User login
Treatment of Axial Psoriatic Arthritis

Psoriatic arthritis (PsA) is a heterogenous inflammatory disease that may involve several different domains, including peripheral joints, entheses, nails, axial skeleton, and skin. A recent increased awareness of PsA has accompanied a large increase in available therapeutic options. In addition to traditional disease-modifying antirheumatic drugs (DMARDs), new biologics and targeted small molecules have now been shown to be effective in PsA. These agents include those targeting pathways involving tumor necrosis factor (TNF), cytotoxic T-lymphocyte–associated protein 4 (CTLA-4), interleukins (IL) 12, 17, 23, janus kinase (JAK), and phosphodiesterase 4 (PDE4). These agents have demonstrated efficacy in outcome measures developed for peripheral arthritis, such as the American College of Rheumatology 20 (ACR20) response. However, an ongoing question is whether these agents are equally effective in axial disease. Based on our experience and the existing literature, we believe that some of these agents, including PDE4 and IL-23 inhibitors, are not effective for axial disease.
Moll and Wright’s original description of PsA estimated that 5% of patients with PsA had axial disease1; however, they were describing patients in whom axial arthritis was the predominant, or the only, manifestation. There are many patients for whom axial symptoms are just one of several domains of disease activity. With this in mind, and depending on the cohort studied, the estimated overall prevalence of axial disease ranges from 7% to 32% in patients with PsA.2 This is in contrast to peripheral arthritis, a domain that occurs in most patients with PsA and is the most common manifestation of PsA.2 We believe there are differences in axial and peripheral response among some of the drugs used to treat PsA; therefore it is critical to consider both the presence and magnitude of axial involvement.
An absence of axial PsA–specific clinical trials complicates navigating this treatment domain. Most considerations regarding treatment options for axial disease in PsA are extrapolated from ankylosing spondylitis (AS) trials and experience, as is the case for the TNF and JAK inhibitors. To our knowledge, only one high-quality randomized trial, MAXIMISE, looked specifically at the treatment of axial PsA, in this case with the IL-17 inhibitor secukinumab.3 This trial demonstrated efficacy of secukinumab in reducing symptoms and acute phase reactants in patients with PsA who were categorized as having active axial disease using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). Other than conclusions drawn from AS trials and from this single axial PsA randomized controlled trial, data on the treatment of axial PsA are drawn entirely from observational and post-hoc analyses. As there are no consensus criteria for axial PsA, the cohorts included in these data may vary. This heterogeneity showcases the diversity in patients with PsA with axial disease but complicates the generalizability of the findings to individual patients.
Another challenge in understanding axial response to medication is the lack of specific, validated outcome measures for axial PsA. The BASDAI and, more recently, the Assessment in Ankylosing Spondylitis (ASAS) and the Ankylosing Spondylitis Disease Activity Score (ASDAS), all developed specifically for AS, are often used to measure treatment response. The BASDAI incorporates patient-reported symptoms which include fatigue, peripheral joint pain/swelling, tenderness, and morning stiffness not specifically localized to the back. The ASDAS also includes a C-reactive protein measurement.
When used to assess response in PsA, however, these patient-reported outcomes may not be precise enough to separate the impact of axial disease or symptoms from that of peripheral disease. Only question 2 on the BASDAI specifically addresses axial complaints: “How would you describe the overall level of AS-related pain you have had in your neck, back, or hips?” Even this question is vulnerable to confounding from noninflammatory causes of back pain. Although these issues exist with patient-reported outcomes, objective spinal mobility measures used in evaluation of AS, including the modified Schober test, lumbar side flexion, and cervical rotation, have been demonstrated also to perform well in axial PsA.4
This was corroborated in the INSPIRE study, which showed adequate interobserver reliability in primary AS that was equally reproducible in axial PsA, with most measures, including occiput to wall, modified Schober test, cervical rotation, lateral bending, and hip mobility, performing in a “good to excellent” manner.5 Therefore, the inclusion of these objective measures in future therapeutic studies may enhance the external validation of available data.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) has established therapeutic guidelines for psoriatic disease based on currently available literature and data. Similar to previous iterations of guidelines, GRAPPA continues to recommend agents with TNF inhibition or IL-17 inhibition for patients with PsA with axial disease who have failed conservative therapy with nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and/or glucocorticoid injections. Newly recommended in the latest iteration of the GRAPPA guidelines, based on the efficacy of these agents in AS, is the use of JAK inhibitors for axial PsA.6
Although TNF, IL-17, and JAK targeted therapies have demonstrated more likely benefit, albeit subject to the trial limitations previously discussed, the question remains whether agents targeting PDE4 and IL-23 are an effective option for axial PsA. Studies of both PDE4 and IL-23 inhibitors in AS have not demonstrated adequate benefit, which, importantly, contrasts with the previously mentioned and recommended therapies. Additionally, there are no primary randomized control trials that have directly evaluated the efficacy of IL-23 therapy in axial PsA.
Existing data about potential benefit come from post-hoc analyses of the PSUMMIT 1 and 2 trials7-10 with ustekinumab (which inhibits IL-12 and IL-23) and the DISCOVER trials11-13 with guselkumab (a pure IL-23 inhibitor). However, these analyses relied on a physician-reported diagnosis of axial disease and not on prespecified entry criteria. This lack of uniform diagnostic criteria may introduce bias into the interpretation of the results and limit external validation. All patients in these trials had a significant burden of peripheral arthritis; therefore it is hard to know whether, even in patients with physician-reported axial disease, improvement in general outcome measures were due to true amelioration of axial disease or were confounded by improvement in peripheral and skin domains. The analysis of these trials did look specifically at patient answers to BASDAI question 2 regarding level of neck, back, or hip pain. However, it remains difficult to be certain that the results are truly a reflection of axial symptoms and are not driven by patient-perceived improvement in other disease domains and an overall positive trajectory in well-being.
In our years of practice, when we turned to biologic agents, the IL-23 inhibitors and the IL-12/23 inhibitor have not been as effective in patients with PsA who have axial-predominant symptoms. The lack of efficacy of these agents in AS, in contrast to their benefit in psoriatic skin and peripheral joint disease, raises questions about the pathophysiologic role of IL-23 in axial disease, which is yet to be fully understood. For patients with a significant burden of axial pain, in concordance with the consensus from GRAPPA,6 our strategy is to start with TNF, IL-17, or JAK targeted therapies, with the choice based on patient-specific factors, including patient comorbidities, patient administration preference, and insurance coverage. We do believe it is reasonable to try IL-23–targeted therapies in patients who have mild axial symptoms when their predominant symptoms are in other domains, such as the peripheral joints or skin. In our opinion, more convincing data supporting IL-23 inhibition are required to move this into the forefront of axial-predominant PsA therapy. Clearly the investigation of axial disease in PsA lags behind that of peripheral and skin domains. Specific classification criteria for axial PsA, as are being currently developed by GRAPPA, should facilitate more focused therapeutic trials that can better inform optimal treatment of patients with this subset of disease.
- Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973;3(1):55-78. doi:10.1016/0049-0172(73)90035-8
- Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum Dis Clin North Am. 2015;41(4):545-568. doi:10.1016/j.rdc.2015.07.001
- Baraliakos X, Gossec L, Pournara E, et al. Secukinumab in patients with psoriatic arthritis and axial manifestations: results from the double-blind, randomised, phase 3 MAXIMISE trial. Ann Rheum Dis. 2021;80(5):582-590. doi:10.1136/annrheumdis-2020-218808
- Fernández-Sueiro JL, Willisch A, Pértega-Díaz S, et al. Evaluation of ankylosing spondylitis spinal mobility measurements in the assessment of spinal involvement in psoriatic arthritis. Arthritis Rheum. 2009;61(3):386-392. doi:10.1002/art.24280
- Gladman DD, Inman RD, Cook RJ, et al. International spondyloarthritis interobserver reliability exercise—the INSPIRE study: I. Assessment of spinal measures. J Rheumatol. 2007;34(8):1733-1739.
- Coates LC, Corp N, van der Windt DA, O’Sullivan D, Soriano ER, Kavanaugh A. GRAPPA treatment recommendations: 2021 update. J Rheumatol. 2022;49(6 suppl 1):52-54. doi:10.3899/jrheum.211331
- McInnes IB, Kavanaugh A, Gottlieb AB, et al; PSUMMIT 1 Study Group. Efficacy and safety of ustekinumab in patients with active psoriatic arthritis: 1 year results of the phase 3, multicentre, double-blind, placebo-controlled PSUMMIT 1 trial. Lancet. 2013;382(9894):780-789. doi:10.1016/S0140-6736(13)60594-2
- Ritchlin C, Rahman P, Kavanaugh A, et al; PSUMMIT 2 Study Group. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999. doi:10.1136/annrheumdis-2013-204655
- Kavanaugh A, Puig L, Gottlieb AB, et al. Efficacy and safety of ustekinumab in psoriatic arthritis patients with peripheral arthritis and physician-reported spondylitis: post-hoc analyses from two phase III, multicentre, double-blind, placebo-controlled studies (PSUMMIT-1/PSUMMIT-2). Ann Rheum Dis. 2016;75(11):1984-1988. doi:10.1136/annrheumdis-2015-209068
- McInnes IB, Chakravarty SD, Apaolaza I, et al. Efficacy of ustekinumab in biologic-naïve patients with psoriatic arthritis by prior treatment exposure and disease duration: data from PSUMMIT 1 and PSUMMIT 2. RMD Open. 2019;5(2):e000990. doi:10.1136/rmdopen-2019-000990
- Deodhar A, Helliwell PS, Boehncke WH, et al; DISCOVER-1 Study Group. Guselkumab in patients with active psoriatic arthritis who were biologic-naive or had previously received TNFα inhibitor treatment (DISCOVER-1): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1115-1125. doi:10.1016/S0140-6736(20)30265-8
- Mease PJ, Rahman P, Gottlieb AB, et al; DISCOVER-2 Study Group. Guselkumab in biologic-naive patients with active psoriatic arthritis (DISCOVER-2): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1126-1136. doi:10.1016/S0140-6736(20)30263-4
- Mease PJ, Helliwell PS, Gladman DD, et al. Efficacy of guselkumab on axial involvement in patients with active psoriatic arthritis and sacroiliitis: a post-hoc analysis of the phase 3 discover-1 and discover-2 studies. Lancet Rheumatol. 2021;3(10). doi:https://doi.org/10.1016/S2665-9913(21)00105-3
Psoriatic arthritis (PsA) is a heterogenous inflammatory disease that may involve several different domains, including peripheral joints, entheses, nails, axial skeleton, and skin. A recent increased awareness of PsA has accompanied a large increase in available therapeutic options. In addition to traditional disease-modifying antirheumatic drugs (DMARDs), new biologics and targeted small molecules have now been shown to be effective in PsA. These agents include those targeting pathways involving tumor necrosis factor (TNF), cytotoxic T-lymphocyte–associated protein 4 (CTLA-4), interleukins (IL) 12, 17, 23, janus kinase (JAK), and phosphodiesterase 4 (PDE4). These agents have demonstrated efficacy in outcome measures developed for peripheral arthritis, such as the American College of Rheumatology 20 (ACR20) response. However, an ongoing question is whether these agents are equally effective in axial disease. Based on our experience and the existing literature, we believe that some of these agents, including PDE4 and IL-23 inhibitors, are not effective for axial disease.
Moll and Wright’s original description of PsA estimated that 5% of patients with PsA had axial disease1; however, they were describing patients in whom axial arthritis was the predominant, or the only, manifestation. There are many patients for whom axial symptoms are just one of several domains of disease activity. With this in mind, and depending on the cohort studied, the estimated overall prevalence of axial disease ranges from 7% to 32% in patients with PsA.2 This is in contrast to peripheral arthritis, a domain that occurs in most patients with PsA and is the most common manifestation of PsA.2 We believe there are differences in axial and peripheral response among some of the drugs used to treat PsA; therefore it is critical to consider both the presence and magnitude of axial involvement.
An absence of axial PsA–specific clinical trials complicates navigating this treatment domain. Most considerations regarding treatment options for axial disease in PsA are extrapolated from ankylosing spondylitis (AS) trials and experience, as is the case for the TNF and JAK inhibitors. To our knowledge, only one high-quality randomized trial, MAXIMISE, looked specifically at the treatment of axial PsA, in this case with the IL-17 inhibitor secukinumab.3 This trial demonstrated efficacy of secukinumab in reducing symptoms and acute phase reactants in patients with PsA who were categorized as having active axial disease using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). Other than conclusions drawn from AS trials and from this single axial PsA randomized controlled trial, data on the treatment of axial PsA are drawn entirely from observational and post-hoc analyses. As there are no consensus criteria for axial PsA, the cohorts included in these data may vary. This heterogeneity showcases the diversity in patients with PsA with axial disease but complicates the generalizability of the findings to individual patients.
Another challenge in understanding axial response to medication is the lack of specific, validated outcome measures for axial PsA. The BASDAI and, more recently, the Assessment in Ankylosing Spondylitis (ASAS) and the Ankylosing Spondylitis Disease Activity Score (ASDAS), all developed specifically for AS, are often used to measure treatment response. The BASDAI incorporates patient-reported symptoms which include fatigue, peripheral joint pain/swelling, tenderness, and morning stiffness not specifically localized to the back. The ASDAS also includes a C-reactive protein measurement.
When used to assess response in PsA, however, these patient-reported outcomes may not be precise enough to separate the impact of axial disease or symptoms from that of peripheral disease. Only question 2 on the BASDAI specifically addresses axial complaints: “How would you describe the overall level of AS-related pain you have had in your neck, back, or hips?” Even this question is vulnerable to confounding from noninflammatory causes of back pain. Although these issues exist with patient-reported outcomes, objective spinal mobility measures used in evaluation of AS, including the modified Schober test, lumbar side flexion, and cervical rotation, have been demonstrated also to perform well in axial PsA.4
This was corroborated in the INSPIRE study, which showed adequate interobserver reliability in primary AS that was equally reproducible in axial PsA, with most measures, including occiput to wall, modified Schober test, cervical rotation, lateral bending, and hip mobility, performing in a “good to excellent” manner.5 Therefore, the inclusion of these objective measures in future therapeutic studies may enhance the external validation of available data.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) has established therapeutic guidelines for psoriatic disease based on currently available literature and data. Similar to previous iterations of guidelines, GRAPPA continues to recommend agents with TNF inhibition or IL-17 inhibition for patients with PsA with axial disease who have failed conservative therapy with nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and/or glucocorticoid injections. Newly recommended in the latest iteration of the GRAPPA guidelines, based on the efficacy of these agents in AS, is the use of JAK inhibitors for axial PsA.6
Although TNF, IL-17, and JAK targeted therapies have demonstrated more likely benefit, albeit subject to the trial limitations previously discussed, the question remains whether agents targeting PDE4 and IL-23 are an effective option for axial PsA. Studies of both PDE4 and IL-23 inhibitors in AS have not demonstrated adequate benefit, which, importantly, contrasts with the previously mentioned and recommended therapies. Additionally, there are no primary randomized control trials that have directly evaluated the efficacy of IL-23 therapy in axial PsA.
Existing data about potential benefit come from post-hoc analyses of the PSUMMIT 1 and 2 trials7-10 with ustekinumab (which inhibits IL-12 and IL-23) and the DISCOVER trials11-13 with guselkumab (a pure IL-23 inhibitor). However, these analyses relied on a physician-reported diagnosis of axial disease and not on prespecified entry criteria. This lack of uniform diagnostic criteria may introduce bias into the interpretation of the results and limit external validation. All patients in these trials had a significant burden of peripheral arthritis; therefore it is hard to know whether, even in patients with physician-reported axial disease, improvement in general outcome measures were due to true amelioration of axial disease or were confounded by improvement in peripheral and skin domains. The analysis of these trials did look specifically at patient answers to BASDAI question 2 regarding level of neck, back, or hip pain. However, it remains difficult to be certain that the results are truly a reflection of axial symptoms and are not driven by patient-perceived improvement in other disease domains and an overall positive trajectory in well-being.
In our years of practice, when we turned to biologic agents, the IL-23 inhibitors and the IL-12/23 inhibitor have not been as effective in patients with PsA who have axial-predominant symptoms. The lack of efficacy of these agents in AS, in contrast to their benefit in psoriatic skin and peripheral joint disease, raises questions about the pathophysiologic role of IL-23 in axial disease, which is yet to be fully understood. For patients with a significant burden of axial pain, in concordance with the consensus from GRAPPA,6 our strategy is to start with TNF, IL-17, or JAK targeted therapies, with the choice based on patient-specific factors, including patient comorbidities, patient administration preference, and insurance coverage. We do believe it is reasonable to try IL-23–targeted therapies in patients who have mild axial symptoms when their predominant symptoms are in other domains, such as the peripheral joints or skin. In our opinion, more convincing data supporting IL-23 inhibition are required to move this into the forefront of axial-predominant PsA therapy. Clearly the investigation of axial disease in PsA lags behind that of peripheral and skin domains. Specific classification criteria for axial PsA, as are being currently developed by GRAPPA, should facilitate more focused therapeutic trials that can better inform optimal treatment of patients with this subset of disease.
Psoriatic arthritis (PsA) is a heterogenous inflammatory disease that may involve several different domains, including peripheral joints, entheses, nails, axial skeleton, and skin. A recent increased awareness of PsA has accompanied a large increase in available therapeutic options. In addition to traditional disease-modifying antirheumatic drugs (DMARDs), new biologics and targeted small molecules have now been shown to be effective in PsA. These agents include those targeting pathways involving tumor necrosis factor (TNF), cytotoxic T-lymphocyte–associated protein 4 (CTLA-4), interleukins (IL) 12, 17, 23, janus kinase (JAK), and phosphodiesterase 4 (PDE4). These agents have demonstrated efficacy in outcome measures developed for peripheral arthritis, such as the American College of Rheumatology 20 (ACR20) response. However, an ongoing question is whether these agents are equally effective in axial disease. Based on our experience and the existing literature, we believe that some of these agents, including PDE4 and IL-23 inhibitors, are not effective for axial disease.
Moll and Wright’s original description of PsA estimated that 5% of patients with PsA had axial disease1; however, they were describing patients in whom axial arthritis was the predominant, or the only, manifestation. There are many patients for whom axial symptoms are just one of several domains of disease activity. With this in mind, and depending on the cohort studied, the estimated overall prevalence of axial disease ranges from 7% to 32% in patients with PsA.2 This is in contrast to peripheral arthritis, a domain that occurs in most patients with PsA and is the most common manifestation of PsA.2 We believe there are differences in axial and peripheral response among some of the drugs used to treat PsA; therefore it is critical to consider both the presence and magnitude of axial involvement.
An absence of axial PsA–specific clinical trials complicates navigating this treatment domain. Most considerations regarding treatment options for axial disease in PsA are extrapolated from ankylosing spondylitis (AS) trials and experience, as is the case for the TNF and JAK inhibitors. To our knowledge, only one high-quality randomized trial, MAXIMISE, looked specifically at the treatment of axial PsA, in this case with the IL-17 inhibitor secukinumab.3 This trial demonstrated efficacy of secukinumab in reducing symptoms and acute phase reactants in patients with PsA who were categorized as having active axial disease using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI). Other than conclusions drawn from AS trials and from this single axial PsA randomized controlled trial, data on the treatment of axial PsA are drawn entirely from observational and post-hoc analyses. As there are no consensus criteria for axial PsA, the cohorts included in these data may vary. This heterogeneity showcases the diversity in patients with PsA with axial disease but complicates the generalizability of the findings to individual patients.
Another challenge in understanding axial response to medication is the lack of specific, validated outcome measures for axial PsA. The BASDAI and, more recently, the Assessment in Ankylosing Spondylitis (ASAS) and the Ankylosing Spondylitis Disease Activity Score (ASDAS), all developed specifically for AS, are often used to measure treatment response. The BASDAI incorporates patient-reported symptoms which include fatigue, peripheral joint pain/swelling, tenderness, and morning stiffness not specifically localized to the back. The ASDAS also includes a C-reactive protein measurement.
When used to assess response in PsA, however, these patient-reported outcomes may not be precise enough to separate the impact of axial disease or symptoms from that of peripheral disease. Only question 2 on the BASDAI specifically addresses axial complaints: “How would you describe the overall level of AS-related pain you have had in your neck, back, or hips?” Even this question is vulnerable to confounding from noninflammatory causes of back pain. Although these issues exist with patient-reported outcomes, objective spinal mobility measures used in evaluation of AS, including the modified Schober test, lumbar side flexion, and cervical rotation, have been demonstrated also to perform well in axial PsA.4
This was corroborated in the INSPIRE study, which showed adequate interobserver reliability in primary AS that was equally reproducible in axial PsA, with most measures, including occiput to wall, modified Schober test, cervical rotation, lateral bending, and hip mobility, performing in a “good to excellent” manner.5 Therefore, the inclusion of these objective measures in future therapeutic studies may enhance the external validation of available data.
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) has established therapeutic guidelines for psoriatic disease based on currently available literature and data. Similar to previous iterations of guidelines, GRAPPA continues to recommend agents with TNF inhibition or IL-17 inhibition for patients with PsA with axial disease who have failed conservative therapy with nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, and/or glucocorticoid injections. Newly recommended in the latest iteration of the GRAPPA guidelines, based on the efficacy of these agents in AS, is the use of JAK inhibitors for axial PsA.6
Although TNF, IL-17, and JAK targeted therapies have demonstrated more likely benefit, albeit subject to the trial limitations previously discussed, the question remains whether agents targeting PDE4 and IL-23 are an effective option for axial PsA. Studies of both PDE4 and IL-23 inhibitors in AS have not demonstrated adequate benefit, which, importantly, contrasts with the previously mentioned and recommended therapies. Additionally, there are no primary randomized control trials that have directly evaluated the efficacy of IL-23 therapy in axial PsA.
Existing data about potential benefit come from post-hoc analyses of the PSUMMIT 1 and 2 trials7-10 with ustekinumab (which inhibits IL-12 and IL-23) and the DISCOVER trials11-13 with guselkumab (a pure IL-23 inhibitor). However, these analyses relied on a physician-reported diagnosis of axial disease and not on prespecified entry criteria. This lack of uniform diagnostic criteria may introduce bias into the interpretation of the results and limit external validation. All patients in these trials had a significant burden of peripheral arthritis; therefore it is hard to know whether, even in patients with physician-reported axial disease, improvement in general outcome measures were due to true amelioration of axial disease or were confounded by improvement in peripheral and skin domains. The analysis of these trials did look specifically at patient answers to BASDAI question 2 regarding level of neck, back, or hip pain. However, it remains difficult to be certain that the results are truly a reflection of axial symptoms and are not driven by patient-perceived improvement in other disease domains and an overall positive trajectory in well-being.
In our years of practice, when we turned to biologic agents, the IL-23 inhibitors and the IL-12/23 inhibitor have not been as effective in patients with PsA who have axial-predominant symptoms. The lack of efficacy of these agents in AS, in contrast to their benefit in psoriatic skin and peripheral joint disease, raises questions about the pathophysiologic role of IL-23 in axial disease, which is yet to be fully understood. For patients with a significant burden of axial pain, in concordance with the consensus from GRAPPA,6 our strategy is to start with TNF, IL-17, or JAK targeted therapies, with the choice based on patient-specific factors, including patient comorbidities, patient administration preference, and insurance coverage. We do believe it is reasonable to try IL-23–targeted therapies in patients who have mild axial symptoms when their predominant symptoms are in other domains, such as the peripheral joints or skin. In our opinion, more convincing data supporting IL-23 inhibition are required to move this into the forefront of axial-predominant PsA therapy. Clearly the investigation of axial disease in PsA lags behind that of peripheral and skin domains. Specific classification criteria for axial PsA, as are being currently developed by GRAPPA, should facilitate more focused therapeutic trials that can better inform optimal treatment of patients with this subset of disease.
- Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973;3(1):55-78. doi:10.1016/0049-0172(73)90035-8
- Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum Dis Clin North Am. 2015;41(4):545-568. doi:10.1016/j.rdc.2015.07.001
- Baraliakos X, Gossec L, Pournara E, et al. Secukinumab in patients with psoriatic arthritis and axial manifestations: results from the double-blind, randomised, phase 3 MAXIMISE trial. Ann Rheum Dis. 2021;80(5):582-590. doi:10.1136/annrheumdis-2020-218808
- Fernández-Sueiro JL, Willisch A, Pértega-Díaz S, et al. Evaluation of ankylosing spondylitis spinal mobility measurements in the assessment of spinal involvement in psoriatic arthritis. Arthritis Rheum. 2009;61(3):386-392. doi:10.1002/art.24280
- Gladman DD, Inman RD, Cook RJ, et al. International spondyloarthritis interobserver reliability exercise—the INSPIRE study: I. Assessment of spinal measures. J Rheumatol. 2007;34(8):1733-1739.
- Coates LC, Corp N, van der Windt DA, O’Sullivan D, Soriano ER, Kavanaugh A. GRAPPA treatment recommendations: 2021 update. J Rheumatol. 2022;49(6 suppl 1):52-54. doi:10.3899/jrheum.211331
- McInnes IB, Kavanaugh A, Gottlieb AB, et al; PSUMMIT 1 Study Group. Efficacy and safety of ustekinumab in patients with active psoriatic arthritis: 1 year results of the phase 3, multicentre, double-blind, placebo-controlled PSUMMIT 1 trial. Lancet. 2013;382(9894):780-789. doi:10.1016/S0140-6736(13)60594-2
- Ritchlin C, Rahman P, Kavanaugh A, et al; PSUMMIT 2 Study Group. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999. doi:10.1136/annrheumdis-2013-204655
- Kavanaugh A, Puig L, Gottlieb AB, et al. Efficacy and safety of ustekinumab in psoriatic arthritis patients with peripheral arthritis and physician-reported spondylitis: post-hoc analyses from two phase III, multicentre, double-blind, placebo-controlled studies (PSUMMIT-1/PSUMMIT-2). Ann Rheum Dis. 2016;75(11):1984-1988. doi:10.1136/annrheumdis-2015-209068
- McInnes IB, Chakravarty SD, Apaolaza I, et al. Efficacy of ustekinumab in biologic-naïve patients with psoriatic arthritis by prior treatment exposure and disease duration: data from PSUMMIT 1 and PSUMMIT 2. RMD Open. 2019;5(2):e000990. doi:10.1136/rmdopen-2019-000990
- Deodhar A, Helliwell PS, Boehncke WH, et al; DISCOVER-1 Study Group. Guselkumab in patients with active psoriatic arthritis who were biologic-naive or had previously received TNFα inhibitor treatment (DISCOVER-1): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1115-1125. doi:10.1016/S0140-6736(20)30265-8
- Mease PJ, Rahman P, Gottlieb AB, et al; DISCOVER-2 Study Group. Guselkumab in biologic-naive patients with active psoriatic arthritis (DISCOVER-2): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1126-1136. doi:10.1016/S0140-6736(20)30263-4
- Mease PJ, Helliwell PS, Gladman DD, et al. Efficacy of guselkumab on axial involvement in patients with active psoriatic arthritis and sacroiliitis: a post-hoc analysis of the phase 3 discover-1 and discover-2 studies. Lancet Rheumatol. 2021;3(10). doi:https://doi.org/10.1016/S2665-9913(21)00105-3
- Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973;3(1):55-78. doi:10.1016/0049-0172(73)90035-8
- Ogdie A, Weiss P. The epidemiology of psoriatic arthritis. Rheum Dis Clin North Am. 2015;41(4):545-568. doi:10.1016/j.rdc.2015.07.001
- Baraliakos X, Gossec L, Pournara E, et al. Secukinumab in patients with psoriatic arthritis and axial manifestations: results from the double-blind, randomised, phase 3 MAXIMISE trial. Ann Rheum Dis. 2021;80(5):582-590. doi:10.1136/annrheumdis-2020-218808
- Fernández-Sueiro JL, Willisch A, Pértega-Díaz S, et al. Evaluation of ankylosing spondylitis spinal mobility measurements in the assessment of spinal involvement in psoriatic arthritis. Arthritis Rheum. 2009;61(3):386-392. doi:10.1002/art.24280
- Gladman DD, Inman RD, Cook RJ, et al. International spondyloarthritis interobserver reliability exercise—the INSPIRE study: I. Assessment of spinal measures. J Rheumatol. 2007;34(8):1733-1739.
- Coates LC, Corp N, van der Windt DA, O’Sullivan D, Soriano ER, Kavanaugh A. GRAPPA treatment recommendations: 2021 update. J Rheumatol. 2022;49(6 suppl 1):52-54. doi:10.3899/jrheum.211331
- McInnes IB, Kavanaugh A, Gottlieb AB, et al; PSUMMIT 1 Study Group. Efficacy and safety of ustekinumab in patients with active psoriatic arthritis: 1 year results of the phase 3, multicentre, double-blind, placebo-controlled PSUMMIT 1 trial. Lancet. 2013;382(9894):780-789. doi:10.1016/S0140-6736(13)60594-2
- Ritchlin C, Rahman P, Kavanaugh A, et al; PSUMMIT 2 Study Group. Efficacy and safety of the anti-IL-12/23 p40 monoclonal antibody, ustekinumab, in patients with active psoriatic arthritis despite conventional non-biological and biological anti-tumour necrosis factor therapy: 6-month and 1-year results of the phase 3, multicentre, double-blind, placebo-controlled, randomised PSUMMIT 2 trial. Ann Rheum Dis. 2014;73(6):990-999. doi:10.1136/annrheumdis-2013-204655
- Kavanaugh A, Puig L, Gottlieb AB, et al. Efficacy and safety of ustekinumab in psoriatic arthritis patients with peripheral arthritis and physician-reported spondylitis: post-hoc analyses from two phase III, multicentre, double-blind, placebo-controlled studies (PSUMMIT-1/PSUMMIT-2). Ann Rheum Dis. 2016;75(11):1984-1988. doi:10.1136/annrheumdis-2015-209068
- McInnes IB, Chakravarty SD, Apaolaza I, et al. Efficacy of ustekinumab in biologic-naïve patients with psoriatic arthritis by prior treatment exposure and disease duration: data from PSUMMIT 1 and PSUMMIT 2. RMD Open. 2019;5(2):e000990. doi:10.1136/rmdopen-2019-000990
- Deodhar A, Helliwell PS, Boehncke WH, et al; DISCOVER-1 Study Group. Guselkumab in patients with active psoriatic arthritis who were biologic-naive or had previously received TNFα inhibitor treatment (DISCOVER-1): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1115-1125. doi:10.1016/S0140-6736(20)30265-8
- Mease PJ, Rahman P, Gottlieb AB, et al; DISCOVER-2 Study Group. Guselkumab in biologic-naive patients with active psoriatic arthritis (DISCOVER-2): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10230):1126-1136. doi:10.1016/S0140-6736(20)30263-4
- Mease PJ, Helliwell PS, Gladman DD, et al. Efficacy of guselkumab on axial involvement in patients with active psoriatic arthritis and sacroiliitis: a post-hoc analysis of the phase 3 discover-1 and discover-2 studies. Lancet Rheumatol. 2021;3(10). doi:https://doi.org/10.1016/S2665-9913(21)00105-3
Culinary medicine guides rural GI doctor’s career
Someone once told Christina Tennyson, MD, that clinical medicine was a grind. Instead of veering away from the profession, she dove in. Medicine will always have its frustrations, she acknowledged.
However, “finding areas that interest me and incorporating those into clinical practice has really helped me enjoy the practice of medicine,” said Dr. Tennyson, who works at Augusta Health in Fishersville, Va.

It has also inspired her to think outside the box in her gastroenterology practice. What her patients eat and the lifestyle choices they make is a central focus of her work.
Q: Why did you choose GI?
Dr. Tennyson: I always had an interest in nutrition. During training at medical school at NYU [New York University], I also really loved learning all I could about internal medicine. I worked with a great surgical team as a student and enjoyed being in the operating room. Although I knew I didn’t want to enter surgery, the experience encouraged me to pursue gastroenterology as it involved nutrition, internal medicine, and procedures as well as my favorite organ, the small bowel. I worked with some great mentors in gastroenterology, such as Dr. David Metz and Dr. Dave Katzka, at the University of Pennsylvania as a resident. I enjoyed taking care of patients with both acute and chronic conditions as well as the mix of doing procedures and seeing patients in the office. It also provided me the opportunity to incorporate nutrition into my clinical practice.
Q: What gives you the most joy in your day-to-day practice?
Dr. Tennyson: I enjoy helping my patients make meaningful lifestyle changes that can positively impact digestive health and well-being. I try to address topics related to lifestyle medicine in most of my clinical visits including eating more fiber/plants, exercise, positive relationships, and stress management. Many of the conditions we treat as gastroenterologists can benefit from addressing aspects of lifestyle along with our conventional medical therapies. I reinforce that attention to these areas can make a difference. I enjoy sharing recipes, books, and websites that I have found helpful.
Q: How has your job changed since you first began your career?
Dr. Tennyson: After fellowship, I joined the faculty at Columbia University and worked at the Celiac Disease Center seeing patients, teaching, and performing clinical research under the mentorship of Peter Green, MD, and Suzanne Lewis, MD. It was a great opportunity to learn and practice in a tertiary center. I later switched roles and joined a general multispecialty community practice in Brooklyn [N.Y.] affiliated with an academic medical center. After practicing in New York for 10 years, I left my clinical practice and performed locums work for several years in underserved rural areas. I enjoyed working in rural areas and took a permanent position at a community hospital in Virginia’s Shenandoah Valley.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Tennyson: The small, rural community hospital where I currently work does not have the same resources and staffing as urban tertiary centers. While we are taking care of the community in our general gastroenterology practice, we’ve also launched an integrated care model in our hospital. We have collaborated with behavioral health, dietitians, nurses, health coaches, exercise physiologists as well as other members of the community, including farmers and a chef. We have performed some innovative, engaging programs, including fermentation workshops, cooking classes, farm walks, and mindfulness programs.
Q: What are you most proud of accomplishing?
Dr. Tennyson: I am proud that I took a nontraditional path after training to do what I enjoy and find rewarding. I received certification during GI fellowship at Mount Sinai [N.Y.] as a physician nutrition specialist. I later completed a fellowship in integrative medicine at the University of Arizona, received certification in lifestyle medicine, and completed coursework in culinary medicine. I really enjoyed doing locums work taking care of patients in other parts of the country, like Mississippi or Maine. I’ve enjoyed working in more rural areas and bringing some innovative programs to the community.
Q: What teacher or mentor had the greatest impact on you?
Dr. Tennyson: Dr. Anthony Grieco while I was a student at NYU. He is an astute clinician, always listened to his patients, loved clinical medicine, and had an endless fund of knowledge. I wanted to be a doctor like him. During my fellowship at Mount Sinai, I was also exposed to many great mentors including Dr. Lloyd Mayer, Dr. Jerome Waye, Dr. Steve Itzkowitz, and Dr. Blair Lewis who encouraged my interest in nutrition and small bowel diseases.
Lightning round
What's your superpower?
Finding fun in mundane things
Favorite movie to quote?
The Princess Bride
What is your favorite form of exercise?
A hike in the woods
Name one thing on your bucket list.
Galapagos Islands trip before my kids grow up
Cats or dogs?
Dogs
Summer or winter?
Summer
Someone once told Christina Tennyson, MD, that clinical medicine was a grind. Instead of veering away from the profession, she dove in. Medicine will always have its frustrations, she acknowledged.
However, “finding areas that interest me and incorporating those into clinical practice has really helped me enjoy the practice of medicine,” said Dr. Tennyson, who works at Augusta Health in Fishersville, Va.
It has also inspired her to think outside the box in her gastroenterology practice. What her patients eat and the lifestyle choices they make is a central focus of her work.
Q: Why did you choose GI?
Dr. Tennyson: I always had an interest in nutrition. During training at medical school at NYU [New York University], I also really loved learning all I could about internal medicine. I worked with a great surgical team as a student and enjoyed being in the operating room. Although I knew I didn’t want to enter surgery, the experience encouraged me to pursue gastroenterology as it involved nutrition, internal medicine, and procedures as well as my favorite organ, the small bowel. I worked with some great mentors in gastroenterology, such as Dr. David Metz and Dr. Dave Katzka, at the University of Pennsylvania as a resident. I enjoyed taking care of patients with both acute and chronic conditions as well as the mix of doing procedures and seeing patients in the office. It also provided me the opportunity to incorporate nutrition into my clinical practice.
Q: What gives you the most joy in your day-to-day practice?
Dr. Tennyson: I enjoy helping my patients make meaningful lifestyle changes that can positively impact digestive health and well-being. I try to address topics related to lifestyle medicine in most of my clinical visits including eating more fiber/plants, exercise, positive relationships, and stress management. Many of the conditions we treat as gastroenterologists can benefit from addressing aspects of lifestyle along with our conventional medical therapies. I reinforce that attention to these areas can make a difference. I enjoy sharing recipes, books, and websites that I have found helpful.
Q: How has your job changed since you first began your career?
Dr. Tennyson: After fellowship, I joined the faculty at Columbia University and worked at the Celiac Disease Center seeing patients, teaching, and performing clinical research under the mentorship of Peter Green, MD, and Suzanne Lewis, MD. It was a great opportunity to learn and practice in a tertiary center. I later switched roles and joined a general multispecialty community practice in Brooklyn [N.Y.] affiliated with an academic medical center. After practicing in New York for 10 years, I left my clinical practice and performed locums work for several years in underserved rural areas. I enjoyed working in rural areas and took a permanent position at a community hospital in Virginia’s Shenandoah Valley.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Tennyson: The small, rural community hospital where I currently work does not have the same resources and staffing as urban tertiary centers. While we are taking care of the community in our general gastroenterology practice, we’ve also launched an integrated care model in our hospital. We have collaborated with behavioral health, dietitians, nurses, health coaches, exercise physiologists as well as other members of the community, including farmers and a chef. We have performed some innovative, engaging programs, including fermentation workshops, cooking classes, farm walks, and mindfulness programs.
Q: What are you most proud of accomplishing?
Dr. Tennyson: I am proud that I took a nontraditional path after training to do what I enjoy and find rewarding. I received certification during GI fellowship at Mount Sinai [N.Y.] as a physician nutrition specialist. I later completed a fellowship in integrative medicine at the University of Arizona, received certification in lifestyle medicine, and completed coursework in culinary medicine. I really enjoyed doing locums work taking care of patients in other parts of the country, like Mississippi or Maine. I’ve enjoyed working in more rural areas and bringing some innovative programs to the community.
Q: What teacher or mentor had the greatest impact on you?
Dr. Tennyson: Dr. Anthony Grieco while I was a student at NYU. He is an astute clinician, always listened to his patients, loved clinical medicine, and had an endless fund of knowledge. I wanted to be a doctor like him. During my fellowship at Mount Sinai, I was also exposed to many great mentors including Dr. Lloyd Mayer, Dr. Jerome Waye, Dr. Steve Itzkowitz, and Dr. Blair Lewis who encouraged my interest in nutrition and small bowel diseases.
Lightning round
What's your superpower?
Finding fun in mundane things
Favorite movie to quote?
The Princess Bride
What is your favorite form of exercise?
A hike in the woods
Name one thing on your bucket list.
Galapagos Islands trip before my kids grow up
Cats or dogs?
Dogs
Summer or winter?
Summer
Someone once told Christina Tennyson, MD, that clinical medicine was a grind. Instead of veering away from the profession, she dove in. Medicine will always have its frustrations, she acknowledged.
However, “finding areas that interest me and incorporating those into clinical practice has really helped me enjoy the practice of medicine,” said Dr. Tennyson, who works at Augusta Health in Fishersville, Va.
It has also inspired her to think outside the box in her gastroenterology practice. What her patients eat and the lifestyle choices they make is a central focus of her work.
Q: Why did you choose GI?
Dr. Tennyson: I always had an interest in nutrition. During training at medical school at NYU [New York University], I also really loved learning all I could about internal medicine. I worked with a great surgical team as a student and enjoyed being in the operating room. Although I knew I didn’t want to enter surgery, the experience encouraged me to pursue gastroenterology as it involved nutrition, internal medicine, and procedures as well as my favorite organ, the small bowel. I worked with some great mentors in gastroenterology, such as Dr. David Metz and Dr. Dave Katzka, at the University of Pennsylvania as a resident. I enjoyed taking care of patients with both acute and chronic conditions as well as the mix of doing procedures and seeing patients in the office. It also provided me the opportunity to incorporate nutrition into my clinical practice.
Q: What gives you the most joy in your day-to-day practice?
Dr. Tennyson: I enjoy helping my patients make meaningful lifestyle changes that can positively impact digestive health and well-being. I try to address topics related to lifestyle medicine in most of my clinical visits including eating more fiber/plants, exercise, positive relationships, and stress management. Many of the conditions we treat as gastroenterologists can benefit from addressing aspects of lifestyle along with our conventional medical therapies. I reinforce that attention to these areas can make a difference. I enjoy sharing recipes, books, and websites that I have found helpful.
Q: How has your job changed since you first began your career?
Dr. Tennyson: After fellowship, I joined the faculty at Columbia University and worked at the Celiac Disease Center seeing patients, teaching, and performing clinical research under the mentorship of Peter Green, MD, and Suzanne Lewis, MD. It was a great opportunity to learn and practice in a tertiary center. I later switched roles and joined a general multispecialty community practice in Brooklyn [N.Y.] affiliated with an academic medical center. After practicing in New York for 10 years, I left my clinical practice and performed locums work for several years in underserved rural areas. I enjoyed working in rural areas and took a permanent position at a community hospital in Virginia’s Shenandoah Valley.
Q: Describe your biggest practice-related challenge and what you are doing to address it.
Dr. Tennyson: The small, rural community hospital where I currently work does not have the same resources and staffing as urban tertiary centers. While we are taking care of the community in our general gastroenterology practice, we’ve also launched an integrated care model in our hospital. We have collaborated with behavioral health, dietitians, nurses, health coaches, exercise physiologists as well as other members of the community, including farmers and a chef. We have performed some innovative, engaging programs, including fermentation workshops, cooking classes, farm walks, and mindfulness programs.
Q: What are you most proud of accomplishing?
Dr. Tennyson: I am proud that I took a nontraditional path after training to do what I enjoy and find rewarding. I received certification during GI fellowship at Mount Sinai [N.Y.] as a physician nutrition specialist. I later completed a fellowship in integrative medicine at the University of Arizona, received certification in lifestyle medicine, and completed coursework in culinary medicine. I really enjoyed doing locums work taking care of patients in other parts of the country, like Mississippi or Maine. I’ve enjoyed working in more rural areas and bringing some innovative programs to the community.
Q: What teacher or mentor had the greatest impact on you?
Dr. Tennyson: Dr. Anthony Grieco while I was a student at NYU. He is an astute clinician, always listened to his patients, loved clinical medicine, and had an endless fund of knowledge. I wanted to be a doctor like him. During my fellowship at Mount Sinai, I was also exposed to many great mentors including Dr. Lloyd Mayer, Dr. Jerome Waye, Dr. Steve Itzkowitz, and Dr. Blair Lewis who encouraged my interest in nutrition and small bowel diseases.
Lightning round
What's your superpower?
Finding fun in mundane things
Favorite movie to quote?
The Princess Bride
What is your favorite form of exercise?
A hike in the woods
Name one thing on your bucket list.
Galapagos Islands trip before my kids grow up
Cats or dogs?
Dogs
Summer or winter?
Summer
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.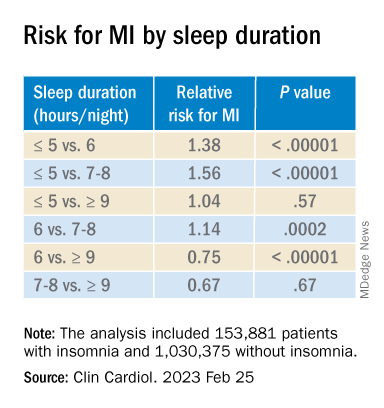
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Question 2
Q2. Correct answer: A - No monitoring of PPI side effects.
Rationale
There are several putative risks associated with long-term PPI use: chronic kidney disease, dementia, vitamin and mineral deficiencies, and others. However, the overall quality of evidence to support these conclusions is low or very low, and the majority of the findings have low effect sizes that may be attributed to confounding. An American Gastroenterological Association clinical practice update recommended against routine monitoring for patients receiving long-term PPI treatment. However, data show that more than one-third of gastroenterologists still check for PPI side effects at least annually in their patients.
References
Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-Term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017;152(4):706-15. doi: 10.1053/j.gastro.2017.01.031.
Leiman DA, Ravi K, Freedberg DE, Gyawali CP. Proton Pump Inhibitor Prescribing and Monitoring Patterns Among Gastroenterology Practitioners (published online ahead of print, 2021 Oct 4). J Clin Gastroenterol. 2021;10.1097/MCG.0000000000001623. doi: 10.1097/MCG.0000000000001623.
Q2. Correct answer: A - No monitoring of PPI side effects.
Rationale
There are several putative risks associated with long-term PPI use: chronic kidney disease, dementia, vitamin and mineral deficiencies, and others. However, the overall quality of evidence to support these conclusions is low or very low, and the majority of the findings have low effect sizes that may be attributed to confounding. An American Gastroenterological Association clinical practice update recommended against routine monitoring for patients receiving long-term PPI treatment. However, data show that more than one-third of gastroenterologists still check for PPI side effects at least annually in their patients.
References
Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-Term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017;152(4):706-15. doi: 10.1053/j.gastro.2017.01.031.
Leiman DA, Ravi K, Freedberg DE, Gyawali CP. Proton Pump Inhibitor Prescribing and Monitoring Patterns Among Gastroenterology Practitioners (published online ahead of print, 2021 Oct 4). J Clin Gastroenterol. 2021;10.1097/MCG.0000000000001623. doi: 10.1097/MCG.0000000000001623.
Q2. Correct answer: A - No monitoring of PPI side effects.
Rationale
There are several putative risks associated with long-term PPI use: chronic kidney disease, dementia, vitamin and mineral deficiencies, and others. However, the overall quality of evidence to support these conclusions is low or very low, and the majority of the findings have low effect sizes that may be attributed to confounding. An American Gastroenterological Association clinical practice update recommended against routine monitoring for patients receiving long-term PPI treatment. However, data show that more than one-third of gastroenterologists still check for PPI side effects at least annually in their patients.
References
Freedberg DE, Kim LS, Yang YX. The Risks and Benefits of Long-Term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology. 2017;152(4):706-15. doi: 10.1053/j.gastro.2017.01.031.
Leiman DA, Ravi K, Freedberg DE, Gyawali CP. Proton Pump Inhibitor Prescribing and Monitoring Patterns Among Gastroenterology Practitioners (published online ahead of print, 2021 Oct 4). J Clin Gastroenterol. 2021;10.1097/MCG.0000000000001623. doi: 10.1097/MCG.0000000000001623.
Q2. A 76-year-old man with atrial fibrillation treated with long-term anticoagulation with warfarin and coronary artery disease treated with aspirin was recently admitted with melena. Upper endoscopy revealed a duodenal ulcer with visible vessel. Endoscopic therapy was performed, and he was started on twice-daily proton-pump inhibitors (PPIs).
Question 1
Q1. Correct answer: B - Adding calcium carbonate (antacid) to her current regimen
Rationale
Compared with proton pump inhibitors (PPIs), vonoprazan is a potassium-competitive acid blocker (PCAB), which inhibits acid secretion by competitively blocking availability of potassium to hydrogen-potassium ATPase. Vonoprazan is rapidly absorbed independent of eating and is not affected by CYP2C19 polymorphisms. Several studies have compared PPIs with vonoprazan. Although vonoprazan is highly effective for treating LA Grade A and B esophagitis, so is lansoprazole, and healing rates at 8 weeks are 100% versus 99.2%, respectively. In contrast, vonoprazan healing of LA Grade C and D esophagitis at 8 weeks is 98.7% compared with 87.5% for lansoprazole.
Sleeping on pillows is not a reliable way to reduce reflux, as patients often move during sleep and lose any benefit from being propped on them. Antacids would not provide superior acid inhibition, compared with vonoprazan, and avoiding spicy foods would not address the underlying permissive reflux barrier that exists (hiatal hernia).
Reference
Graham DY and Dore MP. Update on the Use of Vonoprazan: A Competitive Acid Blocker. Gastroenterology. 2018;154(3):462-6. doi: 10.1053/j.gastro.2018.01.018.
Q1. Correct answer: B - Adding calcium carbonate (antacid) to her current regimen
Rationale
Compared with proton pump inhibitors (PPIs), vonoprazan is a potassium-competitive acid blocker (PCAB), which inhibits acid secretion by competitively blocking availability of potassium to hydrogen-potassium ATPase. Vonoprazan is rapidly absorbed independent of eating and is not affected by CYP2C19 polymorphisms. Several studies have compared PPIs with vonoprazan. Although vonoprazan is highly effective for treating LA Grade A and B esophagitis, so is lansoprazole, and healing rates at 8 weeks are 100% versus 99.2%, respectively. In contrast, vonoprazan healing of LA Grade C and D esophagitis at 8 weeks is 98.7% compared with 87.5% for lansoprazole.
Sleeping on pillows is not a reliable way to reduce reflux, as patients often move during sleep and lose any benefit from being propped on them. Antacids would not provide superior acid inhibition, compared with vonoprazan, and avoiding spicy foods would not address the underlying permissive reflux barrier that exists (hiatal hernia).
Reference
Graham DY and Dore MP. Update on the Use of Vonoprazan: A Competitive Acid Blocker. Gastroenterology. 2018;154(3):462-6. doi: 10.1053/j.gastro.2018.01.018.
Q1. Correct answer: B - Adding calcium carbonate (antacid) to her current regimen
Rationale
Compared with proton pump inhibitors (PPIs), vonoprazan is a potassium-competitive acid blocker (PCAB), which inhibits acid secretion by competitively blocking availability of potassium to hydrogen-potassium ATPase. Vonoprazan is rapidly absorbed independent of eating and is not affected by CYP2C19 polymorphisms. Several studies have compared PPIs with vonoprazan. Although vonoprazan is highly effective for treating LA Grade A and B esophagitis, so is lansoprazole, and healing rates at 8 weeks are 100% versus 99.2%, respectively. In contrast, vonoprazan healing of LA Grade C and D esophagitis at 8 weeks is 98.7% compared with 87.5% for lansoprazole.
Sleeping on pillows is not a reliable way to reduce reflux, as patients often move during sleep and lose any benefit from being propped on them. Antacids would not provide superior acid inhibition, compared with vonoprazan, and avoiding spicy foods would not address the underlying permissive reflux barrier that exists (hiatal hernia).
Reference
Graham DY and Dore MP. Update on the Use of Vonoprazan: A Competitive Acid Blocker. Gastroenterology. 2018;154(3):462-6. doi: 10.1053/j.gastro.2018.01.018.
Q1. A 62-year-old woman with rheumatoid arthritis reports regurgitation, heartburn, and dysphagia. She undergoes upper endoscopy, which reveals a 3-cm hiatal hernia and Los Angeles (LA) Grade D esophagitis. Previously performed esophageal function tests revealed absent contractility and a total acid exposure time of 8.2%. Her thoracic surgeon is concerned about the postoperative risks of dysphagia with hernia repair; therefore, surgery is deferred. Although improved, she continues to have symptoms of heartburn with daily lansoprazole.
FDA warns of potential problems with Abbott Trifecta valves
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
There is a potential risk of early structural valve deterioration with the Abbott Trifecta valve and Trifecta valve with glide technology (Trifecta GT), the U.S. Food and Drug Administration says in a letter to health care professionals posted on its website.
Evidence in the literature suggests a higher cumulative incidence of early structural valve deterioration (SVD) and a lower freedom from reintervention due to SVD with the Trifecta valves, compared with other commercially available bovine pericardial valves, the FDA says.
The Trifecta and Trifecta GT valves are heart valve replacement devices intended to treat diseased, damaged, or malfunctioning native or prosthetic aortic heart valves, the letter notes. The first-generation Trifecta valve was approved in 2011 but is no longer marketed in the United States. The Trifecta GT valve was approved in 2016.
Medical device reports (MDRs) received by the FDA describe early SVD with Trifecta valves, with a peak time to SVD of 3 to 4 years post-implant. “Reported outcomes include surgical valve explant/replacement, transcatheter valve-in-valve intervention, and in some cases death,” the FDA notes.
In a letter to customers, Abbott says a “complaint analysis has shown that most cases of early SVD which occur within 5 years post-implant are characterized as a non-calcific leaflet tear, while most cases of late SVD which occur beyond 5 years post-implant are characterized as a fibrous-calcific SVD.”
The FDA recommends that health care providers take the following actions:
- Be aware of the potential risk of early SVD with Trifecta valves, and current patient management considerations, as communicated by Abbott.
- Discuss the risks and benefits of all available aortic valve treatment options with patients and caregivers as part of shared clinical decision-making prior to surgery.
- Read and carefully follow the Instructions for Use when implanting a Trifecta GT valve.
- Monitor patients who have undergone implantation with Trifecta valves for signs and symptoms of potential SVD.
- Instruct patients to seek medical attention with new onset of symptoms such as shortness of breath or fatigue.
- Ensure lifelong follow-up visits, conducted at least yearly, including transthoracic echocardiogram assessment of the valve beginning 1-year post-implant.
The FDA is working with Abbott to further evaluate the issue and develop additional patient management strategies, if needed. The FDA says it will continue to monitor the literature and reports of adverse events related to the issue.
Clinicians are encouraged to report any adverse events or quality problems with the Trifecta valves to their local Abbott representative or the customer service department at 1-800-544-1664.
Health care professionals can also report adverse reactions or quality problems they experience using these devices to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
To prevent MS, should we target EBV?
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.

EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.

Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.
EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.
Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
SAN DIEGO – Although most adults have been exposed, it is very rare to find MS in an individual with no prior EBV exposure.
That apparent relationship has driven interest in a vaccine against EBV in an effort to reduce MS incidence on a population level.
At a session at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis (ACTRIMS), two researchers debated the potential benefits and pitfalls of such a program. The issues included the possible benefit in MS and other EBV-related conditions such as mononucleosis and various cancers, and whether EBV infection is a sufficient cause for MS, as well as concerns about vaccinating a healthy at-risk population.
Reducing the risk of MS by targeting EBV
Jeffrey I. Cohen, MD, spoke first, and cited several lines of evidence supporting the importance of EBV in MS. One study showed a 32-fold increased risk of MS following primary infection with EBV, and another showed that higher EBV nuclear antigen (EBNA) antibody titers were associated with a 36-fold higher risk of MS. “So we have two completely independent studies suggesting that EBV is really very important as a cofactor for development of MS,” said Dr. Cohen, chief of the laboratory of infectious diseases and chief of the medical virology section at the National Institutes of Health, Bethesda, Md.
EBV is also latent in B cells, and anti-B cell therapy is an effective therapeutic strategy for MS. However, the mechanism remains unknown.
Targeting EBV could involve attacking infected cells, or a therapeutic vaccine could be employed to treat EVB-infected individuals, similar to the shingles vaccine. “In all of these methods, one would end up with fewer EBV infected B cells and as a result, presumably you’d have reduced antigenic stimulation of EBV-infected B cells to stimulate either antibodies or T cells that could damage the nervous system. By reducing this, one might be able to [treat] multiple sclerosis,” said Dr. Cohen.
He did acknowledge concerns. It isn’t yet understood whether destroying EBV-infected cells would actually improve outcomes. It also may be more difficult to reduce a latent infection than to prevent infection, since almost all B cells become latently infected. “Thus we think perhaps a role for preventing infection or modifying the initial infection could be important,” said Dr. Cohen.
The most advanced vaccine candidate is a soluble form of EBV glycoprotein gp 350, which is the dominant glycoprotein on the surface of the virus and infected cells. It reduced the risk of mononucleosis by 78%, but it did not prevent EBV infection. There were no safety concerns. Two more vaccines are currently in clinical trials – an mRNA vaccine against a gp 350 sponsored by Moderna, and a gp 350 nanoparticle vaccine by the NIH.
Dr. Cohen acknowledged that safety is the most important factor, since it would be given to healthy individuals, and probably children. There are worries that a vaccine using EBV proteins could worsen MS. In particular, higher titers of antibodies against EBNA have been linked to developing MS and the anti-EBNA antibody has been implicated in molecular mimicry related to MS. However, the current vaccines avoid EBNA. Another worry is that a vaccine could delay onset of disease to an older age, when infection might be more dangerous. However, no delay in onset has been noted with the varicella vaccine or polio vaccines, which prompted similar concerns.
Vaccinating against EBV could also reduce other conditions such as mononucleosis and several cancers.
Does EBV infection even matter?
In his talk, Peter Calabresi, MD, made the case that EBV is not the sole cause of MS, and thus targeting it may prove ineffective. Dr. Calabresi is director of the division of neuroimmunology at Johns Hopkins Medicine, Baltimore.
Why was he asked to provide a rebuttal? “About this time last year, I commented at a meeting that we should be thoughtful as we think about what to do about EBV and MS. I do believe that constructive dialogue is the foundation of science,” he said. He also stated that he is not opposed to vaccines. “I congratulate Dr. Cohen on all of his vaccine successes,” he said.
Still, he is unconvinced that EBV is solely responsible for MS. “I think it’s hard to draw a straight line between EBV and MS as one might with HPV [human papillomavirus] and cervical cancer. For example, we know that EBV accounts for more than 1% of all cancers, and EBV can also cause other autoimmune diseases such as lupus and Sjogren’s, so it’s complicated. And MS of course has genetic susceptibility that’s not limited to the major histocompatibility complex (MHC) genes that are associated with presenting viral peptides,” said Dr. Calabresi.
Evidence relating MS vulnerability to other genetic and environmental factors, including diet, sunlight, smoking, and even pollution, calls into question a direct causal relationship between EBV and MS, he said.
The age prevalence of EBV would complicate efforts to eradicate it. Seroprevalence is 55% by age 5-11 and 75% among university students. “This is important because the duration of the vaccine response–induced protection in young seronegative children is not lengthy. Vaccinated individuals may become susceptible to natural infection at an age where the consequences of infection are more severe, especially leading to infectious mononucleosis, and hopefully not MS. This then raises the issue of the need for boosters, which we’re all well aware of during the COVID pandemic. This may be a problem, especially in young adults due to noncompliance,” said Dr. Calabresi.
He pointed out that not all vaccine attempts went well. In the 1960s, early respiratory syncytial virus (RSV) vaccines caused enhanced respiratory disease and 2 deaths. “We need to be careful when we think about targeting healthy at-risk young people,” said Dr. Calabresi.
Rather than pursue vaccination, Dr. Calabresi favors research into EBV latency in B cells as well as how EBV-infected B cells may cause or exacerbate MS, with the hopes of developing interventions. “It’s tempting to speculate that the success of the anti-CD 20 monoclonal antibody therapies is related to depletion of EBV infected B cells. In fact, I think that may be the case,” he said.
Dr. Cohen has no relevant financial disclosures. Dr. Calabresi has served on a scientific advisory board or data monitoring board for Biogen and Disarm Therapeutics.
FROM ACTRIMS FORUM 2023
Fewer than 10% of eligible type 2 diabetes patients get new, pricey drugs
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Fewer than 10% of American adults with type 2 diabetes who qualified for treatment with newer agents – such as an SGLT2 inhibitor or GLP-1 agonist – actually received treatment with at least one drug from drug class in 2017-2020, based on a new analysis of just over a thousand adults who participated in a representative, biannual survey and self-reported a diabetes diagnosis.
The cost of these agents, and their uncertain cost-effectiveness at current prices, is likely a key driver of the low usage rate, say the authors of a brief report published in Annals of Internal Medicine.
“Clinical studies have shown that both GLP-1 [glucagonlike peptide–1] receptor agonists and SGLT2 [sodium-glucose cotransporter 2] inhibitors yield additional clinical benefits, compared with older treatments in reducing body weight and progression of cardiovascular disease and chronic kidney disease,” write Shichao Tang, PhD, from the U.S. Centers for Disease Control and Prevention, Atlanta, and colleagues.
“However, these medications come at a substantially higher cost,” they stress.
Dr. Tang explained in an interview that the new study “points to prior studies about the high cost of these medications as a potential barrier to use, but more research is needed to understand cost-effectiveness and any potential barriers to use, including cost.”
The work “did not include research into cost-effectiveness or why the percentage of people already using these medications was low,” he emphasized.
Dr. Tang and colleagues used data collected by the U.S. National Health and Nutrition Examination Survey during two 2-year cycles between 2017 and 2020 that included 1,417 people who self-identified a diagnosis of diabetes.
Excluding those who likely had type 1 diabetes and those with incomplete data left 1,330 survey participants, including 1,133 (85%) who fit criteria for the treatment of type 2 diabetes with an agent from one of the two studied classes, as recommended in 2022 by a panel representing the American Diabetes Association and the European Association for the Study of Diabetes.
Among these 1,133 people – who represent more than 22 million American adults with type 2 diabetes who fit the 2022 criteria – a scant 3.7% were actually taking a GLP-1 agonist and 5.3% were taking an SGLT2 inhibitor.
“While it’s important to note that our data predate the 2022 recommendations, these drugs were offered as second-line therapy for patients with certain diabetes-related complications in 2017-2020” and hence provide potentially useful insights, noted Dr. Tang, a health economist with the CDC National Center for Chronic Disease Prevention and Health Promotion.
Based on retail prices listed on a United States–based website, a 30-day supply of an oral SGLT2 inhibitor can cost about $550-$600 per month, while common subcutaneously injected GLP-1 receptor agonists can run from a few hundred dollars for a daily injection or close to $1,000 for a formulation administered weekly.
“Cost-effectiveness was not formally considered in the current guideline, but an assessment of cost-effectiveness may assist better targeting of interventions to achieve the greatest effect at a sustainable cost,” the researchers conclude.
The study received no commercial funding. None of the authors had relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Optimal Use of Disease-Modifying Therapies in Spinal Muscular Atrophy
Spinal muscular atrophy (SMA) is a hereditary neuromuscular disease that typically begins in infancy or childhood but can manifest at any age.
It is characterized by the irreversible and progressive degeneration of motor neurons in the spinal cord and brainstem. This results in a wide range of symptoms, in addition to which there is substantial variation in the rate of progression and disease prognosis.
Although early diagnosis and timely therapy can slow or prevent disease progression, disease-modifying therapies since 2016 have significantly advanced the management of SMA.
In a clinically focused program, Dr Perry Shieh, a neuromuscular neurologist from the University of California, Los Angeles, discusses the three medications currently approved by the US Food and Drug Administration: nusinersen, risdiplam, and onasemnogene abeparvovec.
He weighs the clinical benefits and key considerations for the use of each drug and emphasizes the need for shared decision-making with the patient.
--
Professor, Departments of Neurology and Pediatrics, University of California, Los Angeles; Neuromuscular Neurologist, Ronald Reagan UCLA Medical Center, Los Angeles, California
Perry Shieh, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Grifolis; Biogen; Genentech; CSL Behring; Alexion; Argenx; Catalyst
Received income in an amount equal to or greater than $250 from: Sarepta; Novartis; Biogen; Genentech; Alexion; Argenx; Catalyst; UCB
Spinal muscular atrophy (SMA) is a hereditary neuromuscular disease that typically begins in infancy or childhood but can manifest at any age.
It is characterized by the irreversible and progressive degeneration of motor neurons in the spinal cord and brainstem. This results in a wide range of symptoms, in addition to which there is substantial variation in the rate of progression and disease prognosis.
Although early diagnosis and timely therapy can slow or prevent disease progression, disease-modifying therapies since 2016 have significantly advanced the management of SMA.
In a clinically focused program, Dr Perry Shieh, a neuromuscular neurologist from the University of California, Los Angeles, discusses the three medications currently approved by the US Food and Drug Administration: nusinersen, risdiplam, and onasemnogene abeparvovec.
He weighs the clinical benefits and key considerations for the use of each drug and emphasizes the need for shared decision-making with the patient.
--
Professor, Departments of Neurology and Pediatrics, University of California, Los Angeles; Neuromuscular Neurologist, Ronald Reagan UCLA Medical Center, Los Angeles, California
Perry Shieh, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Grifolis; Biogen; Genentech; CSL Behring; Alexion; Argenx; Catalyst
Received income in an amount equal to or greater than $250 from: Sarepta; Novartis; Biogen; Genentech; Alexion; Argenx; Catalyst; UCB
Spinal muscular atrophy (SMA) is a hereditary neuromuscular disease that typically begins in infancy or childhood but can manifest at any age.
It is characterized by the irreversible and progressive degeneration of motor neurons in the spinal cord and brainstem. This results in a wide range of symptoms, in addition to which there is substantial variation in the rate of progression and disease prognosis.
Although early diagnosis and timely therapy can slow or prevent disease progression, disease-modifying therapies since 2016 have significantly advanced the management of SMA.
In a clinically focused program, Dr Perry Shieh, a neuromuscular neurologist from the University of California, Los Angeles, discusses the three medications currently approved by the US Food and Drug Administration: nusinersen, risdiplam, and onasemnogene abeparvovec.
He weighs the clinical benefits and key considerations for the use of each drug and emphasizes the need for shared decision-making with the patient.
--
Professor, Departments of Neurology and Pediatrics, University of California, Los Angeles; Neuromuscular Neurologist, Ronald Reagan UCLA Medical Center, Los Angeles, California
Perry Shieh, MD, PhD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Grifolis; Biogen; Genentech; CSL Behring; Alexion; Argenx; Catalyst
Received income in an amount equal to or greater than $250 from: Sarepta; Novartis; Biogen; Genentech; Alexion; Argenx; Catalyst; UCB
