User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Common endoscopic procedure needs quality improvement
One of the most common procedures in gastroenterology – esophagogastroduodenoscopy (EGD) – needs to consistently meet quality measures, but data on interventions to improve them is lacking, according to a recent review.
Researchers, led by Fateh Bazerbachi, MD, with CentraCare, Interventional Endoscopy Program, at St. Cloud (Minn.) Hospital performed a systematic review of the literature to identify which interventions and measures have improved the performance of EGD quality indicators previously identified by the American Society for Gastrointestinal Endoscopy. They also looked for demonstrations of improving compliance with the prioritized indicators. The review appeared in Gastrointestinal Endoscopy.
The authors pointed out that more than 6.1 million EGDs are performed every year in the United States. Although gastroenterologists perform most of them, other providers also perform them, including primary care physicians, surgeons, and sometimes advanced practice providers. Therefore, establishing well-defined quality measures is critical for consistent outcomes.

Daniel C. Buckles, MD, associate professor of gastroenterology, hepatology & motility at the University of Kansas Medical Center in Kansas City, who was not part of the review, said high-quality EGDs are critical for many reasons, including avoiding overuse when results of the procedure are not likely to change a patient’s treatment but add risk to the patient and increase costs to the health care system.
“Lack of training to recognize important GI pathology seen on an EGD and lack of standardized reporting of GI abnormalities using validated classification systems can lead to suboptimal treatment and follow-up for patients,” he noted.
Testing provider adherence to guidelines years after publication helps providers understand what works and can improve outcomes, Dr. Buckles said.
Dr. Buckles said that one of the highlights of the review was that researchers were able to confidently say that use of standardized checklists and frequent auditing had value in improving preprocedural and postprocedural quality indicators.
“The authors also concluded that focused educational interventions might improve endoscopists’ abilities to adhere to standardized Barrett’s esophagus examinations,” he added. “Unfortunately, the authors were not able to find much evidence for interventions that would improve intraprocedural EGD quality indicators.”
The authors pointed to a prospective study that evaluated whether an audit intervention helped in 10,000 consecutive EGDs. They found the audits “improved EGD report quality, such as justification for incompleteness or accurate lesion/segment description, regardless of the endoscopist’s experience documenting the report (specialist vs. trainee).” When audits were used in other studies to evaluate endoscopy overall performance (including EGD and colonoscopy) results showed similar improvement in important endpoints, the authors wrote. Additionally, “use of dictation templates has been demonstrated to improve the completeness of endoscopy report.”
A study led by the European Network for the Investigation of Gastrointestinal Mucosal Alterations found inconsistent compliance with EGD biopsy–sampling guidelines in patients with signs of gastric pathology, even in academic centers. The authors of that study recommended dedicated educational programs to raise awareness of which scenarios warrant gastric sampling during EGD.
The authors of the current study also acknowledge that many sound practices that likely improve quality, for instance time-outs or checklists for administering antibiotics during percutaneous feeding tube placement, are unlikely to be formally studied.
“Nevertheless, such practices should be encouraged and monitored,” they wrote.
“This document synthesizes practices and interventions that may allow for a high-quality upper endoscopy,” they concluded. “Furthermore, the scarcity of strong data to support interventions that can improve important quality indicators in upper-GI endoscopy should be seen as an opportunity.”
Several authors disclosed relationships with commercial interests, such as Boston Scientific, Salix, and Janssen. Dr. Buckles reports no relevant financial relationships.
One of the most common procedures in gastroenterology – esophagogastroduodenoscopy (EGD) – needs to consistently meet quality measures, but data on interventions to improve them is lacking, according to a recent review.
Researchers, led by Fateh Bazerbachi, MD, with CentraCare, Interventional Endoscopy Program, at St. Cloud (Minn.) Hospital performed a systematic review of the literature to identify which interventions and measures have improved the performance of EGD quality indicators previously identified by the American Society for Gastrointestinal Endoscopy. They also looked for demonstrations of improving compliance with the prioritized indicators. The review appeared in Gastrointestinal Endoscopy.
The authors pointed out that more than 6.1 million EGDs are performed every year in the United States. Although gastroenterologists perform most of them, other providers also perform them, including primary care physicians, surgeons, and sometimes advanced practice providers. Therefore, establishing well-defined quality measures is critical for consistent outcomes.
Daniel C. Buckles, MD, associate professor of gastroenterology, hepatology & motility at the University of Kansas Medical Center in Kansas City, who was not part of the review, said high-quality EGDs are critical for many reasons, including avoiding overuse when results of the procedure are not likely to change a patient’s treatment but add risk to the patient and increase costs to the health care system.
“Lack of training to recognize important GI pathology seen on an EGD and lack of standardized reporting of GI abnormalities using validated classification systems can lead to suboptimal treatment and follow-up for patients,” he noted.
Testing provider adherence to guidelines years after publication helps providers understand what works and can improve outcomes, Dr. Buckles said.
Dr. Buckles said that one of the highlights of the review was that researchers were able to confidently say that use of standardized checklists and frequent auditing had value in improving preprocedural and postprocedural quality indicators.
“The authors also concluded that focused educational interventions might improve endoscopists’ abilities to adhere to standardized Barrett’s esophagus examinations,” he added. “Unfortunately, the authors were not able to find much evidence for interventions that would improve intraprocedural EGD quality indicators.”
The authors pointed to a prospective study that evaluated whether an audit intervention helped in 10,000 consecutive EGDs. They found the audits “improved EGD report quality, such as justification for incompleteness or accurate lesion/segment description, regardless of the endoscopist’s experience documenting the report (specialist vs. trainee).” When audits were used in other studies to evaluate endoscopy overall performance (including EGD and colonoscopy) results showed similar improvement in important endpoints, the authors wrote. Additionally, “use of dictation templates has been demonstrated to improve the completeness of endoscopy report.”
A study led by the European Network for the Investigation of Gastrointestinal Mucosal Alterations found inconsistent compliance with EGD biopsy–sampling guidelines in patients with signs of gastric pathology, even in academic centers. The authors of that study recommended dedicated educational programs to raise awareness of which scenarios warrant gastric sampling during EGD.
The authors of the current study also acknowledge that many sound practices that likely improve quality, for instance time-outs or checklists for administering antibiotics during percutaneous feeding tube placement, are unlikely to be formally studied.
“Nevertheless, such practices should be encouraged and monitored,” they wrote.
“This document synthesizes practices and interventions that may allow for a high-quality upper endoscopy,” they concluded. “Furthermore, the scarcity of strong data to support interventions that can improve important quality indicators in upper-GI endoscopy should be seen as an opportunity.”
Several authors disclosed relationships with commercial interests, such as Boston Scientific, Salix, and Janssen. Dr. Buckles reports no relevant financial relationships.
One of the most common procedures in gastroenterology – esophagogastroduodenoscopy (EGD) – needs to consistently meet quality measures, but data on interventions to improve them is lacking, according to a recent review.
Researchers, led by Fateh Bazerbachi, MD, with CentraCare, Interventional Endoscopy Program, at St. Cloud (Minn.) Hospital performed a systematic review of the literature to identify which interventions and measures have improved the performance of EGD quality indicators previously identified by the American Society for Gastrointestinal Endoscopy. They also looked for demonstrations of improving compliance with the prioritized indicators. The review appeared in Gastrointestinal Endoscopy.
The authors pointed out that more than 6.1 million EGDs are performed every year in the United States. Although gastroenterologists perform most of them, other providers also perform them, including primary care physicians, surgeons, and sometimes advanced practice providers. Therefore, establishing well-defined quality measures is critical for consistent outcomes.
Daniel C. Buckles, MD, associate professor of gastroenterology, hepatology & motility at the University of Kansas Medical Center in Kansas City, who was not part of the review, said high-quality EGDs are critical for many reasons, including avoiding overuse when results of the procedure are not likely to change a patient’s treatment but add risk to the patient and increase costs to the health care system.
“Lack of training to recognize important GI pathology seen on an EGD and lack of standardized reporting of GI abnormalities using validated classification systems can lead to suboptimal treatment and follow-up for patients,” he noted.
Testing provider adherence to guidelines years after publication helps providers understand what works and can improve outcomes, Dr. Buckles said.
Dr. Buckles said that one of the highlights of the review was that researchers were able to confidently say that use of standardized checklists and frequent auditing had value in improving preprocedural and postprocedural quality indicators.
“The authors also concluded that focused educational interventions might improve endoscopists’ abilities to adhere to standardized Barrett’s esophagus examinations,” he added. “Unfortunately, the authors were not able to find much evidence for interventions that would improve intraprocedural EGD quality indicators.”
The authors pointed to a prospective study that evaluated whether an audit intervention helped in 10,000 consecutive EGDs. They found the audits “improved EGD report quality, such as justification for incompleteness or accurate lesion/segment description, regardless of the endoscopist’s experience documenting the report (specialist vs. trainee).” When audits were used in other studies to evaluate endoscopy overall performance (including EGD and colonoscopy) results showed similar improvement in important endpoints, the authors wrote. Additionally, “use of dictation templates has been demonstrated to improve the completeness of endoscopy report.”
A study led by the European Network for the Investigation of Gastrointestinal Mucosal Alterations found inconsistent compliance with EGD biopsy–sampling guidelines in patients with signs of gastric pathology, even in academic centers. The authors of that study recommended dedicated educational programs to raise awareness of which scenarios warrant gastric sampling during EGD.
The authors of the current study also acknowledge that many sound practices that likely improve quality, for instance time-outs or checklists for administering antibiotics during percutaneous feeding tube placement, are unlikely to be formally studied.
“Nevertheless, such practices should be encouraged and monitored,” they wrote.
“This document synthesizes practices and interventions that may allow for a high-quality upper endoscopy,” they concluded. “Furthermore, the scarcity of strong data to support interventions that can improve important quality indicators in upper-GI endoscopy should be seen as an opportunity.”
Several authors disclosed relationships with commercial interests, such as Boston Scientific, Salix, and Janssen. Dr. Buckles reports no relevant financial relationships.
FROM GASTROINTESTINAL ENDOSCOPY
FDA orders Juul to stop selling E-cigarettes
The marketing denial order covers all the company’s products in the United States, which means Juul must stop distributing the products and remove everything on the market. That includes the Juul device and flavor replacement pods in the tobacco and menthol flavors.
“Today’s action is further progress on the FDA’s commitment to ensuring that all e-cigarette and electronic nicotine delivery system products currently being marketed to consumers meet our public health standards,” Robert Califf, MD, the FDA commissioner, said in the announcement.
“The agency has dedicated significant resources to review products from the companies that account for most of the U.S. market,” he said. “We recognize these make up a significant part of the available products and many have played a disproportionate role in the rise in youth vaping.”
The marketing denial order covers only the commercial distribution and retail sale of Juul’s products and doesn’t restrict consumer possession or use. The FDA “cannot and will not” enforce actions against consumers, the agency said.
The order comes after a 2-year review of the company’s application seeking authorization to continue selling non–fruit-flavored products, such as menthol and tobacco. The FDA determined the application “lacked sufficient evidence regarding the toxicological profile of the products to demonstrate that marketing of the products would be appropriate for the protection of the public health.”
Some of Juul’s study findings raised concerns because of “insufficient and conflicting data,” the FDA said, including potentially harmful chemicals leaching from the Juul liquid replacement pods.
“To date, the FDA has not received clinical information to suggest an immediate hazard associated with the use of the JUUL device or JUUL pods,” the agency said. “However, the [orders] issued today reflect FDA’s determination that there is insufficient evidence to assess the potential toxicological risks of using the JUUL products.”
Juul is expected to appeal the FDA’s decision, according to The New York Times.
In recent years, the FDA has reviewed marketing applications from Juul and other e-cigarette companies as anti-tobacco groups have called for new rules to limit products that led to a surge in youth vaping during the past decade. At the same time, advocates of e-cigarettes and nicotine-delivery devices have said the products help adult smokers to quit cigarettes and other tobacco products.
Juul, in particular, has been blamed for fueling the surge in underage vaping due to fruity flavors and hip marketing, according to The Wall Street Journal. The company removed sweet and fruity flavors from shelves in 2019 and has been trying to repair its reputation by limiting its marketing and focusing on adult cigarette smokers.
In 2020, all e-cigarette manufacturers in the United States were required to submit their products for FDA review to stay on the market, the newspaper reported. The agency has been weighing the potential benefits for adult cigarette smokers against the harms for young people.
The FDA banned the sale of fruit- and mint-flavored cartridges and juice pods in 2020, but menthol and tobacco-flavored products were left on the market, according to USA Today. In September 2021, the agency also banned the sale of hundreds of thousands of vaping and e-cigarette products but didn’t rule on Juul.
Meanwhile, the FDA has cleared Reynolds American and NJOY Holdings – two of Juul’s biggest rivals – to keep tobacco-flavored products on the market. Industry experts expected Juul to receive similar clearance, the Journal reported.
Juul, which was at the top of the U.S. e-cigarette market in 2018, has moved to second place behind Reynolds’s Vuse brand, the newspaper reported. The United States represents most of the company’s revenue, though its products are also available in Canada, the United Kingdom, France, Italy, and the Philippines.
Underage vaping has fallen in the United States since federal restrictions raised the legal purchase age for tobacco products to 21 and banned the sale of sweet and fruity cartridges, according to the Journal. Juul’s popularity has also dropped among youth, with other products such as Puff Bar, Vuse, and Smok becoming more popular among e-cigarette users in high school.
In a separate decision announced this week, the FDA is also moving forward with a plan to reduce the amount of nicotine in cigarettes. The decision, which has been years in the making, is aimed at prompting millions of cigarette users to quit smoking or switch to alternatives such as e-cigarettes, as well as limit the number of users who pick up smoking at an early age.
A version of this article first appeared on WebMD.com .
The marketing denial order covers all the company’s products in the United States, which means Juul must stop distributing the products and remove everything on the market. That includes the Juul device and flavor replacement pods in the tobacco and menthol flavors.
“Today’s action is further progress on the FDA’s commitment to ensuring that all e-cigarette and electronic nicotine delivery system products currently being marketed to consumers meet our public health standards,” Robert Califf, MD, the FDA commissioner, said in the announcement.
“The agency has dedicated significant resources to review products from the companies that account for most of the U.S. market,” he said. “We recognize these make up a significant part of the available products and many have played a disproportionate role in the rise in youth vaping.”
The marketing denial order covers only the commercial distribution and retail sale of Juul’s products and doesn’t restrict consumer possession or use. The FDA “cannot and will not” enforce actions against consumers, the agency said.
The order comes after a 2-year review of the company’s application seeking authorization to continue selling non–fruit-flavored products, such as menthol and tobacco. The FDA determined the application “lacked sufficient evidence regarding the toxicological profile of the products to demonstrate that marketing of the products would be appropriate for the protection of the public health.”
Some of Juul’s study findings raised concerns because of “insufficient and conflicting data,” the FDA said, including potentially harmful chemicals leaching from the Juul liquid replacement pods.
“To date, the FDA has not received clinical information to suggest an immediate hazard associated with the use of the JUUL device or JUUL pods,” the agency said. “However, the [orders] issued today reflect FDA’s determination that there is insufficient evidence to assess the potential toxicological risks of using the JUUL products.”
Juul is expected to appeal the FDA’s decision, according to The New York Times.
In recent years, the FDA has reviewed marketing applications from Juul and other e-cigarette companies as anti-tobacco groups have called for new rules to limit products that led to a surge in youth vaping during the past decade. At the same time, advocates of e-cigarettes and nicotine-delivery devices have said the products help adult smokers to quit cigarettes and other tobacco products.
Juul, in particular, has been blamed for fueling the surge in underage vaping due to fruity flavors and hip marketing, according to The Wall Street Journal. The company removed sweet and fruity flavors from shelves in 2019 and has been trying to repair its reputation by limiting its marketing and focusing on adult cigarette smokers.
In 2020, all e-cigarette manufacturers in the United States were required to submit their products for FDA review to stay on the market, the newspaper reported. The agency has been weighing the potential benefits for adult cigarette smokers against the harms for young people.
The FDA banned the sale of fruit- and mint-flavored cartridges and juice pods in 2020, but menthol and tobacco-flavored products were left on the market, according to USA Today. In September 2021, the agency also banned the sale of hundreds of thousands of vaping and e-cigarette products but didn’t rule on Juul.
Meanwhile, the FDA has cleared Reynolds American and NJOY Holdings – two of Juul’s biggest rivals – to keep tobacco-flavored products on the market. Industry experts expected Juul to receive similar clearance, the Journal reported.
Juul, which was at the top of the U.S. e-cigarette market in 2018, has moved to second place behind Reynolds’s Vuse brand, the newspaper reported. The United States represents most of the company’s revenue, though its products are also available in Canada, the United Kingdom, France, Italy, and the Philippines.
Underage vaping has fallen in the United States since federal restrictions raised the legal purchase age for tobacco products to 21 and banned the sale of sweet and fruity cartridges, according to the Journal. Juul’s popularity has also dropped among youth, with other products such as Puff Bar, Vuse, and Smok becoming more popular among e-cigarette users in high school.
In a separate decision announced this week, the FDA is also moving forward with a plan to reduce the amount of nicotine in cigarettes. The decision, which has been years in the making, is aimed at prompting millions of cigarette users to quit smoking or switch to alternatives such as e-cigarettes, as well as limit the number of users who pick up smoking at an early age.
A version of this article first appeared on WebMD.com .
The marketing denial order covers all the company’s products in the United States, which means Juul must stop distributing the products and remove everything on the market. That includes the Juul device and flavor replacement pods in the tobacco and menthol flavors.
“Today’s action is further progress on the FDA’s commitment to ensuring that all e-cigarette and electronic nicotine delivery system products currently being marketed to consumers meet our public health standards,” Robert Califf, MD, the FDA commissioner, said in the announcement.
“The agency has dedicated significant resources to review products from the companies that account for most of the U.S. market,” he said. “We recognize these make up a significant part of the available products and many have played a disproportionate role in the rise in youth vaping.”
The marketing denial order covers only the commercial distribution and retail sale of Juul’s products and doesn’t restrict consumer possession or use. The FDA “cannot and will not” enforce actions against consumers, the agency said.
The order comes after a 2-year review of the company’s application seeking authorization to continue selling non–fruit-flavored products, such as menthol and tobacco. The FDA determined the application “lacked sufficient evidence regarding the toxicological profile of the products to demonstrate that marketing of the products would be appropriate for the protection of the public health.”
Some of Juul’s study findings raised concerns because of “insufficient and conflicting data,” the FDA said, including potentially harmful chemicals leaching from the Juul liquid replacement pods.
“To date, the FDA has not received clinical information to suggest an immediate hazard associated with the use of the JUUL device or JUUL pods,” the agency said. “However, the [orders] issued today reflect FDA’s determination that there is insufficient evidence to assess the potential toxicological risks of using the JUUL products.”
Juul is expected to appeal the FDA’s decision, according to The New York Times.
In recent years, the FDA has reviewed marketing applications from Juul and other e-cigarette companies as anti-tobacco groups have called for new rules to limit products that led to a surge in youth vaping during the past decade. At the same time, advocates of e-cigarettes and nicotine-delivery devices have said the products help adult smokers to quit cigarettes and other tobacco products.
Juul, in particular, has been blamed for fueling the surge in underage vaping due to fruity flavors and hip marketing, according to The Wall Street Journal. The company removed sweet and fruity flavors from shelves in 2019 and has been trying to repair its reputation by limiting its marketing and focusing on adult cigarette smokers.
In 2020, all e-cigarette manufacturers in the United States were required to submit their products for FDA review to stay on the market, the newspaper reported. The agency has been weighing the potential benefits for adult cigarette smokers against the harms for young people.
The FDA banned the sale of fruit- and mint-flavored cartridges and juice pods in 2020, but menthol and tobacco-flavored products were left on the market, according to USA Today. In September 2021, the agency also banned the sale of hundreds of thousands of vaping and e-cigarette products but didn’t rule on Juul.
Meanwhile, the FDA has cleared Reynolds American and NJOY Holdings – two of Juul’s biggest rivals – to keep tobacco-flavored products on the market. Industry experts expected Juul to receive similar clearance, the Journal reported.
Juul, which was at the top of the U.S. e-cigarette market in 2018, has moved to second place behind Reynolds’s Vuse brand, the newspaper reported. The United States represents most of the company’s revenue, though its products are also available in Canada, the United Kingdom, France, Italy, and the Philippines.
Underage vaping has fallen in the United States since federal restrictions raised the legal purchase age for tobacco products to 21 and banned the sale of sweet and fruity cartridges, according to the Journal. Juul’s popularity has also dropped among youth, with other products such as Puff Bar, Vuse, and Smok becoming more popular among e-cigarette users in high school.
In a separate decision announced this week, the FDA is also moving forward with a plan to reduce the amount of nicotine in cigarettes. The decision, which has been years in the making, is aimed at prompting millions of cigarette users to quit smoking or switch to alternatives such as e-cigarettes, as well as limit the number of users who pick up smoking at an early age.
A version of this article first appeared on WebMD.com .
Aging HIV patients face comorbidities and hospitalizations
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Thanks to effective treatment, people with HIV are living longer. But as they age, they face higher rates of age-related comorbidities and hospitalizations, according to a recent study of hospitalized patients.
Decision-makers will need to allocate resources, train providers, and plan ways to manage chronic diseases, such as diabetes and cancer, among geriatric HIV inpatients, according to the authors.
“There will be more [HIV] patients with age-related chronic conditions at an earlier age and who will utilize or will have a unique need for [health care for] these geriatric conditions,” first author Khairul A. Siddiqi, PhD, University of Florida, Gainesville, said in an interview. “Eventually, that may increase inpatient resource utilization and costs.”
The study was published online in HIV Medicine.
Aging with HIV
Analyzing the National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project, the authors compared characteristics and comorbidities linked to hospital stays among people with HIV (HSWH) to those linked to hospital stays among people without HIV (HSWOH).
The NIS is a database of hospital records that captures 20% of discharges in the United States and covers all payers. Data in this analysis covered the years 2003-2015.
Among HSWH, patients aged 50 or older accounted for an increasing proportion over time, from fewer than 25% in 2003 to over 50% by 2015, the authors found. The subgroup aged 65-80 had risen from 2.39% to 8.63% by 2015.
The authors also studied rates of eight comorbidities, termed HIV-associated non-AIDS (HANA) conditions: cardiovascular, lung, liver, neurologic, and kidney diseases; diabetes; cancer; and bone loss.
The average number of these conditions among both HSWH and HSWOH rose over time. But this change was disproportionately high among HSWH aged 50-64 and those aged 65 and older.
Over the study period, among patients aged 65 or older, six of the eight age-related conditions the researchers studied rose disproportionately among HSWH in comparison with HSWOH; among those aged 50-64, five conditions did so.
The researchers are now building on the current study of HSWH by examining rates of resource utilization, such as MRIs and procedures, Dr. Siddiqi said.
Study limitations included a lack of data from long-term facilities, potential skewing by patients hospitalized multiple times, and the inherent limitations of administrative data.
A unique group of older people
Among people with HIV (PWH) in the United States, nearly half are aged 50 or older. By 2030, this group is expected to account for some 70% of PWH.
“We need to pay attention to what we know about aging generally. It is also important to study aging in this special population, because we don’t necessarily know a lot about that,” Amy Justice, MD, PhD, professor of medicine and of public health at Yale University, New Haven, Conn., said in an interview. Dr. Justice was not involved in the study.
The HIV epidemic has disproportionately affected people of color, men who have sex with men, and people with a history of injection drug use, Dr. Justice said.
“We don’t know about aging with [a] past history of injection drug use. We don’t even know much about aging with hepatitis C, necessarily,” she said. “So there are lots of reasons to pay some attention to this population to try to optimize their care.”
In addition, compared with their non–HIV-affected counterparts, these individuals are more susceptible to HANA comorbidities. They may experience these conditions at a younger age or more severely. Chronic inflammation and polypharmacy may be to blame, said Dr. Justice.
Given the burden of comorbidities and polypharmacy in this patient population, Dr. Siddiqi said, policy makers will need to focus on developing chronic disease management interventions for them.
However, Dr. Justice added, the risk for multimorbidity is higher among people with HIV throughout the age cycle: “It’s not like I turn 50 with HIV and all of a sudden all the wheels come off. There are ways to successfully age with HIV.”
Geriatric HIV expertise needed
Dr. Justice called the study’s analysis a useful addition to the literature and noted its implications for training.
“One of the biggest challenges with this large bolus of folks who are aging with HIV,” she said, “is to what extent should they be cared for by the people who have been caring for them – largely infectious disease docs – and to what extent should we really be transitioning their care to people with more experience with aging.”
Another key question, Dr. Justice said, relates to nursing homes and assisted-living facilities, whose staff may lack experience caring for HIV patients. Training them and hospital-based providers is crucial, in part to avoid key errors, such as missed antiretroviral doses, she said: “We need to really think about how to get non-HIV providers up to speed.”
That may begin by simply making it clear that this population is here.
“A decade ago, HIV patients used to have a lower life expectancy, so all HIV studies used to use 50 years as the cutoff point for [the] older population,” Dr. Siddiqi said. “Now we know they’re living longer.”
Added Dr. Justice: “Previously, people thought aging and HIV were not coincident findings.”
The study was funded by the Office of the Vice President for Research at the University of South Carolina. The authors and Dr. Justice disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HIV MEDICINE
Study links sleep and objective, subjective cognition
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.

“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”

Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.
“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”
Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
CHARLOTTE, N.C. – , preliminary findings from a pilot study of objective and subjective cognitive measures have shown.
The pilot study underscored the important role of objective sleep measures to better understand discrepancies when patients’ own reports of everyday cognitive function don’t align with objective cognitive profiles, Amy Costa, MA, a graduate student in psychology at the University of Missouri-Columbia, said in reporting the results at the annual meeting of the Associated Professional Sleep Societies.
“Between our previously published paper and these new pilot results, we’re reporting evidence that suggests sleep is playing a role between the objective and subjective cognition relationship,” Ms. Costa said in an interview. “It is possible that these older adults who are sleeping poorly may be worse at understanding how well they’re doing cognitively. That’s really important for doctors. For example, if we can’t diagnose someone with mild cognitive impairment or Alzheimer’s disease or other types of dementia earlier, then we can’t intervene as quickly.”
Sleep efficiency, cognition, and patient complaints
These findings are in agreement with those Ms. Costa and colleagues recently published in the Journal of Clinical Sleep Medicine, she said.
The current pilot study included 35 older adults with an average age of 69 years who had insomnia complaints. They completed one night of home-based polysomnography – specifically with the Sleep Profiler PSG2TM – and a battery of cognitive tests. Their average sleep deficiency was 57%, “indicating potentially pretty severe insomnia,” Ms. Costa said.
“We found that sleep efficiency – that is the percentage of time spent sleeping while in bed – moderated the association between self reports and objective measures of cognitive distractibility,” Ms. Costa said in reporting the results. “In other words, our findings suggest that individuals with lower sleep efficiency who are performing the worst cognitively have the least amount of complaints. Basically, this can be thought of as that they are overestimating their cognitive performance.”
Sleep stage versus working memory and distractibility
The pilot study also focused on how the percentage of lighter-stage sleep, or N1 sleep, moderated the associations between working memory, as measured by Sternberg performance, and memory, distractibility, and blunders measured with the Cognitive Failures Questionnaire.
At the highest percentage of N1 sleep, worse working memory was associated with fewer complaints about memory, distractibility, and blunders, Ms. Costa said.
“The percentage of lighter-stage N1 sleep and sleep efficiency moderated the association between cognitive flexibility and distractibility,” Ms. Costa said. At the lowest percentage of N1 sleep, worse cognitive flexibility was associated with more distractibility, while at the highest percentage of N1 sleep worse cognitive flexibility showed a reverse effect; it was linked to less distractibility. The lowest percentage of sleep efficiency showed an association between worse cognitive flexibility and less distractibility, but the highest percentage of SE showed an association between worse cognitive flexibility and more distractibility.
“So in terms of evaluating their cognitive performance, the worse working memory was associated with more blunder complaints in individuals with the lowest percentage of N1,” she said. “So whenever individuals were spending less time in N1, they were able to better recognized their cognitive ability.”
She added, “Overall, more light and more fragmented sleep moderated the association between worse objective and less cognitive complaints, suggesting that these individuals might be overestimating their cognitive abilities.”
The findings indicate that evaluation of objective sleep should consider objectively measured N1 and sleep efficiency to better understand when subjective cognitive complaints and neurophysiological/objective cognitive profiles don’t align, she said.
Important indicators of cognitive deficits
“Specifically, for an older adult who comes into the clinic with complaints of waking up during the night, low sleep efficiency and more lighter-stage sleep might be really important indicators that they are probably not going to be the best at identifying their cognitive abilities or deficits,” she said.
Future directions for this research include collecting more data and looking at other sleep measures, such as using rapid-eye movement sleep, as potential moderators for the relationship between cognitive outcomes, evaluating sleep architecture more closely, and evaluating outcomes in a longitudinal study, Ms. Costa said.
The importance of objectively measured sleep
“Studies like this one using objectively measured sleep are important because much of the prior literature relied on self-reported sleep measures,” said Brendan P. Lucey, MD, associate professor of neurology and head of the sleep medicine section at Washington University School of Medicine in St. Louis. “This study suggests how objectively measured sleep may mediate discrepancies in objective/subjective cognitive dysfunction. Future studies need to work out if we need to add objective sleep measures when evaluating cognitive complaints in older adults.”
Dr. Lucey, who was not involved in the study, voiced one concern with the pilot study methodology the future research should address: the use of the Sleep Profiler PSG2TM to measure N1 sleep, which, as he noted, records a single-channel electroencephalogram over the forehead. “Scoring N1 sleep relies on attenuation of the alpha rhythm over the occipital region and the Sleep Profiler is not as accurate as in-lab polysomnography for this sleep stage,” he said.
The pilot study received funding from the American Academy of Sleep Medicine Foundation. Ms. Costa and her coauthors have no disclosures. Dr. Lucey disclosed relationships with Merck, Eli Lilly, Eisai, and Beacon Biosignals.
AT SLEEP 2022
Autoimmune disorder drugs top list of meds linked to headache
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.

Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.
Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
DENVER – in a federal side effect database that anyone can contribute to, according to a new study presented at the annual meeting of the American Headache Society.
“Surprising findings included the significant number of immunosuppressants and immunomodulators present in the data,” study lead author Brett Musialowicz, a medical student at Robert Wood Johnson Medical School, New Brunswich, N.J., said in an interview. “Additionally, our data provides evidence that suggests that several medications belonging to these drug classes were less likely to be associated with medication-induced headaches,” raising questions about the mechanism.
Drugs most frequently linked to headaches
The researchers launched their study to better understand headache as a side effect of medication use, Mr. Musialowicz said. They analyzed entries from the Food and Drug Administration’s Adverse Event Reporting System for the period from July 2018 to March 2020 and listed the top 30 most commonly reported medications linked to headaches and their reported odds ratio. According to a website devoted to pharmacovigilance training, ROR refers to “the odds of a certain event occurring with your medicinal product, compared with the odds of the same event occurring with all other medicinal products in the database.”
After generic and brand name data was consolidated, the drug most frequently linked to headaches was apremilast with 8,672 reports, followed by adalimumab (5,357), tofacitinib (4,276), fingolimod (4,123), and etanercept (4,111). These drugs treat autoimmune disorders such as psoriasis, multiple sclerosis, and Crohn’s disease.
The other drugs in the top 15 ranked by frequency are treatments for hepatitis C (4 drugs), pulmonary arterial hypertension (4 drugs), arthritis (1 drug), and asthma (1 drug).
Of the top 30 drugs most frequently linked to headaches, the pulmonary hypertension drug epoprostenol – ranked 23rd – had the highest ROR at 12.8. The next highest were the hepatitis C drugs glecaprevir and pibrentasvir, tied at 10th in the frequency analysis and both with an ROR of 9.4.
“Pulmonary arterial dilators and vasodilators are believed to cause headaches by sensitizing extracranial arteries. Clinical evidence suggests there a vascular component to some types of headache,” Mr. Musialowicz said. “Monoclonal antibodies are suggested to cause headache by means of an immune response. Several monoclonal antibodies are in trials targeting [the calcitonin gene-related peptide] receptor, which is believed to be involved in migraine headache. These trials will help further elucidate the mechanisms of headache and potential drugs to treat these conditions.”
Is the data useful?
Stewart Tepper, MD, a neurologist at Geisel School of Medicine at Dartmouth, Hanover, N.H., who’s familiar with the study findings, discounted the new research in an interview. He noted that any member of the public can contribute to the federal database of adverse effects (drug manufacturers are required to contribute to it), and the data says nothing about denominators.
“It’s not a reasonable way to evaluate adverse effects, to just have everyone and their uncle saying ‘This particular drug did this to me.’ It’s not in any way useful,” he said. However, he added that the database sometimes “gives you a bit of a signal so you can go back and try to get scientifically collected data.”
When asked to respond, study coauthor and neurologist Pengfei (Phil) Zhang, MD, of Robert Wood Johnson Medical School, noted that the FDA created the database “for a reason.” He also noted that the researchers used a statistical analysis technique – ROR – that was invented to adjust for weaknesses in databases.
No study funding is reported. Mr. Musialowicz reported no disclosures. Dr. Zhang has received honorarium from Alder Biopharmaceuticals, Board Vitals, and Fieve Clinical Research. He collaborates with Headache Science Incorporated without receiving financial support, and he has ownership interest in Cymbeline. Another author reports research grant support from the American Epilepsy Society and the New Jersey Health Foundation. Dr. Tepper reported multiple disclosures.
AT AHS 2022
Recommended headache treatments get mixed reception in EDs
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.

“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.
“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
DENVER – a new study finds. But the use of diphenhydramine (Benadryl) more than doubled even though guidelines caution against it, while recommended drugs such triptans and corticosteroids were rarely prescribed.
From 2007-2010 to 2015-2018, researchers reported at the annual meeting of the American Headache Society, a database reveals that opioid use in headache cases at EDs fell from 54% to 28%. Diphenhydramine use grew from 17% to 36% (both (P < .001). The percentage of cases in which EDs sought neuroimaging stayed stable at about 36%, a number that the study authors described as too high.
“Future studies are warranted to identify strategies to promote evidence-based treatments for headaches and appropriate outpatient referrals for follow-up and to reduce unnecessary neuroimaging orders in EDs,” lead author Seonkyeong Yang, MS, of the University of Florida, Gainesville, said in an interview.
Ms. Yang said researchers launched the study to update previous data in light of changes in opioid prescribing and the 2016 release of American Headache Society guidelines for the treatment of acute migraines in the ED setting. The research was published in the Journal of Clinical Medicine.
Headache treatment in the ED
For the study, researchers analyzed data from the U.S. National Hospital Ambulatory Medical Care survey and focused on adults who had a primary discharge diagnosis of headache.
For the 2015-2018 period, per weighted numbers, the survey encompassed 10.2 million headaches mostly among people younger than 50 (71%), female (73%), and White (73%). Migraines made up 33% of the total, with nonspecified headache accounting for almost all of the remainder (63%).
In 68% of cases, two or more medications were administered in the ED. This number rose to 83% among patients with migraine. But most of the time (54%), no medications were prescribed at discharge.
Among recommended medications, antiemetics – the most commonly used class of drugs in these patients – were prescribed 59% of the time in both 2007-2010 and 2015-2018 (P = .88). Usage of acetaminophens and NSAIDs grew from 37% to 52% over that time period.
Despite recommendations, the use of ergot alkaloids/triptans and corticosteroids remained low (less than 6% of the time).
“Several factors may contribute to the underuse of triptans in EDs, including their cardiovascular contraindications, ED physicians’ unfamiliarity with injectable triptans, higher costs, and treatment failures with triptans before ED visits,” Ms. Yang said. “We observed an upward trend in dexamethasone use over time. However, it was still underutilized. [The corticosteroid was only used 3.5% of the time from 2015-2018.] The 2016 AHS guideline strongly recommends dexamethasone use to prevent migraine recurrence after ED discharge. Identifying patients at high risk of headache recurrence for dexamethasone use may further improve patient outcomes of acute headache management in ED settings.”
Ms. Yang also reported that the use of diphenhydramine grew even though it’s not recommended. “Diphenhydramine is more likely to be used to prevent akathisia, a side effect of some antiemetics [that is, dopamine receptor antagonists] in headache-related ED visits,” she said. “However, the 2016 AHS guideline recommends against diphenhydramine use due to its limited efficacy in relieving headache pain. In addition, there is also conflicting evidence on diphenhydramine’s efficacy in preventing akathisia when coadministered with antiemetics. Diphenhydramine use requires caution due to its sedative effect and abuse potential.”
As for medication combinations, Ms. Yang said “the most broadly used therapy among headache-related ED visits in 2007-2010 was an opioid with an antiemetic (21.0%), which decreased to 6.6% in 2015-2018. Meanwhile, the combined use of acetaminophen/NSAIDs with antiemetic and diphenhydramine increased substantially from 3.9% to 15.7% and became the most prevalent therapy in 2015-2018. Opioid monotherapy use gradually decreased during the study period [from 8.8% to 1.9%].”
Evidence-based treatments underutilized
Commenting on the findings, New York University Langone neurologist and headache researcher Mia Tova Minen, MD, MPH, noted in an interview that AHS guidelines do not indicate acetaminophen/NSAIDs, diphenhydramine, and corticosteroids for the acute treatment of migraine. “The recommended treatments are sumatriptan subcutaneous, IV metoclopramide, and IV prochlorperazine. Steroids can be helpful in the prevention of migraine recurrence but not for the acute treatment of the migraine itself,” she said. “We need to ensure that patients with migraine get the top evidence-based treatments for migraine.”
As for diphenhydramine, she said it “is not a treatment for headache disorders. It does not have proven efficacy. It is sometimes given to reduce side effects of more acute treatments of headache, but it can make patients fatigued and keep them in the ED longer.”
Overuse of neuroimaging
Ms. Yang also highlighted study data about the frequency of neuroimaging. “Understandably, ED physicians do not want to miss any life-threatening secondary headaches like stroke,” she said. “However, other factors also contribute to the overuse of neuroimaging in headache-related ED visits: patient demands, financial incentives, a busy ED practice where clinical evaluation is replaced by tests, and ED physicians’ unfamiliarity with ICHD-3 diagnostic criteria for primary headache disorders. There is still much room for improvement in neuroimaging use for headaches in ED settings.”
For her part, Dr. Minen said scans are often performed reflexively and can be overused. “A CT scan is really only good in the case of acute trauma to rule out a fracture or a bleed or if there are signs of an emergent neurologic emergency like herniation or if a MRI is contraindicated. An MRI of the brain is typically the best test to examine brain tissue, though sometimes vessel imaging is also warranted. In the case of no red flags and a normal neurologic exam, the use of neuroimaging is low yield.”
The research has no funding. Ms. Yang and two other authors disclosed research funding from Merck. Dr. Minen reports no disclosures.
AT AHS 2022
Children and COVID: Vaccines now available to all ages
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.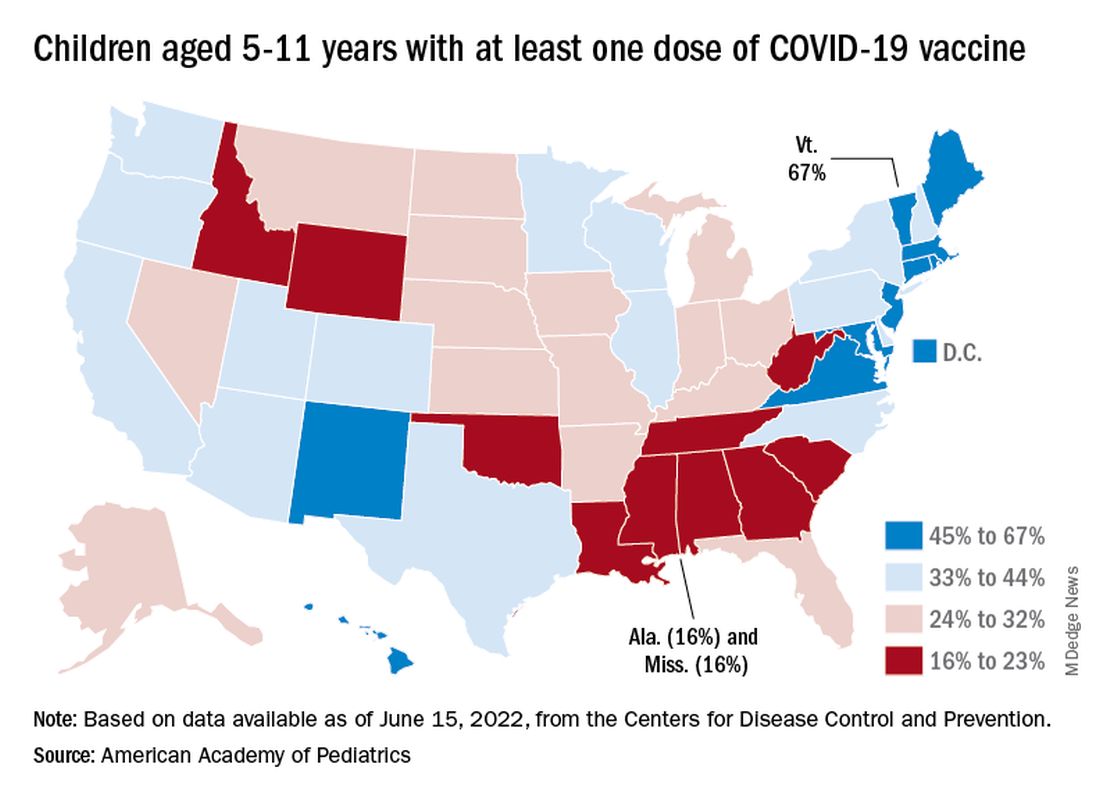
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.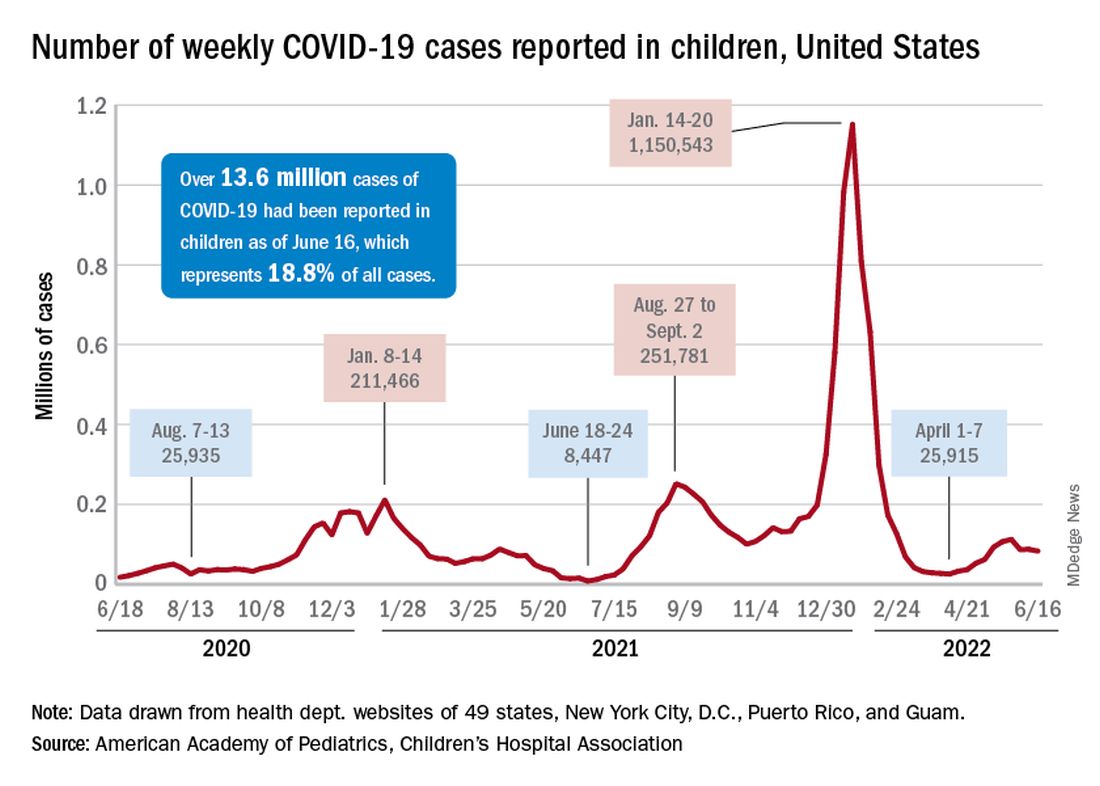
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
The COVID-19 prevention effort in children enters its next phase as June draws to a close, while new pediatric cases continued on a downward trend and hospitalizations continued to rise.
The COVID-19 vaccines from Pfizer-BioNTech and Moderna were approved for use in children as young as 6 months, the Centers for Disease Control and Prevention announced on June 18.
“We know millions of parents and caregivers are eager to get their young children vaccinated. ... I encourage parents and caregivers with questions to talk to their doctor, nurse, or local pharmacist to learn more about the benefits of vaccinations,” CDC Director Rochelle P. Walensky, MD, MPH, said in a written statement.
There are, however, indications that many parents are not that eager. Another 11% said “they will only do so if they are required,” Kaiser noted.
The vaccination experience with children aged 5-11 years seems to agree with those numbers. As of June 16, more than 7 months after the vaccine became available, just over 36% had received at least one dose and about 30% were fully vaccinated, CDC data show.
There are, according to the American Academy of Pediatrics, still five states where less than 20% of eligible 5- to 11-year-olds have received an initial vaccination. Among children aged 12-17, uptake has been much higher: 70% have received at least one dose and 60% are fully vaccinated, the CDC said.
Trends for new cases, hospitalizations diverging
COVID incidence in children, meanwhile, dropped for the second time in 3 weeks. There were 83,000 new cases reported during June 10-16, a decline of 4.8% from the previous week, according to the AAP and the Children’s Hospital Association.
New cases had risen by a very slight 0.31% during the week of June 3-9 after dropping 22% the week before (May 27 to June 2). Total cases in children have surpassed 13.6 million, which represents 18.8% of cases in all ages since the start of the pandemic, the AAP and CHA said in their weekly COVID report.
New admissions of children with confirmed COVID-19, however, have continued to climb since early to mid April. On June 16, the rate for children aged 0-17 years was up to 0.31 per 100,000, compared with the 0.13 per 100,000 recorded as late as April 11, the CDC said on its COVID Data Tracker.
Advance directives for psychiatric care reduce compulsory admissions
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
, new research shows.
Results of a randomized trial showed the peer worker PAD group had a 42% reduction in compulsory admission over the following 12 months. This study group also had lower symptom scores, greater rates of recovery, and increased empowerment, compared with patients assigned to usual care.
In addition to proving that PADs are effective in reducing compulsory admission, the results show that facilitation by peer workers is relevant, study investigator Aurélie Tinland, MD, PhD, Faculté de Médecine Timone, Aix-Marseille University, Marseille, France, told delegates attending the virtual European Psychiatric Association (EPA) 2022 Congress. The study was simultaneously published online in JAMA Psychiatry.
However, Dr. Tinland noted that more research that includes “harder to reach” populations is needed. In addition, greater use of PADs is also key to reducing compulsory admissions.
‘Most coercive’ country
The researchers note that respect for patient autonomy is a strong pillar of health care, such that “involuntary treatment should be unusual.” However, they point out that “compulsory psychiatric admissions are far too common in countries of all income levels.”
In France, said Dr. Tinland, 24% of psychiatric hospitalizations are compulsory. The country is ranked the sixth “most coercive” country in the world, and there are concerns about human rights in French psychiatric facilities.
She added that advance care statements are the most efficient tool for reducing coercion, with one study suggesting they could cut rates by 25%, compared with usual care.
However, she noted there is an “asymmetry” between medical professionals and patients and a risk of “undue influence” when clinicians facilitate the completion of care statements.
To examine the impact on clinical outcomes of peer-worker facilitated PADs, the researchers studied adults with a diagnosis of schizophrenia, bipolar I disorder, or schizoaffective disorder who were admitted to a psychiatric hospital within the previous 12 months. Peer workers are individuals who have lived experience with mental illness and help inform and guide current patients about care options in the event of a mental health crisis.
Study participants were randomly assigned 1:1 to an intervention group or a usual care control group. The intervention group received a PAD document and were assigned a peer worker while the usual care group received comprehensive information about the PAD concept at study entry and were free to complete it, but they were not connected with a peer worker.
The PAD document included information about future treatment and support preferences, early signs of relapse, and coping strategies. Participants could meet the peer worker in a place of their choice and be supported in drafting the document and in sharing it with health care professionals.
In all, 394 individuals completed the study. The majority (61%) of participants were male and 66% had completed post-secondary education. Schizophrenia was diagnosed in 45%, bipolar I disorder in 36%, and schizoaffective disorder in 19%.
Participants in the intervention group were significantly younger than those in the control group, with a mean of 37.4 years versus 41 years (P = .003) and were less likely to have one or more somatic comorbidities, at 61.2% versus 69.2%.
A PAD was completed by 54.6% of individuals in the intervention group versus 7.1% of controls (P < .001). The PAD was written with peer worker support by 41.3% of those in the intervention and by 2% of controls. Of those who completed a PAD, 75.7% met care facilitators, and 27.1% used it during a crisis over the following 12 months.
Results showed that the rate of compulsory admissions was significantly lower in the peer worker PAD group, at 27% versus 39.9% in control participants, at an odds ratio of 0.58 (P = .007).
Participants in the intervention group had lower symptoms on the modified Colorado Symptom Score than usual care patients with an effect size of -0.20 (P = .03) and higher scores on the Empowerment Scale (effect size 0.30, P = .003).
Scores on the Recovery Assessment Scale were also significantly higher in the peer worker PAD group versus controls with an effect size of 0.44 (P < .001). There were no significant differences, however, in overall admission rates, the quality of the therapeutic alliance, or quality of life.
Putting patients in the driver’s seat
Commenting on the findings, Robert Dabney Jr., MA, MDiv, peer apprentice program manager at the Depression and Bipolar Support Alliance, Chicago, said the study “tells us there are many benefits to completing a psychiatric advance directive, but perhaps the most powerful one is putting the person receiving mental health care in the driver’s seat of their own recovery.”
However, he noted that “many people living with mental health conditions don’t know the option exists to decide on their treatment plan in advance of a crisis.”
“This is where peer support specialists can come in. Having a peer who has been through similar experiences and can guide you through the process is as comforting as it is empowering. I have witnessed and experienced firsthand the power of peer support,” he said.
“It’s my personal hope and the goal of the Depression and Bipolar Support Alliance to empower more people to either become peer support specialists or seek out peer support services, because we know it improves and even saves lives,” Mr. Dabney added.
Virginia A. Brown, PhD, department of psychiatry & behavioral sciences, University of Texas at Austin Dell Medical School, noted there are huge differences between the health care systems in France and the United States.
She explained that two of the greatest barriers to PADs in the United States is that until 2016, filling one out was not billable and that “practitioners don’t know anything about advanced care plans.”
Dr. Brown said her own work shows that individuals who support patients during a crisis believe it would be “really helpful if we had some kind of document that we could share with the health care system that says: ‘Hey, look, I’m the designated person to speak for this patient, they’ve identified me through a document.’ So, people were actually describing a need for this document but didn’t know that it existed.”
Another problem is that in the United States, hospitals operate in a “closed system” and cannot talk to an unrelated hospital or to the police department “to get information to those first responders during an emergency about who to talk to about their wishes and preferences.”
“There are a lot of hurdles that we’ve got to get over to make a more robust system that protects the autonomy of people who live with serious mental illness,” Dr. Brown said, as “losing capacity during a crisis is time-limited, and it requires us to respond to it as a medical emergency.”
The study was supported by an institutional grant from the French 2017 National Program of Health Services Research. The Clinical Research Direction of Assistance Publique Hôpitaux de Marseille sponsored the trial. Dr. Tinland declares grants from the French Ministry of Health Directorate General of Health Care Services during the conduct of the study.
A version of this article first appeared on Medscape.com.
FROM EPA 2022
New saliva-based COVID-19 test provides rapid results
A rapid, saliva-based test for COVID-19 could enable testing, diagnosis, and prescribing to take place in a single office visit by immediately confirming whether a patient has the infection and needs to be treated, researchers say. The test has sparked commercial interest and earned additional funding from the Canadian government.
The test uses a DNA aptamer – a short, synthetic oligonucleotide that binds to a specific molecular target – that shows high affinity for the SARS-CoV-2 spike protein and its variants. The approach “can be rapidly adapted to different threats,” as well, Leyla Soleymani, PhD, an associate professor of engineering physics at McMaster University, Hamilton, Ontario, Canada, told this news organization. Her team invented the approach.
Adaptable to other pathogens
Current gold-standard COVID-19 tests are based on reverse transcription-polymerase chain reaction (RT-PCR), which are sensitive but costly, complicated, and require waiting at least a couple of days for results, according to Dr. Soleymani and colleagues. Rapid nucleic acid and antigen tests have only “moderate” sensitivity and specificity, particularly when viral loads are low. None have been shown to work well with saliva samples.
By contrast, the new test “uses a reader and test cartridges, similar to the glucose reader,” said Dr. Soleymani, who is also Canada Research chair in Miniaturized Biomedical Devices. A small sample of saliva is added to a chemical reagent and inserted into the reader, which is attached to a smartphone. Once commercialized, the point-of-care test is expected to be performed quickly in a physician’s office or in a clinic.
“The same reader can be applied to a variety of infectious diseases or infection panels by developing new cartridges,” Dr. Soleymani explained. “Noroviruses and bacteria such as C. difficile are on our list” to examine next.What’s more, she added, “this test is ideally positioned for settings where access to centralized labs is not possible, such as less developed countries.”
The team’s recent studies seem to support the promise. A study published last year in the international edition of Angewandte Chemie documents the development of the test, which at that point could detect wild-type SARS-CoV-2 and its Alpha and Delta variants in unprocessed saliva samples in 10 minutes with 80.5% sensitivity and 100% specificity.
This study was followed in January 2022 by a paper in Chemistry showing that the device also detected Alpha, Gamma, Epsilon, Kappa, and Omicron variants, demonstrating its potential for recognizing rapidly evolving targets such as those found in SARS-CoV-2.
In another demonstration of its versatility, the technology was recently adapted and successfully detected animal viruses from saliva samples.
Commercial and government funding
The findings prompted Zentek, an intellectual property development and commercialization company in Guelph, Ont., to license the technology, with plans to invest more than $1 million in the next 5 years to scale up production of the test components and adapt the technology for other forms of infection.
Furthermore, the collaborative efforts required to develop the test and move it forward gained funding from Canada’s Natural Sciences and Engineering Research Council, which is investing nearly $1.5 million in the form of two grants: $1 million to further streamline the technology development in preparation for the next pandemic and $488,440 (including $140,000 from Zentek) to get the current test to market as quickly as possible.
Meanwhile, Dr. Soleymani is urging clinicians “to be open to nontraditional diagnostic approaches even if the traditional tests do the job. Such tests are more rapid and can be used to enable personalized medicine. Our success relies on collaboration and support from clinicians.”
Further validation needed
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham and Women’s Hospital and the Harriet Ryan Albee Professor of Medicine at Harvard Medical School, Boston, commented on the study in response to a request from this news organization.
While “it’s always good to have more testing options available,” he said, “we don’t yet have very much information about performance characteristics of the test – that is, its sensitivity and specificity. I’d like to see the performance characteristics of this test compared to PCR tests and to the current rapid antigen tests using a large number of patient samples with currently circulating variants, and tests over time to see how soon tests become positive after symptom onset and for how long they remain positive.”
“Further validation studies and emergency use authorization or approval by regulatory authorities are needed before we will see this test implemented in the field,” Dr. Kuritzkes concluded.
A version of this article first appeared on Medscape.com.
A rapid, saliva-based test for COVID-19 could enable testing, diagnosis, and prescribing to take place in a single office visit by immediately confirming whether a patient has the infection and needs to be treated, researchers say. The test has sparked commercial interest and earned additional funding from the Canadian government.
The test uses a DNA aptamer – a short, synthetic oligonucleotide that binds to a specific molecular target – that shows high affinity for the SARS-CoV-2 spike protein and its variants. The approach “can be rapidly adapted to different threats,” as well, Leyla Soleymani, PhD, an associate professor of engineering physics at McMaster University, Hamilton, Ontario, Canada, told this news organization. Her team invented the approach.
Adaptable to other pathogens
Current gold-standard COVID-19 tests are based on reverse transcription-polymerase chain reaction (RT-PCR), which are sensitive but costly, complicated, and require waiting at least a couple of days for results, according to Dr. Soleymani and colleagues. Rapid nucleic acid and antigen tests have only “moderate” sensitivity and specificity, particularly when viral loads are low. None have been shown to work well with saliva samples.
By contrast, the new test “uses a reader and test cartridges, similar to the glucose reader,” said Dr. Soleymani, who is also Canada Research chair in Miniaturized Biomedical Devices. A small sample of saliva is added to a chemical reagent and inserted into the reader, which is attached to a smartphone. Once commercialized, the point-of-care test is expected to be performed quickly in a physician’s office or in a clinic.
“The same reader can be applied to a variety of infectious diseases or infection panels by developing new cartridges,” Dr. Soleymani explained. “Noroviruses and bacteria such as C. difficile are on our list” to examine next.What’s more, she added, “this test is ideally positioned for settings where access to centralized labs is not possible, such as less developed countries.”
The team’s recent studies seem to support the promise. A study published last year in the international edition of Angewandte Chemie documents the development of the test, which at that point could detect wild-type SARS-CoV-2 and its Alpha and Delta variants in unprocessed saliva samples in 10 minutes with 80.5% sensitivity and 100% specificity.
This study was followed in January 2022 by a paper in Chemistry showing that the device also detected Alpha, Gamma, Epsilon, Kappa, and Omicron variants, demonstrating its potential for recognizing rapidly evolving targets such as those found in SARS-CoV-2.
In another demonstration of its versatility, the technology was recently adapted and successfully detected animal viruses from saliva samples.
Commercial and government funding
The findings prompted Zentek, an intellectual property development and commercialization company in Guelph, Ont., to license the technology, with plans to invest more than $1 million in the next 5 years to scale up production of the test components and adapt the technology for other forms of infection.
Furthermore, the collaborative efforts required to develop the test and move it forward gained funding from Canada’s Natural Sciences and Engineering Research Council, which is investing nearly $1.5 million in the form of two grants: $1 million to further streamline the technology development in preparation for the next pandemic and $488,440 (including $140,000 from Zentek) to get the current test to market as quickly as possible.
Meanwhile, Dr. Soleymani is urging clinicians “to be open to nontraditional diagnostic approaches even if the traditional tests do the job. Such tests are more rapid and can be used to enable personalized medicine. Our success relies on collaboration and support from clinicians.”
Further validation needed
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham and Women’s Hospital and the Harriet Ryan Albee Professor of Medicine at Harvard Medical School, Boston, commented on the study in response to a request from this news organization.
While “it’s always good to have more testing options available,” he said, “we don’t yet have very much information about performance characteristics of the test – that is, its sensitivity and specificity. I’d like to see the performance characteristics of this test compared to PCR tests and to the current rapid antigen tests using a large number of patient samples with currently circulating variants, and tests over time to see how soon tests become positive after symptom onset and for how long they remain positive.”
“Further validation studies and emergency use authorization or approval by regulatory authorities are needed before we will see this test implemented in the field,” Dr. Kuritzkes concluded.
A version of this article first appeared on Medscape.com.
A rapid, saliva-based test for COVID-19 could enable testing, diagnosis, and prescribing to take place in a single office visit by immediately confirming whether a patient has the infection and needs to be treated, researchers say. The test has sparked commercial interest and earned additional funding from the Canadian government.
The test uses a DNA aptamer – a short, synthetic oligonucleotide that binds to a specific molecular target – that shows high affinity for the SARS-CoV-2 spike protein and its variants. The approach “can be rapidly adapted to different threats,” as well, Leyla Soleymani, PhD, an associate professor of engineering physics at McMaster University, Hamilton, Ontario, Canada, told this news organization. Her team invented the approach.
Adaptable to other pathogens
Current gold-standard COVID-19 tests are based on reverse transcription-polymerase chain reaction (RT-PCR), which are sensitive but costly, complicated, and require waiting at least a couple of days for results, according to Dr. Soleymani and colleagues. Rapid nucleic acid and antigen tests have only “moderate” sensitivity and specificity, particularly when viral loads are low. None have been shown to work well with saliva samples.
By contrast, the new test “uses a reader and test cartridges, similar to the glucose reader,” said Dr. Soleymani, who is also Canada Research chair in Miniaturized Biomedical Devices. A small sample of saliva is added to a chemical reagent and inserted into the reader, which is attached to a smartphone. Once commercialized, the point-of-care test is expected to be performed quickly in a physician’s office or in a clinic.
“The same reader can be applied to a variety of infectious diseases or infection panels by developing new cartridges,” Dr. Soleymani explained. “Noroviruses and bacteria such as C. difficile are on our list” to examine next.What’s more, she added, “this test is ideally positioned for settings where access to centralized labs is not possible, such as less developed countries.”
The team’s recent studies seem to support the promise. A study published last year in the international edition of Angewandte Chemie documents the development of the test, which at that point could detect wild-type SARS-CoV-2 and its Alpha and Delta variants in unprocessed saliva samples in 10 minutes with 80.5% sensitivity and 100% specificity.
This study was followed in January 2022 by a paper in Chemistry showing that the device also detected Alpha, Gamma, Epsilon, Kappa, and Omicron variants, demonstrating its potential for recognizing rapidly evolving targets such as those found in SARS-CoV-2.
In another demonstration of its versatility, the technology was recently adapted and successfully detected animal viruses from saliva samples.
Commercial and government funding
The findings prompted Zentek, an intellectual property development and commercialization company in Guelph, Ont., to license the technology, with plans to invest more than $1 million in the next 5 years to scale up production of the test components and adapt the technology for other forms of infection.
Furthermore, the collaborative efforts required to develop the test and move it forward gained funding from Canada’s Natural Sciences and Engineering Research Council, which is investing nearly $1.5 million in the form of two grants: $1 million to further streamline the technology development in preparation for the next pandemic and $488,440 (including $140,000 from Zentek) to get the current test to market as quickly as possible.
Meanwhile, Dr. Soleymani is urging clinicians “to be open to nontraditional diagnostic approaches even if the traditional tests do the job. Such tests are more rapid and can be used to enable personalized medicine. Our success relies on collaboration and support from clinicians.”
Further validation needed
Daniel Kuritzkes, MD, chief of infectious diseases at Brigham and Women’s Hospital and the Harriet Ryan Albee Professor of Medicine at Harvard Medical School, Boston, commented on the study in response to a request from this news organization.
While “it’s always good to have more testing options available,” he said, “we don’t yet have very much information about performance characteristics of the test – that is, its sensitivity and specificity. I’d like to see the performance characteristics of this test compared to PCR tests and to the current rapid antigen tests using a large number of patient samples with currently circulating variants, and tests over time to see how soon tests become positive after symptom onset and for how long they remain positive.”
“Further validation studies and emergency use authorization or approval by regulatory authorities are needed before we will see this test implemented in the field,” Dr. Kuritzkes concluded.
A version of this article first appeared on Medscape.com.
Biden moves to limit nicotine levels in cigarettes
The Department of Health and Human Services posted a notice that details plans for a new rule to create a maximum allowed amount of nicotine in certain tobacco products. The Food and Drug Administration would take the action, the notice said, “to reduce addictiveness to certain tobacco products, thus giving addicted users a greater ability to quit.” The product standard would also help keep nonsmokers interested in trying tobacco, mainly youth, from starting to smoke and become regulars.
“Lowering nicotine levels to minimally addictive or non-addictive levels would decrease the likelihood that future generations of young people become addicted to cigarettes and help more currently addicted smokers to quit,” FDA Commissioner Robert Califf, MD, said in a statement.
The FDA, in charge of regulating cigarettes, issues a proposed rule when changes are discussed. That would be followed by a period for public comments before a final rule could be issued.
The proposed rule was first reported by The Washington Post.
The FDA in 2018 published a study in the New England Journal of Medicine that estimated that a potential limit on nicotine in cigarettes could, by the year 2100, prevent more than 33 million people from becoming regular smokers, and prevent the deaths of more than 8 million people from tobacco-related illnesses.
The action to reduce nicotine levels would fit in with President Joe Biden’s goal of reducing cancer death rates by half over 25 years. Each year, according to the American Cancer Society, about 480,000 deaths (about 1 in 5) are related to smoking. Currently, about 34 million American adults still smoke cigarettes.
Matthew Myers, president of the Campaign for Tobacco-Free Kids, called the proposed rule a “truly game-changing proposal.”
“There is no other single action our country can take that would prevent more young people from becoming addicted to tobacco or have a greater impact on reducing deaths from cancer, cardiovascular disease and respiratory disease,” Mr. Myers said in a statement.
However, he said, “these gains will only be realized if the administration and the FDA demonstrate a full-throated commitment to finalizing and implementing this proposal.”
The FDA proposed the nicotine reduction strategy in talks with the White House and the Department of Health and Human Services early in 2021, according to the Post.
Earlier this year, the FDA issued a proposed rule to ban menthol flavoring in cigarettes. The agency is accepting public comments though July 5.
The action of reducing nicotine levels would likely take years to complete, Mitch Zeller, JD, recently retired director of the FDA Center for Tobacco Products, told the Post.
In 2018, the FDA issued a proposed ruling to set a standard for maximum nicotine levels in cigarettes.
Advocates say the action of slashing nicotine, the active – and addictive – ingredient in cigarettes, would save millions of lives for generations to come. Opponents liken it to the prohibition of alcohol in the 1920s and predict the action will fail.
Others say that if limits are put on nicotine levels, adults should have greater access to noncombustible alternatives.
A version of this article first appeared on WebMD.com.
The Department of Health and Human Services posted a notice that details plans for a new rule to create a maximum allowed amount of nicotine in certain tobacco products. The Food and Drug Administration would take the action, the notice said, “to reduce addictiveness to certain tobacco products, thus giving addicted users a greater ability to quit.” The product standard would also help keep nonsmokers interested in trying tobacco, mainly youth, from starting to smoke and become regulars.
“Lowering nicotine levels to minimally addictive or non-addictive levels would decrease the likelihood that future generations of young people become addicted to cigarettes and help more currently addicted smokers to quit,” FDA Commissioner Robert Califf, MD, said in a statement.
The FDA, in charge of regulating cigarettes, issues a proposed rule when changes are discussed. That would be followed by a period for public comments before a final rule could be issued.
The proposed rule was first reported by The Washington Post.
The FDA in 2018 published a study in the New England Journal of Medicine that estimated that a potential limit on nicotine in cigarettes could, by the year 2100, prevent more than 33 million people from becoming regular smokers, and prevent the deaths of more than 8 million people from tobacco-related illnesses.
The action to reduce nicotine levels would fit in with President Joe Biden’s goal of reducing cancer death rates by half over 25 years. Each year, according to the American Cancer Society, about 480,000 deaths (about 1 in 5) are related to smoking. Currently, about 34 million American adults still smoke cigarettes.
Matthew Myers, president of the Campaign for Tobacco-Free Kids, called the proposed rule a “truly game-changing proposal.”
“There is no other single action our country can take that would prevent more young people from becoming addicted to tobacco or have a greater impact on reducing deaths from cancer, cardiovascular disease and respiratory disease,” Mr. Myers said in a statement.
However, he said, “these gains will only be realized if the administration and the FDA demonstrate a full-throated commitment to finalizing and implementing this proposal.”
The FDA proposed the nicotine reduction strategy in talks with the White House and the Department of Health and Human Services early in 2021, according to the Post.
Earlier this year, the FDA issued a proposed rule to ban menthol flavoring in cigarettes. The agency is accepting public comments though July 5.
The action of reducing nicotine levels would likely take years to complete, Mitch Zeller, JD, recently retired director of the FDA Center for Tobacco Products, told the Post.
In 2018, the FDA issued a proposed ruling to set a standard for maximum nicotine levels in cigarettes.
Advocates say the action of slashing nicotine, the active – and addictive – ingredient in cigarettes, would save millions of lives for generations to come. Opponents liken it to the prohibition of alcohol in the 1920s and predict the action will fail.
Others say that if limits are put on nicotine levels, adults should have greater access to noncombustible alternatives.
A version of this article first appeared on WebMD.com.
The Department of Health and Human Services posted a notice that details plans for a new rule to create a maximum allowed amount of nicotine in certain tobacco products. The Food and Drug Administration would take the action, the notice said, “to reduce addictiveness to certain tobacco products, thus giving addicted users a greater ability to quit.” The product standard would also help keep nonsmokers interested in trying tobacco, mainly youth, from starting to smoke and become regulars.
“Lowering nicotine levels to minimally addictive or non-addictive levels would decrease the likelihood that future generations of young people become addicted to cigarettes and help more currently addicted smokers to quit,” FDA Commissioner Robert Califf, MD, said in a statement.
The FDA, in charge of regulating cigarettes, issues a proposed rule when changes are discussed. That would be followed by a period for public comments before a final rule could be issued.
The proposed rule was first reported by The Washington Post.
The FDA in 2018 published a study in the New England Journal of Medicine that estimated that a potential limit on nicotine in cigarettes could, by the year 2100, prevent more than 33 million people from becoming regular smokers, and prevent the deaths of more than 8 million people from tobacco-related illnesses.
The action to reduce nicotine levels would fit in with President Joe Biden’s goal of reducing cancer death rates by half over 25 years. Each year, according to the American Cancer Society, about 480,000 deaths (about 1 in 5) are related to smoking. Currently, about 34 million American adults still smoke cigarettes.
Matthew Myers, president of the Campaign for Tobacco-Free Kids, called the proposed rule a “truly game-changing proposal.”
“There is no other single action our country can take that would prevent more young people from becoming addicted to tobacco or have a greater impact on reducing deaths from cancer, cardiovascular disease and respiratory disease,” Mr. Myers said in a statement.
However, he said, “these gains will only be realized if the administration and the FDA demonstrate a full-throated commitment to finalizing and implementing this proposal.”
The FDA proposed the nicotine reduction strategy in talks with the White House and the Department of Health and Human Services early in 2021, according to the Post.
Earlier this year, the FDA issued a proposed rule to ban menthol flavoring in cigarettes. The agency is accepting public comments though July 5.
The action of reducing nicotine levels would likely take years to complete, Mitch Zeller, JD, recently retired director of the FDA Center for Tobacco Products, told the Post.
In 2018, the FDA issued a proposed ruling to set a standard for maximum nicotine levels in cigarettes.
Advocates say the action of slashing nicotine, the active – and addictive – ingredient in cigarettes, would save millions of lives for generations to come. Opponents liken it to the prohibition of alcohol in the 1920s and predict the action will fail.
Others say that if limits are put on nicotine levels, adults should have greater access to noncombustible alternatives.
A version of this article first appeared on WebMD.com.