User login
Postdischarge Test Results, Acute Renal Failure, Diagnosing PE
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
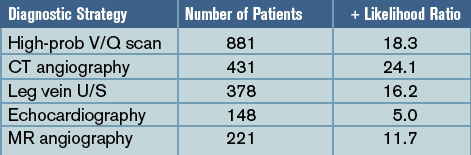
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
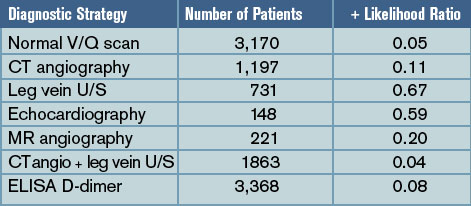
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
Roy PM, Colombet I, Durieux P, et al. Systemic review and meta-analysis of strategies for the diagnosis of suspected pulmonary embolism. BMJ.2005;331:259.
Background: Despite technological advances, the diagnosis of pulmonary embolism remains challenging. A large number of diagnostic tests and strategies have been evaluated and yet the test characteristics of each and their practical use remain unclear.
Methods: Pierre-Marie Roy, MD and colleagues carried out a systematic review and meta-analysis to define the likelihood ratios (LRs) for different diagnostic modalities for pulmonary embolism and provide a simple, evidence-based diagnostic algorithm.
The authors performed a literature search from 1990-2003 identifying all articles that evaluated tests or strategies aimed at diagnosing pulmonary embolism. They only selected papers which were prospective, in which participants were recruited consecutively, and which pulmonary angiography was the reference standard for strategies to confirm pulmonary embolism and clinical follow-up or angiography were used for exclusion strategies.
Results: Forty-eight articles (11,004 patients) met the inclusion criteria and examined ventilation/perfusion (V/Q) lung scanning, computed tomography (CT) angiography, leg vein ultrasound (U/S), echocardiography, magnetic resonance (MR) angiography, and the D-dimer test. For the studies done to evaluate tests to confirm the diagnosis of pulmonary embolism, pooled positive likelihood ratios (+LRs) were calculated and were:
For the studies evaluating tests to exclude the diagnosis of pulmonary embolism, pooled negative likelihood ratios (-LR) were calculated and were:
Discussion: With the pooled positive and negative LRs, Roy and colleagues created a diagnostic algorithm, based on initial pretest probabilities, to help “rule in” and “rule out” the diagnosis of pulmonary embolism. Consistent with prior studies, a calculated post-test probability of >85% confirmed the diagnosis while a post-test probability <5% excluded PE.
In patients with a low or moderate pretest probability, pulmonary embolism is adequately excluded in patients with either 1) negative D-dimers or 2) a normal V/Q scan or 3) a negative CT angiogram in combination with a normal venous ultrasound. In patients with moderate or high pre-test probability, pulmonary embolism is confirmed by either 1) a high-probability V/Q scan or 2) a positive CT angiogram or 3) a positive venous ultrasound. Low-probability V/Q scanning, CT angiogram alone, and MR angiography have higher negative likelihood ratios and can only exclude PE in patients with low pre-test probability.
Many hospitalists are using CT angiography as their sole diagnostic test for pulmonary embolism. Based on the systematic review and meta-analysis by Roy and colleagues, we should proceed with caution as, in some patient populations, a positive or negative “spiral CT” does not adequately confirm or exclude the diagnosis of pulmonary embolism. For those that employ V/Q scanning, MR angiography, or D-dimers, the study also helps define how best to use these tests.
Safdar N, Maki DG. Risk of catheter-related bloodstream infection with peripherally inserted central venous catheters used in hospitalized patients. Chest. 2005;128:489.
Background: In recent years, peripherally inserted central catheters (PICCs) have become more popular, initially for long-term outpatient intravenous therapy but also for inpatient venous access. Traditionally, it was assumed that PICC lines have a lower rate of catheter-related bloodstream infection than conventional central venous catheters (CVCs) placed in the internal jugular, subclavian, or femoral veins.
Methods: One academic medical center prospectively studied the rate of catheter-related bloodstream infection in PICC lines used exclusively in hospitalized patients as part of two trials assessing efficacy of different skin antiseptics. PICC-related bloodstream infection was confirmed when organisms isolated from positive blood cultures matched (by DNA subtyping) organisms isolated from culturing the PICC line at the time of removal. The authors also performed a systematic review of the literature to provide overall estimates of PICC-related bloodstream infection in hospitalized patients.
Results: A total of 115 patients received 251 PICC lines during the study period and the mean duration of catheterization was 11.3 days. More than 40% of the patients were in the intensive care unit (ICU) and most had risk factors for the development of bloodstream infection, including urinary catheterization, mechanical ventilation, prior antibiotic use, and low albumin. Six cases (2.4%) of PICC-related bloodstream infection were confirmed, four with coagulase-negative staphylococcus, one with S. aureus, and one with Klebsiella pneumoniae, a rate of 2.1 per 1,000 catheter-days. In their systematic review, the authors identified 14 studies evaluating the rate of PICC-related bloodstream infection in hospitalized patients; the pooled rate was 1.9 per 1,000 catheter-days.
Discussion: In a small but methodologically sound prospective study and systematic review, Safdar and Maki found a surprisingly high rate of PICC-related bloodstream infection in hospitalized patients. Their calculated rate of 2.1 cases per 1,000 catheter-days is five times the rate seen in PICCs used exclusively in outpatients (0.4 per 1,000 catheter-days). More strikingly, 2.1 cases per 1,000 catheter-days is similar to the rate of catheter-related bloodstream infection in conventional central venous catheters placed in the subclavian or internal jugular veins (two to five per 1,000 catheter-days). Unfortunately, the study didn’t assess the rate of mechanical complications associated with PICC lines or correlate the risk of infection with duration of catheterization.
Hospitalists should be aware that PICC lines likely have the same infection risk as subclavian and internal jugular lines in hospitalized patients and a much higher rate of infection than PICC lines in outpatients. The higher-than-expected rates are likely related to the increased prevalence of risk factors for bloodstream infection in hospitalized patients. Thus, the decision to use PICC lines in hospitalized patients should be made based on factors other than presumed lower infection risk.
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients. A multinational, multicenter study. JAMA. 2005;294:813.
Background: Acute renal failure in critically ill patients is believed common and is associated with a high mortality. The exact prevalence and the calculated risk of death have not been clearly defined across populations.
Methods: A multinational group of investigators conducted a massive prospective observational study of ICU patients who developed renal failure after ICU admission. The study encompassed 54 hospitals in 23 countries with a total of 29,269 admissions over the 14-month study period. Note, acute renal failure was defined as either oliguria (urine output <200cc/12 hours) or BUN >84mg/dL.
Results: Of all ICU patients studied, 5.7% developed acute renal failure after admission and 4.7% of patients received renal replacement therapy (most often continuous replacement). The most common contributing factor to the development of acute renal failure was septic shock (48%), followed by major surgery (34%) and cardiogenic shock (26%). Up to 19% of the cases of acute renal failure were estimated to be drug-related. The in-hospital mortality for critically ill patients with acute renal failure was 60%, which was substantially higher than the mortality estimated by other physiologic scoring systems (45% mortality according to SAPS II). Of those who survived to hospital discharge, only 14% required ongoing hemodialysis.
Discussion: This large, multinational, multicenter prospective observational study helps better define the prevalence and characteristic of acute renal failure that develops in critically ill patients. Overall, acute renal failure in the ICU setting is relatively uncommon, is most often caused by septic shock, and typically does require renal replacement therapy. There was a surprisingly high rate of acute renal failure thought to be secondary to medication or drug effect (19%).
The mortality in patients who develop renal failure in the ICU is high but, surprisingly, if patients survive, they are unlikely to need long-term hemodialysis. The study is limited in that it was not randomized and outcomes associated with particular interventions could not be determined. Yet, the data adds to our understanding of acute renal failure in the ICU and knowledge of the prevalence and expected outcomes could potentially help with prognosis and end-of-life discussions in the intensive care unit.
Roy CL, Poon EG, Karson AS, et al. Patient safety concerns arising from test results that return after hospital discharge. Ann Intern Med. 2005;143:121.
Background: Adequate communication between hospitalists and outpatient providers is essential to patient safety as well as patient and physician satisfaction. It is estimated that more than half of all preventable adverse events occurring soon after hospital discharge have been related to poor communication among providers. With increasing pressure to limit inpatient length of stay, patients are often discharged with numerous laboratory or radiologic test results pending.
Methods: Roy and colleagues at a tertiary care academic medical center prospectively determined the prevalence and characteristics of tests pending at discharge and assessed physician awareness as well as satisfaction. All patients discharged from two hospitalist services over four months in 2004 were followed. Researchers identified all pending test results for these patients and all abnormal tests were reviewed by study physicians and judged to be “potentially actionable” or not (if it could change the management of the patient by requiring a new treatment or diagnostic test, change in a treatment, scheduling of an earlier follow-up, etc).
Results: Of the 2,644 patients discharged, 1,095 (41%) had laboratory or radiographic tests pending. Approximately 43% of all pending tests were abnormal and ~10% of the pending tests were judged by physician-reviewers to be potentially actionable. Examples include a TSH that returned as <0.01 mU/mL after discharge in a patient with new atrial fibrillation, or a urine culture that grew an organism resistant to the antibiotics given at discharge. Of note, outpatient physicians were unaware of two-thirds of the “potentially actionable” results. Finally, when surveyed, the majority of inpatient physicians were concerned about appropriate follow-up of tests and dissatisfied with the system used.
Discussion: Roy and his coauthors attempted to quantify the prevalence of potentially actionable laboratory tests available after discharge and published rather striking findings. Up to half of all patients have some tests pending at discharge and up to 10% of these require some physician action. More frighteningly, outpatient MDs are generally unaware of these tests creating a huge gap in patient safety in the transition back to outpatient care.
How can we do this better? SHM and the Society for General Internal Medicine have convened a Continuity of Care Task Force and found poor communication with outpatient providers was a common and potentially dangerous problem. They outlined the best practices for the discharge of patients to ensure safety as well as maximize patient and physician satisfaction. Their recommendations are available on the SHM Web site. All hospitalists and institutions should be aware of the potential for missed results and put systems in place, electronic and otherwise, to create an appropriate safety net for our discharged patients.
Sharma R, Loomis W, Brown RB. Impact of mandatory inpatient infectious disease consultation on outpatient parenteral antibiotic therapy. Am J Med Sci. 2005;330(2):60.
Background: As the pressure to limit healthcare costs by reducing inpatient length of stay has increased, the use of outpatient parenteral antibiotic therapy has grown. When employed appropriately, home intravenous antibiotic therapy has consistently resulted in cost savings without compromising patient outcomes. As with other healthcare advances, there is some fear that outpatient parenteral antibiotic treatment will be overused or misused, limiting the cost savings or putting patients at risk.
Methods: A single academic medical center instituted mandatory infectious disease consultation on all patients referred to discharge coordinators with plans for outpatient IV antibiotic treatment. The infectious disease consultants helped to determine the need for outpatient parenteral therapy and antibiotic choice. All patients were followed for 30 days.
Results: Over the one-year study period, 44 cases received mandatory infectious disease consultation. Thirty-nine (89%) of these had some change in antibiotic regimen after the consultation. Seventeen patients (39%) were switched to oral antibiotics, 13 (30%) had a change in infectious disease antibiotic, and 5 (11%) had a change in antibiotic dose.
Skin and skin structure and intra-abdominal infections were the most common diagnoses for which antibiotics were changed; a typical change was from intravenous piperacillin/tazobactam to an oral fluoroquinolone plus oral anaerobic coverage. At 30-day follow-up, 98% of patients finished their courses without relapse or complication. The overall costs savings was $27,500 or $1,550 per patient consulted upon.
Discussion: Although from a small, nonrandomized, single-institution study, the results are impressive. Mandatory infectious disease consultation prior to discharge for patients scheduled to received outpatient parenteral antibiotic therapy resulted in substantial cost savings, and streamlined and more appropriate antibiotic regimens without any adverse impact on outcomes. Hospitalists should take two things away from this study: 1) consider consulting infection disease specialists on all patients who might be candidates for home IV antibiotics and 2) be aware that many skin and skin tissue and intra-abdominal infections can often be treated with oral therapy. TH
PEDIATRIC SPECIAL SECTION: Children’s National Medical Center’sHospitalist Division
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Although pediatric resident graduates are well prepared to care for many ill children who require hospitalization, there are clinical, academic, and administrative skills that aren’t a standard part of residency, but are necessary for long-term academic success. The Children’s National Medical Center (CNMC) Hospitalist Fellowship program is structured over three years, through a combination of formal course work, seminars, clinical work, and mentored independent study.
Fellows work under the supervision of faculty in our 20-member Hospitalist Division, with inpatient pediatric services at five hospitals in Washington D.C., and suburban Maryland. A faculty appointment as a clinical instructor of the George Washington University (GWU) School of Medicine and Health Sciences qualifies the fellow to complete a Masters in Public Health, taking 15-18 credits per year. In addition to specific clinical, research, and didactic learning objectives, participation in committees and quality improvement and epidemiologic projects will facilitate study of hospital administration, budget, epidemiology and infection control.
The fellow must be a successful graduate of an American Council of Graduate Medical Education approved pediatric residency.
Clinical Training
Fellows spend approximately three months during the three year fellowship in the pediatric intensive care unit, two weeks in anesthesia, and two months in the emergency department to gain increased confidence, knowledge, and skill in airway management, placement of central lines, evaluation and management of the severely ill/injured child (respiratory failure and shock), conscious sedation, and pain management.
In addition, fellows spend 12 weeks per year on the CNMC hospitalist service. They co-attend with a CNMC hospitalist and lead a team of residents and students to practice an evidence-based approach to the acute evaluation and management of common inpatient problems such as bronchiolitis; asthma; gastroenteritis and dehydration; pneumonia; UTI; ALTE; common head, neck, skin and musculoskeletal infections; metabolic disorders; HIV infection; rheumatologic disease; and child abuse. Fellows also devote eight weeks per year to studying the process of providing coordinated care for the medically complex/technology dependent patients at CNMC and at rehab/subacute care hospital units that focus on improving care for children with multiorgan system disease. They also learn about complications associated with use of technology. Fellows’ elective clinical time may focus on delivery room management skills and well-baby teaching and management issues at one of our community hospital sites with 8,000 deliveries annually.
Research Training
CNMC fellows learn to plan, implement, analyze, and present results of a research study to answer a question relevant to hospitalists. By the end of the fellowship the fellows have an article accepted for publication in a peer-reviewed journal and present findings at a national meeting. To gain knowledge and skill needed to conduct an independent research project the fellows complete coursework in the School of Public Health at GWU and work under faculty mentors at CNMC.
Didactic Training
Four faculty members of our Hospitalist Division have completed the CNMC Master Teacher Certificate program with the GWU School of Education. In seminars taught by master teachers, fellows learn to lead, teach, and develop educational programs effectively. Faculty observe the fellow’s teaching skills in a variety of settings and provide feedback. Fellows have the opportunity to participate and develop computerized and standardized patient simulations to assess residents’ and students’ ability to care for pediatric inpatients.
PEDIATRIC SPECIAL SECTION
In the Literature
Formula Supplementation Prophylaxis for Jaundice in Breastfed Newborns
Gourley GR, Li Z, Kreamer BL, et al. A controlled, randomized, double-blind trial of prophylaxis against jaundice among breastfed newborns. Pediatrics. 2005;116(2):385-391.
Question: In breastfed newborns does oral beta-glucuronidase inhibitors during the first week after birth increase fecal bilirubin excretion and reduce jaundice without affecting breastfeeding deleteriously?
Design: Randomized (randomization table), double-blinded (supplements were prepared by a third party and labeled by a code) controlled trial.
Setting: Clinic.
Patients: 69 newborns, Caucasian, >37 week of gestation who were exclusively breastfed.
Intervention: Patients were randomly assigned to four groups: breastfeeding only (control), L-aspartic acid supplementation (L-aspartic), enzymatically hydrolyzed casein (EHC), and whey/casein-supplement without beta-glucuronidase inhibitor (W/C).
Main outcome measure: Daily transcutaneous and fecal bilirubin levels were obtained. Long-term follow-up assessments included age at first formula feeding, breastfeeding cessation age, and mother’s subjective impression of study.
Main results: Infants in all supplementation groups had significantly lower transcutaneous bilirubin levels in the first week of life than the nonsupplemented infants. The EHC and W/C groups both excreted more bilirubin diglucuronide and bilirubin monoglucuronide than the control group, and the L-aspartic acid had increased bilirubin monoglucuronide excretion compared with the control group. No negative effects from the supplementations were noted.
Conclusions: There is a significant reduction in transcutaneous bilirubin levels, with no negative effects on breastfeeding through the administration of specific supplements that are currently found in infant formulas.
Conflict of interest: None declared.
Commentary: The study describes a possible method of reducing hyperbilirubinemia associated with breastfeeding that employs small-volume supplementations of ingredients found in common infant formulas. The study did not reveal any negative effects on breastfeeding. Though the study was described as blinded the authors do not comment on how the exclusively breastfed infant group was blinded from the researchers and family.
The other control group (W/C) not fed a supplement without a beta-glucuronidase inhibitor yielded the unexpected significant reduction in transcutaneous bilirubin level compared with the control. This may mean that there is at least one other mechanism for the reduction of bilirubin in formula-fed infants than initially proposed by the authors.
In their conclusion, the authors pose a hypothesis explaining this result. They also correctly point out that due to this small study population, larger studies are needed to confirm these results.
This study used transcutaneous bilirubin measurements raising the question of reliability of this method compared to serum bilirubin measurements. A search of Medline using the terms “bilirubin and transcutaneous” produced a technical report.1 One section of this article reviewed available studies on the accuracy of transcutaneous bilirubin measurements concluding that the transcutaneous measurement has a linear correlation to serum bilirubin and its use for hyperbilirubinemia screening is reliable.
Reference
Ip S, Chung M, Kulig J, et al. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. An evidence-based review of important issues concerning neonatal hyperbilirubinemia. Pediatrics. 2004;Jul;114(1):e130-153.
Comparing Controllers: Montelukast and Fluticasone in Mild Persistent Asthma
Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with fluticasone, for control of asthma among 6- to 14-year-old patients with mild asthma: the MOSAIC study. Pediatrics. 2005;116(2):360-369.
Question: In children with mild asthma is the use of an antileukotriene medication as effective as an anti-inflammatory agent in maintaining number of days without the need of a rescue medication or utilization of asthma-related health resources?
Design: Multicenter, double-blind, double-dummy, randomized, parallel-group study. A four-week, single-blind, placebo run-in period was done prior to the initiation of the double-blind portion of the study. This run-in period included three clinic visits. During this time all participants discontinued any asthma controller medications and received image-matching, single-blind, montelukast and fluticasone. A short acting beta-agonist medication (open label) was also provided. Medication usage teaching was done during this time period. There was no placebo control group.
Setting: 104 study sites in 24 countries.
Patients: Patients (six-14 years of age) with mild persistent asthma as defined by the Global Initiative for Asthma (GINA) guidelines and otherwise in good health. Patients were required to have a FEV1 of ≥80% while the beta-receptor agonist was withheld for more than six hours in the first two visits and ≥70% on the third visit of the run-in period.
Intervention: Patients were randomized to receive either montelukast (5 mg oral before bedtime or 10 mg for patients ≥15) or fluticasone (100 mcg through MDI twice a day) and the appropriate placeboes.
Main outcome measures: Percentage of asthma rescue-free days (RFD).
RFD was defined as a day without:
- The use of a rescue medication: defined as any day during which a beta-receptor agonist, a systemic corticosteroid, or other rescue medications were used; and
- The use of an asthma health resource: defined as an unscheduled visit to a physician, an urgent/emergency care center or a hospital.
Main results: The number of RFDs were statistically similar between both groups. Mean percentage of RFD was 84% in the montelukast group and 86.7% in the fluticasone group.
Conflict of interest: Two of the study authors were employees of Merck and Company, which markets montelukast.
Commentary: This is an extensive study with multiple outcome measures. The study mimics actual clinical experience by using clinically relevant end points as primary outcomes. The study does not have a placebo control group. Overall the study showed that there is no significant difference between montelukast and fluticasone with regard to the primary outcome of RFDs, but there were some differences favoring fluticasone in secondary outcome measures, including number of days of beta-receptor agonist use and improvement of the average score of the control domain of the Pediatric Asthma Therapy Assessment Questionnaire.
K. Kingae Causes Osteomyelitis/Septic Arthritis
Kiang KM, Ogunmodede F, Juni BA, et al. Outbreak of osteomyelitis/septic arthritis caused by Kingella kingae among child care center attendees. Pediatrics. 2005;116;e206-213.
Review by Julia Simmons, MD
Kingella kingae (K. kingae), a gram-negative organism known to colonize the oropharynx, may cause invasive diseases, such as septic arthritis and osteomyelitis in children who were previously healthy. In this article, the authors describe the first reported outbreak of K. kingae causing osteomyelitis/septic arthritis.
In October 2003 the Minnesota Department of Health was notified of an outbreak of K. kingae at a daycare facility. There were two culture positive cases and one culture negative but clinically presumed to be secondary to K. kingae. The children were all in the same classroom (toddler classroom 1) and were between the ages of 17 and 21 months. The previously healthy children presented with fever and limp.
In this cohort study, the authors investigated risk factors for invasive disease and for colonization with K. kingae. They also determined the prevalence of asymptomatic colonization at the daycare involving the confirmed cases and at a second daycare facility, which served as the control. Culture samples were analyzed at the Minnesota Department of Health Public Health Laboratory. The laboratory performed confirmation, pulsed-field gel electrophoresis, DNA sequencing, and antimicrobial testing specifically with rifampin, penicillin, and azithromycin.
At the study facility 115/122 (94%) children and 28/29 (97%) adult staff members were cultured. Fifteen (13 %) of the children were colonized. The prevalence of colonization was 45% (9 children) in the toddler 1 classroom, which is the classroom of the confirmed cases. The three case patients had negative oropharyngeal cultures; however, all three had been pretreated with antibiotic therapy. The pulsed-field gel electrophoresis was indistinguishable in the confirmed cases and the colonized students. The authors did not discover any risk factors for invasive disease. This information was gathered from a list of questions regarding past medical history, which the parents discussed on the telephone with the investigators. Rifampin, penicillin, and azithromycin all had low MICs
At the control care center, 45/118 (38%) of people were cultured from the oropharynx. Seven (16%) were colonized. The pulsed-field gel electrophoresis was the same for the control care facility, but varied from the electrophoresis pattern at the study facility.
In conclusion, the authors summarized the findings of K. kingae osteomyelitis/septic arthritis in a daycare facility. There were no identifiable risk factors for invasive disease or for asymptomatic carrier state. It is important to remember that up to 50% of culture negative cases of septic arthritis in patients less than two years of age may be attributed to K. kingae. Thus, the clinician must maintain a high index of suspicion and relay this information to the laboratory so that appropriate measures are taken to ensure the optimal growth environment for the bacteria.
Although the study size was small, the investigators provide initial documentation regarding outbreaks of invasive K. kingae infections. Further studies will be useful to clarify the exact mode of transmission and appropriate duration of antimicrobial therapy.
Systematic Review of Therapy for Pediatric Migraine
Damen L, Bruijn JKJ, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics. 2005;116(2):295-302.
Migraines affect 3%-5% of prepubescent children. The symptoms frequently include unilateral throbbing headache associated with nausea and vomiting. If poorly controlled, the headaches can cause students to miss school and have a decreased quality of life. Symptomatic pharmacologic interventions involve analgesics, triptans, and antiemetics. Nonpharmacologic interventions include dietary changes, biofeedback, and exercise. Treatment is tailored to the patient; however, there are limited studies providing evidence describing the most efficacious pharmacologic treatment for managing symptomatic migraines.
The authors conducted a retrospective literature review to evaluate the evidence from randomized controlled trials (RCT) and clinical controlled trials (CCT) regarding the treatment of symptomatic migraine in children younger than 18. The primary outcome measure was headache clinical improvement defined as a headache decline by >50%. Secondary measures included headache intensity, frequency, duration, and headache index. The authors searched Medline, Embase, PsychInfo, Web of Science, and Cinahl from the start of the databases to June 2004. They used appropriate search terms including “headache,” “migraine,” “child” and variations thereof. Further, they searched reference lists of the articles and the included studies. Two authors independently reviewed the titles and abstracts to determine acceptability in the study. They also used the Delphi list to assess the methodologic quality of the included trials.
Of 3,492 relevant studies, 10 met the inclusion criteria specified by the authors. There were a total of 1,575 patients with a mean age of 11.7 +/- 2.2 years included in the study. A mean of 19.8% of subjects did not complete participation in their respective studies. Overall, the percentage of male and female participants was equal. Six studies were considered to be of high quality by the authors. They found moderate evidence that ibuprofen and acetaminophen were more effective in decreasing headache symptoms one and two hours after ingestion in comparison with a placebo. Further, the nasal spray sumatriptan was more efficacious in diminishing headache than placebo; however, it was associated with more side effects. Intravenous prochlorperazine was more effective than intravenous ketorolac in diminishing symptoms one hour after intake.
While accomplishing a sound systematic review of the available controlled trials, the authors conclude that there are insufficient trials of adequate quality to fully elucidate the most efficacious symptomatic pharmacologic therapy for pediatric patients suffering from migraine headaches. A large randomized prospective trial comparing analgesics, triptans, and antiemetics against placebo is needed. TH
Evidence Based Medicine for The Hospitalist
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
Each of us asks dozens of clinical questions every day. Sometimes the answers are clear: If our question is “Which statin is on formulary?” the answer will be provided to us by a patient’s insurance plan or by our own hospital pharmacy. Many times, however, the answers to our questions aren’t so well defined. Further, these are often the questions that most affect patient care: This is precisely why we ask them in the first place. Many of us give little thought to how we state our questions, but the format of a question can have a dramatic effect on whether or not we will be able to locate an answer. There is an art to asking clinical questions in a manner that maximizes our ability to find a meaningful answer in an efficient way.
Consider an example: We are seeing a 72-year-old man newly diagnosed with a stage II (T2M0N0) renal cell carcinoma. We are curious about treatment options, so we might ask, “Should all cancer patients receive chemotherapy?” It is intuitively clear that the answer to this question depends on a multitude of variables not clarified in the question.
For example, different types of cancer respond differently to chemotherapy and there are innumerable chemotherapy regimens, each having differing mechanisms of action. The patient’s age and gender may matter, and the patient’s medical history will almost certainly affect treatment options. As stated the question is essentially impossible to answer.
A better question might be, “Among men over age 65 with stage II renal cell carcinoma, does post-resection chemotherapy prolong survival compared with nephrectomy alone?” This question is far more specific and therefore more relevant to our individual patient. It is also more likely to yield an answer when we search for one. The point of this somewhat extreme example is that a clear, focused clinical question will usually lead to more precise answers. A vague question will often lead only to frustration.
Construct an Effective Clinical Question
How, then, can we phrase questions to optimize our chances of obtaining clinically helpful answers? One approach is to adopt the PICO or PICOT format. (See “Illustration of PICOT Approach to Clinical Questions,” p. 32.) This format provides a structure for question formation that emphasizes the elements most questions are designed to address: the patients of interest, the intervention in question, what it will be compared with, and what outcome we wish to assess.
The first element (P) represents the patient or population of interest. The aim is to define a group of patients similar to the one prompting the question. For example, our patient is a 72-year-old man with stage II renal cell carcinoma, so we would like to find information on patients that at least approximately fit this description.
The second element (I) represents the intervention, which is usually fairly straightforward to determine if the question relates to a choice of treatments. However, this can also be the prognostic factor or exposure of interest, depending on the type of study and specific question. In our example, the intervention is post-resection chemotherapy, and our clinical question needs to incorporate this information.
The third element (C) is the comparison of interest, if appropriate. For some questions there may not be a comparison, such as when we simply want to know how often a certain side effect occurs. In our example, though, the comparison group is patients treated with surgical resection alone.
The final element (O) is the outcome. The aim here is to define the specific result you are interested in. This will be patient survival in many cases, but it can also be incidence of side effects, correct diagnosis of disease, or any number of other possibilities. In the example, the outcome of interest is survival. We might wish to further refine this by imposing a time at which we would like to assess survival, leading us to look at five-year survival rates, for instance.
An additional element that can be helpful to consider at this stage of the EBM process is what type (T) of question you are asking or what type of study would answer your question. Questions regarding treatment interventions are often questions of therapy and may suggest a search for randomized controlled trials or meta-analyses. Questions regarding the most appropriate diagnostic tests will be best answered by different types of studies. There are many possible types of questions and quite a few types of studies (the Guyatt and Rennie text in “Recommended Reading”(this page, top left) provides many excellent examples), but taking a moment to consider your options can further refine your subsequent search strategy and is well worth the time.
Advantages of the PICOT Question Format
The PICOT approach to constructing clinical questions focuses questions, allowing us to clarify exactly what we hope to answer. This format also provides insight into possible sources that may yield the answers we seek. For example, the question, “How are the stages of renal cell carcinoma defined?” This is a so-called background medical knowledge question and may be answerable by simply reviewing a textbook rather than conducting a complex and exhaustive literature search.
On the other hand, the more specific foreground question outlined in “Illustration of PICOT Approach to Clinical Questions” will likely require a more detailed search of the latest clinical trials.
Finally, this format facilitates the terms we will actually use when conducting the literature search. In many cases, the search terms may be lifted directly from the clinical question, and the PICOT approach typically suggests multiple search terms that can narrow your search. We will explore this further in the next entry of this series.
Summary
Constructing effective clinical questions is an important step in the EBM process. The well-built question makes searching for answers simpler, saving time and effort. The PICOT approach provides a structure flexible enough to accommodate almost any question, and leads directly to more effective search strategies. We will explore search strategies further in the next installment of this series. TH
Dr. West practices in the Division of General Internal Medicine, Mayo Clinic College of Medicine, Rochester, Minn.
The Future of Critical Care
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times

“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times
“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
Critical care is starting to face some tough obstacles, and the ICU of the future will be shaped by these problems—namely an aging population and a shrinking field of expert critical care practitioners. Because of these impending changes, in 20 or 30 years your hospital’s ICU must look different and work differently in order to handle a steady influx of critically ill patients.
This installment of our “Hospital of the Future” series will examine how the hospital of the future will deal effectively with the supply-and-demand quandary that is already becoming apparent in the ICU. It will also examine future possibilities for staffing structure, introduction of critical care guidelines, and groundbreaking technical solutions. Prospects for critical care may look questionable now, but solutions are available. And the future just might be brighter than expected.
Supply and Demand of Critical Care Demands Change
Current trends in both the U.S. population and the demographics of critical care staff dictate that critical care must change—and fast. With millions of baby boomers aging, demand for critical care facilities within hospitals will increase.
“There’s little question that critical care is used disproportionately by the elderly,” says Timothy Buchman, MD, PhD, FACS, FCCM, past president of the Society of Critical Care Medicine (SCCM) and professor at Washington University School of Medicine, St. Louis. “The demand can only increase as the population ages.”
At the same time, there are already too few critical care providers in the United States. “If we designed an ideal ICU for every hospital in the country, we could only staff about one-third of them” right now, says Thomas Rainey, MD, FCCM, president, CriticalMed, Inc., Bethesda, Md.
Critical care experts are, of course, the key to quality care in the ICU. But the population of both specially trained intensivists and experienced ICU nurses is declining. The average age of an ICU nurse is now 47, and they are not replaced fast enough.
“Critical care nursing is brutally hard work; it’s physically, emotionally, and spiritually grueling,” points out Dr. Buchman. “The challenge is keeping experienced nurses from leaving because they’re burned out. We need to keep their knowledge and experience, possibly by creating new positions where their knowledge, experience, and accumulated wisdom can be used to benefit the next generations of patients and providers.”
As for physicians, fewer are choosing critical care, which will likely lead to significant staffing issues. “The number of doctors choosing a career in critical care is leveling off,” says Dr. Buchman. Part of the problem is an educational system that helps medical students choose a specialty.
“We have a direct training path to many specialties through residencies,” he says. “There is no residency in critical care medicine. Instead, we ask people to initially train as something else. We’ve created an educational barrier.”
The upshot of these trends, says Dr. Rainey, is that “the graying population and the loss of [critical care] staff is a collision waiting to happen.”
Dr. Buchman adds, “The question is: How do people organize themselves and leverage technology to address this gap and improve the quality of care?”
How Technology Fits In
In 2001, Richard L. Craft, MSEE, wrote of “Trends in Technology and the Future Intensive Care Unit” ( . 2001;29[8 suppl]): “ … advances in networking are likely to redefine the physical and organizational boundaries of the critical care unit. No longer a self-contained entity … tomorrow’s critical care units are likely to regularly draw on resources—both human and technological—located outside the unit’s physical space.”
The solution to staffing shortages in ICUs lies in using technology that is already available to hospitals.
“Remote monitoring will help leverage existing manpower,” says Dr. Rainey. One option is electronic ICUs—or eICUs, which allow an intensivist and ICU nurse to monitor and manage part or all of the patient population in their organization’s ICU(s) from off-site, if applicable. This remote monitoring supplements on-site hospital staff, but allows fewer specialists access to more patients.
“eICU with smart alerts, physiologic status boards, [and] color-coded assessments of response to protocolized care may help hospitalists and intensivists on-site manage increasingly busy and acute ICUs,” says Dr. Buchman. “The greatest impact will be to facilitate the transformation of data into information and to highlight factors that are of greatest immediate importance.”
In addition to maximizing medical staff, eICU systems can also leverage technical support. Craft writes, “… it is easy to foresee a day when a network of hospitals might centralize its critical care application servers and patient record servers in one location to reduce IT staff overhead, standardize clinical protocols, and automate corporation-wide quality control mechanisms.”
With an eICU system, cameras, monitors, and communication devices provide information on each patient, and can even provide treatment recommendations or guidelines.
“eICU systems are evolving now,” says Dr. Buchman. “They synthesize data streams and allow us to stratify information with respect to how important it is. We’ve [already] had a few components, such as bedside hemodynamic monitors. For each individual patient, a sophisticated system should be able to take data from multiple systems, integrate it, and provide a snapshot of how that patient is doing. Take that throughout the entire ICU and have a display that presents instant pictures of how the ICU is doing. [Have] inventories presented in parallel to providers so they can see where problems are.”
Dr. Buchman predicts that in the future ICU care providers will take on more duties as managers of care.
“ICU providers will go through an evolution like airline pilots did,” he says. “These days, airline transport pilots don’t spend a lot of time actually flying the plane. There are plenty of autopilots and subsystems that do that. The pilot now spends most of her time managing the system, and intervenes as necessary to bring everything into harmony. I think this same type of sophisticated presentation will evolve in the ICU to provide a safer environment that uses the available human resource most efficiently. It won’t save on manpower, but it will greatly increase patient safety.”
J. Christopher Farmer, MD, FCCM, Division of Pulmonary and Critical Care, Mayo Clinic College of Medicine, Rochester, Minn., agrees—especially as relates to disaster response.
“We need technology that doesn’t rely on human factors,” says Dr. Farmer. During a hospital’s disaster response, “we miss things because we don’t notice them. We need automation of systems that will push information to us as computerized analysis; systems that look at everything, including lab results, and postulate on that information. This would help in critical care and could be used in disaster settings as well.”
Dr. Farmer’s vision includes automatic monitoring. “Ideally, I’d like to see every patient have a patch that reads their heart rate, oxygen levels, etc.,” he says. “This 100% monitoring of every patient is applicable in disaster medicine because otherwise you need a person to manually hook up monitors and check vitals on each patient.”
The evolution of ICU technology must focus on bridging the gap between limited staff and growing patient population as well as the gap between adequate care and excellent care.
“Technology is there to serve the patient first, but most importantly, to serve the care alliance of patients and practitioners,” says Dr. Buchman “I think some [advancements] are simply technical toys that are replacing what humans can already do.”
Technology can help identify a disease outbreak or other disaster faster than humans can. Some hospital systems are using surveillance systems that link across their facilities to find patterns. These systems can be used to find medical errors, but they can also act as bio-disease surveillance systems, which can be used to identify a sudden outbreak.
“Say three different hospitals each admit one patient with diarrhea,” says Dr. Farmer. “What if this is the beginning of an outbreak of something? A system that links across hospitals can find these patterns.”
The Critical Care Team of the Future
Today’s most highly developed ICUs are utilizing trained critical care teams to ensure the best possible care. In the future, all ICUs will follow this model in order to improve patient safety and efficiency of care.
These teams can include “not only physicians and nurses, but also respiratory therapists, nutritional support staff, and pharmacists, who collectively function as a highly integrated team, following protocols,” says Dr. Buchman. “This team formulates a patient plan together and evaluates the impact of that plan. I think we’re seeing more of that now, and we’re going to see a lot more of it. It’s a continuum; a growth process.
“This is not restricted to medical care; it will include social and spiritual care as well, with a team of case managers, social workers, and chaplains,” he continues. “These professionals contribute to the integrated care plans.”
Dr. Rainey agrees. “We’ll see a reorganization of physician services into an intensivist team model,” he predicts. “The development we’ve seen over the last 20 years is that outcomes are better with a unit-based special team that manages patients in cooperation with the primary care physician. In fact, this approach has shown something like a 30% decrease in risk for mortality.”
This team approach also applies to hospital disaster preparedness. In his white paper “Hospital Disaster Medical Response: Aligning Everyday Requirements with Emergency Casualty Care,” Dr. Farmer says, “ … we are witnessing the rapid development and emergence of medical emergency teams, or rapid response teams within the hospital. … These teams are intended to monitor inpatients and intervene before physiological deterioration supervenes. One might ask, in the event of a medical disaster, could these teams be repurposed for sophisticated casualty care and ICU expansion? We think it is logical that these types of critical care ‘outreach’ teams, in conjunction with noncritical care hospital personnel, could be leveraged as an effective strategy to extend ICU capabilities during a disaster.”
Having a complete team of ICU providers address each patient’s needs will vastly improve quality of care, but these teams must have some guidelines to follow in order to ensure that they work at maximum efficiency.
Critical Care Guidelines: An Integral Component
Critical care experts shy away from such buzzwords and phrases as “standardization of care” in regard to ICU practices, but they do agree that universal guidelines will be the norm in the future.
“We’ll see the development of drastically improved outcomes, and reduction in harm through reliable processes,” says Dr. Rainey. “We can see, for example, that five things need to be done to every ventilated patient. With development of reliable processes in place, we can see that we will close the gap between intent and actual execution.”
Dr. Farmer agrees. “We do clinical guidelines for everyday issues, so I don’t see why we can’t do the same thing” for critical care and disaster preparedness.
Critical care is ripe for integrating clinical practice guidelines. “There are certain types of interventions that are near universal in ICUs,” says Dr. Buchman. “How we sedate patients, how we relieve pain, how we liberate someone from mechanical support … having touchstones or guidelines for these interventions will help. This is complementary to standardization of care.
“Here’s an example: A patient is admitted with a myocardial infarction. We would treat him with beta-blockers, nitrates, heparin, and aspirin. We don’t think of a standard dose of beta-blockers because the dose must be titrated to [have an] effect on the individual patient,” he continues. “How this individualization is done safely involves organizational guidelines. Systematic implementation of such guidelines will be the difference between good ICUs and great ICUs. The implementation is a continuous four-step process—learn the recommendations, deliver the care, measure the outcomes, and find ways to improve.”
Hospitalists and Critical Care
In concert with technologic advancement and improved guidelines, one major solution to the staffing shortage is hospitalists. According to Dr. Farmer, a large portion of critical care services across the country is provided by family practitioners and general internists. The demographics of the population, combined with the current system of training, ensure inadequate staffing. That shortage could be filled by hospitalists. For many hospitalists ICU care is already an important and satisfying arm of their practice. It may become necessary in the future to define skill sets to work in critical care areas. Hospitalists are well positioned to fill that need.
Looking Ahead
The area of critical care may be moving more quickly toward the future than other hospital functions because it must do so in order to continue to work at all. The success of achieving a future of quality care, patient safety, and adequate staffing rests on a different approach with providers and technology.
“We have to learn to work smarter to leverage new technology and the expertise of all other experts in other fields,” says Dr. Buchman of the future of critical care.TH
Chicago-based Jane Jerrard will write future installments of this series.
FLASHBACK:
An Ill Wind
An 1883 tornado strikes a familiar chord in today’s hurricane-ridden times
“An ill wind”—these were the opening words spoken by William Worrall, MD, at the official opening ceremony for St. Mary’s Hospital in Rochester, Minn. The hospital had been conceived following the destruction wrought on Rochester by a tornado that had left 37 dead and more than 200 injured six years earlier.
Aug. 12, 1883, was a particularly hot day, and many residents must have been hopeful of relief as they saw black clouds looming to the west late that evening. That evening Dr. William Mayo’s sons, Will and Charlie, were headed to the slaughterhouse northwest of town in the part of Rochester then known as the Lower Town to purchase a sheep’s head for eye dissections. The butchers had closed early because of the impending storm and advised the young Mayos to head back posthaste.
The cyclone descended just as they crossed a bridge, which was torn loose of its moorings, over the Zumbro River. They witnessed buildings smashed to bits, a grain elevator toppled, and railroad cars wrecked by the destructive force. They were almost killed by a heavy cornice that had ripped off the Cook House and smashed into their buggy. The Cook House was adjacent to the Cook Block that housed the offices of the Doctors Mayo. Though their buggy was destroyed, they survived and took shelter with their horse in a blacksmith’s shop.
They survived the storm, but others were not so lucky. One-third of the buildings in town were destroyed or damaged with more than half in Lower Town, a predominantly working class neighborhood. They immediately began to care for the wounded brought to the clinic offices. Their father had taken charge of relief efforts in Lower Town, the worst hit part of the city. Victims were brought to a local hotel, where they were quickly triaged and treated according to need.
The physicians in town shared a common goal though they were not always united in their methods. The routine use of an emetic for all trauma patients was advocated by one physician to the opprobrium of the elder Dr. Mayo, who quickly insisted on establishment of clear leadership. He also recruited the assistance of Sister Alfred Moes, who had offered her convent to shelter the sick and homeless and her nuns as nurses for the injured.
The anti-Catholic prejudices of the day necessitated Dr. W. Mayo asking that it be announced that Sister Alfred was offering shelter in her “house” and not in a convent. Other relief efforts such as offering food and provisions to the needy were established in available rooms across town. Recovery of bodies, funeral services, and burials were quickly conducted. Rebuilding efforts were speedily begun with fundraising activities bringing in enough funds to feed and clothe hundreds, rebuild more than 100 houses, and provide money for furniture.
The tornado had highlighted the need for a hospital in Rochester and Sister Alfred ultimately requested that Dr. W. Mayo assist in this venture. The Sisters of Saint Francis raised money and built Saint Mary’s Hospital—the first in Rochester.
The destruction and chaos caused by Hurricane Katrina has brought much pain to our nation. In the early aftermath there appeared to be a dearth of leadership, and questions arose regarding an apparent lack of preparedness and poor response to the carnage caused by the storm. Undoubtedly there will be many investigations into what went wrong. History may help answer these questions, but should also provide reassurance that good can come out of the debris of an ill wind.
—Jamie Newman, MD, FACP, and Adeboye B. Ogunseitan, MD
The Surviving Sepsis Campaign
The incidence of severe sepsis (sepsis with organ dysfunction) is increasing.1 The initial diagnosis and management of severe sepsis may occur in the ED, the ICU, or the hospital ward.
Several recently published studies have demonstrated decreased mortality and morbidity as a result of interventions and therapeutics applied to patients with sepsis.2-5 These new data, resulting from rigorously performed, randomized controlled trials, combined with previous data for beneficial interventions not specific to sepsis management (such as DVT and stress ulcer prophylaxis) and consensus opinion where no evidence exists lend significant weight to the belief that critical care clinicians can now significantly reduce mortality in patients with severe sepsis and septic shock.6-9
Protocolized care now exists for heart attack and stroke, which is based on recent advances as demonstrated by the medical literature. Until now there has been no attempt to reproduce such an approach in severe sepsis. The Surviving Sepsis Campaign hopes to change that.
The Surviving Sepsis Campaign is administered by the Society of Critical Care Medicine (SCCM), the European Society of Intensive Care Medicine (ESICM), and the International Sepsis Forum (ISF) and is open to all industry for funding through unrestricted educational grants. Contributors to date include Baxter, Edwards, and Eli Lilly.
The first phase was the introduction of the campaign at several major international critical care medicine conferences, the ESICM meeting in Barcelona in 2002, and the SCCM meeting in 2003. The stated goal of the campaign is to decrease the mortality from severe sepsis by 25% in five years.
Phase 2 of the campaign was aimed at producing guidelines for the management of sepsis. In 2003, critical care and infectious disease experts representing 11 international organizations developed evidence-based management guidelines for severe sepsis and septic shock for practical use for the bedside clinician, under the auspices of the Surviving Sepsis Campaign.
Pediatric considerations were provided to contrast adult and pediatric management. The resulting recommendations represent an attempt to facilitate a rapid change in the standard of care for management of sepsis, based on the quality of available published data and expert opinion where no literature guidance is available. The guidelines manuscript was published in both Critical Care Medicine and Intensive Care Medicine.10,11 The publication of this manuscript represents an historic step for critical care worldwide. These guidelines represent an international consensus on the best available standard for management of sepsis.
Key Recommendations
Key recommendations (listed by category and not by hierarchy) include:
- Early goal-directed resuscitation of the septic patient during the first six hours after recognition;
- Appropriate diagnostic studies to ascertain causative organisms before starting antibiotics;
- Early administration of broad-spectrum antibiotic therapy;
- Reassessment of antibiotic therapy with microbiology and clinical data to narrow coverage, when appropriate;
- A usual seven to 10 days of antibiotic therapy guided by clinical response;
- Source control with attention to the method that balances risks and benefits;
- Equivalence of crystalloid and colloid resuscitation;
- Aggressive fluid challenge to restore mean circulating filling pressure;
- Vasopressor preference for norepinephrine and dopamine;
- Cautious use of vasopressin pending further studies;
- Avoidance of low-dose dopamine administration for renal protection;
- Consideration of dobutamine inotropic therapy in some clinical situations;
- Avoidance of supranormal oxygen delivery as a goal of therapy;
- Stress-dose steroid therapy for septic shock;
- Use of recombinant activated protein C in patients with severe sepsis and high risk for death;
- Resolution of tissue hypoperfusion and targeting a hemoglobin of 7-9 g/dL in the absence of coronary artery disease or acute hemorrhage;
- Appropriate use of fresh frozen plasma and platelets;
- A low tidal volume and limitation of inspiratory plateau pressure strategy for acute lung injury and acute respiratory distress syndrome;
- Application of a minimal amount of positive end expiratory pressure in acute lung injury/acute respiratory distress syndrome;
- A semi-recumbent bed position unless contraindicated;
- Protocols for weaning and sedation/analgesia, using either intermittent bolus sedation or continuous infusion sedation with daily interruptions/lightening;
- Avoidance of neuromuscular blockers, if at all possible;
- Maintenance of blood glucose <150 mg/dL after initial stabilization;
- Equivalence of continuous veno-veno hemofiltration (CVVH) and intermittent hemodialysis;
- Lack of utility of bicarbonate use for pH 7.15 or greater;
- Use of DVT/stress ulcer prophylaxis; and
- Consideration of limitation of support where appropriate.
Pediatric considerations include a more likely need for intubation due to low functional residual capacity; more difficult intravenous access; fluid resuscitation based on weight with 40-60 mL/kg or higher needed; decreased cardiac output and increased systemic vascular resistance as the most common hemodynamic profile; greater use of physical examination therapeutic endpoints; unsettled issue of high-dose steroids for therapy of septic shock; and greater risk of hypoglycemia with aggressive glucose control.
Operationalizing the Guidelines
Unfortunately, clinicians change slowly. Historically, transfer of research from the bench to the bedside is a long, tortuous process—one that is not driven by anything clear and that seems to be based more on fad and coincidence than on a keen, evidence-based evaluation of the literature. Phase 3 of the campaign hopes to change that.
Phase 3 of the campaign (www.survivingsepsis.org) aims to operationalize the guidelines to create a global standard of care for sepsis management.12 The guidelines will be transformed into user-friendly tools that allow clinicians to easily incorporate these new recommendations into bedside care. The first step in this next phase has been a joint effort with the Institute of Healthcare Improvement (IHI) to deploy a “change bundle” based on a core set of the previous recommendations into the IHI’s collaborative system. Chart review or concurrent data gathering will identify and track changes in practice and clinical outcomes. Engendering evidence-based change through motivational strategies while monitoring and sharing the results with healthcare practitioners is the key to improving outcomes in severe sepsis.
The severe sepsis bundles form the core of the Surviving Sepsis Campaign. A “bundle” is a group of interventions related to a disease process. When executed together, the interventions produce better outcomes than when implemented individually. The individual bundle elements are built on evidence-based practices. The science behind the elements of a bundle is so well established that their implementation should be considered a generally accepted practice. Develop a bundle process in the following way:
- Identify a set of four to six evidence-based interventions that apply to a cohort of patients with a common disease or a common location. An example might be patients with sepsis admitted to the ICU;
- Develop the will in the providers to deliver the interventions every time they are indicated;
- Redesign the delivery system to ensure the interventions in the bundle are delivered; and
- Measure related outcomes to ascertain the effects of the changes in the delivery system.
The sepsis bundles were developed in just such a manner, based on the experience of the ventilator bundle. The goal now is to motivate providers to deliver the sepsis interventions every time they are indicated and measure them in an all-or-nothing way. We believe that if the bundle elements are reliably performed we can achieve the desired outcome of reducing sepsis-related deaths by 25%.
These elements distill the Surviving Sepsis Campaign practice guidelines into a manageable format for use at most institutions. The bundles represent the specific changes the campaign has identified as essential to the care of severely septic patients. Following the severe sepsis bundles will eliminate the piecemeal or inappropriate application of standards for sepsis care that characterize most clinical environments today.
Hospitals should implement two different severe sepsis bundles. Each bundle articulates objectives to be accomplished within specific time frames.
Sepsis Resuscitation Bundle
The severe sepsis resuscitation bundle describes seven tasks that should begin immediately but must be accomplished within the first six hours of presentation for patients with severe sepsis or septic shock. Some items may not be completed if the clinical conditions described in the bundle do not prevail in a particular case, but clinicians must assess for them. The goal is to perform all indicated tasks 100% of the time within the first six hours of identification of severe sepsis. The tasks are:
- Measure serum lactate;
- Obtain blood cultures prior to antibiotic administration;
- Administer broad-spectrum antibiotics within three hours from time of presentation for ED admissions and one hour for non-ED ICU admissions;
- In the event of hypotension and/or lactate >4 mmol/L (36 mg/dL):
- Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent); and
- Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) ≥65 mm Hg;
- In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dL):
- Achieve central venous pressure (CVP) of ≥8-12 mm Hg; and
- Achieve central venous oxygen saturation (ScvO2) of Surviving Sepsis Campaign70%. (Achieving a mixed venous oxygen saturation (SvO2) of 65% is an acceptable alternative.)
Sepsis Management Bundle
The severe sepsis management bundle lists four management goals. Efforts to accomplish these tasks should also begin immediately, but these items may be completed within 24 hours of presentation for patients with severe sepsis or septic shock.
- Administer low-dose steroids for septic shock in accordance with a standardized ICU policy;
- Administer drotrecogin alfa (activated) in accordance with a standardized ICU policy;
- Maintain glucose control ≥ lower limit of normal, but <150 mg/dL (8.3 mmol/L); and
- Maintain inspiratory plateau pressures <30 cm H2O for mechanically ventilated patients.
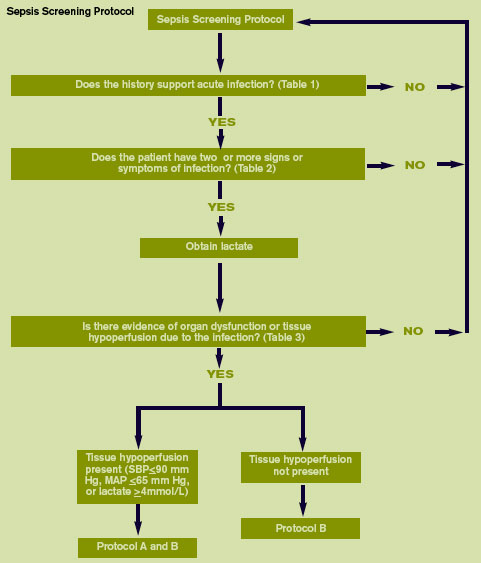
Team Effort
To achieve the goal of reducing mortality by 25% by 2008, everyone involved with the care of severe sepsis patients must be included, work processes must be carefully scripted and standardized, and commitment to this effort must be elevated. This must be a team effort that crosses disciplines and departments; it requires leadership, support from the entire organization, and buy-in from all stakeholders involved with the care of these patients.
Three levels of participation exist in creating successful change:
1) Active working teams are responsible for daily planning, documentation, communication, education, monitoring, and evaluation of activities. The working team must have representation from all departments involved in the change processes ICU, ED, pulmonary department, pharmacy, etc. The team should also be multidisciplinary, comprising physicians, nurses, pharmacists, respiratory therapists, and other staff with roles in the specific change process, such as clerks and technicians. Team members should be knowledgeable about the specific aims, the current local work processes, the associated literature, and any environmental issues that will be affected by these changes.
2) A leadership group or person within the team helps remove barriers, provides resources, monitors global progress, and gives suggestions from an institutional perspective. The working team needs someone with authority in the organization to overcome barriers and to allocate the time and resources the team needs to achieve its aim. Leadership needs to understand how the proposed changes will affect various parts of the system and the more remote consequences such changes might trigger.
3) Providers and stakeholders must be kept informed. Procedures are needed to keep them informed, to receive their feedback, and to ensure them that their responses are respected. This gives stakeholders a sense of ownership and facilitates implementation of the new processes.
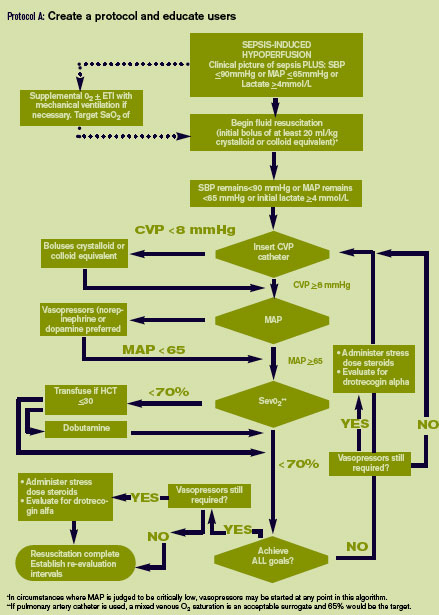
Protocols
Teams should use the bundles to create customized protocols and pathways that will function well within their institutions. However, all of the elements in the bundles must be incorporated into the protocols. The protocols should mirror the bundles but allow flexibility to accommodate the specific needs of a local hospital. The severe sepsis bundles (and thereby the hospital’s protocol) form the basis for the measurements the team will conduct. If all of the elements of the bundles are not incorporated into your customized protocol, your performance on the measures will suffer.
A strong protocol will accomplish all of the items listed in the severe sepsis bundles. If the protocol designer pays careful attention to the details in the bundles, the protocol will score well on the severe sepsis quality indicators. Hospitals will want to publicize their efforts with regard to improving sepsis care and make the protocol an integral part of their rollout strategy. It is imperative to launch an educational initiative regarding the effort.
Examples of sepsis screening and management protocols are available on the Surviving Sepsis Campaign IHI Web site and are rendered on this page as “Protocol A: Create a protocol and educate users” and as “Prot0col B.” The easiest way to get to that page of the IHI Web site is through the home page link from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. These highly visual and easy-to-follow pathways exemplify ways to encourage adherence to a protocol. Notice that the “Sepsis Screening Protocol” (p. 25) complies with the terms of the severe sepsis bundles. Posting these types of algorithms prominently in the ED, hospital wards, and ICU, and making them readily available in laminated and PDA format, can have a significant impact on performance improvement programs.
These flow diagrams may be incorporated into lectures and training programs to support your efforts to change care at the bedside. You can adapt the algorithms to fit the needs of your individual institution, but keep in mind the need to comply with the overall structure of the severe sepsis bundles.
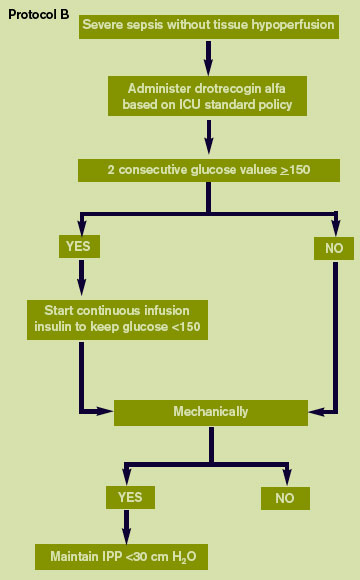
Data Collection
Data collection can seem like an onerous duty in any quality improvement project. Nevertheless, it is essential for improvement. Without attention to measurement, how will you know that your efforts are leading to improvement? At most hospitals, the magnitude of the data collection effort will not be huge as it will be relative to the number of severely septic patients cared for in the ICU.
Generally, hospitals report three to four severely septic patients are treated in one week’s time. This means that zero, one, or two severely septic patients’ charts will need to be abstracted each day in an average-size hospital. If abstraction takes between 20–30 minutes per chart, the daily time for this effort may range from 30–90 minutes daily. This relatively small burden is likely to represent an initial challenge to anyone unfamiliar with the organization of the chart and the measurement forms, or tools, used by the Surviving Sepsis Campaign for data collection. In time, however, data collection will become easier as the chart and the tools provided by the Surviving Sepsis Campaign will become more familiar. Bundle implementation and data collection have begun in hospitals throughout Europe, Latin America, the United Kingdom, and the United States.
The measurement tools were created to achieve a uniform system of data gathering, collation, and calculation across hospitals. Without the measurement tools, teams armed with only the concepts in the severe sepsis bundles would need to decide how to gather data from charts and put it in a format consistent with the calculations listed in the severe sepsis quality indicators. If any hospital were to undertake such a task on its own, it would quickly find that its results were not comparable across institutions because scores of other hospitals would have derived their results by entirely different means.
The Surviving Sepsis Campaign aims to make using the measurement tools as easy as possible for those involved in collecting data. Several basic tools organize data from the patient’s chart. Initially, a paper set of measurement tools was developed to help hospitals orchestrate data collection. Although a database now performs much of the work formerly done on paper, some use of paper tools may be helpful.
For example, the Surviving Sepsis Campaign’s screening tool for severe sepsis is integrated into the database. However, a paper version readily accessible to nurses and clinicians in the ED triage area, the medical and surgical nursing stations, and even the ICU itself will still be practical.
Likewise, some data collectors might find that first capturing on paper the data abstracted from the chart and subsequently entering it into the database is preferable. Most users are likely to find, however, that bringing the database to the ICU on a laptop and directly entering data is the easiest solution.
The most up-to-date paper versions of the tools and the Surviving Sepsis Campaign database can be found on the Institute of Healthcare Improvement Web site. The easiest way to get to that page of the Institute of Healthcare Improvement Web site is by home page linkage from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. An implementation manual is also available that will facilitate initiation of the Surviving Sepsis Campaign performance improvement program as well as installation and use of the associated electronic database.
Conclusion
The Surviving Sepsis Campaign represents an important step for international critical care societies. Recognizing the long history of delay in incorporating research into bedside care, these critical care societies have committed to working together to facilitate bench-to-bedside transfer of recent research. Thus, the campaign represents an ongoing commitment to excellence in patient care. The Surviving Sepsis Campaign has established a target of a 25% reduction in mortality worldwide from sepsis over the next five years. If the Surviving Sepsis Campaign is able to bring the guidelines into routine use, it is possible to achieve this goal. For the campaign to be successful, it will require more than good publicity. It will require a further commitment from bedside clinicians to appraise new research critically and adopt interventions proven to be effective rapidly.
Hospitalists interested in more information about instituting the Surviving Sepsis Campaign and performance improvement package in their hospital should e-mail the Surviving Sepsis Campaign user group program manager at [email protected]. TH
References
- Angus DC, Linde-Zwirble WT, Lidicer J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303-1310.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
- Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862-871.
- Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001;344(10)699-709.
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301-1308.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion in critical care. N Engl J Med. 1999;340:409-4178.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359-1367.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in medical patients with enoxaparin study group. N Engl J Med. 1999;341:793-800.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338:791-797.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858-873.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2004;30:536-55.
- Levy MM, Pronovost PJ, Dellinger RP, et al. Sepsis change bundles: converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004;32(suppl):S595-S597.
The incidence of severe sepsis (sepsis with organ dysfunction) is increasing.1 The initial diagnosis and management of severe sepsis may occur in the ED, the ICU, or the hospital ward.
Several recently published studies have demonstrated decreased mortality and morbidity as a result of interventions and therapeutics applied to patients with sepsis.2-5 These new data, resulting from rigorously performed, randomized controlled trials, combined with previous data for beneficial interventions not specific to sepsis management (such as DVT and stress ulcer prophylaxis) and consensus opinion where no evidence exists lend significant weight to the belief that critical care clinicians can now significantly reduce mortality in patients with severe sepsis and septic shock.6-9
Protocolized care now exists for heart attack and stroke, which is based on recent advances as demonstrated by the medical literature. Until now there has been no attempt to reproduce such an approach in severe sepsis. The Surviving Sepsis Campaign hopes to change that.
The Surviving Sepsis Campaign is administered by the Society of Critical Care Medicine (SCCM), the European Society of Intensive Care Medicine (ESICM), and the International Sepsis Forum (ISF) and is open to all industry for funding through unrestricted educational grants. Contributors to date include Baxter, Edwards, and Eli Lilly.
The first phase was the introduction of the campaign at several major international critical care medicine conferences, the ESICM meeting in Barcelona in 2002, and the SCCM meeting in 2003. The stated goal of the campaign is to decrease the mortality from severe sepsis by 25% in five years.
Phase 2 of the campaign was aimed at producing guidelines for the management of sepsis. In 2003, critical care and infectious disease experts representing 11 international organizations developed evidence-based management guidelines for severe sepsis and septic shock for practical use for the bedside clinician, under the auspices of the Surviving Sepsis Campaign.
Pediatric considerations were provided to contrast adult and pediatric management. The resulting recommendations represent an attempt to facilitate a rapid change in the standard of care for management of sepsis, based on the quality of available published data and expert opinion where no literature guidance is available. The guidelines manuscript was published in both Critical Care Medicine and Intensive Care Medicine.10,11 The publication of this manuscript represents an historic step for critical care worldwide. These guidelines represent an international consensus on the best available standard for management of sepsis.
Key Recommendations
Key recommendations (listed by category and not by hierarchy) include:
- Early goal-directed resuscitation of the septic patient during the first six hours after recognition;
- Appropriate diagnostic studies to ascertain causative organisms before starting antibiotics;
- Early administration of broad-spectrum antibiotic therapy;
- Reassessment of antibiotic therapy with microbiology and clinical data to narrow coverage, when appropriate;
- A usual seven to 10 days of antibiotic therapy guided by clinical response;
- Source control with attention to the method that balances risks and benefits;
- Equivalence of crystalloid and colloid resuscitation;
- Aggressive fluid challenge to restore mean circulating filling pressure;
- Vasopressor preference for norepinephrine and dopamine;
- Cautious use of vasopressin pending further studies;
- Avoidance of low-dose dopamine administration for renal protection;
- Consideration of dobutamine inotropic therapy in some clinical situations;
- Avoidance of supranormal oxygen delivery as a goal of therapy;
- Stress-dose steroid therapy for septic shock;
- Use of recombinant activated protein C in patients with severe sepsis and high risk for death;
- Resolution of tissue hypoperfusion and targeting a hemoglobin of 7-9 g/dL in the absence of coronary artery disease or acute hemorrhage;
- Appropriate use of fresh frozen plasma and platelets;
- A low tidal volume and limitation of inspiratory plateau pressure strategy for acute lung injury and acute respiratory distress syndrome;
- Application of a minimal amount of positive end expiratory pressure in acute lung injury/acute respiratory distress syndrome;
- A semi-recumbent bed position unless contraindicated;
- Protocols for weaning and sedation/analgesia, using either intermittent bolus sedation or continuous infusion sedation with daily interruptions/lightening;
- Avoidance of neuromuscular blockers, if at all possible;
- Maintenance of blood glucose <150 mg/dL after initial stabilization;
- Equivalence of continuous veno-veno hemofiltration (CVVH) and intermittent hemodialysis;
- Lack of utility of bicarbonate use for pH 7.15 or greater;
- Use of DVT/stress ulcer prophylaxis; and
- Consideration of limitation of support where appropriate.
Pediatric considerations include a more likely need for intubation due to low functional residual capacity; more difficult intravenous access; fluid resuscitation based on weight with 40-60 mL/kg or higher needed; decreased cardiac output and increased systemic vascular resistance as the most common hemodynamic profile; greater use of physical examination therapeutic endpoints; unsettled issue of high-dose steroids for therapy of septic shock; and greater risk of hypoglycemia with aggressive glucose control.
Operationalizing the Guidelines
Unfortunately, clinicians change slowly. Historically, transfer of research from the bench to the bedside is a long, tortuous process—one that is not driven by anything clear and that seems to be based more on fad and coincidence than on a keen, evidence-based evaluation of the literature. Phase 3 of the campaign hopes to change that.
Phase 3 of the campaign (www.survivingsepsis.org) aims to operationalize the guidelines to create a global standard of care for sepsis management.12 The guidelines will be transformed into user-friendly tools that allow clinicians to easily incorporate these new recommendations into bedside care. The first step in this next phase has been a joint effort with the Institute of Healthcare Improvement (IHI) to deploy a “change bundle” based on a core set of the previous recommendations into the IHI’s collaborative system. Chart review or concurrent data gathering will identify and track changes in practice and clinical outcomes. Engendering evidence-based change through motivational strategies while monitoring and sharing the results with healthcare practitioners is the key to improving outcomes in severe sepsis.
The severe sepsis bundles form the core of the Surviving Sepsis Campaign. A “bundle” is a group of interventions related to a disease process. When executed together, the interventions produce better outcomes than when implemented individually. The individual bundle elements are built on evidence-based practices. The science behind the elements of a bundle is so well established that their implementation should be considered a generally accepted practice. Develop a bundle process in the following way:
- Identify a set of four to six evidence-based interventions that apply to a cohort of patients with a common disease or a common location. An example might be patients with sepsis admitted to the ICU;
- Develop the will in the providers to deliver the interventions every time they are indicated;
- Redesign the delivery system to ensure the interventions in the bundle are delivered; and
- Measure related outcomes to ascertain the effects of the changes in the delivery system.
The sepsis bundles were developed in just such a manner, based on the experience of the ventilator bundle. The goal now is to motivate providers to deliver the sepsis interventions every time they are indicated and measure them in an all-or-nothing way. We believe that if the bundle elements are reliably performed we can achieve the desired outcome of reducing sepsis-related deaths by 25%.
These elements distill the Surviving Sepsis Campaign practice guidelines into a manageable format for use at most institutions. The bundles represent the specific changes the campaign has identified as essential to the care of severely septic patients. Following the severe sepsis bundles will eliminate the piecemeal or inappropriate application of standards for sepsis care that characterize most clinical environments today.
Hospitals should implement two different severe sepsis bundles. Each bundle articulates objectives to be accomplished within specific time frames.
Sepsis Resuscitation Bundle
The severe sepsis resuscitation bundle describes seven tasks that should begin immediately but must be accomplished within the first six hours of presentation for patients with severe sepsis or septic shock. Some items may not be completed if the clinical conditions described in the bundle do not prevail in a particular case, but clinicians must assess for them. The goal is to perform all indicated tasks 100% of the time within the first six hours of identification of severe sepsis. The tasks are:
- Measure serum lactate;
- Obtain blood cultures prior to antibiotic administration;
- Administer broad-spectrum antibiotics within three hours from time of presentation for ED admissions and one hour for non-ED ICU admissions;
- In the event of hypotension and/or lactate >4 mmol/L (36 mg/dL):
- Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent); and
- Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) ≥65 mm Hg;
- In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dL):
- Achieve central venous pressure (CVP) of ≥8-12 mm Hg; and
- Achieve central venous oxygen saturation (ScvO2) of Surviving Sepsis Campaign70%. (Achieving a mixed venous oxygen saturation (SvO2) of 65% is an acceptable alternative.)
Sepsis Management Bundle
The severe sepsis management bundle lists four management goals. Efforts to accomplish these tasks should also begin immediately, but these items may be completed within 24 hours of presentation for patients with severe sepsis or septic shock.
- Administer low-dose steroids for septic shock in accordance with a standardized ICU policy;
- Administer drotrecogin alfa (activated) in accordance with a standardized ICU policy;
- Maintain glucose control ≥ lower limit of normal, but <150 mg/dL (8.3 mmol/L); and
- Maintain inspiratory plateau pressures <30 cm H2O for mechanically ventilated patients.
Team Effort
To achieve the goal of reducing mortality by 25% by 2008, everyone involved with the care of severe sepsis patients must be included, work processes must be carefully scripted and standardized, and commitment to this effort must be elevated. This must be a team effort that crosses disciplines and departments; it requires leadership, support from the entire organization, and buy-in from all stakeholders involved with the care of these patients.
Three levels of participation exist in creating successful change:
1) Active working teams are responsible for daily planning, documentation, communication, education, monitoring, and evaluation of activities. The working team must have representation from all departments involved in the change processes ICU, ED, pulmonary department, pharmacy, etc. The team should also be multidisciplinary, comprising physicians, nurses, pharmacists, respiratory therapists, and other staff with roles in the specific change process, such as clerks and technicians. Team members should be knowledgeable about the specific aims, the current local work processes, the associated literature, and any environmental issues that will be affected by these changes.
2) A leadership group or person within the team helps remove barriers, provides resources, monitors global progress, and gives suggestions from an institutional perspective. The working team needs someone with authority in the organization to overcome barriers and to allocate the time and resources the team needs to achieve its aim. Leadership needs to understand how the proposed changes will affect various parts of the system and the more remote consequences such changes might trigger.
3) Providers and stakeholders must be kept informed. Procedures are needed to keep them informed, to receive their feedback, and to ensure them that their responses are respected. This gives stakeholders a sense of ownership and facilitates implementation of the new processes.
Protocols
Teams should use the bundles to create customized protocols and pathways that will function well within their institutions. However, all of the elements in the bundles must be incorporated into the protocols. The protocols should mirror the bundles but allow flexibility to accommodate the specific needs of a local hospital. The severe sepsis bundles (and thereby the hospital’s protocol) form the basis for the measurements the team will conduct. If all of the elements of the bundles are not incorporated into your customized protocol, your performance on the measures will suffer.
A strong protocol will accomplish all of the items listed in the severe sepsis bundles. If the protocol designer pays careful attention to the details in the bundles, the protocol will score well on the severe sepsis quality indicators. Hospitals will want to publicize their efforts with regard to improving sepsis care and make the protocol an integral part of their rollout strategy. It is imperative to launch an educational initiative regarding the effort.
Examples of sepsis screening and management protocols are available on the Surviving Sepsis Campaign IHI Web site and are rendered on this page as “Protocol A: Create a protocol and educate users” and as “Prot0col B.” The easiest way to get to that page of the IHI Web site is through the home page link from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. These highly visual and easy-to-follow pathways exemplify ways to encourage adherence to a protocol. Notice that the “Sepsis Screening Protocol” (p. 25) complies with the terms of the severe sepsis bundles. Posting these types of algorithms prominently in the ED, hospital wards, and ICU, and making them readily available in laminated and PDA format, can have a significant impact on performance improvement programs.
These flow diagrams may be incorporated into lectures and training programs to support your efforts to change care at the bedside. You can adapt the algorithms to fit the needs of your individual institution, but keep in mind the need to comply with the overall structure of the severe sepsis bundles.
Data Collection
Data collection can seem like an onerous duty in any quality improvement project. Nevertheless, it is essential for improvement. Without attention to measurement, how will you know that your efforts are leading to improvement? At most hospitals, the magnitude of the data collection effort will not be huge as it will be relative to the number of severely septic patients cared for in the ICU.
Generally, hospitals report three to four severely septic patients are treated in one week’s time. This means that zero, one, or two severely septic patients’ charts will need to be abstracted each day in an average-size hospital. If abstraction takes between 20–30 minutes per chart, the daily time for this effort may range from 30–90 minutes daily. This relatively small burden is likely to represent an initial challenge to anyone unfamiliar with the organization of the chart and the measurement forms, or tools, used by the Surviving Sepsis Campaign for data collection. In time, however, data collection will become easier as the chart and the tools provided by the Surviving Sepsis Campaign will become more familiar. Bundle implementation and data collection have begun in hospitals throughout Europe, Latin America, the United Kingdom, and the United States.
The measurement tools were created to achieve a uniform system of data gathering, collation, and calculation across hospitals. Without the measurement tools, teams armed with only the concepts in the severe sepsis bundles would need to decide how to gather data from charts and put it in a format consistent with the calculations listed in the severe sepsis quality indicators. If any hospital were to undertake such a task on its own, it would quickly find that its results were not comparable across institutions because scores of other hospitals would have derived their results by entirely different means.
The Surviving Sepsis Campaign aims to make using the measurement tools as easy as possible for those involved in collecting data. Several basic tools organize data from the patient’s chart. Initially, a paper set of measurement tools was developed to help hospitals orchestrate data collection. Although a database now performs much of the work formerly done on paper, some use of paper tools may be helpful.
For example, the Surviving Sepsis Campaign’s screening tool for severe sepsis is integrated into the database. However, a paper version readily accessible to nurses and clinicians in the ED triage area, the medical and surgical nursing stations, and even the ICU itself will still be practical.
Likewise, some data collectors might find that first capturing on paper the data abstracted from the chart and subsequently entering it into the database is preferable. Most users are likely to find, however, that bringing the database to the ICU on a laptop and directly entering data is the easiest solution.
The most up-to-date paper versions of the tools and the Surviving Sepsis Campaign database can be found on the Institute of Healthcare Improvement Web site. The easiest way to get to that page of the Institute of Healthcare Improvement Web site is by home page linkage from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. An implementation manual is also available that will facilitate initiation of the Surviving Sepsis Campaign performance improvement program as well as installation and use of the associated electronic database.
Conclusion
The Surviving Sepsis Campaign represents an important step for international critical care societies. Recognizing the long history of delay in incorporating research into bedside care, these critical care societies have committed to working together to facilitate bench-to-bedside transfer of recent research. Thus, the campaign represents an ongoing commitment to excellence in patient care. The Surviving Sepsis Campaign has established a target of a 25% reduction in mortality worldwide from sepsis over the next five years. If the Surviving Sepsis Campaign is able to bring the guidelines into routine use, it is possible to achieve this goal. For the campaign to be successful, it will require more than good publicity. It will require a further commitment from bedside clinicians to appraise new research critically and adopt interventions proven to be effective rapidly.
Hospitalists interested in more information about instituting the Surviving Sepsis Campaign and performance improvement package in their hospital should e-mail the Surviving Sepsis Campaign user group program manager at [email protected]. TH
References
- Angus DC, Linde-Zwirble WT, Lidicer J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303-1310.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
- Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862-871.
- Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001;344(10)699-709.
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301-1308.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion in critical care. N Engl J Med. 1999;340:409-4178.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359-1367.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in medical patients with enoxaparin study group. N Engl J Med. 1999;341:793-800.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338:791-797.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858-873.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2004;30:536-55.
- Levy MM, Pronovost PJ, Dellinger RP, et al. Sepsis change bundles: converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004;32(suppl):S595-S597.
The incidence of severe sepsis (sepsis with organ dysfunction) is increasing.1 The initial diagnosis and management of severe sepsis may occur in the ED, the ICU, or the hospital ward.
Several recently published studies have demonstrated decreased mortality and morbidity as a result of interventions and therapeutics applied to patients with sepsis.2-5 These new data, resulting from rigorously performed, randomized controlled trials, combined with previous data for beneficial interventions not specific to sepsis management (such as DVT and stress ulcer prophylaxis) and consensus opinion where no evidence exists lend significant weight to the belief that critical care clinicians can now significantly reduce mortality in patients with severe sepsis and septic shock.6-9
Protocolized care now exists for heart attack and stroke, which is based on recent advances as demonstrated by the medical literature. Until now there has been no attempt to reproduce such an approach in severe sepsis. The Surviving Sepsis Campaign hopes to change that.
The Surviving Sepsis Campaign is administered by the Society of Critical Care Medicine (SCCM), the European Society of Intensive Care Medicine (ESICM), and the International Sepsis Forum (ISF) and is open to all industry for funding through unrestricted educational grants. Contributors to date include Baxter, Edwards, and Eli Lilly.
The first phase was the introduction of the campaign at several major international critical care medicine conferences, the ESICM meeting in Barcelona in 2002, and the SCCM meeting in 2003. The stated goal of the campaign is to decrease the mortality from severe sepsis by 25% in five years.
Phase 2 of the campaign was aimed at producing guidelines for the management of sepsis. In 2003, critical care and infectious disease experts representing 11 international organizations developed evidence-based management guidelines for severe sepsis and septic shock for practical use for the bedside clinician, under the auspices of the Surviving Sepsis Campaign.
Pediatric considerations were provided to contrast adult and pediatric management. The resulting recommendations represent an attempt to facilitate a rapid change in the standard of care for management of sepsis, based on the quality of available published data and expert opinion where no literature guidance is available. The guidelines manuscript was published in both Critical Care Medicine and Intensive Care Medicine.10,11 The publication of this manuscript represents an historic step for critical care worldwide. These guidelines represent an international consensus on the best available standard for management of sepsis.
Key Recommendations
Key recommendations (listed by category and not by hierarchy) include:
- Early goal-directed resuscitation of the septic patient during the first six hours after recognition;
- Appropriate diagnostic studies to ascertain causative organisms before starting antibiotics;
- Early administration of broad-spectrum antibiotic therapy;
- Reassessment of antibiotic therapy with microbiology and clinical data to narrow coverage, when appropriate;
- A usual seven to 10 days of antibiotic therapy guided by clinical response;
- Source control with attention to the method that balances risks and benefits;
- Equivalence of crystalloid and colloid resuscitation;
- Aggressive fluid challenge to restore mean circulating filling pressure;
- Vasopressor preference for norepinephrine and dopamine;
- Cautious use of vasopressin pending further studies;
- Avoidance of low-dose dopamine administration for renal protection;
- Consideration of dobutamine inotropic therapy in some clinical situations;
- Avoidance of supranormal oxygen delivery as a goal of therapy;
- Stress-dose steroid therapy for septic shock;
- Use of recombinant activated protein C in patients with severe sepsis and high risk for death;
- Resolution of tissue hypoperfusion and targeting a hemoglobin of 7-9 g/dL in the absence of coronary artery disease or acute hemorrhage;
- Appropriate use of fresh frozen plasma and platelets;
- A low tidal volume and limitation of inspiratory plateau pressure strategy for acute lung injury and acute respiratory distress syndrome;
- Application of a minimal amount of positive end expiratory pressure in acute lung injury/acute respiratory distress syndrome;
- A semi-recumbent bed position unless contraindicated;
- Protocols for weaning and sedation/analgesia, using either intermittent bolus sedation or continuous infusion sedation with daily interruptions/lightening;
- Avoidance of neuromuscular blockers, if at all possible;
- Maintenance of blood glucose <150 mg/dL after initial stabilization;
- Equivalence of continuous veno-veno hemofiltration (CVVH) and intermittent hemodialysis;
- Lack of utility of bicarbonate use for pH 7.15 or greater;
- Use of DVT/stress ulcer prophylaxis; and
- Consideration of limitation of support where appropriate.
Pediatric considerations include a more likely need for intubation due to low functional residual capacity; more difficult intravenous access; fluid resuscitation based on weight with 40-60 mL/kg or higher needed; decreased cardiac output and increased systemic vascular resistance as the most common hemodynamic profile; greater use of physical examination therapeutic endpoints; unsettled issue of high-dose steroids for therapy of septic shock; and greater risk of hypoglycemia with aggressive glucose control.
Operationalizing the Guidelines
Unfortunately, clinicians change slowly. Historically, transfer of research from the bench to the bedside is a long, tortuous process—one that is not driven by anything clear and that seems to be based more on fad and coincidence than on a keen, evidence-based evaluation of the literature. Phase 3 of the campaign hopes to change that.
Phase 3 of the campaign (www.survivingsepsis.org) aims to operationalize the guidelines to create a global standard of care for sepsis management.12 The guidelines will be transformed into user-friendly tools that allow clinicians to easily incorporate these new recommendations into bedside care. The first step in this next phase has been a joint effort with the Institute of Healthcare Improvement (IHI) to deploy a “change bundle” based on a core set of the previous recommendations into the IHI’s collaborative system. Chart review or concurrent data gathering will identify and track changes in practice and clinical outcomes. Engendering evidence-based change through motivational strategies while monitoring and sharing the results with healthcare practitioners is the key to improving outcomes in severe sepsis.
The severe sepsis bundles form the core of the Surviving Sepsis Campaign. A “bundle” is a group of interventions related to a disease process. When executed together, the interventions produce better outcomes than when implemented individually. The individual bundle elements are built on evidence-based practices. The science behind the elements of a bundle is so well established that their implementation should be considered a generally accepted practice. Develop a bundle process in the following way:
- Identify a set of four to six evidence-based interventions that apply to a cohort of patients with a common disease or a common location. An example might be patients with sepsis admitted to the ICU;
- Develop the will in the providers to deliver the interventions every time they are indicated;
- Redesign the delivery system to ensure the interventions in the bundle are delivered; and
- Measure related outcomes to ascertain the effects of the changes in the delivery system.
The sepsis bundles were developed in just such a manner, based on the experience of the ventilator bundle. The goal now is to motivate providers to deliver the sepsis interventions every time they are indicated and measure them in an all-or-nothing way. We believe that if the bundle elements are reliably performed we can achieve the desired outcome of reducing sepsis-related deaths by 25%.
These elements distill the Surviving Sepsis Campaign practice guidelines into a manageable format for use at most institutions. The bundles represent the specific changes the campaign has identified as essential to the care of severely septic patients. Following the severe sepsis bundles will eliminate the piecemeal or inappropriate application of standards for sepsis care that characterize most clinical environments today.
Hospitals should implement two different severe sepsis bundles. Each bundle articulates objectives to be accomplished within specific time frames.
Sepsis Resuscitation Bundle
The severe sepsis resuscitation bundle describes seven tasks that should begin immediately but must be accomplished within the first six hours of presentation for patients with severe sepsis or septic shock. Some items may not be completed if the clinical conditions described in the bundle do not prevail in a particular case, but clinicians must assess for them. The goal is to perform all indicated tasks 100% of the time within the first six hours of identification of severe sepsis. The tasks are:
- Measure serum lactate;
- Obtain blood cultures prior to antibiotic administration;
- Administer broad-spectrum antibiotics within three hours from time of presentation for ED admissions and one hour for non-ED ICU admissions;
- In the event of hypotension and/or lactate >4 mmol/L (36 mg/dL):
- Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent); and
- Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) ≥65 mm Hg;
- In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dL):
- Achieve central venous pressure (CVP) of ≥8-12 mm Hg; and
- Achieve central venous oxygen saturation (ScvO2) of Surviving Sepsis Campaign70%. (Achieving a mixed venous oxygen saturation (SvO2) of 65% is an acceptable alternative.)
Sepsis Management Bundle
The severe sepsis management bundle lists four management goals. Efforts to accomplish these tasks should also begin immediately, but these items may be completed within 24 hours of presentation for patients with severe sepsis or septic shock.
- Administer low-dose steroids for septic shock in accordance with a standardized ICU policy;
- Administer drotrecogin alfa (activated) in accordance with a standardized ICU policy;
- Maintain glucose control ≥ lower limit of normal, but <150 mg/dL (8.3 mmol/L); and
- Maintain inspiratory plateau pressures <30 cm H2O for mechanically ventilated patients.
Team Effort
To achieve the goal of reducing mortality by 25% by 2008, everyone involved with the care of severe sepsis patients must be included, work processes must be carefully scripted and standardized, and commitment to this effort must be elevated. This must be a team effort that crosses disciplines and departments; it requires leadership, support from the entire organization, and buy-in from all stakeholders involved with the care of these patients.
Three levels of participation exist in creating successful change:
1) Active working teams are responsible for daily planning, documentation, communication, education, monitoring, and evaluation of activities. The working team must have representation from all departments involved in the change processes ICU, ED, pulmonary department, pharmacy, etc. The team should also be multidisciplinary, comprising physicians, nurses, pharmacists, respiratory therapists, and other staff with roles in the specific change process, such as clerks and technicians. Team members should be knowledgeable about the specific aims, the current local work processes, the associated literature, and any environmental issues that will be affected by these changes.
2) A leadership group or person within the team helps remove barriers, provides resources, monitors global progress, and gives suggestions from an institutional perspective. The working team needs someone with authority in the organization to overcome barriers and to allocate the time and resources the team needs to achieve its aim. Leadership needs to understand how the proposed changes will affect various parts of the system and the more remote consequences such changes might trigger.
3) Providers and stakeholders must be kept informed. Procedures are needed to keep them informed, to receive their feedback, and to ensure them that their responses are respected. This gives stakeholders a sense of ownership and facilitates implementation of the new processes.
Protocols
Teams should use the bundles to create customized protocols and pathways that will function well within their institutions. However, all of the elements in the bundles must be incorporated into the protocols. The protocols should mirror the bundles but allow flexibility to accommodate the specific needs of a local hospital. The severe sepsis bundles (and thereby the hospital’s protocol) form the basis for the measurements the team will conduct. If all of the elements of the bundles are not incorporated into your customized protocol, your performance on the measures will suffer.
A strong protocol will accomplish all of the items listed in the severe sepsis bundles. If the protocol designer pays careful attention to the details in the bundles, the protocol will score well on the severe sepsis quality indicators. Hospitals will want to publicize their efforts with regard to improving sepsis care and make the protocol an integral part of their rollout strategy. It is imperative to launch an educational initiative regarding the effort.
Examples of sepsis screening and management protocols are available on the Surviving Sepsis Campaign IHI Web site and are rendered on this page as “Protocol A: Create a protocol and educate users” and as “Prot0col B.” The easiest way to get to that page of the IHI Web site is through the home page link from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. These highly visual and easy-to-follow pathways exemplify ways to encourage adherence to a protocol. Notice that the “Sepsis Screening Protocol” (p. 25) complies with the terms of the severe sepsis bundles. Posting these types of algorithms prominently in the ED, hospital wards, and ICU, and making them readily available in laminated and PDA format, can have a significant impact on performance improvement programs.
These flow diagrams may be incorporated into lectures and training programs to support your efforts to change care at the bedside. You can adapt the algorithms to fit the needs of your individual institution, but keep in mind the need to comply with the overall structure of the severe sepsis bundles.
Data Collection
Data collection can seem like an onerous duty in any quality improvement project. Nevertheless, it is essential for improvement. Without attention to measurement, how will you know that your efforts are leading to improvement? At most hospitals, the magnitude of the data collection effort will not be huge as it will be relative to the number of severely septic patients cared for in the ICU.
Generally, hospitals report three to four severely septic patients are treated in one week’s time. This means that zero, one, or two severely septic patients’ charts will need to be abstracted each day in an average-size hospital. If abstraction takes between 20–30 minutes per chart, the daily time for this effort may range from 30–90 minutes daily. This relatively small burden is likely to represent an initial challenge to anyone unfamiliar with the organization of the chart and the measurement forms, or tools, used by the Surviving Sepsis Campaign for data collection. In time, however, data collection will become easier as the chart and the tools provided by the Surviving Sepsis Campaign will become more familiar. Bundle implementation and data collection have begun in hospitals throughout Europe, Latin America, the United Kingdom, and the United States.
The measurement tools were created to achieve a uniform system of data gathering, collation, and calculation across hospitals. Without the measurement tools, teams armed with only the concepts in the severe sepsis bundles would need to decide how to gather data from charts and put it in a format consistent with the calculations listed in the severe sepsis quality indicators. If any hospital were to undertake such a task on its own, it would quickly find that its results were not comparable across institutions because scores of other hospitals would have derived their results by entirely different means.
The Surviving Sepsis Campaign aims to make using the measurement tools as easy as possible for those involved in collecting data. Several basic tools organize data from the patient’s chart. Initially, a paper set of measurement tools was developed to help hospitals orchestrate data collection. Although a database now performs much of the work formerly done on paper, some use of paper tools may be helpful.
For example, the Surviving Sepsis Campaign’s screening tool for severe sepsis is integrated into the database. However, a paper version readily accessible to nurses and clinicians in the ED triage area, the medical and surgical nursing stations, and even the ICU itself will still be practical.
Likewise, some data collectors might find that first capturing on paper the data abstracted from the chart and subsequently entering it into the database is preferable. Most users are likely to find, however, that bringing the database to the ICU on a laptop and directly entering data is the easiest solution.
The most up-to-date paper versions of the tools and the Surviving Sepsis Campaign database can be found on the Institute of Healthcare Improvement Web site. The easiest way to get to that page of the Institute of Healthcare Improvement Web site is by home page linkage from the Surviving Sepsis Campaign Web site, www.survivingsepsis.org. An implementation manual is also available that will facilitate initiation of the Surviving Sepsis Campaign performance improvement program as well as installation and use of the associated electronic database.
Conclusion
The Surviving Sepsis Campaign represents an important step for international critical care societies. Recognizing the long history of delay in incorporating research into bedside care, these critical care societies have committed to working together to facilitate bench-to-bedside transfer of recent research. Thus, the campaign represents an ongoing commitment to excellence in patient care. The Surviving Sepsis Campaign has established a target of a 25% reduction in mortality worldwide from sepsis over the next five years. If the Surviving Sepsis Campaign is able to bring the guidelines into routine use, it is possible to achieve this goal. For the campaign to be successful, it will require more than good publicity. It will require a further commitment from bedside clinicians to appraise new research critically and adopt interventions proven to be effective rapidly.
Hospitalists interested in more information about instituting the Surviving Sepsis Campaign and performance improvement package in their hospital should e-mail the Surviving Sepsis Campaign user group program manager at [email protected]. TH
References
- Angus DC, Linde-Zwirble WT, Lidicer J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303-1310.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
- Annane D, Sebille V, Charpentier C, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA. 2002;288:862-871.
- Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001;344(10)699-709.
- Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301-1308.
- Hébert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion in critical care. N Engl J Med. 1999;340:409-4178.
- Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359-1367.
- Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in medical patients with enoxaparin study group. N Engl J Med. 1999;341:793-800.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338:791-797.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858-873.
- Dellinger RP, Carlet JM, Masur H, et al: Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2004;30:536-55.
- Levy MM, Pronovost PJ, Dellinger RP, et al. Sepsis change bundles: converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004;32(suppl):S595-S597.
SHM Establishes Palliative Care Task Force
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at [email protected].
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.

Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at [email protected].
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at [email protected].
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at [email protected].
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care. Yet we often lack the knowledge and skills necessary to provide outstanding palliative care; we may also lack the comfort level we need to take care of patients at that stage of illness.
Steve Pantilat, MD, SHM president and member of the SHM Education Committee, established the Palliative Care Task Force to identify and create opportunities to improve palliative care in the field of hospital medicine. The Palliative Care Task Force had its inaugural meeting in August. Led by founder Dr. Pantilat and Chad Whelan, MD, Palliative Care Task Force chair, the task force established the following goals:
- Promote palliative care as an important skill and activity for hospital medicine physicians and providers;
- Identify and create palliative-care-focused educational activities for hospital medicine physicians and other key stakeholders within hospital medicine;
- Advocate for the creation and or support of hospital-based palliative care services;
- Promote the use of best practices in palliative care; and
- Develop a core community of hospital medicine physicians dedicated to improving our understanding of palliative care.
Our current task force membership is small but energetic. We actively recruit members, particularly nonphysicians and non-SHM members. Palliative care is a multidisciplinary field, and we hope the Palliative Care Task Force membership will reflect this diversity. Potential areas of growth include pharmacists, nurses, social workers, spiritual care providers, and nonhospitalist physicians. We are also looking for a pediatrician with an interest in palliative care to represent the pediatric interests among SHM members.
Since the first meeting in August our members have been developing a plan to achieve our identified goals. While the plan is still early in its development, we have designed a multimodal approach that will rely on traditional CME meetings, print media, as well as electronic media.
The task force’s short-term goals include promoting best practices in palliative care via SHM communication vehicles. For example, we plan to propose a series of articles for the forthcoming Journal of Hospital Medicine to highlight key issues in palliative care.
The 2006 SHM Annual Meeting will feature two workshops with a palliative care focus. One workshop will discuss how to build the case for a palliative care service; the other will address issues in pain management for hospitalized patients. We will learn from the 2006 experience as we look toward the 2007 SHM Annual Meeting in Texas. An electronic CME module is also under development.
Finally, we are planning an electronic compendium of resources and tools for practicing high-quality palliative care. Although the format has not been finalized, the concept is to provide resources that will make caring for palliative care patients as easy as possible.
While we are pleased with the progress of the task force to date, there is still much to do. Hospital medicine physicians can and should serve as leaders to improve palliative care. Traditional medical training focuses our efforts and thoughts of curing and preventing. We’ve all felt the exhilaration of making a life-saving diagnosis on the young, otherwise healthy patient; however, just as there are times to look for a cure at all costs, there are also times when we must treat our patients’ symptoms at all costs.
Often traditional medical training doesn’t provide us with the tools we need to best care for our patients and their families when palliative care goals become the priority. We hope this task force will raise the visibility of palliative care within SHM and provide the opportunities and tools needed for us, as hospital medicine providers, to offer the best palliative care possible to our patients. If successful, we’ll feel the deep personal satisfaction and self-reward of helping a patient and their family transition from hopes of a cure to comfort in the knowledge that their symptoms and needs will be cared for.
Interested in joining the task force or participating in a related work group? Contact Chad Whelan at [email protected].
The Stroke Resource Room
SHM’s Web site features stroke information on call
Online resource rooms comprise an innovative venue within the SHM Web site to focus on essential topics from the forthcoming core curriculum. Specifically, the Web-based resource rooms organize expert opinions, evidence-based literature, clinical tools and guidelines, and recommendations about essential topics in hospital medicine. Initial areas of development include the DVT and stroke resource rooms, with ongoing efforts in other areas including geriatrics, antimicrobial resistance, congestive heart failure, and glycemic control. These interactive rooms help connect hospitalists to information, content experts, and each other.
The Stroke Imperative
Stroke is the third leading cause of death in the United States and a common admission diagnosis. Cerebrovascular disease is a field of great complexity and rapid advance. There is great pressure on the practicing hospitalist to have both a base knowledge of the approach to the patient with stroke as well as an understanding of current best practice.
Traditional internal medicine residencies may not fully prepare one for hospitalist practice. Many patients seen by hospitalists have diagnoses that were managed by internal medicine subspecialties in the past. Most hospitalists feel comfortable managing straightforward gastrointestinal bleeds, myocardial infarctions, and renal failure without consultation. Neurologic cases are somewhat different.
Most medicine residents have rotated on a neurology service, but that limited experience is frequently insufficient in preparing physicians for their future experience as hospitalists. While neurology residencies include one year of internal medicine, the two diverge dramatically afterward. Practitioners of both internal medicine and neurology frequently feel that they speak a different language from one another.
Particularly in the community setting, hospitalists manage the bulk of neurology patients either with or without neurologic consultation. The reasons for this are varied, including poor inpatient reimbursement for neurologists and a tradition of nonaggressive approaches to stroke care.1
The Opportunity
Realizing the need to provide direct access to important information about inpatient stroke management, SHM convened a stroke advisory board, including general hospitalists, a neurologist, and members of the education committee. SHM and Boehringer-Ingelheim provided funding for the resource room through educational funds and an unrestricted grant, respectively.
Stroke Resource Room Content
The Stroke Resource Room is patterned after the template of the DVT Resource Room; the idea being that a standardized format will allow easy navigation and maximal utility. David Likosky, MD, served as content editor, Sandeep Sachdeva, MD, as quality editor, Alpesh Amin, MD as education editor, and Jason Stein, MD, as managing editor.
The rooms are structured to facilitate access to specific types of information. Whether one is looking for the details of a certain study, slide sets to help teach residents, or for input on how to approach a difficult patient, that resource should be readily available. The main sections of the room are summarized below.
The “Awareness” area on the main page of the Stroke Resource Room defines the effects of stroke as well as the hospitalists’ scope of practice.
A separate debate is ongoing within neurology about who should be responsible for the inpatient management of stroke. Interestingly, much of this is about whether general neurologists or vascular/stroke neurologists should primarily manage these patients. One such article referred to the brain as “… the Rolls Royce of the human body” going on to ask, “Would you want your Rolls Royce to be serviced by any ordinary mechanic, who takes care of all kinds of automobiles?”2 Many hospitalists find this argument less than compelling given how difficult it can be in many communities to get a neurologist much less a “vascular neurologist” to see an inpatient.
The “Evidence” section consists of two main parts with the goal of providing a one-stop shop for stroke care literature. The first is a set of links to articles reviewed by the ACP journal club. The second is a concise list of landmark trials, such as the Heparin Acute Embolic Stroke HAEST) trial, which compared low molecular weight heparin versus aspirin in patients with acute stroke and atrial fibrillation.3 These articles help answer questions that come up commonly in clinical practice.
The Experience link capitalizes on the Internet’s ability to disseminate information. There are a limited number of protocols and order sets for ischemic and hemorrhagic stroke available. One can download these and, perhaps more importantly, submit one’s own—including comments on what about that particular tool has been valuable.
Finally, the “Ask the Expert” section features an interactive venue for interacting with a panel of neurologists and neurocritical care physicians. This section answers the more common and more difficult clinical questions in a shared forum. Supportive evidence is cited, with the knowledge that much of stroke care remains in the realm of standard of practice.
The “Improve” section reflects the other roles of hospitalists, such as hospital leader. The three current links include a PowerPoint primer on quality improvement. In addition, there are links to the “Get with the Guidelines” program from the American Stroke Association. This is a continuous quality improvement program focusing on care team protocols and outcome measurement. The final linked site is to the criteria for the disease specific accreditation program from JCAHO. This national effort may drive where patients receive their care for certain conditions.
The “Educate” section caters to multiple audiences. The academic hospitalist may find the “Teaching Pearls” section helpful, as well as the slide sets from the International Stroke Conference and StrokeSTOP, which is aimed at medical students. The patient education links contain a wealth of quality information. The “Professional Development” subsection contains sources for audio lectures with slide sets as well as case presentations and NIH stroke scale training—all with free CME hours. A chapter on stroke from the SHM’s forthcoming core competencies is included as well.
Moving Forward
One of the advantages of an Internet-based resource is the ability to be easily modified. A progressively more robust database will be developed over time as questions are answered in the “Ask the Expert” section and as participants share their stroke care protocols.
The Stroke Resource Room is an excellent forum to improve clinical care and form the basis for future SHM workshops, lectures, and to review articles. By building our collective knowledge, we will be limited only by the energy we put into the adding to and using available information and our desire to apply that energy to patient care.
References
- Likosky DJ, Amin AN. Who will care for our hospitalized patients? Stroke. 2005;36(6): 1113-1114.
- Caplan L. Stroke is best managed by neurologists. Stroke. 2003;34(11):2763.
- Berge E, Abdelnoor M, Nakstad PH, et al. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomized study. HAEST Study Group. Lancet. 2000;355(9211):1205-1210.
Secure the Future
Encourage trainees to consider lifelong careers in hospital medicine
By Vineet Arora, MD, MA, and Margaret C. Fang, MD, MPH, co-chairs of SHM’s Young Physicians Section
Interest in hospital medicine is booming, and it is estimated that the number of hospitalists in the United States is estimated will exceed the number of cardiologists in the near future. Yet, many graduating residents view hospital medicine as a temporary job where they can take time off and work before going on to a subspecialty fellowship. Others perceive hospitalists as “super-residents” susceptible to burnout, and therefore do not consider hospital medicine a sustainable career option. These perceptions may contribute to a high turnover of hospitalists and compromise the accumulation of enough inpatient experience to accomplish many of the benefits associated with the use of hospitalists, including shorter lengths of stay and comparable—if not better—quality of care.
To ensure recruitment and retention of the best and brightest trainees, it’s important to consider ways to educate and encourage them to consider a career in hospital medicine as a rewarding lifelong career. Below, we discuss strategies to encourage trainees to pursue a lifelong career in hospital medicine.
Showcase Your Clinical Work
First, consider your everyday practice an excellent way to showcase the often-exciting world of inpatient medicine. Preclinical students often cherish any opportunity to interact with patients. Inviting first- or second-year medical students to accompany you on rounds is an excellent opportunity to teach clinical medicine and physical exam skills, and a good way to influence their career choice early in their medical career.
If you’re in an academic medical center, accessing preclinical students is as easy as approaching students in an internal medicine interest group or volunteering as a preceptor for a physical diagnosis course for preclinical students. In fact, hospitalists are often acknowledged as some of the best teachers and are highly accessible because of their inpatient duties.
Community-based hospitalists also can provide valuable career advice and opportunities, particularly in exposing students to real-life career experiences often not covered through traditional medical school training. One way for a community-based hospitalist to become involved is to host preclinical students over the summer by contacting a local medical school dean’s office and volunteering as a summer preceptor for interested preclinical students. Your alma mater may be particularly responsive. Or, contact interest groups in internal medicine, family medicine, or pediatrics through the state or local leaders of the American College of Physicians, the American Academy of Family Physicians, and the American Academy of Pediatrics.
Explain Your Nonclinical Work
It’s important to explain your nonclinical roles to residency trainees. Hospitalists increasingly take on numerous administrative, educational, and leadership roles and responsibilities. Whether you are leading a quality improvement effort, interfacing with hospital operations, or running a medical student clerkship, it is crucial that physicians-in-training understand the diverse opportunities within hospital medicine to achieve a healthy work-life balance and avoid clinical burnout.
If you are involved with quality improvement projects at your institution, enlist the help of an interested resident or student. Because student rotations are frequent, their prior experience may be scant and their time limited. So make sure the projects have definite goals and are easily accomplished. Ensure that the projects provide reasonable educational value and experience within a finite time. Lay out explicit goals at the beginning of the project, ask for frequent updates, and then recap the experience and any concrete accomplishments to provide structure and expectations for the process.
For example, the University of California at San Francisco Hospitalist Group is spearheading an educational initiative in which residents learn about both the theory and practice of quality improvement through choosing a project and working with a mentor to design, implement, and measure the results of a quality improvement initiative.
Share Your Passion
In addition to showcasing your clinical and nonclinical activities, share your passion about hospital medicine. Reflect on the reasons you entered hospital medicine, as well as your thoughts on the pros and cons of the field. Perhaps you were drawn to hospital medicine because of a desire to take care of acutely ill patients, or to work on improving the quality of a medical system, or because of a more controllable work schedule with competitive compensation.
In some cases, it may have been a particular interest in medical ethics, palliative care, geriatrics, or perioperative care. Sharing your enthusiasm is the best way to cultivate reciprocal interest. Medical students and residents closely observe your attitudes toward your career, your job satisfaction, and your work-life balance. In addition to mentoring those already entering a medical career, there are endless opportunities to outreach to younger students, including those in high school and college. Many local schools and community organizations offer mentorship programs to area students. Engaging in an informal discussion about your career at a social or community event with younger students can be incredibly rewarding. Younger students often lack realistic career experiences and access to career-specific role models on which to base informed decisions. Although they may express an interest in science or medicine, they may not know how long the training process is or the importance of good grades.
Take a moment to inquire about career interests and explain what a hospitalist is; this can be invaluable in promoting understanding and cultivating interest into the field. More structured interactions with hospitalists can also prepare students for successful entry into the medical field. The University of Chicago Hospitalists, for example, host high-achieving Chicago public school juniors in a summer clinical and research enrichment program in hospital-based medicine called TEACH Research.
Offer Advice and Assistance
Finding your first job can be a nerve-racking situation. Sharing your advice on the process with trainees is always appreciated. For instance, they are interested in hearing how you decided to become a hospitalist and what you did to secure your position.
Offer to meet with them and review their career interests, goals, and curriculum vitae. If you hear of job openings and opportunities, inform the community of trainees by contacting program directors or chief residents at residency programs. Many residency program directors showcase available opportunities in their house-staff office or direct such opportunities to interested residents. Some residency programs invite community-based physicians to give residents insight on securing their first job. This process is particularly foreign to medical trainees who have never had to negotiate such things as benefit packages, compensation, or call schedule. Your candid thoughts on what to expect and how to approach the process are invaluable.
Again, approaching the residency program where you trained is a good starting point. Alternatively, you can locate a nearby residency through the Fellowship and Residency Electronic Interactive Database database offered by the American Medical Association (www.ama-assn.org/vapp/freida/srch/).
Finally, if you know any trainees interested in hospital medicine,encourage them to attend the SHM’s local or national meetings. The annual meeting is an excellent place for medical trainees to hear the latest research and innovations, learn about advanced training and job opportunities, network, and connect with mentors through the Mentorship Breakfast. For the last two years, the Young Physicians Section has organized a Forum for Early Career Hospitalists where we addressed different career paths in hospital medicine and conducted research during training. Continued growth in our field depends on promoting hospital medicine as a vital, sustainable career.
Busy Summer for HQPS
The Health Quality and Patient Safety Committee (HQPS) has developed an array of initiatives to support SHM members in the development, implementation, and evaluation of quality and system improvements at their institutions. Educational programming, tools, and resources are being developed for four specific content areas including prevention of VTE, improving the discharge process, glycemic control, and improving outcomes for hospitalized heart failure patients.
HQPS members and Course Directors Greg Maynard, MD, and Tosha Wetterneck, MD, are developing a quality precourse for the 2006 SHM Annual Meeting. The educational goal for the precourse will be to enable hospitalists to become leaders in quality and safety through the effective implementation of evidence-based, high reliability interventions. Precourse participants will actively participate in small groups to apply techniques for designing, implementing, and evaluating quality improvement projects to address a specific improvement need in one of four areas: heart failure care, glycemic control, and preventing VTE in the hospital or the discharge process. Registration for this precourse will begin in November and space will be limited. Plan to register early.
In June, HQPS convened a multidisciplinary, multiagency Heart Failure Advisory Board to guide the development of a clinical guidelines implementation toolkit (CGIT), resource room, and CME modules related to implementing best practices for care of patients with heart-failure. The advisory board has representatives from several organizations and allied health professions, including the American College of Cardiology, American Medical Directors Association, American Hospital Association, Case Managers Society of America, American Association of Heart Failure Nurses, American Society of Health-System Pharmacists, American Association of Critical Care Nurses, National Association of Social Workers and the Heart Failure Society of America. Currently, the advisory board is completing a needs assessment and will begin development on the CGIT, resource room and CME modules next month.
In July, in collaboration with the Education Committee and SHM staff, HQPS launched the SHM VTE Resource Room (www.hospitalmedicine.org/AM/Template.cfm?Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=6312). The resource room provides users with a workbook, or step-wise process to assess the need for VTE prevention, advocate for local improvements, and implement and evaluate a VTE prevention program. The resource room also provides a useful review of the literature, an “Ask the Expert” forum, slide sets, and bedside teaching tools.
In August, the SHM Executive Committee approved the SHM Discharge Planning Checklist developed by HQPS under the direction of Dennis Manning, MD. This discharge planning checklist and a white paper on guidance for its implementation will be available to members in the near future.
Interested in learning more about these initiatives or becoming involved in an HQPS workgroup? Contact Lakshmi Halasyamani, MD, HQPS chair, at [email protected].
Hartford Grants Awarded
SHM presents Hartford Foundation grant funds to hospitalists for QI demo project
By Kathleen K. Frampton, RN, MPH
Shm remains committed to expanding its efforts to improve inpatient care for older patients. The John A. Hartford Foundation has generously awarded approximately $370,000 to SHM in support of its focus on the geriatric population. This funding will assist SHM in its endeavors related to educational programs and products, hospitalist leadership training, and quality improvement projects. In light of this, SHM allocated a portion of these Hartford grant funds to study a critical aspect of elderly patient care, safety-care transitions.
A competitive request for the proposal (RFP) process was conducted to solicit interest from healthcare institutional providers and SHM members willing to serve as the principle investigator in their work setting. The RFP delineated the requirements for a hospital to serve as a designated study site to implement a discharge planning intervention from hospital-based care to community-based care for elderly patients and to evaluate the facilitating factors, barriers to implementation and outcomes associated with the new approach.
All research proposals submitted by hospitals were evaluated and scored against established criteria. Qualifying hospital finalists were reviewed by a panel consisting of members of three standing SHM Committees: Education, Hospital Quality and Patient Safety, and Research and Executive. In July 2005, this panel selected three hospitals to receive funding for this initiative: Johns Hopkins-Bayview, Baltimore, Md.; Northeast Medical Center, Concord, N.C.; and Geisinger Health System, Danville, Penn.
Johns Hopkins-Bayview (coordinating site): A 355-bed community-based facility located in southeast Baltimore with academic affiliations and approximately 25% of patients over age 65. The hospitalist service consists of nine physicians, five physician assistants, and three nurse practitioners.
Northeast Medical Center: A 457-bed, private, nonprofit community-based facility located in the Charlotte Region with a residency training program and 36% of patients over age 65. The hospitalist service consists of 16 physicians and 24/7 intensivist coverage.
Geisinger Health System: A 366-bed facility and Level 1 Trauma Center, private, nonprofit community based system located in north central Pennsylvania with a residency training program and 70% of patients over age 65. The hospitalist service is staffed by 15 physicians (10 full-time employees).
The QI Demonstration Project will run for 18 months and, according to Tina Budnitz, MPH, SHM senior advisor for planning and development, the study “represents new territory for both SHM and other professional societies … . We have moved beyond developing a best practice to use in the clinical setting to how you can actually change the system so that best practices can be successfully implemented … . It is the intention of SHM to focus on safe practice interventions that can be generalized to other settings.”
Budnitz also explained that near completion of the project SHM plans to convene the advisory board, grantee project teams, representatives of the Hartford Foundation, and the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) to review the data from the demonstration project and design a larger scale quality improvement program.
“Our grantees will work with the SHM Advisory Board to develop a comprehensive toolkit, which will document the lessons learned during the implementation process and any other resources that facilitate adaptation and/or adoption of these safe practice interventions,” explains Budnitz.
Care Transitions in the Treatment of the Elderly
According to the Institute of Medicine (IOM), the healthcare system is poorly organized to meet its current challenges. The delivery of care is often overly complex and uncoordinated, requiring steps and patient hand-offs that slow care and decrease rather than improve patient safety.
An IOM seminal report published in 2001, Crossing the Quality Chasm: A New Health System for the 21st Century, emphasizes that cumbersome processes waste resources, leave unaccountable voids in coverage, lead to loss of information, and fail to build on the strengths of all professionals involved to ensure that care is appropriate, timely, and safe. Right before and after discharge, there often is no one clearly in charge of the transition whom the patient may contact for guidance. Patients are often instructed to contact their primary care provider for follow-up issues or questions, whether or not the primary care provider had been involved in the hospitalization.
A recent study supported by the Agency for Healthcare Research and Quality (AHRQ) showed that high-risk patient targeting, better communications, and better coordination of care and follow-up could potentially prevent some readmissions when transitioning patients from hospital to home.
In 2002, the American Geriatric Society (AGS) issued a Position Statement, Improving the Quality of Transitional Care for Persons with Complex Care Needs, which stressed that both the “sending” and “receiving” health professionals bear responsibility and accountability in this phase. Successful transitions require that there be both a uniform plan of care and procedure for communicating the following:
- An accessible medical record that contains a current problem list;
- A medication regimen;
- A list of allergies;
- Advance directives;
- Baseline physical and cognitive function; and
- Contact information for all professional and informal care providers.
Also, input must be solicited from informal care providers who are involved in the execution of the plan of care. The AGS recommends the use of a “coordinating” health professional who oversees both the sending and receiving aspects of the transition. This professional should be skilled in the identification of health status, assessment and management of multiple chronic conditions, managing medications, and collaboration with members of the interdisciplinary team and caregivers.
The QI Demonstration Project
According to SHM Immediate Past-President Jeanne Huddleston, MD, SHM has structured this demonstration project so that the three study sites in the Hartford Grant Group will implement identical clinical tools while they employ unique processes and procedures at each of the individual sites.
“The what needs to be in common across sites, but the how and who in the implementation will be individually tailored to each specific hospital environment,” she explains.
This is a real strength of the study because standardized interventions can be studied in varied and representative test environments. Dr. Huddleston also stresses that, “SHM envisions its role in quality management to be in the actual implementation realm—rather than in the development of new clinical guidelines. SHM seeks to know whether hospitalists [use] the same tools at different sites and understand their impact at each site.”
The patient care domains selected as a focus for the safe practice implementation tools for the care transition process are:
- Communications;
- Medication reconciliation; and
- Functional status.
Communication tools will be developed for primary care physicians, patients, and their support systems so that important clinical information is transmitted during the discharge process. The implementation tools designed for medication reconciliation will be employed by physicians, care managers, or pharmacists in the hospital. Transmitting the medication regimen is widely recognized as an error-prone element of care. These specific implementation tools will include a method to review and verify any dose/frequency changes of medications that the patient was taking upon admission, as well as those that were added or discontinued during the inpatient episode. Because patient functional status is a critical issue in discharge planning, detailed tools will also be created to standardize content for risk assessment and evaluation of the types of assistance needed for patients to resume activities of daily living.
The demonstration project will also utilize specific metrics to measure patient outcomes as well as the effect that these safe practices have on the discharge and care transition processes. The three study sites will measure referring physician satisfaction with the adequacy of post-hospitalization follow-up information, the accuracy of medication reconciliation, readmission rates, and patient understanding of their treatment plan and medication regimen.
QI Requires Expert Change Management
Hospitalists recognize that the challenge of patient safety is linked to the challenge of organizational change. Patient safety initiatives can succeed only to the extent to which healthcare organizations recognize the need for and develop the means to implement the organizational changes. According to the AHRQ, systemwide improvements in patient safety are possible only if there are coordinated changes in multiple components—clinical procedures, attitudes and behaviors of care providers, incentive systems, coordination structures and processes, patterns of interactions among care providers, and organizational culture.
Senior leadership must play an active role in establishing patient safety as a priority, and staff involved directly in providing care must actively participate in implementing change. The likelihood of successful implementation of even simple change requires multiple tactics or many bullets directed at the same target. Additionally, it is critical to redesign the roles of healthcare workers at the point of care to accommodate the necessary changes and to retrain them to fulfill these roles.
Hospitalists Prepare to Lead
Identifying the facilitating factors and barriers to improvement is essential to effect change because it helps ensure success. It’s also crucial to match the patient safety goals with the change strategies and tactics. Otherwise, mismatches can lead to unintended consequences that will hinder continuous improvements such as employee skepticism, frustration of safety champions, and mislearning or unnecessary ”workarounds“ by staff.
SHM sees this QI Demonstration Project as critical to assisting institutions in the design, implementation, and evaluation of QI programs and systemwide interventions with effectiveness and value. These findings should equip hospitalists with vital tools necessary to provide essential leadership in meeting their institution’s quality and patient safety goals. TH
Writer Kathleen Frampton is based in Columbia, Md
To the Marrow
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
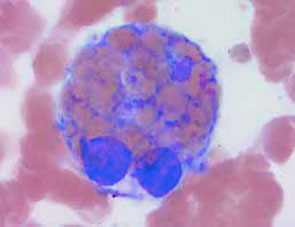
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
A44-year-old male presented with ecthyma gangrenosum and Pseudomonas aeruginosa bacteremia after a two-year history of fever of unknown origin, pancytopenia, hypertriglyceridemia, and splenomegaly. A bone marrow aspirate was performed, as shown.
Based on the bone marrow aspirate, the most likely diagnosis is:
- Acute leukemia
- Myelofibrosis with myeloid metaplasia
- Multiple myeloma
- Myelodysplastic syndrome
- Hemophagocytic syndrome.
Discussion
The answer is e, hemophagocytic syndrome. The bone marrow aspirate shown demonstrates macrophage hemophagocytosis of non-nucleated red blood cells, consistent with hemophagocytic syndrome (HPS). The hemophagocytic syndromes may be classified as either primary or secondary.
Primary HPS is an autosomal recessive disorder most commonly seen in children and characterized by the polyclonal accumulation of T-lymphocytes and activated macrophages. Many of these patients have null mutations in the gene coding for the cytolytic protein perforin.
In contrast, secondary HPS is characterized by the polyclonal accumulation of activated macrophages in patients with underlying infectious, malignant, or rheumatologic diseases. Patients commonly present with fever, splenomegaly, and complications related to pancytopenia. Hypertriglyceridemia (>160 mg/dL) and an elevated serum ferritin (>10,000 ng/mL) are all sensitive and specific (>0.75) for HPS in the appropriate clinical setting, though histologic demonstration of hemophagocytosis (ingestion of red blood cells by cytokine-activated macrophages) in the bone marrow is diagnostic.
Macrophage activation in these disorders may be attributed to dysregulation of cytokines such as IL-1, IL-6, IFN-y and TNF-a. While therapy with corticosteroids, immunosuppressants, intravenous immunoglobulin, and chemotherapeutic agents have provided conflicting results, future therapeutic strategies employing cytokine-specific antagonists (e.g., etanercept) are promising.1,2
In this case, the patient was noted to have a relative lymphocytosis comprising clonal CD16+CD56+ large granular lymphocytes. These large granular lymphocytes stained positive for Epstein-Barr virus (EBV)-encoded RNA by in situ hybridization. This patient with EBV-associated natural killer (NK) cell lymphoma complicated by hemophagocytic syndrome failed to recover, despite treatment with broad spectrum antibiotics, neutrophil transfusions, intravenous immunoglobulin, fludarabine, and cyclophosphamide.
The clinical and laboratory features of HPS, including fever of unknown origin, anemia, and splenomegaly, often mimic other disorders common in hospitalized patients—many of which may be associated with secondary HPS. As this case illustrates, secondary HPS is associated with significant morbidity and mortality, particularly in those patients in which the diagnosis is delayed. Therefore, prompt diagnosis requires a high index of suspicion among hospital-based physicians caring for patients with underlying infectious, rheumatologic or malignant conditions commonly associated with secondary HPS. TH
References
- Ravelli A. Macrophage activation syndrome. Curr Opin Rheumatol. 2002;14:548-552.
- Henter JI, Elinder G, Ost A. Diagnostic guidelines for hemophagocytic lymphohistiocytosis. The FHL Study Group of the Histiocyte Society. Semin Oncol. 1991;18:29.
The Red Badge of Katrina
“If this old ninny-woman, Fate, cannot do better than this, she should be deprived of the management of men’s fortunes. She is an old hen who knows not her intention. If she has decided to drown me, why did she not do it in the beginning and save me all this trouble. The whole affair is absurd. … But, no, she cannot mean to drown me. She dare not drown me. She cannot drown me. Not after all this work.”
—Stephen Crane, The Open Boat
Stephen Crane, the famous 19th-century American author of such works as The Red Badge of Courage, also penned a short story entitled The Open Boat during his illustrious career. The tale is a fictionalized narrative of a traumatic experience in his life. A ship on which he was a passenger sank during a storm off the coast of Florida. He found himself one of four survivors drifting in a tiny open dinghy struggling to stay alive in a tumultuous sea and pounding surf.
As Crane shows in his story, his characters’ salvations depend upon whether or not they will adapt to their surroundings and help their fellow human beings—not whether or not they can conquer nature.
I couldn’t help but think of Crane’s story and its inherent intimations after digesting firsthand accounts from medical staff on duty in ICUs during the recent traumatic experiences of Hurricane Katrina. The circumstances seem so unique and foreign in our modern age of delivering expeditious, accurate, and technologically supported medical care. I invite all physicians to bear witness to these incredulous stories and cleanse their own complacent perceptions, tabula rasa if you will, of functioning as a practitioner of 21st-century healthcare. These tales harken back to a not too distant time in medical practice.
Charity Hospital in New Orleans is one of the oldest continuously operating hospitals in the country. Along with University Hospital, another public facility just up Gravier Street in the Crescent City, Charity dispenses the lion’s share of all medical care in the city to one of the most uninsured populations in the country. Both hospitals are staffed and run jointly by Tulane and Louisiana State University (LSU), whose medical schools sit contiguously with Charity on opposite ends and lie unfavorably in one of the Big Easy’s topographical low points. Here are first-hand accounts from hospital staff who endured Hurricane Katrina from the confines of Charity and University hospitals.
Ben DeBoisblanc, MD, an LSU pulmonary attending physician, was assigned to Charity Hospital’s ICU. What follows is his chronicling of the events surrounding Hurricane Katrina.
“Prior to landfall it was obvious that Katrina had all the characteristics of the hurricane experts for decades had predicted would be the worst natural disaster in U.S. history: A category 5 storm hitting a city that is largely below sea level and completely surrounded by water. We were able to reduce our ICU patient load in Charity Hospital to about 50 prior to the storm hitting.
“After evacuating our own families, our emergency activation team set up to provide medical support for the remaining patients. During the storm windows blew out in the ICU, flooding it with about two inches of water. The power went out, but the emergency generators kicked on and all seemed well.
“But an hour later for some unknown reason we lost all power and began bagging our patients in total darkness. We were able to restart the backup generators late in the day on Monday, which allowed us to start cleaning up the mess in the ICU. Although the city was without power, we were high-fiving each other over a job well done. The day crew went to sleep late Monday, but was suddenly awakened at 3 a.m. on Tuesday to help bag patients when the emergency generators went out again. As dawn began to break we began to understand why: Water was pouring into downtown New Orleans from every direction and had flooded the generators that we located on the first floor.
—Ben DeBoisblanc, MD
“Without power for our life support systems (suction, monitors, vents, dialysis, IV fluid pumps, radiology, laboratory, etc.) we realized that we needed to get our patients out ASAP. Subsequently, a sanitation crisis unfolded when we lost water pressure for toilets. We were not only caring for 300 patients in the hospital but we were also providing refuge for more than 1,000 support staff and their families. Before we lost communication with the outside world on Tuesday FEMA instructed us to prepare for evacuation later that day. Much to our surprise the governor’s office was telling news agencies that we had already been evacuated. Needless to say, no outside help came until Friday, despite FEMA’s instructions.
“It soon became clear that if we were going to get out, we would have to get ourselves out. Our hazmat team had acquired four small diesel generators for field use, but did not have diesel fuel on site to power them. Our ICU respiratory therapist used his ‘Mississippi credit card’ (a hammer and a screwdriver) and some oxygen tubing to siphon diesel from on ambulance flooded on the ED ramp. We were able to power up the ICU to run about six vents. For the others we used gas driven portable vents or continued to hand bag. The roof of Charity Hospital was the only cool place to get a few hours of restorative sleep each night, so we broke away from our 12-on, 12-off usual staffing plan to allow each shift to enjoy a few hours with the rats seeking higher ground.
“By Wednesday we were still without any FEMA presence, and a morale crisis erupted among the employees. Although many staff were incapacitated with fear, grief, and despair, others dug deep and rose to the challenge. We could not communicate with police, National Guard, or FEMA, but our ICU residents were able to text message and get live on-air transmissions to CNN.
“On Wednesday, Francesco Simeone, a colleague from Tulane got a call from private air ambulance services wanting to send in their own helicopters to start the evacuation. The only problem was that the only commercial heliport in the area was at the Superdome, which was in the midst of a security crisis.
“Joe Lasky, the chief of Tulane pulmonary services, paddled a canoe from Charity and found a National Guard five-ton truck with a driver that was not in communication with his command. This actually worked to our advantage because he could not be accused of disobeying an order by helping us.
“Wednesday night we put the first four of our patients in the back of the truck and drove them across the street to Tulane Hospital’s parking garage. One patient was 23-year-old kid with Goodpasture’s and acute renal failure who had not been dialyzed in four days and who being bagged with 100% O2 and a 12 cm PEEP valve. We had to emergently insert a chest tube in the back of the National Guard truck when he desaturated in the middle of riding through the floodwaters.
“We then used a ‘borrowed’ pick-up truck to ferry the patients to the rooftop of a parking lot adjacent to Charity Hospital, where we set up a mini-ICU for the next two days. After removing light poles helicopters were able to begin landing, but the sun set before we could get any ICU patients to the roof, leaving us with four patients and no exit strategy for getting them out of New Orleans. The commercial ambulance personnel were able to communicate with military helicopters and by 11 p.m. Wednesday the clap-clap thunder of a Black Hawk was heard overhead. The Black Hawks were configured only as troop carriers, which meant that we would have to provide patient support for all of the sorties.
“The first ride for me was surreal: a moonless night, unlit buildings and towers, pilots with night vision goggles. A triage landing site had been established on the edge of town on the interstate. Amazingly there were thousands of people waiting, ready to help, but no one had known of our plight. We dumped our patients with brief medical records taped to their forearms into waiting ambulances for dispersion all over the region. A day later I got a call that the 23-year-old patient was alive and doing well.
“We continued the air evacuation all day Thursday, Thursday night, and Friday morning. Nurses cat-napped on the concrete roof by putting their heads on the legs of colleagues who bagged and comforted those waiting for the next helicopter. Not knowing the structural integrity of the rooftop, the Black Hawk pilots stayed powered up while we loaded our patients, docs, and O2 cylinders. After 48 hours of screaming commands over the roaring sound of the Black Hawks our entire ICU staff was both deaf and mute. By Friday afternoon we had completed our mission and walked the three blocks back to Charity in chest-deep sewage just in time to discover that FEMA had arrived to begin evacuating our hospital.
“I cried when I left Charity, perhaps for the last time ever. Some were tears of triumph, some were tears of profound sadness. Triumph for the miracle of human resolve that allowed a group of civilian doctors, nurses, and respiratory therapists to accomplish what the federal government could not. We got all of our patients out alive except two. One we expected to die; the other was an intubated elderly lady with COPD whose husband we were forced to leave behind at Charity.
“I remember how he sat day and night fanning his wife in the sweltering heat of the ICU. Fanning even as he seemed to slip into sleep. She died in the arms of her resident physician who could do no more on the rooftop than comfort her with the touch of a hand. I never saw her husband again because he was evacuated before I got back to the hospital. I don’t even know if he knows that she had died. Even if he does know, I somehow feel that he remains profoundly grateful.
“I feel sad because valuable time was lost both due to the anemic early response and because valuable resources were misused. I personally witnessed dozens and dozens of helicopters—many military—land and fly away with able-bodied citizens while patients died on the rooftop. And sadly, many of those able-bodied citizens were physicians.
“It was an experience that I will never forget. I left with one memento: a set of keys of a John Doe with an unknown medical condition that we loaded into a helicopter to be carried to an unknown place with an uncertain future. If you received a John Doe looking for his keys, let me know, I’d love to one day be able return them.”
Steve McPherson, MD, a third-year Tulane medicine resident was assigned to the ICU of University Hospital. Here is his story.
“I was on a typical every third call schedule for the ICU working that Friday night [August 26, 2005]. As far as I knew, Katrina was in the Gulf at a category 2 and headed for the Panhandle. Friday night as I answered four or five pages, I kept checking the weather channel. The reports kept looking worse. Katrina was growing in strength and had changed course to head right at New Orleans.
“Saturday morning I called my fiancée, informed her of the updated prediction of a direct hit category 4-5 hurricane and asked her to start packing to leave. That afternoon a ‘code gray’ [natural disaster] was called, and we were informed by e-mails and pages. This meant that both the Saturday and Sunday teams had to report on Sunday and would be on duty indefinitely.
“Sunday morning I reported to work under the code gray status. Katrina was bearing down on New Orleans, and it was evident from the media that there was going to be some major damage. [New Orleans] Mayor [Ray] Nagin issued a mandatory evacuation. Katrina was becoming a super-storm, and we were right in her path.
—Steve McPherson, MD
“Our attending rounded as usual that morning. Then he met with the upper echelon of hospital administration. At this meeting the house staff were informed that there was a real possibility that the first two floors of the hospital could be flooded. The administration asked all services to prioritize a list of ‘salvageable’ patients. Essentially this meant asking—assuming we lost power, generators, and elevators—who would be the most appropriate to carry manually up to higher floors. Further, assuming the necessity of economy in allocation of medical resources, who would stand the best chance of survival and would benefit from these resources.
“So, we put our heads together with the SICU teams and developed a triage list. The next step in hurricane preparation involved moving the patients away from vulnerable window areas in into an adjacent recovery area that was more internally located. The rest of Sunday afternoon was business as usual. There was, however, a palpable undercurrent of nervous anticipation. Sunday night we pitched a no-hitter. Of course, this was not due to luck but rather because the town was empty. Aside from zero admissions, the hospital that night from a functional standpoint was essentially normal.
“Monday morning Katrina struck. Despite being in a rather sturdy steel frame, brick-and-mortar public building, you could feel that the wind strength was impressive and the rain was pounding relentlessly like a banshee from hell. At 10 a.m., we lost primary power and generator power kicked in. The ICU was still functioning fairly normally. We were obtaining labs, running vents although we had no computer system, and had to retrieve lab results like an old-fashioned errand boy on the main floor.
“Outside, I could see about three feet of water had flooded Gravier Street. Surrounding houses were missing a few windows and shingles, but otherwise the damage seemed minimal, and it looked like initially we had dodged a bullet. I remember thinking that the levies had done their job. This notion became a pipe dream as the water level surrounding the hospital steadily began to rise sometime between the hours of 12 to 2 p.m. We had no idea about the now-infamous levy breaches, but the burgeoning deluge provided the information that the media or government was unable to give us at that time. The feculent water continued to rise slowly throughout the day. Pretty soon, I saw boats with outboard motors cruising by. I’m not sure if anyone in the hospital knew precisely that our predicament was becoming more precarious by the hour.
“Late Monday, a random boat pulled up to the ED ambulance ramp, which had become a makeshift dock. On board was the boat pilot, a New Orleans police officer, and two chronic ventilator/PEG nursing home residents. Our ED staff informed the cop that there was no way we were able to take these patients and care for them given the rising water levels and impending loss of even backup generator power.
“The cop insisted, stating, ‘This is not my problem.’ He laid the patients on the ED ramp and promptly departed. This incident caused quite a ruckus as no one really knew how to handle it.
“Hospital security quickly stepped in and barked, ‘Everybody inside. We’re locking down the building.’ I guess this was a desperate attempt to control a situation that was obviously way out of control by now and discourage any further ‘dumping’ of patients. All of the staff and residents quickly retreated inside the hospital in a knee-jerk reaction to the mandate. As we filed into the hospital like lemmings, Josh Willis, MD, one of our chiefs, suddenly realized the ethical mistake we were making by abandoning the cast-away patients lying on the ED ramp. ‘What kind of doctors are we anyway?’ I remember hearing him inquire rhetorically.
“This statement seemed to summon forth the quiescent words from the oath of Hippocrates when we had pledged to ‘ … apply dietetic measures for the benefit of the sick according to my ability and judgment … [and] … keep them from harm and injustice.’ We realized our mistake, turned around, and went back outside to bring the two patients into the hospital.
“Through early Monday evening, three to four similar trach/PEG patients were delivered from the same nursing home via watercraft. A piece of tape adhered to their threadbare gowns on which was written the name of the nursing home, the patient’s name, and their social security number. This was hardly a thorough past medical history or active problem list. We situated these patients with the other cast-offs inside the ED. It was apparent by initial observation that several of these patients were in dire medical straits at baseline, let alone having to deal with a natural disaster to boot.
“By early Tuesday morning, our backup generators went down. We had no labs, no chemistries, no ABGs. We were shooting from the hip, so to speak, in terms of treatment. Those nursing home patients brought in by boat remained not only in the ED, but also at the bottom of the ‘salvageable’ list.
“Besides just holding their hands, we could only give them supplemental oxygen. Meanwhile, on the roof of the hospital, a couple of smaller portable generators were running with lines powering three to four vents. Somehow it seemed that all the patients who really needed vents and who had made the salvageable list were getting them. By now, we already had to let one patient die … .
“By Tuesday afternoon the hospital had become—for all intents and purposes—entirely useless. The order was given to evacuate the entire hospital. The first order of business was to evacuate the most critically ill, salvageable patients. The house staff instructed the residents to accompany two patients each to Baton Rouge. One of my patients had West Nile virus and the other had dermatomyositis with ARDS in the fibroproliferative stage. The latter patient had been requiring 50%-75% FIO2. With only supplemental oxygen, trach tubes, and bags, we began our journey through the oppressive heat of late summer New Orleans.
“A boat took us to the Claiborne Avenue/I-10 ramp, which had also become a boat launch with awaiting ambulances. As we drove on the overpass past the drowning city, I could see hordes of wayward and destitute people lining the interstate and around the Superdome. The image was surreal. It looked like some third-world country in the throes of utter civil war chaos. The slings and arrows of outrageous fortune continued their incessant barrage as the ambulance I was riding in ran out of oxygen. The O2 sats on my ARDS patient began dropping precipitously into the low 80s. Before we could reach the safety of Maravich Center [now hospital] in Baton Rouge, we had to stop the ambulance so I could wave down a trailing ambulance and obtain more supplemental oxygen. With a wide-open valve on one tank, I alternated between patients until I was able to drop them off at triage. I called my fiancée who also happens to be an RN to pick me up, and we went to Bunkie, La., to await our next move. After two days, we traveled back to the Maravich Center to volunteer. We were told that our help wasn’t needed.
“It was frustrating to watch TV the next few days and see my colleagues still working at both Charity and University hospitals. I felt I should still be there with my teammates trying to sort through the medical maelstrom. In then end, I guess I took care of my patients and did what my attending ordered us to do. I was lucky because I got out on Tuesday. I’m sure it got ugly in there for everyone who didn’t get to leave until Friday.
“This has proven to be an experience that not many people go through and its lessons I will not soon forget. Leadership is a quality that too often gets overlooked when assessing the qualities of a good physician. When push comes to shove, we as physicians are ultimately responsible for running the patient-care ship. Without a doubt though, I do feel a closer bond with my program colleagues. Jeff Wiese, our program director, even sent out an e-mail stating that there would be no hard feelings if any resident wanted to find a new program. So far, there have been zero transfers.
“Based on the camaraderie being expressed among my fellow residents, I don’t anticipate that there will be any ultimately when all is said and done. This fellowship has truly been inspirational and renewed my own ethical ideals about being a physician.”
Conclusion
The harrowing presence of nature pervades Crane’s The Open Boat as it does the above accounts of two medicine residents during the tragedy of Katrina. But the most significant aspect of these struggles lies in human beings’ attempts to help one another survive despite their backgrounds, vocations, or social status. There is no fighting an angry sea or an incensed hurricane; neither can be conquered. But one can learn to survive the onslaught and to care for to the best of one’s ability those fellow human beings who are also caught in the grip of nature’s immense indifference whether they be castaways on the open ocean or deserted doctors in a drowning city.
“It would be difficult to describe the subtle brotherhood of men that was here established on the seas. No one said that it was so. No one mentioned it. But it dwelt in the boat, and each man felt it warm him. They were a captain, an oiler, a cook, and a correspondent, and they were friends, friends in a more curiously iron-bound degree than may be common.”—Stephen Crane, The Open Boat TH
Dr. Bucci is a psychiatric resident at the Mayo Clinic in Rochester, Minn., and a member of Tulane Medical School’s class of 2003.
“If this old ninny-woman, Fate, cannot do better than this, she should be deprived of the management of men’s fortunes. She is an old hen who knows not her intention. If she has decided to drown me, why did she not do it in the beginning and save me all this trouble. The whole affair is absurd. … But, no, she cannot mean to drown me. She dare not drown me. She cannot drown me. Not after all this work.”
—Stephen Crane, The Open Boat
Stephen Crane, the famous 19th-century American author of such works as The Red Badge of Courage, also penned a short story entitled The Open Boat during his illustrious career. The tale is a fictionalized narrative of a traumatic experience in his life. A ship on which he was a passenger sank during a storm off the coast of Florida. He found himself one of four survivors drifting in a tiny open dinghy struggling to stay alive in a tumultuous sea and pounding surf.
As Crane shows in his story, his characters’ salvations depend upon whether or not they will adapt to their surroundings and help their fellow human beings—not whether or not they can conquer nature.
I couldn’t help but think of Crane’s story and its inherent intimations after digesting firsthand accounts from medical staff on duty in ICUs during the recent traumatic experiences of Hurricane Katrina. The circumstances seem so unique and foreign in our modern age of delivering expeditious, accurate, and technologically supported medical care. I invite all physicians to bear witness to these incredulous stories and cleanse their own complacent perceptions, tabula rasa if you will, of functioning as a practitioner of 21st-century healthcare. These tales harken back to a not too distant time in medical practice.
Charity Hospital in New Orleans is one of the oldest continuously operating hospitals in the country. Along with University Hospital, another public facility just up Gravier Street in the Crescent City, Charity dispenses the lion’s share of all medical care in the city to one of the most uninsured populations in the country. Both hospitals are staffed and run jointly by Tulane and Louisiana State University (LSU), whose medical schools sit contiguously with Charity on opposite ends and lie unfavorably in one of the Big Easy’s topographical low points. Here are first-hand accounts from hospital staff who endured Hurricane Katrina from the confines of Charity and University hospitals.
Ben DeBoisblanc, MD, an LSU pulmonary attending physician, was assigned to Charity Hospital’s ICU. What follows is his chronicling of the events surrounding Hurricane Katrina.
“Prior to landfall it was obvious that Katrina had all the characteristics of the hurricane experts for decades had predicted would be the worst natural disaster in U.S. history: A category 5 storm hitting a city that is largely below sea level and completely surrounded by water. We were able to reduce our ICU patient load in Charity Hospital to about 50 prior to the storm hitting.
“After evacuating our own families, our emergency activation team set up to provide medical support for the remaining patients. During the storm windows blew out in the ICU, flooding it with about two inches of water. The power went out, but the emergency generators kicked on and all seemed well.
“But an hour later for some unknown reason we lost all power and began bagging our patients in total darkness. We were able to restart the backup generators late in the day on Monday, which allowed us to start cleaning up the mess in the ICU. Although the city was without power, we were high-fiving each other over a job well done. The day crew went to sleep late Monday, but was suddenly awakened at 3 a.m. on Tuesday to help bag patients when the emergency generators went out again. As dawn began to break we began to understand why: Water was pouring into downtown New Orleans from every direction and had flooded the generators that we located on the first floor.
—Ben DeBoisblanc, MD
“Without power for our life support systems (suction, monitors, vents, dialysis, IV fluid pumps, radiology, laboratory, etc.) we realized that we needed to get our patients out ASAP. Subsequently, a sanitation crisis unfolded when we lost water pressure for toilets. We were not only caring for 300 patients in the hospital but we were also providing refuge for more than 1,000 support staff and their families. Before we lost communication with the outside world on Tuesday FEMA instructed us to prepare for evacuation later that day. Much to our surprise the governor’s office was telling news agencies that we had already been evacuated. Needless to say, no outside help came until Friday, despite FEMA’s instructions.
“It soon became clear that if we were going to get out, we would have to get ourselves out. Our hazmat team had acquired four small diesel generators for field use, but did not have diesel fuel on site to power them. Our ICU respiratory therapist used his ‘Mississippi credit card’ (a hammer and a screwdriver) and some oxygen tubing to siphon diesel from on ambulance flooded on the ED ramp. We were able to power up the ICU to run about six vents. For the others we used gas driven portable vents or continued to hand bag. The roof of Charity Hospital was the only cool place to get a few hours of restorative sleep each night, so we broke away from our 12-on, 12-off usual staffing plan to allow each shift to enjoy a few hours with the rats seeking higher ground.
“By Wednesday we were still without any FEMA presence, and a morale crisis erupted among the employees. Although many staff were incapacitated with fear, grief, and despair, others dug deep and rose to the challenge. We could not communicate with police, National Guard, or FEMA, but our ICU residents were able to text message and get live on-air transmissions to CNN.
“On Wednesday, Francesco Simeone, a colleague from Tulane got a call from private air ambulance services wanting to send in their own helicopters to start the evacuation. The only problem was that the only commercial heliport in the area was at the Superdome, which was in the midst of a security crisis.
“Joe Lasky, the chief of Tulane pulmonary services, paddled a canoe from Charity and found a National Guard five-ton truck with a driver that was not in communication with his command. This actually worked to our advantage because he could not be accused of disobeying an order by helping us.
“Wednesday night we put the first four of our patients in the back of the truck and drove them across the street to Tulane Hospital’s parking garage. One patient was 23-year-old kid with Goodpasture’s and acute renal failure who had not been dialyzed in four days and who being bagged with 100% O2 and a 12 cm PEEP valve. We had to emergently insert a chest tube in the back of the National Guard truck when he desaturated in the middle of riding through the floodwaters.
“We then used a ‘borrowed’ pick-up truck to ferry the patients to the rooftop of a parking lot adjacent to Charity Hospital, where we set up a mini-ICU for the next two days. After removing light poles helicopters were able to begin landing, but the sun set before we could get any ICU patients to the roof, leaving us with four patients and no exit strategy for getting them out of New Orleans. The commercial ambulance personnel were able to communicate with military helicopters and by 11 p.m. Wednesday the clap-clap thunder of a Black Hawk was heard overhead. The Black Hawks were configured only as troop carriers, which meant that we would have to provide patient support for all of the sorties.
“The first ride for me was surreal: a moonless night, unlit buildings and towers, pilots with night vision goggles. A triage landing site had been established on the edge of town on the interstate. Amazingly there were thousands of people waiting, ready to help, but no one had known of our plight. We dumped our patients with brief medical records taped to their forearms into waiting ambulances for dispersion all over the region. A day later I got a call that the 23-year-old patient was alive and doing well.
“We continued the air evacuation all day Thursday, Thursday night, and Friday morning. Nurses cat-napped on the concrete roof by putting their heads on the legs of colleagues who bagged and comforted those waiting for the next helicopter. Not knowing the structural integrity of the rooftop, the Black Hawk pilots stayed powered up while we loaded our patients, docs, and O2 cylinders. After 48 hours of screaming commands over the roaring sound of the Black Hawks our entire ICU staff was both deaf and mute. By Friday afternoon we had completed our mission and walked the three blocks back to Charity in chest-deep sewage just in time to discover that FEMA had arrived to begin evacuating our hospital.
“I cried when I left Charity, perhaps for the last time ever. Some were tears of triumph, some were tears of profound sadness. Triumph for the miracle of human resolve that allowed a group of civilian doctors, nurses, and respiratory therapists to accomplish what the federal government could not. We got all of our patients out alive except two. One we expected to die; the other was an intubated elderly lady with COPD whose husband we were forced to leave behind at Charity.
“I remember how he sat day and night fanning his wife in the sweltering heat of the ICU. Fanning even as he seemed to slip into sleep. She died in the arms of her resident physician who could do no more on the rooftop than comfort her with the touch of a hand. I never saw her husband again because he was evacuated before I got back to the hospital. I don’t even know if he knows that she had died. Even if he does know, I somehow feel that he remains profoundly grateful.
“I feel sad because valuable time was lost both due to the anemic early response and because valuable resources were misused. I personally witnessed dozens and dozens of helicopters—many military—land and fly away with able-bodied citizens while patients died on the rooftop. And sadly, many of those able-bodied citizens were physicians.
“It was an experience that I will never forget. I left with one memento: a set of keys of a John Doe with an unknown medical condition that we loaded into a helicopter to be carried to an unknown place with an uncertain future. If you received a John Doe looking for his keys, let me know, I’d love to one day be able return them.”
Steve McPherson, MD, a third-year Tulane medicine resident was assigned to the ICU of University Hospital. Here is his story.
“I was on a typical every third call schedule for the ICU working that Friday night [August 26, 2005]. As far as I knew, Katrina was in the Gulf at a category 2 and headed for the Panhandle. Friday night as I answered four or five pages, I kept checking the weather channel. The reports kept looking worse. Katrina was growing in strength and had changed course to head right at New Orleans.
“Saturday morning I called my fiancée, informed her of the updated prediction of a direct hit category 4-5 hurricane and asked her to start packing to leave. That afternoon a ‘code gray’ [natural disaster] was called, and we were informed by e-mails and pages. This meant that both the Saturday and Sunday teams had to report on Sunday and would be on duty indefinitely.
“Sunday morning I reported to work under the code gray status. Katrina was bearing down on New Orleans, and it was evident from the media that there was going to be some major damage. [New Orleans] Mayor [Ray] Nagin issued a mandatory evacuation. Katrina was becoming a super-storm, and we were right in her path.
—Steve McPherson, MD
“Our attending rounded as usual that morning. Then he met with the upper echelon of hospital administration. At this meeting the house staff were informed that there was a real possibility that the first two floors of the hospital could be flooded. The administration asked all services to prioritize a list of ‘salvageable’ patients. Essentially this meant asking—assuming we lost power, generators, and elevators—who would be the most appropriate to carry manually up to higher floors. Further, assuming the necessity of economy in allocation of medical resources, who would stand the best chance of survival and would benefit from these resources.
“So, we put our heads together with the SICU teams and developed a triage list. The next step in hurricane preparation involved moving the patients away from vulnerable window areas in into an adjacent recovery area that was more internally located. The rest of Sunday afternoon was business as usual. There was, however, a palpable undercurrent of nervous anticipation. Sunday night we pitched a no-hitter. Of course, this was not due to luck but rather because the town was empty. Aside from zero admissions, the hospital that night from a functional standpoint was essentially normal.
“Monday morning Katrina struck. Despite being in a rather sturdy steel frame, brick-and-mortar public building, you could feel that the wind strength was impressive and the rain was pounding relentlessly like a banshee from hell. At 10 a.m., we lost primary power and generator power kicked in. The ICU was still functioning fairly normally. We were obtaining labs, running vents although we had no computer system, and had to retrieve lab results like an old-fashioned errand boy on the main floor.
“Outside, I could see about three feet of water had flooded Gravier Street. Surrounding houses were missing a few windows and shingles, but otherwise the damage seemed minimal, and it looked like initially we had dodged a bullet. I remember thinking that the levies had done their job. This notion became a pipe dream as the water level surrounding the hospital steadily began to rise sometime between the hours of 12 to 2 p.m. We had no idea about the now-infamous levy breaches, but the burgeoning deluge provided the information that the media or government was unable to give us at that time. The feculent water continued to rise slowly throughout the day. Pretty soon, I saw boats with outboard motors cruising by. I’m not sure if anyone in the hospital knew precisely that our predicament was becoming more precarious by the hour.
“Late Monday, a random boat pulled up to the ED ambulance ramp, which had become a makeshift dock. On board was the boat pilot, a New Orleans police officer, and two chronic ventilator/PEG nursing home residents. Our ED staff informed the cop that there was no way we were able to take these patients and care for them given the rising water levels and impending loss of even backup generator power.
“The cop insisted, stating, ‘This is not my problem.’ He laid the patients on the ED ramp and promptly departed. This incident caused quite a ruckus as no one really knew how to handle it.
“Hospital security quickly stepped in and barked, ‘Everybody inside. We’re locking down the building.’ I guess this was a desperate attempt to control a situation that was obviously way out of control by now and discourage any further ‘dumping’ of patients. All of the staff and residents quickly retreated inside the hospital in a knee-jerk reaction to the mandate. As we filed into the hospital like lemmings, Josh Willis, MD, one of our chiefs, suddenly realized the ethical mistake we were making by abandoning the cast-away patients lying on the ED ramp. ‘What kind of doctors are we anyway?’ I remember hearing him inquire rhetorically.
“This statement seemed to summon forth the quiescent words from the oath of Hippocrates when we had pledged to ‘ … apply dietetic measures for the benefit of the sick according to my ability and judgment … [and] … keep them from harm and injustice.’ We realized our mistake, turned around, and went back outside to bring the two patients into the hospital.
“Through early Monday evening, three to four similar trach/PEG patients were delivered from the same nursing home via watercraft. A piece of tape adhered to their threadbare gowns on which was written the name of the nursing home, the patient’s name, and their social security number. This was hardly a thorough past medical history or active problem list. We situated these patients with the other cast-offs inside the ED. It was apparent by initial observation that several of these patients were in dire medical straits at baseline, let alone having to deal with a natural disaster to boot.
“By early Tuesday morning, our backup generators went down. We had no labs, no chemistries, no ABGs. We were shooting from the hip, so to speak, in terms of treatment. Those nursing home patients brought in by boat remained not only in the ED, but also at the bottom of the ‘salvageable’ list.
“Besides just holding their hands, we could only give them supplemental oxygen. Meanwhile, on the roof of the hospital, a couple of smaller portable generators were running with lines powering three to four vents. Somehow it seemed that all the patients who really needed vents and who had made the salvageable list were getting them. By now, we already had to let one patient die … .
“By Tuesday afternoon the hospital had become—for all intents and purposes—entirely useless. The order was given to evacuate the entire hospital. The first order of business was to evacuate the most critically ill, salvageable patients. The house staff instructed the residents to accompany two patients each to Baton Rouge. One of my patients had West Nile virus and the other had dermatomyositis with ARDS in the fibroproliferative stage. The latter patient had been requiring 50%-75% FIO2. With only supplemental oxygen, trach tubes, and bags, we began our journey through the oppressive heat of late summer New Orleans.
“A boat took us to the Claiborne Avenue/I-10 ramp, which had also become a boat launch with awaiting ambulances. As we drove on the overpass past the drowning city, I could see hordes of wayward and destitute people lining the interstate and around the Superdome. The image was surreal. It looked like some third-world country in the throes of utter civil war chaos. The slings and arrows of outrageous fortune continued their incessant barrage as the ambulance I was riding in ran out of oxygen. The O2 sats on my ARDS patient began dropping precipitously into the low 80s. Before we could reach the safety of Maravich Center [now hospital] in Baton Rouge, we had to stop the ambulance so I could wave down a trailing ambulance and obtain more supplemental oxygen. With a wide-open valve on one tank, I alternated between patients until I was able to drop them off at triage. I called my fiancée who also happens to be an RN to pick me up, and we went to Bunkie, La., to await our next move. After two days, we traveled back to the Maravich Center to volunteer. We were told that our help wasn’t needed.
“It was frustrating to watch TV the next few days and see my colleagues still working at both Charity and University hospitals. I felt I should still be there with my teammates trying to sort through the medical maelstrom. In then end, I guess I took care of my patients and did what my attending ordered us to do. I was lucky because I got out on Tuesday. I’m sure it got ugly in there for everyone who didn’t get to leave until Friday.
“This has proven to be an experience that not many people go through and its lessons I will not soon forget. Leadership is a quality that too often gets overlooked when assessing the qualities of a good physician. When push comes to shove, we as physicians are ultimately responsible for running the patient-care ship. Without a doubt though, I do feel a closer bond with my program colleagues. Jeff Wiese, our program director, even sent out an e-mail stating that there would be no hard feelings if any resident wanted to find a new program. So far, there have been zero transfers.
“Based on the camaraderie being expressed among my fellow residents, I don’t anticipate that there will be any ultimately when all is said and done. This fellowship has truly been inspirational and renewed my own ethical ideals about being a physician.”
Conclusion
The harrowing presence of nature pervades Crane’s The Open Boat as it does the above accounts of two medicine residents during the tragedy of Katrina. But the most significant aspect of these struggles lies in human beings’ attempts to help one another survive despite their backgrounds, vocations, or social status. There is no fighting an angry sea or an incensed hurricane; neither can be conquered. But one can learn to survive the onslaught and to care for to the best of one’s ability those fellow human beings who are also caught in the grip of nature’s immense indifference whether they be castaways on the open ocean or deserted doctors in a drowning city.
“It would be difficult to describe the subtle brotherhood of men that was here established on the seas. No one said that it was so. No one mentioned it. But it dwelt in the boat, and each man felt it warm him. They were a captain, an oiler, a cook, and a correspondent, and they were friends, friends in a more curiously iron-bound degree than may be common.”—Stephen Crane, The Open Boat TH
Dr. Bucci is a psychiatric resident at the Mayo Clinic in Rochester, Minn., and a member of Tulane Medical School’s class of 2003.
“If this old ninny-woman, Fate, cannot do better than this, she should be deprived of the management of men’s fortunes. She is an old hen who knows not her intention. If she has decided to drown me, why did she not do it in the beginning and save me all this trouble. The whole affair is absurd. … But, no, she cannot mean to drown me. She dare not drown me. She cannot drown me. Not after all this work.”
—Stephen Crane, The Open Boat
Stephen Crane, the famous 19th-century American author of such works as The Red Badge of Courage, also penned a short story entitled The Open Boat during his illustrious career. The tale is a fictionalized narrative of a traumatic experience in his life. A ship on which he was a passenger sank during a storm off the coast of Florida. He found himself one of four survivors drifting in a tiny open dinghy struggling to stay alive in a tumultuous sea and pounding surf.
As Crane shows in his story, his characters’ salvations depend upon whether or not they will adapt to their surroundings and help their fellow human beings—not whether or not they can conquer nature.
I couldn’t help but think of Crane’s story and its inherent intimations after digesting firsthand accounts from medical staff on duty in ICUs during the recent traumatic experiences of Hurricane Katrina. The circumstances seem so unique and foreign in our modern age of delivering expeditious, accurate, and technologically supported medical care. I invite all physicians to bear witness to these incredulous stories and cleanse their own complacent perceptions, tabula rasa if you will, of functioning as a practitioner of 21st-century healthcare. These tales harken back to a not too distant time in medical practice.
Charity Hospital in New Orleans is one of the oldest continuously operating hospitals in the country. Along with University Hospital, another public facility just up Gravier Street in the Crescent City, Charity dispenses the lion’s share of all medical care in the city to one of the most uninsured populations in the country. Both hospitals are staffed and run jointly by Tulane and Louisiana State University (LSU), whose medical schools sit contiguously with Charity on opposite ends and lie unfavorably in one of the Big Easy’s topographical low points. Here are first-hand accounts from hospital staff who endured Hurricane Katrina from the confines of Charity and University hospitals.
Ben DeBoisblanc, MD, an LSU pulmonary attending physician, was assigned to Charity Hospital’s ICU. What follows is his chronicling of the events surrounding Hurricane Katrina.
“Prior to landfall it was obvious that Katrina had all the characteristics of the hurricane experts for decades had predicted would be the worst natural disaster in U.S. history: A category 5 storm hitting a city that is largely below sea level and completely surrounded by water. We were able to reduce our ICU patient load in Charity Hospital to about 50 prior to the storm hitting.
“After evacuating our own families, our emergency activation team set up to provide medical support for the remaining patients. During the storm windows blew out in the ICU, flooding it with about two inches of water. The power went out, but the emergency generators kicked on and all seemed well.
“But an hour later for some unknown reason we lost all power and began bagging our patients in total darkness. We were able to restart the backup generators late in the day on Monday, which allowed us to start cleaning up the mess in the ICU. Although the city was without power, we were high-fiving each other over a job well done. The day crew went to sleep late Monday, but was suddenly awakened at 3 a.m. on Tuesday to help bag patients when the emergency generators went out again. As dawn began to break we began to understand why: Water was pouring into downtown New Orleans from every direction and had flooded the generators that we located on the first floor.
—Ben DeBoisblanc, MD
“Without power for our life support systems (suction, monitors, vents, dialysis, IV fluid pumps, radiology, laboratory, etc.) we realized that we needed to get our patients out ASAP. Subsequently, a sanitation crisis unfolded when we lost water pressure for toilets. We were not only caring for 300 patients in the hospital but we were also providing refuge for more than 1,000 support staff and their families. Before we lost communication with the outside world on Tuesday FEMA instructed us to prepare for evacuation later that day. Much to our surprise the governor’s office was telling news agencies that we had already been evacuated. Needless to say, no outside help came until Friday, despite FEMA’s instructions.
“It soon became clear that if we were going to get out, we would have to get ourselves out. Our hazmat team had acquired four small diesel generators for field use, but did not have diesel fuel on site to power them. Our ICU respiratory therapist used his ‘Mississippi credit card’ (a hammer and a screwdriver) and some oxygen tubing to siphon diesel from on ambulance flooded on the ED ramp. We were able to power up the ICU to run about six vents. For the others we used gas driven portable vents or continued to hand bag. The roof of Charity Hospital was the only cool place to get a few hours of restorative sleep each night, so we broke away from our 12-on, 12-off usual staffing plan to allow each shift to enjoy a few hours with the rats seeking higher ground.
“By Wednesday we were still without any FEMA presence, and a morale crisis erupted among the employees. Although many staff were incapacitated with fear, grief, and despair, others dug deep and rose to the challenge. We could not communicate with police, National Guard, or FEMA, but our ICU residents were able to text message and get live on-air transmissions to CNN.
“On Wednesday, Francesco Simeone, a colleague from Tulane got a call from private air ambulance services wanting to send in their own helicopters to start the evacuation. The only problem was that the only commercial heliport in the area was at the Superdome, which was in the midst of a security crisis.
“Joe Lasky, the chief of Tulane pulmonary services, paddled a canoe from Charity and found a National Guard five-ton truck with a driver that was not in communication with his command. This actually worked to our advantage because he could not be accused of disobeying an order by helping us.
“Wednesday night we put the first four of our patients in the back of the truck and drove them across the street to Tulane Hospital’s parking garage. One patient was 23-year-old kid with Goodpasture’s and acute renal failure who had not been dialyzed in four days and who being bagged with 100% O2 and a 12 cm PEEP valve. We had to emergently insert a chest tube in the back of the National Guard truck when he desaturated in the middle of riding through the floodwaters.
“We then used a ‘borrowed’ pick-up truck to ferry the patients to the rooftop of a parking lot adjacent to Charity Hospital, where we set up a mini-ICU for the next two days. After removing light poles helicopters were able to begin landing, but the sun set before we could get any ICU patients to the roof, leaving us with four patients and no exit strategy for getting them out of New Orleans. The commercial ambulance personnel were able to communicate with military helicopters and by 11 p.m. Wednesday the clap-clap thunder of a Black Hawk was heard overhead. The Black Hawks were configured only as troop carriers, which meant that we would have to provide patient support for all of the sorties.
“The first ride for me was surreal: a moonless night, unlit buildings and towers, pilots with night vision goggles. A triage landing site had been established on the edge of town on the interstate. Amazingly there were thousands of people waiting, ready to help, but no one had known of our plight. We dumped our patients with brief medical records taped to their forearms into waiting ambulances for dispersion all over the region. A day later I got a call that the 23-year-old patient was alive and doing well.
“We continued the air evacuation all day Thursday, Thursday night, and Friday morning. Nurses cat-napped on the concrete roof by putting their heads on the legs of colleagues who bagged and comforted those waiting for the next helicopter. Not knowing the structural integrity of the rooftop, the Black Hawk pilots stayed powered up while we loaded our patients, docs, and O2 cylinders. After 48 hours of screaming commands over the roaring sound of the Black Hawks our entire ICU staff was both deaf and mute. By Friday afternoon we had completed our mission and walked the three blocks back to Charity in chest-deep sewage just in time to discover that FEMA had arrived to begin evacuating our hospital.
“I cried when I left Charity, perhaps for the last time ever. Some were tears of triumph, some were tears of profound sadness. Triumph for the miracle of human resolve that allowed a group of civilian doctors, nurses, and respiratory therapists to accomplish what the federal government could not. We got all of our patients out alive except two. One we expected to die; the other was an intubated elderly lady with COPD whose husband we were forced to leave behind at Charity.
“I remember how he sat day and night fanning his wife in the sweltering heat of the ICU. Fanning even as he seemed to slip into sleep. She died in the arms of her resident physician who could do no more on the rooftop than comfort her with the touch of a hand. I never saw her husband again because he was evacuated before I got back to the hospital. I don’t even know if he knows that she had died. Even if he does know, I somehow feel that he remains profoundly grateful.
“I feel sad because valuable time was lost both due to the anemic early response and because valuable resources were misused. I personally witnessed dozens and dozens of helicopters—many military—land and fly away with able-bodied citizens while patients died on the rooftop. And sadly, many of those able-bodied citizens were physicians.
“It was an experience that I will never forget. I left with one memento: a set of keys of a John Doe with an unknown medical condition that we loaded into a helicopter to be carried to an unknown place with an uncertain future. If you received a John Doe looking for his keys, let me know, I’d love to one day be able return them.”
Steve McPherson, MD, a third-year Tulane medicine resident was assigned to the ICU of University Hospital. Here is his story.
“I was on a typical every third call schedule for the ICU working that Friday night [August 26, 2005]. As far as I knew, Katrina was in the Gulf at a category 2 and headed for the Panhandle. Friday night as I answered four or five pages, I kept checking the weather channel. The reports kept looking worse. Katrina was growing in strength and had changed course to head right at New Orleans.
“Saturday morning I called my fiancée, informed her of the updated prediction of a direct hit category 4-5 hurricane and asked her to start packing to leave. That afternoon a ‘code gray’ [natural disaster] was called, and we were informed by e-mails and pages. This meant that both the Saturday and Sunday teams had to report on Sunday and would be on duty indefinitely.
“Sunday morning I reported to work under the code gray status. Katrina was bearing down on New Orleans, and it was evident from the media that there was going to be some major damage. [New Orleans] Mayor [Ray] Nagin issued a mandatory evacuation. Katrina was becoming a super-storm, and we were right in her path.
—Steve McPherson, MD
“Our attending rounded as usual that morning. Then he met with the upper echelon of hospital administration. At this meeting the house staff were informed that there was a real possibility that the first two floors of the hospital could be flooded. The administration asked all services to prioritize a list of ‘salvageable’ patients. Essentially this meant asking—assuming we lost power, generators, and elevators—who would be the most appropriate to carry manually up to higher floors. Further, assuming the necessity of economy in allocation of medical resources, who would stand the best chance of survival and would benefit from these resources.
“So, we put our heads together with the SICU teams and developed a triage list. The next step in hurricane preparation involved moving the patients away from vulnerable window areas in into an adjacent recovery area that was more internally located. The rest of Sunday afternoon was business as usual. There was, however, a palpable undercurrent of nervous anticipation. Sunday night we pitched a no-hitter. Of course, this was not due to luck but rather because the town was empty. Aside from zero admissions, the hospital that night from a functional standpoint was essentially normal.
“Monday morning Katrina struck. Despite being in a rather sturdy steel frame, brick-and-mortar public building, you could feel that the wind strength was impressive and the rain was pounding relentlessly like a banshee from hell. At 10 a.m., we lost primary power and generator power kicked in. The ICU was still functioning fairly normally. We were obtaining labs, running vents although we had no computer system, and had to retrieve lab results like an old-fashioned errand boy on the main floor.
“Outside, I could see about three feet of water had flooded Gravier Street. Surrounding houses were missing a few windows and shingles, but otherwise the damage seemed minimal, and it looked like initially we had dodged a bullet. I remember thinking that the levies had done their job. This notion became a pipe dream as the water level surrounding the hospital steadily began to rise sometime between the hours of 12 to 2 p.m. We had no idea about the now-infamous levy breaches, but the burgeoning deluge provided the information that the media or government was unable to give us at that time. The feculent water continued to rise slowly throughout the day. Pretty soon, I saw boats with outboard motors cruising by. I’m not sure if anyone in the hospital knew precisely that our predicament was becoming more precarious by the hour.
“Late Monday, a random boat pulled up to the ED ambulance ramp, which had become a makeshift dock. On board was the boat pilot, a New Orleans police officer, and two chronic ventilator/PEG nursing home residents. Our ED staff informed the cop that there was no way we were able to take these patients and care for them given the rising water levels and impending loss of even backup generator power.
“The cop insisted, stating, ‘This is not my problem.’ He laid the patients on the ED ramp and promptly departed. This incident caused quite a ruckus as no one really knew how to handle it.
“Hospital security quickly stepped in and barked, ‘Everybody inside. We’re locking down the building.’ I guess this was a desperate attempt to control a situation that was obviously way out of control by now and discourage any further ‘dumping’ of patients. All of the staff and residents quickly retreated inside the hospital in a knee-jerk reaction to the mandate. As we filed into the hospital like lemmings, Josh Willis, MD, one of our chiefs, suddenly realized the ethical mistake we were making by abandoning the cast-away patients lying on the ED ramp. ‘What kind of doctors are we anyway?’ I remember hearing him inquire rhetorically.
“This statement seemed to summon forth the quiescent words from the oath of Hippocrates when we had pledged to ‘ … apply dietetic measures for the benefit of the sick according to my ability and judgment … [and] … keep them from harm and injustice.’ We realized our mistake, turned around, and went back outside to bring the two patients into the hospital.
“Through early Monday evening, three to four similar trach/PEG patients were delivered from the same nursing home via watercraft. A piece of tape adhered to their threadbare gowns on which was written the name of the nursing home, the patient’s name, and their social security number. This was hardly a thorough past medical history or active problem list. We situated these patients with the other cast-offs inside the ED. It was apparent by initial observation that several of these patients were in dire medical straits at baseline, let alone having to deal with a natural disaster to boot.
“By early Tuesday morning, our backup generators went down. We had no labs, no chemistries, no ABGs. We were shooting from the hip, so to speak, in terms of treatment. Those nursing home patients brought in by boat remained not only in the ED, but also at the bottom of the ‘salvageable’ list.
“Besides just holding their hands, we could only give them supplemental oxygen. Meanwhile, on the roof of the hospital, a couple of smaller portable generators were running with lines powering three to four vents. Somehow it seemed that all the patients who really needed vents and who had made the salvageable list were getting them. By now, we already had to let one patient die … .
“By Tuesday afternoon the hospital had become—for all intents and purposes—entirely useless. The order was given to evacuate the entire hospital. The first order of business was to evacuate the most critically ill, salvageable patients. The house staff instructed the residents to accompany two patients each to Baton Rouge. One of my patients had West Nile virus and the other had dermatomyositis with ARDS in the fibroproliferative stage. The latter patient had been requiring 50%-75% FIO2. With only supplemental oxygen, trach tubes, and bags, we began our journey through the oppressive heat of late summer New Orleans.
“A boat took us to the Claiborne Avenue/I-10 ramp, which had also become a boat launch with awaiting ambulances. As we drove on the overpass past the drowning city, I could see hordes of wayward and destitute people lining the interstate and around the Superdome. The image was surreal. It looked like some third-world country in the throes of utter civil war chaos. The slings and arrows of outrageous fortune continued their incessant barrage as the ambulance I was riding in ran out of oxygen. The O2 sats on my ARDS patient began dropping precipitously into the low 80s. Before we could reach the safety of Maravich Center [now hospital] in Baton Rouge, we had to stop the ambulance so I could wave down a trailing ambulance and obtain more supplemental oxygen. With a wide-open valve on one tank, I alternated between patients until I was able to drop them off at triage. I called my fiancée who also happens to be an RN to pick me up, and we went to Bunkie, La., to await our next move. After two days, we traveled back to the Maravich Center to volunteer. We were told that our help wasn’t needed.
“It was frustrating to watch TV the next few days and see my colleagues still working at both Charity and University hospitals. I felt I should still be there with my teammates trying to sort through the medical maelstrom. In then end, I guess I took care of my patients and did what my attending ordered us to do. I was lucky because I got out on Tuesday. I’m sure it got ugly in there for everyone who didn’t get to leave until Friday.
“This has proven to be an experience that not many people go through and its lessons I will not soon forget. Leadership is a quality that too often gets overlooked when assessing the qualities of a good physician. When push comes to shove, we as physicians are ultimately responsible for running the patient-care ship. Without a doubt though, I do feel a closer bond with my program colleagues. Jeff Wiese, our program director, even sent out an e-mail stating that there would be no hard feelings if any resident wanted to find a new program. So far, there have been zero transfers.
“Based on the camaraderie being expressed among my fellow residents, I don’t anticipate that there will be any ultimately when all is said and done. This fellowship has truly been inspirational and renewed my own ethical ideals about being a physician.”
Conclusion
The harrowing presence of nature pervades Crane’s The Open Boat as it does the above accounts of two medicine residents during the tragedy of Katrina. But the most significant aspect of these struggles lies in human beings’ attempts to help one another survive despite their backgrounds, vocations, or social status. There is no fighting an angry sea or an incensed hurricane; neither can be conquered. But one can learn to survive the onslaught and to care for to the best of one’s ability those fellow human beings who are also caught in the grip of nature’s immense indifference whether they be castaways on the open ocean or deserted doctors in a drowning city.
“It would be difficult to describe the subtle brotherhood of men that was here established on the seas. No one said that it was so. No one mentioned it. But it dwelt in the boat, and each man felt it warm him. They were a captain, an oiler, a cook, and a correspondent, and they were friends, friends in a more curiously iron-bound degree than may be common.”—Stephen Crane, The Open Boat TH
Dr. Bucci is a psychiatric resident at the Mayo Clinic in Rochester, Minn., and a member of Tulane Medical School’s class of 2003.
Where Does Hospital Medicine Begin and End?

It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
It is clear to most of us in hospital medicine that the lines are rapidly blurring between the ED, and the floor, and the ICUs. Some of this has been brought about by the transitional units and the ability to place the patient in the most appropriate area with the correct level of monitoring equipment and nurse-to-patient ratio. Some of this has come about with the increased presence of hospitalists and intensivists in-house to complement the already ever-present ED physicians.
But now there is a movement afoot to both increase the use of observation units (OUs) and to change the physician oversight. Once thought to be an extension of the ED, OUs are now part of the hospitalists’ domain as these patients are thought to be more inpatient-light rather than long-term ED patients. And this makes sense when you realize that hospitalists are better suited to managing patients over time rather than ED physicians who favor shorter term relationships; you’re either admitted or “treated and streeted.”
This is further pushed toward the hospitalists’ realm as some OUs continue to treat patients for up to 48 hours (how can you be in a hospital bed for two days and still not be an inpatient?) and helped by the hospitalist’s 24/7 availability.
Having hospitalists serve as the medical directors for the OUs also makes sense because it gets these patients “out of the ED” from a logistic standpoint and shifts the responsibility to the hospitalist, freeing up the ED physicians to better do their primary job. This is just another in a list of examples of how hospitalists can improve ED throughput.
Further, now that governmental payers require closer on-site management of patients in OUs, this makes it virtually impossible for the outpatient-based primary care physicians to have a significant role.
According to The Advisory Board, Washington, D.C., and others, diseases such as CHF readily treated by hospitalists are well-suited to management in OUs. I thought I’d use CHF as an example of how a well-constructed OU might function. Obviously, there are clear classifications and criteria for those patients who are eligible to have their heart failure managed in an OU. And recent data have shown that appropriate management of CHF in OUs can lead to a lower admission rate, better use of resources, and better outcomes.
The OU setting can deliver a more extended course of therapy than traditionally available in the ED or a physician’s office for patients who may not need an acute hospitalization, but who are decompensating. With the best outcomes, management of CHF in an OU can prevent a hospitalization, delay a revisit to the ED, and improve the quality of the patient’s life by decreasing their symptoms and allowing them more time away form the hospital setting.
Not all patients who present to the ED with worsening CHF are candidates for OU management. Some clearly must be admitted. According to the American Heart Association/American College of Cardiology Guidelines the admission criteria for managing a CHF patient in an OU are:
- Adequate systemic perfusion;
- B-type natriuretic peptide < 100pg/mL;
- CXR consistent with CHF; and
- Demonstration of hemodynamic stability as evidenced by one of the following:
- Heart rate >50 or <130;
- Systolic blood pressure >90 and <175; or
- Oxygen saturation >90%.
As more physicians become aware of the benefits of OU care for these patients, there has been a >9% increase in the number of OU patients in both 2003 and 2004, according to Medicare data. And the increased use is even more dramatic for CHF patients.
As one looks at the elements to design and staff a functioning OU, it is apparent this falls clearly in the hospitalist’s capabilities. The idea is to develop more than just a place to stay longer in the ED, but to create an evidence-based, cost-effective management solution for difficult patients. Key components would include:
- Criteria for admission and exclusion based on risk stratification models;
- Protocols for treatment using evidence-based practice guidelines;
- Clear discharge process supported by patient education materials and discharge criteria; and
- Performance standards and an ongoing data collection and quality improvement process.
CHF is an expensive condition to manage, fraught with frequent episodes of decompensation and admission. This takes an economic toll on the system and results in a poorer quality of life for those patients burdened with the disease. Because many physician offices are not set up to handle patients with increasing symptoms related to CHF, the ED becomes the treatment center of last resort. Thoughtful management of those patients correctly suited to OU care can lead to more directed treatment and avoid hospitalizations that are expensive to the system and unnecessary for the patient.
All data point to an increased prevalence of OUs as more hospitals develop them and more patients are treated in OUs. In addition, professional societies are establishing guidelines and criteria for the appropriate use of OUs for certain ED patients. At the same time, management of patients in the OUs and for the OU itself is evolving to the hospitalist, who is the expert in longitudinal management of the hospitalized (and near hospitalized) patient.
Once again the hospitalist is at the center of new initiatives that are a win-win-win. OUs can minimize the patient’s time away from home, improve their functional capacity, relieve congestion in the ED, allow the ED physicians to concentrate on true ED patients, uncrowd the hospital and the ED and improve throughput, and save the system money. And hospitalists with a plan can make this happen.
Not bad for a specialty that is still the new kid on the block. TH
Dr. Wellikson has been CEO of SHM since 2000.
Tours of Duty
When a hospitalist steps outside during a seemingly unending shift, and a city is silent but for the bark of dogs, something is wrong. When he returns not to a scheduled shift, but to an undefined “tour of duty,” something is very wrong. Such has been the case for many hospitalists and healthcare providers along the Gulf Coast since Hurricane Katrina first devastated miles of the coast in August, and then Hurricane Rita hammered home our vulnerability to natural disasters in September. These sentinel experiences offer learning points for our nation’s healthcare system. “Challenges Hospitals Encountered During the 2005 Hurricane Seasons” (p. 8) lists some of the areas in which hospitals and healthcare providers were tested.

Half the Battle: Getting There
Eniola Otuseso, MD, a hospitalist who works in locum tenens positions across the southeast, calls Atlanta home. Her native Nigeria does not have hurricanes—their natural disasters are dust storms and monsoons—so she had never experienced one. The day before Hurricane Katrina hit, Dr. Otuseso had departed for her next job at Cogent Healthcare’s program at St. Dominic-Jackson Memorial Hospital (Miss.). Unable to take the last flight of the day, she packed a rental car and she, her 22-month-old son, and her teenage niece set off on the 380-mile journey to Jackson, Miss. Her account of the ride gives new meaning to the term “Sunday drive.”
MapQuest directions in hand, Dr. Otuseso took I-20 west toward Mississippi. From the road she called the hotel where she had reservations, only to find them canceled due to overbooking. She proceeded with nervous jitters: She had to report to work at 10 a.m. So she found another hotel, spent the night, and set out again at 6 a.m. Monday.
Then she had another problem: Although she thought she was on I-20 west, she had accidentally taken route 59 south—directly into New Orleans and the brunt of the storm. She notified the hospital that she was on the way, and promptly lost phone service. “I realized I needed to turn around and got off at the next exit, but a tree had blocked the road,” says Dr. Otuseso. “No one was around.”
She took the one-way exit back as trees fell around her. Her nervous jitters escalated to panic.
When a tree fell in front of her car, her attempted circumvention landed the car in the mud, and she ran out of gas trying to dislodge it. Miraculously, she had phone service, but the appalled 9-1-1 operators couldn’t help. Finally, a motorist and his adult passenger stopped and offered a ride. Dr. Otuseso and her wards climbed into the good Samaritan’s vehicle, and they were off again. The frequent need to get out of the car to haul trees from the road slowed their journey.
Finally, the mud was too thick and they became stuck. She managed to reach a nearby house on foot, and the owner used his tractor to move the car. He also offered them respite in his home with his wife and baby. A drenched, discouraged Dr. Otuseso and her children accepted the offer and were ferried there by tractor; her previous companions slogged on.
Dr. Otuseso is a graduate of Medical College of Georgia (Augusta). The rural family that housed her was was uneducated in some of the basics of preventive healthcare. Although culturally and in terms of health beliefs Dr. Otuseso and the family that sheltered her could not have been more different, the host family offered remarkable hospitality by providing food and clothing.
“Tragedy brings different people together,” Dr. Otuseso told her niece. The next day, the hurricane had passed, and the host family transported her to Hattiesburg, Miss., a town a mere 100 miles north of New Orleans. She needed basics: shelter and transportation. Hattiesburg’s hotel lacked power and water, and gas was scarce. Eventually, Dr. Otuseso convinced a service station owner to help her retrieve her rental car and fill it with gas. She then set off for Jackson.
On arrival in Jackson, she checked into another hotel with no water or electricity, but eventually made it to work Tuesday. The hospital had electricity and an endless stream of patients. Dr. Otuseso says that her experience made her more empathetic to patients. She could understand the extent of their loss. And after a lifetime of giving to others, she learned to accept help, hospitality, and assistance from others.
In New Orleans
Rob Minkes, MD, chief of pediatric surgery at Louisiana State University and Children’s Hospital (both of New Orleans) started a shift on Sunday, August 28 that became a four-day tour of duty. With him were more than 700 patients, families, and staff. Throughout the ordeal, they had Internet access and intermittent phone service. It was almost business-as-usual: All employees reported for work, and they even performed procedures in the surgical suite.
Once the storm passed, patients of all ages began to appear needing help. With them came strangers who threatened the hospital’s safety Employees could see looters from the windows. Some visitors who had no official purpose roamed the halls causing fear and despair among employees; although they were few and far between, they created chaos. Once the interlopers were escorted out, the hospital locked down. Lacking armed guards, they contacted local, state, and federal authorities for help, but none came.
“The situation became surreal, like a Stephen King novel,” explains Dr. Minkes. “There was just enough of what was normal, but the workplace and general life began to blend into some kind of limbo.”
He praises staff members who kept doing their jobs. The physicians made rounds, the nurses provided care, the housekeepers cleaned. “People can behave commendably in a crisis,” says Dr. Minkes, who noted that Children’s Hospital was well prepared and their disaster training was effective. The hospital was so prepared, in fact, that it was able to divert a fuel shipment that arrived Monday or Tuesday to a nearby facility that had a greater need.
On Wednesday morning, Children’s Hospital lost water pressure, so running water and air conditioning were history. Hospital leadership made the decision to evacuate patients and staff using any available means. Some neighboring hospitals sent helicopters. A convoy of ambulances and SUVs, staffed with care providers using hand-bag ventilators, set out for Baton Rouge. Those patients well enough were discharged. Hospital leadership received word that the National Guard had aircraft at the airport and could take remaining patients if they could be there by 7 p.m.
John Heaton, MD, chief anesthesiologist for Children’s Hospital, led a caravan of 40 cars, trucks, and SUVs to the interstate and onward to the airport. Staff members returned to the hospital despite worsening violence and health hazards in the city. Wednesday turned to the early hours of Thursday with only a few ICU patients remaining at Children’s.
At 4 a.m. a state trooper who came to support a chopper that was evacuating a patient recommended that staff prepare to evacuate at first light because of increasing danger due to flooding and looting in the city. Until then, Children’s had had very little contact with authorities, and basically made its decisions in isolation. One caravan of employees left with a police escort shortly thereafter. The remaining staff made their way unescorted when the last patient left for safety at 8 a.m., leaving a facility that had operated nobly despite Mother Nature’s wrath and security issues. When staff members left, Children’s Hospital had sustained only two broken windows.
Dr. Minkes praises the staff of every department, and indicates that leadership withstood this test. “The day after the hurricane, we were prepared to stay for two to six weeks,” he says.
When asked if he saw any skill used that surprised him in its utility, he hastens to say that they had power and water for most of the ordeal. He noted, however, that their chief of anesthesiology, an ardent fisher and hunter, calculated how high the waters would rise if the levies broke using a tool he retrieved from the Internet. He assured the staff that the water would not reach Children’s Hospital. It helped people’s spirits immensely.

Back to Jackson
Meanwhile, Dr. Otuseso was seeing an influx of patients in Jackson. With her, Lancy Clark, a registered nurse and Cogent Healthcare Program manager who liaises between St.Dominic-Jackson Memorial Hospital’s hospitalists and community physicians, was frankly shocked. The St.Dominic-Jackson facility staff—150 miles from Gulfport—had not thought that the devastation would reach them. It did.
With no electricity or water, St. Dominic-Jackson’s internal and external communication was in a shambles. Their backup: using the telephone, personal cell phones, and overhead page system. Although the county’s priority was to restore power and water to hospitals, its employees were working in the dark. And county-wide gas shortages meant that staff had difficulty reporting to work. Fortunately, the county gave healthcare providers head-of-the-line privileges for fuel.
“I was amazed at how fast people bounced up and worked,” says Clark. “We were all counselors. We often cried with patients as they told us their stories. We used all the resources we could to help emotionally and financially.”
In all of this, the healthcare providers, too, were victims; many have strong roots and family in the devastated communities.
As the adrenaline rush subsided and things started to be a little more normal, care providers began to feel the effects of the strain. All Clark wanted to do was sit in a chair and sink deep into it. Some experts call this compassion fatigue. It is a unique type of burnout experienced by people in fields that provide care for people under extreme circumstances, or the stress of caring for people who are scared, in pain, and/or suffering. Critical incident stress management and debriefing exercises are two ways to alleviate compassion fatigue. Clark indicates that Cogent Healthcare has plans to hold debriefings so they can apply what they learned.

Westward Bound
Some Hurricane Katrina evacuees found their way to Galveston, Texas. Two physicians on the faculty of the University of Texas Medical Branch (UTMB) at Galveston, Janice Smith, MD, and Donna Weaver, MD, worked in a Red Cross clinic assembled in a Methodist church’s indoor racquetball court.
Like hundreds of others, Dr. Smith responded to the call for volunteers early in the process to help the 300 evacuees. She says that there were many bureaucracies, and their nurse-coordinator handled them all well. In terms of challenges, “Every few hours, policies and procedures would change,” says Dr. Smith. “There was no interclinic communication, and roles were unclear. Although it was emotionally difficult seeing patients who had lost everything, that was the easy part compared to dealing with constant change.”
Dr. Weaver, who is codirector for Center for Training in International Health and teaches the Practice of Medicine course at UTMB at Galveston, responded to a request to describe her previous experience in one word: “Nicaragua.”
She often volunteers in Nicaragua (as does Dr. Smith) and in rural U.S. communities they open clinics in people’s homes. Dr. Weaver says the “organized disorganization” of a pharmacy stocked with samples, borrowed supplies and equipment, and no lab facilities created a situation in which physicians had to rely on medical clinical skills. People came with nothing, and medical records were unavailable. The medical history—just what the patient could tell them—was the cornerstone of treatment.
“The low-tech physicians did well,” she says. Listening skills became key. Dr. Weaver intends to reinforce that lesson with her students.
Both physicians could identify gaps that would have been nice to fill. Dr. Smith said that having an on-site dentist would have helped the many people suffering from toothaches. She also appreciates geographic prescribing differences more now, and would have liked to have had a pharmacist there to tell them what certain drugs were or suggest therapeutic alternatives. Dr. Weaver said privacy was at a premium—a situation that was uncomfortable for providers and patients alike. As each day passed, more barriers and walls were rigged to try to improve privacy.
Desk Jockeys No More
Anthony Campbell, RPh, DO, an internist and a pharmacist, and Joseph Matthews, RS, a sanitarian, were deployed together as part of a United States Public Health Service (USPHS) team. They landed in Louisiana to find their accommodations sufficient: a cot in one of five tents at Camp Allen that housed around 125 responders each. Both of these USPHS-commissioned officers had prior hospital-based practices in one of Washington, D.C.’s poorest neighborhoods. It was perhaps this recent experience that made them prime candidates to be plucked from desk jobs and jettisoned back into a stressed clinical milieu. While experience prepared them for the issues of indigence and poverty, it did not temper their reactions to the devastation and exposure to elements.
Their reunion made the task less challenging but the work they did was grueling. Dr. Campbell and Matthews traveled through parishes conducting needs assessments at Red Cross shelters in Washington Parish during the first week. The days were long—sometimes beginning at 5 a.m. and ending after 11 p.m.—and impossibly hot.
Both were impressed with people’s positive attitudes. Many shelters were overcrowded and lacked bathing facilities. Members of the community welcomed displaced people into their homes to shower and took turns preparing copious quantities of food. In a significantly overcrowded shelter, the Federal Emergency Management Agency (FEMA) tried to move people to hotels; often, unrelated people who had been neighbors or who had weathered the storm together would refuse to go unless they could go together. A group of retirees from Maine who were visiting New Orleans, for example, insisted on staying together even if it was in the crowded shelter. This was an unanticipated dynamic.
Matthews talked about what he called, “the changing theater,” a military term that describes the need to change plans frequently when conditions of austerity dictate it. He indicates that many clinicians were unacquainted with the principle of gathering your assets and regrouping when plans take an about-face. That was the case throughout their deployment.
During the second week, Dr. Campbell moved closer to New Orleans, and Matthews went to the area’s largest animal shelter, a place with five huge barns, two filled with horses and three with smaller pets. In the chaos there, his main concern was not the lack of volunteers—they had plenty—but the frequent disregard for human health risks as they handled hungry pets that had been plucked from toxic floodwaters. The need to take universal precautions is not a universal belief. Just trying to get people to wear gloves was an ordeal. The volunteers were often unaware of their own cuts and bruises, and worked relentlessly.
Matthews laughed as he related a story of the volunteers’ compassion. It was late in the evening, and his transport had not arrived. Concerned, he called the base operation and learned that he’d been forgotten. He started to melt down with anger and fatigue. A group of volunteers quickly surrounded him with comfort and reassurance; they thought he was upset because he couldn’t find his pet! It restored his sense of humor and balance.
Meanwhile, Dr. Campbell was knocking on doors in a housing project, looking for people with health needs. Care was centrally located in Washington Parish, but lacking communication methods and transportation, many residents didn’t know about the help offered there. He relied on the project’s resident manager to help his team. The manager often knew who had been evacuated, how many children lived in units, and who was older and remained.
Dr. Campbell cites the heat and incredible stench as indelible memories. His deployment ended in New Orleans. Even in the French Quarter, which sits on higher ground, the air was thick with the smell of rotting food that had been removed from freezers to prevent it from ruining equipment. (Clark in Mississippi also mentioned the memorable foul odor of rotting food.) He understands now why police officers and forensics workers carry Vicks VapoRub to dab under their nose when they find a decomposed body.
Dr. Campbell indicates that the Red Cross shelters needed more trained medical personnel, although they had ample donations of medication from doctors’ offices in the form of samples, and from hospitals and pharmacies. They did not have a pharmacist, however, and he relied on his dual training to provide some of the services that Dr. Smith in Galveston also identified. He was saddened by the devastation. He visited the Superdome and indicates that the debris and human waste told a sad and shocking story.
Patient Satisfaction
Sixty-year-old patient Emelda Zar evacuated from LaFitte, La., before Hurricane Katrina. She landed in a crowded but hospitable shelter in Jackson, Miss. Some days later, her daughter called an ambulance as Zar’s health deteriorated. She was admitted to St. Dominic-Jackson Memorial Hospital and diagnosed with heart failure.
Recently discharged and about to relocate to an apartment and planning to remain in Jackson, she and her grandchildren have nothing but good things to say about the hospital and, in particular, the hospitalists who provided care.
She arrived with no medical records and a serious health problem. Her hospitalists listened and created a care plan. She left the hospital with not only a clear idea of what she needs to do, but with a scheduled follow-up appointment in the community. Like so many of the people we heard about from healthcare providers, she remains upbeat and optimistic.
Progress Notes
Shortly after Dr. Smith and Dr. Weaver were interviewed in Galveston, the news was full of a new threat: Rita. This time, the hurricane’s target was a few hundred miles west of Katrina’s path. Karen Sexton, RN, PhD, vice president and chief executive officer of Hospitals and Clinics for UTMB shared the story of how Katrina changed their response.
During routine monitoring they saw tropical depression #18 develop on Sunday to the point that it was named Rita on Monday, and began to look like trouble for Galveston. By Tuesday, the city mayor had declared a voluntary evacuation, applying one lesson from Katrina: Residents could take their pets in government evacuation vehicles. The university went on emergency status. UTMB looked at decreasing their activity and reducing the hospital census. They sent the students home.
Tuesday night, their hospitalist service and other key physicians wrote transfer summaries for all patients, beginning with those who were gravely ill. This was a change of policy based on their experience with Katrina. They chose to move critically ill patients while they had the greatest control. The pharmacy prepared medication for all patients, and parts of medical records deemed most important were copied.
Wednesday dawned, and it was clear: Rita was coming in as a level 4 or 5 hurricane. For the first time in 114 years of existence, UTMB evacuated under Dr. Sexton’s direction as the incident commander. Using resources sent in part by the governor, their team discharged and evacuated 427 patients in 12 hours.
“We were all a little teary eyed when the first patient left,” says Dr. Sexton. “We knew we had never evacuated before and we knew were making history.”
Key to the success of UTMB’s evacuation were checklists on the units and at two evacuation stations. This, too, was something they learned from Katrina: Track patient disposition and send as much information as possible. With the goal of improving patient safety, UTMB recently started training staff on an aviation model that mimics what the aviation industry does to ensure safety.
They tracked what went with the patient, where the patient went, and that family notifications were done. The staff’s increased awareness and use of checklists were key components for a successful evacuation. No patients were “lost.” As the last patient left, Dr. Sexton found herself with a hospital staffed to support 500 to 700 patients, no patients, and the realization that staff also needed to evacuate but might not be able to navigate the exodus traffic.
Another request to the Texas governor’s office put two C130 cargo planes at their disposal. Staff were given three options: Stay at the hospital, leave of their own accord, or take the C130 to shelter in Houston. One-hundred-thirty-one staff members chose the latter option and left Thursday; the same planes brought them back the following Monday.
During the storm, UTMB’s ED remained open and staffed. It was the only operating ED for miles. A burn victim and several firemen who were harmed fighting a tremendous blaze during the storm on Friday proved that remaining open was the right thing to do to for the community.
Although UTMB lost some equipment, blocks of air conditioning, and some power, administrators believe that they made good decisions and emerged almost unscathed.
“I never felt prouder of our staff,” says Dr. Sexton. “This will be a different place because we all did this together.”
Less than a week later, they continue to treat patients from the community, have started admitting patients, and have welcomed some of their critically ill neonates back.
Conclusion
Who believes weather analysts? Often, we look at unwelcome weather forecasts and dismiss them, thinking that it always sounds worse than it is. Hospitalists and healthcare providers who weathered Katrina and Rita, and who are still working with the aftermath are probably more apt to listen to future dire weather predictions. “Lessons for Hospitalists from the 2005 Hurricane Season” (left) summarizes some of the lessons learned from the 2005 hurricane season to date. Every hospital will have to look at disaster plans and make changes based on what we’ve learned. Self-sufficiency for 48 hours is probably a less-than-ambitious goal; we may need to think in terms of planning for a week or more. Certainly, hospitalists will need to take leadership roles. TH
Contributor Jeannette Wick, RPh, MBA, is a senior clinical research pharmacist at the NIH in Bethesda, Md. The opinions expressed herein are those of the author and not necessarily those of any government agency.
When a hospitalist steps outside during a seemingly unending shift, and a city is silent but for the bark of dogs, something is wrong. When he returns not to a scheduled shift, but to an undefined “tour of duty,” something is very wrong. Such has been the case for many hospitalists and healthcare providers along the Gulf Coast since Hurricane Katrina first devastated miles of the coast in August, and then Hurricane Rita hammered home our vulnerability to natural disasters in September. These sentinel experiences offer learning points for our nation’s healthcare system. “Challenges Hospitals Encountered During the 2005 Hurricane Seasons” (p. 8) lists some of the areas in which hospitals and healthcare providers were tested.
Half the Battle: Getting There
Eniola Otuseso, MD, a hospitalist who works in locum tenens positions across the southeast, calls Atlanta home. Her native Nigeria does not have hurricanes—their natural disasters are dust storms and monsoons—so she had never experienced one. The day before Hurricane Katrina hit, Dr. Otuseso had departed for her next job at Cogent Healthcare’s program at St. Dominic-Jackson Memorial Hospital (Miss.). Unable to take the last flight of the day, she packed a rental car and she, her 22-month-old son, and her teenage niece set off on the 380-mile journey to Jackson, Miss. Her account of the ride gives new meaning to the term “Sunday drive.”
MapQuest directions in hand, Dr. Otuseso took I-20 west toward Mississippi. From the road she called the hotel where she had reservations, only to find them canceled due to overbooking. She proceeded with nervous jitters: She had to report to work at 10 a.m. So she found another hotel, spent the night, and set out again at 6 a.m. Monday.
Then she had another problem: Although she thought she was on I-20 west, she had accidentally taken route 59 south—directly into New Orleans and the brunt of the storm. She notified the hospital that she was on the way, and promptly lost phone service. “I realized I needed to turn around and got off at the next exit, but a tree had blocked the road,” says Dr. Otuseso. “No one was around.”
She took the one-way exit back as trees fell around her. Her nervous jitters escalated to panic.
When a tree fell in front of her car, her attempted circumvention landed the car in the mud, and she ran out of gas trying to dislodge it. Miraculously, she had phone service, but the appalled 9-1-1 operators couldn’t help. Finally, a motorist and his adult passenger stopped and offered a ride. Dr. Otuseso and her wards climbed into the good Samaritan’s vehicle, and they were off again. The frequent need to get out of the car to haul trees from the road slowed their journey.
Finally, the mud was too thick and they became stuck. She managed to reach a nearby house on foot, and the owner used his tractor to move the car. He also offered them respite in his home with his wife and baby. A drenched, discouraged Dr. Otuseso and her children accepted the offer and were ferried there by tractor; her previous companions slogged on.
Dr. Otuseso is a graduate of Medical College of Georgia (Augusta). The rural family that housed her was was uneducated in some of the basics of preventive healthcare. Although culturally and in terms of health beliefs Dr. Otuseso and the family that sheltered her could not have been more different, the host family offered remarkable hospitality by providing food and clothing.
“Tragedy brings different people together,” Dr. Otuseso told her niece. The next day, the hurricane had passed, and the host family transported her to Hattiesburg, Miss., a town a mere 100 miles north of New Orleans. She needed basics: shelter and transportation. Hattiesburg’s hotel lacked power and water, and gas was scarce. Eventually, Dr. Otuseso convinced a service station owner to help her retrieve her rental car and fill it with gas. She then set off for Jackson.
On arrival in Jackson, she checked into another hotel with no water or electricity, but eventually made it to work Tuesday. The hospital had electricity and an endless stream of patients. Dr. Otuseso says that her experience made her more empathetic to patients. She could understand the extent of their loss. And after a lifetime of giving to others, she learned to accept help, hospitality, and assistance from others.
In New Orleans
Rob Minkes, MD, chief of pediatric surgery at Louisiana State University and Children’s Hospital (both of New Orleans) started a shift on Sunday, August 28 that became a four-day tour of duty. With him were more than 700 patients, families, and staff. Throughout the ordeal, they had Internet access and intermittent phone service. It was almost business-as-usual: All employees reported for work, and they even performed procedures in the surgical suite.
Once the storm passed, patients of all ages began to appear needing help. With them came strangers who threatened the hospital’s safety Employees could see looters from the windows. Some visitors who had no official purpose roamed the halls causing fear and despair among employees; although they were few and far between, they created chaos. Once the interlopers were escorted out, the hospital locked down. Lacking armed guards, they contacted local, state, and federal authorities for help, but none came.
“The situation became surreal, like a Stephen King novel,” explains Dr. Minkes. “There was just enough of what was normal, but the workplace and general life began to blend into some kind of limbo.”
He praises staff members who kept doing their jobs. The physicians made rounds, the nurses provided care, the housekeepers cleaned. “People can behave commendably in a crisis,” says Dr. Minkes, who noted that Children’s Hospital was well prepared and their disaster training was effective. The hospital was so prepared, in fact, that it was able to divert a fuel shipment that arrived Monday or Tuesday to a nearby facility that had a greater need.
On Wednesday morning, Children’s Hospital lost water pressure, so running water and air conditioning were history. Hospital leadership made the decision to evacuate patients and staff using any available means. Some neighboring hospitals sent helicopters. A convoy of ambulances and SUVs, staffed with care providers using hand-bag ventilators, set out for Baton Rouge. Those patients well enough were discharged. Hospital leadership received word that the National Guard had aircraft at the airport and could take remaining patients if they could be there by 7 p.m.
John Heaton, MD, chief anesthesiologist for Children’s Hospital, led a caravan of 40 cars, trucks, and SUVs to the interstate and onward to the airport. Staff members returned to the hospital despite worsening violence and health hazards in the city. Wednesday turned to the early hours of Thursday with only a few ICU patients remaining at Children’s.
At 4 a.m. a state trooper who came to support a chopper that was evacuating a patient recommended that staff prepare to evacuate at first light because of increasing danger due to flooding and looting in the city. Until then, Children’s had had very little contact with authorities, and basically made its decisions in isolation. One caravan of employees left with a police escort shortly thereafter. The remaining staff made their way unescorted when the last patient left for safety at 8 a.m., leaving a facility that had operated nobly despite Mother Nature’s wrath and security issues. When staff members left, Children’s Hospital had sustained only two broken windows.
Dr. Minkes praises the staff of every department, and indicates that leadership withstood this test. “The day after the hurricane, we were prepared to stay for two to six weeks,” he says.
When asked if he saw any skill used that surprised him in its utility, he hastens to say that they had power and water for most of the ordeal. He noted, however, that their chief of anesthesiology, an ardent fisher and hunter, calculated how high the waters would rise if the levies broke using a tool he retrieved from the Internet. He assured the staff that the water would not reach Children’s Hospital. It helped people’s spirits immensely.
Back to Jackson
Meanwhile, Dr. Otuseso was seeing an influx of patients in Jackson. With her, Lancy Clark, a registered nurse and Cogent Healthcare Program manager who liaises between St.Dominic-Jackson Memorial Hospital’s hospitalists and community physicians, was frankly shocked. The St.Dominic-Jackson facility staff—150 miles from Gulfport—had not thought that the devastation would reach them. It did.
With no electricity or water, St. Dominic-Jackson’s internal and external communication was in a shambles. Their backup: using the telephone, personal cell phones, and overhead page system. Although the county’s priority was to restore power and water to hospitals, its employees were working in the dark. And county-wide gas shortages meant that staff had difficulty reporting to work. Fortunately, the county gave healthcare providers head-of-the-line privileges for fuel.
“I was amazed at how fast people bounced up and worked,” says Clark. “We were all counselors. We often cried with patients as they told us their stories. We used all the resources we could to help emotionally and financially.”
In all of this, the healthcare providers, too, were victims; many have strong roots and family in the devastated communities.
As the adrenaline rush subsided and things started to be a little more normal, care providers began to feel the effects of the strain. All Clark wanted to do was sit in a chair and sink deep into it. Some experts call this compassion fatigue. It is a unique type of burnout experienced by people in fields that provide care for people under extreme circumstances, or the stress of caring for people who are scared, in pain, and/or suffering. Critical incident stress management and debriefing exercises are two ways to alleviate compassion fatigue. Clark indicates that Cogent Healthcare has plans to hold debriefings so they can apply what they learned.
Westward Bound
Some Hurricane Katrina evacuees found their way to Galveston, Texas. Two physicians on the faculty of the University of Texas Medical Branch (UTMB) at Galveston, Janice Smith, MD, and Donna Weaver, MD, worked in a Red Cross clinic assembled in a Methodist church’s indoor racquetball court.
Like hundreds of others, Dr. Smith responded to the call for volunteers early in the process to help the 300 evacuees. She says that there were many bureaucracies, and their nurse-coordinator handled them all well. In terms of challenges, “Every few hours, policies and procedures would change,” says Dr. Smith. “There was no interclinic communication, and roles were unclear. Although it was emotionally difficult seeing patients who had lost everything, that was the easy part compared to dealing with constant change.”
Dr. Weaver, who is codirector for Center for Training in International Health and teaches the Practice of Medicine course at UTMB at Galveston, responded to a request to describe her previous experience in one word: “Nicaragua.”
She often volunteers in Nicaragua (as does Dr. Smith) and in rural U.S. communities they open clinics in people’s homes. Dr. Weaver says the “organized disorganization” of a pharmacy stocked with samples, borrowed supplies and equipment, and no lab facilities created a situation in which physicians had to rely on medical clinical skills. People came with nothing, and medical records were unavailable. The medical history—just what the patient could tell them—was the cornerstone of treatment.
“The low-tech physicians did well,” she says. Listening skills became key. Dr. Weaver intends to reinforce that lesson with her students.
Both physicians could identify gaps that would have been nice to fill. Dr. Smith said that having an on-site dentist would have helped the many people suffering from toothaches. She also appreciates geographic prescribing differences more now, and would have liked to have had a pharmacist there to tell them what certain drugs were or suggest therapeutic alternatives. Dr. Weaver said privacy was at a premium—a situation that was uncomfortable for providers and patients alike. As each day passed, more barriers and walls were rigged to try to improve privacy.
Desk Jockeys No More
Anthony Campbell, RPh, DO, an internist and a pharmacist, and Joseph Matthews, RS, a sanitarian, were deployed together as part of a United States Public Health Service (USPHS) team. They landed in Louisiana to find their accommodations sufficient: a cot in one of five tents at Camp Allen that housed around 125 responders each. Both of these USPHS-commissioned officers had prior hospital-based practices in one of Washington, D.C.’s poorest neighborhoods. It was perhaps this recent experience that made them prime candidates to be plucked from desk jobs and jettisoned back into a stressed clinical milieu. While experience prepared them for the issues of indigence and poverty, it did not temper their reactions to the devastation and exposure to elements.
Their reunion made the task less challenging but the work they did was grueling. Dr. Campbell and Matthews traveled through parishes conducting needs assessments at Red Cross shelters in Washington Parish during the first week. The days were long—sometimes beginning at 5 a.m. and ending after 11 p.m.—and impossibly hot.
Both were impressed with people’s positive attitudes. Many shelters were overcrowded and lacked bathing facilities. Members of the community welcomed displaced people into their homes to shower and took turns preparing copious quantities of food. In a significantly overcrowded shelter, the Federal Emergency Management Agency (FEMA) tried to move people to hotels; often, unrelated people who had been neighbors or who had weathered the storm together would refuse to go unless they could go together. A group of retirees from Maine who were visiting New Orleans, for example, insisted on staying together even if it was in the crowded shelter. This was an unanticipated dynamic.
Matthews talked about what he called, “the changing theater,” a military term that describes the need to change plans frequently when conditions of austerity dictate it. He indicates that many clinicians were unacquainted with the principle of gathering your assets and regrouping when plans take an about-face. That was the case throughout their deployment.
During the second week, Dr. Campbell moved closer to New Orleans, and Matthews went to the area’s largest animal shelter, a place with five huge barns, two filled with horses and three with smaller pets. In the chaos there, his main concern was not the lack of volunteers—they had plenty—but the frequent disregard for human health risks as they handled hungry pets that had been plucked from toxic floodwaters. The need to take universal precautions is not a universal belief. Just trying to get people to wear gloves was an ordeal. The volunteers were often unaware of their own cuts and bruises, and worked relentlessly.
Matthews laughed as he related a story of the volunteers’ compassion. It was late in the evening, and his transport had not arrived. Concerned, he called the base operation and learned that he’d been forgotten. He started to melt down with anger and fatigue. A group of volunteers quickly surrounded him with comfort and reassurance; they thought he was upset because he couldn’t find his pet! It restored his sense of humor and balance.
Meanwhile, Dr. Campbell was knocking on doors in a housing project, looking for people with health needs. Care was centrally located in Washington Parish, but lacking communication methods and transportation, many residents didn’t know about the help offered there. He relied on the project’s resident manager to help his team. The manager often knew who had been evacuated, how many children lived in units, and who was older and remained.
Dr. Campbell cites the heat and incredible stench as indelible memories. His deployment ended in New Orleans. Even in the French Quarter, which sits on higher ground, the air was thick with the smell of rotting food that had been removed from freezers to prevent it from ruining equipment. (Clark in Mississippi also mentioned the memorable foul odor of rotting food.) He understands now why police officers and forensics workers carry Vicks VapoRub to dab under their nose when they find a decomposed body.
Dr. Campbell indicates that the Red Cross shelters needed more trained medical personnel, although they had ample donations of medication from doctors’ offices in the form of samples, and from hospitals and pharmacies. They did not have a pharmacist, however, and he relied on his dual training to provide some of the services that Dr. Smith in Galveston also identified. He was saddened by the devastation. He visited the Superdome and indicates that the debris and human waste told a sad and shocking story.
Patient Satisfaction
Sixty-year-old patient Emelda Zar evacuated from LaFitte, La., before Hurricane Katrina. She landed in a crowded but hospitable shelter in Jackson, Miss. Some days later, her daughter called an ambulance as Zar’s health deteriorated. She was admitted to St. Dominic-Jackson Memorial Hospital and diagnosed with heart failure.
Recently discharged and about to relocate to an apartment and planning to remain in Jackson, she and her grandchildren have nothing but good things to say about the hospital and, in particular, the hospitalists who provided care.
She arrived with no medical records and a serious health problem. Her hospitalists listened and created a care plan. She left the hospital with not only a clear idea of what she needs to do, but with a scheduled follow-up appointment in the community. Like so many of the people we heard about from healthcare providers, she remains upbeat and optimistic.
Progress Notes
Shortly after Dr. Smith and Dr. Weaver were interviewed in Galveston, the news was full of a new threat: Rita. This time, the hurricane’s target was a few hundred miles west of Katrina’s path. Karen Sexton, RN, PhD, vice president and chief executive officer of Hospitals and Clinics for UTMB shared the story of how Katrina changed their response.
During routine monitoring they saw tropical depression #18 develop on Sunday to the point that it was named Rita on Monday, and began to look like trouble for Galveston. By Tuesday, the city mayor had declared a voluntary evacuation, applying one lesson from Katrina: Residents could take their pets in government evacuation vehicles. The university went on emergency status. UTMB looked at decreasing their activity and reducing the hospital census. They sent the students home.
Tuesday night, their hospitalist service and other key physicians wrote transfer summaries for all patients, beginning with those who were gravely ill. This was a change of policy based on their experience with Katrina. They chose to move critically ill patients while they had the greatest control. The pharmacy prepared medication for all patients, and parts of medical records deemed most important were copied.
Wednesday dawned, and it was clear: Rita was coming in as a level 4 or 5 hurricane. For the first time in 114 years of existence, UTMB evacuated under Dr. Sexton’s direction as the incident commander. Using resources sent in part by the governor, their team discharged and evacuated 427 patients in 12 hours.
“We were all a little teary eyed when the first patient left,” says Dr. Sexton. “We knew we had never evacuated before and we knew were making history.”
Key to the success of UTMB’s evacuation were checklists on the units and at two evacuation stations. This, too, was something they learned from Katrina: Track patient disposition and send as much information as possible. With the goal of improving patient safety, UTMB recently started training staff on an aviation model that mimics what the aviation industry does to ensure safety.
They tracked what went with the patient, where the patient went, and that family notifications were done. The staff’s increased awareness and use of checklists were key components for a successful evacuation. No patients were “lost.” As the last patient left, Dr. Sexton found herself with a hospital staffed to support 500 to 700 patients, no patients, and the realization that staff also needed to evacuate but might not be able to navigate the exodus traffic.
Another request to the Texas governor’s office put two C130 cargo planes at their disposal. Staff were given three options: Stay at the hospital, leave of their own accord, or take the C130 to shelter in Houston. One-hundred-thirty-one staff members chose the latter option and left Thursday; the same planes brought them back the following Monday.
During the storm, UTMB’s ED remained open and staffed. It was the only operating ED for miles. A burn victim and several firemen who were harmed fighting a tremendous blaze during the storm on Friday proved that remaining open was the right thing to do to for the community.
Although UTMB lost some equipment, blocks of air conditioning, and some power, administrators believe that they made good decisions and emerged almost unscathed.
“I never felt prouder of our staff,” says Dr. Sexton. “This will be a different place because we all did this together.”
Less than a week later, they continue to treat patients from the community, have started admitting patients, and have welcomed some of their critically ill neonates back.
Conclusion
Who believes weather analysts? Often, we look at unwelcome weather forecasts and dismiss them, thinking that it always sounds worse than it is. Hospitalists and healthcare providers who weathered Katrina and Rita, and who are still working with the aftermath are probably more apt to listen to future dire weather predictions. “Lessons for Hospitalists from the 2005 Hurricane Season” (left) summarizes some of the lessons learned from the 2005 hurricane season to date. Every hospital will have to look at disaster plans and make changes based on what we’ve learned. Self-sufficiency for 48 hours is probably a less-than-ambitious goal; we may need to think in terms of planning for a week or more. Certainly, hospitalists will need to take leadership roles. TH
Contributor Jeannette Wick, RPh, MBA, is a senior clinical research pharmacist at the NIH in Bethesda, Md. The opinions expressed herein are those of the author and not necessarily those of any government agency.
When a hospitalist steps outside during a seemingly unending shift, and a city is silent but for the bark of dogs, something is wrong. When he returns not to a scheduled shift, but to an undefined “tour of duty,” something is very wrong. Such has been the case for many hospitalists and healthcare providers along the Gulf Coast since Hurricane Katrina first devastated miles of the coast in August, and then Hurricane Rita hammered home our vulnerability to natural disasters in September. These sentinel experiences offer learning points for our nation’s healthcare system. “Challenges Hospitals Encountered During the 2005 Hurricane Seasons” (p. 8) lists some of the areas in which hospitals and healthcare providers were tested.
Half the Battle: Getting There
Eniola Otuseso, MD, a hospitalist who works in locum tenens positions across the southeast, calls Atlanta home. Her native Nigeria does not have hurricanes—their natural disasters are dust storms and monsoons—so she had never experienced one. The day before Hurricane Katrina hit, Dr. Otuseso had departed for her next job at Cogent Healthcare’s program at St. Dominic-Jackson Memorial Hospital (Miss.). Unable to take the last flight of the day, she packed a rental car and she, her 22-month-old son, and her teenage niece set off on the 380-mile journey to Jackson, Miss. Her account of the ride gives new meaning to the term “Sunday drive.”
MapQuest directions in hand, Dr. Otuseso took I-20 west toward Mississippi. From the road she called the hotel where she had reservations, only to find them canceled due to overbooking. She proceeded with nervous jitters: She had to report to work at 10 a.m. So she found another hotel, spent the night, and set out again at 6 a.m. Monday.
Then she had another problem: Although she thought she was on I-20 west, she had accidentally taken route 59 south—directly into New Orleans and the brunt of the storm. She notified the hospital that she was on the way, and promptly lost phone service. “I realized I needed to turn around and got off at the next exit, but a tree had blocked the road,” says Dr. Otuseso. “No one was around.”
She took the one-way exit back as trees fell around her. Her nervous jitters escalated to panic.
When a tree fell in front of her car, her attempted circumvention landed the car in the mud, and she ran out of gas trying to dislodge it. Miraculously, she had phone service, but the appalled 9-1-1 operators couldn’t help. Finally, a motorist and his adult passenger stopped and offered a ride. Dr. Otuseso and her wards climbed into the good Samaritan’s vehicle, and they were off again. The frequent need to get out of the car to haul trees from the road slowed their journey.
Finally, the mud was too thick and they became stuck. She managed to reach a nearby house on foot, and the owner used his tractor to move the car. He also offered them respite in his home with his wife and baby. A drenched, discouraged Dr. Otuseso and her children accepted the offer and were ferried there by tractor; her previous companions slogged on.
Dr. Otuseso is a graduate of Medical College of Georgia (Augusta). The rural family that housed her was was uneducated in some of the basics of preventive healthcare. Although culturally and in terms of health beliefs Dr. Otuseso and the family that sheltered her could not have been more different, the host family offered remarkable hospitality by providing food and clothing.
“Tragedy brings different people together,” Dr. Otuseso told her niece. The next day, the hurricane had passed, and the host family transported her to Hattiesburg, Miss., a town a mere 100 miles north of New Orleans. She needed basics: shelter and transportation. Hattiesburg’s hotel lacked power and water, and gas was scarce. Eventually, Dr. Otuseso convinced a service station owner to help her retrieve her rental car and fill it with gas. She then set off for Jackson.
On arrival in Jackson, she checked into another hotel with no water or electricity, but eventually made it to work Tuesday. The hospital had electricity and an endless stream of patients. Dr. Otuseso says that her experience made her more empathetic to patients. She could understand the extent of their loss. And after a lifetime of giving to others, she learned to accept help, hospitality, and assistance from others.
In New Orleans
Rob Minkes, MD, chief of pediatric surgery at Louisiana State University and Children’s Hospital (both of New Orleans) started a shift on Sunday, August 28 that became a four-day tour of duty. With him were more than 700 patients, families, and staff. Throughout the ordeal, they had Internet access and intermittent phone service. It was almost business-as-usual: All employees reported for work, and they even performed procedures in the surgical suite.
Once the storm passed, patients of all ages began to appear needing help. With them came strangers who threatened the hospital’s safety Employees could see looters from the windows. Some visitors who had no official purpose roamed the halls causing fear and despair among employees; although they were few and far between, they created chaos. Once the interlopers were escorted out, the hospital locked down. Lacking armed guards, they contacted local, state, and federal authorities for help, but none came.
“The situation became surreal, like a Stephen King novel,” explains Dr. Minkes. “There was just enough of what was normal, but the workplace and general life began to blend into some kind of limbo.”
He praises staff members who kept doing their jobs. The physicians made rounds, the nurses provided care, the housekeepers cleaned. “People can behave commendably in a crisis,” says Dr. Minkes, who noted that Children’s Hospital was well prepared and their disaster training was effective. The hospital was so prepared, in fact, that it was able to divert a fuel shipment that arrived Monday or Tuesday to a nearby facility that had a greater need.
On Wednesday morning, Children’s Hospital lost water pressure, so running water and air conditioning were history. Hospital leadership made the decision to evacuate patients and staff using any available means. Some neighboring hospitals sent helicopters. A convoy of ambulances and SUVs, staffed with care providers using hand-bag ventilators, set out for Baton Rouge. Those patients well enough were discharged. Hospital leadership received word that the National Guard had aircraft at the airport and could take remaining patients if they could be there by 7 p.m.
John Heaton, MD, chief anesthesiologist for Children’s Hospital, led a caravan of 40 cars, trucks, and SUVs to the interstate and onward to the airport. Staff members returned to the hospital despite worsening violence and health hazards in the city. Wednesday turned to the early hours of Thursday with only a few ICU patients remaining at Children’s.
At 4 a.m. a state trooper who came to support a chopper that was evacuating a patient recommended that staff prepare to evacuate at first light because of increasing danger due to flooding and looting in the city. Until then, Children’s had had very little contact with authorities, and basically made its decisions in isolation. One caravan of employees left with a police escort shortly thereafter. The remaining staff made their way unescorted when the last patient left for safety at 8 a.m., leaving a facility that had operated nobly despite Mother Nature’s wrath and security issues. When staff members left, Children’s Hospital had sustained only two broken windows.
Dr. Minkes praises the staff of every department, and indicates that leadership withstood this test. “The day after the hurricane, we were prepared to stay for two to six weeks,” he says.
When asked if he saw any skill used that surprised him in its utility, he hastens to say that they had power and water for most of the ordeal. He noted, however, that their chief of anesthesiology, an ardent fisher and hunter, calculated how high the waters would rise if the levies broke using a tool he retrieved from the Internet. He assured the staff that the water would not reach Children’s Hospital. It helped people’s spirits immensely.
Back to Jackson
Meanwhile, Dr. Otuseso was seeing an influx of patients in Jackson. With her, Lancy Clark, a registered nurse and Cogent Healthcare Program manager who liaises between St.Dominic-Jackson Memorial Hospital’s hospitalists and community physicians, was frankly shocked. The St.Dominic-Jackson facility staff—150 miles from Gulfport—had not thought that the devastation would reach them. It did.
With no electricity or water, St. Dominic-Jackson’s internal and external communication was in a shambles. Their backup: using the telephone, personal cell phones, and overhead page system. Although the county’s priority was to restore power and water to hospitals, its employees were working in the dark. And county-wide gas shortages meant that staff had difficulty reporting to work. Fortunately, the county gave healthcare providers head-of-the-line privileges for fuel.
“I was amazed at how fast people bounced up and worked,” says Clark. “We were all counselors. We often cried with patients as they told us their stories. We used all the resources we could to help emotionally and financially.”
In all of this, the healthcare providers, too, were victims; many have strong roots and family in the devastated communities.
As the adrenaline rush subsided and things started to be a little more normal, care providers began to feel the effects of the strain. All Clark wanted to do was sit in a chair and sink deep into it. Some experts call this compassion fatigue. It is a unique type of burnout experienced by people in fields that provide care for people under extreme circumstances, or the stress of caring for people who are scared, in pain, and/or suffering. Critical incident stress management and debriefing exercises are two ways to alleviate compassion fatigue. Clark indicates that Cogent Healthcare has plans to hold debriefings so they can apply what they learned.
Westward Bound
Some Hurricane Katrina evacuees found their way to Galveston, Texas. Two physicians on the faculty of the University of Texas Medical Branch (UTMB) at Galveston, Janice Smith, MD, and Donna Weaver, MD, worked in a Red Cross clinic assembled in a Methodist church’s indoor racquetball court.
Like hundreds of others, Dr. Smith responded to the call for volunteers early in the process to help the 300 evacuees. She says that there were many bureaucracies, and their nurse-coordinator handled them all well. In terms of challenges, “Every few hours, policies and procedures would change,” says Dr. Smith. “There was no interclinic communication, and roles were unclear. Although it was emotionally difficult seeing patients who had lost everything, that was the easy part compared to dealing with constant change.”
Dr. Weaver, who is codirector for Center for Training in International Health and teaches the Practice of Medicine course at UTMB at Galveston, responded to a request to describe her previous experience in one word: “Nicaragua.”
She often volunteers in Nicaragua (as does Dr. Smith) and in rural U.S. communities they open clinics in people’s homes. Dr. Weaver says the “organized disorganization” of a pharmacy stocked with samples, borrowed supplies and equipment, and no lab facilities created a situation in which physicians had to rely on medical clinical skills. People came with nothing, and medical records were unavailable. The medical history—just what the patient could tell them—was the cornerstone of treatment.
“The low-tech physicians did well,” she says. Listening skills became key. Dr. Weaver intends to reinforce that lesson with her students.
Both physicians could identify gaps that would have been nice to fill. Dr. Smith said that having an on-site dentist would have helped the many people suffering from toothaches. She also appreciates geographic prescribing differences more now, and would have liked to have had a pharmacist there to tell them what certain drugs were or suggest therapeutic alternatives. Dr. Weaver said privacy was at a premium—a situation that was uncomfortable for providers and patients alike. As each day passed, more barriers and walls were rigged to try to improve privacy.
Desk Jockeys No More
Anthony Campbell, RPh, DO, an internist and a pharmacist, and Joseph Matthews, RS, a sanitarian, were deployed together as part of a United States Public Health Service (USPHS) team. They landed in Louisiana to find their accommodations sufficient: a cot in one of five tents at Camp Allen that housed around 125 responders each. Both of these USPHS-commissioned officers had prior hospital-based practices in one of Washington, D.C.’s poorest neighborhoods. It was perhaps this recent experience that made them prime candidates to be plucked from desk jobs and jettisoned back into a stressed clinical milieu. While experience prepared them for the issues of indigence and poverty, it did not temper their reactions to the devastation and exposure to elements.
Their reunion made the task less challenging but the work they did was grueling. Dr. Campbell and Matthews traveled through parishes conducting needs assessments at Red Cross shelters in Washington Parish during the first week. The days were long—sometimes beginning at 5 a.m. and ending after 11 p.m.—and impossibly hot.
Both were impressed with people’s positive attitudes. Many shelters were overcrowded and lacked bathing facilities. Members of the community welcomed displaced people into their homes to shower and took turns preparing copious quantities of food. In a significantly overcrowded shelter, the Federal Emergency Management Agency (FEMA) tried to move people to hotels; often, unrelated people who had been neighbors or who had weathered the storm together would refuse to go unless they could go together. A group of retirees from Maine who were visiting New Orleans, for example, insisted on staying together even if it was in the crowded shelter. This was an unanticipated dynamic.
Matthews talked about what he called, “the changing theater,” a military term that describes the need to change plans frequently when conditions of austerity dictate it. He indicates that many clinicians were unacquainted with the principle of gathering your assets and regrouping when plans take an about-face. That was the case throughout their deployment.
During the second week, Dr. Campbell moved closer to New Orleans, and Matthews went to the area’s largest animal shelter, a place with five huge barns, two filled with horses and three with smaller pets. In the chaos there, his main concern was not the lack of volunteers—they had plenty—but the frequent disregard for human health risks as they handled hungry pets that had been plucked from toxic floodwaters. The need to take universal precautions is not a universal belief. Just trying to get people to wear gloves was an ordeal. The volunteers were often unaware of their own cuts and bruises, and worked relentlessly.
Matthews laughed as he related a story of the volunteers’ compassion. It was late in the evening, and his transport had not arrived. Concerned, he called the base operation and learned that he’d been forgotten. He started to melt down with anger and fatigue. A group of volunteers quickly surrounded him with comfort and reassurance; they thought he was upset because he couldn’t find his pet! It restored his sense of humor and balance.
Meanwhile, Dr. Campbell was knocking on doors in a housing project, looking for people with health needs. Care was centrally located in Washington Parish, but lacking communication methods and transportation, many residents didn’t know about the help offered there. He relied on the project’s resident manager to help his team. The manager often knew who had been evacuated, how many children lived in units, and who was older and remained.
Dr. Campbell cites the heat and incredible stench as indelible memories. His deployment ended in New Orleans. Even in the French Quarter, which sits on higher ground, the air was thick with the smell of rotting food that had been removed from freezers to prevent it from ruining equipment. (Clark in Mississippi also mentioned the memorable foul odor of rotting food.) He understands now why police officers and forensics workers carry Vicks VapoRub to dab under their nose when they find a decomposed body.
Dr. Campbell indicates that the Red Cross shelters needed more trained medical personnel, although they had ample donations of medication from doctors’ offices in the form of samples, and from hospitals and pharmacies. They did not have a pharmacist, however, and he relied on his dual training to provide some of the services that Dr. Smith in Galveston also identified. He was saddened by the devastation. He visited the Superdome and indicates that the debris and human waste told a sad and shocking story.
Patient Satisfaction
Sixty-year-old patient Emelda Zar evacuated from LaFitte, La., before Hurricane Katrina. She landed in a crowded but hospitable shelter in Jackson, Miss. Some days later, her daughter called an ambulance as Zar’s health deteriorated. She was admitted to St. Dominic-Jackson Memorial Hospital and diagnosed with heart failure.
Recently discharged and about to relocate to an apartment and planning to remain in Jackson, she and her grandchildren have nothing but good things to say about the hospital and, in particular, the hospitalists who provided care.
She arrived with no medical records and a serious health problem. Her hospitalists listened and created a care plan. She left the hospital with not only a clear idea of what she needs to do, but with a scheduled follow-up appointment in the community. Like so many of the people we heard about from healthcare providers, she remains upbeat and optimistic.
Progress Notes
Shortly after Dr. Smith and Dr. Weaver were interviewed in Galveston, the news was full of a new threat: Rita. This time, the hurricane’s target was a few hundred miles west of Katrina’s path. Karen Sexton, RN, PhD, vice president and chief executive officer of Hospitals and Clinics for UTMB shared the story of how Katrina changed their response.
During routine monitoring they saw tropical depression #18 develop on Sunday to the point that it was named Rita on Monday, and began to look like trouble for Galveston. By Tuesday, the city mayor had declared a voluntary evacuation, applying one lesson from Katrina: Residents could take their pets in government evacuation vehicles. The university went on emergency status. UTMB looked at decreasing their activity and reducing the hospital census. They sent the students home.
Tuesday night, their hospitalist service and other key physicians wrote transfer summaries for all patients, beginning with those who were gravely ill. This was a change of policy based on their experience with Katrina. They chose to move critically ill patients while they had the greatest control. The pharmacy prepared medication for all patients, and parts of medical records deemed most important were copied.
Wednesday dawned, and it was clear: Rita was coming in as a level 4 or 5 hurricane. For the first time in 114 years of existence, UTMB evacuated under Dr. Sexton’s direction as the incident commander. Using resources sent in part by the governor, their team discharged and evacuated 427 patients in 12 hours.
“We were all a little teary eyed when the first patient left,” says Dr. Sexton. “We knew we had never evacuated before and we knew were making history.”
Key to the success of UTMB’s evacuation were checklists on the units and at two evacuation stations. This, too, was something they learned from Katrina: Track patient disposition and send as much information as possible. With the goal of improving patient safety, UTMB recently started training staff on an aviation model that mimics what the aviation industry does to ensure safety.
They tracked what went with the patient, where the patient went, and that family notifications were done. The staff’s increased awareness and use of checklists were key components for a successful evacuation. No patients were “lost.” As the last patient left, Dr. Sexton found herself with a hospital staffed to support 500 to 700 patients, no patients, and the realization that staff also needed to evacuate but might not be able to navigate the exodus traffic.
Another request to the Texas governor’s office put two C130 cargo planes at their disposal. Staff were given three options: Stay at the hospital, leave of their own accord, or take the C130 to shelter in Houston. One-hundred-thirty-one staff members chose the latter option and left Thursday; the same planes brought them back the following Monday.
During the storm, UTMB’s ED remained open and staffed. It was the only operating ED for miles. A burn victim and several firemen who were harmed fighting a tremendous blaze during the storm on Friday proved that remaining open was the right thing to do to for the community.
Although UTMB lost some equipment, blocks of air conditioning, and some power, administrators believe that they made good decisions and emerged almost unscathed.
“I never felt prouder of our staff,” says Dr. Sexton. “This will be a different place because we all did this together.”
Less than a week later, they continue to treat patients from the community, have started admitting patients, and have welcomed some of their critically ill neonates back.
Conclusion
Who believes weather analysts? Often, we look at unwelcome weather forecasts and dismiss them, thinking that it always sounds worse than it is. Hospitalists and healthcare providers who weathered Katrina and Rita, and who are still working with the aftermath are probably more apt to listen to future dire weather predictions. “Lessons for Hospitalists from the 2005 Hurricane Season” (left) summarizes some of the lessons learned from the 2005 hurricane season to date. Every hospital will have to look at disaster plans and make changes based on what we’ve learned. Self-sufficiency for 48 hours is probably a less-than-ambitious goal; we may need to think in terms of planning for a week or more. Certainly, hospitalists will need to take leadership roles. TH
Contributor Jeannette Wick, RPh, MBA, is a senior clinical research pharmacist at the NIH in Bethesda, Md. The opinions expressed herein are those of the author and not necessarily those of any government agency.