User login
In the Literature
In This Edition
- Pay-for-performance associated with limited benefits on quality in acute myocardial infarction patients.
- Meta-analysis finds increased risk of acute myocardial infarction with use of rosiglitazone.
- Rosiglitazone increases risk of heart failure, but not acute myocardial infarction or death, interim analysis shows.
- Surgery versus prolonged conservative treatment for severe sciatica.
- Predicting poor outcomes in upper gastrointestinal bleeds.
- Discharging patients with unresolved medical issues.
Does Pay for Performance Improve Hospital Quality?
Background: In 2003, the Centers for Medicare and Medicaid Services (CMS) instituted a pay-for-performance (P4P) pilot program in which participating hospitals would be reimbursed more if they met specific quality standards of care for patients with certain conditions, including acute myocardial infarction (AMI). It is unknown if this type of financial incentive produces improvements in the processes or outcomes of care.
Study design: Observational cohort.
Setting: 500 hospitals across the U.S.
Synopsis: This study compared compliance with CMS quality indicators in the treatment of more than 100,000 patients with acute non-ST-elevation myocardial infarction at 54 participating and 446 non-participating hospitals in the P4P pilot. They found no significant difference in mortality or in a composite measure of the six quality indicators but a slight improvement in two of the six quality indicators (aspirin at discharge and smoking cessation counseling). They did not find that P4P adversely affected indicators not subject to financial incentives.
Bottom line: P4P is associated with limited improvements in compliance with CMS quality indicators in patients with AMI.
Citation: Glickman SW, Ou F-S, DeLong ER, et al. Pay for performance, quality of care, and outcomes in acute myocardial infarction. JAMA. 2007 Jun;297(21):2373-2380.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in a Meta-analysis?
Background: Rosiglitazone (Avandia) is one of two approved oral thiazolidinedione drugs used for diabetic control. Muraglitazar, another thiazolidinedione drug, was not approved for market due to adverse cardiovascular outcomes. The cardiovascular effects of rosiglitazone had not previously been evaluated.
Study design: Meta-analysis.
Setting: All clinical trials (published and unpublished) involving rosiglitazone.
Synopsis: The authors reviewed data from all randomized trials of rosiglitazone versus placebo or other drugs for at least 24 weeks. From the 42 included trials (including more than 28,000 patients) researchers found a statistically significant increased risk of the odds of AMI (odds ratio 1.43, confidence interval 1.03-1.98) in the rosiglitazone group, and a non-significant risk of death from any cardiovascular cause (odds ratio 1.64, confidence interval 0.98-2.74) and all-cause mortality (odds ratio 1.18, confidence interval 0.89-1.55). The meta-analysis was criticized due to the small number of events (fewer than 100 acute AMIs in each group) and lack of patient-level data, but one expert wrote that “in view of the potential cardiovascular risks and in the absence of evidence of other health advantages ... the rationale for prescribing rosiglitazone at this time is unclear.”
The study raised larger concerns regarding Food and Drug Administration drug approvals, because the drug was approved due to its effect on lowering blood sugar levels (a surrogate outcome) without enough scrutiny of other patient outcomes.
Bottom line: Rosiglitazone is associated with increased risk of AMI. Alternative oral agents should be considered first for blood sugar control in diabetics.
Citation: Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 Jun;356(24):2457-2471.
Editorial: Psaty BM, Furberg CD. Rosiglitazone and cardiovascular risk. N Engl J Med. 2007 Jun;356(24):2522-2524.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in Interim Analysis?
Background: In response to a meta-analysis, an interim analysis of an ongoing open-label manufacturer-sponsored trial was undertaken to determine the cardiovascular risks of rosiglitazone.
Study design: Unplanned interim analysis of a randomized, multicenter, open-label, non-inferiority trial.
Subjects: Outpatient, inadequately controlled type 2 diabetics.
Synopsis: This was an unplanned interim analysis of an open-label manufacturer-sponsored trial. There were 4,447 inadequately controlled type 2 diabetics on either metformin or sulfonylurea. The patients were randomized to receive both drugs (controls) or add-on rosiglitazone. After a mean follow up of 3.75 years, there was no statistically significant difference between the groups in the primary end point (hospitalization or death from cardiovascular causes), or other end points (MI and death from cardiovascular causes or any cause). However, rosiglitazone was associated with an increased risk of heart failure (hazard ratio 2.15, confidence interval 1.30-3.57). Because this was an unplanned interim analysis for a trial expected to continue for six years, experts caution that the results are inconclusive due to low statistical significance and small event rates.
Bottom line: Rosiglitazone is associated with an increased risk of heart failure, but the risks of hospitalization, death, and acute MI remain unclear.
Citation: Home PD, Phil D, Pockock SJ, et al. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N Engl J Med. 2007 Jul;357(1):28-38.
How Often do Discharged Patients with Unresolved Medical Issues Require Outpatient Workups?
Background: Patients are often discharged from the hospital with incomplete workups, but it is unknown how often and what factors affect the completion of the intended workup.
Study design: Retrospective cohort.
Setting: Single institution teaching hospital.
Synopsis: The authors evaluated the inpatient and outpatient medical records of all patients discharged from the medicine or geriatric service over 18 months. Of almost 700 discharges, 28% of the patients had outpatient workups recommended (48% diagnostic procedures, 35% referrals, and 17% lab tests) by the discharging physician. Completion of the workup did not occur 36% of the time, and the likelihood of non-completion increased with time to the first follow-up appointment and lack of availability of the discharge summary.
Bottom line: Outpatient workups are intended in almost a third of discharged patient, the completion of which can likely be enhanced by timely follow-up and discharge summary availability.
Citation: Moore C, McGinn T, Halm E. Tying up loose ends: discharging patients with unresolved medical issues. Arch Intern Med. 2007;167(12):1305-1311.
Can We Predict Patients at Low Risk for Compli-cations from Acute Upper Gastrointestinal Bleeds?
Background: Although multiple risk-prediction scales exist for patients with upper gastrointestinal (UGI) bleeds, few have been prospectively validated or widely used in clinical practice.
Study design: Prospective cohort.
Setting: Veterans Affairs (VA) hospitals.
Synopsis: VA researchers created and validated a risk predictor in 391 patients with acute upper gastrointestinal bleeding. Data from the derivation set (two-thirds of the patients) was used to create the model tested on the validation set (one-third of the patients). Outcome one (re-bleeding, need for intervention to stop bleeding, or all-cause hospital mortality) was predicted by an APACHE score >11, stigmata of recent bleeding, or varices. Outcome two (outcome one plus new/worsening co-morbidity) was predicted by the above three factors plus an unstable co-morbidity at admission. In the validation group, outcome one occurred in 1%, 5%, and 25% of patients with zero, one, and two or more factors. Outcome two occurred in 6%, 18%, and 49%, respectively. A score of zero accurately identified 93% and 91% of patients for outcomes one and two. The authors speculated that these patients could be safely treated as outpatients. The study excluded patients on anticoagulation, and this VA cohort (99% male) may not be generalizable to other populations.
Bottom line: This validated prediction model can accurately predict more than 90% of patients at low-risk of poor outcomes with UGI bleeding, which could be used to stratify patients in need of hospital admission.
Citation: Imperiale TF, Dominitz JA, Provenzale DT, et al. Predicting poor outcome from acute upper gastrointestinal hemorrhage. Arch Intern Med. 2007 Jun;167(12):1291-1296.
Does Surgery or Conservative Therapy Improve Symptoms of Sciatica Faster?
Background: The optimal timing and benefit of lumbar-disk surgery in patients with symptomatic lumbar disk herniation is unknown.
Study design: Multicenter randomized trial.
Setting: Netherlands.
Synopsis: 283 patients with severe sciatica were randomly chosen to receive early surgery or conservative treatment (with surgery as needed) for six to 12 weeks. The methods for determining the three primary outcomes were: score on the Roland Disability Questionnaire, leg pain score, and self-report of perceived recovery. At one year, 89% of the surgery group and 39% of the control group underwent surgery after a mean of 2.2 and 18.7 weeks, respectively. There was no difference between the groups in the disability score, but time to relief of leg pain and recovery was faster in the surgery group. At one year, 95% in each group reported perceived recovery.
Bottom line: Rates of pain relief and perceived recovery are faster with early surgery than conservative treatment in patients with severe sciatica, but one-year recovery rates are the same. TH
Citation: Peul WC, Van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. NEJM. 2007 May;356(22):2245-2256.
In This Edition
- Pay-for-performance associated with limited benefits on quality in acute myocardial infarction patients.
- Meta-analysis finds increased risk of acute myocardial infarction with use of rosiglitazone.
- Rosiglitazone increases risk of heart failure, but not acute myocardial infarction or death, interim analysis shows.
- Surgery versus prolonged conservative treatment for severe sciatica.
- Predicting poor outcomes in upper gastrointestinal bleeds.
- Discharging patients with unresolved medical issues.
Does Pay for Performance Improve Hospital Quality?
Background: In 2003, the Centers for Medicare and Medicaid Services (CMS) instituted a pay-for-performance (P4P) pilot program in which participating hospitals would be reimbursed more if they met specific quality standards of care for patients with certain conditions, including acute myocardial infarction (AMI). It is unknown if this type of financial incentive produces improvements in the processes or outcomes of care.
Study design: Observational cohort.
Setting: 500 hospitals across the U.S.
Synopsis: This study compared compliance with CMS quality indicators in the treatment of more than 100,000 patients with acute non-ST-elevation myocardial infarction at 54 participating and 446 non-participating hospitals in the P4P pilot. They found no significant difference in mortality or in a composite measure of the six quality indicators but a slight improvement in two of the six quality indicators (aspirin at discharge and smoking cessation counseling). They did not find that P4P adversely affected indicators not subject to financial incentives.
Bottom line: P4P is associated with limited improvements in compliance with CMS quality indicators in patients with AMI.
Citation: Glickman SW, Ou F-S, DeLong ER, et al. Pay for performance, quality of care, and outcomes in acute myocardial infarction. JAMA. 2007 Jun;297(21):2373-2380.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in a Meta-analysis?
Background: Rosiglitazone (Avandia) is one of two approved oral thiazolidinedione drugs used for diabetic control. Muraglitazar, another thiazolidinedione drug, was not approved for market due to adverse cardiovascular outcomes. The cardiovascular effects of rosiglitazone had not previously been evaluated.
Study design: Meta-analysis.
Setting: All clinical trials (published and unpublished) involving rosiglitazone.
Synopsis: The authors reviewed data from all randomized trials of rosiglitazone versus placebo or other drugs for at least 24 weeks. From the 42 included trials (including more than 28,000 patients) researchers found a statistically significant increased risk of the odds of AMI (odds ratio 1.43, confidence interval 1.03-1.98) in the rosiglitazone group, and a non-significant risk of death from any cardiovascular cause (odds ratio 1.64, confidence interval 0.98-2.74) and all-cause mortality (odds ratio 1.18, confidence interval 0.89-1.55). The meta-analysis was criticized due to the small number of events (fewer than 100 acute AMIs in each group) and lack of patient-level data, but one expert wrote that “in view of the potential cardiovascular risks and in the absence of evidence of other health advantages ... the rationale for prescribing rosiglitazone at this time is unclear.”
The study raised larger concerns regarding Food and Drug Administration drug approvals, because the drug was approved due to its effect on lowering blood sugar levels (a surrogate outcome) without enough scrutiny of other patient outcomes.
Bottom line: Rosiglitazone is associated with increased risk of AMI. Alternative oral agents should be considered first for blood sugar control in diabetics.
Citation: Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 Jun;356(24):2457-2471.
Editorial: Psaty BM, Furberg CD. Rosiglitazone and cardiovascular risk. N Engl J Med. 2007 Jun;356(24):2522-2524.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in Interim Analysis?
Background: In response to a meta-analysis, an interim analysis of an ongoing open-label manufacturer-sponsored trial was undertaken to determine the cardiovascular risks of rosiglitazone.
Study design: Unplanned interim analysis of a randomized, multicenter, open-label, non-inferiority trial.
Subjects: Outpatient, inadequately controlled type 2 diabetics.
Synopsis: This was an unplanned interim analysis of an open-label manufacturer-sponsored trial. There were 4,447 inadequately controlled type 2 diabetics on either metformin or sulfonylurea. The patients were randomized to receive both drugs (controls) or add-on rosiglitazone. After a mean follow up of 3.75 years, there was no statistically significant difference between the groups in the primary end point (hospitalization or death from cardiovascular causes), or other end points (MI and death from cardiovascular causes or any cause). However, rosiglitazone was associated with an increased risk of heart failure (hazard ratio 2.15, confidence interval 1.30-3.57). Because this was an unplanned interim analysis for a trial expected to continue for six years, experts caution that the results are inconclusive due to low statistical significance and small event rates.
Bottom line: Rosiglitazone is associated with an increased risk of heart failure, but the risks of hospitalization, death, and acute MI remain unclear.
Citation: Home PD, Phil D, Pockock SJ, et al. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N Engl J Med. 2007 Jul;357(1):28-38.
How Often do Discharged Patients with Unresolved Medical Issues Require Outpatient Workups?
Background: Patients are often discharged from the hospital with incomplete workups, but it is unknown how often and what factors affect the completion of the intended workup.
Study design: Retrospective cohort.
Setting: Single institution teaching hospital.
Synopsis: The authors evaluated the inpatient and outpatient medical records of all patients discharged from the medicine or geriatric service over 18 months. Of almost 700 discharges, 28% of the patients had outpatient workups recommended (48% diagnostic procedures, 35% referrals, and 17% lab tests) by the discharging physician. Completion of the workup did not occur 36% of the time, and the likelihood of non-completion increased with time to the first follow-up appointment and lack of availability of the discharge summary.
Bottom line: Outpatient workups are intended in almost a third of discharged patient, the completion of which can likely be enhanced by timely follow-up and discharge summary availability.
Citation: Moore C, McGinn T, Halm E. Tying up loose ends: discharging patients with unresolved medical issues. Arch Intern Med. 2007;167(12):1305-1311.
Can We Predict Patients at Low Risk for Compli-cations from Acute Upper Gastrointestinal Bleeds?
Background: Although multiple risk-prediction scales exist for patients with upper gastrointestinal (UGI) bleeds, few have been prospectively validated or widely used in clinical practice.
Study design: Prospective cohort.
Setting: Veterans Affairs (VA) hospitals.
Synopsis: VA researchers created and validated a risk predictor in 391 patients with acute upper gastrointestinal bleeding. Data from the derivation set (two-thirds of the patients) was used to create the model tested on the validation set (one-third of the patients). Outcome one (re-bleeding, need for intervention to stop bleeding, or all-cause hospital mortality) was predicted by an APACHE score >11, stigmata of recent bleeding, or varices. Outcome two (outcome one plus new/worsening co-morbidity) was predicted by the above three factors plus an unstable co-morbidity at admission. In the validation group, outcome one occurred in 1%, 5%, and 25% of patients with zero, one, and two or more factors. Outcome two occurred in 6%, 18%, and 49%, respectively. A score of zero accurately identified 93% and 91% of patients for outcomes one and two. The authors speculated that these patients could be safely treated as outpatients. The study excluded patients on anticoagulation, and this VA cohort (99% male) may not be generalizable to other populations.
Bottom line: This validated prediction model can accurately predict more than 90% of patients at low-risk of poor outcomes with UGI bleeding, which could be used to stratify patients in need of hospital admission.
Citation: Imperiale TF, Dominitz JA, Provenzale DT, et al. Predicting poor outcome from acute upper gastrointestinal hemorrhage. Arch Intern Med. 2007 Jun;167(12):1291-1296.
Does Surgery or Conservative Therapy Improve Symptoms of Sciatica Faster?
Background: The optimal timing and benefit of lumbar-disk surgery in patients with symptomatic lumbar disk herniation is unknown.
Study design: Multicenter randomized trial.
Setting: Netherlands.
Synopsis: 283 patients with severe sciatica were randomly chosen to receive early surgery or conservative treatment (with surgery as needed) for six to 12 weeks. The methods for determining the three primary outcomes were: score on the Roland Disability Questionnaire, leg pain score, and self-report of perceived recovery. At one year, 89% of the surgery group and 39% of the control group underwent surgery after a mean of 2.2 and 18.7 weeks, respectively. There was no difference between the groups in the disability score, but time to relief of leg pain and recovery was faster in the surgery group. At one year, 95% in each group reported perceived recovery.
Bottom line: Rates of pain relief and perceived recovery are faster with early surgery than conservative treatment in patients with severe sciatica, but one-year recovery rates are the same. TH
Citation: Peul WC, Van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. NEJM. 2007 May;356(22):2245-2256.
In This Edition
- Pay-for-performance associated with limited benefits on quality in acute myocardial infarction patients.
- Meta-analysis finds increased risk of acute myocardial infarction with use of rosiglitazone.
- Rosiglitazone increases risk of heart failure, but not acute myocardial infarction or death, interim analysis shows.
- Surgery versus prolonged conservative treatment for severe sciatica.
- Predicting poor outcomes in upper gastrointestinal bleeds.
- Discharging patients with unresolved medical issues.
Does Pay for Performance Improve Hospital Quality?
Background: In 2003, the Centers for Medicare and Medicaid Services (CMS) instituted a pay-for-performance (P4P) pilot program in which participating hospitals would be reimbursed more if they met specific quality standards of care for patients with certain conditions, including acute myocardial infarction (AMI). It is unknown if this type of financial incentive produces improvements in the processes or outcomes of care.
Study design: Observational cohort.
Setting: 500 hospitals across the U.S.
Synopsis: This study compared compliance with CMS quality indicators in the treatment of more than 100,000 patients with acute non-ST-elevation myocardial infarction at 54 participating and 446 non-participating hospitals in the P4P pilot. They found no significant difference in mortality or in a composite measure of the six quality indicators but a slight improvement in two of the six quality indicators (aspirin at discharge and smoking cessation counseling). They did not find that P4P adversely affected indicators not subject to financial incentives.
Bottom line: P4P is associated with limited improvements in compliance with CMS quality indicators in patients with AMI.
Citation: Glickman SW, Ou F-S, DeLong ER, et al. Pay for performance, quality of care, and outcomes in acute myocardial infarction. JAMA. 2007 Jun;297(21):2373-2380.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in a Meta-analysis?
Background: Rosiglitazone (Avandia) is one of two approved oral thiazolidinedione drugs used for diabetic control. Muraglitazar, another thiazolidinedione drug, was not approved for market due to adverse cardiovascular outcomes. The cardiovascular effects of rosiglitazone had not previously been evaluated.
Study design: Meta-analysis.
Setting: All clinical trials (published and unpublished) involving rosiglitazone.
Synopsis: The authors reviewed data from all randomized trials of rosiglitazone versus placebo or other drugs for at least 24 weeks. From the 42 included trials (including more than 28,000 patients) researchers found a statistically significant increased risk of the odds of AMI (odds ratio 1.43, confidence interval 1.03-1.98) in the rosiglitazone group, and a non-significant risk of death from any cardiovascular cause (odds ratio 1.64, confidence interval 0.98-2.74) and all-cause mortality (odds ratio 1.18, confidence interval 0.89-1.55). The meta-analysis was criticized due to the small number of events (fewer than 100 acute AMIs in each group) and lack of patient-level data, but one expert wrote that “in view of the potential cardiovascular risks and in the absence of evidence of other health advantages ... the rationale for prescribing rosiglitazone at this time is unclear.”
The study raised larger concerns regarding Food and Drug Administration drug approvals, because the drug was approved due to its effect on lowering blood sugar levels (a surrogate outcome) without enough scrutiny of other patient outcomes.
Bottom line: Rosiglitazone is associated with increased risk of AMI. Alternative oral agents should be considered first for blood sugar control in diabetics.
Citation: Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 Jun;356(24):2457-2471.
Editorial: Psaty BM, Furberg CD. Rosiglitazone and cardiovascular risk. N Engl J Med. 2007 Jun;356(24):2522-2524.
Is Rosiglitazone Associated with Adverse Cardiovascular Outcomes in Interim Analysis?
Background: In response to a meta-analysis, an interim analysis of an ongoing open-label manufacturer-sponsored trial was undertaken to determine the cardiovascular risks of rosiglitazone.
Study design: Unplanned interim analysis of a randomized, multicenter, open-label, non-inferiority trial.
Subjects: Outpatient, inadequately controlled type 2 diabetics.
Synopsis: This was an unplanned interim analysis of an open-label manufacturer-sponsored trial. There were 4,447 inadequately controlled type 2 diabetics on either metformin or sulfonylurea. The patients were randomized to receive both drugs (controls) or add-on rosiglitazone. After a mean follow up of 3.75 years, there was no statistically significant difference between the groups in the primary end point (hospitalization or death from cardiovascular causes), or other end points (MI and death from cardiovascular causes or any cause). However, rosiglitazone was associated with an increased risk of heart failure (hazard ratio 2.15, confidence interval 1.30-3.57). Because this was an unplanned interim analysis for a trial expected to continue for six years, experts caution that the results are inconclusive due to low statistical significance and small event rates.
Bottom line: Rosiglitazone is associated with an increased risk of heart failure, but the risks of hospitalization, death, and acute MI remain unclear.
Citation: Home PD, Phil D, Pockock SJ, et al. Rosiglitazone evaluated for cardiovascular outcomes—an interim analysis. N Engl J Med. 2007 Jul;357(1):28-38.
How Often do Discharged Patients with Unresolved Medical Issues Require Outpatient Workups?
Background: Patients are often discharged from the hospital with incomplete workups, but it is unknown how often and what factors affect the completion of the intended workup.
Study design: Retrospective cohort.
Setting: Single institution teaching hospital.
Synopsis: The authors evaluated the inpatient and outpatient medical records of all patients discharged from the medicine or geriatric service over 18 months. Of almost 700 discharges, 28% of the patients had outpatient workups recommended (48% diagnostic procedures, 35% referrals, and 17% lab tests) by the discharging physician. Completion of the workup did not occur 36% of the time, and the likelihood of non-completion increased with time to the first follow-up appointment and lack of availability of the discharge summary.
Bottom line: Outpatient workups are intended in almost a third of discharged patient, the completion of which can likely be enhanced by timely follow-up and discharge summary availability.
Citation: Moore C, McGinn T, Halm E. Tying up loose ends: discharging patients with unresolved medical issues. Arch Intern Med. 2007;167(12):1305-1311.
Can We Predict Patients at Low Risk for Compli-cations from Acute Upper Gastrointestinal Bleeds?
Background: Although multiple risk-prediction scales exist for patients with upper gastrointestinal (UGI) bleeds, few have been prospectively validated or widely used in clinical practice.
Study design: Prospective cohort.
Setting: Veterans Affairs (VA) hospitals.
Synopsis: VA researchers created and validated a risk predictor in 391 patients with acute upper gastrointestinal bleeding. Data from the derivation set (two-thirds of the patients) was used to create the model tested on the validation set (one-third of the patients). Outcome one (re-bleeding, need for intervention to stop bleeding, or all-cause hospital mortality) was predicted by an APACHE score >11, stigmata of recent bleeding, or varices. Outcome two (outcome one plus new/worsening co-morbidity) was predicted by the above three factors plus an unstable co-morbidity at admission. In the validation group, outcome one occurred in 1%, 5%, and 25% of patients with zero, one, and two or more factors. Outcome two occurred in 6%, 18%, and 49%, respectively. A score of zero accurately identified 93% and 91% of patients for outcomes one and two. The authors speculated that these patients could be safely treated as outpatients. The study excluded patients on anticoagulation, and this VA cohort (99% male) may not be generalizable to other populations.
Bottom line: This validated prediction model can accurately predict more than 90% of patients at low-risk of poor outcomes with UGI bleeding, which could be used to stratify patients in need of hospital admission.
Citation: Imperiale TF, Dominitz JA, Provenzale DT, et al. Predicting poor outcome from acute upper gastrointestinal hemorrhage. Arch Intern Med. 2007 Jun;167(12):1291-1296.
Does Surgery or Conservative Therapy Improve Symptoms of Sciatica Faster?
Background: The optimal timing and benefit of lumbar-disk surgery in patients with symptomatic lumbar disk herniation is unknown.
Study design: Multicenter randomized trial.
Setting: Netherlands.
Synopsis: 283 patients with severe sciatica were randomly chosen to receive early surgery or conservative treatment (with surgery as needed) for six to 12 weeks. The methods for determining the three primary outcomes were: score on the Roland Disability Questionnaire, leg pain score, and self-report of perceived recovery. At one year, 89% of the surgery group and 39% of the control group underwent surgery after a mean of 2.2 and 18.7 weeks, respectively. There was no difference between the groups in the disability score, but time to relief of leg pain and recovery was faster in the surgery group. At one year, 95% in each group reported perceived recovery.
Bottom line: Rates of pain relief and perceived recovery are faster with early surgery than conservative treatment in patients with severe sciatica, but one-year recovery rates are the same. TH
Citation: Peul WC, Van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. NEJM. 2007 May;356(22):2245-2256.
The Life of a Task Force
The Performance and Standards Task Force (PSTF) was formed a little more than a year ago after SHM leadership recognized the need for a coordinated approach to working with external organizations in the performance and standards quality arena.
As SHM’s senior adviser for quality standards and compliance, I work with PSTF Chairman Patrick Torcson, MD, (medical director of hospital medicine at the St. Tammany Parish Hospital in Covington, La.) along with senior staff and leadership of the Public Policy Committee (PPC). We monitor the performance and quality landscape at national organizations charged with measuring development and building consensus. We also develop relationships with other professional medical societies and organizations.
Chapters Summary
Chicago
The Chicago Chapter of SHM met June 7. Attendees came from organizations such as Signature Healthcare Solutions, Advocate Healthcare, Northwestern University, and University of Chicago. The meeting began with an update from the SHM national annual meeting given by Chapter President Tarek Karaman, MD, lead hospitalist, Advocate Health Centers, and hospitalist program director, Department of Internal Medicine, Advocate Illinois Masonic Medical Center, Chicago. This was followed by a presentation on DVT/pulmonary embolism prophylaxis and treatment from SHM board member Alpesh Amin, MD, executive director of the hospitalist program and vice chair for clinical affairs and quality in the department of medicine at the University of California, Irvine. For the first time, the chapter had a panel discussion with two primary care physicians from Northwestern University. John Butter, MD, and Sean O’Conner, MD, shared their thoughts regarding the interaction between primary care physicians and hospitalists. Ideas were given on how to strengthen working relationships between the two.
St. Louis

Since its inception in spring 2006, the PSTF has become engaged in the American Medical Association’s (AMA) Physician Consortium for Performance Improvement (PCPI) and the National Quality Forum (NQF). The NQF is a nonprofit organization instructed by Congress to endorse consensus-based national standards for measurement and public reporting of healthcare performance data. Specifically, NQF aims to influence the development of physician-level performance measures as part of the Centers for Medicare and Medicaid Service’s (CMS) Physician Quality Reporting Initiative (PQRI).
By joining the PCPI, SHM has aligned with other medical specialties to develop performance measures in geriatrics, emergency medicine, outpatient parenteral antimicrobial therapy, and facets of anesthesiology such as perioperative normothermia and critical care.
Additionally, SHM has given feedback during public comment periods on perioperative care, chronic kidney disease, and other measures. The task force continues to evaluate which workgroups it should appoint members to participate in, depending on the topic.
SHM leadership has continued to foster relationships with CMS by sending letters in support of the 2007 PQRI. SHM was able to influence changes to the 2007 measure specifications so hospitalists would have measures to report. Of the 74 measures included in the PQRI, 11 have specifications allowing reporting by hospitalists, underscoring the importance of SHM’s influence and participation in the PCPI process.
Dr. Torcson and Eric Siegal, MD, (regional medical director, Cogent Healthcare, Madison, Wis.) co-chaired a CMS-led SHM member conference call focused on PQRI and how it affects hospitalists. The program was well received by SHM members.
When SHM became a member of the NQF last summer, it nominated several members who were selected to participate on various technical advisory panels overseeing work on the development of consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), is addressing patient safety, pediatrics, and inpatient care.
Last fall, SHM sent Mark Williams, MD (professor of medicine at Emory University School of Medicine in Atlanta and editor of The Journal of Hospital Medicine) to the NQF’s 7th Annual Meeting, a National Policy Conference on Quality. The meeting featured plenary sessions that focused on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, leading professional and trade associations in improving healthcare quality, and efforts under way in the federal government to foster healthcare improvements.
This fall, Greg Seymann, MD, will attend the 8th Annual Meeting. Dr. Seymann is an assistant professor with the Department of Medicine, Hospital Medicine Program, at the University of California San Diego Medical Center.
Goals for 2008, Beyond
By taking an active role in the performance and standard arena, SHM senior staff and leadership have been able to build key relationships. This has paved the way for influencing the current physician reporting program and taking the lead on developing measures that will most reflect hospital medicine in the future.
The task force intends to be at the helm of the development of performance measures that more accurately reflect services provided by hospitalists. Senior staff and leadership have discussed this goal with several national stakeholders including the PCPI and the NQF, whose senior staff have supported its agenda.
In July, SHM, along with the American College of Physicians (ACP), the Society of General Internal Medicine (SGIM), and the American Geriatrics Society (AGS), formed a steering committee to convene a transitions of care consensus conference. This multispecialty, multidisciplinary group reviewed the principles and standards that came from the ABIM Foundation’s Stepping Up to the Plate (SUTTP) Alliance, which met this spring. SHM and PCPI are working to form an expert workgroup that will develop six to eight care transitions measures for inclusion in the 2009 PQRI.
SHM also is exploring collaboration with the American Hospital Association and its Hospital Quality Alliance (HQA), which coordinates the promotion of quality measurement, transparency, and improvement in the hospital setting.
In addition to its work with these external national groups, task force members would also like to start a resource room on the SHM Web site, www.hospitalmedicine.org, which would be devoted to member efforts in research related to quality and performance standards, as well as the member go-to place for tools and references on best practices in performance standards and pay for reporting initiatives.
Finally, Dr. Torcson hopes to shape and disseminate a national research agenda for hospitalist performance measurement and reporting. TH
SHM Behind the Scenes
Quality is our Middle Name
By Geri Barnes
The Education and Quality Initiatives Department’s (EQID) mission is to lead and manage an integrative program that brings resources to improve patient care. With the help of many individuals and partner organizations, SHM is working toward improved care for inpatients. Let’s review our progress as we begin the second quarter of SHM’s fiscal year.
Educational Programs
Our focus over the past few months has been the development of “Hospital Medicine 2008,” which will be held April 3-5 in San Diego. Under the leadership of Sylvia McKean, MD, head of the hospitalist service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School in Boston, the Annual Meeting Committee has developed an innovative program. The session will include a new evidence-based rapid fire track and a new teaching skills pre-course for academic and clinical educators. EQID obtains CMEs, communicates with faculty, and fine-tunes logistical efforts.
Leadership Academy Level I is a mainstay of SHM’s educational efforts. EQID supports Eric Howell, MD, chair of the Leadership Committee, as it focuses on addressing attendee input and encouraging the revision of the program in a continuous quality improvement effort. Dr. Howell is director of the Collaborative Inpatient Medicine Service and director of the Zieve Medical Services for Johns Hopkins Bayview Medical Center in Baltimore.
Along with Level I, Leadership Academy Level II will be presented again this year Nov. 5-8 in San Antonio. It builds on the success of last fall’s first offering by expanding on the concepts presented in the Level I academy.
A new educational initiative, supported by Sanofi-Aventis, provides three training sessions at regional chapters or other designated meetings across the country. The meetings educate hospitalists on best practices for glycemic control, prevention of venous thromboembolism, and transitions of care. Meetings will highlight successful interventions as outlined in the respective quality improvement (QI) implementation guides and resource rooms. Meetings will aim to include 20 to 50 participants.
The last piece of the SHM Heart Failure Quality Improvement Initiative is in its final planning stages, and a third CME module for Team Communications as it relates to the heart failure patient will be developed in the coming months. This initiative is supported in part by Scios Inc. and led by Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.
Quality Initiatives
Over the past several years, SHM has developed initiatives that range from convening a panel to assess the state of the art of a QI intervention to developing a Web-based resource room. Projects EQID is involved with:
- SHM is in the early stages of a three-year effort to develop resources and programs for improving hospital care transitions for older adults. This is supported through a major grant from the John A. Hartford Foundation in New York City, under the leadership of Mark Williams, MD, and Eric Coleman, MD, MPH. Dr. Williams is chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and editor of the Journal of Hospital Medicine. Dr. Coleman is associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora.
- “The Heart Failure Quality Improvement Implementation Guide” has been updated. The Heart Failure Resource Room on SHM’s Web site has been redesigned to make it easier for visitors who wish to follow the process of developing a QI intervention related to care of the hospitalized heart failure patient. We are communicating these changes to the hospital medicine community. Supported in part by Scios Inc., based in Mountain View, Calif., this effort includes presentations at regional meetings. This project was led by Nurcan Ilksoy, MD, assistant professor of Medicine at Emory University School of Medicine in Atlanta.
- The VTE Prevention Collaborative is open to all members implementing a QI program to combat venous thromboembolism in the hospitalized patient. The Sanofi-Aventis-supported collaborative uses seasoned QI leaders as mentors. Greg Maynard, MD, MS, and Jason Stein, MD, lead the enrollees through the QI process. The mentees have the benefit of regularly scheduled calls to ask questions and receive instant feedback on their process and progress. An add-on to this program, funded by the Kettering Foundation of Dayton, Ohio, provides the opportunity for on-site consultations. Dr. Maynard is head of the Division of Hospital Medicine and associate clinical professor of medicine at the University of California-San Diego. Dr. Stein is a hospitalist at Atlanta’s Emory University Hospital, assistant professor of Medicine at Emory University School of Medicine, and director of Quality Improvement for the Emory Hospital Medicine Unit.
- An expert panel convened in July to kick off development of an Acute Coronary Syndrome Resource Room and determine the content the resource room will cover. Content address diagnosis and risk stratification, medication, interventional procedures, patient education, transitions, and care coordination. This initiative is being led by Chad Whelan, MD, and is supported in part by Bristol-Myers Squibb Company, New York City. Dr. Whelan is an academic hospitalist and an assistant professor of medicine at University of Chicago in the Section of General Internal Medicine.
- SHM often studies strategies to improve patient satisfaction, outcomes, length of stay, and other important metrics. An expert panel assesses observation units as they contribute to improved treatment of patients with acute decompensated heart failure, chest pain, and other clinical conditions such as asthma. A white paper is pending on the use and value of observation units. Support for the meeting and development and distribution of the white paper was provided by Scios Inc.
Committee Support
A major staff role is the support of the Education and Hospital Quality and Patient Safety (HQPS) committees, the groups that direct and drive SHM in these important areas. The Education Committee, led by Chairman Bill Rifkin, MD, assistant professor of medicine at Yale University School of Medicine in New Haven, Conn., is focusing on:
- Developing the teaching skills pre-course that will be presented at the 2008 Annual Meeting;
- Defining a workable strategy to promote The Core Competencies in Hospital Medicine;
- Developing educational and/or communication modalities that support maintenance of certification; and
- Further defining the direction of the committee to meet members’ educational needs.
Janet Nagamine, MD, leads the HQPS Committee in the following priorities:
- Planning and holding a quality summit to define goals and priorities for the next three to five years;
- Submitting a grant application to AHRQ to support a multidisciplinary conference in the area of medication reconciliation;
- Developing SHM’s role in care transitions;
- Reviewing quality pre-course information and determining the curriculum for ‘‘Hospital Medicine 2008”; and
- Developing the Quality track for ‘‘Hospital Medicine 2008.”
The Performance and Standards Task Force (PSTF) was formed a little more than a year ago after SHM leadership recognized the need for a coordinated approach to working with external organizations in the performance and standards quality arena.
As SHM’s senior adviser for quality standards and compliance, I work with PSTF Chairman Patrick Torcson, MD, (medical director of hospital medicine at the St. Tammany Parish Hospital in Covington, La.) along with senior staff and leadership of the Public Policy Committee (PPC). We monitor the performance and quality landscape at national organizations charged with measuring development and building consensus. We also develop relationships with other professional medical societies and organizations.
Chapters Summary
Chicago
The Chicago Chapter of SHM met June 7. Attendees came from organizations such as Signature Healthcare Solutions, Advocate Healthcare, Northwestern University, and University of Chicago. The meeting began with an update from the SHM national annual meeting given by Chapter President Tarek Karaman, MD, lead hospitalist, Advocate Health Centers, and hospitalist program director, Department of Internal Medicine, Advocate Illinois Masonic Medical Center, Chicago. This was followed by a presentation on DVT/pulmonary embolism prophylaxis and treatment from SHM board member Alpesh Amin, MD, executive director of the hospitalist program and vice chair for clinical affairs and quality in the department of medicine at the University of California, Irvine. For the first time, the chapter had a panel discussion with two primary care physicians from Northwestern University. John Butter, MD, and Sean O’Conner, MD, shared their thoughts regarding the interaction between primary care physicians and hospitalists. Ideas were given on how to strengthen working relationships between the two.
St. Louis
Since its inception in spring 2006, the PSTF has become engaged in the American Medical Association’s (AMA) Physician Consortium for Performance Improvement (PCPI) and the National Quality Forum (NQF). The NQF is a nonprofit organization instructed by Congress to endorse consensus-based national standards for measurement and public reporting of healthcare performance data. Specifically, NQF aims to influence the development of physician-level performance measures as part of the Centers for Medicare and Medicaid Service’s (CMS) Physician Quality Reporting Initiative (PQRI).
By joining the PCPI, SHM has aligned with other medical specialties to develop performance measures in geriatrics, emergency medicine, outpatient parenteral antimicrobial therapy, and facets of anesthesiology such as perioperative normothermia and critical care.
Additionally, SHM has given feedback during public comment periods on perioperative care, chronic kidney disease, and other measures. The task force continues to evaluate which workgroups it should appoint members to participate in, depending on the topic.
SHM leadership has continued to foster relationships with CMS by sending letters in support of the 2007 PQRI. SHM was able to influence changes to the 2007 measure specifications so hospitalists would have measures to report. Of the 74 measures included in the PQRI, 11 have specifications allowing reporting by hospitalists, underscoring the importance of SHM’s influence and participation in the PCPI process.
Dr. Torcson and Eric Siegal, MD, (regional medical director, Cogent Healthcare, Madison, Wis.) co-chaired a CMS-led SHM member conference call focused on PQRI and how it affects hospitalists. The program was well received by SHM members.
When SHM became a member of the NQF last summer, it nominated several members who were selected to participate on various technical advisory panels overseeing work on the development of consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), is addressing patient safety, pediatrics, and inpatient care.
Last fall, SHM sent Mark Williams, MD (professor of medicine at Emory University School of Medicine in Atlanta and editor of The Journal of Hospital Medicine) to the NQF’s 7th Annual Meeting, a National Policy Conference on Quality. The meeting featured plenary sessions that focused on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, leading professional and trade associations in improving healthcare quality, and efforts under way in the federal government to foster healthcare improvements.
This fall, Greg Seymann, MD, will attend the 8th Annual Meeting. Dr. Seymann is an assistant professor with the Department of Medicine, Hospital Medicine Program, at the University of California San Diego Medical Center.
Goals for 2008, Beyond
By taking an active role in the performance and standard arena, SHM senior staff and leadership have been able to build key relationships. This has paved the way for influencing the current physician reporting program and taking the lead on developing measures that will most reflect hospital medicine in the future.
The task force intends to be at the helm of the development of performance measures that more accurately reflect services provided by hospitalists. Senior staff and leadership have discussed this goal with several national stakeholders including the PCPI and the NQF, whose senior staff have supported its agenda.
In July, SHM, along with the American College of Physicians (ACP), the Society of General Internal Medicine (SGIM), and the American Geriatrics Society (AGS), formed a steering committee to convene a transitions of care consensus conference. This multispecialty, multidisciplinary group reviewed the principles and standards that came from the ABIM Foundation’s Stepping Up to the Plate (SUTTP) Alliance, which met this spring. SHM and PCPI are working to form an expert workgroup that will develop six to eight care transitions measures for inclusion in the 2009 PQRI.
SHM also is exploring collaboration with the American Hospital Association and its Hospital Quality Alliance (HQA), which coordinates the promotion of quality measurement, transparency, and improvement in the hospital setting.
In addition to its work with these external national groups, task force members would also like to start a resource room on the SHM Web site, www.hospitalmedicine.org, which would be devoted to member efforts in research related to quality and performance standards, as well as the member go-to place for tools and references on best practices in performance standards and pay for reporting initiatives.
Finally, Dr. Torcson hopes to shape and disseminate a national research agenda for hospitalist performance measurement and reporting. TH
SHM Behind the Scenes
Quality is our Middle Name
By Geri Barnes
The Education and Quality Initiatives Department’s (EQID) mission is to lead and manage an integrative program that brings resources to improve patient care. With the help of many individuals and partner organizations, SHM is working toward improved care for inpatients. Let’s review our progress as we begin the second quarter of SHM’s fiscal year.
Educational Programs
Our focus over the past few months has been the development of “Hospital Medicine 2008,” which will be held April 3-5 in San Diego. Under the leadership of Sylvia McKean, MD, head of the hospitalist service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School in Boston, the Annual Meeting Committee has developed an innovative program. The session will include a new evidence-based rapid fire track and a new teaching skills pre-course for academic and clinical educators. EQID obtains CMEs, communicates with faculty, and fine-tunes logistical efforts.
Leadership Academy Level I is a mainstay of SHM’s educational efforts. EQID supports Eric Howell, MD, chair of the Leadership Committee, as it focuses on addressing attendee input and encouraging the revision of the program in a continuous quality improvement effort. Dr. Howell is director of the Collaborative Inpatient Medicine Service and director of the Zieve Medical Services for Johns Hopkins Bayview Medical Center in Baltimore.
Along with Level I, Leadership Academy Level II will be presented again this year Nov. 5-8 in San Antonio. It builds on the success of last fall’s first offering by expanding on the concepts presented in the Level I academy.
A new educational initiative, supported by Sanofi-Aventis, provides three training sessions at regional chapters or other designated meetings across the country. The meetings educate hospitalists on best practices for glycemic control, prevention of venous thromboembolism, and transitions of care. Meetings will highlight successful interventions as outlined in the respective quality improvement (QI) implementation guides and resource rooms. Meetings will aim to include 20 to 50 participants.
The last piece of the SHM Heart Failure Quality Improvement Initiative is in its final planning stages, and a third CME module for Team Communications as it relates to the heart failure patient will be developed in the coming months. This initiative is supported in part by Scios Inc. and led by Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.
Quality Initiatives
Over the past several years, SHM has developed initiatives that range from convening a panel to assess the state of the art of a QI intervention to developing a Web-based resource room. Projects EQID is involved with:
- SHM is in the early stages of a three-year effort to develop resources and programs for improving hospital care transitions for older adults. This is supported through a major grant from the John A. Hartford Foundation in New York City, under the leadership of Mark Williams, MD, and Eric Coleman, MD, MPH. Dr. Williams is chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and editor of the Journal of Hospital Medicine. Dr. Coleman is associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora.
- “The Heart Failure Quality Improvement Implementation Guide” has been updated. The Heart Failure Resource Room on SHM’s Web site has been redesigned to make it easier for visitors who wish to follow the process of developing a QI intervention related to care of the hospitalized heart failure patient. We are communicating these changes to the hospital medicine community. Supported in part by Scios Inc., based in Mountain View, Calif., this effort includes presentations at regional meetings. This project was led by Nurcan Ilksoy, MD, assistant professor of Medicine at Emory University School of Medicine in Atlanta.
- The VTE Prevention Collaborative is open to all members implementing a QI program to combat venous thromboembolism in the hospitalized patient. The Sanofi-Aventis-supported collaborative uses seasoned QI leaders as mentors. Greg Maynard, MD, MS, and Jason Stein, MD, lead the enrollees through the QI process. The mentees have the benefit of regularly scheduled calls to ask questions and receive instant feedback on their process and progress. An add-on to this program, funded by the Kettering Foundation of Dayton, Ohio, provides the opportunity for on-site consultations. Dr. Maynard is head of the Division of Hospital Medicine and associate clinical professor of medicine at the University of California-San Diego. Dr. Stein is a hospitalist at Atlanta’s Emory University Hospital, assistant professor of Medicine at Emory University School of Medicine, and director of Quality Improvement for the Emory Hospital Medicine Unit.
- An expert panel convened in July to kick off development of an Acute Coronary Syndrome Resource Room and determine the content the resource room will cover. Content address diagnosis and risk stratification, medication, interventional procedures, patient education, transitions, and care coordination. This initiative is being led by Chad Whelan, MD, and is supported in part by Bristol-Myers Squibb Company, New York City. Dr. Whelan is an academic hospitalist and an assistant professor of medicine at University of Chicago in the Section of General Internal Medicine.
- SHM often studies strategies to improve patient satisfaction, outcomes, length of stay, and other important metrics. An expert panel assesses observation units as they contribute to improved treatment of patients with acute decompensated heart failure, chest pain, and other clinical conditions such as asthma. A white paper is pending on the use and value of observation units. Support for the meeting and development and distribution of the white paper was provided by Scios Inc.
Committee Support
A major staff role is the support of the Education and Hospital Quality and Patient Safety (HQPS) committees, the groups that direct and drive SHM in these important areas. The Education Committee, led by Chairman Bill Rifkin, MD, assistant professor of medicine at Yale University School of Medicine in New Haven, Conn., is focusing on:
- Developing the teaching skills pre-course that will be presented at the 2008 Annual Meeting;
- Defining a workable strategy to promote The Core Competencies in Hospital Medicine;
- Developing educational and/or communication modalities that support maintenance of certification; and
- Further defining the direction of the committee to meet members’ educational needs.
Janet Nagamine, MD, leads the HQPS Committee in the following priorities:
- Planning and holding a quality summit to define goals and priorities for the next three to five years;
- Submitting a grant application to AHRQ to support a multidisciplinary conference in the area of medication reconciliation;
- Developing SHM’s role in care transitions;
- Reviewing quality pre-course information and determining the curriculum for ‘‘Hospital Medicine 2008”; and
- Developing the Quality track for ‘‘Hospital Medicine 2008.”
The Performance and Standards Task Force (PSTF) was formed a little more than a year ago after SHM leadership recognized the need for a coordinated approach to working with external organizations in the performance and standards quality arena.
As SHM’s senior adviser for quality standards and compliance, I work with PSTF Chairman Patrick Torcson, MD, (medical director of hospital medicine at the St. Tammany Parish Hospital in Covington, La.) along with senior staff and leadership of the Public Policy Committee (PPC). We monitor the performance and quality landscape at national organizations charged with measuring development and building consensus. We also develop relationships with other professional medical societies and organizations.
Chapters Summary
Chicago
The Chicago Chapter of SHM met June 7. Attendees came from organizations such as Signature Healthcare Solutions, Advocate Healthcare, Northwestern University, and University of Chicago. The meeting began with an update from the SHM national annual meeting given by Chapter President Tarek Karaman, MD, lead hospitalist, Advocate Health Centers, and hospitalist program director, Department of Internal Medicine, Advocate Illinois Masonic Medical Center, Chicago. This was followed by a presentation on DVT/pulmonary embolism prophylaxis and treatment from SHM board member Alpesh Amin, MD, executive director of the hospitalist program and vice chair for clinical affairs and quality in the department of medicine at the University of California, Irvine. For the first time, the chapter had a panel discussion with two primary care physicians from Northwestern University. John Butter, MD, and Sean O’Conner, MD, shared their thoughts regarding the interaction between primary care physicians and hospitalists. Ideas were given on how to strengthen working relationships between the two.
St. Louis
Since its inception in spring 2006, the PSTF has become engaged in the American Medical Association’s (AMA) Physician Consortium for Performance Improvement (PCPI) and the National Quality Forum (NQF). The NQF is a nonprofit organization instructed by Congress to endorse consensus-based national standards for measurement and public reporting of healthcare performance data. Specifically, NQF aims to influence the development of physician-level performance measures as part of the Centers for Medicare and Medicaid Service’s (CMS) Physician Quality Reporting Initiative (PQRI).
By joining the PCPI, SHM has aligned with other medical specialties to develop performance measures in geriatrics, emergency medicine, outpatient parenteral antimicrobial therapy, and facets of anesthesiology such as perioperative normothermia and critical care.
Additionally, SHM has given feedback during public comment periods on perioperative care, chronic kidney disease, and other measures. The task force continues to evaluate which workgroups it should appoint members to participate in, depending on the topic.
SHM leadership has continued to foster relationships with CMS by sending letters in support of the 2007 PQRI. SHM was able to influence changes to the 2007 measure specifications so hospitalists would have measures to report. Of the 74 measures included in the PQRI, 11 have specifications allowing reporting by hospitalists, underscoring the importance of SHM’s influence and participation in the PCPI process.
Dr. Torcson and Eric Siegal, MD, (regional medical director, Cogent Healthcare, Madison, Wis.) co-chaired a CMS-led SHM member conference call focused on PQRI and how it affects hospitalists. The program was well received by SHM members.
When SHM became a member of the NQF last summer, it nominated several members who were selected to participate on various technical advisory panels overseeing work on the development of consensus standards for hospital care. This project, sponsored by the Agency for Healthcare Research and Quality (AHRQ), is addressing patient safety, pediatrics, and inpatient care.
Last fall, SHM sent Mark Williams, MD (professor of medicine at Emory University School of Medicine in Atlanta and editor of The Journal of Hospital Medicine) to the NQF’s 7th Annual Meeting, a National Policy Conference on Quality. The meeting featured plenary sessions that focused on issues at the forefront of policy discussions, including incentivizing healthcare quality improvement, the role of policymakers, leading professional and trade associations in improving healthcare quality, and efforts under way in the federal government to foster healthcare improvements.
This fall, Greg Seymann, MD, will attend the 8th Annual Meeting. Dr. Seymann is an assistant professor with the Department of Medicine, Hospital Medicine Program, at the University of California San Diego Medical Center.
Goals for 2008, Beyond
By taking an active role in the performance and standard arena, SHM senior staff and leadership have been able to build key relationships. This has paved the way for influencing the current physician reporting program and taking the lead on developing measures that will most reflect hospital medicine in the future.
The task force intends to be at the helm of the development of performance measures that more accurately reflect services provided by hospitalists. Senior staff and leadership have discussed this goal with several national stakeholders including the PCPI and the NQF, whose senior staff have supported its agenda.
In July, SHM, along with the American College of Physicians (ACP), the Society of General Internal Medicine (SGIM), and the American Geriatrics Society (AGS), formed a steering committee to convene a transitions of care consensus conference. This multispecialty, multidisciplinary group reviewed the principles and standards that came from the ABIM Foundation’s Stepping Up to the Plate (SUTTP) Alliance, which met this spring. SHM and PCPI are working to form an expert workgroup that will develop six to eight care transitions measures for inclusion in the 2009 PQRI.
SHM also is exploring collaboration with the American Hospital Association and its Hospital Quality Alliance (HQA), which coordinates the promotion of quality measurement, transparency, and improvement in the hospital setting.
In addition to its work with these external national groups, task force members would also like to start a resource room on the SHM Web site, www.hospitalmedicine.org, which would be devoted to member efforts in research related to quality and performance standards, as well as the member go-to place for tools and references on best practices in performance standards and pay for reporting initiatives.
Finally, Dr. Torcson hopes to shape and disseminate a national research agenda for hospitalist performance measurement and reporting. TH
SHM Behind the Scenes
Quality is our Middle Name
By Geri Barnes
The Education and Quality Initiatives Department’s (EQID) mission is to lead and manage an integrative program that brings resources to improve patient care. With the help of many individuals and partner organizations, SHM is working toward improved care for inpatients. Let’s review our progress as we begin the second quarter of SHM’s fiscal year.
Educational Programs
Our focus over the past few months has been the development of “Hospital Medicine 2008,” which will be held April 3-5 in San Diego. Under the leadership of Sylvia McKean, MD, head of the hospitalist service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School in Boston, the Annual Meeting Committee has developed an innovative program. The session will include a new evidence-based rapid fire track and a new teaching skills pre-course for academic and clinical educators. EQID obtains CMEs, communicates with faculty, and fine-tunes logistical efforts.
Leadership Academy Level I is a mainstay of SHM’s educational efforts. EQID supports Eric Howell, MD, chair of the Leadership Committee, as it focuses on addressing attendee input and encouraging the revision of the program in a continuous quality improvement effort. Dr. Howell is director of the Collaborative Inpatient Medicine Service and director of the Zieve Medical Services for Johns Hopkins Bayview Medical Center in Baltimore.
Along with Level I, Leadership Academy Level II will be presented again this year Nov. 5-8 in San Antonio. It builds on the success of last fall’s first offering by expanding on the concepts presented in the Level I academy.
A new educational initiative, supported by Sanofi-Aventis, provides three training sessions at regional chapters or other designated meetings across the country. The meetings educate hospitalists on best practices for glycemic control, prevention of venous thromboembolism, and transitions of care. Meetings will highlight successful interventions as outlined in the respective quality improvement (QI) implementation guides and resource rooms. Meetings will aim to include 20 to 50 participants.
The last piece of the SHM Heart Failure Quality Improvement Initiative is in its final planning stages, and a third CME module for Team Communications as it relates to the heart failure patient will be developed in the coming months. This initiative is supported in part by Scios Inc. and led by Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.
Quality Initiatives
Over the past several years, SHM has developed initiatives that range from convening a panel to assess the state of the art of a QI intervention to developing a Web-based resource room. Projects EQID is involved with:
- SHM is in the early stages of a three-year effort to develop resources and programs for improving hospital care transitions for older adults. This is supported through a major grant from the John A. Hartford Foundation in New York City, under the leadership of Mark Williams, MD, and Eric Coleman, MD, MPH. Dr. Williams is chief of the new Division of Hospital Medicine at Northwestern Memorial Hospital in Chicago and editor of the Journal of Hospital Medicine. Dr. Coleman is associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora.
- “The Heart Failure Quality Improvement Implementation Guide” has been updated. The Heart Failure Resource Room on SHM’s Web site has been redesigned to make it easier for visitors who wish to follow the process of developing a QI intervention related to care of the hospitalized heart failure patient. We are communicating these changes to the hospital medicine community. Supported in part by Scios Inc., based in Mountain View, Calif., this effort includes presentations at regional meetings. This project was led by Nurcan Ilksoy, MD, assistant professor of Medicine at Emory University School of Medicine in Atlanta.
- The VTE Prevention Collaborative is open to all members implementing a QI program to combat venous thromboembolism in the hospitalized patient. The Sanofi-Aventis-supported collaborative uses seasoned QI leaders as mentors. Greg Maynard, MD, MS, and Jason Stein, MD, lead the enrollees through the QI process. The mentees have the benefit of regularly scheduled calls to ask questions and receive instant feedback on their process and progress. An add-on to this program, funded by the Kettering Foundation of Dayton, Ohio, provides the opportunity for on-site consultations. Dr. Maynard is head of the Division of Hospital Medicine and associate clinical professor of medicine at the University of California-San Diego. Dr. Stein is a hospitalist at Atlanta’s Emory University Hospital, assistant professor of Medicine at Emory University School of Medicine, and director of Quality Improvement for the Emory Hospital Medicine Unit.
- An expert panel convened in July to kick off development of an Acute Coronary Syndrome Resource Room and determine the content the resource room will cover. Content address diagnosis and risk stratification, medication, interventional procedures, patient education, transitions, and care coordination. This initiative is being led by Chad Whelan, MD, and is supported in part by Bristol-Myers Squibb Company, New York City. Dr. Whelan is an academic hospitalist and an assistant professor of medicine at University of Chicago in the Section of General Internal Medicine.
- SHM often studies strategies to improve patient satisfaction, outcomes, length of stay, and other important metrics. An expert panel assesses observation units as they contribute to improved treatment of patients with acute decompensated heart failure, chest pain, and other clinical conditions such as asthma. A white paper is pending on the use and value of observation units. Support for the meeting and development and distribution of the white paper was provided by Scios Inc.
Committee Support
A major staff role is the support of the Education and Hospital Quality and Patient Safety (HQPS) committees, the groups that direct and drive SHM in these important areas. The Education Committee, led by Chairman Bill Rifkin, MD, assistant professor of medicine at Yale University School of Medicine in New Haven, Conn., is focusing on:
- Developing the teaching skills pre-course that will be presented at the 2008 Annual Meeting;
- Defining a workable strategy to promote The Core Competencies in Hospital Medicine;
- Developing educational and/or communication modalities that support maintenance of certification; and
- Further defining the direction of the committee to meet members’ educational needs.
Janet Nagamine, MD, leads the HQPS Committee in the following priorities:
- Planning and holding a quality summit to define goals and priorities for the next three to five years;
- Submitting a grant application to AHRQ to support a multidisciplinary conference in the area of medication reconciliation;
- Developing SHM’s role in care transitions;
- Reviewing quality pre-course information and determining the curriculum for ‘‘Hospital Medicine 2008”; and
- Developing the Quality track for ‘‘Hospital Medicine 2008.”
Boundary crossings: Guard against inappropriate contact
Woman claims improper contact during treatment
Fairfax County (VA) Circuit Court
A 23-year-old woman who received treatment from a psychiatrist for approximately 2½ years claimed that he sexually abused her during that time. She alleged that the inappropriate sexual relationship included holding, hugging, kissing, fondling, and watching pornography. The patient claimed that the relationship led to emotional distress and caused her to attempt suicide.
The psychiatrist admitted that a sexual relationship occurred but contended that the patient suffered no harm.
A $400,000 verdict was returned
Did inappropriate contact cause agoraphobia, anorexia?
Suffolk County (MA) Superior Court
A patient in her 20s had a history of emotional problems and sexual assaults against her. A psychiatrist treated her for obsessive-compulsive disorder for 4 years. He acknowledged giving the patient stuffed animals, cards, and letters and visiting her home several times when she was unable to go to his office. During sessions he touched her hand for comfort and hugged her. The patient claimed they had regular sexual contact.
The patient alleged that the psychiatrist was negligent for engaging in inappropriate sexual conduct, which she claims caused ongoing emotional distress. She claimed she was unable to work and suffered from agoraphobia, intimate relationships difficulties, and anorexia as a result of his actions. The psychiatrist denied any inappropriate sexual conduct.
The psychiatrist’s license was suspended indefinitely, but the suspension was stayed under an agreement that he attend medical education courses.
A $750,000 settlement was reached
Dr. Grant’s observations
Although most physicians would agree that sexual relations with a patient are inappropriate,1 the fact that cases continue to occur suggests a need to emphasize treatment boundaries. Establishing clear boundaries in the doctor-patient relationship creates an atmosphere of safety and predictability that allows treatment to thrive.2
Boundary problems are one of the most frequent reasons for malpractice actions against mental health providers.3 Although much of the literature discusses boundary violations during psychotherapy, issues may arise in all treatment settings, including psychopharmacologic management.
One-half of all psychiatrists will treat at least 1 victim of physician sexual misconduct during their careers.4 One study5 examining sex-related offenses committed by U.S. physicians in all specialties found:
- The number of physicians disciplined for sex-related offenses increased each year from 1989 to 1996.
- 22% of disciplined physicians had sexual intercourse with patients, 15% had sexual contact or touching, 37% committed other sexual abuse that did not fit in either of these 2 categories, and 25% involved nonpatients.
- 28% of disciplined physicians were psychiatrists, the most represented specialty in the study.
The American Medical Association’s Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry states: A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor-patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
“Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.”
Source: Reference 9
In a 1986 survey of psychiatrists, 7% of male and 3% of female clinicians reported having sexual contact with their patients.6 A 1988 survey of fourth-year psychiatry residents found that 1% of respondents acknowledged having sexual relations with a patient.7 In a 1992 study, 9% of physicians across specialties reported engaging in sexual contact with 1 or more current or former patients.8 In that study, 19% of female physicians and 40% of male physicians reported that they did not think physician-patient sexual misconduct was always harmful to patients.8 These views and behaviors are in violation of medical codes of ethics (Box).9
How misconduct harms patients
Trust is essential to establishing a secure therapeutic relationship. Boundary violations may result in missed diagnoses, inappropriate treatment, and/or worsened psychiatric symptoms. Patients might develop complex posttraumatic stress disorder, depression, anxiety, dissociation, sexual dysfunction, somatoform disorders, eating disorders, sleep disorders, or substance use disorders.4 They could lose faith in their treatment providers, have difficulties expressing anger, feel guilty, develop poor self-concept, experience a loss of confidence, and develop problems establishing trusting relationships.4 For these reasons, clinicians can be sued for negligent treatment and sexual misconduct.10
Boundary violations
Although sexual activities with patients are clear boundary violations, what about the second case when the therapist gave the patient stuffed animals and cards and hugged her? Progressive boundary violations often precede and accompany sexual misconduct.10
Five risk factors have been associated with therapist boundary violations:3
- life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts
- transitions—job changes or job loss
- medical illness
- arrogance—the belief that a boundary violation couldn’t happen to him or her and not recognizing the need for consultation
- common stress points with the patient
Although the list is not exhaustive, these factors may be associated with a psychiatrist turning to the patient for solace, gratification, or excitement.
Drawing boundary lines
Not all boundary issues are the same, and Gutheil et al2 suggest 2 categories:
- Boundary crossings—a benign variant where the deviation may advance therapy in a constructive way that does not harm the patient, such as discussion of countertransference.
- Boundary violations—the transgression harms or exploits the patient.
Although some boundary issues may appear benign, even theoretically harmless boundary crossings can be misrepresented or misconstrued by the patient.11 Also, boundary transgressions that do not involve erotic touch might harm the treatment process and the patient.2
When examining “minor” boundary issues that may seem innocuous, ask yourself if the action is for your benefit rather than to advance the patient’s therapy. Also, determine if the intervention is part of a series of progressive boundary violations. If the answer to either question is “yes,” desist immediately and take corrective action.10
The psychiatrist has a professional code of ethics to follow and can be held responsible for failing to set or adhere to boundaries.11 If a patient initiates a boundary violation, you must refuse and then explore the patient’s underlying psychological issues, perhaps aided by consultation with a peer or mentor (Table). Repeated patient demands to breach boundaries requires prompt consultation to determine if you can continue treating the patient or if you should transfer the patient to another clinician. Document the patient’s demands to breach boundaries and your actions when seeking consultation.3
Table 1
How to maintain integrity of the treatment process
| Maintain relative therapist neutrality |
| Foster psychological separateness of the patient |
| Protect confidentiality |
| Obtain informed consent for treatments and procedures |
| Interact verbally with patients |
| Ensure that you do not have any previous, current, or future personal relationships with the patient |
| Minimize physical contact |
| Preserve the therapist’s relative anonymity |
| Establish a stable fee policy |
| Provide a consistent, private, and professional setting |
| Define the time and length of sessions |
| Source: Reference 10 |
1. Herman J, Gartrell N, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, II: psychiatrists’ attitudes. Am J Psychiatry 1987;144:164-9.
2. Gutheil TG, Gabbard GO. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155:409-14.
3. Norris DM, Gutheil TG, Strasburger LH. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
4. Roman B, Kay J. Residency education on the prevention of physician-patient sexual misconduct. Acad Psychiatry 1997;21:26-34.
5. Dehlendorf CE, Wolfe SM. Physicians disciplined for sexrelated offenses. JAMA 1998;279:1883-8.
6. Gartrell NK, Herman J, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, 1: prevalence. Am J Psychiatry 1986;143:1126-31.
7. Gartrell NK, Herman J, Olarte S, et al. Psychiatric residents’ sexual contact with educators and patients: results of a national survey. Am J Psychiatry 1988;145:690-4.
8. Gartrell NK, Milliken M, Goodsen WH, et al. Physicianpatient sexual contact. West J Med 1992;157:139-43.
9. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed August 28, 2007.
10. Simon RI. Boundary violations in psychotherapy. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:195-215.
11. Gutheil TG. Boundaries, blackmail, and double binds: a pattern observed in malpractice consultation. J Am Acad Psychiatry Law 2005;33:476-81.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Woman claims improper contact during treatment
Fairfax County (VA) Circuit Court
A 23-year-old woman who received treatment from a psychiatrist for approximately 2½ years claimed that he sexually abused her during that time. She alleged that the inappropriate sexual relationship included holding, hugging, kissing, fondling, and watching pornography. The patient claimed that the relationship led to emotional distress and caused her to attempt suicide.
The psychiatrist admitted that a sexual relationship occurred but contended that the patient suffered no harm.
A $400,000 verdict was returned
Did inappropriate contact cause agoraphobia, anorexia?
Suffolk County (MA) Superior Court
A patient in her 20s had a history of emotional problems and sexual assaults against her. A psychiatrist treated her for obsessive-compulsive disorder for 4 years. He acknowledged giving the patient stuffed animals, cards, and letters and visiting her home several times when she was unable to go to his office. During sessions he touched her hand for comfort and hugged her. The patient claimed they had regular sexual contact.
The patient alleged that the psychiatrist was negligent for engaging in inappropriate sexual conduct, which she claims caused ongoing emotional distress. She claimed she was unable to work and suffered from agoraphobia, intimate relationships difficulties, and anorexia as a result of his actions. The psychiatrist denied any inappropriate sexual conduct.
The psychiatrist’s license was suspended indefinitely, but the suspension was stayed under an agreement that he attend medical education courses.
A $750,000 settlement was reached
Dr. Grant’s observations
Although most physicians would agree that sexual relations with a patient are inappropriate,1 the fact that cases continue to occur suggests a need to emphasize treatment boundaries. Establishing clear boundaries in the doctor-patient relationship creates an atmosphere of safety and predictability that allows treatment to thrive.2
Boundary problems are one of the most frequent reasons for malpractice actions against mental health providers.3 Although much of the literature discusses boundary violations during psychotherapy, issues may arise in all treatment settings, including psychopharmacologic management.
One-half of all psychiatrists will treat at least 1 victim of physician sexual misconduct during their careers.4 One study5 examining sex-related offenses committed by U.S. physicians in all specialties found:
- The number of physicians disciplined for sex-related offenses increased each year from 1989 to 1996.
- 22% of disciplined physicians had sexual intercourse with patients, 15% had sexual contact or touching, 37% committed other sexual abuse that did not fit in either of these 2 categories, and 25% involved nonpatients.
- 28% of disciplined physicians were psychiatrists, the most represented specialty in the study.
The American Medical Association’s Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry states: A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor-patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
“Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.”
Source: Reference 9
In a 1986 survey of psychiatrists, 7% of male and 3% of female clinicians reported having sexual contact with their patients.6 A 1988 survey of fourth-year psychiatry residents found that 1% of respondents acknowledged having sexual relations with a patient.7 In a 1992 study, 9% of physicians across specialties reported engaging in sexual contact with 1 or more current or former patients.8 In that study, 19% of female physicians and 40% of male physicians reported that they did not think physician-patient sexual misconduct was always harmful to patients.8 These views and behaviors are in violation of medical codes of ethics (Box).9
How misconduct harms patients
Trust is essential to establishing a secure therapeutic relationship. Boundary violations may result in missed diagnoses, inappropriate treatment, and/or worsened psychiatric symptoms. Patients might develop complex posttraumatic stress disorder, depression, anxiety, dissociation, sexual dysfunction, somatoform disorders, eating disorders, sleep disorders, or substance use disorders.4 They could lose faith in their treatment providers, have difficulties expressing anger, feel guilty, develop poor self-concept, experience a loss of confidence, and develop problems establishing trusting relationships.4 For these reasons, clinicians can be sued for negligent treatment and sexual misconduct.10
Boundary violations
Although sexual activities with patients are clear boundary violations, what about the second case when the therapist gave the patient stuffed animals and cards and hugged her? Progressive boundary violations often precede and accompany sexual misconduct.10
Five risk factors have been associated with therapist boundary violations:3
- life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts
- transitions—job changes or job loss
- medical illness
- arrogance—the belief that a boundary violation couldn’t happen to him or her and not recognizing the need for consultation
- common stress points with the patient
Although the list is not exhaustive, these factors may be associated with a psychiatrist turning to the patient for solace, gratification, or excitement.
Drawing boundary lines
Not all boundary issues are the same, and Gutheil et al2 suggest 2 categories:
- Boundary crossings—a benign variant where the deviation may advance therapy in a constructive way that does not harm the patient, such as discussion of countertransference.
- Boundary violations—the transgression harms or exploits the patient.
Although some boundary issues may appear benign, even theoretically harmless boundary crossings can be misrepresented or misconstrued by the patient.11 Also, boundary transgressions that do not involve erotic touch might harm the treatment process and the patient.2
When examining “minor” boundary issues that may seem innocuous, ask yourself if the action is for your benefit rather than to advance the patient’s therapy. Also, determine if the intervention is part of a series of progressive boundary violations. If the answer to either question is “yes,” desist immediately and take corrective action.10
The psychiatrist has a professional code of ethics to follow and can be held responsible for failing to set or adhere to boundaries.11 If a patient initiates a boundary violation, you must refuse and then explore the patient’s underlying psychological issues, perhaps aided by consultation with a peer or mentor (Table). Repeated patient demands to breach boundaries requires prompt consultation to determine if you can continue treating the patient or if you should transfer the patient to another clinician. Document the patient’s demands to breach boundaries and your actions when seeking consultation.3
Table 1
How to maintain integrity of the treatment process
| Maintain relative therapist neutrality |
| Foster psychological separateness of the patient |
| Protect confidentiality |
| Obtain informed consent for treatments and procedures |
| Interact verbally with patients |
| Ensure that you do not have any previous, current, or future personal relationships with the patient |
| Minimize physical contact |
| Preserve the therapist’s relative anonymity |
| Establish a stable fee policy |
| Provide a consistent, private, and professional setting |
| Define the time and length of sessions |
| Source: Reference 10 |
Woman claims improper contact during treatment
Fairfax County (VA) Circuit Court
A 23-year-old woman who received treatment from a psychiatrist for approximately 2½ years claimed that he sexually abused her during that time. She alleged that the inappropriate sexual relationship included holding, hugging, kissing, fondling, and watching pornography. The patient claimed that the relationship led to emotional distress and caused her to attempt suicide.
The psychiatrist admitted that a sexual relationship occurred but contended that the patient suffered no harm.
A $400,000 verdict was returned
Did inappropriate contact cause agoraphobia, anorexia?
Suffolk County (MA) Superior Court
A patient in her 20s had a history of emotional problems and sexual assaults against her. A psychiatrist treated her for obsessive-compulsive disorder for 4 years. He acknowledged giving the patient stuffed animals, cards, and letters and visiting her home several times when she was unable to go to his office. During sessions he touched her hand for comfort and hugged her. The patient claimed they had regular sexual contact.
The patient alleged that the psychiatrist was negligent for engaging in inappropriate sexual conduct, which she claims caused ongoing emotional distress. She claimed she was unable to work and suffered from agoraphobia, intimate relationships difficulties, and anorexia as a result of his actions. The psychiatrist denied any inappropriate sexual conduct.
The psychiatrist’s license was suspended indefinitely, but the suspension was stayed under an agreement that he attend medical education courses.
A $750,000 settlement was reached
Dr. Grant’s observations
Although most physicians would agree that sexual relations with a patient are inappropriate,1 the fact that cases continue to occur suggests a need to emphasize treatment boundaries. Establishing clear boundaries in the doctor-patient relationship creates an atmosphere of safety and predictability that allows treatment to thrive.2
Boundary problems are one of the most frequent reasons for malpractice actions against mental health providers.3 Although much of the literature discusses boundary violations during psychotherapy, issues may arise in all treatment settings, including psychopharmacologic management.
One-half of all psychiatrists will treat at least 1 victim of physician sexual misconduct during their careers.4 One study5 examining sex-related offenses committed by U.S. physicians in all specialties found:
- The number of physicians disciplined for sex-related offenses increased each year from 1989 to 1996.
- 22% of disciplined physicians had sexual intercourse with patients, 15% had sexual contact or touching, 37% committed other sexual abuse that did not fit in either of these 2 categories, and 25% involved nonpatients.
- 28% of disciplined physicians were psychiatrists, the most represented specialty in the study.
The American Medical Association’s Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry states: A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor-patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
“Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.”
Source: Reference 9
In a 1986 survey of psychiatrists, 7% of male and 3% of female clinicians reported having sexual contact with their patients.6 A 1988 survey of fourth-year psychiatry residents found that 1% of respondents acknowledged having sexual relations with a patient.7 In a 1992 study, 9% of physicians across specialties reported engaging in sexual contact with 1 or more current or former patients.8 In that study, 19% of female physicians and 40% of male physicians reported that they did not think physician-patient sexual misconduct was always harmful to patients.8 These views and behaviors are in violation of medical codes of ethics (Box).9
How misconduct harms patients
Trust is essential to establishing a secure therapeutic relationship. Boundary violations may result in missed diagnoses, inappropriate treatment, and/or worsened psychiatric symptoms. Patients might develop complex posttraumatic stress disorder, depression, anxiety, dissociation, sexual dysfunction, somatoform disorders, eating disorders, sleep disorders, or substance use disorders.4 They could lose faith in their treatment providers, have difficulties expressing anger, feel guilty, develop poor self-concept, experience a loss of confidence, and develop problems establishing trusting relationships.4 For these reasons, clinicians can be sued for negligent treatment and sexual misconduct.10
Boundary violations
Although sexual activities with patients are clear boundary violations, what about the second case when the therapist gave the patient stuffed animals and cards and hugged her? Progressive boundary violations often precede and accompany sexual misconduct.10
Five risk factors have been associated with therapist boundary violations:3
- life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts
- transitions—job changes or job loss
- medical illness
- arrogance—the belief that a boundary violation couldn’t happen to him or her and not recognizing the need for consultation
- common stress points with the patient
Although the list is not exhaustive, these factors may be associated with a psychiatrist turning to the patient for solace, gratification, or excitement.
Drawing boundary lines
Not all boundary issues are the same, and Gutheil et al2 suggest 2 categories:
- Boundary crossings—a benign variant where the deviation may advance therapy in a constructive way that does not harm the patient, such as discussion of countertransference.
- Boundary violations—the transgression harms or exploits the patient.
Although some boundary issues may appear benign, even theoretically harmless boundary crossings can be misrepresented or misconstrued by the patient.11 Also, boundary transgressions that do not involve erotic touch might harm the treatment process and the patient.2
When examining “minor” boundary issues that may seem innocuous, ask yourself if the action is for your benefit rather than to advance the patient’s therapy. Also, determine if the intervention is part of a series of progressive boundary violations. If the answer to either question is “yes,” desist immediately and take corrective action.10
The psychiatrist has a professional code of ethics to follow and can be held responsible for failing to set or adhere to boundaries.11 If a patient initiates a boundary violation, you must refuse and then explore the patient’s underlying psychological issues, perhaps aided by consultation with a peer or mentor (Table). Repeated patient demands to breach boundaries requires prompt consultation to determine if you can continue treating the patient or if you should transfer the patient to another clinician. Document the patient’s demands to breach boundaries and your actions when seeking consultation.3
Table 1
How to maintain integrity of the treatment process
| Maintain relative therapist neutrality |
| Foster psychological separateness of the patient |
| Protect confidentiality |
| Obtain informed consent for treatments and procedures |
| Interact verbally with patients |
| Ensure that you do not have any previous, current, or future personal relationships with the patient |
| Minimize physical contact |
| Preserve the therapist’s relative anonymity |
| Establish a stable fee policy |
| Provide a consistent, private, and professional setting |
| Define the time and length of sessions |
| Source: Reference 10 |
1. Herman J, Gartrell N, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, II: psychiatrists’ attitudes. Am J Psychiatry 1987;144:164-9.
2. Gutheil TG, Gabbard GO. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155:409-14.
3. Norris DM, Gutheil TG, Strasburger LH. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
4. Roman B, Kay J. Residency education on the prevention of physician-patient sexual misconduct. Acad Psychiatry 1997;21:26-34.
5. Dehlendorf CE, Wolfe SM. Physicians disciplined for sexrelated offenses. JAMA 1998;279:1883-8.
6. Gartrell NK, Herman J, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, 1: prevalence. Am J Psychiatry 1986;143:1126-31.
7. Gartrell NK, Herman J, Olarte S, et al. Psychiatric residents’ sexual contact with educators and patients: results of a national survey. Am J Psychiatry 1988;145:690-4.
8. Gartrell NK, Milliken M, Goodsen WH, et al. Physicianpatient sexual contact. West J Med 1992;157:139-43.
9. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed August 28, 2007.
10. Simon RI. Boundary violations in psychotherapy. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:195-215.
11. Gutheil TG. Boundaries, blackmail, and double binds: a pattern observed in malpractice consultation. J Am Acad Psychiatry Law 2005;33:476-81.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. Herman J, Gartrell N, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, II: psychiatrists’ attitudes. Am J Psychiatry 1987;144:164-9.
2. Gutheil TG, Gabbard GO. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155:409-14.
3. Norris DM, Gutheil TG, Strasburger LH. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
4. Roman B, Kay J. Residency education on the prevention of physician-patient sexual misconduct. Acad Psychiatry 1997;21:26-34.
5. Dehlendorf CE, Wolfe SM. Physicians disciplined for sexrelated offenses. JAMA 1998;279:1883-8.
6. Gartrell NK, Herman J, Olarte S, et al. Psychiatrist-patient sexual contact: results of a national survey, 1: prevalence. Am J Psychiatry 1986;143:1126-31.
7. Gartrell NK, Herman J, Olarte S, et al. Psychiatric residents’ sexual contact with educators and patients: results of a national survey. Am J Psychiatry 1988;145:690-4.
8. Gartrell NK, Milliken M, Goodsen WH, et al. Physicianpatient sexual contact. West J Med 1992;157:139-43.
9. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association. Available at: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed August 28, 2007.
10. Simon RI. Boundary violations in psychotherapy. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:195-215.
11. Gutheil TG. Boundaries, blackmail, and double binds: a pattern observed in malpractice consultation. J Am Acad Psychiatry Law 2005;33:476-81.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
There is no gold standard for decision-to-incision time
CASE: Primigravida with ruptured membranes
A 21-year-old patient was admitted to the labor and delivery suite in active labor. After a reassuring fetal tracing was documented, active management with oxytocin was initiated.
Five hours later, the nurse noted a prolonged deceleration.
Resuscitative efforts failed to alleviate the deceleration. The nurse notified the attending OB of the situation. An emergency cesarean section was called because:
- of a nonreassuring fetal heart rate tracing and
- delivery was not imminent.
The team is assembled and the patient is moved to the operating room; 34 minutes have elapsed between the time the decision was made to perform the cesarean section and the time the incision is made on the abdomen.
Two minutes later, the baby is delivered. Apgar scores are as follows: 0 at 1 minute; 0 at 5 minutes; 0 at 10 minutes; and 1 at 15 minutes.
Subsequently, the baby is determined to be severely brain-damaged. The parents file a claim of malpractice.
ObGyns have come to depend on ACOG’s Committee Opinions, Educational Bulletins, Practice Bulletins, Policy Statements, and Technology Assessments to help us take the best care of our patients. To quote the College, each of these documents “is reviewed periodically and either reaffirmed, replaced, or withdrawn to ensure its continued appropriateness to practice.”1
Sometimes, however, an ACOG bulletin, statement, or assessment may be misinterpreted and can actually contribute to some of the medicolegal problems that we face. The actual clinical situation just described, relating to ACOG’s statement on the so-called decision-to-incision gold standard, is a case in point.
The parties in the case go to trial
During the subsequent trial, the plaintiff alleges negligence by claiming that the defendant:
- did not anticipate or recognize developing fetal problems
- failed to perform a C-section within 30 minutes after the decision was made to do so.
- There was no fetal indication of hypoxia or cause for concern until the fetal bradycardia was noted
- Brain damage was caused by an unanticipated event that occurred more than 30 minutes before delivery
- The team responded as rapidly as it could given the circumstances of the hospital and staffing patterns.
Are we held to a standard that can’t be met and has no basis in evidence?
To repeat, as reported in hospital records admitted into evidence at trial, the baby was delivered, with a low Apgar score, 34 minutes after the decision was called. The fact that the incision commenced after more than 30 minutes was a major factor contributing to the multimillion-dollar settlement.
That 30-minute mark is taken directly from the fifth edition of ACOG’s Guideline for Perinatal Care:
Any hospital providing obstetric service should have the capability of responding to an obstetric emergency. No data correlate the timing of intervention with outcome, and there is little likelihood that any will be obtained. However, in general, the consensus has been that hospitals should have the capability of beginning a cesarean section within 30 minutes of the decision to operate.2
The interpretation that all C-sections must be performed within 30 minutes of a decision is challenged by a recent study sponsored by The National Institute of Child Health and Human Development (NICHD) Maternal–Fetal Medicine Units Network.3 The design of that study was observational, because no ethical means exist to randomize women to less than or more than 30 minutes from the time of a decision to perform a C-section to the time of the incision.
The data collected came only from primagravid women in active labor who had an infant that had a birth weight of more than 2,500 g. Indications for C-section included: nonreassuring fetal heart rate, umbilical cord prolapse, placental abruption, placenta previa with hemorrhage, and uterine rupture. A total of 11,481 cases were analyzed over a 2-year period, with 2,808 C-sections performed for those indications (a 24.5% rate of C-section). Ninety-four per cent of the C-sections were undertaken because of a nonreassuring fetal heart rate.
In a university setting, where one would expect in-house OB coverage and anesthesia to be available, only 65% of emergency C-sections commenced within 30 minutes of a decision (17% in less than 10 minutes; 27% in less than 20 minutes). Investigators also found that, in cases in which a C-section was performed for a nonreassuring fetal heart rate, only 62% were performed in fewer than 30 minutes.
The data are clear: More than one third of all C-sections for these indications did not comply with the “30-minute rule.”
Notably, the study also found that:
- when the decision-to-incision time was less than 30 minutes, the rates of fetal acidemia and intubation in the delivery room were higher
- 95% of infants delivered in more than 31 minutes did not experience any of the adverse outcomes listed in the accompanying TABLE
- only one of eight neonatal deaths occurred in the group of infants delivered after 31 minutes (at 33 minutes).
TABLE
Outcomes are no better when the decision-to-incision time is less than 30 minutes3
| OUTCOME | INCIDENCE AT | INCIDENCE AT >30 MIN |
|---|---|---|
| Urine pH, | 4.8% | 1.6%* |
| Intubation in delivery | 3.1% | 1.3%* |
| Hypoxic–ischemic encephalopathy | 0.7% | 0.5% |
| Fetal death | 0.2% | 0% |
| Neonatal death | 0.4% | 0.2% |
| Apgar score at 5 min, | 1.0% | 0.9% |
| None of the above | 92.6% | 95.4%* |
| *P .05> | ||
30 minutes? It’s not a mandate
The study supported by NICHD shows that:
- the decision-to-incision interval appears to have no impact on maternal complications
- an infant delivered within 30 minutes for an emergency indication was more likely to be acidemic and to require intubation than an infant delivered in longer than 30 minutes for an emergency indication
- delivery within 30 minutes does not guarantee that there will be no adverse outcome
- 95% of infants delivered in more than 30 minutes did not have compromise.
The ACOG guideline is, as stated, clearly not a requirement. It does not mandate that all C-sections commence within 30 minutes from the time of the decision to perform one. Rather, the guideline clearly states that the hospital should be capable of performing the procedure within 30 minutes.
To be clear, we are not advocating a guideline or policy of waiting to perform a C-section! We believe rapid delivery is proper. But the optimal time, or even minimal time, to delivery has not been defined by data—and may never be.
What should it really mean? Thirty minutes, therefore, should be a goal, not a finite time. Data published by NICHD should now be used to temper notions that exceeding the so-called 30-minute rule necessarily 1) is an indicator of substandard care and 2) has adverse effects on outcome for the newborn.
Perhaps it’s time for ACOG to review these recent data and then reaffirm, replace, or withdraw the statement from the perinatal guidelines proposing that 30 minutes be the maximum time from decision to incision.1
Here’s what you should do until the matter is clarified
If you must defend yourself against an accusation of not having performed a C-section in a timely fashion, data from the NICHD Perinatal Collaborative may offer a helpful defense. Because 38% of C-sections for a nonreassuring fetal heart rate tracing are not performed within 30 minutes of a decision to proceed, even in a university setting, this cannot be considered a standard and not meeting this arbitrary time should be looked on as a frequent occurrence.
Based on current data, therefore, any medicolegal case in which the plaintiff’s attorney implies that failure to conform to this putative standard resulted in a bad outcome should be defended vigorously—and should not be settled.
1. 2006 Compendium of Selected Publications. Washington, DC: American College of Obstetricians and Gynecologists, Women’s Health Care Physicians; 2006:v.
2. Guidelines for Perinatal Care, 5th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2002:147.
3. Bloom SL, Leveno KJ, Spong CY, et al. National Institute of Child Health and Human Development Maternal–Fetal Medicine Units Network. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6-11.
CASE: Primigravida with ruptured membranes
A 21-year-old patient was admitted to the labor and delivery suite in active labor. After a reassuring fetal tracing was documented, active management with oxytocin was initiated.
Five hours later, the nurse noted a prolonged deceleration.
Resuscitative efforts failed to alleviate the deceleration. The nurse notified the attending OB of the situation. An emergency cesarean section was called because:
- of a nonreassuring fetal heart rate tracing and
- delivery was not imminent.
The team is assembled and the patient is moved to the operating room; 34 minutes have elapsed between the time the decision was made to perform the cesarean section and the time the incision is made on the abdomen.
Two minutes later, the baby is delivered. Apgar scores are as follows: 0 at 1 minute; 0 at 5 minutes; 0 at 10 minutes; and 1 at 15 minutes.
Subsequently, the baby is determined to be severely brain-damaged. The parents file a claim of malpractice.
ObGyns have come to depend on ACOG’s Committee Opinions, Educational Bulletins, Practice Bulletins, Policy Statements, and Technology Assessments to help us take the best care of our patients. To quote the College, each of these documents “is reviewed periodically and either reaffirmed, replaced, or withdrawn to ensure its continued appropriateness to practice.”1
Sometimes, however, an ACOG bulletin, statement, or assessment may be misinterpreted and can actually contribute to some of the medicolegal problems that we face. The actual clinical situation just described, relating to ACOG’s statement on the so-called decision-to-incision gold standard, is a case in point.
The parties in the case go to trial
During the subsequent trial, the plaintiff alleges negligence by claiming that the defendant:
- did not anticipate or recognize developing fetal problems
- failed to perform a C-section within 30 minutes after the decision was made to do so.
- There was no fetal indication of hypoxia or cause for concern until the fetal bradycardia was noted
- Brain damage was caused by an unanticipated event that occurred more than 30 minutes before delivery
- The team responded as rapidly as it could given the circumstances of the hospital and staffing patterns.
Are we held to a standard that can’t be met and has no basis in evidence?
To repeat, as reported in hospital records admitted into evidence at trial, the baby was delivered, with a low Apgar score, 34 minutes after the decision was called. The fact that the incision commenced after more than 30 minutes was a major factor contributing to the multimillion-dollar settlement.
That 30-minute mark is taken directly from the fifth edition of ACOG’s Guideline for Perinatal Care:
Any hospital providing obstetric service should have the capability of responding to an obstetric emergency. No data correlate the timing of intervention with outcome, and there is little likelihood that any will be obtained. However, in general, the consensus has been that hospitals should have the capability of beginning a cesarean section within 30 minutes of the decision to operate.2
The interpretation that all C-sections must be performed within 30 minutes of a decision is challenged by a recent study sponsored by The National Institute of Child Health and Human Development (NICHD) Maternal–Fetal Medicine Units Network.3 The design of that study was observational, because no ethical means exist to randomize women to less than or more than 30 minutes from the time of a decision to perform a C-section to the time of the incision.
The data collected came only from primagravid women in active labor who had an infant that had a birth weight of more than 2,500 g. Indications for C-section included: nonreassuring fetal heart rate, umbilical cord prolapse, placental abruption, placenta previa with hemorrhage, and uterine rupture. A total of 11,481 cases were analyzed over a 2-year period, with 2,808 C-sections performed for those indications (a 24.5% rate of C-section). Ninety-four per cent of the C-sections were undertaken because of a nonreassuring fetal heart rate.
In a university setting, where one would expect in-house OB coverage and anesthesia to be available, only 65% of emergency C-sections commenced within 30 minutes of a decision (17% in less than 10 minutes; 27% in less than 20 minutes). Investigators also found that, in cases in which a C-section was performed for a nonreassuring fetal heart rate, only 62% were performed in fewer than 30 minutes.
The data are clear: More than one third of all C-sections for these indications did not comply with the “30-minute rule.”
Notably, the study also found that:
- when the decision-to-incision time was less than 30 minutes, the rates of fetal acidemia and intubation in the delivery room were higher
- 95% of infants delivered in more than 31 minutes did not experience any of the adverse outcomes listed in the accompanying TABLE
- only one of eight neonatal deaths occurred in the group of infants delivered after 31 minutes (at 33 minutes).
TABLE
Outcomes are no better when the decision-to-incision time is less than 30 minutes3
| OUTCOME | INCIDENCE AT | INCIDENCE AT >30 MIN |
|---|---|---|
| Urine pH, | 4.8% | 1.6%* |
| Intubation in delivery | 3.1% | 1.3%* |
| Hypoxic–ischemic encephalopathy | 0.7% | 0.5% |
| Fetal death | 0.2% | 0% |
| Neonatal death | 0.4% | 0.2% |
| Apgar score at 5 min, | 1.0% | 0.9% |
| None of the above | 92.6% | 95.4%* |
| *P .05> | ||
30 minutes? It’s not a mandate
The study supported by NICHD shows that:
- the decision-to-incision interval appears to have no impact on maternal complications
- an infant delivered within 30 minutes for an emergency indication was more likely to be acidemic and to require intubation than an infant delivered in longer than 30 minutes for an emergency indication
- delivery within 30 minutes does not guarantee that there will be no adverse outcome
- 95% of infants delivered in more than 30 minutes did not have compromise.
The ACOG guideline is, as stated, clearly not a requirement. It does not mandate that all C-sections commence within 30 minutes from the time of the decision to perform one. Rather, the guideline clearly states that the hospital should be capable of performing the procedure within 30 minutes.
To be clear, we are not advocating a guideline or policy of waiting to perform a C-section! We believe rapid delivery is proper. But the optimal time, or even minimal time, to delivery has not been defined by data—and may never be.
What should it really mean? Thirty minutes, therefore, should be a goal, not a finite time. Data published by NICHD should now be used to temper notions that exceeding the so-called 30-minute rule necessarily 1) is an indicator of substandard care and 2) has adverse effects on outcome for the newborn.
Perhaps it’s time for ACOG to review these recent data and then reaffirm, replace, or withdraw the statement from the perinatal guidelines proposing that 30 minutes be the maximum time from decision to incision.1
Here’s what you should do until the matter is clarified
If you must defend yourself against an accusation of not having performed a C-section in a timely fashion, data from the NICHD Perinatal Collaborative may offer a helpful defense. Because 38% of C-sections for a nonreassuring fetal heart rate tracing are not performed within 30 minutes of a decision to proceed, even in a university setting, this cannot be considered a standard and not meeting this arbitrary time should be looked on as a frequent occurrence.
Based on current data, therefore, any medicolegal case in which the plaintiff’s attorney implies that failure to conform to this putative standard resulted in a bad outcome should be defended vigorously—and should not be settled.
CASE: Primigravida with ruptured membranes
A 21-year-old patient was admitted to the labor and delivery suite in active labor. After a reassuring fetal tracing was documented, active management with oxytocin was initiated.
Five hours later, the nurse noted a prolonged deceleration.
Resuscitative efforts failed to alleviate the deceleration. The nurse notified the attending OB of the situation. An emergency cesarean section was called because:
- of a nonreassuring fetal heart rate tracing and
- delivery was not imminent.
The team is assembled and the patient is moved to the operating room; 34 minutes have elapsed between the time the decision was made to perform the cesarean section and the time the incision is made on the abdomen.
Two minutes later, the baby is delivered. Apgar scores are as follows: 0 at 1 minute; 0 at 5 minutes; 0 at 10 minutes; and 1 at 15 minutes.
Subsequently, the baby is determined to be severely brain-damaged. The parents file a claim of malpractice.
ObGyns have come to depend on ACOG’s Committee Opinions, Educational Bulletins, Practice Bulletins, Policy Statements, and Technology Assessments to help us take the best care of our patients. To quote the College, each of these documents “is reviewed periodically and either reaffirmed, replaced, or withdrawn to ensure its continued appropriateness to practice.”1
Sometimes, however, an ACOG bulletin, statement, or assessment may be misinterpreted and can actually contribute to some of the medicolegal problems that we face. The actual clinical situation just described, relating to ACOG’s statement on the so-called decision-to-incision gold standard, is a case in point.
The parties in the case go to trial
During the subsequent trial, the plaintiff alleges negligence by claiming that the defendant:
- did not anticipate or recognize developing fetal problems
- failed to perform a C-section within 30 minutes after the decision was made to do so.
- There was no fetal indication of hypoxia or cause for concern until the fetal bradycardia was noted
- Brain damage was caused by an unanticipated event that occurred more than 30 minutes before delivery
- The team responded as rapidly as it could given the circumstances of the hospital and staffing patterns.
Are we held to a standard that can’t be met and has no basis in evidence?
To repeat, as reported in hospital records admitted into evidence at trial, the baby was delivered, with a low Apgar score, 34 minutes after the decision was called. The fact that the incision commenced after more than 30 minutes was a major factor contributing to the multimillion-dollar settlement.
That 30-minute mark is taken directly from the fifth edition of ACOG’s Guideline for Perinatal Care:
Any hospital providing obstetric service should have the capability of responding to an obstetric emergency. No data correlate the timing of intervention with outcome, and there is little likelihood that any will be obtained. However, in general, the consensus has been that hospitals should have the capability of beginning a cesarean section within 30 minutes of the decision to operate.2
The interpretation that all C-sections must be performed within 30 minutes of a decision is challenged by a recent study sponsored by The National Institute of Child Health and Human Development (NICHD) Maternal–Fetal Medicine Units Network.3 The design of that study was observational, because no ethical means exist to randomize women to less than or more than 30 minutes from the time of a decision to perform a C-section to the time of the incision.
The data collected came only from primagravid women in active labor who had an infant that had a birth weight of more than 2,500 g. Indications for C-section included: nonreassuring fetal heart rate, umbilical cord prolapse, placental abruption, placenta previa with hemorrhage, and uterine rupture. A total of 11,481 cases were analyzed over a 2-year period, with 2,808 C-sections performed for those indications (a 24.5% rate of C-section). Ninety-four per cent of the C-sections were undertaken because of a nonreassuring fetal heart rate.
In a university setting, where one would expect in-house OB coverage and anesthesia to be available, only 65% of emergency C-sections commenced within 30 minutes of a decision (17% in less than 10 minutes; 27% in less than 20 minutes). Investigators also found that, in cases in which a C-section was performed for a nonreassuring fetal heart rate, only 62% were performed in fewer than 30 minutes.
The data are clear: More than one third of all C-sections for these indications did not comply with the “30-minute rule.”
Notably, the study also found that:
- when the decision-to-incision time was less than 30 minutes, the rates of fetal acidemia and intubation in the delivery room were higher
- 95% of infants delivered in more than 31 minutes did not experience any of the adverse outcomes listed in the accompanying TABLE
- only one of eight neonatal deaths occurred in the group of infants delivered after 31 minutes (at 33 minutes).
TABLE
Outcomes are no better when the decision-to-incision time is less than 30 minutes3
| OUTCOME | INCIDENCE AT | INCIDENCE AT >30 MIN |
|---|---|---|
| Urine pH, | 4.8% | 1.6%* |
| Intubation in delivery | 3.1% | 1.3%* |
| Hypoxic–ischemic encephalopathy | 0.7% | 0.5% |
| Fetal death | 0.2% | 0% |
| Neonatal death | 0.4% | 0.2% |
| Apgar score at 5 min, | 1.0% | 0.9% |
| None of the above | 92.6% | 95.4%* |
| *P .05> | ||
30 minutes? It’s not a mandate
The study supported by NICHD shows that:
- the decision-to-incision interval appears to have no impact on maternal complications
- an infant delivered within 30 minutes for an emergency indication was more likely to be acidemic and to require intubation than an infant delivered in longer than 30 minutes for an emergency indication
- delivery within 30 minutes does not guarantee that there will be no adverse outcome
- 95% of infants delivered in more than 30 minutes did not have compromise.
The ACOG guideline is, as stated, clearly not a requirement. It does not mandate that all C-sections commence within 30 minutes from the time of the decision to perform one. Rather, the guideline clearly states that the hospital should be capable of performing the procedure within 30 minutes.
To be clear, we are not advocating a guideline or policy of waiting to perform a C-section! We believe rapid delivery is proper. But the optimal time, or even minimal time, to delivery has not been defined by data—and may never be.
What should it really mean? Thirty minutes, therefore, should be a goal, not a finite time. Data published by NICHD should now be used to temper notions that exceeding the so-called 30-minute rule necessarily 1) is an indicator of substandard care and 2) has adverse effects on outcome for the newborn.
Perhaps it’s time for ACOG to review these recent data and then reaffirm, replace, or withdraw the statement from the perinatal guidelines proposing that 30 minutes be the maximum time from decision to incision.1
Here’s what you should do until the matter is clarified
If you must defend yourself against an accusation of not having performed a C-section in a timely fashion, data from the NICHD Perinatal Collaborative may offer a helpful defense. Because 38% of C-sections for a nonreassuring fetal heart rate tracing are not performed within 30 minutes of a decision to proceed, even in a university setting, this cannot be considered a standard and not meeting this arbitrary time should be looked on as a frequent occurrence.
Based on current data, therefore, any medicolegal case in which the plaintiff’s attorney implies that failure to conform to this putative standard resulted in a bad outcome should be defended vigorously—and should not be settled.
1. 2006 Compendium of Selected Publications. Washington, DC: American College of Obstetricians and Gynecologists, Women’s Health Care Physicians; 2006:v.
2. Guidelines for Perinatal Care, 5th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2002:147.
3. Bloom SL, Leveno KJ, Spong CY, et al. National Institute of Child Health and Human Development Maternal–Fetal Medicine Units Network. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6-11.
1. 2006 Compendium of Selected Publications. Washington, DC: American College of Obstetricians and Gynecologists, Women’s Health Care Physicians; 2006:v.
2. Guidelines for Perinatal Care, 5th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2002:147.
3. Bloom SL, Leveno KJ, Spong CY, et al. National Institute of Child Health and Human Development Maternal–Fetal Medicine Units Network. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6-11.
Dare to Compare
A new concept on Capitol Hill could reshape physicians’ treatment choices: comparative effectiveness research, or CER.
CER is a set of standards for examining the effectiveness of different therapies for a specific medical condition or set of patients to determine the best option. It may involve comparing competing medications or analyzing treatment approaches, such as surgery, devices, and drug therapies.
The healthcare community—and Capitol Hill—should keep an eye on CER.
“We need to look at evidence-based medicine and see what is the most effective treatment,” says Andrew Fishmann, MD, FCCP, FACP, co-founder of Cogent Healthcare and director of intensive care at Good Samaritan Hospital in Los Angeles. “The answer may also be the most expensive, but other factors such as decreased length of stay and fewer complications can help bring that cost down.”
One example that CER might address is back surgery—an issue many physicians cannot agree on. “There are billions of dollars spent on back surgery that may not be necessary,” Dr. Fishmann points out.
CER could ultimately provide guidelines that would standardize treatments for all types of conditions: “A big organization like Cogent would like to think that a patient with pneumonia receives the same treatment whether he’s in California or in Mississippi—but there are many reasons this is probably not true,” says Dr. Fishmann.
CER So Far
The Medicare Modernization Act of 2003 gave CER a jumpstart with $65 million in appropriations and authorized the Agency for Healthcare Research and Quality (AHRQ) to conduct research.
“Since 2004, [the AHRQ has] received $15 million a year for CER,” says Emily Rowe, director of government relations for the Coalition for Health Services Research in Washington, D.C., and a member of the Friends of AHRQ coalition. “They’re pretty limited in what they can produce on that budget, but to date they’ve done some interesting work.”
That work includes eight published reports on treatment options for breast cancer, gastroesophageal reflux disease (GERD), cancer-related anemia, low-bone density, depression, and more, with 20 additional reports “in the pipeline,” says Rowe.
All available reports can be downloaded from http://effectivehealthcare. ahrq.gov, where results have been published in separate versions for physicians and consumers.
“The most interesting example of [CER from AHRQ] is synthesized research that shows that drugs can be as effective as surgery for severe heart burn,” or GERD, says Rowe. “This shows the promise of CER.”
So AHRQ is at work on CER projects but, says Rowe, “It needs a more serious investment.” Some in Congress agree.
New Laws, More Money
The Enhanced Health Care Value for All Act of 2007 (HR 2184) was introduced by Reps. Tom Allen, D-Maine, and Jo Ann Emerson, R-Mo, in May. This bill would provide $3 billion over five years to fund CER.
Under the legislation, the AHRQ would remain the federal agency charged with supporting CER, but a new comparative effectiveness advisory board would be established, comprising employers, consumers, healthcare providers, researchers, and others. The board would offer advice on research priorities and methodologies.
Some, including the Blue Cross Blue Shield Association (BCBSA), have called for a new executive-branch agency or a new coalition to oversee CER. Dr. Fishmann, who is serving a second term on the National Advisory Council for AHRQ, strongly disagrees. “This is evidence-based medicine,” he stresses. “AHRQ is the perfect entity for this. What an organization like AHRQ will do is look at everything and address the issue impartially.”
Quality, Costs, Results
Congress views CER as a means of saving costs in healthcare, but CER would not provide immediate savings; rather, it’s a first step toward lowering healthcare costs. In fact, House Ways and Means Subcommittee Chairman Pete Stark, R-Calif., expressed concern about “moving” CER legislation this year, because it would require immediate investment without immediate savings.
“I don’t know where you come up with that money when everyone else in healthcare is fighting for more funds,” Dr. Fishmann says of the current legislation. “But Congress can come up with the funds if they want to.”
Rowe won’t speculate on whether the House bill will pass but does say: “The appropriators and budgeters are getting ready to fund this, so that if the legislation passes the money will be there. And interest in CER is gaining in both parties of Congress.”
While legislators focus on costs and savings, healthcare professionals are interested in improving quality.
“It is a quality issue, but a better term is value,” says Rowe. “The idea is, ‘Let’s get what we pay for.’ The U.S. needs better medical outcomes, and the idea of CER is not what treatments costs less but that it’s worth it if you have to spend more if the outcomes are improved.”
And Dr. Fishmann thinks CER will change how we provide care. “It’s going to standardize the delivery of healthcare,” he predicts. “If you don’t follow these standards, someone is going to ask why not—it might be the payer, your colleagues, your hospital.” Once CER reports are available and shared with the public, he points out, “as patients get educated, and payers too, they’ll stop paying for treatments that go against the standard.”
—Emily Rowe, director of government relations for the Coalition for Health Services Research, Washington, D.C.
Hospitalists and CER
How will comparative effectiveness affect hospital medicine?
“They’re looking at ischemic heart disease, pneumonia, diabetes, stroke—all hospitalized diseases,” says Dr. Fishmann of current CER projects. “Right now, everyone is practicing their trade, and everyone is doing things differently. I think in terms of hospitalists, it clearly will affect how you treat patients, and for how long.”
Regardless of the current House bill, it seems CER is on the horizon, for hospitalists and for all of healthcare.
“The good news is, I don’t think this is going away any time soon,” says Rowe of CER. “The train has left the station and it’s steaming away.” TH
A new concept on Capitol Hill could reshape physicians’ treatment choices: comparative effectiveness research, or CER.
CER is a set of standards for examining the effectiveness of different therapies for a specific medical condition or set of patients to determine the best option. It may involve comparing competing medications or analyzing treatment approaches, such as surgery, devices, and drug therapies.
The healthcare community—and Capitol Hill—should keep an eye on CER.
“We need to look at evidence-based medicine and see what is the most effective treatment,” says Andrew Fishmann, MD, FCCP, FACP, co-founder of Cogent Healthcare and director of intensive care at Good Samaritan Hospital in Los Angeles. “The answer may also be the most expensive, but other factors such as decreased length of stay and fewer complications can help bring that cost down.”
One example that CER might address is back surgery—an issue many physicians cannot agree on. “There are billions of dollars spent on back surgery that may not be necessary,” Dr. Fishmann points out.
CER could ultimately provide guidelines that would standardize treatments for all types of conditions: “A big organization like Cogent would like to think that a patient with pneumonia receives the same treatment whether he’s in California or in Mississippi—but there are many reasons this is probably not true,” says Dr. Fishmann.
CER So Far
The Medicare Modernization Act of 2003 gave CER a jumpstart with $65 million in appropriations and authorized the Agency for Healthcare Research and Quality (AHRQ) to conduct research.
“Since 2004, [the AHRQ has] received $15 million a year for CER,” says Emily Rowe, director of government relations for the Coalition for Health Services Research in Washington, D.C., and a member of the Friends of AHRQ coalition. “They’re pretty limited in what they can produce on that budget, but to date they’ve done some interesting work.”
That work includes eight published reports on treatment options for breast cancer, gastroesophageal reflux disease (GERD), cancer-related anemia, low-bone density, depression, and more, with 20 additional reports “in the pipeline,” says Rowe.
All available reports can be downloaded from http://effectivehealthcare. ahrq.gov, where results have been published in separate versions for physicians and consumers.
“The most interesting example of [CER from AHRQ] is synthesized research that shows that drugs can be as effective as surgery for severe heart burn,” or GERD, says Rowe. “This shows the promise of CER.”
So AHRQ is at work on CER projects but, says Rowe, “It needs a more serious investment.” Some in Congress agree.
New Laws, More Money
The Enhanced Health Care Value for All Act of 2007 (HR 2184) was introduced by Reps. Tom Allen, D-Maine, and Jo Ann Emerson, R-Mo, in May. This bill would provide $3 billion over five years to fund CER.
Under the legislation, the AHRQ would remain the federal agency charged with supporting CER, but a new comparative effectiveness advisory board would be established, comprising employers, consumers, healthcare providers, researchers, and others. The board would offer advice on research priorities and methodologies.
Some, including the Blue Cross Blue Shield Association (BCBSA), have called for a new executive-branch agency or a new coalition to oversee CER. Dr. Fishmann, who is serving a second term on the National Advisory Council for AHRQ, strongly disagrees. “This is evidence-based medicine,” he stresses. “AHRQ is the perfect entity for this. What an organization like AHRQ will do is look at everything and address the issue impartially.”
Quality, Costs, Results
Congress views CER as a means of saving costs in healthcare, but CER would not provide immediate savings; rather, it’s a first step toward lowering healthcare costs. In fact, House Ways and Means Subcommittee Chairman Pete Stark, R-Calif., expressed concern about “moving” CER legislation this year, because it would require immediate investment without immediate savings.
“I don’t know where you come up with that money when everyone else in healthcare is fighting for more funds,” Dr. Fishmann says of the current legislation. “But Congress can come up with the funds if they want to.”
Rowe won’t speculate on whether the House bill will pass but does say: “The appropriators and budgeters are getting ready to fund this, so that if the legislation passes the money will be there. And interest in CER is gaining in both parties of Congress.”
While legislators focus on costs and savings, healthcare professionals are interested in improving quality.
“It is a quality issue, but a better term is value,” says Rowe. “The idea is, ‘Let’s get what we pay for.’ The U.S. needs better medical outcomes, and the idea of CER is not what treatments costs less but that it’s worth it if you have to spend more if the outcomes are improved.”
And Dr. Fishmann thinks CER will change how we provide care. “It’s going to standardize the delivery of healthcare,” he predicts. “If you don’t follow these standards, someone is going to ask why not—it might be the payer, your colleagues, your hospital.” Once CER reports are available and shared with the public, he points out, “as patients get educated, and payers too, they’ll stop paying for treatments that go against the standard.”
—Emily Rowe, director of government relations for the Coalition for Health Services Research, Washington, D.C.
Hospitalists and CER
How will comparative effectiveness affect hospital medicine?
“They’re looking at ischemic heart disease, pneumonia, diabetes, stroke—all hospitalized diseases,” says Dr. Fishmann of current CER projects. “Right now, everyone is practicing their trade, and everyone is doing things differently. I think in terms of hospitalists, it clearly will affect how you treat patients, and for how long.”
Regardless of the current House bill, it seems CER is on the horizon, for hospitalists and for all of healthcare.
“The good news is, I don’t think this is going away any time soon,” says Rowe of CER. “The train has left the station and it’s steaming away.” TH
A new concept on Capitol Hill could reshape physicians’ treatment choices: comparative effectiveness research, or CER.
CER is a set of standards for examining the effectiveness of different therapies for a specific medical condition or set of patients to determine the best option. It may involve comparing competing medications or analyzing treatment approaches, such as surgery, devices, and drug therapies.
The healthcare community—and Capitol Hill—should keep an eye on CER.
“We need to look at evidence-based medicine and see what is the most effective treatment,” says Andrew Fishmann, MD, FCCP, FACP, co-founder of Cogent Healthcare and director of intensive care at Good Samaritan Hospital in Los Angeles. “The answer may also be the most expensive, but other factors such as decreased length of stay and fewer complications can help bring that cost down.”
One example that CER might address is back surgery—an issue many physicians cannot agree on. “There are billions of dollars spent on back surgery that may not be necessary,” Dr. Fishmann points out.
CER could ultimately provide guidelines that would standardize treatments for all types of conditions: “A big organization like Cogent would like to think that a patient with pneumonia receives the same treatment whether he’s in California or in Mississippi—but there are many reasons this is probably not true,” says Dr. Fishmann.
CER So Far
The Medicare Modernization Act of 2003 gave CER a jumpstart with $65 million in appropriations and authorized the Agency for Healthcare Research and Quality (AHRQ) to conduct research.
“Since 2004, [the AHRQ has] received $15 million a year for CER,” says Emily Rowe, director of government relations for the Coalition for Health Services Research in Washington, D.C., and a member of the Friends of AHRQ coalition. “They’re pretty limited in what they can produce on that budget, but to date they’ve done some interesting work.”
That work includes eight published reports on treatment options for breast cancer, gastroesophageal reflux disease (GERD), cancer-related anemia, low-bone density, depression, and more, with 20 additional reports “in the pipeline,” says Rowe.
All available reports can be downloaded from http://effectivehealthcare. ahrq.gov, where results have been published in separate versions for physicians and consumers.
“The most interesting example of [CER from AHRQ] is synthesized research that shows that drugs can be as effective as surgery for severe heart burn,” or GERD, says Rowe. “This shows the promise of CER.”
So AHRQ is at work on CER projects but, says Rowe, “It needs a more serious investment.” Some in Congress agree.
New Laws, More Money
The Enhanced Health Care Value for All Act of 2007 (HR 2184) was introduced by Reps. Tom Allen, D-Maine, and Jo Ann Emerson, R-Mo, in May. This bill would provide $3 billion over five years to fund CER.
Under the legislation, the AHRQ would remain the federal agency charged with supporting CER, but a new comparative effectiveness advisory board would be established, comprising employers, consumers, healthcare providers, researchers, and others. The board would offer advice on research priorities and methodologies.
Some, including the Blue Cross Blue Shield Association (BCBSA), have called for a new executive-branch agency or a new coalition to oversee CER. Dr. Fishmann, who is serving a second term on the National Advisory Council for AHRQ, strongly disagrees. “This is evidence-based medicine,” he stresses. “AHRQ is the perfect entity for this. What an organization like AHRQ will do is look at everything and address the issue impartially.”
Quality, Costs, Results
Congress views CER as a means of saving costs in healthcare, but CER would not provide immediate savings; rather, it’s a first step toward lowering healthcare costs. In fact, House Ways and Means Subcommittee Chairman Pete Stark, R-Calif., expressed concern about “moving” CER legislation this year, because it would require immediate investment without immediate savings.
“I don’t know where you come up with that money when everyone else in healthcare is fighting for more funds,” Dr. Fishmann says of the current legislation. “But Congress can come up with the funds if they want to.”
Rowe won’t speculate on whether the House bill will pass but does say: “The appropriators and budgeters are getting ready to fund this, so that if the legislation passes the money will be there. And interest in CER is gaining in both parties of Congress.”
While legislators focus on costs and savings, healthcare professionals are interested in improving quality.
“It is a quality issue, but a better term is value,” says Rowe. “The idea is, ‘Let’s get what we pay for.’ The U.S. needs better medical outcomes, and the idea of CER is not what treatments costs less but that it’s worth it if you have to spend more if the outcomes are improved.”
And Dr. Fishmann thinks CER will change how we provide care. “It’s going to standardize the delivery of healthcare,” he predicts. “If you don’t follow these standards, someone is going to ask why not—it might be the payer, your colleagues, your hospital.” Once CER reports are available and shared with the public, he points out, “as patients get educated, and payers too, they’ll stop paying for treatments that go against the standard.”
—Emily Rowe, director of government relations for the Coalition for Health Services Research, Washington, D.C.
Hospitalists and CER
How will comparative effectiveness affect hospital medicine?
“They’re looking at ischemic heart disease, pneumonia, diabetes, stroke—all hospitalized diseases,” says Dr. Fishmann of current CER projects. “Right now, everyone is practicing their trade, and everyone is doing things differently. I think in terms of hospitalists, it clearly will affect how you treat patients, and for how long.”
Regardless of the current House bill, it seems CER is on the horizon, for hospitalists and for all of healthcare.
“The good news is, I don’t think this is going away any time soon,” says Rowe of CER. “The train has left the station and it’s steaming away.” TH
Group Growth
This is the last article in a series on the four pillars of career satisfaction in hospital medicine.
What kind of support do you get from your hospital medicine group? From your hospital? How cohesive is your group? Do these things really matter?
The answers can be found in the SHM white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). SHM’s Career Satisfaction Task Force (CSTF) drafted the document to be used by hospitalists and hospital medicine practices as a toolkit for ensuring or improving job satisfaction. It outlines the four pillars of career satisfaction: autonomy/control (see the June edition of The Hospitalist, p. 14), workload/ schedule (July edition, p. 10), reward/ recognition (August edition, p. 10), and community/environment. This article looks at the last of these.
The Fourth Pillar
Hospitalists belong, in some sense, to four communities and must address the expectations of each group: administration, referring and nonreferring physicians, house staff and other healthcare staff, and medical students.
The hospitalist’s community includes his/her practice as well as hospitalists from other groups. The patient community is not just patients and their family members, but the broader public community served by the hospital medicine group and the hospital. The home community, consisting of the hospitalist’s family and friends, is also a vital part of the individual’s environment.
Each of these communities contributes to job satisfaction. A sense of shared values and connection with others, as well as social and work support, can ensure satisfaction; a sense of isolation, lack of support, and unresolved conflict can lead to unhappiness with a job.
Working within a strong community “makes everything else easier,” says CSTF member Noah Harris, MD, a hospitalist at Presbyterian Hospital, Albuquerque, N.M.
“Twenty years ago, there was a medical community in hospitals where physicians came together,” recalls Dr. Harris. “With managed care, physicians have become much less invested in the hospital and you see fewer [primary care] physicians there. Hospitalists have filled that gap. The question is how to restructure the hospital medical community.”
A hospitalist might struggle with the issue this way:
“I’m one of only three hospitalists at a hospital in a rural community. I feel it’s important to work as a team with primary care physicians, the emergency department, and other medical subspecialists.”
“How do hospitalists come in as the new kid on the block and reach out to other physicians?” asks Dr. Harris. “This is important, and if hospitalists feel like they’re more a part of the community, then that makes [their work] easier.”
According to Dr. Harris, the key to building a community in your workplace is communication. Strengthen it or establish it where there is none. When you communicate, focus on common goals with the other parties.
“Community has to do with shared expectations,” Dr. Harris points out. “Everyone—particularly the various types of physicians in the hospital—has to know what they expect from hospitalists.” It may be up to individual hospitalists to educate others as to what those expectations should be.
Of course, communication should start at the top. “On one level, there has to be formal communication with administrators and [physician leaders],” says Dr. Harris. “There has to be some sort of ongoing communication with the hospital administrators because they work with all the other groups as well.”
However, less formal communication is up to the hospitalist. The more you communicate with others, the more you’ll build your community.
Here are tips for how the hospitalist in the aforementioned example might work with each group of physicians:
ED doctors: “This hospitalist needs to get to know the other physicians and healthcare professionals,” Dr. Harris advises. “Make yourself available. When you have a minute, go down to the emergency department to update the ED physicians on admissions they’ve seen. Make a point to chat.”
Primary care physicians (PCPs): It may be more difficult to initiate informal communications with these docs if they’re not often in the hospital.
“One thing that helps is for the hospitalist to focus on communicating by phone, fax, or e-mail to PCPs when their patients are in the hospital,” says Dr. Harris. “In our office, we assigned a secretary to make sure PCPs get discharge summaries. That really helped with the community.”
If you want to strengthen ties to your community PCPs, issue an invitation to an event. “Our group would have an annual holiday party and invite all our referring physicians,” says Dr. Harris. “We’d have a speaker and get to know each other a little better.”
Surgeons: Dr. Harris suggests hospitalists can guide surgeons’ expectations for their working relationship with you and strengthen a sense of community.
“If there’s a particular issue, you can use that,” says Dr. Harris. “We were seeing a lot of elderly patients admitted with hip fractures. One thing we did to get a working relationship [with orthopedic surgeons] is we came up with a set of orders for these patients. The surgeons welcomed this because they wanted help with elderly patients who had multiple conditions. This was a way to work with them in a kind of formal way that helps patients. “It’s good to come up with order sets, but the big part of this is the negotiation with the other physicians that leads up to the order sets,” Dr. Harris says.
If you’re doing something like this to help in obstetrics, neurosurgery, or orthopedics, make it a two-way conversation.
“Above all else, it’s important to work with nonphysician healthcare workers,” says Dr. Harris, “especially nurses and physical therapists.”
The Rural Factor
The example above involves a small hospital medicine program in a rural area. Are there built-in problems with building community in this environment?
“I don’t think [it’s] necessarily more difficult” to build community in this setting, says Dr. Harris, “particularly if the hospital and physicians are on board with bringing in hospitalists. They might even be easier because you have fewer folks to deal with.”
But there may be an underlying problem with working at a smaller hospital. “If you’re the only hospitalist, or even the only hospitalist on a given shift, you’re practicing in a vacuum,” says Dr. Harris. If this is the case, you can broaden your hospitalist community by establishing a network with nearby hospitals and/or hospital medicine groups, and by becoming active in a regional or national group. TH
This is the last article in a series on the four pillars of career satisfaction in hospital medicine.
What kind of support do you get from your hospital medicine group? From your hospital? How cohesive is your group? Do these things really matter?
The answers can be found in the SHM white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). SHM’s Career Satisfaction Task Force (CSTF) drafted the document to be used by hospitalists and hospital medicine practices as a toolkit for ensuring or improving job satisfaction. It outlines the four pillars of career satisfaction: autonomy/control (see the June edition of The Hospitalist, p. 14), workload/ schedule (July edition, p. 10), reward/ recognition (August edition, p. 10), and community/environment. This article looks at the last of these.
The Fourth Pillar
Hospitalists belong, in some sense, to four communities and must address the expectations of each group: administration, referring and nonreferring physicians, house staff and other healthcare staff, and medical students.
The hospitalist’s community includes his/her practice as well as hospitalists from other groups. The patient community is not just patients and their family members, but the broader public community served by the hospital medicine group and the hospital. The home community, consisting of the hospitalist’s family and friends, is also a vital part of the individual’s environment.
Each of these communities contributes to job satisfaction. A sense of shared values and connection with others, as well as social and work support, can ensure satisfaction; a sense of isolation, lack of support, and unresolved conflict can lead to unhappiness with a job.
Working within a strong community “makes everything else easier,” says CSTF member Noah Harris, MD, a hospitalist at Presbyterian Hospital, Albuquerque, N.M.
“Twenty years ago, there was a medical community in hospitals where physicians came together,” recalls Dr. Harris. “With managed care, physicians have become much less invested in the hospital and you see fewer [primary care] physicians there. Hospitalists have filled that gap. The question is how to restructure the hospital medical community.”
A hospitalist might struggle with the issue this way:
“I’m one of only three hospitalists at a hospital in a rural community. I feel it’s important to work as a team with primary care physicians, the emergency department, and other medical subspecialists.”
“How do hospitalists come in as the new kid on the block and reach out to other physicians?” asks Dr. Harris. “This is important, and if hospitalists feel like they’re more a part of the community, then that makes [their work] easier.”
According to Dr. Harris, the key to building a community in your workplace is communication. Strengthen it or establish it where there is none. When you communicate, focus on common goals with the other parties.
“Community has to do with shared expectations,” Dr. Harris points out. “Everyone—particularly the various types of physicians in the hospital—has to know what they expect from hospitalists.” It may be up to individual hospitalists to educate others as to what those expectations should be.
Of course, communication should start at the top. “On one level, there has to be formal communication with administrators and [physician leaders],” says Dr. Harris. “There has to be some sort of ongoing communication with the hospital administrators because they work with all the other groups as well.”
However, less formal communication is up to the hospitalist. The more you communicate with others, the more you’ll build your community.
Here are tips for how the hospitalist in the aforementioned example might work with each group of physicians:
ED doctors: “This hospitalist needs to get to know the other physicians and healthcare professionals,” Dr. Harris advises. “Make yourself available. When you have a minute, go down to the emergency department to update the ED physicians on admissions they’ve seen. Make a point to chat.”
Primary care physicians (PCPs): It may be more difficult to initiate informal communications with these docs if they’re not often in the hospital.
“One thing that helps is for the hospitalist to focus on communicating by phone, fax, or e-mail to PCPs when their patients are in the hospital,” says Dr. Harris. “In our office, we assigned a secretary to make sure PCPs get discharge summaries. That really helped with the community.”
If you want to strengthen ties to your community PCPs, issue an invitation to an event. “Our group would have an annual holiday party and invite all our referring physicians,” says Dr. Harris. “We’d have a speaker and get to know each other a little better.”
Surgeons: Dr. Harris suggests hospitalists can guide surgeons’ expectations for their working relationship with you and strengthen a sense of community.
“If there’s a particular issue, you can use that,” says Dr. Harris. “We were seeing a lot of elderly patients admitted with hip fractures. One thing we did to get a working relationship [with orthopedic surgeons] is we came up with a set of orders for these patients. The surgeons welcomed this because they wanted help with elderly patients who had multiple conditions. This was a way to work with them in a kind of formal way that helps patients. “It’s good to come up with order sets, but the big part of this is the negotiation with the other physicians that leads up to the order sets,” Dr. Harris says.
If you’re doing something like this to help in obstetrics, neurosurgery, or orthopedics, make it a two-way conversation.
“Above all else, it’s important to work with nonphysician healthcare workers,” says Dr. Harris, “especially nurses and physical therapists.”
The Rural Factor
The example above involves a small hospital medicine program in a rural area. Are there built-in problems with building community in this environment?
“I don’t think [it’s] necessarily more difficult” to build community in this setting, says Dr. Harris, “particularly if the hospital and physicians are on board with bringing in hospitalists. They might even be easier because you have fewer folks to deal with.”
But there may be an underlying problem with working at a smaller hospital. “If you’re the only hospitalist, or even the only hospitalist on a given shift, you’re practicing in a vacuum,” says Dr. Harris. If this is the case, you can broaden your hospitalist community by establishing a network with nearby hospitals and/or hospital medicine groups, and by becoming active in a regional or national group. TH
This is the last article in a series on the four pillars of career satisfaction in hospital medicine.
What kind of support do you get from your hospital medicine group? From your hospital? How cohesive is your group? Do these things really matter?
The answers can be found in the SHM white paper “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). SHM’s Career Satisfaction Task Force (CSTF) drafted the document to be used by hospitalists and hospital medicine practices as a toolkit for ensuring or improving job satisfaction. It outlines the four pillars of career satisfaction: autonomy/control (see the June edition of The Hospitalist, p. 14), workload/ schedule (July edition, p. 10), reward/ recognition (August edition, p. 10), and community/environment. This article looks at the last of these.
The Fourth Pillar
Hospitalists belong, in some sense, to four communities and must address the expectations of each group: administration, referring and nonreferring physicians, house staff and other healthcare staff, and medical students.
The hospitalist’s community includes his/her practice as well as hospitalists from other groups. The patient community is not just patients and their family members, but the broader public community served by the hospital medicine group and the hospital. The home community, consisting of the hospitalist’s family and friends, is also a vital part of the individual’s environment.
Each of these communities contributes to job satisfaction. A sense of shared values and connection with others, as well as social and work support, can ensure satisfaction; a sense of isolation, lack of support, and unresolved conflict can lead to unhappiness with a job.
Working within a strong community “makes everything else easier,” says CSTF member Noah Harris, MD, a hospitalist at Presbyterian Hospital, Albuquerque, N.M.
“Twenty years ago, there was a medical community in hospitals where physicians came together,” recalls Dr. Harris. “With managed care, physicians have become much less invested in the hospital and you see fewer [primary care] physicians there. Hospitalists have filled that gap. The question is how to restructure the hospital medical community.”
A hospitalist might struggle with the issue this way:
“I’m one of only three hospitalists at a hospital in a rural community. I feel it’s important to work as a team with primary care physicians, the emergency department, and other medical subspecialists.”
“How do hospitalists come in as the new kid on the block and reach out to other physicians?” asks Dr. Harris. “This is important, and if hospitalists feel like they’re more a part of the community, then that makes [their work] easier.”
According to Dr. Harris, the key to building a community in your workplace is communication. Strengthen it or establish it where there is none. When you communicate, focus on common goals with the other parties.
“Community has to do with shared expectations,” Dr. Harris points out. “Everyone—particularly the various types of physicians in the hospital—has to know what they expect from hospitalists.” It may be up to individual hospitalists to educate others as to what those expectations should be.
Of course, communication should start at the top. “On one level, there has to be formal communication with administrators and [physician leaders],” says Dr. Harris. “There has to be some sort of ongoing communication with the hospital administrators because they work with all the other groups as well.”
However, less formal communication is up to the hospitalist. The more you communicate with others, the more you’ll build your community.
Here are tips for how the hospitalist in the aforementioned example might work with each group of physicians:
ED doctors: “This hospitalist needs to get to know the other physicians and healthcare professionals,” Dr. Harris advises. “Make yourself available. When you have a minute, go down to the emergency department to update the ED physicians on admissions they’ve seen. Make a point to chat.”
Primary care physicians (PCPs): It may be more difficult to initiate informal communications with these docs if they’re not often in the hospital.
“One thing that helps is for the hospitalist to focus on communicating by phone, fax, or e-mail to PCPs when their patients are in the hospital,” says Dr. Harris. “In our office, we assigned a secretary to make sure PCPs get discharge summaries. That really helped with the community.”
If you want to strengthen ties to your community PCPs, issue an invitation to an event. “Our group would have an annual holiday party and invite all our referring physicians,” says Dr. Harris. “We’d have a speaker and get to know each other a little better.”
Surgeons: Dr. Harris suggests hospitalists can guide surgeons’ expectations for their working relationship with you and strengthen a sense of community.
“If there’s a particular issue, you can use that,” says Dr. Harris. “We were seeing a lot of elderly patients admitted with hip fractures. One thing we did to get a working relationship [with orthopedic surgeons] is we came up with a set of orders for these patients. The surgeons welcomed this because they wanted help with elderly patients who had multiple conditions. This was a way to work with them in a kind of formal way that helps patients. “It’s good to come up with order sets, but the big part of this is the negotiation with the other physicians that leads up to the order sets,” Dr. Harris says.
If you’re doing something like this to help in obstetrics, neurosurgery, or orthopedics, make it a two-way conversation.
“Above all else, it’s important to work with nonphysician healthcare workers,” says Dr. Harris, “especially nurses and physical therapists.”
The Rural Factor
The example above involves a small hospital medicine program in a rural area. Are there built-in problems with building community in this environment?
“I don’t think [it’s] necessarily more difficult” to build community in this setting, says Dr. Harris, “particularly if the hospital and physicians are on board with bringing in hospitalists. They might even be easier because you have fewer folks to deal with.”
But there may be an underlying problem with working at a smaller hospital. “If you’re the only hospitalist, or even the only hospitalist on a given shift, you’re practicing in a vacuum,” says Dr. Harris. If this is the case, you can broaden your hospitalist community by establishing a network with nearby hospitals and/or hospital medicine groups, and by becoming active in a regional or national group. TH
After the Discharge
Hospital discharge and transition, whether back into the community or to other levels of care, are burdened by a lack of standardization and can be executed poorly—making them treacherous periods for patients.
Indeed, 20% of discharges are complicated by adverse events within 30 days, often resulting in avoidable trips to the emergency department and rehospitalization. Nationwide, 25% of patients are readmitted within 90 days, often because the fragmented discharge process leaves them vulnerable to iatrogenic complications.
Yet few studies have examined the discharge process in depth. Until now, none have looked at it from the patient’s point of view, lead author Lee Strunin, PhD, and colleagues Meg Stone, MPH, and Brian Jack, MD, write in the September-October edition of the Journal of Hospital Medicine. They interviewed 21 low-income patients in an inner-city hospital in Boston to identify the factors most closely associated with the risk of readmission.
The patients had a mean age of 46, and all had been hospitalized at least once within the previous six months. Twenty of the 21 patients were in the hospital for the same primary problem they were admitted for on their previous stay. The interviews lasted 20 to 45 minutes with each patient and addressed the patient’s ability to obtain follow-up care, care after discharge, and social support.
In most cases, inability to understand discharge instructions was not a problem. All participants could describe those instructions as well as their medical condition, why they were admitted to the hospital, and the medications they were taking.

—Brian Jack, MD, associate professor of family medicine, Boston University Medical Center
“For the participants in this study, difficult life circumstances posed a greater barrier to recuperation than lack of medical knowledge,” the investigators write. Patients complained of little or no support in such areas as child care, transportation to medical appointments, or attempts to overcome alcoholism or drug abuse. Many patients could not follow instructions to rest because they had to work or care for young children.
Half the patients reported psychological conditions such as depression and stress, which interfered with their ability to follow their treatment plan. For example, an 18-year-old black woman with diabetes told of how she would do well for a while, following diet and medication recommendations and monitoring her blood sugar regularly, only to become depressed and lose motivation. She was not receiving treatment for her depression. Another woman with polycystic kidney disease described pain that was sometimes so intense she had to delegate the housekeeping chores to her 5-year-old son.
Even though the patients in this study appeared to understand their illnesses and what to do (under ideal circumstances) after they went home, poor health literacy could be one explanation for these findings, senior author Dr. Jack tells The Hospitalist.
“We have data now that patients with low health literacy are less ready for discharge,” says Dr. Jack, associate professor of family medicine, Boston University Medical Center, and the department’s founding vice chair for academic affairs. He and his colleagues are developing patient-centered interventions to mitigate the discrepancies between people who are more or less health-literate. “To the degree that the middle-class population has higher health literacy, [outcomes after discharge] might vary,” he says.
These findings demonstrate the critical effect life circumstances outside the hospital have on a patient’s recovery, the authors say in the paper, adding that the patients’ experiences “clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain behavior change necessary to improve health, and follow instructions given by clinicians at the time of discharge.”
They further point out that interventions aimed at low-income patients should include social support and assistance with daily responsibilities.
“A focus on each patient’s life circumstance is critical,” Dr. Jack explains. For example, it isn’t sufficient simply to tell the patient when to come back for a stress test. Hospitals or caseworkers should also determine if “it is a day the patient can go, do they have a ride, daycare, do they know where the test is, which doctor will follow up the results, will they be seeing that doctor, and so on. There are now recent data suggesting that most tests ordered after discharge are never done.”
From this and other studies on the subject, it seems intuitive that providing these supports for at-risk patients should reduce rehospitalization rates. Is there any evidence this is the case?
“Not yet,” Dr. Jack says. “But stay tuned.” TH
Norra MacReady is a medical writer based in California.
Hospital discharge and transition, whether back into the community or to other levels of care, are burdened by a lack of standardization and can be executed poorly—making them treacherous periods for patients.
Indeed, 20% of discharges are complicated by adverse events within 30 days, often resulting in avoidable trips to the emergency department and rehospitalization. Nationwide, 25% of patients are readmitted within 90 days, often because the fragmented discharge process leaves them vulnerable to iatrogenic complications.
Yet few studies have examined the discharge process in depth. Until now, none have looked at it from the patient’s point of view, lead author Lee Strunin, PhD, and colleagues Meg Stone, MPH, and Brian Jack, MD, write in the September-October edition of the Journal of Hospital Medicine. They interviewed 21 low-income patients in an inner-city hospital in Boston to identify the factors most closely associated with the risk of readmission.
The patients had a mean age of 46, and all had been hospitalized at least once within the previous six months. Twenty of the 21 patients were in the hospital for the same primary problem they were admitted for on their previous stay. The interviews lasted 20 to 45 minutes with each patient and addressed the patient’s ability to obtain follow-up care, care after discharge, and social support.
In most cases, inability to understand discharge instructions was not a problem. All participants could describe those instructions as well as their medical condition, why they were admitted to the hospital, and the medications they were taking.
—Brian Jack, MD, associate professor of family medicine, Boston University Medical Center
“For the participants in this study, difficult life circumstances posed a greater barrier to recuperation than lack of medical knowledge,” the investigators write. Patients complained of little or no support in such areas as child care, transportation to medical appointments, or attempts to overcome alcoholism or drug abuse. Many patients could not follow instructions to rest because they had to work or care for young children.
Half the patients reported psychological conditions such as depression and stress, which interfered with their ability to follow their treatment plan. For example, an 18-year-old black woman with diabetes told of how she would do well for a while, following diet and medication recommendations and monitoring her blood sugar regularly, only to become depressed and lose motivation. She was not receiving treatment for her depression. Another woman with polycystic kidney disease described pain that was sometimes so intense she had to delegate the housekeeping chores to her 5-year-old son.
Even though the patients in this study appeared to understand their illnesses and what to do (under ideal circumstances) after they went home, poor health literacy could be one explanation for these findings, senior author Dr. Jack tells The Hospitalist.
“We have data now that patients with low health literacy are less ready for discharge,” says Dr. Jack, associate professor of family medicine, Boston University Medical Center, and the department’s founding vice chair for academic affairs. He and his colleagues are developing patient-centered interventions to mitigate the discrepancies between people who are more or less health-literate. “To the degree that the middle-class population has higher health literacy, [outcomes after discharge] might vary,” he says.
These findings demonstrate the critical effect life circumstances outside the hospital have on a patient’s recovery, the authors say in the paper, adding that the patients’ experiences “clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain behavior change necessary to improve health, and follow instructions given by clinicians at the time of discharge.”
They further point out that interventions aimed at low-income patients should include social support and assistance with daily responsibilities.
“A focus on each patient’s life circumstance is critical,” Dr. Jack explains. For example, it isn’t sufficient simply to tell the patient when to come back for a stress test. Hospitals or caseworkers should also determine if “it is a day the patient can go, do they have a ride, daycare, do they know where the test is, which doctor will follow up the results, will they be seeing that doctor, and so on. There are now recent data suggesting that most tests ordered after discharge are never done.”
From this and other studies on the subject, it seems intuitive that providing these supports for at-risk patients should reduce rehospitalization rates. Is there any evidence this is the case?
“Not yet,” Dr. Jack says. “But stay tuned.” TH
Norra MacReady is a medical writer based in California.
Hospital discharge and transition, whether back into the community or to other levels of care, are burdened by a lack of standardization and can be executed poorly—making them treacherous periods for patients.
Indeed, 20% of discharges are complicated by adverse events within 30 days, often resulting in avoidable trips to the emergency department and rehospitalization. Nationwide, 25% of patients are readmitted within 90 days, often because the fragmented discharge process leaves them vulnerable to iatrogenic complications.
Yet few studies have examined the discharge process in depth. Until now, none have looked at it from the patient’s point of view, lead author Lee Strunin, PhD, and colleagues Meg Stone, MPH, and Brian Jack, MD, write in the September-October edition of the Journal of Hospital Medicine. They interviewed 21 low-income patients in an inner-city hospital in Boston to identify the factors most closely associated with the risk of readmission.
The patients had a mean age of 46, and all had been hospitalized at least once within the previous six months. Twenty of the 21 patients were in the hospital for the same primary problem they were admitted for on their previous stay. The interviews lasted 20 to 45 minutes with each patient and addressed the patient’s ability to obtain follow-up care, care after discharge, and social support.
In most cases, inability to understand discharge instructions was not a problem. All participants could describe those instructions as well as their medical condition, why they were admitted to the hospital, and the medications they were taking.
—Brian Jack, MD, associate professor of family medicine, Boston University Medical Center
“For the participants in this study, difficult life circumstances posed a greater barrier to recuperation than lack of medical knowledge,” the investigators write. Patients complained of little or no support in such areas as child care, transportation to medical appointments, or attempts to overcome alcoholism or drug abuse. Many patients could not follow instructions to rest because they had to work or care for young children.
Half the patients reported psychological conditions such as depression and stress, which interfered with their ability to follow their treatment plan. For example, an 18-year-old black woman with diabetes told of how she would do well for a while, following diet and medication recommendations and monitoring her blood sugar regularly, only to become depressed and lose motivation. She was not receiving treatment for her depression. Another woman with polycystic kidney disease described pain that was sometimes so intense she had to delegate the housekeeping chores to her 5-year-old son.
Even though the patients in this study appeared to understand their illnesses and what to do (under ideal circumstances) after they went home, poor health literacy could be one explanation for these findings, senior author Dr. Jack tells The Hospitalist.
“We have data now that patients with low health literacy are less ready for discharge,” says Dr. Jack, associate professor of family medicine, Boston University Medical Center, and the department’s founding vice chair for academic affairs. He and his colleagues are developing patient-centered interventions to mitigate the discrepancies between people who are more or less health-literate. “To the degree that the middle-class population has higher health literacy, [outcomes after discharge] might vary,” he says.
These findings demonstrate the critical effect life circumstances outside the hospital have on a patient’s recovery, the authors say in the paper, adding that the patients’ experiences “clearly demonstrate the ways in which stresses make it difficult or impossible to attain sufficient rest to heal, maintain behavior change necessary to improve health, and follow instructions given by clinicians at the time of discharge.”
They further point out that interventions aimed at low-income patients should include social support and assistance with daily responsibilities.
“A focus on each patient’s life circumstance is critical,” Dr. Jack explains. For example, it isn’t sufficient simply to tell the patient when to come back for a stress test. Hospitals or caseworkers should also determine if “it is a day the patient can go, do they have a ride, daycare, do they know where the test is, which doctor will follow up the results, will they be seeing that doctor, and so on. There are now recent data suggesting that most tests ordered after discharge are never done.”
From this and other studies on the subject, it seems intuitive that providing these supports for at-risk patients should reduce rehospitalization rates. Is there any evidence this is the case?
“Not yet,” Dr. Jack says. “But stay tuned.” TH
Norra MacReady is a medical writer based in California.
Steroid Stress Dosing
Adrenal response to stress can vary broadly from patient to patient. For hospitalists, the challenge is predicting patients’ cortisol needs.
The variability exists whether one is dealing with a healthy patient or a patient with adrenal insufficiency (AI).1 Glucocorticoid use is even more complicated in patients with chronic autoimmune or inflammatory disorders who have been treated with high doses of glucocorticoids, or with those who are hypothalamic-pituitary-adrenal (HPA) axis suppressed.
Additionally, glucocorticoid administration is the most common cause of AI. Guidelines for adrenal supplementation therapy published in JAMA in 2002 note the difficulty in determining exact patient needs. JAMA’s review of guidelines for adrenal supplementation therapy is based on expert opinion, extrapolation from research literature, and clinical experience rather than clinical trials and should be consulted for more specific patient recommendations.2
Around the same time, similar guidelines on the management of rheumatoid arthritis (RA) patients on chronic glucocorticoids were published in the Bulletin on the Rheumatic Diseases.3 The guidelines suggest lower doses and shorter therapy than many textbooks advocate to counter problems associated with excessive steroid dosing. Problems such as immunosuppression, hyperglycemia, hypertension, acute psychosis, and accelerated protein catabolism lead to poor wound healing.
Additionally, the guidelines recommend that all patients receiving chronic glucocorticoids with an illness or while undergoing any procedure continue their normal daily glucocorticoid therapy. The authors caution that in patients with rheumatic disease, discontinuation of even low glucocorticoid doses may lead to a significant disease flare. Patients who receive 5 mg or less of prednisone daily do not require additional supplementation—regardless of whether they are undergoing a procedure or have an intercurrent illness. Patients undergoing superficial surgical procedures while less than an hour under local anesthesia (e.g., routine dental work, skin biopsy, minor orthopedic surgery) require their normal daily glucocorticoid dose without additional supplementation.
Patients with primary AI should receive individualized supplemental homeostatic glucocorticoid replacement therapy—usually with 20 to 30 mg of hydrocortisone two to three times daily in divided doses. Adjust based on patient factors and use of concomitant medications. Also consider that mineralocorticoid replacement may be necessary in these patients.
When considering patients for potential use of corticosteroids in the hospital, identify those who may be HPA-axis suppressed versus those who are not. The time to achieve HPA-axis suppression varies among patients. Patients can be considered not suppressed if:
- They have received any glucocorticoid doses for less than weeks; and
- They have received alternate-day glucocorticoid therapy. 4-6
- On the contrary, patients should be assumed to have HPA-axis suppression if they:
- Have received less than 20 mg of prednisone or its equivalent daily for more than three weeks (e.g., 16 mg/day methylprednisolone, 2 mg/ day dexamethasone, 80 mg/ day hydrocortisone); and/or
- Have clinical Cushing’s syndrome (e.g., centripetal obesity, glucose intolerance, proximal myopathy, hypertension, psychological chan-ges, and easy bruisability).
Intermediate patient categories may require HPA axis function testing with cosyntropin to determine if AI is present. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
References
- Lamberts SWJ, Bruining HA, de Jong FK. Corticosteroid therapy in severe illness. N Engl J Med. 1997 Oct 30;337(18):1285-1292.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002 Jan 9;287(2):236-240.
- Kelley JT, Conn DL. Perioperative management of the rheumatic disease patient. Bull Rheum Dis. 2002;51(6).
- Nieman LK, Kovacs WJ. Pharmacologic use of glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.pharmacologic use of glucocorticoids
- Nieman LK. Clinical manifestations of Cushing’s syndrome. UpToDate. Waltham, Mass. 2007.
- Welsh GA, Manzullo EF, Nieman LK. The surgical patient taking glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.patients.uptodate.com/topic.asp?file=adrenal
NEW WARNINGS

Actos tablets (pioglitazone, Eli Lilly) and Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- They have an increased risk of heart failure. They cause fluid retention, which may lead to or exacerbate congestive heart failure. Their warnings have been updated to reflect this because these agents are sometimes prescribed to patients with heart failure. Monitor patients carefully for the development of adverse cardiac effects.
- Don’t start or continue glitazones in patients with heart failure.
Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- Rosiglitazone has been associated with different rates of ischemic cardiovascular events (fatal and non-fatal). However, diabetic patients have an increased risk of cardiovascular disease.
- Analysis of rosiglitazone safety is ongoing. The Endocrinologic and Metabolic Drugs and the Drug Safety and Risk Management Advisory Committees meet jointly to discuss the cardiovascular ischemic and thrombotic risks of thiazolidinediones, especially focusing on rosiglitazone.
Additional information
- ww.fda.gov/bbs/topics/NEWS/ 2007/NEW01636.html
- www.fda.gov/cder/foi/label/2007/021073s026lbl.pdf
- www.fda.gov/cder/foi/label/2007/021071s023lbl.pdf
- “Rosiglitazone Evaluated for Cardiovascular Outcomes: An Interim Analysis,” New England Journal of Medicine. Published June 5 at www.nejm.org
Injectable Magnetic Resonance Imaging Contrast Agents: Magnevist (gadopentetate dimeglumine), MultiHance (gadobenate dimeglumine), Omniscan (gadodiamide), OptiMARK (gadoversetamide), and ProHance (gadoteridol)
- These are gadolinium-based contrast agents (GBCA).
- Patients with severe kidney insufficiency (a glomerular filtration rate [GLR] <30 mL/min/1.73m2) who receive GBCA are at risk for developing nephrogenic systemic fibrosis (NSF), a debilitating and potentially fatal disease. NSF may result in fatal or debilitating systemic fibrosis.
- Patients who are pre- or post-liver transplantation or have chronic liver disease with renal insufficiency also risk developing NSF.
- Screen patients for kidney problems prior to prescribing one of these GBCA. Do not exceed the recommended dose. Ensure that the recommended time has lapsed between doses of GBCA if it is to be used again.
- Boxed warning includes avoiding use of GBCAs unless the diagnostic information is essential and unavailable with non-contrast enhanced magnetic resonance imaging. Screen all patients for renal dysfunction. For patients receiving hemodialysis (HD), consider prompt HD following use of a GBCA. Published data indicate that GBCA elimination may be enhanced with HD. It has been reported that from the first to third HD sessions that average GBCA clearance rates were 78%, 96%, and 99%, respectively. It is not known whether HD prevents NSF.
- Report possible cases of NSF to the FDA through the FDA’s MedWatch program at www.fda.gov/medwatch/report/hcp.htm.
New Indication
- Apidra (insulin glulisine), Sanofi-Aventis’ rapid-acting insulin, has been FDA approved for intravenous (IV) administration in a clinical setting under medical supervision for glycemic control in adults with Type 1 or Type 2 diabetes mellitus. This approval provides another hospital-based option for diabetic patients, who may benefit from IV therapy in a clinical setting. Apidra is already approved for use subcutaneously from the vial, via external insulin infusion pump, or via the OptiClick reusable insulin pen.
Adrenal response to stress can vary broadly from patient to patient. For hospitalists, the challenge is predicting patients’ cortisol needs.
The variability exists whether one is dealing with a healthy patient or a patient with adrenal insufficiency (AI).1 Glucocorticoid use is even more complicated in patients with chronic autoimmune or inflammatory disorders who have been treated with high doses of glucocorticoids, or with those who are hypothalamic-pituitary-adrenal (HPA) axis suppressed.
Additionally, glucocorticoid administration is the most common cause of AI. Guidelines for adrenal supplementation therapy published in JAMA in 2002 note the difficulty in determining exact patient needs. JAMA’s review of guidelines for adrenal supplementation therapy is based on expert opinion, extrapolation from research literature, and clinical experience rather than clinical trials and should be consulted for more specific patient recommendations.2
Around the same time, similar guidelines on the management of rheumatoid arthritis (RA) patients on chronic glucocorticoids were published in the Bulletin on the Rheumatic Diseases.3 The guidelines suggest lower doses and shorter therapy than many textbooks advocate to counter problems associated with excessive steroid dosing. Problems such as immunosuppression, hyperglycemia, hypertension, acute psychosis, and accelerated protein catabolism lead to poor wound healing.
Additionally, the guidelines recommend that all patients receiving chronic glucocorticoids with an illness or while undergoing any procedure continue their normal daily glucocorticoid therapy. The authors caution that in patients with rheumatic disease, discontinuation of even low glucocorticoid doses may lead to a significant disease flare. Patients who receive 5 mg or less of prednisone daily do not require additional supplementation—regardless of whether they are undergoing a procedure or have an intercurrent illness. Patients undergoing superficial surgical procedures while less than an hour under local anesthesia (e.g., routine dental work, skin biopsy, minor orthopedic surgery) require their normal daily glucocorticoid dose without additional supplementation.
Patients with primary AI should receive individualized supplemental homeostatic glucocorticoid replacement therapy—usually with 20 to 30 mg of hydrocortisone two to three times daily in divided doses. Adjust based on patient factors and use of concomitant medications. Also consider that mineralocorticoid replacement may be necessary in these patients.
When considering patients for potential use of corticosteroids in the hospital, identify those who may be HPA-axis suppressed versus those who are not. The time to achieve HPA-axis suppression varies among patients. Patients can be considered not suppressed if:
- They have received any glucocorticoid doses for less than weeks; and
- They have received alternate-day glucocorticoid therapy. 4-6
- On the contrary, patients should be assumed to have HPA-axis suppression if they:
- Have received less than 20 mg of prednisone or its equivalent daily for more than three weeks (e.g., 16 mg/day methylprednisolone, 2 mg/ day dexamethasone, 80 mg/ day hydrocortisone); and/or
- Have clinical Cushing’s syndrome (e.g., centripetal obesity, glucose intolerance, proximal myopathy, hypertension, psychological chan-ges, and easy bruisability).
Intermediate patient categories may require HPA axis function testing with cosyntropin to determine if AI is present. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
References
- Lamberts SWJ, Bruining HA, de Jong FK. Corticosteroid therapy in severe illness. N Engl J Med. 1997 Oct 30;337(18):1285-1292.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002 Jan 9;287(2):236-240.
- Kelley JT, Conn DL. Perioperative management of the rheumatic disease patient. Bull Rheum Dis. 2002;51(6).
- Nieman LK, Kovacs WJ. Pharmacologic use of glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.pharmacologic use of glucocorticoids
- Nieman LK. Clinical manifestations of Cushing’s syndrome. UpToDate. Waltham, Mass. 2007.
- Welsh GA, Manzullo EF, Nieman LK. The surgical patient taking glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.patients.uptodate.com/topic.asp?file=adrenal
NEW WARNINGS
Actos tablets (pioglitazone, Eli Lilly) and Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- They have an increased risk of heart failure. They cause fluid retention, which may lead to or exacerbate congestive heart failure. Their warnings have been updated to reflect this because these agents are sometimes prescribed to patients with heart failure. Monitor patients carefully for the development of adverse cardiac effects.
- Don’t start or continue glitazones in patients with heart failure.
Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- Rosiglitazone has been associated with different rates of ischemic cardiovascular events (fatal and non-fatal). However, diabetic patients have an increased risk of cardiovascular disease.
- Analysis of rosiglitazone safety is ongoing. The Endocrinologic and Metabolic Drugs and the Drug Safety and Risk Management Advisory Committees meet jointly to discuss the cardiovascular ischemic and thrombotic risks of thiazolidinediones, especially focusing on rosiglitazone.
Additional information
- ww.fda.gov/bbs/topics/NEWS/ 2007/NEW01636.html
- www.fda.gov/cder/foi/label/2007/021073s026lbl.pdf
- www.fda.gov/cder/foi/label/2007/021071s023lbl.pdf
- “Rosiglitazone Evaluated for Cardiovascular Outcomes: An Interim Analysis,” New England Journal of Medicine. Published June 5 at www.nejm.org
Injectable Magnetic Resonance Imaging Contrast Agents: Magnevist (gadopentetate dimeglumine), MultiHance (gadobenate dimeglumine), Omniscan (gadodiamide), OptiMARK (gadoversetamide), and ProHance (gadoteridol)
- These are gadolinium-based contrast agents (GBCA).
- Patients with severe kidney insufficiency (a glomerular filtration rate [GLR] <30 mL/min/1.73m2) who receive GBCA are at risk for developing nephrogenic systemic fibrosis (NSF), a debilitating and potentially fatal disease. NSF may result in fatal or debilitating systemic fibrosis.
- Patients who are pre- or post-liver transplantation or have chronic liver disease with renal insufficiency also risk developing NSF.
- Screen patients for kidney problems prior to prescribing one of these GBCA. Do not exceed the recommended dose. Ensure that the recommended time has lapsed between doses of GBCA if it is to be used again.
- Boxed warning includes avoiding use of GBCAs unless the diagnostic information is essential and unavailable with non-contrast enhanced magnetic resonance imaging. Screen all patients for renal dysfunction. For patients receiving hemodialysis (HD), consider prompt HD following use of a GBCA. Published data indicate that GBCA elimination may be enhanced with HD. It has been reported that from the first to third HD sessions that average GBCA clearance rates were 78%, 96%, and 99%, respectively. It is not known whether HD prevents NSF.
- Report possible cases of NSF to the FDA through the FDA’s MedWatch program at www.fda.gov/medwatch/report/hcp.htm.
New Indication
- Apidra (insulin glulisine), Sanofi-Aventis’ rapid-acting insulin, has been FDA approved for intravenous (IV) administration in a clinical setting under medical supervision for glycemic control in adults with Type 1 or Type 2 diabetes mellitus. This approval provides another hospital-based option for diabetic patients, who may benefit from IV therapy in a clinical setting. Apidra is already approved for use subcutaneously from the vial, via external insulin infusion pump, or via the OptiClick reusable insulin pen.
Adrenal response to stress can vary broadly from patient to patient. For hospitalists, the challenge is predicting patients’ cortisol needs.
The variability exists whether one is dealing with a healthy patient or a patient with adrenal insufficiency (AI).1 Glucocorticoid use is even more complicated in patients with chronic autoimmune or inflammatory disorders who have been treated with high doses of glucocorticoids, or with those who are hypothalamic-pituitary-adrenal (HPA) axis suppressed.
Additionally, glucocorticoid administration is the most common cause of AI. Guidelines for adrenal supplementation therapy published in JAMA in 2002 note the difficulty in determining exact patient needs. JAMA’s review of guidelines for adrenal supplementation therapy is based on expert opinion, extrapolation from research literature, and clinical experience rather than clinical trials and should be consulted for more specific patient recommendations.2
Around the same time, similar guidelines on the management of rheumatoid arthritis (RA) patients on chronic glucocorticoids were published in the Bulletin on the Rheumatic Diseases.3 The guidelines suggest lower doses and shorter therapy than many textbooks advocate to counter problems associated with excessive steroid dosing. Problems such as immunosuppression, hyperglycemia, hypertension, acute psychosis, and accelerated protein catabolism lead to poor wound healing.
Additionally, the guidelines recommend that all patients receiving chronic glucocorticoids with an illness or while undergoing any procedure continue their normal daily glucocorticoid therapy. The authors caution that in patients with rheumatic disease, discontinuation of even low glucocorticoid doses may lead to a significant disease flare. Patients who receive 5 mg or less of prednisone daily do not require additional supplementation—regardless of whether they are undergoing a procedure or have an intercurrent illness. Patients undergoing superficial surgical procedures while less than an hour under local anesthesia (e.g., routine dental work, skin biopsy, minor orthopedic surgery) require their normal daily glucocorticoid dose without additional supplementation.
Patients with primary AI should receive individualized supplemental homeostatic glucocorticoid replacement therapy—usually with 20 to 30 mg of hydrocortisone two to three times daily in divided doses. Adjust based on patient factors and use of concomitant medications. Also consider that mineralocorticoid replacement may be necessary in these patients.
When considering patients for potential use of corticosteroids in the hospital, identify those who may be HPA-axis suppressed versus those who are not. The time to achieve HPA-axis suppression varies among patients. Patients can be considered not suppressed if:
- They have received any glucocorticoid doses for less than weeks; and
- They have received alternate-day glucocorticoid therapy. 4-6
- On the contrary, patients should be assumed to have HPA-axis suppression if they:
- Have received less than 20 mg of prednisone or its equivalent daily for more than three weeks (e.g., 16 mg/day methylprednisolone, 2 mg/ day dexamethasone, 80 mg/ day hydrocortisone); and/or
- Have clinical Cushing’s syndrome (e.g., centripetal obesity, glucose intolerance, proximal myopathy, hypertension, psychological chan-ges, and easy bruisability).
Intermediate patient categories may require HPA axis function testing with cosyntropin to determine if AI is present. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
References
- Lamberts SWJ, Bruining HA, de Jong FK. Corticosteroid therapy in severe illness. N Engl J Med. 1997 Oct 30;337(18):1285-1292.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002 Jan 9;287(2):236-240.
- Kelley JT, Conn DL. Perioperative management of the rheumatic disease patient. Bull Rheum Dis. 2002;51(6).
- Nieman LK, Kovacs WJ. Pharmacologic use of glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.pharmacologic use of glucocorticoids
- Nieman LK. Clinical manifestations of Cushing’s syndrome. UpToDate. Waltham, Mass. 2007.
- Welsh GA, Manzullo EF, Nieman LK. The surgical patient taking glucocorticoids. UpToDate. Waltham, Mass. 2007. Available at: www.patients.uptodate.com/topic.asp?file=adrenal
NEW WARNINGS
Actos tablets (pioglitazone, Eli Lilly) and Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- They have an increased risk of heart failure. They cause fluid retention, which may lead to or exacerbate congestive heart failure. Their warnings have been updated to reflect this because these agents are sometimes prescribed to patients with heart failure. Monitor patients carefully for the development of adverse cardiac effects.
- Don’t start or continue glitazones in patients with heart failure.
Avandia tablets (rosiglitazone, GlaxoSmithKline)
- These are oral thiazolidinediones (glitazones).
- Rosiglitazone has been associated with different rates of ischemic cardiovascular events (fatal and non-fatal). However, diabetic patients have an increased risk of cardiovascular disease.
- Analysis of rosiglitazone safety is ongoing. The Endocrinologic and Metabolic Drugs and the Drug Safety and Risk Management Advisory Committees meet jointly to discuss the cardiovascular ischemic and thrombotic risks of thiazolidinediones, especially focusing on rosiglitazone.
Additional information
- ww.fda.gov/bbs/topics/NEWS/ 2007/NEW01636.html
- www.fda.gov/cder/foi/label/2007/021073s026lbl.pdf
- www.fda.gov/cder/foi/label/2007/021071s023lbl.pdf
- “Rosiglitazone Evaluated for Cardiovascular Outcomes: An Interim Analysis,” New England Journal of Medicine. Published June 5 at www.nejm.org
Injectable Magnetic Resonance Imaging Contrast Agents: Magnevist (gadopentetate dimeglumine), MultiHance (gadobenate dimeglumine), Omniscan (gadodiamide), OptiMARK (gadoversetamide), and ProHance (gadoteridol)
- These are gadolinium-based contrast agents (GBCA).
- Patients with severe kidney insufficiency (a glomerular filtration rate [GLR] <30 mL/min/1.73m2) who receive GBCA are at risk for developing nephrogenic systemic fibrosis (NSF), a debilitating and potentially fatal disease. NSF may result in fatal or debilitating systemic fibrosis.
- Patients who are pre- or post-liver transplantation or have chronic liver disease with renal insufficiency also risk developing NSF.
- Screen patients for kidney problems prior to prescribing one of these GBCA. Do not exceed the recommended dose. Ensure that the recommended time has lapsed between doses of GBCA if it is to be used again.
- Boxed warning includes avoiding use of GBCAs unless the diagnostic information is essential and unavailable with non-contrast enhanced magnetic resonance imaging. Screen all patients for renal dysfunction. For patients receiving hemodialysis (HD), consider prompt HD following use of a GBCA. Published data indicate that GBCA elimination may be enhanced with HD. It has been reported that from the first to third HD sessions that average GBCA clearance rates were 78%, 96%, and 99%, respectively. It is not known whether HD prevents NSF.
- Report possible cases of NSF to the FDA through the FDA’s MedWatch program at www.fda.gov/medwatch/report/hcp.htm.
New Indication
- Apidra (insulin glulisine), Sanofi-Aventis’ rapid-acting insulin, has been FDA approved for intravenous (IV) administration in a clinical setting under medical supervision for glycemic control in adults with Type 1 or Type 2 diabetes mellitus. This approval provides another hospital-based option for diabetic patients, who may benefit from IV therapy in a clinical setting. Apidra is already approved for use subcutaneously from the vial, via external insulin infusion pump, or via the OptiClick reusable insulin pen.
In the Literature
Hematocrit and Perioperative Mortality
Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing noncardiac surgery. JAMA. 2007 Jun 13;297(22):2481-2488.
Several studies have outlined the risk of preoperative anemia prior to noncardiac surgery in elderly patients. These studies have not linked anemia to risk of death unless cardiac disease is present.
Anemia management remains a challenge for many hospitals and is the most important predictor of the need for blood transfusion. Transfusion increases morbidity and mortality in the perioperative setting. At the same time, little is known about the risks of polycythemia in this setting.
This retrospective cohort study used the Veterans’ Affairs National Surgical Quality Improvement Program database of 310,311 veterans 65 or older from 132 VA hospitals. It explores the relationship between abnormal levels of hematocrit and adverse events among elderly surgical patients.
The data suggest an incremental relationship between positive and negative deviation of hematocrit levels with 30-day postoperative mortality in patients 65 and older. Specifically, the study found a 1.6% increase (95% confidence interval, 1.1%-2.2%) in 30-day mortality for every percentage point of increase or decrease in hematocrit from the normal range.
Because this is an observational study of anemia and adverse events, no causal relationship can be established from this data. Hospitalists involved in perioperative care should be careful about drawing conclusions from this study alone and should not necessarily plan interventions to treat abnormal levels of hematocrit without carefully considering the risks and benefits of intervention.
Prognostic Utility of Pre-operative BNP
Feringa HH, Schouten O, Dunkelgrun M, et al. Plasma N-terminal pro-B-type natriuretic peptide as long term prognostic marker after major vascular surgery. Heart. 2007 Feb;93(2):226-231.
Traditional stratification of patients at high risk for cardiac complications and undergoing noncardiac surgery has included clinical risk index scoring and pre-operative stress testing. It is unclear if cardiac biomarkers can be used in conjunction with these measures to improve the identification of patients at risk.
Feringa and colleagues addressed this question by looking prospectively at 335 patients undergoing major vascular surgery over a two-year period. The mean age of patients was 62.2 years; 46% of patients underwent abdominal aortic aneurysm repair, and the remaining 54% received lower-extremity revascularization.
Patients had cardiac risk scores calculated based on the Revised Cardiac Risk Index (RCRI), and all patients had dobutamine stress echocardiogram (DSE) to assess for stress-induced ischemia. N-terminal pro-B-type natriuretic peptide (BNP) was measured at a mean of 12 days before surgery. Patients were followed for all-cause mortality and post-op death for a mean follow-up time of 14 months.
The authors found that NT-pro BNP performed better than the RCRI and DSE for predicting six-month mortality and cardiac events. An NT-pro BNP cut-off level of 319 ng/l was identified as optimal for predicting six-month mortality and cardiac events with 69% sensitivity and 70% specificity for mortality. Patients with levels 319 mg/l had a lower survival during the follow up period (p<0.0001).
Based on this prospective study, it appears that a preoperative elevated NT-Pro BNP is associated with long-term mortality and morbidity and could be used as an additional risk-stratification tool along with clinical risk scoring and stress testing.
Utility of Combination Medications in COPD
Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease. Ann Intern Med. 2007 Feb 19;146:545-555
The appropriateness of multiple long-acting inhaled medications in treating chronic obstructive pulmonary disease (COPD) is poorly studied. This study evaluated whether combining tiotropium with fluticasone-salmeterol or with salmeterol alone improves clinical outcomes in adult patients with moderate to severe COPD, as compared with tiotropium plus placebo.
This randomized, double-blind, placebo-controlled trial was set in academic and community medical centers in Canada. Researchers monitored 449 patients in the three parallel treatment groups for COPD exacerbations for 52 weeks. Analysis was done on an intention-to-treat basis. The rate of COPD exacerbations within the follow-up period (the primary outcome) was not significantly different among the three treatment groups. However, secondary outcomes, such as rates for hospitalization for COPD exacerbations, all-cause hospitalizations, health-related quality of life and lung function were significantly improved in the group receiving tiotropium and fluticasone-salmeterol.
A notable limitation was that more subjects stopped taking the study medications in the tiotropium-placebo and the tiotropium-salmeterol group. Many crossed over to treatments with inhaled corticosteroids or beta-agonists.
The results are in contrast to current guidelines, which recommend adding inhaled steroids to reduce exacerbations in moderate to severe COPD. Whether these results are due to differing statistical analysis among studies remains unclear. The authors postulate that reduction in secondary outcomes may be related to fluticasone reducing the severity of exacerbations rather than the actual number.
COPD exacerbations are among the most common diagnoses encountered by hospitalists. Most patients are treated with multiple inhaled medications to optimize their pulmonary status. Polypharmacy and the added financial burdens on the patient (particularly the elderly) are important considerations when deciding discharge medications, and the evidence of efficacy for combination inhaled medications had not been assessed as a clinical outcome prior to this study.
Benefits of Rapid Response Teams
Winters BD, Pham JC, Hunt EA et al. Rapid response systems: a systematic review. Crit Care Med. 2007 May;35(5):1238-1243.
Although the Institute for Healthcare Improvement has endorsed rapid response teams, and many hospitalist groups are involved with such systems, quality research is lacking.
Following up on the 2006 “First Consensus Conference on Medical Emergency Teams,” this meta-analysis sought to evaluate current literature to identify the effect of rapid response systems (RRS) on rates of hospital mortality and cardiac arrest.
The authors included randomized trials and observational studies in their analysis. Only eight studies met their inclusion criteria (six observational studies, one multicenter randomized trial, and one single-center randomized trial).
The pooled results did not demonstrate a statistically significant benefit of rapid-response systems in rates of hospital mortality. When rates of in-hospital cardiac arrest were analyzed, there was a weak finding in support of RRS, with the relative risk of 0.70 (confidence interval 0.56-0.92) in favor of RRSs. But the confidence interval was wide, and there was substantial heterogeneity among the included studies.
The authors conclude that “it seems premature to declare RRS as the standard of care,” and that data are lacking to justify any particular implementation scheme or composition of RRS or to support the cost-effectiveness of RRS.
Finally, they recognized the need for larger, better-designed randomized trials. However, in an accompanying editorial, Michael DeVita, MD—a pioneer in the development of RRS—rejects the use of techniques of evidence-based medicine such as multicenter trials and meta-analysis in assessing the utility of RRS. Dr. DeVita essentially says that changing the systems and culture of care within the hospital to accommodate patients with unmet critical needs must be effective in improving outcomes.
This meta-analysis is hindered by the suboptimal quality and homogeneity of studies available for assessment. Hospitalists should be aware of the limitations of the data and literature, as well as the empirical arguments raised by Dr. DeVita, when considering involvement in or designing RRS. TH
CLASSIC LIT
Perioperative Statins
Kapoor AS, Kanji H, Buckingham J, et al. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ. 2006 Nov 6;333(7579):1149.
Recent literature and randomized trials have claimed statins decrease morbidity and mortality from cardiovascular events in patients with or at high risk of coronary artery disease. This meta-analysis sought to determine the strength of evidence leading to the recommendations that perioperative statins be used to reduce perioperative cardiovascular events.
The literature search and exclusion criteria identified 18 studies. Two were randomized controlled trials (n=177), 15 were cohort studies (n=799,632), and one was a case-control study (n=480). Of these, 12 studies enrolled patients undergoing noncardiac vascular surgery, four enrolled patients undergoing coronary bypass surgery, and two enrolled patients undergoing various surgical procedures. The 16 nonrandomized studies were rated good. The two randomized trials were rated five and two out of five using the Jadad quality scores.
The results showed that in the randomized trials the summary odds ratio (OR) for death or acute coronary syndrome during the perioperative period with statin use was 0.26 (95% confidence interval 0.07 to 0.99), but this was based on only 13 events in 177 patients and cannot be considered conclusive. In the cohort studies, the OR was 0.70 (95% confidence interval 0.57 to 0.87). Although the pooled cohort data provided a statistically significant result, these cannot be considered conclusive because the statins were not randomly allocated and the results from retrospective studies were more impressive (OR 0.65, 95% confidence interval 0.50 to 0.84) than those in the prospective cohorts (OR 0.91, 95% confidence interval 0.65 to 1.27) and dose, duration, and safety of statin use were not reported.
Limitations of this meta-analysis include that none of the studies reported patient compliance or doses of statins or cholesterol levels before and after surgery, and few reported the duration of therapy before surgery or the which statin was used. Thus, the authors were unable to demonstrate a dose-response association. They were also unable to ascertain if the benefits seen with statins in the observational studies were exaggerated owing to inclusion of patients in the nonstatin group who had their statins stopped prior to surgery, because acute statin withdrawal may be associated with cardiac events.
The authors concluded that although their meta-analysis—which included data from more than 800,000 patients—suggests considerable benefits from perioperative statin use, the evidence from the randomized trials is not definitive. They advocate only that statins be started preoperatively in eligible patients (e.g., patients with coronary artery disease, multiple cardiac risk factors, elevated LDL) who would warrant statin therapy for medical reasons independent of the proposed operation.
Electronic Alerts to Prevent Hospital-acquired VTE
Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005 Mar 10;352(10):969-977
Surveys conducted in North America and Europe have shown that prophylaxis against deep venous thrombosis (DVT) has been consistently underused in hospitalized patients despite consensus guidelines. Studies involving continuing medical education and computerized electronic alerts have shown that physician use of prophylaxis improves when such processes are in place, but have not demonstrated that they can reduce the rate of DVT.
A computer program was developed to identify consecutive hospitalized patients at increased risk for DVT. The program used eight common risk factors to determine each patient’s risk profile for DVT and each risk factor was assigned a score. A cumulative score of four or higher was used to determine patients at high risk for DVT. The computer alert program was screened daily to identify patients whose score increased to four or higher after admission into the hospital. If the cumulative risk score was at least four, the computer program reviewed the current electronic orders and active medications for the use of DVT prophylaxis.
In the study, 2,506 consecutive adult patients were identified as high risk for DVT. Further,1,255 were randomized to the intervention group—in which the responsible physician received one electronic alert about the risk of DVT—and 1,251 patients were randomized to the control group in which no alert was issued. The 120 physicians involved took care of patients in the intervention and control groups. Physicians responsible for the control group were not aware that patients were being followed for clinical events. When physicians received alerts, they had to acknowledge them and could either withhold prophylaxis or order it on the same computer screen.
Patients were followed for 90 days after the index hospitalization. The primary end point was clinically apparent DVT or pulmonary embolism (PE). Safety end points included mortality at 30 days, and the rate of hemorrhagic events at 90 days.
The results showed that prophylactic measures were ordered for 421 of the 1,255 patients in the intervention group (33.5%) and 182 of the 1,251 patients in the control group (14.5%, p <0.001). There were higher rates of both mechanical (10% versus 1.5%, p<0.001) and pharmacological (23.6% versus 13.0%, p<0.001) prophylaxis in the intervention group. The primary end point of DVT or PE at 90 days occurred in 61 patients in the intervention group (4.9%) as compared with 103 patients in the control group (8.2%).
The computer alert reduced the risk of events at 90 days by 41% (HR 0.59; 95% CI 0.43 to 0.81; P=0.001). Of the patients who received prophylaxis 5.1% had DVT or PE compared with 7.0% of those who did not. In the intervention group, DVT or PE occurred in 20 of 421 (4.8%) patients who received prophylaxis compared with 41 of 834 (4.9%) who did not receive any. In the control group, the same numbers were 11 of 182 (6.0%) and 91 of 1,069 (8.5%).
Some of this benefit might be attributed to the additional preventive measures such as physiotherapy and early ambulation in patients assigned to the intervention group. Diagnostic bias also could have played into the results. Not all patients were screened for VTE, and it is likely that symptomatic patients without prophylaxis were screened more frequently than symptomatic patients with prophylaxis. Because physicians took care of both the control and intervention group, alerts received by physicians in the control group could have influenced their decision in the control group as well.
The authors concluded that instituting computer alerts markedly reduced the rates of DVT or PE in hospitalized patients.
Hematocrit and Perioperative Mortality
Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing noncardiac surgery. JAMA. 2007 Jun 13;297(22):2481-2488.
Several studies have outlined the risk of preoperative anemia prior to noncardiac surgery in elderly patients. These studies have not linked anemia to risk of death unless cardiac disease is present.
Anemia management remains a challenge for many hospitals and is the most important predictor of the need for blood transfusion. Transfusion increases morbidity and mortality in the perioperative setting. At the same time, little is known about the risks of polycythemia in this setting.
This retrospective cohort study used the Veterans’ Affairs National Surgical Quality Improvement Program database of 310,311 veterans 65 or older from 132 VA hospitals. It explores the relationship between abnormal levels of hematocrit and adverse events among elderly surgical patients.
The data suggest an incremental relationship between positive and negative deviation of hematocrit levels with 30-day postoperative mortality in patients 65 and older. Specifically, the study found a 1.6% increase (95% confidence interval, 1.1%-2.2%) in 30-day mortality for every percentage point of increase or decrease in hematocrit from the normal range.
Because this is an observational study of anemia and adverse events, no causal relationship can be established from this data. Hospitalists involved in perioperative care should be careful about drawing conclusions from this study alone and should not necessarily plan interventions to treat abnormal levels of hematocrit without carefully considering the risks and benefits of intervention.
Prognostic Utility of Pre-operative BNP
Feringa HH, Schouten O, Dunkelgrun M, et al. Plasma N-terminal pro-B-type natriuretic peptide as long term prognostic marker after major vascular surgery. Heart. 2007 Feb;93(2):226-231.
Traditional stratification of patients at high risk for cardiac complications and undergoing noncardiac surgery has included clinical risk index scoring and pre-operative stress testing. It is unclear if cardiac biomarkers can be used in conjunction with these measures to improve the identification of patients at risk.
Feringa and colleagues addressed this question by looking prospectively at 335 patients undergoing major vascular surgery over a two-year period. The mean age of patients was 62.2 years; 46% of patients underwent abdominal aortic aneurysm repair, and the remaining 54% received lower-extremity revascularization.
Patients had cardiac risk scores calculated based on the Revised Cardiac Risk Index (RCRI), and all patients had dobutamine stress echocardiogram (DSE) to assess for stress-induced ischemia. N-terminal pro-B-type natriuretic peptide (BNP) was measured at a mean of 12 days before surgery. Patients were followed for all-cause mortality and post-op death for a mean follow-up time of 14 months.
The authors found that NT-pro BNP performed better than the RCRI and DSE for predicting six-month mortality and cardiac events. An NT-pro BNP cut-off level of 319 ng/l was identified as optimal for predicting six-month mortality and cardiac events with 69% sensitivity and 70% specificity for mortality. Patients with levels 319 mg/l had a lower survival during the follow up period (p<0.0001).
Based on this prospective study, it appears that a preoperative elevated NT-Pro BNP is associated with long-term mortality and morbidity and could be used as an additional risk-stratification tool along with clinical risk scoring and stress testing.
Utility of Combination Medications in COPD
Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease. Ann Intern Med. 2007 Feb 19;146:545-555
The appropriateness of multiple long-acting inhaled medications in treating chronic obstructive pulmonary disease (COPD) is poorly studied. This study evaluated whether combining tiotropium with fluticasone-salmeterol or with salmeterol alone improves clinical outcomes in adult patients with moderate to severe COPD, as compared with tiotropium plus placebo.
This randomized, double-blind, placebo-controlled trial was set in academic and community medical centers in Canada. Researchers monitored 449 patients in the three parallel treatment groups for COPD exacerbations for 52 weeks. Analysis was done on an intention-to-treat basis. The rate of COPD exacerbations within the follow-up period (the primary outcome) was not significantly different among the three treatment groups. However, secondary outcomes, such as rates for hospitalization for COPD exacerbations, all-cause hospitalizations, health-related quality of life and lung function were significantly improved in the group receiving tiotropium and fluticasone-salmeterol.
A notable limitation was that more subjects stopped taking the study medications in the tiotropium-placebo and the tiotropium-salmeterol group. Many crossed over to treatments with inhaled corticosteroids or beta-agonists.
The results are in contrast to current guidelines, which recommend adding inhaled steroids to reduce exacerbations in moderate to severe COPD. Whether these results are due to differing statistical analysis among studies remains unclear. The authors postulate that reduction in secondary outcomes may be related to fluticasone reducing the severity of exacerbations rather than the actual number.
COPD exacerbations are among the most common diagnoses encountered by hospitalists. Most patients are treated with multiple inhaled medications to optimize their pulmonary status. Polypharmacy and the added financial burdens on the patient (particularly the elderly) are important considerations when deciding discharge medications, and the evidence of efficacy for combination inhaled medications had not been assessed as a clinical outcome prior to this study.
Benefits of Rapid Response Teams
Winters BD, Pham JC, Hunt EA et al. Rapid response systems: a systematic review. Crit Care Med. 2007 May;35(5):1238-1243.
Although the Institute for Healthcare Improvement has endorsed rapid response teams, and many hospitalist groups are involved with such systems, quality research is lacking.
Following up on the 2006 “First Consensus Conference on Medical Emergency Teams,” this meta-analysis sought to evaluate current literature to identify the effect of rapid response systems (RRS) on rates of hospital mortality and cardiac arrest.
The authors included randomized trials and observational studies in their analysis. Only eight studies met their inclusion criteria (six observational studies, one multicenter randomized trial, and one single-center randomized trial).
The pooled results did not demonstrate a statistically significant benefit of rapid-response systems in rates of hospital mortality. When rates of in-hospital cardiac arrest were analyzed, there was a weak finding in support of RRS, with the relative risk of 0.70 (confidence interval 0.56-0.92) in favor of RRSs. But the confidence interval was wide, and there was substantial heterogeneity among the included studies.
The authors conclude that “it seems premature to declare RRS as the standard of care,” and that data are lacking to justify any particular implementation scheme or composition of RRS or to support the cost-effectiveness of RRS.
Finally, they recognized the need for larger, better-designed randomized trials. However, in an accompanying editorial, Michael DeVita, MD—a pioneer in the development of RRS—rejects the use of techniques of evidence-based medicine such as multicenter trials and meta-analysis in assessing the utility of RRS. Dr. DeVita essentially says that changing the systems and culture of care within the hospital to accommodate patients with unmet critical needs must be effective in improving outcomes.
This meta-analysis is hindered by the suboptimal quality and homogeneity of studies available for assessment. Hospitalists should be aware of the limitations of the data and literature, as well as the empirical arguments raised by Dr. DeVita, when considering involvement in or designing RRS. TH
CLASSIC LIT
Perioperative Statins
Kapoor AS, Kanji H, Buckingham J, et al. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ. 2006 Nov 6;333(7579):1149.
Recent literature and randomized trials have claimed statins decrease morbidity and mortality from cardiovascular events in patients with or at high risk of coronary artery disease. This meta-analysis sought to determine the strength of evidence leading to the recommendations that perioperative statins be used to reduce perioperative cardiovascular events.
The literature search and exclusion criteria identified 18 studies. Two were randomized controlled trials (n=177), 15 were cohort studies (n=799,632), and one was a case-control study (n=480). Of these, 12 studies enrolled patients undergoing noncardiac vascular surgery, four enrolled patients undergoing coronary bypass surgery, and two enrolled patients undergoing various surgical procedures. The 16 nonrandomized studies were rated good. The two randomized trials were rated five and two out of five using the Jadad quality scores.
The results showed that in the randomized trials the summary odds ratio (OR) for death or acute coronary syndrome during the perioperative period with statin use was 0.26 (95% confidence interval 0.07 to 0.99), but this was based on only 13 events in 177 patients and cannot be considered conclusive. In the cohort studies, the OR was 0.70 (95% confidence interval 0.57 to 0.87). Although the pooled cohort data provided a statistically significant result, these cannot be considered conclusive because the statins were not randomly allocated and the results from retrospective studies were more impressive (OR 0.65, 95% confidence interval 0.50 to 0.84) than those in the prospective cohorts (OR 0.91, 95% confidence interval 0.65 to 1.27) and dose, duration, and safety of statin use were not reported.
Limitations of this meta-analysis include that none of the studies reported patient compliance or doses of statins or cholesterol levels before and after surgery, and few reported the duration of therapy before surgery or the which statin was used. Thus, the authors were unable to demonstrate a dose-response association. They were also unable to ascertain if the benefits seen with statins in the observational studies were exaggerated owing to inclusion of patients in the nonstatin group who had their statins stopped prior to surgery, because acute statin withdrawal may be associated with cardiac events.
The authors concluded that although their meta-analysis—which included data from more than 800,000 patients—suggests considerable benefits from perioperative statin use, the evidence from the randomized trials is not definitive. They advocate only that statins be started preoperatively in eligible patients (e.g., patients with coronary artery disease, multiple cardiac risk factors, elevated LDL) who would warrant statin therapy for medical reasons independent of the proposed operation.
Electronic Alerts to Prevent Hospital-acquired VTE
Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005 Mar 10;352(10):969-977
Surveys conducted in North America and Europe have shown that prophylaxis against deep venous thrombosis (DVT) has been consistently underused in hospitalized patients despite consensus guidelines. Studies involving continuing medical education and computerized electronic alerts have shown that physician use of prophylaxis improves when such processes are in place, but have not demonstrated that they can reduce the rate of DVT.
A computer program was developed to identify consecutive hospitalized patients at increased risk for DVT. The program used eight common risk factors to determine each patient’s risk profile for DVT and each risk factor was assigned a score. A cumulative score of four or higher was used to determine patients at high risk for DVT. The computer alert program was screened daily to identify patients whose score increased to four or higher after admission into the hospital. If the cumulative risk score was at least four, the computer program reviewed the current electronic orders and active medications for the use of DVT prophylaxis.
In the study, 2,506 consecutive adult patients were identified as high risk for DVT. Further,1,255 were randomized to the intervention group—in which the responsible physician received one electronic alert about the risk of DVT—and 1,251 patients were randomized to the control group in which no alert was issued. The 120 physicians involved took care of patients in the intervention and control groups. Physicians responsible for the control group were not aware that patients were being followed for clinical events. When physicians received alerts, they had to acknowledge them and could either withhold prophylaxis or order it on the same computer screen.
Patients were followed for 90 days after the index hospitalization. The primary end point was clinically apparent DVT or pulmonary embolism (PE). Safety end points included mortality at 30 days, and the rate of hemorrhagic events at 90 days.
The results showed that prophylactic measures were ordered for 421 of the 1,255 patients in the intervention group (33.5%) and 182 of the 1,251 patients in the control group (14.5%, p <0.001). There were higher rates of both mechanical (10% versus 1.5%, p<0.001) and pharmacological (23.6% versus 13.0%, p<0.001) prophylaxis in the intervention group. The primary end point of DVT or PE at 90 days occurred in 61 patients in the intervention group (4.9%) as compared with 103 patients in the control group (8.2%).
The computer alert reduced the risk of events at 90 days by 41% (HR 0.59; 95% CI 0.43 to 0.81; P=0.001). Of the patients who received prophylaxis 5.1% had DVT or PE compared with 7.0% of those who did not. In the intervention group, DVT or PE occurred in 20 of 421 (4.8%) patients who received prophylaxis compared with 41 of 834 (4.9%) who did not receive any. In the control group, the same numbers were 11 of 182 (6.0%) and 91 of 1,069 (8.5%).
Some of this benefit might be attributed to the additional preventive measures such as physiotherapy and early ambulation in patients assigned to the intervention group. Diagnostic bias also could have played into the results. Not all patients were screened for VTE, and it is likely that symptomatic patients without prophylaxis were screened more frequently than symptomatic patients with prophylaxis. Because physicians took care of both the control and intervention group, alerts received by physicians in the control group could have influenced their decision in the control group as well.
The authors concluded that instituting computer alerts markedly reduced the rates of DVT or PE in hospitalized patients.
Hematocrit and Perioperative Mortality
Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing noncardiac surgery. JAMA. 2007 Jun 13;297(22):2481-2488.
Several studies have outlined the risk of preoperative anemia prior to noncardiac surgery in elderly patients. These studies have not linked anemia to risk of death unless cardiac disease is present.
Anemia management remains a challenge for many hospitals and is the most important predictor of the need for blood transfusion. Transfusion increases morbidity and mortality in the perioperative setting. At the same time, little is known about the risks of polycythemia in this setting.
This retrospective cohort study used the Veterans’ Affairs National Surgical Quality Improvement Program database of 310,311 veterans 65 or older from 132 VA hospitals. It explores the relationship between abnormal levels of hematocrit and adverse events among elderly surgical patients.
The data suggest an incremental relationship between positive and negative deviation of hematocrit levels with 30-day postoperative mortality in patients 65 and older. Specifically, the study found a 1.6% increase (95% confidence interval, 1.1%-2.2%) in 30-day mortality for every percentage point of increase or decrease in hematocrit from the normal range.
Because this is an observational study of anemia and adverse events, no causal relationship can be established from this data. Hospitalists involved in perioperative care should be careful about drawing conclusions from this study alone and should not necessarily plan interventions to treat abnormal levels of hematocrit without carefully considering the risks and benefits of intervention.
Prognostic Utility of Pre-operative BNP
Feringa HH, Schouten O, Dunkelgrun M, et al. Plasma N-terminal pro-B-type natriuretic peptide as long term prognostic marker after major vascular surgery. Heart. 2007 Feb;93(2):226-231.
Traditional stratification of patients at high risk for cardiac complications and undergoing noncardiac surgery has included clinical risk index scoring and pre-operative stress testing. It is unclear if cardiac biomarkers can be used in conjunction with these measures to improve the identification of patients at risk.
Feringa and colleagues addressed this question by looking prospectively at 335 patients undergoing major vascular surgery over a two-year period. The mean age of patients was 62.2 years; 46% of patients underwent abdominal aortic aneurysm repair, and the remaining 54% received lower-extremity revascularization.
Patients had cardiac risk scores calculated based on the Revised Cardiac Risk Index (RCRI), and all patients had dobutamine stress echocardiogram (DSE) to assess for stress-induced ischemia. N-terminal pro-B-type natriuretic peptide (BNP) was measured at a mean of 12 days before surgery. Patients were followed for all-cause mortality and post-op death for a mean follow-up time of 14 months.
The authors found that NT-pro BNP performed better than the RCRI and DSE for predicting six-month mortality and cardiac events. An NT-pro BNP cut-off level of 319 ng/l was identified as optimal for predicting six-month mortality and cardiac events with 69% sensitivity and 70% specificity for mortality. Patients with levels 319 mg/l had a lower survival during the follow up period (p<0.0001).
Based on this prospective study, it appears that a preoperative elevated NT-Pro BNP is associated with long-term mortality and morbidity and could be used as an additional risk-stratification tool along with clinical risk scoring and stress testing.
Utility of Combination Medications in COPD
Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease. Ann Intern Med. 2007 Feb 19;146:545-555
The appropriateness of multiple long-acting inhaled medications in treating chronic obstructive pulmonary disease (COPD) is poorly studied. This study evaluated whether combining tiotropium with fluticasone-salmeterol or with salmeterol alone improves clinical outcomes in adult patients with moderate to severe COPD, as compared with tiotropium plus placebo.
This randomized, double-blind, placebo-controlled trial was set in academic and community medical centers in Canada. Researchers monitored 449 patients in the three parallel treatment groups for COPD exacerbations for 52 weeks. Analysis was done on an intention-to-treat basis. The rate of COPD exacerbations within the follow-up period (the primary outcome) was not significantly different among the three treatment groups. However, secondary outcomes, such as rates for hospitalization for COPD exacerbations, all-cause hospitalizations, health-related quality of life and lung function were significantly improved in the group receiving tiotropium and fluticasone-salmeterol.
A notable limitation was that more subjects stopped taking the study medications in the tiotropium-placebo and the tiotropium-salmeterol group. Many crossed over to treatments with inhaled corticosteroids or beta-agonists.
The results are in contrast to current guidelines, which recommend adding inhaled steroids to reduce exacerbations in moderate to severe COPD. Whether these results are due to differing statistical analysis among studies remains unclear. The authors postulate that reduction in secondary outcomes may be related to fluticasone reducing the severity of exacerbations rather than the actual number.
COPD exacerbations are among the most common diagnoses encountered by hospitalists. Most patients are treated with multiple inhaled medications to optimize their pulmonary status. Polypharmacy and the added financial burdens on the patient (particularly the elderly) are important considerations when deciding discharge medications, and the evidence of efficacy for combination inhaled medications had not been assessed as a clinical outcome prior to this study.
Benefits of Rapid Response Teams
Winters BD, Pham JC, Hunt EA et al. Rapid response systems: a systematic review. Crit Care Med. 2007 May;35(5):1238-1243.
Although the Institute for Healthcare Improvement has endorsed rapid response teams, and many hospitalist groups are involved with such systems, quality research is lacking.
Following up on the 2006 “First Consensus Conference on Medical Emergency Teams,” this meta-analysis sought to evaluate current literature to identify the effect of rapid response systems (RRS) on rates of hospital mortality and cardiac arrest.
The authors included randomized trials and observational studies in their analysis. Only eight studies met their inclusion criteria (six observational studies, one multicenter randomized trial, and one single-center randomized trial).
The pooled results did not demonstrate a statistically significant benefit of rapid-response systems in rates of hospital mortality. When rates of in-hospital cardiac arrest were analyzed, there was a weak finding in support of RRS, with the relative risk of 0.70 (confidence interval 0.56-0.92) in favor of RRSs. But the confidence interval was wide, and there was substantial heterogeneity among the included studies.
The authors conclude that “it seems premature to declare RRS as the standard of care,” and that data are lacking to justify any particular implementation scheme or composition of RRS or to support the cost-effectiveness of RRS.
Finally, they recognized the need for larger, better-designed randomized trials. However, in an accompanying editorial, Michael DeVita, MD—a pioneer in the development of RRS—rejects the use of techniques of evidence-based medicine such as multicenter trials and meta-analysis in assessing the utility of RRS. Dr. DeVita essentially says that changing the systems and culture of care within the hospital to accommodate patients with unmet critical needs must be effective in improving outcomes.
This meta-analysis is hindered by the suboptimal quality and homogeneity of studies available for assessment. Hospitalists should be aware of the limitations of the data and literature, as well as the empirical arguments raised by Dr. DeVita, when considering involvement in or designing RRS. TH
CLASSIC LIT
Perioperative Statins
Kapoor AS, Kanji H, Buckingham J, et al. Strength of evidence for perioperative use of statins to reduce cardiovascular risk: systematic review of controlled studies. BMJ. 2006 Nov 6;333(7579):1149.
Recent literature and randomized trials have claimed statins decrease morbidity and mortality from cardiovascular events in patients with or at high risk of coronary artery disease. This meta-analysis sought to determine the strength of evidence leading to the recommendations that perioperative statins be used to reduce perioperative cardiovascular events.
The literature search and exclusion criteria identified 18 studies. Two were randomized controlled trials (n=177), 15 were cohort studies (n=799,632), and one was a case-control study (n=480). Of these, 12 studies enrolled patients undergoing noncardiac vascular surgery, four enrolled patients undergoing coronary bypass surgery, and two enrolled patients undergoing various surgical procedures. The 16 nonrandomized studies were rated good. The two randomized trials were rated five and two out of five using the Jadad quality scores.
The results showed that in the randomized trials the summary odds ratio (OR) for death or acute coronary syndrome during the perioperative period with statin use was 0.26 (95% confidence interval 0.07 to 0.99), but this was based on only 13 events in 177 patients and cannot be considered conclusive. In the cohort studies, the OR was 0.70 (95% confidence interval 0.57 to 0.87). Although the pooled cohort data provided a statistically significant result, these cannot be considered conclusive because the statins were not randomly allocated and the results from retrospective studies were more impressive (OR 0.65, 95% confidence interval 0.50 to 0.84) than those in the prospective cohorts (OR 0.91, 95% confidence interval 0.65 to 1.27) and dose, duration, and safety of statin use were not reported.
Limitations of this meta-analysis include that none of the studies reported patient compliance or doses of statins or cholesterol levels before and after surgery, and few reported the duration of therapy before surgery or the which statin was used. Thus, the authors were unable to demonstrate a dose-response association. They were also unable to ascertain if the benefits seen with statins in the observational studies were exaggerated owing to inclusion of patients in the nonstatin group who had their statins stopped prior to surgery, because acute statin withdrawal may be associated with cardiac events.
The authors concluded that although their meta-analysis—which included data from more than 800,000 patients—suggests considerable benefits from perioperative statin use, the evidence from the randomized trials is not definitive. They advocate only that statins be started preoperatively in eligible patients (e.g., patients with coronary artery disease, multiple cardiac risk factors, elevated LDL) who would warrant statin therapy for medical reasons independent of the proposed operation.
Electronic Alerts to Prevent Hospital-acquired VTE
Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005 Mar 10;352(10):969-977
Surveys conducted in North America and Europe have shown that prophylaxis against deep venous thrombosis (DVT) has been consistently underused in hospitalized patients despite consensus guidelines. Studies involving continuing medical education and computerized electronic alerts have shown that physician use of prophylaxis improves when such processes are in place, but have not demonstrated that they can reduce the rate of DVT.
A computer program was developed to identify consecutive hospitalized patients at increased risk for DVT. The program used eight common risk factors to determine each patient’s risk profile for DVT and each risk factor was assigned a score. A cumulative score of four or higher was used to determine patients at high risk for DVT. The computer alert program was screened daily to identify patients whose score increased to four or higher after admission into the hospital. If the cumulative risk score was at least four, the computer program reviewed the current electronic orders and active medications for the use of DVT prophylaxis.
In the study, 2,506 consecutive adult patients were identified as high risk for DVT. Further,1,255 were randomized to the intervention group—in which the responsible physician received one electronic alert about the risk of DVT—and 1,251 patients were randomized to the control group in which no alert was issued. The 120 physicians involved took care of patients in the intervention and control groups. Physicians responsible for the control group were not aware that patients were being followed for clinical events. When physicians received alerts, they had to acknowledge them and could either withhold prophylaxis or order it on the same computer screen.
Patients were followed for 90 days after the index hospitalization. The primary end point was clinically apparent DVT or pulmonary embolism (PE). Safety end points included mortality at 30 days, and the rate of hemorrhagic events at 90 days.
The results showed that prophylactic measures were ordered for 421 of the 1,255 patients in the intervention group (33.5%) and 182 of the 1,251 patients in the control group (14.5%, p <0.001). There were higher rates of both mechanical (10% versus 1.5%, p<0.001) and pharmacological (23.6% versus 13.0%, p<0.001) prophylaxis in the intervention group. The primary end point of DVT or PE at 90 days occurred in 61 patients in the intervention group (4.9%) as compared with 103 patients in the control group (8.2%).
The computer alert reduced the risk of events at 90 days by 41% (HR 0.59; 95% CI 0.43 to 0.81; P=0.001). Of the patients who received prophylaxis 5.1% had DVT or PE compared with 7.0% of those who did not. In the intervention group, DVT or PE occurred in 20 of 421 (4.8%) patients who received prophylaxis compared with 41 of 834 (4.9%) who did not receive any. In the control group, the same numbers were 11 of 182 (6.0%) and 91 of 1,069 (8.5%).
Some of this benefit might be attributed to the additional preventive measures such as physiotherapy and early ambulation in patients assigned to the intervention group. Diagnostic bias also could have played into the results. Not all patients were screened for VTE, and it is likely that symptomatic patients without prophylaxis were screened more frequently than symptomatic patients with prophylaxis. Because physicians took care of both the control and intervention group, alerts received by physicians in the control group could have influenced their decision in the control group as well.
The authors concluded that instituting computer alerts markedly reduced the rates of DVT or PE in hospitalized patients.
Network of Knowledge
By now almost everyone has heard about the social network site MySpace. More than 50 million people—mostly between ages 14 and 24—post and view online profiles connected by links to friends in the system. It’s one of the most heavily trafficked sites on the Internet.
MySpace is remarkable not only for consistent, double-digit growth rate, but also because visitors average two hours on the site modifying their profiles, and checking out friends’ profiles and commenting on them. MySpace has become ubiquitous to a generation using this public space to create and modify their identity on a daily basis—with technology that only recently has become available.
While recognizing that it may be a long time before www.hospitalmedicine.org becomes a household destination, the SHM Research Committee aims to generate similar excitement among our peers for connecting with each other over hospital medicine research on the Web.
Chapter Summary
Las Vegas

The SHM Las Vegas Chapter held its quarterly administrative meeting June 26 at Roy’s in Las Vegas. Gary Skankey, MD, infectious disease specialist and associate clinical professor at the University of Nevada School of Medicine, presented “Treating Complicated Skin and Skin Infections in an Era of Increasing Resistance.” The chapter will host a CME Program on surviving sepsis Sept. 28-29. Visit the chapter page for further program details.
Nashville
The SHM Nashville Chapter meeting June 6 at Stoney River restaurant was sponsored by Ortho McNeil and HCA Physician Recruitment. Eric Siegal, MD, with the University of Wisconsin Hospital in Madison, was the featured presenter and led an interactive session during “Malpractice for the Hospitalists: Identifying and Mitigating Risks.” The next meeting is scheduled for this month. Details will be posted at a later date.
At the SHM Research Committee meeting in Dallas in May, the conversation covered many topics, including the need for research mentorship, training, and career development. Plans for short- and medium-term measures to support SHM members in these areas are in the works, with a focus on Internet-based resources.
Over the long term, the committee would like to see its efforts result in national, high-impact hospital medicine studies and well-trained researchers. Whether driven by a curiosity in a particular area and/or the desire to provide better care by incorporating the best research, the universal challenge is to free enough time to pursue the answers and for appropriate recognition systems to be in place—be they promotion, funding to support further work, or recognition that leads to new connections.
The 249 abstracts published in a supplement to the Journal of Hospital Medicine only hinted at the depth and enthusiasm behind SHM members’ work. Anyone who walked through the exhibit hall during the poster session at the SHM Annual Meeting and talked with the people behind the research was impressed with their dedication and relative youth. They are the future of hospital medicine and are looking for ways to collaborate and continue to learn. The SHM Research Committee is dedicated to finding ways to support their efforts.
It seems as if many SHM members either engage in research, think about a research project, or wish they could evaluate their everyday practice in a way that can help others. However, it is difficult to discern how best to support individual hospitalists working in diverse settings across the country.
Because clinical responsibilities will not slow down anytime soon, we will have to work within the current, hectic environment and use technology as an equalizer to enable communication. In the spectrum of professional medical societies, SHM could be considered similar to the age 14-24 demographic attracted to the fluidity, instant communication/information and innovation that fuels MySpace.
Our long-term research goals could be powerfully advanced by a peer-catalyzed hospitalist research network.
The term “research network” can refer to many types of collaboration. One type that has been successful is the collection, analysis, and reporting of data in a registry or repository. In this example, medical care can be measured through the collection, analysis, and reporting of data. The National Cardiovascular Data Registry (established in 1998 by the American College of Cardiology Foundation) is a well-known example, but there are many others that have been organized for the purposes of improving quality and providing educational and research activities.
A second type of research network is the developing partnership between the American Medical Association (AMA) and Sermo, an online community where physicians exchange medical opinions. The partnership attempts to use technology to harness innovation, support physicians, and improve the capability of a peer network to influence the care patients receive by letting them share information with each other regarding patient care, pertinent scientific research, and advocacy issues. This is a looser network—without the constraints of data dictionaries—that relies on technology to make the connection between physician peers. While its start-up costs may be lower, its impact will be more difficult to measure.
A third example is the Gotham Prize for Cancer Research, which requires investigators to qualify by logging onto a Web site (www.gothamprize.org), posting a short proposal, and answering questions. If accepted by the expert panel of cancer researchers into this active forum, the new member will not only be eligible to receive the annual prize for the best idea, these individuals and their ideas will be matched to funding agencies and other scientists who may be able to support, assist, and/or collaborate. This limited-access network requires more facilitation than the previous AMA example, and the incentives and outcomes are more clearly defined.
The SHM Research Committee sees potential in exploring a network for hospital medicine researchers, through which members can access resources, collaborate, and innovate. Internet technology has the potential to level the playing field and erase the barriers of time differences and geography. By organizing around areas of interest designed to attract a critical mass of interested hospitalists, the goal of this network is to position SHM to lead hospital medicine research and ensure long-term success and sustainability by enabling powerful, high-impact studies in hospital medicine and supporting well-trained hospitalist researchers. Although this discussion is in the early stages of development, the SHM Research Committee plans to consider the following questions:
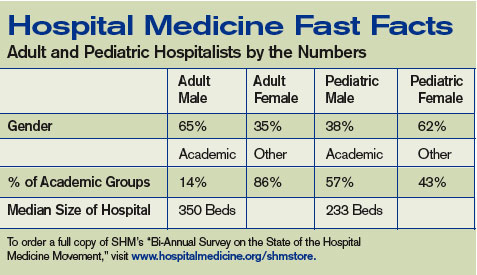
How would a network help hospital medicine and hospitalists? During the meeting in May in Dallas, the SHM Research Committee articulated the need for research mentorship, training, and career development. Any proposed network must further these aims. Hospital medicine investigators and SHM members would be involved in refining these goals at the earliest stages. Opportunities for training a new generation of hospital medicine investigators and strengthening the existing ones through such a network will be explored, including options for training in outcomes research and opportunities to link participants with mentors.
What questions should a network focus on? Hospitalists are well positioned to lead or collaborate on a range of key questions—questions that, in the short term, likely will focus on effectiveness and implementation research (related to quality improvement). Over the longer term, hospitalists should position themselves to be involved in all facets of clinical translational research, including T1 (bench-to-bedside research) and T2 (effectiveness research, such as larger randomized studies, and health services research). As hospital medicine grows, the potential areas where hospitalists might focus their scientific interests will expand. As hospitalists assume greater roles in caring for patients outside general medicine (e.g., surgical, cardiovascular, neurology, and oncology patients), the breadth of scientific inquiry will expand. In many of these cases, research networks exist; SHM will have to facilitate collaboration whenever possible.
How will the network engage a broad swath of hospitalists? By selecting research questions important to public health and anticipating a changing clinical environment, we hope to enhance the interest and relevance of an SHM research network. The SHM Research Committee will focus on how best to design a research network that is practical and useful for hospital medicine researchers and enable straightforward studies. A main goal will be promoting visibility for investigators and coordinators through opportunities for authorship and presentation of results at national meetings.
Healthcare reform has become a hot political issue again—more than a year before the presidential election. All three leading Democratic candidates (Hillary Clinton, Barack Obama, and John Edwards) have proposed some sort of a central institute to assess treatment options and disseminate research and information to providers. Hospitalists (as generalists and team leaders in an arena where approximately 30% of the healthcare dollar is spent) are a key part of any national solution.
Whether this research requires a catalyst such as a hospitalist network—and what that network would look like—remains to be seen. The SHM Research Committee is considering mechanisms to provide research mentorship, training, and career development, and weighing the best use of resources. We count on your input. Contact Carolyn Brennan, director of research program development for SHM, at [email protected] for more information or to get involved. TH
SHM Behind the Scenes
PRIS updates in Salt Lake City
By Todd Von Deak
Each year, one of the premier events in pediatric hospital medicine is a summer conference presented by the American Academy of Pediatrics (AAP), the Ambulatory Pediatric Association (APA), and SHM. This year’s conference, held last month in Salt Lake City under the lead sponsorship of the AAP, was no exception.
More than 300 pediatric hospitalists, medical directors, residents, nurse practitioners, and physician assistants came together for four days to network, get answers, and learn from colleagues at 30 sessions. Charlie Homer, CEO of the National Institute for Children’s HealthCare Quality in Cambridge, Mass., was the keynote speaker. Dr. Homer highlighted the roles hospitalists can and must play to improve children’s health, and challenged all present to create a dashboard that includes quality indicators for care that is efficient, equitable, evidence-based, safe, and family-centered.
Leaders from the AAP, APA, and SHM opened the morning sessions the next day with brief presentations that highlighted the role of pediatric hospitalists in each organization, and the potential to work together to continue to develop pediatric hospital medicine and advance the care of hospitalized children. Participants were then free to choose from more than 16 sessions ranging from clinical issues such as the management of apparent life-threatening events and appropriate maintenance IV fluids, to practice management (Coding 101 and 201), quality improvement, and resident teaching and research.
Capping the schedule of events was a luncheon presentation from Christopher P. Landrigan, MD, director of the Pediatric Research in Inpatient Settings network. He presented “PRIS Update: The Need for Collaborative Hospitalist Research in 2007.” PRIS is an independent collaborative entity established by the same organizations that sponsor the Salt Lake City conference and is designed to allow for collaborative study of key questions in inpatient pediatrics.
Linda Snelling, MD, inpatient director and chief of pediatric critical care at Hasbro Children’s Hospital in Providence, R.I., followed with a talk on how pediatric hospitalists can effectively negotiate for themselves and the field. Her key insights included, “ ‘No.’ is a complete sentence.”
According to Jack Percelay, MD, past chair of SHM’s Pediatric Committee and a practicing pediatric hospitalist in New York and New Jersey, the conference exceeded its goals. “The energy at the conference was tremendous,” he said. “Sessions were filled with attendees learning of and debating cutting-edge issues for pediatric hospitalists. The buzz in the hotel was so intoxicating we were worried that we were violating Salt Lake City liquor laws. The AAP put on a spectacular meeting. SHM is looking forward to following this tradition of excellence as we take the lead for putting on an even larger meeting in Denver July 24-27, 2008.”
Given that the 2008 meeting sold out six weeks in advance, pediatric hospitalists will do well to stay tuned to The Hospitalist and visit SHM’s Web site, www.hospitalmedicine.org, for more details as the 2008 conference approaches. TH
By now almost everyone has heard about the social network site MySpace. More than 50 million people—mostly between ages 14 and 24—post and view online profiles connected by links to friends in the system. It’s one of the most heavily trafficked sites on the Internet.
MySpace is remarkable not only for consistent, double-digit growth rate, but also because visitors average two hours on the site modifying their profiles, and checking out friends’ profiles and commenting on them. MySpace has become ubiquitous to a generation using this public space to create and modify their identity on a daily basis—with technology that only recently has become available.
While recognizing that it may be a long time before www.hospitalmedicine.org becomes a household destination, the SHM Research Committee aims to generate similar excitement among our peers for connecting with each other over hospital medicine research on the Web.
Chapter Summary
Las Vegas
The SHM Las Vegas Chapter held its quarterly administrative meeting June 26 at Roy’s in Las Vegas. Gary Skankey, MD, infectious disease specialist and associate clinical professor at the University of Nevada School of Medicine, presented “Treating Complicated Skin and Skin Infections in an Era of Increasing Resistance.” The chapter will host a CME Program on surviving sepsis Sept. 28-29. Visit the chapter page for further program details.
Nashville
The SHM Nashville Chapter meeting June 6 at Stoney River restaurant was sponsored by Ortho McNeil and HCA Physician Recruitment. Eric Siegal, MD, with the University of Wisconsin Hospital in Madison, was the featured presenter and led an interactive session during “Malpractice for the Hospitalists: Identifying and Mitigating Risks.” The next meeting is scheduled for this month. Details will be posted at a later date.
At the SHM Research Committee meeting in Dallas in May, the conversation covered many topics, including the need for research mentorship, training, and career development. Plans for short- and medium-term measures to support SHM members in these areas are in the works, with a focus on Internet-based resources.
Over the long term, the committee would like to see its efforts result in national, high-impact hospital medicine studies and well-trained researchers. Whether driven by a curiosity in a particular area and/or the desire to provide better care by incorporating the best research, the universal challenge is to free enough time to pursue the answers and for appropriate recognition systems to be in place—be they promotion, funding to support further work, or recognition that leads to new connections.
The 249 abstracts published in a supplement to the Journal of Hospital Medicine only hinted at the depth and enthusiasm behind SHM members’ work. Anyone who walked through the exhibit hall during the poster session at the SHM Annual Meeting and talked with the people behind the research was impressed with their dedication and relative youth. They are the future of hospital medicine and are looking for ways to collaborate and continue to learn. The SHM Research Committee is dedicated to finding ways to support their efforts.
It seems as if many SHM members either engage in research, think about a research project, or wish they could evaluate their everyday practice in a way that can help others. However, it is difficult to discern how best to support individual hospitalists working in diverse settings across the country.
Because clinical responsibilities will not slow down anytime soon, we will have to work within the current, hectic environment and use technology as an equalizer to enable communication. In the spectrum of professional medical societies, SHM could be considered similar to the age 14-24 demographic attracted to the fluidity, instant communication/information and innovation that fuels MySpace.
Our long-term research goals could be powerfully advanced by a peer-catalyzed hospitalist research network.
The term “research network” can refer to many types of collaboration. One type that has been successful is the collection, analysis, and reporting of data in a registry or repository. In this example, medical care can be measured through the collection, analysis, and reporting of data. The National Cardiovascular Data Registry (established in 1998 by the American College of Cardiology Foundation) is a well-known example, but there are many others that have been organized for the purposes of improving quality and providing educational and research activities.
A second type of research network is the developing partnership between the American Medical Association (AMA) and Sermo, an online community where physicians exchange medical opinions. The partnership attempts to use technology to harness innovation, support physicians, and improve the capability of a peer network to influence the care patients receive by letting them share information with each other regarding patient care, pertinent scientific research, and advocacy issues. This is a looser network—without the constraints of data dictionaries—that relies on technology to make the connection between physician peers. While its start-up costs may be lower, its impact will be more difficult to measure.
A third example is the Gotham Prize for Cancer Research, which requires investigators to qualify by logging onto a Web site (www.gothamprize.org), posting a short proposal, and answering questions. If accepted by the expert panel of cancer researchers into this active forum, the new member will not only be eligible to receive the annual prize for the best idea, these individuals and their ideas will be matched to funding agencies and other scientists who may be able to support, assist, and/or collaborate. This limited-access network requires more facilitation than the previous AMA example, and the incentives and outcomes are more clearly defined.
The SHM Research Committee sees potential in exploring a network for hospital medicine researchers, through which members can access resources, collaborate, and innovate. Internet technology has the potential to level the playing field and erase the barriers of time differences and geography. By organizing around areas of interest designed to attract a critical mass of interested hospitalists, the goal of this network is to position SHM to lead hospital medicine research and ensure long-term success and sustainability by enabling powerful, high-impact studies in hospital medicine and supporting well-trained hospitalist researchers. Although this discussion is in the early stages of development, the SHM Research Committee plans to consider the following questions:
How would a network help hospital medicine and hospitalists? During the meeting in May in Dallas, the SHM Research Committee articulated the need for research mentorship, training, and career development. Any proposed network must further these aims. Hospital medicine investigators and SHM members would be involved in refining these goals at the earliest stages. Opportunities for training a new generation of hospital medicine investigators and strengthening the existing ones through such a network will be explored, including options for training in outcomes research and opportunities to link participants with mentors.
What questions should a network focus on? Hospitalists are well positioned to lead or collaborate on a range of key questions—questions that, in the short term, likely will focus on effectiveness and implementation research (related to quality improvement). Over the longer term, hospitalists should position themselves to be involved in all facets of clinical translational research, including T1 (bench-to-bedside research) and T2 (effectiveness research, such as larger randomized studies, and health services research). As hospital medicine grows, the potential areas where hospitalists might focus their scientific interests will expand. As hospitalists assume greater roles in caring for patients outside general medicine (e.g., surgical, cardiovascular, neurology, and oncology patients), the breadth of scientific inquiry will expand. In many of these cases, research networks exist; SHM will have to facilitate collaboration whenever possible.
How will the network engage a broad swath of hospitalists? By selecting research questions important to public health and anticipating a changing clinical environment, we hope to enhance the interest and relevance of an SHM research network. The SHM Research Committee will focus on how best to design a research network that is practical and useful for hospital medicine researchers and enable straightforward studies. A main goal will be promoting visibility for investigators and coordinators through opportunities for authorship and presentation of results at national meetings.
Healthcare reform has become a hot political issue again—more than a year before the presidential election. All three leading Democratic candidates (Hillary Clinton, Barack Obama, and John Edwards) have proposed some sort of a central institute to assess treatment options and disseminate research and information to providers. Hospitalists (as generalists and team leaders in an arena where approximately 30% of the healthcare dollar is spent) are a key part of any national solution.
Whether this research requires a catalyst such as a hospitalist network—and what that network would look like—remains to be seen. The SHM Research Committee is considering mechanisms to provide research mentorship, training, and career development, and weighing the best use of resources. We count on your input. Contact Carolyn Brennan, director of research program development for SHM, at [email protected] for more information or to get involved. TH
SHM Behind the Scenes
PRIS updates in Salt Lake City
By Todd Von Deak
Each year, one of the premier events in pediatric hospital medicine is a summer conference presented by the American Academy of Pediatrics (AAP), the Ambulatory Pediatric Association (APA), and SHM. This year’s conference, held last month in Salt Lake City under the lead sponsorship of the AAP, was no exception.
More than 300 pediatric hospitalists, medical directors, residents, nurse practitioners, and physician assistants came together for four days to network, get answers, and learn from colleagues at 30 sessions. Charlie Homer, CEO of the National Institute for Children’s HealthCare Quality in Cambridge, Mass., was the keynote speaker. Dr. Homer highlighted the roles hospitalists can and must play to improve children’s health, and challenged all present to create a dashboard that includes quality indicators for care that is efficient, equitable, evidence-based, safe, and family-centered.
Leaders from the AAP, APA, and SHM opened the morning sessions the next day with brief presentations that highlighted the role of pediatric hospitalists in each organization, and the potential to work together to continue to develop pediatric hospital medicine and advance the care of hospitalized children. Participants were then free to choose from more than 16 sessions ranging from clinical issues such as the management of apparent life-threatening events and appropriate maintenance IV fluids, to practice management (Coding 101 and 201), quality improvement, and resident teaching and research.
Capping the schedule of events was a luncheon presentation from Christopher P. Landrigan, MD, director of the Pediatric Research in Inpatient Settings network. He presented “PRIS Update: The Need for Collaborative Hospitalist Research in 2007.” PRIS is an independent collaborative entity established by the same organizations that sponsor the Salt Lake City conference and is designed to allow for collaborative study of key questions in inpatient pediatrics.
Linda Snelling, MD, inpatient director and chief of pediatric critical care at Hasbro Children’s Hospital in Providence, R.I., followed with a talk on how pediatric hospitalists can effectively negotiate for themselves and the field. Her key insights included, “ ‘No.’ is a complete sentence.”
According to Jack Percelay, MD, past chair of SHM’s Pediatric Committee and a practicing pediatric hospitalist in New York and New Jersey, the conference exceeded its goals. “The energy at the conference was tremendous,” he said. “Sessions were filled with attendees learning of and debating cutting-edge issues for pediatric hospitalists. The buzz in the hotel was so intoxicating we were worried that we were violating Salt Lake City liquor laws. The AAP put on a spectacular meeting. SHM is looking forward to following this tradition of excellence as we take the lead for putting on an even larger meeting in Denver July 24-27, 2008.”
Given that the 2008 meeting sold out six weeks in advance, pediatric hospitalists will do well to stay tuned to The Hospitalist and visit SHM’s Web site, www.hospitalmedicine.org, for more details as the 2008 conference approaches. TH
By now almost everyone has heard about the social network site MySpace. More than 50 million people—mostly between ages 14 and 24—post and view online profiles connected by links to friends in the system. It’s one of the most heavily trafficked sites on the Internet.
MySpace is remarkable not only for consistent, double-digit growth rate, but also because visitors average two hours on the site modifying their profiles, and checking out friends’ profiles and commenting on them. MySpace has become ubiquitous to a generation using this public space to create and modify their identity on a daily basis—with technology that only recently has become available.
While recognizing that it may be a long time before www.hospitalmedicine.org becomes a household destination, the SHM Research Committee aims to generate similar excitement among our peers for connecting with each other over hospital medicine research on the Web.
Chapter Summary
Las Vegas
The SHM Las Vegas Chapter held its quarterly administrative meeting June 26 at Roy’s in Las Vegas. Gary Skankey, MD, infectious disease specialist and associate clinical professor at the University of Nevada School of Medicine, presented “Treating Complicated Skin and Skin Infections in an Era of Increasing Resistance.” The chapter will host a CME Program on surviving sepsis Sept. 28-29. Visit the chapter page for further program details.
Nashville
The SHM Nashville Chapter meeting June 6 at Stoney River restaurant was sponsored by Ortho McNeil and HCA Physician Recruitment. Eric Siegal, MD, with the University of Wisconsin Hospital in Madison, was the featured presenter and led an interactive session during “Malpractice for the Hospitalists: Identifying and Mitigating Risks.” The next meeting is scheduled for this month. Details will be posted at a later date.
At the SHM Research Committee meeting in Dallas in May, the conversation covered many topics, including the need for research mentorship, training, and career development. Plans for short- and medium-term measures to support SHM members in these areas are in the works, with a focus on Internet-based resources.
Over the long term, the committee would like to see its efforts result in national, high-impact hospital medicine studies and well-trained researchers. Whether driven by a curiosity in a particular area and/or the desire to provide better care by incorporating the best research, the universal challenge is to free enough time to pursue the answers and for appropriate recognition systems to be in place—be they promotion, funding to support further work, or recognition that leads to new connections.
The 249 abstracts published in a supplement to the Journal of Hospital Medicine only hinted at the depth and enthusiasm behind SHM members’ work. Anyone who walked through the exhibit hall during the poster session at the SHM Annual Meeting and talked with the people behind the research was impressed with their dedication and relative youth. They are the future of hospital medicine and are looking for ways to collaborate and continue to learn. The SHM Research Committee is dedicated to finding ways to support their efforts.
It seems as if many SHM members either engage in research, think about a research project, or wish they could evaluate their everyday practice in a way that can help others. However, it is difficult to discern how best to support individual hospitalists working in diverse settings across the country.
Because clinical responsibilities will not slow down anytime soon, we will have to work within the current, hectic environment and use technology as an equalizer to enable communication. In the spectrum of professional medical societies, SHM could be considered similar to the age 14-24 demographic attracted to the fluidity, instant communication/information and innovation that fuels MySpace.
Our long-term research goals could be powerfully advanced by a peer-catalyzed hospitalist research network.
The term “research network” can refer to many types of collaboration. One type that has been successful is the collection, analysis, and reporting of data in a registry or repository. In this example, medical care can be measured through the collection, analysis, and reporting of data. The National Cardiovascular Data Registry (established in 1998 by the American College of Cardiology Foundation) is a well-known example, but there are many others that have been organized for the purposes of improving quality and providing educational and research activities.
A second type of research network is the developing partnership between the American Medical Association (AMA) and Sermo, an online community where physicians exchange medical opinions. The partnership attempts to use technology to harness innovation, support physicians, and improve the capability of a peer network to influence the care patients receive by letting them share information with each other regarding patient care, pertinent scientific research, and advocacy issues. This is a looser network—without the constraints of data dictionaries—that relies on technology to make the connection between physician peers. While its start-up costs may be lower, its impact will be more difficult to measure.
A third example is the Gotham Prize for Cancer Research, which requires investigators to qualify by logging onto a Web site (www.gothamprize.org), posting a short proposal, and answering questions. If accepted by the expert panel of cancer researchers into this active forum, the new member will not only be eligible to receive the annual prize for the best idea, these individuals and their ideas will be matched to funding agencies and other scientists who may be able to support, assist, and/or collaborate. This limited-access network requires more facilitation than the previous AMA example, and the incentives and outcomes are more clearly defined.
The SHM Research Committee sees potential in exploring a network for hospital medicine researchers, through which members can access resources, collaborate, and innovate. Internet technology has the potential to level the playing field and erase the barriers of time differences and geography. By organizing around areas of interest designed to attract a critical mass of interested hospitalists, the goal of this network is to position SHM to lead hospital medicine research and ensure long-term success and sustainability by enabling powerful, high-impact studies in hospital medicine and supporting well-trained hospitalist researchers. Although this discussion is in the early stages of development, the SHM Research Committee plans to consider the following questions:
How would a network help hospital medicine and hospitalists? During the meeting in May in Dallas, the SHM Research Committee articulated the need for research mentorship, training, and career development. Any proposed network must further these aims. Hospital medicine investigators and SHM members would be involved in refining these goals at the earliest stages. Opportunities for training a new generation of hospital medicine investigators and strengthening the existing ones through such a network will be explored, including options for training in outcomes research and opportunities to link participants with mentors.
What questions should a network focus on? Hospitalists are well positioned to lead or collaborate on a range of key questions—questions that, in the short term, likely will focus on effectiveness and implementation research (related to quality improvement). Over the longer term, hospitalists should position themselves to be involved in all facets of clinical translational research, including T1 (bench-to-bedside research) and T2 (effectiveness research, such as larger randomized studies, and health services research). As hospital medicine grows, the potential areas where hospitalists might focus their scientific interests will expand. As hospitalists assume greater roles in caring for patients outside general medicine (e.g., surgical, cardiovascular, neurology, and oncology patients), the breadth of scientific inquiry will expand. In many of these cases, research networks exist; SHM will have to facilitate collaboration whenever possible.
How will the network engage a broad swath of hospitalists? By selecting research questions important to public health and anticipating a changing clinical environment, we hope to enhance the interest and relevance of an SHM research network. The SHM Research Committee will focus on how best to design a research network that is practical and useful for hospital medicine researchers and enable straightforward studies. A main goal will be promoting visibility for investigators and coordinators through opportunities for authorship and presentation of results at national meetings.
Healthcare reform has become a hot political issue again—more than a year before the presidential election. All three leading Democratic candidates (Hillary Clinton, Barack Obama, and John Edwards) have proposed some sort of a central institute to assess treatment options and disseminate research and information to providers. Hospitalists (as generalists and team leaders in an arena where approximately 30% of the healthcare dollar is spent) are a key part of any national solution.
Whether this research requires a catalyst such as a hospitalist network—and what that network would look like—remains to be seen. The SHM Research Committee is considering mechanisms to provide research mentorship, training, and career development, and weighing the best use of resources. We count on your input. Contact Carolyn Brennan, director of research program development for SHM, at [email protected] for more information or to get involved. TH
SHM Behind the Scenes
PRIS updates in Salt Lake City
By Todd Von Deak
Each year, one of the premier events in pediatric hospital medicine is a summer conference presented by the American Academy of Pediatrics (AAP), the Ambulatory Pediatric Association (APA), and SHM. This year’s conference, held last month in Salt Lake City under the lead sponsorship of the AAP, was no exception.
More than 300 pediatric hospitalists, medical directors, residents, nurse practitioners, and physician assistants came together for four days to network, get answers, and learn from colleagues at 30 sessions. Charlie Homer, CEO of the National Institute for Children’s HealthCare Quality in Cambridge, Mass., was the keynote speaker. Dr. Homer highlighted the roles hospitalists can and must play to improve children’s health, and challenged all present to create a dashboard that includes quality indicators for care that is efficient, equitable, evidence-based, safe, and family-centered.
Leaders from the AAP, APA, and SHM opened the morning sessions the next day with brief presentations that highlighted the role of pediatric hospitalists in each organization, and the potential to work together to continue to develop pediatric hospital medicine and advance the care of hospitalized children. Participants were then free to choose from more than 16 sessions ranging from clinical issues such as the management of apparent life-threatening events and appropriate maintenance IV fluids, to practice management (Coding 101 and 201), quality improvement, and resident teaching and research.
Capping the schedule of events was a luncheon presentation from Christopher P. Landrigan, MD, director of the Pediatric Research in Inpatient Settings network. He presented “PRIS Update: The Need for Collaborative Hospitalist Research in 2007.” PRIS is an independent collaborative entity established by the same organizations that sponsor the Salt Lake City conference and is designed to allow for collaborative study of key questions in inpatient pediatrics.
Linda Snelling, MD, inpatient director and chief of pediatric critical care at Hasbro Children’s Hospital in Providence, R.I., followed with a talk on how pediatric hospitalists can effectively negotiate for themselves and the field. Her key insights included, “ ‘No.’ is a complete sentence.”
According to Jack Percelay, MD, past chair of SHM’s Pediatric Committee and a practicing pediatric hospitalist in New York and New Jersey, the conference exceeded its goals. “The energy at the conference was tremendous,” he said. “Sessions were filled with attendees learning of and debating cutting-edge issues for pediatric hospitalists. The buzz in the hotel was so intoxicating we were worried that we were violating Salt Lake City liquor laws. The AAP put on a spectacular meeting. SHM is looking forward to following this tradition of excellence as we take the lead for putting on an even larger meeting in Denver July 24-27, 2008.”
Given that the 2008 meeting sold out six weeks in advance, pediatric hospitalists will do well to stay tuned to The Hospitalist and visit SHM’s Web site, www.hospitalmedicine.org, for more details as the 2008 conference approaches. TH