User login
The Official Newspaper of the American Association for Thoracic Surgery
Cadaveric allograft system used to reconstruct anterior chest wall
PHOENIX – Cadaveric allograft sternal replacement has proven to be safe, providing optimal stability to the chest wall and protection of surrounding organs, an analysis of 18 cases demonstrated.
“The allograft was biologically well tolerated, allowing a perfect integration into the host,” Dr. Giuseppe Marulli said at the annual meeting of the Society of Thoracic Surgeons. “Donor cryopreserved sternochondral allograft may become the ideal way for anterior chest wall reconstruction, particularly for wide resections.”

Dr. Marulli, a thoracic surgeon at the University of Padova, Italy, noted that prior experimental studies have demonstrated that cryopreserved bone allografts preserve osteoconduction and osteoinduction capacity (Eur Spine J. 2001 Oct;10:S96-101). “Therefore, they form the basis for new bone tissue formation, allowing for the capillary and perivascular blood supply,” he said.
Limitations of current materials used for sternal reconstruction include “excessive rigidity with risk of erosion and insufficient support for large chest wall defects,” he said. Perceived advantages of using cadaveric bone allograft include easy incorporation, no risk of rejection, and a low risk of infection. For each procedure used in the current analysis, cadaveric allograft sternums with costal cartilages were harvested with an aseptic method and treated with an antibiotic solution for 72 hours. Next, they were cryopreserved at –80º C and underwent microbiologic testing for at least 1 month to ensure sterility and absence of immunogenic capacity.
Dr. Marulli reported results from 18 patients who underwent the procedure between January 2009 and January 2015, 13 of whom were female. Their median age was 59 years, their median tumor diameter was 4.75 cm, most (88%) had undergone preoperative needle biopsy, and 50% had undergone induction therapy. The main indication for sternectomy was a single-site sternal metastasis (nine patients), primary chondrosarcoma (four cases), sternal dehiscence after cardiac surgery (two cases), malignant fibrous tumor (one case), radioinduced soft-tissue sarcoma (one case), and a thymic carcinoma invading the sternum (one case).
All patients were extubated in the OR, and one patient died in the hospital from a pulmonary embolism. Two patients (11%) developed postoperative complications: one case of Candida urinary infection and one case of bleeding at the site of the muscle flap. The median postoperative length of stay was 11 days.
To date, no infections or rejections of the grafts have occurred, Dr. Marulli said. After a median of 36 months, 13 patients are alive and 4 are dead (3 from a metastatic recurrence and 1 from an unrelated cause). One patient required removal of a clavicular screw for dislocation 4 months after the operation.
Dr. Marulli reported having no financial disclosures.
PHOENIX – Cadaveric allograft sternal replacement has proven to be safe, providing optimal stability to the chest wall and protection of surrounding organs, an analysis of 18 cases demonstrated.
“The allograft was biologically well tolerated, allowing a perfect integration into the host,” Dr. Giuseppe Marulli said at the annual meeting of the Society of Thoracic Surgeons. “Donor cryopreserved sternochondral allograft may become the ideal way for anterior chest wall reconstruction, particularly for wide resections.”
Dr. Marulli, a thoracic surgeon at the University of Padova, Italy, noted that prior experimental studies have demonstrated that cryopreserved bone allografts preserve osteoconduction and osteoinduction capacity (Eur Spine J. 2001 Oct;10:S96-101). “Therefore, they form the basis for new bone tissue formation, allowing for the capillary and perivascular blood supply,” he said.
Limitations of current materials used for sternal reconstruction include “excessive rigidity with risk of erosion and insufficient support for large chest wall defects,” he said. Perceived advantages of using cadaveric bone allograft include easy incorporation, no risk of rejection, and a low risk of infection. For each procedure used in the current analysis, cadaveric allograft sternums with costal cartilages were harvested with an aseptic method and treated with an antibiotic solution for 72 hours. Next, they were cryopreserved at –80º C and underwent microbiologic testing for at least 1 month to ensure sterility and absence of immunogenic capacity.
Dr. Marulli reported results from 18 patients who underwent the procedure between January 2009 and January 2015, 13 of whom were female. Their median age was 59 years, their median tumor diameter was 4.75 cm, most (88%) had undergone preoperative needle biopsy, and 50% had undergone induction therapy. The main indication for sternectomy was a single-site sternal metastasis (nine patients), primary chondrosarcoma (four cases), sternal dehiscence after cardiac surgery (two cases), malignant fibrous tumor (one case), radioinduced soft-tissue sarcoma (one case), and a thymic carcinoma invading the sternum (one case).
All patients were extubated in the OR, and one patient died in the hospital from a pulmonary embolism. Two patients (11%) developed postoperative complications: one case of Candida urinary infection and one case of bleeding at the site of the muscle flap. The median postoperative length of stay was 11 days.
To date, no infections or rejections of the grafts have occurred, Dr. Marulli said. After a median of 36 months, 13 patients are alive and 4 are dead (3 from a metastatic recurrence and 1 from an unrelated cause). One patient required removal of a clavicular screw for dislocation 4 months after the operation.
Dr. Marulli reported having no financial disclosures.
PHOENIX – Cadaveric allograft sternal replacement has proven to be safe, providing optimal stability to the chest wall and protection of surrounding organs, an analysis of 18 cases demonstrated.
“The allograft was biologically well tolerated, allowing a perfect integration into the host,” Dr. Giuseppe Marulli said at the annual meeting of the Society of Thoracic Surgeons. “Donor cryopreserved sternochondral allograft may become the ideal way for anterior chest wall reconstruction, particularly for wide resections.”
Dr. Marulli, a thoracic surgeon at the University of Padova, Italy, noted that prior experimental studies have demonstrated that cryopreserved bone allografts preserve osteoconduction and osteoinduction capacity (Eur Spine J. 2001 Oct;10:S96-101). “Therefore, they form the basis for new bone tissue formation, allowing for the capillary and perivascular blood supply,” he said.
Limitations of current materials used for sternal reconstruction include “excessive rigidity with risk of erosion and insufficient support for large chest wall defects,” he said. Perceived advantages of using cadaveric bone allograft include easy incorporation, no risk of rejection, and a low risk of infection. For each procedure used in the current analysis, cadaveric allograft sternums with costal cartilages were harvested with an aseptic method and treated with an antibiotic solution for 72 hours. Next, they were cryopreserved at –80º C and underwent microbiologic testing for at least 1 month to ensure sterility and absence of immunogenic capacity.
Dr. Marulli reported results from 18 patients who underwent the procedure between January 2009 and January 2015, 13 of whom were female. Their median age was 59 years, their median tumor diameter was 4.75 cm, most (88%) had undergone preoperative needle biopsy, and 50% had undergone induction therapy. The main indication for sternectomy was a single-site sternal metastasis (nine patients), primary chondrosarcoma (four cases), sternal dehiscence after cardiac surgery (two cases), malignant fibrous tumor (one case), radioinduced soft-tissue sarcoma (one case), and a thymic carcinoma invading the sternum (one case).
All patients were extubated in the OR, and one patient died in the hospital from a pulmonary embolism. Two patients (11%) developed postoperative complications: one case of Candida urinary infection and one case of bleeding at the site of the muscle flap. The median postoperative length of stay was 11 days.
To date, no infections or rejections of the grafts have occurred, Dr. Marulli said. After a median of 36 months, 13 patients are alive and 4 are dead (3 from a metastatic recurrence and 1 from an unrelated cause). One patient required removal of a clavicular screw for dislocation 4 months after the operation.
Dr. Marulli reported having no financial disclosures.
AT THE STS ANNUAL MEETING
Key clinical point: Cadaveric allograft sternal replacement appears to be an effective option for reconstructing the anterior chest wall.
Major finding: To date, no infections or rejections of the grafts have occurred in patients who underwent cadaveric allograft sternal replacement.
Data source: An analysis of 18 patients who underwent the procedure between January 2009 and January 2015.
Disclosures: Dr. Marulli reported having no financial disclosures.

Fewer general surgery residents doing thoracic surgery cases
PHOENIX – Over the past 11 years, fewer general surgery residents have participated in important types of general thoracic surgery cases, a retrospective review found.
“These findings may be the result of the work-hours reduction causing less exposure to general thoracic surgery and/or a reluctance to allow general surgery residents to perform the increasingly common minimally invasive procedures,” researchers led by Dr. William S. Ragalie wrote in an abstract presented during a poster session at the annual meeting of the Society of Thoracic Surgeons.

Dr. Ragalie of the Medical College of Wisconsin, Milwaukee, and his associates retrospectively reviewed the Accreditation Council for Graduate Medical Education resident case log database for the most recent 11 years in an effort to quantify and trend the operative experience among general surgery residents. They categorized cases by year, level of resident participation, and level of complexity. Major general thoracic cases were defined as esophagectomy, pneumonectomy, and lobectomy, while cases that did not involve hilar dissection were classified as “other thoracic.”
The researchers found that the 90th percentile of first assist thoracic surgery cases decreased significantly over the study period by an average of 1.46 cases per year (P = .0012). Decreased case volumes in pneumonectomy were also noted at the junior level (–0.012 cases per year; P less than .0001) and at the chief resident level (–0.31 cases per year; P less than .001). This was also true of open lobectomy cases (–0.14 cases per year at the junior level; P less than .001, and –3.41 cases per year at the chief resident level; P less than .0001).
As for video-assisted thoracoscopic surgery (VATS) lobectomy, the researchers observed an increase in average case volume at the junior surgeon level of .13 cases per year, but a decrease at the chief resident level of one case per year (P less than .001 for both).

Dr. Ragalie and his associates also observed a decrease in the following procedures performed by chief residents: open exploratory thoracoscopy (–3.17 cases per year; P less than .001), VATS exploratory thoracoscopy (–2.95 cases per year; P less than .0001), open wedge resection (–1.52 cases per year; P less than .0227), VATS wedge resection (–2.72 cases per year; P less than .0002), “other thoracic” (–6.3 cases per year; P = .0001), and thoracoscopic pleurodesis (–2.09 cases per year; P less than .0001).
At the same time, a significant trend of decreased case volume at the junior surgeon level was noted for open exploratory thoracoscopy (–0.10 cases per year; P less than .0001) and open wedge resection (–0.22 cases per year; P = . 0115).
The researchers reported having no financial disclosures.
PHOENIX – Over the past 11 years, fewer general surgery residents have participated in important types of general thoracic surgery cases, a retrospective review found.
“These findings may be the result of the work-hours reduction causing less exposure to general thoracic surgery and/or a reluctance to allow general surgery residents to perform the increasingly common minimally invasive procedures,” researchers led by Dr. William S. Ragalie wrote in an abstract presented during a poster session at the annual meeting of the Society of Thoracic Surgeons.
Dr. Ragalie of the Medical College of Wisconsin, Milwaukee, and his associates retrospectively reviewed the Accreditation Council for Graduate Medical Education resident case log database for the most recent 11 years in an effort to quantify and trend the operative experience among general surgery residents. They categorized cases by year, level of resident participation, and level of complexity. Major general thoracic cases were defined as esophagectomy, pneumonectomy, and lobectomy, while cases that did not involve hilar dissection were classified as “other thoracic.”
The researchers found that the 90th percentile of first assist thoracic surgery cases decreased significantly over the study period by an average of 1.46 cases per year (P = .0012). Decreased case volumes in pneumonectomy were also noted at the junior level (–0.012 cases per year; P less than .0001) and at the chief resident level (–0.31 cases per year; P less than .001). This was also true of open lobectomy cases (–0.14 cases per year at the junior level; P less than .001, and –3.41 cases per year at the chief resident level; P less than .0001).
As for video-assisted thoracoscopic surgery (VATS) lobectomy, the researchers observed an increase in average case volume at the junior surgeon level of .13 cases per year, but a decrease at the chief resident level of one case per year (P less than .001 for both).
Dr. Ragalie and his associates also observed a decrease in the following procedures performed by chief residents: open exploratory thoracoscopy (–3.17 cases per year; P less than .001), VATS exploratory thoracoscopy (–2.95 cases per year; P less than .0001), open wedge resection (–1.52 cases per year; P less than .0227), VATS wedge resection (–2.72 cases per year; P less than .0002), “other thoracic” (–6.3 cases per year; P = .0001), and thoracoscopic pleurodesis (–2.09 cases per year; P less than .0001).
At the same time, a significant trend of decreased case volume at the junior surgeon level was noted for open exploratory thoracoscopy (–0.10 cases per year; P less than .0001) and open wedge resection (–0.22 cases per year; P = . 0115).
The researchers reported having no financial disclosures.
PHOENIX – Over the past 11 years, fewer general surgery residents have participated in important types of general thoracic surgery cases, a retrospective review found.
“These findings may be the result of the work-hours reduction causing less exposure to general thoracic surgery and/or a reluctance to allow general surgery residents to perform the increasingly common minimally invasive procedures,” researchers led by Dr. William S. Ragalie wrote in an abstract presented during a poster session at the annual meeting of the Society of Thoracic Surgeons.
Dr. Ragalie of the Medical College of Wisconsin, Milwaukee, and his associates retrospectively reviewed the Accreditation Council for Graduate Medical Education resident case log database for the most recent 11 years in an effort to quantify and trend the operative experience among general surgery residents. They categorized cases by year, level of resident participation, and level of complexity. Major general thoracic cases were defined as esophagectomy, pneumonectomy, and lobectomy, while cases that did not involve hilar dissection were classified as “other thoracic.”
The researchers found that the 90th percentile of first assist thoracic surgery cases decreased significantly over the study period by an average of 1.46 cases per year (P = .0012). Decreased case volumes in pneumonectomy were also noted at the junior level (–0.012 cases per year; P less than .0001) and at the chief resident level (–0.31 cases per year; P less than .001). This was also true of open lobectomy cases (–0.14 cases per year at the junior level; P less than .001, and –3.41 cases per year at the chief resident level; P less than .0001).
As for video-assisted thoracoscopic surgery (VATS) lobectomy, the researchers observed an increase in average case volume at the junior surgeon level of .13 cases per year, but a decrease at the chief resident level of one case per year (P less than .001 for both).
Dr. Ragalie and his associates also observed a decrease in the following procedures performed by chief residents: open exploratory thoracoscopy (–3.17 cases per year; P less than .001), VATS exploratory thoracoscopy (–2.95 cases per year; P less than .0001), open wedge resection (–1.52 cases per year; P less than .0227), VATS wedge resection (–2.72 cases per year; P less than .0002), “other thoracic” (–6.3 cases per year; P = .0001), and thoracoscopic pleurodesis (–2.09 cases per year; P less than .0001).
At the same time, a significant trend of decreased case volume at the junior surgeon level was noted for open exploratory thoracoscopy (–0.10 cases per year; P less than .0001) and open wedge resection (–0.22 cases per year; P = . 0115).
The researchers reported having no financial disclosures.
AT THE STS ANNUAL MEETING
Key clinical point: Fewer general surgery residents are participating in important types of general thoracic surgery cases during their residency.
Major finding: The 90th percentile of first-assist thoracic surgery cases decreased significantly over the study period by an average of 1.46 cases per year (P = .0012).
Data source: A retrospective analysis of the Accreditation Council for Graduate Medical Education resident case log database for the most recent 11 years.
Disclosures: The researchers reported having no financial disclosures.

Don’t Miss AATS Week
AATS Week 2016 Registration & Housing Open!
AATS Week 2016 includes Two Terrific Events
Aortic Symposium
May 12–13, 2016
New York, NY
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
Register for AATS Week 2016 today & receive a $100 discount off the AATS Aortic Symposium registration fee
Registration & Housing Now Open: Register online or via phone or mail/fax.
Online
Phone: Customer Service Desk: (US) 800- 424-5249; (International) 847-996-5829
Mail/fax: Get the registration form online. By mail: AATS/Experient, 5202 Presidents Court, Frederick, MD 21705 with check and credit card information. By fax: 301-694-5124.
Take Advantage of These AATS Annual Meeting Opportunities
Annual Meeting Registration Packages
Health Care Professional Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500 — a savings of $300.
Resident/Fellow and Medical Student Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300 — a savings of $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia taking place that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.
AATS Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
The 2016 AATS Aortic Symposium is a two-day symposium focused on the pathophysiology, diagnosis and treatment of aortic aneurysms and dissections. The conference is designed for cardiovascular and thoracic surgeons, residents, perfusionists, ICU and OR nurses and others involved in aortic disease patient care. Faculty members include world leaders in the field who will share their experiences treating difficult aortic disease cases.
View Preliminary Program, Speakers, Presentations & Full Abstracts
AATS 96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting ChaiR
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
View Preliminary Program, Speakers, Presentations and Full Abstracts
The 96th Annual Meeting is a five-day program of state-of-the-art presentations by renowned experts. Attendees will enhance their knowledge and skills in a wide-range of subjects including general and specialized cardiac surgery, emerging technologies, congenital heart disease, critical care and aortic/endovascular surgery.
Don’t miss this year’s exciting program including:
Saturday Skills Courses featuring Combined Luncheon Speaker: Denton A. Cooley, followed by Hands-On Sessions
Sunday Postgraduate Symposia with Legends Luncheons featuring Joel D. Cooper and John L. Ochsner
New: Survival Guide for the Cardiothoracic Surgical Team course following by a Hands-On Session (Available to Residents, Fellows and Health Care Professionals Only)
Presidential Address: Competition: Perspiration to Inspiration “Aut viam inveniam aut faciam”, Joseph S. Coselli, Baylor College of Medicine
Basic Science Lecture: Stopping Incurable Cancers through Eliminating their Anti-Oxidative Defenses, James D. Watson, a Nobel Prize-winning biophysicist and researcher who is credited with co-discovering the double-helix structure of DNA.
Honored Guest Lecture: Brian Kelly, Notre Dame Head Football Coach and a veteran of 23 seasons as a collegiate head coach. Brian Kelly brings a championship tradition to his fifth year as the 29th head football coach at the University of Notre Dame.
Emerging Technologies & Techniques Fora: Adult Cardiac and General Thoracic
VAD/ECMO Session
Masters of Surgery: Video Sessions
AATS Learning Center: Featuring cutting-edge case videos of novel procedures and surgical techniques.
AATS Week 2016 Registration & Housing Open!
AATS Week 2016 includes Two Terrific Events
Aortic Symposium
May 12–13, 2016
New York, NY
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
Register for AATS Week 2016 today & receive a $100 discount off the AATS Aortic Symposium registration fee
Registration & Housing Now Open: Register online or via phone or mail/fax.
Online
Phone: Customer Service Desk: (US) 800- 424-5249; (International) 847-996-5829
Mail/fax: Get the registration form online. By mail: AATS/Experient, 5202 Presidents Court, Frederick, MD 21705 with check and credit card information. By fax: 301-694-5124.
Take Advantage of These AATS Annual Meeting Opportunities
Annual Meeting Registration Packages
Health Care Professional Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500 — a savings of $300.
Resident/Fellow and Medical Student Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300 — a savings of $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia taking place that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.
AATS Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
The 2016 AATS Aortic Symposium is a two-day symposium focused on the pathophysiology, diagnosis and treatment of aortic aneurysms and dissections. The conference is designed for cardiovascular and thoracic surgeons, residents, perfusionists, ICU and OR nurses and others involved in aortic disease patient care. Faculty members include world leaders in the field who will share their experiences treating difficult aortic disease cases.
View Preliminary Program, Speakers, Presentations & Full Abstracts
AATS 96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting ChaiR
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
View Preliminary Program, Speakers, Presentations and Full Abstracts
The 96th Annual Meeting is a five-day program of state-of-the-art presentations by renowned experts. Attendees will enhance their knowledge and skills in a wide-range of subjects including general and specialized cardiac surgery, emerging technologies, congenital heart disease, critical care and aortic/endovascular surgery.
Don’t miss this year’s exciting program including:
Saturday Skills Courses featuring Combined Luncheon Speaker: Denton A. Cooley, followed by Hands-On Sessions
Sunday Postgraduate Symposia with Legends Luncheons featuring Joel D. Cooper and John L. Ochsner
New: Survival Guide for the Cardiothoracic Surgical Team course following by a Hands-On Session (Available to Residents, Fellows and Health Care Professionals Only)
Presidential Address: Competition: Perspiration to Inspiration “Aut viam inveniam aut faciam”, Joseph S. Coselli, Baylor College of Medicine
Basic Science Lecture: Stopping Incurable Cancers through Eliminating their Anti-Oxidative Defenses, James D. Watson, a Nobel Prize-winning biophysicist and researcher who is credited with co-discovering the double-helix structure of DNA.
Honored Guest Lecture: Brian Kelly, Notre Dame Head Football Coach and a veteran of 23 seasons as a collegiate head coach. Brian Kelly brings a championship tradition to his fifth year as the 29th head football coach at the University of Notre Dame.
Emerging Technologies & Techniques Fora: Adult Cardiac and General Thoracic
VAD/ECMO Session
Masters of Surgery: Video Sessions
AATS Learning Center: Featuring cutting-edge case videos of novel procedures and surgical techniques.
AATS Week 2016 Registration & Housing Open!
AATS Week 2016 includes Two Terrific Events
Aortic Symposium
May 12–13, 2016
New York, NY
96th Annual Meeting
May 14-18, 2016
Baltimore, MD
Register for AATS Week 2016 today & receive a $100 discount off the AATS Aortic Symposium registration fee
Registration & Housing Now Open: Register online or via phone or mail/fax.
Online
Phone: Customer Service Desk: (US) 800- 424-5249; (International) 847-996-5829
Mail/fax: Get the registration form online. By mail: AATS/Experient, 5202 Presidents Court, Frederick, MD 21705 with check and credit card information. By fax: 301-694-5124.
Take Advantage of These AATS Annual Meeting Opportunities
Annual Meeting Registration Packages
Health Care Professional Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 for only $400, after which the fee goes up to $500 — a savings of $300.
Resident/Fellow and Medical Student Package: Includes registration for the Saturday Courses, Sunday Symposium and the 96th Annual Meeting (Monday-Wednesday). Register before March 25, 2016 and attend for no charge. After that date, the fee is $300 — a savings of $300.
Saturday Courses and Sunday Symposium Registration: Register for a Saturday course and/or a Sunday symposium and have access to all other courses/symposia taking place that same day. Note: Registration for the Saturday courses and/or Sunday symposium is separate from the Annual Meeting fee.
AATS Aortic Symposium
May 12–13, 2016
New York, NY
Course Directors
Joseph S. Coselli
Steven L. Lansman
The 2016 AATS Aortic Symposium is a two-day symposium focused on the pathophysiology, diagnosis and treatment of aortic aneurysms and dissections. The conference is designed for cardiovascular and thoracic surgeons, residents, perfusionists, ICU and OR nurses and others involved in aortic disease patient care. Faculty members include world leaders in the field who will share their experiences treating difficult aortic disease cases.
View Preliminary Program, Speakers, Presentations & Full Abstracts
AATS 96th Annual Meeting
May 14-18, 2016
Baltimore, MD
President & Annual Meeting ChaiR
Joseph S. Coselli
Annual Meeting Co-Chairs
Charles D. Fraser
David R. Jones
View Preliminary Program, Speakers, Presentations and Full Abstracts
The 96th Annual Meeting is a five-day program of state-of-the-art presentations by renowned experts. Attendees will enhance their knowledge and skills in a wide-range of subjects including general and specialized cardiac surgery, emerging technologies, congenital heart disease, critical care and aortic/endovascular surgery.
Don’t miss this year’s exciting program including:
Saturday Skills Courses featuring Combined Luncheon Speaker: Denton A. Cooley, followed by Hands-On Sessions
Sunday Postgraduate Symposia with Legends Luncheons featuring Joel D. Cooper and John L. Ochsner
New: Survival Guide for the Cardiothoracic Surgical Team course following by a Hands-On Session (Available to Residents, Fellows and Health Care Professionals Only)
Presidential Address: Competition: Perspiration to Inspiration “Aut viam inveniam aut faciam”, Joseph S. Coselli, Baylor College of Medicine
Basic Science Lecture: Stopping Incurable Cancers through Eliminating their Anti-Oxidative Defenses, James D. Watson, a Nobel Prize-winning biophysicist and researcher who is credited with co-discovering the double-helix structure of DNA.
Honored Guest Lecture: Brian Kelly, Notre Dame Head Football Coach and a veteran of 23 seasons as a collegiate head coach. Brian Kelly brings a championship tradition to his fifth year as the 29th head football coach at the University of Notre Dame.
Emerging Technologies & Techniques Fora: Adult Cardiac and General Thoracic
VAD/ECMO Session
Masters of Surgery: Video Sessions
AATS Learning Center: Featuring cutting-edge case videos of novel procedures and surgical techniques.

AATS Graham Foundation Awards Deadline: February 15!
Applications are now open for...
Every Heartbeat Matters Valve Disease Fellowship
Applications for the second award cycle of the Every Heartbeat Matters Valve Fellowship — a joint project of the AATS Graham and Edwards Lifesciences Foundation — are now open. The mission of Every Heartbeat Matters is to impact the global burden of heart valve disease by serving one million people by 2020.
The fellowship’s goal is to enhance the knowledge and skills of practicing cardiothoracic surgeons who are already treating or committed to treating underserved patients worldwide. It provides up to three months of advanced heart valve disease training and education at a host institution.
More information/application
Deadline: February 15, 2016
2016 Graham Surgical Investigator Program
The Graham Surgical Investigator Program supports innovative clinical or translational research for young cardiothoracic surgeons. Topics include, but are not limited to, topics related to outcomes research, as well as robotically assisted surgery, minimally invasive surgery or other applications of new and innovative technologies in cardiothoracic surgery.
Up to four proposals will be funded in 2016.
Thanks to the generosity of Ethicon, Intuitive Surgical, Dr. Mehmet Oz and AATS.
More information/application
Deadline: February 15, 2016
Applications are now open for...
Every Heartbeat Matters Valve Disease Fellowship
Applications for the second award cycle of the Every Heartbeat Matters Valve Fellowship — a joint project of the AATS Graham and Edwards Lifesciences Foundation — are now open. The mission of Every Heartbeat Matters is to impact the global burden of heart valve disease by serving one million people by 2020.
The fellowship’s goal is to enhance the knowledge and skills of practicing cardiothoracic surgeons who are already treating or committed to treating underserved patients worldwide. It provides up to three months of advanced heart valve disease training and education at a host institution.
More information/application
Deadline: February 15, 2016
2016 Graham Surgical Investigator Program
The Graham Surgical Investigator Program supports innovative clinical or translational research for young cardiothoracic surgeons. Topics include, but are not limited to, topics related to outcomes research, as well as robotically assisted surgery, minimally invasive surgery or other applications of new and innovative technologies in cardiothoracic surgery.
Up to four proposals will be funded in 2016.
Thanks to the generosity of Ethicon, Intuitive Surgical, Dr. Mehmet Oz and AATS.
More information/application
Deadline: February 15, 2016
Applications are now open for...
Every Heartbeat Matters Valve Disease Fellowship
Applications for the second award cycle of the Every Heartbeat Matters Valve Fellowship — a joint project of the AATS Graham and Edwards Lifesciences Foundation — are now open. The mission of Every Heartbeat Matters is to impact the global burden of heart valve disease by serving one million people by 2020.
The fellowship’s goal is to enhance the knowledge and skills of practicing cardiothoracic surgeons who are already treating or committed to treating underserved patients worldwide. It provides up to three months of advanced heart valve disease training and education at a host institution.
More information/application
Deadline: February 15, 2016
2016 Graham Surgical Investigator Program
The Graham Surgical Investigator Program supports innovative clinical or translational research for young cardiothoracic surgeons. Topics include, but are not limited to, topics related to outcomes research, as well as robotically assisted surgery, minimally invasive surgery or other applications of new and innovative technologies in cardiothoracic surgery.
Up to four proposals will be funded in 2016.
Thanks to the generosity of Ethicon, Intuitive Surgical, Dr. Mehmet Oz and AATS.
More information/application
Deadline: February 15, 2016
Save the Date: AATS Surgical Patient Safety Course, June 2016
June 24-25, 2016
Renaissance Boston Waterfront Hotel
Boston, MA
Co-Directors
Thoralf M. Sundt, III, MD
Steven Yule, PhD
Program Committee
David J. Bunnell, PA-C, APACVS
David C. Fitzgerald, CCP, AMSECT
Jake Jaquiss, MD
M. Blair Marshall, MD
Shannon Pengel, RN
Kenneth Shann, CCP, LP, AMSECT
Marco Zenati, MD
Improving patient care remains a constant mission for all members of the surgical team. The AATS Surgical Patient Safety Course has been designed to promote a culture of safety and reduce preventable patient harm by engaging, educating, and equipping members of the cardiothoracic surgical team in the multidimensional approach to patient safety.
The course — which features didactic and interactive presentations and focused workshops — will provide attendees with essential patient safety knowledge, skills, and attitudes aimed at improving care in the present and future.
Preliminary Program Now Online
The Patient Safety program includes team training and simulaltion experiences.
Surgical Team Registration
Register three or more members from the same institution and receive one complimentary Healthcare Professional registration. We encourage you to send the entire team to Boston this June for this important course.
June 24-25, 2016
Renaissance Boston Waterfront Hotel
Boston, MA
Co-Directors
Thoralf M. Sundt, III, MD
Steven Yule, PhD
Program Committee
David J. Bunnell, PA-C, APACVS
David C. Fitzgerald, CCP, AMSECT
Jake Jaquiss, MD
M. Blair Marshall, MD
Shannon Pengel, RN
Kenneth Shann, CCP, LP, AMSECT
Marco Zenati, MD
Improving patient care remains a constant mission for all members of the surgical team. The AATS Surgical Patient Safety Course has been designed to promote a culture of safety and reduce preventable patient harm by engaging, educating, and equipping members of the cardiothoracic surgical team in the multidimensional approach to patient safety.
The course — which features didactic and interactive presentations and focused workshops — will provide attendees with essential patient safety knowledge, skills, and attitudes aimed at improving care in the present and future.
Preliminary Program Now Online
The Patient Safety program includes team training and simulaltion experiences.
Surgical Team Registration
Register three or more members from the same institution and receive one complimentary Healthcare Professional registration. We encourage you to send the entire team to Boston this June for this important course.
June 24-25, 2016
Renaissance Boston Waterfront Hotel
Boston, MA
Co-Directors
Thoralf M. Sundt, III, MD
Steven Yule, PhD
Program Committee
David J. Bunnell, PA-C, APACVS
David C. Fitzgerald, CCP, AMSECT
Jake Jaquiss, MD
M. Blair Marshall, MD
Shannon Pengel, RN
Kenneth Shann, CCP, LP, AMSECT
Marco Zenati, MD
Improving patient care remains a constant mission for all members of the surgical team. The AATS Surgical Patient Safety Course has been designed to promote a culture of safety and reduce preventable patient harm by engaging, educating, and equipping members of the cardiothoracic surgical team in the multidimensional approach to patient safety.
The course — which features didactic and interactive presentations and focused workshops — will provide attendees with essential patient safety knowledge, skills, and attitudes aimed at improving care in the present and future.
Preliminary Program Now Online
The Patient Safety program includes team training and simulaltion experiences.
Surgical Team Registration
Register three or more members from the same institution and receive one complimentary Healthcare Professional registration. We encourage you to send the entire team to Boston this June for this important course.

Focus on Thoracic Surgery: Lung and Esophageal Cancer/China This March
March 19-20, 2016
Hilton Shanghai Hongqiao
Shanghai, China
Program Directors
Haiquan Chen
Ke-Neng Chen
G. Alec Patterson
David J. Sugarbaker
Preliminary Program Now Available
Overview
Lung and esophageal disease remain a global concern as two of the deadliest issues facing patients and thoracic surgeons. The 2016 AATS Focus on Thoracic Surgery: Lung and Esophageal Cancer meeting will concentrate on the complex nature of treating both lung and esophageal disease while also discussing innovative approaches to enhancing patient care.
The two-day program features a mixture of lectures, relevant case studies, panel discussions, and videos. The faculty includes local and internationally recognized experts in lung and esophageal disease ensuring that attendees will receive insights from a broad spectrum of leaders thoracic surgery field.
March 19-20, 2016
Hilton Shanghai Hongqiao
Shanghai, China
Program Directors
Haiquan Chen
Ke-Neng Chen
G. Alec Patterson
David J. Sugarbaker
Preliminary Program Now Available
Overview
Lung and esophageal disease remain a global concern as two of the deadliest issues facing patients and thoracic surgeons. The 2016 AATS Focus on Thoracic Surgery: Lung and Esophageal Cancer meeting will concentrate on the complex nature of treating both lung and esophageal disease while also discussing innovative approaches to enhancing patient care.
The two-day program features a mixture of lectures, relevant case studies, panel discussions, and videos. The faculty includes local and internationally recognized experts in lung and esophageal disease ensuring that attendees will receive insights from a broad spectrum of leaders thoracic surgery field.
March 19-20, 2016
Hilton Shanghai Hongqiao
Shanghai, China
Program Directors
Haiquan Chen
Ke-Neng Chen
G. Alec Patterson
David J. Sugarbaker
Preliminary Program Now Available
Overview
Lung and esophageal disease remain a global concern as two of the deadliest issues facing patients and thoracic surgeons. The 2016 AATS Focus on Thoracic Surgery: Lung and Esophageal Cancer meeting will concentrate on the complex nature of treating both lung and esophageal disease while also discussing innovative approaches to enhancing patient care.
The two-day program features a mixture of lectures, relevant case studies, panel discussions, and videos. The faculty includes local and internationally recognized experts in lung and esophageal disease ensuring that attendees will receive insights from a broad spectrum of leaders thoracic surgery field.
Therapeutic hypothermia called biggest recent advance in cardiac arrest
SNOWMASS, COLO. – By far the most-important contributor to improved outcomes following out-of-hospital cardiac arrest during the past decade has been therapeutic hypothermia, Dr. N.A. Mark Estes III said at the Annual Cardiovascular Conference at Snowmass.
The No. 1 cause of in-hospital death in patients who arrive at the hospital with a perfusable rhythm following resuscitation from out-of-hospital cardiac arrest isn’t sepsis, hepatic or renal failure, or cardiogenic shock. It’s neurologic death caused by anoxic brain injury, which begins several hours after cardiac arrest and continues for about 48 hours. This is where therapeutic hypothermia has made a huge difference, said Dr. Estes, professor of medicine and director of cardiac arrhythmia services at Tufts University, Boston.

“One-half of out-of-hospital cardiac arrest survivors experience secondary anoxic brain damage of varying degrees. Until recently, there was no treatment with documented efficacy in preventing this damage. Despite multiple agents being looked at for neuroprevention, none really has worked. But therapeutic hypothermia has drastically improved outcomes. More than half of patients who arrive at the hospital with a perfusable rhythm and receive therapeutic hypothermia are discharged relatively neurologically intact. That’s a huge difference from what we used to see,” the electrophysiologist observed.
Indeed, the proportion of U.S. patients who experience out-of-hospital cardiac arrest and survive to hospital discharge neurologically intact is “dismal” at about 10%, he noted.
Virtually all specialized cardiac arrest centers now provide therapeutic hypothermia using various protocols. The demonstrated effectiveness of this postresuscitation therapy was an impetus for the American Heart Association policy statement calling for creation of regional cardiac resuscitation systems of care (Circulation. 2010 Feb 9;121[5]:709-29). To date, however, such organized systems exist in only a handful of states or portions of states.
Nonetheless, when an out-of-hospital cardiac arrest patient arrives at a community hospital that can’t provide emergency coronary angiography and therapeutic hypothermia, it’s appropriate to stabilize that patient in the emergency department and then transfer to a hospital that can, according to Dr. Estes.
The mechanism by which therapeutic hypothermia works has been well elucidated. The treatment curbs the process by which ischemia as a second blow triggers formation of oxygen free radicals, glutamate release, calcium shifts, and mitochondrial dysfunction, with resultant destruction of brain tissue.
Roughly 250,000 sudden cardiac deaths (SCDs) occur annually in this country. In addition to more widespread availability of therapeutic hypothermia and other forms of specialized postresuscitation care through creation of regional systems of care for out-of-hospital cardiac arrest, there are other opportunities for improving outcomes. These include earlier activation of the chain of survival that begins with a bystander dialing 911 as well as greater availability of public access defibrillation.
Dr. Estes emphasized that while these measures will further improve outcomes of cardiac arrest, they won’t actually reduce its frequency. By far the greatest opportunity in that realm lies in primordial prevention of coronary artery disease; that is, prevention of the risk factors for CAD. After all, he noted, 80% of all SCDs are associated with underlying ischemic heart disease. In 30% of SCDs, the fatal event is the first manifestation of previously unrecognized CAD. Another one-third of SCDs occur in patients with known CAD, but who weren’t considered at high risk for SCD because of their preserved left ventricular ejection fraction.
“There are a number of luminaries in the field who feel that if we’re really going to make an impact on sudden cardiac death, it’s going to be through primordial prevention of CAD,” the cardiologist said.
For this reason, he was thrilled to hear Dr. Robert A. Vogel elsewhere at the conference describe research by investigators at Affiris AG in Vienna who’ve created a peptide-based vaccine that inhibits PCSK9. Moreover, they showed it to be effective in sharply lowering LDL in mice (PLoS One. 2014 Dec 4;9[12]:e114469).
“I believe that in my lifetime, we will have an antiatherosclerotic vaccine that will lower LDL to an extent where this disease will not disappear but may get to a manageable extent, perhaps a 10% lifetime risk instead of the 55% lifetime risk of MI or stroke that we as Americans currently have,” predicted Dr. Vogel of the University of Colorado, Denver.
Dr. Vogel reported serving as a consultant to the National Football League and the Pritikin Longevity Center as well as acting as the national coordinator for the Sanofi-sponsored ODYSSEY Outcomes trial studying the PCSK9 inhibitor alirocumab (Praluent).
Dr. Estes reported serving as a consultant to Boston Scientific, Medtronic, and St. Jude Medical.
SNOWMASS, COLO. – By far the most-important contributor to improved outcomes following out-of-hospital cardiac arrest during the past decade has been therapeutic hypothermia, Dr. N.A. Mark Estes III said at the Annual Cardiovascular Conference at Snowmass.
The No. 1 cause of in-hospital death in patients who arrive at the hospital with a perfusable rhythm following resuscitation from out-of-hospital cardiac arrest isn’t sepsis, hepatic or renal failure, or cardiogenic shock. It’s neurologic death caused by anoxic brain injury, which begins several hours after cardiac arrest and continues for about 48 hours. This is where therapeutic hypothermia has made a huge difference, said Dr. Estes, professor of medicine and director of cardiac arrhythmia services at Tufts University, Boston.
“One-half of out-of-hospital cardiac arrest survivors experience secondary anoxic brain damage of varying degrees. Until recently, there was no treatment with documented efficacy in preventing this damage. Despite multiple agents being looked at for neuroprevention, none really has worked. But therapeutic hypothermia has drastically improved outcomes. More than half of patients who arrive at the hospital with a perfusable rhythm and receive therapeutic hypothermia are discharged relatively neurologically intact. That’s a huge difference from what we used to see,” the electrophysiologist observed.
Indeed, the proportion of U.S. patients who experience out-of-hospital cardiac arrest and survive to hospital discharge neurologically intact is “dismal” at about 10%, he noted.
Virtually all specialized cardiac arrest centers now provide therapeutic hypothermia using various protocols. The demonstrated effectiveness of this postresuscitation therapy was an impetus for the American Heart Association policy statement calling for creation of regional cardiac resuscitation systems of care (Circulation. 2010 Feb 9;121[5]:709-29). To date, however, such organized systems exist in only a handful of states or portions of states.
Nonetheless, when an out-of-hospital cardiac arrest patient arrives at a community hospital that can’t provide emergency coronary angiography and therapeutic hypothermia, it’s appropriate to stabilize that patient in the emergency department and then transfer to a hospital that can, according to Dr. Estes.
The mechanism by which therapeutic hypothermia works has been well elucidated. The treatment curbs the process by which ischemia as a second blow triggers formation of oxygen free radicals, glutamate release, calcium shifts, and mitochondrial dysfunction, with resultant destruction of brain tissue.
Roughly 250,000 sudden cardiac deaths (SCDs) occur annually in this country. In addition to more widespread availability of therapeutic hypothermia and other forms of specialized postresuscitation care through creation of regional systems of care for out-of-hospital cardiac arrest, there are other opportunities for improving outcomes. These include earlier activation of the chain of survival that begins with a bystander dialing 911 as well as greater availability of public access defibrillation.
Dr. Estes emphasized that while these measures will further improve outcomes of cardiac arrest, they won’t actually reduce its frequency. By far the greatest opportunity in that realm lies in primordial prevention of coronary artery disease; that is, prevention of the risk factors for CAD. After all, he noted, 80% of all SCDs are associated with underlying ischemic heart disease. In 30% of SCDs, the fatal event is the first manifestation of previously unrecognized CAD. Another one-third of SCDs occur in patients with known CAD, but who weren’t considered at high risk for SCD because of their preserved left ventricular ejection fraction.
“There are a number of luminaries in the field who feel that if we’re really going to make an impact on sudden cardiac death, it’s going to be through primordial prevention of CAD,” the cardiologist said.
For this reason, he was thrilled to hear Dr. Robert A. Vogel elsewhere at the conference describe research by investigators at Affiris AG in Vienna who’ve created a peptide-based vaccine that inhibits PCSK9. Moreover, they showed it to be effective in sharply lowering LDL in mice (PLoS One. 2014 Dec 4;9[12]:e114469).
“I believe that in my lifetime, we will have an antiatherosclerotic vaccine that will lower LDL to an extent where this disease will not disappear but may get to a manageable extent, perhaps a 10% lifetime risk instead of the 55% lifetime risk of MI or stroke that we as Americans currently have,” predicted Dr. Vogel of the University of Colorado, Denver.
Dr. Vogel reported serving as a consultant to the National Football League and the Pritikin Longevity Center as well as acting as the national coordinator for the Sanofi-sponsored ODYSSEY Outcomes trial studying the PCSK9 inhibitor alirocumab (Praluent).
Dr. Estes reported serving as a consultant to Boston Scientific, Medtronic, and St. Jude Medical.
SNOWMASS, COLO. – By far the most-important contributor to improved outcomes following out-of-hospital cardiac arrest during the past decade has been therapeutic hypothermia, Dr. N.A. Mark Estes III said at the Annual Cardiovascular Conference at Snowmass.
The No. 1 cause of in-hospital death in patients who arrive at the hospital with a perfusable rhythm following resuscitation from out-of-hospital cardiac arrest isn’t sepsis, hepatic or renal failure, or cardiogenic shock. It’s neurologic death caused by anoxic brain injury, which begins several hours after cardiac arrest and continues for about 48 hours. This is where therapeutic hypothermia has made a huge difference, said Dr. Estes, professor of medicine and director of cardiac arrhythmia services at Tufts University, Boston.
“One-half of out-of-hospital cardiac arrest survivors experience secondary anoxic brain damage of varying degrees. Until recently, there was no treatment with documented efficacy in preventing this damage. Despite multiple agents being looked at for neuroprevention, none really has worked. But therapeutic hypothermia has drastically improved outcomes. More than half of patients who arrive at the hospital with a perfusable rhythm and receive therapeutic hypothermia are discharged relatively neurologically intact. That’s a huge difference from what we used to see,” the electrophysiologist observed.
Indeed, the proportion of U.S. patients who experience out-of-hospital cardiac arrest and survive to hospital discharge neurologically intact is “dismal” at about 10%, he noted.
Virtually all specialized cardiac arrest centers now provide therapeutic hypothermia using various protocols. The demonstrated effectiveness of this postresuscitation therapy was an impetus for the American Heart Association policy statement calling for creation of regional cardiac resuscitation systems of care (Circulation. 2010 Feb 9;121[5]:709-29). To date, however, such organized systems exist in only a handful of states or portions of states.
Nonetheless, when an out-of-hospital cardiac arrest patient arrives at a community hospital that can’t provide emergency coronary angiography and therapeutic hypothermia, it’s appropriate to stabilize that patient in the emergency department and then transfer to a hospital that can, according to Dr. Estes.
The mechanism by which therapeutic hypothermia works has been well elucidated. The treatment curbs the process by which ischemia as a second blow triggers formation of oxygen free radicals, glutamate release, calcium shifts, and mitochondrial dysfunction, with resultant destruction of brain tissue.
Roughly 250,000 sudden cardiac deaths (SCDs) occur annually in this country. In addition to more widespread availability of therapeutic hypothermia and other forms of specialized postresuscitation care through creation of regional systems of care for out-of-hospital cardiac arrest, there are other opportunities for improving outcomes. These include earlier activation of the chain of survival that begins with a bystander dialing 911 as well as greater availability of public access defibrillation.
Dr. Estes emphasized that while these measures will further improve outcomes of cardiac arrest, they won’t actually reduce its frequency. By far the greatest opportunity in that realm lies in primordial prevention of coronary artery disease; that is, prevention of the risk factors for CAD. After all, he noted, 80% of all SCDs are associated with underlying ischemic heart disease. In 30% of SCDs, the fatal event is the first manifestation of previously unrecognized CAD. Another one-third of SCDs occur in patients with known CAD, but who weren’t considered at high risk for SCD because of their preserved left ventricular ejection fraction.
“There are a number of luminaries in the field who feel that if we’re really going to make an impact on sudden cardiac death, it’s going to be through primordial prevention of CAD,” the cardiologist said.
For this reason, he was thrilled to hear Dr. Robert A. Vogel elsewhere at the conference describe research by investigators at Affiris AG in Vienna who’ve created a peptide-based vaccine that inhibits PCSK9. Moreover, they showed it to be effective in sharply lowering LDL in mice (PLoS One. 2014 Dec 4;9[12]:e114469).
“I believe that in my lifetime, we will have an antiatherosclerotic vaccine that will lower LDL to an extent where this disease will not disappear but may get to a manageable extent, perhaps a 10% lifetime risk instead of the 55% lifetime risk of MI or stroke that we as Americans currently have,” predicted Dr. Vogel of the University of Colorado, Denver.
Dr. Vogel reported serving as a consultant to the National Football League and the Pritikin Longevity Center as well as acting as the national coordinator for the Sanofi-sponsored ODYSSEY Outcomes trial studying the PCSK9 inhibitor alirocumab (Praluent).
Dr. Estes reported serving as a consultant to Boston Scientific, Medtronic, and St. Jude Medical.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

A better way to relieve rib fracture pain in the ICU
SAN ANTONIO – A new pain relief option for multiple rib fractures means that you might not have to wait around anymore for anesthesiology to place thoracic epidurals.
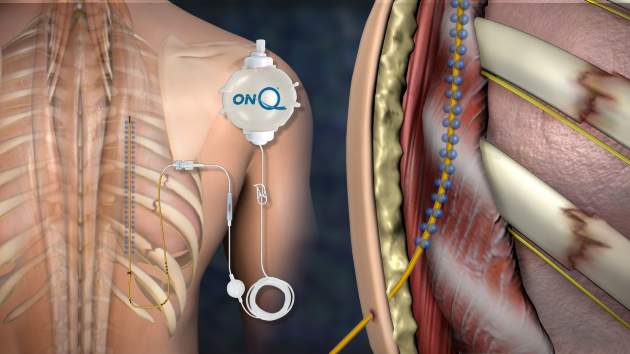
It’s called posterior paramedian subrhomboidal (PoPS) analgesia. A skin incision is made below the lowest fractured rib just paramedian to the spinus processes; a tunneling device is then used to work a catheter upwards under the rhomboids just past the highest fractured rib. The catheter has multiple openings along its length – like a sprinkler hose – so analgesic bathes the intercostal nerves as it runs down from a reservoir into the patient. The reservoir can be set to a desired flow rate or for on-demand use (ON-Q Pain Relief System – Halyard).

A pilot study at the University of Kansas, Kansas City, found that pain control from PoPS was at least equivalent to standard thoracic epidural analgesia (TEA), and that the system can be placed by a variety of hospital staff, not just anesthesiologists.
The 11 PoPS patients also used fewer rescue narcotics than the 19 TEA patients and had less hypotension. Because they weren’t at risk for epidural hematomas, they started venous thromboembolism prophylaxis without delay and at full dose.
“Our results are very promising. PoPS provides pain control similar to that of TEA,” with several “other benefits. You are not relying on one specialty for pain control,” so patients probably get faster relief. “PoPS can also be placed in patients whose injuries prohibit TEA, such as those with spinal cord injuries or increased intracranial pressure,” said investigator Dr. Casey Shelley, a University of Kansas general surgery resident.
PoPS was placed in the study either by anesthesiologists or by a trauma surgeon who practiced placement beforehand in the cadaver lab. The do-it-yourself potential for surgeons “is key. Most of us trauma surgeons are sick of begging anesthesiologists to come place thoracic epidurals,” said an audience member after Dr. Shelley’s presentation at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Ropivacaine 0.2% was used in both PoPS and TEA patients, all of whom had at least three broken ribs.
Median pain scores dropped from 8.5 to 2.5 on a 10-point scale an hour after PoPS placement, versus a median drop from 8 to 5 points an hour after TEA (P = .03). Although not statistically significant, median pain scores were about 1.5 points better with PoPS over the next several days, hovering around 3.5 versus around 5 points with TEA. Anesthesiology “usually won’t place high thoracic epidurals. With PoPS, you can tunnel up as far as you need to go to get to higher ribs,” which might explain the better pain control, Dr. Shelley said.
PoPS patients used about 70 mg/day oral morphine equivalents versus about 90 mg/day with TEA through day 6, but again the difference was not statistically significant. Even so, it might explain why six TEA patients (32%) were hypotensive over that time, compared with two PoPS patients (18%).
PoPS patients were a little older on average (mean 63 versus 55 years), with more fractured ribs (mean eight versus seven), and higher Injury Severity Scale scores (mean 20 versus 16). They were also more likely to have bilateral fractures, longer ICU stays (mean 4.9 versus 3.1 days), and longer overall lengths of stay (mean 14.8 versus 9.8 days), but none of those trends were statistically significant.
Both groups had mean chest Abbreviated Injury Scale scores of 3, and there were no statistical differences in daily spirometry readings. The majority of patients in both groups were men.
Favorable results were also reported in 2010 for ON-Q rib pain control, but the investigators did not compare the system to TEA (World J Surg. 2010 Oct;34:2359-62).
Dr. Shelley said Halyard was not involved in the study, and that she has no disclosures.
SAN ANTONIO – A new pain relief option for multiple rib fractures means that you might not have to wait around anymore for anesthesiology to place thoracic epidurals.
It’s called posterior paramedian subrhomboidal (PoPS) analgesia. A skin incision is made below the lowest fractured rib just paramedian to the spinus processes; a tunneling device is then used to work a catheter upwards under the rhomboids just past the highest fractured rib. The catheter has multiple openings along its length – like a sprinkler hose – so analgesic bathes the intercostal nerves as it runs down from a reservoir into the patient. The reservoir can be set to a desired flow rate or for on-demand use (ON-Q Pain Relief System – Halyard).
A pilot study at the University of Kansas, Kansas City, found that pain control from PoPS was at least equivalent to standard thoracic epidural analgesia (TEA), and that the system can be placed by a variety of hospital staff, not just anesthesiologists.
The 11 PoPS patients also used fewer rescue narcotics than the 19 TEA patients and had less hypotension. Because they weren’t at risk for epidural hematomas, they started venous thromboembolism prophylaxis without delay and at full dose.
“Our results are very promising. PoPS provides pain control similar to that of TEA,” with several “other benefits. You are not relying on one specialty for pain control,” so patients probably get faster relief. “PoPS can also be placed in patients whose injuries prohibit TEA, such as those with spinal cord injuries or increased intracranial pressure,” said investigator Dr. Casey Shelley, a University of Kansas general surgery resident.
PoPS was placed in the study either by anesthesiologists or by a trauma surgeon who practiced placement beforehand in the cadaver lab. The do-it-yourself potential for surgeons “is key. Most of us trauma surgeons are sick of begging anesthesiologists to come place thoracic epidurals,” said an audience member after Dr. Shelley’s presentation at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Ropivacaine 0.2% was used in both PoPS and TEA patients, all of whom had at least three broken ribs.
Median pain scores dropped from 8.5 to 2.5 on a 10-point scale an hour after PoPS placement, versus a median drop from 8 to 5 points an hour after TEA (P = .03). Although not statistically significant, median pain scores were about 1.5 points better with PoPS over the next several days, hovering around 3.5 versus around 5 points with TEA. Anesthesiology “usually won’t place high thoracic epidurals. With PoPS, you can tunnel up as far as you need to go to get to higher ribs,” which might explain the better pain control, Dr. Shelley said.
PoPS patients used about 70 mg/day oral morphine equivalents versus about 90 mg/day with TEA through day 6, but again the difference was not statistically significant. Even so, it might explain why six TEA patients (32%) were hypotensive over that time, compared with two PoPS patients (18%).
PoPS patients were a little older on average (mean 63 versus 55 years), with more fractured ribs (mean eight versus seven), and higher Injury Severity Scale scores (mean 20 versus 16). They were also more likely to have bilateral fractures, longer ICU stays (mean 4.9 versus 3.1 days), and longer overall lengths of stay (mean 14.8 versus 9.8 days), but none of those trends were statistically significant.
Both groups had mean chest Abbreviated Injury Scale scores of 3, and there were no statistical differences in daily spirometry readings. The majority of patients in both groups were men.
Favorable results were also reported in 2010 for ON-Q rib pain control, but the investigators did not compare the system to TEA (World J Surg. 2010 Oct;34:2359-62).
Dr. Shelley said Halyard was not involved in the study, and that she has no disclosures.
SAN ANTONIO – A new pain relief option for multiple rib fractures means that you might not have to wait around anymore for anesthesiology to place thoracic epidurals.
It’s called posterior paramedian subrhomboidal (PoPS) analgesia. A skin incision is made below the lowest fractured rib just paramedian to the spinus processes; a tunneling device is then used to work a catheter upwards under the rhomboids just past the highest fractured rib. The catheter has multiple openings along its length – like a sprinkler hose – so analgesic bathes the intercostal nerves as it runs down from a reservoir into the patient. The reservoir can be set to a desired flow rate or for on-demand use (ON-Q Pain Relief System – Halyard).
A pilot study at the University of Kansas, Kansas City, found that pain control from PoPS was at least equivalent to standard thoracic epidural analgesia (TEA), and that the system can be placed by a variety of hospital staff, not just anesthesiologists.
The 11 PoPS patients also used fewer rescue narcotics than the 19 TEA patients and had less hypotension. Because they weren’t at risk for epidural hematomas, they started venous thromboembolism prophylaxis without delay and at full dose.
“Our results are very promising. PoPS provides pain control similar to that of TEA,” with several “other benefits. You are not relying on one specialty for pain control,” so patients probably get faster relief. “PoPS can also be placed in patients whose injuries prohibit TEA, such as those with spinal cord injuries or increased intracranial pressure,” said investigator Dr. Casey Shelley, a University of Kansas general surgery resident.
PoPS was placed in the study either by anesthesiologists or by a trauma surgeon who practiced placement beforehand in the cadaver lab. The do-it-yourself potential for surgeons “is key. Most of us trauma surgeons are sick of begging anesthesiologists to come place thoracic epidurals,” said an audience member after Dr. Shelley’s presentation at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Ropivacaine 0.2% was used in both PoPS and TEA patients, all of whom had at least three broken ribs.
Median pain scores dropped from 8.5 to 2.5 on a 10-point scale an hour after PoPS placement, versus a median drop from 8 to 5 points an hour after TEA (P = .03). Although not statistically significant, median pain scores were about 1.5 points better with PoPS over the next several days, hovering around 3.5 versus around 5 points with TEA. Anesthesiology “usually won’t place high thoracic epidurals. With PoPS, you can tunnel up as far as you need to go to get to higher ribs,” which might explain the better pain control, Dr. Shelley said.
PoPS patients used about 70 mg/day oral morphine equivalents versus about 90 mg/day with TEA through day 6, but again the difference was not statistically significant. Even so, it might explain why six TEA patients (32%) were hypotensive over that time, compared with two PoPS patients (18%).
PoPS patients were a little older on average (mean 63 versus 55 years), with more fractured ribs (mean eight versus seven), and higher Injury Severity Scale scores (mean 20 versus 16). They were also more likely to have bilateral fractures, longer ICU stays (mean 4.9 versus 3.1 days), and longer overall lengths of stay (mean 14.8 versus 9.8 days), but none of those trends were statistically significant.
Both groups had mean chest Abbreviated Injury Scale scores of 3, and there were no statistical differences in daily spirometry readings. The majority of patients in both groups were men.
Favorable results were also reported in 2010 for ON-Q rib pain control, but the investigators did not compare the system to TEA (World J Surg. 2010 Oct;34:2359-62).
Dr. Shelley said Halyard was not involved in the study, and that she has no disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: You might not have to wait around anymore for anesthesiology to place thoracic epidurals.
Major finding: Median pain scores dropped from 8.5 to 2.5 on a 10-point scale an hour after posterior PoPS placement, versus a median drop from 8 to 5 points an hour after thoracic epidural analgesia (P = .03).
Data source: Pilot study of 30 adults with at least three fractured ribs.
Disclosures: The maker of the PoPS system was not involved in the study, and the presenter had no disclosures.

How to use two new game-changing heart failure drugs
SNOWMASS, COLO. – Ivabradine and sacubitril/valsartan are paradigm-changing drugs approved last year for the treatment of heart failure with reduced ejection fraction – and it’s entirely reasonable to begin using them now in the appropriate patients, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
The impressive positive results seen in the pivotal trials for these novel agents – the SHIFT trial for ivabradine (Corlanor) and PARADIGM-HF for sacubitril/valsartan (Entresto) – have rocked the heart failure world.

The studies showed that, in the right patients, these two medications improve heart failure morbidity and mortality significantly beyond what’s achievable with the current gold standard, guideline-directed medical therapy. That’s exciting because even though great therapeutic strides have been made during the past 15 years, symptomatic patients with heart failure with reduced ejection fraction (HFrEF) treated with optimal guideline-directed pharmacotherapy still have substantial residual risk for heart failure hospitalization and death, noted Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
The U.S. heart failure guidelines panel hasn’t yet addressed the use of either of these recently approved drugs, but Dr. Desai provided his best sense of the data and how he thinks physicians might start using them now.
Ivabradine and sacubitril/valsartan are first-in-class agents with novel mechanisms of action. Ivabradine’s demonstrated safety and efficacy in the SHIFT trial confirmed the hypothesis that elevated heart rate is a legitimate therapeutic target in HFrEF.
Sacubitril/valsartan, an angiotensin II receptor/neprilysin inhibitor formerly known as LCZ696, provides what is to date a unique ability to enhance the activity of endogenous vasoactive peptides, including natriuretic peptides, bradykinin, substance P, adrenomedullin, and calcitonin gene–related peptide. These peptides are antifibrotic, antihypertrophic, and they promote vasodilation and diuresis, thus counteracting the adverse effects of neurohormonal activation. But in HFrEF, these vasoactive peptides are less active and patients are less sensitive to them.
Ivabradine
This selective sinus node inhibitor decreases heart rate and has essentially no other effects. The drug has been available for years in Europe, and the European Society of Cardiology (ESC) has had sufficient time to integrate ivabradine into its guidelines for pharmacotherapy in HFrEF.
The ESC treatment algorithm for HFrEF (Eur Heart J. 2012 Jul;33[14]:1787-847) is built upon a foundation of thiazide diuretics to relieve signs and symptoms of congestion along with a beta-blocker and an ACE inhibitor or angiotensin receptor blocker (ARB). In a patient who still has New York Heart Association class II-IV symptoms after those drugs are titrated to guideline-recommended target levels or maximally tolerated doses, a mineralocorticoid receptor antagonist – either spironolactone or eplerenone – is added. And, in a patient who still remains symptomatic, has a left ventricular ejection fraction of 35% or less, is in sinus rhythm, and has a heart rate of 70 beats per minute or more, it’s time to consider adding ivabradine.
“This is how our own guidelines may elect to incorporate ivabradine, but of course, we don’t know yet,” Dr. Desai observed.
In the randomized, double-blind SHIFT trial involving 6,558 HFrEF patients who fit the description of ivabradine candidates described in the ESC guidelines, those who received ivabradine titrated to a maximum of 7.5 mg twice daily experienced a 26% reduction in hospital admissions for worsening heart failure, compared with placebo, a 26% reduction in deaths from heart failure, and fewer adverse events than the control group (Lancet. 2010 Sep 11;376[9744]:875-85).
The important question is who should get ivabradine and who should just get a little more beta-blocker in order to slow the heart rate. The fact is, many heart failure patients simply can’t tolerate the guideline-recommended target dose of beta-blocker therapy, which is 12.5 mg twice daily of carvedilol or its equivalent. Indeed, only 26% of SHIFT participants were able to do so.
“My interpretation of the SHIFT trial is that the goal is to reduce heart rate by any means necessary; preferentially, with a beta-blocker, and with ivabradine as an adjunct in patients who can’t get to target doses,” the cardiologist said.
Sacubitril/valsartan
In the landmark double-blind, 8,442-patient PARADIGM-HF trial, the group randomized to sacubitril/valsartan had a 20% reduction in the primary endpoint of cardiovascular death or heart failure hospitalization over 27 months of follow-up, compared with controls on enalapril at the guideline-recommended dose of 10 mg twice a day. The number needed to treat (NNT) was 21. Moreover, all-cause mortality was reduced by 16% (N Engl J Med. 2014 Sep 11;37[11]:993-1004).
In a recent follow-up cause of death analysis, Dr. Desai and his coinvestigators reported that 81% of all deaths in PARADIGM-HF were cardiovascular in nature. The NNT for sacubitril/valsartan in order to prevent one cardiovascular death was 32. The risk of sudden cardiac death was reduced by 80%, while the risk of death due to worsening heart failure was decreased by 21% (Eur Heart J 2015 Aug 7;36[30]:1990-7).
In another secondary analysis from the PARADIGM-HF investigators, the use of the angiotensin receptor/neprilysin inhibitor was shown to prevent clinical progression of surviving patients with heart failure much more effectively than enalapril. The sacubitril/valsartan group was 34% less likely to have an emergency department visit for worsening heart failure, 18% less likely to require intensive care, and 22% less likely to receive an implantable heart failure device or undergo cardiac transplantation. The reduction in the rate of heart failure hospitalization became significant within the first 30 days (Circulation. 2015 Jan 6;131[1]:54-61).
Moreover, the absolute benefit of sacubitril/valsartan in PARADIGM-HF was consistent across the full spectrum of patient risk (J Am Coll Cardiol. 2015 Nov 10;66[19]:2059-71).
To put this into perspective, Dr. Desai continued, for every 1,000 HFrEF patients switched from an ACE inhibitor or ARB to sacubitril/valsartan, the absolute benefit over the course of 27 months includes 31 fewer cardiovascular deaths, 28 fewer hospitalizations for heart failure, and 37 fewer hospitalizations for any reason.
“This is potent therapy for patients with HFrEF who have the right phenotype,” he observed.
While substitution of sacubitril/valsartan for an ACE inhibitor or ARB may be appropriate in many patients with chronic HFrEF who continue to have NYHA Class II-IV symptoms on guideline-directed medical therapy, several caveats apply, according to Dr. Desai.
It’s important to be aware of the PARADIGM-HF eligibility criteria, because it’s only in patients who fit that profile that sacubitril/valsartan provides evidence-based therapy. There are as yet no data to support the drug’s use in patients with new-onset HFrEF, acute decompensated HFrEF, in patients who are immediately post-MI, or in those with advanced chronic kidney disease, he emphasized.
“I think you have to be mindful of eligibility because the label that’s applied to this drug is basically ‘patients with HFrEF who are treated with guideline-directed medical therapy.’ There’s no specific requirement that you follow the detailed eligibility criteria of the PARADIGM-HF trial, but you should realize that the drug is known to be effective only in patients who fit the PARADIGM-HF eligibility profile,” he said.
Dr. Desai gave a few clinical pearls for prescribing sacubitril/valsartan. For most patients, the initial recommended dose is 49/51 mg twice daily. In those with low baseline blood pressure and tenuous hemodynamics, it’s appropriate to initiate therapy at 24/26 mg BID. It’s important to halt ACE inhibitor therapy 36 hours prior to starting sacubitril/valsartan so as to avoid overlap and consequent increased risk of angioedema. And while serum n-terminal prohormone brain natriuretic peptide (NT-proBNP) remains a useful biomarker to monitor heart rate severity and response to treatment while a patient is on sacubitril/valsartan, BNP is not because serum levels of that biomarker rise with neprilysin inhibition.
Dr. Desai reported receiving research support from Novartis and St. Jude Medical and serving as a consultant to those companies as well as Merck and Relypsa.
SNOWMASS, COLO. – Ivabradine and sacubitril/valsartan are paradigm-changing drugs approved last year for the treatment of heart failure with reduced ejection fraction – and it’s entirely reasonable to begin using them now in the appropriate patients, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
The impressive positive results seen in the pivotal trials for these novel agents – the SHIFT trial for ivabradine (Corlanor) and PARADIGM-HF for sacubitril/valsartan (Entresto) – have rocked the heart failure world.
The studies showed that, in the right patients, these two medications improve heart failure morbidity and mortality significantly beyond what’s achievable with the current gold standard, guideline-directed medical therapy. That’s exciting because even though great therapeutic strides have been made during the past 15 years, symptomatic patients with heart failure with reduced ejection fraction (HFrEF) treated with optimal guideline-directed pharmacotherapy still have substantial residual risk for heart failure hospitalization and death, noted Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
The U.S. heart failure guidelines panel hasn’t yet addressed the use of either of these recently approved drugs, but Dr. Desai provided his best sense of the data and how he thinks physicians might start using them now.
Ivabradine and sacubitril/valsartan are first-in-class agents with novel mechanisms of action. Ivabradine’s demonstrated safety and efficacy in the SHIFT trial confirmed the hypothesis that elevated heart rate is a legitimate therapeutic target in HFrEF.
Sacubitril/valsartan, an angiotensin II receptor/neprilysin inhibitor formerly known as LCZ696, provides what is to date a unique ability to enhance the activity of endogenous vasoactive peptides, including natriuretic peptides, bradykinin, substance P, adrenomedullin, and calcitonin gene–related peptide. These peptides are antifibrotic, antihypertrophic, and they promote vasodilation and diuresis, thus counteracting the adverse effects of neurohormonal activation. But in HFrEF, these vasoactive peptides are less active and patients are less sensitive to them.
Ivabradine
This selective sinus node inhibitor decreases heart rate and has essentially no other effects. The drug has been available for years in Europe, and the European Society of Cardiology (ESC) has had sufficient time to integrate ivabradine into its guidelines for pharmacotherapy in HFrEF.
The ESC treatment algorithm for HFrEF (Eur Heart J. 2012 Jul;33[14]:1787-847) is built upon a foundation of thiazide diuretics to relieve signs and symptoms of congestion along with a beta-blocker and an ACE inhibitor or angiotensin receptor blocker (ARB). In a patient who still has New York Heart Association class II-IV symptoms after those drugs are titrated to guideline-recommended target levels or maximally tolerated doses, a mineralocorticoid receptor antagonist – either spironolactone or eplerenone – is added. And, in a patient who still remains symptomatic, has a left ventricular ejection fraction of 35% or less, is in sinus rhythm, and has a heart rate of 70 beats per minute or more, it’s time to consider adding ivabradine.
“This is how our own guidelines may elect to incorporate ivabradine, but of course, we don’t know yet,” Dr. Desai observed.
In the randomized, double-blind SHIFT trial involving 6,558 HFrEF patients who fit the description of ivabradine candidates described in the ESC guidelines, those who received ivabradine titrated to a maximum of 7.5 mg twice daily experienced a 26% reduction in hospital admissions for worsening heart failure, compared with placebo, a 26% reduction in deaths from heart failure, and fewer adverse events than the control group (Lancet. 2010 Sep 11;376[9744]:875-85).
The important question is who should get ivabradine and who should just get a little more beta-blocker in order to slow the heart rate. The fact is, many heart failure patients simply can’t tolerate the guideline-recommended target dose of beta-blocker therapy, which is 12.5 mg twice daily of carvedilol or its equivalent. Indeed, only 26% of SHIFT participants were able to do so.
“My interpretation of the SHIFT trial is that the goal is to reduce heart rate by any means necessary; preferentially, with a beta-blocker, and with ivabradine as an adjunct in patients who can’t get to target doses,” the cardiologist said.
Sacubitril/valsartan
In the landmark double-blind, 8,442-patient PARADIGM-HF trial, the group randomized to sacubitril/valsartan had a 20% reduction in the primary endpoint of cardiovascular death or heart failure hospitalization over 27 months of follow-up, compared with controls on enalapril at the guideline-recommended dose of 10 mg twice a day. The number needed to treat (NNT) was 21. Moreover, all-cause mortality was reduced by 16% (N Engl J Med. 2014 Sep 11;37[11]:993-1004).
In a recent follow-up cause of death analysis, Dr. Desai and his coinvestigators reported that 81% of all deaths in PARADIGM-HF were cardiovascular in nature. The NNT for sacubitril/valsartan in order to prevent one cardiovascular death was 32. The risk of sudden cardiac death was reduced by 80%, while the risk of death due to worsening heart failure was decreased by 21% (Eur Heart J 2015 Aug 7;36[30]:1990-7).
In another secondary analysis from the PARADIGM-HF investigators, the use of the angiotensin receptor/neprilysin inhibitor was shown to prevent clinical progression of surviving patients with heart failure much more effectively than enalapril. The sacubitril/valsartan group was 34% less likely to have an emergency department visit for worsening heart failure, 18% less likely to require intensive care, and 22% less likely to receive an implantable heart failure device or undergo cardiac transplantation. The reduction in the rate of heart failure hospitalization became significant within the first 30 days (Circulation. 2015 Jan 6;131[1]:54-61).
Moreover, the absolute benefit of sacubitril/valsartan in PARADIGM-HF was consistent across the full spectrum of patient risk (J Am Coll Cardiol. 2015 Nov 10;66[19]:2059-71).
To put this into perspective, Dr. Desai continued, for every 1,000 HFrEF patients switched from an ACE inhibitor or ARB to sacubitril/valsartan, the absolute benefit over the course of 27 months includes 31 fewer cardiovascular deaths, 28 fewer hospitalizations for heart failure, and 37 fewer hospitalizations for any reason.
“This is potent therapy for patients with HFrEF who have the right phenotype,” he observed.
While substitution of sacubitril/valsartan for an ACE inhibitor or ARB may be appropriate in many patients with chronic HFrEF who continue to have NYHA Class II-IV symptoms on guideline-directed medical therapy, several caveats apply, according to Dr. Desai.
It’s important to be aware of the PARADIGM-HF eligibility criteria, because it’s only in patients who fit that profile that sacubitril/valsartan provides evidence-based therapy. There are as yet no data to support the drug’s use in patients with new-onset HFrEF, acute decompensated HFrEF, in patients who are immediately post-MI, or in those with advanced chronic kidney disease, he emphasized.
“I think you have to be mindful of eligibility because the label that’s applied to this drug is basically ‘patients with HFrEF who are treated with guideline-directed medical therapy.’ There’s no specific requirement that you follow the detailed eligibility criteria of the PARADIGM-HF trial, but you should realize that the drug is known to be effective only in patients who fit the PARADIGM-HF eligibility profile,” he said.
Dr. Desai gave a few clinical pearls for prescribing sacubitril/valsartan. For most patients, the initial recommended dose is 49/51 mg twice daily. In those with low baseline blood pressure and tenuous hemodynamics, it’s appropriate to initiate therapy at 24/26 mg BID. It’s important to halt ACE inhibitor therapy 36 hours prior to starting sacubitril/valsartan so as to avoid overlap and consequent increased risk of angioedema. And while serum n-terminal prohormone brain natriuretic peptide (NT-proBNP) remains a useful biomarker to monitor heart rate severity and response to treatment while a patient is on sacubitril/valsartan, BNP is not because serum levels of that biomarker rise with neprilysin inhibition.
Dr. Desai reported receiving research support from Novartis and St. Jude Medical and serving as a consultant to those companies as well as Merck and Relypsa.
SNOWMASS, COLO. – Ivabradine and sacubitril/valsartan are paradigm-changing drugs approved last year for the treatment of heart failure with reduced ejection fraction – and it’s entirely reasonable to begin using them now in the appropriate patients, Dr. Akshay S. Desai said at the Annual Cardiovascular Conference at Snowmass.
The impressive positive results seen in the pivotal trials for these novel agents – the SHIFT trial for ivabradine (Corlanor) and PARADIGM-HF for sacubitril/valsartan (Entresto) – have rocked the heart failure world.
The studies showed that, in the right patients, these two medications improve heart failure morbidity and mortality significantly beyond what’s achievable with the current gold standard, guideline-directed medical therapy. That’s exciting because even though great therapeutic strides have been made during the past 15 years, symptomatic patients with heart failure with reduced ejection fraction (HFrEF) treated with optimal guideline-directed pharmacotherapy still have substantial residual risk for heart failure hospitalization and death, noted Dr. Desai, director of heart failure disease management at Brigham and Women’s Hospital in Boston.
The U.S. heart failure guidelines panel hasn’t yet addressed the use of either of these recently approved drugs, but Dr. Desai provided his best sense of the data and how he thinks physicians might start using them now.
Ivabradine and sacubitril/valsartan are first-in-class agents with novel mechanisms of action. Ivabradine’s demonstrated safety and efficacy in the SHIFT trial confirmed the hypothesis that elevated heart rate is a legitimate therapeutic target in HFrEF.
Sacubitril/valsartan, an angiotensin II receptor/neprilysin inhibitor formerly known as LCZ696, provides what is to date a unique ability to enhance the activity of endogenous vasoactive peptides, including natriuretic peptides, bradykinin, substance P, adrenomedullin, and calcitonin gene–related peptide. These peptides are antifibrotic, antihypertrophic, and they promote vasodilation and diuresis, thus counteracting the adverse effects of neurohormonal activation. But in HFrEF, these vasoactive peptides are less active and patients are less sensitive to them.
Ivabradine
This selective sinus node inhibitor decreases heart rate and has essentially no other effects. The drug has been available for years in Europe, and the European Society of Cardiology (ESC) has had sufficient time to integrate ivabradine into its guidelines for pharmacotherapy in HFrEF.
The ESC treatment algorithm for HFrEF (Eur Heart J. 2012 Jul;33[14]:1787-847) is built upon a foundation of thiazide diuretics to relieve signs and symptoms of congestion along with a beta-blocker and an ACE inhibitor or angiotensin receptor blocker (ARB). In a patient who still has New York Heart Association class II-IV symptoms after those drugs are titrated to guideline-recommended target levels or maximally tolerated doses, a mineralocorticoid receptor antagonist – either spironolactone or eplerenone – is added. And, in a patient who still remains symptomatic, has a left ventricular ejection fraction of 35% or less, is in sinus rhythm, and has a heart rate of 70 beats per minute or more, it’s time to consider adding ivabradine.
“This is how our own guidelines may elect to incorporate ivabradine, but of course, we don’t know yet,” Dr. Desai observed.
In the randomized, double-blind SHIFT trial involving 6,558 HFrEF patients who fit the description of ivabradine candidates described in the ESC guidelines, those who received ivabradine titrated to a maximum of 7.5 mg twice daily experienced a 26% reduction in hospital admissions for worsening heart failure, compared with placebo, a 26% reduction in deaths from heart failure, and fewer adverse events than the control group (Lancet. 2010 Sep 11;376[9744]:875-85).
The important question is who should get ivabradine and who should just get a little more beta-blocker in order to slow the heart rate. The fact is, many heart failure patients simply can’t tolerate the guideline-recommended target dose of beta-blocker therapy, which is 12.5 mg twice daily of carvedilol or its equivalent. Indeed, only 26% of SHIFT participants were able to do so.
“My interpretation of the SHIFT trial is that the goal is to reduce heart rate by any means necessary; preferentially, with a beta-blocker, and with ivabradine as an adjunct in patients who can’t get to target doses,” the cardiologist said.
Sacubitril/valsartan
In the landmark double-blind, 8,442-patient PARADIGM-HF trial, the group randomized to sacubitril/valsartan had a 20% reduction in the primary endpoint of cardiovascular death or heart failure hospitalization over 27 months of follow-up, compared with controls on enalapril at the guideline-recommended dose of 10 mg twice a day. The number needed to treat (NNT) was 21. Moreover, all-cause mortality was reduced by 16% (N Engl J Med. 2014 Sep 11;37[11]:993-1004).
In a recent follow-up cause of death analysis, Dr. Desai and his coinvestigators reported that 81% of all deaths in PARADIGM-HF were cardiovascular in nature. The NNT for sacubitril/valsartan in order to prevent one cardiovascular death was 32. The risk of sudden cardiac death was reduced by 80%, while the risk of death due to worsening heart failure was decreased by 21% (Eur Heart J 2015 Aug 7;36[30]:1990-7).
In another secondary analysis from the PARADIGM-HF investigators, the use of the angiotensin receptor/neprilysin inhibitor was shown to prevent clinical progression of surviving patients with heart failure much more effectively than enalapril. The sacubitril/valsartan group was 34% less likely to have an emergency department visit for worsening heart failure, 18% less likely to require intensive care, and 22% less likely to receive an implantable heart failure device or undergo cardiac transplantation. The reduction in the rate of heart failure hospitalization became significant within the first 30 days (Circulation. 2015 Jan 6;131[1]:54-61).
Moreover, the absolute benefit of sacubitril/valsartan in PARADIGM-HF was consistent across the full spectrum of patient risk (J Am Coll Cardiol. 2015 Nov 10;66[19]:2059-71).
To put this into perspective, Dr. Desai continued, for every 1,000 HFrEF patients switched from an ACE inhibitor or ARB to sacubitril/valsartan, the absolute benefit over the course of 27 months includes 31 fewer cardiovascular deaths, 28 fewer hospitalizations for heart failure, and 37 fewer hospitalizations for any reason.
“This is potent therapy for patients with HFrEF who have the right phenotype,” he observed.
While substitution of sacubitril/valsartan for an ACE inhibitor or ARB may be appropriate in many patients with chronic HFrEF who continue to have NYHA Class II-IV symptoms on guideline-directed medical therapy, several caveats apply, according to Dr. Desai.
It’s important to be aware of the PARADIGM-HF eligibility criteria, because it’s only in patients who fit that profile that sacubitril/valsartan provides evidence-based therapy. There are as yet no data to support the drug’s use in patients with new-onset HFrEF, acute decompensated HFrEF, in patients who are immediately post-MI, or in those with advanced chronic kidney disease, he emphasized.
“I think you have to be mindful of eligibility because the label that’s applied to this drug is basically ‘patients with HFrEF who are treated with guideline-directed medical therapy.’ There’s no specific requirement that you follow the detailed eligibility criteria of the PARADIGM-HF trial, but you should realize that the drug is known to be effective only in patients who fit the PARADIGM-HF eligibility profile,” he said.
Dr. Desai gave a few clinical pearls for prescribing sacubitril/valsartan. For most patients, the initial recommended dose is 49/51 mg twice daily. In those with low baseline blood pressure and tenuous hemodynamics, it’s appropriate to initiate therapy at 24/26 mg BID. It’s important to halt ACE inhibitor therapy 36 hours prior to starting sacubitril/valsartan so as to avoid overlap and consequent increased risk of angioedema. And while serum n-terminal prohormone brain natriuretic peptide (NT-proBNP) remains a useful biomarker to monitor heart rate severity and response to treatment while a patient is on sacubitril/valsartan, BNP is not because serum levels of that biomarker rise with neprilysin inhibition.
Dr. Desai reported receiving research support from Novartis and St. Jude Medical and serving as a consultant to those companies as well as Merck and Relypsa.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS

Poor adherence to quality indicators found for NSCLC surgery
PHOENIX – National adherence to quality indicators for surgery in stage I non–small cell lung cancer is suboptimal, results from a large analysis of national data suggest.
“Compliance with such guidelines is a strong predictor of long-term survival, and vigorous efforts should be instituted at the level of national societies to improve such adherence,” researchers led by Dr. Pamela P. Samson wrote in an abstract presented at the annual meeting of the Society of Thoracic Surgeons. “National organizations, including American College of Chest Physicians, the National Comprehensive Cancer Network, and the American College of Surgeons Commission on Cancer, have recommended quality standards for surgery in early-stage non–small cell lung cancer (NSCLC). The determinants and outcomes of adherence to these guidelines for early-stage lung cancer patients are largely unknown.”
Dr. Samson, a general surgery resident at Washington University in St. Louis, and her associates used the National Cancer Data Base to evaluate data from 146,908 patients undergoing surgery for clinical stage I NSCLC between 2004 and 2013. They selected the following four quality measures for evaluation: performing an anatomical pulmonary resection, surgery within 8 weeks of diagnosis, R0 resection, and evaluation of 10 or more lymph nodes. Next, the researchers fitted multivariate models to identify variables independently associated with adherence to quality measures, and created a Cox multivariate model to evaluate long-term overall survival.
Dr. Varun Puri, senior author of the study, presented the findings at the STS meeting on behalf of Dr. Samson, and discussed the findings in a video interview. The researchers found that between 2004 and 2013, nearly 100% of patients met at least one of the four recommended criteria, 95% met two, 69% met three, and 22% met all four. Sampling of 10 or more lymph nodes was the least frequently met measure, occurring in only 31% of surgical patients. Patient factors associated with a greater likelihood of receiving all four quality measures included average income in ZIP code of at least $38,000 (odds ratio, 1.20), private insurance (OR, 1.22), or having Medicare (OR, 1.16). Institutional factors associated with a greater likelihood of meeting all four quality measures included higher-volume centers, defined as treating at least 38 cases per year (OR, 1.18), or being an academic institution (OR, 1.31).
At the same time, factors associated with a lower likelihood of recommended surgical care included increasing age (per year increase, OR, 0.99) and a higher Charlson/Deyo comorbidity score (OR, 0.90 for a score of 1 and OR, 0.82 for a score of 2 or more). The strongest determinant of long-term overall survival included pathologic upstaging (HR 1.84) and meeting all four quality indicators (HR 0.39). Every additional quality met was associated with a significant reduction in overall mortality.
“We believe this study can be a starting point to draw attention to institution- and surgeon-specific practice patterns that may vary widely,” Dr. Samson said in an interview prior to the meeting. “At our own institution, we are working to decrease time to surgery, as well as implementing quality improvement measures to increase nodal sampling rates. Improving these trends nationally must start at the local level, with a tailored approach.”
Dr. Samson is currently supported by a T32 NIH training grant for research fellows in cardiothoracic surgery. Study coauthor Dr. Bryan Meyers, has received honoraria from Varian Medical Systems and is a consultant/advisory board member of Ethicon. Senior author Dr. Varun Puri is supported by NIH career awards.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – National adherence to quality indicators for surgery in stage I non–small cell lung cancer is suboptimal, results from a large analysis of national data suggest.
“Compliance with such guidelines is a strong predictor of long-term survival, and vigorous efforts should be instituted at the level of national societies to improve such adherence,” researchers led by Dr. Pamela P. Samson wrote in an abstract presented at the annual meeting of the Society of Thoracic Surgeons. “National organizations, including American College of Chest Physicians, the National Comprehensive Cancer Network, and the American College of Surgeons Commission on Cancer, have recommended quality standards for surgery in early-stage non–small cell lung cancer (NSCLC). The determinants and outcomes of adherence to these guidelines for early-stage lung cancer patients are largely unknown.”
Dr. Samson, a general surgery resident at Washington University in St. Louis, and her associates used the National Cancer Data Base to evaluate data from 146,908 patients undergoing surgery for clinical stage I NSCLC between 2004 and 2013. They selected the following four quality measures for evaluation: performing an anatomical pulmonary resection, surgery within 8 weeks of diagnosis, R0 resection, and evaluation of 10 or more lymph nodes. Next, the researchers fitted multivariate models to identify variables independently associated with adherence to quality measures, and created a Cox multivariate model to evaluate long-term overall survival.
Dr. Varun Puri, senior author of the study, presented the findings at the STS meeting on behalf of Dr. Samson, and discussed the findings in a video interview. The researchers found that between 2004 and 2013, nearly 100% of patients met at least one of the four recommended criteria, 95% met two, 69% met three, and 22% met all four. Sampling of 10 or more lymph nodes was the least frequently met measure, occurring in only 31% of surgical patients. Patient factors associated with a greater likelihood of receiving all four quality measures included average income in ZIP code of at least $38,000 (odds ratio, 1.20), private insurance (OR, 1.22), or having Medicare (OR, 1.16). Institutional factors associated with a greater likelihood of meeting all four quality measures included higher-volume centers, defined as treating at least 38 cases per year (OR, 1.18), or being an academic institution (OR, 1.31).
At the same time, factors associated with a lower likelihood of recommended surgical care included increasing age (per year increase, OR, 0.99) and a higher Charlson/Deyo comorbidity score (OR, 0.90 for a score of 1 and OR, 0.82 for a score of 2 or more). The strongest determinant of long-term overall survival included pathologic upstaging (HR 1.84) and meeting all four quality indicators (HR 0.39). Every additional quality met was associated with a significant reduction in overall mortality.
“We believe this study can be a starting point to draw attention to institution- and surgeon-specific practice patterns that may vary widely,” Dr. Samson said in an interview prior to the meeting. “At our own institution, we are working to decrease time to surgery, as well as implementing quality improvement measures to increase nodal sampling rates. Improving these trends nationally must start at the local level, with a tailored approach.”
Dr. Samson is currently supported by a T32 NIH training grant for research fellows in cardiothoracic surgery. Study coauthor Dr. Bryan Meyers, has received honoraria from Varian Medical Systems and is a consultant/advisory board member of Ethicon. Senior author Dr. Varun Puri is supported by NIH career awards.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
PHOENIX – National adherence to quality indicators for surgery in stage I non–small cell lung cancer is suboptimal, results from a large analysis of national data suggest.
“Compliance with such guidelines is a strong predictor of long-term survival, and vigorous efforts should be instituted at the level of national societies to improve such adherence,” researchers led by Dr. Pamela P. Samson wrote in an abstract presented at the annual meeting of the Society of Thoracic Surgeons. “National organizations, including American College of Chest Physicians, the National Comprehensive Cancer Network, and the American College of Surgeons Commission on Cancer, have recommended quality standards for surgery in early-stage non–small cell lung cancer (NSCLC). The determinants and outcomes of adherence to these guidelines for early-stage lung cancer patients are largely unknown.”
Dr. Samson, a general surgery resident at Washington University in St. Louis, and her associates used the National Cancer Data Base to evaluate data from 146,908 patients undergoing surgery for clinical stage I NSCLC between 2004 and 2013. They selected the following four quality measures for evaluation: performing an anatomical pulmonary resection, surgery within 8 weeks of diagnosis, R0 resection, and evaluation of 10 or more lymph nodes. Next, the researchers fitted multivariate models to identify variables independently associated with adherence to quality measures, and created a Cox multivariate model to evaluate long-term overall survival.
Dr. Varun Puri, senior author of the study, presented the findings at the STS meeting on behalf of Dr. Samson, and discussed the findings in a video interview. The researchers found that between 2004 and 2013, nearly 100% of patients met at least one of the four recommended criteria, 95% met two, 69% met three, and 22% met all four. Sampling of 10 or more lymph nodes was the least frequently met measure, occurring in only 31% of surgical patients. Patient factors associated with a greater likelihood of receiving all four quality measures included average income in ZIP code of at least $38,000 (odds ratio, 1.20), private insurance (OR, 1.22), or having Medicare (OR, 1.16). Institutional factors associated with a greater likelihood of meeting all four quality measures included higher-volume centers, defined as treating at least 38 cases per year (OR, 1.18), or being an academic institution (OR, 1.31).
At the same time, factors associated with a lower likelihood of recommended surgical care included increasing age (per year increase, OR, 0.99) and a higher Charlson/Deyo comorbidity score (OR, 0.90 for a score of 1 and OR, 0.82 for a score of 2 or more). The strongest determinant of long-term overall survival included pathologic upstaging (HR 1.84) and meeting all four quality indicators (HR 0.39). Every additional quality met was associated with a significant reduction in overall mortality.
“We believe this study can be a starting point to draw attention to institution- and surgeon-specific practice patterns that may vary widely,” Dr. Samson said in an interview prior to the meeting. “At our own institution, we are working to decrease time to surgery, as well as implementing quality improvement measures to increase nodal sampling rates. Improving these trends nationally must start at the local level, with a tailored approach.”
Dr. Samson is currently supported by a T32 NIH training grant for research fellows in cardiothoracic surgery. Study coauthor Dr. Bryan Meyers, has received honoraria from Varian Medical Systems and is a consultant/advisory board member of Ethicon. Senior author Dr. Varun Puri is supported by NIH career awards.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT THE STS ANNUAL MEETING
Key clinical point: At the national level, compliance with core indicators for surgery in stage I NSCLC is poor.
Major finding: Between 2004 and 2013, nearly 100% of patients met at least one of four recommended criteria for evaluation of stage I NSCLC, 95% met two, 69% met three, and 22% met all four.
Data source: An analysis of 146,908 patients undergoing surgery for clinical stage I NSCLC between 2004 and 2013.
Disclosures: Dr. Samson is currently supported by a T32 NIH training grant for research fellows in cardiothoracic surgery. Study coauthor Dr. Bryan Meyers, has received honoraria from Varian Medical Systems and is a consultant/advisory board member of Ethicon. Senior author Dr. Varun Puri is supported by NIH career awards.
