User login
The Official Newspaper of the American Association for Thoracic Surgery
“Honoring Our Mentors” Fellowship Open for Submission
The AATS Graham Foundation is calling for submission for its Denton A. Cooley “Honoring Our Mentors” fellowship.
Denton A. Cooley Fellowship
New! Provides a deserving CT surgeon resident or young postgraduate surgeon the opportunity to enrich his/her education during four weeks of study at the Texas Heart Institute and Baylor St. Luke’s Medical Center.
Deadline: December 30, 2016
Share:
The AATS Graham Foundation is calling for submission for its Denton A. Cooley “Honoring Our Mentors” fellowship.
Denton A. Cooley Fellowship
New! Provides a deserving CT surgeon resident or young postgraduate surgeon the opportunity to enrich his/her education during four weeks of study at the Texas Heart Institute and Baylor St. Luke’s Medical Center.
Deadline: December 30, 2016
Share:
The AATS Graham Foundation is calling for submission for its Denton A. Cooley “Honoring Our Mentors” fellowship.
Denton A. Cooley Fellowship
New! Provides a deserving CT surgeon resident or young postgraduate surgeon the opportunity to enrich his/her education during four weeks of study at the Texas Heart Institute and Baylor St. Luke’s Medical Center.
Deadline: December 30, 2016
Share:
AATS Mitral Conclave Call for Abstracts & Videos
AATS invites you to submit your abstracts and videos to the 2017 Mitral Conclave.
AATS Mitral Conclave
April 27-28, 2017
New York, NY
Submission Deadline:
Sunday, January 8, 2017 @ 11.59 pm EST
Share:
AATS invites you to submit your abstracts and videos to the 2017 Mitral Conclave.
AATS Mitral Conclave
April 27-28, 2017
New York, NY
Submission Deadline:
Sunday, January 8, 2017 @ 11.59 pm EST
Share:
AATS invites you to submit your abstracts and videos to the 2017 Mitral Conclave.
AATS Mitral Conclave
April 27-28, 2017
New York, NY
Submission Deadline:
Sunday, January 8, 2017 @ 11.59 pm EST
Share:
TAVR concerns hinder use in younger, lower-risk patients
NEW ORLEANS – Despite increasing use of transcatheter aortic valve replacement for patients with severe aortic stenosis at intermediate risk for surgery, the procedure is meeting selected resistance because of ongoing concerns about the procedure’s limitations.
As more data emerge from randomized trials and registries, cardiologists and cardiothoracic surgeons see the choice between transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) for patients at intermediate surgical risk as something to individualize based on factors that include age, the type of TAVR access possible (transfemoral or an alternative route), and of course, patient preference. An added variable is the constant stream of new data that keeps TAVR in flux, with improved and smaller valves and delivery systems coming onto the market that eclipse the experience and lessons learned from older TAVR systems.
In intermediate-risk patients, usually defined as those with a Society of Thoracic Surgeons (STS) mortality risk score of 4%-8%, “I think you can go either way,” said Frank W. Sellke, MD, at the American Heart Association scientific sessions.
“If a patient is 90 years old and can’t expect to live more than a couple of years, you use TAVR; but if the patient is 55 years old and can expect to live 30 years, I would recommend SAVR,” said Dr. Sellke, professor and chief of cardiothoracic surgery at Brown University in Providence, R.I.
He rattled off four things about TAVR that keep it from being for everyone: periprocedural vascular complications, higher rates of paravalvular leak than with surgery, leaflet thrombosis (a phenomenon with unclear clinical consequences), and undocumented long-term durability.
Dr. Sellke made these comments while discussing the report at the meeting on registry data collected from nearly 6,000 intermediate-risk patients who underwent TAVR or SAVR in Germany during January 2011 through December 2013 and assembled in the German Aortic Valve Registry. During that 3-year period, German TAVR patients could receive either the SAPIEN XT valve or the CoreValve, two TAVR systems that now have been superseded in both Europe and the United States by next-generation systems, SAPIEN 3 and Evolut R.
Limitations of a transthoracic approach
Another factor limiting TAVR is the endovascular approach. The best TAVR results by far have come from using a transfemoral approach for endovascular valve placement, but experts estimate that today at least 10% of patients considered for TAVR have a vascular anatomy that makes the transfemoral TAVR impossible. In the past, when such patients underwent TAVR, it was via either a transapical or transaortic approach (collectively called transthoracic), although additional endovascular entry sites are now being tested.
The limitations of transthoracic TAVR were underscored by results from a prespecified quality-of-life analysis done as part of the PARTNER 2 trial that compared the SAPIEN XT system with SAVR in intermediate-risk patients (N Engl J Med. 2016 April 27;374[17]:1609-20).

In contrast, the patients in the study who had their TAVR done by a transthoracic route had a statistically nonsignificant incremental gain in their KCCQ score, compared with randomized SAVR patients, after 1 month, and their incremental rise in KCCQ score was not clinically meaningful.
The investigators measured KCCQ scores at both 1 and 2 years after treatment, and they were similar regardless of whether patients had undergone TAVR or SAVR in both the transfemoral and transthoracic subgroups. All the quality-of-life benefit from TAVR compared with SAVR occurred only during the first month (and possibly for a few additional months beyond that) and only in TAVR patients treated by the transfemoral route. Dr. Cohen stressed that the SAVR patients in both the transfemoral and transthoracic subgroups had very similar outcomes, showing that patient differences could not explain why the transfemoral patients received a much greater incremental benefit, compared with the SAVR patients, at 1 month than did the transthoracic patients.
“A transthoracic TAVR approach may not be preferable to SAVR, at least in the short to intermediate term,” said Dr. Cohen. “There is no benefit from TAVR, compared with SAVR, if you can’t do it transfemorally, although emerging evidence has suggested that other nontransfemoral approaches that stay out of the chest may provide benefit similar to transfemoral TAVR. The message is, stay out of the chest,” he concluded.

Concerns about durability
The durability of TAVR valves is another concern that has recently been influencing patients as they decide between TAVR and SAVR, said Dr. Smith. “A lot of patients don’t want TAVR because of their concerns about its durability.” These patients usually cite evidence reported in May 2016 at the annual congress of the European Association of Percutaneous Cardiovascular Interventions in Paris by Danny Dvir, MD, on longer-term follow-up of 378 patients who underwent TAVR at either of two pioneering centers. A retrospective review suggested a valve degeneration rate of about 50% after 8 years, Dr. Dvir reported.
This report “has gotten a lot of penetration over the Internet, and a lot of patients don’t like the uncertainty” about TAVR durability that this report produced. “A lot of the time now, patients come in with a fixed idea of whether they want TAVR or SAVR,” Dr. Smith said.
Dr. Smith essentially agreed with Dr. Sellke on the current role for TAVR relative to SAVR in lower-risk patients.
“If the patient is clearly intermediate risk, with an STS mortality risk of more than 6% and is at least 80 years old, then they’ll have TAVR 99% of the time. But if it’s a 75 year old with an STS score of 3.2% and otherwise healthy, the best choice is not as clear.”
Another cardiothoracic surgeon with lots of TAVR experience, Michael J. Reardon, MD, has much more enthusiasm for TAVR. “In my practice, I use TAVR exclusively in patients at least 80 years old. I don‘t care how healthy they look,” said Dr. Reardon, professor of cardiovascular surgery at Houston Methodist. He acknowledged that broader use of TAVR for intermediate-risk patients is getting push back from other cardiothoracic surgeons.
Dr. Sellke is one such surgeon, and he called uncertain TAVR valve durability the deciding factor. “We need longer-term data on [TAVR] valve longevity before we routinely put them into intermediate- or low-risk patients,” he said during a panel discussion at the meeting.
Dr. Reardon highlighted that newer TAVR systems have been reducing problems such as paravalvular leaks and the need for pacemakers following placement of self-expanding TAVR valves. Despite these technical improvements, the final frontier for TAVR for lower-risk patients is valve durability, Dr. Reardon said in an interview.
“I’m convinced the durability is there, and that any 80-year-old patient who is anatomically suited for transfemoral TAVR should get it no matter now healthy they look. If their likely survival is 15 years or less, then they are reasonable candidates for TAVR.”
Dr. Sellke had no relevant disclosures. PARTNER 2 was funded by Edwards, the company that markets Sapient TAVR systems. Dr. Cohen had no relevant disclosures. Dr. Smith has been an investigator in the PARTNER studies. Dr. Reardon has been a consultant to Medtronic, the company that markets the CoreValve and Evolut R TAVR systems.
[email protected]
On Twitter @mitchelzoler
NEW ORLEANS – Despite increasing use of transcatheter aortic valve replacement for patients with severe aortic stenosis at intermediate risk for surgery, the procedure is meeting selected resistance because of ongoing concerns about the procedure’s limitations.
As more data emerge from randomized trials and registries, cardiologists and cardiothoracic surgeons see the choice between transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) for patients at intermediate surgical risk as something to individualize based on factors that include age, the type of TAVR access possible (transfemoral or an alternative route), and of course, patient preference. An added variable is the constant stream of new data that keeps TAVR in flux, with improved and smaller valves and delivery systems coming onto the market that eclipse the experience and lessons learned from older TAVR systems.
In intermediate-risk patients, usually defined as those with a Society of Thoracic Surgeons (STS) mortality risk score of 4%-8%, “I think you can go either way,” said Frank W. Sellke, MD, at the American Heart Association scientific sessions.
“If a patient is 90 years old and can’t expect to live more than a couple of years, you use TAVR; but if the patient is 55 years old and can expect to live 30 years, I would recommend SAVR,” said Dr. Sellke, professor and chief of cardiothoracic surgery at Brown University in Providence, R.I.
He rattled off four things about TAVR that keep it from being for everyone: periprocedural vascular complications, higher rates of paravalvular leak than with surgery, leaflet thrombosis (a phenomenon with unclear clinical consequences), and undocumented long-term durability.
Dr. Sellke made these comments while discussing the report at the meeting on registry data collected from nearly 6,000 intermediate-risk patients who underwent TAVR or SAVR in Germany during January 2011 through December 2013 and assembled in the German Aortic Valve Registry. During that 3-year period, German TAVR patients could receive either the SAPIEN XT valve or the CoreValve, two TAVR systems that now have been superseded in both Europe and the United States by next-generation systems, SAPIEN 3 and Evolut R.
Limitations of a transthoracic approach
Another factor limiting TAVR is the endovascular approach. The best TAVR results by far have come from using a transfemoral approach for endovascular valve placement, but experts estimate that today at least 10% of patients considered for TAVR have a vascular anatomy that makes the transfemoral TAVR impossible. In the past, when such patients underwent TAVR, it was via either a transapical or transaortic approach (collectively called transthoracic), although additional endovascular entry sites are now being tested.
The limitations of transthoracic TAVR were underscored by results from a prespecified quality-of-life analysis done as part of the PARTNER 2 trial that compared the SAPIEN XT system with SAVR in intermediate-risk patients (N Engl J Med. 2016 April 27;374[17]:1609-20).
In contrast, the patients in the study who had their TAVR done by a transthoracic route had a statistically nonsignificant incremental gain in their KCCQ score, compared with randomized SAVR patients, after 1 month, and their incremental rise in KCCQ score was not clinically meaningful.
The investigators measured KCCQ scores at both 1 and 2 years after treatment, and they were similar regardless of whether patients had undergone TAVR or SAVR in both the transfemoral and transthoracic subgroups. All the quality-of-life benefit from TAVR compared with SAVR occurred only during the first month (and possibly for a few additional months beyond that) and only in TAVR patients treated by the transfemoral route. Dr. Cohen stressed that the SAVR patients in both the transfemoral and transthoracic subgroups had very similar outcomes, showing that patient differences could not explain why the transfemoral patients received a much greater incremental benefit, compared with the SAVR patients, at 1 month than did the transthoracic patients.
“A transthoracic TAVR approach may not be preferable to SAVR, at least in the short to intermediate term,” said Dr. Cohen. “There is no benefit from TAVR, compared with SAVR, if you can’t do it transfemorally, although emerging evidence has suggested that other nontransfemoral approaches that stay out of the chest may provide benefit similar to transfemoral TAVR. The message is, stay out of the chest,” he concluded.
Concerns about durability
The durability of TAVR valves is another concern that has recently been influencing patients as they decide between TAVR and SAVR, said Dr. Smith. “A lot of patients don’t want TAVR because of their concerns about its durability.” These patients usually cite evidence reported in May 2016 at the annual congress of the European Association of Percutaneous Cardiovascular Interventions in Paris by Danny Dvir, MD, on longer-term follow-up of 378 patients who underwent TAVR at either of two pioneering centers. A retrospective review suggested a valve degeneration rate of about 50% after 8 years, Dr. Dvir reported.
This report “has gotten a lot of penetration over the Internet, and a lot of patients don’t like the uncertainty” about TAVR durability that this report produced. “A lot of the time now, patients come in with a fixed idea of whether they want TAVR or SAVR,” Dr. Smith said.
Dr. Smith essentially agreed with Dr. Sellke on the current role for TAVR relative to SAVR in lower-risk patients.
“If the patient is clearly intermediate risk, with an STS mortality risk of more than 6% and is at least 80 years old, then they’ll have TAVR 99% of the time. But if it’s a 75 year old with an STS score of 3.2% and otherwise healthy, the best choice is not as clear.”
Another cardiothoracic surgeon with lots of TAVR experience, Michael J. Reardon, MD, has much more enthusiasm for TAVR. “In my practice, I use TAVR exclusively in patients at least 80 years old. I don‘t care how healthy they look,” said Dr. Reardon, professor of cardiovascular surgery at Houston Methodist. He acknowledged that broader use of TAVR for intermediate-risk patients is getting push back from other cardiothoracic surgeons.
Dr. Sellke is one such surgeon, and he called uncertain TAVR valve durability the deciding factor. “We need longer-term data on [TAVR] valve longevity before we routinely put them into intermediate- or low-risk patients,” he said during a panel discussion at the meeting.
Dr. Reardon highlighted that newer TAVR systems have been reducing problems such as paravalvular leaks and the need for pacemakers following placement of self-expanding TAVR valves. Despite these technical improvements, the final frontier for TAVR for lower-risk patients is valve durability, Dr. Reardon said in an interview.
“I’m convinced the durability is there, and that any 80-year-old patient who is anatomically suited for transfemoral TAVR should get it no matter now healthy they look. If their likely survival is 15 years or less, then they are reasonable candidates for TAVR.”
Dr. Sellke had no relevant disclosures. PARTNER 2 was funded by Edwards, the company that markets Sapient TAVR systems. Dr. Cohen had no relevant disclosures. Dr. Smith has been an investigator in the PARTNER studies. Dr. Reardon has been a consultant to Medtronic, the company that markets the CoreValve and Evolut R TAVR systems.
[email protected]
On Twitter @mitchelzoler
NEW ORLEANS – Despite increasing use of transcatheter aortic valve replacement for patients with severe aortic stenosis at intermediate risk for surgery, the procedure is meeting selected resistance because of ongoing concerns about the procedure’s limitations.
As more data emerge from randomized trials and registries, cardiologists and cardiothoracic surgeons see the choice between transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) for patients at intermediate surgical risk as something to individualize based on factors that include age, the type of TAVR access possible (transfemoral or an alternative route), and of course, patient preference. An added variable is the constant stream of new data that keeps TAVR in flux, with improved and smaller valves and delivery systems coming onto the market that eclipse the experience and lessons learned from older TAVR systems.
In intermediate-risk patients, usually defined as those with a Society of Thoracic Surgeons (STS) mortality risk score of 4%-8%, “I think you can go either way,” said Frank W. Sellke, MD, at the American Heart Association scientific sessions.
“If a patient is 90 years old and can’t expect to live more than a couple of years, you use TAVR; but if the patient is 55 years old and can expect to live 30 years, I would recommend SAVR,” said Dr. Sellke, professor and chief of cardiothoracic surgery at Brown University in Providence, R.I.
He rattled off four things about TAVR that keep it from being for everyone: periprocedural vascular complications, higher rates of paravalvular leak than with surgery, leaflet thrombosis (a phenomenon with unclear clinical consequences), and undocumented long-term durability.
Dr. Sellke made these comments while discussing the report at the meeting on registry data collected from nearly 6,000 intermediate-risk patients who underwent TAVR or SAVR in Germany during January 2011 through December 2013 and assembled in the German Aortic Valve Registry. During that 3-year period, German TAVR patients could receive either the SAPIEN XT valve or the CoreValve, two TAVR systems that now have been superseded in both Europe and the United States by next-generation systems, SAPIEN 3 and Evolut R.
Limitations of a transthoracic approach
Another factor limiting TAVR is the endovascular approach. The best TAVR results by far have come from using a transfemoral approach for endovascular valve placement, but experts estimate that today at least 10% of patients considered for TAVR have a vascular anatomy that makes the transfemoral TAVR impossible. In the past, when such patients underwent TAVR, it was via either a transapical or transaortic approach (collectively called transthoracic), although additional endovascular entry sites are now being tested.
The limitations of transthoracic TAVR were underscored by results from a prespecified quality-of-life analysis done as part of the PARTNER 2 trial that compared the SAPIEN XT system with SAVR in intermediate-risk patients (N Engl J Med. 2016 April 27;374[17]:1609-20).
In contrast, the patients in the study who had their TAVR done by a transthoracic route had a statistically nonsignificant incremental gain in their KCCQ score, compared with randomized SAVR patients, after 1 month, and their incremental rise in KCCQ score was not clinically meaningful.
The investigators measured KCCQ scores at both 1 and 2 years after treatment, and they were similar regardless of whether patients had undergone TAVR or SAVR in both the transfemoral and transthoracic subgroups. All the quality-of-life benefit from TAVR compared with SAVR occurred only during the first month (and possibly for a few additional months beyond that) and only in TAVR patients treated by the transfemoral route. Dr. Cohen stressed that the SAVR patients in both the transfemoral and transthoracic subgroups had very similar outcomes, showing that patient differences could not explain why the transfemoral patients received a much greater incremental benefit, compared with the SAVR patients, at 1 month than did the transthoracic patients.
“A transthoracic TAVR approach may not be preferable to SAVR, at least in the short to intermediate term,” said Dr. Cohen. “There is no benefit from TAVR, compared with SAVR, if you can’t do it transfemorally, although emerging evidence has suggested that other nontransfemoral approaches that stay out of the chest may provide benefit similar to transfemoral TAVR. The message is, stay out of the chest,” he concluded.
Concerns about durability
The durability of TAVR valves is another concern that has recently been influencing patients as they decide between TAVR and SAVR, said Dr. Smith. “A lot of patients don’t want TAVR because of their concerns about its durability.” These patients usually cite evidence reported in May 2016 at the annual congress of the European Association of Percutaneous Cardiovascular Interventions in Paris by Danny Dvir, MD, on longer-term follow-up of 378 patients who underwent TAVR at either of two pioneering centers. A retrospective review suggested a valve degeneration rate of about 50% after 8 years, Dr. Dvir reported.
This report “has gotten a lot of penetration over the Internet, and a lot of patients don’t like the uncertainty” about TAVR durability that this report produced. “A lot of the time now, patients come in with a fixed idea of whether they want TAVR or SAVR,” Dr. Smith said.
Dr. Smith essentially agreed with Dr. Sellke on the current role for TAVR relative to SAVR in lower-risk patients.
“If the patient is clearly intermediate risk, with an STS mortality risk of more than 6% and is at least 80 years old, then they’ll have TAVR 99% of the time. But if it’s a 75 year old with an STS score of 3.2% and otherwise healthy, the best choice is not as clear.”
Another cardiothoracic surgeon with lots of TAVR experience, Michael J. Reardon, MD, has much more enthusiasm for TAVR. “In my practice, I use TAVR exclusively in patients at least 80 years old. I don‘t care how healthy they look,” said Dr. Reardon, professor of cardiovascular surgery at Houston Methodist. He acknowledged that broader use of TAVR for intermediate-risk patients is getting push back from other cardiothoracic surgeons.
Dr. Sellke is one such surgeon, and he called uncertain TAVR valve durability the deciding factor. “We need longer-term data on [TAVR] valve longevity before we routinely put them into intermediate- or low-risk patients,” he said during a panel discussion at the meeting.
Dr. Reardon highlighted that newer TAVR systems have been reducing problems such as paravalvular leaks and the need for pacemakers following placement of self-expanding TAVR valves. Despite these technical improvements, the final frontier for TAVR for lower-risk patients is valve durability, Dr. Reardon said in an interview.
“I’m convinced the durability is there, and that any 80-year-old patient who is anatomically suited for transfemoral TAVR should get it no matter now healthy they look. If their likely survival is 15 years or less, then they are reasonable candidates for TAVR.”
Dr. Sellke had no relevant disclosures. PARTNER 2 was funded by Edwards, the company that markets Sapient TAVR systems. Dr. Cohen had no relevant disclosures. Dr. Smith has been an investigator in the PARTNER studies. Dr. Reardon has been a consultant to Medtronic, the company that markets the CoreValve and Evolut R TAVR systems.
[email protected]
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE AHA SCIENTIFIC SESSIONS
Senate sends 21st Century Cures bill to president
With little debate and less dissent, the Senate passed the 21st Century Cures bill and sent it to President Obama for his promised signature.
The legislation passed the House by an overwhelming 392-26 vote on Nov. 30. Key provisions of the bill (H.R. 34) include:
• Food and Drug Administration reforms, including expedited review for certain medical devices, streamlined review for drug/device combinations, and increased patient involvement in the drug approval process, with $500 million to implement the reforms.
• $4.8 billion over 10 years for key biomedical research efforts including the BRAIN Initiative, the Cancer Moonshot, and the Precision Medicine Initiative.
• $1 billion in grants to states over a 2-year period to help supplement opioid abuse prevention and treatment activities.
• Provisions to improve the interoperability of EHRs.
• Provisions to improve treatment of serious mental illness.
“This bipartisan legislation – which [Senate] Majority Leader Mitch McConnell [R-Ky.] has called ‘the most important legislation Congress will pass this year’ – will help us take advantage of the breathtaking advances in biomedical research and bring those innovations to doctors’ offices and patients’ medicine cabinets around the county,” Sen. Lamar Alexander (R-Tenn.), chair of the Senate Health, Education, Labor, and Pensions Committee, said in a statement.
“The most important prescription drug-related crisis facing our country right now is the skyrocketing price of prescription drugs. This bill does not even deal with that issue,” Sen. Sanders said on the Senate floor. “How can we talk about a bill dealing with the pharmaceutical industry without addressing the elephant in the room, which is the fact that we pay the highest prices in the world for medicine?”
In his weekly address on Dec. 3, President Obama promised to “sign [the bill] as soon as it reaches my desk.”
Gregory Twachtman contributed to this report.
[email protected]
On Twitter @denisefulton
With little debate and less dissent, the Senate passed the 21st Century Cures bill and sent it to President Obama for his promised signature.
The legislation passed the House by an overwhelming 392-26 vote on Nov. 30. Key provisions of the bill (H.R. 34) include:
• Food and Drug Administration reforms, including expedited review for certain medical devices, streamlined review for drug/device combinations, and increased patient involvement in the drug approval process, with $500 million to implement the reforms.
• $4.8 billion over 10 years for key biomedical research efforts including the BRAIN Initiative, the Cancer Moonshot, and the Precision Medicine Initiative.
• $1 billion in grants to states over a 2-year period to help supplement opioid abuse prevention and treatment activities.
• Provisions to improve the interoperability of EHRs.
• Provisions to improve treatment of serious mental illness.
“This bipartisan legislation – which [Senate] Majority Leader Mitch McConnell [R-Ky.] has called ‘the most important legislation Congress will pass this year’ – will help us take advantage of the breathtaking advances in biomedical research and bring those innovations to doctors’ offices and patients’ medicine cabinets around the county,” Sen. Lamar Alexander (R-Tenn.), chair of the Senate Health, Education, Labor, and Pensions Committee, said in a statement.
“The most important prescription drug-related crisis facing our country right now is the skyrocketing price of prescription drugs. This bill does not even deal with that issue,” Sen. Sanders said on the Senate floor. “How can we talk about a bill dealing with the pharmaceutical industry without addressing the elephant in the room, which is the fact that we pay the highest prices in the world for medicine?”
In his weekly address on Dec. 3, President Obama promised to “sign [the bill] as soon as it reaches my desk.”
Gregory Twachtman contributed to this report.
[email protected]
On Twitter @denisefulton
With little debate and less dissent, the Senate passed the 21st Century Cures bill and sent it to President Obama for his promised signature.
The legislation passed the House by an overwhelming 392-26 vote on Nov. 30. Key provisions of the bill (H.R. 34) include:
• Food and Drug Administration reforms, including expedited review for certain medical devices, streamlined review for drug/device combinations, and increased patient involvement in the drug approval process, with $500 million to implement the reforms.
• $4.8 billion over 10 years for key biomedical research efforts including the BRAIN Initiative, the Cancer Moonshot, and the Precision Medicine Initiative.
• $1 billion in grants to states over a 2-year period to help supplement opioid abuse prevention and treatment activities.
• Provisions to improve the interoperability of EHRs.
• Provisions to improve treatment of serious mental illness.
“This bipartisan legislation – which [Senate] Majority Leader Mitch McConnell [R-Ky.] has called ‘the most important legislation Congress will pass this year’ – will help us take advantage of the breathtaking advances in biomedical research and bring those innovations to doctors’ offices and patients’ medicine cabinets around the county,” Sen. Lamar Alexander (R-Tenn.), chair of the Senate Health, Education, Labor, and Pensions Committee, said in a statement.
“The most important prescription drug-related crisis facing our country right now is the skyrocketing price of prescription drugs. This bill does not even deal with that issue,” Sen. Sanders said on the Senate floor. “How can we talk about a bill dealing with the pharmaceutical industry without addressing the elephant in the room, which is the fact that we pay the highest prices in the world for medicine?”
In his weekly address on Dec. 3, President Obama promised to “sign [the bill] as soon as it reaches my desk.”
Gregory Twachtman contributed to this report.
[email protected]
On Twitter @denisefulton
Pembrolizumab proves promising for treating advanced SCLC
VIENNA – One third of patients with extensive-stage small-cell lung cancer (SCLC) treated with the checkpoint inhibitor pembrolizumab achieved an objective response, according to updated data from the KEYNOTE-28 trial.
Of the 24 patients with advanced SCLC who received pembrolizumab in the multicohort phase Ib study, one had a complete response, seven had a partial response, and one further patient had stable disease for 6 or more months, giving a clinical benefit rate of 33.3% (95% CI, 15.6-53.3%).
“Pembrolizumab demonstrated meaningful antitumor activity in previously treated patients with PD-L1-positive small-cell lung cancer,” said presenting study author Patrick A. Ott, MD, PhD, of the Dana-Faber Cancer Institute in Boston.

“Responses were durable, with a median duration of response of 19.4 months,” Dr. Ott said at the World Conference on Cancer, which is sponsored by the International Association for the Study of Lung Cancer. About 40% of patients exhibited a decrease in tumor size, he added.
Treatment with pembrolizumab was associated with a progression-free survival (PFS) of 1.2 months, with a range of 1.7-5.9 months. The 6- and 12-month PFS rates were 28.6% and 23.8%, respectively.
The median overall survival (OS) was 9.7 months, ranging from 4.1 months to an upper limit that has not yet been reached. The respective 6- and 12-month OS rates were 66.0% and 37.7%.
“The safety experience was consistent with previous experience for pembrolizumab in other tumor types, and was identical with longer follow-up” Dr. Ott said.
Over a median follow-up duration of 9.8 months, treatment-related adverse events occurred in two-thirds of patients, with arthralgia, asthenia, and rash reported by four (16.7%) patients each, and diarrhea and fatigue by three (12.5%) patients each. There were no cases of pneumonitis.
The mean age of patients recruited into the KEYNOTE-28 trial was 60.5 years; more than half of the patients (58%) were male. Five (20.8%) had stable brain metastases, and 95.8% had small cell histology.
All recruited patients had received prior standard-of-care chemotherapy with cisplatin or carboplatin plus etoposide, 45.8% had received irinotecan or topotecan, and 29.2% had been treated with a taxane. In addition, one patient had received prior radiotherapy, one had been given an investigational tyrosine kinase inhibitor therapy, and another had received another, unspecified, investigational treatment.
After enrollment, all patients were treated with pembrolizumab at an intravenous dose of 10 mg/kg every 2 weeks. Response was assessed every 8 weeks for the first 6 months and then annually, with patients continuing to respond continuing to be treated for up to 2 years or until progression or unacceptable toxicity.
There are two ongoing, phase II trials with pembrolizumab in patients with advanced SCLC. One is looking at maintenance therapy with pembrolizumab after combination chemotherapy and is sponsored by the Barbara Ann Karmanos Cancer Institute in collaboration with the National Cancer Institute (NCT02359019). The other, the REACTION trial sponsored by the European Organisation for Research and Treatment of Cancer, is looking at the use of pembrolizumab together with etoposide and platinum chemotherapy in previously untreated patients (NCT02580994).
Merck funded the KEYNOTE-28 study. Dr. Ott disclosed ties with Bristol-Myers Squibb, Merck, ArmoBiosciences, AstraZeneca/MedImmune, Celldex, Genentech, Alexion, and CytomX.
VIENNA – One third of patients with extensive-stage small-cell lung cancer (SCLC) treated with the checkpoint inhibitor pembrolizumab achieved an objective response, according to updated data from the KEYNOTE-28 trial.
Of the 24 patients with advanced SCLC who received pembrolizumab in the multicohort phase Ib study, one had a complete response, seven had a partial response, and one further patient had stable disease for 6 or more months, giving a clinical benefit rate of 33.3% (95% CI, 15.6-53.3%).
“Pembrolizumab demonstrated meaningful antitumor activity in previously treated patients with PD-L1-positive small-cell lung cancer,” said presenting study author Patrick A. Ott, MD, PhD, of the Dana-Faber Cancer Institute in Boston.
“Responses were durable, with a median duration of response of 19.4 months,” Dr. Ott said at the World Conference on Cancer, which is sponsored by the International Association for the Study of Lung Cancer. About 40% of patients exhibited a decrease in tumor size, he added.
Treatment with pembrolizumab was associated with a progression-free survival (PFS) of 1.2 months, with a range of 1.7-5.9 months. The 6- and 12-month PFS rates were 28.6% and 23.8%, respectively.
The median overall survival (OS) was 9.7 months, ranging from 4.1 months to an upper limit that has not yet been reached. The respective 6- and 12-month OS rates were 66.0% and 37.7%.
“The safety experience was consistent with previous experience for pembrolizumab in other tumor types, and was identical with longer follow-up” Dr. Ott said.
Over a median follow-up duration of 9.8 months, treatment-related adverse events occurred in two-thirds of patients, with arthralgia, asthenia, and rash reported by four (16.7%) patients each, and diarrhea and fatigue by three (12.5%) patients each. There were no cases of pneumonitis.
The mean age of patients recruited into the KEYNOTE-28 trial was 60.5 years; more than half of the patients (58%) were male. Five (20.8%) had stable brain metastases, and 95.8% had small cell histology.
All recruited patients had received prior standard-of-care chemotherapy with cisplatin or carboplatin plus etoposide, 45.8% had received irinotecan or topotecan, and 29.2% had been treated with a taxane. In addition, one patient had received prior radiotherapy, one had been given an investigational tyrosine kinase inhibitor therapy, and another had received another, unspecified, investigational treatment.
After enrollment, all patients were treated with pembrolizumab at an intravenous dose of 10 mg/kg every 2 weeks. Response was assessed every 8 weeks for the first 6 months and then annually, with patients continuing to respond continuing to be treated for up to 2 years or until progression or unacceptable toxicity.
There are two ongoing, phase II trials with pembrolizumab in patients with advanced SCLC. One is looking at maintenance therapy with pembrolizumab after combination chemotherapy and is sponsored by the Barbara Ann Karmanos Cancer Institute in collaboration with the National Cancer Institute (NCT02359019). The other, the REACTION trial sponsored by the European Organisation for Research and Treatment of Cancer, is looking at the use of pembrolizumab together with etoposide and platinum chemotherapy in previously untreated patients (NCT02580994).
Merck funded the KEYNOTE-28 study. Dr. Ott disclosed ties with Bristol-Myers Squibb, Merck, ArmoBiosciences, AstraZeneca/MedImmune, Celldex, Genentech, Alexion, and CytomX.
VIENNA – One third of patients with extensive-stage small-cell lung cancer (SCLC) treated with the checkpoint inhibitor pembrolizumab achieved an objective response, according to updated data from the KEYNOTE-28 trial.
Of the 24 patients with advanced SCLC who received pembrolizumab in the multicohort phase Ib study, one had a complete response, seven had a partial response, and one further patient had stable disease for 6 or more months, giving a clinical benefit rate of 33.3% (95% CI, 15.6-53.3%).
“Pembrolizumab demonstrated meaningful antitumor activity in previously treated patients with PD-L1-positive small-cell lung cancer,” said presenting study author Patrick A. Ott, MD, PhD, of the Dana-Faber Cancer Institute in Boston.
“Responses were durable, with a median duration of response of 19.4 months,” Dr. Ott said at the World Conference on Cancer, which is sponsored by the International Association for the Study of Lung Cancer. About 40% of patients exhibited a decrease in tumor size, he added.
Treatment with pembrolizumab was associated with a progression-free survival (PFS) of 1.2 months, with a range of 1.7-5.9 months. The 6- and 12-month PFS rates were 28.6% and 23.8%, respectively.
The median overall survival (OS) was 9.7 months, ranging from 4.1 months to an upper limit that has not yet been reached. The respective 6- and 12-month OS rates were 66.0% and 37.7%.
“The safety experience was consistent with previous experience for pembrolizumab in other tumor types, and was identical with longer follow-up” Dr. Ott said.
Over a median follow-up duration of 9.8 months, treatment-related adverse events occurred in two-thirds of patients, with arthralgia, asthenia, and rash reported by four (16.7%) patients each, and diarrhea and fatigue by three (12.5%) patients each. There were no cases of pneumonitis.
The mean age of patients recruited into the KEYNOTE-28 trial was 60.5 years; more than half of the patients (58%) were male. Five (20.8%) had stable brain metastases, and 95.8% had small cell histology.
All recruited patients had received prior standard-of-care chemotherapy with cisplatin or carboplatin plus etoposide, 45.8% had received irinotecan or topotecan, and 29.2% had been treated with a taxane. In addition, one patient had received prior radiotherapy, one had been given an investigational tyrosine kinase inhibitor therapy, and another had received another, unspecified, investigational treatment.
After enrollment, all patients were treated with pembrolizumab at an intravenous dose of 10 mg/kg every 2 weeks. Response was assessed every 8 weeks for the first 6 months and then annually, with patients continuing to respond continuing to be treated for up to 2 years or until progression or unacceptable toxicity.
There are two ongoing, phase II trials with pembrolizumab in patients with advanced SCLC. One is looking at maintenance therapy with pembrolizumab after combination chemotherapy and is sponsored by the Barbara Ann Karmanos Cancer Institute in collaboration with the National Cancer Institute (NCT02359019). The other, the REACTION trial sponsored by the European Organisation for Research and Treatment of Cancer, is looking at the use of pembrolizumab together with etoposide and platinum chemotherapy in previously untreated patients (NCT02580994).
Merck funded the KEYNOTE-28 study. Dr. Ott disclosed ties with Bristol-Myers Squibb, Merck, ArmoBiosciences, AstraZeneca/MedImmune, Celldex, Genentech, Alexion, and CytomX.
AT WCLC 2016
Key clinical point: Pembrolizumab has antitumor activity in patients with advanced small-cell lung cancer.
Major finding: The objective response rate was 33.3% (95% CI 15.6-55.3%), including one complete and seven partial responses.
Data source: Phase Ib, nonrandomized, multicohort trial of 24 heavily pretreated patients with extensive-disease small-cell lung cancer.
Disclosures: Merck funded the study. Dr. Ott disclosed ties with Bristol-Myers Squibb, Merck, ArmoBiosciences, AstraZeneca/MedImmune, Celldex, Genentech, Alexion, and CytomX.
Sutureless aortic valve replacement: Is ease worth the cost?
CHICAGO – Rapid deployment sutureless valves can be a good option for some patients, providing a highly functional and nearly leakproof valve with less cardiopulmonary bypass and aortic cross-clamp times than those of conventional procedures.
“Why use a sutureless valve?” asked Vinod H. Thourani, MD, speaking at Heart Valve Summit 2016. He said that for many patients, there are abundant good reasons for the choice. The rapidity of the implantation procedure is a huge plus, he said. Cardiopulmonary bypass times are reduced when sutureless valve replacement is a stand-alone procedure, added Dr. Thourani, chief of cardiovascular surgery at Emory Hospital Midtown and codirector of the Structural Heart and Valve Center at Emory University, Atlanta.

Rapid deployment is also of benefit in combined cases, or when patients have multiple comorbidities or poor left ventricular function. Sutureless valves, he said, are “optimal for multiple valve or concomitant procedures.”
Hemodynamics also are favorable, said Dr. Thourani; sutureless valves produce lower gradients than do their sutured alternatives, and work well in patients with a small aortic root.
Both sutureless valves that are currently available use bovine tissue; one, Sorin’s Perceval, uses a nitinol stent, while the Edwards’ Intuity uses stainless steel. The Perceval stent requires no sutures, while the Intuity requires just three. Also, the Perceval is collapsible, while the Intuity is not.
Removal of the pathologic valve in the sutureless procedure, he said, may contribute to the lower paravalvular leak and stroke rates than are seen in transcatheter aortic valve replacement (TAVR).
Expanded indications for sutureless valves include a calcified aortic root or a homograft; sutureless valves also can be used as an aortic valve redo, with patent grafts. Dr. Thourani said that he favors a transverse incision with a high aortotomy, about 2 cm above the sinotubular junction (STJ). In addition, off-label indications have included bicuspid aortic valve, pure aortic insufficiency, a prior mitral prosthesis or a degenerated aortic bioprosthesis, and a rescue procedure for a failed TAVR.
Dr. Thourani cited results of a trial conducted by Theodor Fischlein, MD, of Paracelsus Medical University in Nuremberg, Germany, and coauthors. These 1-year follow-up data from 628 patients participating in CAVALIER (Perceval S Valve Clinical Trial for Extended CE Mark), an international multicenter prospective trial, were presented at AATS 2016 (J Thorac Cardiovasc Surg. 2016 Jun;51[6]:1617-26.e4).
Of the 658 patients who met enrollment criteria and had a Perceval valve placement attempted, 30 wound up with a different prosthesis, most often because the correct valve size was not available. The remaining 628 patients who received the Perceval valve were included in the study. At 1 year, 549 patients remained; 50 had died, 12 had undergone valve explantation, and the remainder withdrew or were lost to follow-up.
Of the original Perceval recipients, 219 had received their valve via minimally invasive access. At 1 year, effective orifice area remained stable at the same mean 1.5 cm2 that was seen at discharge, an improvement from the mean 0.7 cm2 effective orifice area seen preoperatively. The mean pressure gradient, which was 45 mm Hg preoperatively, dropped precipitously to 10.3 mm Hg at discharge, and dropped a bit more at 1 year, to 9.2 mm Hg.
“This is a rapid and reproducible procedure: Over 20,000 implants have been performed worldwide,” said Dr. Thourani. The procedure looks good for low- to medium-risk patients, and may be the first procedure to consider for patients with a small aortic root, who have had prior coronary artery bypass surgery with patent grafts, or those with a calcified aortic root and homografts.
Questions still to be answered, he said, include whether “the cost will justify the decrease in cross-clamp times.” Also, though midrange results are good, longitudinal follow-up to track long-term valve hemodynamics is still ongoing.
Although patient demand seems to be high for a minimally invasive approach, sutureless valves still have low adoption rates, he said.
Dr. Thourani reported multiple financial relationships with medical device companies.
[email protected]
On Twitter @karioakes
CHICAGO – Rapid deployment sutureless valves can be a good option for some patients, providing a highly functional and nearly leakproof valve with less cardiopulmonary bypass and aortic cross-clamp times than those of conventional procedures.
“Why use a sutureless valve?” asked Vinod H. Thourani, MD, speaking at Heart Valve Summit 2016. He said that for many patients, there are abundant good reasons for the choice. The rapidity of the implantation procedure is a huge plus, he said. Cardiopulmonary bypass times are reduced when sutureless valve replacement is a stand-alone procedure, added Dr. Thourani, chief of cardiovascular surgery at Emory Hospital Midtown and codirector of the Structural Heart and Valve Center at Emory University, Atlanta.
Rapid deployment is also of benefit in combined cases, or when patients have multiple comorbidities or poor left ventricular function. Sutureless valves, he said, are “optimal for multiple valve or concomitant procedures.”
Hemodynamics also are favorable, said Dr. Thourani; sutureless valves produce lower gradients than do their sutured alternatives, and work well in patients with a small aortic root.
Both sutureless valves that are currently available use bovine tissue; one, Sorin’s Perceval, uses a nitinol stent, while the Edwards’ Intuity uses stainless steel. The Perceval stent requires no sutures, while the Intuity requires just three. Also, the Perceval is collapsible, while the Intuity is not.
Removal of the pathologic valve in the sutureless procedure, he said, may contribute to the lower paravalvular leak and stroke rates than are seen in transcatheter aortic valve replacement (TAVR).
Expanded indications for sutureless valves include a calcified aortic root or a homograft; sutureless valves also can be used as an aortic valve redo, with patent grafts. Dr. Thourani said that he favors a transverse incision with a high aortotomy, about 2 cm above the sinotubular junction (STJ). In addition, off-label indications have included bicuspid aortic valve, pure aortic insufficiency, a prior mitral prosthesis or a degenerated aortic bioprosthesis, and a rescue procedure for a failed TAVR.
Dr. Thourani cited results of a trial conducted by Theodor Fischlein, MD, of Paracelsus Medical University in Nuremberg, Germany, and coauthors. These 1-year follow-up data from 628 patients participating in CAVALIER (Perceval S Valve Clinical Trial for Extended CE Mark), an international multicenter prospective trial, were presented at AATS 2016 (J Thorac Cardiovasc Surg. 2016 Jun;51[6]:1617-26.e4).
Of the 658 patients who met enrollment criteria and had a Perceval valve placement attempted, 30 wound up with a different prosthesis, most often because the correct valve size was not available. The remaining 628 patients who received the Perceval valve were included in the study. At 1 year, 549 patients remained; 50 had died, 12 had undergone valve explantation, and the remainder withdrew or were lost to follow-up.
Of the original Perceval recipients, 219 had received their valve via minimally invasive access. At 1 year, effective orifice area remained stable at the same mean 1.5 cm2 that was seen at discharge, an improvement from the mean 0.7 cm2 effective orifice area seen preoperatively. The mean pressure gradient, which was 45 mm Hg preoperatively, dropped precipitously to 10.3 mm Hg at discharge, and dropped a bit more at 1 year, to 9.2 mm Hg.
“This is a rapid and reproducible procedure: Over 20,000 implants have been performed worldwide,” said Dr. Thourani. The procedure looks good for low- to medium-risk patients, and may be the first procedure to consider for patients with a small aortic root, who have had prior coronary artery bypass surgery with patent grafts, or those with a calcified aortic root and homografts.
Questions still to be answered, he said, include whether “the cost will justify the decrease in cross-clamp times.” Also, though midrange results are good, longitudinal follow-up to track long-term valve hemodynamics is still ongoing.
Although patient demand seems to be high for a minimally invasive approach, sutureless valves still have low adoption rates, he said.
Dr. Thourani reported multiple financial relationships with medical device companies.
[email protected]
On Twitter @karioakes
CHICAGO – Rapid deployment sutureless valves can be a good option for some patients, providing a highly functional and nearly leakproof valve with less cardiopulmonary bypass and aortic cross-clamp times than those of conventional procedures.
“Why use a sutureless valve?” asked Vinod H. Thourani, MD, speaking at Heart Valve Summit 2016. He said that for many patients, there are abundant good reasons for the choice. The rapidity of the implantation procedure is a huge plus, he said. Cardiopulmonary bypass times are reduced when sutureless valve replacement is a stand-alone procedure, added Dr. Thourani, chief of cardiovascular surgery at Emory Hospital Midtown and codirector of the Structural Heart and Valve Center at Emory University, Atlanta.
Rapid deployment is also of benefit in combined cases, or when patients have multiple comorbidities or poor left ventricular function. Sutureless valves, he said, are “optimal for multiple valve or concomitant procedures.”
Hemodynamics also are favorable, said Dr. Thourani; sutureless valves produce lower gradients than do their sutured alternatives, and work well in patients with a small aortic root.
Both sutureless valves that are currently available use bovine tissue; one, Sorin’s Perceval, uses a nitinol stent, while the Edwards’ Intuity uses stainless steel. The Perceval stent requires no sutures, while the Intuity requires just three. Also, the Perceval is collapsible, while the Intuity is not.
Removal of the pathologic valve in the sutureless procedure, he said, may contribute to the lower paravalvular leak and stroke rates than are seen in transcatheter aortic valve replacement (TAVR).
Expanded indications for sutureless valves include a calcified aortic root or a homograft; sutureless valves also can be used as an aortic valve redo, with patent grafts. Dr. Thourani said that he favors a transverse incision with a high aortotomy, about 2 cm above the sinotubular junction (STJ). In addition, off-label indications have included bicuspid aortic valve, pure aortic insufficiency, a prior mitral prosthesis or a degenerated aortic bioprosthesis, and a rescue procedure for a failed TAVR.
Dr. Thourani cited results of a trial conducted by Theodor Fischlein, MD, of Paracelsus Medical University in Nuremberg, Germany, and coauthors. These 1-year follow-up data from 628 patients participating in CAVALIER (Perceval S Valve Clinical Trial for Extended CE Mark), an international multicenter prospective trial, were presented at AATS 2016 (J Thorac Cardiovasc Surg. 2016 Jun;51[6]:1617-26.e4).
Of the 658 patients who met enrollment criteria and had a Perceval valve placement attempted, 30 wound up with a different prosthesis, most often because the correct valve size was not available. The remaining 628 patients who received the Perceval valve were included in the study. At 1 year, 549 patients remained; 50 had died, 12 had undergone valve explantation, and the remainder withdrew or were lost to follow-up.
Of the original Perceval recipients, 219 had received their valve via minimally invasive access. At 1 year, effective orifice area remained stable at the same mean 1.5 cm2 that was seen at discharge, an improvement from the mean 0.7 cm2 effective orifice area seen preoperatively. The mean pressure gradient, which was 45 mm Hg preoperatively, dropped precipitously to 10.3 mm Hg at discharge, and dropped a bit more at 1 year, to 9.2 mm Hg.
“This is a rapid and reproducible procedure: Over 20,000 implants have been performed worldwide,” said Dr. Thourani. The procedure looks good for low- to medium-risk patients, and may be the first procedure to consider for patients with a small aortic root, who have had prior coronary artery bypass surgery with patent grafts, or those with a calcified aortic root and homografts.
Questions still to be answered, he said, include whether “the cost will justify the decrease in cross-clamp times.” Also, though midrange results are good, longitudinal follow-up to track long-term valve hemodynamics is still ongoing.
Although patient demand seems to be high for a minimally invasive approach, sutureless valves still have low adoption rates, he said.
Dr. Thourani reported multiple financial relationships with medical device companies.
[email protected]
On Twitter @karioakes
EXPERT ANALYSIS FROM THE HEART VALVE SUMMIT 2016

VIDEO: Pivotal results nail osimertinib’s role in NSCLC
VIENNA – Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor that received U.S. marketing approval in November 2015 as second-line treatment for selected patients with non–small-cell lung cancer based on phase II trial data, now has the pivotal-trial results that completely justify that action.
During a median follow-up of just over 8 months, patients who had progressed on their first-line EGFR tyrosine kinase inhibitor (TKI) and carried the T790M mutation and switched to osimertinib (Tagrisso) had “overwhelmingly” better response rates and progression-free survival, compared with patients put on standard-of-care chemotherapy in a multicenter randomized trial involving 419 patients, Vassiliki A. Papadimitrakopoulou, MD, reported at the World Conference on Lung Cancer.

The AZD9291 Versus Platinum-Based Doublet-Chemotherapy in Locally Advanced or Metastatic Non-Small Cell Lung Cancer (AURA3) trial enrolled 419 patients at 126 international sites during 2014 and 2015. The trial’s primary endpoint was investigator-assessed progression-free survival, which occurred after a median of 10.1 months with osimertinib and 4.4 months with standard chemotherapy, a statistically significant 70% relative risk reduction (P less than .001) in the hazard for death or progressive disease. The drug was as effective for patients with central nervous system metastases as it was for the other patients, which Dr. Papadimitrakopoulou attributed to osimertinib’s good penetration across the blood-brain barrier. The drug’s overall performance in AURA3 was completely consistent with the results of earlier studies that led to its U.S. approval.
Despite that approval, routine testing for T790M mutations and routine prescribing of osimertinib to positive patients “has not fully penetrated U.S. practice,” Dr. Papadimitrakopoulou said, but she hoped that these new confirmatory data will now firmly establish it as standard of care for the tested population.
Osimertinib is now under testing as first-line TKI treatment for EGFR-positive NSCLC regardless of the tumor’s T790M status. It’s going head to head with two first-generation EGFR TKIs, gefitinib and erlotinib, in the FLAURA trial, which should have reportable results in 2017. “We are very encouraged by the AURA3 data that osimertinib could beat the first-generation TKIs” for first-line treatment, she said.
AURA3 was sponsored by AstraZeneca, which markets osimertinib (Tagrisso). Dr. Papadimitrakopoulou is a consultant to, and has received research support from, AstraZeneca and several other companies.
[email protected]
On Twitter @mitchelzoler
Osimertinib overcomes the T790M mutation, which is the cause of about half of the non–small-cell lung cancers that are EGFR positive and develop resistance to a first- or-second generation tyrosine kinase inhibitor. The AURA3 results officially make osimertinib the standard of care for these patients.
Osimertinib’s performance in AURA3 was consistent with what it did in the earlier studies, producing an overall response rate of about 60%-70% and extending progression-free survival out to a median of 10-11 months.

Tetsuya Mitsudomi, MD, is professor of thoracic surgery at Kindai University in Osaka-Sayama, Japan. He has been a consultant to, and has received honoraria and research support from, AstraZeneca and several other companies. He was principal investigator for AURA2, one of the phase II studies of osimertinib. He made these comments as designated discussant for AURA3.
Osimertinib overcomes the T790M mutation, which is the cause of about half of the non–small-cell lung cancers that are EGFR positive and develop resistance to a first- or-second generation tyrosine kinase inhibitor. The AURA3 results officially make osimertinib the standard of care for these patients.
Osimertinib’s performance in AURA3 was consistent with what it did in the earlier studies, producing an overall response rate of about 60%-70% and extending progression-free survival out to a median of 10-11 months.
Tetsuya Mitsudomi, MD, is professor of thoracic surgery at Kindai University in Osaka-Sayama, Japan. He has been a consultant to, and has received honoraria and research support from, AstraZeneca and several other companies. He was principal investigator for AURA2, one of the phase II studies of osimertinib. He made these comments as designated discussant for AURA3.
Osimertinib overcomes the T790M mutation, which is the cause of about half of the non–small-cell lung cancers that are EGFR positive and develop resistance to a first- or-second generation tyrosine kinase inhibitor. The AURA3 results officially make osimertinib the standard of care for these patients.
Osimertinib’s performance in AURA3 was consistent with what it did in the earlier studies, producing an overall response rate of about 60%-70% and extending progression-free survival out to a median of 10-11 months.
Tetsuya Mitsudomi, MD, is professor of thoracic surgery at Kindai University in Osaka-Sayama, Japan. He has been a consultant to, and has received honoraria and research support from, AstraZeneca and several other companies. He was principal investigator for AURA2, one of the phase II studies of osimertinib. He made these comments as designated discussant for AURA3.
VIENNA – Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor that received U.S. marketing approval in November 2015 as second-line treatment for selected patients with non–small-cell lung cancer based on phase II trial data, now has the pivotal-trial results that completely justify that action.
During a median follow-up of just over 8 months, patients who had progressed on their first-line EGFR tyrosine kinase inhibitor (TKI) and carried the T790M mutation and switched to osimertinib (Tagrisso) had “overwhelmingly” better response rates and progression-free survival, compared with patients put on standard-of-care chemotherapy in a multicenter randomized trial involving 419 patients, Vassiliki A. Papadimitrakopoulou, MD, reported at the World Conference on Lung Cancer.
The AZD9291 Versus Platinum-Based Doublet-Chemotherapy in Locally Advanced or Metastatic Non-Small Cell Lung Cancer (AURA3) trial enrolled 419 patients at 126 international sites during 2014 and 2015. The trial’s primary endpoint was investigator-assessed progression-free survival, which occurred after a median of 10.1 months with osimertinib and 4.4 months with standard chemotherapy, a statistically significant 70% relative risk reduction (P less than .001) in the hazard for death or progressive disease. The drug was as effective for patients with central nervous system metastases as it was for the other patients, which Dr. Papadimitrakopoulou attributed to osimertinib’s good penetration across the blood-brain barrier. The drug’s overall performance in AURA3 was completely consistent with the results of earlier studies that led to its U.S. approval.
Despite that approval, routine testing for T790M mutations and routine prescribing of osimertinib to positive patients “has not fully penetrated U.S. practice,” Dr. Papadimitrakopoulou said, but she hoped that these new confirmatory data will now firmly establish it as standard of care for the tested population.
Osimertinib is now under testing as first-line TKI treatment for EGFR-positive NSCLC regardless of the tumor’s T790M status. It’s going head to head with two first-generation EGFR TKIs, gefitinib and erlotinib, in the FLAURA trial, which should have reportable results in 2017. “We are very encouraged by the AURA3 data that osimertinib could beat the first-generation TKIs” for first-line treatment, she said.
AURA3 was sponsored by AstraZeneca, which markets osimertinib (Tagrisso). Dr. Papadimitrakopoulou is a consultant to, and has received research support from, AstraZeneca and several other companies.
[email protected]
On Twitter @mitchelzoler
VIENNA – Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor that received U.S. marketing approval in November 2015 as second-line treatment for selected patients with non–small-cell lung cancer based on phase II trial data, now has the pivotal-trial results that completely justify that action.
During a median follow-up of just over 8 months, patients who had progressed on their first-line EGFR tyrosine kinase inhibitor (TKI) and carried the T790M mutation and switched to osimertinib (Tagrisso) had “overwhelmingly” better response rates and progression-free survival, compared with patients put on standard-of-care chemotherapy in a multicenter randomized trial involving 419 patients, Vassiliki A. Papadimitrakopoulou, MD, reported at the World Conference on Lung Cancer.
The AZD9291 Versus Platinum-Based Doublet-Chemotherapy in Locally Advanced or Metastatic Non-Small Cell Lung Cancer (AURA3) trial enrolled 419 patients at 126 international sites during 2014 and 2015. The trial’s primary endpoint was investigator-assessed progression-free survival, which occurred after a median of 10.1 months with osimertinib and 4.4 months with standard chemotherapy, a statistically significant 70% relative risk reduction (P less than .001) in the hazard for death or progressive disease. The drug was as effective for patients with central nervous system metastases as it was for the other patients, which Dr. Papadimitrakopoulou attributed to osimertinib’s good penetration across the blood-brain barrier. The drug’s overall performance in AURA3 was completely consistent with the results of earlier studies that led to its U.S. approval.
Despite that approval, routine testing for T790M mutations and routine prescribing of osimertinib to positive patients “has not fully penetrated U.S. practice,” Dr. Papadimitrakopoulou said, but she hoped that these new confirmatory data will now firmly establish it as standard of care for the tested population.
Osimertinib is now under testing as first-line TKI treatment for EGFR-positive NSCLC regardless of the tumor’s T790M status. It’s going head to head with two first-generation EGFR TKIs, gefitinib and erlotinib, in the FLAURA trial, which should have reportable results in 2017. “We are very encouraged by the AURA3 data that osimertinib could beat the first-generation TKIs” for first-line treatment, she said.
AURA3 was sponsored by AstraZeneca, which markets osimertinib (Tagrisso). Dr. Papadimitrakopoulou is a consultant to, and has received research support from, AstraZeneca and several other companies.
[email protected]
On Twitter @mitchelzoler
Key clinical point:
Major finding: Progression-free survival averaged 10.1 months with osimertinib and 4.4 months in patients on standard chemotherapy.
Data source: AURA3, which randomized 419 patients at 126 international centers.
Disclosures: AURA3 was sponsored by AstraZeneca, which markets osimertinib (Tagrisso). Dr. Papadimitrakopoulou is a consultant to, and has received research support from, AstraZeneca and several other companies.
‘Vanishing’ role forecast for whole-brain irradiation for NSCLC metastases
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.

Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.

“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.
Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.
“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
VIENNA – Icotinib proved significantly more effective and less toxic than standard therapy with whole-brain irradiation and chemotherapy in patients with multiple brain metastases from epidermal growth factor receptor (EGFR)–mutated non–small cell lung cancer in the phase III BRAIN trial.
“With favorable objective response and disease control rates, icotinib was superior to whole-brain irradiation with chemotherapy, and therefore icotinib should be used as first-line therapy for advanced EGFR-mutant non–small cell lung cancers with brain metastases,” Yi-long Wu, MD, said in presenting the BRAIN results at the World Congress on Lung Cancer.
Patients with brain metastases are often excluded from participation in clinical trials because their prognosis is so poor. BRAIN is the first phase III trial to report results comparing an EGFR tyrosine kinase inhibitor (TKI) – icotinib – to whole-brain irradiation (WBI) plus chemotherapy, regarded in National Comprehensive Cancer Network guidelines as standard therapy in the setting of brain metastases from NSCLC, noted Dr. Wu of the Guangdong Lung Cancer Institute in Guangzhou, China.
BRAIN was a multicenter Chinese trial in which investigators randomized 158 patients with three or more brain metastases from EGFR-mutated NSCLC to oral icotinib at 125 mg t.i.d. or to WBI with four to six cycles of concurrent or sequential platinum-based chemotherapy.
Icotinib outperformed standard therapy with WBI plus chemotherapy on multiple efficacy endpoints. Median intracranial progression-free survival was 10 months with icotinib, compared with only 4.8 months in patients on WBI with chemotherapy. At 6 months, 72% of patients assigned to icotinib remained free of intracranial disease progression, compared with just 48% of controls on WBI and chemotherapy. Six-month overall PFS, intracranial as well as extracranial, was 6.8 months with icotinib and 3.4 months in the WBI group. The intracranial and overall objective response rates were 67% and 55%, respectively, with icotinib, compared with 41% and 11% with WBI.
In addition, the EGFR TKI had a significantly better safety profile: grade 3 or worse toxicities occurred in just 8% of the icotinib group, compared with 26% of controls on standard therapy, Dr. Wu reported at the meeting sponsored by the International Association for the Study of Lung Cancer.
There was, however, no significant difference between the two study arms in overall survival: 18 months with icotinib, 20.5 months with standard therapy, noted Dr. Wu, who is president of the Chinese Society of Clinical Oncology.
Discussant Jacek Jassem, MD, said “This is potentially, and likely, a practice-changing study.” He added that he’s looking forward to planned future presentation of neurotoxicity and quality of life data from BRAIN. Those important endpoints are also incorporated in the ongoing phase III trials of gefitinib and erlotinib, EGFR TKIs which are far more readily accessible at present to physicians outside the Far East.
“Whole-brain radiotherapy for brain metastases from EGFR-mutated non–small cell lung cancer is a vanishing approach. The remaining role in this setting is as salvage in cases of symptomatic primary or secondary resistance to EGFR TKIs,” said Dr. Jassem, head of the department of oncology and radiotherapy at the Medical University of Gdansk, Poland.
By way of background, he noted that 10%-15% of patients already have brain metastases at the time of diagnosis of NSCLC, and 40% develop them eventually. EGFR-mutated primary tumors are particularly likely to metastasize to the brain.
Remaining questions in the wake of the BRAIN trial include the efficacy of gefitinib and erlotinib versus WBI plus chemotherapy, as well as the broader question of the efficacy of EGFR TKIs in non-Asian patients with brain metastases.
“Most of the studies of EGFR TKIs have been in East Asian populations. These agents are particularly active in East Asians. There’s a question as to whether the BRAIN results can be applied to other populations,” Dr. Jassem said.
The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. Dr. Wu reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi. Dr. Jassem reported having no financial conflicts of interest.
AT WCLC 2016
Key clinical point:
Major finding: Median intracranial progression-free survival in patients with multiple brain metastases from EGFR-mutated NSCLC was 10 months in those randomized to icotinib, compared with 4.8 months with standard-of-care whole-brain irradiation plus chemotherapy.
Data source: This phase III multicenter Chinese trial included 158 patients with multiple brain metastases from EGFR-mutated NSCLC.
Disclosures: The BRAIN study was sponsored by the Guangdong Association of Clinical Trials. The presenter reported serving as a consultant to AstraZeneca, Roche, Eli Lilly, Pfizer, and Sanofi.
Ganetespib fails to hit mark in phase III NSCLC trial
VIENNA – The addition of ganetespib to docetaxel for the treatment of advanced non–small cell lung cancer (NSCLC) did not live up to its earlier promise of improved efficacy over docetaxel alone in a phase III study.
Interim results of the GALAXY-2 study, which led to the trial’s termination for futility, showed that there was no difference in the primary endpoint of overall survival (OS). The median OS was a respective 10.9 months and 10.5 months for the combination of ganetespib plus docetaxel versus docetaxel alone (hazard ratio, 1.111, 95% confidence interval, 0.899-1.372, P = .03293).

The combination had looked promising in the phase II GALAXY-1 study (Ann Oncol. 2015;26:1741-8), with a trend towards improved PFS and OS, with patients diagnosed with advanced disease perhaps gaining the most benefit.
“The addition of ganetespib to docetaxel did not result in improved efficacy for the salvage therapy of patients with advanced-stage lung adenocarcinoma,” Rathi Pillai, MD, said at the World Conference on Lung Cancer.
“Based on these findings, further development of Hsp [heat shock protein] 90 inhibitors in lung cancer should be limited to patients with driver mutations with relevant client proteins,” added Dr. Pillai of the Winship Cancer Institute at Emory University in Atlanta.
In GALAXY-2, 672 patients were randomized, 1:1, to receive docetaxel (75 mg/m2 on day 1) with ganetespib (150 mg/m2 on days 1 and 15) or a placebo every 3 weeks. The median number of cycles received was five in the combination arm and four in the docetaxel-only arm. All patients had advanced non–small cell lung adenocarcinoma diagnosed at least 6 months prior to enrollment and had received only one prior treatment regimen.
Response rates were similar between the two groups, with 13.7% and 16% of ganetespib/docetaxel– and docetaxel/placebo–treated patients achieving a partial response (P = .448) and 56.1% and 50.1%, respectively, having stable disease (P = .123).
Almost two-thirds (65%) of patients given ganetespib/docetaxel reported any grade 3-4 adverse event versus 54% of patients given docetaxel/placebo. The most frequent treatment-emergent grade 3-4 adverse event was neutropenia, occurring in 34.6% ad 29.5% of patients in each arm (P = .1807), with only diarrhea (46.2% vs. 14.6%; P less than .0001) and weight loss (11.3% vs. 5.2%; P = .0044) occurring more frequently in the combination than the docetaxel-only arm.

Ganetespib is a second-generation Hsp90 inhibitor and the rationale for using Hsp90 inhibitors as cancer therapy remains sound, Dr. Gandara maintained. One of the issues is finding a biomarker to predict the benefit for these drugs in a clinical setting, he said. In the phase II GALAXY-1 trial it was noted that patients diagnosed with advanced disease more than 6 months prior to study entry fared better than those with more recent diagnosis if they were treated with ganetespib/docetaxel than docetaxel alone. Patients with elevated levels of lactate dehydrogenase (eLDH) also seemed to do better than those with normal LDH levels if they were treated with the combination.
These two subpopulations were specifically looked at the in the phase III study, but again no differences in OS or PFS were observed, nor were differences observed in any of the other subgroups analyzed, which included EGFR- and ALK-negative patients, by response rate or progression because of new metastatic lesions.
“Were these the right surrogates to use as predictive biomarkers for heat shock protein inhibition? Of course, in retrospect, it is easy to say that they were not,” Dr. Gandara said.
“Is there still an opportunity for this class of drugs to make a meaningful impact in NSCLC? In my own opinion I think the answer is yes, but not in this broad page approach and not with these potential surrogates as were used in GALAXY-2,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was sponsored by Synta Pharmaceuticals, which became part of Madrigal Pharmaceuticals in June 2016. Dr. Pillai reported having no financial disclosures. Dr. Gandara disclosed that he had received research grants from several pharmaceutical companies.
VIENNA – The addition of ganetespib to docetaxel for the treatment of advanced non–small cell lung cancer (NSCLC) did not live up to its earlier promise of improved efficacy over docetaxel alone in a phase III study.
Interim results of the GALAXY-2 study, which led to the trial’s termination for futility, showed that there was no difference in the primary endpoint of overall survival (OS). The median OS was a respective 10.9 months and 10.5 months for the combination of ganetespib plus docetaxel versus docetaxel alone (hazard ratio, 1.111, 95% confidence interval, 0.899-1.372, P = .03293).
The combination had looked promising in the phase II GALAXY-1 study (Ann Oncol. 2015;26:1741-8), with a trend towards improved PFS and OS, with patients diagnosed with advanced disease perhaps gaining the most benefit.
“The addition of ganetespib to docetaxel did not result in improved efficacy for the salvage therapy of patients with advanced-stage lung adenocarcinoma,” Rathi Pillai, MD, said at the World Conference on Lung Cancer.
“Based on these findings, further development of Hsp [heat shock protein] 90 inhibitors in lung cancer should be limited to patients with driver mutations with relevant client proteins,” added Dr. Pillai of the Winship Cancer Institute at Emory University in Atlanta.
In GALAXY-2, 672 patients were randomized, 1:1, to receive docetaxel (75 mg/m2 on day 1) with ganetespib (150 mg/m2 on days 1 and 15) or a placebo every 3 weeks. The median number of cycles received was five in the combination arm and four in the docetaxel-only arm. All patients had advanced non–small cell lung adenocarcinoma diagnosed at least 6 months prior to enrollment and had received only one prior treatment regimen.
Response rates were similar between the two groups, with 13.7% and 16% of ganetespib/docetaxel– and docetaxel/placebo–treated patients achieving a partial response (P = .448) and 56.1% and 50.1%, respectively, having stable disease (P = .123).
Almost two-thirds (65%) of patients given ganetespib/docetaxel reported any grade 3-4 adverse event versus 54% of patients given docetaxel/placebo. The most frequent treatment-emergent grade 3-4 adverse event was neutropenia, occurring in 34.6% ad 29.5% of patients in each arm (P = .1807), with only diarrhea (46.2% vs. 14.6%; P less than .0001) and weight loss (11.3% vs. 5.2%; P = .0044) occurring more frequently in the combination than the docetaxel-only arm.
Ganetespib is a second-generation Hsp90 inhibitor and the rationale for using Hsp90 inhibitors as cancer therapy remains sound, Dr. Gandara maintained. One of the issues is finding a biomarker to predict the benefit for these drugs in a clinical setting, he said. In the phase II GALAXY-1 trial it was noted that patients diagnosed with advanced disease more than 6 months prior to study entry fared better than those with more recent diagnosis if they were treated with ganetespib/docetaxel than docetaxel alone. Patients with elevated levels of lactate dehydrogenase (eLDH) also seemed to do better than those with normal LDH levels if they were treated with the combination.
These two subpopulations were specifically looked at the in the phase III study, but again no differences in OS or PFS were observed, nor were differences observed in any of the other subgroups analyzed, which included EGFR- and ALK-negative patients, by response rate or progression because of new metastatic lesions.
“Were these the right surrogates to use as predictive biomarkers for heat shock protein inhibition? Of course, in retrospect, it is easy to say that they were not,” Dr. Gandara said.
“Is there still an opportunity for this class of drugs to make a meaningful impact in NSCLC? In my own opinion I think the answer is yes, but not in this broad page approach and not with these potential surrogates as were used in GALAXY-2,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was sponsored by Synta Pharmaceuticals, which became part of Madrigal Pharmaceuticals in June 2016. Dr. Pillai reported having no financial disclosures. Dr. Gandara disclosed that he had received research grants from several pharmaceutical companies.
VIENNA – The addition of ganetespib to docetaxel for the treatment of advanced non–small cell lung cancer (NSCLC) did not live up to its earlier promise of improved efficacy over docetaxel alone in a phase III study.
Interim results of the GALAXY-2 study, which led to the trial’s termination for futility, showed that there was no difference in the primary endpoint of overall survival (OS). The median OS was a respective 10.9 months and 10.5 months for the combination of ganetespib plus docetaxel versus docetaxel alone (hazard ratio, 1.111, 95% confidence interval, 0.899-1.372, P = .03293).
The combination had looked promising in the phase II GALAXY-1 study (Ann Oncol. 2015;26:1741-8), with a trend towards improved PFS and OS, with patients diagnosed with advanced disease perhaps gaining the most benefit.
“The addition of ganetespib to docetaxel did not result in improved efficacy for the salvage therapy of patients with advanced-stage lung adenocarcinoma,” Rathi Pillai, MD, said at the World Conference on Lung Cancer.
“Based on these findings, further development of Hsp [heat shock protein] 90 inhibitors in lung cancer should be limited to patients with driver mutations with relevant client proteins,” added Dr. Pillai of the Winship Cancer Institute at Emory University in Atlanta.
In GALAXY-2, 672 patients were randomized, 1:1, to receive docetaxel (75 mg/m2 on day 1) with ganetespib (150 mg/m2 on days 1 and 15) or a placebo every 3 weeks. The median number of cycles received was five in the combination arm and four in the docetaxel-only arm. All patients had advanced non–small cell lung adenocarcinoma diagnosed at least 6 months prior to enrollment and had received only one prior treatment regimen.
Response rates were similar between the two groups, with 13.7% and 16% of ganetespib/docetaxel– and docetaxel/placebo–treated patients achieving a partial response (P = .448) and 56.1% and 50.1%, respectively, having stable disease (P = .123).
Almost two-thirds (65%) of patients given ganetespib/docetaxel reported any grade 3-4 adverse event versus 54% of patients given docetaxel/placebo. The most frequent treatment-emergent grade 3-4 adverse event was neutropenia, occurring in 34.6% ad 29.5% of patients in each arm (P = .1807), with only diarrhea (46.2% vs. 14.6%; P less than .0001) and weight loss (11.3% vs. 5.2%; P = .0044) occurring more frequently in the combination than the docetaxel-only arm.
Ganetespib is a second-generation Hsp90 inhibitor and the rationale for using Hsp90 inhibitors as cancer therapy remains sound, Dr. Gandara maintained. One of the issues is finding a biomarker to predict the benefit for these drugs in a clinical setting, he said. In the phase II GALAXY-1 trial it was noted that patients diagnosed with advanced disease more than 6 months prior to study entry fared better than those with more recent diagnosis if they were treated with ganetespib/docetaxel than docetaxel alone. Patients with elevated levels of lactate dehydrogenase (eLDH) also seemed to do better than those with normal LDH levels if they were treated with the combination.
These two subpopulations were specifically looked at the in the phase III study, but again no differences in OS or PFS were observed, nor were differences observed in any of the other subgroups analyzed, which included EGFR- and ALK-negative patients, by response rate or progression because of new metastatic lesions.
“Were these the right surrogates to use as predictive biomarkers for heat shock protein inhibition? Of course, in retrospect, it is easy to say that they were not,” Dr. Gandara said.
“Is there still an opportunity for this class of drugs to make a meaningful impact in NSCLC? In my own opinion I think the answer is yes, but not in this broad page approach and not with these potential surrogates as were used in GALAXY-2,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was sponsored by Synta Pharmaceuticals, which became part of Madrigal Pharmaceuticals in June 2016. Dr. Pillai reported having no financial disclosures. Dr. Gandara disclosed that he had received research grants from several pharmaceutical companies.
AT WCLC 2016
Key clinical point: Adding ganetespib to docetaxel did not improve the survival of the patients studied versus docetaxel alone.
Major finding: Median overall survival was 10.9 months for ganetespib/docetaxel and 10.5 months for docetaxel alone (HR, 1.111; 95% CI, 0.899-1.372; P = .03293).
Data source: International, randomized, phase III, open-label GALAXY-2 study of docetaxel with or without ganetespib in 672 patients with advanced non–small cell lung adenocarcinoma.
Disclosures: The study was sponsored by Synta Pharmaceuticals (Madrigal Pharmaceuticals since June 2016). Dr. Pillai reported having no financial disclosures. Dr. Gandara disclosed that he had received research grants from several pharmaceutical companies.
Trump HHS nominee could curb regulations, reshape health insurance
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.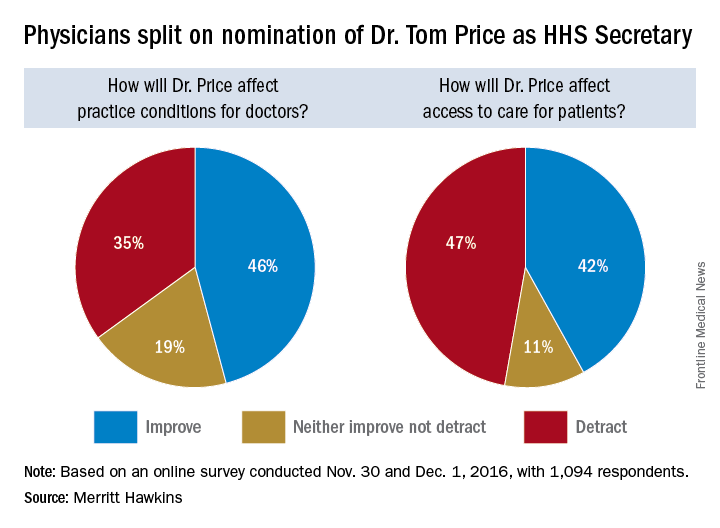
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med
Opinions are mixed on what the nominations of Rep. Tom Price (R-Ga.) as Secretary of Health & Human Services will mean for medicine and health care.
An orthopedic surgeon and six-term congressman, Dr. Price is an outspoken critic of the Affordable Care Act and has sponsored or cosponsored numerous bills to replace it. President-elect Trump called Rep. Price “a renowned physician” who has “earned a reputation for being a tireless problem solver and the go-to expert on health care policy,” according to a statement.
Not everyone agrees.
But Adam Gaffney, MD, a pulmonologist at the Cambridge (Mass.) Health Alliance, said physicians’ ability to care for their patients would be compromised if Rep. Price succeeds with many of his proposals, such as the privatization of Medicare and block grants for Medicaid.
“If these reforms go through, we’re going to see the insurance protections of our patients get worse,” said Dr. Gaffney, a board member for Physicians for a National Health Program, which advocates for a single-payer health care system. “If [his] agenda is successful, I think it’s going to have a detrimental impact on our ability to provide the care that our patients need.”
ACA repeal, malpractice reform
In the House, Rep. Price has introduced the Empowering Patients First Act, legislation, which would allow doctors to opt out of Medicare and enter into private contracts with Medicare patients. The bill is seen by many as a potential blueprint for Trump administration health reform. Rep. Price is also a proponent of malpractice reform that would make it tougher for patients to sue doctors and would lower liability insurance premiums.
The Empowering Patients First Act would repeal the ACA and offer tax credits for the purchase of individual and family health insurance policies. It would also create incentives for patients to contribute to health savings accounts, offer state grants to subsidize coverage for high-risk patients, and authorize businesses to cover members through association health plans.
The American Medical Association praised Rep. Price’s nomination, expressing support for ability to lead HHS.
“Dr. Price has been a leader in the development of health policies to advance patient choice and market-based solutions as well as reduce excessive regulatory burdens that diminish time devoted to patient care and increase costs,” AMA Board of Trustees Chair Patrice A. Harris, MD, said in a statement.
The American College of Surgeons' Executive Director, David B. Hoyt, MD, FACS, issued a supportive statement about the nomination of Dr. Price. "“Dr. Price is a stalwart champion for patients and their surgeons, and the ACS looks forward to working with him on key issues, such as the implementation of the Medicare Access and CHIP Reauthorization Act,” said Dr. Hoyt in a statement. “The ACS encourages the Senate to swiftly confirm Dr. Price’s nomination as Secretary of HHS."
But thousands of physicians disagree. Rep. Price’s proposals on Medicaid and Medicare threaten to harm vulnerable patients and limit access to healthcare, according to an open letter to the AMA published on Medium and credited to Clinician Action Network, a nonpartisan group that supports evidence-based policies. The group was started in opposition to the nomination of Rep. Price.
“We cannot support the dismantling of Medicaid, which has helped 15 million Americans gain health coverage since 2014,” the letter states. “We oppose Dr. Price’s proposals to reduce funding for the Children’s Health Insurance Program, a critical mechanism by which poor children access preventative care.”
Value-based payment or fee for service?
Rep. Price’s experience as a physician fuels his efforts to reduce burdensome regulations for doctors and enhance care efficiency, according to one of his predecessors, Louis W. Sullivan, MD. If confirmed, Rep. Price will become the third physician to be HHS secretary; Dr. Sullivan served in the George H.W. Bush administration and Otis R. Bowen, MD, served in the Reagan administration.
“He is very much aware of the challenges that physicians face in trying to delivery care,” said Dr. Sullivan. “I know that he’ll be working to reduce regulation when feasible so that the cost and delays that some regulatory issues present will hopefully be relieved,”
Some of those regulatory modifications could affect value-based care programs, Dr. Rodriguez said. Rep. Price has been critical of the move from fee for service to quality-based care and has opposed some corresponding programs, such as bundled payment initiatives. Rep. Price and members of the GOP Doctors Caucus wrote to Centers for Medicare & Medicaid Services in October to protest the regulations to implement the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) as too burdensome for smaller practices and calling for flexibility in quality reporting.
Rep. Price voted for passage of MACRA.
“He has been cautious about some of the changes that are being promoted in health care,” Dr. Rodriguez said. “He could slow that down – the processes being put in place. That might delay the impact those systems have in bringing about the improved quality that we want. [This would be] enormous, given the amount of work that we’ve been doing.”
A fair medical liability system also is a priority for Rep. Price, Dr. Sullivan said. His Empowering Patients First bill would require collaboration between HHS and physician associations to develop best practice guidelines that would provide a litigation safe harbor to physicians who practiced in accordance with the standards.
“I know that he will be working to develop strategies to reduce litigation in the health space,” Dr. Sullivan said in an interview. “That is one of the challenges that adds to health care costs, adds tension, and enhances an adversarial relationship between physicians and patients.”
But Dr. Gaffney said that he believes Rep. Price’s views on reproductive rights and gay marriage are regressive and that his agenda regarding health policy issues is bad for medicine.
“The overall [theme] of that agenda can be summed up as ‘take from the poor and sick and give to the rich,’ ” Dr. Gaffney said in an interview. “I think the financing of this [new health reform] system will be much more aggressive, and the result will be greater health care inequity.”
Rep. Price also has supported a ban on federal funding for Planned Parenthood, calling some of their practices barbaric. He has also voted to prohibit the importation of prescription drugs by nonsanctioned importers and has voted to repeal the medical device excise tax.
[email protected]
On Twitter @legal_med