User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Number of cervical cancer screenings linked to higher preterm birth risk
For each additional recommended screening before childbirth, there was a direct increase in absolute PTD risk of 0.073 (95% confidence interval, 0.026-0.120), according to a study led by Rebecca A. Bromley-Dulfano, MS, an MD candidate at Stanford (Calif.) University and a PhD candidate in health policy at Harvard University, Cambridge, Mass.

There was no significant change in very preterm delivery (VPTD) risk, but mothers with hypertension or diabetes were at higher PTD risk.
Women in this younger age group are more prone to PTD. According to the study’s estimate, an additional 73 PTDs per 100,000 women could be expected for every 1 additional recommended screening before childbirth. For the year 2018, that translated to an estimated 1,348 PTDs that could have been averted, with reduced screening requirements (3% relative reduction).
“If you screen someone for cervical cancer and find a cervical lesion, the possible next steps can include a biopsy and an excisional procedure to remove the lesion,” Ms. Bromley-Dulfano explained, “and these procedures which remove a small (mostly diseased) part of the cervix have been shown to slightly increase the risk of PTD. Particularly in young individuals with a cervix who are known to have high rates of lesion regression and who have more potential childbearing years ahead of them, it is important to weigh the oncological benefits with the adverse birth outcome risks.”
Young women are more likely to have false-positive results on Papanicolaou tests and lesion regression within 2 years but may undergo unnecessary treatment, the authors noted.
Cervical excision procedures have previously been associated in clinical trials with an increase in PTB risk.
In their 2017 decision model in a fictive cohort, for example, Kamphuis and colleagues found the most intensive screening program was associated with an increase in maternal life years of 9%, a decrease in cervical cancer incidence of 67%, and a decrease in cervical cancer deaths of 75%. But those gains came at the cost of 250% more preterm births, compared with the least intensive program.
“These results can be used in future simulation models integrating oncological trade-offs to help ascertain optimal screening strategies,” the researchers wrote.
While the optimal screening strategy must trade off the oncologic benefits of cancer detection against the neonatal harms of overtreatment, the ideal age of cervical cancer screening onset and frequency remain uncertain, the authors noted. Recent American Cancer Society guidelines recommending less frequent screening for some diverge from those of other societies.
“The first and foremost priority is for gynecologists to continue to have individualized conversations with patients about all of the benefits and risks of procedures that patients undergo and to understand the benefits and risks influencing screening guidelines,” Ms. Bromley-Dulfano said.
Cross-sectional study
The study used data from the Centers for Disease Control and Prevention’s National Center for Health Statistics to analyze associations between cervical cancer screening guidelines and birth outcomes women who had a singleton nulliparous birth from 19916 to 2018. Gestational age and maternal characteristics were drawn from birth certificates.
The mean age of the 11,333,151 multiracial cohort of women was 20.9 years, and 6.8% had hypertension or diabetes. The mean number of guideline-recommended screenings by time of childbirth was 2.4. Overall, PTD and very PTD occurred in 1,140,490 individuals (10.1%) and 333,040 (2.9%) of births, respectively.
Those with hypertension or diabetes had a somewhat higher PTD risk: 0.26% (95% CI, 0.11-0.4) versus 0.06% (95% CI, 0.01-0.10; Wald test, P < .001).

Offering an outsider’s perspective on the analysis, ob.gyn. Fidel A. Valea, MD, director of gynecologic oncology at the Northwell Health Cancer Institute in New Hyde Park, N.Y., urged caution in drawing conclusions from large population analyses such as this.
“This study had over 11 million data points. Often these large numbers will show statistical differences that are not clinically significant,” he said in an interview. He noted that while small studies have shown a possible impact of frequent Pap tests on cervical function, “this is not 100% proven. Research from Texas showed that screening made a difference only in cases of dysplasia.”
Dr. Valea also noted that screening guidelines have already changed over the lengthy time span of the study and do reflect the concerns of the study authors.
“We know that the HPV virus is cleared more readily by young women than older women and so we have made adjustments and test them less frequently and we test them less early.” He added that conservative options are recommended even in the case of dysplasia.
In defense of the Pap smear test, he added: “It has virtually wiped out cervical cancer in the U.S., bringing it from No. 1 to No. 13.” While broadening HPV vaccination programs may impact guidelines in the future, “vaccination is still in its infancy. We have to wait until women have lived long to enough to see an impact.”
As to why this age group is more vulnerable to PTD, Dr. Valea said, “It’s likely multifactorial, with lifestyle and other factors involved.” Although based on U.S. data, the authors said their results may be useful for other public health entities, particularly in countries where cervical cancer is considerably more prevalent.
This work received no specific funding. The authors and Dr. Valea disclosed no competing interests.
For each additional recommended screening before childbirth, there was a direct increase in absolute PTD risk of 0.073 (95% confidence interval, 0.026-0.120), according to a study led by Rebecca A. Bromley-Dulfano, MS, an MD candidate at Stanford (Calif.) University and a PhD candidate in health policy at Harvard University, Cambridge, Mass.
There was no significant change in very preterm delivery (VPTD) risk, but mothers with hypertension or diabetes were at higher PTD risk.
Women in this younger age group are more prone to PTD. According to the study’s estimate, an additional 73 PTDs per 100,000 women could be expected for every 1 additional recommended screening before childbirth. For the year 2018, that translated to an estimated 1,348 PTDs that could have been averted, with reduced screening requirements (3% relative reduction).
“If you screen someone for cervical cancer and find a cervical lesion, the possible next steps can include a biopsy and an excisional procedure to remove the lesion,” Ms. Bromley-Dulfano explained, “and these procedures which remove a small (mostly diseased) part of the cervix have been shown to slightly increase the risk of PTD. Particularly in young individuals with a cervix who are known to have high rates of lesion regression and who have more potential childbearing years ahead of them, it is important to weigh the oncological benefits with the adverse birth outcome risks.”
Young women are more likely to have false-positive results on Papanicolaou tests and lesion regression within 2 years but may undergo unnecessary treatment, the authors noted.
Cervical excision procedures have previously been associated in clinical trials with an increase in PTB risk.
In their 2017 decision model in a fictive cohort, for example, Kamphuis and colleagues found the most intensive screening program was associated with an increase in maternal life years of 9%, a decrease in cervical cancer incidence of 67%, and a decrease in cervical cancer deaths of 75%. But those gains came at the cost of 250% more preterm births, compared with the least intensive program.
“These results can be used in future simulation models integrating oncological trade-offs to help ascertain optimal screening strategies,” the researchers wrote.
While the optimal screening strategy must trade off the oncologic benefits of cancer detection against the neonatal harms of overtreatment, the ideal age of cervical cancer screening onset and frequency remain uncertain, the authors noted. Recent American Cancer Society guidelines recommending less frequent screening for some diverge from those of other societies.
“The first and foremost priority is for gynecologists to continue to have individualized conversations with patients about all of the benefits and risks of procedures that patients undergo and to understand the benefits and risks influencing screening guidelines,” Ms. Bromley-Dulfano said.
Cross-sectional study
The study used data from the Centers for Disease Control and Prevention’s National Center for Health Statistics to analyze associations between cervical cancer screening guidelines and birth outcomes women who had a singleton nulliparous birth from 19916 to 2018. Gestational age and maternal characteristics were drawn from birth certificates.
The mean age of the 11,333,151 multiracial cohort of women was 20.9 years, and 6.8% had hypertension or diabetes. The mean number of guideline-recommended screenings by time of childbirth was 2.4. Overall, PTD and very PTD occurred in 1,140,490 individuals (10.1%) and 333,040 (2.9%) of births, respectively.
Those with hypertension or diabetes had a somewhat higher PTD risk: 0.26% (95% CI, 0.11-0.4) versus 0.06% (95% CI, 0.01-0.10; Wald test, P < .001).
Offering an outsider’s perspective on the analysis, ob.gyn. Fidel A. Valea, MD, director of gynecologic oncology at the Northwell Health Cancer Institute in New Hyde Park, N.Y., urged caution in drawing conclusions from large population analyses such as this.
“This study had over 11 million data points. Often these large numbers will show statistical differences that are not clinically significant,” he said in an interview. He noted that while small studies have shown a possible impact of frequent Pap tests on cervical function, “this is not 100% proven. Research from Texas showed that screening made a difference only in cases of dysplasia.”
Dr. Valea also noted that screening guidelines have already changed over the lengthy time span of the study and do reflect the concerns of the study authors.
“We know that the HPV virus is cleared more readily by young women than older women and so we have made adjustments and test them less frequently and we test them less early.” He added that conservative options are recommended even in the case of dysplasia.
In defense of the Pap smear test, he added: “It has virtually wiped out cervical cancer in the U.S., bringing it from No. 1 to No. 13.” While broadening HPV vaccination programs may impact guidelines in the future, “vaccination is still in its infancy. We have to wait until women have lived long to enough to see an impact.”
As to why this age group is more vulnerable to PTD, Dr. Valea said, “It’s likely multifactorial, with lifestyle and other factors involved.” Although based on U.S. data, the authors said their results may be useful for other public health entities, particularly in countries where cervical cancer is considerably more prevalent.
This work received no specific funding. The authors and Dr. Valea disclosed no competing interests.
For each additional recommended screening before childbirth, there was a direct increase in absolute PTD risk of 0.073 (95% confidence interval, 0.026-0.120), according to a study led by Rebecca A. Bromley-Dulfano, MS, an MD candidate at Stanford (Calif.) University and a PhD candidate in health policy at Harvard University, Cambridge, Mass.
There was no significant change in very preterm delivery (VPTD) risk, but mothers with hypertension or diabetes were at higher PTD risk.
Women in this younger age group are more prone to PTD. According to the study’s estimate, an additional 73 PTDs per 100,000 women could be expected for every 1 additional recommended screening before childbirth. For the year 2018, that translated to an estimated 1,348 PTDs that could have been averted, with reduced screening requirements (3% relative reduction).
“If you screen someone for cervical cancer and find a cervical lesion, the possible next steps can include a biopsy and an excisional procedure to remove the lesion,” Ms. Bromley-Dulfano explained, “and these procedures which remove a small (mostly diseased) part of the cervix have been shown to slightly increase the risk of PTD. Particularly in young individuals with a cervix who are known to have high rates of lesion regression and who have more potential childbearing years ahead of them, it is important to weigh the oncological benefits with the adverse birth outcome risks.”
Young women are more likely to have false-positive results on Papanicolaou tests and lesion regression within 2 years but may undergo unnecessary treatment, the authors noted.
Cervical excision procedures have previously been associated in clinical trials with an increase in PTB risk.
In their 2017 decision model in a fictive cohort, for example, Kamphuis and colleagues found the most intensive screening program was associated with an increase in maternal life years of 9%, a decrease in cervical cancer incidence of 67%, and a decrease in cervical cancer deaths of 75%. But those gains came at the cost of 250% more preterm births, compared with the least intensive program.
“These results can be used in future simulation models integrating oncological trade-offs to help ascertain optimal screening strategies,” the researchers wrote.
While the optimal screening strategy must trade off the oncologic benefits of cancer detection against the neonatal harms of overtreatment, the ideal age of cervical cancer screening onset and frequency remain uncertain, the authors noted. Recent American Cancer Society guidelines recommending less frequent screening for some diverge from those of other societies.
“The first and foremost priority is for gynecologists to continue to have individualized conversations with patients about all of the benefits and risks of procedures that patients undergo and to understand the benefits and risks influencing screening guidelines,” Ms. Bromley-Dulfano said.
Cross-sectional study
The study used data from the Centers for Disease Control and Prevention’s National Center for Health Statistics to analyze associations between cervical cancer screening guidelines and birth outcomes women who had a singleton nulliparous birth from 19916 to 2018. Gestational age and maternal characteristics were drawn from birth certificates.
The mean age of the 11,333,151 multiracial cohort of women was 20.9 years, and 6.8% had hypertension or diabetes. The mean number of guideline-recommended screenings by time of childbirth was 2.4. Overall, PTD and very PTD occurred in 1,140,490 individuals (10.1%) and 333,040 (2.9%) of births, respectively.
Those with hypertension or diabetes had a somewhat higher PTD risk: 0.26% (95% CI, 0.11-0.4) versus 0.06% (95% CI, 0.01-0.10; Wald test, P < .001).
Offering an outsider’s perspective on the analysis, ob.gyn. Fidel A. Valea, MD, director of gynecologic oncology at the Northwell Health Cancer Institute in New Hyde Park, N.Y., urged caution in drawing conclusions from large population analyses such as this.
“This study had over 11 million data points. Often these large numbers will show statistical differences that are not clinically significant,” he said in an interview. He noted that while small studies have shown a possible impact of frequent Pap tests on cervical function, “this is not 100% proven. Research from Texas showed that screening made a difference only in cases of dysplasia.”
Dr. Valea also noted that screening guidelines have already changed over the lengthy time span of the study and do reflect the concerns of the study authors.
“We know that the HPV virus is cleared more readily by young women than older women and so we have made adjustments and test them less frequently and we test them less early.” He added that conservative options are recommended even in the case of dysplasia.
In defense of the Pap smear test, he added: “It has virtually wiped out cervical cancer in the U.S., bringing it from No. 1 to No. 13.” While broadening HPV vaccination programs may impact guidelines in the future, “vaccination is still in its infancy. We have to wait until women have lived long to enough to see an impact.”
As to why this age group is more vulnerable to PTD, Dr. Valea said, “It’s likely multifactorial, with lifestyle and other factors involved.” Although based on U.S. data, the authors said their results may be useful for other public health entities, particularly in countries where cervical cancer is considerably more prevalent.
This work received no specific funding. The authors and Dr. Valea disclosed no competing interests.
FROM JAMA HEALTH FORUM
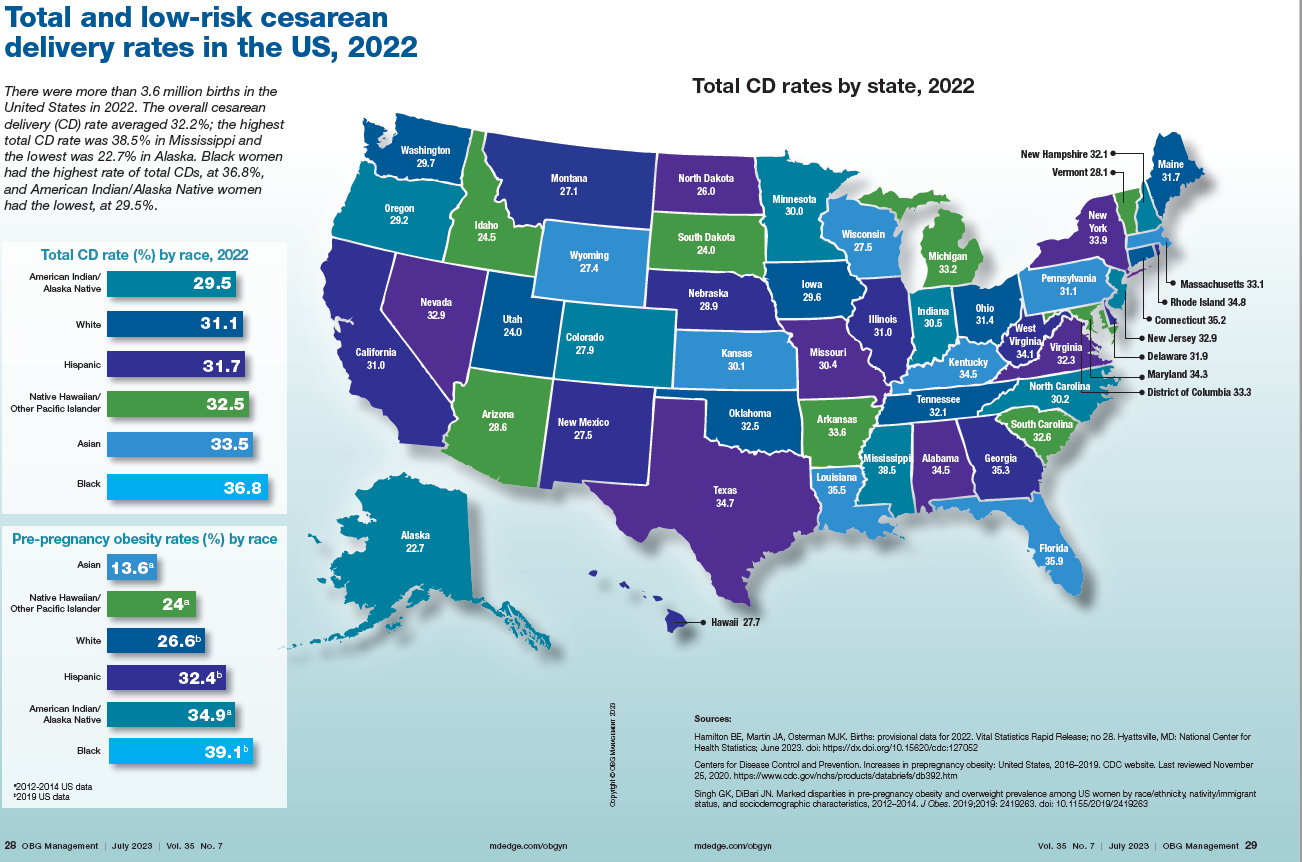
Total cesarean delivery rates in the US, 2022
News & Perspectives from Ob.Gyn. News
REPRODUCTIVE ROUNDS
Applications of office hysteroscopy for the infertility patient
What role does diagnostic office hysteroscopy play in an infertility evaluation?
Performed properly, office hysteroscopy can transform your practice by accurately, gently, and safely assessing the uterine cavity as well as assessing tubal patency.
More specifically, hysteroscopy is the gold standard for assessing the uterine cavity. The sensitivity, specificity, and positive predictive and negative predictive values of hysterosalpingography (HSG) in evaluating uterine cavity abnormalities were 44.83%; 86.67%; 56.52%; and 80.25%, respectively. Given the poor sensitivity of HSG, a diagnosis of endometrial polyps and/or chronic endometritis is more likely to be missed.
Our crossover trial comparing HSG to office hysteroscopy for tubal patency showed that women were 110 times more likely to have the maximum level of pain with HSG than diagnostic hysteroscopy when using a 2.8-mm flexible hysteroscope. Further, infection rates and vasovagal events were far lower with hysteroscopy.
Finally, compared with HSG, we showed 98%-100% sensitivity and 84% specificity for tubal occlusion with hysteroscopy by air-infused saline. Conversely, HSG typically is associated with 76%-96% sensitivity and 67%-100% specificity. Additionally, we can often perform diagnostic hysteroscopies for approximately $35 per procedure for total fixed and disposable equipment costs.
https://www.mdedge.com/obgyn/reproductive-rounds
FEATURE
Is ChatGPT a friend or foe of medical publishing?
Researchers may use artificial intelligence (AI) language models such as ChatGPT to write and revise scientific manuscripts, according to a new announcement from the International Committee of Medical Journal Editors. These tools should not be listed as authors, and researchers must denote how AI-assisted technologies were used, the committee said.
These new guidelines are the latest effort for medical journals to define policies for using these large-scale language models (LLMs) in scientific publication. While these AI-assisted tools can help with tasks such as writing, analyzing data, catching mistakes, and more, they are also prone to errors, noted Casey Greene, PhD, a professor of biomedical informatics at the University of Colorado at Denver, Aurora.
At the same time, experts argue that these AI tools could have a positive impact on the field by limiting some of the linguistic disparities in scientific publishing as well as alleviating the burden of some monotonous or mechanical tasks that come along with manuscript writing.
What experts can agree on, though, is that the use of AI tools is here to stay. “This is going to become a common tool,” Dr. Greene said.
A change in medical publishing
OpenAI released ChatGPT in November 2022. In its own words, ChatGPT is “a deep learning model that has been trained on a massive amount of text data to understand and generate humanlike text.” Enter a question or a prompt, and it will respond. For example, when asked how the AI tool can be used in scientific publishing, ChatGPT responded:
“ChatGPT can aid scientific publishing by generating ideas, clarifying concepts, conducting preliminary literature reviews, providing proofreading and editing suggestions, and assisting with outlining and organizing scientific papers. However, it should be used as a supportive tool alongside domain expertise and validation from trusted scientific sources.”
Just a few months after ChatGPT became available, researchers began using this tool in their own work. One individual, Som Biswas, MD, a radiologist at the University of Tennessee Health Science Center in Memphis, reportedly used ChatGPT to author 16 scientific articles in just 4 months, according to the Daily Beast. Five of these articles have been published in four different journals. Dr. Biswas declined to be interviewed for this article.
There were also reports of papers with ChatGPT as one of the listed authors, which sparked backlash. In response, JAMA, Nature, and Science all published editorials in January outlining their policies for using ChatGPT and other large language models in the scientific authoring process. Editors from the journals of the American College of Cardiology and the American College of Rheumatology also updated their policies to reflect the influence of AI authoring tools.
The consensus is that AI has no place on the author byline.
Continue to: FROM THE JOURNALS...
FROM THE JOURNALS
Review supports continued mask-wearing in health care visits
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
“Masking in interactions between patients and health care personnel should continue to receive serious consideration as a patient safety measure,” Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
https://www.mdedge.com/obgyn/covid-19-updates
CONFERENCE COVERAGE
A ‘one-stop shop’: New guidance on hormones and aging
A new statement from the Endocrine Society on hormones and aging highlights the differences between normal aging and disease, and when treatment is and isn’t appropriate.
The idea of the statement “is to be complete, but also to clarify some misunderstandings. ...We tried to be very clear in the language about what we know, where we can go, where we shouldn’t go, and what we still need to learn,” statement coauthor Cynthia A. Stuenkel, MD, of the University of California, San Diego, said in an interview.
The document is divided into nine parts or axes: growth hormone, adrenal, ovarian, testicular, thyroid, osteoporosis, vitamin D deficiency, type 2 diabetes, and water metabolism. Each section covers natural history and observational data in older individuals, available therapies, clinical trial data on efficacy and safety in older individuals, bulleted “key points,” and research gaps.
“Hormones and Aging: An Endocrine Society Scientific Statement” was presented at the annual meeting of the Endocrine Society and published online in the Journal of Clinical Endocrinology & Metabolism.
During a press briefing, writing group chair Anne R. Cappola, MD, of the University of Pennsylvania, Philadelphia, said the goal is to “provide a really concise summary across each of these areas. ... There are multiple hormonal changes that occur with age, so we really couldn’t limit ourselves to just one gland or the few that we commonly think about. We wanted to cover all the axes.”
The statement tackles several controversial areas, including hormone therapy for menopausal symptoms in women and hypogonadal symptoms in men and diabetes treatment goals in older adults.
“Hormones have these almost mythical qualities to some people. ... ‘If I just had my hormones back the way they were, it would all work out.’ What we want to do is make sure that patients are being treated appropriately and that their symptoms are being heard and managed and ascribed to the appropriate problems and not necessarily to hormonal problems when they are not. ... Part of what we need to do is [provide] the evidence that we have, which includes evidence of when not to prescribe as well as [when] to prescribe,” Dr. Cappola said.
REPRODUCTIVE ROUNDS
Applications of office hysteroscopy for the infertility patient
What role does diagnostic office hysteroscopy play in an infertility evaluation?
Performed properly, office hysteroscopy can transform your practice by accurately, gently, and safely assessing the uterine cavity as well as assessing tubal patency.
More specifically, hysteroscopy is the gold standard for assessing the uterine cavity. The sensitivity, specificity, and positive predictive and negative predictive values of hysterosalpingography (HSG) in evaluating uterine cavity abnormalities were 44.83%; 86.67%; 56.52%; and 80.25%, respectively. Given the poor sensitivity of HSG, a diagnosis of endometrial polyps and/or chronic endometritis is more likely to be missed.
Our crossover trial comparing HSG to office hysteroscopy for tubal patency showed that women were 110 times more likely to have the maximum level of pain with HSG than diagnostic hysteroscopy when using a 2.8-mm flexible hysteroscope. Further, infection rates and vasovagal events were far lower with hysteroscopy.
Finally, compared with HSG, we showed 98%-100% sensitivity and 84% specificity for tubal occlusion with hysteroscopy by air-infused saline. Conversely, HSG typically is associated with 76%-96% sensitivity and 67%-100% specificity. Additionally, we can often perform diagnostic hysteroscopies for approximately $35 per procedure for total fixed and disposable equipment costs.
https://www.mdedge.com/obgyn/reproductive-rounds
FEATURE
Is ChatGPT a friend or foe of medical publishing?
Researchers may use artificial intelligence (AI) language models such as ChatGPT to write and revise scientific manuscripts, according to a new announcement from the International Committee of Medical Journal Editors. These tools should not be listed as authors, and researchers must denote how AI-assisted technologies were used, the committee said.
These new guidelines are the latest effort for medical journals to define policies for using these large-scale language models (LLMs) in scientific publication. While these AI-assisted tools can help with tasks such as writing, analyzing data, catching mistakes, and more, they are also prone to errors, noted Casey Greene, PhD, a professor of biomedical informatics at the University of Colorado at Denver, Aurora.
At the same time, experts argue that these AI tools could have a positive impact on the field by limiting some of the linguistic disparities in scientific publishing as well as alleviating the burden of some monotonous or mechanical tasks that come along with manuscript writing.
What experts can agree on, though, is that the use of AI tools is here to stay. “This is going to become a common tool,” Dr. Greene said.
A change in medical publishing
OpenAI released ChatGPT in November 2022. In its own words, ChatGPT is “a deep learning model that has been trained on a massive amount of text data to understand and generate humanlike text.” Enter a question or a prompt, and it will respond. For example, when asked how the AI tool can be used in scientific publishing, ChatGPT responded:
“ChatGPT can aid scientific publishing by generating ideas, clarifying concepts, conducting preliminary literature reviews, providing proofreading and editing suggestions, and assisting with outlining and organizing scientific papers. However, it should be used as a supportive tool alongside domain expertise and validation from trusted scientific sources.”
Just a few months after ChatGPT became available, researchers began using this tool in their own work. One individual, Som Biswas, MD, a radiologist at the University of Tennessee Health Science Center in Memphis, reportedly used ChatGPT to author 16 scientific articles in just 4 months, according to the Daily Beast. Five of these articles have been published in four different journals. Dr. Biswas declined to be interviewed for this article.
There were also reports of papers with ChatGPT as one of the listed authors, which sparked backlash. In response, JAMA, Nature, and Science all published editorials in January outlining their policies for using ChatGPT and other large language models in the scientific authoring process. Editors from the journals of the American College of Cardiology and the American College of Rheumatology also updated their policies to reflect the influence of AI authoring tools.
The consensus is that AI has no place on the author byline.
Continue to: FROM THE JOURNALS...
FROM THE JOURNALS
Review supports continued mask-wearing in health care visits
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
“Masking in interactions between patients and health care personnel should continue to receive serious consideration as a patient safety measure,” Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
https://www.mdedge.com/obgyn/covid-19-updates
CONFERENCE COVERAGE
A ‘one-stop shop’: New guidance on hormones and aging
A new statement from the Endocrine Society on hormones and aging highlights the differences between normal aging and disease, and when treatment is and isn’t appropriate.
The idea of the statement “is to be complete, but also to clarify some misunderstandings. ...We tried to be very clear in the language about what we know, where we can go, where we shouldn’t go, and what we still need to learn,” statement coauthor Cynthia A. Stuenkel, MD, of the University of California, San Diego, said in an interview.
The document is divided into nine parts or axes: growth hormone, adrenal, ovarian, testicular, thyroid, osteoporosis, vitamin D deficiency, type 2 diabetes, and water metabolism. Each section covers natural history and observational data in older individuals, available therapies, clinical trial data on efficacy and safety in older individuals, bulleted “key points,” and research gaps.
“Hormones and Aging: An Endocrine Society Scientific Statement” was presented at the annual meeting of the Endocrine Society and published online in the Journal of Clinical Endocrinology & Metabolism.
During a press briefing, writing group chair Anne R. Cappola, MD, of the University of Pennsylvania, Philadelphia, said the goal is to “provide a really concise summary across each of these areas. ... There are multiple hormonal changes that occur with age, so we really couldn’t limit ourselves to just one gland or the few that we commonly think about. We wanted to cover all the axes.”
The statement tackles several controversial areas, including hormone therapy for menopausal symptoms in women and hypogonadal symptoms in men and diabetes treatment goals in older adults.
“Hormones have these almost mythical qualities to some people. ... ‘If I just had my hormones back the way they were, it would all work out.’ What we want to do is make sure that patients are being treated appropriately and that their symptoms are being heard and managed and ascribed to the appropriate problems and not necessarily to hormonal problems when they are not. ... Part of what we need to do is [provide] the evidence that we have, which includes evidence of when not to prescribe as well as [when] to prescribe,” Dr. Cappola said.
REPRODUCTIVE ROUNDS
Applications of office hysteroscopy for the infertility patient
What role does diagnostic office hysteroscopy play in an infertility evaluation?
Performed properly, office hysteroscopy can transform your practice by accurately, gently, and safely assessing the uterine cavity as well as assessing tubal patency.
More specifically, hysteroscopy is the gold standard for assessing the uterine cavity. The sensitivity, specificity, and positive predictive and negative predictive values of hysterosalpingography (HSG) in evaluating uterine cavity abnormalities were 44.83%; 86.67%; 56.52%; and 80.25%, respectively. Given the poor sensitivity of HSG, a diagnosis of endometrial polyps and/or chronic endometritis is more likely to be missed.
Our crossover trial comparing HSG to office hysteroscopy for tubal patency showed that women were 110 times more likely to have the maximum level of pain with HSG than diagnostic hysteroscopy when using a 2.8-mm flexible hysteroscope. Further, infection rates and vasovagal events were far lower with hysteroscopy.
Finally, compared with HSG, we showed 98%-100% sensitivity and 84% specificity for tubal occlusion with hysteroscopy by air-infused saline. Conversely, HSG typically is associated with 76%-96% sensitivity and 67%-100% specificity. Additionally, we can often perform diagnostic hysteroscopies for approximately $35 per procedure for total fixed and disposable equipment costs.
https://www.mdedge.com/obgyn/reproductive-rounds
FEATURE
Is ChatGPT a friend or foe of medical publishing?
Researchers may use artificial intelligence (AI) language models such as ChatGPT to write and revise scientific manuscripts, according to a new announcement from the International Committee of Medical Journal Editors. These tools should not be listed as authors, and researchers must denote how AI-assisted technologies were used, the committee said.
These new guidelines are the latest effort for medical journals to define policies for using these large-scale language models (LLMs) in scientific publication. While these AI-assisted tools can help with tasks such as writing, analyzing data, catching mistakes, and more, they are also prone to errors, noted Casey Greene, PhD, a professor of biomedical informatics at the University of Colorado at Denver, Aurora.
At the same time, experts argue that these AI tools could have a positive impact on the field by limiting some of the linguistic disparities in scientific publishing as well as alleviating the burden of some monotonous or mechanical tasks that come along with manuscript writing.
What experts can agree on, though, is that the use of AI tools is here to stay. “This is going to become a common tool,” Dr. Greene said.
A change in medical publishing
OpenAI released ChatGPT in November 2022. In its own words, ChatGPT is “a deep learning model that has been trained on a massive amount of text data to understand and generate humanlike text.” Enter a question or a prompt, and it will respond. For example, when asked how the AI tool can be used in scientific publishing, ChatGPT responded:
“ChatGPT can aid scientific publishing by generating ideas, clarifying concepts, conducting preliminary literature reviews, providing proofreading and editing suggestions, and assisting with outlining and organizing scientific papers. However, it should be used as a supportive tool alongside domain expertise and validation from trusted scientific sources.”
Just a few months after ChatGPT became available, researchers began using this tool in their own work. One individual, Som Biswas, MD, a radiologist at the University of Tennessee Health Science Center in Memphis, reportedly used ChatGPT to author 16 scientific articles in just 4 months, according to the Daily Beast. Five of these articles have been published in four different journals. Dr. Biswas declined to be interviewed for this article.
There were also reports of papers with ChatGPT as one of the listed authors, which sparked backlash. In response, JAMA, Nature, and Science all published editorials in January outlining their policies for using ChatGPT and other large language models in the scientific authoring process. Editors from the journals of the American College of Cardiology and the American College of Rheumatology also updated their policies to reflect the influence of AI authoring tools.
The consensus is that AI has no place on the author byline.
Continue to: FROM THE JOURNALS...
FROM THE JOURNALS
Review supports continued mask-wearing in health care visits
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
“Masking in interactions between patients and health care personnel should continue to receive serious consideration as a patient safety measure,” Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
https://www.mdedge.com/obgyn/covid-19-updates
CONFERENCE COVERAGE
A ‘one-stop shop’: New guidance on hormones and aging
A new statement from the Endocrine Society on hormones and aging highlights the differences between normal aging and disease, and when treatment is and isn’t appropriate.
The idea of the statement “is to be complete, but also to clarify some misunderstandings. ...We tried to be very clear in the language about what we know, where we can go, where we shouldn’t go, and what we still need to learn,” statement coauthor Cynthia A. Stuenkel, MD, of the University of California, San Diego, said in an interview.
The document is divided into nine parts or axes: growth hormone, adrenal, ovarian, testicular, thyroid, osteoporosis, vitamin D deficiency, type 2 diabetes, and water metabolism. Each section covers natural history and observational data in older individuals, available therapies, clinical trial data on efficacy and safety in older individuals, bulleted “key points,” and research gaps.
“Hormones and Aging: An Endocrine Society Scientific Statement” was presented at the annual meeting of the Endocrine Society and published online in the Journal of Clinical Endocrinology & Metabolism.
During a press briefing, writing group chair Anne R. Cappola, MD, of the University of Pennsylvania, Philadelphia, said the goal is to “provide a really concise summary across each of these areas. ... There are multiple hormonal changes that occur with age, so we really couldn’t limit ourselves to just one gland or the few that we commonly think about. We wanted to cover all the axes.”
The statement tackles several controversial areas, including hormone therapy for menopausal symptoms in women and hypogonadal symptoms in men and diabetes treatment goals in older adults.
“Hormones have these almost mythical qualities to some people. ... ‘If I just had my hormones back the way they were, it would all work out.’ What we want to do is make sure that patients are being treated appropriately and that their symptoms are being heard and managed and ascribed to the appropriate problems and not necessarily to hormonal problems when they are not. ... Part of what we need to do is [provide] the evidence that we have, which includes evidence of when not to prescribe as well as [when] to prescribe,” Dr. Cappola said.
Product updates and reviews
Product Update
Newly available single-use vaginal speculum
Ceek Women’s Health introduces the Nella single-use vaginal speculum for use during gynecologic examinations and procedures. Designed “by women for women, along with trusted clinicians to enhance patient comfort,” according to Ceek’s press release, the Nella speculum has a quiet operating mechanism, an LED light, and sidewall retractors. Its narrow shape allows for patient comfort and cervical visualization and because it is single use, it eliminates possibilities of cross contamination, according to the manufacturer. In addition, Ceek says it is an ergonomic tool, made from premium material, and is available in one size.
For more information, visit https://www.nellaspec.com

Product Update
Newly available single-use vaginal speculum
Ceek Women’s Health introduces the Nella single-use vaginal speculum for use during gynecologic examinations and procedures. Designed “by women for women, along with trusted clinicians to enhance patient comfort,” according to Ceek’s press release, the Nella speculum has a quiet operating mechanism, an LED light, and sidewall retractors. Its narrow shape allows for patient comfort and cervical visualization and because it is single use, it eliminates possibilities of cross contamination, according to the manufacturer. In addition, Ceek says it is an ergonomic tool, made from premium material, and is available in one size.
For more information, visit https://www.nellaspec.com
Product Update
Newly available single-use vaginal speculum
Ceek Women’s Health introduces the Nella single-use vaginal speculum for use during gynecologic examinations and procedures. Designed “by women for women, along with trusted clinicians to enhance patient comfort,” according to Ceek’s press release, the Nella speculum has a quiet operating mechanism, an LED light, and sidewall retractors. Its narrow shape allows for patient comfort and cervical visualization and because it is single use, it eliminates possibilities of cross contamination, according to the manufacturer. In addition, Ceek says it is an ergonomic tool, made from premium material, and is available in one size.
For more information, visit https://www.nellaspec.com

Rising patient costs tied to private equity ownership
The report was a collaboration of University of California, Berkeley, staff and researchers from two nonprofits, the American Antitrust Institute and the Washington Center for Equitable Growth. It provides “convincing evidence that incentives to put profits before patients have grown stronger with an increase in private equity ownership of physician practices,” lead author Richard Scheffler, PhD, of UC Berkeley said in a statement.
The report also noted that private equity acquisitions of physician groups have risen sixfold in just a decade, increasing from 75 deals in 2012 to 484 deals in 2021.
Separately, the American Medical Association earlier released a separate report on trends in physician practice arrangements, finding that the percentage of physicians working in private equity–owned groups was 4.5% in 2022, the same as in its previous 2020 report. The share of physicians working in private practices fell by 13 percentage points from 60.1% to 46.7% between 2012 and 2022, the AMA reported.
The Berkeley report and the AMA update come amid rising concerns about the effects of the decline of independent physician practices. The U.S. Senate Finance Committee, which oversees most federal health spending, held a June hearing examining the causes and consequences of increased corporate ownership in health care, including a look at physician practices.
“It’s increasingly clear that consolidation in health care is not lowering costs or increasing the quality of Americans’ health care,” Senate Finance Chairman Ron Wyden (D-Ore.) said in an email. “For private equity in health care in particular, there needs to be more transparency around ownership so the effect on these business relationships can be better understood.”
Federal and state agencies do not generally track acquisitions of physician practices.
The UC Berkeley report impressively documents the rising influence of private equity in health care, for which it’s tough to find good data, said Karen Joynt Maddox, MD, MPH, of Washington University in St. Louis. Dr. Maddox, a cardiologist and policy researcher who also has studied the effects of consolidation in health care, examined the new report at the request of this news organization.
“They did a great job with the data,” Dr. Maddox said. “One of the big issues around private equity, and in general, ‘corporatization’ and consolidation of health care, is that there’s not a great way to track ownership changes. It’s really difficult to study.”
Dr. Scheffler and colleagues used data from the commercial firm PitchBook to identify acquisitions of physician practices by private equity firms. They consulted IQVIA’s physician databases – OneKey and SK&A Office-Based Physicians Database – to learn about the location, size, and specialties of acquired practices. They also used data from the nonprofit Health Care Cost Institute, which tracks commercial health plan claims, to assess how private equity acquisitions affected prices.
The researchers then matched the findings for practices acquired by private equity firms from 2015 to 2021 against those for comparable physician practices that remained independent from 2012 to 2021.
The authors then tied private-equity ownership to the following price increases:
- Gastroenterology (14%; 95% confidence interval, 7.9%-20.4%
- Oncology (16.4%; 95% CI, 5.5%-28.4%)
- Dermatology (4.0%; 95% CI, 1%-7.1%)
- Ob.gyn. (8.8%; 95% CI, 3.8%-14%)
- Ophthalmology (8.7%; 95% CI, 5.1%-12.3%)
- Radiology (8.2%; 95% CI, 0.8%-16.1%)
- Orthopedics (7.1%; 95% CI, 2.2%-12.3%)
- Primary care (4.1%; 95% CI, 1.3%-7%)
The analysis also found higher prices for cardiology (8.7%; 95% CI, –6.4% to 26.1%) and urology (4.2%; 95% CI, –2.3% to 11.1%), but neither of these findings was statistically significant, one of the authors, Daniel R. Arnold, PhD, of UC Berkeley, said in an email. This was most likely caused by smaller sample sizes for these fields.
Factors driving consolidation
The two reports and the Senate Finance consolidation hearing raised similar issues, including calls to look at the factors driving more physicians out of independent practice, including Medicare reimbursement that may not keep up with rising inflation.
The Berkeley report authors called for Congress to add a broad inflation component to the Medicare physician fee schedule. It also called on Congress to add cases where Medicare, the biggest U.S. purchaser of health care, pays less for services when performed in independent practices than in hospital-affiliated ones.
Shawn Martin, executive vice president and CEO of the American Academy of Family Physicians, said his group appreciates how the report from UC Berkeley and nonprofit groups echoed recommendations many clinicians have made, including the call for a broad inflation adjustment for the fee schedule.
“To move the needle forward, Congress must advance site-neutral payment policies while also addressing the administrative requirements that take physicians away from the important work of caring for patients,” Mr. Martin said in an email.
Arnold Ventures provided funding for the report, which was a joint project of the American Antitrust Institute, the Nicholas C. Petris Center on Health Care Markets and Consumer Welfare, UC Berkeley, and the Washington Center for Equitable Growth.
A version of this article appeared on Medscape.com.
The report was a collaboration of University of California, Berkeley, staff and researchers from two nonprofits, the American Antitrust Institute and the Washington Center for Equitable Growth. It provides “convincing evidence that incentives to put profits before patients have grown stronger with an increase in private equity ownership of physician practices,” lead author Richard Scheffler, PhD, of UC Berkeley said in a statement.
The report also noted that private equity acquisitions of physician groups have risen sixfold in just a decade, increasing from 75 deals in 2012 to 484 deals in 2021.
Separately, the American Medical Association earlier released a separate report on trends in physician practice arrangements, finding that the percentage of physicians working in private equity–owned groups was 4.5% in 2022, the same as in its previous 2020 report. The share of physicians working in private practices fell by 13 percentage points from 60.1% to 46.7% between 2012 and 2022, the AMA reported.
The Berkeley report and the AMA update come amid rising concerns about the effects of the decline of independent physician practices. The U.S. Senate Finance Committee, which oversees most federal health spending, held a June hearing examining the causes and consequences of increased corporate ownership in health care, including a look at physician practices.
“It’s increasingly clear that consolidation in health care is not lowering costs or increasing the quality of Americans’ health care,” Senate Finance Chairman Ron Wyden (D-Ore.) said in an email. “For private equity in health care in particular, there needs to be more transparency around ownership so the effect on these business relationships can be better understood.”
Federal and state agencies do not generally track acquisitions of physician practices.
The UC Berkeley report impressively documents the rising influence of private equity in health care, for which it’s tough to find good data, said Karen Joynt Maddox, MD, MPH, of Washington University in St. Louis. Dr. Maddox, a cardiologist and policy researcher who also has studied the effects of consolidation in health care, examined the new report at the request of this news organization.
“They did a great job with the data,” Dr. Maddox said. “One of the big issues around private equity, and in general, ‘corporatization’ and consolidation of health care, is that there’s not a great way to track ownership changes. It’s really difficult to study.”
Dr. Scheffler and colleagues used data from the commercial firm PitchBook to identify acquisitions of physician practices by private equity firms. They consulted IQVIA’s physician databases – OneKey and SK&A Office-Based Physicians Database – to learn about the location, size, and specialties of acquired practices. They also used data from the nonprofit Health Care Cost Institute, which tracks commercial health plan claims, to assess how private equity acquisitions affected prices.
The researchers then matched the findings for practices acquired by private equity firms from 2015 to 2021 against those for comparable physician practices that remained independent from 2012 to 2021.
The authors then tied private-equity ownership to the following price increases:
- Gastroenterology (14%; 95% confidence interval, 7.9%-20.4%
- Oncology (16.4%; 95% CI, 5.5%-28.4%)
- Dermatology (4.0%; 95% CI, 1%-7.1%)
- Ob.gyn. (8.8%; 95% CI, 3.8%-14%)
- Ophthalmology (8.7%; 95% CI, 5.1%-12.3%)
- Radiology (8.2%; 95% CI, 0.8%-16.1%)
- Orthopedics (7.1%; 95% CI, 2.2%-12.3%)
- Primary care (4.1%; 95% CI, 1.3%-7%)
The analysis also found higher prices for cardiology (8.7%; 95% CI, –6.4% to 26.1%) and urology (4.2%; 95% CI, –2.3% to 11.1%), but neither of these findings was statistically significant, one of the authors, Daniel R. Arnold, PhD, of UC Berkeley, said in an email. This was most likely caused by smaller sample sizes for these fields.
Factors driving consolidation
The two reports and the Senate Finance consolidation hearing raised similar issues, including calls to look at the factors driving more physicians out of independent practice, including Medicare reimbursement that may not keep up with rising inflation.
The Berkeley report authors called for Congress to add a broad inflation component to the Medicare physician fee schedule. It also called on Congress to add cases where Medicare, the biggest U.S. purchaser of health care, pays less for services when performed in independent practices than in hospital-affiliated ones.
Shawn Martin, executive vice president and CEO of the American Academy of Family Physicians, said his group appreciates how the report from UC Berkeley and nonprofit groups echoed recommendations many clinicians have made, including the call for a broad inflation adjustment for the fee schedule.
“To move the needle forward, Congress must advance site-neutral payment policies while also addressing the administrative requirements that take physicians away from the important work of caring for patients,” Mr. Martin said in an email.
Arnold Ventures provided funding for the report, which was a joint project of the American Antitrust Institute, the Nicholas C. Petris Center on Health Care Markets and Consumer Welfare, UC Berkeley, and the Washington Center for Equitable Growth.
A version of this article appeared on Medscape.com.
The report was a collaboration of University of California, Berkeley, staff and researchers from two nonprofits, the American Antitrust Institute and the Washington Center for Equitable Growth. It provides “convincing evidence that incentives to put profits before patients have grown stronger with an increase in private equity ownership of physician practices,” lead author Richard Scheffler, PhD, of UC Berkeley said in a statement.
The report also noted that private equity acquisitions of physician groups have risen sixfold in just a decade, increasing from 75 deals in 2012 to 484 deals in 2021.
Separately, the American Medical Association earlier released a separate report on trends in physician practice arrangements, finding that the percentage of physicians working in private equity–owned groups was 4.5% in 2022, the same as in its previous 2020 report. The share of physicians working in private practices fell by 13 percentage points from 60.1% to 46.7% between 2012 and 2022, the AMA reported.
The Berkeley report and the AMA update come amid rising concerns about the effects of the decline of independent physician practices. The U.S. Senate Finance Committee, which oversees most federal health spending, held a June hearing examining the causes and consequences of increased corporate ownership in health care, including a look at physician practices.
“It’s increasingly clear that consolidation in health care is not lowering costs or increasing the quality of Americans’ health care,” Senate Finance Chairman Ron Wyden (D-Ore.) said in an email. “For private equity in health care in particular, there needs to be more transparency around ownership so the effect on these business relationships can be better understood.”
Federal and state agencies do not generally track acquisitions of physician practices.
The UC Berkeley report impressively documents the rising influence of private equity in health care, for which it’s tough to find good data, said Karen Joynt Maddox, MD, MPH, of Washington University in St. Louis. Dr. Maddox, a cardiologist and policy researcher who also has studied the effects of consolidation in health care, examined the new report at the request of this news organization.
“They did a great job with the data,” Dr. Maddox said. “One of the big issues around private equity, and in general, ‘corporatization’ and consolidation of health care, is that there’s not a great way to track ownership changes. It’s really difficult to study.”
Dr. Scheffler and colleagues used data from the commercial firm PitchBook to identify acquisitions of physician practices by private equity firms. They consulted IQVIA’s physician databases – OneKey and SK&A Office-Based Physicians Database – to learn about the location, size, and specialties of acquired practices. They also used data from the nonprofit Health Care Cost Institute, which tracks commercial health plan claims, to assess how private equity acquisitions affected prices.
The researchers then matched the findings for practices acquired by private equity firms from 2015 to 2021 against those for comparable physician practices that remained independent from 2012 to 2021.
The authors then tied private-equity ownership to the following price increases:
- Gastroenterology (14%; 95% confidence interval, 7.9%-20.4%
- Oncology (16.4%; 95% CI, 5.5%-28.4%)
- Dermatology (4.0%; 95% CI, 1%-7.1%)
- Ob.gyn. (8.8%; 95% CI, 3.8%-14%)
- Ophthalmology (8.7%; 95% CI, 5.1%-12.3%)
- Radiology (8.2%; 95% CI, 0.8%-16.1%)
- Orthopedics (7.1%; 95% CI, 2.2%-12.3%)
- Primary care (4.1%; 95% CI, 1.3%-7%)
The analysis also found higher prices for cardiology (8.7%; 95% CI, –6.4% to 26.1%) and urology (4.2%; 95% CI, –2.3% to 11.1%), but neither of these findings was statistically significant, one of the authors, Daniel R. Arnold, PhD, of UC Berkeley, said in an email. This was most likely caused by smaller sample sizes for these fields.
Factors driving consolidation
The two reports and the Senate Finance consolidation hearing raised similar issues, including calls to look at the factors driving more physicians out of independent practice, including Medicare reimbursement that may not keep up with rising inflation.
The Berkeley report authors called for Congress to add a broad inflation component to the Medicare physician fee schedule. It also called on Congress to add cases where Medicare, the biggest U.S. purchaser of health care, pays less for services when performed in independent practices than in hospital-affiliated ones.
Shawn Martin, executive vice president and CEO of the American Academy of Family Physicians, said his group appreciates how the report from UC Berkeley and nonprofit groups echoed recommendations many clinicians have made, including the call for a broad inflation adjustment for the fee schedule.
“To move the needle forward, Congress must advance site-neutral payment policies while also addressing the administrative requirements that take physicians away from the important work of caring for patients,” Mr. Martin said in an email.
Arnold Ventures provided funding for the report, which was a joint project of the American Antitrust Institute, the Nicholas C. Petris Center on Health Care Markets and Consumer Welfare, UC Berkeley, and the Washington Center for Equitable Growth.
A version of this article appeared on Medscape.com.
Clinical index predicts common postpartum mental health disorders
Developed by Canadian researchers, the easily implementable PMH CAREPLAN index “creates a framework for clinically actionable risk stratification that could assist patients and providers in determining an individual’s level of risk for common postpartum mental health disorders and direct them to appropriate intervention,” wrote a group led by Simone N. Vigod, MD, MSc, head of the department of psychiatry at Women’s College Hospital, Toronto, in the British Journal of Psychiatry.

After giving birth, women are especially vulnerable to major depression, anxiety, PTSD, and obsessive-compulsive disorder, which have a general postpartum prevalence of 7%-20%.
Common PMH disorders are to be distinguished from the more rare but severe PMH disorders such as postpartum psychosis and bipolar disorder, the researchers stressed.
“We know there are interventions that can prevent these disorders, but these seem to work best in people who are at high risk for developing the illnesses, “ Dr. Vigod said. “So, we wanted to be able to determine the level of risk that a person might actually experience them.”
In an ideal world, she continued, physicians might be able to say to a patient: “You have a 50% chance of developing postpartum depression and anxiety, so it may be worth investing your time and resources in a course of preventive psychotherapy.” Or: “You have a 90% chance of developing these disorders, so it might be worth going back on your medications even though you are breastfeeding.” Or: “You have only a 1% chance of developing them, so probably it’s not worthwhile to go back on your medication prophylactically.”
A need for a new assessment tool, akin to the Framingham Risk Score for 10-year cardiovascular events and the FRAX scoring system for 10-year fracture risk, was evident since previous indices based largely on patient self-reporting have had moderate predictive capacity, and have not been adopted in clinical practice, Dr. Vigod and associates noted.
Split-cohort design
Using population-based health administrative data and hospital birth records from Ontario during 2012-2015, Dr. Vigod’s group created and internally validated a predictive model for common PMH disorders in a cohort of 152,362 mothers. They then converted it to a risk index after validation in an additional cohort of 75,772 mothers. The women had delivered live infants during 2012-2014.
A common PMH disorder occurred in 13,608 mothers, while 214,526 were unaffected.
Independently associated PMH variables were many: prenatal care provider, mental health diagnosis history and medications during pregnancy, psychiatric hospital admissions or ED visits, conception type and complications, and apprehension of newborn by child services. Other factors were region of maternal origin, extremes of gestational age at birth, primary maternal language, lactation intention, maternal age, and number of prenatal visits.
Based on a broad span of scores from 0 to 39, 1-year common PMH disorder risk ranged from 1.5% to 40.5%, with an overall 1-year prevalence of 6%, consistent with previous studies. That included 11,262 (5%) mothers with an anxiety or related disorder, 3,392 (1.5%) with a depressive episode, and 1,046 (0.5%) with both. The best trade-off of sensitivity/specificity for risk appeared to be at a screening threshold score of 17 or above.
Risk drivers
PMH-affected mothers were slightly younger than unaffected women (mean age, 29.9 years vs. 30.6 years), more likely to be primiparous (45.2% vs. 42%), and less likely to be recent immigrants (16.7% vs. 27.2%).
They were also more likely to have previously experienced postpartum depression (4.4% vs. 1.4%), any depression (15.3% vs. 4.4%), and any anxiety disorder (13.8% vs. 4.3%).
As to lifestyle, smoking was more common in women with PMH (15.0% vs. 10.2%), as were the use of nonprescribed substances (3% vs. 1.4%) and intimate partner violence in pregnancy (2.7% vs. 1.5%).
In addition, the affected group experienced more pregnancy complications than their unaffected peers (16% vs. 13.9%), preterm birth (8.2% vs. 6.8%), and Apgar scores below 7 at 1 or 5 minutes (10.5% vs. 7.6%).
Low income did not appear to have an impact since just over 20% in either group fell into the lowest neighborhood income quintile.

Commenting on the index but not involved in developing it, LaTasha D. Nelson, MD, an associate professor or medicine and a maternal-fetal medicine specialist at Northwestern Medicine in Chicago, doubted the Canadian model would work as well in the more fragmented U.S. health care system, compared with Canada’s universal model with its large provincial health databases.
She also found the large number of variables and broad score range potentially problematic, especially if the risk threshold is set at less than half the maximum score at 17, at which some low-risk mothers might get screening and perhaps intervention. “Are we going to use up the resources we have for those who might not need help, or are we going to treat someone who really needs it?” she asked.
Another concern is the postpartum timing of assessment. At Dr. Nelson’s center, mothers are checked for mental health at two points during pregnancy and those with higher scores are triaged for further care.
Dr. Nelson was also puzzled by the score-lowering impact of prenatal care given by a nurse practitioner and “other” provider : –5 and –2, respectively, versus +3 for a midwife and +1 for a family doctor. “This may capture more relaxed, easy-going multiparous mothers who felt comfortable turning to an NP,” she said.
It may indeed reflect that the risk level of a person who sees those providers is overall lower, Dr. Vigod agreed. “This is one reason why we would want to see replication of these results in other jurisdictions and by other ways of diagnosis before putting it out into clinical practice.”
As to the score-lowering effect of not speaking English as the primary tongue, Dr. Nelson wondered, “is that because we’re taking better care of mothers who speak the main language and missing those who speak other languages? Are they not getting the same level of interrogation?”
It may be that individuals in these groups were less likely to access mental health care, Dr. Vigod agreed, or it might reflect the so-called healthy immigrant effect or culturally different levels of postpartum support. “It might mean that there are more people who benefit from community-level protective factors in these groups. We know that social support is an important protective factor.”
Despite her reservations about the index, Dr. Nelson said that increasing attention to the pre- and postnatal mental health of mothers is an important part of maternal care. “This is an issue that needs to be recognized.”
The next step, Dr. Vigod said, is to determine whether the index holds up in other populations. “Then, we would want to test it out to see if recommending interventions based on a certain level of risk improves outcomes. At what percentage risk would starting an antidepressant medication result in a reduced risk for postpartum depression or anxiety – 90%, 80%, 70%, or less?”
The study received funding from the Canadian Institutes of Health Research. Data were analyzed by ICES, an independent nonprofit research organization that holds population-based data. Dr. Vigod reported royalties from UpToDate for materials related to depression and pregnancy. Dr. Nelson disclosed no relevant competing interests.
Developed by Canadian researchers, the easily implementable PMH CAREPLAN index “creates a framework for clinically actionable risk stratification that could assist patients and providers in determining an individual’s level of risk for common postpartum mental health disorders and direct them to appropriate intervention,” wrote a group led by Simone N. Vigod, MD, MSc, head of the department of psychiatry at Women’s College Hospital, Toronto, in the British Journal of Psychiatry.
After giving birth, women are especially vulnerable to major depression, anxiety, PTSD, and obsessive-compulsive disorder, which have a general postpartum prevalence of 7%-20%.
Common PMH disorders are to be distinguished from the more rare but severe PMH disorders such as postpartum psychosis and bipolar disorder, the researchers stressed.
“We know there are interventions that can prevent these disorders, but these seem to work best in people who are at high risk for developing the illnesses, “ Dr. Vigod said. “So, we wanted to be able to determine the level of risk that a person might actually experience them.”
In an ideal world, she continued, physicians might be able to say to a patient: “You have a 50% chance of developing postpartum depression and anxiety, so it may be worth investing your time and resources in a course of preventive psychotherapy.” Or: “You have a 90% chance of developing these disorders, so it might be worth going back on your medications even though you are breastfeeding.” Or: “You have only a 1% chance of developing them, so probably it’s not worthwhile to go back on your medication prophylactically.”
A need for a new assessment tool, akin to the Framingham Risk Score for 10-year cardiovascular events and the FRAX scoring system for 10-year fracture risk, was evident since previous indices based largely on patient self-reporting have had moderate predictive capacity, and have not been adopted in clinical practice, Dr. Vigod and associates noted.
Split-cohort design
Using population-based health administrative data and hospital birth records from Ontario during 2012-2015, Dr. Vigod’s group created and internally validated a predictive model for common PMH disorders in a cohort of 152,362 mothers. They then converted it to a risk index after validation in an additional cohort of 75,772 mothers. The women had delivered live infants during 2012-2014.
A common PMH disorder occurred in 13,608 mothers, while 214,526 were unaffected.
Independently associated PMH variables were many: prenatal care provider, mental health diagnosis history and medications during pregnancy, psychiatric hospital admissions or ED visits, conception type and complications, and apprehension of newborn by child services. Other factors were region of maternal origin, extremes of gestational age at birth, primary maternal language, lactation intention, maternal age, and number of prenatal visits.
Based on a broad span of scores from 0 to 39, 1-year common PMH disorder risk ranged from 1.5% to 40.5%, with an overall 1-year prevalence of 6%, consistent with previous studies. That included 11,262 (5%) mothers with an anxiety or related disorder, 3,392 (1.5%) with a depressive episode, and 1,046 (0.5%) with both. The best trade-off of sensitivity/specificity for risk appeared to be at a screening threshold score of 17 or above.
Risk drivers
PMH-affected mothers were slightly younger than unaffected women (mean age, 29.9 years vs. 30.6 years), more likely to be primiparous (45.2% vs. 42%), and less likely to be recent immigrants (16.7% vs. 27.2%).
They were also more likely to have previously experienced postpartum depression (4.4% vs. 1.4%), any depression (15.3% vs. 4.4%), and any anxiety disorder (13.8% vs. 4.3%).
As to lifestyle, smoking was more common in women with PMH (15.0% vs. 10.2%), as were the use of nonprescribed substances (3% vs. 1.4%) and intimate partner violence in pregnancy (2.7% vs. 1.5%).
In addition, the affected group experienced more pregnancy complications than their unaffected peers (16% vs. 13.9%), preterm birth (8.2% vs. 6.8%), and Apgar scores below 7 at 1 or 5 minutes (10.5% vs. 7.6%).
Low income did not appear to have an impact since just over 20% in either group fell into the lowest neighborhood income quintile.
Commenting on the index but not involved in developing it, LaTasha D. Nelson, MD, an associate professor or medicine and a maternal-fetal medicine specialist at Northwestern Medicine in Chicago, doubted the Canadian model would work as well in the more fragmented U.S. health care system, compared with Canada’s universal model with its large provincial health databases.
She also found the large number of variables and broad score range potentially problematic, especially if the risk threshold is set at less than half the maximum score at 17, at which some low-risk mothers might get screening and perhaps intervention. “Are we going to use up the resources we have for those who might not need help, or are we going to treat someone who really needs it?” she asked.
Another concern is the postpartum timing of assessment. At Dr. Nelson’s center, mothers are checked for mental health at two points during pregnancy and those with higher scores are triaged for further care.
Dr. Nelson was also puzzled by the score-lowering impact of prenatal care given by a nurse practitioner and “other” provider : –5 and –2, respectively, versus +3 for a midwife and +1 for a family doctor. “This may capture more relaxed, easy-going multiparous mothers who felt comfortable turning to an NP,” she said.
It may indeed reflect that the risk level of a person who sees those providers is overall lower, Dr. Vigod agreed. “This is one reason why we would want to see replication of these results in other jurisdictions and by other ways of diagnosis before putting it out into clinical practice.”
As to the score-lowering effect of not speaking English as the primary tongue, Dr. Nelson wondered, “is that because we’re taking better care of mothers who speak the main language and missing those who speak other languages? Are they not getting the same level of interrogation?”
It may be that individuals in these groups were less likely to access mental health care, Dr. Vigod agreed, or it might reflect the so-called healthy immigrant effect or culturally different levels of postpartum support. “It might mean that there are more people who benefit from community-level protective factors in these groups. We know that social support is an important protective factor.”
Despite her reservations about the index, Dr. Nelson said that increasing attention to the pre- and postnatal mental health of mothers is an important part of maternal care. “This is an issue that needs to be recognized.”
The next step, Dr. Vigod said, is to determine whether the index holds up in other populations. “Then, we would want to test it out to see if recommending interventions based on a certain level of risk improves outcomes. At what percentage risk would starting an antidepressant medication result in a reduced risk for postpartum depression or anxiety – 90%, 80%, 70%, or less?”
The study received funding from the Canadian Institutes of Health Research. Data were analyzed by ICES, an independent nonprofit research organization that holds population-based data. Dr. Vigod reported royalties from UpToDate for materials related to depression and pregnancy. Dr. Nelson disclosed no relevant competing interests.
Developed by Canadian researchers, the easily implementable PMH CAREPLAN index “creates a framework for clinically actionable risk stratification that could assist patients and providers in determining an individual’s level of risk for common postpartum mental health disorders and direct them to appropriate intervention,” wrote a group led by Simone N. Vigod, MD, MSc, head of the department of psychiatry at Women’s College Hospital, Toronto, in the British Journal of Psychiatry.
After giving birth, women are especially vulnerable to major depression, anxiety, PTSD, and obsessive-compulsive disorder, which have a general postpartum prevalence of 7%-20%.
Common PMH disorders are to be distinguished from the more rare but severe PMH disorders such as postpartum psychosis and bipolar disorder, the researchers stressed.
“We know there are interventions that can prevent these disorders, but these seem to work best in people who are at high risk for developing the illnesses, “ Dr. Vigod said. “So, we wanted to be able to determine the level of risk that a person might actually experience them.”
In an ideal world, she continued, physicians might be able to say to a patient: “You have a 50% chance of developing postpartum depression and anxiety, so it may be worth investing your time and resources in a course of preventive psychotherapy.” Or: “You have a 90% chance of developing these disorders, so it might be worth going back on your medications even though you are breastfeeding.” Or: “You have only a 1% chance of developing them, so probably it’s not worthwhile to go back on your medication prophylactically.”
A need for a new assessment tool, akin to the Framingham Risk Score for 10-year cardiovascular events and the FRAX scoring system for 10-year fracture risk, was evident since previous indices based largely on patient self-reporting have had moderate predictive capacity, and have not been adopted in clinical practice, Dr. Vigod and associates noted.
Split-cohort design
Using population-based health administrative data and hospital birth records from Ontario during 2012-2015, Dr. Vigod’s group created and internally validated a predictive model for common PMH disorders in a cohort of 152,362 mothers. They then converted it to a risk index after validation in an additional cohort of 75,772 mothers. The women had delivered live infants during 2012-2014.
A common PMH disorder occurred in 13,608 mothers, while 214,526 were unaffected.
Independently associated PMH variables were many: prenatal care provider, mental health diagnosis history and medications during pregnancy, psychiatric hospital admissions or ED visits, conception type and complications, and apprehension of newborn by child services. Other factors were region of maternal origin, extremes of gestational age at birth, primary maternal language, lactation intention, maternal age, and number of prenatal visits.
Based on a broad span of scores from 0 to 39, 1-year common PMH disorder risk ranged from 1.5% to 40.5%, with an overall 1-year prevalence of 6%, consistent with previous studies. That included 11,262 (5%) mothers with an anxiety or related disorder, 3,392 (1.5%) with a depressive episode, and 1,046 (0.5%) with both. The best trade-off of sensitivity/specificity for risk appeared to be at a screening threshold score of 17 or above.
Risk drivers
PMH-affected mothers were slightly younger than unaffected women (mean age, 29.9 years vs. 30.6 years), more likely to be primiparous (45.2% vs. 42%), and less likely to be recent immigrants (16.7% vs. 27.2%).
They were also more likely to have previously experienced postpartum depression (4.4% vs. 1.4%), any depression (15.3% vs. 4.4%), and any anxiety disorder (13.8% vs. 4.3%).
As to lifestyle, smoking was more common in women with PMH (15.0% vs. 10.2%), as were the use of nonprescribed substances (3% vs. 1.4%) and intimate partner violence in pregnancy (2.7% vs. 1.5%).
In addition, the affected group experienced more pregnancy complications than their unaffected peers (16% vs. 13.9%), preterm birth (8.2% vs. 6.8%), and Apgar scores below 7 at 1 or 5 minutes (10.5% vs. 7.6%).
Low income did not appear to have an impact since just over 20% in either group fell into the lowest neighborhood income quintile.
Commenting on the index but not involved in developing it, LaTasha D. Nelson, MD, an associate professor or medicine and a maternal-fetal medicine specialist at Northwestern Medicine in Chicago, doubted the Canadian model would work as well in the more fragmented U.S. health care system, compared with Canada’s universal model with its large provincial health databases.
She also found the large number of variables and broad score range potentially problematic, especially if the risk threshold is set at less than half the maximum score at 17, at which some low-risk mothers might get screening and perhaps intervention. “Are we going to use up the resources we have for those who might not need help, or are we going to treat someone who really needs it?” she asked.
Another concern is the postpartum timing of assessment. At Dr. Nelson’s center, mothers are checked for mental health at two points during pregnancy and those with higher scores are triaged for further care.
Dr. Nelson was also puzzled by the score-lowering impact of prenatal care given by a nurse practitioner and “other” provider : –5 and –2, respectively, versus +3 for a midwife and +1 for a family doctor. “This may capture more relaxed, easy-going multiparous mothers who felt comfortable turning to an NP,” she said.
It may indeed reflect that the risk level of a person who sees those providers is overall lower, Dr. Vigod agreed. “This is one reason why we would want to see replication of these results in other jurisdictions and by other ways of diagnosis before putting it out into clinical practice.”
As to the score-lowering effect of not speaking English as the primary tongue, Dr. Nelson wondered, “is that because we’re taking better care of mothers who speak the main language and missing those who speak other languages? Are they not getting the same level of interrogation?”
It may be that individuals in these groups were less likely to access mental health care, Dr. Vigod agreed, or it might reflect the so-called healthy immigrant effect or culturally different levels of postpartum support. “It might mean that there are more people who benefit from community-level protective factors in these groups. We know that social support is an important protective factor.”
Despite her reservations about the index, Dr. Nelson said that increasing attention to the pre- and postnatal mental health of mothers is an important part of maternal care. “This is an issue that needs to be recognized.”
The next step, Dr. Vigod said, is to determine whether the index holds up in other populations. “Then, we would want to test it out to see if recommending interventions based on a certain level of risk improves outcomes. At what percentage risk would starting an antidepressant medication result in a reduced risk for postpartum depression or anxiety – 90%, 80%, 70%, or less?”
The study received funding from the Canadian Institutes of Health Research. Data were analyzed by ICES, an independent nonprofit research organization that holds population-based data. Dr. Vigod reported royalties from UpToDate for materials related to depression and pregnancy. Dr. Nelson disclosed no relevant competing interests.
FROM THE BRITISH JOURNAL OF PSYCHIATRY
Nurse practitioners sue state over right to use ‘doctor’ title
, saying it violates their first amendment right to use the honorific title without fear of regulatory repercussions.
The case highlights ongoing scope-creep battles as the American Medical Association tries to preserve the physician-led team model and nursing organizations and some lawmakers push for greater autonomy for allied professionals.
In the complaint filed in district court in June, plaintiffs Jacqueline Palmer, DNP, Heather Lewis, DNP, and Rodolfo Jaravata-Hanson, DNP, say they fear the state will sanction them. They note that “Doctor Sarah,” another DNP, was fined nearly $20,000 by the state last November for false advertising and fraud after using the moniker in her online advertising and social media accounts.
The fine was part of a settlement that the DNP, Sarah Erny, reached with the state to resolve allegations that she failed to identify her supervising physician and inform the public that she was not a medical doctor.
Under California’s Medical Practice Act, individuals cannot refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Instead, nurse practitioners certified by the California Board of Registered Nursing may use titles like “Certified Nurse Practitioner” and “Advanced Practice Registered Nurse,” corresponding letters such as APRN-CNP, RN, and NP, and phrases like pediatric nurse practitioner to identify specialization.
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
The nonprofit Pacific Legal Foundation represents the plaintiffs. In court records, its attorneys argue that after “years earning their advanced degrees and qualifications ... they should be able to speak truthfully about them in their workplaces, on their business cards, the Internet, and social media, so long as they clarify that they are nurse practitioners.”
State lawmakers’ attempts to clarify the roles of physicians and nurse practitioners have seen mixed results. Florida legislators recently passed a bill to prevent advanced practice nurses from using the honorific title, reserving it only for MDs and DOs. Gov. Ron DeSantis vetoed it last month.
In May, Georgia lawmakers passed the Health Care Practitioners Truth and Transparency Act. It requires advanced practice nurses and physician assistants with doctoral degrees who refer to themselves as doctors in a clinical setting to state they are not medical doctors or physicians.
Still, some health professionals say that the designation should only be used in academic settings or among peers, and that all doctoral degree holders should ditch the moniker at the bedside to ease patient communications.
Named as defendants in the suit are three state officials: California Attorney General Rob Bonta, state Medical Board President Kristina Lawson, and California Board of Registered Nursing Executive Officer Loretta Melby.
A version of this article first appeared on Medscape.com.
, saying it violates their first amendment right to use the honorific title without fear of regulatory repercussions.
The case highlights ongoing scope-creep battles as the American Medical Association tries to preserve the physician-led team model and nursing organizations and some lawmakers push for greater autonomy for allied professionals.
In the complaint filed in district court in June, plaintiffs Jacqueline Palmer, DNP, Heather Lewis, DNP, and Rodolfo Jaravata-Hanson, DNP, say they fear the state will sanction them. They note that “Doctor Sarah,” another DNP, was fined nearly $20,000 by the state last November for false advertising and fraud after using the moniker in her online advertising and social media accounts.
The fine was part of a settlement that the DNP, Sarah Erny, reached with the state to resolve allegations that she failed to identify her supervising physician and inform the public that she was not a medical doctor.
Under California’s Medical Practice Act, individuals cannot refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Instead, nurse practitioners certified by the California Board of Registered Nursing may use titles like “Certified Nurse Practitioner” and “Advanced Practice Registered Nurse,” corresponding letters such as APRN-CNP, RN, and NP, and phrases like pediatric nurse practitioner to identify specialization.
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
The nonprofit Pacific Legal Foundation represents the plaintiffs. In court records, its attorneys argue that after “years earning their advanced degrees and qualifications ... they should be able to speak truthfully about them in their workplaces, on their business cards, the Internet, and social media, so long as they clarify that they are nurse practitioners.”
State lawmakers’ attempts to clarify the roles of physicians and nurse practitioners have seen mixed results. Florida legislators recently passed a bill to prevent advanced practice nurses from using the honorific title, reserving it only for MDs and DOs. Gov. Ron DeSantis vetoed it last month.
In May, Georgia lawmakers passed the Health Care Practitioners Truth and Transparency Act. It requires advanced practice nurses and physician assistants with doctoral degrees who refer to themselves as doctors in a clinical setting to state they are not medical doctors or physicians.
Still, some health professionals say that the designation should only be used in academic settings or among peers, and that all doctoral degree holders should ditch the moniker at the bedside to ease patient communications.
Named as defendants in the suit are three state officials: California Attorney General Rob Bonta, state Medical Board President Kristina Lawson, and California Board of Registered Nursing Executive Officer Loretta Melby.
A version of this article first appeared on Medscape.com.
, saying it violates their first amendment right to use the honorific title without fear of regulatory repercussions.
The case highlights ongoing scope-creep battles as the American Medical Association tries to preserve the physician-led team model and nursing organizations and some lawmakers push for greater autonomy for allied professionals.
In the complaint filed in district court in June, plaintiffs Jacqueline Palmer, DNP, Heather Lewis, DNP, and Rodolfo Jaravata-Hanson, DNP, say they fear the state will sanction them. They note that “Doctor Sarah,” another DNP, was fined nearly $20,000 by the state last November for false advertising and fraud after using the moniker in her online advertising and social media accounts.
The fine was part of a settlement that the DNP, Sarah Erny, reached with the state to resolve allegations that she failed to identify her supervising physician and inform the public that she was not a medical doctor.
Under California’s Medical Practice Act, individuals cannot refer to themselves as “doctor, physician, or any other terms or letters indicating or implying that he or she is a physician and surgeon ... without having ... a certificate as a physician and surgeon.”
Instead, nurse practitioners certified by the California Board of Registered Nursing may use titles like “Certified Nurse Practitioner” and “Advanced Practice Registered Nurse,” corresponding letters such as APRN-CNP, RN, and NP, and phrases like pediatric nurse practitioner to identify specialization.
Individuals who misrepresent themselves are subject to misdemeanor charges and civil penalties.
The nonprofit Pacific Legal Foundation represents the plaintiffs. In court records, its attorneys argue that after “years earning their advanced degrees and qualifications ... they should be able to speak truthfully about them in their workplaces, on their business cards, the Internet, and social media, so long as they clarify that they are nurse practitioners.”
State lawmakers’ attempts to clarify the roles of physicians and nurse practitioners have seen mixed results. Florida legislators recently passed a bill to prevent advanced practice nurses from using the honorific title, reserving it only for MDs and DOs. Gov. Ron DeSantis vetoed it last month.
In May, Georgia lawmakers passed the Health Care Practitioners Truth and Transparency Act. It requires advanced practice nurses and physician assistants with doctoral degrees who refer to themselves as doctors in a clinical setting to state they are not medical doctors or physicians.
Still, some health professionals say that the designation should only be used in academic settings or among peers, and that all doctoral degree holders should ditch the moniker at the bedside to ease patient communications.
Named as defendants in the suit are three state officials: California Attorney General Rob Bonta, state Medical Board President Kristina Lawson, and California Board of Registered Nursing Executive Officer Loretta Melby.
A version of this article first appeared on Medscape.com.
U.S. mammogram update sparks concern, reignites debates
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
, while also renewing debates about the timing of these tests and the screening approaches used.
The U.S. Preventive Services Task Force is currently finalizing an update to its recommendations on breast cancer screening. In May, the task force released a proposed update that dropped the initial age for routine mammogram screening from 50 to 40.
The task force intends to give a “B” rating to this recommendation, which covers screening every other year up to age 74 for women deemed average risk for breast cancer.
The task force’s rating carries clout, A. Mark Fendrick, MD, director of the Value-Based Insurance Design at the University of Michigan, Ann Arbor, said in an interview.
For one, the Affordable Care Act requires that private insurers cover services that get top A or B marks from USPSTF without charging copays.
However, Dr. Fendrick noted, such coverage does not necessarily apply to follow-up testing when a routine mammogram comes back with a positive finding. The expense of follow-up testing may deter some women from seeking follow-up diagnostic imaging or biopsies after an abnormal result on a screening mammogram.
A recent analysis in JAMA Network Open found that women facing higher anticipated out-of-pocket costs for breast cancer diagnostic tests, based on their health insurance plan, were less likely to get that follow-up screening. For instance, the use of breast MRI decreased by nearly 24% between patients undergoing subsequent diagnostic testing in plans with the lowest out-of-pocket costs vs. those with the highest.
“The study’s central finding that some women who have an abnormal result on a mammogram may not get appropriate follow-up because of cost is worrisome,” said Dr. Fendrick and Ilana B. Richman, MD, MHS, in an accompanying commentary to the JAMA analysis. “On an individual level, high out-of-pocket costs may directly contribute to worse health outcomes or require individuals to use scarce financial resources that may otherwise be used for critical items such as food or rent.”
For patients to fully benefit from early detection, the USPSTF would also need to make clear that follow-up diagnostic mammograms are covered, Dr. Fendrick said.
The ongoing debates
Concerns over the costs of potential follow-up tests are not the only issues experts have highlighted since USPSTF released its updated draft guidance on screening mammography.
The task force’s proposed update has also reignited questions and uncertainties surrounding when to screen, how often, and what types are best.
When it comes to frequency, the major organizations that provide screening guidance don’t see eye to eye. The USPSTF recommends breast cancer screening every other year, while the American College of Radiology recommends screening every year because that approach leads to saves “the most lives.”
At this time, the American College of Obstetricians and Gynecologists guidance currently teeters in the middle, suggesting either annual or biennial screening and highlighting the pros and cons of either approach. According to ACOG, “annual screening intervals appear to result in the least number of breast cancer deaths, particularly in younger women, but at the cost of additional callbacks and biopsies.”
When to begin screening represents another point of contention. While some experts, such as ACOG, agree with the task force’s decision to lower the screening start age to 40, others point to the need for greater nuance on setting the appropriate screening age. The main issue: the task force’s draft sets a uniform age to begin screening, but the risk for breast cancer and breast cancer mortality is not uniform across different racial and ethnic groups.
A recent study published in JAMA Network Open found that, among women aged 40-49, breast cancer mortality was highest among Black women (27 deaths per 100,000 person-years) followed by White women (15 deaths per 100,000 person-years). Based on a recommended screening age of 50, the authors suggested that Black women should start screening at age 42, whereas White women could start at 51.
“These findings suggest that health policy makers and clinicians could consider an alternative, race and ethnicity–adapted approach in which Black female patients start screening earlier,” writes Tianhui Chen, PhD, of China’s Zhejiang Cancer Hospital and coauthor of the study.
Weighing in on the guidance, the nonprofit National Center for Health Research urged the task force to consider suggesting different screening schedules based on race and ethnicity data. That would mean the recommendation to start at age 40 should only apply to Black women and other groups with higher-than-average risk for breast cancer at a younger age.
“Women are capable of understanding why the age to start mammography screening may be different for women with different risk factors,” the National Center for Health Research wrote in a comment to USPSTF, provided to this news organization by request. “What is confusing is when some physician groups recommend annual mammograms for all women starting at age 40, even though the data do not support that recommendation.”
While the ACR agreed with the task force’s recommendation to lower the screening age, the organization suggested starting risk assessments based on racial variations in breast cancer incidence and death even earlier. Specifically, the ACR recommended that high-risk groups, such as Black women, get risk assessments by age 25 to determine whether mammography before age 40 is needed.
Screening options for women with dense breasts may be some of the most challenging to weigh. Having dense breasts increases an individual’s risk for breast cancer, and mammography alone is not as effective at identifying breast cancer among these women. However, the evidence on the benefits vs. harms of additional screening beyond mammography remains mixed.
As a result, the task force decided to maintain its “I” grade on additional screening beyond mammography for these women – a grade that indicates insufficient evidence to determine the benefits and harms for a service.
The task force largely based its decision on the findings of two key reports. One report from the Cancer Intervention and Surveillance Modeling Network, which modeled potential outcomes of different screening strategies, indicated that extra screening might reduce breast cancer mortality in those with dense breasts, but at a cost of more false-positive reports.
The second report, a review from the Kaiser Permanente Evidence-based Practice Center, reaffirmed the benefits of routine mammography for reducing deaths from breast cancer, but found no solid evidence that different strategies – including supplemental screening in women with denser breasts – lowered breast cancer mortality or the risk of progression to advanced cancer. Further studies may show which approaches work best to reduce breast cancer deaths, the report said.
In this instance, ACOG agreed with USPSTF: “Based on the lack of data, ACOG does not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
Women with dense breasts should still be encouraged to receive regular screening mammography, even if the results they get may not be as accurate as those for women with less dense breasts, said Diana L. Miglioretti, PhD, of the University of California, Davis, who worked on a report for the USPSTF guidelines.
What’s next?
Despite ongoing debate and uncertainties surrounding some breast screening guidance, support for ending copay requirements for follow-up tests after a positive mammogram finding is widespread.
According to Dr. Fendrick, the USPSTF should expand coverage of follow-up testing after a positive mammogram to ensure people receive routine screening and any necessary diagnostic tests, as it did with colon cancer.
Before 2021, patients could face high costs for a colonoscopy following a positive stool-based Cologuard test. But in 2021, the USPSTF said that positive results on stool-based tests would require follow-up with colonoscopy, defining this follow-up as part of the screening benefit. In 2022, Medicare followed by setting a policy that ended the copay for these follow-up colonoscopies.
For breast screening, there are efforts underway in Congress to end copays for breast screening. In May, Rep. Rosa DeLauro (D-Conn.) introduced a bill, the Find It Early Act, that would require both private and government insurers to cover the out-of-pocket costs for many women receiving screening with ultrasound and MRI.
When the USPSTF finalizes its breast screening guidelines, the recommendations will be woven into discussions between primary care physicians and patients about breast cancer screening.
As guidelines and evidence evolve, “we’re learning to adjust” and communicate these changes to patients, said Tochi Iroku-Malize, MD, president of the American Academy of Family Physicians.
However, gaps in the guidance will leave some open-ended questions about optimal screening practices and how much screening may cost.
Given that, Dr. Iroku-Malize takes many factors into account when discussing screening options with her patients. Based on the new information and the patient’s information, she said she will tell her patients, “We’re going to adjust our guidance as to what you need.”
A version of this article first appeared on Medscape.com.
The sacred office space
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.

Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.

Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.
Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.
Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.
Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.
Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
When did medicine become a battleground for everything?
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.

“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”

In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.
“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”
In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.
Like hundreds of other medical experts, Leana Wen, MD, an emergency physician and former Baltimore health commissioner, was an early and avid supporter of COVID vaccines and their ability to prevent severe disease, hospitalization, and death from SARS-CoV-2 infections.
When 51-year-old Scott Eli Harris, of Aubrey, Tex., heard of Dr. Wen’s stance in July 2021, the self-described “fifth-generation U.S. Army veteran and a sniper” sent Dr. Wen an electronic invective laden with racist language and very specific threats to shoot her.
Mr. Harris pled guilty to transmitting threats via interstate commerce last February and began serving 6 months in federal prison in the fall of 2022, but his threats wouldn’t be the last for Dr. Wen. Just 2 days after Mr. Harris was sentenced, charges were unsealed against another man in Massachusetts, who threatened that Dr. Wen would “end up in pieces” if she continued “pushing” her thoughts publicly.’
Dr. Wen has plenty of company. In an August 2022 survey of emergency doctors conducted by the American College of Emergency Physicians, 85% of respondents said violence against them is increasing. One in four doctors said they’re being assaulted by patients and their family and friends multiple times a week, compared with just 8% of doctors who said as much in 2018. About 64% of emergency physicians reported receiving verbal assaults and threats of violence; 40% reported being hit or slapped, and 26% were kicked.
This uptick of violence and threats against physicians didn’t come out of nowhere; violence against health care workers has been gradually increasing over the past decade. Health care providers can attest to the hostility that particular topics have sparked for years: vaccines in pediatrics, abortion in ob.gyn., and gender-affirming care in endocrinology.
But the pandemic fueled the fire. The proliferation of misinformation (often via social media) and the politicization of public health and medicine are at the center of the problem.
‘The people attacking are themselves victims’
The misinformation problem first came to a head in one area of public health: vaccines. The pandemic accelerated antagonism in medicine – thanks, in part, to decades of antivaccine activism.
The antivaccine movement, which has ebbed and flowed in the United States and across the globe since the first vaccine, experienced a new wave in the early 2000s with the combination of concerns about thimerosal in vaccines and a now disproven link between autism and the MMR vaccine. But that movement grew. It picked up steam when activists gained political clout after a 2014 measles outbreak at Disneyland led California schools to tighten up policies regarding vaccinations for kids who enrolled. These stronger public school vaccination laws ran up against religious freedom arguments from antivaccine advocates.
Use of social media continues to grow, and with it, the spread of misinformation. A recent study found that Facebook “users’ social media habits doubled, and in some cases, tripled the amount of fake news they shared.”
In the face of growing confusion, health care providers and public health experts have often struggled to treat their patients – and communicate to the public – without appearing political.
“The people that are doing the attacking are in some ways themselves victims,” said Peter Hotez, MD, PhD, dean of the National School of Tropical Medicine at Baylor College of Medicine, Houston. “They’re victims of the antiscience, antihealth ecosystem coming out of Fox News, the House Freedom Caucus, the CPAC conference, coming out of contrarian intellectuals.”
Many of Dr. Hotez’s colleagues don’t want to talk about the political right as an enabler of scientific disinformation, he said, but that doesn’t change what the evidence shows. The vast majority of state and national bills opposing vaccination, gender-affirming care, comprehensive reproductive care, and other evidence-based medical care often come from Republican legislators.
When politics and health care collide
“We’re in an incredible status quo,” said William Schaffner, MD, the previous director of the Infectious Diseases Society of America and a professor of infectious diseases and preventive medicine at Vanderbilt University, Nashville, Tenn. “You can’t get away from the politics, because you have [political] candidates espousing certain concepts that are antithetical to good public health.”
In March 2023, Florida Gov. Ron DeSantis’s surgeon general, Joseph Ladapo, MD, PhD, warned that COVID vaccines are harmful to young men, prompting rebukes from federal health authorities. It later came out that Dr. Ladapo had changed some of the results of the study before issuing his warning. But long before 2023, there emerged an increasing gap in COVID deaths between red states and blue states, mirroring the vaccination rates in those states. The redder the state, the higher the death toll.
It’s not just Republican Party culture warriors; medical misinformation is also finding increasing purchase on the far left. Robert F. Kennedy Jr. and Marianne Williamson, both of whom have launched long-shot challenges to President Biden for the 2024 Democratic nomination, had promoted antivaccine ideas long before the COVID pandemic. Mr. Kennedy continues to spread misinformation.
In June 2023, Joe Rogan hosted Mr. Kennedy, on his podcast. During the episode, Mr. Rogan listened uncritically as Mr. Kennedy told his millions of listeners that vaccines cause autism and that 5G causes cancer, among other fringe, often-debunked theories.
Dr. Hotez, a prominent misinformation debunker who was also part of a team that designed a low-cost COVID-19 vaccine, wrote on Twitter that the episode was “just awful.”
The backlash began almost immediately. Mr. Rogan, who has over 11 million followers on Twitter, responded with a public challenge for Dr. Hotez to debate Mr. Kennedy on Mr. Rogan’s show, with a reward of $100,000 to the charity of Dr. Hotez’s choice. More offers streamed in, including from Elon Musk, who tweeted that Dr. Hotez was “afraid of a public debate, because he knows he’s wrong.” More supporters of Mr. Kennedy and Mr. Rogan piled on.
Vaccine skeptics even showed up at Dr. Hotez’s house, filming him as he was returning from buying a Father’s Day cake and taunting him to debate Mr. Kennedy.
A turn in the pandemic
For a precious few weeks at the start of the pandemic, it felt as though the country was all in this together. There were arguments against closing schools and shutting down businesses, but for the most part, the nation had about 4 solid weeks of solidarity.
As masking mandates changed and the public health establishment lost the confidence of Americans, the veneer of solidarity began to chip away.
“Things were changing so rapidly during the pandemic that it was very hard for staff and patients to understand the changing guidelines, whether it was visitor constraints or masking,” said Carrie Nelson, the chief medical officer at the telehealth company AmWell, who worked as a supervisor at a large health care system in the Midwest until 2021.
In the midst of the public health crisis, former President Trump was downplaying the severity of the disease and was silencing officials from the Centers for Disease Control and Prevention, such as Nancy Messonier, who warned from the very beginning of the pandemic’s potential.
When the vaccines came out, the latent antivaccine movement flared up once again. And this time – unlike in decades past – the debate over vaccines had become partisan.
“Before the pandemic,” said Christopher Thomas, an emergency physician on the West Coast who requested that a pseudonym be used because of personal threats he has received, “patients wouldn’t really challenge me or throw out weird questions.” It’s not that he never encountered pushback, but the stakes felt lower, and people largely deferred to his medical expertise. “If we got a parent who had not vaccinated their child, I would totally engage back then,” Dr. Thomas said.
But the pandemic – and America’s response to it – changed the conversation. “The rhetoric ... switched from downplaying the virus to demonizing the vaccines,” Dr. Thomas said.
The toll on health care professionals
By the time vaccines were available, the public had begun to conflate doctors with public health experts, since both were “pushing” the vaccine.
“Most people probably don’t really know the difference between clinical medicine and public health,” said Richard Pan, MD, MPH, a pediatrician and California legislator who sponsored two bills – now laws – that strengthened state childhood vaccination requirements.
At first, it was clearly public health officials, such as Anthony Fauci, MD, who were the face of measures to mitigate the virus. But as doctors became the enforcers of those measures, the line between physicians and public health officials blurred.
A lot of the anger then shifted toward doctors, nurses, and other health care professionals, Dr. Pan said, “because we were, of course, the ones who would be administering the vaccines. They don’t really think of their doctor as a government person until your doctor is carrying a [government] message.”
Given the pressures and struggles of the past few years, it’s no surprise that burnout among health care professionals is high. According to an April 2023 study by the National Council of State Boards of Nursing and the National Forum of State Nursing Workforce Centers, an estimated 800,000 nurses expect to leave the profession by 2027, driven first and foremost by “stress and burnout.”
All of these departures in medicine’s “great resignation” have left hospitals and health care organizations even more short staffed, thereby increasing even more the pressure and burnout on those left.
The pandemic had already badly exacerbated the already widespread problem of burnout in the medical field, which Ms. Nelson said has contributed to the tension.
“The burnout problem that we have in health care is not a good basis for the development of a good therapeutic relationship,” Ms. Nelson said. “Burnout is fraught with apathy and desensitization to human emotions. It takes away the empathy that we once had for people that we see.”
What comes next?
Almost exactly 3 years after the world learned about SARS-CoV-2, Biden declared an end to the coronavirus public health emergency in April 2023. Yet, Americans continue to die from COVID, and the anger that bloomed and spread has not abated.
“I think we’re in a new steady state of violence in health care settings,” Ms. Nelson said. “It’s not gone down, because people are still very distressed.” That’s evident from the high prevalence of mental health conditions, the financial strain of first the pandemic and then inflation, and the overall traumatic impact the pandemic had on people, whether they recognize it or not.
The first step to solving any problem is, as the saying goes, to admit that there is a problem.
“I think people need to start stepping out of their comfort bubbles and start to look at things that make them uncomfortable,” Dr. Thomas said, but he doesn’t see that happening any time soon. “I’ve been very let down by physicians and embarrassed by the American physician organizations.”
The medical board in his state, he said, has stood by as some doctors continue misrepresenting medical evidence. “That’s been really, really hard on me. I didn’t think that the medical boards would go so far as to look the other way for something that was this tremendously bad.”
There are others who can take the lead – if they’re willing.
“There are some things the medical societies and academic health centers can do,” Dr. Hotez said, “starting with building up a culture of physicians and health care providers feeling comfortable in the public domain.” He said the messaging when he was getting his degrees was not to engage the public and not to talk to journalists because that was “self-promotion” or “grandstanding.” But the world is different now. Health care professionals need training in public engagement and communication, he said, and the culture needs to change so that health care providers feel comfortable speaking out without feeling “the sword of Damocles over their heads” every time they talk to a reporter, Dr. Hotez said.
There may be no silver bullet to solve the big-picture trust problem in medicine and public health. No TV appearance or quote in an article can solve it. But on an individual level — through careful relationship building with patients – doctors can strengthen that trust.
Telehealth may help with that, but there’s a fine balance there, Ms. Nelson cautioned. On the one hand, with the doctor and the patient each in their own private spaces, where they feel safe and comfortable, the overall experience can be more therapeutic and less stressful. At the same time, telehealth can pile on change-management tasks that can exacerbate burnout, “so it’s a delicate thing we have to approach.”
One very thin silver lining that could emerge from the way in which patients have begun to try to take charge of their care.
“They should fully understand the reasoning behind the recommendations that physicians are making,” Ms. Nelson said. “I’d like to see us get to a happy medium where it’s a partnership. We can’t go back to the old school where the doctor knows best and you don’t ever question him.
“What we need is the partnership, and I would love to see that as the silver lining, but the anger has got to settle down in order for that kind of productive thing to happen.”
As for the big picture? There’s a limit to what even society’s “miracle workers” can do. “The biggest priority right now for the health system is to protect their staff whatever way they can and do some training in deescalation,” Ms. Nelson said. “But I don’t think health care can solve the societal issues that seem to be creating this.”
A version of this article first appeared on Medscape.com.