User login
Utilization of AFP to predict HCC recurrence after liver transplantation in waitlisted patients
Key clinical point: Alpha-fetoprotein (AFP) levels during liver transplantation (LT) and their modulation while on the waitlist are predictors of hepatocellular carcinoma (HCC) recurrence after LT in patients meeting the Milan criteria.
Main finding: An AFP value >25.5 ng/mL (area under the receiver operating characteristic curve, 0.69) could strongly predict HCC recurrence after LT (subdistribution hazard ratio, 2.5; P = .01), which also showed a significant association with an increase in AFP levels by >20.8% while on the waitlist (P = .034).
Study details: The data are derived from a retrospective single-center study that analyzed 207 patients with HCC fulfilling the Milan criteria who were put on the waitlist for LT and had AFP levels >400 ng/mL at transplant.
Disclosures: Financial support for the study was provided by the association Friends of transplantation. The authors reported no conflict of interests.
Source: Magro B et al. Cancers. 2021 Nov 27. doi: 10.3390/cancers13235976.
Key clinical point: Alpha-fetoprotein (AFP) levels during liver transplantation (LT) and their modulation while on the waitlist are predictors of hepatocellular carcinoma (HCC) recurrence after LT in patients meeting the Milan criteria.
Main finding: An AFP value >25.5 ng/mL (area under the receiver operating characteristic curve, 0.69) could strongly predict HCC recurrence after LT (subdistribution hazard ratio, 2.5; P = .01), which also showed a significant association with an increase in AFP levels by >20.8% while on the waitlist (P = .034).
Study details: The data are derived from a retrospective single-center study that analyzed 207 patients with HCC fulfilling the Milan criteria who were put on the waitlist for LT and had AFP levels >400 ng/mL at transplant.
Disclosures: Financial support for the study was provided by the association Friends of transplantation. The authors reported no conflict of interests.
Source: Magro B et al. Cancers. 2021 Nov 27. doi: 10.3390/cancers13235976.
Key clinical point: Alpha-fetoprotein (AFP) levels during liver transplantation (LT) and their modulation while on the waitlist are predictors of hepatocellular carcinoma (HCC) recurrence after LT in patients meeting the Milan criteria.
Main finding: An AFP value >25.5 ng/mL (area under the receiver operating characteristic curve, 0.69) could strongly predict HCC recurrence after LT (subdistribution hazard ratio, 2.5; P = .01), which also showed a significant association with an increase in AFP levels by >20.8% while on the waitlist (P = .034).
Study details: The data are derived from a retrospective single-center study that analyzed 207 patients with HCC fulfilling the Milan criteria who were put on the waitlist for LT and had AFP levels >400 ng/mL at transplant.
Disclosures: Financial support for the study was provided by the association Friends of transplantation. The authors reported no conflict of interests.
Source: Magro B et al. Cancers. 2021 Nov 27. doi: 10.3390/cancers13235976.
Two studies detail the dangers of COVID in pregnancy
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Two new studies show how COVID-19 threatens the health of pregnant people and their newborn infants.
A study conducted in Scotland showed that unvaccinated pregnant people who got COVID were much more likely to have a stillborn infant or one that dies in the first 28 days. The study also found that pregnant women infected with COVID died or needed hospitalization at a much higher rate than vaccinated women who got pregnant.
The University of Edinburgh and Public Health Scotland studied national data in 88,000 pregnancies between Dec. 2020 and Oct. 2021, according to the study published in Nature Medicine.
Overall, 77.4% of infections, 90.9% of COVID-related hospitalizations, and 98% of critical care cases occurred in the unvaccinated people, as did all newborn deaths.
The study said 2,364 babies were born to women infected with COVID, with 2,353 live births. Eleven babies were stillborn and eight live-born babies died within 28 days. Of the live births, 241 were premature.
The problems were more likely if the infection occurred 28 days or less before the delivery date, the researchers said.
The authors said the low vaccination rate among pregnant people was a problem. Only 32% of people giving birth in Oct. 2021 were fully vaccinated, while 77% of the Scottish female population aged 18-44 was fully vaccinated.
“Vaccine hesitancy in pregnancy thus requires addressing, especially in light of new recommendations for booster vaccination administration 3 months after the initial vaccination course to help protect against new variants such as Omicron,” the authors wrote. “Addressing low vaccine uptake rates in pregnant women is imperative to protect the health of women and babies in the ongoing pandemic.”
Vaccinated women who were pregnant had complication rates that were about the same for all pregnant women, the study shows.
The second study, published in The Lancet, found that women who got COVID while pregnant in five Western U.S. states were more likely to have premature births, low birth weights, and stillbirths, even when the COVID cases are mild.
The Institute for Systems Biology researchers in Seattle studied data for women who gave birth in Alaska, California, Montana, Oregon, or Washington from March 5, 2020, to July 4, 2021. About 18,000 of them were tested for COVID, with 882 testing positive. Of the positive tests, 85 came in the first trimester, 226 in the second trimester, and 571 in the third semester. None of the pregnant women had been vaccinated at the time they were infected.
Most of the birth problems occurred with first and second trimester infections, the study noted, and problems occurred even if the pregnant person didn’t have respiratory complications, a major COVID symptom.
“Pregnant people are at an increased risk of adverse outcomes following SARS-CoV-2 infection, even when maternal COVID-19 is less severe, and they may benefit from increased monitoring following infection,” Jennifer Hadlock, MD, an author of the paper, said in a news release.
The study also pointed out continuing inequities in health care, with most of the positive cases occurring among young, non-White people with Medicaid and high body mass index.
A version of this article first appeared on WebMD.com.
Whole blood viscosity as a biomarker for distant metastasis and survival in HCC
Key clinical point: High diastolic whole blood viscosity (WBV) may serve as a new independent factor associated with extrahepatic metastasis and poor survival in patients with hepatocellular carcinoma (HCC).
Main finding: After adjusting for confounding variables, high diastolic WBV was independently associated with extrahepatic metastasis (adjusted odds ratio, 23.41; P < .001) and poor survival (adjusted hazard ratio, 3.81; P < .001) and significantly predicted extrahepatic metastasis at an optimal cutoff of 16 cP (area under the receiver operating characteristic curve, 0.768; P < .001).
Study details: Findings are from a pilot retrospective study including 181 patients with HCC, of which 148 were treatment-naïve having preserved liver function and 33 received nivolumab.
Disclosures: The study was sponsored by Young Medical Scientist Research Grant through the Daewoong Foundation and the Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea. The authors did not declare any conflict of interests.
Source: Han JW et al. PLoS ONE. 2021 Dec 2. doi: 10.1371/journal.pone.0260311.
Key clinical point: High diastolic whole blood viscosity (WBV) may serve as a new independent factor associated with extrahepatic metastasis and poor survival in patients with hepatocellular carcinoma (HCC).
Main finding: After adjusting for confounding variables, high diastolic WBV was independently associated with extrahepatic metastasis (adjusted odds ratio, 23.41; P < .001) and poor survival (adjusted hazard ratio, 3.81; P < .001) and significantly predicted extrahepatic metastasis at an optimal cutoff of 16 cP (area under the receiver operating characteristic curve, 0.768; P < .001).
Study details: Findings are from a pilot retrospective study including 181 patients with HCC, of which 148 were treatment-naïve having preserved liver function and 33 received nivolumab.
Disclosures: The study was sponsored by Young Medical Scientist Research Grant through the Daewoong Foundation and the Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea. The authors did not declare any conflict of interests.
Source: Han JW et al. PLoS ONE. 2021 Dec 2. doi: 10.1371/journal.pone.0260311.
Key clinical point: High diastolic whole blood viscosity (WBV) may serve as a new independent factor associated with extrahepatic metastasis and poor survival in patients with hepatocellular carcinoma (HCC).
Main finding: After adjusting for confounding variables, high diastolic WBV was independently associated with extrahepatic metastasis (adjusted odds ratio, 23.41; P < .001) and poor survival (adjusted hazard ratio, 3.81; P < .001) and significantly predicted extrahepatic metastasis at an optimal cutoff of 16 cP (area under the receiver operating characteristic curve, 0.768; P < .001).
Study details: Findings are from a pilot retrospective study including 181 patients with HCC, of which 148 were treatment-naïve having preserved liver function and 33 received nivolumab.
Disclosures: The study was sponsored by Young Medical Scientist Research Grant through the Daewoong Foundation and the Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea. The authors did not declare any conflict of interests.
Source: Han JW et al. PLoS ONE. 2021 Dec 2. doi: 10.1371/journal.pone.0260311.
Radiologic response to TACE-RT as a prognostic factor in advanced HCC with macroscopic vascular invasion
Key clinical point: The modified Response Evaluation Criteria in Solid Tumors (mRECIST)-determined radiologic response rate of transarterial chemoembolization (TACE) plus radiotherapy (RT) among patients with advanced hepatocellular carcinoma (HCC) showing macroscopic vascular invasion (MVI) is an independent prognosticator for overall survival (OS).
Main finding: Responders vs nonresponders had significantly longer median OS at 2 months (23.1 months vs 8.0 months; adjusted hazard ratio [aHR], 3.194; P < .001) and 4 months (responders vs nonresponders: 26.5 months vs 9.3 months; aHR, 4.534; P < .001).
Study details: This was a retrospective review study including 427 patients with advanced HCC and MVI who received first-line treatment with TACE plus respiratory-gated 3-dimensional conformal RT in the 2-month analysis, whereas the patient number reduced to 355 in the 4-month analysis.
Disclosures: The study was supported by the Asan Institute for Life Sciences of Asan Medical Center, Seoul, Republic of Korea. The authors declared no conflict of interests.
Source: Jung J et al. Liver Cancer. 2021 Dec 7. doi: 10.1159/000521227.
Key clinical point: The modified Response Evaluation Criteria in Solid Tumors (mRECIST)-determined radiologic response rate of transarterial chemoembolization (TACE) plus radiotherapy (RT) among patients with advanced hepatocellular carcinoma (HCC) showing macroscopic vascular invasion (MVI) is an independent prognosticator for overall survival (OS).
Main finding: Responders vs nonresponders had significantly longer median OS at 2 months (23.1 months vs 8.0 months; adjusted hazard ratio [aHR], 3.194; P < .001) and 4 months (responders vs nonresponders: 26.5 months vs 9.3 months; aHR, 4.534; P < .001).
Study details: This was a retrospective review study including 427 patients with advanced HCC and MVI who received first-line treatment with TACE plus respiratory-gated 3-dimensional conformal RT in the 2-month analysis, whereas the patient number reduced to 355 in the 4-month analysis.
Disclosures: The study was supported by the Asan Institute for Life Sciences of Asan Medical Center, Seoul, Republic of Korea. The authors declared no conflict of interests.
Source: Jung J et al. Liver Cancer. 2021 Dec 7. doi: 10.1159/000521227.
Key clinical point: The modified Response Evaluation Criteria in Solid Tumors (mRECIST)-determined radiologic response rate of transarterial chemoembolization (TACE) plus radiotherapy (RT) among patients with advanced hepatocellular carcinoma (HCC) showing macroscopic vascular invasion (MVI) is an independent prognosticator for overall survival (OS).
Main finding: Responders vs nonresponders had significantly longer median OS at 2 months (23.1 months vs 8.0 months; adjusted hazard ratio [aHR], 3.194; P < .001) and 4 months (responders vs nonresponders: 26.5 months vs 9.3 months; aHR, 4.534; P < .001).
Study details: This was a retrospective review study including 427 patients with advanced HCC and MVI who received first-line treatment with TACE plus respiratory-gated 3-dimensional conformal RT in the 2-month analysis, whereas the patient number reduced to 355 in the 4-month analysis.
Disclosures: The study was supported by the Asan Institute for Life Sciences of Asan Medical Center, Seoul, Republic of Korea. The authors declared no conflict of interests.
Source: Jung J et al. Liver Cancer. 2021 Dec 7. doi: 10.1159/000521227.
HAIC-FO outperforms sorafenib against advanced HCC in phase 3
Key clinical point: Hepatic arterial infusion chemotherapy of infusional fluorouracil, leucovorin, and oxaliplatin (HAIC-FO) is better than sorafenib at improving survival in patients with locally advanced hepatocellular carcinoma (HCC).
Main finding: At a median follow-up of 17.1 and 19.8 months, HAIC-FO- and sorafenib-treated patients showed a median overall survival (OS) of 13.9 months (95% CI, 10.6-17.2) and 8.2 months (95% CI, 7.5-9.0), respectively (hazard ratio [HR], 0.408; P = .001), with OS improvements favoring HAIC-FO vs sorafenib in even high-risk patients (10.8 months vs 5.7 months; HR, 0.343; P < .001). Grade 3/4 adverse events were more frequent with sorafenib vs HAIC-FO (48.1% vs20.3%).
Study details: The data come from the open-label, phase 3 FOHAIC-1 trial, which included 262 systemic therapy-naive patients with locally advanced or unresectable HCC who were randomly assigned to receive either HAIC-FO (n=130) or sorafenib (n=132).
Disclosures: The National Natural Science Foundation of China sponsored the study. The authors did not report any potential conflict of interests.
Source: Lyu N et al. J Clin Oncol. 2021 Dec 14. doi: 10.1200/JCO.21.01963.
Key clinical point: Hepatic arterial infusion chemotherapy of infusional fluorouracil, leucovorin, and oxaliplatin (HAIC-FO) is better than sorafenib at improving survival in patients with locally advanced hepatocellular carcinoma (HCC).
Main finding: At a median follow-up of 17.1 and 19.8 months, HAIC-FO- and sorafenib-treated patients showed a median overall survival (OS) of 13.9 months (95% CI, 10.6-17.2) and 8.2 months (95% CI, 7.5-9.0), respectively (hazard ratio [HR], 0.408; P = .001), with OS improvements favoring HAIC-FO vs sorafenib in even high-risk patients (10.8 months vs 5.7 months; HR, 0.343; P < .001). Grade 3/4 adverse events were more frequent with sorafenib vs HAIC-FO (48.1% vs20.3%).
Study details: The data come from the open-label, phase 3 FOHAIC-1 trial, which included 262 systemic therapy-naive patients with locally advanced or unresectable HCC who were randomly assigned to receive either HAIC-FO (n=130) or sorafenib (n=132).
Disclosures: The National Natural Science Foundation of China sponsored the study. The authors did not report any potential conflict of interests.
Source: Lyu N et al. J Clin Oncol. 2021 Dec 14. doi: 10.1200/JCO.21.01963.
Key clinical point: Hepatic arterial infusion chemotherapy of infusional fluorouracil, leucovorin, and oxaliplatin (HAIC-FO) is better than sorafenib at improving survival in patients with locally advanced hepatocellular carcinoma (HCC).
Main finding: At a median follow-up of 17.1 and 19.8 months, HAIC-FO- and sorafenib-treated patients showed a median overall survival (OS) of 13.9 months (95% CI, 10.6-17.2) and 8.2 months (95% CI, 7.5-9.0), respectively (hazard ratio [HR], 0.408; P = .001), with OS improvements favoring HAIC-FO vs sorafenib in even high-risk patients (10.8 months vs 5.7 months; HR, 0.343; P < .001). Grade 3/4 adverse events were more frequent with sorafenib vs HAIC-FO (48.1% vs20.3%).
Study details: The data come from the open-label, phase 3 FOHAIC-1 trial, which included 262 systemic therapy-naive patients with locally advanced or unresectable HCC who were randomly assigned to receive either HAIC-FO (n=130) or sorafenib (n=132).
Disclosures: The National Natural Science Foundation of China sponsored the study. The authors did not report any potential conflict of interests.
Source: Lyu N et al. J Clin Oncol. 2021 Dec 14. doi: 10.1200/JCO.21.01963.
Atezolizumab + bevacizumab shows long-term benefits over sorafenib for unresectable HCC
Key clinical point: Longer follow-up results confirm the survival benefits and consistent safety of first-line atezolizumab + bevacizumab vs sorafenib in patients with locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC).
Major finding: After a 15.6-month median follow-up, the median overall survival (19.2 months vs 13.4 months; stratified hazard ratio [HR] for death, 0.66; P < .001) and progression-free survival (6.9 months vs 4.3 months; HR for death/progression, 0.65; P < .001) were higher with atezolizumab + bevacizumab vs sorafenib. Treatment-related grade 3/4 adverse events occurred in 43% vs 46% of patients receiving atezolizumab + bevacizumab vs sorafenib.
Study details: Findings are from a post hoc analysis of the phase 3 IMbrave150 trial including 501 treatment-naïve patients with locally advanced or metastatic and/or unresectable HCC. Patients were randomly assigned to atezolizumab + bevacizumab or sorafenib.
Disclosures: This study was funded by F. Hoffman-La Roche (FHLR)/Genentech. All investigators reported receiving financial or nonfinancial support, providing expert testimony, being an employee of, or holding shares/stocks in various pharmaceutical companies including FHLR/Genentech.
Source: Cheng AL et al. J Hepatol. 2021 Dec 10. doi: 10.1016/j.jhep.2021.11.030.
Key clinical point: Longer follow-up results confirm the survival benefits and consistent safety of first-line atezolizumab + bevacizumab vs sorafenib in patients with locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC).
Major finding: After a 15.6-month median follow-up, the median overall survival (19.2 months vs 13.4 months; stratified hazard ratio [HR] for death, 0.66; P < .001) and progression-free survival (6.9 months vs 4.3 months; HR for death/progression, 0.65; P < .001) were higher with atezolizumab + bevacizumab vs sorafenib. Treatment-related grade 3/4 adverse events occurred in 43% vs 46% of patients receiving atezolizumab + bevacizumab vs sorafenib.
Study details: Findings are from a post hoc analysis of the phase 3 IMbrave150 trial including 501 treatment-naïve patients with locally advanced or metastatic and/or unresectable HCC. Patients were randomly assigned to atezolizumab + bevacizumab or sorafenib.
Disclosures: This study was funded by F. Hoffman-La Roche (FHLR)/Genentech. All investigators reported receiving financial or nonfinancial support, providing expert testimony, being an employee of, or holding shares/stocks in various pharmaceutical companies including FHLR/Genentech.
Source: Cheng AL et al. J Hepatol. 2021 Dec 10. doi: 10.1016/j.jhep.2021.11.030.
Key clinical point: Longer follow-up results confirm the survival benefits and consistent safety of first-line atezolizumab + bevacizumab vs sorafenib in patients with locally advanced or metastatic and/or unresectable hepatocellular carcinoma (HCC).
Major finding: After a 15.6-month median follow-up, the median overall survival (19.2 months vs 13.4 months; stratified hazard ratio [HR] for death, 0.66; P < .001) and progression-free survival (6.9 months vs 4.3 months; HR for death/progression, 0.65; P < .001) were higher with atezolizumab + bevacizumab vs sorafenib. Treatment-related grade 3/4 adverse events occurred in 43% vs 46% of patients receiving atezolizumab + bevacizumab vs sorafenib.
Study details: Findings are from a post hoc analysis of the phase 3 IMbrave150 trial including 501 treatment-naïve patients with locally advanced or metastatic and/or unresectable HCC. Patients were randomly assigned to atezolizumab + bevacizumab or sorafenib.
Disclosures: This study was funded by F. Hoffman-La Roche (FHLR)/Genentech. All investigators reported receiving financial or nonfinancial support, providing expert testimony, being an employee of, or holding shares/stocks in various pharmaceutical companies including FHLR/Genentech.
Source: Cheng AL et al. J Hepatol. 2021 Dec 10. doi: 10.1016/j.jhep.2021.11.030.
No survival benefits with first-line nivolumab vs sorafenib in advanced HCC
Key clinical point: First-line nivolumab treatment did not improve overall survival in patients with advanced hepatocellular carcinoma (HCC) compared with sorafenib.
Major finding: At a minimum follow-up of 22.8 months, nivolumab vs sorafenib did not meet the prespecified significance boundary for superior overall survival (16.4 months vs 14.7 months; hazard ratio, 0.85; P = .075).
Study details: Findings are from the phase 3 CheckMate 459 trial including 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372).
Disclosures: This study was supported by Bristol Myers Squibb (BMS) and Ono Pharmaceutical. Some investigators including the lead author reported receiving grants and fees from, participation on data safety monitoring board or advisory boards for, owning stocks in, and being an employee of various pharmaceutical companies, including BMS and Ono Pharmaceutical.
Source: Yau T et al. Lancet Oncol. 2021 Dec 13. doi: 10.1016/S1470-2045(21)00604-5.
Key clinical point: First-line nivolumab treatment did not improve overall survival in patients with advanced hepatocellular carcinoma (HCC) compared with sorafenib.
Major finding: At a minimum follow-up of 22.8 months, nivolumab vs sorafenib did not meet the prespecified significance boundary for superior overall survival (16.4 months vs 14.7 months; hazard ratio, 0.85; P = .075).
Study details: Findings are from the phase 3 CheckMate 459 trial including 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372).
Disclosures: This study was supported by Bristol Myers Squibb (BMS) and Ono Pharmaceutical. Some investigators including the lead author reported receiving grants and fees from, participation on data safety monitoring board or advisory boards for, owning stocks in, and being an employee of various pharmaceutical companies, including BMS and Ono Pharmaceutical.
Source: Yau T et al. Lancet Oncol. 2021 Dec 13. doi: 10.1016/S1470-2045(21)00604-5.
Key clinical point: First-line nivolumab treatment did not improve overall survival in patients with advanced hepatocellular carcinoma (HCC) compared with sorafenib.
Major finding: At a minimum follow-up of 22.8 months, nivolumab vs sorafenib did not meet the prespecified significance boundary for superior overall survival (16.4 months vs 14.7 months; hazard ratio, 0.85; P = .075).
Study details: Findings are from the phase 3 CheckMate 459 trial including 743 adult patients with advanced HCC randomly assigned to receive either nivolumab (n=371) or sorafenib (n=372).
Disclosures: This study was supported by Bristol Myers Squibb (BMS) and Ono Pharmaceutical. Some investigators including the lead author reported receiving grants and fees from, participation on data safety monitoring board or advisory boards for, owning stocks in, and being an employee of various pharmaceutical companies, including BMS and Ono Pharmaceutical.
Source: Yau T et al. Lancet Oncol. 2021 Dec 13. doi: 10.1016/S1470-2045(21)00604-5.
Breastfeeding linked to lower CVD risk in later life
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
In a meta-analysis of more than 1 million mothers, those who breastfed their children had an 11% to 17% lower risk of developing cardiovascular disease (CVD), coronary heart disease (CHD), or stroke, and of dying from CVD, in later life than mothers who did not.
On average, the women had two children and had breastfed for 15.9 months in total. Longer breastfeeding was associated with greater CV health benefit.
This meta-analysis of eight studies from different countries was published online Jan. 11 in an issue of the Journal of the American Heart Association devoted to the impact of pregnancy on CV health in the mother and child.
Breastfeeding is known to be associated with a lower risk for death from infectious disease and with fewer respiratory infections in babies, the researchers write, but what is less well known is that it is also associated with a reduced risk for breast and ovarian cancer and type 2 diabetes in mothers.
The current study showed a clear association between breastfeeding and reduced risk for CVD in later life, lead author Lena Tschiderer, Dipl.-Ing., PhD, and senior author Peter Willeit, MD, MPhil, PhD, summarized in a joint email to this news organization.
Specifically, mothers who had breastfed their children at any time had an 11% lower risk for CVD, a 14% lower risk for CHD, a 12% lower risk for stroke, and a 17% lower risk of dying from CVD in later life, compared with other mothers.
On the basis of existing evidence, the researchers write, the World Health Organization recommends exclusive breastfeeding until a baby is 6 months old, followed by breastfeeding plus complementary feeding until the baby is 2 years or older.
“We believe that [breastfeeding] benefits for the mother are communicated poorly,” said Dr. Tschiderer and Dr. Willeit, from the University of Innsbruck, Austria.
“Positive effects of breastfeeding on mothers need to be communicated effectively, awareness for breastfeeding recommendations needs to be raised, and interventions to promote and facilitate breastfeeding need to be implemented and reinforced,” the researchers conclude.
‘Should not be ignored’
Two cardiologists invited to comment, who were not involved with the research, noted that this study provides insight into an important topic.
“This is yet another body of evidence [and the largest population to date] to show that breastfeeding is protective for women and may show important beneficial effects in terms of CV risk,” Roxana Mehran, MD, said in an email.
“The risk reductions were 11% for CVD events and 14% for CHD events; these are impressive numbers,” said Dr. Mehran, from Icahn School of Medicine at Mount Sinai, New York.
“The caveat,” she said, “is that these are data from several trials, but nonetheless, this is a very important observation that should not be ignored.”
The study did not address the definitive amount of time of breastfeeding and its correlation to the improvement of CVD risk, but it did show that for the lifetime duration, the longer the better.
“The beneficial effects,” she noted, “can be linked to hormones during breastfeeding, as well as weight loss associated with breastfeeding, and resetting the maternal metabolism, as the authors suggest.”
Clinicians and employers “must provide ways to educate women about breastfeeding and make it easy for women who are in the workplace to pump, and to provide them with resources” where possible, Dr. Mehran said.
Michelle O’Donoghue, MD, MPH, noted that over the past several years, there has been intense interest in the possible health benefits of breastfeeding for both mother and child.
There is biologic plausibility for some of the possible maternal benefits because the favorable CV effects of both prolactin and oxytocin are only now being better understood, said Dr. O’Donoghue, from Brigham and Women’s Hospital and Harvard Medical School, Boston.
“The current meta-analysis provides a large dataset that helps support the concept that breastfeeding may offer some cardiovascular benefit for the mother,” she agreed.
“However, ultimately more research will be necessary since this method of combining data across trials relies upon the robustness of the statistical method in each study,” Dr. O’Donoghue said. “I applaud the authors for shining a spotlight on this important topic.”
Although the benefits of breastfeeding appear to continue over time, “it is incredibly difficult for women to continue breastfeeding once they return to work,” she added. “Women in some countries outside the U.S. have an advantage due to longer durations of maternity leave.
“If we want to encourage breastfeeding,” Dr. O’Donoghue stressed, “we need to make sure that we put the right supports in place. Women need protected places to breastfeed in the workplace and places to store their milk. Most importantly, women need to be allowed dedicated time to make it happen.”
First large study of CVD in mothers
Emerging individual studies suggest that mothers who breastfeed may have a lower risk for CVD in later life, but studies have been inconsistent, and it is not clear if longer breastfeeding would strengthen this benefit, the authors note.
To examine this, they pooled data from the following eight studies (with study acronym, country, and baseline enrolment dates in brackets): 45&Up (Australia, 2006-2009), China Kadoorie Biobank (CKB, China, 2004-2008), European Prospective Investigation into Cancer and Nutrition (EPIC, multinational, 1992-2000), Gallagher et al. (China, 1989-1991), Nord-Trøndelag Health Survey 2 (HUNT2, Norway, 1995-1997), Japan Public Health Center-based Prospective Study (JPHC, Japan, 1990-1994), Nurses’ Health Study (NHS, U.S., 1986), and the Woman’s Health Initiative (WHI, U.S., 1993-1998).
On average, the women were 51.3 years old (range, 40-65 years) when they enrolled in the study, and they were followed for a median of 10.3 years (range, 7.9-20.9 years, in the individual studies).
On average, they had their first child at age 25 and had two to three children (mean, 2.3); 82% had breastfed at some point (ranging from 58% of women in the two U.S. studies to 97% in CKB and HUNT2).
The women had breastfed for a mean of 7.4 to 18.9 months during their lifetimes (except women in the CKB study, who had breastfed for a median of 24 months).
Among the 1,192,700 women, there were 54,226 incident CVD events, 26,913 incident CHD events, 30,843 incident strokes, and 10,766 deaths from CVD during follow-up.
The researchers acknowledge that study limitations include the fact that there could have been publication bias, since fewer than 10 studies were available for pooling. There was significant between-study heterogeneity for CVD, CHD, and stroke outcomes.
Participant-level data were also lacking, and breastfeeding was self-reported. There may have been unaccounted residual confounding, and the benefits of lifetime breastfeeding that is longer than 2 years are not clear, because few women in this population breastfed that long.
The research was funded by the Austrian Science Fund. The researchers and Dr. Mehran and Dr. O’Donoghue have no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
COVID at 2 years: Preparing for a different ‘normal’
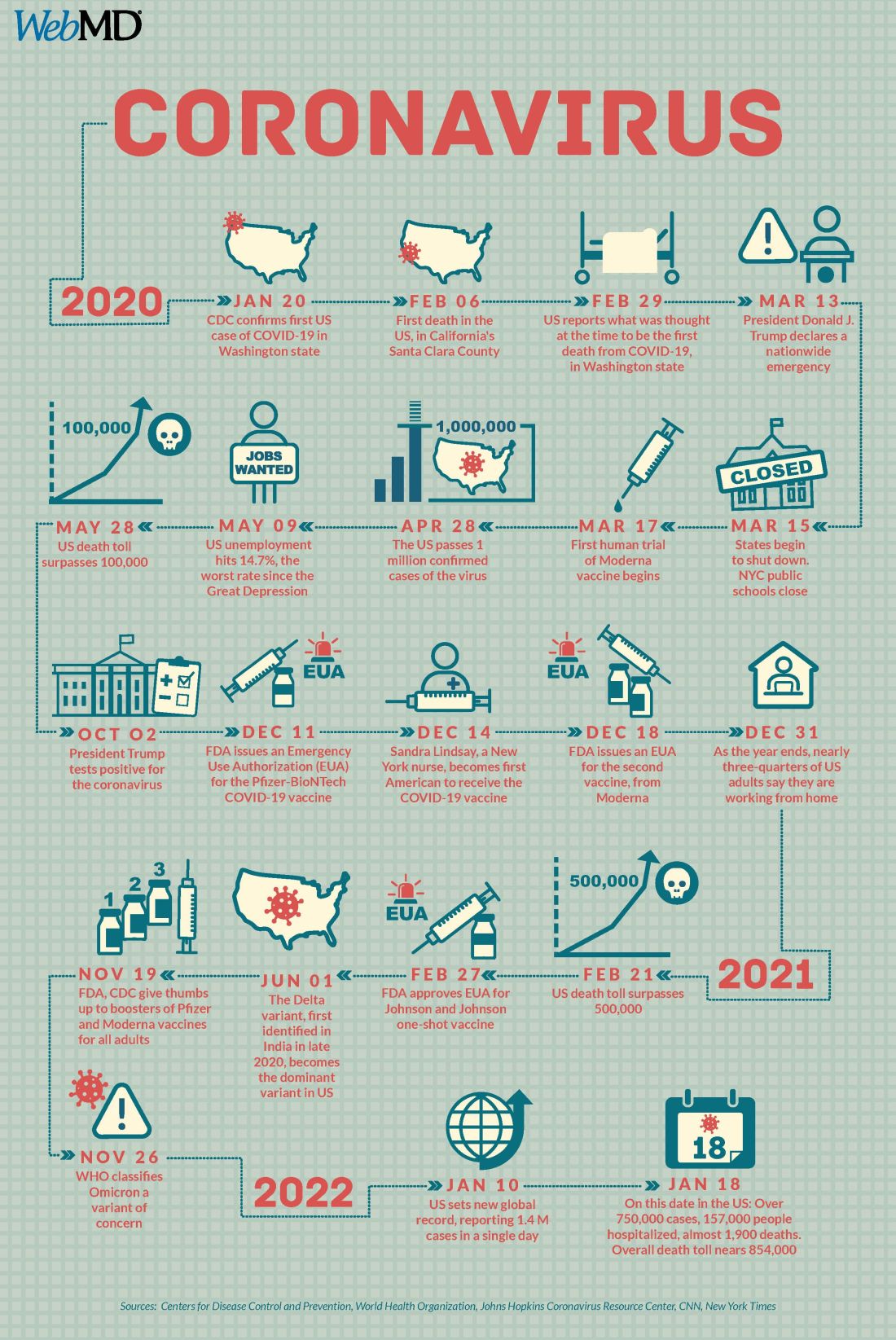
Two years into the COVID-19 pandemic, the United States is still breaking records in hospital overcrowding and new cases.
The United States is logging nearly 800,000 cases a day, hospitals are starting to fray, and deaths have topped 850,000. Schools oscillate from remote to in-person learning, polarizing communities.
The vaccines are lifesaving for many, yet frustration mounts as the numbers of unvaccinated people in this country stays relatively stagnant (63% in the United States are fully vaccinated) and other parts of the world have seen hardly a single dose. Africa has the slowest vaccination rate among continents, with only 14% of the population receiving one shot, according to the New York Times tracker.
Yet
Effective vaccines and treatments that can keep people out of the hospital were developed at an astounding pace, and advances in tracking and testing – in both access and effectiveness – are starting to pay off.
Some experts say it’s possible that the raging Omicron surge will slow by late spring, providing some relief and maybe shifting the pandemic to a slower-burning endemic.
But other experts caution to keep our guard up, saying it’s time to settle into a “new normal” and upend the strategy for fighting COVID-19.
Time to change COVID thinking
Three former members of the Biden-Harris Transition COVID-19 Advisory Board wrote recently in JAMA that COVID-19 has now become one of the many viral respiratory diseases that health care providers and patients will manage each year.
The group of experts from the University of Pennsylvania, University of Minnesota, and New York University write that “many of the measures to reduce transmission of SARS-CoV-2 (for example, ventilation) will also reduce transmission of other respiratory viruses. Thus, policy makers should retire previous public health categorizations, including deaths from pneumonia and influenza or pneumonia, influenza, and COVID-19, and focus on a new category: the aggregate risk of all respiratory virus infections.”
Other experts, including Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security, Baltimore, have said it’s been clear since the early days of SARS-CoV-2 that we must learn to live with the virus because it “will be ever present for the remaining history of our species.”
But that doesn’t mean the virus will always have the upper hand. Although the United States has been reaching record numbers of hospitalizations in January, these hospitalizations differ from those of last year – marked by fewer extreme lifesaving measures, fewer deaths, and shorter hospital stays – caused in part by medical and therapeutic advances and in part to the nature of the Omicron variant itself.
One sign of progress, Dr. Adalja said, will be the widespread decoupling of cases from hospitalizations, something that has already happened in countries such as the United Kingdom.
“That’s a reflection of how well they have vaccinated their high-risk population and how poorly we have vaccinated our high-risk population,” he said.
Omicron will bump up natural immunity
Dr. Adalja said though the numbers of unvaccinated in the United States appear to be stuck, Omicron’s sweep will make the difference, leaving behind more natural immunity in the population.
Currently, hospitals are struggling with staffing concerns as a “direct result” of too many unvaccinated people, he said.
Andrew Badley, MD, an infectious diseases specialist at Mayo Clinic in Rochester, Minn., and director of the clinic’s COVID-19 Task Force, said the good news with Omicron is that nearly all people it infects will recover.
Over time, when the body sees foreign antigens repeatedly, the quantity and quality of the antibodies the immune system produces increase and the body becomes better at fighting disease.
So “a large amount of the population will have recovered and have a degree of immunity,” Dr. Badley said.
His optimism is tempered by his belief that “it’s going to get worse before it gets better.”
But Dr. Badley still predicts a turnaround. “We’ll see a downturn in COVID in late spring or early summer,” and well into the second quarter of 2022, “we’ll see a reemergence of control.”
Right now, with Omicron, one infected person is infecting three to five others, he said. The hope is that it will eventually reach one-to-one endemic levels.
As for the threat of new variants, Badley said, “it’s not predictable whether they will be stronger or weaker.”
Masks may be around for years
Many experts predict that masks will continue to be part of the national wardrobe for the foreseeable future.
“We will continue to see new cases for years and years to come. Some will respond to that with masks in public places for a very long time. I personally will do so,” Dr. Badley said.
Two mindsets: Inside/outside the hospital
Emily Landon, MD, an infectious disease doctor and the executive medical director of infection prevention and control at University of Chicago Medicine, told this news organization she views the pandemic from two different vantage points.
As a health care provider, she sees her hospital, like others worldwide, overwhelmed. Supplies of a major weapon to help prevent hospitalization, the monoclonal antibody sotrovimab, are running out. Dr. Landon said she has been calling other hospitals to see if they have supplies and, if so, whether Omicron patients can transfer there.
Bottom line: The things they relied on a month ago to keep people out of the hospital are no longer there, she said.
Meanwhile, “We have more COVID patients than we have ever had,” Dr. Landon said.
Last year, UChicago hit a high of 170 people hospitalized with COVID. This year, so far, the peak was 270.
Dr. Landon said she is frustrated when she leaves that overburdened world inside the hospital for the outside world, where people wear no masks or ineffective face coverings and gather unsafely. Although some of that behavior reflects an intention to flout the advice of medical experts, some is caused in part, she said, by the lack of a clear national health strategy and garbled communication from those in charge of public safety.
Americans are deciding for themselves, on an a la carte basis, whether to wear a mask or get tested or travel, and school districts decide individually when it’s time to go virtual.
“People are exhausted from having to do a risk-benefit analysis for every single activity they, their friends, their kids want to participate in,” she said.
U.S. behind in several areas
Despite our self-image as the global leader in science and medicine, the United States stumbled badly in its response to the pandemic, with grave consequences both at home and abroad, experts say.
In a recent commentary in JAMA, Lawrence Gostin, JD, from Georgetown University, Washington, and Jennifer Nuzzo, DrPH, at Johns Hopkins University, Baltimore, pointed to several critical shortfalls in the nation’s efforts to control the disease.
One such shortfall is public trust.
This news organization reported in June 2021 that a poll of its readers found that 44% said their trust in the CDC had waned during the pandemic, and 33% said their trust in the FDA had eroded as well.
Health care providers who responded to the poll lost trust as well. About half of the doctors and nurses who responded said they disagreed with the FDA’s decision-making during the pandemic. Nearly 60% of doctors and 65% of nurses said they disagreed with the CDC’s overall pandemic guidance.
Lack of trust can make people resist vaccines and efforts to fight the virus, the authors wrote.
“This will become really relevant when we have ample supply of Pfizer’s antiviral medication,” Mr. Gostin, who directs the O’Neill Institute for National and Global Health Law at Georgetown, told this news organization. “The next phase of the pandemic is not to link testing to contact tracing, because we’re way past that, but to link testing to treatment.”
Lack of regional manufacturing of products is also thwarting global progress.
“It is extraordinarily important that our pharmaceutical industry transfer technology in a pandemic,” Mr. Gostin said. “The most glaring failure to do that is the mRNA vaccines. We’ve got this enormously effective vaccine and the two manufacturers – Pfizer and Moderna – are refusing to share the technology with producers in other countries. That keeps coming back to haunt us.”
Another problem: When the vaccines are shared with other countries, they are being delivered close to the date they expire or arriving at a shipyards without warning, so even some of the doses that get delivered are going to waste, Mr. Gostin said.
“It’s one of the greatest moral failures of my lifetime,” he said.
Also a failure is the “jaw-dropping” state of testing 2 years into the pandemic, he said, as people continue to pay high prices for tests or endure long lines.
The U.S. government updated its calculations and ordered 1 billion tests for the general public. The COVIDtests.gov website to order the free tests is now live.
It’s a step in the right direction. Mr. Gostin and Dr. Nuzzo wrote that there is every reason to expect future epidemics that are as serious or more serious than COVID.
“Failure to address clearly observed weaknesses in the COVID-19 response will have preventable adverse health, social, and economic consequences when the next novel outbreak occurs,” they wrote.
A version of this article first appeared on WebMD.com.
Two years into the COVID-19 pandemic, the United States is still breaking records in hospital overcrowding and new cases.
The United States is logging nearly 800,000 cases a day, hospitals are starting to fray, and deaths have topped 850,000. Schools oscillate from remote to in-person learning, polarizing communities.
The vaccines are lifesaving for many, yet frustration mounts as the numbers of unvaccinated people in this country stays relatively stagnant (63% in the United States are fully vaccinated) and other parts of the world have seen hardly a single dose. Africa has the slowest vaccination rate among continents, with only 14% of the population receiving one shot, according to the New York Times tracker.
Yet
Effective vaccines and treatments that can keep people out of the hospital were developed at an astounding pace, and advances in tracking and testing – in both access and effectiveness – are starting to pay off.
Some experts say it’s possible that the raging Omicron surge will slow by late spring, providing some relief and maybe shifting the pandemic to a slower-burning endemic.
But other experts caution to keep our guard up, saying it’s time to settle into a “new normal” and upend the strategy for fighting COVID-19.
Time to change COVID thinking
Three former members of the Biden-Harris Transition COVID-19 Advisory Board wrote recently in JAMA that COVID-19 has now become one of the many viral respiratory diseases that health care providers and patients will manage each year.
The group of experts from the University of Pennsylvania, University of Minnesota, and New York University write that “many of the measures to reduce transmission of SARS-CoV-2 (for example, ventilation) will also reduce transmission of other respiratory viruses. Thus, policy makers should retire previous public health categorizations, including deaths from pneumonia and influenza or pneumonia, influenza, and COVID-19, and focus on a new category: the aggregate risk of all respiratory virus infections.”
Other experts, including Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security, Baltimore, have said it’s been clear since the early days of SARS-CoV-2 that we must learn to live with the virus because it “will be ever present for the remaining history of our species.”
But that doesn’t mean the virus will always have the upper hand. Although the United States has been reaching record numbers of hospitalizations in January, these hospitalizations differ from those of last year – marked by fewer extreme lifesaving measures, fewer deaths, and shorter hospital stays – caused in part by medical and therapeutic advances and in part to the nature of the Omicron variant itself.
One sign of progress, Dr. Adalja said, will be the widespread decoupling of cases from hospitalizations, something that has already happened in countries such as the United Kingdom.
“That’s a reflection of how well they have vaccinated their high-risk population and how poorly we have vaccinated our high-risk population,” he said.
Omicron will bump up natural immunity
Dr. Adalja said though the numbers of unvaccinated in the United States appear to be stuck, Omicron’s sweep will make the difference, leaving behind more natural immunity in the population.
Currently, hospitals are struggling with staffing concerns as a “direct result” of too many unvaccinated people, he said.
Andrew Badley, MD, an infectious diseases specialist at Mayo Clinic in Rochester, Minn., and director of the clinic’s COVID-19 Task Force, said the good news with Omicron is that nearly all people it infects will recover.
Over time, when the body sees foreign antigens repeatedly, the quantity and quality of the antibodies the immune system produces increase and the body becomes better at fighting disease.
So “a large amount of the population will have recovered and have a degree of immunity,” Dr. Badley said.
His optimism is tempered by his belief that “it’s going to get worse before it gets better.”
But Dr. Badley still predicts a turnaround. “We’ll see a downturn in COVID in late spring or early summer,” and well into the second quarter of 2022, “we’ll see a reemergence of control.”
Right now, with Omicron, one infected person is infecting three to five others, he said. The hope is that it will eventually reach one-to-one endemic levels.
As for the threat of new variants, Badley said, “it’s not predictable whether they will be stronger or weaker.”
Masks may be around for years
Many experts predict that masks will continue to be part of the national wardrobe for the foreseeable future.
“We will continue to see new cases for years and years to come. Some will respond to that with masks in public places for a very long time. I personally will do so,” Dr. Badley said.
Two mindsets: Inside/outside the hospital
Emily Landon, MD, an infectious disease doctor and the executive medical director of infection prevention and control at University of Chicago Medicine, told this news organization she views the pandemic from two different vantage points.
As a health care provider, she sees her hospital, like others worldwide, overwhelmed. Supplies of a major weapon to help prevent hospitalization, the monoclonal antibody sotrovimab, are running out. Dr. Landon said she has been calling other hospitals to see if they have supplies and, if so, whether Omicron patients can transfer there.
Bottom line: The things they relied on a month ago to keep people out of the hospital are no longer there, she said.
Meanwhile, “We have more COVID patients than we have ever had,” Dr. Landon said.
Last year, UChicago hit a high of 170 people hospitalized with COVID. This year, so far, the peak was 270.
Dr. Landon said she is frustrated when she leaves that overburdened world inside the hospital for the outside world, where people wear no masks or ineffective face coverings and gather unsafely. Although some of that behavior reflects an intention to flout the advice of medical experts, some is caused in part, she said, by the lack of a clear national health strategy and garbled communication from those in charge of public safety.
Americans are deciding for themselves, on an a la carte basis, whether to wear a mask or get tested or travel, and school districts decide individually when it’s time to go virtual.
“People are exhausted from having to do a risk-benefit analysis for every single activity they, their friends, their kids want to participate in,” she said.
U.S. behind in several areas
Despite our self-image as the global leader in science and medicine, the United States stumbled badly in its response to the pandemic, with grave consequences both at home and abroad, experts say.
In a recent commentary in JAMA, Lawrence Gostin, JD, from Georgetown University, Washington, and Jennifer Nuzzo, DrPH, at Johns Hopkins University, Baltimore, pointed to several critical shortfalls in the nation’s efforts to control the disease.
One such shortfall is public trust.
This news organization reported in June 2021 that a poll of its readers found that 44% said their trust in the CDC had waned during the pandemic, and 33% said their trust in the FDA had eroded as well.
Health care providers who responded to the poll lost trust as well. About half of the doctors and nurses who responded said they disagreed with the FDA’s decision-making during the pandemic. Nearly 60% of doctors and 65% of nurses said they disagreed with the CDC’s overall pandemic guidance.
Lack of trust can make people resist vaccines and efforts to fight the virus, the authors wrote.
“This will become really relevant when we have ample supply of Pfizer’s antiviral medication,” Mr. Gostin, who directs the O’Neill Institute for National and Global Health Law at Georgetown, told this news organization. “The next phase of the pandemic is not to link testing to contact tracing, because we’re way past that, but to link testing to treatment.”
Lack of regional manufacturing of products is also thwarting global progress.
“It is extraordinarily important that our pharmaceutical industry transfer technology in a pandemic,” Mr. Gostin said. “The most glaring failure to do that is the mRNA vaccines. We’ve got this enormously effective vaccine and the two manufacturers – Pfizer and Moderna – are refusing to share the technology with producers in other countries. That keeps coming back to haunt us.”
Another problem: When the vaccines are shared with other countries, they are being delivered close to the date they expire or arriving at a shipyards without warning, so even some of the doses that get delivered are going to waste, Mr. Gostin said.
“It’s one of the greatest moral failures of my lifetime,” he said.
Also a failure is the “jaw-dropping” state of testing 2 years into the pandemic, he said, as people continue to pay high prices for tests or endure long lines.
The U.S. government updated its calculations and ordered 1 billion tests for the general public. The COVIDtests.gov website to order the free tests is now live.
It’s a step in the right direction. Mr. Gostin and Dr. Nuzzo wrote that there is every reason to expect future epidemics that are as serious or more serious than COVID.
“Failure to address clearly observed weaknesses in the COVID-19 response will have preventable adverse health, social, and economic consequences when the next novel outbreak occurs,” they wrote.
A version of this article first appeared on WebMD.com.
Two years into the COVID-19 pandemic, the United States is still breaking records in hospital overcrowding and new cases.
The United States is logging nearly 800,000 cases a day, hospitals are starting to fray, and deaths have topped 850,000. Schools oscillate from remote to in-person learning, polarizing communities.
The vaccines are lifesaving for many, yet frustration mounts as the numbers of unvaccinated people in this country stays relatively stagnant (63% in the United States are fully vaccinated) and other parts of the world have seen hardly a single dose. Africa has the slowest vaccination rate among continents, with only 14% of the population receiving one shot, according to the New York Times tracker.
Yet
Effective vaccines and treatments that can keep people out of the hospital were developed at an astounding pace, and advances in tracking and testing – in both access and effectiveness – are starting to pay off.
Some experts say it’s possible that the raging Omicron surge will slow by late spring, providing some relief and maybe shifting the pandemic to a slower-burning endemic.
But other experts caution to keep our guard up, saying it’s time to settle into a “new normal” and upend the strategy for fighting COVID-19.
Time to change COVID thinking
Three former members of the Biden-Harris Transition COVID-19 Advisory Board wrote recently in JAMA that COVID-19 has now become one of the many viral respiratory diseases that health care providers and patients will manage each year.
The group of experts from the University of Pennsylvania, University of Minnesota, and New York University write that “many of the measures to reduce transmission of SARS-CoV-2 (for example, ventilation) will also reduce transmission of other respiratory viruses. Thus, policy makers should retire previous public health categorizations, including deaths from pneumonia and influenza or pneumonia, influenza, and COVID-19, and focus on a new category: the aggregate risk of all respiratory virus infections.”
Other experts, including Amesh Adalja, MD, a senior scholar at the Johns Hopkins Center for Health Security, Baltimore, have said it’s been clear since the early days of SARS-CoV-2 that we must learn to live with the virus because it “will be ever present for the remaining history of our species.”
But that doesn’t mean the virus will always have the upper hand. Although the United States has been reaching record numbers of hospitalizations in January, these hospitalizations differ from those of last year – marked by fewer extreme lifesaving measures, fewer deaths, and shorter hospital stays – caused in part by medical and therapeutic advances and in part to the nature of the Omicron variant itself.
One sign of progress, Dr. Adalja said, will be the widespread decoupling of cases from hospitalizations, something that has already happened in countries such as the United Kingdom.
“That’s a reflection of how well they have vaccinated their high-risk population and how poorly we have vaccinated our high-risk population,” he said.
Omicron will bump up natural immunity
Dr. Adalja said though the numbers of unvaccinated in the United States appear to be stuck, Omicron’s sweep will make the difference, leaving behind more natural immunity in the population.
Currently, hospitals are struggling with staffing concerns as a “direct result” of too many unvaccinated people, he said.
Andrew Badley, MD, an infectious diseases specialist at Mayo Clinic in Rochester, Minn., and director of the clinic’s COVID-19 Task Force, said the good news with Omicron is that nearly all people it infects will recover.
Over time, when the body sees foreign antigens repeatedly, the quantity and quality of the antibodies the immune system produces increase and the body becomes better at fighting disease.
So “a large amount of the population will have recovered and have a degree of immunity,” Dr. Badley said.
His optimism is tempered by his belief that “it’s going to get worse before it gets better.”
But Dr. Badley still predicts a turnaround. “We’ll see a downturn in COVID in late spring or early summer,” and well into the second quarter of 2022, “we’ll see a reemergence of control.”
Right now, with Omicron, one infected person is infecting three to five others, he said. The hope is that it will eventually reach one-to-one endemic levels.
As for the threat of new variants, Badley said, “it’s not predictable whether they will be stronger or weaker.”
Masks may be around for years
Many experts predict that masks will continue to be part of the national wardrobe for the foreseeable future.
“We will continue to see new cases for years and years to come. Some will respond to that with masks in public places for a very long time. I personally will do so,” Dr. Badley said.
Two mindsets: Inside/outside the hospital
Emily Landon, MD, an infectious disease doctor and the executive medical director of infection prevention and control at University of Chicago Medicine, told this news organization she views the pandemic from two different vantage points.
As a health care provider, she sees her hospital, like others worldwide, overwhelmed. Supplies of a major weapon to help prevent hospitalization, the monoclonal antibody sotrovimab, are running out. Dr. Landon said she has been calling other hospitals to see if they have supplies and, if so, whether Omicron patients can transfer there.
Bottom line: The things they relied on a month ago to keep people out of the hospital are no longer there, she said.
Meanwhile, “We have more COVID patients than we have ever had,” Dr. Landon said.
Last year, UChicago hit a high of 170 people hospitalized with COVID. This year, so far, the peak was 270.
Dr. Landon said she is frustrated when she leaves that overburdened world inside the hospital for the outside world, where people wear no masks or ineffective face coverings and gather unsafely. Although some of that behavior reflects an intention to flout the advice of medical experts, some is caused in part, she said, by the lack of a clear national health strategy and garbled communication from those in charge of public safety.
Americans are deciding for themselves, on an a la carte basis, whether to wear a mask or get tested or travel, and school districts decide individually when it’s time to go virtual.
“People are exhausted from having to do a risk-benefit analysis for every single activity they, their friends, their kids want to participate in,” she said.
U.S. behind in several areas
Despite our self-image as the global leader in science and medicine, the United States stumbled badly in its response to the pandemic, with grave consequences both at home and abroad, experts say.
In a recent commentary in JAMA, Lawrence Gostin, JD, from Georgetown University, Washington, and Jennifer Nuzzo, DrPH, at Johns Hopkins University, Baltimore, pointed to several critical shortfalls in the nation’s efforts to control the disease.
One such shortfall is public trust.
This news organization reported in June 2021 that a poll of its readers found that 44% said their trust in the CDC had waned during the pandemic, and 33% said their trust in the FDA had eroded as well.
Health care providers who responded to the poll lost trust as well. About half of the doctors and nurses who responded said they disagreed with the FDA’s decision-making during the pandemic. Nearly 60% of doctors and 65% of nurses said they disagreed with the CDC’s overall pandemic guidance.
Lack of trust can make people resist vaccines and efforts to fight the virus, the authors wrote.
“This will become really relevant when we have ample supply of Pfizer’s antiviral medication,” Mr. Gostin, who directs the O’Neill Institute for National and Global Health Law at Georgetown, told this news organization. “The next phase of the pandemic is not to link testing to contact tracing, because we’re way past that, but to link testing to treatment.”
Lack of regional manufacturing of products is also thwarting global progress.
“It is extraordinarily important that our pharmaceutical industry transfer technology in a pandemic,” Mr. Gostin said. “The most glaring failure to do that is the mRNA vaccines. We’ve got this enormously effective vaccine and the two manufacturers – Pfizer and Moderna – are refusing to share the technology with producers in other countries. That keeps coming back to haunt us.”
Another problem: When the vaccines are shared with other countries, they are being delivered close to the date they expire or arriving at a shipyards without warning, so even some of the doses that get delivered are going to waste, Mr. Gostin said.
“It’s one of the greatest moral failures of my lifetime,” he said.
Also a failure is the “jaw-dropping” state of testing 2 years into the pandemic, he said, as people continue to pay high prices for tests or endure long lines.
The U.S. government updated its calculations and ordered 1 billion tests for the general public. The COVIDtests.gov website to order the free tests is now live.
It’s a step in the right direction. Mr. Gostin and Dr. Nuzzo wrote that there is every reason to expect future epidemics that are as serious or more serious than COVID.
“Failure to address clearly observed weaknesses in the COVID-19 response will have preventable adverse health, social, and economic consequences when the next novel outbreak occurs,” they wrote.
A version of this article first appeared on WebMD.com.
Pioneering test predicts return of malignant melanoma
Their research, published in the British Journal of Dermatology, describes how early-stage melanomas at risk of spreading secrete transforming growth factor beta2 (TGF-beta2), which causes the reduction, or down-regulation, of the proteins AMBRA1 and loricrin, both of which are found in the skin overlaying the tumor. TGF-beta2 also causes the loss of claudin-1, which in turn leads to loss of skin integrity, facilitating ulceration.
Senior author Penny Lovat, PhD, professor of cellular dermatology and oncology at Newcastle University, and chief scientific officer at AMLo Biosciences, explained: “AMBRA1, loricrin, and claudin-1 are all proteins key to maintaining the integrity of the upper layer of the skin,” and that the loss of these proteins causes gaps to develop, allowing the tumor to spread and ulcerate – a process associated with high-risk tumors. Dr. Lovat likened the process to that of “mortar and bricks holding together a wall”, with the loss of these proteins being “like the mortar crumbling away in the wall.”
According to Cancer Research UK, there are over 16,000 new cases of melanoma skin cancer each year in the United Kingdom, with over 2,000 deaths annually. After being surgically removed, primary tumors are histologically staged, with even low-risk cases being followed up for a number of years, a process that can be time-consuming for patients and costly for the NHS.
Some reassurance for those with melanoma
The creators of the new test say that it is these low-risk patients that the test is able to identify, offering a degree of reassurance to those diagnosed with the disease, and potentially reducing the number of hospital clinic visits they require.
Dr. Lovat commented: “Our test offers a personalized prognosis as it more accurately predicts if your skin cancer is unlikely to spread.”
She added that the test will aid clinicians to identify genuinely low-risk patients diagnosed with an early-stage melanoma, reducing the number of follow-up appointments for those identified as low risk. It, therefore, offers the opportunity to save the NHS time and money.
Excellent news for those with skin cancer
Phil Brady, chief operating officer of the British Skin Foundation, echoed Dr. Lovat’s comments, saying: “The test can alleviate stress and anxiety for patients caused by this potentially deadly skin cancer, whilst increasing efficiency and reducing costs to the NHS.”
Nick Levell, MD, consultant dermatologist & British Skin Foundation spokesperson, who has not been involved in the research, commented how the arrival of the test was “excellent news,” adding that “people at low risk can be reassured and will not have to attend hospital so often for check-ups”.
The development of the new test AMBLor has been led by Dr. Lovat, in association with the university spin-out company AMLo Biosciences, and is accredited by the National Accreditation Body for the United Kingdom. The test involves tissue sections from the standard biopsy being sent in the post to the lab for analysis and costs £293 plus VAT. Currently available through a private referral service, the Newcastle team have applied for the test to be made available on the NHS.
A version of this article first appeared on Medscape UK.
Their research, published in the British Journal of Dermatology, describes how early-stage melanomas at risk of spreading secrete transforming growth factor beta2 (TGF-beta2), which causes the reduction, or down-regulation, of the proteins AMBRA1 and loricrin, both of which are found in the skin overlaying the tumor. TGF-beta2 also causes the loss of claudin-1, which in turn leads to loss of skin integrity, facilitating ulceration.
Senior author Penny Lovat, PhD, professor of cellular dermatology and oncology at Newcastle University, and chief scientific officer at AMLo Biosciences, explained: “AMBRA1, loricrin, and claudin-1 are all proteins key to maintaining the integrity of the upper layer of the skin,” and that the loss of these proteins causes gaps to develop, allowing the tumor to spread and ulcerate – a process associated with high-risk tumors. Dr. Lovat likened the process to that of “mortar and bricks holding together a wall”, with the loss of these proteins being “like the mortar crumbling away in the wall.”
According to Cancer Research UK, there are over 16,000 new cases of melanoma skin cancer each year in the United Kingdom, with over 2,000 deaths annually. After being surgically removed, primary tumors are histologically staged, with even low-risk cases being followed up for a number of years, a process that can be time-consuming for patients and costly for the NHS.
Some reassurance for those with melanoma
The creators of the new test say that it is these low-risk patients that the test is able to identify, offering a degree of reassurance to those diagnosed with the disease, and potentially reducing the number of hospital clinic visits they require.
Dr. Lovat commented: “Our test offers a personalized prognosis as it more accurately predicts if your skin cancer is unlikely to spread.”
She added that the test will aid clinicians to identify genuinely low-risk patients diagnosed with an early-stage melanoma, reducing the number of follow-up appointments for those identified as low risk. It, therefore, offers the opportunity to save the NHS time and money.
Excellent news for those with skin cancer
Phil Brady, chief operating officer of the British Skin Foundation, echoed Dr. Lovat’s comments, saying: “The test can alleviate stress and anxiety for patients caused by this potentially deadly skin cancer, whilst increasing efficiency and reducing costs to the NHS.”
Nick Levell, MD, consultant dermatologist & British Skin Foundation spokesperson, who has not been involved in the research, commented how the arrival of the test was “excellent news,” adding that “people at low risk can be reassured and will not have to attend hospital so often for check-ups”.
The development of the new test AMBLor has been led by Dr. Lovat, in association with the university spin-out company AMLo Biosciences, and is accredited by the National Accreditation Body for the United Kingdom. The test involves tissue sections from the standard biopsy being sent in the post to the lab for analysis and costs £293 plus VAT. Currently available through a private referral service, the Newcastle team have applied for the test to be made available on the NHS.
A version of this article first appeared on Medscape UK.
Their research, published in the British Journal of Dermatology, describes how early-stage melanomas at risk of spreading secrete transforming growth factor beta2 (TGF-beta2), which causes the reduction, or down-regulation, of the proteins AMBRA1 and loricrin, both of which are found in the skin overlaying the tumor. TGF-beta2 also causes the loss of claudin-1, which in turn leads to loss of skin integrity, facilitating ulceration.
Senior author Penny Lovat, PhD, professor of cellular dermatology and oncology at Newcastle University, and chief scientific officer at AMLo Biosciences, explained: “AMBRA1, loricrin, and claudin-1 are all proteins key to maintaining the integrity of the upper layer of the skin,” and that the loss of these proteins causes gaps to develop, allowing the tumor to spread and ulcerate – a process associated with high-risk tumors. Dr. Lovat likened the process to that of “mortar and bricks holding together a wall”, with the loss of these proteins being “like the mortar crumbling away in the wall.”
According to Cancer Research UK, there are over 16,000 new cases of melanoma skin cancer each year in the United Kingdom, with over 2,000 deaths annually. After being surgically removed, primary tumors are histologically staged, with even low-risk cases being followed up for a number of years, a process that can be time-consuming for patients and costly for the NHS.
Some reassurance for those with melanoma
The creators of the new test say that it is these low-risk patients that the test is able to identify, offering a degree of reassurance to those diagnosed with the disease, and potentially reducing the number of hospital clinic visits they require.
Dr. Lovat commented: “Our test offers a personalized prognosis as it more accurately predicts if your skin cancer is unlikely to spread.”
She added that the test will aid clinicians to identify genuinely low-risk patients diagnosed with an early-stage melanoma, reducing the number of follow-up appointments for those identified as low risk. It, therefore, offers the opportunity to save the NHS time and money.
Excellent news for those with skin cancer
Phil Brady, chief operating officer of the British Skin Foundation, echoed Dr. Lovat’s comments, saying: “The test can alleviate stress and anxiety for patients caused by this potentially deadly skin cancer, whilst increasing efficiency and reducing costs to the NHS.”
Nick Levell, MD, consultant dermatologist & British Skin Foundation spokesperson, who has not been involved in the research, commented how the arrival of the test was “excellent news,” adding that “people at low risk can be reassured and will not have to attend hospital so often for check-ups”.
The development of the new test AMBLor has been led by Dr. Lovat, in association with the university spin-out company AMLo Biosciences, and is accredited by the National Accreditation Body for the United Kingdom. The test involves tissue sections from the standard biopsy being sent in the post to the lab for analysis and costs £293 plus VAT. Currently available through a private referral service, the Newcastle team have applied for the test to be made available on the NHS.
A version of this article first appeared on Medscape UK.
FROM THE BRITISH JOURNAL OF DERMATOLOGY