User login
Liver protein protects against parenteral nutrition liver injury
Hepatic protein PP2A-C-alpha may serve as a protective factor against parenteral nutrition–associated hepatic steatosis by improving liver function, according to a recent study published in Cellular and Molecular Gastroenterology and Hepatology.
Parenteral nutrition–associated hepatic steatosis likely involves the down-regulation of hepatic PP2A-C-alpha and consequent increased phosphorylation of Akt2; this in turn alters hepatic lipid metabolism, promotes triglyceride accumulation, and leads to liver injury, wrote the researchers, led by Gulisudumu Maitiabula and Feng Tian of the Research Institute of General Surgery at Jinling Hospital, Nanjing, China, and the Medical School of Nanjing University.
“Our study provides a strong rationale that PP2A-C-alpha may be involved in the pathogenesis of [parenteral nutrition–associated hepatic steatosis],” they wrote. “Further research is merited to establish whether interventions to enhance PP2A function might suppress the development of hepatic steatosis in patients receiving long-term [parenteral nutrition].”
Parenteral nutrition can be a lifesaving therapy for patients with intestinal failure caused by insufficient bowel length or function, the authors noted However, long-term use can lead to potentially fatal complications such as liver disease, but an understanding of the pathological mechanisms behind parenteral nutrition–associated hepatic steatosis limited.
The research team performed comparative proteomic/phosphoproteomic analyses of liver samples from 10 patients with parenteral nutrition–associated hepatic steatosis, as well as 8 cholelithiasis patients as controls, who were admitted to Jinling Hospital between June 2018 and June 2019. The researchers also assessed the effect of PP2A-C-alpha on liver injury from total parenteral nutrition in mice.
The research team found that PP2A-C-alpha was down-regulated in patients and mice with parenteral nutrition–associated hepatic steatosis. In addition, in patients with parenteral nutrition–associated hepatic steatosis, they found enhanced activation of serine/threonine kinase Akt2 and decreased activation of AMPK.
Mice that were given total parenteral nutrition infusion for 14 days developed hepatic steatosis, down-regulation of PP2A-C-alpha, activation of Akt2, and inhibition of AMPK. Hepatocyte-specific deletion of PP2A-C-alpha in mice given parenteral nutrition exacerbated the Akt2 activation, AMPK inhibition, and hepatic steatosis through an effect on fatty acid degradation.
On the other hand, forced expression of PP2A-C-alpha led to reductions in hepatocyte fat deposition and the pathological score for liver steatosis. Overexpression also significantly improved hepatic steatosis, suppressed Akt2, and activated AMPK. In addition, pharmacological activation of Akt2 in mice overexpressing PP2A-C-alpha led to the aggravation of hepatic steatosis.
“Collectively, these observations suggest that [parenteral nutrition] for [more than] 14 days leads to a down-regulation in PP2A-C-alpha expression that activates Akt2-dependent signaling, which would likely lead to hepatic steatosis,” the study authors wrote.
Intervention trials of PP2A-C-alpha in humans have not been performed because PP2A-C-alpha activators or effector analogs were unavailable for clinical use, they wrote. Additional clinical studies are needed to investigate the effects of PP2A-C-alpha intervention on the development of hepatic steatosis in patients receiving long-term parenteral nutrition.
The study was supported by the National Natural Science Foundation of China, the Science Foundation of Outstanding Youth in Jiangsu Province, the National Science and Technology Research Funding for Public Welfare Medical Projects, “The 13th Five-Year Plan” Foundation of Jiangsu Province for Medical Key Talents, and the Natural Science Foundation of Jiangsu Province. The study authors disclosed no conflicts of interest.
New findings may lead to novel treatments
Parenteral nutrition is a life saver for children and adults with insufficient absorptive capacity of the gastrointestinal tract. Unfortunately, up to two-thirds of patients requiring parenteral nutrition long-term develop liver disease, which can have fatal outcomes. Parenteral nutrition–associated liver disease is characterized by fibrosis and steatosis. While portal inflammation and cholestasis resolve in patients who can be weaned off parenteral nutrition, portal fibrosis and steatosis unfortunately remain in about half of the patients. The development of therapeutic strategies for this condition has thus far been hampered by the fact that the molecular mechanism of parenteral nutrition–associated liver disease was unknown.
This study by Maitiabua and colleagues from Nanjing University Medical School addresses this problem by performing a proteomic and, importantly, phospho-proteomic analysis of liver biopsies from adults treated with parenteral nutrition compared to normally-feeding controls. They discovered that levels of phosphorylated AKT2, the key signaling mediator of insulin in the liver, are increased, while protein levels of the opposing protein phosphatase 2A (PP2A) are decreased in patients receiving parenteral nutrition.
Remarkably, they could reproduce these same pathway changes in a mouse model of parenteral nutrition, which again led to a chronic activation of the insulin signaling pathway, culminating in the phosphorylation of AKT2. They show further that activation of AKT2 inhibits AMPK and alters hepatic lipid metabolism to promote triglyceride accumulation. Using the experimentally tractable mouse model, they demonstrate further that the ablation of a PP2A isoform in the liver is sufficient to cause lipid accumulation and liver injury. Conversely, restoring PP2A expression improved the hepatic phenotype in mice in the parenteral nutrition model. These findings could also be mimicked using pharmacological activation and inhibition of PP2A.
In sum, this experimental study could some day lead the way to novel treatments of parenteral nutrition-induced liver disease through the use of PP2A activators.
Klaus H. Kaestner, PhD, is with the department of genetics and Center for Molecular Studies in Digestive and Liver Diseases, Perelman School of Medicine,University of Pennsylvania, Philadelphia.
New findings may lead to novel treatments
Parenteral nutrition is a life saver for children and adults with insufficient absorptive capacity of the gastrointestinal tract. Unfortunately, up to two-thirds of patients requiring parenteral nutrition long-term develop liver disease, which can have fatal outcomes. Parenteral nutrition–associated liver disease is characterized by fibrosis and steatosis. While portal inflammation and cholestasis resolve in patients who can be weaned off parenteral nutrition, portal fibrosis and steatosis unfortunately remain in about half of the patients. The development of therapeutic strategies for this condition has thus far been hampered by the fact that the molecular mechanism of parenteral nutrition–associated liver disease was unknown.
This study by Maitiabua and colleagues from Nanjing University Medical School addresses this problem by performing a proteomic and, importantly, phospho-proteomic analysis of liver biopsies from adults treated with parenteral nutrition compared to normally-feeding controls. They discovered that levels of phosphorylated AKT2, the key signaling mediator of insulin in the liver, are increased, while protein levels of the opposing protein phosphatase 2A (PP2A) are decreased in patients receiving parenteral nutrition.
Remarkably, they could reproduce these same pathway changes in a mouse model of parenteral nutrition, which again led to a chronic activation of the insulin signaling pathway, culminating in the phosphorylation of AKT2. They show further that activation of AKT2 inhibits AMPK and alters hepatic lipid metabolism to promote triglyceride accumulation. Using the experimentally tractable mouse model, they demonstrate further that the ablation of a PP2A isoform in the liver is sufficient to cause lipid accumulation and liver injury. Conversely, restoring PP2A expression improved the hepatic phenotype in mice in the parenteral nutrition model. These findings could also be mimicked using pharmacological activation and inhibition of PP2A.
In sum, this experimental study could some day lead the way to novel treatments of parenteral nutrition-induced liver disease through the use of PP2A activators.
Klaus H. Kaestner, PhD, is with the department of genetics and Center for Molecular Studies in Digestive and Liver Diseases, Perelman School of Medicine,University of Pennsylvania, Philadelphia.
New findings may lead to novel treatments
Parenteral nutrition is a life saver for children and adults with insufficient absorptive capacity of the gastrointestinal tract. Unfortunately, up to two-thirds of patients requiring parenteral nutrition long-term develop liver disease, which can have fatal outcomes. Parenteral nutrition–associated liver disease is characterized by fibrosis and steatosis. While portal inflammation and cholestasis resolve in patients who can be weaned off parenteral nutrition, portal fibrosis and steatosis unfortunately remain in about half of the patients. The development of therapeutic strategies for this condition has thus far been hampered by the fact that the molecular mechanism of parenteral nutrition–associated liver disease was unknown.
This study by Maitiabua and colleagues from Nanjing University Medical School addresses this problem by performing a proteomic and, importantly, phospho-proteomic analysis of liver biopsies from adults treated with parenteral nutrition compared to normally-feeding controls. They discovered that levels of phosphorylated AKT2, the key signaling mediator of insulin in the liver, are increased, while protein levels of the opposing protein phosphatase 2A (PP2A) are decreased in patients receiving parenteral nutrition.
Remarkably, they could reproduce these same pathway changes in a mouse model of parenteral nutrition, which again led to a chronic activation of the insulin signaling pathway, culminating in the phosphorylation of AKT2. They show further that activation of AKT2 inhibits AMPK and alters hepatic lipid metabolism to promote triglyceride accumulation. Using the experimentally tractable mouse model, they demonstrate further that the ablation of a PP2A isoform in the liver is sufficient to cause lipid accumulation and liver injury. Conversely, restoring PP2A expression improved the hepatic phenotype in mice in the parenteral nutrition model. These findings could also be mimicked using pharmacological activation and inhibition of PP2A.
In sum, this experimental study could some day lead the way to novel treatments of parenteral nutrition-induced liver disease through the use of PP2A activators.
Klaus H. Kaestner, PhD, is with the department of genetics and Center for Molecular Studies in Digestive and Liver Diseases, Perelman School of Medicine,University of Pennsylvania, Philadelphia.
Hepatic protein PP2A-C-alpha may serve as a protective factor against parenteral nutrition–associated hepatic steatosis by improving liver function, according to a recent study published in Cellular and Molecular Gastroenterology and Hepatology.
Parenteral nutrition–associated hepatic steatosis likely involves the down-regulation of hepatic PP2A-C-alpha and consequent increased phosphorylation of Akt2; this in turn alters hepatic lipid metabolism, promotes triglyceride accumulation, and leads to liver injury, wrote the researchers, led by Gulisudumu Maitiabula and Feng Tian of the Research Institute of General Surgery at Jinling Hospital, Nanjing, China, and the Medical School of Nanjing University.
“Our study provides a strong rationale that PP2A-C-alpha may be involved in the pathogenesis of [parenteral nutrition–associated hepatic steatosis],” they wrote. “Further research is merited to establish whether interventions to enhance PP2A function might suppress the development of hepatic steatosis in patients receiving long-term [parenteral nutrition].”
Parenteral nutrition can be a lifesaving therapy for patients with intestinal failure caused by insufficient bowel length or function, the authors noted However, long-term use can lead to potentially fatal complications such as liver disease, but an understanding of the pathological mechanisms behind parenteral nutrition–associated hepatic steatosis limited.
The research team performed comparative proteomic/phosphoproteomic analyses of liver samples from 10 patients with parenteral nutrition–associated hepatic steatosis, as well as 8 cholelithiasis patients as controls, who were admitted to Jinling Hospital between June 2018 and June 2019. The researchers also assessed the effect of PP2A-C-alpha on liver injury from total parenteral nutrition in mice.
The research team found that PP2A-C-alpha was down-regulated in patients and mice with parenteral nutrition–associated hepatic steatosis. In addition, in patients with parenteral nutrition–associated hepatic steatosis, they found enhanced activation of serine/threonine kinase Akt2 and decreased activation of AMPK.
Mice that were given total parenteral nutrition infusion for 14 days developed hepatic steatosis, down-regulation of PP2A-C-alpha, activation of Akt2, and inhibition of AMPK. Hepatocyte-specific deletion of PP2A-C-alpha in mice given parenteral nutrition exacerbated the Akt2 activation, AMPK inhibition, and hepatic steatosis through an effect on fatty acid degradation.
On the other hand, forced expression of PP2A-C-alpha led to reductions in hepatocyte fat deposition and the pathological score for liver steatosis. Overexpression also significantly improved hepatic steatosis, suppressed Akt2, and activated AMPK. In addition, pharmacological activation of Akt2 in mice overexpressing PP2A-C-alpha led to the aggravation of hepatic steatosis.
“Collectively, these observations suggest that [parenteral nutrition] for [more than] 14 days leads to a down-regulation in PP2A-C-alpha expression that activates Akt2-dependent signaling, which would likely lead to hepatic steatosis,” the study authors wrote.
Intervention trials of PP2A-C-alpha in humans have not been performed because PP2A-C-alpha activators or effector analogs were unavailable for clinical use, they wrote. Additional clinical studies are needed to investigate the effects of PP2A-C-alpha intervention on the development of hepatic steatosis in patients receiving long-term parenteral nutrition.
The study was supported by the National Natural Science Foundation of China, the Science Foundation of Outstanding Youth in Jiangsu Province, the National Science and Technology Research Funding for Public Welfare Medical Projects, “The 13th Five-Year Plan” Foundation of Jiangsu Province for Medical Key Talents, and the Natural Science Foundation of Jiangsu Province. The study authors disclosed no conflicts of interest.
Hepatic protein PP2A-C-alpha may serve as a protective factor against parenteral nutrition–associated hepatic steatosis by improving liver function, according to a recent study published in Cellular and Molecular Gastroenterology and Hepatology.
Parenteral nutrition–associated hepatic steatosis likely involves the down-regulation of hepatic PP2A-C-alpha and consequent increased phosphorylation of Akt2; this in turn alters hepatic lipid metabolism, promotes triglyceride accumulation, and leads to liver injury, wrote the researchers, led by Gulisudumu Maitiabula and Feng Tian of the Research Institute of General Surgery at Jinling Hospital, Nanjing, China, and the Medical School of Nanjing University.
“Our study provides a strong rationale that PP2A-C-alpha may be involved in the pathogenesis of [parenteral nutrition–associated hepatic steatosis],” they wrote. “Further research is merited to establish whether interventions to enhance PP2A function might suppress the development of hepatic steatosis in patients receiving long-term [parenteral nutrition].”
Parenteral nutrition can be a lifesaving therapy for patients with intestinal failure caused by insufficient bowel length or function, the authors noted However, long-term use can lead to potentially fatal complications such as liver disease, but an understanding of the pathological mechanisms behind parenteral nutrition–associated hepatic steatosis limited.
The research team performed comparative proteomic/phosphoproteomic analyses of liver samples from 10 patients with parenteral nutrition–associated hepatic steatosis, as well as 8 cholelithiasis patients as controls, who were admitted to Jinling Hospital between June 2018 and June 2019. The researchers also assessed the effect of PP2A-C-alpha on liver injury from total parenteral nutrition in mice.
The research team found that PP2A-C-alpha was down-regulated in patients and mice with parenteral nutrition–associated hepatic steatosis. In addition, in patients with parenteral nutrition–associated hepatic steatosis, they found enhanced activation of serine/threonine kinase Akt2 and decreased activation of AMPK.
Mice that were given total parenteral nutrition infusion for 14 days developed hepatic steatosis, down-regulation of PP2A-C-alpha, activation of Akt2, and inhibition of AMPK. Hepatocyte-specific deletion of PP2A-C-alpha in mice given parenteral nutrition exacerbated the Akt2 activation, AMPK inhibition, and hepatic steatosis through an effect on fatty acid degradation.
On the other hand, forced expression of PP2A-C-alpha led to reductions in hepatocyte fat deposition and the pathological score for liver steatosis. Overexpression also significantly improved hepatic steatosis, suppressed Akt2, and activated AMPK. In addition, pharmacological activation of Akt2 in mice overexpressing PP2A-C-alpha led to the aggravation of hepatic steatosis.
“Collectively, these observations suggest that [parenteral nutrition] for [more than] 14 days leads to a down-regulation in PP2A-C-alpha expression that activates Akt2-dependent signaling, which would likely lead to hepatic steatosis,” the study authors wrote.
Intervention trials of PP2A-C-alpha in humans have not been performed because PP2A-C-alpha activators or effector analogs were unavailable for clinical use, they wrote. Additional clinical studies are needed to investigate the effects of PP2A-C-alpha intervention on the development of hepatic steatosis in patients receiving long-term parenteral nutrition.
The study was supported by the National Natural Science Foundation of China, the Science Foundation of Outstanding Youth in Jiangsu Province, the National Science and Technology Research Funding for Public Welfare Medical Projects, “The 13th Five-Year Plan” Foundation of Jiangsu Province for Medical Key Talents, and the Natural Science Foundation of Jiangsu Province. The study authors disclosed no conflicts of interest.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Vonoprazan-based therapy for resistant H. pylori superior to standard care
A look at the data behind the FDA approval
Vonoprazan, a potassium-competitive acid blocker, appears to be superior to standard proton pump inhibitor–based therapy in clarithromycin-resistant Helicobacter pylori strains, as well as noninferior to standard care in nonresistant infections, according to a recent study that supported a Food and Drug Administration approval of vonoprazan dual and triple therapies in May 2022.
For decades, H. pylori has been mostly treated by proton pump inhibitor–based triple therapy, which includes a proton pump inhibitor, clarithromycin, and amoxicillin or metronidazole. However, eradication rates have dropped below 80% in the United States and Europe, according to the authors, mainly because of rising rates of clarithromycin resistance.

Since H. pylori is a leading cause of peptic ulcer, gastric adenocarcinoma, and gastric mucosa–associated lymphoid tissue lymphoma, better eradication methods should be highlighted, researchers led by William Chey, MD, professor of medicine and director of the GI Physiology Laboratory at Michigan Medicine in Ann Arbor, wrote in Gastroenterology.
In a multicenter, randomized, controlled, phase 3 trial, the research team studied 1,046 treatment-naive adults with H. pylori infection at 103 sites in the U.S., the U.K., Bulgaria, the Czech Republic, Hungary, and Poland between December 2019 and January 2021.
The patients were randomized to receive open-label vonoprazan dual therapy or a double-blind triple therapy twice a day for 14 days. The vonoprazan dual therapy consisted of 20 mg of vonoprazan twice daily and 1 gram of amoxicillin three times per day. The triple therapy consisted of 20 mg of vonoprazan or 30 mg of lansoprazole (standard care), each given with 1 gram of amoxicillin and 500 mg of clarithromycin.
The primary outcome assessed noninferiority in eradication rates in patients without clarithromycin- and amoxicillin-resistant strains, with a noninferiority margin of 10%. Secondary outcomes assessed the superiority in eradication rates in clarithromycin-resistant infections, as well as in all patients.
Eradication rates for nonresistant strains were 84.7% for vonoprazan triple therapy and 78.5% for vonoprazan dual therapy, compared with 78.8% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered noninferior to standard therapy.
The eradication rates in clarithromycin-resistant infections were 65.8% for vonoprazan triple therapy and 69.6% in vonoprazan dual therapy, compared with 31.9% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior to standard therapy, with a difference of 33.9 percentage points for triple therapy and 37.7 percentage points for dual therapy.
In all patients, the eradication rates were 80.8% for vonoprazan triple therapy and 77.2% for vonoprazan dual therapy, compared with 68.5% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior, with a difference of 12.3 percentage points for triple therapy and 8.7 percentage points for dual therapy.
Treatment-emergent adverse events were reported in 34.1% of patients in the vonoprazan triple therapy group and 29.9% of patients in the vonoprazan dual therapy group, compared with 34.5% in the lansoprazole triple-therapy group. Most adverse events were mild to moderate.
Serious adverse events occurred in 1.3% of the overall study population, including 1.7% of the vonoprazan triple therapy group, 1.4% of the vonoprazan dual therapy group, and 0.9% of the lansoprazole triple therapy group. None were considered related to the study drugs.
Vonoprazan was approved for the treatment of H. pylori infections by the FDA in May 2022, and had already been approved for treatment of H. pylori infections and other acid-related diseases in several other countries. It decreases intragastric pH and maintains it to a greater degree than that of proton pump inhibitors, which has been associated with higher eradication rates, the authors wrote.
“Optimizing current regimens offers the potential to increase eradication rates and reduce additional antibiotic usage, thereby promoting and improving antimicrobial stewardship,” the study authors wrote.
The study was funded by Phathom Pharmaceuticals, which contributed to the design and conduct of the trial, collection and interpretation of the data, preparation and review of the manuscript, and the decision to submit the manuscript for publication. The study authors declared various conflicts of interest, including some who have received compensation as a consultant, advisory committee member, or employee for Phathom Pharmaceuticals.
Gastric acid inhibition plays a fundamental role for H. pylori eradication. Proton pump inhibitors (PPIs) are generally used, combined with antibiotics, in this scenario. More recently, vonoprazan, a potassium-competitive acid blocker, has been suggested to enhance H. pylori therapy by optimizing gastric acid suppression. However, clinical experience with vonoprazan has been limited to East Asian countries. The study by Chey et al. reports data from the first clinical trial from the United States and Europe, concluding that vonoprazan triple (together with amoxicillin and clarithromycin) and dual (together with amoxicillin) therapies were superior to PPI-based triple therapy, especially in clarithromycin-resistant strains.
However, some aspects deserve to be taken into consideration. The first one is that the cure rate with the standard triple therapy (with lansoprazole) was as low as 68%, underlining what has been known for a long time: This regimen should no longer be considered standard treatment in Europe or the United States and that it should not be recommended in areas with high (>15%) clarithromycin resistance, such as the United States and most European countries.
Secondly, the overall efficacy considering all patients (both with clarithromycin-susceptible and -resistant strains) with vonoprazan dual and triple regimens were of only 77% and 81%, not reaching the recommended target (≥ 90%) for first-line treatment. Therefore, the fair conclusion of the present article should have been not only that vonoprazan regimens are more effective than PPI ones, but also that all of them are insufficiently effective.
Finally, eradication rates in clarithromycin-resistant infections with the vonoprazan regimens (≤ 70%), although superior to those with lansoprazole (32%), were still clearly suboptimal, emphasizing that both PPI and vonoprazan based treatments would be inadequate if used in high-clarithromycin resistance regions.
Javier P. Gisbert, MD, PhD, is with the Hospital Universitario de La Princesa and the Universidad Autónoma de Madrid, both in Madrid. Dr. Gisbert has served as speaker, consultant, and advisory member for or has received research funding from Mayoly, Allergan, Diasorin, Gebro Pharma, and Richen.
A look at the data behind the FDA approval
A look at the data behind the FDA approval
Gastric acid inhibition plays a fundamental role for H. pylori eradication. Proton pump inhibitors (PPIs) are generally used, combined with antibiotics, in this scenario. More recently, vonoprazan, a potassium-competitive acid blocker, has been suggested to enhance H. pylori therapy by optimizing gastric acid suppression. However, clinical experience with vonoprazan has been limited to East Asian countries. The study by Chey et al. reports data from the first clinical trial from the United States and Europe, concluding that vonoprazan triple (together with amoxicillin and clarithromycin) and dual (together with amoxicillin) therapies were superior to PPI-based triple therapy, especially in clarithromycin-resistant strains.
However, some aspects deserve to be taken into consideration. The first one is that the cure rate with the standard triple therapy (with lansoprazole) was as low as 68%, underlining what has been known for a long time: This regimen should no longer be considered standard treatment in Europe or the United States and that it should not be recommended in areas with high (>15%) clarithromycin resistance, such as the United States and most European countries.
Secondly, the overall efficacy considering all patients (both with clarithromycin-susceptible and -resistant strains) with vonoprazan dual and triple regimens were of only 77% and 81%, not reaching the recommended target (≥ 90%) for first-line treatment. Therefore, the fair conclusion of the present article should have been not only that vonoprazan regimens are more effective than PPI ones, but also that all of them are insufficiently effective.
Finally, eradication rates in clarithromycin-resistant infections with the vonoprazan regimens (≤ 70%), although superior to those with lansoprazole (32%), were still clearly suboptimal, emphasizing that both PPI and vonoprazan based treatments would be inadequate if used in high-clarithromycin resistance regions.
Javier P. Gisbert, MD, PhD, is with the Hospital Universitario de La Princesa and the Universidad Autónoma de Madrid, both in Madrid. Dr. Gisbert has served as speaker, consultant, and advisory member for or has received research funding from Mayoly, Allergan, Diasorin, Gebro Pharma, and Richen.
Gastric acid inhibition plays a fundamental role for H. pylori eradication. Proton pump inhibitors (PPIs) are generally used, combined with antibiotics, in this scenario. More recently, vonoprazan, a potassium-competitive acid blocker, has been suggested to enhance H. pylori therapy by optimizing gastric acid suppression. However, clinical experience with vonoprazan has been limited to East Asian countries. The study by Chey et al. reports data from the first clinical trial from the United States and Europe, concluding that vonoprazan triple (together with amoxicillin and clarithromycin) and dual (together with amoxicillin) therapies were superior to PPI-based triple therapy, especially in clarithromycin-resistant strains.
However, some aspects deserve to be taken into consideration. The first one is that the cure rate with the standard triple therapy (with lansoprazole) was as low as 68%, underlining what has been known for a long time: This regimen should no longer be considered standard treatment in Europe or the United States and that it should not be recommended in areas with high (>15%) clarithromycin resistance, such as the United States and most European countries.
Secondly, the overall efficacy considering all patients (both with clarithromycin-susceptible and -resistant strains) with vonoprazan dual and triple regimens were of only 77% and 81%, not reaching the recommended target (≥ 90%) for first-line treatment. Therefore, the fair conclusion of the present article should have been not only that vonoprazan regimens are more effective than PPI ones, but also that all of them are insufficiently effective.
Finally, eradication rates in clarithromycin-resistant infections with the vonoprazan regimens (≤ 70%), although superior to those with lansoprazole (32%), were still clearly suboptimal, emphasizing that both PPI and vonoprazan based treatments would be inadequate if used in high-clarithromycin resistance regions.
Javier P. Gisbert, MD, PhD, is with the Hospital Universitario de La Princesa and the Universidad Autónoma de Madrid, both in Madrid. Dr. Gisbert has served as speaker, consultant, and advisory member for or has received research funding from Mayoly, Allergan, Diasorin, Gebro Pharma, and Richen.
Vonoprazan, a potassium-competitive acid blocker, appears to be superior to standard proton pump inhibitor–based therapy in clarithromycin-resistant Helicobacter pylori strains, as well as noninferior to standard care in nonresistant infections, according to a recent study that supported a Food and Drug Administration approval of vonoprazan dual and triple therapies in May 2022.
For decades, H. pylori has been mostly treated by proton pump inhibitor–based triple therapy, which includes a proton pump inhibitor, clarithromycin, and amoxicillin or metronidazole. However, eradication rates have dropped below 80% in the United States and Europe, according to the authors, mainly because of rising rates of clarithromycin resistance.
Since H. pylori is a leading cause of peptic ulcer, gastric adenocarcinoma, and gastric mucosa–associated lymphoid tissue lymphoma, better eradication methods should be highlighted, researchers led by William Chey, MD, professor of medicine and director of the GI Physiology Laboratory at Michigan Medicine in Ann Arbor, wrote in Gastroenterology.
In a multicenter, randomized, controlled, phase 3 trial, the research team studied 1,046 treatment-naive adults with H. pylori infection at 103 sites in the U.S., the U.K., Bulgaria, the Czech Republic, Hungary, and Poland between December 2019 and January 2021.
The patients were randomized to receive open-label vonoprazan dual therapy or a double-blind triple therapy twice a day for 14 days. The vonoprazan dual therapy consisted of 20 mg of vonoprazan twice daily and 1 gram of amoxicillin three times per day. The triple therapy consisted of 20 mg of vonoprazan or 30 mg of lansoprazole (standard care), each given with 1 gram of amoxicillin and 500 mg of clarithromycin.
The primary outcome assessed noninferiority in eradication rates in patients without clarithromycin- and amoxicillin-resistant strains, with a noninferiority margin of 10%. Secondary outcomes assessed the superiority in eradication rates in clarithromycin-resistant infections, as well as in all patients.
Eradication rates for nonresistant strains were 84.7% for vonoprazan triple therapy and 78.5% for vonoprazan dual therapy, compared with 78.8% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered noninferior to standard therapy.
The eradication rates in clarithromycin-resistant infections were 65.8% for vonoprazan triple therapy and 69.6% in vonoprazan dual therapy, compared with 31.9% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior to standard therapy, with a difference of 33.9 percentage points for triple therapy and 37.7 percentage points for dual therapy.
In all patients, the eradication rates were 80.8% for vonoprazan triple therapy and 77.2% for vonoprazan dual therapy, compared with 68.5% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior, with a difference of 12.3 percentage points for triple therapy and 8.7 percentage points for dual therapy.
Treatment-emergent adverse events were reported in 34.1% of patients in the vonoprazan triple therapy group and 29.9% of patients in the vonoprazan dual therapy group, compared with 34.5% in the lansoprazole triple-therapy group. Most adverse events were mild to moderate.
Serious adverse events occurred in 1.3% of the overall study population, including 1.7% of the vonoprazan triple therapy group, 1.4% of the vonoprazan dual therapy group, and 0.9% of the lansoprazole triple therapy group. None were considered related to the study drugs.
Vonoprazan was approved for the treatment of H. pylori infections by the FDA in May 2022, and had already been approved for treatment of H. pylori infections and other acid-related diseases in several other countries. It decreases intragastric pH and maintains it to a greater degree than that of proton pump inhibitors, which has been associated with higher eradication rates, the authors wrote.
“Optimizing current regimens offers the potential to increase eradication rates and reduce additional antibiotic usage, thereby promoting and improving antimicrobial stewardship,” the study authors wrote.
The study was funded by Phathom Pharmaceuticals, which contributed to the design and conduct of the trial, collection and interpretation of the data, preparation and review of the manuscript, and the decision to submit the manuscript for publication. The study authors declared various conflicts of interest, including some who have received compensation as a consultant, advisory committee member, or employee for Phathom Pharmaceuticals.
Vonoprazan, a potassium-competitive acid blocker, appears to be superior to standard proton pump inhibitor–based therapy in clarithromycin-resistant Helicobacter pylori strains, as well as noninferior to standard care in nonresistant infections, according to a recent study that supported a Food and Drug Administration approval of vonoprazan dual and triple therapies in May 2022.
For decades, H. pylori has been mostly treated by proton pump inhibitor–based triple therapy, which includes a proton pump inhibitor, clarithromycin, and amoxicillin or metronidazole. However, eradication rates have dropped below 80% in the United States and Europe, according to the authors, mainly because of rising rates of clarithromycin resistance.
Since H. pylori is a leading cause of peptic ulcer, gastric adenocarcinoma, and gastric mucosa–associated lymphoid tissue lymphoma, better eradication methods should be highlighted, researchers led by William Chey, MD, professor of medicine and director of the GI Physiology Laboratory at Michigan Medicine in Ann Arbor, wrote in Gastroenterology.
In a multicenter, randomized, controlled, phase 3 trial, the research team studied 1,046 treatment-naive adults with H. pylori infection at 103 sites in the U.S., the U.K., Bulgaria, the Czech Republic, Hungary, and Poland between December 2019 and January 2021.
The patients were randomized to receive open-label vonoprazan dual therapy or a double-blind triple therapy twice a day for 14 days. The vonoprazan dual therapy consisted of 20 mg of vonoprazan twice daily and 1 gram of amoxicillin three times per day. The triple therapy consisted of 20 mg of vonoprazan or 30 mg of lansoprazole (standard care), each given with 1 gram of amoxicillin and 500 mg of clarithromycin.
The primary outcome assessed noninferiority in eradication rates in patients without clarithromycin- and amoxicillin-resistant strains, with a noninferiority margin of 10%. Secondary outcomes assessed the superiority in eradication rates in clarithromycin-resistant infections, as well as in all patients.
Eradication rates for nonresistant strains were 84.7% for vonoprazan triple therapy and 78.5% for vonoprazan dual therapy, compared with 78.8% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered noninferior to standard therapy.
The eradication rates in clarithromycin-resistant infections were 65.8% for vonoprazan triple therapy and 69.6% in vonoprazan dual therapy, compared with 31.9% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior to standard therapy, with a difference of 33.9 percentage points for triple therapy and 37.7 percentage points for dual therapy.
In all patients, the eradication rates were 80.8% for vonoprazan triple therapy and 77.2% for vonoprazan dual therapy, compared with 68.5% for lansoprazole triple therapy. The rates for both vonoprazan therapies were considered superior, with a difference of 12.3 percentage points for triple therapy and 8.7 percentage points for dual therapy.
Treatment-emergent adverse events were reported in 34.1% of patients in the vonoprazan triple therapy group and 29.9% of patients in the vonoprazan dual therapy group, compared with 34.5% in the lansoprazole triple-therapy group. Most adverse events were mild to moderate.
Serious adverse events occurred in 1.3% of the overall study population, including 1.7% of the vonoprazan triple therapy group, 1.4% of the vonoprazan dual therapy group, and 0.9% of the lansoprazole triple therapy group. None were considered related to the study drugs.
Vonoprazan was approved for the treatment of H. pylori infections by the FDA in May 2022, and had already been approved for treatment of H. pylori infections and other acid-related diseases in several other countries. It decreases intragastric pH and maintains it to a greater degree than that of proton pump inhibitors, which has been associated with higher eradication rates, the authors wrote.
“Optimizing current regimens offers the potential to increase eradication rates and reduce additional antibiotic usage, thereby promoting and improving antimicrobial stewardship,” the study authors wrote.
The study was funded by Phathom Pharmaceuticals, which contributed to the design and conduct of the trial, collection and interpretation of the data, preparation and review of the manuscript, and the decision to submit the manuscript for publication. The study authors declared various conflicts of interest, including some who have received compensation as a consultant, advisory committee member, or employee for Phathom Pharmaceuticals.
FROM GASTROENTEROLOGY

Pancreatic cancer screening in new-onset diabetes appears cost effective
A risk-tailored early-detection strategy for pancreatic cancer that targets patients with new-onset diabetes could be cost effective, according to a recent study.
Screening for pancreatic ductal adenocarcinoma in asymptomatic adults is not recommended, but patients with new-onset diabetes have a risk that’s eight times higher than expected. Screening these patients could improve diagnosis and survival rates if the cancer can be identified at earlier stages, researchers led by Louise Wang, MD, a gastroenterology fellow at the University of Pennsylvania, Philadelphia, wrote in Clinical Gastroenterology and Hepatology.
“As we continue to improve therapies for early-stage pancreatic cancers, especially among the local/resectable stage, the case for the targeted early-detection strategy will be stronger,” they wrote. “Policy makers should take into consideration these novel findings when formulating [pancreatic ductal adenocarcinoma] screening policy and making coverage determinations.”
The research team compared early detection strategies for pancreatic ductal adenocarcinoma that target new-onset diabetes patients at age 50 years and older with standard of care, defined as no early detection strategy. They looked at various minimal predicted cancer risk thresholds versus current standard of care in a Markov state-transition decision model. The analysis assumed a health care sector perspective and a lifetime horizon, with two willingness-to-pay thresholds ($100,000 and $150,000) per quality-adjusted life-year gained.
The researchers used data from one of their previously published studies, which included 89,881 patients with new-onset diabetes diagnosed at age 50 or older. The cumulative incidence of pancreatic cancer was 0.42% during the 3 years after diagnosis.
In the early detection strategy, all patients 50 years and older who were newly diagnosed with diabetes mellitus were placed into low-risk and high-risk cohorts based on their predicted 3-year risk of pancreatic ductal adenocarcinoma under a range of assumed minimum-risk thresholds – 0.5%, 1%, 2%, 3%, 4%, and 5%; these thresholds were based on a previously established prediction model.
The research team found that the early detection strategy that targeted patients with a minimum predicted 3-year pancreatic ductal adenocarcinoma risk of 1% was cost effective, based on a willingness-to-pay threshold of $150,000 per quality-adjusted life-year. The incremental cost-effectiveness ratio was $116,911 per quality-adjusted life-year.
At a willingness-to-pay threshold of $100,000 per quality-adjusted life-year, the early detection strategy at the 2% risk threshold was cost effective. The incremental cost-effectiveness ratio was $63,045 per quality-adjusted life-year.
The most influential factors included the proportion of pancreatic ductal adenocarcinomas detected at the local stage, costs of treatment for metastatic cancer, utilities of local and regional cancers, and sensitivity of screening.
A probabilistic sensitivity analysis confirmed that, at a willingness-to-pay threshold of $150,000, early detection at the 1% risk threshold was favored at 30.6%, followed by the 0.5% risk threshold at 20.4%, compared with the standard of care at 1.7%. In addition, at a willingness-to-pay threshold of $100,000, early detection at the 1% risk threshold was favored at 27.3%, followed by the 2% risk threshold at 22.8%, as compared with the standard of care at 2%.
The two early detection strategies were cost effective, capturing 26%-45% of the pancreatic ductal adenocarcinoma cases in patients with new-onset diabetes.
The study authors noted several limitations, including the inability to incorporate out-of-pocket costs for patients, as well as focusing the analysis on the health care perspective.
“We acknowledge that, by incorporating the full consequences of decisions for all stakeholders, a societal perspective would have offered a more complete view on which to base public policy,” they wrote.
At the same time, “given the substantial prevalence of [new-onset diabetes] among [pancreatic ductal adenocarcinoma] cases, this strategy could improve the survival of a substantial proportion of sporadic PDAC cases in the general population,” they concluded.
The study authors reported various disclosures, including grants and research support from Takeda Pharmaceuticals USA, Janssen Pharmaceuticals, the National Institutes of Health, the Crohn’s and Colitis Foundation, Lilly Oncology, GSK, and Clovis Oncology.
Earlier detection of pancreatic ductal adenocarcinoma (PDAC) is essential to improving the survival for the group of patients diagnosed with PDAC each year. New-onset diabetes in adults 50 years or older is recognized as a risk factor for being diagnosed with PDAC within the following 3 years.

This study by Wang et al. uses previously described clinical prediction models to stratify the risk of PDAC in patients with new-onset diabetes. These models include age, body mass index, weight change, smoking, diabetic medications, and laboratory values (hemoglobin A1c, cholesterol, creatinine, alkaline phosphatase). They ran simulation models to determine the cost-effectiveness of screening for pancreatic cancer at various risk cut-offs. At the $150,000 willingness-to-pay threshold per quality-adjusted life-year, the 1% risk threshold was cost-effective. Stage shifting from a higher-stage cancer to a lower-stage cancer was the driving force behind the cost-effectiveness ratios.
Providers need to have a high index of suspicion when an adult over the age of 50 has had a new diagnosis of diabetes. Abnormalities detected in laboratory data, weight trends, symptoms, a history of underlying smoking or pancreatic disease may appropriately prompt an MRI/MRCP or endoscopic ultrasound. Better and more accessible risk progression calculators for these patients could be used in real time. The current study by Wang et al. will be a helpful tool as well for navigating disputes with payers about the utility of covering screening tests in the subgroup of patients that are higher risk.
Mark A. Gromski, MD, is assistant professor of medicine at Indiana University School of Medicine and a pancreatobiliary specialist and advanced endoscopist at IU Health. He reports having no relevant disclosures.
Earlier detection of pancreatic ductal adenocarcinoma (PDAC) is essential to improving the survival for the group of patients diagnosed with PDAC each year. New-onset diabetes in adults 50 years or older is recognized as a risk factor for being diagnosed with PDAC within the following 3 years.
This study by Wang et al. uses previously described clinical prediction models to stratify the risk of PDAC in patients with new-onset diabetes. These models include age, body mass index, weight change, smoking, diabetic medications, and laboratory values (hemoglobin A1c, cholesterol, creatinine, alkaline phosphatase). They ran simulation models to determine the cost-effectiveness of screening for pancreatic cancer at various risk cut-offs. At the $150,000 willingness-to-pay threshold per quality-adjusted life-year, the 1% risk threshold was cost-effective. Stage shifting from a higher-stage cancer to a lower-stage cancer was the driving force behind the cost-effectiveness ratios.
Providers need to have a high index of suspicion when an adult over the age of 50 has had a new diagnosis of diabetes. Abnormalities detected in laboratory data, weight trends, symptoms, a history of underlying smoking or pancreatic disease may appropriately prompt an MRI/MRCP or endoscopic ultrasound. Better and more accessible risk progression calculators for these patients could be used in real time. The current study by Wang et al. will be a helpful tool as well for navigating disputes with payers about the utility of covering screening tests in the subgroup of patients that are higher risk.
Mark A. Gromski, MD, is assistant professor of medicine at Indiana University School of Medicine and a pancreatobiliary specialist and advanced endoscopist at IU Health. He reports having no relevant disclosures.
Earlier detection of pancreatic ductal adenocarcinoma (PDAC) is essential to improving the survival for the group of patients diagnosed with PDAC each year. New-onset diabetes in adults 50 years or older is recognized as a risk factor for being diagnosed with PDAC within the following 3 years.
This study by Wang et al. uses previously described clinical prediction models to stratify the risk of PDAC in patients with new-onset diabetes. These models include age, body mass index, weight change, smoking, diabetic medications, and laboratory values (hemoglobin A1c, cholesterol, creatinine, alkaline phosphatase). They ran simulation models to determine the cost-effectiveness of screening for pancreatic cancer at various risk cut-offs. At the $150,000 willingness-to-pay threshold per quality-adjusted life-year, the 1% risk threshold was cost-effective. Stage shifting from a higher-stage cancer to a lower-stage cancer was the driving force behind the cost-effectiveness ratios.
Providers need to have a high index of suspicion when an adult over the age of 50 has had a new diagnosis of diabetes. Abnormalities detected in laboratory data, weight trends, symptoms, a history of underlying smoking or pancreatic disease may appropriately prompt an MRI/MRCP or endoscopic ultrasound. Better and more accessible risk progression calculators for these patients could be used in real time. The current study by Wang et al. will be a helpful tool as well for navigating disputes with payers about the utility of covering screening tests in the subgroup of patients that are higher risk.
Mark A. Gromski, MD, is assistant professor of medicine at Indiana University School of Medicine and a pancreatobiliary specialist and advanced endoscopist at IU Health. He reports having no relevant disclosures.
A risk-tailored early-detection strategy for pancreatic cancer that targets patients with new-onset diabetes could be cost effective, according to a recent study.
Screening for pancreatic ductal adenocarcinoma in asymptomatic adults is not recommended, but patients with new-onset diabetes have a risk that’s eight times higher than expected. Screening these patients could improve diagnosis and survival rates if the cancer can be identified at earlier stages, researchers led by Louise Wang, MD, a gastroenterology fellow at the University of Pennsylvania, Philadelphia, wrote in Clinical Gastroenterology and Hepatology.
“As we continue to improve therapies for early-stage pancreatic cancers, especially among the local/resectable stage, the case for the targeted early-detection strategy will be stronger,” they wrote. “Policy makers should take into consideration these novel findings when formulating [pancreatic ductal adenocarcinoma] screening policy and making coverage determinations.”
The research team compared early detection strategies for pancreatic ductal adenocarcinoma that target new-onset diabetes patients at age 50 years and older with standard of care, defined as no early detection strategy. They looked at various minimal predicted cancer risk thresholds versus current standard of care in a Markov state-transition decision model. The analysis assumed a health care sector perspective and a lifetime horizon, with two willingness-to-pay thresholds ($100,000 and $150,000) per quality-adjusted life-year gained.
The researchers used data from one of their previously published studies, which included 89,881 patients with new-onset diabetes diagnosed at age 50 or older. The cumulative incidence of pancreatic cancer was 0.42% during the 3 years after diagnosis.
In the early detection strategy, all patients 50 years and older who were newly diagnosed with diabetes mellitus were placed into low-risk and high-risk cohorts based on their predicted 3-year risk of pancreatic ductal adenocarcinoma under a range of assumed minimum-risk thresholds – 0.5%, 1%, 2%, 3%, 4%, and 5%; these thresholds were based on a previously established prediction model.
The research team found that the early detection strategy that targeted patients with a minimum predicted 3-year pancreatic ductal adenocarcinoma risk of 1% was cost effective, based on a willingness-to-pay threshold of $150,000 per quality-adjusted life-year. The incremental cost-effectiveness ratio was $116,911 per quality-adjusted life-year.
At a willingness-to-pay threshold of $100,000 per quality-adjusted life-year, the early detection strategy at the 2% risk threshold was cost effective. The incremental cost-effectiveness ratio was $63,045 per quality-adjusted life-year.
The most influential factors included the proportion of pancreatic ductal adenocarcinomas detected at the local stage, costs of treatment for metastatic cancer, utilities of local and regional cancers, and sensitivity of screening.
A probabilistic sensitivity analysis confirmed that, at a willingness-to-pay threshold of $150,000, early detection at the 1% risk threshold was favored at 30.6%, followed by the 0.5% risk threshold at 20.4%, compared with the standard of care at 1.7%. In addition, at a willingness-to-pay threshold of $100,000, early detection at the 1% risk threshold was favored at 27.3%, followed by the 2% risk threshold at 22.8%, as compared with the standard of care at 2%.
The two early detection strategies were cost effective, capturing 26%-45% of the pancreatic ductal adenocarcinoma cases in patients with new-onset diabetes.
The study authors noted several limitations, including the inability to incorporate out-of-pocket costs for patients, as well as focusing the analysis on the health care perspective.
“We acknowledge that, by incorporating the full consequences of decisions for all stakeholders, a societal perspective would have offered a more complete view on which to base public policy,” they wrote.
At the same time, “given the substantial prevalence of [new-onset diabetes] among [pancreatic ductal adenocarcinoma] cases, this strategy could improve the survival of a substantial proportion of sporadic PDAC cases in the general population,” they concluded.
The study authors reported various disclosures, including grants and research support from Takeda Pharmaceuticals USA, Janssen Pharmaceuticals, the National Institutes of Health, the Crohn’s and Colitis Foundation, Lilly Oncology, GSK, and Clovis Oncology.
A risk-tailored early-detection strategy for pancreatic cancer that targets patients with new-onset diabetes could be cost effective, according to a recent study.
Screening for pancreatic ductal adenocarcinoma in asymptomatic adults is not recommended, but patients with new-onset diabetes have a risk that’s eight times higher than expected. Screening these patients could improve diagnosis and survival rates if the cancer can be identified at earlier stages, researchers led by Louise Wang, MD, a gastroenterology fellow at the University of Pennsylvania, Philadelphia, wrote in Clinical Gastroenterology and Hepatology.
“As we continue to improve therapies for early-stage pancreatic cancers, especially among the local/resectable stage, the case for the targeted early-detection strategy will be stronger,” they wrote. “Policy makers should take into consideration these novel findings when formulating [pancreatic ductal adenocarcinoma] screening policy and making coverage determinations.”
The research team compared early detection strategies for pancreatic ductal adenocarcinoma that target new-onset diabetes patients at age 50 years and older with standard of care, defined as no early detection strategy. They looked at various minimal predicted cancer risk thresholds versus current standard of care in a Markov state-transition decision model. The analysis assumed a health care sector perspective and a lifetime horizon, with two willingness-to-pay thresholds ($100,000 and $150,000) per quality-adjusted life-year gained.
The researchers used data from one of their previously published studies, which included 89,881 patients with new-onset diabetes diagnosed at age 50 or older. The cumulative incidence of pancreatic cancer was 0.42% during the 3 years after diagnosis.
In the early detection strategy, all patients 50 years and older who were newly diagnosed with diabetes mellitus were placed into low-risk and high-risk cohorts based on their predicted 3-year risk of pancreatic ductal adenocarcinoma under a range of assumed minimum-risk thresholds – 0.5%, 1%, 2%, 3%, 4%, and 5%; these thresholds were based on a previously established prediction model.
The research team found that the early detection strategy that targeted patients with a minimum predicted 3-year pancreatic ductal adenocarcinoma risk of 1% was cost effective, based on a willingness-to-pay threshold of $150,000 per quality-adjusted life-year. The incremental cost-effectiveness ratio was $116,911 per quality-adjusted life-year.
At a willingness-to-pay threshold of $100,000 per quality-adjusted life-year, the early detection strategy at the 2% risk threshold was cost effective. The incremental cost-effectiveness ratio was $63,045 per quality-adjusted life-year.
The most influential factors included the proportion of pancreatic ductal adenocarcinomas detected at the local stage, costs of treatment for metastatic cancer, utilities of local and regional cancers, and sensitivity of screening.
A probabilistic sensitivity analysis confirmed that, at a willingness-to-pay threshold of $150,000, early detection at the 1% risk threshold was favored at 30.6%, followed by the 0.5% risk threshold at 20.4%, compared with the standard of care at 1.7%. In addition, at a willingness-to-pay threshold of $100,000, early detection at the 1% risk threshold was favored at 27.3%, followed by the 2% risk threshold at 22.8%, as compared with the standard of care at 2%.
The two early detection strategies were cost effective, capturing 26%-45% of the pancreatic ductal adenocarcinoma cases in patients with new-onset diabetes.
The study authors noted several limitations, including the inability to incorporate out-of-pocket costs for patients, as well as focusing the analysis on the health care perspective.
“We acknowledge that, by incorporating the full consequences of decisions for all stakeholders, a societal perspective would have offered a more complete view on which to base public policy,” they wrote.
At the same time, “given the substantial prevalence of [new-onset diabetes] among [pancreatic ductal adenocarcinoma] cases, this strategy could improve the survival of a substantial proportion of sporadic PDAC cases in the general population,” they concluded.
The study authors reported various disclosures, including grants and research support from Takeda Pharmaceuticals USA, Janssen Pharmaceuticals, the National Institutes of Health, the Crohn’s and Colitis Foundation, Lilly Oncology, GSK, and Clovis Oncology.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Some GIs receive more industry money than others
Industry payments to U.S. gastroenterologists and hepatologists increased from 2014 to 2016 before beginning to steadily decrease after 2016, but they're largely concentrated among a small few, according to new research published in Gastroenterology.

The study aimed to identify trends in these specialties in the years after the Sunshine Act, enacted in 2010, and the federal program Open Payments, established in 2013.
“Although Open Payments launched in September of 2014, all the joinpoints in our study occurred more than a year later in 2016, suggesting a delay in observable changes in behavior on industry physician relationships,” wrote Xiaohan Ying, MD, of Weill Cornell Medicine in New York, and colleagues. “Since 2016, we have seen a sustained reduction in general industry payments to physicians while research payments remained stable, which is likely the desired outcome of this program.”
That’s also the conclusion of Lawrence Kosinski, MD, MBA, a spokesperson for the American Gastroenterological Association, who was not involved in the study.

“Most all of us are aware of the Sunshine Act and have reacted accordingly, so I am not surprised that reimbursement per physician has declined over the time period,” Dr. Kosinski told this news organization. “Many physicians are very sensitive to their reporting and have decreased their exposures,” said Dr. Kosinski, founder of SonarMD and a member of the Health & Human Services Advisory Committee on Value-Based Payment. “What does surprise me is the marked disparity in payments with a very small number of physicians receiving tremendous reimbursement from speaking engagements and promotions.”
The researchers retrospectively analyzed industry payments to 26,981 practicing pediatric and adults gastroenterologists and hepatologists using the National Plan and Provider Enumeration System and data from Open Payments between January 2014 and December 2020. The researchers excluded education payments and focused on general payments, which “include charitable contribution, speaker fees, consulting fees, ownership and investments, education, entertainment, food and beverages, gift, honoraria, royalty and license, and travel and lodging,” they reported.
Who gets paid, and how much?
While $27.5 million was going to research and grants, most of the payments ($403.3 million) were general payments; out of the total payments to specialists, $30 million went to hepatology, and $400.8 million went to gastroenterology. Nearly all of the general payments ($398.1 million) were for noneducation purposes; 90.5% of general payments went to men and 9.5% went to women, at an average of $17,167 per person. Nearly half the payments (43.8%) were for speaker fees, totaling $174.3 million, followed by 18.4% going to consulting ($73.1 million) and 12.9% going to food and beverages ($51.5 million).
Most of the physicians accepting payments (86.6%) received less than $10,000, but this made up only 8.3% of all payments. Meanwhile, 74% of all the payments, $294.6 million, went to just 3.1% of the physicians, all of whom received more than $100,000.
That breakdown is what most caught Dr. Kosinki’s attention.
“It’s one thing for a speaker to declare that they are receiving funds from pharma, but they never let us know how much,” Dr. Kosinski said. “Some of these speakers are realizing a very significant payment, which could change the opinions of those listening to their presentations.”
The authors reported that a group of 50 top earners (0.2%) received more than $1 million between 2014 and 2020. Their payments totaled $94.8 million and accounted for nearly a quarter (23.8%) of all the payments. All but one of these physicians were men, and one physician has received more than $1 million every year since 2014.
Payments for guideline authors explored
The authors examined payments to practicing U.S. gastroenterologists and hepatologists who helped write clinical guidelines for the following organizations:
- American Gastroenterological Association (AGA).
- American College of Gastroenterology (ACG).
- American Association for the Study of Liver Disease (AASLD).
- North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN).
- American Society for Gastrointestinal Endoscopy (ASGE).
The 186 guidelines published between 2014 and 2020 had 632 physician authors, 415 of whom were practicing gastroenterologists and hepatologists in the United States. Most of these physicians (85.8%) received at least one industry payment, with payments to guideline authors totaling $43.6 million.
Similar to the lopsided breakdown for total payments across all physicians, the majority of the payments (87.4%, or $38.1 million) went to one-quarter of the authors, who each received more than $100,000 per person. Meanwhile, 38.2% of the guideline authors received less than $10,000.
“However, these numbers are likely to decrease in the future as professional societies, such as AASLD, require a majority of the guideline authors to be free of conflict of interest relevant to the subject matter,” the authors wrote. They added that members selected as part of the AGA’s guideline development group (GDG) must report all conflicts of interest, including indirect and intellectual ones, and are recused or excluded when appropriate. These guideline development group participants must also forgo speaking and consulting arrangements until one year after the guideline’s publication.
Trends have been shifting
Total industry payments initially grew at a rate of 11.4% a year between 2014 and 2016 before decreasing at a rate of 5.8% per year after 2016 (P = .03). Though a similar trend occurred at the individual level, it did not reach significance.
However, the trend differed slightly between men and women: Payments to men increased 10.4% annually until 2016 then decreased 6.8% per year thereafter, but women’s payments increased 11.3% per year until 2019. Between 2014 and 2019, the amount per person payment dropped 3.5% annually to physicians overall, but payments to women initially increased 35.4% a year between 2014 and 2016 before decreasing.
Although not statistically significant, trends for types of payments showed that speaker and food/beverage fees have been declining since 2016 while consulting fees have been declining since 2014.
“The reduction in industry payments could be due to the Hawthorne effect, where physicians alter their behavior after becoming aware that their payments were being monitored,” the authors wrote. “Although many physicians see themselves as less vulnerable to be biased by industry compensation, studies have shown that even small payments can affect behavior such as prescription pattern. Additionally, studies have found that patients are less likely to trust physicians who have received industry payments.”
The authors acknowledged the role of industry payments in funding clinical trials but noted that pharmaceutical companies themselves have been taking on more design and execution of trials in recent decades. Further, only 6% of all payments went to research and grant funding, a little more than half the payments for food and beverages.
“While industry research funding is undeniably crucial, it simply plays a very small role in total industry compensation for physicians,” the authors wrote. “While speaker events could be beneficial and educational for physicians and other audiences, these events could also be utilized as means to promote specific products. While it is beneficial to seek input from experienced gastroenterologists for novel therapies and devices, actions should be taken to place limitations on industry payments to physicians, especially for the top earners.”
One author reported speaker fees from W.L. Gore & Associates and Cook Medical. The other two others had no disclosures. No external funding was noted. Dr. Kosinski reported having no relevant disclosures.
This article was updated Aug. 9, 2022.
Industry payments to U.S. gastroenterologists and hepatologists increased from 2014 to 2016 before beginning to steadily decrease after 2016, but they're largely concentrated among a small few, according to new research published in Gastroenterology.
The study aimed to identify trends in these specialties in the years after the Sunshine Act, enacted in 2010, and the federal program Open Payments, established in 2013.
“Although Open Payments launched in September of 2014, all the joinpoints in our study occurred more than a year later in 2016, suggesting a delay in observable changes in behavior on industry physician relationships,” wrote Xiaohan Ying, MD, of Weill Cornell Medicine in New York, and colleagues. “Since 2016, we have seen a sustained reduction in general industry payments to physicians while research payments remained stable, which is likely the desired outcome of this program.”
That’s also the conclusion of Lawrence Kosinski, MD, MBA, a spokesperson for the American Gastroenterological Association, who was not involved in the study.
“Most all of us are aware of the Sunshine Act and have reacted accordingly, so I am not surprised that reimbursement per physician has declined over the time period,” Dr. Kosinski told this news organization. “Many physicians are very sensitive to their reporting and have decreased their exposures,” said Dr. Kosinski, founder of SonarMD and a member of the Health & Human Services Advisory Committee on Value-Based Payment. “What does surprise me is the marked disparity in payments with a very small number of physicians receiving tremendous reimbursement from speaking engagements and promotions.”
The researchers retrospectively analyzed industry payments to 26,981 practicing pediatric and adults gastroenterologists and hepatologists using the National Plan and Provider Enumeration System and data from Open Payments between January 2014 and December 2020. The researchers excluded education payments and focused on general payments, which “include charitable contribution, speaker fees, consulting fees, ownership and investments, education, entertainment, food and beverages, gift, honoraria, royalty and license, and travel and lodging,” they reported.
Who gets paid, and how much?
While $27.5 million was going to research and grants, most of the payments ($403.3 million) were general payments; out of the total payments to specialists, $30 million went to hepatology, and $400.8 million went to gastroenterology. Nearly all of the general payments ($398.1 million) were for noneducation purposes; 90.5% of general payments went to men and 9.5% went to women, at an average of $17,167 per person. Nearly half the payments (43.8%) were for speaker fees, totaling $174.3 million, followed by 18.4% going to consulting ($73.1 million) and 12.9% going to food and beverages ($51.5 million).
Most of the physicians accepting payments (86.6%) received less than $10,000, but this made up only 8.3% of all payments. Meanwhile, 74% of all the payments, $294.6 million, went to just 3.1% of the physicians, all of whom received more than $100,000.
That breakdown is what most caught Dr. Kosinki’s attention.
“It’s one thing for a speaker to declare that they are receiving funds from pharma, but they never let us know how much,” Dr. Kosinski said. “Some of these speakers are realizing a very significant payment, which could change the opinions of those listening to their presentations.”
The authors reported that a group of 50 top earners (0.2%) received more than $1 million between 2014 and 2020. Their payments totaled $94.8 million and accounted for nearly a quarter (23.8%) of all the payments. All but one of these physicians were men, and one physician has received more than $1 million every year since 2014.
Payments for guideline authors explored
The authors examined payments to practicing U.S. gastroenterologists and hepatologists who helped write clinical guidelines for the following organizations:
- American Gastroenterological Association (AGA).
- American College of Gastroenterology (ACG).
- American Association for the Study of Liver Disease (AASLD).
- North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN).
- American Society for Gastrointestinal Endoscopy (ASGE).
The 186 guidelines published between 2014 and 2020 had 632 physician authors, 415 of whom were practicing gastroenterologists and hepatologists in the United States. Most of these physicians (85.8%) received at least one industry payment, with payments to guideline authors totaling $43.6 million.
Similar to the lopsided breakdown for total payments across all physicians, the majority of the payments (87.4%, or $38.1 million) went to one-quarter of the authors, who each received more than $100,000 per person. Meanwhile, 38.2% of the guideline authors received less than $10,000.
“However, these numbers are likely to decrease in the future as professional societies, such as AASLD, require a majority of the guideline authors to be free of conflict of interest relevant to the subject matter,” the authors wrote. They added that members selected as part of the AGA’s guideline development group (GDG) must report all conflicts of interest, including indirect and intellectual ones, and are recused or excluded when appropriate. These guideline development group participants must also forgo speaking and consulting arrangements until one year after the guideline’s publication.
Trends have been shifting
Total industry payments initially grew at a rate of 11.4% a year between 2014 and 2016 before decreasing at a rate of 5.8% per year after 2016 (P = .03). Though a similar trend occurred at the individual level, it did not reach significance.
However, the trend differed slightly between men and women: Payments to men increased 10.4% annually until 2016 then decreased 6.8% per year thereafter, but women’s payments increased 11.3% per year until 2019. Between 2014 and 2019, the amount per person payment dropped 3.5% annually to physicians overall, but payments to women initially increased 35.4% a year between 2014 and 2016 before decreasing.
Although not statistically significant, trends for types of payments showed that speaker and food/beverage fees have been declining since 2016 while consulting fees have been declining since 2014.
“The reduction in industry payments could be due to the Hawthorne effect, where physicians alter their behavior after becoming aware that their payments were being monitored,” the authors wrote. “Although many physicians see themselves as less vulnerable to be biased by industry compensation, studies have shown that even small payments can affect behavior such as prescription pattern. Additionally, studies have found that patients are less likely to trust physicians who have received industry payments.”
The authors acknowledged the role of industry payments in funding clinical trials but noted that pharmaceutical companies themselves have been taking on more design and execution of trials in recent decades. Further, only 6% of all payments went to research and grant funding, a little more than half the payments for food and beverages.
“While industry research funding is undeniably crucial, it simply plays a very small role in total industry compensation for physicians,” the authors wrote. “While speaker events could be beneficial and educational for physicians and other audiences, these events could also be utilized as means to promote specific products. While it is beneficial to seek input from experienced gastroenterologists for novel therapies and devices, actions should be taken to place limitations on industry payments to physicians, especially for the top earners.”
One author reported speaker fees from W.L. Gore & Associates and Cook Medical. The other two others had no disclosures. No external funding was noted. Dr. Kosinski reported having no relevant disclosures.
This article was updated Aug. 9, 2022.
Industry payments to U.S. gastroenterologists and hepatologists increased from 2014 to 2016 before beginning to steadily decrease after 2016, but they're largely concentrated among a small few, according to new research published in Gastroenterology.
The study aimed to identify trends in these specialties in the years after the Sunshine Act, enacted in 2010, and the federal program Open Payments, established in 2013.
“Although Open Payments launched in September of 2014, all the joinpoints in our study occurred more than a year later in 2016, suggesting a delay in observable changes in behavior on industry physician relationships,” wrote Xiaohan Ying, MD, of Weill Cornell Medicine in New York, and colleagues. “Since 2016, we have seen a sustained reduction in general industry payments to physicians while research payments remained stable, which is likely the desired outcome of this program.”
That’s also the conclusion of Lawrence Kosinski, MD, MBA, a spokesperson for the American Gastroenterological Association, who was not involved in the study.
“Most all of us are aware of the Sunshine Act and have reacted accordingly, so I am not surprised that reimbursement per physician has declined over the time period,” Dr. Kosinski told this news organization. “Many physicians are very sensitive to their reporting and have decreased their exposures,” said Dr. Kosinski, founder of SonarMD and a member of the Health & Human Services Advisory Committee on Value-Based Payment. “What does surprise me is the marked disparity in payments with a very small number of physicians receiving tremendous reimbursement from speaking engagements and promotions.”
The researchers retrospectively analyzed industry payments to 26,981 practicing pediatric and adults gastroenterologists and hepatologists using the National Plan and Provider Enumeration System and data from Open Payments between January 2014 and December 2020. The researchers excluded education payments and focused on general payments, which “include charitable contribution, speaker fees, consulting fees, ownership and investments, education, entertainment, food and beverages, gift, honoraria, royalty and license, and travel and lodging,” they reported.
Who gets paid, and how much?
While $27.5 million was going to research and grants, most of the payments ($403.3 million) were general payments; out of the total payments to specialists, $30 million went to hepatology, and $400.8 million went to gastroenterology. Nearly all of the general payments ($398.1 million) were for noneducation purposes; 90.5% of general payments went to men and 9.5% went to women, at an average of $17,167 per person. Nearly half the payments (43.8%) were for speaker fees, totaling $174.3 million, followed by 18.4% going to consulting ($73.1 million) and 12.9% going to food and beverages ($51.5 million).
Most of the physicians accepting payments (86.6%) received less than $10,000, but this made up only 8.3% of all payments. Meanwhile, 74% of all the payments, $294.6 million, went to just 3.1% of the physicians, all of whom received more than $100,000.
That breakdown is what most caught Dr. Kosinki’s attention.
“It’s one thing for a speaker to declare that they are receiving funds from pharma, but they never let us know how much,” Dr. Kosinski said. “Some of these speakers are realizing a very significant payment, which could change the opinions of those listening to their presentations.”
The authors reported that a group of 50 top earners (0.2%) received more than $1 million between 2014 and 2020. Their payments totaled $94.8 million and accounted for nearly a quarter (23.8%) of all the payments. All but one of these physicians were men, and one physician has received more than $1 million every year since 2014.
Payments for guideline authors explored
The authors examined payments to practicing U.S. gastroenterologists and hepatologists who helped write clinical guidelines for the following organizations:
- American Gastroenterological Association (AGA).
- American College of Gastroenterology (ACG).
- American Association for the Study of Liver Disease (AASLD).
- North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN).
- American Society for Gastrointestinal Endoscopy (ASGE).
The 186 guidelines published between 2014 and 2020 had 632 physician authors, 415 of whom were practicing gastroenterologists and hepatologists in the United States. Most of these physicians (85.8%) received at least one industry payment, with payments to guideline authors totaling $43.6 million.
Similar to the lopsided breakdown for total payments across all physicians, the majority of the payments (87.4%, or $38.1 million) went to one-quarter of the authors, who each received more than $100,000 per person. Meanwhile, 38.2% of the guideline authors received less than $10,000.
“However, these numbers are likely to decrease in the future as professional societies, such as AASLD, require a majority of the guideline authors to be free of conflict of interest relevant to the subject matter,” the authors wrote. They added that members selected as part of the AGA’s guideline development group (GDG) must report all conflicts of interest, including indirect and intellectual ones, and are recused or excluded when appropriate. These guideline development group participants must also forgo speaking and consulting arrangements until one year after the guideline’s publication.
Trends have been shifting
Total industry payments initially grew at a rate of 11.4% a year between 2014 and 2016 before decreasing at a rate of 5.8% per year after 2016 (P = .03). Though a similar trend occurred at the individual level, it did not reach significance.
However, the trend differed slightly between men and women: Payments to men increased 10.4% annually until 2016 then decreased 6.8% per year thereafter, but women’s payments increased 11.3% per year until 2019. Between 2014 and 2019, the amount per person payment dropped 3.5% annually to physicians overall, but payments to women initially increased 35.4% a year between 2014 and 2016 before decreasing.
Although not statistically significant, trends for types of payments showed that speaker and food/beverage fees have been declining since 2016 while consulting fees have been declining since 2014.
“The reduction in industry payments could be due to the Hawthorne effect, where physicians alter their behavior after becoming aware that their payments were being monitored,” the authors wrote. “Although many physicians see themselves as less vulnerable to be biased by industry compensation, studies have shown that even small payments can affect behavior such as prescription pattern. Additionally, studies have found that patients are less likely to trust physicians who have received industry payments.”
The authors acknowledged the role of industry payments in funding clinical trials but noted that pharmaceutical companies themselves have been taking on more design and execution of trials in recent decades. Further, only 6% of all payments went to research and grant funding, a little more than half the payments for food and beverages.
“While industry research funding is undeniably crucial, it simply plays a very small role in total industry compensation for physicians,” the authors wrote. “While speaker events could be beneficial and educational for physicians and other audiences, these events could also be utilized as means to promote specific products. While it is beneficial to seek input from experienced gastroenterologists for novel therapies and devices, actions should be taken to place limitations on industry payments to physicians, especially for the top earners.”
One author reported speaker fees from W.L. Gore & Associates and Cook Medical. The other two others had no disclosures. No external funding was noted. Dr. Kosinski reported having no relevant disclosures.
This article was updated Aug. 9, 2022.
FROM GASTROENTEROLOGY
New insights into worldwide biliary tract cancer incidence, mortality
Incidence and mortality for biliary tract cancer (BTC) are both on the rise worldwide, according to a new analysis of data from the International Agency for Research on Cancer and the World Health Organization.
This diverse group of hepatic and perihepatic cancers include gallbladder cancer (GBC), intrahepatic and extrahepatic cholangiocarcinoma (ICC and ECC), and ampulla of Vater cancer. Although BTC is considered rare, incidence of its subtypes can vary significantly by geographic region. Because BTC is typically asymptomatic in its early stage, diagnosis is often made after tumors have spread, when there are few therapeutic options available. In the United States and Europe, 5-year survival is less than 20%.
Although previous studies have examined worldwide BTC incidence, few looked at multiple global regions or at all subtypes. Instead, subtypes may be grouped together and reported as composites, or BTC is lumped together with primary liver cancer. “To our knowledge, this is the first report combining data on worldwide incidence and mortality of all BTC subtypes per the International Classification of Diseases, Tenth Revision,” the authors wrote in the study, published online in Gastro Hep Advances.
The researchers pointed out that classification coding systems have improved at defining BTC subtypes, so that studies using older coding subtypes could cause misinterpretation of incidence rates.
BTC subtypes also have unique sets of risk factors and different prognoses and treatment outcomes. “Thus, there is a need to define accurate epidemiologic trends that will allow specific risk factors to be identified, guiding experts in implementing policies to improve diagnosis and survival,” the authors wrote.
The study included data from 22 countries. BTC incidence ranged from 1.12 cases per 100,000 person-years in Vietnam to 12.42 in Chile. As expected, incidence rates were higher in the Asia-Pacific region (1.12-9.00) and South America (2.73-12.42), compared with Europe (2.00-3.59) and North America (2.33-2.35). Within the United States, Asian Americans had a higher BTC incidence than the general population (2.99 vs. 2.33).
In most countries, new cases were dominated by GBC, while ICC was the most common cause of death.
In each country, older patients were 5-10 times more likely to die than BTC patients generally. The sixth and seventh decades of life are the most common time of diagnosis, and treatment options may be limited in older patients.
Risk factors for BTC may include common comorbidities like obesity, nonalcoholic fatty liver disease, and diabetes. Each is increasing individually, which may in turn contribute to rising BTC incidence. Observational analyses suggest that obesity may contribute to risk of ECC and gallbladder cancer, while diabetes and obesity may raise the risk of ICC. Smoking is associated with increased risk of all BTC subtypes except GBC, and alcohol consumption is associated with ICC.
“This study highlights how each subtype may be vulnerable to specific risk factors and emphasizes the value of separating epidemiologic data by subtype in order to better understand disease etiology,” the researchers wrote.
Risk factors associated with incidence and mortality from BTC aren’t limited to clinical characteristics. Genetic susceptibility may also play a role in incidence and mortality of different subtypes. There is also a relationship between gallstones and BTC risk. In Chile, about 50% of women have gallstones versus 17% of women in the United States. The cancer incidence is 27 per 100,000 person-years in Chile and 2 per 100,000 person-years in the United States. BTC is also the leading cause of cancer death among women in Chile.
The authors also highlighted the high rates of gallbladder cancer in India, despite a low prevalence of gallstones. Incidences can vary with geography along the flow of the Ganges River, which might reflect varying risks from contamination caused by agricultural runoff or industrial or human waste.
Worldwide BTC incidence and mortality was generally higher among women than men, with the exception of ampulla of Vater cancer, which was more common in men.
The study is limited by quality of data, which varied significantly between countries. Mortality data was missing from some countries know to have high BTC incidence. The databases had little survival data, which could have provided insights into treatment efficacy.
The study was funded by AstraZeneca. The authors have extensive financial relationships with pharmaceutical companies.
Biliary tract cancers (BTCs) are understudied malignancies with poor prognoses. A major impediment to a deeper understanding of BTC epidemiology is that the term BTC encompasses a heterogeneous group of cancers including cholangiocarcinoma (both intrahepatic and extrahepatic), as well as ampullary and gallbladder cancer. Studies have often lumped all BTC subgroups together despite differences in their geographic distribution, risk factors, and underlying pathogenesis. Furthermore, epidemiological reporting has often grouped “intrahepatic liver and bile duct cancers” which include hepatocellular carcinoma, a biologically different entity requiring a separate management strategy.

The study highlights the importance of future policy work to address the risk factors for BTCs that vary by region and that will likely evolve over time. It also stresses the urgent need for both early diagnostic strategies and improved biomarker-driven medical therapy, areas of ongoing research requiring accelerated development.
Irun Bhan, MD, is a transplant hepatologist at Massachusetts General Hospital and instructor at Harvard Medical School, Boston. He has no relevant conflicts.
Biliary tract cancers (BTCs) are understudied malignancies with poor prognoses. A major impediment to a deeper understanding of BTC epidemiology is that the term BTC encompasses a heterogeneous group of cancers including cholangiocarcinoma (both intrahepatic and extrahepatic), as well as ampullary and gallbladder cancer. Studies have often lumped all BTC subgroups together despite differences in their geographic distribution, risk factors, and underlying pathogenesis. Furthermore, epidemiological reporting has often grouped “intrahepatic liver and bile duct cancers” which include hepatocellular carcinoma, a biologically different entity requiring a separate management strategy.
The study highlights the importance of future policy work to address the risk factors for BTCs that vary by region and that will likely evolve over time. It also stresses the urgent need for both early diagnostic strategies and improved biomarker-driven medical therapy, areas of ongoing research requiring accelerated development.
Irun Bhan, MD, is a transplant hepatologist at Massachusetts General Hospital and instructor at Harvard Medical School, Boston. He has no relevant conflicts.
Biliary tract cancers (BTCs) are understudied malignancies with poor prognoses. A major impediment to a deeper understanding of BTC epidemiology is that the term BTC encompasses a heterogeneous group of cancers including cholangiocarcinoma (both intrahepatic and extrahepatic), as well as ampullary and gallbladder cancer. Studies have often lumped all BTC subgroups together despite differences in their geographic distribution, risk factors, and underlying pathogenesis. Furthermore, epidemiological reporting has often grouped “intrahepatic liver and bile duct cancers” which include hepatocellular carcinoma, a biologically different entity requiring a separate management strategy.
The study highlights the importance of future policy work to address the risk factors for BTCs that vary by region and that will likely evolve over time. It also stresses the urgent need for both early diagnostic strategies and improved biomarker-driven medical therapy, areas of ongoing research requiring accelerated development.
Irun Bhan, MD, is a transplant hepatologist at Massachusetts General Hospital and instructor at Harvard Medical School, Boston. He has no relevant conflicts.
Incidence and mortality for biliary tract cancer (BTC) are both on the rise worldwide, according to a new analysis of data from the International Agency for Research on Cancer and the World Health Organization.
This diverse group of hepatic and perihepatic cancers include gallbladder cancer (GBC), intrahepatic and extrahepatic cholangiocarcinoma (ICC and ECC), and ampulla of Vater cancer. Although BTC is considered rare, incidence of its subtypes can vary significantly by geographic region. Because BTC is typically asymptomatic in its early stage, diagnosis is often made after tumors have spread, when there are few therapeutic options available. In the United States and Europe, 5-year survival is less than 20%.
Although previous studies have examined worldwide BTC incidence, few looked at multiple global regions or at all subtypes. Instead, subtypes may be grouped together and reported as composites, or BTC is lumped together with primary liver cancer. “To our knowledge, this is the first report combining data on worldwide incidence and mortality of all BTC subtypes per the International Classification of Diseases, Tenth Revision,” the authors wrote in the study, published online in Gastro Hep Advances.
The researchers pointed out that classification coding systems have improved at defining BTC subtypes, so that studies using older coding subtypes could cause misinterpretation of incidence rates.
BTC subtypes also have unique sets of risk factors and different prognoses and treatment outcomes. “Thus, there is a need to define accurate epidemiologic trends that will allow specific risk factors to be identified, guiding experts in implementing policies to improve diagnosis and survival,” the authors wrote.
The study included data from 22 countries. BTC incidence ranged from 1.12 cases per 100,000 person-years in Vietnam to 12.42 in Chile. As expected, incidence rates were higher in the Asia-Pacific region (1.12-9.00) and South America (2.73-12.42), compared with Europe (2.00-3.59) and North America (2.33-2.35). Within the United States, Asian Americans had a higher BTC incidence than the general population (2.99 vs. 2.33).
In most countries, new cases were dominated by GBC, while ICC was the most common cause of death.
In each country, older patients were 5-10 times more likely to die than BTC patients generally. The sixth and seventh decades of life are the most common time of diagnosis, and treatment options may be limited in older patients.
Risk factors for BTC may include common comorbidities like obesity, nonalcoholic fatty liver disease, and diabetes. Each is increasing individually, which may in turn contribute to rising BTC incidence. Observational analyses suggest that obesity may contribute to risk of ECC and gallbladder cancer, while diabetes and obesity may raise the risk of ICC. Smoking is associated with increased risk of all BTC subtypes except GBC, and alcohol consumption is associated with ICC.
“This study highlights how each subtype may be vulnerable to specific risk factors and emphasizes the value of separating epidemiologic data by subtype in order to better understand disease etiology,” the researchers wrote.
Risk factors associated with incidence and mortality from BTC aren’t limited to clinical characteristics. Genetic susceptibility may also play a role in incidence and mortality of different subtypes. There is also a relationship between gallstones and BTC risk. In Chile, about 50% of women have gallstones versus 17% of women in the United States. The cancer incidence is 27 per 100,000 person-years in Chile and 2 per 100,000 person-years in the United States. BTC is also the leading cause of cancer death among women in Chile.
The authors also highlighted the high rates of gallbladder cancer in India, despite a low prevalence of gallstones. Incidences can vary with geography along the flow of the Ganges River, which might reflect varying risks from contamination caused by agricultural runoff or industrial or human waste.
Worldwide BTC incidence and mortality was generally higher among women than men, with the exception of ampulla of Vater cancer, which was more common in men.
The study is limited by quality of data, which varied significantly between countries. Mortality data was missing from some countries know to have high BTC incidence. The databases had little survival data, which could have provided insights into treatment efficacy.
The study was funded by AstraZeneca. The authors have extensive financial relationships with pharmaceutical companies.
Incidence and mortality for biliary tract cancer (BTC) are both on the rise worldwide, according to a new analysis of data from the International Agency for Research on Cancer and the World Health Organization.
This diverse group of hepatic and perihepatic cancers include gallbladder cancer (GBC), intrahepatic and extrahepatic cholangiocarcinoma (ICC and ECC), and ampulla of Vater cancer. Although BTC is considered rare, incidence of its subtypes can vary significantly by geographic region. Because BTC is typically asymptomatic in its early stage, diagnosis is often made after tumors have spread, when there are few therapeutic options available. In the United States and Europe, 5-year survival is less than 20%.
Although previous studies have examined worldwide BTC incidence, few looked at multiple global regions or at all subtypes. Instead, subtypes may be grouped together and reported as composites, or BTC is lumped together with primary liver cancer. “To our knowledge, this is the first report combining data on worldwide incidence and mortality of all BTC subtypes per the International Classification of Diseases, Tenth Revision,” the authors wrote in the study, published online in Gastro Hep Advances.
The researchers pointed out that classification coding systems have improved at defining BTC subtypes, so that studies using older coding subtypes could cause misinterpretation of incidence rates.
BTC subtypes also have unique sets of risk factors and different prognoses and treatment outcomes. “Thus, there is a need to define accurate epidemiologic trends that will allow specific risk factors to be identified, guiding experts in implementing policies to improve diagnosis and survival,” the authors wrote.
The study included data from 22 countries. BTC incidence ranged from 1.12 cases per 100,000 person-years in Vietnam to 12.42 in Chile. As expected, incidence rates were higher in the Asia-Pacific region (1.12-9.00) and South America (2.73-12.42), compared with Europe (2.00-3.59) and North America (2.33-2.35). Within the United States, Asian Americans had a higher BTC incidence than the general population (2.99 vs. 2.33).
In most countries, new cases were dominated by GBC, while ICC was the most common cause of death.
In each country, older patients were 5-10 times more likely to die than BTC patients generally. The sixth and seventh decades of life are the most common time of diagnosis, and treatment options may be limited in older patients.
Risk factors for BTC may include common comorbidities like obesity, nonalcoholic fatty liver disease, and diabetes. Each is increasing individually, which may in turn contribute to rising BTC incidence. Observational analyses suggest that obesity may contribute to risk of ECC and gallbladder cancer, while diabetes and obesity may raise the risk of ICC. Smoking is associated with increased risk of all BTC subtypes except GBC, and alcohol consumption is associated with ICC.
“This study highlights how each subtype may be vulnerable to specific risk factors and emphasizes the value of separating epidemiologic data by subtype in order to better understand disease etiology,” the researchers wrote.
Risk factors associated with incidence and mortality from BTC aren’t limited to clinical characteristics. Genetic susceptibility may also play a role in incidence and mortality of different subtypes. There is also a relationship between gallstones and BTC risk. In Chile, about 50% of women have gallstones versus 17% of women in the United States. The cancer incidence is 27 per 100,000 person-years in Chile and 2 per 100,000 person-years in the United States. BTC is also the leading cause of cancer death among women in Chile.
The authors also highlighted the high rates of gallbladder cancer in India, despite a low prevalence of gallstones. Incidences can vary with geography along the flow of the Ganges River, which might reflect varying risks from contamination caused by agricultural runoff or industrial or human waste.
Worldwide BTC incidence and mortality was generally higher among women than men, with the exception of ampulla of Vater cancer, which was more common in men.
The study is limited by quality of data, which varied significantly between countries. Mortality data was missing from some countries know to have high BTC incidence. The databases had little survival data, which could have provided insights into treatment efficacy.
The study was funded by AstraZeneca. The authors have extensive financial relationships with pharmaceutical companies.
FROM GASTRO HEP ADVANCES
IBD study hints at cause of postacute COVID
A new study among patients with inflammatory bowel disease (IBD) suggests that viral antigen persistence in the gut may contribute to post-acute COVID-19 syndrome.
Postacute COVID-19 syndrome is now understood to be a multiorgan condition with symptoms that may include fatigue, cognitive dysfunction, and pain. Poor baseline health and severe acute infection are risk factors for the condition, but nonhospitalized illness can also lead to persistent symptoms.
Researchers found that nearly two-thirds of IBD patients had persistence of the antigen in infected tissues up to 8 months after a mild (nonhospitalized) acute COVID-19 infection. The study is the first to tie gut antigen persistence to post-acute COVID symptoms, and the results imply that the antigen may lead to immune perturbation and ongoing symptoms.
The study was published online in Gastroenterology.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) uses the membrane-bound angiotensin-converting enzyme 2 to gain entry into cells, which is expressed in the brush border enterocytes, as well as elsewhere in the body.
Previous research using intestinal epithelial organoids confirmed that SARS-CoV-2 is capable of infecting the human epithelium and that the virus can be detected in anal swabs long after it is cleared from nasal passages.
One potential explanation is viral immune perturbation or inflammatory tissue injury. Supporting evidence includes neural accumulation of memory T cells in patients with neuropsychiatric symptoms such as malaise and depression, and similar changes are seen with age-related immune senescence and tissue injury. Hyperactivated B and T cells, as well as other innate immune cells, have also been linked to postacute COVID-19, as has heightened expression of proinflammatory cytokines.
To explore the potential role of persistent viral antigens, the researchers gathered biopsies during upper- and lower-gastrointestinal endoscopy in 46 patients with IBD whose prior COVID-19 infection (mean, 7.3 months previous) had been confirmed by polymerase chain reaction and who were seen at the IBD outpatient unit of the investigators’ institution. In all, 43.5% of patients were female, and the average age was 44.67 years. Overall, 67.4% had been diagnosed with Crohn’s disease, 28.3% with ulcerative colitis, and 4.3% had unclassified IBD; 23.9% had a history of exposure to anti–tumor necrosis factor therapy. Among patients in the study, 32 of the patients tested positive for mucosal SARS-CoV-2 RNA, and there was no association between the presence of viral RNA and IBD type.
The researchers found that 52%-70% of patients had antigen persistence in any gut segment, as measured by nucleocapsid immunofluorescence or expression of one of four viral transcripts. They detected persistence of the nucleocapsid in epithelial cells and CD8+ T cells. Viral antigens persisted in patients with and without exposure to immunosuppressive therapy, and there was no association with antigen persistence and severity of acute COVID-19 infection or the presence of inflammation at the time of the endoscopy.
The researchers believed that the persistent viral antigen reflects incomplete clearance from the original infection rather than a latent or persistent infection because they could not replicate the virus in biopsy samples. Most biopsies within a patient produced some, but not all, of the viral transcripts tested. The authors suggest that immunosuppressive therapy may lead to incomplete viral clearance. Some patients lacked humoral nucleocapsid IgG antibodies, especially among those with gut antigen persistence.
In fact, only patients with gut viral RNA persistence had symptoms of postacute COVID. “This observation strongly argues for a role of viral antigen persistence in postacute COVID-19 and it appears plausible that SARS-CoV-2 antigen persistence, possibly in infected tissues beyond the gut, could impact host immune responses underlying the postacute COVID-19 syndrome,” the researchers wrote.
There is precedent for such a phenomenon in influenza. Mouse models have shown that ineffective clearance can influence adaptive immune responses and memory T-cell formation in lymph nodes of the lung. Another report found that COVID-19 pneumonia survivors have persistent changes to pulmonary CD8+ T cells.
The study is limited by its small sample size and a lack of a replication cohort. The study was also conducted in IBD patients because the researchers believed they were at higher risk of COVID-19 infection, although the researchers note that viral antigen persistence has been observed 2 months after recovery from COVID-19 in patients without IBD or exposure to immunosuppressants.
The researchers call for studies in patients without IBD to determine whether viral antigen persistence is a key mechanism in postacute COVID-19.
The researchers have no relevant financial disclosures.
Understanding the cause and risk factors for the postacute COVID-19 condition is an urgent research priority. The study by Zollner et al. found new clues about the cause of the post–COVID-19 condition in intestinal tissues of patients with IBD. The first important finding was that most adult patients with IBD have persistent viral antigen in their intestine months after even mild acute COVID-19. Importantly, researchers could not recover replicating virus from these tissues, indicating there was unlikely persistent active infection or viral transmissibility. The second major finding was that the presence of persistent viral antigen in intestinal tissue was strongly associated with postacute COVID-19 symptoms. This suggests that persistence of SARS‑CoV‑2 antigen after acute infection could perpetuate an ongoing inflammatory response that causes the postacute COVID-19 condition.

Zollner et al. used the intestine as a window onto how this virus may lead to long-lasting symptoms in IBD patients. However, it does not change our understanding that corticosteroids, poorly controlled IBD, and comorbidities, and not biologic or immunomodulator therapy, increase the risk of severe illness and mortality related to acute COVID-19 in IBD patients.
Michael J. Rosen, MD, MSCI, is Endowed Professor for Pediatric IBD & Celiac Disease and director for the Center for Pediatric IBD & Celiac Disease at Stanford (Calif.) University. Dr. Rosen served on an advisory board for Pfizer.
Understanding the cause and risk factors for the postacute COVID-19 condition is an urgent research priority. The study by Zollner et al. found new clues about the cause of the post–COVID-19 condition in intestinal tissues of patients with IBD. The first important finding was that most adult patients with IBD have persistent viral antigen in their intestine months after even mild acute COVID-19. Importantly, researchers could not recover replicating virus from these tissues, indicating there was unlikely persistent active infection or viral transmissibility. The second major finding was that the presence of persistent viral antigen in intestinal tissue was strongly associated with postacute COVID-19 symptoms. This suggests that persistence of SARS‑CoV‑2 antigen after acute infection could perpetuate an ongoing inflammatory response that causes the postacute COVID-19 condition.
Zollner et al. used the intestine as a window onto how this virus may lead to long-lasting symptoms in IBD patients. However, it does not change our understanding that corticosteroids, poorly controlled IBD, and comorbidities, and not biologic or immunomodulator therapy, increase the risk of severe illness and mortality related to acute COVID-19 in IBD patients.
Michael J. Rosen, MD, MSCI, is Endowed Professor for Pediatric IBD & Celiac Disease and director for the Center for Pediatric IBD & Celiac Disease at Stanford (Calif.) University. Dr. Rosen served on an advisory board for Pfizer.
Understanding the cause and risk factors for the postacute COVID-19 condition is an urgent research priority. The study by Zollner et al. found new clues about the cause of the post–COVID-19 condition in intestinal tissues of patients with IBD. The first important finding was that most adult patients with IBD have persistent viral antigen in their intestine months after even mild acute COVID-19. Importantly, researchers could not recover replicating virus from these tissues, indicating there was unlikely persistent active infection or viral transmissibility. The second major finding was that the presence of persistent viral antigen in intestinal tissue was strongly associated with postacute COVID-19 symptoms. This suggests that persistence of SARS‑CoV‑2 antigen after acute infection could perpetuate an ongoing inflammatory response that causes the postacute COVID-19 condition.
Zollner et al. used the intestine as a window onto how this virus may lead to long-lasting symptoms in IBD patients. However, it does not change our understanding that corticosteroids, poorly controlled IBD, and comorbidities, and not biologic or immunomodulator therapy, increase the risk of severe illness and mortality related to acute COVID-19 in IBD patients.
Michael J. Rosen, MD, MSCI, is Endowed Professor for Pediatric IBD & Celiac Disease and director for the Center for Pediatric IBD & Celiac Disease at Stanford (Calif.) University. Dr. Rosen served on an advisory board for Pfizer.
A new study among patients with inflammatory bowel disease (IBD) suggests that viral antigen persistence in the gut may contribute to post-acute COVID-19 syndrome.
Postacute COVID-19 syndrome is now understood to be a multiorgan condition with symptoms that may include fatigue, cognitive dysfunction, and pain. Poor baseline health and severe acute infection are risk factors for the condition, but nonhospitalized illness can also lead to persistent symptoms.
Researchers found that nearly two-thirds of IBD patients had persistence of the antigen in infected tissues up to 8 months after a mild (nonhospitalized) acute COVID-19 infection. The study is the first to tie gut antigen persistence to post-acute COVID symptoms, and the results imply that the antigen may lead to immune perturbation and ongoing symptoms.
The study was published online in Gastroenterology.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) uses the membrane-bound angiotensin-converting enzyme 2 to gain entry into cells, which is expressed in the brush border enterocytes, as well as elsewhere in the body.
Previous research using intestinal epithelial organoids confirmed that SARS-CoV-2 is capable of infecting the human epithelium and that the virus can be detected in anal swabs long after it is cleared from nasal passages.
One potential explanation is viral immune perturbation or inflammatory tissue injury. Supporting evidence includes neural accumulation of memory T cells in patients with neuropsychiatric symptoms such as malaise and depression, and similar changes are seen with age-related immune senescence and tissue injury. Hyperactivated B and T cells, as well as other innate immune cells, have also been linked to postacute COVID-19, as has heightened expression of proinflammatory cytokines.
To explore the potential role of persistent viral antigens, the researchers gathered biopsies during upper- and lower-gastrointestinal endoscopy in 46 patients with IBD whose prior COVID-19 infection (mean, 7.3 months previous) had been confirmed by polymerase chain reaction and who were seen at the IBD outpatient unit of the investigators’ institution. In all, 43.5% of patients were female, and the average age was 44.67 years. Overall, 67.4% had been diagnosed with Crohn’s disease, 28.3% with ulcerative colitis, and 4.3% had unclassified IBD; 23.9% had a history of exposure to anti–tumor necrosis factor therapy. Among patients in the study, 32 of the patients tested positive for mucosal SARS-CoV-2 RNA, and there was no association between the presence of viral RNA and IBD type.
The researchers found that 52%-70% of patients had antigen persistence in any gut segment, as measured by nucleocapsid immunofluorescence or expression of one of four viral transcripts. They detected persistence of the nucleocapsid in epithelial cells and CD8+ T cells. Viral antigens persisted in patients with and without exposure to immunosuppressive therapy, and there was no association with antigen persistence and severity of acute COVID-19 infection or the presence of inflammation at the time of the endoscopy.
The researchers believed that the persistent viral antigen reflects incomplete clearance from the original infection rather than a latent or persistent infection because they could not replicate the virus in biopsy samples. Most biopsies within a patient produced some, but not all, of the viral transcripts tested. The authors suggest that immunosuppressive therapy may lead to incomplete viral clearance. Some patients lacked humoral nucleocapsid IgG antibodies, especially among those with gut antigen persistence.
In fact, only patients with gut viral RNA persistence had symptoms of postacute COVID. “This observation strongly argues for a role of viral antigen persistence in postacute COVID-19 and it appears plausible that SARS-CoV-2 antigen persistence, possibly in infected tissues beyond the gut, could impact host immune responses underlying the postacute COVID-19 syndrome,” the researchers wrote.
There is precedent for such a phenomenon in influenza. Mouse models have shown that ineffective clearance can influence adaptive immune responses and memory T-cell formation in lymph nodes of the lung. Another report found that COVID-19 pneumonia survivors have persistent changes to pulmonary CD8+ T cells.
The study is limited by its small sample size and a lack of a replication cohort. The study was also conducted in IBD patients because the researchers believed they were at higher risk of COVID-19 infection, although the researchers note that viral antigen persistence has been observed 2 months after recovery from COVID-19 in patients without IBD or exposure to immunosuppressants.
The researchers call for studies in patients without IBD to determine whether viral antigen persistence is a key mechanism in postacute COVID-19.
The researchers have no relevant financial disclosures.
A new study among patients with inflammatory bowel disease (IBD) suggests that viral antigen persistence in the gut may contribute to post-acute COVID-19 syndrome.
Postacute COVID-19 syndrome is now understood to be a multiorgan condition with symptoms that may include fatigue, cognitive dysfunction, and pain. Poor baseline health and severe acute infection are risk factors for the condition, but nonhospitalized illness can also lead to persistent symptoms.
Researchers found that nearly two-thirds of IBD patients had persistence of the antigen in infected tissues up to 8 months after a mild (nonhospitalized) acute COVID-19 infection. The study is the first to tie gut antigen persistence to post-acute COVID symptoms, and the results imply that the antigen may lead to immune perturbation and ongoing symptoms.
The study was published online in Gastroenterology.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) uses the membrane-bound angiotensin-converting enzyme 2 to gain entry into cells, which is expressed in the brush border enterocytes, as well as elsewhere in the body.
Previous research using intestinal epithelial organoids confirmed that SARS-CoV-2 is capable of infecting the human epithelium and that the virus can be detected in anal swabs long after it is cleared from nasal passages.
One potential explanation is viral immune perturbation or inflammatory tissue injury. Supporting evidence includes neural accumulation of memory T cells in patients with neuropsychiatric symptoms such as malaise and depression, and similar changes are seen with age-related immune senescence and tissue injury. Hyperactivated B and T cells, as well as other innate immune cells, have also been linked to postacute COVID-19, as has heightened expression of proinflammatory cytokines.
To explore the potential role of persistent viral antigens, the researchers gathered biopsies during upper- and lower-gastrointestinal endoscopy in 46 patients with IBD whose prior COVID-19 infection (mean, 7.3 months previous) had been confirmed by polymerase chain reaction and who were seen at the IBD outpatient unit of the investigators’ institution. In all, 43.5% of patients were female, and the average age was 44.67 years. Overall, 67.4% had been diagnosed with Crohn’s disease, 28.3% with ulcerative colitis, and 4.3% had unclassified IBD; 23.9% had a history of exposure to anti–tumor necrosis factor therapy. Among patients in the study, 32 of the patients tested positive for mucosal SARS-CoV-2 RNA, and there was no association between the presence of viral RNA and IBD type.
The researchers found that 52%-70% of patients had antigen persistence in any gut segment, as measured by nucleocapsid immunofluorescence or expression of one of four viral transcripts. They detected persistence of the nucleocapsid in epithelial cells and CD8+ T cells. Viral antigens persisted in patients with and without exposure to immunosuppressive therapy, and there was no association with antigen persistence and severity of acute COVID-19 infection or the presence of inflammation at the time of the endoscopy.
The researchers believed that the persistent viral antigen reflects incomplete clearance from the original infection rather than a latent or persistent infection because they could not replicate the virus in biopsy samples. Most biopsies within a patient produced some, but not all, of the viral transcripts tested. The authors suggest that immunosuppressive therapy may lead to incomplete viral clearance. Some patients lacked humoral nucleocapsid IgG antibodies, especially among those with gut antigen persistence.
In fact, only patients with gut viral RNA persistence had symptoms of postacute COVID. “This observation strongly argues for a role of viral antigen persistence in postacute COVID-19 and it appears plausible that SARS-CoV-2 antigen persistence, possibly in infected tissues beyond the gut, could impact host immune responses underlying the postacute COVID-19 syndrome,” the researchers wrote.
There is precedent for such a phenomenon in influenza. Mouse models have shown that ineffective clearance can influence adaptive immune responses and memory T-cell formation in lymph nodes of the lung. Another report found that COVID-19 pneumonia survivors have persistent changes to pulmonary CD8+ T cells.
The study is limited by its small sample size and a lack of a replication cohort. The study was also conducted in IBD patients because the researchers believed they were at higher risk of COVID-19 infection, although the researchers note that viral antigen persistence has been observed 2 months after recovery from COVID-19 in patients without IBD or exposure to immunosuppressants.
The researchers call for studies in patients without IBD to determine whether viral antigen persistence is a key mechanism in postacute COVID-19.
The researchers have no relevant financial disclosures.
FROM GASTROENTEROLOGY
Two genetic intestinal diseases linked
Two genes that have been linked separately to rare intestinal diseases appear to share a functional relationship. The genes have independently been linked to osteo-oto-hepato-enteric (O2HE) syndrome and microvillus inclusion disease (MVID), which are characterized by congenital diarrhea and, in some patients, intrahepatic cholestasis.
It appears that one gene, UNC45A, is directly responsible for the proper function of the protein encoded by the other gene, called MYO5B, according to investigators, who published their findings in Cellular and Molecular Gastroenterology and Hepatology. UNC45A is a chaperone protein that helps proteins fold properly. It has been linked to O2HE patients experiencing congenital diarrhea and intrahepatic cholestasis. The mutation has been identified in four patients from three different families with O2HE, which can also present with sensorineural hearing loss and bone fragility. Cellular analyses have shown that the mutation leads to reduction in protein expression by 70%-90%.
Intestinal symptoms similar to those in O2HE have also been described in diseases caused by mutations in genes that encode the myosin motor proteins that are involved in cellular protein trafficking. This group of disorders includes MVID. The researchers hypothesized that the UNC45A mutation in O2HE might lead to similar symptoms as MVID and others through the altered protein’s failure to assist in the folding of myosin proteins, although to date only the myosin IIa protein has been shown to be a target of UNC45A.
To investigate the possibility, they examined in more detail the relationship between UNC45A and intestinal symptoms. There are various known mutations in myosin proteins. Some have been linked to deafness, but these do not appear to contribute to intestinal symptoms since patients with myelin-related inherited deafness don’t typically have diarrhea. Bone fragility, also sometimes caused by myosin mutations, also appears to be unrelated to intestinal symptoms.
Previous experiments in yeast suggest that the related gene UNC45 may serve as a chaperone for type V myosin: Loss of a yeast version of UNC45 caused a type V myosin called MYO4P to be mislocalized in yeast. In zebrafish, reduction in intestinal levels of the UNC45A gene or the fish’s version of MYO5B interfered with development of intestinal folds.
The researchers used CRISPR-Cas9 gene editing and site-directed mutagenesis in intestinal epithelial and liver cell lines to investigate the relationships between UNC45A and MYO5B mutants. UNC45A depletion or introduction of the UNC45A mutation found in patients led to lower MYO5B expression. Within epithelial cells, loss of UNC45A led to changes in MYO5B–linked processes that are known to play a role in MVID pathogenesis. These included alteration of microvilli development and interference with the location of rat sarcoma–associated binding protein (RAB) 11A–positive recycling endosomes. When normal UNC45A was reintroduced to these cells, MYO5B expression returned. Reintroduction of either UNC45A or MYO5B repaired the alterations to recycling endosome position and microvilli development.
Loss of UNC45A did not appear to affect transcription of the MYO5B gen, which suggests a suggesting a functional interaction between the two at a protein level.
UNC45A has been shown to destabilize microtubules. Exposure of a kidney epithelial cell line to the microtubule-stabilizing drug taxol also led to displacement of RAB11A-positve recycling endosomes, though the specific changes were different than what is seen in MYO5B mutants. The researchers were unable to validate the findings in tissue derived from O2HE patients because of insufficient material, but they maintain that the cell lines used have proven to be highly predictive for the cellular characteristics of MVID.
Overall, the study suggests that reductions in MYO5B and subsequent changes to the cellular processes that depend on it may underlie the intestinal symptoms in O2HE.
The researchers noted that O2HE patients have different phenotypes. Of the four patients they studied, three had severe chronic diarrhea and required parenteral nutrition. One patient later had the diarrhea resolve and her sister did not have diarrhea at all. This heterogeneity in severity and duration of clinical symptoms may be driven by differences in the molecular effects of patient-specific mutations. The two siblings had mutations in a different region of the UNC45A gene than the other two participants.
“Taken together, this study revealed a functional relationship between UNC45A and MYO5B protein expression, thereby connecting two rare congenital diseases with overlapping intestinal symptoms at the molecular level,” the authors wrote.
The authors reported that they had no conflicts of interest.
This article was updated 7/13/22.
Congenital diarrheas and enteropathies (CoDEs) are rare monogenic disorders caused by genes important for intestinal epithelial function. The increasing availability of exome sequencing in clinical practice has accelerated the discovery of new genes associated with these disorders over the past few years. Several CoDE disorders revolve around defects in trafficking of vesicles in epithelial cells. One of these is microvillus inclusion disease which is caused by loss-of-function variants in the gene MYO5B, which encodes an important epithelial motor protein. This study by Li and colleagues reveals that a recently discovered novel CoDE gene and protein, UNC45A, is functionally linked to MYO5B and that loss of UNC45A in cells causes a very similar cellular phenotype to MYO5B-deficient cells.

Jay Thiagarajah, MD, PhD, attending in the division of gastroenterology, hepatology and nutrition and codirector of the congenital enteropathy program at Boston Children’s Hospital, as well as assistant professor in pediatrics at Harvard Medical School, also in Boston. Dr. Thiagarajah stated he had no relevant conflicts to disclose.
Congenital diarrheas and enteropathies (CoDEs) are rare monogenic disorders caused by genes important for intestinal epithelial function. The increasing availability of exome sequencing in clinical practice has accelerated the discovery of new genes associated with these disorders over the past few years. Several CoDE disorders revolve around defects in trafficking of vesicles in epithelial cells. One of these is microvillus inclusion disease which is caused by loss-of-function variants in the gene MYO5B, which encodes an important epithelial motor protein. This study by Li and colleagues reveals that a recently discovered novel CoDE gene and protein, UNC45A, is functionally linked to MYO5B and that loss of UNC45A in cells causes a very similar cellular phenotype to MYO5B-deficient cells.
Jay Thiagarajah, MD, PhD, attending in the division of gastroenterology, hepatology and nutrition and codirector of the congenital enteropathy program at Boston Children’s Hospital, as well as assistant professor in pediatrics at Harvard Medical School, also in Boston. Dr. Thiagarajah stated he had no relevant conflicts to disclose.
Congenital diarrheas and enteropathies (CoDEs) are rare monogenic disorders caused by genes important for intestinal epithelial function. The increasing availability of exome sequencing in clinical practice has accelerated the discovery of new genes associated with these disorders over the past few years. Several CoDE disorders revolve around defects in trafficking of vesicles in epithelial cells. One of these is microvillus inclusion disease which is caused by loss-of-function variants in the gene MYO5B, which encodes an important epithelial motor protein. This study by Li and colleagues reveals that a recently discovered novel CoDE gene and protein, UNC45A, is functionally linked to MYO5B and that loss of UNC45A in cells causes a very similar cellular phenotype to MYO5B-deficient cells.
Jay Thiagarajah, MD, PhD, attending in the division of gastroenterology, hepatology and nutrition and codirector of the congenital enteropathy program at Boston Children’s Hospital, as well as assistant professor in pediatrics at Harvard Medical School, also in Boston. Dr. Thiagarajah stated he had no relevant conflicts to disclose.
Two genes that have been linked separately to rare intestinal diseases appear to share a functional relationship. The genes have independently been linked to osteo-oto-hepato-enteric (O2HE) syndrome and microvillus inclusion disease (MVID), which are characterized by congenital diarrhea and, in some patients, intrahepatic cholestasis.
It appears that one gene, UNC45A, is directly responsible for the proper function of the protein encoded by the other gene, called MYO5B, according to investigators, who published their findings in Cellular and Molecular Gastroenterology and Hepatology. UNC45A is a chaperone protein that helps proteins fold properly. It has been linked to O2HE patients experiencing congenital diarrhea and intrahepatic cholestasis. The mutation has been identified in four patients from three different families with O2HE, which can also present with sensorineural hearing loss and bone fragility. Cellular analyses have shown that the mutation leads to reduction in protein expression by 70%-90%.
Intestinal symptoms similar to those in O2HE have also been described in diseases caused by mutations in genes that encode the myosin motor proteins that are involved in cellular protein trafficking. This group of disorders includes MVID. The researchers hypothesized that the UNC45A mutation in O2HE might lead to similar symptoms as MVID and others through the altered protein’s failure to assist in the folding of myosin proteins, although to date only the myosin IIa protein has been shown to be a target of UNC45A.
To investigate the possibility, they examined in more detail the relationship between UNC45A and intestinal symptoms. There are various known mutations in myosin proteins. Some have been linked to deafness, but these do not appear to contribute to intestinal symptoms since patients with myelin-related inherited deafness don’t typically have diarrhea. Bone fragility, also sometimes caused by myosin mutations, also appears to be unrelated to intestinal symptoms.
Previous experiments in yeast suggest that the related gene UNC45 may serve as a chaperone for type V myosin: Loss of a yeast version of UNC45 caused a type V myosin called MYO4P to be mislocalized in yeast. In zebrafish, reduction in intestinal levels of the UNC45A gene or the fish’s version of MYO5B interfered with development of intestinal folds.
The researchers used CRISPR-Cas9 gene editing and site-directed mutagenesis in intestinal epithelial and liver cell lines to investigate the relationships between UNC45A and MYO5B mutants. UNC45A depletion or introduction of the UNC45A mutation found in patients led to lower MYO5B expression. Within epithelial cells, loss of UNC45A led to changes in MYO5B–linked processes that are known to play a role in MVID pathogenesis. These included alteration of microvilli development and interference with the location of rat sarcoma–associated binding protein (RAB) 11A–positive recycling endosomes. When normal UNC45A was reintroduced to these cells, MYO5B expression returned. Reintroduction of either UNC45A or MYO5B repaired the alterations to recycling endosome position and microvilli development.
Loss of UNC45A did not appear to affect transcription of the MYO5B gen, which suggests a suggesting a functional interaction between the two at a protein level.
UNC45A has been shown to destabilize microtubules. Exposure of a kidney epithelial cell line to the microtubule-stabilizing drug taxol also led to displacement of RAB11A-positve recycling endosomes, though the specific changes were different than what is seen in MYO5B mutants. The researchers were unable to validate the findings in tissue derived from O2HE patients because of insufficient material, but they maintain that the cell lines used have proven to be highly predictive for the cellular characteristics of MVID.
Overall, the study suggests that reductions in MYO5B and subsequent changes to the cellular processes that depend on it may underlie the intestinal symptoms in O2HE.
The researchers noted that O2HE patients have different phenotypes. Of the four patients they studied, three had severe chronic diarrhea and required parenteral nutrition. One patient later had the diarrhea resolve and her sister did not have diarrhea at all. This heterogeneity in severity and duration of clinical symptoms may be driven by differences in the molecular effects of patient-specific mutations. The two siblings had mutations in a different region of the UNC45A gene than the other two participants.
“Taken together, this study revealed a functional relationship between UNC45A and MYO5B protein expression, thereby connecting two rare congenital diseases with overlapping intestinal symptoms at the molecular level,” the authors wrote.
The authors reported that they had no conflicts of interest.
This article was updated 7/13/22.
Two genes that have been linked separately to rare intestinal diseases appear to share a functional relationship. The genes have independently been linked to osteo-oto-hepato-enteric (O2HE) syndrome and microvillus inclusion disease (MVID), which are characterized by congenital diarrhea and, in some patients, intrahepatic cholestasis.
It appears that one gene, UNC45A, is directly responsible for the proper function of the protein encoded by the other gene, called MYO5B, according to investigators, who published their findings in Cellular and Molecular Gastroenterology and Hepatology. UNC45A is a chaperone protein that helps proteins fold properly. It has been linked to O2HE patients experiencing congenital diarrhea and intrahepatic cholestasis. The mutation has been identified in four patients from three different families with O2HE, which can also present with sensorineural hearing loss and bone fragility. Cellular analyses have shown that the mutation leads to reduction in protein expression by 70%-90%.
Intestinal symptoms similar to those in O2HE have also been described in diseases caused by mutations in genes that encode the myosin motor proteins that are involved in cellular protein trafficking. This group of disorders includes MVID. The researchers hypothesized that the UNC45A mutation in O2HE might lead to similar symptoms as MVID and others through the altered protein’s failure to assist in the folding of myosin proteins, although to date only the myosin IIa protein has been shown to be a target of UNC45A.
To investigate the possibility, they examined in more detail the relationship between UNC45A and intestinal symptoms. There are various known mutations in myosin proteins. Some have been linked to deafness, but these do not appear to contribute to intestinal symptoms since patients with myelin-related inherited deafness don’t typically have diarrhea. Bone fragility, also sometimes caused by myosin mutations, also appears to be unrelated to intestinal symptoms.
Previous experiments in yeast suggest that the related gene UNC45 may serve as a chaperone for type V myosin: Loss of a yeast version of UNC45 caused a type V myosin called MYO4P to be mislocalized in yeast. In zebrafish, reduction in intestinal levels of the UNC45A gene or the fish’s version of MYO5B interfered with development of intestinal folds.
The researchers used CRISPR-Cas9 gene editing and site-directed mutagenesis in intestinal epithelial and liver cell lines to investigate the relationships between UNC45A and MYO5B mutants. UNC45A depletion or introduction of the UNC45A mutation found in patients led to lower MYO5B expression. Within epithelial cells, loss of UNC45A led to changes in MYO5B–linked processes that are known to play a role in MVID pathogenesis. These included alteration of microvilli development and interference with the location of rat sarcoma–associated binding protein (RAB) 11A–positive recycling endosomes. When normal UNC45A was reintroduced to these cells, MYO5B expression returned. Reintroduction of either UNC45A or MYO5B repaired the alterations to recycling endosome position and microvilli development.
Loss of UNC45A did not appear to affect transcription of the MYO5B gen, which suggests a suggesting a functional interaction between the two at a protein level.
UNC45A has been shown to destabilize microtubules. Exposure of a kidney epithelial cell line to the microtubule-stabilizing drug taxol also led to displacement of RAB11A-positve recycling endosomes, though the specific changes were different than what is seen in MYO5B mutants. The researchers were unable to validate the findings in tissue derived from O2HE patients because of insufficient material, but they maintain that the cell lines used have proven to be highly predictive for the cellular characteristics of MVID.
Overall, the study suggests that reductions in MYO5B and subsequent changes to the cellular processes that depend on it may underlie the intestinal symptoms in O2HE.
The researchers noted that O2HE patients have different phenotypes. Of the four patients they studied, three had severe chronic diarrhea and required parenteral nutrition. One patient later had the diarrhea resolve and her sister did not have diarrhea at all. This heterogeneity in severity and duration of clinical symptoms may be driven by differences in the molecular effects of patient-specific mutations. The two siblings had mutations in a different region of the UNC45A gene than the other two participants.
“Taken together, this study revealed a functional relationship between UNC45A and MYO5B protein expression, thereby connecting two rare congenital diseases with overlapping intestinal symptoms at the molecular level,” the authors wrote.
The authors reported that they had no conflicts of interest.
This article was updated 7/13/22.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
AGA Clinical Practice Guidelines: Pharmacologic treatment of IBS
The American Gastroenterological Association has issued new guidelines for the medical treatment of irritable bowel syndrome (IBS).
The guidelines, which are separated into one publication for IBS with constipation (IBS-C) and another for IBS with diarrhea (IBS-D), are the first to advise clinicians in the usage of new, old, and over-the-counter drugs for IBS, according to a press release from the AGA.
“With more treatments available, physicians can tailor a personalized approach based on the symptoms a patient with IBS is experiencing,” AGA said.
Published simultaneously in Gastroenterology, the two guidelines describe a shared rationale for their creation, noting how the treatment landscape has changed since the AGA last issued IBS guidelines in 2014.

“New pharmacological treatments have become available and new evidence has accumulated about established treatments,” both guidelines stated. “The purpose of these guidelines is to provide evidence-based recommendations for the pharmacologic management” of individuals with IBS “based on a systematic and comprehensive synthesis of the literature.”
IBS-C
In the IBS-C guidelines, co–first authors Lin Chang, MD, AGAF, of the University of Los Angeles, and Shahnaz Sultan, MD, MHSc, AGAF, of the Minneapolis Veterans Affairs Healthcare System, noted that IBS-C accounts for “more than a third of IBS cases,” with patients frequently reporting “feeling self-conscious, avoiding sex, difficulty concentrating, [and] not feeling able to reach one’s full potential.”
They offered nine pharmacologic recommendations, eight of which are conditional, with certainty in evidence ranging from low to high.
The only strong recommendation with a high certainty in evidence is for linaclotide.
“Across four RCTs [randomized controlled trials], linaclotide improved global assessment of IBS-C symptoms (FDA responder), abdominal pain, complete spontaneous bowel movement response, as well as adequate global response,” Dr. Chang and colleagues wrote.

Conditional recommendations with moderate certainty in evidence are provided for tenapanor, plecanatide, tegaserod, and lubiprostone. Recommendations for polyethylene glycol laxatives, tricyclic antidepressants and antispasmodics are conditional and based on low-certainty evidence, as well as a conditional recommendation against selective serotonin reuptake inhibitors, also based on low-certainty evidence.
IBS-D
The IBS-D guidelines, led by co–first authors Anthony Lembo, MD, AGAF, of Beth Israel Deaconess Medical Center, Boston, and Dr. Sultan, includes eight conditional recommendations with certainty in evidence ranging from very low to moderate.

Drugs recommended based on moderate-certainty evidence include eluxadoline, alosetron, and rifaximin, with the added note that patients who respond to rifaximin but have recurrence should be treated again with rifaximin. Low-certainty evidence supported recommendations for tricyclic antidepressants, and antispasmodics. Very low–certainty evidence stands behind a recommendation for loperamide. Again, the panel made a conditional recommendation against SSRIs, also based on low-certainty evidence.
Shared decision-making
Both publications concluded with similar statements about the importance of shared decision-making, plus a practical mindset, in management of IBS.
“Acknowledging that multimodal treatments that include dietary and behavioral approaches in conjunction with drug therapy may provide maximal benefits and that treatment choices may be influenced by patient preferences, practitioners should engage in shared decision-making with patients when choosing the best therapy,” Dr. Lembo and colleagues wrote. “The importance of the patient-physician relationship is paramount in caring for individuals with IBS, and understanding patient preferences (for side-effect tolerability as well as cost) is valuable in choosing the right therapy.”
Both guidelines noted that some newer drugs for IBS have no generic alternative, and preauthorization may be required. Payer approval may depend on previous treatment failure with generic alternatives, they added.
The guidelines were commissioned and funded by the AGA Institute. The authors disclosed relationships with Ardelyx, Immunic, Protagonist, and others.
The American Gastroenterological Association has issued new guidelines for the medical treatment of irritable bowel syndrome (IBS).
The guidelines, which are separated into one publication for IBS with constipation (IBS-C) and another for IBS with diarrhea (IBS-D), are the first to advise clinicians in the usage of new, old, and over-the-counter drugs for IBS, according to a press release from the AGA.
“With more treatments available, physicians can tailor a personalized approach based on the symptoms a patient with IBS is experiencing,” AGA said.
Published simultaneously in Gastroenterology, the two guidelines describe a shared rationale for their creation, noting how the treatment landscape has changed since the AGA last issued IBS guidelines in 2014.
“New pharmacological treatments have become available and new evidence has accumulated about established treatments,” both guidelines stated. “The purpose of these guidelines is to provide evidence-based recommendations for the pharmacologic management” of individuals with IBS “based on a systematic and comprehensive synthesis of the literature.”
IBS-C
In the IBS-C guidelines, co–first authors Lin Chang, MD, AGAF, of the University of Los Angeles, and Shahnaz Sultan, MD, MHSc, AGAF, of the Minneapolis Veterans Affairs Healthcare System, noted that IBS-C accounts for “more than a third of IBS cases,” with patients frequently reporting “feeling self-conscious, avoiding sex, difficulty concentrating, [and] not feeling able to reach one’s full potential.”
They offered nine pharmacologic recommendations, eight of which are conditional, with certainty in evidence ranging from low to high.
The only strong recommendation with a high certainty in evidence is for linaclotide.
“Across four RCTs [randomized controlled trials], linaclotide improved global assessment of IBS-C symptoms (FDA responder), abdominal pain, complete spontaneous bowel movement response, as well as adequate global response,” Dr. Chang and colleagues wrote.
Conditional recommendations with moderate certainty in evidence are provided for tenapanor, plecanatide, tegaserod, and lubiprostone. Recommendations for polyethylene glycol laxatives, tricyclic antidepressants and antispasmodics are conditional and based on low-certainty evidence, as well as a conditional recommendation against selective serotonin reuptake inhibitors, also based on low-certainty evidence.
IBS-D
The IBS-D guidelines, led by co–first authors Anthony Lembo, MD, AGAF, of Beth Israel Deaconess Medical Center, Boston, and Dr. Sultan, includes eight conditional recommendations with certainty in evidence ranging from very low to moderate.
Drugs recommended based on moderate-certainty evidence include eluxadoline, alosetron, and rifaximin, with the added note that patients who respond to rifaximin but have recurrence should be treated again with rifaximin. Low-certainty evidence supported recommendations for tricyclic antidepressants, and antispasmodics. Very low–certainty evidence stands behind a recommendation for loperamide. Again, the panel made a conditional recommendation against SSRIs, also based on low-certainty evidence.
Shared decision-making
Both publications concluded with similar statements about the importance of shared decision-making, plus a practical mindset, in management of IBS.
“Acknowledging that multimodal treatments that include dietary and behavioral approaches in conjunction with drug therapy may provide maximal benefits and that treatment choices may be influenced by patient preferences, practitioners should engage in shared decision-making with patients when choosing the best therapy,” Dr. Lembo and colleagues wrote. “The importance of the patient-physician relationship is paramount in caring for individuals with IBS, and understanding patient preferences (for side-effect tolerability as well as cost) is valuable in choosing the right therapy.”
Both guidelines noted that some newer drugs for IBS have no generic alternative, and preauthorization may be required. Payer approval may depend on previous treatment failure with generic alternatives, they added.
The guidelines were commissioned and funded by the AGA Institute. The authors disclosed relationships with Ardelyx, Immunic, Protagonist, and others.
The American Gastroenterological Association has issued new guidelines for the medical treatment of irritable bowel syndrome (IBS).
The guidelines, which are separated into one publication for IBS with constipation (IBS-C) and another for IBS with diarrhea (IBS-D), are the first to advise clinicians in the usage of new, old, and over-the-counter drugs for IBS, according to a press release from the AGA.
“With more treatments available, physicians can tailor a personalized approach based on the symptoms a patient with IBS is experiencing,” AGA said.
Published simultaneously in Gastroenterology, the two guidelines describe a shared rationale for their creation, noting how the treatment landscape has changed since the AGA last issued IBS guidelines in 2014.
“New pharmacological treatments have become available and new evidence has accumulated about established treatments,” both guidelines stated. “The purpose of these guidelines is to provide evidence-based recommendations for the pharmacologic management” of individuals with IBS “based on a systematic and comprehensive synthesis of the literature.”
IBS-C
In the IBS-C guidelines, co–first authors Lin Chang, MD, AGAF, of the University of Los Angeles, and Shahnaz Sultan, MD, MHSc, AGAF, of the Minneapolis Veterans Affairs Healthcare System, noted that IBS-C accounts for “more than a third of IBS cases,” with patients frequently reporting “feeling self-conscious, avoiding sex, difficulty concentrating, [and] not feeling able to reach one’s full potential.”
They offered nine pharmacologic recommendations, eight of which are conditional, with certainty in evidence ranging from low to high.
The only strong recommendation with a high certainty in evidence is for linaclotide.
“Across four RCTs [randomized controlled trials], linaclotide improved global assessment of IBS-C symptoms (FDA responder), abdominal pain, complete spontaneous bowel movement response, as well as adequate global response,” Dr. Chang and colleagues wrote.
Conditional recommendations with moderate certainty in evidence are provided for tenapanor, plecanatide, tegaserod, and lubiprostone. Recommendations for polyethylene glycol laxatives, tricyclic antidepressants and antispasmodics are conditional and based on low-certainty evidence, as well as a conditional recommendation against selective serotonin reuptake inhibitors, also based on low-certainty evidence.
IBS-D
The IBS-D guidelines, led by co–first authors Anthony Lembo, MD, AGAF, of Beth Israel Deaconess Medical Center, Boston, and Dr. Sultan, includes eight conditional recommendations with certainty in evidence ranging from very low to moderate.
Drugs recommended based on moderate-certainty evidence include eluxadoline, alosetron, and rifaximin, with the added note that patients who respond to rifaximin but have recurrence should be treated again with rifaximin. Low-certainty evidence supported recommendations for tricyclic antidepressants, and antispasmodics. Very low–certainty evidence stands behind a recommendation for loperamide. Again, the panel made a conditional recommendation against SSRIs, also based on low-certainty evidence.
Shared decision-making
Both publications concluded with similar statements about the importance of shared decision-making, plus a practical mindset, in management of IBS.
“Acknowledging that multimodal treatments that include dietary and behavioral approaches in conjunction with drug therapy may provide maximal benefits and that treatment choices may be influenced by patient preferences, practitioners should engage in shared decision-making with patients when choosing the best therapy,” Dr. Lembo and colleagues wrote. “The importance of the patient-physician relationship is paramount in caring for individuals with IBS, and understanding patient preferences (for side-effect tolerability as well as cost) is valuable in choosing the right therapy.”
Both guidelines noted that some newer drugs for IBS have no generic alternative, and preauthorization may be required. Payer approval may depend on previous treatment failure with generic alternatives, they added.
The guidelines were commissioned and funded by the AGA Institute. The authors disclosed relationships with Ardelyx, Immunic, Protagonist, and others.
FROM GASTROENTEROLOGY
AGA issues position statements on reducing CRC burden
The American Gastroenterological Association has published eight position statements aimed at reducing the burden of colorectal cancer (CRC).
The evidence-based statements, published in Gastroenterology, call for a national approach to CRC screening, outline the elements of a high-quality screening program, and make clear that payers should cover all costs, from bowel prep through pathology, plus follow-up for high-risk patients.
“There is strong evidence that CRC screening is effective [at reducing CRC incidence and mortality] ... but less than 70% of eligible individuals have been screened,” wrote authors led by David Lieberman, MD, who is on the AGA Executive Committee on the Screening Continuum and affiliated with Oregon Health and Science University, Portland, noting the recent expansion of eligibility to include individuals in the 45- to 49-year age group.
“CRC screening saves lives, but only if people get screened,” Dr. Lieberman said in a press release from the AGA. “Cost sharing is an important barrier to screening, which contributes to racial, ethnic and socioeconomic inequities in colorectal cancer outcomes. The full cost of screening – including noninvasive tests and follow-up colonoscopies – should be covered without cost to patients.”
He added: “AGA wishes to collaborate with stakeholders to eliminate obstacles to screening, which disproportionately impact those with low income and lack of insurance.”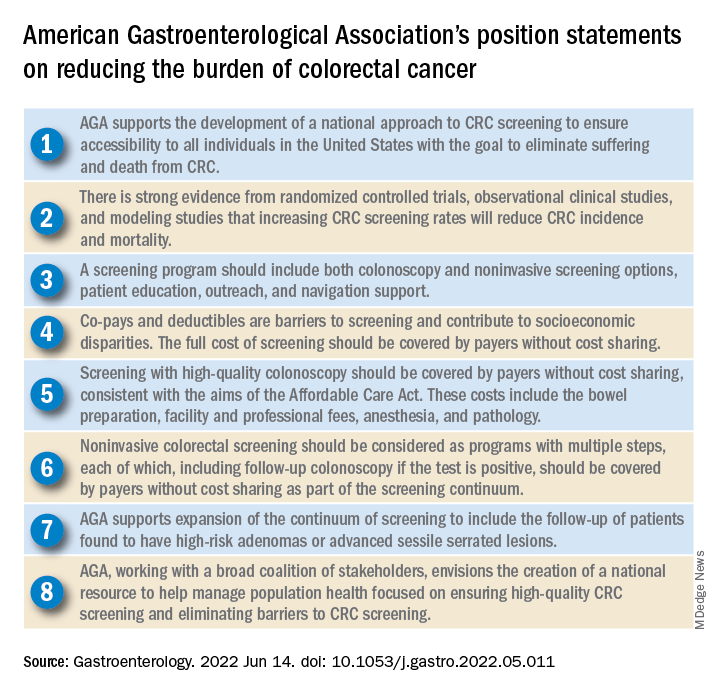
Eliminating disparities in screening
Among the position statements, Dr. Lieberman and colleagues first called for “development of a national approach to CRC screening” to patch gaps in access across the United States.
“Systematic outreach occurs infrequently,” they noted. “CRC screening prevalence is much lower among individuals who do not have access to health care due to lack of insurance, do not have a primary care provider, or are part of a medically underserved community.”
According to Dr. Lieberman and colleagues, the AGA is also “working with a broad coalition of stakeholders,” such as the American Cancer Society, payers, patient advocacy groups, and others, to create a “national resource ... focused on ensuring high-quality CRC screening and eliminating barriers to CRC screening.”
Specifically, the coalition will work to collectively tackle “disparities created by social determinants of health, which includes lack of access to screening, transportation, and even work hours and child care.
“The AGA recognizes that moving the needle to achieve a CRC screening participation goal of 80% will take a village,” they wrote.
Elements of high-quality CRC screening
The investigators went on to describe the key features of a high-quality CRC screening program, including “colonoscopy and noninvasive screening options, patient education, outreach, and navigation support.”
Dr. Lieberman and colleagues pointed out that offering more than one type of screening test “acknowledges patient preferences and improves participation.”
Certain noninvasive methods, such as fecal immunochemical testing (FIT), eliminate “important barriers” to screening, they noted, such as the need for special preparation, time off work, and transportation to a medical facility.
For individuals who have high-risk adenomas (HRAs) or advanced sessile serrated lesions (SSLs), screening should be expanded to include follow-up, the investigators added.
“Evidence from a systematic review demonstrates that individuals with HRAs at baseline have a 3- to 4-fold higher risk of incident CRC during follow-up compared with individuals with no adenoma or low-risk adenomas,” they wrote. “There is also evidence that individuals with advanced SSLs have a three= to fourfold higher risk of CRC, compared with individuals with nonadvanced SSLs.”
Payers should cover costs
To further improve access to care, payers should cover the full costs of CRC screening because “copays and deductibles are barriers to screening and contribute to socioeconomic disparities,” that “disproportionately impact those with low income and lack of insurance,” according to Dr. Lieberman and colleagues.
They noted that the Affordable Care Act “eliminated copayments for preventive services,” yet a recent study showed that almost half of patients with commercial insurance and more than three-quarters of patients with Medicare still share some cost of CRC screening.
The investigators made clear that payers need to cover costs from start to finish, including “bowel preparation, facility and professional fees, anesthesia, and pathology,” as well as follow-up screening for high-risk patients identified by noninvasive methods.
“Noninvasive colorectal screening should be considered as programs with multiple steps, each of which, including follow-up colonoscopy if the test is positive, should be covered by payers without cost sharing as part of the screening continuum,” Dr. Lieberman and colleagues wrote.
Changes underway
According to Steven Itzkowitz, MD, professor of medicine and oncological sciences and director of the gastroenterology fellowship training program at the Icahn School of Medicine at Mount Sinai, New York, the AGA publication is important because it “consolidates many of the critical issues related to decreasing the burden of colorectal cancer in the United States.”
Dr. Itzkowitz noted that changes are already underway to eliminate cost as a barrier to screening.
“The good news is that, in the past year, the Departments of Health & Human Services, Labor, and Treasury declared that cost sharing should not be imposed, and plans are required to cover screening colonoscopy with polyp removal and colonoscopy that is performed to follow-up after an abnormal noninvasive CRC screening test,” Dr. Itzkowitz said in an interview. “Many plans are following suit, but it will take time for this coverage to take effect across all plans.”
For individual gastroenterologists who would like to do their part in reducing screening inequity, Dr. Itzkowitz suggested leveraging noninvasive testing, as the AGA recommends.
“This publication is the latest to call for using noninvasive, stool-based testing in addition to colonoscopy,” Dr. Itzkowitz said. “FIT and multitarget stool DNA tests all have proven efficacy in this regard, so gastroenterologists should have those conversations with their patients. GIs can also make it easier for patients to complete colonoscopy by developing patient navigation programs, direct access referrals, and systems for communicating with primary care providers for easier referrals and communicating colonoscopy results.”
Many practices are already instituting such improvements in response to the restrictions imposed by the COVID-19 pandemic, according to Dr. Itzkowitz.“These changes, plus better coverage by payers, will make a huge impact on health equity when it comes to colorectal cancer screening.”
The publication was supported by the AGA. The investigators disclosed relationships with Geneoscopy, ColoWrap, UniversalDx, and others. Dr. Itzkowitz disclosed no relevant conflicts of interest.
Groups interested in collaborating with AGA should contact Kathleen Teixeira, AGA Vice President, Public Policy and Advocacy, at [email protected].
The American Gastroenterological Association has published eight position statements aimed at reducing the burden of colorectal cancer (CRC).
The evidence-based statements, published in Gastroenterology, call for a national approach to CRC screening, outline the elements of a high-quality screening program, and make clear that payers should cover all costs, from bowel prep through pathology, plus follow-up for high-risk patients.
“There is strong evidence that CRC screening is effective [at reducing CRC incidence and mortality] ... but less than 70% of eligible individuals have been screened,” wrote authors led by David Lieberman, MD, who is on the AGA Executive Committee on the Screening Continuum and affiliated with Oregon Health and Science University, Portland, noting the recent expansion of eligibility to include individuals in the 45- to 49-year age group.
“CRC screening saves lives, but only if people get screened,” Dr. Lieberman said in a press release from the AGA. “Cost sharing is an important barrier to screening, which contributes to racial, ethnic and socioeconomic inequities in colorectal cancer outcomes. The full cost of screening – including noninvasive tests and follow-up colonoscopies – should be covered without cost to patients.”
He added: “AGA wishes to collaborate with stakeholders to eliminate obstacles to screening, which disproportionately impact those with low income and lack of insurance.”
Eliminating disparities in screening
Among the position statements, Dr. Lieberman and colleagues first called for “development of a national approach to CRC screening” to patch gaps in access across the United States.
“Systematic outreach occurs infrequently,” they noted. “CRC screening prevalence is much lower among individuals who do not have access to health care due to lack of insurance, do not have a primary care provider, or are part of a medically underserved community.”
According to Dr. Lieberman and colleagues, the AGA is also “working with a broad coalition of stakeholders,” such as the American Cancer Society, payers, patient advocacy groups, and others, to create a “national resource ... focused on ensuring high-quality CRC screening and eliminating barriers to CRC screening.”
Specifically, the coalition will work to collectively tackle “disparities created by social determinants of health, which includes lack of access to screening, transportation, and even work hours and child care.
“The AGA recognizes that moving the needle to achieve a CRC screening participation goal of 80% will take a village,” they wrote.
Elements of high-quality CRC screening
The investigators went on to describe the key features of a high-quality CRC screening program, including “colonoscopy and noninvasive screening options, patient education, outreach, and navigation support.”
Dr. Lieberman and colleagues pointed out that offering more than one type of screening test “acknowledges patient preferences and improves participation.”
Certain noninvasive methods, such as fecal immunochemical testing (FIT), eliminate “important barriers” to screening, they noted, such as the need for special preparation, time off work, and transportation to a medical facility.
For individuals who have high-risk adenomas (HRAs) or advanced sessile serrated lesions (SSLs), screening should be expanded to include follow-up, the investigators added.
“Evidence from a systematic review demonstrates that individuals with HRAs at baseline have a 3- to 4-fold higher risk of incident CRC during follow-up compared with individuals with no adenoma or low-risk adenomas,” they wrote. “There is also evidence that individuals with advanced SSLs have a three= to fourfold higher risk of CRC, compared with individuals with nonadvanced SSLs.”
Payers should cover costs
To further improve access to care, payers should cover the full costs of CRC screening because “copays and deductibles are barriers to screening and contribute to socioeconomic disparities,” that “disproportionately impact those with low income and lack of insurance,” according to Dr. Lieberman and colleagues.
They noted that the Affordable Care Act “eliminated copayments for preventive services,” yet a recent study showed that almost half of patients with commercial insurance and more than three-quarters of patients with Medicare still share some cost of CRC screening.
The investigators made clear that payers need to cover costs from start to finish, including “bowel preparation, facility and professional fees, anesthesia, and pathology,” as well as follow-up screening for high-risk patients identified by noninvasive methods.
“Noninvasive colorectal screening should be considered as programs with multiple steps, each of which, including follow-up colonoscopy if the test is positive, should be covered by payers without cost sharing as part of the screening continuum,” Dr. Lieberman and colleagues wrote.
Changes underway
According to Steven Itzkowitz, MD, professor of medicine and oncological sciences and director of the gastroenterology fellowship training program at the Icahn School of Medicine at Mount Sinai, New York, the AGA publication is important because it “consolidates many of the critical issues related to decreasing the burden of colorectal cancer in the United States.”
Dr. Itzkowitz noted that changes are already underway to eliminate cost as a barrier to screening.
“The good news is that, in the past year, the Departments of Health & Human Services, Labor, and Treasury declared that cost sharing should not be imposed, and plans are required to cover screening colonoscopy with polyp removal and colonoscopy that is performed to follow-up after an abnormal noninvasive CRC screening test,” Dr. Itzkowitz said in an interview. “Many plans are following suit, but it will take time for this coverage to take effect across all plans.”
For individual gastroenterologists who would like to do their part in reducing screening inequity, Dr. Itzkowitz suggested leveraging noninvasive testing, as the AGA recommends.
“This publication is the latest to call for using noninvasive, stool-based testing in addition to colonoscopy,” Dr. Itzkowitz said. “FIT and multitarget stool DNA tests all have proven efficacy in this regard, so gastroenterologists should have those conversations with their patients. GIs can also make it easier for patients to complete colonoscopy by developing patient navigation programs, direct access referrals, and systems for communicating with primary care providers for easier referrals and communicating colonoscopy results.”
Many practices are already instituting such improvements in response to the restrictions imposed by the COVID-19 pandemic, according to Dr. Itzkowitz.“These changes, plus better coverage by payers, will make a huge impact on health equity when it comes to colorectal cancer screening.”
The publication was supported by the AGA. The investigators disclosed relationships with Geneoscopy, ColoWrap, UniversalDx, and others. Dr. Itzkowitz disclosed no relevant conflicts of interest.
Groups interested in collaborating with AGA should contact Kathleen Teixeira, AGA Vice President, Public Policy and Advocacy, at [email protected].
The American Gastroenterological Association has published eight position statements aimed at reducing the burden of colorectal cancer (CRC).
The evidence-based statements, published in Gastroenterology, call for a national approach to CRC screening, outline the elements of a high-quality screening program, and make clear that payers should cover all costs, from bowel prep through pathology, plus follow-up for high-risk patients.
“There is strong evidence that CRC screening is effective [at reducing CRC incidence and mortality] ... but less than 70% of eligible individuals have been screened,” wrote authors led by David Lieberman, MD, who is on the AGA Executive Committee on the Screening Continuum and affiliated with Oregon Health and Science University, Portland, noting the recent expansion of eligibility to include individuals in the 45- to 49-year age group.
“CRC screening saves lives, but only if people get screened,” Dr. Lieberman said in a press release from the AGA. “Cost sharing is an important barrier to screening, which contributes to racial, ethnic and socioeconomic inequities in colorectal cancer outcomes. The full cost of screening – including noninvasive tests and follow-up colonoscopies – should be covered without cost to patients.”
He added: “AGA wishes to collaborate with stakeholders to eliminate obstacles to screening, which disproportionately impact those with low income and lack of insurance.”
Eliminating disparities in screening
Among the position statements, Dr. Lieberman and colleagues first called for “development of a national approach to CRC screening” to patch gaps in access across the United States.
“Systematic outreach occurs infrequently,” they noted. “CRC screening prevalence is much lower among individuals who do not have access to health care due to lack of insurance, do not have a primary care provider, or are part of a medically underserved community.”
According to Dr. Lieberman and colleagues, the AGA is also “working with a broad coalition of stakeholders,” such as the American Cancer Society, payers, patient advocacy groups, and others, to create a “national resource ... focused on ensuring high-quality CRC screening and eliminating barriers to CRC screening.”
Specifically, the coalition will work to collectively tackle “disparities created by social determinants of health, which includes lack of access to screening, transportation, and even work hours and child care.
“The AGA recognizes that moving the needle to achieve a CRC screening participation goal of 80% will take a village,” they wrote.
Elements of high-quality CRC screening
The investigators went on to describe the key features of a high-quality CRC screening program, including “colonoscopy and noninvasive screening options, patient education, outreach, and navigation support.”
Dr. Lieberman and colleagues pointed out that offering more than one type of screening test “acknowledges patient preferences and improves participation.”
Certain noninvasive methods, such as fecal immunochemical testing (FIT), eliminate “important barriers” to screening, they noted, such as the need for special preparation, time off work, and transportation to a medical facility.
For individuals who have high-risk adenomas (HRAs) or advanced sessile serrated lesions (SSLs), screening should be expanded to include follow-up, the investigators added.
“Evidence from a systematic review demonstrates that individuals with HRAs at baseline have a 3- to 4-fold higher risk of incident CRC during follow-up compared with individuals with no adenoma or low-risk adenomas,” they wrote. “There is also evidence that individuals with advanced SSLs have a three= to fourfold higher risk of CRC, compared with individuals with nonadvanced SSLs.”
Payers should cover costs
To further improve access to care, payers should cover the full costs of CRC screening because “copays and deductibles are barriers to screening and contribute to socioeconomic disparities,” that “disproportionately impact those with low income and lack of insurance,” according to Dr. Lieberman and colleagues.
They noted that the Affordable Care Act “eliminated copayments for preventive services,” yet a recent study showed that almost half of patients with commercial insurance and more than three-quarters of patients with Medicare still share some cost of CRC screening.
The investigators made clear that payers need to cover costs from start to finish, including “bowel preparation, facility and professional fees, anesthesia, and pathology,” as well as follow-up screening for high-risk patients identified by noninvasive methods.
“Noninvasive colorectal screening should be considered as programs with multiple steps, each of which, including follow-up colonoscopy if the test is positive, should be covered by payers without cost sharing as part of the screening continuum,” Dr. Lieberman and colleagues wrote.
Changes underway
According to Steven Itzkowitz, MD, professor of medicine and oncological sciences and director of the gastroenterology fellowship training program at the Icahn School of Medicine at Mount Sinai, New York, the AGA publication is important because it “consolidates many of the critical issues related to decreasing the burden of colorectal cancer in the United States.”
Dr. Itzkowitz noted that changes are already underway to eliminate cost as a barrier to screening.
“The good news is that, in the past year, the Departments of Health & Human Services, Labor, and Treasury declared that cost sharing should not be imposed, and plans are required to cover screening colonoscopy with polyp removal and colonoscopy that is performed to follow-up after an abnormal noninvasive CRC screening test,” Dr. Itzkowitz said in an interview. “Many plans are following suit, but it will take time for this coverage to take effect across all plans.”
For individual gastroenterologists who would like to do their part in reducing screening inequity, Dr. Itzkowitz suggested leveraging noninvasive testing, as the AGA recommends.
“This publication is the latest to call for using noninvasive, stool-based testing in addition to colonoscopy,” Dr. Itzkowitz said. “FIT and multitarget stool DNA tests all have proven efficacy in this regard, so gastroenterologists should have those conversations with their patients. GIs can also make it easier for patients to complete colonoscopy by developing patient navigation programs, direct access referrals, and systems for communicating with primary care providers for easier referrals and communicating colonoscopy results.”
Many practices are already instituting such improvements in response to the restrictions imposed by the COVID-19 pandemic, according to Dr. Itzkowitz.“These changes, plus better coverage by payers, will make a huge impact on health equity when it comes to colorectal cancer screening.”
The publication was supported by the AGA. The investigators disclosed relationships with Geneoscopy, ColoWrap, UniversalDx, and others. Dr. Itzkowitz disclosed no relevant conflicts of interest.
Groups interested in collaborating with AGA should contact Kathleen Teixeira, AGA Vice President, Public Policy and Advocacy, at [email protected].
FROM GASTROENTEROLOGY
AI-based CADe outperforms high-definition white light in colonoscopy
An artificial intelligence (AI)–based computer-aided polyp detection (CADe) system missed fewer adenomas, polyps, and sessile serrated lesions and identified more adenomas per colonoscopy than a high-definition white light (HDWL) colonoscopy, according to findings from a randomized study.
While adenoma detection by colonoscopy is associated with a reduced risk of interval colon cancer, detection rates of adenomas vary among physicians. AI approaches, such as machine learning and deep learning, may improve adenoma detection rates during colonoscopy and thus potentially improve outcomes for patients, suggested study authors led by Jeremy R. Glissen Brown, MD, of the Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, who reported their trial findings in Clinical Gastroenterology and Hepatology.
The investigators explained that, although AI approaches may offer benefits in adenoma detection, there have been no prospective data for U.S. populations on the efficacy of an AI-based CADe system for improving adenoma detection rates (ADRs) and reducing adenoma miss rates (AMRs). To overcome this research gap, the investigators performed a prospective, multicenter, single-blind randomized tandem colonoscopy study which assessed a deep learning–based CADe system in 232 patients.
Individuals who presented to the four included U.S. medical centers for either colorectal cancer screening or surveillance were randomly assigned to the CADe system colonoscopy first (n = 116) or HDWL colonoscopy first (n = 116). This was immediately followed by the other procedure, in tandem fashion, performed by the same endoscopist. AMR was the primary outcome of interest, while secondary outcomes were adenomas per colonoscopy (APC) and the miss rate of sessile serrated lesions (SSL).
The researchers excluded 9 patients, which resulted in a total patient population of 223 patients. Approximately 45.3% of the cohort was female, 67.7% were White, and 21% were Black. Most patients (60%) were indicated for primary colorectal cancer screening.
Compared with the HDWL-first group, the AMR was significantly lower in the CADe-first group (31.25% vs. 20.12%, respectively; P = .0247). The researchers commented that, although the CADe system resulted in a statistically significantly lower AMR, the rate still reflects missed adenomas.
Additionally, the CADe-first group had a lower SSL miss rate, compared with the HDWL-first group (7.14% vs. 42.11%, respectively; P = .0482). The researchers noted that their study is one of the first research studies to show that a computer-assisted polyp detection system can reduce the SSL miss rate. The first-pass APC was also significantly higher in the CADe-first group (1.19 vs. 0.90; P = .0323). No statistically significant difference was observed between the groups in regard to the first-pass ADR (50.44% for the CADe-first group vs. 43.64 % for the HDWL-first group; P = .3091).
A multivariate logistic regression analysis identified three significant factors predictive of missed polyps: use of HDWL first vs. the computer-assisted detection system first (odds ratio, 1.8830; P = .0214), age 65 years or younger (OR, 1.7390; P = .0451), and right colon vs. other location (OR, 1.7865; P = .0436).
According to the researchers, the study was not powered to identify differences in ADR, thereby limiting the interpretation of this analysis. In addition, the investigators noted that the tandem colonoscopy study design is limited in its generalizability to real-world clinical settings. Also, given that endoscopists were not blinded to group assignments while performing each withdrawal, the researchers commented that “it is possible that endoscopist performance was influenced by being observed or that endoscopists who participated for the length of the study became over-reliant on” the CADe system during withdrawal, resulting in an underestimate or overestimation of the system’s performance.
The authors concluded that their findings suggest that an AI-based CADe system with colonoscopy “has the potential to decrease interprovider variability in colonoscopy quality by reducing AMR, even in experienced providers.”
This was an investigator-initiated study, with research software and study funding provided by Wision AI. The investigators reported relationships with Wision AI, as well as Olympus, Fujifilm, and Medtronic.
Several randomized trials testing artificial intelligence (AI)–assisted colonoscopy showed improvement in adenoma detection. This study adds to the growing body of evidence that computer-aided detection (CADe) systems for adenoma augment adenoma detection rates, even among highly skilled endoscopists whose baseline ADRs are much higher than the currently recommended threshold for quality colonoscopy (25%).
This study also highlights the usefulness of CADe in aiding detection of sessile serrated lesions (SSL). Recognition of SSL appears to be challenging for trainees and the most likely type of missed large adenomas overall.

AI-based systems will enhance but will not replace the highly skilled operator. As this study pointed out, despite the superior ADR, adenomas were still missed by CADe. The main reason for this was that the missed polyps were not brought into the visual field by the operator. A combination of a CADe program and a distal attachment mucosa exposure device in the hands of an experienced endoscopists might bring the best results.
Monika Fischer, MD, is an associate professor of medicine at Indiana University, Indianapolis. She reported no relevant conflicts of interest.
Several randomized trials testing artificial intelligence (AI)–assisted colonoscopy showed improvement in adenoma detection. This study adds to the growing body of evidence that computer-aided detection (CADe) systems for adenoma augment adenoma detection rates, even among highly skilled endoscopists whose baseline ADRs are much higher than the currently recommended threshold for quality colonoscopy (25%).
This study also highlights the usefulness of CADe in aiding detection of sessile serrated lesions (SSL). Recognition of SSL appears to be challenging for trainees and the most likely type of missed large adenomas overall.
AI-based systems will enhance but will not replace the highly skilled operator. As this study pointed out, despite the superior ADR, adenomas were still missed by CADe. The main reason for this was that the missed polyps were not brought into the visual field by the operator. A combination of a CADe program and a distal attachment mucosa exposure device in the hands of an experienced endoscopists might bring the best results.
Monika Fischer, MD, is an associate professor of medicine at Indiana University, Indianapolis. She reported no relevant conflicts of interest.
Several randomized trials testing artificial intelligence (AI)–assisted colonoscopy showed improvement in adenoma detection. This study adds to the growing body of evidence that computer-aided detection (CADe) systems for adenoma augment adenoma detection rates, even among highly skilled endoscopists whose baseline ADRs are much higher than the currently recommended threshold for quality colonoscopy (25%).
This study also highlights the usefulness of CADe in aiding detection of sessile serrated lesions (SSL). Recognition of SSL appears to be challenging for trainees and the most likely type of missed large adenomas overall.
AI-based systems will enhance but will not replace the highly skilled operator. As this study pointed out, despite the superior ADR, adenomas were still missed by CADe. The main reason for this was that the missed polyps were not brought into the visual field by the operator. A combination of a CADe program and a distal attachment mucosa exposure device in the hands of an experienced endoscopists might bring the best results.
Monika Fischer, MD, is an associate professor of medicine at Indiana University, Indianapolis. She reported no relevant conflicts of interest.
An artificial intelligence (AI)–based computer-aided polyp detection (CADe) system missed fewer adenomas, polyps, and sessile serrated lesions and identified more adenomas per colonoscopy than a high-definition white light (HDWL) colonoscopy, according to findings from a randomized study.
While adenoma detection by colonoscopy is associated with a reduced risk of interval colon cancer, detection rates of adenomas vary among physicians. AI approaches, such as machine learning and deep learning, may improve adenoma detection rates during colonoscopy and thus potentially improve outcomes for patients, suggested study authors led by Jeremy R. Glissen Brown, MD, of the Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, who reported their trial findings in Clinical Gastroenterology and Hepatology.
The investigators explained that, although AI approaches may offer benefits in adenoma detection, there have been no prospective data for U.S. populations on the efficacy of an AI-based CADe system for improving adenoma detection rates (ADRs) and reducing adenoma miss rates (AMRs). To overcome this research gap, the investigators performed a prospective, multicenter, single-blind randomized tandem colonoscopy study which assessed a deep learning–based CADe system in 232 patients.
Individuals who presented to the four included U.S. medical centers for either colorectal cancer screening or surveillance were randomly assigned to the CADe system colonoscopy first (n = 116) or HDWL colonoscopy first (n = 116). This was immediately followed by the other procedure, in tandem fashion, performed by the same endoscopist. AMR was the primary outcome of interest, while secondary outcomes were adenomas per colonoscopy (APC) and the miss rate of sessile serrated lesions (SSL).
The researchers excluded 9 patients, which resulted in a total patient population of 223 patients. Approximately 45.3% of the cohort was female, 67.7% were White, and 21% were Black. Most patients (60%) were indicated for primary colorectal cancer screening.
Compared with the HDWL-first group, the AMR was significantly lower in the CADe-first group (31.25% vs. 20.12%, respectively; P = .0247). The researchers commented that, although the CADe system resulted in a statistically significantly lower AMR, the rate still reflects missed adenomas.
Additionally, the CADe-first group had a lower SSL miss rate, compared with the HDWL-first group (7.14% vs. 42.11%, respectively; P = .0482). The researchers noted that their study is one of the first research studies to show that a computer-assisted polyp detection system can reduce the SSL miss rate. The first-pass APC was also significantly higher in the CADe-first group (1.19 vs. 0.90; P = .0323). No statistically significant difference was observed between the groups in regard to the first-pass ADR (50.44% for the CADe-first group vs. 43.64 % for the HDWL-first group; P = .3091).
A multivariate logistic regression analysis identified three significant factors predictive of missed polyps: use of HDWL first vs. the computer-assisted detection system first (odds ratio, 1.8830; P = .0214), age 65 years or younger (OR, 1.7390; P = .0451), and right colon vs. other location (OR, 1.7865; P = .0436).
According to the researchers, the study was not powered to identify differences in ADR, thereby limiting the interpretation of this analysis. In addition, the investigators noted that the tandem colonoscopy study design is limited in its generalizability to real-world clinical settings. Also, given that endoscopists were not blinded to group assignments while performing each withdrawal, the researchers commented that “it is possible that endoscopist performance was influenced by being observed or that endoscopists who participated for the length of the study became over-reliant on” the CADe system during withdrawal, resulting in an underestimate or overestimation of the system’s performance.
The authors concluded that their findings suggest that an AI-based CADe system with colonoscopy “has the potential to decrease interprovider variability in colonoscopy quality by reducing AMR, even in experienced providers.”
This was an investigator-initiated study, with research software and study funding provided by Wision AI. The investigators reported relationships with Wision AI, as well as Olympus, Fujifilm, and Medtronic.
An artificial intelligence (AI)–based computer-aided polyp detection (CADe) system missed fewer adenomas, polyps, and sessile serrated lesions and identified more adenomas per colonoscopy than a high-definition white light (HDWL) colonoscopy, according to findings from a randomized study.
While adenoma detection by colonoscopy is associated with a reduced risk of interval colon cancer, detection rates of adenomas vary among physicians. AI approaches, such as machine learning and deep learning, may improve adenoma detection rates during colonoscopy and thus potentially improve outcomes for patients, suggested study authors led by Jeremy R. Glissen Brown, MD, of the Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, who reported their trial findings in Clinical Gastroenterology and Hepatology.
The investigators explained that, although AI approaches may offer benefits in adenoma detection, there have been no prospective data for U.S. populations on the efficacy of an AI-based CADe system for improving adenoma detection rates (ADRs) and reducing adenoma miss rates (AMRs). To overcome this research gap, the investigators performed a prospective, multicenter, single-blind randomized tandem colonoscopy study which assessed a deep learning–based CADe system in 232 patients.
Individuals who presented to the four included U.S. medical centers for either colorectal cancer screening or surveillance were randomly assigned to the CADe system colonoscopy first (n = 116) or HDWL colonoscopy first (n = 116). This was immediately followed by the other procedure, in tandem fashion, performed by the same endoscopist. AMR was the primary outcome of interest, while secondary outcomes were adenomas per colonoscopy (APC) and the miss rate of sessile serrated lesions (SSL).
The researchers excluded 9 patients, which resulted in a total patient population of 223 patients. Approximately 45.3% of the cohort was female, 67.7% were White, and 21% were Black. Most patients (60%) were indicated for primary colorectal cancer screening.
Compared with the HDWL-first group, the AMR was significantly lower in the CADe-first group (31.25% vs. 20.12%, respectively; P = .0247). The researchers commented that, although the CADe system resulted in a statistically significantly lower AMR, the rate still reflects missed adenomas.
Additionally, the CADe-first group had a lower SSL miss rate, compared with the HDWL-first group (7.14% vs. 42.11%, respectively; P = .0482). The researchers noted that their study is one of the first research studies to show that a computer-assisted polyp detection system can reduce the SSL miss rate. The first-pass APC was also significantly higher in the CADe-first group (1.19 vs. 0.90; P = .0323). No statistically significant difference was observed between the groups in regard to the first-pass ADR (50.44% for the CADe-first group vs. 43.64 % for the HDWL-first group; P = .3091).
A multivariate logistic regression analysis identified three significant factors predictive of missed polyps: use of HDWL first vs. the computer-assisted detection system first (odds ratio, 1.8830; P = .0214), age 65 years or younger (OR, 1.7390; P = .0451), and right colon vs. other location (OR, 1.7865; P = .0436).
According to the researchers, the study was not powered to identify differences in ADR, thereby limiting the interpretation of this analysis. In addition, the investigators noted that the tandem colonoscopy study design is limited in its generalizability to real-world clinical settings. Also, given that endoscopists were not blinded to group assignments while performing each withdrawal, the researchers commented that “it is possible that endoscopist performance was influenced by being observed or that endoscopists who participated for the length of the study became over-reliant on” the CADe system during withdrawal, resulting in an underestimate or overestimation of the system’s performance.
The authors concluded that their findings suggest that an AI-based CADe system with colonoscopy “has the potential to decrease interprovider variability in colonoscopy quality by reducing AMR, even in experienced providers.”
This was an investigator-initiated study, with research software and study funding provided by Wision AI. The investigators reported relationships with Wision AI, as well as Olympus, Fujifilm, and Medtronic.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY