User login
Advancing Toward the Ideal Hospital Discharge for the Elderly Patient
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
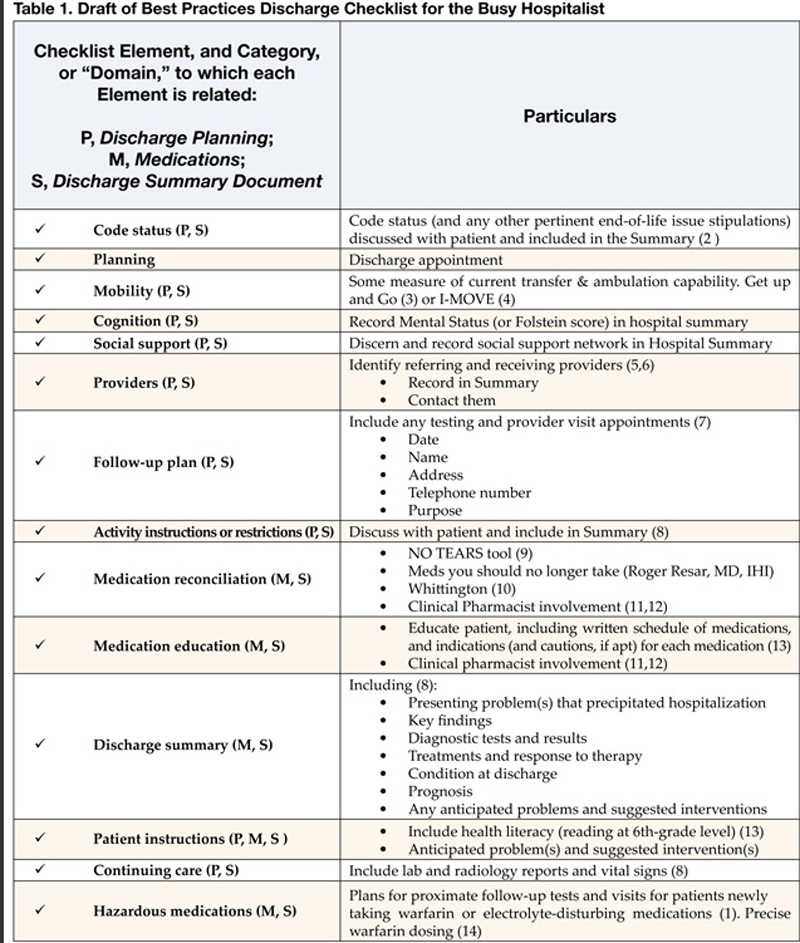
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.
The interval between hospital discharge and the continuity provider’s first post-hospital patient visit is being increasingly recognized as a hazardous hiatus (1). The patient is vulnerable to a variety of factors that may result in morbidity or hospital readmission, including the recurrence of symptoms that prompted the initial hospitalization, adverse drug events from new medications, new drug-drug interactions, or issues of care coordination, such as followup visits and tests. Inadequate social support can further exacerbate the medical complexity of care transition from the inpatient to the outpatient setting.
Many post-discharge adverse events are preventable or “ameliorable” by careful discharge planning and timely followup (1). However, existing guidelines and standards regarding the discharge process have been disease specific and have not focused on populations, such as the elderly, that may be at especially high risk regardless of their specific medical issues. For example, CMS currently requires that all patients have an assessment of cognition, mobility, and family support before final discharge plans are set. Experienced hospitalists know that these basic elements are only the beginning of a more complex and robust algorithm of discharge planning; including trimming and reconciling medications; planning followup tests; engineering followup appointments; and activating any required community resources, durable medical good needs, or home health care. In fact, many SHM members have already begun to implement local strategies to ease the care transition at the time of discharge.
The SHM Hospital Quality & Patient Safety (HQPS) Committee believes that hospitalists will play an important role in shaping the ideal discharge process. With support from the Hartford foundation, HQPS has formulated a strategy to develop “discharge best practices,” integrating evidence-based care with the experience and expert opinion of hospitalist leaders. To our knowledge, no national society or professional organization has undertaken such an activity to improve the quality of care at discharge and after hospitalization.
The process began with a literature review in 2004 that showed no commonly accepted compendium or consolidated list of activities that could form the basis for the ideal discharge. Drawing upon SHM member experience and the literature, HQPS committee members formulated a list of potential best practices, which are presented in Table 1. Although many discharge activities are required and many are done automatically (such as writing a discharge order or prescriptions) the committee chose to focus on important but discretionary activities that may be overlooked by a busy physician. To complement this checklist of activities, the committee is developing a discharge framework with the input of experts in the area of care transitions.
The committee held a consensus-building workshop at the SHM annual meeting entitled “Developing the Ideal Discharge Process.” This session provided a forum to discuss the checklist of best practices and discharge framework with attendees, receive their feedback, and identify hospitalists interested in validating and refining the materials over time. The committee will continue revising the materials in 2005, with the goal of developing a usable and valuable consensus statement addressing the steps involved in the ideal hospital discharge.
References
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138:161-7.
- Guidelines for appropriate use of “Do-Not-Resuscitate” orders. Council on Ethical and Judicial Affairs. American Medical Association. JAMA. 1991;265:1868-71.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “getup and go” test. Arch Phys Med Rehabil. 1986;67:387-9.
- Manning DM, Keller AS, Frank DL. Independent Mobility Validation Exam (IMOVE): A tool for periodic reassessment of fallrisk and discharge planning. Abstract and poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- van Walraven C, Mamdani M, Fang J, Austin PC. Continuity of care and patient outcomes after hospital discharge. J Gen Intern Med. 2004;19:624-31.
- van Walraven C, Seth R, Austin PC, Laupacis A. Effect of discharge summary availability during the post-discharge visits on hospital readmission. J Gen Intern Med. 2002;17:186-92.
- Whitford K, Huddleston JM. Specific appointments after pneumonia hospitalization reduce readmissions. Abstract and Poster presentation at SHM (formerly NAIP) 5th Annual Meeting in Philadelphia, PA, on April 9, 2002.
- JCAHO Manual: Information Management (IM) 6.10 and Patient Care (PC) 15.30.
- Lewis T. Using the NO TEARS tool for medication review. BMJ. 2004;329:434.
- Whittington J, Cohen H. OSF healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-9.
- Kucukarslan SN, Peters M, Mlynarek M, Nafziger D. Pharmacists on rounding teams reduce preventable adverse events in hospital general medicine units. Arch Intern Med. 2003;163:2014-18.
- Dudas V, Bookwalter T, Kerr K, Pantilat SZ. The impact of followup telephone calls to patients after hospitalization. Am J Med. 2001;111(9B):26S-30S.
- Nielsen-Bohlman L, Panzer AM, Kindig DA, eds. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Manning DM. Toward safer warfarin therapy: does precise daily dosing improve international normalized ratio control? Mayo Clin Proc. 2002;77:873-5.
Resources (including Medline Search: “patient discharge” and/ or “quality indicators” and “quality of care”):
- Bull MJ, Hansen HE, Gross CR. Predictors of elder and family caregiver satisfaction with discharge planning. J Cardiovasc Nurs. 2000;14:76-87.
- Charles C, Gauld M, Chambers L, O’Brien B, Haynes RB, Labelle R. How was your hospital stay? Patients’ report about their care in Canadian hospitals. CMAJ. 1994; 150:1813-22.
- Cleary PD. A hospitalization from hell: a patient’s perspective on quality. Ann Intern Med. 2003:138:33-9.
- Demlo LK, Campbell PM. Improving hospital discharge data: lessons from the National Hospital Discharge Survey. Med Care. 1981 Oct;19(10):1030-40.
- Felden JM, scott S, Horne JG. An investigation of patient satisfaction following discharge after total hip replacement surgery. Orthop Nurs. 2003;22:429-36.
- Frain JP, Frain AE, Carr PH. Experience of medical senior house officers in preparing discharge summaries. BMJ. 1996;312:350.
- Gombeski WR, Miller PJ, Hahn JH, et al. Patient callback program. J Health Care Mark 1993;13:60-5.
- Hickey ML, Kleefield SF, Pearson SD, et al. Payer-hospital collaboration to improve patient satisfaction with hospital discharge. Jt Comm J Qual Improv. 1996;22:336-44.
- Kroenke K, Stump T, Clark DO, Callahan CM, McDonald CJ. Symptoms in hospitalized patients: outcome and satisfaction with care. Am J Med 1999;107: 425-31.
- Macaulay EM, Cooper GC, Engeset J, Naylor AR. Prospective audit of discharge summary errors. Br J Surg. 1996;83:788-90.
- Moher D, Weinberg A, Hanlon R, Runnalls K. Effects of a medical team coordinator on length of hospital stay. CMAJ. 1992;146:511-5.
- Minnick A, Young WB. Comparison between reports of care obtained by post-discharge telephone interview and pre-discharge personal interview. Outcomes Manag Nurs Pract 1999;3:32-7.
- Naylor MD, Brooten D, Campbell R, et al. Comprehensive discharge planning and home followup of hospitalized elders: a randomized clinical trial. JAMA. 1999;281:613-20.
- Parkes J, Shepperd S. Discharge planning from hospital to home. Cochrane Database Syst Rev. 2004. Review.
- Reiley P, Pike A, Phipps M, et al. Learning from patients: a discharge planning improvement project. Jt Comm J Qual Improv. 1996;22:31122.
- van Walraven C, Weinberg AL. Quality assessment of a discharge summary system. CMAJ. 1995;152:1437-42.
- van Walraven C, Rokosh E. What is necessary for high-quality discharge summaries? Am J Med Qual. 1999;14: 160-9.
- Zwicker D, Picariello G. Discharge planning for the older adult. In: Mezey M, Fulmer T, Abraaham I, Zwicker D, eds. Geriatric Nursing Protocols for Best Practice. 2nd ed. New York: Springer Publishing 2003;292-316.
Quality Tools: Root Cause Analysis (RCA) and Failure Modes and Effects Analysis (FMEA)
When we speak of “quality” in health care, we generally think of mortality outcomes or regulatory requirements that are mandated by the JCAHO (Joint Commission for Accreditation of Healthcare Organizations). But how do these relate to and impact our everyday lives as hospitalists? At the 8th Annual Meeting of SHM we presented a workshop on RCA and FMEA, taking a practical approach to illustrate how these two JCAHO required methodologies can improve patient care as well as improve the work environment for hospitalists by addressing the systemic issues that can compromise care.
The workshop starts by stepping into the life of a hospitalist and something we all fear: “Something bad happens. Then what?” Depending on the severity of the event, the options include peer review, notifying the Department Chief, calling the Risk Manager, calling your lawyer, or doing nothing. You’ve probably had many experiences when “something wasn’t quite right,” but often there is no obvious bad outcome or obvious solution, so we shrug our shoulders and say, “Oh well, we got lucky this time; no harm, no foul.” The problem is, there are recurring patterns to these types of events, and the same issues may affect the next patient, who may not be so lucky.
Defining “Something Bad”
These types of cases, which have outcomes ranging from no effect on the patient to death, may be approached several different ways. The terms “near miss” or “close call” refer to an incident where a mistake was made but caught in time, so no harm was done to the patient. An example of this is when a physician makes a mistake on a medication order, but it is caught and corrected by a pharmacist or nurse.
When adverse outcomes do occur, think about and define etiologies so that you identify and address underlying causes. Is the outcome an expected or unexpected complication of therapy? Was there an error involved? In asking these questions, remember that you can have harm without error and error without harm. Error is defined as “failure of a planned action to be completed as intended or use of a wrong plan to achieve an aim; the accumulation of errors results in accidents” (Kohn, et al). This definition points out that usually a chain of events rather than a single individual or event results in a bad outcome. The purpose of defining etiologies is not to assign blame but to identify underlying issues and surrounding circumstances that may have contributed to the adverse outcome.
Significant adverse events are called “sentinel events” and defined as an “unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Serious injury specifically includes loss of limb or function” (JCAHO 1998).
How We Approach Error
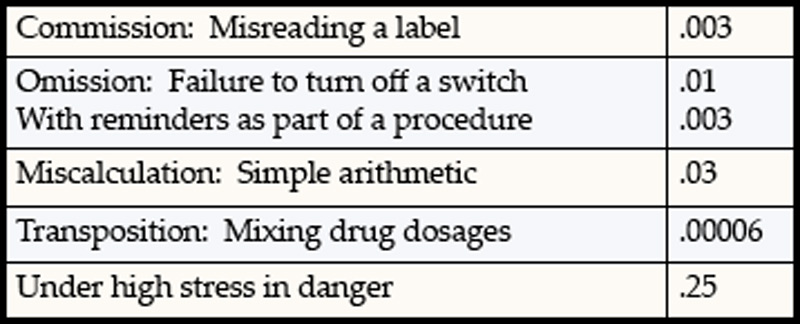
Unfortunately, as humans we are fallible and make errors quite reliably. Table 1 demonstrates types of errors and expected rates of errors. For example, we make errors of omission 0.01% of the time, but the good news is that with reminders or ticklers, we can reduce this rate to 0.003%. Unfortunately, when humans are under high stress in danger, research from the military indicates error rates of 25% (Salvendy 1997). In a complex ICU setting, researchers have documented an average of 178 activities per patient per day with an error rate of 0.95%. Despite an error rate of less than 1%, the yield of errors during the 4-month period of observation was still over 1000 errors, 29% of which were considered to have severe or potentially severe consequences (Donchin, et al).
The reality is that we err. Having the unrealistic expectations developed in medical training of being perfect in all our actions perpetuates the blame cycle when the inevitable mistake occurs, and it prevents us from implementing solutions that prevent errors from ever occurring or catching them before they cause harm.
RCA and FMEA Help Us Create Solutions That Make a Difference
Briefly, Root Cause Analysis (RCA) is a retrospective investigation that is required by JCAHO after a sentinel event: “Root cause analysis is a process for identifying the basic or causal factor(s) that underlies variation in performance, including the occurrence or possible occurrence of a sentinel event. A root cause is that most fundamental reason a problem―a situation where performance does not meet expectations―has occurred” (JCAHO 1998). An RCA looks back in time at an event and asks the question “What
happened?” The utility of this methodology lies in the fact that it not only asks what happened but also asks “Why did this happen” rather than focus on “Who is to blame?” Some hospitals use this methodology for cases that are not sentinel events, because the knowledge gained from these investigations often uncovers system issues previously not known and that negatively impact many departments, not just the departments involved in a particular case.
Failure Modes and Effects Analysis (FMEA) is a prospective investigation aimed at identifying vulnerabilities and preventing failures in the future. It looks forward and asks what could go wrong? Performance of an FMEA is also required yearly by JCAHO and focuses on improving risky processes such as blood transfusions, chemotherapy, and other high risk medications.
Approaching a clinical case clearly demonstrates the differences between RCA and FMEA. Imagine a 72-year-old patient admitted to your hospital with findings of an acute abdomen requiring surgery. The patient is a smoker, with Type 2 diabetes and an admission blood sugar of 465, but no evidence of DKA. She normally takes an oral hypoglycemic to control her diabetes and an ACE inhibitor for high blood pressure but no other medications. She is taken to the OR emergently, where surgery seems to go well, and post-operatively is admitted to the ICU. Subsequently, her blood glucose ranges from 260 to 370 and is “controlled” with sliding scale insulin. Unfortunately, within 18 hours of surgery she suffers an MI and develops a postoperative wound infection 4 days after surgery. She eventually dies from sepsis.
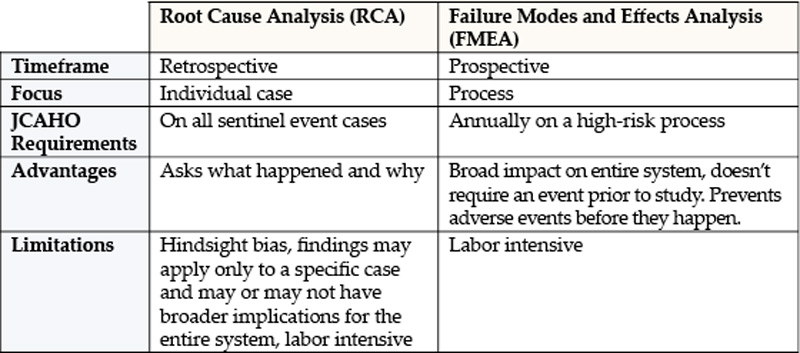
An RCA of this case might reveal causal factors such as lack of use of a beta-blocker preoperatively and lack of use of IV insulin to lower her blood sugars to the 80–110 range. While possibly identifying the root cause of this adverse outcome, an RCA is limited by its hindsight bias and the labor-intensive nature of the investigation that may or may not have broad application, since it is an in-depth study of one case. However, RCA’s do have the salutary effects of building teamwork, identifying needed changes, and if carried out impartially without assigning blame can facilitate a culture of patient safety.
FMEA takes a different approach and proactively aims to prevent failure. It is a systematic method of identifying and preventing product and process failures before they occur. It does not require a specific case or adverse event. Rather, a high-risk process is chosen for study, and an interdisciplinary team asks the question “What can go wrong with this process and how can we prevent failures?” Considering the above case, imagine that before it ever occurred you as the hospitalist concerned with patient safety decided to conduct an FMEA on controlling blood sugar in the ICU or administering beta-blockers perioperatively to patients who are appropriate candidates.
For example, using FMEA methodology to study the process of intensive insulin therapy to achieve tight control of glucose in the ICU would identify potential barriers and failures preventing successful implementation. A significant risk encountered in achieving tight glucose control in the range of 80–110 includes hypoglycemia. Common pitfalls of insulin administration include administration and calculation errors that can result in 10-fold differences in doses of insulin. Other details of administration, such as type of IV tubing used and how the IV tubing is primed, can greatly affect the amount of insulin delivered to the patient and thus the glucose levels. If an inadequate amount of solution is flushed through to prime the tubing, the patient may receive saline rather than insulin for a few hours, resulting in higher-than-expected glucose levels and titration of insulin to higher doses. The result would then be an unexpectedly low glucose several hours later. Once failure modes such as these are identified, a fail-safe system can be designed so that failures are less likely to occur.
The advantages of FMEA include its focus on system design rather than on a single incident such as in RCA. By focusing on systems and processes, the learning and changes implemented are likely to impact a larger number of patients.
Summary and Discussion
To summarize, RCA is retrospective and dissects a case, while FMEA is prospective and dissects a process. It is important to remember that given the right set of circumstances, any physician can make a mistake. It makes sense to apply methodologies that probe into surrounding circumstances and contributing factors so that knowledge gained can be used to prevent the same mistakes from happening to different individuals and have broader impact on healthcare systems.
Resources
- www.patientsafety.gov: VA National Center for Patient Safety. Excellent website with very helpful, practical tools.
- www.ihi.org: Institute for Healthcare Improvement website. Has a nice FMEA toolkit.
- www.jcaho.com: The Joint Commission for Accreditation of Healthcare Organizations website. Has information on sentinel events and use of RCA.
Bibliography
- Kohn LT, Corrigan JM, Eds. To Err is Human. Building a Safer Helath System. Washington, DC: National Academy Press; 1999.
- Joint Commission on Accreditation of Healthcare Organizations. Sentinel events: evaluating cause and planning improvement. 1998. Library of congress catalog number 97-80531.
- Salvendy G, ed. Handbook of Human Factors and Ergonomics. New York: John Wiley & Sons;1997:163
- Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med. 1995;23:294-300.
- McNutt R, Abrams R, Hasler S, et al. Determining medical error: three case reports. Eff Clin Pract. 2002;5:23-8.
- Senders JW. FMEA and RCA: the mantras of modern risk management. Qual Saf Health Care. 2004;13:249-50.
- Spath PL. Investigating Sentinel Events: How to Find and Resolve Root Causes. Forest Grove, OR: Brown Spath and Associates; 1997.
- Wald H, Shojania KG. Root cause analysis. In: Shojania KG, McDonald KM, Wachter RM, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. Available at http://www.ahrq.gov.
- Woodhouse S, Burney B, Coste K. To err is human: improving patient safety through failure mode and effect analysis. Clin leadersh Manag Rev. 2004;18:32-6.
When we speak of “quality” in health care, we generally think of mortality outcomes or regulatory requirements that are mandated by the JCAHO (Joint Commission for Accreditation of Healthcare Organizations). But how do these relate to and impact our everyday lives as hospitalists? At the 8th Annual Meeting of SHM we presented a workshop on RCA and FMEA, taking a practical approach to illustrate how these two JCAHO required methodologies can improve patient care as well as improve the work environment for hospitalists by addressing the systemic issues that can compromise care.
The workshop starts by stepping into the life of a hospitalist and something we all fear: “Something bad happens. Then what?” Depending on the severity of the event, the options include peer review, notifying the Department Chief, calling the Risk Manager, calling your lawyer, or doing nothing. You’ve probably had many experiences when “something wasn’t quite right,” but often there is no obvious bad outcome or obvious solution, so we shrug our shoulders and say, “Oh well, we got lucky this time; no harm, no foul.” The problem is, there are recurring patterns to these types of events, and the same issues may affect the next patient, who may not be so lucky.
Defining “Something Bad”
These types of cases, which have outcomes ranging from no effect on the patient to death, may be approached several different ways. The terms “near miss” or “close call” refer to an incident where a mistake was made but caught in time, so no harm was done to the patient. An example of this is when a physician makes a mistake on a medication order, but it is caught and corrected by a pharmacist or nurse.
When adverse outcomes do occur, think about and define etiologies so that you identify and address underlying causes. Is the outcome an expected or unexpected complication of therapy? Was there an error involved? In asking these questions, remember that you can have harm without error and error without harm. Error is defined as “failure of a planned action to be completed as intended or use of a wrong plan to achieve an aim; the accumulation of errors results in accidents” (Kohn, et al). This definition points out that usually a chain of events rather than a single individual or event results in a bad outcome. The purpose of defining etiologies is not to assign blame but to identify underlying issues and surrounding circumstances that may have contributed to the adverse outcome.
Significant adverse events are called “sentinel events” and defined as an “unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Serious injury specifically includes loss of limb or function” (JCAHO 1998).
How We Approach Error
Unfortunately, as humans we are fallible and make errors quite reliably. Table 1 demonstrates types of errors and expected rates of errors. For example, we make errors of omission 0.01% of the time, but the good news is that with reminders or ticklers, we can reduce this rate to 0.003%. Unfortunately, when humans are under high stress in danger, research from the military indicates error rates of 25% (Salvendy 1997). In a complex ICU setting, researchers have documented an average of 178 activities per patient per day with an error rate of 0.95%. Despite an error rate of less than 1%, the yield of errors during the 4-month period of observation was still over 1000 errors, 29% of which were considered to have severe or potentially severe consequences (Donchin, et al).
The reality is that we err. Having the unrealistic expectations developed in medical training of being perfect in all our actions perpetuates the blame cycle when the inevitable mistake occurs, and it prevents us from implementing solutions that prevent errors from ever occurring or catching them before they cause harm.
RCA and FMEA Help Us Create Solutions That Make a Difference
Briefly, Root Cause Analysis (RCA) is a retrospective investigation that is required by JCAHO after a sentinel event: “Root cause analysis is a process for identifying the basic or causal factor(s) that underlies variation in performance, including the occurrence or possible occurrence of a sentinel event. A root cause is that most fundamental reason a problem―a situation where performance does not meet expectations―has occurred” (JCAHO 1998). An RCA looks back in time at an event and asks the question “What
happened?” The utility of this methodology lies in the fact that it not only asks what happened but also asks “Why did this happen” rather than focus on “Who is to blame?” Some hospitals use this methodology for cases that are not sentinel events, because the knowledge gained from these investigations often uncovers system issues previously not known and that negatively impact many departments, not just the departments involved in a particular case.
Failure Modes and Effects Analysis (FMEA) is a prospective investigation aimed at identifying vulnerabilities and preventing failures in the future. It looks forward and asks what could go wrong? Performance of an FMEA is also required yearly by JCAHO and focuses on improving risky processes such as blood transfusions, chemotherapy, and other high risk medications.
Approaching a clinical case clearly demonstrates the differences between RCA and FMEA. Imagine a 72-year-old patient admitted to your hospital with findings of an acute abdomen requiring surgery. The patient is a smoker, with Type 2 diabetes and an admission blood sugar of 465, but no evidence of DKA. She normally takes an oral hypoglycemic to control her diabetes and an ACE inhibitor for high blood pressure but no other medications. She is taken to the OR emergently, where surgery seems to go well, and post-operatively is admitted to the ICU. Subsequently, her blood glucose ranges from 260 to 370 and is “controlled” with sliding scale insulin. Unfortunately, within 18 hours of surgery she suffers an MI and develops a postoperative wound infection 4 days after surgery. She eventually dies from sepsis.
An RCA of this case might reveal causal factors such as lack of use of a beta-blocker preoperatively and lack of use of IV insulin to lower her blood sugars to the 80–110 range. While possibly identifying the root cause of this adverse outcome, an RCA is limited by its hindsight bias and the labor-intensive nature of the investigation that may or may not have broad application, since it is an in-depth study of one case. However, RCA’s do have the salutary effects of building teamwork, identifying needed changes, and if carried out impartially without assigning blame can facilitate a culture of patient safety.
FMEA takes a different approach and proactively aims to prevent failure. It is a systematic method of identifying and preventing product and process failures before they occur. It does not require a specific case or adverse event. Rather, a high-risk process is chosen for study, and an interdisciplinary team asks the question “What can go wrong with this process and how can we prevent failures?” Considering the above case, imagine that before it ever occurred you as the hospitalist concerned with patient safety decided to conduct an FMEA on controlling blood sugar in the ICU or administering beta-blockers perioperatively to patients who are appropriate candidates.
For example, using FMEA methodology to study the process of intensive insulin therapy to achieve tight control of glucose in the ICU would identify potential barriers and failures preventing successful implementation. A significant risk encountered in achieving tight glucose control in the range of 80–110 includes hypoglycemia. Common pitfalls of insulin administration include administration and calculation errors that can result in 10-fold differences in doses of insulin. Other details of administration, such as type of IV tubing used and how the IV tubing is primed, can greatly affect the amount of insulin delivered to the patient and thus the glucose levels. If an inadequate amount of solution is flushed through to prime the tubing, the patient may receive saline rather than insulin for a few hours, resulting in higher-than-expected glucose levels and titration of insulin to higher doses. The result would then be an unexpectedly low glucose several hours later. Once failure modes such as these are identified, a fail-safe system can be designed so that failures are less likely to occur.
The advantages of FMEA include its focus on system design rather than on a single incident such as in RCA. By focusing on systems and processes, the learning and changes implemented are likely to impact a larger number of patients.
Summary and Discussion
To summarize, RCA is retrospective and dissects a case, while FMEA is prospective and dissects a process. It is important to remember that given the right set of circumstances, any physician can make a mistake. It makes sense to apply methodologies that probe into surrounding circumstances and contributing factors so that knowledge gained can be used to prevent the same mistakes from happening to different individuals and have broader impact on healthcare systems.
Resources
- www.patientsafety.gov: VA National Center for Patient Safety. Excellent website with very helpful, practical tools.
- www.ihi.org: Institute for Healthcare Improvement website. Has a nice FMEA toolkit.
- www.jcaho.com: The Joint Commission for Accreditation of Healthcare Organizations website. Has information on sentinel events and use of RCA.
Bibliography
- Kohn LT, Corrigan JM, Eds. To Err is Human. Building a Safer Helath System. Washington, DC: National Academy Press; 1999.
- Joint Commission on Accreditation of Healthcare Organizations. Sentinel events: evaluating cause and planning improvement. 1998. Library of congress catalog number 97-80531.
- Salvendy G, ed. Handbook of Human Factors and Ergonomics. New York: John Wiley & Sons;1997:163
- Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med. 1995;23:294-300.
- McNutt R, Abrams R, Hasler S, et al. Determining medical error: three case reports. Eff Clin Pract. 2002;5:23-8.
- Senders JW. FMEA and RCA: the mantras of modern risk management. Qual Saf Health Care. 2004;13:249-50.
- Spath PL. Investigating Sentinel Events: How to Find and Resolve Root Causes. Forest Grove, OR: Brown Spath and Associates; 1997.
- Wald H, Shojania KG. Root cause analysis. In: Shojania KG, McDonald KM, Wachter RM, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. Available at http://www.ahrq.gov.
- Woodhouse S, Burney B, Coste K. To err is human: improving patient safety through failure mode and effect analysis. Clin leadersh Manag Rev. 2004;18:32-6.
When we speak of “quality” in health care, we generally think of mortality outcomes or regulatory requirements that are mandated by the JCAHO (Joint Commission for Accreditation of Healthcare Organizations). But how do these relate to and impact our everyday lives as hospitalists? At the 8th Annual Meeting of SHM we presented a workshop on RCA and FMEA, taking a practical approach to illustrate how these two JCAHO required methodologies can improve patient care as well as improve the work environment for hospitalists by addressing the systemic issues that can compromise care.
The workshop starts by stepping into the life of a hospitalist and something we all fear: “Something bad happens. Then what?” Depending on the severity of the event, the options include peer review, notifying the Department Chief, calling the Risk Manager, calling your lawyer, or doing nothing. You’ve probably had many experiences when “something wasn’t quite right,” but often there is no obvious bad outcome or obvious solution, so we shrug our shoulders and say, “Oh well, we got lucky this time; no harm, no foul.” The problem is, there are recurring patterns to these types of events, and the same issues may affect the next patient, who may not be so lucky.
Defining “Something Bad”
These types of cases, which have outcomes ranging from no effect on the patient to death, may be approached several different ways. The terms “near miss” or “close call” refer to an incident where a mistake was made but caught in time, so no harm was done to the patient. An example of this is when a physician makes a mistake on a medication order, but it is caught and corrected by a pharmacist or nurse.
When adverse outcomes do occur, think about and define etiologies so that you identify and address underlying causes. Is the outcome an expected or unexpected complication of therapy? Was there an error involved? In asking these questions, remember that you can have harm without error and error without harm. Error is defined as “failure of a planned action to be completed as intended or use of a wrong plan to achieve an aim; the accumulation of errors results in accidents” (Kohn, et al). This definition points out that usually a chain of events rather than a single individual or event results in a bad outcome. The purpose of defining etiologies is not to assign blame but to identify underlying issues and surrounding circumstances that may have contributed to the adverse outcome.
Significant adverse events are called “sentinel events” and defined as an “unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Serious injury specifically includes loss of limb or function” (JCAHO 1998).
How We Approach Error
Unfortunately, as humans we are fallible and make errors quite reliably. Table 1 demonstrates types of errors and expected rates of errors. For example, we make errors of omission 0.01% of the time, but the good news is that with reminders or ticklers, we can reduce this rate to 0.003%. Unfortunately, when humans are under high stress in danger, research from the military indicates error rates of 25% (Salvendy 1997). In a complex ICU setting, researchers have documented an average of 178 activities per patient per day with an error rate of 0.95%. Despite an error rate of less than 1%, the yield of errors during the 4-month period of observation was still over 1000 errors, 29% of which were considered to have severe or potentially severe consequences (Donchin, et al).
The reality is that we err. Having the unrealistic expectations developed in medical training of being perfect in all our actions perpetuates the blame cycle when the inevitable mistake occurs, and it prevents us from implementing solutions that prevent errors from ever occurring or catching them before they cause harm.
RCA and FMEA Help Us Create Solutions That Make a Difference
Briefly, Root Cause Analysis (RCA) is a retrospective investigation that is required by JCAHO after a sentinel event: “Root cause analysis is a process for identifying the basic or causal factor(s) that underlies variation in performance, including the occurrence or possible occurrence of a sentinel event. A root cause is that most fundamental reason a problem―a situation where performance does not meet expectations―has occurred” (JCAHO 1998). An RCA looks back in time at an event and asks the question “What
happened?” The utility of this methodology lies in the fact that it not only asks what happened but also asks “Why did this happen” rather than focus on “Who is to blame?” Some hospitals use this methodology for cases that are not sentinel events, because the knowledge gained from these investigations often uncovers system issues previously not known and that negatively impact many departments, not just the departments involved in a particular case.
Failure Modes and Effects Analysis (FMEA) is a prospective investigation aimed at identifying vulnerabilities and preventing failures in the future. It looks forward and asks what could go wrong? Performance of an FMEA is also required yearly by JCAHO and focuses on improving risky processes such as blood transfusions, chemotherapy, and other high risk medications.
Approaching a clinical case clearly demonstrates the differences between RCA and FMEA. Imagine a 72-year-old patient admitted to your hospital with findings of an acute abdomen requiring surgery. The patient is a smoker, with Type 2 diabetes and an admission blood sugar of 465, but no evidence of DKA. She normally takes an oral hypoglycemic to control her diabetes and an ACE inhibitor for high blood pressure but no other medications. She is taken to the OR emergently, where surgery seems to go well, and post-operatively is admitted to the ICU. Subsequently, her blood glucose ranges from 260 to 370 and is “controlled” with sliding scale insulin. Unfortunately, within 18 hours of surgery she suffers an MI and develops a postoperative wound infection 4 days after surgery. She eventually dies from sepsis.
An RCA of this case might reveal causal factors such as lack of use of a beta-blocker preoperatively and lack of use of IV insulin to lower her blood sugars to the 80–110 range. While possibly identifying the root cause of this adverse outcome, an RCA is limited by its hindsight bias and the labor-intensive nature of the investigation that may or may not have broad application, since it is an in-depth study of one case. However, RCA’s do have the salutary effects of building teamwork, identifying needed changes, and if carried out impartially without assigning blame can facilitate a culture of patient safety.
FMEA takes a different approach and proactively aims to prevent failure. It is a systematic method of identifying and preventing product and process failures before they occur. It does not require a specific case or adverse event. Rather, a high-risk process is chosen for study, and an interdisciplinary team asks the question “What can go wrong with this process and how can we prevent failures?” Considering the above case, imagine that before it ever occurred you as the hospitalist concerned with patient safety decided to conduct an FMEA on controlling blood sugar in the ICU or administering beta-blockers perioperatively to patients who are appropriate candidates.
For example, using FMEA methodology to study the process of intensive insulin therapy to achieve tight control of glucose in the ICU would identify potential barriers and failures preventing successful implementation. A significant risk encountered in achieving tight glucose control in the range of 80–110 includes hypoglycemia. Common pitfalls of insulin administration include administration and calculation errors that can result in 10-fold differences in doses of insulin. Other details of administration, such as type of IV tubing used and how the IV tubing is primed, can greatly affect the amount of insulin delivered to the patient and thus the glucose levels. If an inadequate amount of solution is flushed through to prime the tubing, the patient may receive saline rather than insulin for a few hours, resulting in higher-than-expected glucose levels and titration of insulin to higher doses. The result would then be an unexpectedly low glucose several hours later. Once failure modes such as these are identified, a fail-safe system can be designed so that failures are less likely to occur.
The advantages of FMEA include its focus on system design rather than on a single incident such as in RCA. By focusing on systems and processes, the learning and changes implemented are likely to impact a larger number of patients.
Summary and Discussion
To summarize, RCA is retrospective and dissects a case, while FMEA is prospective and dissects a process. It is important to remember that given the right set of circumstances, any physician can make a mistake. It makes sense to apply methodologies that probe into surrounding circumstances and contributing factors so that knowledge gained can be used to prevent the same mistakes from happening to different individuals and have broader impact on healthcare systems.
Resources
- www.patientsafety.gov: VA National Center for Patient Safety. Excellent website with very helpful, practical tools.
- www.ihi.org: Institute for Healthcare Improvement website. Has a nice FMEA toolkit.
- www.jcaho.com: The Joint Commission for Accreditation of Healthcare Organizations website. Has information on sentinel events and use of RCA.
Bibliography
- Kohn LT, Corrigan JM, Eds. To Err is Human. Building a Safer Helath System. Washington, DC: National Academy Press; 1999.
- Joint Commission on Accreditation of Healthcare Organizations. Sentinel events: evaluating cause and planning improvement. 1998. Library of congress catalog number 97-80531.
- Salvendy G, ed. Handbook of Human Factors and Ergonomics. New York: John Wiley & Sons;1997:163
- Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med. 1995;23:294-300.
- McNutt R, Abrams R, Hasler S, et al. Determining medical error: three case reports. Eff Clin Pract. 2002;5:23-8.
- Senders JW. FMEA and RCA: the mantras of modern risk management. Qual Saf Health Care. 2004;13:249-50.
- Spath PL. Investigating Sentinel Events: How to Find and Resolve Root Causes. Forest Grove, OR: Brown Spath and Associates; 1997.
- Wald H, Shojania KG. Root cause analysis. In: Shojania KG, McDonald KM, Wachter RM, eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43, AHRQ Publication No. 01-E058; July 2001. Available at http://www.ahrq.gov.
- Woodhouse S, Burney B, Coste K. To err is human: improving patient safety through failure mode and effect analysis. Clin leadersh Manag Rev. 2004;18:32-6.
The Hospital Turned Inside Out

If you’re a “boomer”―one of those Americans born between 1946 and 1964―you have witnessed the most dramatic changes in history in the essential community institution called the hospital. From the technology inside to the kinds of people who deliver the medical care and operate the organization, and from the financial structure that supports it to its image in the eyes of the public, today’s hospital has been radically reformed in the past few decades.
Most Americans don’t like to think about hospitals; they enter our minds only when they must. There’s only one time in the life of a family when they want to be in the hospital. All others are moments of fear at best, human crisis at worst.
As a full-fledged boomer, I remember my early impressions of hospitals: big, mysterious places that sometimes didn’t allow children in. The grownups I knew talked about hospitals with a curious mixture of reverence and fear. If someone died in the hospital, the common notion was that the doctors “did all they could, but Uncle Fred didn’t make it.”
If, heaven forbid, a person faced hospitalization, he or she went wherever the doctor directed. In my small hometown, everybody knew somebody who worked at the hospital, so you at least knew that if you had to go there, you’d see people you knew. And if you knew the people, you trusted the hospital to be a good place where good people did their best for you. And that was about all the information most people had about their local hospital.
Today, the public pressure for information about the inner workings of hospitals is coming from every direction― regulators, politicians at every level, the press, organizations claiming to represent “consumers” and distinct groups such as the elderly and uninsured, unions, the business community, and the list keeps growing. The demand is for an unvarnished took at what occurs in every place, from the boardroom to the billing office to the bedside. How do hospitals govern themselves? Whom do they pay how much? What prevents conflicts of interest? What do they charge for their services, and who actually pays what? What are the policies and practices on charity care, billing, and collections? How many errors do the clinicians make? How many people get infections in the hospital? What are the outcomes of the care? Are patients getting the right care at the right time? Do patients get too much care? Too little? What do you do about inept doctors?
It’s a virtual tsunami for transparency. And hospital people are reacting to this tidal wave in multiple ways. Some are running away from reality. Some are standing their ground. And some are adapting and changing to survive and thrive in an environment vastly different than anything their careers have prepared them for so far.
Because hospitalists are a growing presence and are playing an increasingly important role in all aspects of quality and patient safety, they will be critical to the hospital’s ability to adapt successfully to this new era of transparency and accountability.
The public’s attitudes toward medical error reporting and hospital acquired infections and how hospitals are responding to them today are important clues to the future. In 1999, the Institute of Medicine released its now famous report, To Err Is Human. It estimated that between 45,000 and 98,000 Americans die in hospitals each year from preventable medical errors. The report was nuclear. Not only did it open a national debate on patient safety that continues still, but also it compelled thousands of hospitals to talk with their communities for the first time about what they do to prevent errors.
A recent survey found that 55% of Americans are dissatisfied with the quality of hospital care. In the same poll, 34% said they or a family member had experienced a preventable medical error, and 70% of them said they were not told. Ninety-two percent of the respondents said medical error reporting should be mandatory and public.
Hospitals have agreed that errors should be reported. But unless there’s confidentiality, a culture of blame will discourage reporting and drive errors underground. Caregivers won’t come forward to admit mistakes, making it difficult to get to the root cause and to prevent future incidents. While the national debate goes on, 18 states have passed laws requiring hospitals to report errors to some external body. Some of that data will be made public in some form. Will lawmakers and hospitals be able to resist public pressure over time for public reporting of errors by all hospitals? Can we convince the public that confidentiality will actually lead to safer care and a culture of safety in the nation’s hospitals?
In 2002, the Chicago Tribune reported the results of its investigation into hospital acquired infections, estimating that about 75,000 people died in 2000 from infections that could have been prevented. The Centers for Disease Control and Prevention (CDC) has said that 90,000 patients die annually from hospital acquired infections, adding $5 billion to America’s health care costs. If hospital personnel were more observant of simple infection control procedures, such as regular hand washing, the CDC says thousands of lives and billions of dollars could be saved.
Consumers Union, publisher of the powerful magazine, Consumer Reports, has taken on health care in recent years with the same vigor that it used to get information to the public on autos and appliances. Its current national campaign calls for the reporting and publicizing of hospital acquired infection rates by all hospitals. In 30 states, bills have been introduced to mandate reporting of infection rates. Fifteen states are considering laws to control and oversee hospitals’ infection control practices. The concept that the public should know how well hospitals perform at infection control and prevention resonates strongly. Public reporting of hospital quality measures is in its infancy. Earlier this month, the first public private website opened with information that will allow comparison of hospitals’ performance around pneumonia, heart attack, and heart failure. Soon data on patients’ experience with care―how well they think their doctors and nurses did―will be added. Will infection and infection control statistics be far behind?
And the challenges and tensions are not all in the clinical arena. A recent survey by the American College of Physician Executives found 9 out of 10 physicians concerned about dishonesty, financial conflicts, and unethical behavior among their colleagues.
Eighty percent said they were worried about doctors refusing to treat uninsured patients as part of “on call” responsibilities. And 79% pointed to undue Influence on physicians by medical device companies to perform certain procedures. Physicians’ over treatment of patients to boost income were cited by 78% of the doctors. Another major concern: the influence of drug companies on physicians’ prescribing habits.
In early April, the federal government announced that it would begin investigating the upsurge in tests being ordered for Medicare patients. The issues: medical necessity and rapidly increasing costs.
Hospitals are at a crossroads in their relationships with many publics: their patients, employees and medical staff s, their communities, the government, and the media. The issue is building and retaining trust on so many fronts. Hospitals must be proactive when it comes to accountability and transparency. Doing so will create enormous tensions and challenges inside an institution. This will require leadership and motivation. Hospitalists, given their unique role, are positioned to be powerful catalysts for change―change that will result either in a mountain of cumbersome new laws and regulations or a new culture of openness and trust with the people hospitals exist to serve.
If you’re a “boomer”―one of those Americans born between 1946 and 1964―you have witnessed the most dramatic changes in history in the essential community institution called the hospital. From the technology inside to the kinds of people who deliver the medical care and operate the organization, and from the financial structure that supports it to its image in the eyes of the public, today’s hospital has been radically reformed in the past few decades.
Most Americans don’t like to think about hospitals; they enter our minds only when they must. There’s only one time in the life of a family when they want to be in the hospital. All others are moments of fear at best, human crisis at worst.
As a full-fledged boomer, I remember my early impressions of hospitals: big, mysterious places that sometimes didn’t allow children in. The grownups I knew talked about hospitals with a curious mixture of reverence and fear. If someone died in the hospital, the common notion was that the doctors “did all they could, but Uncle Fred didn’t make it.”
If, heaven forbid, a person faced hospitalization, he or she went wherever the doctor directed. In my small hometown, everybody knew somebody who worked at the hospital, so you at least knew that if you had to go there, you’d see people you knew. And if you knew the people, you trusted the hospital to be a good place where good people did their best for you. And that was about all the information most people had about their local hospital.
Today, the public pressure for information about the inner workings of hospitals is coming from every direction― regulators, politicians at every level, the press, organizations claiming to represent “consumers” and distinct groups such as the elderly and uninsured, unions, the business community, and the list keeps growing. The demand is for an unvarnished took at what occurs in every place, from the boardroom to the billing office to the bedside. How do hospitals govern themselves? Whom do they pay how much? What prevents conflicts of interest? What do they charge for their services, and who actually pays what? What are the policies and practices on charity care, billing, and collections? How many errors do the clinicians make? How many people get infections in the hospital? What are the outcomes of the care? Are patients getting the right care at the right time? Do patients get too much care? Too little? What do you do about inept doctors?
It’s a virtual tsunami for transparency. And hospital people are reacting to this tidal wave in multiple ways. Some are running away from reality. Some are standing their ground. And some are adapting and changing to survive and thrive in an environment vastly different than anything their careers have prepared them for so far.
Because hospitalists are a growing presence and are playing an increasingly important role in all aspects of quality and patient safety, they will be critical to the hospital’s ability to adapt successfully to this new era of transparency and accountability.
The public’s attitudes toward medical error reporting and hospital acquired infections and how hospitals are responding to them today are important clues to the future. In 1999, the Institute of Medicine released its now famous report, To Err Is Human. It estimated that between 45,000 and 98,000 Americans die in hospitals each year from preventable medical errors. The report was nuclear. Not only did it open a national debate on patient safety that continues still, but also it compelled thousands of hospitals to talk with their communities for the first time about what they do to prevent errors.
A recent survey found that 55% of Americans are dissatisfied with the quality of hospital care. In the same poll, 34% said they or a family member had experienced a preventable medical error, and 70% of them said they were not told. Ninety-two percent of the respondents said medical error reporting should be mandatory and public.
Hospitals have agreed that errors should be reported. But unless there’s confidentiality, a culture of blame will discourage reporting and drive errors underground. Caregivers won’t come forward to admit mistakes, making it difficult to get to the root cause and to prevent future incidents. While the national debate goes on, 18 states have passed laws requiring hospitals to report errors to some external body. Some of that data will be made public in some form. Will lawmakers and hospitals be able to resist public pressure over time for public reporting of errors by all hospitals? Can we convince the public that confidentiality will actually lead to safer care and a culture of safety in the nation’s hospitals?
In 2002, the Chicago Tribune reported the results of its investigation into hospital acquired infections, estimating that about 75,000 people died in 2000 from infections that could have been prevented. The Centers for Disease Control and Prevention (CDC) has said that 90,000 patients die annually from hospital acquired infections, adding $5 billion to America’s health care costs. If hospital personnel were more observant of simple infection control procedures, such as regular hand washing, the CDC says thousands of lives and billions of dollars could be saved.
Consumers Union, publisher of the powerful magazine, Consumer Reports, has taken on health care in recent years with the same vigor that it used to get information to the public on autos and appliances. Its current national campaign calls for the reporting and publicizing of hospital acquired infection rates by all hospitals. In 30 states, bills have been introduced to mandate reporting of infection rates. Fifteen states are considering laws to control and oversee hospitals’ infection control practices. The concept that the public should know how well hospitals perform at infection control and prevention resonates strongly. Public reporting of hospital quality measures is in its infancy. Earlier this month, the first public private website opened with information that will allow comparison of hospitals’ performance around pneumonia, heart attack, and heart failure. Soon data on patients’ experience with care―how well they think their doctors and nurses did―will be added. Will infection and infection control statistics be far behind?
And the challenges and tensions are not all in the clinical arena. A recent survey by the American College of Physician Executives found 9 out of 10 physicians concerned about dishonesty, financial conflicts, and unethical behavior among their colleagues.
Eighty percent said they were worried about doctors refusing to treat uninsured patients as part of “on call” responsibilities. And 79% pointed to undue Influence on physicians by medical device companies to perform certain procedures. Physicians’ over treatment of patients to boost income were cited by 78% of the doctors. Another major concern: the influence of drug companies on physicians’ prescribing habits.
In early April, the federal government announced that it would begin investigating the upsurge in tests being ordered for Medicare patients. The issues: medical necessity and rapidly increasing costs.
Hospitals are at a crossroads in their relationships with many publics: their patients, employees and medical staff s, their communities, the government, and the media. The issue is building and retaining trust on so many fronts. Hospitals must be proactive when it comes to accountability and transparency. Doing so will create enormous tensions and challenges inside an institution. This will require leadership and motivation. Hospitalists, given their unique role, are positioned to be powerful catalysts for change―change that will result either in a mountain of cumbersome new laws and regulations or a new culture of openness and trust with the people hospitals exist to serve.
If you’re a “boomer”―one of those Americans born between 1946 and 1964―you have witnessed the most dramatic changes in history in the essential community institution called the hospital. From the technology inside to the kinds of people who deliver the medical care and operate the organization, and from the financial structure that supports it to its image in the eyes of the public, today’s hospital has been radically reformed in the past few decades.
Most Americans don’t like to think about hospitals; they enter our minds only when they must. There’s only one time in the life of a family when they want to be in the hospital. All others are moments of fear at best, human crisis at worst.
As a full-fledged boomer, I remember my early impressions of hospitals: big, mysterious places that sometimes didn’t allow children in. The grownups I knew talked about hospitals with a curious mixture of reverence and fear. If someone died in the hospital, the common notion was that the doctors “did all they could, but Uncle Fred didn’t make it.”
If, heaven forbid, a person faced hospitalization, he or she went wherever the doctor directed. In my small hometown, everybody knew somebody who worked at the hospital, so you at least knew that if you had to go there, you’d see people you knew. And if you knew the people, you trusted the hospital to be a good place where good people did their best for you. And that was about all the information most people had about their local hospital.
Today, the public pressure for information about the inner workings of hospitals is coming from every direction― regulators, politicians at every level, the press, organizations claiming to represent “consumers” and distinct groups such as the elderly and uninsured, unions, the business community, and the list keeps growing. The demand is for an unvarnished took at what occurs in every place, from the boardroom to the billing office to the bedside. How do hospitals govern themselves? Whom do they pay how much? What prevents conflicts of interest? What do they charge for their services, and who actually pays what? What are the policies and practices on charity care, billing, and collections? How many errors do the clinicians make? How many people get infections in the hospital? What are the outcomes of the care? Are patients getting the right care at the right time? Do patients get too much care? Too little? What do you do about inept doctors?
It’s a virtual tsunami for transparency. And hospital people are reacting to this tidal wave in multiple ways. Some are running away from reality. Some are standing their ground. And some are adapting and changing to survive and thrive in an environment vastly different than anything their careers have prepared them for so far.
Because hospitalists are a growing presence and are playing an increasingly important role in all aspects of quality and patient safety, they will be critical to the hospital’s ability to adapt successfully to this new era of transparency and accountability.
The public’s attitudes toward medical error reporting and hospital acquired infections and how hospitals are responding to them today are important clues to the future. In 1999, the Institute of Medicine released its now famous report, To Err Is Human. It estimated that between 45,000 and 98,000 Americans die in hospitals each year from preventable medical errors. The report was nuclear. Not only did it open a national debate on patient safety that continues still, but also it compelled thousands of hospitals to talk with their communities for the first time about what they do to prevent errors.
A recent survey found that 55% of Americans are dissatisfied with the quality of hospital care. In the same poll, 34% said they or a family member had experienced a preventable medical error, and 70% of them said they were not told. Ninety-two percent of the respondents said medical error reporting should be mandatory and public.
Hospitals have agreed that errors should be reported. But unless there’s confidentiality, a culture of blame will discourage reporting and drive errors underground. Caregivers won’t come forward to admit mistakes, making it difficult to get to the root cause and to prevent future incidents. While the national debate goes on, 18 states have passed laws requiring hospitals to report errors to some external body. Some of that data will be made public in some form. Will lawmakers and hospitals be able to resist public pressure over time for public reporting of errors by all hospitals? Can we convince the public that confidentiality will actually lead to safer care and a culture of safety in the nation’s hospitals?
In 2002, the Chicago Tribune reported the results of its investigation into hospital acquired infections, estimating that about 75,000 people died in 2000 from infections that could have been prevented. The Centers for Disease Control and Prevention (CDC) has said that 90,000 patients die annually from hospital acquired infections, adding $5 billion to America’s health care costs. If hospital personnel were more observant of simple infection control procedures, such as regular hand washing, the CDC says thousands of lives and billions of dollars could be saved.
Consumers Union, publisher of the powerful magazine, Consumer Reports, has taken on health care in recent years with the same vigor that it used to get information to the public on autos and appliances. Its current national campaign calls for the reporting and publicizing of hospital acquired infection rates by all hospitals. In 30 states, bills have been introduced to mandate reporting of infection rates. Fifteen states are considering laws to control and oversee hospitals’ infection control practices. The concept that the public should know how well hospitals perform at infection control and prevention resonates strongly. Public reporting of hospital quality measures is in its infancy. Earlier this month, the first public private website opened with information that will allow comparison of hospitals’ performance around pneumonia, heart attack, and heart failure. Soon data on patients’ experience with care―how well they think their doctors and nurses did―will be added. Will infection and infection control statistics be far behind?
And the challenges and tensions are not all in the clinical arena. A recent survey by the American College of Physician Executives found 9 out of 10 physicians concerned about dishonesty, financial conflicts, and unethical behavior among their colleagues.
Eighty percent said they were worried about doctors refusing to treat uninsured patients as part of “on call” responsibilities. And 79% pointed to undue Influence on physicians by medical device companies to perform certain procedures. Physicians’ over treatment of patients to boost income were cited by 78% of the doctors. Another major concern: the influence of drug companies on physicians’ prescribing habits.
In early April, the federal government announced that it would begin investigating the upsurge in tests being ordered for Medicare patients. The issues: medical necessity and rapidly increasing costs.
Hospitals are at a crossroads in their relationships with many publics: their patients, employees and medical staff s, their communities, the government, and the media. The issue is building and retaining trust on so many fronts. Hospitals must be proactive when it comes to accountability and transparency. Doing so will create enormous tensions and challenges inside an institution. This will require leadership and motivation. Hospitalists, given their unique role, are positioned to be powerful catalysts for change―change that will result either in a mountain of cumbersome new laws and regulations or a new culture of openness and trust with the people hospitals exist to serve.
Hospital Medicine: Where We’ve Been and Where We’re Going

Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
Robert M. Wachter, MD, professor and chief of the medical service at the University of California, San Francisco (UCSF) Medical Center and director of its hospital medicine group, addressed the audience at the 8th Annual Meeting of the Society of Hospital Medicine (SHM), along with several other noted leaders. Shortly before the meeting, Wachter shared his insight on the initial years of hospital medicine as well as the complexities, challenges, and opportunities the future holds for hospital medicine groups with The Hospitalist.
Well known for having coined the term “hospitalist” in a 1996 New England Journal of Medicine article, Wachter provided a brief outline of the birth of the hospital medicine discipline. He recalled that the initial growth of the field was slow, but it gained momentum as healthcare facilities began to perceive this specialty as an effective way to fulfill a need. During the last 10 years, hospitalists have made clear their value as agents of throughput, systems management, resource utilization, physician practice improvement, round the clock availability, and medical student education, always placing patient safety, satisfaction, and quality at the forefront of the practice. During the next 10 years―and beyond―Wachter envisions an evolution in the critical role hospitalists will play in the continued delivery of quality health care, although he does admit there are some obstacles in the path.
Surgical Co-management
Having established their core role as managers of medical inpatients, hospitalists are setting their sights on other goals. “It’s logical and inevitable that hospitalists will take on roles in surgical co-management,” Wachter says. “Patients who are sick enough to be inpatients for surgery often have multiple medical illnesses. And surgeons are in the OR for much of the day, in some ways like primary care doctors’ being in the office.” Although the data to support this model are limited presently, he believes that good co-management programs will likely lead to an increase in the quality of care, efficiency and patient satisfaction as well as surgeon satisfaction. “This makes … intuitive sense, just as the whole hospitalist idea made sense 10 years ago,” he says.
Wachter admits that the transition will probably be gradual, because of the many clinical, economic, and political complexities. In many cases, surgeons receive a global fee , linked to the expectation that they will administer preoperative and postoperative care. “It will be tricky to try to figure out how to compensate the hospitalist for surgical co-management,” Wachter says. However, he expects the financial aspect of surgical co-management to eventually work itself out. “If there is a more efficient way to manage patients and a way to free up beds, hospitals will be interested in supporting it,” he says. Wachter anticipates a 5- to 10-year evolution before this model becomes widely embraced.
Patient Safety and Quality Improvement
Timing is everything, and for hospitalists the timing could not have been better. “The hospital medicine movement evolved precisely when American medicine began to care about safety and quality,” says Wachter. ”When I first read the Institute of Medicine report on patient safety, ‘To Err is Human,’ in 1999, I knew that we had a tremendous opportunity to make a difference.” Wachter notes that in the past, incentives for high quality performance were lacking. “That is changing rapidly,” he says. With the profusion of Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates, Centers for Medicare and Medicaid Services (CMS) metrics, Leapfrog initiatives, and other quality measures, patient safety and quality have become top priorities. Since hospital medicine encompasses all the vital aspects of quality improvement and patient safety―from understanding transitions and working collaboratively with other medical specialists to improving systems and more effective oversight―hospitalists are becoming the “goto people,” according to Wachter. This is incredibly healthy for our field, he notes, “but more importantly, it will help save.”
As one measure of how the world has changed in just a few years, Wachter reflects on the experience of editing his textbook, Hospital Medicine, in 2000, and again in 2005 for the second edition. He was particularly struck by the chapter he wrote (in the 2005 edition, with his UCSF colleague Niraj Sehgal) on quality measurement and improvement. “It was staggering how much the area had changed,” he says. In the 2000 edition, there were 2 inpatient quality measures: aspirin and beta blockers for patients with myocardial infarction. In the 2005 edition, “we needed a 2-page table to catalogue all of the hospital quality measures produced by an alphabet soup of agencies and organizations.” In fact, he notes, of the 122 chapters in the book, the chapter that had changed the most in 5 years was the one on quality measurement. “This is a complex science that is still evolving,” Wachter says. “I fully expect that the chapter in the 3rd edition will change even more.”
Wachter has spearheaded several other initiatives designed to improve hospital conditions and care of patients. He leads a team of editors for the website, AHRQ Web M&M: Morbidity and Mortality Rounds on the Web (www.webmm.ahrq.gov), which provides expert analyses on medical errors, as well as a forum and online discussions on patient safety issues. He and his colleagues recently launched a second federally sponsored portal for patient safety, “AHRQ Patient Safety Network” (www.psnet.ahrq.gov), which offers regularly updated tools, new literature, surveys, videos, and links to other useful resources and experts and is customizable according to users’ interests.
Burnout
With all the responsibilities assigned to hospitalists, the issue of burnout might become a concern. Defined as mental and/or physical exhaustion caused by excessive and prolonged stress, burnout can afflict medical professionals who spend long hours caring for complicated patients. Wachter worries about burnout, but not unduly so. “There is nothing fundamental about our field that will cause burnout,” he says. He cites 4 factors that contribute to burnout: doing uninteresting, unimportant work; receiving little or no respect from peers; having little or no time to “catch your breath”; and earning an inadequate and unreasonable income. With the diverse responsibilities and personally and professionally satisfying work in which a hospitalist engages, these risks can be mitigated. “I’ve certainly visited hospital medicine groups that were rife with burned out providers,” he says. “But more often, I’ve seen terrific doctors doing work they love, making a difference in the lives of their patients and their institutions. When that’s the case, you don’t see much burnout.” Wachter believes that the way in which hospital medicine groups are designed influences the potential burnout factor. Considerable thought and planning should precede the creation of a hospital medicine group, he asserts. “Some groups are well constructed,” he says. “They’ve created jobs with reasonable amounts of downtime, an opportunity to earn a good income, and the chance to spend time improving the system and deliver high quality patient care.” On the other hand, groups that care for an unsustainable number of patients with lower recompense might well have burnout; some have even collapsed after the physicians led. “You can be sure,” he notes, “that the second iteration of the hospital medicine programs at these institutions will be structured much more carefully so as not to repeat the same mistakes.”
Using his own UCSF Medical Center as an example, Wachter notes virtually no burnout or attrition among his faculty, even though salaries are on an academic scale, below the prevailing community rate. “We feel supported and have time to catch our breath,” he says. “We are respected by our colleagues and the institution, we have a chance to teach, and we genuinely enjoy each other’s company. And we have a chance to work on other things, not just patient care.” And that makes all the difference.
The Future of Hospital Medicine
Wachter was recently elected to the American Board of Internal Medicine, the only new member and the sole hospitalist to earn this honor. In this role, he will have the opportunity to provide input that will influence the development and expansion of the hospital medicine movement. “The Board is interested in the growth of the hospitalist field and what it means for the future,” he says. “They would like to know how to support the field and how best to attract students to it.” Many members of the Board who were skeptical at first about the hospitalist field have now recognized that “hospitalists have brought back the excitement of being an internist.” Wachter believes that students exposed to hospitalists soon realize that these doctors have fulfilling, diverse careers. “Hospitalists interact with patients, act as leaders to make patient care better, increase quality, and write guidelines,” he says. “This is a rich job description.” At the UCSF Medical Center, students involved in various clerkships have the opportunity to work under the tutelage of hospitalists. These collaborative relationships bring greater understanding of the work a hospitalist does and promotes the future of the field, according to Wachter.
Specialized Certification
As each new specialty evolves, different requirements for certification arise. Since hospital medicine is still a fairly young field, educational and training qualifications have yet to be determined. In his role on the American Board of Internal Medicine, Wachter will probably contribute to the discussion on what certification can and should look like. “This is an area of active investigation,” he says. “Will there be a separate certification for hospitalists? Should it be given at initial certification or when a physician recertifies after having been a practicing hospitalist with demonstrated competency? Right now there is no widespread model for hospitalist training at the residency level,” says Wachter. “I would not be surprised if in 10 or 15 years specialized training evolves for hospitalists. If so, then it would be logical that there be some type of separate certification. It’ll be fascinating working with the Board and SHM to determine the best course in the meantime.”
A View of the SHM Annual Meeting in Chicago
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Editor’s Note:
Having returned from the 8th SHM Annual Meeting at the time of this writing, it is clear that this was not only the biggest but also the best Annual Meeting to date. As Larry Wellikson and Joe Miller describe more fully in this issue, the lectures, workshops and networking activities available far outstripped the ability of attendees to take part in all of them. In fact, it was common to feel that there were 2, 3, or even more “must attend” sessions taking place simultaneously and if this was sometimes frustrating, it also spoke to the fact that the meeting’s quality was strikingly high. With the realization that a collection of articles is unable to fully convey the vibrancy of the meeting, we have assembled in the following section a “Big Picture” from imbedded reporter Joe Miller, overviews of 2 of the plenary lectures, and recaps of several outstanding breakout sessions. A separate monograph that will include other highlights of the Annual Meeting is under development and will be mailed in August.―JP
I was invited to write a short piece for The Hospitalist summarizing SHM’s 8th Annual Meeting on Thursday, April 28 through Saturday, April 30 in Chicago. As I sat on the airplane on my return flight to Boston, I reflected on what would define a “successful” annual meeting for the professional society representing hospitalists. I concluded that three criteria would define success. Specifically that the conference would:
- Demonstrate the strength and resiliency of the hospital medicine movement
- Provide quality content and learning opportunities to a diverse group of attendees
- Demonstrate that SHM is a competent and effective organization meeting the needs of its members.
I believe the meeting measured up extremely well on all three criteria.
With regard to demonstrating the vibrancy of the hospital medicine movement:
- At the conference, there was recognition by three significant stakeholders in the healthcare industry (hospitals, employers, and regulators) of the critical role of hospitalists. In the opening keynote address, Rick Wade, Senior Vice President of the American Hospital Association, described the growing pressure on hospitals to be “transparent,” sharing information with patients and the public on their performance. Mr. Wade’s address was followed by a presentation by Arnold Milstein, MD, Medical Director of the Pacific Business Group on Health and cofounder of the Leapfrog Group. Dr. Milstein used the metaphor of a shark’s jaws to describe the threat of the continued escalation of healthcare costs, and he indicated that the key to addressing this crisis is to “re-engineer” clinical processes to make them more efficient. On Saturday, Dennis O’Leary, CEO of JCAHO, described the challenge of evaluating the performance of hospitals in the era of patient safety. All three speakers indicated that hospitalists will be critical resources to healthcare leaders faced with these challenges. Another measure of the recognition of hospitalists as a force in the healthcare industry was the fact that over 90 exhibitors wanted the opportunity to get the ear of the conference attendees. The exhibit floor was teeming with hospitalists interested in learning about programs, products, and services.
- The growth of the hospital medicine movement was clearly evident to attendees of the conference. This year’s conference had over 1000 attendees,a growth of 15% over the 2004 annual meeting. When Alpesh Amin, MD, co-director of the course, opened the meeting, the attendees responded to a series of questions through the audience response system. For over 50% of the attendees, this was their first SHM Annual Meeting, indicating that the specialty of hospital medicine has a constant influx of “new blood.” And at the President’s Luncheon, the presentation by Larry Wellikson, MD, CEO of SHM, conveyed a broad array of statistics on the status of the hospital medicine movement, including the fact that the 12,000+ hospitalists in the U.S. makes the specialty bigger than gastroenterology and neurology. Approximately 30% of all U.S. Hospitals have hospital medicine programs; for hospitals with over 200 beds, 55% have hospitalists.
- The excellence of the hospital medicine movement was evident through the quality of the 120+ research, innovation, and clinical vignette posters presented on Friday. Furthermore, the accomplishments of the SHM award winners announced at the President’s Luncheon were quite impressive. Joseph Li, MD, won the award for Outstanding Service in Hospital Medicine, Sunil Kripalani, MD, was named the Outstanding Young Investigator, Shaun Frost, MD, won the Clinical Excellence award, and Jeff Wiese, MD, won the award for Excellence in Teaching. Hospitalists are demonstrating their ability to be innovative, high impact physicians.
With regard to providing learning opportunities for a diverse audience:
- The pre-courses on Thursday allowed attendees to gain in-depth knowledge on practice management, perioperative medicine, and critical care medicine.
- There were 35 separate presentations in 7 tracks over the 2 days of the main meeting. The clinical, adult clinical, and pediatric clinical tracks covered a wide array of topics, from maternal fetal medicine to acquired pediatric heart disease to addiction medicine. Tracks on quality and patient safety were very well attended, and the academic track included an important update on the hospitalist core curriculum being developed by SHM.
- There were 10 special interest forums allowing attendees interested in the following subjects to exchange ideas: community based hospitalists, research, education, medical directors, women hospitalists, pediatric hospitalists, family practice hospitalists, geriatric hospitalists, early career hospitalists, and nurse practitioners and physician assistants.
- The plenary sessions on updates in hospital medicine and pediatric hospital medicine provided excellent reviews of recent research relevant to hospitalists. Bob Wachter’s annual presentation, this year entitled “Hospital Medicine: Still Crazy After All These Years” laid out some important challenges for the hospital medicine movement as it moves into adolescence.
Finally, with regard to demonstrating SHM’s competence and its ability to meet the needs of its members:
- At the President’s Luncheon, the depth of SHM leadership was evident. Jeanne Huddleston, MD, reported on the significant accomplishments of the past year and handed the torch to SHM’s new President, Steve Pantilat, MD. Steve described his two goals for the upcoming year, the development ofan SHM Research Foundation and an emphasis on the role of hospitalists in palliative care. And Larry Wellikson, MD, SHM’s CEO, displayed energy and charisma throughout the meeting.
- The power of SHM volunteerism was unmistakable throughout the meeting. Preetha Basaviah, MD, the overall course director, harnessed group of SHM members participating in a planning committee to decide on the topics and choose the speakers for the meeting. A broad cross-section of SHM members participated in over 15 committee meetings in Chicago, as they donated their time to improving the field of hospital medicine.
- The conference was a vehicle to display the public relations capabilities of SHM. Melanie Bloom, wife of NBC newscaster David Bloom who died in Iraq of DVT complications, described the awareness campaign that SHM led. The attendees then viewed a short video of the television appearances by hospitalists in the last year, as hospital medicine has received increasing attention in the media. Larry Wellikson announced that every SHM member will receive a DVD with these video news segments.
- The strength of SHM staff and organization was on display in Chicago. Larry Wellikson reported that the staff has more than doubled and he cited a litany of accomplishments, including a new improved website, electronic registration for meetings, a broad range of educational offerings, and a healthy financial outlook. Furthermore, SHM has continued to experience significant membership growth, as the number of members now exceeds 4700, an increase of more than 40% in the past 12 months.
- Finally, and perhaps most importantly, Wellikson described a wide variety of initiatives that are being pursued to meet the needs of SHM members. These initiatives include a long range plan for the formal certification of hospitalists, strategic partnerships with key organizations, public policy initiatives, and the continued strengthening of historical efforts regarding education, leadership, and surveys.
In summary, the SHM conference was greater than the sum of the parts. It was successfully executed on multiple fronts. However I have not yet discussed perhaps the most important achievement of this meeting. It served as an opportunity for hospitalists to meet new friends and to reconnect with old colleagues. The Annual Meeting in Chicago created a positive energy that will carry SHM members until we have the opportunity to meet again next year in Washington, DC.
Be There or Be Square

The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
The bomb. The franchise. Sine qua non. Must see. Must be there. How do you say it when something or someone just seems to be in the middle of everything? That is hospital medicine, and that is SHM.
Nowhere was this more evident than at the largest gathering of hospitalists to date, the SHM Annual Meeting held in Chicago at the end of April. If you have a stake in hospital medicine or in building and improving the hospital of the future, all roads led to Chicago and SHM.
Not only was the CME content cutting edge and geared specifically for hospitalists, but also the sessions were greeted with standing room attendance. Clearly we struck a nerve with our 1-day in-depth pre-courses on Perioperative Care and Critical Care. The Practice Management course continues to attract 250 to 300 people as everyone tries to figure out how to get the most out of their hospital medicine group.
SHM virtually took over the entire Sheraton Hotel in downtown Chicago. Everywhere you looked, all you saw were hospitalists or people who needed to talk to hospitalists. The exhibit hall was sold out, and the networking between all the industries that support and depend on hospitalists continued well beyond the boundaries of the exhibit hall.
The Research Abstract, Clinical Vignette, and Innovation Poster session had almost 200 entries. On display here was the new thinking that is so characteristic of hospital medicine. As much as anything, this gathering displayed the youthful energy and innovation that will continue to propel hospital medicine into the future.
Important people came to be heard and to hear from hospitalists. Dennis O’Leary, the CEO of JCAHO, challenged hospitalists to lead their hospitals into a future with improved measurable quality. Rick Wade, a senior leader at the American Hospital Association, saw hospitalists as key partners with other stakeholders to meet the increasing demands on hospitals to do a better job. Arnie Milstein, the CMO and one of the founders of the Leapfrog Group, placed hospitalists squarely in the center of delivering the effective and efficient health care now demanded by America’s businesses and patients. And our own Bob Wachter challenged hospitalists to continue to lead the patient safety revolution.
But hospitalists did not just come to Chicago to sit and listen. Hospitalists are faced with so many new and difficult challenges that they clearly came to ask questions and give answers. Networking was both informal and formal and almost constant. With hospitalists everywhere you turned it was clear that people were out seeking the next new idea, the solution to a real life problem back home, and maybe even their next job.
The SHM Special Interest Forums were lively and well attended. This is where SHM gets its ideas. This is where hospitalists have their voices heard. This is where the diversity of hospital medicine can be seen up close and personal. The world of the hospital and our specialty looks different if you are a pediatrician or a family practitioner or a woman or an NP or a PA or a group leader or a young hospitalist. The demands, and your needs to meet them, can be different if you are in academics or a community hospital. SHM must hear your perspective and, boy, did we hear from you in Chicago.
For me personally, it was an opportunity to see and talk to over 1000 people connected in some way to the growing hospital medicine movement. Many of the people I spoke with were frontline hospitalists, earnest and dedicated to making hospital medicine their life’s work. They want to work with SHM to create a specialty and a career that is satisfying and fulfilling.
Some were representatives from publishers or pharmaceutical companies or hospitalist staffing and recruitment companies trying to bring their unique take on hospital medicine to SHM’s attention. Some were key leaders of other national healthcare organizations looking to partner with hospital medicine, the fastest growing workforce component of the hospital of the future and a force for change and improvement.
There were so many good ideas flying around that there is enough to keep SHM busy for years to come. And you will be hearing and reading about these in the coming months and years. It is clear that the energy around hospital medicine is not waning any time in the near future. There will be much for us to do. And if the talent and the drive to succeed of those who came to Chicago last month are any indication, SHM and our nation’s hospitalists are up to the challenge. Stay tuned.
Terri Schiavo and the Pope: My Lessons Learned

As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email ([email protected]). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email ([email protected]). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
As I write first column as President of SHM, palliative care has been much in the news. As a hospitalist who spends much of my time caring for people approaching the end of life and teaching about palliative care, these 2 weeks have kept me busy talking about end of life issues with family, friends, patients, colleagues, and the media. At the same time, these events have reaffirmed for me my choice of a career as a hospitalist and the central role that hospitalists play in providing the highest quality care for the sickest patients, in continually improving that care, and in refining the systems to deliver it.
Terri Schiavo died 2 weeks after her feeding tube was removed. Her life and death sparked protests and political debate. Yet in the end, what seems most profound is the great sadness and loss for her family. Soon after Terri Schiavo died, Pope John Paul II became acutely ill. Several days after a feeding tube was placed, the Pope died in his apartment at the Vatican, triggering a global outpouring of love and grief.
In modern American health care, probably Terri Schiavo and the Pope would have received care from a hospitalist. If she were to arrive in a hospital after a cardiac arrest today, Terri Schiavo would likely be cared for by a hospitalist. It is the hospitalist who would have the first discussions with her family about her condition and prognosis. Similarly, most 84-year-old men with Parkinson’s disease, pneumonia, and a urinary tract infection would be cared for by a hospitalist. Hospitalists are serving as de facto ethicists and palliative care physicians, as we care for increasing numbers of people with serious and terminal illness. This shift in care provides an unprecedented opportunity for us to improve the quality of care for the half of all Americans who die in hospitals. Providing state of the art palliative care reinforces our efforts globally to improve the quality of care for all hospitalized patients. Furthermore, these cases highlight the need for research to define the best ways to deliver that care. As I thought about Terri Schiavo and the Pope, and saw the intense media spotlight on them, I kept thinking, “What does this mean for me?”
I have given this question a great deal of thought over the past week. What, if anything, do the deaths of Terri Schiavo and the Pope teach us? As I see it there are at least 3 important lessons for us as individuals and as hospitalists.
The first lesson is that each of us should consider the kind of care we would want if we were to suffer a devastating injury, as did Terri Schiavo, or be stricken with a progressive, debilitating illness, like the Pope. We should discuss our preferences for care with our loved ones and write them down. As hospitalists we should have these discussions routinely with our patients, document the conversations, notify the patient’s primary care physician, and encourage patients to share their thoughts with their loved ones. As a son, husband, brother, nephew, grandson, and father, I realized that one of the most important obligations I owed to my family was to make my wishes known, and to learn about the wishes of my loved ones. As a hospitalist, I realized that I owed it to my patients to help them express their preferences for care. What I learned echoed what we know about advance directives: You cannot predict what someone will say. Not unexpectedly, my mother, grandmother, and aunt told me that they would never want to live like Terri Schiavo. But in a complete surprise my aunt told me that my favorite uncle, who is blessed with a quick wit and brilliant sense of humor, wants to be kept alive as long as possible.
As a hospitalist, I know that my patients care deeply about these issues and are quite eager to discuss them. Talking with patients about these issues is not just a good thing to do, but ultimately improves quality of care by promoting care that is consistent with patient preferences and emphasizes our commitment to respect patients and advocate on their behalf. I still remember early concerns about hospitalists that we would be cowboys more interested in procedures and yelling “Stat!” than in being caring providers who took time to get to know our patients. Yet an early study of hospitalists that I was involved in found just the opposite. Hospitalists recognized the importance of palliative care and good communication with patients. As I made rounds in the hospital in late March, many patients were watching the vigil outside the hospice in Florida and talking about the Pope. Many patients wanted to know my thoughts. Using the communication skills I have honed over the years, and my cultural background of always answering a question with a question, I turned it around and asked them, “What do you think?” I suspect that patients will be using Terri Schiavo as an example of how they do or do not want to live―and die―for a long time. I will do my best to use this shared touchstone as a starting point for understanding their preferences: “Tell me what it is about Terri Schiavo that worries you?” By helping our patients express their preferences and encouraging them to discuss these with their loved ones, we may ease the burden of families who would otherwise have to make a difficult decision without direct knowledge of the patient’s choice.
The second lesson for us to embrace is that palliative care is a core competency for hospitalists. Palliative care is already identified as a core competency in the Core Curriculum under development by SHM. As part of our goal of improving the quality of care for all of our patients, we have the opportunity to dramatically improve end of life care and to identify people who would benefit from palliative care earlier in the course of illness. This opportunity represents a sacred trust and speaks to the most basic role of the physician to “cure sometimes and comfort always.” Ultimately, the deaths of Terri Schiavo and the Pope, although fundamentally different from each other, and unique in many respects, reaffirmed for me the importance of my role as a hospitalist in providing the highest possible quality of care for people facing serious illness and death. With these skills, we will secure our place as leaders in quality care and reap the rich rewards of using our humanity to help patients and families at one of the most important, profound, and intimate times.
The third lesson for us as hospitalists is that more research is needed to define the optimal ways to care for hospitalized patients. While the case of Terri Schiavo raised particularly thorny family issues that might defy the ability of research to clarify, issues of how best to care for patients like Terri Schiavo and the Pope and the millions of people like them with heart failure, deep vein thromboses, aspiration pneumonia, gastrointestinal bleeding, cancer, and myriad other conditions can be, must be, and will be investigated. The only question will be, by whom? As the providers of an increasingly large percentage of hospital care, we are on the front-lines of recognizing the clinical questions that arise and understanding the systems of care in which solutions must be implemented. Therefore we must play a central role in defining the questions and discovering the answers. Further, because we need research not only in how best to treat patients but also in how to ensure that patients receive these treatments, we need to conduct this research in community hospitals, where the majority of patients are cared for, and not just at academic centers.
In my year as President of SHM, I will continue to develop our organization’s founding mission and to serve hospitalists in their goal of providing the best quality of care to their patients and having satisfying, sustainable, and rewarding jobs. SHM will continue to lead and define the field of hospital medicine in education, leadership, quality, patient safety, and teamwork. In addition, I hope to use my unique skills and insights to focus our members on the central role of research in defining our field and the need for SHM to help direct that research. I will also highlight the importance of hospitalists in providing palliative care and in improving the care of patients with serious and terminal illness. I encourage each hospitalist to embrace these critical issues and invite you to join me in implementing this vision to advance research in hospital medicine and to improve palliative care in hospitals. The research committee has already completed a report on the potential role of SHM in research in hospital medicine that the Board of Directors will discuss at our meeting in May, and I am planning an initiative in palliative care. If you would like to participate in either initiative or simply want to share your thoughts and ideas about these or other important issues in hospital medicine, please contact me by email ([email protected]). My closing wish is that Terri Schiavo’s family will find comfort and closure, out of the media spotlight, and that the memory of the Pope is honored by the ongoing lessons of tolerance and peace that he taught.
Testing for Helicobacter Pylori
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Supplement Editor:
Gary Falk, MD
Contents
Helicobacter pylori: Why it still matters in 2005
M. Brian Fennerty, MD
How to test for Helicobacter pylori in 2005
Nimish Vakil, MD, and A. Mark Fendrick, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Gary Falk, MD; Leonard Ehrlich, MD; A. Mark Fendrick, MD; M. Brian Fennerty, MD; Ben Gold, MD; Nimish Vakil, MD; Derek van Amerongen, MD, MS; and David Wyatt, MD
Pitfalls, pearls, and practicalities in the diagnosis of Helicobacter pylori infection
Other Literature of Interest
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.
1. Carratala J, FernandezSabe N, Ortega L, et al. Outpatient care compared with hospitalization for community-acquired pneumonia: a randomized trial in low-risk patients. Ann Intern Med. 2005;142: 165-72.
The appropriate triage and management of patients with community-acquired pneumonia (CAP) has important implications for patient outcomes and the allocation of health care resources. Despite the availability of validated risk stratification tools significant variability in clinical practice which results in hospitalization rates that are often inconsistent with the severity of illness. In this unblinded, randomized controlled trial, 224 patients with CAP and a low-risk pneumonia severity index (PSI) score between 51 and 90 (class II and III) were randomized to outpatient oral levofloxacin therapy versus inpatient sequential intravenous and oral levofloxacin therapy. Exclusion criteria included quinolone allergy or use within the previous 3 months, PaO2 < 60 mm Hg, complicated pleural effusion, lung abscess, metastatic infection, inability to maintain oral intake, and severe psychosocial problems precluding outpatient therapy. In an intention-to-treat analysis, the primary endpoints, of cure of pneumonia (resolution of signs, symptoms, and radiographic changes at 30 days), absence of adverse drug reactions, medical complications, or need for hospitalization at 30 days were achieved in 83.6% of outpatients and in 80.7% of hospitalized patients. For the secondary endpoint of patient satisfaction, 91.2% of outpatients versus 79.1% of hospitalized patients (p=.03) were satisfied, but there were no differences between groups with respect to the secondary endpoint of health-related quality of life. Mortality was similar between the 2 groups, and although the study was not sufficiently powered to address this outcome, and interestingly there was trend toward increased medical complications in the hospitalized patients.
Limitations of this study include lack of blinding by investigators and questions about whether the results can be generalized given the geographic variation in microbial susceptibility to quinolone antibiotics. As the authors suggest, this study also highlights limitations in the PSI scoring system, given that patients with clinical findings and comorbidities who would never be treated in the outpatient setting may in fact fall into low-risk PSI categories. These concerns notwithstanding, this study adds to our ability to identify an additional subset of patients with CAP who can be safely managed as outpatients.
2. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med. 2005;142:260-73.
Early in the hospital medicine movement, when it was clear that hospitalists provided more efficient care than their colleagues, experience was cited as a reason for this difference. If, for example, a hospitalist cares for patients with community-acquired pneumonia daily, he or she is more likely to make the transition to oral antibiotics sooner, resulting in a shorter length of stay. Everyone recognized the hospitalists were younger, but is it plausible their “inexperience” explained the difference in care?
Choudhry and colleagues explored the available data surrounding clinical experience and quality of care delivered by physicians. They found few studies that specifically evaluated the effects of experience on quality of care. They did find articles that looked at quality of care and included experience or age as part of the physician characteristics
that possibly explained the differences. They reviewed 59 articles, available on MEDLINE, published since 1966. Forty-five studies found an inverse relationship between increasing experience and performance. For example, physicians more recently out of training programs were more familiar with evidence-based therapies for myocardial infarction and more familiar with NIH recommendations for treatment of breast cancer. Experienced physicians were less likely to screen for hypertension and more likely to prescribe inappropriate medications for elderly patients. This led them to the unexpected conclusion that experienced physicians may be at risk for providing lower-quality care and may need improvement interventions. An accompanying editorial by Drs. Weinberger, Duffy, and Cassel of the American Board of Internal Medicine stated, “The profession cannot ignore this striking finding and its implications: Practice does not make perfect, but it must be accompanied by ongoing active effort to maintain competence and quality of care.” They urged all physicians to “embrace the concepts behind maintenance of (board) certification.”
The image of Marcus Welby, MD, would lead one to believe that experience promotes higher quality care. But don’t ask a hospitalist: Many aren’t old enough to remember seeing him on television.
3. Kucher N, Koo S, Quiroz R, et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352:969-77.
March was DVT (deep vein thrombosis) Awareness Month. Despite the availability of numerous guidelines, providers fail to consistently prescribe prophylactic measures against venous thromboembolism (VTE) for their hospitalized patients who meet criteria for prophylaxis.
Kucher and colleagues tested an innovative approach to remind providers to undertake such measures for their patients. They designed a computer program to identify hospitalized patients at increased risk for VTE who were not presently receiving VTE prophylaxis. The program reviewed the records of inpatients on the medical and surgical services and assigned a VTE risk score for each patient based on their history (i.e., history of cancer, hypercoagulability, etc.) and their present medical treatment (i.e., hormone therapy, prescribed bed rest, etc.). For patients considered “high risk” for VTE, the computer reviewed orders to identify ongoing use of VTE prophylactic measures. High-risk patients not receiving prophylactic therapies were randomized into 2 groups. The responsible physician in the intervention group received an electronic alert about the risk of VTE in their patient. No alerts were sent to the physicians in the control group. Physicians who received the alerts were forced to acknowledge the alert by either actively withholding prophylaxis or ordering prophylaxis (mechanical or pharmacologic measures). Patients were followed for 90 days with a primary endpoint of clinically diagnosed, objectively confirmed deep vein thrombosis (DVT) or pulmonary embolism (PE). The primary endpoint occurred in 8.2% of the control group versus 4.9% in the invention group (p<.001). The alert reduced the risk of DVT or PE at 90 days by 41% (p=.001).
The results of the study are interesting. The authors acknowledged that many physicians had patients in both groups. So receiving 1 alert may have affected their use of prophylaxis in both groups. They also could not eliminate the possibility of diagnostic bias. Prophylaxis was not blinded and VTE testing was not routinely performed. Would physicians be more likely to order an imaging study for symptomatic patients on no prophylaxis than patients on prophylaxis? Nevertheless, for hospitals that have sufficient computer resources, implementation of such alerts can elevate physician awareness about VTE and other clinical conditions.
4. Lau DT, Kasper JD, Pofer DE, et al. Hospitalization and death associated with potentially inappropriate medication prescriptions among elderly nursing home residents. Arch Intern Med. 2005;165: 68-74.
Lau and colleagues studied the impact of potentially inappropriate medications among residents of longtermcare facilities. They used information from a 1996 national survey of home residents. The sample included 3372 residents, 65 years and older, who lived in a nursing home for 3 months or longer. Over half of the residents were older than 85 years old and 75% were female. Only 10% were black. Nearly two thirds had dementia or other mental disorders. The study used the Beers Criteria to define potentially inappropriate medications. The potential errors in medications were categorized as 1 of 3 types:
- inappropriate choice of medication
- excessive medication dosage
- drug–disease interactions
Residents were considered to have a potentially inappropriate medication if their medication administration records revealed any of the above findings.
A univariate analysis showed that the risk of hospitalization was almost 30% higher among residents who received potentially inappropriate medications in the preceding month and 33% higher among residents who received potentially inappropriate medications for 2 consecutive months, compared with residents with no inappropriate medication exposure. The odds of death in any month were 21% higher among residents who had inappropriate medication exposure during the month of death or the preceeding month, compared with those with no inappropriate medication exposure.
These findings can be generalized to the inpatient setting, where hospitalists have the opportunity to influence and modify prescribing practices in the elderly population.
5. Lessnau KD. Is chest radiography necessary after uncomplicated insertion of a triplelumen catheter in the right internal jugular vein, using the anterior approach? Chest. 2005;127:220-3.
The routine use of chest radiography to confirm proper triplelumen catheter (TLC) placement may be an unnecessary and costly intervention. Lessnau conducted a prospective observational study of 100 consecutive patients over a 4-month period who required non-urgent TLC placement. The primary operators of the procedure included 18 medical residents, 3 pulmonary fellows, and a pulmonary attending with supervision provided for more junior clinicians. Operators followed a standardized approach to TLC placement utilizing the anterior approach to the right internal jugular vein. Complicated procedures were predefined as any procedure that required more than 3 needle passes, resulted in hemorrhage or hematoma formation (where there was concern for pneumothorax), or an absence of blood return in any of the TLC’s lumens. All subjects underwent routine post-procedure chest radiography to determine proper placement of the catheter and to exclude pneumothorax. A blinded radiologist reviewed these images.
Ninety-eight of the 100 catheters were in proper position. One malpositioned catheter was 7 cm above the right atrium in a patient who was 215 cm (>7 feet) tall. The second was noted to be in an S-shaped position on chest radiography. This procedure had required 20 needle passes and 5 slides of the catheter; additionally, blood return was inadequate in 2 lumens of the catheter. An operator reported a possible complication in 10 other procedures, but the only clinical finding in these cases was the development of a local hematoma in 1 patient. Eighty-eight patients had uncomplicated insertions and had normal chest radiographs. There were no pneumothoraces.
This study demonstrates that in carefully controlled and supervised situations, as described in the study, routine chest radiography may be omitted if the insertion goes smoothly. It is important to note that these results are specific to the technique described in the study (using the anterior approach to the right internal jugular, using a short finder needle to initially locate the vein) and cannot be extrapolated to other methods of TLC insertion. Important limitations of the study include the sample size of only 100 patients and the use of only a single anatomic approach to TLC insertion. These findings, although an important first step, will need to be reproduced on a larger scale before we can recommend the cessation of routine chest radiography after TLC placement on a more widespread basis.
6. Safdar N, Fine JP, Maki DG. Metaanalysis: methods for diagnosing intravascular devicerelated bloodstream infection. Ann Intern Med. 2005;142:451-66.
Intravascular device (IVD)–related blood stream infections are a frequent cause of morbidity and mortality, and yet there is lack of a clear consensus on the most accurate method to make this diagnosis.
In this metaanalysis, Safdar et al. reviewed 185 studies, including 8 different diagnostic tests, for the detection of IVD-related bloodstream infections, of which 51 studies met the inclusion criteria. Tests were divided into IVD-sparing and those requiring IVD removal. Pooled sensitivity and specificity, summary measures of accuracy, and the mean log odds ratio were determined. The most accurate IVD-sparing test was paired quantitative blood cultures (simultaneous blood cultures from the IVD and a peripheral site, with a positive result defined as an IVD-site microorganism concentration 3–5 times greater than peripheral site) with a sensitivity of 0.87 (95% CI: 0.83–0.91) and specificity of 0.98 (95% CI: 0.97–0.99). This was followed by quantitative IVD-drawn blood cultures alone (positive result defined as growth of ≥100 CFU), with a sensitivity of 0.77 (95% CI: 0.69–0.85) and a specificity of 0.90 (95% CI: 0.88–0.92). IVD-drawn qualitative blood cultures had a sensitivity of 0.87 (95% CI: 0.80–0.94) and a specificity of 0.83 (95% CI: 0.78–0.88), and IVD- and peripheral-drawn qualitative blood cultures with differential time to positivity had a sensitivity of 0.85 (95% CI: 0.78–0.92) and specificity of 0.81 (95% CI: 0.81–0.97).
The most accurate test requiring IVD removal was quantitative catheter segment culture (segment of catheter is flushed or sonicated and plated, positive if ≥1000 CFU), with sensitivity of 0.83 (95% CI: 0.78–0.88) and specificity of 0.87 (95% CI: 0.85–0.89), followed by semi-quantitative catheter segment culture (5cm segment plated, positive if ≥ 15 CFU) with sensitivity of 0.82 (95% CI: 0.81–0.89) and specificity of 0.82 (95% CI: 0.80–0.84). The least accurate was qualitative catheter segment culture (positive if any growth) with a sensitivity of 0.90 (95% CI: 0.83–0.97) and specificity of 0.72 (95% CI: 0.66–0.78).
The limitations of this study include heterogeneity of study design, including limited data on the use of antibiotics before culture data was obtained and the baseline prevalence of bacteremia in the study populations. In addition, all data was obtained prior to the widespread use of antibiotic-coated catheters. While these results support the catheter-tip quantitative culture techniques that are already widely in use, they are less applicable to blood culture testing techniques, because quantitative assays are rarely used. Fortunately, all of these assays have a high negative predictive value, and false-positive results can be minimized by reserving testing for patients in whom there is moderate-to-high pretest probability of IVD related bloodstream infection.
7. Sopena N, Sabria M, Neunos 2000 Study Group. Multicenter study of hospital-acquired pneumonia in non-ICU patients. Chest. 2005;127:213-9.
A growing body of literature exists on hospital-acquired pneumonia (HAP) in the ICU setting. Sopena and colleagues extend the HAP literature to the non-ICU setting in a multicenter cross-sectional study. Cases of HAP were identified if clinical or radiographic evidence of pneumonia developed 72 hours after admission or within 10 days of a previous discharge. Patients who developed pneumonia in the ICU were excluded from analysis.
During an 18-month study period, 165 cases were identified with complete clinical and microbiologic data. The incidence of HAP was 3.1 ± 1.4 per 1000 hospital admissions. Ninety-eight (59.4%) patients diagnosed with HAP had severe underlying diseases that were classified as fatal (<1 year) or ultimately fatal (in 5 years). Extrinsic risk factors observed in patients with HAP included concurrent steroid use (29%), antibiotic therapy (53.3%), use of H2 blockers (37%), and hospitalization greater than 5 days (76%). Microbiologic data were positive in 60 (36.4%) cases. Streptococcus pneumoniae was diagnosed in 16 cases (9.7%), enterobacteriaceae in 8 (4.8%), Legionella pneumophila in 7 (4.2%), Aspergillus sp in 7 (4.2%), Pseudomonas aeruginosa in 7 (4.2%). Four cases of Staphylococcus aureus were diagnosed (3%), only one of which was methicillin resistant.
Complications of HAP occurred in 52.1% of cases and included respiratory failure (34.5%), pleural effusion (20.6%), septic shock (9.6%), renal failure (4.8%), and empyema (2.4%). Forty-three (26%) patients died during the hospitalization; 23 of these cases were directly attributed to HAP.
A limitation of the study is that the incidence of HAP was somewhat lower than reported in the literature and thus might represent an unintended sampling bias. Moreover, the study demonstrated underlying factors seen in patients with HAP, but these are not necessarily causative. Results useful to hospitalists include a higher than expected rate of Legionella and Aspergillus sp causing HAP in this population. A Legionella outbreak was not the explanation, as these cases were diagnosed in 5 different hospitals. The high frequency of adverse outcomes associated with HAP should alert hospitalists to the risk of nosocomial pneumonia in the non-ICU setting.