User login
Boston-Area Senior Medical Resident Wins HM13 Scholarship

Josh Allen-Dicker, MD, has received the SHM Boston Chapter’s first HM13 Scholarship. The $1,000 scholarship helped defray Dr. Allen-Dicker’s expenses to attend HM13.
Josh is a senior medical resident at Beth Israel Deaconess Medical Center in Boston. He has taken a job as a hospitalist starting this summer at Mount Sinai Medical Center in New York. He presented a poster as part of the Research, Innovations, and Clinical Vignettes competition at HM13.
"Dr. Allen-Dicker represents the best qualities in the next generation of hospitalists,” says says Kathleen Finn, MD, MGH, of the Boston SHM Chapter. “We are excited and honored to have him join the field of hospital medicine, and are thrilled we could help expose him to the leaders in the field at HM13."
Josh Allen-Dicker, MD, has received the SHM Boston Chapter’s first HM13 Scholarship. The $1,000 scholarship helped defray Dr. Allen-Dicker’s expenses to attend HM13.
Josh is a senior medical resident at Beth Israel Deaconess Medical Center in Boston. He has taken a job as a hospitalist starting this summer at Mount Sinai Medical Center in New York. He presented a poster as part of the Research, Innovations, and Clinical Vignettes competition at HM13.
"Dr. Allen-Dicker represents the best qualities in the next generation of hospitalists,” says says Kathleen Finn, MD, MGH, of the Boston SHM Chapter. “We are excited and honored to have him join the field of hospital medicine, and are thrilled we could help expose him to the leaders in the field at HM13."
Josh Allen-Dicker, MD, has received the SHM Boston Chapter’s first HM13 Scholarship. The $1,000 scholarship helped defray Dr. Allen-Dicker’s expenses to attend HM13.
Josh is a senior medical resident at Beth Israel Deaconess Medical Center in Boston. He has taken a job as a hospitalist starting this summer at Mount Sinai Medical Center in New York. He presented a poster as part of the Research, Innovations, and Clinical Vignettes competition at HM13.
"Dr. Allen-Dicker represents the best qualities in the next generation of hospitalists,” says says Kathleen Finn, MD, MGH, of the Boston SHM Chapter. “We are excited and honored to have him join the field of hospital medicine, and are thrilled we could help expose him to the leaders in the field at HM13."
What to do when pain and addiction coexist
Chronic pain and addictive disorders are each distinct clinical conditions that can be expressed in unique ways in different individuals. Similar to other chronic conditions such as diabetes, hypertension, or asthma, both pain and addictive disease often have biological as well psychobehavioral contributors that may shape clinical expression.1
As with these other illnesses, it is helpful for clinicians to engage the patient in a consistent process of self-care and to provide long-term clinical care while at the same time coordinating the care of other providers and specialists.2,3 In some cases a definitive cure for pain may be possible, but more often, chronic pain, like addiction, is a persistent condition requiring treatment over many years.
It will come as no surprise to learn that the convergence of pain and addiction can complicate recovery from both problems.4 Pain or its associated symptoms may prompt continuing use of substances that provide transient relief, but which sometimes perpetuate distress and reduce quality of life. And addiction may drive the experience of pain and seem to justify use of an addictive substance that the patient craves.
It is also important to recognize that pain and addiction frequently share a number of similar clinical features—including sleep and mood disturbances, substance use, deconditioning, functional losses, and high levels of stress—such that the conditions can reinforce one another. Full evaluation and comprehensive treatment of the biopsychosocial components of both conditions can improve outcomes.
The purpose of this article is to explore a model of multidimensional care that will serve all patients with chronic pain well, including those with addiction disorders.
What drives substance use? How common is it?
Patients with chronic pain may use alcohol, street drugs, or prescribed medications for diverse reasons. Many are self-medicating pain, sleep difficulties, mood fluctuations, or painful, intrusive memories. Others use these psychoactive agents as a form of recreation, as a compulsive act due to addiction, or to avoid withdrawal symptoms when physically dependent. And still others use these agents for diversion and profit.
Sometimes only one motive drives their behavior, but often several are present. As a physician, your goal is to identify the substances being used and the motivators of use (when possible) to better address the underlying causes.
The lifetime prevalence of addictive disorders among US adults is about 12.5% for alcohol dependence, 17.8% for alcohol abuse, 2.6% for drug dependence, and 7.7% for drug abuse.5,6
Research also suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders.7 Many factors may contribute to pain in people with addictions, including injuries8 and traumatic childhood experiences. The latter appears to increase the risk of developing addiction and/or chronic pain later in life.9,10
| Key Point Research suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders. |
Conducting a thorough assessment
In addition to a careful assessment of pain and its consequences for the patient, it is important to conduct a thorough assessment of current and past use of alcohol, street drugs, tobacco, and controlled prescription drugs in a nonjudgmental manner. A number of validated screening tools are available that may help identify substance abuse.
Consider using NIDA-Modified ASSIST (http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf), an excellent assessment tool for primary care providers that inventories substance use and helps monitor it on an ongoing basis. If the patient does not misuse substances, the screen is very brief. If he or she misuses them and acknowledges it, NIDA-Modified ASSIST will provide a comprehensive picture of the nature of the problem. Other assessment tools—including those specifically geared to opioid misuse11—are listed in the TABLE.
TABLE
Screens for addictive disorders
If you are considering the use of opioids to treat a patient’s chronic pain, urine drug testing can provide objective information regarding current substance use and is especially important in patients with known addictive disorders or substance misuse.
A 24-hour inventory of substance and medications use, identifying exactly when and for what symptoms each was used, can reveal important clinical information. It is not unusual, for instance, to identify a pain patient using alcohol at bedtime to induce sleep (although alcohol actually disrupts sleep architecture) or using opioids for stress or anxiety even when pain is not anticipated or present.
Multidimensional treatment approach
Your goals in treating chronic pain include reduction in pain and associated symptoms, enhanced functioning, and a return to a high quality of life with meaning and purpose. The goals of addiction or substance misuse recovery usually include avoiding harmful use of substances and similarly achieving physical, psychological, and spiritual well-being. These goals are entirely compatible.
Unless specific surgeries, procedures, or other interventions are able to eliminate a patient’s pain, treatment usually must address not only the pain, but also coexisting mental health or medical issues, as well as pain sequelae that may increase pain. An interdisciplinary approach often offers the best opportunity for success.12
To effectively address substance misuse in the context of chronic pain requires an understanding of what is driving the misuse and again must address coexisting mental health or other medical issues, as well as the sequelae of the substance problem. A biopsychosocial approach to treatment of both pain and addiction that actively engages the patient in self-management is critical to recovery from both chronic conditions.13 (See “Self-care options for patients with chronic pain and addiction," below.)
Such treatment ideally involves the primary care physician, psychologist or counselor, and physical or occupational therapist—with support from pain or addiction providers. The medical home can play important roles in coordination of care, facilitation of self-management, and promotion of recovery from both conditions.14
The structure of our health care system, however, favors payment for short clinic visits and procedures and may limit access to mental health and substance services. It may be more expedient to prescribe a medication or refer for a pain block than to explore things like stress, diet, exercise, sleep, mood, substance use, and the ability to function at work and home. The “quick solution” approach often omits the development of a foundation of self-care that is important to long-term success.
While patients without co-occurring substance use disorders may get by with this approach, patients with co-occurring addiction-related disorders can be hurt by reliance on medications and other passive therapies.
| SELF-CARE OPTIONS FOR PATIENTS WITH CHRONIC PAIN AND ADDICTION Consider suggesting that your patient:
Remember that chronic pain and addiction are chronic conditions, so it is important to check on self-care at each visit and revise the plan as helpful to the patient. Use selected treatments, such as targeted physical therapy, medications, procedures, or other approaches when appropriate. |
Finding the best treatment approaches
Effective treatment of chronic pain may draw from 4 broad categories: psychobehavioral, physical therapeutic, and interventionalist approaches, as well as medications.
Psychobehavioral and physical therapeutic approaches can provide a foundation for recovery from chronic pain and a context in which strategic use of interventionalist procedures and medications may be more effective. Fortunately, many self-management strategies that have been shown to be effective in pain management are also effective in the treatment of addiction. Among these are: cognitive-behavioral therapy, meditation, emerging 12-step programs for pain, and physical reconditioning.
As you plan out each patient’s therapeutic regimen, consider these options:
Cognitive-behavioral therapy (CBT) aims to change behaviors and thought patterns to help patients gain control over their condition. It has been shown to be effective in improving outcomes in chronic pain and substance abuse treatment.15,16 In the treatment of chronic pain, patients often identify negative self-talk that is impeding their recovery—”My pain is killing me. I’ll never be able to work.” They are encouraged to substitute more positive thoughts that favor recovery, eg, “My pain is hurtful but not harmful. My pain will lead me to new and more meaningful work.”
Patients also examine physical activities, stress, sleep challenges, and mood fluctuations that can increase pain and engage in approaches such as activity pacing, stretching, and relaxation that may mitigate their pain. When CBT is used in addiction treatment, patients similarly explore triggers for drug use (often people, places, and things), and they substitute alternatives that support abstinence and recovery.
For example, patients may elect social opportunities with friends who do not get high, participate in valued activities that don’t involve alcohol or drugs, and frequent places not associated with old drug use patterns. They reframe negative thinking to gain a more positive perspective that favors recovery and prevents relapse. “I can’t live without alcohol forever” becomes “I can enjoy today without alcohol.” They also apply relaxation or meditation skills to reduce stress, and they develop coping skills to address high-risk situations.17
Meditation-relaxation. Despite some scientific debate about the relative merits of different relaxation approaches, such as hypnosis, guided imagery, progressive muscle relaxation, and meditation, there is clear evidence that deep relaxation practices can play an important role in pain management. Recent studies have shown benefit for mindfulness meditation in the treatment of pain.18 Other studies suggest various forms of meditation may help patients recover from addiction.19 The physiologic basis of pain relief associated with meditation or deep relaxation has been variously attributed to muscular relaxation, reduction in sympathetic arousal, and changes in activity of different brain centers that process pain and pain inhibition. Effects on sleep enhancement and reduction in anxiety may also contribute to recovery from pain and substance abuse.
One simple approach to meditation is for the patient to sit comfortably for 10 to 20 minutes while focusing awareness on the natural flow of his or her breath going in and out. The patient is instructed to note thoughts, sounds, and sensations as they pass by and gently bring attention back to the flow of breath. A word or phrase can be silently thought on the outbreath to enhance focus.
12-step programs. Twelve-step programs such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) have been a key element of self-management of recovery from addiction for at least 7 decades. AA and similar meetings engage attendees in a process of self-reflection, reframing of perspectives, interpersonal sharing, and acceptance that for many are powerful supports for substance abuse recovery.20
12-step programs for pain. Recently 12-step programs for chronic pain that use the same basic strategies and paradigm to engage individuals in a process of recovery have begun to proliferate; these meetings are open to people both with pain alone and those with pain and addiction.21 And when pain-specific 12-step groups are not available, many patients find they can adapt the steps in an AA or NA meeting to address their pain.
The strengths of 12-step groups are that they are free and widely available. Patients may need to try different groups, however, to find one at which they feel comfortable.
| Key Point There are now 12-step programs for chronic pain that use the same basic strategies as Alcoholics Anonymous and Narcotics Anonymous to engage in the process of recovery. |
Physical reconditioning. The benefits of exercise and movement therapies in chronic pain management are well documented. Exercise activates central endorphin release and descending pain inhibition. Aerobic exercise, such as cycling, using an elliptical machine, or walking, may improve circulation and tissue oxygenation, which in turn can improve healing. Stretching can relieve muscular tension and normalize joint motion; however, stretches must be tailored to the condition of the particular patient. Improved posture and proper biomechanics during movement reduce physical stress. Similarly, toning or strengthening can provide support for spinal and other joints and reduce propensity for spasm. It is usually important for a patient to initiate exercise under the guidance of a physical therapist.
Clinicians should advise patients with pain to exercise in a manner that is gentle, gradually progressive, and avoids significantly increasing the patient’s pain.22 Some studies suggest exercise can improve outcomes in addiction treatment; it is speculated that enhanced self-esteem and the increase in endogenous endorphins may contribute.23
| Key Point Some studies suggest that exercise can improve outcomes in addiction treatment. |
Adding active treatments to the platform of self-care
Selection of specific procedures and medications for different pain problems is beyond the scope of this article, but it is worth noting that engagement in a biobehavioral self-care program provides a context that supports successful use of procedures and medication. For example, improved posture, muscular support of the spine, and proper biomechanics may reduce disc stresses that can produce recurrent pain after a successful epidural injection of steroids. Similarly, muscular trigger point injections are more likely to result in protracted muscular relaxation if a patient is engaged in regular stress management and stretching.
Similarly, when withdrawal-producing medications are eliminated, when stress, anxiety, and depression are addressed, and when the patient is physically conditioned, he or she may respond better to nonopioid pain medications.
Opioids for pain in substance use disorders
Opioids are rarely first-line medications for chronic pain treatment but they can be valuable components of care for some who have not responded to self-management, interventionalist procedures, and nonopioid medications. But use of opioids in chronic pain patients with addictive disorders requires exceptional care.
As you might expect, the risk of opioid misuse is higher in individuals with a prior history of substance use when compared with a person without this history. But the relative risk for people with different types of addiction is unknown. There’s the potential to become addicted to opioids, for instance, when an individual is in recovery from addiction to alcohol or marijuana. However, observation suggests the risk of addiction to prescribed opioids is more likely in patients with a past history of opioid addiction than other addictions. Duration of recovery is generally inversely related to the risk of relapse, so longer term recovery presents less risk than recent recovery.
Whenever possible, engage any patient with a history of addiction in an active addiction recovery program and have him or her co-managed by an addiction specialist if you plan to prescribe opioids. Patients in recovery from nonopioid addiction who require opioids for pain may benefit from tightening the structure of care. This may include:
-
providing a smaller supply of medications at more frequent intervals;
-
increasing supports for recovery from pain, addiction, and co-occurring disorders;
-
increasing supervision including office visits, urine drug screens, and pill counts;
-
selecting treatments carefully to limit reward (euphoria) when possible, as reward can trigger misuse; and
-
assuring that the setting of care can provide optimal care coordination.24
For those with a history of opioid addiction, the safest option for opioid therapy is engagement in an addiction treatment paradigm of opioid therapy. This will mean either buprenorphine/naloxone with a registered provider or methadone maintenance treatment through a licensed clinic in which medications will be tightly supervised and the patient engaged in psychosocial addiction treatment. Both types of opioid agonist therapy may provide some pain relief while providing pharmacologic treatment of opioid addiction and minimizing the risk of misuse and associated harm (such as overdose).
What’s your role?
The key roles of the primary care physician in managing chronic pain and coexisting substance use disorders are to (1) identify the variables that contribute to the patient’s experience of pain and use of substances, (2) encourage and support the patient as he or she tries to develop a self-care program, (3) strategically implement or refer for active treatment of the various contributing factors, and (4) see the patient regularly to monitor engagement in both self-care and active treatments and to revise the plan as needed.
Coexisting pain and addiction are among the most challenging scenarios encountered in primary care. Recovery is possible, but patience, time, flexibility, and consistent motivational support are critical. The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories.
| Key Point The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories. |
Disclosure The author reported no potential conflict of interest relevant to this article. |
References
- McLellan AT, Lewis DC, O’Brien CP, et al. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284:1689–1695.
- Chelimsky TC, Fischer RL, Levin JB, et al. The primary practice physician program for chronic pain (© 4PCP): outcomes of a primary physician specialist collaboration for community-based training and support. Clin J Pain. 2013 Mar 1. [Epub ahead of print].
- Anderson D, Wang S, Zlateva I. Comprehensive assessment of chronic pain management in primary care: a first phase of a quality improvement initiative at a multisite Community Health Center. Qual Prim Care. 2012;20:421–433.
- Pohl M, Smith L. Chronic pain and addiction: challenging co-occurring disorders. J Psychoactive Drugs. 2012;44:119–124.
- Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:830–842.
- Compton WM, Thomas YF, Stinson FS, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:566–576.
- Clark MR, Stoller KB, Brooner RK. Assessment and management of chronic pain in individuals seeking treatment for opioid dependence disorder. Can J Psychiatry. 2008;53:496–508.
- West SL. Substance use among persons with traumatic brain injury: a review. NeuroRehabilitation. 2011;29:1–8.
- Khoury L, Tang YL, Bradley B, et al. Substance use, childhood traumatic experience, and posttraumatic stress disorder in an urban civilian population. Depress Anxiety. 2010;27:1077–1086.
- Beck JG, Clapp JD. A different kind of co-morbidity: understanding posttraumatic stress disorder and chronic pain. Psychol Trauma. 2011;3:101–108.
- Potter JS, Marino EN. How to avoid opioid misuse. Chronic Pain Perspectives. 2013;62(3):S2–S7.
- Stanos S. Focused review of interdisciplinary pain rehabilitation programs for chronic pain management. Curr Pain Headache Rep. 2012;16:147–152.
- Cheatle MD, Gallagher RM. Chronic pain and comorbid mood and substance use disorders: a biopsychosocial treatment approach. Curr Psychiatry Rep. 2006;8:371–376.
- Chouinard MC, Hudon C, Dubois MF, et al. Case management and self-management support for frequent users with chronic disease in primary care: a pragmatic randomized controlled trial. BMC Health Serv Res. 2013;13:49.
- Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80:1–13.
- McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27:2564–2573.
- SAMHSA/CSAT Treatment Improvement Protocols. Rockville, MD: Substance Abuse and Mental Health Services Administration; 1993-. Available at: http://www.ncbi.nlm.nih.gov/books/NBK82999/. Accessed May 16, 2013.
- Zeidan F, Grant JA, Brown CA, et al. Mindfulness meditation-related pain relief: evidence for unique brain mechanisms in the regulation of pain. Neurosci Lett. 2012;520:165–173.
- Dakwar E, Levin FR. The emerging role of meditation in addressing psychiatric illness, with a focus on substance use disorders. Harv Rev Psychiatry. 2009;17:254–267.
- Kaskutas LA. Alcoholics anonymous effectiveness: faith meets science. J Addict Dis. 2009;28:145–157.
- Colameco S. Chronic Pain: A Way Out. Comprehensive Treatment & 12-Step Recovery Guide. Haddonfield, NJ: Stephen Colameco; 2012.
- Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012;15(3 suppl):ES205–ES213.
- Brown RA, Abrantes AM, Read JP, et al. A pilot study of aerobic exercise as an adjunctive treatment for drug dependence. Ment Health Phys Act. 2010;3:27–34.
- Savage SR, Kirsch KL, Passik SD. Challenges in using opioids to treat pain in persons with substance use disorders. Addict Sci Clin Pract. 2008;4:4–25.
Chronic pain and addictive disorders are each distinct clinical conditions that can be expressed in unique ways in different individuals. Similar to other chronic conditions such as diabetes, hypertension, or asthma, both pain and addictive disease often have biological as well psychobehavioral contributors that may shape clinical expression.1
As with these other illnesses, it is helpful for clinicians to engage the patient in a consistent process of self-care and to provide long-term clinical care while at the same time coordinating the care of other providers and specialists.2,3 In some cases a definitive cure for pain may be possible, but more often, chronic pain, like addiction, is a persistent condition requiring treatment over many years.
It will come as no surprise to learn that the convergence of pain and addiction can complicate recovery from both problems.4 Pain or its associated symptoms may prompt continuing use of substances that provide transient relief, but which sometimes perpetuate distress and reduce quality of life. And addiction may drive the experience of pain and seem to justify use of an addictive substance that the patient craves.
It is also important to recognize that pain and addiction frequently share a number of similar clinical features—including sleep and mood disturbances, substance use, deconditioning, functional losses, and high levels of stress—such that the conditions can reinforce one another. Full evaluation and comprehensive treatment of the biopsychosocial components of both conditions can improve outcomes.
The purpose of this article is to explore a model of multidimensional care that will serve all patients with chronic pain well, including those with addiction disorders.
What drives substance use? How common is it?
Patients with chronic pain may use alcohol, street drugs, or prescribed medications for diverse reasons. Many are self-medicating pain, sleep difficulties, mood fluctuations, or painful, intrusive memories. Others use these psychoactive agents as a form of recreation, as a compulsive act due to addiction, or to avoid withdrawal symptoms when physically dependent. And still others use these agents for diversion and profit.
Sometimes only one motive drives their behavior, but often several are present. As a physician, your goal is to identify the substances being used and the motivators of use (when possible) to better address the underlying causes.
The lifetime prevalence of addictive disorders among US adults is about 12.5% for alcohol dependence, 17.8% for alcohol abuse, 2.6% for drug dependence, and 7.7% for drug abuse.5,6
Research also suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders.7 Many factors may contribute to pain in people with addictions, including injuries8 and traumatic childhood experiences. The latter appears to increase the risk of developing addiction and/or chronic pain later in life.9,10
| Key Point Research suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders. |
Conducting a thorough assessment
In addition to a careful assessment of pain and its consequences for the patient, it is important to conduct a thorough assessment of current and past use of alcohol, street drugs, tobacco, and controlled prescription drugs in a nonjudgmental manner. A number of validated screening tools are available that may help identify substance abuse.
Consider using NIDA-Modified ASSIST (http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf), an excellent assessment tool for primary care providers that inventories substance use and helps monitor it on an ongoing basis. If the patient does not misuse substances, the screen is very brief. If he or she misuses them and acknowledges it, NIDA-Modified ASSIST will provide a comprehensive picture of the nature of the problem. Other assessment tools—including those specifically geared to opioid misuse11—are listed in the TABLE.
TABLE
Screens for addictive disorders
If you are considering the use of opioids to treat a patient’s chronic pain, urine drug testing can provide objective information regarding current substance use and is especially important in patients with known addictive disorders or substance misuse.
A 24-hour inventory of substance and medications use, identifying exactly when and for what symptoms each was used, can reveal important clinical information. It is not unusual, for instance, to identify a pain patient using alcohol at bedtime to induce sleep (although alcohol actually disrupts sleep architecture) or using opioids for stress or anxiety even when pain is not anticipated or present.
Multidimensional treatment approach
Your goals in treating chronic pain include reduction in pain and associated symptoms, enhanced functioning, and a return to a high quality of life with meaning and purpose. The goals of addiction or substance misuse recovery usually include avoiding harmful use of substances and similarly achieving physical, psychological, and spiritual well-being. These goals are entirely compatible.
Unless specific surgeries, procedures, or other interventions are able to eliminate a patient’s pain, treatment usually must address not only the pain, but also coexisting mental health or medical issues, as well as pain sequelae that may increase pain. An interdisciplinary approach often offers the best opportunity for success.12
To effectively address substance misuse in the context of chronic pain requires an understanding of what is driving the misuse and again must address coexisting mental health or other medical issues, as well as the sequelae of the substance problem. A biopsychosocial approach to treatment of both pain and addiction that actively engages the patient in self-management is critical to recovery from both chronic conditions.13 (See “Self-care options for patients with chronic pain and addiction," below.)
Such treatment ideally involves the primary care physician, psychologist or counselor, and physical or occupational therapist—with support from pain or addiction providers. The medical home can play important roles in coordination of care, facilitation of self-management, and promotion of recovery from both conditions.14
The structure of our health care system, however, favors payment for short clinic visits and procedures and may limit access to mental health and substance services. It may be more expedient to prescribe a medication or refer for a pain block than to explore things like stress, diet, exercise, sleep, mood, substance use, and the ability to function at work and home. The “quick solution” approach often omits the development of a foundation of self-care that is important to long-term success.
While patients without co-occurring substance use disorders may get by with this approach, patients with co-occurring addiction-related disorders can be hurt by reliance on medications and other passive therapies.
| SELF-CARE OPTIONS FOR PATIENTS WITH CHRONIC PAIN AND ADDICTION Consider suggesting that your patient:
Remember that chronic pain and addiction are chronic conditions, so it is important to check on self-care at each visit and revise the plan as helpful to the patient. Use selected treatments, such as targeted physical therapy, medications, procedures, or other approaches when appropriate. |
Finding the best treatment approaches
Effective treatment of chronic pain may draw from 4 broad categories: psychobehavioral, physical therapeutic, and interventionalist approaches, as well as medications.
Psychobehavioral and physical therapeutic approaches can provide a foundation for recovery from chronic pain and a context in which strategic use of interventionalist procedures and medications may be more effective. Fortunately, many self-management strategies that have been shown to be effective in pain management are also effective in the treatment of addiction. Among these are: cognitive-behavioral therapy, meditation, emerging 12-step programs for pain, and physical reconditioning.
As you plan out each patient’s therapeutic regimen, consider these options:
Cognitive-behavioral therapy (CBT) aims to change behaviors and thought patterns to help patients gain control over their condition. It has been shown to be effective in improving outcomes in chronic pain and substance abuse treatment.15,16 In the treatment of chronic pain, patients often identify negative self-talk that is impeding their recovery—”My pain is killing me. I’ll never be able to work.” They are encouraged to substitute more positive thoughts that favor recovery, eg, “My pain is hurtful but not harmful. My pain will lead me to new and more meaningful work.”
Patients also examine physical activities, stress, sleep challenges, and mood fluctuations that can increase pain and engage in approaches such as activity pacing, stretching, and relaxation that may mitigate their pain. When CBT is used in addiction treatment, patients similarly explore triggers for drug use (often people, places, and things), and they substitute alternatives that support abstinence and recovery.
For example, patients may elect social opportunities with friends who do not get high, participate in valued activities that don’t involve alcohol or drugs, and frequent places not associated with old drug use patterns. They reframe negative thinking to gain a more positive perspective that favors recovery and prevents relapse. “I can’t live without alcohol forever” becomes “I can enjoy today without alcohol.” They also apply relaxation or meditation skills to reduce stress, and they develop coping skills to address high-risk situations.17
Meditation-relaxation. Despite some scientific debate about the relative merits of different relaxation approaches, such as hypnosis, guided imagery, progressive muscle relaxation, and meditation, there is clear evidence that deep relaxation practices can play an important role in pain management. Recent studies have shown benefit for mindfulness meditation in the treatment of pain.18 Other studies suggest various forms of meditation may help patients recover from addiction.19 The physiologic basis of pain relief associated with meditation or deep relaxation has been variously attributed to muscular relaxation, reduction in sympathetic arousal, and changes in activity of different brain centers that process pain and pain inhibition. Effects on sleep enhancement and reduction in anxiety may also contribute to recovery from pain and substance abuse.
One simple approach to meditation is for the patient to sit comfortably for 10 to 20 minutes while focusing awareness on the natural flow of his or her breath going in and out. The patient is instructed to note thoughts, sounds, and sensations as they pass by and gently bring attention back to the flow of breath. A word or phrase can be silently thought on the outbreath to enhance focus.
12-step programs. Twelve-step programs such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) have been a key element of self-management of recovery from addiction for at least 7 decades. AA and similar meetings engage attendees in a process of self-reflection, reframing of perspectives, interpersonal sharing, and acceptance that for many are powerful supports for substance abuse recovery.20
12-step programs for pain. Recently 12-step programs for chronic pain that use the same basic strategies and paradigm to engage individuals in a process of recovery have begun to proliferate; these meetings are open to people both with pain alone and those with pain and addiction.21 And when pain-specific 12-step groups are not available, many patients find they can adapt the steps in an AA or NA meeting to address their pain.
The strengths of 12-step groups are that they are free and widely available. Patients may need to try different groups, however, to find one at which they feel comfortable.
| Key Point There are now 12-step programs for chronic pain that use the same basic strategies as Alcoholics Anonymous and Narcotics Anonymous to engage in the process of recovery. |
Physical reconditioning. The benefits of exercise and movement therapies in chronic pain management are well documented. Exercise activates central endorphin release and descending pain inhibition. Aerobic exercise, such as cycling, using an elliptical machine, or walking, may improve circulation and tissue oxygenation, which in turn can improve healing. Stretching can relieve muscular tension and normalize joint motion; however, stretches must be tailored to the condition of the particular patient. Improved posture and proper biomechanics during movement reduce physical stress. Similarly, toning or strengthening can provide support for spinal and other joints and reduce propensity for spasm. It is usually important for a patient to initiate exercise under the guidance of a physical therapist.
Clinicians should advise patients with pain to exercise in a manner that is gentle, gradually progressive, and avoids significantly increasing the patient’s pain.22 Some studies suggest exercise can improve outcomes in addiction treatment; it is speculated that enhanced self-esteem and the increase in endogenous endorphins may contribute.23
| Key Point Some studies suggest that exercise can improve outcomes in addiction treatment. |
Adding active treatments to the platform of self-care
Selection of specific procedures and medications for different pain problems is beyond the scope of this article, but it is worth noting that engagement in a biobehavioral self-care program provides a context that supports successful use of procedures and medication. For example, improved posture, muscular support of the spine, and proper biomechanics may reduce disc stresses that can produce recurrent pain after a successful epidural injection of steroids. Similarly, muscular trigger point injections are more likely to result in protracted muscular relaxation if a patient is engaged in regular stress management and stretching.
Similarly, when withdrawal-producing medications are eliminated, when stress, anxiety, and depression are addressed, and when the patient is physically conditioned, he or she may respond better to nonopioid pain medications.
Opioids for pain in substance use disorders
Opioids are rarely first-line medications for chronic pain treatment but they can be valuable components of care for some who have not responded to self-management, interventionalist procedures, and nonopioid medications. But use of opioids in chronic pain patients with addictive disorders requires exceptional care.
As you might expect, the risk of opioid misuse is higher in individuals with a prior history of substance use when compared with a person without this history. But the relative risk for people with different types of addiction is unknown. There’s the potential to become addicted to opioids, for instance, when an individual is in recovery from addiction to alcohol or marijuana. However, observation suggests the risk of addiction to prescribed opioids is more likely in patients with a past history of opioid addiction than other addictions. Duration of recovery is generally inversely related to the risk of relapse, so longer term recovery presents less risk than recent recovery.
Whenever possible, engage any patient with a history of addiction in an active addiction recovery program and have him or her co-managed by an addiction specialist if you plan to prescribe opioids. Patients in recovery from nonopioid addiction who require opioids for pain may benefit from tightening the structure of care. This may include:
-
providing a smaller supply of medications at more frequent intervals;
-
increasing supports for recovery from pain, addiction, and co-occurring disorders;
-
increasing supervision including office visits, urine drug screens, and pill counts;
-
selecting treatments carefully to limit reward (euphoria) when possible, as reward can trigger misuse; and
-
assuring that the setting of care can provide optimal care coordination.24
For those with a history of opioid addiction, the safest option for opioid therapy is engagement in an addiction treatment paradigm of opioid therapy. This will mean either buprenorphine/naloxone with a registered provider or methadone maintenance treatment through a licensed clinic in which medications will be tightly supervised and the patient engaged in psychosocial addiction treatment. Both types of opioid agonist therapy may provide some pain relief while providing pharmacologic treatment of opioid addiction and minimizing the risk of misuse and associated harm (such as overdose).
What’s your role?
The key roles of the primary care physician in managing chronic pain and coexisting substance use disorders are to (1) identify the variables that contribute to the patient’s experience of pain and use of substances, (2) encourage and support the patient as he or she tries to develop a self-care program, (3) strategically implement or refer for active treatment of the various contributing factors, and (4) see the patient regularly to monitor engagement in both self-care and active treatments and to revise the plan as needed.
Coexisting pain and addiction are among the most challenging scenarios encountered in primary care. Recovery is possible, but patience, time, flexibility, and consistent motivational support are critical. The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories.
| Key Point The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories. |
Disclosure The author reported no potential conflict of interest relevant to this article. |
References
- McLellan AT, Lewis DC, O’Brien CP, et al. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284:1689–1695.
- Chelimsky TC, Fischer RL, Levin JB, et al. The primary practice physician program for chronic pain (© 4PCP): outcomes of a primary physician specialist collaboration for community-based training and support. Clin J Pain. 2013 Mar 1. [Epub ahead of print].
- Anderson D, Wang S, Zlateva I. Comprehensive assessment of chronic pain management in primary care: a first phase of a quality improvement initiative at a multisite Community Health Center. Qual Prim Care. 2012;20:421–433.
- Pohl M, Smith L. Chronic pain and addiction: challenging co-occurring disorders. J Psychoactive Drugs. 2012;44:119–124.
- Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:830–842.
- Compton WM, Thomas YF, Stinson FS, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:566–576.
- Clark MR, Stoller KB, Brooner RK. Assessment and management of chronic pain in individuals seeking treatment for opioid dependence disorder. Can J Psychiatry. 2008;53:496–508.
- West SL. Substance use among persons with traumatic brain injury: a review. NeuroRehabilitation. 2011;29:1–8.
- Khoury L, Tang YL, Bradley B, et al. Substance use, childhood traumatic experience, and posttraumatic stress disorder in an urban civilian population. Depress Anxiety. 2010;27:1077–1086.
- Beck JG, Clapp JD. A different kind of co-morbidity: understanding posttraumatic stress disorder and chronic pain. Psychol Trauma. 2011;3:101–108.
- Potter JS, Marino EN. How to avoid opioid misuse. Chronic Pain Perspectives. 2013;62(3):S2–S7.
- Stanos S. Focused review of interdisciplinary pain rehabilitation programs for chronic pain management. Curr Pain Headache Rep. 2012;16:147–152.
- Cheatle MD, Gallagher RM. Chronic pain and comorbid mood and substance use disorders: a biopsychosocial treatment approach. Curr Psychiatry Rep. 2006;8:371–376.
- Chouinard MC, Hudon C, Dubois MF, et al. Case management and self-management support for frequent users with chronic disease in primary care: a pragmatic randomized controlled trial. BMC Health Serv Res. 2013;13:49.
- Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80:1–13.
- McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27:2564–2573.
- SAMHSA/CSAT Treatment Improvement Protocols. Rockville, MD: Substance Abuse and Mental Health Services Administration; 1993-. Available at: http://www.ncbi.nlm.nih.gov/books/NBK82999/. Accessed May 16, 2013.
- Zeidan F, Grant JA, Brown CA, et al. Mindfulness meditation-related pain relief: evidence for unique brain mechanisms in the regulation of pain. Neurosci Lett. 2012;520:165–173.
- Dakwar E, Levin FR. The emerging role of meditation in addressing psychiatric illness, with a focus on substance use disorders. Harv Rev Psychiatry. 2009;17:254–267.
- Kaskutas LA. Alcoholics anonymous effectiveness: faith meets science. J Addict Dis. 2009;28:145–157.
- Colameco S. Chronic Pain: A Way Out. Comprehensive Treatment & 12-Step Recovery Guide. Haddonfield, NJ: Stephen Colameco; 2012.
- Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012;15(3 suppl):ES205–ES213.
- Brown RA, Abrantes AM, Read JP, et al. A pilot study of aerobic exercise as an adjunctive treatment for drug dependence. Ment Health Phys Act. 2010;3:27–34.
- Savage SR, Kirsch KL, Passik SD. Challenges in using opioids to treat pain in persons with substance use disorders. Addict Sci Clin Pract. 2008;4:4–25.
Chronic pain and addictive disorders are each distinct clinical conditions that can be expressed in unique ways in different individuals. Similar to other chronic conditions such as diabetes, hypertension, or asthma, both pain and addictive disease often have biological as well psychobehavioral contributors that may shape clinical expression.1
As with these other illnesses, it is helpful for clinicians to engage the patient in a consistent process of self-care and to provide long-term clinical care while at the same time coordinating the care of other providers and specialists.2,3 In some cases a definitive cure for pain may be possible, but more often, chronic pain, like addiction, is a persistent condition requiring treatment over many years.
It will come as no surprise to learn that the convergence of pain and addiction can complicate recovery from both problems.4 Pain or its associated symptoms may prompt continuing use of substances that provide transient relief, but which sometimes perpetuate distress and reduce quality of life. And addiction may drive the experience of pain and seem to justify use of an addictive substance that the patient craves.
It is also important to recognize that pain and addiction frequently share a number of similar clinical features—including sleep and mood disturbances, substance use, deconditioning, functional losses, and high levels of stress—such that the conditions can reinforce one another. Full evaluation and comprehensive treatment of the biopsychosocial components of both conditions can improve outcomes.
The purpose of this article is to explore a model of multidimensional care that will serve all patients with chronic pain well, including those with addiction disorders.
What drives substance use? How common is it?
Patients with chronic pain may use alcohol, street drugs, or prescribed medications for diverse reasons. Many are self-medicating pain, sleep difficulties, mood fluctuations, or painful, intrusive memories. Others use these psychoactive agents as a form of recreation, as a compulsive act due to addiction, or to avoid withdrawal symptoms when physically dependent. And still others use these agents for diversion and profit.
Sometimes only one motive drives their behavior, but often several are present. As a physician, your goal is to identify the substances being used and the motivators of use (when possible) to better address the underlying causes.
The lifetime prevalence of addictive disorders among US adults is about 12.5% for alcohol dependence, 17.8% for alcohol abuse, 2.6% for drug dependence, and 7.7% for drug abuse.5,6
Research also suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders.7 Many factors may contribute to pain in people with addictions, including injuries8 and traumatic childhood experiences. The latter appears to increase the risk of developing addiction and/or chronic pain later in life.9,10
| Key Point Research suggests that there is a relatively high rate of chronic pain among individuals with addiction disorders. |
Conducting a thorough assessment
In addition to a careful assessment of pain and its consequences for the patient, it is important to conduct a thorough assessment of current and past use of alcohol, street drugs, tobacco, and controlled prescription drugs in a nonjudgmental manner. A number of validated screening tools are available that may help identify substance abuse.
Consider using NIDA-Modified ASSIST (http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf), an excellent assessment tool for primary care providers that inventories substance use and helps monitor it on an ongoing basis. If the patient does not misuse substances, the screen is very brief. If he or she misuses them and acknowledges it, NIDA-Modified ASSIST will provide a comprehensive picture of the nature of the problem. Other assessment tools—including those specifically geared to opioid misuse11—are listed in the TABLE.
TABLE
Screens for addictive disorders
If you are considering the use of opioids to treat a patient’s chronic pain, urine drug testing can provide objective information regarding current substance use and is especially important in patients with known addictive disorders or substance misuse.
A 24-hour inventory of substance and medications use, identifying exactly when and for what symptoms each was used, can reveal important clinical information. It is not unusual, for instance, to identify a pain patient using alcohol at bedtime to induce sleep (although alcohol actually disrupts sleep architecture) or using opioids for stress or anxiety even when pain is not anticipated or present.
Multidimensional treatment approach
Your goals in treating chronic pain include reduction in pain and associated symptoms, enhanced functioning, and a return to a high quality of life with meaning and purpose. The goals of addiction or substance misuse recovery usually include avoiding harmful use of substances and similarly achieving physical, psychological, and spiritual well-being. These goals are entirely compatible.
Unless specific surgeries, procedures, or other interventions are able to eliminate a patient’s pain, treatment usually must address not only the pain, but also coexisting mental health or medical issues, as well as pain sequelae that may increase pain. An interdisciplinary approach often offers the best opportunity for success.12
To effectively address substance misuse in the context of chronic pain requires an understanding of what is driving the misuse and again must address coexisting mental health or other medical issues, as well as the sequelae of the substance problem. A biopsychosocial approach to treatment of both pain and addiction that actively engages the patient in self-management is critical to recovery from both chronic conditions.13 (See “Self-care options for patients with chronic pain and addiction," below.)
Such treatment ideally involves the primary care physician, psychologist or counselor, and physical or occupational therapist—with support from pain or addiction providers. The medical home can play important roles in coordination of care, facilitation of self-management, and promotion of recovery from both conditions.14
The structure of our health care system, however, favors payment for short clinic visits and procedures and may limit access to mental health and substance services. It may be more expedient to prescribe a medication or refer for a pain block than to explore things like stress, diet, exercise, sleep, mood, substance use, and the ability to function at work and home. The “quick solution” approach often omits the development of a foundation of self-care that is important to long-term success.
While patients without co-occurring substance use disorders may get by with this approach, patients with co-occurring addiction-related disorders can be hurt by reliance on medications and other passive therapies.
| SELF-CARE OPTIONS FOR PATIENTS WITH CHRONIC PAIN AND ADDICTION Consider suggesting that your patient:
Remember that chronic pain and addiction are chronic conditions, so it is important to check on self-care at each visit and revise the plan as helpful to the patient. Use selected treatments, such as targeted physical therapy, medications, procedures, or other approaches when appropriate. |
Finding the best treatment approaches
Effective treatment of chronic pain may draw from 4 broad categories: psychobehavioral, physical therapeutic, and interventionalist approaches, as well as medications.
Psychobehavioral and physical therapeutic approaches can provide a foundation for recovery from chronic pain and a context in which strategic use of interventionalist procedures and medications may be more effective. Fortunately, many self-management strategies that have been shown to be effective in pain management are also effective in the treatment of addiction. Among these are: cognitive-behavioral therapy, meditation, emerging 12-step programs for pain, and physical reconditioning.
As you plan out each patient’s therapeutic regimen, consider these options:
Cognitive-behavioral therapy (CBT) aims to change behaviors and thought patterns to help patients gain control over their condition. It has been shown to be effective in improving outcomes in chronic pain and substance abuse treatment.15,16 In the treatment of chronic pain, patients often identify negative self-talk that is impeding their recovery—”My pain is killing me. I’ll never be able to work.” They are encouraged to substitute more positive thoughts that favor recovery, eg, “My pain is hurtful but not harmful. My pain will lead me to new and more meaningful work.”
Patients also examine physical activities, stress, sleep challenges, and mood fluctuations that can increase pain and engage in approaches such as activity pacing, stretching, and relaxation that may mitigate their pain. When CBT is used in addiction treatment, patients similarly explore triggers for drug use (often people, places, and things), and they substitute alternatives that support abstinence and recovery.
For example, patients may elect social opportunities with friends who do not get high, participate in valued activities that don’t involve alcohol or drugs, and frequent places not associated with old drug use patterns. They reframe negative thinking to gain a more positive perspective that favors recovery and prevents relapse. “I can’t live without alcohol forever” becomes “I can enjoy today without alcohol.” They also apply relaxation or meditation skills to reduce stress, and they develop coping skills to address high-risk situations.17
Meditation-relaxation. Despite some scientific debate about the relative merits of different relaxation approaches, such as hypnosis, guided imagery, progressive muscle relaxation, and meditation, there is clear evidence that deep relaxation practices can play an important role in pain management. Recent studies have shown benefit for mindfulness meditation in the treatment of pain.18 Other studies suggest various forms of meditation may help patients recover from addiction.19 The physiologic basis of pain relief associated with meditation or deep relaxation has been variously attributed to muscular relaxation, reduction in sympathetic arousal, and changes in activity of different brain centers that process pain and pain inhibition. Effects on sleep enhancement and reduction in anxiety may also contribute to recovery from pain and substance abuse.
One simple approach to meditation is for the patient to sit comfortably for 10 to 20 minutes while focusing awareness on the natural flow of his or her breath going in and out. The patient is instructed to note thoughts, sounds, and sensations as they pass by and gently bring attention back to the flow of breath. A word or phrase can be silently thought on the outbreath to enhance focus.
12-step programs. Twelve-step programs such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) have been a key element of self-management of recovery from addiction for at least 7 decades. AA and similar meetings engage attendees in a process of self-reflection, reframing of perspectives, interpersonal sharing, and acceptance that for many are powerful supports for substance abuse recovery.20
12-step programs for pain. Recently 12-step programs for chronic pain that use the same basic strategies and paradigm to engage individuals in a process of recovery have begun to proliferate; these meetings are open to people both with pain alone and those with pain and addiction.21 And when pain-specific 12-step groups are not available, many patients find they can adapt the steps in an AA or NA meeting to address their pain.
The strengths of 12-step groups are that they are free and widely available. Patients may need to try different groups, however, to find one at which they feel comfortable.
| Key Point There are now 12-step programs for chronic pain that use the same basic strategies as Alcoholics Anonymous and Narcotics Anonymous to engage in the process of recovery. |
Physical reconditioning. The benefits of exercise and movement therapies in chronic pain management are well documented. Exercise activates central endorphin release and descending pain inhibition. Aerobic exercise, such as cycling, using an elliptical machine, or walking, may improve circulation and tissue oxygenation, which in turn can improve healing. Stretching can relieve muscular tension and normalize joint motion; however, stretches must be tailored to the condition of the particular patient. Improved posture and proper biomechanics during movement reduce physical stress. Similarly, toning or strengthening can provide support for spinal and other joints and reduce propensity for spasm. It is usually important for a patient to initiate exercise under the guidance of a physical therapist.
Clinicians should advise patients with pain to exercise in a manner that is gentle, gradually progressive, and avoids significantly increasing the patient’s pain.22 Some studies suggest exercise can improve outcomes in addiction treatment; it is speculated that enhanced self-esteem and the increase in endogenous endorphins may contribute.23
| Key Point Some studies suggest that exercise can improve outcomes in addiction treatment. |
Adding active treatments to the platform of self-care
Selection of specific procedures and medications for different pain problems is beyond the scope of this article, but it is worth noting that engagement in a biobehavioral self-care program provides a context that supports successful use of procedures and medication. For example, improved posture, muscular support of the spine, and proper biomechanics may reduce disc stresses that can produce recurrent pain after a successful epidural injection of steroids. Similarly, muscular trigger point injections are more likely to result in protracted muscular relaxation if a patient is engaged in regular stress management and stretching.
Similarly, when withdrawal-producing medications are eliminated, when stress, anxiety, and depression are addressed, and when the patient is physically conditioned, he or she may respond better to nonopioid pain medications.
Opioids for pain in substance use disorders
Opioids are rarely first-line medications for chronic pain treatment but they can be valuable components of care for some who have not responded to self-management, interventionalist procedures, and nonopioid medications. But use of opioids in chronic pain patients with addictive disorders requires exceptional care.
As you might expect, the risk of opioid misuse is higher in individuals with a prior history of substance use when compared with a person without this history. But the relative risk for people with different types of addiction is unknown. There’s the potential to become addicted to opioids, for instance, when an individual is in recovery from addiction to alcohol or marijuana. However, observation suggests the risk of addiction to prescribed opioids is more likely in patients with a past history of opioid addiction than other addictions. Duration of recovery is generally inversely related to the risk of relapse, so longer term recovery presents less risk than recent recovery.
Whenever possible, engage any patient with a history of addiction in an active addiction recovery program and have him or her co-managed by an addiction specialist if you plan to prescribe opioids. Patients in recovery from nonopioid addiction who require opioids for pain may benefit from tightening the structure of care. This may include:
-
providing a smaller supply of medications at more frequent intervals;
-
increasing supports for recovery from pain, addiction, and co-occurring disorders;
-
increasing supervision including office visits, urine drug screens, and pill counts;
-
selecting treatments carefully to limit reward (euphoria) when possible, as reward can trigger misuse; and
-
assuring that the setting of care can provide optimal care coordination.24
For those with a history of opioid addiction, the safest option for opioid therapy is engagement in an addiction treatment paradigm of opioid therapy. This will mean either buprenorphine/naloxone with a registered provider or methadone maintenance treatment through a licensed clinic in which medications will be tightly supervised and the patient engaged in psychosocial addiction treatment. Both types of opioid agonist therapy may provide some pain relief while providing pharmacologic treatment of opioid addiction and minimizing the risk of misuse and associated harm (such as overdose).
What’s your role?
The key roles of the primary care physician in managing chronic pain and coexisting substance use disorders are to (1) identify the variables that contribute to the patient’s experience of pain and use of substances, (2) encourage and support the patient as he or she tries to develop a self-care program, (3) strategically implement or refer for active treatment of the various contributing factors, and (4) see the patient regularly to monitor engagement in both self-care and active treatments and to revise the plan as needed.
Coexisting pain and addiction are among the most challenging scenarios encountered in primary care. Recovery is possible, but patience, time, flexibility, and consistent motivational support are critical. The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories.
| Key Point The process is often 2 steps forward, one step back, so clinicians and patients need to celebrate small victories. |
Disclosure The author reported no potential conflict of interest relevant to this article. |
References
- McLellan AT, Lewis DC, O’Brien CP, et al. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284:1689–1695.
- Chelimsky TC, Fischer RL, Levin JB, et al. The primary practice physician program for chronic pain (© 4PCP): outcomes of a primary physician specialist collaboration for community-based training and support. Clin J Pain. 2013 Mar 1. [Epub ahead of print].
- Anderson D, Wang S, Zlateva I. Comprehensive assessment of chronic pain management in primary care: a first phase of a quality improvement initiative at a multisite Community Health Center. Qual Prim Care. 2012;20:421–433.
- Pohl M, Smith L. Chronic pain and addiction: challenging co-occurring disorders. J Psychoactive Drugs. 2012;44:119–124.
- Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:830–842.
- Compton WM, Thomas YF, Stinson FS, Grant BF. Prevalence, correlates, disability, and comorbidity of DSM-IV drug abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2007;64:566–576.
- Clark MR, Stoller KB, Brooner RK. Assessment and management of chronic pain in individuals seeking treatment for opioid dependence disorder. Can J Psychiatry. 2008;53:496–508.
- West SL. Substance use among persons with traumatic brain injury: a review. NeuroRehabilitation. 2011;29:1–8.
- Khoury L, Tang YL, Bradley B, et al. Substance use, childhood traumatic experience, and posttraumatic stress disorder in an urban civilian population. Depress Anxiety. 2010;27:1077–1086.
- Beck JG, Clapp JD. A different kind of co-morbidity: understanding posttraumatic stress disorder and chronic pain. Psychol Trauma. 2011;3:101–108.
- Potter JS, Marino EN. How to avoid opioid misuse. Chronic Pain Perspectives. 2013;62(3):S2–S7.
- Stanos S. Focused review of interdisciplinary pain rehabilitation programs for chronic pain management. Curr Pain Headache Rep. 2012;16:147–152.
- Cheatle MD, Gallagher RM. Chronic pain and comorbid mood and substance use disorders: a biopsychosocial treatment approach. Curr Psychiatry Rep. 2006;8:371–376.
- Chouinard MC, Hudon C, Dubois MF, et al. Case management and self-management support for frequent users with chronic disease in primary care: a pragmatic randomized controlled trial. BMC Health Serv Res. 2013;13:49.
- Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80:1–13.
- McCracken LM, Turk DC. Behavioral and cognitive-behavioral treatment for chronic pain: outcome, predictors of outcome, and treatment process. Spine (Phila Pa 1976). 2002;27:2564–2573.
- SAMHSA/CSAT Treatment Improvement Protocols. Rockville, MD: Substance Abuse and Mental Health Services Administration; 1993-. Available at: http://www.ncbi.nlm.nih.gov/books/NBK82999/. Accessed May 16, 2013.
- Zeidan F, Grant JA, Brown CA, et al. Mindfulness meditation-related pain relief: evidence for unique brain mechanisms in the regulation of pain. Neurosci Lett. 2012;520:165–173.
- Dakwar E, Levin FR. The emerging role of meditation in addressing psychiatric illness, with a focus on substance use disorders. Harv Rev Psychiatry. 2009;17:254–267.
- Kaskutas LA. Alcoholics anonymous effectiveness: faith meets science. J Addict Dis. 2009;28:145–157.
- Colameco S. Chronic Pain: A Way Out. Comprehensive Treatment & 12-Step Recovery Guide. Haddonfield, NJ: Stephen Colameco; 2012.
- Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012;15(3 suppl):ES205–ES213.
- Brown RA, Abrantes AM, Read JP, et al. A pilot study of aerobic exercise as an adjunctive treatment for drug dependence. Ment Health Phys Act. 2010;3:27–34.
- Savage SR, Kirsch KL, Passik SD. Challenges in using opioids to treat pain in persons with substance use disorders. Addict Sci Clin Pract. 2008;4:4–25.
Advanced-Practice Providers Have More to Offer Hospital Medicine Groups

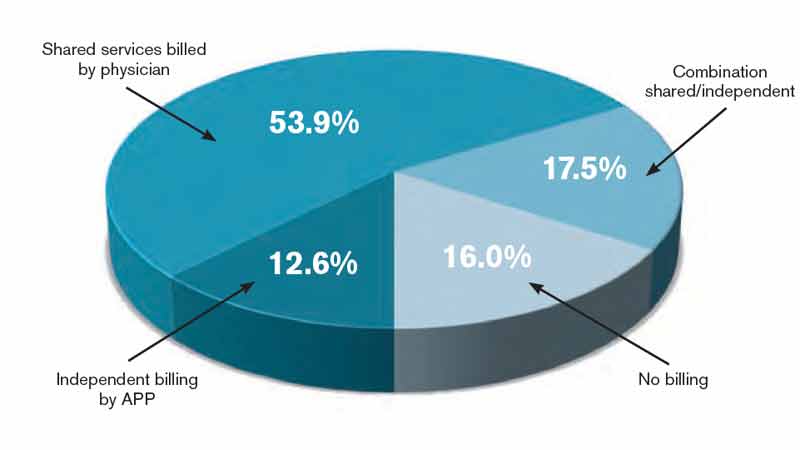
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
Advanced-practice providers (APPs) continue to make their presence felt in the world of hospital medicine. According to survey data from the 2012 State of Hospital Medicine report, more than half (53.9%) of respondent groups serving adults have nurse practitioners (NP) and/or physician assistants (PA) integrated into their practices. The median ratio of APPs to hospitalist physicians in these groups has remained about the same as in previous surveys, with respondents reporting 0.2 FTE NPs per FTE physician, and 0.1 FTE PAs per FTE physician. We’ve also learned that APPs tend to be stable members of most hospitalist practices, with more than 70% of groups reporting no turnover among their APPs during the survey period.
Unfortunately, we don’t yet have much information on the specific roles APPs are filling in HM practices; hopefully, this will be a subject for the next State of Hospital Medicine survey, scheduled to launch in January 2014.
The 2012 survey did provide new information about how APP work is billed by HM groups. More than half the time, APP work is billed as a shared service under a physician’s provider number (see Table 1). Only on rare occasions is APP work billed separately under the APP’s provider number.
Perhaps most surprising of all, 16% of adult HM groups with APPs reported that their APPs don’t generally provide billable services, or no charges were submitted to payors for their services. This figure rose to 23% for hospital-employed groups.
Almost everywhere I go in my consulting work, we are asked about the value APPs can provide to hospitalist practice, and what their optimal roles are. I am extremely supportive of integrating APPs into hospitalist practice and believe they can play valuable roles supporting both excellent patient care and overall group efficiency.
But in my experience, many HM groups fail to execute well on this promise. As the survey results suggest, sometimes APPs are relegated to nonbillable tasks that could be performed by individuals at a lower skill level. Sometimes the hospitalists tend to think of the APPs as “free” help, and no real attempt is made to account for their contribution or capture their billable work. And some groups are so focused on ensuring they capture the 100% reimbursement available by billing under the physician’s name (rather than the 85% reimbursement typically available to APPs) that they lose sight of the fact that the extra physician time and effort involved might cost more than the incremental additional reimbursement received.
As a specialty, we still have a lot to learn about the optimal ways to deploy APPs to support high-quality, effective hospitalist practice. In the meantime, it can be valuable for HM groups to ensure that APPs are functioning in roles that take advantage of their advanced skills and licensure scope, and that efforts are being made to ensure the capture of all billable services provided.
I hope you will plan to participate in the 2014 State of Hospital Medicine survey and share your own practice’s experience with APPs.
Leslie Flores is a partner in Nelson Flores Hospital Medicine Consultants and a member of SHM’s Practice Analysis Committee.
We Welcome the Newest SHM Members
- E. Canady, PA, Alabama
- D. Fico, MD, Alabama
- M. Hazin, DO, Arizona
- K. Ota, DO, Arizona
- T. Phan, Arizona
- M. Poquette, RN, Arizona
- T. Imran, MD, Arkansas
- S. Wooden, MD, Arkansas
- E. Agonafer, California
- S. Badger, MHA, California
- G. Buenaflor, DO, California
- H. Cao, California
- P. Cho, California
- N. Chua, MD, California
- W. Daines, California
- B. Gavi, MD, California
- R. Grant, MD, California
- R. Greysen, MD, California
- V. Hsiao, DO, California
- M. Karube, NP, California
- A. King, MD, California
- M. La, MD, California
- M. Lam, MD, California
- T. Moinizandi, MD, California
- C. Sather, MD, California
- K. Steinberg, MD, California
- S. Woo, MHA, California
- D. Abosh, Canada
- N. Cabilio, MD, Canada
- T. Gepraegs, MD, Canada
- G. Jeffries, CCFP, Canada
- W. Mayhew, MD, Canada
- W. Wilkins, Canada
- M. Braun, ACNP, Colorado
- E. Chu, MD, Colorado
- D. Katz, Colorado
- R. Kumar, Colorado
- A. Maclennan, MD, Colorado
- P. Ryan, Colorado
- O. Akande, MD, Connecticut
- L. Colabelli, Connecticut
- S. Green, ACNP, Connecticut
- S. Lin, Connecticut
- P. Patel, MD, Connecticut
- D. Sewell, MD, Connecticut
- R. Brogan, DO, Florida
- N. Dawson, MD, FACP, Florida
- P. Dhatt, MD, Florida
- N. Griffith, MBA, Florida
- S. Hanson, MD, Florida
- M. Hernandez, MD, Florida
- J. Mennie, MD, Florida
- M. Mohiuddin, MD, Florida
- A. Moynihan, ARNP, Florida
- Y. Patel, MD, Florida
- D. Reto, Florida
- C. Reyes, ARNP, Florida
- B. Fisher, PA-C, Georgia
- S. Fleming, ANP, Georgia
- J. Gilbert, MD, Georgia
- M. Holbrook, FNP, Georgia
- S. Hung, ANP, Georgia
- N. Maignan, MD, Georgia
- P. Nanda, MD, Georgia
- H. Pei, MD, Georgia
- K. Rangnow, NP, Georgia
- S. Shams, MD, Georgia
- L. Wilson, Georgia
- E. Allen, DO, Idaho
- E. Brennan, Illinois
- K. Gul, Illinois
- L. Hansen, MD, Illinois
- D. Nguyen, MD, Illinois
- F. Porter, MD,FACP, Illinois
- A. Ranadive, Illinois
- L. Shahani, MD, Illinois
- J. Tallcott, Illinois
- K. Tulla, Illinois
- N. Wiegley, Illinois
- R. Young, MD, MS, Illinois
- D. Yu, MD, Illinois
- Z. Alba, MD, Indiana
- G. Alcorn, MD, Indiana
- K. Dorairaj, MD, Indiana
- W. Harbin, DO, Indiana
- A. Patel, MD, Indiana
- J. Shamoun, MD, Indiana
- N. Wells, MD, Indiana
- J. Wynn, USA, Indiana
- N. Hartog, MD, Iowa
- K. Emoto, Japan
- M. Sakai, MD, Japan
- P. Poddutoori, MBBS, Kansas
- T. Stofferson, ACMPE, Kansas
- B. Huneycutt, MD, Kentucky
- S. Muldoon, MD, Kentucky
- W. Travis, MD, Kentucky
- B. Molbert, NP, Louisiana
- M. Jacquet, MD, Maine
- P. Pahel, FNP, Maine
- S. Albanez, Maryland
- A. Anigbo, MBBS, Maryland
- A. Antar, PhD, Maryland
- E. Bice, DO, Maryland
- J. Clark, Maryland
- T. Hall, Maryland
- B. Huntley, PA, Maryland
- J. Kaka, Maryland
- D. Kidd, Maryland
- R. Landis, BA, Maryland
- T. Lawgaw, PA-C, Maryland
- M. Singh, Maryland
- M. Baggett, MD, Massachusetts
- E. Barkoudah, MD, Massachusetts
- J. Bortinger, MD, Massachusetts
- J. Bukli, MD, Massachusetts
- S. Dhand, MD, Massachusetts
- L. DiPompo, Massachusetts
- J. Donze, MD, Massachusetts
- S. Ganatra, Massachusetts
- R. Goldberg, MD, Massachusetts
- R. Gumber, MD, Massachusetts
- J. Lawrason, MD, Massachusetts
- N. Lebaka, MD, Massachusetts
- M. Mahmoud, MD, Massachusetts
- G. Mills, Massachusetts
- M. Mohamed, MD, Massachusetts
- J. Parr, MPH, Massachusetts
- D. Ramirez, PA-C, Massachusetts
- L. Solis-Cohen, MD, Massachusetts
- C. Yu, MD, Massachusetts
- E. Bazan, Michigan
- J. Bedore, PA-C, Michigan
- P. Bradley, MD, Michigan
- L. Butz, MD, Michigan
- S. Chase, PharmD, Michigan
- A. Funk, MD, Michigan
- N. Khalid, MD, Michigan
- R. Patel, MD, Michigan
- I. Patsias, MD, Michigan
- P. Sanchez, Michigan
- D. Bowman, Minnesota
- M. Buchner, MD, Minnesota
- S. Mehmood, MD, Minnesota
- J. Ratelle, Minnesota
- M. Werpy, DO, Minnesota
- M. White, MD, Minnesota
- T. Willson, Minnesota
- H. Wood, MD, Minnesota
- S. Altmiller, Mississippi
- R. Andersson, Missouri
- K. Chuu, MD, Missouri
- M. Mullick, MD, Missouri
- C. Obi, MBBS, Missouri
- M. O’Dell, MD, Missouri
- D. Smith, MBA, Missouri
- J. Tyler, DO, Missouri
- S. Riggs, NP, Nebraska
- A. Bose, MD, New Hampshire
- F. Gaffney Comeau, New Hampshire
- C. Raymond, MSN, New Hampshire
- M. Balac, New Jersey
- A. Boa Hocbo, MD, New Jersey
- C. DeLuca, New Jersey
- P. Jadhav, MD, New Jersey
- S. Kishore, MBBS, New Jersey
- P. Krishnamoorthy, MD, New Jersey
- B. LaMotte, PharmD, New Jersey
- C. Maloy, PA-C, New Jersey
- A. Oakley, New Jersey
- K. Pratt, MD, New Jersey
- J. Yacco, New Jersey
- A. Zeff, New Jersey
- K. Caudell, PhD, New Mexico
- G. Ghuneim, MD, New Mexico
- J. Marley, DO, New Mexico
- B. Stricks, New Mexico
- L. Ahmed, New York
- G. Arora, MD, New York
- N. Bangiyeva, MD, New York
- A. Bansal, MD, New York
- L. Belletti, FACP, New York
- N. Bhatt, MPH, New York
- A. Blatt, MD, New York
- T. Chau, New York
- N. Chaudhry, MD, New York
- S. Collins, MD, New York
- L. Coryat, ANP, New York
- R. Dachs, MD, New York
- G. DeCastro, MD, New York
- J. Duffy, ANP, New York
- F. Farzan, MD, New York
- A. Gopal, MD, New York
- S. Hameed, New York
- A. Hanif, MD, New York
- A. Hassan, MD, New York
- A. Howe, New York
- M. Ip, New York
- M. Kelly, MD, New York
- S. Kovtunova, MD, New York
- J. Liu, MD, MPH, New York
- A. Maritato, MD, New York
- K. Mayer, MD, New York
- S. Mehra, New York
- K. Noshiro, MD, New York
- M. Panichas, New York
- V. Rakhvalchuk, DO, New York
- R. Ramkeesoon, New York
- M. Saluja, MD, New York
- P. Shanmugathasan, MD, New York
- S. Sherazi, MD, New York
- J. Shin, MD, New York
- S. Veeramachaneni, MD, New York
- S. Yang, MD, New York
- M. Ardison, MHS, North Carolina
- M. Banks, PA, North Carolina
- W. Brooks, MD, North Carolina
- M. Chadwick, MD, North Carolina
- J. Cowen, DO, North Carolina
- S. Hewitt, North Carolina
- S. Irvin, North Carolina
- J. Kornegay, MD, North Carolina
- K. Larbi-siaw, MD, North Carolina
- J. Pavon, MD, North Carolina
- D. Warner, PA-C, North Carolina
- S. Wells, PA, North Carolina
- S. Abdel-Ghani, MD, Ohio
- D. Abhyankar, Ohio
- A. Alahmar, MD, Ohio
- A. Andreadis, MD, Ohio
- M. Bajwa, Ohio
- A. Blankenship, RN, Ohio
- M. Constantiner, RPh, Ohio
- D. Djigbenou, MD, Ohio
- S. Evans, MD, Ohio
- J. Girard, Ohio
- J. Held, MD, Ohio
- K. Hilder, MD, Ohio
- R. Kanuru, MD, Ohio
- H. Mount, Ohio
- B. Pachmayer, MD, Ohio
- C. Rodehaver, RN, MS, Ohio
- C. Schelzig, MD, FAAP, Ohio
- M. Mathews, Oklahoma
- F. Escaro, Oregon
- S. Hale, MD, Oregon
- E. Meihoff, MD, Oregon
- B. Rainka, Oregon
- A. Behura, MD, Pennsylvania
- B. Bussler, Pennsylvania
- J. Chintanaboina, Pennsylvania
- I. Cirilo, MD, Pennsylvania
- S. Doomra, Pennsylvania
- G. Gabasan, MD, Pennsylvania
- J. Gengaro, DO, Pennsylvania
- D. Gondek, DO, Pennsylvania
- K. Gonzalez, NP, Pennsylvania
- A. Hellyer, Pennsylvania
- J. Julian, MD, MPH, Pennsylvania
- A. Kainz, Pennsylvania
- S. Kaur, MD, Pennsylvania
- P. Lange, MD, Pennsylvania
- S. Leslie, MD, Pennsylvania
- D. McBryan, MD, Pennsylvania
- A. Miller, CRNP, Pennsylvania
- S. Nichuls, PA-C, Pennsylvania
- T. Pellegrino, PharmD, Pennsylvania
- K. Reed, PharmD, Pennsylvania
- A. Seasock, PA-C, BS, Pennsylvania
- S. Soenen, Pennsylvania
- V. Subbiah, MD, Pennsylvania
- N. Thingalaya, MD, Pennsylvania
- E. Tuttle, PA, Pennsylvania
- G. Vadlamudi, MPH, MD, Pennsylvania
- B. Verma, MD, Pennsylvania
- E. Wannebo, MD, Pennsylvania
- A. Wesoly, PA, Pennsylvania
- L. Eddy, FNP, Rhode Island
- M. Antonatos, MD, South Carolina
- S. Connelly, South Carolina
- D. O’Briant, MD, South Carolina
- R. Agarwal, MD, MBA, Tennessee
- A. Aird, MD, Tennessee
- F. Dragila, MD, Tennessee
- S. Duncan, MD, Tennessee
- M. Flint, MPH, Tennessee
- A. Goldfeld, Tennessee
- R. Gusso, MD, Tennessee
- S. Lane, M.H.A., Tennessee
- C. Long, MD, Tennessee
- M. Naeem, MD, PhD, Tennessee
- C. Aiken, RN, Texas
- D. Berhane, Texas
- M. Cabello, MD, Texas
- A. Caruso, MD, Texas
- P. Desai, Texas
- J. Haygood, Texas
- R. Henderson, MD, Texas
- C. Inniss, Texas
- W. Mirza, DO, Texas
- C. Moreland, MD, Texas
- N. Mulukutla, MD, Texas
- G. Neil, MD, Texas
- I. Nwabude, MD, Texas
- T. Onishi, MD, Texas
- K. Patel, MD, Texas
- B. Pomeroy, MD, Texas
- S. Ray, Texas
- J. Tau, MD, Texas
- M. Blankenship, MD, Utah
- L. Porter, RN, Utah
- J. Strong, MD, Utah
- J. Van Blarcom, MD, Utah
- A. Wood, RN, Utah
- M. Wren, Utah
- M. Anawati, MD, Vermont
- S. Lee, Vermont
- C. Cook, MD, Virginia
- E. Deungwe Yonga, MD, Virginia
- F. Dieter, PA, Virginia
- P. Gill, MD, Virginia
- S. Goldwater, PharmD, Virginia
- R. Martin, MD, Virginia
- T. Masterson, Virginia
- P. Ouellette, MD, Virginia
- M. Plazarte, DO, Virginia
- C. Salamanca, NP, Virginia
- B. Seagroves, MD, Virginia
- G. Slitt, MD, Virginia
- F. Williams, MD, Virginia
- S. Won, NP, MSN, Virginia
- L. Alberts, MD, Washington
- E. Lopez, PA-C, Washington
- L. Lubinski, MD, Washington
- J. Oconer, MD, Washington
- K. Shulman, Washington
- S. Carpenter, MD, West Virginia
- Y. Jones, FAAP, West Virginia
- P. Cartier-Neely, PA, Wisconsin
- D. Johnson, MD, Wisconsin
- R. Johnson, MD, Wisconsin
- E. Canady, PA, Alabama
- D. Fico, MD, Alabama
- M. Hazin, DO, Arizona
- K. Ota, DO, Arizona
- T. Phan, Arizona
- M. Poquette, RN, Arizona
- T. Imran, MD, Arkansas
- S. Wooden, MD, Arkansas
- E. Agonafer, California
- S. Badger, MHA, California
- G. Buenaflor, DO, California
- H. Cao, California
- P. Cho, California
- N. Chua, MD, California
- W. Daines, California
- B. Gavi, MD, California
- R. Grant, MD, California
- R. Greysen, MD, California
- V. Hsiao, DO, California
- M. Karube, NP, California
- A. King, MD, California
- M. La, MD, California
- M. Lam, MD, California
- T. Moinizandi, MD, California
- C. Sather, MD, California
- K. Steinberg, MD, California
- S. Woo, MHA, California
- D. Abosh, Canada
- N. Cabilio, MD, Canada
- T. Gepraegs, MD, Canada
- G. Jeffries, CCFP, Canada
- W. Mayhew, MD, Canada
- W. Wilkins, Canada
- M. Braun, ACNP, Colorado
- E. Chu, MD, Colorado
- D. Katz, Colorado
- R. Kumar, Colorado
- A. Maclennan, MD, Colorado
- P. Ryan, Colorado
- O. Akande, MD, Connecticut
- L. Colabelli, Connecticut
- S. Green, ACNP, Connecticut
- S. Lin, Connecticut
- P. Patel, MD, Connecticut
- D. Sewell, MD, Connecticut
- R. Brogan, DO, Florida
- N. Dawson, MD, FACP, Florida
- P. Dhatt, MD, Florida
- N. Griffith, MBA, Florida
- S. Hanson, MD, Florida
- M. Hernandez, MD, Florida
- J. Mennie, MD, Florida
- M. Mohiuddin, MD, Florida
- A. Moynihan, ARNP, Florida
- Y. Patel, MD, Florida
- D. Reto, Florida
- C. Reyes, ARNP, Florida
- B. Fisher, PA-C, Georgia
- S. Fleming, ANP, Georgia
- J. Gilbert, MD, Georgia
- M. Holbrook, FNP, Georgia
- S. Hung, ANP, Georgia
- N. Maignan, MD, Georgia
- P. Nanda, MD, Georgia
- H. Pei, MD, Georgia
- K. Rangnow, NP, Georgia
- S. Shams, MD, Georgia
- L. Wilson, Georgia
- E. Allen, DO, Idaho
- E. Brennan, Illinois
- K. Gul, Illinois
- L. Hansen, MD, Illinois
- D. Nguyen, MD, Illinois
- F. Porter, MD,FACP, Illinois
- A. Ranadive, Illinois
- L. Shahani, MD, Illinois
- J. Tallcott, Illinois
- K. Tulla, Illinois
- N. Wiegley, Illinois
- R. Young, MD, MS, Illinois
- D. Yu, MD, Illinois
- Z. Alba, MD, Indiana
- G. Alcorn, MD, Indiana
- K. Dorairaj, MD, Indiana
- W. Harbin, DO, Indiana
- A. Patel, MD, Indiana
- J. Shamoun, MD, Indiana
- N. Wells, MD, Indiana
- J. Wynn, USA, Indiana
- N. Hartog, MD, Iowa
- K. Emoto, Japan
- M. Sakai, MD, Japan
- P. Poddutoori, MBBS, Kansas
- T. Stofferson, ACMPE, Kansas
- B. Huneycutt, MD, Kentucky
- S. Muldoon, MD, Kentucky
- W. Travis, MD, Kentucky
- B. Molbert, NP, Louisiana
- M. Jacquet, MD, Maine
- P. Pahel, FNP, Maine
- S. Albanez, Maryland
- A. Anigbo, MBBS, Maryland
- A. Antar, PhD, Maryland
- E. Bice, DO, Maryland
- J. Clark, Maryland
- T. Hall, Maryland
- B. Huntley, PA, Maryland
- J. Kaka, Maryland
- D. Kidd, Maryland
- R. Landis, BA, Maryland
- T. Lawgaw, PA-C, Maryland
- M. Singh, Maryland
- M. Baggett, MD, Massachusetts
- E. Barkoudah, MD, Massachusetts
- J. Bortinger, MD, Massachusetts
- J. Bukli, MD, Massachusetts
- S. Dhand, MD, Massachusetts
- L. DiPompo, Massachusetts
- J. Donze, MD, Massachusetts
- S. Ganatra, Massachusetts
- R. Goldberg, MD, Massachusetts
- R. Gumber, MD, Massachusetts
- J. Lawrason, MD, Massachusetts
- N. Lebaka, MD, Massachusetts
- M. Mahmoud, MD, Massachusetts
- G. Mills, Massachusetts
- M. Mohamed, MD, Massachusetts
- J. Parr, MPH, Massachusetts
- D. Ramirez, PA-C, Massachusetts
- L. Solis-Cohen, MD, Massachusetts
- C. Yu, MD, Massachusetts
- E. Bazan, Michigan
- J. Bedore, PA-C, Michigan
- P. Bradley, MD, Michigan
- L. Butz, MD, Michigan
- S. Chase, PharmD, Michigan
- A. Funk, MD, Michigan
- N. Khalid, MD, Michigan
- R. Patel, MD, Michigan
- I. Patsias, MD, Michigan
- P. Sanchez, Michigan
- D. Bowman, Minnesota
- M. Buchner, MD, Minnesota
- S. Mehmood, MD, Minnesota
- J. Ratelle, Minnesota
- M. Werpy, DO, Minnesota
- M. White, MD, Minnesota
- T. Willson, Minnesota
- H. Wood, MD, Minnesota
- S. Altmiller, Mississippi
- R. Andersson, Missouri
- K. Chuu, MD, Missouri
- M. Mullick, MD, Missouri
- C. Obi, MBBS, Missouri
- M. O’Dell, MD, Missouri
- D. Smith, MBA, Missouri
- J. Tyler, DO, Missouri
- S. Riggs, NP, Nebraska
- A. Bose, MD, New Hampshire
- F. Gaffney Comeau, New Hampshire
- C. Raymond, MSN, New Hampshire
- M. Balac, New Jersey
- A. Boa Hocbo, MD, New Jersey
- C. DeLuca, New Jersey
- P. Jadhav, MD, New Jersey
- S. Kishore, MBBS, New Jersey
- P. Krishnamoorthy, MD, New Jersey
- B. LaMotte, PharmD, New Jersey
- C. Maloy, PA-C, New Jersey
- A. Oakley, New Jersey
- K. Pratt, MD, New Jersey
- J. Yacco, New Jersey
- A. Zeff, New Jersey
- K. Caudell, PhD, New Mexico
- G. Ghuneim, MD, New Mexico
- J. Marley, DO, New Mexico
- B. Stricks, New Mexico
- L. Ahmed, New York
- G. Arora, MD, New York
- N. Bangiyeva, MD, New York
- A. Bansal, MD, New York
- L. Belletti, FACP, New York
- N. Bhatt, MPH, New York
- A. Blatt, MD, New York
- T. Chau, New York
- N. Chaudhry, MD, New York
- S. Collins, MD, New York
- L. Coryat, ANP, New York
- R. Dachs, MD, New York
- G. DeCastro, MD, New York
- J. Duffy, ANP, New York
- F. Farzan, MD, New York
- A. Gopal, MD, New York
- S. Hameed, New York
- A. Hanif, MD, New York
- A. Hassan, MD, New York
- A. Howe, New York
- M. Ip, New York
- M. Kelly, MD, New York
- S. Kovtunova, MD, New York
- J. Liu, MD, MPH, New York
- A. Maritato, MD, New York
- K. Mayer, MD, New York
- S. Mehra, New York
- K. Noshiro, MD, New York
- M. Panichas, New York
- V. Rakhvalchuk, DO, New York
- R. Ramkeesoon, New York
- M. Saluja, MD, New York
- P. Shanmugathasan, MD, New York
- S. Sherazi, MD, New York
- J. Shin, MD, New York
- S. Veeramachaneni, MD, New York
- S. Yang, MD, New York
- M. Ardison, MHS, North Carolina
- M. Banks, PA, North Carolina
- W. Brooks, MD, North Carolina
- M. Chadwick, MD, North Carolina
- J. Cowen, DO, North Carolina
- S. Hewitt, North Carolina
- S. Irvin, North Carolina
- J. Kornegay, MD, North Carolina
- K. Larbi-siaw, MD, North Carolina
- J. Pavon, MD, North Carolina
- D. Warner, PA-C, North Carolina
- S. Wells, PA, North Carolina
- S. Abdel-Ghani, MD, Ohio
- D. Abhyankar, Ohio
- A. Alahmar, MD, Ohio
- A. Andreadis, MD, Ohio
- M. Bajwa, Ohio
- A. Blankenship, RN, Ohio
- M. Constantiner, RPh, Ohio
- D. Djigbenou, MD, Ohio
- S. Evans, MD, Ohio
- J. Girard, Ohio
- J. Held, MD, Ohio
- K. Hilder, MD, Ohio
- R. Kanuru, MD, Ohio
- H. Mount, Ohio
- B. Pachmayer, MD, Ohio
- C. Rodehaver, RN, MS, Ohio
- C. Schelzig, MD, FAAP, Ohio
- M. Mathews, Oklahoma
- F. Escaro, Oregon
- S. Hale, MD, Oregon
- E. Meihoff, MD, Oregon
- B. Rainka, Oregon
- A. Behura, MD, Pennsylvania
- B. Bussler, Pennsylvania
- J. Chintanaboina, Pennsylvania
- I. Cirilo, MD, Pennsylvania
- S. Doomra, Pennsylvania
- G. Gabasan, MD, Pennsylvania
- J. Gengaro, DO, Pennsylvania
- D. Gondek, DO, Pennsylvania
- K. Gonzalez, NP, Pennsylvania
- A. Hellyer, Pennsylvania
- J. Julian, MD, MPH, Pennsylvania
- A. Kainz, Pennsylvania
- S. Kaur, MD, Pennsylvania
- P. Lange, MD, Pennsylvania
- S. Leslie, MD, Pennsylvania
- D. McBryan, MD, Pennsylvania
- A. Miller, CRNP, Pennsylvania
- S. Nichuls, PA-C, Pennsylvania
- T. Pellegrino, PharmD, Pennsylvania
- K. Reed, PharmD, Pennsylvania
- A. Seasock, PA-C, BS, Pennsylvania
- S. Soenen, Pennsylvania
- V. Subbiah, MD, Pennsylvania
- N. Thingalaya, MD, Pennsylvania
- E. Tuttle, PA, Pennsylvania
- G. Vadlamudi, MPH, MD, Pennsylvania
- B. Verma, MD, Pennsylvania
- E. Wannebo, MD, Pennsylvania
- A. Wesoly, PA, Pennsylvania
- L. Eddy, FNP, Rhode Island
- M. Antonatos, MD, South Carolina
- S. Connelly, South Carolina
- D. O’Briant, MD, South Carolina
- R. Agarwal, MD, MBA, Tennessee
- A. Aird, MD, Tennessee
- F. Dragila, MD, Tennessee
- S. Duncan, MD, Tennessee
- M. Flint, MPH, Tennessee
- A. Goldfeld, Tennessee
- R. Gusso, MD, Tennessee
- S. Lane, M.H.A., Tennessee
- C. Long, MD, Tennessee
- M. Naeem, MD, PhD, Tennessee
- C. Aiken, RN, Texas
- D. Berhane, Texas
- M. Cabello, MD, Texas
- A. Caruso, MD, Texas
- P. Desai, Texas
- J. Haygood, Texas
- R. Henderson, MD, Texas
- C. Inniss, Texas
- W. Mirza, DO, Texas
- C. Moreland, MD, Texas
- N. Mulukutla, MD, Texas
- G. Neil, MD, Texas
- I. Nwabude, MD, Texas
- T. Onishi, MD, Texas
- K. Patel, MD, Texas
- B. Pomeroy, MD, Texas
- S. Ray, Texas
- J. Tau, MD, Texas
- M. Blankenship, MD, Utah
- L. Porter, RN, Utah
- J. Strong, MD, Utah
- J. Van Blarcom, MD, Utah
- A. Wood, RN, Utah
- M. Wren, Utah
- M. Anawati, MD, Vermont
- S. Lee, Vermont
- C. Cook, MD, Virginia
- E. Deungwe Yonga, MD, Virginia
- F. Dieter, PA, Virginia
- P. Gill, MD, Virginia
- S. Goldwater, PharmD, Virginia
- R. Martin, MD, Virginia
- T. Masterson, Virginia
- P. Ouellette, MD, Virginia
- M. Plazarte, DO, Virginia
- C. Salamanca, NP, Virginia
- B. Seagroves, MD, Virginia
- G. Slitt, MD, Virginia
- F. Williams, MD, Virginia
- S. Won, NP, MSN, Virginia
- L. Alberts, MD, Washington
- E. Lopez, PA-C, Washington
- L. Lubinski, MD, Washington
- J. Oconer, MD, Washington
- K. Shulman, Washington
- S. Carpenter, MD, West Virginia
- Y. Jones, FAAP, West Virginia
- P. Cartier-Neely, PA, Wisconsin
- D. Johnson, MD, Wisconsin
- R. Johnson, MD, Wisconsin
- E. Canady, PA, Alabama
- D. Fico, MD, Alabama
- M. Hazin, DO, Arizona
- K. Ota, DO, Arizona
- T. Phan, Arizona
- M. Poquette, RN, Arizona
- T. Imran, MD, Arkansas
- S. Wooden, MD, Arkansas
- E. Agonafer, California
- S. Badger, MHA, California
- G. Buenaflor, DO, California
- H. Cao, California
- P. Cho, California
- N. Chua, MD, California
- W. Daines, California
- B. Gavi, MD, California
- R. Grant, MD, California
- R. Greysen, MD, California
- V. Hsiao, DO, California
- M. Karube, NP, California
- A. King, MD, California
- M. La, MD, California
- M. Lam, MD, California
- T. Moinizandi, MD, California
- C. Sather, MD, California
- K. Steinberg, MD, California
- S. Woo, MHA, California
- D. Abosh, Canada
- N. Cabilio, MD, Canada
- T. Gepraegs, MD, Canada
- G. Jeffries, CCFP, Canada
- W. Mayhew, MD, Canada
- W. Wilkins, Canada
- M. Braun, ACNP, Colorado
- E. Chu, MD, Colorado
- D. Katz, Colorado
- R. Kumar, Colorado
- A. Maclennan, MD, Colorado
- P. Ryan, Colorado
- O. Akande, MD, Connecticut
- L. Colabelli, Connecticut
- S. Green, ACNP, Connecticut
- S. Lin, Connecticut
- P. Patel, MD, Connecticut
- D. Sewell, MD, Connecticut
- R. Brogan, DO, Florida
- N. Dawson, MD, FACP, Florida
- P. Dhatt, MD, Florida
- N. Griffith, MBA, Florida
- S. Hanson, MD, Florida
- M. Hernandez, MD, Florida
- J. Mennie, MD, Florida
- M. Mohiuddin, MD, Florida
- A. Moynihan, ARNP, Florida
- Y. Patel, MD, Florida
- D. Reto, Florida
- C. Reyes, ARNP, Florida
- B. Fisher, PA-C, Georgia
- S. Fleming, ANP, Georgia
- J. Gilbert, MD, Georgia
- M. Holbrook, FNP, Georgia
- S. Hung, ANP, Georgia
- N. Maignan, MD, Georgia
- P. Nanda, MD, Georgia
- H. Pei, MD, Georgia
- K. Rangnow, NP, Georgia
- S. Shams, MD, Georgia
- L. Wilson, Georgia
- E. Allen, DO, Idaho
- E. Brennan, Illinois
- K. Gul, Illinois
- L. Hansen, MD, Illinois
- D. Nguyen, MD, Illinois
- F. Porter, MD,FACP, Illinois
- A. Ranadive, Illinois
- L. Shahani, MD, Illinois
- J. Tallcott, Illinois
- K. Tulla, Illinois
- N. Wiegley, Illinois
- R. Young, MD, MS, Illinois
- D. Yu, MD, Illinois
- Z. Alba, MD, Indiana
- G. Alcorn, MD, Indiana
- K. Dorairaj, MD, Indiana
- W. Harbin, DO, Indiana
- A. Patel, MD, Indiana
- J. Shamoun, MD, Indiana
- N. Wells, MD, Indiana
- J. Wynn, USA, Indiana
- N. Hartog, MD, Iowa
- K. Emoto, Japan
- M. Sakai, MD, Japan
- P. Poddutoori, MBBS, Kansas
- T. Stofferson, ACMPE, Kansas
- B. Huneycutt, MD, Kentucky
- S. Muldoon, MD, Kentucky
- W. Travis, MD, Kentucky
- B. Molbert, NP, Louisiana
- M. Jacquet, MD, Maine
- P. Pahel, FNP, Maine
- S. Albanez, Maryland
- A. Anigbo, MBBS, Maryland
- A. Antar, PhD, Maryland
- E. Bice, DO, Maryland
- J. Clark, Maryland
- T. Hall, Maryland
- B. Huntley, PA, Maryland
- J. Kaka, Maryland
- D. Kidd, Maryland
- R. Landis, BA, Maryland
- T. Lawgaw, PA-C, Maryland
- M. Singh, Maryland
- M. Baggett, MD, Massachusetts
- E. Barkoudah, MD, Massachusetts
- J. Bortinger, MD, Massachusetts
- J. Bukli, MD, Massachusetts
- S. Dhand, MD, Massachusetts
- L. DiPompo, Massachusetts
- J. Donze, MD, Massachusetts
- S. Ganatra, Massachusetts
- R. Goldberg, MD, Massachusetts
- R. Gumber, MD, Massachusetts
- J. Lawrason, MD, Massachusetts
- N. Lebaka, MD, Massachusetts
- M. Mahmoud, MD, Massachusetts
- G. Mills, Massachusetts
- M. Mohamed, MD, Massachusetts
- J. Parr, MPH, Massachusetts
- D. Ramirez, PA-C, Massachusetts
- L. Solis-Cohen, MD, Massachusetts
- C. Yu, MD, Massachusetts
- E. Bazan, Michigan
- J. Bedore, PA-C, Michigan
- P. Bradley, MD, Michigan
- L. Butz, MD, Michigan
- S. Chase, PharmD, Michigan
- A. Funk, MD, Michigan
- N. Khalid, MD, Michigan
- R. Patel, MD, Michigan
- I. Patsias, MD, Michigan
- P. Sanchez, Michigan
- D. Bowman, Minnesota
- M. Buchner, MD, Minnesota
- S. Mehmood, MD, Minnesota
- J. Ratelle, Minnesota
- M. Werpy, DO, Minnesota
- M. White, MD, Minnesota
- T. Willson, Minnesota
- H. Wood, MD, Minnesota
- S. Altmiller, Mississippi
- R. Andersson, Missouri
- K. Chuu, MD, Missouri
- M. Mullick, MD, Missouri
- C. Obi, MBBS, Missouri
- M. O’Dell, MD, Missouri
- D. Smith, MBA, Missouri
- J. Tyler, DO, Missouri
- S. Riggs, NP, Nebraska
- A. Bose, MD, New Hampshire
- F. Gaffney Comeau, New Hampshire
- C. Raymond, MSN, New Hampshire
- M. Balac, New Jersey
- A. Boa Hocbo, MD, New Jersey
- C. DeLuca, New Jersey
- P. Jadhav, MD, New Jersey
- S. Kishore, MBBS, New Jersey
- P. Krishnamoorthy, MD, New Jersey
- B. LaMotte, PharmD, New Jersey
- C. Maloy, PA-C, New Jersey
- A. Oakley, New Jersey
- K. Pratt, MD, New Jersey
- J. Yacco, New Jersey
- A. Zeff, New Jersey
- K. Caudell, PhD, New Mexico
- G. Ghuneim, MD, New Mexico
- J. Marley, DO, New Mexico
- B. Stricks, New Mexico
- L. Ahmed, New York
- G. Arora, MD, New York
- N. Bangiyeva, MD, New York
- A. Bansal, MD, New York
- L. Belletti, FACP, New York
- N. Bhatt, MPH, New York
- A. Blatt, MD, New York
- T. Chau, New York
- N. Chaudhry, MD, New York
- S. Collins, MD, New York
- L. Coryat, ANP, New York
- R. Dachs, MD, New York
- G. DeCastro, MD, New York
- J. Duffy, ANP, New York
- F. Farzan, MD, New York
- A. Gopal, MD, New York
- S. Hameed, New York
- A. Hanif, MD, New York
- A. Hassan, MD, New York
- A. Howe, New York
- M. Ip, New York
- M. Kelly, MD, New York
- S. Kovtunova, MD, New York
- J. Liu, MD, MPH, New York
- A. Maritato, MD, New York
- K. Mayer, MD, New York
- S. Mehra, New York
- K. Noshiro, MD, New York
- M. Panichas, New York
- V. Rakhvalchuk, DO, New York
- R. Ramkeesoon, New York
- M. Saluja, MD, New York
- P. Shanmugathasan, MD, New York
- S. Sherazi, MD, New York
- J. Shin, MD, New York
- S. Veeramachaneni, MD, New York
- S. Yang, MD, New York
- M. Ardison, MHS, North Carolina
- M. Banks, PA, North Carolina
- W. Brooks, MD, North Carolina
- M. Chadwick, MD, North Carolina
- J. Cowen, DO, North Carolina
- S. Hewitt, North Carolina
- S. Irvin, North Carolina
- J. Kornegay, MD, North Carolina
- K. Larbi-siaw, MD, North Carolina
- J. Pavon, MD, North Carolina
- D. Warner, PA-C, North Carolina
- S. Wells, PA, North Carolina
- S. Abdel-Ghani, MD, Ohio
- D. Abhyankar, Ohio
- A. Alahmar, MD, Ohio
- A. Andreadis, MD, Ohio
- M. Bajwa, Ohio
- A. Blankenship, RN, Ohio
- M. Constantiner, RPh, Ohio
- D. Djigbenou, MD, Ohio
- S. Evans, MD, Ohio
- J. Girard, Ohio
- J. Held, MD, Ohio
- K. Hilder, MD, Ohio
- R. Kanuru, MD, Ohio
- H. Mount, Ohio
- B. Pachmayer, MD, Ohio
- C. Rodehaver, RN, MS, Ohio
- C. Schelzig, MD, FAAP, Ohio
- M. Mathews, Oklahoma
- F. Escaro, Oregon
- S. Hale, MD, Oregon
- E. Meihoff, MD, Oregon
- B. Rainka, Oregon
- A. Behura, MD, Pennsylvania
- B. Bussler, Pennsylvania
- J. Chintanaboina, Pennsylvania
- I. Cirilo, MD, Pennsylvania
- S. Doomra, Pennsylvania
- G. Gabasan, MD, Pennsylvania
- J. Gengaro, DO, Pennsylvania
- D. Gondek, DO, Pennsylvania
- K. Gonzalez, NP, Pennsylvania
- A. Hellyer, Pennsylvania
- J. Julian, MD, MPH, Pennsylvania
- A. Kainz, Pennsylvania
- S. Kaur, MD, Pennsylvania
- P. Lange, MD, Pennsylvania
- S. Leslie, MD, Pennsylvania
- D. McBryan, MD, Pennsylvania
- A. Miller, CRNP, Pennsylvania
- S. Nichuls, PA-C, Pennsylvania
- T. Pellegrino, PharmD, Pennsylvania
- K. Reed, PharmD, Pennsylvania
- A. Seasock, PA-C, BS, Pennsylvania
- S. Soenen, Pennsylvania
- V. Subbiah, MD, Pennsylvania
- N. Thingalaya, MD, Pennsylvania
- E. Tuttle, PA, Pennsylvania
- G. Vadlamudi, MPH, MD, Pennsylvania
- B. Verma, MD, Pennsylvania
- E. Wannebo, MD, Pennsylvania
- A. Wesoly, PA, Pennsylvania
- L. Eddy, FNP, Rhode Island
- M. Antonatos, MD, South Carolina
- S. Connelly, South Carolina
- D. O’Briant, MD, South Carolina
- R. Agarwal, MD, MBA, Tennessee
- A. Aird, MD, Tennessee
- F. Dragila, MD, Tennessee
- S. Duncan, MD, Tennessee
- M. Flint, MPH, Tennessee
- A. Goldfeld, Tennessee
- R. Gusso, MD, Tennessee
- S. Lane, M.H.A., Tennessee
- C. Long, MD, Tennessee
- M. Naeem, MD, PhD, Tennessee
- C. Aiken, RN, Texas
- D. Berhane, Texas
- M. Cabello, MD, Texas
- A. Caruso, MD, Texas
- P. Desai, Texas
- J. Haygood, Texas
- R. Henderson, MD, Texas
- C. Inniss, Texas
- W. Mirza, DO, Texas
- C. Moreland, MD, Texas
- N. Mulukutla, MD, Texas
- G. Neil, MD, Texas
- I. Nwabude, MD, Texas
- T. Onishi, MD, Texas
- K. Patel, MD, Texas
- B. Pomeroy, MD, Texas
- S. Ray, Texas
- J. Tau, MD, Texas
- M. Blankenship, MD, Utah
- L. Porter, RN, Utah
- J. Strong, MD, Utah
- J. Van Blarcom, MD, Utah
- A. Wood, RN, Utah
- M. Wren, Utah
- M. Anawati, MD, Vermont
- S. Lee, Vermont
- C. Cook, MD, Virginia
- E. Deungwe Yonga, MD, Virginia
- F. Dieter, PA, Virginia
- P. Gill, MD, Virginia
- S. Goldwater, PharmD, Virginia
- R. Martin, MD, Virginia
- T. Masterson, Virginia
- P. Ouellette, MD, Virginia
- M. Plazarte, DO, Virginia
- C. Salamanca, NP, Virginia
- B. Seagroves, MD, Virginia
- G. Slitt, MD, Virginia
- F. Williams, MD, Virginia
- S. Won, NP, MSN, Virginia
- L. Alberts, MD, Washington
- E. Lopez, PA-C, Washington
- L. Lubinski, MD, Washington
- J. Oconer, MD, Washington
- K. Shulman, Washington
- S. Carpenter, MD, West Virginia
- Y. Jones, FAAP, West Virginia
- P. Cartier-Neely, PA, Wisconsin
- D. Johnson, MD, Wisconsin
- R. Johnson, MD, Wisconsin
Fellow in Hospital Medicine Spotlight: Rachel Thompson, MD, FHM

Dr. Thompson is an assistant professor in the Department of Medicine and the Department of Neurosurgery at the University of Washington in Seattle. She is director of the medicine consult service and the medicine operative consult clinic at Harborview Medical Center in Seattle. She also is president of SHM’s Pacific Northwest chapter and a member of the National Chapter Support Committee.
Undergraduate education: Amherst College, Amherst, Mass.
Medical school: University of Washington School of Medicine, Seattle.
Notable: Dr. Thompson says one of her greatest career achievements has been the development of collegial services with surgeons and researchers in order to look at surgical outcomes through the lens of a hospitalist. She also developed a glycemic-control center in her hospital to improve insulin ordering, a project for which she has been published and presented locally and nationally. She has served as a resident research project mentor since 2005, helping 13 students achieve their research goals. Dr. Thompson volunteers at the Mathematics Engineering Science Achievement (MESA) Saturday Academy, an inner-city high school program for advancement in math and science, for which she won the 2007 MESA Saturday Academy Outstanding Volunteer Award.
FYI: Dr. Thompson enjoys hiking and takes part in two soccer leagues. Her children are following in her footsteps: Both are on their own soccer teams.
Quotable: “Becoming an SHM fellow shows that you have what it takes to be engaged as a hospitalist. Hospital medicine is not just a job; it’s a career and a dedication.”
Dr. Thompson is an assistant professor in the Department of Medicine and the Department of Neurosurgery at the University of Washington in Seattle. She is director of the medicine consult service and the medicine operative consult clinic at Harborview Medical Center in Seattle. She also is president of SHM’s Pacific Northwest chapter and a member of the National Chapter Support Committee.
Undergraduate education: Amherst College, Amherst, Mass.
Medical school: University of Washington School of Medicine, Seattle.
Notable: Dr. Thompson says one of her greatest career achievements has been the development of collegial services with surgeons and researchers in order to look at surgical outcomes through the lens of a hospitalist. She also developed a glycemic-control center in her hospital to improve insulin ordering, a project for which she has been published and presented locally and nationally. She has served as a resident research project mentor since 2005, helping 13 students achieve their research goals. Dr. Thompson volunteers at the Mathematics Engineering Science Achievement (MESA) Saturday Academy, an inner-city high school program for advancement in math and science, for which she won the 2007 MESA Saturday Academy Outstanding Volunteer Award.
FYI: Dr. Thompson enjoys hiking and takes part in two soccer leagues. Her children are following in her footsteps: Both are on their own soccer teams.
Quotable: “Becoming an SHM fellow shows that you have what it takes to be engaged as a hospitalist. Hospital medicine is not just a job; it’s a career and a dedication.”
Dr. Thompson is an assistant professor in the Department of Medicine and the Department of Neurosurgery at the University of Washington in Seattle. She is director of the medicine consult service and the medicine operative consult clinic at Harborview Medical Center in Seattle. She also is president of SHM’s Pacific Northwest chapter and a member of the National Chapter Support Committee.
Undergraduate education: Amherst College, Amherst, Mass.
Medical school: University of Washington School of Medicine, Seattle.
Notable: Dr. Thompson says one of her greatest career achievements has been the development of collegial services with surgeons and researchers in order to look at surgical outcomes through the lens of a hospitalist. She also developed a glycemic-control center in her hospital to improve insulin ordering, a project for which she has been published and presented locally and nationally. She has served as a resident research project mentor since 2005, helping 13 students achieve their research goals. Dr. Thompson volunteers at the Mathematics Engineering Science Achievement (MESA) Saturday Academy, an inner-city high school program for advancement in math and science, for which she won the 2007 MESA Saturday Academy Outstanding Volunteer Award.
FYI: Dr. Thompson enjoys hiking and takes part in two soccer leagues. Her children are following in her footsteps: Both are on their own soccer teams.
Quotable: “Becoming an SHM fellow shows that you have what it takes to be engaged as a hospitalist. Hospital medicine is not just a job; it’s a career and a dedication.”
Start Planning Now for HM14

Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO

Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
Whether you couldn’t make it to HM13 or you’re bringing back all the energy from the conference back to your hospital, now is the time to start planning for the next national conference exclusively designed for the nation’s 40,000 hospitalists.
For newcomers, HM14 will offer unprecedented access, networking, and CME-accredited educational sessions for hospitalists in all career stages. And for veterans of SHM’s annual meeting, 2014 will introduce two new pre-courses: “Cardiology and Evidence-Based Medicine” and “Bending the Cost Curve,” one of the hottest topics in public health, which will have its own dedicated track as well.
In addition to offering the best CME-accredited educational experience, HM14 will also give hospitalists the chance to enjoy an all-new official headquarters for the meeting: Mandalay Bay Hotel & Casino in Las Vegas.
Pre-Courses
Enhance the HM14 educational experience, broaden your skills, and earn additional CME credits. Choose from one of the following HM-focused topics:
- Medical Procedures for the Hospitalist;
- Portable Ultrasound for the Hospitalist;
- Perioperative Medicine;
- ABIM Maintenance of Certification;
- Practice Management;
- Neurology;
- Cardiology (new); and
- Evidence-Based Medicine (new).
Content Areas
The educational tracks offered at HM14 enable attendees to take courses in various designated tracks designed to better focus and enrich the annual meeting for attendees.
Tracks focus on the following cutting-edge content areas:
- Clinical;
- Rapid Fire;
- Practice Management;
- Academic/Research;
- Quality;
- Bending the Cost Curve (new);
- Pediatric;
- Potpourri;
- Comanagement; and
- Workshops.
Brendon Shank is SHM’s associate vice president of communications.
HM14 HEADQUARTERS: THE MANDALAY BAY HOTEL & CASINO
Enjoy casual elegance and comfort in the main tower’s rooms and suites, or relax in unparalleled sophistication and style at The Hotel at Mandalay Bay. At HM14 in March, hospitalists will:
- Bask in ultimate aquatic relaxation at the unforgettable, 11-acre Mandalay Bay Beach;
- Explore the Shark Reef Aquarium, featuring more than 2,000 exotic animals in a breathtaking 1.6-million-gallon habitat; and
- Taste the variety of foods at the 20-plus restaurants Mandalay Bay has to offer, including beach dining.
RIV Presenters at HM13 Explore Common Hospitalist Concerns
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Two oral research poster presentations at HM13 explored malpractice concerns of hospitalists and the issue of defensive-medicine-related overutilization—popular topics considering how policymakers are attempting to bend the cost curve in the direction of greater efficiency and value.
Hospitalist Alan Kachalia, MD, JD, and colleagues at Brigham and Women’s Hospital in Boston conducted a randomized national survey of 1,020 hospitalists and analyzed their responses to common clinical scenarios. They found evidence of inappropriate overutilization and deviance from scientific evidence or recognized treatment guidelines, which the research team pegged to the practice of defensive medicine.
Dr. Kachalia’s presentation, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists,” was named best of the oral presentations in the research category.
“Our survey found substantial overutilization, frequently caused by defensive medicine,” in response to questions about practice patterns for two common clinical scenarios: preoperative evaluation and syncope, Dr. Kachalia said. Physicians who practiced at Veterans Affairs medical centers had less association with defensive medicine, while those who paid for their own liability insurance reported more. Overall, defensive medicine was reported for 37% of preoperative evaluations and 58% of the syncope scenarios.
More than 800 abstracts were submitted for HM13’s Research, Innovations, and Clinical Vignettes (RIV) competition. Nearly 600 were accepted, put on display at the annual meeting, and published online (www.shmabstracts.com). More than 100 abstracts were judged, with 15 of the Research and Innovations entries invited to make oral presentations of their projects. Three others gave “Best of RIV” plenary presentations at the conference.
The diversity and richness of HM13’s oral and poster presentations also will be highlighted in the Innovations department of The Hospitalist over the next year.
Asked to suggest policy responses to these findings, Dr. Kachalia said reform of the malpractice system is needed. “What a lot of us argue is that to get physicians to follow treatment guidelines, make them more clear and practical,” he said. “We’d also like to see safe harbors [from lawsuits] for following recognized guidelines.”
Adam Schaffer, MD, also a hospitalist at Brigham and Women’s Hospital in Boston, and colleagues reviewed a medical liability insurance carrier’s database of more than 30,000 closed claims for those in which a hospitalist was the attending of record. Dr. Schaffer’s retrospective, observational analysis, “Medical Malpractice: Causes and Outcomes of Claims Against Hospitalists,” of the claims database from 1997 to 2011 found 272 claims—almost 1%—for which the attending was a hospitalist.
“The claims rate was almost four times lower for hospitalists than for nonhospitalist internal-medicine physicians,” he said.
The average payment for claims against hospitalists also was smaller. He noted that the types of claims were similar and tended to fall in three general categories: errors in medical treatment, missed or delayed diagnoses, and medication-related errors (although claims also tended to have multiple contributing factors).
Research like Dr. Schaffer’s could help to inform patient-safety efforts and reduce legal malpractice risk, he said. If hospitalists have fewer malpractice claims, that information might also be used to argue for lower malpractice premium rates.
Larry Beresford is a freelance writer in Oakland, Calif.
Hospitalists Share Information, Insights Through RIV Posters at HM13
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
One of the busiest times of HM13—and, come to think of it, every recent annual meeting—is the poster session for the Research, Innovations, and Clinical Vignettes (RIV) competition. This year, more than 800 abstracts were submitted and reviewed, with nearly 600 being accepted for presentation at HM13. That meant thousands of hospitalists thumbtacking posters to rows and rows of portable bulletin boards in the Gaylord National Resort & Convention Center’s massive exhibit hall.
With all those posters and accompanying oral presentations, it’s impossible for RIV judges to chat with everybody, so they choose finalists based on the abstracts, then listen to quick-hit summaries before choosing a winner on site. And meeting attendees are just as strapped for time, so they do the best they can to see as many posters as they can, taking time to network with old connections and make new ones.
So with all the limitations on how many people will interact with your poster, the small chance of winning Best in Show, and the hundreds of work hours that go into a poster presentation, why do it?
“To share is what I think is really important,” says Todd Hecht, MD, FACP, SFHM, associate professor of clinical medicine at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia. “If you don’t let other people know what you’re doing, they can’t bring it to their institutions, nor can you learn from others and bring their innovations to your own hospital.”
Dr. Hecht, director of the Anticoagulation Management Center and Anticoagulation Management Program at the Hospital of the University of Pennsylvania, takes the poster sessions very seriously. This year, he entered a poster in both the Innovations and Vignette categories. His Innovations poster, “Impact of a Multidisciplinary Safety Checklist on the Rate of Preventable Hospital Complications and Standardization of Care,” was a finalist.
That meant that, at the very least, he’d be able to explain to at least two judges what motivated his research team’s project. And what was the inspiration? A 90-year-old male patient with metastatic melanoma who, in the fall of 2011, refused to take medication for VTE prophylaxis, as lesions on his skin made the process rather painful. After refusing the doses for a bit, though, the high-risk patient unsurprisingly developed a pulmonary embolism (PE).
The man survived the PE, but Dr. Hecht and his colleagues began to wonder how many patients refuse VTE prophylaxis. So they investigated, and it turned out that from December 2010 to February 2011, 26.4% of the prescribed doses of prophylaxis on the medicine floors they studied were missed. Moreover, nearly 80% of all missed doses on the medicine floors were due to patient refusal.
“It was astonishing to me that it was that high,” Dr. Hecht says. “If there were 1,000 doses in a month, 260 of them were not being given—and 205 of them were not given because they were refused.”
Checklist Integration
So Dr. Hecht and colleagues set out to create a checklist that could be used daily on multidisciplinary rounds to help reduce the risk of VTE. First question on the list: Has prophylaxis been ordered, and if so, is the patient refusing it? Knowing that patients are “refusing” medication can lead to discussions about why that is happening, which in turn can lead to ways to convince the patient that the preventative measure is a good idea.
Dr. Hecht says the team also realized a checklist creates the opportunity to improve other quality metrics, such as hospital-associated infections (HAIs). Two questions on the checklist ask whether indwelling urinary catheters (IUCs) and central venous catheters (CVCs) can be removed. Two questions ask if telemetry can be stopped and whether there are any pain-management concerns. A final query asks whether there are any nursing, social work, or discharge-related questions—a step that, according to Dr. Hecht, loops the entire multidisciplinary team into the care-plan discussion.
“An ongoing challenge is making sure it’s not just questions being asked and being answered by rote,” Dr. Hecht says. “Just pause and think for just a second for each question. You can get through the checklist in 10 seconds, but you can’t go through the checklist in two seconds.”
The project’s results are what made it a finalist. After the checklist intervention, the number of missed doses of VTE prophylaxis plummeted 59% to just 10.9% (P<0.001) from September to November 2012; the number of “patient refused” doses dropped to 6.3% (P<0.001).
Not only was Dr. Hecht caught off guard by his findings, but so were the judges who visited his poster—Mangla Gulati, MD, FHM, of the University of Maryland School of Medicine and Rachel George, MD, MBA, FHM, of Cogent HMG.
“I wonder if it’s like that in every hospital,” Dr. George says. “I’d like to know.”
The positive reaction and feedback to Dr. Hecht’s poster, however, was not enough to win the Innovations category. That honor went to “SEPTRIS: Improving Sepsis Recognition and Management Through a Mobile Educational Game,” which was developed by a team of researchers at Stanford University in Palo Alto, Calif. The video game
(http://med.stanford.edu/septris/)—a mashup of sepsis and the once-popular Tetris puzzle game—already has been played 17,000 times and is on its way to being shared in other languages.
“Win or lose, it doesn’t matter,” Dr. Hecht says. “The goal is to share your information with other people and learn from them.”
Peter Watson, MD, FACP, FHM, sees it the same way. That’s why this year he was both judge and judged. The division head of hospital medicine for Henry Ford Medical Group in Detroit was part of a group presenting “Feasibility and Efficacy of a Specialized Pilot Training Program to Enhance Inpatient Communication Skills of Hospitalists.” He was a judge for the Research portion of the contest. He says he’s hard-pressed to say which process he enjoyed more, but one trick of the poster trade he passes along is that “judging actually makes you a better presenter on the back end,” especially when it comes to describing in less than five minutes a poster whose work may date back 12 to 18 months.
“In your brain,” he says, “you have a Tolstoy novel of information, but you have to break that down into a paragraph of CliffsNotes, and actually convince the people that are judging you that you have a really cool project that either is going to have a big impact in the field or may lead to other big studies or is going to impress somebody so much that they’re going to go back to their institution and say, ‘Hey, I’m going to do that.’”
Dr. Watson also urges people not to be discouraged by not winning the poster contest. First, all of the accepted abstracts get published online (www.shmabstracts.com) by the Journal of Hospital Medicine, a high point for medical students, residents, and early-career physicians looking to make a mark. Second, presenting information of value to one’s peers is the definition of a specialty that prides itself on collaboration.
“To see a second-year medical student presenting all the way up to a very senior division chief and everything in between is a really good example for our profession,” he says. “That’s really the magic of this meeting.”
Richard Quinn is a freelance writer in New Jersey.
Quality Improvement (QI) Remains a Central Theme at HM13


Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Like a grinning child at a carnival, Iqbal M. Binoj, MD, steps right up and gives it a try—except instead of tossing rings, he’s gripping an intraosseous infusion drill.
A tutor shows him how the device, which looks remarkably like a glue gun, inserts into the bones of the shoulder or knee and drills down until it hits the marrow. He is guided on using a steady speed to maintain the integrity of the cavity. He’s also taught about the maneuver’s low complication rates and ability to expedite workups.
“I’ve seen it used before, but I never did it,” says Dr. Binoj, a hospitalist with Cogent HMG at Genesis Medical Center in Davenport, Iowa.
Well, he never did it before a hands-on pre-course at HM13 that focused on improving hospitalists’ proficiency at such procedures as lumbar punctures and ultrasound-guided vascular access. Quality improvement (QI) is always a focus of SHM’s annual meeting, but sometimes the science of improving care is viewed from up on high.
Not everything needs to be a national imitative, an institution-wide project, or even a unit-based intervention. Sometimes, it’s as simple as teaching a room full of hospitalists how to use an intraosseous infusion drill, says Michelle Fox, RN, BSN, senior director of clinical affairs with Vidacare, which manufactures the drill used in the demonstration.
“Hospitalists have an increasing role in doing these procedures, not only in the environment they predominantly support but in other areas of the hospital,” Fox says, adding that “the primary goal of this course is to give them the opportunity to perfect those skills.”
Hospitalist Bradley Rosen, MD, MBA, FHM, medical of the inpatient specialty program at Cedars-Sinai in Los Angeles, says the point of hands-on demonstrations is to translate QI to the bedside. Take ultrasound devices, he says. In the past few years, the technology has become less expensive, better in resolution, more common, and more portable. Hospitalists must ensure hands-on training that keeps pace with that technology.
“We actually want people to get gloves on, hands on, learn where they may have challenges in terms of their own dexterity or workflow, which hand is dominant, and how to visualize on the ultrasound machine a three-dimensional structure in 2D,” he says. “We don’t want people watching from the sidelines. ... We try to get people in it and engaged.”
And once hospitalists master procedures or diagnostic maneuvers, they invariably are sought out by other physicians to pass that knowledge on to others, Dr. Rosen says.
“In so doing, we get involved in larger quality initiatives and systemwide changes that can go top-down,” he adds, “but from our perspective, it starts with the individual practitioner. And I think SHM has always advocated and preached the importance of the individual hospitalist doing the best possible job for your patient, and the group, and the institution.”
Shared Excellence
What’s best for individual institutions moving forward is what worries SHM immediate past president Shaun Frost, MD, SFHM. He fears CMS’ Value-Based Payment Modifier (VBPM) program could have the unintended consequence of spurring some hospitals to hang on to innovative ideas in order to keep a competitive business advantage.
In health care, where quality and affordability have long been viewed as valuable for nonmonetary reasons, “the medical profession willingly shares new information” to improve patient care, Dr. Frost said in his farewell speech. But he is concerned that commodification—imbuing monetary value into something that previously had none—could change that dynamic, a situation he says is “ethically not acceptable.”
“When somebody builds a better mousetrap, it should be freely shared so that all patients have the opportunity to benefit,” Dr. Frost said. “The pursuit of economic competitive advantage should not prevent us from collaborating and sharing new ideas that hopefully make the health system better.”
Kendall Rogers, MD, FACP, SFHM, chief of the division of hospital medicine at the University of New Mexico Health Sciences Center in Albuquerque, N.M., says part of that improvement in quality and patient safety will come via hospitalists pushing for improvements to health information technology (HIT), particularly to maximize computerized physician order entry (CPOE) and order sets. He empathizes with those who complain about the operability of existing systems but urges physicians to stop complaining and take action.
“We need to stop accepting what our existing limitations are, and we need to be the innovators,” he says. “Many of us aren’t even thinking about, ‘What are the products we need?’ We’re just reacting to the products we currently have and stating how they don’t meet our needs.”
He suggests people communally report safety or troubleshooting issues, in part via Hospital Medicine Exchange (HMX), an online community SHM launched last year to discuss HM issues (www.hmxchange.org). He also wants hospitalists to push HIT vendors to provide improved functionality, and for institutions to provide necessary training.
“We just need to be vocal,” says Dr. Rogers, chair of SHM’s IT Executive Committee. “I do believe this is all leading us to a good place, but there’s a dip down before we have a swing up.”
Frustration Surge
In the long run, hospitalist Anuj Mehta, MD, medical director of the adult hospitalist program at Nyack Hospital in New York, agrees with Dr. Rogers. But as a provider seeing patients day after day, he says it’s often easier to not engage HIT than it is to slog through it.
“We try to work around the system, and sometimes it’s a much longer workaround,” he says. “So what happens is loss of productivity, greater length of stay, poor patient satisfaction, more screen time, and less bedside time.”
Dr. Mehta says frustration is building as society—outside of medicine—moves rapidly through such technology as smartphones, tablets, and other intuitive devices that make actions easier. He notes that his toddler daughter could learn how to navigate an iPad in a fraction of the time it takes him to complete an HIT training course.
“You cannot have physicians going through learning for four hours, learning a system to do step one before step two before step three,” he laments. “It should flow naturally. I don’t think the IT people have realized that as of yet.”
Richard Quinn is a freelance writer in New Jersey.
Fix for Sustainable Growth Rate Formula a Top Priority
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.
The Improving Access to Medicare Coverage Act isn’t the only legislative proposal on hospitalists’ radar right now. Republican members of the U.S. House of Representatives recently revised their plan to replace the sustainable growth rate (SGR) formula used to determine physician payments. A bill has not been introduced, but Beltway buzz hints one could be forthcoming this year.
“Fixing the flawed SGR physician payment is a top priority for the Committees on Energy and Commerce and Ways and Means,” GOP legislators said in an open letter to the “provider community.”2
The letter requested feedback from physicians and other stakeholders by April 15.
Any proposed fix would look to end the series of time-stamped delays that continue to delay a pending 27% cut to physician payments under Medicare. The latest delay was approved earlier this year, meaning that the new deadline for the SGR cut to be implemented is Dec. 31.
The SGR formula was created in 1997, but the pending cuts tied to the federal sequester were included in the Budget Control Act of 2011. At the time, the massive reduction to Medicare payments was tied to political brinksmanship over the country’s debt ceiling. But the cut also was considered a Draconian penalty that was never likely to actually happen.
Richard Quinn is a freelance writer in New Jersey.
References
- SHM. Letter to Congress members. SHM website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Letters_to_Congress_and_Regulatory_Agencies&Template=/CM/ContentDisplay.cfm&ContentID=33169. Accessed May 3, 2013.
- U.S. House of Representatives' Committee on Ways and Means, Energy and Commerce Committee, Health Subcommittee. Second draft of sustainable growth rate (SGR) repeal and reform proposal—request for feedback letter. U.S. House of Representatives' Committee on Ways and Means website. Available at: http://waysandmeans.house.gov/uploadedfiles/sgr_joint_release_document.pdf. Accessed May 3, 2013.