User login
In the Literature
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
Mission in D.C.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana

Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at [email protected].
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at [email protected].
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at [email protected].
How prenatal genetic testing protects patients—and you
CASE 1 ObGyn fails to scrutinize test results
A woman consulted board-certified ObGyns during the first trimester of her pregnancy and informed one of them that she had recently been given a diagnosis of measles, but was unsure whether the illness was German (rubella virus) measles. The physician examined her and ordered a rubella titer. The results, he noted, “were indicative of past infection.” Instead of performing further testing, he told the patient she “had nothing to worry about because she had become immune to German measles as a child.”1
Soon after birth, her child was diagnosed as suffering from congenital rubella syndrome, including eye lesions, heart disease, and auditory defects.1
Apparently, the physician had failed to consider whether the positive test result was indicative of current, rather than past, infection—and failed to perform further testing to determine whether the titer was falling, stable, or rising.
Is he legally liable for this omission?
The physician in this case violated a simple tenet: If a test is ordered, the clinician must be able to interpret the results or order further testing to ensure that the patient is given valid advice. This physician’s error was compounded by the fact that the patient had notified him of the potential for fetal injury.
Would he be held accountable in a court of law?
The answer to that question depends on:
- the state in which the case arose, and the laws in effect at the time of the incident
- the action initiated by the plaintiff and her attorneys, which may involve “wrongful birth,” “wrongful life,” or other allegation
- the time that transpires between the genetic test (or diagnostic test, such as a rubella titer) and the legal case—in other words, the statute of limitations. In some cases, this period encompasses the time elapsed between omission of a test (or birth of a child) and the filing of a legal claim.
For the purposes of this article, I assume that the facts in the judicial opinion are correct, but focus on legal principle.
Patient testing: ethical issues in selection and counseling. ACOG Committee Opinion No. 363. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2007;109:1021–1023.
Knowledge can be a dangerous thing. At the very least, a bid for genetic data requires careful consideration and preparation, particularly when the information may determine whether a woman continues or terminates her pregnancy.
In April, the American College of Obstetricians and Gynecologists published a Committee Opinion on ethical considerations in the selection and counseling of patients in regard to testing. Although the opinion concerns testing in general—rather than prenatal genetic testing specifically—a number of recommendations are applicable to both:
- Perform testing for the benefit of the patient, not simply because a third party—e.g., her partner, extended family, employer, insurer, or health-care provider—deems it to be necessary. Ensure that she gives consent before proceeding.
- Do not base testing decisions on assumptions about how the patient will respond. “Prejudgments about a patient’s wishes regarding fetal abnormalities, for example, should not preclude her being offered prenatal testing,” the opinion states.
- Tell the patient how the results will be communicated, and to whom.
- Provide or refer the patient for specific counseling whenever planned testing may have multiple medical or psychological implications.
- Respect the patient’s autonomy and involve her in decision-making. If she elects to forego a recommended test, document her refusal in the medical record—and include the reason.
Detectable genetic disorders have increased exponentially
Almost any health-care provider encounters patients who have inheritable disease. Cases have arisen against an oncologist for failure to convey to the patient the potential for genetic transmission of colonic polyposis and against a surgeon for failing to warn a young breast cancer patient that she may carry genes that predispose her offspring to ovarian cancer. But the highest-risk category is reserved for the obstetrician, who must, on a daily basis, consider the need for appropriate screening and proper counseling about the availability of genetic testing that may enable the patient to avoid passing catastrophic disease to her children.
This responsibility is complicated by a dramatic increase in the number of genetic tests. Few areas of medical practice have expanded as rapidly as prenatal genetic testing and counseling. Forty years ago, an obstetrician—or even a nurse—might have discussed the risks of pregnancy at an advanced age, as well as a few possible genetic abnormalities. Today, certified genetic counselors are employed by many clinics and even private practices, and more than 1,000 disorders—as many as 1,300, by some reports—can be detected by the proper test.
Although most of these disorders are uncommon, several dozen or so are more prevalent and, therefore, regularly tested for. They include cystic fibrosis, Down syndrome, and neural tube defects, as well as diseases associated with certain religious, racial, or ethnic groups, such as thalassemia (Mediterranean, Asian, or African heritage), Tay-Sachs (Eastern European or Ashkenazi Jewish descent), and sickle cell disease (African-American ancestry).
Ethical complexity makes resolution difficult
Legal actions are bound to increase as technology evolves, particularly when a child is born with a genetically transmissible disorder that could have been identified with proper counseling and testing. These legal actions are particularly difficult to resolve because they involve complex ethical issues. For example, in “wrongful birth” actions, the parents often allege that they would not have conceived a child if they had known that it might be afflicted with a certain trait or illness, or that they would have terminated the pregnancy if they had learned of the disorder in a timely fashion.
In most of these cases, the plaintiffs are the parents. In a few states, however, successful actions have been brought by the child (“wrongful life”), who, some contend, essentially claims that nonexistence would be better than life with a serious congenital condition. They usually seek the extraordinary expense associated with the condition, as well as other damages.
Similar actions have been brought by children, and parents of children, with acquired conditions such as congenital rubella syndrome, as in the opening case. In that scenario, the parents’ case was declined by attorneys because their state of residence did not allow actions for wrongful birth or wrongful life. The state courts subsequently changed the law to allow wrongful birth actions, but by the time the parents learned of the change in the law, the statute of limitations had expired. They therefore added the attorneys as defendants, alleging that they failed to recall the parents when the law changed, in time to file their lawsuit. By the time the case finally reached the state’s supreme court, the law had changed again, and the child was allowed to proceed with a wrongful life action.
CASE 2 Physician mistakes patient’s tissue for fetus’s
Before becoming pregnant, a woman experienced several medical problems that prompted her and her husband to seek genetic testing and counseling. Testing revealed that she had a balanced translocation of chromosomes 11 and 22.2
After conceiving, the woman underwent chorionic villus sampling, which indicated that the fetus was probably a female with the same chromosomal condition as the mother—therefore, she would develop normally. The mother also underwent several ultrasonographic tests to rule out fetal abnormalities and was told that imaging showed a normally developing fetus.
The woman went on to deliver a boy, and genetic testing revealed that he had trisomy 22, with severe, permanent disabilities.2 The parents sued.
Were the woman’s health-care providers liable?
This case prompts a number of questions:
- Did the physicians seek confirmation that the tissue studied was fetal?
- Did they counsel the parents about the possibility that maternal genetic material might be recovered during sampling? If so, did they consider that possibility when the specimen was identical to the mother’s?
- How is it possible that, on subsequent ultrasonographic evaluations, the male sex of the fetus was not noted? If it was noted, did it register with the providers that the result was inconsistent with the genetic studies?
Despite the dismissal, which was a favorable turn of events for the physicians, they almost certainly lost substantial work time and experienced the emotional roller-coaster ride that accompanies being sued—not to mention the revelation that they may have harmed a patient.
CASE 3 Physician fails to complete testing
The mother of a developmentally delayed daughter delivered another child. Before she conceived, however, she and her husband consulted a physician (a pediatrician) to find out whether there was a genetic reason for the daughter’s developmental delay and the mental retardation of another child, the girl’s half-brother.3 The physician wrote in her notes: “? Chromosomes + fragile X” to indicate testing planned for the daughter.
The testing was performed at a medical center and reported to be normal. The physician relayed this finding to the parents, but failed to mention that fragile X testing had not been conducted. Because they had discussed fragile X testing during the initial consultation, the mother assumed it had been performed and was included in the normal results.3
The latest child was also developmentally delayed, and subsequent testing revealed that all three children were positive for fragile X syndrome. The parents sued, alleging that the physician was negligent for failing to perform the genetic test, and claiming that they would not have conceived another child if they had known of the daughter’s fragile X status.
Are their claims reasonable?
Despite a state statute that prohibited wrongful birth and wrongful life actions that allege that the pregnancy would have been terminated if the parents had known of the genetic impairment, the state supreme court allowed this case to proceed because the issue was whether the mother would have avoided conception. The plaintiffs also argued that the claim did not exceed the statute of limitations. Their reasoning: Although the medical care had been provided more than 4 years earlier (the limitation period), the injury did not occur (i.e., action did not “accrue”) until conception of the child.
Perhaps most telling was the court’s statement that, “[O]ur decision today is informed by the practical reality of the field of genetic testing and counseling; genetic testing and diagnosis [do] not affect only the patient. Both the patient and her family can benefit from accurate testing and diagnosis. And, conversely, both the patient and her family can be harmed by negligent testing and diagnosis.”3
Establishing degree of harm is especially difficult
As you might imagine, allegations involving potential pregnancy termination arouse intense emotions on both sides of the abortion debate. The determination of damages is equally contentious. Among the issues that may arise at the time of trial:
- How much is a parent harmed by the birth of a child with hereditary disease?
- Should damages be offset by the benefit of having any child, even if the child is not “normal”?
- How do you measure the value of a life with Down syndrome, for example, compared with no life at all?
- Should damages include the cost of raising the child, including additional medical expenses, which can be substantial?
Assigning blame for genetic disease is difficult
The arguments in cases involving genetic testing often differ from those made when a fetus sustains injury. In the latter, the injury may be caused by the provider—e.g., after administration of a cytotoxic drug during pregnancy or because of induction of labor at a seriously miscalculated gestational age. Legal actions associated with such injury are widely accepted.
In cases involving genetic counseling, however, the disease is not caused by the practitioner. Rather, the plaintiff alleges that the affected child was born because the provider failed to:
- properly counsel the patient not to conceive
- offer the parents the option of terminating the pregnancy or
- successfully prevent or terminate a pregnancy.
It would be unwise to base one’s conduct on existing law, which is unpredictable. The law can change if a judge determines that a prior opinion was incorrect, a statute was unconstitutional, or a particular injury justifies compensation. Legislative bodies also can change with an election, and the statutes can be amended. The best strategy for you to deal with this uncertainty? Provide comprehensive prenatal care of the highest quality.
Lessons learned
Among the lessons to be gleaned from these cases are:
- Be sure that you understand the limits of any test that you order, and convey those limits to the patient.
- When you inform a patient about a planned test, that test should be completed. If it is not, explain the failure to perform the test (or the lost result, etc.) to the patient so that she can act accordingly. In that regard, a laboratory or other facility can be held liable for a negligently performed test or, as was the case in one lawsuit, a sperm bank may be liable for failing to inform the recipient of donor sperm that the donor had a positive family history of renal disease (i.e., autosomal-dominant polycystic kidney disease).5
- Be aware that, as the amount of information available in the popular literature and on the Web expands, patients will come to question their care more often. An example: A patient recently brought an action against her health-care provider because vitamins containing folate were discontinued shortly before she became pregnant, and the child was born with a neural tube defect.6
- Most court cases, including those cited in this article, are based on the credibility of witnesses recollecting events. Well-documented, legible records written contemporaneously with an event are of enormous benefit in cases involving sometimes widely divergent recollections. When health care meets appropriate standards and is well documented in the records, most plaintiffs’ attorneys will not undertake what can be protracted and expensive litigation. When they do, the health-care provider usually prevails.
Aubrey Milunsky, MD, DSc, DCH
The standard of expected care in clinical genetics is generally the same across most medical specialties. That standard is compounded in obstetrics, however, by critical considerations in three areas in the spectrum of care: future conception, ongoing pregnancy, and postnatal implications. Although guidelines and committee opinions on genetics-related care that are issued by professional societies, such as ACOG, are important in practice, they do not, in fact, set the actual standard of expected care—as those issuing bodies have emphasized in their statements.
Mostly, it is expert opinion that informs a jury about the standard of expected care in genetics. And, ultimately, any action (or inaction) taken by a jury is judged according to what the average, prudent physician would do under the circumstances in question.
Errors tend to be basic
Medical negligence claims relative to genetics in obstetrical practice are usually not a complex matter of failure—for example, failing to diagnose an isodicentric chromosome, misinterpreting a copy number genome variation, mistaking a gene polymorphism as a disease-causing mutation, and failing to order a micro-deletion analysis when a gene sequence is reportedly normal. Rather, errors are usually basic and, invariably, not single; often they result in serious consequences. Space allows only a few, brief (and arbitrary) examples here of where pitfalls can be found:
- genetic counseling
- laboratory interactions
- group practice
- knowledge of practical genetics.
Genetic counseling Simple but critical matters in this area of office practice include taking a family history and not ignoring potential implications in that history of mental retardation, congenital malformations, genetic disorders, specific cancers, and ethnicity. These clues should alert you to offer diagnostic or carrier tests or to refer the patient for a genetics consultation.
Some OBs have the benefit of genetic counselors in their practice, but fail to realize that these members of the staff, albeit very valuable, are not the full and final repository of knowledge about genetic disease. Failure to offer a test, failure to refer for a genetics consultation, and failure to provide accurate information on risk and recurrence all invite litigation.
Laboratory interactions Errors by the office clinician abound in this area. They include failure to obtain the result of a lab test, to provide timely communication, to order the correct test, and to advise the lab about the specific indication for the test (such as a subtle translocation) and misinterpretation of a test result.
Group practice brings with it much benefit but significant risk, too. Assuming that one of your colleagues checked a lab result or communicated important information, without you—personally—having checked the record or obtained the result, can lead to catastrophe. Exercise great care, therefore, in overseeing how lab reports return to the office; who sees them; how, and by whom, they are filed; who is informed, and how, about an abnormal report; and what type of documentation the practice insists upon. Suffice it to say: This territory is replete with litigation.
Knowledge of practical genetics requires your continual learning. Failure to realize (or determine) that a disorder or defect is genetic inevitably raises problems. A lack of awareness of basic advances in medicine—such as preconception folic acid supplementation that provides 70% protection against a neural tube defect—may come to light only after a child is born with spina bifida.
Seek support in your work
Obstetrical practice is exciting and gratifying, but it is ever more challenging in light of the dramatic and continuing advances in human genetics. It is impossible for a busy clinician to keep up with the massive torrent of new information on genetic disease. When possible, establishing linkage—even by telephone—with a clinical genetics group could provide you with the opportunity to practice within the standard of expected care, and without unnecessary anxiety.
Dr. Milunsky is Professor of Human Genetics, Pediatrics, Pathology and Obstetrics and Gynecology, and Director, Center for Human Genetics, Boston University School of Medicine, Boston, Mass. He reports no financial relationships relevant to this article.
1. Procanik by Procanik v Cillo, 97 NJ 339 (1984) 478 A2d 755.
2. Schirmer v Mt. Auburn Obstetrics & Gynecology, 108 Ohio St3d 494 (2006) 2006-Ohio-942, 844 NE2d 1160.
3. Malloy v Meier, 679 NW2d 711 (Minn 2004).
4. A recent summary by a state supreme court reveals the position of various states on wrongful life actions: 27 states have refused to recognize actions by the child by court ruling or statute, or both, while three states do allow them. Willis v Wu, 362 SC 146 (2004), 607 SE2d 63.
5. Johnson v Superior Court, Los Angeles County, 101 Cal App 4th 869 (2002).
6. Brown v US, 462 F3d 609 (6th Cir 2006).
CASE 1 ObGyn fails to scrutinize test results
A woman consulted board-certified ObGyns during the first trimester of her pregnancy and informed one of them that she had recently been given a diagnosis of measles, but was unsure whether the illness was German (rubella virus) measles. The physician examined her and ordered a rubella titer. The results, he noted, “were indicative of past infection.” Instead of performing further testing, he told the patient she “had nothing to worry about because she had become immune to German measles as a child.”1
Soon after birth, her child was diagnosed as suffering from congenital rubella syndrome, including eye lesions, heart disease, and auditory defects.1
Apparently, the physician had failed to consider whether the positive test result was indicative of current, rather than past, infection—and failed to perform further testing to determine whether the titer was falling, stable, or rising.
Is he legally liable for this omission?
The physician in this case violated a simple tenet: If a test is ordered, the clinician must be able to interpret the results or order further testing to ensure that the patient is given valid advice. This physician’s error was compounded by the fact that the patient had notified him of the potential for fetal injury.
Would he be held accountable in a court of law?
The answer to that question depends on:
- the state in which the case arose, and the laws in effect at the time of the incident
- the action initiated by the plaintiff and her attorneys, which may involve “wrongful birth,” “wrongful life,” or other allegation
- the time that transpires between the genetic test (or diagnostic test, such as a rubella titer) and the legal case—in other words, the statute of limitations. In some cases, this period encompasses the time elapsed between omission of a test (or birth of a child) and the filing of a legal claim.
For the purposes of this article, I assume that the facts in the judicial opinion are correct, but focus on legal principle.
Patient testing: ethical issues in selection and counseling. ACOG Committee Opinion No. 363. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2007;109:1021–1023.
Knowledge can be a dangerous thing. At the very least, a bid for genetic data requires careful consideration and preparation, particularly when the information may determine whether a woman continues or terminates her pregnancy.
In April, the American College of Obstetricians and Gynecologists published a Committee Opinion on ethical considerations in the selection and counseling of patients in regard to testing. Although the opinion concerns testing in general—rather than prenatal genetic testing specifically—a number of recommendations are applicable to both:
- Perform testing for the benefit of the patient, not simply because a third party—e.g., her partner, extended family, employer, insurer, or health-care provider—deems it to be necessary. Ensure that she gives consent before proceeding.
- Do not base testing decisions on assumptions about how the patient will respond. “Prejudgments about a patient’s wishes regarding fetal abnormalities, for example, should not preclude her being offered prenatal testing,” the opinion states.
- Tell the patient how the results will be communicated, and to whom.
- Provide or refer the patient for specific counseling whenever planned testing may have multiple medical or psychological implications.
- Respect the patient’s autonomy and involve her in decision-making. If she elects to forego a recommended test, document her refusal in the medical record—and include the reason.
Detectable genetic disorders have increased exponentially
Almost any health-care provider encounters patients who have inheritable disease. Cases have arisen against an oncologist for failure to convey to the patient the potential for genetic transmission of colonic polyposis and against a surgeon for failing to warn a young breast cancer patient that she may carry genes that predispose her offspring to ovarian cancer. But the highest-risk category is reserved for the obstetrician, who must, on a daily basis, consider the need for appropriate screening and proper counseling about the availability of genetic testing that may enable the patient to avoid passing catastrophic disease to her children.
This responsibility is complicated by a dramatic increase in the number of genetic tests. Few areas of medical practice have expanded as rapidly as prenatal genetic testing and counseling. Forty years ago, an obstetrician—or even a nurse—might have discussed the risks of pregnancy at an advanced age, as well as a few possible genetic abnormalities. Today, certified genetic counselors are employed by many clinics and even private practices, and more than 1,000 disorders—as many as 1,300, by some reports—can be detected by the proper test.
Although most of these disorders are uncommon, several dozen or so are more prevalent and, therefore, regularly tested for. They include cystic fibrosis, Down syndrome, and neural tube defects, as well as diseases associated with certain religious, racial, or ethnic groups, such as thalassemia (Mediterranean, Asian, or African heritage), Tay-Sachs (Eastern European or Ashkenazi Jewish descent), and sickle cell disease (African-American ancestry).
Ethical complexity makes resolution difficult
Legal actions are bound to increase as technology evolves, particularly when a child is born with a genetically transmissible disorder that could have been identified with proper counseling and testing. These legal actions are particularly difficult to resolve because they involve complex ethical issues. For example, in “wrongful birth” actions, the parents often allege that they would not have conceived a child if they had known that it might be afflicted with a certain trait or illness, or that they would have terminated the pregnancy if they had learned of the disorder in a timely fashion.
In most of these cases, the plaintiffs are the parents. In a few states, however, successful actions have been brought by the child (“wrongful life”), who, some contend, essentially claims that nonexistence would be better than life with a serious congenital condition. They usually seek the extraordinary expense associated with the condition, as well as other damages.
Similar actions have been brought by children, and parents of children, with acquired conditions such as congenital rubella syndrome, as in the opening case. In that scenario, the parents’ case was declined by attorneys because their state of residence did not allow actions for wrongful birth or wrongful life. The state courts subsequently changed the law to allow wrongful birth actions, but by the time the parents learned of the change in the law, the statute of limitations had expired. They therefore added the attorneys as defendants, alleging that they failed to recall the parents when the law changed, in time to file their lawsuit. By the time the case finally reached the state’s supreme court, the law had changed again, and the child was allowed to proceed with a wrongful life action.
CASE 2 Physician mistakes patient’s tissue for fetus’s
Before becoming pregnant, a woman experienced several medical problems that prompted her and her husband to seek genetic testing and counseling. Testing revealed that she had a balanced translocation of chromosomes 11 and 22.2
After conceiving, the woman underwent chorionic villus sampling, which indicated that the fetus was probably a female with the same chromosomal condition as the mother—therefore, she would develop normally. The mother also underwent several ultrasonographic tests to rule out fetal abnormalities and was told that imaging showed a normally developing fetus.
The woman went on to deliver a boy, and genetic testing revealed that he had trisomy 22, with severe, permanent disabilities.2 The parents sued.
Were the woman’s health-care providers liable?
This case prompts a number of questions:
- Did the physicians seek confirmation that the tissue studied was fetal?
- Did they counsel the parents about the possibility that maternal genetic material might be recovered during sampling? If so, did they consider that possibility when the specimen was identical to the mother’s?
- How is it possible that, on subsequent ultrasonographic evaluations, the male sex of the fetus was not noted? If it was noted, did it register with the providers that the result was inconsistent with the genetic studies?
Despite the dismissal, which was a favorable turn of events for the physicians, they almost certainly lost substantial work time and experienced the emotional roller-coaster ride that accompanies being sued—not to mention the revelation that they may have harmed a patient.
CASE 3 Physician fails to complete testing
The mother of a developmentally delayed daughter delivered another child. Before she conceived, however, she and her husband consulted a physician (a pediatrician) to find out whether there was a genetic reason for the daughter’s developmental delay and the mental retardation of another child, the girl’s half-brother.3 The physician wrote in her notes: “? Chromosomes + fragile X” to indicate testing planned for the daughter.
The testing was performed at a medical center and reported to be normal. The physician relayed this finding to the parents, but failed to mention that fragile X testing had not been conducted. Because they had discussed fragile X testing during the initial consultation, the mother assumed it had been performed and was included in the normal results.3
The latest child was also developmentally delayed, and subsequent testing revealed that all three children were positive for fragile X syndrome. The parents sued, alleging that the physician was negligent for failing to perform the genetic test, and claiming that they would not have conceived another child if they had known of the daughter’s fragile X status.
Are their claims reasonable?
Despite a state statute that prohibited wrongful birth and wrongful life actions that allege that the pregnancy would have been terminated if the parents had known of the genetic impairment, the state supreme court allowed this case to proceed because the issue was whether the mother would have avoided conception. The plaintiffs also argued that the claim did not exceed the statute of limitations. Their reasoning: Although the medical care had been provided more than 4 years earlier (the limitation period), the injury did not occur (i.e., action did not “accrue”) until conception of the child.
Perhaps most telling was the court’s statement that, “[O]ur decision today is informed by the practical reality of the field of genetic testing and counseling; genetic testing and diagnosis [do] not affect only the patient. Both the patient and her family can benefit from accurate testing and diagnosis. And, conversely, both the patient and her family can be harmed by negligent testing and diagnosis.”3
Establishing degree of harm is especially difficult
As you might imagine, allegations involving potential pregnancy termination arouse intense emotions on both sides of the abortion debate. The determination of damages is equally contentious. Among the issues that may arise at the time of trial:
- How much is a parent harmed by the birth of a child with hereditary disease?
- Should damages be offset by the benefit of having any child, even if the child is not “normal”?
- How do you measure the value of a life with Down syndrome, for example, compared with no life at all?
- Should damages include the cost of raising the child, including additional medical expenses, which can be substantial?
Assigning blame for genetic disease is difficult
The arguments in cases involving genetic testing often differ from those made when a fetus sustains injury. In the latter, the injury may be caused by the provider—e.g., after administration of a cytotoxic drug during pregnancy or because of induction of labor at a seriously miscalculated gestational age. Legal actions associated with such injury are widely accepted.
In cases involving genetic counseling, however, the disease is not caused by the practitioner. Rather, the plaintiff alleges that the affected child was born because the provider failed to:
- properly counsel the patient not to conceive
- offer the parents the option of terminating the pregnancy or
- successfully prevent or terminate a pregnancy.
It would be unwise to base one’s conduct on existing law, which is unpredictable. The law can change if a judge determines that a prior opinion was incorrect, a statute was unconstitutional, or a particular injury justifies compensation. Legislative bodies also can change with an election, and the statutes can be amended. The best strategy for you to deal with this uncertainty? Provide comprehensive prenatal care of the highest quality.
Lessons learned
Among the lessons to be gleaned from these cases are:
- Be sure that you understand the limits of any test that you order, and convey those limits to the patient.
- When you inform a patient about a planned test, that test should be completed. If it is not, explain the failure to perform the test (or the lost result, etc.) to the patient so that she can act accordingly. In that regard, a laboratory or other facility can be held liable for a negligently performed test or, as was the case in one lawsuit, a sperm bank may be liable for failing to inform the recipient of donor sperm that the donor had a positive family history of renal disease (i.e., autosomal-dominant polycystic kidney disease).5
- Be aware that, as the amount of information available in the popular literature and on the Web expands, patients will come to question their care more often. An example: A patient recently brought an action against her health-care provider because vitamins containing folate were discontinued shortly before she became pregnant, and the child was born with a neural tube defect.6
- Most court cases, including those cited in this article, are based on the credibility of witnesses recollecting events. Well-documented, legible records written contemporaneously with an event are of enormous benefit in cases involving sometimes widely divergent recollections. When health care meets appropriate standards and is well documented in the records, most plaintiffs’ attorneys will not undertake what can be protracted and expensive litigation. When they do, the health-care provider usually prevails.
Aubrey Milunsky, MD, DSc, DCH
The standard of expected care in clinical genetics is generally the same across most medical specialties. That standard is compounded in obstetrics, however, by critical considerations in three areas in the spectrum of care: future conception, ongoing pregnancy, and postnatal implications. Although guidelines and committee opinions on genetics-related care that are issued by professional societies, such as ACOG, are important in practice, they do not, in fact, set the actual standard of expected care—as those issuing bodies have emphasized in their statements.
Mostly, it is expert opinion that informs a jury about the standard of expected care in genetics. And, ultimately, any action (or inaction) taken by a jury is judged according to what the average, prudent physician would do under the circumstances in question.
Errors tend to be basic
Medical negligence claims relative to genetics in obstetrical practice are usually not a complex matter of failure—for example, failing to diagnose an isodicentric chromosome, misinterpreting a copy number genome variation, mistaking a gene polymorphism as a disease-causing mutation, and failing to order a micro-deletion analysis when a gene sequence is reportedly normal. Rather, errors are usually basic and, invariably, not single; often they result in serious consequences. Space allows only a few, brief (and arbitrary) examples here of where pitfalls can be found:
- genetic counseling
- laboratory interactions
- group practice
- knowledge of practical genetics.
Genetic counseling Simple but critical matters in this area of office practice include taking a family history and not ignoring potential implications in that history of mental retardation, congenital malformations, genetic disorders, specific cancers, and ethnicity. These clues should alert you to offer diagnostic or carrier tests or to refer the patient for a genetics consultation.
Some OBs have the benefit of genetic counselors in their practice, but fail to realize that these members of the staff, albeit very valuable, are not the full and final repository of knowledge about genetic disease. Failure to offer a test, failure to refer for a genetics consultation, and failure to provide accurate information on risk and recurrence all invite litigation.
Laboratory interactions Errors by the office clinician abound in this area. They include failure to obtain the result of a lab test, to provide timely communication, to order the correct test, and to advise the lab about the specific indication for the test (such as a subtle translocation) and misinterpretation of a test result.
Group practice brings with it much benefit but significant risk, too. Assuming that one of your colleagues checked a lab result or communicated important information, without you—personally—having checked the record or obtained the result, can lead to catastrophe. Exercise great care, therefore, in overseeing how lab reports return to the office; who sees them; how, and by whom, they are filed; who is informed, and how, about an abnormal report; and what type of documentation the practice insists upon. Suffice it to say: This territory is replete with litigation.
Knowledge of practical genetics requires your continual learning. Failure to realize (or determine) that a disorder or defect is genetic inevitably raises problems. A lack of awareness of basic advances in medicine—such as preconception folic acid supplementation that provides 70% protection against a neural tube defect—may come to light only after a child is born with spina bifida.
Seek support in your work
Obstetrical practice is exciting and gratifying, but it is ever more challenging in light of the dramatic and continuing advances in human genetics. It is impossible for a busy clinician to keep up with the massive torrent of new information on genetic disease. When possible, establishing linkage—even by telephone—with a clinical genetics group could provide you with the opportunity to practice within the standard of expected care, and without unnecessary anxiety.
Dr. Milunsky is Professor of Human Genetics, Pediatrics, Pathology and Obstetrics and Gynecology, and Director, Center for Human Genetics, Boston University School of Medicine, Boston, Mass. He reports no financial relationships relevant to this article.
CASE 1 ObGyn fails to scrutinize test results
A woman consulted board-certified ObGyns during the first trimester of her pregnancy and informed one of them that she had recently been given a diagnosis of measles, but was unsure whether the illness was German (rubella virus) measles. The physician examined her and ordered a rubella titer. The results, he noted, “were indicative of past infection.” Instead of performing further testing, he told the patient she “had nothing to worry about because she had become immune to German measles as a child.”1
Soon after birth, her child was diagnosed as suffering from congenital rubella syndrome, including eye lesions, heart disease, and auditory defects.1
Apparently, the physician had failed to consider whether the positive test result was indicative of current, rather than past, infection—and failed to perform further testing to determine whether the titer was falling, stable, or rising.
Is he legally liable for this omission?
The physician in this case violated a simple tenet: If a test is ordered, the clinician must be able to interpret the results or order further testing to ensure that the patient is given valid advice. This physician’s error was compounded by the fact that the patient had notified him of the potential for fetal injury.
Would he be held accountable in a court of law?
The answer to that question depends on:
- the state in which the case arose, and the laws in effect at the time of the incident
- the action initiated by the plaintiff and her attorneys, which may involve “wrongful birth,” “wrongful life,” or other allegation
- the time that transpires between the genetic test (or diagnostic test, such as a rubella titer) and the legal case—in other words, the statute of limitations. In some cases, this period encompasses the time elapsed between omission of a test (or birth of a child) and the filing of a legal claim.
For the purposes of this article, I assume that the facts in the judicial opinion are correct, but focus on legal principle.
Patient testing: ethical issues in selection and counseling. ACOG Committee Opinion No. 363. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2007;109:1021–1023.
Knowledge can be a dangerous thing. At the very least, a bid for genetic data requires careful consideration and preparation, particularly when the information may determine whether a woman continues or terminates her pregnancy.
In April, the American College of Obstetricians and Gynecologists published a Committee Opinion on ethical considerations in the selection and counseling of patients in regard to testing. Although the opinion concerns testing in general—rather than prenatal genetic testing specifically—a number of recommendations are applicable to both:
- Perform testing for the benefit of the patient, not simply because a third party—e.g., her partner, extended family, employer, insurer, or health-care provider—deems it to be necessary. Ensure that she gives consent before proceeding.
- Do not base testing decisions on assumptions about how the patient will respond. “Prejudgments about a patient’s wishes regarding fetal abnormalities, for example, should not preclude her being offered prenatal testing,” the opinion states.
- Tell the patient how the results will be communicated, and to whom.
- Provide or refer the patient for specific counseling whenever planned testing may have multiple medical or psychological implications.
- Respect the patient’s autonomy and involve her in decision-making. If she elects to forego a recommended test, document her refusal in the medical record—and include the reason.
Detectable genetic disorders have increased exponentially
Almost any health-care provider encounters patients who have inheritable disease. Cases have arisen against an oncologist for failure to convey to the patient the potential for genetic transmission of colonic polyposis and against a surgeon for failing to warn a young breast cancer patient that she may carry genes that predispose her offspring to ovarian cancer. But the highest-risk category is reserved for the obstetrician, who must, on a daily basis, consider the need for appropriate screening and proper counseling about the availability of genetic testing that may enable the patient to avoid passing catastrophic disease to her children.
This responsibility is complicated by a dramatic increase in the number of genetic tests. Few areas of medical practice have expanded as rapidly as prenatal genetic testing and counseling. Forty years ago, an obstetrician—or even a nurse—might have discussed the risks of pregnancy at an advanced age, as well as a few possible genetic abnormalities. Today, certified genetic counselors are employed by many clinics and even private practices, and more than 1,000 disorders—as many as 1,300, by some reports—can be detected by the proper test.
Although most of these disorders are uncommon, several dozen or so are more prevalent and, therefore, regularly tested for. They include cystic fibrosis, Down syndrome, and neural tube defects, as well as diseases associated with certain religious, racial, or ethnic groups, such as thalassemia (Mediterranean, Asian, or African heritage), Tay-Sachs (Eastern European or Ashkenazi Jewish descent), and sickle cell disease (African-American ancestry).
Ethical complexity makes resolution difficult
Legal actions are bound to increase as technology evolves, particularly when a child is born with a genetically transmissible disorder that could have been identified with proper counseling and testing. These legal actions are particularly difficult to resolve because they involve complex ethical issues. For example, in “wrongful birth” actions, the parents often allege that they would not have conceived a child if they had known that it might be afflicted with a certain trait or illness, or that they would have terminated the pregnancy if they had learned of the disorder in a timely fashion.
In most of these cases, the plaintiffs are the parents. In a few states, however, successful actions have been brought by the child (“wrongful life”), who, some contend, essentially claims that nonexistence would be better than life with a serious congenital condition. They usually seek the extraordinary expense associated with the condition, as well as other damages.
Similar actions have been brought by children, and parents of children, with acquired conditions such as congenital rubella syndrome, as in the opening case. In that scenario, the parents’ case was declined by attorneys because their state of residence did not allow actions for wrongful birth or wrongful life. The state courts subsequently changed the law to allow wrongful birth actions, but by the time the parents learned of the change in the law, the statute of limitations had expired. They therefore added the attorneys as defendants, alleging that they failed to recall the parents when the law changed, in time to file their lawsuit. By the time the case finally reached the state’s supreme court, the law had changed again, and the child was allowed to proceed with a wrongful life action.
CASE 2 Physician mistakes patient’s tissue for fetus’s
Before becoming pregnant, a woman experienced several medical problems that prompted her and her husband to seek genetic testing and counseling. Testing revealed that she had a balanced translocation of chromosomes 11 and 22.2
After conceiving, the woman underwent chorionic villus sampling, which indicated that the fetus was probably a female with the same chromosomal condition as the mother—therefore, she would develop normally. The mother also underwent several ultrasonographic tests to rule out fetal abnormalities and was told that imaging showed a normally developing fetus.
The woman went on to deliver a boy, and genetic testing revealed that he had trisomy 22, with severe, permanent disabilities.2 The parents sued.
Were the woman’s health-care providers liable?
This case prompts a number of questions:
- Did the physicians seek confirmation that the tissue studied was fetal?
- Did they counsel the parents about the possibility that maternal genetic material might be recovered during sampling? If so, did they consider that possibility when the specimen was identical to the mother’s?
- How is it possible that, on subsequent ultrasonographic evaluations, the male sex of the fetus was not noted? If it was noted, did it register with the providers that the result was inconsistent with the genetic studies?
Despite the dismissal, which was a favorable turn of events for the physicians, they almost certainly lost substantial work time and experienced the emotional roller-coaster ride that accompanies being sued—not to mention the revelation that they may have harmed a patient.
CASE 3 Physician fails to complete testing
The mother of a developmentally delayed daughter delivered another child. Before she conceived, however, she and her husband consulted a physician (a pediatrician) to find out whether there was a genetic reason for the daughter’s developmental delay and the mental retardation of another child, the girl’s half-brother.3 The physician wrote in her notes: “? Chromosomes + fragile X” to indicate testing planned for the daughter.
The testing was performed at a medical center and reported to be normal. The physician relayed this finding to the parents, but failed to mention that fragile X testing had not been conducted. Because they had discussed fragile X testing during the initial consultation, the mother assumed it had been performed and was included in the normal results.3
The latest child was also developmentally delayed, and subsequent testing revealed that all three children were positive for fragile X syndrome. The parents sued, alleging that the physician was negligent for failing to perform the genetic test, and claiming that they would not have conceived another child if they had known of the daughter’s fragile X status.
Are their claims reasonable?
Despite a state statute that prohibited wrongful birth and wrongful life actions that allege that the pregnancy would have been terminated if the parents had known of the genetic impairment, the state supreme court allowed this case to proceed because the issue was whether the mother would have avoided conception. The plaintiffs also argued that the claim did not exceed the statute of limitations. Their reasoning: Although the medical care had been provided more than 4 years earlier (the limitation period), the injury did not occur (i.e., action did not “accrue”) until conception of the child.
Perhaps most telling was the court’s statement that, “[O]ur decision today is informed by the practical reality of the field of genetic testing and counseling; genetic testing and diagnosis [do] not affect only the patient. Both the patient and her family can benefit from accurate testing and diagnosis. And, conversely, both the patient and her family can be harmed by negligent testing and diagnosis.”3
Establishing degree of harm is especially difficult
As you might imagine, allegations involving potential pregnancy termination arouse intense emotions on both sides of the abortion debate. The determination of damages is equally contentious. Among the issues that may arise at the time of trial:
- How much is a parent harmed by the birth of a child with hereditary disease?
- Should damages be offset by the benefit of having any child, even if the child is not “normal”?
- How do you measure the value of a life with Down syndrome, for example, compared with no life at all?
- Should damages include the cost of raising the child, including additional medical expenses, which can be substantial?
Assigning blame for genetic disease is difficult
The arguments in cases involving genetic testing often differ from those made when a fetus sustains injury. In the latter, the injury may be caused by the provider—e.g., after administration of a cytotoxic drug during pregnancy or because of induction of labor at a seriously miscalculated gestational age. Legal actions associated with such injury are widely accepted.
In cases involving genetic counseling, however, the disease is not caused by the practitioner. Rather, the plaintiff alleges that the affected child was born because the provider failed to:
- properly counsel the patient not to conceive
- offer the parents the option of terminating the pregnancy or
- successfully prevent or terminate a pregnancy.
It would be unwise to base one’s conduct on existing law, which is unpredictable. The law can change if a judge determines that a prior opinion was incorrect, a statute was unconstitutional, or a particular injury justifies compensation. Legislative bodies also can change with an election, and the statutes can be amended. The best strategy for you to deal with this uncertainty? Provide comprehensive prenatal care of the highest quality.
Lessons learned
Among the lessons to be gleaned from these cases are:
- Be sure that you understand the limits of any test that you order, and convey those limits to the patient.
- When you inform a patient about a planned test, that test should be completed. If it is not, explain the failure to perform the test (or the lost result, etc.) to the patient so that she can act accordingly. In that regard, a laboratory or other facility can be held liable for a negligently performed test or, as was the case in one lawsuit, a sperm bank may be liable for failing to inform the recipient of donor sperm that the donor had a positive family history of renal disease (i.e., autosomal-dominant polycystic kidney disease).5
- Be aware that, as the amount of information available in the popular literature and on the Web expands, patients will come to question their care more often. An example: A patient recently brought an action against her health-care provider because vitamins containing folate were discontinued shortly before she became pregnant, and the child was born with a neural tube defect.6
- Most court cases, including those cited in this article, are based on the credibility of witnesses recollecting events. Well-documented, legible records written contemporaneously with an event are of enormous benefit in cases involving sometimes widely divergent recollections. When health care meets appropriate standards and is well documented in the records, most plaintiffs’ attorneys will not undertake what can be protracted and expensive litigation. When they do, the health-care provider usually prevails.
Aubrey Milunsky, MD, DSc, DCH
The standard of expected care in clinical genetics is generally the same across most medical specialties. That standard is compounded in obstetrics, however, by critical considerations in three areas in the spectrum of care: future conception, ongoing pregnancy, and postnatal implications. Although guidelines and committee opinions on genetics-related care that are issued by professional societies, such as ACOG, are important in practice, they do not, in fact, set the actual standard of expected care—as those issuing bodies have emphasized in their statements.
Mostly, it is expert opinion that informs a jury about the standard of expected care in genetics. And, ultimately, any action (or inaction) taken by a jury is judged according to what the average, prudent physician would do under the circumstances in question.
Errors tend to be basic
Medical negligence claims relative to genetics in obstetrical practice are usually not a complex matter of failure—for example, failing to diagnose an isodicentric chromosome, misinterpreting a copy number genome variation, mistaking a gene polymorphism as a disease-causing mutation, and failing to order a micro-deletion analysis when a gene sequence is reportedly normal. Rather, errors are usually basic and, invariably, not single; often they result in serious consequences. Space allows only a few, brief (and arbitrary) examples here of where pitfalls can be found:
- genetic counseling
- laboratory interactions
- group practice
- knowledge of practical genetics.
Genetic counseling Simple but critical matters in this area of office practice include taking a family history and not ignoring potential implications in that history of mental retardation, congenital malformations, genetic disorders, specific cancers, and ethnicity. These clues should alert you to offer diagnostic or carrier tests or to refer the patient for a genetics consultation.
Some OBs have the benefit of genetic counselors in their practice, but fail to realize that these members of the staff, albeit very valuable, are not the full and final repository of knowledge about genetic disease. Failure to offer a test, failure to refer for a genetics consultation, and failure to provide accurate information on risk and recurrence all invite litigation.
Laboratory interactions Errors by the office clinician abound in this area. They include failure to obtain the result of a lab test, to provide timely communication, to order the correct test, and to advise the lab about the specific indication for the test (such as a subtle translocation) and misinterpretation of a test result.
Group practice brings with it much benefit but significant risk, too. Assuming that one of your colleagues checked a lab result or communicated important information, without you—personally—having checked the record or obtained the result, can lead to catastrophe. Exercise great care, therefore, in overseeing how lab reports return to the office; who sees them; how, and by whom, they are filed; who is informed, and how, about an abnormal report; and what type of documentation the practice insists upon. Suffice it to say: This territory is replete with litigation.
Knowledge of practical genetics requires your continual learning. Failure to realize (or determine) that a disorder or defect is genetic inevitably raises problems. A lack of awareness of basic advances in medicine—such as preconception folic acid supplementation that provides 70% protection against a neural tube defect—may come to light only after a child is born with spina bifida.
Seek support in your work
Obstetrical practice is exciting and gratifying, but it is ever more challenging in light of the dramatic and continuing advances in human genetics. It is impossible for a busy clinician to keep up with the massive torrent of new information on genetic disease. When possible, establishing linkage—even by telephone—with a clinical genetics group could provide you with the opportunity to practice within the standard of expected care, and without unnecessary anxiety.
Dr. Milunsky is Professor of Human Genetics, Pediatrics, Pathology and Obstetrics and Gynecology, and Director, Center for Human Genetics, Boston University School of Medicine, Boston, Mass. He reports no financial relationships relevant to this article.
1. Procanik by Procanik v Cillo, 97 NJ 339 (1984) 478 A2d 755.
2. Schirmer v Mt. Auburn Obstetrics & Gynecology, 108 Ohio St3d 494 (2006) 2006-Ohio-942, 844 NE2d 1160.
3. Malloy v Meier, 679 NW2d 711 (Minn 2004).
4. A recent summary by a state supreme court reveals the position of various states on wrongful life actions: 27 states have refused to recognize actions by the child by court ruling or statute, or both, while three states do allow them. Willis v Wu, 362 SC 146 (2004), 607 SE2d 63.
5. Johnson v Superior Court, Los Angeles County, 101 Cal App 4th 869 (2002).
6. Brown v US, 462 F3d 609 (6th Cir 2006).
1. Procanik by Procanik v Cillo, 97 NJ 339 (1984) 478 A2d 755.
2. Schirmer v Mt. Auburn Obstetrics & Gynecology, 108 Ohio St3d 494 (2006) 2006-Ohio-942, 844 NE2d 1160.
3. Malloy v Meier, 679 NW2d 711 (Minn 2004).
4. A recent summary by a state supreme court reveals the position of various states on wrongful life actions: 27 states have refused to recognize actions by the child by court ruling or statute, or both, while three states do allow them. Willis v Wu, 362 SC 146 (2004), 607 SE2d 63.
5. Johnson v Superior Court, Los Angeles County, 101 Cal App 4th 869 (2002).
6. Brown v US, 462 F3d 609 (6th Cir 2006).
How to protect patients’ confidentiality
Psychiatrist reveals patients’ information to another patient
Alameda County (CA) Superior Court
For several years 2 female patients were treated by the same psychiatrist. Jane Doe, age 56, read a breach of confidentiality report alleging sexual abuse filed by another patient of the psychiatrist. Jane Doe contacted the alleged victim, who informed her that the psychiatrist had disclosed information to her (the victim) regarding Jane Doe’s treatment, emotional problems, sexual preferences, and medication regimen.
Susan Doe, age 64, learned of the sexual abuse accusations against the psychiatrist in the same way and also contacted the alleged victim. She told Susan Doe that the psychiatrist had disclosed to her Susan Doe’s personal information regarding her dificult relationship with her daughter, depression, and instances when she stormed out of counseling sessions.
The patients brought separate claims, and their cases were later consolidated. The psychiatrist denied that he told the alleged sexual abuse victim details of the 2 patients’ treatments. The patients claimed that the victim could not have known their personal details unless the psychiatrist had told her.
- A jury returned a verdict in favor of the 2 patients. Jane Doe was awarded $225,000, and Susan Doe was awarded $47,000.
Dr. Grant’s observations
In the case of Jane Doe and Susan Doe, disclosing a patient’s personal information to another patient violates confidentiality. Patients must consent to the disclosure of information to third parties, and in this case these 2 patients apparently did not provide consent.
Medical practice—and particularly psychiatric practice—is based on the principle that communications between clinicians and patients are private. The Hippocratic oath states, “Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.”1
According to the American Psychiatric Association’s (APA) code of ethics, “Psychiatric records, including even the identification of a person as a patient, must be protected with extreme care. Confidentiality is essential to psychiatric treatment, in part because of the special nature of psychiatric therapy. A psychiatrist may release confidential information only with the patient’s authorization or under proper legal compulsion.”2
Doctor-patient confidentiality is rooted in the belief that potential disclosure of information communicated during psychiatric diagnosis and treatment would discourage patients from seeking medical and mental health care (Table)
Table
Underlying values of confidentiality
| Proper doctor-patient confidentiality aims to: |
|
| Source: U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General—Executive Summary. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, 1999. |
When to disclose
There are circumstances, however, that override the requirement to maintain confidentiality and do not need a patient’s consent. Examples include:3
Duty to protect third parties. In 1976 the California Supreme Court ruled in the landmark Tarasoff case4 that a psychiatrist has a duty to do what is reasonably necessary to protect third parties if a patient presents a serious risk of violence to another person. The specific applications of this principle are governed by other states’ laws, which have extended or limited this duty.5 Be familiar with the law in your jurisdiction before disclosing confidential information to third parties who may be at risk of violence.
The APA’s position on this exception is consistent with legal standards. Its code of ethics states, “When, in the clinical judgment of the treating psychiatrist, the risk of danger is deemed to be significant, the psychiatrist may reveal confidential information disclosed by the patient.”6
Emergency release of information. Psychiatrists can release confidential information during a medical emergency. Releasing the information must be in the patient’s best interests, and the patient’s inability to consent to the release should be the result of a potentially reversible condition that leads the clinician to question the patient’s capacity to consent.3
For example, if a patient in an emergency room is delirious because of ingesting an unknown substance and is unable to consent, a physician can call family members to ask about the patient’s medical problems. Notifying family that the patient is in the hospital could violate confidentiality, however.
Reporting abuse. All clinicians are obligated to report suspected child abuse or neglect. Some state laws also may require physicians to disclose abuse of vulnerable groups such as the elderly or the disabled and report to the local department of health diagnosis of communicable diseases such as HIV.3
Circle of confidentiality. Certain parties— including clinical staff on an inpatient unit or a psychiatrist supervising a resident— are considered to be within a circle of confidentiality.3 You do not need a patient’s consent to share clinical information with those within the circle of confidentiality. Do not release a patient’s information to parties who are not in the circle of confidentiality—such as family members, attorneys representing the patient, and law enforcement personnel—unless you’ve first obtained the patient’s consent.
Document the reasoning behind your decision to disclose your patient’s personal information without the patient’s consent. Show that you engaged in a reasonable clinical decision-making process.3 For example, record the risks and benefits of your decision and how you arrived at your conclusion.3
Other scenarios
Multidisciplinary teams. Members of a multidisciplinary treatment team—such as physicians, nurses, or social workers—should only receive confidential information that is relevant to the patient’s care. Other clinicians who are not involved in the case—although they may be seeing other patients on the same unit—should not have access to the patient’s confidential information. Discussions with these team members must be private so that others do not overhear confidential information.
Insurance companies generally are not party to the patient’s records unless the patient agrees to allow access by signing a release. If the patient’s refusal to allow disclosure results in the insurance company’s refusal to pay, then the patient is responsible for resolving the issue.7
Scientific publications and presentations. When you present a case report for a scientific publication or at a meeting, alter the patient’s biographical data so that someone who knows the patient would be unable to identify him or her based on the information in the case report. If the information is so specific that you cannot prevent patient identification, either do not publish the case or offer the patient the right to veto the manuscript’s distribution. If necessary, have the patient sign a consent form to allow publication or presentation of the case report.
Confidentiality violations
Breach of confidentiality may be intentional, such as disclosing a patient’s personal information to a third party as in this case, or unintentional, such as talking about a patient to a colleague and having someone overhear your discussion.8 Violating confidentiality may result in litigation for malpractice (negligence), invasion of privacy, or breach of contract, and ethical sanctions.8
No aspect of psychiatric practice seems to generate stronger emotions than the potential legal repercussions of our work. Keeping up with patients’ needs, billing issues, and advancements in medicine leaves little time for tracking changing state and federal laws or case precedents. For the past 4 years it has been my pleasure to provide information on the legal issues psychiatrists face and provide possible means of avoiding legal pitfalls.
Although I have decided to pursue other projects, I wish to give readers my thanks and to suggest resources—only a few among many great ones—that may be useful guides for a variety of legal issues.
Jon E. Grant, JD, MD, MPH
- Journal of the American Academy of Psychiatry and the Law.
- Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA:Harvard University Press; 1998.
- Simon RI, Shuman DW.Clinical manual of psychiatry and the law. Washington, DC: American Psychiatric Publishing, Inc. ; 2007.
Editor’s note
Current Psychiatry thanks Dr. Grant for writing the Malpractice Verdicts column since 2004. The column will continue in a new format in the February 2008 issue.
1. National Institutes of Health. The Hippocratic oath. Available at: http://www.nlm.nih.gov/hmd/greek/greek_oath.html. Accessed October 30, 2007.
2. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006: 6. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
3. Lowenthal D. Case studies in confidentiality. J Psychiatr Prac 2002;8:151-9.
4. Tarasoff vs Regents of the University of California 551P 2d 334 (Cal 1976).
5. Appelbaum PS Taras off and the clinician: problems in fulfilling the duty to protect. Am J Psychiatry 1985;142:425-9.
6. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006:7. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
7. Hilliard J. Liability issues with managed care. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:44-51.
8. Berner M. Write smarter, not longer. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:54-71.
Cases are selected by Current Psychiatry fromMedical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.

Jon E. Grant, JD, MD, MPH
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis.
Jon E. Grant, JD, MD, MPH
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis.
Jon E. Grant, JD, MD, MPH
Dr. Grant is associate professor of psychiatry, University of Minnesota Medical Center, Minneapolis.
Psychiatrist reveals patients’ information to another patient
Alameda County (CA) Superior Court
For several years 2 female patients were treated by the same psychiatrist. Jane Doe, age 56, read a breach of confidentiality report alleging sexual abuse filed by another patient of the psychiatrist. Jane Doe contacted the alleged victim, who informed her that the psychiatrist had disclosed information to her (the victim) regarding Jane Doe’s treatment, emotional problems, sexual preferences, and medication regimen.
Susan Doe, age 64, learned of the sexual abuse accusations against the psychiatrist in the same way and also contacted the alleged victim. She told Susan Doe that the psychiatrist had disclosed to her Susan Doe’s personal information regarding her dificult relationship with her daughter, depression, and instances when she stormed out of counseling sessions.
The patients brought separate claims, and their cases were later consolidated. The psychiatrist denied that he told the alleged sexual abuse victim details of the 2 patients’ treatments. The patients claimed that the victim could not have known their personal details unless the psychiatrist had told her.
- A jury returned a verdict in favor of the 2 patients. Jane Doe was awarded $225,000, and Susan Doe was awarded $47,000.
Dr. Grant’s observations
In the case of Jane Doe and Susan Doe, disclosing a patient’s personal information to another patient violates confidentiality. Patients must consent to the disclosure of information to third parties, and in this case these 2 patients apparently did not provide consent.
Medical practice—and particularly psychiatric practice—is based on the principle that communications between clinicians and patients are private. The Hippocratic oath states, “Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.”1
According to the American Psychiatric Association’s (APA) code of ethics, “Psychiatric records, including even the identification of a person as a patient, must be protected with extreme care. Confidentiality is essential to psychiatric treatment, in part because of the special nature of psychiatric therapy. A psychiatrist may release confidential information only with the patient’s authorization or under proper legal compulsion.”2
Doctor-patient confidentiality is rooted in the belief that potential disclosure of information communicated during psychiatric diagnosis and treatment would discourage patients from seeking medical and mental health care (Table)
Table
Underlying values of confidentiality
| Proper doctor-patient confidentiality aims to: |
|
| Source: U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General—Executive Summary. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, 1999. |
When to disclose
There are circumstances, however, that override the requirement to maintain confidentiality and do not need a patient’s consent. Examples include:3
Duty to protect third parties. In 1976 the California Supreme Court ruled in the landmark Tarasoff case4 that a psychiatrist has a duty to do what is reasonably necessary to protect third parties if a patient presents a serious risk of violence to another person. The specific applications of this principle are governed by other states’ laws, which have extended or limited this duty.5 Be familiar with the law in your jurisdiction before disclosing confidential information to third parties who may be at risk of violence.
The APA’s position on this exception is consistent with legal standards. Its code of ethics states, “When, in the clinical judgment of the treating psychiatrist, the risk of danger is deemed to be significant, the psychiatrist may reveal confidential information disclosed by the patient.”6
Emergency release of information. Psychiatrists can release confidential information during a medical emergency. Releasing the information must be in the patient’s best interests, and the patient’s inability to consent to the release should be the result of a potentially reversible condition that leads the clinician to question the patient’s capacity to consent.3
For example, if a patient in an emergency room is delirious because of ingesting an unknown substance and is unable to consent, a physician can call family members to ask about the patient’s medical problems. Notifying family that the patient is in the hospital could violate confidentiality, however.
Reporting abuse. All clinicians are obligated to report suspected child abuse or neglect. Some state laws also may require physicians to disclose abuse of vulnerable groups such as the elderly or the disabled and report to the local department of health diagnosis of communicable diseases such as HIV.3
Circle of confidentiality. Certain parties— including clinical staff on an inpatient unit or a psychiatrist supervising a resident— are considered to be within a circle of confidentiality.3 You do not need a patient’s consent to share clinical information with those within the circle of confidentiality. Do not release a patient’s information to parties who are not in the circle of confidentiality—such as family members, attorneys representing the patient, and law enforcement personnel—unless you’ve first obtained the patient’s consent.
Document the reasoning behind your decision to disclose your patient’s personal information without the patient’s consent. Show that you engaged in a reasonable clinical decision-making process.3 For example, record the risks and benefits of your decision and how you arrived at your conclusion.3
Other scenarios
Multidisciplinary teams. Members of a multidisciplinary treatment team—such as physicians, nurses, or social workers—should only receive confidential information that is relevant to the patient’s care. Other clinicians who are not involved in the case—although they may be seeing other patients on the same unit—should not have access to the patient’s confidential information. Discussions with these team members must be private so that others do not overhear confidential information.
Insurance companies generally are not party to the patient’s records unless the patient agrees to allow access by signing a release. If the patient’s refusal to allow disclosure results in the insurance company’s refusal to pay, then the patient is responsible for resolving the issue.7
Scientific publications and presentations. When you present a case report for a scientific publication or at a meeting, alter the patient’s biographical data so that someone who knows the patient would be unable to identify him or her based on the information in the case report. If the information is so specific that you cannot prevent patient identification, either do not publish the case or offer the patient the right to veto the manuscript’s distribution. If necessary, have the patient sign a consent form to allow publication or presentation of the case report.
Confidentiality violations
Breach of confidentiality may be intentional, such as disclosing a patient’s personal information to a third party as in this case, or unintentional, such as talking about a patient to a colleague and having someone overhear your discussion.8 Violating confidentiality may result in litigation for malpractice (negligence), invasion of privacy, or breach of contract, and ethical sanctions.8
No aspect of psychiatric practice seems to generate stronger emotions than the potential legal repercussions of our work. Keeping up with patients’ needs, billing issues, and advancements in medicine leaves little time for tracking changing state and federal laws or case precedents. For the past 4 years it has been my pleasure to provide information on the legal issues psychiatrists face and provide possible means of avoiding legal pitfalls.
Although I have decided to pursue other projects, I wish to give readers my thanks and to suggest resources—only a few among many great ones—that may be useful guides for a variety of legal issues.
Jon E. Grant, JD, MD, MPH
- Journal of the American Academy of Psychiatry and the Law.
- Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA:Harvard University Press; 1998.
- Simon RI, Shuman DW.Clinical manual of psychiatry and the law. Washington, DC: American Psychiatric Publishing, Inc. ; 2007.
Editor’s note
Current Psychiatry thanks Dr. Grant for writing the Malpractice Verdicts column since 2004. The column will continue in a new format in the February 2008 issue.
Psychiatrist reveals patients’ information to another patient
Alameda County (CA) Superior Court
For several years 2 female patients were treated by the same psychiatrist. Jane Doe, age 56, read a breach of confidentiality report alleging sexual abuse filed by another patient of the psychiatrist. Jane Doe contacted the alleged victim, who informed her that the psychiatrist had disclosed information to her (the victim) regarding Jane Doe’s treatment, emotional problems, sexual preferences, and medication regimen.
Susan Doe, age 64, learned of the sexual abuse accusations against the psychiatrist in the same way and also contacted the alleged victim. She told Susan Doe that the psychiatrist had disclosed to her Susan Doe’s personal information regarding her dificult relationship with her daughter, depression, and instances when she stormed out of counseling sessions.
The patients brought separate claims, and their cases were later consolidated. The psychiatrist denied that he told the alleged sexual abuse victim details of the 2 patients’ treatments. The patients claimed that the victim could not have known their personal details unless the psychiatrist had told her.
- A jury returned a verdict in favor of the 2 patients. Jane Doe was awarded $225,000, and Susan Doe was awarded $47,000.
Dr. Grant’s observations
In the case of Jane Doe and Susan Doe, disclosing a patient’s personal information to another patient violates confidentiality. Patients must consent to the disclosure of information to third parties, and in this case these 2 patients apparently did not provide consent.
Medical practice—and particularly psychiatric practice—is based on the principle that communications between clinicians and patients are private. The Hippocratic oath states, “Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.”1
According to the American Psychiatric Association’s (APA) code of ethics, “Psychiatric records, including even the identification of a person as a patient, must be protected with extreme care. Confidentiality is essential to psychiatric treatment, in part because of the special nature of psychiatric therapy. A psychiatrist may release confidential information only with the patient’s authorization or under proper legal compulsion.”2
Doctor-patient confidentiality is rooted in the belief that potential disclosure of information communicated during psychiatric diagnosis and treatment would discourage patients from seeking medical and mental health care (Table)
Table
Underlying values of confidentiality
| Proper doctor-patient confidentiality aims to: |
|
| Source: U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General—Executive Summary. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, 1999. |
When to disclose
There are circumstances, however, that override the requirement to maintain confidentiality and do not need a patient’s consent. Examples include:3
Duty to protect third parties. In 1976 the California Supreme Court ruled in the landmark Tarasoff case4 that a psychiatrist has a duty to do what is reasonably necessary to protect third parties if a patient presents a serious risk of violence to another person. The specific applications of this principle are governed by other states’ laws, which have extended or limited this duty.5 Be familiar with the law in your jurisdiction before disclosing confidential information to third parties who may be at risk of violence.
The APA’s position on this exception is consistent with legal standards. Its code of ethics states, “When, in the clinical judgment of the treating psychiatrist, the risk of danger is deemed to be significant, the psychiatrist may reveal confidential information disclosed by the patient.”6
Emergency release of information. Psychiatrists can release confidential information during a medical emergency. Releasing the information must be in the patient’s best interests, and the patient’s inability to consent to the release should be the result of a potentially reversible condition that leads the clinician to question the patient’s capacity to consent.3
For example, if a patient in an emergency room is delirious because of ingesting an unknown substance and is unable to consent, a physician can call family members to ask about the patient’s medical problems. Notifying family that the patient is in the hospital could violate confidentiality, however.
Reporting abuse. All clinicians are obligated to report suspected child abuse or neglect. Some state laws also may require physicians to disclose abuse of vulnerable groups such as the elderly or the disabled and report to the local department of health diagnosis of communicable diseases such as HIV.3
Circle of confidentiality. Certain parties— including clinical staff on an inpatient unit or a psychiatrist supervising a resident— are considered to be within a circle of confidentiality.3 You do not need a patient’s consent to share clinical information with those within the circle of confidentiality. Do not release a patient’s information to parties who are not in the circle of confidentiality—such as family members, attorneys representing the patient, and law enforcement personnel—unless you’ve first obtained the patient’s consent.
Document the reasoning behind your decision to disclose your patient’s personal information without the patient’s consent. Show that you engaged in a reasonable clinical decision-making process.3 For example, record the risks and benefits of your decision and how you arrived at your conclusion.3
Other scenarios
Multidisciplinary teams. Members of a multidisciplinary treatment team—such as physicians, nurses, or social workers—should only receive confidential information that is relevant to the patient’s care. Other clinicians who are not involved in the case—although they may be seeing other patients on the same unit—should not have access to the patient’s confidential information. Discussions with these team members must be private so that others do not overhear confidential information.
Insurance companies generally are not party to the patient’s records unless the patient agrees to allow access by signing a release. If the patient’s refusal to allow disclosure results in the insurance company’s refusal to pay, then the patient is responsible for resolving the issue.7
Scientific publications and presentations. When you present a case report for a scientific publication or at a meeting, alter the patient’s biographical data so that someone who knows the patient would be unable to identify him or her based on the information in the case report. If the information is so specific that you cannot prevent patient identification, either do not publish the case or offer the patient the right to veto the manuscript’s distribution. If necessary, have the patient sign a consent form to allow publication or presentation of the case report.
Confidentiality violations
Breach of confidentiality may be intentional, such as disclosing a patient’s personal information to a third party as in this case, or unintentional, such as talking about a patient to a colleague and having someone overhear your discussion.8 Violating confidentiality may result in litigation for malpractice (negligence), invasion of privacy, or breach of contract, and ethical sanctions.8
No aspect of psychiatric practice seems to generate stronger emotions than the potential legal repercussions of our work. Keeping up with patients’ needs, billing issues, and advancements in medicine leaves little time for tracking changing state and federal laws or case precedents. For the past 4 years it has been my pleasure to provide information on the legal issues psychiatrists face and provide possible means of avoiding legal pitfalls.
Although I have decided to pursue other projects, I wish to give readers my thanks and to suggest resources—only a few among many great ones—that may be useful guides for a variety of legal issues.
Jon E. Grant, JD, MD, MPH
- Journal of the American Academy of Psychiatry and the Law.
- Appelbaum PS, Gutheil TG. Clinical handbook of psychiatry and the law. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA:Harvard University Press; 1998.
- Simon RI, Shuman DW.Clinical manual of psychiatry and the law. Washington, DC: American Psychiatric Publishing, Inc. ; 2007.
Editor’s note
Current Psychiatry thanks Dr. Grant for writing the Malpractice Verdicts column since 2004. The column will continue in a new format in the February 2008 issue.
1. National Institutes of Health. The Hippocratic oath. Available at: http://www.nlm.nih.gov/hmd/greek/greek_oath.html. Accessed October 30, 2007.
2. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006: 6. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
3. Lowenthal D. Case studies in confidentiality. J Psychiatr Prac 2002;8:151-9.
4. Tarasoff vs Regents of the University of California 551P 2d 334 (Cal 1976).
5. Appelbaum PS Taras off and the clinician: problems in fulfilling the duty to protect. Am J Psychiatry 1985;142:425-9.
6. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006:7. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
7. Hilliard J. Liability issues with managed care. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:44-51.
8. Berner M. Write smarter, not longer. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:54-71.
Cases are selected by Current Psychiatry fromMedical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
1. National Institutes of Health. The Hippocratic oath. Available at: http://www.nlm.nih.gov/hmd/greek/greek_oath.html. Accessed October 30, 2007.
2. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006: 6. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
3. Lowenthal D. Case studies in confidentiality. J Psychiatr Prac 2002;8:151-9.
4. Tarasoff vs Regents of the University of California 551P 2d 334 (Cal 1976).
5. Appelbaum PS Taras off and the clinician: problems in fulfilling the duty to protect. Am J Psychiatry 1985;142:425-9.
6. Principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2006:7. Availableat: http://www.psych.org/psych_pract/ethics/ppaethics.pdf. Accessed October 30, 2007.
7. Hilliard J. Liability issues with managed care. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:44-51.
8. Berner M. Write smarter, not longer. In: Lifson LE, Simon RI, eds. The mental health practitioner and the law. Cambridge, MA: Harvard University Press; 1998:54-71.
Cases are selected by Current Psychiatry fromMedical Malpractice Verdicts, Settlements & Experts, with permission of its editor, Lewis Laska of Nashville, TN (www.verdictslaska.com). Information may be incomplete in some instances, but these cases represent clinical situations that typically result in litigation.
SHM: BEHIND THE SCENES
Enter text here
Enter text here
Enter text here
What is the best surgical therapy for the secondary prevention of stroke?
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.


Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
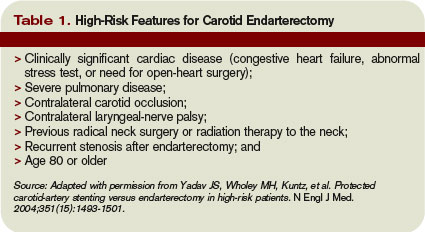
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Demystify Admissions
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Physicians may encounter patients in various ways during the first few days of a hospitalization: admission services, consultations, and medical-surgical co-management.
Submitting claims for these services is often inconsistent and inaccurate because billing education is not a standard part of medical education.
In an attempt to clarify the rules and reduce frustration, I will address billing, coding, and reimbursement guidelines for each type of initial hospital encounter over the next several issues.
Definition
Initial Hospital Care (IHC) comprises all services related to the patient’s admission to an acute care facility. An acute care facility is any that registers inpatients but does not have a corresponding Current Procedural Terminology (CPT) code category for claim reporting. Acute care facilities also include “partial hospitals.”
For example, admissions to inpatient rehabilitation are reported with IHC codes 99221-99223, while nursing facility admissions have a designated category and are best reported with CPT codes 99304-99306 for Initial Nursing Facility Care.
Code Use
IHC codes are reported once per hospitalization and reserved for the physician/group assuming primary responsibility for the patient’s care during that time.
If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99221-99223 are denied or rejected pending review of documentation to ascertain the correct service date and responsible party. This is common because physicians confuse code description IHC with its true intent. They mistakenly report these codes for their first inpatient encounter, regardless of the encounter date or the admitting physician/group.
Specialists assisting in the patient’s management and not primarily responsible for the entire hospitalization report the code category that best reflects the performed service and documentation—as long as the selected category requirements are met. The physician selects from either Inpatient Consultation codes 99251-99255 or Subsequent Hospital Care (SHC) codes 99231-99233. Any physician who provides patient services after the initial encounter, including those by the responsible attending physician/group or a specialist concurrently involved in the patient’s care, reports SHC codes for each date in which a face-to-face encounter occurs.
When services begin in one location (e.g., physician’s office, emergency department, or observation) and end with an inpatient admission on the same calendar day, the physician reports only the most appropriate initial hospital care code. It is not necessary for the physician to duplicate the information from the earlier encounter for the admission service. Instead, the physician can forward a copy of the progress note from the earlier encounter to the inpatient chart, along with the documented decision for admission and pertinent information obtained throughout the day. Auditors consider the culmination of all chart entries in a given date when reviewed. When services begin in one location but end with an admission on different calendar day, the physician separately reports each service provided on each date: 99220 on Day 1 and 99223 on Day 2.
Intrafacility Transfers
Patients may receive different components of inpatient services within the same (uninterrupted) episode of care, all within the same building but treated as separate facility admissions (e.g., rehabilitation or long-term acute care).
It is unlikely the attending physician of record during the acute care phase will also be the attending physician during the second phase of care. Should this occur, Medicare contractors and those payers who follow Medicare guidelines permit the attending physician to separately report the acute care discharge (99238-99239) and the secondary admission (99221-99223), but only in the absence of a shared medical record (see Section 30.6.9.1D,www.cms.hhs.gov/manuals/downloads/clm104c12.pdf). If a common chart is used, the physician reports the secondary admission services as ongoing care, using SHC codes 99231-99233 instead.
Similarly, transfers occur within a single phase of care, such as transfers to and from a medical intensive care unit and a standard medical-surgical unit. Such transfers are not treated as separate admissions, and the receiving physician reports only the SHC codes because the IHC service was previously reported by the admitting physician/group. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia.
Voters Weigh in Early
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.

—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
A poll by the Kaiser Family Foundation in August found that healthcare is the top domestic issue that the public wants presidential candidates to address.
Republicans and independent voters ranked healthcare second only to Iraq in the poll, while for the first time, Democrats ranked the two issues as equally important for the candidates to discuss as they campaign.
With more voters interested in changes to American healthcare—which is really shorthand for affordable access to health insurance coverage—the presidential candidates are also showing interest. Sort of.
Some, including John Edwards, Barack Obama, Hillary Clinton, and Mitt Romney, have a broad plan or opinion in place. Others, such as Mike Huckabee and John McCain, have not yet shared a plan.
As the election progresses—or even after a new president is sworn into office—will we see any real changes to healthcare access? “There has to be [some change],” states Bradley Flansbaum, DO, MPH, chief of hospitalist section at Lenox Hill Hospital in New York, N.Y. “We’ve reached a tipping point. You can’t continue to play kick the can.” The impetus for change, Dr. Flansbaum believes, will not be public opinion so much as money.
“I think that we’re reaching a critical mass, and that premiums will drive the change,” he predicts. “Employers can’t afford insurance benefits any more, and now that employers are changing plans and employees are paying more and faced with higher premiums, I think the house of cards will collapse.”
Laura Allendorf, SHM’s senior adviser for advocacy and government affairs, agrees change is in the air.
“I do think there are better opportunities for action than there have been in the past,” she says. “Various polls show that healthcare [access] is an important issue. That’s why so many candidates are developing proposals on this, or already have a proposal.” She adds, “A U.S. Census Bureau report just came out showing an increase in the number of unemployed—this will lend pressure for policymakers.”
Where Will the Trail Lead?
Campaigning for the 2008 election is in full swing, and no one is surprised the candidates lack firm or detailed opinions on healthcare access. But what can we expect to see in the next year of campaigning?
“As much as Hillary [Clinton] is a lightening rod in some ways, she’s going to be driving the debate on this,” predicts Dr. Flansbaum. “As we get closer to the election and the second- and third-tier candidates start to come apart, she’ll be the one leading the healthcare debate.”
In general, Democrats and Republicans have settled into two camps on the issue.
“It’s easy to say, ‘Don’t listen to the Democrats—they want socialized medicine,’ while the Democrats are saying ‘The Republicans want corporate America to take over,’” says Dr. Flansbaum. “They’re playing games right now. I can’t say if a purely government or a purely corporate system would work, but we probably need and are going to get a mixture of both.” After the election, he says, “There’s got to be some compromise in the middle.”
What about other healthcare issues besides the rising costs and lack of access? “In addition to access, quality improvement is certainly key,” says Allendorf.
For Dr. Flansbaum, everything is connected to access, including healthcare IT, informatics, quality reporting, cost control, and waste reduction.
Hail to the New Chief
Once a new president and his or her administration is in place, will the concerns—and possibly the campaign promises—over healthcare access be dropped?
“Definitely something would—or rather, should—be done,” says Allendorf. “The two parties obviously have different philosophic approaches, but if [the next president] listens to the voters, they’ll act. The voters have spoken.” And if no action is taken on the issues, Allendorf adds, “It’s up to associations like SHM to push for reform.”
But Dr. Flansbaum warns that whatever the change is, it won’t happen overnight.
“There are too many lobbyists and people with their hand in the till to turn this around overnight,” states Dr. Flansbaum. “It will be an incremental change, and it will probably start out like the Massachusetts plan.”
Beginning July 1, Massachusetts enacted a law designed to cover the state’s uninsured population. The law mandates that individuals purchase health insurance with government subsidies to ensure affordability.
—Laura Allendorf, SHM’s senior adviser for advocacy and government affairs
Physician, Educate Thyself
The next year promises more campaigning, including debates and town hall forums, updated Web sites, media interviews, and so on. Allendorf says that as the candidates change and their positions on healthcare issues are fleshed out and become more apparent.
“SHM will provide information through our usual channels and publications about the candidates’ positions as they gel,” she says. “We’ll probably also want to hear from any SHM members who are involved in working with candidates on their positions, crafting proposals or working on healthcare advisory groups.”
For information on the candidates’ healthcare access positions, you can download an August report from the Council for Affordable Health Insurance, “The 2008 Presidential Candidates on Health Care Reform,” from www.cahi.org.
You can also find nonpartisan, up-to-date information about candidates’ healthcare policy, as well as analysis of health policy issues, regular public opinion surveys, and news coverage, on a site hosted by the Kaiser Family Foundation: www.health08.org. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Administrative Ambition
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Interested in a promotion? If you have your eye on an administrative career, go ahead and think big—because the opportunities for today’s hospitalists are there for the taking, with some planning and the careful acquisition of skills, experience, and training.
“Any hospitalist who has any desire to be a leader, whether in a medical practice or in a hospital, has numerous opportunities,” says Patrick Cawley, MD, chief medical officer of Medical University of South Carolina (MUSC) Medical Center in Charleston. “If you’re willing to step up, you can attain that leadership position.”
Plan Your Path
Ambitious hospitalists must consider the administrative positions available to them in the long run.
“Within a hospital medicine practice, you have just one director,” says Joan C. Faro, MD, FACP, MBA, chief medical officer, John T. Mather Memorial Hospital, Port Jefferson, N.Y. “So people working in the ranks need to be creative and come up with ideas on gaining experience, such as creating a QA position.” She advises hospitalists to look at the job description and the performance measures of the director’s position to see what expectations come with the job.
The promotion to director may involve switching practices. “If you want to move quickly, you have to be able to move [to a different group],” explains Dr. Cawley. “In a local community, there will be others ahead of you. If you’re willing to move to a less-than-ideal location, you can find better opportunities.” For community-based hospitalists especially, the director’s position is a necessary one before moving higher up the administrative ladder.
“You need to be managing some people before you become a CMO [chief medical officer] or administrator,” explains Dr. Faro. “You really have to show that you can do some significant work. In academia, you can do this as a division chief or something like that.” As the director of a hospital medicine program, she says, “you can broaden your scope and move higher up into hospital administration.”
First Steps
How do you move from working hospitalist to director or department head? Start small.
“You can start with easy committee assignments,” says Dr. Cawley. “Even while you’re getting leadership training, you can be building those skills on the job. Start with small projects, such as small committee roles or quality management projects. You can then move up, but consider that you’ll need new skills as you do. Before you chair your first committee, you’ll have to brush up on how to run a meeting. You can progressively take on larger, broader roles.”
Enlist the help of your own leaders to help you get started.
“You could go to your CMO or your medical director—if they’re in a position to help—and ask what you need to do to get to the next step,” advises Dr. Faro. “You don’t need formal training at this point; test the waters, find what you’re interested in and make sure that leading change is something you enjoy before you [invest in] formal training.”
Dr. Faro was working as an internist in an academic medical setting when she discovered an affinity for leadership. “I went to my dean and asked to be put on committees,” she recalls. “I also worked in a volunteer capacity and did committee work for the local chapter of the American Heart Association. I ended up chairing a number of committees over the years. It just seemed to happen naturally because I enjoyed it. After these experiences, I knew I had a talent for working with disparate groups and getting things done.”
As you concentrate on committee work and project work, focus on building clinical and administrative skills.
“The most important things are having the right skills and experience,” stresses Dr. Cawley. “In my opinion, experience will count for more than skills, because people tend to assume that your skills improve as you gain experience. Experience is more important than an advanced degree, with the caveat that degrees are one way that leaders can prove themselves. Having that MBA or MPH doesn’t hurt, and it shows that you’re serious; it requires some dedication to earn that.”
Leadership Training A Must
If your committee and project experience assures you that you want to pursue a leadership path, says Dr. Cawley, “you really need leadership training. Now, is that an MBA or simply selective reading and coursework? That depends on what you want and how you want to go about it.”
However you decide to educate yourself, that leadership training should emphasize certain skills.
“You definitely need formal negotiation skills training,” says Dr. Cawley. “You should also train in how to deal with a physician who’s disruptive. You’ll need a little bit of financial training, and then leadership training itself—what is a leader and what are the expectations of a leader? These are the basics.”
Dr. Faro adds that communication skills and presentation skills are important for leaders. “These are things that physicians think they know— after all we all feel we communicate well and we need to talk to our patients—but there’s a difference between teaching your patients about medications and engaging an audience,” she warns. “It’s also important to understand your management or your leadership style.”
Leadership training is easy to find. “Every single organization has now recognized that being a leader is something that requires training,” Dr. Faro points out. Physician leadership training is offered by the American College of Healthcare Executives, the American College of Physician Executives, the American College of Physicians, and SHM.
Opportunities Abound
In the growing field of hospital medicine, opportunities for advancement are growing as well. “Within just a few years, you’d be surprised what level you can reach,” says Dr. Cawley.
“There is a lot of potential for leadership within hospital medicine groups, and for moving from leading a group to a leadership role at a hospital,” says Dr. Cawley. “But the leadership chasm [in healthcare today] extends to every area where physicians are providing care.
“To me, it’s all about opportunities, skills and experience. With these, you’ll find that the sky’s the limit.”
Dr. Faro believes hospitalists are in a perfect position to rise to administrative positions. “You are, by definition, working in an institution,’’ he says. “Hospital medicine is replete with opportunities for leadership—opportunities to start a team for quality endeavors, an IHI [Institute of Healthcare Improvement] campaign, look at medication reconciliation, DVT prophylaxis, or glucose control. There are so many right things for physicians to be doing in a hospital setting. In any hospital today, there are going to be opportunities.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
Drug Stents and Surgery

Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.
Drug-eluting stents (DES) are a medical success story: In the four years since they were approved, in-stent restenosis rates have gone from the 25%-30% associated with bare-metal stents to the single digits.
Thanks to this track record, the world market for stents has doubled to $5 billion—despite the fact patients with DES must take aspirin or clopidogrel to prevent thromboses.
It’s easy to forget not all questions concerning DES have been answered, despite their wide acceptance and good overall outcomes.
One concern is discontinuation of antiplatelet therapy for DES patients who require noncardiac surgery.
In the November-December 2007 Journal of Hospital Medicine, senior author Amir Jaffer, MD, and colleagues at the Cleveland Clinic in Ohio studied the relationship between a patient’s time on antiplatelet medication and the consequences of discontinuing those agents in preparation for surgery.
“This is a common clinical conundrum,” says Dr. Jaffer, director of the Cleveland Clinic’s Internal Medicine Preoperative Assessment Consultation and Treatment (IMPACT) Center. “We face this question almost every day in our practice relative to perioperative care.”
Patients slated for noncardiac surgery are seen first at the IMPACT center, where hospitalists conduct the preoperative evaluation.
Data show that patients with bare-metal stents run a high risk of stent thrombosis if they undergo noncardiac surgery within two to six weeks of stent placement.
But information on DES is hard to come by, “so we decided to try to get a handle on the safety of stopping these drugs,” says Dr. Jaffer.
The authors, led by Daniel J. Brotman, MD, studied all patients who had undergone DES placement and were evaluated for noncardiac surgery at the IMPACT Center from July 2003 to July 2005. They examined 30-day rates of postoperative myocardial infarction (MI), DES thrombosis, major bleeding, and all-cause mortality—all relative to how long the patient had been on and off antiplatelet therapy.
The type of surgery each patient underwent was classified by invasiveness and anticipated blood loss, according to the system developed by L. Reuven Pasternak, MD, vice dean, Bayview Campus, Johns Hopkins University in Baltimore, and his colleagues.1
The categories range from one, which includes cystoscopy, breast biopsy, and other minor procedures that involve little if any blood loss, to five, which encompasses highly invasive procedures with anticipated blood losses in excess of 1,500 cc, such as major vascular repair.
A total of 114 patients met the study criteria. Seventy-five (66%) of the patients were men, and the median age was 71.
The most common comorbidities were diabetes (in 41% of patients), a history of coronary bypass (34%), and chronic renal insufficiency (20%). Most patients (73%) received sirolimus (Rapamune) stents; 28% received paclitaxel (Onxol) stents; and 33% had more than one DES.
Of the patients studied, 69 (61%) underwent surgery more than 180 days after receiving their DES; 30 (26%) had their procedures within 91-180 days of receiving the stent; and 15 (13%) had their operations within 90 days of stenting.
The most common procedures were major orthopedic surgeries such as hip replacement (34.2% of patients), and ophthalmologic procedures like cataract removal (26.3%).
No procedures fell into category five, and only 6.1% fell into category four; the rest were in categories one to three.
In most cases (77%), antiplatelet therapy had been discontinued a median of 10 days before surgery, with patients remaining off the drugs a median of 14 days after surgery.
There were no deaths. The most serious complications were non-ST-elevation myocardial infarction (NSTEMI) in two patients, and retroperitoneal hemorrhage following kidney transplantation in a patient who had been taking aspirin and clopidogrel until a week before surgery.
These findings suggest that “transient termination of antiplatelet agents in the perioperative setting is not associated with high morbidity and mortality in patients with DES, even when patients have had their stents implanted in the previous three to six months,” the authors write.
The study has limitations, Dr. Jaffer warns. “This was a small study, and more than 50% of our patients had surgery more than six months after DES placement,’’ he says. “It is difficult to predict a true relationship between timing of stent placement and subsequent surgery.”
Also, about a third of the patients underwent minor procedures, and roughly one-fifth never discontinued antiplatelet medication.
There were “several issues that may have led to fairly reasonable outcomes, and which could also be related to why we saw a fairly low rate of thrombosis,” he says.
In part because of these remaining questions, he recommends hospitalists take the timing of stent placement into account when evaluating patients with DES for surgery.
If it has been six months or less since the stent was implanted, the risk of thrombosis is still high, and “we can’t accurately say if it’s safe to stop antiplatelet medication,’’ he says. “I would treat those patients cautiously, as the literature suggests they may have a high risk of adverse events.”
But if the patient needs urgent surgery and more than six months have elapsed, “it may be safer to discontinue clopidogrel and continue baby aspirin, or to continue both antiplatelet medications during surgery if an urgent procedure is needed within six months of receiving the DES” he says. TH
Norra MacReady is a medical writer based in California.
Reference
- Pasternak LR. Preoperative assessment: guidelines and challenges. Acta Anaesthesiol Scand Suppl. 1997;111:318-320.