairment (MCI) in primary care are extremely low, with only about 8% of expected cases diagnosed on average, a finding that points to an urgent need to improve early detection in primary care.
METHODOLOGY:
- Researchers estimated MCI detection rates among 226,756 primary care clinicians and 54,597 practices that had at least 25 patients enrolled in Medicare between 2017 and 2019.
- They compared the expected number of MCI cases, based on a predictive model, to actual diagnosed cases as documented in claims and encounter data.
- They accounted for uncertainty in these estimates to determine whether detection rates are within the expected range or significantly higher or lower.
TAKEAWAY:
- More than 25% of clinicians and practices did not have a single patient with diagnosed MCI; the average detection rate was 0.01 for both clinicians and practices.
- The modeled expected MCI detection rate, however, was much higher (average 0.19 for clinicians and 0.20 for practices).
- Average detection rates for clinicians and practices was 0.08, with more than 99% of clinicians and practices underdiagnosing MCI; clinicians practicing geriatric medicine had higher detection rates than others.
IN PRACTICE:
The findings are “concerning not only because patients might not get identified for a disease-modifying AD treatment in time, but also because numerous causes of MCI – such as hypothyroidism and medication side effects – are reversible, and the condition itself can be stabilized by lifestyle modification interventions,” the authors write.
SOURCE:
The study was published online in the Journal of Prevention of Alzheimer’s Disease. The first author was Ying Liu, PhD, of the University of Southern California, Los Angeles.
LIMITATIONS:
The predictive model based on demographic information has only moderate accuracy. Expected prevalence of MCI was based on cognitive test scores, which is not the same as a true clinical diagnosis.
DISCLOSURES:
The study was partially funded by a contract from Genentech to the University of Southern California. Coauthors Soeren Mattke and Christopher Wallick have disclosed relationships with Genentech.
A version of this article appeared on Medscape.com.
TOPLINE:
Detection rates of mild cognitive impairment (MCI) in primary care are extremely low, with only about 8% of expected cases diagnosed on average, a finding that points to an urgent need to improve early detection in primary care.
METHODOLOGY:
- Researchers estimated MCI detection rates among 226,756 primary care clinicians and 54,597 practices that had at least 25 patients enrolled in Medicare between 2017 and 2019.
- They compared the expected number of MCI cases, based on a predictive model, to actual diagnosed cases as documented in claims and encounter data.
- They accounted for uncertainty in these estimates to determine whether detection rates are within the expected range or significantly higher or lower.
TAKEAWAY:
- More than 25% of clinicians and practices did not have a single patient with diagnosed MCI; the average detection rate was 0.01 for both clinicians and practices.
- The modeled expected MCI detection rate, however, was much higher (average 0.19 for clinicians and 0.20 for practices).
- Average detection rates for clinicians and practices was 0.08, with more than 99% of clinicians and practices underdiagnosing MCI; clinicians practicing geriatric medicine had higher detection rates than others.
IN PRACTICE:
The findings are “concerning not only because patients might not get identified for a disease-modifying AD treatment in time, but also because numerous causes of MCI – such as hypothyroidism and medication side effects – are reversible, and the condition itself can be stabilized by lifestyle modification interventions,” the authors write.
SOURCE:
The study was published online in the Journal of Prevention of Alzheimer’s Disease. The first author was Ying Liu, PhD, of the University of Southern California, Los Angeles.
LIMITATIONS:
The predictive model based on demographic information has only moderate accuracy. Expected prevalence of MCI was based on cognitive test scores, which is not the same as a true clinical diagnosis.
DISCLOSURES:
The study was partially funded by a contract from Genentech to the University of Southern California. Coauthors Soeren Mattke and Christopher Wallick have disclosed relationships with Genentech.
A version of this article appeared on Medscape.com.
Is it time to scrap ultraprocessed foods?
Ultraprocessed foods (UPFs) make up nearly three-quarters of the entire U.S. food supply and about 60% of Americans’ daily caloric intake. A significant body of research has tied consumption of these foods – awash in added sugar, salt, fat, artificial colors, or preservatives – to cancer, diabetes, and heart disease.
Now, a growing number of studies also link them to poor brain health, including an increased risk of dementia, depression, and anxiety, and some experts are calling for public health policies aimed at reducing UPF consumption.
Under srutiny
A mainstay of diets in countries around the world, UPFs have come under increasing scrutiny because of their link to major diseases. The ingredients in UPFs add little or no nutritional value. Their primary function is to increase a product’s shelf life and palatability. Some recent evidence suggests these foods may be as addictive as tobacco. In addition, two pooled analysis studies using the Yale Food Addiction Scale showed that 14% of adults and 12% of children in the United States may have a UPF addiction.
The most widely used measure of what is, and what is not, a UPF was developed in 2009 by researchers in Brazil. The NOVA food classification system assigns food and beverages to one of four groups:
- Unprocessed and minimally processed foods, such as fruits, vegetables, milk, and meat.
- Processed culinary ingredients, including white sugar, butter, and oils derived from seeds, nuts, and fruits.
- Processed foods, such as tomato paste, bacon, canned tuna, and wine.
- Ultraprocessed foods, such as soda, ice cream, breakfast cereal, and prepackaged meals.
Those sounding the alarm about the potential harmful effects of UPFs are particularly concerned about their consumption by young people. The National Health and Nutrition Examination Survey showed that from 1999 to 2018, highly processed foods accounted for the majority of energy intake in those aged 2-19 years.
One of the most commonly used additives in UPFs, the artificial sweetener aspartame, garnered headlines this summer when the World Health Organization classified it as a likely carcinogen in humans. Aspartame is used in thousands of products, from soda to chewing gum to chewable vitamins.
The U.S. Food and Drug Administration strongly disagreed with the WHO’s position and is sticking by its recommended daily limit of 50 mg/kg of body weight – equivalent to 75 packets of the sweetener Equal – as safe for human consumption.
“Aspartame is one of the most studied food additives in the human food supply,” FDA officials said in a statement, adding that the agency found “significant shortcomings” in the studies the WHO used to justify the new classification. “FDA scientists do not have safety concerns when aspartame is used under the approved conditions.”
Increased attention to consumption of UPFs in general and aspartame particularly in recent years has yielded several studies pointing to the foods’ association with compromised brain health.
Link to depression, dementia
A recent report on UPF consumption and mental well-being among nearly 300,000 people across 70 countries showed that 53% of those who consumed UPFs several times a day were distressed or were struggling with their mental well-being, compared with 18% of those who rarely or never consumed UPFs.
Part of the Global Mind Project run by the nonprofit Sapien Labs in Arlington, Va., the report also showed that individuals with the highest rates of UPF consumption reported higher levels of confusion, slowed thinking, unwanted or obsessive thoughts, irritability, and feelings of sadness.
“There seems to be a much broader effect than just depression symptoms,” Tara Thiagarajan, PhD, founder and chief scientist of Sapien Labs and coauthor of the report, said in an interview.
The report, which has not been peer reviewed, comes on the heels of several other studies, including one from the Nurses Health Study II that showed that participants who consumed more than eight servings of UPFs daily had about a 50% higher depression risk, compared with those who consumed half that much.
“We found that UPFs in general, and artificial sweeteners and beverages in particular, were associated with increased risk,” said lead investigator Andrew T. Chan, MD, MPH, professor of medicine at Harvard Medical School and chief of the clinical and translational epidemiology unit, Massachusetts General Hospital, both in Boston.
“This was an interesting finding that correlates with data from animal studies that artificial sweeteners may trigger the transmission of particular signaling molecules in the brain that are important for mood,” he told this news organization.
Cognition may also be affected. An analysis of more than 72,000 people in the UK Biobank showed that those who consumed a high levels of UPFs were 50% more likely to develop dementia than those who consumed fewer processed foods. For every 10% increase in UPF consumption, the odds of developing any kind of dementia increased by 25%.
Another study of nearly 11,000 people showed that higher UPF consumption was associated with a significantly faster decline in executive and global cognitive function.
Epigenetic changes
While these and other studies suggest a link between UPF consumption and brain health, they are designed to demonstrate correlation. To date, no human study has proven that eating highly processed foods directly causes a decline in mental health or cognition.
Animal studies could provide that causal link. Earlier this year, researchers at Florida State University in Tallahassee reported learning and memory deficits in two groups of male mice that completed a maze test after being fed water mixed with aspartame for about 20% of their adult lives, compared with a group of mice that drank water only. Animals that ingested aspartame could finish the test, but it took them longer, and they needed help.
The amount of aspartame used in the study was just 7% and 15% of the FDA’s recommended maximum intake of aspartame (equivalent to two to four 8-ounce diet sodas daily).
Most intriguing was that offspring of the mice in the aspartame groups demonstrated the same levels of cognitive decline and anxiety as their fathers, even though they had never ingested the artificial sweetener. Researchers theorize that in addition to changes in brain gene expression, aspartame also caused epigenetic changes in germ cells.
“Epigenetic changes in germ cells due to environmental exposures are both good and bad,” lead investigator Pradeep G. Bhide, PhD, professor of developmental neuroscience and director of the Center for Brain Repair at FSU, told this news organization. “They are bad because the next generation is affected. But they’re good because as long as the exposure no longer occurs, 2 or 3 generations later, that’s gone.”
The mice, which lacked taste receptors for aspartame, were the same age and weight in all three groups. Because the only difference was exposure to the artificial sweetener, Dr. Bhide says it suggests a causal link.
“Extrapolation of data from well-controlled laboratory experiments in mice to humans is always risky,” Dr. Bhide said. “The extrapolations give us insights into what could happen rather than what will happen.”
Potential mechanisms
Although scientists can’t say for certain how UPFs affect brain health, there are several theories. UPFs may influence an inflammatory immune response, which has been linked to depression and dementia. Consumption of highly processed foods may also disrupt the gut microbiome, Dr. Chan said, which, in turn, may increase depression risk.
“This is an important potential mechanism linking ultraprocessed food to depression since there is emerging evidence that microbes in the gut have been linked with mood through their role in metabolizing and producing proteins that have activity in the brain,” he said.
In addition, with UPFs that contain aspartame, there could be a more direct link to brain function. In the gastrointestinal track, the sweetener is quickly broken down into methanol, aspartic acid, and phenylalanine. All three enter the bloodstream, cross the blood-brain barrier, and are neuroactive.
“Phenylalanine is a precursor for neurotransmitters in the brain, and aspartic acid activates the glutamate excitatory neurotransmitter receptor,” Dr. Bhide said. “The effects we’ve seen could be due to these metabolites that have a direct effect on the brain function.”
Time to act?
Some researchers are building a case for classifying UPFs as addictive substances. Others are calling for additional research on UPF safety that is conducted outside the food industry.
There has also been some discussion of placing warning labels on UPFs. However, there is disagreement about what information should be included and how consumers might interpret it. The question of which food products are UPFs and which are not also isn’t settled. The NOVA system may be widely used, but it still has its detractors who believe it misclassifies some healthy foods as ultraprocessed.
Dr. Chan and other experts say the research conducted thus far requires additional corroboration to inform appropriate public health interventions. That would likely take the form of a large, randomized trial with one group of participants eating a healthy diet and the other consuming large amounts of UPFs.
“This type of study is extremely challenging given the number of people that would have to be willing to participate and be willing to eat a very specific diet over a long period of time,” Dr. Chan said. “I am also not sure it would be ethical to assign people to such a diet, given what we already know about the potential health effects of UPFs.”
Dr. Thiagarajan and others have called on funding agencies to direct more grant monies toward studies of UPFs to better understand their effect on brain health.
“Given the magnitude of the problem and given that there is a fair bit of evidence that points to a potential causal link, then we damn well better put money into this and get to the bottom of it,” she said.
Others are looking to the FDA to increase the agency’s scrutiny of food additives. While some additives such as artificial sweeteners have a place in diets of people with diabetes or obesity, Dr. Bhide suggests it may be wise for healthy individuals to reduce their daily intake of UPFs.
“Our data raise this to a different level because of the transgenerational transmission, which has never been shown before,” he said. “We are saying that the FDA should look in preclinical models at germ cells and maybe transgenerational transmission before approving any food additive.”
A version of this article first appeared on Medscape.com.
Ultraprocessed foods (UPFs) make up nearly three-quarters of the entire U.S. food supply and about 60% of Americans’ daily caloric intake. A significant body of research has tied consumption of these foods – awash in added sugar, salt, fat, artificial colors, or preservatives – to cancer, diabetes, and heart disease.
Now, a growing number of studies also link them to poor brain health, including an increased risk of dementia, depression, and anxiety, and some experts are calling for public health policies aimed at reducing UPF consumption.
Under srutiny
A mainstay of diets in countries around the world, UPFs have come under increasing scrutiny because of their link to major diseases. The ingredients in UPFs add little or no nutritional value. Their primary function is to increase a product’s shelf life and palatability. Some recent evidence suggests these foods may be as addictive as tobacco. In addition, two pooled analysis studies using the Yale Food Addiction Scale showed that 14% of adults and 12% of children in the United States may have a UPF addiction.
The most widely used measure of what is, and what is not, a UPF was developed in 2009 by researchers in Brazil. The NOVA food classification system assigns food and beverages to one of four groups:
- Unprocessed and minimally processed foods, such as fruits, vegetables, milk, and meat.
- Processed culinary ingredients, including white sugar, butter, and oils derived from seeds, nuts, and fruits.
- Processed foods, such as tomato paste, bacon, canned tuna, and wine.
- Ultraprocessed foods, such as soda, ice cream, breakfast cereal, and prepackaged meals.
Those sounding the alarm about the potential harmful effects of UPFs are particularly concerned about their consumption by young people. The National Health and Nutrition Examination Survey showed that from 1999 to 2018, highly processed foods accounted for the majority of energy intake in those aged 2-19 years.
One of the most commonly used additives in UPFs, the artificial sweetener aspartame, garnered headlines this summer when the World Health Organization classified it as a likely carcinogen in humans. Aspartame is used in thousands of products, from soda to chewing gum to chewable vitamins.
The U.S. Food and Drug Administration strongly disagreed with the WHO’s position and is sticking by its recommended daily limit of 50 mg/kg of body weight – equivalent to 75 packets of the sweetener Equal – as safe for human consumption.
“Aspartame is one of the most studied food additives in the human food supply,” FDA officials said in a statement, adding that the agency found “significant shortcomings” in the studies the WHO used to justify the new classification. “FDA scientists do not have safety concerns when aspartame is used under the approved conditions.”
Increased attention to consumption of UPFs in general and aspartame particularly in recent years has yielded several studies pointing to the foods’ association with compromised brain health.
Link to depression, dementia
A recent report on UPF consumption and mental well-being among nearly 300,000 people across 70 countries showed that 53% of those who consumed UPFs several times a day were distressed or were struggling with their mental well-being, compared with 18% of those who rarely or never consumed UPFs.
Part of the Global Mind Project run by the nonprofit Sapien Labs in Arlington, Va., the report also showed that individuals with the highest rates of UPF consumption reported higher levels of confusion, slowed thinking, unwanted or obsessive thoughts, irritability, and feelings of sadness.
“There seems to be a much broader effect than just depression symptoms,” Tara Thiagarajan, PhD, founder and chief scientist of Sapien Labs and coauthor of the report, said in an interview.
The report, which has not been peer reviewed, comes on the heels of several other studies, including one from the Nurses Health Study II that showed that participants who consumed more than eight servings of UPFs daily had about a 50% higher depression risk, compared with those who consumed half that much.
“We found that UPFs in general, and artificial sweeteners and beverages in particular, were associated with increased risk,” said lead investigator Andrew T. Chan, MD, MPH, professor of medicine at Harvard Medical School and chief of the clinical and translational epidemiology unit, Massachusetts General Hospital, both in Boston.
“This was an interesting finding that correlates with data from animal studies that artificial sweeteners may trigger the transmission of particular signaling molecules in the brain that are important for mood,” he told this news organization.
Cognition may also be affected. An analysis of more than 72,000 people in the UK Biobank showed that those who consumed a high levels of UPFs were 50% more likely to develop dementia than those who consumed fewer processed foods. For every 10% increase in UPF consumption, the odds of developing any kind of dementia increased by 25%.
Another study of nearly 11,000 people showed that higher UPF consumption was associated with a significantly faster decline in executive and global cognitive function.
Epigenetic changes
While these and other studies suggest a link between UPF consumption and brain health, they are designed to demonstrate correlation. To date, no human study has proven that eating highly processed foods directly causes a decline in mental health or cognition.
Animal studies could provide that causal link. Earlier this year, researchers at Florida State University in Tallahassee reported learning and memory deficits in two groups of male mice that completed a maze test after being fed water mixed with aspartame for about 20% of their adult lives, compared with a group of mice that drank water only. Animals that ingested aspartame could finish the test, but it took them longer, and they needed help.
The amount of aspartame used in the study was just 7% and 15% of the FDA’s recommended maximum intake of aspartame (equivalent to two to four 8-ounce diet sodas daily).
Most intriguing was that offspring of the mice in the aspartame groups demonstrated the same levels of cognitive decline and anxiety as their fathers, even though they had never ingested the artificial sweetener. Researchers theorize that in addition to changes in brain gene expression, aspartame also caused epigenetic changes in germ cells.
“Epigenetic changes in germ cells due to environmental exposures are both good and bad,” lead investigator Pradeep G. Bhide, PhD, professor of developmental neuroscience and director of the Center for Brain Repair at FSU, told this news organization. “They are bad because the next generation is affected. But they’re good because as long as the exposure no longer occurs, 2 or 3 generations later, that’s gone.”
The mice, which lacked taste receptors for aspartame, were the same age and weight in all three groups. Because the only difference was exposure to the artificial sweetener, Dr. Bhide says it suggests a causal link.
“Extrapolation of data from well-controlled laboratory experiments in mice to humans is always risky,” Dr. Bhide said. “The extrapolations give us insights into what could happen rather than what will happen.”
Potential mechanisms
Although scientists can’t say for certain how UPFs affect brain health, there are several theories. UPFs may influence an inflammatory immune response, which has been linked to depression and dementia. Consumption of highly processed foods may also disrupt the gut microbiome, Dr. Chan said, which, in turn, may increase depression risk.
“This is an important potential mechanism linking ultraprocessed food to depression since there is emerging evidence that microbes in the gut have been linked with mood through their role in metabolizing and producing proteins that have activity in the brain,” he said.
In addition, with UPFs that contain aspartame, there could be a more direct link to brain function. In the gastrointestinal track, the sweetener is quickly broken down into methanol, aspartic acid, and phenylalanine. All three enter the bloodstream, cross the blood-brain barrier, and are neuroactive.
“Phenylalanine is a precursor for neurotransmitters in the brain, and aspartic acid activates the glutamate excitatory neurotransmitter receptor,” Dr. Bhide said. “The effects we’ve seen could be due to these metabolites that have a direct effect on the brain function.”
Time to act?
Some researchers are building a case for classifying UPFs as addictive substances. Others are calling for additional research on UPF safety that is conducted outside the food industry.
There has also been some discussion of placing warning labels on UPFs. However, there is disagreement about what information should be included and how consumers might interpret it. The question of which food products are UPFs and which are not also isn’t settled. The NOVA system may be widely used, but it still has its detractors who believe it misclassifies some healthy foods as ultraprocessed.
Dr. Chan and other experts say the research conducted thus far requires additional corroboration to inform appropriate public health interventions. That would likely take the form of a large, randomized trial with one group of participants eating a healthy diet and the other consuming large amounts of UPFs.
“This type of study is extremely challenging given the number of people that would have to be willing to participate and be willing to eat a very specific diet over a long period of time,” Dr. Chan said. “I am also not sure it would be ethical to assign people to such a diet, given what we already know about the potential health effects of UPFs.”
Dr. Thiagarajan and others have called on funding agencies to direct more grant monies toward studies of UPFs to better understand their effect on brain health.
“Given the magnitude of the problem and given that there is a fair bit of evidence that points to a potential causal link, then we damn well better put money into this and get to the bottom of it,” she said.
Others are looking to the FDA to increase the agency’s scrutiny of food additives. While some additives such as artificial sweeteners have a place in diets of people with diabetes or obesity, Dr. Bhide suggests it may be wise for healthy individuals to reduce their daily intake of UPFs.
“Our data raise this to a different level because of the transgenerational transmission, which has never been shown before,” he said. “We are saying that the FDA should look in preclinical models at germ cells and maybe transgenerational transmission before approving any food additive.”
A version of this article first appeared on Medscape.com.
Ultraprocessed foods (UPFs) make up nearly three-quarters of the entire U.S. food supply and about 60% of Americans’ daily caloric intake. A significant body of research has tied consumption of these foods – awash in added sugar, salt, fat, artificial colors, or preservatives – to cancer, diabetes, and heart disease.
Now, a growing number of studies also link them to poor brain health, including an increased risk of dementia, depression, and anxiety, and some experts are calling for public health policies aimed at reducing UPF consumption.
Under srutiny
A mainstay of diets in countries around the world, UPFs have come under increasing scrutiny because of their link to major diseases. The ingredients in UPFs add little or no nutritional value. Their primary function is to increase a product’s shelf life and palatability. Some recent evidence suggests these foods may be as addictive as tobacco. In addition, two pooled analysis studies using the Yale Food Addiction Scale showed that 14% of adults and 12% of children in the United States may have a UPF addiction.
The most widely used measure of what is, and what is not, a UPF was developed in 2009 by researchers in Brazil. The NOVA food classification system assigns food and beverages to one of four groups:
- Unprocessed and minimally processed foods, such as fruits, vegetables, milk, and meat.
- Processed culinary ingredients, including white sugar, butter, and oils derived from seeds, nuts, and fruits.
- Processed foods, such as tomato paste, bacon, canned tuna, and wine.
- Ultraprocessed foods, such as soda, ice cream, breakfast cereal, and prepackaged meals.
Those sounding the alarm about the potential harmful effects of UPFs are particularly concerned about their consumption by young people. The National Health and Nutrition Examination Survey showed that from 1999 to 2018, highly processed foods accounted for the majority of energy intake in those aged 2-19 years.
One of the most commonly used additives in UPFs, the artificial sweetener aspartame, garnered headlines this summer when the World Health Organization classified it as a likely carcinogen in humans. Aspartame is used in thousands of products, from soda to chewing gum to chewable vitamins.
The U.S. Food and Drug Administration strongly disagreed with the WHO’s position and is sticking by its recommended daily limit of 50 mg/kg of body weight – equivalent to 75 packets of the sweetener Equal – as safe for human consumption.
“Aspartame is one of the most studied food additives in the human food supply,” FDA officials said in a statement, adding that the agency found “significant shortcomings” in the studies the WHO used to justify the new classification. “FDA scientists do not have safety concerns when aspartame is used under the approved conditions.”
Increased attention to consumption of UPFs in general and aspartame particularly in recent years has yielded several studies pointing to the foods’ association with compromised brain health.
Link to depression, dementia
A recent report on UPF consumption and mental well-being among nearly 300,000 people across 70 countries showed that 53% of those who consumed UPFs several times a day were distressed or were struggling with their mental well-being, compared with 18% of those who rarely or never consumed UPFs.
Part of the Global Mind Project run by the nonprofit Sapien Labs in Arlington, Va., the report also showed that individuals with the highest rates of UPF consumption reported higher levels of confusion, slowed thinking, unwanted or obsessive thoughts, irritability, and feelings of sadness.
“There seems to be a much broader effect than just depression symptoms,” Tara Thiagarajan, PhD, founder and chief scientist of Sapien Labs and coauthor of the report, said in an interview.
The report, which has not been peer reviewed, comes on the heels of several other studies, including one from the Nurses Health Study II that showed that participants who consumed more than eight servings of UPFs daily had about a 50% higher depression risk, compared with those who consumed half that much.
“We found that UPFs in general, and artificial sweeteners and beverages in particular, were associated with increased risk,” said lead investigator Andrew T. Chan, MD, MPH, professor of medicine at Harvard Medical School and chief of the clinical and translational epidemiology unit, Massachusetts General Hospital, both in Boston.
“This was an interesting finding that correlates with data from animal studies that artificial sweeteners may trigger the transmission of particular signaling molecules in the brain that are important for mood,” he told this news organization.
Cognition may also be affected. An analysis of more than 72,000 people in the UK Biobank showed that those who consumed a high levels of UPFs were 50% more likely to develop dementia than those who consumed fewer processed foods. For every 10% increase in UPF consumption, the odds of developing any kind of dementia increased by 25%.
Another study of nearly 11,000 people showed that higher UPF consumption was associated with a significantly faster decline in executive and global cognitive function.
Epigenetic changes
While these and other studies suggest a link between UPF consumption and brain health, they are designed to demonstrate correlation. To date, no human study has proven that eating highly processed foods directly causes a decline in mental health or cognition.
Animal studies could provide that causal link. Earlier this year, researchers at Florida State University in Tallahassee reported learning and memory deficits in two groups of male mice that completed a maze test after being fed water mixed with aspartame for about 20% of their adult lives, compared with a group of mice that drank water only. Animals that ingested aspartame could finish the test, but it took them longer, and they needed help.
The amount of aspartame used in the study was just 7% and 15% of the FDA’s recommended maximum intake of aspartame (equivalent to two to four 8-ounce diet sodas daily).
Most intriguing was that offspring of the mice in the aspartame groups demonstrated the same levels of cognitive decline and anxiety as their fathers, even though they had never ingested the artificial sweetener. Researchers theorize that in addition to changes in brain gene expression, aspartame also caused epigenetic changes in germ cells.
“Epigenetic changes in germ cells due to environmental exposures are both good and bad,” lead investigator Pradeep G. Bhide, PhD, professor of developmental neuroscience and director of the Center for Brain Repair at FSU, told this news organization. “They are bad because the next generation is affected. But they’re good because as long as the exposure no longer occurs, 2 or 3 generations later, that’s gone.”
The mice, which lacked taste receptors for aspartame, were the same age and weight in all three groups. Because the only difference was exposure to the artificial sweetener, Dr. Bhide says it suggests a causal link.
“Extrapolation of data from well-controlled laboratory experiments in mice to humans is always risky,” Dr. Bhide said. “The extrapolations give us insights into what could happen rather than what will happen.”
Potential mechanisms
Although scientists can’t say for certain how UPFs affect brain health, there are several theories. UPFs may influence an inflammatory immune response, which has been linked to depression and dementia. Consumption of highly processed foods may also disrupt the gut microbiome, Dr. Chan said, which, in turn, may increase depression risk.
“This is an important potential mechanism linking ultraprocessed food to depression since there is emerging evidence that microbes in the gut have been linked with mood through their role in metabolizing and producing proteins that have activity in the brain,” he said.
In addition, with UPFs that contain aspartame, there could be a more direct link to brain function. In the gastrointestinal track, the sweetener is quickly broken down into methanol, aspartic acid, and phenylalanine. All three enter the bloodstream, cross the blood-brain barrier, and are neuroactive.
“Phenylalanine is a precursor for neurotransmitters in the brain, and aspartic acid activates the glutamate excitatory neurotransmitter receptor,” Dr. Bhide said. “The effects we’ve seen could be due to these metabolites that have a direct effect on the brain function.”
Time to act?
Some researchers are building a case for classifying UPFs as addictive substances. Others are calling for additional research on UPF safety that is conducted outside the food industry.
There has also been some discussion of placing warning labels on UPFs. However, there is disagreement about what information should be included and how consumers might interpret it. The question of which food products are UPFs and which are not also isn’t settled. The NOVA system may be widely used, but it still has its detractors who believe it misclassifies some healthy foods as ultraprocessed.
Dr. Chan and other experts say the research conducted thus far requires additional corroboration to inform appropriate public health interventions. That would likely take the form of a large, randomized trial with one group of participants eating a healthy diet and the other consuming large amounts of UPFs.
“This type of study is extremely challenging given the number of people that would have to be willing to participate and be willing to eat a very specific diet over a long period of time,” Dr. Chan said. “I am also not sure it would be ethical to assign people to such a diet, given what we already know about the potential health effects of UPFs.”
Dr. Thiagarajan and others have called on funding agencies to direct more grant monies toward studies of UPFs to better understand their effect on brain health.
“Given the magnitude of the problem and given that there is a fair bit of evidence that points to a potential causal link, then we damn well better put money into this and get to the bottom of it,” she said.
Others are looking to the FDA to increase the agency’s scrutiny of food additives. While some additives such as artificial sweeteners have a place in diets of people with diabetes or obesity, Dr. Bhide suggests it may be wise for healthy individuals to reduce their daily intake of UPFs.
“Our data raise this to a different level because of the transgenerational transmission, which has never been shown before,” he said. “We are saying that the FDA should look in preclinical models at germ cells and maybe transgenerational transmission before approving any food additive.”
A version of this article first appeared on Medscape.com.
Promising topline phase 2 results for novel oral Alzheimer’s drug
Topline results provide “clinical evidence of a modification of multiple AD pathologies associated with amyloid plaque burden,” said John Didsbury, PhD, chief executive officer of T3D Therapeutics Inc., the company developing the drug.
While the primary cognitive endpoints were not met in the overall study population, the data suggest that a “high plasma pTau-217/non–pTau-217 ratio, a marker of AD pathology, likely defines an AD population responsive to T3D-959 therapy,” Dr. Didsbury said.
He said it’s important to note that no PET imaging (amyloid/tau) or biomarkers were used as entry criteria and, in hindsight, some participants likely did not have AD, which likely played a role in the negative primary outcome.
The findings from the PIONEER study were presented at the annual Clinical Trials on Alzheimer’s Disease conference.
‘Surprised and shocked’
The PPAR family of proteins helps regulate blood sugar and triglyceride levels. The rationale for evaluating PPAR agonists in AD is based on the hypothesis that sporadic AD is fundamentally an age-related metabolic disease.
T3D-959 is the first PPAR delta-activating compound to be developed for the treatment of AD. Uniquely, this drug also activates PPAR gamma, which may provide potential additive or synergistic effects in regulating dysfunctional brain glucose energy and lipid metabolism in AD.
The PIONEER tested three doses of T3D-959 (15 mg, 30 mg, and 45 mg) vs. placebo in 250 adults with mild to moderate AD (Mini-Mental State Examination [MMSE] 14-26, Clinical Dementia Rating (CDR)-Global 0.5-2.0, and Sum of Boxes [CDR-SB] ≥ 3.0). T3D-959 or placebo was taken once daily for 24 weeks.
In the overall population, the primary endpoints – Alzheimer Disease Assessment Scale-Cognitive subscale (ADAS-Cog11) and Clinical Global Impression of Change (CGIC) – were not met.
“Plain and simple, when we saw this data, we were surprised and shocked,” said Dr. Didsbury, and wondered, “How can placebo be doing so well on a 6-month AD trial?”
“We suspect the presence of non-AD subjects in the trial based on the lower-than-typical number of ApoE4 positive subjects, increased cognitive performance and learning effects observed, and only 45% of trial subjects having a low pTau-217 ratio, a biomarker indicating that they would have no AD pathology plasma,” he explained.
Plasma baseline pTau-217 ratio correlates with AD risk and severity and is a marker of AD pathology; in the subgroup with high pTau-217 ratio, the ADAS-Cog11 endpoint was met in the 30-mg T3D-959 group vs. the placebo group (–0.74 vs. 1.27; P = .112), “consistent with clinical benefit,” Dr. Didsbury noted.
The secondary endpoint of change in plasma amyloid-beta (Ab)42/40 ratio was also met in the 30-mg T3D-959 group – increasing at week 24 with T3D-959 vs. decreasing with placebo (P = .0206), with even greater improvement in the high pTau-217 ratio group. In this group, improvement of Ab42/40 ratio was nearly twofold greater than the overall group.
T3D-959 had a similar magnitude of effect on Ab42/40 as lecanemab (Leqembi) at 6 months, the researchers point out in their late-breaking abstract.
Biomarkers of all three AD diagnostic criteria (amyloid/tau/neurodegeneration) were improved, as well as markers of inflammation, insulin resistance, and dysfunctional lipid metabolism – results that demonstrate “peripheral targeted engagement,” Dr. Didsbury said.
“Along with the strong safety profile of T3D-959, the evidence supports a larger study evaluating T3D-959 30 mg/day in patients with mild to moderate AD and a baseline plasma p-Tau-217/non–pTau-217 ratio of ≥ 0.015,” the researchers conclude in their abstract.
Lessons learned
Commenting on the research for this article, Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, noted that “the idea behind this treatment is that impaired glucose metabolism in the brain leads to toxic misfolded proteins, including amyloid and tau in people with Alzheimer’s disease.”
“The treatment focuses on improving regulation of glucose and lipid metabolism in the brain. This is one of more than 140 approaches that are being tested today to target the biological drivers and contributors to Alzheimer’s disease,” Dr. Edelmayer said.
Because biomarkers were not used to enroll participants, “there was a high population of people in the trial who did not have Alzheimer’s. This very likely contributed to the negative result,” she noted.
However, the results also suggest that those taking the drug who had a high pTau217 ratio – and are likely to have brain amyloid plaques – had less cognitive decline, she noted.
Lessons learned from this negative trial include “the proper dose to balance efficacy and safety, and how to screen participants for their next study,” Dr. Edelmayer said.
Funding for the study was provided by the National Institute on Aging/National Institutes of Health and the Alzheimer’s Association. Dr. Didsbury and Dr. Edelmayer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Topline results provide “clinical evidence of a modification of multiple AD pathologies associated with amyloid plaque burden,” said John Didsbury, PhD, chief executive officer of T3D Therapeutics Inc., the company developing the drug.
While the primary cognitive endpoints were not met in the overall study population, the data suggest that a “high plasma pTau-217/non–pTau-217 ratio, a marker of AD pathology, likely defines an AD population responsive to T3D-959 therapy,” Dr. Didsbury said.
He said it’s important to note that no PET imaging (amyloid/tau) or biomarkers were used as entry criteria and, in hindsight, some participants likely did not have AD, which likely played a role in the negative primary outcome.
The findings from the PIONEER study were presented at the annual Clinical Trials on Alzheimer’s Disease conference.
‘Surprised and shocked’
The PPAR family of proteins helps regulate blood sugar and triglyceride levels. The rationale for evaluating PPAR agonists in AD is based on the hypothesis that sporadic AD is fundamentally an age-related metabolic disease.
T3D-959 is the first PPAR delta-activating compound to be developed for the treatment of AD. Uniquely, this drug also activates PPAR gamma, which may provide potential additive or synergistic effects in regulating dysfunctional brain glucose energy and lipid metabolism in AD.
The PIONEER tested three doses of T3D-959 (15 mg, 30 mg, and 45 mg) vs. placebo in 250 adults with mild to moderate AD (Mini-Mental State Examination [MMSE] 14-26, Clinical Dementia Rating (CDR)-Global 0.5-2.0, and Sum of Boxes [CDR-SB] ≥ 3.0). T3D-959 or placebo was taken once daily for 24 weeks.
In the overall population, the primary endpoints – Alzheimer Disease Assessment Scale-Cognitive subscale (ADAS-Cog11) and Clinical Global Impression of Change (CGIC) – were not met.
“Plain and simple, when we saw this data, we were surprised and shocked,” said Dr. Didsbury, and wondered, “How can placebo be doing so well on a 6-month AD trial?”
“We suspect the presence of non-AD subjects in the trial based on the lower-than-typical number of ApoE4 positive subjects, increased cognitive performance and learning effects observed, and only 45% of trial subjects having a low pTau-217 ratio, a biomarker indicating that they would have no AD pathology plasma,” he explained.
Plasma baseline pTau-217 ratio correlates with AD risk and severity and is a marker of AD pathology; in the subgroup with high pTau-217 ratio, the ADAS-Cog11 endpoint was met in the 30-mg T3D-959 group vs. the placebo group (–0.74 vs. 1.27; P = .112), “consistent with clinical benefit,” Dr. Didsbury noted.
The secondary endpoint of change in plasma amyloid-beta (Ab)42/40 ratio was also met in the 30-mg T3D-959 group – increasing at week 24 with T3D-959 vs. decreasing with placebo (P = .0206), with even greater improvement in the high pTau-217 ratio group. In this group, improvement of Ab42/40 ratio was nearly twofold greater than the overall group.
T3D-959 had a similar magnitude of effect on Ab42/40 as lecanemab (Leqembi) at 6 months, the researchers point out in their late-breaking abstract.
Biomarkers of all three AD diagnostic criteria (amyloid/tau/neurodegeneration) were improved, as well as markers of inflammation, insulin resistance, and dysfunctional lipid metabolism – results that demonstrate “peripheral targeted engagement,” Dr. Didsbury said.
“Along with the strong safety profile of T3D-959, the evidence supports a larger study evaluating T3D-959 30 mg/day in patients with mild to moderate AD and a baseline plasma p-Tau-217/non–pTau-217 ratio of ≥ 0.015,” the researchers conclude in their abstract.
Lessons learned
Commenting on the research for this article, Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, noted that “the idea behind this treatment is that impaired glucose metabolism in the brain leads to toxic misfolded proteins, including amyloid and tau in people with Alzheimer’s disease.”
“The treatment focuses on improving regulation of glucose and lipid metabolism in the brain. This is one of more than 140 approaches that are being tested today to target the biological drivers and contributors to Alzheimer’s disease,” Dr. Edelmayer said.
Because biomarkers were not used to enroll participants, “there was a high population of people in the trial who did not have Alzheimer’s. This very likely contributed to the negative result,” she noted.
However, the results also suggest that those taking the drug who had a high pTau217 ratio – and are likely to have brain amyloid plaques – had less cognitive decline, she noted.
Lessons learned from this negative trial include “the proper dose to balance efficacy and safety, and how to screen participants for their next study,” Dr. Edelmayer said.
Funding for the study was provided by the National Institute on Aging/National Institutes of Health and the Alzheimer’s Association. Dr. Didsbury and Dr. Edelmayer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Topline results provide “clinical evidence of a modification of multiple AD pathologies associated with amyloid plaque burden,” said John Didsbury, PhD, chief executive officer of T3D Therapeutics Inc., the company developing the drug.
While the primary cognitive endpoints were not met in the overall study population, the data suggest that a “high plasma pTau-217/non–pTau-217 ratio, a marker of AD pathology, likely defines an AD population responsive to T3D-959 therapy,” Dr. Didsbury said.
He said it’s important to note that no PET imaging (amyloid/tau) or biomarkers were used as entry criteria and, in hindsight, some participants likely did not have AD, which likely played a role in the negative primary outcome.
The findings from the PIONEER study were presented at the annual Clinical Trials on Alzheimer’s Disease conference.
‘Surprised and shocked’
The PPAR family of proteins helps regulate blood sugar and triglyceride levels. The rationale for evaluating PPAR agonists in AD is based on the hypothesis that sporadic AD is fundamentally an age-related metabolic disease.
T3D-959 is the first PPAR delta-activating compound to be developed for the treatment of AD. Uniquely, this drug also activates PPAR gamma, which may provide potential additive or synergistic effects in regulating dysfunctional brain glucose energy and lipid metabolism in AD.
The PIONEER tested three doses of T3D-959 (15 mg, 30 mg, and 45 mg) vs. placebo in 250 adults with mild to moderate AD (Mini-Mental State Examination [MMSE] 14-26, Clinical Dementia Rating (CDR)-Global 0.5-2.0, and Sum of Boxes [CDR-SB] ≥ 3.0). T3D-959 or placebo was taken once daily for 24 weeks.
In the overall population, the primary endpoints – Alzheimer Disease Assessment Scale-Cognitive subscale (ADAS-Cog11) and Clinical Global Impression of Change (CGIC) – were not met.
“Plain and simple, when we saw this data, we were surprised and shocked,” said Dr. Didsbury, and wondered, “How can placebo be doing so well on a 6-month AD trial?”
“We suspect the presence of non-AD subjects in the trial based on the lower-than-typical number of ApoE4 positive subjects, increased cognitive performance and learning effects observed, and only 45% of trial subjects having a low pTau-217 ratio, a biomarker indicating that they would have no AD pathology plasma,” he explained.
Plasma baseline pTau-217 ratio correlates with AD risk and severity and is a marker of AD pathology; in the subgroup with high pTau-217 ratio, the ADAS-Cog11 endpoint was met in the 30-mg T3D-959 group vs. the placebo group (–0.74 vs. 1.27; P = .112), “consistent with clinical benefit,” Dr. Didsbury noted.
The secondary endpoint of change in plasma amyloid-beta (Ab)42/40 ratio was also met in the 30-mg T3D-959 group – increasing at week 24 with T3D-959 vs. decreasing with placebo (P = .0206), with even greater improvement in the high pTau-217 ratio group. In this group, improvement of Ab42/40 ratio was nearly twofold greater than the overall group.
T3D-959 had a similar magnitude of effect on Ab42/40 as lecanemab (Leqembi) at 6 months, the researchers point out in their late-breaking abstract.
Biomarkers of all three AD diagnostic criteria (amyloid/tau/neurodegeneration) were improved, as well as markers of inflammation, insulin resistance, and dysfunctional lipid metabolism – results that demonstrate “peripheral targeted engagement,” Dr. Didsbury said.
“Along with the strong safety profile of T3D-959, the evidence supports a larger study evaluating T3D-959 30 mg/day in patients with mild to moderate AD and a baseline plasma p-Tau-217/non–pTau-217 ratio of ≥ 0.015,” the researchers conclude in their abstract.
Lessons learned
Commenting on the research for this article, Rebecca Edelmayer, PhD, senior director of scientific engagement for the Alzheimer’s Association, noted that “the idea behind this treatment is that impaired glucose metabolism in the brain leads to toxic misfolded proteins, including amyloid and tau in people with Alzheimer’s disease.”
“The treatment focuses on improving regulation of glucose and lipid metabolism in the brain. This is one of more than 140 approaches that are being tested today to target the biological drivers and contributors to Alzheimer’s disease,” Dr. Edelmayer said.
Because biomarkers were not used to enroll participants, “there was a high population of people in the trial who did not have Alzheimer’s. This very likely contributed to the negative result,” she noted.
However, the results also suggest that those taking the drug who had a high pTau217 ratio – and are likely to have brain amyloid plaques – had less cognitive decline, she noted.
Lessons learned from this negative trial include “the proper dose to balance efficacy and safety, and how to screen participants for their next study,” Dr. Edelmayer said.
Funding for the study was provided by the National Institute on Aging/National Institutes of Health and the Alzheimer’s Association. Dr. Didsbury and Dr. Edelmayer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CTAD 2023