User login
ONLINE EXCLUSIVE: SHM President, NQF CEO Discuss SHM's Earning National Quality Award
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
ONLINE EXCLUSIVE: Listen to new physician editor Danielle Scheurer's vision for The Hospitalist
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
ONLINE EXCLUSIVE: How the School of Medicine at Stanford University Is Addressing Female Physicians and Leadership
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.

—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
ONLINE EXCLUSIVE: Listen to a Hospitalist and Career Expert Discuss What It Takes to Be a Leader
Geriatric Patients Show Greater Cognitive Decline after Hospitalization
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
A new report that suggests cognitive function tends to decline substantially when older patients are admitted to the hospital could be an opportunity for hospitalists to be proactive in developing interventional therapies to combat the deterioration.
"Cognitive Decline after Hospitalization in a Community Population of Older Persons," published last month in Neurology, found that patients' global cognitive score declined a mean of 0.031 units per year before the first hospitalization, compared with 0.075 units per year thereafter, a more-than-twofold increase. Similar declines were seen in episodic memory (a 3.3-fold increase post-hospitalization) and executive function (a 1.7-fold increase post-hospitalization), according to the survey. More severe illness, longer hospital stay, and older age were associated with even faster cognitive decline after hospitalization.
David Likosky, MD, SFHM, a hospitalist and medical director of The Evergreen Neuroscience Institute in Kirkland, Wash., and a faculty member at HM12 last week in San Diego, says that more research could identify why cognitive functions decrease, as well as assist in developing techniques and therapies that could address the issue.
"A great next step would be to assess short-term cognitive changes post-hospitalization and [watch] how those evolve in the months that follow," Dr. Likosky tells The Hospitalist. "This has implications for discharge planning, and potentially for readmission risk. The step after that will be to determine what strategies might help prevent the cognitive decline seen in the study."
Such a process, he says, has a multiple advantages: First, it can help patients and their families prepare for possible scenarios; second, it provides opportunities for hospitalists to proactively address the issue of cognitive decline.
"If we as hospitalists can intervene to change this rate of decline," says Dr. Likosky, "we can make a great difference in patients' lives."
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Clinical question: Is it safe to perform esophagogastroduodenoscopy (EGD) in patients with upper gastrointestinal (GI) hemorrhage and low hematocrit?
Background: Patients admitted with GI hemorrhage are generally volume-resuscitated aggressively upon admission. After hemodynamic stability has been achieved, some would advocate delaying EGD until the hemoglobin and hematocrit are above 10 g/dL and 30%, respectively. This study attempted to determine whether EGD is safe in the setting of low hematocrit levels.
Study design: Prospective cohort.
Setting: Parkland Memorial Hospital, Dallas.
Synopsis: The 920 patients with upper GI bleeding were divided into two groups: a low (<30%) hematocrit group and a high (>30%) hematocrit group. They were analyzed for differences in rates of cardiovascular events, requirement for surgery, angiography, mortality, or ICU transfer. Overall event rates were extremely low, with no differences between the two groups.
Bottom line: Transfusing to a target hematocrit of >30% should not be a prerequisite for EGD in patients who present with upper GI bleeding.
Citation: Balderas V, Bhore R, Lara LF, Spesivtseva J, Rockey DC. The hematocrit level in upper gastrointestinal hemorrhage: safety of endoscopy and outcomes. Am J Med. 2011;124:970-976.
Pudendal Neuralgia
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.

Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
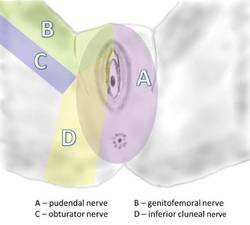
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.
Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
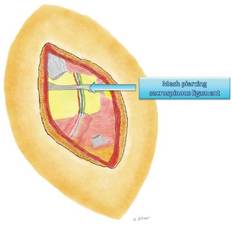
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
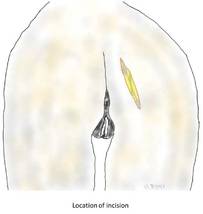
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
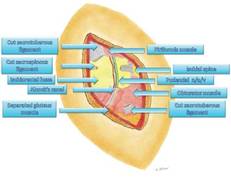
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.
Pudendal neuralgia is an important but often unrecognized and undiagnosed cause of pelvic floor pain.
Its incidence is unknown, and there is relatively little data and scientific evidence in the literature on its diagnosis and treatment. However, I believe that a significant number of women who have burning pain in the vulva, clitoris, vagina, perineum, or rectum – including women who are diagnosed with interstitial cystitis, pelvic floor muscle spasms, vulvodynia, or other conditions – may in fact have pudendal neuralgia.
Indeed, pudendal neuralgia is largely a diagnosis of exclusion, and such conditions often must be ruled out. But the neuropathic condition should be suspected in women who have burning pain in any area along the distribution of the pudendal nerve. Awareness of the nerve’s anatomy and distribution, and of the hallmark characteristics and symptoms of pudendal neuralgia, is important, because earlier identification and treatment appears to provide better outcomes.
Pudendal neuralgia is but one type of pelvic neuralgia; neuropathic pain in the pelvic region also can stem from injury to the obturator, ilioinguinal, iliohypogastric, or genitofemoral nerves, for instance. Most of the patients in our practice, however, have pudendal neuralgia caused by mechanical compression – what is referred to as pudendal nerve entrapment – rather than disease of the nerve.
The condition is sometimes referred to as cyclist syndrome because, historically, the first documented group of patients with symptoms of pudendal neuralgia was competitive cyclists. There is a misconception, however, that the condition only occurs in cyclists. In fact, pudendal neuralgia and pudendal nerve entrapment specifically may be caused by various forms of pelvic trauma, from vaginal delivery (with or without instrumentation) and heavy lifting or falls on the back or pelvis, to previous gynecologic surgery, such as hysterectomy, cystocele repair, and mesh procedures for prolapse and incontinence.
Pudendal neuralgia is multifactorial, involving not only compression of the nerve, for instance, but also muscle spasm and peripheral and central sensitization of pain. Treatment involves a progression of conservative therapies followed by decompression surgery when these conservative treatments fail. We have made several modifications to the transgluteal approach as it was originally described, and believe this approach affords the best outcomes.
Anatomy and Symptoms
The pudendal nerve originates in the S2-S4 sacral foramina, and divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side.
In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
One of my recent patients, for instance, was in a gym class doing a lunge with barbells on her shoulders when her legs gave out and she experienced the start of continuous pain in her vulvar area. Many of our patients trace the onset of their symptoms to immediately after gynecologic surgery, particularly vaginal procedures for prolapse or incontinence. (The pain in these cases is frequently attributed to normal postoperative pain.) Some patients report a more gradual onset of symptoms after surgery.
The pudendal nerve can be compressed in various locations along its course. The nerve runs between the sacrospinous and sacrotuberous ligaments, for instance, and entrapment between these two ligaments is probably the most common cause of pudendal neuralgia. This is where the nerve is compressed by the suturing of mesh placed during prolapse/incontinence surgery.
Another area of compression is Alcock’s canal; entrapment here is characteristic of pudendal neuralgia following vaginal childbirth. Compression also can occur where the clitoral nerve continues underneath the pubic ramus to the clitoris; this is typically where the nerve is compressed by a bicycle seat.
Diagnosis
The most important element of the diagnosis of pudendal neuralgia is the history, particularly regarding the onset of pain, the location of pain, and the nature of symptoms.
History and physical examination both are important for ruling out other reasons for pain, including vulvodynia, pelvic floor tension muscle spasm, and interstitial cystitis. A pelvic exam often will reveal significant tenderness in the pelvic floor muscles, especially in the area of the sacrospinous ligaments. Patients with pudendal neuralgia often have a trigger point – a place of maximal tenderness and pain – at the ischial spine. Palpation of this area to produce what’s known as a Tinel’s sign (with pain and symptoms) thus should be part of the exam.
Also key to diagnosis are computed tomography–guided blocks of the pudendal nerve. In our practice, we consider any degree of pain relief, for any duration of time after the block, as supportive of a diagnosis of pudendal neuralgia. Patients who do not experience immediate relief from a block are thought not to have the condition. These image-guided blocks must be performed by experienced interventional radiologists with a local anesthetic.
To date, there are no imaging studies that are reliable for diagnosis. Ongoing advances in magnetic resonance imaging (MRI) and magnetic resonance neurography (MRN) may make these modalities valuable in the future, but currently these techniques yield too many false negative results. Pudendal nerve motor terminal latency, which measures the conduction velocity of electrical impulses, is not useful given a high rate of intra- and interobserver variability and variations among patients who have had previous vaginal deliveries or pelvic surgery. Sensory threshold testing also has questionable reliability.
Initial Treatments
The initial approach to pudendal neuralgia should be conservative. Surgical decompression is the treatment of choice in patients with likely nerve entrapment, but determining the likelihood and extent of entrapment is a process. First, time must be spent in trying to identify and address the factors causing pain, and in trying to break the vicious cycle that occurs when neuropathic pain causes spasm of the pelvic floor muscles, which in turn leads to increased compression of the nerve and subsequent increases in pain levels.
While there are no official treatment algorithms, we have found – based on available data and our experience in treating more than 500 patients with pudendal neuralgia – that particular therapies can lead to marked improvements for many patients.
For some patients, especially those in whom bicycling or specific exercises initially caused the pain, avoidance of activities that worsen the pain, and other lifestyle modifications, can be helpful. Medical therapy with analgesics/pain management (such as oral pregabalin) and muscle relaxants also may be helpful for some patients. We have tried all kinds of muscle relaxants and have found that a vaginal suppository combining diazepam and baclofen is superior.
The most important treatment modality, however, is pelvic floor physical therapy. Such therapy is key because many patients have significant muscle spasm and subsequent muscle shortening. Therapists who are specially trained to work with pelvic floor muscle dysfunction can address these and other problems largely through various hands-on techniques, exercises, stretching, and education. Therapists can be identified on the International Pelvic Pain Society’s website, www.pelvicpain.org.
Botulinum toxin A (Botox) injections also are often a key part of therapy for patients with significant muscle spasm. In our practice, we administer approximately 200 units in 20 injections using a pudendal nerve block needle, under anesthesia. Not only does the treatment aid in muscle relaxation (thus increasing the patient’s tolerance to physical therapy), it also helps to differentiate between pain caused solely by muscle spasm, and pain caused by nerve injury and muscle spasm.
While patients who do not have neuralgia whose pain is caused solely or almost solely by muscle spasm will benefit significantly more from Botox injections, some patients with pudendal neuralgia will benefit from occasional, repeated Botox treatment in lieu of surgical decompression therapy. Many of our patients have been receiving Botox injections every 3-4 months, for instance.
Similarly, many other patients get significant pain relief from CT-guided injections of the nerve. While an initial CT-guided injection of anesthetic and steroid serves both diagnostic and therapeutic roles, a second and third injection can be performed to deliver more steroid and anesthetic into the pudendal nerve canal (Alcock’s canal) in a patient who responded to the first injection but whose pain has returned. Again, these injections must be performed by an experienced interventional radiologist in a CT scanner.
Injections are offered 6 weeks apart, but some patients have significant pain relief for 4-5 months, or even longer, after CT-guided nerve blocks. Patients who have long-term pain relief from CT-guided blocks will not be offered decompression surgery. One of our patients, for instance, is receiving nerve blocks every 8 months as part of her treatment.
Surgical Decompression
If patients do not have sufficient pain relief from conservative therapies (relief that enables them to return to normal daily function), surgical decompression of the nerve is indicated. An estimated 30%-40% of all patients with pudendal neuralgia will benefit from surgery.
Four different procedures have been described for decompressing an entrapped pudendal nerve: transgluteal, transischiorectal, transperineal, and endoscopic.
The transgluteal approach appears to be the most effective technique, allowing the best visualization of the pudendal nerve and the greatest extent of decompression along the length of the nerve. The main concern with this approach since it was originally described by Professor Roger Robert in Nantes, France, has been the required transection of the sacrotuberous ligament and the possible impact on stability of the sacroiliac joint. In our practice, however, we have made several modifications to the approach that minimize these concerns and, we believe, are improving recovery and outcomes.
The patient is placed in a prone jackknife position, and the electrodes of a NIMS monitor (Nerve Integrity Monitoring System; Medtronic, Minneapolis, Minn.) are placed in the anal sphincter.
An incision of approximately 7-10 cm in length is made across the gluteal region overlying the sacrotuberous ligament. The gluteus muscles are spread, with muscle fibers separated longitudinally, and once the ligament is reached, it is transected at its narrowest point.
The pudendal nerve then can be identified immediately below the ligament with use of a surgical microscope and the NIMS. When the surface of the nerve is touched, we are alerted by the NIMS monitor (part of the nerve runs to the anal center). In some patients, the pudendal nerve may actually be attached to the anterior surface of the sacrotuberous ligament.
The nerve is then decompressed along its entire length, from the piriformis muscle and as close as possible to the spinal cord, to the distal Alcock’s canal. Neurolysis is performed along each of the nerve’s branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve – until the nerve is completely free. In our practice, we most often find the nerve entrapped between the sacrospinous and sacrotuberous ligaments, which form a sort of "V" in the pelvis.
Because the sacrospinous ligament does not serve any anatomic purpose, I transect the ligament so that I can transpose the pudendal nerve anteriorly to give it more room.
Repair of the sacrotuberous ligament was not traditionally performed as part of the transgluteal approach, but we believe that repair is important for stability of the sacroiliac joint. Until recently, we used a graft of cadaver tendon to repair the ligament. Now, however, we transect the ligament with a z-shaped cut; this method allows us to repair the ligament without using any cadaver tissue.
In other modifications to the traditional approach, we wrap a piece of NeuraGen Nerve Guide (Integra LifeSciences, Plainsboro, N.J.), a nerve-protecting sheath made of collagen, around the nerve to prevent the formation or reformation of scar tissue. To promote nerve healing, we then cover the nerve with platelet-rich plasma that has been prepared from the patient’s own blood. The plasma contains growth factors that stimulate the production of myelin-producing cells.
Before closure, we also place a pain pump catheter along the course of the nerve. We believe that infusion of bupivacaine for 10-20 days postoperatively decreases the risk of central sensitization to pain and allows patients to be more mobile after surgery, which we encourage. It also may reduce the risk of scar formation. When neuropathic central pain is believed to be a significant problem, as it often is in patients whose nerves have been injured by surgical mesh, we also administer ketamine. An infusion of this old anesthetic can erase or reverse the troubling phenomena of central sensitization to pain.
Nerve entrapment involving mesh requires lengthy surgery. While other surgeons may trim the mesh, I firmly believe in removing all the mesh because we cannot determine which part of the mesh is causing pain.
Outcomes data from France show that approximately 30%-40% of patients are pain free after surgical decompression, with another 30% reporting improvement in pain and 30% reporting no change in their pain levels (Eur. Urol. 2005;47:403-8).
At our institution, using national scientific standards for the reporting of pain and extent of pain improvement, we have found that 70% of patients who undergo transgluteal surgical decompression have at least a 20% improvement in pain. Within this broad category are a significant number of patients who are pain free, and many who report improvements of 50% or more.
Interestingly, we have found that outcomes are similar among our much smaller number of "re-do" surgical patients. Thus far we have performed approximately 20 such transgluteal procedures – 17 on patients who had re-scarring of the nerve after surgery performed at other institutions, and 3 who had surgery many years ago in our practice, before we were able to optimally visualize the entire nerve and before we made modifications to improve the procedure. Just as with our first-time surgeries, approximately 70% of patients who underwent a second procedure had at least a 20% improvement in pain.
In all cases, the pudendal nerve recovers slowly, especially when it has been entrapped and injured for a long time, and improvements in pain often do not occur until about 4 months after surgery. Improvement typically continues for some time, up to 18 months after surgery. Patients may still have pain related to muscle spasms after surgery, so continued physical therapy and/or more Botox injections are often beneficial. Patients must also, of course, continue to avoid any offending factors or activities.
Dr. Hibner is a former fellow in advanced gynecologic surgery at Mayo Clinic, Scottsdale, Ariz., and is now professor of obstetrics and gynecology, Creighton University, Omaha, Neb., and associate clinical professor of obstetrics and gynecology, University of Arizona, Tucson. He also is director of the Arizona Center for Chronic Pelvic Pain, St. Joseph’s Hospital and Medical Center, Phoenix. To review his surgical procedure, visit SurgeryU at www.aagl.org/mastercourse. Dr. Hibner reported that he has no relevant financial disclosures.
Hyponatremia in Heart Failure
Hyponatremia, defined as a serum [Na+] 135 mEq/L, occurs in 2030% of patients with acute decompensated heart failure (HF)13 and has been independently associated with a poor prognosis. In clinical trials of acute decompensated HF, the reported mean serum sodium is often normal or near normal, but a significant proportion of study subjects can have serum sodium values that approach 130 mEq/L or lower.3 However, despite the association between hyponatremia and clinical outcomes like hospitalization and mortality, data from studies are sparse about the impact of drug or device interventions in the hyponatremic cohort, since patients are generally not stratified at the time of randomization by the value of baseline serum sodium.
HYPONATREMIA AND PROGNOSIS
Hyponatremia has long been recognized as a potential prognostic marker in heart failure, highlighted by Packer and Lee in 1986.4 Subsequently, a wealth of data derived from clinical trials, registries, and observational databases support the concept that hyponatremia is an independent predictor of both short‐ and long‐term outcomes.13, 511 As reviewed by Jao and Chiong,3 this relationship holds in patients on optimal evidence‐based medical therapy, including treatment with antagonists of the renin‐angiotensin system and beta blockers. In the Organized Program To Initiate Lifesaving Treatment In Hospitalized Patients With Heart Failure (OPTIMIZE)2 HF Registry of nearly 50,000 patients, in‐hospital and 60‐day mortality rates were higher in patients with lower serum sodium levels on admission (cut‐off point of 135 mEq/L). In‐hospital death and the combined endpoint of death or re‐hospitalization increased significantly for each 3 mEq/L decrease in serum [Na+] below 140 mEq/L. Patients with hyponatremia were more likely to have lower systolic blood pressures and receive intravenous inotropic agents; lengths of stay were also longer.
Similar findings were reported in the Evaluation Study of Congestive Heart Failure and Pulmonary Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV in CHF)10 trial.11 For example, in the former, Gheorghiade and colleagues tracked serum sodium levels in 433 hospitalized patients who had acute decompensated HF and examined the proportion free from a major event (defined as death and/or HF hospitalization).1 There was a clear association between the event rate and serum sodium level. Patients whose hyponatremia persisted from hospital admission to discharge were at higher risk relative to those whose hyponatremia was corrected during the hospital stay.
However, whether the way in which the serum sodium improvement is achieved has a bearing on outcomes is not known. In the studies comparing outcomes in patients with heart failure and hyponatremia versus normonatremia, no mention is made about how the patient arrived at either state. Despite this limitation, the findings are incontrovertibly consistent. Hyponatremia on discharge (prior to or after the adoption of renin‐angiotensin‐aldosterone system (RAAS) antagonists or beta blockers) is a marker for poorer outcomes, as is another laboratory abnormality frequently observed in patients hospitalized with heart failure: an elevated creatinine.
Additionally, serum sodium obtained shortly after hospitalization is a potent predictor of re‐hospitalization12 and persistently poor health‐related quality‐of‐life.13 The impact on longer‐term outcomes can also be demonstrated in multiple prognostic models6, 8, 9 in which serum sodium is a risk factor for adverse outcomes. For example, using the Seattle Heart Failure Model, overall prognosis worsens for each 1 mEq decline in serum sodium when all other variables are kept constant.8 This observation suggests that, in terms of prognosis, the value of serum sodium functions as a continuous not a binary variable.
HYPONATREMIA AND HF PATHOPHYSIOLOGY
The reasons underlying hyponatremia in heart failure are complex, but a key component is the non‐osmotic release of arginine vasopressin (AVP) in response to stimulation of carotid baroreceptors. This phenomenon occurs as a result of arterial underfilling (both lower blood pressure and lower cardiac output). AVP is one member of a family of neurohormones and cytokines that are upregulated in heart failure (eg, norepinephrine, renin, angiotensin, aldosterone, endothelin, and tumor necrosis factor‐alpha). Levels of AVP are increased most markedly in patients with advanced symptoms (ie, New York Heart Association Class III and IV),14 and this leads to impaired free water handling in the renal tubules and a hypervolemic form of hyponatremia. The reasons underlying the upregulation are debated, but likely reflect a short‐term hemodynamic adaptation that is designed to augment cardiac output by increasing circulating volume. In addition, multiple neurohormones have been shown to promote progressive ventricular dilation, referred to as remodeling. For example, chronic elevations of norepinephrine contribute to a multitude of genotypic and phenotypic changes at the level of the myocyte. The short‐term benefits of neurohormonal upregulation are offset by maladaptive responses in the long term, and this observation likely explains a major part of the clinical benefits seen with drugs such as angiotensin converting enzyme inhibitors, aldosterone antagonists, and beta blockers.
It is also clear that the development and management of patients with hyponatremia and heart failure are frequently complicated by the presence of other factors that impact sodium and water handling. Heart failure often occurs in older patients with renal dysfunction who are on medications that can exacerbate hyponatremia, such as diuretics, non‐steroidal anti‐inflammatory agents, antidepressants, and opiate derivatives. In addition, other conditions like hypothyroidism may coexist and contribute to the hyponatremic state. It is therefore crucial for the clinician to consider these possibilities when a patient with heart failure presents with or develops hyponatremia, and in particular to critically evaluate the potential role of concomitant medications that can cause a syndrome of inappropriate antidiuretic hormone secretion (SIADH)‐like picture.
HYPONATREMIA AND RESOURCE USE
As with other markers of poor outcome in heart failure, such as worsening renal insufficiency, chronic obstructive lung disease, and other comorbidities, hyponatremia is associated with longer lengths of stay (LOS) and cost. In an analysis of approximately 116,000 patients hospitalized with HF and grouped at admission by serum [Na+], risk‐adjusted mortality, LOS, and attributable cost were highest for patients with severe hyponatremia compared to patients with normonatremia.15 In addition, Amin and colleagues recently demonstrated that length of stay in the intensive care unit and associated costs were greater (21% and 23%, respectively) in patients who had an International Classification of Diseases, 9th revision, Clinical Modification (ICD‐9‐CM) code for hyponatremia compared to those that did not.16
CONSIDERATIONS FOR PATIENTS HOSPITALIZED WITH HEART FAILURE WITH AND WITHOUT HYPONATREMIA
A number of significant management challenges exist during the hospitalization phase of acute decompensated heart failure. Among other tasks, the clinician should evaluate the potential cause of the decompensation (eg, medication noncompliance, dietary noncompliance, increased metabolic demand from pneumonia or other infection, worsening renal failure, diuretic resistance, iatrogenic fluid overload) and decide whether the patient is fluid overloaded, in a low cardiac output state contributing to end‐organ perfusion, or both. Manifestations of worsening heart failure other than dyspnea may be present. For example, mental status changes in an elderly patient may reflect fluid overload with or without low cardiac output, but the differential diagnosis also includes impaired clearance of drugs due to liver congestion or worsening renal function (eg, digoxin toxicity), hyponatremia (potentially mediated through cerebral edema), low cardiac output, occult infection, cerebrovascular accident, and other complications of coronary heart disease.
Key components of the physical exam include the presence of jugular venous distention,17 a more sensitive and specific finding than pulmonary rales in chronic or acute‐on‐chronic heart failure. While the mainstay of therapy for fluid overload remains diuretic therapy, we have only recently learned in a definitive way from the Diuretic Optimization Strategies Evaluation (DOSE)18 study that the method of administration (bolus vs continuous intravenous infusion and high dose vs low dose) matters, albeit slightly. Patients who receive high doses of loop diuretic have greater dyspnea relief and weight loss but are at greater risk for developing worsening renal function.
Certain key clinical markers, when present on admission, place the patient in an at‐risk group for a longer length of stay (Table 1). In addition to new or established hyponatremia, these include a creatinine value above baseline, marked antecedent weight gain, and hypotension. During the hospitalization, development of new hyponatremia or worsening of established hyponatremia, worsening renal function (often simply defined by an increase in baseline creatinine by 0.3 mg/dL or more), lack of dyspnea relief, and lack of weight loss, increase the complexity of decision‐making. A proportion of these higher‐risk patients may benefit from the initiation of intravenous vasoactive therapy, mechanical fluid removal (eg, with ultrafiltration), or the use of a vaptan (or aquaretic), depending on the particular presentation and profile. Occasionally, mechanical support will be needed but this option only applies to a limited subgroup.19 However, aside from ventricular assist devices, none of these options have been associated with improved survival.
| Hyponatremia |
| Worsening renal failure |
| Advanced age |
| Comorbidities |
| Marked antecedent weight gain |
| Lack of (early) resolution of weight gain |
| Hypotension |
| Organ hypoperfusion |
Despite this limitation, the immediate goal of care in the acute setting is symptom relief. Thus, although neither intravenous dobutamine nor milrinone have been shown to decrease mortality, both are recognized as palliative options in patients with advanced or end‐stage symptoms20, 21; for example, milrinone, due to its inodilator characteristics, may improve symptoms and end‐organ perfusion while mitigating against an increase in pulmonary vascular resistance. However routine use in the management of acute decompensated heart failure is discouraged, based on the Outcome of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME‐CHF)2 Trial.22 Similarly, the routine use of nesiritide cannot be recommended, based on the neutral findings of the recently published Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND‐HF)23 study, though subsets of patients may still be candidates for this therapy.
Ultrafiltration appears to function well as an adjunct to fluid and salt removal as demonstrated in the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated Congestive Heart Failure (UNLOAD)24 study, though a number of limitations have been cited.25 It should be strongly considered for patients who have developed refractory fluid overload and anasarca, especially if responsiveness to loop diuretics is blunted.
For hypervolemic hyponatremia, the standard approach has been fluid restriction, but this can require a prolonged and at times uncomfortable prescription for patients to follow. Hypertonic saline is contraindicated in most cases, given the salt load and risk of exacerbating fluid overload. Data for demeclocycline are sparse.26 The vaptan class is an interesting option, in large part because of the significant free water loss that can be achieved through the competitive antagonism of V2 receptors in renal tubules. Competitive binding to this receptor leads to a reduction in the deposition of new water channels (or aquaporins) on the luminal side of the tubule, resulting in a marked reduction in water reuptake from the urine.27 Indeed, data for tolvaptan, an orally available vaptan, suggest that short‐term treatment can increase urine output, weight loss, and serum sodium level.28 In both the Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV) and Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study With Tolvaptan (EVEREST)29 studies,28 a number of favorable short‐term effects were seen such as dyspnea relief and weight loss, but in the latter study, the trial did not meet 1 of its 2 prespecified co‐primary endpoints (change on a visual analog scale) in an embedded analysis of acute treatment effects. Further, EVEREST failed to show any meaningful impact on posthospitalization morbidity and mortality when tolvaptan was administered chronically.30 It is also noteworthy that in both trials, inclusion criteria required the presence of symptomatic heart failure rather than hyponatremia; in fact, in EVEREST only 11.5% of patients had a serum sodium level less than 135 mEq/L. To date, there are no long‐term prospectively collected data on the impact of the vaptan class in heart failure accompanied by hyponatremia.
Despite these caveats, the judicious use of vaptans may have a role in heart failure; at the very least, serum sodium increases by, on average, 5.2 mEq/L.31 Fluid restriction should be liberalized and serum sodium should be monitored frequently in the first few days of therapy to avoid rapid correction of serum sodium, which can lead to an unusual neurological complication (osmotic demyelination syndrome).32
OUTPATIENT MANAGEMENT CONSIDERATIONS
Patients who have chronic hyponatremia or who are at risk for worsening of preexisting hyponatremia should be closely monitored during the early postdischarge period, in part to detect further decreases in the serum sodium level and deterioration in overall clinical status. Worsening of hyponatremia may occur in the outpatient setting due to intentional or unintentional increased free water intake, initiation of new medications, exacerbation of the underlying condition, infection, or related conditions. Similar to the inpatient setting, the outpatient management of patients with fluid overload and hyponatremia can be difficult. Further study is required and clinical trials are needed to assess whether the chronic administration of a vaptan in this particular patient population will impact prognosis relative to fluid restriction alone.
Regardless of serum sodium, a frequently advocated intervention in long‐term management is daily weight monitoring which has become a gold standard, especially for patients with advanced symptoms. As shown in EVEREST, lean body weight increases prior to re‐hospitalization for HF were 1.96, 2.07, and 1.97 kg, compared with 0.74, 0.90, and 1.04 kg, respectively, in patients who were not re‐hospitalized (P 0.001 for all groups).33 Recently, use of invasive hemodynamic monitoring, largely on the basis of the CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients (CHAMPION)34 trial, has been advocated as a potential breakthrough in outpatient management because increased right‐sided pressures, rather than weight gain, may precede a heart failure exacerbation.35, 36 It is, however, worthwhile to emphasize that routine hemodynamic monitoring with pulmonary artery catheterization has not been shown to be effective in the inpatient setting,37 despite the attractiveness of knowing the numbers. Additionally, the data supporting the use of serial measurements of biomarkers (in particular, brain natriuretic peptide or its precursor) as a surrogate for filling pressures are conflicting, and therefore this approach is not at present considered standard of care.38
Studies also suggest that postdischarge adherence and the intensity of follow‐up for patients recently admitted for HF may be critical to ensure optimal outcomes. From a practical standpoint, the presence of defined risk factors should lead clinicians to adopt a selective approach to postdischarge monitoring. For those patients deemed to be at risk, reasonable options include outpatient medication titration, more frequent nurse contact, and focused efforts at increasing patient self‐efficacy, all of which can be targeted in the context of a HF disease management program or HF clinic.39, 40 A recent consensus paper outlines the components that should be considered in the establishment of a clinic devoted to the care of patients with heart failure.40 Given increasing reimbursement pressures, these clinics may provide a mechanism to increase quality of care in the outpatient setting while decreasing risk of readmission for preventable heart failure exacerbations. However, other nonphysiological factors influence readmission rates, and not all of these factors can be easily addressed in a traditional medical model.41
SUMMARY
Hyponatremia, in addition to declining renal function, persistent dyspnea, and weight gain, is a major clinical concern during and following hospitalizations for acute decompensated heart failure. Low serum sodium (especially below 130 mEq/L) can contribute to symptoms, complicate diagnostic and therapeutic decision‐making, and significantly prolong length of stay and associated costs. Early recognition of the underlying etiologies, aggressive fluid restriction, and removal of medications that might exacerbate hyponatremia are key steps. The vaptan class is now a useful adjunct in select patients with hyponatremia and fluid overload who do not respond to standard approaches such as fluid restriction.
- ,,, et al.Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial.Arch Intern Med.2007;167:1998–2005.
- ,,, et al,on behalf of the OPTIMIZE‐HF Investigators and Coordinators.Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE‐HF registry.Eur Heart J.2007;28:980–988.
- ,.Hyponatremia in acute decompensated heart failure: mechanisms, prognosis, and treatment options.Clin Cardiol.2010;33:666–671.
- ,.Prognostic importance of serum sodium concentration and its modification by converting enzyme inhibition in patients with severe chronic heart failure.Circulation.1986;73:257–267.
- ,,,,.Risk stratification of in‐hospital mortality in patients hospitalized for chronic congestive heart failure secondary to nonischemic cardiomyopathy.Cardiology.2003;100:136–142.
- ,,,,,.Predicting mortality among patients hospitalized for heart failure. Derivation and validation of a clinical model.JAMA.2003;290:2581–2587.
- ,,.Clinical relevance and management of the major electrolyte abnormalities in congestive heart failure: hyponatremia, hypokalemia, and hypomagnesemia.Am Heart J.1994;128:564–574.
- ,,, et al.The Seattle Heart Failure Model: prediction of survival in heart failure.Circulation.2006;113:1424–1433.
- ,,,,,.Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation.Circulation.1997;95:2660–2667.
- ,,, et alfor the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) Investigators.Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure.JAMA.2004;291:1963–1971.
- ,,, et al.Improvement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trial.Acute Card Care.2007;9:82–86.
- ,,, et al.Critical elements of clinical follow‐up after hospital discharge for heart failure: insights from the EVEREST trial.Eur J Heart Fail.2010;12:367–374.
- ,,, et al.Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life.Circ Cardiovasc Qual Outcomes.2011;4:389–398.
- ,,, et al.Possible vascular role of increased plasma arginine vasopressin in congestive heart failure.Int J Cardiol.2006;106:191–195.
- ,,,,,.Burden of sodium abnormalities in patients hospitalized for heart failure.Congest Heart Fail.2011;17:1–7.
- ,,, et al.Consequences of hyponatremia on cost and length of stay in heart failure patients.J Card Fail.2011;8:S72.
- ,,,.Prognostic importance of elevated jugular venous pressure and a third heart sound in patients with heart failure.N Engl J Med.2001;345:574–581.
- ,,, et alfor the NHLBI Heart Failure Clinical Research Network.Diuretic strategies in patients with acute decompensated heart failure.N Engl J Med.2011;364:797–805.
- ,,.Emerging ventricular assist devices for long‐term cardiac support.Nat Rev Cardiol.2010;7:71–76.
- ,,, et al.Chronic continuous home inotropic therapy in end‐stage heart failure.Am Heart J.2006;152:1096.e1–1096.e8.
- ,.Dobutamine for patients with end‐stage heart failure in a hospice program?J Palliat Med.2003;6:93–97.
- ,,, et al.Short‐term intravenous milrinone for acute exacerbation of chronic heart failure.JAMA.2002;287:1541–1547.
- ,,, et al.Effect of nesiritide in patients with acute decompensated heart failure.N Engl J Med.2011;365:32–43.
- ,,, et alfor the UNLOAD Trial Investigators.Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure.J Am Coll Cardiol.2007;49:675–683.
- ,,.The challenge of correcting volume overload in hospitalized patients with decompensated heart failure.J Am Coll Cardiol.2007;49:684–686.
- ,,.Demeclocycline treatment of water retention in congestive heart failure.Br Med J.1978;1:760.
- ,.Vasopressin antagonists.J Card Fail.2011;17:973–981.
- ,,, et al.A multicenter, randomized, double‐blind, placebo‐controlled study of tolvaptan monotherapy compared to furosemide and the combination of tolvaptan and furosemide in patients with heart failure and systolic dysfunction.JAMA.2004;291:1963–1971.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Short‐term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials.JAMA.2007;297:1332–1343.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial.JAMA.2007;297:1319–1331.
- ,,,,,.Vasopressin receptor antagonists for the treatment of hyponatremia: systematic review and meta‐analysis.Am J Kidney Dis.2010;56:325–337.
- ,,,,.Central pontine myelinolysis and pontine lesions after rapid correction of hyponatremia: a prospective magnetic resonance imaging study.Ann Neurol.1990;27:61–66.
- ,,, et alfor the EVEREST Investigators.Weight changes after hospitalization for worsening heart failure and subsequent re‐hospitalization and mortality in the EVEREST trial.Eur Heart J.2009;30:1666–1673.
- ,,, et alfor the CHAMPION Trial Study Group.Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial.Lancet.2011;377:658–666.
- ,,.Sympathetically mediated changes in capacitance: redistribution of the venous reservoir as a cause of decompensation.Circ Heart Fail.2011;4:669–675.
- ,,, et al.Hemodynamic factors associated with acute decompensated heart failure: part 1—insights into pathophysiology.J Card Fail.2001;17:282–291.
- The ESCAPE Investigators.Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness.JAMA.2005;294:1625–1633.
- ,,, et al.B‐type natriuretic peptide‐guided heart failure therapy: a meta‐analysis.Arch Intern Med.2010;170:507–514.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,, et al.The heart failure clinic: a consensus statement of the Heart Failure Society of America.J Card Fail.2008;14:801–815.
- ,,, et al.An automated model to identify heart failure patients at risk for 30‐day readmission or death using electronic medical record data.Med Care.2010;48:981–988.
Hyponatremia, defined as a serum [Na+] 135 mEq/L, occurs in 2030% of patients with acute decompensated heart failure (HF)13 and has been independently associated with a poor prognosis. In clinical trials of acute decompensated HF, the reported mean serum sodium is often normal or near normal, but a significant proportion of study subjects can have serum sodium values that approach 130 mEq/L or lower.3 However, despite the association between hyponatremia and clinical outcomes like hospitalization and mortality, data from studies are sparse about the impact of drug or device interventions in the hyponatremic cohort, since patients are generally not stratified at the time of randomization by the value of baseline serum sodium.
HYPONATREMIA AND PROGNOSIS
Hyponatremia has long been recognized as a potential prognostic marker in heart failure, highlighted by Packer and Lee in 1986.4 Subsequently, a wealth of data derived from clinical trials, registries, and observational databases support the concept that hyponatremia is an independent predictor of both short‐ and long‐term outcomes.13, 511 As reviewed by Jao and Chiong,3 this relationship holds in patients on optimal evidence‐based medical therapy, including treatment with antagonists of the renin‐angiotensin system and beta blockers. In the Organized Program To Initiate Lifesaving Treatment In Hospitalized Patients With Heart Failure (OPTIMIZE)2 HF Registry of nearly 50,000 patients, in‐hospital and 60‐day mortality rates were higher in patients with lower serum sodium levels on admission (cut‐off point of 135 mEq/L). In‐hospital death and the combined endpoint of death or re‐hospitalization increased significantly for each 3 mEq/L decrease in serum [Na+] below 140 mEq/L. Patients with hyponatremia were more likely to have lower systolic blood pressures and receive intravenous inotropic agents; lengths of stay were also longer.
Similar findings were reported in the Evaluation Study of Congestive Heart Failure and Pulmonary Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV in CHF)10 trial.11 For example, in the former, Gheorghiade and colleagues tracked serum sodium levels in 433 hospitalized patients who had acute decompensated HF and examined the proportion free from a major event (defined as death and/or HF hospitalization).1 There was a clear association between the event rate and serum sodium level. Patients whose hyponatremia persisted from hospital admission to discharge were at higher risk relative to those whose hyponatremia was corrected during the hospital stay.
However, whether the way in which the serum sodium improvement is achieved has a bearing on outcomes is not known. In the studies comparing outcomes in patients with heart failure and hyponatremia versus normonatremia, no mention is made about how the patient arrived at either state. Despite this limitation, the findings are incontrovertibly consistent. Hyponatremia on discharge (prior to or after the adoption of renin‐angiotensin‐aldosterone system (RAAS) antagonists or beta blockers) is a marker for poorer outcomes, as is another laboratory abnormality frequently observed in patients hospitalized with heart failure: an elevated creatinine.
Additionally, serum sodium obtained shortly after hospitalization is a potent predictor of re‐hospitalization12 and persistently poor health‐related quality‐of‐life.13 The impact on longer‐term outcomes can also be demonstrated in multiple prognostic models6, 8, 9 in which serum sodium is a risk factor for adverse outcomes. For example, using the Seattle Heart Failure Model, overall prognosis worsens for each 1 mEq decline in serum sodium when all other variables are kept constant.8 This observation suggests that, in terms of prognosis, the value of serum sodium functions as a continuous not a binary variable.
HYPONATREMIA AND HF PATHOPHYSIOLOGY
The reasons underlying hyponatremia in heart failure are complex, but a key component is the non‐osmotic release of arginine vasopressin (AVP) in response to stimulation of carotid baroreceptors. This phenomenon occurs as a result of arterial underfilling (both lower blood pressure and lower cardiac output). AVP is one member of a family of neurohormones and cytokines that are upregulated in heart failure (eg, norepinephrine, renin, angiotensin, aldosterone, endothelin, and tumor necrosis factor‐alpha). Levels of AVP are increased most markedly in patients with advanced symptoms (ie, New York Heart Association Class III and IV),14 and this leads to impaired free water handling in the renal tubules and a hypervolemic form of hyponatremia. The reasons underlying the upregulation are debated, but likely reflect a short‐term hemodynamic adaptation that is designed to augment cardiac output by increasing circulating volume. In addition, multiple neurohormones have been shown to promote progressive ventricular dilation, referred to as remodeling. For example, chronic elevations of norepinephrine contribute to a multitude of genotypic and phenotypic changes at the level of the myocyte. The short‐term benefits of neurohormonal upregulation are offset by maladaptive responses in the long term, and this observation likely explains a major part of the clinical benefits seen with drugs such as angiotensin converting enzyme inhibitors, aldosterone antagonists, and beta blockers.
It is also clear that the development and management of patients with hyponatremia and heart failure are frequently complicated by the presence of other factors that impact sodium and water handling. Heart failure often occurs in older patients with renal dysfunction who are on medications that can exacerbate hyponatremia, such as diuretics, non‐steroidal anti‐inflammatory agents, antidepressants, and opiate derivatives. In addition, other conditions like hypothyroidism may coexist and contribute to the hyponatremic state. It is therefore crucial for the clinician to consider these possibilities when a patient with heart failure presents with or develops hyponatremia, and in particular to critically evaluate the potential role of concomitant medications that can cause a syndrome of inappropriate antidiuretic hormone secretion (SIADH)‐like picture.
HYPONATREMIA AND RESOURCE USE
As with other markers of poor outcome in heart failure, such as worsening renal insufficiency, chronic obstructive lung disease, and other comorbidities, hyponatremia is associated with longer lengths of stay (LOS) and cost. In an analysis of approximately 116,000 patients hospitalized with HF and grouped at admission by serum [Na+], risk‐adjusted mortality, LOS, and attributable cost were highest for patients with severe hyponatremia compared to patients with normonatremia.15 In addition, Amin and colleagues recently demonstrated that length of stay in the intensive care unit and associated costs were greater (21% and 23%, respectively) in patients who had an International Classification of Diseases, 9th revision, Clinical Modification (ICD‐9‐CM) code for hyponatremia compared to those that did not.16
CONSIDERATIONS FOR PATIENTS HOSPITALIZED WITH HEART FAILURE WITH AND WITHOUT HYPONATREMIA
A number of significant management challenges exist during the hospitalization phase of acute decompensated heart failure. Among other tasks, the clinician should evaluate the potential cause of the decompensation (eg, medication noncompliance, dietary noncompliance, increased metabolic demand from pneumonia or other infection, worsening renal failure, diuretic resistance, iatrogenic fluid overload) and decide whether the patient is fluid overloaded, in a low cardiac output state contributing to end‐organ perfusion, or both. Manifestations of worsening heart failure other than dyspnea may be present. For example, mental status changes in an elderly patient may reflect fluid overload with or without low cardiac output, but the differential diagnosis also includes impaired clearance of drugs due to liver congestion or worsening renal function (eg, digoxin toxicity), hyponatremia (potentially mediated through cerebral edema), low cardiac output, occult infection, cerebrovascular accident, and other complications of coronary heart disease.
Key components of the physical exam include the presence of jugular venous distention,17 a more sensitive and specific finding than pulmonary rales in chronic or acute‐on‐chronic heart failure. While the mainstay of therapy for fluid overload remains diuretic therapy, we have only recently learned in a definitive way from the Diuretic Optimization Strategies Evaluation (DOSE)18 study that the method of administration (bolus vs continuous intravenous infusion and high dose vs low dose) matters, albeit slightly. Patients who receive high doses of loop diuretic have greater dyspnea relief and weight loss but are at greater risk for developing worsening renal function.
Certain key clinical markers, when present on admission, place the patient in an at‐risk group for a longer length of stay (Table 1). In addition to new or established hyponatremia, these include a creatinine value above baseline, marked antecedent weight gain, and hypotension. During the hospitalization, development of new hyponatremia or worsening of established hyponatremia, worsening renal function (often simply defined by an increase in baseline creatinine by 0.3 mg/dL or more), lack of dyspnea relief, and lack of weight loss, increase the complexity of decision‐making. A proportion of these higher‐risk patients may benefit from the initiation of intravenous vasoactive therapy, mechanical fluid removal (eg, with ultrafiltration), or the use of a vaptan (or aquaretic), depending on the particular presentation and profile. Occasionally, mechanical support will be needed but this option only applies to a limited subgroup.19 However, aside from ventricular assist devices, none of these options have been associated with improved survival.
| Hyponatremia |
| Worsening renal failure |
| Advanced age |
| Comorbidities |
| Marked antecedent weight gain |
| Lack of (early) resolution of weight gain |
| Hypotension |
| Organ hypoperfusion |
Despite this limitation, the immediate goal of care in the acute setting is symptom relief. Thus, although neither intravenous dobutamine nor milrinone have been shown to decrease mortality, both are recognized as palliative options in patients with advanced or end‐stage symptoms20, 21; for example, milrinone, due to its inodilator characteristics, may improve symptoms and end‐organ perfusion while mitigating against an increase in pulmonary vascular resistance. However routine use in the management of acute decompensated heart failure is discouraged, based on the Outcome of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME‐CHF)2 Trial.22 Similarly, the routine use of nesiritide cannot be recommended, based on the neutral findings of the recently published Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND‐HF)23 study, though subsets of patients may still be candidates for this therapy.
Ultrafiltration appears to function well as an adjunct to fluid and salt removal as demonstrated in the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated Congestive Heart Failure (UNLOAD)24 study, though a number of limitations have been cited.25 It should be strongly considered for patients who have developed refractory fluid overload and anasarca, especially if responsiveness to loop diuretics is blunted.
For hypervolemic hyponatremia, the standard approach has been fluid restriction, but this can require a prolonged and at times uncomfortable prescription for patients to follow. Hypertonic saline is contraindicated in most cases, given the salt load and risk of exacerbating fluid overload. Data for demeclocycline are sparse.26 The vaptan class is an interesting option, in large part because of the significant free water loss that can be achieved through the competitive antagonism of V2 receptors in renal tubules. Competitive binding to this receptor leads to a reduction in the deposition of new water channels (or aquaporins) on the luminal side of the tubule, resulting in a marked reduction in water reuptake from the urine.27 Indeed, data for tolvaptan, an orally available vaptan, suggest that short‐term treatment can increase urine output, weight loss, and serum sodium level.28 In both the Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV) and Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study With Tolvaptan (EVEREST)29 studies,28 a number of favorable short‐term effects were seen such as dyspnea relief and weight loss, but in the latter study, the trial did not meet 1 of its 2 prespecified co‐primary endpoints (change on a visual analog scale) in an embedded analysis of acute treatment effects. Further, EVEREST failed to show any meaningful impact on posthospitalization morbidity and mortality when tolvaptan was administered chronically.30 It is also noteworthy that in both trials, inclusion criteria required the presence of symptomatic heart failure rather than hyponatremia; in fact, in EVEREST only 11.5% of patients had a serum sodium level less than 135 mEq/L. To date, there are no long‐term prospectively collected data on the impact of the vaptan class in heart failure accompanied by hyponatremia.
Despite these caveats, the judicious use of vaptans may have a role in heart failure; at the very least, serum sodium increases by, on average, 5.2 mEq/L.31 Fluid restriction should be liberalized and serum sodium should be monitored frequently in the first few days of therapy to avoid rapid correction of serum sodium, which can lead to an unusual neurological complication (osmotic demyelination syndrome).32
OUTPATIENT MANAGEMENT CONSIDERATIONS
Patients who have chronic hyponatremia or who are at risk for worsening of preexisting hyponatremia should be closely monitored during the early postdischarge period, in part to detect further decreases in the serum sodium level and deterioration in overall clinical status. Worsening of hyponatremia may occur in the outpatient setting due to intentional or unintentional increased free water intake, initiation of new medications, exacerbation of the underlying condition, infection, or related conditions. Similar to the inpatient setting, the outpatient management of patients with fluid overload and hyponatremia can be difficult. Further study is required and clinical trials are needed to assess whether the chronic administration of a vaptan in this particular patient population will impact prognosis relative to fluid restriction alone.
Regardless of serum sodium, a frequently advocated intervention in long‐term management is daily weight monitoring which has become a gold standard, especially for patients with advanced symptoms. As shown in EVEREST, lean body weight increases prior to re‐hospitalization for HF were 1.96, 2.07, and 1.97 kg, compared with 0.74, 0.90, and 1.04 kg, respectively, in patients who were not re‐hospitalized (P 0.001 for all groups).33 Recently, use of invasive hemodynamic monitoring, largely on the basis of the CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients (CHAMPION)34 trial, has been advocated as a potential breakthrough in outpatient management because increased right‐sided pressures, rather than weight gain, may precede a heart failure exacerbation.35, 36 It is, however, worthwhile to emphasize that routine hemodynamic monitoring with pulmonary artery catheterization has not been shown to be effective in the inpatient setting,37 despite the attractiveness of knowing the numbers. Additionally, the data supporting the use of serial measurements of biomarkers (in particular, brain natriuretic peptide or its precursor) as a surrogate for filling pressures are conflicting, and therefore this approach is not at present considered standard of care.38
Studies also suggest that postdischarge adherence and the intensity of follow‐up for patients recently admitted for HF may be critical to ensure optimal outcomes. From a practical standpoint, the presence of defined risk factors should lead clinicians to adopt a selective approach to postdischarge monitoring. For those patients deemed to be at risk, reasonable options include outpatient medication titration, more frequent nurse contact, and focused efforts at increasing patient self‐efficacy, all of which can be targeted in the context of a HF disease management program or HF clinic.39, 40 A recent consensus paper outlines the components that should be considered in the establishment of a clinic devoted to the care of patients with heart failure.40 Given increasing reimbursement pressures, these clinics may provide a mechanism to increase quality of care in the outpatient setting while decreasing risk of readmission for preventable heart failure exacerbations. However, other nonphysiological factors influence readmission rates, and not all of these factors can be easily addressed in a traditional medical model.41
SUMMARY
Hyponatremia, in addition to declining renal function, persistent dyspnea, and weight gain, is a major clinical concern during and following hospitalizations for acute decompensated heart failure. Low serum sodium (especially below 130 mEq/L) can contribute to symptoms, complicate diagnostic and therapeutic decision‐making, and significantly prolong length of stay and associated costs. Early recognition of the underlying etiologies, aggressive fluid restriction, and removal of medications that might exacerbate hyponatremia are key steps. The vaptan class is now a useful adjunct in select patients with hyponatremia and fluid overload who do not respond to standard approaches such as fluid restriction.
Hyponatremia, defined as a serum [Na+] 135 mEq/L, occurs in 2030% of patients with acute decompensated heart failure (HF)13 and has been independently associated with a poor prognosis. In clinical trials of acute decompensated HF, the reported mean serum sodium is often normal or near normal, but a significant proportion of study subjects can have serum sodium values that approach 130 mEq/L or lower.3 However, despite the association between hyponatremia and clinical outcomes like hospitalization and mortality, data from studies are sparse about the impact of drug or device interventions in the hyponatremic cohort, since patients are generally not stratified at the time of randomization by the value of baseline serum sodium.
HYPONATREMIA AND PROGNOSIS
Hyponatremia has long been recognized as a potential prognostic marker in heart failure, highlighted by Packer and Lee in 1986.4 Subsequently, a wealth of data derived from clinical trials, registries, and observational databases support the concept that hyponatremia is an independent predictor of both short‐ and long‐term outcomes.13, 511 As reviewed by Jao and Chiong,3 this relationship holds in patients on optimal evidence‐based medical therapy, including treatment with antagonists of the renin‐angiotensin system and beta blockers. In the Organized Program To Initiate Lifesaving Treatment In Hospitalized Patients With Heart Failure (OPTIMIZE)2 HF Registry of nearly 50,000 patients, in‐hospital and 60‐day mortality rates were higher in patients with lower serum sodium levels on admission (cut‐off point of 135 mEq/L). In‐hospital death and the combined endpoint of death or re‐hospitalization increased significantly for each 3 mEq/L decrease in serum [Na+] below 140 mEq/L. Patients with hyponatremia were more likely to have lower systolic blood pressures and receive intravenous inotropic agents; lengths of stay were also longer.
Similar findings were reported in the Evaluation Study of Congestive Heart Failure and Pulmonary Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV in CHF)10 trial.11 For example, in the former, Gheorghiade and colleagues tracked serum sodium levels in 433 hospitalized patients who had acute decompensated HF and examined the proportion free from a major event (defined as death and/or HF hospitalization).1 There was a clear association between the event rate and serum sodium level. Patients whose hyponatremia persisted from hospital admission to discharge were at higher risk relative to those whose hyponatremia was corrected during the hospital stay.
However, whether the way in which the serum sodium improvement is achieved has a bearing on outcomes is not known. In the studies comparing outcomes in patients with heart failure and hyponatremia versus normonatremia, no mention is made about how the patient arrived at either state. Despite this limitation, the findings are incontrovertibly consistent. Hyponatremia on discharge (prior to or after the adoption of renin‐angiotensin‐aldosterone system (RAAS) antagonists or beta blockers) is a marker for poorer outcomes, as is another laboratory abnormality frequently observed in patients hospitalized with heart failure: an elevated creatinine.
Additionally, serum sodium obtained shortly after hospitalization is a potent predictor of re‐hospitalization12 and persistently poor health‐related quality‐of‐life.13 The impact on longer‐term outcomes can also be demonstrated in multiple prognostic models6, 8, 9 in which serum sodium is a risk factor for adverse outcomes. For example, using the Seattle Heart Failure Model, overall prognosis worsens for each 1 mEq decline in serum sodium when all other variables are kept constant.8 This observation suggests that, in terms of prognosis, the value of serum sodium functions as a continuous not a binary variable.
HYPONATREMIA AND HF PATHOPHYSIOLOGY
The reasons underlying hyponatremia in heart failure are complex, but a key component is the non‐osmotic release of arginine vasopressin (AVP) in response to stimulation of carotid baroreceptors. This phenomenon occurs as a result of arterial underfilling (both lower blood pressure and lower cardiac output). AVP is one member of a family of neurohormones and cytokines that are upregulated in heart failure (eg, norepinephrine, renin, angiotensin, aldosterone, endothelin, and tumor necrosis factor‐alpha). Levels of AVP are increased most markedly in patients with advanced symptoms (ie, New York Heart Association Class III and IV),14 and this leads to impaired free water handling in the renal tubules and a hypervolemic form of hyponatremia. The reasons underlying the upregulation are debated, but likely reflect a short‐term hemodynamic adaptation that is designed to augment cardiac output by increasing circulating volume. In addition, multiple neurohormones have been shown to promote progressive ventricular dilation, referred to as remodeling. For example, chronic elevations of norepinephrine contribute to a multitude of genotypic and phenotypic changes at the level of the myocyte. The short‐term benefits of neurohormonal upregulation are offset by maladaptive responses in the long term, and this observation likely explains a major part of the clinical benefits seen with drugs such as angiotensin converting enzyme inhibitors, aldosterone antagonists, and beta blockers.
It is also clear that the development and management of patients with hyponatremia and heart failure are frequently complicated by the presence of other factors that impact sodium and water handling. Heart failure often occurs in older patients with renal dysfunction who are on medications that can exacerbate hyponatremia, such as diuretics, non‐steroidal anti‐inflammatory agents, antidepressants, and opiate derivatives. In addition, other conditions like hypothyroidism may coexist and contribute to the hyponatremic state. It is therefore crucial for the clinician to consider these possibilities when a patient with heart failure presents with or develops hyponatremia, and in particular to critically evaluate the potential role of concomitant medications that can cause a syndrome of inappropriate antidiuretic hormone secretion (SIADH)‐like picture.
HYPONATREMIA AND RESOURCE USE
As with other markers of poor outcome in heart failure, such as worsening renal insufficiency, chronic obstructive lung disease, and other comorbidities, hyponatremia is associated with longer lengths of stay (LOS) and cost. In an analysis of approximately 116,000 patients hospitalized with HF and grouped at admission by serum [Na+], risk‐adjusted mortality, LOS, and attributable cost were highest for patients with severe hyponatremia compared to patients with normonatremia.15 In addition, Amin and colleagues recently demonstrated that length of stay in the intensive care unit and associated costs were greater (21% and 23%, respectively) in patients who had an International Classification of Diseases, 9th revision, Clinical Modification (ICD‐9‐CM) code for hyponatremia compared to those that did not.16
CONSIDERATIONS FOR PATIENTS HOSPITALIZED WITH HEART FAILURE WITH AND WITHOUT HYPONATREMIA
A number of significant management challenges exist during the hospitalization phase of acute decompensated heart failure. Among other tasks, the clinician should evaluate the potential cause of the decompensation (eg, medication noncompliance, dietary noncompliance, increased metabolic demand from pneumonia or other infection, worsening renal failure, diuretic resistance, iatrogenic fluid overload) and decide whether the patient is fluid overloaded, in a low cardiac output state contributing to end‐organ perfusion, or both. Manifestations of worsening heart failure other than dyspnea may be present. For example, mental status changes in an elderly patient may reflect fluid overload with or without low cardiac output, but the differential diagnosis also includes impaired clearance of drugs due to liver congestion or worsening renal function (eg, digoxin toxicity), hyponatremia (potentially mediated through cerebral edema), low cardiac output, occult infection, cerebrovascular accident, and other complications of coronary heart disease.
Key components of the physical exam include the presence of jugular venous distention,17 a more sensitive and specific finding than pulmonary rales in chronic or acute‐on‐chronic heart failure. While the mainstay of therapy for fluid overload remains diuretic therapy, we have only recently learned in a definitive way from the Diuretic Optimization Strategies Evaluation (DOSE)18 study that the method of administration (bolus vs continuous intravenous infusion and high dose vs low dose) matters, albeit slightly. Patients who receive high doses of loop diuretic have greater dyspnea relief and weight loss but are at greater risk for developing worsening renal function.
Certain key clinical markers, when present on admission, place the patient in an at‐risk group for a longer length of stay (Table 1). In addition to new or established hyponatremia, these include a creatinine value above baseline, marked antecedent weight gain, and hypotension. During the hospitalization, development of new hyponatremia or worsening of established hyponatremia, worsening renal function (often simply defined by an increase in baseline creatinine by 0.3 mg/dL or more), lack of dyspnea relief, and lack of weight loss, increase the complexity of decision‐making. A proportion of these higher‐risk patients may benefit from the initiation of intravenous vasoactive therapy, mechanical fluid removal (eg, with ultrafiltration), or the use of a vaptan (or aquaretic), depending on the particular presentation and profile. Occasionally, mechanical support will be needed but this option only applies to a limited subgroup.19 However, aside from ventricular assist devices, none of these options have been associated with improved survival.
| Hyponatremia |
| Worsening renal failure |
| Advanced age |
| Comorbidities |
| Marked antecedent weight gain |
| Lack of (early) resolution of weight gain |
| Hypotension |
| Organ hypoperfusion |
Despite this limitation, the immediate goal of care in the acute setting is symptom relief. Thus, although neither intravenous dobutamine nor milrinone have been shown to decrease mortality, both are recognized as palliative options in patients with advanced or end‐stage symptoms20, 21; for example, milrinone, due to its inodilator characteristics, may improve symptoms and end‐organ perfusion while mitigating against an increase in pulmonary vascular resistance. However routine use in the management of acute decompensated heart failure is discouraged, based on the Outcome of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME‐CHF)2 Trial.22 Similarly, the routine use of nesiritide cannot be recommended, based on the neutral findings of the recently published Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND‐HF)23 study, though subsets of patients may still be candidates for this therapy.
Ultrafiltration appears to function well as an adjunct to fluid and salt removal as demonstrated in the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated Congestive Heart Failure (UNLOAD)24 study, though a number of limitations have been cited.25 It should be strongly considered for patients who have developed refractory fluid overload and anasarca, especially if responsiveness to loop diuretics is blunted.
For hypervolemic hyponatremia, the standard approach has been fluid restriction, but this can require a prolonged and at times uncomfortable prescription for patients to follow. Hypertonic saline is contraindicated in most cases, given the salt load and risk of exacerbating fluid overload. Data for demeclocycline are sparse.26 The vaptan class is an interesting option, in large part because of the significant free water loss that can be achieved through the competitive antagonism of V2 receptors in renal tubules. Competitive binding to this receptor leads to a reduction in the deposition of new water channels (or aquaporins) on the luminal side of the tubule, resulting in a marked reduction in water reuptake from the urine.27 Indeed, data for tolvaptan, an orally available vaptan, suggest that short‐term treatment can increase urine output, weight loss, and serum sodium level.28 In both the Acute and Chronic Therapeutic Impact of a Vasopressin 2 Antagonist (Tolvaptan) in Congestive Heart Failure (ACTIV) and Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study With Tolvaptan (EVEREST)29 studies,28 a number of favorable short‐term effects were seen such as dyspnea relief and weight loss, but in the latter study, the trial did not meet 1 of its 2 prespecified co‐primary endpoints (change on a visual analog scale) in an embedded analysis of acute treatment effects. Further, EVEREST failed to show any meaningful impact on posthospitalization morbidity and mortality when tolvaptan was administered chronically.30 It is also noteworthy that in both trials, inclusion criteria required the presence of symptomatic heart failure rather than hyponatremia; in fact, in EVEREST only 11.5% of patients had a serum sodium level less than 135 mEq/L. To date, there are no long‐term prospectively collected data on the impact of the vaptan class in heart failure accompanied by hyponatremia.
Despite these caveats, the judicious use of vaptans may have a role in heart failure; at the very least, serum sodium increases by, on average, 5.2 mEq/L.31 Fluid restriction should be liberalized and serum sodium should be monitored frequently in the first few days of therapy to avoid rapid correction of serum sodium, which can lead to an unusual neurological complication (osmotic demyelination syndrome).32
OUTPATIENT MANAGEMENT CONSIDERATIONS
Patients who have chronic hyponatremia or who are at risk for worsening of preexisting hyponatremia should be closely monitored during the early postdischarge period, in part to detect further decreases in the serum sodium level and deterioration in overall clinical status. Worsening of hyponatremia may occur in the outpatient setting due to intentional or unintentional increased free water intake, initiation of new medications, exacerbation of the underlying condition, infection, or related conditions. Similar to the inpatient setting, the outpatient management of patients with fluid overload and hyponatremia can be difficult. Further study is required and clinical trials are needed to assess whether the chronic administration of a vaptan in this particular patient population will impact prognosis relative to fluid restriction alone.
Regardless of serum sodium, a frequently advocated intervention in long‐term management is daily weight monitoring which has become a gold standard, especially for patients with advanced symptoms. As shown in EVEREST, lean body weight increases prior to re‐hospitalization for HF were 1.96, 2.07, and 1.97 kg, compared with 0.74, 0.90, and 1.04 kg, respectively, in patients who were not re‐hospitalized (P 0.001 for all groups).33 Recently, use of invasive hemodynamic monitoring, largely on the basis of the CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients (CHAMPION)34 trial, has been advocated as a potential breakthrough in outpatient management because increased right‐sided pressures, rather than weight gain, may precede a heart failure exacerbation.35, 36 It is, however, worthwhile to emphasize that routine hemodynamic monitoring with pulmonary artery catheterization has not been shown to be effective in the inpatient setting,37 despite the attractiveness of knowing the numbers. Additionally, the data supporting the use of serial measurements of biomarkers (in particular, brain natriuretic peptide or its precursor) as a surrogate for filling pressures are conflicting, and therefore this approach is not at present considered standard of care.38
Studies also suggest that postdischarge adherence and the intensity of follow‐up for patients recently admitted for HF may be critical to ensure optimal outcomes. From a practical standpoint, the presence of defined risk factors should lead clinicians to adopt a selective approach to postdischarge monitoring. For those patients deemed to be at risk, reasonable options include outpatient medication titration, more frequent nurse contact, and focused efforts at increasing patient self‐efficacy, all of which can be targeted in the context of a HF disease management program or HF clinic.39, 40 A recent consensus paper outlines the components that should be considered in the establishment of a clinic devoted to the care of patients with heart failure.40 Given increasing reimbursement pressures, these clinics may provide a mechanism to increase quality of care in the outpatient setting while decreasing risk of readmission for preventable heart failure exacerbations. However, other nonphysiological factors influence readmission rates, and not all of these factors can be easily addressed in a traditional medical model.41
SUMMARY
Hyponatremia, in addition to declining renal function, persistent dyspnea, and weight gain, is a major clinical concern during and following hospitalizations for acute decompensated heart failure. Low serum sodium (especially below 130 mEq/L) can contribute to symptoms, complicate diagnostic and therapeutic decision‐making, and significantly prolong length of stay and associated costs. Early recognition of the underlying etiologies, aggressive fluid restriction, and removal of medications that might exacerbate hyponatremia are key steps. The vaptan class is now a useful adjunct in select patients with hyponatremia and fluid overload who do not respond to standard approaches such as fluid restriction.
- ,,, et al.Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial.Arch Intern Med.2007;167:1998–2005.
- ,,, et al,on behalf of the OPTIMIZE‐HF Investigators and Coordinators.Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE‐HF registry.Eur Heart J.2007;28:980–988.
- ,.Hyponatremia in acute decompensated heart failure: mechanisms, prognosis, and treatment options.Clin Cardiol.2010;33:666–671.
- ,.Prognostic importance of serum sodium concentration and its modification by converting enzyme inhibition in patients with severe chronic heart failure.Circulation.1986;73:257–267.
- ,,,,.Risk stratification of in‐hospital mortality in patients hospitalized for chronic congestive heart failure secondary to nonischemic cardiomyopathy.Cardiology.2003;100:136–142.
- ,,,,,.Predicting mortality among patients hospitalized for heart failure. Derivation and validation of a clinical model.JAMA.2003;290:2581–2587.
- ,,.Clinical relevance and management of the major electrolyte abnormalities in congestive heart failure: hyponatremia, hypokalemia, and hypomagnesemia.Am Heart J.1994;128:564–574.
- ,,, et al.The Seattle Heart Failure Model: prediction of survival in heart failure.Circulation.2006;113:1424–1433.
- ,,,,,.Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation.Circulation.1997;95:2660–2667.
- ,,, et alfor the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) Investigators.Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure.JAMA.2004;291:1963–1971.
- ,,, et al.Improvement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trial.Acute Card Care.2007;9:82–86.
- ,,, et al.Critical elements of clinical follow‐up after hospital discharge for heart failure: insights from the EVEREST trial.Eur J Heart Fail.2010;12:367–374.
- ,,, et al.Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life.Circ Cardiovasc Qual Outcomes.2011;4:389–398.
- ,,, et al.Possible vascular role of increased plasma arginine vasopressin in congestive heart failure.Int J Cardiol.2006;106:191–195.
- ,,,,,.Burden of sodium abnormalities in patients hospitalized for heart failure.Congest Heart Fail.2011;17:1–7.
- ,,, et al.Consequences of hyponatremia on cost and length of stay in heart failure patients.J Card Fail.2011;8:S72.
- ,,,.Prognostic importance of elevated jugular venous pressure and a third heart sound in patients with heart failure.N Engl J Med.2001;345:574–581.
- ,,, et alfor the NHLBI Heart Failure Clinical Research Network.Diuretic strategies in patients with acute decompensated heart failure.N Engl J Med.2011;364:797–805.
- ,,.Emerging ventricular assist devices for long‐term cardiac support.Nat Rev Cardiol.2010;7:71–76.
- ,,, et al.Chronic continuous home inotropic therapy in end‐stage heart failure.Am Heart J.2006;152:1096.e1–1096.e8.
- ,.Dobutamine for patients with end‐stage heart failure in a hospice program?J Palliat Med.2003;6:93–97.
- ,,, et al.Short‐term intravenous milrinone for acute exacerbation of chronic heart failure.JAMA.2002;287:1541–1547.
- ,,, et al.Effect of nesiritide in patients with acute decompensated heart failure.N Engl J Med.2011;365:32–43.
- ,,, et alfor the UNLOAD Trial Investigators.Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure.J Am Coll Cardiol.2007;49:675–683.
- ,,.The challenge of correcting volume overload in hospitalized patients with decompensated heart failure.J Am Coll Cardiol.2007;49:684–686.
- ,,.Demeclocycline treatment of water retention in congestive heart failure.Br Med J.1978;1:760.
- ,.Vasopressin antagonists.J Card Fail.2011;17:973–981.
- ,,, et al.A multicenter, randomized, double‐blind, placebo‐controlled study of tolvaptan monotherapy compared to furosemide and the combination of tolvaptan and furosemide in patients with heart failure and systolic dysfunction.JAMA.2004;291:1963–1971.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Short‐term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials.JAMA.2007;297:1332–1343.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial.JAMA.2007;297:1319–1331.
- ,,,,,.Vasopressin receptor antagonists for the treatment of hyponatremia: systematic review and meta‐analysis.Am J Kidney Dis.2010;56:325–337.
- ,,,,.Central pontine myelinolysis and pontine lesions after rapid correction of hyponatremia: a prospective magnetic resonance imaging study.Ann Neurol.1990;27:61–66.
- ,,, et alfor the EVEREST Investigators.Weight changes after hospitalization for worsening heart failure and subsequent re‐hospitalization and mortality in the EVEREST trial.Eur Heart J.2009;30:1666–1673.
- ,,, et alfor the CHAMPION Trial Study Group.Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial.Lancet.2011;377:658–666.
- ,,.Sympathetically mediated changes in capacitance: redistribution of the venous reservoir as a cause of decompensation.Circ Heart Fail.2011;4:669–675.
- ,,, et al.Hemodynamic factors associated with acute decompensated heart failure: part 1—insights into pathophysiology.J Card Fail.2001;17:282–291.
- The ESCAPE Investigators.Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness.JAMA.2005;294:1625–1633.
- ,,, et al.B‐type natriuretic peptide‐guided heart failure therapy: a meta‐analysis.Arch Intern Med.2010;170:507–514.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,, et al.The heart failure clinic: a consensus statement of the Heart Failure Society of America.J Card Fail.2008;14:801–815.
- ,,, et al.An automated model to identify heart failure patients at risk for 30‐day readmission or death using electronic medical record data.Med Care.2010;48:981–988.
- ,,, et al.Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial.Arch Intern Med.2007;167:1998–2005.
- ,,, et al,on behalf of the OPTIMIZE‐HF Investigators and Coordinators.Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE‐HF registry.Eur Heart J.2007;28:980–988.
- ,.Hyponatremia in acute decompensated heart failure: mechanisms, prognosis, and treatment options.Clin Cardiol.2010;33:666–671.
- ,.Prognostic importance of serum sodium concentration and its modification by converting enzyme inhibition in patients with severe chronic heart failure.Circulation.1986;73:257–267.
- ,,,,.Risk stratification of in‐hospital mortality in patients hospitalized for chronic congestive heart failure secondary to nonischemic cardiomyopathy.Cardiology.2003;100:136–142.
- ,,,,,.Predicting mortality among patients hospitalized for heart failure. Derivation and validation of a clinical model.JAMA.2003;290:2581–2587.
- ,,.Clinical relevance and management of the major electrolyte abnormalities in congestive heart failure: hyponatremia, hypokalemia, and hypomagnesemia.Am Heart J.1994;128:564–574.
- ,,, et al.The Seattle Heart Failure Model: prediction of survival in heart failure.Circulation.2006;113:1424–1433.
- ,,,,,.Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation.Circulation.1997;95:2660–2667.
- ,,, et alfor the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) Investigators.Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure.JAMA.2004;291:1963–1971.
- ,,, et al.Improvement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trial.Acute Card Care.2007;9:82–86.
- ,,, et al.Critical elements of clinical follow‐up after hospital discharge for heart failure: insights from the EVEREST trial.Eur J Heart Fail.2010;12:367–374.
- ,,, et al.Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life.Circ Cardiovasc Qual Outcomes.2011;4:389–398.
- ,,, et al.Possible vascular role of increased plasma arginine vasopressin in congestive heart failure.Int J Cardiol.2006;106:191–195.
- ,,,,,.Burden of sodium abnormalities in patients hospitalized for heart failure.Congest Heart Fail.2011;17:1–7.
- ,,, et al.Consequences of hyponatremia on cost and length of stay in heart failure patients.J Card Fail.2011;8:S72.
- ,,,.Prognostic importance of elevated jugular venous pressure and a third heart sound in patients with heart failure.N Engl J Med.2001;345:574–581.
- ,,, et alfor the NHLBI Heart Failure Clinical Research Network.Diuretic strategies in patients with acute decompensated heart failure.N Engl J Med.2011;364:797–805.
- ,,.Emerging ventricular assist devices for long‐term cardiac support.Nat Rev Cardiol.2010;7:71–76.
- ,,, et al.Chronic continuous home inotropic therapy in end‐stage heart failure.Am Heart J.2006;152:1096.e1–1096.e8.
- ,.Dobutamine for patients with end‐stage heart failure in a hospice program?J Palliat Med.2003;6:93–97.
- ,,, et al.Short‐term intravenous milrinone for acute exacerbation of chronic heart failure.JAMA.2002;287:1541–1547.
- ,,, et al.Effect of nesiritide in patients with acute decompensated heart failure.N Engl J Med.2011;365:32–43.
- ,,, et alfor the UNLOAD Trial Investigators.Ultrafiltration versus intravenous diuretics for patients hospitalized for acute decompensated heart failure.J Am Coll Cardiol.2007;49:675–683.
- ,,.The challenge of correcting volume overload in hospitalized patients with decompensated heart failure.J Am Coll Cardiol.2007;49:684–686.
- ,,.Demeclocycline treatment of water retention in congestive heart failure.Br Med J.1978;1:760.
- ,.Vasopressin antagonists.J Card Fail.2011;17:973–981.
- ,,, et al.A multicenter, randomized, double‐blind, placebo‐controlled study of tolvaptan monotherapy compared to furosemide and the combination of tolvaptan and furosemide in patients with heart failure and systolic dysfunction.JAMA.2004;291:1963–1971.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Short‐term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials.JAMA.2007;297:1332–1343.
- ,,, et alfor the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators.Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial.JAMA.2007;297:1319–1331.
- ,,,,,.Vasopressin receptor antagonists for the treatment of hyponatremia: systematic review and meta‐analysis.Am J Kidney Dis.2010;56:325–337.
- ,,,,.Central pontine myelinolysis and pontine lesions after rapid correction of hyponatremia: a prospective magnetic resonance imaging study.Ann Neurol.1990;27:61–66.
- ,,, et alfor the EVEREST Investigators.Weight changes after hospitalization for worsening heart failure and subsequent re‐hospitalization and mortality in the EVEREST trial.Eur Heart J.2009;30:1666–1673.
- ,,, et alfor the CHAMPION Trial Study Group.Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial.Lancet.2011;377:658–666.
- ,,.Sympathetically mediated changes in capacitance: redistribution of the venous reservoir as a cause of decompensation.Circ Heart Fail.2011;4:669–675.
- ,,, et al.Hemodynamic factors associated with acute decompensated heart failure: part 1—insights into pathophysiology.J Card Fail.2001;17:282–291.
- The ESCAPE Investigators.Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness.JAMA.2005;294:1625–1633.
- ,,, et al.B‐type natriuretic peptide‐guided heart failure therapy: a meta‐analysis.Arch Intern Med.2010;170:507–514.
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333:1190–1195.
- ,,, et al.The heart failure clinic: a consensus statement of the Heart Failure Society of America.J Card Fail.2008;14:801–815.
- ,,, et al.An automated model to identify heart failure patients at risk for 30‐day readmission or death using electronic medical record data.Med Care.2010;48:981–988.
Hyponatremia in Pneumonia
M.C. is an 82‐year‐old female resident of a skilled nursing facility with a past medical history of moderate dementia, hypertension, type 2 diabetes, and stage 3 chronic kidney disease (baseline creatinine, 1.4 mg/dL; creatinine clearance, 33 mL/min). Her serum sodium concentration ([Na+]) is normal (range, 136139 mEq/L) at baseline. She is brought to the emergency department with a 2‐day history of fever, productive cough, and altered mental status from baseline. She is febrile (38.7C), and has tachycardia (114 bpm), normal blood pressure (128/76 mmHg), and hypoxemia (89% on 2 L). Physical examination suggests euvolemia. Notable laboratory values include: serum [Na+], 127 mEq/L; serum potassium, 4.1 mEq/L; blood urea nitrogen, 14 mg/dL; serum creatinine, 1.5 mg/dL; glucose, 110 mg/dL; plasma osmolality, 253 mOsm/kg; urine [Na+], 92 mEq/L; and urine osmolality, 480 mOsm/kg. Chest radiography shows a right lower lobe infiltrate with prominent air‐bronchograms. The patient is started on intravenous (IV) antibiotics and normal saline (75 mL/hr), and is admitted to the medical service for management of healthcare‐associated pneumonia.
HYPONATREMIA AND PNEUMONIA
The association of hyponatremia with respiratory illness has been recognized for more than 70 years. Winkler and Crankshaw first reported low serum [Na+] in patients with pulmonary tuberculosis in 1938.1 Roughly 25 years later, reports of hyponatremia in patients with pneumonia began to surface in the literature.2 The prevalence of hyponatremia (serum [Na+] 135 mEq/L) is up to 29% of patients with pneumonia.3 Low serum [Na+] is associated with worse outcomes in such patients.36 In a large retrospective cohort (n = 7965), Zilberberg and colleagues found that pneumonia patients with hyponatremia (serum [Na+] 135 mEq/L) had statistically higher rates of intensive care unit (ICU) admission (10.0% vs 6.3%, P 0.001), mechanical ventilation (3.9% vs 2.3%, P = 0.01), longer ICU (6.3 vs 5.3 days, P = 0.07) and hospital lengths of stay (7.6 vs 7.0 days, P 0.001), and a trend toward higher hospital mortality (5.4% vs 4.0%, P = 0.1) as compared with those with normal serum [Na+].4 Hyponatremia is also associated with higher illness severity in a variety of other patient populations. The underlying nature of these associations, however, remains obscure.
The mechanism of hyponatremia in pneumonia is incompletely understood. Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is most often implicated.7 Patients with pneumonia often present with several factors that are associated with nonosmotic stimulation of antidiuretic hormone (ADH), most notably inflammatory cytokines such as interleukin‐6,8 stress, nausea, and hypoxemia.9, 10 Others implicate a reset osmostat, citing evidence for this mechanism in other infectious conditions (ie, tuberculosis and malaria).11, 12 Patients with pneumonia may also have concomitant hypovolemia due to factors such as inadequate oral intake, systemic vasodilation, and extrarenal sodium losses from vomiting and diarrhea.13 In contrast to SIADH, hypovolemia is a potent stimulus for appropriate ADH secretion through activation of the carotid baroreceptors.
CASE STUDY REVISITED
M.C.'s initial laboratory assessment would suggest SIADH. Additional testing rules out endocrinopathy (thyroid‐stimulating hormone, 2.2 mIU/L; AM serum cortisol, 16 g/dL). After 3 days of normal saline infusion (75 mL/hr) and IV vancomycin, cefepime, and levofloxacin, her serum [Na+] has dropped to 125 mEq/L. Her vital signs have normalized and she is now saturating well on ambient air. She remains euvolemic. Notable laboratory values on hospital day 4 include serum [Na+], 125 mEq/L; serum creatinine, 1.3 mg/dL; plasma osmolality, 261 mOsm/kg; urine [Na+], 103 mEq/L; urine potassium, 58 mEq/L; and urine osmolality, 518 mOsm/kg. Her provider invokes a diagnosis of SIADH and appropriately discontinues the normal saline. A fluid restriction of 500 mL/day is then instituted based on her average daily urine volume (1.7 L) and urine/plasma electrolyte ratio (electrolyte‐free water clearance = urine volume {1 [(UNa + UK)/PNa].14 After 48 hours, her serum [Na+] has improved to 128 mEq/L, yet she notes extreme thirst. A trial of increased dietary salt is offered, but she refuses, stating that her primary care physician has advised her for years to avoid salt due to her blood pressure. At this point, the nephrology service is consulted for consideration of a vasopressin receptor antagonist.
MANAGEMENT OF HYPONATREMIA IN PATIENTS WITH PNEUMONIA
As mentioned above, hyponatremia has been identified as a marker of increased disease severity in patients with pneumonia, and as such should serve as a reminder to implement the appropriate level of monitoring and vigilance so as to minimize unfavorable outcomes.
Pneumonia patients with hyponatremia often have concomitant hypovolemia. Administering isotonic fluids at admission is appropriate to treat volume depletion, as well as reduce the risk of hyponatremia developing during hospitalization.3 Nair and colleagues reported that 10.5% of the pneumonia patients with normal serum [Na+] levels at admission developed hyponatremia during their hospital stay.3 The choice of initial IV fluid treatment influenced this risk significantly: 3.9% of patients given isotonic saline developed hyponatremia compared with 14.5% of those given hypotonic fluids and 13.5% given no IV fluids. Volume status must be followed closely in pneumonia patients who are given isotonic fluids such as normal saline. If hyponatremia persists once euvolemia is achieved, isotonic fluids should be discontinued or used with caution in patients with other indications for IV fluids. Although patients with SIADH have impaired free water excretion, their ability to excrete sodium remains intact.15 Therefore, giving normal saline to euvolemic patients with SIADH can lead to free water retention and downward pressure on the serum [Na+].
Once euvolemia is established in this patient group, treatment mirrors the general management principles for SIADH. Many approaches exist to managing this condition, yet the majority of options have significant drawbacks. Although fluid restriction has been promoted for years, the level of restriction must generally be significant and ongoing to be effective. A goal intake of 800 mL/day is usually required to maintain the negative water balance necessary to treat hyponatremia and maintain a normal serum [Na+].16 Patients on such a fluid restriction experience thirst, a fundamentally strong impulse that is difficult to manage. As a result, long‐term compliance is extremely challenging.1719 Diets high in solute (sodium and/or protein) have also been used to manage SIADH. Unfortunately, there are no guidelines to follow, and such diets are generally contraindicated in patients with comorbidities such as heart failure and kidney disease. Demeclocycline has been used successfully to treat hyponatremia, but its effects are variable and it can be nephrotoxic.20 Urea induces an osmotic diuresis and concomitant free water excretion. However, its use is very limited by an unpleasant bitter taste and the lack of availability in many countries.20 Vasopressin receptor antagonists (also known as vaptans) have a US Food and Drug Administration (FDA) indication for the treatment of clinically significant hypervolemic or euvolemic hyponatremia (associated with heart failure, cirrhosis or SIADH) with either a serum [Na+] level 125 mEq/L or less marked hyponatremia that is symptomatic and resistant to fluid restriction. The use of vaptans in patients with pneumonia has not been studied specifically or extensively (unlike patients with heart failure or cirrhosis), and therefore should be used with extra caution in this group, under the supervision of a nephrologist. Additional studies are needed to evaluate long‐term clinical outcomes and cost/benefit ratios for the use of vaptans in patients with SIADH.
SUMMARY
The presence of hyponatremia in patients admitted with pneumonia should be recognized and actively managed. Isotonic fluids are generally appropriate initially to address underlying volume depletion and reduce the risk of hyponatremia developing during hospitalization. If hyponatremia persists once euvolemia is achieved, patients are traditionally then managed with fluid restriction, increased dietary solute, or demeclocycline, each of which has significant limitations. Vasopressin receptor antagonists represent a new option for managing these patients, but must be used carefully under the supervision of a nephrologist.
- ,.Chloride depletion in conditions other than Addison's disease.J Clin Invest.1938;17(1):1–6.
- ,.Severe hyponatremia associated with pneumonia.Metabolism.1962;11:1181–1186.
- ,,,.Hyponatremia in community‐acquired pneumonia.Am J Nephrol.2007;27(2):184–190.
- ,,, et al.Hyponatremia and hospital outcomes among patients with pneumonia: a retrospective cohort study.BMC Pulm Med.2008;8:16.
- ,,, et al.Epidemiology and clinical outcomes of community‐acquired pneumonia in adult patients in Asian countries: a prospective study by the Asian network for surveillance of resistant pathogens.Int J Antimicrob Agents.2008;31:107–114.
- ,.Frequency and significance of electrolyte abnormalities in pneumonia.Indian Pediatr.1992;29(6):735–740.
- ,.Pneumonia and the syndrome of inappropriate antidiuretic hormone secretion: don't pour water on the fire.Am Rev Respir Dis.1988;138:512–513.
- ,,,,.Hypothalamic‐pituitary‐adrenal axis activation and stimulation of systemic vasopressin secretion by recombinant interleukin‐6 in humans: potential implications for the syndrome of inappropriate vasopressin secretion.J Clin Endocrinol Metab.1994;79(4):934–939.
- ,,,,,.Abnormalities of sodium and H2O handling in chronic obstructive lung disease.Arch Intern Med.1982;142(7):1326–1330.
- ,,, et al.Effect of hypoxemia on sodium and water excretion in chronic obstructive lung disease.Am J Med.1985;78(1):87–94.
- ,,,,.Hyponatraemia in malaria.Ann Trop Med Parasitol.1967;61:265–279.
- ,,,.Altered water metabolism in tuberculosis: role of vasopressin.Am J Med.1990;88(4):357–364.
- ,,, et al.Laboratory abnormalities in patients with bacterial pneumonia.Chest.1997;111(3):595–600.
- ,,, et al.The urine/plasma electrolyte ratio: a predictive guide to water restriction.Am J Med Sci.2000;319(4):240–244.
- ,,,,,.Postoperative hyponatremia despite near‐isotonic saline infusion: a phenomenon of desalination.Ann Intern Med.1997;126(1):20–25.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- ,.The syndrome of inappropriate antidiuresis.N Engl J Med.2007;356:2064–2072.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5:S8–S17.
- .Current treatments and novel pharmacologic treatments for hyponatremia in congestive heart failure.Am J Cardiol.2005;95(9A):14B–23B.
- ,.The syndrome of inappropriate antidiuretic hormone: current and future management options.Eur J Endocrinol.2010;162 (suppl 1):S13–S18.
M.C. is an 82‐year‐old female resident of a skilled nursing facility with a past medical history of moderate dementia, hypertension, type 2 diabetes, and stage 3 chronic kidney disease (baseline creatinine, 1.4 mg/dL; creatinine clearance, 33 mL/min). Her serum sodium concentration ([Na+]) is normal (range, 136139 mEq/L) at baseline. She is brought to the emergency department with a 2‐day history of fever, productive cough, and altered mental status from baseline. She is febrile (38.7C), and has tachycardia (114 bpm), normal blood pressure (128/76 mmHg), and hypoxemia (89% on 2 L). Physical examination suggests euvolemia. Notable laboratory values include: serum [Na+], 127 mEq/L; serum potassium, 4.1 mEq/L; blood urea nitrogen, 14 mg/dL; serum creatinine, 1.5 mg/dL; glucose, 110 mg/dL; plasma osmolality, 253 mOsm/kg; urine [Na+], 92 mEq/L; and urine osmolality, 480 mOsm/kg. Chest radiography shows a right lower lobe infiltrate with prominent air‐bronchograms. The patient is started on intravenous (IV) antibiotics and normal saline (75 mL/hr), and is admitted to the medical service for management of healthcare‐associated pneumonia.
HYPONATREMIA AND PNEUMONIA
The association of hyponatremia with respiratory illness has been recognized for more than 70 years. Winkler and Crankshaw first reported low serum [Na+] in patients with pulmonary tuberculosis in 1938.1 Roughly 25 years later, reports of hyponatremia in patients with pneumonia began to surface in the literature.2 The prevalence of hyponatremia (serum [Na+] 135 mEq/L) is up to 29% of patients with pneumonia.3 Low serum [Na+] is associated with worse outcomes in such patients.36 In a large retrospective cohort (n = 7965), Zilberberg and colleagues found that pneumonia patients with hyponatremia (serum [Na+] 135 mEq/L) had statistically higher rates of intensive care unit (ICU) admission (10.0% vs 6.3%, P 0.001), mechanical ventilation (3.9% vs 2.3%, P = 0.01), longer ICU (6.3 vs 5.3 days, P = 0.07) and hospital lengths of stay (7.6 vs 7.0 days, P 0.001), and a trend toward higher hospital mortality (5.4% vs 4.0%, P = 0.1) as compared with those with normal serum [Na+].4 Hyponatremia is also associated with higher illness severity in a variety of other patient populations. The underlying nature of these associations, however, remains obscure.
The mechanism of hyponatremia in pneumonia is incompletely understood. Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is most often implicated.7 Patients with pneumonia often present with several factors that are associated with nonosmotic stimulation of antidiuretic hormone (ADH), most notably inflammatory cytokines such as interleukin‐6,8 stress, nausea, and hypoxemia.9, 10 Others implicate a reset osmostat, citing evidence for this mechanism in other infectious conditions (ie, tuberculosis and malaria).11, 12 Patients with pneumonia may also have concomitant hypovolemia due to factors such as inadequate oral intake, systemic vasodilation, and extrarenal sodium losses from vomiting and diarrhea.13 In contrast to SIADH, hypovolemia is a potent stimulus for appropriate ADH secretion through activation of the carotid baroreceptors.
CASE STUDY REVISITED
M.C.'s initial laboratory assessment would suggest SIADH. Additional testing rules out endocrinopathy (thyroid‐stimulating hormone, 2.2 mIU/L; AM serum cortisol, 16 g/dL). After 3 days of normal saline infusion (75 mL/hr) and IV vancomycin, cefepime, and levofloxacin, her serum [Na+] has dropped to 125 mEq/L. Her vital signs have normalized and she is now saturating well on ambient air. She remains euvolemic. Notable laboratory values on hospital day 4 include serum [Na+], 125 mEq/L; serum creatinine, 1.3 mg/dL; plasma osmolality, 261 mOsm/kg; urine [Na+], 103 mEq/L; urine potassium, 58 mEq/L; and urine osmolality, 518 mOsm/kg. Her provider invokes a diagnosis of SIADH and appropriately discontinues the normal saline. A fluid restriction of 500 mL/day is then instituted based on her average daily urine volume (1.7 L) and urine/plasma electrolyte ratio (electrolyte‐free water clearance = urine volume {1 [(UNa + UK)/PNa].14 After 48 hours, her serum [Na+] has improved to 128 mEq/L, yet she notes extreme thirst. A trial of increased dietary salt is offered, but she refuses, stating that her primary care physician has advised her for years to avoid salt due to her blood pressure. At this point, the nephrology service is consulted for consideration of a vasopressin receptor antagonist.
MANAGEMENT OF HYPONATREMIA IN PATIENTS WITH PNEUMONIA
As mentioned above, hyponatremia has been identified as a marker of increased disease severity in patients with pneumonia, and as such should serve as a reminder to implement the appropriate level of monitoring and vigilance so as to minimize unfavorable outcomes.
Pneumonia patients with hyponatremia often have concomitant hypovolemia. Administering isotonic fluids at admission is appropriate to treat volume depletion, as well as reduce the risk of hyponatremia developing during hospitalization.3 Nair and colleagues reported that 10.5% of the pneumonia patients with normal serum [Na+] levels at admission developed hyponatremia during their hospital stay.3 The choice of initial IV fluid treatment influenced this risk significantly: 3.9% of patients given isotonic saline developed hyponatremia compared with 14.5% of those given hypotonic fluids and 13.5% given no IV fluids. Volume status must be followed closely in pneumonia patients who are given isotonic fluids such as normal saline. If hyponatremia persists once euvolemia is achieved, isotonic fluids should be discontinued or used with caution in patients with other indications for IV fluids. Although patients with SIADH have impaired free water excretion, their ability to excrete sodium remains intact.15 Therefore, giving normal saline to euvolemic patients with SIADH can lead to free water retention and downward pressure on the serum [Na+].
Once euvolemia is established in this patient group, treatment mirrors the general management principles for SIADH. Many approaches exist to managing this condition, yet the majority of options have significant drawbacks. Although fluid restriction has been promoted for years, the level of restriction must generally be significant and ongoing to be effective. A goal intake of 800 mL/day is usually required to maintain the negative water balance necessary to treat hyponatremia and maintain a normal serum [Na+].16 Patients on such a fluid restriction experience thirst, a fundamentally strong impulse that is difficult to manage. As a result, long‐term compliance is extremely challenging.1719 Diets high in solute (sodium and/or protein) have also been used to manage SIADH. Unfortunately, there are no guidelines to follow, and such diets are generally contraindicated in patients with comorbidities such as heart failure and kidney disease. Demeclocycline has been used successfully to treat hyponatremia, but its effects are variable and it can be nephrotoxic.20 Urea induces an osmotic diuresis and concomitant free water excretion. However, its use is very limited by an unpleasant bitter taste and the lack of availability in many countries.20 Vasopressin receptor antagonists (also known as vaptans) have a US Food and Drug Administration (FDA) indication for the treatment of clinically significant hypervolemic or euvolemic hyponatremia (associated with heart failure, cirrhosis or SIADH) with either a serum [Na+] level 125 mEq/L or less marked hyponatremia that is symptomatic and resistant to fluid restriction. The use of vaptans in patients with pneumonia has not been studied specifically or extensively (unlike patients with heart failure or cirrhosis), and therefore should be used with extra caution in this group, under the supervision of a nephrologist. Additional studies are needed to evaluate long‐term clinical outcomes and cost/benefit ratios for the use of vaptans in patients with SIADH.
SUMMARY
The presence of hyponatremia in patients admitted with pneumonia should be recognized and actively managed. Isotonic fluids are generally appropriate initially to address underlying volume depletion and reduce the risk of hyponatremia developing during hospitalization. If hyponatremia persists once euvolemia is achieved, patients are traditionally then managed with fluid restriction, increased dietary solute, or demeclocycline, each of which has significant limitations. Vasopressin receptor antagonists represent a new option for managing these patients, but must be used carefully under the supervision of a nephrologist.
M.C. is an 82‐year‐old female resident of a skilled nursing facility with a past medical history of moderate dementia, hypertension, type 2 diabetes, and stage 3 chronic kidney disease (baseline creatinine, 1.4 mg/dL; creatinine clearance, 33 mL/min). Her serum sodium concentration ([Na+]) is normal (range, 136139 mEq/L) at baseline. She is brought to the emergency department with a 2‐day history of fever, productive cough, and altered mental status from baseline. She is febrile (38.7C), and has tachycardia (114 bpm), normal blood pressure (128/76 mmHg), and hypoxemia (89% on 2 L). Physical examination suggests euvolemia. Notable laboratory values include: serum [Na+], 127 mEq/L; serum potassium, 4.1 mEq/L; blood urea nitrogen, 14 mg/dL; serum creatinine, 1.5 mg/dL; glucose, 110 mg/dL; plasma osmolality, 253 mOsm/kg; urine [Na+], 92 mEq/L; and urine osmolality, 480 mOsm/kg. Chest radiography shows a right lower lobe infiltrate with prominent air‐bronchograms. The patient is started on intravenous (IV) antibiotics and normal saline (75 mL/hr), and is admitted to the medical service for management of healthcare‐associated pneumonia.
HYPONATREMIA AND PNEUMONIA
The association of hyponatremia with respiratory illness has been recognized for more than 70 years. Winkler and Crankshaw first reported low serum [Na+] in patients with pulmonary tuberculosis in 1938.1 Roughly 25 years later, reports of hyponatremia in patients with pneumonia began to surface in the literature.2 The prevalence of hyponatremia (serum [Na+] 135 mEq/L) is up to 29% of patients with pneumonia.3 Low serum [Na+] is associated with worse outcomes in such patients.36 In a large retrospective cohort (n = 7965), Zilberberg and colleagues found that pneumonia patients with hyponatremia (serum [Na+] 135 mEq/L) had statistically higher rates of intensive care unit (ICU) admission (10.0% vs 6.3%, P 0.001), mechanical ventilation (3.9% vs 2.3%, P = 0.01), longer ICU (6.3 vs 5.3 days, P = 0.07) and hospital lengths of stay (7.6 vs 7.0 days, P 0.001), and a trend toward higher hospital mortality (5.4% vs 4.0%, P = 0.1) as compared with those with normal serum [Na+].4 Hyponatremia is also associated with higher illness severity in a variety of other patient populations. The underlying nature of these associations, however, remains obscure.
The mechanism of hyponatremia in pneumonia is incompletely understood. Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is most often implicated.7 Patients with pneumonia often present with several factors that are associated with nonosmotic stimulation of antidiuretic hormone (ADH), most notably inflammatory cytokines such as interleukin‐6,8 stress, nausea, and hypoxemia.9, 10 Others implicate a reset osmostat, citing evidence for this mechanism in other infectious conditions (ie, tuberculosis and malaria).11, 12 Patients with pneumonia may also have concomitant hypovolemia due to factors such as inadequate oral intake, systemic vasodilation, and extrarenal sodium losses from vomiting and diarrhea.13 In contrast to SIADH, hypovolemia is a potent stimulus for appropriate ADH secretion through activation of the carotid baroreceptors.
CASE STUDY REVISITED
M.C.'s initial laboratory assessment would suggest SIADH. Additional testing rules out endocrinopathy (thyroid‐stimulating hormone, 2.2 mIU/L; AM serum cortisol, 16 g/dL). After 3 days of normal saline infusion (75 mL/hr) and IV vancomycin, cefepime, and levofloxacin, her serum [Na+] has dropped to 125 mEq/L. Her vital signs have normalized and she is now saturating well on ambient air. She remains euvolemic. Notable laboratory values on hospital day 4 include serum [Na+], 125 mEq/L; serum creatinine, 1.3 mg/dL; plasma osmolality, 261 mOsm/kg; urine [Na+], 103 mEq/L; urine potassium, 58 mEq/L; and urine osmolality, 518 mOsm/kg. Her provider invokes a diagnosis of SIADH and appropriately discontinues the normal saline. A fluid restriction of 500 mL/day is then instituted based on her average daily urine volume (1.7 L) and urine/plasma electrolyte ratio (electrolyte‐free water clearance = urine volume {1 [(UNa + UK)/PNa].14 After 48 hours, her serum [Na+] has improved to 128 mEq/L, yet she notes extreme thirst. A trial of increased dietary salt is offered, but she refuses, stating that her primary care physician has advised her for years to avoid salt due to her blood pressure. At this point, the nephrology service is consulted for consideration of a vasopressin receptor antagonist.
MANAGEMENT OF HYPONATREMIA IN PATIENTS WITH PNEUMONIA
As mentioned above, hyponatremia has been identified as a marker of increased disease severity in patients with pneumonia, and as such should serve as a reminder to implement the appropriate level of monitoring and vigilance so as to minimize unfavorable outcomes.
Pneumonia patients with hyponatremia often have concomitant hypovolemia. Administering isotonic fluids at admission is appropriate to treat volume depletion, as well as reduce the risk of hyponatremia developing during hospitalization.3 Nair and colleagues reported that 10.5% of the pneumonia patients with normal serum [Na+] levels at admission developed hyponatremia during their hospital stay.3 The choice of initial IV fluid treatment influenced this risk significantly: 3.9% of patients given isotonic saline developed hyponatremia compared with 14.5% of those given hypotonic fluids and 13.5% given no IV fluids. Volume status must be followed closely in pneumonia patients who are given isotonic fluids such as normal saline. If hyponatremia persists once euvolemia is achieved, isotonic fluids should be discontinued or used with caution in patients with other indications for IV fluids. Although patients with SIADH have impaired free water excretion, their ability to excrete sodium remains intact.15 Therefore, giving normal saline to euvolemic patients with SIADH can lead to free water retention and downward pressure on the serum [Na+].
Once euvolemia is established in this patient group, treatment mirrors the general management principles for SIADH. Many approaches exist to managing this condition, yet the majority of options have significant drawbacks. Although fluid restriction has been promoted for years, the level of restriction must generally be significant and ongoing to be effective. A goal intake of 800 mL/day is usually required to maintain the negative water balance necessary to treat hyponatremia and maintain a normal serum [Na+].16 Patients on such a fluid restriction experience thirst, a fundamentally strong impulse that is difficult to manage. As a result, long‐term compliance is extremely challenging.1719 Diets high in solute (sodium and/or protein) have also been used to manage SIADH. Unfortunately, there are no guidelines to follow, and such diets are generally contraindicated in patients with comorbidities such as heart failure and kidney disease. Demeclocycline has been used successfully to treat hyponatremia, but its effects are variable and it can be nephrotoxic.20 Urea induces an osmotic diuresis and concomitant free water excretion. However, its use is very limited by an unpleasant bitter taste and the lack of availability in many countries.20 Vasopressin receptor antagonists (also known as vaptans) have a US Food and Drug Administration (FDA) indication for the treatment of clinically significant hypervolemic or euvolemic hyponatremia (associated with heart failure, cirrhosis or SIADH) with either a serum [Na+] level 125 mEq/L or less marked hyponatremia that is symptomatic and resistant to fluid restriction. The use of vaptans in patients with pneumonia has not been studied specifically or extensively (unlike patients with heart failure or cirrhosis), and therefore should be used with extra caution in this group, under the supervision of a nephrologist. Additional studies are needed to evaluate long‐term clinical outcomes and cost/benefit ratios for the use of vaptans in patients with SIADH.
SUMMARY
The presence of hyponatremia in patients admitted with pneumonia should be recognized and actively managed. Isotonic fluids are generally appropriate initially to address underlying volume depletion and reduce the risk of hyponatremia developing during hospitalization. If hyponatremia persists once euvolemia is achieved, patients are traditionally then managed with fluid restriction, increased dietary solute, or demeclocycline, each of which has significant limitations. Vasopressin receptor antagonists represent a new option for managing these patients, but must be used carefully under the supervision of a nephrologist.
- ,.Chloride depletion in conditions other than Addison's disease.J Clin Invest.1938;17(1):1–6.
- ,.Severe hyponatremia associated with pneumonia.Metabolism.1962;11:1181–1186.
- ,,,.Hyponatremia in community‐acquired pneumonia.Am J Nephrol.2007;27(2):184–190.
- ,,, et al.Hyponatremia and hospital outcomes among patients with pneumonia: a retrospective cohort study.BMC Pulm Med.2008;8:16.
- ,,, et al.Epidemiology and clinical outcomes of community‐acquired pneumonia in adult patients in Asian countries: a prospective study by the Asian network for surveillance of resistant pathogens.Int J Antimicrob Agents.2008;31:107–114.
- ,.Frequency and significance of electrolyte abnormalities in pneumonia.Indian Pediatr.1992;29(6):735–740.
- ,.Pneumonia and the syndrome of inappropriate antidiuretic hormone secretion: don't pour water on the fire.Am Rev Respir Dis.1988;138:512–513.
- ,,,,.Hypothalamic‐pituitary‐adrenal axis activation and stimulation of systemic vasopressin secretion by recombinant interleukin‐6 in humans: potential implications for the syndrome of inappropriate vasopressin secretion.J Clin Endocrinol Metab.1994;79(4):934–939.
- ,,,,,.Abnormalities of sodium and H2O handling in chronic obstructive lung disease.Arch Intern Med.1982;142(7):1326–1330.
- ,,, et al.Effect of hypoxemia on sodium and water excretion in chronic obstructive lung disease.Am J Med.1985;78(1):87–94.
- ,,,,.Hyponatraemia in malaria.Ann Trop Med Parasitol.1967;61:265–279.
- ,,,.Altered water metabolism in tuberculosis: role of vasopressin.Am J Med.1990;88(4):357–364.
- ,,, et al.Laboratory abnormalities in patients with bacterial pneumonia.Chest.1997;111(3):595–600.
- ,,, et al.The urine/plasma electrolyte ratio: a predictive guide to water restriction.Am J Med Sci.2000;319(4):240–244.
- ,,,,,.Postoperative hyponatremia despite near‐isotonic saline infusion: a phenomenon of desalination.Ann Intern Med.1997;126(1):20–25.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- ,.The syndrome of inappropriate antidiuresis.N Engl J Med.2007;356:2064–2072.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5:S8–S17.
- .Current treatments and novel pharmacologic treatments for hyponatremia in congestive heart failure.Am J Cardiol.2005;95(9A):14B–23B.
- ,.The syndrome of inappropriate antidiuretic hormone: current and future management options.Eur J Endocrinol.2010;162 (suppl 1):S13–S18.
- ,.Chloride depletion in conditions other than Addison's disease.J Clin Invest.1938;17(1):1–6.
- ,.Severe hyponatremia associated with pneumonia.Metabolism.1962;11:1181–1186.
- ,,,.Hyponatremia in community‐acquired pneumonia.Am J Nephrol.2007;27(2):184–190.
- ,,, et al.Hyponatremia and hospital outcomes among patients with pneumonia: a retrospective cohort study.BMC Pulm Med.2008;8:16.
- ,,, et al.Epidemiology and clinical outcomes of community‐acquired pneumonia in adult patients in Asian countries: a prospective study by the Asian network for surveillance of resistant pathogens.Int J Antimicrob Agents.2008;31:107–114.
- ,.Frequency and significance of electrolyte abnormalities in pneumonia.Indian Pediatr.1992;29(6):735–740.
- ,.Pneumonia and the syndrome of inappropriate antidiuretic hormone secretion: don't pour water on the fire.Am Rev Respir Dis.1988;138:512–513.
- ,,,,.Hypothalamic‐pituitary‐adrenal axis activation and stimulation of systemic vasopressin secretion by recombinant interleukin‐6 in humans: potential implications for the syndrome of inappropriate vasopressin secretion.J Clin Endocrinol Metab.1994;79(4):934–939.
- ,,,,,.Abnormalities of sodium and H2O handling in chronic obstructive lung disease.Arch Intern Med.1982;142(7):1326–1330.
- ,,, et al.Effect of hypoxemia on sodium and water excretion in chronic obstructive lung disease.Am J Med.1985;78(1):87–94.
- ,,,,.Hyponatraemia in malaria.Ann Trop Med Parasitol.1967;61:265–279.
- ,,,.Altered water metabolism in tuberculosis: role of vasopressin.Am J Med.1990;88(4):357–364.
- ,,, et al.Laboratory abnormalities in patients with bacterial pneumonia.Chest.1997;111(3):595–600.
- ,,, et al.The urine/plasma electrolyte ratio: a predictive guide to water restriction.Am J Med Sci.2000;319(4):240–244.
- ,,,,,.Postoperative hyponatremia despite near‐isotonic saline infusion: a phenomenon of desalination.Ann Intern Med.1997;126(1):20–25.
- ,.Hyponatremia.N Engl J Med.2000;342(21):1581–1589.
- ,.The syndrome of inappropriate antidiuresis.N Engl J Med.2007;356:2064–2072.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5:S8–S17.
- .Current treatments and novel pharmacologic treatments for hyponatremia in congestive heart failure.Am J Cardiol.2005;95(9A):14B–23B.
- ,.The syndrome of inappropriate antidiuretic hormone: current and future management options.Eur J Endocrinol.2010;162 (suppl 1):S13–S18.
Hyponatremia in Cirrhosis
Cirrhosis is one of the main causes of hypervolemic hyponatremia, a dilutional form of hyponatremia that occurs when there is an increase in total body water but a relatively smaller increase in total serum sodium. Portal hypertension is the main precipitating factor in fluid retention that leads to the development of cirrhotic hyponatremia. In cirrhosis, portal hypertension is determined by 2 main factors: increased intrahepatic resistance and increased spanchnic blood flow. The increased intrahepatic resistance is due to both structural (fibrosis, conversion of low resistance fenestrated sinusoids into capillaries) and dynamic (vasoconstriction due to endothelial cell dysfunction) changes.1
The hepatic circulation normally is able to accommodate an increase in portal blood flow associated with postprandial hyperemia. The elevated intrahepatic resistance in cirrhosis results in an inability to accommodate the normal increase in portal blood flow that occurs in the postprandial hyperemia state.3 As a result, portal pressure increases during postprandial hyperemia, leading to reflex vasoconstriction, which creates a shear stress and increases splanchnic nitric oxide (NO) production.4 NO, one of the most important vasodilators in the splanchnic circulation, increases splanchnic blood flow and portal pressures. When this happens repeatedly, it leads to a progressive dilation of preexisting portosystemic vascular channels and the development of varices.5 At the same time, levels of vascular endothelial growth factor rise; this is a very important mediator for angiogenesis because it increases NO, further increasing splanchnic vasodilation.6
Progressive splanchnic vasodilation and increased blood flow into the splanchnic circulation leads to central hypovolemia, arterial underfilling, and decreased blood flow in renal afferent arterioles. Vasoconstrictor norepinephrine and antinatriuretic mechanisms are subsequently activated in an attempt to normalize renal perfusion pressures. Baroreceptor‐mediated nonosmotic release of arginine vasopressin (AVP) is triggered and renin angiotensin‐aldosterone system activity is increased, which increases sodium reabsorption and activates the stellate cells, causing fibrosis, vasoconstriction, and increased portal pressures.6, 7
AVP acts at vasopression‐1A (V1A) receptors to increase arterial vasoconstriction, and at V2 receptors in renal tubule cells for solute‐free water retention.1 The increased sodium and water reabsorption leads to fluid retention, increased central blood volume, venous return to the heart, and an increase in cardiac output to maintain arterial perfusion and create the hyperdynamic circulation that is characteristic of cirrhosis with advanced portal hypertension. Dilutional hyponatremia develops when free water retention is more pronounced than that of sodium retention.
CLINICAL FACTORS ASSOCIATED WITH CIRRHOTIC HYPONATREMIA
Diuretics lead to hyponatremia through several mechanisms.8 First, they induce a contraction of the central blood volume, leading to the nonosmotic release of AVP. In advanced cirrhosis, there is activation of the renin‐angiotensin system in addition to the nonosmotic release of AVP, leading to sodium and free water reabsorption. Diuretics block the sodium reabsorption. However, the water‐retaining effects persist, further contributing to dilutional hyponatremia.8 This cycle is made worse by low sodium intake and frequent thirst experienced by these patients.8 Other medications (eg, non‐steroidal anti‐inflammatory drugs, proton pump inhibitors, and selective serotonin reuptake inhibitors) commonly prescribed for cirrhotic patients may also contribute to the development or worsening of dilutional hyponatremia.8
Increased intrathoracic pressure in patients with tense ascites can also contribute to dilutional hyponatremia by increasing baroreceptor‐mediated release of AVP.9 Large volume paracentesis without the oncotic influence of albumin, an intervention commonly required in patients with cirrhosis and recurrent ascites, may also lead to significant increases in plasma renin activity and plasma aldosterone, which further worsen these pathophysiologic mechanisms, resulting in reduced serum sodium concentration.10 Following removal of excess peritoneal fluid, blood flow to the kidneys is initially improved, but ascitic fluid reaccumulates and the patient becomes intravascularly depleted.10
Infection is an important clinical mediator for the development of both portal hypertension as well as hyponatremia. Bacterial translocation leads to endotoxemia and increased tumor necrosis factor (TNF)‐alpha, resulting in increased splanchnic NO and splanchnic arterial vasodilatation. This process reduces cardiac output, which leads to increased AVP secretion.11, 12 Endotoxin‐mediated splanchnic vasodilatation, especially with spontaneous bacterial peritonitis (SBP), can adversely affect central blood volume status, especially in the presence of severe ascites.1 Clinicians providing care for patients with cirrhosis should be aware of these factors and closely monitor at‐risk patients for the onset or worsening of hyponatremia.1
PROGNOSTIC SIGNIFICANCE OF HYPONATREMIA IN CIRRHOSIS
Hyponatremia has several important clinical implications for patients with cirrhosis.13 Hyponatremia is associated with refractory ascites, greater fluid accumulation, the need for paracentesis, and, importantly, impaired renal function. In patients with ascites and cirrhosis, approximately 50% have some degree of hyponatremia.2 Moreover, the severity of hyponatremia associated with advanced cirrhosis correlates with the degree of cirrhosis complications, especially hyponatremia associated with hepatorenal syndrome, encephalopathy, and SBP (Table 1).2
| Serum [Na+] mEq/L | |||
|---|---|---|---|
| 130 | 131‐135 | >135 | |
| |||
| Hepatorenal syndrome | 3.45 | 1.75 | 1 (reference value) |
| Hepatic encephalopathy | 3.40 | 1.69 | 1 (reference value) |
| Gastrointestinal bleeding | 1.48 | 0.93 | 1 (reference value) |
| Spontaneous bacterial peritonitis | 2.36 | 1.44 | 1 (reference value) |
Similarly, hyponatremia is strongly associated with increasing Child‐Pugh and Model for End‐Stage Liver Disease (MELD) scores.14 In an analysis of data among candidates for liver transplantation from the Organ Procurement and Transplantation Network, the combination of MELD score and serum sodium concentration was a better predictor of death than the MELD score alone.14 In addition, the effect of hyponatremia on clinical outcomes was greater in patients with a low MELD score than those with a relatively high MELD score.. These results suggest that combining serum sodium concentrations with MELD scores to assign transplantation priority might reduce mortality among patients on the waiting list.14
Hyponatremia is also a marker for the development of overt hepatic encephalopathy in patients with cirrhosis.13 One of the proposed mechanisms for encephalopathy is low‐grade cerebral edema. This leads to the conversion of glutamate to glutamine by ammonia, which accumulates within astrocytes, causing astrocyte swelling and dysfunction. Because hyponatremia complicates the management of fluid overload, it increases the risk of developing or exacerbating hepatic encephalopathy.13
Hyponatremia is intimately involved with the development of renal failure in the patient with cirrhosis. It is an earlier and more sensitive marker of renal impairment and/or circulatory dysfunction than serum creatinine.15 It is often the precursor to the development of hepatorenal syndrome.16, 17
Hyponatremia is more common in hospitalized versus ambulatory patients with cirrhosis.1 In a study of 126 patients with cirrhosis admitted to an intensive care unit, patients with serum [Na+] 135 mEq/L had a greater frequency of ascites, illness severity scores, hepatic encephalopathy, sepsis, renal failure, and in‐hospital mortality than normonatremic patients (73.1% vs 55.9%).18 Persistent ascites and low serum sodium identified cirrhotic patients with a high mortality risk, despite low MELD scores, in a study of 507 veterans in the United States with cirrhosis.19 In a retrospective review of 127 patients, hyponatremia was predictive of the development of acute renal failure during hospitalization; among patients with hyponatremia who developed renal failure in the hospital, 72% died.20
Clinical assessment of a patient with cirrhosis who has hyponatremia can be difficult.1 These patients have too much salt and water in the wrong spaces (ie, in the peritoneal cavity and peripheral tissue). As a result, it is possible to have fluid overload with intravascular depletion. A further complication is that dilutional hyponatremia is associated with hepatorenal syndrome. Because these patients have elevated blood urea nitrogen (BUN) and creatinine, and decreased urine output and urine sodium concentration, they appear to be indistinguishable from a patient with prerenal azotemia prior to volume expansion.1 Many of these factors and concerns are illustrated in the following case we handled several years ago.
A 70‐YEAR‐OLD WOMAN WITH CIRRHOSIS
K.R. is a 70‐year‐old white woman recently discharged from the hospital following treatment of recurrent cellulitis. Her past medical history is positive for cirrhosis secondary to active alcohol use, chronic autoimmune hepatitis, and iron overload. Her hospital course was notable for tense ascites, asterixis, and a serum [Na+] of 126 mEq/L at admission. K.R. was managed with large volume paracentesis with 25% salt‐poor albumin, elevation of her lower extremities, discontinuation of diuretics, and 1 L fluid restriction. Her serum [Na+] increased to 128 mEq/L. Although her cellulitis and edema both improved, both persisted. In addition, her mental status also improved, but asterixis persisted. At this point in the hospitalization, effective management of the cellulitis was hindered by the persistent edema, and its treatment with diuretics was limited by the hyponatremia and hepatic encephalopathy.
Today, we have better treatment options for managing this patient. To effectively correct the hyponatremia and facilitate treatment of the other complications of cirrhosis, we can now initiate therapy with one of the vaptans currently available.
TREATMENT OF MILD ASYMPTOMATIC HYPERVOLEMIC HYPONATREMIA
The initial approach to treatment of patients with mild asymptomatic, hypervolemic hyponatremia consists of fluid restriction and a sodium‐restricted diet.1 Fluid restriction, however, has limited efficacy and is often not well tolerated by patients. For patients with severe or progressive hyponatremia, diuretics should be minimized or discontinued to avoid intravascular volume depletion. If patients have severe dilutional hyponatremia and tense ascites, therapeutic paracentesis with plasma expanders is safe.1
The pharmacologic approach to treating hyponatremia has advanced with the discovery of vaptans, drugs that inhibit V2 receptors in cells of the collecting ducts.21 In contrast to conventional diuretics, vaptans do not increase natriuresis. Administration of a vaptan agent for 1 to 2 weeks has been shown to significantly improve low serum sodium levels in patients with hyponatremia, and promote aquaresis without significantly altering renal or circulatory function or activity of the renin‐angiotensin‐aldosterone system. The most frequent side effect of vaptan therapy is thirst.21
Two vaptan agents are currently approved for use in the United States: conivaptan and tolvaptan. Conivaptan is administered intravenously, and is a nonselective vasopressin inhibitor, blocking both V1A and V2 receptors. The course of therapy for conivaptan is 4 days. Tolvaptan, on the other hand, selectively blocks V2 receptors, and is a once‐daily oral vaptan that can be given long‐term.21
The efficacy of tolvaptan was evaluated in the Study of Ascending Levels of Tolvaptan in Hyponatremia 1 and 2 (SALT‐1 and SALT‐2).22 In these multicenter, prospective, randomized, placebo‐controlled trials, patients with dilutional hyponatremia (serum [Na+] 135 mEq/L) associated with cirrhosis (22.4% in SALT‐1, 30.5% in SALT‐2), heart failure, or syndrome of inappropriate antidiuretic hormone (ADH) hypersecretion, and who were hospitalized and clinically stable, received tolvaptan 15 mg daily or placebo. Repeat serum sodium levels were obtained at 8 hours, 2, 3, and 4 days, and then weekly at days 11, 18, 25, and 30. The study drug was discontinued on day 30, with follow‐up serum sodium levels taken 7 days later. (In patients with persistent hyponatremia, the tolvaptan dose was adjusted to 30 mg and then 60 mg with the goal of achieving a serum [Na+] 135 mEq/L.) Increases in serum sodium concentration were seen as early as 8 hours after the first administration of tolvaptan and persisted throughout the study period. After tolvaptan was discontinued, serum sodium levels decreased to baseline within 1 week.22 Tolvaptan was well tolerated, with the most common side effects being increased thirst, dry mouth, and increased urination.22
Longer‐term administration of tolvaptan was shown to maintain a higher serum sodium concentration with an acceptable safety profile in SALTWATER, the open‐label extension of the SALT‐1 and SALT‐2 trials.23 The study included 111 patients with hyponatremia who received oral tolvaptan for a mean follow‐up of 701 days. The most common adverse effects potentially related to tolvaptan were thirst, dry mouth, polydipsia, and polyuria.22, 23 Overall, there were 9 possible and 1 probable serious adverse events, which represents an acceptable safety profile over 77,369 patient‐days of exposure. Over time, 64 patients discontinued tolvaptan, 30 due to adverse reactions or death.22 The results of SALTWATER indicated that most patients received benefit from treatment with tolvaptan, with a decreased need for fluid restriction.23
PATIENT CHARACTERISTICS FOR TOLVAPTAN
In the SALT trials, tolvaptan was administered to clinically stable patients. Based on recommendations by the US Food and Drug Administration (FDA), tolvaptan should be initiated or reinitiated in a hospital setting.1 Patients with severe neurologic symptoms due to hyponatremia should be treated with normal saline instead of tolvaptan; combination therapy with tolvaptan and normal saline should be avoided due to the potential for a too‐rapid correction of hyponatremia and the potential for central pontine myelinolysis. Saline should be discontinued and persistent hyponatremia confirmed before beginning tolvaptan therapy.1
Several additional factors should be considered before patients begin tolvaptan. First, tolvaptan increases thirst, as well as the frequency and volume of urination. Therefore, patients must be able to respond appropriately to thirst with increased water intake. Patients should not be fluid‐restricted during the first day of tolvaptan therapy; instead, they should be instructed to respond to their thirst with increased water ingestion. Because of these factors, caution should be exercised in administering tolvaptan to a confused, restrained patient. In addition, patients should have adequate toileting aids, such as a bedside urinal or commode.1
As with most new drugs, acquisition costs for tolvaptan should be considered in light of the clinical benefits of treatment outcomes. In a retrospective review, median hospital costs for patients with moderate‐to‐severe ($16,606) and mild‐to‐moderate hyponatremia ($14,266) were higher than matched patients without hyponatremia ($13,066).24 In the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trial, in which patients with severe congestive heart failure (including those with and without hyponatremia) were randomized to tolvaptan or placebo, the adjusted mean length of hospital stay for those with hyponatremia at baseline who received tolvaptan was 1.72 days shorter than those who received placebo.25 Although tolvaptan is somewhat expensive, the cost compares favorably with the daily cost of hospitalization.
SUMMARY
Portal hypertension plays a pivotal role in the development of hyponatremia in patients with cirrhosis. Reflex vasodilation in the splanchnic circulation compromises the effective central blood volume, triggering compensatory vasoconstrictor and antinatriuretic mechanisms. The net effect is greater free water accumulation than sodium retention, creating dilutional hyponatremia.
The severity of hyponatremia correlates with the severity of cirrhosis complications, such as hepatorenal syndrome, encephalopathy, SBP, and renal failure. The presence of hyponatremia is a marker for poor outcomes and shortened survival, regardless of MELD scores.
In a hospitalized, acutely ill patient with cirrhosis, such as the person in this case, therapy may involve discontinuation of diuretics, evaluation and treatment of infection, volume expansion with salt‐poor albumin, and tolvaptan for treatment of hyponatremia. Regarding tolvaptan, early morning administration is recommended. At initiation of therapy, fluid restriction should be discontinued, and off‐floor testing should be avoided. Concomitant medications should be reviewed to avoid potentially harmful interactions.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5(suppl 3):S8–S17.
- ,,,; for the CAPPS Investigators.Hyponatremia in cirrhosis: results of a patient population survey.Hepatology.2006;44:1535–1542.
- .Molecular mechanisms of increased intrahepatic resistance in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S259–S261.
- ,,.The pathophysiology of portal hypertension.Dig Dis.2005;23:6–10.
- .The molecules: mechanisms of arterial vasodilatation observed in the splanchnic and systemic circulation in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S288–S294.
- ,.Vascular endothelial dysfunction in cirrhosis.J Hepatol.2007;46:927–934.
- ,, et al.Management of cirrhosis and ascites.N Engl J Med.2004;350(16):1646–1654.
- ,,.A review of drug‐induced hyponatremia.Am J Kidney Dis.2008;52(1):144–153.
- ,,, et al.Effect of intrathoracic pressure on plasma arginine vasopressin levels.Gastroenterology.1991;101:607–617.
- ,,, et al.Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis.Gastroenterol.1988;94:1493–1502.
- ,,, et al.Endogenous cannabinoids: a new system involved in the homeostasis of arterial pressure in experimental cirrhosis in the rat.Gastroenterology.2002;122:85–93.
- ,,, et al.Endocannabinoids acting at CB1 receptors mediate the cardiac contractile dysfunction in in vivo in cirrhotic rats.Am J Physiol Heart Circ Physiol.2007;293:H1689–H1695.
- ,.Pathogenetic mechanisms of hepatic encephalopathy.Gut.2008;57:1156–1165.
- ,,, et al.Hyponatremia and mortality among patients on the liver‐transplant waiting list.N Engl J Med.2008;359:1018–1026.
- ,,, et al.Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone.Liver Transpl.2005;11:336–343.
- ,,, et al.Serum creatinine and bilirubin predict renal failure and mortality in patients with spontaneous bacterial peritonitis: a retrospective study.Liver Int.2009;29:415–419.
- ,,, et al.Natural history of patients hospitalized for management of cirrhotic ascites.Clin Gastroenterol Hepatol.2006;4:1385–1394.
- ,,, et al.Serum sodium predicts prognosis in critically ill cirrhotic patients.J Clin Gastroenterol.2010;44:220–226.
- ,,, et al.Persistent ascites and low serum sodium identify patients with cirrhosis and low MELD scores who are at high risk for early death.Hepatology.2004;40:802–810.
- ,,, et al.Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis.Clin Nephrol.2006;65:28–33.
- ,.Hyponatremia in cirrhosis: pathogenesis, clinical significance, and management.Hepatology.2008;48(3):1002–1010.
- ,,, et al.Tolvaptan, a selective oral vasopressin V2‐receptor antagonist, for hyponatremia.N Engl J Med.2006;355:2099–2112.
- ,,, et al; for the SALTWATER Investigators.Oral tolvaptan is safe and effective in chronic hyponatremia.J Am Soc Nephrol.2010;21:705–712.
- ,,, et al.Economic impact of hyponatremia in hospitalized patients: a retrospective cohort study.Postgrad Med.2009;121(2):186–191.
- ,,, et al.Effect of serum sodium concentration and tolvaptan treatment on length of hospitalization in patients with heart failure.Am J Health Syst Pharm.2011;68(4):328–333.
Cirrhosis is one of the main causes of hypervolemic hyponatremia, a dilutional form of hyponatremia that occurs when there is an increase in total body water but a relatively smaller increase in total serum sodium. Portal hypertension is the main precipitating factor in fluid retention that leads to the development of cirrhotic hyponatremia. In cirrhosis, portal hypertension is determined by 2 main factors: increased intrahepatic resistance and increased spanchnic blood flow. The increased intrahepatic resistance is due to both structural (fibrosis, conversion of low resistance fenestrated sinusoids into capillaries) and dynamic (vasoconstriction due to endothelial cell dysfunction) changes.1
The hepatic circulation normally is able to accommodate an increase in portal blood flow associated with postprandial hyperemia. The elevated intrahepatic resistance in cirrhosis results in an inability to accommodate the normal increase in portal blood flow that occurs in the postprandial hyperemia state.3 As a result, portal pressure increases during postprandial hyperemia, leading to reflex vasoconstriction, which creates a shear stress and increases splanchnic nitric oxide (NO) production.4 NO, one of the most important vasodilators in the splanchnic circulation, increases splanchnic blood flow and portal pressures. When this happens repeatedly, it leads to a progressive dilation of preexisting portosystemic vascular channels and the development of varices.5 At the same time, levels of vascular endothelial growth factor rise; this is a very important mediator for angiogenesis because it increases NO, further increasing splanchnic vasodilation.6
Progressive splanchnic vasodilation and increased blood flow into the splanchnic circulation leads to central hypovolemia, arterial underfilling, and decreased blood flow in renal afferent arterioles. Vasoconstrictor norepinephrine and antinatriuretic mechanisms are subsequently activated in an attempt to normalize renal perfusion pressures. Baroreceptor‐mediated nonosmotic release of arginine vasopressin (AVP) is triggered and renin angiotensin‐aldosterone system activity is increased, which increases sodium reabsorption and activates the stellate cells, causing fibrosis, vasoconstriction, and increased portal pressures.6, 7
AVP acts at vasopression‐1A (V1A) receptors to increase arterial vasoconstriction, and at V2 receptors in renal tubule cells for solute‐free water retention.1 The increased sodium and water reabsorption leads to fluid retention, increased central blood volume, venous return to the heart, and an increase in cardiac output to maintain arterial perfusion and create the hyperdynamic circulation that is characteristic of cirrhosis with advanced portal hypertension. Dilutional hyponatremia develops when free water retention is more pronounced than that of sodium retention.
CLINICAL FACTORS ASSOCIATED WITH CIRRHOTIC HYPONATREMIA
Diuretics lead to hyponatremia through several mechanisms.8 First, they induce a contraction of the central blood volume, leading to the nonosmotic release of AVP. In advanced cirrhosis, there is activation of the renin‐angiotensin system in addition to the nonosmotic release of AVP, leading to sodium and free water reabsorption. Diuretics block the sodium reabsorption. However, the water‐retaining effects persist, further contributing to dilutional hyponatremia.8 This cycle is made worse by low sodium intake and frequent thirst experienced by these patients.8 Other medications (eg, non‐steroidal anti‐inflammatory drugs, proton pump inhibitors, and selective serotonin reuptake inhibitors) commonly prescribed for cirrhotic patients may also contribute to the development or worsening of dilutional hyponatremia.8
Increased intrathoracic pressure in patients with tense ascites can also contribute to dilutional hyponatremia by increasing baroreceptor‐mediated release of AVP.9 Large volume paracentesis without the oncotic influence of albumin, an intervention commonly required in patients with cirrhosis and recurrent ascites, may also lead to significant increases in plasma renin activity and plasma aldosterone, which further worsen these pathophysiologic mechanisms, resulting in reduced serum sodium concentration.10 Following removal of excess peritoneal fluid, blood flow to the kidneys is initially improved, but ascitic fluid reaccumulates and the patient becomes intravascularly depleted.10
Infection is an important clinical mediator for the development of both portal hypertension as well as hyponatremia. Bacterial translocation leads to endotoxemia and increased tumor necrosis factor (TNF)‐alpha, resulting in increased splanchnic NO and splanchnic arterial vasodilatation. This process reduces cardiac output, which leads to increased AVP secretion.11, 12 Endotoxin‐mediated splanchnic vasodilatation, especially with spontaneous bacterial peritonitis (SBP), can adversely affect central blood volume status, especially in the presence of severe ascites.1 Clinicians providing care for patients with cirrhosis should be aware of these factors and closely monitor at‐risk patients for the onset or worsening of hyponatremia.1
PROGNOSTIC SIGNIFICANCE OF HYPONATREMIA IN CIRRHOSIS
Hyponatremia has several important clinical implications for patients with cirrhosis.13 Hyponatremia is associated with refractory ascites, greater fluid accumulation, the need for paracentesis, and, importantly, impaired renal function. In patients with ascites and cirrhosis, approximately 50% have some degree of hyponatremia.2 Moreover, the severity of hyponatremia associated with advanced cirrhosis correlates with the degree of cirrhosis complications, especially hyponatremia associated with hepatorenal syndrome, encephalopathy, and SBP (Table 1).2
| Serum [Na+] mEq/L | |||
|---|---|---|---|
| 130 | 131‐135 | >135 | |
| |||
| Hepatorenal syndrome | 3.45 | 1.75 | 1 (reference value) |
| Hepatic encephalopathy | 3.40 | 1.69 | 1 (reference value) |
| Gastrointestinal bleeding | 1.48 | 0.93 | 1 (reference value) |
| Spontaneous bacterial peritonitis | 2.36 | 1.44 | 1 (reference value) |
Similarly, hyponatremia is strongly associated with increasing Child‐Pugh and Model for End‐Stage Liver Disease (MELD) scores.14 In an analysis of data among candidates for liver transplantation from the Organ Procurement and Transplantation Network, the combination of MELD score and serum sodium concentration was a better predictor of death than the MELD score alone.14 In addition, the effect of hyponatremia on clinical outcomes was greater in patients with a low MELD score than those with a relatively high MELD score.. These results suggest that combining serum sodium concentrations with MELD scores to assign transplantation priority might reduce mortality among patients on the waiting list.14
Hyponatremia is also a marker for the development of overt hepatic encephalopathy in patients with cirrhosis.13 One of the proposed mechanisms for encephalopathy is low‐grade cerebral edema. This leads to the conversion of glutamate to glutamine by ammonia, which accumulates within astrocytes, causing astrocyte swelling and dysfunction. Because hyponatremia complicates the management of fluid overload, it increases the risk of developing or exacerbating hepatic encephalopathy.13
Hyponatremia is intimately involved with the development of renal failure in the patient with cirrhosis. It is an earlier and more sensitive marker of renal impairment and/or circulatory dysfunction than serum creatinine.15 It is often the precursor to the development of hepatorenal syndrome.16, 17
Hyponatremia is more common in hospitalized versus ambulatory patients with cirrhosis.1 In a study of 126 patients with cirrhosis admitted to an intensive care unit, patients with serum [Na+] 135 mEq/L had a greater frequency of ascites, illness severity scores, hepatic encephalopathy, sepsis, renal failure, and in‐hospital mortality than normonatremic patients (73.1% vs 55.9%).18 Persistent ascites and low serum sodium identified cirrhotic patients with a high mortality risk, despite low MELD scores, in a study of 507 veterans in the United States with cirrhosis.19 In a retrospective review of 127 patients, hyponatremia was predictive of the development of acute renal failure during hospitalization; among patients with hyponatremia who developed renal failure in the hospital, 72% died.20
Clinical assessment of a patient with cirrhosis who has hyponatremia can be difficult.1 These patients have too much salt and water in the wrong spaces (ie, in the peritoneal cavity and peripheral tissue). As a result, it is possible to have fluid overload with intravascular depletion. A further complication is that dilutional hyponatremia is associated with hepatorenal syndrome. Because these patients have elevated blood urea nitrogen (BUN) and creatinine, and decreased urine output and urine sodium concentration, they appear to be indistinguishable from a patient with prerenal azotemia prior to volume expansion.1 Many of these factors and concerns are illustrated in the following case we handled several years ago.
A 70‐YEAR‐OLD WOMAN WITH CIRRHOSIS
K.R. is a 70‐year‐old white woman recently discharged from the hospital following treatment of recurrent cellulitis. Her past medical history is positive for cirrhosis secondary to active alcohol use, chronic autoimmune hepatitis, and iron overload. Her hospital course was notable for tense ascites, asterixis, and a serum [Na+] of 126 mEq/L at admission. K.R. was managed with large volume paracentesis with 25% salt‐poor albumin, elevation of her lower extremities, discontinuation of diuretics, and 1 L fluid restriction. Her serum [Na+] increased to 128 mEq/L. Although her cellulitis and edema both improved, both persisted. In addition, her mental status also improved, but asterixis persisted. At this point in the hospitalization, effective management of the cellulitis was hindered by the persistent edema, and its treatment with diuretics was limited by the hyponatremia and hepatic encephalopathy.
Today, we have better treatment options for managing this patient. To effectively correct the hyponatremia and facilitate treatment of the other complications of cirrhosis, we can now initiate therapy with one of the vaptans currently available.
TREATMENT OF MILD ASYMPTOMATIC HYPERVOLEMIC HYPONATREMIA
The initial approach to treatment of patients with mild asymptomatic, hypervolemic hyponatremia consists of fluid restriction and a sodium‐restricted diet.1 Fluid restriction, however, has limited efficacy and is often not well tolerated by patients. For patients with severe or progressive hyponatremia, diuretics should be minimized or discontinued to avoid intravascular volume depletion. If patients have severe dilutional hyponatremia and tense ascites, therapeutic paracentesis with plasma expanders is safe.1
The pharmacologic approach to treating hyponatremia has advanced with the discovery of vaptans, drugs that inhibit V2 receptors in cells of the collecting ducts.21 In contrast to conventional diuretics, vaptans do not increase natriuresis. Administration of a vaptan agent for 1 to 2 weeks has been shown to significantly improve low serum sodium levels in patients with hyponatremia, and promote aquaresis without significantly altering renal or circulatory function or activity of the renin‐angiotensin‐aldosterone system. The most frequent side effect of vaptan therapy is thirst.21
Two vaptan agents are currently approved for use in the United States: conivaptan and tolvaptan. Conivaptan is administered intravenously, and is a nonselective vasopressin inhibitor, blocking both V1A and V2 receptors. The course of therapy for conivaptan is 4 days. Tolvaptan, on the other hand, selectively blocks V2 receptors, and is a once‐daily oral vaptan that can be given long‐term.21
The efficacy of tolvaptan was evaluated in the Study of Ascending Levels of Tolvaptan in Hyponatremia 1 and 2 (SALT‐1 and SALT‐2).22 In these multicenter, prospective, randomized, placebo‐controlled trials, patients with dilutional hyponatremia (serum [Na+] 135 mEq/L) associated with cirrhosis (22.4% in SALT‐1, 30.5% in SALT‐2), heart failure, or syndrome of inappropriate antidiuretic hormone (ADH) hypersecretion, and who were hospitalized and clinically stable, received tolvaptan 15 mg daily or placebo. Repeat serum sodium levels were obtained at 8 hours, 2, 3, and 4 days, and then weekly at days 11, 18, 25, and 30. The study drug was discontinued on day 30, with follow‐up serum sodium levels taken 7 days later. (In patients with persistent hyponatremia, the tolvaptan dose was adjusted to 30 mg and then 60 mg with the goal of achieving a serum [Na+] 135 mEq/L.) Increases in serum sodium concentration were seen as early as 8 hours after the first administration of tolvaptan and persisted throughout the study period. After tolvaptan was discontinued, serum sodium levels decreased to baseline within 1 week.22 Tolvaptan was well tolerated, with the most common side effects being increased thirst, dry mouth, and increased urination.22
Longer‐term administration of tolvaptan was shown to maintain a higher serum sodium concentration with an acceptable safety profile in SALTWATER, the open‐label extension of the SALT‐1 and SALT‐2 trials.23 The study included 111 patients with hyponatremia who received oral tolvaptan for a mean follow‐up of 701 days. The most common adverse effects potentially related to tolvaptan were thirst, dry mouth, polydipsia, and polyuria.22, 23 Overall, there were 9 possible and 1 probable serious adverse events, which represents an acceptable safety profile over 77,369 patient‐days of exposure. Over time, 64 patients discontinued tolvaptan, 30 due to adverse reactions or death.22 The results of SALTWATER indicated that most patients received benefit from treatment with tolvaptan, with a decreased need for fluid restriction.23
PATIENT CHARACTERISTICS FOR TOLVAPTAN
In the SALT trials, tolvaptan was administered to clinically stable patients. Based on recommendations by the US Food and Drug Administration (FDA), tolvaptan should be initiated or reinitiated in a hospital setting.1 Patients with severe neurologic symptoms due to hyponatremia should be treated with normal saline instead of tolvaptan; combination therapy with tolvaptan and normal saline should be avoided due to the potential for a too‐rapid correction of hyponatremia and the potential for central pontine myelinolysis. Saline should be discontinued and persistent hyponatremia confirmed before beginning tolvaptan therapy.1
Several additional factors should be considered before patients begin tolvaptan. First, tolvaptan increases thirst, as well as the frequency and volume of urination. Therefore, patients must be able to respond appropriately to thirst with increased water intake. Patients should not be fluid‐restricted during the first day of tolvaptan therapy; instead, they should be instructed to respond to their thirst with increased water ingestion. Because of these factors, caution should be exercised in administering tolvaptan to a confused, restrained patient. In addition, patients should have adequate toileting aids, such as a bedside urinal or commode.1
As with most new drugs, acquisition costs for tolvaptan should be considered in light of the clinical benefits of treatment outcomes. In a retrospective review, median hospital costs for patients with moderate‐to‐severe ($16,606) and mild‐to‐moderate hyponatremia ($14,266) were higher than matched patients without hyponatremia ($13,066).24 In the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trial, in which patients with severe congestive heart failure (including those with and without hyponatremia) were randomized to tolvaptan or placebo, the adjusted mean length of hospital stay for those with hyponatremia at baseline who received tolvaptan was 1.72 days shorter than those who received placebo.25 Although tolvaptan is somewhat expensive, the cost compares favorably with the daily cost of hospitalization.
SUMMARY
Portal hypertension plays a pivotal role in the development of hyponatremia in patients with cirrhosis. Reflex vasodilation in the splanchnic circulation compromises the effective central blood volume, triggering compensatory vasoconstrictor and antinatriuretic mechanisms. The net effect is greater free water accumulation than sodium retention, creating dilutional hyponatremia.
The severity of hyponatremia correlates with the severity of cirrhosis complications, such as hepatorenal syndrome, encephalopathy, SBP, and renal failure. The presence of hyponatremia is a marker for poor outcomes and shortened survival, regardless of MELD scores.
In a hospitalized, acutely ill patient with cirrhosis, such as the person in this case, therapy may involve discontinuation of diuretics, evaluation and treatment of infection, volume expansion with salt‐poor albumin, and tolvaptan for treatment of hyponatremia. Regarding tolvaptan, early morning administration is recommended. At initiation of therapy, fluid restriction should be discontinued, and off‐floor testing should be avoided. Concomitant medications should be reviewed to avoid potentially harmful interactions.
Cirrhosis is one of the main causes of hypervolemic hyponatremia, a dilutional form of hyponatremia that occurs when there is an increase in total body water but a relatively smaller increase in total serum sodium. Portal hypertension is the main precipitating factor in fluid retention that leads to the development of cirrhotic hyponatremia. In cirrhosis, portal hypertension is determined by 2 main factors: increased intrahepatic resistance and increased spanchnic blood flow. The increased intrahepatic resistance is due to both structural (fibrosis, conversion of low resistance fenestrated sinusoids into capillaries) and dynamic (vasoconstriction due to endothelial cell dysfunction) changes.1
The hepatic circulation normally is able to accommodate an increase in portal blood flow associated with postprandial hyperemia. The elevated intrahepatic resistance in cirrhosis results in an inability to accommodate the normal increase in portal blood flow that occurs in the postprandial hyperemia state.3 As a result, portal pressure increases during postprandial hyperemia, leading to reflex vasoconstriction, which creates a shear stress and increases splanchnic nitric oxide (NO) production.4 NO, one of the most important vasodilators in the splanchnic circulation, increases splanchnic blood flow and portal pressures. When this happens repeatedly, it leads to a progressive dilation of preexisting portosystemic vascular channels and the development of varices.5 At the same time, levels of vascular endothelial growth factor rise; this is a very important mediator for angiogenesis because it increases NO, further increasing splanchnic vasodilation.6
Progressive splanchnic vasodilation and increased blood flow into the splanchnic circulation leads to central hypovolemia, arterial underfilling, and decreased blood flow in renal afferent arterioles. Vasoconstrictor norepinephrine and antinatriuretic mechanisms are subsequently activated in an attempt to normalize renal perfusion pressures. Baroreceptor‐mediated nonosmotic release of arginine vasopressin (AVP) is triggered and renin angiotensin‐aldosterone system activity is increased, which increases sodium reabsorption and activates the stellate cells, causing fibrosis, vasoconstriction, and increased portal pressures.6, 7
AVP acts at vasopression‐1A (V1A) receptors to increase arterial vasoconstriction, and at V2 receptors in renal tubule cells for solute‐free water retention.1 The increased sodium and water reabsorption leads to fluid retention, increased central blood volume, venous return to the heart, and an increase in cardiac output to maintain arterial perfusion and create the hyperdynamic circulation that is characteristic of cirrhosis with advanced portal hypertension. Dilutional hyponatremia develops when free water retention is more pronounced than that of sodium retention.
CLINICAL FACTORS ASSOCIATED WITH CIRRHOTIC HYPONATREMIA
Diuretics lead to hyponatremia through several mechanisms.8 First, they induce a contraction of the central blood volume, leading to the nonosmotic release of AVP. In advanced cirrhosis, there is activation of the renin‐angiotensin system in addition to the nonosmotic release of AVP, leading to sodium and free water reabsorption. Diuretics block the sodium reabsorption. However, the water‐retaining effects persist, further contributing to dilutional hyponatremia.8 This cycle is made worse by low sodium intake and frequent thirst experienced by these patients.8 Other medications (eg, non‐steroidal anti‐inflammatory drugs, proton pump inhibitors, and selective serotonin reuptake inhibitors) commonly prescribed for cirrhotic patients may also contribute to the development or worsening of dilutional hyponatremia.8
Increased intrathoracic pressure in patients with tense ascites can also contribute to dilutional hyponatremia by increasing baroreceptor‐mediated release of AVP.9 Large volume paracentesis without the oncotic influence of albumin, an intervention commonly required in patients with cirrhosis and recurrent ascites, may also lead to significant increases in plasma renin activity and plasma aldosterone, which further worsen these pathophysiologic mechanisms, resulting in reduced serum sodium concentration.10 Following removal of excess peritoneal fluid, blood flow to the kidneys is initially improved, but ascitic fluid reaccumulates and the patient becomes intravascularly depleted.10
Infection is an important clinical mediator for the development of both portal hypertension as well as hyponatremia. Bacterial translocation leads to endotoxemia and increased tumor necrosis factor (TNF)‐alpha, resulting in increased splanchnic NO and splanchnic arterial vasodilatation. This process reduces cardiac output, which leads to increased AVP secretion.11, 12 Endotoxin‐mediated splanchnic vasodilatation, especially with spontaneous bacterial peritonitis (SBP), can adversely affect central blood volume status, especially in the presence of severe ascites.1 Clinicians providing care for patients with cirrhosis should be aware of these factors and closely monitor at‐risk patients for the onset or worsening of hyponatremia.1
PROGNOSTIC SIGNIFICANCE OF HYPONATREMIA IN CIRRHOSIS
Hyponatremia has several important clinical implications for patients with cirrhosis.13 Hyponatremia is associated with refractory ascites, greater fluid accumulation, the need for paracentesis, and, importantly, impaired renal function. In patients with ascites and cirrhosis, approximately 50% have some degree of hyponatremia.2 Moreover, the severity of hyponatremia associated with advanced cirrhosis correlates with the degree of cirrhosis complications, especially hyponatremia associated with hepatorenal syndrome, encephalopathy, and SBP (Table 1).2
| Serum [Na+] mEq/L | |||
|---|---|---|---|
| 130 | 131‐135 | >135 | |
| |||
| Hepatorenal syndrome | 3.45 | 1.75 | 1 (reference value) |
| Hepatic encephalopathy | 3.40 | 1.69 | 1 (reference value) |
| Gastrointestinal bleeding | 1.48 | 0.93 | 1 (reference value) |
| Spontaneous bacterial peritonitis | 2.36 | 1.44 | 1 (reference value) |
Similarly, hyponatremia is strongly associated with increasing Child‐Pugh and Model for End‐Stage Liver Disease (MELD) scores.14 In an analysis of data among candidates for liver transplantation from the Organ Procurement and Transplantation Network, the combination of MELD score and serum sodium concentration was a better predictor of death than the MELD score alone.14 In addition, the effect of hyponatremia on clinical outcomes was greater in patients with a low MELD score than those with a relatively high MELD score.. These results suggest that combining serum sodium concentrations with MELD scores to assign transplantation priority might reduce mortality among patients on the waiting list.14
Hyponatremia is also a marker for the development of overt hepatic encephalopathy in patients with cirrhosis.13 One of the proposed mechanisms for encephalopathy is low‐grade cerebral edema. This leads to the conversion of glutamate to glutamine by ammonia, which accumulates within astrocytes, causing astrocyte swelling and dysfunction. Because hyponatremia complicates the management of fluid overload, it increases the risk of developing or exacerbating hepatic encephalopathy.13
Hyponatremia is intimately involved with the development of renal failure in the patient with cirrhosis. It is an earlier and more sensitive marker of renal impairment and/or circulatory dysfunction than serum creatinine.15 It is often the precursor to the development of hepatorenal syndrome.16, 17
Hyponatremia is more common in hospitalized versus ambulatory patients with cirrhosis.1 In a study of 126 patients with cirrhosis admitted to an intensive care unit, patients with serum [Na+] 135 mEq/L had a greater frequency of ascites, illness severity scores, hepatic encephalopathy, sepsis, renal failure, and in‐hospital mortality than normonatremic patients (73.1% vs 55.9%).18 Persistent ascites and low serum sodium identified cirrhotic patients with a high mortality risk, despite low MELD scores, in a study of 507 veterans in the United States with cirrhosis.19 In a retrospective review of 127 patients, hyponatremia was predictive of the development of acute renal failure during hospitalization; among patients with hyponatremia who developed renal failure in the hospital, 72% died.20
Clinical assessment of a patient with cirrhosis who has hyponatremia can be difficult.1 These patients have too much salt and water in the wrong spaces (ie, in the peritoneal cavity and peripheral tissue). As a result, it is possible to have fluid overload with intravascular depletion. A further complication is that dilutional hyponatremia is associated with hepatorenal syndrome. Because these patients have elevated blood urea nitrogen (BUN) and creatinine, and decreased urine output and urine sodium concentration, they appear to be indistinguishable from a patient with prerenal azotemia prior to volume expansion.1 Many of these factors and concerns are illustrated in the following case we handled several years ago.
A 70‐YEAR‐OLD WOMAN WITH CIRRHOSIS
K.R. is a 70‐year‐old white woman recently discharged from the hospital following treatment of recurrent cellulitis. Her past medical history is positive for cirrhosis secondary to active alcohol use, chronic autoimmune hepatitis, and iron overload. Her hospital course was notable for tense ascites, asterixis, and a serum [Na+] of 126 mEq/L at admission. K.R. was managed with large volume paracentesis with 25% salt‐poor albumin, elevation of her lower extremities, discontinuation of diuretics, and 1 L fluid restriction. Her serum [Na+] increased to 128 mEq/L. Although her cellulitis and edema both improved, both persisted. In addition, her mental status also improved, but asterixis persisted. At this point in the hospitalization, effective management of the cellulitis was hindered by the persistent edema, and its treatment with diuretics was limited by the hyponatremia and hepatic encephalopathy.
Today, we have better treatment options for managing this patient. To effectively correct the hyponatremia and facilitate treatment of the other complications of cirrhosis, we can now initiate therapy with one of the vaptans currently available.
TREATMENT OF MILD ASYMPTOMATIC HYPERVOLEMIC HYPONATREMIA
The initial approach to treatment of patients with mild asymptomatic, hypervolemic hyponatremia consists of fluid restriction and a sodium‐restricted diet.1 Fluid restriction, however, has limited efficacy and is often not well tolerated by patients. For patients with severe or progressive hyponatremia, diuretics should be minimized or discontinued to avoid intravascular volume depletion. If patients have severe dilutional hyponatremia and tense ascites, therapeutic paracentesis with plasma expanders is safe.1
The pharmacologic approach to treating hyponatremia has advanced with the discovery of vaptans, drugs that inhibit V2 receptors in cells of the collecting ducts.21 In contrast to conventional diuretics, vaptans do not increase natriuresis. Administration of a vaptan agent for 1 to 2 weeks has been shown to significantly improve low serum sodium levels in patients with hyponatremia, and promote aquaresis without significantly altering renal or circulatory function or activity of the renin‐angiotensin‐aldosterone system. The most frequent side effect of vaptan therapy is thirst.21
Two vaptan agents are currently approved for use in the United States: conivaptan and tolvaptan. Conivaptan is administered intravenously, and is a nonselective vasopressin inhibitor, blocking both V1A and V2 receptors. The course of therapy for conivaptan is 4 days. Tolvaptan, on the other hand, selectively blocks V2 receptors, and is a once‐daily oral vaptan that can be given long‐term.21
The efficacy of tolvaptan was evaluated in the Study of Ascending Levels of Tolvaptan in Hyponatremia 1 and 2 (SALT‐1 and SALT‐2).22 In these multicenter, prospective, randomized, placebo‐controlled trials, patients with dilutional hyponatremia (serum [Na+] 135 mEq/L) associated with cirrhosis (22.4% in SALT‐1, 30.5% in SALT‐2), heart failure, or syndrome of inappropriate antidiuretic hormone (ADH) hypersecretion, and who were hospitalized and clinically stable, received tolvaptan 15 mg daily or placebo. Repeat serum sodium levels were obtained at 8 hours, 2, 3, and 4 days, and then weekly at days 11, 18, 25, and 30. The study drug was discontinued on day 30, with follow‐up serum sodium levels taken 7 days later. (In patients with persistent hyponatremia, the tolvaptan dose was adjusted to 30 mg and then 60 mg with the goal of achieving a serum [Na+] 135 mEq/L.) Increases in serum sodium concentration were seen as early as 8 hours after the first administration of tolvaptan and persisted throughout the study period. After tolvaptan was discontinued, serum sodium levels decreased to baseline within 1 week.22 Tolvaptan was well tolerated, with the most common side effects being increased thirst, dry mouth, and increased urination.22
Longer‐term administration of tolvaptan was shown to maintain a higher serum sodium concentration with an acceptable safety profile in SALTWATER, the open‐label extension of the SALT‐1 and SALT‐2 trials.23 The study included 111 patients with hyponatremia who received oral tolvaptan for a mean follow‐up of 701 days. The most common adverse effects potentially related to tolvaptan were thirst, dry mouth, polydipsia, and polyuria.22, 23 Overall, there were 9 possible and 1 probable serious adverse events, which represents an acceptable safety profile over 77,369 patient‐days of exposure. Over time, 64 patients discontinued tolvaptan, 30 due to adverse reactions or death.22 The results of SALTWATER indicated that most patients received benefit from treatment with tolvaptan, with a decreased need for fluid restriction.23
PATIENT CHARACTERISTICS FOR TOLVAPTAN
In the SALT trials, tolvaptan was administered to clinically stable patients. Based on recommendations by the US Food and Drug Administration (FDA), tolvaptan should be initiated or reinitiated in a hospital setting.1 Patients with severe neurologic symptoms due to hyponatremia should be treated with normal saline instead of tolvaptan; combination therapy with tolvaptan and normal saline should be avoided due to the potential for a too‐rapid correction of hyponatremia and the potential for central pontine myelinolysis. Saline should be discontinued and persistent hyponatremia confirmed before beginning tolvaptan therapy.1
Several additional factors should be considered before patients begin tolvaptan. First, tolvaptan increases thirst, as well as the frequency and volume of urination. Therefore, patients must be able to respond appropriately to thirst with increased water intake. Patients should not be fluid‐restricted during the first day of tolvaptan therapy; instead, they should be instructed to respond to their thirst with increased water ingestion. Because of these factors, caution should be exercised in administering tolvaptan to a confused, restrained patient. In addition, patients should have adequate toileting aids, such as a bedside urinal or commode.1
As with most new drugs, acquisition costs for tolvaptan should be considered in light of the clinical benefits of treatment outcomes. In a retrospective review, median hospital costs for patients with moderate‐to‐severe ($16,606) and mild‐to‐moderate hyponatremia ($14,266) were higher than matched patients without hyponatremia ($13,066).24 In the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trial, in which patients with severe congestive heart failure (including those with and without hyponatremia) were randomized to tolvaptan or placebo, the adjusted mean length of hospital stay for those with hyponatremia at baseline who received tolvaptan was 1.72 days shorter than those who received placebo.25 Although tolvaptan is somewhat expensive, the cost compares favorably with the daily cost of hospitalization.
SUMMARY
Portal hypertension plays a pivotal role in the development of hyponatremia in patients with cirrhosis. Reflex vasodilation in the splanchnic circulation compromises the effective central blood volume, triggering compensatory vasoconstrictor and antinatriuretic mechanisms. The net effect is greater free water accumulation than sodium retention, creating dilutional hyponatremia.
The severity of hyponatremia correlates with the severity of cirrhosis complications, such as hepatorenal syndrome, encephalopathy, SBP, and renal failure. The presence of hyponatremia is a marker for poor outcomes and shortened survival, regardless of MELD scores.
In a hospitalized, acutely ill patient with cirrhosis, such as the person in this case, therapy may involve discontinuation of diuretics, evaluation and treatment of infection, volume expansion with salt‐poor albumin, and tolvaptan for treatment of hyponatremia. Regarding tolvaptan, early morning administration is recommended. At initiation of therapy, fluid restriction should be discontinued, and off‐floor testing should be avoided. Concomitant medications should be reviewed to avoid potentially harmful interactions.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5(suppl 3):S8–S17.
- ,,,; for the CAPPS Investigators.Hyponatremia in cirrhosis: results of a patient population survey.Hepatology.2006;44:1535–1542.
- .Molecular mechanisms of increased intrahepatic resistance in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S259–S261.
- ,,.The pathophysiology of portal hypertension.Dig Dis.2005;23:6–10.
- .The molecules: mechanisms of arterial vasodilatation observed in the splanchnic and systemic circulation in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S288–S294.
- ,.Vascular endothelial dysfunction in cirrhosis.J Hepatol.2007;46:927–934.
- ,, et al.Management of cirrhosis and ascites.N Engl J Med.2004;350(16):1646–1654.
- ,,.A review of drug‐induced hyponatremia.Am J Kidney Dis.2008;52(1):144–153.
- ,,, et al.Effect of intrathoracic pressure on plasma arginine vasopressin levels.Gastroenterology.1991;101:607–617.
- ,,, et al.Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis.Gastroenterol.1988;94:1493–1502.
- ,,, et al.Endogenous cannabinoids: a new system involved in the homeostasis of arterial pressure in experimental cirrhosis in the rat.Gastroenterology.2002;122:85–93.
- ,,, et al.Endocannabinoids acting at CB1 receptors mediate the cardiac contractile dysfunction in in vivo in cirrhotic rats.Am J Physiol Heart Circ Physiol.2007;293:H1689–H1695.
- ,.Pathogenetic mechanisms of hepatic encephalopathy.Gut.2008;57:1156–1165.
- ,,, et al.Hyponatremia and mortality among patients on the liver‐transplant waiting list.N Engl J Med.2008;359:1018–1026.
- ,,, et al.Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone.Liver Transpl.2005;11:336–343.
- ,,, et al.Serum creatinine and bilirubin predict renal failure and mortality in patients with spontaneous bacterial peritonitis: a retrospective study.Liver Int.2009;29:415–419.
- ,,, et al.Natural history of patients hospitalized for management of cirrhotic ascites.Clin Gastroenterol Hepatol.2006;4:1385–1394.
- ,,, et al.Serum sodium predicts prognosis in critically ill cirrhotic patients.J Clin Gastroenterol.2010;44:220–226.
- ,,, et al.Persistent ascites and low serum sodium identify patients with cirrhosis and low MELD scores who are at high risk for early death.Hepatology.2004;40:802–810.
- ,,, et al.Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis.Clin Nephrol.2006;65:28–33.
- ,.Hyponatremia in cirrhosis: pathogenesis, clinical significance, and management.Hepatology.2008;48(3):1002–1010.
- ,,, et al.Tolvaptan, a selective oral vasopressin V2‐receptor antagonist, for hyponatremia.N Engl J Med.2006;355:2099–2112.
- ,,, et al; for the SALTWATER Investigators.Oral tolvaptan is safe and effective in chronic hyponatremia.J Am Soc Nephrol.2010;21:705–712.
- ,,, et al.Economic impact of hyponatremia in hospitalized patients: a retrospective cohort study.Postgrad Med.2009;121(2):186–191.
- ,,, et al.Effect of serum sodium concentration and tolvaptan treatment on length of hospitalization in patients with heart failure.Am J Health Syst Pharm.2011;68(4):328–333.
- ,.Managing hyponatremia in cirrhosis.J Hosp Med.2010;5(suppl 3):S8–S17.
- ,,,; for the CAPPS Investigators.Hyponatremia in cirrhosis: results of a patient population survey.Hepatology.2006;44:1535–1542.
- .Molecular mechanisms of increased intrahepatic resistance in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S259–S261.
- ,,.The pathophysiology of portal hypertension.Dig Dis.2005;23:6–10.
- .The molecules: mechanisms of arterial vasodilatation observed in the splanchnic and systemic circulation in portal hypertension.J Clin Gastroenterol.2007;41(suppl 3):S288–S294.
- ,.Vascular endothelial dysfunction in cirrhosis.J Hepatol.2007;46:927–934.
- ,, et al.Management of cirrhosis and ascites.N Engl J Med.2004;350(16):1646–1654.
- ,,.A review of drug‐induced hyponatremia.Am J Kidney Dis.2008;52(1):144–153.
- ,,, et al.Effect of intrathoracic pressure on plasma arginine vasopressin levels.Gastroenterology.1991;101:607–617.
- ,,, et al.Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis.Gastroenterol.1988;94:1493–1502.
- ,,, et al.Endogenous cannabinoids: a new system involved in the homeostasis of arterial pressure in experimental cirrhosis in the rat.Gastroenterology.2002;122:85–93.
- ,,, et al.Endocannabinoids acting at CB1 receptors mediate the cardiac contractile dysfunction in in vivo in cirrhotic rats.Am J Physiol Heart Circ Physiol.2007;293:H1689–H1695.
- ,.Pathogenetic mechanisms of hepatic encephalopathy.Gut.2008;57:1156–1165.
- ,,, et al.Hyponatremia and mortality among patients on the liver‐transplant waiting list.N Engl J Med.2008;359:1018–1026.
- ,,, et al.Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone.Liver Transpl.2005;11:336–343.
- ,,, et al.Serum creatinine and bilirubin predict renal failure and mortality in patients with spontaneous bacterial peritonitis: a retrospective study.Liver Int.2009;29:415–419.
- ,,, et al.Natural history of patients hospitalized for management of cirrhotic ascites.Clin Gastroenterol Hepatol.2006;4:1385–1394.
- ,,, et al.Serum sodium predicts prognosis in critically ill cirrhotic patients.J Clin Gastroenterol.2010;44:220–226.
- ,,, et al.Persistent ascites and low serum sodium identify patients with cirrhosis and low MELD scores who are at high risk for early death.Hepatology.2004;40:802–810.
- ,,, et al.Incidence and factors predictive of acute renal failure in patients with advanced liver cirrhosis.Clin Nephrol.2006;65:28–33.
- ,.Hyponatremia in cirrhosis: pathogenesis, clinical significance, and management.Hepatology.2008;48(3):1002–1010.
- ,,, et al.Tolvaptan, a selective oral vasopressin V2‐receptor antagonist, for hyponatremia.N Engl J Med.2006;355:2099–2112.
- ,,, et al; for the SALTWATER Investigators.Oral tolvaptan is safe and effective in chronic hyponatremia.J Am Soc Nephrol.2010;21:705–712.
- ,,, et al.Economic impact of hyponatremia in hospitalized patients: a retrospective cohort study.Postgrad Med.2009;121(2):186–191.
- ,,, et al.Effect of serum sodium concentration and tolvaptan treatment on length of hospitalization in patients with heart failure.Am J Health Syst Pharm.2011;68(4):328–333.