Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease that affects approximately 10% of US children. Colloidal oatmeal has long been used as a topical treatment for AD and modern research confirms the benefits of colloidal oatmeal formulations to significantly improve symptoms. Click to learn more about colloidal oatmeal in combination with oat flour and oat extract as effective and well-tolerated skin-directed therapy for your young AD patients.
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease that affects approximately 10% of US children. Colloidal oatmeal has long been used as a topical treatment for AD and modern research confirms the benefits of colloidal oatmeal formulations to significantly improve symptoms. Click to learn more about colloidal oatmeal in combination with oat flour and oat extract as effective and well-tolerated skin-directed therapy for your young AD patients.
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease that affects approximately 10% of US children. Colloidal oatmeal has long been used as a topical treatment for AD and modern research confirms the benefits of colloidal oatmeal formulations to significantly improve symptoms. Click to learn more about colloidal oatmeal in combination with oat flour and oat extract as effective and well-tolerated skin-directed therapy for your young AD patients.
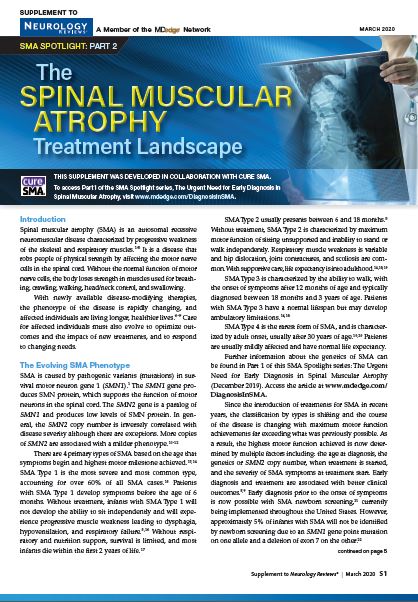
With newly available disease-modifying therapies, the phenotype of spinal muscular atrophy (SMA) is rapidly changing, and affected individuals are living longer, healthier lives.1-4 This supplement discusses therapeutic strategies, FDA-approved treatment options, and the SMA drug pipeline.
To access Part 1 of the SMA Spotlight series, The Urgent Need for Early Diagnosis in Spinal Muscular Atrophy, visit www.mdedge.com/DiagnosisInSMA.
References
Finkel RS, Mercuri E, Darras BT, et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N Engl J Med. 2017;377(18):1723-1732.
Mercuri E, Darras BT, Chiriboga CA, et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378(7):625-635.
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose genereplacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
De Vivo DC, Bertini E, Swoboda KJ, et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: Interim efficacy and safety results from the Phase 2 NURTURE study. Neuromuscul Disord. 2019;29(11):842-856.
Sponsor
This supplement was developed in collaboration with Cure SMA.
With newly available disease-modifying therapies, the phenotype of spinal muscular atrophy (SMA) is rapidly changing, and affected individuals are living longer, healthier lives.1-4 This supplement discusses therapeutic strategies, FDA-approved treatment options, and the SMA drug pipeline.
To access Part 1 of the SMA Spotlight series, The Urgent Need for Early Diagnosis in Spinal Muscular Atrophy, visit www.mdedge.com/DiagnosisInSMA.
References
Finkel RS, Mercuri E, Darras BT, et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N Engl J Med. 2017;377(18):1723-1732.
Mercuri E, Darras BT, Chiriboga CA, et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378(7):625-635.
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose genereplacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
De Vivo DC, Bertini E, Swoboda KJ, et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: Interim efficacy and safety results from the Phase 2 NURTURE study. Neuromuscul Disord. 2019;29(11):842-856.
With newly available disease-modifying therapies, the phenotype of spinal muscular atrophy (SMA) is rapidly changing, and affected individuals are living longer, healthier lives.1-4 This supplement discusses therapeutic strategies, FDA-approved treatment options, and the SMA drug pipeline.
To access Part 1 of the SMA Spotlight series, The Urgent Need for Early Diagnosis in Spinal Muscular Atrophy, visit www.mdedge.com/DiagnosisInSMA.
References
Finkel RS, Mercuri E, Darras BT, et al. Nusinersen versus sham control in infantile-onset spinal muscular atrophy. N Engl J Med. 2017;377(18):1723-1732.
Mercuri E, Darras BT, Chiriboga CA, et al. Nusinersen versus sham control in later-onset spinal muscular atrophy. N Engl J Med. 2018;378(7):625-635.
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose genereplacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
De Vivo DC, Bertini E, Swoboda KJ, et al. Nusinersen initiated in infants during the presymptomatic stage of spinal muscular atrophy: Interim efficacy and safety results from the Phase 2 NURTURE study. Neuromuscul Disord. 2019;29(11):842-856.
Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
Our sixth annual Rare Neurological Disease Special Report is our biggest issue yet. It is very gratifying to know we are part of the rare disease community and witness to some of the exciting developments that are transforming this field. There are many newly approved therapies highlighted in the articles in this issue, as well as brief profiles of a number of research groups within the NIH’s Rare Diseases Clinical Research Network and an intriguing profile of how the Netflix show Diagnosis used crowdsourcing to solve medical mysteries, many of which involved rare neurologic conditions. That’s just a sampling of what this issue has to offer. There are too many articles to mention each one, but I hope you take the time to read the entire issue.
—Glenn S. Williams, vice president, group editor, Neurology Reviews
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this supplement, Paul P. Dobesh, PharmD, examines NVAF in the obese and morbidly obese patient population with a focus on anticoagulant treatment options. Topics include:
Understanding the obesity risk in patients with NVAF
Challenges of anticoagulation with warfarin in patients with obesity
In this issue of CHEST Clinical Perspectives, CHEST is undertaking primary research with pulmonologists to assess perceptions regarding curative intent when it comes to treating patients diagnosed with stage III NSCLC. The objectives of this research are to:
Understand the role of the pulmonologist in diagnostic process, including diagnosis, cell type, staging.
Understand the process of referral for treatment of patients with stage III NSCLC diagnosed in pulmonary practices, including frequency of referral to oncology and barriers to referral.
Understand knowledge levels about stage III NSCLC, including differences between patients with stage III and stage IV and how that impacts referral for treatment.
Understand the extent to which pulmonologists consider stage III patients to be in a curative state.
In this issue of CHEST Clinical Perspectives, CHEST is undertaking primary research with pulmonologists to assess perceptions regarding curative intent when it comes to treating patients diagnosed with stage III NSCLC. The objectives of this research are to:
Understand the role of the pulmonologist in diagnostic process, including diagnosis, cell type, staging.
Understand the process of referral for treatment of patients with stage III NSCLC diagnosed in pulmonary practices, including frequency of referral to oncology and barriers to referral.
Understand knowledge levels about stage III NSCLC, including differences between patients with stage III and stage IV and how that impacts referral for treatment.
Understand the extent to which pulmonologists consider stage III patients to be in a curative state.
In this issue of CHEST Clinical Perspectives, CHEST is undertaking primary research with pulmonologists to assess perceptions regarding curative intent when it comes to treating patients diagnosed with stage III NSCLC. The objectives of this research are to:
Understand the role of the pulmonologist in diagnostic process, including diagnosis, cell type, staging.
Understand the process of referral for treatment of patients with stage III NSCLC diagnosed in pulmonary practices, including frequency of referral to oncology and barriers to referral.
Understand knowledge levels about stage III NSCLC, including differences between patients with stage III and stage IV and how that impacts referral for treatment.
Understand the extent to which pulmonologists consider stage III patients to be in a curative state.
Click here
to read an edited transcript of a mult-disciplinary expert roundtable discussion in which surgeons, pharmacists, anesthesiologists and pain experts discuss insights and best practices for managing peri-operative pain and optimizing patient care.
Chad Brummett, MD Associate Professor, Anesthesiology, Director, Anesthesia Clinical Research, Director, Division of Pain Research, Michigan Medicine Back & Pain Center Ann Arbor, MI
PARTICIPANTS
Andrew C. Eppstein, MD Assistant Professor of Clinical Surgery, Indiana University School of Medicine Chief of General Surgery, Richard L. Roudebush VA Medical Center Indianapolis, IN
Nicholas Giori MD, PhD Professor of Orthopedic Surgery, Stanford University Chief of Orthopedic Surgery, VA Palo Alto Health Care System Palo Alto, CA
Georgine Lamvu, MD, MHP Professor in Obstetrics and Gynecology, University of Central Florida College of Medicine Division of Surgery, Gynecology Section Orlando VA Medical Center Orlando, FL
Bryan Sakamoto, MD, PhD Staff Physician, Richard L. Roudebush VA Medical Center Assistant Professor of Clinical Anesthesia Indiana University School of Medicine Indianapolis, IN
Jack D. Wright, PharmD Chief of Pharmacy, Beckley VA Medical Center Beckley, WV
Sponsor
This roundtable discussion is sponsored by Heron Therapeutics.
This roundtable discussion is sponsored by Heron Therapeutics.
Sponsor
This roundtable discussion is sponsored by Heron Therapeutics.
Click here
to read an edited transcript of a mult-disciplinary expert roundtable discussion in which surgeons, pharmacists, anesthesiologists and pain experts discuss insights and best practices for managing peri-operative pain and optimizing patient care.
Chad Brummett, MD Associate Professor, Anesthesiology, Director, Anesthesia Clinical Research, Director, Division of Pain Research, Michigan Medicine Back & Pain Center Ann Arbor, MI
PARTICIPANTS
Andrew C. Eppstein, MD Assistant Professor of Clinical Surgery, Indiana University School of Medicine Chief of General Surgery, Richard L. Roudebush VA Medical Center Indianapolis, IN
Nicholas Giori MD, PhD Professor of Orthopedic Surgery, Stanford University Chief of Orthopedic Surgery, VA Palo Alto Health Care System Palo Alto, CA
Georgine Lamvu, MD, MHP Professor in Obstetrics and Gynecology, University of Central Florida College of Medicine Division of Surgery, Gynecology Section Orlando VA Medical Center Orlando, FL
Bryan Sakamoto, MD, PhD Staff Physician, Richard L. Roudebush VA Medical Center Assistant Professor of Clinical Anesthesia Indiana University School of Medicine Indianapolis, IN
Jack D. Wright, PharmD Chief of Pharmacy, Beckley VA Medical Center Beckley, WV
Click here
to read an edited transcript of a mult-disciplinary expert roundtable discussion in which surgeons, pharmacists, anesthesiologists and pain experts discuss insights and best practices for managing peri-operative pain and optimizing patient care.
Chad Brummett, MD Associate Professor, Anesthesiology, Director, Anesthesia Clinical Research, Director, Division of Pain Research, Michigan Medicine Back & Pain Center Ann Arbor, MI
PARTICIPANTS
Andrew C. Eppstein, MD Assistant Professor of Clinical Surgery, Indiana University School of Medicine Chief of General Surgery, Richard L. Roudebush VA Medical Center Indianapolis, IN
Nicholas Giori MD, PhD Professor of Orthopedic Surgery, Stanford University Chief of Orthopedic Surgery, VA Palo Alto Health Care System Palo Alto, CA
Georgine Lamvu, MD, MHP Professor in Obstetrics and Gynecology, University of Central Florida College of Medicine Division of Surgery, Gynecology Section Orlando VA Medical Center Orlando, FL
Bryan Sakamoto, MD, PhD Staff Physician, Richard L. Roudebush VA Medical Center Assistant Professor of Clinical Anesthesia Indiana University School of Medicine Indianapolis, IN
Jack D. Wright, PharmD Chief of Pharmacy, Beckley VA Medical Center Beckley, WV
A significant unmet need exists for users of acute medications for the treatment of migraine attacks. These medications can be ineffective or associated with undesirable side effects. However, a novel unique therapy, ubrogepant, has demonstrated efficacy for the acute treatment of migraine.
1. Treatment Patterns and Unmet Needs in the Acute Treatment of Migraine
Audio file
2. Pharmacology and Pharmacokinetics of Ubrogepant: A Potent, Selective Calcitonin Gene-Related Peptide Receptor Antagonist for the Acute Treatment of Migraine
Audio file
3. Clinical Efficacy and Safety of Ubrogepant for the Acute Treatment of Migraine
Audio file
Podcast References
1. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache. 2018;58(4):496-505.
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-858.
3. Evers S, Marziniak M. Clinical features, pathophysiology, and treatment of medication-overuse headache. Lancet Neurol. 2010;9(4):391-401.
4. Ahmed F. Headache disorders: differentiating and managing the common subtypes. Br J Pain. 2012;6(3):124-32.
5. Minen M, Shome A, Halpern A, Tishler L, Brennan KC, Loder E, et al. A migraine management training program for primary care providers: An overview of a survey and pilot study findings, lessons learned, and considerations for further research. Headache. 2016;56(4):725-40.
6. Becker WJ. Acute migraine treatment in adults. Headache. 2015;55(6):778-93.
7. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American Headache Society evidence assessment of migraine pharmacotherapies. Headache. 2015;55(1):3-20.
8. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821-8.
9. Messali AJ, Yang M, Gillard P, Tsai K, Tepper SJ, Bloudek LM, et al. Treatment persistence and switching in triptan users: a systematic literature review. Headache. 2014;54(7):1120-30.
10. Katic BJ, Rajagopalan S, Ho TW, Chen YT, Hu XH. Triptan persistency among newly initiated users in a pharmacy claims database. Cephalalgia. 2011;31(4):488-500.
11. Iyengar S, Ossipov MH, Johnson KW. The role of calcitonin gene-related peptide in peripheral and central pain mechanisms including migraine. Pain. 2017;158(4):543-59.
12. Ho TW, Edvinsson L, Goadsby PJ. CGRP and its receptors provide new insights into migraine pathophysiology. Nat Rev Neurol. 2010;6(10):573-82.
Sponsor
This supplement was sponsored by Allergan plc, with medical writing and editori…
This supplement was sponsored by Allergan plc, with medical writing and editori…
Sponsor
This supplement was sponsored by Allergan plc, with medical writing and editori…
A significant unmet need exists for users of acute medications for the treatment of migraine attacks. These medications can be ineffective or associated with undesirable side effects. However, a novel unique therapy, ubrogepant, has demonstrated efficacy for the acute treatment of migraine.
1. Treatment Patterns and Unmet Needs in the Acute Treatment of Migraine
Audio file
2. Pharmacology and Pharmacokinetics of Ubrogepant: A Potent, Selective Calcitonin Gene-Related Peptide Receptor Antagonist for the Acute Treatment of Migraine
Audio file
3. Clinical Efficacy and Safety of Ubrogepant for the Acute Treatment of Migraine
Audio file
Podcast References
1. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache. 2018;58(4):496-505.
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-858.
3. Evers S, Marziniak M. Clinical features, pathophysiology, and treatment of medication-overuse headache. Lancet Neurol. 2010;9(4):391-401.
4. Ahmed F. Headache disorders: differentiating and managing the common subtypes. Br J Pain. 2012;6(3):124-32.
5. Minen M, Shome A, Halpern A, Tishler L, Brennan KC, Loder E, et al. A migraine management training program for primary care providers: An overview of a survey and pilot study findings, lessons learned, and considerations for further research. Headache. 2016;56(4):725-40.
6. Becker WJ. Acute migraine treatment in adults. Headache. 2015;55(6):778-93.
7. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American Headache Society evidence assessment of migraine pharmacotherapies. Headache. 2015;55(1):3-20.
8. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821-8.
9. Messali AJ, Yang M, Gillard P, Tsai K, Tepper SJ, Bloudek LM, et al. Treatment persistence and switching in triptan users: a systematic literature review. Headache. 2014;54(7):1120-30.
10. Katic BJ, Rajagopalan S, Ho TW, Chen YT, Hu XH. Triptan persistency among newly initiated users in a pharmacy claims database. Cephalalgia. 2011;31(4):488-500.
11. Iyengar S, Ossipov MH, Johnson KW. The role of calcitonin gene-related peptide in peripheral and central pain mechanisms including migraine. Pain. 2017;158(4):543-59.
12. Ho TW, Edvinsson L, Goadsby PJ. CGRP and its receptors provide new insights into migraine pathophysiology. Nat Rev Neurol. 2010;6(10):573-82.
A significant unmet need exists for users of acute medications for the treatment of migraine attacks. These medications can be ineffective or associated with undesirable side effects. However, a novel unique therapy, ubrogepant, has demonstrated efficacy for the acute treatment of migraine.
1. Treatment Patterns and Unmet Needs in the Acute Treatment of Migraine
Audio file
2. Pharmacology and Pharmacokinetics of Ubrogepant: A Potent, Selective Calcitonin Gene-Related Peptide Receptor Antagonist for the Acute Treatment of Migraine
Audio file
3. Clinical Efficacy and Safety of Ubrogepant for the Acute Treatment of Migraine
Audio file
Podcast References
1. Burch R, Rizzoli P, Loder E. The prevalence and impact of migraine and severe headache in the United States: figures and trends from government health studies. Headache. 2018;58(4):496-505.
2. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-858.
3. Evers S, Marziniak M. Clinical features, pathophysiology, and treatment of medication-overuse headache. Lancet Neurol. 2010;9(4):391-401.
4. Ahmed F. Headache disorders: differentiating and managing the common subtypes. Br J Pain. 2012;6(3):124-32.
5. Minen M, Shome A, Halpern A, Tishler L, Brennan KC, Loder E, et al. A migraine management training program for primary care providers: An overview of a survey and pilot study findings, lessons learned, and considerations for further research. Headache. 2016;56(4):725-40.
6. Becker WJ. Acute migraine treatment in adults. Headache. 2015;55(6):778-93.
7. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American Headache Society evidence assessment of migraine pharmacotherapies. Headache. 2015;55(1):3-20.
8. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71(22):1821-8.
9. Messali AJ, Yang M, Gillard P, Tsai K, Tepper SJ, Bloudek LM, et al. Treatment persistence and switching in triptan users: a systematic literature review. Headache. 2014;54(7):1120-30.
10. Katic BJ, Rajagopalan S, Ho TW, Chen YT, Hu XH. Triptan persistency among newly initiated users in a pharmacy claims database. Cephalalgia. 2011;31(4):488-500.
11. Iyengar S, Ossipov MH, Johnson KW. The role of calcitonin gene-related peptide in peripheral and central pain mechanisms including migraine. Pain. 2017;158(4):543-59.
12. Ho TW, Edvinsson L, Goadsby PJ. CGRP and its receptors provide new insights into migraine pathophysiology. Nat Rev Neurol. 2010;6(10):573-82.
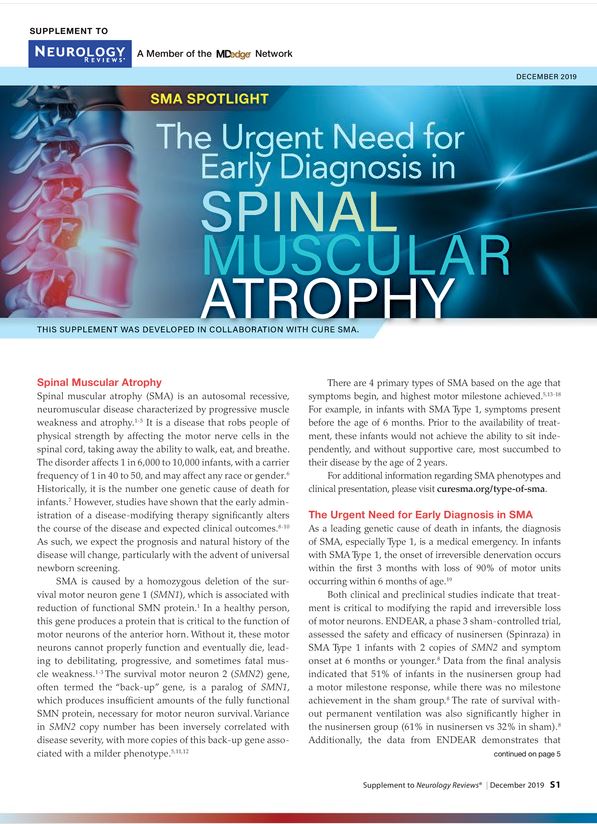
The diagnosis of spinal muscular atrophy (SMA), especially Type 1, is a medical emergency, as SMA is a leading genetic cause of death in infants. In infants with SMA Type 1, the onset of irreversible denervation occurs within the first 3 months with loss of 90% of motor units occurring within 6 months of age.
This supplement examines the clinical implications of delayed diagnosis of SMA, as well as assessment tools, treatment methods, and resources that are available for physicians, patients, and caregivers to better manage this rare disease.
The diagnosis of spinal muscular atrophy (SMA), especially Type 1, is a medical emergency, as SMA is a leading genetic cause of death in infants. In infants with SMA Type 1, the onset of irreversible denervation occurs within the first 3 months with loss of 90% of motor units occurring within 6 months of age.
This supplement examines the clinical implications of delayed diagnosis of SMA, as well as assessment tools, treatment methods, and resources that are available for physicians, patients, and caregivers to better manage this rare disease.
The diagnosis of spinal muscular atrophy (SMA), especially Type 1, is a medical emergency, as SMA is a leading genetic cause of death in infants. In infants with SMA Type 1, the onset of irreversible denervation occurs within the first 3 months with loss of 90% of motor units occurring within 6 months of age.
This supplement examines the clinical implications of delayed diagnosis of SMA, as well as assessment tools, treatment methods, and resources that are available for physicians, patients, and caregivers to better manage this rare disease.