User login
What AI can see in CT scans that humans can’t
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.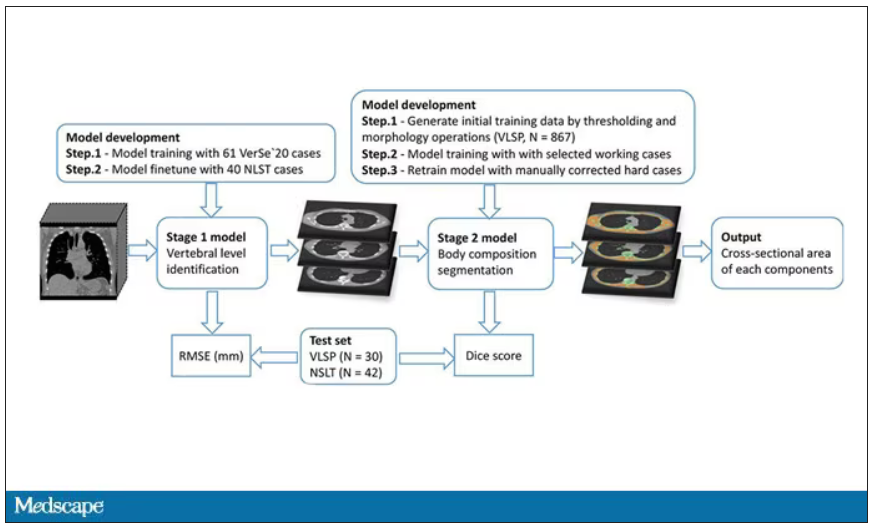
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.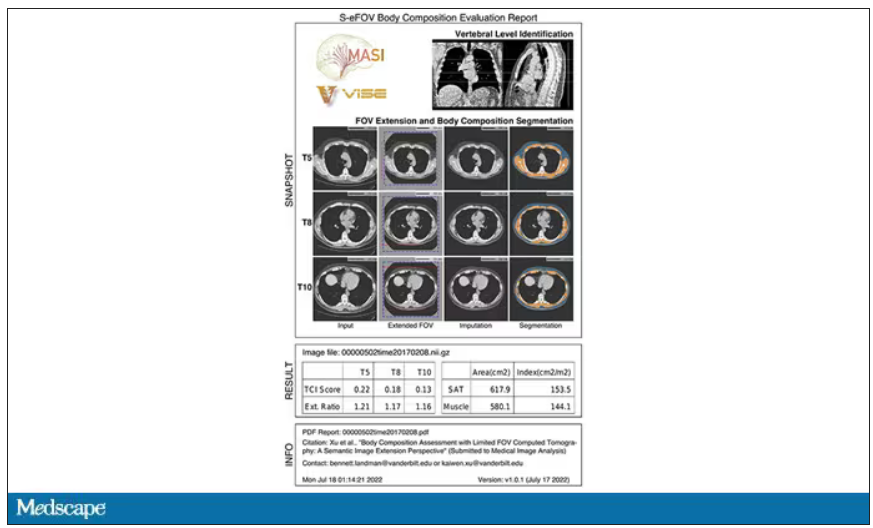
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.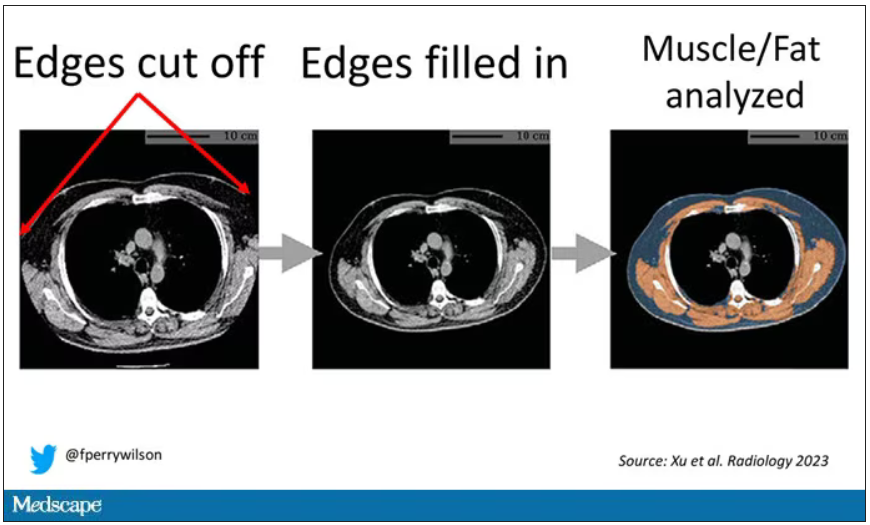
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.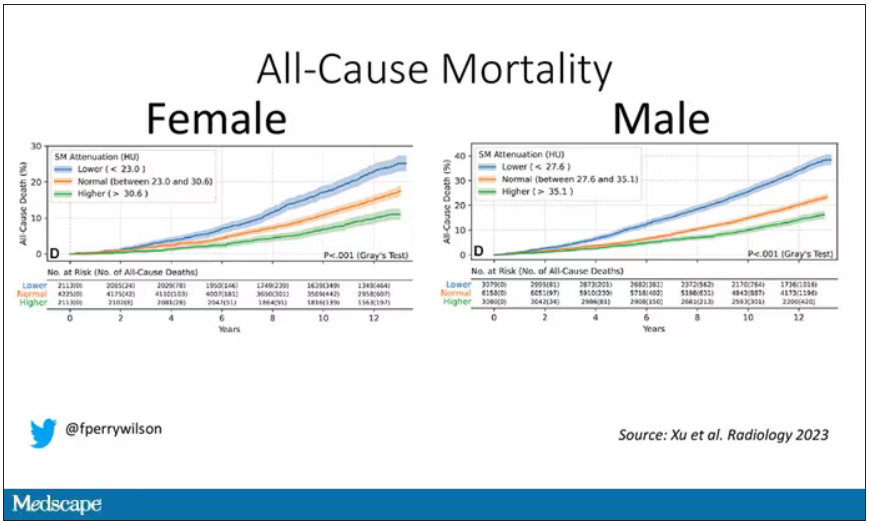
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.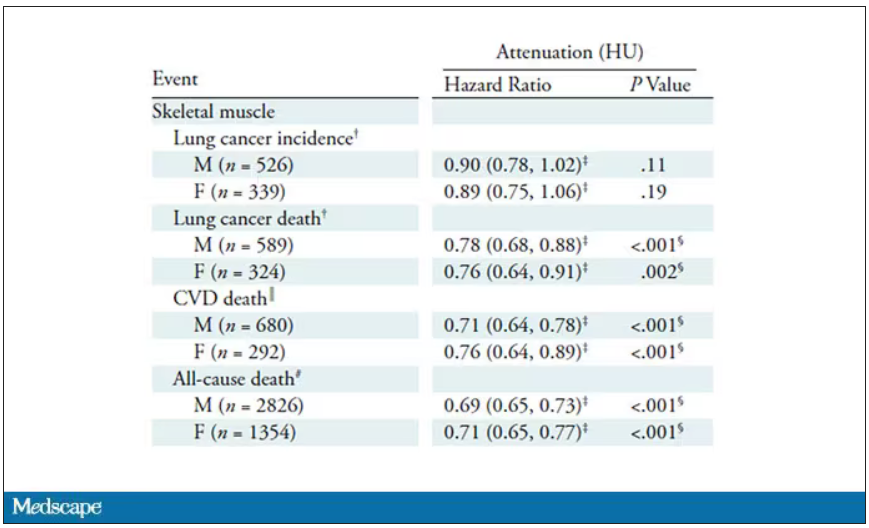
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.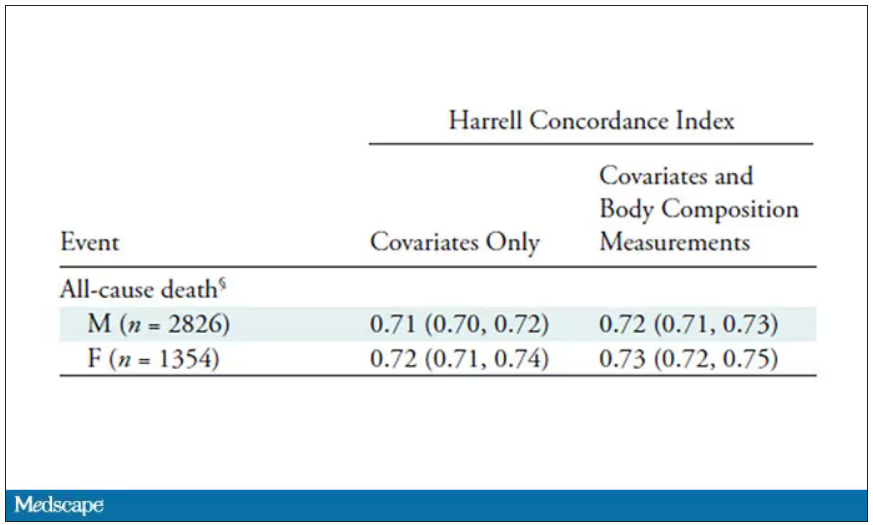
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Commentary: Meningioma, Radiotherapy Interruptions, Therapy Persistence, and Lymphocytes in BC, August 2023

Data are limited regarding the effect of interrupting radiation therapy for patients with BC. A retrospective study by Chow and colleagues looked at 35,845 patients with nonmetastatic triple-negative BC from the National Cancer Database who had received external beam radiation therapy as part of the management of their BC. The analysis showed inferior overall survival in patients with a longer duration of radiation treatment (hazard ratio 1.023; 95% CI 1.015-1.031) The more days of interruption, the higher the likelihood of mortality seen. In reference to 0-1 days of interruption, patients with 2-5 interrupted days (hazard ratio 1.069; 95% CI 1.002-1.140), 6-10 interrupted days (hazard ratio 1.239; 95% CI 1.140-1.348), and 11-15 interrupted days (hazard ratio 1.265; 95% CI 1.126-1.431) did worse. These findings should encourage further studies to explore ways to minimize treatment interruptions among patients with BC.
A lack of adherence to adjuvant endocrine therapy has been associated with increased mortality among women with BC. The retrospective study by Zheng and Thomas included 25,796 older women (> 65 years old) diagnosed with stage I-III hormone receptor–positive BC and looked at associations between adherence to and persistence with adjuvant endocrine therapy and mortality in this cohort. Their findings showed that the risk for all-cause mortality was reduced by 25% in patients with vs without cumulative adherence to endocrine therapy (hazard ratio 0.75; P < .001), although no association was seen with BC-specific mortality. Persistence with endocrine therapy, which was defined as having taken the treatment for ≥ 180 continuous days, was associated with 11% reduction in all-cause mortality and 37% reduction in BC-specific mortality. This study supports prior studies in highlighting the importance of endocrine therapy adherence among women with hormone-positive BC.
Tumor-infiltrating lymphocytes (TIL) are considered significant prognostic markers in patients with BC, although the prognostic effect of TIL in human epidermal growth factor reception 2 (HER2)–low BC has not been identified. A large-cohort, single-institution retrospective analysis by Sun and colleagues investigated the prognostic role of TIL in HER2-low early-stage BC. The analysis included 1763 patients with early-stage BC who underwent surgery, of whom 429 patients were HER2+, 739 were HER2-low, and 595 were HER2-0. No differences in disease-free survival (DFS) were seen between the three cohorts. However, in patients with HER2-low BC, high (>10%) vs low (≤10%) TIL levels were associated with a 53% improvement in DFS overall (hazard ratio 0.47; P = .035), and a 58% improvement in DFS was seen for the hormone receptor–positive/HER2-low cohort (hazard ratio 0.42; P = .032).
Data are limited regarding the effect of interrupting radiation therapy for patients with BC. A retrospective study by Chow and colleagues looked at 35,845 patients with nonmetastatic triple-negative BC from the National Cancer Database who had received external beam radiation therapy as part of the management of their BC. The analysis showed inferior overall survival in patients with a longer duration of radiation treatment (hazard ratio 1.023; 95% CI 1.015-1.031) The more days of interruption, the higher the likelihood of mortality seen. In reference to 0-1 days of interruption, patients with 2-5 interrupted days (hazard ratio 1.069; 95% CI 1.002-1.140), 6-10 interrupted days (hazard ratio 1.239; 95% CI 1.140-1.348), and 11-15 interrupted days (hazard ratio 1.265; 95% CI 1.126-1.431) did worse. These findings should encourage further studies to explore ways to minimize treatment interruptions among patients with BC.
A lack of adherence to adjuvant endocrine therapy has been associated with increased mortality among women with BC. The retrospective study by Zheng and Thomas included 25,796 older women (> 65 years old) diagnosed with stage I-III hormone receptor–positive BC and looked at associations between adherence to and persistence with adjuvant endocrine therapy and mortality in this cohort. Their findings showed that the risk for all-cause mortality was reduced by 25% in patients with vs without cumulative adherence to endocrine therapy (hazard ratio 0.75; P < .001), although no association was seen with BC-specific mortality. Persistence with endocrine therapy, which was defined as having taken the treatment for ≥ 180 continuous days, was associated with 11% reduction in all-cause mortality and 37% reduction in BC-specific mortality. This study supports prior studies in highlighting the importance of endocrine therapy adherence among women with hormone-positive BC.
Tumor-infiltrating lymphocytes (TIL) are considered significant prognostic markers in patients with BC, although the prognostic effect of TIL in human epidermal growth factor reception 2 (HER2)–low BC has not been identified. A large-cohort, single-institution retrospective analysis by Sun and colleagues investigated the prognostic role of TIL in HER2-low early-stage BC. The analysis included 1763 patients with early-stage BC who underwent surgery, of whom 429 patients were HER2+, 739 were HER2-low, and 595 were HER2-0. No differences in disease-free survival (DFS) were seen between the three cohorts. However, in patients with HER2-low BC, high (>10%) vs low (≤10%) TIL levels were associated with a 53% improvement in DFS overall (hazard ratio 0.47; P = .035), and a 58% improvement in DFS was seen for the hormone receptor–positive/HER2-low cohort (hazard ratio 0.42; P = .032).
Data are limited regarding the effect of interrupting radiation therapy for patients with BC. A retrospective study by Chow and colleagues looked at 35,845 patients with nonmetastatic triple-negative BC from the National Cancer Database who had received external beam radiation therapy as part of the management of their BC. The analysis showed inferior overall survival in patients with a longer duration of radiation treatment (hazard ratio 1.023; 95% CI 1.015-1.031) The more days of interruption, the higher the likelihood of mortality seen. In reference to 0-1 days of interruption, patients with 2-5 interrupted days (hazard ratio 1.069; 95% CI 1.002-1.140), 6-10 interrupted days (hazard ratio 1.239; 95% CI 1.140-1.348), and 11-15 interrupted days (hazard ratio 1.265; 95% CI 1.126-1.431) did worse. These findings should encourage further studies to explore ways to minimize treatment interruptions among patients with BC.
A lack of adherence to adjuvant endocrine therapy has been associated with increased mortality among women with BC. The retrospective study by Zheng and Thomas included 25,796 older women (> 65 years old) diagnosed with stage I-III hormone receptor–positive BC and looked at associations between adherence to and persistence with adjuvant endocrine therapy and mortality in this cohort. Their findings showed that the risk for all-cause mortality was reduced by 25% in patients with vs without cumulative adherence to endocrine therapy (hazard ratio 0.75; P < .001), although no association was seen with BC-specific mortality. Persistence with endocrine therapy, which was defined as having taken the treatment for ≥ 180 continuous days, was associated with 11% reduction in all-cause mortality and 37% reduction in BC-specific mortality. This study supports prior studies in highlighting the importance of endocrine therapy adherence among women with hormone-positive BC.
Tumor-infiltrating lymphocytes (TIL) are considered significant prognostic markers in patients with BC, although the prognostic effect of TIL in human epidermal growth factor reception 2 (HER2)–low BC has not been identified. A large-cohort, single-institution retrospective analysis by Sun and colleagues investigated the prognostic role of TIL in HER2-low early-stage BC. The analysis included 1763 patients with early-stage BC who underwent surgery, of whom 429 patients were HER2+, 739 were HER2-low, and 595 were HER2-0. No differences in disease-free survival (DFS) were seen between the three cohorts. However, in patients with HER2-low BC, high (>10%) vs low (≤10%) TIL levels were associated with a 53% improvement in DFS overall (hazard ratio 0.47; P = .035), and a 58% improvement in DFS was seen for the hormone receptor–positive/HER2-low cohort (hazard ratio 0.42; P = .032).
Physician not held liable for child’s necrotizing pancreatitis, jury finds
, according to a report posted on the website of Courtroom View Network.
In 2018, the parents of the then 9-year-old child brought him to Wellstar Paulding Hospital in Hiram, Ga., because of his severe abdominal pain and distention, among other symptoms. Following their examination, medical personnel at the hospital suspected the child’s symptoms were the result of severe constipation.
That evening, he was transferred to Children’s Healthcare of Atlanta, where a pediatric gastroenterologist oversaw his care. (Neither the Atlanta hospital nor Wellstar Paulding were defendants in the subsequent lawsuit.)
Late the following day, the child went into hypovolemic shock, a condition that interrupted the blood supply to his body. Admitted to the pediatric ICU, he was diagnosed with a dangerous complication of acute pancreatitis, necrotizing pancreatitis.
Further complications of his original disease led to a 4-month hospital stay, multiple surgeries, and other interventions. To this point, his medical expenses totaled more than $2.5 million.
His parents then sued the pediatric gastroenterologist who had overseen their child’s care. At issue during the 4-day trial was whether the doctor had properly monitored and treated his patient before his hypovolemic shock set in.
Their attorney sketched the “timeline” of the child’s decline, including his rapid heart rate and repeated vomiting. Given these symptoms, he argued, the standard of care required that steps be taken – including the proper tests and other interventions – to prevent the child’s acute pancreatitis from progressing even further.
“We are not asking you to say, ‘Should [the doctor] have immediately diagnosed pancreatitis,’ “ the attorney told the jury. “But the totality here requires you to think, ‘This might be more than just a backed-up kid.’ ”
The defense pushed back strenuously, however. It argued that the pediatric gastroenterologist had acted appropriately given the prevailing consensus, namely that the child was suffering from extreme constipation. Doctors at Wellstar Paulding, the first hospital where he was seen, suspected this diagnosis – and so, based on his exam and the child’s “non-specific” symptoms, did their client, the pediatric gastroenterologist, who saw him subsequently. “The only clinicians who actually laid hands on [the child] all thought constipation,” the attorney said during his closing argument.
The jury agreed, finding that the pediatric gastroenterologist had acted appropriately, based on the available evidence. Following the jury verdict, the defense attorney noted: Absent the “classic” symptoms of pancreatitis, the jury saw that his client “was working with a reasonable diagnosis until [the child’s] clinical picture deteriorated.”
ED doctors can reduce system errors, study says
Emergency physicians are often blamed for system errors beyond their control, asserts a study in the June issue of Emergency Medicine News.
The study – conducted by Tom Belanger, MD, an emergency physician in Texas and chair-elect of the American College of Emergency Physicians Workforce Section – sought to understand to what extent doctors themselves were aware of systemic problems affecting their job. Dr. Belanger surveyed 99 doctors who were asked to comment on a series of ED–related adverse outcomes.
To mitigate response bias, he randomly manipulated the degree to which system error was a perceived factor in each of the adverse cases. In other words, in some cases, the system was represented as a major factor leading to error, while, in other cases, its role was diminished.
Dr. Belanger also divided his doctor/respondents into two groups: The first was asked about his or her personal experience with systemic issues before being presented with the adverse cases; the second group was queried about this experience after being presented with the cases.
The result confirmed Dr. Belanger’s suspicions: Physicians in the first group – that is, those asked about “system factors” before reading about the cases – “were 1.7 times more likely ... to attribute the adverse outcomes in the cases to system factors. (Other significant variables – including whether their shift was busy – also contributed to doctors’ perceptions of adverse outcomes.)
Concluded Dr. Belanger: Since doctors “can identify factors that increase their chances of making mistakes,” system designers should take heed and make efforts to reduce “the probability of error.” If they drag their heels or continue to point to individual doctor error, “they should be held medically and legally liable.”
A version of this article first appeared on Medscape.com.
, according to a report posted on the website of Courtroom View Network.
In 2018, the parents of the then 9-year-old child brought him to Wellstar Paulding Hospital in Hiram, Ga., because of his severe abdominal pain and distention, among other symptoms. Following their examination, medical personnel at the hospital suspected the child’s symptoms were the result of severe constipation.
That evening, he was transferred to Children’s Healthcare of Atlanta, where a pediatric gastroenterologist oversaw his care. (Neither the Atlanta hospital nor Wellstar Paulding were defendants in the subsequent lawsuit.)
Late the following day, the child went into hypovolemic shock, a condition that interrupted the blood supply to his body. Admitted to the pediatric ICU, he was diagnosed with a dangerous complication of acute pancreatitis, necrotizing pancreatitis.
Further complications of his original disease led to a 4-month hospital stay, multiple surgeries, and other interventions. To this point, his medical expenses totaled more than $2.5 million.
His parents then sued the pediatric gastroenterologist who had overseen their child’s care. At issue during the 4-day trial was whether the doctor had properly monitored and treated his patient before his hypovolemic shock set in.
Their attorney sketched the “timeline” of the child’s decline, including his rapid heart rate and repeated vomiting. Given these symptoms, he argued, the standard of care required that steps be taken – including the proper tests and other interventions – to prevent the child’s acute pancreatitis from progressing even further.
“We are not asking you to say, ‘Should [the doctor] have immediately diagnosed pancreatitis,’ “ the attorney told the jury. “But the totality here requires you to think, ‘This might be more than just a backed-up kid.’ ”
The defense pushed back strenuously, however. It argued that the pediatric gastroenterologist had acted appropriately given the prevailing consensus, namely that the child was suffering from extreme constipation. Doctors at Wellstar Paulding, the first hospital where he was seen, suspected this diagnosis – and so, based on his exam and the child’s “non-specific” symptoms, did their client, the pediatric gastroenterologist, who saw him subsequently. “The only clinicians who actually laid hands on [the child] all thought constipation,” the attorney said during his closing argument.
The jury agreed, finding that the pediatric gastroenterologist had acted appropriately, based on the available evidence. Following the jury verdict, the defense attorney noted: Absent the “classic” symptoms of pancreatitis, the jury saw that his client “was working with a reasonable diagnosis until [the child’s] clinical picture deteriorated.”
ED doctors can reduce system errors, study says
Emergency physicians are often blamed for system errors beyond their control, asserts a study in the June issue of Emergency Medicine News.
The study – conducted by Tom Belanger, MD, an emergency physician in Texas and chair-elect of the American College of Emergency Physicians Workforce Section – sought to understand to what extent doctors themselves were aware of systemic problems affecting their job. Dr. Belanger surveyed 99 doctors who were asked to comment on a series of ED–related adverse outcomes.
To mitigate response bias, he randomly manipulated the degree to which system error was a perceived factor in each of the adverse cases. In other words, in some cases, the system was represented as a major factor leading to error, while, in other cases, its role was diminished.
Dr. Belanger also divided his doctor/respondents into two groups: The first was asked about his or her personal experience with systemic issues before being presented with the adverse cases; the second group was queried about this experience after being presented with the cases.
The result confirmed Dr. Belanger’s suspicions: Physicians in the first group – that is, those asked about “system factors” before reading about the cases – “were 1.7 times more likely ... to attribute the adverse outcomes in the cases to system factors. (Other significant variables – including whether their shift was busy – also contributed to doctors’ perceptions of adverse outcomes.)
Concluded Dr. Belanger: Since doctors “can identify factors that increase their chances of making mistakes,” system designers should take heed and make efforts to reduce “the probability of error.” If they drag their heels or continue to point to individual doctor error, “they should be held medically and legally liable.”
A version of this article first appeared on Medscape.com.
, according to a report posted on the website of Courtroom View Network.
In 2018, the parents of the then 9-year-old child brought him to Wellstar Paulding Hospital in Hiram, Ga., because of his severe abdominal pain and distention, among other symptoms. Following their examination, medical personnel at the hospital suspected the child’s symptoms were the result of severe constipation.
That evening, he was transferred to Children’s Healthcare of Atlanta, where a pediatric gastroenterologist oversaw his care. (Neither the Atlanta hospital nor Wellstar Paulding were defendants in the subsequent lawsuit.)
Late the following day, the child went into hypovolemic shock, a condition that interrupted the blood supply to his body. Admitted to the pediatric ICU, he was diagnosed with a dangerous complication of acute pancreatitis, necrotizing pancreatitis.
Further complications of his original disease led to a 4-month hospital stay, multiple surgeries, and other interventions. To this point, his medical expenses totaled more than $2.5 million.
His parents then sued the pediatric gastroenterologist who had overseen their child’s care. At issue during the 4-day trial was whether the doctor had properly monitored and treated his patient before his hypovolemic shock set in.
Their attorney sketched the “timeline” of the child’s decline, including his rapid heart rate and repeated vomiting. Given these symptoms, he argued, the standard of care required that steps be taken – including the proper tests and other interventions – to prevent the child’s acute pancreatitis from progressing even further.
“We are not asking you to say, ‘Should [the doctor] have immediately diagnosed pancreatitis,’ “ the attorney told the jury. “But the totality here requires you to think, ‘This might be more than just a backed-up kid.’ ”
The defense pushed back strenuously, however. It argued that the pediatric gastroenterologist had acted appropriately given the prevailing consensus, namely that the child was suffering from extreme constipation. Doctors at Wellstar Paulding, the first hospital where he was seen, suspected this diagnosis – and so, based on his exam and the child’s “non-specific” symptoms, did their client, the pediatric gastroenterologist, who saw him subsequently. “The only clinicians who actually laid hands on [the child] all thought constipation,” the attorney said during his closing argument.
The jury agreed, finding that the pediatric gastroenterologist had acted appropriately, based on the available evidence. Following the jury verdict, the defense attorney noted: Absent the “classic” symptoms of pancreatitis, the jury saw that his client “was working with a reasonable diagnosis until [the child’s] clinical picture deteriorated.”
ED doctors can reduce system errors, study says
Emergency physicians are often blamed for system errors beyond their control, asserts a study in the June issue of Emergency Medicine News.
The study – conducted by Tom Belanger, MD, an emergency physician in Texas and chair-elect of the American College of Emergency Physicians Workforce Section – sought to understand to what extent doctors themselves were aware of systemic problems affecting their job. Dr. Belanger surveyed 99 doctors who were asked to comment on a series of ED–related adverse outcomes.
To mitigate response bias, he randomly manipulated the degree to which system error was a perceived factor in each of the adverse cases. In other words, in some cases, the system was represented as a major factor leading to error, while, in other cases, its role was diminished.
Dr. Belanger also divided his doctor/respondents into two groups: The first was asked about his or her personal experience with systemic issues before being presented with the adverse cases; the second group was queried about this experience after being presented with the cases.
The result confirmed Dr. Belanger’s suspicions: Physicians in the first group – that is, those asked about “system factors” before reading about the cases – “were 1.7 times more likely ... to attribute the adverse outcomes in the cases to system factors. (Other significant variables – including whether their shift was busy – also contributed to doctors’ perceptions of adverse outcomes.)
Concluded Dr. Belanger: Since doctors “can identify factors that increase their chances of making mistakes,” system designers should take heed and make efforts to reduce “the probability of error.” If they drag their heels or continue to point to individual doctor error, “they should be held medically and legally liable.”
A version of this article first appeared on Medscape.com.
Pediatric dermatologists encouraged to counter misinformation on TikTok, other social media sites
ASHEVILLE, N.C. – , warned an expert at the annual meeting of the Society for Pediatric Dermatology.
“If we don’t get involved, we are basically letting misinformation win. We need to be there,” said Angelo Landriscina, MD, director of dermatology at a Mount Sinai Doctors Clinic in New York.
Most of the content currently available on medical topics, including dermatology and pediatric dermatology, is not created by health care professionals, Dr. Landriscina noted. Not surprisingly, given that much of the content is based on personal opinion from individuals who have no expertise in medical care, he described the information as being of “low quality” when not fully erroneous.

Dr. Landriscina has been active on social media, including TikTok, for several years. Most of his posts involve responses to misinformation. When he sets the record straight on the basis of existing evidence, he often supports his counterargument with references.
He acknowledged that when he became involved in social media he faced criticism from colleagues about participating on an entertainment platform that many considered unworthy of providing objective information. If that was ever true, he argued, it is no longer the case.
“TikTok has adopted a new strategy. The goal is to unseat Google as a search tool, and it’s working,” he said. He explained that many people now use TikTok and other social media sites as their primary source of information on essentially every topic, from where to eat to whether to be screened for cancer.
The particular problem with TikTok – one of the most popular social media outlets – is that there is no mechanism for vetting the source of information. YouTube, by contrast, now requires some sort of validation for anyone who claims to have a medical degree or any other verifiable qualification, according to Dr. Landriscina. TikTok, like many other platforms, has no such requirement.
“Anyone can buy a pair of scrubs [implying expertise] and then post a video,” Dr. Landriscina said.
Even if information from one content provider is more valid than information from others, the TikTok algorithm is specifically designed to emphasize content that has the potential for going viral, which means it favors videos that are provocative over those that are not.
“The algorithm favors any content that is more controversial, more surprising, and keeps viewers engaged,” Dr. Landriscina pointed out.
This does not mean that objective and factual information is ignored, but the algorithm is indifferent to the validity of information, meaning that it allows videos to be posted without regard to whether the content is true, untrue, purposefully misleading, or utter nonsense. For that reason, it is often easier to attract attention by responding to a post that has already gone viral. Information that is clear and digestible can attract viewers and therefore is distributed more widely with the TikTok algorithm.
Parents are on Tiktok too
There is a misperception that the TikTok audience is younger, according to Dr. Landriscina. While peak use in the United States fell among people between the ages of 25 and 34 years in 2022, he said the number of users falls off relatively slowly with subsequent 10-year increments in age. In 2022, there were nearly 20 million users in the peak 10-year age range, but 7.5 million users were 55 years of age or older.
“Pediatric dermatologists should recognize that it is not just kids who are looking for information about their skin diseases, but also their parents,” Dr. Landriscina said.
The top three dermatology topics searched on TikTok in a recent period were acne, alopecia, and cysts. But top searches are very fluid and are extremely hard to quantify, because the basis of the algorithm, which is a proprietary secret, is not only unknown but produces different results for every user.
“The second you touch the app, it changes,” Dr. Landriscina said. He explained that an inquiry about any subject, including those that are medically related, yields content that is different, or at least ordered differently, “depending on how you behaved on the app in the past.”
The phenomenon that drives social media predates this technology. Dr. Landriscina cited a study in 1956 that described the “parasocial interaction theory.” The theory was based on the observation that those who consume media, such as television, which was relatively new in 1956, believed that they had a personal relationship with media figures.
“The users begin to trust influencers as a source, like a friend providing them advice,” Dr. Landriscina said. As an example, he suggested that a fan of the television show Friends who follows actor Jennifer Aniston on social media platforms may begin to think of her as a trusted source of information on any topic, including those for which she may not have expertise.
The reason that he urges medical professionals to become active on TikTok and other social media platforms is that they have a potentially critical role in responding to information that is not just wrong but harmful.
On TikTok and other social media platforms, “there is a lot of interest in content about dermatologic conditions in children. There is a real need for accurate information,” he said,
In the question-and-answer session following his presentation, Dr. Landriscina’s message was not uniformly embraced. One risk, according to an audience member, is that medical professionals will begin to express their own personal opinions rather than rely on evidence, with the result that they will “just add to the sea of misinformation.”
However, this opinion appeared to be the minority view. Most of those who commented took a “that-ship-has-sailed” stance, recognizing the irreversible ascendancy of social media.
“Whether you like it or not, social media is here to stay. We cannot fight it. Rather, we need to embrace it in a responsible way,” said Dakara R. Wright, MD, a dermatologist at the Mid-Atlantic Kaiser Permanente Group, Halethorpe, Md. She, like others, reported that she has come to recognize that social media is a major source of medical information for her patients.
“We need to be a presence on these platforms for the benefit of our patients and their parents,” she said. She acknowledged that she has not been active in posting on social media in the past but said that she has been speaking with administrators in her organization about how to become involved in a responsible way that can be useful to patients.
Candrice R. Heath, MD, assistant professor of dermatology at Temple University, Philadelphia, has been active on social media for several years, posting content on her own account, which is not related to her academic affiliation. She posts for many reasons, not least of which is drawing attention to her expertise.
Like Dr. Landriscina, she recognizes that users of these platforms are guided by the content to make decisions about health care. She also agreed that physicians should not ignore this phenomenon.
Tips on providing content
Given the fact that the algorithm is intended to produce posts that go viral, Dr. Landriscina urged clinicians to make their content easy to watch. He said it is not necessary to overthink content beyond providing accurate information, but he advised that videos be made with attention to adequate lighting and other simple factors to promote visual quality. He said that accurate information is not necessarily dull.
“Some facts can actually be surprising to patients,” he said. He noted that a calm, coherent video can be particularly effective in attracting an audience when it is in reaction to information that has gone viral but is misleading or patently incorrect.
Dr. Landriscina has been an influencer associated with multiple social media platforms, including TikTok. He has in the past been paid for consulting work for TikTok. Dr. Wright and Dr. Heath reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
ASHEVILLE, N.C. – , warned an expert at the annual meeting of the Society for Pediatric Dermatology.
“If we don’t get involved, we are basically letting misinformation win. We need to be there,” said Angelo Landriscina, MD, director of dermatology at a Mount Sinai Doctors Clinic in New York.
Most of the content currently available on medical topics, including dermatology and pediatric dermatology, is not created by health care professionals, Dr. Landriscina noted. Not surprisingly, given that much of the content is based on personal opinion from individuals who have no expertise in medical care, he described the information as being of “low quality” when not fully erroneous.
Dr. Landriscina has been active on social media, including TikTok, for several years. Most of his posts involve responses to misinformation. When he sets the record straight on the basis of existing evidence, he often supports his counterargument with references.
He acknowledged that when he became involved in social media he faced criticism from colleagues about participating on an entertainment platform that many considered unworthy of providing objective information. If that was ever true, he argued, it is no longer the case.
“TikTok has adopted a new strategy. The goal is to unseat Google as a search tool, and it’s working,” he said. He explained that many people now use TikTok and other social media sites as their primary source of information on essentially every topic, from where to eat to whether to be screened for cancer.
The particular problem with TikTok – one of the most popular social media outlets – is that there is no mechanism for vetting the source of information. YouTube, by contrast, now requires some sort of validation for anyone who claims to have a medical degree or any other verifiable qualification, according to Dr. Landriscina. TikTok, like many other platforms, has no such requirement.
“Anyone can buy a pair of scrubs [implying expertise] and then post a video,” Dr. Landriscina said.
Even if information from one content provider is more valid than information from others, the TikTok algorithm is specifically designed to emphasize content that has the potential for going viral, which means it favors videos that are provocative over those that are not.
“The algorithm favors any content that is more controversial, more surprising, and keeps viewers engaged,” Dr. Landriscina pointed out.
This does not mean that objective and factual information is ignored, but the algorithm is indifferent to the validity of information, meaning that it allows videos to be posted without regard to whether the content is true, untrue, purposefully misleading, or utter nonsense. For that reason, it is often easier to attract attention by responding to a post that has already gone viral. Information that is clear and digestible can attract viewers and therefore is distributed more widely with the TikTok algorithm.
Parents are on Tiktok too
There is a misperception that the TikTok audience is younger, according to Dr. Landriscina. While peak use in the United States fell among people between the ages of 25 and 34 years in 2022, he said the number of users falls off relatively slowly with subsequent 10-year increments in age. In 2022, there were nearly 20 million users in the peak 10-year age range, but 7.5 million users were 55 years of age or older.
“Pediatric dermatologists should recognize that it is not just kids who are looking for information about their skin diseases, but also their parents,” Dr. Landriscina said.
The top three dermatology topics searched on TikTok in a recent period were acne, alopecia, and cysts. But top searches are very fluid and are extremely hard to quantify, because the basis of the algorithm, which is a proprietary secret, is not only unknown but produces different results for every user.
“The second you touch the app, it changes,” Dr. Landriscina said. He explained that an inquiry about any subject, including those that are medically related, yields content that is different, or at least ordered differently, “depending on how you behaved on the app in the past.”
The phenomenon that drives social media predates this technology. Dr. Landriscina cited a study in 1956 that described the “parasocial interaction theory.” The theory was based on the observation that those who consume media, such as television, which was relatively new in 1956, believed that they had a personal relationship with media figures.
“The users begin to trust influencers as a source, like a friend providing them advice,” Dr. Landriscina said. As an example, he suggested that a fan of the television show Friends who follows actor Jennifer Aniston on social media platforms may begin to think of her as a trusted source of information on any topic, including those for which she may not have expertise.
The reason that he urges medical professionals to become active on TikTok and other social media platforms is that they have a potentially critical role in responding to information that is not just wrong but harmful.
On TikTok and other social media platforms, “there is a lot of interest in content about dermatologic conditions in children. There is a real need for accurate information,” he said,
In the question-and-answer session following his presentation, Dr. Landriscina’s message was not uniformly embraced. One risk, according to an audience member, is that medical professionals will begin to express their own personal opinions rather than rely on evidence, with the result that they will “just add to the sea of misinformation.”
However, this opinion appeared to be the minority view. Most of those who commented took a “that-ship-has-sailed” stance, recognizing the irreversible ascendancy of social media.
“Whether you like it or not, social media is here to stay. We cannot fight it. Rather, we need to embrace it in a responsible way,” said Dakara R. Wright, MD, a dermatologist at the Mid-Atlantic Kaiser Permanente Group, Halethorpe, Md. She, like others, reported that she has come to recognize that social media is a major source of medical information for her patients.
“We need to be a presence on these platforms for the benefit of our patients and their parents,” she said. She acknowledged that she has not been active in posting on social media in the past but said that she has been speaking with administrators in her organization about how to become involved in a responsible way that can be useful to patients.
Candrice R. Heath, MD, assistant professor of dermatology at Temple University, Philadelphia, has been active on social media for several years, posting content on her own account, which is not related to her academic affiliation. She posts for many reasons, not least of which is drawing attention to her expertise.
Like Dr. Landriscina, she recognizes that users of these platforms are guided by the content to make decisions about health care. She also agreed that physicians should not ignore this phenomenon.
Tips on providing content
Given the fact that the algorithm is intended to produce posts that go viral, Dr. Landriscina urged clinicians to make their content easy to watch. He said it is not necessary to overthink content beyond providing accurate information, but he advised that videos be made with attention to adequate lighting and other simple factors to promote visual quality. He said that accurate information is not necessarily dull.
“Some facts can actually be surprising to patients,” he said. He noted that a calm, coherent video can be particularly effective in attracting an audience when it is in reaction to information that has gone viral but is misleading or patently incorrect.
Dr. Landriscina has been an influencer associated with multiple social media platforms, including TikTok. He has in the past been paid for consulting work for TikTok. Dr. Wright and Dr. Heath reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
ASHEVILLE, N.C. – , warned an expert at the annual meeting of the Society for Pediatric Dermatology.
“If we don’t get involved, we are basically letting misinformation win. We need to be there,” said Angelo Landriscina, MD, director of dermatology at a Mount Sinai Doctors Clinic in New York.
Most of the content currently available on medical topics, including dermatology and pediatric dermatology, is not created by health care professionals, Dr. Landriscina noted. Not surprisingly, given that much of the content is based on personal opinion from individuals who have no expertise in medical care, he described the information as being of “low quality” when not fully erroneous.
Dr. Landriscina has been active on social media, including TikTok, for several years. Most of his posts involve responses to misinformation. When he sets the record straight on the basis of existing evidence, he often supports his counterargument with references.
He acknowledged that when he became involved in social media he faced criticism from colleagues about participating on an entertainment platform that many considered unworthy of providing objective information. If that was ever true, he argued, it is no longer the case.
“TikTok has adopted a new strategy. The goal is to unseat Google as a search tool, and it’s working,” he said. He explained that many people now use TikTok and other social media sites as their primary source of information on essentially every topic, from where to eat to whether to be screened for cancer.
The particular problem with TikTok – one of the most popular social media outlets – is that there is no mechanism for vetting the source of information. YouTube, by contrast, now requires some sort of validation for anyone who claims to have a medical degree or any other verifiable qualification, according to Dr. Landriscina. TikTok, like many other platforms, has no such requirement.
“Anyone can buy a pair of scrubs [implying expertise] and then post a video,” Dr. Landriscina said.
Even if information from one content provider is more valid than information from others, the TikTok algorithm is specifically designed to emphasize content that has the potential for going viral, which means it favors videos that are provocative over those that are not.
“The algorithm favors any content that is more controversial, more surprising, and keeps viewers engaged,” Dr. Landriscina pointed out.
This does not mean that objective and factual information is ignored, but the algorithm is indifferent to the validity of information, meaning that it allows videos to be posted without regard to whether the content is true, untrue, purposefully misleading, or utter nonsense. For that reason, it is often easier to attract attention by responding to a post that has already gone viral. Information that is clear and digestible can attract viewers and therefore is distributed more widely with the TikTok algorithm.
Parents are on Tiktok too
There is a misperception that the TikTok audience is younger, according to Dr. Landriscina. While peak use in the United States fell among people between the ages of 25 and 34 years in 2022, he said the number of users falls off relatively slowly with subsequent 10-year increments in age. In 2022, there were nearly 20 million users in the peak 10-year age range, but 7.5 million users were 55 years of age or older.
“Pediatric dermatologists should recognize that it is not just kids who are looking for information about their skin diseases, but also their parents,” Dr. Landriscina said.
The top three dermatology topics searched on TikTok in a recent period were acne, alopecia, and cysts. But top searches are very fluid and are extremely hard to quantify, because the basis of the algorithm, which is a proprietary secret, is not only unknown but produces different results for every user.
“The second you touch the app, it changes,” Dr. Landriscina said. He explained that an inquiry about any subject, including those that are medically related, yields content that is different, or at least ordered differently, “depending on how you behaved on the app in the past.”
The phenomenon that drives social media predates this technology. Dr. Landriscina cited a study in 1956 that described the “parasocial interaction theory.” The theory was based on the observation that those who consume media, such as television, which was relatively new in 1956, believed that they had a personal relationship with media figures.
“The users begin to trust influencers as a source, like a friend providing them advice,” Dr. Landriscina said. As an example, he suggested that a fan of the television show Friends who follows actor Jennifer Aniston on social media platforms may begin to think of her as a trusted source of information on any topic, including those for which she may not have expertise.
The reason that he urges medical professionals to become active on TikTok and other social media platforms is that they have a potentially critical role in responding to information that is not just wrong but harmful.
On TikTok and other social media platforms, “there is a lot of interest in content about dermatologic conditions in children. There is a real need for accurate information,” he said,
In the question-and-answer session following his presentation, Dr. Landriscina’s message was not uniformly embraced. One risk, according to an audience member, is that medical professionals will begin to express their own personal opinions rather than rely on evidence, with the result that they will “just add to the sea of misinformation.”
However, this opinion appeared to be the minority view. Most of those who commented took a “that-ship-has-sailed” stance, recognizing the irreversible ascendancy of social media.
“Whether you like it or not, social media is here to stay. We cannot fight it. Rather, we need to embrace it in a responsible way,” said Dakara R. Wright, MD, a dermatologist at the Mid-Atlantic Kaiser Permanente Group, Halethorpe, Md. She, like others, reported that she has come to recognize that social media is a major source of medical information for her patients.
“We need to be a presence on these platforms for the benefit of our patients and their parents,” she said. She acknowledged that she has not been active in posting on social media in the past but said that she has been speaking with administrators in her organization about how to become involved in a responsible way that can be useful to patients.
Candrice R. Heath, MD, assistant professor of dermatology at Temple University, Philadelphia, has been active on social media for several years, posting content on her own account, which is not related to her academic affiliation. She posts for many reasons, not least of which is drawing attention to her expertise.
Like Dr. Landriscina, she recognizes that users of these platforms are guided by the content to make decisions about health care. She also agreed that physicians should not ignore this phenomenon.
Tips on providing content
Given the fact that the algorithm is intended to produce posts that go viral, Dr. Landriscina urged clinicians to make their content easy to watch. He said it is not necessary to overthink content beyond providing accurate information, but he advised that videos be made with attention to adequate lighting and other simple factors to promote visual quality. He said that accurate information is not necessarily dull.
“Some facts can actually be surprising to patients,” he said. He noted that a calm, coherent video can be particularly effective in attracting an audience when it is in reaction to information that has gone viral but is misleading or patently incorrect.
Dr. Landriscina has been an influencer associated with multiple social media platforms, including TikTok. He has in the past been paid for consulting work for TikTok. Dr. Wright and Dr. Heath reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
AT SPD 2023
Commentary: Node irradiation, HER2+ treatment, and diet in BC, August 2023

The addition of pertuzumab to trastuzumab plus chemotherapy has demonstrated improvement in pathologic complete response (pCR) rates compared with trastuzumab plus chemotherapy in early-stage HER2-positive breast cancer.3 The framework of oncology is built on clinical trials through their rigorous design, enrollment, and synthesis of data; however, real-world studies are an integral component of cancer research because they provide a more representative sample of the general population treated in routine clinical practice. Neopearl was a retrospective, observational, real-world study that evaluated the efficacy and safety of trastuzumab plus chemotherapy with or without pertuzumab among 271 patients with stage II-III HER2-positive breast cancer (Fabbri et al). The addition of pertuzumab led to an increase in pCR rate (49% vs 62%; odds ratio 1.74; P = .032) and improvement in 5-year event-free survival (81% vs 93%; hazard ratio 2.22; P = .041), and the benefit on univariate analysis was restricted to patients with positive axillary nodes. Furthermore, there were no significant differences in adverse events, including cardiac, between the two groups. These results serve to strengthen the available data regarding the clinical efficacy and favorable safety profile of dual HER2-targeted therapy combined with neoadjuvant chemotherapy.
Lifestyle factors, including physical activity and diet, are becoming increasingly recognized as important determinants of various cancer-specific outcomes and overall health. Furthermore, because these are modifiable, there is often motivation on behalf of an individual to change behaviors that can affect their outcome. Adherence to the Mediterranean diet (MD) has been associated with reduced risk for breast cancer development and lower mortality among women with breast cancer.4,5 Data from a prospective multicenter European cohort including 13,270 breast cancer survivors demonstrated that low compared with medium adherence to a MD before a breast cancer diagnosis was associated with a 13% higher risk for all-cause mortality (hazard ratio 1.13; 95% CI 1.01-1.26). A three-unit increase in the adapted relative MD score was associated with an 8% reduced risk for overall mortality (hazard ratio3-unit 0.92; 95% CI 0.87-0.97); this result was sustained in the postmenopausal population and strengthened in metastatic disease (Castro-Espin et al). The connection between diet and cancer outcomes is complex, and future research evaluating specific dietary interventions and the underlying biologic pathways by which nutrition exerts its effects will be important to inform our counseling for patients with breast cancer in the survivorship setting.
Additional References
- Whelan TJ, Olivotto IA, Parulekar WR, et al, for the MA.20 Study Investigators. Regional nodal irradiation in early-stage breast cancer. N Engl J Med. 2015;373:307-16. doi:10.1056/NEJMoa1415340
- ClinicalTrials.gov. Regional radiotherapy in biomarker low-risk node positive and T3N0 breast cancer (TAILOR RT). National Library of Medicine. Last updated November 23, 2022. https://www.clinicaltrials.gov/study/NCT03488693
- Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13:25-32. doi:10.1016/S1470-2045(11)70336-9
- Buckland G, Travier N, Cottet V, et al. Adherence to the mediterranean diet and risk of breast cancer in the European prospective investigation into cancer and nutrition cohort study. Int J Cancer. 2013;132:2918-27. doi:10.1002/ijc.27958
- Haslam DE, John EM, Knight JA, et al. Diet quality and all-cause mortality in women with breast cancer from the Breast Cancer Family Registry. Cancer Epidemiol Biomarkers Prev. 2023;32:678-686. doi:10.1158/1055-9965.EPI-22-1198
The addition of pertuzumab to trastuzumab plus chemotherapy has demonstrated improvement in pathologic complete response (pCR) rates compared with trastuzumab plus chemotherapy in early-stage HER2-positive breast cancer.3 The framework of oncology is built on clinical trials through their rigorous design, enrollment, and synthesis of data; however, real-world studies are an integral component of cancer research because they provide a more representative sample of the general population treated in routine clinical practice. Neopearl was a retrospective, observational, real-world study that evaluated the efficacy and safety of trastuzumab plus chemotherapy with or without pertuzumab among 271 patients with stage II-III HER2-positive breast cancer (Fabbri et al). The addition of pertuzumab led to an increase in pCR rate (49% vs 62%; odds ratio 1.74; P = .032) and improvement in 5-year event-free survival (81% vs 93%; hazard ratio 2.22; P = .041), and the benefit on univariate analysis was restricted to patients with positive axillary nodes. Furthermore, there were no significant differences in adverse events, including cardiac, between the two groups. These results serve to strengthen the available data regarding the clinical efficacy and favorable safety profile of dual HER2-targeted therapy combined with neoadjuvant chemotherapy.
Lifestyle factors, including physical activity and diet, are becoming increasingly recognized as important determinants of various cancer-specific outcomes and overall health. Furthermore, because these are modifiable, there is often motivation on behalf of an individual to change behaviors that can affect their outcome. Adherence to the Mediterranean diet (MD) has been associated with reduced risk for breast cancer development and lower mortality among women with breast cancer.4,5 Data from a prospective multicenter European cohort including 13,270 breast cancer survivors demonstrated that low compared with medium adherence to a MD before a breast cancer diagnosis was associated with a 13% higher risk for all-cause mortality (hazard ratio 1.13; 95% CI 1.01-1.26). A three-unit increase in the adapted relative MD score was associated with an 8% reduced risk for overall mortality (hazard ratio3-unit 0.92; 95% CI 0.87-0.97); this result was sustained in the postmenopausal population and strengthened in metastatic disease (Castro-Espin et al). The connection between diet and cancer outcomes is complex, and future research evaluating specific dietary interventions and the underlying biologic pathways by which nutrition exerts its effects will be important to inform our counseling for patients with breast cancer in the survivorship setting.
Additional References
- Whelan TJ, Olivotto IA, Parulekar WR, et al, for the MA.20 Study Investigators. Regional nodal irradiation in early-stage breast cancer. N Engl J Med. 2015;373:307-16. doi:10.1056/NEJMoa1415340
- ClinicalTrials.gov. Regional radiotherapy in biomarker low-risk node positive and T3N0 breast cancer (TAILOR RT). National Library of Medicine. Last updated November 23, 2022. https://www.clinicaltrials.gov/study/NCT03488693
- Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13:25-32. doi:10.1016/S1470-2045(11)70336-9
- Buckland G, Travier N, Cottet V, et al. Adherence to the mediterranean diet and risk of breast cancer in the European prospective investigation into cancer and nutrition cohort study. Int J Cancer. 2013;132:2918-27. doi:10.1002/ijc.27958
- Haslam DE, John EM, Knight JA, et al. Diet quality and all-cause mortality in women with breast cancer from the Breast Cancer Family Registry. Cancer Epidemiol Biomarkers Prev. 2023;32:678-686. doi:10.1158/1055-9965.EPI-22-1198
The addition of pertuzumab to trastuzumab plus chemotherapy has demonstrated improvement in pathologic complete response (pCR) rates compared with trastuzumab plus chemotherapy in early-stage HER2-positive breast cancer.3 The framework of oncology is built on clinical trials through their rigorous design, enrollment, and synthesis of data; however, real-world studies are an integral component of cancer research because they provide a more representative sample of the general population treated in routine clinical practice. Neopearl was a retrospective, observational, real-world study that evaluated the efficacy and safety of trastuzumab plus chemotherapy with or without pertuzumab among 271 patients with stage II-III HER2-positive breast cancer (Fabbri et al). The addition of pertuzumab led to an increase in pCR rate (49% vs 62%; odds ratio 1.74; P = .032) and improvement in 5-year event-free survival (81% vs 93%; hazard ratio 2.22; P = .041), and the benefit on univariate analysis was restricted to patients with positive axillary nodes. Furthermore, there were no significant differences in adverse events, including cardiac, between the two groups. These results serve to strengthen the available data regarding the clinical efficacy and favorable safety profile of dual HER2-targeted therapy combined with neoadjuvant chemotherapy.
Lifestyle factors, including physical activity and diet, are becoming increasingly recognized as important determinants of various cancer-specific outcomes and overall health. Furthermore, because these are modifiable, there is often motivation on behalf of an individual to change behaviors that can affect their outcome. Adherence to the Mediterranean diet (MD) has been associated with reduced risk for breast cancer development and lower mortality among women with breast cancer.4,5 Data from a prospective multicenter European cohort including 13,270 breast cancer survivors demonstrated that low compared with medium adherence to a MD before a breast cancer diagnosis was associated with a 13% higher risk for all-cause mortality (hazard ratio 1.13; 95% CI 1.01-1.26). A three-unit increase in the adapted relative MD score was associated with an 8% reduced risk for overall mortality (hazard ratio3-unit 0.92; 95% CI 0.87-0.97); this result was sustained in the postmenopausal population and strengthened in metastatic disease (Castro-Espin et al). The connection between diet and cancer outcomes is complex, and future research evaluating specific dietary interventions and the underlying biologic pathways by which nutrition exerts its effects will be important to inform our counseling for patients with breast cancer in the survivorship setting.
Additional References
- Whelan TJ, Olivotto IA, Parulekar WR, et al, for the MA.20 Study Investigators. Regional nodal irradiation in early-stage breast cancer. N Engl J Med. 2015;373:307-16. doi:10.1056/NEJMoa1415340
- ClinicalTrials.gov. Regional radiotherapy in biomarker low-risk node positive and T3N0 breast cancer (TAILOR RT). National Library of Medicine. Last updated November 23, 2022. https://www.clinicaltrials.gov/study/NCT03488693
- Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13:25-32. doi:10.1016/S1470-2045(11)70336-9
- Buckland G, Travier N, Cottet V, et al. Adherence to the mediterranean diet and risk of breast cancer in the European prospective investigation into cancer and nutrition cohort study. Int J Cancer. 2013;132:2918-27. doi:10.1002/ijc.27958
- Haslam DE, John EM, Knight JA, et al. Diet quality and all-cause mortality in women with breast cancer from the Breast Cancer Family Registry. Cancer Epidemiol Biomarkers Prev. 2023;32:678-686. doi:10.1158/1055-9965.EPI-22-1198
No cognitive benefit from meditation, learning a language?
The findings are similar to results from another study published last year but are contrary to previous findings showing cognitive benefits for practicing meditation and learning a new language later in life.
“Based on existing literature, which has provided support for the efficacy of meditation and foreign language training in promoting cognition among older adults, perhaps the most surprising outcome of our study was the lack of evidence indicating cognitive benefits after 18 months of either intervention,” lead author Harriet Demnitz-King, MSc, a doctoral candidate at University College London, said in an interview. The findings were published online in JAMA Network Open.

Contradictory findings
For the study, 135 French-speaking, cognitively healthy people were randomized to English-language training, meditation, or a control group. All participants were aged 65 years or older, had been retired for at least 1 year, and had completed at least 7 years of education.
The meditation and English-language training interventions were both 18 months long and included a 2-hour weekly group session, daily home practice of at least 20 minutes, and 1-day intensive 5-hour practice.
Researchers found no significant changes in global cognition, episodic memory, executive function, or attention with either intervention, compared with the control group or to each other.
The findings contradict the researchers’ earlier work that found mindfulness meditation boosted cognitive function in older adults with subjective cognitive decline.
“We are still trying to reconcile these findings,” senior author Natalie Marchant, PhD, associate professor in the division of psychiatry at University College London, said. “It may be that mindfulness meditation may not improve cognition beyond normally functioning levels but may help to preserve cognition in the face of cognitive decline.”

This study was the longest randomized controlled trial in older adults to investigate the effects of non-native language learning on cognition, Dr. Marchant said.
“It may be that language-learning may buffer against age-related cognitive decline but does not boost cognition in high-functioning individuals,” Dr. Marchant said. “While language learning may not improve cognition, we do not want to discard the other possibility without first examining it.”
Dr. Marchant plans to follow participants for years to come to study that very question.
More to learn
The results harken to those of a study last year with a similar participant group and similar results. In that work, mindfulness meditation and exercise also failed to boost cognition in healthy adults. But that may not be the whole story, according to Eric Lenze, MD, professor and chair of psychiatry at Washington University School of Medicine, St. Louis.
Dr. Lenze was a lead author on that earlier research, known as the MEDEX trial, but was not involved with this study. He commented on the new findings for this news organization.
“People may read these results, and ours that were published in JAMA in December, as suggesting that lifestyle and cognitive interventions don’t work in older adults, but that’s not what this shows, in my opinion,” Dr. Lenze said. “It shows that we don’t understand the science of the aging brain as much as we would like to.”
Participants in most of these studies were mostly White, highly educated, and in good cognitive health, all characteristics that could have skewed these findings, he added.
“It may be that interventions to improve cognitive function in older adults would be more likely to help people who have more room to benefit,” Dr. Lenze said. “If you’re already highly educated, healthy, and cognitively normal, why should we expect that you could do even better than that?”
The Age-Well study was funded by European Union in Horizon 2020 program and Inserm, Région Normandie, Fondation d’entreprise MMA des Entrepreneurs du Futur. Dr. Marchant reports grants from Alzheimer’s Society and the U.K. Medical Research Council. Dr. Lenze reports funding from Takeda pharmaceuticals and has been a consultant for Pritikin Intensive Cardiac Rehabilitation.
A version of this article first appeared on Medscape.com.
The findings are similar to results from another study published last year but are contrary to previous findings showing cognitive benefits for practicing meditation and learning a new language later in life.
“Based on existing literature, which has provided support for the efficacy of meditation and foreign language training in promoting cognition among older adults, perhaps the most surprising outcome of our study was the lack of evidence indicating cognitive benefits after 18 months of either intervention,” lead author Harriet Demnitz-King, MSc, a doctoral candidate at University College London, said in an interview. The findings were published online in JAMA Network Open.
Contradictory findings
For the study, 135 French-speaking, cognitively healthy people were randomized to English-language training, meditation, or a control group. All participants were aged 65 years or older, had been retired for at least 1 year, and had completed at least 7 years of education.
The meditation and English-language training interventions were both 18 months long and included a 2-hour weekly group session, daily home practice of at least 20 minutes, and 1-day intensive 5-hour practice.
Researchers found no significant changes in global cognition, episodic memory, executive function, or attention with either intervention, compared with the control group or to each other.
The findings contradict the researchers’ earlier work that found mindfulness meditation boosted cognitive function in older adults with subjective cognitive decline.
“We are still trying to reconcile these findings,” senior author Natalie Marchant, PhD, associate professor in the division of psychiatry at University College London, said. “It may be that mindfulness meditation may not improve cognition beyond normally functioning levels but may help to preserve cognition in the face of cognitive decline.”
This study was the longest randomized controlled trial in older adults to investigate the effects of non-native language learning on cognition, Dr. Marchant said.
“It may be that language-learning may buffer against age-related cognitive decline but does not boost cognition in high-functioning individuals,” Dr. Marchant said. “While language learning may not improve cognition, we do not want to discard the other possibility without first examining it.”
Dr. Marchant plans to follow participants for years to come to study that very question.
More to learn
The results harken to those of a study last year with a similar participant group and similar results. In that work, mindfulness meditation and exercise also failed to boost cognition in healthy adults. But that may not be the whole story, according to Eric Lenze, MD, professor and chair of psychiatry at Washington University School of Medicine, St. Louis.
Dr. Lenze was a lead author on that earlier research, known as the MEDEX trial, but was not involved with this study. He commented on the new findings for this news organization.
“People may read these results, and ours that were published in JAMA in December, as suggesting that lifestyle and cognitive interventions don’t work in older adults, but that’s not what this shows, in my opinion,” Dr. Lenze said. “It shows that we don’t understand the science of the aging brain as much as we would like to.”
Participants in most of these studies were mostly White, highly educated, and in good cognitive health, all characteristics that could have skewed these findings, he added.
“It may be that interventions to improve cognitive function in older adults would be more likely to help people who have more room to benefit,” Dr. Lenze said. “If you’re already highly educated, healthy, and cognitively normal, why should we expect that you could do even better than that?”
The Age-Well study was funded by European Union in Horizon 2020 program and Inserm, Région Normandie, Fondation d’entreprise MMA des Entrepreneurs du Futur. Dr. Marchant reports grants from Alzheimer’s Society and the U.K. Medical Research Council. Dr. Lenze reports funding from Takeda pharmaceuticals and has been a consultant for Pritikin Intensive Cardiac Rehabilitation.
A version of this article first appeared on Medscape.com.
The findings are similar to results from another study published last year but are contrary to previous findings showing cognitive benefits for practicing meditation and learning a new language later in life.
“Based on existing literature, which has provided support for the efficacy of meditation and foreign language training in promoting cognition among older adults, perhaps the most surprising outcome of our study was the lack of evidence indicating cognitive benefits after 18 months of either intervention,” lead author Harriet Demnitz-King, MSc, a doctoral candidate at University College London, said in an interview. The findings were published online in JAMA Network Open.
Contradictory findings
For the study, 135 French-speaking, cognitively healthy people were randomized to English-language training, meditation, or a control group. All participants were aged 65 years or older, had been retired for at least 1 year, and had completed at least 7 years of education.
The meditation and English-language training interventions were both 18 months long and included a 2-hour weekly group session, daily home practice of at least 20 minutes, and 1-day intensive 5-hour practice.
Researchers found no significant changes in global cognition, episodic memory, executive function, or attention with either intervention, compared with the control group or to each other.
The findings contradict the researchers’ earlier work that found mindfulness meditation boosted cognitive function in older adults with subjective cognitive decline.
“We are still trying to reconcile these findings,” senior author Natalie Marchant, PhD, associate professor in the division of psychiatry at University College London, said. “It may be that mindfulness meditation may not improve cognition beyond normally functioning levels but may help to preserve cognition in the face of cognitive decline.”
This study was the longest randomized controlled trial in older adults to investigate the effects of non-native language learning on cognition, Dr. Marchant said.
“It may be that language-learning may buffer against age-related cognitive decline but does not boost cognition in high-functioning individuals,” Dr. Marchant said. “While language learning may not improve cognition, we do not want to discard the other possibility without first examining it.”
Dr. Marchant plans to follow participants for years to come to study that very question.
More to learn
The results harken to those of a study last year with a similar participant group and similar results. In that work, mindfulness meditation and exercise also failed to boost cognition in healthy adults. But that may not be the whole story, according to Eric Lenze, MD, professor and chair of psychiatry at Washington University School of Medicine, St. Louis.
Dr. Lenze was a lead author on that earlier research, known as the MEDEX trial, but was not involved with this study. He commented on the new findings for this news organization.
“People may read these results, and ours that were published in JAMA in December, as suggesting that lifestyle and cognitive interventions don’t work in older adults, but that’s not what this shows, in my opinion,” Dr. Lenze said. “It shows that we don’t understand the science of the aging brain as much as we would like to.”
Participants in most of these studies were mostly White, highly educated, and in good cognitive health, all characteristics that could have skewed these findings, he added.
“It may be that interventions to improve cognitive function in older adults would be more likely to help people who have more room to benefit,” Dr. Lenze said. “If you’re already highly educated, healthy, and cognitively normal, why should we expect that you could do even better than that?”
The Age-Well study was funded by European Union in Horizon 2020 program and Inserm, Région Normandie, Fondation d’entreprise MMA des Entrepreneurs du Futur. Dr. Marchant reports grants from Alzheimer’s Society and the U.K. Medical Research Council. Dr. Lenze reports funding from Takeda pharmaceuticals and has been a consultant for Pritikin Intensive Cardiac Rehabilitation.
A version of this article first appeared on Medscape.com.
FROM JAMA Network Open
‘Treatment holiday’ in prostate cancer with tailored dosing
and improve patient outcomes, new research suggests.
The findings indicate that implementing a personalized dosing strategy with the radioligand therapy “allowed for treatment holidays in excellent responders, continuous 6-weekly treatments in moderate responders, and [allowed us] to consider changing or adding treatment in limited responders,” said study author Andrew Nguyen, MBBS, FRACP, AANMS, senior staff specialist in the department of theranostics and nuclear medicine at St. Vincent’s Hospital in Sydney.
The research was presented at the annual meeting of the Society of Nuclear Medicine and Molecular Imaging.
Although clinical trials have demonstrated that 177Lu-PSMA is an effective treatment for metastatic castration-resistant prostate cancer, the question remains: Can patient outcomes be improved through the use of biomarkers and by escalating or deescalating treatment as appropriate? asked Dr. Nguyen, who presented the findings at the meeting.
Clinical trials use standardized dosing intervals. Adjusting treatment intervals through the use of early-biomarker responses could give some patients a break from treatment and improve overall survival outcomes, Dr. Nguyen explained. For example, the 2021 REALITY study showed that overall survival was significantly better for patients who received 177Lu-PSMA plus standard care, compared with patients who received standard care alone (median, 15.3 vs. 11.3 months), and that overall survival was better among patients with early prostate-specific antigen (PSA) responses.
In the current study, Dr. Nguyen and colleagues used composite early biomarkers of PSA, imaging with 177Lu-PSMA SPECT, and diagnostic CT to guide a personalized dosing interval strategy for patients with metastatic castration-resistant prostate cancer receiving 177Lu-PSMA. The team evaluated progression-free survival and overall survival among these patients to determine whether personalizing dosing on the basis of early biomarker levels was associated with survival outcomes.
The cohort included 125 men who received six weekly doses of 177Lu-PSMA and who underwent imaging with 177Lu-SPECT/CT after each dose. After the second dose, investigators used the composite of PSA and 177Lu SPECT/CT response to determine which patients had a partial response, which had stable disease, and which had progressive disease.
The men were divided into three groups on the basis of their level of response. Group 1, which included 35% of participants, achieved a significant reduction in PSA levels and a partial response on 177Lu-SPECT. These patients were advised to discontinue treatment until PSA levels increased. This treatment holiday lasted a median of about 6 months.
Group 2, which represented 34% of the cohort, had stable or reduced PSA levels as well as stable disease on SPECT imaging. For these patients, the treatment regimen continued.
Group 3 demonstrated rising PSA levels and progressive disease on SPECT imaging. These men were offered an alternative therapy.
Overall, median PSA progression-free survival was 12.1 months in group 1, 6.1 months in group 2, and 2.6 months in group 3. Median overall survival was also significantly better among patients who showed early responses to therapy: 19.2 months in group 1, 13.2 months in group 2, and 11. 2 months in group 3.
Dr. Nguyen noted several limitations to the findings, including the study’s retrospective nature and the fact that some patients in group 1 chose not to resume further treatment after their PSA levels rose.
“Personalizing dosing intervals using early-response biomarkers with 177Lu-PSMA has the potential to achieve similar overall treatment responses to that published for continuous dosing, while allowing treatment holidays in responders and early crossover to potentially more effective therapies in nonresponders,” the authors conclude.
Given the effectiveness of this strategy, Dr. Nguyen says his team “now routinely uses these composite biomarkers when treating clinical patients.”
A version of this article appeared on Medscape.com.
and improve patient outcomes, new research suggests.
The findings indicate that implementing a personalized dosing strategy with the radioligand therapy “allowed for treatment holidays in excellent responders, continuous 6-weekly treatments in moderate responders, and [allowed us] to consider changing or adding treatment in limited responders,” said study author Andrew Nguyen, MBBS, FRACP, AANMS, senior staff specialist in the department of theranostics and nuclear medicine at St. Vincent’s Hospital in Sydney.
The research was presented at the annual meeting of the Society of Nuclear Medicine and Molecular Imaging.
Although clinical trials have demonstrated that 177Lu-PSMA is an effective treatment for metastatic castration-resistant prostate cancer, the question remains: Can patient outcomes be improved through the use of biomarkers and by escalating or deescalating treatment as appropriate? asked Dr. Nguyen, who presented the findings at the meeting.
Clinical trials use standardized dosing intervals. Adjusting treatment intervals through the use of early-biomarker responses could give some patients a break from treatment and improve overall survival outcomes, Dr. Nguyen explained. For example, the 2021 REALITY study showed that overall survival was significantly better for patients who received 177Lu-PSMA plus standard care, compared with patients who received standard care alone (median, 15.3 vs. 11.3 months), and that overall survival was better among patients with early prostate-specific antigen (PSA) responses.
In the current study, Dr. Nguyen and colleagues used composite early biomarkers of PSA, imaging with 177Lu-PSMA SPECT, and diagnostic CT to guide a personalized dosing interval strategy for patients with metastatic castration-resistant prostate cancer receiving 177Lu-PSMA. The team evaluated progression-free survival and overall survival among these patients to determine whether personalizing dosing on the basis of early biomarker levels was associated with survival outcomes.
The cohort included 125 men who received six weekly doses of 177Lu-PSMA and who underwent imaging with 177Lu-SPECT/CT after each dose. After the second dose, investigators used the composite of PSA and 177Lu SPECT/CT response to determine which patients had a partial response, which had stable disease, and which had progressive disease.
The men were divided into three groups on the basis of their level of response. Group 1, which included 35% of participants, achieved a significant reduction in PSA levels and a partial response on 177Lu-SPECT. These patients were advised to discontinue treatment until PSA levels increased. This treatment holiday lasted a median of about 6 months.
Group 2, which represented 34% of the cohort, had stable or reduced PSA levels as well as stable disease on SPECT imaging. For these patients, the treatment regimen continued.
Group 3 demonstrated rising PSA levels and progressive disease on SPECT imaging. These men were offered an alternative therapy.
Overall, median PSA progression-free survival was 12.1 months in group 1, 6.1 months in group 2, and 2.6 months in group 3. Median overall survival was also significantly better among patients who showed early responses to therapy: 19.2 months in group 1, 13.2 months in group 2, and 11. 2 months in group 3.
Dr. Nguyen noted several limitations to the findings, including the study’s retrospective nature and the fact that some patients in group 1 chose not to resume further treatment after their PSA levels rose.
“Personalizing dosing intervals using early-response biomarkers with 177Lu-PSMA has the potential to achieve similar overall treatment responses to that published for continuous dosing, while allowing treatment holidays in responders and early crossover to potentially more effective therapies in nonresponders,” the authors conclude.
Given the effectiveness of this strategy, Dr. Nguyen says his team “now routinely uses these composite biomarkers when treating clinical patients.”
A version of this article appeared on Medscape.com.
and improve patient outcomes, new research suggests.
The findings indicate that implementing a personalized dosing strategy with the radioligand therapy “allowed for treatment holidays in excellent responders, continuous 6-weekly treatments in moderate responders, and [allowed us] to consider changing or adding treatment in limited responders,” said study author Andrew Nguyen, MBBS, FRACP, AANMS, senior staff specialist in the department of theranostics and nuclear medicine at St. Vincent’s Hospital in Sydney.
The research was presented at the annual meeting of the Society of Nuclear Medicine and Molecular Imaging.
Although clinical trials have demonstrated that 177Lu-PSMA is an effective treatment for metastatic castration-resistant prostate cancer, the question remains: Can patient outcomes be improved through the use of biomarkers and by escalating or deescalating treatment as appropriate? asked Dr. Nguyen, who presented the findings at the meeting.
Clinical trials use standardized dosing intervals. Adjusting treatment intervals through the use of early-biomarker responses could give some patients a break from treatment and improve overall survival outcomes, Dr. Nguyen explained. For example, the 2021 REALITY study showed that overall survival was significantly better for patients who received 177Lu-PSMA plus standard care, compared with patients who received standard care alone (median, 15.3 vs. 11.3 months), and that overall survival was better among patients with early prostate-specific antigen (PSA) responses.
In the current study, Dr. Nguyen and colleagues used composite early biomarkers of PSA, imaging with 177Lu-PSMA SPECT, and diagnostic CT to guide a personalized dosing interval strategy for patients with metastatic castration-resistant prostate cancer receiving 177Lu-PSMA. The team evaluated progression-free survival and overall survival among these patients to determine whether personalizing dosing on the basis of early biomarker levels was associated with survival outcomes.
The cohort included 125 men who received six weekly doses of 177Lu-PSMA and who underwent imaging with 177Lu-SPECT/CT after each dose. After the second dose, investigators used the composite of PSA and 177Lu SPECT/CT response to determine which patients had a partial response, which had stable disease, and which had progressive disease.
The men were divided into three groups on the basis of their level of response. Group 1, which included 35% of participants, achieved a significant reduction in PSA levels and a partial response on 177Lu-SPECT. These patients were advised to discontinue treatment until PSA levels increased. This treatment holiday lasted a median of about 6 months.
Group 2, which represented 34% of the cohort, had stable or reduced PSA levels as well as stable disease on SPECT imaging. For these patients, the treatment regimen continued.
Group 3 demonstrated rising PSA levels and progressive disease on SPECT imaging. These men were offered an alternative therapy.
Overall, median PSA progression-free survival was 12.1 months in group 1, 6.1 months in group 2, and 2.6 months in group 3. Median overall survival was also significantly better among patients who showed early responses to therapy: 19.2 months in group 1, 13.2 months in group 2, and 11. 2 months in group 3.
Dr. Nguyen noted several limitations to the findings, including the study’s retrospective nature and the fact that some patients in group 1 chose not to resume further treatment after their PSA levels rose.
“Personalizing dosing intervals using early-response biomarkers with 177Lu-PSMA has the potential to achieve similar overall treatment responses to that published for continuous dosing, while allowing treatment holidays in responders and early crossover to potentially more effective therapies in nonresponders,” the authors conclude.
Given the effectiveness of this strategy, Dr. Nguyen says his team “now routinely uses these composite biomarkers when treating clinical patients.”
A version of this article appeared on Medscape.com.
FROM SNMMI 2023
Early MS treatment tied to a major reduction in severe disability
a new study suggests.
Patients who received early treatment had a 45% lower risk of reaching a disability score of 3 and a 60% lower risk of advancing to secondary progressive MS compared with those who began treatment 18 months or more after symptoms presented.
Those with a score of 3 can still walk unassisted but have moderate disability in one of eight areas, such as motor function, vision or thinking skills, or mild disability in three or four areas.
“With a very early treatment, within 6 months from the first symptoms and even before the MS diagnosis, we are now able to decrease long-term disability. This means the earlier the better – time is brain,” lead author Alvaro Cobo-Calvo, MD, PhD, clinical neurologists and researcher with the Multiple Sclerosis Center of Catalonia in Barcelona and the Universitat Autonoma de Barcelona, said in an interview.
The findings were published online in Neurology.
Measuring disability
The observational, retrospective study included people aged 50 years or younger who received MS treatment within 6 months of their first clinical demyelinating event (n = 194), 6-16 months later (n = 192), or more than 16 months after the initial symptoms presented (n = 194).
The investigators noted that this cohort is one of the few that is considered “deeply phenotyped,” meaning it is followed prospectively over time with strict quality controls and systematic data collection methods.
MRIs were done within 3-5 months of the first symptoms, again at 12 months after the first event, and every 5 years over a median 11.2-year follow-up.
Disability levels were measured using the Expanded Disability Status Scale, with scores ranging from 0-10 and higher scores indicating more disability.
Patients who received treatment within 6 months of first symptoms were 45% less likely to have a disability score of 3 by the end of the study than did those who received treatment more than 16 months after that first event (hazard ratio, 0.55; 95% confidence interval, 0.32-0.97).
The earliest-treatment group also had a 60% lower risk of advancing to secondary progressive MS than did people in the latest-treatment group (HR, 0.40; 95% CI, 0.19-0.85).
Better disease stability
The researchers also found that earlier treatment was associated with a 53% better chance of disease stability 1 year after initial treatment (HR, 0.47; 95% CI, 0.28-0.80).
The early-treatment group also had a lower disability progression rate and lower severe disability in a self-reported test, compared with those who were treated later.
The investigators also found that patients who received early treatment were at lower risk for disability, even those with a higher baseline radiologic burden.
Current guidelines recommend early treatment of MS, but it is unclear whether disease-modifying treatments (DMTs) should be prescribed after the first MS symptoms or after a definitive MS diagnosis.
Earlier studies often evaluated treatment efficacy after MS diagnosis. This study began tracking efficacy when therapy began after the first symptoms. In some cases, that was before a diagnosis was given.
“It is important to be cautious when starting treatment and we need to know if the patient will evolve to MS or if the patient is diagnosed with MS based on current McDonald criteria.
“In our study, 70% of patients had MS at the time of the first symptoms according to McDonald 201, but the remainder started treatment without an ‘official’ diagnosis but with an event highly suggestive of MS,” Dr. Cobo-Calvo said.
He added that very early treatment after first symptoms is key to preserving neurologic functionality.
Controversy remains
Adding MRI results as a clinical variable is a novel approach, but the MRI risk score used in the study is a new tool that has not yet been validated, the authors of an accompanying editorial noted.
“The results of this study show that in order to achieve a balance between compared groups, matching on MRI has little to add to good-quality balancing on patients’ clinical and demographic features,” wrote Erin Longbrake, MD, PhD, of the department of neurology, Yale University, New Haven, Conn., and Tomas Kalincik, MD, PhD, of the Neuroimmunology Centre, department of neurology, Royal Melbourne Hospital and the CORe unit, department of medicine, University of Melbourne.
Despite growing evidence pointing to improved outcomes from administering DMTs soon after diagnosis, the timing and sequence of therapy remains an area of controversy, they added.
“While these uncertain diagnostic scenarios may tempt neurologists to ‘wait and see,’ the data presented here remind us that these patients remain at risk of accumulating disability,” the authors wrote. “Neurologists must therefore remain vigilant to ensure that diagnosis is made promptly, that patients are followed up effectively and that effective treatments are used liberally.”
The study was funded by the European Regional Development Fund, Instituto de Salud Carlos III. Dr. Cobo-Calvo has received a grant from Instituto de Salud Carlos III. Dr. Longbrake has consulted for Genentech and NGM Bio and received research support from Biogen & Genentech. Dr. Kalincik has received conference travel support and/or speaker honoraria from WebMD Global, Eisai, Novartis, Biogen, Roche, Sanofi Genzyme, Teva, BioCSL, and Merck, and has received research or educational event support from Biogen, Novartis, Genzyme, Roche, Celgene, and Merck.
A version of this article first appeared on Medscape.com.
a new study suggests.
Patients who received early treatment had a 45% lower risk of reaching a disability score of 3 and a 60% lower risk of advancing to secondary progressive MS compared with those who began treatment 18 months or more after symptoms presented.
Those with a score of 3 can still walk unassisted but have moderate disability in one of eight areas, such as motor function, vision or thinking skills, or mild disability in three or four areas.
“With a very early treatment, within 6 months from the first symptoms and even before the MS diagnosis, we are now able to decrease long-term disability. This means the earlier the better – time is brain,” lead author Alvaro Cobo-Calvo, MD, PhD, clinical neurologists and researcher with the Multiple Sclerosis Center of Catalonia in Barcelona and the Universitat Autonoma de Barcelona, said in an interview.
The findings were published online in Neurology.
Measuring disability
The observational, retrospective study included people aged 50 years or younger who received MS treatment within 6 months of their first clinical demyelinating event (n = 194), 6-16 months later (n = 192), or more than 16 months after the initial symptoms presented (n = 194).
The investigators noted that this cohort is one of the few that is considered “deeply phenotyped,” meaning it is followed prospectively over time with strict quality controls and systematic data collection methods.
MRIs were done within 3-5 months of the first symptoms, again at 12 months after the first event, and every 5 years over a median 11.2-year follow-up.
Disability levels were measured using the Expanded Disability Status Scale, with scores ranging from 0-10 and higher scores indicating more disability.
Patients who received treatment within 6 months of first symptoms were 45% less likely to have a disability score of 3 by the end of the study than did those who received treatment more than 16 months after that first event (hazard ratio, 0.55; 95% confidence interval, 0.32-0.97).
The earliest-treatment group also had a 60% lower risk of advancing to secondary progressive MS than did people in the latest-treatment group (HR, 0.40; 95% CI, 0.19-0.85).
Better disease stability
The researchers also found that earlier treatment was associated with a 53% better chance of disease stability 1 year after initial treatment (HR, 0.47; 95% CI, 0.28-0.80).
The early-treatment group also had a lower disability progression rate and lower severe disability in a self-reported test, compared with those who were treated later.
The investigators also found that patients who received early treatment were at lower risk for disability, even those with a higher baseline radiologic burden.
Current guidelines recommend early treatment of MS, but it is unclear whether disease-modifying treatments (DMTs) should be prescribed after the first MS symptoms or after a definitive MS diagnosis.
Earlier studies often evaluated treatment efficacy after MS diagnosis. This study began tracking efficacy when therapy began after the first symptoms. In some cases, that was before a diagnosis was given.
“It is important to be cautious when starting treatment and we need to know if the patient will evolve to MS or if the patient is diagnosed with MS based on current McDonald criteria.
“In our study, 70% of patients had MS at the time of the first symptoms according to McDonald 201, but the remainder started treatment without an ‘official’ diagnosis but with an event highly suggestive of MS,” Dr. Cobo-Calvo said.
He added that very early treatment after first symptoms is key to preserving neurologic functionality.
Controversy remains
Adding MRI results as a clinical variable is a novel approach, but the MRI risk score used in the study is a new tool that has not yet been validated, the authors of an accompanying editorial noted.
“The results of this study show that in order to achieve a balance between compared groups, matching on MRI has little to add to good-quality balancing on patients’ clinical and demographic features,” wrote Erin Longbrake, MD, PhD, of the department of neurology, Yale University, New Haven, Conn., and Tomas Kalincik, MD, PhD, of the Neuroimmunology Centre, department of neurology, Royal Melbourne Hospital and the CORe unit, department of medicine, University of Melbourne.
Despite growing evidence pointing to improved outcomes from administering DMTs soon after diagnosis, the timing and sequence of therapy remains an area of controversy, they added.
“While these uncertain diagnostic scenarios may tempt neurologists to ‘wait and see,’ the data presented here remind us that these patients remain at risk of accumulating disability,” the authors wrote. “Neurologists must therefore remain vigilant to ensure that diagnosis is made promptly, that patients are followed up effectively and that effective treatments are used liberally.”
The study was funded by the European Regional Development Fund, Instituto de Salud Carlos III. Dr. Cobo-Calvo has received a grant from Instituto de Salud Carlos III. Dr. Longbrake has consulted for Genentech and NGM Bio and received research support from Biogen & Genentech. Dr. Kalincik has received conference travel support and/or speaker honoraria from WebMD Global, Eisai, Novartis, Biogen, Roche, Sanofi Genzyme, Teva, BioCSL, and Merck, and has received research or educational event support from Biogen, Novartis, Genzyme, Roche, Celgene, and Merck.
A version of this article first appeared on Medscape.com.
a new study suggests.
Patients who received early treatment had a 45% lower risk of reaching a disability score of 3 and a 60% lower risk of advancing to secondary progressive MS compared with those who began treatment 18 months or more after symptoms presented.
Those with a score of 3 can still walk unassisted but have moderate disability in one of eight areas, such as motor function, vision or thinking skills, or mild disability in three or four areas.
“With a very early treatment, within 6 months from the first symptoms and even before the MS diagnosis, we are now able to decrease long-term disability. This means the earlier the better – time is brain,” lead author Alvaro Cobo-Calvo, MD, PhD, clinical neurologists and researcher with the Multiple Sclerosis Center of Catalonia in Barcelona and the Universitat Autonoma de Barcelona, said in an interview.
The findings were published online in Neurology.
Measuring disability
The observational, retrospective study included people aged 50 years or younger who received MS treatment within 6 months of their first clinical demyelinating event (n = 194), 6-16 months later (n = 192), or more than 16 months after the initial symptoms presented (n = 194).
The investigators noted that this cohort is one of the few that is considered “deeply phenotyped,” meaning it is followed prospectively over time with strict quality controls and systematic data collection methods.
MRIs were done within 3-5 months of the first symptoms, again at 12 months after the first event, and every 5 years over a median 11.2-year follow-up.
Disability levels were measured using the Expanded Disability Status Scale, with scores ranging from 0-10 and higher scores indicating more disability.
Patients who received treatment within 6 months of first symptoms were 45% less likely to have a disability score of 3 by the end of the study than did those who received treatment more than 16 months after that first event (hazard ratio, 0.55; 95% confidence interval, 0.32-0.97).
The earliest-treatment group also had a 60% lower risk of advancing to secondary progressive MS than did people in the latest-treatment group (HR, 0.40; 95% CI, 0.19-0.85).
Better disease stability
The researchers also found that earlier treatment was associated with a 53% better chance of disease stability 1 year after initial treatment (HR, 0.47; 95% CI, 0.28-0.80).
The early-treatment group also had a lower disability progression rate and lower severe disability in a self-reported test, compared with those who were treated later.
The investigators also found that patients who received early treatment were at lower risk for disability, even those with a higher baseline radiologic burden.
Current guidelines recommend early treatment of MS, but it is unclear whether disease-modifying treatments (DMTs) should be prescribed after the first MS symptoms or after a definitive MS diagnosis.
Earlier studies often evaluated treatment efficacy after MS diagnosis. This study began tracking efficacy when therapy began after the first symptoms. In some cases, that was before a diagnosis was given.
“It is important to be cautious when starting treatment and we need to know if the patient will evolve to MS or if the patient is diagnosed with MS based on current McDonald criteria.
“In our study, 70% of patients had MS at the time of the first symptoms according to McDonald 201, but the remainder started treatment without an ‘official’ diagnosis but with an event highly suggestive of MS,” Dr. Cobo-Calvo said.
He added that very early treatment after first symptoms is key to preserving neurologic functionality.
Controversy remains
Adding MRI results as a clinical variable is a novel approach, but the MRI risk score used in the study is a new tool that has not yet been validated, the authors of an accompanying editorial noted.
“The results of this study show that in order to achieve a balance between compared groups, matching on MRI has little to add to good-quality balancing on patients’ clinical and demographic features,” wrote Erin Longbrake, MD, PhD, of the department of neurology, Yale University, New Haven, Conn., and Tomas Kalincik, MD, PhD, of the Neuroimmunology Centre, department of neurology, Royal Melbourne Hospital and the CORe unit, department of medicine, University of Melbourne.
Despite growing evidence pointing to improved outcomes from administering DMTs soon after diagnosis, the timing and sequence of therapy remains an area of controversy, they added.
“While these uncertain diagnostic scenarios may tempt neurologists to ‘wait and see,’ the data presented here remind us that these patients remain at risk of accumulating disability,” the authors wrote. “Neurologists must therefore remain vigilant to ensure that diagnosis is made promptly, that patients are followed up effectively and that effective treatments are used liberally.”
The study was funded by the European Regional Development Fund, Instituto de Salud Carlos III. Dr. Cobo-Calvo has received a grant from Instituto de Salud Carlos III. Dr. Longbrake has consulted for Genentech and NGM Bio and received research support from Biogen & Genentech. Dr. Kalincik has received conference travel support and/or speaker honoraria from WebMD Global, Eisai, Novartis, Biogen, Roche, Sanofi Genzyme, Teva, BioCSL, and Merck, and has received research or educational event support from Biogen, Novartis, Genzyme, Roche, Celgene, and Merck.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Vegetarian diets can improve high-risk cardiovascular disease
, a meta-analysis of randomized controlled trials shows.

“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
, a meta-analysis of randomized controlled trials shows.
“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
, a meta-analysis of randomized controlled trials shows.
“To the best of our knowledge, this meta-analysis is the first that generates evidence from randomized controlled trials to assess the association of vegetarian diets with outcomes in people affected by cardiovascular diseases,” report the authors. The study was published online in JAMA Network Open.
“The greatest improvements in hemoglobin A1c and low-density lipoprotein cholesterol (LDL-C) were observed in individuals with type 2 diabetes and people at high risk of cardiovascular disease, highlighting the potential protective and synergistic effects of vegetarian diets for the primary prevention of cardiovascular disease,” they say.
Poor diet is well-established as increasing the morbidity and mortality associated with cardiovascular disease; however, although data has linked vegetarian diets to cardiovascular disease prevention in the general population, research on the effectiveness of such diets in people at high risk of cardiovascular disease is lacking.
“To the best of our knowledge, no meta-analysis of randomized controlled trials has been conducted to investigate the association of vegetarian diets with outcomes among people with CVD – indeed, research here has primarily focused on observational studies,” writes Tian Wang, RD, and colleagues at the University of Sydney.
Greater decreases in LDL-C, A1c, and body weight with vegetarian diets
For the meta-analysis, researchers identified 20 randomized controlled trials involving vegetarian diets that included 1,878 adults with or at a high risk of cardiovascular disease and included measurements of LDL-C, A1c, or systolic blood pressure.
The studies were conducted in the United States, Asia, Europe, and New Zealand between 1990 and 2021. Sample sizes ranged from 12 to 291 participants.
The mean range age of participants was 28-64 years. Studies included patients with cardiovascular disease (four studies), diabetes (seven studies), and those with at least two cardiovascular risk factors (nine studies).
The mean duration of the dietary intervention was 25.4 weeks (range 2-24 months). The most commonly prescribed diets were vegan (plant-based foods only), lacto-ovo-vegetarian (excluded meat, poultry, seafood, and dairy products, but allowed eggs), and lacto-vegetarian (same as previous but allowed dairy products).
Overall, those who consumed a vegetarian diet for an average of 6 months, versus comparison diets, had significantly greater decreases in LDL-C (6.6 mg/dL beyond the reduction achieved with standard therapy); A1c (0.24%); and body weight (3.4 kg), but the reduction in systolic blood pressure (0.1 mmHg) was not significantly greater.
Assessment of the overall certainty of evidence evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool showed a moderate level of evidence for reductions in LDL-C and A1c with the vegetarian diet.
Lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (14.1 mg/dL); however, four out of the five trials restricted energy intake.
Of note, vegetarian diets were most effective for achieving glycemic control among people with type 2 diabetes and leading to improvements in weight among those at high risk of cardiovascular disease as well as those with type 2 diabetes.
The effects “suggest that vegetarian diets might have a synergistic [or at least nonantagonistic] use in potentiating the effects of optimal drug therapy in the prevention and treatment of a range of cardiometabolic diseases,” the authors write.
Although previous studies have shown similar improvements associated with a vegetarian diet, most studies did not stratify populations based on disease status, type of vegetarian diet, or comparison diet, the authors note.
The lack of improvement in systolic blood pressure is consistent with previous meta-analyses of vegetarian diets in general and suggests that salt intake may be the more important factor for those measures.
“[The meta-analysis] suggests that diet quality plays a major role in lowering blood pressure independent of animal food consumption, as the DASH [Dietary Approaches to Stop Hypertension] ... trial demonstrated,” the authors note.
Decreases in medication dose with vegetarian diet
Although most patients were taking medications to manage hypertension, hyperglycemia, and/or dyslipidemia at trial enrollment in as many as eight of the studies, the vegetarian diet intervention resulted in a decrease in medication dose.
In fact, medication use could obscure the favorable effects of vegetarian diets, which could have a larger effect size, the authors speculate.
“This hypothesis is supported by two randomized controlled trials in our meta-analysis that required patients not to take medication that could influence cardiometabolic outcomes, [and] these studies significantly improved systolic blood pressure and LDL-C,” they write.
Not all vegetarian diets are healthy
Although there are numerous variations in vegetarian diets, ranging from vegan diets that eliminate all animal food to pesco-vegetarian diets that allow fish or seafood, most that are well-balanced can provide health benefits including lower saturated fat, L-carnitine, and choline (precursors of the atherogenic TMAO), and other benefits that might explain the improvements seen in the meta-analysis.
The diets may also be high in dietary fiber, mono- and polyunsaturated fatty acids, potassium, magnesium, and phytochemical, and have lower glycemic index scores.
Of note, 12 studies in the meta-analysis emphasized low-fat content, which the authors speculate may have contributed to the improvements observed in LDC-C.
Specifically, lacto-ovo vegetarian diets were associated with the greatest reduction in LDL-C (–14.1 mg/dL); however, four out of five of the trials restricted energy intake, which could have also played a role in improvements.
Importantly, not all vegetarian diets are healthy, and the authors caution about some that allow, for instance, deep-fried foods rich in trans-fatty acids and salt, such as tempura vegetables, potentially increasing the risk of type 2 diabetes and coronary heart disease.
They note that “more than one-third of the studies included in our meta-analysis did not emphasize the importance of consuming minimally processed plant-based whole foods.”
Overall, however, the fact that the greatest improvements in A1c and LDL-C were seen in patients with type 2 diabetes and those at high risk of CVD “highlight[s] the potential protective and synergistic effects of vegetarian diets for the primary prevention of CVD.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Partial immunization leaves children and communities at risk, study finds
TOPLINE
A new American Academy of Pediatrics study reveals that 17.2% of toddlers started but did not finish at least one recommended early childhood vaccine series.
METHODOLOGY
- Examined data collected in 2019 from the National Immunization Survey – Child.
- 16,365 children ages 19-35 months were included.
- Vaccines for diphtheria, tetanus, acellular pertussis, pneumococcal infections, Haemophilus influenzae type b, hepatitis B, polio, measles, mumps, rubella, and varicella were included.
TAKEAWAY
- 72.9% of toddlers completed the seven-vaccine series.
- 17.2% initiated but did not complete one or more of a multidose vaccine series.
- The strongest association with not completing the vaccine series was moving across state lines and not having insurance.
- Children with more siblings at home were less likely to complete a vaccine series.
IN PRACTICE
The study suggests that the “children experienced structural barriers to vaccination,” and the authors urge an “increased focus on strategies to encourage multidose series completion ... to optimize protection from preventable diseases and achieve vaccination coverage goals.”
SOURCE
The study was funded by the National Institutes of Health and published online July 25 in Pediatrics. Sarah Y. Michels, an epidemiology specialist from the University of Montana in Missoula, was the lead author.
LIMITATIONS
Though the researchers studied the risk factors for series noncompletion, they did not have information on the specific reasons why children were missing vaccine doses. Children whose parents chose to participate in the National Immunization Survey – Child may have had higher vaccination coverage than children whose parents declined participation.
DISCLOSURES
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE
A new American Academy of Pediatrics study reveals that 17.2% of toddlers started but did not finish at least one recommended early childhood vaccine series.
METHODOLOGY
- Examined data collected in 2019 from the National Immunization Survey – Child.
- 16,365 children ages 19-35 months were included.
- Vaccines for diphtheria, tetanus, acellular pertussis, pneumococcal infections, Haemophilus influenzae type b, hepatitis B, polio, measles, mumps, rubella, and varicella were included.
TAKEAWAY
- 72.9% of toddlers completed the seven-vaccine series.
- 17.2% initiated but did not complete one or more of a multidose vaccine series.
- The strongest association with not completing the vaccine series was moving across state lines and not having insurance.
- Children with more siblings at home were less likely to complete a vaccine series.
IN PRACTICE
The study suggests that the “children experienced structural barriers to vaccination,” and the authors urge an “increased focus on strategies to encourage multidose series completion ... to optimize protection from preventable diseases and achieve vaccination coverage goals.”
SOURCE
The study was funded by the National Institutes of Health and published online July 25 in Pediatrics. Sarah Y. Michels, an epidemiology specialist from the University of Montana in Missoula, was the lead author.
LIMITATIONS
Though the researchers studied the risk factors for series noncompletion, they did not have information on the specific reasons why children were missing vaccine doses. Children whose parents chose to participate in the National Immunization Survey – Child may have had higher vaccination coverage than children whose parents declined participation.
DISCLOSURES
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE
A new American Academy of Pediatrics study reveals that 17.2% of toddlers started but did not finish at least one recommended early childhood vaccine series.
METHODOLOGY
- Examined data collected in 2019 from the National Immunization Survey – Child.
- 16,365 children ages 19-35 months were included.
- Vaccines for diphtheria, tetanus, acellular pertussis, pneumococcal infections, Haemophilus influenzae type b, hepatitis B, polio, measles, mumps, rubella, and varicella were included.
TAKEAWAY
- 72.9% of toddlers completed the seven-vaccine series.
- 17.2% initiated but did not complete one or more of a multidose vaccine series.
- The strongest association with not completing the vaccine series was moving across state lines and not having insurance.
- Children with more siblings at home were less likely to complete a vaccine series.
IN PRACTICE
The study suggests that the “children experienced structural barriers to vaccination,” and the authors urge an “increased focus on strategies to encourage multidose series completion ... to optimize protection from preventable diseases and achieve vaccination coverage goals.”
SOURCE
The study was funded by the National Institutes of Health and published online July 25 in Pediatrics. Sarah Y. Michels, an epidemiology specialist from the University of Montana in Missoula, was the lead author.
LIMITATIONS
Though the researchers studied the risk factors for series noncompletion, they did not have information on the specific reasons why children were missing vaccine doses. Children whose parents chose to participate in the National Immunization Survey – Child may have had higher vaccination coverage than children whose parents declined participation.
DISCLOSURES
The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.