User login
In Memoriam
CHEST has been informed of the following members’ deaths. We extend our sincere condolences.
Anthony Cosentino, MD, FCCP (January 2016)
Ben Branscomb, MD (July 2016)
Steven Sahn, MD, FCCP (Aug 2016)
Thomas Aldrich, MD (September 2016)
John C. Baldwin, MD, FCCP (September 2016)
David Cugell, MD, FCCP (December 2016)
CHEST has been informed of the following members’ deaths. We extend our sincere condolences.
Anthony Cosentino, MD, FCCP (January 2016)
Ben Branscomb, MD (July 2016)
Steven Sahn, MD, FCCP (Aug 2016)
Thomas Aldrich, MD (September 2016)
John C. Baldwin, MD, FCCP (September 2016)
David Cugell, MD, FCCP (December 2016)
CHEST has been informed of the following members’ deaths. We extend our sincere condolences.
Anthony Cosentino, MD, FCCP (January 2016)
Ben Branscomb, MD (July 2016)
Steven Sahn, MD, FCCP (Aug 2016)
Thomas Aldrich, MD (September 2016)
John C. Baldwin, MD, FCCP (September 2016)
David Cugell, MD, FCCP (December 2016)
Winners-All at CHEST 2016
We all know that, with the great success of CHEST 2016, everyone who shared that event is a winner. But, we would especially like to call out some of the special winners who were recognized during our annual meeting.
CHEST Awards
College Medalist Award
Lewis J. Rubin, MD, FCCP
Distinguished Service Award
Kim D. French, MHSA, CAPPM, FCCP
Alfred Soffer Award for Editorial Excellence
Seth J. Koenig, MD, FCCP
Master Clinician Educator Award
Jack D. Buckley, MD, MPH, FCCP
Distinguished Scientist Honor Lecture
Jay Nadel, MD
Edward C. Rosenow III, MD, Master FCCP/Master Teacher Honor Lecture
Suhail Raoof, MBBS, FCCP
Murray Kornfeld Memorial Founders Lecture
Michael Niederman, MD, FCCP Pasquale Ciaglia Memorial Lecture Kevin L. Kovitz, MD, FCCP
Roger C. Bone Memorial Lecture
Robert A. Berg, MD Thomas L. Petty, MD, Master FCCP Memorial Lecture Nicola A. Hanania, MD, MS, FCCP Margaret Pfrommer Memorial Lecture in Long-term Mechanical Ventilation Thomas G. Keens, MD Om P. Sharma, MD, Master FCCP Memorial Lecture Robert P. Baughman, MD, FCCP
Early Career Educator
Gabriel Bosslet, MD, FCCP
CHEST Challenge Championship 2016
1st Place
The University of Arizona
Huthayfa Ateeli, MBBS Naser Mahmoud, MD
Muna Omar, MD, MBBS
PD: James L. Knepler Jr.
2nd Place
New York Methodist Hospital
Anu R. Jacob, MD
Stephen D. Milan, MD
Jordan Taillon, MD
PD: Anthony G. Saleh, MD, FCCP
3rd Place
Interfaith Medical Center
Chidozie C. Agu, MD
Saroj P. Kandel, MBBS Divya Salhan, MD, MBBS
PD: Marie Frances J. Schmidt, MD, FCCP
CHEST Foundation Grant Winners
GlaxoSmithKline Distinguished Scholar in Respiratory Health
Don Hayes Jr., MD, FCCP The Research Institute at Nationwide Children’s Hospital
Implications of the Lung Allocation Score in Prioritizing Critically Ill Patients for Lung Transplantation
Supported by GlaxoSmithKline.
2016 Research Grantees
Alice Turner, MBChB, MRCP, PhD
University of Birmingham, United Kingdom
CHEST Foundation and the Alpha-1 Foundation Research Grant in Alpha-1 Antitrypsin Deficiency
Improving Access to Augmentation: A Propensity-Matching Study Between the UK AATD Registry and AlphaNet
This grant is jointly supported by the CHEST Foundation and the Alpha-1 Foundation.
Robert Busch, MD
Brigham and Women’s Hospital, Channing Division of Network Medicine
CHEST Foundation Research Grant in Chronic Obstructive Pulmonary Disease
Methylation Quantitative Trait Loci: Markers of Race-Specific Disparities in African Americans With COPD
This grant is supported by AstraZeneca.
Clemens Grassberger, PhD
Massachusetts General Hospital – Harvard University
CHEST Foundation Research Grant in Lung Cancer
Dynamic FLT-PET as Biomarker for Early Response in Locally Advanced Lung Cancer Patients
This grant is supported by Genentech Inc.
Cristina Russo, MD, PhD
Bambino Gesù Children’s Hospital, Rome, Italy
CHEST Foundation Research Grant in Nontuberculous Mycobacteria
A Proteomic-Metaproteomic Analysis Approach Allows Identification of Drug Target Candidates for the Future Design of Preventive, Diagnostic, and Therapeutic Strategies Against Nontuberculous Mycobacteria Diseases
This grant is supported by Insmed.
Peter Leary, MD, MS
University of Washington
CHEST Foundation Research Grant in Pulmonary Arterial Hypertension
Expression Profiling in Pulmonary Arterial Hypertension
This grant is supported by Actelion Pharmaceuticals, US, Inc.
Brett Ley, MD
University of California, San Francisco
CHEST Foundation Research Grant in Pulmonary Fibrosis
Extracellular Circulation RNAs as Predictors of Disease Progression in Idiopathic Pulmonary Fibrosis
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Sydney Montesi, MD
Massachusetts General Hospital
CHEST Foundation Research Grant in Pulmonary Fibrosis
Gadofosveset-Enhanced Lung MRI to Detect Idiopathic Pulmonary Fibrosis Disease Activity
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Farbod Rahaghi, MD, PhD
Brigham and Women’s Hospital
CHEST Foundation Research Grant in Venous Thromboembolism
CT Scan-Based Markers for Prediction of Outcomes in Acute Pulmonary Embolism
This grant is supported by Daiichi Sankyo.
Catherine Oberg, MD
Icahn School of Medicine at Mount Sinai
CHEST Foundation Research Grant in Women’s Lung Health
Effects of Household Air Pollution on Airway Inflammation, Lung Function, and Respiratory Symptoms
This grant is supported in full by the CHEST Foundation.
2016 Community Service Grantee
Ethel Jane Carter, MD, FCCP
Warren Alpert School of Medicine at Brown University
CHEST Foundation Community Service Grant Honoring D. Robert McCaffree, MD, Master FCCP
East African Training Initiative ( EATI) in Pulmonary Medicine
2016 NetWorks Challenge Travel Grantees
Debarsee Banerjee, MS, MD
Women’s Health NetWork
Drew Harris, MD
Occupational and Environmental Health NetWork
Kerry Hena, MD
Occupational and Environmental Health NetWork
Amanpreet Kaur, MD
Women’s Health NetWork
2016 Diversity Travel Grant Winners
John B. Bishara, DO
Renato F. Blanco Jr., MD
Angel Coz-Yataco, MD Sherie A. Gause, MD
Anthony Nebor, MD
James T. Williams, MD
Alfred Soffer Research Award Winners
Kerry Hena, MD
Deepak Pradhan, MD, FCCP
Young Investigator Award Winners
Elizabeth Becker: Clinical Characteristics of Sarcoidosis in World Trade Center (WTC) Exposed Fire Department of the City of New York (FDNY) Firefighters
Daniel Altman, MD : Cost-Effectiveness of Universally Funding Smoking Cessation Pharmacotherapy
Top 3 Poster Winners
Epaminondas Kosmas, MD, PhD, FCCP : Bronchiectasis in Patients With COPD: An Irrelevant Imaging Finding or a Clinically Important Phenotype?
Mark Regala, MD, BS : Evaluation of Outcomes of Post-Extubation Dysphagia in Elderly Patients
Massa Zantah, MD : Correlation of Esophageal Dilatation and Pulmonary Fibrosis in Scleroderma
Runner-up: Alev Gurgun, MD : Pulmonary Rehabilitation Response in Elderly and Younger Patients With COPD
Case Report Slide Winners
John Egan, MD, BA : An Unusual Cause of Tracheal Stenosis Due to a Vascular Anomaly Successfully Managed With Silicone Airway Stenting Prior to Definitive Vascular Repair
Harprett Grewal, MD : Bladder PTLD: First Reported Case of Post-Transplant Lymphoproliferative Disorder (PTLD) in the Bladder in a Lung Transplant Recipient
Michael Fingerhood, MD, MPH : Pulmonary Overlap Histiocytosis: A Rare Case of Interstitial Lung Disease Due to Erdheim Chester Disease in a Patient With Langerhans Cell Histiocytosis and Myelodisplastic Syndrome
Yihenew Negatu, MD : Acute ST Elevation Myocardial Infarction Related to Carbon Monoxide Poisoning in a Young Patient Without Coronary Artery Disease
Stephanie Wappel, MD : False-Negative Pet Imaging in Early Stage Malignant Pleural Mesothelioma
Lina Miyakawa, MD : Restrictive EGFR Mutation
Jeffrey Bonenfant, DO : A Unique Case of Follicular Bronchiolitis
Melissa Myers, MD : Seeing the Forest and Not Just the Trees: A Case of Recurrent Fever, Cough, and Respiratory Failure
Carly Fabrizio, DO : An Unusual Case of Submassive Hemoptysis
Meilinh Thi, DO : A Case to Make Your Skin Crawl
Garrett Harp, MD : Lambertosis: A Lung Cancer Mimic
Malik Khan, MD : Pleural Epithelioid Hemangioendothelioma: A Case Report
Priya Patel, MD : A Troubling Trifecta: Pulmonary Alveolar Proteinosis and Pneumocystis Pneumonia in Acute Myeloid Leukemia
Atul Palkar, MD : SGLT2 Inhibitors: Mind the Gap
Ji Yeon Lee, MD : Making Unusual Connections: Fibrosing Mediastinitis Leading to Bronchoesophageal Fistula
Sailm Daouk, MD : A Rare Form of Invasive Aspergillus Infection in a Severely Immunocompromised Host
Venkata Ravi Kumar Angirekula, MD : Vanishing Lung
Stephen Milan, MD : An Unexpected Mass
Lelia Logue, MD : A Rare Cause of Dysphagia
Daniel Hershberger, MD : Rapidly Progressive Hypoxic Respiratory Failure After a Rash: A Case of Clinically Amyopathic Dermatomyositis (CADM)-Associated ILD
Fellow Case Report Poster Winners
Krishna Siva Sai Kakkera
An Unusual Case of Crypotococcal Pleural Effusion
George Cheng
Use of Laparoscopic Suction Irrigator With Rigid Pleuroscope in Medical Thoracoscopy
Matt Koroscil
Wong Type Dermatomyositis Complicated by Interstitial Lung Disease
Derek Hansen
Acute Fibrinous and Organizing Pneumonia Following Hematopoietic Stem Cell Transplantation Responsive to Corticosteroid Therapy
Ala Eddin Sagar
Pulmonary Embolism Caused by Thrombin-Based Hemostatic Matrix After Discectomy
Sandeep Chennadi
Systemic Lupus Erythematosus (SLE) With Refractory Bilateral Chylothorax and Chylous Ascites
Medical Student/Resident Case Report Poster Winners
Justin Fiala
Pulmonary Presentation Without Concurrent Bone Involvement in Erdheim-Chester Disease: A Report of Two Cases
Navitha Ramesh
A Fatal Migration: A Case of Intra-Cardiac Embolization of a Peripheral Stent
Humna Abid Memon
Use of Extracorporeal Membrane Oxygenation in Postpartum Management of a Patient With PAH
Vanessa Ohleyer
A Case of Unusual Anatomy for an Uncommon Mediastinal Tumor
Tanushree Gahlot
Three Unusual Presentations of Job’s Syndrome (Hyper Immunoglobulin E Syndrome)
NetWorks Challenge Winners
Round 1
Women’s Lung Health NetWork
Round 2
Practice and Operations NetWork-1st place
Home-Based Mechanical Ventilation and Neuromuscular Disease NetWorks – 2nd place
Round 3
Home-Based Mechanical Ventilation, Neuromuscular Disease, and the Women’s Lung Health NetWorks
CHEST Bingo Winners
Youseff Anid, MD, FCCP
Karen Cochran, ACNP
Molly Howsware, DO
Katie Jeans, MD
Genovena Medina, RN
Gregory Eisinger, MD
Saurabh Mittal, MD, MBBS
Navitha Ramesh, MD
Dalvinder Dhillon, MD
Teresita Saylor, MD, FCCP
Carl Kaplan, MD, FCCP
Vishal Patel, MBBS, FCCP
Erin Peterson, CNP
Lilian Pereira, DO
We all know that, with the great success of CHEST 2016, everyone who shared that event is a winner. But, we would especially like to call out some of the special winners who were recognized during our annual meeting.
CHEST Awards
College Medalist Award
Lewis J. Rubin, MD, FCCP
Distinguished Service Award
Kim D. French, MHSA, CAPPM, FCCP
Alfred Soffer Award for Editorial Excellence
Seth J. Koenig, MD, FCCP
Master Clinician Educator Award
Jack D. Buckley, MD, MPH, FCCP
Distinguished Scientist Honor Lecture
Jay Nadel, MD
Edward C. Rosenow III, MD, Master FCCP/Master Teacher Honor Lecture
Suhail Raoof, MBBS, FCCP
Murray Kornfeld Memorial Founders Lecture
Michael Niederman, MD, FCCP Pasquale Ciaglia Memorial Lecture Kevin L. Kovitz, MD, FCCP
Roger C. Bone Memorial Lecture
Robert A. Berg, MD Thomas L. Petty, MD, Master FCCP Memorial Lecture Nicola A. Hanania, MD, MS, FCCP Margaret Pfrommer Memorial Lecture in Long-term Mechanical Ventilation Thomas G. Keens, MD Om P. Sharma, MD, Master FCCP Memorial Lecture Robert P. Baughman, MD, FCCP
Early Career Educator
Gabriel Bosslet, MD, FCCP
CHEST Challenge Championship 2016
1st Place
The University of Arizona
Huthayfa Ateeli, MBBS Naser Mahmoud, MD
Muna Omar, MD, MBBS
PD: James L. Knepler Jr.
2nd Place
New York Methodist Hospital
Anu R. Jacob, MD
Stephen D. Milan, MD
Jordan Taillon, MD
PD: Anthony G. Saleh, MD, FCCP
3rd Place
Interfaith Medical Center
Chidozie C. Agu, MD
Saroj P. Kandel, MBBS Divya Salhan, MD, MBBS
PD: Marie Frances J. Schmidt, MD, FCCP
CHEST Foundation Grant Winners
GlaxoSmithKline Distinguished Scholar in Respiratory Health
Don Hayes Jr., MD, FCCP The Research Institute at Nationwide Children’s Hospital
Implications of the Lung Allocation Score in Prioritizing Critically Ill Patients for Lung Transplantation
Supported by GlaxoSmithKline.
2016 Research Grantees
Alice Turner, MBChB, MRCP, PhD
University of Birmingham, United Kingdom
CHEST Foundation and the Alpha-1 Foundation Research Grant in Alpha-1 Antitrypsin Deficiency
Improving Access to Augmentation: A Propensity-Matching Study Between the UK AATD Registry and AlphaNet
This grant is jointly supported by the CHEST Foundation and the Alpha-1 Foundation.
Robert Busch, MD
Brigham and Women’s Hospital, Channing Division of Network Medicine
CHEST Foundation Research Grant in Chronic Obstructive Pulmonary Disease
Methylation Quantitative Trait Loci: Markers of Race-Specific Disparities in African Americans With COPD
This grant is supported by AstraZeneca.
Clemens Grassberger, PhD
Massachusetts General Hospital – Harvard University
CHEST Foundation Research Grant in Lung Cancer
Dynamic FLT-PET as Biomarker for Early Response in Locally Advanced Lung Cancer Patients
This grant is supported by Genentech Inc.
Cristina Russo, MD, PhD
Bambino Gesù Children’s Hospital, Rome, Italy
CHEST Foundation Research Grant in Nontuberculous Mycobacteria
A Proteomic-Metaproteomic Analysis Approach Allows Identification of Drug Target Candidates for the Future Design of Preventive, Diagnostic, and Therapeutic Strategies Against Nontuberculous Mycobacteria Diseases
This grant is supported by Insmed.
Peter Leary, MD, MS
University of Washington
CHEST Foundation Research Grant in Pulmonary Arterial Hypertension
Expression Profiling in Pulmonary Arterial Hypertension
This grant is supported by Actelion Pharmaceuticals, US, Inc.
Brett Ley, MD
University of California, San Francisco
CHEST Foundation Research Grant in Pulmonary Fibrosis
Extracellular Circulation RNAs as Predictors of Disease Progression in Idiopathic Pulmonary Fibrosis
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Sydney Montesi, MD
Massachusetts General Hospital
CHEST Foundation Research Grant in Pulmonary Fibrosis
Gadofosveset-Enhanced Lung MRI to Detect Idiopathic Pulmonary Fibrosis Disease Activity
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Farbod Rahaghi, MD, PhD
Brigham and Women’s Hospital
CHEST Foundation Research Grant in Venous Thromboembolism
CT Scan-Based Markers for Prediction of Outcomes in Acute Pulmonary Embolism
This grant is supported by Daiichi Sankyo.
Catherine Oberg, MD
Icahn School of Medicine at Mount Sinai
CHEST Foundation Research Grant in Women’s Lung Health
Effects of Household Air Pollution on Airway Inflammation, Lung Function, and Respiratory Symptoms
This grant is supported in full by the CHEST Foundation.
2016 Community Service Grantee
Ethel Jane Carter, MD, FCCP
Warren Alpert School of Medicine at Brown University
CHEST Foundation Community Service Grant Honoring D. Robert McCaffree, MD, Master FCCP
East African Training Initiative ( EATI) in Pulmonary Medicine
2016 NetWorks Challenge Travel Grantees
Debarsee Banerjee, MS, MD
Women’s Health NetWork
Drew Harris, MD
Occupational and Environmental Health NetWork
Kerry Hena, MD
Occupational and Environmental Health NetWork
Amanpreet Kaur, MD
Women’s Health NetWork
2016 Diversity Travel Grant Winners
John B. Bishara, DO
Renato F. Blanco Jr., MD
Angel Coz-Yataco, MD Sherie A. Gause, MD
Anthony Nebor, MD
James T. Williams, MD
Alfred Soffer Research Award Winners
Kerry Hena, MD
Deepak Pradhan, MD, FCCP
Young Investigator Award Winners
Elizabeth Becker: Clinical Characteristics of Sarcoidosis in World Trade Center (WTC) Exposed Fire Department of the City of New York (FDNY) Firefighters
Daniel Altman, MD : Cost-Effectiveness of Universally Funding Smoking Cessation Pharmacotherapy
Top 3 Poster Winners
Epaminondas Kosmas, MD, PhD, FCCP : Bronchiectasis in Patients With COPD: An Irrelevant Imaging Finding or a Clinically Important Phenotype?
Mark Regala, MD, BS : Evaluation of Outcomes of Post-Extubation Dysphagia in Elderly Patients
Massa Zantah, MD : Correlation of Esophageal Dilatation and Pulmonary Fibrosis in Scleroderma
Runner-up: Alev Gurgun, MD : Pulmonary Rehabilitation Response in Elderly and Younger Patients With COPD
Case Report Slide Winners
John Egan, MD, BA : An Unusual Cause of Tracheal Stenosis Due to a Vascular Anomaly Successfully Managed With Silicone Airway Stenting Prior to Definitive Vascular Repair
Harprett Grewal, MD : Bladder PTLD: First Reported Case of Post-Transplant Lymphoproliferative Disorder (PTLD) in the Bladder in a Lung Transplant Recipient
Michael Fingerhood, MD, MPH : Pulmonary Overlap Histiocytosis: A Rare Case of Interstitial Lung Disease Due to Erdheim Chester Disease in a Patient With Langerhans Cell Histiocytosis and Myelodisplastic Syndrome
Yihenew Negatu, MD : Acute ST Elevation Myocardial Infarction Related to Carbon Monoxide Poisoning in a Young Patient Without Coronary Artery Disease
Stephanie Wappel, MD : False-Negative Pet Imaging in Early Stage Malignant Pleural Mesothelioma
Lina Miyakawa, MD : Restrictive EGFR Mutation
Jeffrey Bonenfant, DO : A Unique Case of Follicular Bronchiolitis
Melissa Myers, MD : Seeing the Forest and Not Just the Trees: A Case of Recurrent Fever, Cough, and Respiratory Failure
Carly Fabrizio, DO : An Unusual Case of Submassive Hemoptysis
Meilinh Thi, DO : A Case to Make Your Skin Crawl
Garrett Harp, MD : Lambertosis: A Lung Cancer Mimic
Malik Khan, MD : Pleural Epithelioid Hemangioendothelioma: A Case Report
Priya Patel, MD : A Troubling Trifecta: Pulmonary Alveolar Proteinosis and Pneumocystis Pneumonia in Acute Myeloid Leukemia
Atul Palkar, MD : SGLT2 Inhibitors: Mind the Gap
Ji Yeon Lee, MD : Making Unusual Connections: Fibrosing Mediastinitis Leading to Bronchoesophageal Fistula
Sailm Daouk, MD : A Rare Form of Invasive Aspergillus Infection in a Severely Immunocompromised Host
Venkata Ravi Kumar Angirekula, MD : Vanishing Lung
Stephen Milan, MD : An Unexpected Mass
Lelia Logue, MD : A Rare Cause of Dysphagia
Daniel Hershberger, MD : Rapidly Progressive Hypoxic Respiratory Failure After a Rash: A Case of Clinically Amyopathic Dermatomyositis (CADM)-Associated ILD
Fellow Case Report Poster Winners
Krishna Siva Sai Kakkera
An Unusual Case of Crypotococcal Pleural Effusion
George Cheng
Use of Laparoscopic Suction Irrigator With Rigid Pleuroscope in Medical Thoracoscopy
Matt Koroscil
Wong Type Dermatomyositis Complicated by Interstitial Lung Disease
Derek Hansen
Acute Fibrinous and Organizing Pneumonia Following Hematopoietic Stem Cell Transplantation Responsive to Corticosteroid Therapy
Ala Eddin Sagar
Pulmonary Embolism Caused by Thrombin-Based Hemostatic Matrix After Discectomy
Sandeep Chennadi
Systemic Lupus Erythematosus (SLE) With Refractory Bilateral Chylothorax and Chylous Ascites
Medical Student/Resident Case Report Poster Winners
Justin Fiala
Pulmonary Presentation Without Concurrent Bone Involvement in Erdheim-Chester Disease: A Report of Two Cases
Navitha Ramesh
A Fatal Migration: A Case of Intra-Cardiac Embolization of a Peripheral Stent
Humna Abid Memon
Use of Extracorporeal Membrane Oxygenation in Postpartum Management of a Patient With PAH
Vanessa Ohleyer
A Case of Unusual Anatomy for an Uncommon Mediastinal Tumor
Tanushree Gahlot
Three Unusual Presentations of Job’s Syndrome (Hyper Immunoglobulin E Syndrome)
NetWorks Challenge Winners
Round 1
Women’s Lung Health NetWork
Round 2
Practice and Operations NetWork-1st place
Home-Based Mechanical Ventilation and Neuromuscular Disease NetWorks – 2nd place
Round 3
Home-Based Mechanical Ventilation, Neuromuscular Disease, and the Women’s Lung Health NetWorks
CHEST Bingo Winners
Youseff Anid, MD, FCCP
Karen Cochran, ACNP
Molly Howsware, DO
Katie Jeans, MD
Genovena Medina, RN
Gregory Eisinger, MD
Saurabh Mittal, MD, MBBS
Navitha Ramesh, MD
Dalvinder Dhillon, MD
Teresita Saylor, MD, FCCP
Carl Kaplan, MD, FCCP
Vishal Patel, MBBS, FCCP
Erin Peterson, CNP
Lilian Pereira, DO
We all know that, with the great success of CHEST 2016, everyone who shared that event is a winner. But, we would especially like to call out some of the special winners who were recognized during our annual meeting.
CHEST Awards
College Medalist Award
Lewis J. Rubin, MD, FCCP
Distinguished Service Award
Kim D. French, MHSA, CAPPM, FCCP
Alfred Soffer Award for Editorial Excellence
Seth J. Koenig, MD, FCCP
Master Clinician Educator Award
Jack D. Buckley, MD, MPH, FCCP
Distinguished Scientist Honor Lecture
Jay Nadel, MD
Edward C. Rosenow III, MD, Master FCCP/Master Teacher Honor Lecture
Suhail Raoof, MBBS, FCCP
Murray Kornfeld Memorial Founders Lecture
Michael Niederman, MD, FCCP Pasquale Ciaglia Memorial Lecture Kevin L. Kovitz, MD, FCCP
Roger C. Bone Memorial Lecture
Robert A. Berg, MD Thomas L. Petty, MD, Master FCCP Memorial Lecture Nicola A. Hanania, MD, MS, FCCP Margaret Pfrommer Memorial Lecture in Long-term Mechanical Ventilation Thomas G. Keens, MD Om P. Sharma, MD, Master FCCP Memorial Lecture Robert P. Baughman, MD, FCCP
Early Career Educator
Gabriel Bosslet, MD, FCCP
CHEST Challenge Championship 2016
1st Place
The University of Arizona
Huthayfa Ateeli, MBBS Naser Mahmoud, MD
Muna Omar, MD, MBBS
PD: James L. Knepler Jr.
2nd Place
New York Methodist Hospital
Anu R. Jacob, MD
Stephen D. Milan, MD
Jordan Taillon, MD
PD: Anthony G. Saleh, MD, FCCP
3rd Place
Interfaith Medical Center
Chidozie C. Agu, MD
Saroj P. Kandel, MBBS Divya Salhan, MD, MBBS
PD: Marie Frances J. Schmidt, MD, FCCP
CHEST Foundation Grant Winners
GlaxoSmithKline Distinguished Scholar in Respiratory Health
Don Hayes Jr., MD, FCCP The Research Institute at Nationwide Children’s Hospital
Implications of the Lung Allocation Score in Prioritizing Critically Ill Patients for Lung Transplantation
Supported by GlaxoSmithKline.
2016 Research Grantees
Alice Turner, MBChB, MRCP, PhD
University of Birmingham, United Kingdom
CHEST Foundation and the Alpha-1 Foundation Research Grant in Alpha-1 Antitrypsin Deficiency
Improving Access to Augmentation: A Propensity-Matching Study Between the UK AATD Registry and AlphaNet
This grant is jointly supported by the CHEST Foundation and the Alpha-1 Foundation.
Robert Busch, MD
Brigham and Women’s Hospital, Channing Division of Network Medicine
CHEST Foundation Research Grant in Chronic Obstructive Pulmonary Disease
Methylation Quantitative Trait Loci: Markers of Race-Specific Disparities in African Americans With COPD
This grant is supported by AstraZeneca.
Clemens Grassberger, PhD
Massachusetts General Hospital – Harvard University
CHEST Foundation Research Grant in Lung Cancer
Dynamic FLT-PET as Biomarker for Early Response in Locally Advanced Lung Cancer Patients
This grant is supported by Genentech Inc.
Cristina Russo, MD, PhD
Bambino Gesù Children’s Hospital, Rome, Italy
CHEST Foundation Research Grant in Nontuberculous Mycobacteria
A Proteomic-Metaproteomic Analysis Approach Allows Identification of Drug Target Candidates for the Future Design of Preventive, Diagnostic, and Therapeutic Strategies Against Nontuberculous Mycobacteria Diseases
This grant is supported by Insmed.
Peter Leary, MD, MS
University of Washington
CHEST Foundation Research Grant in Pulmonary Arterial Hypertension
Expression Profiling in Pulmonary Arterial Hypertension
This grant is supported by Actelion Pharmaceuticals, US, Inc.
Brett Ley, MD
University of California, San Francisco
CHEST Foundation Research Grant in Pulmonary Fibrosis
Extracellular Circulation RNAs as Predictors of Disease Progression in Idiopathic Pulmonary Fibrosis
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Sydney Montesi, MD
Massachusetts General Hospital
CHEST Foundation Research Grant in Pulmonary Fibrosis
Gadofosveset-Enhanced Lung MRI to Detect Idiopathic Pulmonary Fibrosis Disease Activity
This grant is supported by Boehringer Ingelheim Pharmaceuticals & Genentech Inc.
Farbod Rahaghi, MD, PhD
Brigham and Women’s Hospital
CHEST Foundation Research Grant in Venous Thromboembolism
CT Scan-Based Markers for Prediction of Outcomes in Acute Pulmonary Embolism
This grant is supported by Daiichi Sankyo.
Catherine Oberg, MD
Icahn School of Medicine at Mount Sinai
CHEST Foundation Research Grant in Women’s Lung Health
Effects of Household Air Pollution on Airway Inflammation, Lung Function, and Respiratory Symptoms
This grant is supported in full by the CHEST Foundation.
2016 Community Service Grantee
Ethel Jane Carter, MD, FCCP
Warren Alpert School of Medicine at Brown University
CHEST Foundation Community Service Grant Honoring D. Robert McCaffree, MD, Master FCCP
East African Training Initiative ( EATI) in Pulmonary Medicine
2016 NetWorks Challenge Travel Grantees
Debarsee Banerjee, MS, MD
Women’s Health NetWork
Drew Harris, MD
Occupational and Environmental Health NetWork
Kerry Hena, MD
Occupational and Environmental Health NetWork
Amanpreet Kaur, MD
Women’s Health NetWork
2016 Diversity Travel Grant Winners
John B. Bishara, DO
Renato F. Blanco Jr., MD
Angel Coz-Yataco, MD Sherie A. Gause, MD
Anthony Nebor, MD
James T. Williams, MD
Alfred Soffer Research Award Winners
Kerry Hena, MD
Deepak Pradhan, MD, FCCP
Young Investigator Award Winners
Elizabeth Becker: Clinical Characteristics of Sarcoidosis in World Trade Center (WTC) Exposed Fire Department of the City of New York (FDNY) Firefighters
Daniel Altman, MD : Cost-Effectiveness of Universally Funding Smoking Cessation Pharmacotherapy
Top 3 Poster Winners
Epaminondas Kosmas, MD, PhD, FCCP : Bronchiectasis in Patients With COPD: An Irrelevant Imaging Finding or a Clinically Important Phenotype?
Mark Regala, MD, BS : Evaluation of Outcomes of Post-Extubation Dysphagia in Elderly Patients
Massa Zantah, MD : Correlation of Esophageal Dilatation and Pulmonary Fibrosis in Scleroderma
Runner-up: Alev Gurgun, MD : Pulmonary Rehabilitation Response in Elderly and Younger Patients With COPD
Case Report Slide Winners
John Egan, MD, BA : An Unusual Cause of Tracheal Stenosis Due to a Vascular Anomaly Successfully Managed With Silicone Airway Stenting Prior to Definitive Vascular Repair
Harprett Grewal, MD : Bladder PTLD: First Reported Case of Post-Transplant Lymphoproliferative Disorder (PTLD) in the Bladder in a Lung Transplant Recipient
Michael Fingerhood, MD, MPH : Pulmonary Overlap Histiocytosis: A Rare Case of Interstitial Lung Disease Due to Erdheim Chester Disease in a Patient With Langerhans Cell Histiocytosis and Myelodisplastic Syndrome
Yihenew Negatu, MD : Acute ST Elevation Myocardial Infarction Related to Carbon Monoxide Poisoning in a Young Patient Without Coronary Artery Disease
Stephanie Wappel, MD : False-Negative Pet Imaging in Early Stage Malignant Pleural Mesothelioma
Lina Miyakawa, MD : Restrictive EGFR Mutation
Jeffrey Bonenfant, DO : A Unique Case of Follicular Bronchiolitis
Melissa Myers, MD : Seeing the Forest and Not Just the Trees: A Case of Recurrent Fever, Cough, and Respiratory Failure
Carly Fabrizio, DO : An Unusual Case of Submassive Hemoptysis
Meilinh Thi, DO : A Case to Make Your Skin Crawl
Garrett Harp, MD : Lambertosis: A Lung Cancer Mimic
Malik Khan, MD : Pleural Epithelioid Hemangioendothelioma: A Case Report
Priya Patel, MD : A Troubling Trifecta: Pulmonary Alveolar Proteinosis and Pneumocystis Pneumonia in Acute Myeloid Leukemia
Atul Palkar, MD : SGLT2 Inhibitors: Mind the Gap
Ji Yeon Lee, MD : Making Unusual Connections: Fibrosing Mediastinitis Leading to Bronchoesophageal Fistula
Sailm Daouk, MD : A Rare Form of Invasive Aspergillus Infection in a Severely Immunocompromised Host
Venkata Ravi Kumar Angirekula, MD : Vanishing Lung
Stephen Milan, MD : An Unexpected Mass
Lelia Logue, MD : A Rare Cause of Dysphagia
Daniel Hershberger, MD : Rapidly Progressive Hypoxic Respiratory Failure After a Rash: A Case of Clinically Amyopathic Dermatomyositis (CADM)-Associated ILD
Fellow Case Report Poster Winners
Krishna Siva Sai Kakkera
An Unusual Case of Crypotococcal Pleural Effusion
George Cheng
Use of Laparoscopic Suction Irrigator With Rigid Pleuroscope in Medical Thoracoscopy
Matt Koroscil
Wong Type Dermatomyositis Complicated by Interstitial Lung Disease
Derek Hansen
Acute Fibrinous and Organizing Pneumonia Following Hematopoietic Stem Cell Transplantation Responsive to Corticosteroid Therapy
Ala Eddin Sagar
Pulmonary Embolism Caused by Thrombin-Based Hemostatic Matrix After Discectomy
Sandeep Chennadi
Systemic Lupus Erythematosus (SLE) With Refractory Bilateral Chylothorax and Chylous Ascites
Medical Student/Resident Case Report Poster Winners
Justin Fiala
Pulmonary Presentation Without Concurrent Bone Involvement in Erdheim-Chester Disease: A Report of Two Cases
Navitha Ramesh
A Fatal Migration: A Case of Intra-Cardiac Embolization of a Peripheral Stent
Humna Abid Memon
Use of Extracorporeal Membrane Oxygenation in Postpartum Management of a Patient With PAH
Vanessa Ohleyer
A Case of Unusual Anatomy for an Uncommon Mediastinal Tumor
Tanushree Gahlot
Three Unusual Presentations of Job’s Syndrome (Hyper Immunoglobulin E Syndrome)
NetWorks Challenge Winners
Round 1
Women’s Lung Health NetWork
Round 2
Practice and Operations NetWork-1st place
Home-Based Mechanical Ventilation and Neuromuscular Disease NetWorks – 2nd place
Round 3
Home-Based Mechanical Ventilation, Neuromuscular Disease, and the Women’s Lung Health NetWorks
CHEST Bingo Winners
Youseff Anid, MD, FCCP
Karen Cochran, ACNP
Molly Howsware, DO
Katie Jeans, MD
Genovena Medina, RN
Gregory Eisinger, MD
Saurabh Mittal, MD, MBBS
Navitha Ramesh, MD
Dalvinder Dhillon, MD
Teresita Saylor, MD, FCCP
Carl Kaplan, MD, FCCP
Vishal Patel, MBBS, FCCP
Erin Peterson, CNP
Lilian Pereira, DO
Joint CHEST-SGP Congress 2017
Basel, Switzerland June 7-9
Join leaders in CHEST medicine for a program designed by clinicians for clinicians.
The Joint Congress organized by CHEST and the Swiss Society of Pneumology will be held from June 7-9 in Basel, Switzerland. The program has been designed by more than 140 faculty members from both the United States and Europe, and it aims to provide a robust overview of all aspects of respiratory medicine through interactive sessions, plenary discussions, critical appraisals on controversial topics, and a review of the last year of published works.
The Joint Congress also provides the opportunity to take part in hands-on simulation in areas such as lung function techniques including body plethysmography, N2 washout techniques, and respiratory physiotherapy. Another hands-on opportunity is the interventional pneumology CHEST experience course, which will be held from 8:00 AM-11:00 AM on June 7 and 8 on site. This course will provide an overview of conventional and EBUS-guided TBNA, an anatomy identification of airway nodes, management of airway bleeding, and management of pneumothorax. This course is ideal for clinicians and health-care professionals with specialties in pulmonary, critical care, and intensive care medicine, as well as thoracic surgery.
The program at the Joint CHEST-SGP Congress aims to improve the patient care abilities of every attendee, as well as provide an ideal environment for networking with leaders in your field.
The call for abstracts remains open until January 24, 2017. The abstract topic areas are:
- Airway disease
- Interstitial lung disease
- Sleep/Breathing
- Lung cancer
- Epidemiology/Rehabilitation
- Interventional pneumology
- Pulmonary hypertension
- Basic science
- Thoracic surgery
- Pediatrics
All abstracts must be submitted via the Joint Congress abstracts web portal www.chest-sgp-switzerland2017.org.
CHEST recognizes the value of international outreach, and this Joint Congress advances that initiative. CHEST aims to standardize the patient care across borders and to encourage international collaboration to build the future of chest medicine. To further this mission, an application has been made to the European Accreditation Council for Continuing Medical Education (EACCME®) for CME accreditation of this event. Additionally, an application has been made to the European Board for Accreditation in Pneumology (EBAP) to provide quality assurance and CME for the event.
For more information or to register, visit the CHEST Joint Congress website www.chest-sgp-switzerland2017.org. Early registration ends on March 16, 2017.
Basel, Switzerland June 7-9
Join leaders in CHEST medicine for a program designed by clinicians for clinicians.
The Joint Congress organized by CHEST and the Swiss Society of Pneumology will be held from June 7-9 in Basel, Switzerland. The program has been designed by more than 140 faculty members from both the United States and Europe, and it aims to provide a robust overview of all aspects of respiratory medicine through interactive sessions, plenary discussions, critical appraisals on controversial topics, and a review of the last year of published works.
The Joint Congress also provides the opportunity to take part in hands-on simulation in areas such as lung function techniques including body plethysmography, N2 washout techniques, and respiratory physiotherapy. Another hands-on opportunity is the interventional pneumology CHEST experience course, which will be held from 8:00 AM-11:00 AM on June 7 and 8 on site. This course will provide an overview of conventional and EBUS-guided TBNA, an anatomy identification of airway nodes, management of airway bleeding, and management of pneumothorax. This course is ideal for clinicians and health-care professionals with specialties in pulmonary, critical care, and intensive care medicine, as well as thoracic surgery.
The program at the Joint CHEST-SGP Congress aims to improve the patient care abilities of every attendee, as well as provide an ideal environment for networking with leaders in your field.
The call for abstracts remains open until January 24, 2017. The abstract topic areas are:
- Airway disease
- Interstitial lung disease
- Sleep/Breathing
- Lung cancer
- Epidemiology/Rehabilitation
- Interventional pneumology
- Pulmonary hypertension
- Basic science
- Thoracic surgery
- Pediatrics
All abstracts must be submitted via the Joint Congress abstracts web portal www.chest-sgp-switzerland2017.org.
CHEST recognizes the value of international outreach, and this Joint Congress advances that initiative. CHEST aims to standardize the patient care across borders and to encourage international collaboration to build the future of chest medicine. To further this mission, an application has been made to the European Accreditation Council for Continuing Medical Education (EACCME®) for CME accreditation of this event. Additionally, an application has been made to the European Board for Accreditation in Pneumology (EBAP) to provide quality assurance and CME for the event.
For more information or to register, visit the CHEST Joint Congress website www.chest-sgp-switzerland2017.org. Early registration ends on March 16, 2017.
Basel, Switzerland June 7-9
Join leaders in CHEST medicine for a program designed by clinicians for clinicians.
The Joint Congress organized by CHEST and the Swiss Society of Pneumology will be held from June 7-9 in Basel, Switzerland. The program has been designed by more than 140 faculty members from both the United States and Europe, and it aims to provide a robust overview of all aspects of respiratory medicine through interactive sessions, plenary discussions, critical appraisals on controversial topics, and a review of the last year of published works.
The Joint Congress also provides the opportunity to take part in hands-on simulation in areas such as lung function techniques including body plethysmography, N2 washout techniques, and respiratory physiotherapy. Another hands-on opportunity is the interventional pneumology CHEST experience course, which will be held from 8:00 AM-11:00 AM on June 7 and 8 on site. This course will provide an overview of conventional and EBUS-guided TBNA, an anatomy identification of airway nodes, management of airway bleeding, and management of pneumothorax. This course is ideal for clinicians and health-care professionals with specialties in pulmonary, critical care, and intensive care medicine, as well as thoracic surgery.
The program at the Joint CHEST-SGP Congress aims to improve the patient care abilities of every attendee, as well as provide an ideal environment for networking with leaders in your field.
The call for abstracts remains open until January 24, 2017. The abstract topic areas are:
- Airway disease
- Interstitial lung disease
- Sleep/Breathing
- Lung cancer
- Epidemiology/Rehabilitation
- Interventional pneumology
- Pulmonary hypertension
- Basic science
- Thoracic surgery
- Pediatrics
All abstracts must be submitted via the Joint Congress abstracts web portal www.chest-sgp-switzerland2017.org.
CHEST recognizes the value of international outreach, and this Joint Congress advances that initiative. CHEST aims to standardize the patient care across borders and to encourage international collaboration to build the future of chest medicine. To further this mission, an application has been made to the European Accreditation Council for Continuing Medical Education (EACCME®) for CME accreditation of this event. Additionally, an application has been made to the European Board for Accreditation in Pneumology (EBAP) to provide quality assurance and CME for the event.
For more information or to register, visit the CHEST Joint Congress website www.chest-sgp-switzerland2017.org. Early registration ends on March 16, 2017.
Macrolide monotherapy works in some NTM lung disease
Patients with cystic fibrosis or bronchiectasis and one form of Mycobacterium abscessus disease can be successfully treated with long-term oral macrolide monotherapy following short-term intravenous combination antibiotic therapy, a Korean research team has shown.
The M. abscessus complex is implicated in between a fifth and half of all cases of lung disease caused by nontuberculous mycobacteria (NTM). Though treatment is notoriously difficult and prolonged in all NTM lung disease, one subspecies of M. abscessus – M. massiliense – lacks the active gene needed for developing resistance to macrolide-based antibiotics, making it potentially more readily treated.
In research published in CHEST, Won-Jung Koh, MD, of Samsung Medical Center and Sungkyunkwan University in Seoul, South Korea, and colleagues, sought to determine the optimal treatment protocol for patients with massiliense disease (Chest. 2016 Dec;150[6]:1211-21). They identified 71 patients with massiliense disease who had initiated antibiotic treatment between January 2007 and December 2012. These patients were part of an ongoing prospective cohort study on NTM lung disease. The first 28 patients in the study were hospitalized for 4 weeks and treated with intravenous amikacin and cefoxitin along with oral clarithromycin and a fluoroquinolone. Following discharge these patients remained on the oral agents for 24 months.
Two years into the study, the protocol changed, and the next 43 patients were treated with a 2-week course of intravenous amikacin and cefoxitin along with the oral agents. In some patients, azithromycin, which came into use in Korea for NTM lung disease in 2011, replaced a fluoroquinolone. After discharge, all patients stayed on the oral macrolides (with seven also taking a fluoroquinolone) until their sputum cultures were negative for 12 months.
For the patients treated for 4 weeks, the response rates after 12 months of treatment were 89% for symptoms, 79% for computed tomography, and 100% for negative sputum cultures. In the patients treated for 2 weeks, they were 100%, 91%, and 91%, respectively. None of these differences between the two groups were statistically significant. Median total treatment duration, however, was significantly shorter – by nearly a year – in the 2-week plus macrolide monotherapy group than in the other group of patients (15.2 months vs. 23.9 months, P less than .001).
Acquired macrolide resistance developed in two patients in the group who received a 2-week course of intravenous amikacin and cefoxitin along with the oral agents, including one case of high-level clarithromycin resistance. Genotyping revealed reinfection with different strains of M. massiliense.
“[Oral] macrolide therapy after an initial 2-week course of combination antibiotics, rather than long-term parenteral antibiotics, might be effective in most patients with M. massiliense lung disease,” Dr. Koh and colleagues wrote, noting that their study’s nonrandomized single-site design was a limitation, and that multicenter randomized trials would be needed “to assess the efficacy” of the findings.
The Korean government funded Dr. Koh and colleagues’ study. None of the authors disclosed conflicts of interest.
“In this study by Koh et al., it is gratifying that most patients had a favorable microbiologic outcome. It is also somewhat surprising that only two patients developed acquired macrolide resistant M. abscessus subsp massiliense isolates. While the absolute number is low, for those two individuals, the consequences of developing macrolide resistance are far from trivial. They have transitioned from having a mycobacterial infection that is relatively easy to treat effectively to a mycobacterial infection that is not,” David E. Griffith, MD, FCCP, and Timothy R. Aksamit, MD, FCCP, wrote in an editorial published in the December issue of CHEST (Chest. 2016 Dec;150[6];1177-8).
The authors noted that they “enthusiastically applaud and acknowledge the prolific and consistently excellent work done by the group in South Korea, but we cannot endorse the widespread adoption of macrolide monotherapy for” this patient group. “In our view, the risk/benefit balance of this approach does not favor macrolide monotherapy even though the majority of patients in this study were adequately treated.”
Dr. Griffith is professor of medicine at University of Texas Health Science Center, Tyler, and Dr. Aksamit is a consultant on pulmonary disease and critical care medicine at the Mayo Clinic, Rochester, Minn. They disclosed no conflicts of interest.
“In this study by Koh et al., it is gratifying that most patients had a favorable microbiologic outcome. It is also somewhat surprising that only two patients developed acquired macrolide resistant M. abscessus subsp massiliense isolates. While the absolute number is low, for those two individuals, the consequences of developing macrolide resistance are far from trivial. They have transitioned from having a mycobacterial infection that is relatively easy to treat effectively to a mycobacterial infection that is not,” David E. Griffith, MD, FCCP, and Timothy R. Aksamit, MD, FCCP, wrote in an editorial published in the December issue of CHEST (Chest. 2016 Dec;150[6];1177-8).
The authors noted that they “enthusiastically applaud and acknowledge the prolific and consistently excellent work done by the group in South Korea, but we cannot endorse the widespread adoption of macrolide monotherapy for” this patient group. “In our view, the risk/benefit balance of this approach does not favor macrolide monotherapy even though the majority of patients in this study were adequately treated.”
Dr. Griffith is professor of medicine at University of Texas Health Science Center, Tyler, and Dr. Aksamit is a consultant on pulmonary disease and critical care medicine at the Mayo Clinic, Rochester, Minn. They disclosed no conflicts of interest.
“In this study by Koh et al., it is gratifying that most patients had a favorable microbiologic outcome. It is also somewhat surprising that only two patients developed acquired macrolide resistant M. abscessus subsp massiliense isolates. While the absolute number is low, for those two individuals, the consequences of developing macrolide resistance are far from trivial. They have transitioned from having a mycobacterial infection that is relatively easy to treat effectively to a mycobacterial infection that is not,” David E. Griffith, MD, FCCP, and Timothy R. Aksamit, MD, FCCP, wrote in an editorial published in the December issue of CHEST (Chest. 2016 Dec;150[6];1177-8).
The authors noted that they “enthusiastically applaud and acknowledge the prolific and consistently excellent work done by the group in South Korea, but we cannot endorse the widespread adoption of macrolide monotherapy for” this patient group. “In our view, the risk/benefit balance of this approach does not favor macrolide monotherapy even though the majority of patients in this study were adequately treated.”
Dr. Griffith is professor of medicine at University of Texas Health Science Center, Tyler, and Dr. Aksamit is a consultant on pulmonary disease and critical care medicine at the Mayo Clinic, Rochester, Minn. They disclosed no conflicts of interest.
Patients with cystic fibrosis or bronchiectasis and one form of Mycobacterium abscessus disease can be successfully treated with long-term oral macrolide monotherapy following short-term intravenous combination antibiotic therapy, a Korean research team has shown.
The M. abscessus complex is implicated in between a fifth and half of all cases of lung disease caused by nontuberculous mycobacteria (NTM). Though treatment is notoriously difficult and prolonged in all NTM lung disease, one subspecies of M. abscessus – M. massiliense – lacks the active gene needed for developing resistance to macrolide-based antibiotics, making it potentially more readily treated.
In research published in CHEST, Won-Jung Koh, MD, of Samsung Medical Center and Sungkyunkwan University in Seoul, South Korea, and colleagues, sought to determine the optimal treatment protocol for patients with massiliense disease (Chest. 2016 Dec;150[6]:1211-21). They identified 71 patients with massiliense disease who had initiated antibiotic treatment between January 2007 and December 2012. These patients were part of an ongoing prospective cohort study on NTM lung disease. The first 28 patients in the study were hospitalized for 4 weeks and treated with intravenous amikacin and cefoxitin along with oral clarithromycin and a fluoroquinolone. Following discharge these patients remained on the oral agents for 24 months.
Two years into the study, the protocol changed, and the next 43 patients were treated with a 2-week course of intravenous amikacin and cefoxitin along with the oral agents. In some patients, azithromycin, which came into use in Korea for NTM lung disease in 2011, replaced a fluoroquinolone. After discharge, all patients stayed on the oral macrolides (with seven also taking a fluoroquinolone) until their sputum cultures were negative for 12 months.
For the patients treated for 4 weeks, the response rates after 12 months of treatment were 89% for symptoms, 79% for computed tomography, and 100% for negative sputum cultures. In the patients treated for 2 weeks, they were 100%, 91%, and 91%, respectively. None of these differences between the two groups were statistically significant. Median total treatment duration, however, was significantly shorter – by nearly a year – in the 2-week plus macrolide monotherapy group than in the other group of patients (15.2 months vs. 23.9 months, P less than .001).
Acquired macrolide resistance developed in two patients in the group who received a 2-week course of intravenous amikacin and cefoxitin along with the oral agents, including one case of high-level clarithromycin resistance. Genotyping revealed reinfection with different strains of M. massiliense.
“[Oral] macrolide therapy after an initial 2-week course of combination antibiotics, rather than long-term parenteral antibiotics, might be effective in most patients with M. massiliense lung disease,” Dr. Koh and colleagues wrote, noting that their study’s nonrandomized single-site design was a limitation, and that multicenter randomized trials would be needed “to assess the efficacy” of the findings.
The Korean government funded Dr. Koh and colleagues’ study. None of the authors disclosed conflicts of interest.
Patients with cystic fibrosis or bronchiectasis and one form of Mycobacterium abscessus disease can be successfully treated with long-term oral macrolide monotherapy following short-term intravenous combination antibiotic therapy, a Korean research team has shown.
The M. abscessus complex is implicated in between a fifth and half of all cases of lung disease caused by nontuberculous mycobacteria (NTM). Though treatment is notoriously difficult and prolonged in all NTM lung disease, one subspecies of M. abscessus – M. massiliense – lacks the active gene needed for developing resistance to macrolide-based antibiotics, making it potentially more readily treated.
In research published in CHEST, Won-Jung Koh, MD, of Samsung Medical Center and Sungkyunkwan University in Seoul, South Korea, and colleagues, sought to determine the optimal treatment protocol for patients with massiliense disease (Chest. 2016 Dec;150[6]:1211-21). They identified 71 patients with massiliense disease who had initiated antibiotic treatment between January 2007 and December 2012. These patients were part of an ongoing prospective cohort study on NTM lung disease. The first 28 patients in the study were hospitalized for 4 weeks and treated with intravenous amikacin and cefoxitin along with oral clarithromycin and a fluoroquinolone. Following discharge these patients remained on the oral agents for 24 months.
Two years into the study, the protocol changed, and the next 43 patients were treated with a 2-week course of intravenous amikacin and cefoxitin along with the oral agents. In some patients, azithromycin, which came into use in Korea for NTM lung disease in 2011, replaced a fluoroquinolone. After discharge, all patients stayed on the oral macrolides (with seven also taking a fluoroquinolone) until their sputum cultures were negative for 12 months.
For the patients treated for 4 weeks, the response rates after 12 months of treatment were 89% for symptoms, 79% for computed tomography, and 100% for negative sputum cultures. In the patients treated for 2 weeks, they were 100%, 91%, and 91%, respectively. None of these differences between the two groups were statistically significant. Median total treatment duration, however, was significantly shorter – by nearly a year – in the 2-week plus macrolide monotherapy group than in the other group of patients (15.2 months vs. 23.9 months, P less than .001).
Acquired macrolide resistance developed in two patients in the group who received a 2-week course of intravenous amikacin and cefoxitin along with the oral agents, including one case of high-level clarithromycin resistance. Genotyping revealed reinfection with different strains of M. massiliense.
“[Oral] macrolide therapy after an initial 2-week course of combination antibiotics, rather than long-term parenteral antibiotics, might be effective in most patients with M. massiliense lung disease,” Dr. Koh and colleagues wrote, noting that their study’s nonrandomized single-site design was a limitation, and that multicenter randomized trials would be needed “to assess the efficacy” of the findings.
The Korean government funded Dr. Koh and colleagues’ study. None of the authors disclosed conflicts of interest.
FROM CHEST
Key clinical point: A short course of intravenous antibiotics followed by oral macrolides may be effective at treating lung disease caused by the massiliense subspecies of M. abscessus.
Major finding: Of 43 patients receiving 2 weeks of combination antibiotics followed by a year of oral macrolides, 39 (91%) converted to negative sputum cultures before 12 months.
Data source: A prospective cohort study enrolling 71 patients at a single treatment center in Korea.
Disclosures: The Korean government sponsored the study and investigators disclosed no conflicts of interest.
Critical Care Commentary
According to IBM, over 2 quintillion bytes of data are generated every day (that’s a 2 with 18 zeros!), with over 90% of the data in the world today generated in the past 2 years alone.
In our private lives, much of this information is generated through online shopping, web surfing, and popular websites such as Facebook and Twitter. Companies are making incredible efforts to collect these data and to use it to improve how they relate to customers and, ultimately, to make more money. For example, companies like Google, Amazon, Facebook, and Netflix collect enormous amounts of data and then use algorithms to provide real-time suggestions for what their customers might want to rent, buy, or click on. These algorithms, which companies use for anything from predicting customer behavior to facial recognition, were developed in the field of machine learning, a branch of computer science that focuses on how to learn from data.

Big data and critical care
Although the “big data” revolution has proliferated across the private sector, medicine has been slow to utilize the data we painstakingly collect in hospitals every day in order to improve patient care.
Clinicians typically rely on their intuition and the few clinical trials that their patients would have been included in to make decisions, and evidence-based clinical decision support tools are often not available or not used. The tools and scores we have at our disposal are often oversimplified so that they can be calculated by hand and usually rely on the clinician to manually gather information from the electronic health record (EHR) to calculate the score. However, this is starting to change. From partnerships between IBM Watson and hospitals, to groups developing and implementing clinical decision support tools in the EHR, it is clear that hospitals are becoming increasingly interested in learning from and using the enormous amount of data that are just sitting in the hospital records.
Although there are many areas in medicine that stand to benefit from harnessing the data available in the EHR to improve patient care, critical care should be one of the specialties that benefits the most. With the variety and frequency of monitoring that critically ill patients receive, there are large swaths of data available to collect, analyze, and harness to improve patient care. The current glut of information results in data overload and alarm fatigue for today’s clinicians, but intelligent use of these data holds promise for making care safer and more efficient and effective.
Groups have already begun using these data to develop tools to identify patients with ARDS (Herasevich V, et al. Intensive Care Med. 2009;35[6]:1018-23), patients at risk of adverse drug reactions (Harinstein LM, et al. J Crit Care. 2012;27[3]:242-9), and those with sepsis (Tafelski S, et al. J Int Med Res. 2010;38:1605-16).
Furthermore, groups have begun “crowdsourcing” critical care problems by making large datasets publicly available, such as the Multi-parameter Intelligent Monitoring in Intensive Care (MIMIC) database, which now holds clinical data from over 40,000 ICU stays from Beth Israel Deaconess Medical Center. Continued efforts to utilize data from patients in the ICU have the potential to revolutionize the care in hospitals today.
An important area of critical care that has seen a rapid rise in the use of EHR data to create decision support tools is in the early detection of critical illness. Given that many in-hospital cardiac arrests occur outside the ICU and delays in transferring critically ill patients to the ICU increase morbidity and mortality (Churpek MM, et al. J Hosp Med. 2016;11[11]:757-62), detecting critical illness early is incredibly important.
For millennia, clinicians have relied on their intuition and experience to determine which patients have a poor prognosis or need increased levels of care. In the 1990s, rapid response teams (RRTs) were developed, with the goal of identifying and treating critical illness earlier. Along with them came early warning scores, which are objective tools that typically use vital sign abnormalities to detect patients at high risk of clinical deterioration. RRTs and the early warning scores used to activate them have proliferated around the world, including in the United States, and scores like the Modified Early Warning Score (MEWS) are available for automatic calculation in the EHR.
However, taking a tool such as the MEWS that can easily be calculated by hand and making our expensive EHRs calculate it is a lot like buying a Ferrari just to drive it around the parking lot. There is no reason to limit our decision support tools to simple algorithms with only a few variables, especially when patients’ lives are at stake.
Several groups around the country have, therefore, begun to utilize other variables in the EHR, such as laboratory values, to create integrated decision support tools for the early identification of critical illness. For example, Kollef and colleagues developed a statistical model to identify critical illness and implemented it on the wards to activate their RRT, which resulted in decreased lengths of stay in the intervention group (Kollef MH, et al. J Hosp Med. 2014;9[7]:424-9).
Escobar et al. developed a model to predict ICU transfer or non-DNR deaths in the Kaiser system and found it to be more accurate than the MEWS in a validation cohort (Escobar GJ, et al. J Hosp Med. 2012;7[5]:388-95). A clinical trial of their system is ongoing.
Finally, our group developed a model called eCART in a multicenter study of over 250,000 patients and has since implemented it in our hospital. An early “black-box” study found that eCART detected more patients who went on to experience a cardiac arrest or ICU transfer than our usual care RRT and it did so 24 hours earlier (Kang MA, et al. Crit Care Med. 2016;44[8]:1468-73). These scores and many more will likely become commonplace in hospitals to provide an objective and accurate way to identify critically ill patients earlier, which may result in decreased preventable morbidity and mortality.
Future directions
There are several important future directions at the intersection of big data and critical care.
First, efforts to collect, store, and share the highly granular data in the ICU are paramount for successful and generalizable research collaborations. Although there are often institutional barriers to data sharing to surmount, efforts such as the MIMIC database provide a roadmap for how ICU data can be shared and problems “crowdsourced” in order to allow researchers access to these data for high quality research.
Second, efforts to fuse randomized controlled trials with big data, such as randomized, embedded, multifactorial, adaptive platform (REMAP) trials, have the potential to greatly enhance the way trials are done in the future. REMAP trials would be embedded in the EHR, provide the ability to study multiple therapies at once, and adapt the randomization scheme to ensure that patients are not harmed by interventions that are clearly detrimental while the study is ongoing (Angus DC. JAMA. 2015;314[8]:767-8).
Finally, it is important that we move beyond the classic statistical methods that are commonly used to develop decision support tools and increase our use of more modern machine learning techniques that companies in the private sector use every day. For example, our group found that classic regression methods were the least accurate of all the methods we studied for detecting clinical deterioration on the wards (Churpek MM, et al. Crit Care Med. 2016;44[2]:368-74). In the future, methods such as the random forest and neural network should become commonplace in the critical care literature.
The big data revolution is here, both in our private lives and in the hospital. The future will bring continued efforts to use data to identify critical illness earlier, improve the care of patients in the ICU, and implement smarter and more efficient clinical trials. This should rapidly increase the generation and utilization of new knowledge and will have a profound impact on the way we care for critically ill patients.
Dr. Churpek is assistant professor, section of pulmonary and critical care medicine, department of medicine at University of Chicago.
Editor’s comment
Why should busy ICU clinicians bother with big data? Isn’t this simply a “flash in the pan” phenomenon that has sprung up in the aftermath of the electronic medical records (EMRs) mandated by the Affordable Care Act? Are concerns valid that clinical data–based algorithms will lead to an endless stream of alerts akin to the ubiquitous pop-up ads for mortgage refinancing, herbal Viagra, and online gambling that has resulted from commercial data mining?
In this Critical Care Commentary, Dr. Matthew Churpek convincingly outlines the potential inherent in the big data generated by our collective ICUs. These benefits are manifesting themselves not just in the data populated within the EMR – but also in the novel ways we can now design and execute studies. And for those who aren’t yet convinced, recall that payers already use the treasure trove of information within our EMRs against us in the forms of self-serving quality metrics, punitive reimbursement, and unvalidated hospital comparison sites.
Lee E. Morrow, MD, FCCP, is the editor of the Critical Care Commentary section of CHEST Physician.
According to IBM, over 2 quintillion bytes of data are generated every day (that’s a 2 with 18 zeros!), with over 90% of the data in the world today generated in the past 2 years alone.
In our private lives, much of this information is generated through online shopping, web surfing, and popular websites such as Facebook and Twitter. Companies are making incredible efforts to collect these data and to use it to improve how they relate to customers and, ultimately, to make more money. For example, companies like Google, Amazon, Facebook, and Netflix collect enormous amounts of data and then use algorithms to provide real-time suggestions for what their customers might want to rent, buy, or click on. These algorithms, which companies use for anything from predicting customer behavior to facial recognition, were developed in the field of machine learning, a branch of computer science that focuses on how to learn from data.
Big data and critical care
Although the “big data” revolution has proliferated across the private sector, medicine has been slow to utilize the data we painstakingly collect in hospitals every day in order to improve patient care.
Clinicians typically rely on their intuition and the few clinical trials that their patients would have been included in to make decisions, and evidence-based clinical decision support tools are often not available or not used. The tools and scores we have at our disposal are often oversimplified so that they can be calculated by hand and usually rely on the clinician to manually gather information from the electronic health record (EHR) to calculate the score. However, this is starting to change. From partnerships between IBM Watson and hospitals, to groups developing and implementing clinical decision support tools in the EHR, it is clear that hospitals are becoming increasingly interested in learning from and using the enormous amount of data that are just sitting in the hospital records.
Although there are many areas in medicine that stand to benefit from harnessing the data available in the EHR to improve patient care, critical care should be one of the specialties that benefits the most. With the variety and frequency of monitoring that critically ill patients receive, there are large swaths of data available to collect, analyze, and harness to improve patient care. The current glut of information results in data overload and alarm fatigue for today’s clinicians, but intelligent use of these data holds promise for making care safer and more efficient and effective.
Groups have already begun using these data to develop tools to identify patients with ARDS (Herasevich V, et al. Intensive Care Med. 2009;35[6]:1018-23), patients at risk of adverse drug reactions (Harinstein LM, et al. J Crit Care. 2012;27[3]:242-9), and those with sepsis (Tafelski S, et al. J Int Med Res. 2010;38:1605-16).
Furthermore, groups have begun “crowdsourcing” critical care problems by making large datasets publicly available, such as the Multi-parameter Intelligent Monitoring in Intensive Care (MIMIC) database, which now holds clinical data from over 40,000 ICU stays from Beth Israel Deaconess Medical Center. Continued efforts to utilize data from patients in the ICU have the potential to revolutionize the care in hospitals today.
An important area of critical care that has seen a rapid rise in the use of EHR data to create decision support tools is in the early detection of critical illness. Given that many in-hospital cardiac arrests occur outside the ICU and delays in transferring critically ill patients to the ICU increase morbidity and mortality (Churpek MM, et al. J Hosp Med. 2016;11[11]:757-62), detecting critical illness early is incredibly important.
For millennia, clinicians have relied on their intuition and experience to determine which patients have a poor prognosis or need increased levels of care. In the 1990s, rapid response teams (RRTs) were developed, with the goal of identifying and treating critical illness earlier. Along with them came early warning scores, which are objective tools that typically use vital sign abnormalities to detect patients at high risk of clinical deterioration. RRTs and the early warning scores used to activate them have proliferated around the world, including in the United States, and scores like the Modified Early Warning Score (MEWS) are available for automatic calculation in the EHR.
However, taking a tool such as the MEWS that can easily be calculated by hand and making our expensive EHRs calculate it is a lot like buying a Ferrari just to drive it around the parking lot. There is no reason to limit our decision support tools to simple algorithms with only a few variables, especially when patients’ lives are at stake.
Several groups around the country have, therefore, begun to utilize other variables in the EHR, such as laboratory values, to create integrated decision support tools for the early identification of critical illness. For example, Kollef and colleagues developed a statistical model to identify critical illness and implemented it on the wards to activate their RRT, which resulted in decreased lengths of stay in the intervention group (Kollef MH, et al. J Hosp Med. 2014;9[7]:424-9).
Escobar et al. developed a model to predict ICU transfer or non-DNR deaths in the Kaiser system and found it to be more accurate than the MEWS in a validation cohort (Escobar GJ, et al. J Hosp Med. 2012;7[5]:388-95). A clinical trial of their system is ongoing.
Finally, our group developed a model called eCART in a multicenter study of over 250,000 patients and has since implemented it in our hospital. An early “black-box” study found that eCART detected more patients who went on to experience a cardiac arrest or ICU transfer than our usual care RRT and it did so 24 hours earlier (Kang MA, et al. Crit Care Med. 2016;44[8]:1468-73). These scores and many more will likely become commonplace in hospitals to provide an objective and accurate way to identify critically ill patients earlier, which may result in decreased preventable morbidity and mortality.
Future directions
There are several important future directions at the intersection of big data and critical care.
First, efforts to collect, store, and share the highly granular data in the ICU are paramount for successful and generalizable research collaborations. Although there are often institutional barriers to data sharing to surmount, efforts such as the MIMIC database provide a roadmap for how ICU data can be shared and problems “crowdsourced” in order to allow researchers access to these data for high quality research.
Second, efforts to fuse randomized controlled trials with big data, such as randomized, embedded, multifactorial, adaptive platform (REMAP) trials, have the potential to greatly enhance the way trials are done in the future. REMAP trials would be embedded in the EHR, provide the ability to study multiple therapies at once, and adapt the randomization scheme to ensure that patients are not harmed by interventions that are clearly detrimental while the study is ongoing (Angus DC. JAMA. 2015;314[8]:767-8).
Finally, it is important that we move beyond the classic statistical methods that are commonly used to develop decision support tools and increase our use of more modern machine learning techniques that companies in the private sector use every day. For example, our group found that classic regression methods were the least accurate of all the methods we studied for detecting clinical deterioration on the wards (Churpek MM, et al. Crit Care Med. 2016;44[2]:368-74). In the future, methods such as the random forest and neural network should become commonplace in the critical care literature.
The big data revolution is here, both in our private lives and in the hospital. The future will bring continued efforts to use data to identify critical illness earlier, improve the care of patients in the ICU, and implement smarter and more efficient clinical trials. This should rapidly increase the generation and utilization of new knowledge and will have a profound impact on the way we care for critically ill patients.
Dr. Churpek is assistant professor, section of pulmonary and critical care medicine, department of medicine at University of Chicago.
Editor’s comment
Why should busy ICU clinicians bother with big data? Isn’t this simply a “flash in the pan” phenomenon that has sprung up in the aftermath of the electronic medical records (EMRs) mandated by the Affordable Care Act? Are concerns valid that clinical data–based algorithms will lead to an endless stream of alerts akin to the ubiquitous pop-up ads for mortgage refinancing, herbal Viagra, and online gambling that has resulted from commercial data mining?
In this Critical Care Commentary, Dr. Matthew Churpek convincingly outlines the potential inherent in the big data generated by our collective ICUs. These benefits are manifesting themselves not just in the data populated within the EMR – but also in the novel ways we can now design and execute studies. And for those who aren’t yet convinced, recall that payers already use the treasure trove of information within our EMRs against us in the forms of self-serving quality metrics, punitive reimbursement, and unvalidated hospital comparison sites.
Lee E. Morrow, MD, FCCP, is the editor of the Critical Care Commentary section of CHEST Physician.
According to IBM, over 2 quintillion bytes of data are generated every day (that’s a 2 with 18 zeros!), with over 90% of the data in the world today generated in the past 2 years alone.
In our private lives, much of this information is generated through online shopping, web surfing, and popular websites such as Facebook and Twitter. Companies are making incredible efforts to collect these data and to use it to improve how they relate to customers and, ultimately, to make more money. For example, companies like Google, Amazon, Facebook, and Netflix collect enormous amounts of data and then use algorithms to provide real-time suggestions for what their customers might want to rent, buy, or click on. These algorithms, which companies use for anything from predicting customer behavior to facial recognition, were developed in the field of machine learning, a branch of computer science that focuses on how to learn from data.
Big data and critical care
Although the “big data” revolution has proliferated across the private sector, medicine has been slow to utilize the data we painstakingly collect in hospitals every day in order to improve patient care.
Clinicians typically rely on their intuition and the few clinical trials that their patients would have been included in to make decisions, and evidence-based clinical decision support tools are often not available or not used. The tools and scores we have at our disposal are often oversimplified so that they can be calculated by hand and usually rely on the clinician to manually gather information from the electronic health record (EHR) to calculate the score. However, this is starting to change. From partnerships between IBM Watson and hospitals, to groups developing and implementing clinical decision support tools in the EHR, it is clear that hospitals are becoming increasingly interested in learning from and using the enormous amount of data that are just sitting in the hospital records.
Although there are many areas in medicine that stand to benefit from harnessing the data available in the EHR to improve patient care, critical care should be one of the specialties that benefits the most. With the variety and frequency of monitoring that critically ill patients receive, there are large swaths of data available to collect, analyze, and harness to improve patient care. The current glut of information results in data overload and alarm fatigue for today’s clinicians, but intelligent use of these data holds promise for making care safer and more efficient and effective.
Groups have already begun using these data to develop tools to identify patients with ARDS (Herasevich V, et al. Intensive Care Med. 2009;35[6]:1018-23), patients at risk of adverse drug reactions (Harinstein LM, et al. J Crit Care. 2012;27[3]:242-9), and those with sepsis (Tafelski S, et al. J Int Med Res. 2010;38:1605-16).
Furthermore, groups have begun “crowdsourcing” critical care problems by making large datasets publicly available, such as the Multi-parameter Intelligent Monitoring in Intensive Care (MIMIC) database, which now holds clinical data from over 40,000 ICU stays from Beth Israel Deaconess Medical Center. Continued efforts to utilize data from patients in the ICU have the potential to revolutionize the care in hospitals today.
An important area of critical care that has seen a rapid rise in the use of EHR data to create decision support tools is in the early detection of critical illness. Given that many in-hospital cardiac arrests occur outside the ICU and delays in transferring critically ill patients to the ICU increase morbidity and mortality (Churpek MM, et al. J Hosp Med. 2016;11[11]:757-62), detecting critical illness early is incredibly important.
For millennia, clinicians have relied on their intuition and experience to determine which patients have a poor prognosis or need increased levels of care. In the 1990s, rapid response teams (RRTs) were developed, with the goal of identifying and treating critical illness earlier. Along with them came early warning scores, which are objective tools that typically use vital sign abnormalities to detect patients at high risk of clinical deterioration. RRTs and the early warning scores used to activate them have proliferated around the world, including in the United States, and scores like the Modified Early Warning Score (MEWS) are available for automatic calculation in the EHR.
However, taking a tool such as the MEWS that can easily be calculated by hand and making our expensive EHRs calculate it is a lot like buying a Ferrari just to drive it around the parking lot. There is no reason to limit our decision support tools to simple algorithms with only a few variables, especially when patients’ lives are at stake.
Several groups around the country have, therefore, begun to utilize other variables in the EHR, such as laboratory values, to create integrated decision support tools for the early identification of critical illness. For example, Kollef and colleagues developed a statistical model to identify critical illness and implemented it on the wards to activate their RRT, which resulted in decreased lengths of stay in the intervention group (Kollef MH, et al. J Hosp Med. 2014;9[7]:424-9).
Escobar et al. developed a model to predict ICU transfer or non-DNR deaths in the Kaiser system and found it to be more accurate than the MEWS in a validation cohort (Escobar GJ, et al. J Hosp Med. 2012;7[5]:388-95). A clinical trial of their system is ongoing.
Finally, our group developed a model called eCART in a multicenter study of over 250,000 patients and has since implemented it in our hospital. An early “black-box” study found that eCART detected more patients who went on to experience a cardiac arrest or ICU transfer than our usual care RRT and it did so 24 hours earlier (Kang MA, et al. Crit Care Med. 2016;44[8]:1468-73). These scores and many more will likely become commonplace in hospitals to provide an objective and accurate way to identify critically ill patients earlier, which may result in decreased preventable morbidity and mortality.
Future directions
There are several important future directions at the intersection of big data and critical care.
First, efforts to collect, store, and share the highly granular data in the ICU are paramount for successful and generalizable research collaborations. Although there are often institutional barriers to data sharing to surmount, efforts such as the MIMIC database provide a roadmap for how ICU data can be shared and problems “crowdsourced” in order to allow researchers access to these data for high quality research.
Second, efforts to fuse randomized controlled trials with big data, such as randomized, embedded, multifactorial, adaptive platform (REMAP) trials, have the potential to greatly enhance the way trials are done in the future. REMAP trials would be embedded in the EHR, provide the ability to study multiple therapies at once, and adapt the randomization scheme to ensure that patients are not harmed by interventions that are clearly detrimental while the study is ongoing (Angus DC. JAMA. 2015;314[8]:767-8).
Finally, it is important that we move beyond the classic statistical methods that are commonly used to develop decision support tools and increase our use of more modern machine learning techniques that companies in the private sector use every day. For example, our group found that classic regression methods were the least accurate of all the methods we studied for detecting clinical deterioration on the wards (Churpek MM, et al. Crit Care Med. 2016;44[2]:368-74). In the future, methods such as the random forest and neural network should become commonplace in the critical care literature.
The big data revolution is here, both in our private lives and in the hospital. The future will bring continued efforts to use data to identify critical illness earlier, improve the care of patients in the ICU, and implement smarter and more efficient clinical trials. This should rapidly increase the generation and utilization of new knowledge and will have a profound impact on the way we care for critically ill patients.
Dr. Churpek is assistant professor, section of pulmonary and critical care medicine, department of medicine at University of Chicago.
Editor’s comment
Why should busy ICU clinicians bother with big data? Isn’t this simply a “flash in the pan” phenomenon that has sprung up in the aftermath of the electronic medical records (EMRs) mandated by the Affordable Care Act? Are concerns valid that clinical data–based algorithms will lead to an endless stream of alerts akin to the ubiquitous pop-up ads for mortgage refinancing, herbal Viagra, and online gambling that has resulted from commercial data mining?
In this Critical Care Commentary, Dr. Matthew Churpek convincingly outlines the potential inherent in the big data generated by our collective ICUs. These benefits are manifesting themselves not just in the data populated within the EMR – but also in the novel ways we can now design and execute studies. And for those who aren’t yet convinced, recall that payers already use the treasure trove of information within our EMRs against us in the forms of self-serving quality metrics, punitive reimbursement, and unvalidated hospital comparison sites.
Lee E. Morrow, MD, FCCP, is the editor of the Critical Care Commentary section of CHEST Physician.

My journey into pulmonary-critical care medicine
Growing up was not easy. Camden, an inner city in southern New Jersey, is known for its abject poverty, constant violence, and drug trafficking and has been notoriously labeled as one of the “most dangerous cities in the US.” It is a daunting place for many, but home for me. My story is one of a single mother high school dropout with eight children, who worked tirelessly to provide my siblings and me with more advantageous circumstances than she had.

They say “home is where the heart is.” I guess this old statement holds true in my case when I think of why I choose to return to Camden for my residency training at Cooper Hospital. Driving to work in Camden is always a memorable event for me. With every corner and bend in the city, I get a short trip down memory lane. I remember fondly walking to the corner store to buy candy with quarters that my sisters and I dredged up from our couch cushions.
Sundays were my favorite days growing up. We all woke up very early with the singular purpose of getting ready for church. As a child, I loved the attention we all gave each other, especially on Sundays. My siblings and I squabbled and played pranks on each other all morning to my mother’s displeasure, but, somehow, we always made it to church on time, dressed in our Sunday best. After church, our home was filled with hours of laughter, good food, and games only children knew how to play. Our house was always a second home to other kids from our block and friends of my mother who stopped by to try her famous chicken dishes. The days always had the feel of a fun holiday, like Halloween, or Christmas without the lights. It is important that people don’t see Camden as a stereotype, as it has more to offer than murder stories, stray cats, and drug dealing. I am a product of this city.
Embarking on pulmonary-critical care medicine is my next chapter. I see the scourge of pulmonary disease in my internal medicine clinic and am looking forward to arming myself with the knowledge to ease my patients’ burdens. Furthermore, I relish the opportunity to learn how to organize a chaos-filled room into an efficient, harmonized resuscitation situation. The process encourages teamwork, mindfulness, and empathy while being a scientist for the sickest patients in the hospital. These are all fundamental qualities I’ve strived to develop over my maturation as an internal medicine resident and traits I’ve also gained through my various life experiences. I am certain that no other field of medicine would better position me to serve in the broadest sense as a clinician, and I am sure that my life experiences will complement my scientific skill set.
It is said that a journey of a thousand miles begins with a single step. Who knew that someday, I would be able to help repay Camden for nurturing me as a child. I am ready for my new challenges and to embark on this new, pulmonary-critical care medicine chapter in my life.
Dr. Lee is an internal medicine resident at Cooper University Hospital at Cooper Medical School of Rowan University, Camden, NJ.
Editor’s Note
Dr. Lee’s thoughtful piece about why she chose to go into pulmonary–critical care medicine is both inspiring and insightful. She deserves commendation for her willingness to share her story, and I am humbled by her words.
Nitin Puri, MD, FCCP, is the editor of the Pulmonary Perspectives section of CHEST Physician.
Growing up was not easy. Camden, an inner city in southern New Jersey, is known for its abject poverty, constant violence, and drug trafficking and has been notoriously labeled as one of the “most dangerous cities in the US.” It is a daunting place for many, but home for me. My story is one of a single mother high school dropout with eight children, who worked tirelessly to provide my siblings and me with more advantageous circumstances than she had.
They say “home is where the heart is.” I guess this old statement holds true in my case when I think of why I choose to return to Camden for my residency training at Cooper Hospital. Driving to work in Camden is always a memorable event for me. With every corner and bend in the city, I get a short trip down memory lane. I remember fondly walking to the corner store to buy candy with quarters that my sisters and I dredged up from our couch cushions.
Sundays were my favorite days growing up. We all woke up very early with the singular purpose of getting ready for church. As a child, I loved the attention we all gave each other, especially on Sundays. My siblings and I squabbled and played pranks on each other all morning to my mother’s displeasure, but, somehow, we always made it to church on time, dressed in our Sunday best. After church, our home was filled with hours of laughter, good food, and games only children knew how to play. Our house was always a second home to other kids from our block and friends of my mother who stopped by to try her famous chicken dishes. The days always had the feel of a fun holiday, like Halloween, or Christmas without the lights. It is important that people don’t see Camden as a stereotype, as it has more to offer than murder stories, stray cats, and drug dealing. I am a product of this city.
Embarking on pulmonary-critical care medicine is my next chapter. I see the scourge of pulmonary disease in my internal medicine clinic and am looking forward to arming myself with the knowledge to ease my patients’ burdens. Furthermore, I relish the opportunity to learn how to organize a chaos-filled room into an efficient, harmonized resuscitation situation. The process encourages teamwork, mindfulness, and empathy while being a scientist for the sickest patients in the hospital. These are all fundamental qualities I’ve strived to develop over my maturation as an internal medicine resident and traits I’ve also gained through my various life experiences. I am certain that no other field of medicine would better position me to serve in the broadest sense as a clinician, and I am sure that my life experiences will complement my scientific skill set.
It is said that a journey of a thousand miles begins with a single step. Who knew that someday, I would be able to help repay Camden for nurturing me as a child. I am ready for my new challenges and to embark on this new, pulmonary-critical care medicine chapter in my life.
Dr. Lee is an internal medicine resident at Cooper University Hospital at Cooper Medical School of Rowan University, Camden, NJ.
Editor’s Note
Dr. Lee’s thoughtful piece about why she chose to go into pulmonary–critical care medicine is both inspiring and insightful. She deserves commendation for her willingness to share her story, and I am humbled by her words.
Nitin Puri, MD, FCCP, is the editor of the Pulmonary Perspectives section of CHEST Physician.
Growing up was not easy. Camden, an inner city in southern New Jersey, is known for its abject poverty, constant violence, and drug trafficking and has been notoriously labeled as one of the “most dangerous cities in the US.” It is a daunting place for many, but home for me. My story is one of a single mother high school dropout with eight children, who worked tirelessly to provide my siblings and me with more advantageous circumstances than she had.
They say “home is where the heart is.” I guess this old statement holds true in my case when I think of why I choose to return to Camden for my residency training at Cooper Hospital. Driving to work in Camden is always a memorable event for me. With every corner and bend in the city, I get a short trip down memory lane. I remember fondly walking to the corner store to buy candy with quarters that my sisters and I dredged up from our couch cushions.
Sundays were my favorite days growing up. We all woke up very early with the singular purpose of getting ready for church. As a child, I loved the attention we all gave each other, especially on Sundays. My siblings and I squabbled and played pranks on each other all morning to my mother’s displeasure, but, somehow, we always made it to church on time, dressed in our Sunday best. After church, our home was filled with hours of laughter, good food, and games only children knew how to play. Our house was always a second home to other kids from our block and friends of my mother who stopped by to try her famous chicken dishes. The days always had the feel of a fun holiday, like Halloween, or Christmas without the lights. It is important that people don’t see Camden as a stereotype, as it has more to offer than murder stories, stray cats, and drug dealing. I am a product of this city.
Embarking on pulmonary-critical care medicine is my next chapter. I see the scourge of pulmonary disease in my internal medicine clinic and am looking forward to arming myself with the knowledge to ease my patients’ burdens. Furthermore, I relish the opportunity to learn how to organize a chaos-filled room into an efficient, harmonized resuscitation situation. The process encourages teamwork, mindfulness, and empathy while being a scientist for the sickest patients in the hospital. These are all fundamental qualities I’ve strived to develop over my maturation as an internal medicine resident and traits I’ve also gained through my various life experiences. I am certain that no other field of medicine would better position me to serve in the broadest sense as a clinician, and I am sure that my life experiences will complement my scientific skill set.
It is said that a journey of a thousand miles begins with a single step. Who knew that someday, I would be able to help repay Camden for nurturing me as a child. I am ready for my new challenges and to embark on this new, pulmonary-critical care medicine chapter in my life.
Dr. Lee is an internal medicine resident at Cooper University Hospital at Cooper Medical School of Rowan University, Camden, NJ.
Editor’s Note
Dr. Lee’s thoughtful piece about why she chose to go into pulmonary–critical care medicine is both inspiring and insightful. She deserves commendation for her willingness to share her story, and I am humbled by her words.
Nitin Puri, MD, FCCP, is the editor of the Pulmonary Perspectives section of CHEST Physician.
This Month in CHEST: Editor’s Picks
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
Oral Macrolide Therapy Following Short-term Combination Antibiotic Treatment of Mycobacterium massiliense Lung Disease. By Dr. Won-Jung Koh, et al.
Impact of Acute Changes in CPAP Flow Route in Sleep Apnea Treatment. By Dr. R. G. Andrade, et al.
Endobronchial Ultrasound: Clinical Uses and Professional Reimbursements. By Dr. T. R. Gildea and Dr. K. Nicolacakis.
Chronic Cough Due to Gastroesophageal Reflux in Adults: CHEST Guideline and Expert Panel Report. By Dr. P. J. Kahrilas, et al., on behalf of the CHEST Expert Cough Panel.
ABIM Pulmonary Medicine Board urges participation in survey
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
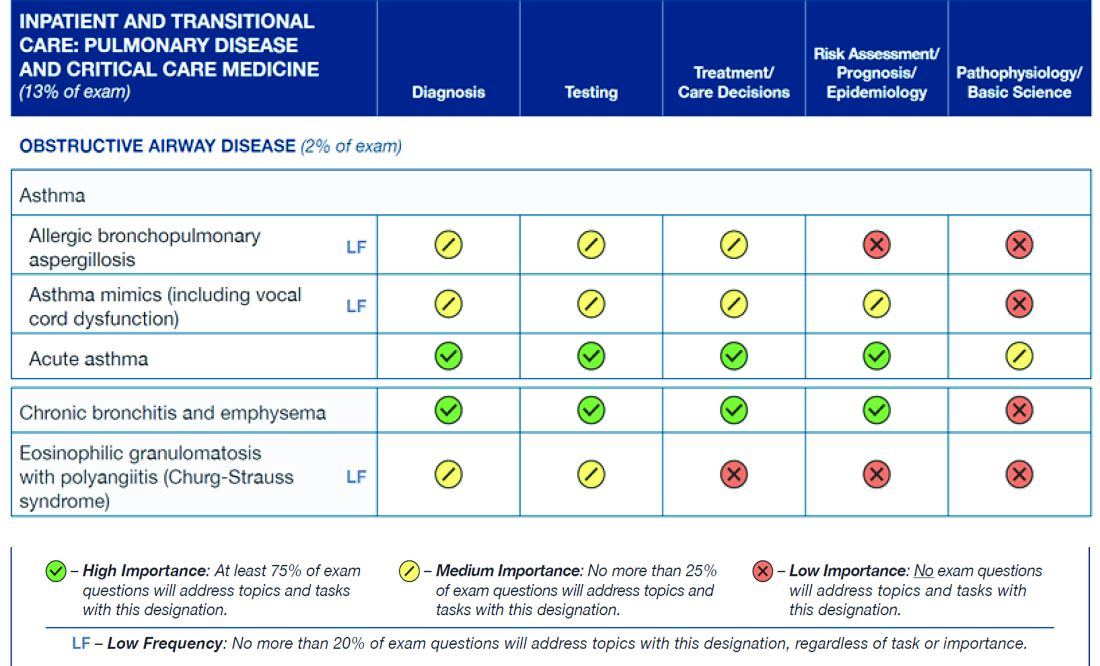
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
The American Board of Internal Medicine (ABIM) has emailed diplomates a survey regarding the blueprint for the Maintenance of Certification (MOC) pulmonary exam.
This survey relates to the content of the exam, as opposed to a prior survey that asked diplomates for their opinion about new proposals for 2- and 5-year cycles for the exam.
Participating in the survey gives diplomates a voice in determining the content of the MOC exam for pulmonary medicine. If enough individuals participate in the survey and the data support changing the distribution of exam content, it is very likely that ABIM will make improvements to the MOC exam.
The figure below illustrates the information provided by diplomates that ABIM used to help them decide the exam content for the Hospital Medicine exam.
Diplomates can find the survey when they log into their respective homepages on the ABIM website at www.abim.org. The survey does not need to be completed in one sitting, but rather can be done one section at a time. It takes approximately 15 minutes to finish each section.
A link to the survey is located in the My Reminders tab.
This is a great opportunity for individuals to make their voices heard.
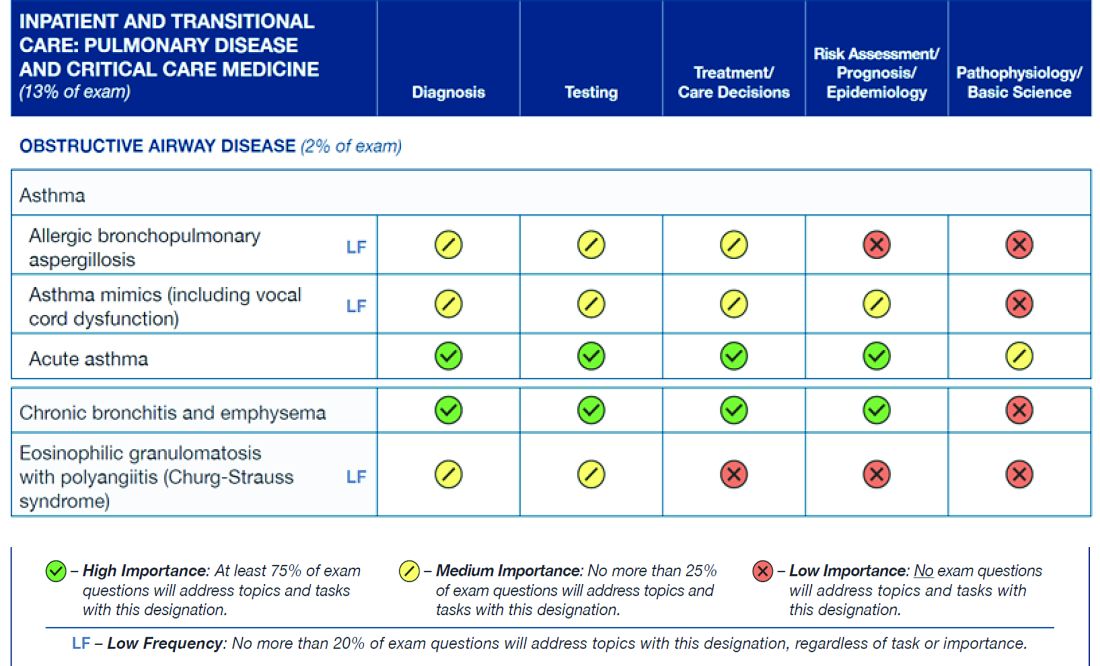
Update on NAMDRC Activities
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.

The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.
The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
The NAMDRC annual meeting will be held March 23-25, 2017, at the Meritage Resort in Napa, California. A variety of excellent speakers and topics of interest to the pulmonary, sleep, and critical care medicine community will be presented, including presentations on the asthma-COPD overlap syndrome, pulmonary hypertension in interstitial lung disease, use of big-data in critical care medicine, cardiovascular risk in obstructive sleep apnea, as well as talks on ICD-10 coding, and updates on practice management and on regulatory topics in pulmonary, critical care, and sleep medicine. Finally, Dr. Mark Kelley, a visiting scholar at the Harvard Business School, will present a special lecture on “What do consumers really value in health care?” Meeting details and a registration form can be found at NAMDRC.org.
The costs of starting a pulmonary rehabilitation program are capital intensive and, generally, only hospitals can afford the start-up and ongoing costs, making pulmonary rehabilitation almost always a hospital service. Cost data from CMS demonstrate that the vast majority of billing for pulmonary rehab comes from hospitals and not from physician practices. By stopping the use of hospital-based clinic billing for new or expanded pulmonary rehabilitation services, this has the likely result of severely limiting the development of new pulmonary rehabilitation programs. If the new site of the rehabilitation program is more than 250 yards away, the hospital must bill under the physician fee schedule for reimbursement. No health care enterprise is likely to expand rehabilitation into new venues with such low reimbursement. The real shame in this scenario is that pulmonary rehabilitation is an effective and very low cost intervention for patients with COPD, and its future is largely being threatened by low reimbursement – making it unattractive for hospitals to open new programs in new space they may have purchased.
What is the fix? NAMDRC has discussed this problem with CMS, pointing out the large likely negative impact on pulmonary rehabilitation. We discussed a possible exemption for pulmonary rehabilitation. The final rule does afford an additional comment period, and we anticipate further discussions with CMS. It is also likely that the American Hospital Association, strongly opposed to this new rule, may seek a legislative fix.
A final area of activity is our ongoing discussion with CMS about updating the archaic guidelines created by CMS that govern how patients can be prescribed a bilevel positive airway pressure (PAP) therapy device for different forms of hypoventilation. The guidelines have been so complicated to follow that many clinicians, often at the request of a durable medical equipment company, have obtained home ventilators for patients for whom it was difficult to get a bilevel PAP. To be sure, hypoventilation disorders are complicated. The different patient types have somewhat different equipment pathways but all are overly complicated and are real barriers to getting these patients the necessary ventilatory equipment, which usually can be a bilevel PAP device. The home ventilator pathway has been easier to use to get therapy provided so many physicians have followed it, but it is also a lot more expensive. However, as of October 2015, CMS has effectively shut down the home ventilator pathway unless the patient has an indwelling invasive airway (i.e., a tracheotomy tube). NAMDRC, working with other sister societies, patient organizations, and others, has developed a strategy to oppose this draconian step. We hope to move CMS in a more rational direction regarding ventilator therapy for a variety of patients with hypoventilation. This work is complicated, but we are determined to do our utmost to bring a contemporary approach to this important area of therapy.
Can We Count on You?
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.
Your donations to the CHEST Foundation unlock knowledge and put it into practice to improve patient outcomes.
CHEST Foundation grant funding for the East African Training Initiative (EATI), for example, will help reduce mortality. Ethiopia bears the burden of high TB and lung disease prevalence. In a country of more than 94 million people, a single pulmonologist was tasked with providing treatment to critically ill patients in a 12-bed ICU. He was armed with a dilapidated facility that had no running water, two functioning ventilators, and no means of performing dialysis. There was no continuity of care at the ICU, and rounds were performed only during the week by rotating departments, few of which were trained in critical care.
This all started to change in 2013, when the EATI, a 2-year fellowship training program in pulmonary and critical care medicine, was launched. With the help of funding from a 2016 CHEST Foundation community service grant, the EATI is establishing infrastructure in Ethiopia to train fellows in pulmonary and critical care medicine for years to come. It is not relief work. The fellows graduating the program go on to set up ICUs in their own hospitals and universities. “As of now, we’ve already graduated five pulmonologists, and we are on track to graduate fifteen by the year 2020,” explained Dr. Joseph Huang, Chairman of Fundraising for the EATI.
The drastic results of reduced mortality rates in the medical ICU have caught the attention of the Ethiopian Ministry of Health. By working directly with the EATI, the ministry established a task force in ICU medicine with a goal to ultimately establish standard protocols in the nation’s ICUs, using the EATI program as a model.
“The CHEST Foundation grant allows us to dive deeper into specialized training and also to sustain and expand the program. Because of this grant, we are able to do workshops on airway management, advanced bronchoscopy, chest tube insertion, and central lines,” Dr. Huang explained. “The fellows have not received this hands-on training before, and allowing them to unlock their knowledge and put it into practice is essential to improving patient outcomes.”
Programs like the EATI are able to continue their work because of generous support from lung health champions like you. Can we count on you to continue your support of the CHEST Foundation during this season of giving? Your tax-deductible gift today will help us reach our goal of $2.5 million to support programs that are changing the future for patients with lung disease all over the world. To make your gift, you can go online to chestnet.org/donate or call the foundation staff at 224/521-9569 to discuss your giving options. Every gift, no matter the size, helps us to achieve our mission to champion lung health by supporting patient education, community service, and clinical research.
As we celebrate our 20th Anniversary this year, we thank you for your steadfast support and dedication to the CHEST Foundation. The last 20 years of success would not have been possible without the tireless commitment of our generous donors and volunteers.