User login
Manage Cancer Drugs
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs

Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
Human epidural growth factor receptor (HER1/EGFR) signaling pathways are crucial in regulating cell proliferation, survival, and differentiation.
HER1/EGFR is a protein tyrosine kinase with therapeutic applications in cancer treatment.1 Two approved drugs categories target HER1/EGFR: anti-HER1/EGFR monoclonal antibodies (mAb) and HER1/EGFR tyrosine kinase inhibitors (TKIs). The drugs have different complex actions, some leading to disruption of cellular processes at the level of cell division, apoptosis, and angiogenesis.
Approximately 30% to 100% of solid tumors express HER1/EGFR on the tumor surface, while some overexpress it. This is thought to lead to tumor growth.2,3 Increased HER1/EGFR activity has been associated with poor survival in some cancers.
The Agents
A number of HER1/EGFR TKIs are FDA approved and administered orally, including erlotinib (Tarceva), gefitinib (Iressa), imatinib (Gleevec), lapatinib (Tykerb), sorafenib (Nexavar), and sunitinib (Sutent).4-6
Cetuximab (Erbitux) and panitumumab (Vectibix) are approved mAbs given intravenously. Both categories treat different cancers including advanced/metastatic non-small cell lung cancer, colorectal cancer, pancreatic cancer, renal cell carcinoma, myelodysplastic syndrome, and others. The HER1/EGFR targeted agents have a more favorable side effect profile compared with more traditional chemotherapeutic agents with primarily dermatologic toxicities and limited hematopoietic effects. Because many patients are being treated with these oral anti-cancer agents, it is important to remain aware of the agents, their toxicities, and their management.
Adverse Effects
The most common adverse effect associated with HER1/EGFR inhibitors is a dose-dependent, folliculitis-like rash.
The rash affects up to two-thirds of treated patients within the first two weeks of therapy. It is usually on the face, neck, and upper torso and is characterized by inter- and intrafollicular papulopustules of mild-to-moderate severity. The rash develops in three phases: sensory disturbance with erythema and edema (weeks zero to one), papulopustular flare (weeks one to three), crusting (weeks three to five), and erythematotelangiectasias (weeks five to eight).
Dry skin and erythema may remain in the areas after resolution. The skin rash appears to be dose-dependent. The mechanism of the rash is not precisely known. However, HER1/EGFR is expressed by normal keratinocytes and skin fibroblasts, along the outer sheath of the hair follicle, and in many epidermal processes, which probably contributes.
Hair effects occur within two to three months of starting treatment. Scalp hair becomes more brittle, fine, and curly. Frontal alopecia gradually develops, and patients experience progressive trichomegaly of the eyelashes and hypertrichosis of the face. Paronychial inflammation can occur on the fingernails or toenails and be so painful it prevents patients from wearing shoes. Its origin is unknown, and it disappears after discontinuation of the drug. Xerosis is also common, which can be treated with topically applied 5% to 10% urea emollient.
New Drugs
Cefotetan Disodium for injection (generic Cefotan) has been FDA approved. It can be used to treat infections due to abdominal or vaginal hysterectomy and/or Caesarean section, as well as colorectal surgery, and others.
IN THE PIPELINE
Gabapentin GR, an extended-release, once-daily formulation, is undergoing Phase III clinical trials for treating postherpetic neuralgia. Depomed recently reported results from a randomized, double-blind, placebo-controlled, multicenter trial using 1,800 mg daily that did not meet the primary endpoint (efficacy to reduce average daily pain). Secondary endpoints of sleep interference were all statistically significant in favor of Gabapentin GR. The most common adverse effects were dizziness and peripheral edema.
Natalizumab (Tysabri) received a favorable recommendation for treating moderate-to-severe Crohn’s disease in patients who have failed tumor necrosis factor inhibitor therapies and are not on immunosuppressive therapy—a narrower indication than that proposed by the manufacturers. The recommendation was made at a joint meeting of the Advisory Committees of Gastrointestinal Drugs and Drug Safety and Risk Management. Natalizumab is FDA-approved for the treatment of relapsing forms of multiple sclerosis (MS). Natalizumab is a recombinant, humanized immunoglobulin G4 mAb against alpha4 integrins that is administered via intravenous infusion. Natalizumab increases the risk of progressive multifocal leukoencephalopathy (PML), an opportunistic viral brain infection that usually leads to severe disability or death. A risk-management program is being developed in case the agent is approved for Crohn’s disease.
Raloxifene (Evista), a selective estrogen receptor modulator, originally approved in December 1997 for the treatment and prevention of postmenopausal osteoporosis has been recommended by an FDA advisory panel to add new indications to its label. The new indications include: (1) reducing the risk of invasive breast cancer in postmenopausal women with osteoporosis, and (2) reducing the risk of invasive breast cancer in postmenopausal women at high risk for developing breast cancer.—MK
Rash as a Marker
There appears to be some evidence of a relationship between HER1/EGFR efficacy and associated rash severity. There have been at least 19 trials and additional compassionate use centers that have found the relationship of a positive correlation between rash and response/survival.
For example, in a Phase II study in 57 patients with non-small cell lung cancer, those with grade zero rashes had a median survival of 1.5 months, those with rash grade one had a median survival of 8.5 months, and those with rash grades two or three had a 19.6 month survival. In another study with erlotinib monotherapy, patients with a skin rash had significantly greater survival rates (approximately 80%) than those without skin rashes. In trials of cetuximab in patients with different cancer types, those who developed a rash lived substantially longer than those who did not.
There are also data supporting gefitinib and cetuximab. Many of the studies note a poorer clinical outcome in those patients without rash. These findings suggest that lack of a rash after a specific period of therapy may be an early indicator of treatment failure and the need for another treatment.
Rash Treatment
While receiving treatment with these agents, patients should be advised to moisturize dry body areas twice daily with a thick alcohol-free emollient. Patients should minimize sun exposure and wear a broad-spectrum sunscreen (SPF 15). Zinc oxide or titanium dioxide is preferred over chemical sunscreens. The following treatment interventions are suggested:
- Mild toxicity: topical hydrocortisone 1% to 2.5% cream or clindamycin 1% gel. The HER1/EGFR dose should not be adjusted;
- Moderate toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. The HER1/EGFR dose should not be adjusted; or
- Severe toxicity: topical hydrocortisone 2.5% cream, clindamycin 1% gel, or pimecrolimus 1% cream (Elidel) with doxycycline 100mg orally twice a day or minocycline 100mg orally twice a day. Also add methylprednisolone dose pack.
Reduce the HER1/EGFR dose, if after two to four weeks the toxicities have not sufficiently abated, then the HER1/EGFR therapy should be interrupted. Once the skin reactions have resolved or diminished in severity, the HER1/EGFR dose may typically be restarted or re-escalated.
Results of a recent double-blind, placebo-controlled study suggest tetracycline may be effective in decreasing EGFR-associated rash severity and improving some quality-of-life parameters (e.g., irritation, burning, stinging).7 Remaining alert to these reactions in patients receiving HER1/EGFRs is important for monitoring treatment and managing patients. TH
Michele B. Kaufman is a freelance medical writer based in New York City.
References
- Castillo L, Etienne-Grimaldi MC, Fischel JL, et al. Pharmacologic background of EGFR targeting. Ann Oncol. 2004;15(7):1007-1012.
- Robert C, Soria JC, Spatz A et al. Cutaneous side effects of kinase inhibitors and blocking antibodies. Lancet Oncol. 2005;6(7):491-500.
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: Is there a silver lining? J Clin Oncol. 2005;23(22):5235-5246.
- Seiverling EV, Fernandez EM, Adams D. Epidermal growth factor receptor inhibitor associated skin eruption. J Drugs Dermatol. 2006;5(4)368-369. Available at http://findarticles.com/p/articles/ mi_m0PDG/ is_4_5/ai_n16361317Accessed August 7, 2007
- Tyrosine Kinase Inhibitors. www.oncolink.com/treatment/article.cfm?c=12&s=90&id=268. Accessed August 7, 2007
- Lynch TJ, Kim ES, Eaby B, et al. Epidermal growth factor receptor inhibitor-associated toxicities: An evolving paradigm in clinical management. Oncologist 2007;12(5):610-621.
- Jatoi A, Rowland K, Sloan JA, et al. J Clin Oncol 2007; ASCO Annual Meeting Proceedings Part I. Vol. 25(18S);June 20:LBA9006.
In the Literature
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
In This Edition
- Cost sharing for prescription medications increases consumption of more costly healthcare services
- Community-acquired pneumonia core measures can lead to unintended consequences
- Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery
- Aspirin resistance correlates with adverse clinical events
- Low-molecular-weight heparin appears to have greater efficacy as a prophylactic agent against deep-vein thrombosis and pulmonary embolism
- Antipsychotic medications appear to be associated with increased risk of death in demented patients
- Anticoagulation plus antiplatelet therapy fails to show benefit for peripheral arterial disease
- Transient atrial fibrillation following myocardial infarction increases the risk of recurrence and stroke
Do Incentives to Encourage Use of Certain Medications Affect Care?
Background: Insurers are increasingly using financial mechanisms to affect pharmaceutical usage. These practices may affect medication use and health outcomes in ways that are poorly defined and difficult to detect.
Study design: Literature review
Synopsis: There are numerous structures for drug-cost sharing, and this study evaluated co-payments, tiers/co-insurance, benefit caps, formulary limitations, and reference pricing strategies for their effect on prescription drug usage and healthcare outcomes.
Included articles varied widely in study design, making generalizable results difficult to isolate, and insurers may have instituted more than one cost-sharing mechanism simultaneously. Overall, for every 10% increase in cost sharing (via copayments or co-insurance) there was an associated 2%-6% decrease in prescription drug spending. Increasing consumer costs for medications clearly decreases usage.
Some studies demonstrated that the decrease in medication utilization was more pronounced for “nonessential” medications over “essential” medications. However, in specific chronic illnesses this is clearly associated with greater usage of inpatient and emergency medical services.
Cost sharing was also more likely to have adverse health consequences in vulnerable populations, particularly the elderly and poor. One in four Medicaid patients couldn’t fill at least one prescription in the past year, as opposed to one in 10 privately insured patients who couldn’t purchase one or more medications.
Further impact on healthcare consumption and outcomes may be masked because it is difficult to determine individual disease severity, and the effect on the more severely ill would be expected to be greater. These authors attempted to sort out a complex interaction between cost, consumption, and health, and they found important trends.
The goal of cost sharing is to align consumption more clearly with appropriate and economic products, thereby using cost sharing as a public health tool. The consequence of creating the incentives for ill patients to forego necessary treatments is a counterbalancing concern that is supported in some, but not all, of the literature.
Bottom line: Cost sharing for prescription medications decreases medication spending and utilization but disproportionately affects the disadvantaged and increases consumption of more costly healthcare services in patients with some chronic illnesses.
Citation: Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-69.
Does Antibiotic Requirement for Suspected CAP Increase Misdiagnosis?
Background: Early administration of antibiotics in community-acquired pneumonia (CAP) improves patient outcomes. The Infectious Disease Society of America instituted guidelines that recommend initiation of antibiotics to all patients with suspected CAP within four hours of triage, and some payors are using this as a quality measure affecting reimbursement. However, this incentive may cause premature diagnosis of CAP and overuse of antibiotics.
Study design: Retrospective chart review
Setting: A large, high-volume teaching hospital with more than 500 beds and more than 112,000 annual emergency department (ED) visits
Synopsis: Charts of all patients with an admitting diagnosis of CAP were reviewed over two six-month periods. The initial review was prior to initiation of a four-hour antibiotics rule; the second was after a financial incentive to initiate antibiotics within four hours of triage was initiated.
After initiation of the four-hour rule, of the patients with an admitting diagnosis of CAP, significantly more patients received antibiotics within four hours of triage (66% versus 54%). However, the number of patients with abnormal chest X-ray findings associated with the diagnosis of CAP decreased from 28.5% to 20.6%, and the proportion of patients with a discharge diagnosis of CAP decreased from 75.9% to 58.9%.
The authors also used two diagnostic paradigms to make an independent diagnosis of CAP based on chart data. With the less rigorous independent analysis 44.7% of patients actually had CAP prior to the four-hour rule, and this fell to 36% after the four-hour rule. Using a more rigorous definition, only 32.7% of patients actually had CAP prior to initiation of the four-hour rule, and this fell to 27%.
There was no difference in length of stay or ICU transfers between the two analysis periods. The authors concluded that a four-hour rule increases premature diagnosis of CAP, presumably because providers felt compelled to initiate antibiotics before they had complete clinical data.
This tendency was associated with misuse and overuse of antibiotics, and increased laboratory testing, such as blood cultures, which had to be obtained before antibiotics were initiated. The authors emphasized the importance of reimbursement-associated quality measures creating incentives to treat the right patients for the correct diagnosis, and the potential harmful consequences of applying a quality-driven protocol to the wrong patient.
They suggest a six-hour rule would decrease the misdiagnosis of CAP. They also feel eliminating a mandatory time frame and requiring only that the first dose of antibiotics be administered in the ED will further ameliorate these effects.
Bottom line: Mandatory administration of antibiotics to patients with suspected CAP within four hours of triage increases the percentage of patients who receive antibiotics within four hours, but also increases the rate of misdiagnosis of CAP, inappropriate administration of antibiotics, and increased use of some laboratory services.
Citation: Kanwar M, Brar N, Khatib R, et al. Misdiagnosis of community-acquired pneumonia and inappropriate utilization of antibiotics: side effects of the 4-hour antibiotic administration rule. Chest. 2007 Jun;131(6):1865-1869.
Does prophylactic cardiac revascularization benefit patients undergoing vascular surgery?
Background: American College of Cardiology/American Heart Association Guidelines recommend referral for patients with multiple cardiac risk factors for non-invasive cardiac stress testing prior to surgery and prophylactic revascularization in high-risk patients. The authors performed a pilot analysis to determine how many patients would be needed to prospectively validate this recommendation in those with more significant ischemic cardiac disease.
Study design: Randomized controlled pilot study of 1,880 consecutive patients undergoing elective vascular surgery
Setting: Brazil, Belgium, the Netherlands, Italy, Serbia, and Montenegro
Synopsis: This was a pilot study to determine the necessary power to prove or disprove the benefit of the recommendation for cardiac revascularization in high-risk patients before major vascular surgery.
Prior research had shown that prophylactic revascularization is not of demonstrable benefit in this cohort. However, the majority of the patients in this previous trial had two-vessel disease and preserved left ventricular function. This study examined a sicker cohort of patients with more significant coronary artery disease and depressed left ventricular function.
This pilot screened all patients undergoing high-risk vascular surgery. All patients with three or more risk factors underwent non-invasive evaluation for cardiac ischemia. Patients with extensive ischemia were randomized to invasive evaluation and revascularization as appropriate or non-invasive management. Both arms received optimal medical management.
Prophylactic revascularization did not improve 30-day outcome after vascular surgery, demonstrated no difference in perioperative cardiac events, and found no difference in all-cause mortality or nonfatal myocardial infarction. Similarly, there was no evidence of long-term (at one year) difference between groups. The sample size needed to definitively establish that coronary revascularization is superior to medical therapy would be 300 patients per arm. That would require screening 9,000 patients.
Bottom line: Prophylactic revascularization has no clear benefit for high-risk patients undergoing vascular surgery, but a much larger sample size would be required to definitively prove or disprove benefit.
Citation: Poldermans D, Schouten O, Vidakovic R, et al. Clinical randomized trial to evaluate the safety of a noninvasive approach in high-risk patients undergoing major vascular surgery: the DECREASE-V pilot study. J. Am Coll Cardiol. 2007;49(17):1763-1769.
How Does Aspirin Resistance Affect Patients with Coronary Artery Disease?
Background: Although aspirin is used to decrease the risk of ischemic events, up to 45% of patients do not derive adequate anti-platelet activity. Few prospective studies have used laboratory-measured aspirin resistance to assess clinical outcomes.
Study design: Blinded cohort
Setting: Patients affiliated with Queen Mary Hospital, the University of Hong Kong.
Synopsis: Aspirin-induced platelet inhibition was measured quantitatively on 468 patients with stable coronary artery disease who take 80-325 mg of aspirin per day. The study found 128 patients were aspirin resistant. Aspirin resistance was more prevalent with increased age, female gender, renal insufficiency, anemia, and with use of low-dose aspirin. At follow up, aspirin-resistant patients were more likely to develop a primary outcome event: cardiovascular deaths, myocardial infarction, stroke, transient ischemic attack, and unstable angina. Aspirin resistance was an independent risk factor for developing the aforementioned outcomes, as are diabetes, prior myocardial infarction, and low hemoglobin.
Bottom line: Aspirin resistance, as defined by an aggregation-based assay, is associated with adverse outcomes in patients with stable coronary artery disease.
Citation: Chen W, Cheng X, Lee PY, et al. Aspirin resistance and adverse clinical events in patients with coronary artery disease. Am J Med. 2007 Jul;120(7):631-635.
Which Agents Best Prevent Venous Thromboembolism?
Background: Pulmonary emboli have been linked to 10% of in-hospital deaths. There continues to be a strong emphasis on prevention. Unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), and selective factor Xa inhibitors are used for prophylaxis.
Study design: A meta-analysis of randomized controlled trials
Synopsis: The meta-analysis included 36 studies of hospitalized medical patients that compared UFH with control, LMWH with control, LMWH with UFH, and a selective factor Xa inhibitor with a placebo.
When each was compared with a control, UFH and LMWH were associated with a decreased risk of deep venous thrombosis (DVT) (risk ratio=0.33; 0.56) and pulmonary embolism (PE) (risk ratio=0.64; 0.37). Compared with control, LMWH three times daily was more effective than twice-daily dosing (risk ratio=0.27, 0.52). Through direct comparison of UFH and LMWH, LMWH was shown to have decreased DVT risk (risk ratio=0.68) and fewer injection site hematomas (risk ratio=0.47).
Neither UFH nor LMWH reduced mortality. LMWH and UFH were associated with significantly more bleeding events than control, but this increased risk was significant only for minor bleeding.
Bottom line: LMWH appears to have greater efficacy than UFH as a prophylactic agent against DVT/PE. If UFH is used, three times daily dosing is preferred.
Citation: Wein L, Wein S, Haas SJ, et al. Pharmacological venous thromboembolism prophylaxis in hospitalized medical patients. Arch Intern Med. 2007;167(14):1476-1486.
What Is the Association Between Antipsychotic Drugs and Mortality?
Background: Atypical antipsychotics prescribed off-label for problematic behaviors in dementia have been associated with risks including diabetes, stroke, and increased mortality. This resulted in the FDA placing a “black box” warning on atypical antipsychotics used for dementia. Subsequent studies have suggested that conventional antipsychotics are perhaps even more problematic.
Study Design: Retrospective cohort study
Synopsis: This trial found a small but significant increase in the risk of death in patients taking an antipsychotic medication.
The adjusted hazard ratio for death with the use of atypical antipsychotics in community dwelling patients with dementia was 1.3 (confidence interval 1.02-1.70). Similar to prior research, the authors found that conventional antipsychotics carried a higher risk than atypical agents.
Patients in long-term care settings also suffered increased risk compared with community dwelling patients. Interestingly, the increased risk of death was apparent after as little as a month of treatment.
As with all retrospective observational cohort trials, there remains the risk that an unanticipated confounding factor could skew the data and create a false association. However, the findings of this research support prior concerns that antipsychotics carry risk of increased mortality. This research bolsters the argument that these agents should not be used lightly or without full discussion of risks and benefits with the patient and/or proxy.
Bottom line: Antipsychotic agents used in patients with dementia may create increased risk of death. Potential benefit needs to be carefully weighted against this serious harm.
Citation: Gill S, Bronskill SE, Normand SL, et al. Antipsychotic drug use and mortality in older adults with dementia. Ann Intern Med. 2007 June 5;146(11):775-786.
Does Combination Therapy Help Prevent Serious Vascular Ischemic Events?
Background: Peripheral arterial disease (PAD) manifests as claudication and limb ischemia affecting 8.5 million Americans. Atherosclerotic disease in the periphery also reflects increased risk for ischemic events in the coronary and cranial circulations. Both antiplatelet agents and anticoagulation will decrease the probability of thrombus formation, although this must be weighed against bleeding risk.
Study design: Randomized, open-label, multicenter trial
Setting: Eighty centers in Europe, Asia, Australia, and North America
Synopsis: This trial randomized more than 2,000 patients with PAD to treatment with antiplatelet therapy (aspirin, ticlopidine, or clopidogrel) with or without additional anticoagulation.
During the next 3.5 years serious vascular events occurred at approximately the same rate in both combination and monotherapy groups (15.9% versus 17.4%, p=0.37). There was no significant difference between the occurrence of the composite ischemic endpoints or any of the individual endpoints. There was, however, a significantly higher rate of both moderate and life-threatening bleeding in the combination therapy group.
The 4% risk of life-threatening hemorrhage in the combination group exceeded the 1.2% rate of the monotherapy group creating a relative risk for bleeding of 3.4.
This trial demonstrates that for patients with PAD on antiplatelet therapy, the increased rate of bleeding without significant added benefit makes addition of warfarin inadvisable.1 Evidence of utility of combination therapy from studies in other arterial systems provides mixed results.2-4 Based on the results of this study, combination therapy cannot be advocated if the primary symptoms are from PAD.
Bottom line: This study provides further evidence that more is not always better when it comes to preventing thrombosis and ischemia in the peripheral arterial system. Antiplatelet agents are preferable for PAD to combination antiplatelet plus anticoagulation.
Citations:
- The Warfarin Antiplatelet Vascular Evaluation Trial Investigators. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007 Jul 19;357(3):217-227.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974.
- Mohr JP, Thompson JL, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15;345(20):1444-1451.
- The ESPRIT Study Group. Medium intensity oral anticoagulants versus aspirin after cerebral ischaemia of arterial origin (ESPRIT): a randomised controlled trial. Lancet Neurol. 2007 Feb;6:115-124.
Does Transient Atrial Fibrillation Increase Stroke Risk After ST-Elevation Myocardial Infarction?
Background: Prior research has demonstrated that 2.1% of patients will suffer a stroke in the year following a heart attack. Persistent and paroxysmal atrial fibrillation (AF) are well recognized as risk factors for stroke, but the significance of transient ischemia-induced AF is less clear.
Study design: Retrospective cohort study
Setting: Queen Mary Hospital, Hong Kong
Synopsis: The study involved patients admitted for acute inferior ST-segment-elevation myocardial infarction (MI) with preserved left ventricular ejection fraction.
Transient AF that had converted back to normal sinus rhythm by discharge was observed in 14% of patients after the MI. Over the next three years the transient AF patients were 15 times more likely than those who remained in sinus rhythm during the index hospitalization to have recurrent AF (34% versus 2%). Despite antiplatelet therapy in both groups, ischemic stroke developed in 22% of patients who had transient AF following their MI, compared with only 4% in patients who did not (HR 5.1, confidence interval 2.4-11.2). Cerebrovascular accidents generally occurred simultaneously with recurrence of paroxysmal AF.1-2
The finding that patients with transient-ischemia-induced AF represents a group with markedly higher risk of ischemic stroke is compelling. It suggests that these patients may be candidates for combined antiplatelet and anticoagulant therapy. Trials of combined therapy following MI demonstrate that this strategy reduces the rate of recurrent cardiac ischemia, stroke, or death but does carry significantly increased risk of bleeding.3-4
Bottom line: The presence of transient AF following MI represents a significant risk factor for the development of subsequent paroxysmal AF. These patients have a five-fold increased risk of ischemic stroke over the next three years and should be considered for combined antiplatelet and anticoagulant therapy.
Citations:
- Chung-Wah S, Man-Hong J, Hee-Hwa H, et al. Transient atrial fibrillation complicating acute inferior myocardial infarction: implications for future risk of ischemic stroke. Chest. 2007 Mar 30;132(1):44-49.
- Witt BJ, Ballman KV, Brown RD Jr., Meverden RA, Jacobsen SJ, Roger VL. The incidence of stroke after myocardial infarction: a meta-analysis. Am J. Med. 2006;119(4):354 e1-9.
- Van Es RF, Jonker J, Verheugt F, et al. Aspirin and Coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002 Jul 13;360(9327):109-113.
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002 Sep 26;347(13):969-974. TH
Renewal Made Easy
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts

JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at [email protected] by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail [email protected].
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
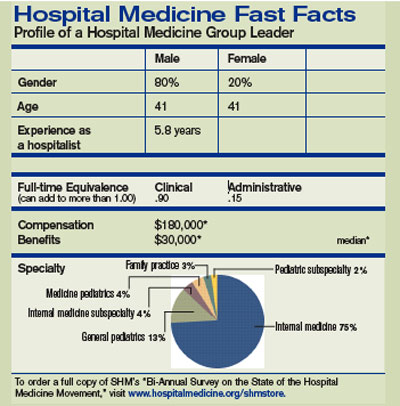
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak

During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is [email protected]. TH
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts
JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at [email protected] by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail [email protected].
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak
During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is [email protected]. TH
Effective April 1, SHM migrated from the fiscal-year renewal process that exists in many medical societies. Now, all members who wish to continue their membership must renew 12 months from the time they joined or last renewed.
As members will recall, SHM’s previous fiscal-year (or calendar-year) renewal process meant dues paid between July 1 and June 30 applied to the current membership year, regardless of the date of joining or renewal. Because full payment could be made in January or February and required again a few months later, this did not sit well with SHM or—more importantly—its members.
Why make the change? Two reasons:
- Fairness. Each membership payment should equal 12 months of member benefits; and
- Simplicity. It will be easier for members to plan for renewal and budget accordingly.
Chapter Summary
Western Massachusetts
JOIN THE SHM TEAM
Interested in being a part of an SHM committee or task force? Now’s your chance. Nominations are open for SHM’s committees and task forces. This is your opportunity to help shape the future of SHM and the hospital medicine movement.
To nominate yourself, visit the SHM Web site, www.hospitalmedicine.org, and click on “About SHM,” then click “Committees.” Here, you will see a full listing of committees, as well as task forces and their current members.
For each committee you would like to serve on, please submit your name and a one-to-two paragraph statement about why you are qualified or interested. E-mail this information to Joi Seabrooks at [email protected] by Dec. 7. Appointments will be made by early February, take effect in April 2008, and last one year.
In the short term, this change means little for current members as long as they renew within the grace period. In the long term, members will receive an expiration date with their payment so they know they’re getting a full year’s worth of benefits.
It’s never too late to join or renew. Whether your membership has lapsed in the past year, two years, or five, renewing is as easy as a phone call or access to the Internet. SHM membership representatives can be reached by calling toll free (800) 843-3360, or by visiting www.joinshm.org. If you’re not sure of your membership status, have questions about membership or the new renewal process, or general feedback as an SHM member, please e-mail [email protected].
Lessons for Leaders
SHM hosted another sold-out Leadership Academy at the Marriott Riverwalk in San Antonio, Texas, Nov. 5-8. The meeting attracted more than 170 hospital medicine leaders for the Level I and Level II courses.
The Leadership Academy Level I was designed to provide leaders in hospital medicine the skills and resources to lead and manage programs. Small group sessions gave attendees a chance to interact with faculty and share personal experiences from their own institutions.
Jack Silversin, DMD, DrPh, president of the consulting firm Amicus in Cambridge, Mass., presented his well-known “broken squares” demonstration to teach the group to work together to learn effective communication. This course allowed attendees to evaluate personal leadership strengths and weaknesses and apply them to everyday leadership and management challenges.
The Level II course focused on discussions about culture change, negotiation skills, and finance. Level II faculty member Leonard Marcus, PhD, described how “meta-leadership” in hospital medicine links individuals through their leader’s vision to create enthusiastic followers. Dr. Marcus is founding director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard School of Public Health. Mike Guthrie, MD, MBA, focused his presentation on finance and taught participants concepts and tools for mastering the case for quality improvement and performance management. Dr. Guthrie is executive-in-residence at the University of Colorado Denver School of Business.
This course is a must-have for those who want to expand upon leadership skills learned in Level I or for those who have an MBA and want to improve their leadership in clinical care.
The skills discussed in this session are essential to developing and implementing quality improvement programs, patient safety initiatives, and other programs to make system changes that improve patient care. Don’t miss out on the next opportunity to attend Level II.
Leadership Academy Level I and II were jam-packed with relevant materials and tools applicable to business and the real world.
This is an outstanding opportunity for those beginning their leadership journey or those wanting to take their skills to the next level.
Don’t miss the next opportunity to become a leader in hospital medicine. The next meeting will take place Feb. 5-8, 2008, at the Loews Lake Las Vegas Resort in Las Vegas. Visit www.hospitalmedicine.org/leadership or call (800) 843-3360 for more information.
SHM BEHIND THE SCENES
The SHM team seeks your feedback at fall conferences
By Todd Von Deak
During my years in association management, I have seen time and time again how easy it is—and how dangerous it can be—to lose touch with your membership. If you truly want to deliver a high-quality product to all who belong to your organization, it is not enough to just read letters or listen to your most active members who serve on committees.
SHM places high value on maintaining a strong connection to all members. To that end, we employ a variety of feedback mechanisms that range from ensuring that all staff have the opportunity to interact with members on the phone, to fielding regular surveys that solicit feedback on a variety of topics.
Each fall, we do something that can easily go unnoticed. But it’s crucial to maintaining a strong connection to the community we serve. Over a four-month span, our staff and volunteer leaders will participate in 10 to 12 hospital medicine conferences ranging from Vancouver, Canada, to Savannah, Ga.
At these conferences, you are likely to find us in the exhibit hall staffing an SHM display. Other times, a physician making a presentation about some facet of hospital medicine will represent us and include a couple of slides about the latest news from within SHM.
No matter our role at a conference, our goal is the same. Whether we’re at an event for one or four days, we want to talk with as many people as possible about everything going on within hospital medicine.
We’re also anxious to hear the latest from the “front lines” and learn new ways we can improve our products and services to better serve your needs. To that end, we keep detailed statistics about the issues you raise and questions you ask when you visit our booth. These metrics are shared with executive management so they have the benefit of direct feedback.
Sure, these events are about signing up new members, selling copies of popular publications, and encouraging registrations for upcoming events. If we didn’t do these things, our dues would be higher.
These events are just as much about making sure we don’t lose touch with the very reason that we all come to work each day: You. You can’t replace the opportunity to look people in the eye, thank them for their support, and hear firsthand how you can make a difference for them personally and professionally.
Next time you’re attending a conference, please take a moment to see if SHM is an exhibitor. If we are, I hope you’ll visit our booth and let us know what’s on your mind and how SHM can continue to improve what we offer.
If you know of an event where hospital medicine is a hot topic and you think we’d benefit from attending, I’d love to hear from you. My e-mail is [email protected]. TH
An idea takes root: Hold those expert witnesses accountable
CASE #1 Suit filed after trauma during home delivery
The facts of the matter. Two parents, whose child was injured during a home delivery, sued the supervising nurse and their obstetrician. An expert witness for the plaintiffs testified that the defendant OB departed from the standard of care under the circumstances. The OB settled the case.
Later, the OB filed a complaint with ACOG’s grievance committee, in which he detailed factual misrepresentations that he claimed were made by the physician–expert witness during that expert’s testimony. (The defendant OB and the expert witness were both members of ACOG.)
The expert witness then sued the OB….
Physician–expert witnesses in medical malpractice litigation have come under increasing scrutiny in recent years. Specifically, many observers worry about “hired guns” who support the testimony of a plaintiff or a defendant in the face (and at the expense) of prevailing medical evidence. That concern is particularly salient in obstetrics, where the cause of a bad outcome that can lead to litigation—such as neurologic birth injury—is, in many cases, still unknown and where malpractice insurance coverage comes at high cost. Many lawsuits often attribute such injury to inappropriate intrapartum management, especially in times of fetal distress, even though leading pediatric neuroepidemiologists have long argued that many of these injuries may be the result of unavoidable antepartum events.1 On the other hand, improper testimony from expert witnesses for the defense may prevent legitimate cases from proceeding.
Medical societies build a place for complaints
Commentators have encouraged medical societies to create venues in which members can bring complaints about the appropriateness of expert witness testimony by other physicians.2 ACOG has established guidelines in its Code of Professional Ethics for members who serve as an expert witness:
…before offering testimony, the obstetrician–gynecologist must thoroughly review the medical facts of the case and all available relevant information…
and, then, during trial:
…the obstetrician–gynecologist testifying as an expert witness must have knowledge and experience about the range of the standard of care and the available scientific evidence for the condition in question during the relevant time and must respond accurately to questions about the range of the standard of care and the available scientific evidence.3
If a member of ACOG considers a fellow member to have violated one of these, or any other, provision of the code, and any litigation has ended, a complaint can be initiated before its grievance committee.
A federal court of appeals recently supported the ability of a professional society to discipline members who violate the society’s code of conduct,4 but such processes can still be subject to judicial review.
Here are three cases that describe professional societies’ role in the oversight of physician–expert witnesses. The cases also reveal how physicians use those review systems and how expert witnesses attempt to rebuff complaints made against them.
A recent study revealed that a small cadre of physicians testified in nearly 90% of a national sample of neurologic birth injury cases. These witnesses tended to act consistently for one side. Frequent witnesses for the plaintiff had fewer markers of expertise than frequent witnesses for the defendant did.1
Reference
1. Kesselheim AS, Studdert DM. Characteristics of physicians who frequently act as expert witnesses in neurological birth injury litigation. Obstet Gynecol. 2006;108:273-279.
CASE #1 continued Birth trauma
The controversy. As described, the physician–expert witness sued the defendant OB after he filed a complaint with ACOG against that expert witness. The suit alleged:
- interference with business contracts— he claimed that ACOG’s grievance committee procedure impaired his ability to obtain more expert witness-related work
- defamation—the complaint damaged his reputation before his peers in ACOG.
What was the outcome? A federal district court ruled for the defendant OB. It found that the OB’s statement to the ACOG grievance committee was not, for a number of reasons, defamatory:
- The complaint constituted a long statement of the obstetrician’s opinions that was supported by a number of underlying facts
- The complaint was submitted to the grievance committee as part of ACOG’s established procedure and was not communicated to other third parties; no apparent effort to intentionally harm the reputation of the expert witness could be inferred.
The court also dismissed the charge of interference with business contracts because, in its jurisdiction, such a claim required an intentionally malicious motive.
To the contrary, according to the court, the defendant OB “limited himself to advancing a confidential complaint to a peer group in which both parties were members, which might have remained confidential but for” the present litigation.5
Ideally, physician–expert witnesses should strive to follow the standards for testimony proposed by any state licensing board or professional society to which they are responsible or belong. Most such standards include being sure to review the entire case history before providing an opinion in court and basing opinions on peer-reviewed evidence when such evidence exists.
The goal of the physician–expert witness should be threefold: to put forth the best medical expertise in litigation, to help secure compensation for deserving plaintiffs in true cases of malpractice, and to reduce the impact of frivolous lawsuits on the medical profession.
CASE #2 Revision of a ventricular shunt
The facts of the matter. A lawsuit charged two neurosurgeons with malpractice in managing a ventricular shunt in a patient who had hydrocephalus. The plaintiff’s expert witness, a neurosurgeon, testified in a deposition that:
- the standard of care for managing a patient after a surgical shunt revision wasn’t met
- communication between the two neurosurgeons was faulty
- he “had difficulty believing” statements made by one of the defendants in the medical chart after the patient’s health declined.
The controversy. At a hearing, the medical board agreed that the expert witness engaged in unprofessional conduct on all counts. It revoked his medical license.
The expert witness appealed the decision to the local state court.
That court found no basis for disciplining the expert for his testimony about the applicable standard of care or the communication between the neurosurgeons. It did uphold the charge of testifying improperly that the defendant had falsified medical records.
The medical board altered its punishment, suspending the expert witness’s medical license for 1 year. The expert witness then appealed this suspension to the North Carolina Court of Appeals.
What was the outcome? The appeals court concluded, after “careful review of the record,” that “the substantial record of evidence does not permit an inference that [the expert witness] made an entirely unfounded statement” about the medical record.
The court held that the expert witness’s opinions were based on a review of multiple aspects of the case, including imaging results and reports of the patient’s behavior. According to the court, “these observations provided a good faith evidentiary basis” for the expert’s opinion. The court reversed the medical board’s suspension of the expert witness’s license.6
CASE #3 Poor care after CVA
The facts of the matter. In a medical malpractice action, a group of physicians were charged with negligence in their care of an elderly diabetic patient who suffered a cerebrovascular accident. During the trial, the plaintiff’s expert witness testified that the defendant physicians’ actions did not meet the standard of care. Ultimately, the case was decided in favor of the defendants.
Afterward, the defendant physicians forwarded a complaint to their state physicians’ association (of which the expert witness was not a member), claiming that the expert witness’s testimony was inappropriate and recommending disciplinary action to prevent the profession “from being terrorized by similar experts.”
The controversy. The expert witness sued the defendants and the state physicians’ association to stop the grievance process, claiming defamation, interference with contract, conspiracy, and other counts. The defendant physicians and the physicians’ association countered that the lawsuit should be dismissed because state and federal laws grant immunity to members of medical peer review committees when there is no evidence of intentional fraud.
The trial court agreed with the defendant physicians. The expert witness appealed.
What was the outcome? The court of appeals overturned the trial court’s opinion. It found that state and federal laws do not clearly provide immunity to the defendants.
The court held that the statutes protecting peer review committees were constructed to help evaluate and improve “the quality of health care rendered by providers of health services”—protection that does not necessarily extend to testimony in a malpractice case. The appeals court also found that the state medical association is not afforded immunity “in its role as an examiner of the quality of a non-member physician’s judicial testimony.”
Ultimately, the court determined that the case could go forward to assess whether there was any validity to the charges made by the expert witness.7
Oversight of physician–expert witnesses is becoming more prevalent among professional specialty societies, state medical societies, and state medical licensing boards. Depending on the region, state, or locale, a physician who notes inappropriate testimony by an expert witness—on behalf of a plaintiff or defendant—may have a better opportunity now to file a complaint with a professional grievance committee established in a pertinent venue.
The cases here teach important lessons for physicians considering bringing a complaint to a grievance committee:
- A physician who files a complaint should be certain not to make unsupported claims or inflammatory statements, or breach any confidentiality provisions in the grievance process
- Complainants’ actions should be well documented because they may be subject to judicial review later
- Physicians should refrain from bringing a complaint against an expert witness to any organization with which that witness is not affiliated because a court might view the role of the organization in that situation differently
- An expert witness who believes that he (or she) has been improperly accused of wrongdoing might not be able to appeal the decision of a professional society to an external court, but he can seek judicial review of actions that affect his medical license and may be able to bring a personal lawsuit in extreme cases of illegal accusation.
- The grievance process should be organized to avoid favoring either party; it should allow both sides to present their opinions and supporting evidence before a set of impartial observers
- An appropriate opportunity should be available for internal appeal
- Although a professional conduct committee can regulate expert witness-related work of its members, that authority may not extend to non-members.
1. Nelson KB, Ellenberg JH. Antecedents of cerebral palsy. Multivariate analysis of risk. N Engl J Med. 1986;315:81-86.
2. Freeman JM, Nelson KB. Expert medical testimony: responsibilities of medical societies. Neurology. 2004;63:1557-1558.
3. Code of professional ethics of the American College of Obstetricians and Gynecologists. Washington, DC: American College of Obstetricians and Gynecologists; 2004. Available at http://www.acog.org/from_home/acogcode.pdf.
4. Austin v. American Association of Neurological Surgeons, 253 F3d 967 (7th Cir 2001).
5. Bundren v. Parriott, 2006 US Dist LEXIS 44591 (D Kansas 2006).
6. In Re: Gary James Lustgarten 629 SE2d 886 (NC Ct App 2006)
7. Fullerton v. Florida Medical Association, 938 So2d 587 (Fla Ct App 2006).
CASE #1 Suit filed after trauma during home delivery
The facts of the matter. Two parents, whose child was injured during a home delivery, sued the supervising nurse and their obstetrician. An expert witness for the plaintiffs testified that the defendant OB departed from the standard of care under the circumstances. The OB settled the case.
Later, the OB filed a complaint with ACOG’s grievance committee, in which he detailed factual misrepresentations that he claimed were made by the physician–expert witness during that expert’s testimony. (The defendant OB and the expert witness were both members of ACOG.)
The expert witness then sued the OB….
Physician–expert witnesses in medical malpractice litigation have come under increasing scrutiny in recent years. Specifically, many observers worry about “hired guns” who support the testimony of a plaintiff or a defendant in the face (and at the expense) of prevailing medical evidence. That concern is particularly salient in obstetrics, where the cause of a bad outcome that can lead to litigation—such as neurologic birth injury—is, in many cases, still unknown and where malpractice insurance coverage comes at high cost. Many lawsuits often attribute such injury to inappropriate intrapartum management, especially in times of fetal distress, even though leading pediatric neuroepidemiologists have long argued that many of these injuries may be the result of unavoidable antepartum events.1 On the other hand, improper testimony from expert witnesses for the defense may prevent legitimate cases from proceeding.
Medical societies build a place for complaints
Commentators have encouraged medical societies to create venues in which members can bring complaints about the appropriateness of expert witness testimony by other physicians.2 ACOG has established guidelines in its Code of Professional Ethics for members who serve as an expert witness:
…before offering testimony, the obstetrician–gynecologist must thoroughly review the medical facts of the case and all available relevant information…
and, then, during trial:
…the obstetrician–gynecologist testifying as an expert witness must have knowledge and experience about the range of the standard of care and the available scientific evidence for the condition in question during the relevant time and must respond accurately to questions about the range of the standard of care and the available scientific evidence.3
If a member of ACOG considers a fellow member to have violated one of these, or any other, provision of the code, and any litigation has ended, a complaint can be initiated before its grievance committee.
A federal court of appeals recently supported the ability of a professional society to discipline members who violate the society’s code of conduct,4 but such processes can still be subject to judicial review.
Here are three cases that describe professional societies’ role in the oversight of physician–expert witnesses. The cases also reveal how physicians use those review systems and how expert witnesses attempt to rebuff complaints made against them.
A recent study revealed that a small cadre of physicians testified in nearly 90% of a national sample of neurologic birth injury cases. These witnesses tended to act consistently for one side. Frequent witnesses for the plaintiff had fewer markers of expertise than frequent witnesses for the defendant did.1
Reference
1. Kesselheim AS, Studdert DM. Characteristics of physicians who frequently act as expert witnesses in neurological birth injury litigation. Obstet Gynecol. 2006;108:273-279.
CASE #1 continued Birth trauma
The controversy. As described, the physician–expert witness sued the defendant OB after he filed a complaint with ACOG against that expert witness. The suit alleged:
- interference with business contracts— he claimed that ACOG’s grievance committee procedure impaired his ability to obtain more expert witness-related work
- defamation—the complaint damaged his reputation before his peers in ACOG.
What was the outcome? A federal district court ruled for the defendant OB. It found that the OB’s statement to the ACOG grievance committee was not, for a number of reasons, defamatory:
- The complaint constituted a long statement of the obstetrician’s opinions that was supported by a number of underlying facts
- The complaint was submitted to the grievance committee as part of ACOG’s established procedure and was not communicated to other third parties; no apparent effort to intentionally harm the reputation of the expert witness could be inferred.
The court also dismissed the charge of interference with business contracts because, in its jurisdiction, such a claim required an intentionally malicious motive.
To the contrary, according to the court, the defendant OB “limited himself to advancing a confidential complaint to a peer group in which both parties were members, which might have remained confidential but for” the present litigation.5
Ideally, physician–expert witnesses should strive to follow the standards for testimony proposed by any state licensing board or professional society to which they are responsible or belong. Most such standards include being sure to review the entire case history before providing an opinion in court and basing opinions on peer-reviewed evidence when such evidence exists.
The goal of the physician–expert witness should be threefold: to put forth the best medical expertise in litigation, to help secure compensation for deserving plaintiffs in true cases of malpractice, and to reduce the impact of frivolous lawsuits on the medical profession.
CASE #2 Revision of a ventricular shunt
The facts of the matter. A lawsuit charged two neurosurgeons with malpractice in managing a ventricular shunt in a patient who had hydrocephalus. The plaintiff’s expert witness, a neurosurgeon, testified in a deposition that:
- the standard of care for managing a patient after a surgical shunt revision wasn’t met
- communication between the two neurosurgeons was faulty
- he “had difficulty believing” statements made by one of the defendants in the medical chart after the patient’s health declined.
The controversy. At a hearing, the medical board agreed that the expert witness engaged in unprofessional conduct on all counts. It revoked his medical license.
The expert witness appealed the decision to the local state court.
That court found no basis for disciplining the expert for his testimony about the applicable standard of care or the communication between the neurosurgeons. It did uphold the charge of testifying improperly that the defendant had falsified medical records.
The medical board altered its punishment, suspending the expert witness’s medical license for 1 year. The expert witness then appealed this suspension to the North Carolina Court of Appeals.
What was the outcome? The appeals court concluded, after “careful review of the record,” that “the substantial record of evidence does not permit an inference that [the expert witness] made an entirely unfounded statement” about the medical record.
The court held that the expert witness’s opinions were based on a review of multiple aspects of the case, including imaging results and reports of the patient’s behavior. According to the court, “these observations provided a good faith evidentiary basis” for the expert’s opinion. The court reversed the medical board’s suspension of the expert witness’s license.6
CASE #3 Poor care after CVA
The facts of the matter. In a medical malpractice action, a group of physicians were charged with negligence in their care of an elderly diabetic patient who suffered a cerebrovascular accident. During the trial, the plaintiff’s expert witness testified that the defendant physicians’ actions did not meet the standard of care. Ultimately, the case was decided in favor of the defendants.
Afterward, the defendant physicians forwarded a complaint to their state physicians’ association (of which the expert witness was not a member), claiming that the expert witness’s testimony was inappropriate and recommending disciplinary action to prevent the profession “from being terrorized by similar experts.”
The controversy. The expert witness sued the defendants and the state physicians’ association to stop the grievance process, claiming defamation, interference with contract, conspiracy, and other counts. The defendant physicians and the physicians’ association countered that the lawsuit should be dismissed because state and federal laws grant immunity to members of medical peer review committees when there is no evidence of intentional fraud.
The trial court agreed with the defendant physicians. The expert witness appealed.
What was the outcome? The court of appeals overturned the trial court’s opinion. It found that state and federal laws do not clearly provide immunity to the defendants.
The court held that the statutes protecting peer review committees were constructed to help evaluate and improve “the quality of health care rendered by providers of health services”—protection that does not necessarily extend to testimony in a malpractice case. The appeals court also found that the state medical association is not afforded immunity “in its role as an examiner of the quality of a non-member physician’s judicial testimony.”
Ultimately, the court determined that the case could go forward to assess whether there was any validity to the charges made by the expert witness.7
Oversight of physician–expert witnesses is becoming more prevalent among professional specialty societies, state medical societies, and state medical licensing boards. Depending on the region, state, or locale, a physician who notes inappropriate testimony by an expert witness—on behalf of a plaintiff or defendant—may have a better opportunity now to file a complaint with a professional grievance committee established in a pertinent venue.
The cases here teach important lessons for physicians considering bringing a complaint to a grievance committee:
- A physician who files a complaint should be certain not to make unsupported claims or inflammatory statements, or breach any confidentiality provisions in the grievance process
- Complainants’ actions should be well documented because they may be subject to judicial review later
- Physicians should refrain from bringing a complaint against an expert witness to any organization with which that witness is not affiliated because a court might view the role of the organization in that situation differently
- An expert witness who believes that he (or she) has been improperly accused of wrongdoing might not be able to appeal the decision of a professional society to an external court, but he can seek judicial review of actions that affect his medical license and may be able to bring a personal lawsuit in extreme cases of illegal accusation.
- The grievance process should be organized to avoid favoring either party; it should allow both sides to present their opinions and supporting evidence before a set of impartial observers
- An appropriate opportunity should be available for internal appeal
- Although a professional conduct committee can regulate expert witness-related work of its members, that authority may not extend to non-members.
CASE #1 Suit filed after trauma during home delivery
The facts of the matter. Two parents, whose child was injured during a home delivery, sued the supervising nurse and their obstetrician. An expert witness for the plaintiffs testified that the defendant OB departed from the standard of care under the circumstances. The OB settled the case.
Later, the OB filed a complaint with ACOG’s grievance committee, in which he detailed factual misrepresentations that he claimed were made by the physician–expert witness during that expert’s testimony. (The defendant OB and the expert witness were both members of ACOG.)
The expert witness then sued the OB….
Physician–expert witnesses in medical malpractice litigation have come under increasing scrutiny in recent years. Specifically, many observers worry about “hired guns” who support the testimony of a plaintiff or a defendant in the face (and at the expense) of prevailing medical evidence. That concern is particularly salient in obstetrics, where the cause of a bad outcome that can lead to litigation—such as neurologic birth injury—is, in many cases, still unknown and where malpractice insurance coverage comes at high cost. Many lawsuits often attribute such injury to inappropriate intrapartum management, especially in times of fetal distress, even though leading pediatric neuroepidemiologists have long argued that many of these injuries may be the result of unavoidable antepartum events.1 On the other hand, improper testimony from expert witnesses for the defense may prevent legitimate cases from proceeding.
Medical societies build a place for complaints
Commentators have encouraged medical societies to create venues in which members can bring complaints about the appropriateness of expert witness testimony by other physicians.2 ACOG has established guidelines in its Code of Professional Ethics for members who serve as an expert witness:
…before offering testimony, the obstetrician–gynecologist must thoroughly review the medical facts of the case and all available relevant information…
and, then, during trial:
…the obstetrician–gynecologist testifying as an expert witness must have knowledge and experience about the range of the standard of care and the available scientific evidence for the condition in question during the relevant time and must respond accurately to questions about the range of the standard of care and the available scientific evidence.3
If a member of ACOG considers a fellow member to have violated one of these, or any other, provision of the code, and any litigation has ended, a complaint can be initiated before its grievance committee.
A federal court of appeals recently supported the ability of a professional society to discipline members who violate the society’s code of conduct,4 but such processes can still be subject to judicial review.
Here are three cases that describe professional societies’ role in the oversight of physician–expert witnesses. The cases also reveal how physicians use those review systems and how expert witnesses attempt to rebuff complaints made against them.
A recent study revealed that a small cadre of physicians testified in nearly 90% of a national sample of neurologic birth injury cases. These witnesses tended to act consistently for one side. Frequent witnesses for the plaintiff had fewer markers of expertise than frequent witnesses for the defendant did.1
Reference
1. Kesselheim AS, Studdert DM. Characteristics of physicians who frequently act as expert witnesses in neurological birth injury litigation. Obstet Gynecol. 2006;108:273-279.
CASE #1 continued Birth trauma
The controversy. As described, the physician–expert witness sued the defendant OB after he filed a complaint with ACOG against that expert witness. The suit alleged:
- interference with business contracts— he claimed that ACOG’s grievance committee procedure impaired his ability to obtain more expert witness-related work
- defamation—the complaint damaged his reputation before his peers in ACOG.
What was the outcome? A federal district court ruled for the defendant OB. It found that the OB’s statement to the ACOG grievance committee was not, for a number of reasons, defamatory:
- The complaint constituted a long statement of the obstetrician’s opinions that was supported by a number of underlying facts
- The complaint was submitted to the grievance committee as part of ACOG’s established procedure and was not communicated to other third parties; no apparent effort to intentionally harm the reputation of the expert witness could be inferred.
The court also dismissed the charge of interference with business contracts because, in its jurisdiction, such a claim required an intentionally malicious motive.
To the contrary, according to the court, the defendant OB “limited himself to advancing a confidential complaint to a peer group in which both parties were members, which might have remained confidential but for” the present litigation.5
Ideally, physician–expert witnesses should strive to follow the standards for testimony proposed by any state licensing board or professional society to which they are responsible or belong. Most such standards include being sure to review the entire case history before providing an opinion in court and basing opinions on peer-reviewed evidence when such evidence exists.
The goal of the physician–expert witness should be threefold: to put forth the best medical expertise in litigation, to help secure compensation for deserving plaintiffs in true cases of malpractice, and to reduce the impact of frivolous lawsuits on the medical profession.
CASE #2 Revision of a ventricular shunt
The facts of the matter. A lawsuit charged two neurosurgeons with malpractice in managing a ventricular shunt in a patient who had hydrocephalus. The plaintiff’s expert witness, a neurosurgeon, testified in a deposition that:
- the standard of care for managing a patient after a surgical shunt revision wasn’t met
- communication between the two neurosurgeons was faulty
- he “had difficulty believing” statements made by one of the defendants in the medical chart after the patient’s health declined.
The controversy. At a hearing, the medical board agreed that the expert witness engaged in unprofessional conduct on all counts. It revoked his medical license.
The expert witness appealed the decision to the local state court.
That court found no basis for disciplining the expert for his testimony about the applicable standard of care or the communication between the neurosurgeons. It did uphold the charge of testifying improperly that the defendant had falsified medical records.
The medical board altered its punishment, suspending the expert witness’s medical license for 1 year. The expert witness then appealed this suspension to the North Carolina Court of Appeals.
What was the outcome? The appeals court concluded, after “careful review of the record,” that “the substantial record of evidence does not permit an inference that [the expert witness] made an entirely unfounded statement” about the medical record.
The court held that the expert witness’s opinions were based on a review of multiple aspects of the case, including imaging results and reports of the patient’s behavior. According to the court, “these observations provided a good faith evidentiary basis” for the expert’s opinion. The court reversed the medical board’s suspension of the expert witness’s license.6
CASE #3 Poor care after CVA
The facts of the matter. In a medical malpractice action, a group of physicians were charged with negligence in their care of an elderly diabetic patient who suffered a cerebrovascular accident. During the trial, the plaintiff’s expert witness testified that the defendant physicians’ actions did not meet the standard of care. Ultimately, the case was decided in favor of the defendants.
Afterward, the defendant physicians forwarded a complaint to their state physicians’ association (of which the expert witness was not a member), claiming that the expert witness’s testimony was inappropriate and recommending disciplinary action to prevent the profession “from being terrorized by similar experts.”
The controversy. The expert witness sued the defendants and the state physicians’ association to stop the grievance process, claiming defamation, interference with contract, conspiracy, and other counts. The defendant physicians and the physicians’ association countered that the lawsuit should be dismissed because state and federal laws grant immunity to members of medical peer review committees when there is no evidence of intentional fraud.
The trial court agreed with the defendant physicians. The expert witness appealed.
What was the outcome? The court of appeals overturned the trial court’s opinion. It found that state and federal laws do not clearly provide immunity to the defendants.
The court held that the statutes protecting peer review committees were constructed to help evaluate and improve “the quality of health care rendered by providers of health services”—protection that does not necessarily extend to testimony in a malpractice case. The appeals court also found that the state medical association is not afforded immunity “in its role as an examiner of the quality of a non-member physician’s judicial testimony.”
Ultimately, the court determined that the case could go forward to assess whether there was any validity to the charges made by the expert witness.7
Oversight of physician–expert witnesses is becoming more prevalent among professional specialty societies, state medical societies, and state medical licensing boards. Depending on the region, state, or locale, a physician who notes inappropriate testimony by an expert witness—on behalf of a plaintiff or defendant—may have a better opportunity now to file a complaint with a professional grievance committee established in a pertinent venue.
The cases here teach important lessons for physicians considering bringing a complaint to a grievance committee:
- A physician who files a complaint should be certain not to make unsupported claims or inflammatory statements, or breach any confidentiality provisions in the grievance process
- Complainants’ actions should be well documented because they may be subject to judicial review later
- Physicians should refrain from bringing a complaint against an expert witness to any organization with which that witness is not affiliated because a court might view the role of the organization in that situation differently
- An expert witness who believes that he (or she) has been improperly accused of wrongdoing might not be able to appeal the decision of a professional society to an external court, but he can seek judicial review of actions that affect his medical license and may be able to bring a personal lawsuit in extreme cases of illegal accusation.
- The grievance process should be organized to avoid favoring either party; it should allow both sides to present their opinions and supporting evidence before a set of impartial observers
- An appropriate opportunity should be available for internal appeal
- Although a professional conduct committee can regulate expert witness-related work of its members, that authority may not extend to non-members.
1. Nelson KB, Ellenberg JH. Antecedents of cerebral palsy. Multivariate analysis of risk. N Engl J Med. 1986;315:81-86.
2. Freeman JM, Nelson KB. Expert medical testimony: responsibilities of medical societies. Neurology. 2004;63:1557-1558.
3. Code of professional ethics of the American College of Obstetricians and Gynecologists. Washington, DC: American College of Obstetricians and Gynecologists; 2004. Available at http://www.acog.org/from_home/acogcode.pdf.
4. Austin v. American Association of Neurological Surgeons, 253 F3d 967 (7th Cir 2001).
5. Bundren v. Parriott, 2006 US Dist LEXIS 44591 (D Kansas 2006).
6. In Re: Gary James Lustgarten 629 SE2d 886 (NC Ct App 2006)
7. Fullerton v. Florida Medical Association, 938 So2d 587 (Fla Ct App 2006).
1. Nelson KB, Ellenberg JH. Antecedents of cerebral palsy. Multivariate analysis of risk. N Engl J Med. 1986;315:81-86.
2. Freeman JM, Nelson KB. Expert medical testimony: responsibilities of medical societies. Neurology. 2004;63:1557-1558.
3. Code of professional ethics of the American College of Obstetricians and Gynecologists. Washington, DC: American College of Obstetricians and Gynecologists; 2004. Available at http://www.acog.org/from_home/acogcode.pdf.
4. Austin v. American Association of Neurological Surgeons, 253 F3d 967 (7th Cir 2001).
5. Bundren v. Parriott, 2006 US Dist LEXIS 44591 (D Kansas 2006).
6. In Re: Gary James Lustgarten 629 SE2d 886 (NC Ct App 2006)
7. Fullerton v. Florida Medical Association, 938 So2d 587 (Fla Ct App 2006).
What is the best medical therapy for the secondary prevention of stroke?
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
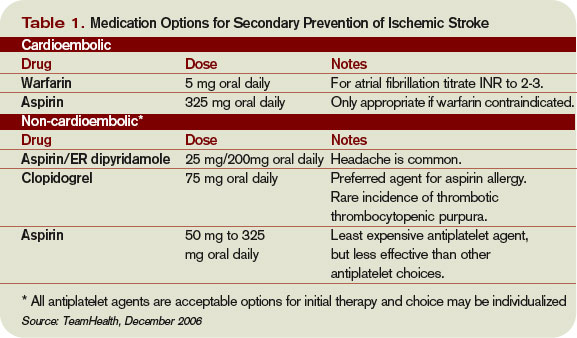
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
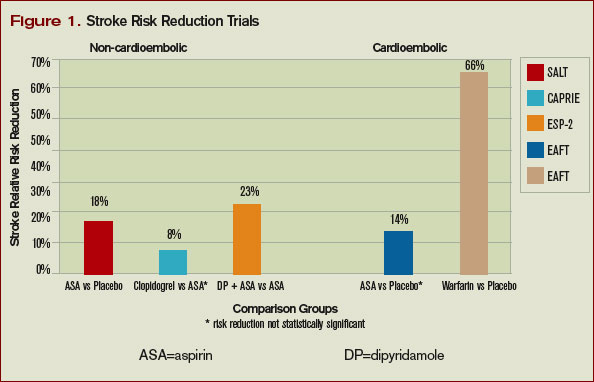
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.

What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
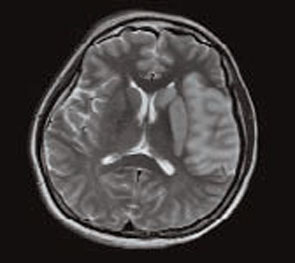
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.
What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
The Case
A 62-year-old obese woman with prior history of type 2 diabetes, hypertension, and a pack-a-day smoking habit presented to the emergency department (ED) for acute onset of right-side weakness and sensory loss noted on awakening from sleep.
She reports taking a baby aspirin daily to “prevent heart attacks” prior to her stroke. Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers with mild hemiparesis and is ready for discharge. What is the best medical therapy for secondary prevention of stroke?
Overview
Cerebrovascular accident (CVA) represents an important diagnosis for the hospitalist, with 700,000 people suffering a stroke in the U.S. each year.1 This translates to a stroke every 45 seconds. About 200,000 of these strokes are recurrent events.
Cardioembolism is the largest cause of ischemic strokes, representing 29% of all infarcts.2 Stasis from impaired contractile function, atrial fibrillation, or mechanical valves are significant risk factors. More rarely, a paradoxical embolus arising in the venous system may pass through a patent foramen ovale.
Large-artery atherosclerosis and lacunar infarcts each account for 16% of strokes. Risk factors for these forms of strokes are the same as those for atherosclerosis and include hypertension and diabetes. Rarer causes such as vasculitis, dissection, hypercoagulability, or hematological disorders account for 3% of strokes. Work-up for these should be driven by historical and atypical features such as young age, family history, or unusual distribution of ischemic zones. Despite appropriate work-up, the mechanism remains uncertain in 36% of strokes.
Regardless of the manifestation and residua of the index event, the hospitalist must initiate appropriate therapy to prevent a disabling CVA. While antithrombotic drugs are the mainstay of secondary prevention, it is a mistake to miss other opportunities for risk modification. Optimal management requires a tailored evaluation for etiology, identification of modifiable risk factors, and initiation of antiplatelet or anticoagulant therapy.
Cardioembolic Stroke
Treatment of stroke depends on the etiology of the original infarct. Evidence is strong that the optimal therapy for cardioembolic stroke is anticoagulation with warfarin.
The European Atrial Fibrillation Trial found that warfarin reduces the risk for second strokes in patients with atrial fibrillation by two-thirds and is superior to antiplatelet agents for preventing cardioembolic strokes.3 Warfarin increases the risk of extracranial bleeding, but not severely enough to negate the benefit of reducing stroke death and disability. The target international normalized ratio (INR) for non-valvular atrial fibrillation is generally two to three, although this may be higher for certain prosthetic valves.
Noncardioembolic Stroke
For large-vessel atherosclerotic and lacunar cerebral ischemia, the oldest—and still effective—treatment for recurrent stroke is aspirin. The use of low-dose aspirin after transient ischemic attack (TIA) or stroke reduces second strokes or death by approximately 15%-18%.4-5 Larger doses do not appear to be more effective, although the rate of gastrointestinal complaints is greater with increased dosage. The use of either 325 mg or 1,200 mg of aspirin produced the same 15% reduction in second ischemic events. Similar efficacy has been seen in comparisons between 30 mg and 283 mg dosing.6
While a subset of patients may experience aspirin resistance, reliable assays in clinical practice are not commonly available to guide management. Current recommendations suggest that use of between 50 mg and 325 mg of aspirin is appropriate for secondary prevention.7
Clopidogrel is another antiplatelet agent that can be given daily at 75 mg as alternate therapy for secondary prevention of non-cardioembolic stroke. The Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events trial comparing clopidogrel with aspirin in patients at risk of ischemic events demonstrated significant reduction in the annual rate of combined endpoint of stroke, myocardial infarction, and vascular death—from 5.83% with aspirin to 5.32% with clopidogrel.8 This study’s applicability to secondary prevention of stroke is limited by the fact that only 19% of the patients in this trial were included because of prior stroke, and the results were not significant for reduction of stroke as a lone endpoint. Clopidogrel is recommended as an acceptable agent for CVA secondary prevention and is preferred for patients with stroke and an aspirin allergy or with recent coronary stent.
The combination of a low-dose aspirin and extended-release dipyridamole has proved superior to aspirin monotherapy in multiple trials. Over two years, the European Stroke Prevention 2 trial found an 18% reduction with aspirin alone compared with 37% reduction with the combination therapy, and the European/Australasian Stroke Prevention in Reversible Ischaemia trial confirmed that the combination reduced the absolute rate of second ischemic events by 1% annually.9-10 Headache is a common side effect of dipyridamole and may limit use. Dypridamole/aspirin is recommended as another acceptable option for secondary prevention of non-cardioembolic stroke.
Evidence suggests that aspirin/dipyridamole and clopidogrel—although significantly more expensive—are more effective than aspirin monotherapy for preventing second cerebral ischemic events. Direct comparison between aspirin/dipyridamole and clopidogrel is ongoing in the Prevention Regimen for Effectively Avoiding Second Stroke trial, with results anticipated in 2008.
Things That Don’t Work
The Warfarin-Aspirin Recurrent Stroke Study trial demonstrated that warfarin was not better than aspirin for prevention of non-cardioembolic stroke, and the Warfarin–Aspirin Symptomatic Intracranial Disease trial found the same result for patients with intracranial stenosis.11-12 There is little evidence that warfarin should have a role in the treatment of most non-cardioembolic strokes. The MATCH trial failed to show benefit to adding aspirin to clopidogrel over clopidogrel monotherapy for secondary preventions of non-cardioembolic cerebral ischemia.13 Despite efficacy following coronary stenting, the combination of clopidogrel and aspirin can not be recommended for stroke prevention.
What To Do
Aggressive risk factor modification is key in the prevention of second ischemic events. One of the most promising therapies is the use of statins following a CVA. Maintaining low-density lipoprotein (LDL) at less than 100 mg/dL (or less than 70 mg/dL in the highest-risk patients) is recommended despite a relatively weak association between stroke and hyperlipidemia.
This stands in contrast to the strong relationship between elevated LDL and coronary disease. However, the Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial utilized high-dose atorvastatin after acute CVA and was able to create an absolute risk reduction for second stroke of 2.2% over the next five years.14 It is possible that the findings of this trial may reflect actions of statin therapy on the endothelium independent of the lipid lowering effect.
Blood pressure commonly has a transient elevation following cerebral ischemia. This is managed permissively to preserve perfusion to the ischemic penumbra. Once the hyperacute period is over, reduction of blood pressure to less than 140/90 mm/Hg (130/80 mm/Hg for diabetics) is recommended.
Interventions to treat chronic hypertension have been demonstrated to reduce the rate of strokes by approximately 30% to 40% over four to five years.15-16 An optimal agent has not been determined, but therapy with angiotensin converting enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB), possibly in combination with a diuretic, have been effective. Close follow-up for titration to goal in the outpatient setting should be arranged. Diabetics should have optimization of glycemic control, and lifestyle counseling should occur regarding recognized risk factors for stroke such as smoking, inactivity, and alcohol abuse.
While antithrombotic therapy is the mainstay of what we think of in secondary prevention of stroke, treatment of these other modifiable risk factors have been shown to affect mortality and second strokes of a similar magnitude and should not be neglected.
How to Treat This Case
The patient described should undergo an MRI with diffusion (to define the area of ischemia) and targeted evaluation for etiology with cardiac monitoring, echocardiogram, and carotid ultrasound.
Assuming atrial fibrillation or intracardiac thrombus is ruled out, this likely represents atherosclerotic disease. MRI will help distinguish between large-vessel atherosclerotic etiology and lacunar infarct. If carotid stenosis of greater than 70% is found in the setting of large vessel atherosclerotic stroke, then she should be referred for carotid endarterectomy. At 50% to 69% stenosis, carotid endarterectomy would still be a consideration. Antithrombotic agent of choice for non-cardioembolic CVA is an anti-platelet agent. With a stroke occurring on a reasonable dose of aspirin, I would not recommend increasing the dose as there is little evidence that 325 mg is more effective than 81mg. The most appropriate step would be to change to an alternate anti-platelet agent such as combination dipyridamole/aspirin or clopidogrel.
In the absence of a direct comparison trial, either choice is acceptable. The evidence supporting dipyridamole/aspirin is stronger for secondary stroke prevention. Atorvastatin 80 mg daily is an evidence-based therapy after acute stroke and can be started immediately. Her hypertension should be managed permissively for the first few days after the acute event, but then an ACE-I or ARB—possibly in combination with a diuretic—would be appropriate. This patient’s goal blood pressure as a diabetic would be at least less than 130/80 mm/Hg.
Finally we would be remiss if we did not stress the importance of smoking cessation, exercise, and weight loss. TH
Dr. Cumbler is an assistant professor in the Section of Hospital Medicine at the University of Colorado, where he is a member of the Acute Stroke Service and serves on the Stroke Council.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007 Feb 6;115(5):e69-e171.
- Petty GW, Brown RD, Whisnant JP, et al. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513-2516.
- European Atrial Fibrillation Trial Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255-1262.
- Swedish Aspirin Low-Dose Trial Collaborative Group. Swedish aspirin low-dose aspirin trial (SALT) of 775 mg aspirin as secondary prophylaxis after cerebrovascular ischaemic events. Lancet. 1991;338(8779):1345-1349.
- Farrell B, Godwin J, Richards S, et al. The United Kingdom Transient Ischaemic Attack (UK-TIA) aspirin trial: final results (abstract). J Neurol Neurosurg. Psychiatry 1991;54:1044-1054.
- Dutch TIA Trial Study Group. A comparison of two doses of aspirin (30 mg versus 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991 Oct 31;325(18):1261-1266.
- Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. Stroke. 2006 Feb;37(2):577-617.
- CAPRIE Steering Committee. A randomized, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events. Lancet 1996 Jan;348:1329-1339.
- Diener H, Cunha L, Forbes C, et al. European stroke prevention study 2: dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1-13.
- ESPRIT Study Group. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665-1673.
- Mohr JP, Thompson JLP, Lazar RM, et al. A comparison of warfarin and aspirin for the prevention of recurrent ischemic stroke. N Engl J Med. 2001 Nov 15; 345(20):1444-1451.
- Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005 Mar 31;352(13):1305-1316.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo controlled trial. Lancet. 2004 Jul 24-30;36499431):331-337.
- Stroke Prevention by Aggressive Reduction in Cholesterol Levels Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559.
- The PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358(9287):1033-1041.
- The Heart Outcomes Prevention Evaluation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000 Jan 20;342:145-153.
The Power of “Sorry”
Like many people, we like to sing while secure in the anonymity of our cars. This morning, one of us was wailing along with Elton John as he sang “Sorry Seems to Be the Hardest Word”:
It’s sad, so sad
Why can’t we talk it over
Oh, it seems to me
That sorry seems to be the hardest word.
That verse frames a critical legal question physicians regularly encounter: how to communicate with patients after an unexpected outcome. More precisely, should a physician apologize to a patient who suffers complications because of that physician’s treatment?
Traditionally, after a patient suffered a complication, defense lawyers were reluctant to allow the physician to express apologies or regret. The defense lawyer feared the apology would be treated as an “admission against interest.” In other words, the defense lawyer wanted to prevent a plaintiff’s lawyer from someday arguing that the physician’s apology was an admission of negligence or wrongdoing.
But the lawyer’s strategy fails. The patient wants the physician to apologize for an error. In fact, the patient distrusts a physician who does not admit errors.
‘‘Although a physician may wish to tell a patient when he has made a mistake, lawyers often order doctors to say nothing,’’ wrote University of Florida law professor Jonathan R. Cohen in the Southern California Law Review.1 “The physician’s silence may then trigger the patient’s anger. This alienation may then prompt the patient to sue.”
These observations are consistent with studies demonstrating that patients are far less to sue when provided with a full explanation and apology.2
Certainly no physician wants to make a statement that a plaintiff’s lawyer will use against him in court. But the same physician rationally wants to take any steps that might prevent the patient from feeling as though he or she needs to consult with a plaintiff’s lawyer. So, what’s a physician to do when caught between the hospital’s lawsuit-fearing attorney and a patient who expects his doctor to communicate with her honestly and forthrightly?
Fortunately, several state legislatures have recognized this tension and passed legislation that encourages physicians to apologize without facing the prospect that a plaintiff’s lawyer will argue that the physician apologized only because he knew he did something wrong. An example best illustrates how such “I’m sorry” statutes work.
Dr. Smith is treating a 22-year-old patient, John Elway, for a fractured fibula. Dr. Smith sees no signs of neurological compromise while the patient is in a cast. After the cast is removed, it appears the patient has lost function in the leg because the cast was too tight. The patient was a star college athlete who was expected to be drafted into the NFL, but now likely won’t be drafted. Dr. Smith tells the patient: “It’s my fault this happened. I’m really sorry that I didn’t pick up on this sooner.”
Does Dr. Smith’s statement come into evidence in court? Does part of it? The answers probably depend upon which state’s apology statute is applied. Massachusetts was one of the first states to pass an apology statute. It reads:
Statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to the person or to the family of such a person shall be inadmissible as evidence of an admission of liability in a civil action.
Significantly, the Massachusetts statute applies to people “involved in an accident,” which might imply that it is limited to automobile accidents or workplace accidents. The Massachusetts statute prevents this limited construction by providing a broad definition of “accident,” including any “occurrence resulting in injury or death to one or more persons which is not the result of a willful action by a party.” This definition would encompass ordinary medical negligence.
It would seem clear that the statute would protect Dr. Smith if he simply stated: “I want you to know how sorry I am this happened. I feel awful that you experienced this complication.”
But if Dr. Smith said, “It’s my fault this happened,” would the Massachusetts statute protect Dr. Smith? That’s a much harder call. Saying “It’s my fault” is technically not an expression of “sympathy or a general act of benevolence.” There no clear answer under Massachusetts law. But we believe the result would probably depend on whether the judge hearing the case thought this statement occurred during an overall act of apology.
The answer is clearer in California. That state’s apology statute reads:
The portion of statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to that person or to the family of that person shall be inadmissible as evidence of an admission of liability in a civil action. A statement of fault, however, which is part of, or in addition to, any of the above shall not be inadmissible pursuant to this section.
California draws a clear distinction between “the portion of statements ... expressing sympathy or a general sense of benevolence” and “a statement of fault.”
In our scenario, the jury would almost certainly be able to hear Dr. Smith’s statement, “It’s my fault this happened.” Critics of California’s law believe it creates too narrow a window for physicians to believe that plaintiff’s lawyers will not use their apology against them in a lawsuit.3
While Dr. Smith’s statement is likely to come into evidence in California, it’s also clear the opposite would occur in Colorado. Colorado’s apology statute, which specifically applies to medical malpractice actions, reads:
In any civil action brought by an alleged victim of an unanticipated outcome of medical care ... any and all statements … expressing apology, fault, sympathy, commiseration, condolence, compassion or a general sense of benevolence ... shall be inadmissible as evidence of an admission of liability or as evidence of an admission against interest.
Because Colorado’s statute specifically renders statements of “fault” inadmissible, a jury would not be able to consider any of Dr. Smith’s statements made during the course of his apology. Colorado’s law provides the physician with the most protection. Critics of Colorado’s law believe it’s unfair for physicians to admit fault to their patients in the hospital, then deny liability after the patient files a lawsuit.
Twenty-six other states have passed apology statutes; each works a bit differently. The choice of words matters. Legally, there is a big difference between a physician telling a patient, “I’m sorry about your pain” or saying, “It’s my fault you’re in pain.”
While apologies are valuable and important in relationships of trust—including the relationship between physicians and patients—we suggest you consult an experienced lawyer when crafting an apology to make sure it conveys your sympathies without opening a door to liability. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, Denver.
References
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1131.
- Hickson GB, Clayton EW, Githens PB, et al. Factors that prompted families to file medical malpractice claims following perinatal injuries. JAMA. 1992 Mar;267(10):1359-1363.
- Eisenberg D. When doctors say, “We’re sorry.” Time. 2005 Aug 15;166(7):50-52.
Like many people, we like to sing while secure in the anonymity of our cars. This morning, one of us was wailing along with Elton John as he sang “Sorry Seems to Be the Hardest Word”:
It’s sad, so sad
Why can’t we talk it over
Oh, it seems to me
That sorry seems to be the hardest word.
That verse frames a critical legal question physicians regularly encounter: how to communicate with patients after an unexpected outcome. More precisely, should a physician apologize to a patient who suffers complications because of that physician’s treatment?
Traditionally, after a patient suffered a complication, defense lawyers were reluctant to allow the physician to express apologies or regret. The defense lawyer feared the apology would be treated as an “admission against interest.” In other words, the defense lawyer wanted to prevent a plaintiff’s lawyer from someday arguing that the physician’s apology was an admission of negligence or wrongdoing.
But the lawyer’s strategy fails. The patient wants the physician to apologize for an error. In fact, the patient distrusts a physician who does not admit errors.
‘‘Although a physician may wish to tell a patient when he has made a mistake, lawyers often order doctors to say nothing,’’ wrote University of Florida law professor Jonathan R. Cohen in the Southern California Law Review.1 “The physician’s silence may then trigger the patient’s anger. This alienation may then prompt the patient to sue.”
These observations are consistent with studies demonstrating that patients are far less to sue when provided with a full explanation and apology.2
Certainly no physician wants to make a statement that a plaintiff’s lawyer will use against him in court. But the same physician rationally wants to take any steps that might prevent the patient from feeling as though he or she needs to consult with a plaintiff’s lawyer. So, what’s a physician to do when caught between the hospital’s lawsuit-fearing attorney and a patient who expects his doctor to communicate with her honestly and forthrightly?
Fortunately, several state legislatures have recognized this tension and passed legislation that encourages physicians to apologize without facing the prospect that a plaintiff’s lawyer will argue that the physician apologized only because he knew he did something wrong. An example best illustrates how such “I’m sorry” statutes work.
Dr. Smith is treating a 22-year-old patient, John Elway, for a fractured fibula. Dr. Smith sees no signs of neurological compromise while the patient is in a cast. After the cast is removed, it appears the patient has lost function in the leg because the cast was too tight. The patient was a star college athlete who was expected to be drafted into the NFL, but now likely won’t be drafted. Dr. Smith tells the patient: “It’s my fault this happened. I’m really sorry that I didn’t pick up on this sooner.”
Does Dr. Smith’s statement come into evidence in court? Does part of it? The answers probably depend upon which state’s apology statute is applied. Massachusetts was one of the first states to pass an apology statute. It reads:
Statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to the person or to the family of such a person shall be inadmissible as evidence of an admission of liability in a civil action.
Significantly, the Massachusetts statute applies to people “involved in an accident,” which might imply that it is limited to automobile accidents or workplace accidents. The Massachusetts statute prevents this limited construction by providing a broad definition of “accident,” including any “occurrence resulting in injury or death to one or more persons which is not the result of a willful action by a party.” This definition would encompass ordinary medical negligence.
It would seem clear that the statute would protect Dr. Smith if he simply stated: “I want you to know how sorry I am this happened. I feel awful that you experienced this complication.”
But if Dr. Smith said, “It’s my fault this happened,” would the Massachusetts statute protect Dr. Smith? That’s a much harder call. Saying “It’s my fault” is technically not an expression of “sympathy or a general act of benevolence.” There no clear answer under Massachusetts law. But we believe the result would probably depend on whether the judge hearing the case thought this statement occurred during an overall act of apology.
The answer is clearer in California. That state’s apology statute reads:
The portion of statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to that person or to the family of that person shall be inadmissible as evidence of an admission of liability in a civil action. A statement of fault, however, which is part of, or in addition to, any of the above shall not be inadmissible pursuant to this section.
California draws a clear distinction between “the portion of statements ... expressing sympathy or a general sense of benevolence” and “a statement of fault.”
In our scenario, the jury would almost certainly be able to hear Dr. Smith’s statement, “It’s my fault this happened.” Critics of California’s law believe it creates too narrow a window for physicians to believe that plaintiff’s lawyers will not use their apology against them in a lawsuit.3
While Dr. Smith’s statement is likely to come into evidence in California, it’s also clear the opposite would occur in Colorado. Colorado’s apology statute, which specifically applies to medical malpractice actions, reads:
In any civil action brought by an alleged victim of an unanticipated outcome of medical care ... any and all statements … expressing apology, fault, sympathy, commiseration, condolence, compassion or a general sense of benevolence ... shall be inadmissible as evidence of an admission of liability or as evidence of an admission against interest.
Because Colorado’s statute specifically renders statements of “fault” inadmissible, a jury would not be able to consider any of Dr. Smith’s statements made during the course of his apology. Colorado’s law provides the physician with the most protection. Critics of Colorado’s law believe it’s unfair for physicians to admit fault to their patients in the hospital, then deny liability after the patient files a lawsuit.
Twenty-six other states have passed apology statutes; each works a bit differently. The choice of words matters. Legally, there is a big difference between a physician telling a patient, “I’m sorry about your pain” or saying, “It’s my fault you’re in pain.”
While apologies are valuable and important in relationships of trust—including the relationship between physicians and patients—we suggest you consult an experienced lawyer when crafting an apology to make sure it conveys your sympathies without opening a door to liability. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, Denver.
References
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1131.
- Hickson GB, Clayton EW, Githens PB, et al. Factors that prompted families to file medical malpractice claims following perinatal injuries. JAMA. 1992 Mar;267(10):1359-1363.
- Eisenberg D. When doctors say, “We’re sorry.” Time. 2005 Aug 15;166(7):50-52.
Like many people, we like to sing while secure in the anonymity of our cars. This morning, one of us was wailing along with Elton John as he sang “Sorry Seems to Be the Hardest Word”:
It’s sad, so sad
Why can’t we talk it over
Oh, it seems to me
That sorry seems to be the hardest word.
That verse frames a critical legal question physicians regularly encounter: how to communicate with patients after an unexpected outcome. More precisely, should a physician apologize to a patient who suffers complications because of that physician’s treatment?
Traditionally, after a patient suffered a complication, defense lawyers were reluctant to allow the physician to express apologies or regret. The defense lawyer feared the apology would be treated as an “admission against interest.” In other words, the defense lawyer wanted to prevent a plaintiff’s lawyer from someday arguing that the physician’s apology was an admission of negligence or wrongdoing.
But the lawyer’s strategy fails. The patient wants the physician to apologize for an error. In fact, the patient distrusts a physician who does not admit errors.
‘‘Although a physician may wish to tell a patient when he has made a mistake, lawyers often order doctors to say nothing,’’ wrote University of Florida law professor Jonathan R. Cohen in the Southern California Law Review.1 “The physician’s silence may then trigger the patient’s anger. This alienation may then prompt the patient to sue.”
These observations are consistent with studies demonstrating that patients are far less to sue when provided with a full explanation and apology.2
Certainly no physician wants to make a statement that a plaintiff’s lawyer will use against him in court. But the same physician rationally wants to take any steps that might prevent the patient from feeling as though he or she needs to consult with a plaintiff’s lawyer. So, what’s a physician to do when caught between the hospital’s lawsuit-fearing attorney and a patient who expects his doctor to communicate with her honestly and forthrightly?
Fortunately, several state legislatures have recognized this tension and passed legislation that encourages physicians to apologize without facing the prospect that a plaintiff’s lawyer will argue that the physician apologized only because he knew he did something wrong. An example best illustrates how such “I’m sorry” statutes work.
Dr. Smith is treating a 22-year-old patient, John Elway, for a fractured fibula. Dr. Smith sees no signs of neurological compromise while the patient is in a cast. After the cast is removed, it appears the patient has lost function in the leg because the cast was too tight. The patient was a star college athlete who was expected to be drafted into the NFL, but now likely won’t be drafted. Dr. Smith tells the patient: “It’s my fault this happened. I’m really sorry that I didn’t pick up on this sooner.”
Does Dr. Smith’s statement come into evidence in court? Does part of it? The answers probably depend upon which state’s apology statute is applied. Massachusetts was one of the first states to pass an apology statute. It reads:
Statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to the person or to the family of such a person shall be inadmissible as evidence of an admission of liability in a civil action.
Significantly, the Massachusetts statute applies to people “involved in an accident,” which might imply that it is limited to automobile accidents or workplace accidents. The Massachusetts statute prevents this limited construction by providing a broad definition of “accident,” including any “occurrence resulting in injury or death to one or more persons which is not the result of a willful action by a party.” This definition would encompass ordinary medical negligence.
It would seem clear that the statute would protect Dr. Smith if he simply stated: “I want you to know how sorry I am this happened. I feel awful that you experienced this complication.”
But if Dr. Smith said, “It’s my fault this happened,” would the Massachusetts statute protect Dr. Smith? That’s a much harder call. Saying “It’s my fault” is technically not an expression of “sympathy or a general act of benevolence.” There no clear answer under Massachusetts law. But we believe the result would probably depend on whether the judge hearing the case thought this statement occurred during an overall act of apology.
The answer is clearer in California. That state’s apology statute reads:
The portion of statements, writings, or benevolent gestures expressing sympathy or a general sense of benevolence relating to the pain, suffering or death of a person involved in an accident and made to that person or to the family of that person shall be inadmissible as evidence of an admission of liability in a civil action. A statement of fault, however, which is part of, or in addition to, any of the above shall not be inadmissible pursuant to this section.
California draws a clear distinction between “the portion of statements ... expressing sympathy or a general sense of benevolence” and “a statement of fault.”
In our scenario, the jury would almost certainly be able to hear Dr. Smith’s statement, “It’s my fault this happened.” Critics of California’s law believe it creates too narrow a window for physicians to believe that plaintiff’s lawyers will not use their apology against them in a lawsuit.3
While Dr. Smith’s statement is likely to come into evidence in California, it’s also clear the opposite would occur in Colorado. Colorado’s apology statute, which specifically applies to medical malpractice actions, reads:
In any civil action brought by an alleged victim of an unanticipated outcome of medical care ... any and all statements … expressing apology, fault, sympathy, commiseration, condolence, compassion or a general sense of benevolence ... shall be inadmissible as evidence of an admission of liability or as evidence of an admission against interest.
Because Colorado’s statute specifically renders statements of “fault” inadmissible, a jury would not be able to consider any of Dr. Smith’s statements made during the course of his apology. Colorado’s law provides the physician with the most protection. Critics of Colorado’s law believe it’s unfair for physicians to admit fault to their patients in the hospital, then deny liability after the patient files a lawsuit.
Twenty-six other states have passed apology statutes; each works a bit differently. The choice of words matters. Legally, there is a big difference between a physician telling a patient, “I’m sorry about your pain” or saying, “It’s my fault you’re in pain.”
While apologies are valuable and important in relationships of trust—including the relationship between physicians and patients—we suggest you consult an experienced lawyer when crafting an apology to make sure it conveys your sympathies without opening a door to liability. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, Denver.
References
- Cohen JR. Advising clients to apologize. Southern California Law Review. 1999;72:1009-1131.
- Hickson GB, Clayton EW, Githens PB, et al. Factors that prompted families to file medical malpractice claims following perinatal injuries. JAMA. 1992 Mar;267(10):1359-1363.
- Eisenberg D. When doctors say, “We’re sorry.” Time. 2005 Aug 15;166(7):50-52.
Is P4P Paying off?
Pay for performance (P4P) has been the hottest topic among physicians for quite a while. Perhaps the time has come to ask: Is it worth the hype?
“In terms of organized pay-for-performance programs, we’re at the very beginning of seeing pay for performance in action,” says Patrick J. Torcson, MD, MMM, FACP, member of SHM’s Public Policy Committee and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
Although P4P is still in its infancy, one major demonstration trial is complete, and researchers have begun to mine results for indications of success.
The largest national P4P trial to date is the Centers for Medicare and Medicaid (CMS)/Premier Hospital Quality Incentive Demonstration Project, which involved more than 260 hospitals reporting on 34 quality measures from October 2003 through September 2006. The measures were grouped in five clinical areas: acute myocardial infarction, heart failure, coronary artery bypass graft, pneumonia, and hip and knee replacement.
Hospitals in the top 10% for each of the quality measures received a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% received a 1% bonus; and hospitals in the bottom 20% returned 1% to 2% of their diagnosis-related group (DRG) payments.
CMS has paid $17.55 million in incentives to the top-tier, participating hospitals and reported savings of $1.4 billion in terms of avoidable deaths, complications and readmissions prevented, and shortened lengths of stay.
As for quality improvements, results from the first two years of the demonstration project show proven improvement across all five clinical focus areas. The average improvement of the composite quality scores (CQS), an aggregate of all quality measures within each clinical area, in the project’s second year was 6.7%, for total gains of 11.8% over the project’s first two years.
The CQS improved significantly between the start date and the end of the second year in all five clinical focus areas:
- From 87.5% to 94.4% for patients with acute myocardial infarction;
- From 64.5% to 82.4% for patients with heart failure;
- From 69.3% to 85.8% for patients with community acquired pneumonia;
- From 84.8% to 93.8% for patients with coronary artery bypass graft; and
- From 84.6% to 93.4% for patients with hip and knee replacement.
“In many circles, this is proof positive that pay for performance works,” Dr. Torcson says of the results of the Premier demo. “However, this was hospital-level P4P and involves a different methodology than physician-level P4P. I don’t think it’s safe or accurate to extrapolate these results.”
What the Research Says
Various researchers have examined available P4P data to see if incentives improve care.
Recent studies include one led by hospitalist Peter Lindenauer, MD, MSc, FACP, medical director, clinical and quality informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston.1 Dr. Lindenauer and his colleagues examined data from the CMS data warehouse gathered as part of the Hospital Quality Alliance (Hospital Compare) project. Specifically, they compared P4P CMS Premier hospitals with 408 hospitals that participated only in public reporting, with no compensation.
They found that the P4P hospitals showed modestly greater improvement in all composite measures of quality than hospitals that simply reported on measures. Specifically, improvements in the P4P hospitals ranged from 2.6% to 4.1% over two years. “The small gains in process of care measures observed in the study are unlikely to have translated into meaningful improvements in outcomes,” Dr. Lindenauer says.
Other studies of P4P are inconclusive. A literature review on the subject finds “little evidence to support the effectiveness of paying for quality.”2
A second literature review out of the Baylor College of Medicine in Houston based on 17 studies “suggests some positive effects of financial incentives at the physician level, the provider group level, and the healthcare payment system level. The findings also suggest that ongoing monitoring of incentive programs is critical to determine whether incentives are having unintended effects on quality of care.”3
Finally, a study of P4P programs for family practices in the United Kingdom revealed that serious financial incentives for physicians resulted in 83.4% achieving goals for 10 chronic diseases in a year.4
“There is no conclusive evidence that physician-level P4P works to improve quality of care and reduce cost of care,” concludes Dr. Torcson. “The U.K. experience demonstrates that given a sufficient incentive, physicians will adhere to and report on performance measures. Further study is being done to see if this translates into quality improvement for patients.”
The next phase of P4P is pay for reporting—which may help pin down the true value of P4P.
The Physician Quality Reporting Initiative (PQRI), now well under way, “is the first nationwide pay-for-performance program, and one of the first to include hospitalists,” says Dr. Torcson. “This is the first taste we’re all having of physician-level pay-for-performance since the PQRI started on July 1.”
The incentives for participating in the trial aren’t high. “Based on projections of PQRI reporting, hospitalists can earn a bonus of $807,” says Dr. Torcson. “This may not be a strong motivator to participate in PQRI. However, it’s a beginning. If you’re going to fail [at reporting], this is the time to do it.”
The PQRI trial is short; it will end Dec. 31. And early next year, it’s guaranteed that all eyes will be on outcomes from this program. “Private payers are watching this very closely; they’re ready to jump into the game,” says Dr. Torcson. Healthcare organizations and professionals should be ready to jump as well, because next steps for P4P and other payment factors are still unknown.
“What happens after Dec. 31 is wide open,” Dr. Torcson says. “We don’t know what to expect from Congress. Right now we’re looking at a proposed 9.8% cut to physician fees. Will this cut be made up by pay-for-performance bonuses? Congress determines what will happen, and the [2008] election could change everything.”
To date, P4P has not lived up to its hype; however, the use of incentives to improve quality is in the early stages. Time will tell if P4P pays off in improved care—but CMS and many physicians seem committed to the idea.
“I think there’s a lot to be said for the concept of providing incentives that encourage hospitals to invest in quality of care,” says Dr. Lindenauer. “Our current system of healthcare hasn’t done that.”
Dr. Lindenauer’s advice for moving ahead with P4P? “We need to proceed cautiously and be mindful of some of the unintended consequences,” he concludes. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
References
- Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007 Feb 1;356(5):486-496.
- Rosenthal MB, Frank RG. What is the empirical basis for paying for quality in health care? Med Care Res Rev. 2006;63(2):135-137.
- Petersen LA, Woodard LD, Urech T, et al. Does pay-for-performance improve the quality of health care? Ann Intern Med. 2006;145(4):265-272.
- Doran T, Fullwood C, Gravelle H, et al. Pay-for-performance programs in family practices in the United Kingdom. N Engl J Med. 2006;355(4):375-384.
Pay for performance (P4P) has been the hottest topic among physicians for quite a while. Perhaps the time has come to ask: Is it worth the hype?
“In terms of organized pay-for-performance programs, we’re at the very beginning of seeing pay for performance in action,” says Patrick J. Torcson, MD, MMM, FACP, member of SHM’s Public Policy Committee and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
Although P4P is still in its infancy, one major demonstration trial is complete, and researchers have begun to mine results for indications of success.
The largest national P4P trial to date is the Centers for Medicare and Medicaid (CMS)/Premier Hospital Quality Incentive Demonstration Project, which involved more than 260 hospitals reporting on 34 quality measures from October 2003 through September 2006. The measures were grouped in five clinical areas: acute myocardial infarction, heart failure, coronary artery bypass graft, pneumonia, and hip and knee replacement.
Hospitals in the top 10% for each of the quality measures received a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% received a 1% bonus; and hospitals in the bottom 20% returned 1% to 2% of their diagnosis-related group (DRG) payments.
CMS has paid $17.55 million in incentives to the top-tier, participating hospitals and reported savings of $1.4 billion in terms of avoidable deaths, complications and readmissions prevented, and shortened lengths of stay.
As for quality improvements, results from the first two years of the demonstration project show proven improvement across all five clinical focus areas. The average improvement of the composite quality scores (CQS), an aggregate of all quality measures within each clinical area, in the project’s second year was 6.7%, for total gains of 11.8% over the project’s first two years.
The CQS improved significantly between the start date and the end of the second year in all five clinical focus areas:
- From 87.5% to 94.4% for patients with acute myocardial infarction;
- From 64.5% to 82.4% for patients with heart failure;
- From 69.3% to 85.8% for patients with community acquired pneumonia;
- From 84.8% to 93.8% for patients with coronary artery bypass graft; and
- From 84.6% to 93.4% for patients with hip and knee replacement.
“In many circles, this is proof positive that pay for performance works,” Dr. Torcson says of the results of the Premier demo. “However, this was hospital-level P4P and involves a different methodology than physician-level P4P. I don’t think it’s safe or accurate to extrapolate these results.”
What the Research Says
Various researchers have examined available P4P data to see if incentives improve care.
Recent studies include one led by hospitalist Peter Lindenauer, MD, MSc, FACP, medical director, clinical and quality informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston.1 Dr. Lindenauer and his colleagues examined data from the CMS data warehouse gathered as part of the Hospital Quality Alliance (Hospital Compare) project. Specifically, they compared P4P CMS Premier hospitals with 408 hospitals that participated only in public reporting, with no compensation.
They found that the P4P hospitals showed modestly greater improvement in all composite measures of quality than hospitals that simply reported on measures. Specifically, improvements in the P4P hospitals ranged from 2.6% to 4.1% over two years. “The small gains in process of care measures observed in the study are unlikely to have translated into meaningful improvements in outcomes,” Dr. Lindenauer says.
Other studies of P4P are inconclusive. A literature review on the subject finds “little evidence to support the effectiveness of paying for quality.”2
A second literature review out of the Baylor College of Medicine in Houston based on 17 studies “suggests some positive effects of financial incentives at the physician level, the provider group level, and the healthcare payment system level. The findings also suggest that ongoing monitoring of incentive programs is critical to determine whether incentives are having unintended effects on quality of care.”3
Finally, a study of P4P programs for family practices in the United Kingdom revealed that serious financial incentives for physicians resulted in 83.4% achieving goals for 10 chronic diseases in a year.4
“There is no conclusive evidence that physician-level P4P works to improve quality of care and reduce cost of care,” concludes Dr. Torcson. “The U.K. experience demonstrates that given a sufficient incentive, physicians will adhere to and report on performance measures. Further study is being done to see if this translates into quality improvement for patients.”
The next phase of P4P is pay for reporting—which may help pin down the true value of P4P.
The Physician Quality Reporting Initiative (PQRI), now well under way, “is the first nationwide pay-for-performance program, and one of the first to include hospitalists,” says Dr. Torcson. “This is the first taste we’re all having of physician-level pay-for-performance since the PQRI started on July 1.”
The incentives for participating in the trial aren’t high. “Based on projections of PQRI reporting, hospitalists can earn a bonus of $807,” says Dr. Torcson. “This may not be a strong motivator to participate in PQRI. However, it’s a beginning. If you’re going to fail [at reporting], this is the time to do it.”
The PQRI trial is short; it will end Dec. 31. And early next year, it’s guaranteed that all eyes will be on outcomes from this program. “Private payers are watching this very closely; they’re ready to jump into the game,” says Dr. Torcson. Healthcare organizations and professionals should be ready to jump as well, because next steps for P4P and other payment factors are still unknown.
“What happens after Dec. 31 is wide open,” Dr. Torcson says. “We don’t know what to expect from Congress. Right now we’re looking at a proposed 9.8% cut to physician fees. Will this cut be made up by pay-for-performance bonuses? Congress determines what will happen, and the [2008] election could change everything.”
To date, P4P has not lived up to its hype; however, the use of incentives to improve quality is in the early stages. Time will tell if P4P pays off in improved care—but CMS and many physicians seem committed to the idea.
“I think there’s a lot to be said for the concept of providing incentives that encourage hospitals to invest in quality of care,” says Dr. Lindenauer. “Our current system of healthcare hasn’t done that.”
Dr. Lindenauer’s advice for moving ahead with P4P? “We need to proceed cautiously and be mindful of some of the unintended consequences,” he concludes. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
References
- Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007 Feb 1;356(5):486-496.
- Rosenthal MB, Frank RG. What is the empirical basis for paying for quality in health care? Med Care Res Rev. 2006;63(2):135-137.
- Petersen LA, Woodard LD, Urech T, et al. Does pay-for-performance improve the quality of health care? Ann Intern Med. 2006;145(4):265-272.
- Doran T, Fullwood C, Gravelle H, et al. Pay-for-performance programs in family practices in the United Kingdom. N Engl J Med. 2006;355(4):375-384.
Pay for performance (P4P) has been the hottest topic among physicians for quite a while. Perhaps the time has come to ask: Is it worth the hype?
“In terms of organized pay-for-performance programs, we’re at the very beginning of seeing pay for performance in action,” says Patrick J. Torcson, MD, MMM, FACP, member of SHM’s Public Policy Committee and director of hospital medicine at St. Tammany Parish Hospital in Covington, La.
Although P4P is still in its infancy, one major demonstration trial is complete, and researchers have begun to mine results for indications of success.
The largest national P4P trial to date is the Centers for Medicare and Medicaid (CMS)/Premier Hospital Quality Incentive Demonstration Project, which involved more than 260 hospitals reporting on 34 quality measures from October 2003 through September 2006. The measures were grouped in five clinical areas: acute myocardial infarction, heart failure, coronary artery bypass graft, pneumonia, and hip and knee replacement.
Hospitals in the top 10% for each of the quality measures received a 2% bonus of their Medicare payments for the measured condition; hospitals in the top 20% received a 1% bonus; and hospitals in the bottom 20% returned 1% to 2% of their diagnosis-related group (DRG) payments.
CMS has paid $17.55 million in incentives to the top-tier, participating hospitals and reported savings of $1.4 billion in terms of avoidable deaths, complications and readmissions prevented, and shortened lengths of stay.
As for quality improvements, results from the first two years of the demonstration project show proven improvement across all five clinical focus areas. The average improvement of the composite quality scores (CQS), an aggregate of all quality measures within each clinical area, in the project’s second year was 6.7%, for total gains of 11.8% over the project’s first two years.
The CQS improved significantly between the start date and the end of the second year in all five clinical focus areas:
- From 87.5% to 94.4% for patients with acute myocardial infarction;
- From 64.5% to 82.4% for patients with heart failure;
- From 69.3% to 85.8% for patients with community acquired pneumonia;
- From 84.8% to 93.8% for patients with coronary artery bypass graft; and
- From 84.6% to 93.4% for patients with hip and knee replacement.
“In many circles, this is proof positive that pay for performance works,” Dr. Torcson says of the results of the Premier demo. “However, this was hospital-level P4P and involves a different methodology than physician-level P4P. I don’t think it’s safe or accurate to extrapolate these results.”
What the Research Says
Various researchers have examined available P4P data to see if incentives improve care.
Recent studies include one led by hospitalist Peter Lindenauer, MD, MSc, FACP, medical director, clinical and quality informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston.1 Dr. Lindenauer and his colleagues examined data from the CMS data warehouse gathered as part of the Hospital Quality Alliance (Hospital Compare) project. Specifically, they compared P4P CMS Premier hospitals with 408 hospitals that participated only in public reporting, with no compensation.
They found that the P4P hospitals showed modestly greater improvement in all composite measures of quality than hospitals that simply reported on measures. Specifically, improvements in the P4P hospitals ranged from 2.6% to 4.1% over two years. “The small gains in process of care measures observed in the study are unlikely to have translated into meaningful improvements in outcomes,” Dr. Lindenauer says.
Other studies of P4P are inconclusive. A literature review on the subject finds “little evidence to support the effectiveness of paying for quality.”2
A second literature review out of the Baylor College of Medicine in Houston based on 17 studies “suggests some positive effects of financial incentives at the physician level, the provider group level, and the healthcare payment system level. The findings also suggest that ongoing monitoring of incentive programs is critical to determine whether incentives are having unintended effects on quality of care.”3
Finally, a study of P4P programs for family practices in the United Kingdom revealed that serious financial incentives for physicians resulted in 83.4% achieving goals for 10 chronic diseases in a year.4
“There is no conclusive evidence that physician-level P4P works to improve quality of care and reduce cost of care,” concludes Dr. Torcson. “The U.K. experience demonstrates that given a sufficient incentive, physicians will adhere to and report on performance measures. Further study is being done to see if this translates into quality improvement for patients.”
The next phase of P4P is pay for reporting—which may help pin down the true value of P4P.
The Physician Quality Reporting Initiative (PQRI), now well under way, “is the first nationwide pay-for-performance program, and one of the first to include hospitalists,” says Dr. Torcson. “This is the first taste we’re all having of physician-level pay-for-performance since the PQRI started on July 1.”
The incentives for participating in the trial aren’t high. “Based on projections of PQRI reporting, hospitalists can earn a bonus of $807,” says Dr. Torcson. “This may not be a strong motivator to participate in PQRI. However, it’s a beginning. If you’re going to fail [at reporting], this is the time to do it.”
The PQRI trial is short; it will end Dec. 31. And early next year, it’s guaranteed that all eyes will be on outcomes from this program. “Private payers are watching this very closely; they’re ready to jump into the game,” says Dr. Torcson. Healthcare organizations and professionals should be ready to jump as well, because next steps for P4P and other payment factors are still unknown.
“What happens after Dec. 31 is wide open,” Dr. Torcson says. “We don’t know what to expect from Congress. Right now we’re looking at a proposed 9.8% cut to physician fees. Will this cut be made up by pay-for-performance bonuses? Congress determines what will happen, and the [2008] election could change everything.”
To date, P4P has not lived up to its hype; however, the use of incentives to improve quality is in the early stages. Time will tell if P4P pays off in improved care—but CMS and many physicians seem committed to the idea.
“I think there’s a lot to be said for the concept of providing incentives that encourage hospitals to invest in quality of care,” says Dr. Lindenauer. “Our current system of healthcare hasn’t done that.”
Dr. Lindenauer’s advice for moving ahead with P4P? “We need to proceed cautiously and be mindful of some of the unintended consequences,” he concludes. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
References
- Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007 Feb 1;356(5):486-496.
- Rosenthal MB, Frank RG. What is the empirical basis for paying for quality in health care? Med Care Res Rev. 2006;63(2):135-137.
- Petersen LA, Woodard LD, Urech T, et al. Does pay-for-performance improve the quality of health care? Ann Intern Med. 2006;145(4):265-272.
- Doran T, Fullwood C, Gravelle H, et al. Pay-for-performance programs in family practices in the United Kingdom. N Engl J Med. 2006;355(4):375-384.
Group Growth
Ambitious hospitalists may be eager to add an MBA or a PhD to their credentials, in the belief those magic letters will open doors to leadership positions or higher compensation. But before you fork over tuition for an advanced degree program, consider whether that degree will pay off.
Choose Your Career Path
If you’re considering pursuing a Master of Business Administration (MBA), Master of Public Health (MPH), Master of Health Administration (MPH), or even a doctorate degree, the first thing you should consider is which career path within hospital medicine you’re interested in. What position would you ultimately like to hold? And which, if any, advanced degree can help you get there?
“Explore the idea [of earning an advanced degree], but the most important steps are to try to get some work experience and set some goals,” says Mary Jo Gorman, MD, MBA, the CEO of Advanced ICU Care, St. Louis, Mo. “Along the way, find out what you have an aptitude for.” Once you know your general or specific career goals, you can consider whether to earn an advanced degree.
“It’s a significant monetary and time commitment, so make sure it makes sense for where you want to go,” advises Dr. Gorman. “I’d also advise career counseling to help with this. Great people to talk to are recruiters. They’ll tell you what you need in order to apply for certain positions.”
It should be obvious that some positions will require certain degrees beyond an MD or a DO. Look at the next—or final—job you want. Is the job held by someone with an MBA, a PhD, or another degree? Is that person’s successor likely to need specific education?
“If you want to be the chief operating officer of a hospital, or the CEO of a large medical group, you’re not getting that without an MBA,” Dr. Gorman says. “In fact, if you’re planning to apply for a position that requires strong financial expertise, they’re not going to accept you without [an MBA] unless you’re of a certain age and have a great track record that shows you can do the job.”
On the other hand, many experienced hospitalist leaders don’t have an MBA and won’t need one. “A lot of community-based hospitalists are already doing these things and don’t need the degree,” Dr. Gorman points out. “They created the job, or they created the group.”
A New Way of Thinking
Perhaps the most valuable aspect of any higher degree is the training one receives, which can provide new ways to approach one’s work, problem solving and general thought processes.
“The degree alone won’t help if you haven’t learned while getting it,” explains Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor Veterans Affairs (VA) Medical Center and University of Michigan Medical School. “That’s the real value: Learn the material and it will alter how you approach things.”
Fred A. McCurdy, MD, who holds a PhD and an MBA, was recently promoted from pediatric department chair at Texas Tech University Health Sciences Center at Amarillo to associate dean for faculty development. He earned his MBA with an eye on becoming department chair and says that the MBA program “gave me a background in thought process. From there, I could build on that foundation.”
As for his PhD, Dr. McCurdy says the degree “has its place. The program taught me methodology and scientific process. It taught me how to break down a problem into researchable questions, and I can apply that to areas like education. If your job calls for thinking logically and critically, a PhD gives experience in using scientific methods.”
Earning an MPH also bears fruit.
“Having an MPH is helpful,” says Dr. Saint. “In addition to helping you learn how to research, how to be a better user of literature, it helps prepare someone for taking a leadership role.”

—Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor VA Medical Center and University of Michigan Medical School, Ann Arbor
Your Dream Job
While an additional degree can improve your knowledge and skills, it’s no guarantee you’ll move to the top of a list for a promotion or new job.
“It’s not a given that it will necessarily help your career,” warns Dr. Gorman. “You need to first do an analysis about what you want to achieve, then work toward that goal. A lot of doctors don’t really realize that they need to think in terms of their total career plan.”
Dr. Saint agrees, saying of an MPH, “It may open the door, but you still have to walk through it. You still have to do the work yourself. You cannot hide behind the MPH. You have to be productive and even be an overperformer. But it does give you the tools you need, and it can help you get that first job.”
Dr. McCurdy believes a degree such as an MBA can be helpful for today’s hospitalists: “For a hospitalist with a strong interest in rising up through the hospital administrative ranks, having an MBA early in their career could definitely be beneficial,” speculates Dr. McCurdy. “Holding an MBA [in academia] is becoming the norm rather than the exception. There’s an increasing awareness in academics that this is a business.”
Does an advanced degree make a new hospitalist more hirable? “That depends,” says Dr. McCurdy. “For hospitalists working in a large hospital system, it becomes a matter of choice. I don’t think you’d be hired based on an advanced degree [such as a PhD] unless the job has something to do with a scholarly pursuit such as research or teaching. If you’re competing for a job in an academic health science center, a PhD degree can help if it has to do with scholarship.”
The Final Answer
Follow this sound advice: Chart your hospital medicine career path, and then work backward to see whether you’ll benefit from obtaining a specific degree.
“It has to do with what you intend to do in a five- or 10-year timeframe, with the course direction of your career,” says Dr. McCurdy. “If you plan to pursue academic scholarship, a PhD can be very helpful. If you aspire to become medical director at Maryland Shock Trauma, an MBA is the ticket you’re definitely going to need to punch.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Ambitious hospitalists may be eager to add an MBA or a PhD to their credentials, in the belief those magic letters will open doors to leadership positions or higher compensation. But before you fork over tuition for an advanced degree program, consider whether that degree will pay off.
Choose Your Career Path
If you’re considering pursuing a Master of Business Administration (MBA), Master of Public Health (MPH), Master of Health Administration (MPH), or even a doctorate degree, the first thing you should consider is which career path within hospital medicine you’re interested in. What position would you ultimately like to hold? And which, if any, advanced degree can help you get there?
“Explore the idea [of earning an advanced degree], but the most important steps are to try to get some work experience and set some goals,” says Mary Jo Gorman, MD, MBA, the CEO of Advanced ICU Care, St. Louis, Mo. “Along the way, find out what you have an aptitude for.” Once you know your general or specific career goals, you can consider whether to earn an advanced degree.
“It’s a significant monetary and time commitment, so make sure it makes sense for where you want to go,” advises Dr. Gorman. “I’d also advise career counseling to help with this. Great people to talk to are recruiters. They’ll tell you what you need in order to apply for certain positions.”
It should be obvious that some positions will require certain degrees beyond an MD or a DO. Look at the next—or final—job you want. Is the job held by someone with an MBA, a PhD, or another degree? Is that person’s successor likely to need specific education?
“If you want to be the chief operating officer of a hospital, or the CEO of a large medical group, you’re not getting that without an MBA,” Dr. Gorman says. “In fact, if you’re planning to apply for a position that requires strong financial expertise, they’re not going to accept you without [an MBA] unless you’re of a certain age and have a great track record that shows you can do the job.”
On the other hand, many experienced hospitalist leaders don’t have an MBA and won’t need one. “A lot of community-based hospitalists are already doing these things and don’t need the degree,” Dr. Gorman points out. “They created the job, or they created the group.”
A New Way of Thinking
Perhaps the most valuable aspect of any higher degree is the training one receives, which can provide new ways to approach one’s work, problem solving and general thought processes.
“The degree alone won’t help if you haven’t learned while getting it,” explains Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor Veterans Affairs (VA) Medical Center and University of Michigan Medical School. “That’s the real value: Learn the material and it will alter how you approach things.”
Fred A. McCurdy, MD, who holds a PhD and an MBA, was recently promoted from pediatric department chair at Texas Tech University Health Sciences Center at Amarillo to associate dean for faculty development. He earned his MBA with an eye on becoming department chair and says that the MBA program “gave me a background in thought process. From there, I could build on that foundation.”
As for his PhD, Dr. McCurdy says the degree “has its place. The program taught me methodology and scientific process. It taught me how to break down a problem into researchable questions, and I can apply that to areas like education. If your job calls for thinking logically and critically, a PhD gives experience in using scientific methods.”
Earning an MPH also bears fruit.
“Having an MPH is helpful,” says Dr. Saint. “In addition to helping you learn how to research, how to be a better user of literature, it helps prepare someone for taking a leadership role.”
—Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor VA Medical Center and University of Michigan Medical School, Ann Arbor
Your Dream Job
While an additional degree can improve your knowledge and skills, it’s no guarantee you’ll move to the top of a list for a promotion or new job.
“It’s not a given that it will necessarily help your career,” warns Dr. Gorman. “You need to first do an analysis about what you want to achieve, then work toward that goal. A lot of doctors don’t really realize that they need to think in terms of their total career plan.”
Dr. Saint agrees, saying of an MPH, “It may open the door, but you still have to walk through it. You still have to do the work yourself. You cannot hide behind the MPH. You have to be productive and even be an overperformer. But it does give you the tools you need, and it can help you get that first job.”
Dr. McCurdy believes a degree such as an MBA can be helpful for today’s hospitalists: “For a hospitalist with a strong interest in rising up through the hospital administrative ranks, having an MBA early in their career could definitely be beneficial,” speculates Dr. McCurdy. “Holding an MBA [in academia] is becoming the norm rather than the exception. There’s an increasing awareness in academics that this is a business.”
Does an advanced degree make a new hospitalist more hirable? “That depends,” says Dr. McCurdy. “For hospitalists working in a large hospital system, it becomes a matter of choice. I don’t think you’d be hired based on an advanced degree [such as a PhD] unless the job has something to do with a scholarly pursuit such as research or teaching. If you’re competing for a job in an academic health science center, a PhD degree can help if it has to do with scholarship.”
The Final Answer
Follow this sound advice: Chart your hospital medicine career path, and then work backward to see whether you’ll benefit from obtaining a specific degree.
“It has to do with what you intend to do in a five- or 10-year timeframe, with the course direction of your career,” says Dr. McCurdy. “If you plan to pursue academic scholarship, a PhD can be very helpful. If you aspire to become medical director at Maryland Shock Trauma, an MBA is the ticket you’re definitely going to need to punch.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Ambitious hospitalists may be eager to add an MBA or a PhD to their credentials, in the belief those magic letters will open doors to leadership positions or higher compensation. But before you fork over tuition for an advanced degree program, consider whether that degree will pay off.
Choose Your Career Path
If you’re considering pursuing a Master of Business Administration (MBA), Master of Public Health (MPH), Master of Health Administration (MPH), or even a doctorate degree, the first thing you should consider is which career path within hospital medicine you’re interested in. What position would you ultimately like to hold? And which, if any, advanced degree can help you get there?
“Explore the idea [of earning an advanced degree], but the most important steps are to try to get some work experience and set some goals,” says Mary Jo Gorman, MD, MBA, the CEO of Advanced ICU Care, St. Louis, Mo. “Along the way, find out what you have an aptitude for.” Once you know your general or specific career goals, you can consider whether to earn an advanced degree.
“It’s a significant monetary and time commitment, so make sure it makes sense for where you want to go,” advises Dr. Gorman. “I’d also advise career counseling to help with this. Great people to talk to are recruiters. They’ll tell you what you need in order to apply for certain positions.”
It should be obvious that some positions will require certain degrees beyond an MD or a DO. Look at the next—or final—job you want. Is the job held by someone with an MBA, a PhD, or another degree? Is that person’s successor likely to need specific education?
“If you want to be the chief operating officer of a hospital, or the CEO of a large medical group, you’re not getting that without an MBA,” Dr. Gorman says. “In fact, if you’re planning to apply for a position that requires strong financial expertise, they’re not going to accept you without [an MBA] unless you’re of a certain age and have a great track record that shows you can do the job.”
On the other hand, many experienced hospitalist leaders don’t have an MBA and won’t need one. “A lot of community-based hospitalists are already doing these things and don’t need the degree,” Dr. Gorman points out. “They created the job, or they created the group.”
A New Way of Thinking
Perhaps the most valuable aspect of any higher degree is the training one receives, which can provide new ways to approach one’s work, problem solving and general thought processes.
“The degree alone won’t help if you haven’t learned while getting it,” explains Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor Veterans Affairs (VA) Medical Center and University of Michigan Medical School. “That’s the real value: Learn the material and it will alter how you approach things.”
Fred A. McCurdy, MD, who holds a PhD and an MBA, was recently promoted from pediatric department chair at Texas Tech University Health Sciences Center at Amarillo to associate dean for faculty development. He earned his MBA with an eye on becoming department chair and says that the MBA program “gave me a background in thought process. From there, I could build on that foundation.”
As for his PhD, Dr. McCurdy says the degree “has its place. The program taught me methodology and scientific process. It taught me how to break down a problem into researchable questions, and I can apply that to areas like education. If your job calls for thinking logically and critically, a PhD gives experience in using scientific methods.”
Earning an MPH also bears fruit.
“Having an MPH is helpful,” says Dr. Saint. “In addition to helping you learn how to research, how to be a better user of literature, it helps prepare someone for taking a leadership role.”
—Sanjay Saint, MD, MPH, hospitalist and professor of internal medicine, Ann Arbor VA Medical Center and University of Michigan Medical School, Ann Arbor
Your Dream Job
While an additional degree can improve your knowledge and skills, it’s no guarantee you’ll move to the top of a list for a promotion or new job.
“It’s not a given that it will necessarily help your career,” warns Dr. Gorman. “You need to first do an analysis about what you want to achieve, then work toward that goal. A lot of doctors don’t really realize that they need to think in terms of their total career plan.”
Dr. Saint agrees, saying of an MPH, “It may open the door, but you still have to walk through it. You still have to do the work yourself. You cannot hide behind the MPH. You have to be productive and even be an overperformer. But it does give you the tools you need, and it can help you get that first job.”
Dr. McCurdy believes a degree such as an MBA can be helpful for today’s hospitalists: “For a hospitalist with a strong interest in rising up through the hospital administrative ranks, having an MBA early in their career could definitely be beneficial,” speculates Dr. McCurdy. “Holding an MBA [in academia] is becoming the norm rather than the exception. There’s an increasing awareness in academics that this is a business.”
Does an advanced degree make a new hospitalist more hirable? “That depends,” says Dr. McCurdy. “For hospitalists working in a large hospital system, it becomes a matter of choice. I don’t think you’d be hired based on an advanced degree [such as a PhD] unless the job has something to do with a scholarly pursuit such as research or teaching. If you’re competing for a job in an academic health science center, a PhD degree can help if it has to do with scholarship.”
The Final Answer
Follow this sound advice: Chart your hospital medicine career path, and then work backward to see whether you’ll benefit from obtaining a specific degree.
“It has to do with what you intend to do in a five- or 10-year timeframe, with the course direction of your career,” says Dr. McCurdy. “If you plan to pursue academic scholarship, a PhD can be very helpful. If you aspire to become medical director at Maryland Shock Trauma, an MBA is the ticket you’re definitely going to need to punch.” TH
Jane Jerrard has been writing for The Hospitalist since 2005.
When Discharge Fails
A significant percentage of patients do not remember or understand the instructions they receive before leaving the hospital, according to a study in this month’s Journal of Hospital Medicine.
“Anyone who’s taken care of patients or put together a discharge plan only to have things not work out knows how frustrating that can be,” says lead author Jonathan Flacker, MD.

Dr. Flacker, assistant professor of medicine in the Division of Geriatric Medicine and Gerontology, Emory University School of Medicine, Atlanta, and coauthors Wansoo Park, PhD, and Addie Sims, MSW, surveyed a group of elderly patients shortly after discharge to determine their recall and comprehension of their pre-discharge instructions. Dr. Park is an assistant professor of social work at the University of Windsor in Ontario, Canada. Dr. Sims is director of Senior Services at Grady Health System in Atlanta.
They conducted telephone interviews with 269 patients 70 or older, or their caregivers, within 10 days of discharge from Grady Memorial Hospital in Atlanta. Most interviews were conducted within a mean of three days of discharge and lasted 20 to 30 minutes. No effort was made to determine the patients’ cognitive status or degree of health literacy.
The survey was an offshoot of Aging Atlanta, a project funded by the Robert Wood Johnson Foundation to study the overall care of older adults in the community. It asked 37 questions covering patients’ financial resources and activities of daily living as well as the nature of their discharge instructions.
The authors found the survey “feasible and easily administered,” but its results were somewhat discouraging. In 52% of the cases, respondents claimed no one spoke to them prior to discharge about caring for themselves at home. Almost as many (47%) says they were not given a phone number or the name of a person to call if they experienced problems at home. “Yet the number was on the discharge papers; 100% of the people received it,” says Dr. Flacker.
Also, 41% says they were not told what to do if they experienced problems at home. On a more positive note, only 13% of the patients had to call concerning problems, and 84% felt they had received enough help after returning home.
Of the 115 (43%) patients who said the received instructions prior to discharge, 103 (90%) remembered how they were delivered: verbally in 68 cases (63%), written in 11 cases (11%), and both ways in 24 cases (23%).
“Patients receiving instructions both verbally and in writing were more likely to report that they understood care instruction ‘very well’ versus ‘somewhat’ or ‘very little,’ ” the authors wrote. Of those who recalled being instructed on how to take their medication, 86% says they took their medicine correctly, compared with 62% who had no such recollection.
To those who can’t understand how someone might completely forget receiving discharge instructions, Dr. Flacker suggests thinking back to the first day of residency or medical school when “you’re handed a whole pile of stuff” while trying to acclimate to unfamiliar surroundings. “Add to that being uncomfortable, sick, and uncertain about the future, and a lot of what is said goes untransferred,” he says.
In an elderly population, cognitive status and poor health literacy are certainly important potential confounders, but “based on my experience, our results are not a whole lot different than those of other investigators who accounted for those factors,” says Dr. Flacker.
These findings suggest that merely transmitting information is not sufficient. Some follow-up is needed to ensure that patients understand the information as their healthcare providers intend, Dr. Flacker and his colleagues wrote. Anything less might violate the spirit of Joint Commission on Accreditation of Healthcare Organization (JCAHO) standards requiring the clear and routine provision of information to patients.
Because of this study, Grady has revised its discharge sheet so information concerning telephone numbers, medication, and other important details are displayed more prominently. The hospital has retrained its nurses to deliver the information more effectively. Follow-up studies will assess how these changes affect patient comprehension and outcomes.
If hospitalists perceive their responsibility to the patient ending not at hospital discharge, but when the patient resumes seeing his or her primary care physician, then “their job is to ensure that the patient understands the discharge instructions,” Dr. Flacker points out.
He suggests they have a social worker or other staff member call patients within a few days after discharge to see how they’re doing and nip any problems in the bud. Admittedly, “a lot depends on where you want to put your resources,” he says. Time and budgets can be stretched only so far. Nevertheless, he maintains, “Post discharge contact is a critically important piece of the process.” TH
Norra MacReady is a medical writer based in California.
A significant percentage of patients do not remember or understand the instructions they receive before leaving the hospital, according to a study in this month’s Journal of Hospital Medicine.
“Anyone who’s taken care of patients or put together a discharge plan only to have things not work out knows how frustrating that can be,” says lead author Jonathan Flacker, MD.
Dr. Flacker, assistant professor of medicine in the Division of Geriatric Medicine and Gerontology, Emory University School of Medicine, Atlanta, and coauthors Wansoo Park, PhD, and Addie Sims, MSW, surveyed a group of elderly patients shortly after discharge to determine their recall and comprehension of their pre-discharge instructions. Dr. Park is an assistant professor of social work at the University of Windsor in Ontario, Canada. Dr. Sims is director of Senior Services at Grady Health System in Atlanta.
They conducted telephone interviews with 269 patients 70 or older, or their caregivers, within 10 days of discharge from Grady Memorial Hospital in Atlanta. Most interviews were conducted within a mean of three days of discharge and lasted 20 to 30 minutes. No effort was made to determine the patients’ cognitive status or degree of health literacy.
The survey was an offshoot of Aging Atlanta, a project funded by the Robert Wood Johnson Foundation to study the overall care of older adults in the community. It asked 37 questions covering patients’ financial resources and activities of daily living as well as the nature of their discharge instructions.
The authors found the survey “feasible and easily administered,” but its results were somewhat discouraging. In 52% of the cases, respondents claimed no one spoke to them prior to discharge about caring for themselves at home. Almost as many (47%) says they were not given a phone number or the name of a person to call if they experienced problems at home. “Yet the number was on the discharge papers; 100% of the people received it,” says Dr. Flacker.
Also, 41% says they were not told what to do if they experienced problems at home. On a more positive note, only 13% of the patients had to call concerning problems, and 84% felt they had received enough help after returning home.
Of the 115 (43%) patients who said the received instructions prior to discharge, 103 (90%) remembered how they were delivered: verbally in 68 cases (63%), written in 11 cases (11%), and both ways in 24 cases (23%).
“Patients receiving instructions both verbally and in writing were more likely to report that they understood care instruction ‘very well’ versus ‘somewhat’ or ‘very little,’ ” the authors wrote. Of those who recalled being instructed on how to take their medication, 86% says they took their medicine correctly, compared with 62% who had no such recollection.
To those who can’t understand how someone might completely forget receiving discharge instructions, Dr. Flacker suggests thinking back to the first day of residency or medical school when “you’re handed a whole pile of stuff” while trying to acclimate to unfamiliar surroundings. “Add to that being uncomfortable, sick, and uncertain about the future, and a lot of what is said goes untransferred,” he says.
In an elderly population, cognitive status and poor health literacy are certainly important potential confounders, but “based on my experience, our results are not a whole lot different than those of other investigators who accounted for those factors,” says Dr. Flacker.
These findings suggest that merely transmitting information is not sufficient. Some follow-up is needed to ensure that patients understand the information as their healthcare providers intend, Dr. Flacker and his colleagues wrote. Anything less might violate the spirit of Joint Commission on Accreditation of Healthcare Organization (JCAHO) standards requiring the clear and routine provision of information to patients.
Because of this study, Grady has revised its discharge sheet so information concerning telephone numbers, medication, and other important details are displayed more prominently. The hospital has retrained its nurses to deliver the information more effectively. Follow-up studies will assess how these changes affect patient comprehension and outcomes.
If hospitalists perceive their responsibility to the patient ending not at hospital discharge, but when the patient resumes seeing his or her primary care physician, then “their job is to ensure that the patient understands the discharge instructions,” Dr. Flacker points out.
He suggests they have a social worker or other staff member call patients within a few days after discharge to see how they’re doing and nip any problems in the bud. Admittedly, “a lot depends on where you want to put your resources,” he says. Time and budgets can be stretched only so far. Nevertheless, he maintains, “Post discharge contact is a critically important piece of the process.” TH
Norra MacReady is a medical writer based in California.
A significant percentage of patients do not remember or understand the instructions they receive before leaving the hospital, according to a study in this month’s Journal of Hospital Medicine.
“Anyone who’s taken care of patients or put together a discharge plan only to have things not work out knows how frustrating that can be,” says lead author Jonathan Flacker, MD.
Dr. Flacker, assistant professor of medicine in the Division of Geriatric Medicine and Gerontology, Emory University School of Medicine, Atlanta, and coauthors Wansoo Park, PhD, and Addie Sims, MSW, surveyed a group of elderly patients shortly after discharge to determine their recall and comprehension of their pre-discharge instructions. Dr. Park is an assistant professor of social work at the University of Windsor in Ontario, Canada. Dr. Sims is director of Senior Services at Grady Health System in Atlanta.
They conducted telephone interviews with 269 patients 70 or older, or their caregivers, within 10 days of discharge from Grady Memorial Hospital in Atlanta. Most interviews were conducted within a mean of three days of discharge and lasted 20 to 30 minutes. No effort was made to determine the patients’ cognitive status or degree of health literacy.
The survey was an offshoot of Aging Atlanta, a project funded by the Robert Wood Johnson Foundation to study the overall care of older adults in the community. It asked 37 questions covering patients’ financial resources and activities of daily living as well as the nature of their discharge instructions.
The authors found the survey “feasible and easily administered,” but its results were somewhat discouraging. In 52% of the cases, respondents claimed no one spoke to them prior to discharge about caring for themselves at home. Almost as many (47%) says they were not given a phone number or the name of a person to call if they experienced problems at home. “Yet the number was on the discharge papers; 100% of the people received it,” says Dr. Flacker.
Also, 41% says they were not told what to do if they experienced problems at home. On a more positive note, only 13% of the patients had to call concerning problems, and 84% felt they had received enough help after returning home.
Of the 115 (43%) patients who said the received instructions prior to discharge, 103 (90%) remembered how they were delivered: verbally in 68 cases (63%), written in 11 cases (11%), and both ways in 24 cases (23%).
“Patients receiving instructions both verbally and in writing were more likely to report that they understood care instruction ‘very well’ versus ‘somewhat’ or ‘very little,’ ” the authors wrote. Of those who recalled being instructed on how to take their medication, 86% says they took their medicine correctly, compared with 62% who had no such recollection.
To those who can’t understand how someone might completely forget receiving discharge instructions, Dr. Flacker suggests thinking back to the first day of residency or medical school when “you’re handed a whole pile of stuff” while trying to acclimate to unfamiliar surroundings. “Add to that being uncomfortable, sick, and uncertain about the future, and a lot of what is said goes untransferred,” he says.
In an elderly population, cognitive status and poor health literacy are certainly important potential confounders, but “based on my experience, our results are not a whole lot different than those of other investigators who accounted for those factors,” says Dr. Flacker.
These findings suggest that merely transmitting information is not sufficient. Some follow-up is needed to ensure that patients understand the information as their healthcare providers intend, Dr. Flacker and his colleagues wrote. Anything less might violate the spirit of Joint Commission on Accreditation of Healthcare Organization (JCAHO) standards requiring the clear and routine provision of information to patients.
Because of this study, Grady has revised its discharge sheet so information concerning telephone numbers, medication, and other important details are displayed more prominently. The hospital has retrained its nurses to deliver the information more effectively. Follow-up studies will assess how these changes affect patient comprehension and outcomes.
If hospitalists perceive their responsibility to the patient ending not at hospital discharge, but when the patient resumes seeing his or her primary care physician, then “their job is to ensure that the patient understands the discharge instructions,” Dr. Flacker points out.
He suggests they have a social worker or other staff member call patients within a few days after discharge to see how they’re doing and nip any problems in the bud. Admittedly, “a lot depends on where you want to put your resources,” he says. Time and budgets can be stretched only so far. Nevertheless, he maintains, “Post discharge contact is a critically important piece of the process.” TH
Norra MacReady is a medical writer based in California.
Stress Ulcer Agents
An article published this year in the American Journal of Health-Systems Pharmacy defined stress ulcers as “acute superficial inflammatory lesions of the gastric mucosa induced when an individual is subjected to abnormally high physiologic demands.”1
These stress ulcers are believed to be caused by an imbalance between gastric acid production and the normal physiologic protective mucosal mechanisms in the gastrointestinal (GI) tract. Reduction of blood flow to the gastric mucosa may also lead to ischemic damage to the GI mucosa.
The development of stress ulcers, or stress-related mucosal disease (SRMD), occurs in 75% to 100% of critically ill patients within 24 hours of intensive care unit (ICU) admission. Although bleeding risk has decreased over the years, mortality from stress-related bleeding nears 50%. According a peer-reviewed guideline from the American Society of Health-System Pharmacists (ASHP), indications for SRMD in the ICU setting include:2
- Coagulopathy;
- Mechanical ventilation longer than 48 hours;
- History of GI ulceration or bleeding within one year of the current admission;
- Glasgow Coma score of 10 or less (or if unable to obey simple commands);
- Thermal injury to more than 35% of the body surface area;
- Partial hepatectomy;
- Multiple trauma;
- Transplantation perioperatively in the ICU;
- Spinal cord injury;
- Hepatic failure; and
- Two or more of the following risk factors: sepsis, ICU stay of a week or longer, occult bleeding for more than six days, or high-dose corticosteroids (more than 250 mg a day of hydrocortisone or the equivalent).
Other risk factors for SRMD in ICU patients include multiorgan failure, chronic renal failure, major surgical procedures, shock, and tetraplegia.3,4
Recommended SRMD prophylaxis agents should be institution-based, taking into account the administration route (e.g., functioning GI tract), daily dosing regimens, adverse effect profile, drug interactions, and total costs. Classes that can be used include sucralfate, antacids, H2 receptor antagonists (H2RA), and proton-pump inhibitors (PPIs).
Some patients may prefer the oral route. Some agents can be given in solution or suspension and administered via a nasogastric tube—but be aware of drug interactions. There are limited comparative data for preventing SRMD with these classes. The H2RA and PPI classes of agents are available in intravenous forms, which may be preferable in critically ill patients. However, none of the PPIs are FDA-approved for SRMD prophylaxis.
In the general patient population, SRMD prophylaxis with H2RAs or PPIs is common in 30% to 50% of patients without clear evidence of benefit. Qadeer, et al., identified a 0.4% bleeding rate in their retrospective case-control study of nearly 18,000 patients over a four-year period. In their study, the key risk factor for development of nosocomial GI bleeding was treatment with full-dose anticoagulation or clopidogrel.
Another concern they identified is that when a patient commences an SRMD prophylaxis agent in the hospital, they continue on it post-discharge when it is not needed. This creates an unnecessary cost burden and risks adverse drug interactions.
Todd Janicki, MD, and Scott Stewart, MD, both with the department of medicine at the State University of New York at Buffalo, this year reported on a review of evidence for SRMD prophylaxis in general medicine patients from the peer-reviewed literature.5 They found limited data, identifying only five citations meeting their evaluation criteria. Two of these studies noted only a 3% to 6% reduction in clinically significant bleeding utilizing SRMD prophylaxis. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
New Indications
![]()
Its other FDA-approved uses:
- Prophylaxis of DVT (which may lead to PE) in patients undergoing hip replacement surgery;
- Prophylaxis of DVT in patients undergoing abdominal surgery who are at risk for thromboembolic (TE) complications;
- Prophylaxis of DVT in patients who are at-risk for TE complications due to severely restricted mobility during acute illness; and
- Prophylaxis of ischemic complications due to unstable angina and non-Q-wave myocardial infarction (MI) when used along with aspirin.
Lovenox is now also indicated for treatment of patients with acute ST-segment elevation MI (STEMI), managed medically or with subsequent percutaneous coronary intervention (PCI).
Its other FDA-approved uses:
- Prophylaxis of DVT in abdominal surgery;
- Prophylaxis of DVT in hip replacement surgery;
- Prophylaxis of DVT in knee replacement surgery;
- Prophylaxis of DVT in medical patients with severely restricted mobility during acute illness;
- Inpatient treatment of acute DVT with or without PE;
- Outpatient treatment of acute DVT without PE; and
- Prophylaxis of ischemic complication of unstable angina and non-Q-wave STEMI managed medically or with subsequent PCI.
References
- Grube RRA, May DB. Stress ulcer prophylaxis in hospitalized patients not in intensive care units. Am J Health-Syst Pharm. 2007;64:1396-400.
- ASHP Commission on Therapeutics. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health-Syst Pharm. 1999;56:347-379.
- Qadeer MA, Richter JE, Brotman DJ. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1(1):13-20.
- Weinhouse GL, Manaker S. Stress ulcer prophylaxis in the intensive care unit. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass. 2007.
- Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2(2):86-92.
An article published this year in the American Journal of Health-Systems Pharmacy defined stress ulcers as “acute superficial inflammatory lesions of the gastric mucosa induced when an individual is subjected to abnormally high physiologic demands.”1
These stress ulcers are believed to be caused by an imbalance between gastric acid production and the normal physiologic protective mucosal mechanisms in the gastrointestinal (GI) tract. Reduction of blood flow to the gastric mucosa may also lead to ischemic damage to the GI mucosa.
The development of stress ulcers, or stress-related mucosal disease (SRMD), occurs in 75% to 100% of critically ill patients within 24 hours of intensive care unit (ICU) admission. Although bleeding risk has decreased over the years, mortality from stress-related bleeding nears 50%. According a peer-reviewed guideline from the American Society of Health-System Pharmacists (ASHP), indications for SRMD in the ICU setting include:2
- Coagulopathy;
- Mechanical ventilation longer than 48 hours;
- History of GI ulceration or bleeding within one year of the current admission;
- Glasgow Coma score of 10 or less (or if unable to obey simple commands);
- Thermal injury to more than 35% of the body surface area;
- Partial hepatectomy;
- Multiple trauma;
- Transplantation perioperatively in the ICU;
- Spinal cord injury;
- Hepatic failure; and
- Two or more of the following risk factors: sepsis, ICU stay of a week or longer, occult bleeding for more than six days, or high-dose corticosteroids (more than 250 mg a day of hydrocortisone or the equivalent).
Other risk factors for SRMD in ICU patients include multiorgan failure, chronic renal failure, major surgical procedures, shock, and tetraplegia.3,4
Recommended SRMD prophylaxis agents should be institution-based, taking into account the administration route (e.g., functioning GI tract), daily dosing regimens, adverse effect profile, drug interactions, and total costs. Classes that can be used include sucralfate, antacids, H2 receptor antagonists (H2RA), and proton-pump inhibitors (PPIs).
Some patients may prefer the oral route. Some agents can be given in solution or suspension and administered via a nasogastric tube—but be aware of drug interactions. There are limited comparative data for preventing SRMD with these classes. The H2RA and PPI classes of agents are available in intravenous forms, which may be preferable in critically ill patients. However, none of the PPIs are FDA-approved for SRMD prophylaxis.
In the general patient population, SRMD prophylaxis with H2RAs or PPIs is common in 30% to 50% of patients without clear evidence of benefit. Qadeer, et al., identified a 0.4% bleeding rate in their retrospective case-control study of nearly 18,000 patients over a four-year period. In their study, the key risk factor for development of nosocomial GI bleeding was treatment with full-dose anticoagulation or clopidogrel.
Another concern they identified is that when a patient commences an SRMD prophylaxis agent in the hospital, they continue on it post-discharge when it is not needed. This creates an unnecessary cost burden and risks adverse drug interactions.
Todd Janicki, MD, and Scott Stewart, MD, both with the department of medicine at the State University of New York at Buffalo, this year reported on a review of evidence for SRMD prophylaxis in general medicine patients from the peer-reviewed literature.5 They found limited data, identifying only five citations meeting their evaluation criteria. Two of these studies noted only a 3% to 6% reduction in clinically significant bleeding utilizing SRMD prophylaxis. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
New Indications
![]()
Its other FDA-approved uses:
- Prophylaxis of DVT (which may lead to PE) in patients undergoing hip replacement surgery;
- Prophylaxis of DVT in patients undergoing abdominal surgery who are at risk for thromboembolic (TE) complications;
- Prophylaxis of DVT in patients who are at-risk for TE complications due to severely restricted mobility during acute illness; and
- Prophylaxis of ischemic complications due to unstable angina and non-Q-wave myocardial infarction (MI) when used along with aspirin.
Lovenox is now also indicated for treatment of patients with acute ST-segment elevation MI (STEMI), managed medically or with subsequent percutaneous coronary intervention (PCI).
Its other FDA-approved uses:
- Prophylaxis of DVT in abdominal surgery;
- Prophylaxis of DVT in hip replacement surgery;
- Prophylaxis of DVT in knee replacement surgery;
- Prophylaxis of DVT in medical patients with severely restricted mobility during acute illness;
- Inpatient treatment of acute DVT with or without PE;
- Outpatient treatment of acute DVT without PE; and
- Prophylaxis of ischemic complication of unstable angina and non-Q-wave STEMI managed medically or with subsequent PCI.
References
- Grube RRA, May DB. Stress ulcer prophylaxis in hospitalized patients not in intensive care units. Am J Health-Syst Pharm. 2007;64:1396-400.
- ASHP Commission on Therapeutics. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health-Syst Pharm. 1999;56:347-379.
- Qadeer MA, Richter JE, Brotman DJ. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1(1):13-20.
- Weinhouse GL, Manaker S. Stress ulcer prophylaxis in the intensive care unit. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass. 2007.
- Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2(2):86-92.
An article published this year in the American Journal of Health-Systems Pharmacy defined stress ulcers as “acute superficial inflammatory lesions of the gastric mucosa induced when an individual is subjected to abnormally high physiologic demands.”1
These stress ulcers are believed to be caused by an imbalance between gastric acid production and the normal physiologic protective mucosal mechanisms in the gastrointestinal (GI) tract. Reduction of blood flow to the gastric mucosa may also lead to ischemic damage to the GI mucosa.
The development of stress ulcers, or stress-related mucosal disease (SRMD), occurs in 75% to 100% of critically ill patients within 24 hours of intensive care unit (ICU) admission. Although bleeding risk has decreased over the years, mortality from stress-related bleeding nears 50%. According a peer-reviewed guideline from the American Society of Health-System Pharmacists (ASHP), indications for SRMD in the ICU setting include:2
- Coagulopathy;
- Mechanical ventilation longer than 48 hours;
- History of GI ulceration or bleeding within one year of the current admission;
- Glasgow Coma score of 10 or less (or if unable to obey simple commands);
- Thermal injury to more than 35% of the body surface area;
- Partial hepatectomy;
- Multiple trauma;
- Transplantation perioperatively in the ICU;
- Spinal cord injury;
- Hepatic failure; and
- Two or more of the following risk factors: sepsis, ICU stay of a week or longer, occult bleeding for more than six days, or high-dose corticosteroids (more than 250 mg a day of hydrocortisone or the equivalent).
Other risk factors for SRMD in ICU patients include multiorgan failure, chronic renal failure, major surgical procedures, shock, and tetraplegia.3,4
Recommended SRMD prophylaxis agents should be institution-based, taking into account the administration route (e.g., functioning GI tract), daily dosing regimens, adverse effect profile, drug interactions, and total costs. Classes that can be used include sucralfate, antacids, H2 receptor antagonists (H2RA), and proton-pump inhibitors (PPIs).
Some patients may prefer the oral route. Some agents can be given in solution or suspension and administered via a nasogastric tube—but be aware of drug interactions. There are limited comparative data for preventing SRMD with these classes. The H2RA and PPI classes of agents are available in intravenous forms, which may be preferable in critically ill patients. However, none of the PPIs are FDA-approved for SRMD prophylaxis.
In the general patient population, SRMD prophylaxis with H2RAs or PPIs is common in 30% to 50% of patients without clear evidence of benefit. Qadeer, et al., identified a 0.4% bleeding rate in their retrospective case-control study of nearly 18,000 patients over a four-year period. In their study, the key risk factor for development of nosocomial GI bleeding was treatment with full-dose anticoagulation or clopidogrel.
Another concern they identified is that when a patient commences an SRMD prophylaxis agent in the hospital, they continue on it post-discharge when it is not needed. This creates an unnecessary cost burden and risks adverse drug interactions.
Todd Janicki, MD, and Scott Stewart, MD, both with the department of medicine at the State University of New York at Buffalo, this year reported on a review of evidence for SRMD prophylaxis in general medicine patients from the peer-reviewed literature.5 They found limited data, identifying only five citations meeting their evaluation criteria. Two of these studies noted only a 3% to 6% reduction in clinically significant bleeding utilizing SRMD prophylaxis. TH
Michele Kaufman is a clinical/managed care consultant and medical writer based in New York City.
New Indications
![]()
Its other FDA-approved uses:
- Prophylaxis of DVT (which may lead to PE) in patients undergoing hip replacement surgery;
- Prophylaxis of DVT in patients undergoing abdominal surgery who are at risk for thromboembolic (TE) complications;
- Prophylaxis of DVT in patients who are at-risk for TE complications due to severely restricted mobility during acute illness; and
- Prophylaxis of ischemic complications due to unstable angina and non-Q-wave myocardial infarction (MI) when used along with aspirin.
Lovenox is now also indicated for treatment of patients with acute ST-segment elevation MI (STEMI), managed medically or with subsequent percutaneous coronary intervention (PCI).
Its other FDA-approved uses:
- Prophylaxis of DVT in abdominal surgery;
- Prophylaxis of DVT in hip replacement surgery;
- Prophylaxis of DVT in knee replacement surgery;
- Prophylaxis of DVT in medical patients with severely restricted mobility during acute illness;
- Inpatient treatment of acute DVT with or without PE;
- Outpatient treatment of acute DVT without PE; and
- Prophylaxis of ischemic complication of unstable angina and non-Q-wave STEMI managed medically or with subsequent PCI.
References
- Grube RRA, May DB. Stress ulcer prophylaxis in hospitalized patients not in intensive care units. Am J Health-Syst Pharm. 2007;64:1396-400.
- ASHP Commission on Therapeutics. ASHP therapeutic guidelines on stress ulcer prophylaxis. Am J Health-Syst Pharm. 1999;56:347-379.
- Qadeer MA, Richter JE, Brotman DJ. Hospital-acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006;1(1):13-20.
- Weinhouse GL, Manaker S. Stress ulcer prophylaxis in the intensive care unit. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass. 2007.
- Janicki T, Stewart S. Stress-ulcer prophylaxis for general medical patients: a review of the evidence. J Hosp Med. 2007;2(2):86-92.