User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Children and COVID: New cases hold steady in nonholiday week
The new-case count for the most recent reporting week – 87,644 for June 3-9 – did go up from the previous week, but by only 270 cases, the American Academy of Pediatrics and Children’s Hospital Association said in their weekly COVID report. That’s just 0.31% higher than a week ago and probably is affected by reduced testing and reporting because of Memorial Day, as the AAP and CHA noted earlier.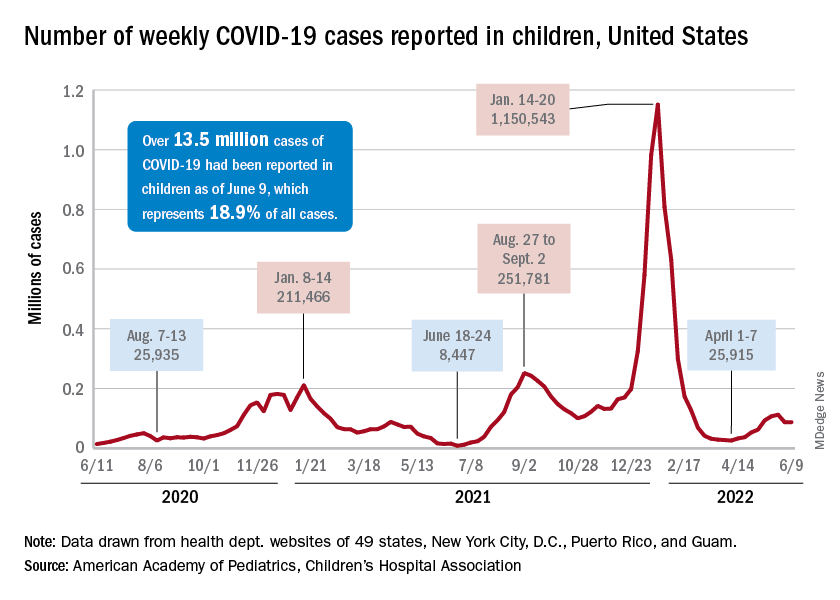
That hint of a continued decline accompanies the latest trend for new cases for all age groups: They have leveled out over the last month, with the moving 7-day daily average hovering around 100,000-110,000 since mid-May, data from the Centers for Disease Control and Prevention show.
The Food and Drug Administration, meanwhile, is in the news this week as two of its advisory panels take the next steps toward pediatric approvals of vaccines from Pfizer/BioNTtech and Moderna. The panels could advance the approvals of the Pfizer vaccine for children under the age of 5 years and the Moderna vaccine for children aged 6 months to 17 years.
Matthew Harris, MD, medical director of the COVID-19 vaccination program for Northwell Health in New Hyde Park, N.Y., emphasized the importance of vaccinations, as well as the continued challenge of convincing parents to get the shots for eligible children. “We still have a long way to go for primary vaccines and boosters for children 5 years and above,” he said in an interview.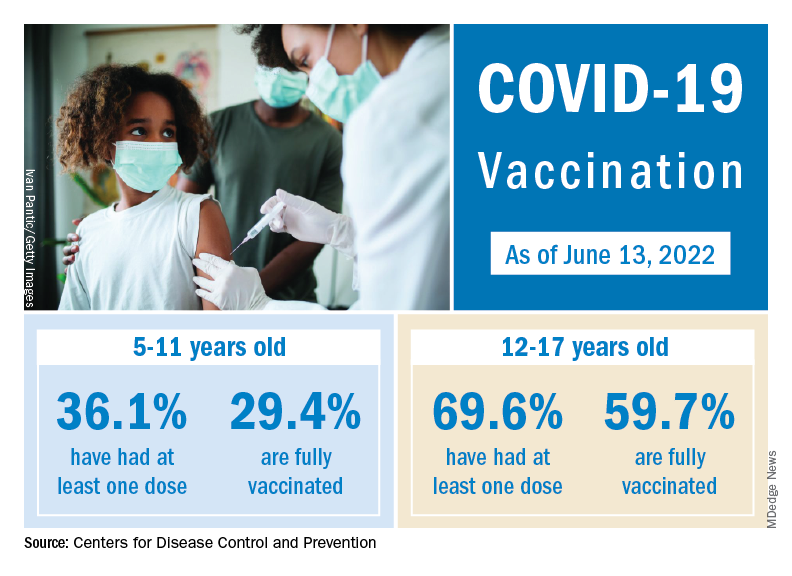
The vaccination effort against COVID-19 has stalled somewhat as interest has waned since the Omicron surge. Weekly initial vaccinations for children aged 5-11 years, which topped 100,000 as recently as mid-March, have been about 43,000 a week for the last 3 weeks, while 12- to 17-year-olds had around 27,000 or 28,000 initial vaccinations per week over that span, the AAP said in a separate report.
The latest data available from the CDC show that overall vaccine coverage levels for the younger group are only about half those of the 12- to 17-year-olds, both in terms of initial doses and completions. The 5- to 11-year-olds are not eligible for boosters yet, but 26.5% of the older children had received one as of June 13, according to the CDC’s COVID Data Tracker.
The new-case count for the most recent reporting week – 87,644 for June 3-9 – did go up from the previous week, but by only 270 cases, the American Academy of Pediatrics and Children’s Hospital Association said in their weekly COVID report. That’s just 0.31% higher than a week ago and probably is affected by reduced testing and reporting because of Memorial Day, as the AAP and CHA noted earlier.
That hint of a continued decline accompanies the latest trend for new cases for all age groups: They have leveled out over the last month, with the moving 7-day daily average hovering around 100,000-110,000 since mid-May, data from the Centers for Disease Control and Prevention show.
The Food and Drug Administration, meanwhile, is in the news this week as two of its advisory panels take the next steps toward pediatric approvals of vaccines from Pfizer/BioNTtech and Moderna. The panels could advance the approvals of the Pfizer vaccine for children under the age of 5 years and the Moderna vaccine for children aged 6 months to 17 years.
Matthew Harris, MD, medical director of the COVID-19 vaccination program for Northwell Health in New Hyde Park, N.Y., emphasized the importance of vaccinations, as well as the continued challenge of convincing parents to get the shots for eligible children. “We still have a long way to go for primary vaccines and boosters for children 5 years and above,” he said in an interview.
The vaccination effort against COVID-19 has stalled somewhat as interest has waned since the Omicron surge. Weekly initial vaccinations for children aged 5-11 years, which topped 100,000 as recently as mid-March, have been about 43,000 a week for the last 3 weeks, while 12- to 17-year-olds had around 27,000 or 28,000 initial vaccinations per week over that span, the AAP said in a separate report.
The latest data available from the CDC show that overall vaccine coverage levels for the younger group are only about half those of the 12- to 17-year-olds, both in terms of initial doses and completions. The 5- to 11-year-olds are not eligible for boosters yet, but 26.5% of the older children had received one as of June 13, according to the CDC’s COVID Data Tracker.
The new-case count for the most recent reporting week – 87,644 for June 3-9 – did go up from the previous week, but by only 270 cases, the American Academy of Pediatrics and Children’s Hospital Association said in their weekly COVID report. That’s just 0.31% higher than a week ago and probably is affected by reduced testing and reporting because of Memorial Day, as the AAP and CHA noted earlier.
That hint of a continued decline accompanies the latest trend for new cases for all age groups: They have leveled out over the last month, with the moving 7-day daily average hovering around 100,000-110,000 since mid-May, data from the Centers for Disease Control and Prevention show.
The Food and Drug Administration, meanwhile, is in the news this week as two of its advisory panels take the next steps toward pediatric approvals of vaccines from Pfizer/BioNTtech and Moderna. The panels could advance the approvals of the Pfizer vaccine for children under the age of 5 years and the Moderna vaccine for children aged 6 months to 17 years.
Matthew Harris, MD, medical director of the COVID-19 vaccination program for Northwell Health in New Hyde Park, N.Y., emphasized the importance of vaccinations, as well as the continued challenge of convincing parents to get the shots for eligible children. “We still have a long way to go for primary vaccines and boosters for children 5 years and above,” he said in an interview.
The vaccination effort against COVID-19 has stalled somewhat as interest has waned since the Omicron surge. Weekly initial vaccinations for children aged 5-11 years, which topped 100,000 as recently as mid-March, have been about 43,000 a week for the last 3 weeks, while 12- to 17-year-olds had around 27,000 or 28,000 initial vaccinations per week over that span, the AAP said in a separate report.
The latest data available from the CDC show that overall vaccine coverage levels for the younger group are only about half those of the 12- to 17-year-olds, both in terms of initial doses and completions. The 5- to 11-year-olds are not eligible for boosters yet, but 26.5% of the older children had received one as of June 13, according to the CDC’s COVID Data Tracker.
Surgery during a pandemic? COVID vaccination status matters – or not
An online survey captured mixed information about people’s willingness to undergo surgery during a viral pandemic in relation to the vaccine status of the patient and staff. The findings showcase opportunities for public education and “skillful messaging,” researchers report.
In survey scenarios that asked people to imagine their vaccination status, people were more willing to undergo surgery if it was lifesaving, rather than elective, especially if vaccinated. The prospect of no hospital stay tipped the scales further toward surgery. The vaccination status of hospital staff played only a minor role in decision making, according to the study, which was published in Vaccine.
But as a post hoc analysis revealed, it was participants who were not vaccinated against COVID-19 in real life who were more willing to undergo surgery, compared with those who had one or two shots.
In either case, too many people were unwilling to undergo lifesaving surgery, even though the risk of hospital-acquired COVID-19 is low. “Making this choice for an actual health problem would result in an unacceptably high rate of potential morbidity attributable to pandemic-related fears, the authors wrote.
In an unusual approach, the researchers used Amazon’s Mechanical Turk to electronically recruit 2,006 adults. The participants answered a 26-item survey about a hypothetical surgery in an unnamed pandemic with different combinations of vaccine status for patient and staff.
Coauthor and anesthesiologist Keith J. Ruskin, MD, of the University of Chicago, told this news organization that they “wanted to make this timeless” and independent of COVID “so that when the next thing came about, the paper would still be relevant.”
The researchers were surprised by the findings at the extreme ends of attitudes toward surgery. Some were still willing to have elective surgery with (hypothetically) unvaccinated patients and staff.
“And people at the other end, even though they are vaccinated, the hospital staff is vaccinated, and the surgery is lifesaving, they absolutely won’t have surgery,” Dr. Ruskin said.
He viewed these two groups as opportunities for education. “You can present information in the most positive light to get them to do the right thing with what’s best for themselves,” he said.
As an example, Dr. Ruskin pointed to an ad in Illinois. “It’s not only people saying I’m getting vaccinated for myself and my family, but there are people who said I got vaccinated and I still got COVID, but it could have been much worse. Please, if you’re on the fence, just get vaccinated,” he said.
Coauthor Anna Clebone Ruskin, MD, an anesthesiologist at the University of Chicago, said, “Humans are programmed to see things in extremes. With surgery, people tend to think of surgery as a monolith – surgery is all good, or surgery is all bad, where there is a huge in between. So we saw those extremes. ... Seeing that dichotomy with people on either end was pretty surprising.
“Getting surgery is not always good. Getting surgery is not always bad. It’s a risk-versus-benefit analysis and educating the public to consider the risks and benefits of medical decisions, in general, would be enormously beneficial,” she said.
A post hoc analysis found that “participants who were not actually vaccinated against COVID-19 were generally more willing to undergo surgery compared to those who had one vaccination or two vaccinations,” the authors wrote.
In a second post hoc finding, participants who reported high wariness of vaccines were generally more likely to be willing to undergo surgery. Notably, 15% of participants “were unwilling to undergo lifesaving surgery during a pandemic even when they and the health care staff were vaccinated,” the authors wrote.
Dr. Keith J. Ruskin hypothesized about this result, saying, “What we think is that potentially actually getting vaccinated against COVID-19 may indicate that you have a lower risk tolerance. So you may be less likely to do anything you perceive to be risky if you’re vaccinated against COVID-19.”
The authors stated that “the risk of hospital-acquired COVID-19 even prior to vaccination is vanishingly small.” The risk of nosocomial COVID varies among different studies. An EPIC-based study between April 2020 and October 2021 found the risk to be 1.8%; EPIC describes the fears of a patient catching COVID at a hospital as “likely unfounded.”
In the United Kingdom, the risk was as high as 24% earlier in the pandemic and then declined to approximately 5% a year ago. Omicron also brought more infections. Rates varied significantly among hospitals – and, notably, the risk of death from a nosocomial COVID infection was 21% in April-September 2020.
Emily Landon, MD, an epidemiologist and executive medical director for infection prevention and control at the University of Chicago Medicine, told this news organization that the study’s data were collected during Delta, a “time when we thought that this was a pandemic of the unvaccinated. But there was serious politicization of the vaccine.”
Dr. Landon said one of the study’s strengths was the large number of participants. A limitation was, “You’re going to have less participants who are generally poor and indigent, and fewer old participants, probably because they’re less likely to respond to an online survey.
“But the most interesting results are that people who were wary of vaccines or who hadn’t been vaccinated, were much more willing to undergo surgical procedures in the time of a pandemic, regardless of status, which reflects the fact that not being vaccinated correlates with not worrying much about COVID. Vaccinated individuals had a lot more wariness about undergoing surgical procedures during a pandemic.”
It appeared “individuals who were vaccinated in real life [were] worried about staff vaccination,” Dr. Landon noted. She concluded, “I think it supports the need for mandatory vaccinations in health care workers.”
The study has implications for hospital vaccination policies and practices. In Cumberland, Md., when COVID was high and vaccines first became available, the Maryland Hospital Association said that all health care staff should be vaccinated. The local hospital, UPMC–Western Maryland Hospital, refused.
Two months later, the local news reporter, Teresa McMinn, wrote, “While Maryland’s largest hospital systems have ‘led by example by mandating vaccines for all of their hospital staff,’ other facilities – including UPMC Western Maryland and Garrett Regional Medical Center – have taken no such action even though it’s been 8 months since vaccines were made available to health care workers.”
The hospital would not tell patients whether staff were vaccinated, either. An ongoing concern for members of the community is the lack of communication with UPMC, which erodes trust in the health system – the only hospital available in this rural community.
This vaccine study supports that the vaccination status of the staff may influence some patients’ decision on whether to have surgery.
The Ruskins and Dr. Landon have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An online survey captured mixed information about people’s willingness to undergo surgery during a viral pandemic in relation to the vaccine status of the patient and staff. The findings showcase opportunities for public education and “skillful messaging,” researchers report.
In survey scenarios that asked people to imagine their vaccination status, people were more willing to undergo surgery if it was lifesaving, rather than elective, especially if vaccinated. The prospect of no hospital stay tipped the scales further toward surgery. The vaccination status of hospital staff played only a minor role in decision making, according to the study, which was published in Vaccine.
But as a post hoc analysis revealed, it was participants who were not vaccinated against COVID-19 in real life who were more willing to undergo surgery, compared with those who had one or two shots.
In either case, too many people were unwilling to undergo lifesaving surgery, even though the risk of hospital-acquired COVID-19 is low. “Making this choice for an actual health problem would result in an unacceptably high rate of potential morbidity attributable to pandemic-related fears, the authors wrote.
In an unusual approach, the researchers used Amazon’s Mechanical Turk to electronically recruit 2,006 adults. The participants answered a 26-item survey about a hypothetical surgery in an unnamed pandemic with different combinations of vaccine status for patient and staff.
Coauthor and anesthesiologist Keith J. Ruskin, MD, of the University of Chicago, told this news organization that they “wanted to make this timeless” and independent of COVID “so that when the next thing came about, the paper would still be relevant.”
The researchers were surprised by the findings at the extreme ends of attitudes toward surgery. Some were still willing to have elective surgery with (hypothetically) unvaccinated patients and staff.
“And people at the other end, even though they are vaccinated, the hospital staff is vaccinated, and the surgery is lifesaving, they absolutely won’t have surgery,” Dr. Ruskin said.
He viewed these two groups as opportunities for education. “You can present information in the most positive light to get them to do the right thing with what’s best for themselves,” he said.
As an example, Dr. Ruskin pointed to an ad in Illinois. “It’s not only people saying I’m getting vaccinated for myself and my family, but there are people who said I got vaccinated and I still got COVID, but it could have been much worse. Please, if you’re on the fence, just get vaccinated,” he said.
Coauthor Anna Clebone Ruskin, MD, an anesthesiologist at the University of Chicago, said, “Humans are programmed to see things in extremes. With surgery, people tend to think of surgery as a monolith – surgery is all good, or surgery is all bad, where there is a huge in between. So we saw those extremes. ... Seeing that dichotomy with people on either end was pretty surprising.
“Getting surgery is not always good. Getting surgery is not always bad. It’s a risk-versus-benefit analysis and educating the public to consider the risks and benefits of medical decisions, in general, would be enormously beneficial,” she said.
A post hoc analysis found that “participants who were not actually vaccinated against COVID-19 were generally more willing to undergo surgery compared to those who had one vaccination or two vaccinations,” the authors wrote.
In a second post hoc finding, participants who reported high wariness of vaccines were generally more likely to be willing to undergo surgery. Notably, 15% of participants “were unwilling to undergo lifesaving surgery during a pandemic even when they and the health care staff were vaccinated,” the authors wrote.
Dr. Keith J. Ruskin hypothesized about this result, saying, “What we think is that potentially actually getting vaccinated against COVID-19 may indicate that you have a lower risk tolerance. So you may be less likely to do anything you perceive to be risky if you’re vaccinated against COVID-19.”
The authors stated that “the risk of hospital-acquired COVID-19 even prior to vaccination is vanishingly small.” The risk of nosocomial COVID varies among different studies. An EPIC-based study between April 2020 and October 2021 found the risk to be 1.8%; EPIC describes the fears of a patient catching COVID at a hospital as “likely unfounded.”
In the United Kingdom, the risk was as high as 24% earlier in the pandemic and then declined to approximately 5% a year ago. Omicron also brought more infections. Rates varied significantly among hospitals – and, notably, the risk of death from a nosocomial COVID infection was 21% in April-September 2020.
Emily Landon, MD, an epidemiologist and executive medical director for infection prevention and control at the University of Chicago Medicine, told this news organization that the study’s data were collected during Delta, a “time when we thought that this was a pandemic of the unvaccinated. But there was serious politicization of the vaccine.”
Dr. Landon said one of the study’s strengths was the large number of participants. A limitation was, “You’re going to have less participants who are generally poor and indigent, and fewer old participants, probably because they’re less likely to respond to an online survey.
“But the most interesting results are that people who were wary of vaccines or who hadn’t been vaccinated, were much more willing to undergo surgical procedures in the time of a pandemic, regardless of status, which reflects the fact that not being vaccinated correlates with not worrying much about COVID. Vaccinated individuals had a lot more wariness about undergoing surgical procedures during a pandemic.”
It appeared “individuals who were vaccinated in real life [were] worried about staff vaccination,” Dr. Landon noted. She concluded, “I think it supports the need for mandatory vaccinations in health care workers.”
The study has implications for hospital vaccination policies and practices. In Cumberland, Md., when COVID was high and vaccines first became available, the Maryland Hospital Association said that all health care staff should be vaccinated. The local hospital, UPMC–Western Maryland Hospital, refused.
Two months later, the local news reporter, Teresa McMinn, wrote, “While Maryland’s largest hospital systems have ‘led by example by mandating vaccines for all of their hospital staff,’ other facilities – including UPMC Western Maryland and Garrett Regional Medical Center – have taken no such action even though it’s been 8 months since vaccines were made available to health care workers.”
The hospital would not tell patients whether staff were vaccinated, either. An ongoing concern for members of the community is the lack of communication with UPMC, which erodes trust in the health system – the only hospital available in this rural community.
This vaccine study supports that the vaccination status of the staff may influence some patients’ decision on whether to have surgery.
The Ruskins and Dr. Landon have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An online survey captured mixed information about people’s willingness to undergo surgery during a viral pandemic in relation to the vaccine status of the patient and staff. The findings showcase opportunities for public education and “skillful messaging,” researchers report.
In survey scenarios that asked people to imagine their vaccination status, people were more willing to undergo surgery if it was lifesaving, rather than elective, especially if vaccinated. The prospect of no hospital stay tipped the scales further toward surgery. The vaccination status of hospital staff played only a minor role in decision making, according to the study, which was published in Vaccine.
But as a post hoc analysis revealed, it was participants who were not vaccinated against COVID-19 in real life who were more willing to undergo surgery, compared with those who had one or two shots.
In either case, too many people were unwilling to undergo lifesaving surgery, even though the risk of hospital-acquired COVID-19 is low. “Making this choice for an actual health problem would result in an unacceptably high rate of potential morbidity attributable to pandemic-related fears, the authors wrote.
In an unusual approach, the researchers used Amazon’s Mechanical Turk to electronically recruit 2,006 adults. The participants answered a 26-item survey about a hypothetical surgery in an unnamed pandemic with different combinations of vaccine status for patient and staff.
Coauthor and anesthesiologist Keith J. Ruskin, MD, of the University of Chicago, told this news organization that they “wanted to make this timeless” and independent of COVID “so that when the next thing came about, the paper would still be relevant.”
The researchers were surprised by the findings at the extreme ends of attitudes toward surgery. Some were still willing to have elective surgery with (hypothetically) unvaccinated patients and staff.
“And people at the other end, even though they are vaccinated, the hospital staff is vaccinated, and the surgery is lifesaving, they absolutely won’t have surgery,” Dr. Ruskin said.
He viewed these two groups as opportunities for education. “You can present information in the most positive light to get them to do the right thing with what’s best for themselves,” he said.
As an example, Dr. Ruskin pointed to an ad in Illinois. “It’s not only people saying I’m getting vaccinated for myself and my family, but there are people who said I got vaccinated and I still got COVID, but it could have been much worse. Please, if you’re on the fence, just get vaccinated,” he said.
Coauthor Anna Clebone Ruskin, MD, an anesthesiologist at the University of Chicago, said, “Humans are programmed to see things in extremes. With surgery, people tend to think of surgery as a monolith – surgery is all good, or surgery is all bad, where there is a huge in between. So we saw those extremes. ... Seeing that dichotomy with people on either end was pretty surprising.
“Getting surgery is not always good. Getting surgery is not always bad. It’s a risk-versus-benefit analysis and educating the public to consider the risks and benefits of medical decisions, in general, would be enormously beneficial,” she said.
A post hoc analysis found that “participants who were not actually vaccinated against COVID-19 were generally more willing to undergo surgery compared to those who had one vaccination or two vaccinations,” the authors wrote.
In a second post hoc finding, participants who reported high wariness of vaccines were generally more likely to be willing to undergo surgery. Notably, 15% of participants “were unwilling to undergo lifesaving surgery during a pandemic even when they and the health care staff were vaccinated,” the authors wrote.
Dr. Keith J. Ruskin hypothesized about this result, saying, “What we think is that potentially actually getting vaccinated against COVID-19 may indicate that you have a lower risk tolerance. So you may be less likely to do anything you perceive to be risky if you’re vaccinated against COVID-19.”
The authors stated that “the risk of hospital-acquired COVID-19 even prior to vaccination is vanishingly small.” The risk of nosocomial COVID varies among different studies. An EPIC-based study between April 2020 and October 2021 found the risk to be 1.8%; EPIC describes the fears of a patient catching COVID at a hospital as “likely unfounded.”
In the United Kingdom, the risk was as high as 24% earlier in the pandemic and then declined to approximately 5% a year ago. Omicron also brought more infections. Rates varied significantly among hospitals – and, notably, the risk of death from a nosocomial COVID infection was 21% in April-September 2020.
Emily Landon, MD, an epidemiologist and executive medical director for infection prevention and control at the University of Chicago Medicine, told this news organization that the study’s data were collected during Delta, a “time when we thought that this was a pandemic of the unvaccinated. But there was serious politicization of the vaccine.”
Dr. Landon said one of the study’s strengths was the large number of participants. A limitation was, “You’re going to have less participants who are generally poor and indigent, and fewer old participants, probably because they’re less likely to respond to an online survey.
“But the most interesting results are that people who were wary of vaccines or who hadn’t been vaccinated, were much more willing to undergo surgical procedures in the time of a pandemic, regardless of status, which reflects the fact that not being vaccinated correlates with not worrying much about COVID. Vaccinated individuals had a lot more wariness about undergoing surgical procedures during a pandemic.”
It appeared “individuals who were vaccinated in real life [were] worried about staff vaccination,” Dr. Landon noted. She concluded, “I think it supports the need for mandatory vaccinations in health care workers.”
The study has implications for hospital vaccination policies and practices. In Cumberland, Md., when COVID was high and vaccines first became available, the Maryland Hospital Association said that all health care staff should be vaccinated. The local hospital, UPMC–Western Maryland Hospital, refused.
Two months later, the local news reporter, Teresa McMinn, wrote, “While Maryland’s largest hospital systems have ‘led by example by mandating vaccines for all of their hospital staff,’ other facilities – including UPMC Western Maryland and Garrett Regional Medical Center – have taken no such action even though it’s been 8 months since vaccines were made available to health care workers.”
The hospital would not tell patients whether staff were vaccinated, either. An ongoing concern for members of the community is the lack of communication with UPMC, which erodes trust in the health system – the only hospital available in this rural community.
This vaccine study supports that the vaccination status of the staff may influence some patients’ decision on whether to have surgery.
The Ruskins and Dr. Landon have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surprising link between herpes zoster and dementia
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Herpes zoster does not appear to increase dementia risk – on the contrary, the viral infection may offer some protection, a large population-based study suggests.
“We were surprised by these results [and] the reasons for the decreased risk are unclear,” study author Sigrun Alba Johannesdottir Schmidt, MD, PhD, with Aarhus (Denmark) University Hospital, said in a news release.
The study was published online in Neurology.
Conflicting findings
Herpes zoster (HZ) is an acute, cutaneous viral infection caused by the reactivation of varicella-zoster virus (VZV). Previous population-based studies have reported both decreased and increased risks of dementia after having HZ.
It’s thought that HZ may contribute to the development of dementia through neuroinflammation, cerebral vasculopathy, or direct neural damage, but epidemiologic evidence is limited.
To investigate further, Dr. Schmidt and colleagues used Danish medical registries to identify 247,305 people who had visited a hospital for HZ or were prescribed antiviral medication for HZ over a 20-year period and matched them to 1,235,890 people who did not have HZ. For both cohorts, the median age was 64 years, and 61% were women.
Dementia was diagnosed in 9.7% of zoster patients and 10.3% of matched control persons during up to 21 years of follow-up.
Contrary to the researchers’ expectation, HZ was associated with a small (7%) decreased relative risk of all-cause dementia during follow-up (hazard ratio, 0.93; 95% confidence interval, 0.90-0.95).
There was no increased long-term risk of dementia in subgroup analyses, except possibly among those with HZ that involved the central nervous system (HR, 1.94; 95% CI, 0.78-4.80), which has been shown before.
However, the population attributable fraction of dementia caused by this rare complication is low (< 1%), suggesting that universal vaccination against VZV in the elderly has limited potential to reduce dementia risk, the investigators noted.
Nonetheless, Dr. Schmidt said shingles vaccination should be encouraged in older people because it can prevent complications from the disease.
The research team admitted that the slightly decreased long-term risk of dementia, including Alzheimer’s disease, was “unexpected.” The reasons for this decreased risk are unclear, they say, and could be explained by missed diagnoses of shingles in people with undiagnosed dementia.
They were not able to examine whether antiviral treatment modifies the association between HZ and dementia and said that this topic merits further research.
The study was supported by the Edel and Wilhelm Daubenmerkls Charitable Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Severe COVID-19 and blood cancer: Plasma therapy may help
, new research shows.
The study demonstrated that “plasma from convalescent or vaccinated individuals shortens the time to improvement in hematological and solid cancer patients with severe COVID-19” and “prolongs overall survival,” said study coauthor Maike Janssen, MD, of the department of internal medicine at Heidelberg (Germany) University Hospital.
Dr. Janssen presented the study findings at the annual congress of the European Hematology Association held in Vienna.
Although people with COVID-19 do not appear to benefit from treatment with convalescent plasma, some data indicate that certain patients who cannot mount a strong immune response to SARS-CoV-2 infection may benefit.
In this recent multicenter study, 134 patients with confirmed COVID-19 whose oxygen saturation was 94% or lower were randomly assigned to undergo treatment with convalescent or vaccinated SARS-CoV-2 plasma (n = 68) or to receive standard of care (n = 66). Patients fell into four clinical groups: those with a hematologic malignancy or who had undergone active cancer therapy for any cancer within the past 24 months; those with chronic immunosuppression; those between the ages of 50 and 75 with lymphopenia and/or elevated D-dimer levels; and those older than 75 years.
The convalescent or vaccinated SARS-CoV-2 plasma was administered in two bags (238-337 mL plasma each) from different donors on days 1 and 2. Only plasma from donors with high levels of neutralizing activity (titers above 1:80) were included. The primary endpoint was time to improvement by 2 points on a 7-point scale or discharge from the hospital. The secondary endpoint was improvement in overall survival.
The authors found that overall, patients in the plasma group demonstrated a shorter time to improvement – median of 12.5 days, vs. 18 days – but the difference was not significant (P = .29).
However, for the subgroup of 56 patients with hematologic/solid cancers, the time to improvement was significantly shorter: 13 days vs. 31 days (hazard ratio [HR], 2.5; P = .003).
Similarly, plasma therapy did not improve overall survival in the study population overall – there were 12 deaths in the plasma group over 80 days, vs. 15 in the control group (P = .80). Patients in the hematologic/solid cancer subgroup who received plasma therapy did demonstrate significantly better overall survival (HR, 0.28; P = .042).
No similar significant differences in time to improvement or overall survival were observed in the other three groups. “We found that plasma did not improve outcomes in immune-competent patients with other risk factors and/or older age,” Dr. Janssen said.
Although study enrollment ended when the Omicron variant began surging, Dr. Janssen noted that plasma from Omicron patients may also be of benefit to those with hematologic cancers.
“We have treated some patients in individual cases using plasma from Omicron patients who were already vaccinated or with breakthrough infections, and we did see benefits in those cases,” she noted.
The study was funded by the Federal Ministry of Education and Research, Germany. Dr. Janssen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
The study demonstrated that “plasma from convalescent or vaccinated individuals shortens the time to improvement in hematological and solid cancer patients with severe COVID-19” and “prolongs overall survival,” said study coauthor Maike Janssen, MD, of the department of internal medicine at Heidelberg (Germany) University Hospital.
Dr. Janssen presented the study findings at the annual congress of the European Hematology Association held in Vienna.
Although people with COVID-19 do not appear to benefit from treatment with convalescent plasma, some data indicate that certain patients who cannot mount a strong immune response to SARS-CoV-2 infection may benefit.
In this recent multicenter study, 134 patients with confirmed COVID-19 whose oxygen saturation was 94% or lower were randomly assigned to undergo treatment with convalescent or vaccinated SARS-CoV-2 plasma (n = 68) or to receive standard of care (n = 66). Patients fell into four clinical groups: those with a hematologic malignancy or who had undergone active cancer therapy for any cancer within the past 24 months; those with chronic immunosuppression; those between the ages of 50 and 75 with lymphopenia and/or elevated D-dimer levels; and those older than 75 years.
The convalescent or vaccinated SARS-CoV-2 plasma was administered in two bags (238-337 mL plasma each) from different donors on days 1 and 2. Only plasma from donors with high levels of neutralizing activity (titers above 1:80) were included. The primary endpoint was time to improvement by 2 points on a 7-point scale or discharge from the hospital. The secondary endpoint was improvement in overall survival.
The authors found that overall, patients in the plasma group demonstrated a shorter time to improvement – median of 12.5 days, vs. 18 days – but the difference was not significant (P = .29).
However, for the subgroup of 56 patients with hematologic/solid cancers, the time to improvement was significantly shorter: 13 days vs. 31 days (hazard ratio [HR], 2.5; P = .003).
Similarly, plasma therapy did not improve overall survival in the study population overall – there were 12 deaths in the plasma group over 80 days, vs. 15 in the control group (P = .80). Patients in the hematologic/solid cancer subgroup who received plasma therapy did demonstrate significantly better overall survival (HR, 0.28; P = .042).
No similar significant differences in time to improvement or overall survival were observed in the other three groups. “We found that plasma did not improve outcomes in immune-competent patients with other risk factors and/or older age,” Dr. Janssen said.
Although study enrollment ended when the Omicron variant began surging, Dr. Janssen noted that plasma from Omicron patients may also be of benefit to those with hematologic cancers.
“We have treated some patients in individual cases using plasma from Omicron patients who were already vaccinated or with breakthrough infections, and we did see benefits in those cases,” she noted.
The study was funded by the Federal Ministry of Education and Research, Germany. Dr. Janssen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
The study demonstrated that “plasma from convalescent or vaccinated individuals shortens the time to improvement in hematological and solid cancer patients with severe COVID-19” and “prolongs overall survival,” said study coauthor Maike Janssen, MD, of the department of internal medicine at Heidelberg (Germany) University Hospital.
Dr. Janssen presented the study findings at the annual congress of the European Hematology Association held in Vienna.
Although people with COVID-19 do not appear to benefit from treatment with convalescent plasma, some data indicate that certain patients who cannot mount a strong immune response to SARS-CoV-2 infection may benefit.
In this recent multicenter study, 134 patients with confirmed COVID-19 whose oxygen saturation was 94% or lower were randomly assigned to undergo treatment with convalescent or vaccinated SARS-CoV-2 plasma (n = 68) or to receive standard of care (n = 66). Patients fell into four clinical groups: those with a hematologic malignancy or who had undergone active cancer therapy for any cancer within the past 24 months; those with chronic immunosuppression; those between the ages of 50 and 75 with lymphopenia and/or elevated D-dimer levels; and those older than 75 years.
The convalescent or vaccinated SARS-CoV-2 plasma was administered in two bags (238-337 mL plasma each) from different donors on days 1 and 2. Only plasma from donors with high levels of neutralizing activity (titers above 1:80) were included. The primary endpoint was time to improvement by 2 points on a 7-point scale or discharge from the hospital. The secondary endpoint was improvement in overall survival.
The authors found that overall, patients in the plasma group demonstrated a shorter time to improvement – median of 12.5 days, vs. 18 days – but the difference was not significant (P = .29).
However, for the subgroup of 56 patients with hematologic/solid cancers, the time to improvement was significantly shorter: 13 days vs. 31 days (hazard ratio [HR], 2.5; P = .003).
Similarly, plasma therapy did not improve overall survival in the study population overall – there were 12 deaths in the plasma group over 80 days, vs. 15 in the control group (P = .80). Patients in the hematologic/solid cancer subgroup who received plasma therapy did demonstrate significantly better overall survival (HR, 0.28; P = .042).
No similar significant differences in time to improvement or overall survival were observed in the other three groups. “We found that plasma did not improve outcomes in immune-competent patients with other risk factors and/or older age,” Dr. Janssen said.
Although study enrollment ended when the Omicron variant began surging, Dr. Janssen noted that plasma from Omicron patients may also be of benefit to those with hematologic cancers.
“We have treated some patients in individual cases using plasma from Omicron patients who were already vaccinated or with breakthrough infections, and we did see benefits in those cases,” she noted.
The study was funded by the Federal Ministry of Education and Research, Germany. Dr. Janssen has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM EHA 2022
‘My malpractice insurance doubled!’ Why, when fewer patients are suing?
Angela Intili, MD, an ob.gyn., was used to seeing her medical malpractice insurance premium rise slightly every couple of years. But she was shocked by the drastic rise she recently experienced.
In the last 2 years, Dr. Intili’s premiums shot from $60,000 to $130,000, she said.
“After 30 years of practice, this is the first time I’ve asked myself if I can even afford to continue practicing obstetrics and gynecology,” said Dr. Intili, 62, of Joliet, Ill. “It’s gotten very difficult to make ends meet as far as overhead because of the liability costs. I still love what I’m doing but I don’t know if I can afford to do it anymore.”
Even more frustrating for Dr. Intili was learning that claims in Illinois have sharply declined. From 2016 to 2020, tort filings in Illinois decreased by 43%, according to a state report.
“If claims are going down, I don’t understand why premium payments are going up,” she said.
Physicians across the country are experiencing a similar paradox. Claims are down, yet premiums are rising.
Medscape’s Malpractice Report 2021 found that 42% of primary care physicians were sued in 2020 through mid-2021, down from 52% in 2019. Fifty-six percent of specialists were sued in 2020 through mid-2021 compared with 62% in 2019, the report found. The pandemic was undoubtedly behind the decrease in suits, according to legal experts.
Yet, physicians paid higher premiums in 2021 and are on track for increases again in 2022, according to data and analysts.
According to Conning, direct premiums written for physicians increased 7.0% in 2021 (from $5.01 billion to $5.36 billion). Conning, an investment management firm that serves the insurance industry, analyzes annual financial reports filed by insurers to state insurance departments. The Medical Liability Monitor’s 2021 report found that premiums for internists, surgeons, and ob.gyns. in states without Patient Compensation Funds rose by an average of 2% in 2021.
The disparities raise questions about why physicians are paying higher premiums when having fewer claims is likely saving insurers’ money. Shouldn’t physicians’ rates reflect the reduction in claims?
Cases plummet during pandemic
During the pandemic, the volume of new medical malpractice claims dwindled to nearly nothing, said Michael Matray, editor of the Medical Liability Monitor, a national publication that analyzes medical liability insurance premiums.
“The court system closed for a while,” he said. “No elective procedures were being done in 2020 and the early parts of 2021. If you have no treatment, you have no malpractice, so of course, claims frequency tumbled down to a trickle.”
The number of large awards also decreased during the pandemic, noted Bill Burns, a director of insurance research at Conning.
“For claims that were already in the system, many of them could not be resolved because of the court closures, inability to take statements and depositions, etc.,” he said. “This resulted in a drop in verdicts.”
In 2021, there were 16 medical malpractice verdicts of $10 million or more in the United States, according to TransRe, an international reinsurance company that tracks large verdicts. In 2020, there were six verdicts of $10 million or more, TransRe research found. This is down from 52 verdicts of $10 million or more in 2019 and 46 verdicts of $10 million or more in 2018.
But although the pandemic lowered claims and decreased the number of payouts, one important aspect was untouched by the COVID era, said Richard E. Anderson, MD, chairman and CEO for The Doctors Company, a national medical liability insurer, and TDC Group.
“It’s a fair question: If claims are down, why are premiums continuing to go up?” Dr. Anderson said. “The answer is severity.”
High-dollar verdicts pave expensive path
The upward trend in severity has continued for about 6 years and has not slowed, Dr. Anderson said. Severity refers to high-dollar verdicts and settlements.
“We’re seeing record-high verdicts all over the country,” he said. “We used to have maps that showed the top 10 medical malpractice verdicts or awards, and they would be clustered where you’d expect them to be, New York, Florida, Illinois, and so forth. Now, if you look at those top 10 verdicts, they could be anywhere in the country.”
In Minnesota for instance, a jury awarded a record $111 million in damages to a college student in May after finding a hospital and an orthopedic surgeon negligent in treating his broken leg. In April, a Kansas City jury awarded a family $25 million after finding that an ob.gyn. and hospital failed to properly treat a mother in labor, causing brain damage to her infant.
Such record payouts factor into premium costs, said Ned Rand Jr., CEO for ProAssurance, a national medical liability insurer. Though only a minority of claims reach that level, when a high award occurs, it puts pressure on the ultimate cost to resolve claims, he said. The frequency of claims filed is also expected to soon rebound, he noted.
“As we price the product sitting here today, we have to factor both of those in,” Mr. Rand said. “That’s why we, as an industry, continue to see, by and large, rates going up. And we fell behind. Some of this severity, in particular, as an industry, we weren’t pricing fully for, so we’ve been playing catch-up.”
High-dollar awards – also called nuclear verdicts – set the arena for future settlements in similar cases, Dr. Anderson added.
“If it was an orthopedic case for instance, and there was a similar injury in another case, that’s the trial lawyers’ starting point for the award,” he said. “Now, they’re not going to get it, but it distorts the negotiations. As we have more and more nuclear verdicts, it becomes harder to settle claims for reasonable amounts.”
What does 2022 have in store?
Analysts say the backlog of malpractice claims in the court system could prove calamitous for premiums and the liability landscape.
Courts are slogging through the pileup caused by the pandemic, but it’s estimated that there is still about a one-third larger case backlog than normal, according to Mr. Matray.
Such delayed claims may end up costing more because of social inflation, said Mr. Burns.
“People look at the world differently than they did 2 years ago,” he said. “A jury may have awarded $5 million for a claim a few years ago. But then the pandemic hits, and we have the George Floyd incident, and we have people out of work and a shortage in baby formula. Yet, companies are still making a lot of money and many insurance companies are turning record profits. Today, that jury may look at a sympathetic malpractice victim and award $10 million for the same claim.”
Concerns also exist about a potential surge of new malpractice claims. Mr. Rand compares the possible wave to a large bubble.
“I liken it to a cartoon, when one character grabs the hose and a big bubble forms as the water builds up,” he said. “Then the character releases, and water comes flooding out. As an industry, we wait, wondering: Is there going to be this flood of claims as the court systems reopen and the statute of limitations approach around some of these claims? That’s an ongoing concern.”
As for impending premiums, physicians can expect rises in 2022 and again in 2023, according to Chris Wojciechowski, a partner at TigerRisk Partners, a reinsurance broker.
“In general, there is a lot of uncertainty around the state of the economy, the tort environment, litigation post COVID, and overall volatility across the capital markets,” he said. “Furthermore, thanks to social and financial inflation, the potential for very severe verdicts has increased dramatically, and as courthouses reopen, the trends are not looking favorable. While many of the physician carriers have strong balance sheets, they can’t lose money on an underwriting basis forever.”
For Dr. Intili, the Illinois ob.gyn., news of another impending increase in 2022 is distressing. She expects another 10%-20% rise in 2022, she said. If she were younger and earlier in her career, she might’ve considered moving, she said, but her family lives in Illinois and she cares for her older parents.
“I’m not ready to retire,” Dr. Intili said. “I’m looking into options, possibly becoming a hospitalist or doing locum tenens work. I’ve been a solo practitioner for 27 years and I love the autonomy. But these high premiums are making it almost impossible to continue.”
A version of this article first appeared on Medscape.com.
Angela Intili, MD, an ob.gyn., was used to seeing her medical malpractice insurance premium rise slightly every couple of years. But she was shocked by the drastic rise she recently experienced.
In the last 2 years, Dr. Intili’s premiums shot from $60,000 to $130,000, she said.
“After 30 years of practice, this is the first time I’ve asked myself if I can even afford to continue practicing obstetrics and gynecology,” said Dr. Intili, 62, of Joliet, Ill. “It’s gotten very difficult to make ends meet as far as overhead because of the liability costs. I still love what I’m doing but I don’t know if I can afford to do it anymore.”
Even more frustrating for Dr. Intili was learning that claims in Illinois have sharply declined. From 2016 to 2020, tort filings in Illinois decreased by 43%, according to a state report.
“If claims are going down, I don’t understand why premium payments are going up,” she said.
Physicians across the country are experiencing a similar paradox. Claims are down, yet premiums are rising.
Medscape’s Malpractice Report 2021 found that 42% of primary care physicians were sued in 2020 through mid-2021, down from 52% in 2019. Fifty-six percent of specialists were sued in 2020 through mid-2021 compared with 62% in 2019, the report found. The pandemic was undoubtedly behind the decrease in suits, according to legal experts.
Yet, physicians paid higher premiums in 2021 and are on track for increases again in 2022, according to data and analysts.
According to Conning, direct premiums written for physicians increased 7.0% in 2021 (from $5.01 billion to $5.36 billion). Conning, an investment management firm that serves the insurance industry, analyzes annual financial reports filed by insurers to state insurance departments. The Medical Liability Monitor’s 2021 report found that premiums for internists, surgeons, and ob.gyns. in states without Patient Compensation Funds rose by an average of 2% in 2021.
The disparities raise questions about why physicians are paying higher premiums when having fewer claims is likely saving insurers’ money. Shouldn’t physicians’ rates reflect the reduction in claims?
Cases plummet during pandemic
During the pandemic, the volume of new medical malpractice claims dwindled to nearly nothing, said Michael Matray, editor of the Medical Liability Monitor, a national publication that analyzes medical liability insurance premiums.
“The court system closed for a while,” he said. “No elective procedures were being done in 2020 and the early parts of 2021. If you have no treatment, you have no malpractice, so of course, claims frequency tumbled down to a trickle.”
The number of large awards also decreased during the pandemic, noted Bill Burns, a director of insurance research at Conning.
“For claims that were already in the system, many of them could not be resolved because of the court closures, inability to take statements and depositions, etc.,” he said. “This resulted in a drop in verdicts.”
In 2021, there were 16 medical malpractice verdicts of $10 million or more in the United States, according to TransRe, an international reinsurance company that tracks large verdicts. In 2020, there were six verdicts of $10 million or more, TransRe research found. This is down from 52 verdicts of $10 million or more in 2019 and 46 verdicts of $10 million or more in 2018.
But although the pandemic lowered claims and decreased the number of payouts, one important aspect was untouched by the COVID era, said Richard E. Anderson, MD, chairman and CEO for The Doctors Company, a national medical liability insurer, and TDC Group.
“It’s a fair question: If claims are down, why are premiums continuing to go up?” Dr. Anderson said. “The answer is severity.”
High-dollar verdicts pave expensive path
The upward trend in severity has continued for about 6 years and has not slowed, Dr. Anderson said. Severity refers to high-dollar verdicts and settlements.
“We’re seeing record-high verdicts all over the country,” he said. “We used to have maps that showed the top 10 medical malpractice verdicts or awards, and they would be clustered where you’d expect them to be, New York, Florida, Illinois, and so forth. Now, if you look at those top 10 verdicts, they could be anywhere in the country.”
In Minnesota for instance, a jury awarded a record $111 million in damages to a college student in May after finding a hospital and an orthopedic surgeon negligent in treating his broken leg. In April, a Kansas City jury awarded a family $25 million after finding that an ob.gyn. and hospital failed to properly treat a mother in labor, causing brain damage to her infant.
Such record payouts factor into premium costs, said Ned Rand Jr., CEO for ProAssurance, a national medical liability insurer. Though only a minority of claims reach that level, when a high award occurs, it puts pressure on the ultimate cost to resolve claims, he said. The frequency of claims filed is also expected to soon rebound, he noted.
“As we price the product sitting here today, we have to factor both of those in,” Mr. Rand said. “That’s why we, as an industry, continue to see, by and large, rates going up. And we fell behind. Some of this severity, in particular, as an industry, we weren’t pricing fully for, so we’ve been playing catch-up.”
High-dollar awards – also called nuclear verdicts – set the arena for future settlements in similar cases, Dr. Anderson added.
“If it was an orthopedic case for instance, and there was a similar injury in another case, that’s the trial lawyers’ starting point for the award,” he said. “Now, they’re not going to get it, but it distorts the negotiations. As we have more and more nuclear verdicts, it becomes harder to settle claims for reasonable amounts.”
What does 2022 have in store?
Analysts say the backlog of malpractice claims in the court system could prove calamitous for premiums and the liability landscape.
Courts are slogging through the pileup caused by the pandemic, but it’s estimated that there is still about a one-third larger case backlog than normal, according to Mr. Matray.
Such delayed claims may end up costing more because of social inflation, said Mr. Burns.
“People look at the world differently than they did 2 years ago,” he said. “A jury may have awarded $5 million for a claim a few years ago. But then the pandemic hits, and we have the George Floyd incident, and we have people out of work and a shortage in baby formula. Yet, companies are still making a lot of money and many insurance companies are turning record profits. Today, that jury may look at a sympathetic malpractice victim and award $10 million for the same claim.”
Concerns also exist about a potential surge of new malpractice claims. Mr. Rand compares the possible wave to a large bubble.
“I liken it to a cartoon, when one character grabs the hose and a big bubble forms as the water builds up,” he said. “Then the character releases, and water comes flooding out. As an industry, we wait, wondering: Is there going to be this flood of claims as the court systems reopen and the statute of limitations approach around some of these claims? That’s an ongoing concern.”
As for impending premiums, physicians can expect rises in 2022 and again in 2023, according to Chris Wojciechowski, a partner at TigerRisk Partners, a reinsurance broker.
“In general, there is a lot of uncertainty around the state of the economy, the tort environment, litigation post COVID, and overall volatility across the capital markets,” he said. “Furthermore, thanks to social and financial inflation, the potential for very severe verdicts has increased dramatically, and as courthouses reopen, the trends are not looking favorable. While many of the physician carriers have strong balance sheets, they can’t lose money on an underwriting basis forever.”
For Dr. Intili, the Illinois ob.gyn., news of another impending increase in 2022 is distressing. She expects another 10%-20% rise in 2022, she said. If she were younger and earlier in her career, she might’ve considered moving, she said, but her family lives in Illinois and she cares for her older parents.
“I’m not ready to retire,” Dr. Intili said. “I’m looking into options, possibly becoming a hospitalist or doing locum tenens work. I’ve been a solo practitioner for 27 years and I love the autonomy. But these high premiums are making it almost impossible to continue.”
A version of this article first appeared on Medscape.com.
Angela Intili, MD, an ob.gyn., was used to seeing her medical malpractice insurance premium rise slightly every couple of years. But she was shocked by the drastic rise she recently experienced.
In the last 2 years, Dr. Intili’s premiums shot from $60,000 to $130,000, she said.
“After 30 years of practice, this is the first time I’ve asked myself if I can even afford to continue practicing obstetrics and gynecology,” said Dr. Intili, 62, of Joliet, Ill. “It’s gotten very difficult to make ends meet as far as overhead because of the liability costs. I still love what I’m doing but I don’t know if I can afford to do it anymore.”
Even more frustrating for Dr. Intili was learning that claims in Illinois have sharply declined. From 2016 to 2020, tort filings in Illinois decreased by 43%, according to a state report.
“If claims are going down, I don’t understand why premium payments are going up,” she said.
Physicians across the country are experiencing a similar paradox. Claims are down, yet premiums are rising.
Medscape’s Malpractice Report 2021 found that 42% of primary care physicians were sued in 2020 through mid-2021, down from 52% in 2019. Fifty-six percent of specialists were sued in 2020 through mid-2021 compared with 62% in 2019, the report found. The pandemic was undoubtedly behind the decrease in suits, according to legal experts.
Yet, physicians paid higher premiums in 2021 and are on track for increases again in 2022, according to data and analysts.
According to Conning, direct premiums written for physicians increased 7.0% in 2021 (from $5.01 billion to $5.36 billion). Conning, an investment management firm that serves the insurance industry, analyzes annual financial reports filed by insurers to state insurance departments. The Medical Liability Monitor’s 2021 report found that premiums for internists, surgeons, and ob.gyns. in states without Patient Compensation Funds rose by an average of 2% in 2021.
The disparities raise questions about why physicians are paying higher premiums when having fewer claims is likely saving insurers’ money. Shouldn’t physicians’ rates reflect the reduction in claims?
Cases plummet during pandemic
During the pandemic, the volume of new medical malpractice claims dwindled to nearly nothing, said Michael Matray, editor of the Medical Liability Monitor, a national publication that analyzes medical liability insurance premiums.
“The court system closed for a while,” he said. “No elective procedures were being done in 2020 and the early parts of 2021. If you have no treatment, you have no malpractice, so of course, claims frequency tumbled down to a trickle.”
The number of large awards also decreased during the pandemic, noted Bill Burns, a director of insurance research at Conning.
“For claims that were already in the system, many of them could not be resolved because of the court closures, inability to take statements and depositions, etc.,” he said. “This resulted in a drop in verdicts.”
In 2021, there were 16 medical malpractice verdicts of $10 million or more in the United States, according to TransRe, an international reinsurance company that tracks large verdicts. In 2020, there were six verdicts of $10 million or more, TransRe research found. This is down from 52 verdicts of $10 million or more in 2019 and 46 verdicts of $10 million or more in 2018.
But although the pandemic lowered claims and decreased the number of payouts, one important aspect was untouched by the COVID era, said Richard E. Anderson, MD, chairman and CEO for The Doctors Company, a national medical liability insurer, and TDC Group.
“It’s a fair question: If claims are down, why are premiums continuing to go up?” Dr. Anderson said. “The answer is severity.”
High-dollar verdicts pave expensive path
The upward trend in severity has continued for about 6 years and has not slowed, Dr. Anderson said. Severity refers to high-dollar verdicts and settlements.
“We’re seeing record-high verdicts all over the country,” he said. “We used to have maps that showed the top 10 medical malpractice verdicts or awards, and they would be clustered where you’d expect them to be, New York, Florida, Illinois, and so forth. Now, if you look at those top 10 verdicts, they could be anywhere in the country.”
In Minnesota for instance, a jury awarded a record $111 million in damages to a college student in May after finding a hospital and an orthopedic surgeon negligent in treating his broken leg. In April, a Kansas City jury awarded a family $25 million after finding that an ob.gyn. and hospital failed to properly treat a mother in labor, causing brain damage to her infant.
Such record payouts factor into premium costs, said Ned Rand Jr., CEO for ProAssurance, a national medical liability insurer. Though only a minority of claims reach that level, when a high award occurs, it puts pressure on the ultimate cost to resolve claims, he said. The frequency of claims filed is also expected to soon rebound, he noted.
“As we price the product sitting here today, we have to factor both of those in,” Mr. Rand said. “That’s why we, as an industry, continue to see, by and large, rates going up. And we fell behind. Some of this severity, in particular, as an industry, we weren’t pricing fully for, so we’ve been playing catch-up.”
High-dollar awards – also called nuclear verdicts – set the arena for future settlements in similar cases, Dr. Anderson added.
“If it was an orthopedic case for instance, and there was a similar injury in another case, that’s the trial lawyers’ starting point for the award,” he said. “Now, they’re not going to get it, but it distorts the negotiations. As we have more and more nuclear verdicts, it becomes harder to settle claims for reasonable amounts.”
What does 2022 have in store?
Analysts say the backlog of malpractice claims in the court system could prove calamitous for premiums and the liability landscape.
Courts are slogging through the pileup caused by the pandemic, but it’s estimated that there is still about a one-third larger case backlog than normal, according to Mr. Matray.
Such delayed claims may end up costing more because of social inflation, said Mr. Burns.
“People look at the world differently than they did 2 years ago,” he said. “A jury may have awarded $5 million for a claim a few years ago. But then the pandemic hits, and we have the George Floyd incident, and we have people out of work and a shortage in baby formula. Yet, companies are still making a lot of money and many insurance companies are turning record profits. Today, that jury may look at a sympathetic malpractice victim and award $10 million for the same claim.”
Concerns also exist about a potential surge of new malpractice claims. Mr. Rand compares the possible wave to a large bubble.
“I liken it to a cartoon, when one character grabs the hose and a big bubble forms as the water builds up,” he said. “Then the character releases, and water comes flooding out. As an industry, we wait, wondering: Is there going to be this flood of claims as the court systems reopen and the statute of limitations approach around some of these claims? That’s an ongoing concern.”
As for impending premiums, physicians can expect rises in 2022 and again in 2023, according to Chris Wojciechowski, a partner at TigerRisk Partners, a reinsurance broker.
“In general, there is a lot of uncertainty around the state of the economy, the tort environment, litigation post COVID, and overall volatility across the capital markets,” he said. “Furthermore, thanks to social and financial inflation, the potential for very severe verdicts has increased dramatically, and as courthouses reopen, the trends are not looking favorable. While many of the physician carriers have strong balance sheets, they can’t lose money on an underwriting basis forever.”
For Dr. Intili, the Illinois ob.gyn., news of another impending increase in 2022 is distressing. She expects another 10%-20% rise in 2022, she said. If she were younger and earlier in her career, she might’ve considered moving, she said, but her family lives in Illinois and she cares for her older parents.
“I’m not ready to retire,” Dr. Intili said. “I’m looking into options, possibly becoming a hospitalist or doing locum tenens work. I’ve been a solo practitioner for 27 years and I love the autonomy. But these high premiums are making it almost impossible to continue.”
A version of this article first appeared on Medscape.com.
Insurer told to pay $5.2 million to woman who caught STD in a car
A Missouri lawsuit adds a new twist to the kind of “bodily harm” in a car that’s covered by insurance.
On June 7,
The woman, identified in court documents as M.O., said she contracted human papillomavirus from her boyfriend. She said he knew he had the disease but didn’t tell her.
An arbitrator found in May 2021 that the in-car sex had “directly caused, or directly contributed to cause” the STD transmission. The man was found liable. The woman was awarded $5.2 million to be paid by GEICO, which insured the man’s vehicle.
GEICO filed for the award to be overturned, alleging it had been denied due process and that the arbitration deal was unenforceable.
Court documents show that GEICO claimed the man’s policy covered only injuries that came “out of the ownership, maintenance or use of the ... auto” and that the woman’s “injuries arose from an intervening cause – namely, her failure to prevent transmission of STDs by having unprotected sex.”
The state appellate panel ruled that the lower court made no mistake in the case and upheld the decision.
The Kansas City Star reported that one of the judges concurred but said GEICO was offered “no meaningful opportunity to participate” in the lawsuit and existing law “relegat(es) the insurer to the status of a bystander.”
“This case presents novel and potentially important issues about whether an insurance carrier can be held liable under such policies for the consequences of two adults voluntarily having unprotected sex in the insured’s automobile,” noted U.S. Magistrate Judge Angel D. Mitchell in court documents. “Interpretation of these policies could have far-reaching implications for other policies with similar terms.”
A version of this article first appeared on WebMD.com.
A Missouri lawsuit adds a new twist to the kind of “bodily harm” in a car that’s covered by insurance.
On June 7,
The woman, identified in court documents as M.O., said she contracted human papillomavirus from her boyfriend. She said he knew he had the disease but didn’t tell her.
An arbitrator found in May 2021 that the in-car sex had “directly caused, or directly contributed to cause” the STD transmission. The man was found liable. The woman was awarded $5.2 million to be paid by GEICO, which insured the man’s vehicle.
GEICO filed for the award to be overturned, alleging it had been denied due process and that the arbitration deal was unenforceable.
Court documents show that GEICO claimed the man’s policy covered only injuries that came “out of the ownership, maintenance or use of the ... auto” and that the woman’s “injuries arose from an intervening cause – namely, her failure to prevent transmission of STDs by having unprotected sex.”
The state appellate panel ruled that the lower court made no mistake in the case and upheld the decision.
The Kansas City Star reported that one of the judges concurred but said GEICO was offered “no meaningful opportunity to participate” in the lawsuit and existing law “relegat(es) the insurer to the status of a bystander.”
“This case presents novel and potentially important issues about whether an insurance carrier can be held liable under such policies for the consequences of two adults voluntarily having unprotected sex in the insured’s automobile,” noted U.S. Magistrate Judge Angel D. Mitchell in court documents. “Interpretation of these policies could have far-reaching implications for other policies with similar terms.”
A version of this article first appeared on WebMD.com.
A Missouri lawsuit adds a new twist to the kind of “bodily harm” in a car that’s covered by insurance.
On June 7,
The woman, identified in court documents as M.O., said she contracted human papillomavirus from her boyfriend. She said he knew he had the disease but didn’t tell her.
An arbitrator found in May 2021 that the in-car sex had “directly caused, or directly contributed to cause” the STD transmission. The man was found liable. The woman was awarded $5.2 million to be paid by GEICO, which insured the man’s vehicle.
GEICO filed for the award to be overturned, alleging it had been denied due process and that the arbitration deal was unenforceable.
Court documents show that GEICO claimed the man’s policy covered only injuries that came “out of the ownership, maintenance or use of the ... auto” and that the woman’s “injuries arose from an intervening cause – namely, her failure to prevent transmission of STDs by having unprotected sex.”
The state appellate panel ruled that the lower court made no mistake in the case and upheld the decision.
The Kansas City Star reported that one of the judges concurred but said GEICO was offered “no meaningful opportunity to participate” in the lawsuit and existing law “relegat(es) the insurer to the status of a bystander.”
“This case presents novel and potentially important issues about whether an insurance carrier can be held liable under such policies for the consequences of two adults voluntarily having unprotected sex in the insured’s automobile,” noted U.S. Magistrate Judge Angel D. Mitchell in court documents. “Interpretation of these policies could have far-reaching implications for other policies with similar terms.”
A version of this article first appeared on WebMD.com.
People with HIV may need an additional COVID vaccine dose
People with HIV have an increased risk of breakthrough SARS-CoV-2 infections, a new study finds, and the authors say an additional primary vaccine dose should be considered for all who are living with the disease.
Currently, an additional primary dose administered 28 days after a second dose of the mRNA (Moderna or Pfizer) vaccines or after the first dose of the Johnson & Johnson (J&J) vaccine is recommended only for those with advanced or untreated HIV.
The Centers for Disease Control and Prevention recommends boosters for all adults with or without HIV.
Sally B. Coburn, PhD, of the department of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, led the study, which was published online in JAMA Network Open. In their study, the researchers estimate the risk of breakthrough infections among fully vaccinated adults on the basis of HIV status in the United States.
Adults with HIV who were fully vaccinated before June 30, 2021, were matched with adults without HIV with regard to date of full vaccination, age, race/ethnicity, and sex. All were followed through Dec. 31, 2021.
Patients were considered fully vaccinated either 14 days after the second dose of the Pfizer or Moderna shots or 14 days after the single dose of the J&J shot.
Breakthrough risk 28% higher
In the study of 113,994 patients, researchers found that risk of breakthrough SARS-CoV-2 infection was low overall (3.8%) but was 28% higher among people with HIV in comparison with people without HIV (adjusted hazard ratio, 1.28; 95% confidence interval, 1.19-1.37).
The breakthrough rate was also higher in the HIV group (55 cases per 1,000 person-years, vs. 43 cases per 1,000 person-years in people without HIV).
Patients were drawn from the Corona-Infectious-Virus Epidemiology Team (CIVET)–II of the North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD), which is part of the International Epidemiology Databases to Evaluate AIDS (IeDEA) collaboration involving four cohorts.
Among people with HIV, those younger than 45 years (vs. those aged 45-54) and those with a history of COVID-19 were more likely to experience breakthrough infections. Those who did not get any additional shots after the primary vaccination were more likely to have breakthrough infections, amplifying the need to get boosters, the authors wrote.
There was no link between breakthrough infections and HIV viral load suppression, but high CD4 counts (> 500 cells/mm3) were associated with fewer breakthrough cases among people with HIV, they noted.
Monica Gandhi, MD, professor of medicine and associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, praised the study, noting that until now, large studies have not examined the rate of breakthrough infections among vaccinated people with HIV and people without HIV in the United States.
She told this news organization she agrees with the authors that a third dose for all who are living with HIV is needed because rates of breakthrough infections were high across all populations during the Omicron surge (which largely occurred after the period of this study).
She said she was not convinced the third shot was needed before Omicron, because breakthrough rates in both HIV and non-HIV groups were low.
“However, the most interesting part of this study for me was how well the vaccines worked in people with HIV with generally higher CD4 counts and virologic suppression, again telling us as HIV providers how well the HIV medicines work and how our patients with HIV have relatively normal immune systems if treated,” she said.
One limitation was that the study population was 92% male. Also, those without regular access to health care (who may be at greater risk for COVID-19) were less likely to be included in the study. People engaged in care may seek more frequent COVID-19 testing, which could lead to higher detection of breakthrough infections than in the general population.
“Future analyses should account for testing practices and include a larger proportion of women with HIV,” the authors wrote. “Ultimately, policy makers must determine the appropriate balance between preventing further COVID-19 infections and possibly unnecessary additional vaccinations.”
Coauthor Keri N. Althoff, PhD, told this news organization that there’s one unanswered question that would strengthen the call to action by the CDC: Do people with HIV have more severe postvaccination COVID-19 breakthrough illness?
“We have a second paper that is a preprint and currently under peer review,” she said. “In this paper, we found that people with HIV with a CD4 count less than 350 cells/mm3 were more likely to be hospitalized with postvaccination COVID-19 breakthrough illness compared to similar people without HIV. “
At a minimum, Dr. Althoff said, policymakers should consider including people with HIV with a CD4 less than 350 cells/mm3 (loosening the restriction to less than 200 cells/mm3) in their recommendations for people who are moderately or severely immunocompromised.
The research was funded with supplemental funds to the North American AIDS Cohort Collaboration on Research and Design. Dr. Coburn reports no relevant financial relationships. A coauthor has received grants from the Canadian Institutes of Health Research, Alberta Innovates, and University of Calgary/Alberta Health Services outside the submitted work. One coauthor reports serving as a consultant to Trio Health, Kennedy Dundas, and MedIQ outside the submitted work.
A version of this article first appeared on Medscape.com.
People with HIV have an increased risk of breakthrough SARS-CoV-2 infections, a new study finds, and the authors say an additional primary vaccine dose should be considered for all who are living with the disease.
Currently, an additional primary dose administered 28 days after a second dose of the mRNA (Moderna or Pfizer) vaccines or after the first dose of the Johnson & Johnson (J&J) vaccine is recommended only for those with advanced or untreated HIV.
The Centers for Disease Control and Prevention recommends boosters for all adults with or without HIV.
Sally B. Coburn, PhD, of the department of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, led the study, which was published online in JAMA Network Open. In their study, the researchers estimate the risk of breakthrough infections among fully vaccinated adults on the basis of HIV status in the United States.
Adults with HIV who were fully vaccinated before June 30, 2021, were matched with adults without HIV with regard to date of full vaccination, age, race/ethnicity, and sex. All were followed through Dec. 31, 2021.
Patients were considered fully vaccinated either 14 days after the second dose of the Pfizer or Moderna shots or 14 days after the single dose of the J&J shot.
Breakthrough risk 28% higher
In the study of 113,994 patients, researchers found that risk of breakthrough SARS-CoV-2 infection was low overall (3.8%) but was 28% higher among people with HIV in comparison with people without HIV (adjusted hazard ratio, 1.28; 95% confidence interval, 1.19-1.37).
The breakthrough rate was also higher in the HIV group (55 cases per 1,000 person-years, vs. 43 cases per 1,000 person-years in people without HIV).
Patients were drawn from the Corona-Infectious-Virus Epidemiology Team (CIVET)–II of the North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD), which is part of the International Epidemiology Databases to Evaluate AIDS (IeDEA) collaboration involving four cohorts.
Among people with HIV, those younger than 45 years (vs. those aged 45-54) and those with a history of COVID-19 were more likely to experience breakthrough infections. Those who did not get any additional shots after the primary vaccination were more likely to have breakthrough infections, amplifying the need to get boosters, the authors wrote.
There was no link between breakthrough infections and HIV viral load suppression, but high CD4 counts (> 500 cells/mm3) were associated with fewer breakthrough cases among people with HIV, they noted.
Monica Gandhi, MD, professor of medicine and associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, praised the study, noting that until now, large studies have not examined the rate of breakthrough infections among vaccinated people with HIV and people without HIV in the United States.
She told this news organization she agrees with the authors that a third dose for all who are living with HIV is needed because rates of breakthrough infections were high across all populations during the Omicron surge (which largely occurred after the period of this study).
She said she was not convinced the third shot was needed before Omicron, because breakthrough rates in both HIV and non-HIV groups were low.
“However, the most interesting part of this study for me was how well the vaccines worked in people with HIV with generally higher CD4 counts and virologic suppression, again telling us as HIV providers how well the HIV medicines work and how our patients with HIV have relatively normal immune systems if treated,” she said.
One limitation was that the study population was 92% male. Also, those without regular access to health care (who may be at greater risk for COVID-19) were less likely to be included in the study. People engaged in care may seek more frequent COVID-19 testing, which could lead to higher detection of breakthrough infections than in the general population.
“Future analyses should account for testing practices and include a larger proportion of women with HIV,” the authors wrote. “Ultimately, policy makers must determine the appropriate balance between preventing further COVID-19 infections and possibly unnecessary additional vaccinations.”
Coauthor Keri N. Althoff, PhD, told this news organization that there’s one unanswered question that would strengthen the call to action by the CDC: Do people with HIV have more severe postvaccination COVID-19 breakthrough illness?
“We have a second paper that is a preprint and currently under peer review,” she said. “In this paper, we found that people with HIV with a CD4 count less than 350 cells/mm3 were more likely to be hospitalized with postvaccination COVID-19 breakthrough illness compared to similar people without HIV. “
At a minimum, Dr. Althoff said, policymakers should consider including people with HIV with a CD4 less than 350 cells/mm3 (loosening the restriction to less than 200 cells/mm3) in their recommendations for people who are moderately or severely immunocompromised.
The research was funded with supplemental funds to the North American AIDS Cohort Collaboration on Research and Design. Dr. Coburn reports no relevant financial relationships. A coauthor has received grants from the Canadian Institutes of Health Research, Alberta Innovates, and University of Calgary/Alberta Health Services outside the submitted work. One coauthor reports serving as a consultant to Trio Health, Kennedy Dundas, and MedIQ outside the submitted work.
A version of this article first appeared on Medscape.com.
People with HIV have an increased risk of breakthrough SARS-CoV-2 infections, a new study finds, and the authors say an additional primary vaccine dose should be considered for all who are living with the disease.
Currently, an additional primary dose administered 28 days after a second dose of the mRNA (Moderna or Pfizer) vaccines or after the first dose of the Johnson & Johnson (J&J) vaccine is recommended only for those with advanced or untreated HIV.
The Centers for Disease Control and Prevention recommends boosters for all adults with or without HIV.
Sally B. Coburn, PhD, of the department of epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, led the study, which was published online in JAMA Network Open. In their study, the researchers estimate the risk of breakthrough infections among fully vaccinated adults on the basis of HIV status in the United States.
Adults with HIV who were fully vaccinated before June 30, 2021, were matched with adults without HIV with regard to date of full vaccination, age, race/ethnicity, and sex. All were followed through Dec. 31, 2021.
Patients were considered fully vaccinated either 14 days after the second dose of the Pfizer or Moderna shots or 14 days after the single dose of the J&J shot.
Breakthrough risk 28% higher
In the study of 113,994 patients, researchers found that risk of breakthrough SARS-CoV-2 infection was low overall (3.8%) but was 28% higher among people with HIV in comparison with people without HIV (adjusted hazard ratio, 1.28; 95% confidence interval, 1.19-1.37).
The breakthrough rate was also higher in the HIV group (55 cases per 1,000 person-years, vs. 43 cases per 1,000 person-years in people without HIV).
Patients were drawn from the Corona-Infectious-Virus Epidemiology Team (CIVET)–II of the North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD), which is part of the International Epidemiology Databases to Evaluate AIDS (IeDEA) collaboration involving four cohorts.
Among people with HIV, those younger than 45 years (vs. those aged 45-54) and those with a history of COVID-19 were more likely to experience breakthrough infections. Those who did not get any additional shots after the primary vaccination were more likely to have breakthrough infections, amplifying the need to get boosters, the authors wrote.
There was no link between breakthrough infections and HIV viral load suppression, but high CD4 counts (> 500 cells/mm3) were associated with fewer breakthrough cases among people with HIV, they noted.
Monica Gandhi, MD, professor of medicine and associate division chief of HIV, infectious diseases, and global medicine at the University of California, San Francisco, praised the study, noting that until now, large studies have not examined the rate of breakthrough infections among vaccinated people with HIV and people without HIV in the United States.
She told this news organization she agrees with the authors that a third dose for all who are living with HIV is needed because rates of breakthrough infections were high across all populations during the Omicron surge (which largely occurred after the period of this study).
She said she was not convinced the third shot was needed before Omicron, because breakthrough rates in both HIV and non-HIV groups were low.
“However, the most interesting part of this study for me was how well the vaccines worked in people with HIV with generally higher CD4 counts and virologic suppression, again telling us as HIV providers how well the HIV medicines work and how our patients with HIV have relatively normal immune systems if treated,” she said.
One limitation was that the study population was 92% male. Also, those without regular access to health care (who may be at greater risk for COVID-19) were less likely to be included in the study. People engaged in care may seek more frequent COVID-19 testing, which could lead to higher detection of breakthrough infections than in the general population.
“Future analyses should account for testing practices and include a larger proportion of women with HIV,” the authors wrote. “Ultimately, policy makers must determine the appropriate balance between preventing further COVID-19 infections and possibly unnecessary additional vaccinations.”
Coauthor Keri N. Althoff, PhD, told this news organization that there’s one unanswered question that would strengthen the call to action by the CDC: Do people with HIV have more severe postvaccination COVID-19 breakthrough illness?
“We have a second paper that is a preprint and currently under peer review,” she said. “In this paper, we found that people with HIV with a CD4 count less than 350 cells/mm3 were more likely to be hospitalized with postvaccination COVID-19 breakthrough illness compared to similar people without HIV. “
At a minimum, Dr. Althoff said, policymakers should consider including people with HIV with a CD4 less than 350 cells/mm3 (loosening the restriction to less than 200 cells/mm3) in their recommendations for people who are moderately or severely immunocompromised.
The research was funded with supplemental funds to the North American AIDS Cohort Collaboration on Research and Design. Dr. Coburn reports no relevant financial relationships. A coauthor has received grants from the Canadian Institutes of Health Research, Alberta Innovates, and University of Calgary/Alberta Health Services outside the submitted work. One coauthor reports serving as a consultant to Trio Health, Kennedy Dundas, and MedIQ outside the submitted work.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
COVID tied to a profound impact on children’s sleep
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
During the first year of the pandemic, profound changes in screen use and sleep timing occurred among U.S. adolescents as a result of spending more time using electronic devices, going to bed later, and getting up later, compared with before the pandemic, new research indicates.
The excessive screen time negatively affected sleep, said lead investigator Orsolya Kiss, PhD, with the Center for Health Sciences at SRI International, Menlo Park, Calif.
And what’s “concerning,” she told this news organization, is that there is no indication of any spontaneous decline in screen use in 2021, when there were fewer restrictions.
Dr. Kiss said she is “very much interested to see what future studies will show.”
The findings were presented at the annual meeting of the Associated Professional Sleep Societies.
Sleep takes a pandemic hit
“Adolescents and families have turned to online activities and social platforms more than ever before to maintain wellbeing, [to] connect with friends and family, and for online schooling,” Dr. Kiss said in a conference statement.
She and her colleagues examined longitudinal data from 5,027 adolescents aged 11-14 years who are participating in the ongoing Adolescent Brain Cognitive Development (ABCD) study.
As part of the study, participants reported sleep and daily screen time use prior to and at six time points during the first year of the pandemic (May 2020 to March 2021).
During the first year of the pandemic, relative to before the pandemic, recreational screen time was dramatically higher, with adolescents spending about 45 minutes more on social media and 20 minutes more playing video games, Dr. Kiss reported.
The jump in screen time was coupled with changes in sleep patterns.
Adolescents’ wake up times were delayed about 1.5 hours during May and August 2020, relative to prepandemic levels. The delay was partly due to summer break; wake-up times returned to earlier times in the fall of 2020.
During all pandemic assessments, bedtimes were delayed by about 1 hour, even when the new school year started. This was particularly the case in older adolescents and girls.
The findings highlight the need to promote “balanced and informed use of social media platforms, video games, and other digital technology to ensure adequate opportunity to sleep and maintain other healthy behaviors during this critical period of developmental change,” the authors wrote in their conference abstract.
Mental illness risk
In an interview, Ruth Benca, MD, PhD, co-chair of the Alliance for Sleep, noted that “during adolescence, the tendency to become more of a night owl naturally worsens, and when kids have no sleep schedule imposed on them, these patterns become exacerbated.”
Dr. Benca, who was not involved in the study, also noted that altered sleep patterns are risk factors for psychiatric illness.
“Adolescence, in particular, is so critical for brain development, and it really raises the question of whether sleep disturbances in adolescence or poor sleep patterns are contributing to the increase psychiatric epidemic we’re seeing in adolescents and children these days,” said Dr. Benca, with Wake Forest University School of Medicine and Atrium Health Wake Forest Baptist, Winston-Salem, N.C.
Also weighing in on the study, journalist and author Lisa Lewis, MS, based in Southern California, said, “It’s not surprising that tech use and social media – which is such an important part of their social worlds – went up during the pandemic.”
Ms. Lewis, a parent of two teenagers, played a key role in California’s new healthy school start times law, the first of its kind in the nation, and is the author of the newly released book, The Sleep-Deprived Teen (Mango Publishing).
“Far too many adolescents aren’t getting anywhere close to the 8-10 hours of nightly sleep they need,” Ms. Lewis said in an interview.
She noted that the the American Academy of Pediatrics recommends no tech use an hour before bed.
“And there are other house rules parents can implement, such as charging all devices in a central location, like the kitchen. Making sleep a priority helps teens, but it helps parents too: No one functions well when they’re sleep-deprived,” Ms. Lewis added.
Support for the study was provided by the National Institutes of Health. The authors have disclosed no relevant financial relationships. Dr. Benca is a consultant for Idorsia Pharmaceuticals. Ms. Lewis has no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM SLEEP 2022
Parkinson’s disease could be hiding behind those nightmares
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.

For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Pregnant women with monkeypox advised to have C-section
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
FROM ULTRASOUND IN OBSTETRICS & GYNECOLOGY