Exclude this publication from publication selection on articles and quiz
Challenge Center
Disable Inline Native ads
survey writer start date
Current Issue
Title
Latest Issue
Description
A peer-reviewed clinical journal serving healthcare professionals working with the Department of Veterans Affairs, the Department of Defense, and the Public Health Service.
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
The US Department of Veterans Affairs (VA) has announced that tele-emergency care (tele-EC) is now available nationwide. According to the VA, the expansion has already helped > 61,000 callers with a 59.4% case resolution rate, meaning veterans’ needs were resolved without them having to travel to urgent care or an emergency department.
Tele-EC does not replace the need for in-person emergency evaluation, but offers quick, virtual triage assessments for veterans in rural areas or those with mobility and transportation challenges when in-person immediate care can be difficult to access. The program is a part of VA Health Connect, which connects the caller to a clinical triage nurse, who connects the veteran to tele-emergency care when clinically appropriate. Tele-EC practitioners evaluate the veteran over the phone or on video and recommend treatment or follow-up, including in-person care if needed. In life-threatening emergencies, the clinical triage nurse will call 911 and stay on the phone with the veteran until help arrives. The VA however, says the best step for a veteran experiencing a life-threatening emergency is to immediately contact 911 as opposed to seeking support via tele-EC.
The program can save time not only through on-the-spot evaluation, but by avoiding drive and wait times. “Sometimes, you’re not sure whether what you’re experiencing is a minor emergency or not — and tele-emergency care can help you resolve those questions,” VA Under Secretary for Health Shereef Elnahal, MD, says. “Veterans can get immediate, virtual triage with a VA medical provider who has direct access to their medical records. This avoids having to potentially drive to the nearest emergency department and wait to be evaluated, if appropriate.”
Testing for mismatch repair (MMR) and microsatellite instability (MSI) among patients with colorectal cancer (CRC) increased from 22.7% in 2012 to 71.5% in 2021, but variations in access remain, with testing rates differing by cancer stage, individual hospital, patient sex, race, and insurance status.
METHODOLOGY:
In 2017, the National Comprehensive Cancer Network (NCCN) recommended universal testing for MMR and MSI among patients with CRC, but studies suggest that testing may still be underused.
To assess trends and factors associated with MMR/MSI testing in the United States, researchers evaluated 834,797 patients diagnosed with stage I-IV CRC between 2012 and 2021 across 1366 Commission on Cancer–accredited hospitals in the National Cancer Database.
The variability in MMR/MSI testing was assessed in relation to both patient and hospital-level factors.
Overall, 70.7% patients had colon cancer, 7.3% had rectosigmoid cancer, and 22.0% had rectal cancer. The median patient age was 66 years; just over half (53%) were men, 81.8% were White, and 11.9% were Black.
TAKEAWAY:
Overall, 43.9% patients underwent MMR/MSI testing, but testing rates increased more than threefold between 2012 and 2021 — from 22.7% to 71.5%. Still, testing rates varied depending on a range of factors.
About 22% variability in MMR/MSI testing was attributed to hospital-level variations, with the best vs worst performing hospitals reporting testing rates of 90% vs 2%. This hospital-level variation may be caused by testing protocol differences at individual institutions, the authors said.
The likelihood of undergoing MMR/MSI testing was lower in patients with stage IV vs stage I disease (adjusted odds ratio [aOR], 0.78) but higher in those with stage II (aOR, 1.53) and III (aOR, 1.40) disease.
The likelihood of undergoing MMR/MSI testing was slightly lower for men than for women (aOR, 0.98) and for Black patients than for White patients (aOR, 0.97). Having a lower household income, public or no insurance (vs private insurance), or living a longer distance (more than 5 miles) from the treatment facility was also associated with lower odds of testing.
IN PRACTICE:
“This cohort study indicated that MMR/MSI testing increased markedly, suggesting increased NCCN guideline adherence,” the authors said. However, variations still exist by cancer stage, hospital, and patient factors. Implementing “widespread institution-level reflexive testing for every initial diagnostic biopsy” can improve testing rates and reduce disparities, the authors suggested.
SOURCE:
This study, led by Totadri Dhimal, MD, University of Rochester Medical Center in New York, was published onlinein JAMA Oncology.
LIMITATIONS:
The study lacked clinical granularity, and potential coding inaccuracies and incomplete data could have affected the interpretation and generalizability of the findings.
DISCLOSURES:
No funding information was provided for the study. One author reported receiving author royalties from UpToDate outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Testing for mismatch repair (MMR) and microsatellite instability (MSI) among patients with colorectal cancer (CRC) increased from 22.7% in 2012 to 71.5% in 2021, but variations in access remain, with testing rates differing by cancer stage, individual hospital, patient sex, race, and insurance status.
METHODOLOGY:
In 2017, the National Comprehensive Cancer Network (NCCN) recommended universal testing for MMR and MSI among patients with CRC, but studies suggest that testing may still be underused.
To assess trends and factors associated with MMR/MSI testing in the United States, researchers evaluated 834,797 patients diagnosed with stage I-IV CRC between 2012 and 2021 across 1366 Commission on Cancer–accredited hospitals in the National Cancer Database.
The variability in MMR/MSI testing was assessed in relation to both patient and hospital-level factors.
Overall, 70.7% patients had colon cancer, 7.3% had rectosigmoid cancer, and 22.0% had rectal cancer. The median patient age was 66 years; just over half (53%) were men, 81.8% were White, and 11.9% were Black.
TAKEAWAY:
Overall, 43.9% patients underwent MMR/MSI testing, but testing rates increased more than threefold between 2012 and 2021 — from 22.7% to 71.5%. Still, testing rates varied depending on a range of factors.
About 22% variability in MMR/MSI testing was attributed to hospital-level variations, with the best vs worst performing hospitals reporting testing rates of 90% vs 2%. This hospital-level variation may be caused by testing protocol differences at individual institutions, the authors said.
The likelihood of undergoing MMR/MSI testing was lower in patients with stage IV vs stage I disease (adjusted odds ratio [aOR], 0.78) but higher in those with stage II (aOR, 1.53) and III (aOR, 1.40) disease.
The likelihood of undergoing MMR/MSI testing was slightly lower for men than for women (aOR, 0.98) and for Black patients than for White patients (aOR, 0.97). Having a lower household income, public or no insurance (vs private insurance), or living a longer distance (more than 5 miles) from the treatment facility was also associated with lower odds of testing.
IN PRACTICE:
“This cohort study indicated that MMR/MSI testing increased markedly, suggesting increased NCCN guideline adherence,” the authors said. However, variations still exist by cancer stage, hospital, and patient factors. Implementing “widespread institution-level reflexive testing for every initial diagnostic biopsy” can improve testing rates and reduce disparities, the authors suggested.
SOURCE:
This study, led by Totadri Dhimal, MD, University of Rochester Medical Center in New York, was published onlinein JAMA Oncology.
LIMITATIONS:
The study lacked clinical granularity, and potential coding inaccuracies and incomplete data could have affected the interpretation and generalizability of the findings.
DISCLOSURES:
No funding information was provided for the study. One author reported receiving author royalties from UpToDate outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Testing for mismatch repair (MMR) and microsatellite instability (MSI) among patients with colorectal cancer (CRC) increased from 22.7% in 2012 to 71.5% in 2021, but variations in access remain, with testing rates differing by cancer stage, individual hospital, patient sex, race, and insurance status.
METHODOLOGY:
In 2017, the National Comprehensive Cancer Network (NCCN) recommended universal testing for MMR and MSI among patients with CRC, but studies suggest that testing may still be underused.
To assess trends and factors associated with MMR/MSI testing in the United States, researchers evaluated 834,797 patients diagnosed with stage I-IV CRC between 2012 and 2021 across 1366 Commission on Cancer–accredited hospitals in the National Cancer Database.
The variability in MMR/MSI testing was assessed in relation to both patient and hospital-level factors.
Overall, 70.7% patients had colon cancer, 7.3% had rectosigmoid cancer, and 22.0% had rectal cancer. The median patient age was 66 years; just over half (53%) were men, 81.8% were White, and 11.9% were Black.
TAKEAWAY:
Overall, 43.9% patients underwent MMR/MSI testing, but testing rates increased more than threefold between 2012 and 2021 — from 22.7% to 71.5%. Still, testing rates varied depending on a range of factors.
About 22% variability in MMR/MSI testing was attributed to hospital-level variations, with the best vs worst performing hospitals reporting testing rates of 90% vs 2%. This hospital-level variation may be caused by testing protocol differences at individual institutions, the authors said.
The likelihood of undergoing MMR/MSI testing was lower in patients with stage IV vs stage I disease (adjusted odds ratio [aOR], 0.78) but higher in those with stage II (aOR, 1.53) and III (aOR, 1.40) disease.
The likelihood of undergoing MMR/MSI testing was slightly lower for men than for women (aOR, 0.98) and for Black patients than for White patients (aOR, 0.97). Having a lower household income, public or no insurance (vs private insurance), or living a longer distance (more than 5 miles) from the treatment facility was also associated with lower odds of testing.
IN PRACTICE:
“This cohort study indicated that MMR/MSI testing increased markedly, suggesting increased NCCN guideline adherence,” the authors said. However, variations still exist by cancer stage, hospital, and patient factors. Implementing “widespread institution-level reflexive testing for every initial diagnostic biopsy” can improve testing rates and reduce disparities, the authors suggested.
SOURCE:
This study, led by Totadri Dhimal, MD, University of Rochester Medical Center in New York, was published onlinein JAMA Oncology.
LIMITATIONS:
The study lacked clinical granularity, and potential coding inaccuracies and incomplete data could have affected the interpretation and generalizability of the findings.
DISCLOSURES:
No funding information was provided for the study. One author reported receiving author royalties from UpToDate outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Potassium-competitive acid blocker vonoprazan is safe and effective for patients with heartburn from nonerosive reflux disease (NERD), according to investigators.
Benefits of vonoprazan were seen as soon as the first day of treatment and persisted through the 20-week extension period, lead author Loren Laine, MD, AGAF, of Yale School of Medicine, New Haven, Connecticut, and colleagues reported.
Yale School of Medicine
Dr. Loren Laine
“A potential alternative to PPI therapy is a potassium-competitive acid blocker, a new class of antisecretory agents that provide more potent inhibition of gastric acid secretion than PPIs,” the investigators wrote in Clinical Gastroenterology and Hepatology.
While a small observational study found that 18 out of 26 patients (69%) with PPI-resistant NERD had improved symptoms with vonoprazan, subsequent randomized trials in Japan failed to meet their primary endpoints, Laine and colleagues noted. The present randomized trial was therefore conducted to determine how vonoprazan might help a US patient population.
The study involved 772 patients who reported heartburn at least 4 days per week during screening, but without erosive esophagitis on endoscopy. Participants were randomized into three groups: placebo, vonoprazan 10 mg, or vonoprazan 20 mg. These protocols were administered for 4 weeks, followed by a 20-week extension, in which placebo patients were rerandomized to receive one of the two vonoprazan dose levels.
The primary endpoint was the percentage of days without daytime or nighttime heartburn (24-hour heartburn-free days) during the initial 4-week treatment period. The secondary endpoint, assessed during the same timeframe, was percentage of days without need for a rescue antacid.
In the 4-week placebo-controlled period, patients treated with vonoprazan 10 mg and 20 mg showed a significant improvement in heartburn-free days, compared with placebo. The percentage of 24-hour heartburn-free days was 27.7% in the placebo group vs 44.8% in the 10-mg vonoprazan group (least squares mean difference 17.1%; P < .0001) and 44.4% in the 20 mg vonoprazan group (least squares mean difference 16.7%; P < .0001).
Benefits of vonoprazan were seen as early as the first day of treatment, with 8.3% and 11.6% more patients in the 10-mg and 20-mg groups, respectively, experiencing a heartburn-free day, compared with placebo. By day 2, these differences increased to 18.1% and 23.2%, respectively.
The percentage of days without rescue antacid use was also significantly higher in both vonoprazan groups. Patients in the 10 mg and 20 mg groups had 63.3% and 61.2% of days without antacid use, respectively, compared with 47.6% in the placebo group (P < .0001 for both comparisons).
These benefits persisted throughout the 20-week extension period, with similar percentages of heartburn-free days across all groups. Mean percentages of 24-hour heartburn-free days ranged from 61% to 63% in the extension phase, while median percentages spanned 76%-79%.
Adverse events were infrequent and comparable across all groups. The most common adverse event was nausea, occurring slightly more frequently in the vonoprazan groups (2.3% in the 10-mg group and 3.1% in the 20-mg group) vs placebo (0.4%). Serious adverse events were rare and were deemed unrelated to treatment. No new safety signals were identified during the 20-week extension period. Increases in serum gastrin levels, a marker of acid suppression, returned to near baseline after discontinuation of vonoprazan.
“In conclusion, the potassium-competitive acid blocker vonoprazan was efficacious in reducing heartburn symptoms in patients with NERD, with the benefit appearing to begin as early as the first day of therapy,” Laine and colleagues wrote.
In July 2024, the Food and Drug Administration approved vonoprazan for treating heartburn in patients with nonerosive gastroesophageal reflux disease.This study was funded by Phathom Pharmaceuticals. The investigators disclosed additional relationships with Takeda, Medtronic, Carnot, and others.
Body
Proton pump inhibitors (PPIs) have revolutionized the treatment of gastroesophageal reflux disease (GERD). One might ask what the reason would be to challenge this giant of the pharmacopeia with another medication for GERD.
Dr. David A. Katzka
Enter vonoprazan, which competitively binds to the H+, K+-ATPase alpha-subunit (PCAB), has a more rapid and sustained onset of gastric acid inhibition, is resistant to degradation by acid and remains active at a neutral pH, has a t ½ four times longer than a PPI, and is not metabolized through the CYP2C19 or CYP3A4 enzyme. But do these pharmacokinetic advantages translate to clinical advantages in the treatment of GERD?
In this important study by Laine et al, vonoprazan is expectedly efficacious in treating nonerosive GERD (NERD) but notably less so when compared with the authors’ trial for erosive GERD. This is not surprising owing to the multiple and common acid independent etiologies of NERD, such as esophageal hypersensitivity. The high placebo response supports this. Two notable results, however, merit emphasis in potential advantages over PPIs.
First, vonoprazan is effective at day 1 of therapy by eliminating the need for loading. Second, nocturnal reflux, a purer form of GERD, is better controlled with a morning dose of vonopazan mitigating against nocturnal acid breakthrough and the need for twice-daily dosing with PPIs and/or addition of an H2 antagonist. These results by no means advocate for replacement of PPIs with PCABs, but at least suggest specific populations of GERD patients who may specifically benefit from PCAB use. The study also indirectly emphasizes that careful selection of NERD patients whose GERD symptoms are predominantly caused by increased esophageal acid exposure are the most appropriate candidates. The ultimate answer as to where vonoprazan will be used in our practice is evolving.
David Katzka, MD, is based in the Division of Digestive and Liver Diseases, Columbia University Medical Center, New York City. He has received research support from Takeda, Sanofi, and Regeneron. He is also an associate editor for GI & Hepatology News.
Proton pump inhibitors (PPIs) have revolutionized the treatment of gastroesophageal reflux disease (GERD). One might ask what the reason would be to challenge this giant of the pharmacopeia with another medication for GERD.
Dr. David A. Katzka
Enter vonoprazan, which competitively binds to the H+, K+-ATPase alpha-subunit (PCAB), has a more rapid and sustained onset of gastric acid inhibition, is resistant to degradation by acid and remains active at a neutral pH, has a t ½ four times longer than a PPI, and is not metabolized through the CYP2C19 or CYP3A4 enzyme. But do these pharmacokinetic advantages translate to clinical advantages in the treatment of GERD?
In this important study by Laine et al, vonoprazan is expectedly efficacious in treating nonerosive GERD (NERD) but notably less so when compared with the authors’ trial for erosive GERD. This is not surprising owing to the multiple and common acid independent etiologies of NERD, such as esophageal hypersensitivity. The high placebo response supports this. Two notable results, however, merit emphasis in potential advantages over PPIs.
First, vonoprazan is effective at day 1 of therapy by eliminating the need for loading. Second, nocturnal reflux, a purer form of GERD, is better controlled with a morning dose of vonopazan mitigating against nocturnal acid breakthrough and the need for twice-daily dosing with PPIs and/or addition of an H2 antagonist. These results by no means advocate for replacement of PPIs with PCABs, but at least suggest specific populations of GERD patients who may specifically benefit from PCAB use. The study also indirectly emphasizes that careful selection of NERD patients whose GERD symptoms are predominantly caused by increased esophageal acid exposure are the most appropriate candidates. The ultimate answer as to where vonoprazan will be used in our practice is evolving.
David Katzka, MD, is based in the Division of Digestive and Liver Diseases, Columbia University Medical Center, New York City. He has received research support from Takeda, Sanofi, and Regeneron. He is also an associate editor for GI & Hepatology News.
Body
Proton pump inhibitors (PPIs) have revolutionized the treatment of gastroesophageal reflux disease (GERD). One might ask what the reason would be to challenge this giant of the pharmacopeia with another medication for GERD.
Dr. David A. Katzka
Enter vonoprazan, which competitively binds to the H+, K+-ATPase alpha-subunit (PCAB), has a more rapid and sustained onset of gastric acid inhibition, is resistant to degradation by acid and remains active at a neutral pH, has a t ½ four times longer than a PPI, and is not metabolized through the CYP2C19 or CYP3A4 enzyme. But do these pharmacokinetic advantages translate to clinical advantages in the treatment of GERD?
In this important study by Laine et al, vonoprazan is expectedly efficacious in treating nonerosive GERD (NERD) but notably less so when compared with the authors’ trial for erosive GERD. This is not surprising owing to the multiple and common acid independent etiologies of NERD, such as esophageal hypersensitivity. The high placebo response supports this. Two notable results, however, merit emphasis in potential advantages over PPIs.
First, vonoprazan is effective at day 1 of therapy by eliminating the need for loading. Second, nocturnal reflux, a purer form of GERD, is better controlled with a morning dose of vonopazan mitigating against nocturnal acid breakthrough and the need for twice-daily dosing with PPIs and/or addition of an H2 antagonist. These results by no means advocate for replacement of PPIs with PCABs, but at least suggest specific populations of GERD patients who may specifically benefit from PCAB use. The study also indirectly emphasizes that careful selection of NERD patients whose GERD symptoms are predominantly caused by increased esophageal acid exposure are the most appropriate candidates. The ultimate answer as to where vonoprazan will be used in our practice is evolving.
David Katzka, MD, is based in the Division of Digestive and Liver Diseases, Columbia University Medical Center, New York City. He has received research support from Takeda, Sanofi, and Regeneron. He is also an associate editor for GI & Hepatology News.
Title
Effective at Day 1
Effective at Day 1
Potassium-competitive acid blocker vonoprazan is safe and effective for patients with heartburn from nonerosive reflux disease (NERD), according to investigators.
Benefits of vonoprazan were seen as soon as the first day of treatment and persisted through the 20-week extension period, lead author Loren Laine, MD, AGAF, of Yale School of Medicine, New Haven, Connecticut, and colleagues reported.
Yale School of Medicine
Dr. Loren Laine
“A potential alternative to PPI therapy is a potassium-competitive acid blocker, a new class of antisecretory agents that provide more potent inhibition of gastric acid secretion than PPIs,” the investigators wrote in Clinical Gastroenterology and Hepatology.
While a small observational study found that 18 out of 26 patients (69%) with PPI-resistant NERD had improved symptoms with vonoprazan, subsequent randomized trials in Japan failed to meet their primary endpoints, Laine and colleagues noted. The present randomized trial was therefore conducted to determine how vonoprazan might help a US patient population.
The study involved 772 patients who reported heartburn at least 4 days per week during screening, but without erosive esophagitis on endoscopy. Participants were randomized into three groups: placebo, vonoprazan 10 mg, or vonoprazan 20 mg. These protocols were administered for 4 weeks, followed by a 20-week extension, in which placebo patients were rerandomized to receive one of the two vonoprazan dose levels.
The primary endpoint was the percentage of days without daytime or nighttime heartburn (24-hour heartburn-free days) during the initial 4-week treatment period. The secondary endpoint, assessed during the same timeframe, was percentage of days without need for a rescue antacid.
In the 4-week placebo-controlled period, patients treated with vonoprazan 10 mg and 20 mg showed a significant improvement in heartburn-free days, compared with placebo. The percentage of 24-hour heartburn-free days was 27.7% in the placebo group vs 44.8% in the 10-mg vonoprazan group (least squares mean difference 17.1%; P < .0001) and 44.4% in the 20 mg vonoprazan group (least squares mean difference 16.7%; P < .0001).
Benefits of vonoprazan were seen as early as the first day of treatment, with 8.3% and 11.6% more patients in the 10-mg and 20-mg groups, respectively, experiencing a heartburn-free day, compared with placebo. By day 2, these differences increased to 18.1% and 23.2%, respectively.
The percentage of days without rescue antacid use was also significantly higher in both vonoprazan groups. Patients in the 10 mg and 20 mg groups had 63.3% and 61.2% of days without antacid use, respectively, compared with 47.6% in the placebo group (P < .0001 for both comparisons).
These benefits persisted throughout the 20-week extension period, with similar percentages of heartburn-free days across all groups. Mean percentages of 24-hour heartburn-free days ranged from 61% to 63% in the extension phase, while median percentages spanned 76%-79%.
Adverse events were infrequent and comparable across all groups. The most common adverse event was nausea, occurring slightly more frequently in the vonoprazan groups (2.3% in the 10-mg group and 3.1% in the 20-mg group) vs placebo (0.4%). Serious adverse events were rare and were deemed unrelated to treatment. No new safety signals were identified during the 20-week extension period. Increases in serum gastrin levels, a marker of acid suppression, returned to near baseline after discontinuation of vonoprazan.
“In conclusion, the potassium-competitive acid blocker vonoprazan was efficacious in reducing heartburn symptoms in patients with NERD, with the benefit appearing to begin as early as the first day of therapy,” Laine and colleagues wrote.
In July 2024, the Food and Drug Administration approved vonoprazan for treating heartburn in patients with nonerosive gastroesophageal reflux disease.This study was funded by Phathom Pharmaceuticals. The investigators disclosed additional relationships with Takeda, Medtronic, Carnot, and others.
Potassium-competitive acid blocker vonoprazan is safe and effective for patients with heartburn from nonerosive reflux disease (NERD), according to investigators.
Benefits of vonoprazan were seen as soon as the first day of treatment and persisted through the 20-week extension period, lead author Loren Laine, MD, AGAF, of Yale School of Medicine, New Haven, Connecticut, and colleagues reported.
Yale School of Medicine
Dr. Loren Laine
“A potential alternative to PPI therapy is a potassium-competitive acid blocker, a new class of antisecretory agents that provide more potent inhibition of gastric acid secretion than PPIs,” the investigators wrote in Clinical Gastroenterology and Hepatology.
While a small observational study found that 18 out of 26 patients (69%) with PPI-resistant NERD had improved symptoms with vonoprazan, subsequent randomized trials in Japan failed to meet their primary endpoints, Laine and colleagues noted. The present randomized trial was therefore conducted to determine how vonoprazan might help a US patient population.
The study involved 772 patients who reported heartburn at least 4 days per week during screening, but without erosive esophagitis on endoscopy. Participants were randomized into three groups: placebo, vonoprazan 10 mg, or vonoprazan 20 mg. These protocols were administered for 4 weeks, followed by a 20-week extension, in which placebo patients were rerandomized to receive one of the two vonoprazan dose levels.
The primary endpoint was the percentage of days without daytime or nighttime heartburn (24-hour heartburn-free days) during the initial 4-week treatment period. The secondary endpoint, assessed during the same timeframe, was percentage of days without need for a rescue antacid.
In the 4-week placebo-controlled period, patients treated with vonoprazan 10 mg and 20 mg showed a significant improvement in heartburn-free days, compared with placebo. The percentage of 24-hour heartburn-free days was 27.7% in the placebo group vs 44.8% in the 10-mg vonoprazan group (least squares mean difference 17.1%; P < .0001) and 44.4% in the 20 mg vonoprazan group (least squares mean difference 16.7%; P < .0001).
Benefits of vonoprazan were seen as early as the first day of treatment, with 8.3% and 11.6% more patients in the 10-mg and 20-mg groups, respectively, experiencing a heartburn-free day, compared with placebo. By day 2, these differences increased to 18.1% and 23.2%, respectively.
The percentage of days without rescue antacid use was also significantly higher in both vonoprazan groups. Patients in the 10 mg and 20 mg groups had 63.3% and 61.2% of days without antacid use, respectively, compared with 47.6% in the placebo group (P < .0001 for both comparisons).
These benefits persisted throughout the 20-week extension period, with similar percentages of heartburn-free days across all groups. Mean percentages of 24-hour heartburn-free days ranged from 61% to 63% in the extension phase, while median percentages spanned 76%-79%.
Adverse events were infrequent and comparable across all groups. The most common adverse event was nausea, occurring slightly more frequently in the vonoprazan groups (2.3% in the 10-mg group and 3.1% in the 20-mg group) vs placebo (0.4%). Serious adverse events were rare and were deemed unrelated to treatment. No new safety signals were identified during the 20-week extension period. Increases in serum gastrin levels, a marker of acid suppression, returned to near baseline after discontinuation of vonoprazan.
“In conclusion, the potassium-competitive acid blocker vonoprazan was efficacious in reducing heartburn symptoms in patients with NERD, with the benefit appearing to begin as early as the first day of therapy,” Laine and colleagues wrote.
In July 2024, the Food and Drug Administration approved vonoprazan for treating heartburn in patients with nonerosive gastroesophageal reflux disease.This study was funded by Phathom Pharmaceuticals. The investigators disclosed additional relationships with Takeda, Medtronic, Carnot, and others.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
One of the things I picked up on was a nice mini-symposium on gastrointestinal cancer led by Sara Lonardi, who made an excellent presentation, picking out three abstracts. They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
One of the things I picked up on was a nice mini-symposium on gastrointestinal cancer led by Sara Lonardi, who made an excellent presentation, picking out three abstracts. They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
One of the things I picked up on was a nice mini-symposium on gastrointestinal cancer led by Sara Lonardi, who made an excellent presentation, picking out three abstracts. They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
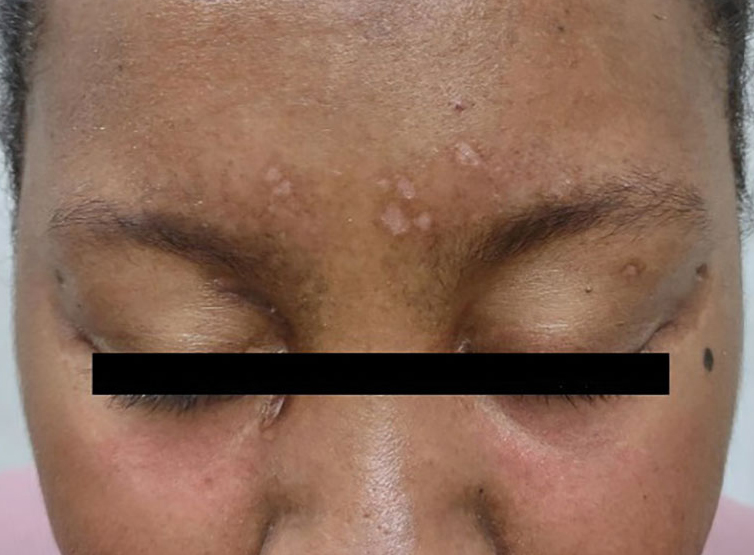
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
Author and Disclosure Information
LT Logan Oliver, MD, USNa; CAPT Rachel Lee, MD, FACP, USNa; MAJ Michael Loncharich, MD, USAb; CPT Shena Kravitz, MD, USAb; MAJ Rebecca Wetzel, DO, USAb; CPT Jon Heald, DO, USAb
Author affiliations aNaval Medical Center San Diego, California bWalter Reed National Military Medical Center, Bethesda, Maryland
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article
Fed Pract. 2024;41(10) Published online October 16. doi:10.12788/fp0517
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
A previously healthy 31-year-old female active-duty Navy sailor working as a calibration technician developed a painful, erythematous, pruritic, indurated plaque on her left breast. The sailor was not lactating and had no known family history of malignancy. Initially, she was treated by her primary care practitioner for presumed mastitis with oral cephalexin and then with oral clindamycin with no symptom improvement. About 2 weeks after the completion of both antibiotic courses, she developed angioedema and periorbital edema (Figure 1), requiring highdose corticosteroids and antihistamines with a corticosteroid course of prednisone 40 mg daily tapered to 10 mg daily over 12 days and diphenhydramine 25 mg to use up to 4 times daily. Workup for both was acquired and hereditary angioedema was unremarkable. Two months later, the patient developed patches of alopecia, oral ulcerations, and hypopigmented plaques with a peripheral hyperpigmented rim on the central face and bilateral conchal bowls (Figure 2). She also developed hypopigmented papules with peripheral hyperpigmentation on the bilateral dorsal hands overlying the metacarpal and proximal interphalangeal joints, which eventually ulcerated (Figure 3). Laboratory evaluation, including tests for creatine kinase, aldolase, transaminases, lactate dehydrogenase, and autoantibodies (antiJo-1, anti-Mi-2, anti-MDA-5, anti-TIF-1, anti-NXP-2, and anti-SAEP), were unremarkable. A punch biopsy from a papule on the right dorsal hand showed superficial perivascular lymphohistiocytic inflammation with a subtle focal increase in dermal mucin, highlighted by the colloidal iron stain. Further evaluation of the left breast plaque revealed ER/PR+ HER2- stage IIIB inflammatory breast cancer.
FIGURE 1 Angioedema With Notable Periorbital Edema
FIGURE 2 Alopecia Patches, Hypopigmented Plaques, and Peripheral Hyperpigmented Rim on Central Face
FIGURE 3 Ulcerative Papules Overlying the Metacarpal and Proximal Interphalangeal Joints
DISCUSSION
Based on the clinical presentation and diagnosis of inflammatory breast cancer, the patient was diagnosed with paraneoplastic clinically amyopathic dermatomyositis (CADM). She was treated for her breast cancer with an initial chemotherapy regimen consisting of dose-dense cyclophosphamide and doxorubicin followed by paclitaxel. The patient underwent a mastectomy, axillary lymph node dissection, and 25 sessions of radiation therapy, and is currently continuing therapy with anastrozole 1 mg daily and ovarian suppression with leuprorelin 11.25 mg every 3 months. For the severe angioedema and dermatomyositis-like cutaneous findings, the patient was continued on high-dose corticosteroids at prednisone 60 mg daily with a prolonged taper to prednisone 10 mg daily. After about 10 months, she transitioned from prednisone 10 mg daily to hydrocortisone 30 mg daily and is currently tapering her hydrocortisone dosing. She was additionally started on monthly intravenous immunoglobulin, hydroxychloroquine 300 mg daily, and amlodipine 5 mg daily. The ulcerated papules on her hands were treated with topical clobetasol 0.05% ointment applied daily, topical tacrolimus 0.1% ointment applied daily, and multiple intralesional triamcinolone 5 mg/mL injections. With this regimen, the patient experienced significant improvement in her cutaneous symptoms.
CADM is a rare autoimmune inflammatory disease featuring classic dermatomyositis-like cutaneous findings such as a heliotrope rash and Gottron papules. Ulcerative Gottron papules are less common than the typical erythematous papules and are associated more strongly with amyopathic disease.1 Paraneoplastic myositis poses a diagnostic challenge because it presents like an idiopathic dermatomyositis and often has a heterogeneous clinical presentation with additional manifestations, including periorbital edema, myalgias, dysphagia, and shortness of breath. If clinically suspected, laboratory tests (eg, creatine kinase, aldolase, transaminases, and lactate dehydrogenase) can assist in diagnosing paraneoplastic myositis. Additionally, serologic testing for autoantibodies such as anti-CADM-140, anti-Jo-1, anti-Mi-2, antiMDA-5, anti-TIF-1, anti-NXP-2, and antiSAE can assist the diagnosis and predict disease phenotype.1,2
Malignancy can precede, occur during, or develop after the diagnosis of CADM.3 Malignancies most often associated with CADM include ovarian, breast, and lung cancers.4 Despite the strong correlation with malignancy, there are currently no screening guidelines for malignancy upon inflammatory myositis diagnosis. Therefore, it is important to consider the entirety of a patient’s clinical presentation in establishing further evaluation in the initial diagnostic workup.
There are numerous systemic complications associated with inflammatory myositis and imaging modalities can help to rule out some of these conditions. CADM is strongly associated with the development of interstitial lung disease, so chest radiography and pulmonary function testing are often checked.1 Though cardiac and esophageal involvement are more commonly associated with classic dermatomyositis, it may be useful to obtain an electrocardiogram to rule out conduction abnormalities from myocardial involvement, along with esophageal manometry to evaluate for esophageal dysmotility.1,5
In the management of paraneoplastic CADM, the underlying malignancy should be treated first.6 If symptoms persist after the cancer is in remission, then CADM is treated with immunosuppressive medications such as methotrexate, mycophenolate mofetil, or azathioprine. Physical therapy can also provide further symptom relief for those suffering from proximal weakness.
CONCLUSIONS
Presumed mastitis, angioedema, and eczematous lesions for this patient were dermatologic manifestations of an underlying inflammatory breast cancer. This case highlights the importance of early recognition, the diagnosis of CADM and awareness of its association with underlying malignancy, especially within the primary care setting where most skin concerns are addressed. Early clinical suspicion and a swift diagnostic workup can further optimize multidisciplinary management, which is often required to treat malignancies.
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
References
Cao H, Xia Q, Pan M, et al. Gottron papules and gottron sign with ulceration: a distinctive cutaneous feature in a subset of patients with classic dermatomyositis and clinically amyopathic dermatomyositis. J Rheumatol. 2016;43(9):1735-1742. doi:10.3899/jrheum.160024
Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. 2017;52(1):1-19. doi:10.1007/s12016-015-8510-y
Zahr ZA, Baer AN. Malignancy in myositis. Curr Rheumatol Rep. 2011;13(3):208-215. doi:10.1007/s11926-011-0169-7
Udkoff J, Cohen PR. Amyopathic dermatomyositis: a concise review of clinical manifestations and associated malignancies. Am J Clin Dermatol. 2016;17(5): 509-518. doi:10.1007/s40257-016-0199-z
Fathi M, Lundberg IE, Tornling G. Pulmonary complications of polymyositis and dermatomyositis. Semin Respir Crit Care Med. 2007;28(4):451-458. doi:10.1055/s-2007-985666
Hendren E, Vinik O, Faragalla H, Haq R. Breast cancer and dermatomyositis: a case study and literature review. Curr Oncol. 2017;24(5):e429-e433. doi:10.3747/co.24.3696
Antimicrobial resistance is a global threat and burden to health care, with > 2.8 million antibiotic-resistant infections occurring annually in the United States.1 To combat this issue and improve patient care, the US Department of Veterans Affairs (VA) has implemented antimicrobial stewardship programs (ASPs) across its health care systems. ASPs are multidisciplinary teams that promote evidence-based use of antimicrobials through activities supporting appropriate selection, dosing, route, and duration of antimicrobial therapy. ASP best practices are also included in the Joint Commission and Centers for Medicare and Medicaid Services accreditation standards.2
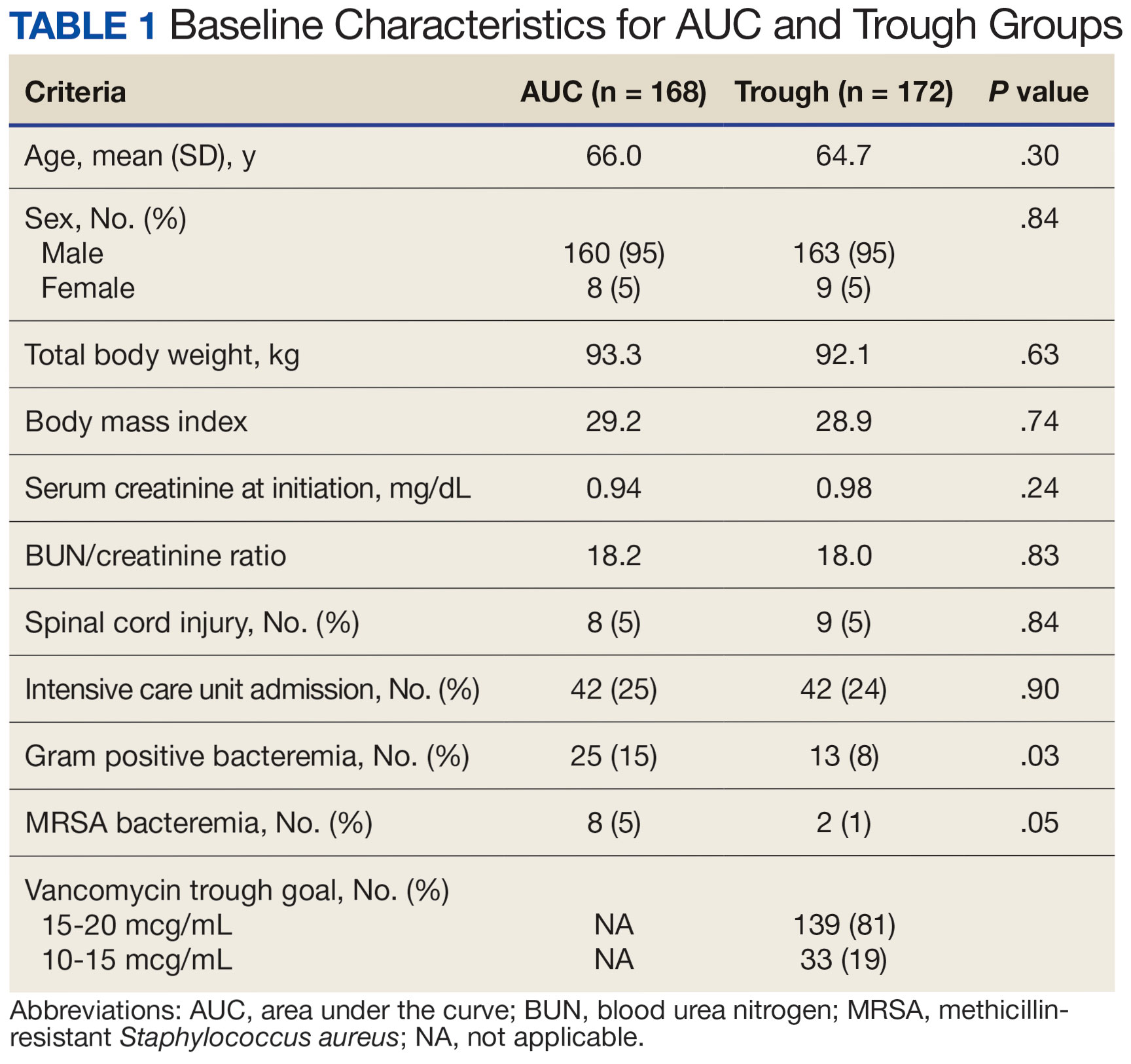
The foundational charge for VA facilities to develop and maintain ASPs was outlined in 2014 and updated in 2023 in the Veterans Health Administration (VHA) Directive 1031 on antimicrobial stewardship programs.2 This directive outlines specific requirements for all VA ASPs, including personnel, staffing levels, and the roles and responsibilities of all team members. VHA now requires that Veterans Integrated Services Networks (VISNs) establish robust ASP collaboratives. A VISN ASP collaborative consists of stewardship champions from each VA medical center in the VISN and is designed to support, develop, and enhance ASP programs across all facilities within that VISN.2 Some VISNs may lack an ASP collaborative altogether, and others with existing groups may seek ways to expand their collaboratives in line with the updated directive. Prior to VHA Directive 1031, the VA Sunshine Healthcare Network (VISN 8) established an ASP collaborative. This article describes the structure and activities of the VISN 8 ASP collaborative and highlights a recent VISN 8 quality assurance initiative related to vancomycin area under the curve (AUC) dosing that illustrates how ASP collaboratives can enhance stewardship and clinical care across broad geographic areas.
VISN 8 ASP
The VHA, the largest integrated US health care system, is divided into 18 VISNs that provide regional systems of care to enhance access and meet the local health care needs of veterans.3 VISN 8 serves > 1.5 million veterans across 165,759 km2 in Florida, South Georgia, Puerto Rico, and the US Virgin Islands.4 The network is composed of 7 health systems with 8 medical centers and > 60 outpatient clinics. These facilities provide comprehensive acute, primary, and specialty care, as well as mental health and extended care services in inpatient, outpatient, nursing home, and home care settings.4
The 2023 VHA Directive 1031 update recognizes the importance of VISN-level coordination of ASP activities to enhance the standardization of care and build partnerships in stewardship across all levels of care. The VISN 8 ASP collaborative workgroup (ASPWG) was established in 2015. Consistent with Directive 1031, the ASPWG is guided by clinician and pharmacist VISN leads. These leads serve as subject matter experts, facilitate access to resources, establish VISN-level consensus, and enhance communication among local ASP champions at medical centers within the VISN. All 7 health systems include = 1 ASP champion (clinician or pharmacist) in the ASPWG. Ad hoc members, whose routine duties are not solely focused on antimicrobial stewardship, contribute to specific stewardship projects as needed. For example, the ASPWG has included internal medicine, emergency department, community living center pharmacists, representatives from pharmacy administration, and trainees (pharmacy students and residents, and infectious diseases fellows) in antimicrobial stewardship initiatives. The inclusion of non-ASP champions is not discussed in VHA Directive 1031. However, these members have made valuable contributions to the ASPWG.
The ASPWG meets monthly. Agendas and priorities are developed by the VISN pharmacist and health care practitioner (HCP) leads. Monthly discussions may include but are not limited to a review of national formulary decisions, VISN goals and metrics, infectious diseases hot topics, pharmacoeconomic initiatives, strong practice presentations, regulatory and accreditation preparation, preparation of tracking reports, as well as the development of both patient-level and HCPlevel tools, resources, and education materials. This forum facilitates collaborative learning: members process and synthesize information, share and reframe ideas, and listen to other viewpoints to gain a complete understanding as a group.5 For example, ASPWG members have leaned on each other to prepare for Joint Commission accreditation surveys and strengthen the VISN 8 COVID-19 program through the rollout of vaccines and treatments. Other collaborative projects completed over the past few years included a penicillin allergy testing initiative and anti-methicillin-resistant Staphylococcus aureus (MRSA) and pseudomonal medication use evaluations. This team-centric problem-solving approach is highly effective while also fostering professional and social relationships. However, collaboratives could be perceived to have drawbacks. There may be opportunity costs if ASP time is allocated for issues that have already been addressed locally or concerns that standardization might hinder rapid adoption of practices at individual sites. Therefore, participation in each distinct group initiative is optional. This allows sites to choose projects related to their high priority areas and maintain bandwidth to implement practices not yet adopted by the larger group.
The ASPWG tracks metrics related to antimicrobial use with quarterly data presented by the VISN pharmacist lead. Both inpatient and outpatient metrics are evaluated, such as days of therapy per 1000 days and outpatient antibiotic prescriptions per 1000 unique patients. Facilities are benchmarked against their own historical data and other VISN sites, as well as other VISNs across the country. When outliers are identified, facilities are encouraged to conduct local projects to identify reasons for different antimicrobial use patterns and subsequent initiatives to optimize antimicrobial use. Benchmarking against VISN facilities can be useful since VISN facilities may be more similar than facilities in different geographic regions. Each year, the ASPWG reviews the current metrics, makes adjustments to address VISN priorities, and votes for approval of the metrics that will be tracked in the coming year.
Participation in an ASP collaborative streamlines the rollout of ASP and quality improvement initiatives across multiple sites, allowing ASPs to impact a greater number of veterans and evaluate initiatives on a larger scale. In 2019, with the anticipation of revised vancomycin dosing and monitoring guidelines, our ASPWG began to strategize the transition to AUC-based vancomycin monitoring.6 This multisite initiative showcases the strengths of implementing and evaluating practice changes as part of an ASP collaborative.
Vancomycin Dosing
The antibiotic vancomycin is used primarily for the treatment of MRSA infections.6 The 2020 consensus guidelines for vancomycin therapeutic monitoring recommend using the AUC to minimum inhibitory concentration (MIC) ratio as the pharmacodynamic target for serious MRSA infections, with an AUC/MIC goal of 400 to 600 mcg*h/mL.6 Prior guidelines recommended using vancomycin trough concentrations of 15 to 20 mcg/mL as a surrogate for this AUC target. However, subsequent studies have shown that trough-based dosing is associated with higher vancomycin exposures, supratherapeutic AUCs, and increased risk of vancomycin-associated acute kidney injury (AKI).7,8 Therefore, more direct AUC estimation is now recommended.6 The preferred approach for AUC calculations is through Bayesian modeling. Due to limited resources and software availability, many facilities use an alternative method involving 2 postdistributive serum vancomycin concentrations and first-order pharmacokinetic equations. This approach can optimize vancomycin dosing but is more mathematically and logistically challenging. Transitioning from troughto AUC-based vancomycin monitoring requires careful planning and comprehensive staff education.
In 2019, the VISN 8 ASPWG created a comprehensive vancomycin AUC toolkit to facilitate implementation. Components included a pharmacokinetic management policy and procedure, a vancomycin dosing guide, a progress note template, educational materials specific to pharmacy, nursing, laboratory, and medical services, a pharmacist competency examination, and a vancomycin AUC calculator (eAppendix). Each component was developed by a subgroup with the understanding that sites could incorporate variations based on local practices and needs.
FIGURE Vancomycin Area Under the Curve Dosing Calculator
The vancomycin AUC calculator was developed to be user-friendly and included safety validation protocols to prevent the entry of erroneous data (eg, unrealistic patient weight or laboratory values). The calculator allowed users to copy data into the electronic health record to avoid manual transcription errors and improve operational efficiency. It offered suggested volume of distribution estimates and 2 methods to estimate elimination constant (Ke ) depending on the patient’s weight.9,10 Creatinine clearance could be estimated using serum creatinine or cystatin C and considered amputation history. The default AUC goal in the calculator was 400 to 550 mcg*h/mL. This range was chosen based on consensus guidelines, data suggesting increased risk of AKI with AUCs > 515 mcg*h/mL, and the preference for conservative empiric dosing in the generally older VA population.11 The calculator suggested loading doses of about 25 mg/kg with a 2500 mg limit. VHA facilities could make limited modifications to the calculator based on local policies and procedures (eg, adjusting default infusion times or a dosing intervals).
The VISN 8 Pharmacy Pharmacokinetic Dosing Manual was developed as a comprehensive document to guide pharmacy staff with dosing vancomycin across diverse patient populations. This document included recommendations for renal function assessment, patient-specific considerations when choosing an empiric vancomycin dose, methods of ordering vancomycin peak, trough, and surveillance levels, dose determination based on 2 levels, and other clinical insights or frequently asked questions.
ASPWG members presented an accredited continuing education webinar for pharmacists, which reviewed the rationale for AUC-targeted dosing, changes to the current pharmacokinetic dosing program, case-based scenarios across various patient populations, and potential challenges associated with vancomycin AUC-based dosing. A recording of the live training was also made available. A vancomycin AUC dosing competency test was developed with 11 basic pharmacokinetic and case-based questions and comprehensive explanations provided for each answer.
VHA facilities implemented AUC dosing in a staggered manner, allowing for lessons learned at earlier adopters to be addressed proactively at later sites. The dosing calculator and education documents were updated iteratively as opportunities for improvement were discovered. ASPWG members held local office hours to address questions or concerns from staff at their facilities. Sharing standardized materials across the VISN reduced individual site workload and complications in rolling out this complex new process.
VISN-WIDE QUALITY ASSURANCE
At the time of project conception, 4 of 7 VISN 8 health systems had transitioned to AUC-based dosing. A quality assurance protocol to compare patient outcomes before and after changing to AUC dosing was developed. Each site followed local protocols for project approval and data were deidentified, collected, and aggregated for analysis.
The primary objectives were to compare the incidence of AKI and persistent bacteremia and assess rates of AUC target attainment (400-600 mcg*h/mL) in the AUC-based and trough-based dosing groups.6 Data for both groups included anthropomorphic measurements, serum creatinine, amputation status, vancomycin dosing, and infection characteristics. The X2 test was used for categorical data and the t test was used for continuous data. A 2-tailed α of 0.05 was used to determine significance. Each site sequentially reviewed all patients receiving ≥ 48 hours of intravenous vancomycin over a 3-month period and contributed up to 50 patients for each group. Due to staggered implementation, the study periods for sites spanned 2018 to 2023. A minimum 6-month washout period was observed between the trough and AUC groups at each site. Patients were excluded if pregnant, receiving renal replacement therapy, or presenting with AKI at the time of vancomycin initiation.
There were 168 patients in the AUC group and 172 patients in the trough group (Table 1). The rate of AUC target attainment with the initial dosing regimen varied across sites from 18% to 69% (mean, 48%). Total daily vancomycin exposure was lower in the AUC group compared with the trough group (2402 mg vs 2605 mg, respectively), with AUC-dosed patients being less likely to experience troughs level ≥ 15 or 20 mcg/mL (Table 2). There was a statistically significant lower rate of AKI in the AUC group: 2.4% in the AUC group (range, 2%-3%) vs 10.4% (range 7%-12%) in the trough group (P = .002). Rates of AKI were comparable to those observed in previous interventions.6 There was no statistical difference in length of stay, time to blood culture clearance, or rate of persistent bacteremia in the 2 groups, but these assessments were limited by sample size.
We did not anticipate such variability in initial target attainment across sites. The multisite quality assurance design allowed for qualitative evaluation of variability in dosing practices, which likely arose from sites and individual pharmacists having some flexibility in adjusting dosing tool parameters. Further analysis revealed that the facility with low initial target attainment was not routinely utilizing vancomycin loading doses. Sites routinely use robust loading doses achieved earlier and more consistent target attainment. Some sites used a narrower AUC target range in certain clinical scenarios (eg, > 500 mcg*h/mL for septic patients and < 500 mcg*h/mL for patients with less severe infections) rather than the 400 to 550 mcg*h/mL range for all patients. Sites targeting broader AUC ranges for all patients had higher rates of target attainment. Reviewing differences among sites allowed the ASPWG to identify best practices to optimize future care.
CONCLUSIONS
VHA ASPs must meet the standards outlined in VHA Directive 1031, including the new requirement for each VISN to develop an ASP collaborative. The VISN 8 ASPWG demonstrates how ASP champions can collaborate to solve common issues, complete tasks, explore new infectious diseases concepts, and impact large veteran populations. Furthermore, ASP collaboratives can harness their collective size to complete robust quality assurance evaluations that might otherwise be underpowered if completed at a single center. A limitation of the collaborative model is that a site with a robust ASP may already have specific practices in place. Expanding the ASP collaborative model further highlights the VHA role as a nationwide leader in ASP best practices.
US Department of Veterans Affairs, Veteran Health Administration. Veterans Integrated Service Networks (VISNs). Accessed September 13, 2024. https://www.va.gov/HEALTH/visns.asp
Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2020;77(11):835-864. doi:10.1093/ajhp/zxaa036
Finch NA, Zasowski EJ, Murray KP, et al. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycinassociated nephrotoxicity. Antimicrob Agents Chemother. 2017;61(12):e01293-17. doi:10.1128/AAC.01293-17
Zasowski EJ, Murray KP, Trinh TD, et al. Identification of vancomycin exposure-toxicity thresholds in hospitalized patients receiving intravenous vancomycin. Antimicrob Agents Chemother. 2017;62(1):e01684-17. doi:10.1128/AAC.01684-17
Matzke GR, Kovarik JM, Rybak MJ, Boike SC. Evaluation of the vancomycin-clearance: creatinine-clearance relationship for predicting vancomycin dosage. Clin Pharm. 1985;4(3):311-315.
Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081-3086. doi:10.1093/jac/dky310
Lodise TP, Rosenkranz SL, Finnemeyer M, et al. The emperor’s new clothes: prospective observational evaluation of the association between initial vancomycIn exposure and failure rates among adult hospitalized patients with methicillin-resistant staphylococcus aureus bloodstream infections (PROVIDE). Clin Infect Dis. 2020;70(8):1536-1545. doi:10.1093/cid/ciz460
Author affiliations: aBay Pines Veterans Affairs Healthcare System, Florida bVeterans Affairs North Florida/South Georgia Veterans Health System, Gainesville c James A. Haley Veterans Hospital, Tampa, Florida dBruce W. Carter Veterans Affairs Medical Center, Miami, Florida eVISN 8 Pharmacy Benefits Management, Tampa, Florida f Enanta Pharmaceuticals, Miami, Florida
Author disclosuresThe authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 18. doi:10.12788/fp0520
Author affiliations: aBay Pines Veterans Affairs Healthcare System, Florida bVeterans Affairs North Florida/South Georgia Veterans Health System, Gainesville c James A. Haley Veterans Hospital, Tampa, Florida dBruce W. Carter Veterans Affairs Medical Center, Miami, Florida eVISN 8 Pharmacy Benefits Management, Tampa, Florida f Enanta Pharmaceuticals, Miami, Florida
Author disclosuresThe authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 18. doi:10.12788/fp0520
Author and Disclosure Information
Peter Pasek, PharmD, BCPS, BCGPa; Joseph Hong, PharmDa; Joe Pardo, PharmD, BCIDPb; Sidorela Gllava, PharmDc; Lauren Bjork, PharmDd,e; Linda Cheung, PharmD, BCPS, MBAe
Author affiliations: aBay Pines Veterans Affairs Healthcare System, Florida bVeterans Affairs North Florida/South Georgia Veterans Health System, Gainesville c James A. Haley Veterans Hospital, Tampa, Florida dBruce W. Carter Veterans Affairs Medical Center, Miami, Florida eVISN 8 Pharmacy Benefits Management, Tampa, Florida f Enanta Pharmaceuticals, Miami, Florida
Author disclosuresThe authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 18. doi:10.12788/fp0520
Antimicrobial resistance is a global threat and burden to health care, with > 2.8 million antibiotic-resistant infections occurring annually in the United States.1 To combat this issue and improve patient care, the US Department of Veterans Affairs (VA) has implemented antimicrobial stewardship programs (ASPs) across its health care systems. ASPs are multidisciplinary teams that promote evidence-based use of antimicrobials through activities supporting appropriate selection, dosing, route, and duration of antimicrobial therapy. ASP best practices are also included in the Joint Commission and Centers for Medicare and Medicaid Services accreditation standards.2
The foundational charge for VA facilities to develop and maintain ASPs was outlined in 2014 and updated in 2023 in the Veterans Health Administration (VHA) Directive 1031 on antimicrobial stewardship programs.2 This directive outlines specific requirements for all VA ASPs, including personnel, staffing levels, and the roles and responsibilities of all team members. VHA now requires that Veterans Integrated Services Networks (VISNs) establish robust ASP collaboratives. A VISN ASP collaborative consists of stewardship champions from each VA medical center in the VISN and is designed to support, develop, and enhance ASP programs across all facilities within that VISN.2 Some VISNs may lack an ASP collaborative altogether, and others with existing groups may seek ways to expand their collaboratives in line with the updated directive. Prior to VHA Directive 1031, the VA Sunshine Healthcare Network (VISN 8) established an ASP collaborative. This article describes the structure and activities of the VISN 8 ASP collaborative and highlights a recent VISN 8 quality assurance initiative related to vancomycin area under the curve (AUC) dosing that illustrates how ASP collaboratives can enhance stewardship and clinical care across broad geographic areas.
VISN 8 ASP
The VHA, the largest integrated US health care system, is divided into 18 VISNs that provide regional systems of care to enhance access and meet the local health care needs of veterans.3 VISN 8 serves > 1.5 million veterans across 165,759 km2 in Florida, South Georgia, Puerto Rico, and the US Virgin Islands.4 The network is composed of 7 health systems with 8 medical centers and > 60 outpatient clinics. These facilities provide comprehensive acute, primary, and specialty care, as well as mental health and extended care services in inpatient, outpatient, nursing home, and home care settings.4
The 2023 VHA Directive 1031 update recognizes the importance of VISN-level coordination of ASP activities to enhance the standardization of care and build partnerships in stewardship across all levels of care. The VISN 8 ASP collaborative workgroup (ASPWG) was established in 2015. Consistent with Directive 1031, the ASPWG is guided by clinician and pharmacist VISN leads. These leads serve as subject matter experts, facilitate access to resources, establish VISN-level consensus, and enhance communication among local ASP champions at medical centers within the VISN. All 7 health systems include = 1 ASP champion (clinician or pharmacist) in the ASPWG. Ad hoc members, whose routine duties are not solely focused on antimicrobial stewardship, contribute to specific stewardship projects as needed. For example, the ASPWG has included internal medicine, emergency department, community living center pharmacists, representatives from pharmacy administration, and trainees (pharmacy students and residents, and infectious diseases fellows) in antimicrobial stewardship initiatives. The inclusion of non-ASP champions is not discussed in VHA Directive 1031. However, these members have made valuable contributions to the ASPWG.
The ASPWG meets monthly. Agendas and priorities are developed by the VISN pharmacist and health care practitioner (HCP) leads. Monthly discussions may include but are not limited to a review of national formulary decisions, VISN goals and metrics, infectious diseases hot topics, pharmacoeconomic initiatives, strong practice presentations, regulatory and accreditation preparation, preparation of tracking reports, as well as the development of both patient-level and HCPlevel tools, resources, and education materials. This forum facilitates collaborative learning: members process and synthesize information, share and reframe ideas, and listen to other viewpoints to gain a complete understanding as a group.5 For example, ASPWG members have leaned on each other to prepare for Joint Commission accreditation surveys and strengthen the VISN 8 COVID-19 program through the rollout of vaccines and treatments. Other collaborative projects completed over the past few years included a penicillin allergy testing initiative and anti-methicillin-resistant Staphylococcus aureus (MRSA) and pseudomonal medication use evaluations. This team-centric problem-solving approach is highly effective while also fostering professional and social relationships. However, collaboratives could be perceived to have drawbacks. There may be opportunity costs if ASP time is allocated for issues that have already been addressed locally or concerns that standardization might hinder rapid adoption of practices at individual sites. Therefore, participation in each distinct group initiative is optional. This allows sites to choose projects related to their high priority areas and maintain bandwidth to implement practices not yet adopted by the larger group.
The ASPWG tracks metrics related to antimicrobial use with quarterly data presented by the VISN pharmacist lead. Both inpatient and outpatient metrics are evaluated, such as days of therapy per 1000 days and outpatient antibiotic prescriptions per 1000 unique patients. Facilities are benchmarked against their own historical data and other VISN sites, as well as other VISNs across the country. When outliers are identified, facilities are encouraged to conduct local projects to identify reasons for different antimicrobial use patterns and subsequent initiatives to optimize antimicrobial use. Benchmarking against VISN facilities can be useful since VISN facilities may be more similar than facilities in different geographic regions. Each year, the ASPWG reviews the current metrics, makes adjustments to address VISN priorities, and votes for approval of the metrics that will be tracked in the coming year.
Participation in an ASP collaborative streamlines the rollout of ASP and quality improvement initiatives across multiple sites, allowing ASPs to impact a greater number of veterans and evaluate initiatives on a larger scale. In 2019, with the anticipation of revised vancomycin dosing and monitoring guidelines, our ASPWG began to strategize the transition to AUC-based vancomycin monitoring.6 This multisite initiative showcases the strengths of implementing and evaluating practice changes as part of an ASP collaborative.
Vancomycin Dosing
The antibiotic vancomycin is used primarily for the treatment of MRSA infections.6 The 2020 consensus guidelines for vancomycin therapeutic monitoring recommend using the AUC to minimum inhibitory concentration (MIC) ratio as the pharmacodynamic target for serious MRSA infections, with an AUC/MIC goal of 400 to 600 mcg*h/mL.6 Prior guidelines recommended using vancomycin trough concentrations of 15 to 20 mcg/mL as a surrogate for this AUC target. However, subsequent studies have shown that trough-based dosing is associated with higher vancomycin exposures, supratherapeutic AUCs, and increased risk of vancomycin-associated acute kidney injury (AKI).7,8 Therefore, more direct AUC estimation is now recommended.6 The preferred approach for AUC calculations is through Bayesian modeling. Due to limited resources and software availability, many facilities use an alternative method involving 2 postdistributive serum vancomycin concentrations and first-order pharmacokinetic equations. This approach can optimize vancomycin dosing but is more mathematically and logistically challenging. Transitioning from troughto AUC-based vancomycin monitoring requires careful planning and comprehensive staff education.
In 2019, the VISN 8 ASPWG created a comprehensive vancomycin AUC toolkit to facilitate implementation. Components included a pharmacokinetic management policy and procedure, a vancomycin dosing guide, a progress note template, educational materials specific to pharmacy, nursing, laboratory, and medical services, a pharmacist competency examination, and a vancomycin AUC calculator (eAppendix). Each component was developed by a subgroup with the understanding that sites could incorporate variations based on local practices and needs.
FIGURE Vancomycin Area Under the Curve Dosing Calculator
The vancomycin AUC calculator was developed to be user-friendly and included safety validation protocols to prevent the entry of erroneous data (eg, unrealistic patient weight or laboratory values). The calculator allowed users to copy data into the electronic health record to avoid manual transcription errors and improve operational efficiency. It offered suggested volume of distribution estimates and 2 methods to estimate elimination constant (Ke ) depending on the patient’s weight.9,10 Creatinine clearance could be estimated using serum creatinine or cystatin C and considered amputation history. The default AUC goal in the calculator was 400 to 550 mcg*h/mL. This range was chosen based on consensus guidelines, data suggesting increased risk of AKI with AUCs > 515 mcg*h/mL, and the preference for conservative empiric dosing in the generally older VA population.11 The calculator suggested loading doses of about 25 mg/kg with a 2500 mg limit. VHA facilities could make limited modifications to the calculator based on local policies and procedures (eg, adjusting default infusion times or a dosing intervals).
The VISN 8 Pharmacy Pharmacokinetic Dosing Manual was developed as a comprehensive document to guide pharmacy staff with dosing vancomycin across diverse patient populations. This document included recommendations for renal function assessment, patient-specific considerations when choosing an empiric vancomycin dose, methods of ordering vancomycin peak, trough, and surveillance levels, dose determination based on 2 levels, and other clinical insights or frequently asked questions.
ASPWG members presented an accredited continuing education webinar for pharmacists, which reviewed the rationale for AUC-targeted dosing, changes to the current pharmacokinetic dosing program, case-based scenarios across various patient populations, and potential challenges associated with vancomycin AUC-based dosing. A recording of the live training was also made available. A vancomycin AUC dosing competency test was developed with 11 basic pharmacokinetic and case-based questions and comprehensive explanations provided for each answer.
VHA facilities implemented AUC dosing in a staggered manner, allowing for lessons learned at earlier adopters to be addressed proactively at later sites. The dosing calculator and education documents were updated iteratively as opportunities for improvement were discovered. ASPWG members held local office hours to address questions or concerns from staff at their facilities. Sharing standardized materials across the VISN reduced individual site workload and complications in rolling out this complex new process.
VISN-WIDE QUALITY ASSURANCE
At the time of project conception, 4 of 7 VISN 8 health systems had transitioned to AUC-based dosing. A quality assurance protocol to compare patient outcomes before and after changing to AUC dosing was developed. Each site followed local protocols for project approval and data were deidentified, collected, and aggregated for analysis.
The primary objectives were to compare the incidence of AKI and persistent bacteremia and assess rates of AUC target attainment (400-600 mcg*h/mL) in the AUC-based and trough-based dosing groups.6 Data for both groups included anthropomorphic measurements, serum creatinine, amputation status, vancomycin dosing, and infection characteristics. The X2 test was used for categorical data and the t test was used for continuous data. A 2-tailed α of 0.05 was used to determine significance. Each site sequentially reviewed all patients receiving ≥ 48 hours of intravenous vancomycin over a 3-month period and contributed up to 50 patients for each group. Due to staggered implementation, the study periods for sites spanned 2018 to 2023. A minimum 6-month washout period was observed between the trough and AUC groups at each site. Patients were excluded if pregnant, receiving renal replacement therapy, or presenting with AKI at the time of vancomycin initiation.
There were 168 patients in the AUC group and 172 patients in the trough group (Table 1). The rate of AUC target attainment with the initial dosing regimen varied across sites from 18% to 69% (mean, 48%). Total daily vancomycin exposure was lower in the AUC group compared with the trough group (2402 mg vs 2605 mg, respectively), with AUC-dosed patients being less likely to experience troughs level ≥ 15 or 20 mcg/mL (Table 2). There was a statistically significant lower rate of AKI in the AUC group: 2.4% in the AUC group (range, 2%-3%) vs 10.4% (range 7%-12%) in the trough group (P = .002). Rates of AKI were comparable to those observed in previous interventions.6 There was no statistical difference in length of stay, time to blood culture clearance, or rate of persistent bacteremia in the 2 groups, but these assessments were limited by sample size.
We did not anticipate such variability in initial target attainment across sites. The multisite quality assurance design allowed for qualitative evaluation of variability in dosing practices, which likely arose from sites and individual pharmacists having some flexibility in adjusting dosing tool parameters. Further analysis revealed that the facility with low initial target attainment was not routinely utilizing vancomycin loading doses. Sites routinely use robust loading doses achieved earlier and more consistent target attainment. Some sites used a narrower AUC target range in certain clinical scenarios (eg, > 500 mcg*h/mL for septic patients and < 500 mcg*h/mL for patients with less severe infections) rather than the 400 to 550 mcg*h/mL range for all patients. Sites targeting broader AUC ranges for all patients had higher rates of target attainment. Reviewing differences among sites allowed the ASPWG to identify best practices to optimize future care.
CONCLUSIONS
VHA ASPs must meet the standards outlined in VHA Directive 1031, including the new requirement for each VISN to develop an ASP collaborative. The VISN 8 ASPWG demonstrates how ASP champions can collaborate to solve common issues, complete tasks, explore new infectious diseases concepts, and impact large veteran populations. Furthermore, ASP collaboratives can harness their collective size to complete robust quality assurance evaluations that might otherwise be underpowered if completed at a single center. A limitation of the collaborative model is that a site with a robust ASP may already have specific practices in place. Expanding the ASP collaborative model further highlights the VHA role as a nationwide leader in ASP best practices.
Antimicrobial resistance is a global threat and burden to health care, with > 2.8 million antibiotic-resistant infections occurring annually in the United States.1 To combat this issue and improve patient care, the US Department of Veterans Affairs (VA) has implemented antimicrobial stewardship programs (ASPs) across its health care systems. ASPs are multidisciplinary teams that promote evidence-based use of antimicrobials through activities supporting appropriate selection, dosing, route, and duration of antimicrobial therapy. ASP best practices are also included in the Joint Commission and Centers for Medicare and Medicaid Services accreditation standards.2
The foundational charge for VA facilities to develop and maintain ASPs was outlined in 2014 and updated in 2023 in the Veterans Health Administration (VHA) Directive 1031 on antimicrobial stewardship programs.2 This directive outlines specific requirements for all VA ASPs, including personnel, staffing levels, and the roles and responsibilities of all team members. VHA now requires that Veterans Integrated Services Networks (VISNs) establish robust ASP collaboratives. A VISN ASP collaborative consists of stewardship champions from each VA medical center in the VISN and is designed to support, develop, and enhance ASP programs across all facilities within that VISN.2 Some VISNs may lack an ASP collaborative altogether, and others with existing groups may seek ways to expand their collaboratives in line with the updated directive. Prior to VHA Directive 1031, the VA Sunshine Healthcare Network (VISN 8) established an ASP collaborative. This article describes the structure and activities of the VISN 8 ASP collaborative and highlights a recent VISN 8 quality assurance initiative related to vancomycin area under the curve (AUC) dosing that illustrates how ASP collaboratives can enhance stewardship and clinical care across broad geographic areas.
VISN 8 ASP
The VHA, the largest integrated US health care system, is divided into 18 VISNs that provide regional systems of care to enhance access and meet the local health care needs of veterans.3 VISN 8 serves > 1.5 million veterans across 165,759 km2 in Florida, South Georgia, Puerto Rico, and the US Virgin Islands.4 The network is composed of 7 health systems with 8 medical centers and > 60 outpatient clinics. These facilities provide comprehensive acute, primary, and specialty care, as well as mental health and extended care services in inpatient, outpatient, nursing home, and home care settings.4
The 2023 VHA Directive 1031 update recognizes the importance of VISN-level coordination of ASP activities to enhance the standardization of care and build partnerships in stewardship across all levels of care. The VISN 8 ASP collaborative workgroup (ASPWG) was established in 2015. Consistent with Directive 1031, the ASPWG is guided by clinician and pharmacist VISN leads. These leads serve as subject matter experts, facilitate access to resources, establish VISN-level consensus, and enhance communication among local ASP champions at medical centers within the VISN. All 7 health systems include = 1 ASP champion (clinician or pharmacist) in the ASPWG. Ad hoc members, whose routine duties are not solely focused on antimicrobial stewardship, contribute to specific stewardship projects as needed. For example, the ASPWG has included internal medicine, emergency department, community living center pharmacists, representatives from pharmacy administration, and trainees (pharmacy students and residents, and infectious diseases fellows) in antimicrobial stewardship initiatives. The inclusion of non-ASP champions is not discussed in VHA Directive 1031. However, these members have made valuable contributions to the ASPWG.
The ASPWG meets monthly. Agendas and priorities are developed by the VISN pharmacist and health care practitioner (HCP) leads. Monthly discussions may include but are not limited to a review of national formulary decisions, VISN goals and metrics, infectious diseases hot topics, pharmacoeconomic initiatives, strong practice presentations, regulatory and accreditation preparation, preparation of tracking reports, as well as the development of both patient-level and HCPlevel tools, resources, and education materials. This forum facilitates collaborative learning: members process and synthesize information, share and reframe ideas, and listen to other viewpoints to gain a complete understanding as a group.5 For example, ASPWG members have leaned on each other to prepare for Joint Commission accreditation surveys and strengthen the VISN 8 COVID-19 program through the rollout of vaccines and treatments. Other collaborative projects completed over the past few years included a penicillin allergy testing initiative and anti-methicillin-resistant Staphylococcus aureus (MRSA) and pseudomonal medication use evaluations. This team-centric problem-solving approach is highly effective while also fostering professional and social relationships. However, collaboratives could be perceived to have drawbacks. There may be opportunity costs if ASP time is allocated for issues that have already been addressed locally or concerns that standardization might hinder rapid adoption of practices at individual sites. Therefore, participation in each distinct group initiative is optional. This allows sites to choose projects related to their high priority areas and maintain bandwidth to implement practices not yet adopted by the larger group.
The ASPWG tracks metrics related to antimicrobial use with quarterly data presented by the VISN pharmacist lead. Both inpatient and outpatient metrics are evaluated, such as days of therapy per 1000 days and outpatient antibiotic prescriptions per 1000 unique patients. Facilities are benchmarked against their own historical data and other VISN sites, as well as other VISNs across the country. When outliers are identified, facilities are encouraged to conduct local projects to identify reasons for different antimicrobial use patterns and subsequent initiatives to optimize antimicrobial use. Benchmarking against VISN facilities can be useful since VISN facilities may be more similar than facilities in different geographic regions. Each year, the ASPWG reviews the current metrics, makes adjustments to address VISN priorities, and votes for approval of the metrics that will be tracked in the coming year.
Participation in an ASP collaborative streamlines the rollout of ASP and quality improvement initiatives across multiple sites, allowing ASPs to impact a greater number of veterans and evaluate initiatives on a larger scale. In 2019, with the anticipation of revised vancomycin dosing and monitoring guidelines, our ASPWG began to strategize the transition to AUC-based vancomycin monitoring.6 This multisite initiative showcases the strengths of implementing and evaluating practice changes as part of an ASP collaborative.
Vancomycin Dosing
The antibiotic vancomycin is used primarily for the treatment of MRSA infections.6 The 2020 consensus guidelines for vancomycin therapeutic monitoring recommend using the AUC to minimum inhibitory concentration (MIC) ratio as the pharmacodynamic target for serious MRSA infections, with an AUC/MIC goal of 400 to 600 mcg*h/mL.6 Prior guidelines recommended using vancomycin trough concentrations of 15 to 20 mcg/mL as a surrogate for this AUC target. However, subsequent studies have shown that trough-based dosing is associated with higher vancomycin exposures, supratherapeutic AUCs, and increased risk of vancomycin-associated acute kidney injury (AKI).7,8 Therefore, more direct AUC estimation is now recommended.6 The preferred approach for AUC calculations is through Bayesian modeling. Due to limited resources and software availability, many facilities use an alternative method involving 2 postdistributive serum vancomycin concentrations and first-order pharmacokinetic equations. This approach can optimize vancomycin dosing but is more mathematically and logistically challenging. Transitioning from troughto AUC-based vancomycin monitoring requires careful planning and comprehensive staff education.
In 2019, the VISN 8 ASPWG created a comprehensive vancomycin AUC toolkit to facilitate implementation. Components included a pharmacokinetic management policy and procedure, a vancomycin dosing guide, a progress note template, educational materials specific to pharmacy, nursing, laboratory, and medical services, a pharmacist competency examination, and a vancomycin AUC calculator (eAppendix). Each component was developed by a subgroup with the understanding that sites could incorporate variations based on local practices and needs.
FIGURE Vancomycin Area Under the Curve Dosing Calculator
The vancomycin AUC calculator was developed to be user-friendly and included safety validation protocols to prevent the entry of erroneous data (eg, unrealistic patient weight or laboratory values). The calculator allowed users to copy data into the electronic health record to avoid manual transcription errors and improve operational efficiency. It offered suggested volume of distribution estimates and 2 methods to estimate elimination constant (Ke ) depending on the patient’s weight.9,10 Creatinine clearance could be estimated using serum creatinine or cystatin C and considered amputation history. The default AUC goal in the calculator was 400 to 550 mcg*h/mL. This range was chosen based on consensus guidelines, data suggesting increased risk of AKI with AUCs > 515 mcg*h/mL, and the preference for conservative empiric dosing in the generally older VA population.11 The calculator suggested loading doses of about 25 mg/kg with a 2500 mg limit. VHA facilities could make limited modifications to the calculator based on local policies and procedures (eg, adjusting default infusion times or a dosing intervals).
The VISN 8 Pharmacy Pharmacokinetic Dosing Manual was developed as a comprehensive document to guide pharmacy staff with dosing vancomycin across diverse patient populations. This document included recommendations for renal function assessment, patient-specific considerations when choosing an empiric vancomycin dose, methods of ordering vancomycin peak, trough, and surveillance levels, dose determination based on 2 levels, and other clinical insights or frequently asked questions.
ASPWG members presented an accredited continuing education webinar for pharmacists, which reviewed the rationale for AUC-targeted dosing, changes to the current pharmacokinetic dosing program, case-based scenarios across various patient populations, and potential challenges associated with vancomycin AUC-based dosing. A recording of the live training was also made available. A vancomycin AUC dosing competency test was developed with 11 basic pharmacokinetic and case-based questions and comprehensive explanations provided for each answer.
VHA facilities implemented AUC dosing in a staggered manner, allowing for lessons learned at earlier adopters to be addressed proactively at later sites. The dosing calculator and education documents were updated iteratively as opportunities for improvement were discovered. ASPWG members held local office hours to address questions or concerns from staff at their facilities. Sharing standardized materials across the VISN reduced individual site workload and complications in rolling out this complex new process.
VISN-WIDE QUALITY ASSURANCE
At the time of project conception, 4 of 7 VISN 8 health systems had transitioned to AUC-based dosing. A quality assurance protocol to compare patient outcomes before and after changing to AUC dosing was developed. Each site followed local protocols for project approval and data were deidentified, collected, and aggregated for analysis.
The primary objectives were to compare the incidence of AKI and persistent bacteremia and assess rates of AUC target attainment (400-600 mcg*h/mL) in the AUC-based and trough-based dosing groups.6 Data for both groups included anthropomorphic measurements, serum creatinine, amputation status, vancomycin dosing, and infection characteristics. The X2 test was used for categorical data and the t test was used for continuous data. A 2-tailed α of 0.05 was used to determine significance. Each site sequentially reviewed all patients receiving ≥ 48 hours of intravenous vancomycin over a 3-month period and contributed up to 50 patients for each group. Due to staggered implementation, the study periods for sites spanned 2018 to 2023. A minimum 6-month washout period was observed between the trough and AUC groups at each site. Patients were excluded if pregnant, receiving renal replacement therapy, or presenting with AKI at the time of vancomycin initiation.
There were 168 patients in the AUC group and 172 patients in the trough group (Table 1). The rate of AUC target attainment with the initial dosing regimen varied across sites from 18% to 69% (mean, 48%). Total daily vancomycin exposure was lower in the AUC group compared with the trough group (2402 mg vs 2605 mg, respectively), with AUC-dosed patients being less likely to experience troughs level ≥ 15 or 20 mcg/mL (Table 2). There was a statistically significant lower rate of AKI in the AUC group: 2.4% in the AUC group (range, 2%-3%) vs 10.4% (range 7%-12%) in the trough group (P = .002). Rates of AKI were comparable to those observed in previous interventions.6 There was no statistical difference in length of stay, time to blood culture clearance, or rate of persistent bacteremia in the 2 groups, but these assessments were limited by sample size.
We did not anticipate such variability in initial target attainment across sites. The multisite quality assurance design allowed for qualitative evaluation of variability in dosing practices, which likely arose from sites and individual pharmacists having some flexibility in adjusting dosing tool parameters. Further analysis revealed that the facility with low initial target attainment was not routinely utilizing vancomycin loading doses. Sites routinely use robust loading doses achieved earlier and more consistent target attainment. Some sites used a narrower AUC target range in certain clinical scenarios (eg, > 500 mcg*h/mL for septic patients and < 500 mcg*h/mL for patients with less severe infections) rather than the 400 to 550 mcg*h/mL range for all patients. Sites targeting broader AUC ranges for all patients had higher rates of target attainment. Reviewing differences among sites allowed the ASPWG to identify best practices to optimize future care.
CONCLUSIONS
VHA ASPs must meet the standards outlined in VHA Directive 1031, including the new requirement for each VISN to develop an ASP collaborative. The VISN 8 ASPWG demonstrates how ASP champions can collaborate to solve common issues, complete tasks, explore new infectious diseases concepts, and impact large veteran populations. Furthermore, ASP collaboratives can harness their collective size to complete robust quality assurance evaluations that might otherwise be underpowered if completed at a single center. A limitation of the collaborative model is that a site with a robust ASP may already have specific practices in place. Expanding the ASP collaborative model further highlights the VHA role as a nationwide leader in ASP best practices.
US Department of Veterans Affairs, Veteran Health Administration. Veterans Integrated Service Networks (VISNs). Accessed September 13, 2024. https://www.va.gov/HEALTH/visns.asp
Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2020;77(11):835-864. doi:10.1093/ajhp/zxaa036
Finch NA, Zasowski EJ, Murray KP, et al. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycinassociated nephrotoxicity. Antimicrob Agents Chemother. 2017;61(12):e01293-17. doi:10.1128/AAC.01293-17
Zasowski EJ, Murray KP, Trinh TD, et al. Identification of vancomycin exposure-toxicity thresholds in hospitalized patients receiving intravenous vancomycin. Antimicrob Agents Chemother. 2017;62(1):e01684-17. doi:10.1128/AAC.01684-17
Matzke GR, Kovarik JM, Rybak MJ, Boike SC. Evaluation of the vancomycin-clearance: creatinine-clearance relationship for predicting vancomycin dosage. Clin Pharm. 1985;4(3):311-315.
Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081-3086. doi:10.1093/jac/dky310
Lodise TP, Rosenkranz SL, Finnemeyer M, et al. The emperor’s new clothes: prospective observational evaluation of the association between initial vancomycIn exposure and failure rates among adult hospitalized patients with methicillin-resistant staphylococcus aureus bloodstream infections (PROVIDE). Clin Infect Dis. 2020;70(8):1536-1545. doi:10.1093/cid/ciz460
US Department of Veterans Affairs, Veteran Health Administration. Veterans Integrated Service Networks (VISNs). Accessed September 13, 2024. https://www.va.gov/HEALTH/visns.asp
Rybak MJ, Le J, Lodise TP, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant staphylococcus aureus infections: a revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm. 2020;77(11):835-864. doi:10.1093/ajhp/zxaa036
Finch NA, Zasowski EJ, Murray KP, et al. A quasi-experiment to study the impact of vancomycin area under the concentration-time curve-guided dosing on vancomycinassociated nephrotoxicity. Antimicrob Agents Chemother. 2017;61(12):e01293-17. doi:10.1128/AAC.01293-17
Zasowski EJ, Murray KP, Trinh TD, et al. Identification of vancomycin exposure-toxicity thresholds in hospitalized patients receiving intravenous vancomycin. Antimicrob Agents Chemother. 2017;62(1):e01684-17. doi:10.1128/AAC.01684-17
Matzke GR, Kovarik JM, Rybak MJ, Boike SC. Evaluation of the vancomycin-clearance: creatinine-clearance relationship for predicting vancomycin dosage. Clin Pharm. 1985;4(3):311-315.
Crass RL, Dunn R, Hong J, Krop LC, Pai MP. Dosing vancomycin in the super obese: less is more. J Antimicrob Chemother. 2018;73(11):3081-3086. doi:10.1093/jac/dky310
Lodise TP, Rosenkranz SL, Finnemeyer M, et al. The emperor’s new clothes: prospective observational evaluation of the association between initial vancomycIn exposure and failure rates among adult hospitalized patients with methicillin-resistant staphylococcus aureus bloodstream infections (PROVIDE). Clin Infect Dis. 2020;70(8):1536-1545. doi:10.1093/cid/ciz460
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Fed Pract. 2024;41(10). Published online October 15. doi:10.12788/fp.0516
Author and Disclosure Information
Lindsey Ulin, MDa,b; Meghan Hickey, MDb,c; Caroline Ross, MDb,c; Alan Manivannan, MDb,c; Jay Orlander, MD, MPHb,d; Rahul B. Ganatra, MD, MPHb
Author affiliationsa Brigham and Women’s Hospital, Boston, Massachusetts bVeterans Affairs Boston Healthcare System, West Roxbury, Massachusetts c Boston Medical Center, Massachusetts dBoston University Chobanian & Avedisian School of Medicine, Massachusetts
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
Case Presentation:A 65-year-old male veteran presented to the Veterans Affairs Boston Healthcare System (VABHS) emergency department with progressive fatigue, dyspnea on exertion, lightheadedness, and falls over the last month. New bilateral lower extremity numbness up to his knees developed in the week prior to admission and prompted him to seek care. Additional history included 2 episodes of transient loss of consciousness resulting in falls and a week of diarrhea, which had resolved. His medical history was notable for hypothyroidism secondary to Hashimoto thyroiditis, seizure disorder, vitiligo, treated hepatitis C virus (HCV) infection, alcohol use disorder in remission, diabetes mellitus, posttraumatic stress disorder, and traumatic brain injury. His medications included levothyroxine and carbamazepine. He previously worked as a barber but recently had stopped due to cognitive impairment. On initial evaluation, the patient's vital signs included a temperature of 36.3 °C, heart rate of 77 beats per minute, blood pressure of 139/83 mm Hg, respiratory rate of 18 breaths per minute, and 99% oxygen saturation while breathing ambient air. Physical examination was notable for a frail-appearing man in no acute distress. His conjunctivae were pale, and cardiac auscultation revealed a normal heart rate and irregularly irregular heart rhythm. A neurologic examination revealed decreased vibratory sensation in both feet, delayed and minimal speech, and a blunted affect. His skin was warm and dry with patchy hypopigmentation across the face and forehead. Laboratory results are shown in the Table. Testing 2 years previously found the patient's hemoglobin to be 11.4 g/dL and serum creatinine to be 1.7 mg/dL. A peripheral blood smear showed anisocytosis, hypochromia, decreased platelets, ovalocytes, elliptocytes, and rare teardrop cells, with no schistocytes present. Chest radiography and computed tomography of the head were unremarkable. An abdominal ultrasound revealed a complex hypoechoic mass with peripheral rim vascularity in the right hepatic lobe measuring 3.9 cm × 3.6 cm × 3.9 cm.
Lindsey Ulin, MD, Chief Medical Resident, VABHS and Brigham and Women’s Hospital (BWH):
To build the initial differential diagnosis, we are joined today by 3 internal medicine residents who were not involved in the care of this patient. Dr. Hickey, Dr. Ross and Dr. Manivannan, how did you approach this case?
Meghan Hickey, MD, Senior Internal Medicine Resident, VABHS and Boston Medical Center (BMC):
The constellation of fatigue, weakness, blunted affect, and delayed, minimal speech suggested central nervous system involvement, which I sought to unify with hemolytic anemia and his liver mass. The first diagnosis I considered was Wilson disease; however, this genetic disorder of copper metabolism often presents with liver failure or cirrhosis in young or middle-aged women, so this presentation would be atypical. Next, given the hypopigmentation was reported only on sun-exposed areas of the patient’s face, I considered possibilities other than vitiligo to avoid diagnostic anchoring. One such alternate diagnosis is porphyria cutanea tarda (PCT), which presents in middle-aged and older adults with a photosensitive dermatitis that can include acute sensory deficits. Manifestations of PCT can be triggered by alcohol consumption, though his alcohol use disorder was thought to be in remission, as well as HCV, for which he previously received treatment. However, anemia is uncommon in PCT, so the patient’s low hemoglobin would not be explained by this diagnosis. Lastly, I considered thrombotic thrombocytopenic purpura (TTP) given his anemia, thrombocytopenia, and neurologic symptoms; however, the patient did not have fever or a clear inciting cause, his renal dysfunction was relatively mild, and the peripheral blood smear revealed no schistocytes, which should be present in TTP.
TABLE Laboratory Results
Caroline Ross, MD, and Alan Manivannan, MD; Senior Internal Medicine Residents, VABHS and BMC:
We noted several salient features in the history and physical examination. First, we sought to explain the bilateral lower extremity numbness and decreased vibratory sensation in the feet leading to falls. We also considered his anemia and thrombocytopenia with signs of hemolysis including elevated lactate dehydrogenase (LDH), low haptoglobin, and elevated total bilirubin; however, with normal coagulation parameters. These results initially raised our concern for a thrombotic microangiopathy (TMA) such as TTP. However, the peripheral smear lacked schistocytes, making this less likely. The combination of his neurologic symptoms and TMA-like laboratory findings but without schistocytes raised our concern for vitamin B12 deficiency. Vitamin B12 deficiency can cause a pseudo-TMA picture with laboratory finding similar to TTP; however, schistocytes are typically absent. We also considered the possibility of hepatocellular carcinoma (HCC) with bone marrow infiltration leading to anemia given the finding of a liver mass on his abdominal ultrasound and low reticulocyte index. However, this would not explain his hemolysis. We also considered chronic disseminated intravascular coagulation in the setting of a malignancy as a contributor, but again, the smear lacked schistocytes and his coagulation parameters were normal. Finally, we considered a primary bone marrow process such as myelodysplastic syndrome due to the bicytopenia with poor bone marrow response and smear with tear drop cells and elliptocytes. However, we felt this was less likely as this would not explain his hemolytic anemia.
Dr. Ulin:
To refine the differential diagnosis, we are joined by an expert clinician who was also not involved in the care of this patient to describe his approach to this case. Dr. Orlander, can you walk us through your clinical reasoning?
Jay Orlander, MD, MPH: Professor of Medicine, Section of General Internal Medicine, Boston University Chobanian & Avedisian School of Medicine, Associate Chief, Medical Service, VABHS:
I will first comment on the hepatic mass. The hypoechoic liver mass with peripheral vascularity suggests a growing tumor. The patient has a history of substance use disorder with alcohol and treated HCV. He remains at increased risk for HCC even after prior successful HCV treatment and has 2 of 4 known risk factors for developing HCC— diabetes mellitus and alcohol use—the other 2 being underlying metabolic dysfunctionassociated steatotic liver disease (MASLD) and the presence of hepatic fibrosis, which we have not yet assessed. Worsening liver function can lead to cognitive issues and alcohol to peripheral neuropathy, but his story is not consistent with this. For his liver mass, I recommend a nonurgent magnetic resonance image for further evaluation.
Next, let’s consider his markedly elevated thyrotropin (TSH). Cognitive impairment along with lethargy, fatigue, and decreased exercise tolerance can be prominent features in severe hypothyroidism, but this diagnosis would not explain his hematologic findings.1
I view the principal finding of his laboratory testing as being that his bone marrow is failing to maintain adequate blood elements. He has a markedly low hematocrit along with low platelets and low-normal white blood cell counts. There is an absence of schistocytes on the blood smear, and after correcting his reticulocyte count for his degree of anemia (observed reticulocyte percentage [0.8%] x observed hematocrit [15.3%] / expected hematocrit [40%]), results in a reticulocyte index of 0.12, which is low. This suggests his bone marrow is failing to manufacture red blood cells at an appropriate rate. His haptoglobin is unmeasurable, so there is some free heme circulating. Hence, I infer that hemolysis and ineffective erythropoiesis are both occurring within the bone marrow, which also explains the slight elevation in bilirubin.
Intramedullary hemolysis with a markedly elevated LDH can be seen in severe vitamin B12 deficiency, which has many causes, but one cause in particular warrants consideration in this case: pernicious anemia. Pernicious anemia has an overall prevalence of about 0.1%, but is more common in older adults, and is estimated to be present in 2% to 3% of adults aged > 65 years.2 Prevalence is also increased in patients with other autoimmune diseases such as vitiligo and hypothyroidism, which our patient has.3 The pathophysiology of pernicious anemia relates to either autoimmune gastric parietal cell destruction and/or the development of antibodies against intrinsic factor, which is required for absorption of vitamin B12. Early disease may present with macrocytosis and a normal hemoglobin initially, but anemia develops over time if left untreated. When the primary cause of pernicious anemia is gastric parietal cell destruction, there is also an associated lack of stomach acid production (achlorhydria) with resulting poor micronutrient absorption; specifically, vitamin D, vitamin C, and iron. Hence, 30% of patients diagnosed with pernicious anemia have concurrent iron deficiency, which may counteract macrocytosis and result in a normal mean corpuscular volume. 4 Some medications are also poorly absorbed in achlorhydric states, such as levothyroxine, and treatment doses need to be increased, which could explain his markedly elevated TSH despite presumed medication adherence.
Vitamin B12 is essential for both the peripheral and central nervous systems. Longstanding severe B12 deficiency can explain all of his neurological and neurocognitive changes. The most common neurologic findings in B12 deficiency are symmetric paresthesias or numbness and gait problems. The sensory neuropathy affects the lower extremities more commonly than the upper. Untreated, patients can develop progressive weakness, ataxia, and orthostatic hypotension with syncope, as well as neuropsychiatric changes including depression or mood impairment, cognitive slowing, forgetfulness, and dementia.
Dr. Ulin:
Dr. Orlander, which pieces of objective data are most important in forming your differential diagnosis, and what tests would you obtain next?
Dr. Orlander:
The 3 most salient laboratory tests to me are a complete blood count, with all cell lines impacted but the hemoglobin and hematocrit most dramatically impacted, reticulocyte count of 0.8%, which is inappropriately low and hence suggests a hypoproliferative anemia, and the elevated LDH > 5000 IU/L.
Since my suspected diagnosis is pernicious anemia, I would obtain a blood smear looking for hypersegmented neutrophils, > 1 white blood cells with 5 lobes, or 1 with 6 lobes, which should clinch the diagnosis. Methylmalonic acid (MMA) levels are the most sensitive test for B12 deficiency, so I would also obtain that. Finally, I would check a B12 level, since in a patient with pernicious anemia, I would expect the level to be < 200 pg/mL.
Dr. Ulin:
Before we reveal the results of the patient’s additional workup, how do you approach interpreting B12 levels?
Dr. Orlander:
Measuring B12 can sometimes be problematic: the normal range is considered 200 to 900 pg/mL, but patients with measured low-normal levels in the range of 200 to 400 pg/mL can actually be physiologically deficient. There are also several common causes of falsely low and falsely high B12 levels in the absence of B12 deficiency. Hence, for patients with mild symptoms that could be due to B12 deficiency, many clinicians choose to just treat with B12 supplementation, deeming it safer to treat than miss an early diagnosis. B12 is involved in hydrogen transfer to convert MMA into succinyl-CoA and hence true vitamin B12 deficiency causes an increase in MMA.
Decreased production of vitamin B12 binding proteins, like haptocorrin, has been proposed as the mechanism for spurious low values.5 Certain conditions or medications can also cause spurious low serum vitamin B12 levels and thus might cause the appearance of vitamin B12 deficiency when the patient is not deficient. Examples include multiple myeloma, HIV infection, pregnancy, oral contraceptives, and phenytoin use. An example of spuriously low vitamin B12 level in pregnancy was demonstrated in a series of 50 pregnant individuals with low vitamin B12 levels (45-199 pg/mL), in whom metabolite testing for MMA and homocysteine showed no correlation with vitamin B12 level.6
Further complicating things, some conditions can cause spuriously increased vitamin B12 levels and thus might cause the appearance of normal vitamin B12 levels when the patient is actually deficient.7 Examples include occult malignancy, myeloproliferative neoplasms, alcoholic liver disease, kidney disease, and nitrous oxide exposure (the latter of which is unique in that it can also cause true vitamin B12 deficiency, as evidenced by clinical symptoms and high MMA levels).8,9
Lastly, autoantibodies to intrinsic factor in individuals with pernicious anemia may compete with intrinsic factor in the chemiluminescence assay and result in spuriously normal vitamin B12 levels in the presence of true deficiency.10-12 If the vitamin B12 level is very high (eg, 800 pg/mL), we do not worry about this effect in the absence of clinical features suggesting vitamin B12 deficiency; however, if the vitamin B12 level is borderline or low-normal and/or other clinical features suggest vitamin B12 deficiency, it is prudent to obtain other testing such as an MMA level.
Dr. Ulin:
We are also joined by Dr. Rahul Ganatra, who cared for the patient at the time the diagnosis was made. Dr. Ganatra, can you share the final diagnosis and provide an update on the patient?
Rahul Ganatra, MD, MPH, Director of Continuing Medical Education, VABHS:
The patient’s hemoglobin rose to 6.9 g/dL after transfusion of 2 units of packed red blood cells, and his dyspnea on exertion and fatigue improved. Iron studies, serum thiamine, serum folate, ADAMTS13 activity levels, and AM cortisol level were normal. Upon closer examination of the peripheral blood smear, rare hypersegmented neutrophils were noted. Serum B12 level returned below assay (< 146 pg/mL), and serum MMA was 50,800 nmol/L, confirming the diagnosis of severe vitamin B12 deficiency. Antibodies against intrinsic factor were detected, confirming the diagnosis of pernicious anemia. Treatment was initiated with intramuscular cyanocobalamin every other day and was transitioned to weekly dosing at the time of hospital discharge. After excluding adrenal insufficiency, his levothyroxine dose was increased. Finally, a liver mass biopsy confirmed a concomitant diagnosis of HCC. The patient was discharged home. Five weeks after discharge, his serum B12 level rose to > 1000 pg/mL, and 10 months after discharge, his TSH fell to 0.97 uIU/mL. Several months later, he underwent stereotactic body radiotherapy for the HCC. One year after his initial presentation, he has not resumed work as a barber.
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
References
Leigh H, Kramer SI. The psychiatric manifestations of endocrine disease. Adv Intern Med. 1984;29:413-445
Lenti MV, Rugge M, Lahner E, et al. Autoimmune gastritis. Nat Rev Dis Primers. 2020;6(1):56.doi:10.1038/s41572-020-0187-8
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441-1448. doi:10.1056/NEJM199711133372007
. Hershko C, Ronson A, Souroujon M, Maschler I, Heyd J, Patz J. Variable hematologic presentation of autoimmune gastritis: age-related progression from iron deficiency to cobalamin depletion. Blood. 2006;107(4):1673-1679. doi:10.1182/blood-2005-09-3534
Morkbak AL, Hvas AM, Milman N, Nexo E. Holotranscobalamin remains unchanged during pregnancy. Longitudinal changes of cobalamins and their binding proteins during pregnancy and postpartum. Haematologica. 2007;92(12):1711-1712. doi:10.3324/haematol.11636
Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995;48(4):251-255. doi:10.1002/ajh.2830480409
Marsden P, Sharma AA, Rotella JA. Review article: clinical manifestations and outcomes of chronic nitrous oxide misuse: a systematic review. Emerg Med Australas. 2022;34(4):492- 503. doi:10.1111/1742-6723.13997
Hamilton MS, Blackmore S, Lee A. Possible cause of false normal B-12 assays. BMJ. 2006;333(7569):654-655. doi:10.1136/bmj.333.7569.654-c
Yang DT, Cook RJ. Spurious elevations of vitamin B12 with pernicious anemia. N Engl J Med. 2012;366(18):1742-1743. doi:10.1056/NEJMc1201655
Carmel R, Agrawal YP. Failures of cobalamin assays in pernicious anemia. N Engl J Med. 2012;367(4):385-386. doi:10.1056/NEJMc1204070
Green R. Vitamin B12 deficiency from the perspective of a practicing hematologist. Blood. May 11 2017;129(19):2603- 2611. doi:10.1182/blood-2016-10-569186
Miceli E, Lenti MV, Padula D, et al. Common features of patients with autoimmune atrophic gastritis. Clin Gastroenterol Hepatol. 2012;10(7):812-814.doi:10.1016/j.cgh.2012.02.018
The COVID-19 pandemic established a new normal for health care delivery, with leaders rethinking core practices to survive and thrive in a changing environment and improve the health and well-being of patients. The Veterans Health Administration (VHA) is embracing a shift in focus from “what is the matter” to “what really matters” to address pre- and postpandemic challenges through a whole health approach.1 Initially conceptualized by the VHA in 2011, whole health “is an approach to health care that empowers and equips people to take charge of their health and well-being so that they can live their life to the fullest.”1 Whole health integrates evidence-based complementary and integrative health (CIH) therapies to manage pain; this includes acupuncture, meditation, tai chi, yoga, massage therapy, guided imagery, biofeedback, and clinical hypnosis.1 The VHA now recognizes well-being as a core value, helping clinicians respond to emerging challenges related to the social determinants of health (eg, access to health care, physical activity, and healthy foods) and guiding health care decision making.1,2
Well-being through empowerment—elements of whole health and Age-Friendly Health Systems (AFHS)—encourages health care institutions to work with employees, patients, and other stakeholders to address global challenges, clinician burnout, and social issues faced by their communities. This approach focuses on life’s purpose and meaning for individuals and inspires leaders to engage with patients, staff, and communities in new, impactful ways by focusing on wellbeing and wholeness rather than illness and disease. Having a higher sense of purpose is associated with lower all-cause mortality, reduced risk of specific diseases, better health behaviors, greater use of preventive services, and fewer hospital days of care.3
This article describes how AFHS supports the well-being of older adults and aligns with the whole health model of care. It also outlines the VHA investment to transform health care to be more person-centered by documenting what matters in the electronic health record (EHR).
AGE-FRIENDLY CARE
Given that nearly half of veterans enrolled in the VHA are aged ≥ 65 years, there is an increased need to identify models of care to support this aging population.4 This is especially critical because older veterans often have multiple chronic conditions and complex care needs that benefit from a whole person approach. The AFHS movement aims to provide evidence-based care aligned with what matters to older adults and provides a mechanism for transforming care to meet the needs of older veterans. This includes addressing age-related health concerns while promoting optimal health outcomes and quality of life. AFHS follows the 4Ms framework: what matters, medication, mentation, and mobility.5 The 4Ms serve as a guide for the health care of older adults in any setting, where each “M” is assessed and acted on to support what matters.5 Since 2020, > 390 teams have developed a plan to implement the 4Ms at 156 VHA facilities, demonstrating the VHA commitment to transforming health care for veterans.6
When VHA teams join the AFHS movement, they may also engage older veterans in a whole health system (WHS) (Figure). While AFHS is designed to improve care for patients aged ≥ 65 years, it also complements whole health, a person-centered approach available to all veterans enrolled in the VHA. Through the WHS and AFHS, veterans are empowered and equipped to take charge of their health and well-being through conversations about their unique goals, preferences, and health priorities.4 Clinicians are challenged to assess what matters by asking questions like, “What brings you joy?” and, “How can we help you meet your health goals?”1,5 These questions shift the conversation from disease-based treatment and enable clinicians to better understand the veteran as a person.1,5
FIGURE The Whole Health System and the Circle of Health19
For whole health and AFHS, conversations about what matters are anchored in the veteran’s goals and preferences, especially those facing a significant health change (ie, a new diagnosis or treatment decision).5,7 Together, the veteran’s goals and priorities serve as the foundation for developing person-centered care plans that often go beyond conventional medical treatments to address the physical, mental, emotional, and social aspects of health.
SYSTEM-WIDE DIRECTIVE
The WHS enhances AFHS discussions about what matters to veterans by adding a system-level lens for conceptualizing health care delivery by leveraging the 3 components of WHS: the “pathway,” well-being programs, and whole health clinical care.
The Pathway
Discovering what matters, or the veteran’s “mission, aspiration, and purpose,” begins with the WHS pathway. When stepping into the pathway, veterans begin completing a personal health inventory, or “walking the circle of health,” which encourages self-reflection that focuses on components of their life that can influence health and well-being.1,8 The circle of health offers a visual representation of the 4 most important aspects of health and well-being: First, “Me” at the center as an individual who is the expert on their life, values, goals, and priorities. Only the individual can know what really matters through mindful awareness and what works for their life. Second, self-care consists of 8 areas that impact health and wellbeing: working your body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind. Third, professional care consists of prevention, conventional care, and complementary care. Finally, the community that supports the individual.
Well-Being Programs
VHA provides WHS programs that support veterans in building self-care skills and improving their quality of life, often through integrative care clinics that offer coaching and CIH therapies. For example, a veteran who prioritizes mobility when seeking care at an integrative care clinic will not only receive conventional medical treatment for their physical symptoms but may also be offered CIH therapies depending on their goals. The veteran may set a daily mobility goal with their care team that supports what matters, incorporating CIH approaches, such as yoga and tai chi into the care plan.5 These holistic approaches for moving the body can help alleviate physical symptoms, reduce stress, improve mindful awareness, and provide opportunities for self-discovery and growth, thus promote overall well-being
Whole Health Clinical Care
AFHS and the 4Ms embody the clinical care component of the WHS. Because what matters is the driver of the 4Ms, every action taken by the care team supports wellbeing and quality of life by promoting independence, connection, and support, and addressing external factors, such as social determinants of health. At a minimum, well-being includes “functioning well: the experience of positive emotions such as happiness and contentment as well as the development of one’s potential, having some control over one’s life, having a sense of purpose, and experiencing positive relationships.”9 From a system perspective, the VHA has begun to normalize focusing on what matters to veterans, using an interprofessional approach, one of the first steps to implementing AFHS.
As the programs expand, AFHS teams can learn from whole health well-being programs and increase the capacity for self-care in older veterans. Learning about the key elements included in the circle of health helps clinicians understand each veteran’s perceived strengths and weaknesses to support their self-care. From there, teams can act on the 4Ms and connect older veterans with the most appropriate programs and services at their facility, ensuring continuum of care.
DOCUMENTATION
The VHA leverages several tools and evidence-based practices to assess and act on what matters for veterans of all ages (Table).5,10-16 The VHA EHR and associated dashboards contain a wealth of information about whole health and AFHS implementation, scale up, and spread. A national AFHS 4Ms note template contains standardized data elements called health factors, which provide a mechanism for monitoring 4Ms care via its related dashboard. This template was developed by an interprofessional workgroup of VHA staff and underwent a thorough human factors engineering review and testing process prior to its release. Although teams continue to personalize care based on what matters to the veteran, data from the standardized 4Ms note template and dashboard provide a way to establish consistent, equitable care across multiple care settings.17
Between January 2022 and December 2023, > 612,000 participants aged ≥ 65 years identified what matters to them through 1.35 million assessments. During that period, > 36,000 veterans aged ≥ 65 years participated in AFHS and had what matters conversations documented. A personalized health plan was completed by 585,270 veterans for a total of 1.1 million assessments.11 Whole health coaching has been documented for > 57,000 veterans with > 200,000 assessments completed.13 In fiscal year 2023, a total of 1,802,131 veterans participated in whole health.
When teams share information about what matters to the veteran in a clinicianfacing format in the EHR, this helps ensure that the VHA honors veteran preferences throughout transitions of care and across all phases of health care. Although the EHR captures data on what matters, measurement of the overall impact on veteran and health system outcomes is essential. Further evaluation and ongoing education are needed to ensure clinicians are accurately and efficiently capturing the care provided by completing the appropriate EHR. Additional challenges include identifying ways to balance the documentation burden, while ensuring notes include valuable patient-centered information to guide care. EHR tools and templates have helped to unlock important insights on health care delivery in the VHA; however, health systems must consider how these clinical practices support the overall well-being of patients. How leaders empower frontline clinicians in any care setting to use these data to drive meaningful change is also important.
TRANSFORMING VHA CARE DELIVERY
In Achieving Whole Health: A New Approach for Veterans and the Nation, the National Academy of Science proposes a framework for the transformation of health care institutions to provide better whole health to veterans.3 Transformation requires change in entire systems and leaders who mobilize people “for participation in the process of change, encouraging a sense of collective identity and collective efficacy, which in turn brings stronger feelings of self-worth and self-efficacy,” and an enhanced sense of meaningfulness in their work and lives.18
Shifting health care approaches to equipping and empowering veterans and employees with whole health and AFHS resources is transformational and requires radically different assumptions and approaches that cannot be realized through traditional approaches. This change requires robust and multifaceted cultural transformation spanning all levels of the organization. Whole health and AFHS are facilitating this transformation by supporting documentation and data needs, tracking outcomes across settings, and accelerating spread to new facilities and care settings nationwide to support older veterans in improving their health and well-being.
Whole health and AFHS are complementary approaches to care that can work to empower veterans (as well as caregivers and clinicians) to align services with what matters most to veterans. Lessons such as standardizing person-centered assessments of what matters, creating supportive structures to better align care with veterans’ priorities, and identifying meaningful veteran and system-level outcomes to help sustain transformational change can be applied from whole health to AFHS. Together these programs have the potential to enhance overall health outcomes and quality of life for veterans.
References
Kligler B, Hyde J, Gantt C, Bokhour B. The Whole Health transformation at the Veterans Health Administration: moving from “what’s the matter with you?” to “what matters to you?” Med Care. 2022;60(5):387-391. doi:10.1097/MLR.0000000000001706
National Academies of Sciences, Engineering, and Medicine. Achieving Whole Health: A New Approach for Veterans and the Nation. The National Academies Press; 2023. Accessed September 9, 2024. doi:10.17226/26854
Church K, Munro S, Shaughnessy M, Clancy C. Age-friendly health systems: improving care for older adults in the Veterans Health Administration. Health Serv Res. 2023;58 Suppl 1(Suppl 1):5-8. doi:10.1111/1475-6773.14110
Brown TT, Hurley VB, Rodriguez HP, et al. Shared dec i s i o n - m a k i n g l o w e r s m e d i c a l e x p e n d i t u re s a n d the effect is amplified in racially-ethnically concordant relationships. Med Care. 2023;61(8):528-535. doi:10.1097/MLR.0000000000001881
Kligler B. Whole Health in the Veterans Health Administration. Glob Adv Health Med. 2022;11:2164957X221077214.
Ruggeri K, Garcia-Garzon E, Maguire Á, Matz S, Huppert FA. Well-being is more than happiness and life satisfaction: a multidimensional analysis of 21 countries. Health Qual Life Outcomes. 2020;18(1):192. doi:10.1186/s12955-020-01423-y
Munro S, Church K, Berner C, et al. Implementation of an agefriendly template in the Veterans Health Administration electronic health record. J Inform Nurs. 2023;8(3):6-11.
Burns JM. Transforming Leadership: A New Pursuit of Happiness. Grove Press; 2003.
Kimberly Wozneak, MSa; Shannon Munro, PhD, APRN, NPa; Kirstin Manges Piazza, PhD, MSHP, RNb; Kelly J. Cummings, RN, PhDa
Author affiliationsa Veterans Health Administration, Washington, DC bCorporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, Pennsylvania
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Funding Kimberly Wozneak acknowledges receiving funding from John A. Hartford Foundation and the Institute for Healthcare Improvement that supported the first VA Action Community.
Kimberly Wozneak, MSa; Shannon Munro, PhD, APRN, NPa; Kirstin Manges Piazza, PhD, MSHP, RNb; Kelly J. Cummings, RN, PhDa
Author affiliationsa Veterans Health Administration, Washington, DC bCorporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, Pennsylvania
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Funding Kimberly Wozneak acknowledges receiving funding from John A. Hartford Foundation and the Institute for Healthcare Improvement that supported the first VA Action Community.
Fed Pract. 2024;41(10). Published online October 18. doi:10.12788/fp0518
Author and Disclosure Information
Kimberly Wozneak, MSa; Shannon Munro, PhD, APRN, NPa; Kirstin Manges Piazza, PhD, MSHP, RNb; Kelly J. Cummings, RN, PhDa
Author affiliationsa Veterans Health Administration, Washington, DC bCorporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, Pennsylvania
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Funding Kimberly Wozneak acknowledges receiving funding from John A. Hartford Foundation and the Institute for Healthcare Improvement that supported the first VA Action Community.
The COVID-19 pandemic established a new normal for health care delivery, with leaders rethinking core practices to survive and thrive in a changing environment and improve the health and well-being of patients. The Veterans Health Administration (VHA) is embracing a shift in focus from “what is the matter” to “what really matters” to address pre- and postpandemic challenges through a whole health approach.1 Initially conceptualized by the VHA in 2011, whole health “is an approach to health care that empowers and equips people to take charge of their health and well-being so that they can live their life to the fullest.”1 Whole health integrates evidence-based complementary and integrative health (CIH) therapies to manage pain; this includes acupuncture, meditation, tai chi, yoga, massage therapy, guided imagery, biofeedback, and clinical hypnosis.1 The VHA now recognizes well-being as a core value, helping clinicians respond to emerging challenges related to the social determinants of health (eg, access to health care, physical activity, and healthy foods) and guiding health care decision making.1,2
Well-being through empowerment—elements of whole health and Age-Friendly Health Systems (AFHS)—encourages health care institutions to work with employees, patients, and other stakeholders to address global challenges, clinician burnout, and social issues faced by their communities. This approach focuses on life’s purpose and meaning for individuals and inspires leaders to engage with patients, staff, and communities in new, impactful ways by focusing on wellbeing and wholeness rather than illness and disease. Having a higher sense of purpose is associated with lower all-cause mortality, reduced risk of specific diseases, better health behaviors, greater use of preventive services, and fewer hospital days of care.3
This article describes how AFHS supports the well-being of older adults and aligns with the whole health model of care. It also outlines the VHA investment to transform health care to be more person-centered by documenting what matters in the electronic health record (EHR).
AGE-FRIENDLY CARE
Given that nearly half of veterans enrolled in the VHA are aged ≥ 65 years, there is an increased need to identify models of care to support this aging population.4 This is especially critical because older veterans often have multiple chronic conditions and complex care needs that benefit from a whole person approach. The AFHS movement aims to provide evidence-based care aligned with what matters to older adults and provides a mechanism for transforming care to meet the needs of older veterans. This includes addressing age-related health concerns while promoting optimal health outcomes and quality of life. AFHS follows the 4Ms framework: what matters, medication, mentation, and mobility.5 The 4Ms serve as a guide for the health care of older adults in any setting, where each “M” is assessed and acted on to support what matters.5 Since 2020, > 390 teams have developed a plan to implement the 4Ms at 156 VHA facilities, demonstrating the VHA commitment to transforming health care for veterans.6
When VHA teams join the AFHS movement, they may also engage older veterans in a whole health system (WHS) (Figure). While AFHS is designed to improve care for patients aged ≥ 65 years, it also complements whole health, a person-centered approach available to all veterans enrolled in the VHA. Through the WHS and AFHS, veterans are empowered and equipped to take charge of their health and well-being through conversations about their unique goals, preferences, and health priorities.4 Clinicians are challenged to assess what matters by asking questions like, “What brings you joy?” and, “How can we help you meet your health goals?”1,5 These questions shift the conversation from disease-based treatment and enable clinicians to better understand the veteran as a person.1,5
FIGURE The Whole Health System and the Circle of Health19
For whole health and AFHS, conversations about what matters are anchored in the veteran’s goals and preferences, especially those facing a significant health change (ie, a new diagnosis or treatment decision).5,7 Together, the veteran’s goals and priorities serve as the foundation for developing person-centered care plans that often go beyond conventional medical treatments to address the physical, mental, emotional, and social aspects of health.
SYSTEM-WIDE DIRECTIVE
The WHS enhances AFHS discussions about what matters to veterans by adding a system-level lens for conceptualizing health care delivery by leveraging the 3 components of WHS: the “pathway,” well-being programs, and whole health clinical care.
The Pathway
Discovering what matters, or the veteran’s “mission, aspiration, and purpose,” begins with the WHS pathway. When stepping into the pathway, veterans begin completing a personal health inventory, or “walking the circle of health,” which encourages self-reflection that focuses on components of their life that can influence health and well-being.1,8 The circle of health offers a visual representation of the 4 most important aspects of health and well-being: First, “Me” at the center as an individual who is the expert on their life, values, goals, and priorities. Only the individual can know what really matters through mindful awareness and what works for their life. Second, self-care consists of 8 areas that impact health and wellbeing: working your body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind. Third, professional care consists of prevention, conventional care, and complementary care. Finally, the community that supports the individual.
Well-Being Programs
VHA provides WHS programs that support veterans in building self-care skills and improving their quality of life, often through integrative care clinics that offer coaching and CIH therapies. For example, a veteran who prioritizes mobility when seeking care at an integrative care clinic will not only receive conventional medical treatment for their physical symptoms but may also be offered CIH therapies depending on their goals. The veteran may set a daily mobility goal with their care team that supports what matters, incorporating CIH approaches, such as yoga and tai chi into the care plan.5 These holistic approaches for moving the body can help alleviate physical symptoms, reduce stress, improve mindful awareness, and provide opportunities for self-discovery and growth, thus promote overall well-being
Whole Health Clinical Care
AFHS and the 4Ms embody the clinical care component of the WHS. Because what matters is the driver of the 4Ms, every action taken by the care team supports wellbeing and quality of life by promoting independence, connection, and support, and addressing external factors, such as social determinants of health. At a minimum, well-being includes “functioning well: the experience of positive emotions such as happiness and contentment as well as the development of one’s potential, having some control over one’s life, having a sense of purpose, and experiencing positive relationships.”9 From a system perspective, the VHA has begun to normalize focusing on what matters to veterans, using an interprofessional approach, one of the first steps to implementing AFHS.
As the programs expand, AFHS teams can learn from whole health well-being programs and increase the capacity for self-care in older veterans. Learning about the key elements included in the circle of health helps clinicians understand each veteran’s perceived strengths and weaknesses to support their self-care. From there, teams can act on the 4Ms and connect older veterans with the most appropriate programs and services at their facility, ensuring continuum of care.
DOCUMENTATION
The VHA leverages several tools and evidence-based practices to assess and act on what matters for veterans of all ages (Table).5,10-16 The VHA EHR and associated dashboards contain a wealth of information about whole health and AFHS implementation, scale up, and spread. A national AFHS 4Ms note template contains standardized data elements called health factors, which provide a mechanism for monitoring 4Ms care via its related dashboard. This template was developed by an interprofessional workgroup of VHA staff and underwent a thorough human factors engineering review and testing process prior to its release. Although teams continue to personalize care based on what matters to the veteran, data from the standardized 4Ms note template and dashboard provide a way to establish consistent, equitable care across multiple care settings.17
Between January 2022 and December 2023, > 612,000 participants aged ≥ 65 years identified what matters to them through 1.35 million assessments. During that period, > 36,000 veterans aged ≥ 65 years participated in AFHS and had what matters conversations documented. A personalized health plan was completed by 585,270 veterans for a total of 1.1 million assessments.11 Whole health coaching has been documented for > 57,000 veterans with > 200,000 assessments completed.13 In fiscal year 2023, a total of 1,802,131 veterans participated in whole health.
When teams share information about what matters to the veteran in a clinicianfacing format in the EHR, this helps ensure that the VHA honors veteran preferences throughout transitions of care and across all phases of health care. Although the EHR captures data on what matters, measurement of the overall impact on veteran and health system outcomes is essential. Further evaluation and ongoing education are needed to ensure clinicians are accurately and efficiently capturing the care provided by completing the appropriate EHR. Additional challenges include identifying ways to balance the documentation burden, while ensuring notes include valuable patient-centered information to guide care. EHR tools and templates have helped to unlock important insights on health care delivery in the VHA; however, health systems must consider how these clinical practices support the overall well-being of patients. How leaders empower frontline clinicians in any care setting to use these data to drive meaningful change is also important.
TRANSFORMING VHA CARE DELIVERY
In Achieving Whole Health: A New Approach for Veterans and the Nation, the National Academy of Science proposes a framework for the transformation of health care institutions to provide better whole health to veterans.3 Transformation requires change in entire systems and leaders who mobilize people “for participation in the process of change, encouraging a sense of collective identity and collective efficacy, which in turn brings stronger feelings of self-worth and self-efficacy,” and an enhanced sense of meaningfulness in their work and lives.18
Shifting health care approaches to equipping and empowering veterans and employees with whole health and AFHS resources is transformational and requires radically different assumptions and approaches that cannot be realized through traditional approaches. This change requires robust and multifaceted cultural transformation spanning all levels of the organization. Whole health and AFHS are facilitating this transformation by supporting documentation and data needs, tracking outcomes across settings, and accelerating spread to new facilities and care settings nationwide to support older veterans in improving their health and well-being.
Whole health and AFHS are complementary approaches to care that can work to empower veterans (as well as caregivers and clinicians) to align services with what matters most to veterans. Lessons such as standardizing person-centered assessments of what matters, creating supportive structures to better align care with veterans’ priorities, and identifying meaningful veteran and system-level outcomes to help sustain transformational change can be applied from whole health to AFHS. Together these programs have the potential to enhance overall health outcomes and quality of life for veterans.
The COVID-19 pandemic established a new normal for health care delivery, with leaders rethinking core practices to survive and thrive in a changing environment and improve the health and well-being of patients. The Veterans Health Administration (VHA) is embracing a shift in focus from “what is the matter” to “what really matters” to address pre- and postpandemic challenges through a whole health approach.1 Initially conceptualized by the VHA in 2011, whole health “is an approach to health care that empowers and equips people to take charge of their health and well-being so that they can live their life to the fullest.”1 Whole health integrates evidence-based complementary and integrative health (CIH) therapies to manage pain; this includes acupuncture, meditation, tai chi, yoga, massage therapy, guided imagery, biofeedback, and clinical hypnosis.1 The VHA now recognizes well-being as a core value, helping clinicians respond to emerging challenges related to the social determinants of health (eg, access to health care, physical activity, and healthy foods) and guiding health care decision making.1,2
Well-being through empowerment—elements of whole health and Age-Friendly Health Systems (AFHS)—encourages health care institutions to work with employees, patients, and other stakeholders to address global challenges, clinician burnout, and social issues faced by their communities. This approach focuses on life’s purpose and meaning for individuals and inspires leaders to engage with patients, staff, and communities in new, impactful ways by focusing on wellbeing and wholeness rather than illness and disease. Having a higher sense of purpose is associated with lower all-cause mortality, reduced risk of specific diseases, better health behaviors, greater use of preventive services, and fewer hospital days of care.3
This article describes how AFHS supports the well-being of older adults and aligns with the whole health model of care. It also outlines the VHA investment to transform health care to be more person-centered by documenting what matters in the electronic health record (EHR).
AGE-FRIENDLY CARE
Given that nearly half of veterans enrolled in the VHA are aged ≥ 65 years, there is an increased need to identify models of care to support this aging population.4 This is especially critical because older veterans often have multiple chronic conditions and complex care needs that benefit from a whole person approach. The AFHS movement aims to provide evidence-based care aligned with what matters to older adults and provides a mechanism for transforming care to meet the needs of older veterans. This includes addressing age-related health concerns while promoting optimal health outcomes and quality of life. AFHS follows the 4Ms framework: what matters, medication, mentation, and mobility.5 The 4Ms serve as a guide for the health care of older adults in any setting, where each “M” is assessed and acted on to support what matters.5 Since 2020, > 390 teams have developed a plan to implement the 4Ms at 156 VHA facilities, demonstrating the VHA commitment to transforming health care for veterans.6
When VHA teams join the AFHS movement, they may also engage older veterans in a whole health system (WHS) (Figure). While AFHS is designed to improve care for patients aged ≥ 65 years, it also complements whole health, a person-centered approach available to all veterans enrolled in the VHA. Through the WHS and AFHS, veterans are empowered and equipped to take charge of their health and well-being through conversations about their unique goals, preferences, and health priorities.4 Clinicians are challenged to assess what matters by asking questions like, “What brings you joy?” and, “How can we help you meet your health goals?”1,5 These questions shift the conversation from disease-based treatment and enable clinicians to better understand the veteran as a person.1,5
FIGURE The Whole Health System and the Circle of Health19
For whole health and AFHS, conversations about what matters are anchored in the veteran’s goals and preferences, especially those facing a significant health change (ie, a new diagnosis or treatment decision).5,7 Together, the veteran’s goals and priorities serve as the foundation for developing person-centered care plans that often go beyond conventional medical treatments to address the physical, mental, emotional, and social aspects of health.
SYSTEM-WIDE DIRECTIVE
The WHS enhances AFHS discussions about what matters to veterans by adding a system-level lens for conceptualizing health care delivery by leveraging the 3 components of WHS: the “pathway,” well-being programs, and whole health clinical care.
The Pathway
Discovering what matters, or the veteran’s “mission, aspiration, and purpose,” begins with the WHS pathway. When stepping into the pathway, veterans begin completing a personal health inventory, or “walking the circle of health,” which encourages self-reflection that focuses on components of their life that can influence health and well-being.1,8 The circle of health offers a visual representation of the 4 most important aspects of health and well-being: First, “Me” at the center as an individual who is the expert on their life, values, goals, and priorities. Only the individual can know what really matters through mindful awareness and what works for their life. Second, self-care consists of 8 areas that impact health and wellbeing: working your body; surroundings; personal development; food and drink; recharge; family, friends, and coworkers; spirit and soul; and power of the mind. Third, professional care consists of prevention, conventional care, and complementary care. Finally, the community that supports the individual.
Well-Being Programs
VHA provides WHS programs that support veterans in building self-care skills and improving their quality of life, often through integrative care clinics that offer coaching and CIH therapies. For example, a veteran who prioritizes mobility when seeking care at an integrative care clinic will not only receive conventional medical treatment for their physical symptoms but may also be offered CIH therapies depending on their goals. The veteran may set a daily mobility goal with their care team that supports what matters, incorporating CIH approaches, such as yoga and tai chi into the care plan.5 These holistic approaches for moving the body can help alleviate physical symptoms, reduce stress, improve mindful awareness, and provide opportunities for self-discovery and growth, thus promote overall well-being
Whole Health Clinical Care
AFHS and the 4Ms embody the clinical care component of the WHS. Because what matters is the driver of the 4Ms, every action taken by the care team supports wellbeing and quality of life by promoting independence, connection, and support, and addressing external factors, such as social determinants of health. At a minimum, well-being includes “functioning well: the experience of positive emotions such as happiness and contentment as well as the development of one’s potential, having some control over one’s life, having a sense of purpose, and experiencing positive relationships.”9 From a system perspective, the VHA has begun to normalize focusing on what matters to veterans, using an interprofessional approach, one of the first steps to implementing AFHS.
As the programs expand, AFHS teams can learn from whole health well-being programs and increase the capacity for self-care in older veterans. Learning about the key elements included in the circle of health helps clinicians understand each veteran’s perceived strengths and weaknesses to support their self-care. From there, teams can act on the 4Ms and connect older veterans with the most appropriate programs and services at their facility, ensuring continuum of care.
DOCUMENTATION
The VHA leverages several tools and evidence-based practices to assess and act on what matters for veterans of all ages (Table).5,10-16 The VHA EHR and associated dashboards contain a wealth of information about whole health and AFHS implementation, scale up, and spread. A national AFHS 4Ms note template contains standardized data elements called health factors, which provide a mechanism for monitoring 4Ms care via its related dashboard. This template was developed by an interprofessional workgroup of VHA staff and underwent a thorough human factors engineering review and testing process prior to its release. Although teams continue to personalize care based on what matters to the veteran, data from the standardized 4Ms note template and dashboard provide a way to establish consistent, equitable care across multiple care settings.17
Between January 2022 and December 2023, > 612,000 participants aged ≥ 65 years identified what matters to them through 1.35 million assessments. During that period, > 36,000 veterans aged ≥ 65 years participated in AFHS and had what matters conversations documented. A personalized health plan was completed by 585,270 veterans for a total of 1.1 million assessments.11 Whole health coaching has been documented for > 57,000 veterans with > 200,000 assessments completed.13 In fiscal year 2023, a total of 1,802,131 veterans participated in whole health.
When teams share information about what matters to the veteran in a clinicianfacing format in the EHR, this helps ensure that the VHA honors veteran preferences throughout transitions of care and across all phases of health care. Although the EHR captures data on what matters, measurement of the overall impact on veteran and health system outcomes is essential. Further evaluation and ongoing education are needed to ensure clinicians are accurately and efficiently capturing the care provided by completing the appropriate EHR. Additional challenges include identifying ways to balance the documentation burden, while ensuring notes include valuable patient-centered information to guide care. EHR tools and templates have helped to unlock important insights on health care delivery in the VHA; however, health systems must consider how these clinical practices support the overall well-being of patients. How leaders empower frontline clinicians in any care setting to use these data to drive meaningful change is also important.
TRANSFORMING VHA CARE DELIVERY
In Achieving Whole Health: A New Approach for Veterans and the Nation, the National Academy of Science proposes a framework for the transformation of health care institutions to provide better whole health to veterans.3 Transformation requires change in entire systems and leaders who mobilize people “for participation in the process of change, encouraging a sense of collective identity and collective efficacy, which in turn brings stronger feelings of self-worth and self-efficacy,” and an enhanced sense of meaningfulness in their work and lives.18
Shifting health care approaches to equipping and empowering veterans and employees with whole health and AFHS resources is transformational and requires radically different assumptions and approaches that cannot be realized through traditional approaches. This change requires robust and multifaceted cultural transformation spanning all levels of the organization. Whole health and AFHS are facilitating this transformation by supporting documentation and data needs, tracking outcomes across settings, and accelerating spread to new facilities and care settings nationwide to support older veterans in improving their health and well-being.
Whole health and AFHS are complementary approaches to care that can work to empower veterans (as well as caregivers and clinicians) to align services with what matters most to veterans. Lessons such as standardizing person-centered assessments of what matters, creating supportive structures to better align care with veterans’ priorities, and identifying meaningful veteran and system-level outcomes to help sustain transformational change can be applied from whole health to AFHS. Together these programs have the potential to enhance overall health outcomes and quality of life for veterans.
References
Kligler B, Hyde J, Gantt C, Bokhour B. The Whole Health transformation at the Veterans Health Administration: moving from “what’s the matter with you?” to “what matters to you?” Med Care. 2022;60(5):387-391. doi:10.1097/MLR.0000000000001706
National Academies of Sciences, Engineering, and Medicine. Achieving Whole Health: A New Approach for Veterans and the Nation. The National Academies Press; 2023. Accessed September 9, 2024. doi:10.17226/26854
Church K, Munro S, Shaughnessy M, Clancy C. Age-friendly health systems: improving care for older adults in the Veterans Health Administration. Health Serv Res. 2023;58 Suppl 1(Suppl 1):5-8. doi:10.1111/1475-6773.14110
Brown TT, Hurley VB, Rodriguez HP, et al. Shared dec i s i o n - m a k i n g l o w e r s m e d i c a l e x p e n d i t u re s a n d the effect is amplified in racially-ethnically concordant relationships. Med Care. 2023;61(8):528-535. doi:10.1097/MLR.0000000000001881
Kligler B. Whole Health in the Veterans Health Administration. Glob Adv Health Med. 2022;11:2164957X221077214.
Ruggeri K, Garcia-Garzon E, Maguire Á, Matz S, Huppert FA. Well-being is more than happiness and life satisfaction: a multidimensional analysis of 21 countries. Health Qual Life Outcomes. 2020;18(1):192. doi:10.1186/s12955-020-01423-y
Munro S, Church K, Berner C, et al. Implementation of an agefriendly template in the Veterans Health Administration electronic health record. J Inform Nurs. 2023;8(3):6-11.
Burns JM. Transforming Leadership: A New Pursuit of Happiness. Grove Press; 2003.
Kligler B, Hyde J, Gantt C, Bokhour B. The Whole Health transformation at the Veterans Health Administration: moving from “what’s the matter with you?” to “what matters to you?” Med Care. 2022;60(5):387-391. doi:10.1097/MLR.0000000000001706
National Academies of Sciences, Engineering, and Medicine. Achieving Whole Health: A New Approach for Veterans and the Nation. The National Academies Press; 2023. Accessed September 9, 2024. doi:10.17226/26854
Church K, Munro S, Shaughnessy M, Clancy C. Age-friendly health systems: improving care for older adults in the Veterans Health Administration. Health Serv Res. 2023;58 Suppl 1(Suppl 1):5-8. doi:10.1111/1475-6773.14110
Brown TT, Hurley VB, Rodriguez HP, et al. Shared dec i s i o n - m a k i n g l o w e r s m e d i c a l e x p e n d i t u re s a n d the effect is amplified in racially-ethnically concordant relationships. Med Care. 2023;61(8):528-535. doi:10.1097/MLR.0000000000001881
Kligler B. Whole Health in the Veterans Health Administration. Glob Adv Health Med. 2022;11:2164957X221077214.
Ruggeri K, Garcia-Garzon E, Maguire Á, Matz S, Huppert FA. Well-being is more than happiness and life satisfaction: a multidimensional analysis of 21 countries. Health Qual Life Outcomes. 2020;18(1):192. doi:10.1186/s12955-020-01423-y
Munro S, Church K, Berner C, et al. Implementation of an agefriendly template in the Veterans Health Administration electronic health record. J Inform Nurs. 2023;8(3):6-11.
Burns JM. Transforming Leadership: A New Pursuit of Happiness. Grove Press; 2003.
Acute otitis media (AOM) is caused by Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Since the introduction of pneumococcal conjugate vaccines (PCVs) shifts in the proportion of these three bacteria as causes of AOM and their antibiotic susceptibility profiles and strain diversity have occurred due to multiple factors including the PCVs and antibiotic selection pressure.
The 7-valent PCV (PCV7) was introduced in 2000 and was proven to be efficacious in preventing AOM, but no subsequent PCV has received an indication for prevention of AOM because the FDA required a tympanocentesis study to prove efficacy and that approval was not achieved for PCV13, PCV15, or PCV20. This is a little known fact. After introduction of PCV7, replacement pneumococcal strains expressing serotypes not in PCV7 emerged and antibiotic non-susceptible strains became predominant causes of AOM, especially antibiotic-resistant serotype 19A. To address the phenomena of pneumococcal serotype replacement, PCV13 was introduced in 2010. But serotype replacement continued to occur under PCV13 pressure, replacement serotypes increasingly caused AOM, and antibiotic-resistant serotype 35B emerged. Now we have two new higher valency PCVs: PCV15 (Merck) where serotypes 22F and 33F were added to the PCV13 serotypes and PCV20 (Pfizer) where 22F, 33F, 8, 10A, 11A, 12F, 15B were added to PCV13. Note that neither PCV15 nor PCV20 includes the most common serotype causing AOM – serotype 35B.1
While PCV15 and PCV20 should provide protection against more pneumococcal serotypes, increasing serotypes in both vaccines decreased immunogenicity of certain shared serotypes, more so with the addition of seven more in PCV20 than two more in PCV15, compared with PCV13. Whether lower antibody concentrations will make a difference clinically in terms of vaccine failure to prevent nasopharyngeal colonization, AOM, and/or invasive pneumococcal infections is currently unknown.
Our group from greater Rochester, New York, is the only one in the United States performing tympanocentesis to determine the etiology of AOM infections. Children between ages 6 and 36 months are studied. We recently reported our results for the time span September 2021 to September 2023, the immediate 2 years prior to recommendations for use of PCV15 and PCV20 in young children.2 Tympanocentesis was performed in 139 (78%) of 179 episodes of AOM, yielding 216 middle ear fluid samples (the higher number of middle ear fluids was due to bilateral tympanocentesis in some children). H. influenzae (40%) was the most common bacterial isolate, followed by S. pneumonia (19%) and M. catarrhalis (17%), with the remainder no growth. Polymerase chain reactions (PCR) was positive in many of those culture negative samples, suggesting prior use of antibiotics before tympanocentesis was performed. Among the pneumococcal isolates, 46% were oxacillin non-susceptible. Among the H. influenzae isolates, 27% were beta-lactamase producing and all M. catarrhalis were beta-lactamase-producing.
As we previously reported,1 we once again found that serotype 35B was the most frequent non-PCV15, non-PCV20, serotype. Other frequently detected non-PCV20 pneumococcal serotypes were 23A, 23B, 35D, 35F and 15C.2
Projected Pneumococcal Serotype Coverage by PCV15 and PCV20
PCV13 serotypes were identified in 9% of middle ear fluids, consistent with vaccine failure. As we commence use of PCV15 and PCV20 in the United States, our data provide insights regarding estimation of the projected effects of these vaccines on AOM. Assuming 100% vaccine-type effectiveness, PCV15 will provide about 11% coverage of pneumococci causing AOM, the same PCV13 and PCV20 will provide 30% coverage, leaving 70% of pneumococci causing AOM in young children uncovered (Figure).
MDedge News
Thus, the high proportion of pneumococcal serotype 35B and other non-PCV15 or non-PCV20 serotypes will result in a relatively small incremental benefit over PCV13 in young children for AOM.
AOM is the most common cause of pediatric outpatient visits and antibiotic prescriptions in the United States that contributes to selection of antibiotic-resistant microbes.3 The economic burden of AOM is high, estimated at about $3 billion annually in the United States, when direct and indirect costs are calculated,4 thereby making AOM a major factor in calculations of cost effectiveness analyses of PCV immunizations in children.
While PCV15 and PCV20 include common serotypes associated with invasive pneumococcal diseases, their effectiveness in preventing AOM, acute sinusitis, and non-bacteremic community-acquired pneumonia is currently unknown because these vaccines were licensed based on safety and immunogenicity data, not proven efficacy.
The data on antibiotic susceptibility of pneumococci and H. influenza and M. catarrhalis isolated in the late post PCV13 era from young children in a pediatric primary-care setting raise a question about empiric antibiotic choice for AOM today. For penicillin non-susceptible pneumococcal strains, higher dosages of amoxicillin can improve eradication. However, higher dosages of amoxicillin cannot overcome beta-lactamase production by H. influenza and M. catarrhalis. Based on the mix of pathogens causing AOM and the antibiotic susceptibility of those bacteria, high-dose amoxicillin/clavulanate or alternative cephalosporin drugs active against pneumococci and beta-lactamase producing H. influenza and M. catarrhalis would be a better empiric choice over high-dose amoxicillin.
Dr. Michael E. Pichichero
Limitations of our study include that it occurred in one center in New York, although we have previously shown results of tympanocentesis at our center are similar to those in Virginia and Pennsylvania5 and our study population was composed of children living in urban, suburban, and rural households of all economic levels. Because this study was conducted during a relatively short time frame (2021-2023), the numbers of subjects and samples were sometimes insufficient to identify statistically significant differences in some comparisons. Some children were lost to follow-up, and not every participant was consented for tympanocentesis. Some participants received antibiotics prior to middle ear fluid specimen collection.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Dynamic Changes in Otopathogens Colonizing the Nasopharynx and Causing Acute Otitis Media in Children After 13-Valent (PCV13) Pneumococcal Conjugate Vaccination During 2015-2019. Eur J Clin Microbiol Infect Dis. 2022 Jan;41(1):37-44. doi: 10.1007/s10096-021-04324-0.
2. Kaur R et al. Anticipated Effects of Higher-valency Pneumococcal Conjugate Vaccines on Colonization and Acute Otitis Media. Pediatr Infect Dis J. 2024 Oct 1;43(10):1004-1010. doi: 10.1097/INF.0000000000004413.
3. King LM et al. Pediatric Outpatient Visits and Antibiotic Use Attributable to Higher Valency Pneumococcal Conjugate Vaccine Serotypes. medRxiv [Preprint]. 2023 Aug 25:2023.08.24.23294570. doi: 10.1101/2023.08.24.23294570.
4. Ahmed S et al. Incremental Health Care Utilization and Costs for Acute Otitis Media in Children. Laryngoscope. 2014 Jan;124(1):301-5. doi: 10.1002/lary.24190.
5. Pichichero ME et al. Pathogens Causing Recurrent and Difficult-to-Treat Acute Otitis Media, 2003-2006. Clin Pediatr (Phila). 2008 Nov;47(9):901-6. doi: 10.1177/0009922808319966.
Acute otitis media (AOM) is caused by Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Since the introduction of pneumococcal conjugate vaccines (PCVs) shifts in the proportion of these three bacteria as causes of AOM and their antibiotic susceptibility profiles and strain diversity have occurred due to multiple factors including the PCVs and antibiotic selection pressure.
The 7-valent PCV (PCV7) was introduced in 2000 and was proven to be efficacious in preventing AOM, but no subsequent PCV has received an indication for prevention of AOM because the FDA required a tympanocentesis study to prove efficacy and that approval was not achieved for PCV13, PCV15, or PCV20. This is a little known fact. After introduction of PCV7, replacement pneumococcal strains expressing serotypes not in PCV7 emerged and antibiotic non-susceptible strains became predominant causes of AOM, especially antibiotic-resistant serotype 19A. To address the phenomena of pneumococcal serotype replacement, PCV13 was introduced in 2010. But serotype replacement continued to occur under PCV13 pressure, replacement serotypes increasingly caused AOM, and antibiotic-resistant serotype 35B emerged. Now we have two new higher valency PCVs: PCV15 (Merck) where serotypes 22F and 33F were added to the PCV13 serotypes and PCV20 (Pfizer) where 22F, 33F, 8, 10A, 11A, 12F, 15B were added to PCV13. Note that neither PCV15 nor PCV20 includes the most common serotype causing AOM – serotype 35B.1
While PCV15 and PCV20 should provide protection against more pneumococcal serotypes, increasing serotypes in both vaccines decreased immunogenicity of certain shared serotypes, more so with the addition of seven more in PCV20 than two more in PCV15, compared with PCV13. Whether lower antibody concentrations will make a difference clinically in terms of vaccine failure to prevent nasopharyngeal colonization, AOM, and/or invasive pneumococcal infections is currently unknown.
Our group from greater Rochester, New York, is the only one in the United States performing tympanocentesis to determine the etiology of AOM infections. Children between ages 6 and 36 months are studied. We recently reported our results for the time span September 2021 to September 2023, the immediate 2 years prior to recommendations for use of PCV15 and PCV20 in young children.2 Tympanocentesis was performed in 139 (78%) of 179 episodes of AOM, yielding 216 middle ear fluid samples (the higher number of middle ear fluids was due to bilateral tympanocentesis in some children). H. influenzae (40%) was the most common bacterial isolate, followed by S. pneumonia (19%) and M. catarrhalis (17%), with the remainder no growth. Polymerase chain reactions (PCR) was positive in many of those culture negative samples, suggesting prior use of antibiotics before tympanocentesis was performed. Among the pneumococcal isolates, 46% were oxacillin non-susceptible. Among the H. influenzae isolates, 27% were beta-lactamase producing and all M. catarrhalis were beta-lactamase-producing.
As we previously reported,1 we once again found that serotype 35B was the most frequent non-PCV15, non-PCV20, serotype. Other frequently detected non-PCV20 pneumococcal serotypes were 23A, 23B, 35D, 35F and 15C.2
Projected Pneumococcal Serotype Coverage by PCV15 and PCV20
PCV13 serotypes were identified in 9% of middle ear fluids, consistent with vaccine failure. As we commence use of PCV15 and PCV20 in the United States, our data provide insights regarding estimation of the projected effects of these vaccines on AOM. Assuming 100% vaccine-type effectiveness, PCV15 will provide about 11% coverage of pneumococci causing AOM, the same PCV13 and PCV20 will provide 30% coverage, leaving 70% of pneumococci causing AOM in young children uncovered (Figure).
MDedge News
Thus, the high proportion of pneumococcal serotype 35B and other non-PCV15 or non-PCV20 serotypes will result in a relatively small incremental benefit over PCV13 in young children for AOM.
AOM is the most common cause of pediatric outpatient visits and antibiotic prescriptions in the United States that contributes to selection of antibiotic-resistant microbes.3 The economic burden of AOM is high, estimated at about $3 billion annually in the United States, when direct and indirect costs are calculated,4 thereby making AOM a major factor in calculations of cost effectiveness analyses of PCV immunizations in children.
While PCV15 and PCV20 include common serotypes associated with invasive pneumococcal diseases, their effectiveness in preventing AOM, acute sinusitis, and non-bacteremic community-acquired pneumonia is currently unknown because these vaccines were licensed based on safety and immunogenicity data, not proven efficacy.
The data on antibiotic susceptibility of pneumococci and H. influenza and M. catarrhalis isolated in the late post PCV13 era from young children in a pediatric primary-care setting raise a question about empiric antibiotic choice for AOM today. For penicillin non-susceptible pneumococcal strains, higher dosages of amoxicillin can improve eradication. However, higher dosages of amoxicillin cannot overcome beta-lactamase production by H. influenza and M. catarrhalis. Based on the mix of pathogens causing AOM and the antibiotic susceptibility of those bacteria, high-dose amoxicillin/clavulanate or alternative cephalosporin drugs active against pneumococci and beta-lactamase producing H. influenza and M. catarrhalis would be a better empiric choice over high-dose amoxicillin.
Dr. Michael E. Pichichero
Limitations of our study include that it occurred in one center in New York, although we have previously shown results of tympanocentesis at our center are similar to those in Virginia and Pennsylvania5 and our study population was composed of children living in urban, suburban, and rural households of all economic levels. Because this study was conducted during a relatively short time frame (2021-2023), the numbers of subjects and samples were sometimes insufficient to identify statistically significant differences in some comparisons. Some children were lost to follow-up, and not every participant was consented for tympanocentesis. Some participants received antibiotics prior to middle ear fluid specimen collection.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Dynamic Changes in Otopathogens Colonizing the Nasopharynx and Causing Acute Otitis Media in Children After 13-Valent (PCV13) Pneumococcal Conjugate Vaccination During 2015-2019. Eur J Clin Microbiol Infect Dis. 2022 Jan;41(1):37-44. doi: 10.1007/s10096-021-04324-0.
2. Kaur R et al. Anticipated Effects of Higher-valency Pneumococcal Conjugate Vaccines on Colonization and Acute Otitis Media. Pediatr Infect Dis J. 2024 Oct 1;43(10):1004-1010. doi: 10.1097/INF.0000000000004413.
3. King LM et al. Pediatric Outpatient Visits and Antibiotic Use Attributable to Higher Valency Pneumococcal Conjugate Vaccine Serotypes. medRxiv [Preprint]. 2023 Aug 25:2023.08.24.23294570. doi: 10.1101/2023.08.24.23294570.
4. Ahmed S et al. Incremental Health Care Utilization and Costs for Acute Otitis Media in Children. Laryngoscope. 2014 Jan;124(1):301-5. doi: 10.1002/lary.24190.
5. Pichichero ME et al. Pathogens Causing Recurrent and Difficult-to-Treat Acute Otitis Media, 2003-2006. Clin Pediatr (Phila). 2008 Nov;47(9):901-6. doi: 10.1177/0009922808319966.
Acute otitis media (AOM) is caused by Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Since the introduction of pneumococcal conjugate vaccines (PCVs) shifts in the proportion of these three bacteria as causes of AOM and their antibiotic susceptibility profiles and strain diversity have occurred due to multiple factors including the PCVs and antibiotic selection pressure.
The 7-valent PCV (PCV7) was introduced in 2000 and was proven to be efficacious in preventing AOM, but no subsequent PCV has received an indication for prevention of AOM because the FDA required a tympanocentesis study to prove efficacy and that approval was not achieved for PCV13, PCV15, or PCV20. This is a little known fact. After introduction of PCV7, replacement pneumococcal strains expressing serotypes not in PCV7 emerged and antibiotic non-susceptible strains became predominant causes of AOM, especially antibiotic-resistant serotype 19A. To address the phenomena of pneumococcal serotype replacement, PCV13 was introduced in 2010. But serotype replacement continued to occur under PCV13 pressure, replacement serotypes increasingly caused AOM, and antibiotic-resistant serotype 35B emerged. Now we have two new higher valency PCVs: PCV15 (Merck) where serotypes 22F and 33F were added to the PCV13 serotypes and PCV20 (Pfizer) where 22F, 33F, 8, 10A, 11A, 12F, 15B were added to PCV13. Note that neither PCV15 nor PCV20 includes the most common serotype causing AOM – serotype 35B.1
While PCV15 and PCV20 should provide protection against more pneumococcal serotypes, increasing serotypes in both vaccines decreased immunogenicity of certain shared serotypes, more so with the addition of seven more in PCV20 than two more in PCV15, compared with PCV13. Whether lower antibody concentrations will make a difference clinically in terms of vaccine failure to prevent nasopharyngeal colonization, AOM, and/or invasive pneumococcal infections is currently unknown.
Our group from greater Rochester, New York, is the only one in the United States performing tympanocentesis to determine the etiology of AOM infections. Children between ages 6 and 36 months are studied. We recently reported our results for the time span September 2021 to September 2023, the immediate 2 years prior to recommendations for use of PCV15 and PCV20 in young children.2 Tympanocentesis was performed in 139 (78%) of 179 episodes of AOM, yielding 216 middle ear fluid samples (the higher number of middle ear fluids was due to bilateral tympanocentesis in some children). H. influenzae (40%) was the most common bacterial isolate, followed by S. pneumonia (19%) and M. catarrhalis (17%), with the remainder no growth. Polymerase chain reactions (PCR) was positive in many of those culture negative samples, suggesting prior use of antibiotics before tympanocentesis was performed. Among the pneumococcal isolates, 46% were oxacillin non-susceptible. Among the H. influenzae isolates, 27% were beta-lactamase producing and all M. catarrhalis were beta-lactamase-producing.
As we previously reported,1 we once again found that serotype 35B was the most frequent non-PCV15, non-PCV20, serotype. Other frequently detected non-PCV20 pneumococcal serotypes were 23A, 23B, 35D, 35F and 15C.2
Projected Pneumococcal Serotype Coverage by PCV15 and PCV20
PCV13 serotypes were identified in 9% of middle ear fluids, consistent with vaccine failure. As we commence use of PCV15 and PCV20 in the United States, our data provide insights regarding estimation of the projected effects of these vaccines on AOM. Assuming 100% vaccine-type effectiveness, PCV15 will provide about 11% coverage of pneumococci causing AOM, the same PCV13 and PCV20 will provide 30% coverage, leaving 70% of pneumococci causing AOM in young children uncovered (Figure).
MDedge News
Thus, the high proportion of pneumococcal serotype 35B and other non-PCV15 or non-PCV20 serotypes will result in a relatively small incremental benefit over PCV13 in young children for AOM.
AOM is the most common cause of pediatric outpatient visits and antibiotic prescriptions in the United States that contributes to selection of antibiotic-resistant microbes.3 The economic burden of AOM is high, estimated at about $3 billion annually in the United States, when direct and indirect costs are calculated,4 thereby making AOM a major factor in calculations of cost effectiveness analyses of PCV immunizations in children.
While PCV15 and PCV20 include common serotypes associated with invasive pneumococcal diseases, their effectiveness in preventing AOM, acute sinusitis, and non-bacteremic community-acquired pneumonia is currently unknown because these vaccines were licensed based on safety and immunogenicity data, not proven efficacy.
The data on antibiotic susceptibility of pneumococci and H. influenza and M. catarrhalis isolated in the late post PCV13 era from young children in a pediatric primary-care setting raise a question about empiric antibiotic choice for AOM today. For penicillin non-susceptible pneumococcal strains, higher dosages of amoxicillin can improve eradication. However, higher dosages of amoxicillin cannot overcome beta-lactamase production by H. influenza and M. catarrhalis. Based on the mix of pathogens causing AOM and the antibiotic susceptibility of those bacteria, high-dose amoxicillin/clavulanate or alternative cephalosporin drugs active against pneumococci and beta-lactamase producing H. influenza and M. catarrhalis would be a better empiric choice over high-dose amoxicillin.
Dr. Michael E. Pichichero
Limitations of our study include that it occurred in one center in New York, although we have previously shown results of tympanocentesis at our center are similar to those in Virginia and Pennsylvania5 and our study population was composed of children living in urban, suburban, and rural households of all economic levels. Because this study was conducted during a relatively short time frame (2021-2023), the numbers of subjects and samples were sometimes insufficient to identify statistically significant differences in some comparisons. Some children were lost to follow-up, and not every participant was consented for tympanocentesis. Some participants received antibiotics prior to middle ear fluid specimen collection.
Dr. Pichichero is a specialist in pediatric infectious diseases, Center for Infectious Diseases and Immunology, and director of the Research Institute, at Rochester (N.Y.) General Hospital. He has no conflicts of interest to declare.
References
1. Kaur R et al. Dynamic Changes in Otopathogens Colonizing the Nasopharynx and Causing Acute Otitis Media in Children After 13-Valent (PCV13) Pneumococcal Conjugate Vaccination During 2015-2019. Eur J Clin Microbiol Infect Dis. 2022 Jan;41(1):37-44. doi: 10.1007/s10096-021-04324-0.
2. Kaur R et al. Anticipated Effects of Higher-valency Pneumococcal Conjugate Vaccines on Colonization and Acute Otitis Media. Pediatr Infect Dis J. 2024 Oct 1;43(10):1004-1010. doi: 10.1097/INF.0000000000004413.
3. King LM et al. Pediatric Outpatient Visits and Antibiotic Use Attributable to Higher Valency Pneumococcal Conjugate Vaccine Serotypes. medRxiv [Preprint]. 2023 Aug 25:2023.08.24.23294570. doi: 10.1101/2023.08.24.23294570.
4. Ahmed S et al. Incremental Health Care Utilization and Costs for Acute Otitis Media in Children. Laryngoscope. 2014 Jan;124(1):301-5. doi: 10.1002/lary.24190.
5. Pichichero ME et al. Pathogens Causing Recurrent and Difficult-to-Treat Acute Otitis Media, 2003-2006. Clin Pediatr (Phila). 2008 Nov;47(9):901-6. doi: 10.1177/0009922808319966.