User login
The Hospitalist only
Battling physician burnout delivers monetary benefits for health care organizations
The financial impact of physician burnout can provide a guide to help organizations address the problem, according to a special communication published online in JAMA Internal Medicine.
Approximately half of U.S. physicians experience some degree of professional burnout, but health care organizations have done little to respond, wrote Tait Shanafelt, MD, of Stanford (Calif.) University, and colleagues (JAMA Intern Med. 2017 Sep 25. doi: 10.1001/jamainternmed.2017.4340).
The researchers cited “a lack of awareness regarding the economic costs of physician burnout” and a lack of confidence that anything can be done as key factors in why the organizational response to burnout has been so limited.
The business end of physician burnout includes the costs associated with physician turnover and decreased productivity, as well as “financial risks to the organization’s long-term viability due to the relationship between burnout and lower quality of care, decreased patient satisfaction, and problems with patient safety,” the researchers said.
Organizations can combat physician burnout, the authors noted, and the effort is financially worthwhile, as well as morally and ethically important. “Burnout is primarily a system-level problem driven by excess job demands and inadequate resources and support, not an individual problem triggered by personal limitations,” they wrote.
The researchers developed a model outlining “Typical Steps in an Organization’s Journey Toward Expertise in Physician Well-being.” The steps begin with strategies that have a minor impact, including awareness of the problem of physician burnout and a focus on individual interventions such as mindfulness training, exercise, and nutrition.
However, the “transformative” changes in an organization include developing a “culture of wellness,” strategic investment in physician well-being, the presence of a “chief well-being officer” at the executive level, and accountability for physician wellness shared among organizational leaders.
The cost of such strategies varies among institutions, and the researchers provided worksheets to calculate the organizational cost of burnout and the return on investment if intervention steps are taken.
For example, an organization employing 450 physicians could potentially spend $1 million per year on an intervention to reduce physician burnout from 50% to 40%. The intervention investment could yield organizational cost savings of $1.125 million per year, with a 12.5% return on investment, as well as the potential financial benefits of improved patient satisfaction and quality of care.
“Understanding the business case to reduce burnout and promote engagement, as well as overcoming the misperception that nothing meaningful can be done, are key steps for organizations to begin to take action,” the researchers concluded.
“Improvement is possible, investment is justified, and return on investment measurable,” they said.
Dr. Shanafelt is a coinventor of the Physician Well-Being Index, Medical Student Well-Being Index, and Well-Being Index; copyright and licensing rights for these tools belong to the Mayo Clinic, and Dr. Shanafelt receives part of the royalties. The researchers had no other financial conflicts to disclose.
The financial impact of physician burnout can provide a guide to help organizations address the problem, according to a special communication published online in JAMA Internal Medicine.
Approximately half of U.S. physicians experience some degree of professional burnout, but health care organizations have done little to respond, wrote Tait Shanafelt, MD, of Stanford (Calif.) University, and colleagues (JAMA Intern Med. 2017 Sep 25. doi: 10.1001/jamainternmed.2017.4340).
The researchers cited “a lack of awareness regarding the economic costs of physician burnout” and a lack of confidence that anything can be done as key factors in why the organizational response to burnout has been so limited.
The business end of physician burnout includes the costs associated with physician turnover and decreased productivity, as well as “financial risks to the organization’s long-term viability due to the relationship between burnout and lower quality of care, decreased patient satisfaction, and problems with patient safety,” the researchers said.
Organizations can combat physician burnout, the authors noted, and the effort is financially worthwhile, as well as morally and ethically important. “Burnout is primarily a system-level problem driven by excess job demands and inadequate resources and support, not an individual problem triggered by personal limitations,” they wrote.
The researchers developed a model outlining “Typical Steps in an Organization’s Journey Toward Expertise in Physician Well-being.” The steps begin with strategies that have a minor impact, including awareness of the problem of physician burnout and a focus on individual interventions such as mindfulness training, exercise, and nutrition.
However, the “transformative” changes in an organization include developing a “culture of wellness,” strategic investment in physician well-being, the presence of a “chief well-being officer” at the executive level, and accountability for physician wellness shared among organizational leaders.
The cost of such strategies varies among institutions, and the researchers provided worksheets to calculate the organizational cost of burnout and the return on investment if intervention steps are taken.
For example, an organization employing 450 physicians could potentially spend $1 million per year on an intervention to reduce physician burnout from 50% to 40%. The intervention investment could yield organizational cost savings of $1.125 million per year, with a 12.5% return on investment, as well as the potential financial benefits of improved patient satisfaction and quality of care.
“Understanding the business case to reduce burnout and promote engagement, as well as overcoming the misperception that nothing meaningful can be done, are key steps for organizations to begin to take action,” the researchers concluded.
“Improvement is possible, investment is justified, and return on investment measurable,” they said.
Dr. Shanafelt is a coinventor of the Physician Well-Being Index, Medical Student Well-Being Index, and Well-Being Index; copyright and licensing rights for these tools belong to the Mayo Clinic, and Dr. Shanafelt receives part of the royalties. The researchers had no other financial conflicts to disclose.
The financial impact of physician burnout can provide a guide to help organizations address the problem, according to a special communication published online in JAMA Internal Medicine.
Approximately half of U.S. physicians experience some degree of professional burnout, but health care organizations have done little to respond, wrote Tait Shanafelt, MD, of Stanford (Calif.) University, and colleagues (JAMA Intern Med. 2017 Sep 25. doi: 10.1001/jamainternmed.2017.4340).
The researchers cited “a lack of awareness regarding the economic costs of physician burnout” and a lack of confidence that anything can be done as key factors in why the organizational response to burnout has been so limited.
The business end of physician burnout includes the costs associated with physician turnover and decreased productivity, as well as “financial risks to the organization’s long-term viability due to the relationship between burnout and lower quality of care, decreased patient satisfaction, and problems with patient safety,” the researchers said.
Organizations can combat physician burnout, the authors noted, and the effort is financially worthwhile, as well as morally and ethically important. “Burnout is primarily a system-level problem driven by excess job demands and inadequate resources and support, not an individual problem triggered by personal limitations,” they wrote.
The researchers developed a model outlining “Typical Steps in an Organization’s Journey Toward Expertise in Physician Well-being.” The steps begin with strategies that have a minor impact, including awareness of the problem of physician burnout and a focus on individual interventions such as mindfulness training, exercise, and nutrition.
However, the “transformative” changes in an organization include developing a “culture of wellness,” strategic investment in physician well-being, the presence of a “chief well-being officer” at the executive level, and accountability for physician wellness shared among organizational leaders.
The cost of such strategies varies among institutions, and the researchers provided worksheets to calculate the organizational cost of burnout and the return on investment if intervention steps are taken.
For example, an organization employing 450 physicians could potentially spend $1 million per year on an intervention to reduce physician burnout from 50% to 40%. The intervention investment could yield organizational cost savings of $1.125 million per year, with a 12.5% return on investment, as well as the potential financial benefits of improved patient satisfaction and quality of care.
“Understanding the business case to reduce burnout and promote engagement, as well as overcoming the misperception that nothing meaningful can be done, are key steps for organizations to begin to take action,” the researchers concluded.
“Improvement is possible, investment is justified, and return on investment measurable,” they said.
Dr. Shanafelt is a coinventor of the Physician Well-Being Index, Medical Student Well-Being Index, and Well-Being Index; copyright and licensing rights for these tools belong to the Mayo Clinic, and Dr. Shanafelt receives part of the royalties. The researchers had no other financial conflicts to disclose.
FROM JAMA INTERNAL MEDICINE
New hospitalist unit has stellar patient satisfaction scores
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at [email protected]
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at [email protected]
It’s very unusual for hospitalists to achieve top quartile performance on the Physician Communication domain of the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. This is the story of a group that did just that for patients on one unit of a large hospital.
I’m not sure how reproducible this would be at other hospitals, or even on other units in the same hospital, and wonder whether performance will stay at this remarkably high level much longer than the current 5-month track record of success. Even so, five months of success suggests they’re on to something.
There is another hospitalist group at that hospital, but I’m discussing work done only by MedOne hospitalists, who together with hospital personnel, developed what they call the Comprehensive Medical Unit (CMU). Their goal was to involve multiple disciplines and use Lean principles to design a new approach to care on 5-Orange, a 20-bed unit in OhioHealth’s Riverside Methodist Hospital in Columbus. The CMU model went live in October 2016.
MedOne Hospital Physicians is a private hospitalist group of 35 physicians and 12 advanced practice clinicians, which comprise nurse practitioners (NPs) and physician assistants (PAs), constituting 46 full-time–equivalent clinical staffing. The group contracts with Riverside, which has approximately 710 staffed beds. MedOne also works in area skilled nursing facilities, helps a long-term acute care and rehabilitation hospital, and provides support to two other hospitals that are not part of OhioHealth.
Features of the model
At its core, this model is a variation of the increasingly common combination of geographically assigned hospitalists (who in this case don’t have patients elsewhere in the hospital) and multidisciplinary rounds (that is, the physician and NP hospitalists make bedside rounds with a nurse and pharmacist). But their model also incorporates a few less-common features.
Only 4 of the 35 MedOne hospitalists are eligible to provide care on the CMU, and each still spends a significant portion of time in the regular hospitalist rotation working in the rest of the hospital. These doctors weren’t selected as the highest performers or because they had the best patient satisfaction track record. Instead, five MedOne doctors volunteered to work on the unit, and four were chosen. A MedOne hospitalist NP also works on the unit, since any NP in the group is eligible to work there.
This is a hospitalist-only unit; no non–hospitalist patients are placed on the unit. There is no deliberate attempt to assign patients to the unit based on how sick they are or complicated their cases are. All are general medicine patients, including up to six intermediate care patients (e.g., “ICU step-down” patients requiring mask ventilation, etc.). While configured for 20 patients, the unit can flex to as many as 24 patients and has done so numerous times. The hospitalists (physician and NP combined) have averaged 18.9 daily encounters since the CMU opened.
Nurse staffing on the unit was reconfigured to comprise bedside nurses – known as Clinical Nurses (CNs) – and more experienced RNs – in the role of Comprehensive Charge Nurses (CCNs), who attend rounds and coordinate the patients’ hospitalizations rather than doing bedside care. 5-Orange has one more Charge Nurse than is typical for other units in the hospital, so total RN-to-patient staffing levels and nurse staffing costs are higher. But the CNs care for the same number of patients as do their counterparts in other hospital units.
In order to try to discharge patients early in the day, the NP sees only the patients who are being discharged, while the physician makes all other visits. When possible, I think it’s best to minimize the incidence of a provider’s first visit with a patient being a discharge visit; this may increase the risk of misunderstandings and errors. Instead, in this model, the physician working on the CMU will already know the patient from the preceding days and will be on the unit and readily accessible to the NP all day, which might mitigate some of these concerns.
Outcomes
I think the most notable outcome is the top quartile patient satisfaction scores from the 37 patients cared for on the unit who returned a survey, some of whom have asked to return to the CMU if they’re hospitalized again. Specifically, 86% of responses were “top box,” which places the hospitalists at the 84th percentile of performance for all hospitals. Physician Communication scores on the HCAHPS survey for hospitalists on other units at this hospital are in the bottom deciles, which is more typical for hospitalists.
Length of stay is half a day shorter than comparable units with similar readmission rates, and more patients are discharged earlier in the day. The four hospitalists who work on the unit report higher satisfaction, in part because they get an average of only 1 page a day – compared with the typical 15-40 pages their colleagues get working elsewhere in the hospital.
Cautions
I’m not sure why the MedOne model has yielded such impressive patient satisfaction and other results. While there are some relatively unique features of their model – only four hospitalists are eligible to work there and nursing roles have been reconfigured – I wouldn’t expect these to yield such remarkable results. So far, they have roughly 5 months of data and just 37 returned patient satisfaction surveys, so it’s possible that random variation and/or the Hawthorne effect are playing a meaningful role. It will be really informative to see their outcomes a year or 2 from now and to gauge how they fare if and when they implement the same model in other units of the hospital.
I suspect MedOne’s precise configuration for staffing and roles of nurses, NPs, and physicians is important, but I’m guessing the most valuable thing they implemented was the creation of a powerful sense of teamwork and shared purpose among those working on the unit. The interpersonal bonding and feeling of shared purpose that likely occurred as they worked to devise and go live with the model, as well as the tremendous satisfaction at seeing their early results, have probably led to terrific enthusiasm within their team.
That enthusiasm may be the key ingredient contributing to their early success.
Dr. Nelson has been working in clinical practice as a hospitalist since 1988. He is a cofounder and past president of Society of Hospital Medicine and a principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice-management courses. Contact him at [email protected]
More studies show Medicaid expansion has benefited hospitals
In 2016, a series of studies showed the impact of Medicaid expansion on hospitals.1 The news was good: Hospitals in states that accepted Medicaid expansion through the Affordable Care Act saw dramatic reductions in their uninsured patient populations, increases in their Medicaid stays, and reductions in uncompensated care costs.1,2
In 2017, additional data continue to show that Medicaid expansion has been a boon to hospitals, including an April 2017 report published by the Urban Institute and a May 2017 analysis from The Commonwealth Fund.3,4 Both show that some of the hospitals that need it most are reaping the greatest benefits of expansion.

At the same time, Craig Garthwaite, PhD, MPP, lead author of The Commonwealth Fund report, said Medicaid expansion “wiped out roughly half of the uncompensated care faced by hospitals, with relatively little or no decline in nonexpansion states.” To date, 19 states have not expanded Medicaid.
With Medicaid facing an uncertain future, Dr. Blavin said some experts are concerned about what could happen to vulnerable hospitals if Medicaid expansion is repealed or scaled back. Indeed, President Trump and Congressional Republicans have proposed significantly altering Medicaid by either transitioning it to block grants or by capping federal funding for the entitlement.6,7
“We wanted to give people a sense of the stakes of what you’re talking about with repeal of the Affordable Care Act and go back to a system where patients are able to get emergency care at the hospital but not the complete care they get if they’re insured. We’re not going to be paying hospitals for that care, so the hospital has that coming out of their profit margin,” said Dr. Garthwaite, professor of strategy and codirector of the Health Enterprise Management Program in the Kellogg School of Management at Northwestern University, Evanston, Ill.
The Commonwealth Fund report used data from the Centers for Medicare & Medicaid Services (CMS) Hospital Cost Reports to examine 1,154 hospitals in expansion and nonexpansion states. It built on a Health Affairs study Dr. Garthwaite and his coauthors published in 2016.2 The analysis found that between 2013 and 2014, uncompensated care costs declined dramatically in expansion states and continued into 2015, falling from 3.9% to 2.3% of operating costs. Meanwhile, hospitals in nonexpansion states saw uncompensated care costs drop just 0.3-0.4 percentage points. The largest reductions were seen by hospitals providing the highest proportion of care to low-income and uninsured patients and overall savings to hospitals in expansion states amounted to $6.2 billion.
“Any contraction of the Medicaid expansion will reduce overall health insurance coverage and could have important financial implications for hospitals,” Dr. Blavin said. “We are likely to see large increases in expenses attributable to uninsured patients, declines in Medicaid revenue, and increases in uncompensated care burdens that can be a significant financial strain to hospitals.”
As part of a project supported by the Robert Wood Johnson Foundation, the Urban Institute in May 2011 began to track and study the impact of health reform. The report Dr. Blavin authored is part of this endeavor and utilized data from the American Hospital Association Annual Survey and the CMS Health Care Cost Reports to update the 2016 JAMA study. It compared hospitals in expansion states to those in nonexpansion states between fiscal years 2011 and 2015, excluding hospitals in states that expanded before January 2014. It examined hospital-reported data on uncompensated care, uncompensated care as a percentage of total hospital expenses, Medicaid revenue, Medicaid as a percentage of total revenue, operating margins, and excess margins.
The analysis found that Medicaid expansion resulted in a $3.2 million reduction in uncompensated care and a $5.0 million increase in mean annual Medicaid revenue per hospital. Expansion-state hospitals also saw improvements in excess and operating margins relative to nonexpansion state hospitals.

In Connecticut, Medicaid reimbursement rates are among the lowest in the country.8 The state uses a provider tax to finance Medicaid but, facing a budget deficit, state leaders have dramatically reduced the amount of money returned to hospitals in recent years.9
“Our Medicaid patient volume has gone up but our margins have declined because the return on investment is so low,” added Dr. Kumar, a practicing hospitalist and member of the SHM Public Policy Committee. He is concerned about what happens if Medicaid is capped or transitioned to a block grant, since “block grants have not been favorable so far … It would further squeeze us.”
In Arizona, Steve Narang, MD, MHCM, a hospitalist and CEO of Banner–University Medical Center Phoenix (B-UMCP), already knows what it’s like when Medicaid funding expands and then contracts. In 2001, the state expanded Medicaid to 100% of the federal poverty level for childless adults but then in 2011, in the throes of recession, the state froze its match on federal dollars. Prior to the freeze, charity care and bad debt made up 9% of B-UMCP’s net revenue. After the state cut to Medicaid, the hospital’s uncompensated care doubled; charity care and bad debt spiked to 20% of net revenue. Once the freeze was lifted and the state expanded Medicaid through the ACA in 2014, bad debt and charity care plummeted to 7% of revenue and remains in the single digits, Dr. Narang said.
“You hear a lot, especially in debates, about Medicaid being bad coverage … From a hospital perspective, if you’re taking care of a patient who is uninsured versus a patient with Medicaid coverage, that hospital is likely better off financially treating the patient with Medicaid coverage,” said Dr. Blavin.

“From a basic commitment to our fellow human beings, are we doing the right thing as a country?” he asked, noting that states and the federal government must address the economic realities of health care while also providing safety nets for patients. “We have to do both. But I have faith that the state and federal government will find a model and we will continue to focus on what we can control.”
References
1. Tyrrell K. Benefits of Medicaid Expansion for Hospitalists. The Hospitalist. 2016 March;2016(3). http://www.the-hospitalist.org/hospitalist/article/121832/benefits-medicaid-expansion-hospitalists. Accessed May 25, 2017.
2. Dranove D., Garthwaite C., Ody C. Uncompensated Care Decreased at Hospitals in Medicaid Expansion States but Not at Hospitals in Nonexpansion States. Health Affairs, Aug. 2016 35(8):1471-9. http://content.healthaffairs.org/content/35/8/1471.abstract. Accessed May 25, 2017.
3. Blavin F. How Has the ACA Changed Finances for Different Types of Hospitals? Updated Insights from 2015 Cost Report Data. Urban Institute. Published April 2017. Accessed May 25, 2017. http://www.urban.org/sites/default/files/publication/89446/2001215-how-has-the-aca-changed-finances-for-different-types-of-hospitals.pdf.
4. Dranove D., Garthwaite C., Ody C. The Impact of the ACA’s Medicaid Expansion on Hospitals’ Uncompensated Care Burden and the Potential Effects of Repeal. Published May 3, 2017. Accessed May 25, 2017. http://www.commonwealthfund.org/publications/issue-briefs/2017/may/aca-medicaid-expansion-hospital-uncompensated-care.
5. Blavin F. Association Between the 2014 Medicaid Expansion and US Hospital Finances. http://jamanetwork.com/journals/jama/fullarticle/2565750. JAMA 2016;316(14):1475-1483. doi:10.1001/jama.2016.14765
6. President Trump’s 2018 Budget Proposal Reduces Federal Funding for Coverage of Children in Medicaid and CHIP. Kaiser Family Foundation. Published March 23, 2017. Accessed May 25, 2017. http://kff.org/medicaid/fact-sheet/presidents-2018-budget-proposal-reduces-federal-funding-for-coverage-of-children-in-medicaid-and-chip/
7. Paradise J. Restructuring Medicaid in the American Health Care Act: Five Key Considerations. Kaiser Family Foundation. Published March 15, 2017. Accessed May 25, 2017. http://kff.org/medicaid/issue-brief/restructuring-medicaid-in-the-american-health-care-act-five-key-considerations/
8. Medicaid Hospital Payment: A comparison across states and to Medicare. MACPAC Issue Brief. Published April 2017.
9. Levin Becker A. Hospitals blast Malloy’s proposal to subject them to property taxes. Published Feb. 8, 2017. Accessed May 25, 2017. https://ctmirror.org/2017/02/08/hospitals-blast-malloys-proposal-to-subject-them-to-property-taxes/
In 2016, a series of studies showed the impact of Medicaid expansion on hospitals.1 The news was good: Hospitals in states that accepted Medicaid expansion through the Affordable Care Act saw dramatic reductions in their uninsured patient populations, increases in their Medicaid stays, and reductions in uncompensated care costs.1,2
In 2017, additional data continue to show that Medicaid expansion has been a boon to hospitals, including an April 2017 report published by the Urban Institute and a May 2017 analysis from The Commonwealth Fund.3,4 Both show that some of the hospitals that need it most are reaping the greatest benefits of expansion.
At the same time, Craig Garthwaite, PhD, MPP, lead author of The Commonwealth Fund report, said Medicaid expansion “wiped out roughly half of the uncompensated care faced by hospitals, with relatively little or no decline in nonexpansion states.” To date, 19 states have not expanded Medicaid.
With Medicaid facing an uncertain future, Dr. Blavin said some experts are concerned about what could happen to vulnerable hospitals if Medicaid expansion is repealed or scaled back. Indeed, President Trump and Congressional Republicans have proposed significantly altering Medicaid by either transitioning it to block grants or by capping federal funding for the entitlement.6,7
“We wanted to give people a sense of the stakes of what you’re talking about with repeal of the Affordable Care Act and go back to a system where patients are able to get emergency care at the hospital but not the complete care they get if they’re insured. We’re not going to be paying hospitals for that care, so the hospital has that coming out of their profit margin,” said Dr. Garthwaite, professor of strategy and codirector of the Health Enterprise Management Program in the Kellogg School of Management at Northwestern University, Evanston, Ill.
The Commonwealth Fund report used data from the Centers for Medicare & Medicaid Services (CMS) Hospital Cost Reports to examine 1,154 hospitals in expansion and nonexpansion states. It built on a Health Affairs study Dr. Garthwaite and his coauthors published in 2016.2 The analysis found that between 2013 and 2014, uncompensated care costs declined dramatically in expansion states and continued into 2015, falling from 3.9% to 2.3% of operating costs. Meanwhile, hospitals in nonexpansion states saw uncompensated care costs drop just 0.3-0.4 percentage points. The largest reductions were seen by hospitals providing the highest proportion of care to low-income and uninsured patients and overall savings to hospitals in expansion states amounted to $6.2 billion.
“Any contraction of the Medicaid expansion will reduce overall health insurance coverage and could have important financial implications for hospitals,” Dr. Blavin said. “We are likely to see large increases in expenses attributable to uninsured patients, declines in Medicaid revenue, and increases in uncompensated care burdens that can be a significant financial strain to hospitals.”
As part of a project supported by the Robert Wood Johnson Foundation, the Urban Institute in May 2011 began to track and study the impact of health reform. The report Dr. Blavin authored is part of this endeavor and utilized data from the American Hospital Association Annual Survey and the CMS Health Care Cost Reports to update the 2016 JAMA study. It compared hospitals in expansion states to those in nonexpansion states between fiscal years 2011 and 2015, excluding hospitals in states that expanded before January 2014. It examined hospital-reported data on uncompensated care, uncompensated care as a percentage of total hospital expenses, Medicaid revenue, Medicaid as a percentage of total revenue, operating margins, and excess margins.
The analysis found that Medicaid expansion resulted in a $3.2 million reduction in uncompensated care and a $5.0 million increase in mean annual Medicaid revenue per hospital. Expansion-state hospitals also saw improvements in excess and operating margins relative to nonexpansion state hospitals.
In Connecticut, Medicaid reimbursement rates are among the lowest in the country.8 The state uses a provider tax to finance Medicaid but, facing a budget deficit, state leaders have dramatically reduced the amount of money returned to hospitals in recent years.9
“Our Medicaid patient volume has gone up but our margins have declined because the return on investment is so low,” added Dr. Kumar, a practicing hospitalist and member of the SHM Public Policy Committee. He is concerned about what happens if Medicaid is capped or transitioned to a block grant, since “block grants have not been favorable so far … It would further squeeze us.”
In Arizona, Steve Narang, MD, MHCM, a hospitalist and CEO of Banner–University Medical Center Phoenix (B-UMCP), already knows what it’s like when Medicaid funding expands and then contracts. In 2001, the state expanded Medicaid to 100% of the federal poverty level for childless adults but then in 2011, in the throes of recession, the state froze its match on federal dollars. Prior to the freeze, charity care and bad debt made up 9% of B-UMCP’s net revenue. After the state cut to Medicaid, the hospital’s uncompensated care doubled; charity care and bad debt spiked to 20% of net revenue. Once the freeze was lifted and the state expanded Medicaid through the ACA in 2014, bad debt and charity care plummeted to 7% of revenue and remains in the single digits, Dr. Narang said.
“You hear a lot, especially in debates, about Medicaid being bad coverage … From a hospital perspective, if you’re taking care of a patient who is uninsured versus a patient with Medicaid coverage, that hospital is likely better off financially treating the patient with Medicaid coverage,” said Dr. Blavin.
“From a basic commitment to our fellow human beings, are we doing the right thing as a country?” he asked, noting that states and the federal government must address the economic realities of health care while also providing safety nets for patients. “We have to do both. But I have faith that the state and federal government will find a model and we will continue to focus on what we can control.”
References
1. Tyrrell K. Benefits of Medicaid Expansion for Hospitalists. The Hospitalist. 2016 March;2016(3). http://www.the-hospitalist.org/hospitalist/article/121832/benefits-medicaid-expansion-hospitalists. Accessed May 25, 2017.
2. Dranove D., Garthwaite C., Ody C. Uncompensated Care Decreased at Hospitals in Medicaid Expansion States but Not at Hospitals in Nonexpansion States. Health Affairs, Aug. 2016 35(8):1471-9. http://content.healthaffairs.org/content/35/8/1471.abstract. Accessed May 25, 2017.
3. Blavin F. How Has the ACA Changed Finances for Different Types of Hospitals? Updated Insights from 2015 Cost Report Data. Urban Institute. Published April 2017. Accessed May 25, 2017. http://www.urban.org/sites/default/files/publication/89446/2001215-how-has-the-aca-changed-finances-for-different-types-of-hospitals.pdf.
4. Dranove D., Garthwaite C., Ody C. The Impact of the ACA’s Medicaid Expansion on Hospitals’ Uncompensated Care Burden and the Potential Effects of Repeal. Published May 3, 2017. Accessed May 25, 2017. http://www.commonwealthfund.org/publications/issue-briefs/2017/may/aca-medicaid-expansion-hospital-uncompensated-care.
5. Blavin F. Association Between the 2014 Medicaid Expansion and US Hospital Finances. http://jamanetwork.com/journals/jama/fullarticle/2565750. JAMA 2016;316(14):1475-1483. doi:10.1001/jama.2016.14765
6. President Trump’s 2018 Budget Proposal Reduces Federal Funding for Coverage of Children in Medicaid and CHIP. Kaiser Family Foundation. Published March 23, 2017. Accessed May 25, 2017. http://kff.org/medicaid/fact-sheet/presidents-2018-budget-proposal-reduces-federal-funding-for-coverage-of-children-in-medicaid-and-chip/
7. Paradise J. Restructuring Medicaid in the American Health Care Act: Five Key Considerations. Kaiser Family Foundation. Published March 15, 2017. Accessed May 25, 2017. http://kff.org/medicaid/issue-brief/restructuring-medicaid-in-the-american-health-care-act-five-key-considerations/
8. Medicaid Hospital Payment: A comparison across states and to Medicare. MACPAC Issue Brief. Published April 2017.
9. Levin Becker A. Hospitals blast Malloy’s proposal to subject them to property taxes. Published Feb. 8, 2017. Accessed May 25, 2017. https://ctmirror.org/2017/02/08/hospitals-blast-malloys-proposal-to-subject-them-to-property-taxes/
In 2016, a series of studies showed the impact of Medicaid expansion on hospitals.1 The news was good: Hospitals in states that accepted Medicaid expansion through the Affordable Care Act saw dramatic reductions in their uninsured patient populations, increases in their Medicaid stays, and reductions in uncompensated care costs.1,2
In 2017, additional data continue to show that Medicaid expansion has been a boon to hospitals, including an April 2017 report published by the Urban Institute and a May 2017 analysis from The Commonwealth Fund.3,4 Both show that some of the hospitals that need it most are reaping the greatest benefits of expansion.
At the same time, Craig Garthwaite, PhD, MPP, lead author of The Commonwealth Fund report, said Medicaid expansion “wiped out roughly half of the uncompensated care faced by hospitals, with relatively little or no decline in nonexpansion states.” To date, 19 states have not expanded Medicaid.
With Medicaid facing an uncertain future, Dr. Blavin said some experts are concerned about what could happen to vulnerable hospitals if Medicaid expansion is repealed or scaled back. Indeed, President Trump and Congressional Republicans have proposed significantly altering Medicaid by either transitioning it to block grants or by capping federal funding for the entitlement.6,7
“We wanted to give people a sense of the stakes of what you’re talking about with repeal of the Affordable Care Act and go back to a system where patients are able to get emergency care at the hospital but not the complete care they get if they’re insured. We’re not going to be paying hospitals for that care, so the hospital has that coming out of their profit margin,” said Dr. Garthwaite, professor of strategy and codirector of the Health Enterprise Management Program in the Kellogg School of Management at Northwestern University, Evanston, Ill.
The Commonwealth Fund report used data from the Centers for Medicare & Medicaid Services (CMS) Hospital Cost Reports to examine 1,154 hospitals in expansion and nonexpansion states. It built on a Health Affairs study Dr. Garthwaite and his coauthors published in 2016.2 The analysis found that between 2013 and 2014, uncompensated care costs declined dramatically in expansion states and continued into 2015, falling from 3.9% to 2.3% of operating costs. Meanwhile, hospitals in nonexpansion states saw uncompensated care costs drop just 0.3-0.4 percentage points. The largest reductions were seen by hospitals providing the highest proportion of care to low-income and uninsured patients and overall savings to hospitals in expansion states amounted to $6.2 billion.
“Any contraction of the Medicaid expansion will reduce overall health insurance coverage and could have important financial implications for hospitals,” Dr. Blavin said. “We are likely to see large increases in expenses attributable to uninsured patients, declines in Medicaid revenue, and increases in uncompensated care burdens that can be a significant financial strain to hospitals.”
As part of a project supported by the Robert Wood Johnson Foundation, the Urban Institute in May 2011 began to track and study the impact of health reform. The report Dr. Blavin authored is part of this endeavor and utilized data from the American Hospital Association Annual Survey and the CMS Health Care Cost Reports to update the 2016 JAMA study. It compared hospitals in expansion states to those in nonexpansion states between fiscal years 2011 and 2015, excluding hospitals in states that expanded before January 2014. It examined hospital-reported data on uncompensated care, uncompensated care as a percentage of total hospital expenses, Medicaid revenue, Medicaid as a percentage of total revenue, operating margins, and excess margins.
The analysis found that Medicaid expansion resulted in a $3.2 million reduction in uncompensated care and a $5.0 million increase in mean annual Medicaid revenue per hospital. Expansion-state hospitals also saw improvements in excess and operating margins relative to nonexpansion state hospitals.
In Connecticut, Medicaid reimbursement rates are among the lowest in the country.8 The state uses a provider tax to finance Medicaid but, facing a budget deficit, state leaders have dramatically reduced the amount of money returned to hospitals in recent years.9
“Our Medicaid patient volume has gone up but our margins have declined because the return on investment is so low,” added Dr. Kumar, a practicing hospitalist and member of the SHM Public Policy Committee. He is concerned about what happens if Medicaid is capped or transitioned to a block grant, since “block grants have not been favorable so far … It would further squeeze us.”
In Arizona, Steve Narang, MD, MHCM, a hospitalist and CEO of Banner–University Medical Center Phoenix (B-UMCP), already knows what it’s like when Medicaid funding expands and then contracts. In 2001, the state expanded Medicaid to 100% of the federal poverty level for childless adults but then in 2011, in the throes of recession, the state froze its match on federal dollars. Prior to the freeze, charity care and bad debt made up 9% of B-UMCP’s net revenue. After the state cut to Medicaid, the hospital’s uncompensated care doubled; charity care and bad debt spiked to 20% of net revenue. Once the freeze was lifted and the state expanded Medicaid through the ACA in 2014, bad debt and charity care plummeted to 7% of revenue and remains in the single digits, Dr. Narang said.
“You hear a lot, especially in debates, about Medicaid being bad coverage … From a hospital perspective, if you’re taking care of a patient who is uninsured versus a patient with Medicaid coverage, that hospital is likely better off financially treating the patient with Medicaid coverage,” said Dr. Blavin.
“From a basic commitment to our fellow human beings, are we doing the right thing as a country?” he asked, noting that states and the federal government must address the economic realities of health care while also providing safety nets for patients. “We have to do both. But I have faith that the state and federal government will find a model and we will continue to focus on what we can control.”
References
1. Tyrrell K. Benefits of Medicaid Expansion for Hospitalists. The Hospitalist. 2016 March;2016(3). http://www.the-hospitalist.org/hospitalist/article/121832/benefits-medicaid-expansion-hospitalists. Accessed May 25, 2017.
2. Dranove D., Garthwaite C., Ody C. Uncompensated Care Decreased at Hospitals in Medicaid Expansion States but Not at Hospitals in Nonexpansion States. Health Affairs, Aug. 2016 35(8):1471-9. http://content.healthaffairs.org/content/35/8/1471.abstract. Accessed May 25, 2017.
3. Blavin F. How Has the ACA Changed Finances for Different Types of Hospitals? Updated Insights from 2015 Cost Report Data. Urban Institute. Published April 2017. Accessed May 25, 2017. http://www.urban.org/sites/default/files/publication/89446/2001215-how-has-the-aca-changed-finances-for-different-types-of-hospitals.pdf.
4. Dranove D., Garthwaite C., Ody C. The Impact of the ACA’s Medicaid Expansion on Hospitals’ Uncompensated Care Burden and the Potential Effects of Repeal. Published May 3, 2017. Accessed May 25, 2017. http://www.commonwealthfund.org/publications/issue-briefs/2017/may/aca-medicaid-expansion-hospital-uncompensated-care.
5. Blavin F. Association Between the 2014 Medicaid Expansion and US Hospital Finances. http://jamanetwork.com/journals/jama/fullarticle/2565750. JAMA 2016;316(14):1475-1483. doi:10.1001/jama.2016.14765
6. President Trump’s 2018 Budget Proposal Reduces Federal Funding for Coverage of Children in Medicaid and CHIP. Kaiser Family Foundation. Published March 23, 2017. Accessed May 25, 2017. http://kff.org/medicaid/fact-sheet/presidents-2018-budget-proposal-reduces-federal-funding-for-coverage-of-children-in-medicaid-and-chip/
7. Paradise J. Restructuring Medicaid in the American Health Care Act: Five Key Considerations. Kaiser Family Foundation. Published March 15, 2017. Accessed May 25, 2017. http://kff.org/medicaid/issue-brief/restructuring-medicaid-in-the-american-health-care-act-five-key-considerations/
8. Medicaid Hospital Payment: A comparison across states and to Medicare. MACPAC Issue Brief. Published April 2017.
9. Levin Becker A. Hospitals blast Malloy’s proposal to subject them to property taxes. Published Feb. 8, 2017. Accessed May 25, 2017. https://ctmirror.org/2017/02/08/hospitals-blast-malloys-proposal-to-subject-them-to-property-taxes/
Hospital value-based purchasing is largely ineffective
Over the last 5 years, I’ve periodically devoted this column to providing updates to the Hospital Value-Based Purchasing program. HVBP launched in 2013 as a 5-year mixed upside/downside incentive program with mandatory participation for all U.S. acute care hospitals (critical access, acute inpatient rehabilitation, and long-term acute care hospitals are exempt). The program initially included process and patient experience measures. It later added measures for mortality, efficiency, and patient safety.
For the 2017 version of HVBP, the measures are allocated as follows: eight for patient experience, seven for patient safety (1 of which is a roll up of 11 claims-based measures), three for process, and three for mortality. HVBP uses a budget-neutral funding approach with some winners and some losers but overall net zero spending on the program. It initially put hospitals at risk for 1% of their Medicare inpatient payments (in 2013), with a progressive increase to 2% by this year. HVBP has used a complex approach to determining incentives and penalties, rewarding either improvement or achievement, depending on the baseline performance of the hospital.

Has HVBP improved quality? Two studies looking at the early period of HVBP failed to show improvements in process or patient experience measures and demonstrated no change in mortality for heart failure, pneumonia, or heart attack.1,2 Now that the program is in its 5th and final year, thanks to a recent study by Ryan et al., we have an idea if HVBP is associated with longer-term improvements in quality.3
In the study, Ryan et al. compared hospitals participating in HVBP with critical access hospitals, which are exempt from the program. The study yielded some disappointing, if not surprising, results. Improvements in process and patient experience measures for HVBP hospitals were no greater than those for the control group. HVBP was not associated with a significant reduction in mortality for heart failure or heart attack, but was associated with a mortality reduction for pneumonia. In sum, HVBP was not associated with improvements in process or patient experience, and was not associated with lower mortality, except in pneumonia.
As a program designed to incentivize better quality, where did HVBP go wrong? I believe HVBP simply had too many measures for the cognitive bandwidth of an individual or a team looking to improve quality. The total measure count for 2017 is 21! I submit that a hospitalist working to improve quality can keep top-of-mind one or two measures, possibly three at most. While others have postulated that the amount of dollars at risk are too small, I don’t think that’s the problem. Instead, my sense is that hospitalists and other members of the hospital team have quality improvement in their DNA and, regardless of the size of the financial incentives, will work to improve it as long as they have the right tools. Chief among these are good performance data and the time to focus on a finite number of projects.
What lessons can inform better design in the future? As of January 2017, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – representing the biggest change in reimbursement in a generation – progressively exposes doctors and other professionals to upside/downside incentives for quality, resource utilization, use of a certified electronic health record (hospitalists are exempt as they already use the hospital’s EHR), and practice improvement activities.
It would be wise to learn from the shortcomings of HVBP. Namely, if MACRA keeps on its course to incentivize physicians using a complicated formula based on four domains and many more subdomains, it will repeat the mistakes of HVBP and – while creating more administrative burden – likely improve quality very little, if at all. Instead, MACRA should delineate a simple measure set representing improvement activities that physicians and teams can incorporate into their regular work flow without more time taken away from patient care.
The reality is that complicated pay-for-performance programs divert limited available resources away from meaningful improvement activities in order to comply with onerous reporting requirements. As we gain a more nuanced understanding of how these programs work, policy makers should pay attention to the elements of “low-value” and “high-value” incentive systems and apply the “less is more” ethos of high-value care to the next generation of pay-for-performance programs.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Ryan AM, Burgess JF, Pesko MF, Borden WB, Dimick JB. “The early effects of Medicare’s mandatory hospital pay-for-performance program” Health Serv Res. 2015;50:81-97.
2. Figueroa JF, Tsugawa Y, Zheng J, Orav EJ, Jha AK. “Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study” BMJ. 2016;353:i2214.
3. Ryan AM, Krinsky S, Maurer KA, Dimick JB. “Changes in Hospital Quality Associated with Hospital Value-Based Purchasing” N Engl J Med. 2017;376:2358-66.
Over the last 5 years, I’ve periodically devoted this column to providing updates to the Hospital Value-Based Purchasing program. HVBP launched in 2013 as a 5-year mixed upside/downside incentive program with mandatory participation for all U.S. acute care hospitals (critical access, acute inpatient rehabilitation, and long-term acute care hospitals are exempt). The program initially included process and patient experience measures. It later added measures for mortality, efficiency, and patient safety.
For the 2017 version of HVBP, the measures are allocated as follows: eight for patient experience, seven for patient safety (1 of which is a roll up of 11 claims-based measures), three for process, and three for mortality. HVBP uses a budget-neutral funding approach with some winners and some losers but overall net zero spending on the program. It initially put hospitals at risk for 1% of their Medicare inpatient payments (in 2013), with a progressive increase to 2% by this year. HVBP has used a complex approach to determining incentives and penalties, rewarding either improvement or achievement, depending on the baseline performance of the hospital.
Has HVBP improved quality? Two studies looking at the early period of HVBP failed to show improvements in process or patient experience measures and demonstrated no change in mortality for heart failure, pneumonia, or heart attack.1,2 Now that the program is in its 5th and final year, thanks to a recent study by Ryan et al., we have an idea if HVBP is associated with longer-term improvements in quality.3
In the study, Ryan et al. compared hospitals participating in HVBP with critical access hospitals, which are exempt from the program. The study yielded some disappointing, if not surprising, results. Improvements in process and patient experience measures for HVBP hospitals were no greater than those for the control group. HVBP was not associated with a significant reduction in mortality for heart failure or heart attack, but was associated with a mortality reduction for pneumonia. In sum, HVBP was not associated with improvements in process or patient experience, and was not associated with lower mortality, except in pneumonia.
As a program designed to incentivize better quality, where did HVBP go wrong? I believe HVBP simply had too many measures for the cognitive bandwidth of an individual or a team looking to improve quality. The total measure count for 2017 is 21! I submit that a hospitalist working to improve quality can keep top-of-mind one or two measures, possibly three at most. While others have postulated that the amount of dollars at risk are too small, I don’t think that’s the problem. Instead, my sense is that hospitalists and other members of the hospital team have quality improvement in their DNA and, regardless of the size of the financial incentives, will work to improve it as long as they have the right tools. Chief among these are good performance data and the time to focus on a finite number of projects.
What lessons can inform better design in the future? As of January 2017, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – representing the biggest change in reimbursement in a generation – progressively exposes doctors and other professionals to upside/downside incentives for quality, resource utilization, use of a certified electronic health record (hospitalists are exempt as they already use the hospital’s EHR), and practice improvement activities.
It would be wise to learn from the shortcomings of HVBP. Namely, if MACRA keeps on its course to incentivize physicians using a complicated formula based on four domains and many more subdomains, it will repeat the mistakes of HVBP and – while creating more administrative burden – likely improve quality very little, if at all. Instead, MACRA should delineate a simple measure set representing improvement activities that physicians and teams can incorporate into their regular work flow without more time taken away from patient care.
The reality is that complicated pay-for-performance programs divert limited available resources away from meaningful improvement activities in order to comply with onerous reporting requirements. As we gain a more nuanced understanding of how these programs work, policy makers should pay attention to the elements of “low-value” and “high-value” incentive systems and apply the “less is more” ethos of high-value care to the next generation of pay-for-performance programs.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Ryan AM, Burgess JF, Pesko MF, Borden WB, Dimick JB. “The early effects of Medicare’s mandatory hospital pay-for-performance program” Health Serv Res. 2015;50:81-97.
2. Figueroa JF, Tsugawa Y, Zheng J, Orav EJ, Jha AK. “Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study” BMJ. 2016;353:i2214.
3. Ryan AM, Krinsky S, Maurer KA, Dimick JB. “Changes in Hospital Quality Associated with Hospital Value-Based Purchasing” N Engl J Med. 2017;376:2358-66.
Over the last 5 years, I’ve periodically devoted this column to providing updates to the Hospital Value-Based Purchasing program. HVBP launched in 2013 as a 5-year mixed upside/downside incentive program with mandatory participation for all U.S. acute care hospitals (critical access, acute inpatient rehabilitation, and long-term acute care hospitals are exempt). The program initially included process and patient experience measures. It later added measures for mortality, efficiency, and patient safety.
For the 2017 version of HVBP, the measures are allocated as follows: eight for patient experience, seven for patient safety (1 of which is a roll up of 11 claims-based measures), three for process, and three for mortality. HVBP uses a budget-neutral funding approach with some winners and some losers but overall net zero spending on the program. It initially put hospitals at risk for 1% of their Medicare inpatient payments (in 2013), with a progressive increase to 2% by this year. HVBP has used a complex approach to determining incentives and penalties, rewarding either improvement or achievement, depending on the baseline performance of the hospital.
Has HVBP improved quality? Two studies looking at the early period of HVBP failed to show improvements in process or patient experience measures and demonstrated no change in mortality for heart failure, pneumonia, or heart attack.1,2 Now that the program is in its 5th and final year, thanks to a recent study by Ryan et al., we have an idea if HVBP is associated with longer-term improvements in quality.3
In the study, Ryan et al. compared hospitals participating in HVBP with critical access hospitals, which are exempt from the program. The study yielded some disappointing, if not surprising, results. Improvements in process and patient experience measures for HVBP hospitals were no greater than those for the control group. HVBP was not associated with a significant reduction in mortality for heart failure or heart attack, but was associated with a mortality reduction for pneumonia. In sum, HVBP was not associated with improvements in process or patient experience, and was not associated with lower mortality, except in pneumonia.
As a program designed to incentivize better quality, where did HVBP go wrong? I believe HVBP simply had too many measures for the cognitive bandwidth of an individual or a team looking to improve quality. The total measure count for 2017 is 21! I submit that a hospitalist working to improve quality can keep top-of-mind one or two measures, possibly three at most. While others have postulated that the amount of dollars at risk are too small, I don’t think that’s the problem. Instead, my sense is that hospitalists and other members of the hospital team have quality improvement in their DNA and, regardless of the size of the financial incentives, will work to improve it as long as they have the right tools. Chief among these are good performance data and the time to focus on a finite number of projects.
What lessons can inform better design in the future? As of January 2017, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) – representing the biggest change in reimbursement in a generation – progressively exposes doctors and other professionals to upside/downside incentives for quality, resource utilization, use of a certified electronic health record (hospitalists are exempt as they already use the hospital’s EHR), and practice improvement activities.
It would be wise to learn from the shortcomings of HVBP. Namely, if MACRA keeps on its course to incentivize physicians using a complicated formula based on four domains and many more subdomains, it will repeat the mistakes of HVBP and – while creating more administrative burden – likely improve quality very little, if at all. Instead, MACRA should delineate a simple measure set representing improvement activities that physicians and teams can incorporate into their regular work flow without more time taken away from patient care.
The reality is that complicated pay-for-performance programs divert limited available resources away from meaningful improvement activities in order to comply with onerous reporting requirements. As we gain a more nuanced understanding of how these programs work, policy makers should pay attention to the elements of “low-value” and “high-value” incentive systems and apply the “less is more” ethos of high-value care to the next generation of pay-for-performance programs.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Ryan AM, Burgess JF, Pesko MF, Borden WB, Dimick JB. “The early effects of Medicare’s mandatory hospital pay-for-performance program” Health Serv Res. 2015;50:81-97.
2. Figueroa JF, Tsugawa Y, Zheng J, Orav EJ, Jha AK. “Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study” BMJ. 2016;353:i2214.
3. Ryan AM, Krinsky S, Maurer KA, Dimick JB. “Changes in Hospital Quality Associated with Hospital Value-Based Purchasing” N Engl J Med. 2017;376:2358-66.
VIP services linked to unnecessary care
Clinical Question: Does “very important person” (VIP) status impact physician decision making and lead to unnecessary care?
Background: In many centers, VIP patients avail VIP services, which involve extra services beyond the standard of care. No prior studies assess the impact of such VIP services on these patients.
Setting: Centers associated with the Hospital Medicine Reengineering Network (HOMERuN).
Synopsis: Of the 160 hospitalists across eight sites, 45% felt that VIP services were present at their hospital. These patients often had personal ties with the hospital. The majority of hospitalists (78%) felt VIP patients received similar medical care, compared with non-VIP patients. However, 63% felt pressured by VIP patients or families to order unnecessary tests. Moreover, 36% perceived pressure from hospital administration to comply with VIP patient wishes. Most hospitalists (56%) reported being more likely to comply with requests from VIP patients than from other patients.
The survey questions were not validated, so the responses might not reflect actual perceptions of hospitalists. These results are purely qualitative, so the burden of unnecessary care cannot be quantified.
Bottom Line: Most hospitalists perceive VIP services to lead to pressure to deliver unnecessary care.
Citation: Allen-Dicker J, Auerbach A, Herzig SJ. Perceived Safety and Value of Inpatient “Very Important Person” Services. J Hosp Med. 2017 Mar;12(3):177-179.
Dr. Suman is clinical instructor of medicine in the University of Kentucky division of hospital medicine.
Clinical Question: Does “very important person” (VIP) status impact physician decision making and lead to unnecessary care?
Background: In many centers, VIP patients avail VIP services, which involve extra services beyond the standard of care. No prior studies assess the impact of such VIP services on these patients.
Setting: Centers associated with the Hospital Medicine Reengineering Network (HOMERuN).
Synopsis: Of the 160 hospitalists across eight sites, 45% felt that VIP services were present at their hospital. These patients often had personal ties with the hospital. The majority of hospitalists (78%) felt VIP patients received similar medical care, compared with non-VIP patients. However, 63% felt pressured by VIP patients or families to order unnecessary tests. Moreover, 36% perceived pressure from hospital administration to comply with VIP patient wishes. Most hospitalists (56%) reported being more likely to comply with requests from VIP patients than from other patients.
The survey questions were not validated, so the responses might not reflect actual perceptions of hospitalists. These results are purely qualitative, so the burden of unnecessary care cannot be quantified.
Bottom Line: Most hospitalists perceive VIP services to lead to pressure to deliver unnecessary care.
Citation: Allen-Dicker J, Auerbach A, Herzig SJ. Perceived Safety and Value of Inpatient “Very Important Person” Services. J Hosp Med. 2017 Mar;12(3):177-179.
Dr. Suman is clinical instructor of medicine in the University of Kentucky division of hospital medicine.
Clinical Question: Does “very important person” (VIP) status impact physician decision making and lead to unnecessary care?
Background: In many centers, VIP patients avail VIP services, which involve extra services beyond the standard of care. No prior studies assess the impact of such VIP services on these patients.
Setting: Centers associated with the Hospital Medicine Reengineering Network (HOMERuN).
Synopsis: Of the 160 hospitalists across eight sites, 45% felt that VIP services were present at their hospital. These patients often had personal ties with the hospital. The majority of hospitalists (78%) felt VIP patients received similar medical care, compared with non-VIP patients. However, 63% felt pressured by VIP patients or families to order unnecessary tests. Moreover, 36% perceived pressure from hospital administration to comply with VIP patient wishes. Most hospitalists (56%) reported being more likely to comply with requests from VIP patients than from other patients.
The survey questions were not validated, so the responses might not reflect actual perceptions of hospitalists. These results are purely qualitative, so the burden of unnecessary care cannot be quantified.
Bottom Line: Most hospitalists perceive VIP services to lead to pressure to deliver unnecessary care.
Citation: Allen-Dicker J, Auerbach A, Herzig SJ. Perceived Safety and Value of Inpatient “Very Important Person” Services. J Hosp Med. 2017 Mar;12(3):177-179.
Dr. Suman is clinical instructor of medicine in the University of Kentucky division of hospital medicine.
Communication tools improve patient experience and satisfaction
How hospitalists and other clinicians communicate with patients impacts a patient’s overall experience and satisfaction. But according to the authors of “Communication the Cleveland Way,”1 a book about how the clinic created and applied communication skills training, “in a culture prioritizing clinical outcomes above all, there can be a tendency to lose sight of one of the most critical aspects of providing effective care: the communication skills that build and foster physician-patient relationships.”
“Studies2,3 have shown that good communication between doctors and patients and among all caregivers who interface with patients directly results in better clinical outcomes, reduced costs, greater patient satisfaction, and lower rates of physician burnout,” the authors wrote.

“It places a special focus on empathy in relationships, and in our case, the provider-patient relationship rather than patient-centered care. The former acknowledges that the thoughts and feelings in both sides of a relationship are important. We know that clinicians, too, can suffer as a result of the care they provide,” Dr. Velez wrote in “Communication the Cleveland Way.”1
“Healthy relationships are based on balance and mutual respect,” Dr Velez said. “Courses made a strong point to practice empathy in order to teach empathy. Clinician participants were gifted with a safe space, an opportunity to share their own skills and expertise, and a chance to be appreciated for what they already do effectively. Most of all, activities were designed to be fun and engaging.” For example, CEHC encouraged and fostered an attitude of exploration, experimentation, and adventure. Various warm-up activities effectively helped the participants enter a more playful space and get into character portrayal.
Dr. Velez credits the CEHC model’s sustainability and success to the early realization that an appreciative approach is effective. In a study3 about the strategy, hospital-employed attending physicians participated in the 8-hour experiential communication skills training course on REDE. The study compared approximately 1,500 “intervention” physicians who attended and 1,900 “nonintervention” physicians who did not attend.
Following the course, scores for physician communication and respect were higher for intervention physicians. Furthermore, physicians showed significant improvement in self-perceptions of empathy and burnout. Some of these gains were sustained for at least 3 months. “This is especially important because in the current health care climate, physicians experience increased burnout,” Dr. Velez notes.
How it works
Because a provider’s connection with a patient occurs when a relationship is established, the REDE course focuses on the beginning of the conversation. “It’s important for clinicians to exhibit value and respect through words and actions when welcoming patients,” Dr. Velez said. “Further, instead of guiding the medical interview with a series of close-ended questions like an interrogator would, we invite the use of open-ended questions and setting an agenda for the visit early on, by asking the patient what they wish to discuss.”
Another key component is empathy, which plays a huge role in patient satisfaction. “Learning how to express empathy is very important,” Dr. Velez said. “A patient may not remember all of the medical details discussed, but human interactions, rapport, expressions of care, support, validation, and acknowledgment of emotions tend to be more indelible.”
Dr. Velez notes that decades of literature regarding effective communication have demonstrated improved outcomes. “If trust in a therapeutic relationship is strong, a patient is more likely to follow instructions and have better engagement with their care plan,” he said. “If a clinician ensures that the patient understands the diagnosis and recommendations, then compliance will increase, especially if the plan is tailored to the patient’s goals and perspective.”
One surprising effect of the REDE course was how it improved relationships among professionals. “Many participants have shared that having a day out of one’s normal schedule, not only to learn, but also to share their own experiences, is quite therapeutic,” Dr. Velez said. “We can extend the same communication strategies to team building, interprofessional interactions, and challenging encounters.”
Study focuses on comportment and communication
In an effort to define optimal care in hospital medicine, a team from Johns Hopkins Health System set out to establish a metric that would comprehensively assess hospitalists’ comportment (which includes behavior as well as general demeanor) and communication to establish norms and expectations when they saw patients at the bedside.
To perform the study,4 chiefs of hospital medicine divisions at five independent hospitals located in Baltimore and Washington identified their most clinically excellent hospitalists. Then, an investigator observed each hospitalist during a routine clinical shift and recorded behaviors believed to be associated with excellent behavior and communication using the hospital medicine comportment and communication observation tool (HMCCOT), said Susrutha Kotwal, MD, assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, and lead author. The investigators collected basic demographic information while observing hospitalists for an average of 280 minutes; 26 physicians were observed for 181 separate clinical encounters. Each provider’s mean HMCCOT score was compared with patient satisfaction surveys such as Press Ganey (PG) scores.

Noteworthy is the fact that the distribution of HMCCOT scores were similar when analyzed by age, gender, race, amount of clinical experience, the hospitalist’s clinical workload, hospital, or time spent observing the hospitalist. But the distribution of HMCCOT scores was quite different in new patient encounters, compared with follow-ups (68.1% versus 39.7%). Encounters with patients that generated HMCCOT scores above versus below the mean were longer (13 minutes versus 8.7 minutes). The physicians’ HMCCOT scores were also associated with their PG scores. These findings suggest that improved bedside communication and comportment with patients might also translate into enhanced patient satisfaction.
As a result of the study, a comportment and communication tool was established and validated by following clinically excellent hospitalists at the bedside. “Even among clinically respected hospitalists, the results reveal that there is wide variability in behaviors and communication practices at the bedside,” Dr. Kotwal said.
Employing the tool
Hospitalists can choose whether to perform behaviors in the HMCCOT themselves, while others may wish to watch other hospitalists to give them feedback tied to specific behaviors. “These simple behaviors are intimately linked to excellent communication and comportment, which can serve as the foundation for delivering patient-centered care,” Dr. Kotwal said.
A positive correlation was found between spending more time with patients and higher HMCCOT scores. “Patients’ complaints about doctors often relate to feeling rushed, that their physicians did not listen to them, or that they did not convey information in a clear manner,” Dr. Kotwal said. “When successfully achieved, patient-centered communication has been associated with improved clinical outcomes, including adherence to recommended treatment and better self-management of chronic disease. Many of the components of the HMCCOT described in our study are at the heart of patient-centered care.”
Dr. Kotwal believes HMCCOT is a better strategy to improve patient satisfaction than patient satisfaction surveys because patients can’t always recall which specific provider saw them. In addition, patients’ recall about the provider may be poor because surveys are sent to patients days after they return home. In addition, patients’ recovery and health outcomes are likely to influence their assessment of the doctor. Finally, feedback is known to be most valuable and transformative when it is specific and given in real time. Therefore, a tool that is able to provide feedback at the encounter level should be more helpful than a tool that offers assessment at the level of the admission, particularly when it can be also delivered immediately after the data are collected.5
The study authors conclude that, “Future studies are necessary to determine whether hospitalists of all levels of experience and clinical skill can improve when given data and feedback using the HMCCOT. Larger studies are then needed to assess whether enhancing comportment and communication can truly improve patient satisfaction and clinical outcomes in the hospital. Because hospitalists spend only a small proportion of their clinical time in direct patient care, it is imperative that excellent comportment and communication be established as a goal for every encounter.”
The effectiveness of care team rounds at the bedside
Investigators at the UMass Memorial Medical Center, in Worcester, Mass., studied the effectiveness of assembling the entire care team (i.e., physicians, including residents and attendings, nursing, and clinical pharmacy) to round at the patient’s bedside each morning – in lieu of its traditionally separate rounding strategies – on one unit of its academic hospitalist service for an internal quality program, said Patricia Seymour, MD, FAAFP, assistant professor and family medicine hospitalist education director.
Additionally, academic presentations and discussions were all done in front of patients and their families (with a few exceptions) rather than traditional hallway rounds or sit rounds. Over the course of the project, the hospital also offered residents training around physician behaviors that improve patient satisfaction; provided incentives for nurses and residents to work as a team; and created a welcome visit template for the nursing manager and instruments for patients to enhance engagement. Through all of these cycles, the collaborative rounding strategy continued.
Because Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey scores yielded low response rates for the singular test unit and service, the investigators used a validated patient satisfaction instrument and surveyed patients from the intervention group and patients on the same unit who did not experience this collaborative rounding on their day of discharge. The intervention group had higher satisfaction scores at most of the time points. The unit-based HCAHPS scores (not just study patients) improved during this time period.
“We think the strategy of collaborative rounding yielded positive results for obvious reasons – the entire team was on the same page and the information given to the patient was consistent,” said Dr. Seymour, who notes that the study’s findings weren’t published and the project was completed for an internal quality program. “Doctors had an increased understanding about nursing concerns and the nursing staff expressed improved understanding of patients’ care plans.”
Certainly, face time with the patient was extended because much of the academic discussion occurred at the bedside instead of at another physical location without patient awareness, Dr. Seymour said. She believes the strategy boosted patient satisfaction because it was patient centered. “While this rounding strategy is not the most convenient rounding strategy for nurses or doctors, it consolidates the discussion about the patient’s clinical condition and the plan for the day. The patient experiences a strong sense of being cared for by a unified team and receives consistent messaging,” she said.
Also noteworthy is that job satisfaction for residents and nurses improved on the unit over the study time period because of the expected collaboration that was built into the work flow.
Although the facility is no longer using this communication strategy to the same degree, teaching attendings have seen the value of true bedside rounding and continue to teach this skill to learners. “We have had some challenges with geographic cohorting at our institution, which is essential for this type of team-based strategy,” Dr. Seymour said. “Sustainability requires constant encouragement, oversight, and auditing from team leaders which is also challenging and fluctuates with competing demands.”
The results of this study, and others, show that employing tools to improve communication can also result in improved patient satisfaction and experience.
Karen Appold is a medical writer in Pennsylvania.
References
1. Boissy A, Gilligan T. “Communication the Cleveland Clinic Way: How to drive a relationship-centered strategy for superior patient experience.” New York: McGraw-Hill Education. 2016.
2. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45:835-42.
3. Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016 Jul;31(7):755-761. doi: 10.1007/s11606-016-3597-2. Epub 2016 Feb 26.
4. Kotwal S, Khaliq W, Landis R, Wright S. Developing a comportment and communication tool for use in hospital medicine. J Hosp Med. 2016 Dec;11(12):853-858. doi: 10.1002/jhm.2647. Epub 2016 Aug 13.
5. Fong Ha J, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010 Spring; 10(1):38-43.
6. Bodenheimer T, Sinsky C. From Triple to Quadruple Aim: care of the patient requires care of the provider. Ann Fam Med. 2014 Nov;12(6): 573-6. doi: 10.1370/afm.1713.
Bonus Content
Clinicians wary of course's worthiness
Before clinicians took Cleveland Clinic’s Relationship Establishment, Development, and Engagement (REDE) course, only 20% strongly agreed that the course would be valuable, whereas afterward 58% strongly agreed that it was indeed valuable. Less than 1% said it wasn’t valuable.4 “Most likely clinicians had a preconceived notion about how communication courses go, but they were probably surprised at how much these sessions were equally about them as providers as they were about caring for patients,” said Vicente J. Velez, MD, FACP, FHM, a hospitalist who serves as the director of faculty enrichment for the leadership team of CEHC. “This is the power of relationship-centered care, and also why I think the model has been sustainable.”
Physicians also reported that before taking the course, they had moderate levels of burnout and low levels of empathy. After taking it, burnout metrics (i.e., emotional exhaustion, depersonalization, and personal achievement) and empathy improved significantly. “I observed that most are surprised to find out that empathy is a discreet set of skills that can be learned, practiced, observed, measured, and improved upon,” Dr. Velez said. “If taught in a safe and validating environment and if principles of adult learning are followed, improvement can be optimized and sustained.”
Since the REDE course rolled out in 2012, all attending physicians and medical staff members have been trained in it.
Why empathy is preferred over patient-centered care
The Cleveland Clinic intentionally puts a focus on relationship-centered care.
“When there’s an emphasis on patient-centered care, some physicians have a hard time figuring out what to do when the patient wants something that the physician doesn’t feel is appropriate,” said Katie Neuendorf, MD, director for the Center for Excellence in Healthcare Communication. “Patient-centered implies that the patient is always right and that their opinion should win out over the physician’s opinion. In that same scenario, relationship-centered care implies that the relationship should be prioritized, even when there’s disagreement in the plan of care. I can tell my patients that I hear what they are saying, that I empathize with their struggles, that I care about the way the illness is affecting their lives, and that I am here to support them. I can do all of that and still not prescribe a treatment that I feel is inappropriate just because it happens to be what the patient wants.”

The Cleveland Clinic’s Relationship Establishment, Development and Engagement (REDE) course helps clinicians to see the individual that exists beyond a diagnosis. “Having empathy, or putting yourself in the other person’s shoes, is a key step in that process,” Dr. Neuendorf said. “Once a physician understands the patient’s perspective, the treatment for the diagnosis is more meaningful to both the patient and physician. Finding meaning in their work addresses the Quadruple Aim.”
How hospitalists and other clinicians communicate with patients impacts a patient’s overall experience and satisfaction. But according to the authors of “Communication the Cleveland Way,”1 a book about how the clinic created and applied communication skills training, “in a culture prioritizing clinical outcomes above all, there can be a tendency to lose sight of one of the most critical aspects of providing effective care: the communication skills that build and foster physician-patient relationships.”
“Studies2,3 have shown that good communication between doctors and patients and among all caregivers who interface with patients directly results in better clinical outcomes, reduced costs, greater patient satisfaction, and lower rates of physician burnout,” the authors wrote.
“It places a special focus on empathy in relationships, and in our case, the provider-patient relationship rather than patient-centered care. The former acknowledges that the thoughts and feelings in both sides of a relationship are important. We know that clinicians, too, can suffer as a result of the care they provide,” Dr. Velez wrote in “Communication the Cleveland Way.”1
“Healthy relationships are based on balance and mutual respect,” Dr Velez said. “Courses made a strong point to practice empathy in order to teach empathy. Clinician participants were gifted with a safe space, an opportunity to share their own skills and expertise, and a chance to be appreciated for what they already do effectively. Most of all, activities were designed to be fun and engaging.” For example, CEHC encouraged and fostered an attitude of exploration, experimentation, and adventure. Various warm-up activities effectively helped the participants enter a more playful space and get into character portrayal.
Dr. Velez credits the CEHC model’s sustainability and success to the early realization that an appreciative approach is effective. In a study3 about the strategy, hospital-employed attending physicians participated in the 8-hour experiential communication skills training course on REDE. The study compared approximately 1,500 “intervention” physicians who attended and 1,900 “nonintervention” physicians who did not attend.
Following the course, scores for physician communication and respect were higher for intervention physicians. Furthermore, physicians showed significant improvement in self-perceptions of empathy and burnout. Some of these gains were sustained for at least 3 months. “This is especially important because in the current health care climate, physicians experience increased burnout,” Dr. Velez notes.
How it works
Because a provider’s connection with a patient occurs when a relationship is established, the REDE course focuses on the beginning of the conversation. “It’s important for clinicians to exhibit value and respect through words and actions when welcoming patients,” Dr. Velez said. “Further, instead of guiding the medical interview with a series of close-ended questions like an interrogator would, we invite the use of open-ended questions and setting an agenda for the visit early on, by asking the patient what they wish to discuss.”
Another key component is empathy, which plays a huge role in patient satisfaction. “Learning how to express empathy is very important,” Dr. Velez said. “A patient may not remember all of the medical details discussed, but human interactions, rapport, expressions of care, support, validation, and acknowledgment of emotions tend to be more indelible.”
Dr. Velez notes that decades of literature regarding effective communication have demonstrated improved outcomes. “If trust in a therapeutic relationship is strong, a patient is more likely to follow instructions and have better engagement with their care plan,” he said. “If a clinician ensures that the patient understands the diagnosis and recommendations, then compliance will increase, especially if the plan is tailored to the patient’s goals and perspective.”
One surprising effect of the REDE course was how it improved relationships among professionals. “Many participants have shared that having a day out of one’s normal schedule, not only to learn, but also to share their own experiences, is quite therapeutic,” Dr. Velez said. “We can extend the same communication strategies to team building, interprofessional interactions, and challenging encounters.”
Study focuses on comportment and communication
In an effort to define optimal care in hospital medicine, a team from Johns Hopkins Health System set out to establish a metric that would comprehensively assess hospitalists’ comportment (which includes behavior as well as general demeanor) and communication to establish norms and expectations when they saw patients at the bedside.
To perform the study,4 chiefs of hospital medicine divisions at five independent hospitals located in Baltimore and Washington identified their most clinically excellent hospitalists. Then, an investigator observed each hospitalist during a routine clinical shift and recorded behaviors believed to be associated with excellent behavior and communication using the hospital medicine comportment and communication observation tool (HMCCOT), said Susrutha Kotwal, MD, assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, and lead author. The investigators collected basic demographic information while observing hospitalists for an average of 280 minutes; 26 physicians were observed for 181 separate clinical encounters. Each provider’s mean HMCCOT score was compared with patient satisfaction surveys such as Press Ganey (PG) scores.
Noteworthy is the fact that the distribution of HMCCOT scores were similar when analyzed by age, gender, race, amount of clinical experience, the hospitalist’s clinical workload, hospital, or time spent observing the hospitalist. But the distribution of HMCCOT scores was quite different in new patient encounters, compared with follow-ups (68.1% versus 39.7%). Encounters with patients that generated HMCCOT scores above versus below the mean were longer (13 minutes versus 8.7 minutes). The physicians’ HMCCOT scores were also associated with their PG scores. These findings suggest that improved bedside communication and comportment with patients might also translate into enhanced patient satisfaction.
As a result of the study, a comportment and communication tool was established and validated by following clinically excellent hospitalists at the bedside. “Even among clinically respected hospitalists, the results reveal that there is wide variability in behaviors and communication practices at the bedside,” Dr. Kotwal said.
Employing the tool
Hospitalists can choose whether to perform behaviors in the HMCCOT themselves, while others may wish to watch other hospitalists to give them feedback tied to specific behaviors. “These simple behaviors are intimately linked to excellent communication and comportment, which can serve as the foundation for delivering patient-centered care,” Dr. Kotwal said.
A positive correlation was found between spending more time with patients and higher HMCCOT scores. “Patients’ complaints about doctors often relate to feeling rushed, that their physicians did not listen to them, or that they did not convey information in a clear manner,” Dr. Kotwal said. “When successfully achieved, patient-centered communication has been associated with improved clinical outcomes, including adherence to recommended treatment and better self-management of chronic disease. Many of the components of the HMCCOT described in our study are at the heart of patient-centered care.”
Dr. Kotwal believes HMCCOT is a better strategy to improve patient satisfaction than patient satisfaction surveys because patients can’t always recall which specific provider saw them. In addition, patients’ recall about the provider may be poor because surveys are sent to patients days after they return home. In addition, patients’ recovery and health outcomes are likely to influence their assessment of the doctor. Finally, feedback is known to be most valuable and transformative when it is specific and given in real time. Therefore, a tool that is able to provide feedback at the encounter level should be more helpful than a tool that offers assessment at the level of the admission, particularly when it can be also delivered immediately after the data are collected.5
The study authors conclude that, “Future studies are necessary to determine whether hospitalists of all levels of experience and clinical skill can improve when given data and feedback using the HMCCOT. Larger studies are then needed to assess whether enhancing comportment and communication can truly improve patient satisfaction and clinical outcomes in the hospital. Because hospitalists spend only a small proportion of their clinical time in direct patient care, it is imperative that excellent comportment and communication be established as a goal for every encounter.”
The effectiveness of care team rounds at the bedside
Investigators at the UMass Memorial Medical Center, in Worcester, Mass., studied the effectiveness of assembling the entire care team (i.e., physicians, including residents and attendings, nursing, and clinical pharmacy) to round at the patient’s bedside each morning – in lieu of its traditionally separate rounding strategies – on one unit of its academic hospitalist service for an internal quality program, said Patricia Seymour, MD, FAAFP, assistant professor and family medicine hospitalist education director.
Additionally, academic presentations and discussions were all done in front of patients and their families (with a few exceptions) rather than traditional hallway rounds or sit rounds. Over the course of the project, the hospital also offered residents training around physician behaviors that improve patient satisfaction; provided incentives for nurses and residents to work as a team; and created a welcome visit template for the nursing manager and instruments for patients to enhance engagement. Through all of these cycles, the collaborative rounding strategy continued.
Because Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey scores yielded low response rates for the singular test unit and service, the investigators used a validated patient satisfaction instrument and surveyed patients from the intervention group and patients on the same unit who did not experience this collaborative rounding on their day of discharge. The intervention group had higher satisfaction scores at most of the time points. The unit-based HCAHPS scores (not just study patients) improved during this time period.
“We think the strategy of collaborative rounding yielded positive results for obvious reasons – the entire team was on the same page and the information given to the patient was consistent,” said Dr. Seymour, who notes that the study’s findings weren’t published and the project was completed for an internal quality program. “Doctors had an increased understanding about nursing concerns and the nursing staff expressed improved understanding of patients’ care plans.”
Certainly, face time with the patient was extended because much of the academic discussion occurred at the bedside instead of at another physical location without patient awareness, Dr. Seymour said. She believes the strategy boosted patient satisfaction because it was patient centered. “While this rounding strategy is not the most convenient rounding strategy for nurses or doctors, it consolidates the discussion about the patient’s clinical condition and the plan for the day. The patient experiences a strong sense of being cared for by a unified team and receives consistent messaging,” she said.
Also noteworthy is that job satisfaction for residents and nurses improved on the unit over the study time period because of the expected collaboration that was built into the work flow.
Although the facility is no longer using this communication strategy to the same degree, teaching attendings have seen the value of true bedside rounding and continue to teach this skill to learners. “We have had some challenges with geographic cohorting at our institution, which is essential for this type of team-based strategy,” Dr. Seymour said. “Sustainability requires constant encouragement, oversight, and auditing from team leaders which is also challenging and fluctuates with competing demands.”
The results of this study, and others, show that employing tools to improve communication can also result in improved patient satisfaction and experience.
Karen Appold is a medical writer in Pennsylvania.
References
1. Boissy A, Gilligan T. “Communication the Cleveland Clinic Way: How to drive a relationship-centered strategy for superior patient experience.” New York: McGraw-Hill Education. 2016.
2. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45:835-42.
3. Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016 Jul;31(7):755-761. doi: 10.1007/s11606-016-3597-2. Epub 2016 Feb 26.
4. Kotwal S, Khaliq W, Landis R, Wright S. Developing a comportment and communication tool for use in hospital medicine. J Hosp Med. 2016 Dec;11(12):853-858. doi: 10.1002/jhm.2647. Epub 2016 Aug 13.
5. Fong Ha J, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010 Spring; 10(1):38-43.
6. Bodenheimer T, Sinsky C. From Triple to Quadruple Aim: care of the patient requires care of the provider. Ann Fam Med. 2014 Nov;12(6): 573-6. doi: 10.1370/afm.1713.
Bonus Content
Clinicians wary of course's worthiness
Before clinicians took Cleveland Clinic’s Relationship Establishment, Development, and Engagement (REDE) course, only 20% strongly agreed that the course would be valuable, whereas afterward 58% strongly agreed that it was indeed valuable. Less than 1% said it wasn’t valuable.4 “Most likely clinicians had a preconceived notion about how communication courses go, but they were probably surprised at how much these sessions were equally about them as providers as they were about caring for patients,” said Vicente J. Velez, MD, FACP, FHM, a hospitalist who serves as the director of faculty enrichment for the leadership team of CEHC. “This is the power of relationship-centered care, and also why I think the model has been sustainable.”
Physicians also reported that before taking the course, they had moderate levels of burnout and low levels of empathy. After taking it, burnout metrics (i.e., emotional exhaustion, depersonalization, and personal achievement) and empathy improved significantly. “I observed that most are surprised to find out that empathy is a discreet set of skills that can be learned, practiced, observed, measured, and improved upon,” Dr. Velez said. “If taught in a safe and validating environment and if principles of adult learning are followed, improvement can be optimized and sustained.”
Since the REDE course rolled out in 2012, all attending physicians and medical staff members have been trained in it.
Why empathy is preferred over patient-centered care
The Cleveland Clinic intentionally puts a focus on relationship-centered care.
“When there’s an emphasis on patient-centered care, some physicians have a hard time figuring out what to do when the patient wants something that the physician doesn’t feel is appropriate,” said Katie Neuendorf, MD, director for the Center for Excellence in Healthcare Communication. “Patient-centered implies that the patient is always right and that their opinion should win out over the physician’s opinion. In that same scenario, relationship-centered care implies that the relationship should be prioritized, even when there’s disagreement in the plan of care. I can tell my patients that I hear what they are saying, that I empathize with their struggles, that I care about the way the illness is affecting their lives, and that I am here to support them. I can do all of that and still not prescribe a treatment that I feel is inappropriate just because it happens to be what the patient wants.”
The Cleveland Clinic’s Relationship Establishment, Development and Engagement (REDE) course helps clinicians to see the individual that exists beyond a diagnosis. “Having empathy, or putting yourself in the other person’s shoes, is a key step in that process,” Dr. Neuendorf said. “Once a physician understands the patient’s perspective, the treatment for the diagnosis is more meaningful to both the patient and physician. Finding meaning in their work addresses the Quadruple Aim.”
How hospitalists and other clinicians communicate with patients impacts a patient’s overall experience and satisfaction. But according to the authors of “Communication the Cleveland Way,”1 a book about how the clinic created and applied communication skills training, “in a culture prioritizing clinical outcomes above all, there can be a tendency to lose sight of one of the most critical aspects of providing effective care: the communication skills that build and foster physician-patient relationships.”
“Studies2,3 have shown that good communication between doctors and patients and among all caregivers who interface with patients directly results in better clinical outcomes, reduced costs, greater patient satisfaction, and lower rates of physician burnout,” the authors wrote.
“It places a special focus on empathy in relationships, and in our case, the provider-patient relationship rather than patient-centered care. The former acknowledges that the thoughts and feelings in both sides of a relationship are important. We know that clinicians, too, can suffer as a result of the care they provide,” Dr. Velez wrote in “Communication the Cleveland Way.”1
“Healthy relationships are based on balance and mutual respect,” Dr Velez said. “Courses made a strong point to practice empathy in order to teach empathy. Clinician participants were gifted with a safe space, an opportunity to share their own skills and expertise, and a chance to be appreciated for what they already do effectively. Most of all, activities were designed to be fun and engaging.” For example, CEHC encouraged and fostered an attitude of exploration, experimentation, and adventure. Various warm-up activities effectively helped the participants enter a more playful space and get into character portrayal.
Dr. Velez credits the CEHC model’s sustainability and success to the early realization that an appreciative approach is effective. In a study3 about the strategy, hospital-employed attending physicians participated in the 8-hour experiential communication skills training course on REDE. The study compared approximately 1,500 “intervention” physicians who attended and 1,900 “nonintervention” physicians who did not attend.
Following the course, scores for physician communication and respect were higher for intervention physicians. Furthermore, physicians showed significant improvement in self-perceptions of empathy and burnout. Some of these gains were sustained for at least 3 months. “This is especially important because in the current health care climate, physicians experience increased burnout,” Dr. Velez notes.
How it works
Because a provider’s connection with a patient occurs when a relationship is established, the REDE course focuses on the beginning of the conversation. “It’s important for clinicians to exhibit value and respect through words and actions when welcoming patients,” Dr. Velez said. “Further, instead of guiding the medical interview with a series of close-ended questions like an interrogator would, we invite the use of open-ended questions and setting an agenda for the visit early on, by asking the patient what they wish to discuss.”
Another key component is empathy, which plays a huge role in patient satisfaction. “Learning how to express empathy is very important,” Dr. Velez said. “A patient may not remember all of the medical details discussed, but human interactions, rapport, expressions of care, support, validation, and acknowledgment of emotions tend to be more indelible.”
Dr. Velez notes that decades of literature regarding effective communication have demonstrated improved outcomes. “If trust in a therapeutic relationship is strong, a patient is more likely to follow instructions and have better engagement with their care plan,” he said. “If a clinician ensures that the patient understands the diagnosis and recommendations, then compliance will increase, especially if the plan is tailored to the patient’s goals and perspective.”
One surprising effect of the REDE course was how it improved relationships among professionals. “Many participants have shared that having a day out of one’s normal schedule, not only to learn, but also to share their own experiences, is quite therapeutic,” Dr. Velez said. “We can extend the same communication strategies to team building, interprofessional interactions, and challenging encounters.”
Study focuses on comportment and communication
In an effort to define optimal care in hospital medicine, a team from Johns Hopkins Health System set out to establish a metric that would comprehensively assess hospitalists’ comportment (which includes behavior as well as general demeanor) and communication to establish norms and expectations when they saw patients at the bedside.
To perform the study,4 chiefs of hospital medicine divisions at five independent hospitals located in Baltimore and Washington identified their most clinically excellent hospitalists. Then, an investigator observed each hospitalist during a routine clinical shift and recorded behaviors believed to be associated with excellent behavior and communication using the hospital medicine comportment and communication observation tool (HMCCOT), said Susrutha Kotwal, MD, assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, and lead author. The investigators collected basic demographic information while observing hospitalists for an average of 280 minutes; 26 physicians were observed for 181 separate clinical encounters. Each provider’s mean HMCCOT score was compared with patient satisfaction surveys such as Press Ganey (PG) scores.
Noteworthy is the fact that the distribution of HMCCOT scores were similar when analyzed by age, gender, race, amount of clinical experience, the hospitalist’s clinical workload, hospital, or time spent observing the hospitalist. But the distribution of HMCCOT scores was quite different in new patient encounters, compared with follow-ups (68.1% versus 39.7%). Encounters with patients that generated HMCCOT scores above versus below the mean were longer (13 minutes versus 8.7 minutes). The physicians’ HMCCOT scores were also associated with their PG scores. These findings suggest that improved bedside communication and comportment with patients might also translate into enhanced patient satisfaction.
As a result of the study, a comportment and communication tool was established and validated by following clinically excellent hospitalists at the bedside. “Even among clinically respected hospitalists, the results reveal that there is wide variability in behaviors and communication practices at the bedside,” Dr. Kotwal said.
Employing the tool
Hospitalists can choose whether to perform behaviors in the HMCCOT themselves, while others may wish to watch other hospitalists to give them feedback tied to specific behaviors. “These simple behaviors are intimately linked to excellent communication and comportment, which can serve as the foundation for delivering patient-centered care,” Dr. Kotwal said.
A positive correlation was found between spending more time with patients and higher HMCCOT scores. “Patients’ complaints about doctors often relate to feeling rushed, that their physicians did not listen to them, or that they did not convey information in a clear manner,” Dr. Kotwal said. “When successfully achieved, patient-centered communication has been associated with improved clinical outcomes, including adherence to recommended treatment and better self-management of chronic disease. Many of the components of the HMCCOT described in our study are at the heart of patient-centered care.”
Dr. Kotwal believes HMCCOT is a better strategy to improve patient satisfaction than patient satisfaction surveys because patients can’t always recall which specific provider saw them. In addition, patients’ recall about the provider may be poor because surveys are sent to patients days after they return home. In addition, patients’ recovery and health outcomes are likely to influence their assessment of the doctor. Finally, feedback is known to be most valuable and transformative when it is specific and given in real time. Therefore, a tool that is able to provide feedback at the encounter level should be more helpful than a tool that offers assessment at the level of the admission, particularly when it can be also delivered immediately after the data are collected.5
The study authors conclude that, “Future studies are necessary to determine whether hospitalists of all levels of experience and clinical skill can improve when given data and feedback using the HMCCOT. Larger studies are then needed to assess whether enhancing comportment and communication can truly improve patient satisfaction and clinical outcomes in the hospital. Because hospitalists spend only a small proportion of their clinical time in direct patient care, it is imperative that excellent comportment and communication be established as a goal for every encounter.”
The effectiveness of care team rounds at the bedside
Investigators at the UMass Memorial Medical Center, in Worcester, Mass., studied the effectiveness of assembling the entire care team (i.e., physicians, including residents and attendings, nursing, and clinical pharmacy) to round at the patient’s bedside each morning – in lieu of its traditionally separate rounding strategies – on one unit of its academic hospitalist service for an internal quality program, said Patricia Seymour, MD, FAAFP, assistant professor and family medicine hospitalist education director.
Additionally, academic presentations and discussions were all done in front of patients and their families (with a few exceptions) rather than traditional hallway rounds or sit rounds. Over the course of the project, the hospital also offered residents training around physician behaviors that improve patient satisfaction; provided incentives for nurses and residents to work as a team; and created a welcome visit template for the nursing manager and instruments for patients to enhance engagement. Through all of these cycles, the collaborative rounding strategy continued.
Because Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey scores yielded low response rates for the singular test unit and service, the investigators used a validated patient satisfaction instrument and surveyed patients from the intervention group and patients on the same unit who did not experience this collaborative rounding on their day of discharge. The intervention group had higher satisfaction scores at most of the time points. The unit-based HCAHPS scores (not just study patients) improved during this time period.
“We think the strategy of collaborative rounding yielded positive results for obvious reasons – the entire team was on the same page and the information given to the patient was consistent,” said Dr. Seymour, who notes that the study’s findings weren’t published and the project was completed for an internal quality program. “Doctors had an increased understanding about nursing concerns and the nursing staff expressed improved understanding of patients’ care plans.”
Certainly, face time with the patient was extended because much of the academic discussion occurred at the bedside instead of at another physical location without patient awareness, Dr. Seymour said. She believes the strategy boosted patient satisfaction because it was patient centered. “While this rounding strategy is not the most convenient rounding strategy for nurses or doctors, it consolidates the discussion about the patient’s clinical condition and the plan for the day. The patient experiences a strong sense of being cared for by a unified team and receives consistent messaging,” she said.
Also noteworthy is that job satisfaction for residents and nurses improved on the unit over the study time period because of the expected collaboration that was built into the work flow.
Although the facility is no longer using this communication strategy to the same degree, teaching attendings have seen the value of true bedside rounding and continue to teach this skill to learners. “We have had some challenges with geographic cohorting at our institution, which is essential for this type of team-based strategy,” Dr. Seymour said. “Sustainability requires constant encouragement, oversight, and auditing from team leaders which is also challenging and fluctuates with competing demands.”
The results of this study, and others, show that employing tools to improve communication can also result in improved patient satisfaction and experience.
Karen Appold is a medical writer in Pennsylvania.
References
1. Boissy A, Gilligan T. “Communication the Cleveland Clinic Way: How to drive a relationship-centered strategy for superior patient experience.” New York: McGraw-Hill Education. 2016.
2. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45:835-42.
3. Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016 Jul;31(7):755-761. doi: 10.1007/s11606-016-3597-2. Epub 2016 Feb 26.
4. Kotwal S, Khaliq W, Landis R, Wright S. Developing a comportment and communication tool for use in hospital medicine. J Hosp Med. 2016 Dec;11(12):853-858. doi: 10.1002/jhm.2647. Epub 2016 Aug 13.
5. Fong Ha J, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010 Spring; 10(1):38-43.
6. Bodenheimer T, Sinsky C. From Triple to Quadruple Aim: care of the patient requires care of the provider. Ann Fam Med. 2014 Nov;12(6): 573-6. doi: 10.1370/afm.1713.
Bonus Content
Clinicians wary of course's worthiness
Before clinicians took Cleveland Clinic’s Relationship Establishment, Development, and Engagement (REDE) course, only 20% strongly agreed that the course would be valuable, whereas afterward 58% strongly agreed that it was indeed valuable. Less than 1% said it wasn’t valuable.4 “Most likely clinicians had a preconceived notion about how communication courses go, but they were probably surprised at how much these sessions were equally about them as providers as they were about caring for patients,” said Vicente J. Velez, MD, FACP, FHM, a hospitalist who serves as the director of faculty enrichment for the leadership team of CEHC. “This is the power of relationship-centered care, and also why I think the model has been sustainable.”
Physicians also reported that before taking the course, they had moderate levels of burnout and low levels of empathy. After taking it, burnout metrics (i.e., emotional exhaustion, depersonalization, and personal achievement) and empathy improved significantly. “I observed that most are surprised to find out that empathy is a discreet set of skills that can be learned, practiced, observed, measured, and improved upon,” Dr. Velez said. “If taught in a safe and validating environment and if principles of adult learning are followed, improvement can be optimized and sustained.”
Since the REDE course rolled out in 2012, all attending physicians and medical staff members have been trained in it.
Why empathy is preferred over patient-centered care
The Cleveland Clinic intentionally puts a focus on relationship-centered care.
“When there’s an emphasis on patient-centered care, some physicians have a hard time figuring out what to do when the patient wants something that the physician doesn’t feel is appropriate,” said Katie Neuendorf, MD, director for the Center for Excellence in Healthcare Communication. “Patient-centered implies that the patient is always right and that their opinion should win out over the physician’s opinion. In that same scenario, relationship-centered care implies that the relationship should be prioritized, even when there’s disagreement in the plan of care. I can tell my patients that I hear what they are saying, that I empathize with their struggles, that I care about the way the illness is affecting their lives, and that I am here to support them. I can do all of that and still not prescribe a treatment that I feel is inappropriate just because it happens to be what the patient wants.”
The Cleveland Clinic’s Relationship Establishment, Development and Engagement (REDE) course helps clinicians to see the individual that exists beyond a diagnosis. “Having empathy, or putting yourself in the other person’s shoes, is a key step in that process,” Dr. Neuendorf said. “Once a physician understands the patient’s perspective, the treatment for the diagnosis is more meaningful to both the patient and physician. Finding meaning in their work addresses the Quadruple Aim.”
Standardized infection ratio for CLABSI almost halved since 2009
The standardized infection ratio (SIR) for central line–associated bloodstream infections dropped 42% from 2009 to 2014, according to the Agency for Healthcare Research and Quality.
For acute care hospitalizations, the SIR for central line–associated bloodstream infections (CLABSIs) fell from 0.854 in 2009 to 0.495 in 2014. Over that same time period, the SIR for surgical site infections involving Surgical Care Improvement Project procedures decreased from 0.981 to 0.827 – almost 16%, the AHRQ said in its annual National Healthcare Quality and Disparities Report.
From 2010 to 2014, the SIR for catheter-associated urinary tract infections increased 6.7% from 0.937 to 1.000, but that change was not significant. For laboratory-identified hospital-onset Clostridium difficile infection, the SIR dropped from 0.963 to 0.924 – about 4% – from 2012 to 2014, the AHRQ reported using data from the National Center for Emerging and Zoonotic Infectious Diseases and the National Healthcare Safety Network.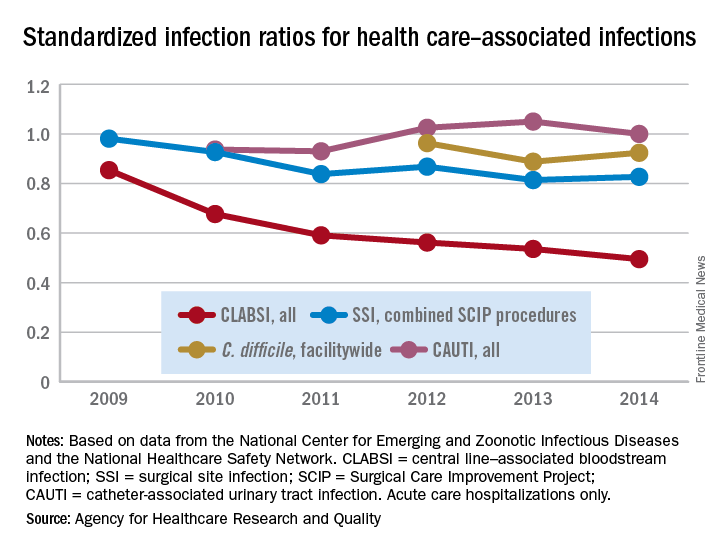
The standardized infection ratio (SIR) for central line–associated bloodstream infections dropped 42% from 2009 to 2014, according to the Agency for Healthcare Research and Quality.
For acute care hospitalizations, the SIR for central line–associated bloodstream infections (CLABSIs) fell from 0.854 in 2009 to 0.495 in 2014. Over that same time period, the SIR for surgical site infections involving Surgical Care Improvement Project procedures decreased from 0.981 to 0.827 – almost 16%, the AHRQ said in its annual National Healthcare Quality and Disparities Report.
From 2010 to 2014, the SIR for catheter-associated urinary tract infections increased 6.7% from 0.937 to 1.000, but that change was not significant. For laboratory-identified hospital-onset Clostridium difficile infection, the SIR dropped from 0.963 to 0.924 – about 4% – from 2012 to 2014, the AHRQ reported using data from the National Center for Emerging and Zoonotic Infectious Diseases and the National Healthcare Safety Network.
The standardized infection ratio (SIR) for central line–associated bloodstream infections dropped 42% from 2009 to 2014, according to the Agency for Healthcare Research and Quality.
For acute care hospitalizations, the SIR for central line–associated bloodstream infections (CLABSIs) fell from 0.854 in 2009 to 0.495 in 2014. Over that same time period, the SIR for surgical site infections involving Surgical Care Improvement Project procedures decreased from 0.981 to 0.827 – almost 16%, the AHRQ said in its annual National Healthcare Quality and Disparities Report.
From 2010 to 2014, the SIR for catheter-associated urinary tract infections increased 6.7% from 0.937 to 1.000, but that change was not significant. For laboratory-identified hospital-onset Clostridium difficile infection, the SIR dropped from 0.963 to 0.924 – about 4% – from 2012 to 2014, the AHRQ reported using data from the National Center for Emerging and Zoonotic Infectious Diseases and the National Healthcare Safety Network.
Immigration reforms: Repercussions for hospitalists and the health care industry
International medical graduates (IMGs) have been playing a crucial role in clinician staffing needs for U.S. hospitals, especially in hospital medicine and internal medicine. According to a study, IMGs comprise 25% of the total U.S. physician workforce and 36% of internists.1,2 According to data from the 2008 Today’s Hospitalist Compensation & Career Survey, 32% of practicing hospitalists are IMGs.3
Many IMGs come to work in the U.S. via one of three paths. Just like all roads lead to Rome, all visas lead to a permanent residency pathway, eventually based on the country of origin and number of years waiting. The first path is a green card – cases where IMGs were on a visa and within a certain amount of time they received a green card. The second path is J-1 visa waivers for physicians who trained in the U.S. under a J-1 Visa. Typically, physicians on J-1 Visa waivers need to provide their services for a minimum of 3 years working in underserved areas – where there’s a shortage of health professionals – before they can apply for permanent residency.
The third and most popular path is the H-1B visa, which hospitalists traditionally use as a springboard to apply for permanent residency. Studies have shown that IMGs are more likely to practice medicine in rural and underserved areas. In many instances, physicians end up working in these areas for long periods of time.4

The Department of Homeland Security has considered creating another visa pathway for the technology industry, whereby an alien graduating from a U.S. university with an advanced degree in a STEM (Science, Technology, Engineering, and Math) course of study would receive a new visa and pathway to permanent residency. We believe hospitalists and other physicians should also have an expedited pathway to permanent residency. This step benefits both the U.S. health care system and hospitalists in many ways. It increases hospitalists’ portability and flexibility with schedules. With a traditional H-1B visa, hospitalists are bound to work with the one hospital/system that sponsors the H-1B, and would not be able to work at any other hospital without another extension/addendum to current visa status, even in cases where a physician had time off and would like to offer services at another facility. It is a well-known fact that hospitalist teams are understaffed and try to bring on per-diem staff to fill holes in schedules. The majority of hospitalists are working week-on/week-off schedules, and with an expedited pathway to a green card they would be able to work in different hospitals. They would also be able to move to remote places, or “doctor deserts,” and offer their services, helping to ensure the quality and safety of patient care to which all Americans are entitled.
In 2016 alone, around 1,500 H-1B visas were filed for hospitalist physicians.7 Each hospitalist has an average of 15 patient encounters per day, and for 1,500 physicians that amounts to about 4 million patient encounters annually.8 These data account for only new 2016 visa-holding physicians, and do not account for already approved or renewed visas. It would be very challenging to count the number of patient encounters by hospitalists who are on a visa, but 1 billion patient encounters is not overestimating. Recent studies show that quality of care provided by IMGs is not inferior to that of U.S. medical graduates. The study showed that patients cared for by IMGs have lesser mortality, compared with those cared by U.S. medical graduates.9
In this era of hospital medicine, hospitalists are focusing not only on clinical aspects of patient care but also on efficacy, quality of care, and patient safety and satisfaction, and they are working with the Centers for Medicare & Medicaid Services to develop cost-cutting programs to save billions of dollars in health care expenses. This is the primary reason a majority of hospitals are focused on developing a hospitalist track, and encouraging hospitalists to pursue leadership roles in managing hospitals effectively.
The U.S. health care system is starved for hospitalists and primary care physicians, and IMGs will continue to play a pivotal role. Yet IMGs must deal with shifting trends in immigration policy, and in some recent instances immigrant physicians have been asked to leave the U.S. because of immigration reforms.10,11 We would like the Society of Hospital Medicine to take a stand on behalf of IMG hospitalists and ask the U.S. Department of Labor and Homeland Security for an expedited permanent residency pathway for IMG hospitalists. We are certain that our request will get a fair hearing, as the former U.S. surgeon general was a hospitalist and, indeed, an immigrant.
Dr. Medarametla is medical director, Intermediate Care Unit, Baystate Medical Center, Springfield, Mass., and assistant professor of medicine, University of Massachusetts Medical School. Dr. Pamerla is a hospitalist at Wilson Medical Center, Wilson, N.C.
References
1. Educational Commission for Foreign Medical Graduates; ECFMG 2015 Annual Report. April 2016 http://www.ecfmg.org/resources/ECFMG-2015-annual-report.pdf.
2. Pinsky WW. The Importance of International Medical Graduates in the United States. Ann Intern Med. 2017. doi: 10.7326/M17-0505.
3. Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-69.
4. Goodfellow A1, Ulloa JG, Dowling PT, et al. Predictors of Primary Care Physician Practice Location in Underserved Urban or Rural Areas in the United States: A Systematic Literature Review. Acad Med. 2016 Sep;91(9):1313-21.
5. https://www.uscis.gov/working-united-states/temporary-workers/h-1b-specialty-occupations-and-fashion-models/h-1b-fiscal-year-fy-2018-cap-season#count
6. https://www.graphiq.com/vlp/bCIqXCpVqF7
7. http://www.myvisajobs.com/Reports/2017-H1B-Visa-Category.aspx?T=JT&P=2
8. Steven M Harris: http://www.the-hospitalist.org/hospitalist/article/125455/appropriate-patient-census-hospital-medicines-holy-grail
9. Tsugawa Y, Jena AB, Orav EJ, Jha AK. Quality of care delivered by general internists in US hospitals who graduated from foreign versus US medical schools: observational study. BMJ. 2017;356:j273.
10. https://www.propublica.org/article/cleveland-clinic-doctor-forced-to-leave-country-after-trump-order
11. http://www.houstonchronicle.com/news/houston-texas/houston/article/Houston-immigrant-doctors-given-24-hours-to-leave-11040259.php
International medical graduates (IMGs) have been playing a crucial role in clinician staffing needs for U.S. hospitals, especially in hospital medicine and internal medicine. According to a study, IMGs comprise 25% of the total U.S. physician workforce and 36% of internists.1,2 According to data from the 2008 Today’s Hospitalist Compensation & Career Survey, 32% of practicing hospitalists are IMGs.3
Many IMGs come to work in the U.S. via one of three paths. Just like all roads lead to Rome, all visas lead to a permanent residency pathway, eventually based on the country of origin and number of years waiting. The first path is a green card – cases where IMGs were on a visa and within a certain amount of time they received a green card. The second path is J-1 visa waivers for physicians who trained in the U.S. under a J-1 Visa. Typically, physicians on J-1 Visa waivers need to provide their services for a minimum of 3 years working in underserved areas – where there’s a shortage of health professionals – before they can apply for permanent residency.
The third and most popular path is the H-1B visa, which hospitalists traditionally use as a springboard to apply for permanent residency. Studies have shown that IMGs are more likely to practice medicine in rural and underserved areas. In many instances, physicians end up working in these areas for long periods of time.4
The Department of Homeland Security has considered creating another visa pathway for the technology industry, whereby an alien graduating from a U.S. university with an advanced degree in a STEM (Science, Technology, Engineering, and Math) course of study would receive a new visa and pathway to permanent residency. We believe hospitalists and other physicians should also have an expedited pathway to permanent residency. This step benefits both the U.S. health care system and hospitalists in many ways. It increases hospitalists’ portability and flexibility with schedules. With a traditional H-1B visa, hospitalists are bound to work with the one hospital/system that sponsors the H-1B, and would not be able to work at any other hospital without another extension/addendum to current visa status, even in cases where a physician had time off and would like to offer services at another facility. It is a well-known fact that hospitalist teams are understaffed and try to bring on per-diem staff to fill holes in schedules. The majority of hospitalists are working week-on/week-off schedules, and with an expedited pathway to a green card they would be able to work in different hospitals. They would also be able to move to remote places, or “doctor deserts,” and offer their services, helping to ensure the quality and safety of patient care to which all Americans are entitled.
In 2016 alone, around 1,500 H-1B visas were filed for hospitalist physicians.7 Each hospitalist has an average of 15 patient encounters per day, and for 1,500 physicians that amounts to about 4 million patient encounters annually.8 These data account for only new 2016 visa-holding physicians, and do not account for already approved or renewed visas. It would be very challenging to count the number of patient encounters by hospitalists who are on a visa, but 1 billion patient encounters is not overestimating. Recent studies show that quality of care provided by IMGs is not inferior to that of U.S. medical graduates. The study showed that patients cared for by IMGs have lesser mortality, compared with those cared by U.S. medical graduates.9
In this era of hospital medicine, hospitalists are focusing not only on clinical aspects of patient care but also on efficacy, quality of care, and patient safety and satisfaction, and they are working with the Centers for Medicare & Medicaid Services to develop cost-cutting programs to save billions of dollars in health care expenses. This is the primary reason a majority of hospitals are focused on developing a hospitalist track, and encouraging hospitalists to pursue leadership roles in managing hospitals effectively.
The U.S. health care system is starved for hospitalists and primary care physicians, and IMGs will continue to play a pivotal role. Yet IMGs must deal with shifting trends in immigration policy, and in some recent instances immigrant physicians have been asked to leave the U.S. because of immigration reforms.10,11 We would like the Society of Hospital Medicine to take a stand on behalf of IMG hospitalists and ask the U.S. Department of Labor and Homeland Security for an expedited permanent residency pathway for IMG hospitalists. We are certain that our request will get a fair hearing, as the former U.S. surgeon general was a hospitalist and, indeed, an immigrant.
Dr. Medarametla is medical director, Intermediate Care Unit, Baystate Medical Center, Springfield, Mass., and assistant professor of medicine, University of Massachusetts Medical School. Dr. Pamerla is a hospitalist at Wilson Medical Center, Wilson, N.C.
References
1. Educational Commission for Foreign Medical Graduates; ECFMG 2015 Annual Report. April 2016 http://www.ecfmg.org/resources/ECFMG-2015-annual-report.pdf.
2. Pinsky WW. The Importance of International Medical Graduates in the United States. Ann Intern Med. 2017. doi: 10.7326/M17-0505.
3. Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-69.
4. Goodfellow A1, Ulloa JG, Dowling PT, et al. Predictors of Primary Care Physician Practice Location in Underserved Urban or Rural Areas in the United States: A Systematic Literature Review. Acad Med. 2016 Sep;91(9):1313-21.
5. https://www.uscis.gov/working-united-states/temporary-workers/h-1b-specialty-occupations-and-fashion-models/h-1b-fiscal-year-fy-2018-cap-season#count
6. https://www.graphiq.com/vlp/bCIqXCpVqF7
7. http://www.myvisajobs.com/Reports/2017-H1B-Visa-Category.aspx?T=JT&P=2
8. Steven M Harris: http://www.the-hospitalist.org/hospitalist/article/125455/appropriate-patient-census-hospital-medicines-holy-grail
9. Tsugawa Y, Jena AB, Orav EJ, Jha AK. Quality of care delivered by general internists in US hospitals who graduated from foreign versus US medical schools: observational study. BMJ. 2017;356:j273.
10. https://www.propublica.org/article/cleveland-clinic-doctor-forced-to-leave-country-after-trump-order
11. http://www.houstonchronicle.com/news/houston-texas/houston/article/Houston-immigrant-doctors-given-24-hours-to-leave-11040259.php
International medical graduates (IMGs) have been playing a crucial role in clinician staffing needs for U.S. hospitals, especially in hospital medicine and internal medicine. According to a study, IMGs comprise 25% of the total U.S. physician workforce and 36% of internists.1,2 According to data from the 2008 Today’s Hospitalist Compensation & Career Survey, 32% of practicing hospitalists are IMGs.3
Many IMGs come to work in the U.S. via one of three paths. Just like all roads lead to Rome, all visas lead to a permanent residency pathway, eventually based on the country of origin and number of years waiting. The first path is a green card – cases where IMGs were on a visa and within a certain amount of time they received a green card. The second path is J-1 visa waivers for physicians who trained in the U.S. under a J-1 Visa. Typically, physicians on J-1 Visa waivers need to provide their services for a minimum of 3 years working in underserved areas – where there’s a shortage of health professionals – before they can apply for permanent residency.
The third and most popular path is the H-1B visa, which hospitalists traditionally use as a springboard to apply for permanent residency. Studies have shown that IMGs are more likely to practice medicine in rural and underserved areas. In many instances, physicians end up working in these areas for long periods of time.4
The Department of Homeland Security has considered creating another visa pathway for the technology industry, whereby an alien graduating from a U.S. university with an advanced degree in a STEM (Science, Technology, Engineering, and Math) course of study would receive a new visa and pathway to permanent residency. We believe hospitalists and other physicians should also have an expedited pathway to permanent residency. This step benefits both the U.S. health care system and hospitalists in many ways. It increases hospitalists’ portability and flexibility with schedules. With a traditional H-1B visa, hospitalists are bound to work with the one hospital/system that sponsors the H-1B, and would not be able to work at any other hospital without another extension/addendum to current visa status, even in cases where a physician had time off and would like to offer services at another facility. It is a well-known fact that hospitalist teams are understaffed and try to bring on per-diem staff to fill holes in schedules. The majority of hospitalists are working week-on/week-off schedules, and with an expedited pathway to a green card they would be able to work in different hospitals. They would also be able to move to remote places, or “doctor deserts,” and offer their services, helping to ensure the quality and safety of patient care to which all Americans are entitled.
In 2016 alone, around 1,500 H-1B visas were filed for hospitalist physicians.7 Each hospitalist has an average of 15 patient encounters per day, and for 1,500 physicians that amounts to about 4 million patient encounters annually.8 These data account for only new 2016 visa-holding physicians, and do not account for already approved or renewed visas. It would be very challenging to count the number of patient encounters by hospitalists who are on a visa, but 1 billion patient encounters is not overestimating. Recent studies show that quality of care provided by IMGs is not inferior to that of U.S. medical graduates. The study showed that patients cared for by IMGs have lesser mortality, compared with those cared by U.S. medical graduates.9
In this era of hospital medicine, hospitalists are focusing not only on clinical aspects of patient care but also on efficacy, quality of care, and patient safety and satisfaction, and they are working with the Centers for Medicare & Medicaid Services to develop cost-cutting programs to save billions of dollars in health care expenses. This is the primary reason a majority of hospitals are focused on developing a hospitalist track, and encouraging hospitalists to pursue leadership roles in managing hospitals effectively.
The U.S. health care system is starved for hospitalists and primary care physicians, and IMGs will continue to play a pivotal role. Yet IMGs must deal with shifting trends in immigration policy, and in some recent instances immigrant physicians have been asked to leave the U.S. because of immigration reforms.10,11 We would like the Society of Hospital Medicine to take a stand on behalf of IMG hospitalists and ask the U.S. Department of Labor and Homeland Security for an expedited permanent residency pathway for IMG hospitalists. We are certain that our request will get a fair hearing, as the former U.S. surgeon general was a hospitalist and, indeed, an immigrant.
Dr. Medarametla is medical director, Intermediate Care Unit, Baystate Medical Center, Springfield, Mass., and assistant professor of medicine, University of Massachusetts Medical School. Dr. Pamerla is a hospitalist at Wilson Medical Center, Wilson, N.C.
References
1. Educational Commission for Foreign Medical Graduates; ECFMG 2015 Annual Report. April 2016 http://www.ecfmg.org/resources/ECFMG-2015-annual-report.pdf.
2. Pinsky WW. The Importance of International Medical Graduates in the United States. Ann Intern Med. 2017. doi: 10.7326/M17-0505.
3. Hart LG, Skillman SM, Fordyce M, et al. International medical graduate physicians in the United States: changes since 1981. Health Aff. 2007 July/August;26(4):1159-69.
4. Goodfellow A1, Ulloa JG, Dowling PT, et al. Predictors of Primary Care Physician Practice Location in Underserved Urban or Rural Areas in the United States: A Systematic Literature Review. Acad Med. 2016 Sep;91(9):1313-21.
5. https://www.uscis.gov/working-united-states/temporary-workers/h-1b-specialty-occupations-and-fashion-models/h-1b-fiscal-year-fy-2018-cap-season#count
6. https://www.graphiq.com/vlp/bCIqXCpVqF7
7. http://www.myvisajobs.com/Reports/2017-H1B-Visa-Category.aspx?T=JT&P=2
8. Steven M Harris: http://www.the-hospitalist.org/hospitalist/article/125455/appropriate-patient-census-hospital-medicines-holy-grail
9. Tsugawa Y, Jena AB, Orav EJ, Jha AK. Quality of care delivered by general internists in US hospitals who graduated from foreign versus US medical schools: observational study. BMJ. 2017;356:j273.
10. https://www.propublica.org/article/cleveland-clinic-doctor-forced-to-leave-country-after-trump-order
11. http://www.houstonchronicle.com/news/houston-texas/houston/article/Houston-immigrant-doctors-given-24-hours-to-leave-11040259.php