User login
How to get paid if your patient passes on
The death of a patient comes with many challenges for physicians, including a range of emotional and professional issues. Beyond those concerns,
“When a patient passes away, obviously there is, unfortunately, a lot of paperwork and stress for families, and it’s a very difficult situation,” says Shikha Jain, MD, an oncologist and associate professor of medicine at the University of Illinois at Chicago. “Talking about finances in that moment can be difficult and uncomfortable, and one thing I’d recommend is that the physicians themselves not get involved.”
Instead, Dr. Jain said, someone in the billing department in the practice or the hospital should take a lead on dealing with any outstanding debts.
“That doctor-patient relationship is a very precious relationship, so you don’t want to mix that financial aspect of providing care with the doctor-patient relationship,” Dr. Jain said. “That’s one thing that’s really important.”
The best approach in such situations is for practices to have a standing policy in place that dictates how to handle bills once a patient has died.
In most cases, the executor of the patient’s will must inform all creditors, including doctors, that the decedent has died, but sometimes there’s a delay.
Hoping the doctor’s office writes it off
“Even though the person in charge of the estate is supposed to contact the doctor’s office and let them know when a patient has passed, that doesn’t always happen,” says Hope Wen, head of billing at practice management platform Soundry Health. “It can be very challenging to track down that information, and sometimes they’re just crossing their fingers hoping that the doctor’s office will just write off the balance, which they often do.”
Some offices use a service that compares accounts receivable lists to Social Security death files and state records to identify deaths more quickly. Some physicians might also use a debt collection agency or an attorney who has experience collecting decedent debts and dealing with executors and probate courts.
Once the practice becomes aware that a patient has died, it can no longer send communications to the name and address on file, although it can continue to go through the billing process with the insurer for any bills incurred up to the date of the death.
At that point, the estate becomes responsible for the debt, and all communication must go to the executor of the estate (in some states, this might be called a personal representative). The office can reach out to any contacts on file to see if they are able to identify the executor.
“You want to do that in a compassionate way,” says Jack Brown III, JD, MBA, president of Gulf Coast Collection Bureau. “You’ll tell them you’re sorry for their loss, but you’re wondering who is responsible for the estate. Once you’ve identified that person and gotten their letter of administration from the probate court or a power of attorney, then you can speak with that person as if they were the patient.”
The names of executors are also public record and are available through the probate court (sometimes called the surrogate court) in the county where the decedent lived.
“Even if there’s no will or no executive named, the court will appoint an administrator for the estate, which is usually a family member,” said Robert Bernstein, an estate lawyer in Parsippany, N.J. “Their information will be on file in the court.”
Insurance coverage
Typically, insurance will pay for treatment (after deductibles and copays) up until the date of the patient’s death. But, of course, it can take months for some insurance companies to make their final payments, allowing physicians to know exactly how much they’re owed by that estate. In such cases, it’s important for physicians to know the rules in the decedent’s state for how long they have to file a claim.
Most states require that claims occur within 6-9 months of the person’s death. However, in some states, claimants can continue to file for much longer if the estate has not yet paid out all of its assets.
“Sometimes there is real estate to sell or a business to wind down, and it can take years for the estate to distribute all of the assets,” Mr. Bernstein says. “If it’s a year later and they still haven’t distributed the assets, the physician can still file the claim and should be paid.”
In some cases, especially if the decedent received compassionate, quality care, their family will want to make good on any outstanding debts to the health care providers who took care of their loved ones in their final days. In other cases, especially when a family member has had a long illness, their assets have been depleted over time or were transferred to other family members so that there is little left in the estate itself when the patient dies.
Regardless of other circumstances, the estate alone is responsible for such payments, and family members, including spouses and children, typically have no liability. (Though rarely enforced, some states do have filial responsibility laws that could hold children responsible for their parents’ debts, including unpaid medical bills. In addition, states with community property laws might require a surviving spouse to cover their partner’s debt, even after death.)
The probate process varies from state to state, but in general, the probate system and the executor will gather all existing assets and then notify all creditors about how to submit a claim. Typically, the claim will need to include information about how much is owed and documentation, such as bills and an explanation of benefits to back up the claim. It should be borne in mind that even those who’ve passed away have privacy protections under the Health Insurance Portability and Accountability Act, so practices must be careful as to how much information they’re sharing through their claim.
Once the estate has received all the claims, the executor will follow a priority of claims, starting with secured creditors. Typically, medical bills, especially those incurred in the last 90 days of the decedent’s life, have priority in the probate process, Mr. Brown says.
How to minimize losses
In that case, the practice would write off the unpaid debt as a business loss. If there are not enough assets in the estate to pay all claims, the executor will follow a state schedule that apportions those assets that are available.
There are some steps that practices can take to protect themselves from incurring such losses. For example, before beginning treatment, practices might consider asking patients to name a guarantor, who will essentially promise to cover any outstanding debts that the patient incurs.
To be binding, the office will need a signature from both the patient and the guarantor. Some offices may also keep a patient credit card number on file with written authorization that they can use to pay bills that are past due, although this payment method would no longer be valid after a patient dies.
While it’s important for all physicians to document and verify the financial information for their patients, oncologists often must consider an additional layer of fiduciary responsibility when it comes to their patients. Ms. Wen suggests that oncology offices check in with insurance companies to determine whether a patient has exhausted their benefits.
“That can happen with cancer patients, depending on how long they’ve been receiving treatment and what type of treatment they’ve been getting,” she said. “Some of the clinical trials, insurance will pay for them, but they’re really expensive and can get toward that max. So knowing where they are with their insurance coverage is big.”
When time is of the essence, some patients will choose to go forward with a treatment before receiving insurance approval. In those cases, the office must have an additional conversation in which the costs of the treatment are discussed. The office should obtain written confirmation of who will pay if the insurer does not, Ms. Wen said. While it’s the patient’s responsibility to keep track of their insurance benefits, oncology practices and hospitals must also exercise due diligence in monitoring the benefits that are available.
“That’s part of their contract with insurance companies if they’re in network, helping patients understand their benefits,” Ms. Wen saids.
It’s also important for practices to keep clear, consistent records to make it easier to identify outstanding bills and the correct contact information for them. If bills had gone unpaid prior to a patient’s death and the office started legal action and received a judgment, that claim would typically go ahead of other creditors’ claims.
Dr. Jain says that some practices might also consider keeping a financial adviser or social worker on staff who can assist patients and their families with understanding their out-of-pocket costs for treatment.
“Financial toxicity in oncology and medical care is a very real problem,” she says. “At the beginning of the relationship, I recommend that my patients get set up with a financial specialist that can help them navigate that aspect, not only when a patient passes away but during the process of receiving treatment, so they’re not shocked by the bills.”
A version of this article first appeared on Medscape.com.
The death of a patient comes with many challenges for physicians, including a range of emotional and professional issues. Beyond those concerns,
“When a patient passes away, obviously there is, unfortunately, a lot of paperwork and stress for families, and it’s a very difficult situation,” says Shikha Jain, MD, an oncologist and associate professor of medicine at the University of Illinois at Chicago. “Talking about finances in that moment can be difficult and uncomfortable, and one thing I’d recommend is that the physicians themselves not get involved.”
Instead, Dr. Jain said, someone in the billing department in the practice or the hospital should take a lead on dealing with any outstanding debts.
“That doctor-patient relationship is a very precious relationship, so you don’t want to mix that financial aspect of providing care with the doctor-patient relationship,” Dr. Jain said. “That’s one thing that’s really important.”
The best approach in such situations is for practices to have a standing policy in place that dictates how to handle bills once a patient has died.
In most cases, the executor of the patient’s will must inform all creditors, including doctors, that the decedent has died, but sometimes there’s a delay.
Hoping the doctor’s office writes it off
“Even though the person in charge of the estate is supposed to contact the doctor’s office and let them know when a patient has passed, that doesn’t always happen,” says Hope Wen, head of billing at practice management platform Soundry Health. “It can be very challenging to track down that information, and sometimes they’re just crossing their fingers hoping that the doctor’s office will just write off the balance, which they often do.”
Some offices use a service that compares accounts receivable lists to Social Security death files and state records to identify deaths more quickly. Some physicians might also use a debt collection agency or an attorney who has experience collecting decedent debts and dealing with executors and probate courts.
Once the practice becomes aware that a patient has died, it can no longer send communications to the name and address on file, although it can continue to go through the billing process with the insurer for any bills incurred up to the date of the death.
At that point, the estate becomes responsible for the debt, and all communication must go to the executor of the estate (in some states, this might be called a personal representative). The office can reach out to any contacts on file to see if they are able to identify the executor.
“You want to do that in a compassionate way,” says Jack Brown III, JD, MBA, president of Gulf Coast Collection Bureau. “You’ll tell them you’re sorry for their loss, but you’re wondering who is responsible for the estate. Once you’ve identified that person and gotten their letter of administration from the probate court or a power of attorney, then you can speak with that person as if they were the patient.”
The names of executors are also public record and are available through the probate court (sometimes called the surrogate court) in the county where the decedent lived.
“Even if there’s no will or no executive named, the court will appoint an administrator for the estate, which is usually a family member,” said Robert Bernstein, an estate lawyer in Parsippany, N.J. “Their information will be on file in the court.”
Insurance coverage
Typically, insurance will pay for treatment (after deductibles and copays) up until the date of the patient’s death. But, of course, it can take months for some insurance companies to make their final payments, allowing physicians to know exactly how much they’re owed by that estate. In such cases, it’s important for physicians to know the rules in the decedent’s state for how long they have to file a claim.
Most states require that claims occur within 6-9 months of the person’s death. However, in some states, claimants can continue to file for much longer if the estate has not yet paid out all of its assets.
“Sometimes there is real estate to sell or a business to wind down, and it can take years for the estate to distribute all of the assets,” Mr. Bernstein says. “If it’s a year later and they still haven’t distributed the assets, the physician can still file the claim and should be paid.”
In some cases, especially if the decedent received compassionate, quality care, their family will want to make good on any outstanding debts to the health care providers who took care of their loved ones in their final days. In other cases, especially when a family member has had a long illness, their assets have been depleted over time or were transferred to other family members so that there is little left in the estate itself when the patient dies.
Regardless of other circumstances, the estate alone is responsible for such payments, and family members, including spouses and children, typically have no liability. (Though rarely enforced, some states do have filial responsibility laws that could hold children responsible for their parents’ debts, including unpaid medical bills. In addition, states with community property laws might require a surviving spouse to cover their partner’s debt, even after death.)
The probate process varies from state to state, but in general, the probate system and the executor will gather all existing assets and then notify all creditors about how to submit a claim. Typically, the claim will need to include information about how much is owed and documentation, such as bills and an explanation of benefits to back up the claim. It should be borne in mind that even those who’ve passed away have privacy protections under the Health Insurance Portability and Accountability Act, so practices must be careful as to how much information they’re sharing through their claim.
Once the estate has received all the claims, the executor will follow a priority of claims, starting with secured creditors. Typically, medical bills, especially those incurred in the last 90 days of the decedent’s life, have priority in the probate process, Mr. Brown says.
How to minimize losses
In that case, the practice would write off the unpaid debt as a business loss. If there are not enough assets in the estate to pay all claims, the executor will follow a state schedule that apportions those assets that are available.
There are some steps that practices can take to protect themselves from incurring such losses. For example, before beginning treatment, practices might consider asking patients to name a guarantor, who will essentially promise to cover any outstanding debts that the patient incurs.
To be binding, the office will need a signature from both the patient and the guarantor. Some offices may also keep a patient credit card number on file with written authorization that they can use to pay bills that are past due, although this payment method would no longer be valid after a patient dies.
While it’s important for all physicians to document and verify the financial information for their patients, oncologists often must consider an additional layer of fiduciary responsibility when it comes to their patients. Ms. Wen suggests that oncology offices check in with insurance companies to determine whether a patient has exhausted their benefits.
“That can happen with cancer patients, depending on how long they’ve been receiving treatment and what type of treatment they’ve been getting,” she said. “Some of the clinical trials, insurance will pay for them, but they’re really expensive and can get toward that max. So knowing where they are with their insurance coverage is big.”
When time is of the essence, some patients will choose to go forward with a treatment before receiving insurance approval. In those cases, the office must have an additional conversation in which the costs of the treatment are discussed. The office should obtain written confirmation of who will pay if the insurer does not, Ms. Wen said. While it’s the patient’s responsibility to keep track of their insurance benefits, oncology practices and hospitals must also exercise due diligence in monitoring the benefits that are available.
“That’s part of their contract with insurance companies if they’re in network, helping patients understand their benefits,” Ms. Wen saids.
It’s also important for practices to keep clear, consistent records to make it easier to identify outstanding bills and the correct contact information for them. If bills had gone unpaid prior to a patient’s death and the office started legal action and received a judgment, that claim would typically go ahead of other creditors’ claims.
Dr. Jain says that some practices might also consider keeping a financial adviser or social worker on staff who can assist patients and their families with understanding their out-of-pocket costs for treatment.
“Financial toxicity in oncology and medical care is a very real problem,” she says. “At the beginning of the relationship, I recommend that my patients get set up with a financial specialist that can help them navigate that aspect, not only when a patient passes away but during the process of receiving treatment, so they’re not shocked by the bills.”
A version of this article first appeared on Medscape.com.
The death of a patient comes with many challenges for physicians, including a range of emotional and professional issues. Beyond those concerns,
“When a patient passes away, obviously there is, unfortunately, a lot of paperwork and stress for families, and it’s a very difficult situation,” says Shikha Jain, MD, an oncologist and associate professor of medicine at the University of Illinois at Chicago. “Talking about finances in that moment can be difficult and uncomfortable, and one thing I’d recommend is that the physicians themselves not get involved.”
Instead, Dr. Jain said, someone in the billing department in the practice or the hospital should take a lead on dealing with any outstanding debts.
“That doctor-patient relationship is a very precious relationship, so you don’t want to mix that financial aspect of providing care with the doctor-patient relationship,” Dr. Jain said. “That’s one thing that’s really important.”
The best approach in such situations is for practices to have a standing policy in place that dictates how to handle bills once a patient has died.
In most cases, the executor of the patient’s will must inform all creditors, including doctors, that the decedent has died, but sometimes there’s a delay.
Hoping the doctor’s office writes it off
“Even though the person in charge of the estate is supposed to contact the doctor’s office and let them know when a patient has passed, that doesn’t always happen,” says Hope Wen, head of billing at practice management platform Soundry Health. “It can be very challenging to track down that information, and sometimes they’re just crossing their fingers hoping that the doctor’s office will just write off the balance, which they often do.”
Some offices use a service that compares accounts receivable lists to Social Security death files and state records to identify deaths more quickly. Some physicians might also use a debt collection agency or an attorney who has experience collecting decedent debts and dealing with executors and probate courts.
Once the practice becomes aware that a patient has died, it can no longer send communications to the name and address on file, although it can continue to go through the billing process with the insurer for any bills incurred up to the date of the death.
At that point, the estate becomes responsible for the debt, and all communication must go to the executor of the estate (in some states, this might be called a personal representative). The office can reach out to any contacts on file to see if they are able to identify the executor.
“You want to do that in a compassionate way,” says Jack Brown III, JD, MBA, president of Gulf Coast Collection Bureau. “You’ll tell them you’re sorry for their loss, but you’re wondering who is responsible for the estate. Once you’ve identified that person and gotten their letter of administration from the probate court or a power of attorney, then you can speak with that person as if they were the patient.”
The names of executors are also public record and are available through the probate court (sometimes called the surrogate court) in the county where the decedent lived.
“Even if there’s no will or no executive named, the court will appoint an administrator for the estate, which is usually a family member,” said Robert Bernstein, an estate lawyer in Parsippany, N.J. “Their information will be on file in the court.”
Insurance coverage
Typically, insurance will pay for treatment (after deductibles and copays) up until the date of the patient’s death. But, of course, it can take months for some insurance companies to make their final payments, allowing physicians to know exactly how much they’re owed by that estate. In such cases, it’s important for physicians to know the rules in the decedent’s state for how long they have to file a claim.
Most states require that claims occur within 6-9 months of the person’s death. However, in some states, claimants can continue to file for much longer if the estate has not yet paid out all of its assets.
“Sometimes there is real estate to sell or a business to wind down, and it can take years for the estate to distribute all of the assets,” Mr. Bernstein says. “If it’s a year later and they still haven’t distributed the assets, the physician can still file the claim and should be paid.”
In some cases, especially if the decedent received compassionate, quality care, their family will want to make good on any outstanding debts to the health care providers who took care of their loved ones in their final days. In other cases, especially when a family member has had a long illness, their assets have been depleted over time or were transferred to other family members so that there is little left in the estate itself when the patient dies.
Regardless of other circumstances, the estate alone is responsible for such payments, and family members, including spouses and children, typically have no liability. (Though rarely enforced, some states do have filial responsibility laws that could hold children responsible for their parents’ debts, including unpaid medical bills. In addition, states with community property laws might require a surviving spouse to cover their partner’s debt, even after death.)
The probate process varies from state to state, but in general, the probate system and the executor will gather all existing assets and then notify all creditors about how to submit a claim. Typically, the claim will need to include information about how much is owed and documentation, such as bills and an explanation of benefits to back up the claim. It should be borne in mind that even those who’ve passed away have privacy protections under the Health Insurance Portability and Accountability Act, so practices must be careful as to how much information they’re sharing through their claim.
Once the estate has received all the claims, the executor will follow a priority of claims, starting with secured creditors. Typically, medical bills, especially those incurred in the last 90 days of the decedent’s life, have priority in the probate process, Mr. Brown says.
How to minimize losses
In that case, the practice would write off the unpaid debt as a business loss. If there are not enough assets in the estate to pay all claims, the executor will follow a state schedule that apportions those assets that are available.
There are some steps that practices can take to protect themselves from incurring such losses. For example, before beginning treatment, practices might consider asking patients to name a guarantor, who will essentially promise to cover any outstanding debts that the patient incurs.
To be binding, the office will need a signature from both the patient and the guarantor. Some offices may also keep a patient credit card number on file with written authorization that they can use to pay bills that are past due, although this payment method would no longer be valid after a patient dies.
While it’s important for all physicians to document and verify the financial information for their patients, oncologists often must consider an additional layer of fiduciary responsibility when it comes to their patients. Ms. Wen suggests that oncology offices check in with insurance companies to determine whether a patient has exhausted their benefits.
“That can happen with cancer patients, depending on how long they’ve been receiving treatment and what type of treatment they’ve been getting,” she said. “Some of the clinical trials, insurance will pay for them, but they’re really expensive and can get toward that max. So knowing where they are with their insurance coverage is big.”
When time is of the essence, some patients will choose to go forward with a treatment before receiving insurance approval. In those cases, the office must have an additional conversation in which the costs of the treatment are discussed. The office should obtain written confirmation of who will pay if the insurer does not, Ms. Wen said. While it’s the patient’s responsibility to keep track of their insurance benefits, oncology practices and hospitals must also exercise due diligence in monitoring the benefits that are available.
“That’s part of their contract with insurance companies if they’re in network, helping patients understand their benefits,” Ms. Wen saids.
It’s also important for practices to keep clear, consistent records to make it easier to identify outstanding bills and the correct contact information for them. If bills had gone unpaid prior to a patient’s death and the office started legal action and received a judgment, that claim would typically go ahead of other creditors’ claims.
Dr. Jain says that some practices might also consider keeping a financial adviser or social worker on staff who can assist patients and their families with understanding their out-of-pocket costs for treatment.
“Financial toxicity in oncology and medical care is a very real problem,” she says. “At the beginning of the relationship, I recommend that my patients get set up with a financial specialist that can help them navigate that aspect, not only when a patient passes away but during the process of receiving treatment, so they’re not shocked by the bills.”
A version of this article first appeared on Medscape.com.
People with long COVID have specific blood biomarkers, study says
The findings may be a step toward creating blood tests to positively identify people with long COVID so specialized treatments can be employed, researchers said.
“This is a decisive step forward in the development of valid and reliable blood testing protocols for long COVID,” said David Putrino, PhD., lead author and professor of rehabilitation and human performance and director of the Abilities Research Center at Icahn Mount Sinai Health System, New York.
Researchers from the Icahn School of Medicine at Mount Sinai and Yale School of Medicine looked at blood samples from about 270 people between January 2021 and June 2022. The people had never been infected with COVID, had fully recovered from an infection, or still showed symptoms at least four months after infection.
Using machine learning, the research teams were able to differentiate between people with and without long COVID with 96% accuracy based on distinctive features in the blood samples, according to a news release from Mount Sinai.
People with long COVID had abnormal T-cell activity and low levels of the hormone cortisol. Cortisol helps people feel alert and awake, which would explain why people with long COVID often report fatigue, NBC News said in a report on the study.
“It was one of the findings that most definitively separated the folks with long Covid from the people without long Covid,” Dr. Putrino told NBC News.
The study also found that long COVID appears to reactivate latent viruses including Epstein-Barr and mononucleosis, the study said.
The blood tests could allow doctors to come up with specialized treatments in people who report a wide variety of long COVID symptoms, Dr. Putrino said.
“There is no ‘silver bullet’ for treating long COVID, because it is an illness that infiltrates complex systems such as the immune and hormonal regulation,” he said.
The Centers for Disease Control and Prevention says about one in five Americans who had COVID still have long COVID. Symptoms include fatigue, brain fog, dizziness, digestive problems, and loss of smell and taste.
A version of this article appeared on WebMD.com.
The findings may be a step toward creating blood tests to positively identify people with long COVID so specialized treatments can be employed, researchers said.
“This is a decisive step forward in the development of valid and reliable blood testing protocols for long COVID,” said David Putrino, PhD., lead author and professor of rehabilitation and human performance and director of the Abilities Research Center at Icahn Mount Sinai Health System, New York.
Researchers from the Icahn School of Medicine at Mount Sinai and Yale School of Medicine looked at blood samples from about 270 people between January 2021 and June 2022. The people had never been infected with COVID, had fully recovered from an infection, or still showed symptoms at least four months after infection.
Using machine learning, the research teams were able to differentiate between people with and without long COVID with 96% accuracy based on distinctive features in the blood samples, according to a news release from Mount Sinai.
People with long COVID had abnormal T-cell activity and low levels of the hormone cortisol. Cortisol helps people feel alert and awake, which would explain why people with long COVID often report fatigue, NBC News said in a report on the study.
“It was one of the findings that most definitively separated the folks with long Covid from the people without long Covid,” Dr. Putrino told NBC News.
The study also found that long COVID appears to reactivate latent viruses including Epstein-Barr and mononucleosis, the study said.
The blood tests could allow doctors to come up with specialized treatments in people who report a wide variety of long COVID symptoms, Dr. Putrino said.
“There is no ‘silver bullet’ for treating long COVID, because it is an illness that infiltrates complex systems such as the immune and hormonal regulation,” he said.
The Centers for Disease Control and Prevention says about one in five Americans who had COVID still have long COVID. Symptoms include fatigue, brain fog, dizziness, digestive problems, and loss of smell and taste.
A version of this article appeared on WebMD.com.
The findings may be a step toward creating blood tests to positively identify people with long COVID so specialized treatments can be employed, researchers said.
“This is a decisive step forward in the development of valid and reliable blood testing protocols for long COVID,” said David Putrino, PhD., lead author and professor of rehabilitation and human performance and director of the Abilities Research Center at Icahn Mount Sinai Health System, New York.
Researchers from the Icahn School of Medicine at Mount Sinai and Yale School of Medicine looked at blood samples from about 270 people between January 2021 and June 2022. The people had never been infected with COVID, had fully recovered from an infection, or still showed symptoms at least four months after infection.
Using machine learning, the research teams were able to differentiate between people with and without long COVID with 96% accuracy based on distinctive features in the blood samples, according to a news release from Mount Sinai.
People with long COVID had abnormal T-cell activity and low levels of the hormone cortisol. Cortisol helps people feel alert and awake, which would explain why people with long COVID often report fatigue, NBC News said in a report on the study.
“It was one of the findings that most definitively separated the folks with long Covid from the people without long Covid,” Dr. Putrino told NBC News.
The study also found that long COVID appears to reactivate latent viruses including Epstein-Barr and mononucleosis, the study said.
The blood tests could allow doctors to come up with specialized treatments in people who report a wide variety of long COVID symptoms, Dr. Putrino said.
“There is no ‘silver bullet’ for treating long COVID, because it is an illness that infiltrates complex systems such as the immune and hormonal regulation,” he said.
The Centers for Disease Control and Prevention says about one in five Americans who had COVID still have long COVID. Symptoms include fatigue, brain fog, dizziness, digestive problems, and loss of smell and taste.
A version of this article appeared on WebMD.com.
Hypotrichosis and Hair Loss on the Occipital Scalp
The Diagnosis: Monilethrix
A diagnosis of monilethrix was rendered based on the clinical and trichoscopic findings. Simple surveillance of the patient’s condition and prevention of further hair trauma were proposed as management options.
Monilethrix is a hair shaft disorder that is inherited in a predominantly autosomal-dominant pattern with variable expressiveness and penetrance resulting from heterozygous mutations in hair keratin genes KRT81, KRT83, and KRT86 in a region of chromosome 12q13.13.1,2 An autosomalrecessive form has been described with mutation in desmoglein 4, but it differs from the classical form by the variable periodicity of the region between the nodules.3,4
The morphologic alteration consists of the formation of fusiform nodules of normal structure alternated with narrow and dystrophic constrictions (Figure). These internodes are fragile areas that cause breakage at constricted points.5 Clinically, monilethrix presents as areas of focal or diffuse alopecia with frequent involvement of the terminal follicles, mainly in areas of friction. The hair is normal at birth due to the predominance of lanugo in the neonatal period, but it subsequently is replaced by abnormal hairs in the first months of life.6 Initial clinical signs begin to appear when the terminal hairs begin to form.7 Although rarer, the eyebrows and eyelashes, as well as the axillary, pubic, and body hair, may be involved.5
.")
Other hair shaft anomalies merit consideration in the differential diagnosis of monilethrix, including pseudomonilethrix, pressure alopecia, trichorrhexis invaginata, ectodermal dysplasia, tinea capitis, and trichothiodystrophy.6 The diagnosis is reached by clinical history and physical examination. Trichoscopy and light microscopy are used to confirm the diagnosis. Trichoscopic examination shows markedly higher rates of anagen hair. The shafts examined in our patient revealed 0.7- to 1-mm intervals between nodes. Hair can be better visualized under a polarized microscope, and the condition can be distinguished from pseudomonilethrix using this approach.5,6 In our patient, the diagnosis was made based on light microscopy and trichoscopic findings with no genetic testing; however, genetic testing for the classic mutations of the keratin genes would be desirable to confirm the diagnosis but was not done in our patient.6 The prognosis of monilethrix is variable; most cases persist into adulthood, though spontaneous improvement may occur with advancing age, during summer, and during pregnancy.8
There is no definitive therapy for monilethrix. Although there have been reports of cases treated with systemic corticosteroids, oral retinoids, topical minoxidil, vitamins, and peeling ointments (desquamative oil), the cornerstone of management is protecting the hair against traumatic procedures such as excessive combing, brushing, and friction, as well as parent and patient education about the benign nature of the condition.9 Additionally, some cases have shown improvement with minoxidil solution at 2% and 5% concentrations, oral minoxidil, or acitretin.7-9
- Fontenelle de Oliveira E, Cotta de Alencar Araripe AL. Monilethrix: a typical case report with microscopic and dermatoscopic findings. An Bras Dermatol. 2015;90:126-127.
- de Cruz R, Horev L, Green J, et al. A novel monilethrix mutation in coil 2A of KRT86 causing autosomal dominant monilethrix with incomplete penetrance. Br J Dermatol. 2012;166(suppl 2):20-26.
- Baltazard T, Dhaille F, Chaby G, et al. Value of dermoscopy for the diagnosis of monilethrix. Dermatol Online J. 2017;23:13030 /qt9hf1p3xm.
- Kato M, Shimizu A, Yokoyama Y, et al. An autosomal recessive mutation of DSG4 causes monilethrix through the ER stress response. J Invest Dermatol. 2015;135:1253-1260.
- Gummer CL, Dawber RP, Swift JA. Monilethrix: an electron microscopic and electron histochemical study. Br J Dermatol. 1981;105:529-541.
- Sharma VK, Chiramel MJ, Rao A. Dermoscopy: a rapid bedside tool to assess monilethrix. Indian J Dermatol Venereol Leprol. 2016;82:73-74.
- Sinclair R. Treatment of monilethrix with oral minoxidil. JAAD Case Rep. 2016;2:212-215.
- Rakowska A, Slowinska M, Czuwara J, et al. Dermoscopy as a tool for rapid diagnosis of monilethrix. J Drugs Dermatol. 2007;6:222-224.
- Karincaoglu Y, Coskun BK, Seyhan ME, et al. Monilethrix. Am J Clin Dermatol. 2005;6:407-410.
The Diagnosis: Monilethrix
A diagnosis of monilethrix was rendered based on the clinical and trichoscopic findings. Simple surveillance of the patient’s condition and prevention of further hair trauma were proposed as management options.
Monilethrix is a hair shaft disorder that is inherited in a predominantly autosomal-dominant pattern with variable expressiveness and penetrance resulting from heterozygous mutations in hair keratin genes KRT81, KRT83, and KRT86 in a region of chromosome 12q13.13.1,2 An autosomalrecessive form has been described with mutation in desmoglein 4, but it differs from the classical form by the variable periodicity of the region between the nodules.3,4
The morphologic alteration consists of the formation of fusiform nodules of normal structure alternated with narrow and dystrophic constrictions (Figure). These internodes are fragile areas that cause breakage at constricted points.5 Clinically, monilethrix presents as areas of focal or diffuse alopecia with frequent involvement of the terminal follicles, mainly in areas of friction. The hair is normal at birth due to the predominance of lanugo in the neonatal period, but it subsequently is replaced by abnormal hairs in the first months of life.6 Initial clinical signs begin to appear when the terminal hairs begin to form.7 Although rarer, the eyebrows and eyelashes, as well as the axillary, pubic, and body hair, may be involved.5
Other hair shaft anomalies merit consideration in the differential diagnosis of monilethrix, including pseudomonilethrix, pressure alopecia, trichorrhexis invaginata, ectodermal dysplasia, tinea capitis, and trichothiodystrophy.6 The diagnosis is reached by clinical history and physical examination. Trichoscopy and light microscopy are used to confirm the diagnosis. Trichoscopic examination shows markedly higher rates of anagen hair. The shafts examined in our patient revealed 0.7- to 1-mm intervals between nodes. Hair can be better visualized under a polarized microscope, and the condition can be distinguished from pseudomonilethrix using this approach.5,6 In our patient, the diagnosis was made based on light microscopy and trichoscopic findings with no genetic testing; however, genetic testing for the classic mutations of the keratin genes would be desirable to confirm the diagnosis but was not done in our patient.6 The prognosis of monilethrix is variable; most cases persist into adulthood, though spontaneous improvement may occur with advancing age, during summer, and during pregnancy.8
There is no definitive therapy for monilethrix. Although there have been reports of cases treated with systemic corticosteroids, oral retinoids, topical minoxidil, vitamins, and peeling ointments (desquamative oil), the cornerstone of management is protecting the hair against traumatic procedures such as excessive combing, brushing, and friction, as well as parent and patient education about the benign nature of the condition.9 Additionally, some cases have shown improvement with minoxidil solution at 2% and 5% concentrations, oral minoxidil, or acitretin.7-9
The Diagnosis: Monilethrix
A diagnosis of monilethrix was rendered based on the clinical and trichoscopic findings. Simple surveillance of the patient’s condition and prevention of further hair trauma were proposed as management options.
Monilethrix is a hair shaft disorder that is inherited in a predominantly autosomal-dominant pattern with variable expressiveness and penetrance resulting from heterozygous mutations in hair keratin genes KRT81, KRT83, and KRT86 in a region of chromosome 12q13.13.1,2 An autosomalrecessive form has been described with mutation in desmoglein 4, but it differs from the classical form by the variable periodicity of the region between the nodules.3,4
The morphologic alteration consists of the formation of fusiform nodules of normal structure alternated with narrow and dystrophic constrictions (Figure). These internodes are fragile areas that cause breakage at constricted points.5 Clinically, monilethrix presents as areas of focal or diffuse alopecia with frequent involvement of the terminal follicles, mainly in areas of friction. The hair is normal at birth due to the predominance of lanugo in the neonatal period, but it subsequently is replaced by abnormal hairs in the first months of life.6 Initial clinical signs begin to appear when the terminal hairs begin to form.7 Although rarer, the eyebrows and eyelashes, as well as the axillary, pubic, and body hair, may be involved.5
Other hair shaft anomalies merit consideration in the differential diagnosis of monilethrix, including pseudomonilethrix, pressure alopecia, trichorrhexis invaginata, ectodermal dysplasia, tinea capitis, and trichothiodystrophy.6 The diagnosis is reached by clinical history and physical examination. Trichoscopy and light microscopy are used to confirm the diagnosis. Trichoscopic examination shows markedly higher rates of anagen hair. The shafts examined in our patient revealed 0.7- to 1-mm intervals between nodes. Hair can be better visualized under a polarized microscope, and the condition can be distinguished from pseudomonilethrix using this approach.5,6 In our patient, the diagnosis was made based on light microscopy and trichoscopic findings with no genetic testing; however, genetic testing for the classic mutations of the keratin genes would be desirable to confirm the diagnosis but was not done in our patient.6 The prognosis of monilethrix is variable; most cases persist into adulthood, though spontaneous improvement may occur with advancing age, during summer, and during pregnancy.8
There is no definitive therapy for monilethrix. Although there have been reports of cases treated with systemic corticosteroids, oral retinoids, topical minoxidil, vitamins, and peeling ointments (desquamative oil), the cornerstone of management is protecting the hair against traumatic procedures such as excessive combing, brushing, and friction, as well as parent and patient education about the benign nature of the condition.9 Additionally, some cases have shown improvement with minoxidil solution at 2% and 5% concentrations, oral minoxidil, or acitretin.7-9
- Fontenelle de Oliveira E, Cotta de Alencar Araripe AL. Monilethrix: a typical case report with microscopic and dermatoscopic findings. An Bras Dermatol. 2015;90:126-127.
- de Cruz R, Horev L, Green J, et al. A novel monilethrix mutation in coil 2A of KRT86 causing autosomal dominant monilethrix with incomplete penetrance. Br J Dermatol. 2012;166(suppl 2):20-26.
- Baltazard T, Dhaille F, Chaby G, et al. Value of dermoscopy for the diagnosis of monilethrix. Dermatol Online J. 2017;23:13030 /qt9hf1p3xm.
- Kato M, Shimizu A, Yokoyama Y, et al. An autosomal recessive mutation of DSG4 causes monilethrix through the ER stress response. J Invest Dermatol. 2015;135:1253-1260.
- Gummer CL, Dawber RP, Swift JA. Monilethrix: an electron microscopic and electron histochemical study. Br J Dermatol. 1981;105:529-541.
- Sharma VK, Chiramel MJ, Rao A. Dermoscopy: a rapid bedside tool to assess monilethrix. Indian J Dermatol Venereol Leprol. 2016;82:73-74.
- Sinclair R. Treatment of monilethrix with oral minoxidil. JAAD Case Rep. 2016;2:212-215.
- Rakowska A, Slowinska M, Czuwara J, et al. Dermoscopy as a tool for rapid diagnosis of monilethrix. J Drugs Dermatol. 2007;6:222-224.
- Karincaoglu Y, Coskun BK, Seyhan ME, et al. Monilethrix. Am J Clin Dermatol. 2005;6:407-410.
- Fontenelle de Oliveira E, Cotta de Alencar Araripe AL. Monilethrix: a typical case report with microscopic and dermatoscopic findings. An Bras Dermatol. 2015;90:126-127.
- de Cruz R, Horev L, Green J, et al. A novel monilethrix mutation in coil 2A of KRT86 causing autosomal dominant monilethrix with incomplete penetrance. Br J Dermatol. 2012;166(suppl 2):20-26.
- Baltazard T, Dhaille F, Chaby G, et al. Value of dermoscopy for the diagnosis of monilethrix. Dermatol Online J. 2017;23:13030 /qt9hf1p3xm.
- Kato M, Shimizu A, Yokoyama Y, et al. An autosomal recessive mutation of DSG4 causes monilethrix through the ER stress response. J Invest Dermatol. 2015;135:1253-1260.
- Gummer CL, Dawber RP, Swift JA. Monilethrix: an electron microscopic and electron histochemical study. Br J Dermatol. 1981;105:529-541.
- Sharma VK, Chiramel MJ, Rao A. Dermoscopy: a rapid bedside tool to assess monilethrix. Indian J Dermatol Venereol Leprol. 2016;82:73-74.
- Sinclair R. Treatment of monilethrix with oral minoxidil. JAAD Case Rep. 2016;2:212-215.
- Rakowska A, Slowinska M, Czuwara J, et al. Dermoscopy as a tool for rapid diagnosis of monilethrix. J Drugs Dermatol. 2007;6:222-224.
- Karincaoglu Y, Coskun BK, Seyhan ME, et al. Monilethrix. Am J Clin Dermatol. 2005;6:407-410.
A 6-month-old infant girl was referred to the dermatology service with hypotrichosis and hair loss on the occipital region of the scalp of 4 months’ duration (top). The patient was born at full term by cesarean delivery without complications. There were no comorbidities or family history of alopecia. Clinical examination revealed an alopecic plaque in the occipital region with broken hairs and some dystrophic hairs associated with follicular papules and perifollicular hyperkeratosis. A hair pull test was positive for telogen hairs. Trichoscopy revealed black dots and broken hairs resembling Morse code (bottom). Hair microscopy showed regular alternation of constriction zones separated by intervals of normal thickness.


Endoscopic monitoring may not be needed for nonerosive GERD
Patients with confirmed nonerosive gastroesophageal reflux disease (GERD) are not at greater risk for esophageal cancer compared with the general population and are unlikely to need additional endoscopic monitoring for cancer, new research suggests.
By contrast, patients with erosive disease had more than double the incidence of esophageal cancer.
“We expected a less-strong association with cancer among patients with nonerosive GERD compared to those with erosive GERD, [and] the results do make sense in view of the fact that the nonerosive GERD patients had normal esophageal mucosa at endoscopy,” Jesper Lagergren, MD, PhD, of Karolinska Institutet, Stockholm, told this news organization.
The findings “suggest that in patients with GERD, a normal endoscopy indicates that the risk of cancer development in the esophagus is low,” he said. “If future research confirms our results, no monitoring would be needed for patients with known nonerosive GERD.”
However, a related editorial suggests there may be other reasons to endoscopically monitor patients with nonerosive GERD.
The study was published online in the BMJ, as was the editorial.
Erosive GERD raises risk
To assess the incidence rate of esophageal cancer among patients with nonerosive GERD compared with the general population, the investigators analyzed records from 486,556 patients in hospital and specialized outpatient centers in Denmark, Finland, and Sweden who underwent endoscopy from 1987 to 2019.
A total of 285,811 patients were included in the nonerosive GERD cohort, and 200,745 were included in a validation cohort of patients with erosive GERD.
Nonerosive GERD was defined by the absence of esophagitis and any other esophageal disorder at endoscopy. Erosive GERD was defined by esophagitis at endoscopy.
The incidence rate of esophageal cancer was assessed for up to 31 years of follow-up, with the median being 6.3 years.
In the nonerosive GERD cohort, 228 patients developed esophageal cancer during nearly 2.1 million person-years of follow-up. The incidence rate was 11 per 100,000 person-years, similar to that of the general population (standardized incidence ratio, 1.04) and did not increase with longer follow-up.
In the erosive GERD cohort, 542 patients developed esophageal cancer over almost 1.8 million person-years. This corresponded to an incidence rate of 31 per 100,000 person-years, or an increased overall standardized incidence ratio of 2.36, which became more pronounced with longer follow-up.
“This finding suggests that endoscopically confirmed non-erosive [GERD] does not require additional endoscopic monitoring for esophageal adenocarcinoma,” the authors concluded.
‘Dynamic’ progression
In a related editorial, Jerry Zhou, PhD, and Vincent Ho, MD, both of Western Sydney University, Penrith, New South Wales, Australia, wrote that the finding that patients with nonerosive disease do not have to undergo additional endoscopic evaluations for cancer is in line with previous research.
However, they added, “the more pressing rationale for reevaluating these patients would be the potential for progression to conditions such as erosive reflux disease or Barrett’s esophagus.” Longitudinal studies have shown that GERD progression is dynamic, and so the development of erosive disease after nonerosive disease is feasible.
“Widespread use of proton-pump inhibitors complicates our understanding” of GERD progression, they noted. Although study participants were advised not to take antireflux medications in the weeks prior to their endoscopy, “uncertainties about previous treatments remain due to the study’s design.” Some participants without erosive disease at baseline may have had it in the past.
Dr. Zhou and Dr. Ho also postulated that rather than being a progressive disease, nonerosive and erosive GERD might be two distinct conditions with different features and underpinnings.
Although valuable, the study “prompts reflection on the limitations of relying on the absence of esophageal erosions as the sole diagnostic criterion for non-erosive disease. The changing progression of gastroesophageal reflux disease, the complex influence of proton pump inhibitors, and the potential for a range of underlying pathophysiological causes requires a more comprehensive diagnostic perspective,” they concluded.
Dr. Lagergren said that his group plans to assess whether treatment of nonerosive GERD should be different from erosive GERD.
The study was funded by the Swedish Research Council, Swedish Cancer Society, and Nordic Cancer Union. No competing interests were declared.
A version of this article appeared on Medscape.com.
Patients with confirmed nonerosive gastroesophageal reflux disease (GERD) are not at greater risk for esophageal cancer compared with the general population and are unlikely to need additional endoscopic monitoring for cancer, new research suggests.
By contrast, patients with erosive disease had more than double the incidence of esophageal cancer.
“We expected a less-strong association with cancer among patients with nonerosive GERD compared to those with erosive GERD, [and] the results do make sense in view of the fact that the nonerosive GERD patients had normal esophageal mucosa at endoscopy,” Jesper Lagergren, MD, PhD, of Karolinska Institutet, Stockholm, told this news organization.
The findings “suggest that in patients with GERD, a normal endoscopy indicates that the risk of cancer development in the esophagus is low,” he said. “If future research confirms our results, no monitoring would be needed for patients with known nonerosive GERD.”
However, a related editorial suggests there may be other reasons to endoscopically monitor patients with nonerosive GERD.
The study was published online in the BMJ, as was the editorial.
Erosive GERD raises risk
To assess the incidence rate of esophageal cancer among patients with nonerosive GERD compared with the general population, the investigators analyzed records from 486,556 patients in hospital and specialized outpatient centers in Denmark, Finland, and Sweden who underwent endoscopy from 1987 to 2019.
A total of 285,811 patients were included in the nonerosive GERD cohort, and 200,745 were included in a validation cohort of patients with erosive GERD.
Nonerosive GERD was defined by the absence of esophagitis and any other esophageal disorder at endoscopy. Erosive GERD was defined by esophagitis at endoscopy.
The incidence rate of esophageal cancer was assessed for up to 31 years of follow-up, with the median being 6.3 years.
In the nonerosive GERD cohort, 228 patients developed esophageal cancer during nearly 2.1 million person-years of follow-up. The incidence rate was 11 per 100,000 person-years, similar to that of the general population (standardized incidence ratio, 1.04) and did not increase with longer follow-up.
In the erosive GERD cohort, 542 patients developed esophageal cancer over almost 1.8 million person-years. This corresponded to an incidence rate of 31 per 100,000 person-years, or an increased overall standardized incidence ratio of 2.36, which became more pronounced with longer follow-up.
“This finding suggests that endoscopically confirmed non-erosive [GERD] does not require additional endoscopic monitoring for esophageal adenocarcinoma,” the authors concluded.
‘Dynamic’ progression
In a related editorial, Jerry Zhou, PhD, and Vincent Ho, MD, both of Western Sydney University, Penrith, New South Wales, Australia, wrote that the finding that patients with nonerosive disease do not have to undergo additional endoscopic evaluations for cancer is in line with previous research.
However, they added, “the more pressing rationale for reevaluating these patients would be the potential for progression to conditions such as erosive reflux disease or Barrett’s esophagus.” Longitudinal studies have shown that GERD progression is dynamic, and so the development of erosive disease after nonerosive disease is feasible.
“Widespread use of proton-pump inhibitors complicates our understanding” of GERD progression, they noted. Although study participants were advised not to take antireflux medications in the weeks prior to their endoscopy, “uncertainties about previous treatments remain due to the study’s design.” Some participants without erosive disease at baseline may have had it in the past.
Dr. Zhou and Dr. Ho also postulated that rather than being a progressive disease, nonerosive and erosive GERD might be two distinct conditions with different features and underpinnings.
Although valuable, the study “prompts reflection on the limitations of relying on the absence of esophageal erosions as the sole diagnostic criterion for non-erosive disease. The changing progression of gastroesophageal reflux disease, the complex influence of proton pump inhibitors, and the potential for a range of underlying pathophysiological causes requires a more comprehensive diagnostic perspective,” they concluded.
Dr. Lagergren said that his group plans to assess whether treatment of nonerosive GERD should be different from erosive GERD.
The study was funded by the Swedish Research Council, Swedish Cancer Society, and Nordic Cancer Union. No competing interests were declared.
A version of this article appeared on Medscape.com.
Patients with confirmed nonerosive gastroesophageal reflux disease (GERD) are not at greater risk for esophageal cancer compared with the general population and are unlikely to need additional endoscopic monitoring for cancer, new research suggests.
By contrast, patients with erosive disease had more than double the incidence of esophageal cancer.
“We expected a less-strong association with cancer among patients with nonerosive GERD compared to those with erosive GERD, [and] the results do make sense in view of the fact that the nonerosive GERD patients had normal esophageal mucosa at endoscopy,” Jesper Lagergren, MD, PhD, of Karolinska Institutet, Stockholm, told this news organization.
The findings “suggest that in patients with GERD, a normal endoscopy indicates that the risk of cancer development in the esophagus is low,” he said. “If future research confirms our results, no monitoring would be needed for patients with known nonerosive GERD.”
However, a related editorial suggests there may be other reasons to endoscopically monitor patients with nonerosive GERD.
The study was published online in the BMJ, as was the editorial.
Erosive GERD raises risk
To assess the incidence rate of esophageal cancer among patients with nonerosive GERD compared with the general population, the investigators analyzed records from 486,556 patients in hospital and specialized outpatient centers in Denmark, Finland, and Sweden who underwent endoscopy from 1987 to 2019.
A total of 285,811 patients were included in the nonerosive GERD cohort, and 200,745 were included in a validation cohort of patients with erosive GERD.
Nonerosive GERD was defined by the absence of esophagitis and any other esophageal disorder at endoscopy. Erosive GERD was defined by esophagitis at endoscopy.
The incidence rate of esophageal cancer was assessed for up to 31 years of follow-up, with the median being 6.3 years.
In the nonerosive GERD cohort, 228 patients developed esophageal cancer during nearly 2.1 million person-years of follow-up. The incidence rate was 11 per 100,000 person-years, similar to that of the general population (standardized incidence ratio, 1.04) and did not increase with longer follow-up.
In the erosive GERD cohort, 542 patients developed esophageal cancer over almost 1.8 million person-years. This corresponded to an incidence rate of 31 per 100,000 person-years, or an increased overall standardized incidence ratio of 2.36, which became more pronounced with longer follow-up.
“This finding suggests that endoscopically confirmed non-erosive [GERD] does not require additional endoscopic monitoring for esophageal adenocarcinoma,” the authors concluded.
‘Dynamic’ progression
In a related editorial, Jerry Zhou, PhD, and Vincent Ho, MD, both of Western Sydney University, Penrith, New South Wales, Australia, wrote that the finding that patients with nonerosive disease do not have to undergo additional endoscopic evaluations for cancer is in line with previous research.
However, they added, “the more pressing rationale for reevaluating these patients would be the potential for progression to conditions such as erosive reflux disease or Barrett’s esophagus.” Longitudinal studies have shown that GERD progression is dynamic, and so the development of erosive disease after nonerosive disease is feasible.
“Widespread use of proton-pump inhibitors complicates our understanding” of GERD progression, they noted. Although study participants were advised not to take antireflux medications in the weeks prior to their endoscopy, “uncertainties about previous treatments remain due to the study’s design.” Some participants without erosive disease at baseline may have had it in the past.
Dr. Zhou and Dr. Ho also postulated that rather than being a progressive disease, nonerosive and erosive GERD might be two distinct conditions with different features and underpinnings.
Although valuable, the study “prompts reflection on the limitations of relying on the absence of esophageal erosions as the sole diagnostic criterion for non-erosive disease. The changing progression of gastroesophageal reflux disease, the complex influence of proton pump inhibitors, and the potential for a range of underlying pathophysiological causes requires a more comprehensive diagnostic perspective,” they concluded.
Dr. Lagergren said that his group plans to assess whether treatment of nonerosive GERD should be different from erosive GERD.
The study was funded by the Swedish Research Council, Swedish Cancer Society, and Nordic Cancer Union. No competing interests were declared.
A version of this article appeared on Medscape.com.
No need to restrict hep C DAA therapy based on alcohol use
TOPLINE:
Alcohol use at any level, including alcohol use disorder (AUD), is not associated with decreased odds of a sustained virologic response (SVR) to direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection. Therefore, DAA therapy should not be withheld from patients who consume alcohol.
METHODOLOGY:
- The researchers examined electronic health records for 69,229 patients (mean age, 63 years; 97% men; 50% non-Hispanic White) who started DAA therapy through the Department of Veterans Affairs between 2014 and 2018.
- Alcohol use categories were abstinent without history of AUD, abstinent with history of AUD, lower-risk consumption, moderate-risk consumption, and high-risk consumption or AUD.
- The primary outcome was SVR, which was defined as undetectable HCV RNA for 12 weeks to 6 months after completion of DAA treatment.
TAKEAWAY:
- Close to half (46.6%) of patients were abstinent without AUD, 13.3% were abstinent with AUD, 19.4% had lower-risk consumption, 4.5% had moderate-risk consumption, and 16.2% had high-risk consumption or AUD.
- Overall, 94.4% of those who started on DAA treatment achieved SVR.
- After adjustment, there was no evidence that any alcohol category was significantly associated with decreased odds of achieving SVR. The odds ratios were 1.09 for abstinent without AUD history, 0.92 for abstinent with AUD history, 0.96 for moderate-risk consumption, and 0.95 for high-risk consumption or AUD.
- SVR did not differ by baseline stage of hepatic fibrosis, as measured by Fibrosis-4 score of 3.25 or less versus greater than 3.25.
IN PRACTICE:
“Achieving SVR has been shown to be associated with reduced risk of post-SVR outcomes, including hepatocellular carcinoma, liver-related mortality, and all-cause mortality. Our findings suggest that DAA therapy should be provided and reimbursed despite alcohol consumption or history of AUD. Restricting access to DAA therapy according to alcohol consumption or AUD creates an unnecessary barrier to patients accessing DAA therapy and challenges HCV elimination goals,” the investigators wrote.
SOURCE:
Emily J. Cartwright, MD, of Emory University, Atlanta, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
The study was observational and subject to potential residual confounding. To define SVR, HCV RNA was measured 6 months after DAA treatment ended, which may have resulted in a misclassification of patients who experienced viral relapse. Most participants were men born between 1945 and 1965, and the results may not be generalizable to women and/or older and younger patients.
DISCLOSURES:
The study was supported by grants from the National Institute on Alcohol Abuse and Alcoholism. Dr. Cartwright reported no disclosures. Two coauthors disclosed fees from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
TOPLINE:
Alcohol use at any level, including alcohol use disorder (AUD), is not associated with decreased odds of a sustained virologic response (SVR) to direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection. Therefore, DAA therapy should not be withheld from patients who consume alcohol.
METHODOLOGY:
- The researchers examined electronic health records for 69,229 patients (mean age, 63 years; 97% men; 50% non-Hispanic White) who started DAA therapy through the Department of Veterans Affairs between 2014 and 2018.
- Alcohol use categories were abstinent without history of AUD, abstinent with history of AUD, lower-risk consumption, moderate-risk consumption, and high-risk consumption or AUD.
- The primary outcome was SVR, which was defined as undetectable HCV RNA for 12 weeks to 6 months after completion of DAA treatment.
TAKEAWAY:
- Close to half (46.6%) of patients were abstinent without AUD, 13.3% were abstinent with AUD, 19.4% had lower-risk consumption, 4.5% had moderate-risk consumption, and 16.2% had high-risk consumption or AUD.
- Overall, 94.4% of those who started on DAA treatment achieved SVR.
- After adjustment, there was no evidence that any alcohol category was significantly associated with decreased odds of achieving SVR. The odds ratios were 1.09 for abstinent without AUD history, 0.92 for abstinent with AUD history, 0.96 for moderate-risk consumption, and 0.95 for high-risk consumption or AUD.
- SVR did not differ by baseline stage of hepatic fibrosis, as measured by Fibrosis-4 score of 3.25 or less versus greater than 3.25.
IN PRACTICE:
“Achieving SVR has been shown to be associated with reduced risk of post-SVR outcomes, including hepatocellular carcinoma, liver-related mortality, and all-cause mortality. Our findings suggest that DAA therapy should be provided and reimbursed despite alcohol consumption or history of AUD. Restricting access to DAA therapy according to alcohol consumption or AUD creates an unnecessary barrier to patients accessing DAA therapy and challenges HCV elimination goals,” the investigators wrote.
SOURCE:
Emily J. Cartwright, MD, of Emory University, Atlanta, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
The study was observational and subject to potential residual confounding. To define SVR, HCV RNA was measured 6 months after DAA treatment ended, which may have resulted in a misclassification of patients who experienced viral relapse. Most participants were men born between 1945 and 1965, and the results may not be generalizable to women and/or older and younger patients.
DISCLOSURES:
The study was supported by grants from the National Institute on Alcohol Abuse and Alcoholism. Dr. Cartwright reported no disclosures. Two coauthors disclosed fees from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
TOPLINE:
Alcohol use at any level, including alcohol use disorder (AUD), is not associated with decreased odds of a sustained virologic response (SVR) to direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection. Therefore, DAA therapy should not be withheld from patients who consume alcohol.
METHODOLOGY:
- The researchers examined electronic health records for 69,229 patients (mean age, 63 years; 97% men; 50% non-Hispanic White) who started DAA therapy through the Department of Veterans Affairs between 2014 and 2018.
- Alcohol use categories were abstinent without history of AUD, abstinent with history of AUD, lower-risk consumption, moderate-risk consumption, and high-risk consumption or AUD.
- The primary outcome was SVR, which was defined as undetectable HCV RNA for 12 weeks to 6 months after completion of DAA treatment.
TAKEAWAY:
- Close to half (46.6%) of patients were abstinent without AUD, 13.3% were abstinent with AUD, 19.4% had lower-risk consumption, 4.5% had moderate-risk consumption, and 16.2% had high-risk consumption or AUD.
- Overall, 94.4% of those who started on DAA treatment achieved SVR.
- After adjustment, there was no evidence that any alcohol category was significantly associated with decreased odds of achieving SVR. The odds ratios were 1.09 for abstinent without AUD history, 0.92 for abstinent with AUD history, 0.96 for moderate-risk consumption, and 0.95 for high-risk consumption or AUD.
- SVR did not differ by baseline stage of hepatic fibrosis, as measured by Fibrosis-4 score of 3.25 or less versus greater than 3.25.
IN PRACTICE:
“Achieving SVR has been shown to be associated with reduced risk of post-SVR outcomes, including hepatocellular carcinoma, liver-related mortality, and all-cause mortality. Our findings suggest that DAA therapy should be provided and reimbursed despite alcohol consumption or history of AUD. Restricting access to DAA therapy according to alcohol consumption or AUD creates an unnecessary barrier to patients accessing DAA therapy and challenges HCV elimination goals,” the investigators wrote.
SOURCE:
Emily J. Cartwright, MD, of Emory University, Atlanta, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
The study was observational and subject to potential residual confounding. To define SVR, HCV RNA was measured 6 months after DAA treatment ended, which may have resulted in a misclassification of patients who experienced viral relapse. Most participants were men born between 1945 and 1965, and the results may not be generalizable to women and/or older and younger patients.
DISCLOSURES:
The study was supported by grants from the National Institute on Alcohol Abuse and Alcoholism. Dr. Cartwright reported no disclosures. Two coauthors disclosed fees from pharmaceutical companies outside the submitted work.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
No benefit of EC/IC bypass versus meds in large-artery stroke
in the latest randomized trial comparing the two interventions.
However, subgroup analyses suggest a potential benefit of surgery for certain patients, such as those with MCA vs. ICA occlusion, mean transit time greater than 6 seconds, or regional blood flow of 0.8 or less.
“We were disappointed by the results,” Liqun Jiao, MD, of the National Center for Neurological Disorders in Beijing, told this news organization. “We were expecting to demonstrate a benefit from EC-IC bypass surgery over medical treatment alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, per our original hypothesis.”
Although the study showed improved efficacy and safety for the surgical procedure, he said, “The progress of medical treatment is even better.”
The study was published online in JAMA.
Subgroup analyses promising
Previous randomized clinical trials, including the EC/IC Bypass Study and the Carotid Occlusion Surgery Study (COSS), showed no benefit in stroke prevention for patients with atherosclerotic occlusion of the ICA or MCA.
However, in light of improvements over the years in surgical techniques and patient selection, the authors conducted the Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS), a multicenter, randomized, open-label trial comparing EC-IC bypass surgery plus medical therapy, consisting of antiplatelet therapy and control of stroke risk factors, with medical therapy alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, with refined patient and operator selection.
A total of 324 patients (median age, 52.7 years; 79% men) in 13 centers in China were included; 309 patients (95%) completed the study.
The primary outcome was a composite of stroke or death within 30 days or ipsilateral ischemic stroke beyond 30 days through 2 years after randomization.
Secondary outcomes included, among others, any stroke or death within 2 years and fatal stroke within 2 years.
No significant difference was found for the primary outcome between the surgical group (8.6%) and the medical group (12.3%).
The 30-day risk of stroke or death was 6.2% in the surgery group, versus 1.8% (3/163) for the medical group. The risk of ipsilateral ischemic stroke beyond 30 days through 2 years was 2%, versus 10.3% – nonsignificant differences.
Furthermore, none of the prespecified secondary endpoints showed a significant difference, including any stroke or death within 2 years (9.9% vs. 15.3%; hazard ratio, 0.69) and fatal stroke within 2 years (2% vs. none).
Despite the findings, “We are encouraged by the subgroup analysis and the trend of long-term outcomes,” Dr. Jiao said. “We will continue to finish 5-10 years of follow-up to see whether the benefit of bypass surgery can be identified.”
The team has also launched the CMOSS-2 trial with a refined study design based on the results of subgroup analysis of the CMOSS study.
CMOSS-2 is recruiting patients with symptomatic chronic occlusion of the MCA and severe hemodynamic insufficiency in 13 sites in China. The primary outcome is ischemic stroke in the territory of the target artery within 24 months after randomization.
Can’t exclude benefit
Thomas Jeerakathil, MD, a professor at the University of Alberta and Northern Stroke Lead, Cardiovascular and Stroke Strategic Clinical Network, Alberta Health Services, Edmonton, commented on the study for this news organization. Like the authors, he said, “I don’t consider this study to definitively exclude the benefit of EC/IC bypass. More studies are required.”
Dr. Jeerakathil would like to see a study of a higher-risk group based on both clinical and hemodynamic blood flow criteria. In the current study, he said, “The trial group overall may not have been at high enough stroke risk to justify the up-front risks of the EC-IC bypass procedure.”
In addition, “The analysis method of Cox proportional hazards regression for the primary outcome did not fit the data when the perioperative period was combined with the period beyond 30 days,” he noted. “The researchers were open about this and did pivot and included a post hoc relative risk-based analysis, but the validity of their primary analysis is questionable.”
Furthermore, the study was “somewhat underpowered with a relatively small sample size and had the potential to miss clinically significant differences between groups,” he said. “It would be good to see a longer follow-up period of at least 5 years added to this trial and used in future trials, rather than 2 years.”
“Lastly,” he said, “it’s difficult to ignore the reduction in recurrent stroke events over the 30-day to 2-year time period associated with EC-IC bypass (from 10.3% down to 2%). This reduction alone shows the procedure has some potential to prevent stroke and would argue for more trials.”
EC-IC could be considered for patients who have failed other medical therapies and have more substantial evidence of compromised blood flow to the brain than those in the CMOSS trial, he noted, as many of these patients have few other options. “In our center and many other centers, the approach to EC-IC bypass is probably much more selective than used in the trial.”
Dr. Jeerakathil concluded, “Clinicians should be cautious about offering the procedure to patients with just mildly delayed blood flow in the hemisphere affected by the occluded artery and those who have not yet failed maximal medical therapy.”
But Seemant Chaturvedi, MD, and J. Marc Simard, MD, PhD, both of the University of Maryland, Baltimore, are not as optimistic about the potential for EC-IC.
Writing in a related editorial, they conclude that the results with EC-IC bypass surgery in randomized trials “remain unimpressive. Until a better understanding of the unique hemodynamic features of the brain is achieved, it will be difficult for neurosurgeons to continue offering this procedure to patients with ICA or MCA occlusion. Intensive, multifaceted medical therapy remains the first-line treatment for [these] patients.”
The study was supported by a research grant from the National Health Commission of the People’s Republic of China. Dr. Jiao, Dr. Jeerakathil, Dr. Chaturvedi, and Dr. Simard reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
in the latest randomized trial comparing the two interventions.
However, subgroup analyses suggest a potential benefit of surgery for certain patients, such as those with MCA vs. ICA occlusion, mean transit time greater than 6 seconds, or regional blood flow of 0.8 or less.
“We were disappointed by the results,” Liqun Jiao, MD, of the National Center for Neurological Disorders in Beijing, told this news organization. “We were expecting to demonstrate a benefit from EC-IC bypass surgery over medical treatment alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, per our original hypothesis.”
Although the study showed improved efficacy and safety for the surgical procedure, he said, “The progress of medical treatment is even better.”
The study was published online in JAMA.
Subgroup analyses promising
Previous randomized clinical trials, including the EC/IC Bypass Study and the Carotid Occlusion Surgery Study (COSS), showed no benefit in stroke prevention for patients with atherosclerotic occlusion of the ICA or MCA.
However, in light of improvements over the years in surgical techniques and patient selection, the authors conducted the Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS), a multicenter, randomized, open-label trial comparing EC-IC bypass surgery plus medical therapy, consisting of antiplatelet therapy and control of stroke risk factors, with medical therapy alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, with refined patient and operator selection.
A total of 324 patients (median age, 52.7 years; 79% men) in 13 centers in China were included; 309 patients (95%) completed the study.
The primary outcome was a composite of stroke or death within 30 days or ipsilateral ischemic stroke beyond 30 days through 2 years after randomization.
Secondary outcomes included, among others, any stroke or death within 2 years and fatal stroke within 2 years.
No significant difference was found for the primary outcome between the surgical group (8.6%) and the medical group (12.3%).
The 30-day risk of stroke or death was 6.2% in the surgery group, versus 1.8% (3/163) for the medical group. The risk of ipsilateral ischemic stroke beyond 30 days through 2 years was 2%, versus 10.3% – nonsignificant differences.
Furthermore, none of the prespecified secondary endpoints showed a significant difference, including any stroke or death within 2 years (9.9% vs. 15.3%; hazard ratio, 0.69) and fatal stroke within 2 years (2% vs. none).
Despite the findings, “We are encouraged by the subgroup analysis and the trend of long-term outcomes,” Dr. Jiao said. “We will continue to finish 5-10 years of follow-up to see whether the benefit of bypass surgery can be identified.”
The team has also launched the CMOSS-2 trial with a refined study design based on the results of subgroup analysis of the CMOSS study.
CMOSS-2 is recruiting patients with symptomatic chronic occlusion of the MCA and severe hemodynamic insufficiency in 13 sites in China. The primary outcome is ischemic stroke in the territory of the target artery within 24 months after randomization.
Can’t exclude benefit
Thomas Jeerakathil, MD, a professor at the University of Alberta and Northern Stroke Lead, Cardiovascular and Stroke Strategic Clinical Network, Alberta Health Services, Edmonton, commented on the study for this news organization. Like the authors, he said, “I don’t consider this study to definitively exclude the benefit of EC/IC bypass. More studies are required.”
Dr. Jeerakathil would like to see a study of a higher-risk group based on both clinical and hemodynamic blood flow criteria. In the current study, he said, “The trial group overall may not have been at high enough stroke risk to justify the up-front risks of the EC-IC bypass procedure.”
In addition, “The analysis method of Cox proportional hazards regression for the primary outcome did not fit the data when the perioperative period was combined with the period beyond 30 days,” he noted. “The researchers were open about this and did pivot and included a post hoc relative risk-based analysis, but the validity of their primary analysis is questionable.”
Furthermore, the study was “somewhat underpowered with a relatively small sample size and had the potential to miss clinically significant differences between groups,” he said. “It would be good to see a longer follow-up period of at least 5 years added to this trial and used in future trials, rather than 2 years.”
“Lastly,” he said, “it’s difficult to ignore the reduction in recurrent stroke events over the 30-day to 2-year time period associated with EC-IC bypass (from 10.3% down to 2%). This reduction alone shows the procedure has some potential to prevent stroke and would argue for more trials.”
EC-IC could be considered for patients who have failed other medical therapies and have more substantial evidence of compromised blood flow to the brain than those in the CMOSS trial, he noted, as many of these patients have few other options. “In our center and many other centers, the approach to EC-IC bypass is probably much more selective than used in the trial.”
Dr. Jeerakathil concluded, “Clinicians should be cautious about offering the procedure to patients with just mildly delayed blood flow in the hemisphere affected by the occluded artery and those who have not yet failed maximal medical therapy.”
But Seemant Chaturvedi, MD, and J. Marc Simard, MD, PhD, both of the University of Maryland, Baltimore, are not as optimistic about the potential for EC-IC.
Writing in a related editorial, they conclude that the results with EC-IC bypass surgery in randomized trials “remain unimpressive. Until a better understanding of the unique hemodynamic features of the brain is achieved, it will be difficult for neurosurgeons to continue offering this procedure to patients with ICA or MCA occlusion. Intensive, multifaceted medical therapy remains the first-line treatment for [these] patients.”
The study was supported by a research grant from the National Health Commission of the People’s Republic of China. Dr. Jiao, Dr. Jeerakathil, Dr. Chaturvedi, and Dr. Simard reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
in the latest randomized trial comparing the two interventions.
However, subgroup analyses suggest a potential benefit of surgery for certain patients, such as those with MCA vs. ICA occlusion, mean transit time greater than 6 seconds, or regional blood flow of 0.8 or less.
“We were disappointed by the results,” Liqun Jiao, MD, of the National Center for Neurological Disorders in Beijing, told this news organization. “We were expecting to demonstrate a benefit from EC-IC bypass surgery over medical treatment alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, per our original hypothesis.”
Although the study showed improved efficacy and safety for the surgical procedure, he said, “The progress of medical treatment is even better.”
The study was published online in JAMA.
Subgroup analyses promising
Previous randomized clinical trials, including the EC/IC Bypass Study and the Carotid Occlusion Surgery Study (COSS), showed no benefit in stroke prevention for patients with atherosclerotic occlusion of the ICA or MCA.
However, in light of improvements over the years in surgical techniques and patient selection, the authors conducted the Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS), a multicenter, randomized, open-label trial comparing EC-IC bypass surgery plus medical therapy, consisting of antiplatelet therapy and control of stroke risk factors, with medical therapy alone in symptomatic patients with ICA or MCA occlusion and hemodynamic insufficiency, with refined patient and operator selection.
A total of 324 patients (median age, 52.7 years; 79% men) in 13 centers in China were included; 309 patients (95%) completed the study.
The primary outcome was a composite of stroke or death within 30 days or ipsilateral ischemic stroke beyond 30 days through 2 years after randomization.
Secondary outcomes included, among others, any stroke or death within 2 years and fatal stroke within 2 years.
No significant difference was found for the primary outcome between the surgical group (8.6%) and the medical group (12.3%).
The 30-day risk of stroke or death was 6.2% in the surgery group, versus 1.8% (3/163) for the medical group. The risk of ipsilateral ischemic stroke beyond 30 days through 2 years was 2%, versus 10.3% – nonsignificant differences.
Furthermore, none of the prespecified secondary endpoints showed a significant difference, including any stroke or death within 2 years (9.9% vs. 15.3%; hazard ratio, 0.69) and fatal stroke within 2 years (2% vs. none).
Despite the findings, “We are encouraged by the subgroup analysis and the trend of long-term outcomes,” Dr. Jiao said. “We will continue to finish 5-10 years of follow-up to see whether the benefit of bypass surgery can be identified.”
The team has also launched the CMOSS-2 trial with a refined study design based on the results of subgroup analysis of the CMOSS study.
CMOSS-2 is recruiting patients with symptomatic chronic occlusion of the MCA and severe hemodynamic insufficiency in 13 sites in China. The primary outcome is ischemic stroke in the territory of the target artery within 24 months after randomization.
Can’t exclude benefit
Thomas Jeerakathil, MD, a professor at the University of Alberta and Northern Stroke Lead, Cardiovascular and Stroke Strategic Clinical Network, Alberta Health Services, Edmonton, commented on the study for this news organization. Like the authors, he said, “I don’t consider this study to definitively exclude the benefit of EC/IC bypass. More studies are required.”
Dr. Jeerakathil would like to see a study of a higher-risk group based on both clinical and hemodynamic blood flow criteria. In the current study, he said, “The trial group overall may not have been at high enough stroke risk to justify the up-front risks of the EC-IC bypass procedure.”
In addition, “The analysis method of Cox proportional hazards regression for the primary outcome did not fit the data when the perioperative period was combined with the period beyond 30 days,” he noted. “The researchers were open about this and did pivot and included a post hoc relative risk-based analysis, but the validity of their primary analysis is questionable.”
Furthermore, the study was “somewhat underpowered with a relatively small sample size and had the potential to miss clinically significant differences between groups,” he said. “It would be good to see a longer follow-up period of at least 5 years added to this trial and used in future trials, rather than 2 years.”
“Lastly,” he said, “it’s difficult to ignore the reduction in recurrent stroke events over the 30-day to 2-year time period associated with EC-IC bypass (from 10.3% down to 2%). This reduction alone shows the procedure has some potential to prevent stroke and would argue for more trials.”
EC-IC could be considered for patients who have failed other medical therapies and have more substantial evidence of compromised blood flow to the brain than those in the CMOSS trial, he noted, as many of these patients have few other options. “In our center and many other centers, the approach to EC-IC bypass is probably much more selective than used in the trial.”
Dr. Jeerakathil concluded, “Clinicians should be cautious about offering the procedure to patients with just mildly delayed blood flow in the hemisphere affected by the occluded artery and those who have not yet failed maximal medical therapy.”
But Seemant Chaturvedi, MD, and J. Marc Simard, MD, PhD, both of the University of Maryland, Baltimore, are not as optimistic about the potential for EC-IC.
Writing in a related editorial, they conclude that the results with EC-IC bypass surgery in randomized trials “remain unimpressive. Until a better understanding of the unique hemodynamic features of the brain is achieved, it will be difficult for neurosurgeons to continue offering this procedure to patients with ICA or MCA occlusion. Intensive, multifaceted medical therapy remains the first-line treatment for [these] patients.”
The study was supported by a research grant from the National Health Commission of the People’s Republic of China. Dr. Jiao, Dr. Jeerakathil, Dr. Chaturvedi, and Dr. Simard reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA
Study: Antiviral med linked to COVID mutations that can spread
published in the online journal Nature.
There’s no evidence that molnupiravir, sold under the brand name Lagevrio, has caused the creation of more transmissible or severe variants of COVID, the study says, but researchers called for more scrutiny of the drug.
Researchers looked at 15 million COVID genomes and discovered that hallmark mutations linked to molnupiravir increased in 2022, especially in places where the drug was widely used, such as the United States and the United Kingdom. Levels of the mutations were also found in populations where the drug was heavily prescribed, such as seniors.
Molnupiravir is an antiviral given to people after they show signs of having COVID-19. It interferes with the COVID-19 virus’s ability to make copies of itself, thus stopping the spread of the virus throughout the body and keeping the virus level low.
The study found the virus can sometimes survive molnupiravir, resulting in mutations that have spread to other people.
Theo Sanderson, PhD, the lead author on the study and a postdoctoral researcher at the Francis Crick Institute in London, told The Guardian that the implications of the mutations were unclear.
“The signature is very clear, but there aren’t any widely circulating variants that have the signature. At the moment there’s nothing that’s transmitted very widely that’s due to molnupiravir,” he said.
The study doesn’t say people should not use molnupiravir but calls for public health officials to scrutinize it.
“The observation that molnupiravir treatment has left a visible trace in global sequencing databases, including onwards transmission of molnupiravir-derived sequences, will be an important consideration for assessing the effects and evolutionary safety of this drug,” the researchers concluded.
When reached for comment, Merck questioned the evidence.
“The authors assume these mutations were associated with viral spread from molnupiravir-treated patients without documented evidence of that transmission. Instead, the authors rely on circumstantial associations between the region from which the sequence was identified and time frame of sequence collection in countries where molnupiravir is available to draw their conclusions,” the company said.
The Food and Drug Administration authorized the use of molnupiravir for the treatment of mild to moderate COVID-19 in adults in December 2021. The FDA has also authorized the use of nirmatrelvir/ritonavir (Paxlovid), an antiviral made by Pfizer.
A version of this article appeared on WebMD.com.
published in the online journal Nature.
There’s no evidence that molnupiravir, sold under the brand name Lagevrio, has caused the creation of more transmissible or severe variants of COVID, the study says, but researchers called for more scrutiny of the drug.
Researchers looked at 15 million COVID genomes and discovered that hallmark mutations linked to molnupiravir increased in 2022, especially in places where the drug was widely used, such as the United States and the United Kingdom. Levels of the mutations were also found in populations where the drug was heavily prescribed, such as seniors.
Molnupiravir is an antiviral given to people after they show signs of having COVID-19. It interferes with the COVID-19 virus’s ability to make copies of itself, thus stopping the spread of the virus throughout the body and keeping the virus level low.
The study found the virus can sometimes survive molnupiravir, resulting in mutations that have spread to other people.
Theo Sanderson, PhD, the lead author on the study and a postdoctoral researcher at the Francis Crick Institute in London, told The Guardian that the implications of the mutations were unclear.
“The signature is very clear, but there aren’t any widely circulating variants that have the signature. At the moment there’s nothing that’s transmitted very widely that’s due to molnupiravir,” he said.
The study doesn’t say people should not use molnupiravir but calls for public health officials to scrutinize it.
“The observation that molnupiravir treatment has left a visible trace in global sequencing databases, including onwards transmission of molnupiravir-derived sequences, will be an important consideration for assessing the effects and evolutionary safety of this drug,” the researchers concluded.
When reached for comment, Merck questioned the evidence.
“The authors assume these mutations were associated with viral spread from molnupiravir-treated patients without documented evidence of that transmission. Instead, the authors rely on circumstantial associations between the region from which the sequence was identified and time frame of sequence collection in countries where molnupiravir is available to draw their conclusions,” the company said.
The Food and Drug Administration authorized the use of molnupiravir for the treatment of mild to moderate COVID-19 in adults in December 2021. The FDA has also authorized the use of nirmatrelvir/ritonavir (Paxlovid), an antiviral made by Pfizer.
A version of this article appeared on WebMD.com.
published in the online journal Nature.
There’s no evidence that molnupiravir, sold under the brand name Lagevrio, has caused the creation of more transmissible or severe variants of COVID, the study says, but researchers called for more scrutiny of the drug.
Researchers looked at 15 million COVID genomes and discovered that hallmark mutations linked to molnupiravir increased in 2022, especially in places where the drug was widely used, such as the United States and the United Kingdom. Levels of the mutations were also found in populations where the drug was heavily prescribed, such as seniors.
Molnupiravir is an antiviral given to people after they show signs of having COVID-19. It interferes with the COVID-19 virus’s ability to make copies of itself, thus stopping the spread of the virus throughout the body and keeping the virus level low.
The study found the virus can sometimes survive molnupiravir, resulting in mutations that have spread to other people.
Theo Sanderson, PhD, the lead author on the study and a postdoctoral researcher at the Francis Crick Institute in London, told The Guardian that the implications of the mutations were unclear.
“The signature is very clear, but there aren’t any widely circulating variants that have the signature. At the moment there’s nothing that’s transmitted very widely that’s due to molnupiravir,” he said.
The study doesn’t say people should not use molnupiravir but calls for public health officials to scrutinize it.
“The observation that molnupiravir treatment has left a visible trace in global sequencing databases, including onwards transmission of molnupiravir-derived sequences, will be an important consideration for assessing the effects and evolutionary safety of this drug,” the researchers concluded.
When reached for comment, Merck questioned the evidence.
“The authors assume these mutations were associated with viral spread from molnupiravir-treated patients without documented evidence of that transmission. Instead, the authors rely on circumstantial associations between the region from which the sequence was identified and time frame of sequence collection in countries where molnupiravir is available to draw their conclusions,” the company said.
The Food and Drug Administration authorized the use of molnupiravir for the treatment of mild to moderate COVID-19 in adults in December 2021. The FDA has also authorized the use of nirmatrelvir/ritonavir (Paxlovid), an antiviral made by Pfizer.
A version of this article appeared on WebMD.com.
FROM NATURE
Long COVID and the Gastrointestinal System: Emerging Evidence
- Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
- Choudhury A et al. Therap Adv Gastroenterol. 2022;15:17562848221118403. doi:10.1177/17562848221118403
- Xu E et al. Nat Commun. 2023;14(1):983. doi:10.1038/s41467-023-36223-7
- Freedberg DE, Chang L. Curr Opin Gastroenterol. 2022;38(6):555-561. doi:10.1097/MOG.0000000000000876
- Blackett JW et al. Gastroenterology. 2022;162(2):648-650.e2. doi:10.1053/j.gastro.2021.10.040
- Chey WD et al. Gastroenterology. 2021;160(1):47-62. doi:10.1053/j.gastro.2020.06.099
- Líška D et al. Front Public Health. 2022;10:975992. doi:10.3389/fpubh.2022.975992
- Moens M et al. Front Public Health. 2022;10:991572. doi:10.3389/fpubh.2022.991572
- Cutler DM. The economic cost of long COVID: an update. Scholars at Harvard. Published July 2022. Accessed July 20, 2023. https://scholar.harvard.edu/sites/scholar.harvard.edu/files/cutler/files/long_covid_update_7-22.pdf
- National Center for Education Statistics (2023). Public School Expenditures. Condition of Education. US Department of Education, Institute of Education Sciences. Accessed August 4, 2023. https://nces.ed.gov/programs/coe/indicator/cmb
- Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
- Choudhury A et al. Therap Adv Gastroenterol. 2022;15:17562848221118403. doi:10.1177/17562848221118403
- Xu E et al. Nat Commun. 2023;14(1):983. doi:10.1038/s41467-023-36223-7
- Freedberg DE, Chang L. Curr Opin Gastroenterol. 2022;38(6):555-561. doi:10.1097/MOG.0000000000000876
- Blackett JW et al. Gastroenterology. 2022;162(2):648-650.e2. doi:10.1053/j.gastro.2021.10.040
- Chey WD et al. Gastroenterology. 2021;160(1):47-62. doi:10.1053/j.gastro.2020.06.099
- Líška D et al. Front Public Health. 2022;10:975992. doi:10.3389/fpubh.2022.975992
- Moens M et al. Front Public Health. 2022;10:991572. doi:10.3389/fpubh.2022.991572
- Cutler DM. The economic cost of long COVID: an update. Scholars at Harvard. Published July 2022. Accessed July 20, 2023. https://scholar.harvard.edu/sites/scholar.harvard.edu/files/cutler/files/long_covid_update_7-22.pdf
- National Center for Education Statistics (2023). Public School Expenditures. Condition of Education. US Department of Education, Institute of Education Sciences. Accessed August 4, 2023. https://nces.ed.gov/programs/coe/indicator/cmb
- Lutchmansingh DD et al. Semin Respir Crit Care Med. 2023;44(1):130-142. doi:10.1055/s-0042-1759568
- Choudhury A et al. Therap Adv Gastroenterol. 2022;15:17562848221118403. doi:10.1177/17562848221118403
- Xu E et al. Nat Commun. 2023;14(1):983. doi:10.1038/s41467-023-36223-7
- Freedberg DE, Chang L. Curr Opin Gastroenterol. 2022;38(6):555-561. doi:10.1097/MOG.0000000000000876
- Blackett JW et al. Gastroenterology. 2022;162(2):648-650.e2. doi:10.1053/j.gastro.2021.10.040
- Chey WD et al. Gastroenterology. 2021;160(1):47-62. doi:10.1053/j.gastro.2020.06.099
- Líška D et al. Front Public Health. 2022;10:975992. doi:10.3389/fpubh.2022.975992
- Moens M et al. Front Public Health. 2022;10:991572. doi:10.3389/fpubh.2022.991572
- Cutler DM. The economic cost of long COVID: an update. Scholars at Harvard. Published July 2022. Accessed July 20, 2023. https://scholar.harvard.edu/sites/scholar.harvard.edu/files/cutler/files/long_covid_update_7-22.pdf
- National Center for Education Statistics (2023). Public School Expenditures. Condition of Education. US Department of Education, Institute of Education Sciences. Accessed August 4, 2023. https://nces.ed.gov/programs/coe/indicator/cmb
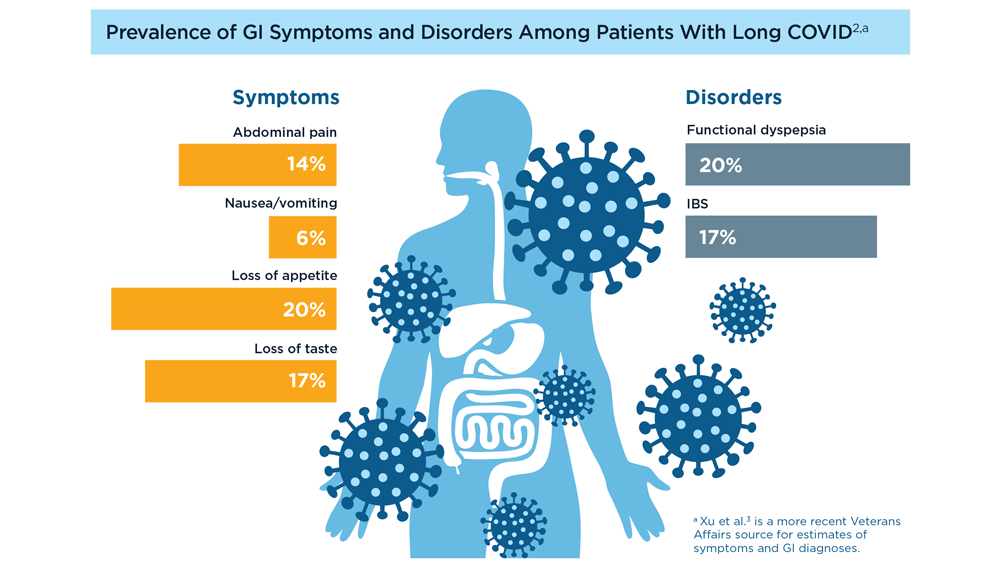
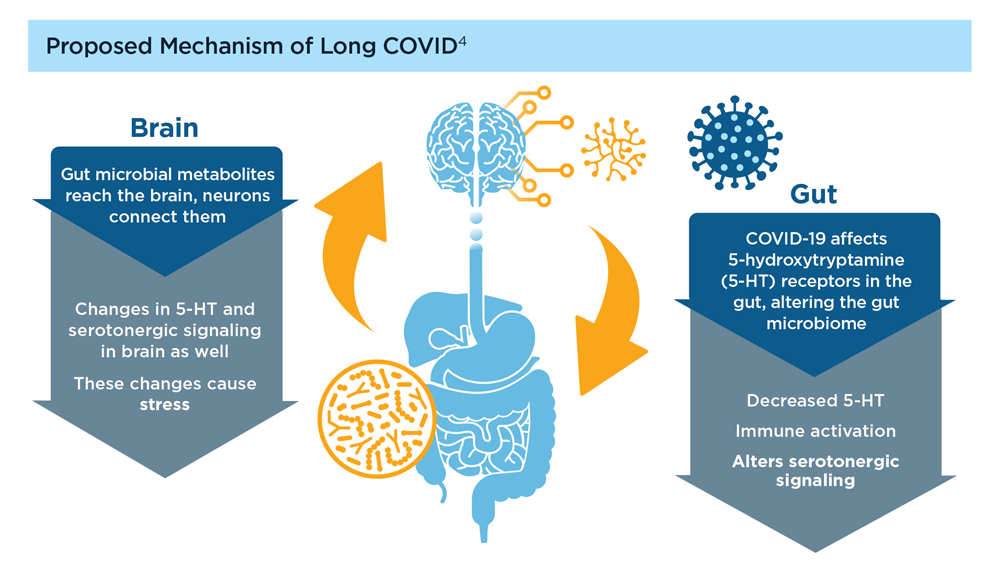
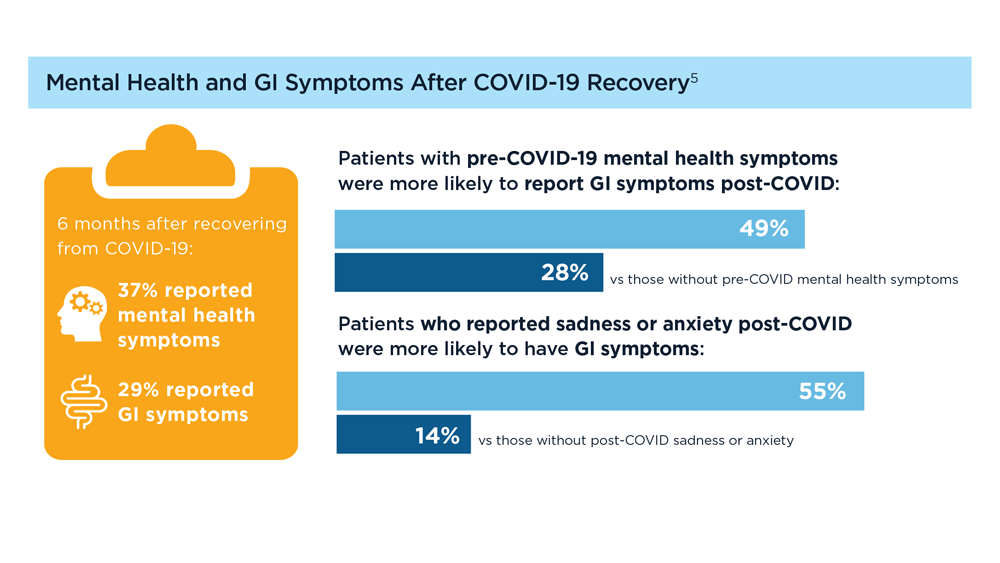
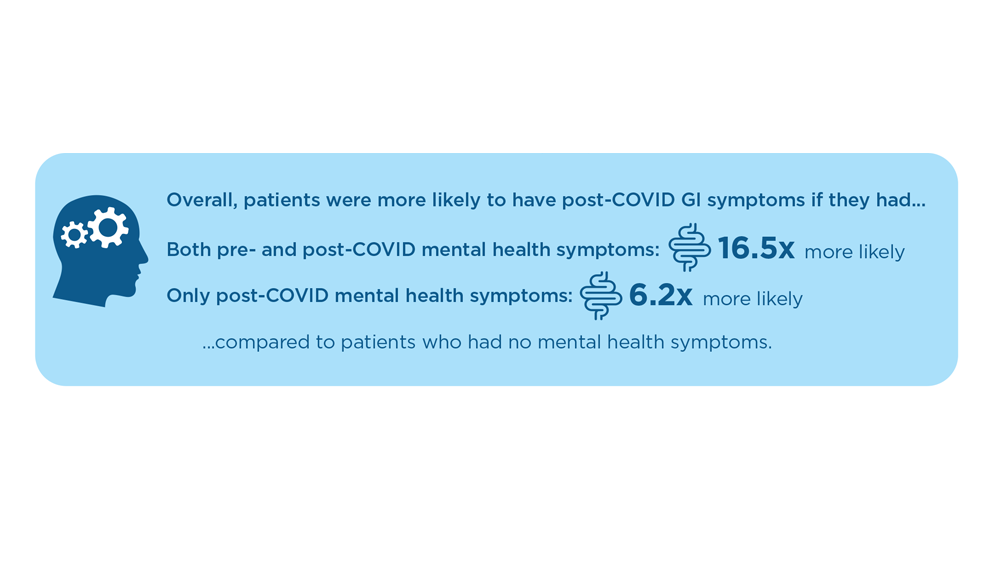
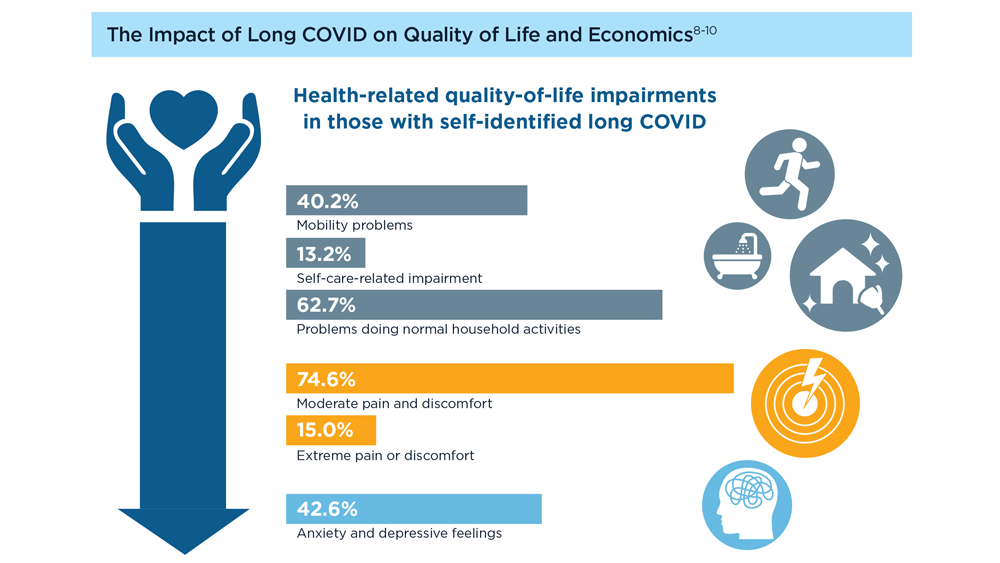
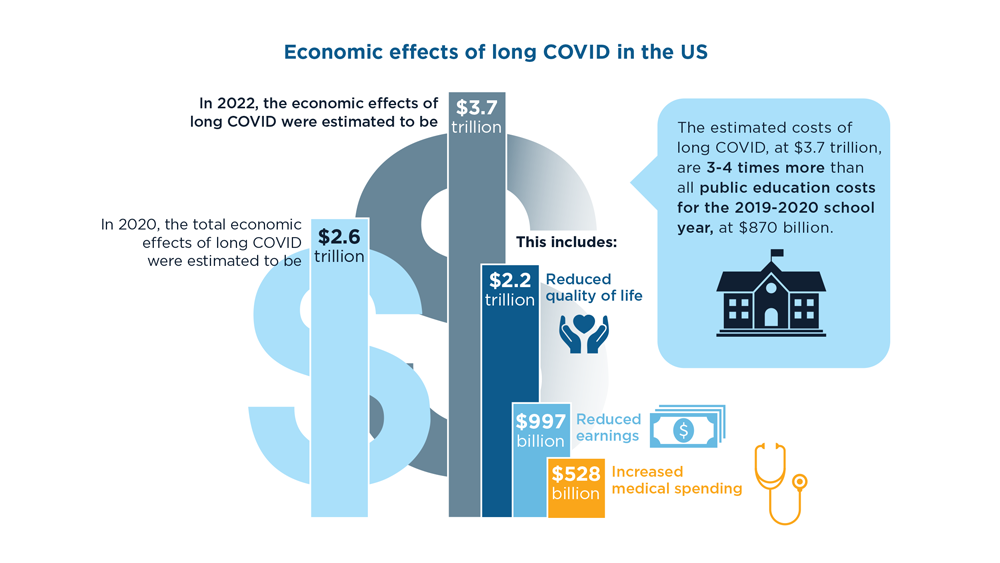
Digital Tools in the Management of IBS/ Functional GI Disorders
- Hasan SS et al. Neurogastroenterol Motil. 2023;35(4):e14554. doi:10.1111/nmo.14554
- Peters SL et al. Neurogastroenterol Motil. 2023;35(4):e14533. doi:10.1111/nmo.14533
- Zhou C et al. Neurogastroenterol Motil. 2019;31(2):e13461. doi:10.1111/nmo.13461
- Staudacher HM et al. Nat Rev Gastroenterol Hepatol. 2023;1-15. doi:10.1038/s41575-023-00794-z
- Qin HY et al. World J Gastroenterol. 2014;20(39):14126-14131. doi:10.3748/wjg.v20.i39.14126
- Varjú P et al. PLoS One. 2017;12(8):e0182942. doi:10.1371/journal.pone.0182942
- Saleh ZM et al. Am J Gastroenterol. 2023. doi:10.14309/ajg.0000000000002220
- Yu C et al. Clin Transl Gastroenterol. 2022;13(9):e00515. doi:10.14309/ctg.0000000000000515
- Jagannath B et al. Inflamm Bowel Dis. 2020;26(10):1533-1542. doi:10.1093/ibd/izaa191
- Zhang H et al. J Nutr. 2023;153(4):924-939. doi:10.1016/j.tjnut.2023.01.026
- Karakan T et al. Gut Microbes. 2022;14(1):2138672. doi:10.1080/19490976.2022.2138672
- Kordi M et al. Inform Med Unlocked. 2022;29:100891. doi:10.1016/j.imu.2022.100891
- Gubatan J et al. World J Gastroenterol. 2021;27(17):1920-1935. doi:10.3748/wjg.v27.i17.1920
- Boucher EM et al. Expert Rev Med Devices. 2021;18(suppl 1):37-49. doi:10.1080/17434440.2021.2013200
- Babel A et al. Front Digit Health. 2021;3:669869. doi:10.3389/fdgth.2021.669869
- Hasan SS et al. Neurogastroenterol Motil. 2023;35(4):e14554. doi:10.1111/nmo.14554
- Peters SL et al. Neurogastroenterol Motil. 2023;35(4):e14533. doi:10.1111/nmo.14533
- Zhou C et al. Neurogastroenterol Motil. 2019;31(2):e13461. doi:10.1111/nmo.13461
- Staudacher HM et al. Nat Rev Gastroenterol Hepatol. 2023;1-15. doi:10.1038/s41575-023-00794-z
- Qin HY et al. World J Gastroenterol. 2014;20(39):14126-14131. doi:10.3748/wjg.v20.i39.14126
- Varjú P et al. PLoS One. 2017;12(8):e0182942. doi:10.1371/journal.pone.0182942
- Saleh ZM et al. Am J Gastroenterol. 2023. doi:10.14309/ajg.0000000000002220
- Yu C et al. Clin Transl Gastroenterol. 2022;13(9):e00515. doi:10.14309/ctg.0000000000000515
- Jagannath B et al. Inflamm Bowel Dis. 2020;26(10):1533-1542. doi:10.1093/ibd/izaa191
- Zhang H et al. J Nutr. 2023;153(4):924-939. doi:10.1016/j.tjnut.2023.01.026
- Karakan T et al. Gut Microbes. 2022;14(1):2138672. doi:10.1080/19490976.2022.2138672
- Kordi M et al. Inform Med Unlocked. 2022;29:100891. doi:10.1016/j.imu.2022.100891
- Gubatan J et al. World J Gastroenterol. 2021;27(17):1920-1935. doi:10.3748/wjg.v27.i17.1920
- Boucher EM et al. Expert Rev Med Devices. 2021;18(suppl 1):37-49. doi:10.1080/17434440.2021.2013200
- Babel A et al. Front Digit Health. 2021;3:669869. doi:10.3389/fdgth.2021.669869
- Hasan SS et al. Neurogastroenterol Motil. 2023;35(4):e14554. doi:10.1111/nmo.14554
- Peters SL et al. Neurogastroenterol Motil. 2023;35(4):e14533. doi:10.1111/nmo.14533
- Zhou C et al. Neurogastroenterol Motil. 2019;31(2):e13461. doi:10.1111/nmo.13461
- Staudacher HM et al. Nat Rev Gastroenterol Hepatol. 2023;1-15. doi:10.1038/s41575-023-00794-z
- Qin HY et al. World J Gastroenterol. 2014;20(39):14126-14131. doi:10.3748/wjg.v20.i39.14126
- Varjú P et al. PLoS One. 2017;12(8):e0182942. doi:10.1371/journal.pone.0182942
- Saleh ZM et al. Am J Gastroenterol. 2023. doi:10.14309/ajg.0000000000002220
- Yu C et al. Clin Transl Gastroenterol. 2022;13(9):e00515. doi:10.14309/ctg.0000000000000515
- Jagannath B et al. Inflamm Bowel Dis. 2020;26(10):1533-1542. doi:10.1093/ibd/izaa191
- Zhang H et al. J Nutr. 2023;153(4):924-939. doi:10.1016/j.tjnut.2023.01.026
- Karakan T et al. Gut Microbes. 2022;14(1):2138672. doi:10.1080/19490976.2022.2138672
- Kordi M et al. Inform Med Unlocked. 2022;29:100891. doi:10.1016/j.imu.2022.100891
- Gubatan J et al. World J Gastroenterol. 2021;27(17):1920-1935. doi:10.3748/wjg.v27.i17.1920
- Boucher EM et al. Expert Rev Med Devices. 2021;18(suppl 1):37-49. doi:10.1080/17434440.2021.2013200
- Babel A et al. Front Digit Health. 2021;3:669869. doi:10.3389/fdgth.2021.669869
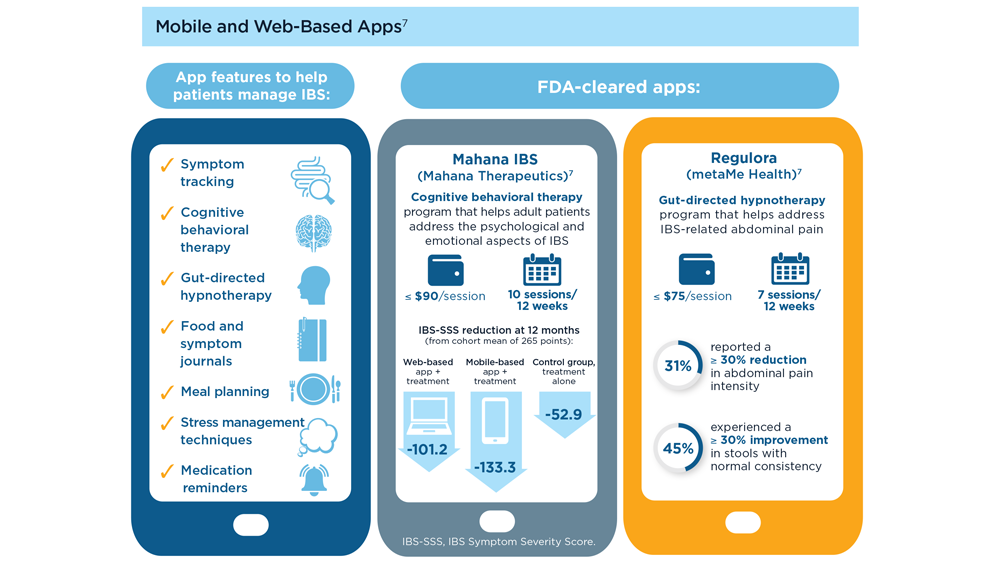
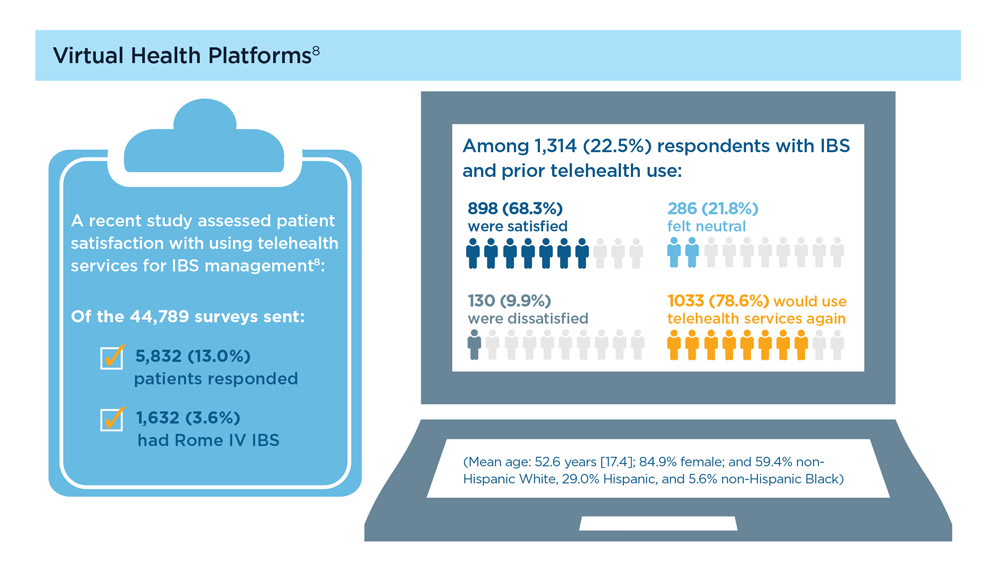
‘Old school’ laser resurfacing remains an effective option for rejuvenation
SAN DIEGO – , according to Arisa E. Ortiz, MD.

“Fractional resurfacing is great because there is less downtime, but the results are not as dramatic as with fully ablative resurfacing,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. In her practice, she said, “we do a combination,” which can include “fully ablative around the mouth and eyes and fractional everywhere else.”
Key drawbacks to fully ablative laser resurfacing include significant downtime and extensive wound care, “so it’s not for everybody,” she said. Prolonged erythema following treatment is expected, “so patients need to plan for this. It can last 3-4 months, and it will continue to fade and can be covered up with makeup, but it does last a while,” she noted. “One of the things that made ablative resurfacing fall out of favor was the delayed and permanent hypopigmentation where there’s a stark line of demarcation because you can’t treat the neck [with this modality], so patients have this pearly white looking face that appears 6 months after the treatment,” she added.
Preoperatively, Dr. Ortiz asks patients what other cosmetic procedures they have had in the past. For example, if they have had a facelift, they might have neck skin on their jawline, which will react differently to fully ablative resurfacing than facial skin. “I don’t perform fully ablative resurfacing on the neck or body, or in patients with darker skin types,” she said.
To optimize results, she recommends pretreatment of the area with a neuromodulator a week or 2 before the procedure, “so that they’re not actively contracting and recreating creases,” she said. Studies, she noted, have shown that this approach results in better outcomes. She also asks patients to apply a tripeptide serum daily a week or 2 prior to their procedure to stimulate wound healing and collagen remodeling.
For antibiotic and antiviral prophylaxis, Dr. Ortiz typically prescribes doxycycline 100 mg b.i.d. for 7 days and valacyclovir 500 mg b.i.d. for 7 days and asks patients to start the course the night before the procedure. “If they break through the antiviral, I increase to zoster dosing,” she said. “I make sure they have my cell phone number and call me right away if that happens. I don’t routinely prescribe an antifungal, but you can if you want to.”
For anesthesia, Dr. Ortiz applies lidocaine 23%/tetracaine 7% an hour before the procedure and performs nerve blocks at the mentalis, infraorbital, supraorbital, and nasalis muscles. “I also do local infiltration with a three-pronged Mesoram adapter,” she said. “That has changed the comfort level for these patients. I don’t offer any sedation in my practice but that is an option if you have it available. If you’re going to be resurfacing within the orbital rim you need to know how to place corneal shields. Only use injectable lidocaine in this area because if topical lidocaine gets into the eye, it can cause a chemical corneal abrasion. Nothing happens to their vision permanently, but it’s extremely painful for 24-48 hours.”
Dr. Ortiz described postoperative wound care as “the hardest part” of fully ablative laser resurfacing treatments. The treated area will look “bloody and crusty” for 1-2 weeks. She instructs patients to do vinegar soaks four times per day for 2-3 weeks, “depending on how quickly they heal,” she said. She also counsels patients to apply petrolatum ointment to the area and provides them with a bottle of hypochlorous acid spray, an antiseptic – which also helps with the itching they may experience. “They need to avoid the sun, so I recommend full face visors,” she added.
In her clinical experience, postoperative pain medications are not required. “If the patient calls you on day 3 with increased pain, that’s usually a sign of infection; don’t ignore that,” said Dr. Ortiz, who is also president-elect of the American Society for Laser Medicine and Surgery. In a case of suspected infection, she asks the patient to come in right away, and obtains a bacterial culture. “If they break through the doxycycline, it’s usually a gram-negative infection, so I’ll treat them prophylactically for that,” she said.
“Significant itching may be a sign of Candida infection,” she noted. “Because the epidermis has been disrupted, if they have systemic symptoms then you want to consider IV antibiotics because the infection can spread rapidly.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
SAN DIEGO – , according to Arisa E. Ortiz, MD.
“Fractional resurfacing is great because there is less downtime, but the results are not as dramatic as with fully ablative resurfacing,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. In her practice, she said, “we do a combination,” which can include “fully ablative around the mouth and eyes and fractional everywhere else.”
Key drawbacks to fully ablative laser resurfacing include significant downtime and extensive wound care, “so it’s not for everybody,” she said. Prolonged erythema following treatment is expected, “so patients need to plan for this. It can last 3-4 months, and it will continue to fade and can be covered up with makeup, but it does last a while,” she noted. “One of the things that made ablative resurfacing fall out of favor was the delayed and permanent hypopigmentation where there’s a stark line of demarcation because you can’t treat the neck [with this modality], so patients have this pearly white looking face that appears 6 months after the treatment,” she added.
Preoperatively, Dr. Ortiz asks patients what other cosmetic procedures they have had in the past. For example, if they have had a facelift, they might have neck skin on their jawline, which will react differently to fully ablative resurfacing than facial skin. “I don’t perform fully ablative resurfacing on the neck or body, or in patients with darker skin types,” she said.
To optimize results, she recommends pretreatment of the area with a neuromodulator a week or 2 before the procedure, “so that they’re not actively contracting and recreating creases,” she said. Studies, she noted, have shown that this approach results in better outcomes. She also asks patients to apply a tripeptide serum daily a week or 2 prior to their procedure to stimulate wound healing and collagen remodeling.
For antibiotic and antiviral prophylaxis, Dr. Ortiz typically prescribes doxycycline 100 mg b.i.d. for 7 days and valacyclovir 500 mg b.i.d. for 7 days and asks patients to start the course the night before the procedure. “If they break through the antiviral, I increase to zoster dosing,” she said. “I make sure they have my cell phone number and call me right away if that happens. I don’t routinely prescribe an antifungal, but you can if you want to.”
For anesthesia, Dr. Ortiz applies lidocaine 23%/tetracaine 7% an hour before the procedure and performs nerve blocks at the mentalis, infraorbital, supraorbital, and nasalis muscles. “I also do local infiltration with a three-pronged Mesoram adapter,” she said. “That has changed the comfort level for these patients. I don’t offer any sedation in my practice but that is an option if you have it available. If you’re going to be resurfacing within the orbital rim you need to know how to place corneal shields. Only use injectable lidocaine in this area because if topical lidocaine gets into the eye, it can cause a chemical corneal abrasion. Nothing happens to their vision permanently, but it’s extremely painful for 24-48 hours.”
Dr. Ortiz described postoperative wound care as “the hardest part” of fully ablative laser resurfacing treatments. The treated area will look “bloody and crusty” for 1-2 weeks. She instructs patients to do vinegar soaks four times per day for 2-3 weeks, “depending on how quickly they heal,” she said. She also counsels patients to apply petrolatum ointment to the area and provides them with a bottle of hypochlorous acid spray, an antiseptic – which also helps with the itching they may experience. “They need to avoid the sun, so I recommend full face visors,” she added.
In her clinical experience, postoperative pain medications are not required. “If the patient calls you on day 3 with increased pain, that’s usually a sign of infection; don’t ignore that,” said Dr. Ortiz, who is also president-elect of the American Society for Laser Medicine and Surgery. In a case of suspected infection, she asks the patient to come in right away, and obtains a bacterial culture. “If they break through the doxycycline, it’s usually a gram-negative infection, so I’ll treat them prophylactically for that,” she said.
“Significant itching may be a sign of Candida infection,” she noted. “Because the epidermis has been disrupted, if they have systemic symptoms then you want to consider IV antibiotics because the infection can spread rapidly.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
SAN DIEGO – , according to Arisa E. Ortiz, MD.
“Fractional resurfacing is great because there is less downtime, but the results are not as dramatic as with fully ablative resurfacing,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. In her practice, she said, “we do a combination,” which can include “fully ablative around the mouth and eyes and fractional everywhere else.”
Key drawbacks to fully ablative laser resurfacing include significant downtime and extensive wound care, “so it’s not for everybody,” she said. Prolonged erythema following treatment is expected, “so patients need to plan for this. It can last 3-4 months, and it will continue to fade and can be covered up with makeup, but it does last a while,” she noted. “One of the things that made ablative resurfacing fall out of favor was the delayed and permanent hypopigmentation where there’s a stark line of demarcation because you can’t treat the neck [with this modality], so patients have this pearly white looking face that appears 6 months after the treatment,” she added.
Preoperatively, Dr. Ortiz asks patients what other cosmetic procedures they have had in the past. For example, if they have had a facelift, they might have neck skin on their jawline, which will react differently to fully ablative resurfacing than facial skin. “I don’t perform fully ablative resurfacing on the neck or body, or in patients with darker skin types,” she said.
To optimize results, she recommends pretreatment of the area with a neuromodulator a week or 2 before the procedure, “so that they’re not actively contracting and recreating creases,” she said. Studies, she noted, have shown that this approach results in better outcomes. She also asks patients to apply a tripeptide serum daily a week or 2 prior to their procedure to stimulate wound healing and collagen remodeling.
For antibiotic and antiviral prophylaxis, Dr. Ortiz typically prescribes doxycycline 100 mg b.i.d. for 7 days and valacyclovir 500 mg b.i.d. for 7 days and asks patients to start the course the night before the procedure. “If they break through the antiviral, I increase to zoster dosing,” she said. “I make sure they have my cell phone number and call me right away if that happens. I don’t routinely prescribe an antifungal, but you can if you want to.”
For anesthesia, Dr. Ortiz applies lidocaine 23%/tetracaine 7% an hour before the procedure and performs nerve blocks at the mentalis, infraorbital, supraorbital, and nasalis muscles. “I also do local infiltration with a three-pronged Mesoram adapter,” she said. “That has changed the comfort level for these patients. I don’t offer any sedation in my practice but that is an option if you have it available. If you’re going to be resurfacing within the orbital rim you need to know how to place corneal shields. Only use injectable lidocaine in this area because if topical lidocaine gets into the eye, it can cause a chemical corneal abrasion. Nothing happens to their vision permanently, but it’s extremely painful for 24-48 hours.”
Dr. Ortiz described postoperative wound care as “the hardest part” of fully ablative laser resurfacing treatments. The treated area will look “bloody and crusty” for 1-2 weeks. She instructs patients to do vinegar soaks four times per day for 2-3 weeks, “depending on how quickly they heal,” she said. She also counsels patients to apply petrolatum ointment to the area and provides them with a bottle of hypochlorous acid spray, an antiseptic – which also helps with the itching they may experience. “They need to avoid the sun, so I recommend full face visors,” she added.
In her clinical experience, postoperative pain medications are not required. “If the patient calls you on day 3 with increased pain, that’s usually a sign of infection; don’t ignore that,” said Dr. Ortiz, who is also president-elect of the American Society for Laser Medicine and Surgery. In a case of suspected infection, she asks the patient to come in right away, and obtains a bacterial culture. “If they break through the doxycycline, it’s usually a gram-negative infection, so I’ll treat them prophylactically for that,” she said.
“Significant itching may be a sign of Candida infection,” she noted. “Because the epidermis has been disrupted, if they have systemic symptoms then you want to consider IV antibiotics because the infection can spread rapidly.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
AT MOAS 2023