User login
Promote the Generalists
Isn’t it ironic that just as America is waking up to the importance of primary care medicine, our own representative organizations are selling us down the river?
The training of primary care physicians has for decades allowed us to branch out and follow our patients in multiple sites of care. We are the masters of managing care across this continuum.
Government and big business are finally recognizing that they need to bolster primary care to manage patients in the new chronic care medical home models. They are finally recognizing the need to better supply, equip, and finance primary care physicians.
The American College of Physicians (ACP), the American Academy of Family Practice (AAFP), and the American Medical Association all appear to support this concept. So where is the irony?
The American Board of Internal Medicine (ABIM), along with the aforementioned groups and others, continues to carve medicine into ever increasing sub areas, based on sites of care and interests. Hospitalists (who already have three branches—general hospitalists, proceduralists, and nocturnists) are seeking special certification recognition through ABIM. Palliative care is a new certification. These branches of medicine deserve recognition, but do we need all these fractured certifications?
Soon, no primary care physicians will be certified as capable of practicing in multiple sites of care without multiple certifications for each separate site and individual function. Soon there will be no “general” primary care physicians. Can hospitalists equally manage the whole continuum of care, or will they need to become generalists again to do the job?
Medicine teaches us to care for the whole person—body, mind, and spirit—not just individual parts. I urge the ABIM, the ACP, the AAFP, the AMA, SHM, and others to stop this fracturing of primary care. Now is the time to promote the generalists. Now is the time to lift all primary care-related areas of medicine together, leaving no one behind.
John M. Colombo, MD
HAN/Colombo
Crozer Keystone Health Network
Isn’t it ironic that just as America is waking up to the importance of primary care medicine, our own representative organizations are selling us down the river?
The training of primary care physicians has for decades allowed us to branch out and follow our patients in multiple sites of care. We are the masters of managing care across this continuum.
Government and big business are finally recognizing that they need to bolster primary care to manage patients in the new chronic care medical home models. They are finally recognizing the need to better supply, equip, and finance primary care physicians.
The American College of Physicians (ACP), the American Academy of Family Practice (AAFP), and the American Medical Association all appear to support this concept. So where is the irony?
The American Board of Internal Medicine (ABIM), along with the aforementioned groups and others, continues to carve medicine into ever increasing sub areas, based on sites of care and interests. Hospitalists (who already have three branches—general hospitalists, proceduralists, and nocturnists) are seeking special certification recognition through ABIM. Palliative care is a new certification. These branches of medicine deserve recognition, but do we need all these fractured certifications?
Soon, no primary care physicians will be certified as capable of practicing in multiple sites of care without multiple certifications for each separate site and individual function. Soon there will be no “general” primary care physicians. Can hospitalists equally manage the whole continuum of care, or will they need to become generalists again to do the job?
Medicine teaches us to care for the whole person—body, mind, and spirit—not just individual parts. I urge the ABIM, the ACP, the AAFP, the AMA, SHM, and others to stop this fracturing of primary care. Now is the time to promote the generalists. Now is the time to lift all primary care-related areas of medicine together, leaving no one behind.
John M. Colombo, MD
HAN/Colombo
Crozer Keystone Health Network
Isn’t it ironic that just as America is waking up to the importance of primary care medicine, our own representative organizations are selling us down the river?
The training of primary care physicians has for decades allowed us to branch out and follow our patients in multiple sites of care. We are the masters of managing care across this continuum.
Government and big business are finally recognizing that they need to bolster primary care to manage patients in the new chronic care medical home models. They are finally recognizing the need to better supply, equip, and finance primary care physicians.
The American College of Physicians (ACP), the American Academy of Family Practice (AAFP), and the American Medical Association all appear to support this concept. So where is the irony?
The American Board of Internal Medicine (ABIM), along with the aforementioned groups and others, continues to carve medicine into ever increasing sub areas, based on sites of care and interests. Hospitalists (who already have three branches—general hospitalists, proceduralists, and nocturnists) are seeking special certification recognition through ABIM. Palliative care is a new certification. These branches of medicine deserve recognition, but do we need all these fractured certifications?
Soon, no primary care physicians will be certified as capable of practicing in multiple sites of care without multiple certifications for each separate site and individual function. Soon there will be no “general” primary care physicians. Can hospitalists equally manage the whole continuum of care, or will they need to become generalists again to do the job?
Medicine teaches us to care for the whole person—body, mind, and spirit—not just individual parts. I urge the ABIM, the ACP, the AAFP, the AMA, SHM, and others to stop this fracturing of primary care. Now is the time to promote the generalists. Now is the time to lift all primary care-related areas of medicine together, leaving no one behind.
John M. Colombo, MD
HAN/Colombo
Crozer Keystone Health Network
Traumatic childbirth: Address the great emotional pain, too
Her letter has been abbreviated, with names and dates altered.
Eric David Foster
Born: May 15, 2003, Died: May 18, 2003
Does that name or do those dates mean anything to you? They should, but I doubt that they do. I, on the other hand, have been haunted by painful and awful memories of those 4 days, as I will be every day for the rest of my life. I hope that you have the courage and integrity to read this letter completely, because this is the only chance I have to reach you.
Do you remember my first visit? I had the impression then that you listened and understood when I related my complicated obstetric history, but that was the first and last time I felt that way. You seemed to forget about the uterine septum until I called you at 25 weeks’ gestation to report that I had gone into labor. My husband and I were so terrified, we left our sleeping 2-year-old son alone in the house to await the nanny in order to get to the hospital as soon as possible. Although we arrived there at 7 AM, we had to wait 2 horrifying hours for you to show up. By then it was too late, and Eric was delivered prematurely with extensive brain damage from ischemia and hemorrhage. Distraught, my heart breaking and my brain dazed from shock, trauma, surgery, and lack of sleep, I then had to plead and fight at the ethics committee meeting for the discontinuation of life support so Eric’s suffering could end.
A strongly worded letter if ever there was one; the patient’s emotional pain comes through loud and clear. Bear in mind that the obstetrician’s voice is silent; we do not hear his perspective.
That is intentional. The aim of this article is not to pass judgment or offer defense, but to draw attention to two specific consequences of a major traumatic experience—incomplete mourning and traumatic stress disorder.
In an earlier article, “The nightmare of litigation: A survivor’s true story,”1 I presented the case of an obstetrician who was sued for medical malpractice. The trauma of the experience led him to develop an acute stress disorder, which evolved into posttraumatic stress disorder (PTSD). In this article, the focus is on the patient, who also develops PTSD after an adverse outcome—specifically, premature delivery and neonatal death.
A mourning process stuck in the anger stage
Letter continued
For the past year I have wanted to ask you…
- Why did you make me feel invisible during my pregnancy, after I went to so much trouble to explain my special situation?
- Why didn’t you seem to notice how terrified we were when I started bleeding? Instead, you took your time getting to the ER.
- Why didn’t you come to talk to me later in the day after the cesarean section? When you spoke to my husband, you mentioned that you had removed the uterine septum so I could go on to have a normal full-term pregnancy. How could you begin to talk about another pregnancy while my son was in pain, bleeding into his brain? You wrote him off the minute you left the OR, just like you peeled off your gloves and dropped them into the trash.
- Why didn’t you ask the chaplain to be at the ethics hearing as a support for us?
- At my postoperative checkup, why did you rip off the dressing and declare me “beautifully healed”? And why did you walk off before I could say anything?
When the obstetrician ripped off the dressing and declared the patient healed, he was addressing the physical abdominal wound, but he completely overlooked the deeper, invisible, psychospiritual wounds arising from loss of a child—and from loss of safety, power, trust, faith, and meaning. The patient’s feelings are striking in their potency, but the obstetrician remained unaware of them. At the time of her postoperative visit, these psychological wounds had not even begun to heal. The self that had been preparing to be a mother had not yet integrated all the losses and realigned to the grim reality that she was now the parent of a dead baby.
Rather than further her healing, the obstetrician’s words alienated her and added yet another layer of wounding.
Letter continued
That hospital was my personal place in hell from the moment I entered until the day I was discharged. You and your office staff seemed totally oblivious to this fact. Now a year has passed—a year of pure devastation—and I still have pain and sadness that cannot be understood by anyone who has not experienced the death of a child. And I have anger at the incompetent ER staff and at myself for being “a good patient” and ignoring my intuition.
I deserved a physician who can remember who I am and my relevant history—one who would come to see me immediately and reassure me that everything possible would be done for my baby and me. I deserved a physician who can acknowledge the awfulness of such a loss and offer sympathy and support. And to make matters worse, you immediately retreated behind the fear of a lawsuit.
Grief, interrupted: When the business-as-usual world interferes
An outpouring of grief in the face of loss is normal; it mobilizes energy and is an integral part of the healing process. Emotional healing may seem protracted when it is viewed in the context of chronological time, and pressing demands frequently interfere with the process. In this case, demands included the need to attend an ethics meeting, arrange a funeral, care for a 2-year-old son, host parents-in-law who had arrived from out of town, and, the following week, throw a birthday party for her son.
Disenfranchised grief: How wrong words, or none, can slow healing
This patient found little validation or support for her grief from those who were around her:
- Medical personnel acted defensively and insensitively.
- Her in-laws kept busy, making idle chitchat while they fussed over the party and memorial arrangements.
- Her friends plied her with platitudes: “God needs an angel in heaven,” “God needed your son more than you do,” “We can’t know why God makes these decisions.”
- The priest performed the memorial service in ritualistic fashion. “He couldn’t even get Eric’s name right,” she lamented.
- Her return to work was marked by awkward cheeriness, “as if I had been on vacation.” Her boss’s comment? “Best hop right back in the saddle.”
Three symptom clusters signal PTSD
Dr. Foster’s description of her postdelivery experience suggests to me that she sustained an acute stress disorder—a condition that involves feelings of intense fear, horror, disorientation, and helplessness in response to an unusually traumatic experience that threatens death or serious physical injury to self or others. In Dr. Foster’s case, the stress disorder progressed to PTSD—a pervasive chronic anxiety disorder characterized by three clusters of symptoms:
- Recurrent, intrusive recollections of events; recurrent flashbacks and dreams. “At night, after going to bed, I would see the fetal monitor showing my child’s heart rate running like a video stream in front of my eyes. This went on for months. It would take me 1 to 2 hours to force myself to fall asleep.”
- Persistent avoidance of stimuli associated with the event; numbness and detachment. “I had feelings of numbness and unreality but couldn’t really understand or process them. Eating became difficult, and I was unable to experience any pleasure. Survivor’s guilt plagued me. Why am I alive? I asked myself. I had some 30 years, but my son didn’t even have a chance.”
- Persistent symptoms of increased arousal; insomnia, hypervigilance, irritability, difficulty with concentration. “I returned to work after a month but could not focus or concentrate, so I took 2 additional months off. Whenever I heard the obstetrician paged at the hospital, I had a physical reaction. My muscles clenched, my skin flushed, and my heart raced. Eventually, I stopped working at that hospital because I couldn’t stand being there.”
In Dr. Foster’s case, PTSD went unrecognized and untreated.
How to avert, and alleviate, PTSD
As with any disaster, careful planning can mitigate consequences even though it cannot necessarily prevent PTSD. Prenatal visits offer a unique opportunity to build a trusting partnership with your patient and her partner. Skilled professional communication is essential. Anticipate common themes:
- Fear of failure and shame is an issue for many mothers-to-be. Here, your affirmations and good humor are helpful. Be very respectful of the patient’s interpersonal boundaries, both physical and emotional.
- Disempowerment is an inherent part of the patient experience; trauma aggravates this dynamic. Whenever feasible, shift some of your power to the patient by eliciting her wishes and offering her choices. Together, create a plan for delivery and postnatal care that reflects her desires. As you demonstrate competence and control, consciously deconstruct the image your patient may have of you as an infallible authority figure by selectively revealing a little of the personality behind the white coat.
- Feelings of isolation always occur with trauma. The bonds you cultivate with the patient during her pregnancy will alleviate this isolation, as will your message: You are not alone in this experience; we will deal with this together.
Other helpful practices
Allow the grieving couple space and privacy to ventilate and mourn any way they need to. This may include expressions of anger.
Listen silently and attentively even if you feel passive or uncomfortable doing so. Resist the urge to comfort the patient; even well-intentioned comforting can interrupt healing.
Validate the patient’s trauma. Be careful to avoid making the suggestion that you understand. No one but the patient can understand—suffering is always unique and personal.
Express a genuine and carefully worded sense of regret for the patient’s loss. Take care not to express personal negative feelings, such as those regarding a baby’s deformity. Your words may become permanently imprinted.9
Present any information and recommendations the patient needs in writing because, when a person is in shock, she may be unable to recall verbal messages. Also give written recommendations to one of the patient’s family members, if possible.
Avoid well-intentioned attempts to reassure a patient or to rationalize or offer premature hope. There is time for such things later.
Cultivate a referral network that includes social workers, chaplains, and psychotherapists trained to work with trauma victims, and when they are necessary, involve them as early as possible. Also familiarize yourself with local support groups and short-term cognitive group-therapy programs for grieving parents.10
Frame the gesture carefully if you feel the need to refer the patient to a psychotherapist or psychiatrist. It is better to emphasize to the patient that she has sustained a major trauma than to suggest there is something wrong with her. The latter will only add to her sense of personal failure and may trigger resistance or anger.
Take care of yourself! You need your own practices and rituals to sustain you in the work you do. Create your own network of support. Concentrate on expanding your resilience and strive to be comfortable with your emotions. If symptoms of burnout appear, seek help quickly.
The author thanks Amy Hyams and Anne-Marie Jackson, MD, for their assistance.
Recommended reading
- Bub B. Communication Skills That Heal: A Practical Approach to a New Professionalism in Medicine. Abington, UK: Radcliffe Publishing–Oxford; 2005.
- Herman J. Trauma and Recovery. London: Rivers Oram Press; 1997.
- Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wisc: Seasons; 1994.
1. Bub B. The nightmare of litigation: a survivor’s true story. OBG Management. 2005;17(1):21-27.
2. Mundy E, Baum A. Medical disorders as a cause of psychological trauma and posttraumatic stress disorder. Curr Opin Psychiatry. 2004;17(2):123-128.
3. Bowles SV, James LC, Solursh D, et al. Acute and post traumatic stress disorder after spontaneous abortion. Am Fam Physician. 2000;61:1689-1696.
4. Reynolds JL. Post-traumatic stress disorder after childbirth: the phenomenon of traumatic birth. CMAJ. 1997;156:831-835.
5. Ayers S, Pickering A. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth. 2001;28:111-118.
6. Pantien A, Rohde A. Psychologic effects of traumatic live deliveries [article in German]. Zentralbl Gynakol. 2001;123:42-47.
7. Soet J, Brack G, Dilorio C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth. 2003;30:36-46.
8. Beck C. Post-traumatic stress disorder due to childbirth: the aftermath. Nurs Res. 2004;53:216-224.
9. Bub B. Sam and the perfect world. Acad Med. 2007;82:201.-
10. Sorenson D. Healing traumatizing provider interactions among women through short-term group therapy. Arch Psych Nurs. 2003;17:259-269.
Her letter has been abbreviated, with names and dates altered.
Eric David Foster
Born: May 15, 2003, Died: May 18, 2003
Does that name or do those dates mean anything to you? They should, but I doubt that they do. I, on the other hand, have been haunted by painful and awful memories of those 4 days, as I will be every day for the rest of my life. I hope that you have the courage and integrity to read this letter completely, because this is the only chance I have to reach you.
Do you remember my first visit? I had the impression then that you listened and understood when I related my complicated obstetric history, but that was the first and last time I felt that way. You seemed to forget about the uterine septum until I called you at 25 weeks’ gestation to report that I had gone into labor. My husband and I were so terrified, we left our sleeping 2-year-old son alone in the house to await the nanny in order to get to the hospital as soon as possible. Although we arrived there at 7 AM, we had to wait 2 horrifying hours for you to show up. By then it was too late, and Eric was delivered prematurely with extensive brain damage from ischemia and hemorrhage. Distraught, my heart breaking and my brain dazed from shock, trauma, surgery, and lack of sleep, I then had to plead and fight at the ethics committee meeting for the discontinuation of life support so Eric’s suffering could end.
A strongly worded letter if ever there was one; the patient’s emotional pain comes through loud and clear. Bear in mind that the obstetrician’s voice is silent; we do not hear his perspective.
That is intentional. The aim of this article is not to pass judgment or offer defense, but to draw attention to two specific consequences of a major traumatic experience—incomplete mourning and traumatic stress disorder.
In an earlier article, “The nightmare of litigation: A survivor’s true story,”1 I presented the case of an obstetrician who was sued for medical malpractice. The trauma of the experience led him to develop an acute stress disorder, which evolved into posttraumatic stress disorder (PTSD). In this article, the focus is on the patient, who also develops PTSD after an adverse outcome—specifically, premature delivery and neonatal death.
A mourning process stuck in the anger stage
Letter continued
For the past year I have wanted to ask you…
- Why did you make me feel invisible during my pregnancy, after I went to so much trouble to explain my special situation?
- Why didn’t you seem to notice how terrified we were when I started bleeding? Instead, you took your time getting to the ER.
- Why didn’t you come to talk to me later in the day after the cesarean section? When you spoke to my husband, you mentioned that you had removed the uterine septum so I could go on to have a normal full-term pregnancy. How could you begin to talk about another pregnancy while my son was in pain, bleeding into his brain? You wrote him off the minute you left the OR, just like you peeled off your gloves and dropped them into the trash.
- Why didn’t you ask the chaplain to be at the ethics hearing as a support for us?
- At my postoperative checkup, why did you rip off the dressing and declare me “beautifully healed”? And why did you walk off before I could say anything?
When the obstetrician ripped off the dressing and declared the patient healed, he was addressing the physical abdominal wound, but he completely overlooked the deeper, invisible, psychospiritual wounds arising from loss of a child—and from loss of safety, power, trust, faith, and meaning. The patient’s feelings are striking in their potency, but the obstetrician remained unaware of them. At the time of her postoperative visit, these psychological wounds had not even begun to heal. The self that had been preparing to be a mother had not yet integrated all the losses and realigned to the grim reality that she was now the parent of a dead baby.
Rather than further her healing, the obstetrician’s words alienated her and added yet another layer of wounding.
Letter continued
That hospital was my personal place in hell from the moment I entered until the day I was discharged. You and your office staff seemed totally oblivious to this fact. Now a year has passed—a year of pure devastation—and I still have pain and sadness that cannot be understood by anyone who has not experienced the death of a child. And I have anger at the incompetent ER staff and at myself for being “a good patient” and ignoring my intuition.
I deserved a physician who can remember who I am and my relevant history—one who would come to see me immediately and reassure me that everything possible would be done for my baby and me. I deserved a physician who can acknowledge the awfulness of such a loss and offer sympathy and support. And to make matters worse, you immediately retreated behind the fear of a lawsuit.
Grief, interrupted: When the business-as-usual world interferes
An outpouring of grief in the face of loss is normal; it mobilizes energy and is an integral part of the healing process. Emotional healing may seem protracted when it is viewed in the context of chronological time, and pressing demands frequently interfere with the process. In this case, demands included the need to attend an ethics meeting, arrange a funeral, care for a 2-year-old son, host parents-in-law who had arrived from out of town, and, the following week, throw a birthday party for her son.
Disenfranchised grief: How wrong words, or none, can slow healing
This patient found little validation or support for her grief from those who were around her:
- Medical personnel acted defensively and insensitively.
- Her in-laws kept busy, making idle chitchat while they fussed over the party and memorial arrangements.
- Her friends plied her with platitudes: “God needs an angel in heaven,” “God needed your son more than you do,” “We can’t know why God makes these decisions.”
- The priest performed the memorial service in ritualistic fashion. “He couldn’t even get Eric’s name right,” she lamented.
- Her return to work was marked by awkward cheeriness, “as if I had been on vacation.” Her boss’s comment? “Best hop right back in the saddle.”
Three symptom clusters signal PTSD
Dr. Foster’s description of her postdelivery experience suggests to me that she sustained an acute stress disorder—a condition that involves feelings of intense fear, horror, disorientation, and helplessness in response to an unusually traumatic experience that threatens death or serious physical injury to self or others. In Dr. Foster’s case, the stress disorder progressed to PTSD—a pervasive chronic anxiety disorder characterized by three clusters of symptoms:
- Recurrent, intrusive recollections of events; recurrent flashbacks and dreams. “At night, after going to bed, I would see the fetal monitor showing my child’s heart rate running like a video stream in front of my eyes. This went on for months. It would take me 1 to 2 hours to force myself to fall asleep.”
- Persistent avoidance of stimuli associated with the event; numbness and detachment. “I had feelings of numbness and unreality but couldn’t really understand or process them. Eating became difficult, and I was unable to experience any pleasure. Survivor’s guilt plagued me. Why am I alive? I asked myself. I had some 30 years, but my son didn’t even have a chance.”
- Persistent symptoms of increased arousal; insomnia, hypervigilance, irritability, difficulty with concentration. “I returned to work after a month but could not focus or concentrate, so I took 2 additional months off. Whenever I heard the obstetrician paged at the hospital, I had a physical reaction. My muscles clenched, my skin flushed, and my heart raced. Eventually, I stopped working at that hospital because I couldn’t stand being there.”
In Dr. Foster’s case, PTSD went unrecognized and untreated.
How to avert, and alleviate, PTSD
As with any disaster, careful planning can mitigate consequences even though it cannot necessarily prevent PTSD. Prenatal visits offer a unique opportunity to build a trusting partnership with your patient and her partner. Skilled professional communication is essential. Anticipate common themes:
- Fear of failure and shame is an issue for many mothers-to-be. Here, your affirmations and good humor are helpful. Be very respectful of the patient’s interpersonal boundaries, both physical and emotional.
- Disempowerment is an inherent part of the patient experience; trauma aggravates this dynamic. Whenever feasible, shift some of your power to the patient by eliciting her wishes and offering her choices. Together, create a plan for delivery and postnatal care that reflects her desires. As you demonstrate competence and control, consciously deconstruct the image your patient may have of you as an infallible authority figure by selectively revealing a little of the personality behind the white coat.
- Feelings of isolation always occur with trauma. The bonds you cultivate with the patient during her pregnancy will alleviate this isolation, as will your message: You are not alone in this experience; we will deal with this together.
Other helpful practices
Allow the grieving couple space and privacy to ventilate and mourn any way they need to. This may include expressions of anger.
Listen silently and attentively even if you feel passive or uncomfortable doing so. Resist the urge to comfort the patient; even well-intentioned comforting can interrupt healing.
Validate the patient’s trauma. Be careful to avoid making the suggestion that you understand. No one but the patient can understand—suffering is always unique and personal.
Express a genuine and carefully worded sense of regret for the patient’s loss. Take care not to express personal negative feelings, such as those regarding a baby’s deformity. Your words may become permanently imprinted.9
Present any information and recommendations the patient needs in writing because, when a person is in shock, she may be unable to recall verbal messages. Also give written recommendations to one of the patient’s family members, if possible.
Avoid well-intentioned attempts to reassure a patient or to rationalize or offer premature hope. There is time for such things later.
Cultivate a referral network that includes social workers, chaplains, and psychotherapists trained to work with trauma victims, and when they are necessary, involve them as early as possible. Also familiarize yourself with local support groups and short-term cognitive group-therapy programs for grieving parents.10
Frame the gesture carefully if you feel the need to refer the patient to a psychotherapist or psychiatrist. It is better to emphasize to the patient that she has sustained a major trauma than to suggest there is something wrong with her. The latter will only add to her sense of personal failure and may trigger resistance or anger.
Take care of yourself! You need your own practices and rituals to sustain you in the work you do. Create your own network of support. Concentrate on expanding your resilience and strive to be comfortable with your emotions. If symptoms of burnout appear, seek help quickly.
The author thanks Amy Hyams and Anne-Marie Jackson, MD, for their assistance.
Recommended reading
- Bub B. Communication Skills That Heal: A Practical Approach to a New Professionalism in Medicine. Abington, UK: Radcliffe Publishing–Oxford; 2005.
- Herman J. Trauma and Recovery. London: Rivers Oram Press; 1997.
- Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wisc: Seasons; 1994.
Her letter has been abbreviated, with names and dates altered.
Eric David Foster
Born: May 15, 2003, Died: May 18, 2003
Does that name or do those dates mean anything to you? They should, but I doubt that they do. I, on the other hand, have been haunted by painful and awful memories of those 4 days, as I will be every day for the rest of my life. I hope that you have the courage and integrity to read this letter completely, because this is the only chance I have to reach you.
Do you remember my first visit? I had the impression then that you listened and understood when I related my complicated obstetric history, but that was the first and last time I felt that way. You seemed to forget about the uterine septum until I called you at 25 weeks’ gestation to report that I had gone into labor. My husband and I were so terrified, we left our sleeping 2-year-old son alone in the house to await the nanny in order to get to the hospital as soon as possible. Although we arrived there at 7 AM, we had to wait 2 horrifying hours for you to show up. By then it was too late, and Eric was delivered prematurely with extensive brain damage from ischemia and hemorrhage. Distraught, my heart breaking and my brain dazed from shock, trauma, surgery, and lack of sleep, I then had to plead and fight at the ethics committee meeting for the discontinuation of life support so Eric’s suffering could end.
A strongly worded letter if ever there was one; the patient’s emotional pain comes through loud and clear. Bear in mind that the obstetrician’s voice is silent; we do not hear his perspective.
That is intentional. The aim of this article is not to pass judgment or offer defense, but to draw attention to two specific consequences of a major traumatic experience—incomplete mourning and traumatic stress disorder.
In an earlier article, “The nightmare of litigation: A survivor’s true story,”1 I presented the case of an obstetrician who was sued for medical malpractice. The trauma of the experience led him to develop an acute stress disorder, which evolved into posttraumatic stress disorder (PTSD). In this article, the focus is on the patient, who also develops PTSD after an adverse outcome—specifically, premature delivery and neonatal death.
A mourning process stuck in the anger stage
Letter continued
For the past year I have wanted to ask you…
- Why did you make me feel invisible during my pregnancy, after I went to so much trouble to explain my special situation?
- Why didn’t you seem to notice how terrified we were when I started bleeding? Instead, you took your time getting to the ER.
- Why didn’t you come to talk to me later in the day after the cesarean section? When you spoke to my husband, you mentioned that you had removed the uterine septum so I could go on to have a normal full-term pregnancy. How could you begin to talk about another pregnancy while my son was in pain, bleeding into his brain? You wrote him off the minute you left the OR, just like you peeled off your gloves and dropped them into the trash.
- Why didn’t you ask the chaplain to be at the ethics hearing as a support for us?
- At my postoperative checkup, why did you rip off the dressing and declare me “beautifully healed”? And why did you walk off before I could say anything?
When the obstetrician ripped off the dressing and declared the patient healed, he was addressing the physical abdominal wound, but he completely overlooked the deeper, invisible, psychospiritual wounds arising from loss of a child—and from loss of safety, power, trust, faith, and meaning. The patient’s feelings are striking in their potency, but the obstetrician remained unaware of them. At the time of her postoperative visit, these psychological wounds had not even begun to heal. The self that had been preparing to be a mother had not yet integrated all the losses and realigned to the grim reality that she was now the parent of a dead baby.
Rather than further her healing, the obstetrician’s words alienated her and added yet another layer of wounding.
Letter continued
That hospital was my personal place in hell from the moment I entered until the day I was discharged. You and your office staff seemed totally oblivious to this fact. Now a year has passed—a year of pure devastation—and I still have pain and sadness that cannot be understood by anyone who has not experienced the death of a child. And I have anger at the incompetent ER staff and at myself for being “a good patient” and ignoring my intuition.
I deserved a physician who can remember who I am and my relevant history—one who would come to see me immediately and reassure me that everything possible would be done for my baby and me. I deserved a physician who can acknowledge the awfulness of such a loss and offer sympathy and support. And to make matters worse, you immediately retreated behind the fear of a lawsuit.
Grief, interrupted: When the business-as-usual world interferes
An outpouring of grief in the face of loss is normal; it mobilizes energy and is an integral part of the healing process. Emotional healing may seem protracted when it is viewed in the context of chronological time, and pressing demands frequently interfere with the process. In this case, demands included the need to attend an ethics meeting, arrange a funeral, care for a 2-year-old son, host parents-in-law who had arrived from out of town, and, the following week, throw a birthday party for her son.
Disenfranchised grief: How wrong words, or none, can slow healing
This patient found little validation or support for her grief from those who were around her:
- Medical personnel acted defensively and insensitively.
- Her in-laws kept busy, making idle chitchat while they fussed over the party and memorial arrangements.
- Her friends plied her with platitudes: “God needs an angel in heaven,” “God needed your son more than you do,” “We can’t know why God makes these decisions.”
- The priest performed the memorial service in ritualistic fashion. “He couldn’t even get Eric’s name right,” she lamented.
- Her return to work was marked by awkward cheeriness, “as if I had been on vacation.” Her boss’s comment? “Best hop right back in the saddle.”
Three symptom clusters signal PTSD
Dr. Foster’s description of her postdelivery experience suggests to me that she sustained an acute stress disorder—a condition that involves feelings of intense fear, horror, disorientation, and helplessness in response to an unusually traumatic experience that threatens death or serious physical injury to self or others. In Dr. Foster’s case, the stress disorder progressed to PTSD—a pervasive chronic anxiety disorder characterized by three clusters of symptoms:
- Recurrent, intrusive recollections of events; recurrent flashbacks and dreams. “At night, after going to bed, I would see the fetal monitor showing my child’s heart rate running like a video stream in front of my eyes. This went on for months. It would take me 1 to 2 hours to force myself to fall asleep.”
- Persistent avoidance of stimuli associated with the event; numbness and detachment. “I had feelings of numbness and unreality but couldn’t really understand or process them. Eating became difficult, and I was unable to experience any pleasure. Survivor’s guilt plagued me. Why am I alive? I asked myself. I had some 30 years, but my son didn’t even have a chance.”
- Persistent symptoms of increased arousal; insomnia, hypervigilance, irritability, difficulty with concentration. “I returned to work after a month but could not focus or concentrate, so I took 2 additional months off. Whenever I heard the obstetrician paged at the hospital, I had a physical reaction. My muscles clenched, my skin flushed, and my heart raced. Eventually, I stopped working at that hospital because I couldn’t stand being there.”
In Dr. Foster’s case, PTSD went unrecognized and untreated.
How to avert, and alleviate, PTSD
As with any disaster, careful planning can mitigate consequences even though it cannot necessarily prevent PTSD. Prenatal visits offer a unique opportunity to build a trusting partnership with your patient and her partner. Skilled professional communication is essential. Anticipate common themes:
- Fear of failure and shame is an issue for many mothers-to-be. Here, your affirmations and good humor are helpful. Be very respectful of the patient’s interpersonal boundaries, both physical and emotional.
- Disempowerment is an inherent part of the patient experience; trauma aggravates this dynamic. Whenever feasible, shift some of your power to the patient by eliciting her wishes and offering her choices. Together, create a plan for delivery and postnatal care that reflects her desires. As you demonstrate competence and control, consciously deconstruct the image your patient may have of you as an infallible authority figure by selectively revealing a little of the personality behind the white coat.
- Feelings of isolation always occur with trauma. The bonds you cultivate with the patient during her pregnancy will alleviate this isolation, as will your message: You are not alone in this experience; we will deal with this together.
Other helpful practices
Allow the grieving couple space and privacy to ventilate and mourn any way they need to. This may include expressions of anger.
Listen silently and attentively even if you feel passive or uncomfortable doing so. Resist the urge to comfort the patient; even well-intentioned comforting can interrupt healing.
Validate the patient’s trauma. Be careful to avoid making the suggestion that you understand. No one but the patient can understand—suffering is always unique and personal.
Express a genuine and carefully worded sense of regret for the patient’s loss. Take care not to express personal negative feelings, such as those regarding a baby’s deformity. Your words may become permanently imprinted.9
Present any information and recommendations the patient needs in writing because, when a person is in shock, she may be unable to recall verbal messages. Also give written recommendations to one of the patient’s family members, if possible.
Avoid well-intentioned attempts to reassure a patient or to rationalize or offer premature hope. There is time for such things later.
Cultivate a referral network that includes social workers, chaplains, and psychotherapists trained to work with trauma victims, and when they are necessary, involve them as early as possible. Also familiarize yourself with local support groups and short-term cognitive group-therapy programs for grieving parents.10
Frame the gesture carefully if you feel the need to refer the patient to a psychotherapist or psychiatrist. It is better to emphasize to the patient that she has sustained a major trauma than to suggest there is something wrong with her. The latter will only add to her sense of personal failure and may trigger resistance or anger.
Take care of yourself! You need your own practices and rituals to sustain you in the work you do. Create your own network of support. Concentrate on expanding your resilience and strive to be comfortable with your emotions. If symptoms of burnout appear, seek help quickly.
The author thanks Amy Hyams and Anne-Marie Jackson, MD, for their assistance.
Recommended reading
- Bub B. Communication Skills That Heal: A Practical Approach to a New Professionalism in Medicine. Abington, UK: Radcliffe Publishing–Oxford; 2005.
- Herman J. Trauma and Recovery. London: Rivers Oram Press; 1997.
- Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wisc: Seasons; 1994.
1. Bub B. The nightmare of litigation: a survivor’s true story. OBG Management. 2005;17(1):21-27.
2. Mundy E, Baum A. Medical disorders as a cause of psychological trauma and posttraumatic stress disorder. Curr Opin Psychiatry. 2004;17(2):123-128.
3. Bowles SV, James LC, Solursh D, et al. Acute and post traumatic stress disorder after spontaneous abortion. Am Fam Physician. 2000;61:1689-1696.
4. Reynolds JL. Post-traumatic stress disorder after childbirth: the phenomenon of traumatic birth. CMAJ. 1997;156:831-835.
5. Ayers S, Pickering A. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth. 2001;28:111-118.
6. Pantien A, Rohde A. Psychologic effects of traumatic live deliveries [article in German]. Zentralbl Gynakol. 2001;123:42-47.
7. Soet J, Brack G, Dilorio C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth. 2003;30:36-46.
8. Beck C. Post-traumatic stress disorder due to childbirth: the aftermath. Nurs Res. 2004;53:216-224.
9. Bub B. Sam and the perfect world. Acad Med. 2007;82:201.-
10. Sorenson D. Healing traumatizing provider interactions among women through short-term group therapy. Arch Psych Nurs. 2003;17:259-269.
1. Bub B. The nightmare of litigation: a survivor’s true story. OBG Management. 2005;17(1):21-27.
2. Mundy E, Baum A. Medical disorders as a cause of psychological trauma and posttraumatic stress disorder. Curr Opin Psychiatry. 2004;17(2):123-128.
3. Bowles SV, James LC, Solursh D, et al. Acute and post traumatic stress disorder after spontaneous abortion. Am Fam Physician. 2000;61:1689-1696.
4. Reynolds JL. Post-traumatic stress disorder after childbirth: the phenomenon of traumatic birth. CMAJ. 1997;156:831-835.
5. Ayers S, Pickering A. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth. 2001;28:111-118.
6. Pantien A, Rohde A. Psychologic effects of traumatic live deliveries [article in German]. Zentralbl Gynakol. 2001;123:42-47.
7. Soet J, Brack G, Dilorio C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth. 2003;30:36-46.
8. Beck C. Post-traumatic stress disorder due to childbirth: the aftermath. Nurs Res. 2004;53:216-224.
9. Bub B. Sam and the perfect world. Acad Med. 2007;82:201.-
10. Sorenson D. Healing traumatizing provider interactions among women through short-term group therapy. Arch Psych Nurs. 2003;17:259-269.
In the Literature

Retrospective Study of Symptoms in Post-Discharge Patients
Epstein K, Juarez E, Loya K, et al. Frequency of new or worsening symptoms in the posthospitalization period. J Hosp Med. March/April 2007;2(2):58-68.
As hospital stays shorten and acuity rises, patients often are discharged with complex instructions and discharge plans including home health services, physical therapy, hospice service, antibiotic infusions, and follow-up appointments. The potential for new or progressive symptoms in the days following discharge is an important parameter in assessing whether our planning is safe and effective.
The researchers in this study investigated the post-discharge period using a retrospective analysis of new or worsening symptoms within two to five days of hospital discharge among 15,767 patients surveyed between May 1 and Oct. 31, 2003. Patients were all under the care of hospitalists employed by IPC, a large private hospitalist group based in North Hollywood, Calif. Total discharges from which this cohort was selected numbered 48,236.
Staff with medical backgrounds conducted a scripted survey by phone. Licensed nursing personnel contacted those patients whose answers to initial questions suggested they were at high risk for postdischarge complications. A five-point Likert scale was used so patients could rate their overall health status in addition to specific symptomatology ranging from abdominal pain to bleeding. Other questions targeted pick-up and administration of prescribed medications, insulin regimen adherence, and implementation of home health services.
Among all patients discharged, 32.7% were contacted within two days of discharge. The mean age was 60.1 years, and 57% were female. Ethnicity and socioeconomic status were not reported. Medicare and HMOs were the most common type of insurance. Of the 15,767 patients contacted, 11.9% reported symptoms that were new or worsening since discharge; of this subgroup, 64% had new symptoms whereas 36% had “worse” symptoms.
Women were more likely than men to report new or worsening symptoms, and patients who rated themselves as having a poor health status were more likely to have new or worsening symptoms. Younger patients were less likely to report new or worsening symptoms, particularly younger men. Those with new or worse symptoms were slightly more likely to have made a follow-up appointment but also more likely to have a problem with their medications. Interestingly, there was no correlation between self-rated health status and reported severity of illness based on the diagnosis related group (DRG) score. Patients discharged with a DRG of chest pain were less likely to report symptoms than all other patients.
The authors acknowledge the low response rate (32.7%) relative to the 48,236 discharges during the study period. Logistic challenges, resource limitations, and erroneous contact information precluded successful contact for the remainder of patients. The magnitude of this exclusion effect essentially precludes statistically valid extrapolation to the inception cohort (all discharges). For example, in a sensitivity analysis where all the excluded patients are assumed to have developed new or worsening symptoms, the actual rate overall would have been 71%. If none developed new or worsening symptoms, that rate would be 3.8%. The rate for the inception cohort may or may not approximate the 11.9% found among the studied patients. There is insufficient evidence to determine whether the studied cohort reflects the entire population of discharged patients.
To their credit, no such analysis or interpretation is claimed or intended by the authors, and the information derived from the included cohort nonetheless provides interesting and important descriptive data.
Ethnicity and cultural factors were not taken into consideration. One might postulate that language barriers could affect compliance and symptom reporting. Day-of-the-week and holiday status also were not reported with regard to discharge. It would be interesting and useful to know whether access to pharmacy and other resources varied in this regard and whether symptom reporting was affected by such timing.
In the final analysis, this study suggests hospitalists remain alert to possible problems that might develop during the vulnerable first few days following discharge. It reminds us to advise patients how to receive prompt and knowledgeable medical advice from someone familiar with their hospital care prior to their first scheduled follow-up.
Based on the reported rate of new or worsening symptoms, should a post-discharge clinic be part of hospitalists’ scope of practice, at least for selected patients? Can subsets of patients who would benefit most from such intervention be identified? These and many more questions are raised by this study. We look forward to further research into the best process for ensuring optimal outcomes in the immediate post-discharge period.
Rosiglitazone’s Effect on MI Risk in Diabetes Patients
Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 June 14;356(24):2457-2471.
Cardiovascular causes account for more than 65% of deaths in diabetic patients. Rosiglitazone—a thiazolidinedione-class drug—has been broadly used in diabetes, but its effect on cardiovascular morbidity and mortality has not been conclusively determined. The authors initiated this meta-analysis to determine the effect of rosiglitazone on the risk of myocardial infarction (MI) and death from cardiovascular causes in diabetics.
The meta-analysis included 42 trials from three data sources. Forty trials were obtained from the Food and Drug Administration (FDA) Web site and the GlaxoSmithKline clinical trials registry. The third data source comprised two recent large, well-known trials: the Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medication (DREAM) and the A Diabetes Outcome Prevention Trial (ADOPT).1-2 The authors’ inclusion criteria were a study with a duration of more than 24 weeks, the use of a randomized control group not receiving rosiglitazone (placebo or comparator drug), and the availability of outcome data for MI and death from cardiovascular causes.
The studies included 15,560 patients randomly assigned to regimens that included rosiglitazone and 12,283 patients to comparator groups that did not include rosiglitazone.
The authors reviewed the data summaries of the 42 trials and tabulated adverse events (not reported as outcomes) of MI and death from cardiovascular causes. Hazard ratios could not be calculated since time-to-event data were lacking. Summary data also precluded the ability to determine whether the same patient suffered both an MI and death from cardiovascular causes.
Results of the authors’ statistical analyses included odds ratios and 95% confidence intervals to assess the risk associated with the rosiglitazone group as well as the subgroups of metformin, sulfonylurea, insulin, and placebo versus rosiglitazone.
The authors tabulated 86 MIs and 39 unadjudicated deaths from cardiovascular causes in the rosiglitazone group, and 72 MIs plus 22 deaths from cardiovascular causes in the control group.
The main conclusion was that rosiglitazone was associated with a statistically significant increase in the risk of MI (odds ratio 1.43, 95% confidence interval 1.03 to 1.98, p=0.03), but was not associated with a statistically significant increase in the risk of death from cardiovascular causes (odds ratio 1.64, 95% confidence interval 0.98 to 2.74, p=0.06).
Additionally, there were no statistical differences between rosiglitazone versus placebo or the individual antidiabetics in the subanalyses.
The authors have recognized the following major limitations in this meta-analysis:
- The low rate of MI is 0.55% (86 of 15,560 cases) in the rosiglitazone group and 0.59% (72 of 12,283 cases) in the control group. The odds ratio of 1.43 was statistically significant in the rosiglitazone group, although the event rate was higher in the control group. The risk of cardiovascular death was not significant, though a trend toward a higher death rate is noted;
- The lack of source data did not allow the use of time event analysis including hazard ratios;
- The definition of MI was unavailable; and
- MI and cardiovascular events were recorded in the trials as adverse events, not outcomes. Therefore, deaths from the latter were unadjudicated.
The authors suggested that the potential mechanism for increased MI in the rosiglitazone group could be its known effects on increasing low-density lipoproteins (LDL), precipitating congestive heart failure and reducing hemoglobin levels.
Rosiglitazone is one of two peroxisome proliferation activated receptor y (PPAR-y) agonists licensed for use in the United States; the other is pioglitazone. The third drug was troglitazone; it was taken off the market in March of 2000 due to hepatotoxicity.
The PPAR-y agonists decrease plasma glycemia by increasing insulin sensitivity in the peripheral tissues. These drugs have complex physiologic effects in activating and suppressing multiple genes, with most target genes being unknown. The observed side effects with rosiglitazone are not necessarily a class effect. Pioglitazone showed a trend toward reducing triglycerides and cardiovascular events, including MI and CVA, in a prospective, randomized trial called Prospective Pioglitazone Clinical Trial in Macrovascular Events (PROACTIVE).
This meta-analysis precipitated an interim analysis of the ongoing Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycemia in Diabetes (RECORD) trial.3 The RECORD trial is a randomized, open-label, multicenter, non-inferiority trial of 4,427 patients; 2,220 received add-on rosiglitazone, and 2,227 received a combination of metformin plus sulfonylurea (control group). The primary end point was hospitalization or death from cardiovascular causes. Interim findings were inconclusive for the rosiglitazone group. There was also no evidence of any increase in death from cardiovascular causes or all causes. However, rosiglitazone was found to be associated with an increased risk of congestive heart failure. The data were insufficient to determine whether the drug was associated with increased MI risk.
This important meta-analysis raises concerns about the association of rosiglitazone with cardiovascular events—but do not consider it definitive. For now, patients with comparable alternatives to rosiglitazone (indeed all patients on this medication) should be advised of the undetermined safety concerns. For those who consider rosiglitazone a compelling choice, abrupt discontinuation on the basis of this study may be premature.
Finally, we need to remain cognizant of the proven negative side effects of rosiglitazone—it increases fracture risks in women, precipitates congestive heart failure, increases LDL, and decreases hemoglobin levels. We should consider alternative anti-hyperglycemic agents in selected patients at risk until there are solid data from large randomized control trials with rosiglitazone that pre-empt its use altogether.
References
- Gerstein HC, Yusuf S, Bosch J, et al. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomized controlled trial. Lancet 2006 Sep 23; 368(9547):1096-1105.
- Kahn SE, Haffner SM, Heise MA, et al; ADOPT Study Group. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006 Dec 7;355(23):2427-2443.
- Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiac outcomes and regulation of glycemia in diabetes (RECORD): study design and protocol. Diabetologia. 2005;48:1726-1735.
Statins and Sepsis in Dialysis Patients
Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA. 2007 Apr 4;297(13):1455-1464.
Epidemiological data has revealed an increase in the rate of sepsis in the U.S. during the past two decades.1 In individuals with chronic kidney disease who are on dialysis, sepsis is a significant cause of morbidity and mortality. Various studies have looked at risk factors associated with septicemia in patients with chronic kidney disease; however, no preventive treatments have been identified.
Recent research has shown the use of statins has been associated with a decreased rate of sepsis and improved sepsis outcomes. The authors of this study investigated whether statin use may help reduce the incidence of sepsis in patients with chronic kidney disease on dialysis.
This prospective cohort study enrolled 1,041 participants attending dialysis clinics from October 1995 to June 1998, with a follow-up through Jan. 1, 2005. Statin use at baseline was determined by review of medical records. The primary outcome was hospitalization for sepsis, indicated by hospital data from the U.S. Renal Data System (mean follow-up 3.4 years).
The association of statin use and sepsis was assessed using two analyses. A multivariate regression analysis was performed on the entire cohort, and adjustments were made for potential confounders. An analysis was performed on a sub-cohort comparing sepsis rates in statin users with a control group identified through the likelihood of having been prescribed a statin (propensity matching).
There were 303 hospitalizations for sepsis among the 1,041 patients enrolled, with 14% of participants receiving a statin at baseline. The crude incidence rate of sepsis was 41/1,000 patient-years among statin users compared with 110/1,000 patient-years in the control group (p<0.001). The fully adjusted incidence ratio for sepsis among statin users versus nonusers was 0.38, or 62% lower among statin users.
In the propensity-matched subcohort group, there were 54 hospitalizations during follow-up. The relative risk of sepsis was 0.24 (95% confidence interval, 0.11-0.49) for statin users compared with nonusers.
A strong and independent association exists between statin use and reduced incidence of sepsis in chronic kidney disease patients. This association remained statistically significant after controlling for potential confounding. Why the statins might have this effect is not definitively known.
This national study further demonstrates the potential protective effect of statins on the occurrence of sepsis, which has been observed in previous research in a non-renal population. The author mentions that this is the first study to show a strong and significant effect of a medication administered long term on lower rates of sepsis among patients with chronic kidney disease.
Because this is an observational study, it is limited due to lack of randomization. As such, this study cannot prove causality. Further limitations include the assessment of patient and treatment factors at baseline, which can lead to a misclassification of factors that change over time. It is important to point out the study was dependent on U.S. Renal Data System and Medicare data to determine outcome, and the use of their ICD-9 coding information may have resulted in decreased reporting of sepsis.
Still, the relevant results of this investigation warrant further examination of statins and the prevention of sepsis in a prospective randomized trial. TH
Reference
- Sarnak MJ, Jaber BL. Mortality caused by sepsis in patients with end-stage renal disease compared with the general population. Kidney Int. 2000 Oct;58(4):1758-1764.
Retrospective Study of Symptoms in Post-Discharge Patients
Epstein K, Juarez E, Loya K, et al. Frequency of new or worsening symptoms in the posthospitalization period. J Hosp Med. March/April 2007;2(2):58-68.
As hospital stays shorten and acuity rises, patients often are discharged with complex instructions and discharge plans including home health services, physical therapy, hospice service, antibiotic infusions, and follow-up appointments. The potential for new or progressive symptoms in the days following discharge is an important parameter in assessing whether our planning is safe and effective.
The researchers in this study investigated the post-discharge period using a retrospective analysis of new or worsening symptoms within two to five days of hospital discharge among 15,767 patients surveyed between May 1 and Oct. 31, 2003. Patients were all under the care of hospitalists employed by IPC, a large private hospitalist group based in North Hollywood, Calif. Total discharges from which this cohort was selected numbered 48,236.
Staff with medical backgrounds conducted a scripted survey by phone. Licensed nursing personnel contacted those patients whose answers to initial questions suggested they were at high risk for postdischarge complications. A five-point Likert scale was used so patients could rate their overall health status in addition to specific symptomatology ranging from abdominal pain to bleeding. Other questions targeted pick-up and administration of prescribed medications, insulin regimen adherence, and implementation of home health services.
Among all patients discharged, 32.7% were contacted within two days of discharge. The mean age was 60.1 years, and 57% were female. Ethnicity and socioeconomic status were not reported. Medicare and HMOs were the most common type of insurance. Of the 15,767 patients contacted, 11.9% reported symptoms that were new or worsening since discharge; of this subgroup, 64% had new symptoms whereas 36% had “worse” symptoms.
Women were more likely than men to report new or worsening symptoms, and patients who rated themselves as having a poor health status were more likely to have new or worsening symptoms. Younger patients were less likely to report new or worsening symptoms, particularly younger men. Those with new or worse symptoms were slightly more likely to have made a follow-up appointment but also more likely to have a problem with their medications. Interestingly, there was no correlation between self-rated health status and reported severity of illness based on the diagnosis related group (DRG) score. Patients discharged with a DRG of chest pain were less likely to report symptoms than all other patients.
The authors acknowledge the low response rate (32.7%) relative to the 48,236 discharges during the study period. Logistic challenges, resource limitations, and erroneous contact information precluded successful contact for the remainder of patients. The magnitude of this exclusion effect essentially precludes statistically valid extrapolation to the inception cohort (all discharges). For example, in a sensitivity analysis where all the excluded patients are assumed to have developed new or worsening symptoms, the actual rate overall would have been 71%. If none developed new or worsening symptoms, that rate would be 3.8%. The rate for the inception cohort may or may not approximate the 11.9% found among the studied patients. There is insufficient evidence to determine whether the studied cohort reflects the entire population of discharged patients.
To their credit, no such analysis or interpretation is claimed or intended by the authors, and the information derived from the included cohort nonetheless provides interesting and important descriptive data.
Ethnicity and cultural factors were not taken into consideration. One might postulate that language barriers could affect compliance and symptom reporting. Day-of-the-week and holiday status also were not reported with regard to discharge. It would be interesting and useful to know whether access to pharmacy and other resources varied in this regard and whether symptom reporting was affected by such timing.
In the final analysis, this study suggests hospitalists remain alert to possible problems that might develop during the vulnerable first few days following discharge. It reminds us to advise patients how to receive prompt and knowledgeable medical advice from someone familiar with their hospital care prior to their first scheduled follow-up.
Based on the reported rate of new or worsening symptoms, should a post-discharge clinic be part of hospitalists’ scope of practice, at least for selected patients? Can subsets of patients who would benefit most from such intervention be identified? These and many more questions are raised by this study. We look forward to further research into the best process for ensuring optimal outcomes in the immediate post-discharge period.
Rosiglitazone’s Effect on MI Risk in Diabetes Patients
Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 June 14;356(24):2457-2471.
Cardiovascular causes account for more than 65% of deaths in diabetic patients. Rosiglitazone—a thiazolidinedione-class drug—has been broadly used in diabetes, but its effect on cardiovascular morbidity and mortality has not been conclusively determined. The authors initiated this meta-analysis to determine the effect of rosiglitazone on the risk of myocardial infarction (MI) and death from cardiovascular causes in diabetics.
The meta-analysis included 42 trials from three data sources. Forty trials were obtained from the Food and Drug Administration (FDA) Web site and the GlaxoSmithKline clinical trials registry. The third data source comprised two recent large, well-known trials: the Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medication (DREAM) and the A Diabetes Outcome Prevention Trial (ADOPT).1-2 The authors’ inclusion criteria were a study with a duration of more than 24 weeks, the use of a randomized control group not receiving rosiglitazone (placebo or comparator drug), and the availability of outcome data for MI and death from cardiovascular causes.
The studies included 15,560 patients randomly assigned to regimens that included rosiglitazone and 12,283 patients to comparator groups that did not include rosiglitazone.
The authors reviewed the data summaries of the 42 trials and tabulated adverse events (not reported as outcomes) of MI and death from cardiovascular causes. Hazard ratios could not be calculated since time-to-event data were lacking. Summary data also precluded the ability to determine whether the same patient suffered both an MI and death from cardiovascular causes.
Results of the authors’ statistical analyses included odds ratios and 95% confidence intervals to assess the risk associated with the rosiglitazone group as well as the subgroups of metformin, sulfonylurea, insulin, and placebo versus rosiglitazone.
The authors tabulated 86 MIs and 39 unadjudicated deaths from cardiovascular causes in the rosiglitazone group, and 72 MIs plus 22 deaths from cardiovascular causes in the control group.
The main conclusion was that rosiglitazone was associated with a statistically significant increase in the risk of MI (odds ratio 1.43, 95% confidence interval 1.03 to 1.98, p=0.03), but was not associated with a statistically significant increase in the risk of death from cardiovascular causes (odds ratio 1.64, 95% confidence interval 0.98 to 2.74, p=0.06).
Additionally, there were no statistical differences between rosiglitazone versus placebo or the individual antidiabetics in the subanalyses.
The authors have recognized the following major limitations in this meta-analysis:
- The low rate of MI is 0.55% (86 of 15,560 cases) in the rosiglitazone group and 0.59% (72 of 12,283 cases) in the control group. The odds ratio of 1.43 was statistically significant in the rosiglitazone group, although the event rate was higher in the control group. The risk of cardiovascular death was not significant, though a trend toward a higher death rate is noted;
- The lack of source data did not allow the use of time event analysis including hazard ratios;
- The definition of MI was unavailable; and
- MI and cardiovascular events were recorded in the trials as adverse events, not outcomes. Therefore, deaths from the latter were unadjudicated.
The authors suggested that the potential mechanism for increased MI in the rosiglitazone group could be its known effects on increasing low-density lipoproteins (LDL), precipitating congestive heart failure and reducing hemoglobin levels.
Rosiglitazone is one of two peroxisome proliferation activated receptor y (PPAR-y) agonists licensed for use in the United States; the other is pioglitazone. The third drug was troglitazone; it was taken off the market in March of 2000 due to hepatotoxicity.
The PPAR-y agonists decrease plasma glycemia by increasing insulin sensitivity in the peripheral tissues. These drugs have complex physiologic effects in activating and suppressing multiple genes, with most target genes being unknown. The observed side effects with rosiglitazone are not necessarily a class effect. Pioglitazone showed a trend toward reducing triglycerides and cardiovascular events, including MI and CVA, in a prospective, randomized trial called Prospective Pioglitazone Clinical Trial in Macrovascular Events (PROACTIVE).
This meta-analysis precipitated an interim analysis of the ongoing Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycemia in Diabetes (RECORD) trial.3 The RECORD trial is a randomized, open-label, multicenter, non-inferiority trial of 4,427 patients; 2,220 received add-on rosiglitazone, and 2,227 received a combination of metformin plus sulfonylurea (control group). The primary end point was hospitalization or death from cardiovascular causes. Interim findings were inconclusive for the rosiglitazone group. There was also no evidence of any increase in death from cardiovascular causes or all causes. However, rosiglitazone was found to be associated with an increased risk of congestive heart failure. The data were insufficient to determine whether the drug was associated with increased MI risk.
This important meta-analysis raises concerns about the association of rosiglitazone with cardiovascular events—but do not consider it definitive. For now, patients with comparable alternatives to rosiglitazone (indeed all patients on this medication) should be advised of the undetermined safety concerns. For those who consider rosiglitazone a compelling choice, abrupt discontinuation on the basis of this study may be premature.
Finally, we need to remain cognizant of the proven negative side effects of rosiglitazone—it increases fracture risks in women, precipitates congestive heart failure, increases LDL, and decreases hemoglobin levels. We should consider alternative anti-hyperglycemic agents in selected patients at risk until there are solid data from large randomized control trials with rosiglitazone that pre-empt its use altogether.
References
- Gerstein HC, Yusuf S, Bosch J, et al. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomized controlled trial. Lancet 2006 Sep 23; 368(9547):1096-1105.
- Kahn SE, Haffner SM, Heise MA, et al; ADOPT Study Group. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006 Dec 7;355(23):2427-2443.
- Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiac outcomes and regulation of glycemia in diabetes (RECORD): study design and protocol. Diabetologia. 2005;48:1726-1735.
Statins and Sepsis in Dialysis Patients
Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA. 2007 Apr 4;297(13):1455-1464.
Epidemiological data has revealed an increase in the rate of sepsis in the U.S. during the past two decades.1 In individuals with chronic kidney disease who are on dialysis, sepsis is a significant cause of morbidity and mortality. Various studies have looked at risk factors associated with septicemia in patients with chronic kidney disease; however, no preventive treatments have been identified.
Recent research has shown the use of statins has been associated with a decreased rate of sepsis and improved sepsis outcomes. The authors of this study investigated whether statin use may help reduce the incidence of sepsis in patients with chronic kidney disease on dialysis.
This prospective cohort study enrolled 1,041 participants attending dialysis clinics from October 1995 to June 1998, with a follow-up through Jan. 1, 2005. Statin use at baseline was determined by review of medical records. The primary outcome was hospitalization for sepsis, indicated by hospital data from the U.S. Renal Data System (mean follow-up 3.4 years).
The association of statin use and sepsis was assessed using two analyses. A multivariate regression analysis was performed on the entire cohort, and adjustments were made for potential confounders. An analysis was performed on a sub-cohort comparing sepsis rates in statin users with a control group identified through the likelihood of having been prescribed a statin (propensity matching).
There were 303 hospitalizations for sepsis among the 1,041 patients enrolled, with 14% of participants receiving a statin at baseline. The crude incidence rate of sepsis was 41/1,000 patient-years among statin users compared with 110/1,000 patient-years in the control group (p<0.001). The fully adjusted incidence ratio for sepsis among statin users versus nonusers was 0.38, or 62% lower among statin users.
In the propensity-matched subcohort group, there were 54 hospitalizations during follow-up. The relative risk of sepsis was 0.24 (95% confidence interval, 0.11-0.49) for statin users compared with nonusers.
A strong and independent association exists between statin use and reduced incidence of sepsis in chronic kidney disease patients. This association remained statistically significant after controlling for potential confounding. Why the statins might have this effect is not definitively known.
This national study further demonstrates the potential protective effect of statins on the occurrence of sepsis, which has been observed in previous research in a non-renal population. The author mentions that this is the first study to show a strong and significant effect of a medication administered long term on lower rates of sepsis among patients with chronic kidney disease.
Because this is an observational study, it is limited due to lack of randomization. As such, this study cannot prove causality. Further limitations include the assessment of patient and treatment factors at baseline, which can lead to a misclassification of factors that change over time. It is important to point out the study was dependent on U.S. Renal Data System and Medicare data to determine outcome, and the use of their ICD-9 coding information may have resulted in decreased reporting of sepsis.
Still, the relevant results of this investigation warrant further examination of statins and the prevention of sepsis in a prospective randomized trial. TH
Reference
- Sarnak MJ, Jaber BL. Mortality caused by sepsis in patients with end-stage renal disease compared with the general population. Kidney Int. 2000 Oct;58(4):1758-1764.
Retrospective Study of Symptoms in Post-Discharge Patients
Epstein K, Juarez E, Loya K, et al. Frequency of new or worsening symptoms in the posthospitalization period. J Hosp Med. March/April 2007;2(2):58-68.
As hospital stays shorten and acuity rises, patients often are discharged with complex instructions and discharge plans including home health services, physical therapy, hospice service, antibiotic infusions, and follow-up appointments. The potential for new or progressive symptoms in the days following discharge is an important parameter in assessing whether our planning is safe and effective.
The researchers in this study investigated the post-discharge period using a retrospective analysis of new or worsening symptoms within two to five days of hospital discharge among 15,767 patients surveyed between May 1 and Oct. 31, 2003. Patients were all under the care of hospitalists employed by IPC, a large private hospitalist group based in North Hollywood, Calif. Total discharges from which this cohort was selected numbered 48,236.
Staff with medical backgrounds conducted a scripted survey by phone. Licensed nursing personnel contacted those patients whose answers to initial questions suggested they were at high risk for postdischarge complications. A five-point Likert scale was used so patients could rate their overall health status in addition to specific symptomatology ranging from abdominal pain to bleeding. Other questions targeted pick-up and administration of prescribed medications, insulin regimen adherence, and implementation of home health services.
Among all patients discharged, 32.7% were contacted within two days of discharge. The mean age was 60.1 years, and 57% were female. Ethnicity and socioeconomic status were not reported. Medicare and HMOs were the most common type of insurance. Of the 15,767 patients contacted, 11.9% reported symptoms that were new or worsening since discharge; of this subgroup, 64% had new symptoms whereas 36% had “worse” symptoms.
Women were more likely than men to report new or worsening symptoms, and patients who rated themselves as having a poor health status were more likely to have new or worsening symptoms. Younger patients were less likely to report new or worsening symptoms, particularly younger men. Those with new or worse symptoms were slightly more likely to have made a follow-up appointment but also more likely to have a problem with their medications. Interestingly, there was no correlation between self-rated health status and reported severity of illness based on the diagnosis related group (DRG) score. Patients discharged with a DRG of chest pain were less likely to report symptoms than all other patients.
The authors acknowledge the low response rate (32.7%) relative to the 48,236 discharges during the study period. Logistic challenges, resource limitations, and erroneous contact information precluded successful contact for the remainder of patients. The magnitude of this exclusion effect essentially precludes statistically valid extrapolation to the inception cohort (all discharges). For example, in a sensitivity analysis where all the excluded patients are assumed to have developed new or worsening symptoms, the actual rate overall would have been 71%. If none developed new or worsening symptoms, that rate would be 3.8%. The rate for the inception cohort may or may not approximate the 11.9% found among the studied patients. There is insufficient evidence to determine whether the studied cohort reflects the entire population of discharged patients.
To their credit, no such analysis or interpretation is claimed or intended by the authors, and the information derived from the included cohort nonetheless provides interesting and important descriptive data.
Ethnicity and cultural factors were not taken into consideration. One might postulate that language barriers could affect compliance and symptom reporting. Day-of-the-week and holiday status also were not reported with regard to discharge. It would be interesting and useful to know whether access to pharmacy and other resources varied in this regard and whether symptom reporting was affected by such timing.
In the final analysis, this study suggests hospitalists remain alert to possible problems that might develop during the vulnerable first few days following discharge. It reminds us to advise patients how to receive prompt and knowledgeable medical advice from someone familiar with their hospital care prior to their first scheduled follow-up.
Based on the reported rate of new or worsening symptoms, should a post-discharge clinic be part of hospitalists’ scope of practice, at least for selected patients? Can subsets of patients who would benefit most from such intervention be identified? These and many more questions are raised by this study. We look forward to further research into the best process for ensuring optimal outcomes in the immediate post-discharge period.
Rosiglitazone’s Effect on MI Risk in Diabetes Patients
Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med. 2007 June 14;356(24):2457-2471.
Cardiovascular causes account for more than 65% of deaths in diabetic patients. Rosiglitazone—a thiazolidinedione-class drug—has been broadly used in diabetes, but its effect on cardiovascular morbidity and mortality has not been conclusively determined. The authors initiated this meta-analysis to determine the effect of rosiglitazone on the risk of myocardial infarction (MI) and death from cardiovascular causes in diabetics.
The meta-analysis included 42 trials from three data sources. Forty trials were obtained from the Food and Drug Administration (FDA) Web site and the GlaxoSmithKline clinical trials registry. The third data source comprised two recent large, well-known trials: the Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medication (DREAM) and the A Diabetes Outcome Prevention Trial (ADOPT).1-2 The authors’ inclusion criteria were a study with a duration of more than 24 weeks, the use of a randomized control group not receiving rosiglitazone (placebo or comparator drug), and the availability of outcome data for MI and death from cardiovascular causes.
The studies included 15,560 patients randomly assigned to regimens that included rosiglitazone and 12,283 patients to comparator groups that did not include rosiglitazone.
The authors reviewed the data summaries of the 42 trials and tabulated adverse events (not reported as outcomes) of MI and death from cardiovascular causes. Hazard ratios could not be calculated since time-to-event data were lacking. Summary data also precluded the ability to determine whether the same patient suffered both an MI and death from cardiovascular causes.
Results of the authors’ statistical analyses included odds ratios and 95% confidence intervals to assess the risk associated with the rosiglitazone group as well as the subgroups of metformin, sulfonylurea, insulin, and placebo versus rosiglitazone.
The authors tabulated 86 MIs and 39 unadjudicated deaths from cardiovascular causes in the rosiglitazone group, and 72 MIs plus 22 deaths from cardiovascular causes in the control group.
The main conclusion was that rosiglitazone was associated with a statistically significant increase in the risk of MI (odds ratio 1.43, 95% confidence interval 1.03 to 1.98, p=0.03), but was not associated with a statistically significant increase in the risk of death from cardiovascular causes (odds ratio 1.64, 95% confidence interval 0.98 to 2.74, p=0.06).
Additionally, there were no statistical differences between rosiglitazone versus placebo or the individual antidiabetics in the subanalyses.
The authors have recognized the following major limitations in this meta-analysis:
- The low rate of MI is 0.55% (86 of 15,560 cases) in the rosiglitazone group and 0.59% (72 of 12,283 cases) in the control group. The odds ratio of 1.43 was statistically significant in the rosiglitazone group, although the event rate was higher in the control group. The risk of cardiovascular death was not significant, though a trend toward a higher death rate is noted;
- The lack of source data did not allow the use of time event analysis including hazard ratios;
- The definition of MI was unavailable; and
- MI and cardiovascular events were recorded in the trials as adverse events, not outcomes. Therefore, deaths from the latter were unadjudicated.
The authors suggested that the potential mechanism for increased MI in the rosiglitazone group could be its known effects on increasing low-density lipoproteins (LDL), precipitating congestive heart failure and reducing hemoglobin levels.
Rosiglitazone is one of two peroxisome proliferation activated receptor y (PPAR-y) agonists licensed for use in the United States; the other is pioglitazone. The third drug was troglitazone; it was taken off the market in March of 2000 due to hepatotoxicity.
The PPAR-y agonists decrease plasma glycemia by increasing insulin sensitivity in the peripheral tissues. These drugs have complex physiologic effects in activating and suppressing multiple genes, with most target genes being unknown. The observed side effects with rosiglitazone are not necessarily a class effect. Pioglitazone showed a trend toward reducing triglycerides and cardiovascular events, including MI and CVA, in a prospective, randomized trial called Prospective Pioglitazone Clinical Trial in Macrovascular Events (PROACTIVE).
This meta-analysis precipitated an interim analysis of the ongoing Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycemia in Diabetes (RECORD) trial.3 The RECORD trial is a randomized, open-label, multicenter, non-inferiority trial of 4,427 patients; 2,220 received add-on rosiglitazone, and 2,227 received a combination of metformin plus sulfonylurea (control group). The primary end point was hospitalization or death from cardiovascular causes. Interim findings were inconclusive for the rosiglitazone group. There was also no evidence of any increase in death from cardiovascular causes or all causes. However, rosiglitazone was found to be associated with an increased risk of congestive heart failure. The data were insufficient to determine whether the drug was associated with increased MI risk.
This important meta-analysis raises concerns about the association of rosiglitazone with cardiovascular events—but do not consider it definitive. For now, patients with comparable alternatives to rosiglitazone (indeed all patients on this medication) should be advised of the undetermined safety concerns. For those who consider rosiglitazone a compelling choice, abrupt discontinuation on the basis of this study may be premature.
Finally, we need to remain cognizant of the proven negative side effects of rosiglitazone—it increases fracture risks in women, precipitates congestive heart failure, increases LDL, and decreases hemoglobin levels. We should consider alternative anti-hyperglycemic agents in selected patients at risk until there are solid data from large randomized control trials with rosiglitazone that pre-empt its use altogether.
References
- Gerstein HC, Yusuf S, Bosch J, et al. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomized controlled trial. Lancet 2006 Sep 23; 368(9547):1096-1105.
- Kahn SE, Haffner SM, Heise MA, et al; ADOPT Study Group. Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med. 2006 Dec 7;355(23):2427-2443.
- Home PD, Pocock SJ, Beck-Nielsen H, et al. Rosiglitazone evaluated for cardiac outcomes and regulation of glycemia in diabetes (RECORD): study design and protocol. Diabetologia. 2005;48:1726-1735.
Statins and Sepsis in Dialysis Patients
Gupta R, Plantinga LC, Fink NE, et al. Statin use and hospitalization for sepsis in patients with chronic kidney disease. JAMA. 2007 Apr 4;297(13):1455-1464.
Epidemiological data has revealed an increase in the rate of sepsis in the U.S. during the past two decades.1 In individuals with chronic kidney disease who are on dialysis, sepsis is a significant cause of morbidity and mortality. Various studies have looked at risk factors associated with septicemia in patients with chronic kidney disease; however, no preventive treatments have been identified.
Recent research has shown the use of statins has been associated with a decreased rate of sepsis and improved sepsis outcomes. The authors of this study investigated whether statin use may help reduce the incidence of sepsis in patients with chronic kidney disease on dialysis.
This prospective cohort study enrolled 1,041 participants attending dialysis clinics from October 1995 to June 1998, with a follow-up through Jan. 1, 2005. Statin use at baseline was determined by review of medical records. The primary outcome was hospitalization for sepsis, indicated by hospital data from the U.S. Renal Data System (mean follow-up 3.4 years).
The association of statin use and sepsis was assessed using two analyses. A multivariate regression analysis was performed on the entire cohort, and adjustments were made for potential confounders. An analysis was performed on a sub-cohort comparing sepsis rates in statin users with a control group identified through the likelihood of having been prescribed a statin (propensity matching).
There were 303 hospitalizations for sepsis among the 1,041 patients enrolled, with 14% of participants receiving a statin at baseline. The crude incidence rate of sepsis was 41/1,000 patient-years among statin users compared with 110/1,000 patient-years in the control group (p<0.001). The fully adjusted incidence ratio for sepsis among statin users versus nonusers was 0.38, or 62% lower among statin users.
In the propensity-matched subcohort group, there were 54 hospitalizations during follow-up. The relative risk of sepsis was 0.24 (95% confidence interval, 0.11-0.49) for statin users compared with nonusers.
A strong and independent association exists between statin use and reduced incidence of sepsis in chronic kidney disease patients. This association remained statistically significant after controlling for potential confounding. Why the statins might have this effect is not definitively known.
This national study further demonstrates the potential protective effect of statins on the occurrence of sepsis, which has been observed in previous research in a non-renal population. The author mentions that this is the first study to show a strong and significant effect of a medication administered long term on lower rates of sepsis among patients with chronic kidney disease.
Because this is an observational study, it is limited due to lack of randomization. As such, this study cannot prove causality. Further limitations include the assessment of patient and treatment factors at baseline, which can lead to a misclassification of factors that change over time. It is important to point out the study was dependent on U.S. Renal Data System and Medicare data to determine outcome, and the use of their ICD-9 coding information may have resulted in decreased reporting of sepsis.
Still, the relevant results of this investigation warrant further examination of statins and the prevention of sepsis in a prospective randomized trial. TH
Reference
- Sarnak MJ, Jaber BL. Mortality caused by sepsis in patients with end-stage renal disease compared with the general population. Kidney Int. 2000 Oct;58(4):1758-1764.
SHM Behind the Scenes
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.

“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.

More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.

To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.
“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.
More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.
To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.
“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.
More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.
To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
Rewards and Recognition

This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
Benefit Quest

The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
For the Team

Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
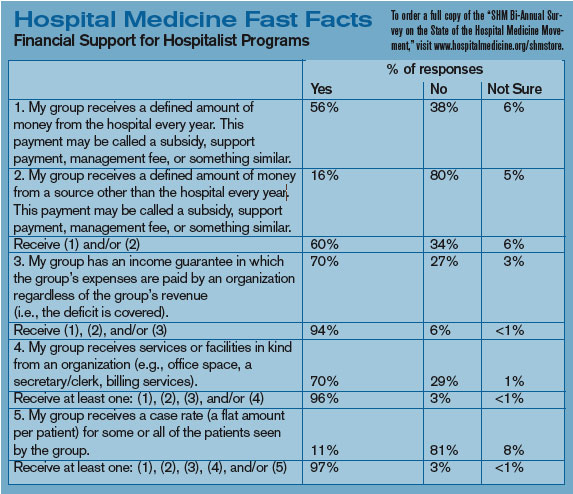
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at [email protected].
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at [email protected].
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH
Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at [email protected].
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at [email protected].
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH
Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at [email protected].
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at [email protected].
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH
Hospitalists Have Full Range of Career Opportunities
Jane Jerrard covered some potential career paths for academic hospitalists in her article “How to Navigate Hospital Medicine” (May 2007, p. 9). But I believe her account was incomplete. I would like to add detail to the opportunities in community-based and other programs.
Community-based medical groups offer a number of opportunities in hospitals or hospital systems. These include:
- Committee chairman. Most hospitals want interested, dedicated individuals to chair traditional medical staff committees. Hospitalists are well suited because our unique perspective lets us identify processes or products that can help many patients. Begin by serving on a committee, such as ethics, pharmacy and therapeutics, IRB, or departmental peer review. As you get comfortable, discuss potential chairmanships with the chief of staff or the vice president of medical affairs (VPMA). Don’t expect to advance if you don’t show up or don’t come prepared to committee meetings.
- Department chairperson. These positions are often elected and may allow one to serve on the credentials committee and the medical executive committee.
- Medical staff officers. Hospitalists often are elected to these key positions and gain access to administration and various committees.
- Project manager. Installing and using electronic medical records and devices calls for physician involvement in design and support. These are great chances to work on interesting projects and affect the tools you work with.
- Hospital administrative positions. Many hospitals have a VPMA or a chief medical officer (CMO), and some are developing the role of vice president of quality. These can be full- or part-time positions. You will be expected to help members of the medical staff implement change, and you should have experience and proven effectiveness in prior roles. Several predict that hospital COOs and CEOs of the future will be hospitalists.
Another path of opportunity is within your organization, depending on your employer. These roles may overlap with hospital positions:
- Group leader. Generally responsible for working on scheduling, recruitment, and organizational structure. The job may involve responsibility for one or more facilities.
- Compliance officer. Someone in the group must understand billing, coding, and proper use of rules and legislation.
- Quality and safety officer.
- Group president.
Hospitalists can also participate on committees that deal with such areas as pension plans, contracts, or other business.
Health insurance companies provide opportunities for individuals to practice part-time and serve as medical directors. They also have career paths for VPMAs and CMOs.
Also, many healthcare companies have been started and run by physicians. Invent something; start a company. The opportunities are endless.
Some other tips:
- Educate yourself. Take courses like the SHM Leadership Academy. Learn how to interact in a businesslike manner. Some on-the-job training is OK, but management and leadership are new fields that require new learning.
- Read. There are many great books on being an executive. Learn how to run a meeting, make an agenda, work with other professionals, and delegate.
- Ask for help. Find an individual or individuals with whom you can discuss ideas. Some of your best mentors will be managers in other fields.
Mary Jo Gorman, MD, MBA
Immediate Past President, SHM
Consequences of Locum Tenens Work
I feel one piece of advice in the Career Development section in the May issue of The Hospitalist (“How to Navigate Hospital Medicine,” p. 9) is not complete and may adversely affect a new hospitalist’s career.
The article recommends exploring locum tenens work. We have found two unintended consequences of such action. First, the locum companies usually have a buyout clause for the physician. Should he decide he likes a location and wishes to stay, the potential employer faces an additional cost in the $20,000-$30,000 range. It makes budgeting difficult. Also, there is usually a clause in the locum contract that this policy is in place for two years after leaving the locum company.
Second, frequent job changes lead to prolonged processing of credentials at hospitals as they verify good standing at all previous practice sites. This means delays that force a hospitalist company to look for more readily available docs. The physician may be unable to find hospitals in highly desirable areas.
The article was otherwise well balanced and timely.
George Block, MD
CMO, Galen Inpatient Physicians Medical Group
Emeryville, Calif.
Jane Jerrard covered some potential career paths for academic hospitalists in her article “How to Navigate Hospital Medicine” (May 2007, p. 9). But I believe her account was incomplete. I would like to add detail to the opportunities in community-based and other programs.
Community-based medical groups offer a number of opportunities in hospitals or hospital systems. These include:
- Committee chairman. Most hospitals want interested, dedicated individuals to chair traditional medical staff committees. Hospitalists are well suited because our unique perspective lets us identify processes or products that can help many patients. Begin by serving on a committee, such as ethics, pharmacy and therapeutics, IRB, or departmental peer review. As you get comfortable, discuss potential chairmanships with the chief of staff or the vice president of medical affairs (VPMA). Don’t expect to advance if you don’t show up or don’t come prepared to committee meetings.
- Department chairperson. These positions are often elected and may allow one to serve on the credentials committee and the medical executive committee.
- Medical staff officers. Hospitalists often are elected to these key positions and gain access to administration and various committees.
- Project manager. Installing and using electronic medical records and devices calls for physician involvement in design and support. These are great chances to work on interesting projects and affect the tools you work with.
- Hospital administrative positions. Many hospitals have a VPMA or a chief medical officer (CMO), and some are developing the role of vice president of quality. These can be full- or part-time positions. You will be expected to help members of the medical staff implement change, and you should have experience and proven effectiveness in prior roles. Several predict that hospital COOs and CEOs of the future will be hospitalists.
Another path of opportunity is within your organization, depending on your employer. These roles may overlap with hospital positions:
- Group leader. Generally responsible for working on scheduling, recruitment, and organizational structure. The job may involve responsibility for one or more facilities.
- Compliance officer. Someone in the group must understand billing, coding, and proper use of rules and legislation.
- Quality and safety officer.
- Group president.
Hospitalists can also participate on committees that deal with such areas as pension plans, contracts, or other business.
Health insurance companies provide opportunities for individuals to practice part-time and serve as medical directors. They also have career paths for VPMAs and CMOs.
Also, many healthcare companies have been started and run by physicians. Invent something; start a company. The opportunities are endless.
Some other tips:
- Educate yourself. Take courses like the SHM Leadership Academy. Learn how to interact in a businesslike manner. Some on-the-job training is OK, but management and leadership are new fields that require new learning.
- Read. There are many great books on being an executive. Learn how to run a meeting, make an agenda, work with other professionals, and delegate.
- Ask for help. Find an individual or individuals with whom you can discuss ideas. Some of your best mentors will be managers in other fields.
Mary Jo Gorman, MD, MBA
Immediate Past President, SHM
Consequences of Locum Tenens Work
I feel one piece of advice in the Career Development section in the May issue of The Hospitalist (“How to Navigate Hospital Medicine,” p. 9) is not complete and may adversely affect a new hospitalist’s career.
The article recommends exploring locum tenens work. We have found two unintended consequences of such action. First, the locum companies usually have a buyout clause for the physician. Should he decide he likes a location and wishes to stay, the potential employer faces an additional cost in the $20,000-$30,000 range. It makes budgeting difficult. Also, there is usually a clause in the locum contract that this policy is in place for two years after leaving the locum company.
Second, frequent job changes lead to prolonged processing of credentials at hospitals as they verify good standing at all previous practice sites. This means delays that force a hospitalist company to look for more readily available docs. The physician may be unable to find hospitals in highly desirable areas.
The article was otherwise well balanced and timely.
George Block, MD
CMO, Galen Inpatient Physicians Medical Group
Emeryville, Calif.
Jane Jerrard covered some potential career paths for academic hospitalists in her article “How to Navigate Hospital Medicine” (May 2007, p. 9). But I believe her account was incomplete. I would like to add detail to the opportunities in community-based and other programs.
Community-based medical groups offer a number of opportunities in hospitals or hospital systems. These include:
- Committee chairman. Most hospitals want interested, dedicated individuals to chair traditional medical staff committees. Hospitalists are well suited because our unique perspective lets us identify processes or products that can help many patients. Begin by serving on a committee, such as ethics, pharmacy and therapeutics, IRB, or departmental peer review. As you get comfortable, discuss potential chairmanships with the chief of staff or the vice president of medical affairs (VPMA). Don’t expect to advance if you don’t show up or don’t come prepared to committee meetings.
- Department chairperson. These positions are often elected and may allow one to serve on the credentials committee and the medical executive committee.
- Medical staff officers. Hospitalists often are elected to these key positions and gain access to administration and various committees.
- Project manager. Installing and using electronic medical records and devices calls for physician involvement in design and support. These are great chances to work on interesting projects and affect the tools you work with.
- Hospital administrative positions. Many hospitals have a VPMA or a chief medical officer (CMO), and some are developing the role of vice president of quality. These can be full- or part-time positions. You will be expected to help members of the medical staff implement change, and you should have experience and proven effectiveness in prior roles. Several predict that hospital COOs and CEOs of the future will be hospitalists.
Another path of opportunity is within your organization, depending on your employer. These roles may overlap with hospital positions:
- Group leader. Generally responsible for working on scheduling, recruitment, and organizational structure. The job may involve responsibility for one or more facilities.
- Compliance officer. Someone in the group must understand billing, coding, and proper use of rules and legislation.
- Quality and safety officer.
- Group president.
Hospitalists can also participate on committees that deal with such areas as pension plans, contracts, or other business.
Health insurance companies provide opportunities for individuals to practice part-time and serve as medical directors. They also have career paths for VPMAs and CMOs.
Also, many healthcare companies have been started and run by physicians. Invent something; start a company. The opportunities are endless.
Some other tips:
- Educate yourself. Take courses like the SHM Leadership Academy. Learn how to interact in a businesslike manner. Some on-the-job training is OK, but management and leadership are new fields that require new learning.
- Read. There are many great books on being an executive. Learn how to run a meeting, make an agenda, work with other professionals, and delegate.
- Ask for help. Find an individual or individuals with whom you can discuss ideas. Some of your best mentors will be managers in other fields.
Mary Jo Gorman, MD, MBA
Immediate Past President, SHM
Consequences of Locum Tenens Work
I feel one piece of advice in the Career Development section in the May issue of The Hospitalist (“How to Navigate Hospital Medicine,” p. 9) is not complete and may adversely affect a new hospitalist’s career.
The article recommends exploring locum tenens work. We have found two unintended consequences of such action. First, the locum companies usually have a buyout clause for the physician. Should he decide he likes a location and wishes to stay, the potential employer faces an additional cost in the $20,000-$30,000 range. It makes budgeting difficult. Also, there is usually a clause in the locum contract that this policy is in place for two years after leaving the locum company.
Second, frequent job changes lead to prolonged processing of credentials at hospitals as they verify good standing at all previous practice sites. This means delays that force a hospitalist company to look for more readily available docs. The physician may be unable to find hospitals in highly desirable areas.
The article was otherwise well balanced and timely.
George Block, MD
CMO, Galen Inpatient Physicians Medical Group
Emeryville, Calif.
How to monitor medication side effects
Woman prescribed a stimulant suffers stroke and disability
Harris County (TX) District Court
A 39-year-old patient was diagnosed with attention-deficit/hyperactivity disorder (ADHD) by a psychologist, who referred her to a psychiatrist. The psychiatrist prescribed amphetamine/dextroamphetamine, which the patient took for 9 months. During this time her blood pressure and other vital signs were not monitored. The patient then suffered a stroke, is now a paraplegic, and must use a wheelchair.
The patient claimed that negligent misdiagnosis and monitoring caused the stroke. The psychiatrist maintained that diagnosis and monitoring were appropriate, and the drug did not cause the stroke. The psychiatrist also claimed that the patient had a transient ischemic attack (TIA) before taking amphetamine/dextroamphetamine and another stroke after discontinuing the drug.
- A defense verdict was returned
Improper dose of lamotrigine blamed for liver failure
San Diego County (CA) Superior Court
The patient, age 35, was involuntarily admitted to an inpatient psychiatric facility after the police found her acting bizarrely and hallucinating. The admitting and treating psychiatrist learned that the patient had been admitted for psychiatric treatment 9 times in the previous 12 months, had a long history of polysubstance abuse, and had been largely nonadherent with medication. The psychiatrist diagnosed rapid-cycling bipolar disorder and started the patient on lamotrigine with an escalating dosage schedule. The patient was released from the psychiatric facility.
Later that month, the patient developed a urinary tract infection and was readmitted to the hospital. She agreed to lab testing and all results were within normal limits, but throughout a 2-month stay the patient intermittently complained of a sore throat, cough, and nausea. Two weeks later, the psychiatrist reviewed lab tests that showed a mild elevation of the patient’s liver enzymes.
The next day the patient reported a rash on her chest and a high fever. She was transferred to an acute care facility. The patient’s liver enzymes continued to rise, and the psychiatrist discontinued lamotrigine. The patient continued to deteriorate and was transferred to another hospital to consult with a liver specialist. About 3 weeks later the patient went into a coma and died.
Autopsy showed massive liver necrosis. The patient’s family claimed the psychiatrist was negligent in giving the patient lamotrigine, which caused the liver failure. They contended the dose prescribed was too high, the patient was not properly monitored, and other psychiatric drugs could have been used with more gradual increases.
The psychiatrist maintained that the lamotrigine dosage used was appropriate, lamotrigine was not known to cause liver problems, and it did not cause the patient’s liver failure.
- A defense verdict was returned
Dr. Grant’s observations
These cases reflect a clinician’s worst nightmare—using an appropriate medication, experiencing a disastrous outcome, and then being sued for malpractice. Clinicians need to remember:
- anyone can be sued
- a lawsuit does not mean that the clinician did anything inappropriate.
Meeting standards of care
Medical malpractice claims could be based on a physician diverging from 1 of 2 standards of care:
- The “average practitioner” or “customary practice” standard means the treatment practice is consistent with others in the field. Courts might allow the medical profession to define the standard of care according to medical custom.
- The “reasonably prudent physician” standard means what a reasonable physician would have done under the circumstances. The jury determines if the physician acted reasonably, not whether the physician conformed to existing standards.1
In these cases, using amphetamine/ dextroamphetamine for ADHD and lamotrigine for bipolar disorder appears to meet either standard. These 2 drugs are FDA-approved to treat the disorders for which they were prescribed. Although we do not know what doses the physicians prescribed in these 2 cases, in general if the dosing adheres to the FDA-approved range or can be based on credible research, the treatment will meet the 2 standards.
Choosing a treatment plan
The American Psychiatric Association’s practice guidelines (available at http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm) state “the ultimate judgment regarding a particular clinical procedure or treatment plan must be made by the psychiatrist in light of the clinical data presented by the patient and the diagnostic and treatment options available.”3
Regardless of the treatment used—even if the medication is “off-label” and not FDA-approved for a particular disorder or the dose is not within the FDA-approved dosing range—you should be able to document your rationale for using a medication and dosing by showing that it is part of good clinical practice.
A clinician’s scientific rationale for medication and dosing choice should be based on the psychiatric evaluation and known risks and benefits of the treatment. In addition, the patient should:
- understand pertinent information regarding the medication and its side effects
- and freely give consent to treatment.4
Monitoring for side effects
In these cases, the court also had to determine whether clinicians’ monitoring for side effects was appropriate. For several years, case reports have raised speculation about a link between strokes and amphetamine/ dextroamphetamine4,5 In 2005, Adderall XR was taken off the Canadian market because of reports of strokes and sudden deaths.7
The FDA’s Adverse Event Reporting System database identified 12 cases of sudden death in pediatric patents treated for ADHD with Adderall or Adderall XR.8 lthough the drug has returned to the Canadian market and a clear link between stroke or sudden death and Adderall has not been established, The Physicians’ Desk Reference (PDR)9 advises physicians to monitor blood pressure in individuals taking amphetamine/dextroamphetamine, particularly those with hypertension. The FDA has issued new labeling instructions for all stimulants advising prescribing clinicians to monitor blood pressure regularly.10
Even so, if you fail to monitor blood pressure and a patient has a stroke—such as in the first case—you are not necessarily negligent. Successful malpractice cases need to demonstrate causation. The plaintiff must prove:
- The physician’s act or omission was the cause-in-fact of the harm. Without the act, the harm would not have occurred.
- The act was the proximate cause of the harm. In a natural, unbroken sequence of events, the act produces a foreseeable result. A physician should not be liable for the far-reaching and improbable consequences of an act or omission.1
- lack of foreseeability—the consequences of the act were not reasonably foreseeable, or
- an intervening event that supersedes all others in causing the injury.1
Foreseeability
A defendant may be liable only if the consequences of the act or omission were reasonably foreseeable. Foreseeability is a vague legal concept and is not the same as predictability. Foreseeability should be understood in context of what information was available at the time. For example, the FDA black box warnings about the link between stimulants and stroke or sudden death did not appear until 2006.11 What light be considered foreseeable now might not have been before 2006 (it is unclear when the above case was litigated).
Intervening events
An intervening event is one that takes effect after the defendant’s negligence and breaks the chain of causation. In the first case, the patient had a history of TIAs before taking amphetamine/dextroamphetamine. The condition that caused the TIAs, such as atherosclerosis in an artery, may also have caused the stroke independent of the use of stimulants, and therefore could be considered an intervening event.
In the lamotrigine case, elevations of aspartate transaminase and alanine transaminase are infrequent or rare. Several case reports have discussed possible hepatotoxicity associated with the drug.13
A reasonably prudent physician should warn patients about and monitor for symptoms of Stevens-Johnson syndrome, a serious disorder of the skin and mucous membranes sometimes seen with lamotrigine that can begin with cough, fever, and sore throat. Although hepatitis is a possible complication of Stevens-Johnson, the first step of treatment is to hospitalize the patient in an intensive care unit, which the physician did. The PDR and FDA guidelines do not recommend monitoring liver function tests as a way to assess for Stevens-Johnson or for liver dysfunction as an independent problem with lamotrigine.9,12
Given the lack of guidelines and the scant literature on this topic, the psychiatrist in this case would not have been expected to monitor liver function, which would meet either the “average practitioner” or “reasonably prudent physician” standard. Although the literature suggests that liver toxicity might have been foreseeable, the patient had a history of polysubstance abuse, which may be determined to be an intervening event. Substance abuse could have caused liver toxicity, depending on the drugs the patient abused.
Drug brand names
- Amphetamine/Dextroamphetamine • Adderall
- Lamotrigine • Lamictal
1. Knoll J, Gerbasi J. Psychiatric malpractice case analysis: striving for objectivity. J Am Acad Psychiatry Law 2006;34:215-223.
2. Lewis MH, Gohagan JK, Merensteine DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA 2007;297:2633-7.
3. American Psychiatric Association Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed June 27, 2007.
4. Berner M. Informed consent. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press 1998:23-43.
5. Toffol GJ, Biller J, Adams HP. Nontraumtic intracerebral hemorrhage in young adults. Arch Neurol 1987;44:483-5.
6. Bakheit AM. Intracerebral haemorrhage in previously healthy young adults. Postgrad Med J 1999;75:499-500.
7. McMillen M. Adderall: a stroke of bad news. The Washington Post. February 15, 2005. Available at: http://www.washingtonpost.com/wp-dyn/articles/A24764-2005Feb14.html. Accessed June 27, 2007.
8. U.S. Food and Drug Administration. Alert for healthcare professionals Adderall and Adderall XT (amphetamines). September 23, 2005. Available at: http://www.fda.gov/cder/drug/infosheets/hcp/adderalhcp.htm. Accessed July 5, 2007.
9. Physicians’ desk reference Montvale, NJ: Thompson PDR; 2007.
10. U.S. Food and Drug Administration. Adderall and Adderall XR (amphetamines) information. February 22, 2007. Available at: http://www.fda.gov/cder/drug/infopage/adderall/default.htm. Accessed June 27, 2007.
11. Charatan F. FDA committee votes for warning labels on stimulant drugs. BMJ 2006;332:380-
12. Lamictal prescribing information. Food and Drug Administration Web site. Available at http://www.fda.gov/cder/foi/label/2006020241s10s21s25s26s27,020764s3s14s18s19s20lbl.pdf. Accessed July 9, 2007.
13. Overstreet K, Costanza C, Behling C, et al. Fatal progressive hepatic necrosis associated with lamotrigine treatment: a case report and literature review. Dig Dis Sci 2002;47:1921-5.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
Woman prescribed a stimulant suffers stroke and disability
Harris County (TX) District Court
A 39-year-old patient was diagnosed with attention-deficit/hyperactivity disorder (ADHD) by a psychologist, who referred her to a psychiatrist. The psychiatrist prescribed amphetamine/dextroamphetamine, which the patient took for 9 months. During this time her blood pressure and other vital signs were not monitored. The patient then suffered a stroke, is now a paraplegic, and must use a wheelchair.
The patient claimed that negligent misdiagnosis and monitoring caused the stroke. The psychiatrist maintained that diagnosis and monitoring were appropriate, and the drug did not cause the stroke. The psychiatrist also claimed that the patient had a transient ischemic attack (TIA) before taking amphetamine/dextroamphetamine and another stroke after discontinuing the drug.
- A defense verdict was returned
Improper dose of lamotrigine blamed for liver failure
San Diego County (CA) Superior Court
The patient, age 35, was involuntarily admitted to an inpatient psychiatric facility after the police found her acting bizarrely and hallucinating. The admitting and treating psychiatrist learned that the patient had been admitted for psychiatric treatment 9 times in the previous 12 months, had a long history of polysubstance abuse, and had been largely nonadherent with medication. The psychiatrist diagnosed rapid-cycling bipolar disorder and started the patient on lamotrigine with an escalating dosage schedule. The patient was released from the psychiatric facility.
Later that month, the patient developed a urinary tract infection and was readmitted to the hospital. She agreed to lab testing and all results were within normal limits, but throughout a 2-month stay the patient intermittently complained of a sore throat, cough, and nausea. Two weeks later, the psychiatrist reviewed lab tests that showed a mild elevation of the patient’s liver enzymes.
The next day the patient reported a rash on her chest and a high fever. She was transferred to an acute care facility. The patient’s liver enzymes continued to rise, and the psychiatrist discontinued lamotrigine. The patient continued to deteriorate and was transferred to another hospital to consult with a liver specialist. About 3 weeks later the patient went into a coma and died.
Autopsy showed massive liver necrosis. The patient’s family claimed the psychiatrist was negligent in giving the patient lamotrigine, which caused the liver failure. They contended the dose prescribed was too high, the patient was not properly monitored, and other psychiatric drugs could have been used with more gradual increases.
The psychiatrist maintained that the lamotrigine dosage used was appropriate, lamotrigine was not known to cause liver problems, and it did not cause the patient’s liver failure.
- A defense verdict was returned
Dr. Grant’s observations
These cases reflect a clinician’s worst nightmare—using an appropriate medication, experiencing a disastrous outcome, and then being sued for malpractice. Clinicians need to remember:
- anyone can be sued
- a lawsuit does not mean that the clinician did anything inappropriate.
Meeting standards of care
Medical malpractice claims could be based on a physician diverging from 1 of 2 standards of care:
- The “average practitioner” or “customary practice” standard means the treatment practice is consistent with others in the field. Courts might allow the medical profession to define the standard of care according to medical custom.
- The “reasonably prudent physician” standard means what a reasonable physician would have done under the circumstances. The jury determines if the physician acted reasonably, not whether the physician conformed to existing standards.1
In these cases, using amphetamine/ dextroamphetamine for ADHD and lamotrigine for bipolar disorder appears to meet either standard. These 2 drugs are FDA-approved to treat the disorders for which they were prescribed. Although we do not know what doses the physicians prescribed in these 2 cases, in general if the dosing adheres to the FDA-approved range or can be based on credible research, the treatment will meet the 2 standards.
Choosing a treatment plan
The American Psychiatric Association’s practice guidelines (available at http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm) state “the ultimate judgment regarding a particular clinical procedure or treatment plan must be made by the psychiatrist in light of the clinical data presented by the patient and the diagnostic and treatment options available.”3
Regardless of the treatment used—even if the medication is “off-label” and not FDA-approved for a particular disorder or the dose is not within the FDA-approved dosing range—you should be able to document your rationale for using a medication and dosing by showing that it is part of good clinical practice.
A clinician’s scientific rationale for medication and dosing choice should be based on the psychiatric evaluation and known risks and benefits of the treatment. In addition, the patient should:
- understand pertinent information regarding the medication and its side effects
- and freely give consent to treatment.4
Monitoring for side effects
In these cases, the court also had to determine whether clinicians’ monitoring for side effects was appropriate. For several years, case reports have raised speculation about a link between strokes and amphetamine/ dextroamphetamine4,5 In 2005, Adderall XR was taken off the Canadian market because of reports of strokes and sudden deaths.7
The FDA’s Adverse Event Reporting System database identified 12 cases of sudden death in pediatric patents treated for ADHD with Adderall or Adderall XR.8 lthough the drug has returned to the Canadian market and a clear link between stroke or sudden death and Adderall has not been established, The Physicians’ Desk Reference (PDR)9 advises physicians to monitor blood pressure in individuals taking amphetamine/dextroamphetamine, particularly those with hypertension. The FDA has issued new labeling instructions for all stimulants advising prescribing clinicians to monitor blood pressure regularly.10
Even so, if you fail to monitor blood pressure and a patient has a stroke—such as in the first case—you are not necessarily negligent. Successful malpractice cases need to demonstrate causation. The plaintiff must prove:
- The physician’s act or omission was the cause-in-fact of the harm. Without the act, the harm would not have occurred.
- The act was the proximate cause of the harm. In a natural, unbroken sequence of events, the act produces a foreseeable result. A physician should not be liable for the far-reaching and improbable consequences of an act or omission.1
- lack of foreseeability—the consequences of the act were not reasonably foreseeable, or
- an intervening event that supersedes all others in causing the injury.1
Foreseeability
A defendant may be liable only if the consequences of the act or omission were reasonably foreseeable. Foreseeability is a vague legal concept and is not the same as predictability. Foreseeability should be understood in context of what information was available at the time. For example, the FDA black box warnings about the link between stimulants and stroke or sudden death did not appear until 2006.11 What light be considered foreseeable now might not have been before 2006 (it is unclear when the above case was litigated).
Intervening events
An intervening event is one that takes effect after the defendant’s negligence and breaks the chain of causation. In the first case, the patient had a history of TIAs before taking amphetamine/dextroamphetamine. The condition that caused the TIAs, such as atherosclerosis in an artery, may also have caused the stroke independent of the use of stimulants, and therefore could be considered an intervening event.
In the lamotrigine case, elevations of aspartate transaminase and alanine transaminase are infrequent or rare. Several case reports have discussed possible hepatotoxicity associated with the drug.13
A reasonably prudent physician should warn patients about and monitor for symptoms of Stevens-Johnson syndrome, a serious disorder of the skin and mucous membranes sometimes seen with lamotrigine that can begin with cough, fever, and sore throat. Although hepatitis is a possible complication of Stevens-Johnson, the first step of treatment is to hospitalize the patient in an intensive care unit, which the physician did. The PDR and FDA guidelines do not recommend monitoring liver function tests as a way to assess for Stevens-Johnson or for liver dysfunction as an independent problem with lamotrigine.9,12
Given the lack of guidelines and the scant literature on this topic, the psychiatrist in this case would not have been expected to monitor liver function, which would meet either the “average practitioner” or “reasonably prudent physician” standard. Although the literature suggests that liver toxicity might have been foreseeable, the patient had a history of polysubstance abuse, which may be determined to be an intervening event. Substance abuse could have caused liver toxicity, depending on the drugs the patient abused.
Drug brand names
- Amphetamine/Dextroamphetamine • Adderall
- Lamotrigine • Lamictal
Woman prescribed a stimulant suffers stroke and disability
Harris County (TX) District Court
A 39-year-old patient was diagnosed with attention-deficit/hyperactivity disorder (ADHD) by a psychologist, who referred her to a psychiatrist. The psychiatrist prescribed amphetamine/dextroamphetamine, which the patient took for 9 months. During this time her blood pressure and other vital signs were not monitored. The patient then suffered a stroke, is now a paraplegic, and must use a wheelchair.
The patient claimed that negligent misdiagnosis and monitoring caused the stroke. The psychiatrist maintained that diagnosis and monitoring were appropriate, and the drug did not cause the stroke. The psychiatrist also claimed that the patient had a transient ischemic attack (TIA) before taking amphetamine/dextroamphetamine and another stroke after discontinuing the drug.
- A defense verdict was returned
Improper dose of lamotrigine blamed for liver failure
San Diego County (CA) Superior Court
The patient, age 35, was involuntarily admitted to an inpatient psychiatric facility after the police found her acting bizarrely and hallucinating. The admitting and treating psychiatrist learned that the patient had been admitted for psychiatric treatment 9 times in the previous 12 months, had a long history of polysubstance abuse, and had been largely nonadherent with medication. The psychiatrist diagnosed rapid-cycling bipolar disorder and started the patient on lamotrigine with an escalating dosage schedule. The patient was released from the psychiatric facility.
Later that month, the patient developed a urinary tract infection and was readmitted to the hospital. She agreed to lab testing and all results were within normal limits, but throughout a 2-month stay the patient intermittently complained of a sore throat, cough, and nausea. Two weeks later, the psychiatrist reviewed lab tests that showed a mild elevation of the patient’s liver enzymes.
The next day the patient reported a rash on her chest and a high fever. She was transferred to an acute care facility. The patient’s liver enzymes continued to rise, and the psychiatrist discontinued lamotrigine. The patient continued to deteriorate and was transferred to another hospital to consult with a liver specialist. About 3 weeks later the patient went into a coma and died.
Autopsy showed massive liver necrosis. The patient’s family claimed the psychiatrist was negligent in giving the patient lamotrigine, which caused the liver failure. They contended the dose prescribed was too high, the patient was not properly monitored, and other psychiatric drugs could have been used with more gradual increases.
The psychiatrist maintained that the lamotrigine dosage used was appropriate, lamotrigine was not known to cause liver problems, and it did not cause the patient’s liver failure.
- A defense verdict was returned
Dr. Grant’s observations
These cases reflect a clinician’s worst nightmare—using an appropriate medication, experiencing a disastrous outcome, and then being sued for malpractice. Clinicians need to remember:
- anyone can be sued
- a lawsuit does not mean that the clinician did anything inappropriate.
Meeting standards of care
Medical malpractice claims could be based on a physician diverging from 1 of 2 standards of care:
- The “average practitioner” or “customary practice” standard means the treatment practice is consistent with others in the field. Courts might allow the medical profession to define the standard of care according to medical custom.
- The “reasonably prudent physician” standard means what a reasonable physician would have done under the circumstances. The jury determines if the physician acted reasonably, not whether the physician conformed to existing standards.1
In these cases, using amphetamine/ dextroamphetamine for ADHD and lamotrigine for bipolar disorder appears to meet either standard. These 2 drugs are FDA-approved to treat the disorders for which they were prescribed. Although we do not know what doses the physicians prescribed in these 2 cases, in general if the dosing adheres to the FDA-approved range or can be based on credible research, the treatment will meet the 2 standards.
Choosing a treatment plan
The American Psychiatric Association’s practice guidelines (available at http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm) state “the ultimate judgment regarding a particular clinical procedure or treatment plan must be made by the psychiatrist in light of the clinical data presented by the patient and the diagnostic and treatment options available.”3
Regardless of the treatment used—even if the medication is “off-label” and not FDA-approved for a particular disorder or the dose is not within the FDA-approved dosing range—you should be able to document your rationale for using a medication and dosing by showing that it is part of good clinical practice.
A clinician’s scientific rationale for medication and dosing choice should be based on the psychiatric evaluation and known risks and benefits of the treatment. In addition, the patient should:
- understand pertinent information regarding the medication and its side effects
- and freely give consent to treatment.4
Monitoring for side effects
In these cases, the court also had to determine whether clinicians’ monitoring for side effects was appropriate. For several years, case reports have raised speculation about a link between strokes and amphetamine/ dextroamphetamine4,5 In 2005, Adderall XR was taken off the Canadian market because of reports of strokes and sudden deaths.7
The FDA’s Adverse Event Reporting System database identified 12 cases of sudden death in pediatric patents treated for ADHD with Adderall or Adderall XR.8 lthough the drug has returned to the Canadian market and a clear link between stroke or sudden death and Adderall has not been established, The Physicians’ Desk Reference (PDR)9 advises physicians to monitor blood pressure in individuals taking amphetamine/dextroamphetamine, particularly those with hypertension. The FDA has issued new labeling instructions for all stimulants advising prescribing clinicians to monitor blood pressure regularly.10
Even so, if you fail to monitor blood pressure and a patient has a stroke—such as in the first case—you are not necessarily negligent. Successful malpractice cases need to demonstrate causation. The plaintiff must prove:
- The physician’s act or omission was the cause-in-fact of the harm. Without the act, the harm would not have occurred.
- The act was the proximate cause of the harm. In a natural, unbroken sequence of events, the act produces a foreseeable result. A physician should not be liable for the far-reaching and improbable consequences of an act or omission.1
- lack of foreseeability—the consequences of the act were not reasonably foreseeable, or
- an intervening event that supersedes all others in causing the injury.1
Foreseeability
A defendant may be liable only if the consequences of the act or omission were reasonably foreseeable. Foreseeability is a vague legal concept and is not the same as predictability. Foreseeability should be understood in context of what information was available at the time. For example, the FDA black box warnings about the link between stimulants and stroke or sudden death did not appear until 2006.11 What light be considered foreseeable now might not have been before 2006 (it is unclear when the above case was litigated).
Intervening events
An intervening event is one that takes effect after the defendant’s negligence and breaks the chain of causation. In the first case, the patient had a history of TIAs before taking amphetamine/dextroamphetamine. The condition that caused the TIAs, such as atherosclerosis in an artery, may also have caused the stroke independent of the use of stimulants, and therefore could be considered an intervening event.
In the lamotrigine case, elevations of aspartate transaminase and alanine transaminase are infrequent or rare. Several case reports have discussed possible hepatotoxicity associated with the drug.13
A reasonably prudent physician should warn patients about and monitor for symptoms of Stevens-Johnson syndrome, a serious disorder of the skin and mucous membranes sometimes seen with lamotrigine that can begin with cough, fever, and sore throat. Although hepatitis is a possible complication of Stevens-Johnson, the first step of treatment is to hospitalize the patient in an intensive care unit, which the physician did. The PDR and FDA guidelines do not recommend monitoring liver function tests as a way to assess for Stevens-Johnson or for liver dysfunction as an independent problem with lamotrigine.9,12
Given the lack of guidelines and the scant literature on this topic, the psychiatrist in this case would not have been expected to monitor liver function, which would meet either the “average practitioner” or “reasonably prudent physician” standard. Although the literature suggests that liver toxicity might have been foreseeable, the patient had a history of polysubstance abuse, which may be determined to be an intervening event. Substance abuse could have caused liver toxicity, depending on the drugs the patient abused.
Drug brand names
- Amphetamine/Dextroamphetamine • Adderall
- Lamotrigine • Lamictal
1. Knoll J, Gerbasi J. Psychiatric malpractice case analysis: striving for objectivity. J Am Acad Psychiatry Law 2006;34:215-223.
2. Lewis MH, Gohagan JK, Merensteine DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA 2007;297:2633-7.
3. American Psychiatric Association Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed June 27, 2007.
4. Berner M. Informed consent. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press 1998:23-43.
5. Toffol GJ, Biller J, Adams HP. Nontraumtic intracerebral hemorrhage in young adults. Arch Neurol 1987;44:483-5.
6. Bakheit AM. Intracerebral haemorrhage in previously healthy young adults. Postgrad Med J 1999;75:499-500.
7. McMillen M. Adderall: a stroke of bad news. The Washington Post. February 15, 2005. Available at: http://www.washingtonpost.com/wp-dyn/articles/A24764-2005Feb14.html. Accessed June 27, 2007.
8. U.S. Food and Drug Administration. Alert for healthcare professionals Adderall and Adderall XT (amphetamines). September 23, 2005. Available at: http://www.fda.gov/cder/drug/infosheets/hcp/adderalhcp.htm. Accessed July 5, 2007.
9. Physicians’ desk reference Montvale, NJ: Thompson PDR; 2007.
10. U.S. Food and Drug Administration. Adderall and Adderall XR (amphetamines) information. February 22, 2007. Available at: http://www.fda.gov/cder/drug/infopage/adderall/default.htm. Accessed June 27, 2007.
11. Charatan F. FDA committee votes for warning labels on stimulant drugs. BMJ 2006;332:380-
12. Lamictal prescribing information. Food and Drug Administration Web site. Available at http://www.fda.gov/cder/foi/label/2006020241s10s21s25s26s27,020764s3s14s18s19s20lbl.pdf. Accessed July 9, 2007.
13. Overstreet K, Costanza C, Behling C, et al. Fatal progressive hepatic necrosis associated with lamotrigine treatment: a case report and literature review. Dig Dis Sci 2002;47:1921-5.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. Knoll J, Gerbasi J. Psychiatric malpractice case analysis: striving for objectivity. J Am Acad Psychiatry Law 2006;34:215-223.
2. Lewis MH, Gohagan JK, Merensteine DJ. The locality rule and the physician’s dilemma: local medical practices vs the national standard of care. JAMA 2007;297:2633-7.
3. American Psychiatric Association Practice guidelines. Available at: http://www.psych.org/psych_pract/treatg/pg/prac_guide.cfm. Accessed June 27, 2007.
4. Berner M. Informed consent. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press 1998:23-43.
5. Toffol GJ, Biller J, Adams HP. Nontraumtic intracerebral hemorrhage in young adults. Arch Neurol 1987;44:483-5.
6. Bakheit AM. Intracerebral haemorrhage in previously healthy young adults. Postgrad Med J 1999;75:499-500.
7. McMillen M. Adderall: a stroke of bad news. The Washington Post. February 15, 2005. Available at: http://www.washingtonpost.com/wp-dyn/articles/A24764-2005Feb14.html. Accessed June 27, 2007.
8. U.S. Food and Drug Administration. Alert for healthcare professionals Adderall and Adderall XT (amphetamines). September 23, 2005. Available at: http://www.fda.gov/cder/drug/infosheets/hcp/adderalhcp.htm. Accessed July 5, 2007.
9. Physicians’ desk reference Montvale, NJ: Thompson PDR; 2007.
10. U.S. Food and Drug Administration. Adderall and Adderall XR (amphetamines) information. February 22, 2007. Available at: http://www.fda.gov/cder/drug/infopage/adderall/default.htm. Accessed June 27, 2007.
11. Charatan F. FDA committee votes for warning labels on stimulant drugs. BMJ 2006;332:380-
12. Lamictal prescribing information. Food and Drug Administration Web site. Available at http://www.fda.gov/cder/foi/label/2006020241s10s21s25s26s27,020764s3s14s18s19s20lbl.pdf. Accessed July 9, 2007.
13. Overstreet K, Costanza C, Behling C, et al. Fatal progressive hepatic necrosis associated with lamotrigine treatment: a case report and literature review. Dig Dis Sci 2002;47:1921-5.
Cases are selected by Current Psychiatry from Medical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
SHM Wins $1.4 Million Grant from Hartford

On March 16, the John A. Hartford Foundation awarded SHM a $1.4 million grant to develop interventions to improve care transitions for older adults at the time of hospital discharge.
One of the core values of SHM and hospital medicine is to implement changes that improve the care older Americans receive. With this grant support from The Hartford Foundation, SHM can help define and set standards for best practices in discharge and provide a continuum of training opportunities to support those practices.
As part of this three-year project, SHM will partner with national leaders in care coordination to form a national advisory board, create clinical tools, implement guidelines, and provide technical support and training tools to hospitals across the U.S. The project aims to build capacity in at least 200 hospital sites to improve the discharge process and, ultimately, health outcomes for older adults.
Chapter Report

National Advisory Board AND Project Team
SHM has assembled a national advisory board to inform and guide the project. The board will be chaired by Eric Coleman, MD, MPH, associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora. At press time, members included:
- Barbara Berkman, DSW, PhD, professor of health and mental health, University School of Social Work, Mount Sinai School of Medicine;
- Tom Bookwalter, PharmD, clinical pharmacist, American Society of Health-System Pharmacists (ASHP);
- Alan Korn, MD, chief medical officer and senior vice president for clinical affairs, Blue Cross Blue Shield Association;
- Chuck Denham, MD, chair, National Quality Forum (NQF);
- Gavin Hougham, PhD, senior program officer, John A. Hartford Foundation;
- Seth Landefeld, MD, director, American Geriatrics Society (AGS);
- Cheri Lattimer, RN, BSN, executive director, Case Management Society of America (CMSA);
- William Lyons, MD, AGS; Nebraska Medical Center in Omaha;
- Lorraine Mion, PhD, RN, FAAN, director of nursing services for geriatrics, Metro Health Medical Center in Cleveland, Ohio;
- Mary Naylor, PhD, RN, FAANS, Marian S. Ware professor in gerontology, University of Pennsylvania;
- Gail Povar, MD, MPH, chair, George Washington School of Medicine, Cameron Medical Group;
- Deborah Queenan, national advisory council coordinator, Agency for Healthcare Research and Quality (AHRQ);
- Pat Rutherford, RN, MS, vice president, Institute for Healthcare Improvement (IHI), Transforming Care at the Bedside (TCAB);
- Eric Warm, MD, Society General Internal Medicine (SGIM); and
- Larry Wellikson, MD, CEO of SHM.
Dr. Williams will serve as principal investigator, leading a team of co-investigators including Jeffrey Greenwald, MD, (Boston University co-investigator, AHRQ, Project ReEngineering Discharge); Eric Howell, MD (Johns Hopkins Bayview, SHM/Hartford Safe Steps Demonstration Project); Param Dedhia, MD (Johns Hopkins Bayview, SHM/Hartford Safe STEPS Demonstration Project); Lakshmi Halasyamani, MD (St. Joseph Mercy Hospital); Kathleen Kerr (SHM); and Tina Budnitz, MPH (SHM).
The project team includes investigators from the SHM/Hartford Foundation Safe STEPS project and two AHRQ-funded projects. All three projects aim to pilot test discharge-planning toolkits and interventions and develop implementation strategies for adoption. The current project will leverage the findings of all three projects with the insights of the advisory board to create a transitions bundle to optimize the discharge process. Following development of this bundle, SHM will develop a toolkit for implementation with corresponding training programs, and other technical support.
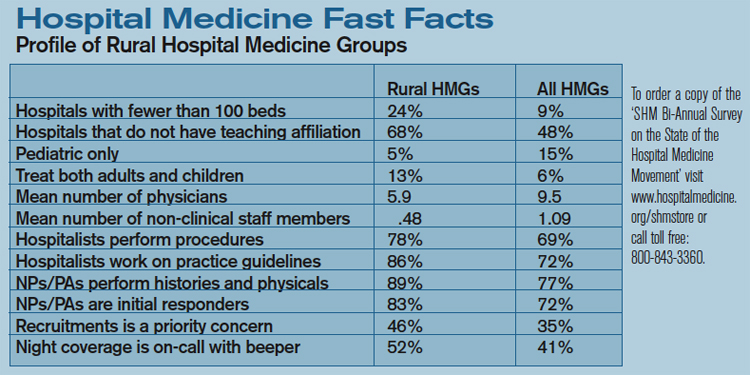
Capacity Building Via Continuum of Training Options
SHM has designed a range of technical support and training options to meet the needs of member institutions aiming to implement and sustain the transitions bundle. Strategies include:
- A Web-based resource room for care transitions in older adults: The transitions bundle, field guide, and related interventional materials will be freely available in the SHM online resource room.
- A Quality Pre-Course for QI Teams: The course is scheduled for 2008 and 2009 SHM Annual Meetings.
- A Transition Planning Mentored Implementation Program (TPMI): This yearlong mentoring program will support sites as they implement and evaluate transitions bundle interventions. The program includes a training conference, monthly teleconferences with expert mentors and peer support mechanisms.
- A consultation service: This will provide on-site consultation and technical assistance to sites planning, implementing, and evaluating discharge interventions. The service includes site visit, follow-up report of findings, recommendations and resources, and post-visit follow-up to review progress, successes and unforeseen barriers.
These support mechanisms are intended to assist those who lead improvement teams at their institutions. Enrollment will begin in the fall. For more information, contact [email protected].
A Seat at the Table
SHM active in shaping new performance standards
By Jane Jerrard
Healthcare providers are in the midst of important changes in how they work and how they’re rewarded for that work. Recent initiatives including Medicare’s Physician Quality Reporting Initiative and a Medicare hospital value-based purchasing program mandated by the Deficit Reduction Act spell change for practitioners, including hospitalists.
SHM is working to add a hospitalist voice to discussions and decisions that shape these initiatives. By participating in organizations such as the American Medical Association’s (AMA) Physician consortium for Performance Improvement (PCPI), SHM has a seat at the table where decisions are made.
How Participation Works
The PCPI was convened in 2001 by the AMA, with the mission of physician-led performance improvement. While the primary focus is on improving quality, the Consortium’s performance measures are ultimately those used in CMS and other pay-for-performance (P4P) programs and value-based purchasing initiatives.
SHM didn’t get involved when the PCPI was first formed because the issues weren’t relevant to hospitalists. “SHM was invited to participate at that time, but the focus was really on outpatient care,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. “More recently, when the PCPI began looking at the relation between hospital-level measures and physician-level measures, SHM CEO Larry Wellikson said we need to get involved.”
Dr. Torcson is SHM’s representative on the consortium. “For the last year and a half, I’ve been attending the PCPI meetings to represent SHM and have been involved in various PCPI work groups,” he says. “I had previously served on the SHM HQPS [Healthcare Quality and Patient Safety Task Force] and now serve on the PPC [Public Policy Committee], and I think the SHM leadership thought that combination of interests would be good for a PCPI representative.”
What about the Work Groups?
Work groups within the PCPI are assigned specific areas. These groups are responsible for creating performance measures within an area, which are then reviewed by the entire consortium.
“I participated on a work group to develop performance measures for emergency medicine physicians,” says Dr. Torcson. “This group thought that the current disease-specific measures weren’t relevant for them, and that the current hospital measures were also not relevant. I provided a hospitalist’s perspective on hand-offs and discharge which was really focused on a process of care that begins in the ED [emergency department].”
Each work group has representation from various areas of healthcare. “My work group had about 20 or 25 people, which is probably typical,” says Dr. Torcson. “The AMA provided a methodologist, and there was a CMS representative on the work group.” The work group first met face to face to review relevant evidence-based clinical guidelines and scame up with five to eight measures. These were then reworked through phone calls and e-mails before going before the entire PCPI for approval.
Other SHM representatives participated in relevant PCPI work groups as well. “PPC member Greg Seymann from San Diego participated in a geriatric work group that was convened for the same reason” as the ED group, says Dr. Torcson. “His group looked at creating a number of measures that were relative to both inpatient and outpatient geriatric patients. Some of these measures are now part of the Medicare Physician Quality Reporting Initiative.”
Another SHM member, James C. Pile. MD, FACP, participated in a work group on developing measures for outpatient administration of IV antibiotics. Pile is a staff physician in the Department of General Internal Medicine, Section of Hospital Medicine, at The Cleveland Clinic in Ohio.
In each group, SHM representatives were able to help shape measures that reflect the unique knowledge and perspective of hospital medicine.
“A hospitalist brings the perspective of having seen how these measures are actually incorporated into a practice, how they are actually applied to patient care,” Dr. Torcson points out. “These work groups to develop additional performance measures are ongoing. The PCPI has a rigorous agenda for what they want to accomplish over the next few years.”
SHM to Lead the Way on Care Transitions
The PCPI has asked SHM to be the lead organization for a performance measure development work group on care coordination and care transitions.
“This will be groundbreaking work around this important aspect of care that is very process-focused as opposed to disease-focused,” says Dr. Torcson. “It’s very appropriate that SHM was asked to be the lead group for this. This area of performance improvement is perfect for what hospitalists do.”
The PCPI plans to have care transition performance measures ready for adoption by 2009.
SHM and the Big Three
CMS is also collaborating with the National Quality Forum (NQF) and Ambulatory Quality Alliance (AQA). “The PCPI, AQA, and NQF are the most influential organizations right now for quality and performance measures,” says Dr. Torcson.
The NQF, a unique public and private collaborative, develops consensus standards on different measures submitted to it. “I have had the opportunity to participate on an NQF Steering Committee for performance measure endorsement,” says Dr. Torcson.
The AQA is responsible for standardizing performance measurement and reporting, and developing measures for efficiency to be included in forthcoming Medicare P4P programs. “The AQA is charged with implementing performance measures and bringing them to the marketplace,” explains Dr. Torcson. “SHM is not involved in the AQA process yet.”
Membership in SHM means you are able to access the latest information on issues like CMS reporting initiatives and have representation in the decision-making process.
“I think it’s the responsibility of a professional society to not only be informed on what’s happening on a national level, but to have some influence,” says Dr. Torcson. “And SHM has done a great job in being well-positioned to influence the national agenda on quality and performance improvement.” TH
Jane Jerrard writes frequently for The Hospitalist.
On March 16, the John A. Hartford Foundation awarded SHM a $1.4 million grant to develop interventions to improve care transitions for older adults at the time of hospital discharge.
One of the core values of SHM and hospital medicine is to implement changes that improve the care older Americans receive. With this grant support from The Hartford Foundation, SHM can help define and set standards for best practices in discharge and provide a continuum of training opportunities to support those practices.
As part of this three-year project, SHM will partner with national leaders in care coordination to form a national advisory board, create clinical tools, implement guidelines, and provide technical support and training tools to hospitals across the U.S. The project aims to build capacity in at least 200 hospital sites to improve the discharge process and, ultimately, health outcomes for older adults.
Chapter Report
National Advisory Board AND Project Team
SHM has assembled a national advisory board to inform and guide the project. The board will be chaired by Eric Coleman, MD, MPH, associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora. At press time, members included:
- Barbara Berkman, DSW, PhD, professor of health and mental health, University School of Social Work, Mount Sinai School of Medicine;
- Tom Bookwalter, PharmD, clinical pharmacist, American Society of Health-System Pharmacists (ASHP);
- Alan Korn, MD, chief medical officer and senior vice president for clinical affairs, Blue Cross Blue Shield Association;
- Chuck Denham, MD, chair, National Quality Forum (NQF);
- Gavin Hougham, PhD, senior program officer, John A. Hartford Foundation;
- Seth Landefeld, MD, director, American Geriatrics Society (AGS);
- Cheri Lattimer, RN, BSN, executive director, Case Management Society of America (CMSA);
- William Lyons, MD, AGS; Nebraska Medical Center in Omaha;
- Lorraine Mion, PhD, RN, FAAN, director of nursing services for geriatrics, Metro Health Medical Center in Cleveland, Ohio;
- Mary Naylor, PhD, RN, FAANS, Marian S. Ware professor in gerontology, University of Pennsylvania;
- Gail Povar, MD, MPH, chair, George Washington School of Medicine, Cameron Medical Group;
- Deborah Queenan, national advisory council coordinator, Agency for Healthcare Research and Quality (AHRQ);
- Pat Rutherford, RN, MS, vice president, Institute for Healthcare Improvement (IHI), Transforming Care at the Bedside (TCAB);
- Eric Warm, MD, Society General Internal Medicine (SGIM); and
- Larry Wellikson, MD, CEO of SHM.
Dr. Williams will serve as principal investigator, leading a team of co-investigators including Jeffrey Greenwald, MD, (Boston University co-investigator, AHRQ, Project ReEngineering Discharge); Eric Howell, MD (Johns Hopkins Bayview, SHM/Hartford Safe Steps Demonstration Project); Param Dedhia, MD (Johns Hopkins Bayview, SHM/Hartford Safe STEPS Demonstration Project); Lakshmi Halasyamani, MD (St. Joseph Mercy Hospital); Kathleen Kerr (SHM); and Tina Budnitz, MPH (SHM).
The project team includes investigators from the SHM/Hartford Foundation Safe STEPS project and two AHRQ-funded projects. All three projects aim to pilot test discharge-planning toolkits and interventions and develop implementation strategies for adoption. The current project will leverage the findings of all three projects with the insights of the advisory board to create a transitions bundle to optimize the discharge process. Following development of this bundle, SHM will develop a toolkit for implementation with corresponding training programs, and other technical support.
Capacity Building Via Continuum of Training Options
SHM has designed a range of technical support and training options to meet the needs of member institutions aiming to implement and sustain the transitions bundle. Strategies include:
- A Web-based resource room for care transitions in older adults: The transitions bundle, field guide, and related interventional materials will be freely available in the SHM online resource room.
- A Quality Pre-Course for QI Teams: The course is scheduled for 2008 and 2009 SHM Annual Meetings.
- A Transition Planning Mentored Implementation Program (TPMI): This yearlong mentoring program will support sites as they implement and evaluate transitions bundle interventions. The program includes a training conference, monthly teleconferences with expert mentors and peer support mechanisms.
- A consultation service: This will provide on-site consultation and technical assistance to sites planning, implementing, and evaluating discharge interventions. The service includes site visit, follow-up report of findings, recommendations and resources, and post-visit follow-up to review progress, successes and unforeseen barriers.
These support mechanisms are intended to assist those who lead improvement teams at their institutions. Enrollment will begin in the fall. For more information, contact [email protected].
A Seat at the Table
SHM active in shaping new performance standards
By Jane Jerrard
Healthcare providers are in the midst of important changes in how they work and how they’re rewarded for that work. Recent initiatives including Medicare’s Physician Quality Reporting Initiative and a Medicare hospital value-based purchasing program mandated by the Deficit Reduction Act spell change for practitioners, including hospitalists.
SHM is working to add a hospitalist voice to discussions and decisions that shape these initiatives. By participating in organizations such as the American Medical Association’s (AMA) Physician consortium for Performance Improvement (PCPI), SHM has a seat at the table where decisions are made.
How Participation Works
The PCPI was convened in 2001 by the AMA, with the mission of physician-led performance improvement. While the primary focus is on improving quality, the Consortium’s performance measures are ultimately those used in CMS and other pay-for-performance (P4P) programs and value-based purchasing initiatives.
SHM didn’t get involved when the PCPI was first formed because the issues weren’t relevant to hospitalists. “SHM was invited to participate at that time, but the focus was really on outpatient care,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. “More recently, when the PCPI began looking at the relation between hospital-level measures and physician-level measures, SHM CEO Larry Wellikson said we need to get involved.”
Dr. Torcson is SHM’s representative on the consortium. “For the last year and a half, I’ve been attending the PCPI meetings to represent SHM and have been involved in various PCPI work groups,” he says. “I had previously served on the SHM HQPS [Healthcare Quality and Patient Safety Task Force] and now serve on the PPC [Public Policy Committee], and I think the SHM leadership thought that combination of interests would be good for a PCPI representative.”
What about the Work Groups?
Work groups within the PCPI are assigned specific areas. These groups are responsible for creating performance measures within an area, which are then reviewed by the entire consortium.
“I participated on a work group to develop performance measures for emergency medicine physicians,” says Dr. Torcson. “This group thought that the current disease-specific measures weren’t relevant for them, and that the current hospital measures were also not relevant. I provided a hospitalist’s perspective on hand-offs and discharge which was really focused on a process of care that begins in the ED [emergency department].”
Each work group has representation from various areas of healthcare. “My work group had about 20 or 25 people, which is probably typical,” says Dr. Torcson. “The AMA provided a methodologist, and there was a CMS representative on the work group.” The work group first met face to face to review relevant evidence-based clinical guidelines and scame up with five to eight measures. These were then reworked through phone calls and e-mails before going before the entire PCPI for approval.
Other SHM representatives participated in relevant PCPI work groups as well. “PPC member Greg Seymann from San Diego participated in a geriatric work group that was convened for the same reason” as the ED group, says Dr. Torcson. “His group looked at creating a number of measures that were relative to both inpatient and outpatient geriatric patients. Some of these measures are now part of the Medicare Physician Quality Reporting Initiative.”
Another SHM member, James C. Pile. MD, FACP, participated in a work group on developing measures for outpatient administration of IV antibiotics. Pile is a staff physician in the Department of General Internal Medicine, Section of Hospital Medicine, at The Cleveland Clinic in Ohio.
In each group, SHM representatives were able to help shape measures that reflect the unique knowledge and perspective of hospital medicine.
“A hospitalist brings the perspective of having seen how these measures are actually incorporated into a practice, how they are actually applied to patient care,” Dr. Torcson points out. “These work groups to develop additional performance measures are ongoing. The PCPI has a rigorous agenda for what they want to accomplish over the next few years.”
SHM to Lead the Way on Care Transitions
The PCPI has asked SHM to be the lead organization for a performance measure development work group on care coordination and care transitions.
“This will be groundbreaking work around this important aspect of care that is very process-focused as opposed to disease-focused,” says Dr. Torcson. “It’s very appropriate that SHM was asked to be the lead group for this. This area of performance improvement is perfect for what hospitalists do.”
The PCPI plans to have care transition performance measures ready for adoption by 2009.
SHM and the Big Three
CMS is also collaborating with the National Quality Forum (NQF) and Ambulatory Quality Alliance (AQA). “The PCPI, AQA, and NQF are the most influential organizations right now for quality and performance measures,” says Dr. Torcson.
The NQF, a unique public and private collaborative, develops consensus standards on different measures submitted to it. “I have had the opportunity to participate on an NQF Steering Committee for performance measure endorsement,” says Dr. Torcson.
The AQA is responsible for standardizing performance measurement and reporting, and developing measures for efficiency to be included in forthcoming Medicare P4P programs. “The AQA is charged with implementing performance measures and bringing them to the marketplace,” explains Dr. Torcson. “SHM is not involved in the AQA process yet.”
Membership in SHM means you are able to access the latest information on issues like CMS reporting initiatives and have representation in the decision-making process.
“I think it’s the responsibility of a professional society to not only be informed on what’s happening on a national level, but to have some influence,” says Dr. Torcson. “And SHM has done a great job in being well-positioned to influence the national agenda on quality and performance improvement.” TH
Jane Jerrard writes frequently for The Hospitalist.
On March 16, the John A. Hartford Foundation awarded SHM a $1.4 million grant to develop interventions to improve care transitions for older adults at the time of hospital discharge.
One of the core values of SHM and hospital medicine is to implement changes that improve the care older Americans receive. With this grant support from The Hartford Foundation, SHM can help define and set standards for best practices in discharge and provide a continuum of training opportunities to support those practices.
As part of this three-year project, SHM will partner with national leaders in care coordination to form a national advisory board, create clinical tools, implement guidelines, and provide technical support and training tools to hospitals across the U.S. The project aims to build capacity in at least 200 hospital sites to improve the discharge process and, ultimately, health outcomes for older adults.
Chapter Report
National Advisory Board AND Project Team
SHM has assembled a national advisory board to inform and guide the project. The board will be chaired by Eric Coleman, MD, MPH, associate professor of medicine within the divisions of healthcare policy and research and geriatric medicine at the University of Colorado Health Sciences Center in Aurora. At press time, members included:
- Barbara Berkman, DSW, PhD, professor of health and mental health, University School of Social Work, Mount Sinai School of Medicine;
- Tom Bookwalter, PharmD, clinical pharmacist, American Society of Health-System Pharmacists (ASHP);
- Alan Korn, MD, chief medical officer and senior vice president for clinical affairs, Blue Cross Blue Shield Association;
- Chuck Denham, MD, chair, National Quality Forum (NQF);
- Gavin Hougham, PhD, senior program officer, John A. Hartford Foundation;
- Seth Landefeld, MD, director, American Geriatrics Society (AGS);
- Cheri Lattimer, RN, BSN, executive director, Case Management Society of America (CMSA);
- William Lyons, MD, AGS; Nebraska Medical Center in Omaha;
- Lorraine Mion, PhD, RN, FAAN, director of nursing services for geriatrics, Metro Health Medical Center in Cleveland, Ohio;
- Mary Naylor, PhD, RN, FAANS, Marian S. Ware professor in gerontology, University of Pennsylvania;
- Gail Povar, MD, MPH, chair, George Washington School of Medicine, Cameron Medical Group;
- Deborah Queenan, national advisory council coordinator, Agency for Healthcare Research and Quality (AHRQ);
- Pat Rutherford, RN, MS, vice president, Institute for Healthcare Improvement (IHI), Transforming Care at the Bedside (TCAB);
- Eric Warm, MD, Society General Internal Medicine (SGIM); and
- Larry Wellikson, MD, CEO of SHM.
Dr. Williams will serve as principal investigator, leading a team of co-investigators including Jeffrey Greenwald, MD, (Boston University co-investigator, AHRQ, Project ReEngineering Discharge); Eric Howell, MD (Johns Hopkins Bayview, SHM/Hartford Safe Steps Demonstration Project); Param Dedhia, MD (Johns Hopkins Bayview, SHM/Hartford Safe STEPS Demonstration Project); Lakshmi Halasyamani, MD (St. Joseph Mercy Hospital); Kathleen Kerr (SHM); and Tina Budnitz, MPH (SHM).
The project team includes investigators from the SHM/Hartford Foundation Safe STEPS project and two AHRQ-funded projects. All three projects aim to pilot test discharge-planning toolkits and interventions and develop implementation strategies for adoption. The current project will leverage the findings of all three projects with the insights of the advisory board to create a transitions bundle to optimize the discharge process. Following development of this bundle, SHM will develop a toolkit for implementation with corresponding training programs, and other technical support.
Capacity Building Via Continuum of Training Options
SHM has designed a range of technical support and training options to meet the needs of member institutions aiming to implement and sustain the transitions bundle. Strategies include:
- A Web-based resource room for care transitions in older adults: The transitions bundle, field guide, and related interventional materials will be freely available in the SHM online resource room.
- A Quality Pre-Course for QI Teams: The course is scheduled for 2008 and 2009 SHM Annual Meetings.
- A Transition Planning Mentored Implementation Program (TPMI): This yearlong mentoring program will support sites as they implement and evaluate transitions bundle interventions. The program includes a training conference, monthly teleconferences with expert mentors and peer support mechanisms.
- A consultation service: This will provide on-site consultation and technical assistance to sites planning, implementing, and evaluating discharge interventions. The service includes site visit, follow-up report of findings, recommendations and resources, and post-visit follow-up to review progress, successes and unforeseen barriers.
These support mechanisms are intended to assist those who lead improvement teams at their institutions. Enrollment will begin in the fall. For more information, contact [email protected].
A Seat at the Table
SHM active in shaping new performance standards
By Jane Jerrard
Healthcare providers are in the midst of important changes in how they work and how they’re rewarded for that work. Recent initiatives including Medicare’s Physician Quality Reporting Initiative and a Medicare hospital value-based purchasing program mandated by the Deficit Reduction Act spell change for practitioners, including hospitalists.
SHM is working to add a hospitalist voice to discussions and decisions that shape these initiatives. By participating in organizations such as the American Medical Association’s (AMA) Physician consortium for Performance Improvement (PCPI), SHM has a seat at the table where decisions are made.
How Participation Works
The PCPI was convened in 2001 by the AMA, with the mission of physician-led performance improvement. While the primary focus is on improving quality, the Consortium’s performance measures are ultimately those used in CMS and other pay-for-performance (P4P) programs and value-based purchasing initiatives.
SHM didn’t get involved when the PCPI was first formed because the issues weren’t relevant to hospitalists. “SHM was invited to participate at that time, but the focus was really on outpatient care,” says Patrick J. Torcson, MD, MMM, FACP, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. “More recently, when the PCPI began looking at the relation between hospital-level measures and physician-level measures, SHM CEO Larry Wellikson said we need to get involved.”
Dr. Torcson is SHM’s representative on the consortium. “For the last year and a half, I’ve been attending the PCPI meetings to represent SHM and have been involved in various PCPI work groups,” he says. “I had previously served on the SHM HQPS [Healthcare Quality and Patient Safety Task Force] and now serve on the PPC [Public Policy Committee], and I think the SHM leadership thought that combination of interests would be good for a PCPI representative.”
What about the Work Groups?
Work groups within the PCPI are assigned specific areas. These groups are responsible for creating performance measures within an area, which are then reviewed by the entire consortium.
“I participated on a work group to develop performance measures for emergency medicine physicians,” says Dr. Torcson. “This group thought that the current disease-specific measures weren’t relevant for them, and that the current hospital measures were also not relevant. I provided a hospitalist’s perspective on hand-offs and discharge which was really focused on a process of care that begins in the ED [emergency department].”
Each work group has representation from various areas of healthcare. “My work group had about 20 or 25 people, which is probably typical,” says Dr. Torcson. “The AMA provided a methodologist, and there was a CMS representative on the work group.” The work group first met face to face to review relevant evidence-based clinical guidelines and scame up with five to eight measures. These were then reworked through phone calls and e-mails before going before the entire PCPI for approval.
Other SHM representatives participated in relevant PCPI work groups as well. “PPC member Greg Seymann from San Diego participated in a geriatric work group that was convened for the same reason” as the ED group, says Dr. Torcson. “His group looked at creating a number of measures that were relative to both inpatient and outpatient geriatric patients. Some of these measures are now part of the Medicare Physician Quality Reporting Initiative.”
Another SHM member, James C. Pile. MD, FACP, participated in a work group on developing measures for outpatient administration of IV antibiotics. Pile is a staff physician in the Department of General Internal Medicine, Section of Hospital Medicine, at The Cleveland Clinic in Ohio.
In each group, SHM representatives were able to help shape measures that reflect the unique knowledge and perspective of hospital medicine.
“A hospitalist brings the perspective of having seen how these measures are actually incorporated into a practice, how they are actually applied to patient care,” Dr. Torcson points out. “These work groups to develop additional performance measures are ongoing. The PCPI has a rigorous agenda for what they want to accomplish over the next few years.”
SHM to Lead the Way on Care Transitions
The PCPI has asked SHM to be the lead organization for a performance measure development work group on care coordination and care transitions.
“This will be groundbreaking work around this important aspect of care that is very process-focused as opposed to disease-focused,” says Dr. Torcson. “It’s very appropriate that SHM was asked to be the lead group for this. This area of performance improvement is perfect for what hospitalists do.”
The PCPI plans to have care transition performance measures ready for adoption by 2009.
SHM and the Big Three
CMS is also collaborating with the National Quality Forum (NQF) and Ambulatory Quality Alliance (AQA). “The PCPI, AQA, and NQF are the most influential organizations right now for quality and performance measures,” says Dr. Torcson.
The NQF, a unique public and private collaborative, develops consensus standards on different measures submitted to it. “I have had the opportunity to participate on an NQF Steering Committee for performance measure endorsement,” says Dr. Torcson.
The AQA is responsible for standardizing performance measurement and reporting, and developing measures for efficiency to be included in forthcoming Medicare P4P programs. “The AQA is charged with implementing performance measures and bringing them to the marketplace,” explains Dr. Torcson. “SHM is not involved in the AQA process yet.”
Membership in SHM means you are able to access the latest information on issues like CMS reporting initiatives and have representation in the decision-making process.
“I think it’s the responsibility of a professional society to not only be informed on what’s happening on a national level, but to have some influence,” says Dr. Torcson. “And SHM has done a great job in being well-positioned to influence the national agenda on quality and performance improvement.” TH
Jane Jerrard writes frequently for The Hospitalist.