User login
AVAHO
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Oncologist stars in film and shares philosophy on death
When New York oncologist Gabriel Sara, MD, approached the French actress and film director Emmanuelle Bercot after a screening of one of her films in Manhattan, he was thinking big.
He never dreamed she would think bigger.
“I thought maybe she will do a movie about some of my beliefs,” he said.
“Ma’am, would you like to go in the trenches of cancer?” he asked her, inviting her to tour the oncology department at Mount Sinai West.
Whether it was the Lebanese-born doctor’s Parisian French, his gentle, double-handed handshake, or the perpetual twinkle in his eye, something convinced Ms. Bercot to go. After the visit, she decided to base an entire film on the doctor’s philosophy about death, and she even cast him as one of the leads.
With no formal training in acting, “it’s incredible and prodigious what he did,” Ms. Bercot said in an interview at the 2021 Cannes Film Festival, where the film, “Peaceful” (“De Son Vivant”) premiered.
she said.
Dr. Sara said that authenticity came easily, given that “a lot of my dialogue – maybe most – came from things I shared with Emmanuelle,” he said in an interview with this news organization. “She took the information from me, and she created the whole story. She studied my character and came up with really all the messages that I was hoping to share.”
He said that acting alongside professionals was not intimidating once he realized he was simply playing himself. “At some point ... it clicked in my head. Let me stop acting – I should just be me,” he recalled.
“Peaceful,” performed in French with English subtitles, was nominated for Best Film at the 2022 Lumières Awards.
It tells the story of a 39-year-old man (played by French actor Beno
It is also the story of an oncologist, played by Dr. Sara as himself, who takes his patient by the hand, and refuses to sugarcoat the truth, because he believes that it is only by facing the facts that patients can continue to live – and then die – in peace.
“You’ll never hear me say I’ll cure your cancer. I’d be a liar if I did,” he tells his patient in the film.
“Patients put their life in your hands, so if you don’t tell them the truth you are betraying them,” he explained in the interview. “I have refused to see patients whose family did not allow them to come to the consultation to hear the truth. ... Nobody hears the truth and feels great about it the next day, but the truth helps them focus on what they need to deal with. And once they focus, they’re in control ... a big part of what is terrible for patients is that loss of control.”
The approach may sound harsh, but it is conveyed tenderly in the film. “[Your mother] thinks that half-truths will hurt you half as much,” he tells his patient gently, but “the scariest thing is realizing someone is lying to you. ... We have a tough journey ahead, there’s no room for lies. ... For me, truth is nonnegotiable.”
Dr. Sara is brimming with stories of real-life patients whose lives were enriched and empowered by the clarity they gained in knowing the full truth.
However, not all oncologists agree with his style.
After screenings of the film in other parts of the world, and even in the United States, he has encountered some physicians who strongly disagree with his uncompromising honesty. “You always have somebody who says you know, in America, you will receive the truth but not in our culture – people are not used to it. I hear this all the time,” he said.
“And a long time ago, I decided I’m not going to accept that conversation. Truth works with all patients across all cultures,” Dr. Sara insisted.
“However, as caregivers, we have to be sensitive and present to the kind of culture we are dealing with. The content has to be always 100% honest but we adapt our language to the cultural and emotional state of the patient in order to successfully transmit the message,” he added.
Helping patients digest the news of their diagnosis and prognosis has been Dr. Sara’s recipe for his own survival at work. Now 68 and recently retired as medical director of the chemotherapy infusion suite and executive director of the patient services initiative at Mount Sinai West, he says he emerged from 40 years of practice without burning out by learning to step in time with each patient.
“My recipe for it is tango,” he said. Regular tango performances on his cancer ward were among his many real-life techniques that Ms. Bercot incorporated into the film. “I feel that we have to dance closely with our patients’ emotion,” he explained. “We have to feel our patients’ emotion and work with that. If you don’t move in harmony with your partner, you trip together and both of you will fall,” he told an audience after a screening of his film in New York City.
“I completely try to isolate my mind from anything else in order to be with the patient – this is what presence is about for me – to be right there for them, close to them. To spend that whole moment with them. That’s what will make the consultation really helpful, and will make me feel that I can move to the next page without feeling exhausted from the first one.”
A key scene in the film comes after the patient’s mother is stunned to discover a cheerful tango performance on her son’s ward, and confronts the doctor angrily.
“It’s like I’m abandoning him,” she says tearfully, when the doctor urges her to accept that her son’s chemotherapy is no longer working and let him live what life he has left.
“Give him permission to go,” he urges her. “It would be your greatest gift of love.”
Dr. Sara encourages a similar approach in his staff. He warns them about the “hero syndrome,” in which dying patients are made to feel they need to “hang on” and “fight” for the sake of their caregivers and families.
“The patient never asked to be the hero, but our attitude is telling him that he’s the hero,” he says in the film. “That puts him in an intolerable impasse because he figures that if he gives up, if he dies, he’s betraying his fans. He needs the exact opposite: to be set free. He needs the permission to die. That permission is given by two people: his doctor and his family.”
Of course, not all cancer patients have such a dim prognosis, and Dr. Sara is the first to forge ahead if he feels it’s appropriate. “If, if there is no option for them, I’m going to be aggressive to protect them. But when there is a curable disease, I will go broke to try to treat my patient. I’m willing to give them toxic drugs and hold their hand, get them through the storm if I believe it’s going to cure what they have, and I will coach them to accept being sick.”
He also believes in physical contact with the patient. “If we have some intimacy with the patient, we can at least palpate the kind of person they are,” he said. But his wife Nada pointed out that physical examinations can sometimes make patients nervous. “She told me, if you have a tie, they might have fun looking at it.” Thus began Dr. Sara’s collection of about 30 fun ties decorated with unicorns or jellyfish tailored to various patients’ preferences.
In the film, his patient teases him about this quirk, but Dr. Sara insists it is a small gesture that carries meaning. “One patient told me a story about lovebugs. She would see them in her kitchen when she was feeling well – so lovebugs became a sign of hope for her. I was telling the story to my wife ... so she got me a tie with lovebugs on it, and my patient was so happy when she saw me wearing that.”
In the film – and in real life – Dr. Sara often played guitar at breakfast music sessions with his staff in which he encouraged them to express their feelings about patients’ struggles. “If you cry, don’t be ashamed. Your patient will feel you’re with him,” he said in the film. In the final scenes, wearing a cloud-covered tie, he says goodbye to his patient with tears in his eyes. “They [the tears] are sincere,” he recalled. “Because I really felt I was looking at a dying patient. I really did.”
A version of this article first appeared on Medscape.com.
When New York oncologist Gabriel Sara, MD, approached the French actress and film director Emmanuelle Bercot after a screening of one of her films in Manhattan, he was thinking big.
He never dreamed she would think bigger.
“I thought maybe she will do a movie about some of my beliefs,” he said.
“Ma’am, would you like to go in the trenches of cancer?” he asked her, inviting her to tour the oncology department at Mount Sinai West.
Whether it was the Lebanese-born doctor’s Parisian French, his gentle, double-handed handshake, or the perpetual twinkle in his eye, something convinced Ms. Bercot to go. After the visit, she decided to base an entire film on the doctor’s philosophy about death, and she even cast him as one of the leads.
With no formal training in acting, “it’s incredible and prodigious what he did,” Ms. Bercot said in an interview at the 2021 Cannes Film Festival, where the film, “Peaceful” (“De Son Vivant”) premiered.
she said.
Dr. Sara said that authenticity came easily, given that “a lot of my dialogue – maybe most – came from things I shared with Emmanuelle,” he said in an interview with this news organization. “She took the information from me, and she created the whole story. She studied my character and came up with really all the messages that I was hoping to share.”
He said that acting alongside professionals was not intimidating once he realized he was simply playing himself. “At some point ... it clicked in my head. Let me stop acting – I should just be me,” he recalled.
“Peaceful,” performed in French with English subtitles, was nominated for Best Film at the 2022 Lumières Awards.
It tells the story of a 39-year-old man (played by French actor Beno
It is also the story of an oncologist, played by Dr. Sara as himself, who takes his patient by the hand, and refuses to sugarcoat the truth, because he believes that it is only by facing the facts that patients can continue to live – and then die – in peace.
“You’ll never hear me say I’ll cure your cancer. I’d be a liar if I did,” he tells his patient in the film.
“Patients put their life in your hands, so if you don’t tell them the truth you are betraying them,” he explained in the interview. “I have refused to see patients whose family did not allow them to come to the consultation to hear the truth. ... Nobody hears the truth and feels great about it the next day, but the truth helps them focus on what they need to deal with. And once they focus, they’re in control ... a big part of what is terrible for patients is that loss of control.”
The approach may sound harsh, but it is conveyed tenderly in the film. “[Your mother] thinks that half-truths will hurt you half as much,” he tells his patient gently, but “the scariest thing is realizing someone is lying to you. ... We have a tough journey ahead, there’s no room for lies. ... For me, truth is nonnegotiable.”
Dr. Sara is brimming with stories of real-life patients whose lives were enriched and empowered by the clarity they gained in knowing the full truth.
However, not all oncologists agree with his style.
After screenings of the film in other parts of the world, and even in the United States, he has encountered some physicians who strongly disagree with his uncompromising honesty. “You always have somebody who says you know, in America, you will receive the truth but not in our culture – people are not used to it. I hear this all the time,” he said.
“And a long time ago, I decided I’m not going to accept that conversation. Truth works with all patients across all cultures,” Dr. Sara insisted.
“However, as caregivers, we have to be sensitive and present to the kind of culture we are dealing with. The content has to be always 100% honest but we adapt our language to the cultural and emotional state of the patient in order to successfully transmit the message,” he added.
Helping patients digest the news of their diagnosis and prognosis has been Dr. Sara’s recipe for his own survival at work. Now 68 and recently retired as medical director of the chemotherapy infusion suite and executive director of the patient services initiative at Mount Sinai West, he says he emerged from 40 years of practice without burning out by learning to step in time with each patient.
“My recipe for it is tango,” he said. Regular tango performances on his cancer ward were among his many real-life techniques that Ms. Bercot incorporated into the film. “I feel that we have to dance closely with our patients’ emotion,” he explained. “We have to feel our patients’ emotion and work with that. If you don’t move in harmony with your partner, you trip together and both of you will fall,” he told an audience after a screening of his film in New York City.
“I completely try to isolate my mind from anything else in order to be with the patient – this is what presence is about for me – to be right there for them, close to them. To spend that whole moment with them. That’s what will make the consultation really helpful, and will make me feel that I can move to the next page without feeling exhausted from the first one.”
A key scene in the film comes after the patient’s mother is stunned to discover a cheerful tango performance on her son’s ward, and confronts the doctor angrily.
“It’s like I’m abandoning him,” she says tearfully, when the doctor urges her to accept that her son’s chemotherapy is no longer working and let him live what life he has left.
“Give him permission to go,” he urges her. “It would be your greatest gift of love.”
Dr. Sara encourages a similar approach in his staff. He warns them about the “hero syndrome,” in which dying patients are made to feel they need to “hang on” and “fight” for the sake of their caregivers and families.
“The patient never asked to be the hero, but our attitude is telling him that he’s the hero,” he says in the film. “That puts him in an intolerable impasse because he figures that if he gives up, if he dies, he’s betraying his fans. He needs the exact opposite: to be set free. He needs the permission to die. That permission is given by two people: his doctor and his family.”
Of course, not all cancer patients have such a dim prognosis, and Dr. Sara is the first to forge ahead if he feels it’s appropriate. “If, if there is no option for them, I’m going to be aggressive to protect them. But when there is a curable disease, I will go broke to try to treat my patient. I’m willing to give them toxic drugs and hold their hand, get them through the storm if I believe it’s going to cure what they have, and I will coach them to accept being sick.”
He also believes in physical contact with the patient. “If we have some intimacy with the patient, we can at least palpate the kind of person they are,” he said. But his wife Nada pointed out that physical examinations can sometimes make patients nervous. “She told me, if you have a tie, they might have fun looking at it.” Thus began Dr. Sara’s collection of about 30 fun ties decorated with unicorns or jellyfish tailored to various patients’ preferences.
In the film, his patient teases him about this quirk, but Dr. Sara insists it is a small gesture that carries meaning. “One patient told me a story about lovebugs. She would see them in her kitchen when she was feeling well – so lovebugs became a sign of hope for her. I was telling the story to my wife ... so she got me a tie with lovebugs on it, and my patient was so happy when she saw me wearing that.”
In the film – and in real life – Dr. Sara often played guitar at breakfast music sessions with his staff in which he encouraged them to express their feelings about patients’ struggles. “If you cry, don’t be ashamed. Your patient will feel you’re with him,” he said in the film. In the final scenes, wearing a cloud-covered tie, he says goodbye to his patient with tears in his eyes. “They [the tears] are sincere,” he recalled. “Because I really felt I was looking at a dying patient. I really did.”
A version of this article first appeared on Medscape.com.
When New York oncologist Gabriel Sara, MD, approached the French actress and film director Emmanuelle Bercot after a screening of one of her films in Manhattan, he was thinking big.
He never dreamed she would think bigger.
“I thought maybe she will do a movie about some of my beliefs,” he said.
“Ma’am, would you like to go in the trenches of cancer?” he asked her, inviting her to tour the oncology department at Mount Sinai West.
Whether it was the Lebanese-born doctor’s Parisian French, his gentle, double-handed handshake, or the perpetual twinkle in his eye, something convinced Ms. Bercot to go. After the visit, she decided to base an entire film on the doctor’s philosophy about death, and she even cast him as one of the leads.
With no formal training in acting, “it’s incredible and prodigious what he did,” Ms. Bercot said in an interview at the 2021 Cannes Film Festival, where the film, “Peaceful” (“De Son Vivant”) premiered.
she said.
Dr. Sara said that authenticity came easily, given that “a lot of my dialogue – maybe most – came from things I shared with Emmanuelle,” he said in an interview with this news organization. “She took the information from me, and she created the whole story. She studied my character and came up with really all the messages that I was hoping to share.”
He said that acting alongside professionals was not intimidating once he realized he was simply playing himself. “At some point ... it clicked in my head. Let me stop acting – I should just be me,” he recalled.
“Peaceful,” performed in French with English subtitles, was nominated for Best Film at the 2022 Lumières Awards.
It tells the story of a 39-year-old man (played by French actor Beno
It is also the story of an oncologist, played by Dr. Sara as himself, who takes his patient by the hand, and refuses to sugarcoat the truth, because he believes that it is only by facing the facts that patients can continue to live – and then die – in peace.
“You’ll never hear me say I’ll cure your cancer. I’d be a liar if I did,” he tells his patient in the film.
“Patients put their life in your hands, so if you don’t tell them the truth you are betraying them,” he explained in the interview. “I have refused to see patients whose family did not allow them to come to the consultation to hear the truth. ... Nobody hears the truth and feels great about it the next day, but the truth helps them focus on what they need to deal with. And once they focus, they’re in control ... a big part of what is terrible for patients is that loss of control.”
The approach may sound harsh, but it is conveyed tenderly in the film. “[Your mother] thinks that half-truths will hurt you half as much,” he tells his patient gently, but “the scariest thing is realizing someone is lying to you. ... We have a tough journey ahead, there’s no room for lies. ... For me, truth is nonnegotiable.”
Dr. Sara is brimming with stories of real-life patients whose lives were enriched and empowered by the clarity they gained in knowing the full truth.
However, not all oncologists agree with his style.
After screenings of the film in other parts of the world, and even in the United States, he has encountered some physicians who strongly disagree with his uncompromising honesty. “You always have somebody who says you know, in America, you will receive the truth but not in our culture – people are not used to it. I hear this all the time,” he said.
“And a long time ago, I decided I’m not going to accept that conversation. Truth works with all patients across all cultures,” Dr. Sara insisted.
“However, as caregivers, we have to be sensitive and present to the kind of culture we are dealing with. The content has to be always 100% honest but we adapt our language to the cultural and emotional state of the patient in order to successfully transmit the message,” he added.
Helping patients digest the news of their diagnosis and prognosis has been Dr. Sara’s recipe for his own survival at work. Now 68 and recently retired as medical director of the chemotherapy infusion suite and executive director of the patient services initiative at Mount Sinai West, he says he emerged from 40 years of practice without burning out by learning to step in time with each patient.
“My recipe for it is tango,” he said. Regular tango performances on his cancer ward were among his many real-life techniques that Ms. Bercot incorporated into the film. “I feel that we have to dance closely with our patients’ emotion,” he explained. “We have to feel our patients’ emotion and work with that. If you don’t move in harmony with your partner, you trip together and both of you will fall,” he told an audience after a screening of his film in New York City.
“I completely try to isolate my mind from anything else in order to be with the patient – this is what presence is about for me – to be right there for them, close to them. To spend that whole moment with them. That’s what will make the consultation really helpful, and will make me feel that I can move to the next page without feeling exhausted from the first one.”
A key scene in the film comes after the patient’s mother is stunned to discover a cheerful tango performance on her son’s ward, and confronts the doctor angrily.
“It’s like I’m abandoning him,” she says tearfully, when the doctor urges her to accept that her son’s chemotherapy is no longer working and let him live what life he has left.
“Give him permission to go,” he urges her. “It would be your greatest gift of love.”
Dr. Sara encourages a similar approach in his staff. He warns them about the “hero syndrome,” in which dying patients are made to feel they need to “hang on” and “fight” for the sake of their caregivers and families.
“The patient never asked to be the hero, but our attitude is telling him that he’s the hero,” he says in the film. “That puts him in an intolerable impasse because he figures that if he gives up, if he dies, he’s betraying his fans. He needs the exact opposite: to be set free. He needs the permission to die. That permission is given by two people: his doctor and his family.”
Of course, not all cancer patients have such a dim prognosis, and Dr. Sara is the first to forge ahead if he feels it’s appropriate. “If, if there is no option for them, I’m going to be aggressive to protect them. But when there is a curable disease, I will go broke to try to treat my patient. I’m willing to give them toxic drugs and hold their hand, get them through the storm if I believe it’s going to cure what they have, and I will coach them to accept being sick.”
He also believes in physical contact with the patient. “If we have some intimacy with the patient, we can at least palpate the kind of person they are,” he said. But his wife Nada pointed out that physical examinations can sometimes make patients nervous. “She told me, if you have a tie, they might have fun looking at it.” Thus began Dr. Sara’s collection of about 30 fun ties decorated with unicorns or jellyfish tailored to various patients’ preferences.
In the film, his patient teases him about this quirk, but Dr. Sara insists it is a small gesture that carries meaning. “One patient told me a story about lovebugs. She would see them in her kitchen when she was feeling well – so lovebugs became a sign of hope for her. I was telling the story to my wife ... so she got me a tie with lovebugs on it, and my patient was so happy when she saw me wearing that.”
In the film – and in real life – Dr. Sara often played guitar at breakfast music sessions with his staff in which he encouraged them to express their feelings about patients’ struggles. “If you cry, don’t be ashamed. Your patient will feel you’re with him,” he said in the film. In the final scenes, wearing a cloud-covered tie, he says goodbye to his patient with tears in his eyes. “They [the tears] are sincere,” he recalled. “Because I really felt I was looking at a dying patient. I really did.”
A version of this article first appeared on Medscape.com.
Maternal infection in pregnancy ups risk for childhood leukemia?
Children born to mothers who had urinary or genital tract infections during pregnancy appear to have an increased risk for childhood leukemia, said researchers reporting a Danish registry analysis that may point to preventive strategies for the disease.
The research was published online in JAMA Network Open.
The team studied more than 2.2 million children born in Denmark over more than 3 decades, linking their records across multiple national registries to examine both later cancer risk and maternal infection rates.
They found that, overall, at least one maternal infection during pregnancy was associated with a 35% increased risk for leukemia in the children, rising to 65% for urinary tract infections, and 142% for genital infections.
“The findings of this large population-based cohort study suggest that maternal urinary and genital tract infections during pregnancy are associated with a higher risk of childhood leukemia in offspring,” said lead author Jian-Rong He, DPhil, division of birth cohort study, Guangzhou (China) Women and Children’s Medical Center.
However, he added, “the associated absolute risk remained small given the rarity” of the disease. In absolute terms, the risk difference between exposed and unexposed children was 1.8 cases per 100,000 person-years for any infection, 3.4 cases per 100,000 person-years for urinary traction infection, and 7.1 cases per 100,000 person-years for genital tract infection.
Maternal infections during pregnancy may be associated with chromosomal and immunologic alterations in the fetus, the authors speculated.
“Given that little is known about the etiology of childhood leukemia,” these results “suggest an important direction for research on the etiology of childhood leukemia as well as development of potential preventive measures,” they wrote.
In many countries, pregnant women are tested for urinary tract infection and bacterial vaginosis, and treated with antibiotics in antenatal care, as these infections are linked to adverse perinatal outcomes, they pointed out.
Study details
The team conducted a large population-based study that included all live births in Denmark between 1978 and 2015.
After exclusions, they gathered information on 2,222,797 children, linking data from several national registries, including the Danish Medical Birth Register, the Danish National Patient Registry, and the Danish National Cancer Registry, to identify cases of childhood cancers and maternal infection during pregnancy.
The results were then validated by comparing them with those in 2.6 million live births in Sweden between 1988 and 2014, for whom similar data were available through linkage with several Swedish registries.
The Danish cohort was followed up for a mean of 12 years per person, yielding a total of 27 million person-years. Just over half (51.3%) were boys.
Cancer was diagnosed in 4,362 children before 15 years of age, of whom 1,307 had leukemia (1,050 had acute lymphocytic leukemia), 1,267 had a brain tumor, 224 had lymphoma, and 1,564 had other cancers.
At least one infection during pregnancy was diagnosed in 81,717 mothers (3.7%). Urinary tract infections were the most common (in 1.7% of women), followed by genital tract infection (in 0.7%), digestive system infection (in 0.5%), and respiratory tract infection (in 0.3%).
Women with any infection during pregnancy were more likely to be younger and primiparous than were women who did not have infections, and they were also more likely to have fewer years of education, higher prepregnancy BMI, diabetes, and to smoke during early pregnancy.
Preterm delivery and low-birth-weight infants were also more common in women with infections during pregnancy.
Cox proportional hazards regression models revealed that, after adjustment for confounders, any maternal infection was associated with a hazard ratio of childhood leukemia of 1.35.
Further analysis revealed that the association was driven by genital tract infection, at a hazard ratio for childhood leukemia of 2.42, and urinary tract infection, at a hazard ratio 1.65.
Moreover, children born to women who had a sexually transmitted infection during pregnancy had a hazard ratio for developing leukemia of 3.13 compared with unexposed children.
There were no associations between other maternal infections and childhood leukemia.
The patterns of association between maternal infections and childhood leukemia were similar when looking at disease subtypes, as well as in the Swedish validation cohort, they added.
When interpreting the results, the researchers caution that, as data on maternal infection were drawn from hospital data, “milder infections and those not diagnosed or treated in specialized health care facilities were not captured.”
“Also, some infections could be captured because the mother sought care for other, more serious conditions, which might bias the association of maternal infections and childhood leukemia.”
The study was supported by grants from the China Scholarship Council–University of Oxford; National Natural Science Foundation of China; Danish Council for Independent Research; Nordic Cancer Union; Novo Nordisk Fonden; and the Swedish Council for Working Life and Social Research. Dr He reported receiving a PhD scholarship from the China Scholarship Council during the conduct of the study. Several other coauthors have disclosures; the full list can be found with the original article.
A version of this article originally appeared on Medscape.com.
Children born to mothers who had urinary or genital tract infections during pregnancy appear to have an increased risk for childhood leukemia, said researchers reporting a Danish registry analysis that may point to preventive strategies for the disease.
The research was published online in JAMA Network Open.
The team studied more than 2.2 million children born in Denmark over more than 3 decades, linking their records across multiple national registries to examine both later cancer risk and maternal infection rates.
They found that, overall, at least one maternal infection during pregnancy was associated with a 35% increased risk for leukemia in the children, rising to 65% for urinary tract infections, and 142% for genital infections.
“The findings of this large population-based cohort study suggest that maternal urinary and genital tract infections during pregnancy are associated with a higher risk of childhood leukemia in offspring,” said lead author Jian-Rong He, DPhil, division of birth cohort study, Guangzhou (China) Women and Children’s Medical Center.
However, he added, “the associated absolute risk remained small given the rarity” of the disease. In absolute terms, the risk difference between exposed and unexposed children was 1.8 cases per 100,000 person-years for any infection, 3.4 cases per 100,000 person-years for urinary traction infection, and 7.1 cases per 100,000 person-years for genital tract infection.
Maternal infections during pregnancy may be associated with chromosomal and immunologic alterations in the fetus, the authors speculated.
“Given that little is known about the etiology of childhood leukemia,” these results “suggest an important direction for research on the etiology of childhood leukemia as well as development of potential preventive measures,” they wrote.
In many countries, pregnant women are tested for urinary tract infection and bacterial vaginosis, and treated with antibiotics in antenatal care, as these infections are linked to adverse perinatal outcomes, they pointed out.
Study details
The team conducted a large population-based study that included all live births in Denmark between 1978 and 2015.
After exclusions, they gathered information on 2,222,797 children, linking data from several national registries, including the Danish Medical Birth Register, the Danish National Patient Registry, and the Danish National Cancer Registry, to identify cases of childhood cancers and maternal infection during pregnancy.
The results were then validated by comparing them with those in 2.6 million live births in Sweden between 1988 and 2014, for whom similar data were available through linkage with several Swedish registries.
The Danish cohort was followed up for a mean of 12 years per person, yielding a total of 27 million person-years. Just over half (51.3%) were boys.
Cancer was diagnosed in 4,362 children before 15 years of age, of whom 1,307 had leukemia (1,050 had acute lymphocytic leukemia), 1,267 had a brain tumor, 224 had lymphoma, and 1,564 had other cancers.
At least one infection during pregnancy was diagnosed in 81,717 mothers (3.7%). Urinary tract infections were the most common (in 1.7% of women), followed by genital tract infection (in 0.7%), digestive system infection (in 0.5%), and respiratory tract infection (in 0.3%).
Women with any infection during pregnancy were more likely to be younger and primiparous than were women who did not have infections, and they were also more likely to have fewer years of education, higher prepregnancy BMI, diabetes, and to smoke during early pregnancy.
Preterm delivery and low-birth-weight infants were also more common in women with infections during pregnancy.
Cox proportional hazards regression models revealed that, after adjustment for confounders, any maternal infection was associated with a hazard ratio of childhood leukemia of 1.35.
Further analysis revealed that the association was driven by genital tract infection, at a hazard ratio for childhood leukemia of 2.42, and urinary tract infection, at a hazard ratio 1.65.
Moreover, children born to women who had a sexually transmitted infection during pregnancy had a hazard ratio for developing leukemia of 3.13 compared with unexposed children.
There were no associations between other maternal infections and childhood leukemia.
The patterns of association between maternal infections and childhood leukemia were similar when looking at disease subtypes, as well as in the Swedish validation cohort, they added.
When interpreting the results, the researchers caution that, as data on maternal infection were drawn from hospital data, “milder infections and those not diagnosed or treated in specialized health care facilities were not captured.”
“Also, some infections could be captured because the mother sought care for other, more serious conditions, which might bias the association of maternal infections and childhood leukemia.”
The study was supported by grants from the China Scholarship Council–University of Oxford; National Natural Science Foundation of China; Danish Council for Independent Research; Nordic Cancer Union; Novo Nordisk Fonden; and the Swedish Council for Working Life and Social Research. Dr He reported receiving a PhD scholarship from the China Scholarship Council during the conduct of the study. Several other coauthors have disclosures; the full list can be found with the original article.
A version of this article originally appeared on Medscape.com.
Children born to mothers who had urinary or genital tract infections during pregnancy appear to have an increased risk for childhood leukemia, said researchers reporting a Danish registry analysis that may point to preventive strategies for the disease.
The research was published online in JAMA Network Open.
The team studied more than 2.2 million children born in Denmark over more than 3 decades, linking their records across multiple national registries to examine both later cancer risk and maternal infection rates.
They found that, overall, at least one maternal infection during pregnancy was associated with a 35% increased risk for leukemia in the children, rising to 65% for urinary tract infections, and 142% for genital infections.
“The findings of this large population-based cohort study suggest that maternal urinary and genital tract infections during pregnancy are associated with a higher risk of childhood leukemia in offspring,” said lead author Jian-Rong He, DPhil, division of birth cohort study, Guangzhou (China) Women and Children’s Medical Center.
However, he added, “the associated absolute risk remained small given the rarity” of the disease. In absolute terms, the risk difference between exposed and unexposed children was 1.8 cases per 100,000 person-years for any infection, 3.4 cases per 100,000 person-years for urinary traction infection, and 7.1 cases per 100,000 person-years for genital tract infection.
Maternal infections during pregnancy may be associated with chromosomal and immunologic alterations in the fetus, the authors speculated.
“Given that little is known about the etiology of childhood leukemia,” these results “suggest an important direction for research on the etiology of childhood leukemia as well as development of potential preventive measures,” they wrote.
In many countries, pregnant women are tested for urinary tract infection and bacterial vaginosis, and treated with antibiotics in antenatal care, as these infections are linked to adverse perinatal outcomes, they pointed out.
Study details
The team conducted a large population-based study that included all live births in Denmark between 1978 and 2015.
After exclusions, they gathered information on 2,222,797 children, linking data from several national registries, including the Danish Medical Birth Register, the Danish National Patient Registry, and the Danish National Cancer Registry, to identify cases of childhood cancers and maternal infection during pregnancy.
The results were then validated by comparing them with those in 2.6 million live births in Sweden between 1988 and 2014, for whom similar data were available through linkage with several Swedish registries.
The Danish cohort was followed up for a mean of 12 years per person, yielding a total of 27 million person-years. Just over half (51.3%) were boys.
Cancer was diagnosed in 4,362 children before 15 years of age, of whom 1,307 had leukemia (1,050 had acute lymphocytic leukemia), 1,267 had a brain tumor, 224 had lymphoma, and 1,564 had other cancers.
At least one infection during pregnancy was diagnosed in 81,717 mothers (3.7%). Urinary tract infections were the most common (in 1.7% of women), followed by genital tract infection (in 0.7%), digestive system infection (in 0.5%), and respiratory tract infection (in 0.3%).
Women with any infection during pregnancy were more likely to be younger and primiparous than were women who did not have infections, and they were also more likely to have fewer years of education, higher prepregnancy BMI, diabetes, and to smoke during early pregnancy.
Preterm delivery and low-birth-weight infants were also more common in women with infections during pregnancy.
Cox proportional hazards regression models revealed that, after adjustment for confounders, any maternal infection was associated with a hazard ratio of childhood leukemia of 1.35.
Further analysis revealed that the association was driven by genital tract infection, at a hazard ratio for childhood leukemia of 2.42, and urinary tract infection, at a hazard ratio 1.65.
Moreover, children born to women who had a sexually transmitted infection during pregnancy had a hazard ratio for developing leukemia of 3.13 compared with unexposed children.
There were no associations between other maternal infections and childhood leukemia.
The patterns of association between maternal infections and childhood leukemia were similar when looking at disease subtypes, as well as in the Swedish validation cohort, they added.
When interpreting the results, the researchers caution that, as data on maternal infection were drawn from hospital data, “milder infections and those not diagnosed or treated in specialized health care facilities were not captured.”
“Also, some infections could be captured because the mother sought care for other, more serious conditions, which might bias the association of maternal infections and childhood leukemia.”
The study was supported by grants from the China Scholarship Council–University of Oxford; National Natural Science Foundation of China; Danish Council for Independent Research; Nordic Cancer Union; Novo Nordisk Fonden; and the Swedish Council for Working Life and Social Research. Dr He reported receiving a PhD scholarship from the China Scholarship Council during the conduct of the study. Several other coauthors have disclosures; the full list can be found with the original article.
A version of this article originally appeared on Medscape.com.
CML: Preventing chemo-induced vascular toxicity
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
PARIS –
Cardiologist Gabrielle Sarlon, MD, PhD, a professor at Marseille (France) University Hospital, offered her recommendations at the European Days of the French Society of Cardiology Conference 2023.
In the literature, we find many hypotheses that seek to explain why these drugs bring about the formation of atheromatous plaque. The findings of one French study led Dr. Sarlon to state, “I firmly believe that, in some patients, these treatments make LDL cholesterol go up.” This would be the main cause of the coronary and peripheral arterial diseases that are being seen.
Therefore, “LDL-C should start being monitored when the therapy starts, and a statin may have to be prescribed,” she said.
Arterial diseases
By bringing about a marked improvement in patients’ chances of survival, TKIs “have revolutionized the management of chronic myeloid leukemia,” Dr. Sarlon added. But these treatments have side effects. The most common is high blood pressure, “an effect that attests to the efficacy of targeted therapies and that must be quickly treated” with antihypertensives.
It is well known that the targeted therapies cause the rise in blood pressure. What was unexpected, though, was the vascular toxicity seen with the latest generation of TKIs. “This is a real toxicity that we need to know about, detect, and manage,” said Dr. Sarlon.
The prevalence of arterial diseases induced by nilotinib, a second-generation TKI, can be as high as 10%. Single-center studies have indicated much higher numbers. In a small study that Dr. Sarlon and her team conducted at Marseille University Hospital, atherosclerotic-type arterial injuries were observed in more than 30% of patients treated with nilotinib.
Dr. Sarlon noted that the signs of arterial toxicity occurring with this treatment have not appeared in clinical trials. Observations of the real-life use of nilotinib led French and German teams to sound the alarm. They noticed that some patients treated for CML had developed claudication and progression to critical limb ischemia of the lower extremities.
Risk factors uncovered
The first retrospective analysis to explore this risk was carried out by a German team. They included 179 patients who received nilotinib and found that 11 (6.2%) developed severe and previously unrecognized lower-extremity peripheral arterial disease (PAD) that required invasive therapy. The mean time from initiation of nilotinib to the first PAD event was 105.1 weeks (range = 16-212 weeks).
The following have emerged as major risk factors for nilotinib-induced PAD: the presence of cardiovascular risk factors, age older than 60 years, and long duration of exposure to nilotinib. Some of these factors were confirmed in the more recent study conducted at Marseille University Hospital involving patients treated with nilotinib. According to other research, there seems to be a correlation between this risk and the dose administered.
In the case of ponatinib, the side effects are even more common – so much so that, a few months after this third-generation TKI was authorized, a warning was issued about its use. A long-term follow-up study reported a 28% prevalence of cardiovascular events, while arterial diseases were observed in 20% of cases after 1-2 years on the treatment.
In terms of pathophysiology, the Marseilles University Hospital study found that arterial injuries were associated with stenosis greater than 50% in almost half of cases. “The atheromatous plaques were found where they typically are,” with the carotid bulb being the most involved territory, according to the researchers. But they’re also found in other arteries – femoral, vertebral, even renal – “sometimes in patients without cardiovascular risk factors.”
One distinctive characteristic to keep in mind is that “lipid-rich atheromatous plaques appear very dark on imaging” and thus can go unnoticed during a Doppler ultrasound. And, Dr. Sarlon added, “surprisingly, the thickening can extend to the external carotid artery.”
Ankle-brachial index
Published last year, the first European Society of Cardiology Guidelines on Cardio-Oncology present specific baseline risk-assessment and monitoring recommendations regarding patients treated with nilotinib and ponatinib. One suggests that a cardiovascular risk assessment be done every 3 months during the first year and every 6-12 months thereafter. This assessment would include such items as ECGs, blood pressure measurements, and lipid profile tests.
In addition, it is advised that every 6 months an ankle-brachial index test be performed to check for PAD. At Marseille University Hospital, a Doppler ultrasound is also done at each follow-up appointment to look for arterial plaques, “even for patients at low risk for cardiovascular disease,” said Dr. Sarlon. “It seems, above all, absolutely necessary that hematologists order an LDL-C test and, if needed, consider statin therapy,” all the while keeping in mind that “the target LDL-C level is 1 gram per liter.”
This article was translated from the Medscape French edition. A version of this article first appeared on Medscape.com.
New cancer screen, same issues: Physicians confront Galleri test
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
In January 2022, Anthony Arenz, a 51-year-old living in Mesa, Ariz., breathed a small sigh of relief.
The Galleri blood test, which screens for 50 types of cancer, hadn’t detected any positive signs.
It would be welcome news to anyone but especially to a firefighter with a 9% greater risk of developing cancer and a 14% greater risk of dying from it than the average person. The Mesa unit had lost two servicemen to cancer in the past 3 years. Both were more than a decade younger than Mr. Arenz.
When the city of Mesa offered additional free screening – including a full-body MRI – to firefighters over 50, Mr. Arenz initially shrugged it off. With a negative Galleri test in hand, he didn’t want to spend more time dwelling on it.
Still, he began to feel a creeping guilt for skipping a test that many of his fallen colleagues hadn’t been offered. He tried to soothe his anxiety with research. A look through the company’s website didn’t set him at ease. According to Grail Bio, a test result of “no cancer signal detected” does not rule out cancer.
Mr. Arenz booked his free MRI.
The results left him heavy: stage I kidney cancer. The Galleri test had missed it.
Mr. Arenz received his free Galleri test through a cancer screening program funded by the city of Mesa. The program is housed at Vincere Cancer Center in Scottsdale, Ariz. Under the leadership of radiation oncologist and Vincere co-owner Vershalee Shukla, MD, the program currently screens first responders in more than 10 Arizona cities at no cost to them.
Vincere began using Galleri shortly after the test launched for consumers in June 2021. Since then, the first responder program has become the largest commercial user of the test in North America.
The Galleri test, which has not yet been approved by the Food and Drug Administration, is so new that few know what incorrect results look like in practice and how often they might occur.
After running the test on about 2,000 servicemen and servicewomen, Dr. Shukla can offer some insight about the test’s real-world value in a high-risk population.
“Cancer screening is a very complicated issue,” Dr. Shukla said in an interview. “Being honest, the tests are good but are not ready yet [for wider use].”
Mr. Arenz was not the only firefighter who got a surprise after taking a Galleri test.
In nearby Phoenix, 51-year-old firefighter Mike Curtis knew his risk for cancer was high, but he wasn’t that worried. Mr. Curtis had been running into fires since he was 17. His dad, also a firefighter, had died of cancer at age 58.
Mr. Curtis had taken the Vincere Cancer Center up on every free screening service since the program began in late 2018 – well before Dr. Shukla started using Galleri in 2021. His most recent lung CT was clear. But he underwent the Galleri test just to stay vigilant.
His result was a shock. The test detected signs of cancer.
Mr. Curtis decided to tell no one, not even his wife. He’d bear the bad news alone until he was certain.
Dr. Shukla, however, immediately doubted the blood test result. She expedited several follow-up tests. One week, a PET, and CT of the abdomen and pelvis later, her hunch was confirmed. The Galleri test result was wrong, Mr. Curtis did not have cancer.
The price of his peace of mind: an extensive workup with a $4,000 price tag. Fortunately, the bill was covered by the screening program.
Overall, in just over 18 months of using the blood test, Dr. Shukla has only encountered 1 other false positive out of about 2,000 Galleri results.
She also discovered two positive signals for cancer using Galleri that were confirmed with follow-up tests. One was a chordoma, a rare type of bone cancer, and the other was a squamous cell carcinoma of the head and neck. The Galleri test caught both remarkably early, in time for treatment.
For Dr. Shukla, however, false negatives were particularly “horrible.” Mr. Arenz’s was just 1 of 28 cancers that the blood test missed. And because 500 negative tests are yet to be validated, the 28 false negatives may be an underestimate.
In her experience, the binary test result – a simple positive or negative cancer signal – is an oversimplification of risk, she said. It “gives a false perception that you have cancer or you don’t,” although the test itself is not definitive.
Grail senior medical director Whitney Jones, MD, agreed that the test is not meant to be a stand-alone screening test for cancer. The purpose of the Galleri test is to “complement other screenings, not replace them,” Dr. Jones told this news organization.
According to an analysis of Galleri data and Dr. Shukla’s experience, the test’s specificity was over 99%. That means the test successfully minimizes false positives.
But the test’s sensitivity was much lower. From data from first responders, Dr. Shukla determined the sensitivity to be 6.7%. That means the test misses about 93 of every 100 cancers. According to Grail’s latest data from more than 6,300 people older than 50, the test’s sensitivity was 29%.
Specificity and sensitivity are metrics used to credential a test and establish confidence in its ability to detect the target disease. A test with high specificity can correctly identify patients who do not have the condition in question, while a test with high sensitivity can correctly identify patients who do have the disease. But there are trade-offs between sensitivity and specificity. One value is increased at the expense of the other.
It’s normal for a cancer screening test to prioritize specificity, according to Aparna Parikh, MD, an oncologist at Mass General Cancer Center in Boston. In a test like Galleri, which is meant to be an adjunct to other screening modalities, “at least we are seeing a good specificity, which is important, because we don’t want false positives, where the downstream impact on the patient can be high.”
Overall, Dr. Jones said, Grail Bio’s aim is to build a test that’s sensitive enough to catch the most dangerous cancers without inundating the healthcare system with false positives. In addition, Dr. Jones explained, sensitivity varies by cancer type. It tends to be lower for cancers for which other screening modalities are available, as well as for earlier-stage disease.
However, the Galleri sensitivity values are “a little bit scary,” said Ji-Hyun Lee, DrPH, professor of biostatistics at the University of Florida and director of the division of quantitative sciences at the University of Florida Health Cancer Center, both in Gainesville. Dr. Lee, who is not affiliated with Grail, reviewed the company’s publicly available data as well as Dr. Shukla’s data at the request of this news organization.
While there’s no definitive threshold for sensitivity, miss rates as high as 93% and 71% “provide little confidence in the [accuracy of the] test,” Dr. Lee said.
Positive and negative predictive values, however, are more clinically relevant measures of a screening test. These numbers indicate how likely it is that a patient’s results are true and therefore how worried they should be about a positive result and how much they should trust a negative result.
Galleri’s data in the over-50 population and Dr. Shukla’s in first responders suggest the test’s negative predictive value is very high – 98.6% and 98.1%, respectively – which means most people can trust a negative test result.
The positive predictive value, however, was less straightforward. In first responders, Dr. Shukla found that only half of positive Galleri tests were confirmed cases of cancer. And an analysis of Grail’s data found that only 38% of positive Galleri tests – 35 of 92 tests – represented a validated cancer diagnosis.
“In a clinical setting, positive predictive value is more usable for decision-making for the patient,” said Dr. Lee. “Positive predictive value isn’t always high, because everything doesn’t always transfer perfectly to the clinic.” But in the general population, if only 38% of patients with positive Galleri results truly have cancer, the test is “not quite useful to make a decision for the patient or the providers.”
Galleri may also be a costly prospect for patients, no matter the result, cautioned Electra Paskett, PhD, an epidemiologist and cancer screening expert at Ohio State University, Columbus. A positive Galleri test leads to a cascade of follow-up diagnostic tests, which payers may not cover. For a negative result, Galleri recommends that the patient undergo screening again in a year, at an annual cost of $950 plus the cost of any follow-up testing when Galleri does pick something up.
“If a provider wants to offer the Galleri test, all those things need to be made abundantly clear, in my opinion,” Dr. Paskett said.
Following the negative Galleri test, Mr. Arenz’s cancer didn’t slip through the cracks because he received other advanced imaging free of charge. But whether all doctors will go to such lengths to back up Galleri results, even for patients with negative results, is unknown.
A negative result can give patients “a huge false sense of security,” said Dr. Shukla. And if a test is positive, the workup isn’t simple. Chasing cancer, especially one that’s not really there, can be nerve-wracking and expensive.
The question, then, is why perform the Galleri test at all if results require so much validation?
Dr. Parikh explained that a high-risk group such as firefighters represents an ideal-use case for Galleri and other liquid biopsy tests. But she noted that she would be “wary of the ability of the system to manage this test en masse” were the test to be used more widely in the general population.
Dr. Shukla said it’s less about the results she’s getting today and more about making the test more effective for her patients in the future. First responders need a test such as this that can quickly identify multiple cancers. However, to improve the test, Grail needs more data from this high-risk population. That’s what she’s after.
Mr. Curtis doesn’t regret taking the Galleri test. The emotional toll of thinking he had cancer for a few days wasn’t too high a price, in his opinion. It’s part of cancer screening. But he acknowledged that it would have been a much more burdensome experience had he’d been financially responsible for the workup or if he hadn’t had Dr. Shukla to manage his case from start to finish.
Because it was free, Mr. Arenz doesn’t regret undergoing the Galleri test either. But he tells his coworkers to check the site, do their research, and get more screening.
“Any medical center that’s just doing this one test, you just have to be careful,” Dr. Shukla said. “It’s not that easy.”
A version of this article first appeared on Medscape.com.
‘Financial toxicity’ from breast cancer is a worldwide phenomenon
Women across the world face high levels of financial burden from breast cancer, a new systematic review and analysis finds. While the burden of the disease is much higher in less-developed countries, about a third of women in Western nations like the United States say the disease has hurt their financial well-being.
When it comes to financial burden, patients with breast cancer are “a highly vulnerable patient population,” said study coauthor Kavitha Ranganathan, MD, of Brigham and Women’s Hospital, Boston, in an interview. “We need to be both strategic and comprehensive with our approach and use evidence-based methods to come up with these comprehensive solutions,” said Dr. Ranganathan, who noted that she’s hearing more from patients who face monetary hurdles.
The findings were published online in JAMA Network Open.
The researchers believe their analysis is the first to attempt to understand financial toxicity (FT) – excessive financial burden – in breast cancer on a global level. This turned out to be a challenge since there’s no standard way to measure FT.
One approach is to look at financial burden in terms of whether patients are suffering from “catastrophic expenditure,” Dr. Ranganathan said. “That’s what the World Bank and other top health and economic organizations have focused on. It means that the cost of care and – whatever it takes to get care – exceeds 10% of total annual household income.”
Another approach is more subjective and based on patient-reported outcomes, she said: “Are patients having to forgo basic subsistence needs like rent and food?”
For the report, researchers analyzed studies that use both approaches to measure FT from breast cancer. The studies came from high-income countries (n = 24, including 19 from the United States) and middle- and low-income countries (n = 10), and ranged in size from 5 to 2,445 subjects.
The analyzed studies were a range of cross-sectional (n = 26), prospective (n = 7), and retrospective designs (n = 1).
The authors pooled the data from 18 studies and estimated that the rate of patients with FT was 35.3% (14 studies, 27.3%-44.4%) in high-income countries and 78.8% (4 studies, 60.4%-90.0%) in the other countries.
The researchers also conducted a separate pooled analysis of only the U.S. studies (n = 11). It found that 34% (27%-43%) of subjects reported FT. The researchers also conducted a new analysis of Canada-only studies (n = 2) and found that 19% (9%-35%) reported FT.
The researchers weren’t able to provide insight into trends in FT in the United States prior to the period of the studies (2014-2021). But raw numbers suggest the percentage of patients facing financial challenges rose over that time, suggesting a possible increase in burden.
Previous research has suggested that breast cancer poses a higher financial burden than other chronic conditions. “Breast cancer care in particular may be associated with high FT given the need for screening and diagnosis, multidisciplinary care, and longitudinal follow-up,” the researchers write. They add that “notably, gender also affects financial security.”
As for limitations, the researchers report that they only analyzed studies in English, and there was a wide variation in approaches used to analyze FT. The analysis “did not account for different health care systems or control for health care–dedicated gross domestic product,” meaning that there’s no way to know for sure that rates were lower in nations with universal health care.
How could the new findings be useful? “They’re eye-opening for health policymakers. Whenever they see these numbers, they will say, ‘Wow, it is really a problem,’ and they’ll start thinking about solutions,” said study coauthor Rania A. Mekary, PhD, MSc, MSc, of Massachusetts College of Pharmacy and Health Sciences in Boston. “When you give them evidence-based data, then they will take it more seriously.”
The researchers call for interventions in several areas including education about early diagnosis and treatment of breast cancer, expansion of health care coverage, programs to help with nonmedical costs, and better resources for breast cancer care.
In an interview, Mary C. Politi, PhD, of Washington University, St. Louis, said the new report is useful “because it examines financial hardship internationally. Some people wonder whether financial hardship is a U.S. problem because of our health care system, which often relies on insurance and a lot of cost-sharing between insurance and patients. However, financial toxicity is prevalent across countries.”
And, she said, “the study is also useful because it encourages us to measure financial hardship and burden in a more uniform way so we can better compare and pool studies.”
Dr. Politi noted that there are ways to help patients now. “Most hospitals and health centers have staff who can talk to patients about their bills. Sometimes, a payment plan can be set up to space out payments,” she said. “Health care teams can try to consolidate care for patients on the same day to reduce parking expenses or time off for work or child care. Sometimes, changing to less expensive but effective generic medications is an option.”
The study authors received support from the National Cancer Institute, the United Nations Institute for Training and Research, the Global Surgery Foundation, the Harvard Global Health Institute, the Connors Center for Women’s Health and Gender Biology, the Center for Surgery and Public Health, and the National Endowment for Plastic Surgery. Dr. Ranganathan and Dr. Mekary report no disclosures. One coauthor reported a patent (BREAST-Q) and codevelopment of QPROMS, owned by Memorial Sloan Kettering Cancer Center. Another author reports salary support from Blue Cross Blue Shield of Michigan through the collaborative quality initiative known as Michigan Social Health Interventions to Eliminate Disparities. Dr. Politi has no disclosures.
Women across the world face high levels of financial burden from breast cancer, a new systematic review and analysis finds. While the burden of the disease is much higher in less-developed countries, about a third of women in Western nations like the United States say the disease has hurt their financial well-being.
When it comes to financial burden, patients with breast cancer are “a highly vulnerable patient population,” said study coauthor Kavitha Ranganathan, MD, of Brigham and Women’s Hospital, Boston, in an interview. “We need to be both strategic and comprehensive with our approach and use evidence-based methods to come up with these comprehensive solutions,” said Dr. Ranganathan, who noted that she’s hearing more from patients who face monetary hurdles.
The findings were published online in JAMA Network Open.
The researchers believe their analysis is the first to attempt to understand financial toxicity (FT) – excessive financial burden – in breast cancer on a global level. This turned out to be a challenge since there’s no standard way to measure FT.
One approach is to look at financial burden in terms of whether patients are suffering from “catastrophic expenditure,” Dr. Ranganathan said. “That’s what the World Bank and other top health and economic organizations have focused on. It means that the cost of care and – whatever it takes to get care – exceeds 10% of total annual household income.”
Another approach is more subjective and based on patient-reported outcomes, she said: “Are patients having to forgo basic subsistence needs like rent and food?”
For the report, researchers analyzed studies that use both approaches to measure FT from breast cancer. The studies came from high-income countries (n = 24, including 19 from the United States) and middle- and low-income countries (n = 10), and ranged in size from 5 to 2,445 subjects.
The analyzed studies were a range of cross-sectional (n = 26), prospective (n = 7), and retrospective designs (n = 1).
The authors pooled the data from 18 studies and estimated that the rate of patients with FT was 35.3% (14 studies, 27.3%-44.4%) in high-income countries and 78.8% (4 studies, 60.4%-90.0%) in the other countries.
The researchers also conducted a separate pooled analysis of only the U.S. studies (n = 11). It found that 34% (27%-43%) of subjects reported FT. The researchers also conducted a new analysis of Canada-only studies (n = 2) and found that 19% (9%-35%) reported FT.
The researchers weren’t able to provide insight into trends in FT in the United States prior to the period of the studies (2014-2021). But raw numbers suggest the percentage of patients facing financial challenges rose over that time, suggesting a possible increase in burden.
Previous research has suggested that breast cancer poses a higher financial burden than other chronic conditions. “Breast cancer care in particular may be associated with high FT given the need for screening and diagnosis, multidisciplinary care, and longitudinal follow-up,” the researchers write. They add that “notably, gender also affects financial security.”
As for limitations, the researchers report that they only analyzed studies in English, and there was a wide variation in approaches used to analyze FT. The analysis “did not account for different health care systems or control for health care–dedicated gross domestic product,” meaning that there’s no way to know for sure that rates were lower in nations with universal health care.
How could the new findings be useful? “They’re eye-opening for health policymakers. Whenever they see these numbers, they will say, ‘Wow, it is really a problem,’ and they’ll start thinking about solutions,” said study coauthor Rania A. Mekary, PhD, MSc, MSc, of Massachusetts College of Pharmacy and Health Sciences in Boston. “When you give them evidence-based data, then they will take it more seriously.”
The researchers call for interventions in several areas including education about early diagnosis and treatment of breast cancer, expansion of health care coverage, programs to help with nonmedical costs, and better resources for breast cancer care.
In an interview, Mary C. Politi, PhD, of Washington University, St. Louis, said the new report is useful “because it examines financial hardship internationally. Some people wonder whether financial hardship is a U.S. problem because of our health care system, which often relies on insurance and a lot of cost-sharing between insurance and patients. However, financial toxicity is prevalent across countries.”
And, she said, “the study is also useful because it encourages us to measure financial hardship and burden in a more uniform way so we can better compare and pool studies.”
Dr. Politi noted that there are ways to help patients now. “Most hospitals and health centers have staff who can talk to patients about their bills. Sometimes, a payment plan can be set up to space out payments,” she said. “Health care teams can try to consolidate care for patients on the same day to reduce parking expenses or time off for work or child care. Sometimes, changing to less expensive but effective generic medications is an option.”
The study authors received support from the National Cancer Institute, the United Nations Institute for Training and Research, the Global Surgery Foundation, the Harvard Global Health Institute, the Connors Center for Women’s Health and Gender Biology, the Center for Surgery and Public Health, and the National Endowment for Plastic Surgery. Dr. Ranganathan and Dr. Mekary report no disclosures. One coauthor reported a patent (BREAST-Q) and codevelopment of QPROMS, owned by Memorial Sloan Kettering Cancer Center. Another author reports salary support from Blue Cross Blue Shield of Michigan through the collaborative quality initiative known as Michigan Social Health Interventions to Eliminate Disparities. Dr. Politi has no disclosures.
Women across the world face high levels of financial burden from breast cancer, a new systematic review and analysis finds. While the burden of the disease is much higher in less-developed countries, about a third of women in Western nations like the United States say the disease has hurt their financial well-being.
When it comes to financial burden, patients with breast cancer are “a highly vulnerable patient population,” said study coauthor Kavitha Ranganathan, MD, of Brigham and Women’s Hospital, Boston, in an interview. “We need to be both strategic and comprehensive with our approach and use evidence-based methods to come up with these comprehensive solutions,” said Dr. Ranganathan, who noted that she’s hearing more from patients who face monetary hurdles.
The findings were published online in JAMA Network Open.
The researchers believe their analysis is the first to attempt to understand financial toxicity (FT) – excessive financial burden – in breast cancer on a global level. This turned out to be a challenge since there’s no standard way to measure FT.
One approach is to look at financial burden in terms of whether patients are suffering from “catastrophic expenditure,” Dr. Ranganathan said. “That’s what the World Bank and other top health and economic organizations have focused on. It means that the cost of care and – whatever it takes to get care – exceeds 10% of total annual household income.”
Another approach is more subjective and based on patient-reported outcomes, she said: “Are patients having to forgo basic subsistence needs like rent and food?”
For the report, researchers analyzed studies that use both approaches to measure FT from breast cancer. The studies came from high-income countries (n = 24, including 19 from the United States) and middle- and low-income countries (n = 10), and ranged in size from 5 to 2,445 subjects.
The analyzed studies were a range of cross-sectional (n = 26), prospective (n = 7), and retrospective designs (n = 1).
The authors pooled the data from 18 studies and estimated that the rate of patients with FT was 35.3% (14 studies, 27.3%-44.4%) in high-income countries and 78.8% (4 studies, 60.4%-90.0%) in the other countries.
The researchers also conducted a separate pooled analysis of only the U.S. studies (n = 11). It found that 34% (27%-43%) of subjects reported FT. The researchers also conducted a new analysis of Canada-only studies (n = 2) and found that 19% (9%-35%) reported FT.
The researchers weren’t able to provide insight into trends in FT in the United States prior to the period of the studies (2014-2021). But raw numbers suggest the percentage of patients facing financial challenges rose over that time, suggesting a possible increase in burden.
Previous research has suggested that breast cancer poses a higher financial burden than other chronic conditions. “Breast cancer care in particular may be associated with high FT given the need for screening and diagnosis, multidisciplinary care, and longitudinal follow-up,” the researchers write. They add that “notably, gender also affects financial security.”
As for limitations, the researchers report that they only analyzed studies in English, and there was a wide variation in approaches used to analyze FT. The analysis “did not account for different health care systems or control for health care–dedicated gross domestic product,” meaning that there’s no way to know for sure that rates were lower in nations with universal health care.
How could the new findings be useful? “They’re eye-opening for health policymakers. Whenever they see these numbers, they will say, ‘Wow, it is really a problem,’ and they’ll start thinking about solutions,” said study coauthor Rania A. Mekary, PhD, MSc, MSc, of Massachusetts College of Pharmacy and Health Sciences in Boston. “When you give them evidence-based data, then they will take it more seriously.”
The researchers call for interventions in several areas including education about early diagnosis and treatment of breast cancer, expansion of health care coverage, programs to help with nonmedical costs, and better resources for breast cancer care.
In an interview, Mary C. Politi, PhD, of Washington University, St. Louis, said the new report is useful “because it examines financial hardship internationally. Some people wonder whether financial hardship is a U.S. problem because of our health care system, which often relies on insurance and a lot of cost-sharing between insurance and patients. However, financial toxicity is prevalent across countries.”
And, she said, “the study is also useful because it encourages us to measure financial hardship and burden in a more uniform way so we can better compare and pool studies.”
Dr. Politi noted that there are ways to help patients now. “Most hospitals and health centers have staff who can talk to patients about their bills. Sometimes, a payment plan can be set up to space out payments,” she said. “Health care teams can try to consolidate care for patients on the same day to reduce parking expenses or time off for work or child care. Sometimes, changing to less expensive but effective generic medications is an option.”
The study authors received support from the National Cancer Institute, the United Nations Institute for Training and Research, the Global Surgery Foundation, the Harvard Global Health Institute, the Connors Center for Women’s Health and Gender Biology, the Center for Surgery and Public Health, and the National Endowment for Plastic Surgery. Dr. Ranganathan and Dr. Mekary report no disclosures. One coauthor reported a patent (BREAST-Q) and codevelopment of QPROMS, owned by Memorial Sloan Kettering Cancer Center. Another author reports salary support from Blue Cross Blue Shield of Michigan through the collaborative quality initiative known as Michigan Social Health Interventions to Eliminate Disparities. Dr. Politi has no disclosures.
FROM JAMA NETWORK OPEN
Expert discusses pros, cons of molecular tests for melanoma
SAN DIEGO – , according to Gregory A. Hosler, MD, PhD.
At the annual Cutaneous Malignancy Update, Dr. Hosler, director of dermatopathology for ProPath, highlighted the following molecular tests currently used for the diagnosis of challenging melanocytic lesions:
Comparative genomic hybridization (CGH). This technique allows for the detection of chromosomal copy number changes throughout the tumor genome. “With CGH, test (tumor) DNA and normal DNA are differentially labeled and compared to a reference library. Gains and losses of portions of the tumor genome are determined by comparing the relative signals from these two groups,” said Dr. Hosler, clinical professor of pathology and dermatology at the University of Texas Southwestern Medical Center, Dallas.
“In the past, your library was a metaphase of spread of chromosomes, which introduced technical challenges and made performance of the assay labor intensive. Because of this, CGH is not routinely performed by clinical laboratories and is used more as an exploratory/research technique.”
Array CGH (also known as SNP array). Newer versions of CGH use short DNA sequences that are tiled onto a chip. “The interesting thing about these chips is that you can purchase them or design them on your own,” Dr. Hosler said. “The chips may cover the entire genome or cover specific areas of the genome at higher resolution.” One upside of array CGH, he continued, is that it allows one to detect essentially all gains or losses of chromosomal material in a single reaction. “It is not subject to the artifacts associated with cutting thin sections like with fluorescence in situ hybridization (FISH); it can detect copy number neutral loss of heterozygosity, and it is more scalable,” Dr. Hosler said at the meeting, which was hosted by Scripps MD Anderson Cancer Center.

One downside of array CGH is that does not allow one to analyze specific cells, “so if you have a tumor that’s heterogeneous, the assay is agnostic to this and spits out a result based on all the material provided,” he said. “You can’t parse out different areas of the lesion. It also does not track balanced translocations.” In addition, he said, “there are also questions about reimbursement and these are lab-developed tests, so each lab’s assay is different. Finally, it requires specialized equipment and expertise for interpretation.”
FISH. First-generation melanoma FISH assays, which became available in 2009, used six probes and four colors and had a sensitivity of about 87% and specificity of about 95%, Dr. Hosler said, but there were problems with those assays, particularly related to Spitz nevi. Spitz nevi often duplicate their chromosomes, “so instead of being diploid they’re tetraploid,” he said.
“The second-generation melanoma FISH assays addressed this by adding centromeres to the assay, and targeted probes could be compared to the centromeres on the same chromosome to determine if these were true copy number gains, due to genetic instability, or gains or losses of entire arms or whole chromosomes. This modification and the addition of new targets really improved upon the sensitivity and specificity (94% and 98%, respectively),” he said, noting that this assay is widely used.
Upsides of melanoma FISH assays are that they are a “fairly routine methodology” in large clinical laboratories, he said, and that many labs are familiar with interpretation. “I would say the biggest advantage to FISH is its ability to analyze specific cells, which is useful with small or heterogeneous tumors,” Dr. Hosler said. “Also, there is a genetic reimbursement code for it, and it yields diagnostic and potentially prognostic information.” For example, certain copy number changes have shown to portend a worse prognosis if they’re present in a melanocytic tumor, including alterations in CDKN2A, CCND1, MYC, topoisomerase, and BAP1.
Downsides of melanoma FISH assays are that they are expensive, labor-intensive, and require experts to interpret the results. “The stacking and truncation of cell nuclei innate to paraffin-embedded FISH make interpretation difficult,” he said. “Also, all colors cannot be viewed simultaneously, and each lab’s assay potentially is different, requiring validation. These are not [Food and Drug Administration]-approved tests.”
Next generation sequencing (NGS). Also known as high-throughput sequencing, this technique allows for the generation of millions of sequencing reads that are aligned to a standard human genome, and likely represents the wave of the future. “With NGS you can increase breadth, so you can sequence the entire genome if you want, but you can also increase depth, meaning increasing the number of reads over a single target of the genome,” Dr. Hosler said. “That’s useful if you’re looking for a low frequency mutation.”
For example, NGS allows one to detect alterations of BRAF and KIT and other potentially actionable alterations. It can also be used to detect mutations in benign and malignant melanocytic lesions, including historically diagnostically challenging Spitz and desmoplastic subgroups. Several different NGS technologies exist, and there are different strategies behind each assay, including whole genome sequencing, whole exome sequencing, transcriptome sequencing, and targeted panels. “I’ve seen panels of 10 and I’ve seen panels of 1,500; there’s a wide range,” Dr. Hosler said. “The biggest challenge with NGS, currently, is that it’s difficult to interpret. Trying to figure out what’s important and what’s not important can be challenging. Often you need a team of people who are experts in bioinformatics to interpret these results.”
Slow turnaround time is another downside. “It can take a month to get results, and sometimes clinicians don’t want to wait that long, especially if they think a lesion is melanoma, so that’s an area of focus for NGS laboratories,” he said. “And there are questions on reimbursement. If you run NGS on every unusual melanocytic lesion, that’s not a good use of health care dollars. Who’s paying for it? I don’t have an answer for you. It’s all over the map right now. Each lab’s test and billing practice is different.”
Dr. Hosler reported having no relevant financial disclosures. ProPath is a nationwide pathology practice.
SAN DIEGO – , according to Gregory A. Hosler, MD, PhD.
At the annual Cutaneous Malignancy Update, Dr. Hosler, director of dermatopathology for ProPath, highlighted the following molecular tests currently used for the diagnosis of challenging melanocytic lesions:
Comparative genomic hybridization (CGH). This technique allows for the detection of chromosomal copy number changes throughout the tumor genome. “With CGH, test (tumor) DNA and normal DNA are differentially labeled and compared to a reference library. Gains and losses of portions of the tumor genome are determined by comparing the relative signals from these two groups,” said Dr. Hosler, clinical professor of pathology and dermatology at the University of Texas Southwestern Medical Center, Dallas.
“In the past, your library was a metaphase of spread of chromosomes, which introduced technical challenges and made performance of the assay labor intensive. Because of this, CGH is not routinely performed by clinical laboratories and is used more as an exploratory/research technique.”
Array CGH (also known as SNP array). Newer versions of CGH use short DNA sequences that are tiled onto a chip. “The interesting thing about these chips is that you can purchase them or design them on your own,” Dr. Hosler said. “The chips may cover the entire genome or cover specific areas of the genome at higher resolution.” One upside of array CGH, he continued, is that it allows one to detect essentially all gains or losses of chromosomal material in a single reaction. “It is not subject to the artifacts associated with cutting thin sections like with fluorescence in situ hybridization (FISH); it can detect copy number neutral loss of heterozygosity, and it is more scalable,” Dr. Hosler said at the meeting, which was hosted by Scripps MD Anderson Cancer Center.
One downside of array CGH is that does not allow one to analyze specific cells, “so if you have a tumor that’s heterogeneous, the assay is agnostic to this and spits out a result based on all the material provided,” he said. “You can’t parse out different areas of the lesion. It also does not track balanced translocations.” In addition, he said, “there are also questions about reimbursement and these are lab-developed tests, so each lab’s assay is different. Finally, it requires specialized equipment and expertise for interpretation.”
FISH. First-generation melanoma FISH assays, which became available in 2009, used six probes and four colors and had a sensitivity of about 87% and specificity of about 95%, Dr. Hosler said, but there were problems with those assays, particularly related to Spitz nevi. Spitz nevi often duplicate their chromosomes, “so instead of being diploid they’re tetraploid,” he said.
“The second-generation melanoma FISH assays addressed this by adding centromeres to the assay, and targeted probes could be compared to the centromeres on the same chromosome to determine if these were true copy number gains, due to genetic instability, or gains or losses of entire arms or whole chromosomes. This modification and the addition of new targets really improved upon the sensitivity and specificity (94% and 98%, respectively),” he said, noting that this assay is widely used.
Upsides of melanoma FISH assays are that they are a “fairly routine methodology” in large clinical laboratories, he said, and that many labs are familiar with interpretation. “I would say the biggest advantage to FISH is its ability to analyze specific cells, which is useful with small or heterogeneous tumors,” Dr. Hosler said. “Also, there is a genetic reimbursement code for it, and it yields diagnostic and potentially prognostic information.” For example, certain copy number changes have shown to portend a worse prognosis if they’re present in a melanocytic tumor, including alterations in CDKN2A, CCND1, MYC, topoisomerase, and BAP1.
Downsides of melanoma FISH assays are that they are expensive, labor-intensive, and require experts to interpret the results. “The stacking and truncation of cell nuclei innate to paraffin-embedded FISH make interpretation difficult,” he said. “Also, all colors cannot be viewed simultaneously, and each lab’s assay potentially is different, requiring validation. These are not [Food and Drug Administration]-approved tests.”
Next generation sequencing (NGS). Also known as high-throughput sequencing, this technique allows for the generation of millions of sequencing reads that are aligned to a standard human genome, and likely represents the wave of the future. “With NGS you can increase breadth, so you can sequence the entire genome if you want, but you can also increase depth, meaning increasing the number of reads over a single target of the genome,” Dr. Hosler said. “That’s useful if you’re looking for a low frequency mutation.”
For example, NGS allows one to detect alterations of BRAF and KIT and other potentially actionable alterations. It can also be used to detect mutations in benign and malignant melanocytic lesions, including historically diagnostically challenging Spitz and desmoplastic subgroups. Several different NGS technologies exist, and there are different strategies behind each assay, including whole genome sequencing, whole exome sequencing, transcriptome sequencing, and targeted panels. “I’ve seen panels of 10 and I’ve seen panels of 1,500; there’s a wide range,” Dr. Hosler said. “The biggest challenge with NGS, currently, is that it’s difficult to interpret. Trying to figure out what’s important and what’s not important can be challenging. Often you need a team of people who are experts in bioinformatics to interpret these results.”
Slow turnaround time is another downside. “It can take a month to get results, and sometimes clinicians don’t want to wait that long, especially if they think a lesion is melanoma, so that’s an area of focus for NGS laboratories,” he said. “And there are questions on reimbursement. If you run NGS on every unusual melanocytic lesion, that’s not a good use of health care dollars. Who’s paying for it? I don’t have an answer for you. It’s all over the map right now. Each lab’s test and billing practice is different.”
Dr. Hosler reported having no relevant financial disclosures. ProPath is a nationwide pathology practice.
SAN DIEGO – , according to Gregory A. Hosler, MD, PhD.
At the annual Cutaneous Malignancy Update, Dr. Hosler, director of dermatopathology for ProPath, highlighted the following molecular tests currently used for the diagnosis of challenging melanocytic lesions:
Comparative genomic hybridization (CGH). This technique allows for the detection of chromosomal copy number changes throughout the tumor genome. “With CGH, test (tumor) DNA and normal DNA are differentially labeled and compared to a reference library. Gains and losses of portions of the tumor genome are determined by comparing the relative signals from these two groups,” said Dr. Hosler, clinical professor of pathology and dermatology at the University of Texas Southwestern Medical Center, Dallas.
“In the past, your library was a metaphase of spread of chromosomes, which introduced technical challenges and made performance of the assay labor intensive. Because of this, CGH is not routinely performed by clinical laboratories and is used more as an exploratory/research technique.”
Array CGH (also known as SNP array). Newer versions of CGH use short DNA sequences that are tiled onto a chip. “The interesting thing about these chips is that you can purchase them or design them on your own,” Dr. Hosler said. “The chips may cover the entire genome or cover specific areas of the genome at higher resolution.” One upside of array CGH, he continued, is that it allows one to detect essentially all gains or losses of chromosomal material in a single reaction. “It is not subject to the artifacts associated with cutting thin sections like with fluorescence in situ hybridization (FISH); it can detect copy number neutral loss of heterozygosity, and it is more scalable,” Dr. Hosler said at the meeting, which was hosted by Scripps MD Anderson Cancer Center.
One downside of array CGH is that does not allow one to analyze specific cells, “so if you have a tumor that’s heterogeneous, the assay is agnostic to this and spits out a result based on all the material provided,” he said. “You can’t parse out different areas of the lesion. It also does not track balanced translocations.” In addition, he said, “there are also questions about reimbursement and these are lab-developed tests, so each lab’s assay is different. Finally, it requires specialized equipment and expertise for interpretation.”
FISH. First-generation melanoma FISH assays, which became available in 2009, used six probes and four colors and had a sensitivity of about 87% and specificity of about 95%, Dr. Hosler said, but there were problems with those assays, particularly related to Spitz nevi. Spitz nevi often duplicate their chromosomes, “so instead of being diploid they’re tetraploid,” he said.
“The second-generation melanoma FISH assays addressed this by adding centromeres to the assay, and targeted probes could be compared to the centromeres on the same chromosome to determine if these were true copy number gains, due to genetic instability, or gains or losses of entire arms or whole chromosomes. This modification and the addition of new targets really improved upon the sensitivity and specificity (94% and 98%, respectively),” he said, noting that this assay is widely used.
Upsides of melanoma FISH assays are that they are a “fairly routine methodology” in large clinical laboratories, he said, and that many labs are familiar with interpretation. “I would say the biggest advantage to FISH is its ability to analyze specific cells, which is useful with small or heterogeneous tumors,” Dr. Hosler said. “Also, there is a genetic reimbursement code for it, and it yields diagnostic and potentially prognostic information.” For example, certain copy number changes have shown to portend a worse prognosis if they’re present in a melanocytic tumor, including alterations in CDKN2A, CCND1, MYC, topoisomerase, and BAP1.
Downsides of melanoma FISH assays are that they are expensive, labor-intensive, and require experts to interpret the results. “The stacking and truncation of cell nuclei innate to paraffin-embedded FISH make interpretation difficult,” he said. “Also, all colors cannot be viewed simultaneously, and each lab’s assay potentially is different, requiring validation. These are not [Food and Drug Administration]-approved tests.”
Next generation sequencing (NGS). Also known as high-throughput sequencing, this technique allows for the generation of millions of sequencing reads that are aligned to a standard human genome, and likely represents the wave of the future. “With NGS you can increase breadth, so you can sequence the entire genome if you want, but you can also increase depth, meaning increasing the number of reads over a single target of the genome,” Dr. Hosler said. “That’s useful if you’re looking for a low frequency mutation.”
For example, NGS allows one to detect alterations of BRAF and KIT and other potentially actionable alterations. It can also be used to detect mutations in benign and malignant melanocytic lesions, including historically diagnostically challenging Spitz and desmoplastic subgroups. Several different NGS technologies exist, and there are different strategies behind each assay, including whole genome sequencing, whole exome sequencing, transcriptome sequencing, and targeted panels. “I’ve seen panels of 10 and I’ve seen panels of 1,500; there’s a wide range,” Dr. Hosler said. “The biggest challenge with NGS, currently, is that it’s difficult to interpret. Trying to figure out what’s important and what’s not important can be challenging. Often you need a team of people who are experts in bioinformatics to interpret these results.”
Slow turnaround time is another downside. “It can take a month to get results, and sometimes clinicians don’t want to wait that long, especially if they think a lesion is melanoma, so that’s an area of focus for NGS laboratories,” he said. “And there are questions on reimbursement. If you run NGS on every unusual melanocytic lesion, that’s not a good use of health care dollars. Who’s paying for it? I don’t have an answer for you. It’s all over the map right now. Each lab’s test and billing practice is different.”
Dr. Hosler reported having no relevant financial disclosures. ProPath is a nationwide pathology practice.
AT MELANOMA 2023
Progress in breast cancer screening over the past 50 years: A remarkable story, but still work to do
Meaningful progress has been made in reducing deaths due to breast cancer over the last half century, with a 43% decrease in mortality rate (breast cancer deaths per 100,000 population).1 Screening mammography (SM) has contributed greatly to that success, accounting for 30% to 70% of the reduced mortality rate, with the remainder due to advancements in breast cancer treatment.2 Despite these improvements, invasive breast cancer remains the highest incident cancer in the United States and in the world, is the second leading cause of cancer death in the United States, and results in more years of life lost than any other cancer (TABLE 1).1,3
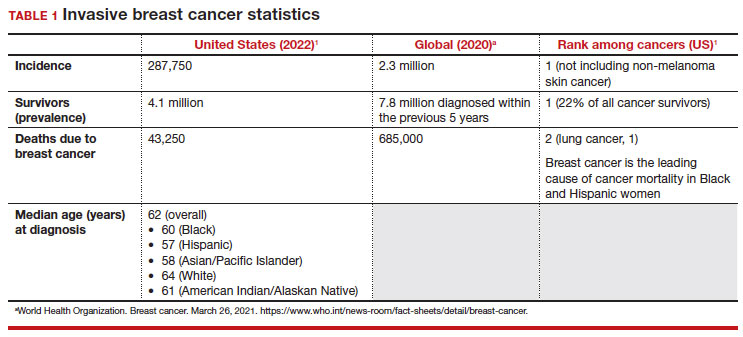
While the benefits and harms of SM are reasonably well understood, different guidelines groups have approached the relative value of the risks and benefits differently, which has led to challenges in implementation of shared decision making, particularly around the age to initiate routine screening.4-6 In this article, we will focus on the data behind the controversy, current gaps in knowledge, challenges related to breast density and screening in diverse groups, and emerging technologies to address these gaps and provide a construct for appropriate counseling of the patient across the risk spectrum.
In recognition of 35 years of publication of OBG Management, this article on breast cancer screening by Mark D. Pearlman, MD, kicks off a series that focuses on various cancer screening modalities and expert recommendations.
Stay tuned for articles on the future of cervical cancer screening and genetic testing for cancer risk beyond BRCA testing.
We look forward to continuing OBG Management’s mission of enhancing the quality of reproductive health care and the professional development of ObGyns and all women’s health care clinicians.
Breast cancer risk
Variables that affect risk
While female sex and older age are the 2 greatest risks for the development of breast cancer, many other factors can either increase or decrease breast cancer risk in a person’s lifetime. The importance of identifying risk factors is 3-fold:
- to perform risk assessment to determine if individuals would benefit from average-risk versus high-risk breast cancer surveillance
- to identify persons who might benefit from BRCA genetic counseling and screening, risk reduction medications or procedures, and
- to allow patients to determine whether any modification in their lifestyle or reproductive choices would make sense to them to reduce their future breast cancer risk.
Most of these risk variables are largely inalterable (for example, family history of breast cancer, carriage of genetic pathogenic variants such as BRCA1 and BRCA2, age of menarche and menopause), but some are potentially modifiable, such as parity, age at first birth, lactation and duration, and dietary factors, among others. TABLE 2 lists common breast cancer risk factors.
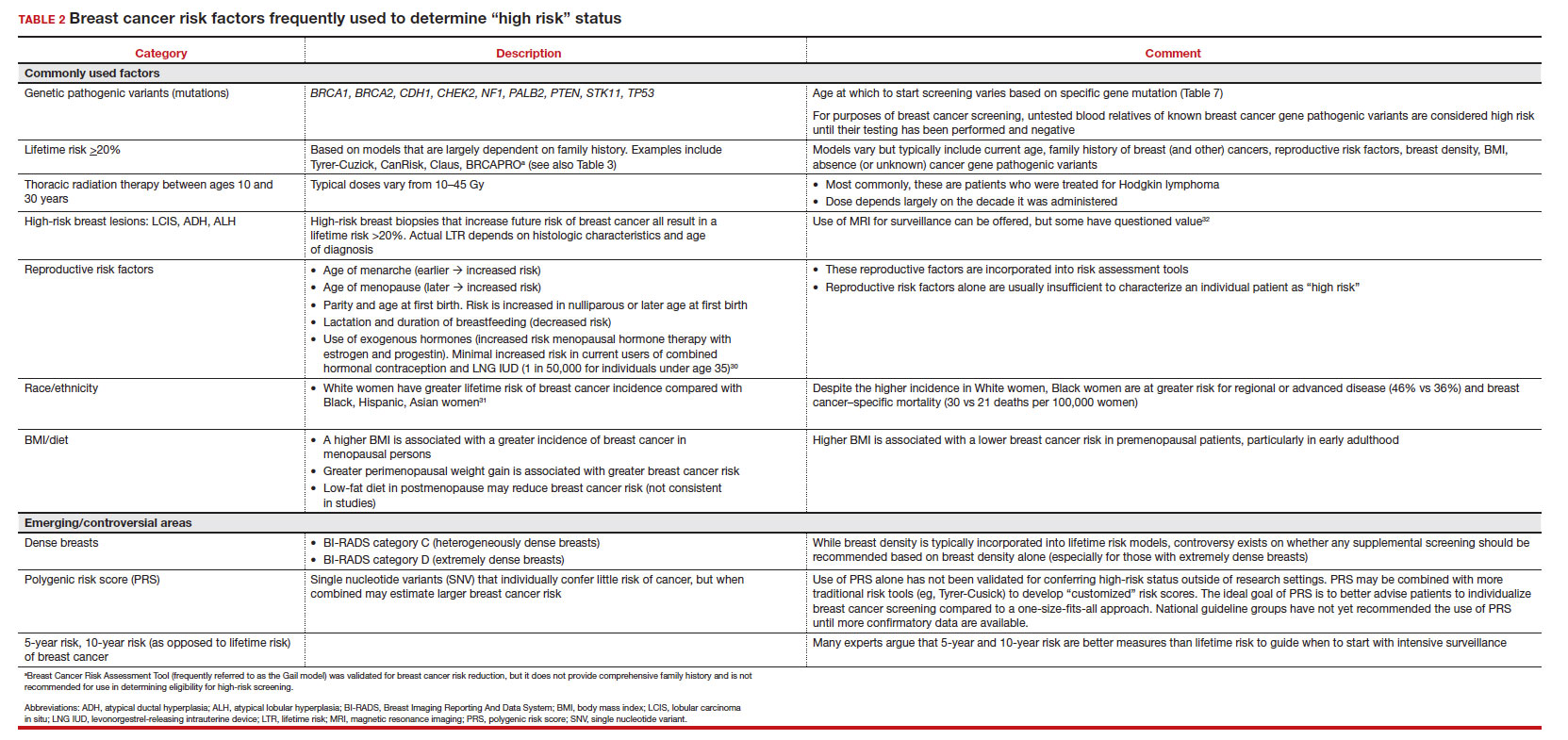
Breast cancer risk assessment
Several validated tools have been developed to estimate a person’s breast cancer risk (TABLE 3). These tools combine known risk factors and, depending on the specific tool, can provide estimates of 5-year, 10-year, or lifetime risk of breast cancer. Patients at highest risk can benefit from earlier screening, supplemental screening with breast magnetic resonance imaging (MRI), or risk reduction (see the section, “High-risk screening”). Ideally, a risk assessment should be done by age 30 so that patients at high risk can be identified for earlier or more intensive screening and for possible genetic testing in those at risk for carriage of the BRCA or other breast cancer gene pathogenic variants.5,7
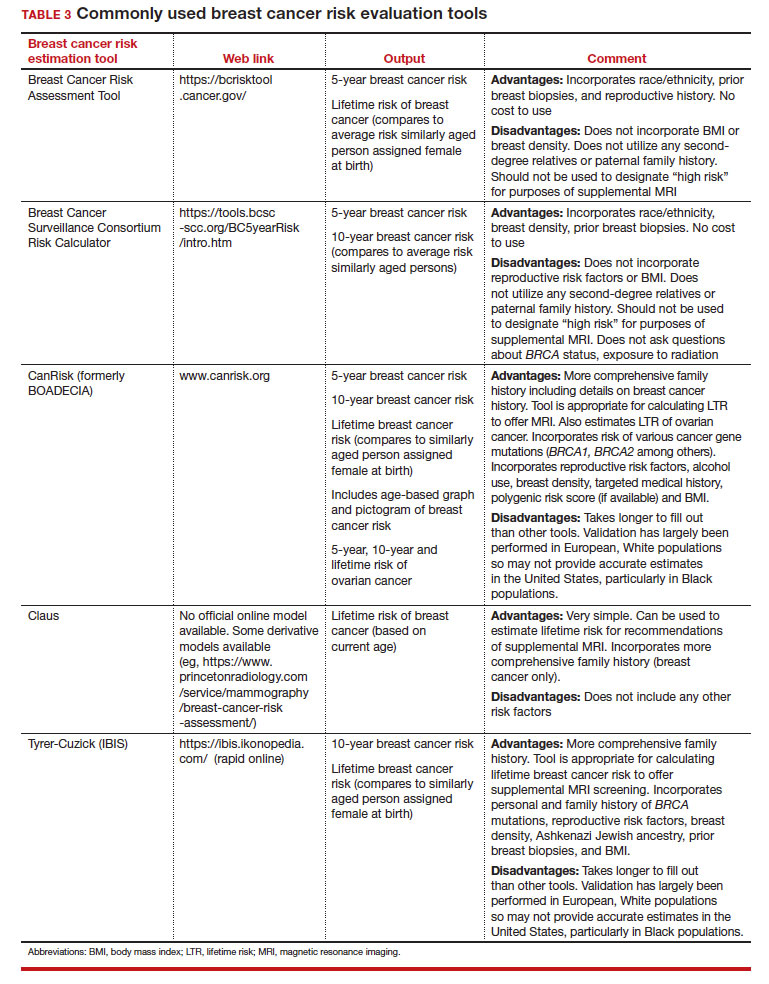
Continue to: Breast cancer screening: Efficacy and harms...
Breast cancer screening: Efficacy and harms
The earliest studies of breast cancer screening with mammography were randomized controlled trials (RCTs) that compared screened and unscreened patients aged 40 to 74. Nearly all the RCTs and numerous well-designed incidence-based and case-control studies have demonstrated that SM results in a clinically and statistically significant reduction in breast cancer mortality (TABLE 4).4,6,8 Since the mid-1980s and continuing to the current day, SM programs are routinely recommended in the United States. In addition to the mortality benefit outlined in TABLE 4, SM also is associated with a need for less invasive treatments if breast cancer is diagnosed.9,10
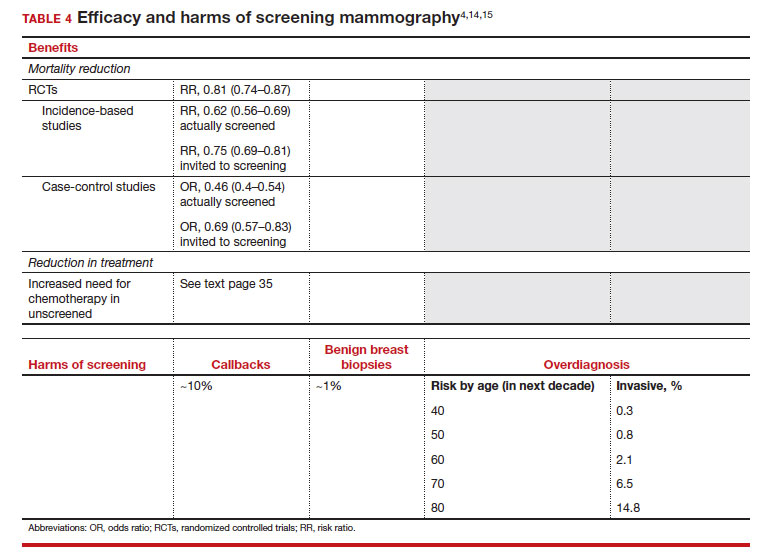
With several decades of experience, SM programs have demonstrated that multiple harms are associated with SM, including callbacks, false-positive mammograms that result in a benign biopsy, and overdiagnosis of breast cancer (TABLE 4). Overdiagnosis is a mammographic detection of a breast cancer that would not have harmed that woman in her lifetime. Overdiagnosis leads to overtreatment of breast cancers with its attendant side effects, the emotional harms of a breast cancer diagnosis, and the substantial financial cost of cancer treatment. Estimates of overdiagnosis range from 0% to 50%, with the most likely estimate of invasive breast cancer overdiagnosis from SM between 5% and 15%.11-13 Some of these overdiagnosed cancers are due to very slow growing cancers or breast cancers that may even regress. However, the higher rates of overdiagnosis occur in older persons who are screened and in whom competing causes of mortality become more prevalent. It is estimated that overdiagnosis of invasive breast cancer in patients younger than age 60 is less than 1%, but it exceeds 14% in those older than age 80 (TABLE 4).14
A structured approach is needed to counsel patients about SM so that they understand both the substantial benefit (earlier-stage diagnosis, reduced need for treatment, reduced breast cancer and all-cause mortality) and the potential harms (callback, false-positive results, and overdiagnosis). Moreover, the relative balance of the benefits and harms are influenced throughout their lifetime by both aging and changes in their personal and family medical history.
Counseling should consider factors beyond just the performance of mammography (sensitivity and specificity), such as the patient’s current health and age (competing causes of mortality), likelihood of developing breast cancer based on risk assessment (more benefit in higher-risk persons), and the individual patient’s values on the importance of the benefits and harms. The differing emphases on mammography performance and the relative value of the benefits and harms have led experts to produce disparate national guideline recommendations (TABLE 5).
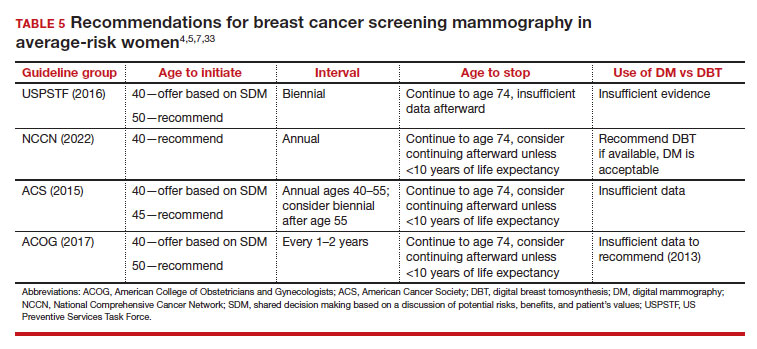
Should SM start at age 40, 45, or 50 in average-risk persons?
There is not clear consensus about the age at which to begin to recommend routine SM in patients at average risk. The National Comprehensive Cancer Network (NCCN),7 American Cancer Society (ACS),4 and the US Preventive Services Task Force (USPSTF)5 recommend that those at average risk start SM at age 40, 45, and 50, respectively (TABLE 5). While the guideline groups listed in TABLE 5 agree that there is level 1 evidence that SM reduces breast cancer mortality in the general population for persons starting at age 40, because the incidence of breast cancer is lower in younger persons (TABLE 6),4 the net population-based screening benefit is lower in this group, and the number needed to invite to screening to save a single life due to breast cancer varies.
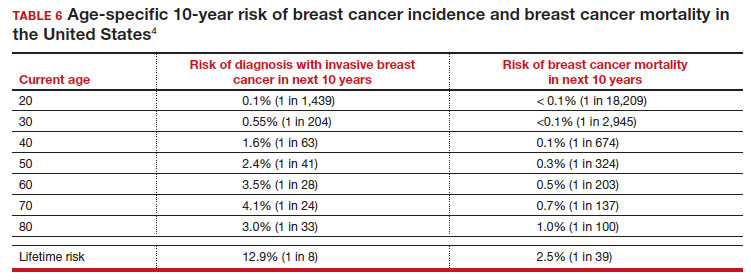
For patients in their 40s, it is estimated that 1,904 individuals need to be invited to SM to save 1 life, whereas for patients in their 50s, it is 1,339.15 However, for patients in their 40s, the number needed to screen to save 1 life due to breast cancer decreases from 1 in 1,904 if invited to be screened to 1 in 588 if they are actually screened.16 Furthermore, if a patient is diagnosed with breast cancer at age 40–50, the likelihood of dying is reduced at least 22% and perhaps as high as 48% if her cancer was diagnosed on SM compared with an unscreened individual with a symptomatic presentation (for example, palpable mass).4,15,17,18 Another benefit of SM in the fifth decade of life (40s) is the decreased need for more extensive treatment, including a higher risk of need for chemotherapy (odds ratio [OR], 2.81; 95% confidence interval [CI], 1.16–6.84); need for mastectomy (OR, 3.41; 95% CI, 1.36–8.52); and need for axillary lymph node dissection (OR, 5.76; 95% CI, 2.40–13.82) in unscreened (compared with screened) patients diagnosed with breast cancer.10
The harms associated with SM are not inconsequential and include callbacks (approximately 1 in 10), false-positive biopsy (approximately 1 in 100), and overdiagnosis (likely <1% of all breast cancers in persons younger than age 50). Because most patients in their 40s will not develop breast cancer (TABLE 6), the benefit of reduced breast cancer mortality will not be experienced by most in this decade of life, but they are still just as likely to experience a callback, false-positive biopsy, or the possibility of overdiagnosis. Interpretation of this balance on a population level is the crux of the various guideline groups’ development of differing recommendations as to when screening should start. Despite this seeming disagreement, all the guideline groups listed in TABLE 5 concur that persons at average risk for breast cancer should be offered SM if they desire starting at age 40 after a shared decision-making conversation that incorporates the patient’s view on the relative value of the benefits and risks.
Continue to: High-risk screening...
High-risk screening
Unlike in screening average-risk patients, there is less disagreement about screening in high-risk groups. TABLE 7 outlines the various categories and recommended strategies that qualify for screening at younger ages or more intensive screening. Adding breast MRI to SM in high-risk individuals results in both higher cancer detection rates and less interval breast cancers (cancers diagnosed between screening rounds) diagnosed compared with SM alone.19,20 Interval breast cancer tends to be more aggressive and is used as a surrogate marker for more recognized factors, such as breast cancer mortality. In addition to less interval breast cancers, high-risk patients are more likely to be diagnosed with node-negative disease if screening breast MRI is added to SM.
Long-term mortality benefit studies using MRI have not been conducted due to the prolonged follow-up times needed. Expense, lower specificity compared with mammography (that is, more false-positive results), and need for the use of gadolinium limit more widespread use of breast MRI screening in average-risk persons.
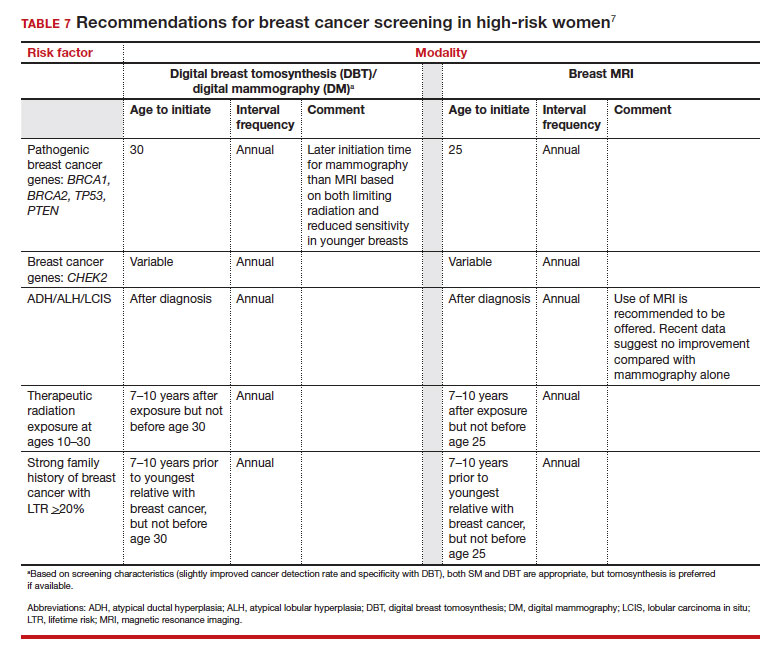
Screening in patients with dense breasts
Half of patients undergoing SM in the United States have dense breasts (heterogeneously dense breasts, 40%; extremely dense breasts, 10%). Importantly, increasing breast density is associated with a lower cancer detection rate with SM and is an independent risk factor for developing breast cancer. While most states already require patients to be notified if they have dense breasts identified on SM, the US Food and Drug Administration will soon make breast density patient notification a national standard (see: https://delauro.house.gov/media-center/press-releases/delauro-secures-timeline-fda-rollout-breast-density-notification-rule).
Most of the risk assessment tools listed in TABLE 3 incorporate breast density into their calculation of breast cancer risk. If that calculation places a patient into one of the highest-risk groups (based on additional factors like strong family history of breast cancer, reproductive risk factors, BRCA carriage, and so on), more intensive surveillance should be recommended (TABLE 7).7 However, once these risk calculations are done, most persons with dense breasts will remain in an average-risk category.
Because of the frequency and risks associated with dense breasts, different and alternative strategies have been recommended for screening persons who are at average risk with dense breasts. Supplemental screening with MRI, ultrasonography, contrast-enhanced mammography, and molecular breast imaging are all being considered but have not been studied sufficiently to demonstrate mortality benefit or cost-effectiveness.
Of all the supplemental modalities used to screen patients with dense breasts, MRI has been the best studied. A large RCT in the Netherlands evaluated supplemental MRI screening in persons with extremely dense breasts after a negative mammogram.21 Compared with no supplemental screening, the MRI group had 17 additional cancers detected per 1,000 screened and a 50% reduction in interval breast cancers; in addition, MRI was associated with a positive predictive value of 26% for biopsies. At present, high cost and limited access to standard breast MRI has not allowed its routine use for persons with dense breasts in the United States, but this may change with more experience and more widespread introduction and experience with abbreviated (or rapid) breast MRI in the future (TABLE 8).
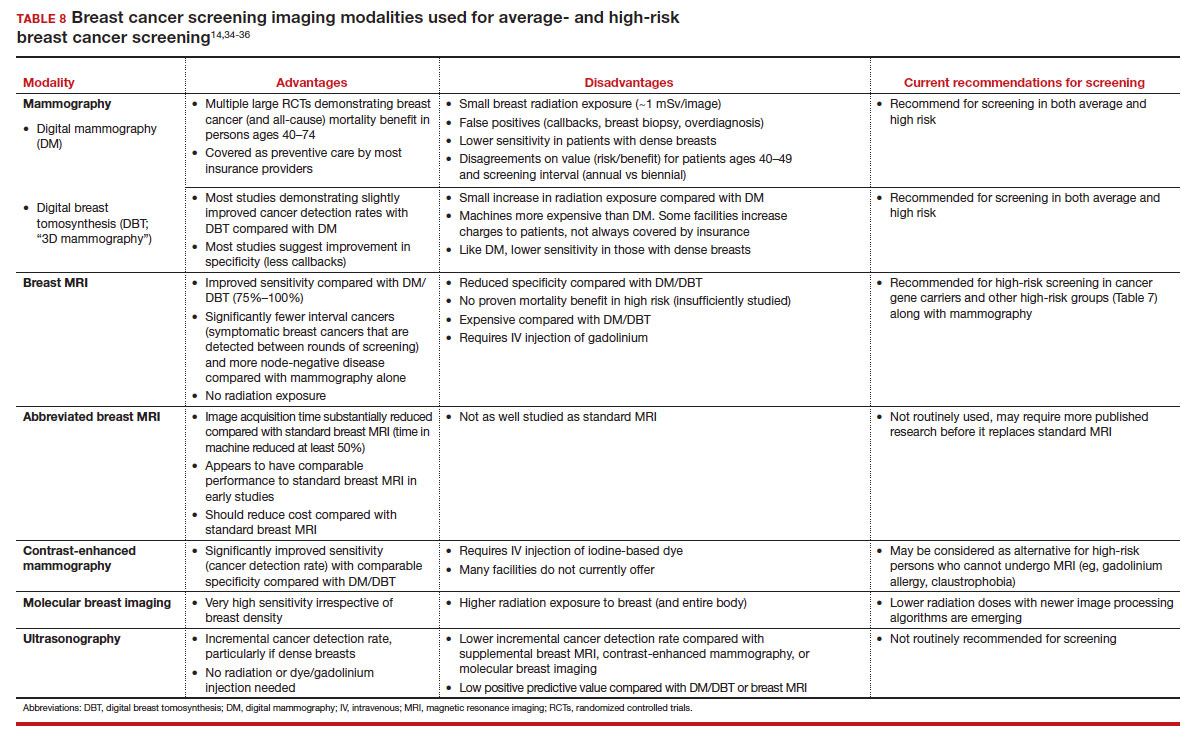
Equitable screening
Black persons who are diagnosed with breast cancer have a 40% higher risk of dying than White patients due to multiple factors, including systemic racial factors (implicit and unconscious bias), reduced access to care, and a lower likelihood of receiving standard of care once diagnosed.22-24 In addition, Black patients have twice the likelihood of being diagnosed with triple-negative breast cancers, a biologically more aggressive tumor.22-24 Among Black, Asian, and Hispanic persons diagnosed with breast cancer, one-third are diagnosed younger than age 50, which is higher than for non-Hispanic White persons. Prior to the age of 50, Black, Asian, and Hispanic patients also have a 72% more likelihood of being diagnosed with invasive breast cancer, have a 58% greater risk of advanced-stage disease, and have a 127% higher risk of dying from breast cancer compared with White patients.25,26 Based on all of these factors, delaying SM until age 50 may adversely affect the Black, Asian, and Hispanic populations.
Persons in the LGBTQ+ community do not present for SM as frequently as the general population, often because they feel threatened or unwelcome.27 Clinicians and breast imaging units should review their inclusivity policies and training to provide a welcoming and respectful environment to all persons in an effort to reduce these barriers. While data are limited and largely depend on expert opinion, current recommendations for screening in the transgender patient depend on sex assigned at birth, the type and duration of hormone use, and surgical history. In patients assigned female sex at birth, average-risk and high-risk screening recommendations are similar to those for the general population unless bilateral mastectomy has been performed.28 In transfeminine patients who have used hormones for longer than 5 years, some groups recommend annual screening starting at age 40, although well-designed studies are lacking.29
Continue to: We have done well, can we do better?...
We have done well, can we do better?
Screening mammography clearly has been an important and effective tool in the effort to reduce breast cancer mortality, but there are clear limitations. These include moderate sensitivity of mammography, particularly in patients with dense breasts, and a specificity that results in either callbacks (10%), breast biopsies for benign disease (1%), or the reality of overdiagnosis, which becomes increasingly important in older patients.
With the introduction of mammography in the mid-1980s, a one-size-fits-all approach has proved challenging more recently due to an increased recognition of the harms of screening. As a result of this evolving understanding, different recommendations for average-risk screening have emerged. With the advent of breast MRI, risk-based screening is an important but underutilized tool to identify highest-risk individuals, which is associated with improved cancer detection rates, reduced node-positive disease, and fewer diagnosed interval breast cancers. Assuring that nearly all of this highest-risk group is identified through routine breast cancer risk assessment remains a challenge for clinicians.
But what SM recommendations should be offered to persons who fall into an intermediate-risk group (15%–20%), very low-risk groups (<5%), or patients with dense breasts? These are challenges that could be met through novel and individualized approaches (for example, polygenic risk scoring, further research on newer modalities of screening [TABLE 8]), improved screening algorithms for persons with dense breasts, and enhanced clinician engagement to achieve universal breast cancer and BRCA risk assessment of patients by age 25 to 30.
In 2023, best practice and consensus guidelines for intermediate- and low-risk breast cancer groups remain unclear, and one of the many ongoing challenges is to further reduce the impact of breast cancer on the lives of persons affected and the recognized harms of SM.
In the meantime, there is consensus in average-risk patients to provide counseling about SM by age 40. My approach has been to counsel all average-risk patients on the risks and benefits of mammography using the acronym TIP-V:
- Use a Tool to calculate breast cancer risk (TABLE 3). If they are at high risk, provide recommendations for high-risk management (TABLE 7).7
- For average-risk patients, counsel that their Incidence of developing breast cancer in the next decade is approximately 1 in 70 (TABLE 6).4
- Provide data and guidance on the benefits of SM for patients in their 40s (mortality improvement, decreased treatment) and the likelihood of harm from breast cancer screening (10% callback, 1% benign biopsy, and <1% likelihood of overdiagnosis [TABLE 4]).4,14,15
- Engage the patient to better understand their relative Values of the benefits and harms and make a shared decision on screening starting at age 40, 45, or 50.
Looking forward
In summary, SM remains an important tool in the effort to decrease the risk of mortality due to breast cancer. Given the limitations of SM, however, newer tools and methods—abbreviated MRI, contrast-enhanced mammography, molecular breast imaging, customized screening intervals depending on individual risk/polygenic risk score, and customized counseling and screening based on risk factors (TABLES 2 and 7)—will play an increased role in recommendations for breast cancer screening in the future. ●
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541.
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-249.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Drist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force Recommendation statement. JAMA. 2019;322:652-665.
- Nelson HD, Cantor A, Humphrey L, et al. Screening for breast cancer: a systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence synthesis no 124. AHRQ publication no 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Karzai S, Port E, Siderides C, et al. Impact of screening mammography on treatment in young women diagnosed with breast cancer. Ann Surg Oncol. 2022. doi:10.1245/ s10434-022-11581-6.
- Ahn S, Wooster M, Valente C, et al. Impact of screening mammography on treatment in women diagnosed with breast cancer. Ann Surg Oncol. 2018;25:2979-2986.
- Coldman A, Phillips N. Incidence of breast cancer and estimates of overdiagnosis after the initiation of a population-based mammography screening program. CMAJ. 2013;185:E492-E498.
- Etzioni R, Gulati R, Mallinger L, et al. Influence of study features and methods on overdiagnosis estimates in breast and prostate cancer screening. Ann Internal Med. 2013;158:831-838.
- Ryser MD, Lange J, Inoue LY, et al. Estimation of breast cancer overdiagnosis in a US breast screening cohort. Ann Intern Med. 2022;175:471-478.
- Monticciolo DL, Malak SF, Friedewald SM, et al. Breast cancer screening recommendations inclusive of all women at average risk: update from the ACR and Society of Breast Imaging. J Am Coll Radiol. 2021;18:1280-1288.
- Nelson HD, Fu R, Cantor A, Pappas M, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Internal Med. 2016;164:244-255.
- Hendrick RE, Helvie MA, Hardesty LA. Implications of CISNET modeling on number needed to screen and mortality reduction with digital mammography in women 40–49 years old. Am J Roentgenol. 2014;203:1379-1381.
- Broeders M, Moss S, Nyström L, et al; EUROSCREEN Working Group. The impact of mammographic screening on breast cancer mortality in Europe: a review of observational studies. J Med Screen. 2012;19(suppl 1):14-25.
- Tabár L, Yen AMF, Wu WYY, et al. Insights from the breast cancer screening trials: how screening affects the natural history of breast cancer and implications for evaluating service screening programs. Breast J. 2015;21:13-20.
- Kriege M, Brekelmans CTM, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351:427-437.
- Vreemann S, Gubern-Merida A, Lardenoije S, et al. The frequency of missed breast cancers in women participating in a high-risk MRI screening program. Breast Cancer Res Treat. 2018;169:323-331.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Amirikia KC, Mills P, Bush J, et al. Higher population‐based incidence rates of triple‐negative breast cancer among young African‐American women: implications for breast cancer screening recommendations. Cancer. 2011;117:2747-2753.
- Kohler BA, Sherman RL, Howlader N, et al. Annual report to the nation on the status of cancer, 1975-2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J Natl Cancer Inst. 2015;107:djv048.
- Newman LA, Kaljee LM. Health disparities and triple-negative breast cancer in African American women: a review. JAMA Surg. 2017;152:485-493.
- Stapleton SM, Oseni TO, Bababekov YJ, et al. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. 2018;153:594-595.
- Hendrick RE, Monticciolo DL, Biggs KW, et al. Age distributions of breast cancer diagnosis and mortality by race and ethnicity in US women. Cancer. 2021;127:4384-4392.
- Perry H, Fang AJ, Tsai EM, et al. Imaging health and radiology care of transgender patients: a call to build evidence-based best practices. J Am Coll Radiol. 2021;18(3 pt B):475-480.
- Lockhart R, Kamaya A. Patient-friendly summary of the ACR Appropriateness Criteria: transgender breast cancer screening. J Am Coll Radiol. 2022;19:e19.
- Expert Panel on Breast Imaging; Brown A, Lourenco AP, Niell BL, et al. ACR Appropriateness Criteria transgender breast cancer screening. J Am Coll Radiol. 2021;18:S502-S515.
- Mørch LS, Skovlund CW, Hannaford PC, et al. Contemporary hormonal contraception and the risk of breast cancer. N Engl J Med. 2017;377:2228-2239.
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33.
- Laws A, Katlin F, Hans M, et al. Screening MRI does not increase cancer detection or result in an earlier stage at diagnosis for patients with high-risk breast lesions: a propensity score analysis. Ann Surg Oncol. 2023;30;68-77.
- American College of Obstetricians and Gynecologists. Practice bulletin no 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Grimm LJ, Mango VL, Harvey JA, et al. Implementation of abbreviated breast MRI for screening: AJR expert panel narrative review. AJR Am J Roentgenol. 2022;218:202-212.
- Potsch N, Vatteroini G, Clauser P, et al. Contrast-enhanced mammography versus contrast-enhanced breast MRI: a systematic review and meta-analysis. Radiology. 2022;305:94-103.
- Covington MF, Parent EE, Dibble EH, et al. Advances and future directions in molecular breast imaging. J Nucl Med. 2022;63:17-21.
Disclaimer: Gender-neutral terms (“persons,” “people,” “patients,” “individuals,” “they,” etc) are used throughout this article, but the use of screening mammography and other breast cancer screening tools generally references persons who were assigned female sex at birth.

Dr. Pearlman is Professor Emeritus,
Departments of Obstetrics and
Gynecology, Department of Surgery,
University of Michigan Health
System, Ann Arbor, Michigan.
The author reports no financial relationships relevant to this article.
Disclaimer: Gender-neutral terms (“persons,” “people,” “patients,” “individuals,” “they,” etc) are used throughout this article, but the use of screening mammography and other breast cancer screening tools generally references persons who were assigned female sex at birth.
Dr. Pearlman is Professor Emeritus,
Departments of Obstetrics and
Gynecology, Department of Surgery,
University of Michigan Health
System, Ann Arbor, Michigan.
The author reports no financial relationships relevant to this article.
Disclaimer: Gender-neutral terms (“persons,” “people,” “patients,” “individuals,” “they,” etc) are used throughout this article, but the use of screening mammography and other breast cancer screening tools generally references persons who were assigned female sex at birth.
Dr. Pearlman is Professor Emeritus,
Departments of Obstetrics and
Gynecology, Department of Surgery,
University of Michigan Health
System, Ann Arbor, Michigan.
The author reports no financial relationships relevant to this article.
Meaningful progress has been made in reducing deaths due to breast cancer over the last half century, with a 43% decrease in mortality rate (breast cancer deaths per 100,000 population).1 Screening mammography (SM) has contributed greatly to that success, accounting for 30% to 70% of the reduced mortality rate, with the remainder due to advancements in breast cancer treatment.2 Despite these improvements, invasive breast cancer remains the highest incident cancer in the United States and in the world, is the second leading cause of cancer death in the United States, and results in more years of life lost than any other cancer (TABLE 1).1,3
While the benefits and harms of SM are reasonably well understood, different guidelines groups have approached the relative value of the risks and benefits differently, which has led to challenges in implementation of shared decision making, particularly around the age to initiate routine screening.4-6 In this article, we will focus on the data behind the controversy, current gaps in knowledge, challenges related to breast density and screening in diverse groups, and emerging technologies to address these gaps and provide a construct for appropriate counseling of the patient across the risk spectrum.
In recognition of 35 years of publication of OBG Management, this article on breast cancer screening by Mark D. Pearlman, MD, kicks off a series that focuses on various cancer screening modalities and expert recommendations.
Stay tuned for articles on the future of cervical cancer screening and genetic testing for cancer risk beyond BRCA testing.
We look forward to continuing OBG Management’s mission of enhancing the quality of reproductive health care and the professional development of ObGyns and all women’s health care clinicians.
Breast cancer risk
Variables that affect risk
While female sex and older age are the 2 greatest risks for the development of breast cancer, many other factors can either increase or decrease breast cancer risk in a person’s lifetime. The importance of identifying risk factors is 3-fold:
- to perform risk assessment to determine if individuals would benefit from average-risk versus high-risk breast cancer surveillance
- to identify persons who might benefit from BRCA genetic counseling and screening, risk reduction medications or procedures, and
- to allow patients to determine whether any modification in their lifestyle or reproductive choices would make sense to them to reduce their future breast cancer risk.
Most of these risk variables are largely inalterable (for example, family history of breast cancer, carriage of genetic pathogenic variants such as BRCA1 and BRCA2, age of menarche and menopause), but some are potentially modifiable, such as parity, age at first birth, lactation and duration, and dietary factors, among others. TABLE 2 lists common breast cancer risk factors.
Breast cancer risk assessment
Several validated tools have been developed to estimate a person’s breast cancer risk (TABLE 3). These tools combine known risk factors and, depending on the specific tool, can provide estimates of 5-year, 10-year, or lifetime risk of breast cancer. Patients at highest risk can benefit from earlier screening, supplemental screening with breast magnetic resonance imaging (MRI), or risk reduction (see the section, “High-risk screening”). Ideally, a risk assessment should be done by age 30 so that patients at high risk can be identified for earlier or more intensive screening and for possible genetic testing in those at risk for carriage of the BRCA or other breast cancer gene pathogenic variants.5,7
Continue to: Breast cancer screening: Efficacy and harms...
Breast cancer screening: Efficacy and harms
The earliest studies of breast cancer screening with mammography were randomized controlled trials (RCTs) that compared screened and unscreened patients aged 40 to 74. Nearly all the RCTs and numerous well-designed incidence-based and case-control studies have demonstrated that SM results in a clinically and statistically significant reduction in breast cancer mortality (TABLE 4).4,6,8 Since the mid-1980s and continuing to the current day, SM programs are routinely recommended in the United States. In addition to the mortality benefit outlined in TABLE 4, SM also is associated with a need for less invasive treatments if breast cancer is diagnosed.9,10
With several decades of experience, SM programs have demonstrated that multiple harms are associated with SM, including callbacks, false-positive mammograms that result in a benign biopsy, and overdiagnosis of breast cancer (TABLE 4). Overdiagnosis is a mammographic detection of a breast cancer that would not have harmed that woman in her lifetime. Overdiagnosis leads to overtreatment of breast cancers with its attendant side effects, the emotional harms of a breast cancer diagnosis, and the substantial financial cost of cancer treatment. Estimates of overdiagnosis range from 0% to 50%, with the most likely estimate of invasive breast cancer overdiagnosis from SM between 5% and 15%.11-13 Some of these overdiagnosed cancers are due to very slow growing cancers or breast cancers that may even regress. However, the higher rates of overdiagnosis occur in older persons who are screened and in whom competing causes of mortality become more prevalent. It is estimated that overdiagnosis of invasive breast cancer in patients younger than age 60 is less than 1%, but it exceeds 14% in those older than age 80 (TABLE 4).14
A structured approach is needed to counsel patients about SM so that they understand both the substantial benefit (earlier-stage diagnosis, reduced need for treatment, reduced breast cancer and all-cause mortality) and the potential harms (callback, false-positive results, and overdiagnosis). Moreover, the relative balance of the benefits and harms are influenced throughout their lifetime by both aging and changes in their personal and family medical history.
Counseling should consider factors beyond just the performance of mammography (sensitivity and specificity), such as the patient’s current health and age (competing causes of mortality), likelihood of developing breast cancer based on risk assessment (more benefit in higher-risk persons), and the individual patient’s values on the importance of the benefits and harms. The differing emphases on mammography performance and the relative value of the benefits and harms have led experts to produce disparate national guideline recommendations (TABLE 5).
Should SM start at age 40, 45, or 50 in average-risk persons?
There is not clear consensus about the age at which to begin to recommend routine SM in patients at average risk. The National Comprehensive Cancer Network (NCCN),7 American Cancer Society (ACS),4 and the US Preventive Services Task Force (USPSTF)5 recommend that those at average risk start SM at age 40, 45, and 50, respectively (TABLE 5). While the guideline groups listed in TABLE 5 agree that there is level 1 evidence that SM reduces breast cancer mortality in the general population for persons starting at age 40, because the incidence of breast cancer is lower in younger persons (TABLE 6),4 the net population-based screening benefit is lower in this group, and the number needed to invite to screening to save a single life due to breast cancer varies.
For patients in their 40s, it is estimated that 1,904 individuals need to be invited to SM to save 1 life, whereas for patients in their 50s, it is 1,339.15 However, for patients in their 40s, the number needed to screen to save 1 life due to breast cancer decreases from 1 in 1,904 if invited to be screened to 1 in 588 if they are actually screened.16 Furthermore, if a patient is diagnosed with breast cancer at age 40–50, the likelihood of dying is reduced at least 22% and perhaps as high as 48% if her cancer was diagnosed on SM compared with an unscreened individual with a symptomatic presentation (for example, palpable mass).4,15,17,18 Another benefit of SM in the fifth decade of life (40s) is the decreased need for more extensive treatment, including a higher risk of need for chemotherapy (odds ratio [OR], 2.81; 95% confidence interval [CI], 1.16–6.84); need for mastectomy (OR, 3.41; 95% CI, 1.36–8.52); and need for axillary lymph node dissection (OR, 5.76; 95% CI, 2.40–13.82) in unscreened (compared with screened) patients diagnosed with breast cancer.10
The harms associated with SM are not inconsequential and include callbacks (approximately 1 in 10), false-positive biopsy (approximately 1 in 100), and overdiagnosis (likely <1% of all breast cancers in persons younger than age 50). Because most patients in their 40s will not develop breast cancer (TABLE 6), the benefit of reduced breast cancer mortality will not be experienced by most in this decade of life, but they are still just as likely to experience a callback, false-positive biopsy, or the possibility of overdiagnosis. Interpretation of this balance on a population level is the crux of the various guideline groups’ development of differing recommendations as to when screening should start. Despite this seeming disagreement, all the guideline groups listed in TABLE 5 concur that persons at average risk for breast cancer should be offered SM if they desire starting at age 40 after a shared decision-making conversation that incorporates the patient’s view on the relative value of the benefits and risks.
Continue to: High-risk screening...
High-risk screening
Unlike in screening average-risk patients, there is less disagreement about screening in high-risk groups. TABLE 7 outlines the various categories and recommended strategies that qualify for screening at younger ages or more intensive screening. Adding breast MRI to SM in high-risk individuals results in both higher cancer detection rates and less interval breast cancers (cancers diagnosed between screening rounds) diagnosed compared with SM alone.19,20 Interval breast cancer tends to be more aggressive and is used as a surrogate marker for more recognized factors, such as breast cancer mortality. In addition to less interval breast cancers, high-risk patients are more likely to be diagnosed with node-negative disease if screening breast MRI is added to SM.
Long-term mortality benefit studies using MRI have not been conducted due to the prolonged follow-up times needed. Expense, lower specificity compared with mammography (that is, more false-positive results), and need for the use of gadolinium limit more widespread use of breast MRI screening in average-risk persons.
Screening in patients with dense breasts
Half of patients undergoing SM in the United States have dense breasts (heterogeneously dense breasts, 40%; extremely dense breasts, 10%). Importantly, increasing breast density is associated with a lower cancer detection rate with SM and is an independent risk factor for developing breast cancer. While most states already require patients to be notified if they have dense breasts identified on SM, the US Food and Drug Administration will soon make breast density patient notification a national standard (see: https://delauro.house.gov/media-center/press-releases/delauro-secures-timeline-fda-rollout-breast-density-notification-rule).
Most of the risk assessment tools listed in TABLE 3 incorporate breast density into their calculation of breast cancer risk. If that calculation places a patient into one of the highest-risk groups (based on additional factors like strong family history of breast cancer, reproductive risk factors, BRCA carriage, and so on), more intensive surveillance should be recommended (TABLE 7).7 However, once these risk calculations are done, most persons with dense breasts will remain in an average-risk category.
Because of the frequency and risks associated with dense breasts, different and alternative strategies have been recommended for screening persons who are at average risk with dense breasts. Supplemental screening with MRI, ultrasonography, contrast-enhanced mammography, and molecular breast imaging are all being considered but have not been studied sufficiently to demonstrate mortality benefit or cost-effectiveness.
Of all the supplemental modalities used to screen patients with dense breasts, MRI has been the best studied. A large RCT in the Netherlands evaluated supplemental MRI screening in persons with extremely dense breasts after a negative mammogram.21 Compared with no supplemental screening, the MRI group had 17 additional cancers detected per 1,000 screened and a 50% reduction in interval breast cancers; in addition, MRI was associated with a positive predictive value of 26% for biopsies. At present, high cost and limited access to standard breast MRI has not allowed its routine use for persons with dense breasts in the United States, but this may change with more experience and more widespread introduction and experience with abbreviated (or rapid) breast MRI in the future (TABLE 8).
Equitable screening
Black persons who are diagnosed with breast cancer have a 40% higher risk of dying than White patients due to multiple factors, including systemic racial factors (implicit and unconscious bias), reduced access to care, and a lower likelihood of receiving standard of care once diagnosed.22-24 In addition, Black patients have twice the likelihood of being diagnosed with triple-negative breast cancers, a biologically more aggressive tumor.22-24 Among Black, Asian, and Hispanic persons diagnosed with breast cancer, one-third are diagnosed younger than age 50, which is higher than for non-Hispanic White persons. Prior to the age of 50, Black, Asian, and Hispanic patients also have a 72% more likelihood of being diagnosed with invasive breast cancer, have a 58% greater risk of advanced-stage disease, and have a 127% higher risk of dying from breast cancer compared with White patients.25,26 Based on all of these factors, delaying SM until age 50 may adversely affect the Black, Asian, and Hispanic populations.
Persons in the LGBTQ+ community do not present for SM as frequently as the general population, often because they feel threatened or unwelcome.27 Clinicians and breast imaging units should review their inclusivity policies and training to provide a welcoming and respectful environment to all persons in an effort to reduce these barriers. While data are limited and largely depend on expert opinion, current recommendations for screening in the transgender patient depend on sex assigned at birth, the type and duration of hormone use, and surgical history. In patients assigned female sex at birth, average-risk and high-risk screening recommendations are similar to those for the general population unless bilateral mastectomy has been performed.28 In transfeminine patients who have used hormones for longer than 5 years, some groups recommend annual screening starting at age 40, although well-designed studies are lacking.29
Continue to: We have done well, can we do better?...
We have done well, can we do better?
Screening mammography clearly has been an important and effective tool in the effort to reduce breast cancer mortality, but there are clear limitations. These include moderate sensitivity of mammography, particularly in patients with dense breasts, and a specificity that results in either callbacks (10%), breast biopsies for benign disease (1%), or the reality of overdiagnosis, which becomes increasingly important in older patients.
With the introduction of mammography in the mid-1980s, a one-size-fits-all approach has proved challenging more recently due to an increased recognition of the harms of screening. As a result of this evolving understanding, different recommendations for average-risk screening have emerged. With the advent of breast MRI, risk-based screening is an important but underutilized tool to identify highest-risk individuals, which is associated with improved cancer detection rates, reduced node-positive disease, and fewer diagnosed interval breast cancers. Assuring that nearly all of this highest-risk group is identified through routine breast cancer risk assessment remains a challenge for clinicians.
But what SM recommendations should be offered to persons who fall into an intermediate-risk group (15%–20%), very low-risk groups (<5%), or patients with dense breasts? These are challenges that could be met through novel and individualized approaches (for example, polygenic risk scoring, further research on newer modalities of screening [TABLE 8]), improved screening algorithms for persons with dense breasts, and enhanced clinician engagement to achieve universal breast cancer and BRCA risk assessment of patients by age 25 to 30.
In 2023, best practice and consensus guidelines for intermediate- and low-risk breast cancer groups remain unclear, and one of the many ongoing challenges is to further reduce the impact of breast cancer on the lives of persons affected and the recognized harms of SM.
In the meantime, there is consensus in average-risk patients to provide counseling about SM by age 40. My approach has been to counsel all average-risk patients on the risks and benefits of mammography using the acronym TIP-V:
- Use a Tool to calculate breast cancer risk (TABLE 3). If they are at high risk, provide recommendations for high-risk management (TABLE 7).7
- For average-risk patients, counsel that their Incidence of developing breast cancer in the next decade is approximately 1 in 70 (TABLE 6).4
- Provide data and guidance on the benefits of SM for patients in their 40s (mortality improvement, decreased treatment) and the likelihood of harm from breast cancer screening (10% callback, 1% benign biopsy, and <1% likelihood of overdiagnosis [TABLE 4]).4,14,15
- Engage the patient to better understand their relative Values of the benefits and harms and make a shared decision on screening starting at age 40, 45, or 50.
Looking forward
In summary, SM remains an important tool in the effort to decrease the risk of mortality due to breast cancer. Given the limitations of SM, however, newer tools and methods—abbreviated MRI, contrast-enhanced mammography, molecular breast imaging, customized screening intervals depending on individual risk/polygenic risk score, and customized counseling and screening based on risk factors (TABLES 2 and 7)—will play an increased role in recommendations for breast cancer screening in the future. ●
Meaningful progress has been made in reducing deaths due to breast cancer over the last half century, with a 43% decrease in mortality rate (breast cancer deaths per 100,000 population).1 Screening mammography (SM) has contributed greatly to that success, accounting for 30% to 70% of the reduced mortality rate, with the remainder due to advancements in breast cancer treatment.2 Despite these improvements, invasive breast cancer remains the highest incident cancer in the United States and in the world, is the second leading cause of cancer death in the United States, and results in more years of life lost than any other cancer (TABLE 1).1,3
While the benefits and harms of SM are reasonably well understood, different guidelines groups have approached the relative value of the risks and benefits differently, which has led to challenges in implementation of shared decision making, particularly around the age to initiate routine screening.4-6 In this article, we will focus on the data behind the controversy, current gaps in knowledge, challenges related to breast density and screening in diverse groups, and emerging technologies to address these gaps and provide a construct for appropriate counseling of the patient across the risk spectrum.
In recognition of 35 years of publication of OBG Management, this article on breast cancer screening by Mark D. Pearlman, MD, kicks off a series that focuses on various cancer screening modalities and expert recommendations.
Stay tuned for articles on the future of cervical cancer screening and genetic testing for cancer risk beyond BRCA testing.
We look forward to continuing OBG Management’s mission of enhancing the quality of reproductive health care and the professional development of ObGyns and all women’s health care clinicians.
Breast cancer risk
Variables that affect risk
While female sex and older age are the 2 greatest risks for the development of breast cancer, many other factors can either increase or decrease breast cancer risk in a person’s lifetime. The importance of identifying risk factors is 3-fold:
- to perform risk assessment to determine if individuals would benefit from average-risk versus high-risk breast cancer surveillance
- to identify persons who might benefit from BRCA genetic counseling and screening, risk reduction medications or procedures, and
- to allow patients to determine whether any modification in their lifestyle or reproductive choices would make sense to them to reduce their future breast cancer risk.
Most of these risk variables are largely inalterable (for example, family history of breast cancer, carriage of genetic pathogenic variants such as BRCA1 and BRCA2, age of menarche and menopause), but some are potentially modifiable, such as parity, age at first birth, lactation and duration, and dietary factors, among others. TABLE 2 lists common breast cancer risk factors.
Breast cancer risk assessment
Several validated tools have been developed to estimate a person’s breast cancer risk (TABLE 3). These tools combine known risk factors and, depending on the specific tool, can provide estimates of 5-year, 10-year, or lifetime risk of breast cancer. Patients at highest risk can benefit from earlier screening, supplemental screening with breast magnetic resonance imaging (MRI), or risk reduction (see the section, “High-risk screening”). Ideally, a risk assessment should be done by age 30 so that patients at high risk can be identified for earlier or more intensive screening and for possible genetic testing in those at risk for carriage of the BRCA or other breast cancer gene pathogenic variants.5,7
Continue to: Breast cancer screening: Efficacy and harms...
Breast cancer screening: Efficacy and harms
The earliest studies of breast cancer screening with mammography were randomized controlled trials (RCTs) that compared screened and unscreened patients aged 40 to 74. Nearly all the RCTs and numerous well-designed incidence-based and case-control studies have demonstrated that SM results in a clinically and statistically significant reduction in breast cancer mortality (TABLE 4).4,6,8 Since the mid-1980s and continuing to the current day, SM programs are routinely recommended in the United States. In addition to the mortality benefit outlined in TABLE 4, SM also is associated with a need for less invasive treatments if breast cancer is diagnosed.9,10
With several decades of experience, SM programs have demonstrated that multiple harms are associated with SM, including callbacks, false-positive mammograms that result in a benign biopsy, and overdiagnosis of breast cancer (TABLE 4). Overdiagnosis is a mammographic detection of a breast cancer that would not have harmed that woman in her lifetime. Overdiagnosis leads to overtreatment of breast cancers with its attendant side effects, the emotional harms of a breast cancer diagnosis, and the substantial financial cost of cancer treatment. Estimates of overdiagnosis range from 0% to 50%, with the most likely estimate of invasive breast cancer overdiagnosis from SM between 5% and 15%.11-13 Some of these overdiagnosed cancers are due to very slow growing cancers or breast cancers that may even regress. However, the higher rates of overdiagnosis occur in older persons who are screened and in whom competing causes of mortality become more prevalent. It is estimated that overdiagnosis of invasive breast cancer in patients younger than age 60 is less than 1%, but it exceeds 14% in those older than age 80 (TABLE 4).14
A structured approach is needed to counsel patients about SM so that they understand both the substantial benefit (earlier-stage diagnosis, reduced need for treatment, reduced breast cancer and all-cause mortality) and the potential harms (callback, false-positive results, and overdiagnosis). Moreover, the relative balance of the benefits and harms are influenced throughout their lifetime by both aging and changes in their personal and family medical history.
Counseling should consider factors beyond just the performance of mammography (sensitivity and specificity), such as the patient’s current health and age (competing causes of mortality), likelihood of developing breast cancer based on risk assessment (more benefit in higher-risk persons), and the individual patient’s values on the importance of the benefits and harms. The differing emphases on mammography performance and the relative value of the benefits and harms have led experts to produce disparate national guideline recommendations (TABLE 5).
Should SM start at age 40, 45, or 50 in average-risk persons?
There is not clear consensus about the age at which to begin to recommend routine SM in patients at average risk. The National Comprehensive Cancer Network (NCCN),7 American Cancer Society (ACS),4 and the US Preventive Services Task Force (USPSTF)5 recommend that those at average risk start SM at age 40, 45, and 50, respectively (TABLE 5). While the guideline groups listed in TABLE 5 agree that there is level 1 evidence that SM reduces breast cancer mortality in the general population for persons starting at age 40, because the incidence of breast cancer is lower in younger persons (TABLE 6),4 the net population-based screening benefit is lower in this group, and the number needed to invite to screening to save a single life due to breast cancer varies.
For patients in their 40s, it is estimated that 1,904 individuals need to be invited to SM to save 1 life, whereas for patients in their 50s, it is 1,339.15 However, for patients in their 40s, the number needed to screen to save 1 life due to breast cancer decreases from 1 in 1,904 if invited to be screened to 1 in 588 if they are actually screened.16 Furthermore, if a patient is diagnosed with breast cancer at age 40–50, the likelihood of dying is reduced at least 22% and perhaps as high as 48% if her cancer was diagnosed on SM compared with an unscreened individual with a symptomatic presentation (for example, palpable mass).4,15,17,18 Another benefit of SM in the fifth decade of life (40s) is the decreased need for more extensive treatment, including a higher risk of need for chemotherapy (odds ratio [OR], 2.81; 95% confidence interval [CI], 1.16–6.84); need for mastectomy (OR, 3.41; 95% CI, 1.36–8.52); and need for axillary lymph node dissection (OR, 5.76; 95% CI, 2.40–13.82) in unscreened (compared with screened) patients diagnosed with breast cancer.10
The harms associated with SM are not inconsequential and include callbacks (approximately 1 in 10), false-positive biopsy (approximately 1 in 100), and overdiagnosis (likely <1% of all breast cancers in persons younger than age 50). Because most patients in their 40s will not develop breast cancer (TABLE 6), the benefit of reduced breast cancer mortality will not be experienced by most in this decade of life, but they are still just as likely to experience a callback, false-positive biopsy, or the possibility of overdiagnosis. Interpretation of this balance on a population level is the crux of the various guideline groups’ development of differing recommendations as to when screening should start. Despite this seeming disagreement, all the guideline groups listed in TABLE 5 concur that persons at average risk for breast cancer should be offered SM if they desire starting at age 40 after a shared decision-making conversation that incorporates the patient’s view on the relative value of the benefits and risks.
Continue to: High-risk screening...
High-risk screening
Unlike in screening average-risk patients, there is less disagreement about screening in high-risk groups. TABLE 7 outlines the various categories and recommended strategies that qualify for screening at younger ages or more intensive screening. Adding breast MRI to SM in high-risk individuals results in both higher cancer detection rates and less interval breast cancers (cancers diagnosed between screening rounds) diagnosed compared with SM alone.19,20 Interval breast cancer tends to be more aggressive and is used as a surrogate marker for more recognized factors, such as breast cancer mortality. In addition to less interval breast cancers, high-risk patients are more likely to be diagnosed with node-negative disease if screening breast MRI is added to SM.
Long-term mortality benefit studies using MRI have not been conducted due to the prolonged follow-up times needed. Expense, lower specificity compared with mammography (that is, more false-positive results), and need for the use of gadolinium limit more widespread use of breast MRI screening in average-risk persons.
Screening in patients with dense breasts
Half of patients undergoing SM in the United States have dense breasts (heterogeneously dense breasts, 40%; extremely dense breasts, 10%). Importantly, increasing breast density is associated with a lower cancer detection rate with SM and is an independent risk factor for developing breast cancer. While most states already require patients to be notified if they have dense breasts identified on SM, the US Food and Drug Administration will soon make breast density patient notification a national standard (see: https://delauro.house.gov/media-center/press-releases/delauro-secures-timeline-fda-rollout-breast-density-notification-rule).
Most of the risk assessment tools listed in TABLE 3 incorporate breast density into their calculation of breast cancer risk. If that calculation places a patient into one of the highest-risk groups (based on additional factors like strong family history of breast cancer, reproductive risk factors, BRCA carriage, and so on), more intensive surveillance should be recommended (TABLE 7).7 However, once these risk calculations are done, most persons with dense breasts will remain in an average-risk category.
Because of the frequency and risks associated with dense breasts, different and alternative strategies have been recommended for screening persons who are at average risk with dense breasts. Supplemental screening with MRI, ultrasonography, contrast-enhanced mammography, and molecular breast imaging are all being considered but have not been studied sufficiently to demonstrate mortality benefit or cost-effectiveness.
Of all the supplemental modalities used to screen patients with dense breasts, MRI has been the best studied. A large RCT in the Netherlands evaluated supplemental MRI screening in persons with extremely dense breasts after a negative mammogram.21 Compared with no supplemental screening, the MRI group had 17 additional cancers detected per 1,000 screened and a 50% reduction in interval breast cancers; in addition, MRI was associated with a positive predictive value of 26% for biopsies. At present, high cost and limited access to standard breast MRI has not allowed its routine use for persons with dense breasts in the United States, but this may change with more experience and more widespread introduction and experience with abbreviated (or rapid) breast MRI in the future (TABLE 8).
Equitable screening
Black persons who are diagnosed with breast cancer have a 40% higher risk of dying than White patients due to multiple factors, including systemic racial factors (implicit and unconscious bias), reduced access to care, and a lower likelihood of receiving standard of care once diagnosed.22-24 In addition, Black patients have twice the likelihood of being diagnosed with triple-negative breast cancers, a biologically more aggressive tumor.22-24 Among Black, Asian, and Hispanic persons diagnosed with breast cancer, one-third are diagnosed younger than age 50, which is higher than for non-Hispanic White persons. Prior to the age of 50, Black, Asian, and Hispanic patients also have a 72% more likelihood of being diagnosed with invasive breast cancer, have a 58% greater risk of advanced-stage disease, and have a 127% higher risk of dying from breast cancer compared with White patients.25,26 Based on all of these factors, delaying SM until age 50 may adversely affect the Black, Asian, and Hispanic populations.
Persons in the LGBTQ+ community do not present for SM as frequently as the general population, often because they feel threatened or unwelcome.27 Clinicians and breast imaging units should review their inclusivity policies and training to provide a welcoming and respectful environment to all persons in an effort to reduce these barriers. While data are limited and largely depend on expert opinion, current recommendations for screening in the transgender patient depend on sex assigned at birth, the type and duration of hormone use, and surgical history. In patients assigned female sex at birth, average-risk and high-risk screening recommendations are similar to those for the general population unless bilateral mastectomy has been performed.28 In transfeminine patients who have used hormones for longer than 5 years, some groups recommend annual screening starting at age 40, although well-designed studies are lacking.29
Continue to: We have done well, can we do better?...
We have done well, can we do better?
Screening mammography clearly has been an important and effective tool in the effort to reduce breast cancer mortality, but there are clear limitations. These include moderate sensitivity of mammography, particularly in patients with dense breasts, and a specificity that results in either callbacks (10%), breast biopsies for benign disease (1%), or the reality of overdiagnosis, which becomes increasingly important in older patients.
With the introduction of mammography in the mid-1980s, a one-size-fits-all approach has proved challenging more recently due to an increased recognition of the harms of screening. As a result of this evolving understanding, different recommendations for average-risk screening have emerged. With the advent of breast MRI, risk-based screening is an important but underutilized tool to identify highest-risk individuals, which is associated with improved cancer detection rates, reduced node-positive disease, and fewer diagnosed interval breast cancers. Assuring that nearly all of this highest-risk group is identified through routine breast cancer risk assessment remains a challenge for clinicians.
But what SM recommendations should be offered to persons who fall into an intermediate-risk group (15%–20%), very low-risk groups (<5%), or patients with dense breasts? These are challenges that could be met through novel and individualized approaches (for example, polygenic risk scoring, further research on newer modalities of screening [TABLE 8]), improved screening algorithms for persons with dense breasts, and enhanced clinician engagement to achieve universal breast cancer and BRCA risk assessment of patients by age 25 to 30.
In 2023, best practice and consensus guidelines for intermediate- and low-risk breast cancer groups remain unclear, and one of the many ongoing challenges is to further reduce the impact of breast cancer on the lives of persons affected and the recognized harms of SM.
In the meantime, there is consensus in average-risk patients to provide counseling about SM by age 40. My approach has been to counsel all average-risk patients on the risks and benefits of mammography using the acronym TIP-V:
- Use a Tool to calculate breast cancer risk (TABLE 3). If they are at high risk, provide recommendations for high-risk management (TABLE 7).7
- For average-risk patients, counsel that their Incidence of developing breast cancer in the next decade is approximately 1 in 70 (TABLE 6).4
- Provide data and guidance on the benefits of SM for patients in their 40s (mortality improvement, decreased treatment) and the likelihood of harm from breast cancer screening (10% callback, 1% benign biopsy, and <1% likelihood of overdiagnosis [TABLE 4]).4,14,15
- Engage the patient to better understand their relative Values of the benefits and harms and make a shared decision on screening starting at age 40, 45, or 50.
Looking forward
In summary, SM remains an important tool in the effort to decrease the risk of mortality due to breast cancer. Given the limitations of SM, however, newer tools and methods—abbreviated MRI, contrast-enhanced mammography, molecular breast imaging, customized screening intervals depending on individual risk/polygenic risk score, and customized counseling and screening based on risk factors (TABLES 2 and 7)—will play an increased role in recommendations for breast cancer screening in the future. ●
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541.
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-249.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Drist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force Recommendation statement. JAMA. 2019;322:652-665.
- Nelson HD, Cantor A, Humphrey L, et al. Screening for breast cancer: a systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence synthesis no 124. AHRQ publication no 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Karzai S, Port E, Siderides C, et al. Impact of screening mammography on treatment in young women diagnosed with breast cancer. Ann Surg Oncol. 2022. doi:10.1245/ s10434-022-11581-6.
- Ahn S, Wooster M, Valente C, et al. Impact of screening mammography on treatment in women diagnosed with breast cancer. Ann Surg Oncol. 2018;25:2979-2986.
- Coldman A, Phillips N. Incidence of breast cancer and estimates of overdiagnosis after the initiation of a population-based mammography screening program. CMAJ. 2013;185:E492-E498.
- Etzioni R, Gulati R, Mallinger L, et al. Influence of study features and methods on overdiagnosis estimates in breast and prostate cancer screening. Ann Internal Med. 2013;158:831-838.
- Ryser MD, Lange J, Inoue LY, et al. Estimation of breast cancer overdiagnosis in a US breast screening cohort. Ann Intern Med. 2022;175:471-478.
- Monticciolo DL, Malak SF, Friedewald SM, et al. Breast cancer screening recommendations inclusive of all women at average risk: update from the ACR and Society of Breast Imaging. J Am Coll Radiol. 2021;18:1280-1288.
- Nelson HD, Fu R, Cantor A, Pappas M, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Internal Med. 2016;164:244-255.
- Hendrick RE, Helvie MA, Hardesty LA. Implications of CISNET modeling on number needed to screen and mortality reduction with digital mammography in women 40–49 years old. Am J Roentgenol. 2014;203:1379-1381.
- Broeders M, Moss S, Nyström L, et al; EUROSCREEN Working Group. The impact of mammographic screening on breast cancer mortality in Europe: a review of observational studies. J Med Screen. 2012;19(suppl 1):14-25.
- Tabár L, Yen AMF, Wu WYY, et al. Insights from the breast cancer screening trials: how screening affects the natural history of breast cancer and implications for evaluating service screening programs. Breast J. 2015;21:13-20.
- Kriege M, Brekelmans CTM, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351:427-437.
- Vreemann S, Gubern-Merida A, Lardenoije S, et al. The frequency of missed breast cancers in women participating in a high-risk MRI screening program. Breast Cancer Res Treat. 2018;169:323-331.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Amirikia KC, Mills P, Bush J, et al. Higher population‐based incidence rates of triple‐negative breast cancer among young African‐American women: implications for breast cancer screening recommendations. Cancer. 2011;117:2747-2753.
- Kohler BA, Sherman RL, Howlader N, et al. Annual report to the nation on the status of cancer, 1975-2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J Natl Cancer Inst. 2015;107:djv048.
- Newman LA, Kaljee LM. Health disparities and triple-negative breast cancer in African American women: a review. JAMA Surg. 2017;152:485-493.
- Stapleton SM, Oseni TO, Bababekov YJ, et al. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. 2018;153:594-595.
- Hendrick RE, Monticciolo DL, Biggs KW, et al. Age distributions of breast cancer diagnosis and mortality by race and ethnicity in US women. Cancer. 2021;127:4384-4392.
- Perry H, Fang AJ, Tsai EM, et al. Imaging health and radiology care of transgender patients: a call to build evidence-based best practices. J Am Coll Radiol. 2021;18(3 pt B):475-480.
- Lockhart R, Kamaya A. Patient-friendly summary of the ACR Appropriateness Criteria: transgender breast cancer screening. J Am Coll Radiol. 2022;19:e19.
- Expert Panel on Breast Imaging; Brown A, Lourenco AP, Niell BL, et al. ACR Appropriateness Criteria transgender breast cancer screening. J Am Coll Radiol. 2021;18:S502-S515.
- Mørch LS, Skovlund CW, Hannaford PC, et al. Contemporary hormonal contraception and the risk of breast cancer. N Engl J Med. 2017;377:2228-2239.
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33.
- Laws A, Katlin F, Hans M, et al. Screening MRI does not increase cancer detection or result in an earlier stage at diagnosis for patients with high-risk breast lesions: a propensity score analysis. Ann Surg Oncol. 2023;30;68-77.
- American College of Obstetricians and Gynecologists. Practice bulletin no 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Grimm LJ, Mango VL, Harvey JA, et al. Implementation of abbreviated breast MRI for screening: AJR expert panel narrative review. AJR Am J Roentgenol. 2022;218:202-212.
- Potsch N, Vatteroini G, Clauser P, et al. Contrast-enhanced mammography versus contrast-enhanced breast MRI: a systematic review and meta-analysis. Radiology. 2022;305:94-103.
- Covington MF, Parent EE, Dibble EH, et al. Advances and future directions in molecular breast imaging. J Nucl Med. 2022;63:17-21.
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541.
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353:1784-1792.
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-249.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314:1599-1614.
- US Preventive Services Task Force; Owens DK, Davidson KW, Drist AH, et al. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer: US Preventive Services Task Force Recommendation statement. JAMA. 2019;322:652-665.
- Nelson HD, Cantor A, Humphrey L, et al. Screening for breast cancer: a systematic review to update the 2009 US Preventive Services Task Force recommendation. Evidence synthesis no 124. AHRQ publication no 14-05201-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
- Bevers TB, Helvie M, Bonaccio E, et al. Breast cancer screening and diagnosis, version 3.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:1362-1389.
- Duffy SW, Vulkan D, Cuckle H, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165-1172.
- Karzai S, Port E, Siderides C, et al. Impact of screening mammography on treatment in young women diagnosed with breast cancer. Ann Surg Oncol. 2022. doi:10.1245/ s10434-022-11581-6.
- Ahn S, Wooster M, Valente C, et al. Impact of screening mammography on treatment in women diagnosed with breast cancer. Ann Surg Oncol. 2018;25:2979-2986.
- Coldman A, Phillips N. Incidence of breast cancer and estimates of overdiagnosis after the initiation of a population-based mammography screening program. CMAJ. 2013;185:E492-E498.
- Etzioni R, Gulati R, Mallinger L, et al. Influence of study features and methods on overdiagnosis estimates in breast and prostate cancer screening. Ann Internal Med. 2013;158:831-838.
- Ryser MD, Lange J, Inoue LY, et al. Estimation of breast cancer overdiagnosis in a US breast screening cohort. Ann Intern Med. 2022;175:471-478.
- Monticciolo DL, Malak SF, Friedewald SM, et al. Breast cancer screening recommendations inclusive of all women at average risk: update from the ACR and Society of Breast Imaging. J Am Coll Radiol. 2021;18:1280-1288.
- Nelson HD, Fu R, Cantor A, Pappas M, et al. Effectiveness of breast cancer screening: systematic review and meta-analysis to update the 2009 US Preventive Services Task Force recommendation. Ann Internal Med. 2016;164:244-255.
- Hendrick RE, Helvie MA, Hardesty LA. Implications of CISNET modeling on number needed to screen and mortality reduction with digital mammography in women 40–49 years old. Am J Roentgenol. 2014;203:1379-1381.
- Broeders M, Moss S, Nyström L, et al; EUROSCREEN Working Group. The impact of mammographic screening on breast cancer mortality in Europe: a review of observational studies. J Med Screen. 2012;19(suppl 1):14-25.
- Tabár L, Yen AMF, Wu WYY, et al. Insights from the breast cancer screening trials: how screening affects the natural history of breast cancer and implications for evaluating service screening programs. Breast J. 2015;21:13-20.
- Kriege M, Brekelmans CTM, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351:427-437.
- Vreemann S, Gubern-Merida A, Lardenoije S, et al. The frequency of missed breast cancers in women participating in a high-risk MRI screening program. Breast Cancer Res Treat. 2018;169:323-331.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Amirikia KC, Mills P, Bush J, et al. Higher population‐based incidence rates of triple‐negative breast cancer among young African‐American women: implications for breast cancer screening recommendations. Cancer. 2011;117:2747-2753.
- Kohler BA, Sherman RL, Howlader N, et al. Annual report to the nation on the status of cancer, 1975-2011, featuring incidence of breast cancer subtypes by race/ethnicity, poverty, and state. J Natl Cancer Inst. 2015;107:djv048.
- Newman LA, Kaljee LM. Health disparities and triple-negative breast cancer in African American women: a review. JAMA Surg. 2017;152:485-493.
- Stapleton SM, Oseni TO, Bababekov YJ, et al. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. 2018;153:594-595.
- Hendrick RE, Monticciolo DL, Biggs KW, et al. Age distributions of breast cancer diagnosis and mortality by race and ethnicity in US women. Cancer. 2021;127:4384-4392.
- Perry H, Fang AJ, Tsai EM, et al. Imaging health and radiology care of transgender patients: a call to build evidence-based best practices. J Am Coll Radiol. 2021;18(3 pt B):475-480.
- Lockhart R, Kamaya A. Patient-friendly summary of the ACR Appropriateness Criteria: transgender breast cancer screening. J Am Coll Radiol. 2022;19:e19.
- Expert Panel on Breast Imaging; Brown A, Lourenco AP, Niell BL, et al. ACR Appropriateness Criteria transgender breast cancer screening. J Am Coll Radiol. 2021;18:S502-S515.
- Mørch LS, Skovlund CW, Hannaford PC, et al. Contemporary hormonal contraception and the risk of breast cancer. N Engl J Med. 2017;377:2228-2239.
- Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7-33.
- Laws A, Katlin F, Hans M, et al. Screening MRI does not increase cancer detection or result in an earlier stage at diagnosis for patients with high-risk breast lesions: a propensity score analysis. Ann Surg Oncol. 2023;30;68-77.
- American College of Obstetricians and Gynecologists. Practice bulletin no 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1-e16.
- Grimm LJ, Mango VL, Harvey JA, et al. Implementation of abbreviated breast MRI for screening: AJR expert panel narrative review. AJR Am J Roentgenol. 2022;218:202-212.
- Potsch N, Vatteroini G, Clauser P, et al. Contrast-enhanced mammography versus contrast-enhanced breast MRI: a systematic review and meta-analysis. Radiology. 2022;305:94-103.
- Covington MF, Parent EE, Dibble EH, et al. Advances and future directions in molecular breast imaging. J Nucl Med. 2022;63:17-21.

Rucaparib benefit in BRCA+ prostate cancer confirmed
The finding, which comes from the TRITON3 clinical trial, provides evidence of clinical benefit for an indication for rucaparib that was granted an accelerated approval in May 2020.
“Rucaparib reduced the risk of progression or death by half in patients with BRCA alterations,” said lead author Alan H. Bryce, MD, medical director of the Genomic Oncology Clinic at Mayo Clinic Arizona, in Phoenix.
For the subgroup of patients with BRCA alterations, the median PFS was 11.2 months with rucaparib vs. 6.4 months (hazard ratio, 0.50; P < .001) among those who received physician’s choice of therapy, which included docetaxel or a second-generation ARPI, such as abiraterone or enzalutamide.
In another subgroup of patients whose disease had ATM alterations, the median PFS was 8.1 months with rucaparib vs. 6.8 months with physician’s choice of drug. The difference was not statistically significant.
However, the difference was significant in the intention-to-treat (ITT) population (comprising both subgroups), for whom the median PFS was 10.2 months with rucaparib vs. 6.4 months with physician’s choice of drug (HR, 0.61; P < .001 by log-rank test).
Dr. Bryce pointed out that three-quarters of the patients in the physician’s-choice arm who had progressive disease crossed over to rucaparib upon progression and that overall survival (OS) results are immature. At 62 months, median OS did not significantly differ in the BRCA subgroup (24.3 vs. 20.8 months favoring rucaparib; P = .21) or in the ITT group (23.6 vs. 20.9 months; P = .67).
Importantly, rucaparib was well tolerated. In all treatment groups, the most frequent adverse events were asthenia and fatigue, Bryce said. “There were no cases of myelodysplastic syndrome or acute myeloid leukemia reported.”
These results from the TRITON3 trial were presented at the 2023 ASCO Genitourinary Cancers Symposium and were published simultaneously in the New England Journal of Medicine.
Suggested benefit
Rucaparib is the first PARP inhibitor approved for use in patients with mCRPC that harbors deleterious BRCA mutations (germline and/or somatic) who have already been treated with androgen receptor–directed therapy and a taxane-based chemotherapy. This prostate cancer indication was granted an accelerated approval in May 2020 by the U.S. Food and Drug Administration on the basis of response rates and effect on levels of prostate-specific antigen (PSA) from the TRITON2 clinical trial, the forerunner of the current study.
The TRITON2 study was a single-arm clinical trial that involved three cohorts: 62 patients with a BRCA mutation (germline and/or somatic) and measurable disease; 115 patients with a BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease; and 209 patients with homologous recombination deficiency–positive mCRPC.
In an analysis of 115 patients with a deleterious BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease, the confirmed PSA response rate was 55%. For the patients with measurable disease and a BRCA mutation, the objective response rate was 44%. The objective response rate was similar for those with a germline BRCA mutation.
Study details
The current phase 3 randomized TRITON3 clinical trial was conducted to confirm the earlier findings and to expand upon the data in mCRPC. The participants in this trial were patients with mCRPC who had specific gene alterations, including BRCA and ATM alterations, who had experienced disease progression after androgen receptor–directed therapy but who had not yet received chemotherapy.
A total of 270 men were assigned to receive rucaparib (600 mg twice daily); 135 patients received their physician’s choice of medication. Within the two study arms, 302 patients had a BRCA alteration, and 103 patients had an ATM alteration. The ITT population consisted of all the patients who had been randomly assigned to either of the two groups. A prespecified subgroup included patients with a BRCA alteration.
The primary outcome was the median duration of imaging-based PSF, as determined through independent review. Key secondary outcomes were overall survival and objective response rate.
The most common adverse events in the rucaparib group were fatigue, nausea, and anemia or decreased hemoglobin. In the control group, the most common adverse events were fatigue, diarrhea, and neuropathy. The most common events of grade 3 or higher were anemia or decreased hemoglobin, neutropenia or a decreased neutrophil count, and fatigue in the rucaparib group, and fatigue and neutropenia or a decreased neutrophil count among control patients.
No changes in standard of care
In a discussion of the study, Elena Castro, MD, PhD, of the Instituto de Investigación Biomédica de Málaga, Campanillas, Spain, emphasized that there is a clear benefit from the use of PARP inhibitors (such as rucaparib) for patients with BRCA alterations.
However, she highlighted the absence of convincing overall survival data and the absence of a clear benefit on PFS in the subgroup of patients with ATM alterations.
“These data raise several questions,” she noted, “such as, do patients with ATM alterations benefit at all? And should PARP inhibitors [such as rucaparib] precede or follow docetaxel therapy?”
Because of the high crossover rate, it may be possible to evaluate the directionality of docetaxel followed by PARP inhibitors and the other way around, she suggested.
Dr. Castro said that patients with BRCA alterations benefit from PARP inhibitors and are likely to derive more benefit from them than from taxanes.
“But those with ATM alterations are unlikely to benefit from rucaparib more than from taxanes,” she said.
In a comment, Hank Ng, MD, medical oncologist, NYU Langone Perlmutter Cancer Center, New York, said he is not convinced that the findings from TRITON 3 represent a new standard of care in BRCA 1/2 mutations or ATM.
“Currently, we know that, for patients with prostate cancer with BRCA1/2 or ATM, the standard of care is an androgen receptor pathway inhibitor (ARPI), such as abiraterone or enzalutamide, then docetaxel, and then a PARP inhibitor like rucaparib,” he said.
(Currently, rucaparib is indicated for use in patients with mCRPC with BRCA alterations after they have already received an ARPI and taxane-based chemotherapy.)
Dr. Ng also questioned the control arm of the TRITON 3 trial. All the participants in the trial had already experienced disease progression after treatment with a second-generation ARPI. But the physician’s choice of therapy allowed them to move on to another ARPI or to docetaxel.
Dr. NG commented that, “in almost all cases, after progression of one ARPI, switching to another ARPI does not provide much benefit – from what is visible from this abstract – and only 56% patients received docetaxel, and thus 44% received a not-beneficial treatment,” he said.
“I am not sure what the docetaxel subgroup showed, but potentially, if those numbers are convincing, we could move this [rucaparib] ahead of docetaxel,” he speculated.
However, he also pointed out that an overall survival benefit has not yet been shown; so far, the benefit that has been shown is with respect to imaging-based PFS.
Dr. Ng does agree that rucaparib is indicated in the second line after progression with one ARPI for patients who are not candidates for chemotherapy. “But this has not yet shown me that we should absolutely be offering rucaparib before docetaxel,” he said.
TRITON3 was supported by Clovis Oncology, manufacturer of rucaparib. Dr. Bryce has relationships with Bayer, Foundation Medicine, Janssen, Merck, Myovant Sciences, and Novartis and holds a patent for therapeutic targeting of cancer patients with NRG1 rearrangements. Dr. Castro has relationships with Astellas Pharma, AstraZeneca, Bayer, Clovis Oncology, Janssen-Cilag, Merck, MSD Oncology, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.
The finding, which comes from the TRITON3 clinical trial, provides evidence of clinical benefit for an indication for rucaparib that was granted an accelerated approval in May 2020.
“Rucaparib reduced the risk of progression or death by half in patients with BRCA alterations,” said lead author Alan H. Bryce, MD, medical director of the Genomic Oncology Clinic at Mayo Clinic Arizona, in Phoenix.
For the subgroup of patients with BRCA alterations, the median PFS was 11.2 months with rucaparib vs. 6.4 months (hazard ratio, 0.50; P < .001) among those who received physician’s choice of therapy, which included docetaxel or a second-generation ARPI, such as abiraterone or enzalutamide.
In another subgroup of patients whose disease had ATM alterations, the median PFS was 8.1 months with rucaparib vs. 6.8 months with physician’s choice of drug. The difference was not statistically significant.
However, the difference was significant in the intention-to-treat (ITT) population (comprising both subgroups), for whom the median PFS was 10.2 months with rucaparib vs. 6.4 months with physician’s choice of drug (HR, 0.61; P < .001 by log-rank test).
Dr. Bryce pointed out that three-quarters of the patients in the physician’s-choice arm who had progressive disease crossed over to rucaparib upon progression and that overall survival (OS) results are immature. At 62 months, median OS did not significantly differ in the BRCA subgroup (24.3 vs. 20.8 months favoring rucaparib; P = .21) or in the ITT group (23.6 vs. 20.9 months; P = .67).
Importantly, rucaparib was well tolerated. In all treatment groups, the most frequent adverse events were asthenia and fatigue, Bryce said. “There were no cases of myelodysplastic syndrome or acute myeloid leukemia reported.”
These results from the TRITON3 trial were presented at the 2023 ASCO Genitourinary Cancers Symposium and were published simultaneously in the New England Journal of Medicine.
Suggested benefit
Rucaparib is the first PARP inhibitor approved for use in patients with mCRPC that harbors deleterious BRCA mutations (germline and/or somatic) who have already been treated with androgen receptor–directed therapy and a taxane-based chemotherapy. This prostate cancer indication was granted an accelerated approval in May 2020 by the U.S. Food and Drug Administration on the basis of response rates and effect on levels of prostate-specific antigen (PSA) from the TRITON2 clinical trial, the forerunner of the current study.
The TRITON2 study was a single-arm clinical trial that involved three cohorts: 62 patients with a BRCA mutation (germline and/or somatic) and measurable disease; 115 patients with a BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease; and 209 patients with homologous recombination deficiency–positive mCRPC.
In an analysis of 115 patients with a deleterious BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease, the confirmed PSA response rate was 55%. For the patients with measurable disease and a BRCA mutation, the objective response rate was 44%. The objective response rate was similar for those with a germline BRCA mutation.
Study details
The current phase 3 randomized TRITON3 clinical trial was conducted to confirm the earlier findings and to expand upon the data in mCRPC. The participants in this trial were patients with mCRPC who had specific gene alterations, including BRCA and ATM alterations, who had experienced disease progression after androgen receptor–directed therapy but who had not yet received chemotherapy.
A total of 270 men were assigned to receive rucaparib (600 mg twice daily); 135 patients received their physician’s choice of medication. Within the two study arms, 302 patients had a BRCA alteration, and 103 patients had an ATM alteration. The ITT population consisted of all the patients who had been randomly assigned to either of the two groups. A prespecified subgroup included patients with a BRCA alteration.
The primary outcome was the median duration of imaging-based PSF, as determined through independent review. Key secondary outcomes were overall survival and objective response rate.
The most common adverse events in the rucaparib group were fatigue, nausea, and anemia or decreased hemoglobin. In the control group, the most common adverse events were fatigue, diarrhea, and neuropathy. The most common events of grade 3 or higher were anemia or decreased hemoglobin, neutropenia or a decreased neutrophil count, and fatigue in the rucaparib group, and fatigue and neutropenia or a decreased neutrophil count among control patients.
No changes in standard of care
In a discussion of the study, Elena Castro, MD, PhD, of the Instituto de Investigación Biomédica de Málaga, Campanillas, Spain, emphasized that there is a clear benefit from the use of PARP inhibitors (such as rucaparib) for patients with BRCA alterations.
However, she highlighted the absence of convincing overall survival data and the absence of a clear benefit on PFS in the subgroup of patients with ATM alterations.
“These data raise several questions,” she noted, “such as, do patients with ATM alterations benefit at all? And should PARP inhibitors [such as rucaparib] precede or follow docetaxel therapy?”
Because of the high crossover rate, it may be possible to evaluate the directionality of docetaxel followed by PARP inhibitors and the other way around, she suggested.
Dr. Castro said that patients with BRCA alterations benefit from PARP inhibitors and are likely to derive more benefit from them than from taxanes.
“But those with ATM alterations are unlikely to benefit from rucaparib more than from taxanes,” she said.
In a comment, Hank Ng, MD, medical oncologist, NYU Langone Perlmutter Cancer Center, New York, said he is not convinced that the findings from TRITON 3 represent a new standard of care in BRCA 1/2 mutations or ATM.
“Currently, we know that, for patients with prostate cancer with BRCA1/2 or ATM, the standard of care is an androgen receptor pathway inhibitor (ARPI), such as abiraterone or enzalutamide, then docetaxel, and then a PARP inhibitor like rucaparib,” he said.
(Currently, rucaparib is indicated for use in patients with mCRPC with BRCA alterations after they have already received an ARPI and taxane-based chemotherapy.)
Dr. Ng also questioned the control arm of the TRITON 3 trial. All the participants in the trial had already experienced disease progression after treatment with a second-generation ARPI. But the physician’s choice of therapy allowed them to move on to another ARPI or to docetaxel.
Dr. NG commented that, “in almost all cases, after progression of one ARPI, switching to another ARPI does not provide much benefit – from what is visible from this abstract – and only 56% patients received docetaxel, and thus 44% received a not-beneficial treatment,” he said.
“I am not sure what the docetaxel subgroup showed, but potentially, if those numbers are convincing, we could move this [rucaparib] ahead of docetaxel,” he speculated.
However, he also pointed out that an overall survival benefit has not yet been shown; so far, the benefit that has been shown is with respect to imaging-based PFS.
Dr. Ng does agree that rucaparib is indicated in the second line after progression with one ARPI for patients who are not candidates for chemotherapy. “But this has not yet shown me that we should absolutely be offering rucaparib before docetaxel,” he said.
TRITON3 was supported by Clovis Oncology, manufacturer of rucaparib. Dr. Bryce has relationships with Bayer, Foundation Medicine, Janssen, Merck, Myovant Sciences, and Novartis and holds a patent for therapeutic targeting of cancer patients with NRG1 rearrangements. Dr. Castro has relationships with Astellas Pharma, AstraZeneca, Bayer, Clovis Oncology, Janssen-Cilag, Merck, MSD Oncology, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.
The finding, which comes from the TRITON3 clinical trial, provides evidence of clinical benefit for an indication for rucaparib that was granted an accelerated approval in May 2020.
“Rucaparib reduced the risk of progression or death by half in patients with BRCA alterations,” said lead author Alan H. Bryce, MD, medical director of the Genomic Oncology Clinic at Mayo Clinic Arizona, in Phoenix.
For the subgroup of patients with BRCA alterations, the median PFS was 11.2 months with rucaparib vs. 6.4 months (hazard ratio, 0.50; P < .001) among those who received physician’s choice of therapy, which included docetaxel or a second-generation ARPI, such as abiraterone or enzalutamide.
In another subgroup of patients whose disease had ATM alterations, the median PFS was 8.1 months with rucaparib vs. 6.8 months with physician’s choice of drug. The difference was not statistically significant.
However, the difference was significant in the intention-to-treat (ITT) population (comprising both subgroups), for whom the median PFS was 10.2 months with rucaparib vs. 6.4 months with physician’s choice of drug (HR, 0.61; P < .001 by log-rank test).
Dr. Bryce pointed out that three-quarters of the patients in the physician’s-choice arm who had progressive disease crossed over to rucaparib upon progression and that overall survival (OS) results are immature. At 62 months, median OS did not significantly differ in the BRCA subgroup (24.3 vs. 20.8 months favoring rucaparib; P = .21) or in the ITT group (23.6 vs. 20.9 months; P = .67).
Importantly, rucaparib was well tolerated. In all treatment groups, the most frequent adverse events were asthenia and fatigue, Bryce said. “There were no cases of myelodysplastic syndrome or acute myeloid leukemia reported.”
These results from the TRITON3 trial were presented at the 2023 ASCO Genitourinary Cancers Symposium and were published simultaneously in the New England Journal of Medicine.
Suggested benefit
Rucaparib is the first PARP inhibitor approved for use in patients with mCRPC that harbors deleterious BRCA mutations (germline and/or somatic) who have already been treated with androgen receptor–directed therapy and a taxane-based chemotherapy. This prostate cancer indication was granted an accelerated approval in May 2020 by the U.S. Food and Drug Administration on the basis of response rates and effect on levels of prostate-specific antigen (PSA) from the TRITON2 clinical trial, the forerunner of the current study.
The TRITON2 study was a single-arm clinical trial that involved three cohorts: 62 patients with a BRCA mutation (germline and/or somatic) and measurable disease; 115 patients with a BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease; and 209 patients with homologous recombination deficiency–positive mCRPC.
In an analysis of 115 patients with a deleterious BRCA mutation (germline and/or somatic) and measurable or nonmeasurable disease, the confirmed PSA response rate was 55%. For the patients with measurable disease and a BRCA mutation, the objective response rate was 44%. The objective response rate was similar for those with a germline BRCA mutation.
Study details
The current phase 3 randomized TRITON3 clinical trial was conducted to confirm the earlier findings and to expand upon the data in mCRPC. The participants in this trial were patients with mCRPC who had specific gene alterations, including BRCA and ATM alterations, who had experienced disease progression after androgen receptor–directed therapy but who had not yet received chemotherapy.
A total of 270 men were assigned to receive rucaparib (600 mg twice daily); 135 patients received their physician’s choice of medication. Within the two study arms, 302 patients had a BRCA alteration, and 103 patients had an ATM alteration. The ITT population consisted of all the patients who had been randomly assigned to either of the two groups. A prespecified subgroup included patients with a BRCA alteration.
The primary outcome was the median duration of imaging-based PSF, as determined through independent review. Key secondary outcomes were overall survival and objective response rate.
The most common adverse events in the rucaparib group were fatigue, nausea, and anemia or decreased hemoglobin. In the control group, the most common adverse events were fatigue, diarrhea, and neuropathy. The most common events of grade 3 or higher were anemia or decreased hemoglobin, neutropenia or a decreased neutrophil count, and fatigue in the rucaparib group, and fatigue and neutropenia or a decreased neutrophil count among control patients.
No changes in standard of care
In a discussion of the study, Elena Castro, MD, PhD, of the Instituto de Investigación Biomédica de Málaga, Campanillas, Spain, emphasized that there is a clear benefit from the use of PARP inhibitors (such as rucaparib) for patients with BRCA alterations.
However, she highlighted the absence of convincing overall survival data and the absence of a clear benefit on PFS in the subgroup of patients with ATM alterations.
“These data raise several questions,” she noted, “such as, do patients with ATM alterations benefit at all? And should PARP inhibitors [such as rucaparib] precede or follow docetaxel therapy?”
Because of the high crossover rate, it may be possible to evaluate the directionality of docetaxel followed by PARP inhibitors and the other way around, she suggested.
Dr. Castro said that patients with BRCA alterations benefit from PARP inhibitors and are likely to derive more benefit from them than from taxanes.
“But those with ATM alterations are unlikely to benefit from rucaparib more than from taxanes,” she said.
In a comment, Hank Ng, MD, medical oncologist, NYU Langone Perlmutter Cancer Center, New York, said he is not convinced that the findings from TRITON 3 represent a new standard of care in BRCA 1/2 mutations or ATM.
“Currently, we know that, for patients with prostate cancer with BRCA1/2 or ATM, the standard of care is an androgen receptor pathway inhibitor (ARPI), such as abiraterone or enzalutamide, then docetaxel, and then a PARP inhibitor like rucaparib,” he said.
(Currently, rucaparib is indicated for use in patients with mCRPC with BRCA alterations after they have already received an ARPI and taxane-based chemotherapy.)
Dr. Ng also questioned the control arm of the TRITON 3 trial. All the participants in the trial had already experienced disease progression after treatment with a second-generation ARPI. But the physician’s choice of therapy allowed them to move on to another ARPI or to docetaxel.
Dr. NG commented that, “in almost all cases, after progression of one ARPI, switching to another ARPI does not provide much benefit – from what is visible from this abstract – and only 56% patients received docetaxel, and thus 44% received a not-beneficial treatment,” he said.
“I am not sure what the docetaxel subgroup showed, but potentially, if those numbers are convincing, we could move this [rucaparib] ahead of docetaxel,” he speculated.
However, he also pointed out that an overall survival benefit has not yet been shown; so far, the benefit that has been shown is with respect to imaging-based PFS.
Dr. Ng does agree that rucaparib is indicated in the second line after progression with one ARPI for patients who are not candidates for chemotherapy. “But this has not yet shown me that we should absolutely be offering rucaparib before docetaxel,” he said.
TRITON3 was supported by Clovis Oncology, manufacturer of rucaparib. Dr. Bryce has relationships with Bayer, Foundation Medicine, Janssen, Merck, Myovant Sciences, and Novartis and holds a patent for therapeutic targeting of cancer patients with NRG1 rearrangements. Dr. Castro has relationships with Astellas Pharma, AstraZeneca, Bayer, Clovis Oncology, Janssen-Cilag, Merck, MSD Oncology, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.
AT ASCO GU 2023
Transplant vs. chemo: Similar AML survival rates
Notably, all patients who relapsed after consolidation chemotherapy were able to receive allogeneic HCT, suggesting that transplantation may be safely delayed in some patients until their first relapse.
“The results of this randomized clinical trial indicate that the probability of survival after [allogeneic] HCT is not superior to that of conventional consolidation chemotherapy” among patients 60 years or younger with intermediate-risk AML, the authors concluded.
However, two experts highlighted several caveats to the study, which suggest the results may not translate to current clinical practice.
The study was published online in JAMA Oncology.
Approximately 50%-70% of patients with AML who receive intensive induction chemotherapy for AML and achieve a first complete remission are referred for post-remission therapy.
While consolidation chemotherapy with high-dose cytarabine has shown a benefit for those with a favorable risk profile, patients considered high-risk with adequate performance status may be candidates for allogeneic HCT.
However, determining the optimal post-remission treatment option for patients who fall into the intermediate-risk category can be more challenging.
To compare outcomes among intermediate-risk patients, researchers from Germany conducted a multicenter trial, enrolling 143 adults aged 60 or younger with intermediate-risk AML who had achieved first complete remission or complete remission with incomplete blood cell count recovery following conventional induction therapy.
The patients, who had a mean age of 48.2 years, were randomly assigned to consolidation treatment with allogeneic HCT (n = 76) or chemotherapy with high-dose cytarabine (n = 67), with the option for salvage HCT in the case of relapse. Overall, 12 patients in the HCT group received one consolidation course of high-dose cytarabine after achieving complete remission to bridge until allogeneic HCT, while all other patients in this group received allogeneic HCT directly after induction therapy.
Overall, disease-free survival at 2 years was significantly higher in the allogeneic HCT group (69%), compared with the consolidation therapy group (40%; P = .001). And the cumulative incidence of relapse at 2 years in the allogeneic HCT group was also lower, at 20%, compared with 58% in the consolidation therapy group (P < .001).
The overall survival data, however, painted a slightly more complex picture. In the intention-to-treat analysis, the probability of survival at 2 years was similar between the allogeneic HCT group (74%, or 56 of 76 patients), compared with consolidation chemotherapy (84%, or 56 of 67 patients; P = .22).
In addition, the rates of nonrelapse mortality at 2 years were higher in the allogeneic HCT group (9%) versus chemotherapy (2%; P = .005).
Although the rate of nonrelapse mortality was higher with allogeneic HCT, the relatively low rate with each treatment strategies was “an important and rewarding finding,” the authors noted. “This achievement is clearly due to the availability of less toxic but still effective conditioning therapies and modern antiviral and antifungal prophylaxis.”
In addition, among the 41 patients who relapsed after consolidation chemotherapy, all received allogeneic HCT, and the authors observed no significant differences between the groups in terms of health-related quality of life measures.
Results ‘may not translate to real-life clinical practice’
An important caveat is that the findings do not reflect some key updated strategies currently used in clinical practice, said Diego Adrianzen Herrera, MD, from the University of Vermont’s Larner College of Medicine, Burlington, who was not involved in the study.
“A charitable interpretation of the results is that a clear, large survival benefit of transplant in first complete remission is not apparent, which in turn can inform decision-making in certain circumstances for patients meeting the trial criteria, [including] younger patients with a readily available donor,” he told this news organization.
“However, risk stratification strategies currently used were not followed,” he said.
For instance, molecular risk stratification was not universally used, which may have led the researchers to overrepresent the number of patients considered to have favorable risk disease and “could have skewed the results in favor of the chemotherapy arm,” he explained.
In addition, minimal residual disease surveillance by flow cytometry was not used. Plus, Dr. Herrera added, in practice, not all patients can be salvaged and taken to HCT when in their second complete remission, or even achieve complete remission again.
“Unfortunately, these issues make the clinical significance of these results limited,” he concluded.
Margaret Kasner, MD, who was not associated with the research, agreed that aspects of the study design may not translate to real-life clinical practice, particularly in terms of quality-of-life outcomes.
“Although the [study] showed no difference in quality of life in the patient groups, this is likely due to the patient selection,” Dr. Kasner, of the Sidney Kimmel Cancer Center, Thomas Jefferson University, Philadelphia, said in an interview. “Most patients do not allow themselves to be randomized between these two very different strategies, so those who are willing to be randomized may be a different population in terms how their quality of life is affected by relapse.”
The authors acknowledged some of these limitations, adding that the routine use of minimal residual disease monitoring in some patients was only established once the trial was underway, and the number of patients with complete minimal residual disease was therefore limited.
In addition, Dr. Herrera explained that because HCT involves significant disruptions to daily life and extensive follow-up and monitoring, decisions to use the strategy are not taken lightly by clinicians or patients.
“This is a major issue,” he said. “HCT remains a therapeutic option which causes significant apprehension to patients.”
Nevertheless, “in my experience most patients would prefer an upfront strategy if there is a definitive need for transplant,” he added. “I think the main question patients have is whether they absolutely need an HCT and how can we better identify up front who will be in the relapse-free group at 2 years.”
The study received grant funding from the Deutsche Forschungsgemeinschaft. The authors’ disclosures are detailed in the original article. Dr. Herrera and Dr. Kasner report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Notably, all patients who relapsed after consolidation chemotherapy were able to receive allogeneic HCT, suggesting that transplantation may be safely delayed in some patients until their first relapse.
“The results of this randomized clinical trial indicate that the probability of survival after [allogeneic] HCT is not superior to that of conventional consolidation chemotherapy” among patients 60 years or younger with intermediate-risk AML, the authors concluded.
However, two experts highlighted several caveats to the study, which suggest the results may not translate to current clinical practice.
The study was published online in JAMA Oncology.
Approximately 50%-70% of patients with AML who receive intensive induction chemotherapy for AML and achieve a first complete remission are referred for post-remission therapy.
While consolidation chemotherapy with high-dose cytarabine has shown a benefit for those with a favorable risk profile, patients considered high-risk with adequate performance status may be candidates for allogeneic HCT.
However, determining the optimal post-remission treatment option for patients who fall into the intermediate-risk category can be more challenging.
To compare outcomes among intermediate-risk patients, researchers from Germany conducted a multicenter trial, enrolling 143 adults aged 60 or younger with intermediate-risk AML who had achieved first complete remission or complete remission with incomplete blood cell count recovery following conventional induction therapy.
The patients, who had a mean age of 48.2 years, were randomly assigned to consolidation treatment with allogeneic HCT (n = 76) or chemotherapy with high-dose cytarabine (n = 67), with the option for salvage HCT in the case of relapse. Overall, 12 patients in the HCT group received one consolidation course of high-dose cytarabine after achieving complete remission to bridge until allogeneic HCT, while all other patients in this group received allogeneic HCT directly after induction therapy.
Overall, disease-free survival at 2 years was significantly higher in the allogeneic HCT group (69%), compared with the consolidation therapy group (40%; P = .001). And the cumulative incidence of relapse at 2 years in the allogeneic HCT group was also lower, at 20%, compared with 58% in the consolidation therapy group (P < .001).
The overall survival data, however, painted a slightly more complex picture. In the intention-to-treat analysis, the probability of survival at 2 years was similar between the allogeneic HCT group (74%, or 56 of 76 patients), compared with consolidation chemotherapy (84%, or 56 of 67 patients; P = .22).
In addition, the rates of nonrelapse mortality at 2 years were higher in the allogeneic HCT group (9%) versus chemotherapy (2%; P = .005).
Although the rate of nonrelapse mortality was higher with allogeneic HCT, the relatively low rate with each treatment strategies was “an important and rewarding finding,” the authors noted. “This achievement is clearly due to the availability of less toxic but still effective conditioning therapies and modern antiviral and antifungal prophylaxis.”
In addition, among the 41 patients who relapsed after consolidation chemotherapy, all received allogeneic HCT, and the authors observed no significant differences between the groups in terms of health-related quality of life measures.
Results ‘may not translate to real-life clinical practice’
An important caveat is that the findings do not reflect some key updated strategies currently used in clinical practice, said Diego Adrianzen Herrera, MD, from the University of Vermont’s Larner College of Medicine, Burlington, who was not involved in the study.
“A charitable interpretation of the results is that a clear, large survival benefit of transplant in first complete remission is not apparent, which in turn can inform decision-making in certain circumstances for patients meeting the trial criteria, [including] younger patients with a readily available donor,” he told this news organization.
“However, risk stratification strategies currently used were not followed,” he said.
For instance, molecular risk stratification was not universally used, which may have led the researchers to overrepresent the number of patients considered to have favorable risk disease and “could have skewed the results in favor of the chemotherapy arm,” he explained.
In addition, minimal residual disease surveillance by flow cytometry was not used. Plus, Dr. Herrera added, in practice, not all patients can be salvaged and taken to HCT when in their second complete remission, or even achieve complete remission again.
“Unfortunately, these issues make the clinical significance of these results limited,” he concluded.
Margaret Kasner, MD, who was not associated with the research, agreed that aspects of the study design may not translate to real-life clinical practice, particularly in terms of quality-of-life outcomes.
“Although the [study] showed no difference in quality of life in the patient groups, this is likely due to the patient selection,” Dr. Kasner, of the Sidney Kimmel Cancer Center, Thomas Jefferson University, Philadelphia, said in an interview. “Most patients do not allow themselves to be randomized between these two very different strategies, so those who are willing to be randomized may be a different population in terms how their quality of life is affected by relapse.”
The authors acknowledged some of these limitations, adding that the routine use of minimal residual disease monitoring in some patients was only established once the trial was underway, and the number of patients with complete minimal residual disease was therefore limited.
In addition, Dr. Herrera explained that because HCT involves significant disruptions to daily life and extensive follow-up and monitoring, decisions to use the strategy are not taken lightly by clinicians or patients.
“This is a major issue,” he said. “HCT remains a therapeutic option which causes significant apprehension to patients.”
Nevertheless, “in my experience most patients would prefer an upfront strategy if there is a definitive need for transplant,” he added. “I think the main question patients have is whether they absolutely need an HCT and how can we better identify up front who will be in the relapse-free group at 2 years.”
The study received grant funding from the Deutsche Forschungsgemeinschaft. The authors’ disclosures are detailed in the original article. Dr. Herrera and Dr. Kasner report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Notably, all patients who relapsed after consolidation chemotherapy were able to receive allogeneic HCT, suggesting that transplantation may be safely delayed in some patients until their first relapse.
“The results of this randomized clinical trial indicate that the probability of survival after [allogeneic] HCT is not superior to that of conventional consolidation chemotherapy” among patients 60 years or younger with intermediate-risk AML, the authors concluded.
However, two experts highlighted several caveats to the study, which suggest the results may not translate to current clinical practice.
The study was published online in JAMA Oncology.
Approximately 50%-70% of patients with AML who receive intensive induction chemotherapy for AML and achieve a first complete remission are referred for post-remission therapy.
While consolidation chemotherapy with high-dose cytarabine has shown a benefit for those with a favorable risk profile, patients considered high-risk with adequate performance status may be candidates for allogeneic HCT.
However, determining the optimal post-remission treatment option for patients who fall into the intermediate-risk category can be more challenging.
To compare outcomes among intermediate-risk patients, researchers from Germany conducted a multicenter trial, enrolling 143 adults aged 60 or younger with intermediate-risk AML who had achieved first complete remission or complete remission with incomplete blood cell count recovery following conventional induction therapy.
The patients, who had a mean age of 48.2 years, were randomly assigned to consolidation treatment with allogeneic HCT (n = 76) or chemotherapy with high-dose cytarabine (n = 67), with the option for salvage HCT in the case of relapse. Overall, 12 patients in the HCT group received one consolidation course of high-dose cytarabine after achieving complete remission to bridge until allogeneic HCT, while all other patients in this group received allogeneic HCT directly after induction therapy.
Overall, disease-free survival at 2 years was significantly higher in the allogeneic HCT group (69%), compared with the consolidation therapy group (40%; P = .001). And the cumulative incidence of relapse at 2 years in the allogeneic HCT group was also lower, at 20%, compared with 58% in the consolidation therapy group (P < .001).
The overall survival data, however, painted a slightly more complex picture. In the intention-to-treat analysis, the probability of survival at 2 years was similar between the allogeneic HCT group (74%, or 56 of 76 patients), compared with consolidation chemotherapy (84%, or 56 of 67 patients; P = .22).
In addition, the rates of nonrelapse mortality at 2 years were higher in the allogeneic HCT group (9%) versus chemotherapy (2%; P = .005).
Although the rate of nonrelapse mortality was higher with allogeneic HCT, the relatively low rate with each treatment strategies was “an important and rewarding finding,” the authors noted. “This achievement is clearly due to the availability of less toxic but still effective conditioning therapies and modern antiviral and antifungal prophylaxis.”
In addition, among the 41 patients who relapsed after consolidation chemotherapy, all received allogeneic HCT, and the authors observed no significant differences between the groups in terms of health-related quality of life measures.
Results ‘may not translate to real-life clinical practice’
An important caveat is that the findings do not reflect some key updated strategies currently used in clinical practice, said Diego Adrianzen Herrera, MD, from the University of Vermont’s Larner College of Medicine, Burlington, who was not involved in the study.
“A charitable interpretation of the results is that a clear, large survival benefit of transplant in first complete remission is not apparent, which in turn can inform decision-making in certain circumstances for patients meeting the trial criteria, [including] younger patients with a readily available donor,” he told this news organization.
“However, risk stratification strategies currently used were not followed,” he said.
For instance, molecular risk stratification was not universally used, which may have led the researchers to overrepresent the number of patients considered to have favorable risk disease and “could have skewed the results in favor of the chemotherapy arm,” he explained.
In addition, minimal residual disease surveillance by flow cytometry was not used. Plus, Dr. Herrera added, in practice, not all patients can be salvaged and taken to HCT when in their second complete remission, or even achieve complete remission again.
“Unfortunately, these issues make the clinical significance of these results limited,” he concluded.
Margaret Kasner, MD, who was not associated with the research, agreed that aspects of the study design may not translate to real-life clinical practice, particularly in terms of quality-of-life outcomes.
“Although the [study] showed no difference in quality of life in the patient groups, this is likely due to the patient selection,” Dr. Kasner, of the Sidney Kimmel Cancer Center, Thomas Jefferson University, Philadelphia, said in an interview. “Most patients do not allow themselves to be randomized between these two very different strategies, so those who are willing to be randomized may be a different population in terms how their quality of life is affected by relapse.”
The authors acknowledged some of these limitations, adding that the routine use of minimal residual disease monitoring in some patients was only established once the trial was underway, and the number of patients with complete minimal residual disease was therefore limited.
In addition, Dr. Herrera explained that because HCT involves significant disruptions to daily life and extensive follow-up and monitoring, decisions to use the strategy are not taken lightly by clinicians or patients.
“This is a major issue,” he said. “HCT remains a therapeutic option which causes significant apprehension to patients.”
Nevertheless, “in my experience most patients would prefer an upfront strategy if there is a definitive need for transplant,” he added. “I think the main question patients have is whether they absolutely need an HCT and how can we better identify up front who will be in the relapse-free group at 2 years.”
The study received grant funding from the Deutsche Forschungsgemeinschaft. The authors’ disclosures are detailed in the original article. Dr. Herrera and Dr. Kasner report no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Surviving CLL: Higher risk of other cancer DXs
The report, which appeared in January in Blood Cancer Journal, found that patients diagnosed with CLL between 1989 and 2019 were 63% more likely to were diagnosed with SPM than a matched population: standardized incidence ratio = 1.63, 95% confidence interval (CI), 1.59-1.68.
“Our results provide patients and their treating physicians with an overview of the risk of SPM development. This information can be used in treatment decision-making and for planning appropriate surveillance activities and interventions,” study lead author Lina van der Straten, MD, PhD, of the Albert Schweitzer Hospital and Erasmus University Medical Center in the Netherlands, said in an interview.
Ohio State University hematologist David Bond, MD, who’s familiar with the findings, said in an interview that “it’s been well-established that patients with CLL are at increased risk for second primary malignancies. This is thought to be due to impaired immune surveillance and possibly carcinogenic effects of CLL treatments.” It’s not clear, he said, “whether the rate of second cancers differs between chemoimmunotherapy-treated patients and those receiving newer oral kinase inhibitors.”
Previous research into CLL and SPM has been sparse, Dr. van der Straten said, and most studies haven’t looked at SPM over time and taken into account the widespread use of chemoimmunotherapy and agents such as ibrutinib and venetoclax.
It’s important to study this topic, she said, since “cancers diagnosed after the CLL diagnosis can outweigh the improved longevity and contribute to excess morbidity and mortality in long-term CLL survivors.”
With the help of the Netherlands Cancer Registry, researchers tracked 24,815 patients with CLL who were diagnosed over the 20-year period; 4,369 developed SPM. “We demonstrated that the risk of SPM development was higher than in the general population with an excess of 125 malignancies per 10,000 person-years in the CLL cohort,” Dr. van der Straten said. “The risk of SPM development was found to be heightened in solid and hematological cancers. Patients with CLL had an increased risk of developing cancers at the following sites or types: skin, acute myeloid leukemia, soft-tissue sarcomas, thyroid, kidney, unknown primary localization, non-Hodgkin lymphomas, lung and bronchus, and colon and rectum.”
Specifically, the study reports that “elevated risk was observed for solid (SIR = 1.67; 95% CI, 1.65-1.75) and hematological SPMs (SIR = 1.42; 95% CI, 1.24-1.62). The highest risk for SPMs was noted beyond 5 years post diagnosis (SIR = 1.70; 95% CI, 1.62-1.77), for male individuals (SIR = 1.70; 95% CI, 1.64-1.77), and patients aged 18-69 years (SR = 1.92; 95% CI, 1.79-2.05).
“Patients with CLL exposed to treatment have a higher risk of SPM development than patients who will never receive therapy,” Dr. van der Straten said. Research has shown that “treatment with fludarabine, cyclophosphamide, and rituximab has been associated with a 2.38 increased risk for SPM development, particularly acute myeloid leukemia. Indeed, we found an increased risk for hematological malignancies in patients diagnosed between 2003-2009 and 2010-2019, which might be explained by the broader administration of fludarabine-based strategies in these calendar periods.”
Multiple factors could explain the higher risk of SPM in patients with CLL, including “a dysregulated immune system, treatment-related effects, and surveillance bias,” Dr. van der Straten said. “In addition, it is proposed that the immune dysfunctional nature of CLL might enhance the effect of common carcinogens, such as UV exposure and smoking, in increasing the probability of skin and respiratory cancers.”
She added that “the risk and the spectrum of SPMs were comparable for the 2003-2009 and 2010-2019 periods, suggesting that both the introduction of chemoimmunotherapy and, in part, targeted therapies did not dramatically alter the SPM landscape. However, due to the short follow-up period for the small cohort of patients receiving targeted therapies, further research is warranted.”
Dr. Bond said the findings “are largely in line with prior studies and strengthen their conclusions. Immune surveillance appears to be critical to reducing the risk for some but not all malignancies including lung cancer and melanoma, and the treatments given for CLL can cause immune suppression and thus may increase the risk.”
Moving forward, he said, “this research highlights the importance of second cancers to patients with CLL. It also highlights the need for secondary cancer screening for CLL patients, patient education to avoid known cancer risk factors including smoking and excess UV light exposure, and the need as a field to continue to invest in research into characteristics of second cancers and mitigation strategies.”
Study funding was not reported. The authors and Dr. Bond report no disclosures.
The report, which appeared in January in Blood Cancer Journal, found that patients diagnosed with CLL between 1989 and 2019 were 63% more likely to were diagnosed with SPM than a matched population: standardized incidence ratio = 1.63, 95% confidence interval (CI), 1.59-1.68.
“Our results provide patients and their treating physicians with an overview of the risk of SPM development. This information can be used in treatment decision-making and for planning appropriate surveillance activities and interventions,” study lead author Lina van der Straten, MD, PhD, of the Albert Schweitzer Hospital and Erasmus University Medical Center in the Netherlands, said in an interview.
Ohio State University hematologist David Bond, MD, who’s familiar with the findings, said in an interview that “it’s been well-established that patients with CLL are at increased risk for second primary malignancies. This is thought to be due to impaired immune surveillance and possibly carcinogenic effects of CLL treatments.” It’s not clear, he said, “whether the rate of second cancers differs between chemoimmunotherapy-treated patients and those receiving newer oral kinase inhibitors.”
Previous research into CLL and SPM has been sparse, Dr. van der Straten said, and most studies haven’t looked at SPM over time and taken into account the widespread use of chemoimmunotherapy and agents such as ibrutinib and venetoclax.
It’s important to study this topic, she said, since “cancers diagnosed after the CLL diagnosis can outweigh the improved longevity and contribute to excess morbidity and mortality in long-term CLL survivors.”
With the help of the Netherlands Cancer Registry, researchers tracked 24,815 patients with CLL who were diagnosed over the 20-year period; 4,369 developed SPM. “We demonstrated that the risk of SPM development was higher than in the general population with an excess of 125 malignancies per 10,000 person-years in the CLL cohort,” Dr. van der Straten said. “The risk of SPM development was found to be heightened in solid and hematological cancers. Patients with CLL had an increased risk of developing cancers at the following sites or types: skin, acute myeloid leukemia, soft-tissue sarcomas, thyroid, kidney, unknown primary localization, non-Hodgkin lymphomas, lung and bronchus, and colon and rectum.”
Specifically, the study reports that “elevated risk was observed for solid (SIR = 1.67; 95% CI, 1.65-1.75) and hematological SPMs (SIR = 1.42; 95% CI, 1.24-1.62). The highest risk for SPMs was noted beyond 5 years post diagnosis (SIR = 1.70; 95% CI, 1.62-1.77), for male individuals (SIR = 1.70; 95% CI, 1.64-1.77), and patients aged 18-69 years (SR = 1.92; 95% CI, 1.79-2.05).
“Patients with CLL exposed to treatment have a higher risk of SPM development than patients who will never receive therapy,” Dr. van der Straten said. Research has shown that “treatment with fludarabine, cyclophosphamide, and rituximab has been associated with a 2.38 increased risk for SPM development, particularly acute myeloid leukemia. Indeed, we found an increased risk for hematological malignancies in patients diagnosed between 2003-2009 and 2010-2019, which might be explained by the broader administration of fludarabine-based strategies in these calendar periods.”
Multiple factors could explain the higher risk of SPM in patients with CLL, including “a dysregulated immune system, treatment-related effects, and surveillance bias,” Dr. van der Straten said. “In addition, it is proposed that the immune dysfunctional nature of CLL might enhance the effect of common carcinogens, such as UV exposure and smoking, in increasing the probability of skin and respiratory cancers.”
She added that “the risk and the spectrum of SPMs were comparable for the 2003-2009 and 2010-2019 periods, suggesting that both the introduction of chemoimmunotherapy and, in part, targeted therapies did not dramatically alter the SPM landscape. However, due to the short follow-up period for the small cohort of patients receiving targeted therapies, further research is warranted.”
Dr. Bond said the findings “are largely in line with prior studies and strengthen their conclusions. Immune surveillance appears to be critical to reducing the risk for some but not all malignancies including lung cancer and melanoma, and the treatments given for CLL can cause immune suppression and thus may increase the risk.”
Moving forward, he said, “this research highlights the importance of second cancers to patients with CLL. It also highlights the need for secondary cancer screening for CLL patients, patient education to avoid known cancer risk factors including smoking and excess UV light exposure, and the need as a field to continue to invest in research into characteristics of second cancers and mitigation strategies.”
Study funding was not reported. The authors and Dr. Bond report no disclosures.
The report, which appeared in January in Blood Cancer Journal, found that patients diagnosed with CLL between 1989 and 2019 were 63% more likely to were diagnosed with SPM than a matched population: standardized incidence ratio = 1.63, 95% confidence interval (CI), 1.59-1.68.
“Our results provide patients and their treating physicians with an overview of the risk of SPM development. This information can be used in treatment decision-making and for planning appropriate surveillance activities and interventions,” study lead author Lina van der Straten, MD, PhD, of the Albert Schweitzer Hospital and Erasmus University Medical Center in the Netherlands, said in an interview.
Ohio State University hematologist David Bond, MD, who’s familiar with the findings, said in an interview that “it’s been well-established that patients with CLL are at increased risk for second primary malignancies. This is thought to be due to impaired immune surveillance and possibly carcinogenic effects of CLL treatments.” It’s not clear, he said, “whether the rate of second cancers differs between chemoimmunotherapy-treated patients and those receiving newer oral kinase inhibitors.”
Previous research into CLL and SPM has been sparse, Dr. van der Straten said, and most studies haven’t looked at SPM over time and taken into account the widespread use of chemoimmunotherapy and agents such as ibrutinib and venetoclax.
It’s important to study this topic, she said, since “cancers diagnosed after the CLL diagnosis can outweigh the improved longevity and contribute to excess morbidity and mortality in long-term CLL survivors.”
With the help of the Netherlands Cancer Registry, researchers tracked 24,815 patients with CLL who were diagnosed over the 20-year period; 4,369 developed SPM. “We demonstrated that the risk of SPM development was higher than in the general population with an excess of 125 malignancies per 10,000 person-years in the CLL cohort,” Dr. van der Straten said. “The risk of SPM development was found to be heightened in solid and hematological cancers. Patients with CLL had an increased risk of developing cancers at the following sites or types: skin, acute myeloid leukemia, soft-tissue sarcomas, thyroid, kidney, unknown primary localization, non-Hodgkin lymphomas, lung and bronchus, and colon and rectum.”
Specifically, the study reports that “elevated risk was observed for solid (SIR = 1.67; 95% CI, 1.65-1.75) and hematological SPMs (SIR = 1.42; 95% CI, 1.24-1.62). The highest risk for SPMs was noted beyond 5 years post diagnosis (SIR = 1.70; 95% CI, 1.62-1.77), for male individuals (SIR = 1.70; 95% CI, 1.64-1.77), and patients aged 18-69 years (SR = 1.92; 95% CI, 1.79-2.05).
“Patients with CLL exposed to treatment have a higher risk of SPM development than patients who will never receive therapy,” Dr. van der Straten said. Research has shown that “treatment with fludarabine, cyclophosphamide, and rituximab has been associated with a 2.38 increased risk for SPM development, particularly acute myeloid leukemia. Indeed, we found an increased risk for hematological malignancies in patients diagnosed between 2003-2009 and 2010-2019, which might be explained by the broader administration of fludarabine-based strategies in these calendar periods.”
Multiple factors could explain the higher risk of SPM in patients with CLL, including “a dysregulated immune system, treatment-related effects, and surveillance bias,” Dr. van der Straten said. “In addition, it is proposed that the immune dysfunctional nature of CLL might enhance the effect of common carcinogens, such as UV exposure and smoking, in increasing the probability of skin and respiratory cancers.”
She added that “the risk and the spectrum of SPMs were comparable for the 2003-2009 and 2010-2019 periods, suggesting that both the introduction of chemoimmunotherapy and, in part, targeted therapies did not dramatically alter the SPM landscape. However, due to the short follow-up period for the small cohort of patients receiving targeted therapies, further research is warranted.”
Dr. Bond said the findings “are largely in line with prior studies and strengthen their conclusions. Immune surveillance appears to be critical to reducing the risk for some but not all malignancies including lung cancer and melanoma, and the treatments given for CLL can cause immune suppression and thus may increase the risk.”
Moving forward, he said, “this research highlights the importance of second cancers to patients with CLL. It also highlights the need for secondary cancer screening for CLL patients, patient education to avoid known cancer risk factors including smoking and excess UV light exposure, and the need as a field to continue to invest in research into characteristics of second cancers and mitigation strategies.”
Study funding was not reported. The authors and Dr. Bond report no disclosures.
FROM BLOOD CANCER JOURNAL