User login
CNS Events Not Immediately Fatal in Mantle Cell Lymphomas
AMSTERDAM – Although it is rare and the prognosis for patients is often poor, the presence of central nervous system involvement at the time of diagnosis of mantle cell lymphoma is not always immediately fatal, according to findings from an international study.
According to the European Mantle Cell Lymphoma Network (EMCLN) findings, the crude prevalence of CNS events was 0.9% at the time of diagnosis and 4.1% at any time. The multicenter, retrospective study found that the median time to a CNS event’s occurring was 15.2 months, with an overall survival of 3.9 months after the event was identified, but some patients were still alive 2 years later.

"We now have some better descriptors about what the expectations and outcome of patients with central nervous system involvement are," Dr. John Seymour said in an interview at the annual congress of the European Hematology Association.
Dr. Seymour, professor and chair of the hematology service at Australia’s Peter MacCallum Cancer Centre in East Melbourne, Victoria, added that even though the overall prognosis of patients who develop CNS involvement is very poor, there are some patients who do better than others.
There is "a subgroup [of patients] who are able to receive high-dose ara-c [cytarabine] or high-dose methotrexate treatment, who are young and fit enough, who do somewhat better," Dr. Seymour said. "A proportion will be alive at 2 years, so it’s not an inevitably, rapidly fatal, and ... futile situation."
Mantle cell lymphomas are a rare type of non-Hodgkin’s lymphoma (NHL), accounting for just less than 3% of all NHL cases in the United States and affecting primarily more elderly patients (Cancer 2008;113:791-8).CNS involvement is also a rare and often devastating event, but it has not previously been very well characterized. As a result, it’s not known whether CNS prophylaxis is of benefit to patients.
The aim of the EMCLN study, therefore, was to look at the problem in more detail, to determine the prevalence of CNS involvement, and to look for any clinically defining features, effect of treatment, and patient outcomes.
A retrospective database review by EMCLN members in 12 centers identified 1,396 patients with mantle cell lymphoma, of whom 1,339 had no CNS involvement. Of the 57 patients with CNS involvement, most (44) developed it at some point during the course of their follow-up.
At diagnosis of mantle cell lymphoma, the patients who developed CNS involvement had a median age of 61 years, but this ranged from 38 years to 82 years; patients were predominantly men (70%), with stage IV (91%) disease, and 28% had blastoid histology. Isolated CNS involvement occurred in 15 cases.
Prominent features were a high MIPI (Mantle Cell Lymphoma International Prognostic Index) score (61% of cases), a Ki-67 greater than 30% in 69% of patients, and increased beta2-microglobulin and lactate dehydrogenase in 77% and 75% of cases, respectively. The bone marrow and the peripheral blood were the most common extranodal sites involved, affecting two or more sites in 61% of patients.
At diagnosis of CNS involvement, patients’ neurologic symptoms included weakness, altered mental state, headache, and ocular problems such as double vision. Other symptoms – such as sensory disturbances, pain, sciatica, dizziness, vertigo, ataxia, seizure, and dysphagia – occurred but were less frequent.
CSF cytology and flow cytometry showed a high sensitivity for identifying CNS involvement, with 85% having positive cytology and 91% a positive flow cytometry result.
"Patients had a range of chemotherapies prior to developing central nervous system involvement, but receipt of these regimens was not totally protective," Dr. Seymour said. Data were not collected to enable the relative risk of CNS development with the regimens received.
Chemotherapy was the most frequent treatment strategy to allay CNS disease (67%), and some patients did appear to achieve a complete remission of the CNS disease as a result. In an exploratory analysis, these patients also tended to have improved overall survival, as did those with lower white cell counts (less than 10.9 x 109/L), and who received treatment with high-dose antimetabolites.
"In the longer term, these data will provide a foundation for us to identify predictive factors, to identify – ahead of the event – those people at increased risk," Dr. Seymour said, adding his hope that this will allow preventive steps to be taken.
Dr. Seymour had no conflicts of interest.
AMSTERDAM – Although it is rare and the prognosis for patients is often poor, the presence of central nervous system involvement at the time of diagnosis of mantle cell lymphoma is not always immediately fatal, according to findings from an international study.
According to the European Mantle Cell Lymphoma Network (EMCLN) findings, the crude prevalence of CNS events was 0.9% at the time of diagnosis and 4.1% at any time. The multicenter, retrospective study found that the median time to a CNS event’s occurring was 15.2 months, with an overall survival of 3.9 months after the event was identified, but some patients were still alive 2 years later.
"We now have some better descriptors about what the expectations and outcome of patients with central nervous system involvement are," Dr. John Seymour said in an interview at the annual congress of the European Hematology Association.
Dr. Seymour, professor and chair of the hematology service at Australia’s Peter MacCallum Cancer Centre in East Melbourne, Victoria, added that even though the overall prognosis of patients who develop CNS involvement is very poor, there are some patients who do better than others.
There is "a subgroup [of patients] who are able to receive high-dose ara-c [cytarabine] or high-dose methotrexate treatment, who are young and fit enough, who do somewhat better," Dr. Seymour said. "A proportion will be alive at 2 years, so it’s not an inevitably, rapidly fatal, and ... futile situation."
Mantle cell lymphomas are a rare type of non-Hodgkin’s lymphoma (NHL), accounting for just less than 3% of all NHL cases in the United States and affecting primarily more elderly patients (Cancer 2008;113:791-8).CNS involvement is also a rare and often devastating event, but it has not previously been very well characterized. As a result, it’s not known whether CNS prophylaxis is of benefit to patients.
The aim of the EMCLN study, therefore, was to look at the problem in more detail, to determine the prevalence of CNS involvement, and to look for any clinically defining features, effect of treatment, and patient outcomes.
A retrospective database review by EMCLN members in 12 centers identified 1,396 patients with mantle cell lymphoma, of whom 1,339 had no CNS involvement. Of the 57 patients with CNS involvement, most (44) developed it at some point during the course of their follow-up.
At diagnosis of mantle cell lymphoma, the patients who developed CNS involvement had a median age of 61 years, but this ranged from 38 years to 82 years; patients were predominantly men (70%), with stage IV (91%) disease, and 28% had blastoid histology. Isolated CNS involvement occurred in 15 cases.
Prominent features were a high MIPI (Mantle Cell Lymphoma International Prognostic Index) score (61% of cases), a Ki-67 greater than 30% in 69% of patients, and increased beta2-microglobulin and lactate dehydrogenase in 77% and 75% of cases, respectively. The bone marrow and the peripheral blood were the most common extranodal sites involved, affecting two or more sites in 61% of patients.
At diagnosis of CNS involvement, patients’ neurologic symptoms included weakness, altered mental state, headache, and ocular problems such as double vision. Other symptoms – such as sensory disturbances, pain, sciatica, dizziness, vertigo, ataxia, seizure, and dysphagia – occurred but were less frequent.
CSF cytology and flow cytometry showed a high sensitivity for identifying CNS involvement, with 85% having positive cytology and 91% a positive flow cytometry result.
"Patients had a range of chemotherapies prior to developing central nervous system involvement, but receipt of these regimens was not totally protective," Dr. Seymour said. Data were not collected to enable the relative risk of CNS development with the regimens received.
Chemotherapy was the most frequent treatment strategy to allay CNS disease (67%), and some patients did appear to achieve a complete remission of the CNS disease as a result. In an exploratory analysis, these patients also tended to have improved overall survival, as did those with lower white cell counts (less than 10.9 x 109/L), and who received treatment with high-dose antimetabolites.
"In the longer term, these data will provide a foundation for us to identify predictive factors, to identify – ahead of the event – those people at increased risk," Dr. Seymour said, adding his hope that this will allow preventive steps to be taken.
Dr. Seymour had no conflicts of interest.
AMSTERDAM – Although it is rare and the prognosis for patients is often poor, the presence of central nervous system involvement at the time of diagnosis of mantle cell lymphoma is not always immediately fatal, according to findings from an international study.
According to the European Mantle Cell Lymphoma Network (EMCLN) findings, the crude prevalence of CNS events was 0.9% at the time of diagnosis and 4.1% at any time. The multicenter, retrospective study found that the median time to a CNS event’s occurring was 15.2 months, with an overall survival of 3.9 months after the event was identified, but some patients were still alive 2 years later.
"We now have some better descriptors about what the expectations and outcome of patients with central nervous system involvement are," Dr. John Seymour said in an interview at the annual congress of the European Hematology Association.
Dr. Seymour, professor and chair of the hematology service at Australia’s Peter MacCallum Cancer Centre in East Melbourne, Victoria, added that even though the overall prognosis of patients who develop CNS involvement is very poor, there are some patients who do better than others.
There is "a subgroup [of patients] who are able to receive high-dose ara-c [cytarabine] or high-dose methotrexate treatment, who are young and fit enough, who do somewhat better," Dr. Seymour said. "A proportion will be alive at 2 years, so it’s not an inevitably, rapidly fatal, and ... futile situation."
Mantle cell lymphomas are a rare type of non-Hodgkin’s lymphoma (NHL), accounting for just less than 3% of all NHL cases in the United States and affecting primarily more elderly patients (Cancer 2008;113:791-8).CNS involvement is also a rare and often devastating event, but it has not previously been very well characterized. As a result, it’s not known whether CNS prophylaxis is of benefit to patients.
The aim of the EMCLN study, therefore, was to look at the problem in more detail, to determine the prevalence of CNS involvement, and to look for any clinically defining features, effect of treatment, and patient outcomes.
A retrospective database review by EMCLN members in 12 centers identified 1,396 patients with mantle cell lymphoma, of whom 1,339 had no CNS involvement. Of the 57 patients with CNS involvement, most (44) developed it at some point during the course of their follow-up.
At diagnosis of mantle cell lymphoma, the patients who developed CNS involvement had a median age of 61 years, but this ranged from 38 years to 82 years; patients were predominantly men (70%), with stage IV (91%) disease, and 28% had blastoid histology. Isolated CNS involvement occurred in 15 cases.
Prominent features were a high MIPI (Mantle Cell Lymphoma International Prognostic Index) score (61% of cases), a Ki-67 greater than 30% in 69% of patients, and increased beta2-microglobulin and lactate dehydrogenase in 77% and 75% of cases, respectively. The bone marrow and the peripheral blood were the most common extranodal sites involved, affecting two or more sites in 61% of patients.
At diagnosis of CNS involvement, patients’ neurologic symptoms included weakness, altered mental state, headache, and ocular problems such as double vision. Other symptoms – such as sensory disturbances, pain, sciatica, dizziness, vertigo, ataxia, seizure, and dysphagia – occurred but were less frequent.
CSF cytology and flow cytometry showed a high sensitivity for identifying CNS involvement, with 85% having positive cytology and 91% a positive flow cytometry result.
"Patients had a range of chemotherapies prior to developing central nervous system involvement, but receipt of these regimens was not totally protective," Dr. Seymour said. Data were not collected to enable the relative risk of CNS development with the regimens received.
Chemotherapy was the most frequent treatment strategy to allay CNS disease (67%), and some patients did appear to achieve a complete remission of the CNS disease as a result. In an exploratory analysis, these patients also tended to have improved overall survival, as did those with lower white cell counts (less than 10.9 x 109/L), and who received treatment with high-dose antimetabolites.
"In the longer term, these data will provide a foundation for us to identify predictive factors, to identify – ahead of the event – those people at increased risk," Dr. Seymour said, adding his hope that this will allow preventive steps to be taken.
Dr. Seymour had no conflicts of interest.
AT THE ANNUAL CONGRESS OF THE EUROPEAN HEMATOLOGY ASSOCIATION
Major Finding: Crude prevalences of CNS involvement at diagnosis and overall were 0.9% and 4.1%, respectively, with a median time to an event of 15.2 months and overall survival thereafter of 3.9 months.
Data Source: The EMCLN conducted a retrospective database review of 1,396 patients with mantle cell lymphoma in 12 centers.
Disclosures: Dr. Seymour had no conflicts of interest.
Public Reacts to Supreme Court ACA Ruling
The U.S. Supreme Court, in a 5-4 ruling, upheld the constitutionality of most provisions of the Affordable Care Act on June 28. Democrats claimed victory while Republicans resolved to repeal the law in Congress and use the justice's comments as ammunition against President Obama in the coming election. See our video for more details.
The U.S. Supreme Court, in a 5-4 ruling, upheld the constitutionality of most provisions of the Affordable Care Act on June 28. Democrats claimed victory while Republicans resolved to repeal the law in Congress and use the justice's comments as ammunition against President Obama in the coming election. See our video for more details.
The U.S. Supreme Court, in a 5-4 ruling, upheld the constitutionality of most provisions of the Affordable Care Act on June 28. Democrats claimed victory while Republicans resolved to repeal the law in Congress and use the justice's comments as ammunition against President Obama in the coming election. See our video for more details.
Statin Withdrawal After Major Surgery
Accumulating evidence suggests that perioperative treatment with 3‐hydroxy‐3‐methylglutaryl coenzyme‐A (HMG‐CoA) reductase inhibitors (or, statins) reduces the incidence of cardiovascular events during noncardiac surgery.16 This evidence has lead the European Society of Cardiology (ESC) and American College of Cardiology Foundation/American Heart Association (ACCF/AHA) to endorse the use of perioperative statins in patients already on this treatment or those at high‐risk of cardiovascular events.7, 8
However, statins are available only in oral formulation. Consequently, prolonged bowel recovery or clinical instability may interfere with use during surgery. Furthermore, many clinicians may not recognize the imperative of postoperative statin resumption, viewing them principally as lipid‐lowering entities and not as agents of perioperative benefit. Failure to resume statins postoperatively can be catastrophic, as the ensuing inflammation and thrombosis frequently culminates in myocardial infarction (MI) or death.9, 10
In this article, we review the potent anti‐inflammatory properties of statins and their role in preventing perioperative cardiac events. We outline the biochemical basis for perioperative statin benefit, summarizing the basic, clinical, and experimental evidence regarding statin withdrawal. We conclude by presenting strategies to avert postoperative statin cessation and outline a research agenda dedicated to informing this practice.
METHODS
We performed a literature search using MEDLINE via Ovid (1946present), EMBASE (1946present), Biosis (1926present), and Cochrane CENTRAL (1960present). We used Boolean logic to search for key terms including statins, 3‐hydroxy‐3‐methylglutaryl CoA reductase inhibitors, death, MI, stroke, acute coronary syndrome (ACS), and statin withdrawal or cessation. All studies published in full‐text or abstract form were included. A total of 489 articles were retrieved by this search (last updated March 15, 2012). For this narrative review, we focused on studies that examined adverse outcomes associated with statin withdrawal.
BIOCHEMICAL BASIS OF STATIN PLEIOTROPICITY
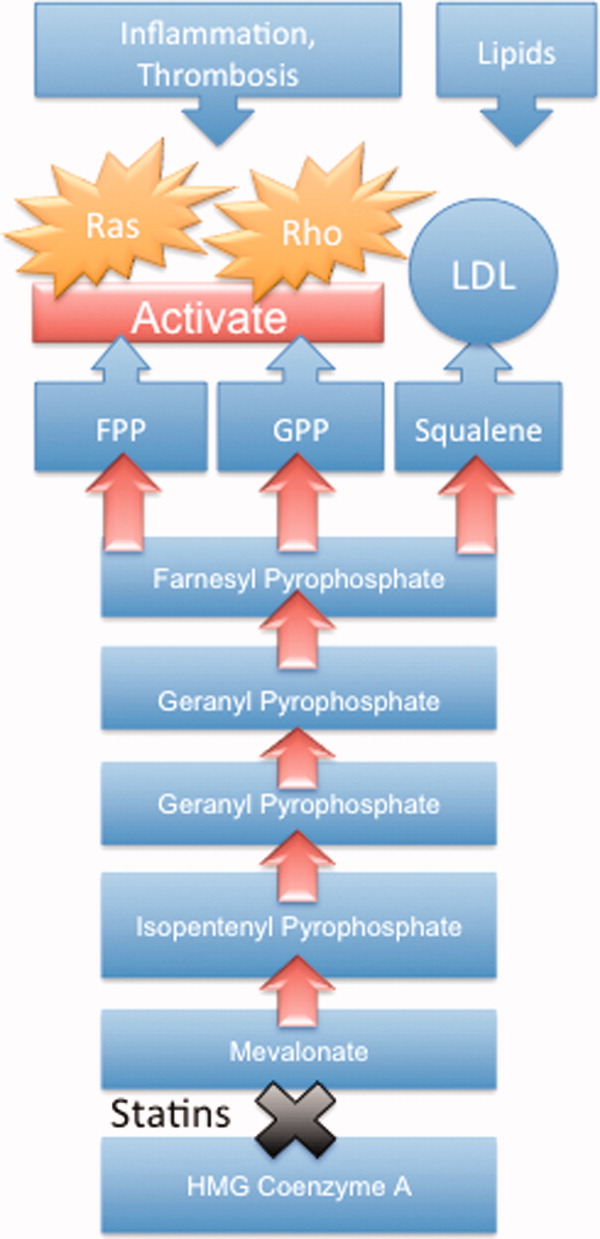
The nonlipid‐lowering or pleiotropic properties of statins are especially valuable in the perioperative setting.16, 11 Perioperative cardiac complications occur due to oxygen supply:demand mismatch, vascular inflammation, or a combination of these states. A significant perisurgical catecholamine surge produces unopposed sympathetic effects,12 increasing the risk of rupture of vulnerable coronary plaques, thrombus formation, and adverse cardiac events.13, 14 Similarly, augmented inflammatory responses and increased circulating coagulation factors further predispose to a hazardous perioperative milieu.15 Statins attenuate this vascular inflammatory response by suppressing the synthesis of mevalonate by inhibiting HMG‐CoA reductase. Suppression of mevalonate synthesis reduces the bioavailability of 2 important isoprenoid molecules: farnesyl‐pyrophosphate and geranylgeranyl‐pyrophosphate.16 Diminution of these isoprenoid intermediaries leads to reductions in the active intracellular signaling molecules Ras, Rho, and Rac, which play critical roles in vascular reactivity, endothelial function, and coagulation and inflammatory pathways.1723 The cumulative effect of these cellular changes is diminished inflammation during periods of surgical stress (Figure 1).
While the perioperative pleiotropicity of statins is of inherent clinical value, several studies have shown that these effects are lost and even reversed when statins are withdrawn.2428 During statin treatment, absence of isoprenoid intermediaries induces cytosolic accumulation of nonactivated Rho and Rac proteins. Abrupt cessation of statins activates Rho/Rac‐kinase pathways, leading to unregulated inflammation, platelet hyper‐activation, and endothelial dysfunction.24, 25, 28, 29 For instance, statin withdrawal in mice‐models leads to an overshoot activation of Rho, resulting in down‐regulation of endothelial nitric oxide production,25 activation of nicotinamide adenine dinucleotide phosphate (NAD[P]H)‐oxidase, and increased superoxide production.29 In another mouse‐model, statin withdrawal was associated with up‐regulation of key pro‐thrombotic molecules including platelet factor 4 and beta‐thromboglobulin.24 In human studies, a platelet hyper‐activation state (manifested by increased platelet P‐selectin expression and enhanced platelet aggregation) occurs after statin discontinuation.27 Furthermore, withdrawal of statins in patients with hyperlipidemia increases inflammatory markers such as C‐reactive protein and interleukin‐6.26 In the perioperative context, absence of these important anti‐inflammatory properties increases the risk of cardiac events.9, 10
EVIDENCE SUGGESTING BENEFIT FROM PERIOPERATIVE STATIN TREATMENT
Retrospective studies first suggested clinical benefit from perioperative statin treatment. In a case‐control study involving 2816 patients undergoing vascular surgery at Erasmus Medical Center, statin use was associated with substantially decreased postoperative mortality (adjusted odd ratio [OR] 0.22, 95% confidence interval [CI] 0.100.47).5 In a subsequent retrospective cohort study of 780,591 patients who underwent major noncardiac surgery, the risk of postoperative mortality was considerably lower among statin users (unadjusted OR 0.68, 95% CI 0.640.72) compared to patients who did not receive, or received delayed treatment with statins.3 A third retrospective study of 1163 vascular surgery patients found that statins prevented perioperative cardiac complications including death, MI, congestive heart failure, and ventricular tachyarrhythmias (OR 0.52, 95% CI 0.350.76).4
The benefit from statin treatment found in retrospective studies prompted the first double‐blinded, randomized controlled trial (RCT) of perioperative statin use. In 2004, Durazzo and colleagues1 randomized 100 statin‐naive patients scheduled to undergo elective aortic, femoro‐popliteal, or carotid surgery to receive either 20 mg of atorvastatin or placebo for 45 days. Vascular surgery was performed, on average, 31 days after randomization. Atorvastatin therapy reduced the incidence of death from cardiac causes, nonfatal acute MI, ischemic stroke, and unstable angina (26% in the placebo group vs 8% in the atorvastatin group; P = 0.031).1 Although the small size of the trial rendered it underpowered to show a mortality benefit, this remains the first RCT to demonstrate a protective perioperative effect of statins.
In the 2009 Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE)‐III trial, Schouten and colleagues6 randomized 497 high‐risk, statin‐naive patients undergoing vascular surgery to receive, in addition to a beta‐blocker, either fluvastatin or placebo before surgery (median of 37 days). Postoperative myocardial ischemia (hazard ratio [HR] 0.55, 95% CI 0.340.88), and combined death from cardiovascular causes or nonfatal MI (HR 0.47, 95% CI 0.240.94), occurred less frequently in the treatment group.6 In 2009, the same group published DECREASE‐IV, a multicenter, prospective, open‐label, 2 2 factorial design trial of 1066 intermediate‐risk patients, scheduled to undergo elective, noncardiac surgery. Patients were assigned to bisoprolol, fluvastatin, combination treatment, or control therapy before surgery (median of 34 days). Although those randomized to fluvastatin demonstrated lower incidence of 30‐day cardiac death and MI than control (HR 0.65, 95% CI 0.351.10), these outcomes failed to reach statistical significance as the trial was principally powered to examine the effects of perioperative beta‐blockade.30
Using this pool of data, a meta‐analysis of 15 studies (223,010 patients) found a substantial 38% reduction in the risk of mortality after cardiac surgery (1.9% vs 3.1%; P = 0.0001) and an even greater 59% reduction in the risk of mortality following vascular surgery (1.7% vs 6.1%; P = 0.0001) with perioperative statin therapy. When including noncardiac surgery, a 44% reduction in mortality was observed (2.2% vs 3.2%; P 0.01).2 We performed a similar meta‐analysis of 15 RCTs involving 2292 patients to determine whether perioperative statin treatment in statin‐naive patients, undergoing either cardiac or noncardiac surgery, improved clinical outcomes. Our analysis also found statistically significant reductions in the risk of MI associated with perioperative statin use in both cardiac and noncardiac surgery (risk reduction [RR] 0.53, 95% CI 0.380.74) and atrial fibrillation in statin‐naive patients undergoing cardiac surgery (RR 0.56, 95% CI 0.450.69).31 Taken together, a large volume of evidence supports the use of statins in surgical settings.
In view of this evidence, the ACCF/AHA perioperative guidelines for noncardiac surgery endorsed statins as an important risk‐reducing intervention in those undergoing noncardiac surgery, and recommended continued use in patients on chronic statin treatment scheduled for noncardiac surgery (Level of Evidence B, Class I; Benefits >>> Risk). Initiating statins in patients undergoing vascular surgery, with or without risk factors, was considered reasonable (Level of Evidence B, Class IIa; Benefits >> Risk).7 Current ESC perioperative guidelines in noncardiac surgery offer similar recommendations to those of ACCF/AHA, but differ by categorizing the recommendation to initiate statins in patients at high cardiovascular risk as a Class I recommendation.8
CLINICAL CONSEQUENCES OF STATIN WITHDRAWAL
Although statins provide important cardiac benefits, an important limitation to their perioperative use remains their oral‐only formulation. Thus, patients who are unable to resume oral intake may fail to resume treatment. Perioperative statin cessation has been hypothesized to lead to a statin withdrawal phenomenon. The evidence that supports the existence of this phenomenon comes from 3 distinct populations: ACS, ischemic stroke, and perioperative patients (Table 1).
| Author (ref) Year | Design | Study Population | Sample Size (N) (Total/ Continuation/Discontinuation) | Clinical Setting and Context | Timing of Statin Discontinuation | Study Outcome | Results (Withdrawal vs Continuation) |
|---|---|---|---|---|---|---|---|
| |||||||
| Heeschen et al33 2002 | Retrospective cohort | Mostly men (68%) in early 60s | 1616/379/86 | Chest pain in ACS | During or after admission | Incidence of death and nonfatal MI | OR (95% CI) |
| 2.93 (1.646.27) | |||||||
| Spencer et al32 2004 | Retrospective cohort | Mostly men (62%) in late 60s | 68,506/9001/487 | NonST‐segment elevation MI | During the first 24 hr of hospitalization | In‐hospital death | HR (95% CI) |
| 1.83 (1.582.13) | |||||||
| Daskalopoulou et al34 2008 | Retrospective cohort | 60% men in late 60s | 9939/2026/137 Non‐users 2124 (reference group) | Acute MI | Within 1 yr of the coronary event | 1‐yr all‐cause mortality | HR (95% CI) |
| 1.88 (1.133.07)* | |||||||
| Colivicchi et al36 2007 | Prospective cohort | 51% men in early 70s | 631/385/246 | Ischemic stroke | Mean 48.6 days | 1‐yr all‐cause mortality | HR (95% CI) |
| 2.78 (1.963.72) | |||||||
| Blanco et al37 2007 | RCT | 51% men in mid‐60s | 215/46/43 | Ischemic stroke | N/A | Risk of death or dependency at 3 mo | OR (95% CI) |
| 4.66 (1.4614.91) | |||||||
| Early neurologic deterioration | OR (95% CI) | ||||||
| 7.08 (2.7318.37) | |||||||
| Le Manach et al9 2007 | Quasi‐experimental (prepost) | Mostly men (89%) in late‐60s | 669/178/491 | Infra‐renal aortic surgery | Median of 4 days off statins | Postoperative troponin release, MI | OR (95% CI) |
| 2.9 (1.65.5) | |||||||
| Schouten et al10 2007 | Prospective cohort | Mostly men (75%) in mid‐60s | 298/228/70 | Aortic and lower extremity vascular surgery | Median of 3 days off statins | Postoperative troponin release | HR (95% CI) |
| 4.6 (2.29.6) | |||||||
| Combination of postoperative MI and CV death | HR (95% CI) | ||||||
| 7.5 (2.820.1) | |||||||
| Schouten et al6 2009 | RCT | Mostly men (75%) in mid‐60s | 250/189/61 | Vascular surgery (carotid, abdominal aortic, endovascular, and lower extremity arterial) | Median of 2 days off statins | Postoperative myocardial ischemia and combined death from cardiovascular causes or nonfatal MI | OR (95% CI) |
| 1.1 (0.482.52) | |||||||
Statin Withdrawal in Acute Coronary Syndromes
Several studies have demonstrated an association between statin withdrawal and heightened risk of cardiovascular events in ACS.3234 In a retrospective analysis of 1616 patients presenting with ACS, withdrawal of statins during or after admission was associated with more frequent death and nonfatal MI compared to those who continued therapy (OR 2.93, 95% CI 1.646.27).33 In another retrospective observational study of 68,606 nonST‐segment elevation MI patients, statin cessation during the first 24 hours of hospitalization was independently associated with adverse outcomes including in‐hospital death (adjusted HR 1.83; 95% CI 1.582.13), cardiac arrest, and cardiogenic shock.32 In a population‐based, cohort study in the United Kingdom, statin cessation following an acute MI was independently associated with greater all‐cause mortality at 1‐year (adjusted HR 1.88, 95% CI 1.133.07).34
The significantly increased risk of adverse outcomes associated with the interruption of statins in ACS may be moderated by vascular inflammation related to the inciting coronary event, as statin discontinuation in patients with stable cardiac conditions was not associated with increased risk of cardiovascular events in a large‐scale, double‐blind, parallel‐group study.35
Statin Withdrawal in Ischemic Stroke
Adverse events associated with statin withdrawal have also been reported in patients with cerebrovascular disease. In a prospective observational study of 631 consecutive stroke survivors, those who discontinued statins (owing to mild adverse effects or unclear reasons) experienced increased mortality during the first year after the event (adjusted HR 2.78, 95% CI 1.963.72).36 Using a controversial study design aimed at evaluating the effects of stopping oral intake (including chronic medications) during the first days of acute stroke, Blanco and colleagues37 randomized 89 stroke victims on chronic statins to either continue medications or experience statin withdrawal following admission. Statin withdrawal was independently associated with increased risk of mortality and dependency at 3 months (OR 4.66, 95% CI 1.4614.91).37
Perioperative Statin Withdrawal
In the perioperative setting, statin withdrawal has also been associated with adverse outcomes. Using a quasi‐experimental design, Le Manach et al.9 evaluated the risk of cardiac complications after infra‐renal aortic surgery when immediate, postoperative resumption of statins was adopted at their institution. The investigators compared the risk of developing MI, cardiac death, or abnormal troponin release in 491 patients who did not get early postoperative statin resumption (pre‐intervention group) to 178 patients who did. Statin withdrawal for 4 days was demonstrated to be an independent predictor of postoperative troponin leak and MI (OR 2.9, 95% CI 1.65.5). Similarly, Schouten et al.10 investigated the risk of adverse events related to interruption of long‐term statins by examining cardiac outcomes in 298 statin users undergoing major vascular surgery. Among the 70 patients who experienced statin withdrawal, an increased risk of postoperative troponin release (HR 4.6, 95% CI 2.29.6), and the composite endpoint of MI and cardiovascular death (HR 7.5, 95% CI 2.820.1), was observed compared to those who resumed treatment. Not unexpectedly, the most common reason for statin cessation was inability to take oral medications after surgery. However, even in patients who discontinued statins, the use of extended‐release fluvastatin was associated with fewer perioperative cardiac events than other statins. Furthermore, extended‐release fluvastatin was also held for 2 days following surgery (owing to inability to take the drug orally), in 25% of patients in the DECREASE‐III study. However, no impact in the rate of adverse outcomes was noted despite this interruption (OR 1.1, 95% CI 0.482.52).6 Although the authors surmised that the extended formulation of fluvastatin had provided sustained levels of statin activity despite lack of timely oral intake, it is important to note that this theory may not be generalizable to chronic statin users, as they were not enrolled in this study. Conversely, some patients may have experienced postoperative ileus for longer than 2 days, perhaps resulting in confounding or attenuation of the effect noted in the study.
CLINICAL INSIGHTS INTO FAILURE OF POSTOPERATIVE STATIN RESUMPTION
We hypothesize that failure to resume perioperative statins may occur for 4 cardinal reasons. First, resumption of an oral agent frequently proves clinically challenging when complications such as postoperative ileus, nausea, and vomiting peak. To date, no intravenous statin formulations are available, although phase‐I studies are currently underway.38 Second, it is not inconceivable that perioperative clinical instability may overshadow the resumption of statin treatment. Third, clinicians may also remain concerned regarding adverse effects of statins, a thought compounded by US Food and Drug Administration statin package inserts that specifically advocate for statins to be withheld during surgery. However, although the occurrence of elevated liver function tests and myopathy are theoretically important, the overwhelming majority of perioperative statin studies in noncardiac surgery have not found this to be a major occurrence.39 Nonetheless, a lack of uniform definitions and appropriate surveillance for adverse events are important limitations to this finding. In our recent systematic review, we were unable to provide refined estimates of these important side effects owing to differences in definition, variations in screening, and absence of standardized cutoffs used in studies.31 Finally, an important reason for failing to resume postoperative statins is that many physicians simply fail to recognize the perioperative importance of these agents.
STRATEGIES TO IMPROVE PERIOPERATIVE STATIN RESUMPTION
Using the existing evidence, we propose the following 4 clinical strategies to assist in avoiding a statin withdrawal state.
Nasogastric Administration
Utilizing a post‐pyloric nasogastric tube is a straightforward solution to provide statins in those who cannot otherwise tolerate oral intake due to nausea or emesis. Although this solution is hardly innovative, it is relevant as it forces consideration of the need to resume postoperative statins by available means. While the development of a high nasogastric output or a prolonged ileus may limit the applicability of this intervention, it is important that this option be considered as opposed to expectant watching for the clinical return of bowel function. Simvastatin, atorvastatin, rosuvastatin, and pravastatin can be crushed and delivered through this route.40
Development of Reminder Systems
Computerized reminder systems have proved important in ensuring the resumption of deep venous thrombosis prophylaxis and other preventative care compliance in hospitalized patients.41, 42 Using this process, pharmacist‐ or electronic health record‐based reminder systems could be implemented to ensure that statins are restarted when clinically feasible. Further studies are needed to test whether this approach can lead to improved outcomes.
Medication Reconciliation Prior to Hospital Discharge
Statin withdrawal highlights the pertinence of a robust, medical reconciliation process prior to the patient's departure from the hospital. In this context, the development of policies using single‐ or multi‐faceted interventions that promote cooperation between inpatient physicians, surgeons, and pharmacists with outpatient primary care providers are necessary.43
Preoperative Transition to Extended Release Statin Formulations
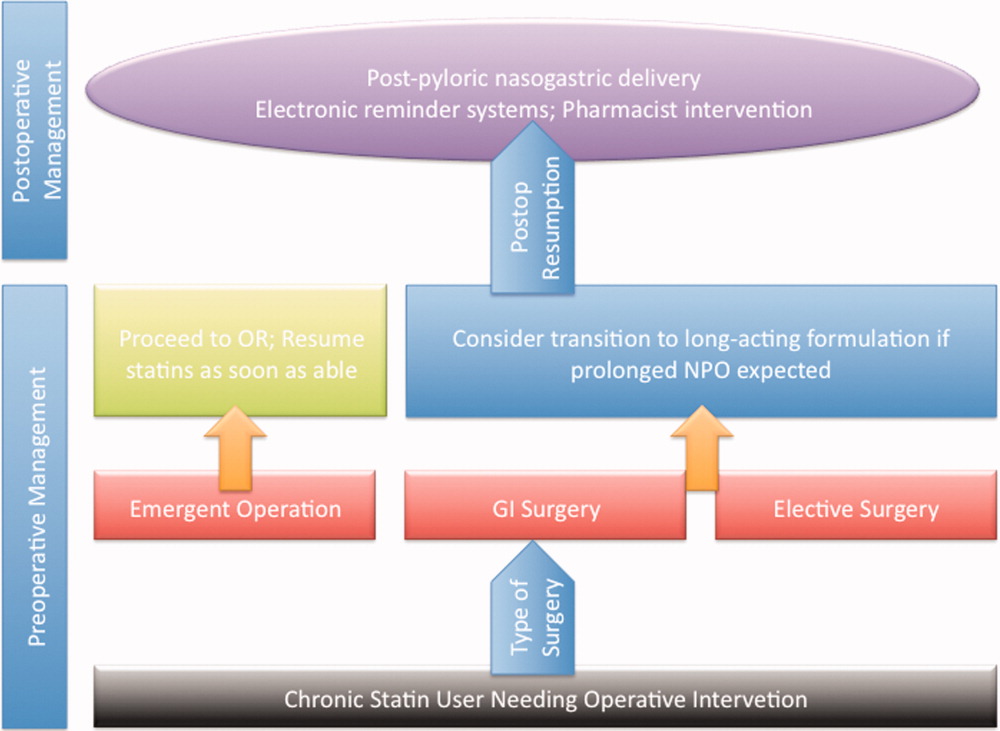
An innovative approach to minimizing statin withdrawal involves preoperative transition to an extended‐release statin formulation. This strategy may be of particular value in patients where prolonged bowel nonavailability is likely, such as those undergoing gastrointestinal surgery, or when prolonged postoperative dietary restriction (eg, NPO [nil per os]: nothing by mouth) status is expected (Figure 2).
CONCLUSIONS AND FUTURE DIRECTIONS
Sudden withdrawal of perioperative statins results in adverse clinical outcomes. Individuals engaged in the care of patients during surgery such as hospitalists, anesthesiologists, and surgeons must become more cognizant of a statin withdrawal state.
An important limitation associated with the study of perioperative statin withdrawal remains the ambiguity regarding the extent of the problem in the United States. Therefore, a logical first step could be the use of infrastructure within the National Surgical Quality Improvement Program (NSQIP) to understand the epidemiology of perioperative statin use and consequences associated with statin discontinuation.44 Mandating such quality reporting could easily be built into current NSQIP performance metrics. These data would help inform a research agenda targeting patients that experience statin withdrawal and strategies most likely to prevent it.
Note Added in Proof
Disclosure: Nothing to report.
- , , , et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg. 2004;39(5):967–975.
- , , , , , . Improved postoperative outcomes associated with preoperative statin therapy. Anesthesiology. 2006;105(6):1260–1272; quiz 1289–1290.
- , , , , . Lipid‐lowering therapy and in‐hospital mortality following major noncardiac surgery. JAMA. 2004;291(17):2092–2099.
- , , , et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS) study. J Am Coll Cardiol. 2005;45(3):336–342.
- , , , et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation. 2003;107(14):1848–1851.
- , , , et al. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med. 2009;361(10):980–989.
- , , , et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418–e499.
- , , , et al. Guidelines for pre‐operative cardiac risk assessment and perioperative cardiac management in non‐cardiac surgery. Eur Heart J. 2009;30(22):2769–2812.
- , , , et al. The impact of postoperative discontinuation or continuation of chronic statin therapy on cardiac outcome after major vascular surgery. Anesth Analg. 2007;104(6):1326–1333.
- , , , et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol. 2007;100(2):316–320.
- . Beneficial cardiovascular pleiotropic effects of statins. Circulation. 2004;109(23 suppl 1):III39–III43.
- , , , , , . Persistent endocrine stress response in patients undergoing cardiac surgery. J Endocrinol Invest. 1998;21(1):12–19.
- , , , , , . Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol. 1996;57(1):37–44.
- , , , , , . Perioperative cardiac events in patients undergoing noncardiac surgery: a review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. Can Med Assoc J. 2005;173(6):627–634.
- . Perioperative cardiac morbidity. Anesthesiology. 1990;72(1):153–184.
- , . Isoprenoid metabolism and the pleiotropic effects of statins. Curr Atheroscler Rep. 2003;5(5):372–378.
- , , , . Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97(12):1129–1135.
- , , , et al. Roles of rho‐associated kinase and oxidative stress in the pathogenesis of aortic stiffness. J Am Coll Cardiol. 2007;49(6):698–705.
- , , , et al. Inhibition of rho‐associated kinase results in suppression of neointimal formation of balloon‐injured arteries. Circulation. 2000;101(17):2030–2033.
- , , , . Reduced expression of endothelial cell markers after 1 year treatment with simvastatin and atorvastatin in patients with coronary heart disease. Atherosclerosis. 2002;162(1):179–185.
- , , , et al. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest. 2001;108(10):1429–1437.
- , , . Pleiotropic effects of statin therapy: molecular mechanisms and clinical results. Trends Mol Med. 2008;14(1):37–44.
- , , , et al. Inhibition of geranylgeranylation reduces angiotensin II‐mediated free radical production in vascular smooth muscle cells: involvement of angiotensin AT1 receptor expression and Rac1 GTPase. Mol Pharmacol. 2001;59(3):646–654.
- , , , et al. Withdrawal of statin treatment abrogates stroke protection in mice. Stroke. 2003;34(2):551–557.
- , , , et al. Suppression of endothelial nitric oxide production after withdrawal of statin treatment is mediated by negative feedback regulation of rho GTPase gene transcription. Circulation. 2000;102(25):3104–3110.
- , , , et al. Changes of plasma inflammatory markers after withdrawal of statin therapy in patients with hyperlipidemia. Clin Chim Acta. 2006;366(1–2):269–273.
- , , , et al. Platelet hyperactivity after statin treatment discontinuation. Thromb Haemost. 2003;90(3):476–482.
- , , , et al. Rebound inflammatory response during the acute phase of myocardial infarction after simvastatin withdrawal. Atherosclerosis. 2009;207(1):191–194.
- , . Effects of statins on endothelium and signaling mechanisms. Stroke. 2004;35(11 suppl 1):2708–2711.
- , , , et al. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate‐risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE‐IV). Ann Surg. 2009;249(6):921–926.
- , , , et al. Effect of perioperative statins on death, myocardial infarction, atrial fibrillation, and length of stay: a systematic review and meta‐analysis. Arch Surg. 2012;147(2):181–189.
- , , , et al. Early withdrawal of statin therapy in patients with non‐ST‐segment elevation myocardial infarction: National Registry of Myocardial Infarction. Arch Intern Med. 2004;164(19):2162–2168.
- , , , , , . Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation. 2002;105(12):1446–1452.
- , , , , , . Discontinuation of statin therapy following an acute myocardial infarction: a population‐based study. Eur Heart J. 2008;29(17):2083–2091.
- . There is no evidence for an increase in acute coronary syndromes after short‐term abrupt discontinuation of statins in stable cardiac patients. Circulation. 2004;110(16):2333–2335.
- , , , . Discontinuation of statin therapy and clinical outcome after ischemic stroke. Stroke. 2007;38(10):2652–2657.
- , , , et al. Statin treatment withdrawal in ischemic stroke: a controlled randomized study. Neurology. 2007;69(9):904–910.
- , , , et al. Intravenous rosuvastatin for acute stroke treatment: an animal study. Stroke. 2008;39(2):433–438.
- , , , et al. Safety of perioperative statin use in high‐risk patients undergoing major vascular surgery. Am J Cardiol. 2005;95(5):658–660.
- Lexi‐Comp Online™, Lexi‐Drugs™, Hudson, OH: Lexi‐Comp, Inc; December 7, 2011.
- , , , , , . A computerized reminder system to increase the use of preventive care for hospitalized patients. N Engl J Med. 2001;345(13):965–970.
- , , , et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969–977.
- , , , . Medication review and reconciliation with cooperation between pharmacist and general practitioner and the benefit for the patient: a systematic review. Br J Clin Pharmacol. January 13, 2012. doi: 10.1111/j.1365–2125.2012.04178.x.
- American College of Surgeons National Surgical Quality Improvement Program. Available at: http://www.acsnsqip.org. Accessed December 15, 2012.
Accumulating evidence suggests that perioperative treatment with 3‐hydroxy‐3‐methylglutaryl coenzyme‐A (HMG‐CoA) reductase inhibitors (or, statins) reduces the incidence of cardiovascular events during noncardiac surgery.16 This evidence has lead the European Society of Cardiology (ESC) and American College of Cardiology Foundation/American Heart Association (ACCF/AHA) to endorse the use of perioperative statins in patients already on this treatment or those at high‐risk of cardiovascular events.7, 8
However, statins are available only in oral formulation. Consequently, prolonged bowel recovery or clinical instability may interfere with use during surgery. Furthermore, many clinicians may not recognize the imperative of postoperative statin resumption, viewing them principally as lipid‐lowering entities and not as agents of perioperative benefit. Failure to resume statins postoperatively can be catastrophic, as the ensuing inflammation and thrombosis frequently culminates in myocardial infarction (MI) or death.9, 10
In this article, we review the potent anti‐inflammatory properties of statins and their role in preventing perioperative cardiac events. We outline the biochemical basis for perioperative statin benefit, summarizing the basic, clinical, and experimental evidence regarding statin withdrawal. We conclude by presenting strategies to avert postoperative statin cessation and outline a research agenda dedicated to informing this practice.
METHODS
We performed a literature search using MEDLINE via Ovid (1946present), EMBASE (1946present), Biosis (1926present), and Cochrane CENTRAL (1960present). We used Boolean logic to search for key terms including statins, 3‐hydroxy‐3‐methylglutaryl CoA reductase inhibitors, death, MI, stroke, acute coronary syndrome (ACS), and statin withdrawal or cessation. All studies published in full‐text or abstract form were included. A total of 489 articles were retrieved by this search (last updated March 15, 2012). For this narrative review, we focused on studies that examined adverse outcomes associated with statin withdrawal.
BIOCHEMICAL BASIS OF STATIN PLEIOTROPICITY
The nonlipid‐lowering or pleiotropic properties of statins are especially valuable in the perioperative setting.16, 11 Perioperative cardiac complications occur due to oxygen supply:demand mismatch, vascular inflammation, or a combination of these states. A significant perisurgical catecholamine surge produces unopposed sympathetic effects,12 increasing the risk of rupture of vulnerable coronary plaques, thrombus formation, and adverse cardiac events.13, 14 Similarly, augmented inflammatory responses and increased circulating coagulation factors further predispose to a hazardous perioperative milieu.15 Statins attenuate this vascular inflammatory response by suppressing the synthesis of mevalonate by inhibiting HMG‐CoA reductase. Suppression of mevalonate synthesis reduces the bioavailability of 2 important isoprenoid molecules: farnesyl‐pyrophosphate and geranylgeranyl‐pyrophosphate.16 Diminution of these isoprenoid intermediaries leads to reductions in the active intracellular signaling molecules Ras, Rho, and Rac, which play critical roles in vascular reactivity, endothelial function, and coagulation and inflammatory pathways.1723 The cumulative effect of these cellular changes is diminished inflammation during periods of surgical stress (Figure 1).
While the perioperative pleiotropicity of statins is of inherent clinical value, several studies have shown that these effects are lost and even reversed when statins are withdrawn.2428 During statin treatment, absence of isoprenoid intermediaries induces cytosolic accumulation of nonactivated Rho and Rac proteins. Abrupt cessation of statins activates Rho/Rac‐kinase pathways, leading to unregulated inflammation, platelet hyper‐activation, and endothelial dysfunction.24, 25, 28, 29 For instance, statin withdrawal in mice‐models leads to an overshoot activation of Rho, resulting in down‐regulation of endothelial nitric oxide production,25 activation of nicotinamide adenine dinucleotide phosphate (NAD[P]H)‐oxidase, and increased superoxide production.29 In another mouse‐model, statin withdrawal was associated with up‐regulation of key pro‐thrombotic molecules including platelet factor 4 and beta‐thromboglobulin.24 In human studies, a platelet hyper‐activation state (manifested by increased platelet P‐selectin expression and enhanced platelet aggregation) occurs after statin discontinuation.27 Furthermore, withdrawal of statins in patients with hyperlipidemia increases inflammatory markers such as C‐reactive protein and interleukin‐6.26 In the perioperative context, absence of these important anti‐inflammatory properties increases the risk of cardiac events.9, 10
EVIDENCE SUGGESTING BENEFIT FROM PERIOPERATIVE STATIN TREATMENT
Retrospective studies first suggested clinical benefit from perioperative statin treatment. In a case‐control study involving 2816 patients undergoing vascular surgery at Erasmus Medical Center, statin use was associated with substantially decreased postoperative mortality (adjusted odd ratio [OR] 0.22, 95% confidence interval [CI] 0.100.47).5 In a subsequent retrospective cohort study of 780,591 patients who underwent major noncardiac surgery, the risk of postoperative mortality was considerably lower among statin users (unadjusted OR 0.68, 95% CI 0.640.72) compared to patients who did not receive, or received delayed treatment with statins.3 A third retrospective study of 1163 vascular surgery patients found that statins prevented perioperative cardiac complications including death, MI, congestive heart failure, and ventricular tachyarrhythmias (OR 0.52, 95% CI 0.350.76).4
The benefit from statin treatment found in retrospective studies prompted the first double‐blinded, randomized controlled trial (RCT) of perioperative statin use. In 2004, Durazzo and colleagues1 randomized 100 statin‐naive patients scheduled to undergo elective aortic, femoro‐popliteal, or carotid surgery to receive either 20 mg of atorvastatin or placebo for 45 days. Vascular surgery was performed, on average, 31 days after randomization. Atorvastatin therapy reduced the incidence of death from cardiac causes, nonfatal acute MI, ischemic stroke, and unstable angina (26% in the placebo group vs 8% in the atorvastatin group; P = 0.031).1 Although the small size of the trial rendered it underpowered to show a mortality benefit, this remains the first RCT to demonstrate a protective perioperative effect of statins.
In the 2009 Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE)‐III trial, Schouten and colleagues6 randomized 497 high‐risk, statin‐naive patients undergoing vascular surgery to receive, in addition to a beta‐blocker, either fluvastatin or placebo before surgery (median of 37 days). Postoperative myocardial ischemia (hazard ratio [HR] 0.55, 95% CI 0.340.88), and combined death from cardiovascular causes or nonfatal MI (HR 0.47, 95% CI 0.240.94), occurred less frequently in the treatment group.6 In 2009, the same group published DECREASE‐IV, a multicenter, prospective, open‐label, 2 2 factorial design trial of 1066 intermediate‐risk patients, scheduled to undergo elective, noncardiac surgery. Patients were assigned to bisoprolol, fluvastatin, combination treatment, or control therapy before surgery (median of 34 days). Although those randomized to fluvastatin demonstrated lower incidence of 30‐day cardiac death and MI than control (HR 0.65, 95% CI 0.351.10), these outcomes failed to reach statistical significance as the trial was principally powered to examine the effects of perioperative beta‐blockade.30
Using this pool of data, a meta‐analysis of 15 studies (223,010 patients) found a substantial 38% reduction in the risk of mortality after cardiac surgery (1.9% vs 3.1%; P = 0.0001) and an even greater 59% reduction in the risk of mortality following vascular surgery (1.7% vs 6.1%; P = 0.0001) with perioperative statin therapy. When including noncardiac surgery, a 44% reduction in mortality was observed (2.2% vs 3.2%; P 0.01).2 We performed a similar meta‐analysis of 15 RCTs involving 2292 patients to determine whether perioperative statin treatment in statin‐naive patients, undergoing either cardiac or noncardiac surgery, improved clinical outcomes. Our analysis also found statistically significant reductions in the risk of MI associated with perioperative statin use in both cardiac and noncardiac surgery (risk reduction [RR] 0.53, 95% CI 0.380.74) and atrial fibrillation in statin‐naive patients undergoing cardiac surgery (RR 0.56, 95% CI 0.450.69).31 Taken together, a large volume of evidence supports the use of statins in surgical settings.
In view of this evidence, the ACCF/AHA perioperative guidelines for noncardiac surgery endorsed statins as an important risk‐reducing intervention in those undergoing noncardiac surgery, and recommended continued use in patients on chronic statin treatment scheduled for noncardiac surgery (Level of Evidence B, Class I; Benefits >>> Risk). Initiating statins in patients undergoing vascular surgery, with or without risk factors, was considered reasonable (Level of Evidence B, Class IIa; Benefits >> Risk).7 Current ESC perioperative guidelines in noncardiac surgery offer similar recommendations to those of ACCF/AHA, but differ by categorizing the recommendation to initiate statins in patients at high cardiovascular risk as a Class I recommendation.8
CLINICAL CONSEQUENCES OF STATIN WITHDRAWAL
Although statins provide important cardiac benefits, an important limitation to their perioperative use remains their oral‐only formulation. Thus, patients who are unable to resume oral intake may fail to resume treatment. Perioperative statin cessation has been hypothesized to lead to a statin withdrawal phenomenon. The evidence that supports the existence of this phenomenon comes from 3 distinct populations: ACS, ischemic stroke, and perioperative patients (Table 1).
| Author (ref) Year | Design | Study Population | Sample Size (N) (Total/ Continuation/Discontinuation) | Clinical Setting and Context | Timing of Statin Discontinuation | Study Outcome | Results (Withdrawal vs Continuation) |
|---|---|---|---|---|---|---|---|
| |||||||
| Heeschen et al33 2002 | Retrospective cohort | Mostly men (68%) in early 60s | 1616/379/86 | Chest pain in ACS | During or after admission | Incidence of death and nonfatal MI | OR (95% CI) |
| 2.93 (1.646.27) | |||||||
| Spencer et al32 2004 | Retrospective cohort | Mostly men (62%) in late 60s | 68,506/9001/487 | NonST‐segment elevation MI | During the first 24 hr of hospitalization | In‐hospital death | HR (95% CI) |
| 1.83 (1.582.13) | |||||||
| Daskalopoulou et al34 2008 | Retrospective cohort | 60% men in late 60s | 9939/2026/137 Non‐users 2124 (reference group) | Acute MI | Within 1 yr of the coronary event | 1‐yr all‐cause mortality | HR (95% CI) |
| 1.88 (1.133.07)* | |||||||
| Colivicchi et al36 2007 | Prospective cohort | 51% men in early 70s | 631/385/246 | Ischemic stroke | Mean 48.6 days | 1‐yr all‐cause mortality | HR (95% CI) |
| 2.78 (1.963.72) | |||||||
| Blanco et al37 2007 | RCT | 51% men in mid‐60s | 215/46/43 | Ischemic stroke | N/A | Risk of death or dependency at 3 mo | OR (95% CI) |
| 4.66 (1.4614.91) | |||||||
| Early neurologic deterioration | OR (95% CI) | ||||||
| 7.08 (2.7318.37) | |||||||
| Le Manach et al9 2007 | Quasi‐experimental (prepost) | Mostly men (89%) in late‐60s | 669/178/491 | Infra‐renal aortic surgery | Median of 4 days off statins | Postoperative troponin release, MI | OR (95% CI) |
| 2.9 (1.65.5) | |||||||
| Schouten et al10 2007 | Prospective cohort | Mostly men (75%) in mid‐60s | 298/228/70 | Aortic and lower extremity vascular surgery | Median of 3 days off statins | Postoperative troponin release | HR (95% CI) |
| 4.6 (2.29.6) | |||||||
| Combination of postoperative MI and CV death | HR (95% CI) | ||||||
| 7.5 (2.820.1) | |||||||
| Schouten et al6 2009 | RCT | Mostly men (75%) in mid‐60s | 250/189/61 | Vascular surgery (carotid, abdominal aortic, endovascular, and lower extremity arterial) | Median of 2 days off statins | Postoperative myocardial ischemia and combined death from cardiovascular causes or nonfatal MI | OR (95% CI) |
| 1.1 (0.482.52) | |||||||
Statin Withdrawal in Acute Coronary Syndromes
Several studies have demonstrated an association between statin withdrawal and heightened risk of cardiovascular events in ACS.3234 In a retrospective analysis of 1616 patients presenting with ACS, withdrawal of statins during or after admission was associated with more frequent death and nonfatal MI compared to those who continued therapy (OR 2.93, 95% CI 1.646.27).33 In another retrospective observational study of 68,606 nonST‐segment elevation MI patients, statin cessation during the first 24 hours of hospitalization was independently associated with adverse outcomes including in‐hospital death (adjusted HR 1.83; 95% CI 1.582.13), cardiac arrest, and cardiogenic shock.32 In a population‐based, cohort study in the United Kingdom, statin cessation following an acute MI was independently associated with greater all‐cause mortality at 1‐year (adjusted HR 1.88, 95% CI 1.133.07).34
The significantly increased risk of adverse outcomes associated with the interruption of statins in ACS may be moderated by vascular inflammation related to the inciting coronary event, as statin discontinuation in patients with stable cardiac conditions was not associated with increased risk of cardiovascular events in a large‐scale, double‐blind, parallel‐group study.35
Statin Withdrawal in Ischemic Stroke
Adverse events associated with statin withdrawal have also been reported in patients with cerebrovascular disease. In a prospective observational study of 631 consecutive stroke survivors, those who discontinued statins (owing to mild adverse effects or unclear reasons) experienced increased mortality during the first year after the event (adjusted HR 2.78, 95% CI 1.963.72).36 Using a controversial study design aimed at evaluating the effects of stopping oral intake (including chronic medications) during the first days of acute stroke, Blanco and colleagues37 randomized 89 stroke victims on chronic statins to either continue medications or experience statin withdrawal following admission. Statin withdrawal was independently associated with increased risk of mortality and dependency at 3 months (OR 4.66, 95% CI 1.4614.91).37
Perioperative Statin Withdrawal
In the perioperative setting, statin withdrawal has also been associated with adverse outcomes. Using a quasi‐experimental design, Le Manach et al.9 evaluated the risk of cardiac complications after infra‐renal aortic surgery when immediate, postoperative resumption of statins was adopted at their institution. The investigators compared the risk of developing MI, cardiac death, or abnormal troponin release in 491 patients who did not get early postoperative statin resumption (pre‐intervention group) to 178 patients who did. Statin withdrawal for 4 days was demonstrated to be an independent predictor of postoperative troponin leak and MI (OR 2.9, 95% CI 1.65.5). Similarly, Schouten et al.10 investigated the risk of adverse events related to interruption of long‐term statins by examining cardiac outcomes in 298 statin users undergoing major vascular surgery. Among the 70 patients who experienced statin withdrawal, an increased risk of postoperative troponin release (HR 4.6, 95% CI 2.29.6), and the composite endpoint of MI and cardiovascular death (HR 7.5, 95% CI 2.820.1), was observed compared to those who resumed treatment. Not unexpectedly, the most common reason for statin cessation was inability to take oral medications after surgery. However, even in patients who discontinued statins, the use of extended‐release fluvastatin was associated with fewer perioperative cardiac events than other statins. Furthermore, extended‐release fluvastatin was also held for 2 days following surgery (owing to inability to take the drug orally), in 25% of patients in the DECREASE‐III study. However, no impact in the rate of adverse outcomes was noted despite this interruption (OR 1.1, 95% CI 0.482.52).6 Although the authors surmised that the extended formulation of fluvastatin had provided sustained levels of statin activity despite lack of timely oral intake, it is important to note that this theory may not be generalizable to chronic statin users, as they were not enrolled in this study. Conversely, some patients may have experienced postoperative ileus for longer than 2 days, perhaps resulting in confounding or attenuation of the effect noted in the study.
CLINICAL INSIGHTS INTO FAILURE OF POSTOPERATIVE STATIN RESUMPTION
We hypothesize that failure to resume perioperative statins may occur for 4 cardinal reasons. First, resumption of an oral agent frequently proves clinically challenging when complications such as postoperative ileus, nausea, and vomiting peak. To date, no intravenous statin formulations are available, although phase‐I studies are currently underway.38 Second, it is not inconceivable that perioperative clinical instability may overshadow the resumption of statin treatment. Third, clinicians may also remain concerned regarding adverse effects of statins, a thought compounded by US Food and Drug Administration statin package inserts that specifically advocate for statins to be withheld during surgery. However, although the occurrence of elevated liver function tests and myopathy are theoretically important, the overwhelming majority of perioperative statin studies in noncardiac surgery have not found this to be a major occurrence.39 Nonetheless, a lack of uniform definitions and appropriate surveillance for adverse events are important limitations to this finding. In our recent systematic review, we were unable to provide refined estimates of these important side effects owing to differences in definition, variations in screening, and absence of standardized cutoffs used in studies.31 Finally, an important reason for failing to resume postoperative statins is that many physicians simply fail to recognize the perioperative importance of these agents.
STRATEGIES TO IMPROVE PERIOPERATIVE STATIN RESUMPTION
Using the existing evidence, we propose the following 4 clinical strategies to assist in avoiding a statin withdrawal state.
Nasogastric Administration
Utilizing a post‐pyloric nasogastric tube is a straightforward solution to provide statins in those who cannot otherwise tolerate oral intake due to nausea or emesis. Although this solution is hardly innovative, it is relevant as it forces consideration of the need to resume postoperative statins by available means. While the development of a high nasogastric output or a prolonged ileus may limit the applicability of this intervention, it is important that this option be considered as opposed to expectant watching for the clinical return of bowel function. Simvastatin, atorvastatin, rosuvastatin, and pravastatin can be crushed and delivered through this route.40
Development of Reminder Systems
Computerized reminder systems have proved important in ensuring the resumption of deep venous thrombosis prophylaxis and other preventative care compliance in hospitalized patients.41, 42 Using this process, pharmacist‐ or electronic health record‐based reminder systems could be implemented to ensure that statins are restarted when clinically feasible. Further studies are needed to test whether this approach can lead to improved outcomes.
Medication Reconciliation Prior to Hospital Discharge
Statin withdrawal highlights the pertinence of a robust, medical reconciliation process prior to the patient's departure from the hospital. In this context, the development of policies using single‐ or multi‐faceted interventions that promote cooperation between inpatient physicians, surgeons, and pharmacists with outpatient primary care providers are necessary.43
Preoperative Transition to Extended Release Statin Formulations
An innovative approach to minimizing statin withdrawal involves preoperative transition to an extended‐release statin formulation. This strategy may be of particular value in patients where prolonged bowel nonavailability is likely, such as those undergoing gastrointestinal surgery, or when prolonged postoperative dietary restriction (eg, NPO [nil per os]: nothing by mouth) status is expected (Figure 2).
CONCLUSIONS AND FUTURE DIRECTIONS
Sudden withdrawal of perioperative statins results in adverse clinical outcomes. Individuals engaged in the care of patients during surgery such as hospitalists, anesthesiologists, and surgeons must become more cognizant of a statin withdrawal state.
An important limitation associated with the study of perioperative statin withdrawal remains the ambiguity regarding the extent of the problem in the United States. Therefore, a logical first step could be the use of infrastructure within the National Surgical Quality Improvement Program (NSQIP) to understand the epidemiology of perioperative statin use and consequences associated with statin discontinuation.44 Mandating such quality reporting could easily be built into current NSQIP performance metrics. These data would help inform a research agenda targeting patients that experience statin withdrawal and strategies most likely to prevent it.
Note Added in Proof
Disclosure: Nothing to report.
Accumulating evidence suggests that perioperative treatment with 3‐hydroxy‐3‐methylglutaryl coenzyme‐A (HMG‐CoA) reductase inhibitors (or, statins) reduces the incidence of cardiovascular events during noncardiac surgery.16 This evidence has lead the European Society of Cardiology (ESC) and American College of Cardiology Foundation/American Heart Association (ACCF/AHA) to endorse the use of perioperative statins in patients already on this treatment or those at high‐risk of cardiovascular events.7, 8
However, statins are available only in oral formulation. Consequently, prolonged bowel recovery or clinical instability may interfere with use during surgery. Furthermore, many clinicians may not recognize the imperative of postoperative statin resumption, viewing them principally as lipid‐lowering entities and not as agents of perioperative benefit. Failure to resume statins postoperatively can be catastrophic, as the ensuing inflammation and thrombosis frequently culminates in myocardial infarction (MI) or death.9, 10
In this article, we review the potent anti‐inflammatory properties of statins and their role in preventing perioperative cardiac events. We outline the biochemical basis for perioperative statin benefit, summarizing the basic, clinical, and experimental evidence regarding statin withdrawal. We conclude by presenting strategies to avert postoperative statin cessation and outline a research agenda dedicated to informing this practice.
METHODS
We performed a literature search using MEDLINE via Ovid (1946present), EMBASE (1946present), Biosis (1926present), and Cochrane CENTRAL (1960present). We used Boolean logic to search for key terms including statins, 3‐hydroxy‐3‐methylglutaryl CoA reductase inhibitors, death, MI, stroke, acute coronary syndrome (ACS), and statin withdrawal or cessation. All studies published in full‐text or abstract form were included. A total of 489 articles were retrieved by this search (last updated March 15, 2012). For this narrative review, we focused on studies that examined adverse outcomes associated with statin withdrawal.
BIOCHEMICAL BASIS OF STATIN PLEIOTROPICITY
The nonlipid‐lowering or pleiotropic properties of statins are especially valuable in the perioperative setting.16, 11 Perioperative cardiac complications occur due to oxygen supply:demand mismatch, vascular inflammation, or a combination of these states. A significant perisurgical catecholamine surge produces unopposed sympathetic effects,12 increasing the risk of rupture of vulnerable coronary plaques, thrombus formation, and adverse cardiac events.13, 14 Similarly, augmented inflammatory responses and increased circulating coagulation factors further predispose to a hazardous perioperative milieu.15 Statins attenuate this vascular inflammatory response by suppressing the synthesis of mevalonate by inhibiting HMG‐CoA reductase. Suppression of mevalonate synthesis reduces the bioavailability of 2 important isoprenoid molecules: farnesyl‐pyrophosphate and geranylgeranyl‐pyrophosphate.16 Diminution of these isoprenoid intermediaries leads to reductions in the active intracellular signaling molecules Ras, Rho, and Rac, which play critical roles in vascular reactivity, endothelial function, and coagulation and inflammatory pathways.1723 The cumulative effect of these cellular changes is diminished inflammation during periods of surgical stress (Figure 1).
While the perioperative pleiotropicity of statins is of inherent clinical value, several studies have shown that these effects are lost and even reversed when statins are withdrawn.2428 During statin treatment, absence of isoprenoid intermediaries induces cytosolic accumulation of nonactivated Rho and Rac proteins. Abrupt cessation of statins activates Rho/Rac‐kinase pathways, leading to unregulated inflammation, platelet hyper‐activation, and endothelial dysfunction.24, 25, 28, 29 For instance, statin withdrawal in mice‐models leads to an overshoot activation of Rho, resulting in down‐regulation of endothelial nitric oxide production,25 activation of nicotinamide adenine dinucleotide phosphate (NAD[P]H)‐oxidase, and increased superoxide production.29 In another mouse‐model, statin withdrawal was associated with up‐regulation of key pro‐thrombotic molecules including platelet factor 4 and beta‐thromboglobulin.24 In human studies, a platelet hyper‐activation state (manifested by increased platelet P‐selectin expression and enhanced platelet aggregation) occurs after statin discontinuation.27 Furthermore, withdrawal of statins in patients with hyperlipidemia increases inflammatory markers such as C‐reactive protein and interleukin‐6.26 In the perioperative context, absence of these important anti‐inflammatory properties increases the risk of cardiac events.9, 10
EVIDENCE SUGGESTING BENEFIT FROM PERIOPERATIVE STATIN TREATMENT
Retrospective studies first suggested clinical benefit from perioperative statin treatment. In a case‐control study involving 2816 patients undergoing vascular surgery at Erasmus Medical Center, statin use was associated with substantially decreased postoperative mortality (adjusted odd ratio [OR] 0.22, 95% confidence interval [CI] 0.100.47).5 In a subsequent retrospective cohort study of 780,591 patients who underwent major noncardiac surgery, the risk of postoperative mortality was considerably lower among statin users (unadjusted OR 0.68, 95% CI 0.640.72) compared to patients who did not receive, or received delayed treatment with statins.3 A third retrospective study of 1163 vascular surgery patients found that statins prevented perioperative cardiac complications including death, MI, congestive heart failure, and ventricular tachyarrhythmias (OR 0.52, 95% CI 0.350.76).4
The benefit from statin treatment found in retrospective studies prompted the first double‐blinded, randomized controlled trial (RCT) of perioperative statin use. In 2004, Durazzo and colleagues1 randomized 100 statin‐naive patients scheduled to undergo elective aortic, femoro‐popliteal, or carotid surgery to receive either 20 mg of atorvastatin or placebo for 45 days. Vascular surgery was performed, on average, 31 days after randomization. Atorvastatin therapy reduced the incidence of death from cardiac causes, nonfatal acute MI, ischemic stroke, and unstable angina (26% in the placebo group vs 8% in the atorvastatin group; P = 0.031).1 Although the small size of the trial rendered it underpowered to show a mortality benefit, this remains the first RCT to demonstrate a protective perioperative effect of statins.
In the 2009 Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE)‐III trial, Schouten and colleagues6 randomized 497 high‐risk, statin‐naive patients undergoing vascular surgery to receive, in addition to a beta‐blocker, either fluvastatin or placebo before surgery (median of 37 days). Postoperative myocardial ischemia (hazard ratio [HR] 0.55, 95% CI 0.340.88), and combined death from cardiovascular causes or nonfatal MI (HR 0.47, 95% CI 0.240.94), occurred less frequently in the treatment group.6 In 2009, the same group published DECREASE‐IV, a multicenter, prospective, open‐label, 2 2 factorial design trial of 1066 intermediate‐risk patients, scheduled to undergo elective, noncardiac surgery. Patients were assigned to bisoprolol, fluvastatin, combination treatment, or control therapy before surgery (median of 34 days). Although those randomized to fluvastatin demonstrated lower incidence of 30‐day cardiac death and MI than control (HR 0.65, 95% CI 0.351.10), these outcomes failed to reach statistical significance as the trial was principally powered to examine the effects of perioperative beta‐blockade.30
Using this pool of data, a meta‐analysis of 15 studies (223,010 patients) found a substantial 38% reduction in the risk of mortality after cardiac surgery (1.9% vs 3.1%; P = 0.0001) and an even greater 59% reduction in the risk of mortality following vascular surgery (1.7% vs 6.1%; P = 0.0001) with perioperative statin therapy. When including noncardiac surgery, a 44% reduction in mortality was observed (2.2% vs 3.2%; P 0.01).2 We performed a similar meta‐analysis of 15 RCTs involving 2292 patients to determine whether perioperative statin treatment in statin‐naive patients, undergoing either cardiac or noncardiac surgery, improved clinical outcomes. Our analysis also found statistically significant reductions in the risk of MI associated with perioperative statin use in both cardiac and noncardiac surgery (risk reduction [RR] 0.53, 95% CI 0.380.74) and atrial fibrillation in statin‐naive patients undergoing cardiac surgery (RR 0.56, 95% CI 0.450.69).31 Taken together, a large volume of evidence supports the use of statins in surgical settings.
In view of this evidence, the ACCF/AHA perioperative guidelines for noncardiac surgery endorsed statins as an important risk‐reducing intervention in those undergoing noncardiac surgery, and recommended continued use in patients on chronic statin treatment scheduled for noncardiac surgery (Level of Evidence B, Class I; Benefits >>> Risk). Initiating statins in patients undergoing vascular surgery, with or without risk factors, was considered reasonable (Level of Evidence B, Class IIa; Benefits >> Risk).7 Current ESC perioperative guidelines in noncardiac surgery offer similar recommendations to those of ACCF/AHA, but differ by categorizing the recommendation to initiate statins in patients at high cardiovascular risk as a Class I recommendation.8
CLINICAL CONSEQUENCES OF STATIN WITHDRAWAL
Although statins provide important cardiac benefits, an important limitation to their perioperative use remains their oral‐only formulation. Thus, patients who are unable to resume oral intake may fail to resume treatment. Perioperative statin cessation has been hypothesized to lead to a statin withdrawal phenomenon. The evidence that supports the existence of this phenomenon comes from 3 distinct populations: ACS, ischemic stroke, and perioperative patients (Table 1).
| Author (ref) Year | Design | Study Population | Sample Size (N) (Total/ Continuation/Discontinuation) | Clinical Setting and Context | Timing of Statin Discontinuation | Study Outcome | Results (Withdrawal vs Continuation) |
|---|---|---|---|---|---|---|---|
| |||||||
| Heeschen et al33 2002 | Retrospective cohort | Mostly men (68%) in early 60s | 1616/379/86 | Chest pain in ACS | During or after admission | Incidence of death and nonfatal MI | OR (95% CI) |
| 2.93 (1.646.27) | |||||||
| Spencer et al32 2004 | Retrospective cohort | Mostly men (62%) in late 60s | 68,506/9001/487 | NonST‐segment elevation MI | During the first 24 hr of hospitalization | In‐hospital death | HR (95% CI) |
| 1.83 (1.582.13) | |||||||
| Daskalopoulou et al34 2008 | Retrospective cohort | 60% men in late 60s | 9939/2026/137 Non‐users 2124 (reference group) | Acute MI | Within 1 yr of the coronary event | 1‐yr all‐cause mortality | HR (95% CI) |
| 1.88 (1.133.07)* | |||||||
| Colivicchi et al36 2007 | Prospective cohort | 51% men in early 70s | 631/385/246 | Ischemic stroke | Mean 48.6 days | 1‐yr all‐cause mortality | HR (95% CI) |
| 2.78 (1.963.72) | |||||||
| Blanco et al37 2007 | RCT | 51% men in mid‐60s | 215/46/43 | Ischemic stroke | N/A | Risk of death or dependency at 3 mo | OR (95% CI) |
| 4.66 (1.4614.91) | |||||||
| Early neurologic deterioration | OR (95% CI) | ||||||
| 7.08 (2.7318.37) | |||||||
| Le Manach et al9 2007 | Quasi‐experimental (prepost) | Mostly men (89%) in late‐60s | 669/178/491 | Infra‐renal aortic surgery | Median of 4 days off statins | Postoperative troponin release, MI | OR (95% CI) |
| 2.9 (1.65.5) | |||||||
| Schouten et al10 2007 | Prospective cohort | Mostly men (75%) in mid‐60s | 298/228/70 | Aortic and lower extremity vascular surgery | Median of 3 days off statins | Postoperative troponin release | HR (95% CI) |
| 4.6 (2.29.6) | |||||||
| Combination of postoperative MI and CV death | HR (95% CI) | ||||||
| 7.5 (2.820.1) | |||||||
| Schouten et al6 2009 | RCT | Mostly men (75%) in mid‐60s | 250/189/61 | Vascular surgery (carotid, abdominal aortic, endovascular, and lower extremity arterial) | Median of 2 days off statins | Postoperative myocardial ischemia and combined death from cardiovascular causes or nonfatal MI | OR (95% CI) |
| 1.1 (0.482.52) | |||||||
Statin Withdrawal in Acute Coronary Syndromes
Several studies have demonstrated an association between statin withdrawal and heightened risk of cardiovascular events in ACS.3234 In a retrospective analysis of 1616 patients presenting with ACS, withdrawal of statins during or after admission was associated with more frequent death and nonfatal MI compared to those who continued therapy (OR 2.93, 95% CI 1.646.27).33 In another retrospective observational study of 68,606 nonST‐segment elevation MI patients, statin cessation during the first 24 hours of hospitalization was independently associated with adverse outcomes including in‐hospital death (adjusted HR 1.83; 95% CI 1.582.13), cardiac arrest, and cardiogenic shock.32 In a population‐based, cohort study in the United Kingdom, statin cessation following an acute MI was independently associated with greater all‐cause mortality at 1‐year (adjusted HR 1.88, 95% CI 1.133.07).34
The significantly increased risk of adverse outcomes associated with the interruption of statins in ACS may be moderated by vascular inflammation related to the inciting coronary event, as statin discontinuation in patients with stable cardiac conditions was not associated with increased risk of cardiovascular events in a large‐scale, double‐blind, parallel‐group study.35
Statin Withdrawal in Ischemic Stroke
Adverse events associated with statin withdrawal have also been reported in patients with cerebrovascular disease. In a prospective observational study of 631 consecutive stroke survivors, those who discontinued statins (owing to mild adverse effects or unclear reasons) experienced increased mortality during the first year after the event (adjusted HR 2.78, 95% CI 1.963.72).36 Using a controversial study design aimed at evaluating the effects of stopping oral intake (including chronic medications) during the first days of acute stroke, Blanco and colleagues37 randomized 89 stroke victims on chronic statins to either continue medications or experience statin withdrawal following admission. Statin withdrawal was independently associated with increased risk of mortality and dependency at 3 months (OR 4.66, 95% CI 1.4614.91).37
Perioperative Statin Withdrawal
In the perioperative setting, statin withdrawal has also been associated with adverse outcomes. Using a quasi‐experimental design, Le Manach et al.9 evaluated the risk of cardiac complications after infra‐renal aortic surgery when immediate, postoperative resumption of statins was adopted at their institution. The investigators compared the risk of developing MI, cardiac death, or abnormal troponin release in 491 patients who did not get early postoperative statin resumption (pre‐intervention group) to 178 patients who did. Statin withdrawal for 4 days was demonstrated to be an independent predictor of postoperative troponin leak and MI (OR 2.9, 95% CI 1.65.5). Similarly, Schouten et al.10 investigated the risk of adverse events related to interruption of long‐term statins by examining cardiac outcomes in 298 statin users undergoing major vascular surgery. Among the 70 patients who experienced statin withdrawal, an increased risk of postoperative troponin release (HR 4.6, 95% CI 2.29.6), and the composite endpoint of MI and cardiovascular death (HR 7.5, 95% CI 2.820.1), was observed compared to those who resumed treatment. Not unexpectedly, the most common reason for statin cessation was inability to take oral medications after surgery. However, even in patients who discontinued statins, the use of extended‐release fluvastatin was associated with fewer perioperative cardiac events than other statins. Furthermore, extended‐release fluvastatin was also held for 2 days following surgery (owing to inability to take the drug orally), in 25% of patients in the DECREASE‐III study. However, no impact in the rate of adverse outcomes was noted despite this interruption (OR 1.1, 95% CI 0.482.52).6 Although the authors surmised that the extended formulation of fluvastatin had provided sustained levels of statin activity despite lack of timely oral intake, it is important to note that this theory may not be generalizable to chronic statin users, as they were not enrolled in this study. Conversely, some patients may have experienced postoperative ileus for longer than 2 days, perhaps resulting in confounding or attenuation of the effect noted in the study.
CLINICAL INSIGHTS INTO FAILURE OF POSTOPERATIVE STATIN RESUMPTION
We hypothesize that failure to resume perioperative statins may occur for 4 cardinal reasons. First, resumption of an oral agent frequently proves clinically challenging when complications such as postoperative ileus, nausea, and vomiting peak. To date, no intravenous statin formulations are available, although phase‐I studies are currently underway.38 Second, it is not inconceivable that perioperative clinical instability may overshadow the resumption of statin treatment. Third, clinicians may also remain concerned regarding adverse effects of statins, a thought compounded by US Food and Drug Administration statin package inserts that specifically advocate for statins to be withheld during surgery. However, although the occurrence of elevated liver function tests and myopathy are theoretically important, the overwhelming majority of perioperative statin studies in noncardiac surgery have not found this to be a major occurrence.39 Nonetheless, a lack of uniform definitions and appropriate surveillance for adverse events are important limitations to this finding. In our recent systematic review, we were unable to provide refined estimates of these important side effects owing to differences in definition, variations in screening, and absence of standardized cutoffs used in studies.31 Finally, an important reason for failing to resume postoperative statins is that many physicians simply fail to recognize the perioperative importance of these agents.
STRATEGIES TO IMPROVE PERIOPERATIVE STATIN RESUMPTION
Using the existing evidence, we propose the following 4 clinical strategies to assist in avoiding a statin withdrawal state.
Nasogastric Administration
Utilizing a post‐pyloric nasogastric tube is a straightforward solution to provide statins in those who cannot otherwise tolerate oral intake due to nausea or emesis. Although this solution is hardly innovative, it is relevant as it forces consideration of the need to resume postoperative statins by available means. While the development of a high nasogastric output or a prolonged ileus may limit the applicability of this intervention, it is important that this option be considered as opposed to expectant watching for the clinical return of bowel function. Simvastatin, atorvastatin, rosuvastatin, and pravastatin can be crushed and delivered through this route.40
Development of Reminder Systems
Computerized reminder systems have proved important in ensuring the resumption of deep venous thrombosis prophylaxis and other preventative care compliance in hospitalized patients.41, 42 Using this process, pharmacist‐ or electronic health record‐based reminder systems could be implemented to ensure that statins are restarted when clinically feasible. Further studies are needed to test whether this approach can lead to improved outcomes.
Medication Reconciliation Prior to Hospital Discharge
Statin withdrawal highlights the pertinence of a robust, medical reconciliation process prior to the patient's departure from the hospital. In this context, the development of policies using single‐ or multi‐faceted interventions that promote cooperation between inpatient physicians, surgeons, and pharmacists with outpatient primary care providers are necessary.43
Preoperative Transition to Extended Release Statin Formulations
An innovative approach to minimizing statin withdrawal involves preoperative transition to an extended‐release statin formulation. This strategy may be of particular value in patients where prolonged bowel nonavailability is likely, such as those undergoing gastrointestinal surgery, or when prolonged postoperative dietary restriction (eg, NPO [nil per os]: nothing by mouth) status is expected (Figure 2).
CONCLUSIONS AND FUTURE DIRECTIONS
Sudden withdrawal of perioperative statins results in adverse clinical outcomes. Individuals engaged in the care of patients during surgery such as hospitalists, anesthesiologists, and surgeons must become more cognizant of a statin withdrawal state.
An important limitation associated with the study of perioperative statin withdrawal remains the ambiguity regarding the extent of the problem in the United States. Therefore, a logical first step could be the use of infrastructure within the National Surgical Quality Improvement Program (NSQIP) to understand the epidemiology of perioperative statin use and consequences associated with statin discontinuation.44 Mandating such quality reporting could easily be built into current NSQIP performance metrics. These data would help inform a research agenda targeting patients that experience statin withdrawal and strategies most likely to prevent it.
Note Added in Proof
Disclosure: Nothing to report.
- , , , et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg. 2004;39(5):967–975.
- , , , , , . Improved postoperative outcomes associated with preoperative statin therapy. Anesthesiology. 2006;105(6):1260–1272; quiz 1289–1290.
- , , , , . Lipid‐lowering therapy and in‐hospital mortality following major noncardiac surgery. JAMA. 2004;291(17):2092–2099.
- , , , et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS) study. J Am Coll Cardiol. 2005;45(3):336–342.
- , , , et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation. 2003;107(14):1848–1851.
- , , , et al. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med. 2009;361(10):980–989.
- , , , et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418–e499.
- , , , et al. Guidelines for pre‐operative cardiac risk assessment and perioperative cardiac management in non‐cardiac surgery. Eur Heart J. 2009;30(22):2769–2812.
- , , , et al. The impact of postoperative discontinuation or continuation of chronic statin therapy on cardiac outcome after major vascular surgery. Anesth Analg. 2007;104(6):1326–1333.
- , , , et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol. 2007;100(2):316–320.
- . Beneficial cardiovascular pleiotropic effects of statins. Circulation. 2004;109(23 suppl 1):III39–III43.
- , , , , , . Persistent endocrine stress response in patients undergoing cardiac surgery. J Endocrinol Invest. 1998;21(1):12–19.
- , , , , , . Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol. 1996;57(1):37–44.
- , , , , , . Perioperative cardiac events in patients undergoing noncardiac surgery: a review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. Can Med Assoc J. 2005;173(6):627–634.
- . Perioperative cardiac morbidity. Anesthesiology. 1990;72(1):153–184.
- , . Isoprenoid metabolism and the pleiotropic effects of statins. Curr Atheroscler Rep. 2003;5(5):372–378.
- , , , . Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97(12):1129–1135.
- , , , et al. Roles of rho‐associated kinase and oxidative stress in the pathogenesis of aortic stiffness. J Am Coll Cardiol. 2007;49(6):698–705.
- , , , et al. Inhibition of rho‐associated kinase results in suppression of neointimal formation of balloon‐injured arteries. Circulation. 2000;101(17):2030–2033.
- , , , . Reduced expression of endothelial cell markers after 1 year treatment with simvastatin and atorvastatin in patients with coronary heart disease. Atherosclerosis. 2002;162(1):179–185.
- , , , et al. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest. 2001;108(10):1429–1437.
- , , . Pleiotropic effects of statin therapy: molecular mechanisms and clinical results. Trends Mol Med. 2008;14(1):37–44.
- , , , et al. Inhibition of geranylgeranylation reduces angiotensin II‐mediated free radical production in vascular smooth muscle cells: involvement of angiotensin AT1 receptor expression and Rac1 GTPase. Mol Pharmacol. 2001;59(3):646–654.
- , , , et al. Withdrawal of statin treatment abrogates stroke protection in mice. Stroke. 2003;34(2):551–557.
- , , , et al. Suppression of endothelial nitric oxide production after withdrawal of statin treatment is mediated by negative feedback regulation of rho GTPase gene transcription. Circulation. 2000;102(25):3104–3110.
- , , , et al. Changes of plasma inflammatory markers after withdrawal of statin therapy in patients with hyperlipidemia. Clin Chim Acta. 2006;366(1–2):269–273.
- , , , et al. Platelet hyperactivity after statin treatment discontinuation. Thromb Haemost. 2003;90(3):476–482.
- , , , et al. Rebound inflammatory response during the acute phase of myocardial infarction after simvastatin withdrawal. Atherosclerosis. 2009;207(1):191–194.
- , . Effects of statins on endothelium and signaling mechanisms. Stroke. 2004;35(11 suppl 1):2708–2711.
- , , , et al. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate‐risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE‐IV). Ann Surg. 2009;249(6):921–926.
- , , , et al. Effect of perioperative statins on death, myocardial infarction, atrial fibrillation, and length of stay: a systematic review and meta‐analysis. Arch Surg. 2012;147(2):181–189.
- , , , et al. Early withdrawal of statin therapy in patients with non‐ST‐segment elevation myocardial infarction: National Registry of Myocardial Infarction. Arch Intern Med. 2004;164(19):2162–2168.
- , , , , , . Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation. 2002;105(12):1446–1452.
- , , , , , . Discontinuation of statin therapy following an acute myocardial infarction: a population‐based study. Eur Heart J. 2008;29(17):2083–2091.
- . There is no evidence for an increase in acute coronary syndromes after short‐term abrupt discontinuation of statins in stable cardiac patients. Circulation. 2004;110(16):2333–2335.
- , , , . Discontinuation of statin therapy and clinical outcome after ischemic stroke. Stroke. 2007;38(10):2652–2657.
- , , , et al. Statin treatment withdrawal in ischemic stroke: a controlled randomized study. Neurology. 2007;69(9):904–910.
- , , , et al. Intravenous rosuvastatin for acute stroke treatment: an animal study. Stroke. 2008;39(2):433–438.
- , , , et al. Safety of perioperative statin use in high‐risk patients undergoing major vascular surgery. Am J Cardiol. 2005;95(5):658–660.
- Lexi‐Comp Online™, Lexi‐Drugs™, Hudson, OH: Lexi‐Comp, Inc; December 7, 2011.
- , , , , , . A computerized reminder system to increase the use of preventive care for hospitalized patients. N Engl J Med. 2001;345(13):965–970.
- , , , et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969–977.
- , , , . Medication review and reconciliation with cooperation between pharmacist and general practitioner and the benefit for the patient: a systematic review. Br J Clin Pharmacol. January 13, 2012. doi: 10.1111/j.1365–2125.2012.04178.x.
- American College of Surgeons National Surgical Quality Improvement Program. Available at: http://www.acsnsqip.org. Accessed December 15, 2012.
- , , , et al. Reduction in cardiovascular events after vascular surgery with atorvastatin: a randomized trial. J Vasc Surg. 2004;39(5):967–975.
- , , , , , . Improved postoperative outcomes associated with preoperative statin therapy. Anesthesiology. 2006;105(6):1260–1272; quiz 1289–1290.
- , , , , . Lipid‐lowering therapy and in‐hospital mortality following major noncardiac surgery. JAMA. 2004;291(17):2092–2099.
- , , , et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS) study. J Am Coll Cardiol. 2005;45(3):336–342.
- , , , et al. Statins are associated with a reduced incidence of perioperative mortality in patients undergoing major noncardiac vascular surgery. Circulation. 2003;107(14):1848–1851.
- , , , et al. Fluvastatin and perioperative events in patients undergoing vascular surgery. N Engl J Med. 2009;361(10):980–989.
- , , , et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation. 2007;116(17):e418–e499.
- , , , et al. Guidelines for pre‐operative cardiac risk assessment and perioperative cardiac management in non‐cardiac surgery. Eur Heart J. 2009;30(22):2769–2812.
- , , , et al. The impact of postoperative discontinuation or continuation of chronic statin therapy on cardiac outcome after major vascular surgery. Anesth Analg. 2007;104(6):1326–1333.
- , , , et al. Effect of statin withdrawal on frequency of cardiac events after vascular surgery. Am J Cardiol. 2007;100(2):316–320.
- . Beneficial cardiovascular pleiotropic effects of statins. Circulation. 2004;109(23 suppl 1):III39–III43.
- , , , , , . Persistent endocrine stress response in patients undergoing cardiac surgery. J Endocrinol Invest. 1998;21(1):12–19.
- , , , , , . Pathology of fatal perioperative myocardial infarction: implications regarding pathophysiology and prevention. Int J Cardiol. 1996;57(1):37–44.
- , , , , , . Perioperative cardiac events in patients undergoing noncardiac surgery: a review of the magnitude of the problem, the pathophysiology of the events and methods to estimate and communicate risk. Can Med Assoc J. 2005;173(6):627–634.
- . Perioperative cardiac morbidity. Anesthesiology. 1990;72(1):153–184.
- , . Isoprenoid metabolism and the pleiotropic effects of statins. Curr Atheroscler Rep. 2003;5(5):372–378.
- , , , . Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97(12):1129–1135.
- , , , et al. Roles of rho‐associated kinase and oxidative stress in the pathogenesis of aortic stiffness. J Am Coll Cardiol. 2007;49(6):698–705.
- , , , et al. Inhibition of rho‐associated kinase results in suppression of neointimal formation of balloon‐injured arteries. Circulation. 2000;101(17):2030–2033.
- , , , . Reduced expression of endothelial cell markers after 1 year treatment with simvastatin and atorvastatin in patients with coronary heart disease. Atherosclerosis. 2002;162(1):179–185.
- , , , et al. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest. 2001;108(10):1429–1437.
- , , . Pleiotropic effects of statin therapy: molecular mechanisms and clinical results. Trends Mol Med. 2008;14(1):37–44.
- , , , et al. Inhibition of geranylgeranylation reduces angiotensin II‐mediated free radical production in vascular smooth muscle cells: involvement of angiotensin AT1 receptor expression and Rac1 GTPase. Mol Pharmacol. 2001;59(3):646–654.
- , , , et al. Withdrawal of statin treatment abrogates stroke protection in mice. Stroke. 2003;34(2):551–557.
- , , , et al. Suppression of endothelial nitric oxide production after withdrawal of statin treatment is mediated by negative feedback regulation of rho GTPase gene transcription. Circulation. 2000;102(25):3104–3110.
- , , , et al. Changes of plasma inflammatory markers after withdrawal of statin therapy in patients with hyperlipidemia. Clin Chim Acta. 2006;366(1–2):269–273.
- , , , et al. Platelet hyperactivity after statin treatment discontinuation. Thromb Haemost. 2003;90(3):476–482.
- , , , et al. Rebound inflammatory response during the acute phase of myocardial infarction after simvastatin withdrawal. Atherosclerosis. 2009;207(1):191–194.
- , . Effects of statins on endothelium and signaling mechanisms. Stroke. 2004;35(11 suppl 1):2708–2711.
- , , , et al. Bisoprolol and fluvastatin for the reduction of perioperative cardiac mortality and myocardial infarction in intermediate‐risk patients undergoing noncardiovascular surgery: a randomized controlled trial (DECREASE‐IV). Ann Surg. 2009;249(6):921–926.
- , , , et al. Effect of perioperative statins on death, myocardial infarction, atrial fibrillation, and length of stay: a systematic review and meta‐analysis. Arch Surg. 2012;147(2):181–189.
- , , , et al. Early withdrawal of statin therapy in patients with non‐ST‐segment elevation myocardial infarction: National Registry of Myocardial Infarction. Arch Intern Med. 2004;164(19):2162–2168.
- , , , , , . Withdrawal of statins increases event rates in patients with acute coronary syndromes. Circulation. 2002;105(12):1446–1452.
- , , , , , . Discontinuation of statin therapy following an acute myocardial infarction: a population‐based study. Eur Heart J. 2008;29(17):2083–2091.
- . There is no evidence for an increase in acute coronary syndromes after short‐term abrupt discontinuation of statins in stable cardiac patients. Circulation. 2004;110(16):2333–2335.
- , , , . Discontinuation of statin therapy and clinical outcome after ischemic stroke. Stroke. 2007;38(10):2652–2657.
- , , , et al. Statin treatment withdrawal in ischemic stroke: a controlled randomized study. Neurology. 2007;69(9):904–910.
- , , , et al. Intravenous rosuvastatin for acute stroke treatment: an animal study. Stroke. 2008;39(2):433–438.
- , , , et al. Safety of perioperative statin use in high‐risk patients undergoing major vascular surgery. Am J Cardiol. 2005;95(5):658–660.
- Lexi‐Comp Online™, Lexi‐Drugs™, Hudson, OH: Lexi‐Comp, Inc; December 7, 2011.
- , , , , , . A computerized reminder system to increase the use of preventive care for hospitalized patients. N Engl J Med. 2001;345(13):965–970.
- , , , et al. Electronic alerts to prevent venous thromboembolism among hospitalized patients. N Engl J Med. 2005;352(10):969–977.
- , , , . Medication review and reconciliation with cooperation between pharmacist and general practitioner and the benefit for the patient: a systematic review. Br J Clin Pharmacol. January 13, 2012. doi: 10.1111/j.1365–2125.2012.04178.x.
- American College of Surgeons National Surgical Quality Improvement Program. Available at: http://www.acsnsqip.org. Accessed December 15, 2012.

Smartphone Use During Attending Rounds
Healthcare market research has predicted that over 80% of physicians will use smartphones by 2012.1 These handheld devices allow users immediate access to various forms of electronic media such as Internet, instant messaging, and e‐mail. Smartphones provide numerous benefits to physicians, including rapid access to medical references, research applications, and patient information.2 These devices have been used for teleconsultation3 and patient education,4 and applications have been developed for numerous clinical specialties.48
Housestaff perceive that communication improves when they use smartphones rather than traditional pagers on the inpatient service,9 and patients may have a positive view of physicians' use of handheld computers.10 Medical schools and residency programs are increasingly requiring smartphone ownership for their trainees, with the expectation that smartphone use will enhance the educational experience, ensure the highest level of patient care, improve user efficiency, and help control the costs associated with purchasing updated textbooks.7, 1113 In the future, hospitals may rely on smartphone technologies to help reduce the enormous economic burden created by inefficient communication.14
Despite their numerous benefits for physicians and patients, little is known about the potential for smartphones to distract users in clinical care settings. Studies from the psychology and traffic safety fields have documented untoward consequences when individuals use electronic devices to multitask.1519 Given these concerns, we investigated the prevalence and patterns of smartphone use during inpatient attending rounds, and whether these devices can distract team members in this period of important information transfer.
METHODS
At our institution, attending rounds are faculty‐led inpatient teaching rounds that focus on clinical care and patient management; these sessions may be conducted either in the classroom or at the bedside, depending on patient and learner needs, and faculty preference. Inpatient teams are comprised of 1 attending, housestaff, and third and fourth year medical students. Each team conducts attending rounds independently; these rounds range in length from 1 hour (Pediatrics) to 2 hours (Medicine).
A survey instrument was designed to evaluate smartphone usage patterns during hospital inpatient attending rounds, and perceived distraction from smartphones in this setting. A preliminary version of the survey was pilot tested by a group of housestaff for face validity, redundancy, and ease of use, and it was subsequently revised. For the purposes of this study, a smartphone was defined broadly as any mobile, personal communication device (cellphone, iPhone, Android, Blackberry, iPad, etc). Residents were asked about their own smartphone use, as well as their observations of supervising attendings and other learners' devices use during rounds (see Supporting Appendix 1 in the online version of this article).
In February 2011, the anonymous online survey was administered using Survey Monkey (
Respondents were not required to answer each question in order to complete the survey. With the exception of free‐text comments, all responses were either yes/no or were graded on a 5‐point frequency scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always). This scale was chosen because it allowed for adequate dispersion of responses, and for the identification of meaningful smartphone usage among respondents (score 3) and data dichotomization. The z test was used to compare the proportions between independent groups.
All free‐text comments were imported into a Microsoft Word table. Comments were separated into 2 groups: housestaff and attending. Each comment was hand‐coded by 2 authors (R.J.K.‐S. and R.S.) to reach consensus for 1 of the following 4 categories: the comment was a positive statement; a negative statement; a positive/negative statement; or a neutral one, ie, neither positive nor negative. The terms positive and negative here refer to whether the statement explicitly highlighted benefits of smartphone use or a negative aspect of smartphone use, respectively. A comment was coded as positive/negative if it highlighted both benefits and drawbacks in the same comment. In addition, each comment that mentioned texting or call functions was secondarily coded as personal, patient, both, or unknown depending on the purpose of the texting or calls described in each comment. Comments were also reviewed for possible subthemes.
RESULTS
The overall response rate was 73% (156/214), with 81% (116/143) of housestaff and 56% (40/71) of faculty participating. The mean tenure of faculty respondents was 13 years. Eighty‐nine percent (103/116) of residents and 98% (39/40) of faculty owned devices, with 57% of housestaff and 28% of attendings reporting regular personal use of smartphones during attending rounds (Table 1).
| Smartphone User | Self‐Report % (n/N) | Resident Observations of Other Team Members % (n/N) | Faculty Observations of Trainees % (n/N) |
|---|---|---|---|
| |||
| Resident | 57% (59/103) | 91% (103/113)* | 73% (29/40) |
| Faculty | 28% (11/39) | 43% (49/113)* | n/a |
Respondents reported that they used their smartphones during attending rounds for the following reasons: 1) patient care (85% residents, 48% faculty); 2) reading/responding to personal texts/e‐mails (37% residents, 12% faculty); and 3) other non‐patient care uses, such as Web surfing (15% residents, 0% faculty) (Tables 2 and 3). Nineteen percent of residents reported that they missed important clinical information due to distraction from smartphone use, as did 12% of attendings (Table 4). Respondents reported observing other team members using smartphones and missing important clinical data at higher rates than they reported for themselves (see Tables 1, 4, and 5). A majority of both residents (56%) and faculty (73%) agreed (score >3) that smartphones can be a serious distraction during attending rounds, and 77% of attendings affirmed that teaching hospitals should establish smartphone use codes of conduct in order to minimize unnecessary distraction during attending rounds.
| Reason | Based on Housestaff Self‐Report (n = 85)* | Based on Trainee Observations of One Another (n = 112) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 85% | 86% | NS |
| Reading or responding to personal texts or e‐mail | 37% | 55% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 15% | 37% | <0.01 |
| Reason | Based on Faculty Self‐Report (n = 25)* | Based on Housestaff Observations of Faculty (n = 91) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 48% | 48% | NS |
| Reading or responding to personal texts or e‐mail | 12% | 47% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 0% | 20% | <0.05 |
| Smartphone User | Self‐Report % (n/N) |
|---|---|
| |
| Housestaff | 19% (18/85)* |
| Faculty | 12% (3/25)* |
| Smartphone User | Based on Housestaff Observation % (n/N) | Based on Faculty Observation % (n/N) |
|---|---|---|
| ||
| Trainee | 34% (38/112)* | 43% (17/40) |
| Faculty | 20% (18/91)* | n/a |
Despite not requiring responses in order to complete the questionnaires, we found that, in general, few eligible faculty or residents skipped questions on the survey. Nevertheless, there was a substantial drop in responses (91/116) for the last 2 questions on the housestaff survey. These questions asked for resident observations of attending smartphone usage patterns during rounds, and whether they had seen attendings miss clinical information because of distractions from smartphone use.
There were 25 free‐text comments from residents and 11 from attendings. The resultant comments highlight differences in residents' and attendings' perspectives toward smartphone use during attending rounds. Housestaff comments included 7 positive comments, 7 positive/negative comments, 1 negative comment, and 10 neutral comments. A subtheme that emerged in 2 of the housestaff comments was the importance of personal autonomy in being able to use one's smartphone. Attending comments included 2 positive comments, 0 positive/negative comments, 4 negative comments, and 5 neutral comments. Faculty comments revealed that attendings use their smartphones' e‐mail/texting and call capabilities during rounds both for patient care issues (3 comments) and/or urgent family concerns (2 comments). In 2 other attending comments, the reason for calls/texts during rounds was not specified.
Housestaff comments included: I do not know why it is that attendings never use it these phones are so easy to use and [enhance] patient care in a number of ways, Depending on how they are used, if strictly for pt care then they can be a great mobile tool, Of course they can be a distraction, but they are also a very good tool. You take the good with the bad, If you are bored you will find other things to occupy your mind. If you can look up some info at the time of rounding you are actively participating. Please, do not make it worse than it is already, and It is a personal choice. Faculty negative comments highlighted the potential for distraction from the e‐mail beeps, the fact that some of the housestaff will be tuned into their SmartPhones, that residents frequently check their phones during roundsa distraction and frankly rude when the attending or fellow are giving a brief lecture, and that sometimes more focus is on the SmartPhone than rounds.
DISCUSSION
Physicians and their patients benefit from the wide‐ranging capabilities of personal, mobile communication devices in the healthcare environment. Smartphones house the latest medical references, provide access to patients' medical records and imaging studies, can photograph or video physical findings, and educate and monitor patients.28 Smartphones can facilitate information transfer in the medical setting and may improve housestaff efficiency and communication.9
Despite their significant benefits, smartphones introduce another source of interruption, multitasking, and distraction into the hospital environment. There is increasing awareness that breaks‐in‐task in the clinical setting may have negative consequences.2024 While some types of interruptions are beneficial and can facilitate patient care (eg, an alarm ringing to indicate abnormal vitals signs on a patient),2024 other forms of interruptions, even those that are self‐initiated,22 can be distracting and detrimental. Along these lines, recommendations for safe handoffs and information transfer have specifically included advice to minimize potential distractions.25
In addition, studies from the psychology and education literature have previously documented negative consequences on learning when individuals use electronic devices to multitask.1517 Students who used a laptop in class were likely to multitask, become distracted, and distract others; the more a student used the laptop in class, the lower the student's class performance.15 Multitasking with a cellphone during driving can be especially hazardous.18, 19 According to National Highway Traffic Safety Administration data, 20% of injury crashes in 2009 involved reports of distracted driving, and cellphones were implicated in 18% of distracted driving deaths that year.18
Little is known about any negative effects of using personal electronic devices in the context of patient care. A 2011 study of Internal Medicine residents who used smartphones for team communication documented both positive and negative consequences of smartphone use in the hospital setting. Negative consequences included frequent interruptions, a weakening of interprofessional behaviors as housestaff relied on texting over direct communication with nurses, and unprofessional housestaff behaviors.26 The Agency for Healthcare Quality and Research published a case report in which a resident's smartphone use during clinical care resulted in patient harm.27 To our knowledge, this is the first study to detail housestaff and faculty smartphone usage patterns and potential for user distractibility during inpatient attending rounds.
Our data show that device use during attending rounds is prevalent among residents and faculty alike, with the majority of use related to patient care. However, attendings were half as likely as residents to report using devices regularly during rounds. This finding may reflect attendings' inability to multitask while leading the rounds, or a deliberate role‐modeling of desired conduct during rounds. Generational differences may also play a role, with residents more likely than their older attendings to multitask and self‐interrupt. Along these lines, traffic safety research has found that younger drivers are more likely to text during driving; approximately 30% of drivers under 30 years old reported texting while driving in the previous 30 days, compared to 9% of respondents over 30 years old.19 Increased smartphone use by housestaff during rounds may also reflect attitudinal differences between the 2 groups. As seen in the free‐text comments, housestaff tended to emphasize the benefits of smartphone use, and with 1 exception, all negative housestaff comments were balanced by a positive statement. Faculty more commonly underscored the negative aspects of smartphone use during rounds, including the devices' adverse effects on housestaff professional behavior in this setting.
Faculty and housestaff consistently reported observing others using smartphones at higher rates than they reported for themselves. This discrepancy may reflect underrecognition of self‐use, or a discomfort in reporting self‐use during attending rounds. In addition, residents' observations of other trainees' usage of smartphones (91%) was higher than faculty observation of the same group (73%). Trainees' smartphone use may be less obvious to attendings who are involved in facilitating rounds. Alternatively, trainees may use their smartphones in subtle ways to prevent attending awareness.
There are several limitations to our study. Our research focused specifically on attending rounds. Smartphone usage patterns by faculty and housestaff at other times in the work day, such as during resident handoffs, at a patient's bedside, or during academic conferences, may differ. Nevertheless, we specifically chose to study smartphone use during attending rounds, as these sessions are discrete time frames during which important teaching occurs and clinical management decisions are made. With recent Accreditation Council for Graduate Medical Education (ACGME) work hour restrictions, these faculty‐led rounds may become increasingly important in ensuring the safe transition of patient care. Secondly, despite asking respondents how often they use their smartphones for personal texts or e‐mails, it was clear from the free‐text comments that respondents use their smartphone e‐mail/texting capabilities and take urgent calls during rounds for both patient care and/or family issues. It is not possible from the data to sort out the subset of respondents who use texting or e‐mailing exclusively for patient care during rounds. Third, we did not survey medical students on the teams, so it is possible that their device use on rounds differs from that of housestaff and faculty. Fourth, since the survey could be completed without answering every question, response rates for some items varied slightly; there was a substantial reduction in the number of eligible residents who answered the final 2 questions on the survey about their observations of attendings' smartphone usage patterns and distraction during rounds. While the flexibility in survey completion was intended to enhance overall study participation, it is unknown how nonresponders might have affected the study results; as such, those specific results should be interpreted with some caution. Finally, our findings were based on respondents' retrospective recall, and therefore may not accurately reflect true usage patterns. Timemotion studies with real‐time observation of smartphone use would provide more accurate data.
A majority of residents and attendings in our study agreed that smartphones can pose a serious distraction during attending rounds, and attendings strongly favored the institution of formal codes of conduct for smartphone use during inpatient attending rounds. The development of such policies are important for patient safety; at the same time, they are in line with medical institutions' increasing awareness about the need for guidelines regarding other aspects of digital professionalism.28 In February 2012, our hospital instituted a policy regarding appropriate device use during inpatient attending rounds (see Supporting Appendix 3 in the online version of this article). Because our research found differences in housestaff and faculty attitudes toward smartphone use during rounds, we developed our policy after discussion with, and feedback from, all members of the inpatient team, including faculty, residents, and medical students. Incorporating the various perspectives of all stakeholders can be helpful to institutions in developing guidelines that maximize the benefits of smartphone use in the learning environment, while reducing the potential for distraction and adverse outcomes.
Acknowledgements
Disclosure: Nothing to report.
- . 72 percent of US physicians use smartphones. MobiHealthNews. Available at: http://mobihealthnews.com/7505/72‐percent‐of‐us‐physicians‐use‐smartphones/. Accessed April 16, 2012.
- . Smartphones in clinical practice, medical education, and research. Arch Intern Med. 2011;171(14):1294–1296.
- ,. Telemedicine using smartphones for oral and maxillofacial surgery consultation, communication, and treatment planning.J Oral Maxillofac Surg.2009;67:2505–2509.
- . Mobile phones to improve the practice of neurology. Neurol Clin. 2010;28(2):395–410.
- , , . Infectious diseases resources for the iPhone. Clin Infect Dis. 2010;50(9):1268–1274.
- , , , . Novel uses of smartphones in ophthalmology. Ophthalmology. 2010;117:1274–1274.e3.
- , , . The uses of the iPhone for surgeons. Surgeon. 2011;9(1):44–48.
- . Smartphone apps for orthopaedic surgeons. Clin Orthop Relat Res. 2011;469(7):2042–2048.
- , , , et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553–559.
- , , , . Patient attitudes toward physician use of tablet computers in the exam room. Fam Med. 2010;42(9):643–647.
- . iPads to be distributed to incoming class by Stanford Medical School. Available at: http://med.stanford.edu/ism/2010/august/ipad.html. Accessed April 16, 2012.
- University of Virginia School of Medicine. Third year medical student mobile device requirement. Available at: http://www.medicine.virginia.edu/education/medical‐students/ome/edtech/pda_recom‐page/. Accessed April 16, 2012.
- . Tablet computers in the hospital. ACP Hospitalist 2011. Available at: http://www.acphospitalist.org/archives/2011/08/tablet. htm. Accessed April 16, 2012.
- , , . Quantifying the economic impact of communication inefficiencies in US hospitals. Available at: http://www.rhsmith.umd.edu/chids/pdfs_docs/ResearchBriefings/CHIDS‐ResearchBriefing‐Vol3Issue1b.pdf. Accessed April 16, 2012.
- . In‐class laptop use and its effects on student learning. Computers 50(3):906–914.
- , , . Distractions, distractions: does instant messaging affect college students' performance on a concurrent reading comprehension task? CyberPsychology 12(1):51–53.
- , , , . Can students really multitask? An experimental study of instant messaging while reading. Computers 54(4):927–931.
- US Department of Transportation. Statistics and facts about distracted driving. Available at: http://www.distraction.gov/stats‐and‐facts/index.html. Accessed November 17, 2011.
- Driving distracted. Consumer Reports. April 2011:22–25. See also: http://www.distraction.gov/files/for‐media/2011/2011–03‐04‐cr‐dot‐distracted‐driving‐initiative.pdf. Accessed November 25, 2011.
- , , , . Emergency department workplace interruptions: are emergency physicians “interrupt‐driven” and “multitasking”? Acad Emerg Med. 2000;7(11):1239–1243.
- , . Interruptions and multitasking in nursing care. Jt Comm J Qual Paient Saf. 2010;36(3):126–132.
- , . Interruptions and distractions in healthcare: review and reappraisal. Qual Saf Health Care. 2010;19(4):304–312.
- , , . How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88–93.
- , , , , . Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683–690.
- , , , . Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs. Acad Med. 2005;80(12):1094–1099.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- Agency for Healthcare Research and Quality. Spotlight case. Order interrupted by text: multitasking mishap. Commentary by Halamka J. December 2011. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=257. Accessed April 16, 2012.
- , , , . Social media policies at US medical schools. Med Educ Online. 2010;15:5324. DOI: 10.3402/meo.v15i0.5324.
Healthcare market research has predicted that over 80% of physicians will use smartphones by 2012.1 These handheld devices allow users immediate access to various forms of electronic media such as Internet, instant messaging, and e‐mail. Smartphones provide numerous benefits to physicians, including rapid access to medical references, research applications, and patient information.2 These devices have been used for teleconsultation3 and patient education,4 and applications have been developed for numerous clinical specialties.48
Housestaff perceive that communication improves when they use smartphones rather than traditional pagers on the inpatient service,9 and patients may have a positive view of physicians' use of handheld computers.10 Medical schools and residency programs are increasingly requiring smartphone ownership for their trainees, with the expectation that smartphone use will enhance the educational experience, ensure the highest level of patient care, improve user efficiency, and help control the costs associated with purchasing updated textbooks.7, 1113 In the future, hospitals may rely on smartphone technologies to help reduce the enormous economic burden created by inefficient communication.14
Despite their numerous benefits for physicians and patients, little is known about the potential for smartphones to distract users in clinical care settings. Studies from the psychology and traffic safety fields have documented untoward consequences when individuals use electronic devices to multitask.1519 Given these concerns, we investigated the prevalence and patterns of smartphone use during inpatient attending rounds, and whether these devices can distract team members in this period of important information transfer.
METHODS
At our institution, attending rounds are faculty‐led inpatient teaching rounds that focus on clinical care and patient management; these sessions may be conducted either in the classroom or at the bedside, depending on patient and learner needs, and faculty preference. Inpatient teams are comprised of 1 attending, housestaff, and third and fourth year medical students. Each team conducts attending rounds independently; these rounds range in length from 1 hour (Pediatrics) to 2 hours (Medicine).
A survey instrument was designed to evaluate smartphone usage patterns during hospital inpatient attending rounds, and perceived distraction from smartphones in this setting. A preliminary version of the survey was pilot tested by a group of housestaff for face validity, redundancy, and ease of use, and it was subsequently revised. For the purposes of this study, a smartphone was defined broadly as any mobile, personal communication device (cellphone, iPhone, Android, Blackberry, iPad, etc). Residents were asked about their own smartphone use, as well as their observations of supervising attendings and other learners' devices use during rounds (see Supporting Appendix 1 in the online version of this article).
In February 2011, the anonymous online survey was administered using Survey Monkey (
Respondents were not required to answer each question in order to complete the survey. With the exception of free‐text comments, all responses were either yes/no or were graded on a 5‐point frequency scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always). This scale was chosen because it allowed for adequate dispersion of responses, and for the identification of meaningful smartphone usage among respondents (score 3) and data dichotomization. The z test was used to compare the proportions between independent groups.
All free‐text comments were imported into a Microsoft Word table. Comments were separated into 2 groups: housestaff and attending. Each comment was hand‐coded by 2 authors (R.J.K.‐S. and R.S.) to reach consensus for 1 of the following 4 categories: the comment was a positive statement; a negative statement; a positive/negative statement; or a neutral one, ie, neither positive nor negative. The terms positive and negative here refer to whether the statement explicitly highlighted benefits of smartphone use or a negative aspect of smartphone use, respectively. A comment was coded as positive/negative if it highlighted both benefits and drawbacks in the same comment. In addition, each comment that mentioned texting or call functions was secondarily coded as personal, patient, both, or unknown depending on the purpose of the texting or calls described in each comment. Comments were also reviewed for possible subthemes.
RESULTS
The overall response rate was 73% (156/214), with 81% (116/143) of housestaff and 56% (40/71) of faculty participating. The mean tenure of faculty respondents was 13 years. Eighty‐nine percent (103/116) of residents and 98% (39/40) of faculty owned devices, with 57% of housestaff and 28% of attendings reporting regular personal use of smartphones during attending rounds (Table 1).
| Smartphone User | Self‐Report % (n/N) | Resident Observations of Other Team Members % (n/N) | Faculty Observations of Trainees % (n/N) |
|---|---|---|---|
| |||
| Resident | 57% (59/103) | 91% (103/113)* | 73% (29/40) |
| Faculty | 28% (11/39) | 43% (49/113)* | n/a |
Respondents reported that they used their smartphones during attending rounds for the following reasons: 1) patient care (85% residents, 48% faculty); 2) reading/responding to personal texts/e‐mails (37% residents, 12% faculty); and 3) other non‐patient care uses, such as Web surfing (15% residents, 0% faculty) (Tables 2 and 3). Nineteen percent of residents reported that they missed important clinical information due to distraction from smartphone use, as did 12% of attendings (Table 4). Respondents reported observing other team members using smartphones and missing important clinical data at higher rates than they reported for themselves (see Tables 1, 4, and 5). A majority of both residents (56%) and faculty (73%) agreed (score >3) that smartphones can be a serious distraction during attending rounds, and 77% of attendings affirmed that teaching hospitals should establish smartphone use codes of conduct in order to minimize unnecessary distraction during attending rounds.
| Reason | Based on Housestaff Self‐Report (n = 85)* | Based on Trainee Observations of One Another (n = 112) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 85% | 86% | NS |
| Reading or responding to personal texts or e‐mail | 37% | 55% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 15% | 37% | <0.01 |
| Reason | Based on Faculty Self‐Report (n = 25)* | Based on Housestaff Observations of Faculty (n = 91) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 48% | 48% | NS |
| Reading or responding to personal texts or e‐mail | 12% | 47% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 0% | 20% | <0.05 |
| Smartphone User | Self‐Report % (n/N) |
|---|---|
| |
| Housestaff | 19% (18/85)* |
| Faculty | 12% (3/25)* |
| Smartphone User | Based on Housestaff Observation % (n/N) | Based on Faculty Observation % (n/N) |
|---|---|---|
| ||
| Trainee | 34% (38/112)* | 43% (17/40) |
| Faculty | 20% (18/91)* | n/a |
Despite not requiring responses in order to complete the questionnaires, we found that, in general, few eligible faculty or residents skipped questions on the survey. Nevertheless, there was a substantial drop in responses (91/116) for the last 2 questions on the housestaff survey. These questions asked for resident observations of attending smartphone usage patterns during rounds, and whether they had seen attendings miss clinical information because of distractions from smartphone use.
There were 25 free‐text comments from residents and 11 from attendings. The resultant comments highlight differences in residents' and attendings' perspectives toward smartphone use during attending rounds. Housestaff comments included 7 positive comments, 7 positive/negative comments, 1 negative comment, and 10 neutral comments. A subtheme that emerged in 2 of the housestaff comments was the importance of personal autonomy in being able to use one's smartphone. Attending comments included 2 positive comments, 0 positive/negative comments, 4 negative comments, and 5 neutral comments. Faculty comments revealed that attendings use their smartphones' e‐mail/texting and call capabilities during rounds both for patient care issues (3 comments) and/or urgent family concerns (2 comments). In 2 other attending comments, the reason for calls/texts during rounds was not specified.
Housestaff comments included: I do not know why it is that attendings never use it these phones are so easy to use and [enhance] patient care in a number of ways, Depending on how they are used, if strictly for pt care then they can be a great mobile tool, Of course they can be a distraction, but they are also a very good tool. You take the good with the bad, If you are bored you will find other things to occupy your mind. If you can look up some info at the time of rounding you are actively participating. Please, do not make it worse than it is already, and It is a personal choice. Faculty negative comments highlighted the potential for distraction from the e‐mail beeps, the fact that some of the housestaff will be tuned into their SmartPhones, that residents frequently check their phones during roundsa distraction and frankly rude when the attending or fellow are giving a brief lecture, and that sometimes more focus is on the SmartPhone than rounds.
DISCUSSION
Physicians and their patients benefit from the wide‐ranging capabilities of personal, mobile communication devices in the healthcare environment. Smartphones house the latest medical references, provide access to patients' medical records and imaging studies, can photograph or video physical findings, and educate and monitor patients.28 Smartphones can facilitate information transfer in the medical setting and may improve housestaff efficiency and communication.9
Despite their significant benefits, smartphones introduce another source of interruption, multitasking, and distraction into the hospital environment. There is increasing awareness that breaks‐in‐task in the clinical setting may have negative consequences.2024 While some types of interruptions are beneficial and can facilitate patient care (eg, an alarm ringing to indicate abnormal vitals signs on a patient),2024 other forms of interruptions, even those that are self‐initiated,22 can be distracting and detrimental. Along these lines, recommendations for safe handoffs and information transfer have specifically included advice to minimize potential distractions.25
In addition, studies from the psychology and education literature have previously documented negative consequences on learning when individuals use electronic devices to multitask.1517 Students who used a laptop in class were likely to multitask, become distracted, and distract others; the more a student used the laptop in class, the lower the student's class performance.15 Multitasking with a cellphone during driving can be especially hazardous.18, 19 According to National Highway Traffic Safety Administration data, 20% of injury crashes in 2009 involved reports of distracted driving, and cellphones were implicated in 18% of distracted driving deaths that year.18
Little is known about any negative effects of using personal electronic devices in the context of patient care. A 2011 study of Internal Medicine residents who used smartphones for team communication documented both positive and negative consequences of smartphone use in the hospital setting. Negative consequences included frequent interruptions, a weakening of interprofessional behaviors as housestaff relied on texting over direct communication with nurses, and unprofessional housestaff behaviors.26 The Agency for Healthcare Quality and Research published a case report in which a resident's smartphone use during clinical care resulted in patient harm.27 To our knowledge, this is the first study to detail housestaff and faculty smartphone usage patterns and potential for user distractibility during inpatient attending rounds.
Our data show that device use during attending rounds is prevalent among residents and faculty alike, with the majority of use related to patient care. However, attendings were half as likely as residents to report using devices regularly during rounds. This finding may reflect attendings' inability to multitask while leading the rounds, or a deliberate role‐modeling of desired conduct during rounds. Generational differences may also play a role, with residents more likely than their older attendings to multitask and self‐interrupt. Along these lines, traffic safety research has found that younger drivers are more likely to text during driving; approximately 30% of drivers under 30 years old reported texting while driving in the previous 30 days, compared to 9% of respondents over 30 years old.19 Increased smartphone use by housestaff during rounds may also reflect attitudinal differences between the 2 groups. As seen in the free‐text comments, housestaff tended to emphasize the benefits of smartphone use, and with 1 exception, all negative housestaff comments were balanced by a positive statement. Faculty more commonly underscored the negative aspects of smartphone use during rounds, including the devices' adverse effects on housestaff professional behavior in this setting.
Faculty and housestaff consistently reported observing others using smartphones at higher rates than they reported for themselves. This discrepancy may reflect underrecognition of self‐use, or a discomfort in reporting self‐use during attending rounds. In addition, residents' observations of other trainees' usage of smartphones (91%) was higher than faculty observation of the same group (73%). Trainees' smartphone use may be less obvious to attendings who are involved in facilitating rounds. Alternatively, trainees may use their smartphones in subtle ways to prevent attending awareness.
There are several limitations to our study. Our research focused specifically on attending rounds. Smartphone usage patterns by faculty and housestaff at other times in the work day, such as during resident handoffs, at a patient's bedside, or during academic conferences, may differ. Nevertheless, we specifically chose to study smartphone use during attending rounds, as these sessions are discrete time frames during which important teaching occurs and clinical management decisions are made. With recent Accreditation Council for Graduate Medical Education (ACGME) work hour restrictions, these faculty‐led rounds may become increasingly important in ensuring the safe transition of patient care. Secondly, despite asking respondents how often they use their smartphones for personal texts or e‐mails, it was clear from the free‐text comments that respondents use their smartphone e‐mail/texting capabilities and take urgent calls during rounds for both patient care and/or family issues. It is not possible from the data to sort out the subset of respondents who use texting or e‐mailing exclusively for patient care during rounds. Third, we did not survey medical students on the teams, so it is possible that their device use on rounds differs from that of housestaff and faculty. Fourth, since the survey could be completed without answering every question, response rates for some items varied slightly; there was a substantial reduction in the number of eligible residents who answered the final 2 questions on the survey about their observations of attendings' smartphone usage patterns and distraction during rounds. While the flexibility in survey completion was intended to enhance overall study participation, it is unknown how nonresponders might have affected the study results; as such, those specific results should be interpreted with some caution. Finally, our findings were based on respondents' retrospective recall, and therefore may not accurately reflect true usage patterns. Timemotion studies with real‐time observation of smartphone use would provide more accurate data.
A majority of residents and attendings in our study agreed that smartphones can pose a serious distraction during attending rounds, and attendings strongly favored the institution of formal codes of conduct for smartphone use during inpatient attending rounds. The development of such policies are important for patient safety; at the same time, they are in line with medical institutions' increasing awareness about the need for guidelines regarding other aspects of digital professionalism.28 In February 2012, our hospital instituted a policy regarding appropriate device use during inpatient attending rounds (see Supporting Appendix 3 in the online version of this article). Because our research found differences in housestaff and faculty attitudes toward smartphone use during rounds, we developed our policy after discussion with, and feedback from, all members of the inpatient team, including faculty, residents, and medical students. Incorporating the various perspectives of all stakeholders can be helpful to institutions in developing guidelines that maximize the benefits of smartphone use in the learning environment, while reducing the potential for distraction and adverse outcomes.
Acknowledgements
Disclosure: Nothing to report.
Healthcare market research has predicted that over 80% of physicians will use smartphones by 2012.1 These handheld devices allow users immediate access to various forms of electronic media such as Internet, instant messaging, and e‐mail. Smartphones provide numerous benefits to physicians, including rapid access to medical references, research applications, and patient information.2 These devices have been used for teleconsultation3 and patient education,4 and applications have been developed for numerous clinical specialties.48
Housestaff perceive that communication improves when they use smartphones rather than traditional pagers on the inpatient service,9 and patients may have a positive view of physicians' use of handheld computers.10 Medical schools and residency programs are increasingly requiring smartphone ownership for their trainees, with the expectation that smartphone use will enhance the educational experience, ensure the highest level of patient care, improve user efficiency, and help control the costs associated with purchasing updated textbooks.7, 1113 In the future, hospitals may rely on smartphone technologies to help reduce the enormous economic burden created by inefficient communication.14
Despite their numerous benefits for physicians and patients, little is known about the potential for smartphones to distract users in clinical care settings. Studies from the psychology and traffic safety fields have documented untoward consequences when individuals use electronic devices to multitask.1519 Given these concerns, we investigated the prevalence and patterns of smartphone use during inpatient attending rounds, and whether these devices can distract team members in this period of important information transfer.
METHODS
At our institution, attending rounds are faculty‐led inpatient teaching rounds that focus on clinical care and patient management; these sessions may be conducted either in the classroom or at the bedside, depending on patient and learner needs, and faculty preference. Inpatient teams are comprised of 1 attending, housestaff, and third and fourth year medical students. Each team conducts attending rounds independently; these rounds range in length from 1 hour (Pediatrics) to 2 hours (Medicine).
A survey instrument was designed to evaluate smartphone usage patterns during hospital inpatient attending rounds, and perceived distraction from smartphones in this setting. A preliminary version of the survey was pilot tested by a group of housestaff for face validity, redundancy, and ease of use, and it was subsequently revised. For the purposes of this study, a smartphone was defined broadly as any mobile, personal communication device (cellphone, iPhone, Android, Blackberry, iPad, etc). Residents were asked about their own smartphone use, as well as their observations of supervising attendings and other learners' devices use during rounds (see Supporting Appendix 1 in the online version of this article).
In February 2011, the anonymous online survey was administered using Survey Monkey (
Respondents were not required to answer each question in order to complete the survey. With the exception of free‐text comments, all responses were either yes/no or were graded on a 5‐point frequency scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always). This scale was chosen because it allowed for adequate dispersion of responses, and for the identification of meaningful smartphone usage among respondents (score 3) and data dichotomization. The z test was used to compare the proportions between independent groups.
All free‐text comments were imported into a Microsoft Word table. Comments were separated into 2 groups: housestaff and attending. Each comment was hand‐coded by 2 authors (R.J.K.‐S. and R.S.) to reach consensus for 1 of the following 4 categories: the comment was a positive statement; a negative statement; a positive/negative statement; or a neutral one, ie, neither positive nor negative. The terms positive and negative here refer to whether the statement explicitly highlighted benefits of smartphone use or a negative aspect of smartphone use, respectively. A comment was coded as positive/negative if it highlighted both benefits and drawbacks in the same comment. In addition, each comment that mentioned texting or call functions was secondarily coded as personal, patient, both, or unknown depending on the purpose of the texting or calls described in each comment. Comments were also reviewed for possible subthemes.
RESULTS
The overall response rate was 73% (156/214), with 81% (116/143) of housestaff and 56% (40/71) of faculty participating. The mean tenure of faculty respondents was 13 years. Eighty‐nine percent (103/116) of residents and 98% (39/40) of faculty owned devices, with 57% of housestaff and 28% of attendings reporting regular personal use of smartphones during attending rounds (Table 1).
| Smartphone User | Self‐Report % (n/N) | Resident Observations of Other Team Members % (n/N) | Faculty Observations of Trainees % (n/N) |
|---|---|---|---|
| |||
| Resident | 57% (59/103) | 91% (103/113)* | 73% (29/40) |
| Faculty | 28% (11/39) | 43% (49/113)* | n/a |
Respondents reported that they used their smartphones during attending rounds for the following reasons: 1) patient care (85% residents, 48% faculty); 2) reading/responding to personal texts/e‐mails (37% residents, 12% faculty); and 3) other non‐patient care uses, such as Web surfing (15% residents, 0% faculty) (Tables 2 and 3). Nineteen percent of residents reported that they missed important clinical information due to distraction from smartphone use, as did 12% of attendings (Table 4). Respondents reported observing other team members using smartphones and missing important clinical data at higher rates than they reported for themselves (see Tables 1, 4, and 5). A majority of both residents (56%) and faculty (73%) agreed (score >3) that smartphones can be a serious distraction during attending rounds, and 77% of attendings affirmed that teaching hospitals should establish smartphone use codes of conduct in order to minimize unnecessary distraction during attending rounds.
| Reason | Based on Housestaff Self‐Report (n = 85)* | Based on Trainee Observations of One Another (n = 112) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 85% | 86% | NS |
| Reading or responding to personal texts or e‐mail | 37% | 55% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 15% | 37% | <0.01 |
| Reason | Based on Faculty Self‐Report (n = 25)* | Based on Housestaff Observations of Faculty (n = 91) | P Value |
|---|---|---|---|
| |||
| Patient care‐related use (ePocrates, MedCalc, Medline, Google Scholar) | 48% | 48% | NS |
| Reading or responding to personal texts or e‐mail | 12% | 47% | <0.01 |
| Other non‐patient care‐related use, Web surfing | 0% | 20% | <0.05 |
| Smartphone User | Self‐Report % (n/N) |
|---|---|
| |
| Housestaff | 19% (18/85)* |
| Faculty | 12% (3/25)* |
| Smartphone User | Based on Housestaff Observation % (n/N) | Based on Faculty Observation % (n/N) |
|---|---|---|
| ||
| Trainee | 34% (38/112)* | 43% (17/40) |
| Faculty | 20% (18/91)* | n/a |
Despite not requiring responses in order to complete the questionnaires, we found that, in general, few eligible faculty or residents skipped questions on the survey. Nevertheless, there was a substantial drop in responses (91/116) for the last 2 questions on the housestaff survey. These questions asked for resident observations of attending smartphone usage patterns during rounds, and whether they had seen attendings miss clinical information because of distractions from smartphone use.
There were 25 free‐text comments from residents and 11 from attendings. The resultant comments highlight differences in residents' and attendings' perspectives toward smartphone use during attending rounds. Housestaff comments included 7 positive comments, 7 positive/negative comments, 1 negative comment, and 10 neutral comments. A subtheme that emerged in 2 of the housestaff comments was the importance of personal autonomy in being able to use one's smartphone. Attending comments included 2 positive comments, 0 positive/negative comments, 4 negative comments, and 5 neutral comments. Faculty comments revealed that attendings use their smartphones' e‐mail/texting and call capabilities during rounds both for patient care issues (3 comments) and/or urgent family concerns (2 comments). In 2 other attending comments, the reason for calls/texts during rounds was not specified.
Housestaff comments included: I do not know why it is that attendings never use it these phones are so easy to use and [enhance] patient care in a number of ways, Depending on how they are used, if strictly for pt care then they can be a great mobile tool, Of course they can be a distraction, but they are also a very good tool. You take the good with the bad, If you are bored you will find other things to occupy your mind. If you can look up some info at the time of rounding you are actively participating. Please, do not make it worse than it is already, and It is a personal choice. Faculty negative comments highlighted the potential for distraction from the e‐mail beeps, the fact that some of the housestaff will be tuned into their SmartPhones, that residents frequently check their phones during roundsa distraction and frankly rude when the attending or fellow are giving a brief lecture, and that sometimes more focus is on the SmartPhone than rounds.
DISCUSSION
Physicians and their patients benefit from the wide‐ranging capabilities of personal, mobile communication devices in the healthcare environment. Smartphones house the latest medical references, provide access to patients' medical records and imaging studies, can photograph or video physical findings, and educate and monitor patients.28 Smartphones can facilitate information transfer in the medical setting and may improve housestaff efficiency and communication.9
Despite their significant benefits, smartphones introduce another source of interruption, multitasking, and distraction into the hospital environment. There is increasing awareness that breaks‐in‐task in the clinical setting may have negative consequences.2024 While some types of interruptions are beneficial and can facilitate patient care (eg, an alarm ringing to indicate abnormal vitals signs on a patient),2024 other forms of interruptions, even those that are self‐initiated,22 can be distracting and detrimental. Along these lines, recommendations for safe handoffs and information transfer have specifically included advice to minimize potential distractions.25
In addition, studies from the psychology and education literature have previously documented negative consequences on learning when individuals use electronic devices to multitask.1517 Students who used a laptop in class were likely to multitask, become distracted, and distract others; the more a student used the laptop in class, the lower the student's class performance.15 Multitasking with a cellphone during driving can be especially hazardous.18, 19 According to National Highway Traffic Safety Administration data, 20% of injury crashes in 2009 involved reports of distracted driving, and cellphones were implicated in 18% of distracted driving deaths that year.18
Little is known about any negative effects of using personal electronic devices in the context of patient care. A 2011 study of Internal Medicine residents who used smartphones for team communication documented both positive and negative consequences of smartphone use in the hospital setting. Negative consequences included frequent interruptions, a weakening of interprofessional behaviors as housestaff relied on texting over direct communication with nurses, and unprofessional housestaff behaviors.26 The Agency for Healthcare Quality and Research published a case report in which a resident's smartphone use during clinical care resulted in patient harm.27 To our knowledge, this is the first study to detail housestaff and faculty smartphone usage patterns and potential for user distractibility during inpatient attending rounds.
Our data show that device use during attending rounds is prevalent among residents and faculty alike, with the majority of use related to patient care. However, attendings were half as likely as residents to report using devices regularly during rounds. This finding may reflect attendings' inability to multitask while leading the rounds, or a deliberate role‐modeling of desired conduct during rounds. Generational differences may also play a role, with residents more likely than their older attendings to multitask and self‐interrupt. Along these lines, traffic safety research has found that younger drivers are more likely to text during driving; approximately 30% of drivers under 30 years old reported texting while driving in the previous 30 days, compared to 9% of respondents over 30 years old.19 Increased smartphone use by housestaff during rounds may also reflect attitudinal differences between the 2 groups. As seen in the free‐text comments, housestaff tended to emphasize the benefits of smartphone use, and with 1 exception, all negative housestaff comments were balanced by a positive statement. Faculty more commonly underscored the negative aspects of smartphone use during rounds, including the devices' adverse effects on housestaff professional behavior in this setting.
Faculty and housestaff consistently reported observing others using smartphones at higher rates than they reported for themselves. This discrepancy may reflect underrecognition of self‐use, or a discomfort in reporting self‐use during attending rounds. In addition, residents' observations of other trainees' usage of smartphones (91%) was higher than faculty observation of the same group (73%). Trainees' smartphone use may be less obvious to attendings who are involved in facilitating rounds. Alternatively, trainees may use their smartphones in subtle ways to prevent attending awareness.
There are several limitations to our study. Our research focused specifically on attending rounds. Smartphone usage patterns by faculty and housestaff at other times in the work day, such as during resident handoffs, at a patient's bedside, or during academic conferences, may differ. Nevertheless, we specifically chose to study smartphone use during attending rounds, as these sessions are discrete time frames during which important teaching occurs and clinical management decisions are made. With recent Accreditation Council for Graduate Medical Education (ACGME) work hour restrictions, these faculty‐led rounds may become increasingly important in ensuring the safe transition of patient care. Secondly, despite asking respondents how often they use their smartphones for personal texts or e‐mails, it was clear from the free‐text comments that respondents use their smartphone e‐mail/texting capabilities and take urgent calls during rounds for both patient care and/or family issues. It is not possible from the data to sort out the subset of respondents who use texting or e‐mailing exclusively for patient care during rounds. Third, we did not survey medical students on the teams, so it is possible that their device use on rounds differs from that of housestaff and faculty. Fourth, since the survey could be completed without answering every question, response rates for some items varied slightly; there was a substantial reduction in the number of eligible residents who answered the final 2 questions on the survey about their observations of attendings' smartphone usage patterns and distraction during rounds. While the flexibility in survey completion was intended to enhance overall study participation, it is unknown how nonresponders might have affected the study results; as such, those specific results should be interpreted with some caution. Finally, our findings were based on respondents' retrospective recall, and therefore may not accurately reflect true usage patterns. Timemotion studies with real‐time observation of smartphone use would provide more accurate data.
A majority of residents and attendings in our study agreed that smartphones can pose a serious distraction during attending rounds, and attendings strongly favored the institution of formal codes of conduct for smartphone use during inpatient attending rounds. The development of such policies are important for patient safety; at the same time, they are in line with medical institutions' increasing awareness about the need for guidelines regarding other aspects of digital professionalism.28 In February 2012, our hospital instituted a policy regarding appropriate device use during inpatient attending rounds (see Supporting Appendix 3 in the online version of this article). Because our research found differences in housestaff and faculty attitudes toward smartphone use during rounds, we developed our policy after discussion with, and feedback from, all members of the inpatient team, including faculty, residents, and medical students. Incorporating the various perspectives of all stakeholders can be helpful to institutions in developing guidelines that maximize the benefits of smartphone use in the learning environment, while reducing the potential for distraction and adverse outcomes.
Acknowledgements
Disclosure: Nothing to report.
- . 72 percent of US physicians use smartphones. MobiHealthNews. Available at: http://mobihealthnews.com/7505/72‐percent‐of‐us‐physicians‐use‐smartphones/. Accessed April 16, 2012.
- . Smartphones in clinical practice, medical education, and research. Arch Intern Med. 2011;171(14):1294–1296.
- ,. Telemedicine using smartphones for oral and maxillofacial surgery consultation, communication, and treatment planning.J Oral Maxillofac Surg.2009;67:2505–2509.
- . Mobile phones to improve the practice of neurology. Neurol Clin. 2010;28(2):395–410.
- , , . Infectious diseases resources for the iPhone. Clin Infect Dis. 2010;50(9):1268–1274.
- , , , . Novel uses of smartphones in ophthalmology. Ophthalmology. 2010;117:1274–1274.e3.
- , , . The uses of the iPhone for surgeons. Surgeon. 2011;9(1):44–48.
- . Smartphone apps for orthopaedic surgeons. Clin Orthop Relat Res. 2011;469(7):2042–2048.
- , , , et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553–559.
- , , , . Patient attitudes toward physician use of tablet computers in the exam room. Fam Med. 2010;42(9):643–647.
- . iPads to be distributed to incoming class by Stanford Medical School. Available at: http://med.stanford.edu/ism/2010/august/ipad.html. Accessed April 16, 2012.
- University of Virginia School of Medicine. Third year medical student mobile device requirement. Available at: http://www.medicine.virginia.edu/education/medical‐students/ome/edtech/pda_recom‐page/. Accessed April 16, 2012.
- . Tablet computers in the hospital. ACP Hospitalist 2011. Available at: http://www.acphospitalist.org/archives/2011/08/tablet. htm. Accessed April 16, 2012.
- , , . Quantifying the economic impact of communication inefficiencies in US hospitals. Available at: http://www.rhsmith.umd.edu/chids/pdfs_docs/ResearchBriefings/CHIDS‐ResearchBriefing‐Vol3Issue1b.pdf. Accessed April 16, 2012.
- . In‐class laptop use and its effects on student learning. Computers 50(3):906–914.
- , , . Distractions, distractions: does instant messaging affect college students' performance on a concurrent reading comprehension task? CyberPsychology 12(1):51–53.
- , , , . Can students really multitask? An experimental study of instant messaging while reading. Computers 54(4):927–931.
- US Department of Transportation. Statistics and facts about distracted driving. Available at: http://www.distraction.gov/stats‐and‐facts/index.html. Accessed November 17, 2011.
- Driving distracted. Consumer Reports. April 2011:22–25. See also: http://www.distraction.gov/files/for‐media/2011/2011–03‐04‐cr‐dot‐distracted‐driving‐initiative.pdf. Accessed November 25, 2011.
- , , , . Emergency department workplace interruptions: are emergency physicians “interrupt‐driven” and “multitasking”? Acad Emerg Med. 2000;7(11):1239–1243.
- , . Interruptions and multitasking in nursing care. Jt Comm J Qual Paient Saf. 2010;36(3):126–132.
- , . Interruptions and distractions in healthcare: review and reappraisal. Qual Saf Health Care. 2010;19(4):304–312.
- , , . How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88–93.
- , , , , . Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683–690.
- , , , . Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs. Acad Med. 2005;80(12):1094–1099.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- Agency for Healthcare Research and Quality. Spotlight case. Order interrupted by text: multitasking mishap. Commentary by Halamka J. December 2011. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=257. Accessed April 16, 2012.
- , , , . Social media policies at US medical schools. Med Educ Online. 2010;15:5324. DOI: 10.3402/meo.v15i0.5324.
- . 72 percent of US physicians use smartphones. MobiHealthNews. Available at: http://mobihealthnews.com/7505/72‐percent‐of‐us‐physicians‐use‐smartphones/. Accessed April 16, 2012.
- . Smartphones in clinical practice, medical education, and research. Arch Intern Med. 2011;171(14):1294–1296.
- ,. Telemedicine using smartphones for oral and maxillofacial surgery consultation, communication, and treatment planning.J Oral Maxillofac Surg.2009;67:2505–2509.
- . Mobile phones to improve the practice of neurology. Neurol Clin. 2010;28(2):395–410.
- , , . Infectious diseases resources for the iPhone. Clin Infect Dis. 2010;50(9):1268–1274.
- , , , . Novel uses of smartphones in ophthalmology. Ophthalmology. 2010;117:1274–1274.e3.
- , , . The uses of the iPhone for surgeons. Surgeon. 2011;9(1):44–48.
- . Smartphone apps for orthopaedic surgeons. Clin Orthop Relat Res. 2011;469(7):2042–2048.
- , , , et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553–559.
- , , , . Patient attitudes toward physician use of tablet computers in the exam room. Fam Med. 2010;42(9):643–647.
- . iPads to be distributed to incoming class by Stanford Medical School. Available at: http://med.stanford.edu/ism/2010/august/ipad.html. Accessed April 16, 2012.
- University of Virginia School of Medicine. Third year medical student mobile device requirement. Available at: http://www.medicine.virginia.edu/education/medical‐students/ome/edtech/pda_recom‐page/. Accessed April 16, 2012.
- . Tablet computers in the hospital. ACP Hospitalist 2011. Available at: http://www.acphospitalist.org/archives/2011/08/tablet. htm. Accessed April 16, 2012.
- , , . Quantifying the economic impact of communication inefficiencies in US hospitals. Available at: http://www.rhsmith.umd.edu/chids/pdfs_docs/ResearchBriefings/CHIDS‐ResearchBriefing‐Vol3Issue1b.pdf. Accessed April 16, 2012.
- . In‐class laptop use and its effects on student learning. Computers 50(3):906–914.
- , , . Distractions, distractions: does instant messaging affect college students' performance on a concurrent reading comprehension task? CyberPsychology 12(1):51–53.
- , , , . Can students really multitask? An experimental study of instant messaging while reading. Computers 54(4):927–931.
- US Department of Transportation. Statistics and facts about distracted driving. Available at: http://www.distraction.gov/stats‐and‐facts/index.html. Accessed November 17, 2011.
- Driving distracted. Consumer Reports. April 2011:22–25. See also: http://www.distraction.gov/files/for‐media/2011/2011–03‐04‐cr‐dot‐distracted‐driving‐initiative.pdf. Accessed November 25, 2011.
- , , , . Emergency department workplace interruptions: are emergency physicians “interrupt‐driven” and “multitasking”? Acad Emerg Med. 2000;7(11):1239–1243.
- , . Interruptions and multitasking in nursing care. Jt Comm J Qual Paient Saf. 2010;36(3):126–132.
- , . Interruptions and distractions in healthcare: review and reappraisal. Qual Saf Health Care. 2010;19(4):304–312.
- , , . How hospitalists spend their time: insights on efficiency and safety. J Hosp Med. 2006;1(2):88–93.
- , , , , . Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683–690.
- , , , . Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs. Acad Med. 2005;80(12):1094–1099.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- Agency for Healthcare Research and Quality. Spotlight case. Order interrupted by text: multitasking mishap. Commentary by Halamka J. December 2011. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=257. Accessed April 16, 2012.
- , , , . Social media policies at US medical schools. Med Educ Online. 2010;15:5324. DOI: 10.3402/meo.v15i0.5324.
Copyright © 2012 Society of Hospital Medicine
New Study on Anticoagulation Therapies “Definitive Word” on Topic, Hospitalist Says
A recent report that states the choice between warfarin and aspirin in patients with heart failure and sinus rhythm should be individualized is the most definitive word to date on the topic, says a hospitalist focused on anticoagulation therapies.
The report, “Warfarin and Aspirin in Patients with Heart Failure and Sinus Rhythm,” focused on patients in sinus rhythm who had reduced left ventricular ejection fraction (LVEF). The authors concluded that the reduced risk of ischemic stroke with warfarin was offset by an increased risk of major hemorrhage.
“The new thing about this study is it’s really the definitive, well-designed, large trial that provides guidance to us as to what is right,” says Margaret Fang, MD, MPH, an associate professor of medicine at the University of California at San Francisco (UCSF) and medical director of the UCSF Anticoagulation Clinic. “Is warfarin really the right decision?”
Dr. Fang notes that the report, known more commonly as the Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction (WARCEF) trial, did find that, over time, warfarin began to show improvement over aspirin. But the improvements, which favored warfarin by the fourth year of the six-year trial, were deemed only marginally significant (P=.046).
A recent report that states the choice between warfarin and aspirin in patients with heart failure and sinus rhythm should be individualized is the most definitive word to date on the topic, says a hospitalist focused on anticoagulation therapies.
The report, “Warfarin and Aspirin in Patients with Heart Failure and Sinus Rhythm,” focused on patients in sinus rhythm who had reduced left ventricular ejection fraction (LVEF). The authors concluded that the reduced risk of ischemic stroke with warfarin was offset by an increased risk of major hemorrhage.
“The new thing about this study is it’s really the definitive, well-designed, large trial that provides guidance to us as to what is right,” says Margaret Fang, MD, MPH, an associate professor of medicine at the University of California at San Francisco (UCSF) and medical director of the UCSF Anticoagulation Clinic. “Is warfarin really the right decision?”
Dr. Fang notes that the report, known more commonly as the Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction (WARCEF) trial, did find that, over time, warfarin began to show improvement over aspirin. But the improvements, which favored warfarin by the fourth year of the six-year trial, were deemed only marginally significant (P=.046).
A recent report that states the choice between warfarin and aspirin in patients with heart failure and sinus rhythm should be individualized is the most definitive word to date on the topic, says a hospitalist focused on anticoagulation therapies.
The report, “Warfarin and Aspirin in Patients with Heart Failure and Sinus Rhythm,” focused on patients in sinus rhythm who had reduced left ventricular ejection fraction (LVEF). The authors concluded that the reduced risk of ischemic stroke with warfarin was offset by an increased risk of major hemorrhage.
“The new thing about this study is it’s really the definitive, well-designed, large trial that provides guidance to us as to what is right,” says Margaret Fang, MD, MPH, an associate professor of medicine at the University of California at San Francisco (UCSF) and medical director of the UCSF Anticoagulation Clinic. “Is warfarin really the right decision?”
Dr. Fang notes that the report, known more commonly as the Warfarin versus Aspirin in Reduced Cardiac Ejection Fraction (WARCEF) trial, did find that, over time, warfarin began to show improvement over aspirin. But the improvements, which favored warfarin by the fourth year of the six-year trial, were deemed only marginally significant (P=.046).
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Is the risk of recurrence of Clostridium difficile infection (CDI) increased by the use of “non-CDI” antimicrobial agents (inactive against C. diff) during or after CDI therapy?
Background: Recurrence of CDI is expected to increase with use of non-CDI antimicrobials. Previous studies have not distinguished between the timing of non-CDI agents during and after CDI treatment, nor examined the effect of frequency, duration, or type of non-CDI antibiotic therapy.
Study design: Retrospective cohort.
Setting: Academic Veterans Affairs medical center.
Synopsis: All patients with CDI over a three-year period were evaluated to determine the association between non-CDI antimicrobial during or within 30 days following CDI therapy and 90-day CDI recurrence. Of 246 patients, 57% received concurrent or subsequent non-CDI antimicrobials. CDI recurred in 40% of patients who received non-CDI antimicrobials and in 16% of those who did not (OR: 3.5, 95% CI: 1.9 to 6.5).
After multivariable adjustment (including age, duration of CDI treatment, comorbidity, hospital and ICU admission, and gastric acid suppression), those who received non-CDI antimicrobials during CDI therapy had no increased risk of recurrence. However, those who received any non-CDI antimicrobials after initial CDI treatment had an absolute recurrence rate of 48% with an adjusted OR of 3.02 (95% CI: 1.65 to 5.52). This increased risk of recurrence was unaffected by the number or duration of non-CDI antimicrobial prescriptions. Subgroup analysis by antimicrobial class revealed statistically significant associations only with beta-lactams and fluoroquinolones.
Bottom line: The risk of recurrence of CDI is tripled by exposure to non-CDI antimicrobials within 30 days after CDI treatment, irrespective of the number or duration of such exposures.
Citation: Drekonja DM, Amundson WH, DeCarolis DD, Kuskowski MA, Lederle FA, Johnson JR. Antimicrobial use and risk for recurrent Clostridium difficile infection. Am J Med. 2011;124:1081.e1-1081.e7.
Clinical question: Is the risk of recurrence of Clostridium difficile infection (CDI) increased by the use of “non-CDI” antimicrobial agents (inactive against C. diff) during or after CDI therapy?
Background: Recurrence of CDI is expected to increase with use of non-CDI antimicrobials. Previous studies have not distinguished between the timing of non-CDI agents during and after CDI treatment, nor examined the effect of frequency, duration, or type of non-CDI antibiotic therapy.
Study design: Retrospective cohort.
Setting: Academic Veterans Affairs medical center.
Synopsis: All patients with CDI over a three-year period were evaluated to determine the association between non-CDI antimicrobial during or within 30 days following CDI therapy and 90-day CDI recurrence. Of 246 patients, 57% received concurrent or subsequent non-CDI antimicrobials. CDI recurred in 40% of patients who received non-CDI antimicrobials and in 16% of those who did not (OR: 3.5, 95% CI: 1.9 to 6.5).
After multivariable adjustment (including age, duration of CDI treatment, comorbidity, hospital and ICU admission, and gastric acid suppression), those who received non-CDI antimicrobials during CDI therapy had no increased risk of recurrence. However, those who received any non-CDI antimicrobials after initial CDI treatment had an absolute recurrence rate of 48% with an adjusted OR of 3.02 (95% CI: 1.65 to 5.52). This increased risk of recurrence was unaffected by the number or duration of non-CDI antimicrobial prescriptions. Subgroup analysis by antimicrobial class revealed statistically significant associations only with beta-lactams and fluoroquinolones.
Bottom line: The risk of recurrence of CDI is tripled by exposure to non-CDI antimicrobials within 30 days after CDI treatment, irrespective of the number or duration of such exposures.
Citation: Drekonja DM, Amundson WH, DeCarolis DD, Kuskowski MA, Lederle FA, Johnson JR. Antimicrobial use and risk for recurrent Clostridium difficile infection. Am J Med. 2011;124:1081.e1-1081.e7.
Clinical question: Is the risk of recurrence of Clostridium difficile infection (CDI) increased by the use of “non-CDI” antimicrobial agents (inactive against C. diff) during or after CDI therapy?
Background: Recurrence of CDI is expected to increase with use of non-CDI antimicrobials. Previous studies have not distinguished between the timing of non-CDI agents during and after CDI treatment, nor examined the effect of frequency, duration, or type of non-CDI antibiotic therapy.
Study design: Retrospective cohort.
Setting: Academic Veterans Affairs medical center.
Synopsis: All patients with CDI over a three-year period were evaluated to determine the association between non-CDI antimicrobial during or within 30 days following CDI therapy and 90-day CDI recurrence. Of 246 patients, 57% received concurrent or subsequent non-CDI antimicrobials. CDI recurred in 40% of patients who received non-CDI antimicrobials and in 16% of those who did not (OR: 3.5, 95% CI: 1.9 to 6.5).
After multivariable adjustment (including age, duration of CDI treatment, comorbidity, hospital and ICU admission, and gastric acid suppression), those who received non-CDI antimicrobials during CDI therapy had no increased risk of recurrence. However, those who received any non-CDI antimicrobials after initial CDI treatment had an absolute recurrence rate of 48% with an adjusted OR of 3.02 (95% CI: 1.65 to 5.52). This increased risk of recurrence was unaffected by the number or duration of non-CDI antimicrobial prescriptions. Subgroup analysis by antimicrobial class revealed statistically significant associations only with beta-lactams and fluoroquinolones.
Bottom line: The risk of recurrence of CDI is tripled by exposure to non-CDI antimicrobials within 30 days after CDI treatment, irrespective of the number or duration of such exposures.
Citation: Drekonja DM, Amundson WH, DeCarolis DD, Kuskowski MA, Lederle FA, Johnson JR. Antimicrobial use and risk for recurrent Clostridium difficile infection. Am J Med. 2011;124:1081.e1-1081.e7.
Drug for aHUS effective but expensive

Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Congress of the EHA
Photo courtesy of EHA
AMSTERDAM—Eculizumab elicits “phenomenal” results in atypical hemolytic uremic syndrome (aHUS), according to two presentations given at the 17th Annual Congress of the European Hematology Association.
But, as one speaker pointed out, the drug may prove too expensive for a lot of patients.
“It’s the most expensive drug I’ve ever come across in my entire life,” said Adrian Newland, MD, of Barts and The London School of Medicine and Dentistry in the UK.
He noted that the drug costs about £400,000 per year in the UK. And reports have listed the US cost at around $400,000 per year.
Expense aside, the drug elicits “dramatic” improvements in aHUS patients, according to Dr Newland. And he presented data to support that statement during an EHA-JSH joint symposium on platelet disorders.
Ramon Vilalta, MD, of Hospital Vall d’Hebron in Barcelona, Spain, also presented favorable results with eculizumab at the meeting, as abstract 1155.
Dr Vilalta began his presentation by pointing out that aHUS is a life-threatening disease that results in multi-organ damage caused by thrombotic microangiopathy (TMA). And plasma exchange/plasma infusion (PE/PI) therapy does little to alter the poor prognosis in this patient population.
“Our patients—pediatric patients mainly—develop end-stage renal failure and even die, despite treatment [with PE/PI],” he said. “[E]culizumab is an anti-C5 terminal complement blocker that could give some hope in the treatment of these patients.”
In an attempt to prove this theory, Dr Vilalta and his colleagues retrospectively analyzed 19 patients with aHUS. Patients—who ranged in age from 2 months to 17 years—received eculizumab for a median of 6 months (range, less than 1 month to 16 months).
All 19 patients had renal complications prior to receiving eculizumab, and 10 had renal and extra-renal complications. Eight patients had baseline platelet counts less than 150 x 109/L. Eight patients were on dialysis at the start of therapy, and 6 patients had undergone kidney transplant.
The first thing the researchers noticed was that eculizumab increased patients’ platelet counts within a week of administration. And this effect was maintained throughout the study period.
Seven of the 8 patients (88%) with abnormal platelet counts at baseline achieved normalized platelet counts. And 89% of all the patients (17/19) had platelet counts of 150 x 109/L or greater at the data cutoff point.
Eculizumab also reduced the burden of disease, Dr Vilalta said. He and his colleagues observed a significant reduction in the TMA intervention rate, which included the number of PE/PIs and new dialysis events. There were a median of 2 interventions per patient per week before treatment initiation, and a median of 0 interventions during treatment (P<0.0001).
None of the patients required new dialysis, and eculizumab eliminated the need for dialysis in 50% of patients (4/8).
Dr Vilalta also pointed out that eculizumab demonstrated similar efficacy regardless of patients’ mutation status or age. He added that the drug appeared to be well-tolerated, although the retrospective nature of the study did not allow for the full collection of drug-specific adverse events.
Of the side effects the researchers did observe, most were mild or moderate. Nine patients experienced pyrexia, 6 had diarrhea, 6 developed an upper respiratory tract infection, 5 developed a cough, 4 experienced vomiting, 4 had nasal congestion, 4 had tachycardia, and 1 patient developed a meningococcal infection during follow-up.
Dr Newland presented similar results from another study of eculizumab in aHUS. He discussed the results during an EHA-JSH joint symposium on platelet disorders, but the study was also presented at ASH last year as abstract 193.
The study included 17 aHUS patients who received eculizumab for a mean of 58 weeks. All of the patients achieved event-free status, which was defined as 12 weeks or more of stable platelet count, no PE/PI, and no new dialysis. Additionally, 4 of 5 patients were able to discontinue dialysis as a result of treatment with eculizumab.
As in Dr Vilalta’s study, treatment was similarly effective in patients with or without complement regulatory factor mutations. And the drug was generally well-tolerated. Twelve patients experienced adverse events, 1 of which was severe.
“[Eculizumab] showed phenomenal results here,” Dr Newland said. “Patients, particularly those treated earlier in their disease, were able to normalize their renal function.”
He said such an improvement is “dramatic” for this patient population, as 25% of aHUS patients die with the first attack, and 50% go into end-stage renal disease. Therefore, eculizumab can be considered the standard of care for aHUS patients—“if [they] can afford it.” ![]()
Perceived Levels of Pain Associated with Bone Marrow Aspirates and Biopsies
Perceived Levels of Pain Associated with Bone Marrow Aspirates and Biopsies
Perceived Levels of Pain Associated with Bone Marrow Aspirates and Biopsies
Perceived Levels of Pain Associated with Bone Marrow Aspirates and Biopsies
Physicians' Undecided Attitudes Toward Posthumous Reproduction: Fertility Preservation in Cancer Patients with a Poor Prognosis
Physicians' Undecided Attitudes Toward Posthumous Reproduction: Fertility Preservation in Cancer Patients with a Poor Prognosis
Physicians' Undecided Attitudes Toward Posthumous Reproduction: Fertility Preservation in Cancer Patients with a Poor Prognosis
Physicians' Undecided Attitudes Toward Posthumous Reproduction: Fertility Preservation in Cancer Patients with a Poor Prognosis
Acyclovir Prophylaxis Against Varicella Zoster Virus Reactivation in Multiple Myeloma Patients Treated With Bortezomib-Based Therapies: A Retrospective Analysis of 100 Patients
Acyclovir Prophylaxis Against Varicella Zoster Virus Reactivation in Multiple Myeloma Patients Treated With Bortezomib-Based Therapies: A Retrospective Analysis of 100 Patients
Acyclovir Prophylaxis Against Varicella Zoster Virus Reactivation in Multiple Myeloma Patients Treated With Bortezomib-Based Therapies: A Retrospective Analysis of 100 Patients
Acyclovir Prophylaxis Against Varicella Zoster Virus Reactivation in Multiple Myeloma Patients Treated With Bortezomib-Based Therapies: A Retrospective Analysis of 100 Patients