User login
mRNA Cancer Vaccines: Pipeline Insights for Clinicians
Since 1965, messenger RNA (mRNA) vaccines have been studied for cancer treatment, but it was the technological advances in vaccines during the COVID pandemic that helped accelerate research. Currently, no vaccine has been approved for tumor treatment, although many clinical studies are ongoing worldwide. According to experts consulted by Medscape’s Portuguese edition, the outlook is very promising, and these studies are expected to open doors for personalized therapies.
In cancer treatment, the vaccine would function as an immunotherapy, in which the immune system can be “trained” to act against an invader. Just as with pathogens, the platform would use parts of the tumor — which have altered proteins or are expressed at abnormal levels — to teach the body to defend itself against cancer.
Vladmir Lima, MD, PhD, clinical oncologist at A.C. Camargo Cancer Center, São Paulo, Brazil, explained that with this technology it will be possible to produce personalized vaccines, which prevents, for example, large-scale manufacturing. “In theory, these vaccines can be developed for any tumor type, but this does not mean that efficacy will be the same for all,” he said. Because cancer has specific characteristics in each individual, it is difficult to envision a single vaccine that works for all cancers.
Current evidence suggests the vaccine could be administered after chemotherapy or radiotherapy, with the goal of reducing tumor mass and increasing the effectiveness of mRNA-based treatment, according to Ana Paula Lepique, professor and researcher in tumor immunology at the Institute of Biomedical Sciences, University of São Paulo, São Paulo.
“There is also a study with pancreatic cancer patients, in which the vaccine was administered after surgery,” she explained. “It would not work, for example, to give chemotherapy or radiotherapy while the immune response is being triggered by the vaccine. This would make the vaccine ineffective, since chemotherapy and radiotherapy are toxic to lymphocytes.”
Lepique also clarified that it is possible to combine the vaccine with immunotherapy targeting immune regulatory molecules. “In this case, in addition to administering the mRNA with the antigen, a strategy is used to improve the patient’s immune response.”
Challenges With mRNA Vaccines
Despite being a promising technology, there are challenges, warned Lepique. mRNA molecules degrade quickly when injected into the body, which can compromise vaccine efficacy. To overcome this, researchers have developed nanoencapsulation technologies that protect the molecules and allow safe use in vaccines. “Another alternative is transferring the mRNA into dendritic cells, known as antigen-presenting cells, and then administering these cells to the patient,” she explained.
Global Research Status
According to a study published this year in Med, over 120 clinical trials are exploring mRNA vaccines to treat lung, breast, prostate, and pancreatic tumors, as well as melanoma.
Lepique noted that the countries leading this research are the US, UK, Germany, China, and Japan. “Unfortunately, the US government recently cut funding for mRNA vaccine development and testing, which will likely have significant consequences,” she said.
Lepique reported that Brazilian researchers are collaborating with international institutions to develop these vaccines. “The Brazilian government, through the Ministry of Health and the Ministry of Science, Technology, and Innovation, recently announced investments in mRNA technologies for vaccines. While not specifically targeting cancer, these investments could also benefit this field,” she clarified.
Leading Studies
Lepique highlighted the most advanced studies to date:
- Pancreatic cancer: A study published in Nature in February demonstrated that a personalized mRNA vaccine reduced the risk for recurrence after surgery in 16 patients, with 3 years of follow-up.
- Melanoma: A study published in The Lancet reported improved survival in melanoma patients after mRNA vaccine administration combined with the checkpoint inhibitor pembrolizumab applied after surgical tumor resection.
- Universal vaccine: A study in Nature Biomedical Engineering described the creation of a “generic” vaccine capable of activating the patient’s immune system and inducing tumor regression. Lepique explained that this vaccine acts more as an immune response modulator than a classical neoantigen-specific vaccine. “Because it is not limited to a single neoantigen, it could potentially be universal, though further testing is needed to determine efficacy across all cancer types,” she added.
Lima highlighted a 2024 study being conducted by MSD and Moderna against lung cancer, with results yet to be published. “Patients first receive immunotherapy after surgery. Once the vaccine is ready, it is added to the ongoing immunotherapy,” he explained. The global phase 3 study involves 868 patients with resected lung cancer who previously underwent chemotherapy. Participants receive the vaccine (1 mg every 3 weeks, up to nine doses) alongside pembrolizumab (400 mg every 6 weeks, up to nine cycles) over approximately 1 year.
Other mRNA vaccines remain in early-stage development. For example, in May 2024, the UK National Health Service recruited participants for a personalized colorectal cancer mRNA vaccine trial.
Advantages of mRNA Technology
Experts noted that mRNA-based cancer vaccines are considered safer for patients because the tumor mRNA is synthesized in the laboratory. According to Lepique, these vaccines are more specific than many other cancer therapies, and therefore carry a lower risk for serious side effects.
“Clinical studies have shown that these vaccines can generate immunological memory, meaning lymphocytes that recognize tumor antigens remain in the body and can respond to recurrence,” she explained.
It is also possible to combine multiple mRNA molecules in a single vaccine, creating a platform that targets several tumor antigens simultaneously. “Formulations can additionally include adjuvants to further enhance immune responses against tumors,” she said. However, as a personalized therapy, costs are high, and vaccine formulation requires considerable time.
Lima emphasized the customization advantage: “We can take a portion of the patient’s tumor, sequence it to identify alterations, and develop a vaccine specifically for that tumor.” He also highlighted safety data, noting that the platform has been widely used in SARS-CoV-2 vaccine development, providing confidence in large-scale application. “The potential exists to achieve more personalized, tumor-directed immunotherapy with greater scalability,” he explained.
Outlook and Limitations
Lima noted that although the projected efficacy is promising, definitive results are still pending.
“We have very positive expectations, but we must wait for study outcomes. Efficacy may vary across scenarios and among patients. The immune system may also respond against the vaccine itself, potentially reducing effectiveness at times,” he explained.
According to Lima, mRNA vaccines are expected to complement current treatments, enhancing outcomes without replacing conventional approaches entirely.
“It will not be a panacea. These vaccines are likely to add to and improve strategies we already use, but they will not work for all patients in every scenario,” he concluded.
Lepique highlighted the promise of combination strategies. “The outlook is positive, particularly because multiple mRNA types can be combined in a single formulation and used alongside drugs that enhance immune responses,” she explained.
Although mRNA vaccine research has been ongoing for many years, prior results have brought both progress and setbacks. “This new protocol appears more effective [and] capable of generating immunological memory and is also safe,” she noted. Still, she cautioned that cancer presents unique challenges: “The disease has multiple mechanisms to evade immune responses. Additionally, some tumors are naturally unrecognized by the immune system, the so-called ‘cold tumors.’”
This story was translated from Medscape’s Portuguese edition. A version of this article appeared on Medscape.com.
Since 1965, messenger RNA (mRNA) vaccines have been studied for cancer treatment, but it was the technological advances in vaccines during the COVID pandemic that helped accelerate research. Currently, no vaccine has been approved for tumor treatment, although many clinical studies are ongoing worldwide. According to experts consulted by Medscape’s Portuguese edition, the outlook is very promising, and these studies are expected to open doors for personalized therapies.
In cancer treatment, the vaccine would function as an immunotherapy, in which the immune system can be “trained” to act against an invader. Just as with pathogens, the platform would use parts of the tumor — which have altered proteins or are expressed at abnormal levels — to teach the body to defend itself against cancer.
Vladmir Lima, MD, PhD, clinical oncologist at A.C. Camargo Cancer Center, São Paulo, Brazil, explained that with this technology it will be possible to produce personalized vaccines, which prevents, for example, large-scale manufacturing. “In theory, these vaccines can be developed for any tumor type, but this does not mean that efficacy will be the same for all,” he said. Because cancer has specific characteristics in each individual, it is difficult to envision a single vaccine that works for all cancers.
Current evidence suggests the vaccine could be administered after chemotherapy or radiotherapy, with the goal of reducing tumor mass and increasing the effectiveness of mRNA-based treatment, according to Ana Paula Lepique, professor and researcher in tumor immunology at the Institute of Biomedical Sciences, University of São Paulo, São Paulo.
“There is also a study with pancreatic cancer patients, in which the vaccine was administered after surgery,” she explained. “It would not work, for example, to give chemotherapy or radiotherapy while the immune response is being triggered by the vaccine. This would make the vaccine ineffective, since chemotherapy and radiotherapy are toxic to lymphocytes.”
Lepique also clarified that it is possible to combine the vaccine with immunotherapy targeting immune regulatory molecules. “In this case, in addition to administering the mRNA with the antigen, a strategy is used to improve the patient’s immune response.”
Challenges With mRNA Vaccines
Despite being a promising technology, there are challenges, warned Lepique. mRNA molecules degrade quickly when injected into the body, which can compromise vaccine efficacy. To overcome this, researchers have developed nanoencapsulation technologies that protect the molecules and allow safe use in vaccines. “Another alternative is transferring the mRNA into dendritic cells, known as antigen-presenting cells, and then administering these cells to the patient,” she explained.
Global Research Status
According to a study published this year in Med, over 120 clinical trials are exploring mRNA vaccines to treat lung, breast, prostate, and pancreatic tumors, as well as melanoma.
Lepique noted that the countries leading this research are the US, UK, Germany, China, and Japan. “Unfortunately, the US government recently cut funding for mRNA vaccine development and testing, which will likely have significant consequences,” she said.
Lepique reported that Brazilian researchers are collaborating with international institutions to develop these vaccines. “The Brazilian government, through the Ministry of Health and the Ministry of Science, Technology, and Innovation, recently announced investments in mRNA technologies for vaccines. While not specifically targeting cancer, these investments could also benefit this field,” she clarified.
Leading Studies
Lepique highlighted the most advanced studies to date:
- Pancreatic cancer: A study published in Nature in February demonstrated that a personalized mRNA vaccine reduced the risk for recurrence after surgery in 16 patients, with 3 years of follow-up.
- Melanoma: A study published in The Lancet reported improved survival in melanoma patients after mRNA vaccine administration combined with the checkpoint inhibitor pembrolizumab applied after surgical tumor resection.
- Universal vaccine: A study in Nature Biomedical Engineering described the creation of a “generic” vaccine capable of activating the patient’s immune system and inducing tumor regression. Lepique explained that this vaccine acts more as an immune response modulator than a classical neoantigen-specific vaccine. “Because it is not limited to a single neoantigen, it could potentially be universal, though further testing is needed to determine efficacy across all cancer types,” she added.
Lima highlighted a 2024 study being conducted by MSD and Moderna against lung cancer, with results yet to be published. “Patients first receive immunotherapy after surgery. Once the vaccine is ready, it is added to the ongoing immunotherapy,” he explained. The global phase 3 study involves 868 patients with resected lung cancer who previously underwent chemotherapy. Participants receive the vaccine (1 mg every 3 weeks, up to nine doses) alongside pembrolizumab (400 mg every 6 weeks, up to nine cycles) over approximately 1 year.
Other mRNA vaccines remain in early-stage development. For example, in May 2024, the UK National Health Service recruited participants for a personalized colorectal cancer mRNA vaccine trial.
Advantages of mRNA Technology
Experts noted that mRNA-based cancer vaccines are considered safer for patients because the tumor mRNA is synthesized in the laboratory. According to Lepique, these vaccines are more specific than many other cancer therapies, and therefore carry a lower risk for serious side effects.
“Clinical studies have shown that these vaccines can generate immunological memory, meaning lymphocytes that recognize tumor antigens remain in the body and can respond to recurrence,” she explained.
It is also possible to combine multiple mRNA molecules in a single vaccine, creating a platform that targets several tumor antigens simultaneously. “Formulations can additionally include adjuvants to further enhance immune responses against tumors,” she said. However, as a personalized therapy, costs are high, and vaccine formulation requires considerable time.
Lima emphasized the customization advantage: “We can take a portion of the patient’s tumor, sequence it to identify alterations, and develop a vaccine specifically for that tumor.” He also highlighted safety data, noting that the platform has been widely used in SARS-CoV-2 vaccine development, providing confidence in large-scale application. “The potential exists to achieve more personalized, tumor-directed immunotherapy with greater scalability,” he explained.
Outlook and Limitations
Lima noted that although the projected efficacy is promising, definitive results are still pending.
“We have very positive expectations, but we must wait for study outcomes. Efficacy may vary across scenarios and among patients. The immune system may also respond against the vaccine itself, potentially reducing effectiveness at times,” he explained.
According to Lima, mRNA vaccines are expected to complement current treatments, enhancing outcomes without replacing conventional approaches entirely.
“It will not be a panacea. These vaccines are likely to add to and improve strategies we already use, but they will not work for all patients in every scenario,” he concluded.
Lepique highlighted the promise of combination strategies. “The outlook is positive, particularly because multiple mRNA types can be combined in a single formulation and used alongside drugs that enhance immune responses,” she explained.
Although mRNA vaccine research has been ongoing for many years, prior results have brought both progress and setbacks. “This new protocol appears more effective [and] capable of generating immunological memory and is also safe,” she noted. Still, she cautioned that cancer presents unique challenges: “The disease has multiple mechanisms to evade immune responses. Additionally, some tumors are naturally unrecognized by the immune system, the so-called ‘cold tumors.’”
This story was translated from Medscape’s Portuguese edition. A version of this article appeared on Medscape.com.
Since 1965, messenger RNA (mRNA) vaccines have been studied for cancer treatment, but it was the technological advances in vaccines during the COVID pandemic that helped accelerate research. Currently, no vaccine has been approved for tumor treatment, although many clinical studies are ongoing worldwide. According to experts consulted by Medscape’s Portuguese edition, the outlook is very promising, and these studies are expected to open doors for personalized therapies.
In cancer treatment, the vaccine would function as an immunotherapy, in which the immune system can be “trained” to act against an invader. Just as with pathogens, the platform would use parts of the tumor — which have altered proteins or are expressed at abnormal levels — to teach the body to defend itself against cancer.
Vladmir Lima, MD, PhD, clinical oncologist at A.C. Camargo Cancer Center, São Paulo, Brazil, explained that with this technology it will be possible to produce personalized vaccines, which prevents, for example, large-scale manufacturing. “In theory, these vaccines can be developed for any tumor type, but this does not mean that efficacy will be the same for all,” he said. Because cancer has specific characteristics in each individual, it is difficult to envision a single vaccine that works for all cancers.
Current evidence suggests the vaccine could be administered after chemotherapy or radiotherapy, with the goal of reducing tumor mass and increasing the effectiveness of mRNA-based treatment, according to Ana Paula Lepique, professor and researcher in tumor immunology at the Institute of Biomedical Sciences, University of São Paulo, São Paulo.
“There is also a study with pancreatic cancer patients, in which the vaccine was administered after surgery,” she explained. “It would not work, for example, to give chemotherapy or radiotherapy while the immune response is being triggered by the vaccine. This would make the vaccine ineffective, since chemotherapy and radiotherapy are toxic to lymphocytes.”
Lepique also clarified that it is possible to combine the vaccine with immunotherapy targeting immune regulatory molecules. “In this case, in addition to administering the mRNA with the antigen, a strategy is used to improve the patient’s immune response.”
Challenges With mRNA Vaccines
Despite being a promising technology, there are challenges, warned Lepique. mRNA molecules degrade quickly when injected into the body, which can compromise vaccine efficacy. To overcome this, researchers have developed nanoencapsulation technologies that protect the molecules and allow safe use in vaccines. “Another alternative is transferring the mRNA into dendritic cells, known as antigen-presenting cells, and then administering these cells to the patient,” she explained.
Global Research Status
According to a study published this year in Med, over 120 clinical trials are exploring mRNA vaccines to treat lung, breast, prostate, and pancreatic tumors, as well as melanoma.
Lepique noted that the countries leading this research are the US, UK, Germany, China, and Japan. “Unfortunately, the US government recently cut funding for mRNA vaccine development and testing, which will likely have significant consequences,” she said.
Lepique reported that Brazilian researchers are collaborating with international institutions to develop these vaccines. “The Brazilian government, through the Ministry of Health and the Ministry of Science, Technology, and Innovation, recently announced investments in mRNA technologies for vaccines. While not specifically targeting cancer, these investments could also benefit this field,” she clarified.
Leading Studies
Lepique highlighted the most advanced studies to date:
- Pancreatic cancer: A study published in Nature in February demonstrated that a personalized mRNA vaccine reduced the risk for recurrence after surgery in 16 patients, with 3 years of follow-up.
- Melanoma: A study published in The Lancet reported improved survival in melanoma patients after mRNA vaccine administration combined with the checkpoint inhibitor pembrolizumab applied after surgical tumor resection.
- Universal vaccine: A study in Nature Biomedical Engineering described the creation of a “generic” vaccine capable of activating the patient’s immune system and inducing tumor regression. Lepique explained that this vaccine acts more as an immune response modulator than a classical neoantigen-specific vaccine. “Because it is not limited to a single neoantigen, it could potentially be universal, though further testing is needed to determine efficacy across all cancer types,” she added.
Lima highlighted a 2024 study being conducted by MSD and Moderna against lung cancer, with results yet to be published. “Patients first receive immunotherapy after surgery. Once the vaccine is ready, it is added to the ongoing immunotherapy,” he explained. The global phase 3 study involves 868 patients with resected lung cancer who previously underwent chemotherapy. Participants receive the vaccine (1 mg every 3 weeks, up to nine doses) alongside pembrolizumab (400 mg every 6 weeks, up to nine cycles) over approximately 1 year.
Other mRNA vaccines remain in early-stage development. For example, in May 2024, the UK National Health Service recruited participants for a personalized colorectal cancer mRNA vaccine trial.
Advantages of mRNA Technology
Experts noted that mRNA-based cancer vaccines are considered safer for patients because the tumor mRNA is synthesized in the laboratory. According to Lepique, these vaccines are more specific than many other cancer therapies, and therefore carry a lower risk for serious side effects.
“Clinical studies have shown that these vaccines can generate immunological memory, meaning lymphocytes that recognize tumor antigens remain in the body and can respond to recurrence,” she explained.
It is also possible to combine multiple mRNA molecules in a single vaccine, creating a platform that targets several tumor antigens simultaneously. “Formulations can additionally include adjuvants to further enhance immune responses against tumors,” she said. However, as a personalized therapy, costs are high, and vaccine formulation requires considerable time.
Lima emphasized the customization advantage: “We can take a portion of the patient’s tumor, sequence it to identify alterations, and develop a vaccine specifically for that tumor.” He also highlighted safety data, noting that the platform has been widely used in SARS-CoV-2 vaccine development, providing confidence in large-scale application. “The potential exists to achieve more personalized, tumor-directed immunotherapy with greater scalability,” he explained.
Outlook and Limitations
Lima noted that although the projected efficacy is promising, definitive results are still pending.
“We have very positive expectations, but we must wait for study outcomes. Efficacy may vary across scenarios and among patients. The immune system may also respond against the vaccine itself, potentially reducing effectiveness at times,” he explained.
According to Lima, mRNA vaccines are expected to complement current treatments, enhancing outcomes without replacing conventional approaches entirely.
“It will not be a panacea. These vaccines are likely to add to and improve strategies we already use, but they will not work for all patients in every scenario,” he concluded.
Lepique highlighted the promise of combination strategies. “The outlook is positive, particularly because multiple mRNA types can be combined in a single formulation and used alongside drugs that enhance immune responses,” she explained.
Although mRNA vaccine research has been ongoing for many years, prior results have brought both progress and setbacks. “This new protocol appears more effective [and] capable of generating immunological memory and is also safe,” she noted. Still, she cautioned that cancer presents unique challenges: “The disease has multiple mechanisms to evade immune responses. Additionally, some tumors are naturally unrecognized by the immune system, the so-called ‘cold tumors.’”
This story was translated from Medscape’s Portuguese edition. A version of this article appeared on Medscape.com.

Hepatitis D Virus Classified as Carcinogenic: Implications
The International Agency for Research on Cancer (IARC) of the World Health Organization has classified hepatitis D virus (HDV) as carcinogenic, citing sufficient evidence and placing it alongside hepatitis B virus (HBV) and hepatitis C virus (HCV) as a cause of hepatocellular carcinoma (HCC).
Individuals with HBV-HDV coinfection face an elevated risk for liver cancer, highlighting the need for HBV vaccination, systematic screening, and early antiviral treatment to reduce the progression to cirrhosis and HCC.
About 12 million people globally have HBV-HDV coinfection, representing 5% of all chronic HBV cases. The prevalence of this condition varies regionally, with a likely underdiagnosis. True coinfection rates may reach 13%-14%, the highest in Europe’s Mediterranean region.
Virus Biology
HDV is an incomplete virus that infects hepatocytes and requires the envelope protein of hepatitis B surface antigen (HBsAg) for cell exit. Infection occurs only with chronic HBV infection, either as a superinfection or simultaneous acquisition. Humans are the only known natural host.
HDV coinfection worsens HBV-induced hepatic inflammation and prognosis, and up to 80% of patients develop cirrhosis. Triple infection with the HBV virus, HDV, and HIV further increases this risk, and the global prevalence is likely underestimated.
Cancer Risk
HDV infection significantly increases the risk for HCC compared with HBV infection alone. Many patients die from decompensated cirrhosis or HCC, reflecting the aggressive nature of coinfection.
The molecular mechanisms underlying HDV oncogenesis remain unclear. Research conducted over the past 15 years has provided insights that could inform the development of more effective treatments.
Early vaccination prophylaxis is critical for reducing the risk for HCC, despite limited options.
Treatment Options
Randomized controlled trials have demonstrated antiviral efficacy for:
- Pegylated interferon alpha (Peg-IFN) is approved for HBV and is active against HDV.
- Bulevirtide, a synthetic myristoylated lipopeptide entry inhibitor, is used alone or in combination with Peg-IFN.
Suppression of HBV remains central. Nucleoside and nucleotide analogs, such as entecavir, tenofovir alafenamide fumarate, and tenofovir disoproxil fumarate, significantly reduce HCC progression in treated patients compared with untreated patients at risk.
Promising therapeutics include lonafarnib, a farnesyltransferase inhibitor that blocks HDV particle formation, and nucleic acid polymers targeting the host chaperone DNAJB12 to inhibit HBV and HDV replication.
Guideline Updates
The 2023 addendum to the S3 guidelines covers the prophylaxis, diagnosis, and treatment of HBV, including HDV management.
IARC experts also re-evaluated the human cytomegalovirus and Merkel cell polyomavirus. Complete assessments are expected in the next edition of IARC Monographs.
HBV Vaccination
HBV vaccination is the only effective prophylaxis against HBV and HDV. Introduced in 1982 for high-risk groups, it reduced chronic infections, with the WHO expanding its recommendations from 1992 onward.
Infants and young children are at the highest risk of developing this disease. Acute HBV infection often resolves in adults, but infants face up to a 90% risk of developing chronic infection. Newborns of mothers with chronic or undiagnosed HBV infections are particularly vulnerable.
Routine infant immunization includes three doses, with the first dose administered within 12 hours of birth. In Germany, the Standing Committee on Vaccination (STIKO) recommends the administration of combination vaccines, with the hexavalent vaccine administered at 2, 4, and 11 months in a 2 + 1 schedule.
Timely vaccination is crucial because undetected chronic infections often lead to late-stage HCC diagnosis. Adults in high-risk groups should receive HBV vaccination counseling.
STIKO recommends vaccination for close contacts of individuals who are HBsAg-positive, individuals with high-risk sexual contacts, immunocompromised persons, and those with preexisting conditions that increase the risk for severe HBV infection.
Since 2021, insured adults aged 35 years or older in Germany have undergone one-time HBV and HCV screening. HDV testing is recommended for all HBsAg-positive patients. Current frameworks may miss cases, and additional or personalized screening could improve the detection of previously unrecognized infections.
This story was translated from Univadis Germany.
A version of this article appeared on Medscape.com.
The International Agency for Research on Cancer (IARC) of the World Health Organization has classified hepatitis D virus (HDV) as carcinogenic, citing sufficient evidence and placing it alongside hepatitis B virus (HBV) and hepatitis C virus (HCV) as a cause of hepatocellular carcinoma (HCC).
Individuals with HBV-HDV coinfection face an elevated risk for liver cancer, highlighting the need for HBV vaccination, systematic screening, and early antiviral treatment to reduce the progression to cirrhosis and HCC.
About 12 million people globally have HBV-HDV coinfection, representing 5% of all chronic HBV cases. The prevalence of this condition varies regionally, with a likely underdiagnosis. True coinfection rates may reach 13%-14%, the highest in Europe’s Mediterranean region.
Virus Biology
HDV is an incomplete virus that infects hepatocytes and requires the envelope protein of hepatitis B surface antigen (HBsAg) for cell exit. Infection occurs only with chronic HBV infection, either as a superinfection or simultaneous acquisition. Humans are the only known natural host.
HDV coinfection worsens HBV-induced hepatic inflammation and prognosis, and up to 80% of patients develop cirrhosis. Triple infection with the HBV virus, HDV, and HIV further increases this risk, and the global prevalence is likely underestimated.
Cancer Risk
HDV infection significantly increases the risk for HCC compared with HBV infection alone. Many patients die from decompensated cirrhosis or HCC, reflecting the aggressive nature of coinfection.
The molecular mechanisms underlying HDV oncogenesis remain unclear. Research conducted over the past 15 years has provided insights that could inform the development of more effective treatments.
Early vaccination prophylaxis is critical for reducing the risk for HCC, despite limited options.
Treatment Options
Randomized controlled trials have demonstrated antiviral efficacy for:
- Pegylated interferon alpha (Peg-IFN) is approved for HBV and is active against HDV.
- Bulevirtide, a synthetic myristoylated lipopeptide entry inhibitor, is used alone or in combination with Peg-IFN.
Suppression of HBV remains central. Nucleoside and nucleotide analogs, such as entecavir, tenofovir alafenamide fumarate, and tenofovir disoproxil fumarate, significantly reduce HCC progression in treated patients compared with untreated patients at risk.
Promising therapeutics include lonafarnib, a farnesyltransferase inhibitor that blocks HDV particle formation, and nucleic acid polymers targeting the host chaperone DNAJB12 to inhibit HBV and HDV replication.
Guideline Updates
The 2023 addendum to the S3 guidelines covers the prophylaxis, diagnosis, and treatment of HBV, including HDV management.
IARC experts also re-evaluated the human cytomegalovirus and Merkel cell polyomavirus. Complete assessments are expected in the next edition of IARC Monographs.
HBV Vaccination
HBV vaccination is the only effective prophylaxis against HBV and HDV. Introduced in 1982 for high-risk groups, it reduced chronic infections, with the WHO expanding its recommendations from 1992 onward.
Infants and young children are at the highest risk of developing this disease. Acute HBV infection often resolves in adults, but infants face up to a 90% risk of developing chronic infection. Newborns of mothers with chronic or undiagnosed HBV infections are particularly vulnerable.
Routine infant immunization includes three doses, with the first dose administered within 12 hours of birth. In Germany, the Standing Committee on Vaccination (STIKO) recommends the administration of combination vaccines, with the hexavalent vaccine administered at 2, 4, and 11 months in a 2 + 1 schedule.
Timely vaccination is crucial because undetected chronic infections often lead to late-stage HCC diagnosis. Adults in high-risk groups should receive HBV vaccination counseling.
STIKO recommends vaccination for close contacts of individuals who are HBsAg-positive, individuals with high-risk sexual contacts, immunocompromised persons, and those with preexisting conditions that increase the risk for severe HBV infection.
Since 2021, insured adults aged 35 years or older in Germany have undergone one-time HBV and HCV screening. HDV testing is recommended for all HBsAg-positive patients. Current frameworks may miss cases, and additional or personalized screening could improve the detection of previously unrecognized infections.
This story was translated from Univadis Germany.
A version of this article appeared on Medscape.com.
The International Agency for Research on Cancer (IARC) of the World Health Organization has classified hepatitis D virus (HDV) as carcinogenic, citing sufficient evidence and placing it alongside hepatitis B virus (HBV) and hepatitis C virus (HCV) as a cause of hepatocellular carcinoma (HCC).
Individuals with HBV-HDV coinfection face an elevated risk for liver cancer, highlighting the need for HBV vaccination, systematic screening, and early antiviral treatment to reduce the progression to cirrhosis and HCC.
About 12 million people globally have HBV-HDV coinfection, representing 5% of all chronic HBV cases. The prevalence of this condition varies regionally, with a likely underdiagnosis. True coinfection rates may reach 13%-14%, the highest in Europe’s Mediterranean region.
Virus Biology
HDV is an incomplete virus that infects hepatocytes and requires the envelope protein of hepatitis B surface antigen (HBsAg) for cell exit. Infection occurs only with chronic HBV infection, either as a superinfection or simultaneous acquisition. Humans are the only known natural host.
HDV coinfection worsens HBV-induced hepatic inflammation and prognosis, and up to 80% of patients develop cirrhosis. Triple infection with the HBV virus, HDV, and HIV further increases this risk, and the global prevalence is likely underestimated.
Cancer Risk
HDV infection significantly increases the risk for HCC compared with HBV infection alone. Many patients die from decompensated cirrhosis or HCC, reflecting the aggressive nature of coinfection.
The molecular mechanisms underlying HDV oncogenesis remain unclear. Research conducted over the past 15 years has provided insights that could inform the development of more effective treatments.
Early vaccination prophylaxis is critical for reducing the risk for HCC, despite limited options.
Treatment Options
Randomized controlled trials have demonstrated antiviral efficacy for:
- Pegylated interferon alpha (Peg-IFN) is approved for HBV and is active against HDV.
- Bulevirtide, a synthetic myristoylated lipopeptide entry inhibitor, is used alone or in combination with Peg-IFN.
Suppression of HBV remains central. Nucleoside and nucleotide analogs, such as entecavir, tenofovir alafenamide fumarate, and tenofovir disoproxil fumarate, significantly reduce HCC progression in treated patients compared with untreated patients at risk.
Promising therapeutics include lonafarnib, a farnesyltransferase inhibitor that blocks HDV particle formation, and nucleic acid polymers targeting the host chaperone DNAJB12 to inhibit HBV and HDV replication.
Guideline Updates
The 2023 addendum to the S3 guidelines covers the prophylaxis, diagnosis, and treatment of HBV, including HDV management.
IARC experts also re-evaluated the human cytomegalovirus and Merkel cell polyomavirus. Complete assessments are expected in the next edition of IARC Monographs.
HBV Vaccination
HBV vaccination is the only effective prophylaxis against HBV and HDV. Introduced in 1982 for high-risk groups, it reduced chronic infections, with the WHO expanding its recommendations from 1992 onward.
Infants and young children are at the highest risk of developing this disease. Acute HBV infection often resolves in adults, but infants face up to a 90% risk of developing chronic infection. Newborns of mothers with chronic or undiagnosed HBV infections are particularly vulnerable.
Routine infant immunization includes three doses, with the first dose administered within 12 hours of birth. In Germany, the Standing Committee on Vaccination (STIKO) recommends the administration of combination vaccines, with the hexavalent vaccine administered at 2, 4, and 11 months in a 2 + 1 schedule.
Timely vaccination is crucial because undetected chronic infections often lead to late-stage HCC diagnosis. Adults in high-risk groups should receive HBV vaccination counseling.
STIKO recommends vaccination for close contacts of individuals who are HBsAg-positive, individuals with high-risk sexual contacts, immunocompromised persons, and those with preexisting conditions that increase the risk for severe HBV infection.
Since 2021, insured adults aged 35 years or older in Germany have undergone one-time HBV and HCV screening. HDV testing is recommended for all HBsAg-positive patients. Current frameworks may miss cases, and additional or personalized screening could improve the detection of previously unrecognized infections.
This story was translated from Univadis Germany.
A version of this article appeared on Medscape.com.

Physician Compensation: Gains Small, Gaps Large
Few would deny that physicians today face many challenges: a growing and aging patient population, personnel shortages, mounting paperwork, regulatory and reimbursement pressures, and personal burnout. Collectively these could work to worsen patient access to care. Yet despite these headwinds, Doximity’s survey-based Physician Compensation Report 2025 found that more than three-quarters of physicians polled would still choose to enter their profession.
“Physician burnout isn’t new. It’s been a persistent problem over the past decade,” said Amit Phull, MD, chief clinical experience officer at Doximity. “In a Doximity poll of nearly 2,000 physicians conducted in May 2025, 85% reported they feel overworked, up from 73% just four years ago. As a result, about 68% of physicians said they are looking for an employment change or considering early retirement.”

Greater awareness of contemporary trends may help physicians make more-informed career decisions and more effectively advocate for both themselves and the patients who need them, the report’s authors stated.
Compensation Lag May Impact Care
A small overall average compensation increase of 3.7% from 2023 to 2024 – a slightly lower increase than the 5.9% in the prior year – has done little to close existing pay gaps across the profession.
In 2024, average compensation for men rose 5.7% over 2023, compared with just 1.7% for women – widening the gender pay gap to 26% vs 23% in 2023 and matching the gender gap seen in 2022. And significant disparities persist between physicians caring for adults vs children. In some specialties, the pay gap between pediatric and adult specialists exceeded 80% despite practitioners’ similar levels of training and clinical complexity.
Nearly 60% of respondents said reimbursement pressures could affect their ability to serve Medicare or Medicaid patients in the next year. Additionally, 81% reported that reimbursement policies have significantly contributed to the decline of private practices, and more than a third said they could stifle practice growth with compensation concerns forcing them to delay or cancel hiring or expansion plans. Almost 90% reported an adverse impact from physician shortages, with more citing an inability or limited ability to accept new patients.
Narrowing the Gap for Primary Care?
Over the past three years, the percent pay gap between primary care and specialist medicine declined modestly, the report noted. In 2024, surgical specialists earned 87% more than primary care physicians, down from 100% in 2022. Non-surgical specialists, emergency medicine physicians, and Ob/Gyns also continued to earn significantly more than primary care physicians, though the gaps have narrowed slightly.
“These trends come at a time when primary care remains critical to meeting high patient demand, especially amid ongoing physician shortages,” the report stated. “Primary care physicians continue to earn considerably less than many of their medical colleagues despite their essential role in the healthcare system.”
Significantly, many physicians believe that current reimbursement policies have contributed to the steady decline of independent practices in their fields. According to the American Medical Association, the share of physicians working in private practices dropped by 18 percentage points from 60.1% to 42.2% from 2012 to 2024.
The Specialties
This year’s review found that among 20 specialties, the highest average compensation occurred in surgical and procedural specialties, while the lowest paid were, as mentioned, pediatric medicine and primary care. Pediatric nephrology saw the largest average compensation growth in 2024 at 15.6%, yet compensation still lagged behind adult nephrology with a 40% pay gap.
By medical discipline, gastroenterologists ranked 13th overall in average annual compensation. Gastroenterology remained in the top 20 compensated specialties, with average annual compensation of $537,870 – an increase from $514,208 in 2024, representing a 4.5% growth rate over 2023. Neurosurgeons topped the list at $749,140, followed by thoracic surgeons at $689,969 and orthopedic surgeons at $679,517.
The three lowest-paid branches were all pediatric: endocrinology at $230,426, rheumatology at $231,574, and infectious diseases at $248,322. Pediatric gastroenterology paid somewhat higher at $298,457.
The largest disparities were seen in hematology and oncology, where adult specialists earned 93% more than their pediatric peers. Pediatric gastroenterology showed an 80% pay gap. There were also substantial pay differences across cardiology, pulmonology, and rheumatology. “These gaps appear to reflect a systemic lag in pay for pediatric specialty care, even as demand for pediatric subspecialists continues to rise,” the report stated.
Practice Setting and Location
Where a doctor practices impacts the bottom line, too: in 2024 the highest compensation reported for a metro area was in Rochester, Minnesota (the Mayo Clinic effect?), at $495,532, while the lowest reported was in Durham-Chapel Hill, North Carolina, at $368,782. St. Louis, Missouri ($484,883) and Los Angeles, California ($470,198) were 2nd and 3rd at the top of the list. Rochester, Minnesota, also emerged as best for annual compensation after cost-of-living adjustment, while Boston, Massachusetts, occupied the bottom rung.
The Gender Effect
With a women’s pay increase in 2024 of just 1.7%, the gender gap returned to its 2022-level disparity of 26%, with women physicians earning an average of $120,917 less than men after adjusting for specialty, location, and years of experience.
Doximity’s analysis of data from 2014 to 2019 estimated that on average men make at least $2 million more than women over the course of a 40-year career. This gap is often attributed to the fewer hours worked by female physician with their generally heavier familial responsibilities, “but Doximity’s gender wage gap analysis controls for the number of hours worked and career stage, along with specialty, work type, employment status, region, and credentials,” Phull said.
Women physicians had lower average earnings than men physicians across all specialties, a trend consistent with prior years. As a percentage of pay, the largest gender disparity was seen in pediatric nephrology (16.5%), a specialty that in fact saw the largest annual growth in physician pay. Neurosurgery had the smallest gender gap at 11.3%, while infectious diseases came in at 11.5% and oncology at 12%.
According to Maria T. Abreu, MD, AGAF, executive director of the F. Widjaja Inflammatory Bowel Disease Institute at Cedars-Sinai Medical Center in Los Angeles and past president of AGA, the remuneration gender gap in gastroenterology is being taken seriously by AGA and several other GI societies. “The discrepancies in pay start from the beginning and therefore are magnified over time. We are helping to empower women to negotiate better as well as to gather data on the roots of inequity, she told GI & Hepatology News.

The AGA Women’s Committee has developed a project to support the advancement of women in gastroenterology, Abreu said. The initiative, which includes the AGA Gender Equity Framework and Gender Equity Road Map. focuses attention on disparities in the workplace and promotes opportunities for women’s leadership, career advancement, mentorship and physician health and wellness, she added.
Are these disparities due mainly to the “motherhood penalty,” with career interruption and time lost to maternity leave and fewer hours worked owing to the greater parenting burden of physician mothers? Or are they due to the systemic effects of gender expectations around compensation?
Hours worked appear to be a factor. A 2017 study of dual physician couples found that among childless respondents men worked an average of 57 hours and women 52 hours weekly. Compared with childless men, men with children worked similar numbers of hours weekly. However, compared with childless physicians, mothers worked significantly fewer hours – roughly 40 to 43 hours weekly – depending on the age of their youngest child.
Abreu pushed back on this stereotype. “Most women physicians, including gastroenterologists, do not take the maternity leave they are allowed because they are concerned about burdening their colleagues,” she said. “Thus, it is unlikely to explain the disparities. Many systemic issues remain challenging, but we want women to be empowered to advocate for themselves at the time of hiring and along the arc of their career paths.”
In Abreu’s view, having women assume more leadership roles in the field of gastroenterology provides an opportunity to focus on reducing the disparities in compensation.
Regardless of gender, among all physicians surveyed, autonomy and work-life balance appeared to be a high priority: 77% of doctors said they would be willing to accept or have already accepted lower pay for more autonomy or work-life balance. “Overwork appears to be especially prevalent among women physicians,” said Phull, noting that 91% of women respondents reported being overworked compared with 80% of men. “This overwork has compelled 74% of women to consider making a career change, compared with 62% of men.” Differences emerged among specialties as well: 90% of primary care physicians said they are overworked compared with 84% of surgeons and 83% of non-surgical specialists.
Looking ahead, the report raised an important question. Are we relying too heavily on physicians rather than addressing the underlying need for policies that support a healthier, more sustainable future for all? “Building that future will take more than physician dedication alone,” Phull said. “It will require meaningful collaboration across the entire health care ecosystem – including health systems, hospitals, payors, and policymakers. And physicians must not only have a voice in shaping the path forward; they must have a seat at the table.”
Abreu reported no conflicts of interest in regard to her comments.
Few would deny that physicians today face many challenges: a growing and aging patient population, personnel shortages, mounting paperwork, regulatory and reimbursement pressures, and personal burnout. Collectively these could work to worsen patient access to care. Yet despite these headwinds, Doximity’s survey-based Physician Compensation Report 2025 found that more than three-quarters of physicians polled would still choose to enter their profession.
“Physician burnout isn’t new. It’s been a persistent problem over the past decade,” said Amit Phull, MD, chief clinical experience officer at Doximity. “In a Doximity poll of nearly 2,000 physicians conducted in May 2025, 85% reported they feel overworked, up from 73% just four years ago. As a result, about 68% of physicians said they are looking for an employment change or considering early retirement.”
Greater awareness of contemporary trends may help physicians make more-informed career decisions and more effectively advocate for both themselves and the patients who need them, the report’s authors stated.
Compensation Lag May Impact Care
A small overall average compensation increase of 3.7% from 2023 to 2024 – a slightly lower increase than the 5.9% in the prior year – has done little to close existing pay gaps across the profession.
In 2024, average compensation for men rose 5.7% over 2023, compared with just 1.7% for women – widening the gender pay gap to 26% vs 23% in 2023 and matching the gender gap seen in 2022. And significant disparities persist between physicians caring for adults vs children. In some specialties, the pay gap between pediatric and adult specialists exceeded 80% despite practitioners’ similar levels of training and clinical complexity.
Nearly 60% of respondents said reimbursement pressures could affect their ability to serve Medicare or Medicaid patients in the next year. Additionally, 81% reported that reimbursement policies have significantly contributed to the decline of private practices, and more than a third said they could stifle practice growth with compensation concerns forcing them to delay or cancel hiring or expansion plans. Almost 90% reported an adverse impact from physician shortages, with more citing an inability or limited ability to accept new patients.
Narrowing the Gap for Primary Care?
Over the past three years, the percent pay gap between primary care and specialist medicine declined modestly, the report noted. In 2024, surgical specialists earned 87% more than primary care physicians, down from 100% in 2022. Non-surgical specialists, emergency medicine physicians, and Ob/Gyns also continued to earn significantly more than primary care physicians, though the gaps have narrowed slightly.
“These trends come at a time when primary care remains critical to meeting high patient demand, especially amid ongoing physician shortages,” the report stated. “Primary care physicians continue to earn considerably less than many of their medical colleagues despite their essential role in the healthcare system.”
Significantly, many physicians believe that current reimbursement policies have contributed to the steady decline of independent practices in their fields. According to the American Medical Association, the share of physicians working in private practices dropped by 18 percentage points from 60.1% to 42.2% from 2012 to 2024.
The Specialties
This year’s review found that among 20 specialties, the highest average compensation occurred in surgical and procedural specialties, while the lowest paid were, as mentioned, pediatric medicine and primary care. Pediatric nephrology saw the largest average compensation growth in 2024 at 15.6%, yet compensation still lagged behind adult nephrology with a 40% pay gap.
By medical discipline, gastroenterologists ranked 13th overall in average annual compensation. Gastroenterology remained in the top 20 compensated specialties, with average annual compensation of $537,870 – an increase from $514,208 in 2024, representing a 4.5% growth rate over 2023. Neurosurgeons topped the list at $749,140, followed by thoracic surgeons at $689,969 and orthopedic surgeons at $679,517.
The three lowest-paid branches were all pediatric: endocrinology at $230,426, rheumatology at $231,574, and infectious diseases at $248,322. Pediatric gastroenterology paid somewhat higher at $298,457.
The largest disparities were seen in hematology and oncology, where adult specialists earned 93% more than their pediatric peers. Pediatric gastroenterology showed an 80% pay gap. There were also substantial pay differences across cardiology, pulmonology, and rheumatology. “These gaps appear to reflect a systemic lag in pay for pediatric specialty care, even as demand for pediatric subspecialists continues to rise,” the report stated.
Practice Setting and Location
Where a doctor practices impacts the bottom line, too: in 2024 the highest compensation reported for a metro area was in Rochester, Minnesota (the Mayo Clinic effect?), at $495,532, while the lowest reported was in Durham-Chapel Hill, North Carolina, at $368,782. St. Louis, Missouri ($484,883) and Los Angeles, California ($470,198) were 2nd and 3rd at the top of the list. Rochester, Minnesota, also emerged as best for annual compensation after cost-of-living adjustment, while Boston, Massachusetts, occupied the bottom rung.
The Gender Effect
With a women’s pay increase in 2024 of just 1.7%, the gender gap returned to its 2022-level disparity of 26%, with women physicians earning an average of $120,917 less than men after adjusting for specialty, location, and years of experience.
Doximity’s analysis of data from 2014 to 2019 estimated that on average men make at least $2 million more than women over the course of a 40-year career. This gap is often attributed to the fewer hours worked by female physician with their generally heavier familial responsibilities, “but Doximity’s gender wage gap analysis controls for the number of hours worked and career stage, along with specialty, work type, employment status, region, and credentials,” Phull said.
Women physicians had lower average earnings than men physicians across all specialties, a trend consistent with prior years. As a percentage of pay, the largest gender disparity was seen in pediatric nephrology (16.5%), a specialty that in fact saw the largest annual growth in physician pay. Neurosurgery had the smallest gender gap at 11.3%, while infectious diseases came in at 11.5% and oncology at 12%.
According to Maria T. Abreu, MD, AGAF, executive director of the F. Widjaja Inflammatory Bowel Disease Institute at Cedars-Sinai Medical Center in Los Angeles and past president of AGA, the remuneration gender gap in gastroenterology is being taken seriously by AGA and several other GI societies. “The discrepancies in pay start from the beginning and therefore are magnified over time. We are helping to empower women to negotiate better as well as to gather data on the roots of inequity, she told GI & Hepatology News.
The AGA Women’s Committee has developed a project to support the advancement of women in gastroenterology, Abreu said. The initiative, which includes the AGA Gender Equity Framework and Gender Equity Road Map. focuses attention on disparities in the workplace and promotes opportunities for women’s leadership, career advancement, mentorship and physician health and wellness, she added.
Are these disparities due mainly to the “motherhood penalty,” with career interruption and time lost to maternity leave and fewer hours worked owing to the greater parenting burden of physician mothers? Or are they due to the systemic effects of gender expectations around compensation?
Hours worked appear to be a factor. A 2017 study of dual physician couples found that among childless respondents men worked an average of 57 hours and women 52 hours weekly. Compared with childless men, men with children worked similar numbers of hours weekly. However, compared with childless physicians, mothers worked significantly fewer hours – roughly 40 to 43 hours weekly – depending on the age of their youngest child.
Abreu pushed back on this stereotype. “Most women physicians, including gastroenterologists, do not take the maternity leave they are allowed because they are concerned about burdening their colleagues,” she said. “Thus, it is unlikely to explain the disparities. Many systemic issues remain challenging, but we want women to be empowered to advocate for themselves at the time of hiring and along the arc of their career paths.”
In Abreu’s view, having women assume more leadership roles in the field of gastroenterology provides an opportunity to focus on reducing the disparities in compensation.
Regardless of gender, among all physicians surveyed, autonomy and work-life balance appeared to be a high priority: 77% of doctors said they would be willing to accept or have already accepted lower pay for more autonomy or work-life balance. “Overwork appears to be especially prevalent among women physicians,” said Phull, noting that 91% of women respondents reported being overworked compared with 80% of men. “This overwork has compelled 74% of women to consider making a career change, compared with 62% of men.” Differences emerged among specialties as well: 90% of primary care physicians said they are overworked compared with 84% of surgeons and 83% of non-surgical specialists.
Looking ahead, the report raised an important question. Are we relying too heavily on physicians rather than addressing the underlying need for policies that support a healthier, more sustainable future for all? “Building that future will take more than physician dedication alone,” Phull said. “It will require meaningful collaboration across the entire health care ecosystem – including health systems, hospitals, payors, and policymakers. And physicians must not only have a voice in shaping the path forward; they must have a seat at the table.”
Abreu reported no conflicts of interest in regard to her comments.
Few would deny that physicians today face many challenges: a growing and aging patient population, personnel shortages, mounting paperwork, regulatory and reimbursement pressures, and personal burnout. Collectively these could work to worsen patient access to care. Yet despite these headwinds, Doximity’s survey-based Physician Compensation Report 2025 found that more than three-quarters of physicians polled would still choose to enter their profession.
“Physician burnout isn’t new. It’s been a persistent problem over the past decade,” said Amit Phull, MD, chief clinical experience officer at Doximity. “In a Doximity poll of nearly 2,000 physicians conducted in May 2025, 85% reported they feel overworked, up from 73% just four years ago. As a result, about 68% of physicians said they are looking for an employment change or considering early retirement.”
Greater awareness of contemporary trends may help physicians make more-informed career decisions and more effectively advocate for both themselves and the patients who need them, the report’s authors stated.
Compensation Lag May Impact Care
A small overall average compensation increase of 3.7% from 2023 to 2024 – a slightly lower increase than the 5.9% in the prior year – has done little to close existing pay gaps across the profession.
In 2024, average compensation for men rose 5.7% over 2023, compared with just 1.7% for women – widening the gender pay gap to 26% vs 23% in 2023 and matching the gender gap seen in 2022. And significant disparities persist between physicians caring for adults vs children. In some specialties, the pay gap between pediatric and adult specialists exceeded 80% despite practitioners’ similar levels of training and clinical complexity.
Nearly 60% of respondents said reimbursement pressures could affect their ability to serve Medicare or Medicaid patients in the next year. Additionally, 81% reported that reimbursement policies have significantly contributed to the decline of private practices, and more than a third said they could stifle practice growth with compensation concerns forcing them to delay or cancel hiring or expansion plans. Almost 90% reported an adverse impact from physician shortages, with more citing an inability or limited ability to accept new patients.
Narrowing the Gap for Primary Care?
Over the past three years, the percent pay gap between primary care and specialist medicine declined modestly, the report noted. In 2024, surgical specialists earned 87% more than primary care physicians, down from 100% in 2022. Non-surgical specialists, emergency medicine physicians, and Ob/Gyns also continued to earn significantly more than primary care physicians, though the gaps have narrowed slightly.
“These trends come at a time when primary care remains critical to meeting high patient demand, especially amid ongoing physician shortages,” the report stated. “Primary care physicians continue to earn considerably less than many of their medical colleagues despite their essential role in the healthcare system.”
Significantly, many physicians believe that current reimbursement policies have contributed to the steady decline of independent practices in their fields. According to the American Medical Association, the share of physicians working in private practices dropped by 18 percentage points from 60.1% to 42.2% from 2012 to 2024.
The Specialties
This year’s review found that among 20 specialties, the highest average compensation occurred in surgical and procedural specialties, while the lowest paid were, as mentioned, pediatric medicine and primary care. Pediatric nephrology saw the largest average compensation growth in 2024 at 15.6%, yet compensation still lagged behind adult nephrology with a 40% pay gap.
By medical discipline, gastroenterologists ranked 13th overall in average annual compensation. Gastroenterology remained in the top 20 compensated specialties, with average annual compensation of $537,870 – an increase from $514,208 in 2024, representing a 4.5% growth rate over 2023. Neurosurgeons topped the list at $749,140, followed by thoracic surgeons at $689,969 and orthopedic surgeons at $679,517.
The three lowest-paid branches were all pediatric: endocrinology at $230,426, rheumatology at $231,574, and infectious diseases at $248,322. Pediatric gastroenterology paid somewhat higher at $298,457.
The largest disparities were seen in hematology and oncology, where adult specialists earned 93% more than their pediatric peers. Pediatric gastroenterology showed an 80% pay gap. There were also substantial pay differences across cardiology, pulmonology, and rheumatology. “These gaps appear to reflect a systemic lag in pay for pediatric specialty care, even as demand for pediatric subspecialists continues to rise,” the report stated.
Practice Setting and Location
Where a doctor practices impacts the bottom line, too: in 2024 the highest compensation reported for a metro area was in Rochester, Minnesota (the Mayo Clinic effect?), at $495,532, while the lowest reported was in Durham-Chapel Hill, North Carolina, at $368,782. St. Louis, Missouri ($484,883) and Los Angeles, California ($470,198) were 2nd and 3rd at the top of the list. Rochester, Minnesota, also emerged as best for annual compensation after cost-of-living adjustment, while Boston, Massachusetts, occupied the bottom rung.
The Gender Effect
With a women’s pay increase in 2024 of just 1.7%, the gender gap returned to its 2022-level disparity of 26%, with women physicians earning an average of $120,917 less than men after adjusting for specialty, location, and years of experience.
Doximity’s analysis of data from 2014 to 2019 estimated that on average men make at least $2 million more than women over the course of a 40-year career. This gap is often attributed to the fewer hours worked by female physician with their generally heavier familial responsibilities, “but Doximity’s gender wage gap analysis controls for the number of hours worked and career stage, along with specialty, work type, employment status, region, and credentials,” Phull said.
Women physicians had lower average earnings than men physicians across all specialties, a trend consistent with prior years. As a percentage of pay, the largest gender disparity was seen in pediatric nephrology (16.5%), a specialty that in fact saw the largest annual growth in physician pay. Neurosurgery had the smallest gender gap at 11.3%, while infectious diseases came in at 11.5% and oncology at 12%.
According to Maria T. Abreu, MD, AGAF, executive director of the F. Widjaja Inflammatory Bowel Disease Institute at Cedars-Sinai Medical Center in Los Angeles and past president of AGA, the remuneration gender gap in gastroenterology is being taken seriously by AGA and several other GI societies. “The discrepancies in pay start from the beginning and therefore are magnified over time. We are helping to empower women to negotiate better as well as to gather data on the roots of inequity, she told GI & Hepatology News.
The AGA Women’s Committee has developed a project to support the advancement of women in gastroenterology, Abreu said. The initiative, which includes the AGA Gender Equity Framework and Gender Equity Road Map. focuses attention on disparities in the workplace and promotes opportunities for women’s leadership, career advancement, mentorship and physician health and wellness, she added.
Are these disparities due mainly to the “motherhood penalty,” with career interruption and time lost to maternity leave and fewer hours worked owing to the greater parenting burden of physician mothers? Or are they due to the systemic effects of gender expectations around compensation?
Hours worked appear to be a factor. A 2017 study of dual physician couples found that among childless respondents men worked an average of 57 hours and women 52 hours weekly. Compared with childless men, men with children worked similar numbers of hours weekly. However, compared with childless physicians, mothers worked significantly fewer hours – roughly 40 to 43 hours weekly – depending on the age of their youngest child.
Abreu pushed back on this stereotype. “Most women physicians, including gastroenterologists, do not take the maternity leave they are allowed because they are concerned about burdening their colleagues,” she said. “Thus, it is unlikely to explain the disparities. Many systemic issues remain challenging, but we want women to be empowered to advocate for themselves at the time of hiring and along the arc of their career paths.”
In Abreu’s view, having women assume more leadership roles in the field of gastroenterology provides an opportunity to focus on reducing the disparities in compensation.
Regardless of gender, among all physicians surveyed, autonomy and work-life balance appeared to be a high priority: 77% of doctors said they would be willing to accept or have already accepted lower pay for more autonomy or work-life balance. “Overwork appears to be especially prevalent among women physicians,” said Phull, noting that 91% of women respondents reported being overworked compared with 80% of men. “This overwork has compelled 74% of women to consider making a career change, compared with 62% of men.” Differences emerged among specialties as well: 90% of primary care physicians said they are overworked compared with 84% of surgeons and 83% of non-surgical specialists.
Looking ahead, the report raised an important question. Are we relying too heavily on physicians rather than addressing the underlying need for policies that support a healthier, more sustainable future for all? “Building that future will take more than physician dedication alone,” Phull said. “It will require meaningful collaboration across the entire health care ecosystem – including health systems, hospitals, payors, and policymakers. And physicians must not only have a voice in shaping the path forward; they must have a seat at the table.”
Abreu reported no conflicts of interest in regard to her comments.
Supporting Exceptional Researchers
Did you know that the AGA Research Foundation helped support 74 researchers this past May?

But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: [email protected] or contact us at [email protected].
Did you know that the AGA Research Foundation helped support 74 researchers this past May?
But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: [email protected] or contact us at [email protected].
Did you know that the AGA Research Foundation helped support 74 researchers this past May?
But we can’t do it without you. We depend on the generosity of our supporters to make our vision for the future a reality.
When you donate to AGA Research Foundation, you don’t just give funds – you personally give our beneficiaries grant funding that will lead to new discoveries in GI. Your support goes directly towards funding GI research, helping us address immediate needs while building the foundation for long-term solutions. Plus, you’ll become part of a community full of passionate members like you.
It’s easy to make your mark on our efforts to support investigators. Simply visit our website or learn more ways to give here: [email protected] or contact us at [email protected].
Streamlined Testosterone Order Template to Improve the Diagnosis and Evaluation of Hypogonadism in Veterans
Streamlined Testosterone Order Template to Improve the Diagnosis and Evaluation of Hypogonadism in Veterans
Testosterone therapy is administered following pragmatic diagnostic evaluation and workup to assess whether an adult male is hypogonadal, based on symptoms consistent with androgen deficiency and low morning serum testosterone concentrations on ≥ 2 occasions. Effects of testosterone administration include the development or maintenance of secondary sexual characteristics and increases in libido, muscle strength, fat-free mass, and bone density.
Testosterone prescriptions have markedly increased in the past 20 years, including within the US Department of Veterans Affairs (VA) health care system.1-3 This trend may be influenced by various factors, including patient perceptions of benefit, an increase in marketing, and the availability of more user-friendly formulations.
Since 2006, evidence-based clinical practice guidelines have recommended specific clinical and laboratory evaluation and counseling prior to starting testosterone replacement therapy (TRT).4-8 However, research has shown poor adherence to these recommendations, including at the VA, which raises concerns about inappropriate TRT initiation without proper diagnostic evaluation.9,10 Observational research has suggested a possible link between testosterone therapy and increased risk of cardiovascular (CV) events. The US Food and Drug Administration prescribing information includes boxed warnings about potential risks of high blood pressure, myocardial infarction, stroke, and CV-related mortality with testosterone treatment, contact transfer of transdermal testosterone, and pulmonary oil microembolism with testosterone undecanoate injections.11-15
A VA Office of Inspector General (OIG) review of VA clinician adherence to clinical and laboratory evaluation guidelines for testosterone deficiency found poor adherence among VA practitioners and made recommendations for improvement.4,15 These focused on establishing clinical signs and symptoms consistent with testosterone deficiency, confirming hypogonadism by repeated testosterone testing, determining the etiology of hypogonadism by measuring gonadotropins, initiating a discussion of risks and benefits of TRT, and assessing clinical improvement and obtaining an updated hematocrit test within 3 to 6 months of initiation.
The VA Puget Sound Health Care System (VAPSHCS) developed a local prior authorization template to assist health care practitioners (HCPs) to address the OIG recommendations. This testosterone order template (TOT) aimed to improve the diagnosis, evaluation, and monitoring of TRT in males with hypogonadism, combined with existing VA pharmacy criteria for the use of testosterone based on Endocrine Society guidelines. A version of the VAPSHCS TOT was approved as the national VA Computerized Patient Record System (CPRS) template.
Preliminary evaluation of the TOT suggested improved short-term adherence to guideline recommendations following implementation.16 This quality improvement study sought to assess the long-term effectiveness of the TOT with respect to clinical practice guideline adherence. The OIG did not address prostate-specific antigen (PSA) monitoring because understanding of the relationship between TRT and the risks of elevated PSA levels remains incomplete.6,17 This project hypothesized that implementation of a pharmacy-managed TOT incorporated into CPRS would result in higher adherence rates to guideline-recommended clinical and laboratory evaluation, in addition to counseling of men with hypogonadism prior to initiation of TRT.
Methods
Eligible participants were cisgender males who received a new testosterone prescription, had ≥ 2 clinic visits at VAPSHCS, and no previous testosterone prescription in the previous 2 years. Individuals were excluded if they had testosterone administered at VAPSHCS; were prescribed testosterone at another facility (VA or community-based); pilot tested an initial version of the TOT prior to November 30, 2019; or had an International Classification of Diseases, Tenth Revision codes for hypopituitarism, gender identity disorder, history of sexual assignment, or Klinefelter syndrome for which testosterone therapy was already approved. Patients who met the inclusion criteria were identified by an algorithm developed by the VAPSHCS pharmacoeconomist.
This quality improvement project used a retrospective, pre-post experimental design. Electronic chart review and systematic manual review of all eligible patient charts were performed for the pretemplate period (December 1, 2018, to November 30, 2019) and after the template implementation, (December 1, 2021, to November 30, 2022).
An initial version of the TOT was implemented on July 1, 2019, but was not fully integrated into CPRS until early 2020; individuals in whom the TOT was used prior to November 30, 2019, were excluded. Data from the initial period of the COVID-19 pandemic were avoided because of alterations in clinic and prescribing practices. As a quality improvement project, the TOT evaluation was exempt from formal review by the VAPSHCS Institutional Review Board, as determined by the Director of the Office of Transformation/Quality/Safety/Value.
Interventions
Testosterone is a Schedule III controlled substance with potential risks and a propensity for varied prescribing practices. It was designated as a restricted drug requiring a prior authorization drug request (PADR) for which a specific TOT was developed, approved by the VAPSHCS Pharmacy and Therapeutics Committee, and incorporated into CPRS. A team of pharmacists, primary care physicians, geriatricians, endocrinologists, and health informatics experts created and developed the TOT. Pharmacists managed and monitored its completion.
The process for prescribing testosterone via the TOT is outlined in the eAppendix. When an HCP orders testosterone in CPRS, reminders prompt them to use the TOT and indicate required laboratory measurements (an order set is provided). Completion of TOT is not necessary to order testosterone for patients with an existing diagnosis of an organic cause of hypogonadism (eg, Klinefelter syndrome or hypopituitarism) or transgender women (assigned male at birth). In the TOT, the prescriber must also indicate signs and symptoms of testosterone deficiency; required laboratory tests; and counseling regarding potential risks and benefits of TRT. A pharmacist reviews the TOT and either approves or rejects the testosterone prescription and provides follow-up guidance to the prescriber. The completed TOT serves as documentation of guideline adherence in CPRS. The TOT also includes sections for first renewal testosterone prescriptions, addressing guideline recommendations for follow-up laboratory evaluation and clinical response to TRT. Due to limited completion of this section in the posttemplate period, evaluating adherence to follow-up recommendations was not feasible.
Measures
This project assessed the percentage of patients in the posttemplate period vs pretemplate period with an approved PADR. Documentation of specific guideline-recommended measures was assessed: signs and symptoms of testosterone deficiency; ≥ 2 serum testosterone measurements (≥ 2 total, free and total, or 2 free testosterone levels, and ≥ 1 testosterone level before 10
The project also assessed the proportion of patients in the posttemplate period vs pretemplate period who had all hormone tests (≥ 2 serum testosterone and LH and FSH concentrations), all laboratory tests (hormone tests and hematocrit), and all 5 guideline-recommended measures.
Analysis
Statistical comparisons between the proportions of patients in the pretemplate and posttemplate periods for each measure were performed using a χ2 test, without correction for multiple comparisons. All analyses were conducted using Stata version 10.0. A P value < .05 was considered significant for all comparisons.
Results
Chart review identified 189 patients in the pretemplate period and 113 patients in the posttemplate period with a new testosterone prescription (Figure). After exclusions, 91 and 49 patients, respectively, met eligibility criteria (Table 1). Fifty-six patients (62%) pretemplate and 40 patients (82%) posttemplate (P = .015) had approved PADRs and comprised the groups that were analyzed (Table 2).
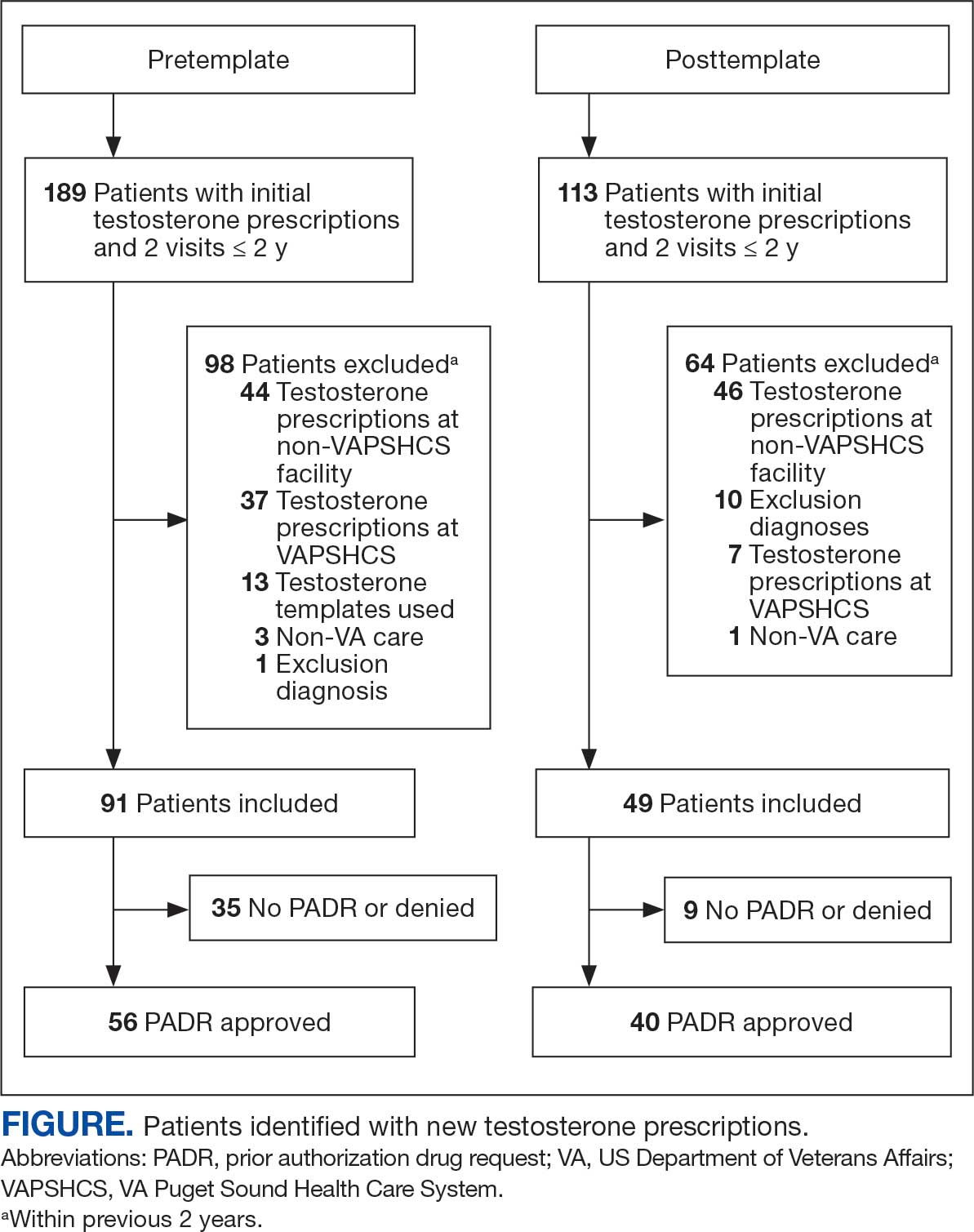
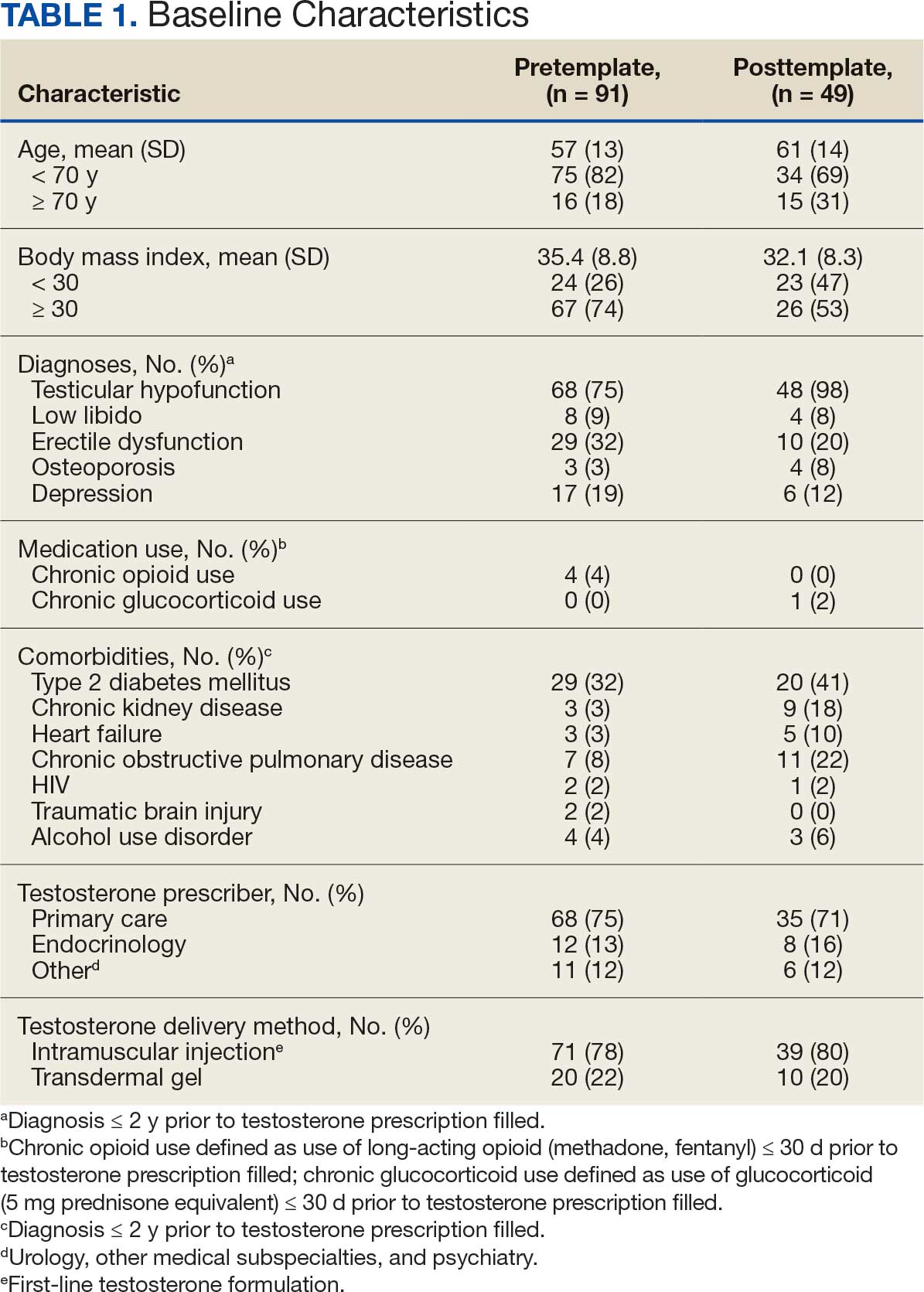

The mean age and body mass index were similar in the pretemplate and posttemplate periods, but there was variation in the proportions of patients aged < 70 years and those with a body mass index < 30 between the groups. The most common diagnosis in both groups was testicular hypofunction, and the most common comorbidity was type 2 diabetes mellitus. Concomitant use of opioids or glucocorticoids that can lower testosterone levels was rare. Most testosterone prescriptions originated from primary care clinics in both periods: 68 (75%) in the pretemplate period and 35 (71%) in the posttemplate period. Most testosterone treatment was delivered by intramuscular injection.
In the posttemplate period vs pretemplate period, the proportion of patients with an approved PADR (82% vs 62%, P = .02), and documentation of signs and symptoms of hypogonadism (93% vs 71%, P = .002) prior to starting TRT were higher, while the percentage of patients having ≥ 2 testosterone measurements (85% vs 89%, P = .53), ≥ 1 testosterone level before 10 AM (78% vs 75%, P = .70), and hematocrit measured (95% vs 91%, P = .47) were similar. Rates of LH and FSH testing were higher in the posttemplate period (80%) vs the pretemplate period (63%) but did not achieve statistical significance (P = .07), and discussion of the risks and benefits of TRT was higher in the posttemplate period (58%) vs the pretemplate period (34%) (P = .02). The percentage of patients who had all hormone measurements (total and/or free testosterone, LH, and FSH) was higher in the posttemplate period (78%) vs the pretemplate period (59%) but did not achieve statistical significance (P = .06). The rates of all guideline-recommended laboratory test orders were higher in the posttemplate period (78%) vs the pretemplate period (55%) (P = .03), and all 5 guideline-recommended clinical and laboratory measures were higher in the posttemplate period (45%) vs the pretemplate period (18%) (P = .004).
Discussion
The implementation of a pharmacy-managed TOT in CPRS demonstrated higher adherence to evidence-based guidelines for diagnosing and evaluating hypogonadism before TRT. After TOT implementation, a higher proportion of patients had documented signs and symptoms of testosterone deficiency, underwent all recommended laboratory tests, and had discussions about the risks and benefits of TRT. Adherence to 5 clinical and laboratory measures recommended by Endocrine Society guidelines was higher after TOT implementation, indicating improved prescribing practices.4
The requirement for TOT completion before testosterone prescription and its management by trained pharmacists likely contributed to higher adherence to guideline recommendations than previously reported. Integration of the TOT into CPRS with pharmacy oversight may have enhanced adherence by summarizing and codifying evidence-based guideline recommendations for clinical and biochemical evaluation prior to TRT initiation, offering relevant education to clinicians and pharmacists, automatically importing pertinent clinical information and laboratory results, and generating CPRS documentation to reduce clinician burden during patient care.
The proportion of patients with documented signs and symptoms of testosterone deficiency before TRT increased from the pretemplate period (71%) to the posttemplate period (93%), indicating that most patients receiving TRT had clinical manifestations of hypogonadism. This aligns with Endocrine Society guidelines, which define hypogonadism as a clinical disorder characterized by clinical manifestations of testosterone deficiency and persistently low serum testosterone levels on ≥ 2 separate occasions.4,6 However, recent trends in direct-to-consumer advertising for testosterone and the rise of “low T” clinics may contribute to increased testing, varied practices, and inappropriate testosterone therapy initiation (eg, in men with low testosterone levels who lack symptoms of hypogonadism).18 Improved adherence in documenting clinical hypogonadism with implementation of the TOT reinforces the value of incorporating educational material, as previously reported.11
Adherence to guideline recommendations following implementation of the TOT in this project was higher than those previously reported. In a study of 111,631 outpatient veterans prescribed testosterone from 2009 to 2012, only 18.3% had ≥ 2 testosterone prescriptions, and 3.5% had ≥ 2 testosterone, LH, and FSH levels measured prior to the initiation of a TRT.9 In a report of 63,534 insured patients who received TRT from 2010 to 2012, 40.3% had ≥ 2 testosterone prescriptions, and 12% had LH and/or FSH measured prior to the initiation.8
Low rates of guideline-recommended laboratory tests prior to initiation of testosterone treatment were reported in prior non-VA studies.19,20 Poor guideline adherence reinforces the need for clinician education or other methods to improve TRT and ensure appropriate prescribing practices across health care systems. The TOT described in this project is a sustainable clinical tool with the potential to improve testosterone prescribing practices.
The high rates of adherence to guideline recommendations at VAPSHCS likely stem from local endocrine expertise and ongoing educational initiatives, as well as the requirement for template completion before testosterone prescription. However, most testosterone prescriptions were initiated by primary care and monitored by pharmacists with varying degrees of training and clinical experience in hypogonadism and TRT.
However, adherence to guideline recommendations was modest, suggesting there is still an opportunity for improvement. The decision to initiate therapy should be made only after appropriate counseling with patients regarding its potential benefits and risks. Reports on the CV risk of TRT have been mixed. The 2023 TRAVERSE study found no increase in major adverse CV events among older men with hypogonadism and pre-existing CV risks undergoing TRT, but noted higher instances of pulmonary embolism, atrial fibrillation, and acute kidney injury.21 This highlights the need for clinicians to continue to engage in informed decision-making with patients. Effective pretreatment counseling is important but time-consuming; future TOT monitoring and modifications could consider mandatory checkboxes to document counseling on TRT risks and benefits.
The TOT described in this study could be adapted and incorporated into the prescribing process and electronic health record of larger health care systems. Use of an electronic template allows for automatic real-time dashboard monitoring of organization performance. The TOT described could be modified or simplified for specialty or primary care clinics or individual practitioners to improve adherence to evidence-based guideline recommendations and quality of care.
Strengths
A strength of this study is the multidisciplinary team (composed of stakeholders with experience in VA health care system and subject matter experts in hypogonadism) that developed and incorporated a user-friendly template for testosterone prescriptions; the use of evidence-based guideline recommendations; and the use of a structured chart review permitted accurate assessment of adherence to recommendations to document signs and symptoms of testosterone deficiency and a discussion of potential risks and benefits prior to TRT. To our knowledge, these recommendations have not been assessed in previous reports.
Limitations
The retrospective pre-post design of this study precludes a conclusion that implementation of the TOT caused the increase in adherence to guideline recommendations. Improved adherence could have resulted from the ongoing development of the preauthorization process for testosterone prescriptions or other changes over time. However, the preauthorization process had already been established for many years prior to template implementation. Forty-nine patients had new prescriptions for testosterone in the posttemplate period compared to 91 in the pretemplate period, but TRT was initiated in accordance with guideline recommendations more appropriately in the posttemplate period. The study’s sample size was small, and many eligible patients were excluded; however, exclusions were necessary to evaluate men who had new testosterone prescriptions for which the template was designed. Most men excluded were already taking testosterone.
Conclusions
The implementation of a CPRS-based TOT improved adherence to evidence-based guidelines for the diagnosis, evaluation, and counseling of patients with hypogonadism before starting TRT. While there were improvements in adherence with the TOT, the relatively low proportion of patients with documentation of TRT risks and benefits and all guideline recommendations highlights the need for additional efforts to further strengthen adherence to guideline recommendations and ensure appropriate evaluation, counseling, and prescribing practices before initiating TRT.
- Layton JB, Li D, Meier CR, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab. 2014;99:835-842. doi:10.1210/jc.2013-3570
- Baillargeon J, Kuo YF, Westra JR, et al. Testosterone prescribing in the United States, 2002-2016. JAMA. 2018;320:200-202. doi:10.1001/jama.2018.7999
- Jasuja GK, Bhasin S, Rose AJ. Patterns of testosterone prescription overuse. Curr Opin Endocrinol Diabetes Obes. 2017;24:240-245. doi:10.1097/MED.0000000000000336
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010. doi:10.1210/jc.2005-2847
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95:2536-2559. doi:10.1210/jc.2009-2354
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103:1715-1744. doi:10.1210/jc.2018-00229
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200:423-432. doi:10.1016/j.juro.2018.03.115
- Muram D, Zhang X, Cui Z, et al. Use of hormone testing for the diagnosis and evaluation of male hypogonadism and monitoring of testosterone therapy: application of hormone testing guideline recommendations in clinical practice. J Sex Med. 2015;12:1886-1894. doi:10.1111/jsm.12968
- Jasuja GK, Bhasin S, Reisman JI, et al. Ascertainment of testosterone prescribing practices in the VA. Med Care. 2015;53:746-752. doi:10.1097/MLR.0000000000000398?
- Jasuja GK, Bhasin S, Reisman JI, et al. Who gets testosterone? Patient characteristics associated with testosterone prescribing in the Veteran Affairs system: a cross-sectional study. J Gen Intern Med. 2017;32:304-311. doi:10.1007/s11606-016-3940-7
- Basaria S, Coviello AD, Travison TG, et al. Adverse events associated with testosterone administration. N Engl J Med. 2010;363:109-122. doi:10.1056/NEJMoa1000485
- Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829-1836. doi:10.1001/jama.2013.280386
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of non-fatal myocardial infarction following testosterone therapy prescription in men. PLoS One. 2014;9:e85805. doi:10.1371/journal.pone.0085805
- US Food and Drug Administration. FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. FDA.gov. March 3, 2015. Updated February 28, 2025. Accessed July 8, 2025. http://www.fda.gov/Drugs/DrugSafety/ucm436259.htm
- US Dept of Veterans Affairs, Office of Inspector General. Healthcare inspection – testosterone replacement therapy initiation and follow-up evaluation in VA male patients. April 11, 2018. Accessed July 8, 2025. https://www.vaoig.gov/reports/national-healthcare-review/healthcare-inspection-testosterone-replacement-therapy
- Narla R, Mobley D, Nguyen EHK, et al. Preliminary evaluation of an order template to improve diagnosis and testosterone therapy of hypogonadism in veterans. Fed Pract. 2021;38:121-127. doi:10.12788/fp.0103
- Bhasin S, Travison TG, Pencina KM, et al. Prostate safety events during testosterone replacement therapy in men with hypogonadism: a randomized clinical trial. JAMA Netw Open. 2023;6:e2348692. doi:10.1001/jamanetworkopen.2023.48692
- Dubin JM, Jesse E, Fantus RJ, et al. Guideline-discordant care among direct-to-consumer testosterone therapy platforms. JAMA Intern Med. 2022;182:1321-1323. doi:10.1001/jamainternmed.2022.4928
- Baillargeon J, Urban RJ, Ottenbacher KJ, et al. Trends in androgen prescribing in the United States, 2001 to 2011. JAMA Intern Med. 2013;173:1465-1466. doi:10.1001/jamainternmed.2013.6895
- Locke JA, Flannigan R, Günther OP, et al. Testosterone therapy: prescribing and monitoring patterns of practice in British Columbia. Can Urol Assoc J. 2021;15:e110-e117. doi:10.5489/cuaj.6586
- Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. N Engl J Med. 2023;389:107-117. doi:10.1056/NEJMoa2215025
Testosterone therapy is administered following pragmatic diagnostic evaluation and workup to assess whether an adult male is hypogonadal, based on symptoms consistent with androgen deficiency and low morning serum testosterone concentrations on ≥ 2 occasions. Effects of testosterone administration include the development or maintenance of secondary sexual characteristics and increases in libido, muscle strength, fat-free mass, and bone density.
Testosterone prescriptions have markedly increased in the past 20 years, including within the US Department of Veterans Affairs (VA) health care system.1-3 This trend may be influenced by various factors, including patient perceptions of benefit, an increase in marketing, and the availability of more user-friendly formulations.
Since 2006, evidence-based clinical practice guidelines have recommended specific clinical and laboratory evaluation and counseling prior to starting testosterone replacement therapy (TRT).4-8 However, research has shown poor adherence to these recommendations, including at the VA, which raises concerns about inappropriate TRT initiation without proper diagnostic evaluation.9,10 Observational research has suggested a possible link between testosterone therapy and increased risk of cardiovascular (CV) events. The US Food and Drug Administration prescribing information includes boxed warnings about potential risks of high blood pressure, myocardial infarction, stroke, and CV-related mortality with testosterone treatment, contact transfer of transdermal testosterone, and pulmonary oil microembolism with testosterone undecanoate injections.11-15
A VA Office of Inspector General (OIG) review of VA clinician adherence to clinical and laboratory evaluation guidelines for testosterone deficiency found poor adherence among VA practitioners and made recommendations for improvement.4,15 These focused on establishing clinical signs and symptoms consistent with testosterone deficiency, confirming hypogonadism by repeated testosterone testing, determining the etiology of hypogonadism by measuring gonadotropins, initiating a discussion of risks and benefits of TRT, and assessing clinical improvement and obtaining an updated hematocrit test within 3 to 6 months of initiation.
The VA Puget Sound Health Care System (VAPSHCS) developed a local prior authorization template to assist health care practitioners (HCPs) to address the OIG recommendations. This testosterone order template (TOT) aimed to improve the diagnosis, evaluation, and monitoring of TRT in males with hypogonadism, combined with existing VA pharmacy criteria for the use of testosterone based on Endocrine Society guidelines. A version of the VAPSHCS TOT was approved as the national VA Computerized Patient Record System (CPRS) template.
Preliminary evaluation of the TOT suggested improved short-term adherence to guideline recommendations following implementation.16 This quality improvement study sought to assess the long-term effectiveness of the TOT with respect to clinical practice guideline adherence. The OIG did not address prostate-specific antigen (PSA) monitoring because understanding of the relationship between TRT and the risks of elevated PSA levels remains incomplete.6,17 This project hypothesized that implementation of a pharmacy-managed TOT incorporated into CPRS would result in higher adherence rates to guideline-recommended clinical and laboratory evaluation, in addition to counseling of men with hypogonadism prior to initiation of TRT.
Methods
Eligible participants were cisgender males who received a new testosterone prescription, had ≥ 2 clinic visits at VAPSHCS, and no previous testosterone prescription in the previous 2 years. Individuals were excluded if they had testosterone administered at VAPSHCS; were prescribed testosterone at another facility (VA or community-based); pilot tested an initial version of the TOT prior to November 30, 2019; or had an International Classification of Diseases, Tenth Revision codes for hypopituitarism, gender identity disorder, history of sexual assignment, or Klinefelter syndrome for which testosterone therapy was already approved. Patients who met the inclusion criteria were identified by an algorithm developed by the VAPSHCS pharmacoeconomist.
This quality improvement project used a retrospective, pre-post experimental design. Electronic chart review and systematic manual review of all eligible patient charts were performed for the pretemplate period (December 1, 2018, to November 30, 2019) and after the template implementation, (December 1, 2021, to November 30, 2022).
An initial version of the TOT was implemented on July 1, 2019, but was not fully integrated into CPRS until early 2020; individuals in whom the TOT was used prior to November 30, 2019, were excluded. Data from the initial period of the COVID-19 pandemic were avoided because of alterations in clinic and prescribing practices. As a quality improvement project, the TOT evaluation was exempt from formal review by the VAPSHCS Institutional Review Board, as determined by the Director of the Office of Transformation/Quality/Safety/Value.
Interventions
Testosterone is a Schedule III controlled substance with potential risks and a propensity for varied prescribing practices. It was designated as a restricted drug requiring a prior authorization drug request (PADR) for which a specific TOT was developed, approved by the VAPSHCS Pharmacy and Therapeutics Committee, and incorporated into CPRS. A team of pharmacists, primary care physicians, geriatricians, endocrinologists, and health informatics experts created and developed the TOT. Pharmacists managed and monitored its completion.
The process for prescribing testosterone via the TOT is outlined in the eAppendix. When an HCP orders testosterone in CPRS, reminders prompt them to use the TOT and indicate required laboratory measurements (an order set is provided). Completion of TOT is not necessary to order testosterone for patients with an existing diagnosis of an organic cause of hypogonadism (eg, Klinefelter syndrome or hypopituitarism) or transgender women (assigned male at birth). In the TOT, the prescriber must also indicate signs and symptoms of testosterone deficiency; required laboratory tests; and counseling regarding potential risks and benefits of TRT. A pharmacist reviews the TOT and either approves or rejects the testosterone prescription and provides follow-up guidance to the prescriber. The completed TOT serves as documentation of guideline adherence in CPRS. The TOT also includes sections for first renewal testosterone prescriptions, addressing guideline recommendations for follow-up laboratory evaluation and clinical response to TRT. Due to limited completion of this section in the posttemplate period, evaluating adherence to follow-up recommendations was not feasible.
Measures
This project assessed the percentage of patients in the posttemplate period vs pretemplate period with an approved PADR. Documentation of specific guideline-recommended measures was assessed: signs and symptoms of testosterone deficiency; ≥ 2 serum testosterone measurements (≥ 2 total, free and total, or 2 free testosterone levels, and ≥ 1 testosterone level before 10
The project also assessed the proportion of patients in the posttemplate period vs pretemplate period who had all hormone tests (≥ 2 serum testosterone and LH and FSH concentrations), all laboratory tests (hormone tests and hematocrit), and all 5 guideline-recommended measures.
Analysis
Statistical comparisons between the proportions of patients in the pretemplate and posttemplate periods for each measure were performed using a χ2 test, without correction for multiple comparisons. All analyses were conducted using Stata version 10.0. A P value < .05 was considered significant for all comparisons.
Results
Chart review identified 189 patients in the pretemplate period and 113 patients in the posttemplate period with a new testosterone prescription (Figure). After exclusions, 91 and 49 patients, respectively, met eligibility criteria (Table 1). Fifty-six patients (62%) pretemplate and 40 patients (82%) posttemplate (P = .015) had approved PADRs and comprised the groups that were analyzed (Table 2).
The mean age and body mass index were similar in the pretemplate and posttemplate periods, but there was variation in the proportions of patients aged < 70 years and those with a body mass index < 30 between the groups. The most common diagnosis in both groups was testicular hypofunction, and the most common comorbidity was type 2 diabetes mellitus. Concomitant use of opioids or glucocorticoids that can lower testosterone levels was rare. Most testosterone prescriptions originated from primary care clinics in both periods: 68 (75%) in the pretemplate period and 35 (71%) in the posttemplate period. Most testosterone treatment was delivered by intramuscular injection.
In the posttemplate period vs pretemplate period, the proportion of patients with an approved PADR (82% vs 62%, P = .02), and documentation of signs and symptoms of hypogonadism (93% vs 71%, P = .002) prior to starting TRT were higher, while the percentage of patients having ≥ 2 testosterone measurements (85% vs 89%, P = .53), ≥ 1 testosterone level before 10 AM (78% vs 75%, P = .70), and hematocrit measured (95% vs 91%, P = .47) were similar. Rates of LH and FSH testing were higher in the posttemplate period (80%) vs the pretemplate period (63%) but did not achieve statistical significance (P = .07), and discussion of the risks and benefits of TRT was higher in the posttemplate period (58%) vs the pretemplate period (34%) (P = .02). The percentage of patients who had all hormone measurements (total and/or free testosterone, LH, and FSH) was higher in the posttemplate period (78%) vs the pretemplate period (59%) but did not achieve statistical significance (P = .06). The rates of all guideline-recommended laboratory test orders were higher in the posttemplate period (78%) vs the pretemplate period (55%) (P = .03), and all 5 guideline-recommended clinical and laboratory measures were higher in the posttemplate period (45%) vs the pretemplate period (18%) (P = .004).
Discussion
The implementation of a pharmacy-managed TOT in CPRS demonstrated higher adherence to evidence-based guidelines for diagnosing and evaluating hypogonadism before TRT. After TOT implementation, a higher proportion of patients had documented signs and symptoms of testosterone deficiency, underwent all recommended laboratory tests, and had discussions about the risks and benefits of TRT. Adherence to 5 clinical and laboratory measures recommended by Endocrine Society guidelines was higher after TOT implementation, indicating improved prescribing practices.4
The requirement for TOT completion before testosterone prescription and its management by trained pharmacists likely contributed to higher adherence to guideline recommendations than previously reported. Integration of the TOT into CPRS with pharmacy oversight may have enhanced adherence by summarizing and codifying evidence-based guideline recommendations for clinical and biochemical evaluation prior to TRT initiation, offering relevant education to clinicians and pharmacists, automatically importing pertinent clinical information and laboratory results, and generating CPRS documentation to reduce clinician burden during patient care.
The proportion of patients with documented signs and symptoms of testosterone deficiency before TRT increased from the pretemplate period (71%) to the posttemplate period (93%), indicating that most patients receiving TRT had clinical manifestations of hypogonadism. This aligns with Endocrine Society guidelines, which define hypogonadism as a clinical disorder characterized by clinical manifestations of testosterone deficiency and persistently low serum testosterone levels on ≥ 2 separate occasions.4,6 However, recent trends in direct-to-consumer advertising for testosterone and the rise of “low T” clinics may contribute to increased testing, varied practices, and inappropriate testosterone therapy initiation (eg, in men with low testosterone levels who lack symptoms of hypogonadism).18 Improved adherence in documenting clinical hypogonadism with implementation of the TOT reinforces the value of incorporating educational material, as previously reported.11
Adherence to guideline recommendations following implementation of the TOT in this project was higher than those previously reported. In a study of 111,631 outpatient veterans prescribed testosterone from 2009 to 2012, only 18.3% had ≥ 2 testosterone prescriptions, and 3.5% had ≥ 2 testosterone, LH, and FSH levels measured prior to the initiation of a TRT.9 In a report of 63,534 insured patients who received TRT from 2010 to 2012, 40.3% had ≥ 2 testosterone prescriptions, and 12% had LH and/or FSH measured prior to the initiation.8
Low rates of guideline-recommended laboratory tests prior to initiation of testosterone treatment were reported in prior non-VA studies.19,20 Poor guideline adherence reinforces the need for clinician education or other methods to improve TRT and ensure appropriate prescribing practices across health care systems. The TOT described in this project is a sustainable clinical tool with the potential to improve testosterone prescribing practices.
The high rates of adherence to guideline recommendations at VAPSHCS likely stem from local endocrine expertise and ongoing educational initiatives, as well as the requirement for template completion before testosterone prescription. However, most testosterone prescriptions were initiated by primary care and monitored by pharmacists with varying degrees of training and clinical experience in hypogonadism and TRT.
However, adherence to guideline recommendations was modest, suggesting there is still an opportunity for improvement. The decision to initiate therapy should be made only after appropriate counseling with patients regarding its potential benefits and risks. Reports on the CV risk of TRT have been mixed. The 2023 TRAVERSE study found no increase in major adverse CV events among older men with hypogonadism and pre-existing CV risks undergoing TRT, but noted higher instances of pulmonary embolism, atrial fibrillation, and acute kidney injury.21 This highlights the need for clinicians to continue to engage in informed decision-making with patients. Effective pretreatment counseling is important but time-consuming; future TOT monitoring and modifications could consider mandatory checkboxes to document counseling on TRT risks and benefits.
The TOT described in this study could be adapted and incorporated into the prescribing process and electronic health record of larger health care systems. Use of an electronic template allows for automatic real-time dashboard monitoring of organization performance. The TOT described could be modified or simplified for specialty or primary care clinics or individual practitioners to improve adherence to evidence-based guideline recommendations and quality of care.
Strengths
A strength of this study is the multidisciplinary team (composed of stakeholders with experience in VA health care system and subject matter experts in hypogonadism) that developed and incorporated a user-friendly template for testosterone prescriptions; the use of evidence-based guideline recommendations; and the use of a structured chart review permitted accurate assessment of adherence to recommendations to document signs and symptoms of testosterone deficiency and a discussion of potential risks and benefits prior to TRT. To our knowledge, these recommendations have not been assessed in previous reports.
Limitations
The retrospective pre-post design of this study precludes a conclusion that implementation of the TOT caused the increase in adherence to guideline recommendations. Improved adherence could have resulted from the ongoing development of the preauthorization process for testosterone prescriptions or other changes over time. However, the preauthorization process had already been established for many years prior to template implementation. Forty-nine patients had new prescriptions for testosterone in the posttemplate period compared to 91 in the pretemplate period, but TRT was initiated in accordance with guideline recommendations more appropriately in the posttemplate period. The study’s sample size was small, and many eligible patients were excluded; however, exclusions were necessary to evaluate men who had new testosterone prescriptions for which the template was designed. Most men excluded were already taking testosterone.
Conclusions
The implementation of a CPRS-based TOT improved adherence to evidence-based guidelines for the diagnosis, evaluation, and counseling of patients with hypogonadism before starting TRT. While there were improvements in adherence with the TOT, the relatively low proportion of patients with documentation of TRT risks and benefits and all guideline recommendations highlights the need for additional efforts to further strengthen adherence to guideline recommendations and ensure appropriate evaluation, counseling, and prescribing practices before initiating TRT.
Testosterone therapy is administered following pragmatic diagnostic evaluation and workup to assess whether an adult male is hypogonadal, based on symptoms consistent with androgen deficiency and low morning serum testosterone concentrations on ≥ 2 occasions. Effects of testosterone administration include the development or maintenance of secondary sexual characteristics and increases in libido, muscle strength, fat-free mass, and bone density.
Testosterone prescriptions have markedly increased in the past 20 years, including within the US Department of Veterans Affairs (VA) health care system.1-3 This trend may be influenced by various factors, including patient perceptions of benefit, an increase in marketing, and the availability of more user-friendly formulations.
Since 2006, evidence-based clinical practice guidelines have recommended specific clinical and laboratory evaluation and counseling prior to starting testosterone replacement therapy (TRT).4-8 However, research has shown poor adherence to these recommendations, including at the VA, which raises concerns about inappropriate TRT initiation without proper diagnostic evaluation.9,10 Observational research has suggested a possible link between testosterone therapy and increased risk of cardiovascular (CV) events. The US Food and Drug Administration prescribing information includes boxed warnings about potential risks of high blood pressure, myocardial infarction, stroke, and CV-related mortality with testosterone treatment, contact transfer of transdermal testosterone, and pulmonary oil microembolism with testosterone undecanoate injections.11-15
A VA Office of Inspector General (OIG) review of VA clinician adherence to clinical and laboratory evaluation guidelines for testosterone deficiency found poor adherence among VA practitioners and made recommendations for improvement.4,15 These focused on establishing clinical signs and symptoms consistent with testosterone deficiency, confirming hypogonadism by repeated testosterone testing, determining the etiology of hypogonadism by measuring gonadotropins, initiating a discussion of risks and benefits of TRT, and assessing clinical improvement and obtaining an updated hematocrit test within 3 to 6 months of initiation.
The VA Puget Sound Health Care System (VAPSHCS) developed a local prior authorization template to assist health care practitioners (HCPs) to address the OIG recommendations. This testosterone order template (TOT) aimed to improve the diagnosis, evaluation, and monitoring of TRT in males with hypogonadism, combined with existing VA pharmacy criteria for the use of testosterone based on Endocrine Society guidelines. A version of the VAPSHCS TOT was approved as the national VA Computerized Patient Record System (CPRS) template.
Preliminary evaluation of the TOT suggested improved short-term adherence to guideline recommendations following implementation.16 This quality improvement study sought to assess the long-term effectiveness of the TOT with respect to clinical practice guideline adherence. The OIG did not address prostate-specific antigen (PSA) monitoring because understanding of the relationship between TRT and the risks of elevated PSA levels remains incomplete.6,17 This project hypothesized that implementation of a pharmacy-managed TOT incorporated into CPRS would result in higher adherence rates to guideline-recommended clinical and laboratory evaluation, in addition to counseling of men with hypogonadism prior to initiation of TRT.
Methods
Eligible participants were cisgender males who received a new testosterone prescription, had ≥ 2 clinic visits at VAPSHCS, and no previous testosterone prescription in the previous 2 years. Individuals were excluded if they had testosterone administered at VAPSHCS; were prescribed testosterone at another facility (VA or community-based); pilot tested an initial version of the TOT prior to November 30, 2019; or had an International Classification of Diseases, Tenth Revision codes for hypopituitarism, gender identity disorder, history of sexual assignment, or Klinefelter syndrome for which testosterone therapy was already approved. Patients who met the inclusion criteria were identified by an algorithm developed by the VAPSHCS pharmacoeconomist.
This quality improvement project used a retrospective, pre-post experimental design. Electronic chart review and systematic manual review of all eligible patient charts were performed for the pretemplate period (December 1, 2018, to November 30, 2019) and after the template implementation, (December 1, 2021, to November 30, 2022).
An initial version of the TOT was implemented on July 1, 2019, but was not fully integrated into CPRS until early 2020; individuals in whom the TOT was used prior to November 30, 2019, were excluded. Data from the initial period of the COVID-19 pandemic were avoided because of alterations in clinic and prescribing practices. As a quality improvement project, the TOT evaluation was exempt from formal review by the VAPSHCS Institutional Review Board, as determined by the Director of the Office of Transformation/Quality/Safety/Value.
Interventions
Testosterone is a Schedule III controlled substance with potential risks and a propensity for varied prescribing practices. It was designated as a restricted drug requiring a prior authorization drug request (PADR) for which a specific TOT was developed, approved by the VAPSHCS Pharmacy and Therapeutics Committee, and incorporated into CPRS. A team of pharmacists, primary care physicians, geriatricians, endocrinologists, and health informatics experts created and developed the TOT. Pharmacists managed and monitored its completion.
The process for prescribing testosterone via the TOT is outlined in the eAppendix. When an HCP orders testosterone in CPRS, reminders prompt them to use the TOT and indicate required laboratory measurements (an order set is provided). Completion of TOT is not necessary to order testosterone for patients with an existing diagnosis of an organic cause of hypogonadism (eg, Klinefelter syndrome or hypopituitarism) or transgender women (assigned male at birth). In the TOT, the prescriber must also indicate signs and symptoms of testosterone deficiency; required laboratory tests; and counseling regarding potential risks and benefits of TRT. A pharmacist reviews the TOT and either approves or rejects the testosterone prescription and provides follow-up guidance to the prescriber. The completed TOT serves as documentation of guideline adherence in CPRS. The TOT also includes sections for first renewal testosterone prescriptions, addressing guideline recommendations for follow-up laboratory evaluation and clinical response to TRT. Due to limited completion of this section in the posttemplate period, evaluating adherence to follow-up recommendations was not feasible.
Measures
This project assessed the percentage of patients in the posttemplate period vs pretemplate period with an approved PADR. Documentation of specific guideline-recommended measures was assessed: signs and symptoms of testosterone deficiency; ≥ 2 serum testosterone measurements (≥ 2 total, free and total, or 2 free testosterone levels, and ≥ 1 testosterone level before 10
The project also assessed the proportion of patients in the posttemplate period vs pretemplate period who had all hormone tests (≥ 2 serum testosterone and LH and FSH concentrations), all laboratory tests (hormone tests and hematocrit), and all 5 guideline-recommended measures.
Analysis
Statistical comparisons between the proportions of patients in the pretemplate and posttemplate periods for each measure were performed using a χ2 test, without correction for multiple comparisons. All analyses were conducted using Stata version 10.0. A P value < .05 was considered significant for all comparisons.
Results
Chart review identified 189 patients in the pretemplate period and 113 patients in the posttemplate period with a new testosterone prescription (Figure). After exclusions, 91 and 49 patients, respectively, met eligibility criteria (Table 1). Fifty-six patients (62%) pretemplate and 40 patients (82%) posttemplate (P = .015) had approved PADRs and comprised the groups that were analyzed (Table 2).
The mean age and body mass index were similar in the pretemplate and posttemplate periods, but there was variation in the proportions of patients aged < 70 years and those with a body mass index < 30 between the groups. The most common diagnosis in both groups was testicular hypofunction, and the most common comorbidity was type 2 diabetes mellitus. Concomitant use of opioids or glucocorticoids that can lower testosterone levels was rare. Most testosterone prescriptions originated from primary care clinics in both periods: 68 (75%) in the pretemplate period and 35 (71%) in the posttemplate period. Most testosterone treatment was delivered by intramuscular injection.
In the posttemplate period vs pretemplate period, the proportion of patients with an approved PADR (82% vs 62%, P = .02), and documentation of signs and symptoms of hypogonadism (93% vs 71%, P = .002) prior to starting TRT were higher, while the percentage of patients having ≥ 2 testosterone measurements (85% vs 89%, P = .53), ≥ 1 testosterone level before 10 AM (78% vs 75%, P = .70), and hematocrit measured (95% vs 91%, P = .47) were similar. Rates of LH and FSH testing were higher in the posttemplate period (80%) vs the pretemplate period (63%) but did not achieve statistical significance (P = .07), and discussion of the risks and benefits of TRT was higher in the posttemplate period (58%) vs the pretemplate period (34%) (P = .02). The percentage of patients who had all hormone measurements (total and/or free testosterone, LH, and FSH) was higher in the posttemplate period (78%) vs the pretemplate period (59%) but did not achieve statistical significance (P = .06). The rates of all guideline-recommended laboratory test orders were higher in the posttemplate period (78%) vs the pretemplate period (55%) (P = .03), and all 5 guideline-recommended clinical and laboratory measures were higher in the posttemplate period (45%) vs the pretemplate period (18%) (P = .004).
Discussion
The implementation of a pharmacy-managed TOT in CPRS demonstrated higher adherence to evidence-based guidelines for diagnosing and evaluating hypogonadism before TRT. After TOT implementation, a higher proportion of patients had documented signs and symptoms of testosterone deficiency, underwent all recommended laboratory tests, and had discussions about the risks and benefits of TRT. Adherence to 5 clinical and laboratory measures recommended by Endocrine Society guidelines was higher after TOT implementation, indicating improved prescribing practices.4
The requirement for TOT completion before testosterone prescription and its management by trained pharmacists likely contributed to higher adherence to guideline recommendations than previously reported. Integration of the TOT into CPRS with pharmacy oversight may have enhanced adherence by summarizing and codifying evidence-based guideline recommendations for clinical and biochemical evaluation prior to TRT initiation, offering relevant education to clinicians and pharmacists, automatically importing pertinent clinical information and laboratory results, and generating CPRS documentation to reduce clinician burden during patient care.
The proportion of patients with documented signs and symptoms of testosterone deficiency before TRT increased from the pretemplate period (71%) to the posttemplate period (93%), indicating that most patients receiving TRT had clinical manifestations of hypogonadism. This aligns with Endocrine Society guidelines, which define hypogonadism as a clinical disorder characterized by clinical manifestations of testosterone deficiency and persistently low serum testosterone levels on ≥ 2 separate occasions.4,6 However, recent trends in direct-to-consumer advertising for testosterone and the rise of “low T” clinics may contribute to increased testing, varied practices, and inappropriate testosterone therapy initiation (eg, in men with low testosterone levels who lack symptoms of hypogonadism).18 Improved adherence in documenting clinical hypogonadism with implementation of the TOT reinforces the value of incorporating educational material, as previously reported.11
Adherence to guideline recommendations following implementation of the TOT in this project was higher than those previously reported. In a study of 111,631 outpatient veterans prescribed testosterone from 2009 to 2012, only 18.3% had ≥ 2 testosterone prescriptions, and 3.5% had ≥ 2 testosterone, LH, and FSH levels measured prior to the initiation of a TRT.9 In a report of 63,534 insured patients who received TRT from 2010 to 2012, 40.3% had ≥ 2 testosterone prescriptions, and 12% had LH and/or FSH measured prior to the initiation.8
Low rates of guideline-recommended laboratory tests prior to initiation of testosterone treatment were reported in prior non-VA studies.19,20 Poor guideline adherence reinforces the need for clinician education or other methods to improve TRT and ensure appropriate prescribing practices across health care systems. The TOT described in this project is a sustainable clinical tool with the potential to improve testosterone prescribing practices.
The high rates of adherence to guideline recommendations at VAPSHCS likely stem from local endocrine expertise and ongoing educational initiatives, as well as the requirement for template completion before testosterone prescription. However, most testosterone prescriptions were initiated by primary care and monitored by pharmacists with varying degrees of training and clinical experience in hypogonadism and TRT.
However, adherence to guideline recommendations was modest, suggesting there is still an opportunity for improvement. The decision to initiate therapy should be made only after appropriate counseling with patients regarding its potential benefits and risks. Reports on the CV risk of TRT have been mixed. The 2023 TRAVERSE study found no increase in major adverse CV events among older men with hypogonadism and pre-existing CV risks undergoing TRT, but noted higher instances of pulmonary embolism, atrial fibrillation, and acute kidney injury.21 This highlights the need for clinicians to continue to engage in informed decision-making with patients. Effective pretreatment counseling is important but time-consuming; future TOT monitoring and modifications could consider mandatory checkboxes to document counseling on TRT risks and benefits.
The TOT described in this study could be adapted and incorporated into the prescribing process and electronic health record of larger health care systems. Use of an electronic template allows for automatic real-time dashboard monitoring of organization performance. The TOT described could be modified or simplified for specialty or primary care clinics or individual practitioners to improve adherence to evidence-based guideline recommendations and quality of care.
Strengths
A strength of this study is the multidisciplinary team (composed of stakeholders with experience in VA health care system and subject matter experts in hypogonadism) that developed and incorporated a user-friendly template for testosterone prescriptions; the use of evidence-based guideline recommendations; and the use of a structured chart review permitted accurate assessment of adherence to recommendations to document signs and symptoms of testosterone deficiency and a discussion of potential risks and benefits prior to TRT. To our knowledge, these recommendations have not been assessed in previous reports.
Limitations
The retrospective pre-post design of this study precludes a conclusion that implementation of the TOT caused the increase in adherence to guideline recommendations. Improved adherence could have resulted from the ongoing development of the preauthorization process for testosterone prescriptions or other changes over time. However, the preauthorization process had already been established for many years prior to template implementation. Forty-nine patients had new prescriptions for testosterone in the posttemplate period compared to 91 in the pretemplate period, but TRT was initiated in accordance with guideline recommendations more appropriately in the posttemplate period. The study’s sample size was small, and many eligible patients were excluded; however, exclusions were necessary to evaluate men who had new testosterone prescriptions for which the template was designed. Most men excluded were already taking testosterone.
Conclusions
The implementation of a CPRS-based TOT improved adherence to evidence-based guidelines for the diagnosis, evaluation, and counseling of patients with hypogonadism before starting TRT. While there were improvements in adherence with the TOT, the relatively low proportion of patients with documentation of TRT risks and benefits and all guideline recommendations highlights the need for additional efforts to further strengthen adherence to guideline recommendations and ensure appropriate evaluation, counseling, and prescribing practices before initiating TRT.
- Layton JB, Li D, Meier CR, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab. 2014;99:835-842. doi:10.1210/jc.2013-3570
- Baillargeon J, Kuo YF, Westra JR, et al. Testosterone prescribing in the United States, 2002-2016. JAMA. 2018;320:200-202. doi:10.1001/jama.2018.7999
- Jasuja GK, Bhasin S, Rose AJ. Patterns of testosterone prescription overuse. Curr Opin Endocrinol Diabetes Obes. 2017;24:240-245. doi:10.1097/MED.0000000000000336
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010. doi:10.1210/jc.2005-2847
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95:2536-2559. doi:10.1210/jc.2009-2354
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103:1715-1744. doi:10.1210/jc.2018-00229
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200:423-432. doi:10.1016/j.juro.2018.03.115
- Muram D, Zhang X, Cui Z, et al. Use of hormone testing for the diagnosis and evaluation of male hypogonadism and monitoring of testosterone therapy: application of hormone testing guideline recommendations in clinical practice. J Sex Med. 2015;12:1886-1894. doi:10.1111/jsm.12968
- Jasuja GK, Bhasin S, Reisman JI, et al. Ascertainment of testosterone prescribing practices in the VA. Med Care. 2015;53:746-752. doi:10.1097/MLR.0000000000000398?
- Jasuja GK, Bhasin S, Reisman JI, et al. Who gets testosterone? Patient characteristics associated with testosterone prescribing in the Veteran Affairs system: a cross-sectional study. J Gen Intern Med. 2017;32:304-311. doi:10.1007/s11606-016-3940-7
- Basaria S, Coviello AD, Travison TG, et al. Adverse events associated with testosterone administration. N Engl J Med. 2010;363:109-122. doi:10.1056/NEJMoa1000485
- Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829-1836. doi:10.1001/jama.2013.280386
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of non-fatal myocardial infarction following testosterone therapy prescription in men. PLoS One. 2014;9:e85805. doi:10.1371/journal.pone.0085805
- US Food and Drug Administration. FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. FDA.gov. March 3, 2015. Updated February 28, 2025. Accessed July 8, 2025. http://www.fda.gov/Drugs/DrugSafety/ucm436259.htm
- US Dept of Veterans Affairs, Office of Inspector General. Healthcare inspection – testosterone replacement therapy initiation and follow-up evaluation in VA male patients. April 11, 2018. Accessed July 8, 2025. https://www.vaoig.gov/reports/national-healthcare-review/healthcare-inspection-testosterone-replacement-therapy
- Narla R, Mobley D, Nguyen EHK, et al. Preliminary evaluation of an order template to improve diagnosis and testosterone therapy of hypogonadism in veterans. Fed Pract. 2021;38:121-127. doi:10.12788/fp.0103
- Bhasin S, Travison TG, Pencina KM, et al. Prostate safety events during testosterone replacement therapy in men with hypogonadism: a randomized clinical trial. JAMA Netw Open. 2023;6:e2348692. doi:10.1001/jamanetworkopen.2023.48692
- Dubin JM, Jesse E, Fantus RJ, et al. Guideline-discordant care among direct-to-consumer testosterone therapy platforms. JAMA Intern Med. 2022;182:1321-1323. doi:10.1001/jamainternmed.2022.4928
- Baillargeon J, Urban RJ, Ottenbacher KJ, et al. Trends in androgen prescribing in the United States, 2001 to 2011. JAMA Intern Med. 2013;173:1465-1466. doi:10.1001/jamainternmed.2013.6895
- Locke JA, Flannigan R, Günther OP, et al. Testosterone therapy: prescribing and monitoring patterns of practice in British Columbia. Can Urol Assoc J. 2021;15:e110-e117. doi:10.5489/cuaj.6586
- Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. N Engl J Med. 2023;389:107-117. doi:10.1056/NEJMoa2215025
- Layton JB, Li D, Meier CR, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab. 2014;99:835-842. doi:10.1210/jc.2013-3570
- Baillargeon J, Kuo YF, Westra JR, et al. Testosterone prescribing in the United States, 2002-2016. JAMA. 2018;320:200-202. doi:10.1001/jama.2018.7999
- Jasuja GK, Bhasin S, Rose AJ. Patterns of testosterone prescription overuse. Curr Opin Endocrinol Diabetes Obes. 2017;24:240-245. doi:10.1097/MED.0000000000000336
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in adult men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995-2010. doi:10.1210/jc.2005-2847
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95:2536-2559. doi:10.1210/jc.2009-2354
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103:1715-1744. doi:10.1210/jc.2018-00229
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200:423-432. doi:10.1016/j.juro.2018.03.115
- Muram D, Zhang X, Cui Z, et al. Use of hormone testing for the diagnosis and evaluation of male hypogonadism and monitoring of testosterone therapy: application of hormone testing guideline recommendations in clinical practice. J Sex Med. 2015;12:1886-1894. doi:10.1111/jsm.12968
- Jasuja GK, Bhasin S, Reisman JI, et al. Ascertainment of testosterone prescribing practices in the VA. Med Care. 2015;53:746-752. doi:10.1097/MLR.0000000000000398?
- Jasuja GK, Bhasin S, Reisman JI, et al. Who gets testosterone? Patient characteristics associated with testosterone prescribing in the Veteran Affairs system: a cross-sectional study. J Gen Intern Med. 2017;32:304-311. doi:10.1007/s11606-016-3940-7
- Basaria S, Coviello AD, Travison TG, et al. Adverse events associated with testosterone administration. N Engl J Med. 2010;363:109-122. doi:10.1056/NEJMoa1000485
- Vigen R, O’Donnell CI, Barón AE, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829-1836. doi:10.1001/jama.2013.280386
- Finkle WD, Greenland S, Ridgeway GK, et al. Increased risk of non-fatal myocardial infarction following testosterone therapy prescription in men. PLoS One. 2014;9:e85805. doi:10.1371/journal.pone.0085805
- US Food and Drug Administration. FDA Drug Safety Communication: FDA cautions about using testosterone products for low testosterone due to aging; requires labeling change to inform of possible increased risk of heart attack and stroke with use. FDA.gov. March 3, 2015. Updated February 28, 2025. Accessed July 8, 2025. http://www.fda.gov/Drugs/DrugSafety/ucm436259.htm
- US Dept of Veterans Affairs, Office of Inspector General. Healthcare inspection – testosterone replacement therapy initiation and follow-up evaluation in VA male patients. April 11, 2018. Accessed July 8, 2025. https://www.vaoig.gov/reports/national-healthcare-review/healthcare-inspection-testosterone-replacement-therapy
- Narla R, Mobley D, Nguyen EHK, et al. Preliminary evaluation of an order template to improve diagnosis and testosterone therapy of hypogonadism in veterans. Fed Pract. 2021;38:121-127. doi:10.12788/fp.0103
- Bhasin S, Travison TG, Pencina KM, et al. Prostate safety events during testosterone replacement therapy in men with hypogonadism: a randomized clinical trial. JAMA Netw Open. 2023;6:e2348692. doi:10.1001/jamanetworkopen.2023.48692
- Dubin JM, Jesse E, Fantus RJ, et al. Guideline-discordant care among direct-to-consumer testosterone therapy platforms. JAMA Intern Med. 2022;182:1321-1323. doi:10.1001/jamainternmed.2022.4928
- Baillargeon J, Urban RJ, Ottenbacher KJ, et al. Trends in androgen prescribing in the United States, 2001 to 2011. JAMA Intern Med. 2013;173:1465-1466. doi:10.1001/jamainternmed.2013.6895
- Locke JA, Flannigan R, Günther OP, et al. Testosterone therapy: prescribing and monitoring patterns of practice in British Columbia. Can Urol Assoc J. 2021;15:e110-e117. doi:10.5489/cuaj.6586
- Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. N Engl J Med. 2023;389:107-117. doi:10.1056/NEJMoa2215025
Streamlined Testosterone Order Template to Improve the Diagnosis and Evaluation of Hypogonadism in Veterans
Streamlined Testosterone Order Template to Improve the Diagnosis and Evaluation of Hypogonadism in Veterans

Simpler Approach Increases Diagnostic Accuracy of Timed Barium Esophagram for Achalasia
, according to investigators.
The classification tree offers a practical alternative for evaluating esophagogastric junction (EGJ) outflow disorders when more advanced methods like high-resolution manometry (HRM) or functional lumen imaging probe (FLIP) panometry are unavailable, lead author Ofer Z. Fass, MD, of Northwestern University, Chicago, and colleagues reported.
“[T]here are limited data on normative TBE values,” the investigators wrote in Gastroenterology. “Furthermore, data supporting the accuracy of TBE as a screening test for esophageal motility disorders, as well as clinically relevant test thresholds, remains limited.”
TBE is conventionally interpreted using a handful of single measurements, most often the barium column height at 1, 2, or 5 minutes. Although these metrics are simple to obtain, variability in technique, cutoff values, and interpretation across centers limits reproducibility and weakens diagnostic accuracy, according to the investigators. The role of TBE has therefore been largely confined to adjudicating inconclusive manometry findings, but even in that setting, the absence of validated reference standards constrains its utility as a reliable screening tool.
To address this gap, Fass and colleagues conducted a prospective analysis of 290 patients who underwent TBE at Northwestern Memorial Hospital, Chicago, with HRM and FLIP panometry, interpreted according to the Chicago Classification version 4.0 (CCv4.0), serving as the diagnostic reference standards.
Patients were included if they had both TBE and manometry performed within a short interval, ensuring that the two tests could be meaningfully compared. The study population represented a broad spectrum of esophageal motility presentations, allowing the model to be trained on clinically relevant variation.
Beyond column height, the investigators measured barium height at multiple timepoints, maximal esophageal body width, maximum EGJ diameter, and tablet passage. These variables were incorporated into a recursive partitioning algorithm to build a multimetric classification tree aimed at distinguishing EGJ outflow obstruction from other motility disorders.
The optimal tree incorporated three sequential decision levels. At the top was maximum esophageal body width, followed by EGJ diameter and barium height at the second level, and tablet passage at the third. This stepwise structure allowed the model to refine diagnoses by combining simple, reproducible TBE metrics that are already collected in routine practice.
Among the 290 patients, 121 (42%) had EGJ outflow disorders, 151 (52%) had no outflow disorder, and 18 (6%) had inconclusive manometry findings. Using conventional interpretation with column height and tablet passage, TBE demonstrated a sensitivity of 77.8%, a specificity of 86.0%, and an accuracy of 82.2%. The multimetric classification tree improved diagnostic performance across all parameters, with a sensitivity of 84.2%, a specificity of 92.1%, and an accuracy of 88.3%.
The advantages of multimetric interpretation were most notable in patients with borderline column heights, which single-metric approaches often misclassify, underscoring the value of integrating multiple measurements into a unified model.
“[T]his study demonstrated that TBE can accurately identify achalasia when analyzed using multiple metrics in a classification tree model,” Fass and colleagues wrote. “Future studies should explore the use of TBE metrics and models to identify more specific esophageal motor disorders (such as esophageal spasm and absent contractility), as well as validation in a larger, multicenter cohort.”
Clinical Takeaways
Rishi Naik, MD, of the Center for Swallowing and Esophageal Disorders, Vanderbilt University Medical Center, Nashville, Tennessee, said the study represents a step forward in how clinicians can use a widely accessible esophageal imaging test.
“This study is important in that it has updated the way we use a very common, readily available imaging test and compared it to the current gold standard of HRM and FLIP,” he told GI & Hepatology News. “This provides a practical, standardized framework for clinicians evaluating patients with suspected esophageal motility disorders.”
Naik noted that while HRM and FLIP provide highly detailed information, both carry drawbacks that limit their universal adoption.
“Practically, HRM is a transnasal test that can be cumbersome, and FLIP is performed during a sedated procedure,” he said. “From a comfort and cost perspective, the esophagram outcompetes. What the TBE lacked was adequate sensitivity and specificity when just looking at column height, which is how the authors overcame this by leveraging the comparisons using CCv4.0.”
Implementation, however, requires discipline.
“A timed barium esophagram is a protocol, not a single esophagram,” Naik said. “Without proper measurements, you can’t follow the decision tree.”
Still, he pointed to radiology’s increasing adoption of artificial intelligence (AI) as a promising way forward.
“AI has already transformed radiological reads, and I’m optimistic it will eventually allow us to incorporate not only width, height, and tablet clearance but also 3D [three-dimensional] reconstructions of bolus retention and pressure to enhance predictive modeling,” Naik said.
This study was supported by the Public Health Service.
The investigators disclosed having relationships with Takeda, Phathom Pharmaceuticals, Medtronic, and others. Naik is a consultant for Sanofi/Regeneron, Eli Lilly and Company, and Renexxion.
A version of this article appeared on Medscape.com.
, according to investigators.
The classification tree offers a practical alternative for evaluating esophagogastric junction (EGJ) outflow disorders when more advanced methods like high-resolution manometry (HRM) or functional lumen imaging probe (FLIP) panometry are unavailable, lead author Ofer Z. Fass, MD, of Northwestern University, Chicago, and colleagues reported.
“[T]here are limited data on normative TBE values,” the investigators wrote in Gastroenterology. “Furthermore, data supporting the accuracy of TBE as a screening test for esophageal motility disorders, as well as clinically relevant test thresholds, remains limited.”
TBE is conventionally interpreted using a handful of single measurements, most often the barium column height at 1, 2, or 5 minutes. Although these metrics are simple to obtain, variability in technique, cutoff values, and interpretation across centers limits reproducibility and weakens diagnostic accuracy, according to the investigators. The role of TBE has therefore been largely confined to adjudicating inconclusive manometry findings, but even in that setting, the absence of validated reference standards constrains its utility as a reliable screening tool.
To address this gap, Fass and colleagues conducted a prospective analysis of 290 patients who underwent TBE at Northwestern Memorial Hospital, Chicago, with HRM and FLIP panometry, interpreted according to the Chicago Classification version 4.0 (CCv4.0), serving as the diagnostic reference standards.
Patients were included if they had both TBE and manometry performed within a short interval, ensuring that the two tests could be meaningfully compared. The study population represented a broad spectrum of esophageal motility presentations, allowing the model to be trained on clinically relevant variation.
Beyond column height, the investigators measured barium height at multiple timepoints, maximal esophageal body width, maximum EGJ diameter, and tablet passage. These variables were incorporated into a recursive partitioning algorithm to build a multimetric classification tree aimed at distinguishing EGJ outflow obstruction from other motility disorders.
The optimal tree incorporated three sequential decision levels. At the top was maximum esophageal body width, followed by EGJ diameter and barium height at the second level, and tablet passage at the third. This stepwise structure allowed the model to refine diagnoses by combining simple, reproducible TBE metrics that are already collected in routine practice.
Among the 290 patients, 121 (42%) had EGJ outflow disorders, 151 (52%) had no outflow disorder, and 18 (6%) had inconclusive manometry findings. Using conventional interpretation with column height and tablet passage, TBE demonstrated a sensitivity of 77.8%, a specificity of 86.0%, and an accuracy of 82.2%. The multimetric classification tree improved diagnostic performance across all parameters, with a sensitivity of 84.2%, a specificity of 92.1%, and an accuracy of 88.3%.
The advantages of multimetric interpretation were most notable in patients with borderline column heights, which single-metric approaches often misclassify, underscoring the value of integrating multiple measurements into a unified model.
“[T]his study demonstrated that TBE can accurately identify achalasia when analyzed using multiple metrics in a classification tree model,” Fass and colleagues wrote. “Future studies should explore the use of TBE metrics and models to identify more specific esophageal motor disorders (such as esophageal spasm and absent contractility), as well as validation in a larger, multicenter cohort.”
Clinical Takeaways
Rishi Naik, MD, of the Center for Swallowing and Esophageal Disorders, Vanderbilt University Medical Center, Nashville, Tennessee, said the study represents a step forward in how clinicians can use a widely accessible esophageal imaging test.
“This study is important in that it has updated the way we use a very common, readily available imaging test and compared it to the current gold standard of HRM and FLIP,” he told GI & Hepatology News. “This provides a practical, standardized framework for clinicians evaluating patients with suspected esophageal motility disorders.”
Naik noted that while HRM and FLIP provide highly detailed information, both carry drawbacks that limit their universal adoption.
“Practically, HRM is a transnasal test that can be cumbersome, and FLIP is performed during a sedated procedure,” he said. “From a comfort and cost perspective, the esophagram outcompetes. What the TBE lacked was adequate sensitivity and specificity when just looking at column height, which is how the authors overcame this by leveraging the comparisons using CCv4.0.”
Implementation, however, requires discipline.
“A timed barium esophagram is a protocol, not a single esophagram,” Naik said. “Without proper measurements, you can’t follow the decision tree.”
Still, he pointed to radiology’s increasing adoption of artificial intelligence (AI) as a promising way forward.
“AI has already transformed radiological reads, and I’m optimistic it will eventually allow us to incorporate not only width, height, and tablet clearance but also 3D [three-dimensional] reconstructions of bolus retention and pressure to enhance predictive modeling,” Naik said.
This study was supported by the Public Health Service.
The investigators disclosed having relationships with Takeda, Phathom Pharmaceuticals, Medtronic, and others. Naik is a consultant for Sanofi/Regeneron, Eli Lilly and Company, and Renexxion.
A version of this article appeared on Medscape.com.
, according to investigators.
The classification tree offers a practical alternative for evaluating esophagogastric junction (EGJ) outflow disorders when more advanced methods like high-resolution manometry (HRM) or functional lumen imaging probe (FLIP) panometry are unavailable, lead author Ofer Z. Fass, MD, of Northwestern University, Chicago, and colleagues reported.
“[T]here are limited data on normative TBE values,” the investigators wrote in Gastroenterology. “Furthermore, data supporting the accuracy of TBE as a screening test for esophageal motility disorders, as well as clinically relevant test thresholds, remains limited.”
TBE is conventionally interpreted using a handful of single measurements, most often the barium column height at 1, 2, or 5 minutes. Although these metrics are simple to obtain, variability in technique, cutoff values, and interpretation across centers limits reproducibility and weakens diagnostic accuracy, according to the investigators. The role of TBE has therefore been largely confined to adjudicating inconclusive manometry findings, but even in that setting, the absence of validated reference standards constrains its utility as a reliable screening tool.
To address this gap, Fass and colleagues conducted a prospective analysis of 290 patients who underwent TBE at Northwestern Memorial Hospital, Chicago, with HRM and FLIP panometry, interpreted according to the Chicago Classification version 4.0 (CCv4.0), serving as the diagnostic reference standards.
Patients were included if they had both TBE and manometry performed within a short interval, ensuring that the two tests could be meaningfully compared. The study population represented a broad spectrum of esophageal motility presentations, allowing the model to be trained on clinically relevant variation.
Beyond column height, the investigators measured barium height at multiple timepoints, maximal esophageal body width, maximum EGJ diameter, and tablet passage. These variables were incorporated into a recursive partitioning algorithm to build a multimetric classification tree aimed at distinguishing EGJ outflow obstruction from other motility disorders.
The optimal tree incorporated three sequential decision levels. At the top was maximum esophageal body width, followed by EGJ diameter and barium height at the second level, and tablet passage at the third. This stepwise structure allowed the model to refine diagnoses by combining simple, reproducible TBE metrics that are already collected in routine practice.
Among the 290 patients, 121 (42%) had EGJ outflow disorders, 151 (52%) had no outflow disorder, and 18 (6%) had inconclusive manometry findings. Using conventional interpretation with column height and tablet passage, TBE demonstrated a sensitivity of 77.8%, a specificity of 86.0%, and an accuracy of 82.2%. The multimetric classification tree improved diagnostic performance across all parameters, with a sensitivity of 84.2%, a specificity of 92.1%, and an accuracy of 88.3%.
The advantages of multimetric interpretation were most notable in patients with borderline column heights, which single-metric approaches often misclassify, underscoring the value of integrating multiple measurements into a unified model.
“[T]his study demonstrated that TBE can accurately identify achalasia when analyzed using multiple metrics in a classification tree model,” Fass and colleagues wrote. “Future studies should explore the use of TBE metrics and models to identify more specific esophageal motor disorders (such as esophageal spasm and absent contractility), as well as validation in a larger, multicenter cohort.”
Clinical Takeaways
Rishi Naik, MD, of the Center for Swallowing and Esophageal Disorders, Vanderbilt University Medical Center, Nashville, Tennessee, said the study represents a step forward in how clinicians can use a widely accessible esophageal imaging test.
“This study is important in that it has updated the way we use a very common, readily available imaging test and compared it to the current gold standard of HRM and FLIP,” he told GI & Hepatology News. “This provides a practical, standardized framework for clinicians evaluating patients with suspected esophageal motility disorders.”
Naik noted that while HRM and FLIP provide highly detailed information, both carry drawbacks that limit their universal adoption.
“Practically, HRM is a transnasal test that can be cumbersome, and FLIP is performed during a sedated procedure,” he said. “From a comfort and cost perspective, the esophagram outcompetes. What the TBE lacked was adequate sensitivity and specificity when just looking at column height, which is how the authors overcame this by leveraging the comparisons using CCv4.0.”
Implementation, however, requires discipline.
“A timed barium esophagram is a protocol, not a single esophagram,” Naik said. “Without proper measurements, you can’t follow the decision tree.”
Still, he pointed to radiology’s increasing adoption of artificial intelligence (AI) as a promising way forward.
“AI has already transformed radiological reads, and I’m optimistic it will eventually allow us to incorporate not only width, height, and tablet clearance but also 3D [three-dimensional] reconstructions of bolus retention and pressure to enhance predictive modeling,” Naik said.
This study was supported by the Public Health Service.
The investigators disclosed having relationships with Takeda, Phathom Pharmaceuticals, Medtronic, and others. Naik is a consultant for Sanofi/Regeneron, Eli Lilly and Company, and Renexxion.
A version of this article appeared on Medscape.com.
FROM GASTROENTEROLOGY
Medicolegal Concerns in Contemporary Private GI Practice
The need for gastroenterology (GI) services is on the rise in the US, with growing rates of colonoscopy, earlier-onset colon cancer, and inflammatory bowel disease. This increase is taking place in the context of a changing regulatory landscape.
, and to that end, a recent educational practice management update was published in Clinical Gastroenterology and Hepatology by Erin Smith Aebel, JD, a health law specialist with Trenam Law in Tampa, Florida. Aebel has been a speaker at several national GI conferences and has addressed GI trainees on these issues in medical schools.

“Healthcare regulation continues to evolve and it’s a complicated area,” Aebel told GI & Hepatology News. “Some physician investors in healthcare ventures see the potential profits but are not fully aware of how a physician’s license and livelihood could be affected by noncompliance.”
Aebel has seen some medical business owners and institutions pushing physicians to their limits in order to maximize profits. “They’re failing to allow them the meaningful things that allow for a long-term productive and successful practice that provides great patient care,” she said. “A current issue I’m dealing with is employers’ taking away physicians’ administrative time and not respecting the work that is necessary for the physician to be efficient and provide great care,” she said. “If too many physicians get squeezed in this manner, they will eventually walk away from big employers to something they can better control.”
Aebel noted that private-equity acquisitions of medical practices — a fast-growing US trend — are often targeted at quick profits and quick exits, which can be inconsistent with quality long-term patient care. “A question to be asked by physicians and patients is who is benefiting from this transaction?” she said. “Sometimes retired physicians can see a great benefit in private equity, but newer physicians can get tied up with a strong noncompete agreement. The best deals are ones that try to find wins for all involved, including patients.”
Many independent gastroenterologists focusing on the demands of daily practice are less aware than they should be of the legal and business administration sides. “I often get clients who come to me complaining about their contracts after they’ve signed them. I don’t have leverage to do as much for them,” she admitted.
From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control. These could relate to compensation and bonuses, as well as opportunities to invest in the practice, the practice management company, and possibly real estate or ambulatory surgery centers (ASCs).
Aebel’s overarching messages to gastroenterologists are as follows: “Be aware. Learn basic health law. Read your contracts before you sign them. And invest in good counsel before you sign agreements,” she said. “In addition, GI practitioners need to have a working knowledge of the federal Anti-Kickback Statute and the federal Stark Law and how they could be commonly applied in their practices.”
These are designed to protect government-funded patient care from monetary influence. The False Claims Act is another federal buttress against fraud and abuse, she said.
Update Details
Though not intended to be legal advice, Aebel’s update touches on several important medicolegal areas.
Stark Law on Self-Referrals
Gastroenterologists should be familiar with this federal law, a self-referral civil penalty statute regulating how physicians can pay themselves in practices that provide designated health services covered by federal healthcare programs such as Medicare or Medicaid.
For a Stark penalty to apply, there must be a physician referral to an entity (eg, lab, hospital, nutrition service, physiotherapy or radiotherapy center) in which the physician or a close family member has a financial interest.
Ambulatory Surgery Centers
Another common area vulnerable to federal fraud and abuse regulation is investment in ASCs. “Generally speaking, it is a felony to pay or be paid anything of value for Medicare or Medicaid business referrals,” Aebel wrote. This provision relates to the general restriction of the federal AKB statute.
A gastroenterologist referring Medicare patients to a center where that physician has an investment could technically violate this law because the physician will receive profit distributions from the referral. In addition to constituting a felony with potential jail time, violation of this statute is grounds for substantial civil monetary penalties and/or exclusion from the government coverage program.
Fortunately, Aebel noted, legal safe harbors cover many financial relationships, including investment in an ASC. The financial arrangement is protected from prosecution if it meets five safe harbor requirements, including nondiscriminatory treatment of government-insured patients and physician investment unrelated to a center’s volume or the value of referrals. If even one aspect is not met, that will automatically constitute a crime.
“However, the government will look at facts and circumstances to determine whether there was an intent to pay for a referral,” Aebel wrote.
The safe harbor designates requirements for four types of ASCs: surgeon-owned, single-specialty, multispecialty, and hospital/physician ASCs.
Private-Equity Investment
With mergers and acquisitions of US medical practices and networks by private-equity firms becoming more common, gastroenterologists need to be aware of the legal issues involved in such investment.
Most states abide by corporate practice of medicine doctrines, which prohibit unlicensed people from direct ownership in a medical practice. These doctrines vary by state, but their primary goal is to ensure that medical decisions are made solely based on patient care and not influenced by corporate interests. The aim is to shield the physician-patient relationship from commercial influence.
“Accordingly, this creates additional complicated structures necessary for private-equity investment in gastroenterology practices,” Aebel wrote. Usually, such investors will invest in a management services organization (MSO), which takes much of the practice’s value via management fees. Gastroenterologists may or may not have an opportunity to invest in the practice and the MSO in this scenario.
Under corporate practice of medicine doctrine, physicians must control the clinical aspects of patient care. Therefore, some states may have restrictions on private-equity companies’ control of the use of medical devices, pricing, medical protocols, or other issues of patient care.
“This needs to be considered when reviewing the investment documents and structural documents proposed by private equity companies,” the advisory stated. From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control over their clinical practice. “This could relate to their compensation, bonuses, and investment opportunities in the practice, the practice management company, and possibly real estate or ASCs.”

Offering a gastroenterologist’s perspective on the paper, Camille Thélin, MD, MSc, an associate professor in the Division of Digestive Diseases and Health at the University of South Florida, Tampa, Florida, who also practices privately, said, that “what Erin Aebel reminds us is that the business side of GI can be just as tricky as the clinical side. Ancillary services like capsule studies or office labs fall under strict Stark rules, ASC ownership has Anti-Kickback Law restrictions, and private-equity deals may affect both your paycheck and your autonomy.”
Thélin’s main takeaway advice is that business opportunities can be valuable but carry real legal risks if not structured correctly. “This isn’t just abstract compliance law — it’s about protecting one’s ability to practice medicine, earn fairly, and avoid devastating penalties,” she told GI & Hepatology News. “This article reinforces the need for proactive legal review and careful structuring of business arrangements so physicians can focus on patient care without stumbling into avoidable legal pitfalls. With the right legal structure, ancillaries, ASCs, and private equity can strengthen your GI practice without risking compliance.”
The bottom line, said Aebel, is that gastroenterologists already in private practice or considering entering one must navigate a complex landscape of compliance and regulatory requirements — particularly when providing ancillary services, investing in ASCs, or engaging with private equity.
Understanding the Stark law, the AKB statute, and the intricacies of private-equity investment is essential to mitigate risks and avoid severe penalties, the advisory stressed. By proactively seeking expert legal and business guidance, gastroenterologists can structure their financial and ownership arrangements in a compliant manner, safeguarding their practices while capitalizing on growth opportunities.
This paper listed no external funding. Neither Aebel nor Thélin had any relevant conflicts of interest.
A version of this article appeared on Medscape.com.
The need for gastroenterology (GI) services is on the rise in the US, with growing rates of colonoscopy, earlier-onset colon cancer, and inflammatory bowel disease. This increase is taking place in the context of a changing regulatory landscape.
, and to that end, a recent educational practice management update was published in Clinical Gastroenterology and Hepatology by Erin Smith Aebel, JD, a health law specialist with Trenam Law in Tampa, Florida. Aebel has been a speaker at several national GI conferences and has addressed GI trainees on these issues in medical schools.
“Healthcare regulation continues to evolve and it’s a complicated area,” Aebel told GI & Hepatology News. “Some physician investors in healthcare ventures see the potential profits but are not fully aware of how a physician’s license and livelihood could be affected by noncompliance.”
Aebel has seen some medical business owners and institutions pushing physicians to their limits in order to maximize profits. “They’re failing to allow them the meaningful things that allow for a long-term productive and successful practice that provides great patient care,” she said. “A current issue I’m dealing with is employers’ taking away physicians’ administrative time and not respecting the work that is necessary for the physician to be efficient and provide great care,” she said. “If too many physicians get squeezed in this manner, they will eventually walk away from big employers to something they can better control.”
Aebel noted that private-equity acquisitions of medical practices — a fast-growing US trend — are often targeted at quick profits and quick exits, which can be inconsistent with quality long-term patient care. “A question to be asked by physicians and patients is who is benefiting from this transaction?” she said. “Sometimes retired physicians can see a great benefit in private equity, but newer physicians can get tied up with a strong noncompete agreement. The best deals are ones that try to find wins for all involved, including patients.”
Many independent gastroenterologists focusing on the demands of daily practice are less aware than they should be of the legal and business administration sides. “I often get clients who come to me complaining about their contracts after they’ve signed them. I don’t have leverage to do as much for them,” she admitted.
From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control. These could relate to compensation and bonuses, as well as opportunities to invest in the practice, the practice management company, and possibly real estate or ambulatory surgery centers (ASCs).
Aebel’s overarching messages to gastroenterologists are as follows: “Be aware. Learn basic health law. Read your contracts before you sign them. And invest in good counsel before you sign agreements,” she said. “In addition, GI practitioners need to have a working knowledge of the federal Anti-Kickback Statute and the federal Stark Law and how they could be commonly applied in their practices.”
These are designed to protect government-funded patient care from monetary influence. The False Claims Act is another federal buttress against fraud and abuse, she said.
Update Details
Though not intended to be legal advice, Aebel’s update touches on several important medicolegal areas.
Stark Law on Self-Referrals
Gastroenterologists should be familiar with this federal law, a self-referral civil penalty statute regulating how physicians can pay themselves in practices that provide designated health services covered by federal healthcare programs such as Medicare or Medicaid.
For a Stark penalty to apply, there must be a physician referral to an entity (eg, lab, hospital, nutrition service, physiotherapy or radiotherapy center) in which the physician or a close family member has a financial interest.
Ambulatory Surgery Centers
Another common area vulnerable to federal fraud and abuse regulation is investment in ASCs. “Generally speaking, it is a felony to pay or be paid anything of value for Medicare or Medicaid business referrals,” Aebel wrote. This provision relates to the general restriction of the federal AKB statute.
A gastroenterologist referring Medicare patients to a center where that physician has an investment could technically violate this law because the physician will receive profit distributions from the referral. In addition to constituting a felony with potential jail time, violation of this statute is grounds for substantial civil monetary penalties and/or exclusion from the government coverage program.
Fortunately, Aebel noted, legal safe harbors cover many financial relationships, including investment in an ASC. The financial arrangement is protected from prosecution if it meets five safe harbor requirements, including nondiscriminatory treatment of government-insured patients and physician investment unrelated to a center’s volume or the value of referrals. If even one aspect is not met, that will automatically constitute a crime.
“However, the government will look at facts and circumstances to determine whether there was an intent to pay for a referral,” Aebel wrote.
The safe harbor designates requirements for four types of ASCs: surgeon-owned, single-specialty, multispecialty, and hospital/physician ASCs.
Private-Equity Investment
With mergers and acquisitions of US medical practices and networks by private-equity firms becoming more common, gastroenterologists need to be aware of the legal issues involved in such investment.
Most states abide by corporate practice of medicine doctrines, which prohibit unlicensed people from direct ownership in a medical practice. These doctrines vary by state, but their primary goal is to ensure that medical decisions are made solely based on patient care and not influenced by corporate interests. The aim is to shield the physician-patient relationship from commercial influence.
“Accordingly, this creates additional complicated structures necessary for private-equity investment in gastroenterology practices,” Aebel wrote. Usually, such investors will invest in a management services organization (MSO), which takes much of the practice’s value via management fees. Gastroenterologists may or may not have an opportunity to invest in the practice and the MSO in this scenario.
Under corporate practice of medicine doctrine, physicians must control the clinical aspects of patient care. Therefore, some states may have restrictions on private-equity companies’ control of the use of medical devices, pricing, medical protocols, or other issues of patient care.
“This needs to be considered when reviewing the investment documents and structural documents proposed by private equity companies,” the advisory stated. From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control over their clinical practice. “This could relate to their compensation, bonuses, and investment opportunities in the practice, the practice management company, and possibly real estate or ASCs.”
Offering a gastroenterologist’s perspective on the paper, Camille Thélin, MD, MSc, an associate professor in the Division of Digestive Diseases and Health at the University of South Florida, Tampa, Florida, who also practices privately, said, that “what Erin Aebel reminds us is that the business side of GI can be just as tricky as the clinical side. Ancillary services like capsule studies or office labs fall under strict Stark rules, ASC ownership has Anti-Kickback Law restrictions, and private-equity deals may affect both your paycheck and your autonomy.”
Thélin’s main takeaway advice is that business opportunities can be valuable but carry real legal risks if not structured correctly. “This isn’t just abstract compliance law — it’s about protecting one’s ability to practice medicine, earn fairly, and avoid devastating penalties,” she told GI & Hepatology News. “This article reinforces the need for proactive legal review and careful structuring of business arrangements so physicians can focus on patient care without stumbling into avoidable legal pitfalls. With the right legal structure, ancillaries, ASCs, and private equity can strengthen your GI practice without risking compliance.”
The bottom line, said Aebel, is that gastroenterologists already in private practice or considering entering one must navigate a complex landscape of compliance and regulatory requirements — particularly when providing ancillary services, investing in ASCs, or engaging with private equity.
Understanding the Stark law, the AKB statute, and the intricacies of private-equity investment is essential to mitigate risks and avoid severe penalties, the advisory stressed. By proactively seeking expert legal and business guidance, gastroenterologists can structure their financial and ownership arrangements in a compliant manner, safeguarding their practices while capitalizing on growth opportunities.
This paper listed no external funding. Neither Aebel nor Thélin had any relevant conflicts of interest.
A version of this article appeared on Medscape.com.
The need for gastroenterology (GI) services is on the rise in the US, with growing rates of colonoscopy, earlier-onset colon cancer, and inflammatory bowel disease. This increase is taking place in the context of a changing regulatory landscape.
, and to that end, a recent educational practice management update was published in Clinical Gastroenterology and Hepatology by Erin Smith Aebel, JD, a health law specialist with Trenam Law in Tampa, Florida. Aebel has been a speaker at several national GI conferences and has addressed GI trainees on these issues in medical schools.
“Healthcare regulation continues to evolve and it’s a complicated area,” Aebel told GI & Hepatology News. “Some physician investors in healthcare ventures see the potential profits but are not fully aware of how a physician’s license and livelihood could be affected by noncompliance.”
Aebel has seen some medical business owners and institutions pushing physicians to their limits in order to maximize profits. “They’re failing to allow them the meaningful things that allow for a long-term productive and successful practice that provides great patient care,” she said. “A current issue I’m dealing with is employers’ taking away physicians’ administrative time and not respecting the work that is necessary for the physician to be efficient and provide great care,” she said. “If too many physicians get squeezed in this manner, they will eventually walk away from big employers to something they can better control.”
Aebel noted that private-equity acquisitions of medical practices — a fast-growing US trend — are often targeted at quick profits and quick exits, which can be inconsistent with quality long-term patient care. “A question to be asked by physicians and patients is who is benefiting from this transaction?” she said. “Sometimes retired physicians can see a great benefit in private equity, but newer physicians can get tied up with a strong noncompete agreement. The best deals are ones that try to find wins for all involved, including patients.”
Many independent gastroenterologists focusing on the demands of daily practice are less aware than they should be of the legal and business administration sides. “I often get clients who come to me complaining about their contracts after they’ve signed them. I don’t have leverage to do as much for them,” she admitted.
From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control. These could relate to compensation and bonuses, as well as opportunities to invest in the practice, the practice management company, and possibly real estate or ambulatory surgery centers (ASCs).
Aebel’s overarching messages to gastroenterologists are as follows: “Be aware. Learn basic health law. Read your contracts before you sign them. And invest in good counsel before you sign agreements,” she said. “In addition, GI practitioners need to have a working knowledge of the federal Anti-Kickback Statute and the federal Stark Law and how they could be commonly applied in their practices.”
These are designed to protect government-funded patient care from monetary influence. The False Claims Act is another federal buttress against fraud and abuse, she said.
Update Details
Though not intended to be legal advice, Aebel’s update touches on several important medicolegal areas.
Stark Law on Self-Referrals
Gastroenterologists should be familiar with this federal law, a self-referral civil penalty statute regulating how physicians can pay themselves in practices that provide designated health services covered by federal healthcare programs such as Medicare or Medicaid.
For a Stark penalty to apply, there must be a physician referral to an entity (eg, lab, hospital, nutrition service, physiotherapy or radiotherapy center) in which the physician or a close family member has a financial interest.
Ambulatory Surgery Centers
Another common area vulnerable to federal fraud and abuse regulation is investment in ASCs. “Generally speaking, it is a felony to pay or be paid anything of value for Medicare or Medicaid business referrals,” Aebel wrote. This provision relates to the general restriction of the federal AKB statute.
A gastroenterologist referring Medicare patients to a center where that physician has an investment could technically violate this law because the physician will receive profit distributions from the referral. In addition to constituting a felony with potential jail time, violation of this statute is grounds for substantial civil monetary penalties and/or exclusion from the government coverage program.
Fortunately, Aebel noted, legal safe harbors cover many financial relationships, including investment in an ASC. The financial arrangement is protected from prosecution if it meets five safe harbor requirements, including nondiscriminatory treatment of government-insured patients and physician investment unrelated to a center’s volume or the value of referrals. If even one aspect is not met, that will automatically constitute a crime.
“However, the government will look at facts and circumstances to determine whether there was an intent to pay for a referral,” Aebel wrote.
The safe harbor designates requirements for four types of ASCs: surgeon-owned, single-specialty, multispecialty, and hospital/physician ASCs.
Private-Equity Investment
With mergers and acquisitions of US medical practices and networks by private-equity firms becoming more common, gastroenterologists need to be aware of the legal issues involved in such investment.
Most states abide by corporate practice of medicine doctrines, which prohibit unlicensed people from direct ownership in a medical practice. These doctrines vary by state, but their primary goal is to ensure that medical decisions are made solely based on patient care and not influenced by corporate interests. The aim is to shield the physician-patient relationship from commercial influence.
“Accordingly, this creates additional complicated structures necessary for private-equity investment in gastroenterology practices,” Aebel wrote. Usually, such investors will invest in a management services organization (MSO), which takes much of the practice’s value via management fees. Gastroenterologists may or may not have an opportunity to invest in the practice and the MSO in this scenario.
Under corporate practice of medicine doctrine, physicians must control the clinical aspects of patient care. Therefore, some states may have restrictions on private-equity companies’ control of the use of medical devices, pricing, medical protocols, or other issues of patient care.
“This needs to be considered when reviewing the investment documents and structural documents proposed by private equity companies,” the advisory stated. From a business standpoint, gastroenterologists need to understand where they can negotiate for financial gain and control over their clinical practice. “This could relate to their compensation, bonuses, and investment opportunities in the practice, the practice management company, and possibly real estate or ASCs.”
Offering a gastroenterologist’s perspective on the paper, Camille Thélin, MD, MSc, an associate professor in the Division of Digestive Diseases and Health at the University of South Florida, Tampa, Florida, who also practices privately, said, that “what Erin Aebel reminds us is that the business side of GI can be just as tricky as the clinical side. Ancillary services like capsule studies or office labs fall under strict Stark rules, ASC ownership has Anti-Kickback Law restrictions, and private-equity deals may affect both your paycheck and your autonomy.”
Thélin’s main takeaway advice is that business opportunities can be valuable but carry real legal risks if not structured correctly. “This isn’t just abstract compliance law — it’s about protecting one’s ability to practice medicine, earn fairly, and avoid devastating penalties,” she told GI & Hepatology News. “This article reinforces the need for proactive legal review and careful structuring of business arrangements so physicians can focus on patient care without stumbling into avoidable legal pitfalls. With the right legal structure, ancillaries, ASCs, and private equity can strengthen your GI practice without risking compliance.”
The bottom line, said Aebel, is that gastroenterologists already in private practice or considering entering one must navigate a complex landscape of compliance and regulatory requirements — particularly when providing ancillary services, investing in ASCs, or engaging with private equity.
Understanding the Stark law, the AKB statute, and the intricacies of private-equity investment is essential to mitigate risks and avoid severe penalties, the advisory stressed. By proactively seeking expert legal and business guidance, gastroenterologists can structure their financial and ownership arrangements in a compliant manner, safeguarding their practices while capitalizing on growth opportunities.
This paper listed no external funding. Neither Aebel nor Thélin had any relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Fecal Transplant Benefits in Primary C Difficile Infection Similar to Vancomycin
, with efficacy that is comparable to the standard treatment of vancomycin, and in some measures, showing even stronger efficacy, new research showed.
“FMT, prepared and administered according to international guidelines, is an effective and safe treatment option for C difficile infections, which should be considered for all patients with the infection,” first author Frederik Emil Juul, MD, PhD, of the Clinical Effectiveness Research Group, University of Oslo, in Oslo, Norway, told GI & Hepatology News.
FMT even showed a numerical superiority to vancomycin, which, though not statistically significant, “indicates that FMT has the potential to change the current practice of antibiotic therapy and may establish FMT as a first-line treatment for primary CDI,” the authors further asserted in the study, published recently in the Annals of Internal Medicine.
In the treatment of antibiotic-associated colitis due to CDI, vancomycin or fidaxomicin are the standard therapies, yet up to 20% of patients experience one or more symptom recurrences following successful initial antibiotic treatment, prompting the need for continued antibiotic regimens, resulting in increased costs and potential adverse events, while contributing to antibiotic resistance.
FMT, designed to restore a normal functional colonic microenvironment with the transfer of a healthy person’s stool, though still somewhat controversial, has gained acceptance and favor in recent years in the treatment of recurrent CDI, however, research has been lacking on its efficacy in the treatment of primary CDI.
With a previous proof-of-concept trial and observational study showing promising results in primary CDI, Juul and colleagues conducted the current randomized, open-label noninferiority trial.
For the multi-center study, 100 adult patients with CDI, defined as C diff toxin in stool and at least three loose stools daily, and no previous CDI within 1 year prior to enrollment, were randomized at 20 hospitals in Norway to receive either FMT, administered as an enema, without antibiotic pretreatment, or oral vancomycin at a dose of 125 mg, four times daily for 10 days.
The patients had a median age of about 70 years; more than 40% of patients had a Charlson Comorbidity Index score of ≥ 4, indicating severe comorbidity, and a third had severe CDI.
With the trial showing favorable results, a data and safety monitoring board recommended stopping the trial for efficacy and noninferiority after about half of the planned enrollment was reached.
The primary endpoint of a clinical cure, defined as firm stools or less than three bowel movements daily and no disease recurrence within 60 days without additional treatment, was observed in 34 of 51 patients who received FMT (66.7%) compared with 30 of 49 of those receiving vancomycin (61.2%; difference, 5.4 percentage points; P for noninferiority < .001).
The results contradict the theory that response to FMT is 25 percentage points lower than response to vancomycin, the authors noted.
The proportion of patients with clinical cure at day 14 was 70.6% in the FMT group and 77.6% in the vancomycin group, and among those patients, two (5.6%) in the FMT group had disease recurrence compared with eight (21.1%) in the vancomycin group between days 15 and 60.
In the FMT group, 11 patients received additional treatment compared with four in the vancomycin group, predominantly oral vancomycin in both groups.
Despite the high rates of severe comorbidity among the patients at baseline, a subgroup analyses showed no significant differences in treatment effects based on factors including sex, age group, Charlson Comorbidity Index score, or CDI severity.
Importantly, there were also no significant differences in adverse events between the groups.
“Our results indicate that it is reasonable to treat patients with primary CDI with FMT and provide antibiotics only to patients with ongoing symptoms or recurrence after FMT,” the authors concluded.
FMT Faces Challenges in the US
FMT specifically consists of direct instillation of fecal matter to the upper gastrointestinal tract, via capsules or duodenal infusion, or the lower gastrointestinal tract via colonoscopy or enema.
While an AGA guideline issued in 2024 endorsed FMT for the prevention of recurrent, refractory, or fulminant CDI in select adults not responding to standard antibiotics, the association underscored important caveats, including a low quality of evidence, and concluded that FMT could not yet be recommended for other gastrointestinal conditions.
The treatment meanwhile has faced an uphill battle in the US. The provision of screened FMT inocula through the nonprofit OpenBiome, previously the country’s largest stool bank, was recently suspended amid FDA policy changes.
And while other commercial-grade biotherapeutic products Rebyota and Vowst, have received FDA approval, cost and insurance coverage can be significant barriers, said Elizabeth Hohmann, MD, of the Infectious Disease Division at Massachusetts General Hospital, Boston, in an editorial published with the study.
“Currently approved options are expensive and are not available to many who might benefit for various reasons, primarily cost,” she said.
Acceptance Higher in Europe
In Europe, and particularly Norway, acceptance of FMT for CDI and other indications has been more favorable, and while regulation of the treatment has varied among European countries, a new regulation to be implemented by the European Union in 2027 will improve standardization of the production, handling, storage, and other factors of FMT, Juul told GI & Hepatology News.
“I believe the new regulations will make the treatment more available to patients, and a standardization of the FMT production will make future trials more comparable and useful across countries,” he said.
Juul said he further expects that “our results will lower the threshold for choosing FMT as treatment in primary infections. I know that Denmark also gives FMT to patients with primary CDI.”
Quality of Life
Hohmann, who has treated many patients with recurrent CDI with FMT, noted that a key factor that should be underscored is how much better patients can feel after the treatment.
“Although there are no quality of life surveys in [the current study], had they been done, I suspect quality of life might have been higher in the FMT group; in my experience, people feel better after microbiome restoration.”
She added that her patients “report feeling much better, and that’s why I keep doing it,” she said. “I’ve had an 80-year-old patient tell me he’s going back to snow shoveling; another saying she can return to yoga classes.”
“When you have had bad gut microbiome dysbiosis that becomes normal, you feel a lot better,” Hohmann said.
In the treatment of primary CDI, however, Hohmann said the prospects, at least in the US, are likely slim.
“I do not believe that we in the United States will see FMT as a primary treatment of C difficile infection anytime soon,” she wrote in the editorial.
Nevertheless, Hohmann asserted that “FMT should remain available, with appropriate sources of carefully screened inocula for care and for further research into the many illnesses and therapies that are influenced by the health of the gut microbiome.”
This study received funding from the South-East Norway Health Trust. Hohmann had no disclosures to report.
A version of this article appeared on Medscape.com.
, with efficacy that is comparable to the standard treatment of vancomycin, and in some measures, showing even stronger efficacy, new research showed.
“FMT, prepared and administered according to international guidelines, is an effective and safe treatment option for C difficile infections, which should be considered for all patients with the infection,” first author Frederik Emil Juul, MD, PhD, of the Clinical Effectiveness Research Group, University of Oslo, in Oslo, Norway, told GI & Hepatology News.
FMT even showed a numerical superiority to vancomycin, which, though not statistically significant, “indicates that FMT has the potential to change the current practice of antibiotic therapy and may establish FMT as a first-line treatment for primary CDI,” the authors further asserted in the study, published recently in the Annals of Internal Medicine.
In the treatment of antibiotic-associated colitis due to CDI, vancomycin or fidaxomicin are the standard therapies, yet up to 20% of patients experience one or more symptom recurrences following successful initial antibiotic treatment, prompting the need for continued antibiotic regimens, resulting in increased costs and potential adverse events, while contributing to antibiotic resistance.
FMT, designed to restore a normal functional colonic microenvironment with the transfer of a healthy person’s stool, though still somewhat controversial, has gained acceptance and favor in recent years in the treatment of recurrent CDI, however, research has been lacking on its efficacy in the treatment of primary CDI.
With a previous proof-of-concept trial and observational study showing promising results in primary CDI, Juul and colleagues conducted the current randomized, open-label noninferiority trial.
For the multi-center study, 100 adult patients with CDI, defined as C diff toxin in stool and at least three loose stools daily, and no previous CDI within 1 year prior to enrollment, were randomized at 20 hospitals in Norway to receive either FMT, administered as an enema, without antibiotic pretreatment, or oral vancomycin at a dose of 125 mg, four times daily for 10 days.
The patients had a median age of about 70 years; more than 40% of patients had a Charlson Comorbidity Index score of ≥ 4, indicating severe comorbidity, and a third had severe CDI.
With the trial showing favorable results, a data and safety monitoring board recommended stopping the trial for efficacy and noninferiority after about half of the planned enrollment was reached.
The primary endpoint of a clinical cure, defined as firm stools or less than three bowel movements daily and no disease recurrence within 60 days without additional treatment, was observed in 34 of 51 patients who received FMT (66.7%) compared with 30 of 49 of those receiving vancomycin (61.2%; difference, 5.4 percentage points; P for noninferiority < .001).
The results contradict the theory that response to FMT is 25 percentage points lower than response to vancomycin, the authors noted.
The proportion of patients with clinical cure at day 14 was 70.6% in the FMT group and 77.6% in the vancomycin group, and among those patients, two (5.6%) in the FMT group had disease recurrence compared with eight (21.1%) in the vancomycin group between days 15 and 60.
In the FMT group, 11 patients received additional treatment compared with four in the vancomycin group, predominantly oral vancomycin in both groups.
Despite the high rates of severe comorbidity among the patients at baseline, a subgroup analyses showed no significant differences in treatment effects based on factors including sex, age group, Charlson Comorbidity Index score, or CDI severity.
Importantly, there were also no significant differences in adverse events between the groups.
“Our results indicate that it is reasonable to treat patients with primary CDI with FMT and provide antibiotics only to patients with ongoing symptoms or recurrence after FMT,” the authors concluded.
FMT Faces Challenges in the US
FMT specifically consists of direct instillation of fecal matter to the upper gastrointestinal tract, via capsules or duodenal infusion, or the lower gastrointestinal tract via colonoscopy or enema.
While an AGA guideline issued in 2024 endorsed FMT for the prevention of recurrent, refractory, or fulminant CDI in select adults not responding to standard antibiotics, the association underscored important caveats, including a low quality of evidence, and concluded that FMT could not yet be recommended for other gastrointestinal conditions.
The treatment meanwhile has faced an uphill battle in the US. The provision of screened FMT inocula through the nonprofit OpenBiome, previously the country’s largest stool bank, was recently suspended amid FDA policy changes.
And while other commercial-grade biotherapeutic products Rebyota and Vowst, have received FDA approval, cost and insurance coverage can be significant barriers, said Elizabeth Hohmann, MD, of the Infectious Disease Division at Massachusetts General Hospital, Boston, in an editorial published with the study.
“Currently approved options are expensive and are not available to many who might benefit for various reasons, primarily cost,” she said.
Acceptance Higher in Europe
In Europe, and particularly Norway, acceptance of FMT for CDI and other indications has been more favorable, and while regulation of the treatment has varied among European countries, a new regulation to be implemented by the European Union in 2027 will improve standardization of the production, handling, storage, and other factors of FMT, Juul told GI & Hepatology News.
“I believe the new regulations will make the treatment more available to patients, and a standardization of the FMT production will make future trials more comparable and useful across countries,” he said.
Juul said he further expects that “our results will lower the threshold for choosing FMT as treatment in primary infections. I know that Denmark also gives FMT to patients with primary CDI.”
Quality of Life
Hohmann, who has treated many patients with recurrent CDI with FMT, noted that a key factor that should be underscored is how much better patients can feel after the treatment.
“Although there are no quality of life surveys in [the current study], had they been done, I suspect quality of life might have been higher in the FMT group; in my experience, people feel better after microbiome restoration.”
She added that her patients “report feeling much better, and that’s why I keep doing it,” she said. “I’ve had an 80-year-old patient tell me he’s going back to snow shoveling; another saying she can return to yoga classes.”
“When you have had bad gut microbiome dysbiosis that becomes normal, you feel a lot better,” Hohmann said.
In the treatment of primary CDI, however, Hohmann said the prospects, at least in the US, are likely slim.
“I do not believe that we in the United States will see FMT as a primary treatment of C difficile infection anytime soon,” she wrote in the editorial.
Nevertheless, Hohmann asserted that “FMT should remain available, with appropriate sources of carefully screened inocula for care and for further research into the many illnesses and therapies that are influenced by the health of the gut microbiome.”
This study received funding from the South-East Norway Health Trust. Hohmann had no disclosures to report.
A version of this article appeared on Medscape.com.
, with efficacy that is comparable to the standard treatment of vancomycin, and in some measures, showing even stronger efficacy, new research showed.
“FMT, prepared and administered according to international guidelines, is an effective and safe treatment option for C difficile infections, which should be considered for all patients with the infection,” first author Frederik Emil Juul, MD, PhD, of the Clinical Effectiveness Research Group, University of Oslo, in Oslo, Norway, told GI & Hepatology News.
FMT even showed a numerical superiority to vancomycin, which, though not statistically significant, “indicates that FMT has the potential to change the current practice of antibiotic therapy and may establish FMT as a first-line treatment for primary CDI,” the authors further asserted in the study, published recently in the Annals of Internal Medicine.
In the treatment of antibiotic-associated colitis due to CDI, vancomycin or fidaxomicin are the standard therapies, yet up to 20% of patients experience one or more symptom recurrences following successful initial antibiotic treatment, prompting the need for continued antibiotic regimens, resulting in increased costs and potential adverse events, while contributing to antibiotic resistance.
FMT, designed to restore a normal functional colonic microenvironment with the transfer of a healthy person’s stool, though still somewhat controversial, has gained acceptance and favor in recent years in the treatment of recurrent CDI, however, research has been lacking on its efficacy in the treatment of primary CDI.
With a previous proof-of-concept trial and observational study showing promising results in primary CDI, Juul and colleagues conducted the current randomized, open-label noninferiority trial.
For the multi-center study, 100 adult patients with CDI, defined as C diff toxin in stool and at least three loose stools daily, and no previous CDI within 1 year prior to enrollment, were randomized at 20 hospitals in Norway to receive either FMT, administered as an enema, without antibiotic pretreatment, or oral vancomycin at a dose of 125 mg, four times daily for 10 days.
The patients had a median age of about 70 years; more than 40% of patients had a Charlson Comorbidity Index score of ≥ 4, indicating severe comorbidity, and a third had severe CDI.
With the trial showing favorable results, a data and safety monitoring board recommended stopping the trial for efficacy and noninferiority after about half of the planned enrollment was reached.
The primary endpoint of a clinical cure, defined as firm stools or less than three bowel movements daily and no disease recurrence within 60 days without additional treatment, was observed in 34 of 51 patients who received FMT (66.7%) compared with 30 of 49 of those receiving vancomycin (61.2%; difference, 5.4 percentage points; P for noninferiority < .001).
The results contradict the theory that response to FMT is 25 percentage points lower than response to vancomycin, the authors noted.
The proportion of patients with clinical cure at day 14 was 70.6% in the FMT group and 77.6% in the vancomycin group, and among those patients, two (5.6%) in the FMT group had disease recurrence compared with eight (21.1%) in the vancomycin group between days 15 and 60.
In the FMT group, 11 patients received additional treatment compared with four in the vancomycin group, predominantly oral vancomycin in both groups.
Despite the high rates of severe comorbidity among the patients at baseline, a subgroup analyses showed no significant differences in treatment effects based on factors including sex, age group, Charlson Comorbidity Index score, or CDI severity.
Importantly, there were also no significant differences in adverse events between the groups.
“Our results indicate that it is reasonable to treat patients with primary CDI with FMT and provide antibiotics only to patients with ongoing symptoms or recurrence after FMT,” the authors concluded.
FMT Faces Challenges in the US
FMT specifically consists of direct instillation of fecal matter to the upper gastrointestinal tract, via capsules or duodenal infusion, or the lower gastrointestinal tract via colonoscopy or enema.
While an AGA guideline issued in 2024 endorsed FMT for the prevention of recurrent, refractory, or fulminant CDI in select adults not responding to standard antibiotics, the association underscored important caveats, including a low quality of evidence, and concluded that FMT could not yet be recommended for other gastrointestinal conditions.
The treatment meanwhile has faced an uphill battle in the US. The provision of screened FMT inocula through the nonprofit OpenBiome, previously the country’s largest stool bank, was recently suspended amid FDA policy changes.
And while other commercial-grade biotherapeutic products Rebyota and Vowst, have received FDA approval, cost and insurance coverage can be significant barriers, said Elizabeth Hohmann, MD, of the Infectious Disease Division at Massachusetts General Hospital, Boston, in an editorial published with the study.
“Currently approved options are expensive and are not available to many who might benefit for various reasons, primarily cost,” she said.
Acceptance Higher in Europe
In Europe, and particularly Norway, acceptance of FMT for CDI and other indications has been more favorable, and while regulation of the treatment has varied among European countries, a new regulation to be implemented by the European Union in 2027 will improve standardization of the production, handling, storage, and other factors of FMT, Juul told GI & Hepatology News.
“I believe the new regulations will make the treatment more available to patients, and a standardization of the FMT production will make future trials more comparable and useful across countries,” he said.
Juul said he further expects that “our results will lower the threshold for choosing FMT as treatment in primary infections. I know that Denmark also gives FMT to patients with primary CDI.”
Quality of Life
Hohmann, who has treated many patients with recurrent CDI with FMT, noted that a key factor that should be underscored is how much better patients can feel after the treatment.
“Although there are no quality of life surveys in [the current study], had they been done, I suspect quality of life might have been higher in the FMT group; in my experience, people feel better after microbiome restoration.”
She added that her patients “report feeling much better, and that’s why I keep doing it,” she said. “I’ve had an 80-year-old patient tell me he’s going back to snow shoveling; another saying she can return to yoga classes.”
“When you have had bad gut microbiome dysbiosis that becomes normal, you feel a lot better,” Hohmann said.
In the treatment of primary CDI, however, Hohmann said the prospects, at least in the US, are likely slim.
“I do not believe that we in the United States will see FMT as a primary treatment of C difficile infection anytime soon,” she wrote in the editorial.
Nevertheless, Hohmann asserted that “FMT should remain available, with appropriate sources of carefully screened inocula for care and for further research into the many illnesses and therapies that are influenced by the health of the gut microbiome.”
This study received funding from the South-East Norway Health Trust. Hohmann had no disclosures to report.
A version of this article appeared on Medscape.com.