User login
Uveal melanoma: NCCN provides first pathway-based guidelines
ORLANDO – Uveal melanoma has little in common with it’s cutaneous namesake, and its distinct characteristics necessitated the development of specific guidelines for diagnosis and management, which were released earlier this year by the National Comprehensive Cancer Network (NCCN).
Unlike cutaneous melanoma, uveal melanoma is usually treated with radiotherapy rather than surgery, and primary treatment is based on tumor size, according to Christopher A. Barker, MD, a radiation oncologist and director of clinical investigations in the department of radiation at Memorial Sloan Kettering Cancer Center, New York.
Further, molecular testing aids in prognosis in uveal melanoma but not in predicting treatment response as it can in cutaneous disease, and recurrences of uveal melanoma are typically distant – usually occurring in the liver – rather than in the skin or lymph nodes as with cutaneous melanoma.
These and other diagnosis- and treatment-related issues are outlined in the new guidelines, which are the first developed by the NCCN for uveal melanoma.
Guidelines exist in several countries, including Australia, the United Kingdom, Canada, and the United States (published by The American Brachytherapy Society), but until now none have provided pathway-based strategies for the management of all stages of this rare disease that affects about 1 in 200,000 Americans, typically Caucasians in their 50s, 60s, or 70s, Dr. Barker, a member of the NCCN Melanoma guidelines panel and the uveal melanoma subcommittee, said at the NCCN’s annual meeting where he presented the guidelines.
The median age of diagnosis is 60 years, he noted.
The NCCN guidelines specifically address melanoma arising in the choroid and ciliary body of the uvea. The choroid is the predominant site of uveal melanoma origin, and tumors arising there may involve the ciliary body as well, although the latter is a rare site of melanoma origin. The iris is also a rare site of origin, and tumors arising there are typically indolent in nature and thus are not part of the new guidelines, he explained.
Risk factors include choroidal nevi, ocular melanocytosis, and familial uveal melanoma associated with germline BAP1 mutation, neurofibromatosis, or dysplastic nevus syndrome; cutaneous melanoma is not a risk factor, he said.
The guidelines address clinical presentation, diagnostic work-up, and staging; primary treatments; and metastatic risks and follow-up imaging.
Presentation, diagnosis, and staging
About two-thirds of patients with uveal melanoma present because of changes in their vision, and about a third present with no new symptoms and are diagnosed during routine evaluation, Dr. Barker said.
“History and physical exam, and specifically attention to any prior malignancies, is important,” he said. “A comprehensive eye examination is absolutely vital to the evaluation and staging of patients with uveal melanoma.”
Numerous additional testing options, including autofluorescence of the ocular fundus, retinal fluorescein angiography of the ocular fundus, and transillumination, among others, are listed in the guidelines, which note that MRI is sometimes needed to confirm diagnosis.
Biopsies, however, are generally only performed to confirm diagnosis if needed or for prognostic analysis for risk stratification.
Staging is determined mainly by tumor size, which is known to be associated with outcomes in patients with uveal melanoma, and is based on criteria from both the Collaborative Ocular Melanoma Study (COMS) staging system and the American Joint Committee on Cancer (AJCC) staging manual, Dr. Barker said.
The COMS system was developed based on separate studies of small, medium, and large tumors and helped define primary tumor management and establish existing standards of care. The AJCC system was developed subsequently and focuses more on tumor features that may improve clinical predictions.
Primary treatments
Options for primary treatment for small tumors (largest diameter 5-16 mm and thickness less than 2.5 mm) include plaque brachytherapy, partical beam radiation, and laser ablation in highly select patients. For medium tumors (18mm or less at largest diameter and thickness of 2.5-10 mm), they include plaque brachytherapy, particle beam radiation, and enucleation, according to the guidelines.
Large tumors can be treated with radiotherapy (preferably particle beam radiation, Dr. Barker said) or enucleation. Large tumors are those greater than 18mm with any thickness, those with thickness greater than 10mm with any diameter, and those with thickness greater than 8mm with optic nerve involvement.
In patients for whom surgical removal is selected, “ there are a few unusual situations where additional local adjuvant therapy might be considered,” Dr. Barker said, explaining, for example, that the presence of microscopically positive or close margins after enucleation without evidence of gross residual disease in the orbit may be observed or may warrant map biopsy and/or particle beam or photon beam radiotherapy to the orbit.
For visible extraocular tumors or suspicion of gross disease in the orbit, biopsy of the extraocular tissue is recommended when possible, along with either intraoperative cryotherapy, orbital exenteration, or particle beam or photon beam radiotherapy to the orbit, he added.
Metastatic risks and follow-up imaging
Recent studies, including Cancer Genome Atlas Research Network studies, have elucidated the genomics of both uveal and cutaneous melanomas, and they show “a completely different mutation spectrum” for uveal melanoma, Dr. Barker said.
These genomic studies demonstrate that cutaneous melanoma involves mutations that predict response to certain treatments, while those found in uveal melanoma do not, but they are, however, associated with the probability of metastasis, he said.
For example, various studies have shown that BRAF mutation in cutaneous melanoma predicts response to RAF or MEK inhibition and that the overall number of mutations in cutaneous melanoma may predict response to immunotherapy.
In uveal melanoma, alterations in ElFAX1, SF3B1, or BAP1 have been shown to indicate low, intermediate, and high risk of metastasis, respectively.
Other factors associated with the risk of metastasis after primary tumor treatment in uveal melanoma include clinical factors (tumor size, ciliary body involvement, and extraocular extension); histopathologic factors (spindle or epithelioid cell type); and cytogenetics (status of chromosomes 3, 6, and 8), he said.
An AJCC Ophthalmic Oncology Task Force study published in 2015, for example, showed that the 5-year metastasis-free survival was 97% for AJCC stage T1 disease, 85% for stage T2, 77% for stage T3, and 61% for stage T4. T-stage modifiers, which are based on particular tumor characteristics, such as ciliary body involvement (CBI) and extraocular extension (EXE), were also associated with the risk of distant metastasis: 5-year metastasis-free survival was 90%, 72%, 54% and 33% for AJCC T_a (no CBI or EXE), T_b (CBI only), T_c (EXE only), and T_d tumors (CBI and EXE), respectively.
Follow-up imaging after primary tumor treatment should be based on the most likely site of metastatic recurrence, which is the liver in 90% of uveal melanoma metastases.
“For this reason, surveillance of high-risk patients with uveal melanoma should include specific imaging of the liver,” Dr. Barker said, who noted that the NCCN risk stratification–based surveillance guidelines categorize patients as either low, medium, or high risk for metastasis based on the various characteristics that can affect risk.
“These risk groups help clinicians identify how often imaging should be performed in their surveillance strategy,” he said, adding that those who are high risk based on BAP1 mutation, PRAME mutation, CBI, or EXE, for example, should undergo imaging to evaluate signs or symptoms every 3-6 months for 5 years, every 6-12 months for 10 years, and then as clinically indicated thereafter.
The guideline calls for less stringent imaging for low- and medium-risk patients.
“Now, what happens when distant metastases are identified? Unfortunately there is no single systemic therapy that has proven to be most effective for uveal melanoma,” he said. “For this reason, the NCCN guideline encourages clinical trial participation whenever possible for patients who develop distant metastasis.”
This is because drugs effective for cutaneous melanoma are far less effective for uveal melanoma, but do elicit response in some patients and can be considered, he explained.
“Moreover, because the liver is the site of metastasis most often, and is often the exclusive site of metastasis, liver metastasis–directed therapy is considered part of the management of patients with uveal melanoma,” he said, adding that this can involve resection, ablation, chemo/radio embolization, or regional perfusion.”
The NCCN Uveal Melanoma Guidelines were developed by a panel of experts from various institutions based on the available evidence and on consensus; they are category 2A (based on lower-level evidence with uniform NCCN consensus that the intervention is appropriate).
Dr. Barker reported receiving clinical research support from Amgen, Bristol-Myers Squibb, Elekta, Merck, University of California San Francisco, and University of Florida Health Cancer Center Orlando, and serving as an advisor, consultant, or expert witness for Pfizer.
ORLANDO – Uveal melanoma has little in common with it’s cutaneous namesake, and its distinct characteristics necessitated the development of specific guidelines for diagnosis and management, which were released earlier this year by the National Comprehensive Cancer Network (NCCN).
Unlike cutaneous melanoma, uveal melanoma is usually treated with radiotherapy rather than surgery, and primary treatment is based on tumor size, according to Christopher A. Barker, MD, a radiation oncologist and director of clinical investigations in the department of radiation at Memorial Sloan Kettering Cancer Center, New York.
Further, molecular testing aids in prognosis in uveal melanoma but not in predicting treatment response as it can in cutaneous disease, and recurrences of uveal melanoma are typically distant – usually occurring in the liver – rather than in the skin or lymph nodes as with cutaneous melanoma.
These and other diagnosis- and treatment-related issues are outlined in the new guidelines, which are the first developed by the NCCN for uveal melanoma.
Guidelines exist in several countries, including Australia, the United Kingdom, Canada, and the United States (published by The American Brachytherapy Society), but until now none have provided pathway-based strategies for the management of all stages of this rare disease that affects about 1 in 200,000 Americans, typically Caucasians in their 50s, 60s, or 70s, Dr. Barker, a member of the NCCN Melanoma guidelines panel and the uveal melanoma subcommittee, said at the NCCN’s annual meeting where he presented the guidelines.
The median age of diagnosis is 60 years, he noted.
The NCCN guidelines specifically address melanoma arising in the choroid and ciliary body of the uvea. The choroid is the predominant site of uveal melanoma origin, and tumors arising there may involve the ciliary body as well, although the latter is a rare site of melanoma origin. The iris is also a rare site of origin, and tumors arising there are typically indolent in nature and thus are not part of the new guidelines, he explained.
Risk factors include choroidal nevi, ocular melanocytosis, and familial uveal melanoma associated with germline BAP1 mutation, neurofibromatosis, or dysplastic nevus syndrome; cutaneous melanoma is not a risk factor, he said.
The guidelines address clinical presentation, diagnostic work-up, and staging; primary treatments; and metastatic risks and follow-up imaging.
Presentation, diagnosis, and staging
About two-thirds of patients with uveal melanoma present because of changes in their vision, and about a third present with no new symptoms and are diagnosed during routine evaluation, Dr. Barker said.
“History and physical exam, and specifically attention to any prior malignancies, is important,” he said. “A comprehensive eye examination is absolutely vital to the evaluation and staging of patients with uveal melanoma.”
Numerous additional testing options, including autofluorescence of the ocular fundus, retinal fluorescein angiography of the ocular fundus, and transillumination, among others, are listed in the guidelines, which note that MRI is sometimes needed to confirm diagnosis.
Biopsies, however, are generally only performed to confirm diagnosis if needed or for prognostic analysis for risk stratification.
Staging is determined mainly by tumor size, which is known to be associated with outcomes in patients with uveal melanoma, and is based on criteria from both the Collaborative Ocular Melanoma Study (COMS) staging system and the American Joint Committee on Cancer (AJCC) staging manual, Dr. Barker said.
The COMS system was developed based on separate studies of small, medium, and large tumors and helped define primary tumor management and establish existing standards of care. The AJCC system was developed subsequently and focuses more on tumor features that may improve clinical predictions.
Primary treatments
Options for primary treatment for small tumors (largest diameter 5-16 mm and thickness less than 2.5 mm) include plaque brachytherapy, partical beam radiation, and laser ablation in highly select patients. For medium tumors (18mm or less at largest diameter and thickness of 2.5-10 mm), they include plaque brachytherapy, particle beam radiation, and enucleation, according to the guidelines.
Large tumors can be treated with radiotherapy (preferably particle beam radiation, Dr. Barker said) or enucleation. Large tumors are those greater than 18mm with any thickness, those with thickness greater than 10mm with any diameter, and those with thickness greater than 8mm with optic nerve involvement.
In patients for whom surgical removal is selected, “ there are a few unusual situations where additional local adjuvant therapy might be considered,” Dr. Barker said, explaining, for example, that the presence of microscopically positive or close margins after enucleation without evidence of gross residual disease in the orbit may be observed or may warrant map biopsy and/or particle beam or photon beam radiotherapy to the orbit.
For visible extraocular tumors or suspicion of gross disease in the orbit, biopsy of the extraocular tissue is recommended when possible, along with either intraoperative cryotherapy, orbital exenteration, or particle beam or photon beam radiotherapy to the orbit, he added.
Metastatic risks and follow-up imaging
Recent studies, including Cancer Genome Atlas Research Network studies, have elucidated the genomics of both uveal and cutaneous melanomas, and they show “a completely different mutation spectrum” for uveal melanoma, Dr. Barker said.
These genomic studies demonstrate that cutaneous melanoma involves mutations that predict response to certain treatments, while those found in uveal melanoma do not, but they are, however, associated with the probability of metastasis, he said.
For example, various studies have shown that BRAF mutation in cutaneous melanoma predicts response to RAF or MEK inhibition and that the overall number of mutations in cutaneous melanoma may predict response to immunotherapy.
In uveal melanoma, alterations in ElFAX1, SF3B1, or BAP1 have been shown to indicate low, intermediate, and high risk of metastasis, respectively.
Other factors associated with the risk of metastasis after primary tumor treatment in uveal melanoma include clinical factors (tumor size, ciliary body involvement, and extraocular extension); histopathologic factors (spindle or epithelioid cell type); and cytogenetics (status of chromosomes 3, 6, and 8), he said.
An AJCC Ophthalmic Oncology Task Force study published in 2015, for example, showed that the 5-year metastasis-free survival was 97% for AJCC stage T1 disease, 85% for stage T2, 77% for stage T3, and 61% for stage T4. T-stage modifiers, which are based on particular tumor characteristics, such as ciliary body involvement (CBI) and extraocular extension (EXE), were also associated with the risk of distant metastasis: 5-year metastasis-free survival was 90%, 72%, 54% and 33% for AJCC T_a (no CBI or EXE), T_b (CBI only), T_c (EXE only), and T_d tumors (CBI and EXE), respectively.
Follow-up imaging after primary tumor treatment should be based on the most likely site of metastatic recurrence, which is the liver in 90% of uveal melanoma metastases.
“For this reason, surveillance of high-risk patients with uveal melanoma should include specific imaging of the liver,” Dr. Barker said, who noted that the NCCN risk stratification–based surveillance guidelines categorize patients as either low, medium, or high risk for metastasis based on the various characteristics that can affect risk.
“These risk groups help clinicians identify how often imaging should be performed in their surveillance strategy,” he said, adding that those who are high risk based on BAP1 mutation, PRAME mutation, CBI, or EXE, for example, should undergo imaging to evaluate signs or symptoms every 3-6 months for 5 years, every 6-12 months for 10 years, and then as clinically indicated thereafter.
The guideline calls for less stringent imaging for low- and medium-risk patients.
“Now, what happens when distant metastases are identified? Unfortunately there is no single systemic therapy that has proven to be most effective for uveal melanoma,” he said. “For this reason, the NCCN guideline encourages clinical trial participation whenever possible for patients who develop distant metastasis.”
This is because drugs effective for cutaneous melanoma are far less effective for uveal melanoma, but do elicit response in some patients and can be considered, he explained.
“Moreover, because the liver is the site of metastasis most often, and is often the exclusive site of metastasis, liver metastasis–directed therapy is considered part of the management of patients with uveal melanoma,” he said, adding that this can involve resection, ablation, chemo/radio embolization, or regional perfusion.”
The NCCN Uveal Melanoma Guidelines were developed by a panel of experts from various institutions based on the available evidence and on consensus; they are category 2A (based on lower-level evidence with uniform NCCN consensus that the intervention is appropriate).
Dr. Barker reported receiving clinical research support from Amgen, Bristol-Myers Squibb, Elekta, Merck, University of California San Francisco, and University of Florida Health Cancer Center Orlando, and serving as an advisor, consultant, or expert witness for Pfizer.
ORLANDO – Uveal melanoma has little in common with it’s cutaneous namesake, and its distinct characteristics necessitated the development of specific guidelines for diagnosis and management, which were released earlier this year by the National Comprehensive Cancer Network (NCCN).
Unlike cutaneous melanoma, uveal melanoma is usually treated with radiotherapy rather than surgery, and primary treatment is based on tumor size, according to Christopher A. Barker, MD, a radiation oncologist and director of clinical investigations in the department of radiation at Memorial Sloan Kettering Cancer Center, New York.
Further, molecular testing aids in prognosis in uveal melanoma but not in predicting treatment response as it can in cutaneous disease, and recurrences of uveal melanoma are typically distant – usually occurring in the liver – rather than in the skin or lymph nodes as with cutaneous melanoma.
These and other diagnosis- and treatment-related issues are outlined in the new guidelines, which are the first developed by the NCCN for uveal melanoma.
Guidelines exist in several countries, including Australia, the United Kingdom, Canada, and the United States (published by The American Brachytherapy Society), but until now none have provided pathway-based strategies for the management of all stages of this rare disease that affects about 1 in 200,000 Americans, typically Caucasians in their 50s, 60s, or 70s, Dr. Barker, a member of the NCCN Melanoma guidelines panel and the uveal melanoma subcommittee, said at the NCCN’s annual meeting where he presented the guidelines.
The median age of diagnosis is 60 years, he noted.
The NCCN guidelines specifically address melanoma arising in the choroid and ciliary body of the uvea. The choroid is the predominant site of uveal melanoma origin, and tumors arising there may involve the ciliary body as well, although the latter is a rare site of melanoma origin. The iris is also a rare site of origin, and tumors arising there are typically indolent in nature and thus are not part of the new guidelines, he explained.
Risk factors include choroidal nevi, ocular melanocytosis, and familial uveal melanoma associated with germline BAP1 mutation, neurofibromatosis, or dysplastic nevus syndrome; cutaneous melanoma is not a risk factor, he said.
The guidelines address clinical presentation, diagnostic work-up, and staging; primary treatments; and metastatic risks and follow-up imaging.
Presentation, diagnosis, and staging
About two-thirds of patients with uveal melanoma present because of changes in their vision, and about a third present with no new symptoms and are diagnosed during routine evaluation, Dr. Barker said.
“History and physical exam, and specifically attention to any prior malignancies, is important,” he said. “A comprehensive eye examination is absolutely vital to the evaluation and staging of patients with uveal melanoma.”
Numerous additional testing options, including autofluorescence of the ocular fundus, retinal fluorescein angiography of the ocular fundus, and transillumination, among others, are listed in the guidelines, which note that MRI is sometimes needed to confirm diagnosis.
Biopsies, however, are generally only performed to confirm diagnosis if needed or for prognostic analysis for risk stratification.
Staging is determined mainly by tumor size, which is known to be associated with outcomes in patients with uveal melanoma, and is based on criteria from both the Collaborative Ocular Melanoma Study (COMS) staging system and the American Joint Committee on Cancer (AJCC) staging manual, Dr. Barker said.
The COMS system was developed based on separate studies of small, medium, and large tumors and helped define primary tumor management and establish existing standards of care. The AJCC system was developed subsequently and focuses more on tumor features that may improve clinical predictions.
Primary treatments
Options for primary treatment for small tumors (largest diameter 5-16 mm and thickness less than 2.5 mm) include plaque brachytherapy, partical beam radiation, and laser ablation in highly select patients. For medium tumors (18mm or less at largest diameter and thickness of 2.5-10 mm), they include plaque brachytherapy, particle beam radiation, and enucleation, according to the guidelines.
Large tumors can be treated with radiotherapy (preferably particle beam radiation, Dr. Barker said) or enucleation. Large tumors are those greater than 18mm with any thickness, those with thickness greater than 10mm with any diameter, and those with thickness greater than 8mm with optic nerve involvement.
In patients for whom surgical removal is selected, “ there are a few unusual situations where additional local adjuvant therapy might be considered,” Dr. Barker said, explaining, for example, that the presence of microscopically positive or close margins after enucleation without evidence of gross residual disease in the orbit may be observed or may warrant map biopsy and/or particle beam or photon beam radiotherapy to the orbit.
For visible extraocular tumors or suspicion of gross disease in the orbit, biopsy of the extraocular tissue is recommended when possible, along with either intraoperative cryotherapy, orbital exenteration, or particle beam or photon beam radiotherapy to the orbit, he added.
Metastatic risks and follow-up imaging
Recent studies, including Cancer Genome Atlas Research Network studies, have elucidated the genomics of both uveal and cutaneous melanomas, and they show “a completely different mutation spectrum” for uveal melanoma, Dr. Barker said.
These genomic studies demonstrate that cutaneous melanoma involves mutations that predict response to certain treatments, while those found in uveal melanoma do not, but they are, however, associated with the probability of metastasis, he said.
For example, various studies have shown that BRAF mutation in cutaneous melanoma predicts response to RAF or MEK inhibition and that the overall number of mutations in cutaneous melanoma may predict response to immunotherapy.
In uveal melanoma, alterations in ElFAX1, SF3B1, or BAP1 have been shown to indicate low, intermediate, and high risk of metastasis, respectively.
Other factors associated with the risk of metastasis after primary tumor treatment in uveal melanoma include clinical factors (tumor size, ciliary body involvement, and extraocular extension); histopathologic factors (spindle or epithelioid cell type); and cytogenetics (status of chromosomes 3, 6, and 8), he said.
An AJCC Ophthalmic Oncology Task Force study published in 2015, for example, showed that the 5-year metastasis-free survival was 97% for AJCC stage T1 disease, 85% for stage T2, 77% for stage T3, and 61% for stage T4. T-stage modifiers, which are based on particular tumor characteristics, such as ciliary body involvement (CBI) and extraocular extension (EXE), were also associated with the risk of distant metastasis: 5-year metastasis-free survival was 90%, 72%, 54% and 33% for AJCC T_a (no CBI or EXE), T_b (CBI only), T_c (EXE only), and T_d tumors (CBI and EXE), respectively.
Follow-up imaging after primary tumor treatment should be based on the most likely site of metastatic recurrence, which is the liver in 90% of uveal melanoma metastases.
“For this reason, surveillance of high-risk patients with uveal melanoma should include specific imaging of the liver,” Dr. Barker said, who noted that the NCCN risk stratification–based surveillance guidelines categorize patients as either low, medium, or high risk for metastasis based on the various characteristics that can affect risk.
“These risk groups help clinicians identify how often imaging should be performed in their surveillance strategy,” he said, adding that those who are high risk based on BAP1 mutation, PRAME mutation, CBI, or EXE, for example, should undergo imaging to evaluate signs or symptoms every 3-6 months for 5 years, every 6-12 months for 10 years, and then as clinically indicated thereafter.
The guideline calls for less stringent imaging for low- and medium-risk patients.
“Now, what happens when distant metastases are identified? Unfortunately there is no single systemic therapy that has proven to be most effective for uveal melanoma,” he said. “For this reason, the NCCN guideline encourages clinical trial participation whenever possible for patients who develop distant metastasis.”
This is because drugs effective for cutaneous melanoma are far less effective for uveal melanoma, but do elicit response in some patients and can be considered, he explained.
“Moreover, because the liver is the site of metastasis most often, and is often the exclusive site of metastasis, liver metastasis–directed therapy is considered part of the management of patients with uveal melanoma,” he said, adding that this can involve resection, ablation, chemo/radio embolization, or regional perfusion.”
The NCCN Uveal Melanoma Guidelines were developed by a panel of experts from various institutions based on the available evidence and on consensus; they are category 2A (based on lower-level evidence with uniform NCCN consensus that the intervention is appropriate).
Dr. Barker reported receiving clinical research support from Amgen, Bristol-Myers Squibb, Elekta, Merck, University of California San Francisco, and University of Florida Health Cancer Center Orlando, and serving as an advisor, consultant, or expert witness for Pfizer.
EXPERT ANALYSIS FROM THE NCCN ANNUAL CONFERENCE
Task force advises behavioral intervention for obese adults
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.

Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
For most primary care clinicians, referring obese patients for more advanced behavioral therapy will be the most practical integration of the recommendation, Susan Z. Yanovski, MD, wrote in an accompanying editorial. Clinicians with training in motivational interviewing or counseling may help assess a patient’s readiness for treatment, but even being familiar with weight-management resources in the community can help patients find the right fit.
“Clinicians can do their patients a great service by showing respect for their patients’ struggles with weight management, screening for obesity-related comorbidities, and providing treatment for identified conditions regardless of the patient’s motivation for, or success with, weight-loss treatment,” she said.
Dr. Yanovski noted that pharmacotherapy options have increased since the 2012 recommendations, when orlistat was the only approved drug for long-term treatment of obesity. Five medications are currently available for this indication.
The USPSTF review was limited in scope for both drug and behavior therapy, noted Dr. Yanovski. “Because the recommendations are meant to apply to adults without diseases for which weight loss is part of disease management, some large and long-term clinical trials conducted among patients with type 2 diabetes or cardiovascular disease were not included.”
Another limitation was the exclusion of surgical treatments as being outside the primary care setting, but bariatric surgery remains a viable option for many patients, especially for prevention or resolution of type 2 diabetes. Primary care clinicians are in a position to identify patients who might benefit and to provide referrals to surgeons if appropriate, she wrote.
Dr. Yanovski agreed with the recommendations but concluded that early strategies to prevent obesity should not be neglected. “Research to develop effective prevention strategies throughout the life course, including infancy and early childhood, could ultimately decrease the number of adults who must confront the difficult challenge of losing excess weight.”
Dr. Yanovski is affiliated with the National Institute of Diabetes and Digestive and Kidney Diseases. She disclosed that her spouse has received research funding from Zafgen and Rhythm Pharmaceuticals for studies of investigational products to treat obesity. Her comments are summarized from an editorial accompanying the articles by Curry SJ et al. and LeBlanc ES et al. (JAMA. 2018;320[11]:1111-3).
For most primary care clinicians, referring obese patients for more advanced behavioral therapy will be the most practical integration of the recommendation, Susan Z. Yanovski, MD, wrote in an accompanying editorial. Clinicians with training in motivational interviewing or counseling may help assess a patient’s readiness for treatment, but even being familiar with weight-management resources in the community can help patients find the right fit.
“Clinicians can do their patients a great service by showing respect for their patients’ struggles with weight management, screening for obesity-related comorbidities, and providing treatment for identified conditions regardless of the patient’s motivation for, or success with, weight-loss treatment,” she said.
Dr. Yanovski noted that pharmacotherapy options have increased since the 2012 recommendations, when orlistat was the only approved drug for long-term treatment of obesity. Five medications are currently available for this indication.
The USPSTF review was limited in scope for both drug and behavior therapy, noted Dr. Yanovski. “Because the recommendations are meant to apply to adults without diseases for which weight loss is part of disease management, some large and long-term clinical trials conducted among patients with type 2 diabetes or cardiovascular disease were not included.”
Another limitation was the exclusion of surgical treatments as being outside the primary care setting, but bariatric surgery remains a viable option for many patients, especially for prevention or resolution of type 2 diabetes. Primary care clinicians are in a position to identify patients who might benefit and to provide referrals to surgeons if appropriate, she wrote.
Dr. Yanovski agreed with the recommendations but concluded that early strategies to prevent obesity should not be neglected. “Research to develop effective prevention strategies throughout the life course, including infancy and early childhood, could ultimately decrease the number of adults who must confront the difficult challenge of losing excess weight.”
Dr. Yanovski is affiliated with the National Institute of Diabetes and Digestive and Kidney Diseases. She disclosed that her spouse has received research funding from Zafgen and Rhythm Pharmaceuticals for studies of investigational products to treat obesity. Her comments are summarized from an editorial accompanying the articles by Curry SJ et al. and LeBlanc ES et al. (JAMA. 2018;320[11]:1111-3).
For most primary care clinicians, referring obese patients for more advanced behavioral therapy will be the most practical integration of the recommendation, Susan Z. Yanovski, MD, wrote in an accompanying editorial. Clinicians with training in motivational interviewing or counseling may help assess a patient’s readiness for treatment, but even being familiar with weight-management resources in the community can help patients find the right fit.
“Clinicians can do their patients a great service by showing respect for their patients’ struggles with weight management, screening for obesity-related comorbidities, and providing treatment for identified conditions regardless of the patient’s motivation for, or success with, weight-loss treatment,” she said.
Dr. Yanovski noted that pharmacotherapy options have increased since the 2012 recommendations, when orlistat was the only approved drug for long-term treatment of obesity. Five medications are currently available for this indication.
The USPSTF review was limited in scope for both drug and behavior therapy, noted Dr. Yanovski. “Because the recommendations are meant to apply to adults without diseases for which weight loss is part of disease management, some large and long-term clinical trials conducted among patients with type 2 diabetes or cardiovascular disease were not included.”
Another limitation was the exclusion of surgical treatments as being outside the primary care setting, but bariatric surgery remains a viable option for many patients, especially for prevention or resolution of type 2 diabetes. Primary care clinicians are in a position to identify patients who might benefit and to provide referrals to surgeons if appropriate, she wrote.
Dr. Yanovski agreed with the recommendations but concluded that early strategies to prevent obesity should not be neglected. “Research to develop effective prevention strategies throughout the life course, including infancy and early childhood, could ultimately decrease the number of adults who must confront the difficult challenge of losing excess weight.”
Dr. Yanovski is affiliated with the National Institute of Diabetes and Digestive and Kidney Diseases. She disclosed that her spouse has received research funding from Zafgen and Rhythm Pharmaceuticals for studies of investigational products to treat obesity. Her comments are summarized from an editorial accompanying the articles by Curry SJ et al. and LeBlanc ES et al. (JAMA. 2018;320[11]:1111-3).
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.
Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
The U.S. Preventive Services Task Force advises clinicians to refer or offer intensive behavioral weight-loss interventions to obese adults, according to an updated recommendation statement published in JAMA.
Obesity affects more than one-third of U.S. adults, according to federal statistics. It carries increased risk for comorbidities including heart disease, diabetes, and various cancers, as well as increased risk of death among adults younger than 65 years, noted lead author Susan J. Curry, PhD, of the University of Iowa, Iowa City, and members of the Task Force.
The B recommendation applies to obese adults; obesity was defined as a body mass index of 30 kg/m2 or higher. The evidence review focused on interventions for weight loss and weight maintenance that could be provided in primary care or referred from primary care, such as nutrition counseling, exercise strategies, and goal setting.
The Task Force found adequate evidence that behavior-based weight-loss interventions improved weight, reduced incidence of type 2 diabetes, and helped maintain weight loss after interventions ended.
The Task Force found small to no evidence of harm associated with any of the behavioral weight-loss interventions, which included group sessions, personal sessions, print-based interventions, and technology-based interventions (such as text messages). Although interventions that combined drug therapy with behavioral intervention resulted in greater weight loss over 12-18 months, compared with behavioral interventions alone, the attrition rates were high and data on weight-loss maintenance after discontinuation of the drugs were limited, the Task Force noted.
“As a result, the USPSTF encourages clinicians to promote behavioral interventions as the primary focus of effective interventions for weight loss in adults,” they wrote.
The Task Force acknowledged the need for future research in subgroups and to explore whether factors such as genetics and untreated conditions are barriers to behavior-based weight loss interventions.
In the evidence review published in JAMA, Erin S. LeBlanc, MD, of Kaiser Permanente in Portland, Ore., and her colleagues reviewed data from 122 randomized, controlled trials including more than 62,000 persons and 2 observational studies including more than 209,000 persons.
The researchers found behavioral interventions were associated with greater weight loss and less risk of developing diabetes, compared with control interventions.
Intensive behavioral interventions included counseling patients about healthy eating, encouraging physical activity, setting weight and health goals, and assisting with weight monitoring. The interventions ranged from text messaging to in-person sessions for individuals or groups. The average absolute weight loss in the trials included in the review ranged from –0.5 kg to –9.3 kg (–1.1 lb to –20.5 lb) for intervention patients and from +1.4 kg to –5.6 kg (+3.1 lb to –12.3 lb) in controls.
Limitations of the review included a lack of data on population subgroups and a lack of long-term data on weight and health outcomes, the researchers noted. However, the results support the value of behavior-based therapy for obesity treatment.
The final recommendation is consistent with the 2018 draft recommendation and updates the 2012 final recommendation on obesity management.
The researchers and Task Force members had no relevant financial conflicts to disclose.
SOURCE: U.S. Preventive Services Task Force. JAMA. 2018;320(11):1163-71. doi: 10.1001/jama.2018.13022.
FROM JAMA
ASCO addresses financial barriers to cancer clinical trials
The American Society of Clinical Oncology (ASCO) has released a policy statement addressing financial barriers that may prevent cancer patients from participating in clinical trials.
The four main recommendations in ASCO’s policy statement are:
- Payers should create clear, consistent, streamlined, and transparent policies regarding clinical trial coverage.
- Patients should receive easy-to-understand information about potential out-of-pocket costs.
- “Ethically appropriate” financial compensation for out-of-pocket costs should be allowed.
- Researchers should be incentivized to investigate and “better characterize” costs incurred by cancer patients in clinical trials as well as identify ways to “mitigate the risk of trial-associated financial hardship.”
ASCO’s full policy statement, “Addressing Financial Barriers to Patient Participation in Clinical Trials,” is available on the Journal of Clinical Oncology website.
SOURCE: Winkfield KM et al. J Clin Oncol. 2018 Sep 13:JCO1801132. doi: 10.1200/JCO.18.01132.
The American Society of Clinical Oncology (ASCO) has released a policy statement addressing financial barriers that may prevent cancer patients from participating in clinical trials.
The four main recommendations in ASCO’s policy statement are:
- Payers should create clear, consistent, streamlined, and transparent policies regarding clinical trial coverage.
- Patients should receive easy-to-understand information about potential out-of-pocket costs.
- “Ethically appropriate” financial compensation for out-of-pocket costs should be allowed.
- Researchers should be incentivized to investigate and “better characterize” costs incurred by cancer patients in clinical trials as well as identify ways to “mitigate the risk of trial-associated financial hardship.”
ASCO’s full policy statement, “Addressing Financial Barriers to Patient Participation in Clinical Trials,” is available on the Journal of Clinical Oncology website.
SOURCE: Winkfield KM et al. J Clin Oncol. 2018 Sep 13:JCO1801132. doi: 10.1200/JCO.18.01132.
The American Society of Clinical Oncology (ASCO) has released a policy statement addressing financial barriers that may prevent cancer patients from participating in clinical trials.
The four main recommendations in ASCO’s policy statement are:
- Payers should create clear, consistent, streamlined, and transparent policies regarding clinical trial coverage.
- Patients should receive easy-to-understand information about potential out-of-pocket costs.
- “Ethically appropriate” financial compensation for out-of-pocket costs should be allowed.
- Researchers should be incentivized to investigate and “better characterize” costs incurred by cancer patients in clinical trials as well as identify ways to “mitigate the risk of trial-associated financial hardship.”
ASCO’s full policy statement, “Addressing Financial Barriers to Patient Participation in Clinical Trials,” is available on the Journal of Clinical Oncology website.
SOURCE: Winkfield KM et al. J Clin Oncol. 2018 Sep 13:JCO1801132. doi: 10.1200/JCO.18.01132.
FROM JOURNAL OF CLINICAL ONCOLOGY
Best practices defined for proton therapy in mediastinal lymphomas
Proton therapy can help mitigate toxicity in adults with mediastinal lymphomas, but only when this modality offers a clear advantage over intensity-modulated radiotherapy, according to new guidelines from the International Lymphoma Radiation Oncology Group.
Proton therapy reduces radiation dose to organs at risk in certain clinical presentations, such as when the mediastinal target is on both sides of the heart. The advantages are not always clear in other situations, such as when the target spans the right side of the heart, or when the target is above the heart with no axillary involvement, according to guideline authors Bouthaina Dabaja, MD, professor and section chief of hematology in the department of radiation oncology at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues.
“The limited availability of proton therapy calls for case selection based on a clear understanding of which cases will derive most benefit from proton therapy as compared to advanced photon techniques,” Dr. Dabaja and her coauthors said in the guidelines, which were published in the journal Blood (doi: 10.1182/blood-2018-03-837633).
Along with intensity-modulated radiotherapy and 3-dimensional conformal radiotherapy, proton therapy presents “another opportunity” for more conformal dose distribution and better sparing of organs at risk, according to the consensus recommendations. Proton therapy can greatly benefit certain patients with mediastinal disease. These include young female patients to reduce breast dose and risk of a secondary breast cancer, patients at high risk of radiation-related toxicity due to previous treatment, and patients with disease spanning below the origin of the left main stem coronary artery that is anterior to, posterior to, or on the left side of the heart.
“The relation of disease to organs at risk determines the situations in which proton therapy is most beneficial,” the experts said in the guidelines. However, the consideration of proton therapy needs to factor the complexities of proton therapy planning, the need to manage uncertainties, and the “evolving nature of the technology,” which includes the development of pencil beam scanning.
While passive scattering proton therapy (PSPT) is the least complex delivery technique, it is challenging because beams can conform only to one side of the target; by contrast, the experts said, active mode pencil beam scanning proton therapy (PBSPT) potentially provides better conformity and sparing of organs at risk.
“Because treatment involves delivery of individual controlled spots, inhomogenous doses can be created deliberately,” the guideline authors said in their report.
However, motion management is “of prime importance” with PBSPT, which is more sensitive to density changes in the beam path as compared to PSPT, they added. Toward that end, physicians should pay close attention to evaluating intrafractional movement, which is frequently tied to the breathing cycle.
The guidelines list a total of 11 authors representing The University of Texas MD Anderson Cancer Center; University of Florida, Jacksonville; University of Pennsylvania, Philadelphia; University of Louisiana, Baton Rouge; Proton Therapy Center Czech, Prague; Motol University Hospital, Czech Republic; St. Thomas and Guy Hospital, London; Institut Curie, Paris; and Rigshospitalet, Copenhagen.
Dr. Dabaja and her guideline coauthors reported no funding or conflicts of interest.
Proton therapy can help mitigate toxicity in adults with mediastinal lymphomas, but only when this modality offers a clear advantage over intensity-modulated radiotherapy, according to new guidelines from the International Lymphoma Radiation Oncology Group.
Proton therapy reduces radiation dose to organs at risk in certain clinical presentations, such as when the mediastinal target is on both sides of the heart. The advantages are not always clear in other situations, such as when the target spans the right side of the heart, or when the target is above the heart with no axillary involvement, according to guideline authors Bouthaina Dabaja, MD, professor and section chief of hematology in the department of radiation oncology at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues.
“The limited availability of proton therapy calls for case selection based on a clear understanding of which cases will derive most benefit from proton therapy as compared to advanced photon techniques,” Dr. Dabaja and her coauthors said in the guidelines, which were published in the journal Blood (doi: 10.1182/blood-2018-03-837633).
Along with intensity-modulated radiotherapy and 3-dimensional conformal radiotherapy, proton therapy presents “another opportunity” for more conformal dose distribution and better sparing of organs at risk, according to the consensus recommendations. Proton therapy can greatly benefit certain patients with mediastinal disease. These include young female patients to reduce breast dose and risk of a secondary breast cancer, patients at high risk of radiation-related toxicity due to previous treatment, and patients with disease spanning below the origin of the left main stem coronary artery that is anterior to, posterior to, or on the left side of the heart.
“The relation of disease to organs at risk determines the situations in which proton therapy is most beneficial,” the experts said in the guidelines. However, the consideration of proton therapy needs to factor the complexities of proton therapy planning, the need to manage uncertainties, and the “evolving nature of the technology,” which includes the development of pencil beam scanning.
While passive scattering proton therapy (PSPT) is the least complex delivery technique, it is challenging because beams can conform only to one side of the target; by contrast, the experts said, active mode pencil beam scanning proton therapy (PBSPT) potentially provides better conformity and sparing of organs at risk.
“Because treatment involves delivery of individual controlled spots, inhomogenous doses can be created deliberately,” the guideline authors said in their report.
However, motion management is “of prime importance” with PBSPT, which is more sensitive to density changes in the beam path as compared to PSPT, they added. Toward that end, physicians should pay close attention to evaluating intrafractional movement, which is frequently tied to the breathing cycle.
The guidelines list a total of 11 authors representing The University of Texas MD Anderson Cancer Center; University of Florida, Jacksonville; University of Pennsylvania, Philadelphia; University of Louisiana, Baton Rouge; Proton Therapy Center Czech, Prague; Motol University Hospital, Czech Republic; St. Thomas and Guy Hospital, London; Institut Curie, Paris; and Rigshospitalet, Copenhagen.
Dr. Dabaja and her guideline coauthors reported no funding or conflicts of interest.
Proton therapy can help mitigate toxicity in adults with mediastinal lymphomas, but only when this modality offers a clear advantage over intensity-modulated radiotherapy, according to new guidelines from the International Lymphoma Radiation Oncology Group.
Proton therapy reduces radiation dose to organs at risk in certain clinical presentations, such as when the mediastinal target is on both sides of the heart. The advantages are not always clear in other situations, such as when the target spans the right side of the heart, or when the target is above the heart with no axillary involvement, according to guideline authors Bouthaina Dabaja, MD, professor and section chief of hematology in the department of radiation oncology at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues.
“The limited availability of proton therapy calls for case selection based on a clear understanding of which cases will derive most benefit from proton therapy as compared to advanced photon techniques,” Dr. Dabaja and her coauthors said in the guidelines, which were published in the journal Blood (doi: 10.1182/blood-2018-03-837633).
Along with intensity-modulated radiotherapy and 3-dimensional conformal radiotherapy, proton therapy presents “another opportunity” for more conformal dose distribution and better sparing of organs at risk, according to the consensus recommendations. Proton therapy can greatly benefit certain patients with mediastinal disease. These include young female patients to reduce breast dose and risk of a secondary breast cancer, patients at high risk of radiation-related toxicity due to previous treatment, and patients with disease spanning below the origin of the left main stem coronary artery that is anterior to, posterior to, or on the left side of the heart.
“The relation of disease to organs at risk determines the situations in which proton therapy is most beneficial,” the experts said in the guidelines. However, the consideration of proton therapy needs to factor the complexities of proton therapy planning, the need to manage uncertainties, and the “evolving nature of the technology,” which includes the development of pencil beam scanning.
While passive scattering proton therapy (PSPT) is the least complex delivery technique, it is challenging because beams can conform only to one side of the target; by contrast, the experts said, active mode pencil beam scanning proton therapy (PBSPT) potentially provides better conformity and sparing of organs at risk.
“Because treatment involves delivery of individual controlled spots, inhomogenous doses can be created deliberately,” the guideline authors said in their report.
However, motion management is “of prime importance” with PBSPT, which is more sensitive to density changes in the beam path as compared to PSPT, they added. Toward that end, physicians should pay close attention to evaluating intrafractional movement, which is frequently tied to the breathing cycle.
The guidelines list a total of 11 authors representing The University of Texas MD Anderson Cancer Center; University of Florida, Jacksonville; University of Pennsylvania, Philadelphia; University of Louisiana, Baton Rouge; Proton Therapy Center Czech, Prague; Motol University Hospital, Czech Republic; St. Thomas and Guy Hospital, London; Institut Curie, Paris; and Rigshospitalet, Copenhagen.
Dr. Dabaja and her guideline coauthors reported no funding or conflicts of interest.
FROM BLOOD
U.S. perspective: Euro hypertension guidelines look a lot like ours
MUNICH – The “overwhelming impression” that Paul K. Whelton, MD, has of the newly revised hypertension diagnosis and management guidelines of the European Society of Cardiology is their similarity to hypertension guidelines released by the American College of Cardiology and American Heart Association in November 2017.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“We both recommend the same treatment target, of less than 130/80 mm Hg,” noted Dr. Whelton, professor at Tulane University in New Orleans, although the European guidelines (Euro J Cardiology. 2018 Sep 1; 39[33]:3021-104) put more qualifications on this target and specify treating to no lower than 130 mm Hg systolic pressure in patients who are at least 65 years old as well as in patients with chronic kidney disease at any age. In a video interview, Dr. Whelton also cited areas of disagreement, such as how patients with an untreated blood pressure of 130-139 mm Hg are classified (high normal in the European guidelines, stage 1 hypertension in the U.S. guidelines), and whether initial drug monotherapy is a reasonable treatment strategy (U.S. says yes, Europe says no).
Dr. Whelton noted that recent modeling studies have documented the potential public health benefits from following the diagnosis and management approaches set forth in the 2017 U.S. guidelines (J Am Coll Cardiol. 2018 May;71[19]:e127-e248). For example, an analysis based on data collected by the U.S. National Health and Nutrition Examination Survey during 2013-2016 showed that following the 2017 guidelines for diagnosing and treating hypertension would have resulted in prevention of more than twice the number of cardiovascular disease events nationally as compared with application of the prior, 2014 U.S. hypertension guideline (JAMA. 2014 Feb 5;311[5]:507-20): 610,000 events prevented, compared with 270,000 events prevented. The same study showed that the 2017 guidelines would have nearly doubled the number of all-cause deaths prevented, with 334,000 deaths prevented, compared with 177,000 prevented by applying the 2014 guidelines (JAMA Cardiology. 2018 July;3[7]:572-81).
Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MUNICH – The “overwhelming impression” that Paul K. Whelton, MD, has of the newly revised hypertension diagnosis and management guidelines of the European Society of Cardiology is their similarity to hypertension guidelines released by the American College of Cardiology and American Heart Association in November 2017.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“We both recommend the same treatment target, of less than 130/80 mm Hg,” noted Dr. Whelton, professor at Tulane University in New Orleans, although the European guidelines (Euro J Cardiology. 2018 Sep 1; 39[33]:3021-104) put more qualifications on this target and specify treating to no lower than 130 mm Hg systolic pressure in patients who are at least 65 years old as well as in patients with chronic kidney disease at any age. In a video interview, Dr. Whelton also cited areas of disagreement, such as how patients with an untreated blood pressure of 130-139 mm Hg are classified (high normal in the European guidelines, stage 1 hypertension in the U.S. guidelines), and whether initial drug monotherapy is a reasonable treatment strategy (U.S. says yes, Europe says no).
Dr. Whelton noted that recent modeling studies have documented the potential public health benefits from following the diagnosis and management approaches set forth in the 2017 U.S. guidelines (J Am Coll Cardiol. 2018 May;71[19]:e127-e248). For example, an analysis based on data collected by the U.S. National Health and Nutrition Examination Survey during 2013-2016 showed that following the 2017 guidelines for diagnosing and treating hypertension would have resulted in prevention of more than twice the number of cardiovascular disease events nationally as compared with application of the prior, 2014 U.S. hypertension guideline (JAMA. 2014 Feb 5;311[5]:507-20): 610,000 events prevented, compared with 270,000 events prevented. The same study showed that the 2017 guidelines would have nearly doubled the number of all-cause deaths prevented, with 334,000 deaths prevented, compared with 177,000 prevented by applying the 2014 guidelines (JAMA Cardiology. 2018 July;3[7]:572-81).
Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MUNICH – The “overwhelming impression” that Paul K. Whelton, MD, has of the newly revised hypertension diagnosis and management guidelines of the European Society of Cardiology is their similarity to hypertension guidelines released by the American College of Cardiology and American Heart Association in November 2017.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“We both recommend the same treatment target, of less than 130/80 mm Hg,” noted Dr. Whelton, professor at Tulane University in New Orleans, although the European guidelines (Euro J Cardiology. 2018 Sep 1; 39[33]:3021-104) put more qualifications on this target and specify treating to no lower than 130 mm Hg systolic pressure in patients who are at least 65 years old as well as in patients with chronic kidney disease at any age. In a video interview, Dr. Whelton also cited areas of disagreement, such as how patients with an untreated blood pressure of 130-139 mm Hg are classified (high normal in the European guidelines, stage 1 hypertension in the U.S. guidelines), and whether initial drug monotherapy is a reasonable treatment strategy (U.S. says yes, Europe says no).
Dr. Whelton noted that recent modeling studies have documented the potential public health benefits from following the diagnosis and management approaches set forth in the 2017 U.S. guidelines (J Am Coll Cardiol. 2018 May;71[19]:e127-e248). For example, an analysis based on data collected by the U.S. National Health and Nutrition Examination Survey during 2013-2016 showed that following the 2017 guidelines for diagnosing and treating hypertension would have resulted in prevention of more than twice the number of cardiovascular disease events nationally as compared with application of the prior, 2014 U.S. hypertension guideline (JAMA. 2014 Feb 5;311[5]:507-20): 610,000 events prevented, compared with 270,000 events prevented. The same study showed that the 2017 guidelines would have nearly doubled the number of all-cause deaths prevented, with 334,000 deaths prevented, compared with 177,000 prevented by applying the 2014 guidelines (JAMA Cardiology. 2018 July;3[7]:572-81).
Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM THE ESC CONGRESS 2018
New Euro hypertension guidelines target most adults to less than 130/80 mm Hg
MUNICH – The European Society of Cardiology joined other international cardiology groups in endorsing lower targets for blood pressure treatment and lower pressure thresholds for starting drug treatment in its revised hypertension diagnosis and management guidelines released in August during the Society’s annual congress here.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Provided that treatment is well tolerated, treated blood pressure should be targeted to 130/80 mm Hg or lower in most patients,” Giuseppe Mancia, MD, said as he and his colleagues presented the new guidelines at the annual congress of the European Society of Cardiology.
Although the new European guidelines further buttress this more aggressive approach to blood pressure management that first appeared almost a year ago in U.S. guidelines from the American College of Cardiology and the American Heart Association, an approach that remains controversial among U.S. primary care physicians, the European strategy (Eur Heart J. 2018 Sep 1;39[33]:3021-104) was generally more cautious than the broader endorsement of lower blood pressure goals advanced by the U.S. recommendations (J Am Coll Cardiol. 2018 May;71[19]:e127-e248).
In the European approach, “the first objective is to treat to less than 140/90 mm Hg. If this is well tolerated, then treat to less than 130/80 mm Hg in most patients,” said Dr. Mancia, cochair of the European writing panel. Further pressure reductions to less than 130/80 mm Hg are usually harder, the incremental benefit from further reduction is less than when pressures first fall below 140/90 mm Hg, and the evidence for incremental benefit of any size from further pressure reduction is less strong for certain key patient subgroups: people at least 80 years old, and patients with diabetes, chronic kidney disease, or coronary artery disease, said Dr. Mancia, an emeritus professor at the University of Milan.
“The consistency between two major guidelines is important, but there are differences that may look subtle but are not subtle,” he said in a video interview. “If a patient gets to less than 140 mm Hg, the doctor should not think that’s a failure; it’s a very important result.”
One striking example of how the two guidelines differ on treatment targets is for people at least 80 years old. The overall blood pressure threshold for starting drug treatment in patients this age in the European guidelines is 160/90 mm Hg, although it remains at 140/90 for people aged 65-79 years old “provided that treatment is well tolerated” and the patients are “fit.” The 2017 U.S. guidelines, by contrast, say that considering drug treatment for everyone with a pressure at or above 130/80 mm Hg is a class I recommendation regardless of age as long as the person is “noninstitutionalized, ambulatory, [and] community-dwelling.” Once an older patient of any age, 65 years or older, starts drug treatment to reduce blood pressure, the European guidelines allow for treating to a target systolic blood pressure of 130-139 mm Hg as long as the regimen is well tolerated, and the guidelines say that a diastolic pressure target of less than 80 mm Hg should be considered for all adults regardless of age.
The new European guidelines also define adults with an untreated pressure of 130-139/85-89 mm Hg as “high normal,” rather than the “stage 1 hypertension” designation given to people with pressures of 130-139/80-89 mm Hg in the U.S. guidelines. Robert M. Carey, MD, vice chair of the U.S. guidelines panel, minimized this as a “semantic” difference, and he highlighted that management of people with pressures in this range is roughly similar in the two sets of recommendations. “The name is different, but treatment is the same,” Dr. Carey said.
The European guidelines call for initial lifestyle interventions, followed by drug treatment “that may be considered” for patients who have “very-high” cardiovascular risk because of established cardiovascular disease, especially coronary artery disease, and detail the specific clinical conditions that fall into the very-high-risk category. The U.S. guidelines say that stage 1 hypertension patients should get lifestyle interventions, followed by drug treatment for the roughly 30% of patients in this category who score at least a 10% 10-year risk on the American College of Cardiology’s Atherosclerotic Cardiovascular Disease Risk Estimator Plus.The new European guidelines are a “validation” of the ACC/AHA 2017 guidelines, commented Dr. Carey, a professor of medicine at the University of Virginia in Charlottesville. “Overall, we’re delighted to have these two major groups” agree, he said in an interview. “There is a tremendous amount of concurrence.”
Other areas of agreement between the two guidelines include their emphasis on careful and repeated blood pressure measurement, including out-of-office measurement, before settling on a diagnosis of hypertension; systematic assessment of possible masked or white-coat hypertension in selected people; and frequent use of combined drug treatment including initiation of a dual-drug, single-pill regimen when starting drug treatment and aggressive follow-up by adding a third drug when needed. However, in another divergence the U.S. guidelines give a much stronger endorsement to starting treatment with monotherapy, a strategy the European guidelines scrapped.


Dr. Carey also noted that the European endorsement of three antihypertensives formulated into a single pill for patients who need more than two drugs would be difficult for American clinicians to follow as virtually no such formulations are approved for U.S. use.
Dr. Mancini has received honoraria from Boehringer Ingelheim, CVRx, Daiichi Sankyo, Ferrer, Medtronic, Menarini, Merck, Novartis, Recordati, and Servier. Dr. Williams has been a consultant to Novartis, Relypsa, and Vascular Dynamics, and he has spoken on behalf of Boehringer Ingelheim, Daiichi Sankyo, Novartis, and Servier. Dr. Carey and Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MUNICH – The European Society of Cardiology joined other international cardiology groups in endorsing lower targets for blood pressure treatment and lower pressure thresholds for starting drug treatment in its revised hypertension diagnosis and management guidelines released in August during the Society’s annual congress here.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Provided that treatment is well tolerated, treated blood pressure should be targeted to 130/80 mm Hg or lower in most patients,” Giuseppe Mancia, MD, said as he and his colleagues presented the new guidelines at the annual congress of the European Society of Cardiology.
Although the new European guidelines further buttress this more aggressive approach to blood pressure management that first appeared almost a year ago in U.S. guidelines from the American College of Cardiology and the American Heart Association, an approach that remains controversial among U.S. primary care physicians, the European strategy (Eur Heart J. 2018 Sep 1;39[33]:3021-104) was generally more cautious than the broader endorsement of lower blood pressure goals advanced by the U.S. recommendations (J Am Coll Cardiol. 2018 May;71[19]:e127-e248).
In the European approach, “the first objective is to treat to less than 140/90 mm Hg. If this is well tolerated, then treat to less than 130/80 mm Hg in most patients,” said Dr. Mancia, cochair of the European writing panel. Further pressure reductions to less than 130/80 mm Hg are usually harder, the incremental benefit from further reduction is less than when pressures first fall below 140/90 mm Hg, and the evidence for incremental benefit of any size from further pressure reduction is less strong for certain key patient subgroups: people at least 80 years old, and patients with diabetes, chronic kidney disease, or coronary artery disease, said Dr. Mancia, an emeritus professor at the University of Milan.
“The consistency between two major guidelines is important, but there are differences that may look subtle but are not subtle,” he said in a video interview. “If a patient gets to less than 140 mm Hg, the doctor should not think that’s a failure; it’s a very important result.”
One striking example of how the two guidelines differ on treatment targets is for people at least 80 years old. The overall blood pressure threshold for starting drug treatment in patients this age in the European guidelines is 160/90 mm Hg, although it remains at 140/90 for people aged 65-79 years old “provided that treatment is well tolerated” and the patients are “fit.” The 2017 U.S. guidelines, by contrast, say that considering drug treatment for everyone with a pressure at or above 130/80 mm Hg is a class I recommendation regardless of age as long as the person is “noninstitutionalized, ambulatory, [and] community-dwelling.” Once an older patient of any age, 65 years or older, starts drug treatment to reduce blood pressure, the European guidelines allow for treating to a target systolic blood pressure of 130-139 mm Hg as long as the regimen is well tolerated, and the guidelines say that a diastolic pressure target of less than 80 mm Hg should be considered for all adults regardless of age.
The new European guidelines also define adults with an untreated pressure of 130-139/85-89 mm Hg as “high normal,” rather than the “stage 1 hypertension” designation given to people with pressures of 130-139/80-89 mm Hg in the U.S. guidelines. Robert M. Carey, MD, vice chair of the U.S. guidelines panel, minimized this as a “semantic” difference, and he highlighted that management of people with pressures in this range is roughly similar in the two sets of recommendations. “The name is different, but treatment is the same,” Dr. Carey said.
The European guidelines call for initial lifestyle interventions, followed by drug treatment “that may be considered” for patients who have “very-high” cardiovascular risk because of established cardiovascular disease, especially coronary artery disease, and detail the specific clinical conditions that fall into the very-high-risk category. The U.S. guidelines say that stage 1 hypertension patients should get lifestyle interventions, followed by drug treatment for the roughly 30% of patients in this category who score at least a 10% 10-year risk on the American College of Cardiology’s Atherosclerotic Cardiovascular Disease Risk Estimator Plus.The new European guidelines are a “validation” of the ACC/AHA 2017 guidelines, commented Dr. Carey, a professor of medicine at the University of Virginia in Charlottesville. “Overall, we’re delighted to have these two major groups” agree, he said in an interview. “There is a tremendous amount of concurrence.”
Other areas of agreement between the two guidelines include their emphasis on careful and repeated blood pressure measurement, including out-of-office measurement, before settling on a diagnosis of hypertension; systematic assessment of possible masked or white-coat hypertension in selected people; and frequent use of combined drug treatment including initiation of a dual-drug, single-pill regimen when starting drug treatment and aggressive follow-up by adding a third drug when needed. However, in another divergence the U.S. guidelines give a much stronger endorsement to starting treatment with monotherapy, a strategy the European guidelines scrapped.
Dr. Carey also noted that the European endorsement of three antihypertensives formulated into a single pill for patients who need more than two drugs would be difficult for American clinicians to follow as virtually no such formulations are approved for U.S. use.
Dr. Mancini has received honoraria from Boehringer Ingelheim, CVRx, Daiichi Sankyo, Ferrer, Medtronic, Menarini, Merck, Novartis, Recordati, and Servier. Dr. Williams has been a consultant to Novartis, Relypsa, and Vascular Dynamics, and he has spoken on behalf of Boehringer Ingelheim, Daiichi Sankyo, Novartis, and Servier. Dr. Carey and Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MUNICH – The European Society of Cardiology joined other international cardiology groups in endorsing lower targets for blood pressure treatment and lower pressure thresholds for starting drug treatment in its revised hypertension diagnosis and management guidelines released in August during the Society’s annual congress here.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
“Provided that treatment is well tolerated, treated blood pressure should be targeted to 130/80 mm Hg or lower in most patients,” Giuseppe Mancia, MD, said as he and his colleagues presented the new guidelines at the annual congress of the European Society of Cardiology.
Although the new European guidelines further buttress this more aggressive approach to blood pressure management that first appeared almost a year ago in U.S. guidelines from the American College of Cardiology and the American Heart Association, an approach that remains controversial among U.S. primary care physicians, the European strategy (Eur Heart J. 2018 Sep 1;39[33]:3021-104) was generally more cautious than the broader endorsement of lower blood pressure goals advanced by the U.S. recommendations (J Am Coll Cardiol. 2018 May;71[19]:e127-e248).
In the European approach, “the first objective is to treat to less than 140/90 mm Hg. If this is well tolerated, then treat to less than 130/80 mm Hg in most patients,” said Dr. Mancia, cochair of the European writing panel. Further pressure reductions to less than 130/80 mm Hg are usually harder, the incremental benefit from further reduction is less than when pressures first fall below 140/90 mm Hg, and the evidence for incremental benefit of any size from further pressure reduction is less strong for certain key patient subgroups: people at least 80 years old, and patients with diabetes, chronic kidney disease, or coronary artery disease, said Dr. Mancia, an emeritus professor at the University of Milan.
“The consistency between two major guidelines is important, but there are differences that may look subtle but are not subtle,” he said in a video interview. “If a patient gets to less than 140 mm Hg, the doctor should not think that’s a failure; it’s a very important result.”
One striking example of how the two guidelines differ on treatment targets is for people at least 80 years old. The overall blood pressure threshold for starting drug treatment in patients this age in the European guidelines is 160/90 mm Hg, although it remains at 140/90 for people aged 65-79 years old “provided that treatment is well tolerated” and the patients are “fit.” The 2017 U.S. guidelines, by contrast, say that considering drug treatment for everyone with a pressure at or above 130/80 mm Hg is a class I recommendation regardless of age as long as the person is “noninstitutionalized, ambulatory, [and] community-dwelling.” Once an older patient of any age, 65 years or older, starts drug treatment to reduce blood pressure, the European guidelines allow for treating to a target systolic blood pressure of 130-139 mm Hg as long as the regimen is well tolerated, and the guidelines say that a diastolic pressure target of less than 80 mm Hg should be considered for all adults regardless of age.
The new European guidelines also define adults with an untreated pressure of 130-139/85-89 mm Hg as “high normal,” rather than the “stage 1 hypertension” designation given to people with pressures of 130-139/80-89 mm Hg in the U.S. guidelines. Robert M. Carey, MD, vice chair of the U.S. guidelines panel, minimized this as a “semantic” difference, and he highlighted that management of people with pressures in this range is roughly similar in the two sets of recommendations. “The name is different, but treatment is the same,” Dr. Carey said.
The European guidelines call for initial lifestyle interventions, followed by drug treatment “that may be considered” for patients who have “very-high” cardiovascular risk because of established cardiovascular disease, especially coronary artery disease, and detail the specific clinical conditions that fall into the very-high-risk category. The U.S. guidelines say that stage 1 hypertension patients should get lifestyle interventions, followed by drug treatment for the roughly 30% of patients in this category who score at least a 10% 10-year risk on the American College of Cardiology’s Atherosclerotic Cardiovascular Disease Risk Estimator Plus.The new European guidelines are a “validation” of the ACC/AHA 2017 guidelines, commented Dr. Carey, a professor of medicine at the University of Virginia in Charlottesville. “Overall, we’re delighted to have these two major groups” agree, he said in an interview. “There is a tremendous amount of concurrence.”
Other areas of agreement between the two guidelines include their emphasis on careful and repeated blood pressure measurement, including out-of-office measurement, before settling on a diagnosis of hypertension; systematic assessment of possible masked or white-coat hypertension in selected people; and frequent use of combined drug treatment including initiation of a dual-drug, single-pill regimen when starting drug treatment and aggressive follow-up by adding a third drug when needed. However, in another divergence the U.S. guidelines give a much stronger endorsement to starting treatment with monotherapy, a strategy the European guidelines scrapped.
Dr. Carey also noted that the European endorsement of three antihypertensives formulated into a single pill for patients who need more than two drugs would be difficult for American clinicians to follow as virtually no such formulations are approved for U.S. use.
Dr. Mancini has received honoraria from Boehringer Ingelheim, CVRx, Daiichi Sankyo, Ferrer, Medtronic, Menarini, Merck, Novartis, Recordati, and Servier. Dr. Williams has been a consultant to Novartis, Relypsa, and Vascular Dynamics, and he has spoken on behalf of Boehringer Ingelheim, Daiichi Sankyo, Novartis, and Servier. Dr. Carey and Dr. Whelton had no commercial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
REPORTING FROM THE ESC CONGRESS 2018

Updated AHA recommendations favor nonstatin therapy for cholesterol control
Importance
While statins remain the foundation for treating high cholesterol in order to reduce cardiovascular risk, new evidence has lead to important revisions in the American Heart Association’s recommendations for treatment of hypercholesterolemia in patients at very high cardiovascular risk (secondary prevention) with the addition of specific nonstatin agents. We will briefly review the AHA 2013 guideline recommendations, the relevant new information, and the updated AHA recommendations.
American Heart Association 2013 guidelines
The 2013 American College of Cardiology/AHA cholesterol guidelines recommend either high- or moderate-intensity statin therapy for patients in the four statin benefit groups:
1. Adult patients older than 21 years of age with clinical atherosclerotic cardiovascular disease (ASCVD).
2. Adults older than 21 years of age with low-density lipoprotein cholesterol (LDL-C) above 190 mg/dL.
3. Adults aged 40-75 years without ASCVD but with diabetes and with LDL-C 70-189 mg/dL.
4. Adults aged 40-75 years without either ASCVD or diabetes, with LDL-C 70-189 mg/dL and an estimated 10-year risk for ASCVD of over 7.5% as determined by the Pooled Cohort Equations.
At the time of the 2013 guidelines, there was little evidence to recommend the use of medications other than statins.
Recent evidence
The IMPROVE-IT trial1 was a double-blind, randomized trial involving 18,144 men and women who were older than 50 years and hospitalized for an acute coronary syndrome within the preceding 10 days. They were randomized to either simvastatin plus ezetimibe or simvastatin plus placebo. The primary endpoints were a composite of death from cardiovascular disease, a major coronary event (nonfatal MI, unstable angina requiring admission, or coronary revascularization), or nonfatal stroke. At 1 year, the mean LDL was 69.9 mg/dL in the simvastatin-monotherapy group and 53.2 mg/dL in the simvastatin-ezetimibe group (P under .001), representing a 24% decrease in LDL between the two groups. The rate of the primary endpoints was significantly lower in the simvastatin plus ezetimibe group with a hazard ratio of 0.936 (P = .016). The risk of MI was significantly decreased with an HR of 0.87 (P = .002), and the risk of ischemic stroke significantly decreased with an HR of 0.79 (P = .008). Prespecified safety endpoints showed no significant difference between the two groups.
The FOURIER trial2 examined the PCSK-9 inhibitor, evolocumab. FOURIER was a randomized, double-blind, placebo-controlled study involving 27,564 patients with atherosclerotic cardiovascular disease and LDL levels of 70 mg/dL or higher who were receiving statin therapy (at least atorvastatin 20 mg or equivalent with/without ezetimibe). Patients were between 45 and 80 years old with a history of history of MI, nonhemorrhagic stroke, or symptomatic peripheral artery disease. Patients were randomized to receive subcutaneous injections of evolocumab or matching placebo. The primary endpoints were similar to that of IMPROVE-IT: a composite of cardiovascular death, myocardial infarction, stroke, unstable angina hospitalization, and coronary revascularization. The median LDL on entry was 92 mg/dL for both groups. At 48 weeks, the evolocumab group showed a 59% decrease in LDL, compared with placebo, with a decrease in median LDL from 92 mg/dL to 30 mg/dL. The primary endpoint occurred in 9.8% of the evolocumab group and 11.3% in the placebo group for a hazard ratio of 0.85 (P less than .001) representing a total risk reduction of 13.2%. The risk of MI or stroke and need for revascularization were significantly lower values in the evolocumab group, compared with placebo. Cardiovascular death did not show significant changes. There was no significant difference in rate of serious events.
The ODYSSEY trial3 reported on another PCSK-9 inhibitor, alirocumab, in a randomized, double-blind, placebo-controlled trial involving 18,924 patients who had an ACS in the prior 12 months. At the median follow-up (2.8 years), the LDL of the alirocumab group was 53.3 mg/dL, compared with 101.4 mg/dL in the placebo group. The primary endpoints for cardiovascular risks were similar to those in the FOURIER trial: a risk of 9.5% in the alirocumab group and 11.1% in the placebo group for a total risk reduction of 14.4%. This suggests the class of PCSK-9 inhibitors have a strong correlation with reducing LDL levels 54%-59% and reducing major cardiac adverse events by 13%-15%.
Recommendations
The American College of Cardiology released a focused update that integrated the new evidence regarding the use of nonstatin therapy. The current focused update recommends an overall 50% or greater reduction in LDL for patients with clinical ASCVD. If this reduction is not achieved, ACC suggests that one consider the addition of nonstatin therapy with either ezetimibe or a PCSK-9 inhibitor.4 If a patient requires less than 25% additional LDL reduction, consider ezetimibe; if a patient requires more than 25% additional LDL reduction, consider a PCSK-9 inhibitor. Specifically, the guideline states: “If the patient still has less than 50% reduction in LDL-C (and may consider LDL-C above 70 mg/dL or non–HDL-C above 100 mg/dL), the patient and clinician should enter into a discussion focused on shared decision making regarding the addition of a nonstatin medication to the current regimen.”
The other group that is mentioned in the recommendations, with an acknowledgment that the evidence for benefit in primary prevention is not available, is individuals who have an LDL above 190 mg/dL even while compliant with a maximally effective statin regimen. The guidelines make further but less strong recommendations about a number of risk groups, but the largest and strongest change, based on strong evidence, is the recommendation to consider nonstatin therapy in individuals with established ASCVD, as described above.
Bottom line
Recent trials show significant reductions in LDL, leading to significant reductions in cardiovascular endpoints with ezetimibe and PCSK-9 inhibitors. This has led to an additional ACC recommendation to consider the use of nonstatin therapy in addition to maximal statin therapy in selected patients with established cardiovascular disease.
References
1. Cannon C et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387-97.
2. Sabatine M et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713-22.
3. ODYSSEY Outcomes: Results suggest use of PCSK9 inhibitor reduces CV events, LDL-C in ACS patients. Article from American College of Cardiology. ACC News Story. 2018 Mar 10.
4. Lloyd-Jones DM et al. 2017 Focused update of the 2016 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology task force on expert consensus decision pathways. J Am Coll Cardiol. 2017 Oct 3;70(14):1785-1822. Epub 2017 Sep 5.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Plako is a second-year resident in the family medicine residency program at Abington Jefferson Hospital.
Importance
While statins remain the foundation for treating high cholesterol in order to reduce cardiovascular risk, new evidence has lead to important revisions in the American Heart Association’s recommendations for treatment of hypercholesterolemia in patients at very high cardiovascular risk (secondary prevention) with the addition of specific nonstatin agents. We will briefly review the AHA 2013 guideline recommendations, the relevant new information, and the updated AHA recommendations.
American Heart Association 2013 guidelines
The 2013 American College of Cardiology/AHA cholesterol guidelines recommend either high- or moderate-intensity statin therapy for patients in the four statin benefit groups:
1. Adult patients older than 21 years of age with clinical atherosclerotic cardiovascular disease (ASCVD).
2. Adults older than 21 years of age with low-density lipoprotein cholesterol (LDL-C) above 190 mg/dL.
3. Adults aged 40-75 years without ASCVD but with diabetes and with LDL-C 70-189 mg/dL.
4. Adults aged 40-75 years without either ASCVD or diabetes, with LDL-C 70-189 mg/dL and an estimated 10-year risk for ASCVD of over 7.5% as determined by the Pooled Cohort Equations.
At the time of the 2013 guidelines, there was little evidence to recommend the use of medications other than statins.
Recent evidence
The IMPROVE-IT trial1 was a double-blind, randomized trial involving 18,144 men and women who were older than 50 years and hospitalized for an acute coronary syndrome within the preceding 10 days. They were randomized to either simvastatin plus ezetimibe or simvastatin plus placebo. The primary endpoints were a composite of death from cardiovascular disease, a major coronary event (nonfatal MI, unstable angina requiring admission, or coronary revascularization), or nonfatal stroke. At 1 year, the mean LDL was 69.9 mg/dL in the simvastatin-monotherapy group and 53.2 mg/dL in the simvastatin-ezetimibe group (P under .001), representing a 24% decrease in LDL between the two groups. The rate of the primary endpoints was significantly lower in the simvastatin plus ezetimibe group with a hazard ratio of 0.936 (P = .016). The risk of MI was significantly decreased with an HR of 0.87 (P = .002), and the risk of ischemic stroke significantly decreased with an HR of 0.79 (P = .008). Prespecified safety endpoints showed no significant difference between the two groups.
The FOURIER trial2 examined the PCSK-9 inhibitor, evolocumab. FOURIER was a randomized, double-blind, placebo-controlled study involving 27,564 patients with atherosclerotic cardiovascular disease and LDL levels of 70 mg/dL or higher who were receiving statin therapy (at least atorvastatin 20 mg or equivalent with/without ezetimibe). Patients were between 45 and 80 years old with a history of history of MI, nonhemorrhagic stroke, or symptomatic peripheral artery disease. Patients were randomized to receive subcutaneous injections of evolocumab or matching placebo. The primary endpoints were similar to that of IMPROVE-IT: a composite of cardiovascular death, myocardial infarction, stroke, unstable angina hospitalization, and coronary revascularization. The median LDL on entry was 92 mg/dL for both groups. At 48 weeks, the evolocumab group showed a 59% decrease in LDL, compared with placebo, with a decrease in median LDL from 92 mg/dL to 30 mg/dL. The primary endpoint occurred in 9.8% of the evolocumab group and 11.3% in the placebo group for a hazard ratio of 0.85 (P less than .001) representing a total risk reduction of 13.2%. The risk of MI or stroke and need for revascularization were significantly lower values in the evolocumab group, compared with placebo. Cardiovascular death did not show significant changes. There was no significant difference in rate of serious events.
The ODYSSEY trial3 reported on another PCSK-9 inhibitor, alirocumab, in a randomized, double-blind, placebo-controlled trial involving 18,924 patients who had an ACS in the prior 12 months. At the median follow-up (2.8 years), the LDL of the alirocumab group was 53.3 mg/dL, compared with 101.4 mg/dL in the placebo group. The primary endpoints for cardiovascular risks were similar to those in the FOURIER trial: a risk of 9.5% in the alirocumab group and 11.1% in the placebo group for a total risk reduction of 14.4%. This suggests the class of PCSK-9 inhibitors have a strong correlation with reducing LDL levels 54%-59% and reducing major cardiac adverse events by 13%-15%.
Recommendations
The American College of Cardiology released a focused update that integrated the new evidence regarding the use of nonstatin therapy. The current focused update recommends an overall 50% or greater reduction in LDL for patients with clinical ASCVD. If this reduction is not achieved, ACC suggests that one consider the addition of nonstatin therapy with either ezetimibe or a PCSK-9 inhibitor.4 If a patient requires less than 25% additional LDL reduction, consider ezetimibe; if a patient requires more than 25% additional LDL reduction, consider a PCSK-9 inhibitor. Specifically, the guideline states: “If the patient still has less than 50% reduction in LDL-C (and may consider LDL-C above 70 mg/dL or non–HDL-C above 100 mg/dL), the patient and clinician should enter into a discussion focused on shared decision making regarding the addition of a nonstatin medication to the current regimen.”
The other group that is mentioned in the recommendations, with an acknowledgment that the evidence for benefit in primary prevention is not available, is individuals who have an LDL above 190 mg/dL even while compliant with a maximally effective statin regimen. The guidelines make further but less strong recommendations about a number of risk groups, but the largest and strongest change, based on strong evidence, is the recommendation to consider nonstatin therapy in individuals with established ASCVD, as described above.
Bottom line
Recent trials show significant reductions in LDL, leading to significant reductions in cardiovascular endpoints with ezetimibe and PCSK-9 inhibitors. This has led to an additional ACC recommendation to consider the use of nonstatin therapy in addition to maximal statin therapy in selected patients with established cardiovascular disease.
References
1. Cannon C et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387-97.
2. Sabatine M et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713-22.
3. ODYSSEY Outcomes: Results suggest use of PCSK9 inhibitor reduces CV events, LDL-C in ACS patients. Article from American College of Cardiology. ACC News Story. 2018 Mar 10.
4. Lloyd-Jones DM et al. 2017 Focused update of the 2016 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology task force on expert consensus decision pathways. J Am Coll Cardiol. 2017 Oct 3;70(14):1785-1822. Epub 2017 Sep 5.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Plako is a second-year resident in the family medicine residency program at Abington Jefferson Hospital.
Importance
While statins remain the foundation for treating high cholesterol in order to reduce cardiovascular risk, new evidence has lead to important revisions in the American Heart Association’s recommendations for treatment of hypercholesterolemia in patients at very high cardiovascular risk (secondary prevention) with the addition of specific nonstatin agents. We will briefly review the AHA 2013 guideline recommendations, the relevant new information, and the updated AHA recommendations.
American Heart Association 2013 guidelines
The 2013 American College of Cardiology/AHA cholesterol guidelines recommend either high- or moderate-intensity statin therapy for patients in the four statin benefit groups:
1. Adult patients older than 21 years of age with clinical atherosclerotic cardiovascular disease (ASCVD).
2. Adults older than 21 years of age with low-density lipoprotein cholesterol (LDL-C) above 190 mg/dL.
3. Adults aged 40-75 years without ASCVD but with diabetes and with LDL-C 70-189 mg/dL.
4. Adults aged 40-75 years without either ASCVD or diabetes, with LDL-C 70-189 mg/dL and an estimated 10-year risk for ASCVD of over 7.5% as determined by the Pooled Cohort Equations.
At the time of the 2013 guidelines, there was little evidence to recommend the use of medications other than statins.
Recent evidence
The IMPROVE-IT trial1 was a double-blind, randomized trial involving 18,144 men and women who were older than 50 years and hospitalized for an acute coronary syndrome within the preceding 10 days. They were randomized to either simvastatin plus ezetimibe or simvastatin plus placebo. The primary endpoints were a composite of death from cardiovascular disease, a major coronary event (nonfatal MI, unstable angina requiring admission, or coronary revascularization), or nonfatal stroke. At 1 year, the mean LDL was 69.9 mg/dL in the simvastatin-monotherapy group and 53.2 mg/dL in the simvastatin-ezetimibe group (P under .001), representing a 24% decrease in LDL between the two groups. The rate of the primary endpoints was significantly lower in the simvastatin plus ezetimibe group with a hazard ratio of 0.936 (P = .016). The risk of MI was significantly decreased with an HR of 0.87 (P = .002), and the risk of ischemic stroke significantly decreased with an HR of 0.79 (P = .008). Prespecified safety endpoints showed no significant difference between the two groups.
The FOURIER trial2 examined the PCSK-9 inhibitor, evolocumab. FOURIER was a randomized, double-blind, placebo-controlled study involving 27,564 patients with atherosclerotic cardiovascular disease and LDL levels of 70 mg/dL or higher who were receiving statin therapy (at least atorvastatin 20 mg or equivalent with/without ezetimibe). Patients were between 45 and 80 years old with a history of history of MI, nonhemorrhagic stroke, or symptomatic peripheral artery disease. Patients were randomized to receive subcutaneous injections of evolocumab or matching placebo. The primary endpoints were similar to that of IMPROVE-IT: a composite of cardiovascular death, myocardial infarction, stroke, unstable angina hospitalization, and coronary revascularization. The median LDL on entry was 92 mg/dL for both groups. At 48 weeks, the evolocumab group showed a 59% decrease in LDL, compared with placebo, with a decrease in median LDL from 92 mg/dL to 30 mg/dL. The primary endpoint occurred in 9.8% of the evolocumab group and 11.3% in the placebo group for a hazard ratio of 0.85 (P less than .001) representing a total risk reduction of 13.2%. The risk of MI or stroke and need for revascularization were significantly lower values in the evolocumab group, compared with placebo. Cardiovascular death did not show significant changes. There was no significant difference in rate of serious events.
The ODYSSEY trial3 reported on another PCSK-9 inhibitor, alirocumab, in a randomized, double-blind, placebo-controlled trial involving 18,924 patients who had an ACS in the prior 12 months. At the median follow-up (2.8 years), the LDL of the alirocumab group was 53.3 mg/dL, compared with 101.4 mg/dL in the placebo group. The primary endpoints for cardiovascular risks were similar to those in the FOURIER trial: a risk of 9.5% in the alirocumab group and 11.1% in the placebo group for a total risk reduction of 14.4%. This suggests the class of PCSK-9 inhibitors have a strong correlation with reducing LDL levels 54%-59% and reducing major cardiac adverse events by 13%-15%.
Recommendations
The American College of Cardiology released a focused update that integrated the new evidence regarding the use of nonstatin therapy. The current focused update recommends an overall 50% or greater reduction in LDL for patients with clinical ASCVD. If this reduction is not achieved, ACC suggests that one consider the addition of nonstatin therapy with either ezetimibe or a PCSK-9 inhibitor.4 If a patient requires less than 25% additional LDL reduction, consider ezetimibe; if a patient requires more than 25% additional LDL reduction, consider a PCSK-9 inhibitor. Specifically, the guideline states: “If the patient still has less than 50% reduction in LDL-C (and may consider LDL-C above 70 mg/dL or non–HDL-C above 100 mg/dL), the patient and clinician should enter into a discussion focused on shared decision making regarding the addition of a nonstatin medication to the current regimen.”
The other group that is mentioned in the recommendations, with an acknowledgment that the evidence for benefit in primary prevention is not available, is individuals who have an LDL above 190 mg/dL even while compliant with a maximally effective statin regimen. The guidelines make further but less strong recommendations about a number of risk groups, but the largest and strongest change, based on strong evidence, is the recommendation to consider nonstatin therapy in individuals with established ASCVD, as described above.
Bottom line
Recent trials show significant reductions in LDL, leading to significant reductions in cardiovascular endpoints with ezetimibe and PCSK-9 inhibitors. This has led to an additional ACC recommendation to consider the use of nonstatin therapy in addition to maximal statin therapy in selected patients with established cardiovascular disease.
References
1. Cannon C et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387-97.
2. Sabatine M et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713-22.
3. ODYSSEY Outcomes: Results suggest use of PCSK9 inhibitor reduces CV events, LDL-C in ACS patients. Article from American College of Cardiology. ACC News Story. 2018 Mar 10.
4. Lloyd-Jones DM et al. 2017 Focused update of the 2016 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology task force on expert consensus decision pathways. J Am Coll Cardiol. 2017 Oct 3;70(14):1785-1822. Epub 2017 Sep 5.
Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Plako is a second-year resident in the family medicine residency program at Abington Jefferson Hospital.

Updated IPF guideline refines diagnostic criteria with HRCT
A recently updated guideline for idiopathic pulmonary fibrosis (IPF) provides refined diagnostic criteria in an effort to improve clinical application and diagnostic accuracy.
Of note, the guideline recommends that high-resolution CT (HRCT) patterns be used to dictate management course. The guideline also calls for detailed medical history, serological testing to exclude connective tissue disease, and multidisciplinary discussion. Serum biomarkers are recommended against as a means of distinguishing between IPF and other interstitial lung diseases (ILDs).
“Diagnosing IPF is challenging because these symptoms are nonspecific: They occur with all other interstitial lung diseases and with other respiratory problems,” Ganesh Raghu, MD, chair of the guideline committee and professor of medicine and director of the Center for Interstitial Lung Disease at the University of Washington, Seattle, said in a written statement. “Because drugs may slow the progression of IPF, an early and accurate diagnosis is essential for prompt and appropriate treatment for this fatal disease.”
The 2018 guideline represents a second collaborative effort from the American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society. The guideline committee consisted of 29 clinicians, scientists, and a patient with IPF. They evaluated all IPF-related evidence and rated the quality of findings with the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) system. The first IPF guideline was published 7 years ago; the intervening time has revealed some clinical limitations that the 2018 guideline aims to fix.
“The 2011 guideline provided the first evidence-based, formal criteria for diagnosis of IPF and allowed patients with a well-defined diagnosis of IPF to participate in numerous clinical studies and randomized controlled trials that enhanced our understanding of the disease,” Dr. Raghu said. “However, it became clear that there were significant challenges in ascertaining the diagnosis per the 2011 criteria, and abundant evidence accumulated since then allowed the committee to refine the diagnostic criteria now.”
“This [updated] guideline is intended to help clinicians make an accurate diagnosis of IPF,” the authors wrote in the American Journal of Respiratory and Critical Care Medicine, “and to empower them to implement recommended courses of action in the context of individual patient values and preferences, particularly decisions regarding which diagnostic interventions to pursue.”
While the 2011 guideline did not distinguish between patients with different HRCT patterns, the 2018 guideline emphasizes the use of HRCT. It is now recommended that patients undergo HRCT to determine the pattern of usual interstitial pneumonia (UIP). Broadly, patients exhibit the UIP pattern or one of three possible non-UIP patterns (probable UIP, indeterminate UIP, or an alternative diagnosis). Recommendations are specific for UIP and non-UIP.
Patients with probable UIP, indeterminate UIP, or an alternative diagnosis should undergo bronchoalveolar lavage (BAL) and surgical lung biopsy (SLB). Transbronchial lung biopsy (TBBx) and lung cryobiopsy recommendations were not described in these patients because of a lack of evidence. However, patients with UIP should not undergo BAL, SLB, TBBx, or cryobiopsy.
For all patients, the 2018 guideline recommends that medical histories include environmental exposure and medication use, and that serological testing is performed to exclude connective tissue disease. Multidisciplinary discussion is conditionally recommended for diagnostic decision making, particularly when a patient has probable UIP, indeterminate UIP, or an alternative diagnosis.
Finally, the guideline recommends against the use of serum biomarkers as a means of distinguishing between IPF and other ILDs because of weak data on this point. “For the time being, the guideline panel dismissed serum biomarker measurement as an approach to distinguishing IPF from other ILDs because of the high false-positive and false-negative result rates,” the panel wrote.
“Our hope is that this new guideline will bridge the gap between the experienced IPF experts and general pulmonologists in making a prompt and accurate diagnosis of IPF for the individual unfortunately confronted with the disease,” Dr. Raghu said. “This will allow patients to make well-informed decisions about treatment options and participation in clinical trials.”
Looking to the future, the panel described an “urgent need to refine and validate diagnostic approaches to ILD. These needs can be roughly categorized as investigations into the roles of clinical observations, HRCT, bronchoscopy, histopathology, and biomarkers.” The authors also emphasized “the need to refine prognostic approaches, identify risk factors for the development of IPF, and determine the impact and approach to the diagnosis of comorbid illness in the patient with IPF.”
The authors reported funding from Bellerophon, Gilead, Roche, Sanofi, and others.
SOURCE: Raghu G et al. Am J Respir Crit Care Med. 2018 Sep 1. doi: 10.1164/rccm.201807-1255ST.
A recently updated guideline for idiopathic pulmonary fibrosis (IPF) provides refined diagnostic criteria in an effort to improve clinical application and diagnostic accuracy.
Of note, the guideline recommends that high-resolution CT (HRCT) patterns be used to dictate management course. The guideline also calls for detailed medical history, serological testing to exclude connective tissue disease, and multidisciplinary discussion. Serum biomarkers are recommended against as a means of distinguishing between IPF and other interstitial lung diseases (ILDs).
“Diagnosing IPF is challenging because these symptoms are nonspecific: They occur with all other interstitial lung diseases and with other respiratory problems,” Ganesh Raghu, MD, chair of the guideline committee and professor of medicine and director of the Center for Interstitial Lung Disease at the University of Washington, Seattle, said in a written statement. “Because drugs may slow the progression of IPF, an early and accurate diagnosis is essential for prompt and appropriate treatment for this fatal disease.”
The 2018 guideline represents a second collaborative effort from the American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society. The guideline committee consisted of 29 clinicians, scientists, and a patient with IPF. They evaluated all IPF-related evidence and rated the quality of findings with the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) system. The first IPF guideline was published 7 years ago; the intervening time has revealed some clinical limitations that the 2018 guideline aims to fix.
“The 2011 guideline provided the first evidence-based, formal criteria for diagnosis of IPF and allowed patients with a well-defined diagnosis of IPF to participate in numerous clinical studies and randomized controlled trials that enhanced our understanding of the disease,” Dr. Raghu said. “However, it became clear that there were significant challenges in ascertaining the diagnosis per the 2011 criteria, and abundant evidence accumulated since then allowed the committee to refine the diagnostic criteria now.”
“This [updated] guideline is intended to help clinicians make an accurate diagnosis of IPF,” the authors wrote in the American Journal of Respiratory and Critical Care Medicine, “and to empower them to implement recommended courses of action in the context of individual patient values and preferences, particularly decisions regarding which diagnostic interventions to pursue.”
While the 2011 guideline did not distinguish between patients with different HRCT patterns, the 2018 guideline emphasizes the use of HRCT. It is now recommended that patients undergo HRCT to determine the pattern of usual interstitial pneumonia (UIP). Broadly, patients exhibit the UIP pattern or one of three possible non-UIP patterns (probable UIP, indeterminate UIP, or an alternative diagnosis). Recommendations are specific for UIP and non-UIP.
Patients with probable UIP, indeterminate UIP, or an alternative diagnosis should undergo bronchoalveolar lavage (BAL) and surgical lung biopsy (SLB). Transbronchial lung biopsy (TBBx) and lung cryobiopsy recommendations were not described in these patients because of a lack of evidence. However, patients with UIP should not undergo BAL, SLB, TBBx, or cryobiopsy.
For all patients, the 2018 guideline recommends that medical histories include environmental exposure and medication use, and that serological testing is performed to exclude connective tissue disease. Multidisciplinary discussion is conditionally recommended for diagnostic decision making, particularly when a patient has probable UIP, indeterminate UIP, or an alternative diagnosis.
Finally, the guideline recommends against the use of serum biomarkers as a means of distinguishing between IPF and other ILDs because of weak data on this point. “For the time being, the guideline panel dismissed serum biomarker measurement as an approach to distinguishing IPF from other ILDs because of the high false-positive and false-negative result rates,” the panel wrote.
“Our hope is that this new guideline will bridge the gap between the experienced IPF experts and general pulmonologists in making a prompt and accurate diagnosis of IPF for the individual unfortunately confronted with the disease,” Dr. Raghu said. “This will allow patients to make well-informed decisions about treatment options and participation in clinical trials.”
Looking to the future, the panel described an “urgent need to refine and validate diagnostic approaches to ILD. These needs can be roughly categorized as investigations into the roles of clinical observations, HRCT, bronchoscopy, histopathology, and biomarkers.” The authors also emphasized “the need to refine prognostic approaches, identify risk factors for the development of IPF, and determine the impact and approach to the diagnosis of comorbid illness in the patient with IPF.”
The authors reported funding from Bellerophon, Gilead, Roche, Sanofi, and others.
SOURCE: Raghu G et al. Am J Respir Crit Care Med. 2018 Sep 1. doi: 10.1164/rccm.201807-1255ST.
A recently updated guideline for idiopathic pulmonary fibrosis (IPF) provides refined diagnostic criteria in an effort to improve clinical application and diagnostic accuracy.
Of note, the guideline recommends that high-resolution CT (HRCT) patterns be used to dictate management course. The guideline also calls for detailed medical history, serological testing to exclude connective tissue disease, and multidisciplinary discussion. Serum biomarkers are recommended against as a means of distinguishing between IPF and other interstitial lung diseases (ILDs).
“Diagnosing IPF is challenging because these symptoms are nonspecific: They occur with all other interstitial lung diseases and with other respiratory problems,” Ganesh Raghu, MD, chair of the guideline committee and professor of medicine and director of the Center for Interstitial Lung Disease at the University of Washington, Seattle, said in a written statement. “Because drugs may slow the progression of IPF, an early and accurate diagnosis is essential for prompt and appropriate treatment for this fatal disease.”
The 2018 guideline represents a second collaborative effort from the American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society. The guideline committee consisted of 29 clinicians, scientists, and a patient with IPF. They evaluated all IPF-related evidence and rated the quality of findings with the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) system. The first IPF guideline was published 7 years ago; the intervening time has revealed some clinical limitations that the 2018 guideline aims to fix.
“The 2011 guideline provided the first evidence-based, formal criteria for diagnosis of IPF and allowed patients with a well-defined diagnosis of IPF to participate in numerous clinical studies and randomized controlled trials that enhanced our understanding of the disease,” Dr. Raghu said. “However, it became clear that there were significant challenges in ascertaining the diagnosis per the 2011 criteria, and abundant evidence accumulated since then allowed the committee to refine the diagnostic criteria now.”
“This [updated] guideline is intended to help clinicians make an accurate diagnosis of IPF,” the authors wrote in the American Journal of Respiratory and Critical Care Medicine, “and to empower them to implement recommended courses of action in the context of individual patient values and preferences, particularly decisions regarding which diagnostic interventions to pursue.”
While the 2011 guideline did not distinguish between patients with different HRCT patterns, the 2018 guideline emphasizes the use of HRCT. It is now recommended that patients undergo HRCT to determine the pattern of usual interstitial pneumonia (UIP). Broadly, patients exhibit the UIP pattern or one of three possible non-UIP patterns (probable UIP, indeterminate UIP, or an alternative diagnosis). Recommendations are specific for UIP and non-UIP.
Patients with probable UIP, indeterminate UIP, or an alternative diagnosis should undergo bronchoalveolar lavage (BAL) and surgical lung biopsy (SLB). Transbronchial lung biopsy (TBBx) and lung cryobiopsy recommendations were not described in these patients because of a lack of evidence. However, patients with UIP should not undergo BAL, SLB, TBBx, or cryobiopsy.
For all patients, the 2018 guideline recommends that medical histories include environmental exposure and medication use, and that serological testing is performed to exclude connective tissue disease. Multidisciplinary discussion is conditionally recommended for diagnostic decision making, particularly when a patient has probable UIP, indeterminate UIP, or an alternative diagnosis.
Finally, the guideline recommends against the use of serum biomarkers as a means of distinguishing between IPF and other ILDs because of weak data on this point. “For the time being, the guideline panel dismissed serum biomarker measurement as an approach to distinguishing IPF from other ILDs because of the high false-positive and false-negative result rates,” the panel wrote.
“Our hope is that this new guideline will bridge the gap between the experienced IPF experts and general pulmonologists in making a prompt and accurate diagnosis of IPF for the individual unfortunately confronted with the disease,” Dr. Raghu said. “This will allow patients to make well-informed decisions about treatment options and participation in clinical trials.”
Looking to the future, the panel described an “urgent need to refine and validate diagnostic approaches to ILD. These needs can be roughly categorized as investigations into the roles of clinical observations, HRCT, bronchoscopy, histopathology, and biomarkers.” The authors also emphasized “the need to refine prognostic approaches, identify risk factors for the development of IPF, and determine the impact and approach to the diagnosis of comorbid illness in the patient with IPF.”
The authors reported funding from Bellerophon, Gilead, Roche, Sanofi, and others.
SOURCE: Raghu G et al. Am J Respir Crit Care Med. 2018 Sep 1. doi: 10.1164/rccm.201807-1255ST.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
AAP guidelines emphasize gender-affirmative care
according to an American Academy of Pediatrics policy statement published in Pediatrics.

The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.

Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
The AAP policy offers a more detailed overview of the health care needs of transgender and gender-diverse (TGD) youth than was previously available, with data to support these recommendations.
Future efforts should focus on expanding the definition and components of gender-affirmative care, as well as training providers to be more competent in providing this care by introducing these concepts earlier in medical training so that pediatricians feel comfortable with implementation.
The new guidelines “emphasize that care for TGD youth is a rapidly evolving field,” and that “continued support is needed for research, education, and advocacy in this arena so we can provide the best level of evidence-based care to TGD youth.”
Gayathri Chelvakumar, MD, is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at Ohio State University, both in Columbus. She was asked to comment on the AAP guidelines.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
according to an American Academy of Pediatrics policy statement published in Pediatrics.
The policy statement defines the gender-affirmative care model as one that provide “developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience,” wrote Jason Rafferty, MD, of the department of pediatrics at Hasbro Children’s Hospital in Providence, R.I., and the department of child psychiatryf at Emma Pendleton Bradley Hospital, East Providence, R.I. Dr. Rafferty serves on the AAP Committee on Psychosocial Aspects of Child and Family Health. The AAP Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness also participated in writing this policy statement.
The model emphasizes four main points, according to the statement:
- Transgender and gender-diverse identities are not mental disorders.
- Variations in gender identity are “normal aspects of human diversity.”
- Gender identity “evolves as a result of the interaction between biology, development, socialization, and culture.”
- Any mental health issue “most often stems from stigma and negative experiences” rather than being “intrinsic” to the child.
In the gender-affirmative approach, a supportive, nonjudgmental partnership between you, the patient, and the patient’s family is encouraged to “facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised,” Dr. Rafferty said. This contrasts with “reparative” or “conversion” treatment, which seeks to change rather than accept the patient’s gender identity.
The AAP statement also recommends accessibility of family therapy, addressing the emotional and mental health needs not only of the patient, but also the parents, caregivers, and siblings.
The policy statement provides definitions for common terminology and distinguishes between “sex” as assigned at birth, based on anatomy, and “gender identity,” described as one’s internal sense of self. It also emphasizes that gender identity is not synonymous with sexual orientation, although the two may be interrelated. “The Gender Book” website is a resource that explains these terms and concepts.
A 2015 study revealed that 25% of transgender adults avoided a necessary doctor appointment because they feared mistreatment. Creating an environment at your office where TGD patients feel safe is key. This can be done by displaying posters or having flyers about lesbian, gay, bisexual, transgender, and questioning (LGBTQ) issues and having a gender-neutral bathroom. Educate staff by having diversity training that makes them sensitive to the needs of LGBTQ youth and their families. Patient-asserted names and pronouns should be used by staff and reflected in the EHR. “Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ,” according to the statement. “Maintaining a safe clinical space can provide at least one consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.”
Barriers to care cited in the report include fear of discrimination by providers, lack of access to physical and sexual health services, inadequate mental health resources, and lack of provider continuity. The AAP recommends that EHRs respect the gender identity of the patient. Further research into health disparities, as well as establishment of standards of care, also are needed, the author notes.
The stigma and discrimination often experienced by TGD youth lead to feelings of rejection and isolation. Prior research has shown that transgender adolescents and adults have high rates of depression, anxiety, eating disorders, self-harm, and suicide, the report noted. One retrospective study found that 56% of transgender youth reported previous suicidal ideation, compared with 20% of those who identified as cisgender, and 31% reported a prior suicide attempt, compared with 11% cisgender youth. TGD youth also experience high rates of homelessness, violence, substance abuse, and high-risk sexual behaviors, studies have shown.
The statement also addresses issues such as medical interventions for pubertal suppression, surgical affirmation, difficulties with obtaining insurance coverage because of being transgender, family acceptance, safety in schools and communities, and medical education.
No disclosures or funding sources were reported.
SOURCE: Rafferty J et al. Pediatrics. 2018;142(4):e20182162.
FROM PEDATRICS

How to screen for, manage FASD in a medical home
providing early intervention and accessing community resources, according to a clinical report from the American Academy of Pediatrics.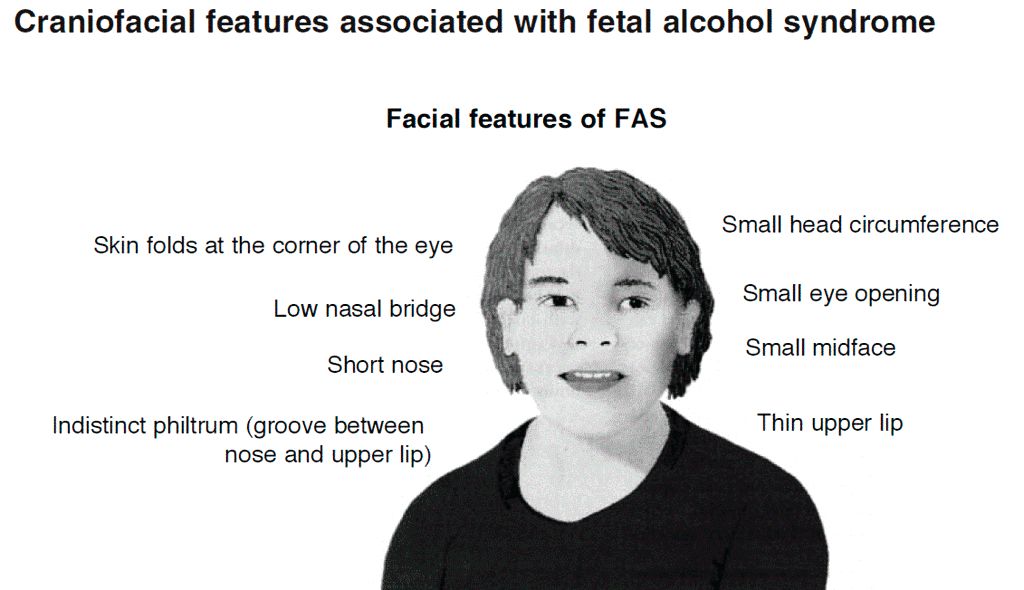
After the AAP released its guidelines on fetal alcohol spectrum disorder (FASD) in 2015, some pediatricians asked for further guidance on how to care for patients with FASD within the medical home, as many had a knowledge gap on how to best manage these patients.
“For some pediatricians, it can seem like a daunting task to care for an individual with an FASD, but there are aspects of integrated care and providing a medical home that can be instituted as with all children with complex medical diagnoses,” wrote Renee M. Turchi, MD, MPH, of the department of pediatrics at St. Christopher’s Hospital for Children and Drexel Dornsife School of Public Health in Philadelphia, and her colleagues on the AAP Committee on Substance Abuse and the Council on Children with Disabilities. Their report is in Pediatrics. “In addition, not recognizing an FASD can lead to inadequate treatment and less-than-optimal outcomes for the patient and family.”
Dr. Turchi and her colleagues released the FASD clinical report with “strategies to support families who are interacting with early intervention services, the educational system, the behavioral and/or mental health system, other community resources, and the transition to adult-oriented heath care systems when appropriate.” They noted the prevalence of FASD is increasing, with 1 in 10 pregnant women using alcohol within the past 30 days and 1 in 33 pregnant women reporting binge drinking in the past 30 days. They reaffirmed the AAP’s endorsement from the 2015 clinical report on FASD regarding abstinence of alcohol for pregnant women, emphasizing that there is no amount or kind of alcohol that is risk free during pregnancy, nor is there a time in pregnancy when drinking alcohol is risk free.
Providers in a medical home should communicate any prenatal alcohol exposure (PAE) to obstetric providers so they can review risk factors, optimize screening, and monitor children, Dr. Turchi and her colleagues said. They also should understand the diagnostic criteria and classifications for FASDs, including physical features such as low weight, short palpebral features, smooth philtrum, a thin upper lip, abnormalities in the central nervous system, and any alcohol use during pregnancy. Any child – regardless of age – is a candidate for universal PAE screening at initial visits or when “additional cognitive and behavioral concerns arise.”
The federal Child Abuse Prevention and Treatment Act “does not require clinicians to report to child protective services if a child has been exposed prenatally to alcohol (i.e., for a positive PAE screening result). Referral to child protective services is required if the child has been diagnosed with an FASD in the period between birth and 3 years. The intent of this referral is to develop safe care and possible treatment plans for the infant and caregiver if needed, not to initiate punitive actions,” according to the report. States have their own definitions about child abuse and neglect, so the report encourages providers to know the mandates and reporting laws in the states where they practice.
Monitoring children in a medical home for the signs and symptoms of FASD is important, the authors said, because research has shown an increased chance at reducing adverse life outcomes if a child is diagnosed before age 6 and is in a stable home with access to support services.
Management of children with FASD is individual, as symptoms for each child will uniquely present not just in terms of physical issues such as growth or congenital defects affecting the heart, eyes, kidneys, or bones, but also as developmental, cognitive, and behavioral problems. Children with FASD also may receive a concomitant diagnosis when evaluated, such as ADHD or depression, that will require additional accommodation. The use of evidence-based diagnostic and standard screening approaches and referring when necessary will help reevaluate whether a child has a condition such as ADHD, oppositional defiant disorder, or another diagnosis, or is displaying symptoms of FASD such as a receptive or expressive language disorder.
Pediatricians must work together with the families, educational professionals, the mental health community, and therapists to help manage FASD in children. In cases where a child is in foster care, partnering with the foster care partners and child welfare agencies to gain access to the medical information of the biological parents is important to determine whether there is parental history of substance abuse and to provide appropriate treatment and interventions.
“Given the complex array of systems and services requiring navigation and coordination for children with an FASD and their families, a high-quality primary care medical home with partnerships with families, specialists, therapists, mental and/or behavioral health professionals, and community partners is critical, as it is for all children with special health care needs,” Dr. Turchi and her colleagues said.
The authors reported no relevant conflicts of interest.
SOURCE: Turchi RM et al. Pediatrics. 2018 Sept 10. doi:10.1542/peds.2018-2333.
providing early intervention and accessing community resources, according to a clinical report from the American Academy of Pediatrics.
After the AAP released its guidelines on fetal alcohol spectrum disorder (FASD) in 2015, some pediatricians asked for further guidance on how to care for patients with FASD within the medical home, as many had a knowledge gap on how to best manage these patients.
“For some pediatricians, it can seem like a daunting task to care for an individual with an FASD, but there are aspects of integrated care and providing a medical home that can be instituted as with all children with complex medical diagnoses,” wrote Renee M. Turchi, MD, MPH, of the department of pediatrics at St. Christopher’s Hospital for Children and Drexel Dornsife School of Public Health in Philadelphia, and her colleagues on the AAP Committee on Substance Abuse and the Council on Children with Disabilities. Their report is in Pediatrics. “In addition, not recognizing an FASD can lead to inadequate treatment and less-than-optimal outcomes for the patient and family.”
Dr. Turchi and her colleagues released the FASD clinical report with “strategies to support families who are interacting with early intervention services, the educational system, the behavioral and/or mental health system, other community resources, and the transition to adult-oriented heath care systems when appropriate.” They noted the prevalence of FASD is increasing, with 1 in 10 pregnant women using alcohol within the past 30 days and 1 in 33 pregnant women reporting binge drinking in the past 30 days. They reaffirmed the AAP’s endorsement from the 2015 clinical report on FASD regarding abstinence of alcohol for pregnant women, emphasizing that there is no amount or kind of alcohol that is risk free during pregnancy, nor is there a time in pregnancy when drinking alcohol is risk free.
Providers in a medical home should communicate any prenatal alcohol exposure (PAE) to obstetric providers so they can review risk factors, optimize screening, and monitor children, Dr. Turchi and her colleagues said. They also should understand the diagnostic criteria and classifications for FASDs, including physical features such as low weight, short palpebral features, smooth philtrum, a thin upper lip, abnormalities in the central nervous system, and any alcohol use during pregnancy. Any child – regardless of age – is a candidate for universal PAE screening at initial visits or when “additional cognitive and behavioral concerns arise.”
The federal Child Abuse Prevention and Treatment Act “does not require clinicians to report to child protective services if a child has been exposed prenatally to alcohol (i.e., for a positive PAE screening result). Referral to child protective services is required if the child has been diagnosed with an FASD in the period between birth and 3 years. The intent of this referral is to develop safe care and possible treatment plans for the infant and caregiver if needed, not to initiate punitive actions,” according to the report. States have their own definitions about child abuse and neglect, so the report encourages providers to know the mandates and reporting laws in the states where they practice.
Monitoring children in a medical home for the signs and symptoms of FASD is important, the authors said, because research has shown an increased chance at reducing adverse life outcomes if a child is diagnosed before age 6 and is in a stable home with access to support services.
Management of children with FASD is individual, as symptoms for each child will uniquely present not just in terms of physical issues such as growth or congenital defects affecting the heart, eyes, kidneys, or bones, but also as developmental, cognitive, and behavioral problems. Children with FASD also may receive a concomitant diagnosis when evaluated, such as ADHD or depression, that will require additional accommodation. The use of evidence-based diagnostic and standard screening approaches and referring when necessary will help reevaluate whether a child has a condition such as ADHD, oppositional defiant disorder, or another diagnosis, or is displaying symptoms of FASD such as a receptive or expressive language disorder.
Pediatricians must work together with the families, educational professionals, the mental health community, and therapists to help manage FASD in children. In cases where a child is in foster care, partnering with the foster care partners and child welfare agencies to gain access to the medical information of the biological parents is important to determine whether there is parental history of substance abuse and to provide appropriate treatment and interventions.
“Given the complex array of systems and services requiring navigation and coordination for children with an FASD and their families, a high-quality primary care medical home with partnerships with families, specialists, therapists, mental and/or behavioral health professionals, and community partners is critical, as it is for all children with special health care needs,” Dr. Turchi and her colleagues said.
The authors reported no relevant conflicts of interest.
SOURCE: Turchi RM et al. Pediatrics. 2018 Sept 10. doi:10.1542/peds.2018-2333.
providing early intervention and accessing community resources, according to a clinical report from the American Academy of Pediatrics.
After the AAP released its guidelines on fetal alcohol spectrum disorder (FASD) in 2015, some pediatricians asked for further guidance on how to care for patients with FASD within the medical home, as many had a knowledge gap on how to best manage these patients.
“For some pediatricians, it can seem like a daunting task to care for an individual with an FASD, but there are aspects of integrated care and providing a medical home that can be instituted as with all children with complex medical diagnoses,” wrote Renee M. Turchi, MD, MPH, of the department of pediatrics at St. Christopher’s Hospital for Children and Drexel Dornsife School of Public Health in Philadelphia, and her colleagues on the AAP Committee on Substance Abuse and the Council on Children with Disabilities. Their report is in Pediatrics. “In addition, not recognizing an FASD can lead to inadequate treatment and less-than-optimal outcomes for the patient and family.”
Dr. Turchi and her colleagues released the FASD clinical report with “strategies to support families who are interacting with early intervention services, the educational system, the behavioral and/or mental health system, other community resources, and the transition to adult-oriented heath care systems when appropriate.” They noted the prevalence of FASD is increasing, with 1 in 10 pregnant women using alcohol within the past 30 days and 1 in 33 pregnant women reporting binge drinking in the past 30 days. They reaffirmed the AAP’s endorsement from the 2015 clinical report on FASD regarding abstinence of alcohol for pregnant women, emphasizing that there is no amount or kind of alcohol that is risk free during pregnancy, nor is there a time in pregnancy when drinking alcohol is risk free.
Providers in a medical home should communicate any prenatal alcohol exposure (PAE) to obstetric providers so they can review risk factors, optimize screening, and monitor children, Dr. Turchi and her colleagues said. They also should understand the diagnostic criteria and classifications for FASDs, including physical features such as low weight, short palpebral features, smooth philtrum, a thin upper lip, abnormalities in the central nervous system, and any alcohol use during pregnancy. Any child – regardless of age – is a candidate for universal PAE screening at initial visits or when “additional cognitive and behavioral concerns arise.”
The federal Child Abuse Prevention and Treatment Act “does not require clinicians to report to child protective services if a child has been exposed prenatally to alcohol (i.e., for a positive PAE screening result). Referral to child protective services is required if the child has been diagnosed with an FASD in the period between birth and 3 years. The intent of this referral is to develop safe care and possible treatment plans for the infant and caregiver if needed, not to initiate punitive actions,” according to the report. States have their own definitions about child abuse and neglect, so the report encourages providers to know the mandates and reporting laws in the states where they practice.
Monitoring children in a medical home for the signs and symptoms of FASD is important, the authors said, because research has shown an increased chance at reducing adverse life outcomes if a child is diagnosed before age 6 and is in a stable home with access to support services.
Management of children with FASD is individual, as symptoms for each child will uniquely present not just in terms of physical issues such as growth or congenital defects affecting the heart, eyes, kidneys, or bones, but also as developmental, cognitive, and behavioral problems. Children with FASD also may receive a concomitant diagnosis when evaluated, such as ADHD or depression, that will require additional accommodation. The use of evidence-based diagnostic and standard screening approaches and referring when necessary will help reevaluate whether a child has a condition such as ADHD, oppositional defiant disorder, or another diagnosis, or is displaying symptoms of FASD such as a receptive or expressive language disorder.
Pediatricians must work together with the families, educational professionals, the mental health community, and therapists to help manage FASD in children. In cases where a child is in foster care, partnering with the foster care partners and child welfare agencies to gain access to the medical information of the biological parents is important to determine whether there is parental history of substance abuse and to provide appropriate treatment and interventions.
“Given the complex array of systems and services requiring navigation and coordination for children with an FASD and their families, a high-quality primary care medical home with partnerships with families, specialists, therapists, mental and/or behavioral health professionals, and community partners is critical, as it is for all children with special health care needs,” Dr. Turchi and her colleagues said.
The authors reported no relevant conflicts of interest.
SOURCE: Turchi RM et al. Pediatrics. 2018 Sept 10. doi:10.1542/peds.2018-2333.
FROM PEDIATRICS