User login
Undercover, MD

I had a baby. OK, that may not be entirely accurate: My wife, ever the stickler for details, likes to irritatingly point out that she had the baby and I just stood around, unearthing innovative means to get in the way while nervously asking inappropriate questions seemingly aimed only at annoying the hospital staff.
A baby was had, nonetheless.
And while that is remarkable, the really notable story is what happened during our hospital stay.
An Inauspicious Start
It’s hard to read a newspaper, view a television news program, or have a conversation in public without knowing the situation: The U.S. healthcare system is in shambles—nearly 50 million uninsured, 16% of GDP spent on healthcare, and a World Health Organization (WHO) overall ranking of 37th in the world based on multiple health indicators. And, of course, there’s the thorny data suggesting that as many as 98,000 patients die annually from hospital-induced medical errors.
As such, I was prepared and ever vigilant for this admission. This was my chance to see, from the patient’s perspective, this massive, impersonal, error-riddled, sputtering system. I would expose it for what it was, and take names.
We started our odyssey a bit early, as these things are wont to happen—two weeks early, in fact. A somewhat inauspicious start, some would say. Admittedly, that’s what my buddy grumbled as I called him 90 minutes before the first pitch of Game 4 of the National League Divisional Series to tell him he’d have to watch the Phillies play the Rockies without me.
The Death Trap Beckons
My wife went to check in while I parked the car. Well, sort of park the car. It turns out this unwelcoming beast known as “the hospital” actually employed valets to park my car. “Parking is the last thing you need to worry about right now,” the attendant said. I, however, saw through this ruse. Aaron—according to his nametag—is up to no good, or so I thought, counting the pennies in my ashtray.
After checking in, the first person my wife and I encountered was Jane, our nurse. She came in all bubbly, effusing that “things will go well and you’ll be with your new addition very soon.” All heart-warming encouragement and smiles aside, she actually appeared unaware of this death trap cavorting as a hospital—a jumbo jet’s worth of patients dying from medical errors every day is no laughing matter, missy. “I’ve got my eye on you,” I whispered conspiratorially to no one; a knowing smirk appeared as I took down her name.
Later, this Jane would interrupt my attempts to make my wife laugh through expertly executed 1980s dance moves. Jane implored her to just “let it out and cry for a few minutes—then you’ll feel better.” Somewhat embarrassingly, this automaton was so caught up in her own medical world that she misinterpreted my wife’s tears of laughter for tears of apprehension. Oh, how misguided these medical personnel can be. “Stick to the nursing and I’ll comfort my wife,” I thought to myself. My wife, meanwhile, was in the process of “letting it out,” after which she did indeed report feeling better. Oh, she’s good. If I didn’t know her so well, she would have led me to believe Nurse Jane’s advice was sage, caring, and spot-on. I wasn’t fooled; my wife’s a sucker for my dance moves.
Procedural Missteps: I’ll Be Outside
Next up: Steve, a second-year anesthesia resident intent on plunging a catheter into my wife’s spine for pain relief. Little did young Steve know that I was on to him and his attempts to give my wife Brown-Séquard syndrome. After all, procedures are a common source of hospital error. Under the guise of “informed consent,” he spouted the pros and cons of the procedure, all the while failing to mention the near certainty with which my wife would develop paralysis from a spinal hematoma.
Of course, I am no boob. I relentlessly exposed this neophyte with my knowing questions, finishing the undressing with a curt “there is no way you’re coming near my wife with that needle!” To which my wife, in her ever-tender way, ordered me to get the hell out of the room so she could get some (unprintable expletive) pain relief. See, this young doctor was getting to her as well.
Undeterred, I continued to prowl for medical errors. Knowing communication to be fertile ground for hospital slip-ups, I watched intently the handoff of care the day nurse, Jane, gave to the night nurse, Sarah. Surprisingly, Jane appeared to get it all right—at least that’s how it would appear to the untrained eye. She succinctly overviewed our history and course, documented the medications my wife received, gave the plan, and told her what to do if things didn’t follow that plan. Sarah repeated back the salient points as she reviewed the written chart and asked a few questions.
All good on the surface, but she spent so much time doting over my wife’s emotional needs that she failed to notice my discontent over the Rockies’ series-ending loss to the Phillies. I helpfully pointed out this blunder to her, at which time my wife rolled her eyes and asked, “Why can’t guys have babies?” Assuming my wife missed that class in medical school, I immediately began to overview basic reproductive physiology, at which point I was again asked to leave the room—this time by Nurse Sarah.
Waiting-Room Reflections
Not one to be satisfied with my victories, I stalked the halls looking for a less-than-15-second hand wash or an HIPAA violation. Seeing none, I pondered my wife’s fate at the hands of this massive, impersonal, error-riddled healthcare machine. I just couldn’t surmise a scenario in which she’d get out of there alive.
Just then, Susan, our obstetrician, came out to let me know that my daughter would soon be making her entrance. She informed me that it would be OK to film the procedure, if I liked. “But what about malpractice? Aren’t you worried about having this on film?” I asked. “Not a bit,” she replied. “What I’m worried about is your horsing around causing us both to miss this delivery.”
With that, we were back in the room, reunited in our common purpose. Moments later, I was the proud owner of a freshly minted baby girl.
Putting down the video camera, the state of the healthcare system finally came into focus. To be certain, we have our problems. But this wasn’t the massive, impersonal, sputtering system I was led to expect. Rather, I found it filled with caring, compassionate, highly skilled professionals with names like Aaron, Jane, Sarah, Steve, and Susan. Together, they had engineered a true miracle.
A miracle named Kaiya. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I had a baby. OK, that may not be entirely accurate: My wife, ever the stickler for details, likes to irritatingly point out that she had the baby and I just stood around, unearthing innovative means to get in the way while nervously asking inappropriate questions seemingly aimed only at annoying the hospital staff.
A baby was had, nonetheless.
And while that is remarkable, the really notable story is what happened during our hospital stay.
An Inauspicious Start
It’s hard to read a newspaper, view a television news program, or have a conversation in public without knowing the situation: The U.S. healthcare system is in shambles—nearly 50 million uninsured, 16% of GDP spent on healthcare, and a World Health Organization (WHO) overall ranking of 37th in the world based on multiple health indicators. And, of course, there’s the thorny data suggesting that as many as 98,000 patients die annually from hospital-induced medical errors.
As such, I was prepared and ever vigilant for this admission. This was my chance to see, from the patient’s perspective, this massive, impersonal, error-riddled, sputtering system. I would expose it for what it was, and take names.
We started our odyssey a bit early, as these things are wont to happen—two weeks early, in fact. A somewhat inauspicious start, some would say. Admittedly, that’s what my buddy grumbled as I called him 90 minutes before the first pitch of Game 4 of the National League Divisional Series to tell him he’d have to watch the Phillies play the Rockies without me.
The Death Trap Beckons
My wife went to check in while I parked the car. Well, sort of park the car. It turns out this unwelcoming beast known as “the hospital” actually employed valets to park my car. “Parking is the last thing you need to worry about right now,” the attendant said. I, however, saw through this ruse. Aaron—according to his nametag—is up to no good, or so I thought, counting the pennies in my ashtray.
After checking in, the first person my wife and I encountered was Jane, our nurse. She came in all bubbly, effusing that “things will go well and you’ll be with your new addition very soon.” All heart-warming encouragement and smiles aside, she actually appeared unaware of this death trap cavorting as a hospital—a jumbo jet’s worth of patients dying from medical errors every day is no laughing matter, missy. “I’ve got my eye on you,” I whispered conspiratorially to no one; a knowing smirk appeared as I took down her name.
Later, this Jane would interrupt my attempts to make my wife laugh through expertly executed 1980s dance moves. Jane implored her to just “let it out and cry for a few minutes—then you’ll feel better.” Somewhat embarrassingly, this automaton was so caught up in her own medical world that she misinterpreted my wife’s tears of laughter for tears of apprehension. Oh, how misguided these medical personnel can be. “Stick to the nursing and I’ll comfort my wife,” I thought to myself. My wife, meanwhile, was in the process of “letting it out,” after which she did indeed report feeling better. Oh, she’s good. If I didn’t know her so well, she would have led me to believe Nurse Jane’s advice was sage, caring, and spot-on. I wasn’t fooled; my wife’s a sucker for my dance moves.
Procedural Missteps: I’ll Be Outside
Next up: Steve, a second-year anesthesia resident intent on plunging a catheter into my wife’s spine for pain relief. Little did young Steve know that I was on to him and his attempts to give my wife Brown-Séquard syndrome. After all, procedures are a common source of hospital error. Under the guise of “informed consent,” he spouted the pros and cons of the procedure, all the while failing to mention the near certainty with which my wife would develop paralysis from a spinal hematoma.
Of course, I am no boob. I relentlessly exposed this neophyte with my knowing questions, finishing the undressing with a curt “there is no way you’re coming near my wife with that needle!” To which my wife, in her ever-tender way, ordered me to get the hell out of the room so she could get some (unprintable expletive) pain relief. See, this young doctor was getting to her as well.
Undeterred, I continued to prowl for medical errors. Knowing communication to be fertile ground for hospital slip-ups, I watched intently the handoff of care the day nurse, Jane, gave to the night nurse, Sarah. Surprisingly, Jane appeared to get it all right—at least that’s how it would appear to the untrained eye. She succinctly overviewed our history and course, documented the medications my wife received, gave the plan, and told her what to do if things didn’t follow that plan. Sarah repeated back the salient points as she reviewed the written chart and asked a few questions.
All good on the surface, but she spent so much time doting over my wife’s emotional needs that she failed to notice my discontent over the Rockies’ series-ending loss to the Phillies. I helpfully pointed out this blunder to her, at which time my wife rolled her eyes and asked, “Why can’t guys have babies?” Assuming my wife missed that class in medical school, I immediately began to overview basic reproductive physiology, at which point I was again asked to leave the room—this time by Nurse Sarah.
Waiting-Room Reflections
Not one to be satisfied with my victories, I stalked the halls looking for a less-than-15-second hand wash or an HIPAA violation. Seeing none, I pondered my wife’s fate at the hands of this massive, impersonal, error-riddled healthcare machine. I just couldn’t surmise a scenario in which she’d get out of there alive.
Just then, Susan, our obstetrician, came out to let me know that my daughter would soon be making her entrance. She informed me that it would be OK to film the procedure, if I liked. “But what about malpractice? Aren’t you worried about having this on film?” I asked. “Not a bit,” she replied. “What I’m worried about is your horsing around causing us both to miss this delivery.”
With that, we were back in the room, reunited in our common purpose. Moments later, I was the proud owner of a freshly minted baby girl.
Putting down the video camera, the state of the healthcare system finally came into focus. To be certain, we have our problems. But this wasn’t the massive, impersonal, sputtering system I was led to expect. Rather, I found it filled with caring, compassionate, highly skilled professionals with names like Aaron, Jane, Sarah, Steve, and Susan. Together, they had engineered a true miracle.
A miracle named Kaiya. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
I had a baby. OK, that may not be entirely accurate: My wife, ever the stickler for details, likes to irritatingly point out that she had the baby and I just stood around, unearthing innovative means to get in the way while nervously asking inappropriate questions seemingly aimed only at annoying the hospital staff.
A baby was had, nonetheless.
And while that is remarkable, the really notable story is what happened during our hospital stay.
An Inauspicious Start
It’s hard to read a newspaper, view a television news program, or have a conversation in public without knowing the situation: The U.S. healthcare system is in shambles—nearly 50 million uninsured, 16% of GDP spent on healthcare, and a World Health Organization (WHO) overall ranking of 37th in the world based on multiple health indicators. And, of course, there’s the thorny data suggesting that as many as 98,000 patients die annually from hospital-induced medical errors.
As such, I was prepared and ever vigilant for this admission. This was my chance to see, from the patient’s perspective, this massive, impersonal, error-riddled, sputtering system. I would expose it for what it was, and take names.
We started our odyssey a bit early, as these things are wont to happen—two weeks early, in fact. A somewhat inauspicious start, some would say. Admittedly, that’s what my buddy grumbled as I called him 90 minutes before the first pitch of Game 4 of the National League Divisional Series to tell him he’d have to watch the Phillies play the Rockies without me.
The Death Trap Beckons
My wife went to check in while I parked the car. Well, sort of park the car. It turns out this unwelcoming beast known as “the hospital” actually employed valets to park my car. “Parking is the last thing you need to worry about right now,” the attendant said. I, however, saw through this ruse. Aaron—according to his nametag—is up to no good, or so I thought, counting the pennies in my ashtray.
After checking in, the first person my wife and I encountered was Jane, our nurse. She came in all bubbly, effusing that “things will go well and you’ll be with your new addition very soon.” All heart-warming encouragement and smiles aside, she actually appeared unaware of this death trap cavorting as a hospital—a jumbo jet’s worth of patients dying from medical errors every day is no laughing matter, missy. “I’ve got my eye on you,” I whispered conspiratorially to no one; a knowing smirk appeared as I took down her name.
Later, this Jane would interrupt my attempts to make my wife laugh through expertly executed 1980s dance moves. Jane implored her to just “let it out and cry for a few minutes—then you’ll feel better.” Somewhat embarrassingly, this automaton was so caught up in her own medical world that she misinterpreted my wife’s tears of laughter for tears of apprehension. Oh, how misguided these medical personnel can be. “Stick to the nursing and I’ll comfort my wife,” I thought to myself. My wife, meanwhile, was in the process of “letting it out,” after which she did indeed report feeling better. Oh, she’s good. If I didn’t know her so well, she would have led me to believe Nurse Jane’s advice was sage, caring, and spot-on. I wasn’t fooled; my wife’s a sucker for my dance moves.
Procedural Missteps: I’ll Be Outside
Next up: Steve, a second-year anesthesia resident intent on plunging a catheter into my wife’s spine for pain relief. Little did young Steve know that I was on to him and his attempts to give my wife Brown-Séquard syndrome. After all, procedures are a common source of hospital error. Under the guise of “informed consent,” he spouted the pros and cons of the procedure, all the while failing to mention the near certainty with which my wife would develop paralysis from a spinal hematoma.
Of course, I am no boob. I relentlessly exposed this neophyte with my knowing questions, finishing the undressing with a curt “there is no way you’re coming near my wife with that needle!” To which my wife, in her ever-tender way, ordered me to get the hell out of the room so she could get some (unprintable expletive) pain relief. See, this young doctor was getting to her as well.
Undeterred, I continued to prowl for medical errors. Knowing communication to be fertile ground for hospital slip-ups, I watched intently the handoff of care the day nurse, Jane, gave to the night nurse, Sarah. Surprisingly, Jane appeared to get it all right—at least that’s how it would appear to the untrained eye. She succinctly overviewed our history and course, documented the medications my wife received, gave the plan, and told her what to do if things didn’t follow that plan. Sarah repeated back the salient points as she reviewed the written chart and asked a few questions.
All good on the surface, but she spent so much time doting over my wife’s emotional needs that she failed to notice my discontent over the Rockies’ series-ending loss to the Phillies. I helpfully pointed out this blunder to her, at which time my wife rolled her eyes and asked, “Why can’t guys have babies?” Assuming my wife missed that class in medical school, I immediately began to overview basic reproductive physiology, at which point I was again asked to leave the room—this time by Nurse Sarah.
Waiting-Room Reflections
Not one to be satisfied with my victories, I stalked the halls looking for a less-than-15-second hand wash or an HIPAA violation. Seeing none, I pondered my wife’s fate at the hands of this massive, impersonal, error-riddled healthcare machine. I just couldn’t surmise a scenario in which she’d get out of there alive.
Just then, Susan, our obstetrician, came out to let me know that my daughter would soon be making her entrance. She informed me that it would be OK to film the procedure, if I liked. “But what about malpractice? Aren’t you worried about having this on film?” I asked. “Not a bit,” she replied. “What I’m worried about is your horsing around causing us both to miss this delivery.”
With that, we were back in the room, reunited in our common purpose. Moments later, I was the proud owner of a freshly minted baby girl.
Putting down the video camera, the state of the healthcare system finally came into focus. To be certain, we have our problems. But this wasn’t the massive, impersonal, sputtering system I was led to expect. Rather, I found it filled with caring, compassionate, highly skilled professionals with names like Aaron, Jane, Sarah, Steve, and Susan. Together, they had engineered a true miracle.
A miracle named Kaiya. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
A Watershed Moment

The announcement was made Sept. 23, 2009. The American Board of Medical Specialties (ABMS) had approved a “pilot program” for Recognition of Focused Practice (RFP) in Hospital Medicine. ABMS-sanctioned board certification for hospitalists had finally arrived.
When the announcement came, I was at the University of California at San Francisco’s CME conference with 600 other hospitalists. Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, announced the RFP in HM to the audience—it received resounding applause. Dr. Wachter, the UCSF conference chair, then went on to recap the history behind RFP and how we got here. As he spoke, I realized that I had forgotten how long this process had taken and how much work had been done by so many people.
To practicing hospitalists, the creation of some sort of certification in HM seems like the proverbial no-brainer. But think about it from the American Board of Internal Medicine (ABIM) perspective: All “specialties” with board certification have training programs or fellowships that help define them. We do not have hospitalist residency programs or fellowships that are necessary for practicing as a hospitalist. Our expertise is acquired during practice.
So if the training path for hospitalists is not different—at least for now—from that of other general internists, how do we create board certification? When a group, such as hospitalists, “asks” to be recognized as a specialty with their own certification, the ABIM needs to consider the implications of creating such recognition. For hospitalists, the question was: If we do this for hospitalists, do we have to create a certificate for officists or outpatient physicians? For the broader questions around recognition of focused practice, the board needed to ask, “What if a group comes forward and asks for recognition of their focus and expertise in caring for diabetes or sepsis?”
ABIM thought very carefully about these questions. For the latter, ABIM says the field asking for recognition of focused practice must have a lot of physicians who only practice in this field while also having large numbers of physicians who never practice in the field. And they said, “Yes, if we do this for hospitalists, we will ultimately need to create a similar pathway for outpatient physicians.” Fortunately for us, they did not wait for RFP in outpatient medicine to be developed before proceeding with RFP for HM. (Figuring out how to do this on the outpatient side is even harder, and even though ABIM has been very supportive of RFP for hospitalists, the ABMS, which oversees all the specialty boards, still had to sign off on this approach. In September, they did.)
RFP Formula
So what will RFP in HM look like? The process is described on ABIM’s Web site (www.abim.org/news/news/focused-practice-hospital-medicine-qa.aspx), but to qualify, a hospitalist must:
- Be certified in internal medicine;
- Have practiced for a sufficient period of time to have achieved certain volume thresholds for patients with inpatient diagnoses;
- Participate in hospitalist-based practice improvement and self-assessment modules; and
- Pass a secure exam, which SHM president-elect Jeff Wiese, MD, FHM, and his committee have been hard at work in creating.
All told, the bar has been set high. And from what I hear, the exam has a strong QI focus—a discipline most residency programs skimp on when designing their curriculums.
SHM recognizes that we will have to ramp up our educational efforts to prepare hospitalists for RFP. We will need to develop QI assessment modules, continue developing and enhancing QI education at our annual meeting, and we’ll need to consider more regional efforts at providing the education hospitalists need to do this QI work in their hospitals.
A Bright Future
So what does this really mean for our field? Quite a bit, actually.
We have long tracked all the elements traditionally required to call HM a specialty, and one by one we have ticked them off: large numbers of physicians in the field, a separate body of knowledge (i.e., core competencies), textbooks, a journal, national meetings, training programs. But the one element that remained unchecked was a separate certification. Cross that one off the list. Granted, training programs remain few and underdeveloped, but I expect that, too, will change and grow over time.
There are additional questions raised by this new certification. One might ask: “Will hospitals or payors require RFP in HM in order to practice or be paid for what we do?” Maybe. I expect this will not happen rapidly, as many hospitalists are likely to wait until they need to recertify before choosing to pursue RFP in HM. But if all of our colleagues start getting certified, or programs hiring hospitalists begin to require this certification (e.g., advertise the fact that all of their physicians are “certified hospitalists”), the floodgates will open.
Questions also arise about what happens now for family practice or pediatrics. Well, I am pleased to say that the American Board of Family Medicine (ABFM) has announced its intent to collaborate with ABIM to establish a similar pilot program for RFP in HM for family-practice physicians. And the pediatric societies and board-certifying agencies are watching closely to see if they might consider the same approach for pediatric hospitalists. Stay tuned.
ABMS’ recent approval of the RFP pathway is what many have been working tirelessly toward for years. It is a testament to the maturity, breadth, and importance of our field. And it validates what many of us have known for years: Hospitalists have unique skill sets that are vital to the U.S. healthcare system, and, as a result, we have been integrated into the fabric of hospital care delivery in every state.
With the coming redesign of the healthcare system, hospitalists will be counted on to lead and facilitate the work required to deliver high-quality, efficient hospital care across the country. RFP provides both a means to get hospitalists up to speed to do this important work and recognizes those who are ready to go out and lead.
This truly is a watershed moment for HM. TH
Dr. Flanders is president of SHM.
The announcement was made Sept. 23, 2009. The American Board of Medical Specialties (ABMS) had approved a “pilot program” for Recognition of Focused Practice (RFP) in Hospital Medicine. ABMS-sanctioned board certification for hospitalists had finally arrived.
When the announcement came, I was at the University of California at San Francisco’s CME conference with 600 other hospitalists. Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, announced the RFP in HM to the audience—it received resounding applause. Dr. Wachter, the UCSF conference chair, then went on to recap the history behind RFP and how we got here. As he spoke, I realized that I had forgotten how long this process had taken and how much work had been done by so many people.
To practicing hospitalists, the creation of some sort of certification in HM seems like the proverbial no-brainer. But think about it from the American Board of Internal Medicine (ABIM) perspective: All “specialties” with board certification have training programs or fellowships that help define them. We do not have hospitalist residency programs or fellowships that are necessary for practicing as a hospitalist. Our expertise is acquired during practice.
So if the training path for hospitalists is not different—at least for now—from that of other general internists, how do we create board certification? When a group, such as hospitalists, “asks” to be recognized as a specialty with their own certification, the ABIM needs to consider the implications of creating such recognition. For hospitalists, the question was: If we do this for hospitalists, do we have to create a certificate for officists or outpatient physicians? For the broader questions around recognition of focused practice, the board needed to ask, “What if a group comes forward and asks for recognition of their focus and expertise in caring for diabetes or sepsis?”
ABIM thought very carefully about these questions. For the latter, ABIM says the field asking for recognition of focused practice must have a lot of physicians who only practice in this field while also having large numbers of physicians who never practice in the field. And they said, “Yes, if we do this for hospitalists, we will ultimately need to create a similar pathway for outpatient physicians.” Fortunately for us, they did not wait for RFP in outpatient medicine to be developed before proceeding with RFP for HM. (Figuring out how to do this on the outpatient side is even harder, and even though ABIM has been very supportive of RFP for hospitalists, the ABMS, which oversees all the specialty boards, still had to sign off on this approach. In September, they did.)
RFP Formula
So what will RFP in HM look like? The process is described on ABIM’s Web site (www.abim.org/news/news/focused-practice-hospital-medicine-qa.aspx), but to qualify, a hospitalist must:
- Be certified in internal medicine;
- Have practiced for a sufficient period of time to have achieved certain volume thresholds for patients with inpatient diagnoses;
- Participate in hospitalist-based practice improvement and self-assessment modules; and
- Pass a secure exam, which SHM president-elect Jeff Wiese, MD, FHM, and his committee have been hard at work in creating.
All told, the bar has been set high. And from what I hear, the exam has a strong QI focus—a discipline most residency programs skimp on when designing their curriculums.
SHM recognizes that we will have to ramp up our educational efforts to prepare hospitalists for RFP. We will need to develop QI assessment modules, continue developing and enhancing QI education at our annual meeting, and we’ll need to consider more regional efforts at providing the education hospitalists need to do this QI work in their hospitals.
A Bright Future
So what does this really mean for our field? Quite a bit, actually.
We have long tracked all the elements traditionally required to call HM a specialty, and one by one we have ticked them off: large numbers of physicians in the field, a separate body of knowledge (i.e., core competencies), textbooks, a journal, national meetings, training programs. But the one element that remained unchecked was a separate certification. Cross that one off the list. Granted, training programs remain few and underdeveloped, but I expect that, too, will change and grow over time.
There are additional questions raised by this new certification. One might ask: “Will hospitals or payors require RFP in HM in order to practice or be paid for what we do?” Maybe. I expect this will not happen rapidly, as many hospitalists are likely to wait until they need to recertify before choosing to pursue RFP in HM. But if all of our colleagues start getting certified, or programs hiring hospitalists begin to require this certification (e.g., advertise the fact that all of their physicians are “certified hospitalists”), the floodgates will open.
Questions also arise about what happens now for family practice or pediatrics. Well, I am pleased to say that the American Board of Family Medicine (ABFM) has announced its intent to collaborate with ABIM to establish a similar pilot program for RFP in HM for family-practice physicians. And the pediatric societies and board-certifying agencies are watching closely to see if they might consider the same approach for pediatric hospitalists. Stay tuned.
ABMS’ recent approval of the RFP pathway is what many have been working tirelessly toward for years. It is a testament to the maturity, breadth, and importance of our field. And it validates what many of us have known for years: Hospitalists have unique skill sets that are vital to the U.S. healthcare system, and, as a result, we have been integrated into the fabric of hospital care delivery in every state.
With the coming redesign of the healthcare system, hospitalists will be counted on to lead and facilitate the work required to deliver high-quality, efficient hospital care across the country. RFP provides both a means to get hospitalists up to speed to do this important work and recognizes those who are ready to go out and lead.
This truly is a watershed moment for HM. TH
Dr. Flanders is president of SHM.
The announcement was made Sept. 23, 2009. The American Board of Medical Specialties (ABMS) had approved a “pilot program” for Recognition of Focused Practice (RFP) in Hospital Medicine. ABMS-sanctioned board certification for hospitalists had finally arrived.
When the announcement came, I was at the University of California at San Francisco’s CME conference with 600 other hospitalists. Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World, announced the RFP in HM to the audience—it received resounding applause. Dr. Wachter, the UCSF conference chair, then went on to recap the history behind RFP and how we got here. As he spoke, I realized that I had forgotten how long this process had taken and how much work had been done by so many people.
To practicing hospitalists, the creation of some sort of certification in HM seems like the proverbial no-brainer. But think about it from the American Board of Internal Medicine (ABIM) perspective: All “specialties” with board certification have training programs or fellowships that help define them. We do not have hospitalist residency programs or fellowships that are necessary for practicing as a hospitalist. Our expertise is acquired during practice.
So if the training path for hospitalists is not different—at least for now—from that of other general internists, how do we create board certification? When a group, such as hospitalists, “asks” to be recognized as a specialty with their own certification, the ABIM needs to consider the implications of creating such recognition. For hospitalists, the question was: If we do this for hospitalists, do we have to create a certificate for officists or outpatient physicians? For the broader questions around recognition of focused practice, the board needed to ask, “What if a group comes forward and asks for recognition of their focus and expertise in caring for diabetes or sepsis?”
ABIM thought very carefully about these questions. For the latter, ABIM says the field asking for recognition of focused practice must have a lot of physicians who only practice in this field while also having large numbers of physicians who never practice in the field. And they said, “Yes, if we do this for hospitalists, we will ultimately need to create a similar pathway for outpatient physicians.” Fortunately for us, they did not wait for RFP in outpatient medicine to be developed before proceeding with RFP for HM. (Figuring out how to do this on the outpatient side is even harder, and even though ABIM has been very supportive of RFP for hospitalists, the ABMS, which oversees all the specialty boards, still had to sign off on this approach. In September, they did.)
RFP Formula
So what will RFP in HM look like? The process is described on ABIM’s Web site (www.abim.org/news/news/focused-practice-hospital-medicine-qa.aspx), but to qualify, a hospitalist must:
- Be certified in internal medicine;
- Have practiced for a sufficient period of time to have achieved certain volume thresholds for patients with inpatient diagnoses;
- Participate in hospitalist-based practice improvement and self-assessment modules; and
- Pass a secure exam, which SHM president-elect Jeff Wiese, MD, FHM, and his committee have been hard at work in creating.
All told, the bar has been set high. And from what I hear, the exam has a strong QI focus—a discipline most residency programs skimp on when designing their curriculums.
SHM recognizes that we will have to ramp up our educational efforts to prepare hospitalists for RFP. We will need to develop QI assessment modules, continue developing and enhancing QI education at our annual meeting, and we’ll need to consider more regional efforts at providing the education hospitalists need to do this QI work in their hospitals.
A Bright Future
So what does this really mean for our field? Quite a bit, actually.
We have long tracked all the elements traditionally required to call HM a specialty, and one by one we have ticked them off: large numbers of physicians in the field, a separate body of knowledge (i.e., core competencies), textbooks, a journal, national meetings, training programs. But the one element that remained unchecked was a separate certification. Cross that one off the list. Granted, training programs remain few and underdeveloped, but I expect that, too, will change and grow over time.
There are additional questions raised by this new certification. One might ask: “Will hospitals or payors require RFP in HM in order to practice or be paid for what we do?” Maybe. I expect this will not happen rapidly, as many hospitalists are likely to wait until they need to recertify before choosing to pursue RFP in HM. But if all of our colleagues start getting certified, or programs hiring hospitalists begin to require this certification (e.g., advertise the fact that all of their physicians are “certified hospitalists”), the floodgates will open.
Questions also arise about what happens now for family practice or pediatrics. Well, I am pleased to say that the American Board of Family Medicine (ABFM) has announced its intent to collaborate with ABIM to establish a similar pilot program for RFP in HM for family-practice physicians. And the pediatric societies and board-certifying agencies are watching closely to see if they might consider the same approach for pediatric hospitalists. Stay tuned.
ABMS’ recent approval of the RFP pathway is what many have been working tirelessly toward for years. It is a testament to the maturity, breadth, and importance of our field. And it validates what many of us have known for years: Hospitalists have unique skill sets that are vital to the U.S. healthcare system, and, as a result, we have been integrated into the fabric of hospital care delivery in every state.
With the coming redesign of the healthcare system, hospitalists will be counted on to lead and facilitate the work required to deliver high-quality, efficient hospital care across the country. RFP provides both a means to get hospitalists up to speed to do this important work and recognizes those who are ready to go out and lead.
This truly is a watershed moment for HM. TH
Dr. Flanders is president of SHM.
(Fish) Food for Thought

The putrid smell of vomit wafted behind me, flowing in and out of my nostrils with each up and down of our boat. Two in our deep-sea-fishing party already had lost their breakfast; I was focused on keeping mine down. The ocean seemed fairly calm, but I didn’t feel very steady. In fact, I felt like I was on a bamboo raft that had been tied together with palm fronds.
In between thoughts of how I would have been ostracized as a seafaring Polynesian, I had one thought on my mind. “Keep your eyes on the horizon,” our captain had said as we boarded the boat. My eyes were not going anywhere else that day. The horizon, whether the coastline of Oahu or just the thin line between ocean blue and sky blue, provided an unwavering constant as the waves changed our position minute by minute.
Our daily work as hospitalists is filled with ups and downs—waves, if you will. At times they threaten to capsize us; at others, they provide a short boost of momentum. These waves come in many forms, whether a busy teaching service, an interaction with a consultant, or your personal schedule. And all too often, that constant cyclical motion becomes hypnotizing. All of us have encountered colleagues that get lost at sea; they seem to always focus on that constant sense of unsteadiness. We recognize this form of despair as whining, and it’s not far removed from motion sickness. The only difference is the specific sense that is assaulted when the victim can no longer handle the ride.
Chart a Course to Success
If the captain of our fishing charter had been a business instructor, the lesson for the day would have been strategic planning. If he had been a medical school professor—well, there probably is no suitable analogy, as the path to organizational success isn’t yet a part of our core curriculum. Strategic planning is the deceptively simple process by which you ensure that you are headed toward your ultimate vision; it’s how you, your group, or your field charts its course toward the horizon.
Medicine has been in the habit of learning from business lately. Toyota’s strategy is a prime example. Their core strategic plan is termed “Lean” production or practices. Continuous quality improvement, though an oversimplification, is a substitute phrase that all hospitalists should recognize. Amazingly, Toyota’s strategic plan extends 50 to 100 years into the future and is intertwined into each and every phase of the company. Although the Lean system is being carefully studied and applied by many in the healthcare industry, the true hidden curriculum lies not in the details of their practices, but rather in their choice and execution of strategy. Toyota’s impressive history of achievement contains a few valuable lessons applicable to your own future success.
At one time, Toyota was a newcomer to the established field of automobile manufacturing, not dissimilar to the current state of most pediatric hospitalists. Like us, they undoubtedly faced uphill battles surrounding established cultural barriers and rigid practice patterns. And despite giving up more than half a century to Ford and the concept of mass production, Toyota has become the leading manufacturer of automobiles in the world.
How did Toyota choose and execute a strategy that allowed it to thrive in the face of such obstacles? In the beginning, there probably were many strategic options. They could have decided to focus on creating a specific product, such as the “ultimate driving machine,” or cars that are boxy but safe. They could have opted to cater to a specific consumer class, perhaps building a strong fleet of affordable autos. Or they could have looked to improve their purchasing power and distribution methods (think Dell and Walmart).
Instead, they made a conscious decision to pursue excellence in reliability, quality, and value (sound familiar?), then followed through beautifully.
Strategy at Home
Despite differences in industry and scale, all of these same sorts of decisions are critical to the success of your career, your HM group, or even the field of pediatric HM. Are you aware of the specific strategies in place for your group’s success? Have you been involved in the process? Before this year, I was probably like most of you. I had some vague notion of success. It involved increasing relative value units, making everyone happy, and completing a big QI or research project.
In the past 12 months, however, I have taken part in three strategic planning sessions: one for a regional pediatric society, one for my hospital, and one for my hospitalist group. The importance of these processes crystallized for me. Apparently, the leaders in our field have had the same thoughts. They convened the Pediatric Hospital Medicine Roundtable, a strategic planning session for our field (see “All Grown Up,” p. 1). Clearly, 2009 is the year of the strategic plan.
Despite the unifying theme, the processes and products of all of these plans have been unique. Strategic plans must be developed organically, out of local context and environment, and can only be created by those who live and breathe the work. What works for group safety at the university hospital of quality focus might not work for group communication experts at suburban community hospitals. Differences in institutional, organizational, and cultural beliefs should affect the decision-making process. When a strategy has been devised, it should be carefully chosen and explicitly implemented.
Does your group’s strategy come to mind? Or are you just treading water, unable to see beyond the next looming wave? If you have a vision of what you want, whether it’s money, fame, or protected time, then this same line of reasoning should apply to the strategic plan for your individual career, as well as the future of pediatric HM.
The lesson here is simple: Success requires a plan. Strategic planning is how you set a vision for the future and chart that course. Unexpected political waves are sure to come, and not every victory will come with a prize catch. But if you can create that beautiful Impressionist painting on the horizon and maintain that course, you are less likely to lose your breakfast and go without lunch. TH
Dr. Shen is The Hospitalist’s pediatric editor.
The putrid smell of vomit wafted behind me, flowing in and out of my nostrils with each up and down of our boat. Two in our deep-sea-fishing party already had lost their breakfast; I was focused on keeping mine down. The ocean seemed fairly calm, but I didn’t feel very steady. In fact, I felt like I was on a bamboo raft that had been tied together with palm fronds.
In between thoughts of how I would have been ostracized as a seafaring Polynesian, I had one thought on my mind. “Keep your eyes on the horizon,” our captain had said as we boarded the boat. My eyes were not going anywhere else that day. The horizon, whether the coastline of Oahu or just the thin line between ocean blue and sky blue, provided an unwavering constant as the waves changed our position minute by minute.
Our daily work as hospitalists is filled with ups and downs—waves, if you will. At times they threaten to capsize us; at others, they provide a short boost of momentum. These waves come in many forms, whether a busy teaching service, an interaction with a consultant, or your personal schedule. And all too often, that constant cyclical motion becomes hypnotizing. All of us have encountered colleagues that get lost at sea; they seem to always focus on that constant sense of unsteadiness. We recognize this form of despair as whining, and it’s not far removed from motion sickness. The only difference is the specific sense that is assaulted when the victim can no longer handle the ride.
Chart a Course to Success
If the captain of our fishing charter had been a business instructor, the lesson for the day would have been strategic planning. If he had been a medical school professor—well, there probably is no suitable analogy, as the path to organizational success isn’t yet a part of our core curriculum. Strategic planning is the deceptively simple process by which you ensure that you are headed toward your ultimate vision; it’s how you, your group, or your field charts its course toward the horizon.
Medicine has been in the habit of learning from business lately. Toyota’s strategy is a prime example. Their core strategic plan is termed “Lean” production or practices. Continuous quality improvement, though an oversimplification, is a substitute phrase that all hospitalists should recognize. Amazingly, Toyota’s strategic plan extends 50 to 100 years into the future and is intertwined into each and every phase of the company. Although the Lean system is being carefully studied and applied by many in the healthcare industry, the true hidden curriculum lies not in the details of their practices, but rather in their choice and execution of strategy. Toyota’s impressive history of achievement contains a few valuable lessons applicable to your own future success.
At one time, Toyota was a newcomer to the established field of automobile manufacturing, not dissimilar to the current state of most pediatric hospitalists. Like us, they undoubtedly faced uphill battles surrounding established cultural barriers and rigid practice patterns. And despite giving up more than half a century to Ford and the concept of mass production, Toyota has become the leading manufacturer of automobiles in the world.
How did Toyota choose and execute a strategy that allowed it to thrive in the face of such obstacles? In the beginning, there probably were many strategic options. They could have decided to focus on creating a specific product, such as the “ultimate driving machine,” or cars that are boxy but safe. They could have opted to cater to a specific consumer class, perhaps building a strong fleet of affordable autos. Or they could have looked to improve their purchasing power and distribution methods (think Dell and Walmart).
Instead, they made a conscious decision to pursue excellence in reliability, quality, and value (sound familiar?), then followed through beautifully.
Strategy at Home
Despite differences in industry and scale, all of these same sorts of decisions are critical to the success of your career, your HM group, or even the field of pediatric HM. Are you aware of the specific strategies in place for your group’s success? Have you been involved in the process? Before this year, I was probably like most of you. I had some vague notion of success. It involved increasing relative value units, making everyone happy, and completing a big QI or research project.
In the past 12 months, however, I have taken part in three strategic planning sessions: one for a regional pediatric society, one for my hospital, and one for my hospitalist group. The importance of these processes crystallized for me. Apparently, the leaders in our field have had the same thoughts. They convened the Pediatric Hospital Medicine Roundtable, a strategic planning session for our field (see “All Grown Up,” p. 1). Clearly, 2009 is the year of the strategic plan.
Despite the unifying theme, the processes and products of all of these plans have been unique. Strategic plans must be developed organically, out of local context and environment, and can only be created by those who live and breathe the work. What works for group safety at the university hospital of quality focus might not work for group communication experts at suburban community hospitals. Differences in institutional, organizational, and cultural beliefs should affect the decision-making process. When a strategy has been devised, it should be carefully chosen and explicitly implemented.
Does your group’s strategy come to mind? Or are you just treading water, unable to see beyond the next looming wave? If you have a vision of what you want, whether it’s money, fame, or protected time, then this same line of reasoning should apply to the strategic plan for your individual career, as well as the future of pediatric HM.
The lesson here is simple: Success requires a plan. Strategic planning is how you set a vision for the future and chart that course. Unexpected political waves are sure to come, and not every victory will come with a prize catch. But if you can create that beautiful Impressionist painting on the horizon and maintain that course, you are less likely to lose your breakfast and go without lunch. TH
Dr. Shen is The Hospitalist’s pediatric editor.
The putrid smell of vomit wafted behind me, flowing in and out of my nostrils with each up and down of our boat. Two in our deep-sea-fishing party already had lost their breakfast; I was focused on keeping mine down. The ocean seemed fairly calm, but I didn’t feel very steady. In fact, I felt like I was on a bamboo raft that had been tied together with palm fronds.
In between thoughts of how I would have been ostracized as a seafaring Polynesian, I had one thought on my mind. “Keep your eyes on the horizon,” our captain had said as we boarded the boat. My eyes were not going anywhere else that day. The horizon, whether the coastline of Oahu or just the thin line between ocean blue and sky blue, provided an unwavering constant as the waves changed our position minute by minute.
Our daily work as hospitalists is filled with ups and downs—waves, if you will. At times they threaten to capsize us; at others, they provide a short boost of momentum. These waves come in many forms, whether a busy teaching service, an interaction with a consultant, or your personal schedule. And all too often, that constant cyclical motion becomes hypnotizing. All of us have encountered colleagues that get lost at sea; they seem to always focus on that constant sense of unsteadiness. We recognize this form of despair as whining, and it’s not far removed from motion sickness. The only difference is the specific sense that is assaulted when the victim can no longer handle the ride.
Chart a Course to Success
If the captain of our fishing charter had been a business instructor, the lesson for the day would have been strategic planning. If he had been a medical school professor—well, there probably is no suitable analogy, as the path to organizational success isn’t yet a part of our core curriculum. Strategic planning is the deceptively simple process by which you ensure that you are headed toward your ultimate vision; it’s how you, your group, or your field charts its course toward the horizon.
Medicine has been in the habit of learning from business lately. Toyota’s strategy is a prime example. Their core strategic plan is termed “Lean” production or practices. Continuous quality improvement, though an oversimplification, is a substitute phrase that all hospitalists should recognize. Amazingly, Toyota’s strategic plan extends 50 to 100 years into the future and is intertwined into each and every phase of the company. Although the Lean system is being carefully studied and applied by many in the healthcare industry, the true hidden curriculum lies not in the details of their practices, but rather in their choice and execution of strategy. Toyota’s impressive history of achievement contains a few valuable lessons applicable to your own future success.
At one time, Toyota was a newcomer to the established field of automobile manufacturing, not dissimilar to the current state of most pediatric hospitalists. Like us, they undoubtedly faced uphill battles surrounding established cultural barriers and rigid practice patterns. And despite giving up more than half a century to Ford and the concept of mass production, Toyota has become the leading manufacturer of automobiles in the world.
How did Toyota choose and execute a strategy that allowed it to thrive in the face of such obstacles? In the beginning, there probably were many strategic options. They could have decided to focus on creating a specific product, such as the “ultimate driving machine,” or cars that are boxy but safe. They could have opted to cater to a specific consumer class, perhaps building a strong fleet of affordable autos. Or they could have looked to improve their purchasing power and distribution methods (think Dell and Walmart).
Instead, they made a conscious decision to pursue excellence in reliability, quality, and value (sound familiar?), then followed through beautifully.
Strategy at Home
Despite differences in industry and scale, all of these same sorts of decisions are critical to the success of your career, your HM group, or even the field of pediatric HM. Are you aware of the specific strategies in place for your group’s success? Have you been involved in the process? Before this year, I was probably like most of you. I had some vague notion of success. It involved increasing relative value units, making everyone happy, and completing a big QI or research project.
In the past 12 months, however, I have taken part in three strategic planning sessions: one for a regional pediatric society, one for my hospital, and one for my hospitalist group. The importance of these processes crystallized for me. Apparently, the leaders in our field have had the same thoughts. They convened the Pediatric Hospital Medicine Roundtable, a strategic planning session for our field (see “All Grown Up,” p. 1). Clearly, 2009 is the year of the strategic plan.
Despite the unifying theme, the processes and products of all of these plans have been unique. Strategic plans must be developed organically, out of local context and environment, and can only be created by those who live and breathe the work. What works for group safety at the university hospital of quality focus might not work for group communication experts at suburban community hospitals. Differences in institutional, organizational, and cultural beliefs should affect the decision-making process. When a strategy has been devised, it should be carefully chosen and explicitly implemented.
Does your group’s strategy come to mind? Or are you just treading water, unable to see beyond the next looming wave? If you have a vision of what you want, whether it’s money, fame, or protected time, then this same line of reasoning should apply to the strategic plan for your individual career, as well as the future of pediatric HM.
The lesson here is simple: Success requires a plan. Strategic planning is how you set a vision for the future and chart that course. Unexpected political waves are sure to come, and not every victory will come with a prize catch. But if you can create that beautiful Impressionist painting on the horizon and maintain that course, you are less likely to lose your breakfast and go without lunch. TH
Dr. Shen is The Hospitalist’s pediatric editor.
Quality over Quantity
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
The Mayo Clinic is technically one. So are Pennsylvania’s Geisinger Health System, California-based Kaiser Permanente, and the Cleveland Clinic. Beyond the handful of long-established and well-integrated sites being labeled as de facto accountable care organizations (ACOs), advocates are seizing the moment and pushing for a bold vision of what role ACOs will play in the movement to reform the healthcare payment system across the country. In at least two major pilot projects in the works, hospitalists are expected to be front and center in leading the transition.
An ACO is an agreed-upon group of providers bands together to assume joint responsibility for both the quality and cost of healthcare for a specific population of beneficiaries. “What an ACO is trying to do is defragment healthcare,” says Mark Werner, MD, chief medical officer for southwest Virginia’s Carilion Clinic. As long as the group meets defined quality benchmarks, its providers can share in any financial rewards that spring from cost savings. But the providers also share in the collective risk of penalties for poor performance. Using the buzzwords of the moment, an “alignment of incentives” could help “bend the curve” of the sharp upturn in healthcare delivery costs.
ACO advocates argue that by pushing quantity over quality, the current fee-for-service payment system actually punishes providers that coordinate care or promote greater efficiencies; policy analysts are nearly unanimous in decreeing that the current model is fundamentally broken and must be replaced. “Well, actually, it’s not broken,” says Alfred Tallia, MD, MPH, professor and chair of the department of family medicine at the Robert Wood Johnson Medical School in New Brunswick, N.J. “It’s working very well for delivering what we’ve got now, which is not what we need, unfortunately.”
—Ralph Whatley, MD, chair, department of medicine, Carilion Clinic, Roanoke, Va.
Perfect Timing
The current push for healthcare reform offers the opportunity to make the case for a more equitable, outcome-oriented payment system as a necessary component of any structure that emerges. Many reform advocates in Massachusetts already have moved from asking how to provide more healthcare coverage to asking how the government can afford it, and ACOs have become a favored mechanism for controlling costs.
The general ACO concept has been backed by the nonpartisan Medicare Payment Advisory Commission, and received another boost when the Accountable Care Promotion Act, initially co-sponsored by Rep. Peter Welch (D-Vt.) and Rep. Earl Pomeroy (D-N.D.) in May, was incorporated in its entirety into the healthcare reform bill introduced in the House of Representatives. The bill would launch a pilot program for ACOs for Medicare beneficiaries, while similar provisions within the Senate healthcare reform bill would set up pilot projects for both Medicare beneficiaries and pediatric beneficiaries of Medicaid or the Children’s Health Insurance Program.
Among the pilot projects already planned, healthcare officials at Robert Wood Johnson are hoping to create an academic-health-center-related ACO to link the disparate elements of healthcare delivery across a large swath. “Our vision is really to build the finest 21st-century integrated delivery system for New Jersey,” Dr. Tallia says. “And that would include everything from advanced, personalized in-home and outpatient primary care to high-tech, leading-edge inpatient quaternary care—and everything in between.”
Virginia’s Carilion Clinic was the first to announce its participation in a separate pilot involving the Engelberg Center for Health Care Reform at the Brookings Institution in Washington, D.C., and the Dartmouth Institute for Health Policy and Clinical Practice in Lebanon, N.H. Both institutions have been heavyweights in championing the ACO cause. Dr. Werner says Carilion actually began transforming itself into a more coordinated and integrated organization about three years ago, well before the current ACO buzz began. “We always said from the beginning that we were creating an accountable physicians group, where the physician group had accountability for all of the outcomes important in healthcare,” he says.
The Nitty-Gritty
So how would such organizations actually work? Dr. Tallia sees three absolutes: local accountability, shared savings, and performance measurements. Beyond those necessities, the details begin to blur. The bad taste left by the widely despised capitation payment systems of the 1980s and ’90s has made experts wary of dwelling on the similarities between ACOs and fixed, prepaid capitation plans. Any mention of the C-word, in fact, is followed almost immediately by a caveat: This is a flexible, big-tent strategy that avoids any one-size-fits-all payment prescriptions. And most advocates are emphasizing that ACOs should be voluntary.
Analyses have suggested that in order to succeed, an ACO should enroll 5,000 or more Medicare beneficiaries, or at least 15,000 privately insured patients. Which combination of patients and providers should be included has been left vague to allow emerging networks to tailor the model to their own needs. Some experts differ as to whether hospitals are a necessary component, though almost all agree on the need to include primary-care providers.
Dr. Tallia envisions his medical-school-based linkup as a marriage between New Jersey’s largest multispecialty medical network, the Robert Wood Johnson Medical Group, and the 30% to 40% of primary-care practices in the state that already have relationships with the school. “If you marry the primary-care relationships to the subspecialty care in the Robert Wood Johnson Medical Group and then tie in the area hospitals, by golly, you’ve got an ACO,” he says.
Robert Wood Johnson University Hospital is building an inpatient hospitalist service that will become an integral part of that mission, he says, with its focus on increasing efficiency, reducing the length of hospital stays, appropriate testing and handoffs, and proper communication with other care providers prior to hospital discharges.
ACO Outreach
But any system in which success leads to fewer hospitalizations also needs buy-in from those who stand to lose business. In short, hospitalists and other specialists will need financial incentives, too. That reward system, in turn, requires the right formula for setting and regularly measuring quality standards.
Based on initial savings estimates, however, Dr. Tallia isn’t worried about anyone missing out on a slice of the pie. “We’re looking at somewhere between 15% and 25% cost reductions,” he says, adding participants should gain sizable rewards. Initially, he says, he hopes to start with 5,000 to 10,000 enrollees and launch demonstration projects targeting patient subsets like Medicare beneficiaries and those insured by large employer groups. Ultimately, he’d love to have half of the state’s insured population.
From its own database models, Virginia’s Carilion Clinic estimates that its doctor group takes care of as many as 60,000 Medicare patients per year, with a strong tilt toward primary-care providers. For the past six months, the clinic has been working to identify the geographical scope and specific subset of beneficiaries that would work best for the pilot.
Once it settles on the best combination, Dr. Werner says, the clinic can look at that group’s historical spend rate over the past few years, then agree on a reduction in the rate of growth by, say, 1.5%. “If we’re able to have reductions that exceed 1.5 percent, we would have an opportunity to share in those reductions,” he says.
HM Front and Center
If all goes well, the first pieces of the Carilion ACO will be in place by Jan. 1, and Ralph Whatley, MD, chair of the department of medicine, says the hospitalist program will be “ground zero” in helping to smooth the transition through the proper handling of admissions, discharges, and handoffs of care. “If we do our job as an accountable care organization well, one of the things we should see is that we have less admissions to our hospitalist service,” Dr. Whatley says, especially as the management of such conditions as chronic diseases moves to outpatient settings. Nevertheless, “we can have our hospitalists front and center in the efforts to make the acute management of illness that requires the inpatient setting more efficient, less costly, and with better outcomes.”
Carilion’s hospitalists have played prominent roles in many of the clinic’s quality, safety, and efficiency initiatives. “I would have difficulty imagining that a health system that didn’t have a widespread, cohesive hospitalist service could pull off the kind of inpatient management efficiency, even preventive medicine, that a hospitalist model like ours is going to be able to do,” Dr. Whatley says.
Similarly, he has difficulty imagining how an organization could pull off a successful ACO without ready access to patient information through electronic health records, as Carilion now does. Unsurprisingly, many healthcare payment reform advocates are pushing for the technology needed for ACO-style startups to flourish.
As Dr. Werner says, “You need to give the group of physicians that are going to be part of an accountable group the necessary infrastructure and tools to be able to provide care together.” TH
Bryn Nelson is a freelance writer based in Seattle.
Submission Support
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
Physicians receive requests for documentation on a daily basis. Insurer requests need particular attention, as they can be directly related to reimbursement. If the documentation supports the service, payment is rendered (pre-payment request) or maintained (post-payment request). If the documentation is not supportive, payment is denied (pre-payment request) or refunded (post-payment request).
The two most common reasons submitted documentation is not supportive: It lacks information or only a portion of the documentation was submitted.
Not Enough Documentation
“Insufficient documentation” can take many forms. Each visit category (e.g., initial hospital care or subsequent hospital care) and level of service (e.g., 99221-99233) has corresponding documentation requirements. A full list of requirements is available on the Centers for Medicare and Medicaid Services Web site (www.cms.hhs.gov/MLNProducts/Downloads/1995dg.pdf). Selecting an evaluation and management (E/M) level is focused on either upon the content of three key components: history, exam, and decision-making; time can also be a consideration but only when counseling or coordination of care dominate more than 50% of the physician’s total visit time.1 Failure to document any essential element in a given visit level (e.g., family history required but missing for 99222 and 99223) might result in a reviewer down-coding or denying the service.
Dates and signatures are vital to each encounter. The reviewer must be able to identify each individual who performs, documents, and bills for a service, as well as when the service occurred. Notes that lack dates or signatures are not considered in support of a billed service. Notes that contain an illegible signature are equally problematic. If the legibility of a signature prevents the reviewer from correctly identifying the rendering physician, the service can be denied.
It is advisable for the physician to print their name alongside the signature on the encounter note, or include a separate signature sheet with the requested documentation to assist the reviewer in deciphering the physician’s scrawl. Keep in mind that stamped signatures are not acceptable. Medicare accepts handwritten signatures, electronic signatures, or facsimiles of original written or electronic signatures.2
A service is questioned when two different sets of handwriting appear on a note and only one signature is provided. Because the reviewer cannot confirm the credentials of the unidentified individual and cannot be sure which portion belongs to the identified individual, the entire note is disregarded.
Incomplete Submission
Many times, an encounter note does not contain the cumulative information representing the reported service. For example, other pieces of pertinent information might be included in the data section or order section of the chart. If the individual responsible for gathering the requested documentation does not review the information before submitting it, those other important entries could be missed, and the complexity of the billed service might not be justified.
To avoid this, have the designated individual review the note for specific references to information housed in different areas of the chart. The provider should submit any entry with the same date as the requested documentation: labs, diagnostic testing, physician orders, patient instructions, nursing notes, resident notes, notes by other physicians in the same group, discharge summaries, etc.
Legibility is crucial when the documentation is sent for review. Note that the reviewer will not contact the provider if the information is not readable. Most reviewers seek another reviewer’s assistance in translating the handwriting, but they are not obligated to do this. If the note is deemed incomprehensible, the service is denied.
Electronic health records (EHR) are assisting physicians and other providers with legibility issues, and can help take the guesswork out of the note’s content. If a physician is still writing notes by hand, a transcription could be sent along with the documentation to prevent unnecessary denials. It is not advisable to do this for all requests, but only for requests involving providers who have particularly problematic handwriting.
Timeliness of Response
Once the documentation request is received, the physician has a small window of opportunity to review the request, collect the information, and issue a response. A lack of physician response always results in a service denial or a refund request. Once denied, the physician must go through the proper channels of appeal (with a different insurer reviewing department). Requests for refunds are more difficult to overturn. It is difficult to “open” a case that has been “closed.” Denials resulting from a failure to respond to a pre-payment request are a bit easier to resolve because the resulting denial is typically the payor’s initial determination of the claim. The physician usually is allowed an appeal of the payor’s initial determination. However, it is not a cost-effective process to handle prepayment requests in this manner. Always attempt to respond to the initial request within the designated time frame. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008;79-109.
- Centers for Medicare and Medicaid Services: CR 5971 Clarification-Signature Requirements. Medicare Learning Network Web site. Available at: www.cms.hhs.gov/MLNMattersArticles/downloads/SE0829.pdf. Accessed Sept. 1, 2009.
- Pohlig C. Evaluation and Management Services: An Overview. In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians, 2008; 65-78.
What is the best initial treatment of an adult patient with healthcare-associated pneumonia?
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?

Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
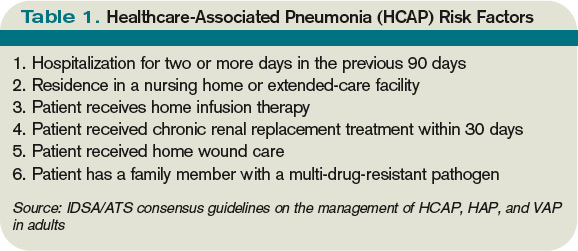
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
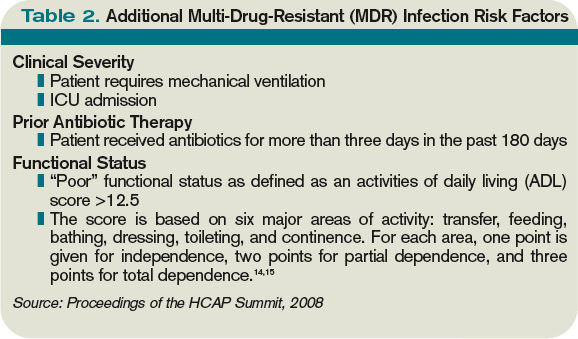
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
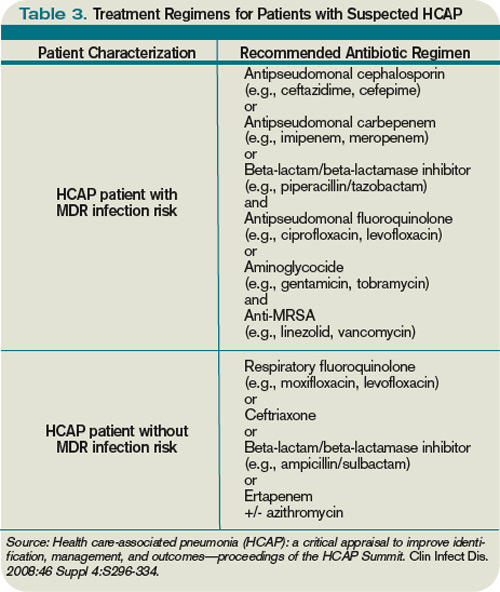
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?
Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Case
A 68-year-old man with hypertension, diabetes, and recent hip fracture with poor functional status presents from a nursing home with a productive cough, shortness of breath, and chills of two-day duration. He finished a five-day course of cephalexin for a urinary tract infection one week ago. His vital signs reveal a blood pressure of 162/80 mm/Hg, temperature of 101.9°F, respirations of 26 breaths per minute, and oxygen saturation of 88% on room air. Coarse breath sounds are noted in the right lung field and his chest X-ray reveals a right-middle-lobe infiltrate.
He is admitted to the hospital with a diagnosis of healthcare-associated pneumonia. What is the best empiric antibiotic coverage for this patient?
Overview
Modern medicine exists over a continuum of care that is delivered in a manifold of different settings. Patients routinely receive complex medical care at home, including wound care and infusion of intravenous antibiotics. Additionally, many patients are interfacing with the healthcare system on a regular basis via hemodialysis centers or sub-acute rehabilitation centers. As a result of these interactions, patients are exposed to—and colonized by—different bacterial pathogens that can result in a variety of infections.1
While patients with healthcare-associated pneumonia (HCAP) can present similarly to those with community-acquired pneumonia (CAP)—patients with CAP normally present with a lower-respiratory-tract infection—the differences in the likely etiological pathogens dictate that these patients be considered for broader-spectrum empiric antibiotics. Hospitalists will continue to be responsible for choosing the initial antibiotic regimen for these patients, and they need to be able to recognize this disease process in order to treat it appropriately.
The joint American Thoracic Society (ATS) and Infectious Diseases Society of America (IDSA) guidelines released in 2005 emphasize that certain clinical HCAP risk factors center on increased interactions and encounters with healthcare facilities.2 These risk factors are evolving over time to include a patient’s functional status, recent antibiotic use, and clinical severity.
Review of the Data
Differences between HCAP and CAP
HCAP represents a diagnostic category of pneumonia created to differentiate patients with infections caused by a different microbiological subset of bacteria, including possible multi-drug-resistant (MDR) organisms, from patients with CAP. Thus far, culture data support this dichotomy.3,4
Kollef and colleagues performed a multicenter, retrospective cohort study of 4,543 patients with bacterial respiratory culture-positive pneumonia between 2002 and 2003. The study examined the bacteriological differences between CAP and HCAP. In this study, HCAP patients were defined as having: transfer from another healthcare facility; long-term hemodialysis; or prior hospitalization within 30 days in which they had non-ventilator-associated pneumonia (VAP). CAP patients were defined as having non-VAP and non-HCAP.
The study showed that the frequency of Pseudomonas aeurginosa (25% HCAP vs. 17% CAP) and Staphylococcus aureus (46% vs. 25%), which included methicillin-resistant Staphylococcus aureus (MRSA) (18% vs. 6%), was significantly higher in patients with HCAP than those with CAP. Additionally, frequency of Streptococcus pneumoniae (5% vs. 16%) and Haemophilus influenza (5% vs. 16%) infections were noted as significantly lower.3
A single-center, retrospective cohort analysis of 639 patients done by Micek et al yielded similar culture differences between CAP and HCAP patients. In this study, criteria for HCAP were defined as hospitalization in the past year, immunosuppression, nursing-home resident, or hemodialysis. The study authors found that a significantly higher percentage of HCAP patients were infected with MRSA (30% vs. 12%), Pseudomonas aeurginosa (25% vs. 4%), and other non-fermenting gram-negative rods (GNR) (10% vs. 2%). HCAP patients again were noted as having significantly fewer infections with S. pneumoniae (10% vs. 40%) and Haemophilus influenza (4% vs. 17%).
In addition to showing a difference in the bacteriology of CAP and HCAP, the Kollef study also evaluated mortality rates, length of stay, and hospital charges. Mortality rates for HCAP (19.8%) were similar to those of hospital-acquired pneumonia (HAP) (18.8%), and both of these were significantly higher than CAP (10%). Length of stay and hospital cost increased across the spectrum, from CAP to HCAP to HAP, with significant differences between each.3
ATS/IDSA Guidelines
In 2005, a joint committee of the ATS and ISDA updated its initial 1996 nosocomial pneumonia guidelines. The guideline update included the new HCAP category.2 The No. 1 goal of these guidelines was to emphasize early and appropriate antibiotics, followed by tailoring of the treatment regimen based upon culture and clinical data. To this end, HCAP risk factors were developed via extrapolation from observational data generated from HAP and VAP patients.5,6,7
The risk factors are summarized in Table 1 (see p. 19).2 Guidelines dictated that the identification of any of these risk factors in pneumonia patients at the time of admission indicates increased risk for infection with an MDR organism. These high-risk patients require placement into the diagnostic category of HCAP.
Once a patient has been diagnosed with HCAP, the guidelines recommended obtaining lower-respiratory-tract cultures and initiating broad-spectrum antibiotic therapy. Appropriate empiric antibiotic therapy was suggested to be the same as for HAP. This regimen requires coverage with two anti-pseudomonal agents, as well as an agent with activity against MRSA.
The rationale behind initial coverage with two anti-pseudomonal agents stems from the finding that pseudomonas has a high rate of resistance to many antibiotics, and that if two agents are empirically started, chances of appropriate coverage increase from the outset. This is important, as timely administration of appropriate antibiotics has been shown to decrease mortality in infections.8
Additional considerations for empiric antibiotic treatment include sensitivities of local microbiologic data, as well as any recent antibiotic regimens given to the patient. Following this broad primary antibiotic coverage, de-escalation was recommended based on results of lower respiratory cultures and clinical improvement.2
Evolution of Diagnostic Criteria and Empiric Antibiotic Coverage
Since the publication of the 2005 ATS/IDSA guidelines, the aforementioned risk factors for HCAP have been brought into question, as they have yet to be validated by prospective trials. There is a growing concern that these criteria may not be adequately specific and, therefore, might call for too many patients to be treated with a broader spectrum of antibiotic coverage, thereby increasing the likelihood of developing MDR bacteria.
In order to further analyze HCAP criteria, Poch and Ost wrote a review earlier this year examining the data behind each of the risk factors cited in the ATS/IDSA guidelines; they found considerable heterogeneity in magnitude of MDR infection risk for these criteria.9 The authors also reviewed studies looking at other risk factors for MDR infections in patients living in nursing homes or afflicted with CAP. They proposed that such additional factors as patient specific risks (including functional status and previous antibiotic exposure) and contextual risks (including nurse-to-patient ratio) be evaluated and possibly incorporated into criteria.
Of all the patients with HCAP criteria, residents in nursing homes have been studied the best. Loeb et al, while looking for a way to decrease hospitalizations for nursing-home residents, showed that patients who get pneumonia (by guideline definition HCAP) can be effectively treated as outpatients with a single antibiotic agent.10 This randomized controlled trial of 680 patients, all with HCAP, were treated with oral levofloxacin at the nursing home or admitted to the hospital. There were no significant differences between mortality (8% vs. 9%) and quality-of-life measures between the two groups. Furthermore, analysis of data from the 1980s showed that nursing-home-acquired pneumonia could be treated effectively with single agents.11,12
To address some of the questions regarding HCAP, national infectious-disease leaders were brought together to respond to a number of HCAP questions.13 One of the questions centered on the recommended empiric coverage for HCAP. Given the above noted studies in nursing-home patients, disagreement emerged about the need to empirically treat all HCAP patients with broad-spectrum antibiotics. Therefore, another assessment of risk factors for MDR infections was proposed (see Table 2, p. 20) and a consensus was reached, resulting in the current recommendations. The current guidelines state that once a patient has met HCAP criteria, if they have additional MDR risk factors, then broad antibiotic coverage is recommended; however, if no additional MDR risk is found, then more conservative, narrower coverage could be given (see Table 3, p. 31).13
Additional considerations
More studies are needed to refine and validate the specific diagnostic criteria for HCAP, as well as the MDR infectious risk factors. Moreover, current recommendations are for lower respiratory cultures to be obtained on all patients with pneumonia and antibiotic coverage to be titrated according to these results. This practice, however, appears to be uncommon. More data are needed to further guide treatment following initiation of empiric antibiotic coverage without the guidance of culture data, with reliance upon clinical parameters instead.
Back to the Case
This patient met initial criteria for HCAP because he was a nursing home resident, and was found to have additional MDR risk factors (poor functional status and a recent course of antibiotics). Therefore, lower respiratory cultures were obtained, supplemental oxygen was started, and piperacillin/tazobactam plus levofloxacin and vancomycin (with consideration made for local resistance patterns) was administered. He clinically improved over the next two days. His sputum cultures grew Pseudomonas aeuroginosa, which was sensitive to piperacillin/tazobactam but resistant to levofloxacin.
The vancomycin and levofloxacin were discontinued, and he was treated with a seven-day course of piperacillin/tazobactam.
Bottom Line
For adults who present with pneumonia from the community, special attention must be paid to certain parts of the patient’s history to determine if they have HCAP.
Patients who have HCAP can benefit from broad-spectrum empiric antibiotic coverage, which current expert consensus believes is dependent upon further MDR infection risk factors. TH
Dr. Rohde is medicine faculty hospitalist at the University of Michigan in Ann Arbor.
References
- Jernigan JA, Pullen AL, Flowers L, Bell M, Jarvis WR. Prevalence of and risk factors for colonization with methicillin-resistant Staphylococcus aureus at the time of hospital admission. Infect Control Hosp Epidemiol. 2003;24(6):409-414.
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388-416.
- Kollef MH, Shorr A, Tabak YP, Gupta V, Liu LZ, Johannes RS. Epidemiology and outcomes of health-care-associated pneumonia: results from a large US database of culture-positive pneumonia. Chest. 2005;128(5):3854-3862.
- Micek ST, Kollef KE, Reichley RM, Roubinian N, Kollef MH. Health care-associated pneumonia and community-acquired pneumonia: a single-center experience. Antimicrob Agents Chemother. 2007;51(10):3568-3573.
- Chastre J, Fagon JY. Ventilator-associated pneumonia. Am J Respir Crit Care Med. 2002;165(7):867-903.
- Celis R, Torres A, Gatell JM, Almela M, Rodríguez-Roisin R, Augustí-Vidal A. Nosocomial pneumonia: a multivariate analysis of risk and prognosis. Chest. 1988;93(2):318-324.
- Lim WS, Macfarlane JT. A prospective comparison of nursing home acquired pneumonia with community acquired pneumonia. Eur Respir J. 2001;18(2):362-368.
- Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31 Supple 4:S131-S138.
- Poch DS, Ost DE. What are the important risk factors for healthcare-associated pneumonia? Semin Respir Crit Care Med. 2009;30(1):26-35.
- Loeb M, Carusone SC, Goeree R, et al. Effect of clinical pathway to reduce hospitalizations in nursing home residents with pneumonia: a randomized controlled trial. JAMA. 2006;295(21):2503-2510.
- Peterson PK, Stein D, Guay DR, et al. Prospective study of lower respiratory tract infections in an extended-care nursing home program: potential role of oral ciprofloxacin. Am J Med. 1988;85(2):164-171.
- Trenholme GM, Schmitt BA, Spear J, Gvazdinskas LC, Levin S. Randomized study of intravenous/oral ciprofloxacin versus ceftazidime in the treatment of hospital and nursing home patients with lower respiratory tract infections. Am J Med. 1989(5A);87:116S-118S.
- Kollef MH, Morrow LE, Baughman RP, et al. Healthcare-associated pneumonia (HCAP): a critical appraisal to improve identification, management and outcomes—proceedings of the HCAP summit. Clin Infect Dis. 2008;46 Suppl 4:S296-S334.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919.
- El Solh AA, Pietrantoni C, Bhat A, Bhora M, Berbary E. Indicators of potentially drug-resistant bacteria in severe nursing home-acquired pneumonia. Clin Infect Dis. 2004;39(4):474-480.
If you are interested in joining our reader-involvement program, e-mail Editor Jason Carris at [email protected].
Should group directors continue clinical practice?
PRO
Clinical practice is beneficial to patients, the group, and your career

Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading

I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.
PRO
Clinical practice is beneficial to patients, the group, and your career
Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading
I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.
PRO
Clinical practice is beneficial to patients, the group, and your career
Finding a balance between clinical care and leadership duties truly is a challenge for hospitalist directors. Changes in the landscape of inpatient care delivery, rapid growth of HM groups, and expansion of hospitalist roles have resulted in a substantial increase in a director’s responsibilities. Today’s hospitalist leader squarely faces the dilemma of continuing clinical practice and performing administrative efforts while demonstrating competence in each. To be effective, this is precisely what physician leaders must strive to do.
Maintaining clinical practice alongside directorship duties conveys advantages in critical leadership areas. You must consider the benefits to your patient, your career, and the hospitalist group.
The Patient, Director, Group
Physician leaders offer clinical experience combined with a unique perspective on systems of care, or “the big picture.”
Likewise, caring for patients provides the opportunity to interact with and listen to the customer, which is necessary for important outcomes, such as patient satisfaction. It reminds us that we are here to care for and about patients, keeping our efforts patient-centered.
Direct patient care refocuses directors on the fundamental reason they are in leadership. It offers intrinsic professional rewards and intellectual satisfaction that will sustain and strengthen the leadership role. The effective leader strategically finds balance by delegating, prioritizing, and focusing on time management.
Continuing your clinical practice affords physician leaders leverage with their constituents—the hospitalists. Working in the trenches, especially during critical times, yields legitimacy and credibility. It also allows the leader to identify with and respond to concerns raised by members. This can connect the leader to the group, avoiding the “suit vs. white coat” dynamic. The same principle extends to other stakeholders who are part of the care team, such as nurses and referring physicians.
Other Factors
Maintaining clinical aptitude ensures that leaders stay apprised of current practices, and are aware of the latest techniques, data, and evidence. This is critical for ensuring group performance in quality initiatives, and for setting standards of clinical excellence in the group practice.
In academic centers, ward teaching allows leaders to train future physicians, pass on knowledge, and gain an understanding of the next generation and its priorities, thus keeping an eye on the future and having a clear vision.
Perhaps the most important benefit direct patient care provides in leadership is the ability to accomplish the group’s mission. A firsthand experience brings understanding of issues around workflow, efficiency, and career satisfaction. It allows leaders to audit best practices. It inspires innovative ideas for healthcare delivery and processing improvement changes.
The model of successful physician leadership is based on clinical excellence. The construct of a separation between clinical and administrative roles is a false dichotomy; the two are interdependent. HM directors have a duty to perform both, as it is the combination that makes leaders successful. TH
Dr. Wright is associate clinical professor and chief of the division of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
CON
Physician leaders should relinquish clinical practice, focus on leading
I believe the vast majority of hospitalists agree with the “pro” side of this debate, but I also believe that this kind of knee-jerk reaction reflects the core deficiency that plagues physicians’ thinking regarding leadership.
The way medicine is being practiced and delivered in the hospital setting is rapidly changing. In fact, our specialty is based on this premise. Yet hospitalists still have a stone-age mentality when it comes to physician leaders. The concept of leadership, in most cases, is an afterthought.
Our Role as Leaders
The HM leader is expected to act as a caretaker: set the schedule, organize and implement QI programs, and represent the hospitalists to administration. Most HM directors are accidental leaders who sheepishly step into a position when the opportunity presents itself. This usually happens as programs grow. Few industries would accept this business model. Leadership should be considered critical and given its due respect in terms of resources, training, and experience. Rarely are supervisory positions rewarded to accidental, part-time volunteers. Leaders are chosen, groomed, and given the sufficient time and resources to carry out their mandate.
When HM programs become dysfunctional, hospitalists are quick to blame the administration—some refer to it as the “evil empire” or “the dark side.” But interesting research by Gallup Inc. has shown that the majority of employees who leave their jobs actually are leaving their manager.1
Wants vs. Needs
Leaders face dilemmas every work day. For instance, leaders need to communicate the administration’s goals and weave them into HM department systems and policies. Conversely, HM leaders have to negotiate with administration to secure the resources they need to execute those goals. Technologies are mere facilitators; people actually produce results. Yet many administrators and HM leaders are fixated on the latest software without giving much thought about how staff will implement the changes.
HM leaders need time and resources to be effective. As hospitalists, we’ve been bombarded by the evidence-based medicine mantra. But most hospitalists have never heard of, or they laugh at, evidence-based techniques that were first documented in the 1970s.2 Data is available regarding management skills that can be used to effect positive organization behavior.
We also need to be authentic leaders to combat internal disruptions from medical staff. Gallup Management research has shown that 42% of physicians on medical staffs are actively disengaged.3 Physicians not only are distant, they also actively sabotage and poison new efforts introduced by administration or physician leaders.
The hospitalist leader should only perform clinical responsibilities if they are absolutely necessary. The HM director should be given all the time, resources, due respect, and training to be a dynamic leader. The hospitalist movement would be better for it. TH
References
- Buckingham, M, Coffman C. First, Break All the Rules: How Managers Trump Companies. 1999. New York City: Simon & Schuster.
- Luthans F. Organizational Behavior. 1973. New York City: McGraw-Hill.
- Paller D. What the doctor ordered. Gallup Management Web site. Available at: http://gmj.gallup.com/content/18361/What-Doctor-Ordered.aspx. Accessed Nov. 9, 2009.
Dr. Yu is medical director of hospitalist services at Decatur (Ill.) Memorial Hospital.
In the Literature
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of VTE with travel
- Hyponatremia and mortality
- Clopidogrel and aspirin for atrial fibrillation
- Cost-effective evaluation of syncope
- Early vs. delayed intervention in STEMI patients receiving fibrinolytics
- Predictors of prolonged SSU length of stay
- Rates of survival for in-hospital CPR
- Hospitalists and hospital quality measures
Travel Increases Risk for Venous Thromboembolism in a Dose-Response Relationship
Clinical question: What is the association between travel and the risk of venous thromboembolism (VTE)?
Background: Previous studies evaluating the relationship between long-distance travel and VTE have been heterogeneous and inconclusive. Though a relationship is often discussed, only about half of prior investigations have identified an elevated VTE risk in those who travel, and the impact of duration on VTE risk is unclear.
Study design: Meta-analysis.
Setting: Western countries.
Synopsis: Studies were included if they investigated the association between travel and VTE for persons using any mode of transportation and if nontraveling persons were included for comparison. Fourteen studies met the criteria, and included 4,055 patients with VTE. Compared with nontravelers, the overall pooled relative risk for VTE in travelers was 2.0 (95% CI, 1.5-2.7).
Significant heterogeneity was present among these 14 studies, specifically with regard to the method used for selecting control participants. Six case-control studies used control patients who had been referred for VTE evaluation. When these studies were excluded, the pooled relative risk for VTE in travelers was 2.8 (95% CI, 2.2-3.7).
A dose-response relationship was identified. There was an 18% higher risk for VTE for each two-hour increase in duration of travel among all modes of transportation (P=0.010). When studies evaluating only air travel were analyzed, a 26% higher risk was found for every two-hour increase in air travel (P=0.005).
Bottom line: Travel is associated with a three-fold increase in the risk for VTE, and for each two-hour increase in travel duration, the risk increases approximately 18%.
Citation: Chandra D, Parisini E, Mozaffarian D. Meta-analysis: travel and risk for venous thromboembolism. Ann Intern Med. 2009;151(3):180-190.
Hyponatremia in Hospitalized Patients is Associated with Increased Mortality
Clinical question: Is hyponatremia in hospitalized patients associated with increased mortality?
Background: Hyponatremia is the most common electrolyte abnormality in hospitalized patients. Patients admitted with hyponatremia have increased in-hospital mortality. Long-term mortality in hospitalized patients with hyponatremia is not known. Further, the effects of the degree of hyponatremia on mortality are not known.
Study design: Prospective cohort.
Setting: Two teaching hospitals in Boston.
Synopsis: The study identified 14,290 patients with hyponatremia (serum sodium <135 mEq/L) at admission (14.5%) and an additional 5,093 patients (19,383 total patients, or 19.7% of the 98,411 study patients) with hyponatremia at some point during their hospital stay. After multivariable adjustments and correction for hyperglycemia, patients with hyponatremia had increased mortality in the hospital (OR 1.47, 95% CI, 1.33-1.62), at one year (HR 1.38, 95% CI, 1.32-1.46), and at five years (HR 1.25, 95% CI, 1.21-1.30) compared with normonatremic patients. These mortality differences were seen in patients with mild, moderate, and moderately severe hyponatremia (serum sodium concentrations 130-134, 125-129, and 120-124 mEq/L, respectively), but not in patients with severe hyponatremia (serum sodium <120 mEq/L).
This study is limited by its post-hoc identification and classification of patients using ICD-9-CM codes, which could have resulted in some misclassification. Also, this study includes only two teaching hospitals in an urban setting; the prevalence of hyponatremia might differ in other settings. Causality cannot be determined based on these results.
Bottom line: Hospitalized patients with hyponatremia have increased in-hospital and long-term mortality.
Citation: Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122(9):857-865.
Clopidogrel Plus Aspirin in Patients with Atrial Fibrillation Reduces Risk of Major Vascular Events
Clinical question: Does the addition of clopidogrel to aspirin therapy reduce the risk of major vascular events in patients with atrial fibrillation for whom vitamin K antagonists (VKAs) are unsuitable?
Background: Although VKAs reduce the risk of stroke in atrial fibrillation, many patients are unable to use VKAs and are treated with aspirin instead. The potential benefits of adding clopidogrel to aspirin therapy in this population are unknown.
Study design: Randomized controlled trial.
Setting: Five hundred eighty medical centers in 33 countries.
Synopsis: More than 7,500 patients with atrial fibrillation who were also at high risk for stroke were randomly assigned to receive either clopidogrel or placebo once daily. All patients also received aspirin at a dose of 75 mg to 100 mg daily. A major vascular event occurred in 6.8% of patients per year who received clopidogrel and in 7.6% of patients per year who received placebo (RR 0.89, 95% CI, 0.89-0.98, P=0.01). This reduction primarily was due to a reduction in stroke, which occurred in 2.4% of patients per year who received clopidogrel, compared with 3.3% of patients per year who received placebo (RR 0.72, 95% CI, 0.62-0.83, P<0.001).
Major bleeding occurred in 2% of patients per year who received clopidogrel and in 1.3% of patients per year who received placebo (RR 1.57, 95% CI, 1.29-1.92, P<0.001).
Bottom line: Adding clopidogrel to aspirin in patients with atrial fibrillation who are not eligible for VKAs decreases the risk of major vascular events, including stroke, but increases risk of major hemorrhage compared with aspirin alone.
Citation: ACTIVE Investigators, Connolly SJ, Pogue J, et al. Effect of clopidogrel added to aspirin in patients with atrial fibrillation. N Engl J Med. 2009;360(20):2066-2078.
Prioritize Syncope Testing by Diagnostic Yield and Cost Effectiveness
Clinical question: What are the utilization, yield, and cost effectiveness of tests used for evaluation of syncope in older patients?
Background: Clinicians utilize multiple diagnostic tests to help delineate the cause of syncope, but the yield and cost effectiveness of many of these tests are unclear. Further, it is unknown if considering patient characteristics, as in the San Francisco syncope rule (SFSR), can improve the yield of diagnostic tests.
Study design: Retrospective cohort.
Setting: Single acute-care hospital.
Synopsis: Review of 2,106 admissions in patients 65 and older with syncope revealed that the most common tests were electrocardiogram (99%), telemetry (95%), cardiac enzymes (95%), and head computed tomography (CT) scan (63%). The majority of tests did not affect diagnosis or management.
Postural blood pressure (BP) reading was infrequently recorded (38%) but had the highest yield. BP influenced diagnosis at least 18% of the time and management at least 25% of the time. Tests with the lowest likelihood of affecting diagnosis and management were head CT, carotid ultrasound, electroencephalography (EEG), and cardiac enzymes.
EEG had the highest cost per test affecting the diagnosis or management ($32,973), followed by head CT. The cost per test affecting diagnosis or management for postural BP was $17. Cardiac testing, including telemetry, echocardiogram, and cardiac enzymes, had significantly better yield in patients who met SFSR criteria.
Bottom line: In patients with syncope, the history and exam should guide evaluation, and tests with high yield and low cost per test, such as postural BP, should be prioritized.
Citation: Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14): 1299-1305.
Early PCI is Superior to Delayed Intervention in Patients with STEMI Receiving Fibrinolytic Therapy
Clinical question: Does early percutaneous coronary intervention (PCI) improve clinical outcomes compared with standard management in patients with ST elevation myocardial infarction (STEMI) who receive fibrinolysis?
Background: Prior research has demonstrated the benefit of timely PCI in the management of acute coronary syndrome, specifically with ST elevation. However, many hospitals do not have this capability and utilize fibrinolysis as a standard alternative. The optimal timing of subsequent invasive intervention following fibrinolysis has not been established.
Study design: Multicenter randomized trial.
Setting: Fifty-two sites in three provinces in Canada.
Synopsis: This study randomized 1,059 patients presenting with STEMI and receiving fibrinolysis to early intervention (immediate transfer to another hospital with PCI less than six hours after fibrinolysis) versus standard intervention (rescue PCI if needed, or delayed angiography at more than 24 hours). The primary outcome was the composite of death, reinfarction, recurrent ischemia, new or worsening congestive heart failure, or cardiogenic shock within 30 days.
The primary outcome occurred in 11% of patients in the early intervention group, compared with 17.2% of patients randomized to standard intervention (RR 0.64, 95% CI, 0.47-0.87, P=0.004). Urgent catheterization was performed within 12 hours of fibrinolysis in 34.9% of patients randomized to the standard treatment group.
This study was not powered to detect differences in mortality and other individual components of the primary endpoint.
Bottom line: STEMI patients who received fibrinolysis had a lower risk of adverse outcomes when receiving transfer and PCI within six hours, compared with standard delayed intervention.
Citation: Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360(26):2705-2718.
Specialty Consultation and Limited Access Tests Predict Unsuccessful SSU Admissions
Clinical question: In patients admitted to short-stay units (SSUs), what characteristics are associated with unsuccessful SSU admission?
Background: Short-stay units have become prevalent in U.S. hospitals, but it is unclear which patient populations are best served by SSUs.
Study design: Prospective cohort.
Setting: Fourteen-bed SSU in a 500-bed public teaching hospital in Chicago.
Synopsis: More than 700 patients admitted to the Cook County Hospital SSU over a four-month period were interviewed and examined, and their ED and inpatient records were reviewed. An SSU admission was defined as “successful” if the length of stay (LOS) was less than 72 hours and the patient was discharged directly from the SSU.
Overall, 79% of patients had a successful SSU admission. In multivariate analysis, the strongest predictors of an unsuccessful SSU stay were subspecialty consultation (OR 8.1, P<0.001), a provisional diagnosis of heart failure (OR 1.9, P=0.02), and limited availability of a diagnostic test (OR 2.5, P<0.001).
The study was limited primarily to patients with cardiovascular diagnoses.
Bottom line: Patients admitted to SSUs who receive specialty consultation, carry a diagnosis of heart failure, or require diagnostic testing that is not readily available might have a longer LOS or eventual inpatient admission.
Citation: Lucas BP, Kumapley R, Mba B, et al. A hospitalist-run short-stay unit: features that predict length-of-stay and eventual admission to traditional inpatient services. J Hosp Med. 2009;4(5):276-284.
Lack of Significant Gains in Survival Rates Following In-Hospital CPR
Clinical question: Is survival after in-hospital CPR improving over time, and what are the factors associated with survival?
Background: Advances in out-of-hospital CPR have improved outcomes. However, it is unknown whether the survival rate after in-hospital CPR is improving over time, and it is unclear which patient and/or hospital characteristics predict post-CPR survival.
Study design: Retrospective cohort.
Setting: Inpatient Medicare beneficiaries from 1992 to 2005.
Synopsis: The study examined more than 150 million Medicare admissions, 433,985 of which underwent in-hospital CPR. Survival to discharge occurred in 18.3% of CPR events and did not change significantly from 1992 to 2005. The cumulative incidence of in-hospital CPR events was 2.73 per 1,000 admissions; it did not change substantially over time.
The survival rate was lower among black patients (OR 0.76, 95% CI, 0.74-0.79), which is partially explained due to the fact they tended to receive CPR at hospitals with lower post-CPR survival. Gender (specifically male), older age, race (specifically other nonwhite patients), higher burden of chronic illness, and admission from a skilled nursing facility were significantly associated with decreased survival to hospital discharge following CPR.
Limitations of this study included the identification of CPR by ICD-9 codes, which have not been validated for this purpose and could vary among hospitals. Other factors that might explain variations in survival were not available, including severity of acute illness and the presence (or absence) of a shockable rhythm at initial presentation.
Bottom line: Rates of survival to hospital discharge among Medicare beneficiaries receiving in-hospital CPR have remained constant over time, with poorer survival rates among blacks and other nonwhite patients.
Citation: Ehlenbach WJ, Barnato AE, Curtis JR, et al. Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly. N Engl J Med. 2009;361(1):22-31.
Hospitalists Are Associated with Improved Performance on Quality Metrics
Clinical question: Is the presence of hospitalist physicians associated with improved performance on standard quality measures for acute myocardial infarction (AMI), congestive heart failure (CHF), and pneumonia?
Background: Previous investigations have demonstrated significant improvements in cost and LOS for patients under the care of hospitalists compared with other inpatient providers. The association between hospitalist prevalence and quality of care, as measured by standard quality process measures, is unknown.
Study design: Cross-sectional.
Setting: More than 3,600 hospitals participating in the Health Quality Alliance (HQA) program.
Synopsis: Investigators looked at a large sample of HQA hospitals in the American Hospital Association survey, and identified facilities with hospitalist services and those without. The primary endpoint was the adherence to composites of standard quality process measures across three disease categories (AMI, CHF, and pneumonia) and two domains of care (disease treatment/diagnosis and counseling/prevention).
Multivariable analyses revealed a statistically significant association between the presence of hospitalists and adherence to composite quality measures for AMI and pneumonia. This association was demonstrated for both treatment and counseling domains.
The study is cross-sectional, so conclusions cannot be drawn about causality. Also, there are likely unmeasured differences between hospitals that utilize hospitalists compared with those that do not, which could further confound the relationship between the presence of hospitalists and adherence to quality measures.
Finally, this study only evaluated hospital-level performance, and it cannot offer insight on the quality of individual patient care by hospitalist providers.
Bottom line: The presence of hospitalists is associated with improvement in adherence to quality measures for both AMI and pneumonia, and across clinical domains of treatment and counseling.
Citation: López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394. TH
PEDIATRIC HM LITerature
Inpatient Curriculum Implicit, but Aligns with ACGME Competencies
By Mark Shen, MD

Clinical question: Does implicit resident learning on an inpatient unit correspond to the explicit Accreditation Council for Graduate Medical Education (ACGME) competencies?
Background: The ACGME competency-based model of education places an emphasis on task-oriented ability as a translation of skills and knowledge. Although it is recognized that most learning occurs through the process of daily patient care, it is unclear how much learning is explicit and linked to ACGME competencies, as defined in the goals and objectives of an inpatient rotation.
Study design: Qualitative, ethnographic case study.
Setting: One general pediatric floor in a large, urban pediatric hospital.
Synopsis: Over an eight-month period, one researcher directly observed and asked questions of inpatient teams as they worked on a general pediatric service. There was a particular emphasis on morning rounds. Data coding was completed in an iterative manner, and both data and method triangulation were used to enhance trustworthiness.
Curricular convergence occurred and was most obvious in the patient-care domain; however, the explicit curriculum was not formally referred to during the study period. The implicit curriculum was ill-structured and unpredictable, typically dictated by the patients’ socioclinical environment.
The primary limitations of this work are the focus on one service on one hospital floor, and that the study authors were former trainees or employees of that institution. This institution-specific bias, however, might be gauged by the degree to which the themes in this research will resonate with clinician-educators who read this article. Given the increasing time constraints on explicit inpatient didactic teaching, the vignettes and conclusions within this report are likely to find many a sympathetic ear. Illumination of the hidden curriculum could further support learner-centered education.
Bottom line: The inpatient service is a fertile and primarily implicit training ground for the ACGME competencies.
Citation: Balmer DF, Master CL, Richards B, Giardino AP. Implicit versus explicit curricula in general pediatrics education: is there a convergence? Pediatrics. 2009;124(2):e347-354.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of VTE with travel
- Hyponatremia and mortality
- Clopidogrel and aspirin for atrial fibrillation
- Cost-effective evaluation of syncope
- Early vs. delayed intervention in STEMI patients receiving fibrinolytics
- Predictors of prolonged SSU length of stay
- Rates of survival for in-hospital CPR
- Hospitalists and hospital quality measures
Travel Increases Risk for Venous Thromboembolism in a Dose-Response Relationship
Clinical question: What is the association between travel and the risk of venous thromboembolism (VTE)?
Background: Previous studies evaluating the relationship between long-distance travel and VTE have been heterogeneous and inconclusive. Though a relationship is often discussed, only about half of prior investigations have identified an elevated VTE risk in those who travel, and the impact of duration on VTE risk is unclear.
Study design: Meta-analysis.
Setting: Western countries.
Synopsis: Studies were included if they investigated the association between travel and VTE for persons using any mode of transportation and if nontraveling persons were included for comparison. Fourteen studies met the criteria, and included 4,055 patients with VTE. Compared with nontravelers, the overall pooled relative risk for VTE in travelers was 2.0 (95% CI, 1.5-2.7).
Significant heterogeneity was present among these 14 studies, specifically with regard to the method used for selecting control participants. Six case-control studies used control patients who had been referred for VTE evaluation. When these studies were excluded, the pooled relative risk for VTE in travelers was 2.8 (95% CI, 2.2-3.7).
A dose-response relationship was identified. There was an 18% higher risk for VTE for each two-hour increase in duration of travel among all modes of transportation (P=0.010). When studies evaluating only air travel were analyzed, a 26% higher risk was found for every two-hour increase in air travel (P=0.005).
Bottom line: Travel is associated with a three-fold increase in the risk for VTE, and for each two-hour increase in travel duration, the risk increases approximately 18%.
Citation: Chandra D, Parisini E, Mozaffarian D. Meta-analysis: travel and risk for venous thromboembolism. Ann Intern Med. 2009;151(3):180-190.
Hyponatremia in Hospitalized Patients is Associated with Increased Mortality
Clinical question: Is hyponatremia in hospitalized patients associated with increased mortality?
Background: Hyponatremia is the most common electrolyte abnormality in hospitalized patients. Patients admitted with hyponatremia have increased in-hospital mortality. Long-term mortality in hospitalized patients with hyponatremia is not known. Further, the effects of the degree of hyponatremia on mortality are not known.
Study design: Prospective cohort.
Setting: Two teaching hospitals in Boston.
Synopsis: The study identified 14,290 patients with hyponatremia (serum sodium <135 mEq/L) at admission (14.5%) and an additional 5,093 patients (19,383 total patients, or 19.7% of the 98,411 study patients) with hyponatremia at some point during their hospital stay. After multivariable adjustments and correction for hyperglycemia, patients with hyponatremia had increased mortality in the hospital (OR 1.47, 95% CI, 1.33-1.62), at one year (HR 1.38, 95% CI, 1.32-1.46), and at five years (HR 1.25, 95% CI, 1.21-1.30) compared with normonatremic patients. These mortality differences were seen in patients with mild, moderate, and moderately severe hyponatremia (serum sodium concentrations 130-134, 125-129, and 120-124 mEq/L, respectively), but not in patients with severe hyponatremia (serum sodium <120 mEq/L).
This study is limited by its post-hoc identification and classification of patients using ICD-9-CM codes, which could have resulted in some misclassification. Also, this study includes only two teaching hospitals in an urban setting; the prevalence of hyponatremia might differ in other settings. Causality cannot be determined based on these results.
Bottom line: Hospitalized patients with hyponatremia have increased in-hospital and long-term mortality.
Citation: Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122(9):857-865.
Clopidogrel Plus Aspirin in Patients with Atrial Fibrillation Reduces Risk of Major Vascular Events
Clinical question: Does the addition of clopidogrel to aspirin therapy reduce the risk of major vascular events in patients with atrial fibrillation for whom vitamin K antagonists (VKAs) are unsuitable?
Background: Although VKAs reduce the risk of stroke in atrial fibrillation, many patients are unable to use VKAs and are treated with aspirin instead. The potential benefits of adding clopidogrel to aspirin therapy in this population are unknown.
Study design: Randomized controlled trial.
Setting: Five hundred eighty medical centers in 33 countries.
Synopsis: More than 7,500 patients with atrial fibrillation who were also at high risk for stroke were randomly assigned to receive either clopidogrel or placebo once daily. All patients also received aspirin at a dose of 75 mg to 100 mg daily. A major vascular event occurred in 6.8% of patients per year who received clopidogrel and in 7.6% of patients per year who received placebo (RR 0.89, 95% CI, 0.89-0.98, P=0.01). This reduction primarily was due to a reduction in stroke, which occurred in 2.4% of patients per year who received clopidogrel, compared with 3.3% of patients per year who received placebo (RR 0.72, 95% CI, 0.62-0.83, P<0.001).
Major bleeding occurred in 2% of patients per year who received clopidogrel and in 1.3% of patients per year who received placebo (RR 1.57, 95% CI, 1.29-1.92, P<0.001).
Bottom line: Adding clopidogrel to aspirin in patients with atrial fibrillation who are not eligible for VKAs decreases the risk of major vascular events, including stroke, but increases risk of major hemorrhage compared with aspirin alone.
Citation: ACTIVE Investigators, Connolly SJ, Pogue J, et al. Effect of clopidogrel added to aspirin in patients with atrial fibrillation. N Engl J Med. 2009;360(20):2066-2078.
Prioritize Syncope Testing by Diagnostic Yield and Cost Effectiveness
Clinical question: What are the utilization, yield, and cost effectiveness of tests used for evaluation of syncope in older patients?
Background: Clinicians utilize multiple diagnostic tests to help delineate the cause of syncope, but the yield and cost effectiveness of many of these tests are unclear. Further, it is unknown if considering patient characteristics, as in the San Francisco syncope rule (SFSR), can improve the yield of diagnostic tests.
Study design: Retrospective cohort.
Setting: Single acute-care hospital.
Synopsis: Review of 2,106 admissions in patients 65 and older with syncope revealed that the most common tests were electrocardiogram (99%), telemetry (95%), cardiac enzymes (95%), and head computed tomography (CT) scan (63%). The majority of tests did not affect diagnosis or management.
Postural blood pressure (BP) reading was infrequently recorded (38%) but had the highest yield. BP influenced diagnosis at least 18% of the time and management at least 25% of the time. Tests with the lowest likelihood of affecting diagnosis and management were head CT, carotid ultrasound, electroencephalography (EEG), and cardiac enzymes.
EEG had the highest cost per test affecting the diagnosis or management ($32,973), followed by head CT. The cost per test affecting diagnosis or management for postural BP was $17. Cardiac testing, including telemetry, echocardiogram, and cardiac enzymes, had significantly better yield in patients who met SFSR criteria.
Bottom line: In patients with syncope, the history and exam should guide evaluation, and tests with high yield and low cost per test, such as postural BP, should be prioritized.
Citation: Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14): 1299-1305.
Early PCI is Superior to Delayed Intervention in Patients with STEMI Receiving Fibrinolytic Therapy
Clinical question: Does early percutaneous coronary intervention (PCI) improve clinical outcomes compared with standard management in patients with ST elevation myocardial infarction (STEMI) who receive fibrinolysis?
Background: Prior research has demonstrated the benefit of timely PCI in the management of acute coronary syndrome, specifically with ST elevation. However, many hospitals do not have this capability and utilize fibrinolysis as a standard alternative. The optimal timing of subsequent invasive intervention following fibrinolysis has not been established.
Study design: Multicenter randomized trial.
Setting: Fifty-two sites in three provinces in Canada.
Synopsis: This study randomized 1,059 patients presenting with STEMI and receiving fibrinolysis to early intervention (immediate transfer to another hospital with PCI less than six hours after fibrinolysis) versus standard intervention (rescue PCI if needed, or delayed angiography at more than 24 hours). The primary outcome was the composite of death, reinfarction, recurrent ischemia, new or worsening congestive heart failure, or cardiogenic shock within 30 days.
The primary outcome occurred in 11% of patients in the early intervention group, compared with 17.2% of patients randomized to standard intervention (RR 0.64, 95% CI, 0.47-0.87, P=0.004). Urgent catheterization was performed within 12 hours of fibrinolysis in 34.9% of patients randomized to the standard treatment group.
This study was not powered to detect differences in mortality and other individual components of the primary endpoint.
Bottom line: STEMI patients who received fibrinolysis had a lower risk of adverse outcomes when receiving transfer and PCI within six hours, compared with standard delayed intervention.
Citation: Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360(26):2705-2718.
Specialty Consultation and Limited Access Tests Predict Unsuccessful SSU Admissions
Clinical question: In patients admitted to short-stay units (SSUs), what characteristics are associated with unsuccessful SSU admission?
Background: Short-stay units have become prevalent in U.S. hospitals, but it is unclear which patient populations are best served by SSUs.
Study design: Prospective cohort.
Setting: Fourteen-bed SSU in a 500-bed public teaching hospital in Chicago.
Synopsis: More than 700 patients admitted to the Cook County Hospital SSU over a four-month period were interviewed and examined, and their ED and inpatient records were reviewed. An SSU admission was defined as “successful” if the length of stay (LOS) was less than 72 hours and the patient was discharged directly from the SSU.
Overall, 79% of patients had a successful SSU admission. In multivariate analysis, the strongest predictors of an unsuccessful SSU stay were subspecialty consultation (OR 8.1, P<0.001), a provisional diagnosis of heart failure (OR 1.9, P=0.02), and limited availability of a diagnostic test (OR 2.5, P<0.001).
The study was limited primarily to patients with cardiovascular diagnoses.
Bottom line: Patients admitted to SSUs who receive specialty consultation, carry a diagnosis of heart failure, or require diagnostic testing that is not readily available might have a longer LOS or eventual inpatient admission.
Citation: Lucas BP, Kumapley R, Mba B, et al. A hospitalist-run short-stay unit: features that predict length-of-stay and eventual admission to traditional inpatient services. J Hosp Med. 2009;4(5):276-284.
Lack of Significant Gains in Survival Rates Following In-Hospital CPR
Clinical question: Is survival after in-hospital CPR improving over time, and what are the factors associated with survival?
Background: Advances in out-of-hospital CPR have improved outcomes. However, it is unknown whether the survival rate after in-hospital CPR is improving over time, and it is unclear which patient and/or hospital characteristics predict post-CPR survival.
Study design: Retrospective cohort.
Setting: Inpatient Medicare beneficiaries from 1992 to 2005.
Synopsis: The study examined more than 150 million Medicare admissions, 433,985 of which underwent in-hospital CPR. Survival to discharge occurred in 18.3% of CPR events and did not change significantly from 1992 to 2005. The cumulative incidence of in-hospital CPR events was 2.73 per 1,000 admissions; it did not change substantially over time.
The survival rate was lower among black patients (OR 0.76, 95% CI, 0.74-0.79), which is partially explained due to the fact they tended to receive CPR at hospitals with lower post-CPR survival. Gender (specifically male), older age, race (specifically other nonwhite patients), higher burden of chronic illness, and admission from a skilled nursing facility were significantly associated with decreased survival to hospital discharge following CPR.
Limitations of this study included the identification of CPR by ICD-9 codes, which have not been validated for this purpose and could vary among hospitals. Other factors that might explain variations in survival were not available, including severity of acute illness and the presence (or absence) of a shockable rhythm at initial presentation.
Bottom line: Rates of survival to hospital discharge among Medicare beneficiaries receiving in-hospital CPR have remained constant over time, with poorer survival rates among blacks and other nonwhite patients.
Citation: Ehlenbach WJ, Barnato AE, Curtis JR, et al. Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly. N Engl J Med. 2009;361(1):22-31.
Hospitalists Are Associated with Improved Performance on Quality Metrics
Clinical question: Is the presence of hospitalist physicians associated with improved performance on standard quality measures for acute myocardial infarction (AMI), congestive heart failure (CHF), and pneumonia?
Background: Previous investigations have demonstrated significant improvements in cost and LOS for patients under the care of hospitalists compared with other inpatient providers. The association between hospitalist prevalence and quality of care, as measured by standard quality process measures, is unknown.
Study design: Cross-sectional.
Setting: More than 3,600 hospitals participating in the Health Quality Alliance (HQA) program.
Synopsis: Investigators looked at a large sample of HQA hospitals in the American Hospital Association survey, and identified facilities with hospitalist services and those without. The primary endpoint was the adherence to composites of standard quality process measures across three disease categories (AMI, CHF, and pneumonia) and two domains of care (disease treatment/diagnosis and counseling/prevention).
Multivariable analyses revealed a statistically significant association between the presence of hospitalists and adherence to composite quality measures for AMI and pneumonia. This association was demonstrated for both treatment and counseling domains.
The study is cross-sectional, so conclusions cannot be drawn about causality. Also, there are likely unmeasured differences between hospitals that utilize hospitalists compared with those that do not, which could further confound the relationship between the presence of hospitalists and adherence to quality measures.
Finally, this study only evaluated hospital-level performance, and it cannot offer insight on the quality of individual patient care by hospitalist providers.
Bottom line: The presence of hospitalists is associated with improvement in adherence to quality measures for both AMI and pneumonia, and across clinical domains of treatment and counseling.
Citation: López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394. TH
PEDIATRIC HM LITerature
Inpatient Curriculum Implicit, but Aligns with ACGME Competencies
By Mark Shen, MD
Clinical question: Does implicit resident learning on an inpatient unit correspond to the explicit Accreditation Council for Graduate Medical Education (ACGME) competencies?
Background: The ACGME competency-based model of education places an emphasis on task-oriented ability as a translation of skills and knowledge. Although it is recognized that most learning occurs through the process of daily patient care, it is unclear how much learning is explicit and linked to ACGME competencies, as defined in the goals and objectives of an inpatient rotation.
Study design: Qualitative, ethnographic case study.
Setting: One general pediatric floor in a large, urban pediatric hospital.
Synopsis: Over an eight-month period, one researcher directly observed and asked questions of inpatient teams as they worked on a general pediatric service. There was a particular emphasis on morning rounds. Data coding was completed in an iterative manner, and both data and method triangulation were used to enhance trustworthiness.
Curricular convergence occurred and was most obvious in the patient-care domain; however, the explicit curriculum was not formally referred to during the study period. The implicit curriculum was ill-structured and unpredictable, typically dictated by the patients’ socioclinical environment.
The primary limitations of this work are the focus on one service on one hospital floor, and that the study authors were former trainees or employees of that institution. This institution-specific bias, however, might be gauged by the degree to which the themes in this research will resonate with clinician-educators who read this article. Given the increasing time constraints on explicit inpatient didactic teaching, the vignettes and conclusions within this report are likely to find many a sympathetic ear. Illumination of the hidden curriculum could further support learner-centered education.
Bottom line: The inpatient service is a fertile and primarily implicit training ground for the ACGME competencies.
Citation: Balmer DF, Master CL, Richards B, Giardino AP. Implicit versus explicit curricula in general pediatrics education: is there a convergence? Pediatrics. 2009;124(2):e347-354.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Risk of VTE with travel
- Hyponatremia and mortality
- Clopidogrel and aspirin for atrial fibrillation
- Cost-effective evaluation of syncope
- Early vs. delayed intervention in STEMI patients receiving fibrinolytics
- Predictors of prolonged SSU length of stay
- Rates of survival for in-hospital CPR
- Hospitalists and hospital quality measures
Travel Increases Risk for Venous Thromboembolism in a Dose-Response Relationship
Clinical question: What is the association between travel and the risk of venous thromboembolism (VTE)?
Background: Previous studies evaluating the relationship between long-distance travel and VTE have been heterogeneous and inconclusive. Though a relationship is often discussed, only about half of prior investigations have identified an elevated VTE risk in those who travel, and the impact of duration on VTE risk is unclear.
Study design: Meta-analysis.
Setting: Western countries.
Synopsis: Studies were included if they investigated the association between travel and VTE for persons using any mode of transportation and if nontraveling persons were included for comparison. Fourteen studies met the criteria, and included 4,055 patients with VTE. Compared with nontravelers, the overall pooled relative risk for VTE in travelers was 2.0 (95% CI, 1.5-2.7).
Significant heterogeneity was present among these 14 studies, specifically with regard to the method used for selecting control participants. Six case-control studies used control patients who had been referred for VTE evaluation. When these studies were excluded, the pooled relative risk for VTE in travelers was 2.8 (95% CI, 2.2-3.7).
A dose-response relationship was identified. There was an 18% higher risk for VTE for each two-hour increase in duration of travel among all modes of transportation (P=0.010). When studies evaluating only air travel were analyzed, a 26% higher risk was found for every two-hour increase in air travel (P=0.005).
Bottom line: Travel is associated with a three-fold increase in the risk for VTE, and for each two-hour increase in travel duration, the risk increases approximately 18%.
Citation: Chandra D, Parisini E, Mozaffarian D. Meta-analysis: travel and risk for venous thromboembolism. Ann Intern Med. 2009;151(3):180-190.
Hyponatremia in Hospitalized Patients is Associated with Increased Mortality
Clinical question: Is hyponatremia in hospitalized patients associated with increased mortality?
Background: Hyponatremia is the most common electrolyte abnormality in hospitalized patients. Patients admitted with hyponatremia have increased in-hospital mortality. Long-term mortality in hospitalized patients with hyponatremia is not known. Further, the effects of the degree of hyponatremia on mortality are not known.
Study design: Prospective cohort.
Setting: Two teaching hospitals in Boston.
Synopsis: The study identified 14,290 patients with hyponatremia (serum sodium <135 mEq/L) at admission (14.5%) and an additional 5,093 patients (19,383 total patients, or 19.7% of the 98,411 study patients) with hyponatremia at some point during their hospital stay. After multivariable adjustments and correction for hyperglycemia, patients with hyponatremia had increased mortality in the hospital (OR 1.47, 95% CI, 1.33-1.62), at one year (HR 1.38, 95% CI, 1.32-1.46), and at five years (HR 1.25, 95% CI, 1.21-1.30) compared with normonatremic patients. These mortality differences were seen in patients with mild, moderate, and moderately severe hyponatremia (serum sodium concentrations 130-134, 125-129, and 120-124 mEq/L, respectively), but not in patients with severe hyponatremia (serum sodium <120 mEq/L).
This study is limited by its post-hoc identification and classification of patients using ICD-9-CM codes, which could have resulted in some misclassification. Also, this study includes only two teaching hospitals in an urban setting; the prevalence of hyponatremia might differ in other settings. Causality cannot be determined based on these results.
Bottom line: Hospitalized patients with hyponatremia have increased in-hospital and long-term mortality.
Citation: Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122(9):857-865.
Clopidogrel Plus Aspirin in Patients with Atrial Fibrillation Reduces Risk of Major Vascular Events
Clinical question: Does the addition of clopidogrel to aspirin therapy reduce the risk of major vascular events in patients with atrial fibrillation for whom vitamin K antagonists (VKAs) are unsuitable?
Background: Although VKAs reduce the risk of stroke in atrial fibrillation, many patients are unable to use VKAs and are treated with aspirin instead. The potential benefits of adding clopidogrel to aspirin therapy in this population are unknown.
Study design: Randomized controlled trial.
Setting: Five hundred eighty medical centers in 33 countries.
Synopsis: More than 7,500 patients with atrial fibrillation who were also at high risk for stroke were randomly assigned to receive either clopidogrel or placebo once daily. All patients also received aspirin at a dose of 75 mg to 100 mg daily. A major vascular event occurred in 6.8% of patients per year who received clopidogrel and in 7.6% of patients per year who received placebo (RR 0.89, 95% CI, 0.89-0.98, P=0.01). This reduction primarily was due to a reduction in stroke, which occurred in 2.4% of patients per year who received clopidogrel, compared with 3.3% of patients per year who received placebo (RR 0.72, 95% CI, 0.62-0.83, P<0.001).
Major bleeding occurred in 2% of patients per year who received clopidogrel and in 1.3% of patients per year who received placebo (RR 1.57, 95% CI, 1.29-1.92, P<0.001).
Bottom line: Adding clopidogrel to aspirin in patients with atrial fibrillation who are not eligible for VKAs decreases the risk of major vascular events, including stroke, but increases risk of major hemorrhage compared with aspirin alone.
Citation: ACTIVE Investigators, Connolly SJ, Pogue J, et al. Effect of clopidogrel added to aspirin in patients with atrial fibrillation. N Engl J Med. 2009;360(20):2066-2078.
Prioritize Syncope Testing by Diagnostic Yield and Cost Effectiveness
Clinical question: What are the utilization, yield, and cost effectiveness of tests used for evaluation of syncope in older patients?
Background: Clinicians utilize multiple diagnostic tests to help delineate the cause of syncope, but the yield and cost effectiveness of many of these tests are unclear. Further, it is unknown if considering patient characteristics, as in the San Francisco syncope rule (SFSR), can improve the yield of diagnostic tests.
Study design: Retrospective cohort.
Setting: Single acute-care hospital.
Synopsis: Review of 2,106 admissions in patients 65 and older with syncope revealed that the most common tests were electrocardiogram (99%), telemetry (95%), cardiac enzymes (95%), and head computed tomography (CT) scan (63%). The majority of tests did not affect diagnosis or management.
Postural blood pressure (BP) reading was infrequently recorded (38%) but had the highest yield. BP influenced diagnosis at least 18% of the time and management at least 25% of the time. Tests with the lowest likelihood of affecting diagnosis and management were head CT, carotid ultrasound, electroencephalography (EEG), and cardiac enzymes.
EEG had the highest cost per test affecting the diagnosis or management ($32,973), followed by head CT. The cost per test affecting diagnosis or management for postural BP was $17. Cardiac testing, including telemetry, echocardiogram, and cardiac enzymes, had significantly better yield in patients who met SFSR criteria.
Bottom line: In patients with syncope, the history and exam should guide evaluation, and tests with high yield and low cost per test, such as postural BP, should be prioritized.
Citation: Mendu ML, McAvay G, Lampert R, Stoehr J, Tinetti ME. Yield of diagnostic tests in evaluating syncopal episodes in older patients. Arch Intern Med. 2009;169(14): 1299-1305.
Early PCI is Superior to Delayed Intervention in Patients with STEMI Receiving Fibrinolytic Therapy
Clinical question: Does early percutaneous coronary intervention (PCI) improve clinical outcomes compared with standard management in patients with ST elevation myocardial infarction (STEMI) who receive fibrinolysis?
Background: Prior research has demonstrated the benefit of timely PCI in the management of acute coronary syndrome, specifically with ST elevation. However, many hospitals do not have this capability and utilize fibrinolysis as a standard alternative. The optimal timing of subsequent invasive intervention following fibrinolysis has not been established.
Study design: Multicenter randomized trial.
Setting: Fifty-two sites in three provinces in Canada.
Synopsis: This study randomized 1,059 patients presenting with STEMI and receiving fibrinolysis to early intervention (immediate transfer to another hospital with PCI less than six hours after fibrinolysis) versus standard intervention (rescue PCI if needed, or delayed angiography at more than 24 hours). The primary outcome was the composite of death, reinfarction, recurrent ischemia, new or worsening congestive heart failure, or cardiogenic shock within 30 days.
The primary outcome occurred in 11% of patients in the early intervention group, compared with 17.2% of patients randomized to standard intervention (RR 0.64, 95% CI, 0.47-0.87, P=0.004). Urgent catheterization was performed within 12 hours of fibrinolysis in 34.9% of patients randomized to the standard treatment group.
This study was not powered to detect differences in mortality and other individual components of the primary endpoint.
Bottom line: STEMI patients who received fibrinolysis had a lower risk of adverse outcomes when receiving transfer and PCI within six hours, compared with standard delayed intervention.
Citation: Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360(26):2705-2718.
Specialty Consultation and Limited Access Tests Predict Unsuccessful SSU Admissions
Clinical question: In patients admitted to short-stay units (SSUs), what characteristics are associated with unsuccessful SSU admission?
Background: Short-stay units have become prevalent in U.S. hospitals, but it is unclear which patient populations are best served by SSUs.
Study design: Prospective cohort.
Setting: Fourteen-bed SSU in a 500-bed public teaching hospital in Chicago.
Synopsis: More than 700 patients admitted to the Cook County Hospital SSU over a four-month period were interviewed and examined, and their ED and inpatient records were reviewed. An SSU admission was defined as “successful” if the length of stay (LOS) was less than 72 hours and the patient was discharged directly from the SSU.
Overall, 79% of patients had a successful SSU admission. In multivariate analysis, the strongest predictors of an unsuccessful SSU stay were subspecialty consultation (OR 8.1, P<0.001), a provisional diagnosis of heart failure (OR 1.9, P=0.02), and limited availability of a diagnostic test (OR 2.5, P<0.001).
The study was limited primarily to patients with cardiovascular diagnoses.
Bottom line: Patients admitted to SSUs who receive specialty consultation, carry a diagnosis of heart failure, or require diagnostic testing that is not readily available might have a longer LOS or eventual inpatient admission.
Citation: Lucas BP, Kumapley R, Mba B, et al. A hospitalist-run short-stay unit: features that predict length-of-stay and eventual admission to traditional inpatient services. J Hosp Med. 2009;4(5):276-284.
Lack of Significant Gains in Survival Rates Following In-Hospital CPR
Clinical question: Is survival after in-hospital CPR improving over time, and what are the factors associated with survival?
Background: Advances in out-of-hospital CPR have improved outcomes. However, it is unknown whether the survival rate after in-hospital CPR is improving over time, and it is unclear which patient and/or hospital characteristics predict post-CPR survival.
Study design: Retrospective cohort.
Setting: Inpatient Medicare beneficiaries from 1992 to 2005.
Synopsis: The study examined more than 150 million Medicare admissions, 433,985 of which underwent in-hospital CPR. Survival to discharge occurred in 18.3% of CPR events and did not change significantly from 1992 to 2005. The cumulative incidence of in-hospital CPR events was 2.73 per 1,000 admissions; it did not change substantially over time.
The survival rate was lower among black patients (OR 0.76, 95% CI, 0.74-0.79), which is partially explained due to the fact they tended to receive CPR at hospitals with lower post-CPR survival. Gender (specifically male), older age, race (specifically other nonwhite patients), higher burden of chronic illness, and admission from a skilled nursing facility were significantly associated with decreased survival to hospital discharge following CPR.
Limitations of this study included the identification of CPR by ICD-9 codes, which have not been validated for this purpose and could vary among hospitals. Other factors that might explain variations in survival were not available, including severity of acute illness and the presence (or absence) of a shockable rhythm at initial presentation.
Bottom line: Rates of survival to hospital discharge among Medicare beneficiaries receiving in-hospital CPR have remained constant over time, with poorer survival rates among blacks and other nonwhite patients.
Citation: Ehlenbach WJ, Barnato AE, Curtis JR, et al. Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly. N Engl J Med. 2009;361(1):22-31.
Hospitalists Are Associated with Improved Performance on Quality Metrics
Clinical question: Is the presence of hospitalist physicians associated with improved performance on standard quality measures for acute myocardial infarction (AMI), congestive heart failure (CHF), and pneumonia?
Background: Previous investigations have demonstrated significant improvements in cost and LOS for patients under the care of hospitalists compared with other inpatient providers. The association between hospitalist prevalence and quality of care, as measured by standard quality process measures, is unknown.
Study design: Cross-sectional.
Setting: More than 3,600 hospitals participating in the Health Quality Alliance (HQA) program.
Synopsis: Investigators looked at a large sample of HQA hospitals in the American Hospital Association survey, and identified facilities with hospitalist services and those without. The primary endpoint was the adherence to composites of standard quality process measures across three disease categories (AMI, CHF, and pneumonia) and two domains of care (disease treatment/diagnosis and counseling/prevention).
Multivariable analyses revealed a statistically significant association between the presence of hospitalists and adherence to composite quality measures for AMI and pneumonia. This association was demonstrated for both treatment and counseling domains.
The study is cross-sectional, so conclusions cannot be drawn about causality. Also, there are likely unmeasured differences between hospitals that utilize hospitalists compared with those that do not, which could further confound the relationship between the presence of hospitalists and adherence to quality measures.
Finally, this study only evaluated hospital-level performance, and it cannot offer insight on the quality of individual patient care by hospitalist providers.
Bottom line: The presence of hospitalists is associated with improvement in adherence to quality measures for both AMI and pneumonia, and across clinical domains of treatment and counseling.
Citation: López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394. TH
PEDIATRIC HM LITerature
Inpatient Curriculum Implicit, but Aligns with ACGME Competencies
By Mark Shen, MD
Clinical question: Does implicit resident learning on an inpatient unit correspond to the explicit Accreditation Council for Graduate Medical Education (ACGME) competencies?
Background: The ACGME competency-based model of education places an emphasis on task-oriented ability as a translation of skills and knowledge. Although it is recognized that most learning occurs through the process of daily patient care, it is unclear how much learning is explicit and linked to ACGME competencies, as defined in the goals and objectives of an inpatient rotation.
Study design: Qualitative, ethnographic case study.
Setting: One general pediatric floor in a large, urban pediatric hospital.
Synopsis: Over an eight-month period, one researcher directly observed and asked questions of inpatient teams as they worked on a general pediatric service. There was a particular emphasis on morning rounds. Data coding was completed in an iterative manner, and both data and method triangulation were used to enhance trustworthiness.
Curricular convergence occurred and was most obvious in the patient-care domain; however, the explicit curriculum was not formally referred to during the study period. The implicit curriculum was ill-structured and unpredictable, typically dictated by the patients’ socioclinical environment.
The primary limitations of this work are the focus on one service on one hospital floor, and that the study authors were former trainees or employees of that institution. This institution-specific bias, however, might be gauged by the degree to which the themes in this research will resonate with clinician-educators who read this article. Given the increasing time constraints on explicit inpatient didactic teaching, the vignettes and conclusions within this report are likely to find many a sympathetic ear. Illumination of the hidden curriculum could further support learner-centered education.
Bottom line: The inpatient service is a fertile and primarily implicit training ground for the ACGME competencies.
Citation: Balmer DF, Master CL, Richards B, Giardino AP. Implicit versus explicit curricula in general pediatrics education: is there a convergence? Pediatrics. 2009;124(2):e347-354.
Market Watch
New Generics
- Nateglinide (generic Starlix) tablets1
New Drugs, Indications, and Dosage Forms
- Abatacept (Orencia), a selective costimulation modulator used in treating moderate to severe juvenile idiopathic arthritis and rheumatoid arthritis (RA), has undergone a label change regarding earlier use in methotrexate-naïve patients with moderate to severe RA of less than two years’ disease duration.2,3
- Aliskiren/valsartan (Valturna) has been approved by the FDA for treating hypertension in patients with inadequate hypertension control using aliskiren or valsartan alone. It’s also approved for first-line treatment of patients who are likely to need multiple agents to manage their hypertension.4
- Cethromycin (Restanza) has been granted orphan drug approval as a once-daily agent for the prophylaxis of anthrax, tularemia, and the plague. Studies are being conducted on the drug as a potential bioterrorism countermeasure agent through a Department of Defense contract.5
- Ganciclovir ophthalmic gel 0.15% (Zirgan) has been approved by the FDA for treating acute herpetic keratitis. It held orphan drug status for this indication since April 2007. Comparable clinical resolution of herpetic keratitis was obtained compared with acyclovir at day seven in an open-label, multicenter study of 213 patients (77% ganciclovir; 72% acyclovir). The most common adverse effects in clinical trials were blurred vision, eye irritation, punctate keratitis, and conjunctival hyperemia. Dosing recommendations are to instill one drop of ganciclovir in the affected eye five times daily until the ulcer heals, then instill one drop three times daily for seven days. It is anticipated that this product will be available in a 5-g tube in early 2010.6
- Glycerol phenylbutyrate (HPN-100), an experimental intermittent or chronic treatment for patients with cirrhosis and hepatic encephalopathy, has received orphan drug status. A phase-2 trial is planned for late 2009 or early 2010.7 Glycerol phenylbutyrate is a pre-pro-drug of phenylacetic acid, the active component of buphenyl (approved by the FDA to treat urea cycle disorders). Glycerol phenylbutyrate is administered in liquid form and also has orphan drug status for treating urea cycle disorders.
- Guanfacine extended-release tablets (Intuiv), a once-daily, nonstimulant treatment for attention deficit hyperactivity disorder (ADHD), has been approved by the FDA for treating patients 6 to 17 years old. Because guanfacine is not a controlled substance, a 90-day supply can be prescribed.8
- Pancrelipase (Zenpep), a delayed-release pancrelipase enzyme product, has been approved by the FDA for treating adults and children (ages 1 to 12) with cystic fibrosis. The most common adverse effects reported in clinical trials were flatulence, abdominal pain, headache, and cough. The product is available in four prescription strengths: “Eurand 5” is 5,000 USP units of lipase, 17,000 USP units of protease, and 27,000 USP units of amylase; “Eurand 10” is 10,000 units lipase, 34,000 units protease, and 55,000 units amylase; “Eurand 15” is 15,000 units lipase, 51,000 units protease, and 82,000 units amylase; and “Eurand 20” is 20,000 units lipase, 68,000 units protease, and 109,000 units amylase.9,10
- Vigabatrin (Sabril) has been approved by the FDA in an oral solution as monotherapy for treating infantile spasms in children ages one month to 2 years. The tablets also are approved for adjunctive therapy for refractory complex partial seizures in adults who have not adequately responded to other treatments. It is available in 500-mg powder packets for oral solution preparation and 500-mg tablets.11 One severe adverse effect is progressive peripheral vision loss with the potential to decrease visual acuity. Due to this risk of permanent vision loss, vigabatrin is available only through a restricted distribution program.
Pipeline
- Human papillomavirus quadrivalent (Types 6, 11, 16 and 18; Gardasil) has been recommended for approval to prevent genital warts in boys and young men 9 to 26 years old. The FDA is expected to make a decision by the end of 2009.12,13 This vaccine already is approved for use in men in 112 countries.
- Oral insulin (Ora-Lyn) is a proprietary formulation that delivers insulin spray through the buccal mucosa.14 In September, Ora-Lyn was approved under the FDA’s Treatment Investigational New Drug (IND) program for both Type 1 and Type 2 diabetes mellitus. This program allows manufacturers to provide early medication access to investigational drugs for patients with life-threatening or other serious conditions for which there are no satisfactory treatment alternatives. Doctors must register with the IND program to obtain the medication for their patients.15Ora-Lyn already is approved abroad.
Drug Information
- On Sept. 22, the FDA banned candy- and fruit-flavored cigarettes under the Family Smoking Prevention and Tobacco Control Act. The goal is to reduce smoking in America.16 Menthol cigarettes and flavored tobacco products are not part of this ban, but they are being evaluated as many of these products are seen as a gateway for children and young adults to begin smoking. More information is available at www.fda.gov/flavoredtobacco. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Par Pharma to begin marketing Starlix generic. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/news/news64185.html. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/125118s0086lbl.pdf Accessed Sept. 23, 2009.
- Bratulic A. Bristol Myers Squibb: Orencia label updated to support earlier use in adults with RA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=DA78CDE71605485C9BC1B3B40392B1C0&logRowId=323904. Accessed Sept. 23, 2009.
- Bratulic A. FDA approves Novartis’ Valturna for hypertension. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=4D45881D26B8447D950A4D63E80B806C&logRowId=327307. Accessed Sept. 23, 2009.
- Advanced Life Sciences’ Restanza could treat plague and anthrax. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News64553.html. Accessed Sept. 23, 2009.
- FDA approves Zirgan. Drugs.com Web site. Available at: www.drugs.com/newdrugs/sirion-therapeutics-announces-fda-approval-zirgan-ganciclovir-ophthalmic-gel-0-15-herpetic-keratitis-1657.html. Accessed Sept. 23, 2009.
- 7. Hyperion Therapeutics receives orphan drug designation for HPN-100 for the treatment of hepatic encephalopathy. Hyperion Therapeutics Web site. Available at: www.hyperiontx.com/press/release/pr_1253144476. Accessed Sept. 23, 2009.
- George J. FDA approves nonstimulant Shire ADHD drug. Philadelphia Business Journal Web site. Available at: philadelphia.bizjournals.com/philadelphia/stories/2009/08/31/daily40.html?surround=etf&ana=e_article. Accessed Sept. 23, 2009.
- Petrochko C. FDA approves first EPI drug for kids. Medpage Today Web site. Available at: www.medpagetoday.com/Gastroenterology/GeneralGastroenterology/15734. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022210s000lbl.pdf. Accessed Sept. 23, 2009.
- Sabril approved for infantile spasms and adult epileptic seizures. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sabril-approved-for-infantile-spasms-and-adult-epileptic-seizures/article/147148/. Accessed Sept. 23, 2009.
- FDA advisory committee recommends approval for use of Gardasil in boys and men. Merck Web site. Available at: www.merck.com/newsroom/press_releases/product/2009_0909.html. Accessed Sept. 23, 2009.
- Bratulic A. Merck & Co.’s Gardasil recommended by FDA panel for use in boys and men. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=352E8E6109E14925B0168FF465E27C1F&logRowId=325991. Accessed Sept. 23, 2009.
- Generex technology. Generex Biotechnology Web site. Available at: www.generex.com/technology.php. Accessed Sept. 23, 2009.
- Reidy C. Generex Drug is OK’d under special FDA program. The Boston Globe Web site. www.generex.com/fckuploads/file/Boston_Globe_09_10_09.pdf. Accessed Sept. 23, 2009.
- Quinn K. Candy and fruit flavored cigarettes now illegal in United States; step is first under new tobacco law. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm183211.htm. Accessed Sept. 23, 2009.
New Generics
- Nateglinide (generic Starlix) tablets1
New Drugs, Indications, and Dosage Forms
- Abatacept (Orencia), a selective costimulation modulator used in treating moderate to severe juvenile idiopathic arthritis and rheumatoid arthritis (RA), has undergone a label change regarding earlier use in methotrexate-naïve patients with moderate to severe RA of less than two years’ disease duration.2,3
- Aliskiren/valsartan (Valturna) has been approved by the FDA for treating hypertension in patients with inadequate hypertension control using aliskiren or valsartan alone. It’s also approved for first-line treatment of patients who are likely to need multiple agents to manage their hypertension.4
- Cethromycin (Restanza) has been granted orphan drug approval as a once-daily agent for the prophylaxis of anthrax, tularemia, and the plague. Studies are being conducted on the drug as a potential bioterrorism countermeasure agent through a Department of Defense contract.5
- Ganciclovir ophthalmic gel 0.15% (Zirgan) has been approved by the FDA for treating acute herpetic keratitis. It held orphan drug status for this indication since April 2007. Comparable clinical resolution of herpetic keratitis was obtained compared with acyclovir at day seven in an open-label, multicenter study of 213 patients (77% ganciclovir; 72% acyclovir). The most common adverse effects in clinical trials were blurred vision, eye irritation, punctate keratitis, and conjunctival hyperemia. Dosing recommendations are to instill one drop of ganciclovir in the affected eye five times daily until the ulcer heals, then instill one drop three times daily for seven days. It is anticipated that this product will be available in a 5-g tube in early 2010.6
- Glycerol phenylbutyrate (HPN-100), an experimental intermittent or chronic treatment for patients with cirrhosis and hepatic encephalopathy, has received orphan drug status. A phase-2 trial is planned for late 2009 or early 2010.7 Glycerol phenylbutyrate is a pre-pro-drug of phenylacetic acid, the active component of buphenyl (approved by the FDA to treat urea cycle disorders). Glycerol phenylbutyrate is administered in liquid form and also has orphan drug status for treating urea cycle disorders.
- Guanfacine extended-release tablets (Intuiv), a once-daily, nonstimulant treatment for attention deficit hyperactivity disorder (ADHD), has been approved by the FDA for treating patients 6 to 17 years old. Because guanfacine is not a controlled substance, a 90-day supply can be prescribed.8
- Pancrelipase (Zenpep), a delayed-release pancrelipase enzyme product, has been approved by the FDA for treating adults and children (ages 1 to 12) with cystic fibrosis. The most common adverse effects reported in clinical trials were flatulence, abdominal pain, headache, and cough. The product is available in four prescription strengths: “Eurand 5” is 5,000 USP units of lipase, 17,000 USP units of protease, and 27,000 USP units of amylase; “Eurand 10” is 10,000 units lipase, 34,000 units protease, and 55,000 units amylase; “Eurand 15” is 15,000 units lipase, 51,000 units protease, and 82,000 units amylase; and “Eurand 20” is 20,000 units lipase, 68,000 units protease, and 109,000 units amylase.9,10
- Vigabatrin (Sabril) has been approved by the FDA in an oral solution as monotherapy for treating infantile spasms in children ages one month to 2 years. The tablets also are approved for adjunctive therapy for refractory complex partial seizures in adults who have not adequately responded to other treatments. It is available in 500-mg powder packets for oral solution preparation and 500-mg tablets.11 One severe adverse effect is progressive peripheral vision loss with the potential to decrease visual acuity. Due to this risk of permanent vision loss, vigabatrin is available only through a restricted distribution program.
Pipeline
- Human papillomavirus quadrivalent (Types 6, 11, 16 and 18; Gardasil) has been recommended for approval to prevent genital warts in boys and young men 9 to 26 years old. The FDA is expected to make a decision by the end of 2009.12,13 This vaccine already is approved for use in men in 112 countries.
- Oral insulin (Ora-Lyn) is a proprietary formulation that delivers insulin spray through the buccal mucosa.14 In September, Ora-Lyn was approved under the FDA’s Treatment Investigational New Drug (IND) program for both Type 1 and Type 2 diabetes mellitus. This program allows manufacturers to provide early medication access to investigational drugs for patients with life-threatening or other serious conditions for which there are no satisfactory treatment alternatives. Doctors must register with the IND program to obtain the medication for their patients.15Ora-Lyn already is approved abroad.
Drug Information
- On Sept. 22, the FDA banned candy- and fruit-flavored cigarettes under the Family Smoking Prevention and Tobacco Control Act. The goal is to reduce smoking in America.16 Menthol cigarettes and flavored tobacco products are not part of this ban, but they are being evaluated as many of these products are seen as a gateway for children and young adults to begin smoking. More information is available at www.fda.gov/flavoredtobacco. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Par Pharma to begin marketing Starlix generic. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/news/news64185.html. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/125118s0086lbl.pdf Accessed Sept. 23, 2009.
- Bratulic A. Bristol Myers Squibb: Orencia label updated to support earlier use in adults with RA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=DA78CDE71605485C9BC1B3B40392B1C0&logRowId=323904. Accessed Sept. 23, 2009.
- Bratulic A. FDA approves Novartis’ Valturna for hypertension. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=4D45881D26B8447D950A4D63E80B806C&logRowId=327307. Accessed Sept. 23, 2009.
- Advanced Life Sciences’ Restanza could treat plague and anthrax. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News64553.html. Accessed Sept. 23, 2009.
- FDA approves Zirgan. Drugs.com Web site. Available at: www.drugs.com/newdrugs/sirion-therapeutics-announces-fda-approval-zirgan-ganciclovir-ophthalmic-gel-0-15-herpetic-keratitis-1657.html. Accessed Sept. 23, 2009.
- 7. Hyperion Therapeutics receives orphan drug designation for HPN-100 for the treatment of hepatic encephalopathy. Hyperion Therapeutics Web site. Available at: www.hyperiontx.com/press/release/pr_1253144476. Accessed Sept. 23, 2009.
- George J. FDA approves nonstimulant Shire ADHD drug. Philadelphia Business Journal Web site. Available at: philadelphia.bizjournals.com/philadelphia/stories/2009/08/31/daily40.html?surround=etf&ana=e_article. Accessed Sept. 23, 2009.
- Petrochko C. FDA approves first EPI drug for kids. Medpage Today Web site. Available at: www.medpagetoday.com/Gastroenterology/GeneralGastroenterology/15734. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022210s000lbl.pdf. Accessed Sept. 23, 2009.
- Sabril approved for infantile spasms and adult epileptic seizures. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sabril-approved-for-infantile-spasms-and-adult-epileptic-seizures/article/147148/. Accessed Sept. 23, 2009.
- FDA advisory committee recommends approval for use of Gardasil in boys and men. Merck Web site. Available at: www.merck.com/newsroom/press_releases/product/2009_0909.html. Accessed Sept. 23, 2009.
- Bratulic A. Merck & Co.’s Gardasil recommended by FDA panel for use in boys and men. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=352E8E6109E14925B0168FF465E27C1F&logRowId=325991. Accessed Sept. 23, 2009.
- Generex technology. Generex Biotechnology Web site. Available at: www.generex.com/technology.php. Accessed Sept. 23, 2009.
- Reidy C. Generex Drug is OK’d under special FDA program. The Boston Globe Web site. www.generex.com/fckuploads/file/Boston_Globe_09_10_09.pdf. Accessed Sept. 23, 2009.
- Quinn K. Candy and fruit flavored cigarettes now illegal in United States; step is first under new tobacco law. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm183211.htm. Accessed Sept. 23, 2009.
New Generics
- Nateglinide (generic Starlix) tablets1
New Drugs, Indications, and Dosage Forms
- Abatacept (Orencia), a selective costimulation modulator used in treating moderate to severe juvenile idiopathic arthritis and rheumatoid arthritis (RA), has undergone a label change regarding earlier use in methotrexate-naïve patients with moderate to severe RA of less than two years’ disease duration.2,3
- Aliskiren/valsartan (Valturna) has been approved by the FDA for treating hypertension in patients with inadequate hypertension control using aliskiren or valsartan alone. It’s also approved for first-line treatment of patients who are likely to need multiple agents to manage their hypertension.4
- Cethromycin (Restanza) has been granted orphan drug approval as a once-daily agent for the prophylaxis of anthrax, tularemia, and the plague. Studies are being conducted on the drug as a potential bioterrorism countermeasure agent through a Department of Defense contract.5
- Ganciclovir ophthalmic gel 0.15% (Zirgan) has been approved by the FDA for treating acute herpetic keratitis. It held orphan drug status for this indication since April 2007. Comparable clinical resolution of herpetic keratitis was obtained compared with acyclovir at day seven in an open-label, multicenter study of 213 patients (77% ganciclovir; 72% acyclovir). The most common adverse effects in clinical trials were blurred vision, eye irritation, punctate keratitis, and conjunctival hyperemia. Dosing recommendations are to instill one drop of ganciclovir in the affected eye five times daily until the ulcer heals, then instill one drop three times daily for seven days. It is anticipated that this product will be available in a 5-g tube in early 2010.6
- Glycerol phenylbutyrate (HPN-100), an experimental intermittent or chronic treatment for patients with cirrhosis and hepatic encephalopathy, has received orphan drug status. A phase-2 trial is planned for late 2009 or early 2010.7 Glycerol phenylbutyrate is a pre-pro-drug of phenylacetic acid, the active component of buphenyl (approved by the FDA to treat urea cycle disorders). Glycerol phenylbutyrate is administered in liquid form and also has orphan drug status for treating urea cycle disorders.
- Guanfacine extended-release tablets (Intuiv), a once-daily, nonstimulant treatment for attention deficit hyperactivity disorder (ADHD), has been approved by the FDA for treating patients 6 to 17 years old. Because guanfacine is not a controlled substance, a 90-day supply can be prescribed.8
- Pancrelipase (Zenpep), a delayed-release pancrelipase enzyme product, has been approved by the FDA for treating adults and children (ages 1 to 12) with cystic fibrosis. The most common adverse effects reported in clinical trials were flatulence, abdominal pain, headache, and cough. The product is available in four prescription strengths: “Eurand 5” is 5,000 USP units of lipase, 17,000 USP units of protease, and 27,000 USP units of amylase; “Eurand 10” is 10,000 units lipase, 34,000 units protease, and 55,000 units amylase; “Eurand 15” is 15,000 units lipase, 51,000 units protease, and 82,000 units amylase; and “Eurand 20” is 20,000 units lipase, 68,000 units protease, and 109,000 units amylase.9,10
- Vigabatrin (Sabril) has been approved by the FDA in an oral solution as monotherapy for treating infantile spasms in children ages one month to 2 years. The tablets also are approved for adjunctive therapy for refractory complex partial seizures in adults who have not adequately responded to other treatments. It is available in 500-mg powder packets for oral solution preparation and 500-mg tablets.11 One severe adverse effect is progressive peripheral vision loss with the potential to decrease visual acuity. Due to this risk of permanent vision loss, vigabatrin is available only through a restricted distribution program.
Pipeline
- Human papillomavirus quadrivalent (Types 6, 11, 16 and 18; Gardasil) has been recommended for approval to prevent genital warts in boys and young men 9 to 26 years old. The FDA is expected to make a decision by the end of 2009.12,13 This vaccine already is approved for use in men in 112 countries.
- Oral insulin (Ora-Lyn) is a proprietary formulation that delivers insulin spray through the buccal mucosa.14 In September, Ora-Lyn was approved under the FDA’s Treatment Investigational New Drug (IND) program for both Type 1 and Type 2 diabetes mellitus. This program allows manufacturers to provide early medication access to investigational drugs for patients with life-threatening or other serious conditions for which there are no satisfactory treatment alternatives. Doctors must register with the IND program to obtain the medication for their patients.15Ora-Lyn already is approved abroad.
Drug Information
- On Sept. 22, the FDA banned candy- and fruit-flavored cigarettes under the Family Smoking Prevention and Tobacco Control Act. The goal is to reduce smoking in America.16 Menthol cigarettes and flavored tobacco products are not part of this ban, but they are being evaluated as many of these products are seen as a gateway for children and young adults to begin smoking. More information is available at www.fda.gov/flavoredtobacco. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Par Pharma to begin marketing Starlix generic. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/news/news64185.html. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/125118s0086lbl.pdf Accessed Sept. 23, 2009.
- Bratulic A. Bristol Myers Squibb: Orencia label updated to support earlier use in adults with RA. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=DA78CDE71605485C9BC1B3B40392B1C0&logRowId=323904. Accessed Sept. 23, 2009.
- Bratulic A. FDA approves Novartis’ Valturna for hypertension. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=4D45881D26B8447D950A4D63E80B806C&logRowId=327307. Accessed Sept. 23, 2009.
- Advanced Life Sciences’ Restanza could treat plague and anthrax. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News64553.html. Accessed Sept. 23, 2009.
- FDA approves Zirgan. Drugs.com Web site. Available at: www.drugs.com/newdrugs/sirion-therapeutics-announces-fda-approval-zirgan-ganciclovir-ophthalmic-gel-0-15-herpetic-keratitis-1657.html. Accessed Sept. 23, 2009.
- 7. Hyperion Therapeutics receives orphan drug designation for HPN-100 for the treatment of hepatic encephalopathy. Hyperion Therapeutics Web site. Available at: www.hyperiontx.com/press/release/pr_1253144476. Accessed Sept. 23, 2009.
- George J. FDA approves nonstimulant Shire ADHD drug. Philadelphia Business Journal Web site. Available at: philadelphia.bizjournals.com/philadelphia/stories/2009/08/31/daily40.html?surround=etf&ana=e_article. Accessed Sept. 23, 2009.
- Petrochko C. FDA approves first EPI drug for kids. Medpage Today Web site. Available at: www.medpagetoday.com/Gastroenterology/GeneralGastroenterology/15734. Accessed Sept. 23, 2009.
- Highlights of prescribing information. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022210s000lbl.pdf. Accessed Sept. 23, 2009.
- Sabril approved for infantile spasms and adult epileptic seizures. Monthly Prescribing Reference Web site. Available at: www.empr.com/Sabril-approved-for-infantile-spasms-and-adult-epileptic-seizures/article/147148/. Accessed Sept. 23, 2009.
- FDA advisory committee recommends approval for use of Gardasil in boys and men. Merck Web site. Available at: www.merck.com/newsroom/press_releases/product/2009_0909.html. Accessed Sept. 23, 2009.
- Bratulic A. Merck & Co.’s Gardasil recommended by FDA panel for use in boys and men. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=352E8E6109E14925B0168FF465E27C1F&logRowId=325991. Accessed Sept. 23, 2009.
- Generex technology. Generex Biotechnology Web site. Available at: www.generex.com/technology.php. Accessed Sept. 23, 2009.
- Reidy C. Generex Drug is OK’d under special FDA program. The Boston Globe Web site. www.generex.com/fckuploads/file/Boston_Globe_09_10_09.pdf. Accessed Sept. 23, 2009.
- Quinn K. Candy and fruit flavored cigarettes now illegal in United States; step is first under new tobacco law. Food and Drug Administration Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm183211.htm. Accessed Sept. 23, 2009.
2009: Year in Review
From continued membership growth to increased visibility in the national media, SHM and its members have been influencing healthcare for more than a decade. But even by the highest of standards, 2009 has been a landmark year—one that demonstrated hospitalists’ collective ability to transform healthcare and improve care to the hospitalized patient.
“The momentum of the hospital medicine movement has been growing for years, and 2009 has been no exception,” says Scott Flanders, MD, FHM, president of SHM. “This year built on the successes of the past and plainly illustrated the impact that hospital medicine will have on the future of healthcare.”
Groundbreaking QI Programs Go Nationwide
This year, SHM and its members began to tackle some of the most pressing QI issues in healthcare: reducing readmissions to the hospital and glycemic control. New research in the New England Journal of Medicine couldn’t have made the need for reducing readmissions any clearer: Unplanned hospital readmissions cost Medicare $17.4 billion annually.1
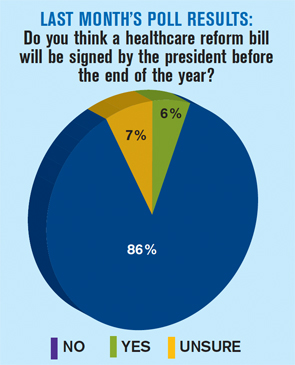
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) helps hospitals implement customized programs to reduce readmissions through improved discharge processes. Hospitalists who enroll in the yearlong program take advantage of a one-on-one mentorship arrangement with experts in the field. Participants can also access the Project BOOST resource toolkit.
Project BOOST began in six pilot hospital sites in 2008 and added 24 new sites in March 2009. The program’s leaders are looking forward to further expansion in 2010. “The response to Project BOOST has been overwhelmingly positive. Given today’s healthcare climate, we know its impact will be even greater in years to come,” says Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives. “There is a very serious need to improve discharge processes in hospitals across the country. With Project BOOST, hospitalists are taking the initiative to ensure a smooth transition from hospital to home.”
SHM also launched the Glycemic Control Mentored Implementation (GCMI) program. Like Project BOOST, GCMI uses a combination of one-on-one mentorships and customized resources to assist hospitalists with QI program implementation.
GCMI takes on another common chronic issue hospitalists face daily: managing glycemic levels in hospitalized patients. The GCMI program is currently in 30 sites across the country.

—Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives
HM09 Draws Capacity Crowd in Chicago
In an economic climate that forced many industries’ annual meetings to be canceled, delayed, or scaled back, Hospital Medicine 2009 (HM09) in Chicago exceeded expectations. SHM had expected about 1,500 participants in the annual conference; organizers were pleasantly surprised to receive more than 2,000 registrations for the May event. The demand for exhibition space also surpassed projections.
“We’ve long known that hospitalists see real value in a meeting specifically designed for them, with relevant educational sessions and plenty of time for networking,” says Geri Barnes, SHM’s senior director of education and meetings. “Each year, we’ve received more and more interest in the annual conference, but the response to our 2009 conference was unprecedented.”
HM10 is April 8-11 at the Gaylord National Hotel and Convention Center in Washington, D.C.
SHM, MGMA Form Research Partnership
Beginning in 2010, SHM and the Medical Group Management Association (MGMA) will team up to give hospitalists and healthcare executives an even clearer picture on hospitalist compensation and productivity.
Prior to the partnership, SHM had conducted its own research. Now, hospitals and HM managers will have new data at their fingertips, and additional analysis and name-brand recognition of one of the leaders in medical practice research. The first round of research will be available in summer 2010. SHM and MGMA already have collaborated on educational webinars for hospitalists, and SHM is offering books published by MGMA on its Web site.
“This new alliance will pay dividends for years to come,” says Leslie Flores, the director of SHM’s Practice Management Institute. “The information from our compensation and productivity surveys has always been valuable to hospitals. Having the MGMA name attached to next year’s product will only increase its significance and usefulness.”
Hospitalists will receive the joint survey questionnaire from SHM and MGMA in January.
Fellow in Hospital medicine Spotlight
Penny McDonald, MD, FACP, FHM

Undergraduate education: High Point University, High Point, N.C.
Medical school: East Carolina University School of Medicine, Greenville, N.C.
Notable: Dr. McDonald has been a practicing hospitalist since 1997 and an SHM member since 1999. She has served on the physician leadership board and ethics committee at Forsyth. She has been published in the Archives of Internal Medicine.
FYI: Outside the hospital, Dr. McDonald is an avid hiker and loves to travel. Last year, she reached her own personal goal of visiting all 50 states. Her new goal is to visit every national park in the U.S.
Quotable: “I have a secret desire that our specialty be renamed. Describing us as ‘hospitalists,’ based on where we practice, doesn’t seem to cover it. I think ‘medical complexity specialist’ would be more fitting and would encompass all of what we do.”
For more information about the FHM program, visit www.hospitalmedicine.org/fellows.
HM Fellows
Three letters can mean a lot, especially for hospitalists looking for ways to demonstrate their commitment to the specialty. This year was the first in which qualified hospitalists could earn the Fellow in Hospital Medicine (FHM) designation. The first class of more than 500 FHM designees was introduced in an on-stage ceremony at HM09.
“This is a special way for SHM—and the healthcare industry as a whole—to recognize the unique achievements and dedication that hospital medicine requires,” says Todd Von Deak, MBA, CAE, SHM’s vice president for marketing and membership. “As the specialty grows in number and influence, so will the fellows program.”
In 2010, SHM will induct the first class of Senior Fellows in Hospital Medicine (SFHM). While the process for applying for the senior designation will be similar to the FHM designation, the SFHM will require additional years of practice and leadership in the specialty.
The fellows program also features the Master in Hospital Medicine (MHM) designation, the highest level of recognition available. The MHM will be available in 2011, and the nomination process will be invitation-only.
Outside Recognition
SHM isn’t the only group recognizing the impact hospitalists are making on healthcare. In September, the American Board of Internal Medicine (ABIM) announced that hospitalists will be able to apply for Recognition of Focused Practice (RFP) in Hospital Medicine as part of ABIM’s maintenance of certification (MOC) program. The application process will be available as early as next month.
SHM will be assisting hospitalists in the application process through online resources and the MOC pre-course, which will be offered before HM10. Hospitalists with three years of experience in the field can apply for the RFP program. Although most physicians are required to recertify every 10 years, hospitalists won’t have to wait until their certification is up to apply for focused recognition. For more information about the RFP in HM program, visit www.abim.org.
Hospital-Provider Partners
Treating hospitalized patients has always been a team sport. From caseworkers and pharmacists to physicians and critical-care nurses, the diverse and specialized needs of hospital care demand collaboration and coordination.
That’s the idea behind the Hospital Care Collaborative (HCC), which convened for the first time in 2009. The group is made up of six national organizations that represent hundreds of thousands of care providers. The HCC has developed and published “Common Principles for Team-Based Healthcare.” The principles emphasize the need for teamwork within the hospital setting and a focus on the patient.
As part of its goals for the future, the HCC will identify best practices in teamwork and promote educational programs that encourage interdisciplinary teams.
Look Back, Look Forward
For SHM CEO Larry Wellikson, MD, FHM, the end of 2009 is an opportunity to look forward to 2010 and beyond. “Ten years ago, hospital medicine was little more than an idea,” he says. “Today, it is a growing medical specialty, recognized by leaders in healthcare and public policy, with thousands of experienced and enthusiastic hospitalists throughout the country.
“I am confident that when we look back ten years from now, we will see a hospital landscape transformed for the better, and that hospitalists and the rest of the new healthcare team will have played an important role.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman A. Rehospitaliza- tions among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Chapter Updates
Los Angeles
The Los Angeles chapter met Sept. 24 at Craft restaurant. The event was hosted by Manoj K. Mathew, MD, FHM. The presentation, “An Update in Hospital Medicine,” was offered by Joseph Li, MD, FHM, director of hospitalist services at Beth Israel Deaconess Medical Center in Boston and an SHM board member. Nearly 30 attendees from 10 hospitalist organizations attended the meeting. The next Los Angeles chapter meeting is scheduled for January 2010.
Southwest Wisconsin
Transitions of care was the featured topic at the Aug. 6 Southwest Wisconsin chapter meeting. Monica Anderson, director of business development at Select Specialty Hospital in Madison, presented valuable information about the role long-term acute-care hospitals play in a patient’s continuum of care. Following the presentation, attendees discussed ways in which hospitalists can collaborate across HM groups to address patient care and quality issues that are common to hospitalist practices.
Philadelphia Tri-State Area
The Philadelphia Tri-State Area chapter met Sept. 30 at Ristorante Panorama. About 20 hospitalists attended the event, which was sponsored by the France Foundation.
Todd Hecht, MD, of the University of Pennsylvania lectured on DVT prophylaxis. Chapter founder Jennifer Myers, MD, FHM, preceded the lecture by announcing she was stepping down as co-president after a six-year tenure. She thanked the audience for their support and introduced Susan Krekun, MD, chair of the division of hospital medicine at Jefferson University Hospital in Philadelphia, as the new chapter co-president.
The chapter sponsored a job fair Nov. 19 at the downtown Marriott. Medical directors from more than 10 programs attended the event to meet aspiring hospitalists and discuss the state of hospital medicine in the Philadelphia area.
Indiana

The Indiana chapter held a meeting Sept. 2 at Maggiano’s Italian Restaurant in Indianapolis. The meeting was sponsored by AstraZeneca and featured a meet-and-greet before the regular program. Attendees were treated to a report about SHM’s recent Leadership Academy in Miami, and election results were revealed.
Angela Corea, MD, announced the 2010 chapter election nomination results: vice president, John Gilbert, MD, unopposed; secretary, Robert Blessing, MD, unopposed; president, Angela Corea, MD, Raphael Villavicencio, MD, and Gordon Reed, MD, FHM. All three chapter president nominees addressed the attendees.
David Mares, MD, held a question-and-answer session to discuss “New Maintenance Options for the Treatment of COPD.” Drs. Reed and Corea discussed the results of the SHM survey. The meeting concluded with a secret ballot.
Nashville and Middle Tennessee
The Nashville and Middle Tennessee chapter met Oct. 27, with 16 attendees representing eight local hospitals. The speaker, Anton Maki, MD, of Kingsport, presented a thorough review of the microbiology and antimicrobial treatment recommendations for community-acquired pneumonia (CAP). Attendees also were provided information about upcoming SHM conferences and training academies, the application process for the fellowship program, and plans for the ABIM Recognition of Focused Practice in Hospital Medicine certification.
Boston
Anita Barry, the infectious-disease bureau chief and director of communicable-disease control for the Boston Public Health Commission, spoke to nearly 60 hospitalists and guests during the Sept. 10 Boston chapter meeting at Legal Sea Foods. Dr. Barry’s topic was the H1N1 virus. The next chapter event is a clinical investigator training course Dec. 10-11 at Beth Israel Deaconess Medical Center in Boston. Anyone interested in learning more about conducting clinical trials can attend. This course is not limited to physicians; nurses and others are encouraged to attend. There is no fee to attend Boston chapter events. For more information or to RSVP, contact Dr. Li at [email protected] or 617-632-0205.
From continued membership growth to increased visibility in the national media, SHM and its members have been influencing healthcare for more than a decade. But even by the highest of standards, 2009 has been a landmark year—one that demonstrated hospitalists’ collective ability to transform healthcare and improve care to the hospitalized patient.
“The momentum of the hospital medicine movement has been growing for years, and 2009 has been no exception,” says Scott Flanders, MD, FHM, president of SHM. “This year built on the successes of the past and plainly illustrated the impact that hospital medicine will have on the future of healthcare.”
Groundbreaking QI Programs Go Nationwide
This year, SHM and its members began to tackle some of the most pressing QI issues in healthcare: reducing readmissions to the hospital and glycemic control. New research in the New England Journal of Medicine couldn’t have made the need for reducing readmissions any clearer: Unplanned hospital readmissions cost Medicare $17.4 billion annually.1
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) helps hospitals implement customized programs to reduce readmissions through improved discharge processes. Hospitalists who enroll in the yearlong program take advantage of a one-on-one mentorship arrangement with experts in the field. Participants can also access the Project BOOST resource toolkit.
Project BOOST began in six pilot hospital sites in 2008 and added 24 new sites in March 2009. The program’s leaders are looking forward to further expansion in 2010. “The response to Project BOOST has been overwhelmingly positive. Given today’s healthcare climate, we know its impact will be even greater in years to come,” says Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives. “There is a very serious need to improve discharge processes in hospitals across the country. With Project BOOST, hospitalists are taking the initiative to ensure a smooth transition from hospital to home.”
SHM also launched the Glycemic Control Mentored Implementation (GCMI) program. Like Project BOOST, GCMI uses a combination of one-on-one mentorships and customized resources to assist hospitalists with QI program implementation.
GCMI takes on another common chronic issue hospitalists face daily: managing glycemic levels in hospitalized patients. The GCMI program is currently in 30 sites across the country.
—Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives
HM09 Draws Capacity Crowd in Chicago
In an economic climate that forced many industries’ annual meetings to be canceled, delayed, or scaled back, Hospital Medicine 2009 (HM09) in Chicago exceeded expectations. SHM had expected about 1,500 participants in the annual conference; organizers were pleasantly surprised to receive more than 2,000 registrations for the May event. The demand for exhibition space also surpassed projections.
“We’ve long known that hospitalists see real value in a meeting specifically designed for them, with relevant educational sessions and plenty of time for networking,” says Geri Barnes, SHM’s senior director of education and meetings. “Each year, we’ve received more and more interest in the annual conference, but the response to our 2009 conference was unprecedented.”
HM10 is April 8-11 at the Gaylord National Hotel and Convention Center in Washington, D.C.
SHM, MGMA Form Research Partnership
Beginning in 2010, SHM and the Medical Group Management Association (MGMA) will team up to give hospitalists and healthcare executives an even clearer picture on hospitalist compensation and productivity.
Prior to the partnership, SHM had conducted its own research. Now, hospitals and HM managers will have new data at their fingertips, and additional analysis and name-brand recognition of one of the leaders in medical practice research. The first round of research will be available in summer 2010. SHM and MGMA already have collaborated on educational webinars for hospitalists, and SHM is offering books published by MGMA on its Web site.
“This new alliance will pay dividends for years to come,” says Leslie Flores, the director of SHM’s Practice Management Institute. “The information from our compensation and productivity surveys has always been valuable to hospitals. Having the MGMA name attached to next year’s product will only increase its significance and usefulness.”
Hospitalists will receive the joint survey questionnaire from SHM and MGMA in January.
Fellow in Hospital medicine Spotlight
Penny McDonald, MD, FACP, FHM
Undergraduate education: High Point University, High Point, N.C.
Medical school: East Carolina University School of Medicine, Greenville, N.C.
Notable: Dr. McDonald has been a practicing hospitalist since 1997 and an SHM member since 1999. She has served on the physician leadership board and ethics committee at Forsyth. She has been published in the Archives of Internal Medicine.
FYI: Outside the hospital, Dr. McDonald is an avid hiker and loves to travel. Last year, she reached her own personal goal of visiting all 50 states. Her new goal is to visit every national park in the U.S.
Quotable: “I have a secret desire that our specialty be renamed. Describing us as ‘hospitalists,’ based on where we practice, doesn’t seem to cover it. I think ‘medical complexity specialist’ would be more fitting and would encompass all of what we do.”
For more information about the FHM program, visit www.hospitalmedicine.org/fellows.
HM Fellows
Three letters can mean a lot, especially for hospitalists looking for ways to demonstrate their commitment to the specialty. This year was the first in which qualified hospitalists could earn the Fellow in Hospital Medicine (FHM) designation. The first class of more than 500 FHM designees was introduced in an on-stage ceremony at HM09.
“This is a special way for SHM—and the healthcare industry as a whole—to recognize the unique achievements and dedication that hospital medicine requires,” says Todd Von Deak, MBA, CAE, SHM’s vice president for marketing and membership. “As the specialty grows in number and influence, so will the fellows program.”
In 2010, SHM will induct the first class of Senior Fellows in Hospital Medicine (SFHM). While the process for applying for the senior designation will be similar to the FHM designation, the SFHM will require additional years of practice and leadership in the specialty.
The fellows program also features the Master in Hospital Medicine (MHM) designation, the highest level of recognition available. The MHM will be available in 2011, and the nomination process will be invitation-only.
Outside Recognition
SHM isn’t the only group recognizing the impact hospitalists are making on healthcare. In September, the American Board of Internal Medicine (ABIM) announced that hospitalists will be able to apply for Recognition of Focused Practice (RFP) in Hospital Medicine as part of ABIM’s maintenance of certification (MOC) program. The application process will be available as early as next month.
SHM will be assisting hospitalists in the application process through online resources and the MOC pre-course, which will be offered before HM10. Hospitalists with three years of experience in the field can apply for the RFP program. Although most physicians are required to recertify every 10 years, hospitalists won’t have to wait until their certification is up to apply for focused recognition. For more information about the RFP in HM program, visit www.abim.org.
Hospital-Provider Partners
Treating hospitalized patients has always been a team sport. From caseworkers and pharmacists to physicians and critical-care nurses, the diverse and specialized needs of hospital care demand collaboration and coordination.
That’s the idea behind the Hospital Care Collaborative (HCC), which convened for the first time in 2009. The group is made up of six national organizations that represent hundreds of thousands of care providers. The HCC has developed and published “Common Principles for Team-Based Healthcare.” The principles emphasize the need for teamwork within the hospital setting and a focus on the patient.
As part of its goals for the future, the HCC will identify best practices in teamwork and promote educational programs that encourage interdisciplinary teams.
Look Back, Look Forward
For SHM CEO Larry Wellikson, MD, FHM, the end of 2009 is an opportunity to look forward to 2010 and beyond. “Ten years ago, hospital medicine was little more than an idea,” he says. “Today, it is a growing medical specialty, recognized by leaders in healthcare and public policy, with thousands of experienced and enthusiastic hospitalists throughout the country.
“I am confident that when we look back ten years from now, we will see a hospital landscape transformed for the better, and that hospitalists and the rest of the new healthcare team will have played an important role.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman A. Rehospitaliza- tions among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Chapter Updates
Los Angeles
The Los Angeles chapter met Sept. 24 at Craft restaurant. The event was hosted by Manoj K. Mathew, MD, FHM. The presentation, “An Update in Hospital Medicine,” was offered by Joseph Li, MD, FHM, director of hospitalist services at Beth Israel Deaconess Medical Center in Boston and an SHM board member. Nearly 30 attendees from 10 hospitalist organizations attended the meeting. The next Los Angeles chapter meeting is scheduled for January 2010.
Southwest Wisconsin
Transitions of care was the featured topic at the Aug. 6 Southwest Wisconsin chapter meeting. Monica Anderson, director of business development at Select Specialty Hospital in Madison, presented valuable information about the role long-term acute-care hospitals play in a patient’s continuum of care. Following the presentation, attendees discussed ways in which hospitalists can collaborate across HM groups to address patient care and quality issues that are common to hospitalist practices.
Philadelphia Tri-State Area
The Philadelphia Tri-State Area chapter met Sept. 30 at Ristorante Panorama. About 20 hospitalists attended the event, which was sponsored by the France Foundation.
Todd Hecht, MD, of the University of Pennsylvania lectured on DVT prophylaxis. Chapter founder Jennifer Myers, MD, FHM, preceded the lecture by announcing she was stepping down as co-president after a six-year tenure. She thanked the audience for their support and introduced Susan Krekun, MD, chair of the division of hospital medicine at Jefferson University Hospital in Philadelphia, as the new chapter co-president.
The chapter sponsored a job fair Nov. 19 at the downtown Marriott. Medical directors from more than 10 programs attended the event to meet aspiring hospitalists and discuss the state of hospital medicine in the Philadelphia area.
Indiana
The Indiana chapter held a meeting Sept. 2 at Maggiano’s Italian Restaurant in Indianapolis. The meeting was sponsored by AstraZeneca and featured a meet-and-greet before the regular program. Attendees were treated to a report about SHM’s recent Leadership Academy in Miami, and election results were revealed.
Angela Corea, MD, announced the 2010 chapter election nomination results: vice president, John Gilbert, MD, unopposed; secretary, Robert Blessing, MD, unopposed; president, Angela Corea, MD, Raphael Villavicencio, MD, and Gordon Reed, MD, FHM. All three chapter president nominees addressed the attendees.
David Mares, MD, held a question-and-answer session to discuss “New Maintenance Options for the Treatment of COPD.” Drs. Reed and Corea discussed the results of the SHM survey. The meeting concluded with a secret ballot.
Nashville and Middle Tennessee
The Nashville and Middle Tennessee chapter met Oct. 27, with 16 attendees representing eight local hospitals. The speaker, Anton Maki, MD, of Kingsport, presented a thorough review of the microbiology and antimicrobial treatment recommendations for community-acquired pneumonia (CAP). Attendees also were provided information about upcoming SHM conferences and training academies, the application process for the fellowship program, and plans for the ABIM Recognition of Focused Practice in Hospital Medicine certification.
Boston
Anita Barry, the infectious-disease bureau chief and director of communicable-disease control for the Boston Public Health Commission, spoke to nearly 60 hospitalists and guests during the Sept. 10 Boston chapter meeting at Legal Sea Foods. Dr. Barry’s topic was the H1N1 virus. The next chapter event is a clinical investigator training course Dec. 10-11 at Beth Israel Deaconess Medical Center in Boston. Anyone interested in learning more about conducting clinical trials can attend. This course is not limited to physicians; nurses and others are encouraged to attend. There is no fee to attend Boston chapter events. For more information or to RSVP, contact Dr. Li at [email protected] or 617-632-0205.
From continued membership growth to increased visibility in the national media, SHM and its members have been influencing healthcare for more than a decade. But even by the highest of standards, 2009 has been a landmark year—one that demonstrated hospitalists’ collective ability to transform healthcare and improve care to the hospitalized patient.
“The momentum of the hospital medicine movement has been growing for years, and 2009 has been no exception,” says Scott Flanders, MD, FHM, president of SHM. “This year built on the successes of the past and plainly illustrated the impact that hospital medicine will have on the future of healthcare.”
Groundbreaking QI Programs Go Nationwide
This year, SHM and its members began to tackle some of the most pressing QI issues in healthcare: reducing readmissions to the hospital and glycemic control. New research in the New England Journal of Medicine couldn’t have made the need for reducing readmissions any clearer: Unplanned hospital readmissions cost Medicare $17.4 billion annually.1
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) helps hospitals implement customized programs to reduce readmissions through improved discharge processes. Hospitalists who enroll in the yearlong program take advantage of a one-on-one mentorship arrangement with experts in the field. Participants can also access the Project BOOST resource toolkit.
Project BOOST began in six pilot hospital sites in 2008 and added 24 new sites in March 2009. The program’s leaders are looking forward to further expansion in 2010. “The response to Project BOOST has been overwhelmingly positive. Given today’s healthcare climate, we know its impact will be even greater in years to come,” says Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives. “There is a very serious need to improve discharge processes in hospitals across the country. With Project BOOST, hospitalists are taking the initiative to ensure a smooth transition from hospital to home.”
SHM also launched the Glycemic Control Mentored Implementation (GCMI) program. Like Project BOOST, GCMI uses a combination of one-on-one mentorships and customized resources to assist hospitalists with QI program implementation.
GCMI takes on another common chronic issue hospitalists face daily: managing glycemic levels in hospitalized patients. The GCMI program is currently in 30 sites across the country.
—Jane Kelly-Cummings, RN, CPHQ, SHM’s senior director of quality initiatives
HM09 Draws Capacity Crowd in Chicago
In an economic climate that forced many industries’ annual meetings to be canceled, delayed, or scaled back, Hospital Medicine 2009 (HM09) in Chicago exceeded expectations. SHM had expected about 1,500 participants in the annual conference; organizers were pleasantly surprised to receive more than 2,000 registrations for the May event. The demand for exhibition space also surpassed projections.
“We’ve long known that hospitalists see real value in a meeting specifically designed for them, with relevant educational sessions and plenty of time for networking,” says Geri Barnes, SHM’s senior director of education and meetings. “Each year, we’ve received more and more interest in the annual conference, but the response to our 2009 conference was unprecedented.”
HM10 is April 8-11 at the Gaylord National Hotel and Convention Center in Washington, D.C.
SHM, MGMA Form Research Partnership
Beginning in 2010, SHM and the Medical Group Management Association (MGMA) will team up to give hospitalists and healthcare executives an even clearer picture on hospitalist compensation and productivity.
Prior to the partnership, SHM had conducted its own research. Now, hospitals and HM managers will have new data at their fingertips, and additional analysis and name-brand recognition of one of the leaders in medical practice research. The first round of research will be available in summer 2010. SHM and MGMA already have collaborated on educational webinars for hospitalists, and SHM is offering books published by MGMA on its Web site.
“This new alliance will pay dividends for years to come,” says Leslie Flores, the director of SHM’s Practice Management Institute. “The information from our compensation and productivity surveys has always been valuable to hospitals. Having the MGMA name attached to next year’s product will only increase its significance and usefulness.”
Hospitalists will receive the joint survey questionnaire from SHM and MGMA in January.
Fellow in Hospital medicine Spotlight
Penny McDonald, MD, FACP, FHM
Undergraduate education: High Point University, High Point, N.C.
Medical school: East Carolina University School of Medicine, Greenville, N.C.
Notable: Dr. McDonald has been a practicing hospitalist since 1997 and an SHM member since 1999. She has served on the physician leadership board and ethics committee at Forsyth. She has been published in the Archives of Internal Medicine.
FYI: Outside the hospital, Dr. McDonald is an avid hiker and loves to travel. Last year, she reached her own personal goal of visiting all 50 states. Her new goal is to visit every national park in the U.S.
Quotable: “I have a secret desire that our specialty be renamed. Describing us as ‘hospitalists,’ based on where we practice, doesn’t seem to cover it. I think ‘medical complexity specialist’ would be more fitting and would encompass all of what we do.”
For more information about the FHM program, visit www.hospitalmedicine.org/fellows.
HM Fellows
Three letters can mean a lot, especially for hospitalists looking for ways to demonstrate their commitment to the specialty. This year was the first in which qualified hospitalists could earn the Fellow in Hospital Medicine (FHM) designation. The first class of more than 500 FHM designees was introduced in an on-stage ceremony at HM09.
“This is a special way for SHM—and the healthcare industry as a whole—to recognize the unique achievements and dedication that hospital medicine requires,” says Todd Von Deak, MBA, CAE, SHM’s vice president for marketing and membership. “As the specialty grows in number and influence, so will the fellows program.”
In 2010, SHM will induct the first class of Senior Fellows in Hospital Medicine (SFHM). While the process for applying for the senior designation will be similar to the FHM designation, the SFHM will require additional years of practice and leadership in the specialty.
The fellows program also features the Master in Hospital Medicine (MHM) designation, the highest level of recognition available. The MHM will be available in 2011, and the nomination process will be invitation-only.
Outside Recognition
SHM isn’t the only group recognizing the impact hospitalists are making on healthcare. In September, the American Board of Internal Medicine (ABIM) announced that hospitalists will be able to apply for Recognition of Focused Practice (RFP) in Hospital Medicine as part of ABIM’s maintenance of certification (MOC) program. The application process will be available as early as next month.
SHM will be assisting hospitalists in the application process through online resources and the MOC pre-course, which will be offered before HM10. Hospitalists with three years of experience in the field can apply for the RFP program. Although most physicians are required to recertify every 10 years, hospitalists won’t have to wait until their certification is up to apply for focused recognition. For more information about the RFP in HM program, visit www.abim.org.
Hospital-Provider Partners
Treating hospitalized patients has always been a team sport. From caseworkers and pharmacists to physicians and critical-care nurses, the diverse and specialized needs of hospital care demand collaboration and coordination.
That’s the idea behind the Hospital Care Collaborative (HCC), which convened for the first time in 2009. The group is made up of six national organizations that represent hundreds of thousands of care providers. The HCC has developed and published “Common Principles for Team-Based Healthcare.” The principles emphasize the need for teamwork within the hospital setting and a focus on the patient.
As part of its goals for the future, the HCC will identify best practices in teamwork and promote educational programs that encourage interdisciplinary teams.
Look Back, Look Forward
For SHM CEO Larry Wellikson, MD, FHM, the end of 2009 is an opportunity to look forward to 2010 and beyond. “Ten years ago, hospital medicine was little more than an idea,” he says. “Today, it is a growing medical specialty, recognized by leaders in healthcare and public policy, with thousands of experienced and enthusiastic hospitalists throughout the country.
“I am confident that when we look back ten years from now, we will see a hospital landscape transformed for the better, and that hospitalists and the rest of the new healthcare team will have played an important role.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Reference
- Jencks SF, Williams MV, Coleman A. Rehospitaliza- tions among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Chapter Updates
Los Angeles
The Los Angeles chapter met Sept. 24 at Craft restaurant. The event was hosted by Manoj K. Mathew, MD, FHM. The presentation, “An Update in Hospital Medicine,” was offered by Joseph Li, MD, FHM, director of hospitalist services at Beth Israel Deaconess Medical Center in Boston and an SHM board member. Nearly 30 attendees from 10 hospitalist organizations attended the meeting. The next Los Angeles chapter meeting is scheduled for January 2010.
Southwest Wisconsin
Transitions of care was the featured topic at the Aug. 6 Southwest Wisconsin chapter meeting. Monica Anderson, director of business development at Select Specialty Hospital in Madison, presented valuable information about the role long-term acute-care hospitals play in a patient’s continuum of care. Following the presentation, attendees discussed ways in which hospitalists can collaborate across HM groups to address patient care and quality issues that are common to hospitalist practices.
Philadelphia Tri-State Area
The Philadelphia Tri-State Area chapter met Sept. 30 at Ristorante Panorama. About 20 hospitalists attended the event, which was sponsored by the France Foundation.
Todd Hecht, MD, of the University of Pennsylvania lectured on DVT prophylaxis. Chapter founder Jennifer Myers, MD, FHM, preceded the lecture by announcing she was stepping down as co-president after a six-year tenure. She thanked the audience for their support and introduced Susan Krekun, MD, chair of the division of hospital medicine at Jefferson University Hospital in Philadelphia, as the new chapter co-president.
The chapter sponsored a job fair Nov. 19 at the downtown Marriott. Medical directors from more than 10 programs attended the event to meet aspiring hospitalists and discuss the state of hospital medicine in the Philadelphia area.
Indiana
The Indiana chapter held a meeting Sept. 2 at Maggiano’s Italian Restaurant in Indianapolis. The meeting was sponsored by AstraZeneca and featured a meet-and-greet before the regular program. Attendees were treated to a report about SHM’s recent Leadership Academy in Miami, and election results were revealed.
Angela Corea, MD, announced the 2010 chapter election nomination results: vice president, John Gilbert, MD, unopposed; secretary, Robert Blessing, MD, unopposed; president, Angela Corea, MD, Raphael Villavicencio, MD, and Gordon Reed, MD, FHM. All three chapter president nominees addressed the attendees.
David Mares, MD, held a question-and-answer session to discuss “New Maintenance Options for the Treatment of COPD.” Drs. Reed and Corea discussed the results of the SHM survey. The meeting concluded with a secret ballot.
Nashville and Middle Tennessee
The Nashville and Middle Tennessee chapter met Oct. 27, with 16 attendees representing eight local hospitals. The speaker, Anton Maki, MD, of Kingsport, presented a thorough review of the microbiology and antimicrobial treatment recommendations for community-acquired pneumonia (CAP). Attendees also were provided information about upcoming SHM conferences and training academies, the application process for the fellowship program, and plans for the ABIM Recognition of Focused Practice in Hospital Medicine certification.
Boston
Anita Barry, the infectious-disease bureau chief and director of communicable-disease control for the Boston Public Health Commission, spoke to nearly 60 hospitalists and guests during the Sept. 10 Boston chapter meeting at Legal Sea Foods. Dr. Barry’s topic was the H1N1 virus. The next chapter event is a clinical investigator training course Dec. 10-11 at Beth Israel Deaconess Medical Center in Boston. Anyone interested in learning more about conducting clinical trials can attend. This course is not limited to physicians; nurses and others are encouraged to attend. There is no fee to attend Boston chapter events. For more information or to RSVP, contact Dr. Li at [email protected] or 617-632-0205.