User login
Obesity Affects More Than 1 Billion Around the World
TOPLINE:
More than a billion children, adolescents, and adults are living with obesity, globally, with rates of obesity among children and adolescents quadrupling between 1990 and 2022.
Obesity rates nearly tripled among adult men and more than doubled among women during the time period, according to results from a collaboration between the NCD Risk Factor Collaboration and the World Health Organization (WHO).
The rates of being underweight have meanwhile declined, making obesity now the most common form of malnutrition in most regions.
METHODOLOGY:
In this global analysis, the authors evaluated 3663 population-based studies conducted in 200 countries and territories, with data on 222 million participants in the general population, including height and weight.
Trends were established according to categories of body mass index (BMI) in groups of adults aged 20 years or older, representing 150 million individuals, and 63 million school-aged children and adolescents aged 5-19 years, spanning from 1990 to 2022.
Assessments of adults focus on the individual and combined prevalence of underweight (BMI < 18.5 kg/m2) and obesity (BMI ≥ 30 kg/m2).
For school-aged children and adolescents, assessments were for thinness (BMI < 2 standard deviation [SD] below the median of the WHO growth reference) and obesity (BMI > 2 SD above the median).
TAKEAWAY:
In 2022, obesity rates were higher than underweight in 177 countries (89%) for women and 145 countries (73%) for men.
Likewise, among school-aged children and adolescents, obesity in 2022 was more prevalent than thinness among girls in 130 countries (67%) and boys in 125 countries (63%), while thinness was more prevalent in only 18% and 21% of the countries, respectively.
In 2022, the combined prevalence of underweight and obesity was highest in island nations in the Caribbean and Polynesia and Micronesia, as well as in countries in the Middle East and North Africa.
Among school-aged children, the countries with the highest combined prevalence of underweight and obesity were Polynesia and Micronesia and the Caribbean for both sexes and Chile and Qatar for boys.
The prevalence of obesity surpassed 60% among women in eight countries (4%) and men in six countries (3%), all in Polynesia and Micronesia.
In the United States, the obesity rate increased from 21.2% in 1990 to 43.8% in 2022 for women and from 16.9% to 41.6% in 2022 for men.
As of 2022, the prevalence of obesity in the United States ranked 36th highest in the world for women and 10th highest in the world for men.
IN PRACTICE:
“It is very concerning that the epidemic of obesity that was evident among adults in much of the world in 1990 is now mirrored in school-aged children and adolescents,” senior author Majid Ezzati, PhD, of Imperial College of London, said in a press statement.
“At the same time, hundreds of millions are still affected by undernutrition, particularly in some of the poorest parts of the world,” he said. “To successfully tackle both forms of malnutrition, it is vital we significantly improve the availability and affordability of healthy, nutritious foods.”
Tedros Adhanom Ghebreyesus, PhD, WHO Director-General, added in the press statement that “this new study highlights the importance of preventing and managing obesity from early life to adulthood, through diet, physical activity, and adequate care, as needed.
“Getting back on track to meet the global targets for curbing obesity will take the work of governments and communities, supported by evidence-based policies from WHO and national public health agencies,” he said.
“Importantly, it requires the cooperation of the private sector, which must be accountable for the health impacts of their products.”
SOURCE:
The study was published on February 29, 2024, in The Lancet. The study was conducted by the NCD Risk Factor Collaboration and the WHO.
LIMITATIONS:
Data differences in countries included that some had limited data and three had none, requiring some estimates to be formed using data from other countries. Data availability was also lower among the youngest and oldest patients, increasing uncertainty of data in those age groups. In addition, data from health surveys can be subject to error, and BMI can be an imperfect measure of the extent or distribution of body fat.
DISCLOSURES:
The study was funded by UK Medical Research Council, UK Research and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.
TOPLINE:
More than a billion children, adolescents, and adults are living with obesity, globally, with rates of obesity among children and adolescents quadrupling between 1990 and 2022.
Obesity rates nearly tripled among adult men and more than doubled among women during the time period, according to results from a collaboration between the NCD Risk Factor Collaboration and the World Health Organization (WHO).
The rates of being underweight have meanwhile declined, making obesity now the most common form of malnutrition in most regions.
METHODOLOGY:
In this global analysis, the authors evaluated 3663 population-based studies conducted in 200 countries and territories, with data on 222 million participants in the general population, including height and weight.
Trends were established according to categories of body mass index (BMI) in groups of adults aged 20 years or older, representing 150 million individuals, and 63 million school-aged children and adolescents aged 5-19 years, spanning from 1990 to 2022.
Assessments of adults focus on the individual and combined prevalence of underweight (BMI < 18.5 kg/m2) and obesity (BMI ≥ 30 kg/m2).
For school-aged children and adolescents, assessments were for thinness (BMI < 2 standard deviation [SD] below the median of the WHO growth reference) and obesity (BMI > 2 SD above the median).
TAKEAWAY:
In 2022, obesity rates were higher than underweight in 177 countries (89%) for women and 145 countries (73%) for men.
Likewise, among school-aged children and adolescents, obesity in 2022 was more prevalent than thinness among girls in 130 countries (67%) and boys in 125 countries (63%), while thinness was more prevalent in only 18% and 21% of the countries, respectively.
In 2022, the combined prevalence of underweight and obesity was highest in island nations in the Caribbean and Polynesia and Micronesia, as well as in countries in the Middle East and North Africa.
Among school-aged children, the countries with the highest combined prevalence of underweight and obesity were Polynesia and Micronesia and the Caribbean for both sexes and Chile and Qatar for boys.
The prevalence of obesity surpassed 60% among women in eight countries (4%) and men in six countries (3%), all in Polynesia and Micronesia.
In the United States, the obesity rate increased from 21.2% in 1990 to 43.8% in 2022 for women and from 16.9% to 41.6% in 2022 for men.
As of 2022, the prevalence of obesity in the United States ranked 36th highest in the world for women and 10th highest in the world for men.
IN PRACTICE:
“It is very concerning that the epidemic of obesity that was evident among adults in much of the world in 1990 is now mirrored in school-aged children and adolescents,” senior author Majid Ezzati, PhD, of Imperial College of London, said in a press statement.
“At the same time, hundreds of millions are still affected by undernutrition, particularly in some of the poorest parts of the world,” he said. “To successfully tackle both forms of malnutrition, it is vital we significantly improve the availability and affordability of healthy, nutritious foods.”
Tedros Adhanom Ghebreyesus, PhD, WHO Director-General, added in the press statement that “this new study highlights the importance of preventing and managing obesity from early life to adulthood, through diet, physical activity, and adequate care, as needed.
“Getting back on track to meet the global targets for curbing obesity will take the work of governments and communities, supported by evidence-based policies from WHO and national public health agencies,” he said.
“Importantly, it requires the cooperation of the private sector, which must be accountable for the health impacts of their products.”
SOURCE:
The study was published on February 29, 2024, in The Lancet. The study was conducted by the NCD Risk Factor Collaboration and the WHO.
LIMITATIONS:
Data differences in countries included that some had limited data and three had none, requiring some estimates to be formed using data from other countries. Data availability was also lower among the youngest and oldest patients, increasing uncertainty of data in those age groups. In addition, data from health surveys can be subject to error, and BMI can be an imperfect measure of the extent or distribution of body fat.
DISCLOSURES:
The study was funded by UK Medical Research Council, UK Research and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.
TOPLINE:
More than a billion children, adolescents, and adults are living with obesity, globally, with rates of obesity among children and adolescents quadrupling between 1990 and 2022.
Obesity rates nearly tripled among adult men and more than doubled among women during the time period, according to results from a collaboration between the NCD Risk Factor Collaboration and the World Health Organization (WHO).
The rates of being underweight have meanwhile declined, making obesity now the most common form of malnutrition in most regions.
METHODOLOGY:
In this global analysis, the authors evaluated 3663 population-based studies conducted in 200 countries and territories, with data on 222 million participants in the general population, including height and weight.
Trends were established according to categories of body mass index (BMI) in groups of adults aged 20 years or older, representing 150 million individuals, and 63 million school-aged children and adolescents aged 5-19 years, spanning from 1990 to 2022.
Assessments of adults focus on the individual and combined prevalence of underweight (BMI < 18.5 kg/m2) and obesity (BMI ≥ 30 kg/m2).
For school-aged children and adolescents, assessments were for thinness (BMI < 2 standard deviation [SD] below the median of the WHO growth reference) and obesity (BMI > 2 SD above the median).
TAKEAWAY:
In 2022, obesity rates were higher than underweight in 177 countries (89%) for women and 145 countries (73%) for men.
Likewise, among school-aged children and adolescents, obesity in 2022 was more prevalent than thinness among girls in 130 countries (67%) and boys in 125 countries (63%), while thinness was more prevalent in only 18% and 21% of the countries, respectively.
In 2022, the combined prevalence of underweight and obesity was highest in island nations in the Caribbean and Polynesia and Micronesia, as well as in countries in the Middle East and North Africa.
Among school-aged children, the countries with the highest combined prevalence of underweight and obesity were Polynesia and Micronesia and the Caribbean for both sexes and Chile and Qatar for boys.
The prevalence of obesity surpassed 60% among women in eight countries (4%) and men in six countries (3%), all in Polynesia and Micronesia.
In the United States, the obesity rate increased from 21.2% in 1990 to 43.8% in 2022 for women and from 16.9% to 41.6% in 2022 for men.
As of 2022, the prevalence of obesity in the United States ranked 36th highest in the world for women and 10th highest in the world for men.
IN PRACTICE:
“It is very concerning that the epidemic of obesity that was evident among adults in much of the world in 1990 is now mirrored in school-aged children and adolescents,” senior author Majid Ezzati, PhD, of Imperial College of London, said in a press statement.
“At the same time, hundreds of millions are still affected by undernutrition, particularly in some of the poorest parts of the world,” he said. “To successfully tackle both forms of malnutrition, it is vital we significantly improve the availability and affordability of healthy, nutritious foods.”
Tedros Adhanom Ghebreyesus, PhD, WHO Director-General, added in the press statement that “this new study highlights the importance of preventing and managing obesity from early life to adulthood, through diet, physical activity, and adequate care, as needed.
“Getting back on track to meet the global targets for curbing obesity will take the work of governments and communities, supported by evidence-based policies from WHO and national public health agencies,” he said.
“Importantly, it requires the cooperation of the private sector, which must be accountable for the health impacts of their products.”
SOURCE:
The study was published on February 29, 2024, in The Lancet. The study was conducted by the NCD Risk Factor Collaboration and the WHO.
LIMITATIONS:
Data differences in countries included that some had limited data and three had none, requiring some estimates to be formed using data from other countries. Data availability was also lower among the youngest and oldest patients, increasing uncertainty of data in those age groups. In addition, data from health surveys can be subject to error, and BMI can be an imperfect measure of the extent or distribution of body fat.
DISCLOSURES:
The study was funded by UK Medical Research Council, UK Research and Innovation, and the European Commission.
A version of this article appeared on Medscape.com.
Diabetes Complication Risk Larger in US Small Towns
TOPLINE:
METHODOLOGY:
Retrospective cohort study using the OptumLabs Data Warehouse used a deidentified data set of US commercial and Medicare Advantage beneficiaries including 2,901,563 adults with diabetes between 2012 and 2021.
Overall, 2.6% lived in remote areas (population < 2500), 14.1% in small towns (2500-50,000), and 83.3% in cities (> 50,000).
Multivariable analysis adjusted for age, sex, health plan type, index year, diabetes type, baseline comorbidities, and medication use.
TAKEAWAY:
Relative to people living in cities, people in remote areas had significantly greater risks for myocardial infarction (hazard ratio, 1.06) and revascularization (1.04) but lower risks for hypoglycemia (0.90) and stroke (0.91).
Compared with cities, people living in small towns had significantly more hyperglycemia (1.06), hypoglycemia (1.15), end-stage kidney disease (1.04), myocardial infarction (1.10), heart failure (1.05), amputation (1.05), other lower-extremity complications (1.02), and revascularization (1.05), but a lower risk for stroke (0.95).
Compared with small towns, people living in remote areas had lower risks for hyperglycemia (0.85), hypoglycemia (0.92), and heart failure (0.94).
No geographic differences were found for retinopathy or atrial fibrillation/flutter.
The results didn’t differ significantly when the 2.5% overall with type 1 diabetes were removed from the dataset.
IN PRACTICE:
“While more research is needed to better understand the underlying causes of disparate diabetes outcomes along the rural-urban continuum, this study establishes the foundational differences to guide improvement efforts and helps to identify complications with the greatest disparities to which policy interventions may be targeted.”
SOURCE:
The study was conducted by Kyle Steiger, MD, Internal Medicine Residency, Mayo Clinic, Rochester, Minnesota, and colleagues, and published February 22 in Diabetes Care.
LIMITATIONS:
Claims data were from a single national health insurance provider that administers multiple private and Medicare Advantage health plans with disproportionate representation of urban populations and without people who have Medicaid or traditional Medicare fee-for-service or who are without insurance (and would be expected to have higher complication rates). There were no data on race/ethnicity. Potential for residual confounding.
DISCLOSURES:
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Steiger had no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
Retrospective cohort study using the OptumLabs Data Warehouse used a deidentified data set of US commercial and Medicare Advantage beneficiaries including 2,901,563 adults with diabetes between 2012 and 2021.
Overall, 2.6% lived in remote areas (population < 2500), 14.1% in small towns (2500-50,000), and 83.3% in cities (> 50,000).
Multivariable analysis adjusted for age, sex, health plan type, index year, diabetes type, baseline comorbidities, and medication use.
TAKEAWAY:
Relative to people living in cities, people in remote areas had significantly greater risks for myocardial infarction (hazard ratio, 1.06) and revascularization (1.04) but lower risks for hypoglycemia (0.90) and stroke (0.91).
Compared with cities, people living in small towns had significantly more hyperglycemia (1.06), hypoglycemia (1.15), end-stage kidney disease (1.04), myocardial infarction (1.10), heart failure (1.05), amputation (1.05), other lower-extremity complications (1.02), and revascularization (1.05), but a lower risk for stroke (0.95).
Compared with small towns, people living in remote areas had lower risks for hyperglycemia (0.85), hypoglycemia (0.92), and heart failure (0.94).
No geographic differences were found for retinopathy or atrial fibrillation/flutter.
The results didn’t differ significantly when the 2.5% overall with type 1 diabetes were removed from the dataset.
IN PRACTICE:
“While more research is needed to better understand the underlying causes of disparate diabetes outcomes along the rural-urban continuum, this study establishes the foundational differences to guide improvement efforts and helps to identify complications with the greatest disparities to which policy interventions may be targeted.”
SOURCE:
The study was conducted by Kyle Steiger, MD, Internal Medicine Residency, Mayo Clinic, Rochester, Minnesota, and colleagues, and published February 22 in Diabetes Care.
LIMITATIONS:
Claims data were from a single national health insurance provider that administers multiple private and Medicare Advantage health plans with disproportionate representation of urban populations and without people who have Medicaid or traditional Medicare fee-for-service or who are without insurance (and would be expected to have higher complication rates). There were no data on race/ethnicity. Potential for residual confounding.
DISCLOSURES:
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Steiger had no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
Retrospective cohort study using the OptumLabs Data Warehouse used a deidentified data set of US commercial and Medicare Advantage beneficiaries including 2,901,563 adults with diabetes between 2012 and 2021.
Overall, 2.6% lived in remote areas (population < 2500), 14.1% in small towns (2500-50,000), and 83.3% in cities (> 50,000).
Multivariable analysis adjusted for age, sex, health plan type, index year, diabetes type, baseline comorbidities, and medication use.
TAKEAWAY:
Relative to people living in cities, people in remote areas had significantly greater risks for myocardial infarction (hazard ratio, 1.06) and revascularization (1.04) but lower risks for hypoglycemia (0.90) and stroke (0.91).
Compared with cities, people living in small towns had significantly more hyperglycemia (1.06), hypoglycemia (1.15), end-stage kidney disease (1.04), myocardial infarction (1.10), heart failure (1.05), amputation (1.05), other lower-extremity complications (1.02), and revascularization (1.05), but a lower risk for stroke (0.95).
Compared with small towns, people living in remote areas had lower risks for hyperglycemia (0.85), hypoglycemia (0.92), and heart failure (0.94).
No geographic differences were found for retinopathy or atrial fibrillation/flutter.
The results didn’t differ significantly when the 2.5% overall with type 1 diabetes were removed from the dataset.
IN PRACTICE:
“While more research is needed to better understand the underlying causes of disparate diabetes outcomes along the rural-urban continuum, this study establishes the foundational differences to guide improvement efforts and helps to identify complications with the greatest disparities to which policy interventions may be targeted.”
SOURCE:
The study was conducted by Kyle Steiger, MD, Internal Medicine Residency, Mayo Clinic, Rochester, Minnesota, and colleagues, and published February 22 in Diabetes Care.
LIMITATIONS:
Claims data were from a single national health insurance provider that administers multiple private and Medicare Advantage health plans with disproportionate representation of urban populations and without people who have Medicaid or traditional Medicare fee-for-service or who are without insurance (and would be expected to have higher complication rates). There were no data on race/ethnicity. Potential for residual confounding.
DISCLOSURES:
This study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Steiger had no disclosures.
A version of this article appeared on Medscape.com.
How Good are Tools to Screen for Spondyloarthritis in Patients With Psoriasis, Uveitis, IBD?
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Osteoporosis Drug Denosumab May Confer Lower Risk for Diabetes
TOPLINE:
Continued denosumab treatment is associated with a lower risk for diabetes in adults with osteoporosis older than 65 years, found a large-scale cohort study in Taiwan.
METHODOLOGY:
- Denosumab, used in osteoporosis treatment, has been suggested to improve glycemic parameters, but clinical evidence of its effects on diabetes risk is limited and inconsistent.
- Using data from Taiwan’s National Health Insurance Research Database (NHIRD), the study asked if continued denosumab treatment (60 mg) for osteoporosis reduced the risk for diabetes compared to those who discontinued denosumab.
- Researchers included all new users of denosumab between 2012 and 2019 who had no prior history of malignant neoplasms, Paget disease, or diabetes requiring antidiabetic medication.
- Patients in the treatment group (n = 34,255), who received a second dose of denosumab within 225 days, were 1:1 propensity matched with a control group (n = 34,255) of patients who had discontinued denosumab after the first dose.
- The 68,510 patients (mean age, 77.7 years; 84.3% women) were followed up for a mean of 1.9 years. The primary outcome was new-onset diabetes that required treatment with any antidiabetic drug.
TAKEAWAY:
- Continued denosumab treatment vs its discontinuation was associated with a lower risk for incident diabetes (hazard ratio [HR], 0.84; 95% CI, 0.78-0.90).
- In patients aged 65 years or older who were on continued treatment of denosumab, the risk for diabetes was lower (HR, 0.80; 95% CI, 0.75-0.85) but not among those younger than 65 years.
- A reduced risk for diabetes with continued denosumab treatment was observed in both men (HR, 0.85; 95% CI, 0.73-0.97) and women (HR, 0.81; 95% CI, 0.76-0.86).
- Lower diabetes risk with continued denosumab treatment was observed regardless of comorbidities, such as dyslipidemia, hypertension, ischemic heart disease, or kidney failure.
IN PRACTICE:
“Given the high osteoporosis prevalence, the extensive use of antiosteoporosis medications, and the negative effect of diabetes on both patient health and healthcare system burdens in the global aging population, our findings possess substantial clinical and public health significance,” the authors wrote.
SOURCE:
This study was led by Huei-Kai Huang, MD, Department of Family Medicine and Department of Medical Research, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan, and published online in JAMA Network Open.
LIMITATIONS:
The research used claims-based data, so some clinical details, such as lifestyle, substance use, prediabetes weight status, and laboratory results, were not included. Owing to the anonymity policy of the NHIRD, patients could not be directly evaluated to validate incident diabetes. The study included the Taiwanese population, so the findings may not be generalizable to other populations. In Taiwan, the threshold for reimbursement of initiating denosumab treatment for osteoporosis includes below-normal bone density scores and a hip or vertebral fracture.
DISCLOSURES:
This study was supported by grants from the National Science and Technology Council of Taiwan and the National Health Research Institutes of Taiwan and a grant from the Buddhist Tzu Chi Medical Foundation. The corresponding author and a coauthor disclosed receiving funds from Amgen, Novartis, Pfizer, Sanofi, Takeda, and AbbVie, all outside the submitted work.
A version of this article appeared on Medscape.com.
TOPLINE:
Continued denosumab treatment is associated with a lower risk for diabetes in adults with osteoporosis older than 65 years, found a large-scale cohort study in Taiwan.
METHODOLOGY:
- Denosumab, used in osteoporosis treatment, has been suggested to improve glycemic parameters, but clinical evidence of its effects on diabetes risk is limited and inconsistent.
- Using data from Taiwan’s National Health Insurance Research Database (NHIRD), the study asked if continued denosumab treatment (60 mg) for osteoporosis reduced the risk for diabetes compared to those who discontinued denosumab.
- Researchers included all new users of denosumab between 2012 and 2019 who had no prior history of malignant neoplasms, Paget disease, or diabetes requiring antidiabetic medication.
- Patients in the treatment group (n = 34,255), who received a second dose of denosumab within 225 days, were 1:1 propensity matched with a control group (n = 34,255) of patients who had discontinued denosumab after the first dose.
- The 68,510 patients (mean age, 77.7 years; 84.3% women) were followed up for a mean of 1.9 years. The primary outcome was new-onset diabetes that required treatment with any antidiabetic drug.
TAKEAWAY:
- Continued denosumab treatment vs its discontinuation was associated with a lower risk for incident diabetes (hazard ratio [HR], 0.84; 95% CI, 0.78-0.90).
- In patients aged 65 years or older who were on continued treatment of denosumab, the risk for diabetes was lower (HR, 0.80; 95% CI, 0.75-0.85) but not among those younger than 65 years.
- A reduced risk for diabetes with continued denosumab treatment was observed in both men (HR, 0.85; 95% CI, 0.73-0.97) and women (HR, 0.81; 95% CI, 0.76-0.86).
- Lower diabetes risk with continued denosumab treatment was observed regardless of comorbidities, such as dyslipidemia, hypertension, ischemic heart disease, or kidney failure.
IN PRACTICE:
“Given the high osteoporosis prevalence, the extensive use of antiosteoporosis medications, and the negative effect of diabetes on both patient health and healthcare system burdens in the global aging population, our findings possess substantial clinical and public health significance,” the authors wrote.
SOURCE:
This study was led by Huei-Kai Huang, MD, Department of Family Medicine and Department of Medical Research, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan, and published online in JAMA Network Open.
LIMITATIONS:
The research used claims-based data, so some clinical details, such as lifestyle, substance use, prediabetes weight status, and laboratory results, were not included. Owing to the anonymity policy of the NHIRD, patients could not be directly evaluated to validate incident diabetes. The study included the Taiwanese population, so the findings may not be generalizable to other populations. In Taiwan, the threshold for reimbursement of initiating denosumab treatment for osteoporosis includes below-normal bone density scores and a hip or vertebral fracture.
DISCLOSURES:
This study was supported by grants from the National Science and Technology Council of Taiwan and the National Health Research Institutes of Taiwan and a grant from the Buddhist Tzu Chi Medical Foundation. The corresponding author and a coauthor disclosed receiving funds from Amgen, Novartis, Pfizer, Sanofi, Takeda, and AbbVie, all outside the submitted work.
A version of this article appeared on Medscape.com.
TOPLINE:
Continued denosumab treatment is associated with a lower risk for diabetes in adults with osteoporosis older than 65 years, found a large-scale cohort study in Taiwan.
METHODOLOGY:
- Denosumab, used in osteoporosis treatment, has been suggested to improve glycemic parameters, but clinical evidence of its effects on diabetes risk is limited and inconsistent.
- Using data from Taiwan’s National Health Insurance Research Database (NHIRD), the study asked if continued denosumab treatment (60 mg) for osteoporosis reduced the risk for diabetes compared to those who discontinued denosumab.
- Researchers included all new users of denosumab between 2012 and 2019 who had no prior history of malignant neoplasms, Paget disease, or diabetes requiring antidiabetic medication.
- Patients in the treatment group (n = 34,255), who received a second dose of denosumab within 225 days, were 1:1 propensity matched with a control group (n = 34,255) of patients who had discontinued denosumab after the first dose.
- The 68,510 patients (mean age, 77.7 years; 84.3% women) were followed up for a mean of 1.9 years. The primary outcome was new-onset diabetes that required treatment with any antidiabetic drug.
TAKEAWAY:
- Continued denosumab treatment vs its discontinuation was associated with a lower risk for incident diabetes (hazard ratio [HR], 0.84; 95% CI, 0.78-0.90).
- In patients aged 65 years or older who were on continued treatment of denosumab, the risk for diabetes was lower (HR, 0.80; 95% CI, 0.75-0.85) but not among those younger than 65 years.
- A reduced risk for diabetes with continued denosumab treatment was observed in both men (HR, 0.85; 95% CI, 0.73-0.97) and women (HR, 0.81; 95% CI, 0.76-0.86).
- Lower diabetes risk with continued denosumab treatment was observed regardless of comorbidities, such as dyslipidemia, hypertension, ischemic heart disease, or kidney failure.
IN PRACTICE:
“Given the high osteoporosis prevalence, the extensive use of antiosteoporosis medications, and the negative effect of diabetes on both patient health and healthcare system burdens in the global aging population, our findings possess substantial clinical and public health significance,” the authors wrote.
SOURCE:
This study was led by Huei-Kai Huang, MD, Department of Family Medicine and Department of Medical Research, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan, and published online in JAMA Network Open.
LIMITATIONS:
The research used claims-based data, so some clinical details, such as lifestyle, substance use, prediabetes weight status, and laboratory results, were not included. Owing to the anonymity policy of the NHIRD, patients could not be directly evaluated to validate incident diabetes. The study included the Taiwanese population, so the findings may not be generalizable to other populations. In Taiwan, the threshold for reimbursement of initiating denosumab treatment for osteoporosis includes below-normal bone density scores and a hip or vertebral fracture.
DISCLOSURES:
This study was supported by grants from the National Science and Technology Council of Taiwan and the National Health Research Institutes of Taiwan and a grant from the Buddhist Tzu Chi Medical Foundation. The corresponding author and a coauthor disclosed receiving funds from Amgen, Novartis, Pfizer, Sanofi, Takeda, and AbbVie, all outside the submitted work.
A version of this article appeared on Medscape.com.
Promising New Wearable Could Retrain the Brain After Stroke
A new and deceptively simple advance in chronic stroke treatment could be a vibrating glove.
Researchers at Stanford University and Georgia Tech have developed a wearable device that straps around the wrist and hand, delivering subtle vibrations (akin to a vibrating cellphone) that may relieve spasticity as well as or better than the standard Botox injections.
“The vibro-tactile stimulation can be used at home, and we’re hoping it can be relatively low cost,” said senior study author Allison Okamura, PhD, a mechanical engineer at Stanford University, Stanford, California.
For now, the device is available only to clinical trial patients. But the researchers hope to get the glove into — or rather onto — more patients’ hands within a few years. A recent grant from the National Science Foundation’s Convergence Accelerator program could help pave the way to a commercial product. The team also hopes to expand access in the meantime through larger clinical trials with patients in additional locations.
The work builds on accumulating research exploring vibration and other stimulation therapies as treatments for neurological conditions. Other vibrating gloves have helped reduce involuntary movement for patients with Parkinson’s. And the University of Kansas Medical Center, Kansas City, will soon trial the Food and Drug Administration–approved vagal nerve stimulator, an implantable device intended to treat motor function in stroke survivors. Dr. Okamura noted that devices use “different types of vibration patterns and intensities,” depending on the disease state they target.
Spasticity often develops or worsens months after a stroke. By then, patients may have run out of insurance coverage for rehabilitation. And the effectiveness of Botox injections can “wear out over time,” Dr. Okamura said.
In a clinical trial, patients wore the device for 3 hours a day for 8 weeks, while doing their usual activities. The researchers continued testing their spasticity for 2 more weeks.
How Vibro-Tactile Stimulation May Rewire the Brain
The device originated at Georgia Tech, where Dr. Okamura’s postdoctoral research fellow Caitlyn Seim, PhD, was using vibro-tactile stimulation (VTS) to teach people skills, such as playing the piano, using touch-feedback training. The team decided to target spasticity, which VTS had helped in previousstudies of in-clinic (non-wearable) devices.
How does the device work? The researchers point to neuroplasticity, the ability of neurons to create new synapses or strengthen existing ones in the brain.
“The stimulation is sending additional sensory signals to the brain, which helps the brain interpret and reconnect any lost circuits,” Dr. Okamura said.
Spasticity is driven by “an imbalance in the excitatory drive to the muscles,” she continued. This can lead to worsening contractions, until a hand closes into a fist or a foot curls up. (The team has also done preliminary research on a similar device for foot spasticity, which they hope to continue developing.) Previous studies by Okamura and others suggest that vibration stimulation may prevent these contractions, both in the short and long term.
“Immediately, we do see some softening of the muscles,” Dr. Okamura said. “But in our longer-term study, where we compared to Botox, I also think that the vibration may be retraining the brain to send inhibitory signals. And that can restore balance that’s lost due to the damaged neural circuits from a stroke.”
When the team did a separate study comparing the effects of muscle and skin stimulation, they hypothesized that the vibration could be having a biomechanical effect on the muscle. Instead, they found that stimulating the skin had a greater impact — a “somewhat unexpected” result, Dr. Okamura said. That led them to the brain.
“Stimulating the skin is really about creating sensory signals that get sent to the brain,” Dr. Okamura said, “which is why we think it’s actually a brain-retraining effect and not a direct biomechanical effect.”
What’s Next?
The researchers are seeking funding for longer-term clinical studies to find out if effects persist beyond 2 weeks. They also want to explore how long and often patients should wear the glove for best results.
The researchers also want to study how movement might enhance the effects of the device.
“One of the treatments for spasticity — medications aside, this vibration machine aside — is more exercise, more passive range of motion,” said Oluwole O. Awosika, MD, associate professor at the University of Cincinnati College of Medicine, who was not involved in the study. “It would have been nice to have a control group that didn’t get any of this stimulation or that was only encouraged to do 3 hours of movement a day. What would the difference be?”
Dr. Awosika also wondered how easy it would be for stroke patients without in-home assistance to use the device. “Sometimes wearing these devices requires someone to put it on,” he said.
Of course, if all goes well, patients wouldn’t have to deal with that forever. “The dream would be that you reach true rehabilitation, which is no longer needing the device,” Dr. Okamura said.
A version of this article appeared on Medscape.com.
A new and deceptively simple advance in chronic stroke treatment could be a vibrating glove.
Researchers at Stanford University and Georgia Tech have developed a wearable device that straps around the wrist and hand, delivering subtle vibrations (akin to a vibrating cellphone) that may relieve spasticity as well as or better than the standard Botox injections.
“The vibro-tactile stimulation can be used at home, and we’re hoping it can be relatively low cost,” said senior study author Allison Okamura, PhD, a mechanical engineer at Stanford University, Stanford, California.
For now, the device is available only to clinical trial patients. But the researchers hope to get the glove into — or rather onto — more patients’ hands within a few years. A recent grant from the National Science Foundation’s Convergence Accelerator program could help pave the way to a commercial product. The team also hopes to expand access in the meantime through larger clinical trials with patients in additional locations.
The work builds on accumulating research exploring vibration and other stimulation therapies as treatments for neurological conditions. Other vibrating gloves have helped reduce involuntary movement for patients with Parkinson’s. And the University of Kansas Medical Center, Kansas City, will soon trial the Food and Drug Administration–approved vagal nerve stimulator, an implantable device intended to treat motor function in stroke survivors. Dr. Okamura noted that devices use “different types of vibration patterns and intensities,” depending on the disease state they target.
Spasticity often develops or worsens months after a stroke. By then, patients may have run out of insurance coverage for rehabilitation. And the effectiveness of Botox injections can “wear out over time,” Dr. Okamura said.
In a clinical trial, patients wore the device for 3 hours a day for 8 weeks, while doing their usual activities. The researchers continued testing their spasticity for 2 more weeks.
How Vibro-Tactile Stimulation May Rewire the Brain
The device originated at Georgia Tech, where Dr. Okamura’s postdoctoral research fellow Caitlyn Seim, PhD, was using vibro-tactile stimulation (VTS) to teach people skills, such as playing the piano, using touch-feedback training. The team decided to target spasticity, which VTS had helped in previousstudies of in-clinic (non-wearable) devices.
How does the device work? The researchers point to neuroplasticity, the ability of neurons to create new synapses or strengthen existing ones in the brain.
“The stimulation is sending additional sensory signals to the brain, which helps the brain interpret and reconnect any lost circuits,” Dr. Okamura said.
Spasticity is driven by “an imbalance in the excitatory drive to the muscles,” she continued. This can lead to worsening contractions, until a hand closes into a fist or a foot curls up. (The team has also done preliminary research on a similar device for foot spasticity, which they hope to continue developing.) Previous studies by Okamura and others suggest that vibration stimulation may prevent these contractions, both in the short and long term.
“Immediately, we do see some softening of the muscles,” Dr. Okamura said. “But in our longer-term study, where we compared to Botox, I also think that the vibration may be retraining the brain to send inhibitory signals. And that can restore balance that’s lost due to the damaged neural circuits from a stroke.”
When the team did a separate study comparing the effects of muscle and skin stimulation, they hypothesized that the vibration could be having a biomechanical effect on the muscle. Instead, they found that stimulating the skin had a greater impact — a “somewhat unexpected” result, Dr. Okamura said. That led them to the brain.
“Stimulating the skin is really about creating sensory signals that get sent to the brain,” Dr. Okamura said, “which is why we think it’s actually a brain-retraining effect and not a direct biomechanical effect.”
What’s Next?
The researchers are seeking funding for longer-term clinical studies to find out if effects persist beyond 2 weeks. They also want to explore how long and often patients should wear the glove for best results.
The researchers also want to study how movement might enhance the effects of the device.
“One of the treatments for spasticity — medications aside, this vibration machine aside — is more exercise, more passive range of motion,” said Oluwole O. Awosika, MD, associate professor at the University of Cincinnati College of Medicine, who was not involved in the study. “It would have been nice to have a control group that didn’t get any of this stimulation or that was only encouraged to do 3 hours of movement a day. What would the difference be?”
Dr. Awosika also wondered how easy it would be for stroke patients without in-home assistance to use the device. “Sometimes wearing these devices requires someone to put it on,” he said.
Of course, if all goes well, patients wouldn’t have to deal with that forever. “The dream would be that you reach true rehabilitation, which is no longer needing the device,” Dr. Okamura said.
A version of this article appeared on Medscape.com.
A new and deceptively simple advance in chronic stroke treatment could be a vibrating glove.
Researchers at Stanford University and Georgia Tech have developed a wearable device that straps around the wrist and hand, delivering subtle vibrations (akin to a vibrating cellphone) that may relieve spasticity as well as or better than the standard Botox injections.
“The vibro-tactile stimulation can be used at home, and we’re hoping it can be relatively low cost,” said senior study author Allison Okamura, PhD, a mechanical engineer at Stanford University, Stanford, California.
For now, the device is available only to clinical trial patients. But the researchers hope to get the glove into — or rather onto — more patients’ hands within a few years. A recent grant from the National Science Foundation’s Convergence Accelerator program could help pave the way to a commercial product. The team also hopes to expand access in the meantime through larger clinical trials with patients in additional locations.
The work builds on accumulating research exploring vibration and other stimulation therapies as treatments for neurological conditions. Other vibrating gloves have helped reduce involuntary movement for patients with Parkinson’s. And the University of Kansas Medical Center, Kansas City, will soon trial the Food and Drug Administration–approved vagal nerve stimulator, an implantable device intended to treat motor function in stroke survivors. Dr. Okamura noted that devices use “different types of vibration patterns and intensities,” depending on the disease state they target.
Spasticity often develops or worsens months after a stroke. By then, patients may have run out of insurance coverage for rehabilitation. And the effectiveness of Botox injections can “wear out over time,” Dr. Okamura said.
In a clinical trial, patients wore the device for 3 hours a day for 8 weeks, while doing their usual activities. The researchers continued testing their spasticity for 2 more weeks.
How Vibro-Tactile Stimulation May Rewire the Brain
The device originated at Georgia Tech, where Dr. Okamura’s postdoctoral research fellow Caitlyn Seim, PhD, was using vibro-tactile stimulation (VTS) to teach people skills, such as playing the piano, using touch-feedback training. The team decided to target spasticity, which VTS had helped in previousstudies of in-clinic (non-wearable) devices.
How does the device work? The researchers point to neuroplasticity, the ability of neurons to create new synapses or strengthen existing ones in the brain.
“The stimulation is sending additional sensory signals to the brain, which helps the brain interpret and reconnect any lost circuits,” Dr. Okamura said.
Spasticity is driven by “an imbalance in the excitatory drive to the muscles,” she continued. This can lead to worsening contractions, until a hand closes into a fist or a foot curls up. (The team has also done preliminary research on a similar device for foot spasticity, which they hope to continue developing.) Previous studies by Okamura and others suggest that vibration stimulation may prevent these contractions, both in the short and long term.
“Immediately, we do see some softening of the muscles,” Dr. Okamura said. “But in our longer-term study, where we compared to Botox, I also think that the vibration may be retraining the brain to send inhibitory signals. And that can restore balance that’s lost due to the damaged neural circuits from a stroke.”
When the team did a separate study comparing the effects of muscle and skin stimulation, they hypothesized that the vibration could be having a biomechanical effect on the muscle. Instead, they found that stimulating the skin had a greater impact — a “somewhat unexpected” result, Dr. Okamura said. That led them to the brain.
“Stimulating the skin is really about creating sensory signals that get sent to the brain,” Dr. Okamura said, “which is why we think it’s actually a brain-retraining effect and not a direct biomechanical effect.”
What’s Next?
The researchers are seeking funding for longer-term clinical studies to find out if effects persist beyond 2 weeks. They also want to explore how long and often patients should wear the glove for best results.
The researchers also want to study how movement might enhance the effects of the device.
“One of the treatments for spasticity — medications aside, this vibration machine aside — is more exercise, more passive range of motion,” said Oluwole O. Awosika, MD, associate professor at the University of Cincinnati College of Medicine, who was not involved in the study. “It would have been nice to have a control group that didn’t get any of this stimulation or that was only encouraged to do 3 hours of movement a day. What would the difference be?”
Dr. Awosika also wondered how easy it would be for stroke patients without in-home assistance to use the device. “Sometimes wearing these devices requires someone to put it on,” he said.
Of course, if all goes well, patients wouldn’t have to deal with that forever. “The dream would be that you reach true rehabilitation, which is no longer needing the device,” Dr. Okamura said.
A version of this article appeared on Medscape.com.
FDA Approves Amivantamab First-line Indication for NSCLC
Specifically, the FDA approved the first-line use of the agent in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with epidermal growth factor receptor (EGFR) exon 20 insertion mutations, as detected by an FDA-approved test.
The FDA also granted traditional approval for use in these patients after their cancer has progressed on or following platinum-based chemotherapy. The original accelerated approval for this indication occurred in 2021. At that time, the FDA also approved Guardant360® CDx (Guardant Health, Inc.) as a companion diagnostic test for amivantamab-vmjw.
The first-line approval, which followed priority review, was based on the randomized, open-label PAPILLON trial, which revealed a statistically significant improvement in progression-free survival (PFS) among the 153 patients who received amivantamab-vmjw plus carboplatin and pemetrexed vs the 155 who received the chemotherapy combination alone. Median PFS was 11.4 months in the amivantamab-vmjw arm vs 6.7 months in the control arm (hazard ratio, 0.40).
Data for overall survival, a key secondary endpoint of the study, were immature at the time of the latest analysis, but “no trend toward a detriment was observed,” according to an FDA approval announcement.
Common adverse reactions, occurring in at least 20% of patients in the study, were rash, nail toxicity, stomatitis, infusion-related reaction, fatigue, edema, constipation, decreased appetite, nausea, diarrhea, and vomiting. Weight-based dosing guidance can be found in the full prescribing information.
A version of this article appeared on Medscape.com.
Specifically, the FDA approved the first-line use of the agent in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with epidermal growth factor receptor (EGFR) exon 20 insertion mutations, as detected by an FDA-approved test.
The FDA also granted traditional approval for use in these patients after their cancer has progressed on or following platinum-based chemotherapy. The original accelerated approval for this indication occurred in 2021. At that time, the FDA also approved Guardant360® CDx (Guardant Health, Inc.) as a companion diagnostic test for amivantamab-vmjw.
The first-line approval, which followed priority review, was based on the randomized, open-label PAPILLON trial, which revealed a statistically significant improvement in progression-free survival (PFS) among the 153 patients who received amivantamab-vmjw plus carboplatin and pemetrexed vs the 155 who received the chemotherapy combination alone. Median PFS was 11.4 months in the amivantamab-vmjw arm vs 6.7 months in the control arm (hazard ratio, 0.40).
Data for overall survival, a key secondary endpoint of the study, were immature at the time of the latest analysis, but “no trend toward a detriment was observed,” according to an FDA approval announcement.
Common adverse reactions, occurring in at least 20% of patients in the study, were rash, nail toxicity, stomatitis, infusion-related reaction, fatigue, edema, constipation, decreased appetite, nausea, diarrhea, and vomiting. Weight-based dosing guidance can be found in the full prescribing information.
A version of this article appeared on Medscape.com.
Specifically, the FDA approved the first-line use of the agent in combination with carboplatin and pemetrexed in patients with locally advanced or metastatic NSCLC with epidermal growth factor receptor (EGFR) exon 20 insertion mutations, as detected by an FDA-approved test.
The FDA also granted traditional approval for use in these patients after their cancer has progressed on or following platinum-based chemotherapy. The original accelerated approval for this indication occurred in 2021. At that time, the FDA also approved Guardant360® CDx (Guardant Health, Inc.) as a companion diagnostic test for amivantamab-vmjw.
The first-line approval, which followed priority review, was based on the randomized, open-label PAPILLON trial, which revealed a statistically significant improvement in progression-free survival (PFS) among the 153 patients who received amivantamab-vmjw plus carboplatin and pemetrexed vs the 155 who received the chemotherapy combination alone. Median PFS was 11.4 months in the amivantamab-vmjw arm vs 6.7 months in the control arm (hazard ratio, 0.40).
Data for overall survival, a key secondary endpoint of the study, were immature at the time of the latest analysis, but “no trend toward a detriment was observed,” according to an FDA approval announcement.
Common adverse reactions, occurring in at least 20% of patients in the study, were rash, nail toxicity, stomatitis, infusion-related reaction, fatigue, edema, constipation, decreased appetite, nausea, diarrhea, and vomiting. Weight-based dosing guidance can be found in the full prescribing information.
A version of this article appeared on Medscape.com.
New Biomarkers Identified to Help Predict Cardiovascular Risk in RA
TOPLINE:
Researchers have identified six blood biomarkers tied to changes in arterial inflammation in patients with rheumatoid arthritis (RA).
METHODOLOGY:
- Researchers selected 24 candidate blood biomarkers previously associated with both RA and systemic inflammation.
- They measured biomarkers in 109 patients in the , which tested whether different treatments for RA reduced arterial inflammation.
- Along with biomarkers, they measured arterial inflammation via [18F] fluorodeoxyglucose (FDG)-PET/CT scans at baseline and 24 weeks.
TAKEAWAY:
- Baseline levels of the biomarkers serum amyloid A, C-reactive protein, soluble tumor necrosis factor receptor 1, adiponectin, YKL-4, and osteoprotegerin were associated with significant changes in arterial inflammation on FDG-PET/CT scans.
- Adding these biomarkers to predictive models improved the adjusted R2 from 0.20 to 0.32 (likelihood ratio test, P = .0005).
- Researchers plan to validate these associations in a larger, external patient cohort.
IN PRACTICE:
This study is too preliminary to have practical applications.
SOURCE:
The study, led by Daniel Solomon, MD, of Brigham and Women’s Hospital, Boston, was published on February 28 in the Journal of the American Heart Association.
DISCLOSURES:
The research was funded by a National Institutes of Health grant as well as the Foundation for the National Institutes of Health Biomarkers Consortium. Several authors reported salary support or consulting fees from pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Researchers have identified six blood biomarkers tied to changes in arterial inflammation in patients with rheumatoid arthritis (RA).
METHODOLOGY:
- Researchers selected 24 candidate blood biomarkers previously associated with both RA and systemic inflammation.
- They measured biomarkers in 109 patients in the , which tested whether different treatments for RA reduced arterial inflammation.
- Along with biomarkers, they measured arterial inflammation via [18F] fluorodeoxyglucose (FDG)-PET/CT scans at baseline and 24 weeks.
TAKEAWAY:
- Baseline levels of the biomarkers serum amyloid A, C-reactive protein, soluble tumor necrosis factor receptor 1, adiponectin, YKL-4, and osteoprotegerin were associated with significant changes in arterial inflammation on FDG-PET/CT scans.
- Adding these biomarkers to predictive models improved the adjusted R2 from 0.20 to 0.32 (likelihood ratio test, P = .0005).
- Researchers plan to validate these associations in a larger, external patient cohort.
IN PRACTICE:
This study is too preliminary to have practical applications.
SOURCE:
The study, led by Daniel Solomon, MD, of Brigham and Women’s Hospital, Boston, was published on February 28 in the Journal of the American Heart Association.
DISCLOSURES:
The research was funded by a National Institutes of Health grant as well as the Foundation for the National Institutes of Health Biomarkers Consortium. Several authors reported salary support or consulting fees from pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Researchers have identified six blood biomarkers tied to changes in arterial inflammation in patients with rheumatoid arthritis (RA).
METHODOLOGY:
- Researchers selected 24 candidate blood biomarkers previously associated with both RA and systemic inflammation.
- They measured biomarkers in 109 patients in the , which tested whether different treatments for RA reduced arterial inflammation.
- Along with biomarkers, they measured arterial inflammation via [18F] fluorodeoxyglucose (FDG)-PET/CT scans at baseline and 24 weeks.
TAKEAWAY:
- Baseline levels of the biomarkers serum amyloid A, C-reactive protein, soluble tumor necrosis factor receptor 1, adiponectin, YKL-4, and osteoprotegerin were associated with significant changes in arterial inflammation on FDG-PET/CT scans.
- Adding these biomarkers to predictive models improved the adjusted R2 from 0.20 to 0.32 (likelihood ratio test, P = .0005).
- Researchers plan to validate these associations in a larger, external patient cohort.
IN PRACTICE:
This study is too preliminary to have practical applications.
SOURCE:
The study, led by Daniel Solomon, MD, of Brigham and Women’s Hospital, Boston, was published on February 28 in the Journal of the American Heart Association.
DISCLOSURES:
The research was funded by a National Institutes of Health grant as well as the Foundation for the National Institutes of Health Biomarkers Consortium. Several authors reported salary support or consulting fees from pharmaceutical companies.
A version of this article appeared on Medscape.com.
Find your community with CHEST Interest Groups
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.



To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
To learn more about Interest Groups and how to join, go to chestnet.org/interest-groups.
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
Learn about the LGBTQ+ at CHEST, Respiratory Care, and Women in Chest Medicine Interest Groups
, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.
To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
To learn more about Interest Groups and how to join, go to chestnet.org/interest-groups.
, we were proud to add Interest Groups to our member offerings in 2023.
The introduction of Interest Groups has proven to be an effective way to organically connect CHEST members with shared interests and passions. Membership in one of these groups allows for networking in a smaller setting, with the goals of supporting career development and enriching an individual’s professional path.
To learn more about the three existing Interest Groups, we spoke with each group’s chair: Margaret Pisani, MD, FCCP, Chair of the Women in Chest Medicine Interest Group; Kevin O’Neil, MD, FCCP, Chair of the Respiratory Care Interest Group; and Mauricio Danckers, MD, FCCP, Chair of the LGBTQ+ at CHEST Interest Group.
1) Tell us about the key issues that your Interest Group is trying to address and who should join this group.
Mauricio Danckers: Our LGBTQ+ community continues to be the target of unrelenting discrimination. Current disparities toward sexual and gender-diverse individuals persistently hinder their personal and professional growth. There are several key issues currently affecting the LGBTQ+ community; among those are ongoing health care disparities, lack of education of our providers on LGBTQ+ health issues, underrepresentation of scientific research in the LGBTQ+ community, and scarce opportunities for mentorship and networking among LGBTQ+ health professionals. Our Interest Group seeks to provide a space to work together to overcome these shortcomings. Through the exchange of ideas, the opportunity for interprofessional collaborations, resource development and dissemination, scholar productivity, organic mentoring, and patient and provider advocacy, we seek to create change and better serve the LGBTQ+ identity in our CHEST community.
Anyone who is ready to make a change for the LGBTQ+ community, their care, and their well-being is encouraged to join. Self-identification as a member of the LGBTQ+ community is not a prerequisite for joining our group. We welcome individuals committed to advancing gender-affirming health, wellness, and education approaches to reduce health disparities.
Kevin O’Neil: The Respiratory Care Interest Group is invested in a number of focus areas, including improving collaboration between pulmonary/critical care/sleep physicians and respiratory care providers with a goal of improved and more efficient patient care, addressing critical shortages in the respiratory therapist (RT) workforce in collaboration with respiratory care organizations by identifying and supporting strategies to grow the workforce, and promoting wellness in all members of the community by providing tools and resources to mitigate stress and reduce burnout.
This Interest Group is for any CHEST member with an interest in respiratory care education or care delivery.
Margaret Pisani: The Women in Chest Medicine Interest Group has two overarching goals. The first is focused on ensuring that content around sex as a biologic variable and the impact of gender—as they relate to lung disease and critical care—are addressed in the educational activities of CHEST. The second is to provide mentorship and aid with career advancement for women in pulmonary, critical care, and sleep medicine (PCCSM) who are members of CHEST.
Anyone who does research on the impact of sex and gender as biologic variables—and the importance of these variables in lung disease—is welcome in this Interest Group. Persons who would like to be involved in mentoring the next generation of women and junior members who would like to learn more about how to be active at CHEST are also encouraged to join.
2) What motivated you to lead an Interest Group?
Danckers: My path in medicine as an LGBTQ+ individual has been unique and personal. It has opened the opportunity to witness the urgency of the changes needed to serve our LGBTQ+ community better. I wanted to lead this Interest Group to connect to other members interested in advancing health care equity for LGBTQ+ individuals, to inspire one another to achieve major changes in LGBTQ+ health education, and to ignite an educational and social initiative supported by CHEST to witness the LGBTQ+ medical community thriving while grounded on mentoring and advocacy.
O’Neil: I’ve been a CHEST member for more than 35 years and involved with respiratory care almost as long. The relationship between pulmonary/critical care physicians and RTs is unique, and RTs are critically important to my ability to care for my patients. I am committed to facilitating opportunities for collaboration between the two groups.
Pisani: I am motivated by my passion to ensure we are providing the best possible education to our members and patients and supporting the next generation of leaders in the PCCSM community.
3) What are the goals for your Interest Group in 2024?
Danckers: 2024 will be an exciting year, no doubt about it! Our goals for 2024 are: 1) to connect talented individuals with professional goals that align with the ones from the Interest Group and CHEST, 2) to increase the presence of the LGBTQ+ identity representation in our CHEST scientific meetings and educational offerings, 3) to build a resource platform for LGBTQ+ health education with the innovative approach CHEST is known to provide, and 4) to provide venues to inspire and support scholarly work within the LGBTQ+ community.
O’Neil: Growing the Interest Group membership and increasing opportunities for RTs to participate in CHEST activities by providing a landing space for new RT members are key initiatives for us. We are also hoping to increase the visibility of the Interest Group through events at the annual meeting, educational offerings, and other opportunities as they arise. We will also focus on improving communication between CHEST and other respiratory organizations.
Pisani: We are focused on ensuring that sex and gender topics are addressed during scientific presentations when relevant to research and patient care and developing resources on specific topics where there is data regarding the impact of sex and gender in lung disease.
To learn more about Interest Groups and how to join, go to chestnet.org/interest-groups.
Leading with integrity: A values-driven year
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.

As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at [email protected]. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
Until next time,
Jack D. Buckley, MD, MPH, FCCP
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.
As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at [email protected]. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
Until next time,
Jack D. Buckley, MD, MPH, FCCP
As the President of the American College of Chest Physicians (CHEST), I have the privilege of regularly addressing CHEST members through a quarterly column where I can share updates and expand on topics that we hold in high regard.
As such, I’d like to focus on the CHEST commitment to social responsibility and the work we have done and will continue to do throughout this year and beyond.
In 2023, under the leadership of my predecessor, Doreen Addrizzo-Harris, MD, FCCP, CHEST made strong changes to our organizational focus, including cementing Social Responsibility as a formal pillar of CHEST. In addition to our other four pillars—Education, People, Products, and Growth—this new pillar is a sign of our stronger commitment to be more explicit in our aspirations, measure our success, and move the bar higher.
As part of the new social responsibility pillar, CHEST philanthropy evolved from what was known as the CHEST Foundation and defined a new giving strategy that reflects our organizational commitment to clinical research, community impact, support for the profession, and fostering education. Through growth in our research support and furthering community impact, 2024 will be a strong year of providing grant support aligned to this new giving strategy.
In addition, we formalized how CHEST will pursue our new social responsibility pillar. In 2023, we articulated our organizational values—Community, Inclusivity, Innovation, Advocacy, and Integrity—which will serve as a consistent reminder of who we are as an organization and guide us in decisions as we pursue our mission.
Led by these values, CHEST will use its voice and capabilities to promote change that equitably impacts our community. In 2024 specifically, the organization looks forward to engaging actively with social responsibility by expanding volunteer opportunities local to CHEST headquarters and in conjunction with the location of the annual meeting.
It is also my hope that 2024 will be known as a year of member input, starring feedback from none other than you, our members.
For those who recall my address from the Opening Session at CHEST 2023, I very much encourage you to reach out to share with me your thoughts, your CHEST experience, and more at [email protected]. I look forward to having this regular touchpoint with all of you, and I welcome your input on topics you’d like to hear more on.
Until next time,
Jack D. Buckley, MD, MPH, FCCP
Implementing a critical care TEE program at your institution
Starting from the ground up!
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.

In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).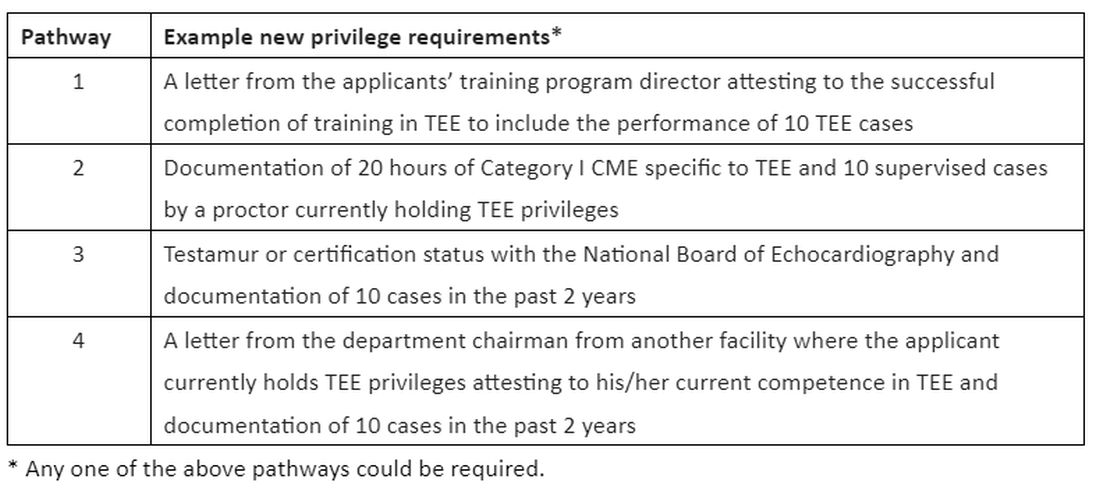
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.
Starting from the ground up!
Starting from the ground up!
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.
In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.
Bedside-focused cardiac ultrasound assessment, or cardiac point-of-care ultrasound (POCUS), has become common in intensive care units throughout the US and the world.
However, obtaining images adequate for decision making via standard transthoracic echo (TTE) is not possible in a significant number of patients; as high as 30% of critically ill patients, according to The American Society of Echocardiography (ASE) guidelines.1 Factors common to critically ill patients, such as invasive mechanical ventilation, external dressings, and limited mobility, contribute to poor image acquisition.
In almost all these cases, the factors limiting image acquisition can be eliminated by utilizing a transesophageal approach. In a recent study, researchers were able to demonstrate that adding transesophageal echocardiography (TEE) to TTE in critically ill patients yielded a new diagnosis or a change in management about 45% of the time.2
Using transesophageal ultrasound for a focused cardiac assessment in hemodynamically unstable patients is not new—and is often referred to as rescue TEE or resuscitative TEE. A broader term, transesophageal ultrasound, has also been used to include sonographic evaluation of the lungs in patients with poor acoustic windows. At my institution, we use the term critical care TEE to define TEE performed by a noncardiology-trained intensivist in an intubated critically ill patient.
Regardless of the term, the use of transesophageal ultrasound by the noncardiologist in the ICU appears to be a developing trend. As with other uses of POCUS, ultrasound machines continue to be able to “do more” at a lower price point. In 2024, several cart-based ultrasound machines are compatible with transesophageal probes and contain software packages capable of common cardiac measurements.
Despite this growing interest, intensivists are likely to encounter barriers to implementing critical care TEE. Our division recently implemented adding TEE to our practice. Our practice involves two separate systems: a Veterans Administration hospital and a university-based county hospital. Our division has integrated the use of TEE in the medical ICU at both institutions. Having navigated the process at both institutions, I can offer some guidance in navigating barriers.
The development of a critical care TEE program must start with a strong base in transthoracic cardiac POCUS, at least for the foreseeable future. Having a strong background in TTE gives learners a solid foundation in cardiac anatomy, cardiac function, and ultrasound properties. Obtaining testamur status or board certification in critical care echocardiography is not an absolute must but is a definite benefit. Having significant experience in TTE image acquisition and interpretation will flatten the learning curve for TEE. Interestingly, image acquisition in TEE is often easier than in TTE, so the paradigm of learning TTE before TEE may reverse in the years to come.
Two barriers often work together to create a vicious cycle that stops the development of a TEE program at its start. These barriers include the lack of training and lack of equipment, specifically a TEE probe. Those who do not understand the value of TEE may ask, “Why purchase equipment for a procedure that you do not yet know how to do?” The opposite question can also be asked, “Why get trained to do something you don’t have the equipment to perform?”
My best advice to break this cycle is to “dive in” to whichever barrier seems easier to overcome first. I started with obtaining knowledge and training. Obtaining training and education in a procedure that is historically not done in your specialty is challenging but is not impossible. It takes a combination of high levels of self-motivation and at least one colleague with the training to support you. I approached a cardiac anesthesiologist, whom I knew from the surgical ICU. Cardiologists can also be a resource, but working with cardiac anesthesiologists offers several advantages. TEEs done by cardiac anesthesiologists are similar to those done in ICU patients (ie, all patients are intubated and sedated). The procedures are also scheduled several days in advance, making it easier to integrate training into your daily work schedule. Lastly, the TEE probe remains in place for several hours, so repeating the probe manipulations again as a learner does not add additional risk to the patient. In my case, we somewhat arbitrarily agreed that I participate in 25 TEE exams. (CME courses, both online and in-person simulation, exist and greatly supplement self-study.)
Obtaining equipment is also a common barrier, though this has become less restrictive in the last several years. As previously mentioned, many cart-based ultrasound machines can accommodate a TEE probe. This changes the request from purchasing a new machine to “just a probe.” Despite the higher cost than most other probes, those in charge of purchasing are often more open to purchasing “a probe” than to purchasing an ultrasound machine.
Additionally, the purchasing decision regarding probes may fall to a different person than it does for an ultrasound machine. If available, POCUS image archiving into the medical record can help offset the cost of equipment, both by increasing revenue via billing and by demonstrating that equipment is being used. If initially declined, continue to ask and work to integrate the purchase into the next year’s budget. Inquire about the process of making a formal request and follow that process. This will often involve obtaining a quote or quotes from the ultrasound manufacturer(s).
Keep in mind that the probe will require a special storage cabinet specifically designed for TEE probes. It is prudent to include this in budget requests. If needed, the echocardiography lab can be a useful resource for additional information regarding the cabinet requirements. It is strongly recommended to discuss TEE probe models with sterile processing before any purchasing. If options are available, it is wise to choose a model the hospital already uses, as the cleaning protocol is well established. Our unit purchased a model that did not have an established protocol, which took nearly 6 months to develop. If probe options are limited, involving sterile processing early to start developing a protocol will help decrease delays.
Obtaining hospital privileges is also a common barrier, though this may not be as challenging as expected. Hospitals typically have well-outlined policies on obtaining privileges for established procedures. One of our hospital systems had four different options; the most straightforward required 20 hours of CME specific to TEE and 10 supervised cases by a proctor currently holding TEE privileges (see Table 1).
Discussions about obtaining privileges should involve your division chief, chair of medicine, and the cardiology division chief. Clearly outlining the plan to perform this procedure only in critically ill patients who are already intubated for other reasons made these conversations go much more smoothly. In the development of delineation of privileges, we used the term critical care TEE to clearly define this patient population. During these conversations, highlight the safety of the procedure; ASE guidelines3 estimate a severe complication rate of less than 1 in 10,000 cases and explain the anticipated benefits to critically ill patients.
In conclusion, at an institution that is already adept at the use of POCUS in the ICU, the additional of critical care TEE within 1 to 2 years is a very realistic achievement. It will undoubtedly require patience, persistence, and self-motivation, but the barriers are becoming smaller every day. Stay motivated!
Dr. Proud is Associate Professor of Medicine, Division of Pulmonary and Critical Care Medicine, Pulmonary and Critical Care Medicine Program Director, UT Health San Antonio.
References:
1. Porter TR, Abdelmoneim S, Belcik FT, et al. Guidelines for the cardiac sonographer in the performance of contrast echocardiography: a focused update from the American Society of Echocardiography. J Am Soc Echocardiogr. 2024;27(8):797-810.
2. Si X, Ma J, Cao DY, et al. Transesophageal echocardiography instead or in addition to transthoracic echocardiography in evaluating haemodynamic problems in intubated critically ill patients. Ann Transl Med. 2020;8(12):785.
3. Hahn RT, Abraham T, Adams MS, et al. Guidelines for performing a cmprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardioraphy and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. 2013;26(9):921-964.