User login
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
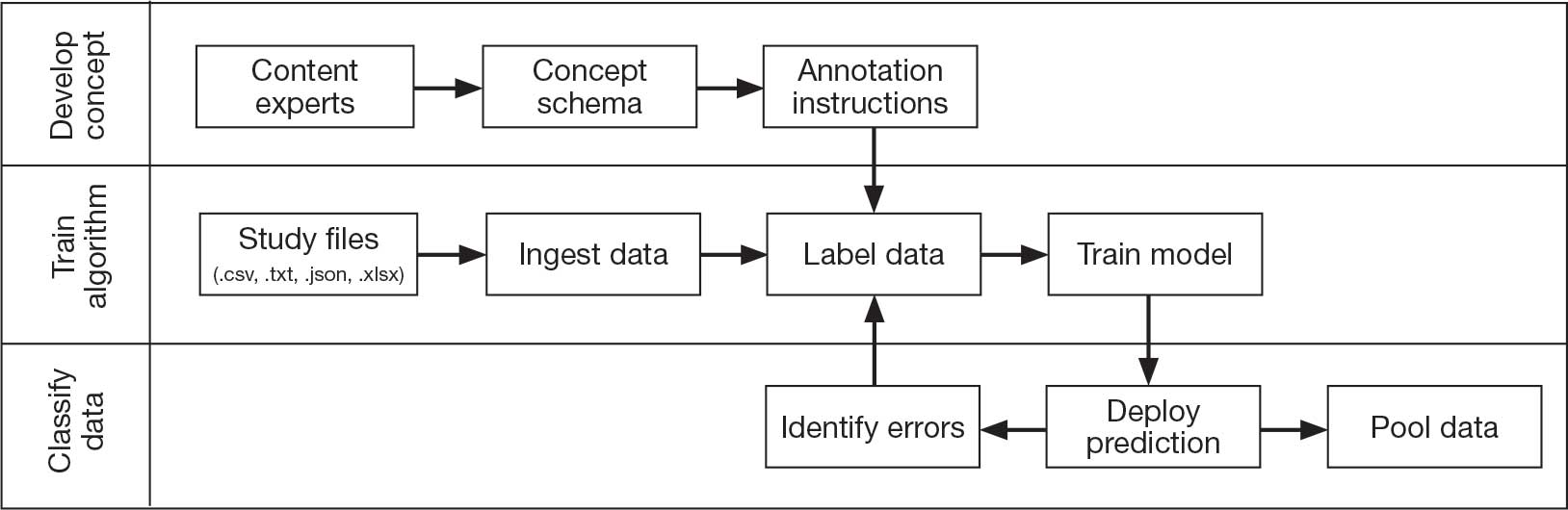
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
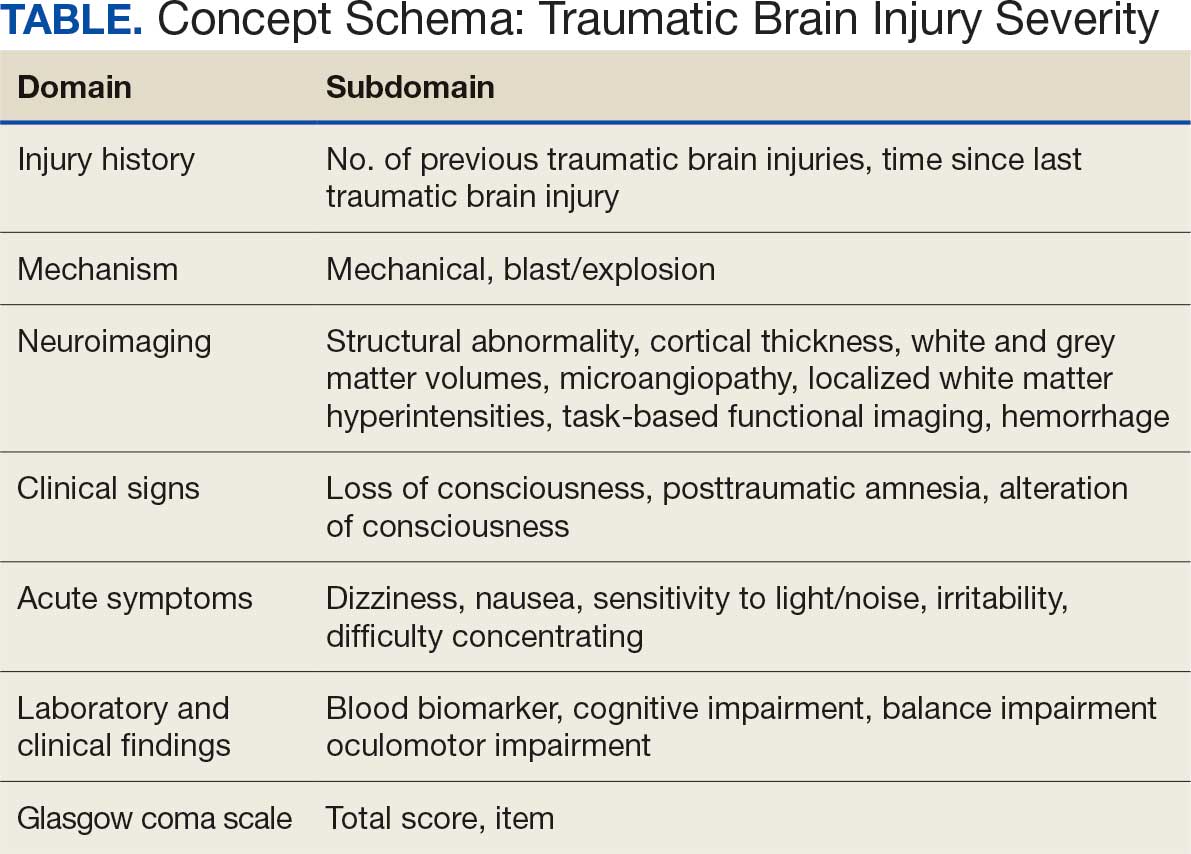
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
In leveraging existing, readily available evidence-based health care information (eg, systematic reviews, clinical practice guidelines), clinicians have historically made recommendations based on treatment responses of the average patient.1 Recently, this approach has been expanded into data-driven, evidence-based precision medical care for individuals across a wide range of disciplines and care settings. These precision medicine approaches use information related to an individual’s genes, environment, and lifestyle to tailor recommendations regarding prevention, diagnosis, and treatment.
Applying precision medicine approaches to the unique exposures and experiences of service members and veterans—particularly those who served in combat environments—through the incorporation of biopsychosocial factors into medical decision-making may be even more pertinent. This sentiment is reflected in Section 305 of the Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, which outlines the Precision Medicine Initiative of the US Department of Veterans Affairs (VA) to identify and validate brain and mental health biomarkers.2 Despite widespread consensus regarding the promise of precision medicine, large, rich datasets with elements pertaining to common military exposures such as traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) are limited.
Existing datasets, most of which are relatively small or focus on specific cohorts (eg, older veterans, transitioning veterans), continue to create barriers to advancing precision medicine. For example, in classically designed clinical trials, analyses are generally conducted in a manner that may obfuscate efficacy among subcohorts of individuals, thereby underscoring the need to explore alternative strategies to unify existing datasets capable of revealing such heterogeneity.3 The evidence base for precision medical care is limited, drawing from published trials with relatively small sample sizes and even larger cohort studies have limited biomarker data. Additionally, these models are often exploratory during development, and to avoid statistical overfitting of an exploratory model, validation in similar datasets is needed—an added burden when data sources are small or underpowered to begin with.
A promising approach is to combine and harmonize the largest, most deeply characterized data sources from similar samples. Although combining such datasets may appear to require minimal time and effort, harmonizing similar variables in an evidence-based and replicable manner requires time and expertise, even when participant characteristics and outcomes are similar.4-7
Challenges related to harmonization are related to the wide range of strategies (eg, self-report questionnaires, clinical interviews, electronic health record review) used to measure common brain and mental health constructs, such as depression. Even when similar methods (eg, self-report measures) are implemented, challenges persist. For example, if a study used a depression measure that focused primarily on cognitive symptoms (eg, pessimism, self-dislike, suicidal ideation) and another study used a depression measure composed of items more heavily weighted towards somatic symptoms (eg, insomnia, loss of appetite, weight loss, decreased libido), combining their data could be challenging, particularly if researchers, clinicians, or administrators are interested in more than dichotomous outcomes (eg, depression vs no depression).8,9
To address this knowledge gap and harmonize multimodal data from varied sources, well-planned and reproducible curation is needed. Longitudinal cohort studies of service members and veterans with military combat and training exposure histories provide researchers and other stakeholders access to extant biopsychosocial data shown to affect risk for adverse health outcomes; however, efforts to facilitate individually tailored treatment or other precision medicine approaches would benefit from the synthesis of such datasets.10
Members of the VA Total Brain Diagnostics (TBD) team are engaged in harmonizing variables from the Long-Term Impact of Military-Relevant Brain Injury Consortium–Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC)11 and the Translational Research Center for TBI and Stress Disorders (TRACTS).12-21 While there is overlap across LIMBIC-CENC and TRACTS with respect to data domains, considerable data harmonization is needed to allow for future valid and meaningful analyses, particularly those involving multivariable predictors.
Data Sources
Both data sources for the TBD harmonization project, LIMBIC-CENC and TRACTS, include extensive, longitudinal data collected from relatively large cohorts of veterans and service members with combat exposure. Both studies collect detailed data related to potential brain injury history and include participants with and without a history of TBI. Similarly, both include extensive collection of fluid biomarkers and imaging data, as well as measures of biopsychosocial functioning.
Data collection sites for LIMBIC-CENC include 16 recruitment sites, 9 at VA medical centers (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego) and 7 at military treatment sites (Alexandria, San Diego, Tampa, Tacoma, Columbia, Coronado, Hinesville), in addition to 11 assessment sites (Richmond, Houston, Tampa, San Antonio, Portland, Minneapolis, Boston, Salisbury, San Diego, Alexandria, Augusta). Data for TRACTS are collected at sites in Boston and Houston.
LIMBIC-CENC is a 12-year, 17-site cohort of service members and veteran participants with combat exposure who are well characterized at baseline and undergo annual reassessments. As of December 2025, > 3100 participants have been recruited, and nearly 90% remain in follow-up. Data collection includes > 6200 annual follow-up evaluations and > 1550 5-year re-evaluations, with 400 enrolled participants followed up annually.
TRACTS is a 16-year, 2-site cohort of veterans with combat exposure who complete comprehensive assessments at enrollment, undergo annual reassessments, and complete comprehensive reassessment every 5 years thereafter. As of December 2025, > 1075 participants have completed baseline (Time 1) assessments, > 600 have completed the 2-year re-evaluation (Time 2), > 175 have completed the 5-year re-evaluation (Time 3), and > 35 have completed 10-year evaluations (Time 4), with about 50 new participants added and 100 enrolled participants followed up annually. More data on participant characteristics are available for both LIMBIC-CENC and TRACTS in previous publications.11,22These 2 ongoing, prospective, longitudinal cohorts of service members and veterans offer access to a wide range of potential risk factors that can affect response to care and outcomes, including demographics (eg, age, sex), injury characteristics (eg, pre-exposure factors, exposure factors), biomarkers (eg, serum, saliva, brain imaging, evoked potentials), and functional measures (eg, computerized posturography, computerized eye tracking, sensory testing, clinical examination, neuropsychological assessments, symptom questionnaires).
Harmonization Strategy
Pooling and harmonizing data from large studies evaluating similar participant cohorts and conditions involves numerous steps to appropriately handle a variety of measurements and disparate variable names. The TBD team adapted a model data harmonization system developed by O’Neil et al through initial work harmonizing the Federal Interagency Traumatic Brain Injury Research Informatics System (FITBIR).4-7 This process was expanded and generalized by the research team to combine data from LIMBIC-CENC and TRACTS to create a single pooled dataset for analysis (Figure).
Injury Research database.
This approach was selected because it accommodates heterogeneous study designs (eg, cross-sectional, longitudinal, case-control), data collection methods (eg, clinical assessment, self-reported, objective blood, and imaging biomarkers), and various assessments of the same construct (ie, different measures of brain injury). While exact matches for data collection methods and measures may be easily harmonized, the timing of assessment, number of assessments, assessment tool version, and other factors must be considered. The goal was to harmonize data from LIMBIC-CENC and TRACTS to allow additional data sources to be harmonized and incorporated in the future.
Original data files from each study were reshaped to represent participant-level observations with 1 unique measurement per row. The measurement represents what information was collected and the value recorded represents the unique observation. These data are linked to metadata from the original study, which includes the study’s definition of each measurement, how it was collected, and any available information regarding when it was collected in reference to study enrollment or injury. Additional information on the file source, row, and column position of each data point was added to enable recreation of the original data as needed.
The resulting dataset was used to harmonize measurements from LIMBIC-CENC and TRACTS into a priori-defined schemas for brain- and mental health-relevant concepts, including TBI severity, PTSD, substance use, depression, suicidal ideation, and functioning (including cognitive, physical, and social functioning). This process was facilitated using natural language processing (NLP). Each study uniquely defines all measurements and provides written definitions with the data. Measurement definitions serve as records describing what was collected, how it was collected, and how the study may have uniquely defined information for its purposes. For example, definitions of exposure to brain injury and severity of brain injury may differ between studies, and the study-provided definition defines these differences.
Definitions were converted into numeric vectors through sentence embedding, a process that preserves the semantic meaning of the definition.23 Cosine similarity was used as the primary metric to compare the semantic textual similarity between pairs of measurement definitions. Cosine similarity ranges from 0 to 1, where 0 indicates no meaningful similarity and 1 indicates they have identical meanings.24 This approach leverages the relationship between the definitions of each measurement provided by a study and enables quick comparison of all pairwise combinations of measurement definitions between studies.
Subsets of similar measurements across studies were organized into a priori-defined schema. Clinical experts then reviewed each schema and further refined them into domains, (eg, mechanism of injury, clinical signs, acute symptoms) and subdomains (children), such as loss of consciousness, amnesia, and alteration of consciousness. This approach allows efficient handling of 2 specific cases that commonly occur when pooling and harmonizing datasets: (1) identifying the same measurement with differing names; and (2) identifying different measurements with definitions that each relate to the same domain.
The Table provides a general example of the schema for TBI severity. This was an iterative process in which clinical experts reviewed study-defined measurement definitions to develop general harmonized domains, and NLP techniques facilitated and accelerated identification and organization of measurements within these domains.
Expected Impact
Harmonization combining LIMBIC-CENC and TRACTS datasets is ongoing. Preliminary descriptive analyses of baseline cohort data indicate that harmonization across data sources is appropriate, given the lack of significant heterogeneity across sites and studies for most domains. Work by members of the TBD team is expected to lay the foundation for the use of existing and ongoing prospective, longitudinal datasets (eg, LIMBIC-CENC, TRACTS) and linked large datasets (eg, VA Informatics and Computing Infrastructure including electronic health records, VA Million Veteran Program, DaVINCI [US Department of Defense and VA Infrastructure for Clinical Intelligence]) to generate generalizable, clinically relevant information to advance precision brain and mental health care among service members and veterans.
By enhancing existing practice, this synthesized dataset has the potential to inform tailored and personalized medicine approaches designed to meet the needs of veterans and service members. These data will serve as the starting point for multivariable models examining the intersection of physiologic, behavioral, and environmental factors. The goal of this data harmonization effort is to better elucidate how clinicians and researchers can select optimal approaches for veterans and service members with TBI histories by accounting for a comprehensive set of physiologic, behavioral, and environmental factors in an individually tailored manner. These data may further extend existing clinical practice guideline approaches, inform shared decision-making, and enhance functional outcomes beyond those currently available.
Conclusions
Individuals who have served in the military have unique biopsychosocial exposures that are associated with brain and mental health disorders. To address these needs, the nationwide TBD team has initiated the creation of a unified, longitudinal dataset that includes harmonized measures from existing LIMBIC-CENC and TRACTS protocols. Initial data harmonization efforts are required to facilitate precision prognostics, diagnostics, and tailored interventions, with the goal of improving veterans’ brain and mental health and psychosocial functioning and enabling tailored and evidence-informed, individualized clinical care.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
- The Promise of Precision Medicine. National Institutes of Health (NIH). Updated January 21, 2025. Accessed January 5, 2026. https://www.nih.gov/about-nih/nih-turning-discovery-into-health/promise-precision-medicine.
- Commander John Scott Hannon Veterans Mental Health Care Improvement Act of 2019, S 785, 116th Cong (2019-2020) Accessed January 5, 2026. https://www.congress.gov/bill/116th-congress/senate-bill/785
- Cheng C, Messerschmidt L, Bravo I, et al. A general primer for data harmonization. Sci Data. 2024;11:152. doi:10.1038/s41597-024-02956-3
- Neil M, Cameron D, Clauss K, et al. A proof-of-concept study demonstrating how FITBIR datasets can be harmonized to examine posttraumatic stress disorder-traumatic brain injury associations. J Behav Data Sci. 2024;4:45-62. doi:10.35566/jbds/oneil
- O’Neil ME, Cameron D, Krushnic D, et al. Using harmonized FITBIR datasets to examine associations between TBI history and cognitive functioning. Appl Neuropsychol Adult. doi:10.1080/23279095.2024.2401974
- O’Neil ME, Krushnic D, Clauss K, et al. Harmonizing federal interagency traumatic brain injury research data to examine depression and suicide-related outcomes. Rehabil Psychol. 2024;69:159-170. doi:10.1037/rep0000547
- O’Neil ME, Krushnic D, Walker WC, et al. Increased risk for clinically significant sleep disturbances in mild traumatic brain injury: an approach to leveraging the federal interagency traumatic brain injury research database. Brain Sci. 2024;14:921. doi:10.3390/brainsci14090921
- Uher R, Perlis RH, Placentino A, et al. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29:1043-1049. doi:10.1002/da.21993
- Hung CI, Weng LJ, Su YJ, et al. Depression and somatic symptoms scale: a new scale with both depression and somatic symptoms emphasized. Psychiatry Clin Neurosci. 2006;60:700-708. doi:10.1111/j.1440-1819.2006.01585.x
- Stewart IJ, Howard JT, Amuan ME, et al. Traumatic brain injury is associated with the subsequent risk of atrial fibrillation or atrial flutter. Heart Rhythm. 2025;22:661-667. doi:10.1016/j.hrthm.2024.09.019
- Cifu DX. Clinical research findings from the long-term impact of military-relevant brain injury consortium-chronic effects of neurotrauma consortium (LIMBIC-CENC) 2013-2021. Brain Inj. 2022;36:587-597.doi:10.1080/02699052.2022.2033843
- Fonda JR, Fredman L, Brogly SB, et al. Traumatic brain injury and attempted suicide among veterans of the wars in Iraq and Afghanistan. Am J Epidemiol. 2017;186:220-226. doi:10.1093/aje/kwx044
- Fortier CB, Amick MM, Kenna A, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) clinical interview and the VA TBI screen. J Head Trauma Rehabil. 2015;30:E1-7. doi:10.1097/htr.0000000000000008
- Grande LJ, Robinson ME, Radigan LJ, et al. Verbal memory deficits in OEF/OIF/OND veterans exposed to blasts at close range. J Int Neuropsychol Soc. 2018;24:466-475. doi:10.1017/S1355617717001242
- Hayes JP, Logue MW, Sadeh N, et al. Mild traumatic brain injury is associated with reduced cortical thickness in those at risk for Alzheimer’s disease. Brain. 2017;140:813-825. doi:10.1093/brain/aww344
- Lippa SM, Fonda JR, Fortier CB, et al. Deployment-related psychiatric and behavioral conditions and their association with functional disability in OEF/OIF/OND veterans. J Trauma Stress. 2015;28:25-33. doi:10.1002/jts.21979
- McGlinchey RE, Milberg WP, Fonda JR, et al. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudinal prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Radigan LJ, McGlinchey RE, Milberg WP, et al. Correspondence of the Boston Assessment of Traumatic Brain Injury-Lifetime and the VA Comprehensive TBI Evaluation. J Head Trauma Rehabil. 2018;33:E51-E55. doi:10.1097/htr.0000000000000361
- Sydnor VJ, Bouix S, Pasternak O, et al. Mild traumatic brain injury impacts associations between limbic system microstructure and post-traumatic stress disorder symptomatology. Neuroimage Clin. 2020;26:102190. doi:10.1016/j.nicl.2020.102190
- Van Etten EJ, Knight AR, Colaizzi TA, et al. Peritraumatic context and long-term outcomes of concussion. JAMA Netw Open. 2025;8:e2455622. doi:10.1001/jamanetworkopen.2024.55622
- Andrews RJ, Fonda JR, Levin LK, et al. Comprehensive analysis of the predictors of neurobehavioral symptom reporting in veterans. Neurology. 2018;91:e732-e745. doi:10.1212/wnl.0000000000006034
- McGlinchey RE, Milberg WP, Fonda JR, Fortier CB. A methodology for assessing deployment trauma and its consequences in OEF/OIF/OND veterans: the TRACTS longitudional prospective cohort study. Int J Methods Psychiatr Res. 2017;26:e1556. doi:10.1002/mpr.1556
- Reimers N, Gurevych I. Sentence-BERT: Sentence embeddings using Siamese BERT-Networks. 2019. Conference on Empirical Methods in Natural Language Processing.
- Singhal A. Modern information retrieval: a brief overview. IEEE Data Eng Bull. 2001;24:34-43.
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs
Total Brain Diagnostics: Advancing Precision Brain and Mental Health at the Department of Veterans Affairs

Implementation of Harm Reduction Syringe Services Programs at 2 Veterans Affairs Medical Centers
Implementation of Harm Reduction Syringe Services Programs at 2 Veterans Affairs Medical Centers
A syringe services program (SSP) is a harm reduction strategy designed to improve the quality of care provided to people who use drugs (PWUD). SSPs not only provide sterile syringes but establish a connection to medical services and resources for the safe disposal of syringes. By engaging with an SSP, patients may receive naloxone, condoms, fentanyl test strips, opioid use disorder medications, vaccinations, or testing for infectious diseases such as HIV and hepatitis C virus (HCV). Patients may also be connected to housing or social work services.
SSPs do not lead to increased drug use,1 increased improperly disposed supplies needed for drug use in the community, or increased crime.2,3 New users of SSPs are 5 times more likely to enter treatment for drug use than those who do not use SSPs.4-8 Further, SSPs have been found to reduce HIV and HCV transmission and are cost-effective in HIV prevention.9-11
Syringe Services Program
SSPs were implemented at the US Department of Veterans Affairs (VA) Alaska VA Healthcare System (AVAHCS) and VA Southern Oregon Healthcare System (VASOHCS). AVAHCS provides outpatient care across Alaska, with sites in Anchorage, Fairbanks, Homer, Juneau, Wasilla, and Soldotna. VASOHCS provides outpatient care to Southern Oregon and Northern California, with sites in White City, Grants Pass, and Klamath Falls, Oregon. Both are part of Veterans Integrated Service Network 20
Workgroups at AVAHCS and VASOHCS developed SSPs to reduce risks associated with drug use, promote positive outcomes for PWUD, and increase availability of harm reduction resources. During the July 2023 to June 2024 pharmacy residency cycle, an ambulatory care pharmacy resident from the Veterans Integrated Services Network 20 Clinical Resource Hub—a regional resource for clinical services—joined the workgroups. The workgroups established a goal that SSP resources would be made available to enrolled patients without any exclusions, prioritizing health equity.
SSP implementation needed buy-in from AVAHCS and VASOHCS leadership and key stakeholders who could participate in the workgroups. Following AVAHCS and VASOHCS leadership approval, each facility workgroup drafted standard operating procedures (SOPs). Both facilities planned to implement the program using prepackaged kits (sterile syringes, alcohol pads, cotton swabs, a sharps container, and an educational brochure on safe injection practices) supplied by the VA National Harm Reduction Program.
Each SSP offered patients direct links to additional care options at the time of kit distribution, including information regarding medications/supplies (ie, hepatitis A/B vaccines, HIV preexposure prophylaxis, substance use disorder pharmacotherapy, naloxone, and condoms), laboratory tests for infectious and sexually transmitted diseases, and referrals to substance use disorder treatment, social work, suicide prevention, mental health, and primary care.
The goal was to implement both SSPs during the July 2023 to June 2024 residency year. Other goals included tracking the quantity of supplies distributed, the number of patients reached, the impact of clinician education on the distribution of supplies, and comparing the implementation of the SSPs in the electronic health record (EHR) systems.
Alaska VA Healthcare System
An SOP was approved on December 20, 2023, and national supply kits were stocked in collaboration with the logistics department at the Anchorage AVAHCS campus. Social and behavioral health teams, primary care social workers, primary care clinicians, and nursing staff received training on the resources available through the SSP. A local adaptation of a template was created in the Computerized Patient Records System (CPRS) EHR. The template facilitates SSP kit distribution and patient screening for additional resources. Patients can engage with the SSP through any trained staff member. The staff member then completes the template and helps to distribute the SSP kit, in collaboration with the logistics department. The SSP does not operate in a dedicated physical space. The behavioral health team is most actively engaged in the SSP. The goal of SSP is to have resources available anywhere a patient requests services, including primary care and specialty clinics and to empower staff to meet patients’ needs. One patient has utilized the SSP as of June 2025.
Southern Oregon Healthcare System
Kits were ordered and stocked as pharmacy items in preparation for dispensing while awaiting medical center policy approval. Education began with the primary care mental health integration team. After initial education, an interdisciplinary presentation was given to VASOHCS clinicians to increase knowledge of the SSP. To enable documentation of SSP engagement, a local template was developed in the Cerner EHR to be shared among care team members at the facility. Similar to AVAHCS, the SSP does not have a physical space. All trained facility staff may engage in the SSP and distribute SSP kits. The workgroup that implemented this program remains available to support staff. Five patients have accessed the SSP since November 2024 and 7 SSP kits have been distributed as of June 2025.
Discussion
The SSP workgroups sought to expand the program through additional education. A number of factors should be considered when implementing an SSP. Across facilities, program implementation can be time-consuming and the timeline for administrative processes may be long. The workgroups met weekly or monthly depending on the status of the program and the administrative processes. Materials developed included SOP and MCP documents, a 1-page educational handout on SSP offerings, and a PowerPoint presentation for initial clinician education. Involving a pharmacy resident supported professional development and accelerated implementation timelines.
The facilities differed in implementation. AVAHCS collaborated with the logistics department to distribute kits, while VASOHCS worked with the Pharmacy service. A benefit of collaborating with logistics is that patients can receive a kit at the point of contact with the health care system, receiving it directly from the clinic the patient is visiting while eliminating the need to make an additional stop at the pharmacy. Conversely, partnering with the Pharmacy service allowed supply kits to be distributed by mail, enabling patients direct access to kits without having to present in-person. This is particularly valuable considering the large geographical area and remote care services available at VASOHCS.
Implementation varied significantly because AVAHCS operated on CPRS while VASOHCS used Cerner, a newer EHR. AVAHCS adapted a national template produced for CPRS sites, while VASOHCS had to prepare a local template (auto-text) for SSP documentation. Future plans at AVAHCS may include adding fentanyl test strips as an orderable item in the EHR given that AVAHCS has a local instance of CPRS; however, VASOHCS cannot order fentanyl test strips through the Pharmacy service due to legal restrictions. While Oregon permits fentanyl test strip use, the Cerner instance used by VA is a national program, and therefore the addition of fentanyl test strips as an orderable item in the EHR would carry national implications, including for VA health care systems in states where fentanyl test strip legality is variable. Despite the challenges, efforts to include fentanyl test strips in both SSPs are ongoing.
No significant EHR changes were needed to make the national supply kits available in the Cerner EHR through the VASOHCS Pharmacy service. To have national supply kits available through the AVAHCS Pharmacy service, the EHR would need to be manipulated by adding a local drug file in CPRS. Differences between the EHRs often facilitated the need for adaptation from existing models of SSPs within VA, which were all based in CPRS.
Conclusions
The implementation of SSPs at AVAHCS and VASOHCS enable clinicians to provide quality harm reduction services to PWUD. Despite variations in EHR systems, AVAHCS and VASOHCS implemented SSP within 1 year. Tracking of program engagement via the number of patients interacting with the program and the number of SSP kits distributed will continue. SSP implementation in states where it is permitted may help provide optimal patient care for PWUD.
- Hagan H, McGough JP, Thiede H, Hopkins S, Duchin J, Alexander ER. Reduced injection frequency and increased entry and retention in drug treatment associated with needle-exchange participation in Seattle drug injectors. J Subst Abuse Treat. 2000;19(3):247-252. doi:10.1016/s0740-5472(00)00104-5
- Marx MA, Crape B, Brookmeyer RS, et al. Trends in crime and the introduction of a needle exchange program. Am J Public Health. 2000;90(12):1933-1936. doi:10.2105/ajph.90.12.1933
- Galea S, Ahern J, Fuller C, Freudenberg N, Vlahov D. Needle exchange programs and experience of violence in an inner city neighborhood. J Acquir Immune Defic Syndr. 2001;28(3):282-288. doi:10.1097/00042560-200111010-00014
- Des Jarlais DC, Nugent A, Solberg A, Feelemyer J, Mermin J, Holtzman D. Syringe service programs for persons who inject drugs in urban, suburban, and rural areas — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(48):1337-1341. doi:10.15585/ mmwr.mm6448a3
- Tookes HE, Kral AH, Wenger LD, et al. A comparison of syringe disposal practices among injection drug users in a city with versus a city without needle and syringe programs. Drug Alcohol Depend. 2012;123(1-3):255-259. doi:10.1016/j.drugalcdep.2011.12.001
- Klein SJ, Candelas AR, Cooper JG, et al. Increasing safe syringe collection sites in New York State. Public Health Rep. 2008;123(4):433-440. doi:10.1177/003335490812300404
- de Montigny L, Vernez Moudon A, Leigh B, Kim SY. Assessing a drop box programme: a spatial analysis of discarded needles. Int J Drug Policy. 2010;21(3):208-214. doi:10.1016/j.drugpo.2009.07.003
- Bluthenthal RN, Anderson R, Flynn NM, Kral AH. Higher syringe coverage is associated with lower odds of HIV risk and does not increase unsafe syringe disposal among syringe exchange program clients. Drug Alcohol Depend. 2007;89(2-3):214-222. doi:10.1016/j.drugalcdep.2006.12.035
- Platt L, Minozzi S, Reed J, et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs. Cochrane Database Syst Rev. 2017;9(9):CD012021. doi:10.1002/14651858.CD012021.pub2
- Fernandes RM, Cary M, Duarte G, et al. Effectiveness of needle and syringe programmes in people who inject drugs — an overview of systematic reviews. BMC Public Health. 2017;17(1):309. doi:10.1186/s12889-017-4210-2
- Bernard CL, Owens DK, Goldhaber-Fiebert JD, Brandeau ML. Estimation of the cost-effectiveness of HIV prevention portfolios for people who inject drugs in the United States: a model-based analysis. PLoS Med. 2017;14(5):e1002312. doi:10.1371/journal.pmed.1002312
A syringe services program (SSP) is a harm reduction strategy designed to improve the quality of care provided to people who use drugs (PWUD). SSPs not only provide sterile syringes but establish a connection to medical services and resources for the safe disposal of syringes. By engaging with an SSP, patients may receive naloxone, condoms, fentanyl test strips, opioid use disorder medications, vaccinations, or testing for infectious diseases such as HIV and hepatitis C virus (HCV). Patients may also be connected to housing or social work services.
SSPs do not lead to increased drug use,1 increased improperly disposed supplies needed for drug use in the community, or increased crime.2,3 New users of SSPs are 5 times more likely to enter treatment for drug use than those who do not use SSPs.4-8 Further, SSPs have been found to reduce HIV and HCV transmission and are cost-effective in HIV prevention.9-11
Syringe Services Program
SSPs were implemented at the US Department of Veterans Affairs (VA) Alaska VA Healthcare System (AVAHCS) and VA Southern Oregon Healthcare System (VASOHCS). AVAHCS provides outpatient care across Alaska, with sites in Anchorage, Fairbanks, Homer, Juneau, Wasilla, and Soldotna. VASOHCS provides outpatient care to Southern Oregon and Northern California, with sites in White City, Grants Pass, and Klamath Falls, Oregon. Both are part of Veterans Integrated Service Network 20
Workgroups at AVAHCS and VASOHCS developed SSPs to reduce risks associated with drug use, promote positive outcomes for PWUD, and increase availability of harm reduction resources. During the July 2023 to June 2024 pharmacy residency cycle, an ambulatory care pharmacy resident from the Veterans Integrated Services Network 20 Clinical Resource Hub—a regional resource for clinical services—joined the workgroups. The workgroups established a goal that SSP resources would be made available to enrolled patients without any exclusions, prioritizing health equity.
SSP implementation needed buy-in from AVAHCS and VASOHCS leadership and key stakeholders who could participate in the workgroups. Following AVAHCS and VASOHCS leadership approval, each facility workgroup drafted standard operating procedures (SOPs). Both facilities planned to implement the program using prepackaged kits (sterile syringes, alcohol pads, cotton swabs, a sharps container, and an educational brochure on safe injection practices) supplied by the VA National Harm Reduction Program.
Each SSP offered patients direct links to additional care options at the time of kit distribution, including information regarding medications/supplies (ie, hepatitis A/B vaccines, HIV preexposure prophylaxis, substance use disorder pharmacotherapy, naloxone, and condoms), laboratory tests for infectious and sexually transmitted diseases, and referrals to substance use disorder treatment, social work, suicide prevention, mental health, and primary care.
The goal was to implement both SSPs during the July 2023 to June 2024 residency year. Other goals included tracking the quantity of supplies distributed, the number of patients reached, the impact of clinician education on the distribution of supplies, and comparing the implementation of the SSPs in the electronic health record (EHR) systems.
Alaska VA Healthcare System
An SOP was approved on December 20, 2023, and national supply kits were stocked in collaboration with the logistics department at the Anchorage AVAHCS campus. Social and behavioral health teams, primary care social workers, primary care clinicians, and nursing staff received training on the resources available through the SSP. A local adaptation of a template was created in the Computerized Patient Records System (CPRS) EHR. The template facilitates SSP kit distribution and patient screening for additional resources. Patients can engage with the SSP through any trained staff member. The staff member then completes the template and helps to distribute the SSP kit, in collaboration with the logistics department. The SSP does not operate in a dedicated physical space. The behavioral health team is most actively engaged in the SSP. The goal of SSP is to have resources available anywhere a patient requests services, including primary care and specialty clinics and to empower staff to meet patients’ needs. One patient has utilized the SSP as of June 2025.
Southern Oregon Healthcare System
Kits were ordered and stocked as pharmacy items in preparation for dispensing while awaiting medical center policy approval. Education began with the primary care mental health integration team. After initial education, an interdisciplinary presentation was given to VASOHCS clinicians to increase knowledge of the SSP. To enable documentation of SSP engagement, a local template was developed in the Cerner EHR to be shared among care team members at the facility. Similar to AVAHCS, the SSP does not have a physical space. All trained facility staff may engage in the SSP and distribute SSP kits. The workgroup that implemented this program remains available to support staff. Five patients have accessed the SSP since November 2024 and 7 SSP kits have been distributed as of June 2025.
Discussion
The SSP workgroups sought to expand the program through additional education. A number of factors should be considered when implementing an SSP. Across facilities, program implementation can be time-consuming and the timeline for administrative processes may be long. The workgroups met weekly or monthly depending on the status of the program and the administrative processes. Materials developed included SOP and MCP documents, a 1-page educational handout on SSP offerings, and a PowerPoint presentation for initial clinician education. Involving a pharmacy resident supported professional development and accelerated implementation timelines.
The facilities differed in implementation. AVAHCS collaborated with the logistics department to distribute kits, while VASOHCS worked with the Pharmacy service. A benefit of collaborating with logistics is that patients can receive a kit at the point of contact with the health care system, receiving it directly from the clinic the patient is visiting while eliminating the need to make an additional stop at the pharmacy. Conversely, partnering with the Pharmacy service allowed supply kits to be distributed by mail, enabling patients direct access to kits without having to present in-person. This is particularly valuable considering the large geographical area and remote care services available at VASOHCS.
Implementation varied significantly because AVAHCS operated on CPRS while VASOHCS used Cerner, a newer EHR. AVAHCS adapted a national template produced for CPRS sites, while VASOHCS had to prepare a local template (auto-text) for SSP documentation. Future plans at AVAHCS may include adding fentanyl test strips as an orderable item in the EHR given that AVAHCS has a local instance of CPRS; however, VASOHCS cannot order fentanyl test strips through the Pharmacy service due to legal restrictions. While Oregon permits fentanyl test strip use, the Cerner instance used by VA is a national program, and therefore the addition of fentanyl test strips as an orderable item in the EHR would carry national implications, including for VA health care systems in states where fentanyl test strip legality is variable. Despite the challenges, efforts to include fentanyl test strips in both SSPs are ongoing.
No significant EHR changes were needed to make the national supply kits available in the Cerner EHR through the VASOHCS Pharmacy service. To have national supply kits available through the AVAHCS Pharmacy service, the EHR would need to be manipulated by adding a local drug file in CPRS. Differences between the EHRs often facilitated the need for adaptation from existing models of SSPs within VA, which were all based in CPRS.
Conclusions
The implementation of SSPs at AVAHCS and VASOHCS enable clinicians to provide quality harm reduction services to PWUD. Despite variations in EHR systems, AVAHCS and VASOHCS implemented SSP within 1 year. Tracking of program engagement via the number of patients interacting with the program and the number of SSP kits distributed will continue. SSP implementation in states where it is permitted may help provide optimal patient care for PWUD.
A syringe services program (SSP) is a harm reduction strategy designed to improve the quality of care provided to people who use drugs (PWUD). SSPs not only provide sterile syringes but establish a connection to medical services and resources for the safe disposal of syringes. By engaging with an SSP, patients may receive naloxone, condoms, fentanyl test strips, opioid use disorder medications, vaccinations, or testing for infectious diseases such as HIV and hepatitis C virus (HCV). Patients may also be connected to housing or social work services.
SSPs do not lead to increased drug use,1 increased improperly disposed supplies needed for drug use in the community, or increased crime.2,3 New users of SSPs are 5 times more likely to enter treatment for drug use than those who do not use SSPs.4-8 Further, SSPs have been found to reduce HIV and HCV transmission and are cost-effective in HIV prevention.9-11
Syringe Services Program
SSPs were implemented at the US Department of Veterans Affairs (VA) Alaska VA Healthcare System (AVAHCS) and VA Southern Oregon Healthcare System (VASOHCS). AVAHCS provides outpatient care across Alaska, with sites in Anchorage, Fairbanks, Homer, Juneau, Wasilla, and Soldotna. VASOHCS provides outpatient care to Southern Oregon and Northern California, with sites in White City, Grants Pass, and Klamath Falls, Oregon. Both are part of Veterans Integrated Service Network 20
Workgroups at AVAHCS and VASOHCS developed SSPs to reduce risks associated with drug use, promote positive outcomes for PWUD, and increase availability of harm reduction resources. During the July 2023 to June 2024 pharmacy residency cycle, an ambulatory care pharmacy resident from the Veterans Integrated Services Network 20 Clinical Resource Hub—a regional resource for clinical services—joined the workgroups. The workgroups established a goal that SSP resources would be made available to enrolled patients without any exclusions, prioritizing health equity.
SSP implementation needed buy-in from AVAHCS and VASOHCS leadership and key stakeholders who could participate in the workgroups. Following AVAHCS and VASOHCS leadership approval, each facility workgroup drafted standard operating procedures (SOPs). Both facilities planned to implement the program using prepackaged kits (sterile syringes, alcohol pads, cotton swabs, a sharps container, and an educational brochure on safe injection practices) supplied by the VA National Harm Reduction Program.
Each SSP offered patients direct links to additional care options at the time of kit distribution, including information regarding medications/supplies (ie, hepatitis A/B vaccines, HIV preexposure prophylaxis, substance use disorder pharmacotherapy, naloxone, and condoms), laboratory tests for infectious and sexually transmitted diseases, and referrals to substance use disorder treatment, social work, suicide prevention, mental health, and primary care.
The goal was to implement both SSPs during the July 2023 to June 2024 residency year. Other goals included tracking the quantity of supplies distributed, the number of patients reached, the impact of clinician education on the distribution of supplies, and comparing the implementation of the SSPs in the electronic health record (EHR) systems.
Alaska VA Healthcare System
An SOP was approved on December 20, 2023, and national supply kits were stocked in collaboration with the logistics department at the Anchorage AVAHCS campus. Social and behavioral health teams, primary care social workers, primary care clinicians, and nursing staff received training on the resources available through the SSP. A local adaptation of a template was created in the Computerized Patient Records System (CPRS) EHR. The template facilitates SSP kit distribution and patient screening for additional resources. Patients can engage with the SSP through any trained staff member. The staff member then completes the template and helps to distribute the SSP kit, in collaboration with the logistics department. The SSP does not operate in a dedicated physical space. The behavioral health team is most actively engaged in the SSP. The goal of SSP is to have resources available anywhere a patient requests services, including primary care and specialty clinics and to empower staff to meet patients’ needs. One patient has utilized the SSP as of June 2025.
Southern Oregon Healthcare System
Kits were ordered and stocked as pharmacy items in preparation for dispensing while awaiting medical center policy approval. Education began with the primary care mental health integration team. After initial education, an interdisciplinary presentation was given to VASOHCS clinicians to increase knowledge of the SSP. To enable documentation of SSP engagement, a local template was developed in the Cerner EHR to be shared among care team members at the facility. Similar to AVAHCS, the SSP does not have a physical space. All trained facility staff may engage in the SSP and distribute SSP kits. The workgroup that implemented this program remains available to support staff. Five patients have accessed the SSP since November 2024 and 7 SSP kits have been distributed as of June 2025.
Discussion
The SSP workgroups sought to expand the program through additional education. A number of factors should be considered when implementing an SSP. Across facilities, program implementation can be time-consuming and the timeline for administrative processes may be long. The workgroups met weekly or monthly depending on the status of the program and the administrative processes. Materials developed included SOP and MCP documents, a 1-page educational handout on SSP offerings, and a PowerPoint presentation for initial clinician education. Involving a pharmacy resident supported professional development and accelerated implementation timelines.
The facilities differed in implementation. AVAHCS collaborated with the logistics department to distribute kits, while VASOHCS worked with the Pharmacy service. A benefit of collaborating with logistics is that patients can receive a kit at the point of contact with the health care system, receiving it directly from the clinic the patient is visiting while eliminating the need to make an additional stop at the pharmacy. Conversely, partnering with the Pharmacy service allowed supply kits to be distributed by mail, enabling patients direct access to kits without having to present in-person. This is particularly valuable considering the large geographical area and remote care services available at VASOHCS.
Implementation varied significantly because AVAHCS operated on CPRS while VASOHCS used Cerner, a newer EHR. AVAHCS adapted a national template produced for CPRS sites, while VASOHCS had to prepare a local template (auto-text) for SSP documentation. Future plans at AVAHCS may include adding fentanyl test strips as an orderable item in the EHR given that AVAHCS has a local instance of CPRS; however, VASOHCS cannot order fentanyl test strips through the Pharmacy service due to legal restrictions. While Oregon permits fentanyl test strip use, the Cerner instance used by VA is a national program, and therefore the addition of fentanyl test strips as an orderable item in the EHR would carry national implications, including for VA health care systems in states where fentanyl test strip legality is variable. Despite the challenges, efforts to include fentanyl test strips in both SSPs are ongoing.
No significant EHR changes were needed to make the national supply kits available in the Cerner EHR through the VASOHCS Pharmacy service. To have national supply kits available through the AVAHCS Pharmacy service, the EHR would need to be manipulated by adding a local drug file in CPRS. Differences between the EHRs often facilitated the need for adaptation from existing models of SSPs within VA, which were all based in CPRS.
Conclusions
The implementation of SSPs at AVAHCS and VASOHCS enable clinicians to provide quality harm reduction services to PWUD. Despite variations in EHR systems, AVAHCS and VASOHCS implemented SSP within 1 year. Tracking of program engagement via the number of patients interacting with the program and the number of SSP kits distributed will continue. SSP implementation in states where it is permitted may help provide optimal patient care for PWUD.
- Hagan H, McGough JP, Thiede H, Hopkins S, Duchin J, Alexander ER. Reduced injection frequency and increased entry and retention in drug treatment associated with needle-exchange participation in Seattle drug injectors. J Subst Abuse Treat. 2000;19(3):247-252. doi:10.1016/s0740-5472(00)00104-5
- Marx MA, Crape B, Brookmeyer RS, et al. Trends in crime and the introduction of a needle exchange program. Am J Public Health. 2000;90(12):1933-1936. doi:10.2105/ajph.90.12.1933
- Galea S, Ahern J, Fuller C, Freudenberg N, Vlahov D. Needle exchange programs and experience of violence in an inner city neighborhood. J Acquir Immune Defic Syndr. 2001;28(3):282-288. doi:10.1097/00042560-200111010-00014
- Des Jarlais DC, Nugent A, Solberg A, Feelemyer J, Mermin J, Holtzman D. Syringe service programs for persons who inject drugs in urban, suburban, and rural areas — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(48):1337-1341. doi:10.15585/ mmwr.mm6448a3
- Tookes HE, Kral AH, Wenger LD, et al. A comparison of syringe disposal practices among injection drug users in a city with versus a city without needle and syringe programs. Drug Alcohol Depend. 2012;123(1-3):255-259. doi:10.1016/j.drugalcdep.2011.12.001
- Klein SJ, Candelas AR, Cooper JG, et al. Increasing safe syringe collection sites in New York State. Public Health Rep. 2008;123(4):433-440. doi:10.1177/003335490812300404
- de Montigny L, Vernez Moudon A, Leigh B, Kim SY. Assessing a drop box programme: a spatial analysis of discarded needles. Int J Drug Policy. 2010;21(3):208-214. doi:10.1016/j.drugpo.2009.07.003
- Bluthenthal RN, Anderson R, Flynn NM, Kral AH. Higher syringe coverage is associated with lower odds of HIV risk and does not increase unsafe syringe disposal among syringe exchange program clients. Drug Alcohol Depend. 2007;89(2-3):214-222. doi:10.1016/j.drugalcdep.2006.12.035
- Platt L, Minozzi S, Reed J, et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs. Cochrane Database Syst Rev. 2017;9(9):CD012021. doi:10.1002/14651858.CD012021.pub2
- Fernandes RM, Cary M, Duarte G, et al. Effectiveness of needle and syringe programmes in people who inject drugs — an overview of systematic reviews. BMC Public Health. 2017;17(1):309. doi:10.1186/s12889-017-4210-2
- Bernard CL, Owens DK, Goldhaber-Fiebert JD, Brandeau ML. Estimation of the cost-effectiveness of HIV prevention portfolios for people who inject drugs in the United States: a model-based analysis. PLoS Med. 2017;14(5):e1002312. doi:10.1371/journal.pmed.1002312
- Hagan H, McGough JP, Thiede H, Hopkins S, Duchin J, Alexander ER. Reduced injection frequency and increased entry and retention in drug treatment associated with needle-exchange participation in Seattle drug injectors. J Subst Abuse Treat. 2000;19(3):247-252. doi:10.1016/s0740-5472(00)00104-5
- Marx MA, Crape B, Brookmeyer RS, et al. Trends in crime and the introduction of a needle exchange program. Am J Public Health. 2000;90(12):1933-1936. doi:10.2105/ajph.90.12.1933
- Galea S, Ahern J, Fuller C, Freudenberg N, Vlahov D. Needle exchange programs and experience of violence in an inner city neighborhood. J Acquir Immune Defic Syndr. 2001;28(3):282-288. doi:10.1097/00042560-200111010-00014
- Des Jarlais DC, Nugent A, Solberg A, Feelemyer J, Mermin J, Holtzman D. Syringe service programs for persons who inject drugs in urban, suburban, and rural areas — United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(48):1337-1341. doi:10.15585/ mmwr.mm6448a3
- Tookes HE, Kral AH, Wenger LD, et al. A comparison of syringe disposal practices among injection drug users in a city with versus a city without needle and syringe programs. Drug Alcohol Depend. 2012;123(1-3):255-259. doi:10.1016/j.drugalcdep.2011.12.001
- Klein SJ, Candelas AR, Cooper JG, et al. Increasing safe syringe collection sites in New York State. Public Health Rep. 2008;123(4):433-440. doi:10.1177/003335490812300404
- de Montigny L, Vernez Moudon A, Leigh B, Kim SY. Assessing a drop box programme: a spatial analysis of discarded needles. Int J Drug Policy. 2010;21(3):208-214. doi:10.1016/j.drugpo.2009.07.003
- Bluthenthal RN, Anderson R, Flynn NM, Kral AH. Higher syringe coverage is associated with lower odds of HIV risk and does not increase unsafe syringe disposal among syringe exchange program clients. Drug Alcohol Depend. 2007;89(2-3):214-222. doi:10.1016/j.drugalcdep.2006.12.035
- Platt L, Minozzi S, Reed J, et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs. Cochrane Database Syst Rev. 2017;9(9):CD012021. doi:10.1002/14651858.CD012021.pub2
- Fernandes RM, Cary M, Duarte G, et al. Effectiveness of needle and syringe programmes in people who inject drugs — an overview of systematic reviews. BMC Public Health. 2017;17(1):309. doi:10.1186/s12889-017-4210-2
- Bernard CL, Owens DK, Goldhaber-Fiebert JD, Brandeau ML. Estimation of the cost-effectiveness of HIV prevention portfolios for people who inject drugs in the United States: a model-based analysis. PLoS Med. 2017;14(5):e1002312. doi:10.1371/journal.pmed.1002312
Implementation of Harm Reduction Syringe Services Programs at 2 Veterans Affairs Medical Centers
Implementation of Harm Reduction Syringe Services Programs at 2 Veterans Affairs Medical Centers
VA Cancer Clinical Trials as a Strategy for Increasing Accrual of Racial and Ethnic Underrepresented Groups
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Background
Cancer clinical trials (CCTs) are central to improving cancer care. However, generalizability of findings from CCTs is difficult due to the lack of diversity in most United States CCTs. Clinical trial accrual of underrepresented groups, is low throughout the United States and is approximately 4-5% in most CCTs. Reasons for low accrual in this population are multifactorial. Despite numerous factors related to accruing racial and ethnic underrepresented groups, many institutions have sought to address these barriers. We conducted a scoping review to identify evidence-based approaches to increase participation in cancer treatment clinical trials.
Methods
We reviewed the Salisbury VA Medical Center Oncology clinical trial database from October 2019 to June 2024. The participants in these clinical trials required consent. These clinical trials included treatment interventional as well as non-treatment interventional. Fifteen studies were included and over 260 Veterans participated.
Results
Key themes emerged that included a focus on patient education, cultural competency, and building capacity in the clinics to care for the Veteran population at three separate sites in the Salisbury VA system. The Black Veteran accrual rate of 29% was achieved. This accrual rate is representative of our VA catchment population of 33% for Black Veterans, and is five times the national average.
Conclusions
The research team’s success in enrolling Black Veterans in clinical trials is attributed to several factors. The demographic composition of Veterans served by the Salisbury, Charlotte, and Kernersville VA provided a diverse population that included a 33% Black group. The type of clinical trials focused on patients who were most impacted by the disease. The VA did afford less barriers to access to health care.
Improving Colorectal Cancer Screening via Mailed Fecal Immunochemical Testing in a Veterans Affairs Health System
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
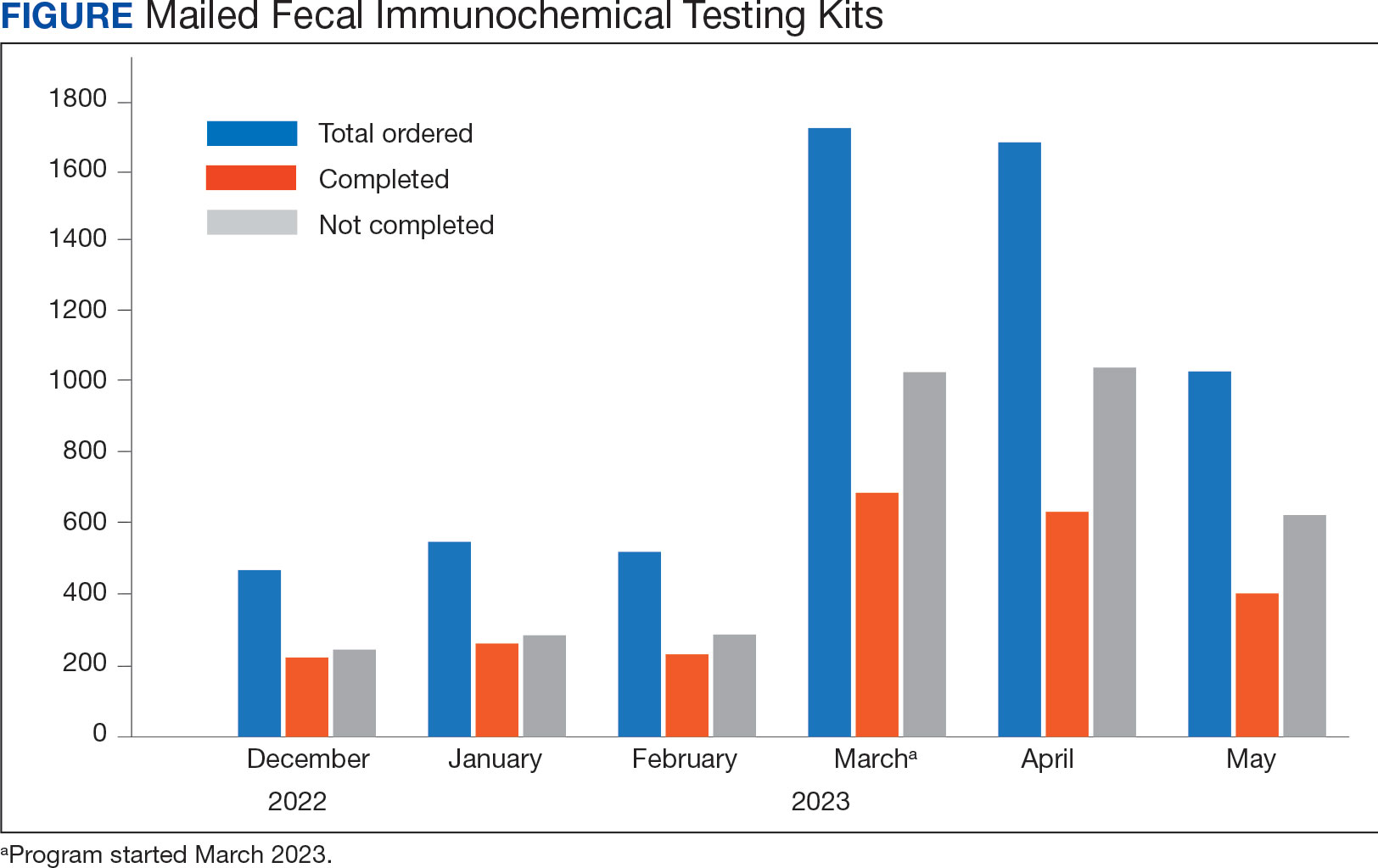
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
Colorectal cancer (CRC) is among the most common cancers and causes of cancer-related deaths in the United States.1 Reflective of a nationwide trend, CRC screening rates at the Veterans Affairs Connecticut Healthcare System (VACHS) decreased during the COVID-19 pandemic.2-5 Contributing factors to this decrease included cancellations of elective colonoscopies during the initial phase of the pandemic and concurrent turnover of endoscopists. In 2021, the US Preventive Services Task Force lowered the recommended initial CRC screening age from 50 years to 45 years, further increasing the backlog of unscreened patients.6
Fecal immunochemical testing (FIT) is a noninvasive screening method in which antibodies are used to detect hemoglobin in the stool. The sensitivity and specificity of 1-time FIT are 79% to 80% and 94%, respectively, for the detection of CRC, with sensitivity improving with successive testing.7,8 Annual FIT is recognized as a tier 1 preferred screening method by the US Multi-Society Task Force on Colorectal Cancer.7,9 Programs that mail FIT kits to eligible patients outside of physician visits have been successfully implemented in health care systems.10,11
The VACHS designed and implemented a mailed FIT program using existing infrastructure and staffing.
Program Description
A team of local stakeholders comprised of VACHS leadership, primary care, nursing, and gastroenterology staff, as well as representatives from laboratory, informatics, mail services, and group practice management, was established to execute the project. The team met monthly to plan the project.
The team developed a dataset consisting of patients aged 45 to 75 years who were at average risk for CRC and due for CRC screening. Patients were defined as due for CRC screening if they had not had a colonoscopy in the previous 9 years or a FIT or fecal occult blood test in the previous 11 months. Average risk for CRC was defined by excluding patients with associated diagnosis codes for CRC, colectomy, inflammatory bowel disease, and anemia. The program also excluded patients with diagnosis codes associated with dementia, deferring discussions about cancer screening to their primary care practitioners (PCPs). Patients with invalid mailing addresses were also excluded, as well as those whose PCPs had indicated in the electronic health record that the patient received CRC screening outside the US Department of Veterans Affairs (VA) system.
Letter Templates
Two patient letter electronic health record templates were developed. The first was a primer letter, which was mailed to patients 2 to 3 weeks before the mailed FIT kit as an introduction to the program.12 The purpose of the primer letter was to give advance notice to patients that they could expect a FIT kit to arrive in the mail. The goal was to prepare patients to complete FIT when the kit arrived and prompt them to call the VA to opt out of the mailed FIT program if they were up to date with CRC screening or if they had a condition which made them at high risk for CRC.
The second FIT letter arrived with the FIT kit, introduced FIT and described the importance of CRC screening. The letter detailed instructions for completing FIT and automatically created a FIT order. It also included a list of common conditions that may exclude patients, with a recommendation for patients to contact their medical team if they felt they were not candidates for FIT.
Staff Education
A previous VACHS pilot project demonstrated the success of a mailed FIT program to increase FIT use. Implemented as part of the pilot program, staff education consisted of a session for clinicians about the role of FIT in CRC screening and an all-staff education session. An additional education session about CRC and FIT for all staff was repeated with the program launch.
Program Launch
The mailed FIT program was introduced during a VACHS primary care all-staff meeting. After the meeting, each patient aligned care team (PACT) received an encrypted email that included a list of the patients on their team who were candidates for the program, a patient-facing FIT instruction sheet, detailed instructions on how to send the FIT primer letter, and a FIT package consisting of the labeled FIT kit, FIT letter, and patient instruction sheet. A reminder letter was sent to each patient 3 weeks after the FIT package was mailed. The patient lists were populated into a shared, encrypted Microsoft Teams folder that was edited in real time by PACT teams and viewed by VACHS leadership to track progress.
Program Metrics
At program launch, the VACHS had 4642 patients due for CRC screening who were eligible for the mailed FIT program. On March 7, 2023, the data consisting of FIT tests ordered between December 2022 and May 2023—3 months before and after the launch of the program—were reviewed and categorized. In the 3 months before program launch, 1528 FIT were ordered and 714 were returned (46.7%). In the 3 months after the launch of the program, 4383 FIT were ordered and 1712 were returned (39.1%) (Figure). Test orders increased 287% from the preintervention to the postintervention period. The mean (SD) number of monthly FIT tests prelaunch was 509 (32.7), which increased to 1461 (331.6) postlaunch.
At the VACHS, 61.4% of patients aged 45 to 75 years were up to date with CRC screening before the program launch. In the 3 months after program launch, the rate increased to 63.8% among patients aged 45 to 75 years, the highest rate in our Veterans Integrated Services Network and exceeding the VA national average CRC screening rate, according to unpublished VA Monthly Management Report data.
In the 3 months following the program launch, 139 FIT kits tested positive for potential CRC. Of these, 79 (56.8%) patients had completed a diagnostic colonoscopy. PACT PCPs and nurses received reports on patients with positive FIT tests and those with no colonoscopy scheduled or completed and were asked to follow up.
Discussion
Through a proactive, population-based CRC screening program centered on mailed FIT kits outside of the traditional patient visit, the VACHS increased the use of FIT and rates of CRC screening. The numbers of FIT kits ordered and completed substantially increased in the 3 months after program launch.
Compared to mailed FIT programs described in the literature that rely on centralized processes in that a separate team operates the mailed FIT program for the entire organization, this program used existing PACT infrastructure and staff.10,11 This strategy allowed VACHS to design and implement the program in several months. Not needing to hire new staff or create a central team for the sole purpose of implementing the program allowed us to save on any organizational funding and efforts that would have accompanied the additional staff. The program described in this article may be more attainable for primary care practices or smaller health systems that do not have the capacity for the creation of a centralized process.
Limitations
Although the total number of FIT completions substantially increased during the program, the rate of FIT completion during the mailed FIT program was lower than the rate of completion prior to program launch. This decreased rate of FIT kit completion may be related to separation from a patient visit and potential loss of real-time education with a clinician. The program’s decentralized design increased the existing workload for primary care staff, and as a result, consideration must be given to local staffing levels. Additionally, the report of eligible patients depended on diagnosis codes and may have captured patients with higher-than-average risk of CRC, such as patients with prior history of adenomatous polyps, family history of CRC, or other medical or genetic conditions. We attempted to mitigate this by including a list of conditions that would exclude patients from FIT eligibility in the FIT letter and giving them the option to opt out.
Conclusions
CRC screening rates improved following implementation of a primary care team-centered quality improvement process to proactively identify patients appropriate for FIT and mail them FIT kits. This project highlights that population-health interventions around CRC screening via use of FIT can be successful within a primary care patient-centered medical home model, considering the increases in both CRC screening rates and increase in FIT tests ordered.
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
1. American Cancer Society. Key statistics for colorectal cancer. Revised January 29, 2024. Accessed June 11, 2024. https://www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
2. Chen RC, Haynes K, Du S, Barron J, Katz AJ. Association of cancer screening deficit in the United States with the COVID-19 pandemic. JAMA Oncol. 2021;7(6):878-884. doi:10.1001/jamaoncol.2021.0884
3. Mazidimoradi A, Tiznobaik A, Salehiniya H. Impact of the COVID-19 pandemic on colorectal cancer screening: a systematic review. J Gastrointest Cancer. 2022;53(3):730-744. doi:10.1007/s12029-021-00679-x
4. Adams MA, Kurlander JE, Gao Y, Yankey N, Saini SD. Impact of coronavirus disease 2019 on screening colonoscopy utilization in a large integrated health system. Gastroenterology. 2022;162(7):2098-2100.e2. doi:10.1053/j.gastro.2022.02.034
5. Sundaram S, Olson S, Sharma P, Rajendra S. A review of the impact of the COVID-19 pandemic on colorectal cancer screening: implications and solutions. Pathogens. 2021;10(11):558. doi:10.3390/pathogens10111508
6. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(19):1965-1977. doi:10.1001/jama.2021.6238
7. Robertson DJ, Lee JK, Boland CR, et al. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: a consensus statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc. 2017;85(1):2-21.e3. doi:10.1016/j.gie.2016.09.025
8. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immunochemical tests for colorectal cancer: systematic review and meta-analysis. Ann Intern Med. 2014;160(3):171. doi:10.7326/M13-1484
9. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307-323. doi:10.1053/j.gastro.2017.05.013
10. Deeds SA, Moore CB, Gunnink EJ, et al. Implementation of a mailed faecal immunochemical test programme for colorectal cancer screening among veterans. BMJ Open Qual. 2022;11(4):e001927. doi:10.1136/bmjoq-2022-001927
11. Selby K, Jensen CD, Levin TR, et al. Program components and results from an organized colorectal cancer screening program using annual fecal immunochemical testing. Clin Gastroenterol Hepatol. 2022;20(1):145-152. doi:10.1016/j.cgh.2020.09.042
12. Deeds S, Liu T, Schuttner L, et al. A postcard primer prior to mailed fecal immunochemical test among veterans: a randomized controlled trial. J Gen Intern Med. 2023:38(14):3235-3241. doi:10.1007/s11606-023-08248-7
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
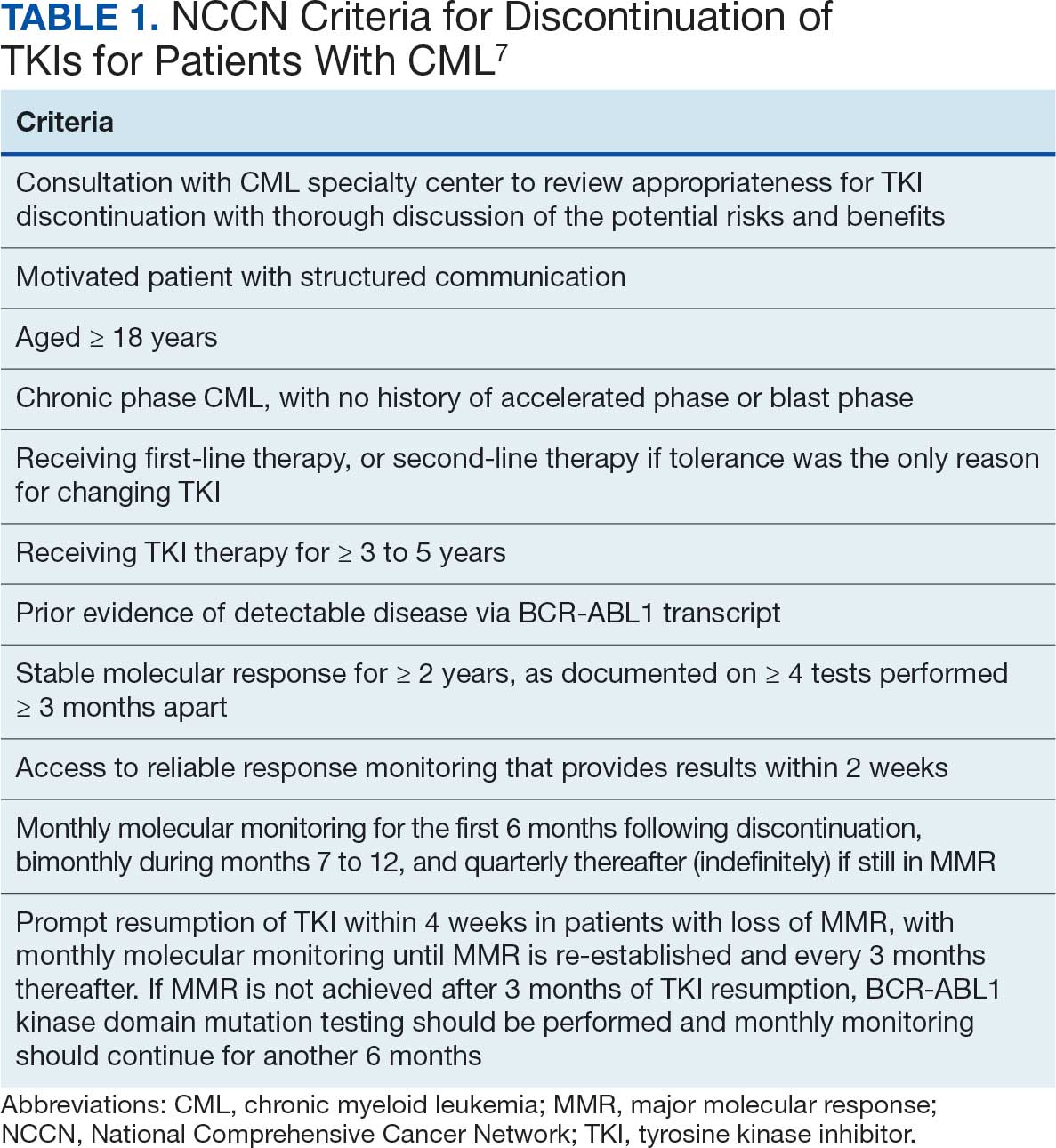
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
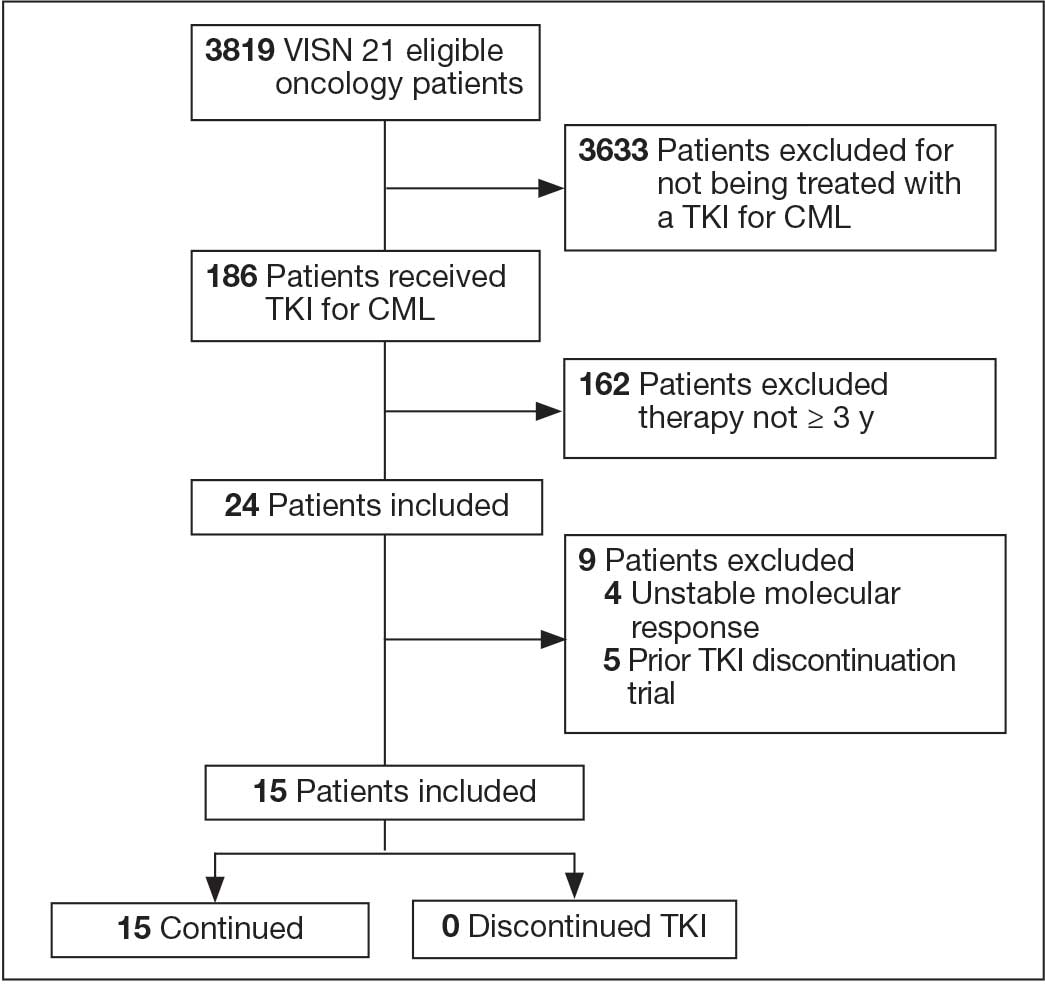
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
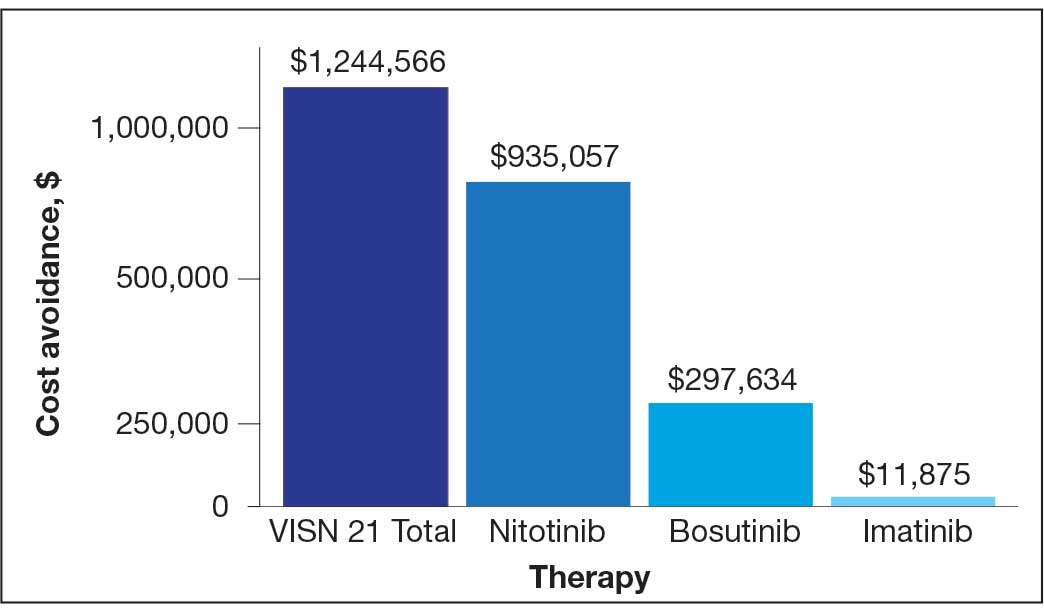
for 15 patients at Veterans Integrated Services Network 21.
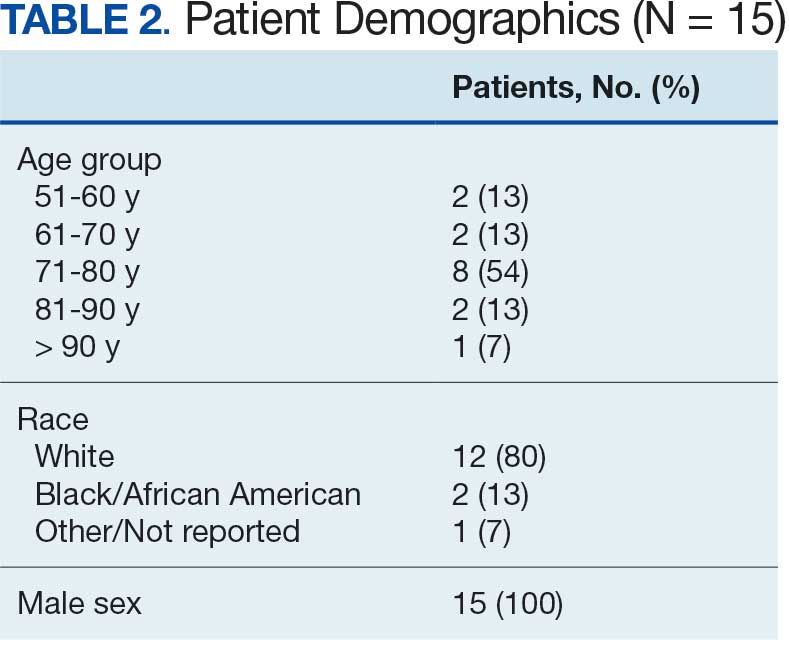
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
Chronic myeloid leukemia (CML) is a hematologic malignancy resulting from an acquired mutation. The mutation results in a reciprocal translocation between the long arms of chromosomes 9 and 22 and is known as the Philadelphia chromosome (Ph), or Ph-positive (Ph+) when present. The translocation results in the formation of a BCR-ABL fusion oncogene, which leads to continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.1,2
Until the 1980s, CML was considered fatal.3 The mainstay of treatment consisted of 2 oral chemotherapeutic agents, busulfan and hydroxyurea. These medications did not prevent blast crisis, a fatal form of leukemia.4,5 The introduction of tyrosine kinase inhibitors (TKIs) transformed CML management and improved 10-year overall survival from about 20% to > 80% by delaying the transition to blast crisis. Now, the risk of death from general health conditions or comorbidities is higher than that of CML.6
TKIs target the root cause of CML through inhibition of the BCR-ABL oncoprotein.1,2 For CML, the goals of treatment include maintaining hematologic, cytogenetic, and molecular remission; preventing progression to accelerated phase or blast crisis; minimizing toxicity; and enabling potential cessation of therapy in carefully selected patients.7,8
Small cohort studies suggest that dose reduction of TKIs in patients who achieve optimal responses may reduce the risk of long-term adverse effects (AEs). However, optimal dose-reduction and minimum effective dose of each agent are unknown.7 The ability to maintain undetectable minimal residual disease or disease detectable at a stable low level after TKI discontinuation has been called treatment-free remission. Studies suggest that about 40% to 50% of patients who have achieved a stable deep molecular response remain in treatment-free remission after stopping first-line treatment.9,10 Of the patients who relapse following TKI discontinuation, 80% relapse within the first 6 months of treatment cessation. Molecular response is regained in almost all patients when treatment is resumed with the same TKI.11
The National Comprehensive Cancer Network (NCCN) recommends considering discontinuation of TKI therapy only outside the setting of a clinical trial and only in patients who consent to discontinuation after a thorough discussion of the potential risks and benefits. The NCCN criteria for patients who may be eligible for discontinuation are listed in Table 1. The Life After Stopping TKIs study reported that 80% of patients with well-controlled chronic phase CML who discontinued TKIs had a clinically meaningful improvement in fatigue. Patients also reported clinically meaningful improvements in depression, diarrhea, sleep disturbance, and pain interference. These symptoms worsened after restarting TKI therapy.12
TKI DISCONTINUATION
Electronic health record data were extracted using structured query language from the US Department of Veterans Affairs (VA) Corporate Data Warehouse (CDW). To be eligible for discontinuation, veterans had to be aged > 18 years, receive oncology care within a Veterans Integrated Services Network (VISN) 21 health care system (HCS) (VA Sierra Nevada HCS, VA Southern Nevada HCS, VA Central California HCS, VA Palo Alto HCS, VA Northern California HCS, and VA San Francisco HCS) or be a veteran referred to a community-based oncology practitioner. Patients had to have a documented diagnosis of chronic phase CML, have an active order for a TKI, be on TKI therapy for ≥ 3 years, and have a stable molecular response (BCR-ABL1 ≤ 0.01% on the International Scale for ≥ 2 years with ≥ 4 tests done ≥ 3 months apart) as of October 1, 2024. Veterans were excluded if they had a history of advanced accelerated phase CML, previous TKI discontinuation trials, nonadherence to the TKI, or if they did not want to consider TKI discontinuation.
This analysis evaluated the potential cost avoidance associated with TKI discontinuation. Cost avoidance was calculated using the average wholesale price of each TKI. Secondary objectives evaluated health outcomes of TKI discontinuation including CML relapse, reported AEs, long-term remission, and TKI withdrawal syndrome. Health outcomes were determined through chart review of AEs and clinic notes documented in the electronic health record during the study time frame.
Baseline information for eligible patients was collected, including age, sex, and race, and chart reviews were completed to evaluate reported AEs associated with therapy. Oncology clinical pharmacy practitioners (CPPs) at each VISN 21 facility were notified of eligible patients to facilitate discussion with oncologists and establish monitoring if therapy was discontinued. Following TKI discontinuation, health outcomes were evaluated, including CML relapse, changes in reported AEs, long-term remission, and TKI withdrawal syndrome. Descriptive statistics were used to analyze the baseline characteristics. Cost avoidance was calculated using the average wholesale price for each TKI. The number of tablets required to reach each patient’s individual dose was taken into consideration when determining the cost avoidance. A dashboard was created using the query from the CDW and was developed in Microsoft Power BI.
Preliminary Results
In FY 2024, VISN 21 had 3819 oncology patients. Twenty-four patients had taken a TKI for ≥ 3 years, 20 had a stable molecular response, and 15 had not previously attempted to discontinue their TKI (Figure 1). Fifteen veterans were eligible for therapy discontinuation for a total potential annual cost avoidance of $1.2 million (Figure 2). Most of the cost avoidance, $935,057 (78%), was attributed to 3 patients on nilotinib. The mean age of the population was 74 years. All patients were male, and 12 (80%) were White. (Table 2). At baseline, 11 patients (73%) were taking imatinib. One patient received oncology care from a community care clinician. All 15 patients decided to remain on therapy.
Abbreviations: CML, chronic myeloid leukemia; TKI, tyrosine kinase inhibitor;
VISN, Veterans Integrated Service Network.
for 15 patients at Veterans Integrated Services Network 21.
DISCUSSION
As a multisite quality improvement initiative, this project raised awareness of TKI therapy discontinuation in select patients with CML. It also sparked collaboration among oncology CPPs and clinicians and stimulated conversations about CML treatment. The development of the TKI discontinuation dashboard provides a population health management tool for CPPs and clinicians to identify eligible patients in the future.
Adherence to TKIs is crucial for disease control and survival in patients with CML. Patients are counseled that poor adherence to therapy may contribute to worsening disease or suboptimal response, the development of resistance, and greater health care costs.13 Therefore, it was a challenge for patients to understand and accept that they could stop TKI therapy after achieving a stable deep molecular response. Discussions with patients about the goal of therapy—suppressing the BCR-ABL oncogene, which they have achieved—could encourage patients to trial therapy discontinuation.
Only small cohort studies have been completed to evaluate the outcomes of therapy discontinuation. Much remains unknown regarding the optimal dose-reduction strategy and the minimum effective dose of each agent. Additionally, understanding the qualities of a good candidate for TKI discontinuation remains a barrier. A similar project was conducted in VISN 17. Five patients were counseled on TKI discontinuation; however, only 1 discontinued TKI therapy. Unfortunately, soon after discontinuing treatment, the patient had to restart therapy. Additional literature will enhance understanding of therapy discontinuation.
An unexpected finding of TKI discontinuation trials has been a reversible phenomenon known as TKI withdrawal syndrome.9 It can occur regardless of the TKI used and results in pruritus and new or worsening musculoskeletal pain within several weeks of TKI discontinuation in about 30% of patients. Symptoms may last several months and may require acetaminophen or nonsteroidal anti-inflammatory drugs for pain control.9,10,14
The potential cost avoidance of $1.2 million is an underestimation because VA contracts allow for greater cost savings. However, that information is confidential and therefore average wholesale price had to be used for this project. Most of the cost avoidance was due to 4 patients who could not tolerate imatinib and used nilotinib, which is more expensive.
Limitations
The small sample size presented some limitations. Of the 3819 oncology patients within VISN 21 in FY 2024, 186 received a TKI and only 15 were eligible for discontinuation. Additionally, challenges emerged when discussing discontinuation with community care clinicians and patients. Community care clinicians were difficult to contact, making it challenging to discuss the project with them. CPPs noted hesitancy among VA clinicians and patients to discontinue a medication for which adherence was continually emphasized.
Conclusions
Discussions about CML TKI discontinuation led to collaboration with the oncology care team and could lead to significant cost avoidance. Barriers to TKI discontinuation included patients’ concern for relapse, risk of discontinuation syndrome, the requirement for close monitoring, and clinician buy-in. Outcome studies are needed to gain a greater understanding of the benefits and risks of therapy discontinuation. In the future, evaluation of possible clinical and biological predictors of successful TKI discontinuation may be beneficial.
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
- Schiffer CA. BCR-ABL tyrosine kinase inhibitors for chronic myelogenous leukemia. N Engl J Med. 2007;357:258-265. doi:10.1056/NEJMct071828
- Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet. Chronic myeloid leukaemia. Lancet. 2007;370:342-350. doi:10.1016/S0140-6736(07)61165-9
- Goldman JM, Melo JV. Chronic myeloid leukemia--advances in biology and new approaches to treatment. N Engl J Med. 2003;349:1451-1464. doi:10.1056/NEJMra020777
- Pasic I, Lipton JH. Current approach to the treatment of chronic myeloid leukaemia. Leuk Res. 2017;55:65-78. doi:10.1016/j.leukres.2017.01.005
- Rao KV, Iannucci A, Jabbour E. Current and future clinical strategies in the management of chronic myeloid leukemia. Pharmacotherapy. 2010;30:77S-101S. doi:10.1592/phco.30.pt2.77S
- Cortes J, Pavlovsky C, Saußele S. Chronic myeloid leukaemia. Lancet. 2021;398:1914-1926. doi:10.1016/S0140-6736(21)01204-6
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Chronic myeloid leukemia. Version 1.2026. July 16, 2025. Accessed February 8, 2026. https://www.nccn.org /guidelines/guidelines-detail?id=1427
- Hochhaus A, Baccarani M, Silver RT, et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia. 2020;34:966-984. doi:10.1038/s41375-020-0776-2
- Saußele S, Richter J, Hochhaus A, Mahon F-X. The concept of treatment-free remission in chronic myeloid leukemia. Leukemia. 2016;30:1638-1647. doi:10.1038/leu.2016.115
- Atallah E, Sweet K. Treatment-free remission: the new goal in CML therapy. Curr Hematol Malig Rep. 2021;16:433-439. doi:10.1007/s11899-021-00653-1
- Hehlmann R. The new ELN recommendations for treating CML. J Clin Med. 2020;9:3671. doi:10.3390/jcm9113671
- Atallah E, Schiffer CA, Radich JP , et al. Assessment of outcomes after stopping tyrosine kinase inhibitors among patients with chronic myeloid leukemia: a non-randomized clinical trial. JAMA Oncol. 2021;7:42-50. doi:10.1001/jamaoncol.2020.5774
- Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: what have we learned so far? Cancer Lett. 2011;300:115-121. doi:10.1016/j.canlet.2010.10.018
- Berman E. How I treat chronic-phase chronic myelogenous leukemia. Blood. 2022;139:3138-3147. doi:10.1182/blood.2021011722
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Potential Tyrosine Kinase Inhibitor Therapy Discontinuation for Patients With Chronic Myeloid Leukemia in a VA Regional Network
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
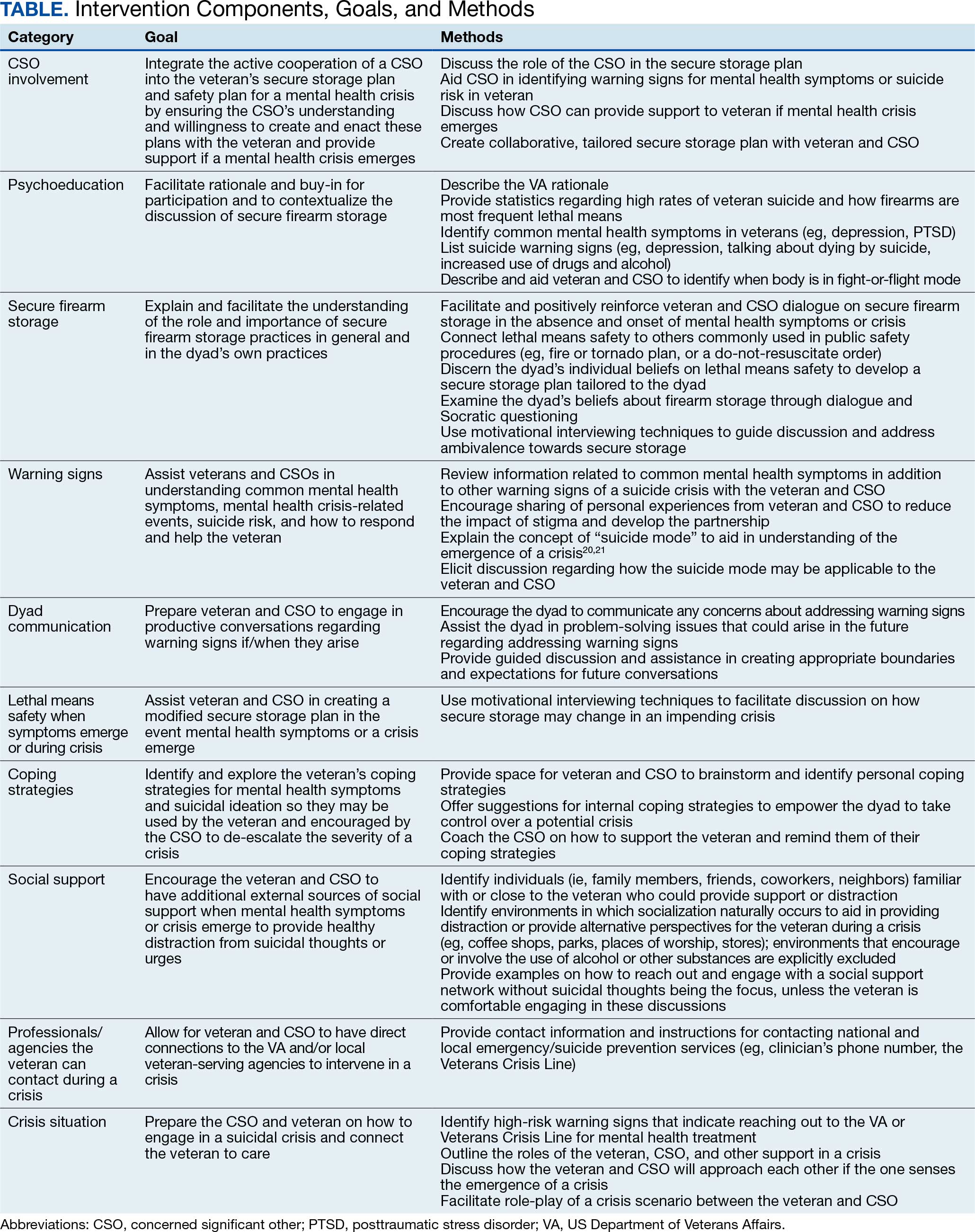
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
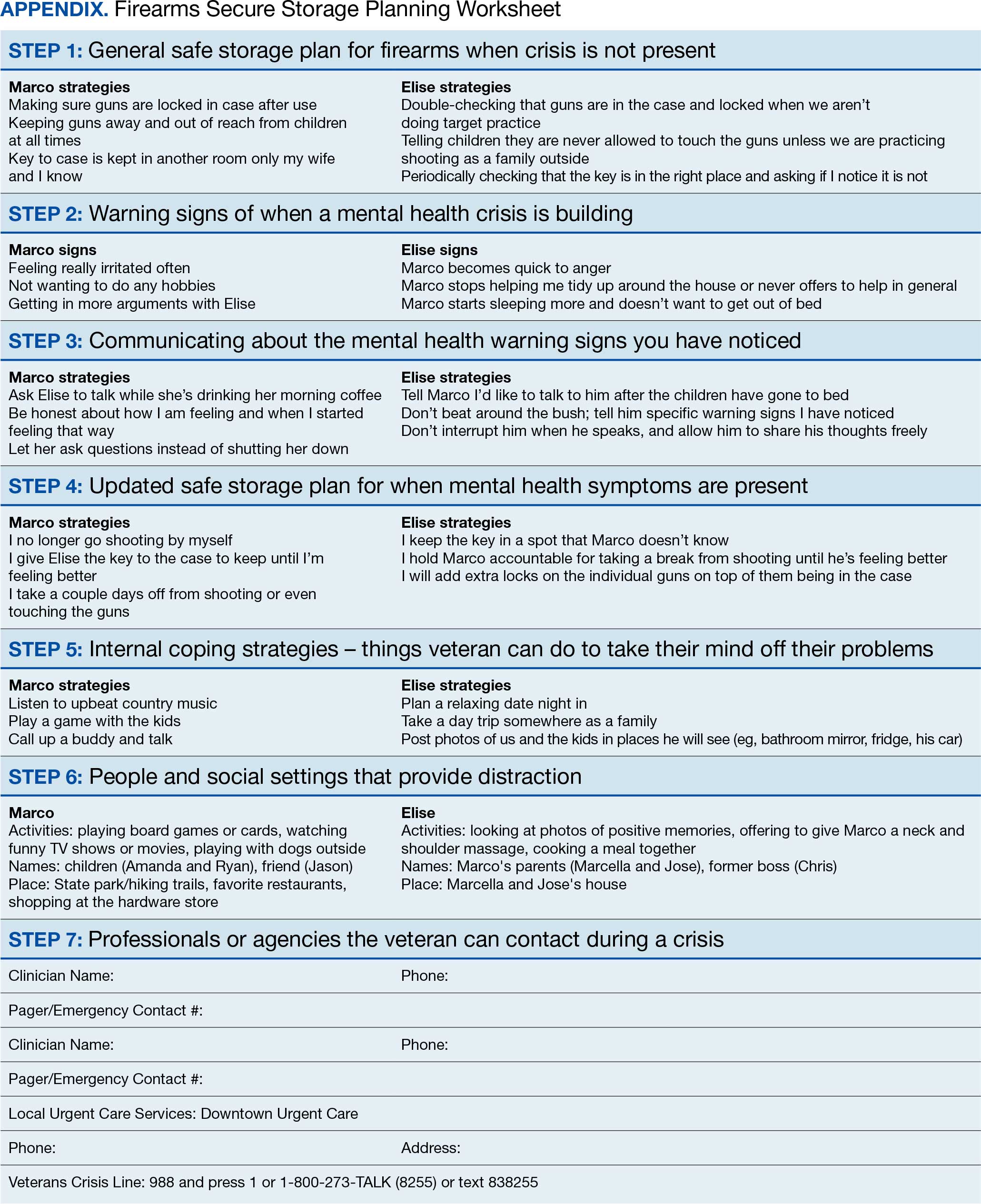
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
Veterans are at higher risk for suicide compared with civilian populations.1 Firearms are the most frequent cause of death in veteran deaths by suicide, likely because about 51% of veterans own ≥ 1 firearms and firearms are the most lethal and readily available mechanism.1-3 Unsecure firearm storage practices (eg, storing firearms unlocked, in an unsecure location, or loaded with ammunition) are associated with increased suicide risk.4 Conversely, secure firearm storage (ie, storing firearms locked and unloaded) is associated with lower suicide risk.5
A 2019 study of veterans who own firearms found that only 22.2% store all their firearms unloaded and locked, while 32.7% store ≥ 1 firearm unlocked and loaded, and 45.2% store firearms both unlocked and loaded or locked and unloaded. Only 6.3% of veterans strongly agreed that having a firearm at home increased suicide risk among household members; however, 77.2% indicated they would ensure a household member could not access firearms if they were concerned about their suicidal ideation.6
Another study found that 9.2% of veterans receive lethal means safety counseling from their US Department of Veterans Affairs (VA)-affiliated or non-VA health care professional.7 These data highlight a need to educate veterans about the increased risk for suicide associated with storing an unsecured firearm in the household and to connect this understanding to their values of service and protection of others, while simultaneously preparing them and their family members for a potential mental health crisis.
Consistent with the government’s public health approach to suicide prevention, prevention efforts should also enlist the participation of individuals outside health care.8 For example, prior research has found that family members are considered highly credible, and engaging them could expand the reach of lethal means safety conversations. A qualitative analysis of 29 veterans found that 17 (57%) said they preferred having a concerned significant other (CSO) (eg, spouse, adult friend, or relative) involved in their suicide prevention care, while 21 (72%) said they would prefer having a CSO assisting in the secure storage of firearms.9,10 Some veterans may be more amenable to a conversation about firearm access and suicide risk concerns initiated by a CSO rather than by a clinician, indicating the potential benefits of educating and involving CSOs in suicide prevention.11 Involving CSOs in secure firearm storage planning may also strengthen the veteran’s sense of social support, a key protective factor against suicidal ideation.12
CSO involvement in secure firearm storage can provide the following benefits: (1) helping the veteran create a secure storage plan, including developing approaches to secure storage; (2) understanding warning signs of suicide; (3) helping the veteran limit access to firearms during a suicidal crisis; (4) helping the veteran remember the secure storage plan; (5) helping the veteran connect with mental health services; and (6) enhancing social support. In most instances, CSOs are physically close to the veteran (eg, live in the same household) and have a greater practical ability to support and affect change with respect to changes in firearm storage practices.
This article describes the development of an intervention that incorporates CSO involvement in firearms safety efforts for veterans with guidance from VA mental health care practitioners (HCPs). The goal is to provide HCPs and other key stakeholders with a detailed description of the intervention and to suggest potential strategies for how to involve CSOs in suicide prevention.
This article follows the Guideline for Reporting Evidence-based Practice Educational interventions and Teaching checklist, which was developed to facilitate standardized reporting and replication for education interventions.13 Applicable portions of the checklist are outlined, with others (ie, incentives, planned/unplanned changes, attendance, and other outcomes) to be addressed in future research.
FFAST INTERVENTION
Training (FFAST) intervention promotes voluntary secure firearm storage, engages CSOs in veteran mental health care, and provides psychoeducation and skills to support crisis management. The intervention was developed for all veterans who do not securely store firearms.
Theory
The intervention incorporates motivational interviewing techniques, as ambivalence about changing firearm storage behaviors is common, particularly when veterans own firearms for safety or protection.6,14 Motivational interviewing is a collaborative approach that addresses a client’s ambivalence to change by eliciting and exploring the client’s own arguments related to change.14 An important aspect of developing this intervention was to ensure it would be culturally relevant to veteran firearm owners and their CSOs.15 Further, involvement of the CSO is intentional and meant to boost social support, a known buffering factor against suicide risk.12
Objectives
This intervention’s primary objective was for veteran participants to identify secure firearm storage practices and develop a plan for implementing them, including when a veteran or other household member experiences a mental health crisis. For CSOs, the primary objective is to learn how to help the veteran connect with mental health resources if needed and support secure firearm storage as necessary. The overall goal is to learn how to identify warning signs for suicide and how to respond to a mental health crisis through a collaborative process, including securing firearms in a crisis situation.
Materials, Educational Strategies, and Instructors
Training for delivering the intervention was provided via direct consultation with the developer of the intervention and manual. The manual contains pertinent background information to provide context for the intervention’s significance and rationale, including the role of firearms in suicides and current lethal means safety initiatives. It also describes the purpose and objective of each intervention component in detail in addition to providing a script for interventionists to follow to complete each objective.
Training materials for veterans and CSOs include a single Firearms Secure Storage Planning worksheet completed during the intervention, with which the interventionist guides participants through the creation of a secure firearm storage plan (Table). Educational strategies include psychoeducation and Socratic questioning (eg, questioning focused on guiding participants toward the intervention goals) delivered verbally by the interventionist.
The intervention is delivered in person or virtually during a single 90-minute session with a veteran and CSO. Veterans and CSOs work with the interventionist to complete collaborative activities during the session and have self-directive learning activities or homework.
The intervention has 4 primary components: (1) CSO involvement; (2) psychoeducation; (3) secure firearm storage; and (4) how to respond to a mental health crisis. Each CSO should have an established relationship with the veteran, be willing and able to be present during the intervention, and remain an encouraging support person for the veteran. The interventionist emphasizes that it is part of the VA mission for staff to care about the veteran, and that initiating such contact with a CSO is meant to prioritize veteran safety and the safety of their family. Psychoeducation on mental health symptoms, suicide warning signs, veteran suicide rates and lethal means, and the benefits of secure firearm storage, is incorporated in the intervention.
The secure firearm storage component consists of 7 subcomponents: (1) general lethal means secure storage; (2) warning signs; (3) dyad communication; (4) lethal means safety when symptoms emerge; (5) coping strategies; (6) social support; and (7) emergency contacts. A lethal means safety worksheet rooted in the Stanley and Brown suicide safety plan model and implemented in VA health care settings is used to facilitate discussions of secure storage (Appendix).16
CSOs typically have little or no suicidal crisis response training, yet they likely have more interaction with the veteran on a daily basis than HCPs, putting them in a vital position to identify a crisis early and connect the veteran with the proper care. The crisis component prepares the CSO and veteran to navigate a crisis scenario so they can practice their newly developed safety plan and increase their comfort in discussing mental health and suicidal crisis.
FICTIONAL CASE STUDY
Cole, aged 59 years, is a Persian Gulf War veteran and retired police officer. His medical history includes hypothyroidism, hypertension, type 2 diabetes mellitus, chronic posttraumatic stress disorder, major depressive disorder, and insomnia.
Cole's wife of > 30 years, Sheila, joined him for the FFAST intervention. They report having 4 firearms in the home, 3 of which are loaded but stored in a lockbox and 1 that Cole reports is kept on his person for protection. Cole reports passive suicidal ideation, but no plans or intent. When discussing warning signs that a mental health crisis is building, Cole describes feeling anxious, having a change in his speech patterns, and isolating himself. Sheila agrees, but also mentions that Cole is easily angered and becomes nonverbal. Cole and Sheila express difficulty communicating and appear to have a breakthrough moment when Cole says he does not like when Sheila repeats herself, as he feels like she is “poking” at him. Sheila shares concerns for his safety and that she only repeats herself because he refuses to talk.
Cole agrees to verbalize that he is safe but needs time to process his thoughts. Sheila agrees to give him space with a plan to revisit the conversation within an agreed upon timeline. When discussing an updated secure storage plan for their firearms when a mental health crisis is building, Cole commits to allowing Sheila to store the firearm currently on his person in their gun safe, with the ammunition stored separately, and to giving her the gun safe key. They agree to implement this practice until the mental health crisis has passed.
To mitigate a potential crisis, the interventionist discusses possible internal coping strategies for Cole, including writing, reading, walking the dog, listening to music, and baking. People and social settings that could provide distraction involve going to the gym, talking to his friend Carl or his daughter Kelly, and attending the men’s ministry at church. The intervention concludes by discussing professionals or agencies that Cole and Sheila could contact during a crisis. After the intervention, Cole and Sheila are asked to rate their likelihood of using the plan they established during the conversation on a scale of 0 to 10, with 0 being highly unlikely and 10 being extremely likely. Cole responds with 9 and Sheila responds with 10.
DISCUSSION
Lethal means safety remains a critical component of veteran suicide prevention. However, lethal means safety discussions are often implemented after suicide risk has been identified, which may be too late. Thus, having these conversations early and before a crisis may be imperative. Veterans have expressed a desire to have CSOs involved in their suicide prevention treatment, and CSOs can play a key role in recognizing risk factors during everyday life. The FFAST intervention addresses many of these gaps.
Having discussions in advance of a crisis allows veterans to consider an effective secure firearm storage plan outside of the context of a crisis. Including a CSO galvanizes another person to understand a veteran’s needs and assist with secure firearm storage, identify warning signs, and support them during a crisis. These discussions occur in a context where there is less pressure than during a crisis. Features that were more appealing to veterans and their CSOs were also incorporated, such as having the dyad build a plan that is conceptually similar to other public safety initiatives (eg, a fire safety plan, tornado plan, or hurricane plan). Previous research demonstrates that veterans appreciated the nonjudgmental approach and some preferred that clinicians approach the discussion of secure firearm storage within the context of general home and family safety.17 Additionally, this intervention can build on veterans’ prior military training in preparedness.
Other potential benefits associated with the FFAST intervention include creating an opportunity to strengthen communication between the veteran and CSO. While FFAST is intended to be used with all types of CSOs, this work is consistent with preliminary data from a couples-based suicide prevention study that indicated veterans and their partners reported increases in relationship functioning and marginal decreases in suicidal ideation.18 It is possible that communication strategies gained from the current intervention could improve veterans’ relationships with their CSOs, which are associated with a greater sense of social support and reduced suicide risk.12
The intervention is a brief, single session that may be appealing to veterans and CSOs with full schedules. Evidence suggests that even brief, single-session interventions have a significant impact on beliefs about secure firearm storage, knowledge of lethal means safety, and confidence in having secure firearm storage conversations.19 However, clinicians should be cautious when extrapolating from the findings of the current case example, which was a one-time intervention with no follow-up.
Future Directions
Pilot testing of the proposed intervention is underway, and future research will include feedback from veterans and CSOs, as well as feasibility and acceptability data collected during the pilot process. The pilot study uses a successive cohort design with an initial 2 sets of 5 veteran and CSO dyads, and subsequent funding has expanded the pilot study to include an additional 30 dyads. Qualitative interviews will be conducted separately with each veteran and CSO, and additional constructs such as feasibility, acceptability, barriers and facilitators to implementation, and changes in secure storage will be examined. This future research may provide a deeper understanding of the broader acceptability, feasibility, and satisfaction associated with a suicide prevention intervention focused on securing firearms and involving veterans and their CSOs. These data could be used to inform future implementation trials and inform the development of an implementation strategy. In the interim, the nature of the manual is summarized in the context of the urgency of suicide prevention in this at-risk population.
Conclusions
FFAST is a novel approach to veteran firearm suicide prevention. By involving CSOs and emphasizing mental health crisis preparedness between them and veterans, the dyad can work in association with HCPs to establish and exercise secure firearm storage practices as part of an at-home safety plan. Implementation of FFAST may be beneficial for all veterans, not only those who have been identified as being at high suicide risk.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
- US Dept of Veterans Affairs Office of Suicide Prevention. 2024 national veteran suicide prevention annual report. December 2024. Accessed February 5, 2026. https://www.mentalhealth.va.gov/docs/data-sheets/2024/2024-Annual-Report-Part-2-of-2_508.pdf
- Fischer IC, Aunon FM, Nichter B, et al. Firearm ownership among a nationally representative sample of U.S. veterans. Am J Prev Med. 2023;65:1129-1133. doi:10.1016/j.amepre.2023.06.013
- Conner A, Azrael D, Miller M. Suicide case-fatality rates in the United States, 2007-2014: a nationwide population-based study. Ann Intern Med. 2019;171(12):885-895. doi:10.7326/M19-1324
- Dempsey CL, Benedek DM, Zuromski KL, et al. Association of firearm ownership, use, accessibility, and storage practices with suicide risk among US army soldiers. JAMA Netw Open. 2019;2:e195383. doi:10.1001/jamanetworkopen.2019.5383
- Butterworth SE, Daruwala SE, Anestis MD. Firearm storage and shooting experience: factors relevant to the practical capability for suicide. J Psychiatr Res. 2018;102:52-56. doi:10.1016/j.jpsychires.2018.03.010
- Simonetti JA, Azrael D, Miller M. Firearm storage practices and risk perceptions among a nationally representative sample of U.S. veterans with and without self-harm risk factors. Suicide Life Threat Behav. 2019;49:653-664. doi:10.1111/sltb.12463
- Simonetti JA, Azrael D, Zhang W, Miller M. Receipt of clinician-delivered firearm safety counseling among U.S. veterans: results from a 2019 national survey. Suicide Life Threat Behav. 2022;52:1121-1125. doi:10.1111/sltb.12906
- US Office of the Surgeon General. The surgeon general’s call to action to implement the national strategy for suicide prevention. January 2021. Accessed February 5, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- DeBeer BB, Matthieu MM, Kittel JA, et al. Quality Improvement Evaluation of the Feasibility and Acceptability of Adding a Concerned Significant Other to Safety Planning for Suicide Prevention With Veterans. J Ment Health Couns. 2019;41:4-20. doi:10.17744/mehc.41.1.02
- DeBeer BB, Matthieu MM, Degutis LC, et al. Firearms lethal means safety among veterans: attitudes toward involving a concerned significant other. J Mil Veteran Fam Health. 2025;11:23-31.
- Monteith LL, Holliday R, Dorsey Holliman BA, et al. Understanding female veterans’ experiences and perspectives of firearms. J Clin Psychol. 2020;76:1736-1753. doi:10.1002/jclp.22952
- DeBeer BB, Kimbrel NA, Meyer EC, et al. Combined PTSD and depressive symptoms interact with post-deployment social support to predict suicidal ideation in Operation Enduring Freedom and Operation Iraqi Freedom veterans. Psychiatry Res. 2014;216:357-362. doi:10.1016/j.psychres.2014.02.010
- Phillips AC, Lewis LK, McEvoy MP, et al. Development and validation of the guideline for reporting evidence-based practice educational interventions and teaching (GREET). BMC Med Educ. 2016;16:237. doi:10.1186/s12909-016-0759-1
- Miller WR, Rollnick S. Motivational Interviewing: Helping People Change. 3rd ed. Guilford Press; 2013.
- Khazanov GK, Keddem S, Hoskins K, et al. Stakeholder perceptions of lethal means safety counseling: a qualitative systematic review. Front Psychiatry. 2022;13:993415. doi:10.3389/fpsyt.2022.993415
- Stanley B, Brown GK, Karlin B, et al. US Dept of Veterans Affairs. Safety plan treatment manual to reduce suicide risk: veteran version. August 20, 2008. Accessed February 5, 2026. https://www.mentalhealth.va.gov/mentalhealth/docs/va_safety_planning_manual.doc
- Dobscha SK, Clark KD, Newell S, et al. Strategies for discussing firearms storage safety in primary care: veteran perspectives. J Gen Intern Med. 2021;36:1492-1502. doi:10.1007/s11606-020-06412-x
- Khalifian CE, Leifker FR, Knopp K, et al. Utilizing the couple relationship to prevent suicide: a preliminary examination of treatment for relationships and safety together. J Clin Psych. 2022;78:747-757. doi:10.1002/jclp.23251
- Walsh A, Friedman K, Morrissey BH, et al. Project Safe Guard: evaluating a lethal means safety intervention to reduce firearm suicide in the National Guard. Mil Med. 2024;189:510-516. doi:10.1093/milmed/usae172
- Beck AT. Beyond belief: a theory of modes, personality, and psychopathology. In: Salkovkis PM, ed. Frontiers of Cognitive Therapy. Guilford Press;1996:1-25.
- Rudd MD. The suicidal mode: a cognitive-behavioral model of suicidality. Suicide Life Threat Behav. 2000;30(1):18-33.
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Involving Concerned Significant Others in Firearm Suicide Prevention: Development of the Family FireArms Secure Storage Training Intervention
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
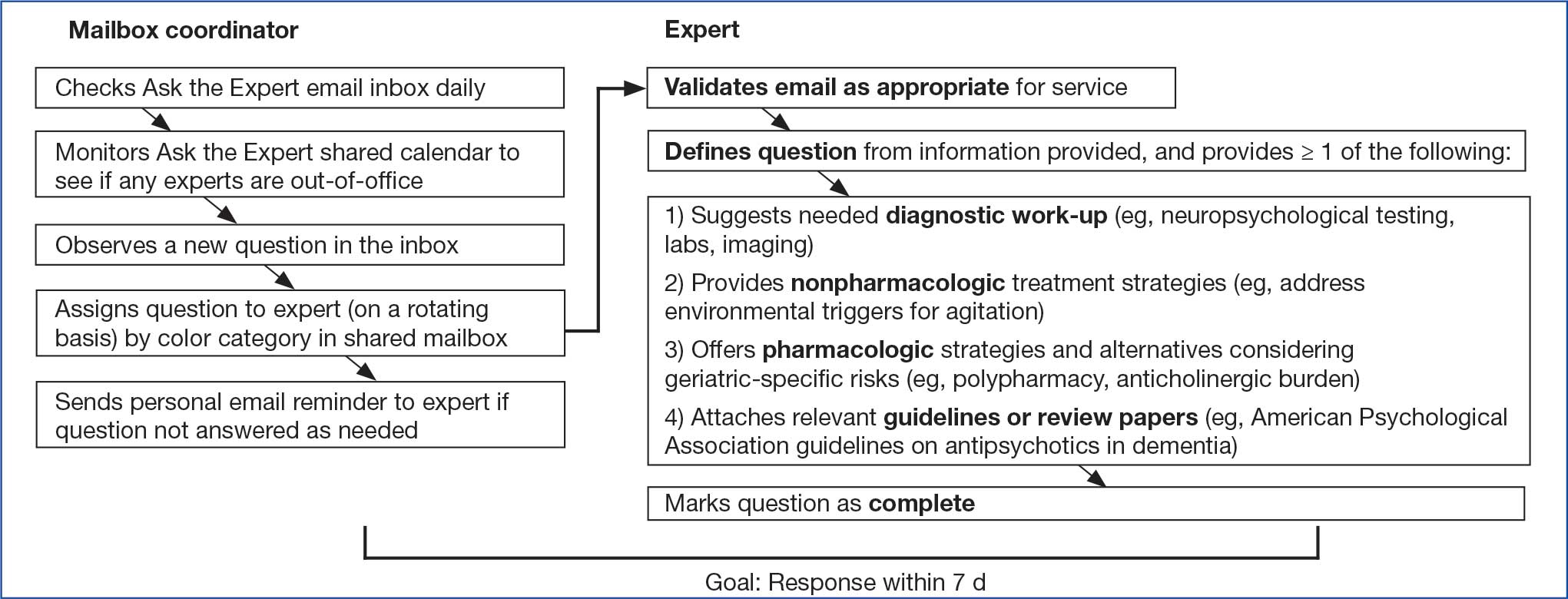
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
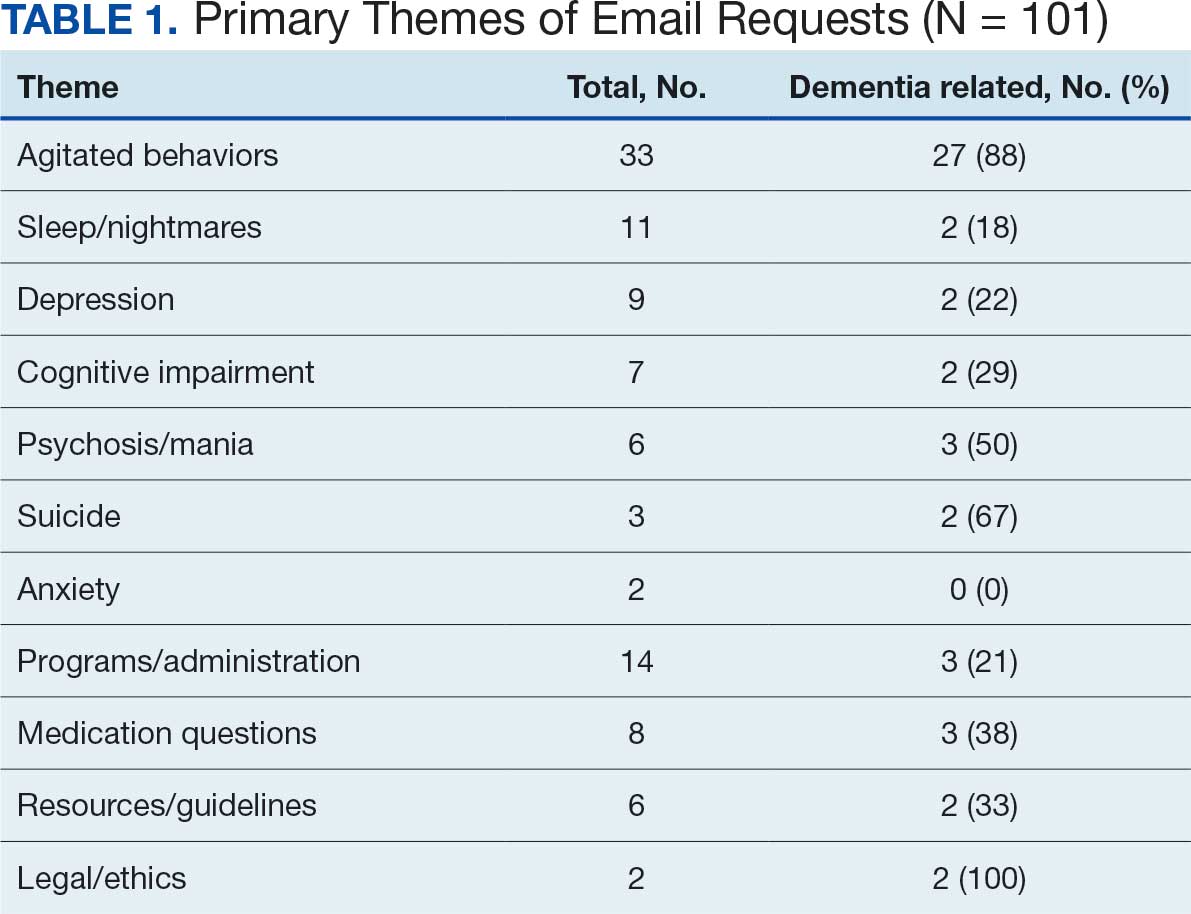
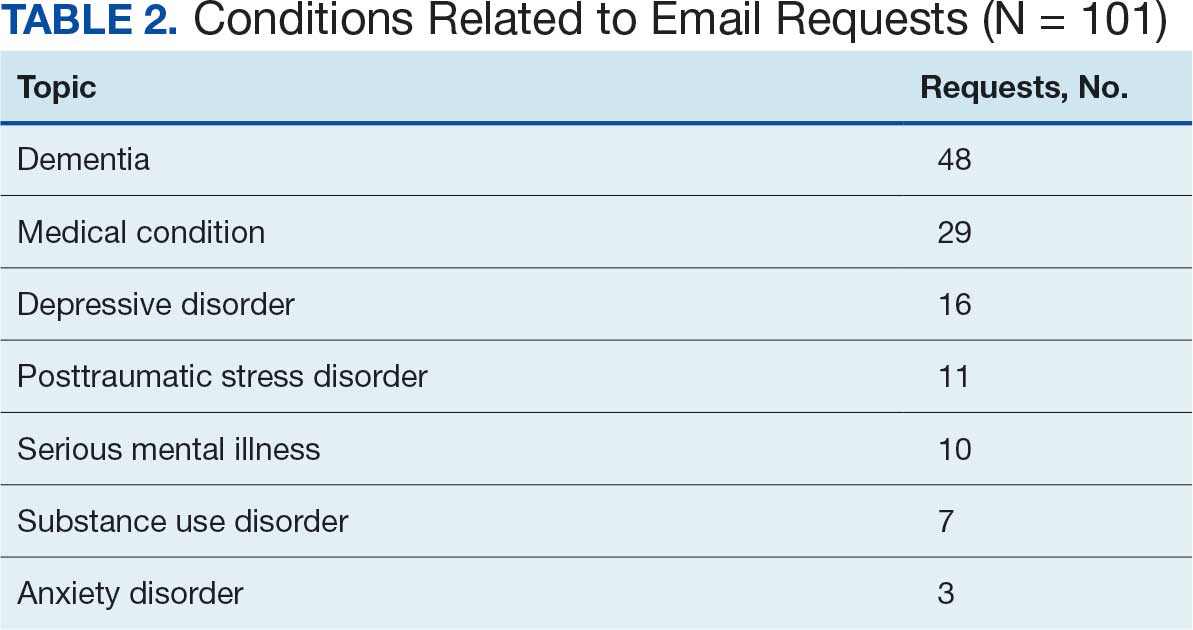
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
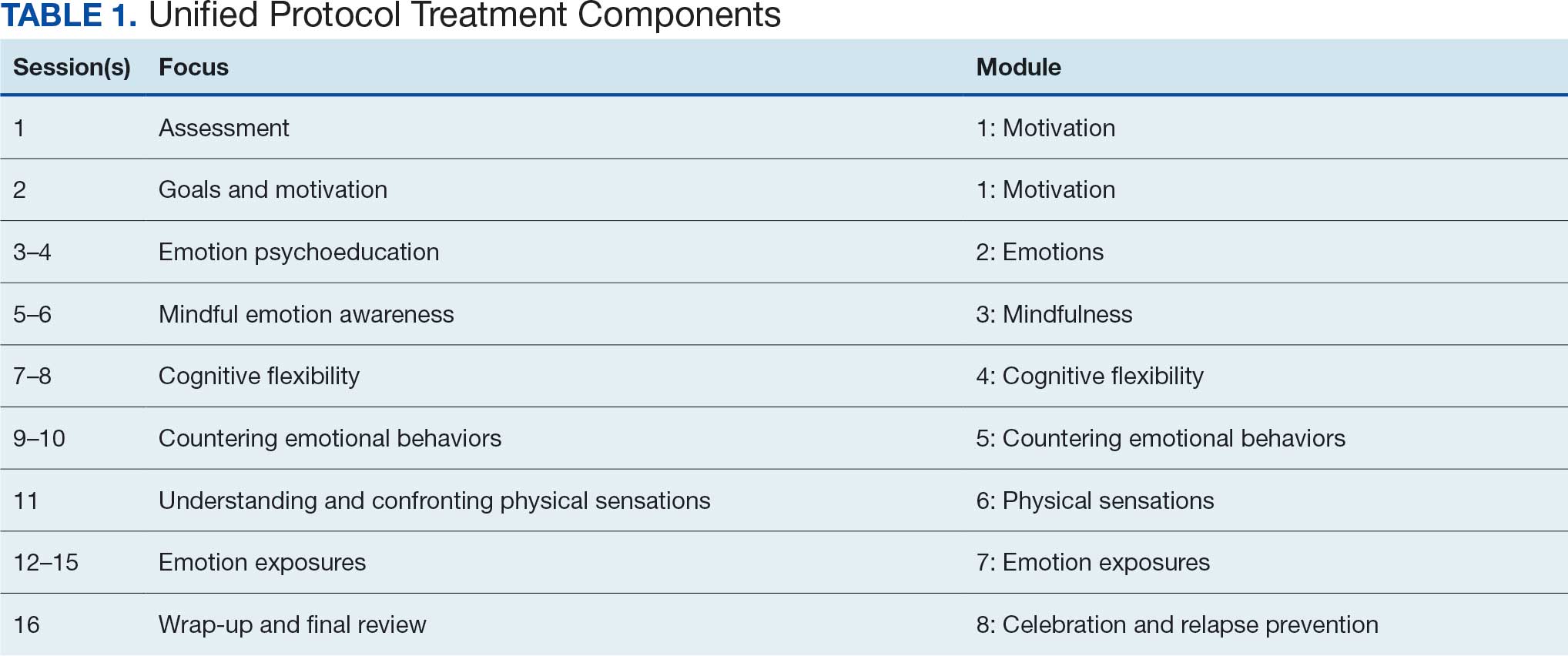
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
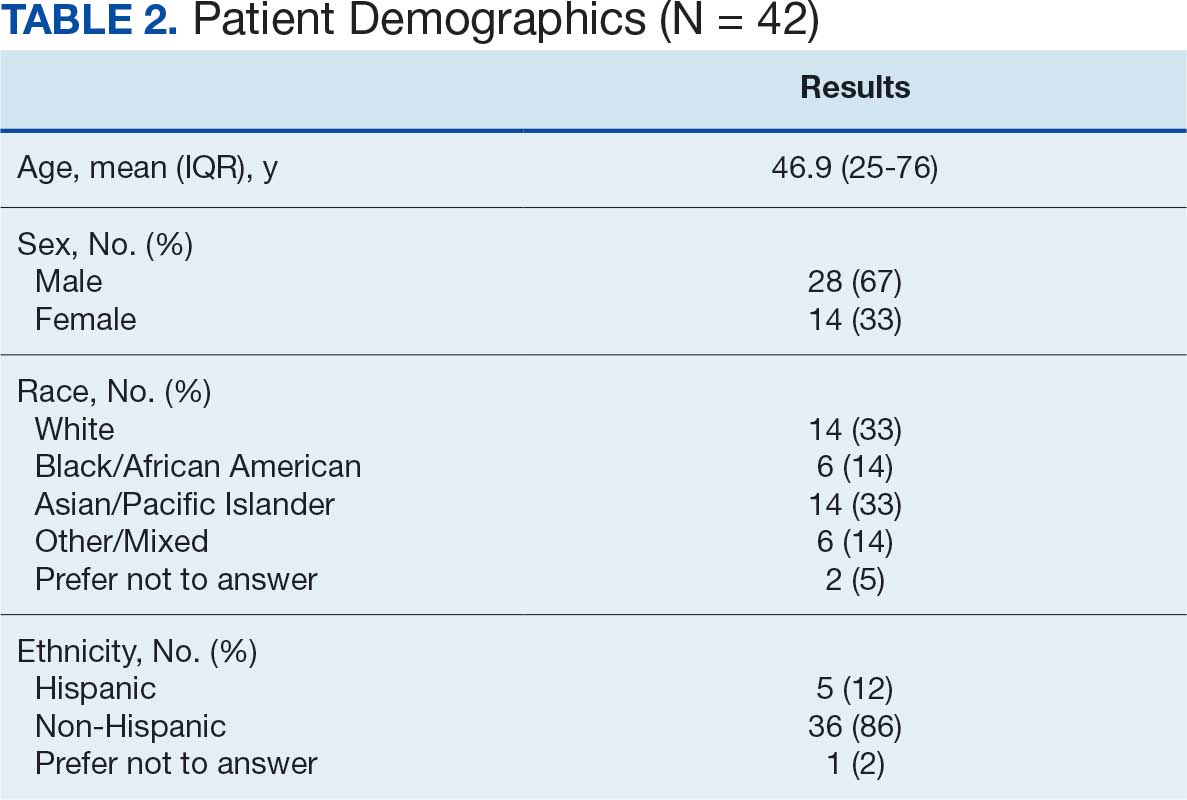
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
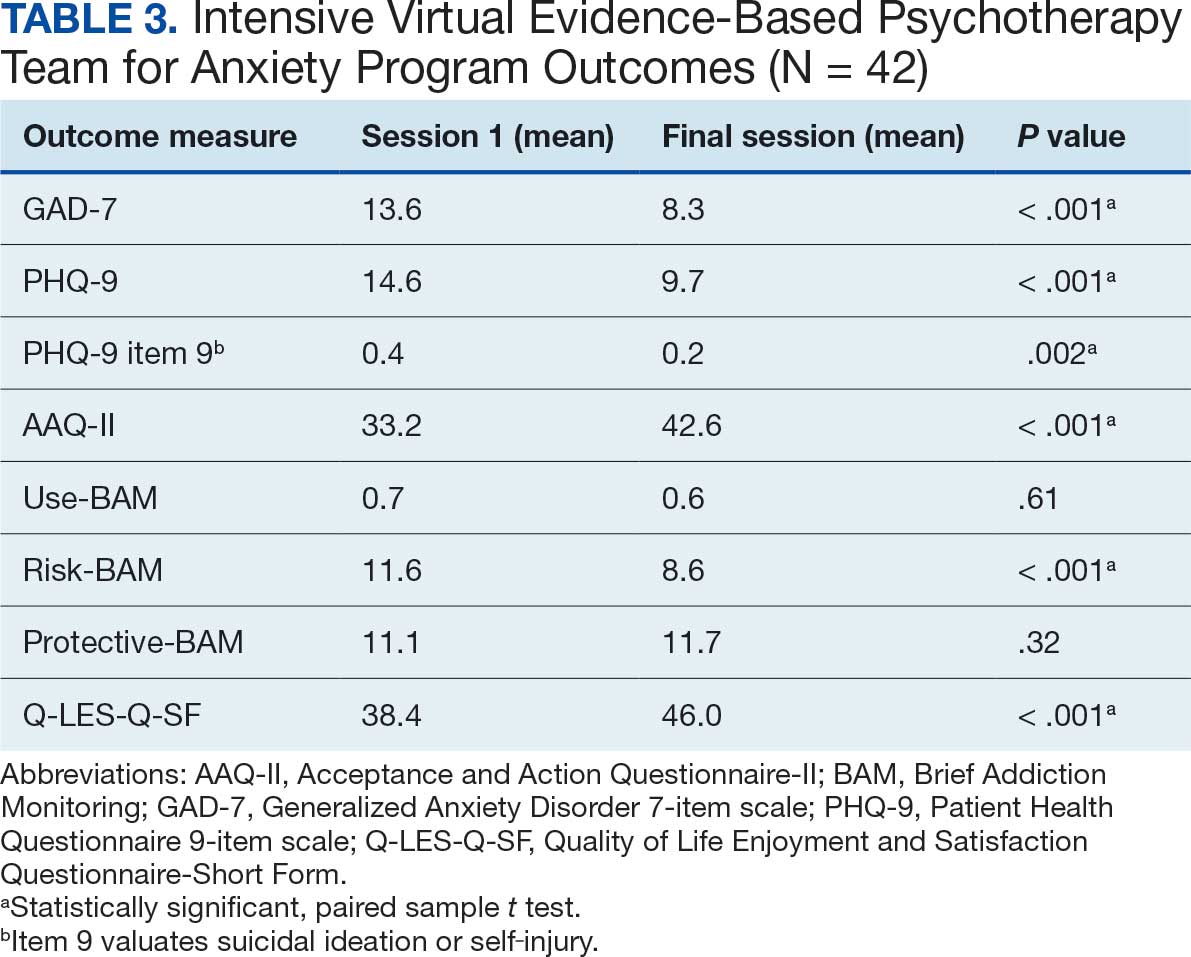
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
Cognitive behavioral therapy (CBT) is supported as an effective treatment for depression by clinical practice guidelines from the US Department of Veterans Affairs (VA) and US Department of Defense.1-3 Despite research supporting the use of evidence-based CBT for anxiety, mood, and emotional disorders, patient access to these interventions is limited.4 One barrier to CBT for anxiety, mood, and emotional disorders is the traditional use of single-disorder protocols (SDPs) to separately treat each disorder (eg, major depression, generalized anxiety disorder, panic disorder).
Use of SDPs places a high burden on clinicians, requiring them to learn and competently implement multiple different manualized interventions for each anxiety, mood, or emotional disorder encountered in practice.4 It is common for individuals who present with an anxiety, mood, or emotional disorder to experience co-occurring disorders.5 Traditional SDP-based CBT may require multiple SDPs to address co-occurring disorders, extending time in treatment and increasing training burden. There is evidence that even when an SDP is used, co-occurring difficulties may decrease in intensity.6 Thus, evidence-based CBT for 1 presenting concern may positively affect co-occurring difficulties that are not the primary treatment target.6
Unified Protocol (UP) is a transdiagnostic CBT intervention for anxiety and mood disorders. UP targets emotional experiences (eg, negative affect and emotional distress) that are present in multiple anxiety, depression, and emotional disorders. UP is organized into 8 modules and uses interventions present in other CBT SDPs, such as teaching objective assessment methods to clients, motivational enhancement and goal setting, emotion psychoeducation, mindful awareness, cognitive reframing, and exposure principles as mechanisms of change (Table 1).4 UP is an ideal intervention for addressing a number of anxiety, mood, and emotional disorders as well as addressing cooccurring disorders within the same course of treatment.
UP has been compared to SDPs; studies illustrate that UP is equivalent to SDPs at the end of treatment and at 6 months posttreatment.4,7 Additionally, patients who received UP experienced symptom reduction for multiple co-occurring disorders.7 Furthermore, patients were less likely to drop out of UP when compared with SDPs.4
Studies have reported positive impacts on affective disorders with UP. A 2019 meta-analysis found significant reductions in depression and anxiety-related disorders.8 Additionally, UP has been shown to be effective when delivered in person and via telehealth.9,10 UP has also been successfully used in veterans.11 While traditional models of UP (1-2 sessions weekly) have a lower dropout rate than SDPs, UP and CBT dropout rates still leave room for improvement.12-14 Specifically, rates of attrition from SDP CBT and transdiagnostic CBT protocols range from 9% to 35%, and dropout reduces the likelihood of attaining a full therapeutic dose of any course of CBT. Notably, accelerated delivery of CBT (ie, ≥ 3 sessions/wk) has been shown to reduce risk of dropout.14,15
Veterans are at increased risk for suicide, and anxiety and mood disorders are associated with increased risk of suicide attempt and death.16,17 Very few veterans who could benefit from high-quality CBT interventions, whether SDP or UP, are able to access them. Only 6.3% of veterans received ≥1 session of an evidence-based CBT SDP for posttraumatic stress disorder (PTSD) at 6 clinics evaluated in 2010.18
We identified 2 strategies to increase access to and completion of an evidence-based CBT course. First, the use of transdiagnostic UP instead of SDPs reduced burden on therapists and allowed them to address presenting and co-occurring disorders within the same course of care. Second, the use of an accelerated model of service delivery reduced dropout risk. Training clinicians to deliver UP is efficient and cost-effective, considering clinicians use core strategies that can be tailored and flexibly applied to a range of emotional difficulties. Thus, implementing UP may decrease barriers to receiving an optimal dose of an evidence-based CBT delivered with fidelity in a time- and cost-efficient manner.4 Two studies have found no evidence of differences in outcomes between UP and SDPs, suggesting that training and supervising clinicians in a single transdiagnostic UP intervention may prepare them to treat heterogeneous and co-occurring anxiety, mood, and emotional disorders with less burden than learning multiple SDPs.7,19
Delivering UP in an accelerated or massed format (≥4 sessions/wk) instead of the traditional spaced model (1 session/wk) has empirical support but has not been widely implemented. This approach, sometimes referred to as a UP-intensive outpatient program (UP-IOP) or UP-intensive outpatient track (UP-IOT), has been shown to be feasible, acceptable, and effective, with increased completion rates compared with traditional UP delivery (1-2 sessions/wk).20-22
Ragsdale et al describe a 2-week IOP with multiple treatment tracks, including a general track.20 The general track includes massed UP and additional standard services, including case management, wellness services, family services, and a single session effective behaviors group. Additional augmentation services are available when clinically indicated (eg, repetitive transcranial magnetic stimulation, transcranial direct current stimulation, psychoeducation, motivational interviewing, relapse prevention). In other words, this was an UP-IOP.20
Thompson-Brenner et al described a successful implementation of massed UP applied in intensive treatment settings, such as residential and day-hospital programs, for eating disorders. Patients reported improvements in 3 UP targets: experiential avoidance, mindfulness, and anxiety.21 Watkins et al evaluated a 2-week IOP using CBT for comorbid substance use and mental health disorders, including prolonged exposure, UP, and relapse prevention for substance use disorders. Participants were post-9/11 veterans and activeduty personnel. Results indicated that UP reduced PTSD and depressive symptoms following treatment. Furthermore, the retention rate (91%) was higher than retention in outpatient treatment (39%-65%), supporting the IOP model as a strategy to reduce dropout.22
Massed psychotherapy has been extended to IOP programs for PTSD treatment within the Veterans Health Administration (VHA). Yamokoski et al found that patients who completed an IOP that included massed CBT for PTSD had high retention, high satisfaction, and significant reduction in self-reported co-occurring depression symptoms. The authors also found that this model of care could be implemented and sustained within a VHA facility using minimal staffing resources.23
The UP-IOP models described by Ragsdale et al and Watkins et al included massed UP as the primary evidence-based practice (EBP) with adjunctive groups (eg, wellness and educational groups and access to complementary interventions such as mindfulness and yoga); they found that adding these groups increased retention and patient- reported satisfaction (ie, UP-IOP).20,22 The addition of wellness education alongside a primary EBP aligns with the VHA focus on whole health well-being and wellness. This includes understanding factors that motivate a patient toward health and well-being, providing health education, and offering access to complementary interventions such as mindfulness.24
Dryden et al described the whole health transformation within VHA as a proactive approach to addressing both employee and patient wellness. Their research found that the whole health model promoted wellbeing in patients and staff and these improvements were sustained during the COVID-19 pandemic. Dryden et al also noted that virtual technologies facilitated continued whole health implementation.25
The literature illustrates that (1) massed UP can be delivered with complementary education and wellness offerings that may increase retention and satisfaction by enriching treatment (eg, delivering UP-IOP); (2) whole health, including wellness education and complementary interventions (eg, mindfulness, motivational enhancement), promotes well-being in patients and clinicians; and (3) whole health education and complementary interventions can be delivered virtually.
IVET
Health Care Need
Veterans Affairs Pacific Islands Health Care System (VAPIHCS) provides medical services to veterans in the Hawaiian Islands, American Samoa, Guam, and Saipan spanning nearly 4000 miles across the Pacific Ocean. Prior to implementation of this program, veterans who received care at VAPIHCS had little to no access to UP in outpatient settings and no access to UP in residential settings. Access to UP depended on the presence of a therapist trained in UP within a given clinic and was geographically limited to the location of the UP-trained therapist. The limited outpatient access to UP was restricted to the traditional UP delivery model (eg, about 1 session/wk); thus, there was no access to accelerated UP for veterans served at VAPIHCS. In the fiscal year prior to implementation of the massed UP program, > 1000 VAPIHCS veterans had been diagnosed with obsessive-compulsive related disorder or anxiety. A massed-UP program with weekly rolling admissions would support access to UP for more veterans over 12 months, and the virtual treatment modality would reduce barriers for diverse and underserved veterans, making care more equitable and inclusive.
Successful implementation and sustainment of an EBP prompted the establishment of this UP program. In 2022, VAPIHCS launched the Intensive Virtual Evidence- Based Psychotherapy Team (iVET) for treatment of PTSD. This clinic and associated EBP project demonstrated that massed (≥3 individual sessions/wk) of prolonged exposure (PE) therapy, delivered virtually to a geographically diverse veteran population with PTSD, resulted in significant reductions in PTSD, depression, and anxiety symptoms and substance use risk factors, with very high retention rates. The iVET for PTSD program was feasible, acceptable, and effective, with veterans reporting significant improvement in quality of life and high satisfaction with their mental health services.15 Given the known benefits of transdiagnostic UP treatment (vs SDPs), the need for accelerated UP, and success with accelerated PE, our goal was to spread the EBP of massed (≥3 sessions/ wk) virtual psychotherapy to other presenting problems (eg, anxiety disorders with or without co-occurring unipolar depression) using transdiagnostic UP.
Program Description
The program implemented within outpatient mental health services at VAPIHCS was iVET for the treatment of anxiety with or without co-occurring depression. The program model consists of an accelerated course of UP and whole health education provided via VA Video Connect (VVC), the VA video telehealth platform. iVET is a 2- to 4-week program and consists of 3 parts: (1) massed individual UP for transdiagnostic treatment of anxiety and co-occurring depression, (2) group whole health and wellness classes, and (3) individual health coaching to address personal wellness goals. Programming is offered over 10-hour days to increase access across multiple time zones, especially to allow participation from Guam and Saipan.
When a patient is referred to iVET, the first contact is a video (or telephone) appointment with a registered nurse (RN) for a screening session. The screening session is designed to provide education about the program (including interventions, time commitment, and resources required for participation). Following education, the RN completes a safety screening, including screening for suicidal ideation and risk, as well as intimate partner violence risk. If urgent safety concerns are present, a licensed social worker or psychologist joins the screening to complete further risk assessment and address any safety concerns.
Following screening, patients are scheduled for a VVC telehealth intake with a licensed therapist (social worker or psychologist) to complete a diagnostic interview. Patients are sent a secure link to complete a measurement-based care (MBC) battery of self-report measures, including assessments of demographics, anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care. The results of the diagnostic interview and self-report measures are discussed with the patient during the intake session to plan next steps and support shared decision-making. This initial VVC intake not only allows for fit assessment but also serves to troubleshoot technical difficulties with the virtual platforms.
Notably, there are minimal exclusion criteria for participation in iVET. These include active unmanaged psychosis or manic symptoms, recent suicidal crises (attempt within 8 weeks), active nonsuicidal self-injury (within 8 weeks), and moderate to severe cognitive impairment. Following intake, patients are scheduled to begin their course of care with iVET. Upon completion of intake, patients receive program materials for individual and group classes and are told they will receive email links for all VVC telehealth appointments. Patients are admitted to the iVET on a rolling basis, thereby increasing access compared with closed group and/or cohort models of care.
Patients receiving iVET attend 2 to 4 telehealth appointments daily and complete exercises between sessions. The primary iVET for Anxiety program EBP intervention is a massed or accelerated individual course of UP, which includes 8 primary components: assessment, goals and motivation, understanding emotions, mindful emotion awareness, cognitive flexibility, countering emotional behaviors, understanding and confronting physical sensations, and emotional exposures. UP is delivered in 4 to 8 individual sessions weekly (60-90 minutes each), allowing completion of the full UP protocol with fidelity in 2 to 4 weeks. In addition to primary EBP intervention, patients participate in 4 group sessions weekly (50 minutes each) of a whole health and wellness education class and have access to 1 individual health coaching session weekly (30- 60 minutes) to set wellness goals and receive coaching. During iVET, patients are invited to complete MBC batteries of self-report measures assessing anxiety symptoms, depression symptoms, substance use, psychological flexibility, quality of life, and satisfaction with mental health care at sessions 1, 5, 9, 13, and the final UP session. Following discharge from the iVET, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with a therapist, during which they are invited to complete MBC measures and review relapse prevention and maintenance of treatment gains. Likewise, patients are offered 1-, 3-, and 6-month individual postdischarge check-up sessions with an RN focused on maintaining wellness gains.
The iVET for Anxiety staff has 3 therapists (psychologists or social workers) and 1 RN. Additionally, the iVET for Anxiety is supported by a program manager and a program support assistant who support 2 programs total (the iVET for Anxiety plus another mental health program). The primary cost of the program is staff salary. Additional resources included computer equipment for staff and supplies (eg, printed materials for patients and office supplies). Due to the virtual environment of care, iVET staff telework and do not require physical space within VAPIHCS.
Outcomes
Veterans receiving iVET for Anxiety are invited to complete MBC multiple times, including pretreatment, during UP treatment (sessions 1, 5, 9, 13, and the final session), and posttreatment (1, 3, and 6 months). MBC measures include self-reported demographics; a 2-item measure of satisfaction with mental health services; the Acceptance and Action Questionnaire II,26 the Brief Addiction Monitor-Intensive Outpatient Program, 27 the Generalized Anxiety Disorder-7,28 the Patient Health Questionnaire (PHQ-9),29 and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form.30
Forty-two veterans completed the iVET for Anxiety program, with a retention rate of 87.5% completing . 16 sessions of massed UP (Table 2). Veterans reported reduced anxiety (P < .001), depression (P < .001), and substance use risk (P < .001). Veterans experienced improved acceptance of emotional experiences (P < .001) and quality of life (P < .001), based on paired sample t tests comparing session 1 vs final session scores on the self-reported measures. Veterans also reported high satisfaction with mental health care in iVET for Anxiety.
Veterans experienced reduced thoughts of death or suicidal ideation (SI) based on responses to item 9 of PHQ-9. When SI was categorically analyzed (presence vs absence) using PHQ-9 item 9, there was an association observed between absence of SI and completion of a course of massed UP that does not appear to be due to chance, (X2 [1, N = 42) = 3.94; P = .047). In addition, veterans who completed the program showed a significant decrease in SI severity measured continuously (range, 0-3) on PHQ-9 item 9 (P < .05) (Table 3).
Future Directions
The aim of this program is to see sustained patient outcomes as iVET continues to serve more veterans. Another line of inquiry is longer- term follow-up, given that long-term follow- up was not addressed in this project. We also hope that the accelerated model of care can be applied to treatment of other presenting concerns (eg, relationship difficulties, insomnia). Expansion of accelerated mental health treatment into other federal and nonfederal health care settings is another area worthy of future inquiry. Exploration of staff satisfaction and burnout related to providing accelerated UP is another important future direction. Relatedly, assessment of the staff burden to learn 1 transdiagnostic EBP vs learning multiple SDPs is another future direction. Likewise, exploration of institutional benefits of investment in transdiagnostic training, supervision, and consultation for UP vs multiple SDPs may be important. These areas could also result in insightful, beneficial evidence of the effectiveness of massed UP to add to the existing literature.
Conclusions
UP for transdiagnostic treatment of anxiety, depressive, and emotional disorders has demonstrated reduced suffering and improved functioning and is supported by multiple clinical practice guidelines.1-4 Federal practitioners are positioned to improve access to this intervention, thereby reducing pain and improving lives. Indeed, it is crucial to envision a future state in which access to UP for a range of anxiety and depressive disorders is improved and broad, retention rates are dramatically improved, and clinicians providing UP do not experience the high burden and burnout associated with needing to learn and implement a variety of SDPs. Development of these programs, or similar tracks within existing programs, that provide massed or accelerated UP for transdiagnostic treatment of a range of anxiety and depressive disorders with virtual delivery options, is imperative to advance improved care for patients and clinicians.
Federal health care settings treating patients with anxiety and depression, such as those within the US Department of Defense, Indian Health Services, Bureau of Prisons, and VHA, are positioned to implement programs like iVET. Moreover, at the institutional level, investment in training and supervision in the transdiagnostic UP as opposed to multiple SDPs warrants consideration. We believe this model of care has great merit and foresee a future where all patients seeking treatment for anxiety and depression have the option to complete an accelerated or massed course of transdiagnostic care with UP if they so desire. Our experiences with iVET illustrate the feasibility, acceptability, and sustainability of such programs without requiring substantial staffing and financial resources.
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
- US Department of Veterans Affairs, US Department of Defense. VA/DoD clinical practice guideline for the management of major depressive disorder. Version 4. 2022. Accessed February 1, 2026. https://www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFinal508.pdf
- American Psychological Association. Clinical practice guideline for the treatment of depression across three age cohorts. February 2019. Accessed February 4, 2026. https://www.apa.org/depression-guideline/guideline.pdf
- Katzman MA, Bleau P, Blier P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive compulsive disorders. BMC Psychiatry. 2014;14:S1. doi:10.1186/1471-244X-14-S1-S1
- Barlow DH, Farchione TJ, Bullis JR, et al. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders: a randomized clinical trial. JAMA Psychiatry. 2017;74:875-884. doi:10.1001/jamapsychiatry.2017.2164
- Calkins AW, et al. Comorbidity of anxiety and depression. In: Ressler KJ, Pine DS, Rothbaum BO, eds. Anxiety Disorders, Primer On. Oxford Academic; 2015. https://doi.org/10.1093/med/9780199395125.003.0021
- Manber R, Edinger JD, Gress JL, et al. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489-495. doi:10.1093/sleep/31.4.489
- Steele SJ, Farchione TJ, Cassiello-Robbins C, et al. Efficacy of the Unified Protocol for transdiagnostic treatment of comorbid psychopathology accompanying emotional disorders compared to treatments targeting single disorders. J Psychiatr Res. 2018;104:211-216. doi:10.1016/j.jpsychires.2018.08.005
- Sakiris N, Berle D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. doi:10.1016/j.cpr.2019.101751
- Cassiello-Robbins C, Rosenthal MZ, Ammirati RJ. Delivering transdiagnostic treatment over telehealth during the COVID-19 pandemic: application of the unified protocol. Cogn Behav Pract. 2021;28:555-572. doi:10.1016/j.cbpra.2021.04.007
- Meyer EC, Coe E, Pennington ML, et al. The unified protocol for transdiagnostic treatment of emotional disorders delivered to firefighters via videoconferencing: pilot outcomes highlighting improvements in alcohol use disorder and posttraumatic stress disorder symptoms. Cogn Behav Pract. 2024;31:215-229. doi:10.1016/j.cbpra.2022.08.004
- Varkovitzky RL, Sherrill AM, Reger GM. Effectiveness of the unified protocol for transdiagnostic treatment of emotional disorders among veterans with posttraumatic stress disorder: a pilot study. Behav Modif. 2018;42:210-230. doi:10.1177/0145445517724539
- Oliveira JT, Sousa I, Ribeiro AP, et al. Premature termination of the unified protocol for the transdiagnostic treatment of emotional disorders: The role of ambivalence towards change. Clin Psychol Psychother. 2022;29:1089-1100. doi:10.1002/cpp.2694
- Schaeuffele C, Homeyer S, Perea L, et al. The unified protocol as an internet-based intervention for emotional disorders: Randomized controlled trial. PLoS One. 2022;17:e0270178. doi:10.1371/journal.pone.0270178
- Bentley KH, Cohen ZD, Kim T, et al. The nature, timing, and symptom trajectories of dropout from transdiagnostic and single-diagnosis cognitive-behavioral therapy for anxiety disorders. Behav Ther. 2021;52:1364-1376. doi:10.1016/j.beth.2021.03.007
- Aosved AC, Brown TB, Bell JC, et al. Accelerated prolonged exposure therapy for posttraumatic stress disorder in a Veterans Health Administration system. Fed Pract. 2025;42:S6-S11. doi:10.12788/fp.0568
- Nepon J, Belik SL, Bolton J, et al. The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety. 2010;27:791-798. doi:10.1002/da.20674
- Shiner B, D’Avolio LW, Nguyen TM, et al. Measuring use of evidence based psychotherapy for posttraumatic stress disorder. Adm Policy Ment Health. 2013;40:311-318. doi:10.1007/s10488-012-0421-0
- Nichter B, Stein MB, Monteith LL, et al. Risk factors for suicide attempts among U.S. military veterans: A 7-year population-based, longitudinal cohort study. Suicide Life Threat Behav. 2022;52:303-316. doi:10.1111/sltb.12822
- McHugh RK, Barlow DH. The dissemination and implementation of evidence-based psychological treatments. A review of current efforts. Am Psychol. 2010;65:73-84. doi:10.1037/a0018121
- Ragsdale KA, Nichols AA, Mehta M, et al. Comorbid treatment of traumatic brain injury and mental health disorders. NeuroRehabilitation. 2024;55:375-384. doi:10.3233/NRE-230235
- Thompson-Brenner H, Brooks GE, Boswell JF, et al. Evidence-based implementation practices applied to the intensive treatment of eating disorders: summary of research and illustration of principles using a case example. Clin Psychol Sci Pract. 2018;25:e12221. doi:10.1111/cpsp.12221
- Watkins LE, Patton SC, Drexler K, et al. Clinical effectiveness of an intensive outpatient program for integrated treatment of comorbid substance abuse and mental health disorders. Cog Behav Pract. 2023;30:354-366.
- Yamokoski C, Flores H, Facemire V, et al. Feasibility of an intensive outpatient treatment program for post-traumatic stress disorder within the veterans health care administration. Psychol Serv. 2023;20:506-515. doi:10.1037/ser0000628
- Gaudet T, Kligler B. Whole health in the whole system of the Veterans Administration: how will we know we have reached this future state?. J Altern Complement Med. 2019;25:S7-S11. doi:10.1089/acm.2018.29061.gau
- Dryden EM, Bolton RE, Bokhour BG, et al. Leaning into whole health: sustaining system transformation while supporting patients and employees during COVID-19. Glob Adv Health Med. 2021;10:21649561211021047. doi:10.1177/21649561211021047
- Bond FW, Hayes SC, Baer RA, et al. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676-688. doi:10.1016/j.beth.2011.03.007
- Cacciola JS, Alterman AI, Dephilippis D, et al. Development and initial evaluation of the Brief Addiction Monitor (BAM). J Subst Abuse Treat. 2013;44:256-263. doi:10.1016/j.jsat.2012.07.013
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092-1097. doi:10.1001/archinte.166.10.1092
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Stevanovic D. Quality of life enjoyment and satisfaction questionnaire-short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18:744-750. doi:10.1111/j.1365-2850.2011.01735.x
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Accelerated Unified Protocol for Transdiagnostic Treatment of Anxiety Disorders in a VHA System
Whole Health(y) Aging With Gerofit: The Development of a Pilot Wellness Program for Older Veterans
Whole Health(y) Aging With Gerofit: The Development of a Pilot Wellness Program for Older Veterans
About half of the > 9 million veterans served by the Veterans Health Administration (VHA) are aged ≥ 65 years.1 Veterans are at a higher risk for comorbidities, which may contribute to increased health care costs, mobility limitations and disability, poor quality of life, and mortality. 2-5 Programs and policies that promote health maintenance, independent living, and quality of life are needed among older veterans. To support veterans’ overall health and well-being, the VHA has shifted to whole health, a patient-centered care model.6
The whole health paradigm employs personalized, proactive, and patient-driven care, emphasizing complementary and integrative health practices, and prioritizing health promotion and disease prevention over disease treatment.7 The veteran is empowered to decide “what matters to [me],” reflect on life and health, and define mission, aspiration, and purpose. This approach gives veterans a more active and direct role in their care, distinguishing it from traditional care models. In turn, it helps reduce the burden on clinicians and fosters a more collaborative environment in which both the clinician and veteran work together to shape the care process.7 Veterans utilize the Circle of Health to identify skills and support needed to implement changes in self-care. The Circle of Health includes 8 self-care components: moving the body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind.6 This process drives the creation of a personal health plan, creating opportunities for individuals to engage in well-being programs that matter to them and help them meet their goals.
Gerofit is a VHA best practice and whole health outpatient exercise program for veterans aged ≥65 years.8 Gerofit has focused primarily on exercise within the moving the body self-care component.9 A longitudinal study followed 691 Gerofit participants across 6 US Department of Veterans Affairs (VA) medical centers who on average were 73 years old, had 16 different medical conditions, and took 10 medications. Most were obese and had a mean gait speed of 1.04 m/s, suggesting functional impairment.10 Prior studies have shown that Gerofit participation is associated with a range of health benefits. Two studies reported improvements in psychological well-being and sustained gains in endurance, strength, and flexibility following early Gerofit program participation. 11,12 A 10-year analysis of 115 veterans found that long-term Gerofit participation reduced mortality risk, while another study of 452 veterans showed decreased medication use following 1 year in the program.13,14
The VHA whole health model comprises 3 components: (1) The Pathway, (2) well-being programs, and (3) whole health clinical care.6 The Pathway engages veterans in identifying personal health goals, while well-being programs offer selfcare and skill-building activities. Traditional clinical settings often focus primarily on the third component due to time and resource constraints. The Gerofit platform addresses all 3 components. Its existing infrastructure, including a supportive community and dedicated facilities, provides a setting for implementing The Pathway and well-being programs. The Gerofit structure allows for the time and continuity necessary for these components, which are often limited during standard clinical visits.
By expanding the Gerofit exercise regimen to include additional wellness activities, it can holistically support older veterans. Research supports this integrative approach. For example, a 2020 study found that incorporating a holistic health program into an existing exercise program within a church setting led to improved physical activity and overall health among women participants.15 This article describes the integration of Whole Health(y) Aging with Gerofit (WHAG), a pilot program in Baltimore, Maryland, that integrates whole health components into the established Gerofit framework to enhance the overall well-being of participating veterans (Figure 1).

WHOLE HEALTH(Y) AGING WITH GEROFIT
Gerofit enrollment has been described elsewhere in detail.16 Patients aged ≥ 65 years are eligible to participate with clinician approval if they are medically stable. Following VHA clinician referral and primary care approval, veterans completed a telephone visit to determine eligibility and discuss their exercise history, goals, and preferences. Veterans dependent in activities of daily living and those with cognitive impairment, unstable angina, active proliferative diabetic retinopathy, oxygen dependence, frank incontinence, active open wounds, active substance abuse, volatile behavioral issues, or who are experiencing homelessness are not eligible for Gerofit.
The exercise physiologist identified veteran barriers and incentives to participation and assisted with a plan to maximize SMART goals (specific, measurable, achievable, relevant, and time-bound). Veterans then completed an assessment visit, either in person or virtually, depending on the selected programming. Functional assessments conducted by trained Gerofit exercise physiologists include testing of lower and upper body strength and submaximal endurance.9,17,18 Participation in Gerofit is voluntary and not time limited.
Prior to these newly expanded offerings, veterans could only enroll in a personalized, structured exercise program. Based on feedback from Gerofit participants indicating areas of interest, WHAG was developed to provide additional wellness offerings aligned with other Circle of Health components.6 This included virtual group nutrition education and cooking interventions with optional fresh produce delivery; wellness classes, the Companion Dog Fostering & Adoption program, and Gerofit in the Mind, which included mindfulness classes and relaxation seminars (Figure 1). Programs were virtual (except dog fostering and adoption) and rotated throughout the year. Not all programs are offered simultaneously.
Attendance, completion of selected questions from the individual Personal Health Inventory (PHI) Short Form, measured physical function, self-reported physical activity levels, physical and mental health status, and program satisfaction were measured for all WHAG subprograms.18 Selected questions from the PHI Short Form use a 5-point Likert scale to rate the following whole health components: physical activity; sleep, relaxation, and recovery; healthy eating habits; and positive outlook, healthy relationships, and caring for mental health. Physical function was assessed using 30-second arm curls (upper body strength), 30-second chair stands (lower body strength), and the 2-minute step test (virtual) or 6-minute walk test (in person) (submaximal cardiovascular endurance).
Self-reported physical activity was assessed by asking frequency (days per week) and duration (minutes per session) of cardiovascular and strength exercises to calculate total minutes per week. Physical and mental health status was assessed using the Patient Reported Outcomes Measurement Information System (PROMIS) Global Health Scale.19 Demographic data included sex, race and ethnicity, and age at baseline visit. Mean (SD) was calculated for continuous variables and presented unless otherwise specified, and frequencies were calculated for categorical variables. Subsequent reports will describe additional assessments and detailed outcomes unique to individual programs.
Overview
Veterans chose the programs that best suited their needs without limitations.7 Staff provided guidance on newly available programs based on an individual’s specified goals. Gerofit staff assisted veterans with development of individualized personal health plans, monitoring progress towards their goals, supporting program participation, and connecting veterans with additional whole health resources.
Gerofit Exercise Group. Exercise was designed to address the Moving the Body component of whole health. Veterans could elect to schedule 1-hour, 3-times-weekly in-person gym appointments, participate in 3-times-weekly livestreamed virtual group exercise classes through VA Video Connect, or receive a self-directed at-home exercise plan.
Gerofit Learning Opportunities for Wellness Classes. These virtual health education sessions addressed the personal development component of whole health and were designed to increase self-efficacy and empower veterans to take an active role in their health care. Topics focused broadly on issues related to healthy aging (eg, importance of sleep, goal setting, self-care, and comorbidity education). Veterans could participate in any classes of interest, which were led by health care professionals and offered twice monthly. Sessions encouraged participant questions and peer interaction.
Nutrition. Improving dietary quality is a frequently reported goal of Gerofit participants. WHAG incorporated multiple strategies to assist veterans in meeting these goals. For example, through a partnership with Therapeutic Alternative of Maryland Farm, Gerofit provided veterans free, locally grown fresh produce. This initiative addressed barriers to healthy eating by improving access to fresh produce, which has been shown to influence cooking frequency and diet quality.20-22 Participation in nutrition classes was not required. In 2021, veterans received produce weekly; however, many reported excess quantities. Beginning in 2022, veterans could select both produce items and quantities desired.
In addition, a registered dietitian led a 14-week virtual nutrition education program guided by the social cognitive theory framework and focused on self-regulation skills such as goal setting, overcoming barriers, and identifying triggers.23 Prior research highlighted low health literacy as a common barrier among older veterans, which informed several key components of the curriculum.24 These included how to read and interpret nutrition labels, define balanced meals and snacks, and understand the classification of various food groups such as fats, carbohydrates, and proteins. The online program curriculum included an instructor guide and participant materials for each individual lesson, including an educational handout on the specific week’s topic, applied activity (group or individual), and recipes related to the produce shares. Structured group discussion promoted camaraderie and recipe sharing, and additional instruction on produce preparation and storage.
Reported lack of self-efficacy and knowledge regarding produce preparation prompted a 5-week virtual cooking series, led by a medical student and supervised by a registered dietitian. Sessions combined brief nutrition education with live cooking demonstrations adapted from the VA Healthy Teaching Kitchen curriculum. Recipes emphasized low-cost, commonly found food items. The Healthy Teaching Kitchen modifications focused on Dietary Approaches to Stop Hypertension diets, diabetes, and the importance of protein for older adults. Participants were allowed time to discuss recipes and food preparation tips, and other household members were allowed to observe.
Dog Fostering and Adoption. Veterans could foster or adopt a rescue dog through a partnership with local rescue groups. This program allowed participating veterans to have a companion, which addressed the surroundings, moving the body, and spirit and soul whole health components. The Companion Dog Fostering and Adoption Program and results on physical function and daily physical activity from the first 3 months were recently published. Positive effects on physical activity, physical function, and quality of life were observed at 3 months as compared to baseline in veterans who received a companion dog.25
Gerofit in the Garden. Veterans could opt to receive an EarthBox containing soil and seedlings for 1 vegetable and 1 herb. The boxes are designed to fit on a small tabletop, regardless of home type or availability of backyard. In-person instruction for veterans on care and maintenance was provided by a farm employee with experience in gardening and farming practices.
Gerofit in the Mind. Online relaxation seminars were offered twice monthly for 4 months. Led by a certified sound health guide, sessions incorporated sound baths, crystal bowls, Tibetan bowls, tuning forks, and breath work. Virtual mindfulness classes led by a certified yoga instructor were offered weekly for 1 month. Veterans could drop in and participate based on their availability. Classes were designed to introduce veterans to the practice of mindfulness, improve mood, and lower stress and anxiety.
Pilot Program Outcomes
Sixteen male veterans participated in WHAG. Participants were 62% Black, with a mean age of 76 years. Veterans collaborated with Gerofit staff to develop personal health plans, which ultimately guided program participation (Figure 2).
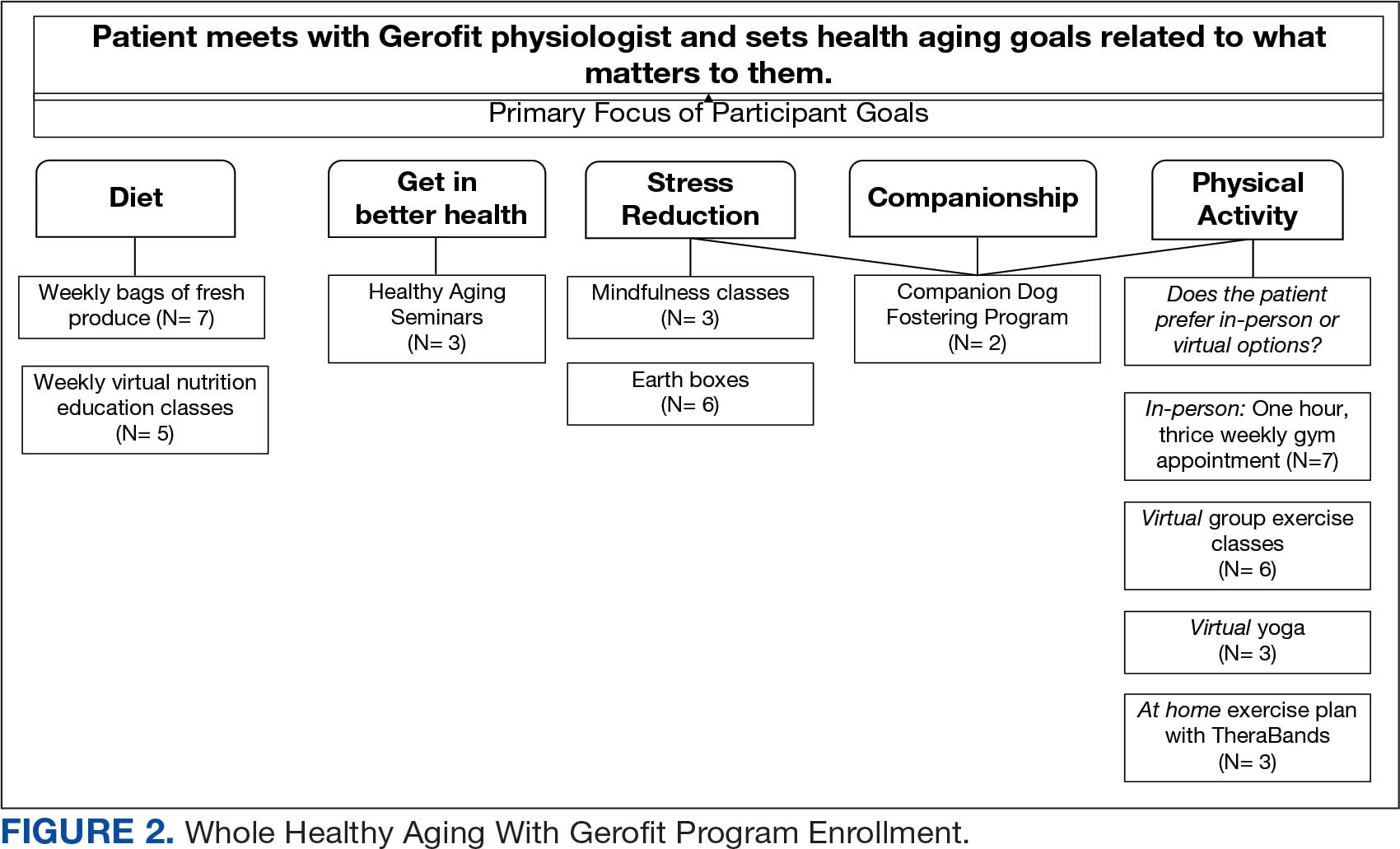
Five participants enrolled in 1 WHAG program, 11 enrolled in 2, and 8 enrolled in ≥ 3 (Table 1). Sixteen veterans completed baseline testing and 12 completed 3-month follow-up assessments (Table 2). At baseline, participants were below the reference range for physical functioning and physical activity levels. After 3 months, improvements were observed in endurance self-reported physical activity, and strength with many values in the reference range. However, physical and mental global health scores did not change.
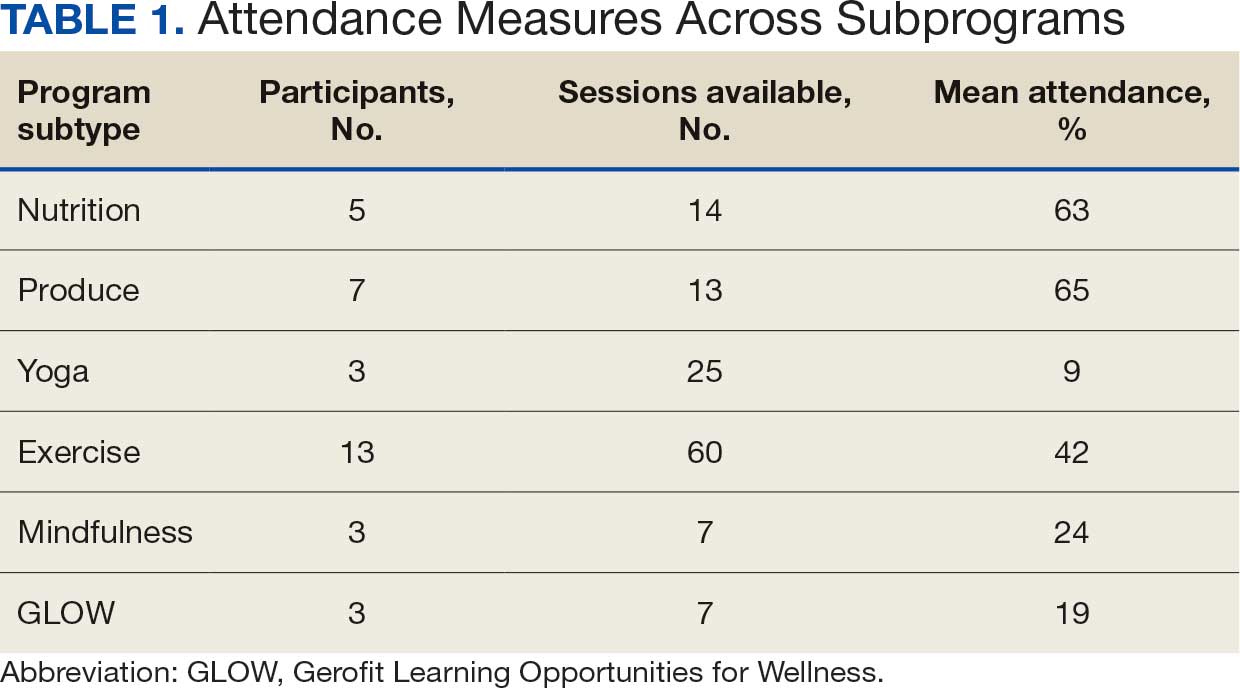

Ten veterans completed the PHI Short Form. Veterans most frequently identified multiple areas they wished to improve, including moving the body (n = 10), recharge (n = 10), food and drink (n = 9), and power of the mind (n = 7). Baseline self-ratings on each whole health component, along with follow-up ratings at the program’s conclusion, are presented in Figure 3. Some participants aimed to maintain current levels rather than seek improvement. At the 3-month mark, most veterans perceived themselves as improving in ≥1 health component.

Discussion Programs that target holistic wellness are needed to ensure the health of a rapidly aging population. The WHAG pilot program is an example of a comprehensive, patient-centered wellness program that supports participants in defining personal wellness goals to promote healthy aging. Gerofit addresses the continuum by beginning with goal-oriented discussions with veterans to guide program participation and support desired outcomes.
Gerofit provided a strong pre-existing framework of virtual social support and physical infrastructure for the addition of WHAG. Gerofit staff were responsible for recruitment and engagement, program oversight, and outcome data collection. Additionally, VHA facilities provide physical space for in-person and virtual programming. Integrating WHAG into Gerofit allows veterans to prioritize “what matters” and engage with peers in a nontraditional way, such as the dog fostering and adoption program provides veterans with an opportunity to increase physical activity levels and improve mental and physical health through the human-animal bond.25
By providing virtual options, WHAG enhances access to health care in medically underserved areas. WHAG also improves the veteran experience with the VA, building on Gerofit’s track record of high patient satisfaction, strong adherence, high retention, and consistent consults for veterans to join.10 The program allows veterans to be at the forefront of their VHA care, choosing to participate in the various offerings based on their personal preferences.
In this population of older veterans from Baltimore, Maryland, the majority of whom reside in disadvantaged areas, we observed that the programs with the highest participation were related to diet, stress reduction, and physical activity. These 3 areas align with common barriers faced by individuals in underserved communities. Many of these communities are food deserts, lack space or resources for gardening, and have limited or unsafe access to opportunities for physical activity, making gyms or even neighborhood exercise difficult to access.26-28 Offering produce delivery and virtual nutrition classes may potentially alleviate this barrier by providing economic stability by increasing access to healthy foods paired with nutrition education to promote use of free, fresh food. Teaching older adults with impaired mobility how to overcome barriers to consuming a healthy diet may improve their dietary intake.23,29,30 Future evaluations aim to examine how these various nutrition programs impact dietary intake and how changes in dietary intake may impact functional outcomes among this group.
Group classes provide opportunities for social connection and mutual support, both of which are powerful motivators for older adults. Frequent contact with others may help reduce the risk of depression, loneliness, and social isolation.28 Routine contact with staff allows for observation of short-term changes in behavior and mood, giving staff the chance to follow up when needed. The addition of these new programs gives participants more opportunities to engage with Gerofit staff and fellow veterans beyond traditional exercise sessions. This WHAG model could expand to other Gerofit sites; however, future whole health programs should take into account the unique needs and barriers specific to each location. Doing so will help ensure offerings align with participant preferences. Programs should be thoughtfully selected and designed to directly address local challenges to promote optimal engagement and support the greatest potential for success.
CONCLUSIONS
Programs that promote and support functional independence in older adults are needed, particularly given the rapidly growing and aging population. Identifying comprehensive strategies that promote healthy aging is likely to be beneficial not only for chronic disease management and social engagement but may also promote functional independence and reduce the risk of further functional decline.
- US Department of Veterans Affairs. Veterans Health Administration– About VHA. Veterans Health Administration. 2023. Accessed December 4, 2025. https://www.va.gov/health/aboutvha.asp
- Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006;21:915- 919. doi:10.1111/j.1525-1497.2006.00526.x
- Koepsell TD, Forsberg CW, Littman AJ. Obesity, overweight, and weight control practices in U.S. veterans. Prev Med. 2009;48:267-271. doi:10.1016/j.ypmed.2009.01.008
- Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28:291-294. doi:10.1016/j.amepre.2004.12.007
- Agha Z, Lofgren RP, VanRuiswyk JV, et al. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160:3252-3257. doi:10.1001/archinte.160.21.3252
- Bokhour BG, Haun JN, Hyde J, et al. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295-300. doi:10.1097/MLR.0000000000001316
- Marchand WR, Beckstrom J, Nazarenko E, et al. The Veterans Health Administration whole health model of care: early implementation and utilization at a large healthcare system. Mil Med. 2020;185:2150-2157. doi:10.1093/milmed/usaa198
- Shulkin D, Elnahal S, Maddock E, Shaheen M. Best Care Everywhere by VA Professionals Across the Nation. US Dept of Veterans Affairs; 2017.
- Morey MC, Lee CC, Castle S, et al. Should structured exercise be promoted as a model of care? Dissemination of the Department of Veterans Affairs Gerofit Program. J Am Geriatr Soc. 2018;66:1009-1016. doi:10.1111/jgs.15276
- Cowper PA, Morey MC, Bearon LB, et al. The impact of supervised exercise on the psychological well-being and health status of older veterans. J Appl Gerontol. 1991;10:469-485. doi:10.1177/073346489101000408
- Pepin MJ, Valencia WM, Bettger JP, et al. Impact of supervised exercise on one-year medication use in older veterans with multiple morbidities. Gerontol Geriatr Med. 2020;6:2333721420956751. doi:10.1177/073346489101000408
- Morey MC, Pieper CF, Sullivan RJ Jr, et al. Fiveyear performance trends for older exercisers: a hierarchical model of endurance, strength, and flexibility. J Am Geriatr Soc. 1996;44:1226-1231. doi:10.1111/j.1532-5415.1996.tb01374.x
- Morey MC, Pieper CF, Crowley GM, et al. Exercise adherence and 10-year mortality in chronically ill older adults. J Am Geriatr Soc. 2002;50:1929-1933. doi:10.1046/j.1532-5415.2002.50602.x
- Jorna M, Ball K, Salmon J. Effects of a holistic health program on women’s physical activity and mental and spiritual health. J Sci Med Sport. 2006;9:395-401. doi:10.1016/j.jsams.2006.06.011
- Jennings SC, Manning KM, Bettger JP, et al. Rapid transition to telehealth group exercise and functional assessments in response to COVID-19. Gerontol Geriatr Med. 2020;6:2333721420980313. doi:10.1177/2333721420980313
- Morey MC, Crowley GM, Robbins MS, et al. The Gerofit program: a VA innovation. South Med J. 1994;87:S83-87.
- Addison O, Serra MC, Katzel L, et al. Mobility improvements are found in older veterans after 6 months of Gerofit regardless of BMI classification. J Aging Phys Act. 2019;27:848-854. doi:10.1123/japa.2018-0317
- Veterans Health Administration Office of Patient Centered Care and Cultural Transformation. Making your plan— whole health. November 14, 2023. Accessed December 4, 2025. https://www.va.gov/WHOLEHEALTH/phi.asp
- Hays RD, Bjorner JB, Revicki DA, et al. Development of physical and mental health summary scores from the Patient-Reported Outcomes Measurement Information System (PROMIS) global items. Qual Life Res. 2009;18:873-880. doi:10.1007/s11136-009-9496-9
- Aktary ML, Caron-Roy S, Sajobi T, et al. Impact of a farmers’ market nutrition coupon programme on diet quality and psychosocial well-being among low-income adults: protocol for a randomised controlled trial and a longitudinal qualitative investigation. BMJ Open. 2020;10:e035143. doi:10.1136/bmjopen-2019-035143
- Afshin A, Penalvo JL, Del Gobbo L, et al. The prospective impact of food pricing on improving dietary consumption: a systematic review and meta-analysis. PLoS One. 2017;12:e0172277. doi:10.1371/journal.pone.0172277
- Singleton CR, Kessee N, Chatman C, et al. Racial/ ethnic differences in the shopping behaviors and fruit and vegetable consumption of farmers’ market incentive program users in Illinois. Ethn Dis. 2020;30:109. doi:10.18865/ed.30.1.109
- Cassatt S, Giffuni J, Ortmeyer H, et al. A pilot study to evaluate the development and implementation of a virtual nutrition education program in older veterans. Abstract presented at: American Heart Association Epidemiology and Prevention/Lifestyle and Cardiometabolic Health 2022 Scientific Sessions; March 1-4, 2022; Chicago, IL. https:// www.ahajournals.org/doi/10.1161/circ.145.suppl_1.P002
- Parker EA, Perez WJ, Phipps B, et al. Dietary quality and perceived barriers to weight loss among older overweight veterans with dysmobility. Int J Environ Res Public Health. 2022;19:9153. doi:10.3390/ijerph19159153
- Ortmeyer HK, Giffuni J, Etchberger D, et al. The role of companion dogs in the VA Maryland Health Care System Whole Health(y) GeroFit Program. Animals (Basel). 2023;13:19. doi:10.3390/ani13193047
- Milaneschi Y, Tanaka T, Ferrucci L. Nutritional determinants of mobility. Curr Opin Clin Nutr Metab Care. 2010;13:625- 629.
- Lane JM, Davis BA. Food, physical activity, and health deserts in Alabama: the spatial link between healthy eating, exercise, and socioeconomic factors. GeoJournal. 2022;87:5229-5249.
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Wolfson JA, Ramsing R, Richardson CR, et al. Barriers to healthy food access: associations with household income and cooking behavior. Prev Med Rep. 2019;13:298-305. doi:10.1016/j.pmedr.2019.01.023
About half of the > 9 million veterans served by the Veterans Health Administration (VHA) are aged ≥ 65 years.1 Veterans are at a higher risk for comorbidities, which may contribute to increased health care costs, mobility limitations and disability, poor quality of life, and mortality. 2-5 Programs and policies that promote health maintenance, independent living, and quality of life are needed among older veterans. To support veterans’ overall health and well-being, the VHA has shifted to whole health, a patient-centered care model.6
The whole health paradigm employs personalized, proactive, and patient-driven care, emphasizing complementary and integrative health practices, and prioritizing health promotion and disease prevention over disease treatment.7 The veteran is empowered to decide “what matters to [me],” reflect on life and health, and define mission, aspiration, and purpose. This approach gives veterans a more active and direct role in their care, distinguishing it from traditional care models. In turn, it helps reduce the burden on clinicians and fosters a more collaborative environment in which both the clinician and veteran work together to shape the care process.7 Veterans utilize the Circle of Health to identify skills and support needed to implement changes in self-care. The Circle of Health includes 8 self-care components: moving the body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind.6 This process drives the creation of a personal health plan, creating opportunities for individuals to engage in well-being programs that matter to them and help them meet their goals.
Gerofit is a VHA best practice and whole health outpatient exercise program for veterans aged ≥65 years.8 Gerofit has focused primarily on exercise within the moving the body self-care component.9 A longitudinal study followed 691 Gerofit participants across 6 US Department of Veterans Affairs (VA) medical centers who on average were 73 years old, had 16 different medical conditions, and took 10 medications. Most were obese and had a mean gait speed of 1.04 m/s, suggesting functional impairment.10 Prior studies have shown that Gerofit participation is associated with a range of health benefits. Two studies reported improvements in psychological well-being and sustained gains in endurance, strength, and flexibility following early Gerofit program participation. 11,12 A 10-year analysis of 115 veterans found that long-term Gerofit participation reduced mortality risk, while another study of 452 veterans showed decreased medication use following 1 year in the program.13,14
The VHA whole health model comprises 3 components: (1) The Pathway, (2) well-being programs, and (3) whole health clinical care.6 The Pathway engages veterans in identifying personal health goals, while well-being programs offer selfcare and skill-building activities. Traditional clinical settings often focus primarily on the third component due to time and resource constraints. The Gerofit platform addresses all 3 components. Its existing infrastructure, including a supportive community and dedicated facilities, provides a setting for implementing The Pathway and well-being programs. The Gerofit structure allows for the time and continuity necessary for these components, which are often limited during standard clinical visits.
By expanding the Gerofit exercise regimen to include additional wellness activities, it can holistically support older veterans. Research supports this integrative approach. For example, a 2020 study found that incorporating a holistic health program into an existing exercise program within a church setting led to improved physical activity and overall health among women participants.15 This article describes the integration of Whole Health(y) Aging with Gerofit (WHAG), a pilot program in Baltimore, Maryland, that integrates whole health components into the established Gerofit framework to enhance the overall well-being of participating veterans (Figure 1).
WHOLE HEALTH(Y) AGING WITH GEROFIT
Gerofit enrollment has been described elsewhere in detail.16 Patients aged ≥ 65 years are eligible to participate with clinician approval if they are medically stable. Following VHA clinician referral and primary care approval, veterans completed a telephone visit to determine eligibility and discuss their exercise history, goals, and preferences. Veterans dependent in activities of daily living and those with cognitive impairment, unstable angina, active proliferative diabetic retinopathy, oxygen dependence, frank incontinence, active open wounds, active substance abuse, volatile behavioral issues, or who are experiencing homelessness are not eligible for Gerofit.
The exercise physiologist identified veteran barriers and incentives to participation and assisted with a plan to maximize SMART goals (specific, measurable, achievable, relevant, and time-bound). Veterans then completed an assessment visit, either in person or virtually, depending on the selected programming. Functional assessments conducted by trained Gerofit exercise physiologists include testing of lower and upper body strength and submaximal endurance.9,17,18 Participation in Gerofit is voluntary and not time limited.
Prior to these newly expanded offerings, veterans could only enroll in a personalized, structured exercise program. Based on feedback from Gerofit participants indicating areas of interest, WHAG was developed to provide additional wellness offerings aligned with other Circle of Health components.6 This included virtual group nutrition education and cooking interventions with optional fresh produce delivery; wellness classes, the Companion Dog Fostering & Adoption program, and Gerofit in the Mind, which included mindfulness classes and relaxation seminars (Figure 1). Programs were virtual (except dog fostering and adoption) and rotated throughout the year. Not all programs are offered simultaneously.
Attendance, completion of selected questions from the individual Personal Health Inventory (PHI) Short Form, measured physical function, self-reported physical activity levels, physical and mental health status, and program satisfaction were measured for all WHAG subprograms.18 Selected questions from the PHI Short Form use a 5-point Likert scale to rate the following whole health components: physical activity; sleep, relaxation, and recovery; healthy eating habits; and positive outlook, healthy relationships, and caring for mental health. Physical function was assessed using 30-second arm curls (upper body strength), 30-second chair stands (lower body strength), and the 2-minute step test (virtual) or 6-minute walk test (in person) (submaximal cardiovascular endurance).
Self-reported physical activity was assessed by asking frequency (days per week) and duration (minutes per session) of cardiovascular and strength exercises to calculate total minutes per week. Physical and mental health status was assessed using the Patient Reported Outcomes Measurement Information System (PROMIS) Global Health Scale.19 Demographic data included sex, race and ethnicity, and age at baseline visit. Mean (SD) was calculated for continuous variables and presented unless otherwise specified, and frequencies were calculated for categorical variables. Subsequent reports will describe additional assessments and detailed outcomes unique to individual programs.
Overview
Veterans chose the programs that best suited their needs without limitations.7 Staff provided guidance on newly available programs based on an individual’s specified goals. Gerofit staff assisted veterans with development of individualized personal health plans, monitoring progress towards their goals, supporting program participation, and connecting veterans with additional whole health resources.
Gerofit Exercise Group. Exercise was designed to address the Moving the Body component of whole health. Veterans could elect to schedule 1-hour, 3-times-weekly in-person gym appointments, participate in 3-times-weekly livestreamed virtual group exercise classes through VA Video Connect, or receive a self-directed at-home exercise plan.
Gerofit Learning Opportunities for Wellness Classes. These virtual health education sessions addressed the personal development component of whole health and were designed to increase self-efficacy and empower veterans to take an active role in their health care. Topics focused broadly on issues related to healthy aging (eg, importance of sleep, goal setting, self-care, and comorbidity education). Veterans could participate in any classes of interest, which were led by health care professionals and offered twice monthly. Sessions encouraged participant questions and peer interaction.
Nutrition. Improving dietary quality is a frequently reported goal of Gerofit participants. WHAG incorporated multiple strategies to assist veterans in meeting these goals. For example, through a partnership with Therapeutic Alternative of Maryland Farm, Gerofit provided veterans free, locally grown fresh produce. This initiative addressed barriers to healthy eating by improving access to fresh produce, which has been shown to influence cooking frequency and diet quality.20-22 Participation in nutrition classes was not required. In 2021, veterans received produce weekly; however, many reported excess quantities. Beginning in 2022, veterans could select both produce items and quantities desired.
In addition, a registered dietitian led a 14-week virtual nutrition education program guided by the social cognitive theory framework and focused on self-regulation skills such as goal setting, overcoming barriers, and identifying triggers.23 Prior research highlighted low health literacy as a common barrier among older veterans, which informed several key components of the curriculum.24 These included how to read and interpret nutrition labels, define balanced meals and snacks, and understand the classification of various food groups such as fats, carbohydrates, and proteins. The online program curriculum included an instructor guide and participant materials for each individual lesson, including an educational handout on the specific week’s topic, applied activity (group or individual), and recipes related to the produce shares. Structured group discussion promoted camaraderie and recipe sharing, and additional instruction on produce preparation and storage.
Reported lack of self-efficacy and knowledge regarding produce preparation prompted a 5-week virtual cooking series, led by a medical student and supervised by a registered dietitian. Sessions combined brief nutrition education with live cooking demonstrations adapted from the VA Healthy Teaching Kitchen curriculum. Recipes emphasized low-cost, commonly found food items. The Healthy Teaching Kitchen modifications focused on Dietary Approaches to Stop Hypertension diets, diabetes, and the importance of protein for older adults. Participants were allowed time to discuss recipes and food preparation tips, and other household members were allowed to observe.
Dog Fostering and Adoption. Veterans could foster or adopt a rescue dog through a partnership with local rescue groups. This program allowed participating veterans to have a companion, which addressed the surroundings, moving the body, and spirit and soul whole health components. The Companion Dog Fostering and Adoption Program and results on physical function and daily physical activity from the first 3 months were recently published. Positive effects on physical activity, physical function, and quality of life were observed at 3 months as compared to baseline in veterans who received a companion dog.25
Gerofit in the Garden. Veterans could opt to receive an EarthBox containing soil and seedlings for 1 vegetable and 1 herb. The boxes are designed to fit on a small tabletop, regardless of home type or availability of backyard. In-person instruction for veterans on care and maintenance was provided by a farm employee with experience in gardening and farming practices.
Gerofit in the Mind. Online relaxation seminars were offered twice monthly for 4 months. Led by a certified sound health guide, sessions incorporated sound baths, crystal bowls, Tibetan bowls, tuning forks, and breath work. Virtual mindfulness classes led by a certified yoga instructor were offered weekly for 1 month. Veterans could drop in and participate based on their availability. Classes were designed to introduce veterans to the practice of mindfulness, improve mood, and lower stress and anxiety.
Pilot Program Outcomes
Sixteen male veterans participated in WHAG. Participants were 62% Black, with a mean age of 76 years. Veterans collaborated with Gerofit staff to develop personal health plans, which ultimately guided program participation (Figure 2).
Five participants enrolled in 1 WHAG program, 11 enrolled in 2, and 8 enrolled in ≥ 3 (Table 1). Sixteen veterans completed baseline testing and 12 completed 3-month follow-up assessments (Table 2). At baseline, participants were below the reference range for physical functioning and physical activity levels. After 3 months, improvements were observed in endurance self-reported physical activity, and strength with many values in the reference range. However, physical and mental global health scores did not change.
Ten veterans completed the PHI Short Form. Veterans most frequently identified multiple areas they wished to improve, including moving the body (n = 10), recharge (n = 10), food and drink (n = 9), and power of the mind (n = 7). Baseline self-ratings on each whole health component, along with follow-up ratings at the program’s conclusion, are presented in Figure 3. Some participants aimed to maintain current levels rather than seek improvement. At the 3-month mark, most veterans perceived themselves as improving in ≥1 health component.
Discussion Programs that target holistic wellness are needed to ensure the health of a rapidly aging population. The WHAG pilot program is an example of a comprehensive, patient-centered wellness program that supports participants in defining personal wellness goals to promote healthy aging. Gerofit addresses the continuum by beginning with goal-oriented discussions with veterans to guide program participation and support desired outcomes.
Gerofit provided a strong pre-existing framework of virtual social support and physical infrastructure for the addition of WHAG. Gerofit staff were responsible for recruitment and engagement, program oversight, and outcome data collection. Additionally, VHA facilities provide physical space for in-person and virtual programming. Integrating WHAG into Gerofit allows veterans to prioritize “what matters” and engage with peers in a nontraditional way, such as the dog fostering and adoption program provides veterans with an opportunity to increase physical activity levels and improve mental and physical health through the human-animal bond.25
By providing virtual options, WHAG enhances access to health care in medically underserved areas. WHAG also improves the veteran experience with the VA, building on Gerofit’s track record of high patient satisfaction, strong adherence, high retention, and consistent consults for veterans to join.10 The program allows veterans to be at the forefront of their VHA care, choosing to participate in the various offerings based on their personal preferences.
In this population of older veterans from Baltimore, Maryland, the majority of whom reside in disadvantaged areas, we observed that the programs with the highest participation were related to diet, stress reduction, and physical activity. These 3 areas align with common barriers faced by individuals in underserved communities. Many of these communities are food deserts, lack space or resources for gardening, and have limited or unsafe access to opportunities for physical activity, making gyms or even neighborhood exercise difficult to access.26-28 Offering produce delivery and virtual nutrition classes may potentially alleviate this barrier by providing economic stability by increasing access to healthy foods paired with nutrition education to promote use of free, fresh food. Teaching older adults with impaired mobility how to overcome barriers to consuming a healthy diet may improve their dietary intake.23,29,30 Future evaluations aim to examine how these various nutrition programs impact dietary intake and how changes in dietary intake may impact functional outcomes among this group.
Group classes provide opportunities for social connection and mutual support, both of which are powerful motivators for older adults. Frequent contact with others may help reduce the risk of depression, loneliness, and social isolation.28 Routine contact with staff allows for observation of short-term changes in behavior and mood, giving staff the chance to follow up when needed. The addition of these new programs gives participants more opportunities to engage with Gerofit staff and fellow veterans beyond traditional exercise sessions. This WHAG model could expand to other Gerofit sites; however, future whole health programs should take into account the unique needs and barriers specific to each location. Doing so will help ensure offerings align with participant preferences. Programs should be thoughtfully selected and designed to directly address local challenges to promote optimal engagement and support the greatest potential for success.
CONCLUSIONS
Programs that promote and support functional independence in older adults are needed, particularly given the rapidly growing and aging population. Identifying comprehensive strategies that promote healthy aging is likely to be beneficial not only for chronic disease management and social engagement but may also promote functional independence and reduce the risk of further functional decline.
About half of the > 9 million veterans served by the Veterans Health Administration (VHA) are aged ≥ 65 years.1 Veterans are at a higher risk for comorbidities, which may contribute to increased health care costs, mobility limitations and disability, poor quality of life, and mortality. 2-5 Programs and policies that promote health maintenance, independent living, and quality of life are needed among older veterans. To support veterans’ overall health and well-being, the VHA has shifted to whole health, a patient-centered care model.6
The whole health paradigm employs personalized, proactive, and patient-driven care, emphasizing complementary and integrative health practices, and prioritizing health promotion and disease prevention over disease treatment.7 The veteran is empowered to decide “what matters to [me],” reflect on life and health, and define mission, aspiration, and purpose. This approach gives veterans a more active and direct role in their care, distinguishing it from traditional care models. In turn, it helps reduce the burden on clinicians and fosters a more collaborative environment in which both the clinician and veteran work together to shape the care process.7 Veterans utilize the Circle of Health to identify skills and support needed to implement changes in self-care. The Circle of Health includes 8 self-care components: moving the body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind.6 This process drives the creation of a personal health plan, creating opportunities for individuals to engage in well-being programs that matter to them and help them meet their goals.
Gerofit is a VHA best practice and whole health outpatient exercise program for veterans aged ≥65 years.8 Gerofit has focused primarily on exercise within the moving the body self-care component.9 A longitudinal study followed 691 Gerofit participants across 6 US Department of Veterans Affairs (VA) medical centers who on average were 73 years old, had 16 different medical conditions, and took 10 medications. Most were obese and had a mean gait speed of 1.04 m/s, suggesting functional impairment.10 Prior studies have shown that Gerofit participation is associated with a range of health benefits. Two studies reported improvements in psychological well-being and sustained gains in endurance, strength, and flexibility following early Gerofit program participation. 11,12 A 10-year analysis of 115 veterans found that long-term Gerofit participation reduced mortality risk, while another study of 452 veterans showed decreased medication use following 1 year in the program.13,14
The VHA whole health model comprises 3 components: (1) The Pathway, (2) well-being programs, and (3) whole health clinical care.6 The Pathway engages veterans in identifying personal health goals, while well-being programs offer selfcare and skill-building activities. Traditional clinical settings often focus primarily on the third component due to time and resource constraints. The Gerofit platform addresses all 3 components. Its existing infrastructure, including a supportive community and dedicated facilities, provides a setting for implementing The Pathway and well-being programs. The Gerofit structure allows for the time and continuity necessary for these components, which are often limited during standard clinical visits.
By expanding the Gerofit exercise regimen to include additional wellness activities, it can holistically support older veterans. Research supports this integrative approach. For example, a 2020 study found that incorporating a holistic health program into an existing exercise program within a church setting led to improved physical activity and overall health among women participants.15 This article describes the integration of Whole Health(y) Aging with Gerofit (WHAG), a pilot program in Baltimore, Maryland, that integrates whole health components into the established Gerofit framework to enhance the overall well-being of participating veterans (Figure 1).
WHOLE HEALTH(Y) AGING WITH GEROFIT
Gerofit enrollment has been described elsewhere in detail.16 Patients aged ≥ 65 years are eligible to participate with clinician approval if they are medically stable. Following VHA clinician referral and primary care approval, veterans completed a telephone visit to determine eligibility and discuss their exercise history, goals, and preferences. Veterans dependent in activities of daily living and those with cognitive impairment, unstable angina, active proliferative diabetic retinopathy, oxygen dependence, frank incontinence, active open wounds, active substance abuse, volatile behavioral issues, or who are experiencing homelessness are not eligible for Gerofit.
The exercise physiologist identified veteran barriers and incentives to participation and assisted with a plan to maximize SMART goals (specific, measurable, achievable, relevant, and time-bound). Veterans then completed an assessment visit, either in person or virtually, depending on the selected programming. Functional assessments conducted by trained Gerofit exercise physiologists include testing of lower and upper body strength and submaximal endurance.9,17,18 Participation in Gerofit is voluntary and not time limited.
Prior to these newly expanded offerings, veterans could only enroll in a personalized, structured exercise program. Based on feedback from Gerofit participants indicating areas of interest, WHAG was developed to provide additional wellness offerings aligned with other Circle of Health components.6 This included virtual group nutrition education and cooking interventions with optional fresh produce delivery; wellness classes, the Companion Dog Fostering & Adoption program, and Gerofit in the Mind, which included mindfulness classes and relaxation seminars (Figure 1). Programs were virtual (except dog fostering and adoption) and rotated throughout the year. Not all programs are offered simultaneously.
Attendance, completion of selected questions from the individual Personal Health Inventory (PHI) Short Form, measured physical function, self-reported physical activity levels, physical and mental health status, and program satisfaction were measured for all WHAG subprograms.18 Selected questions from the PHI Short Form use a 5-point Likert scale to rate the following whole health components: physical activity; sleep, relaxation, and recovery; healthy eating habits; and positive outlook, healthy relationships, and caring for mental health. Physical function was assessed using 30-second arm curls (upper body strength), 30-second chair stands (lower body strength), and the 2-minute step test (virtual) or 6-minute walk test (in person) (submaximal cardiovascular endurance).
Self-reported physical activity was assessed by asking frequency (days per week) and duration (minutes per session) of cardiovascular and strength exercises to calculate total minutes per week. Physical and mental health status was assessed using the Patient Reported Outcomes Measurement Information System (PROMIS) Global Health Scale.19 Demographic data included sex, race and ethnicity, and age at baseline visit. Mean (SD) was calculated for continuous variables and presented unless otherwise specified, and frequencies were calculated for categorical variables. Subsequent reports will describe additional assessments and detailed outcomes unique to individual programs.
Overview
Veterans chose the programs that best suited their needs without limitations.7 Staff provided guidance on newly available programs based on an individual’s specified goals. Gerofit staff assisted veterans with development of individualized personal health plans, monitoring progress towards their goals, supporting program participation, and connecting veterans with additional whole health resources.
Gerofit Exercise Group. Exercise was designed to address the Moving the Body component of whole health. Veterans could elect to schedule 1-hour, 3-times-weekly in-person gym appointments, participate in 3-times-weekly livestreamed virtual group exercise classes through VA Video Connect, or receive a self-directed at-home exercise plan.
Gerofit Learning Opportunities for Wellness Classes. These virtual health education sessions addressed the personal development component of whole health and were designed to increase self-efficacy and empower veterans to take an active role in their health care. Topics focused broadly on issues related to healthy aging (eg, importance of sleep, goal setting, self-care, and comorbidity education). Veterans could participate in any classes of interest, which were led by health care professionals and offered twice monthly. Sessions encouraged participant questions and peer interaction.
Nutrition. Improving dietary quality is a frequently reported goal of Gerofit participants. WHAG incorporated multiple strategies to assist veterans in meeting these goals. For example, through a partnership with Therapeutic Alternative of Maryland Farm, Gerofit provided veterans free, locally grown fresh produce. This initiative addressed barriers to healthy eating by improving access to fresh produce, which has been shown to influence cooking frequency and diet quality.20-22 Participation in nutrition classes was not required. In 2021, veterans received produce weekly; however, many reported excess quantities. Beginning in 2022, veterans could select both produce items and quantities desired.
In addition, a registered dietitian led a 14-week virtual nutrition education program guided by the social cognitive theory framework and focused on self-regulation skills such as goal setting, overcoming barriers, and identifying triggers.23 Prior research highlighted low health literacy as a common barrier among older veterans, which informed several key components of the curriculum.24 These included how to read and interpret nutrition labels, define balanced meals and snacks, and understand the classification of various food groups such as fats, carbohydrates, and proteins. The online program curriculum included an instructor guide and participant materials for each individual lesson, including an educational handout on the specific week’s topic, applied activity (group or individual), and recipes related to the produce shares. Structured group discussion promoted camaraderie and recipe sharing, and additional instruction on produce preparation and storage.
Reported lack of self-efficacy and knowledge regarding produce preparation prompted a 5-week virtual cooking series, led by a medical student and supervised by a registered dietitian. Sessions combined brief nutrition education with live cooking demonstrations adapted from the VA Healthy Teaching Kitchen curriculum. Recipes emphasized low-cost, commonly found food items. The Healthy Teaching Kitchen modifications focused on Dietary Approaches to Stop Hypertension diets, diabetes, and the importance of protein for older adults. Participants were allowed time to discuss recipes and food preparation tips, and other household members were allowed to observe.
Dog Fostering and Adoption. Veterans could foster or adopt a rescue dog through a partnership with local rescue groups. This program allowed participating veterans to have a companion, which addressed the surroundings, moving the body, and spirit and soul whole health components. The Companion Dog Fostering and Adoption Program and results on physical function and daily physical activity from the first 3 months were recently published. Positive effects on physical activity, physical function, and quality of life were observed at 3 months as compared to baseline in veterans who received a companion dog.25
Gerofit in the Garden. Veterans could opt to receive an EarthBox containing soil and seedlings for 1 vegetable and 1 herb. The boxes are designed to fit on a small tabletop, regardless of home type or availability of backyard. In-person instruction for veterans on care and maintenance was provided by a farm employee with experience in gardening and farming practices.
Gerofit in the Mind. Online relaxation seminars were offered twice monthly for 4 months. Led by a certified sound health guide, sessions incorporated sound baths, crystal bowls, Tibetan bowls, tuning forks, and breath work. Virtual mindfulness classes led by a certified yoga instructor were offered weekly for 1 month. Veterans could drop in and participate based on their availability. Classes were designed to introduce veterans to the practice of mindfulness, improve mood, and lower stress and anxiety.
Pilot Program Outcomes
Sixteen male veterans participated in WHAG. Participants were 62% Black, with a mean age of 76 years. Veterans collaborated with Gerofit staff to develop personal health plans, which ultimately guided program participation (Figure 2).
Five participants enrolled in 1 WHAG program, 11 enrolled in 2, and 8 enrolled in ≥ 3 (Table 1). Sixteen veterans completed baseline testing and 12 completed 3-month follow-up assessments (Table 2). At baseline, participants were below the reference range for physical functioning and physical activity levels. After 3 months, improvements were observed in endurance self-reported physical activity, and strength with many values in the reference range. However, physical and mental global health scores did not change.
Ten veterans completed the PHI Short Form. Veterans most frequently identified multiple areas they wished to improve, including moving the body (n = 10), recharge (n = 10), food and drink (n = 9), and power of the mind (n = 7). Baseline self-ratings on each whole health component, along with follow-up ratings at the program’s conclusion, are presented in Figure 3. Some participants aimed to maintain current levels rather than seek improvement. At the 3-month mark, most veterans perceived themselves as improving in ≥1 health component.
Discussion Programs that target holistic wellness are needed to ensure the health of a rapidly aging population. The WHAG pilot program is an example of a comprehensive, patient-centered wellness program that supports participants in defining personal wellness goals to promote healthy aging. Gerofit addresses the continuum by beginning with goal-oriented discussions with veterans to guide program participation and support desired outcomes.
Gerofit provided a strong pre-existing framework of virtual social support and physical infrastructure for the addition of WHAG. Gerofit staff were responsible for recruitment and engagement, program oversight, and outcome data collection. Additionally, VHA facilities provide physical space for in-person and virtual programming. Integrating WHAG into Gerofit allows veterans to prioritize “what matters” and engage with peers in a nontraditional way, such as the dog fostering and adoption program provides veterans with an opportunity to increase physical activity levels and improve mental and physical health through the human-animal bond.25
By providing virtual options, WHAG enhances access to health care in medically underserved areas. WHAG also improves the veteran experience with the VA, building on Gerofit’s track record of high patient satisfaction, strong adherence, high retention, and consistent consults for veterans to join.10 The program allows veterans to be at the forefront of their VHA care, choosing to participate in the various offerings based on their personal preferences.
In this population of older veterans from Baltimore, Maryland, the majority of whom reside in disadvantaged areas, we observed that the programs with the highest participation were related to diet, stress reduction, and physical activity. These 3 areas align with common barriers faced by individuals in underserved communities. Many of these communities are food deserts, lack space or resources for gardening, and have limited or unsafe access to opportunities for physical activity, making gyms or even neighborhood exercise difficult to access.26-28 Offering produce delivery and virtual nutrition classes may potentially alleviate this barrier by providing economic stability by increasing access to healthy foods paired with nutrition education to promote use of free, fresh food. Teaching older adults with impaired mobility how to overcome barriers to consuming a healthy diet may improve their dietary intake.23,29,30 Future evaluations aim to examine how these various nutrition programs impact dietary intake and how changes in dietary intake may impact functional outcomes among this group.
Group classes provide opportunities for social connection and mutual support, both of which are powerful motivators for older adults. Frequent contact with others may help reduce the risk of depression, loneliness, and social isolation.28 Routine contact with staff allows for observation of short-term changes in behavior and mood, giving staff the chance to follow up when needed. The addition of these new programs gives participants more opportunities to engage with Gerofit staff and fellow veterans beyond traditional exercise sessions. This WHAG model could expand to other Gerofit sites; however, future whole health programs should take into account the unique needs and barriers specific to each location. Doing so will help ensure offerings align with participant preferences. Programs should be thoughtfully selected and designed to directly address local challenges to promote optimal engagement and support the greatest potential for success.
CONCLUSIONS
Programs that promote and support functional independence in older adults are needed, particularly given the rapidly growing and aging population. Identifying comprehensive strategies that promote healthy aging is likely to be beneficial not only for chronic disease management and social engagement but may also promote functional independence and reduce the risk of further functional decline.
- US Department of Veterans Affairs. Veterans Health Administration– About VHA. Veterans Health Administration. 2023. Accessed December 4, 2025. https://www.va.gov/health/aboutvha.asp
- Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006;21:915- 919. doi:10.1111/j.1525-1497.2006.00526.x
- Koepsell TD, Forsberg CW, Littman AJ. Obesity, overweight, and weight control practices in U.S. veterans. Prev Med. 2009;48:267-271. doi:10.1016/j.ypmed.2009.01.008
- Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28:291-294. doi:10.1016/j.amepre.2004.12.007
- Agha Z, Lofgren RP, VanRuiswyk JV, et al. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160:3252-3257. doi:10.1001/archinte.160.21.3252
- Bokhour BG, Haun JN, Hyde J, et al. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295-300. doi:10.1097/MLR.0000000000001316
- Marchand WR, Beckstrom J, Nazarenko E, et al. The Veterans Health Administration whole health model of care: early implementation and utilization at a large healthcare system. Mil Med. 2020;185:2150-2157. doi:10.1093/milmed/usaa198
- Shulkin D, Elnahal S, Maddock E, Shaheen M. Best Care Everywhere by VA Professionals Across the Nation. US Dept of Veterans Affairs; 2017.
- Morey MC, Lee CC, Castle S, et al. Should structured exercise be promoted as a model of care? Dissemination of the Department of Veterans Affairs Gerofit Program. J Am Geriatr Soc. 2018;66:1009-1016. doi:10.1111/jgs.15276
- Cowper PA, Morey MC, Bearon LB, et al. The impact of supervised exercise on the psychological well-being and health status of older veterans. J Appl Gerontol. 1991;10:469-485. doi:10.1177/073346489101000408
- Pepin MJ, Valencia WM, Bettger JP, et al. Impact of supervised exercise on one-year medication use in older veterans with multiple morbidities. Gerontol Geriatr Med. 2020;6:2333721420956751. doi:10.1177/073346489101000408
- Morey MC, Pieper CF, Sullivan RJ Jr, et al. Fiveyear performance trends for older exercisers: a hierarchical model of endurance, strength, and flexibility. J Am Geriatr Soc. 1996;44:1226-1231. doi:10.1111/j.1532-5415.1996.tb01374.x
- Morey MC, Pieper CF, Crowley GM, et al. Exercise adherence and 10-year mortality in chronically ill older adults. J Am Geriatr Soc. 2002;50:1929-1933. doi:10.1046/j.1532-5415.2002.50602.x
- Jorna M, Ball K, Salmon J. Effects of a holistic health program on women’s physical activity and mental and spiritual health. J Sci Med Sport. 2006;9:395-401. doi:10.1016/j.jsams.2006.06.011
- Jennings SC, Manning KM, Bettger JP, et al. Rapid transition to telehealth group exercise and functional assessments in response to COVID-19. Gerontol Geriatr Med. 2020;6:2333721420980313. doi:10.1177/2333721420980313
- Morey MC, Crowley GM, Robbins MS, et al. The Gerofit program: a VA innovation. South Med J. 1994;87:S83-87.
- Addison O, Serra MC, Katzel L, et al. Mobility improvements are found in older veterans after 6 months of Gerofit regardless of BMI classification. J Aging Phys Act. 2019;27:848-854. doi:10.1123/japa.2018-0317
- Veterans Health Administration Office of Patient Centered Care and Cultural Transformation. Making your plan— whole health. November 14, 2023. Accessed December 4, 2025. https://www.va.gov/WHOLEHEALTH/phi.asp
- Hays RD, Bjorner JB, Revicki DA, et al. Development of physical and mental health summary scores from the Patient-Reported Outcomes Measurement Information System (PROMIS) global items. Qual Life Res. 2009;18:873-880. doi:10.1007/s11136-009-9496-9
- Aktary ML, Caron-Roy S, Sajobi T, et al. Impact of a farmers’ market nutrition coupon programme on diet quality and psychosocial well-being among low-income adults: protocol for a randomised controlled trial and a longitudinal qualitative investigation. BMJ Open. 2020;10:e035143. doi:10.1136/bmjopen-2019-035143
- Afshin A, Penalvo JL, Del Gobbo L, et al. The prospective impact of food pricing on improving dietary consumption: a systematic review and meta-analysis. PLoS One. 2017;12:e0172277. doi:10.1371/journal.pone.0172277
- Singleton CR, Kessee N, Chatman C, et al. Racial/ ethnic differences in the shopping behaviors and fruit and vegetable consumption of farmers’ market incentive program users in Illinois. Ethn Dis. 2020;30:109. doi:10.18865/ed.30.1.109
- Cassatt S, Giffuni J, Ortmeyer H, et al. A pilot study to evaluate the development and implementation of a virtual nutrition education program in older veterans. Abstract presented at: American Heart Association Epidemiology and Prevention/Lifestyle and Cardiometabolic Health 2022 Scientific Sessions; March 1-4, 2022; Chicago, IL. https:// www.ahajournals.org/doi/10.1161/circ.145.suppl_1.P002
- Parker EA, Perez WJ, Phipps B, et al. Dietary quality and perceived barriers to weight loss among older overweight veterans with dysmobility. Int J Environ Res Public Health. 2022;19:9153. doi:10.3390/ijerph19159153
- Ortmeyer HK, Giffuni J, Etchberger D, et al. The role of companion dogs in the VA Maryland Health Care System Whole Health(y) GeroFit Program. Animals (Basel). 2023;13:19. doi:10.3390/ani13193047
- Milaneschi Y, Tanaka T, Ferrucci L. Nutritional determinants of mobility. Curr Opin Clin Nutr Metab Care. 2010;13:625- 629.
- Lane JM, Davis BA. Food, physical activity, and health deserts in Alabama: the spatial link between healthy eating, exercise, and socioeconomic factors. GeoJournal. 2022;87:5229-5249.
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Wolfson JA, Ramsing R, Richardson CR, et al. Barriers to healthy food access: associations with household income and cooking behavior. Prev Med Rep. 2019;13:298-305. doi:10.1016/j.pmedr.2019.01.023
- US Department of Veterans Affairs. Veterans Health Administration– About VHA. Veterans Health Administration. 2023. Accessed December 4, 2025. https://www.va.gov/health/aboutvha.asp
- Nelson KM. The burden of obesity among a national probability sample of veterans. J Gen Intern Med. 2006;21:915- 919. doi:10.1111/j.1525-1497.2006.00526.x
- Koepsell TD, Forsberg CW, Littman AJ. Obesity, overweight, and weight control practices in U.S. veterans. Prev Med. 2009;48:267-271. doi:10.1016/j.ypmed.2009.01.008
- Das SR, Kinsinger LS, Yancy WS Jr, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28:291-294. doi:10.1016/j.amepre.2004.12.007
- Agha Z, Lofgren RP, VanRuiswyk JV, et al. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch Intern Med. 2000;160:3252-3257. doi:10.1001/archinte.160.21.3252
- Bokhour BG, Haun JN, Hyde J, et al. Transforming the Veterans Affairs to a whole health system of care: time for action and research. Med Care. 2020;58:295-300. doi:10.1097/MLR.0000000000001316
- Marchand WR, Beckstrom J, Nazarenko E, et al. The Veterans Health Administration whole health model of care: early implementation and utilization at a large healthcare system. Mil Med. 2020;185:2150-2157. doi:10.1093/milmed/usaa198
- Shulkin D, Elnahal S, Maddock E, Shaheen M. Best Care Everywhere by VA Professionals Across the Nation. US Dept of Veterans Affairs; 2017.
- Morey MC, Lee CC, Castle S, et al. Should structured exercise be promoted as a model of care? Dissemination of the Department of Veterans Affairs Gerofit Program. J Am Geriatr Soc. 2018;66:1009-1016. doi:10.1111/jgs.15276
- Cowper PA, Morey MC, Bearon LB, et al. The impact of supervised exercise on the psychological well-being and health status of older veterans. J Appl Gerontol. 1991;10:469-485. doi:10.1177/073346489101000408
- Pepin MJ, Valencia WM, Bettger JP, et al. Impact of supervised exercise on one-year medication use in older veterans with multiple morbidities. Gerontol Geriatr Med. 2020;6:2333721420956751. doi:10.1177/073346489101000408
- Morey MC, Pieper CF, Sullivan RJ Jr, et al. Fiveyear performance trends for older exercisers: a hierarchical model of endurance, strength, and flexibility. J Am Geriatr Soc. 1996;44:1226-1231. doi:10.1111/j.1532-5415.1996.tb01374.x
- Morey MC, Pieper CF, Crowley GM, et al. Exercise adherence and 10-year mortality in chronically ill older adults. J Am Geriatr Soc. 2002;50:1929-1933. doi:10.1046/j.1532-5415.2002.50602.x
- Jorna M, Ball K, Salmon J. Effects of a holistic health program on women’s physical activity and mental and spiritual health. J Sci Med Sport. 2006;9:395-401. doi:10.1016/j.jsams.2006.06.011
- Jennings SC, Manning KM, Bettger JP, et al. Rapid transition to telehealth group exercise and functional assessments in response to COVID-19. Gerontol Geriatr Med. 2020;6:2333721420980313. doi:10.1177/2333721420980313
- Morey MC, Crowley GM, Robbins MS, et al. The Gerofit program: a VA innovation. South Med J. 1994;87:S83-87.
- Addison O, Serra MC, Katzel L, et al. Mobility improvements are found in older veterans after 6 months of Gerofit regardless of BMI classification. J Aging Phys Act. 2019;27:848-854. doi:10.1123/japa.2018-0317
- Veterans Health Administration Office of Patient Centered Care and Cultural Transformation. Making your plan— whole health. November 14, 2023. Accessed December 4, 2025. https://www.va.gov/WHOLEHEALTH/phi.asp
- Hays RD, Bjorner JB, Revicki DA, et al. Development of physical and mental health summary scores from the Patient-Reported Outcomes Measurement Information System (PROMIS) global items. Qual Life Res. 2009;18:873-880. doi:10.1007/s11136-009-9496-9
- Aktary ML, Caron-Roy S, Sajobi T, et al. Impact of a farmers’ market nutrition coupon programme on diet quality and psychosocial well-being among low-income adults: protocol for a randomised controlled trial and a longitudinal qualitative investigation. BMJ Open. 2020;10:e035143. doi:10.1136/bmjopen-2019-035143
- Afshin A, Penalvo JL, Del Gobbo L, et al. The prospective impact of food pricing on improving dietary consumption: a systematic review and meta-analysis. PLoS One. 2017;12:e0172277. doi:10.1371/journal.pone.0172277
- Singleton CR, Kessee N, Chatman C, et al. Racial/ ethnic differences in the shopping behaviors and fruit and vegetable consumption of farmers’ market incentive program users in Illinois. Ethn Dis. 2020;30:109. doi:10.18865/ed.30.1.109
- Cassatt S, Giffuni J, Ortmeyer H, et al. A pilot study to evaluate the development and implementation of a virtual nutrition education program in older veterans. Abstract presented at: American Heart Association Epidemiology and Prevention/Lifestyle and Cardiometabolic Health 2022 Scientific Sessions; March 1-4, 2022; Chicago, IL. https:// www.ahajournals.org/doi/10.1161/circ.145.suppl_1.P002
- Parker EA, Perez WJ, Phipps B, et al. Dietary quality and perceived barriers to weight loss among older overweight veterans with dysmobility. Int J Environ Res Public Health. 2022;19:9153. doi:10.3390/ijerph19159153
- Ortmeyer HK, Giffuni J, Etchberger D, et al. The role of companion dogs in the VA Maryland Health Care System Whole Health(y) GeroFit Program. Animals (Basel). 2023;13:19. doi:10.3390/ani13193047
- Milaneschi Y, Tanaka T, Ferrucci L. Nutritional determinants of mobility. Curr Opin Clin Nutr Metab Care. 2010;13:625- 629.
- Lane JM, Davis BA. Food, physical activity, and health deserts in Alabama: the spatial link between healthy eating, exercise, and socioeconomic factors. GeoJournal. 2022;87:5229-5249.
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Komatsu H, Yagasaki K, Saito Y, et al. Regular group exercise contributes to balanced health in older adults in Japan: a qualitative study. BMC Geriatr. 2017;17:190. doi:10.1186/s12877-017-0584-3
- Wolfson JA, Ramsing R, Richardson CR, et al. Barriers to healthy food access: associations with household income and cooking behavior. Prev Med Rep. 2019;13:298-305. doi:10.1016/j.pmedr.2019.01.023
Whole Health(y) Aging With Gerofit: The Development of a Pilot Wellness Program for Older Veterans
Whole Health(y) Aging With Gerofit: The Development of a Pilot Wellness Program for Older Veterans

Daily Double! Assessing the Effectiveness of Game-Based Learning on the Pharmacy Knowledge of US Coast Guard Health Services Technicians
Daily Double! Assessing the Effectiveness of Game-Based Learning on the Pharmacy Knowledge of US Coast Guard Health Services Technicians
The US Coast Guard (USCG) operates within the US Department of Homeland Security and represents a force of > 50,000 servicemembers.1 The missions of the service include maritime law enforcement (drug interdiction), search and rescue, and defense readiness.2
The USCG operates 42 clinics and numerous smaller sick bays of varying sizes and medical capabilities throughout the country to provide acute and routine medical services. Health services technicians (HSs) are the most common staffing component and provide much of the support services in each USCG health care setting. The HS rating, colloquially referred to as corpsmen, is achieved through a 22-week course known as “A” school that trains servicemembers in outpatient and acute care, including emergency medical technician training.3 There are about 750 USCG HSs.
Within USCG clinics, HSs conduct ambulatory intakes for outpatient appointments, administer immunizations and blood draws, requisition medical equipment and supplies, serve as a pharmacy technician, complete physical examinations, and manage referrals, among other duties. Their familiarity with different aspects of clinic operations and medical practice must be broad. To that end, corpsmen develop and reinforce their medical knowledge through various trainings, including additional courses to specialize in certain medical skills, such as pharmacy technician “C” school or dental assistant “C” school.
The USCG employs < 15 field pharmacists, most of whom serve in an ambulatory care environment.4 Responsibilities of USCG pharmacists include the routine reinforcement of pharmacy knowledge with HSs. For the corpsmen who are not pharmacy technicians or who have not attended pharmacy technician “C” school, the extent of their pharmacy instruction primarily came from the “A” school curriculum, of which only 1 class is specific to pharmacy. Providing routine pharmacy-related training to the HSs further cultivates their pharmacy knowledge and confidence so that they can practice more holistically. These trainings do not need to follow any specific format.
In this study, 3 pharmacists at 3 separate USCG clinics conducted a training inspired by the Jeopardy! game show with the corpsmen at their respective clinics. This study examined the effectiveness of game-based learning on the pharmacy knowledge retention of HSs at 3 USCG clinics. A secondary objective was to evaluate the baseline pharmacy knowledge of corpsmen based on specific corpsmen demographics.
Methods
As part of a USCG quality improvement study in 2024, 28 HSs at the 3 USCG clinics were provided a preintervention assessment, completed game-based educational program (intervention), and then were assessed again following the intervention.
The HSs were presented with a 25-question assessment that included 10 knowledge questions (3 on over-the-counter medications, 2 on use of medications in pregnancy, 2 on precautions and contraindications, 2 on indications, and 1 on immunizations) and 15 brand-generic matching questions. These questions were developed and reviewed by the 3 participating pharmacists to ensure that their scope was commensurate with the overall pharmacy knowledge that could be reasonably expected of corpsmen spanning various points of their HS career.
One to 7 days after the preintervention assessment, the pharmacists hosted the game-based learning modeled after Jeopardy!. The Jeopardy! categories mirrored the assessment knowledge question categories, and brand-generic nomenclature was freely discussed throughout. About 2 weeks later, the same HSs who completed the preintervention assessment and participated in the game were presented with the same assessment.
In addition to capturing the difference in scores between the 2 assessments, additional demographic data were gathered, including service time as an HS and whether they received formalized pharmacy technician training and if so, how long they have served in that capacity. Demographic data were collected to identify potential correlations between demographic characteristics and results.
Results
Twenty-eight HSs at the 3 clinics completed the game-based training and both assessments. The mean score increased from 15.1 preintervention to 17.4 postintervention (Table). Preintervention scores ranged from 1 to 24 and postintervention scores ranged from 6 to 25.
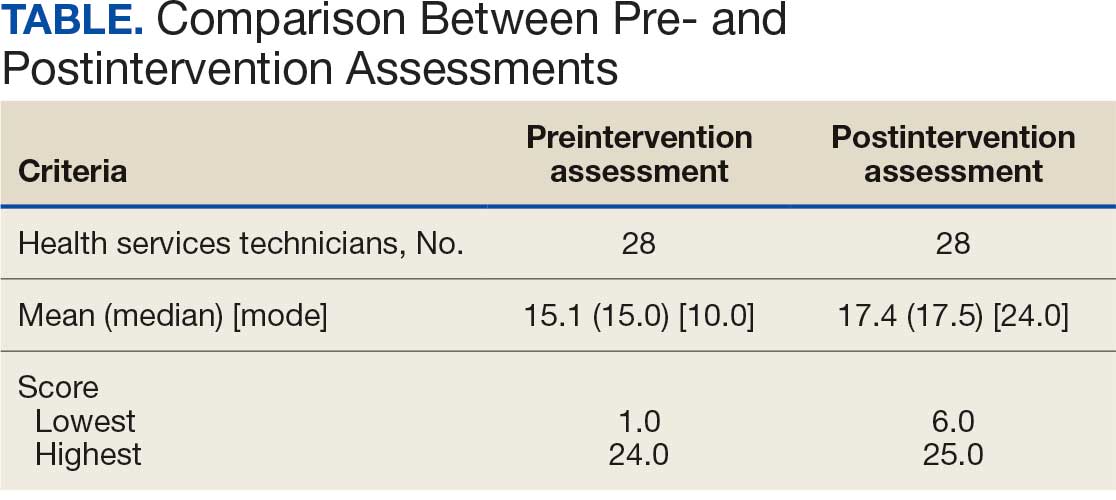
There were 19 HSs (68%) whose score increased from preintervention to postintervention and 5 (18%) had decreased scores. The largest score decrease was 4 (from 18 to 14), and the largest score increase was 11 (from 13 to 24). The mean improvement was 3.9 among the 19 HSs with increased scores
Twenty-one HSs reported no formal pharmacy technician training, 3 completed pharmacy technician “C” school, and 4 received informal on-the-job training. The mean score for the “C” school trained HSs was 23.0 preintervention and 23.7 postintervention. The mean score for HSs trained on the job was 16.0 preintervention and 18.5 postintervention. The mean score for HSs with no training was 13.9 preintervention and 16.3 postintervention.
As HSs advance in their careers, they typically assume roles with increasing technical knowledge, responsibility, and oversight, thus aligning with advancement from E-4 (third class petty officer) to E-6 (first class petty officer) and beyond. In this study, there was 1 E-3, 12 E-4s (mean time as an HS, 1.3 years), 8 E-5s (mean time as an HS, 4.8 years), and 7 E-6s (mean time as an HS, 8.6 years). The E-3 had a preintervention score of 1.0 and a postintervention score of 6.0. The E-4s had a mean change in score from pre- to postintervention of 2.4. The E-5s had a mean change in score from pre- to postintervention of 1.6. The E-6s had a mean change in score from pre- to postintervention of 2.3.
Discussion
This study is novel in its examination of the impact of game-based learning on the retention of the pharmacy knowledge of USCG corpsmen. A PubMed literature search of the phrase “((Corpsman) OR (Corpsmen)) AND (Coast Guard)” yields 135 results, though none were relevant to the USCG population described in this study. A PubMed literature search of the phrase “(Jeopardy!) AND (pharmacy)” yields 28 results, only 1 of which discusses using the game-based approach as an instructional tool.5 A PubMed literature search of the phrase “(game) AND (Coast Guard)” yields 55 results, none of which were specifically relevant to game-based learning in the USCG. This study appears to be among the first to discuss results and trends in game-based learning with USCG corpsmen.
The preponderance of literature for game-based learning strategies exists in children; more research in adults is needed.6,7 With studies showing that game-based learning may impact motivation to learn and learning gains, it is unsurprising that there is some research in professional health care education. Games modeled after everything from simulated clinical scenarios to Family Feud and Chutes and Ladders-style games have been compared with traditional learning strategies. However, the results of whether game-based learning strategies improve knowledge, clinical decision-making, and motivation to learn vary, suggesting the need for more research in this field.8
The results of this study suggest that Jeopardy! is likely an effective instructional method for USCG corpsmen on pharmacy topics. While there were some HSs whose postintervention scores decreased, 19 (68%) had increased scores. Because the second assessment was administered about 2 weeks after the game-based learning, the results suggest some level of knowledge retention. Between these results and the informally perceived level of engagement, game-based learning could be a more stimulating alternative training method to a standard slide-based presentation.
Stratifying the data by demographics revealed additional trends, although they should be interpreted with caution due to the small sample size. The baseline results strongly illustrate the value of formalized training. It is generally expected that HSs who have completed the “C” school pharmacy technician training program should have more pharmacy knowledge than those with on-the-job or less training. The results indicate that “C” school trained and on-the-job trained HSs scored higher on the preintervention assessment (mean, 23.0 and 16.0, respectively), than those with no such experiences (mean, 13.9). Such results underscore the value of formalized training—whether as a pharmacy technician or in any other “C” school—in enhancing the medical knowledge of HSs that may allow them to hold roles of increased responsibility and medical scope.
In addition to stratification by pharmacy technician training, stratification by years of HS experience (roughly correlated to rank) yields a similar result. It would be expected that as HSs advance in their careers, they gain more exposure to various medical topics, including pharmacy. That is not always the case, however, as it is possible an HS never rotated through a pharmacy technician position or has not been recently exposed to pharmacy knowledge. Nevertheless, the results suggest that increased HS experience was likely associated with an increased baseline pharmacy knowledge, with mean preintervention scores increasing from 11.9 to 18.1 to 19.3 for E-4, E-5, and E-6, respectively.
While there are many explanations for these results, the authors hypothesize that when HSs are E-4s, they might not yet have exposure to all aspects of the clinic and are perhaps not as well-versed in pharmacy practice. An E-5—now a few years into their career—would have completed pharmacy technician “C” school or on-the-job training (if applicable), which could account for the significant jump in pharmacy knowledge scores. An E-6 can still engage in direct patient care activities but take on leadership and supervisory roles within the clinic, perhaps explaining the smaller increase in score.
In terms of increasing responsibility, many USCG corpsmen complete another schooling opportunity—Independent Duty Health Services Technician (IDHS)—so they can serve in independent duty roles, many of which are on USCG cutters. While cutters are deployed, that IDHS could be the sole medical personnel on the cutter and function in a midlevel practitioner extender role. Formalized training in pharmacy—the benefits of which are suggested through these results—or another field of medical practice would strengthen the skillset and confidence of IDHSs.
Though not formally assessed, the 3 pharmacists noted that the game-based learning was met with overwhelmingly positive feedback in terms of excitement, energy, and overall engagement.
Limitations
This cohort of individuals represents a small proportion of the total number of USCG corpsmen, and it is not fully representative of all practice settings. HSs can be assigned to USCG cutters as IDHSs, which would not be captured in this cohort. Even within a single clinic, the knowledge of HSs varies, as not all HS duties consist solely of clinical skills. Additionally, while the overall game framework was consistent among the 3 sites, there may have been unquantifiable differences in overall teaching style by the 3 pharmacists that may have resulted in different levels of content retention. Given the lack of similar studies in this population, this study can best be described as a quantitative descriptor of results rather than a statistical comparison of what instructional method works best.
Conclusions
The USCG greatly benefits from having trained and experienced HSs fulfilling mission support roles in the organization. In addition to traditional slide-based trainings, game-based learning can be considered to create engaging learning environments to support the knowledge retention of pharmacy and other medical topics for USCG corpsmen.
- US Coast Guard. Organizational overview. About the US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About
- US Coast Guard. Missions. About US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About/Missions/
- US Coast Guard. Health services technician. Accessed October 14, 2025. https://www.gocoastguard.com/careers/enlisted/hs
- Zhou F, Woodward Z. Impact of pharmacist interventions at an outpatient US Coast Guard clinic. Fed Pract. 2023;40(6):174-177. doi:10.12788/fp.0383
- Cusick J. A Jeopardy-style review game using team clickers. MedEdPORTAL. 2016;12:10485. doi:10.15766/mep_2374-8265.10485
- Dahalan F, Alias N, Shaharom MSN. Gamification and game based learning for vocational education and training: a systematic literature review. Educ Inf Technol (Dordr). 2023:1-39. doi:10.1007/s10639-022-11548-w
- Wesselink LA. Testing the Effectiveness of Game-Based Learning for Adults by Designing an Educational Game: A Design and Research Study to Investigate the Effectiveness of Educational Games for Adults to Learn Basic Skills of Microsoft Excel. Master’s thesis. University of Twente; 2020. Accessed October 22, 2025. http://essay.utwentw.nl/88229
- Del Cura-González I, Ariza-Cardiel G, Polentinos-Castro E, et al. Effectiveness of a game-based educational strategy e-EDUCAGUIA for implementing antimicrobial clinical practice guidelines in family medicine residents in Spain: a randomized clinical trial by cluster. BMC Med Educ. 2022;22:893. doi:10.1186/s12909-022-03843-4
The US Coast Guard (USCG) operates within the US Department of Homeland Security and represents a force of > 50,000 servicemembers.1 The missions of the service include maritime law enforcement (drug interdiction), search and rescue, and defense readiness.2
The USCG operates 42 clinics and numerous smaller sick bays of varying sizes and medical capabilities throughout the country to provide acute and routine medical services. Health services technicians (HSs) are the most common staffing component and provide much of the support services in each USCG health care setting. The HS rating, colloquially referred to as corpsmen, is achieved through a 22-week course known as “A” school that trains servicemembers in outpatient and acute care, including emergency medical technician training.3 There are about 750 USCG HSs.
Within USCG clinics, HSs conduct ambulatory intakes for outpatient appointments, administer immunizations and blood draws, requisition medical equipment and supplies, serve as a pharmacy technician, complete physical examinations, and manage referrals, among other duties. Their familiarity with different aspects of clinic operations and medical practice must be broad. To that end, corpsmen develop and reinforce their medical knowledge through various trainings, including additional courses to specialize in certain medical skills, such as pharmacy technician “C” school or dental assistant “C” school.
The USCG employs < 15 field pharmacists, most of whom serve in an ambulatory care environment.4 Responsibilities of USCG pharmacists include the routine reinforcement of pharmacy knowledge with HSs. For the corpsmen who are not pharmacy technicians or who have not attended pharmacy technician “C” school, the extent of their pharmacy instruction primarily came from the “A” school curriculum, of which only 1 class is specific to pharmacy. Providing routine pharmacy-related training to the HSs further cultivates their pharmacy knowledge and confidence so that they can practice more holistically. These trainings do not need to follow any specific format.
In this study, 3 pharmacists at 3 separate USCG clinics conducted a training inspired by the Jeopardy! game show with the corpsmen at their respective clinics. This study examined the effectiveness of game-based learning on the pharmacy knowledge retention of HSs at 3 USCG clinics. A secondary objective was to evaluate the baseline pharmacy knowledge of corpsmen based on specific corpsmen demographics.
Methods
As part of a USCG quality improvement study in 2024, 28 HSs at the 3 USCG clinics were provided a preintervention assessment, completed game-based educational program (intervention), and then were assessed again following the intervention.
The HSs were presented with a 25-question assessment that included 10 knowledge questions (3 on over-the-counter medications, 2 on use of medications in pregnancy, 2 on precautions and contraindications, 2 on indications, and 1 on immunizations) and 15 brand-generic matching questions. These questions were developed and reviewed by the 3 participating pharmacists to ensure that their scope was commensurate with the overall pharmacy knowledge that could be reasonably expected of corpsmen spanning various points of their HS career.
One to 7 days after the preintervention assessment, the pharmacists hosted the game-based learning modeled after Jeopardy!. The Jeopardy! categories mirrored the assessment knowledge question categories, and brand-generic nomenclature was freely discussed throughout. About 2 weeks later, the same HSs who completed the preintervention assessment and participated in the game were presented with the same assessment.
In addition to capturing the difference in scores between the 2 assessments, additional demographic data were gathered, including service time as an HS and whether they received formalized pharmacy technician training and if so, how long they have served in that capacity. Demographic data were collected to identify potential correlations between demographic characteristics and results.
Results
Twenty-eight HSs at the 3 clinics completed the game-based training and both assessments. The mean score increased from 15.1 preintervention to 17.4 postintervention (Table). Preintervention scores ranged from 1 to 24 and postintervention scores ranged from 6 to 25.
There were 19 HSs (68%) whose score increased from preintervention to postintervention and 5 (18%) had decreased scores. The largest score decrease was 4 (from 18 to 14), and the largest score increase was 11 (from 13 to 24). The mean improvement was 3.9 among the 19 HSs with increased scores
Twenty-one HSs reported no formal pharmacy technician training, 3 completed pharmacy technician “C” school, and 4 received informal on-the-job training. The mean score for the “C” school trained HSs was 23.0 preintervention and 23.7 postintervention. The mean score for HSs trained on the job was 16.0 preintervention and 18.5 postintervention. The mean score for HSs with no training was 13.9 preintervention and 16.3 postintervention.
As HSs advance in their careers, they typically assume roles with increasing technical knowledge, responsibility, and oversight, thus aligning with advancement from E-4 (third class petty officer) to E-6 (first class petty officer) and beyond. In this study, there was 1 E-3, 12 E-4s (mean time as an HS, 1.3 years), 8 E-5s (mean time as an HS, 4.8 years), and 7 E-6s (mean time as an HS, 8.6 years). The E-3 had a preintervention score of 1.0 and a postintervention score of 6.0. The E-4s had a mean change in score from pre- to postintervention of 2.4. The E-5s had a mean change in score from pre- to postintervention of 1.6. The E-6s had a mean change in score from pre- to postintervention of 2.3.
Discussion
This study is novel in its examination of the impact of game-based learning on the retention of the pharmacy knowledge of USCG corpsmen. A PubMed literature search of the phrase “((Corpsman) OR (Corpsmen)) AND (Coast Guard)” yields 135 results, though none were relevant to the USCG population described in this study. A PubMed literature search of the phrase “(Jeopardy!) AND (pharmacy)” yields 28 results, only 1 of which discusses using the game-based approach as an instructional tool.5 A PubMed literature search of the phrase “(game) AND (Coast Guard)” yields 55 results, none of which were specifically relevant to game-based learning in the USCG. This study appears to be among the first to discuss results and trends in game-based learning with USCG corpsmen.
The preponderance of literature for game-based learning strategies exists in children; more research in adults is needed.6,7 With studies showing that game-based learning may impact motivation to learn and learning gains, it is unsurprising that there is some research in professional health care education. Games modeled after everything from simulated clinical scenarios to Family Feud and Chutes and Ladders-style games have been compared with traditional learning strategies. However, the results of whether game-based learning strategies improve knowledge, clinical decision-making, and motivation to learn vary, suggesting the need for more research in this field.8
The results of this study suggest that Jeopardy! is likely an effective instructional method for USCG corpsmen on pharmacy topics. While there were some HSs whose postintervention scores decreased, 19 (68%) had increased scores. Because the second assessment was administered about 2 weeks after the game-based learning, the results suggest some level of knowledge retention. Between these results and the informally perceived level of engagement, game-based learning could be a more stimulating alternative training method to a standard slide-based presentation.
Stratifying the data by demographics revealed additional trends, although they should be interpreted with caution due to the small sample size. The baseline results strongly illustrate the value of formalized training. It is generally expected that HSs who have completed the “C” school pharmacy technician training program should have more pharmacy knowledge than those with on-the-job or less training. The results indicate that “C” school trained and on-the-job trained HSs scored higher on the preintervention assessment (mean, 23.0 and 16.0, respectively), than those with no such experiences (mean, 13.9). Such results underscore the value of formalized training—whether as a pharmacy technician or in any other “C” school—in enhancing the medical knowledge of HSs that may allow them to hold roles of increased responsibility and medical scope.
In addition to stratification by pharmacy technician training, stratification by years of HS experience (roughly correlated to rank) yields a similar result. It would be expected that as HSs advance in their careers, they gain more exposure to various medical topics, including pharmacy. That is not always the case, however, as it is possible an HS never rotated through a pharmacy technician position or has not been recently exposed to pharmacy knowledge. Nevertheless, the results suggest that increased HS experience was likely associated with an increased baseline pharmacy knowledge, with mean preintervention scores increasing from 11.9 to 18.1 to 19.3 for E-4, E-5, and E-6, respectively.
While there are many explanations for these results, the authors hypothesize that when HSs are E-4s, they might not yet have exposure to all aspects of the clinic and are perhaps not as well-versed in pharmacy practice. An E-5—now a few years into their career—would have completed pharmacy technician “C” school or on-the-job training (if applicable), which could account for the significant jump in pharmacy knowledge scores. An E-6 can still engage in direct patient care activities but take on leadership and supervisory roles within the clinic, perhaps explaining the smaller increase in score.
In terms of increasing responsibility, many USCG corpsmen complete another schooling opportunity—Independent Duty Health Services Technician (IDHS)—so they can serve in independent duty roles, many of which are on USCG cutters. While cutters are deployed, that IDHS could be the sole medical personnel on the cutter and function in a midlevel practitioner extender role. Formalized training in pharmacy—the benefits of which are suggested through these results—or another field of medical practice would strengthen the skillset and confidence of IDHSs.
Though not formally assessed, the 3 pharmacists noted that the game-based learning was met with overwhelmingly positive feedback in terms of excitement, energy, and overall engagement.
Limitations
This cohort of individuals represents a small proportion of the total number of USCG corpsmen, and it is not fully representative of all practice settings. HSs can be assigned to USCG cutters as IDHSs, which would not be captured in this cohort. Even within a single clinic, the knowledge of HSs varies, as not all HS duties consist solely of clinical skills. Additionally, while the overall game framework was consistent among the 3 sites, there may have been unquantifiable differences in overall teaching style by the 3 pharmacists that may have resulted in different levels of content retention. Given the lack of similar studies in this population, this study can best be described as a quantitative descriptor of results rather than a statistical comparison of what instructional method works best.
Conclusions
The USCG greatly benefits from having trained and experienced HSs fulfilling mission support roles in the organization. In addition to traditional slide-based trainings, game-based learning can be considered to create engaging learning environments to support the knowledge retention of pharmacy and other medical topics for USCG corpsmen.
The US Coast Guard (USCG) operates within the US Department of Homeland Security and represents a force of > 50,000 servicemembers.1 The missions of the service include maritime law enforcement (drug interdiction), search and rescue, and defense readiness.2
The USCG operates 42 clinics and numerous smaller sick bays of varying sizes and medical capabilities throughout the country to provide acute and routine medical services. Health services technicians (HSs) are the most common staffing component and provide much of the support services in each USCG health care setting. The HS rating, colloquially referred to as corpsmen, is achieved through a 22-week course known as “A” school that trains servicemembers in outpatient and acute care, including emergency medical technician training.3 There are about 750 USCG HSs.
Within USCG clinics, HSs conduct ambulatory intakes for outpatient appointments, administer immunizations and blood draws, requisition medical equipment and supplies, serve as a pharmacy technician, complete physical examinations, and manage referrals, among other duties. Their familiarity with different aspects of clinic operations and medical practice must be broad. To that end, corpsmen develop and reinforce their medical knowledge through various trainings, including additional courses to specialize in certain medical skills, such as pharmacy technician “C” school or dental assistant “C” school.
The USCG employs < 15 field pharmacists, most of whom serve in an ambulatory care environment.4 Responsibilities of USCG pharmacists include the routine reinforcement of pharmacy knowledge with HSs. For the corpsmen who are not pharmacy technicians or who have not attended pharmacy technician “C” school, the extent of their pharmacy instruction primarily came from the “A” school curriculum, of which only 1 class is specific to pharmacy. Providing routine pharmacy-related training to the HSs further cultivates their pharmacy knowledge and confidence so that they can practice more holistically. These trainings do not need to follow any specific format.
In this study, 3 pharmacists at 3 separate USCG clinics conducted a training inspired by the Jeopardy! game show with the corpsmen at their respective clinics. This study examined the effectiveness of game-based learning on the pharmacy knowledge retention of HSs at 3 USCG clinics. A secondary objective was to evaluate the baseline pharmacy knowledge of corpsmen based on specific corpsmen demographics.
Methods
As part of a USCG quality improvement study in 2024, 28 HSs at the 3 USCG clinics were provided a preintervention assessment, completed game-based educational program (intervention), and then were assessed again following the intervention.
The HSs were presented with a 25-question assessment that included 10 knowledge questions (3 on over-the-counter medications, 2 on use of medications in pregnancy, 2 on precautions and contraindications, 2 on indications, and 1 on immunizations) and 15 brand-generic matching questions. These questions were developed and reviewed by the 3 participating pharmacists to ensure that their scope was commensurate with the overall pharmacy knowledge that could be reasonably expected of corpsmen spanning various points of their HS career.
One to 7 days after the preintervention assessment, the pharmacists hosted the game-based learning modeled after Jeopardy!. The Jeopardy! categories mirrored the assessment knowledge question categories, and brand-generic nomenclature was freely discussed throughout. About 2 weeks later, the same HSs who completed the preintervention assessment and participated in the game were presented with the same assessment.
In addition to capturing the difference in scores between the 2 assessments, additional demographic data were gathered, including service time as an HS and whether they received formalized pharmacy technician training and if so, how long they have served in that capacity. Demographic data were collected to identify potential correlations between demographic characteristics and results.
Results
Twenty-eight HSs at the 3 clinics completed the game-based training and both assessments. The mean score increased from 15.1 preintervention to 17.4 postintervention (Table). Preintervention scores ranged from 1 to 24 and postintervention scores ranged from 6 to 25.
There were 19 HSs (68%) whose score increased from preintervention to postintervention and 5 (18%) had decreased scores. The largest score decrease was 4 (from 18 to 14), and the largest score increase was 11 (from 13 to 24). The mean improvement was 3.9 among the 19 HSs with increased scores
Twenty-one HSs reported no formal pharmacy technician training, 3 completed pharmacy technician “C” school, and 4 received informal on-the-job training. The mean score for the “C” school trained HSs was 23.0 preintervention and 23.7 postintervention. The mean score for HSs trained on the job was 16.0 preintervention and 18.5 postintervention. The mean score for HSs with no training was 13.9 preintervention and 16.3 postintervention.
As HSs advance in their careers, they typically assume roles with increasing technical knowledge, responsibility, and oversight, thus aligning with advancement from E-4 (third class petty officer) to E-6 (first class petty officer) and beyond. In this study, there was 1 E-3, 12 E-4s (mean time as an HS, 1.3 years), 8 E-5s (mean time as an HS, 4.8 years), and 7 E-6s (mean time as an HS, 8.6 years). The E-3 had a preintervention score of 1.0 and a postintervention score of 6.0. The E-4s had a mean change in score from pre- to postintervention of 2.4. The E-5s had a mean change in score from pre- to postintervention of 1.6. The E-6s had a mean change in score from pre- to postintervention of 2.3.
Discussion
This study is novel in its examination of the impact of game-based learning on the retention of the pharmacy knowledge of USCG corpsmen. A PubMed literature search of the phrase “((Corpsman) OR (Corpsmen)) AND (Coast Guard)” yields 135 results, though none were relevant to the USCG population described in this study. A PubMed literature search of the phrase “(Jeopardy!) AND (pharmacy)” yields 28 results, only 1 of which discusses using the game-based approach as an instructional tool.5 A PubMed literature search of the phrase “(game) AND (Coast Guard)” yields 55 results, none of which were specifically relevant to game-based learning in the USCG. This study appears to be among the first to discuss results and trends in game-based learning with USCG corpsmen.
The preponderance of literature for game-based learning strategies exists in children; more research in adults is needed.6,7 With studies showing that game-based learning may impact motivation to learn and learning gains, it is unsurprising that there is some research in professional health care education. Games modeled after everything from simulated clinical scenarios to Family Feud and Chutes and Ladders-style games have been compared with traditional learning strategies. However, the results of whether game-based learning strategies improve knowledge, clinical decision-making, and motivation to learn vary, suggesting the need for more research in this field.8
The results of this study suggest that Jeopardy! is likely an effective instructional method for USCG corpsmen on pharmacy topics. While there were some HSs whose postintervention scores decreased, 19 (68%) had increased scores. Because the second assessment was administered about 2 weeks after the game-based learning, the results suggest some level of knowledge retention. Between these results and the informally perceived level of engagement, game-based learning could be a more stimulating alternative training method to a standard slide-based presentation.
Stratifying the data by demographics revealed additional trends, although they should be interpreted with caution due to the small sample size. The baseline results strongly illustrate the value of formalized training. It is generally expected that HSs who have completed the “C” school pharmacy technician training program should have more pharmacy knowledge than those with on-the-job or less training. The results indicate that “C” school trained and on-the-job trained HSs scored higher on the preintervention assessment (mean, 23.0 and 16.0, respectively), than those with no such experiences (mean, 13.9). Such results underscore the value of formalized training—whether as a pharmacy technician or in any other “C” school—in enhancing the medical knowledge of HSs that may allow them to hold roles of increased responsibility and medical scope.
In addition to stratification by pharmacy technician training, stratification by years of HS experience (roughly correlated to rank) yields a similar result. It would be expected that as HSs advance in their careers, they gain more exposure to various medical topics, including pharmacy. That is not always the case, however, as it is possible an HS never rotated through a pharmacy technician position or has not been recently exposed to pharmacy knowledge. Nevertheless, the results suggest that increased HS experience was likely associated with an increased baseline pharmacy knowledge, with mean preintervention scores increasing from 11.9 to 18.1 to 19.3 for E-4, E-5, and E-6, respectively.
While there are many explanations for these results, the authors hypothesize that when HSs are E-4s, they might not yet have exposure to all aspects of the clinic and are perhaps not as well-versed in pharmacy practice. An E-5—now a few years into their career—would have completed pharmacy technician “C” school or on-the-job training (if applicable), which could account for the significant jump in pharmacy knowledge scores. An E-6 can still engage in direct patient care activities but take on leadership and supervisory roles within the clinic, perhaps explaining the smaller increase in score.
In terms of increasing responsibility, many USCG corpsmen complete another schooling opportunity—Independent Duty Health Services Technician (IDHS)—so they can serve in independent duty roles, many of which are on USCG cutters. While cutters are deployed, that IDHS could be the sole medical personnel on the cutter and function in a midlevel practitioner extender role. Formalized training in pharmacy—the benefits of which are suggested through these results—or another field of medical practice would strengthen the skillset and confidence of IDHSs.
Though not formally assessed, the 3 pharmacists noted that the game-based learning was met with overwhelmingly positive feedback in terms of excitement, energy, and overall engagement.
Limitations
This cohort of individuals represents a small proportion of the total number of USCG corpsmen, and it is not fully representative of all practice settings. HSs can be assigned to USCG cutters as IDHSs, which would not be captured in this cohort. Even within a single clinic, the knowledge of HSs varies, as not all HS duties consist solely of clinical skills. Additionally, while the overall game framework was consistent among the 3 sites, there may have been unquantifiable differences in overall teaching style by the 3 pharmacists that may have resulted in different levels of content retention. Given the lack of similar studies in this population, this study can best be described as a quantitative descriptor of results rather than a statistical comparison of what instructional method works best.
Conclusions
The USCG greatly benefits from having trained and experienced HSs fulfilling mission support roles in the organization. In addition to traditional slide-based trainings, game-based learning can be considered to create engaging learning environments to support the knowledge retention of pharmacy and other medical topics for USCG corpsmen.
- US Coast Guard. Organizational overview. About the US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About
- US Coast Guard. Missions. About US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About/Missions/
- US Coast Guard. Health services technician. Accessed October 14, 2025. https://www.gocoastguard.com/careers/enlisted/hs
- Zhou F, Woodward Z. Impact of pharmacist interventions at an outpatient US Coast Guard clinic. Fed Pract. 2023;40(6):174-177. doi:10.12788/fp.0383
- Cusick J. A Jeopardy-style review game using team clickers. MedEdPORTAL. 2016;12:10485. doi:10.15766/mep_2374-8265.10485
- Dahalan F, Alias N, Shaharom MSN. Gamification and game based learning for vocational education and training: a systematic literature review. Educ Inf Technol (Dordr). 2023:1-39. doi:10.1007/s10639-022-11548-w
- Wesselink LA. Testing the Effectiveness of Game-Based Learning for Adults by Designing an Educational Game: A Design and Research Study to Investigate the Effectiveness of Educational Games for Adults to Learn Basic Skills of Microsoft Excel. Master’s thesis. University of Twente; 2020. Accessed October 22, 2025. http://essay.utwentw.nl/88229
- Del Cura-González I, Ariza-Cardiel G, Polentinos-Castro E, et al. Effectiveness of a game-based educational strategy e-EDUCAGUIA for implementing antimicrobial clinical practice guidelines in family medicine residents in Spain: a randomized clinical trial by cluster. BMC Med Educ. 2022;22:893. doi:10.1186/s12909-022-03843-4
- US Coast Guard. Organizational overview. About the US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About
- US Coast Guard. Missions. About US Coast Guard. Accessed October 14, 2025. https://www.uscg.mil/About/Missions/
- US Coast Guard. Health services technician. Accessed October 14, 2025. https://www.gocoastguard.com/careers/enlisted/hs
- Zhou F, Woodward Z. Impact of pharmacist interventions at an outpatient US Coast Guard clinic. Fed Pract. 2023;40(6):174-177. doi:10.12788/fp.0383
- Cusick J. A Jeopardy-style review game using team clickers. MedEdPORTAL. 2016;12:10485. doi:10.15766/mep_2374-8265.10485
- Dahalan F, Alias N, Shaharom MSN. Gamification and game based learning for vocational education and training: a systematic literature review. Educ Inf Technol (Dordr). 2023:1-39. doi:10.1007/s10639-022-11548-w
- Wesselink LA. Testing the Effectiveness of Game-Based Learning for Adults by Designing an Educational Game: A Design and Research Study to Investigate the Effectiveness of Educational Games for Adults to Learn Basic Skills of Microsoft Excel. Master’s thesis. University of Twente; 2020. Accessed October 22, 2025. http://essay.utwentw.nl/88229
- Del Cura-González I, Ariza-Cardiel G, Polentinos-Castro E, et al. Effectiveness of a game-based educational strategy e-EDUCAGUIA for implementing antimicrobial clinical practice guidelines in family medicine residents in Spain: a randomized clinical trial by cluster. BMC Med Educ. 2022;22:893. doi:10.1186/s12909-022-03843-4
Daily Double! Assessing the Effectiveness of Game-Based Learning on the Pharmacy Knowledge of US Coast Guard Health Services Technicians
Daily Double! Assessing the Effectiveness of Game-Based Learning on the Pharmacy Knowledge of US Coast Guard Health Services Technicians