User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
How can we make medical training less ‘toxic’?
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
Suicidality risk in youth at highest at night
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators found that suicidal ideation and attempts were lowest in the mornings and highest in the evenings, particularly among youth with higher levels of self-critical rumination.
“These are preliminary findings, and there is a need for more data, but they signal potentially that there’s a need for support, particularly at nighttime, and that there might be a potential of targeting self-critical rumination in daily lives of youth,” said lead researcher Anastacia Kudinova, PhD, with the department of psychiatry and human behavior, Alpert Medical School of Brown University, Providence, R.I.
The findings were presented at the late-breaker session at the annual meeting of the Associated Professional Sleep Societies.
Urgent need
Suicidal ideation (SI) is a “robust” predictor of suicidal behavior and, “alarmingly,” both suicidal ideation and suicidal behavior have been increasing, Dr. Kudinova said.
“There is an urgent need to describe proximal time-period risk factors for suicide so that we can identify who is at a greater suicide risk on the time scale of weeks, days, or even hours,” she told attendees.
The researchers asked 165 psychiatrically hospitalized youth aged 11-18 (72% female) about the time of day of their most recent suicide attempt.
More than half (58%) said it occurred in the evenings and nights, followed by daytime (35%) and mornings (7%).
They also assessed the timing of suicidal ideation at home in 61 youth aged 12-15 (61% female) who were discharged after a partial hospitalization program.
They did this using ecological momentary assessments (EMAs) three times a day over 2 weeks. EMAs study people’s thoughts and behavior in their daily lives by repeatedly collecting data in an individual’s normal environment at or close to the time they carry out that behavior.
As in the other sample, youth in this sample also experienced significantly more frequent suicidal ideation later in the day (P < .01).
There was also a significant moderating effect of self-criticism (P < .01), such that more self-critical youth evidenced the highest levels of suicidal ideation later in the day.
True variation or mechanics?
Reached for comment, Paul Nestadt, MD, with Johns Hopkins Bloomberg School of Public Health, Baltimore, noted that EMA is becoming “an interesting way to track high-resolution temporal variation in suicidal ideation and other psych symptoms.”
Dr. Nestadt, who was not involved in the study, said that “it’s not surprising” that the majority of youth attempted suicide in evenings and nights, “as adolescents are generally being supervised in a school setting during daytime hours. It may not be the fluctuation in suicidality that impacts attempt timing so much as the mechanics – it is very hard to attempt suicide in math class.”
The same may be true for the youth in the second sample who were in the partial hospital program. “During the day, they were in therapy groups where feelings of suicidal ideation would have been solicited and addressed in real time,” Dr. Nestadt noted.
“Again, suicidal ideation later in the day may be a practical effect of how they are occupied in the partial hospital program, as opposed to some inherent suicidal ideation increase linked to something endogenous, such as circadian rhythm or cortisol level rises. That said, we do often see more attempts in the evenings in adults as well,” he added.
A vulnerable time
Also weighing in, Casey O’Brien, PsyD, a psychologist in the department of psychiatry at Columbia University Irving Medical Center, New York, said the findings in this study “track” with what she sees in the clinic.
Teens often report in session that the “unstructured time of night – especially the time when they usually should be getting to bed but are kind of staying up – tends to be a very vulnerable time for them,” Dr. O’Brien said in an interview.
“It’s really nice to have research confirm a lot of what we see reported anecdotally from the teens we work with,” said Dr. O’Brien.
Dr. O’Brien heads the intensive adolescent dialectical behavior therapy (DBT) program at Columbia for young people struggling with mental health issues.
“Within the DBT framework, we try to really focus on accepting that this is a vulnerable time and then planning ahead for what the strategies are that they can use to help them transition to bed quickly and smoothly,” Dr. O’Brien said.
These strategies may include spending time with their parents before bed, reading, or building into their bedtime routines things that they find soothing and comforting, like taking a longer shower or having comfortable pajamas to change into, she explained.
“We also work a lot on sleep hygiene strategies to help develop a regular bedtime and have a consistent sleep-wake cycle. We also will plan ahead for using distress tolerance skills during times of emotional vulnerability,” Dr. O’Brien said.
The Columbia DBT program also offers phone coaching “so teens can reach out to a therapist for help using skills outside of a therapeutic hour, and we do find that we get more coaching calls closer to around bedtime,” Dr. O’Brien said.
Support for the study was provided by the National Institute of Mental Health and Bradley Hospital COBRE Center. Dr. Kudinova, Dr. Nestadt, and Dr. O’Brien have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2023
Ketamine may be a viable alternative to ECT for severe depression
“The take-home message right now is that if somebody is being referred for ECT, the treating clinician should think of offering ketamine first,” study investigator Amit Anand, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
The study was published online in the New England Journal of Medicine.
‘Preferred treatment’
More than one-third of cases of depression are treatment resistant, said Dr. Anand, who is also director of Psychiatry Translational Clinical Trials at Mass General Brigham. He noted that ECT has been the “gold standard for treating severe depression for over 80 years.”
He added that although ECT is very effective and is fast acting, “it requires anesthesia, can be socially stigmatizing, and is associated with memory problems following the treatment.”
An anesthetic agent, ketamine has been shown to have rapid antidepressant effects and does not cause memory loss or carry the stigma associated with ECT, he added. For these reasons, the investigators examined whether it may be a viable alternative to ECT.
To date, no large, head-to-head trials have compared ECT to intravenous ketamine. A recent meta-analysis showed that ECT was superior to ketamine for major depression, but the total number of patients included in the analysis was small, Dr. Anand said.
In addition, most of the participants in that trial were drawn from a single center. Approximately 95 patients were enrolled in each arm of the trial, which included some participants with features of psychosis. “ECT is very effective for depression associated with psychotic features, which may be one reason ECT had a better response in that trial,” said Dr. Anand.
The investigators compared ECT to ketamine in a larger sample that excluded patients with psychosis. They randomly assigned 403 patients at five clinical sites in a 1:1 ratio to receive either ketamine or ECT (n = 200 and 203, respectively; 53% and 49.3% women, respectively; aged 45.6 ± 14.8 and 47.1 ± 14.1 years, respectively).
Patients were required to have had an unsatisfactory response to two or more adequate trials of antidepressant treatment.
Prior to initiation of the assigned treatment, 38 patients withdrew, leaving 195 in the ketamine group and 170 in the ECT group.
Treatment was administered over a 3-week period, during which patients received either ECT three times per week or ketamine (0.5 mg/kg of body weight) twice per week.
The primary outcome was treatment response, defined as a decrease of 50% or more from baseline in the16-item Quick Inventory of Depressive Symptomatology–Self-Report (QIDS-SR-16). Secondary outcomes included scores on memory tests and patient-reported quality of life.
Patients who had a response were followed for 6 months after the initial treatment phase.
More research needed
Following the 3-week treatment period, a total of 55.4% patients who received ketamine and 41.2% of patients who underwent ECT responded to treatment, which translates into a difference of 14.2 percentage points (95% confidence interval, 3.9-24.2; P < .001) – a finding that fell within the noninferiority threshold set by the investigators.
ECT was associated with decreased memory recall after the 3 weeks of treatment, with a mean (standard deviation) decrease in the T-score for delayed recall on the Hopkins Verbal Learning Test–Revised of –0.9 (1.1) in the ketamine group vs. –9.7 (1.2) in the ECT group (difference, –1.8 points [–2.8 to –0.8]).
Remission, determined on the basis of QIDS-SR-16 score, occurred in 32% of the ketamine group and in 20% in the ECT group. Similar findings were seen on the Montgomery-Åsberg Depression Rating Scale.
Both groups showed significant improvements in quality of life, with changes of 12.3 and 12.9 points, respectively, on the 16-item Quality of Life Scale.
“ECT was associated with musculoskeletal adverse events, whereas ketamine was associated with dissociation,” the investigators note.
During the 6-month follow-up period, there were differences in relapse rates between the groups (defined as QIDS-SRS-16 score > 11). At 1 month, the rates were 19.0% for those receiving ketamine and 35.4% for those receiving ECT. At 3 months, the rates were 25.0% and 50.9%, respectively; at 6 months, the rates were 34.5% and 56.3%, respectively.
ECT has been shown to be effective for older adults, patients with MDD and psychosis, and in inpatient and research settings. Future studies are needed to determine the comparative effectiveness of ketamine in these populations, the authors note.
Not life-changing
In a comment, Dan Iosifescu, MD, professor of psychiatry, NYU Langone Health, New York, called it an “extraordinarily important and clinically relevant study, large, well-designed, and well-conducted.”
Dr. Iosifescu, director of the clinical research division, Nathan Kline Institute, Orangeburg, N.Y., who was not involved with the study, noted that the study wasn’t powered to determine whether one treatment was superior to the other, but rather it assessed noninferiority.
“The main point of this study is that the two treatments are largely equivalent, although numerically, ketamine was slightly associated with more beneficial outcomes and fewer cognitive side effects,” he said.
The findings suggest “that people who have no contraindications and are candidates for both ketamine and ECT – which is the vast majority of people with treatment-resistant depression – should consider getting ketamine first because it is somewhat easier in terms of side effects and logistics and consider ECT afterwards if the ketamine doesn’t work.”
In an accompanying editorial, Robert Freedman, MD, clinical professor, University of Colorado at Denver, Aurora, noted that although “3 weeks of lightened mood is undoubtedly a gift ... the results of this current trial suggests that the 3-week treatment was not life-changing,” since effects had largely worn off by 6 months in both groups.
Longer-term treatment with ketamine “increases the likelihood of both drug dependence and cognitive adverse effects, including dissociation, paranoia, and other psychotic symptoms,” Dr. Freedman said.
He recommends that informed consent documents be used to caution patients and clinicians considering ketamine “that temporary relief may come with longer-term costs.”
The study was supported by a grant from PCORI to Dr. Anand. Dr. Freedman has disclosed no relevant financial relationships. In the past 2 years, Dr. Iosifescu has been a consultant for Axsome, Allergan, Biogen, Clexio, Jazz, Neumora, Relmada, and Sage. He has also received a research grant from Otsuka.
A version of this article first appeared on Medscape.com.
“The take-home message right now is that if somebody is being referred for ECT, the treating clinician should think of offering ketamine first,” study investigator Amit Anand, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
The study was published online in the New England Journal of Medicine.
‘Preferred treatment’
More than one-third of cases of depression are treatment resistant, said Dr. Anand, who is also director of Psychiatry Translational Clinical Trials at Mass General Brigham. He noted that ECT has been the “gold standard for treating severe depression for over 80 years.”
He added that although ECT is very effective and is fast acting, “it requires anesthesia, can be socially stigmatizing, and is associated with memory problems following the treatment.”
An anesthetic agent, ketamine has been shown to have rapid antidepressant effects and does not cause memory loss or carry the stigma associated with ECT, he added. For these reasons, the investigators examined whether it may be a viable alternative to ECT.
To date, no large, head-to-head trials have compared ECT to intravenous ketamine. A recent meta-analysis showed that ECT was superior to ketamine for major depression, but the total number of patients included in the analysis was small, Dr. Anand said.
In addition, most of the participants in that trial were drawn from a single center. Approximately 95 patients were enrolled in each arm of the trial, which included some participants with features of psychosis. “ECT is very effective for depression associated with psychotic features, which may be one reason ECT had a better response in that trial,” said Dr. Anand.
The investigators compared ECT to ketamine in a larger sample that excluded patients with psychosis. They randomly assigned 403 patients at five clinical sites in a 1:1 ratio to receive either ketamine or ECT (n = 200 and 203, respectively; 53% and 49.3% women, respectively; aged 45.6 ± 14.8 and 47.1 ± 14.1 years, respectively).
Patients were required to have had an unsatisfactory response to two or more adequate trials of antidepressant treatment.
Prior to initiation of the assigned treatment, 38 patients withdrew, leaving 195 in the ketamine group and 170 in the ECT group.
Treatment was administered over a 3-week period, during which patients received either ECT three times per week or ketamine (0.5 mg/kg of body weight) twice per week.
The primary outcome was treatment response, defined as a decrease of 50% or more from baseline in the16-item Quick Inventory of Depressive Symptomatology–Self-Report (QIDS-SR-16). Secondary outcomes included scores on memory tests and patient-reported quality of life.
Patients who had a response were followed for 6 months after the initial treatment phase.
More research needed
Following the 3-week treatment period, a total of 55.4% patients who received ketamine and 41.2% of patients who underwent ECT responded to treatment, which translates into a difference of 14.2 percentage points (95% confidence interval, 3.9-24.2; P < .001) – a finding that fell within the noninferiority threshold set by the investigators.
ECT was associated with decreased memory recall after the 3 weeks of treatment, with a mean (standard deviation) decrease in the T-score for delayed recall on the Hopkins Verbal Learning Test–Revised of –0.9 (1.1) in the ketamine group vs. –9.7 (1.2) in the ECT group (difference, –1.8 points [–2.8 to –0.8]).
Remission, determined on the basis of QIDS-SR-16 score, occurred in 32% of the ketamine group and in 20% in the ECT group. Similar findings were seen on the Montgomery-Åsberg Depression Rating Scale.
Both groups showed significant improvements in quality of life, with changes of 12.3 and 12.9 points, respectively, on the 16-item Quality of Life Scale.
“ECT was associated with musculoskeletal adverse events, whereas ketamine was associated with dissociation,” the investigators note.
During the 6-month follow-up period, there were differences in relapse rates between the groups (defined as QIDS-SRS-16 score > 11). At 1 month, the rates were 19.0% for those receiving ketamine and 35.4% for those receiving ECT. At 3 months, the rates were 25.0% and 50.9%, respectively; at 6 months, the rates were 34.5% and 56.3%, respectively.
ECT has been shown to be effective for older adults, patients with MDD and psychosis, and in inpatient and research settings. Future studies are needed to determine the comparative effectiveness of ketamine in these populations, the authors note.
Not life-changing
In a comment, Dan Iosifescu, MD, professor of psychiatry, NYU Langone Health, New York, called it an “extraordinarily important and clinically relevant study, large, well-designed, and well-conducted.”
Dr. Iosifescu, director of the clinical research division, Nathan Kline Institute, Orangeburg, N.Y., who was not involved with the study, noted that the study wasn’t powered to determine whether one treatment was superior to the other, but rather it assessed noninferiority.
“The main point of this study is that the two treatments are largely equivalent, although numerically, ketamine was slightly associated with more beneficial outcomes and fewer cognitive side effects,” he said.
The findings suggest “that people who have no contraindications and are candidates for both ketamine and ECT – which is the vast majority of people with treatment-resistant depression – should consider getting ketamine first because it is somewhat easier in terms of side effects and logistics and consider ECT afterwards if the ketamine doesn’t work.”
In an accompanying editorial, Robert Freedman, MD, clinical professor, University of Colorado at Denver, Aurora, noted that although “3 weeks of lightened mood is undoubtedly a gift ... the results of this current trial suggests that the 3-week treatment was not life-changing,” since effects had largely worn off by 6 months in both groups.
Longer-term treatment with ketamine “increases the likelihood of both drug dependence and cognitive adverse effects, including dissociation, paranoia, and other psychotic symptoms,” Dr. Freedman said.
He recommends that informed consent documents be used to caution patients and clinicians considering ketamine “that temporary relief may come with longer-term costs.”
The study was supported by a grant from PCORI to Dr. Anand. Dr. Freedman has disclosed no relevant financial relationships. In the past 2 years, Dr. Iosifescu has been a consultant for Axsome, Allergan, Biogen, Clexio, Jazz, Neumora, Relmada, and Sage. He has also received a research grant from Otsuka.
A version of this article first appeared on Medscape.com.
“The take-home message right now is that if somebody is being referred for ECT, the treating clinician should think of offering ketamine first,” study investigator Amit Anand, MD, professor of psychiatry, Harvard Medical School, Boston, said in an interview.
The study was published online in the New England Journal of Medicine.
‘Preferred treatment’
More than one-third of cases of depression are treatment resistant, said Dr. Anand, who is also director of Psychiatry Translational Clinical Trials at Mass General Brigham. He noted that ECT has been the “gold standard for treating severe depression for over 80 years.”
He added that although ECT is very effective and is fast acting, “it requires anesthesia, can be socially stigmatizing, and is associated with memory problems following the treatment.”
An anesthetic agent, ketamine has been shown to have rapid antidepressant effects and does not cause memory loss or carry the stigma associated with ECT, he added. For these reasons, the investigators examined whether it may be a viable alternative to ECT.
To date, no large, head-to-head trials have compared ECT to intravenous ketamine. A recent meta-analysis showed that ECT was superior to ketamine for major depression, but the total number of patients included in the analysis was small, Dr. Anand said.
In addition, most of the participants in that trial were drawn from a single center. Approximately 95 patients were enrolled in each arm of the trial, which included some participants with features of psychosis. “ECT is very effective for depression associated with psychotic features, which may be one reason ECT had a better response in that trial,” said Dr. Anand.
The investigators compared ECT to ketamine in a larger sample that excluded patients with psychosis. They randomly assigned 403 patients at five clinical sites in a 1:1 ratio to receive either ketamine or ECT (n = 200 and 203, respectively; 53% and 49.3% women, respectively; aged 45.6 ± 14.8 and 47.1 ± 14.1 years, respectively).
Patients were required to have had an unsatisfactory response to two or more adequate trials of antidepressant treatment.
Prior to initiation of the assigned treatment, 38 patients withdrew, leaving 195 in the ketamine group and 170 in the ECT group.
Treatment was administered over a 3-week period, during which patients received either ECT three times per week or ketamine (0.5 mg/kg of body weight) twice per week.
The primary outcome was treatment response, defined as a decrease of 50% or more from baseline in the16-item Quick Inventory of Depressive Symptomatology–Self-Report (QIDS-SR-16). Secondary outcomes included scores on memory tests and patient-reported quality of life.
Patients who had a response were followed for 6 months after the initial treatment phase.
More research needed
Following the 3-week treatment period, a total of 55.4% patients who received ketamine and 41.2% of patients who underwent ECT responded to treatment, which translates into a difference of 14.2 percentage points (95% confidence interval, 3.9-24.2; P < .001) – a finding that fell within the noninferiority threshold set by the investigators.
ECT was associated with decreased memory recall after the 3 weeks of treatment, with a mean (standard deviation) decrease in the T-score for delayed recall on the Hopkins Verbal Learning Test–Revised of –0.9 (1.1) in the ketamine group vs. –9.7 (1.2) in the ECT group (difference, –1.8 points [–2.8 to –0.8]).
Remission, determined on the basis of QIDS-SR-16 score, occurred in 32% of the ketamine group and in 20% in the ECT group. Similar findings were seen on the Montgomery-Åsberg Depression Rating Scale.
Both groups showed significant improvements in quality of life, with changes of 12.3 and 12.9 points, respectively, on the 16-item Quality of Life Scale.
“ECT was associated with musculoskeletal adverse events, whereas ketamine was associated with dissociation,” the investigators note.
During the 6-month follow-up period, there were differences in relapse rates between the groups (defined as QIDS-SRS-16 score > 11). At 1 month, the rates were 19.0% for those receiving ketamine and 35.4% for those receiving ECT. At 3 months, the rates were 25.0% and 50.9%, respectively; at 6 months, the rates were 34.5% and 56.3%, respectively.
ECT has been shown to be effective for older adults, patients with MDD and psychosis, and in inpatient and research settings. Future studies are needed to determine the comparative effectiveness of ketamine in these populations, the authors note.
Not life-changing
In a comment, Dan Iosifescu, MD, professor of psychiatry, NYU Langone Health, New York, called it an “extraordinarily important and clinically relevant study, large, well-designed, and well-conducted.”
Dr. Iosifescu, director of the clinical research division, Nathan Kline Institute, Orangeburg, N.Y., who was not involved with the study, noted that the study wasn’t powered to determine whether one treatment was superior to the other, but rather it assessed noninferiority.
“The main point of this study is that the two treatments are largely equivalent, although numerically, ketamine was slightly associated with more beneficial outcomes and fewer cognitive side effects,” he said.
The findings suggest “that people who have no contraindications and are candidates for both ketamine and ECT – which is the vast majority of people with treatment-resistant depression – should consider getting ketamine first because it is somewhat easier in terms of side effects and logistics and consider ECT afterwards if the ketamine doesn’t work.”
In an accompanying editorial, Robert Freedman, MD, clinical professor, University of Colorado at Denver, Aurora, noted that although “3 weeks of lightened mood is undoubtedly a gift ... the results of this current trial suggests that the 3-week treatment was not life-changing,” since effects had largely worn off by 6 months in both groups.
Longer-term treatment with ketamine “increases the likelihood of both drug dependence and cognitive adverse effects, including dissociation, paranoia, and other psychotic symptoms,” Dr. Freedman said.
He recommends that informed consent documents be used to caution patients and clinicians considering ketamine “that temporary relief may come with longer-term costs.”
The study was supported by a grant from PCORI to Dr. Anand. Dr. Freedman has disclosed no relevant financial relationships. In the past 2 years, Dr. Iosifescu has been a consultant for Axsome, Allergan, Biogen, Clexio, Jazz, Neumora, Relmada, and Sage. He has also received a research grant from Otsuka.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Treatment-resistant depression? Don’t forget about MAOIs
SAN FRANCISCO – University of California, San Diego, psychiatrist Stephen M. Stahl, MD, PhD, has heard the scary stories about monoamine oxidase inhibitors (MAOIs): Patients supposedly need to be on restrictive diets free of culinary joys like cheese, beer, and wine; they can’t take cold medicines; and they can just forget about anesthesia for dental work or surgery.

Wrong, wrong, and wrong, Dr. Stahl told an audience at the annual meeting of the American Psychiatric Association. While the venerable antidepressants can transform the lives of patients with treatment-resistant depression, he said, .
“These are good options,” he said. “Everybody who prescribes these today, without exception, has seen patients respond after nothing else has – including ECT (electroconvulsive therapy).”
Still, MAOIs, which were first developed in the 1950s, remain little-used in the United States. While an average of six selective serotonin reuptake inhibitors (SSRIs) are prescribed every second in the United States each day, Dr. Stahl said, “there are only a few hundred MAOI prescribers for a few thousand patients.”
The main barrier to the use of the drugs is unfamiliarity, he said. Despite their low profile, they’re appropriate to use after failures of monotherapy with SSRIs/serotonin and norepinephrine reuptake inhibitors (SNRIs) and augmentation with atypical antipsychotics. And they can be used in conjunction with ketamine/esketamine and ECT, which are other options for treatment-resistant depression, he said.
As for the myths about MAOIs, Dr. Stahl said the drugs can indeed interact with tyramine, which is found in foods like cheese, beer, and wine. The interaction can lead to potentially fatal hypertensive crises, Dr. Stahl said, noting that patients should avoid aged cheeses, tap and unpasteurized beer, soy products, and certain other foods. (Patients taking 6 mg transdermal or low-dose oral selegiline can ignore these restrictions.)
But canned beer, certain wines, yogurt, fresh American cheese, mozzarella/pizza chain cheese, cream cheese, and fresh or processed meat/poultry/fish are fine, he said. “Selectively, you can have a pretty high tyramine diet,” he added, although it’s a good idea for patients to have a blood pressure monitor at home.
As for cold medicines, sympathomimetic decongestants and stimulants should be used cautiously with blood pressure monitoring or not at all, he said, but those with codeine or expectorants are OK. Dextromethorphan, a weak serotonin reuptake inhibitor in some cough medicine, should be avoided. However, antihistamines other than chlorpheniramine/brompheniramine are OK to use, he added, and they may be the ideal choice for cold relief.
As for anesthesia, he cautioned that local anesthetics with epinephrine and general anesthesia can disrupt blood pressure. Choose a local anesthetic that does not contain vasoconstrictors, he said, and if surgery with general anesthesia is needed, “you can wash [the MAOI] out if you want” ahead of time.
Benzodiazepines, mivacurium, rapacuronium, morphine, or codeine can be used cautiously, he said, in urgent or elective surgery in a patient on an MAOI.
As for other myths, he said tricyclic antidepressants and related drugs aren’t as troublesome as psychiatrists may assume. Clomipramine and imipramine should be avoided. But other tricyclic antidepressants can be used with caution.
As for painkillers, he said it’s not true that they must be avoided, although MAIOs shouldn’t be taken with meperidine, fentanyl, methadone, tramadol, or tapentadol. Other painkillers, including over-the-counter products like aspirin, NSAIDs, and acetaminophen, should be used with caution, he said. And expert guidance is advised for use of hydromorphone, morphine, oxycodone, or oxymorphone.
In the big picture, he noted, myths are so prevalent “that you have more calls from patients – and other doctors, dentists, and anesthesiologists – about MAO inhibitors then you will ever have about any other drug there.”
Columbia University, New York, psychiatrist Jonathan W. Stewart, MD, also spoke at the presentation on MAIOs at the APA conference. He recommended that colleagues consider the drugs if two or more antidepressants that work in different ways fail to provide relief after 4 weeks at a sufficient dose. Start low with one pill a day, he recommended, and seek full remission – no depressed mood – instead of simply “better.”
Ultimately, he said, “we do patients a disservice” if MAOIs aren’t considered in the appropriate patients.
Dr. Stahl discloses grant/research support (Acadia, Allergan/AbbVie, Avanir, Boehringer Ingelheim Braeburn, Daiichi Sankyo-Brazil Eisai, Eli Lilly, Harmony, Indivior, Intra-Cellular Therapies, Ironshore, Neurocrine, Otsuka, Pear Therapeutics, Sage, Shire Sunovion, Supernus, and Torrent), consultant/advisor support (Acadia, Alkermes, Allergan, AbbVie, Axsome, Clearview, Done, Eisai Pharmaceuticals, Gedeon Richter, Intra-Cellular Therapies, Karuna, Levo, Lundbeck, Neurocrine, Neurawell, Otsuka, Relmada, Sage, Sunovion, Supernus, Taliaz, Teva, Tris Pharma, and VistaGen), speakers bureau payments (Acadia, Lundbeck, Neurocrine, Otsuka, Servier, Sunovion, and Teva), and options in Genomind, Lipidio, Neurawell and Delix. Dr. Stewart discloses unspecified relationships with Eli Lilly, Pfizer, Merck, Boeringer- Ingleheim, Bristol-Myers, Sinolfi-Aventis, Amilyn, Novartis, Organon, GlaxoSmithKlein, Shire, and Somerset.
SAN FRANCISCO – University of California, San Diego, psychiatrist Stephen M. Stahl, MD, PhD, has heard the scary stories about monoamine oxidase inhibitors (MAOIs): Patients supposedly need to be on restrictive diets free of culinary joys like cheese, beer, and wine; they can’t take cold medicines; and they can just forget about anesthesia for dental work or surgery.
Wrong, wrong, and wrong, Dr. Stahl told an audience at the annual meeting of the American Psychiatric Association. While the venerable antidepressants can transform the lives of patients with treatment-resistant depression, he said, .
“These are good options,” he said. “Everybody who prescribes these today, without exception, has seen patients respond after nothing else has – including ECT (electroconvulsive therapy).”
Still, MAOIs, which were first developed in the 1950s, remain little-used in the United States. While an average of six selective serotonin reuptake inhibitors (SSRIs) are prescribed every second in the United States each day, Dr. Stahl said, “there are only a few hundred MAOI prescribers for a few thousand patients.”
The main barrier to the use of the drugs is unfamiliarity, he said. Despite their low profile, they’re appropriate to use after failures of monotherapy with SSRIs/serotonin and norepinephrine reuptake inhibitors (SNRIs) and augmentation with atypical antipsychotics. And they can be used in conjunction with ketamine/esketamine and ECT, which are other options for treatment-resistant depression, he said.
As for the myths about MAOIs, Dr. Stahl said the drugs can indeed interact with tyramine, which is found in foods like cheese, beer, and wine. The interaction can lead to potentially fatal hypertensive crises, Dr. Stahl said, noting that patients should avoid aged cheeses, tap and unpasteurized beer, soy products, and certain other foods. (Patients taking 6 mg transdermal or low-dose oral selegiline can ignore these restrictions.)
But canned beer, certain wines, yogurt, fresh American cheese, mozzarella/pizza chain cheese, cream cheese, and fresh or processed meat/poultry/fish are fine, he said. “Selectively, you can have a pretty high tyramine diet,” he added, although it’s a good idea for patients to have a blood pressure monitor at home.
As for cold medicines, sympathomimetic decongestants and stimulants should be used cautiously with blood pressure monitoring or not at all, he said, but those with codeine or expectorants are OK. Dextromethorphan, a weak serotonin reuptake inhibitor in some cough medicine, should be avoided. However, antihistamines other than chlorpheniramine/brompheniramine are OK to use, he added, and they may be the ideal choice for cold relief.
As for anesthesia, he cautioned that local anesthetics with epinephrine and general anesthesia can disrupt blood pressure. Choose a local anesthetic that does not contain vasoconstrictors, he said, and if surgery with general anesthesia is needed, “you can wash [the MAOI] out if you want” ahead of time.
Benzodiazepines, mivacurium, rapacuronium, morphine, or codeine can be used cautiously, he said, in urgent or elective surgery in a patient on an MAOI.
As for other myths, he said tricyclic antidepressants and related drugs aren’t as troublesome as psychiatrists may assume. Clomipramine and imipramine should be avoided. But other tricyclic antidepressants can be used with caution.
As for painkillers, he said it’s not true that they must be avoided, although MAIOs shouldn’t be taken with meperidine, fentanyl, methadone, tramadol, or tapentadol. Other painkillers, including over-the-counter products like aspirin, NSAIDs, and acetaminophen, should be used with caution, he said. And expert guidance is advised for use of hydromorphone, morphine, oxycodone, or oxymorphone.
In the big picture, he noted, myths are so prevalent “that you have more calls from patients – and other doctors, dentists, and anesthesiologists – about MAO inhibitors then you will ever have about any other drug there.”
Columbia University, New York, psychiatrist Jonathan W. Stewart, MD, also spoke at the presentation on MAIOs at the APA conference. He recommended that colleagues consider the drugs if two or more antidepressants that work in different ways fail to provide relief after 4 weeks at a sufficient dose. Start low with one pill a day, he recommended, and seek full remission – no depressed mood – instead of simply “better.”
Ultimately, he said, “we do patients a disservice” if MAOIs aren’t considered in the appropriate patients.
Dr. Stahl discloses grant/research support (Acadia, Allergan/AbbVie, Avanir, Boehringer Ingelheim Braeburn, Daiichi Sankyo-Brazil Eisai, Eli Lilly, Harmony, Indivior, Intra-Cellular Therapies, Ironshore, Neurocrine, Otsuka, Pear Therapeutics, Sage, Shire Sunovion, Supernus, and Torrent), consultant/advisor support (Acadia, Alkermes, Allergan, AbbVie, Axsome, Clearview, Done, Eisai Pharmaceuticals, Gedeon Richter, Intra-Cellular Therapies, Karuna, Levo, Lundbeck, Neurocrine, Neurawell, Otsuka, Relmada, Sage, Sunovion, Supernus, Taliaz, Teva, Tris Pharma, and VistaGen), speakers bureau payments (Acadia, Lundbeck, Neurocrine, Otsuka, Servier, Sunovion, and Teva), and options in Genomind, Lipidio, Neurawell and Delix. Dr. Stewart discloses unspecified relationships with Eli Lilly, Pfizer, Merck, Boeringer- Ingleheim, Bristol-Myers, Sinolfi-Aventis, Amilyn, Novartis, Organon, GlaxoSmithKlein, Shire, and Somerset.
SAN FRANCISCO – University of California, San Diego, psychiatrist Stephen M. Stahl, MD, PhD, has heard the scary stories about monoamine oxidase inhibitors (MAOIs): Patients supposedly need to be on restrictive diets free of culinary joys like cheese, beer, and wine; they can’t take cold medicines; and they can just forget about anesthesia for dental work or surgery.
Wrong, wrong, and wrong, Dr. Stahl told an audience at the annual meeting of the American Psychiatric Association. While the venerable antidepressants can transform the lives of patients with treatment-resistant depression, he said, .
“These are good options,” he said. “Everybody who prescribes these today, without exception, has seen patients respond after nothing else has – including ECT (electroconvulsive therapy).”
Still, MAOIs, which were first developed in the 1950s, remain little-used in the United States. While an average of six selective serotonin reuptake inhibitors (SSRIs) are prescribed every second in the United States each day, Dr. Stahl said, “there are only a few hundred MAOI prescribers for a few thousand patients.”
The main barrier to the use of the drugs is unfamiliarity, he said. Despite their low profile, they’re appropriate to use after failures of monotherapy with SSRIs/serotonin and norepinephrine reuptake inhibitors (SNRIs) and augmentation with atypical antipsychotics. And they can be used in conjunction with ketamine/esketamine and ECT, which are other options for treatment-resistant depression, he said.
As for the myths about MAOIs, Dr. Stahl said the drugs can indeed interact with tyramine, which is found in foods like cheese, beer, and wine. The interaction can lead to potentially fatal hypertensive crises, Dr. Stahl said, noting that patients should avoid aged cheeses, tap and unpasteurized beer, soy products, and certain other foods. (Patients taking 6 mg transdermal or low-dose oral selegiline can ignore these restrictions.)
But canned beer, certain wines, yogurt, fresh American cheese, mozzarella/pizza chain cheese, cream cheese, and fresh or processed meat/poultry/fish are fine, he said. “Selectively, you can have a pretty high tyramine diet,” he added, although it’s a good idea for patients to have a blood pressure monitor at home.
As for cold medicines, sympathomimetic decongestants and stimulants should be used cautiously with blood pressure monitoring or not at all, he said, but those with codeine or expectorants are OK. Dextromethorphan, a weak serotonin reuptake inhibitor in some cough medicine, should be avoided. However, antihistamines other than chlorpheniramine/brompheniramine are OK to use, he added, and they may be the ideal choice for cold relief.
As for anesthesia, he cautioned that local anesthetics with epinephrine and general anesthesia can disrupt blood pressure. Choose a local anesthetic that does not contain vasoconstrictors, he said, and if surgery with general anesthesia is needed, “you can wash [the MAOI] out if you want” ahead of time.
Benzodiazepines, mivacurium, rapacuronium, morphine, or codeine can be used cautiously, he said, in urgent or elective surgery in a patient on an MAOI.
As for other myths, he said tricyclic antidepressants and related drugs aren’t as troublesome as psychiatrists may assume. Clomipramine and imipramine should be avoided. But other tricyclic antidepressants can be used with caution.
As for painkillers, he said it’s not true that they must be avoided, although MAIOs shouldn’t be taken with meperidine, fentanyl, methadone, tramadol, or tapentadol. Other painkillers, including over-the-counter products like aspirin, NSAIDs, and acetaminophen, should be used with caution, he said. And expert guidance is advised for use of hydromorphone, morphine, oxycodone, or oxymorphone.
In the big picture, he noted, myths are so prevalent “that you have more calls from patients – and other doctors, dentists, and anesthesiologists – about MAO inhibitors then you will ever have about any other drug there.”
Columbia University, New York, psychiatrist Jonathan W. Stewart, MD, also spoke at the presentation on MAIOs at the APA conference. He recommended that colleagues consider the drugs if two or more antidepressants that work in different ways fail to provide relief after 4 weeks at a sufficient dose. Start low with one pill a day, he recommended, and seek full remission – no depressed mood – instead of simply “better.”
Ultimately, he said, “we do patients a disservice” if MAOIs aren’t considered in the appropriate patients.
Dr. Stahl discloses grant/research support (Acadia, Allergan/AbbVie, Avanir, Boehringer Ingelheim Braeburn, Daiichi Sankyo-Brazil Eisai, Eli Lilly, Harmony, Indivior, Intra-Cellular Therapies, Ironshore, Neurocrine, Otsuka, Pear Therapeutics, Sage, Shire Sunovion, Supernus, and Torrent), consultant/advisor support (Acadia, Alkermes, Allergan, AbbVie, Axsome, Clearview, Done, Eisai Pharmaceuticals, Gedeon Richter, Intra-Cellular Therapies, Karuna, Levo, Lundbeck, Neurocrine, Neurawell, Otsuka, Relmada, Sage, Sunovion, Supernus, Taliaz, Teva, Tris Pharma, and VistaGen), speakers bureau payments (Acadia, Lundbeck, Neurocrine, Otsuka, Servier, Sunovion, and Teva), and options in Genomind, Lipidio, Neurawell and Delix. Dr. Stewart discloses unspecified relationships with Eli Lilly, Pfizer, Merck, Boeringer- Ingleheim, Bristol-Myers, Sinolfi-Aventis, Amilyn, Novartis, Organon, GlaxoSmithKlein, Shire, and Somerset.
AT APA 2023

Unlocking the riddle of REM sleep
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.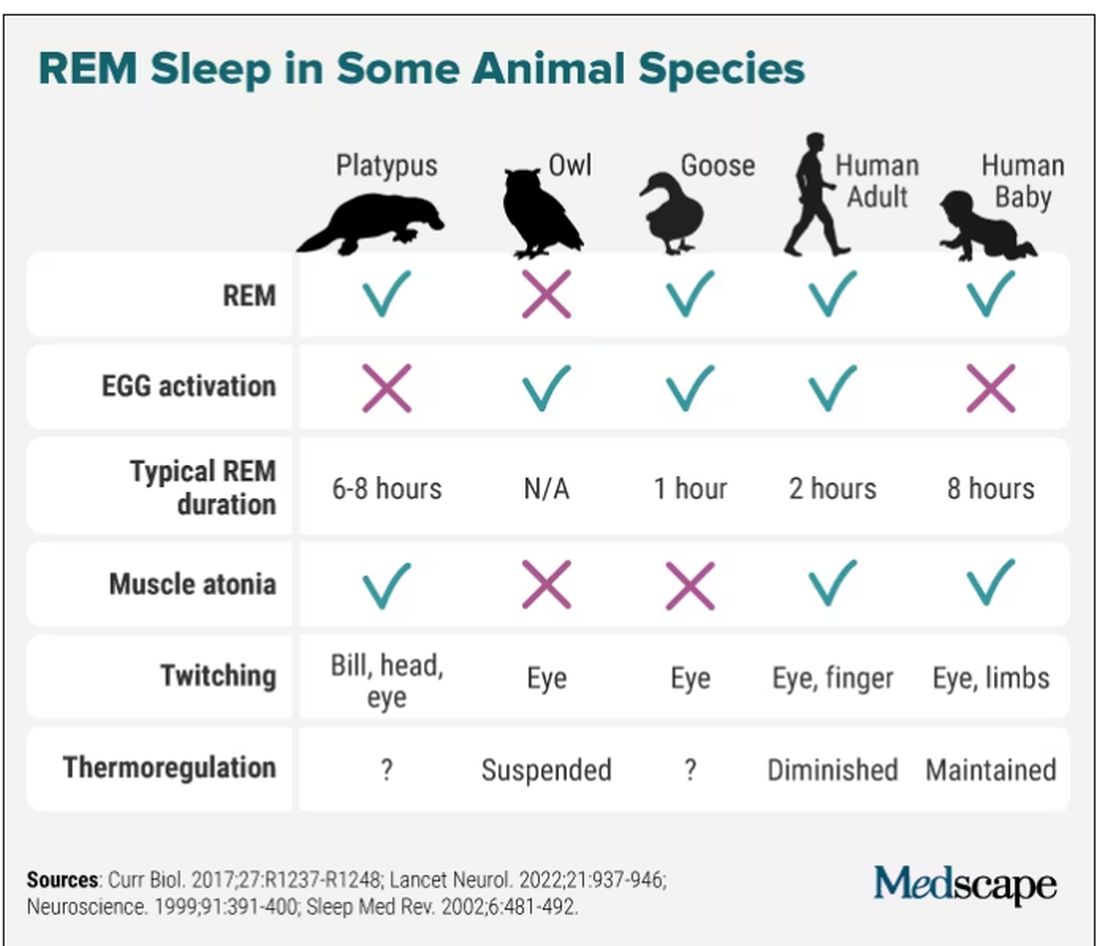
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Music therapy helps motivate patients with schizophrenia
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”

She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.

The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”
She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.
The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”
She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.
The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
AT APA 2023
Community workers may address psychiatrist shortage
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.

A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.

“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.
A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.
“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.
A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.
“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM APA 2023
U.S. psychiatrist shortage causing months-long wait times
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.

“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.

“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.
“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.
“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.
“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.
“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Psychiatrists: Don’t fear clozapine in treatment-resistant schizophrenia
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.

T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.
T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.
T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
AT APA 2023
Higher buprenorphine doses help OUD patients stay in treatment
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
AT APA 2023