User login
Bill Seeks to Enhance Patient Access to Post-Hospital Benefit
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
New national legislation proposed in March would change Medicare billing rules to allow patients to more easily access Medicare’s institutional skilled nursing care benefit following a hospital discharge. Currently, patients can get the benefit only after a qualifying three-day hospital stay. If they don’t qualify, they often have to pay out of pocket for the subsequent skilled nursing facility placement.
The Improving Access to Medicare Coverage Act, introduced by Reps. Joe Courtney (D-Conn.) and Tom Latham (R-Iowa) and Sen. Sherrod Brown (D-Ohio), would allow the time patients spend inside the hospital on “observation status” to count toward their required three-day hospital stay. It also would establish a 90-day appeal period for those who have been denied this benefit.
SHM is one of a dozen endorsing organizations, joining the American Medical Association, American Medical Directors Association, and AARP. For more information, check out this month’s “Policy Corner”.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Quinn K, Neeman N, Mourad M, Sliwka D. Communication coaching: A multifaceted intervention to improve physician-patient communication [abstract]. J Hosp Med. 2012;7 Suppl 2:S108.
- Sokol PE, Wynia MK. There and Home Again, Safely: Five Responsibilities of Ambulatory Practices in High Quality Care Transitions. American Medical Association website. http://www.ama-assn.org/resources/doc/patient-safety/ambulatory-practices.pdf. Accessed February 12, 2013.
- Dharmarajan K, Hsieh AF, Lin Z, et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
- JAMA Internal Medicine. Nearly one-third of physicians report missing electronic notification of test results. JAMA Internal Medicine website. Available at: http://media.jamanetwork.com/news-item/nearly-one-third-of-physicians-report-missing-electronic-notification-of-test-results/.Accessed April 8, 2013.
- Miliard M. VA enlists telehealth for disasters. Healthcare IT News website. http://www.healthcareitnews.com/news/va-enlists-telehealth-disasters. Published February 27, 2013. Accessed April 1, 2013.
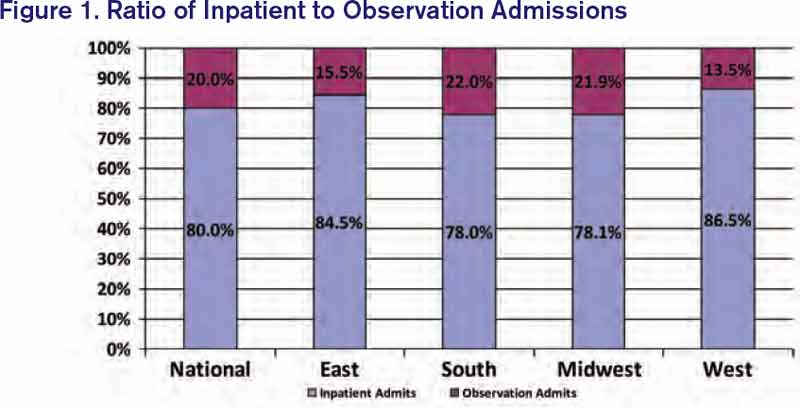
SHM Tallies Ratio of Hospital Respondents' Observation Admissions to Inpatient Admission Encounters

SHM added a new item to its 2012 State of Hospital Medicine report: the ratio of respondents’ observation admissions to inpatient admission encounters. This metric was added because observation encounters have been increasing, with financial effects on hospitals and patients. SHM survey respondents reported a 20% observation rate for both adult and pediatric practice groups (see Figure 1).
Under observation status, services that used to be billed as inpatient status (e.g. chest pain evaluation, treatment of asthma exacerbation) must be billed by the hospital at much lower outpatient rates. Some hospitals have responded to this financial pressure by creating observation units or making other operational adjustments. One recent analysis suggested that nationwide adoption of such efforts could save billions of dollars.1
Becoming lean enough to do short work in short time, though, does not address all of the observation-related issues facing hospitals. When the Centers for Medicare & Medicaid Services’ (CMS) Recovery Audit Contractors (RACs) determine retrospectively that an inpatient admission should have been an observation encounter, the hospital’s payment is not downgraded but forfeited.2 This development has prompted hospitals to preemptively opt for observation status for certain patients. Case managers and providers increasingly are spending time reviewing inpatient versus observation status throughout a patient’s stay. Many hospitals have turned to third-party contractors to help review observation status.
Observation status has financial implications for patients as well. In the past year, USA Today, The Wall Street Journal, and CNN Money all have reported on patients hit with unexpected out-of-pocket expenses related to observation care.3,4,5 A common theme: Medicare patient hospitalized with an acute fracture, managed nonoperatively but requiring rehabilitation prior to returning home. These patients found out too late that observation, a status they were often unaware of, did not qualify for CMS’ three-day inpatient requirement to cover rehabilitation costs. Some patients were charged exorbitant prices for noncovered “outpatient” services, such as providing their routine medications.
Advocacy groups have joined the fray on patients’ behalf, and legal challenges have ensued. AARP and others are educating patients about observation status—and their right to challenge it. The Center for Medicare Advocacy (www.kslaw.com/Library/publication/HH111411_Bagnall.pdf) has filed a lawsuit against the U.S. Department of Health and Human Services on behalf of patients hit with uncovered rehabilitation costs, and the American Hospital Association has teamed with several hospitals to sue over funds forfeited in RAC audits (www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf). Both houses of Congress have legislation (H.R. 1543 and S. 818) seeking to count observation days toward the Medicare three-day rule. For its part, CMS has promised to review observation status and, hopefully, clarify the rules.
Hospitalists, meanwhile, are gearing up for more observation care. The 2012 State of Hospital Medicine report shows that 37% of adult groups and 28% of pediatric groups reported having primary responsibility for observation or short-stay units. My own hospital runs both a clinical decision unit in the ED and a short-stay unit staffed by our hospitalist group. As SHM tracks observation status in future surveys, HM groups will be able to follow this phenomenon among their colleagues and benchmark their own rates of observation encounters.
Dr. Creamer is medical director of the short-stay unit at MetroHealth Medical Center in Cleveland and a member of SHM’s Practice Analysis Committee.
References
- Feng Z, Wright DB, Mor V. Sharp rise in Medicare enrollees being held in hospitals for observation raises concerns about causes and consequences. Health Aff (Millwood). 2012;31(6):1251-1259.
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Gengler A. The painful new trend in Medicare. CNN Money website. Available at: http://money.cnn.com/2012/08/07/pf/medicare-rehab-costs.moneymag/index.htm. Accessed March 6, 2013.
- Jaffe S. Patients held for observation can face steep drug bills. USA Today website. Available at: http://usatoday30.usatoday.com/money/industries/health/drugs/story/2012-04-30/drugs-can-be-expensive-in-observation-care/54646378/1. Accessed March 6, 2013.
- Landro L. Filling a gap between ERs and inpatient rooms. The Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052970204349404578101060863887052.html. Accessed March 6, 2013.
SHM added a new item to its 2012 State of Hospital Medicine report: the ratio of respondents’ observation admissions to inpatient admission encounters. This metric was added because observation encounters have been increasing, with financial effects on hospitals and patients. SHM survey respondents reported a 20% observation rate for both adult and pediatric practice groups (see Figure 1).
Under observation status, services that used to be billed as inpatient status (e.g. chest pain evaluation, treatment of asthma exacerbation) must be billed by the hospital at much lower outpatient rates. Some hospitals have responded to this financial pressure by creating observation units or making other operational adjustments. One recent analysis suggested that nationwide adoption of such efforts could save billions of dollars.1
Becoming lean enough to do short work in short time, though, does not address all of the observation-related issues facing hospitals. When the Centers for Medicare & Medicaid Services’ (CMS) Recovery Audit Contractors (RACs) determine retrospectively that an inpatient admission should have been an observation encounter, the hospital’s payment is not downgraded but forfeited.2 This development has prompted hospitals to preemptively opt for observation status for certain patients. Case managers and providers increasingly are spending time reviewing inpatient versus observation status throughout a patient’s stay. Many hospitals have turned to third-party contractors to help review observation status.
Observation status has financial implications for patients as well. In the past year, USA Today, The Wall Street Journal, and CNN Money all have reported on patients hit with unexpected out-of-pocket expenses related to observation care.3,4,5 A common theme: Medicare patient hospitalized with an acute fracture, managed nonoperatively but requiring rehabilitation prior to returning home. These patients found out too late that observation, a status they were often unaware of, did not qualify for CMS’ three-day inpatient requirement to cover rehabilitation costs. Some patients were charged exorbitant prices for noncovered “outpatient” services, such as providing their routine medications.
Advocacy groups have joined the fray on patients’ behalf, and legal challenges have ensued. AARP and others are educating patients about observation status—and their right to challenge it. The Center for Medicare Advocacy (www.kslaw.com/Library/publication/HH111411_Bagnall.pdf) has filed a lawsuit against the U.S. Department of Health and Human Services on behalf of patients hit with uncovered rehabilitation costs, and the American Hospital Association has teamed with several hospitals to sue over funds forfeited in RAC audits (www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf). Both houses of Congress have legislation (H.R. 1543 and S. 818) seeking to count observation days toward the Medicare three-day rule. For its part, CMS has promised to review observation status and, hopefully, clarify the rules.
Hospitalists, meanwhile, are gearing up for more observation care. The 2012 State of Hospital Medicine report shows that 37% of adult groups and 28% of pediatric groups reported having primary responsibility for observation or short-stay units. My own hospital runs both a clinical decision unit in the ED and a short-stay unit staffed by our hospitalist group. As SHM tracks observation status in future surveys, HM groups will be able to follow this phenomenon among their colleagues and benchmark their own rates of observation encounters.
Dr. Creamer is medical director of the short-stay unit at MetroHealth Medical Center in Cleveland and a member of SHM’s Practice Analysis Committee.
References
- Feng Z, Wright DB, Mor V. Sharp rise in Medicare enrollees being held in hospitals for observation raises concerns about causes and consequences. Health Aff (Millwood). 2012;31(6):1251-1259.
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Gengler A. The painful new trend in Medicare. CNN Money website. Available at: http://money.cnn.com/2012/08/07/pf/medicare-rehab-costs.moneymag/index.htm. Accessed March 6, 2013.
- Jaffe S. Patients held for observation can face steep drug bills. USA Today website. Available at: http://usatoday30.usatoday.com/money/industries/health/drugs/story/2012-04-30/drugs-can-be-expensive-in-observation-care/54646378/1. Accessed March 6, 2013.
- Landro L. Filling a gap between ERs and inpatient rooms. The Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052970204349404578101060863887052.html. Accessed March 6, 2013.
SHM added a new item to its 2012 State of Hospital Medicine report: the ratio of respondents’ observation admissions to inpatient admission encounters. This metric was added because observation encounters have been increasing, with financial effects on hospitals and patients. SHM survey respondents reported a 20% observation rate for both adult and pediatric practice groups (see Figure 1).
Under observation status, services that used to be billed as inpatient status (e.g. chest pain evaluation, treatment of asthma exacerbation) must be billed by the hospital at much lower outpatient rates. Some hospitals have responded to this financial pressure by creating observation units or making other operational adjustments. One recent analysis suggested that nationwide adoption of such efforts could save billions of dollars.1
Becoming lean enough to do short work in short time, though, does not address all of the observation-related issues facing hospitals. When the Centers for Medicare & Medicaid Services’ (CMS) Recovery Audit Contractors (RACs) determine retrospectively that an inpatient admission should have been an observation encounter, the hospital’s payment is not downgraded but forfeited.2 This development has prompted hospitals to preemptively opt for observation status for certain patients. Case managers and providers increasingly are spending time reviewing inpatient versus observation status throughout a patient’s stay. Many hospitals have turned to third-party contractors to help review observation status.
Observation status has financial implications for patients as well. In the past year, USA Today, The Wall Street Journal, and CNN Money all have reported on patients hit with unexpected out-of-pocket expenses related to observation care.3,4,5 A common theme: Medicare patient hospitalized with an acute fracture, managed nonoperatively but requiring rehabilitation prior to returning home. These patients found out too late that observation, a status they were often unaware of, did not qualify for CMS’ three-day inpatient requirement to cover rehabilitation costs. Some patients were charged exorbitant prices for noncovered “outpatient” services, such as providing their routine medications.
Advocacy groups have joined the fray on patients’ behalf, and legal challenges have ensued. AARP and others are educating patients about observation status—and their right to challenge it. The Center for Medicare Advocacy (www.kslaw.com/Library/publication/HH111411_Bagnall.pdf) has filed a lawsuit against the U.S. Department of Health and Human Services on behalf of patients hit with uncovered rehabilitation costs, and the American Hospital Association has teamed with several hospitals to sue over funds forfeited in RAC audits (www.aha.org/content/12/121101-aha-hhs-medicare-com.pdf). Both houses of Congress have legislation (H.R. 1543 and S. 818) seeking to count observation days toward the Medicare three-day rule. For its part, CMS has promised to review observation status and, hopefully, clarify the rules.
Hospitalists, meanwhile, are gearing up for more observation care. The 2012 State of Hospital Medicine report shows that 37% of adult groups and 28% of pediatric groups reported having primary responsibility for observation or short-stay units. My own hospital runs both a clinical decision unit in the ED and a short-stay unit staffed by our hospitalist group. As SHM tracks observation status in future surveys, HM groups will be able to follow this phenomenon among their colleagues and benchmark their own rates of observation encounters.
Dr. Creamer is medical director of the short-stay unit at MetroHealth Medical Center in Cleveland and a member of SHM’s Practice Analysis Committee.
References
- Feng Z, Wright DB, Mor V. Sharp rise in Medicare enrollees being held in hospitals for observation raises concerns about causes and consequences. Health Aff (Millwood). 2012;31(6):1251-1259.
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Gengler A. The painful new trend in Medicare. CNN Money website. Available at: http://money.cnn.com/2012/08/07/pf/medicare-rehab-costs.moneymag/index.htm. Accessed March 6, 2013.
- Jaffe S. Patients held for observation can face steep drug bills. USA Today website. Available at: http://usatoday30.usatoday.com/money/industries/health/drugs/story/2012-04-30/drugs-can-be-expensive-in-observation-care/54646378/1. Accessed March 6, 2013.
- Landro L. Filling a gap between ERs and inpatient rooms. The Wall Street Journal website. Available at: http://online.wsj.com/article/SB10001424052970204349404578101060863887052.html. Accessed March 6, 2013.
Affordable Care Act (ACA) Provision Carries Pay Raise for Some Hospitalists
For those who remain unaware, hospitalists who care for Medicaid patients will be getting a raise in 2013 and 2014. The reason is that the Affordable Care Act (ACA) requires Medicaid rates for specified primary-care services to be equal to those of Medicare rates during those two years, with the federal government paying the difference. Hospitalists generally meet the requirements and, therefore, will see this pay increase for their applicable Medicaid billing. For some context of the scope of this change, on average, Medicaid pays physicians at 66% of the national Medicare rates, although there is significant variation among the states.
To qualify, a physician must have a specialty designation of family medicine, internal medicine, or pediatrics, then further attest to board certification in one of those specialties or related subspecialties. Alternatively, the physician must have a 60% claims history for the specified evaluation and management (E&M) codes.
Multiple parties who have heard reports about state plans for Medicaid parity recently have contacted SHM; the plans, they report, intentionally would exclude hospitalists from the promised increase. There are variations on the explanation for the exclusion and where the idea is coming from, but the inquiries follow this general theme: “Since the definition of eligible physicians remains a grey area, states are developing alternative plans with a more narrow interpretation of the qualifying factors for the increase. These plans are only including physicians who practice in the community setting (i.e. not the hospital setting).”
This is demonstrably wrong. Even if states are having these discussions, such a plan is not going to come to fruition. The final rule for Medicaid parity, which essentially has the effect of law, is very clear: It does not allow for differing eligibility or alternate state plans.
The Centers for Medicare & Medicaid Services (CMS) specifically stated in the final rule that the increase is not limited to office-based primary-care services, but it will also include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services. In other words, a hospitalist who attests eligibility for their respective state Medicaid agency and bills 99231-3, 99221-3, 99238-9, etc., will receive the increased payment for these codes.
In response to an SHM inquiry for further clarification, CMS officials have stated, “The regulation requires that qualified physicians billing eligible codes receive higher payment. States do not have the latitude to exclude physicians simply because they practice in hospitals.”
It is possible that some confusion might be arising due to the recent controversies around the upcoming Medicaid expansion, which would extend Medicaid eligibility to individuals who earn up to 138% of the federal poverty line. Some states have chosen to opt out of this expansion and have publicly fought its implementation. The Medicaid parity provision is parallel to, but independent of, Medicaid expansion. Even if a state opts out of the expansion, the Medicaid payment increase for primary-care services should remain unaffected.
This isn’t to say that the Medicaid parity provision is a certainty. With the eyes of Congress turned toward budget cuts and austerity, the funds allocated for this temporary increase could easily be targeted. Regardless, any change in eligibility would require a rule change at the federal level, which is unlikely.
Many states have already devoted much time and effort on plans to implement the provision, and the plans were due to be submitted to CMS on March 31. It is pretty late in the game to consider changes. Barring an unlikely rule change or total elimination of funding, it is clear that hospitalists are eligible for the payment bump and should remain so.
Josh Boswell is SHM’s senior manager of government relations.
For those who remain unaware, hospitalists who care for Medicaid patients will be getting a raise in 2013 and 2014. The reason is that the Affordable Care Act (ACA) requires Medicaid rates for specified primary-care services to be equal to those of Medicare rates during those two years, with the federal government paying the difference. Hospitalists generally meet the requirements and, therefore, will see this pay increase for their applicable Medicaid billing. For some context of the scope of this change, on average, Medicaid pays physicians at 66% of the national Medicare rates, although there is significant variation among the states.
To qualify, a physician must have a specialty designation of family medicine, internal medicine, or pediatrics, then further attest to board certification in one of those specialties or related subspecialties. Alternatively, the physician must have a 60% claims history for the specified evaluation and management (E&M) codes.
Multiple parties who have heard reports about state plans for Medicaid parity recently have contacted SHM; the plans, they report, intentionally would exclude hospitalists from the promised increase. There are variations on the explanation for the exclusion and where the idea is coming from, but the inquiries follow this general theme: “Since the definition of eligible physicians remains a grey area, states are developing alternative plans with a more narrow interpretation of the qualifying factors for the increase. These plans are only including physicians who practice in the community setting (i.e. not the hospital setting).”
This is demonstrably wrong. Even if states are having these discussions, such a plan is not going to come to fruition. The final rule for Medicaid parity, which essentially has the effect of law, is very clear: It does not allow for differing eligibility or alternate state plans.
The Centers for Medicare & Medicaid Services (CMS) specifically stated in the final rule that the increase is not limited to office-based primary-care services, but it will also include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services. In other words, a hospitalist who attests eligibility for their respective state Medicaid agency and bills 99231-3, 99221-3, 99238-9, etc., will receive the increased payment for these codes.
In response to an SHM inquiry for further clarification, CMS officials have stated, “The regulation requires that qualified physicians billing eligible codes receive higher payment. States do not have the latitude to exclude physicians simply because they practice in hospitals.”
It is possible that some confusion might be arising due to the recent controversies around the upcoming Medicaid expansion, which would extend Medicaid eligibility to individuals who earn up to 138% of the federal poverty line. Some states have chosen to opt out of this expansion and have publicly fought its implementation. The Medicaid parity provision is parallel to, but independent of, Medicaid expansion. Even if a state opts out of the expansion, the Medicaid payment increase for primary-care services should remain unaffected.
This isn’t to say that the Medicaid parity provision is a certainty. With the eyes of Congress turned toward budget cuts and austerity, the funds allocated for this temporary increase could easily be targeted. Regardless, any change in eligibility would require a rule change at the federal level, which is unlikely.
Many states have already devoted much time and effort on plans to implement the provision, and the plans were due to be submitted to CMS on March 31. It is pretty late in the game to consider changes. Barring an unlikely rule change or total elimination of funding, it is clear that hospitalists are eligible for the payment bump and should remain so.
Josh Boswell is SHM’s senior manager of government relations.
For those who remain unaware, hospitalists who care for Medicaid patients will be getting a raise in 2013 and 2014. The reason is that the Affordable Care Act (ACA) requires Medicaid rates for specified primary-care services to be equal to those of Medicare rates during those two years, with the federal government paying the difference. Hospitalists generally meet the requirements and, therefore, will see this pay increase for their applicable Medicaid billing. For some context of the scope of this change, on average, Medicaid pays physicians at 66% of the national Medicare rates, although there is significant variation among the states.
To qualify, a physician must have a specialty designation of family medicine, internal medicine, or pediatrics, then further attest to board certification in one of those specialties or related subspecialties. Alternatively, the physician must have a 60% claims history for the specified evaluation and management (E&M) codes.
Multiple parties who have heard reports about state plans for Medicaid parity recently have contacted SHM; the plans, they report, intentionally would exclude hospitalists from the promised increase. There are variations on the explanation for the exclusion and where the idea is coming from, but the inquiries follow this general theme: “Since the definition of eligible physicians remains a grey area, states are developing alternative plans with a more narrow interpretation of the qualifying factors for the increase. These plans are only including physicians who practice in the community setting (i.e. not the hospital setting).”
This is demonstrably wrong. Even if states are having these discussions, such a plan is not going to come to fruition. The final rule for Medicaid parity, which essentially has the effect of law, is very clear: It does not allow for differing eligibility or alternate state plans.
The Centers for Medicare & Medicaid Services (CMS) specifically stated in the final rule that the increase is not limited to office-based primary-care services, but it will also include hospital observation and consultation for inpatient services provided by nonadmitting physicians, ED services, and critical-care services. In other words, a hospitalist who attests eligibility for their respective state Medicaid agency and bills 99231-3, 99221-3, 99238-9, etc., will receive the increased payment for these codes.
In response to an SHM inquiry for further clarification, CMS officials have stated, “The regulation requires that qualified physicians billing eligible codes receive higher payment. States do not have the latitude to exclude physicians simply because they practice in hospitals.”
It is possible that some confusion might be arising due to the recent controversies around the upcoming Medicaid expansion, which would extend Medicaid eligibility to individuals who earn up to 138% of the federal poverty line. Some states have chosen to opt out of this expansion and have publicly fought its implementation. The Medicaid parity provision is parallel to, but independent of, Medicaid expansion. Even if a state opts out of the expansion, the Medicaid payment increase for primary-care services should remain unaffected.
This isn’t to say that the Medicaid parity provision is a certainty. With the eyes of Congress turned toward budget cuts and austerity, the funds allocated for this temporary increase could easily be targeted. Regardless, any change in eligibility would require a rule change at the federal level, which is unlikely.
Many states have already devoted much time and effort on plans to implement the provision, and the plans were due to be submitted to CMS on March 31. It is pretty late in the game to consider changes. Barring an unlikely rule change or total elimination of funding, it is clear that hospitalists are eligible for the payment bump and should remain so.
Josh Boswell is SHM’s senior manager of government relations.
Medicare Billing Regulations for Nonphysician Providers Vary by State, Facility
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders

Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.

Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation

Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Nurse practitioners (NPs) and physician assistants (PAs), referred to as nonphysician providers (NPPs) in billing policy, provide many different services in the hospital setting. Roles include:
- Rounding independently and following patients of varying acuity with physician supervision. The NPP may ask the physician to see the patient, as necessary, if a change in the patient’s condition arises and warrants physician evaluation.
- Providing prompt consultative
- services when the physician is not
- readily available.
- Rounding alongside the physician and expediting the work of admission services through a combined effort.
Hospitalist programs may elect one model over another, or utilize NPPs according to existing need and shifting census. Employers must be aware of state and federal regulations, facility-imposed standards of care, and billing requirements surrounding NPP services.
Medicare Enrollment and Billing Eligibility
Certified PAs and NPs may provide covered services to Medicare beneficiaries in accordance with their state scope of practice under state law and corresponding supervision/collaboration requirements. They can submit claims for these services, providing they meet enrollment qualifications.1
PAs must have:
- Graduated from a PA educational program accredited by the Accreditation Review Commission on Education for the Physician Assistant (or its predecessor agencies, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) and the Committee on Allied Health Education and Accreditation (CAHEA); or
- Passed the national certification examination administered by the National Commission on Certification of Physician Assistants (NCCPA); and
- A license as a PA in the practicing state.
NPs must:
- Be a registered nurse who is authorized and licensed by the state to practice as a nurse practitioner by Dec. 31, 2000; or
- After Jan. 1, 2001, be a registered nurse who is authorized and licensed by the state to practice as an NP and be certified by a recognized national certifying body that has established standards for NPs (e.g. American Academy of Nurse Practitioners, American Nurses Credentialing Center, AACN Certification Corp., or National Board on Certification of Hospice and Palliative Nurses); and
- Possess a master’s degree in nursing.
Independent Billing
NPPs can see patients in any setting without the presence of a physician. The physician is not required to see the patient but must be available by phone or beeper in accordance with supervisory/collaborative guidelines. Physician cosignature is not required unless mandated by state law or the facility.
NPPs document and report their services according to the Centers for Medicare & Medicaid Services (CMS) Documentation Guidelines (available at www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/EMDOC.html). The NPP should be listed as the rendering provider on the claim form. Currently, insurance programs Medicare and Aetna Inc. consistently enroll and recognize NPPs as billing providers and reimburse these services at 85% of the allowable physician rate.2
Shared/Split Billing
When two providers (a physician and NPP) from the same group (direct employment or a lease arrangement contractually linking the providers) perform a service for the same patient on the same calendar day, CMS allows the combined services to be reported under a single provider’s name.
Allowable services. NPPs are only limited by the state scope of practice under state law, and the facility rules in which the NPPs practice. Services must be performed under the appropriate level of supervision or collaboration. Medicare reimburses reasonable and necessary services not otherwise excluded from coverage.
However, shared/split rules restrict the services reported under this billing model, recognizing only evaluation and management (E/M) services (and not procedures) provided in the ED, outpatient hospital clinics, or inpatient hospital (i.e. facility-based services). Shared/split rules do not involve all types of E/M services. For hospitalist programs, critical-care services (99291-99292) are excluded.3
Physician requirement. Shared/split rules require a face-to-face patient encounter by each provider on the same calendar day. There are no billing mandates requiring the NPP to see the patient before the physician does, although practice style might govern this decision.4 CMS does not specify the extent of provider involvement, but it could be established by local Medicare contractor requirements. Some contractors reference physician participation as a “substantive” service without further elaboration on specific parameters. Therefore, the physician determines the critical or key portion of his/her personal service. Minimalistic documentation can be problematic for quality or medicolegal aspects of patient care, and physicians might benefit from a more detailed notation of participation.
Documentation. Physician documentation must include an attestation that supports the physician encounter (e.g. “Patient seen and examined by me”), the individual with whom the service is shared (e.g. “Agree with note by X”), their portion of the rendered service (e.g. “Pulse oximetry 94% on room air. Audible rhonchi at bilateral lung bases. Start O2 2L nasal cannula. Obtain CXR”), the date, and a legible signature. NPP documentation should include as similar reference to the physician with whom the service is being shared for better charge capture. It alerts coders, auditors, and payor representatives to consider both notes in support of the billed service and ensures that the correct notes are sent to the payor in the event of claim denial and subsequent appeal.
Although the visit level is supported by both provider services, only one claim may be submitted for a shared/split service. The rendering provider listed on the claim can be the physician (reimbursed at 100% of the Medicare allowable physician rate) or the NPP (reimbursed at 85% of the allowable physician rate).
Non-Medicare Claims
Shared/split billing policy only applies to Medicare beneficiaries, while independent billing policy applies to Medicare and Aetna. Excessive costs prevent most other non-Medicare insurers from credentialing and enrollment NPPs. Absence of payor policy does not disqualify reimbursement for shared services, but it does require additional measures to establish recognition of NPP services and a corresponding reimbursement model.
After determining payor mix, develop a reasonable guideline for those payors who do not enroll NPPs. Delineate, in writing, a predetermined time frame for guideline implementation unless the payor can provide an alternate billing option. Some experts suggest physician groups outline the following key issues when structuring a billing option5:
- Type of NPPs involved in patient care;
- Category of services provided;
- Service location(s);
- Physician involvement;
- Mechanism for reporting services; and
- Documentation requirements.
Guidelines can be developed for any of the billing options (independent, “incident-to,” shared/split). Be sure to obtain written payor response before initiating the billing process.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
NPP Billing Reminders
Discharge day management (99238-99239) often is delegated to qualified NPPs.3 Because this service is time-based, the final code selection is based upon the total time spent with the patient, and on the patient’s unit/floor, coordinating care prior to the patient leaving the hospital on the day of discharge. If this service is solely provided by the NPP, the NPP must report the appropriate code under his/her own name on the claim form (for eligible payors). If this service is shared with the physician, report the code representing the cumulative, documented time in both notes, provided that each note identifies the face-toface service from each provider, and his/her corresponding participation.
Many questions arise about NPPs performing the admission service because NPPs might not be given “admitting” privileges by the facility in which they practice. NPPs may provide and/or participate in services according to their state scope practice and facility-imposed guidelines. Billing policy supports state law and will reimburse any “independent” service permitted by the state. Facilities may limit NPP scope of practice by disallowing independent admission service but permittin a shared service with the physician. If this service is shared with the physician, report the code representing the cumulative, documented encounter, provided that each note identifies the face-to-face service from each provider, and his/her corresponding participation
Prior to Medicare’s elimination of consultation services (99241-99245, 99251-99255), shared/split billing rules excluded consultations from this claim-reporting model.3 Since the elimination of consults, “consultations” are reported as initial hospital care services (99221-99223).3 Therefore, consultative services can be shared by NPPs and physicians, and reported as a cumulative initial hospital service through the shared/ split billing model. Other payors still accept consultation codes and do not have a specified shared/split model. This allows for the consultative service to be reported as a cumulative NPP/physician effort under the physician name, as long as a written contractual agreement exists allowing this billing option.
References
- Centers for Medicare & Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 190-200. Centers for Medicare & Medicaid website. Available at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf. Accessed Nov. 5, 2012.
- Aetna Inc. Aetna office links updates. Reminder: Reimbursement change for mid-level practitioners. Aetna Inc. website. Available at www.aetna.com/provider/data/OLU_MA_JUN2010_final.pdf. Accessed Nov. 6, 2012.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare & Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. Centers for Medicare & Medicaid website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan 21, 2013.
- Pohlig, C. Nonphysician Providers in Your Practice. In: Coding for Chest Medicine 2011. Northbrook, Ill.: American College of Chest Physicians, 2010.
Affordable Care Act Provides Two-Year Increase in Medicaid Payments for Primary-Care Services
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”

Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”

—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Some hospitalist groups can expect a bump in total revenue over the next two years, thanks to the Medicaid-to-Medicare parity regulation that was included in the Affordable Care Act. But whether the increase in reimbursement lasts beyond 2014 is anyone’s guess.
The regulation, which the Centers for Medicare & Medicaid Services (CMS) released in November and made effective Jan. 1, increases Medicaid payments for certain primary-care services to 100% of Medicare levels this year and next. States will receive an estimated $11 billion over the next two years to fund the program, according to the American Academy of Family Physicians (AAFP). Eligible providers include physicians, physician assistants (PAs), and nurse practitioners (NPs), who self-attest they are board-certified in family, pediatric, or general internal medicine; it also includes those doctors, PAs, or NPs who self-attest that at least 60% of all Medicaid services they bill or provide in a managed-care environment are for specific evaluation and management (E&M) and vaccine administration codes.1
The concept is to boost Medicaid participation by improving historically lagging reimbursement rates.2 To wit, CMS’ Office of the Actuary estimates the parity rule will add more than 10,000 new primary-care physicians (PCPs) to the Medicaid participation ranks.3
SHM Public Policy Committee member Brad Flansbaum, DO, MPH, SFHM, says that hospitalists who deal with Medicaid populations can expect at least some increase in their revenue over the next two years. For example, he says, take an HM group earning $100,000 a year in Medicaid revenue. Now consider Urban Institute figures that show, in 2012, Medicaid physician fees on average were 66% of Medicare physician fees (with wide state variations). The parity rule now pays that hypothetical HM group about $150,000.
“It’s simple math,” Dr. Flansbaum says. “I would emphasize that the bump in pay is going to be proportional to the percentage of Medicaid patients that you see. There are some doctors who see an awful lot of Medicaid patients in safety-net and public hospitals, and that money, when it comes back to departments and divisions, can be used for things that a lot of these places never had the means to do before. It could be salary, but it could also mean hiring more people, more resources. It makes a difference.”
Public Policy Committee chair Ron Greeno, MD, FCCP, MHM, says SHM advocated for the parity regulation, as Medicaid has historically paid for only about 70% of the healthcare delivered to patients. Although the parity issue has not gathered as much attention as other facets of the healthcare reform movement, having CMS recognize that delivery of primary care is not restricted to traditional offices is one he and SHM are particularly proud of.
“This is a correction long in coming,” Dr. Greeno says. “We’re happy hospitalists were included in the group of people that will achieve that parity.”
Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City, says few physicians are even aware of the provision, in part because of a widespread frustration with Medicaid’s historic reimbursements rates.
“It’s almost a foregone conclusion that Medicaid never pays, reimbursement always goes down, and the interactions with Medicaid are always increasingly difficult,” Dr. Flansbaum adds.
The question for physicians and policy wonks now is what happens to the parity regulation after its scheduled expiration Dec. 31, 2014. Several medical societies, including SHM and the American College of Physicians (ACP), lobbied Congress to make sure the parity regulation was not impacted by the “fiscal cliff” negotiations. The next step is to craft a permanent funding source to pay for it.
“Unless Congress acts to permanently extend and fund this provision, a sudden return to disparate and inadequate payment for primary services needed by Medicaid patients after only two years will again threaten to restrict their access to such needed services,” AAFP said in a statement after the rule was implemented. “It would once again shut out people who have come to know and depend on their primary care physicians. Only by extending Medicaid parity with Medicare can we ensure that these Americans continue to have uninterrupted medical care in the future.”
—Brad Flansbaum, DO, MPH, SFHM, Lenox Hill Hospital, New York City, SHM Public Policy Committee member
SHM recommended that CMS work with the states to facilitate timely data collection designed to determine the effects on the quality and efficiency of care being received under Medicaid as a result of the enhanced fees. CMS agreed with this recommendation and the resulting data, hopefully, will make the case for continuing the enhanced payment following 2014.
Dr. Flansbaum says SHM’s policy team will continue to work on the issue, but given the precarious state of federal budgets and political dysfunction in Washington, it’s too early to know whether a funding source will be identified to pay for parity in 2015 and beyond—especially as politicians have yet to craft long-term solutions to issues including the sustainable-growth rate formula and other specialists, including radiologists and obstetricians, lobby to be eligible for the parity pay. However, he is hopeful that physicians who see the added impact of parity pay in the next two years will lobby Congress to find a way to continue the higher reimbursement.
“I can’t tell you whether or not when you put on the scale of all the priorities whether it’s going to be a new Air Force bomber, another $50 billion into Medicare for physicians, or an educational system upgrade,” he says. “I don’t know where the government is going to assign its priorities. Will the money be there to extend both the two-year Medicaid and the reprieve? And if the answer is yes, will it be extended to other providers beyond just primary-care practitioners? It’s anyone’s guess.”
Richard Quinn is a freelance writer in New Jersey.
References
- FAQ: Medicaid/Medicare Parity Regulation. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Images/Advocacy_Image/pdf/Parity_FAQ_Final.pdf. Accessed Jan. 27, 2013.
- Centers for Medicare & Medicaid Services. Medicaid program; payments for services furnished by certain primary care physicians and charges for vaccine administration under the Vaccines for Children program. Federal Register website. Available at: http://www.gpo.gov/fdsys/pkg/FR-2012-11-06/pdf/2012-26507.pdf. Accessed Jan. 15, 2013.
- Bindman A. JAMA Forum: Warning: Dangerous physician payment cliffs ahead. Journal of the American Medical Association website. Available at: http://newsatjama.jama.com/2013/01/10/jama-forum-warning-dangerous-physician-payment-cliffs-ahead/.Accessed Jan. 15, 2013.
Hospitalists Get Answers to Tough Healthcare Questions
When it comes to Medicare, the Affordable Care Act, and a host of other healthcare-reform-related topics, hospitalists have lots of good questions, such as:
- When does the Physician Value-Based Payment Modifier (VBPM) take effect? And will I be included?
- Which primary-care services are covered by the increased Medicaid payments?
- Are hospitalists eligible to bill for Medicare’s new CPT Transitional Care Management (TCM) codes? (see “New Codes Bridge Billing Gap,”).
Now, SHM’s Public Policy Committee has answered all of the above—and many more—in a set of three “Frequently Asked Questions” documents available at www.hospitalmedicine.org/advocacy. Each document goes in-depth on the most cutting-edge policy issues that are top of mind for hospitalists and the hospitals they serve on these issues:
The Physician Value-Based Payment Modifier (VBPM): The VBPM seeks to connect cost and quality of services in order to begin reimbursement for the value, rather than the quantity, of care. It combines the quality measuring in the Physician Quality Reporting System (PQRS), cost measures, and a payment adjustment for physicians. Measurement begins this year, and many hospitalists will be included.
Medicaid/Medicare parity regulation: On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulations implementing Section 1202 of the Affordable Care Act, which increases Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
New CPT Transitional Care Management (TCM) codes 99495-99496: CMS has created two new CPT Transitional Care Management (TCM) codes designed to improve care coordination and provide better incentives to ensure patients are seen in a physician’s office, rather than be at risk for readmission.
New Action: Getting Involved Just Got Easier
SHM’s Legislative Action Center also makes getting involved easier with a new grassroots outreach tool called Voter Voice. SHM’s first action alert on Voter Voice was sent to members in December. Hospitalists’ willingness to take a few minutes and contact their congressional leaders using Voter Voice increased SHM’s visibility to Congress by nearly five times compared with prior similar alerts.
Getting involved is easy and only takes a few seconds. You can use either your ZIP code to look up your members of Congress or search active legislation by keyword. SHM members can sign up for SHM Legislative Action Center alerts by entering their email address.
To download the new SHM advocacy FAQs or use the improved Legislative Action Center, visit www.hospitalmedicine.org/advocacy.
When it comes to Medicare, the Affordable Care Act, and a host of other healthcare-reform-related topics, hospitalists have lots of good questions, such as:
- When does the Physician Value-Based Payment Modifier (VBPM) take effect? And will I be included?
- Which primary-care services are covered by the increased Medicaid payments?
- Are hospitalists eligible to bill for Medicare’s new CPT Transitional Care Management (TCM) codes? (see “New Codes Bridge Billing Gap,”).
Now, SHM’s Public Policy Committee has answered all of the above—and many more—in a set of three “Frequently Asked Questions” documents available at www.hospitalmedicine.org/advocacy. Each document goes in-depth on the most cutting-edge policy issues that are top of mind for hospitalists and the hospitals they serve on these issues:
The Physician Value-Based Payment Modifier (VBPM): The VBPM seeks to connect cost and quality of services in order to begin reimbursement for the value, rather than the quantity, of care. It combines the quality measuring in the Physician Quality Reporting System (PQRS), cost measures, and a payment adjustment for physicians. Measurement begins this year, and many hospitalists will be included.
Medicaid/Medicare parity regulation: On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulations implementing Section 1202 of the Affordable Care Act, which increases Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
New CPT Transitional Care Management (TCM) codes 99495-99496: CMS has created two new CPT Transitional Care Management (TCM) codes designed to improve care coordination and provide better incentives to ensure patients are seen in a physician’s office, rather than be at risk for readmission.
New Action: Getting Involved Just Got Easier
SHM’s Legislative Action Center also makes getting involved easier with a new grassroots outreach tool called Voter Voice. SHM’s first action alert on Voter Voice was sent to members in December. Hospitalists’ willingness to take a few minutes and contact their congressional leaders using Voter Voice increased SHM’s visibility to Congress by nearly five times compared with prior similar alerts.
Getting involved is easy and only takes a few seconds. You can use either your ZIP code to look up your members of Congress or search active legislation by keyword. SHM members can sign up for SHM Legislative Action Center alerts by entering their email address.
To download the new SHM advocacy FAQs or use the improved Legislative Action Center, visit www.hospitalmedicine.org/advocacy.
When it comes to Medicare, the Affordable Care Act, and a host of other healthcare-reform-related topics, hospitalists have lots of good questions, such as:
- When does the Physician Value-Based Payment Modifier (VBPM) take effect? And will I be included?
- Which primary-care services are covered by the increased Medicaid payments?
- Are hospitalists eligible to bill for Medicare’s new CPT Transitional Care Management (TCM) codes? (see “New Codes Bridge Billing Gap,”).
Now, SHM’s Public Policy Committee has answered all of the above—and many more—in a set of three “Frequently Asked Questions” documents available at www.hospitalmedicine.org/advocacy. Each document goes in-depth on the most cutting-edge policy issues that are top of mind for hospitalists and the hospitals they serve on these issues:
The Physician Value-Based Payment Modifier (VBPM): The VBPM seeks to connect cost and quality of services in order to begin reimbursement for the value, rather than the quantity, of care. It combines the quality measuring in the Physician Quality Reporting System (PQRS), cost measures, and a payment adjustment for physicians. Measurement begins this year, and many hospitalists will be included.
Medicaid/Medicare parity regulation: On Nov. 1, 2012, the Centers for Medicare & Medicaid Services (CMS) released the final regulations implementing Section 1202 of the Affordable Care Act, which increases Medicaid payments for specified primary-care services to 100% of Medicare levels in 2013 and 2014.
New CPT Transitional Care Management (TCM) codes 99495-99496: CMS has created two new CPT Transitional Care Management (TCM) codes designed to improve care coordination and provide better incentives to ensure patients are seen in a physician’s office, rather than be at risk for readmission.
New Action: Getting Involved Just Got Easier
SHM’s Legislative Action Center also makes getting involved easier with a new grassroots outreach tool called Voter Voice. SHM’s first action alert on Voter Voice was sent to members in December. Hospitalists’ willingness to take a few minutes and contact their congressional leaders using Voter Voice increased SHM’s visibility to Congress by nearly five times compared with prior similar alerts.
Getting involved is easy and only takes a few seconds. You can use either your ZIP code to look up your members of Congress or search active legislation by keyword. SHM members can sign up for SHM Legislative Action Center alerts by entering their email address.
To download the new SHM advocacy FAQs or use the improved Legislative Action Center, visit www.hospitalmedicine.org/advocacy.
New Codes Bridge Hospitals' Post-Discharge Billing Gap

In November 2012, the Center for Medicare & Medicaid Services (CMS) finalized its 2013 physician fee schedule with two new transitional-care-management (TCM) codes, 99495 and 99496. These codes provide reimbursement for transitional-care services to patients for 30 days after hospital discharge. CMS estimates that two-thirds of the 10 million Medicare patients discharged annually from hospitals will have TCM services provided by an outpatient doctor. Why might hospitalists be interested in these outpatient codes? Read on.
As a post-discharge provider in a primary-care-based discharge clinic, I can say the new Medicare transitional codes read like our job description. Because I’ve worked in a post-discharge clinic for the past three years, I have learned that post-discharge care requires time and resource allocation beyond routine outpatient care. Because of the unique population we see, on average we bill at a higher level than the rest of the practice. Yet we, like all outpatient providers, remain constrained by the existing billing structure, which is intimately connected to physician face-to-face visits.
Here’s an illustration of a typical afternoon in the post-discharge clinic: A schizophrenic patient presents with renal failure, hypoglycemia, and confusion. Her home visiting nurse (VNA) administers her medications; the patient cannot tell you any of them. While you are calling the VNA to clarify her medications, trying to identify her healthcare proxy, and stopping her ACE inhibitor because her potassium is 5.6, the next patient arrives. She has end-stage liver disease and was recently in the hospital for liver failure, and now has worsening recurrent ascites. After clinic, you call interventional radiology to coordinate a therapeutic paracentesis and change diuretic doses after her labs return. Two weeks later, you arrange a repeat paracentesis, and subsequently a transition to comfort care in a hospice house. For this work, right now, you can at most bill a high-complexity office visit (99215), and the rest of the care coordination—by you, your nurse, or your administrative staff—is not compensated.
How Do the New Codes Work?
CMS created the new TCM codes to begin to change the outpatient fee schedule to emphasize primary care and care coordination for beneficiaries, particularly in the post-hospitalization period. The new TCM codes are a first step toward reimbursement for non-face-to-face activities, which are increasingly important in the evolving healthcare system.
The investment is estimated at more than $1 billion in 2013. The new codes are available to physicians, physician assistants, nurse practitioners, and other advanced-practice nurses only once within the 30 days after hospital discharge. During the 30 days after discharge, the two codes, 99495 and 99496, require a single face-to-face visit within seven days of discharge for the highest-risk patients and within 14 days of discharge for moderate-risk patients. The face-to-face visit is not billed separately. The codes also mandate telephone communication with the patient or caregiver within two business days of hospital discharge; the medical decision-making must be of either moderate or high complexity.
The average reimbursement for the codes will be $132.96 for 99495 and $231.11 for 99496, reflecting a higher wRVU than either hospital discharge day management or high-acuity outpatient visits. The code is billed at the end of the 30 days. The TCM code cannot be billed a second time if a patient is readmitted within the 30 days. Other E/M codes can be billed during the same time period for additional visits as necessary.
What’s the Impact on Hospitalists?
The new codes affect hospitalists in two ways. First, the hospitalists in the growing group of “transitionalists,” many of whom practice in outpatient clinics seeing patients after discharge, will be able to use these codes. As the codes require no pre-existing relationship with the patient, non-primary-care providers will be able to bill these codes, assuming that they fulfill the designated requirements. This concession enables hospitalists to fill a vital role for those patients who have inadequate access to immediate primary care post-hospitalization. It also provides a necessary bridge to appropriate primary care for those patients. This group of patients might be particularly vulnerable to adverse events, including hospital readmission, given their suboptimal connection with their primary-care providers.
Hospitalists who practice entirely as inpatient physicians will not be able to bill these new codes, but they will provide a valuable service to patients by helping identify the physicians who will provide their TCM and documenting this in the discharge documentation, already seen as a key element of discharge day management services.
Do These Codes Change the Business Case for Discharge Clinics?
Discharge clinics, either hospitalist-staffed or otherwise, have been actively discussed in the media in recent years.1 Even without these transitional codes, discharge clinics have arisen where primary-care access is limited and as a potential, but as yet unproven, solution to high readmission rates. Despite this proliferation, discharge clinics have not yet proven to be cost-effective.
Implementation of these codes could change the calculus for organizations considering dedicating resources to a discharge clinic. The new codes could make discharge clinics more financially viable by increasing the reimbursement for care that often requires more than 30 minutes. However, based on the experience in our clinic, the increased revenue accurately reflects the intensity of service necessary to coordinate care in the post-discharge period.
The time intensity of care already is obvious from the structure of established discharge clinics. Examples include the comprehensive care centers at HealthCare Partners in Southern California, where multidisciplinary visits average 90 minutes, or at our clinic at Beth Israel Deaconess Medical Center in Boston.2 While the visits in our clinic are less than half as long as those at HealthCare Partners, we are not including the time spent reviewing the discharge documentation, outstanding tests, and medication changes in advance of the visit, and the time spent after the visit, coordinating the patient’s care with visiting nurses and elder service agencies.3
What’s Next?
Whether these codes lead to an increased interest in hospitalist-staffed discharge clinics or to primary-care development of robust transitional-care structures, these new codes will help focus resources and attention on increasing services, with the goal of improving patient care during a period of extreme vulnerability. This alone is something to be grateful for, whether you are a transitionalist, hospitalist, primary-care doctor, caregiver, or patient.
Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center in Boston and an instructor in medicine at Harvard Medical School. She is medical director of BIDMC’s Health Care Associates Post Discharge Clinic.
References
- Andrews M. Post-discharge clinics try to cut hospital readmissions by helping patients. Washington Post website. Available at: http://articles.washingtonpost.com/2011-12-19/national/35288219_1_readmissions-discharge-vulnerable-patients. Accessed Jan. 7, 2013.
- Feder JL. Predictive modeling and team care for high-need patients at HealthCare Partners. Health Aff (Millwood). 2011;30(3):416-418.
- Doctoroff L. Interval examination: establishment of a hospitalist-staffed discharge clinic. J Gen Intern Med. 2012;27(10):1377-1382.
In November 2012, the Center for Medicare & Medicaid Services (CMS) finalized its 2013 physician fee schedule with two new transitional-care-management (TCM) codes, 99495 and 99496. These codes provide reimbursement for transitional-care services to patients for 30 days after hospital discharge. CMS estimates that two-thirds of the 10 million Medicare patients discharged annually from hospitals will have TCM services provided by an outpatient doctor. Why might hospitalists be interested in these outpatient codes? Read on.
As a post-discharge provider in a primary-care-based discharge clinic, I can say the new Medicare transitional codes read like our job description. Because I’ve worked in a post-discharge clinic for the past three years, I have learned that post-discharge care requires time and resource allocation beyond routine outpatient care. Because of the unique population we see, on average we bill at a higher level than the rest of the practice. Yet we, like all outpatient providers, remain constrained by the existing billing structure, which is intimately connected to physician face-to-face visits.
Here’s an illustration of a typical afternoon in the post-discharge clinic: A schizophrenic patient presents with renal failure, hypoglycemia, and confusion. Her home visiting nurse (VNA) administers her medications; the patient cannot tell you any of them. While you are calling the VNA to clarify her medications, trying to identify her healthcare proxy, and stopping her ACE inhibitor because her potassium is 5.6, the next patient arrives. She has end-stage liver disease and was recently in the hospital for liver failure, and now has worsening recurrent ascites. After clinic, you call interventional radiology to coordinate a therapeutic paracentesis and change diuretic doses after her labs return. Two weeks later, you arrange a repeat paracentesis, and subsequently a transition to comfort care in a hospice house. For this work, right now, you can at most bill a high-complexity office visit (99215), and the rest of the care coordination—by you, your nurse, or your administrative staff—is not compensated.
How Do the New Codes Work?
CMS created the new TCM codes to begin to change the outpatient fee schedule to emphasize primary care and care coordination for beneficiaries, particularly in the post-hospitalization period. The new TCM codes are a first step toward reimbursement for non-face-to-face activities, which are increasingly important in the evolving healthcare system.
The investment is estimated at more than $1 billion in 2013. The new codes are available to physicians, physician assistants, nurse practitioners, and other advanced-practice nurses only once within the 30 days after hospital discharge. During the 30 days after discharge, the two codes, 99495 and 99496, require a single face-to-face visit within seven days of discharge for the highest-risk patients and within 14 days of discharge for moderate-risk patients. The face-to-face visit is not billed separately. The codes also mandate telephone communication with the patient or caregiver within two business days of hospital discharge; the medical decision-making must be of either moderate or high complexity.
The average reimbursement for the codes will be $132.96 for 99495 and $231.11 for 99496, reflecting a higher wRVU than either hospital discharge day management or high-acuity outpatient visits. The code is billed at the end of the 30 days. The TCM code cannot be billed a second time if a patient is readmitted within the 30 days. Other E/M codes can be billed during the same time period for additional visits as necessary.
What’s the Impact on Hospitalists?
The new codes affect hospitalists in two ways. First, the hospitalists in the growing group of “transitionalists,” many of whom practice in outpatient clinics seeing patients after discharge, will be able to use these codes. As the codes require no pre-existing relationship with the patient, non-primary-care providers will be able to bill these codes, assuming that they fulfill the designated requirements. This concession enables hospitalists to fill a vital role for those patients who have inadequate access to immediate primary care post-hospitalization. It also provides a necessary bridge to appropriate primary care for those patients. This group of patients might be particularly vulnerable to adverse events, including hospital readmission, given their suboptimal connection with their primary-care providers.
Hospitalists who practice entirely as inpatient physicians will not be able to bill these new codes, but they will provide a valuable service to patients by helping identify the physicians who will provide their TCM and documenting this in the discharge documentation, already seen as a key element of discharge day management services.
Do These Codes Change the Business Case for Discharge Clinics?
Discharge clinics, either hospitalist-staffed or otherwise, have been actively discussed in the media in recent years.1 Even without these transitional codes, discharge clinics have arisen where primary-care access is limited and as a potential, but as yet unproven, solution to high readmission rates. Despite this proliferation, discharge clinics have not yet proven to be cost-effective.
Implementation of these codes could change the calculus for organizations considering dedicating resources to a discharge clinic. The new codes could make discharge clinics more financially viable by increasing the reimbursement for care that often requires more than 30 minutes. However, based on the experience in our clinic, the increased revenue accurately reflects the intensity of service necessary to coordinate care in the post-discharge period.
The time intensity of care already is obvious from the structure of established discharge clinics. Examples include the comprehensive care centers at HealthCare Partners in Southern California, where multidisciplinary visits average 90 minutes, or at our clinic at Beth Israel Deaconess Medical Center in Boston.2 While the visits in our clinic are less than half as long as those at HealthCare Partners, we are not including the time spent reviewing the discharge documentation, outstanding tests, and medication changes in advance of the visit, and the time spent after the visit, coordinating the patient’s care with visiting nurses and elder service agencies.3
What’s Next?
Whether these codes lead to an increased interest in hospitalist-staffed discharge clinics or to primary-care development of robust transitional-care structures, these new codes will help focus resources and attention on increasing services, with the goal of improving patient care during a period of extreme vulnerability. This alone is something to be grateful for, whether you are a transitionalist, hospitalist, primary-care doctor, caregiver, or patient.
Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center in Boston and an instructor in medicine at Harvard Medical School. She is medical director of BIDMC’s Health Care Associates Post Discharge Clinic.
References
- Andrews M. Post-discharge clinics try to cut hospital readmissions by helping patients. Washington Post website. Available at: http://articles.washingtonpost.com/2011-12-19/national/35288219_1_readmissions-discharge-vulnerable-patients. Accessed Jan. 7, 2013.
- Feder JL. Predictive modeling and team care for high-need patients at HealthCare Partners. Health Aff (Millwood). 2011;30(3):416-418.
- Doctoroff L. Interval examination: establishment of a hospitalist-staffed discharge clinic. J Gen Intern Med. 2012;27(10):1377-1382.
In November 2012, the Center for Medicare & Medicaid Services (CMS) finalized its 2013 physician fee schedule with two new transitional-care-management (TCM) codes, 99495 and 99496. These codes provide reimbursement for transitional-care services to patients for 30 days after hospital discharge. CMS estimates that two-thirds of the 10 million Medicare patients discharged annually from hospitals will have TCM services provided by an outpatient doctor. Why might hospitalists be interested in these outpatient codes? Read on.
As a post-discharge provider in a primary-care-based discharge clinic, I can say the new Medicare transitional codes read like our job description. Because I’ve worked in a post-discharge clinic for the past three years, I have learned that post-discharge care requires time and resource allocation beyond routine outpatient care. Because of the unique population we see, on average we bill at a higher level than the rest of the practice. Yet we, like all outpatient providers, remain constrained by the existing billing structure, which is intimately connected to physician face-to-face visits.
Here’s an illustration of a typical afternoon in the post-discharge clinic: A schizophrenic patient presents with renal failure, hypoglycemia, and confusion. Her home visiting nurse (VNA) administers her medications; the patient cannot tell you any of them. While you are calling the VNA to clarify her medications, trying to identify her healthcare proxy, and stopping her ACE inhibitor because her potassium is 5.6, the next patient arrives. She has end-stage liver disease and was recently in the hospital for liver failure, and now has worsening recurrent ascites. After clinic, you call interventional radiology to coordinate a therapeutic paracentesis and change diuretic doses after her labs return. Two weeks later, you arrange a repeat paracentesis, and subsequently a transition to comfort care in a hospice house. For this work, right now, you can at most bill a high-complexity office visit (99215), and the rest of the care coordination—by you, your nurse, or your administrative staff—is not compensated.
How Do the New Codes Work?
CMS created the new TCM codes to begin to change the outpatient fee schedule to emphasize primary care and care coordination for beneficiaries, particularly in the post-hospitalization period. The new TCM codes are a first step toward reimbursement for non-face-to-face activities, which are increasingly important in the evolving healthcare system.
The investment is estimated at more than $1 billion in 2013. The new codes are available to physicians, physician assistants, nurse practitioners, and other advanced-practice nurses only once within the 30 days after hospital discharge. During the 30 days after discharge, the two codes, 99495 and 99496, require a single face-to-face visit within seven days of discharge for the highest-risk patients and within 14 days of discharge for moderate-risk patients. The face-to-face visit is not billed separately. The codes also mandate telephone communication with the patient or caregiver within two business days of hospital discharge; the medical decision-making must be of either moderate or high complexity.
The average reimbursement for the codes will be $132.96 for 99495 and $231.11 for 99496, reflecting a higher wRVU than either hospital discharge day management or high-acuity outpatient visits. The code is billed at the end of the 30 days. The TCM code cannot be billed a second time if a patient is readmitted within the 30 days. Other E/M codes can be billed during the same time period for additional visits as necessary.
What’s the Impact on Hospitalists?
The new codes affect hospitalists in two ways. First, the hospitalists in the growing group of “transitionalists,” many of whom practice in outpatient clinics seeing patients after discharge, will be able to use these codes. As the codes require no pre-existing relationship with the patient, non-primary-care providers will be able to bill these codes, assuming that they fulfill the designated requirements. This concession enables hospitalists to fill a vital role for those patients who have inadequate access to immediate primary care post-hospitalization. It also provides a necessary bridge to appropriate primary care for those patients. This group of patients might be particularly vulnerable to adverse events, including hospital readmission, given their suboptimal connection with their primary-care providers.
Hospitalists who practice entirely as inpatient physicians will not be able to bill these new codes, but they will provide a valuable service to patients by helping identify the physicians who will provide their TCM and documenting this in the discharge documentation, already seen as a key element of discharge day management services.
Do These Codes Change the Business Case for Discharge Clinics?
Discharge clinics, either hospitalist-staffed or otherwise, have been actively discussed in the media in recent years.1 Even without these transitional codes, discharge clinics have arisen where primary-care access is limited and as a potential, but as yet unproven, solution to high readmission rates. Despite this proliferation, discharge clinics have not yet proven to be cost-effective.
Implementation of these codes could change the calculus for organizations considering dedicating resources to a discharge clinic. The new codes could make discharge clinics more financially viable by increasing the reimbursement for care that often requires more than 30 minutes. However, based on the experience in our clinic, the increased revenue accurately reflects the intensity of service necessary to coordinate care in the post-discharge period.
The time intensity of care already is obvious from the structure of established discharge clinics. Examples include the comprehensive care centers at HealthCare Partners in Southern California, where multidisciplinary visits average 90 minutes, or at our clinic at Beth Israel Deaconess Medical Center in Boston.2 While the visits in our clinic are less than half as long as those at HealthCare Partners, we are not including the time spent reviewing the discharge documentation, outstanding tests, and medication changes in advance of the visit, and the time spent after the visit, coordinating the patient’s care with visiting nurses and elder service agencies.3
What’s Next?
Whether these codes lead to an increased interest in hospitalist-staffed discharge clinics or to primary-care development of robust transitional-care structures, these new codes will help focus resources and attention on increasing services, with the goal of improving patient care during a period of extreme vulnerability. This alone is something to be grateful for, whether you are a transitionalist, hospitalist, primary-care doctor, caregiver, or patient.
Dr. Doctoroff is a hospitalist at Beth Israel Deaconess Medical Center in Boston and an instructor in medicine at Harvard Medical School. She is medical director of BIDMC’s Health Care Associates Post Discharge Clinic.
References
- Andrews M. Post-discharge clinics try to cut hospital readmissions by helping patients. Washington Post website. Available at: http://articles.washingtonpost.com/2011-12-19/national/35288219_1_readmissions-discharge-vulnerable-patients. Accessed Jan. 7, 2013.
- Feder JL. Predictive modeling and team care for high-need patients at HealthCare Partners. Health Aff (Millwood). 2011;30(3):416-418.
- Doctoroff L. Interval examination: establishment of a hospitalist-staffed discharge clinic. J Gen Intern Med. 2012;27(10):1377-1382.
ONLINE EXCLUSIVE: Billing Expert Explains Why Documentation, Education, and Feedback Are Crucial to Reimbursement
12 Things Hospitalists Need to Know About Billing and Coding
Documentation, CPT codes, modifiers—it’s not glamorous, but it’s an integral part of a 21st-century physician’s job description. The Hospitalist queried more than a handful of billing and coding experts about the advice they would dispense to clinicians navigating the reimbursement maze.
“Physicians often do more than what is reflected in the documentation,” says Barb Pierce, CCS-P, ACS-EM, a national coding consultant based in West Des Moines, Iowa, and CODE-H faculty. “They can’t always bill for everything they do, but they certainly can document and code to obtain the appropriate levels of service.”
Meanwhile, hospitalists have to be careful they aren’t excessive in their billing practices. “The name of the game isn’t just to bill higher,” Pierce adds, “but to make sure that your documentation supports the service being billed, and Medicare is watching. They’re doing a lot of focused audits.”
Some hospitalists might opt for a lower level of service, suspecting they’re less likely to be audited. Other hospitalists might seek reimbursement for more of their time and efforts.
“You have both ends of the spectrum,” says Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education for AAPC, formerly known as the American Academy of Professional Coders. “There are a lot of factors that would go into why a provider would code something incorrectly.”
Here’s how to land somewhere in the middle.
1 Be thorough in documenting the initial hospital visit.
When selecting the level of service for an initial hospital visit, the documentation consists of three key components: history, physical examination, and medical decision-making. The history includes the chief complaint as well as the review of systems. This is “an inventory of the patient’s organ systems.” Both the complaint and the systems review are often incorporated in the history of present illness, says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist in the Department of Medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.
A patient’s family history is commonly overlooked in a hospitalist’s notes, primarily when they know the patient from previous admissions for chronic diseases and when the family history will likely not have an impact on treatment. “If they do not document a complete review of systems or miss one of the histories, the service will definitely be down-coded,” Mulholland says, “no matter how complete the exam and medical decision-making documentation.”
2 Familiarize yourself with Medicare reimbursement rules in the state where you practice.
In some states, Medicare contractors require providers to document the status of each organ system reviewed individually. In other states, it’s acceptable to document a system review with pertinent findings, “whether positive or negative,” and the statement of “all other systems negative,” Mulholland says.
The auditor will give credit for the review based on the number of organ systems documented. “If you miss one system review, it will take down what otherwise would be a Level Three hospital admission to a Level One,” she says. “So there would be a significant financial impact.”
Medicare reimbursement for a Level Three initial visit in Mulholland’s area of practice—Philadelphia County in Pennsylvania—is $206.57, compared with $104.69 for a Level One. During this visit, each of the key components—history, exam, and medical decision-making—need to be documented completely for the provider to receive the highest level of reimbursement.
3 Ask about a patient’s social history.
Social history can be obtained by querying the patient about smoking, drug and alcohol use, his or her occupation, marital status, and type of living arrangement.
“Knowing the social history helps the hospitalist understand the home situation or social circumstances that may have contributed to the hospitalization or may complicate the discharge plan,” Mulholland says.
This is particularly important in decision-making that involves elderly patients. The clinician should “think down the road” as to where the patient will be discharged and if a social worker’s assistance will be needed. It’s about “seeing the whole patient,” she says, “not just the disease.”
4 Remember to include the actual diagnosis.
“As coders, we can see all the clinical indicators of a particular diagnosis,” says Kathryn DeVault, RHIA, CCS, CCS-P, a director at HIM Solutions at the American Health Management Association. However, “unless [physicians] write down the diagnosis, we can’t code it.”
Documents without a diagnosis are more common than one would expect. For example, if a patient has pain when urinating, the hospitalist typically orders a culture. If the result is positive, the hospitalist prescribes an antibiotic for the infection, and too often “the story ends there.” From experience, DeVault can decipher that the patient is being treated for a urinary tract infection, but she can’t assign a code without querying the physician. Hospitalists, she suggests, should try to “close the loop in their documentation.”
5 Be specific in your written assessment of the patient’s condition.
“The main thing that we see is missing documentation,” says Angie Comfort, RHIT, CCS, a director at HIM Solutions. For instance, if a hospitalist documents congestive heart failure, it’s important to indicate whether the condition is chronic or acute and systolic or diastolic.
In the case of a diabetic patient, the notes should specify the type of diabetes. Not doing so “could be a reimbursement-changer,” Comfort says. In contrast, documenting such specifics could result in higher reimbursement, especially if a patient has complications from Type 1 diabetes.
6 Note the severity of the patient’s case.
Hospitalists’ documentation doesn’t always capture everything they’re evaluating for patients. “I’ve seen notes to the extent of ‘patient doing well; waiting on test results,’” the AAPC’s Jimenez says. “If they’re doing certain tests, why are they doing them? What are they trying to diagnose for the patient? What treatment are they considering?”
The reasons for the tests need to be explained. When a provider is monitoring someone in the hospital, the documentation should elaborate on the patient’s response to a treatment, and whether the patient’s condition is better, stable, or worse. This information helps put the severity in perspective.
“A diabetic could be a diabetic out of control. It could be a diabetic who’s not responding or who has comorbidities,” Jimenez says. “No one diagnosis is the same for every patient.”

—Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist, department of medicine, University of Pennsylvania, Philadelphia
7 Indicate which aspect of the patient’s condition you are treating.
When multiple providers are involved in a hospitalized patient’s care, it’s important to document your specific role apart from the services rendered by specialists, Jimenez says. The codes billed must be supported by the documentation for each service. Many providers contribute to the inpatient documentation, so it must be clear what each clinician personally performs.
Only report the diagnosis you are treating or the diagnoses that affect the ones you are managing. If a specialist has been brought in to take over treatment for a specific condition, a hospitalist would not bill for that diagnosis code.

—Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education, AAPC Salt Lake City
8 Note your personal review of medical records and reports from other clinicians.
Hospitalists should document their review of lab data or radiology reports, discussion of the case with other providers, or collection of the history from someone other than the patient. It’s also helpful to document your personal review of any images, such as a chest X-ray or MRI. Examining the images yourself might lead to higher reimbursement, Mulholland says.
Providers also should note when they request or review old records, and they should include a short synopsis of the information obtained and how it contributed to the current treatment plan.
9 Learn the correct coding for patients being transferred.
A transfer can occur either from a different facility or from a hospital floor to a rehabilitation unit. Either way, the patient is seen twice in one day, with each visit covered by the same hospitalist practice.
“Both physicians often report a separate independent visit. However, because these services occurred on the same day, it is not appropriate to bill for two separate subsequent or initial hospital codes,” says Sherri Dumford, MBA, CHBME, director of operations and past president of the Healthcare Billing and Management Association. “Often what will happen is both services will be reported and get through the billing system. The second claim is just written off as a denied service, when, in fact, you could combine the elements of service of both visits and possibly bill for a single higher level of visit.”
10 Consider delegating to a coding expert.
While smaller hospitalist groups can turn to a coding consultant on an as-needed basis, larger groups might consider bringing a certified coder on staff. This person would inform physicians about proper coding, review their documentation, and “give real-time feedback,” Pierce says.
An internal audit would show if the documentation meets selected evaluation management codes. Also, it usually takes a coding professional to determine whether prolonged services are an option for the team on any given date of service. Someone would need to internally “add together” multiple services on one date to see if there is sufficient time documented to allow billing for these add-on codes, Pierce says. Similarly, critical-care time needs to be accumulated during a date of service.

—Barb Pierce, CCS-P, ACS-EM, national coding consultant, West Des Moines, Iowa
11 Indicate the number of minutes spent arranging for a patient’s discharge.
Discharging a patient involves various steps, says Peter Thompson, MD, chief of clinical operations at the Phoenix headquarters of Apogee Physicians, a hospitalist management company that employs about 750 hospitalists across the country. Hospitalists discuss the hospital stay with the patient and family members, prescribe medications, issue discharge recommendations, set up follow-up care, and coordinate with the case manager, specialists, and primary-care physician.
“It generally is one sequential event after the other,” lasting between 20 and 40 minutes and leading up to discharge, Thompson says. Reimbursement for a high-level discharge constitutes more than 30 minutes. However, without proper documentation, he cautions, the claim could be downgraded or denied.
12 Don’t forget to sign, date, and time your progress note.
Last but not least, when it comes to reimbursement, your signature really does matter.
“For an illegible signature, Medicare and the insurance companies have the option of not paying for the service,” Mulholland says. “They’re trying to establish or authenticate who provided the service.”
And they want to know when the hospitalist saw the patient, so it’s a good idea to indicate the exact time of your visit.
Susan Kreimer is a freelance medical writer in New York.
Documentation, CPT codes, modifiers—it’s not glamorous, but it’s an integral part of a 21st-century physician’s job description. The Hospitalist queried more than a handful of billing and coding experts about the advice they would dispense to clinicians navigating the reimbursement maze.
“Physicians often do more than what is reflected in the documentation,” says Barb Pierce, CCS-P, ACS-EM, a national coding consultant based in West Des Moines, Iowa, and CODE-H faculty. “They can’t always bill for everything they do, but they certainly can document and code to obtain the appropriate levels of service.”
Meanwhile, hospitalists have to be careful they aren’t excessive in their billing practices. “The name of the game isn’t just to bill higher,” Pierce adds, “but to make sure that your documentation supports the service being billed, and Medicare is watching. They’re doing a lot of focused audits.”
Some hospitalists might opt for a lower level of service, suspecting they’re less likely to be audited. Other hospitalists might seek reimbursement for more of their time and efforts.
“You have both ends of the spectrum,” says Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education for AAPC, formerly known as the American Academy of Professional Coders. “There are a lot of factors that would go into why a provider would code something incorrectly.”
Here’s how to land somewhere in the middle.
1 Be thorough in documenting the initial hospital visit.
When selecting the level of service for an initial hospital visit, the documentation consists of three key components: history, physical examination, and medical decision-making. The history includes the chief complaint as well as the review of systems. This is “an inventory of the patient’s organ systems.” Both the complaint and the systems review are often incorporated in the history of present illness, says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist in the Department of Medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.
A patient’s family history is commonly overlooked in a hospitalist’s notes, primarily when they know the patient from previous admissions for chronic diseases and when the family history will likely not have an impact on treatment. “If they do not document a complete review of systems or miss one of the histories, the service will definitely be down-coded,” Mulholland says, “no matter how complete the exam and medical decision-making documentation.”
2 Familiarize yourself with Medicare reimbursement rules in the state where you practice.
In some states, Medicare contractors require providers to document the status of each organ system reviewed individually. In other states, it’s acceptable to document a system review with pertinent findings, “whether positive or negative,” and the statement of “all other systems negative,” Mulholland says.
The auditor will give credit for the review based on the number of organ systems documented. “If you miss one system review, it will take down what otherwise would be a Level Three hospital admission to a Level One,” she says. “So there would be a significant financial impact.”
Medicare reimbursement for a Level Three initial visit in Mulholland’s area of practice—Philadelphia County in Pennsylvania—is $206.57, compared with $104.69 for a Level One. During this visit, each of the key components—history, exam, and medical decision-making—need to be documented completely for the provider to receive the highest level of reimbursement.
3 Ask about a patient’s social history.
Social history can be obtained by querying the patient about smoking, drug and alcohol use, his or her occupation, marital status, and type of living arrangement.
“Knowing the social history helps the hospitalist understand the home situation or social circumstances that may have contributed to the hospitalization or may complicate the discharge plan,” Mulholland says.
This is particularly important in decision-making that involves elderly patients. The clinician should “think down the road” as to where the patient will be discharged and if a social worker’s assistance will be needed. It’s about “seeing the whole patient,” she says, “not just the disease.”
4 Remember to include the actual diagnosis.
“As coders, we can see all the clinical indicators of a particular diagnosis,” says Kathryn DeVault, RHIA, CCS, CCS-P, a director at HIM Solutions at the American Health Management Association. However, “unless [physicians] write down the diagnosis, we can’t code it.”
Documents without a diagnosis are more common than one would expect. For example, if a patient has pain when urinating, the hospitalist typically orders a culture. If the result is positive, the hospitalist prescribes an antibiotic for the infection, and too often “the story ends there.” From experience, DeVault can decipher that the patient is being treated for a urinary tract infection, but she can’t assign a code without querying the physician. Hospitalists, she suggests, should try to “close the loop in their documentation.”
5 Be specific in your written assessment of the patient’s condition.
“The main thing that we see is missing documentation,” says Angie Comfort, RHIT, CCS, a director at HIM Solutions. For instance, if a hospitalist documents congestive heart failure, it’s important to indicate whether the condition is chronic or acute and systolic or diastolic.
In the case of a diabetic patient, the notes should specify the type of diabetes. Not doing so “could be a reimbursement-changer,” Comfort says. In contrast, documenting such specifics could result in higher reimbursement, especially if a patient has complications from Type 1 diabetes.
6 Note the severity of the patient’s case.
Hospitalists’ documentation doesn’t always capture everything they’re evaluating for patients. “I’ve seen notes to the extent of ‘patient doing well; waiting on test results,’” the AAPC’s Jimenez says. “If they’re doing certain tests, why are they doing them? What are they trying to diagnose for the patient? What treatment are they considering?”
The reasons for the tests need to be explained. When a provider is monitoring someone in the hospital, the documentation should elaborate on the patient’s response to a treatment, and whether the patient’s condition is better, stable, or worse. This information helps put the severity in perspective.
“A diabetic could be a diabetic out of control. It could be a diabetic who’s not responding or who has comorbidities,” Jimenez says. “No one diagnosis is the same for every patient.”
—Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist, department of medicine, University of Pennsylvania, Philadelphia
7 Indicate which aspect of the patient’s condition you are treating.
When multiple providers are involved in a hospitalized patient’s care, it’s important to document your specific role apart from the services rendered by specialists, Jimenez says. The codes billed must be supported by the documentation for each service. Many providers contribute to the inpatient documentation, so it must be clear what each clinician personally performs.
Only report the diagnosis you are treating or the diagnoses that affect the ones you are managing. If a specialist has been brought in to take over treatment for a specific condition, a hospitalist would not bill for that diagnosis code.
—Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education, AAPC Salt Lake City
8 Note your personal review of medical records and reports from other clinicians.
Hospitalists should document their review of lab data or radiology reports, discussion of the case with other providers, or collection of the history from someone other than the patient. It’s also helpful to document your personal review of any images, such as a chest X-ray or MRI. Examining the images yourself might lead to higher reimbursement, Mulholland says.
Providers also should note when they request or review old records, and they should include a short synopsis of the information obtained and how it contributed to the current treatment plan.
9 Learn the correct coding for patients being transferred.
A transfer can occur either from a different facility or from a hospital floor to a rehabilitation unit. Either way, the patient is seen twice in one day, with each visit covered by the same hospitalist practice.
“Both physicians often report a separate independent visit. However, because these services occurred on the same day, it is not appropriate to bill for two separate subsequent or initial hospital codes,” says Sherri Dumford, MBA, CHBME, director of operations and past president of the Healthcare Billing and Management Association. “Often what will happen is both services will be reported and get through the billing system. The second claim is just written off as a denied service, when, in fact, you could combine the elements of service of both visits and possibly bill for a single higher level of visit.”
10 Consider delegating to a coding expert.
While smaller hospitalist groups can turn to a coding consultant on an as-needed basis, larger groups might consider bringing a certified coder on staff. This person would inform physicians about proper coding, review their documentation, and “give real-time feedback,” Pierce says.
An internal audit would show if the documentation meets selected evaluation management codes. Also, it usually takes a coding professional to determine whether prolonged services are an option for the team on any given date of service. Someone would need to internally “add together” multiple services on one date to see if there is sufficient time documented to allow billing for these add-on codes, Pierce says. Similarly, critical-care time needs to be accumulated during a date of service.
—Barb Pierce, CCS-P, ACS-EM, national coding consultant, West Des Moines, Iowa
11 Indicate the number of minutes spent arranging for a patient’s discharge.
Discharging a patient involves various steps, says Peter Thompson, MD, chief of clinical operations at the Phoenix headquarters of Apogee Physicians, a hospitalist management company that employs about 750 hospitalists across the country. Hospitalists discuss the hospital stay with the patient and family members, prescribe medications, issue discharge recommendations, set up follow-up care, and coordinate with the case manager, specialists, and primary-care physician.
“It generally is one sequential event after the other,” lasting between 20 and 40 minutes and leading up to discharge, Thompson says. Reimbursement for a high-level discharge constitutes more than 30 minutes. However, without proper documentation, he cautions, the claim could be downgraded or denied.
12 Don’t forget to sign, date, and time your progress note.
Last but not least, when it comes to reimbursement, your signature really does matter.
“For an illegible signature, Medicare and the insurance companies have the option of not paying for the service,” Mulholland says. “They’re trying to establish or authenticate who provided the service.”
And they want to know when the hospitalist saw the patient, so it’s a good idea to indicate the exact time of your visit.
Susan Kreimer is a freelance medical writer in New York.
Documentation, CPT codes, modifiers—it’s not glamorous, but it’s an integral part of a 21st-century physician’s job description. The Hospitalist queried more than a handful of billing and coding experts about the advice they would dispense to clinicians navigating the reimbursement maze.
“Physicians often do more than what is reflected in the documentation,” says Barb Pierce, CCS-P, ACS-EM, a national coding consultant based in West Des Moines, Iowa, and CODE-H faculty. “They can’t always bill for everything they do, but they certainly can document and code to obtain the appropriate levels of service.”
Meanwhile, hospitalists have to be careful they aren’t excessive in their billing practices. “The name of the game isn’t just to bill higher,” Pierce adds, “but to make sure that your documentation supports the service being billed, and Medicare is watching. They’re doing a lot of focused audits.”
Some hospitalists might opt for a lower level of service, suspecting they’re less likely to be audited. Other hospitalists might seek reimbursement for more of their time and efforts.
“You have both ends of the spectrum,” says Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education for AAPC, formerly known as the American Academy of Professional Coders. “There are a lot of factors that would go into why a provider would code something incorrectly.”
Here’s how to land somewhere in the middle.
1 Be thorough in documenting the initial hospital visit.
When selecting the level of service for an initial hospital visit, the documentation consists of three key components: history, physical examination, and medical decision-making. The history includes the chief complaint as well as the review of systems. This is “an inventory of the patient’s organ systems.” Both the complaint and the systems review are often incorporated in the history of present illness, says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist in the Department of Medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.
A patient’s family history is commonly overlooked in a hospitalist’s notes, primarily when they know the patient from previous admissions for chronic diseases and when the family history will likely not have an impact on treatment. “If they do not document a complete review of systems or miss one of the histories, the service will definitely be down-coded,” Mulholland says, “no matter how complete the exam and medical decision-making documentation.”
2 Familiarize yourself with Medicare reimbursement rules in the state where you practice.
In some states, Medicare contractors require providers to document the status of each organ system reviewed individually. In other states, it’s acceptable to document a system review with pertinent findings, “whether positive or negative,” and the statement of “all other systems negative,” Mulholland says.
The auditor will give credit for the review based on the number of organ systems documented. “If you miss one system review, it will take down what otherwise would be a Level Three hospital admission to a Level One,” she says. “So there would be a significant financial impact.”
Medicare reimbursement for a Level Three initial visit in Mulholland’s area of practice—Philadelphia County in Pennsylvania—is $206.57, compared with $104.69 for a Level One. During this visit, each of the key components—history, exam, and medical decision-making—need to be documented completely for the provider to receive the highest level of reimbursement.
3 Ask about a patient’s social history.
Social history can be obtained by querying the patient about smoking, drug and alcohol use, his or her occupation, marital status, and type of living arrangement.
“Knowing the social history helps the hospitalist understand the home situation or social circumstances that may have contributed to the hospitalization or may complicate the discharge plan,” Mulholland says.
This is particularly important in decision-making that involves elderly patients. The clinician should “think down the road” as to where the patient will be discharged and if a social worker’s assistance will be needed. It’s about “seeing the whole patient,” she says, “not just the disease.”
4 Remember to include the actual diagnosis.
“As coders, we can see all the clinical indicators of a particular diagnosis,” says Kathryn DeVault, RHIA, CCS, CCS-P, a director at HIM Solutions at the American Health Management Association. However, “unless [physicians] write down the diagnosis, we can’t code it.”
Documents without a diagnosis are more common than one would expect. For example, if a patient has pain when urinating, the hospitalist typically orders a culture. If the result is positive, the hospitalist prescribes an antibiotic for the infection, and too often “the story ends there.” From experience, DeVault can decipher that the patient is being treated for a urinary tract infection, but she can’t assign a code without querying the physician. Hospitalists, she suggests, should try to “close the loop in their documentation.”
5 Be specific in your written assessment of the patient’s condition.
“The main thing that we see is missing documentation,” says Angie Comfort, RHIT, CCS, a director at HIM Solutions. For instance, if a hospitalist documents congestive heart failure, it’s important to indicate whether the condition is chronic or acute and systolic or diastolic.
In the case of a diabetic patient, the notes should specify the type of diabetes. Not doing so “could be a reimbursement-changer,” Comfort says. In contrast, documenting such specifics could result in higher reimbursement, especially if a patient has complications from Type 1 diabetes.
6 Note the severity of the patient’s case.
Hospitalists’ documentation doesn’t always capture everything they’re evaluating for patients. “I’ve seen notes to the extent of ‘patient doing well; waiting on test results,’” the AAPC’s Jimenez says. “If they’re doing certain tests, why are they doing them? What are they trying to diagnose for the patient? What treatment are they considering?”
The reasons for the tests need to be explained. When a provider is monitoring someone in the hospital, the documentation should elaborate on the patient’s response to a treatment, and whether the patient’s condition is better, stable, or worse. This information helps put the severity in perspective.
“A diabetic could be a diabetic out of control. It could be a diabetic who’s not responding or who has comorbidities,” Jimenez says. “No one diagnosis is the same for every patient.”
—Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist, department of medicine, University of Pennsylvania, Philadelphia
7 Indicate which aspect of the patient’s condition you are treating.
When multiple providers are involved in a hospitalized patient’s care, it’s important to document your specific role apart from the services rendered by specialists, Jimenez says. The codes billed must be supported by the documentation for each service. Many providers contribute to the inpatient documentation, so it must be clear what each clinician personally performs.
Only report the diagnosis you are treating or the diagnoses that affect the ones you are managing. If a specialist has been brought in to take over treatment for a specific condition, a hospitalist would not bill for that diagnosis code.
—Raemarie Jimenez, CPC, CPMA, CPC-I, CANPC, CRHC, director of education, AAPC Salt Lake City
8 Note your personal review of medical records and reports from other clinicians.
Hospitalists should document their review of lab data or radiology reports, discussion of the case with other providers, or collection of the history from someone other than the patient. It’s also helpful to document your personal review of any images, such as a chest X-ray or MRI. Examining the images yourself might lead to higher reimbursement, Mulholland says.
Providers also should note when they request or review old records, and they should include a short synopsis of the information obtained and how it contributed to the current treatment plan.
9 Learn the correct coding for patients being transferred.
A transfer can occur either from a different facility or from a hospital floor to a rehabilitation unit. Either way, the patient is seen twice in one day, with each visit covered by the same hospitalist practice.
“Both physicians often report a separate independent visit. However, because these services occurred on the same day, it is not appropriate to bill for two separate subsequent or initial hospital codes,” says Sherri Dumford, MBA, CHBME, director of operations and past president of the Healthcare Billing and Management Association. “Often what will happen is both services will be reported and get through the billing system. The second claim is just written off as a denied service, when, in fact, you could combine the elements of service of both visits and possibly bill for a single higher level of visit.”
10 Consider delegating to a coding expert.
While smaller hospitalist groups can turn to a coding consultant on an as-needed basis, larger groups might consider bringing a certified coder on staff. This person would inform physicians about proper coding, review their documentation, and “give real-time feedback,” Pierce says.
An internal audit would show if the documentation meets selected evaluation management codes. Also, it usually takes a coding professional to determine whether prolonged services are an option for the team on any given date of service. Someone would need to internally “add together” multiple services on one date to see if there is sufficient time documented to allow billing for these add-on codes, Pierce says. Similarly, critical-care time needs to be accumulated during a date of service.
—Barb Pierce, CCS-P, ACS-EM, national coding consultant, West Des Moines, Iowa
11 Indicate the number of minutes spent arranging for a patient’s discharge.
Discharging a patient involves various steps, says Peter Thompson, MD, chief of clinical operations at the Phoenix headquarters of Apogee Physicians, a hospitalist management company that employs about 750 hospitalists across the country. Hospitalists discuss the hospital stay with the patient and family members, prescribe medications, issue discharge recommendations, set up follow-up care, and coordinate with the case manager, specialists, and primary-care physician.
“It generally is one sequential event after the other,” lasting between 20 and 40 minutes and leading up to discharge, Thompson says. Reimbursement for a high-level discharge constitutes more than 30 minutes. However, without proper documentation, he cautions, the claim could be downgraded or denied.
12 Don’t forget to sign, date, and time your progress note.
Last but not least, when it comes to reimbursement, your signature really does matter.
“For an illegible signature, Medicare and the insurance companies have the option of not paying for the service,” Mulholland says. “They’re trying to establish or authenticate who provided the service.”
And they want to know when the hospitalist saw the patient, so it’s a good idea to indicate the exact time of your visit.
Susan Kreimer is a freelance medical writer in New York.
Paying Attention to Detail Critical in Medical Coding
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer
Documentation demands attention to detail. For a patient with abdominal pain, be sure to ask: How long has the patient experienced pain? Is it generalized or in a particular quadrant? Sharp or dull? And does it radiate? And jot down the answers.
“Try to use adjectives that would give specifics regarding the complaint,” says Mary Mulholland, MHA, BSN, RN, CPC, senior coding and education specialist at the University of Pennsylvania’s department of medicine. She also suggests hospitalists find out which medications a patient is taking or has taken and indicate whether symptoms have improved or deteriorated. Here’s how Mulholland would document such a case:
Initial hospital admission, level of service:
Code 99223
83-year-old male admitted from the emergency room, complaining of intermittent crampy lower abdominal pain (severe at times), blood in stool and increased weakness for three weeks, worse when getting up or standing. Patient has decreased appetite and progressive shortness of breath. His review of systems is otherwise negative.
Past medical history: Coronary artery disease and hypertension
Family history: Mother with Type 2 diabetes
Social history: Quit smoking 20 years ago
Alert: Blood pressure (90/68), pulse (88), and respiratory (24)
Eyes: Non-icteric
ENT: Dry oral mucosa
Lymphatic: Palpable nodes—right auxilla and right inguinal areas
Lungs: Clear
Cardio: Slight tachycardia, no murmurs, rubs or gallops
Abdomen: Slightly distended, tender on palpation
Skin: Slightly diaphoretic, no rashes or bruising
Neurologic: Cranial nerves intact, alert and conversant
Psychiatric: Anxious
Lab results: Blood in stool, hemoglobin (6.7), serum blood glucose (120), serum sodium (132), serum potassium (4.3), chest X-ray clear (my interpretation). Old records requested.
Assessment: Gastrointestional bleeding, tachycardia, and mild dehydration
Treatment plan: Check hemoglobin and hematocrit every six hours. Also check prothrombin time and partial prothrombin time. Repeat electrolytes in the morning. Order an X-ray of the lower gastrointestinal tract. Type and screen for 2 units of packed red blood cells, and transfuse pending repeat hemoglobin and hematocrit values. Infuse intravenous fluids at 80 cc per minute. Check electrocardiogram. Consult GI regarding endoscopy.
—Susan Kreimer