User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Children and COVID: Weekly cases rise again, but more slowly
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.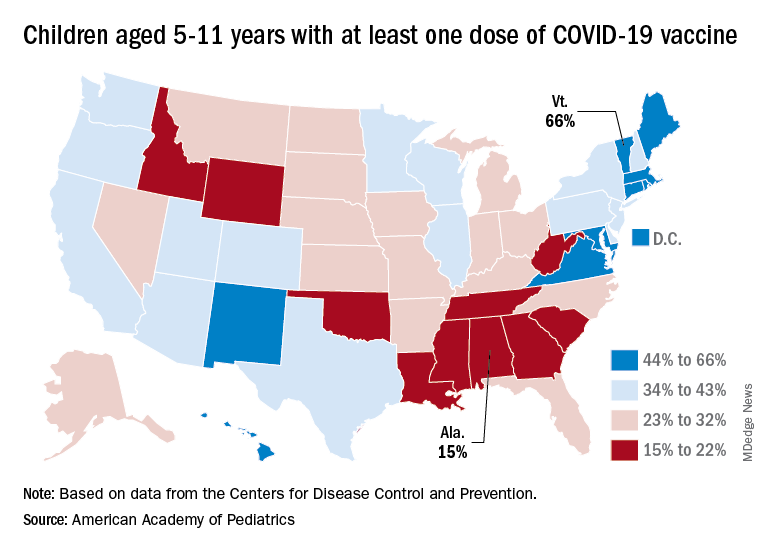
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
One in four feel fully recovered following COVID-19 hospitalization
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
FROM THE LANCET RESPIRATORY MEDICINE
2020 presidential election tied to spike in cardiac events
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Firearm counseling in the ED could be lifesaving for teens
Caregivers who brought suicidal adolescents to the emergency department reported safer gun storage practices after firearm counseling – a crucial way to cut gun deaths among children, according to researchers from Cincinnati Children’s Hospital.
In the study, which took place between June 2021 and Feb 2022, gun safety counseling and handouts were provided to 99 families of children who had come to the ED with mental health problems. A separate set of 101 families in similar situations received counseling and handouts, along with two cable-style gun locks.
Four weeks later, parents in both groups reported an increase in safe storage practices in which they locked away all guns in the household. Those offered only counseling increased safe storage by 7.2% – from 89.9% to 97.1%.
The gains were greater for families that received locks in addition to counseling. The number of those who locked away all guns rose from 82.2% to 98.5% – a 16.3% increase. (Roughly one-third of families in both arms of the study were lost to follow-up, according to the researchers, which left 68 families in each group for analysis.)
Several caregivers in each group reported that guns had been removed entirely from the home, and more than 60% in each group said they had bought additional gun locks to secure their weapons.
“The main point of our study is that just-in-time counseling is very effective in helping these families of children with mental health concerns in securing all their guns, and an emergency department visit is a great time to do that,” said Bijan Ketabchi, MD, a clinical fellow in the division of emergency medicine at Cincinnati Children’s Hospital Medical Center, who presented the findings at the Pediatric Academic Societies annual meeting.
Dr. Ketabchi said his department sees 500-700 children each month with mental health concerns, most commonly depression. The mean age of adolescent patients in the study was 14 years.
Suicide is the second-leading cause of death among children in the United States. Both pediatric suicides and firearm suicides have increased in the past 2 decades, Dr. Ketabchi said. The number of youth suicides who use guns has risen 90% since 2008. One in three U.S. families own a firearm, and 4.6 million children live in a home with loaded, unlocked guns.
Among children aged 17 years and younger who die by firearm suicide, 82% used guns belonging to a family member.
The right time for the message
Interventions to encourage safe gun storage – at a time when caregivers are really listening – can be lifesaving, Dr. Ketabchi said.
“We know that counseling is really helpful for these families, because when they come to the emergency department with a concern, they can have a teachable moment,” he said in an interview. “It resonates with them a lot more than it normally would because they have experienced something traumatic.”
The importance of safe gun storage in households with adolescents can’t be overstated, even if the children are not at risk of suicide, said Naoka Carey, a doctoral candidate at Boston College.
Ms. Carey authored an article on the prevalence of handguns among adolescents that will be published in May in Pediatrics.
“Three kinds of harm for adolescents with access to guns are accidental injury, homicide, and suicide,” she said. “Families who own guns don’t always know their teens have access to the guns.”
The problem is getting worse. Ms. Carey and colleagues found that, between 2002 and 2019, the rate of children aged 12-17 who reported carrying handguns increased 41%. Most of them were White, and their families were in high-income brackets. New data show that firearm injuries have become the leading cause of death among youth in the United States, eclipsing auto accidents for the first time.
“Preventing tragedy in your family is more than reason enough to secure guns you have,” she said.
Dr. Ketabchi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Caregivers who brought suicidal adolescents to the emergency department reported safer gun storage practices after firearm counseling – a crucial way to cut gun deaths among children, according to researchers from Cincinnati Children’s Hospital.
In the study, which took place between June 2021 and Feb 2022, gun safety counseling and handouts were provided to 99 families of children who had come to the ED with mental health problems. A separate set of 101 families in similar situations received counseling and handouts, along with two cable-style gun locks.
Four weeks later, parents in both groups reported an increase in safe storage practices in which they locked away all guns in the household. Those offered only counseling increased safe storage by 7.2% – from 89.9% to 97.1%.
The gains were greater for families that received locks in addition to counseling. The number of those who locked away all guns rose from 82.2% to 98.5% – a 16.3% increase. (Roughly one-third of families in both arms of the study were lost to follow-up, according to the researchers, which left 68 families in each group for analysis.)
Several caregivers in each group reported that guns had been removed entirely from the home, and more than 60% in each group said they had bought additional gun locks to secure their weapons.
“The main point of our study is that just-in-time counseling is very effective in helping these families of children with mental health concerns in securing all their guns, and an emergency department visit is a great time to do that,” said Bijan Ketabchi, MD, a clinical fellow in the division of emergency medicine at Cincinnati Children’s Hospital Medical Center, who presented the findings at the Pediatric Academic Societies annual meeting.
Dr. Ketabchi said his department sees 500-700 children each month with mental health concerns, most commonly depression. The mean age of adolescent patients in the study was 14 years.
Suicide is the second-leading cause of death among children in the United States. Both pediatric suicides and firearm suicides have increased in the past 2 decades, Dr. Ketabchi said. The number of youth suicides who use guns has risen 90% since 2008. One in three U.S. families own a firearm, and 4.6 million children live in a home with loaded, unlocked guns.
Among children aged 17 years and younger who die by firearm suicide, 82% used guns belonging to a family member.
The right time for the message
Interventions to encourage safe gun storage – at a time when caregivers are really listening – can be lifesaving, Dr. Ketabchi said.
“We know that counseling is really helpful for these families, because when they come to the emergency department with a concern, they can have a teachable moment,” he said in an interview. “It resonates with them a lot more than it normally would because they have experienced something traumatic.”
The importance of safe gun storage in households with adolescents can’t be overstated, even if the children are not at risk of suicide, said Naoka Carey, a doctoral candidate at Boston College.
Ms. Carey authored an article on the prevalence of handguns among adolescents that will be published in May in Pediatrics.
“Three kinds of harm for adolescents with access to guns are accidental injury, homicide, and suicide,” she said. “Families who own guns don’t always know their teens have access to the guns.”
The problem is getting worse. Ms. Carey and colleagues found that, between 2002 and 2019, the rate of children aged 12-17 who reported carrying handguns increased 41%. Most of them were White, and their families were in high-income brackets. New data show that firearm injuries have become the leading cause of death among youth in the United States, eclipsing auto accidents for the first time.
“Preventing tragedy in your family is more than reason enough to secure guns you have,” she said.
Dr. Ketabchi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Caregivers who brought suicidal adolescents to the emergency department reported safer gun storage practices after firearm counseling – a crucial way to cut gun deaths among children, according to researchers from Cincinnati Children’s Hospital.
In the study, which took place between June 2021 and Feb 2022, gun safety counseling and handouts were provided to 99 families of children who had come to the ED with mental health problems. A separate set of 101 families in similar situations received counseling and handouts, along with two cable-style gun locks.
Four weeks later, parents in both groups reported an increase in safe storage practices in which they locked away all guns in the household. Those offered only counseling increased safe storage by 7.2% – from 89.9% to 97.1%.
The gains were greater for families that received locks in addition to counseling. The number of those who locked away all guns rose from 82.2% to 98.5% – a 16.3% increase. (Roughly one-third of families in both arms of the study were lost to follow-up, according to the researchers, which left 68 families in each group for analysis.)
Several caregivers in each group reported that guns had been removed entirely from the home, and more than 60% in each group said they had bought additional gun locks to secure their weapons.
“The main point of our study is that just-in-time counseling is very effective in helping these families of children with mental health concerns in securing all their guns, and an emergency department visit is a great time to do that,” said Bijan Ketabchi, MD, a clinical fellow in the division of emergency medicine at Cincinnati Children’s Hospital Medical Center, who presented the findings at the Pediatric Academic Societies annual meeting.
Dr. Ketabchi said his department sees 500-700 children each month with mental health concerns, most commonly depression. The mean age of adolescent patients in the study was 14 years.
Suicide is the second-leading cause of death among children in the United States. Both pediatric suicides and firearm suicides have increased in the past 2 decades, Dr. Ketabchi said. The number of youth suicides who use guns has risen 90% since 2008. One in three U.S. families own a firearm, and 4.6 million children live in a home with loaded, unlocked guns.
Among children aged 17 years and younger who die by firearm suicide, 82% used guns belonging to a family member.
The right time for the message
Interventions to encourage safe gun storage – at a time when caregivers are really listening – can be lifesaving, Dr. Ketabchi said.
“We know that counseling is really helpful for these families, because when they come to the emergency department with a concern, they can have a teachable moment,” he said in an interview. “It resonates with them a lot more than it normally would because they have experienced something traumatic.”
The importance of safe gun storage in households with adolescents can’t be overstated, even if the children are not at risk of suicide, said Naoka Carey, a doctoral candidate at Boston College.
Ms. Carey authored an article on the prevalence of handguns among adolescents that will be published in May in Pediatrics.
“Three kinds of harm for adolescents with access to guns are accidental injury, homicide, and suicide,” she said. “Families who own guns don’t always know their teens have access to the guns.”
The problem is getting worse. Ms. Carey and colleagues found that, between 2002 and 2019, the rate of children aged 12-17 who reported carrying handguns increased 41%. Most of them were White, and their families were in high-income brackets. New data show that firearm injuries have become the leading cause of death among youth in the United States, eclipsing auto accidents for the first time.
“Preventing tragedy in your family is more than reason enough to secure guns you have,” she said.
Dr. Ketabchi disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PAS 2022
COVID-19 again the third-leading cause of U.S. deaths
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
FROM THE MMWR
Experts decry CDC’s long pause on neglected tropical disease testing
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has long been the premier reference lab for the United States and, for some diseases, internationally.
In September 2021, the CDC stated on its website that it would stop testing for parasites, herpesvirus encephalitis, human herpesvirus 6 and 7, Epstein-Barr virus, and other viruses, saying, “We are working diligently to implement laboratory system improvements.”
At the time, the CDC said testing would be halted only for a few months.
In response to a query from this news organization, a CDC spokesperson replied, “While at present we are unable to share a detailed timeline, our highest priority is to resume high-quality testing operations in a phased, prioritized approach as soon as possible and to offer the same tests that were available before the pause.”
Several global health clinicians told this news organization that they were not aware of the halt and that they are now uncertain about the specific diagnosis and best treatment for some patients. Other patients have been lost to follow-up.
In response, a group of tropical disease specialists who focus on neglected tropical diseases (NTDs) wrote an editorial, “Neglected Testing for Neglected Tropical Diseases at the CDC,” which recently appeared in the American Journal of Tropical Medicine and Hygiene (AJTMH).
NTDs are caused by viruses, bacteria, and parasites. They include leprosy and worms; many such diseases are disfiguring, such as filariasis (which causes the hugely swollen extremities of elephantiasis) and onchocerciasis (river blindness). They also include some viral and bacterial diseases. Their common denominator is that they are diseases of poverty, primarily in Africa, Asia, and Latin America, so they garner little attention from “first world” countries.
The loss of testing for two devastating parasites – Chagas and Leishmania – was particularly significant. Few other labs in the United States test for these, and the tests can be expensive and of variable quality, experts said.
Norman Beatty, MD, a global health physician at the University of Florida, told this news organization, “Chagas confirmatory testing is only available at the CDC and is the most reliable testing we have access to in the United States. Leishmania species identification is also only available at the CDC and is important in determining which antiparasitic medications we will use.”
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs, also known as kissing bugs. Chagas is a major cause of an enlarged heart and congestive heart failure, as well as a dramatically enlarged esophagus or colon.
Prior to the cuts and before COVID-19, the CDC reported that they ran 10,000 to 15,000 tests for parasitic diseases annually. Testing requests declined during COVID. In 2021, they ran 1,003 tests for Chagas.
Dr. Beatty said that he first became aware of the CDC’s testing cuts last fall when he sought care for a patient. He was first told the delay would be 2-3 weeks, then another 2-3 weeks. It’s now been 7 months, and only three tests have been resumed.
Dr. Beatty added that for Chagas disease in particular, there is urgency in testing because cardiac complications can be life-threatening. He said that “a lot of these diseases can be considered rare, but they also have a tremendous ability to cause morbidity and mortality.”
Leishmania infections are also serious. Following the bite of an infected sandfly, they can cause disfiguring skin infections, but, more importantly, they can affect the liver, spleen, and bone marrow. Dr. Beatty said that since testing was dropped at the CDC, some colleagues had to send specimens outside of the country.
Dr. Beatty emphasized that the cuts in testing at the CDC highlight disparities in our society. “There are other commercial reference laboratories who may have some of these tests available, but the vast majority of people who suffer from diseases are underserved and vulnerable. [My patients] most definitely will not have access to advanced testing commercial laboratories,” Dr. Beatty said. Those laboratories include Associated Regional University Pathologists laboratories, Quest Diagnostics, and LabCorp Diagnostics. But for some parasitic infections, there will simply be no testing, and patients will not receive appropriate therapy.
The CDC’s website says, “USAID and CDC work together on a shared agenda to advance global progress towards the control and elimination of NTDs that can be addressed with preventive chemotherapy. ... CDC has strong working relationships with WHO, regional reference laboratories/bodies, [and] national NTD programs ... working with these partners through the provision of unique laboratory, diagnostic, and epidemiological technical assistance.”
The WHO Roadmap for 2030 aims to prevent and control many NTDs, in part by “providing new interventions and effective, standardized, and affordable diagnostics.” Last year, the CDC said that they “will continue working with WHO and other global partners to meet the established goals.”
But testing for a number of NTDs is not currently available at the CDC. In response to questions from this news organization, a CDC spokesperson said the agency “supports the development of country capacity for NTD testing required ... but does not perform testing related to the WHO Roadmap.”
A group of CDC officials wrote an editorial response that was published in AJTMH, saying the agency has “three main priorities: reducing parasitic disease-related death, illness, and disability in the United States; reducing the global burden of malaria; and eliminating targeted neglected tropical diseases.”
In response to this news organization’s interview request, a CDC spokesperson wrote, “CDC is unwavering in our commitment to provide the highest quality laboratory diagnostic services for parasitic diseases. We understand the concerns expressed in the editorial and the challenges the pause in testing for parasitic diseases presents for health care providers, particularly those treating people at elevated risk for parasitic diseases.”
Michael Reich, PhD, Dr. Beatty’s co-author, is an international health policy expert at Harvard. He and the physicians had approached CDC about the elimination of services. He said in an interview, “We’re still unable to get clear responses except for something along the lines of, ‘We are working on it. It is complicated. It takes time. We’re doing our best.’”
Dr. Reich added, “For me, this raises troubling issues both of transparency and accountability – transparency about what is going on and what the problems are, and accountability in terms of who’s being held responsible for the closures and the impacts on both public health and patient treatment.”
Dr. Beatty concluded, “I think the goal of our group was to bring more awareness to the importance of having a national laboratory that can service all people, even the most underserved and vulnerable populations.” He added, “Chagas disease is a disease of inequity in Latin Americans. Without having access to an appropriate laboratory such as the CDC, we would be taking a backwards approach to tackle neglected tropical diseases in our country and worldwide.”
Dr. Beatty and Dr. Reich report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Three in four U.S. doctors are employed by hospitals, corporate entities: Report
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Myocarditis higher with Moderna COVID vax in young men
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.

They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.
They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.
They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY

Gun violence now leading cause of death for U.S. children
In 2020, 4,357 children aged 1-19, or approximately 6 in 100,000, died from a gun-related injury, the researchers reported, modestly exceeding the number for auto accidents (3,913) and greatly exceeding deaths caused by suffocation (1,411) or drowning (966).
To observers of gun violence in this country, the grim statistical marker has been all but inevitable. Gunshots were the second-leading cause of death in 2016 among children aged 1-19, the researchers reported. But sharp rises in such fatalities since then, especially in 2020 as the COVID-19 pandemic began, pushed the death toll above all other causes among Americans in this age group.
Guns accounted for more than 45,000 deaths among all age groups in 2020, also a record, according to the U.S. Centers for Disease Control and Prevention.
Although gun deaths rose across nearly every racial and ethnic group, the increase was greatest among Black children. In this group, firearms accounted for more than 15 deaths per 100,000 children in 2020 – up from about 12 such deaths in 2019.
Homicide was the leading cause of gun deaths, followed by suicide and then accidental shootings, although the reason for some deaths could not be determined, according to the researchers.
The researchers reported their findings in the New England Journal of Medicine.
Gun deaths among children are preventable, both researchers and advocates said.
“There are ways to reduce injuries without banning guns,” said Jason Goldstick, PhD, a statistician at the University of Michigan, Ann Arbor, who led the study.
Dr. Goldstick pointed to significant investments in car vehicle safety as a model for policy makers to follow today for making gun injuries less frequent and deadly.
“More people drive today than in the 1970s, and motor vehicle–related injury rates are much lower,” Dr. Goldstick said. Innovations like seatbelt laws and changes in how cars are built have made them less deadly during a crash. Similar innovations are possible in how guns are managed.
More than 4.6 million U.S. children live in homes with unsecured firearms, according to Shannon Watts of the advocacy organization Moms Demand Action. “Securely storing firearms unloaded, locked and separate from ammunition is a simple yet lifesaving action that all gun owners should follow – and lawmakers should require,” she said in a statement to this news organization.
“The effects of gun violence ripple far beyond the child who was struck by a bullet,” said Sarah Burd-Sharps, the senior director of research for the advocacy organization Everytown for Gun Safety. Children might grieve their friends who are now lost or worry that they will be next.
The data in this study aren’t surprising, Ms. Burd-Sharps said, given the large number of homes in which guns are unsecured and the sharp rise in gun sales during the pandemic. On average one child per day in the United States accesses an unsecured gun that ends up injuring or killing themself or someone else.
“Gun owners want to be responsible. These deaths are really preventable,” Ms. Burd-Sharps said. In addition to securing ammunition and firearms separately, she recommended wider use of biometric guns that can only be used by someone with a specific fingerprint. If a young person got ahold of such a gun, even if it was loaded, they couldn’t use it.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
In 2020, 4,357 children aged 1-19, or approximately 6 in 100,000, died from a gun-related injury, the researchers reported, modestly exceeding the number for auto accidents (3,913) and greatly exceeding deaths caused by suffocation (1,411) or drowning (966).
To observers of gun violence in this country, the grim statistical marker has been all but inevitable. Gunshots were the second-leading cause of death in 2016 among children aged 1-19, the researchers reported. But sharp rises in such fatalities since then, especially in 2020 as the COVID-19 pandemic began, pushed the death toll above all other causes among Americans in this age group.
Guns accounted for more than 45,000 deaths among all age groups in 2020, also a record, according to the U.S. Centers for Disease Control and Prevention.
Although gun deaths rose across nearly every racial and ethnic group, the increase was greatest among Black children. In this group, firearms accounted for more than 15 deaths per 100,000 children in 2020 – up from about 12 such deaths in 2019.
Homicide was the leading cause of gun deaths, followed by suicide and then accidental shootings, although the reason for some deaths could not be determined, according to the researchers.
The researchers reported their findings in the New England Journal of Medicine.
Gun deaths among children are preventable, both researchers and advocates said.
“There are ways to reduce injuries without banning guns,” said Jason Goldstick, PhD, a statistician at the University of Michigan, Ann Arbor, who led the study.
Dr. Goldstick pointed to significant investments in car vehicle safety as a model for policy makers to follow today for making gun injuries less frequent and deadly.
“More people drive today than in the 1970s, and motor vehicle–related injury rates are much lower,” Dr. Goldstick said. Innovations like seatbelt laws and changes in how cars are built have made them less deadly during a crash. Similar innovations are possible in how guns are managed.
More than 4.6 million U.S. children live in homes with unsecured firearms, according to Shannon Watts of the advocacy organization Moms Demand Action. “Securely storing firearms unloaded, locked and separate from ammunition is a simple yet lifesaving action that all gun owners should follow – and lawmakers should require,” she said in a statement to this news organization.
“The effects of gun violence ripple far beyond the child who was struck by a bullet,” said Sarah Burd-Sharps, the senior director of research for the advocacy organization Everytown for Gun Safety. Children might grieve their friends who are now lost or worry that they will be next.
The data in this study aren’t surprising, Ms. Burd-Sharps said, given the large number of homes in which guns are unsecured and the sharp rise in gun sales during the pandemic. On average one child per day in the United States accesses an unsecured gun that ends up injuring or killing themself or someone else.
“Gun owners want to be responsible. These deaths are really preventable,” Ms. Burd-Sharps said. In addition to securing ammunition and firearms separately, she recommended wider use of biometric guns that can only be used by someone with a specific fingerprint. If a young person got ahold of such a gun, even if it was loaded, they couldn’t use it.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
In 2020, 4,357 children aged 1-19, or approximately 6 in 100,000, died from a gun-related injury, the researchers reported, modestly exceeding the number for auto accidents (3,913) and greatly exceeding deaths caused by suffocation (1,411) or drowning (966).
To observers of gun violence in this country, the grim statistical marker has been all but inevitable. Gunshots were the second-leading cause of death in 2016 among children aged 1-19, the researchers reported. But sharp rises in such fatalities since then, especially in 2020 as the COVID-19 pandemic began, pushed the death toll above all other causes among Americans in this age group.
Guns accounted for more than 45,000 deaths among all age groups in 2020, also a record, according to the U.S. Centers for Disease Control and Prevention.
Although gun deaths rose across nearly every racial and ethnic group, the increase was greatest among Black children. In this group, firearms accounted for more than 15 deaths per 100,000 children in 2020 – up from about 12 such deaths in 2019.
Homicide was the leading cause of gun deaths, followed by suicide and then accidental shootings, although the reason for some deaths could not be determined, according to the researchers.
The researchers reported their findings in the New England Journal of Medicine.
Gun deaths among children are preventable, both researchers and advocates said.
“There are ways to reduce injuries without banning guns,” said Jason Goldstick, PhD, a statistician at the University of Michigan, Ann Arbor, who led the study.
Dr. Goldstick pointed to significant investments in car vehicle safety as a model for policy makers to follow today for making gun injuries less frequent and deadly.
“More people drive today than in the 1970s, and motor vehicle–related injury rates are much lower,” Dr. Goldstick said. Innovations like seatbelt laws and changes in how cars are built have made them less deadly during a crash. Similar innovations are possible in how guns are managed.
More than 4.6 million U.S. children live in homes with unsecured firearms, according to Shannon Watts of the advocacy organization Moms Demand Action. “Securely storing firearms unloaded, locked and separate from ammunition is a simple yet lifesaving action that all gun owners should follow – and lawmakers should require,” she said in a statement to this news organization.
“The effects of gun violence ripple far beyond the child who was struck by a bullet,” said Sarah Burd-Sharps, the senior director of research for the advocacy organization Everytown for Gun Safety. Children might grieve their friends who are now lost or worry that they will be next.
The data in this study aren’t surprising, Ms. Burd-Sharps said, given the large number of homes in which guns are unsecured and the sharp rise in gun sales during the pandemic. On average one child per day in the United States accesses an unsecured gun that ends up injuring or killing themself or someone else.
“Gun owners want to be responsible. These deaths are really preventable,” Ms. Burd-Sharps said. In addition to securing ammunition and firearms separately, she recommended wider use of biometric guns that can only be used by someone with a specific fingerprint. If a young person got ahold of such a gun, even if it was loaded, they couldn’t use it.
The researchers reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Doc accused of killing 14 patients found not guilty
In an unprecedented murder case about end-of-life care, a physician accused of killing 14 critically ill patients with opioid overdoses in a Columbus, Ohio, hospital ICU over a period of 4 years was found not guilty by a jury April 20.
The jury, after a 7-week trial featuring more than 50 witnesses in the Franklin County Court of Common Pleas, declared William Husel, DO, not guilty on 14 counts of murder and attempted murder.
In a news conference after the verdict was announced, lead defense attorney Jose Baez said Dr. Husel, whom he called a “great doctor,” hopes to practice medicine again in the future. “They don’t need to be looking over their shoulders worrying about whether they’ll get charged with crimes,” he said.
The prosecutors in the case declined to comment, other than to say they “accept” the verdict.
Legal experts said it’s highly unlikely that Ohio or any other state would restore Dr. Husel’s suspended medical license. “I doubt he could ever work in medicine again,” said Mark Schumacher, a Columbus medical malpractice defense attorney who retired in 2020 after practicing for 39 years. Mr. Schumacher followed the trial closely.
The trial raised the specific issue of what constitutes a medically justifiable dose of opioid painkillers during the end-of-life procedure known as palliative extubation, in which critically ill patients are withdrawn from the ventilator when they are expected to die. Under medicine’s so-called double-effect principle, physicians must weigh the benefits and risks of ordering potentially lethal doses of painkillers and sedatives to provide comfort care for critically ill patients.
To many observers, however, the case really centered on the largely hidden debate over whether it’s acceptable to hasten the deaths of dying patients who haven’t chosen that path. That’s called euthanasia, which is illegal in the United States. In contrast, 10 states plus the District of Columbia allow physicians to prescribe lethal drugs to terminally ill, mentally competent adults who can self-administer them. That’s called medical aid in dying, or physician-assisted dying or suicide.
“Maybe this is a wake-up call that people believe this is the right thing to do,” said Lewis Nelson, MD, chair of emergency medicine at New Jersey Medical School in Newark. “The medical community has a sense that we often prolong life unnecessarily. But a physician cannot unilaterally decide it’s time for someone to die. It sounds like [Dr. Husel] took that decision into his own hands.”
The case also exposed major gaps in the patient safety culture at Mount Carmel West Hospital in Columbus, which is owned by the Catholic chain Trinity Health. Experts say failures by hospital staff to question physicians’ orders and raise patient safety concerns, as happened at Mount Carmel, occur at many hospitals around the country. Experts say the Husel case offers vital lessons for health care professionals about improving safety procedures.
“This is an extreme example, that everyone should learn from, about what not to do,” said Michael Cohen, RPh, founder and president emeritus of the Institute for Safe Medication Practices. “Husel was giving massive overdoses of drugs, people knew it was problematic, and someone didn’t put their foot down. You’ve got to have a process in place to address these situations where there is disagreement over the safety of a medication order.”
Dr. Husel was charged with killing the 14 patients from 2015 through 2018 by ordering single large doses of the painkiller fentanyl – from 500 to 2,000 micrograms – often in combination with other opioids and sedatives, while working as the solo physician on the overnight shift in the ICU at Mount Carmel West Hospital and at Mount Carmel St. Ann’s Hospital in Westerville, Ohio.
Dr. Husel ordered administration of the drugs while his patients were having an endotracheal tube removed as part of palliative extubation. There was conflicting testimony during the trial about whether the patients were showing signs of pain or were even capable of feeling pain.
Prosecutors argued that Dr. Husel, who did a residency and fellowship in critical care medicine at Cleveland Clinic and started working at Mount Carmel in 2013 in his first job as a full-fledged physician, intended to kill the patients or hasten their deaths. They contended that the inexperienced nurses in the ICU went along with his large drug doses because they were “in thrall” to him because of his prestigious background at the Cleveland Clinic and his willingness to take the time to teach them.
“With his training in anesthesiology, he knew what those drugs do,” assistant prosecutor David Zeyen said in closing arguments. “This isn’t negligence. This is on purpose ... Euthanizing animals with the intent to kill is fine in veterinary medicine. It’s not fine in the ICU at Mount Carmel or anywhere.”
The defense team argued that Dr. Husel was a caring and compassionate physician who ordered the drugs to relieve the patients’ pain and discomfort during the extubation process. He did not testify.
“Common sense says Dr Husel had no motive to harm patients,” defense attorney Baez said in his closing. “He dedicated his life to taking care of patients and saving lives, not taking them. ... Why would this man risk his family, career, and 17 years of trying to be a doctor to hasten someone’s death or kill them?”
There were 35 Mount Carmel patients who died in the ICU under Dr. Husel’s care after receiving large fentanyl doses during palliative extubation. The state originally charged him with murder in 25 of those cases, then reduced that to 14.
Many of Dr. Husel’s drug orders were given verbally instead of through the regular process of being entered into the electronic health record. He and the nurses on duty also skipped the standard nonemergency process of getting approval from the pharmacist on duty, instead using the override function on Mount Carmel’s automated Pyxis drug dispensing system.
Dr. Husel’s unusual dosing patterns were first reported to Mount Carmel officials by pharmacists in October 2018, spurring an investigation. The hospital system let him go in December 2018, after concluding that the opioid dosages he used were “significantly excessive and potentially fatal” and “went beyond providing comfort.”
Nearly two dozen RNs and two pharmacists involved in these cases have faced state disciplinary action, mostly license suspension. Federal and state agencies have cited the Mount Carmel system for faults in its patient safety processes and culture that were exposed by the Husel cases.
The Mount Carmel CEO; the chief clinical officer; other physician, nursing, and pharmacy leaders; and dozens of nurses and pharmacists were forced out following the Husel investigation.
In 2019, the Centers for Medicare & Medicaid Services, after threatening to cut off federal reimbursements to Mount Carmel, accepted the hospital system’s correction plan restricting the use of verbal drug orders and prohibiting Pyxis system overrides for opioids except in life-threatening emergencies. The Ohio Board of Pharmacy hit Mount Carmel with $477,000 in fines and costs for pharmacy rules violations.
Mount Carmel and Trinity have settled a number of civil wrongful death lawsuits filed by the families of Dr. Husel’s patients for nearly $20 million, with many more suits pending. Gerry Leeseberg, a Columbus medical malpractice plaintiff attorney who is representing 17 of the families, said a number of the cases are set for trial starting in June.
During the trial, family members of many of the 14 patients whom Dr. Husel allegedly murdered testified that Dr. Husel told them their loved ones were dying. Some said they felt rushed into making a decision to extubate the person.
Before performing a palliative extubation, physicians commonly administer opioids and/or sedatives to ease pain and discomfort, and spare family members from witnessing their loved ones gasping for breath. But most medical experts – including the state’s two physician expert witnesses – say the fentanyl doses Dr. Husel ordered were 5-20 times larger than doses normally used in palliative extubation. Such doses, they say, will quickly kill most patients – except those with high opioid tolerance – by stopping their breathing.
Physicians say they typically give much smaller doses of fentanyl or morphine, then administer more as needed if they observe the patient experiencing pain or distress. Mount Carmel’s 2016 guidelines for IV administration of fentanyl specified a dosage range of 50-100 micrograms for relieving pain, and its 2018 guidelines reduced that to 25-50 micrograms.
The doses Dr. Husel ordered are lethal, even for most patients with some tolerance to opioids, said Rutgers EM chair Dr. Nelson, who practices medical toxicology and addiction medicine. “Those are doses to provide euthanasia, not to relieve pain.”
At trial, the prosecutors had to overcome two big challenges to win murder convictions against Dr. Husel: They had to prove beyond a reasonable doubt that the drugs Dr. Husel ordered are what directly caused these critically ill patients to die, and that he intended to kill them.
Late in the trial, at the state’s request, the judge ruled to allow the jury to also consider attempted murder charges, which require proof of intent but not that the defendant’s actions directly caused the deaths.
Another challenge was that physicians have certain legal protections for administering drugs to patients for the purpose of relieving pain and suffering, even if the drugs hasten the patients’ deaths – as long the intent was not to cause death and the drugs were properly used. This is known as the double-effect principle. In contrast, intentional killing to relieve pain and suffering is called euthanasia. That’s what prosecutors accused Dr. Husel of doing.
“If you hasten a person’s death, even if their death is as sure as the sun is going to rise in the morning ... you have caused their death in the eyes of the law,” assistant prosecutor Mr. Zeyen said in his closing. “You don’t get a pass for killing a dying man ...”
Mr. Leeseberg said it was always going to be extremely hard to convince a jury to convict a physician of murder, with the potential of life in prison, in a case where the physician’s acts occurred openly over 4 years in a hospital setting where no one did anything to stop him. It would have been much easier to convince a jury to convict him of reckless homicide, a lesser offense with a shorter prison term. That would have required proving that he acted in reckless disregard for his patients’ health and safety.
In post-verdict comments to the news media, Judge Michael Holbrook said jurors told him that the procedures for the dispensing of fentanyl and other drugs at Mount Carmel weren’t properly explained to them during the trial, and that they were confused by the large number of prosecution witnesses. He also said they were confused that no one had stated a maximum dosage for fentanyl.
Mr. Schumacher, the retired malpractice defense lawyer who followed the trial, disagreed with defense attorney Baez’s takeaway about the impact of the case on pain-relief practices. In his view, the case likely will heighten rather than reduce the anxiety of physicians and nurses about administering opioids, even when the dosages are clearly needed and appropriate. He doesn’t think Dr. Husel’s dosages can be justified, however.
“Physicians have a naive overreaction to any legal development, and overgeneralize from a particular case to everyday practice,” he said.
There is only one known prior case that’s somewhat comparable of a physician tried for murder or attempted murder for giving a critically ill patient opioids for pain relief. In 1996, a Kansas jury convicted Lloyd Stanley Naramore, DO, of attempted murder in the death of a patient to whom he gave an opioid, and of second-degree murder for removing a patient from a ventilator. After Dr. Naramore served 6 months in prison, an appellate court reversed the convictions for lack of evidence.
In March, RaDonda Vaught, a nurse who worked at Vanderbilt University Medical Center in Nashville, Tenn., was convicted of criminal neglect and negligent homicide for mistakenly administering a fatal dose of the paralyzing drug vecuronium, instead of the prescribed drug Versed (midazolam), to a patient. Providers around the country were alarmed by her criminal prosecution for what was clearly an unintentional error.
But legal and medical experts said Dr. Husel’s case was sharply different from Vaught’s and Dr. Naramore’s because he deliberately and repeatedly ordered large doses of fentanyl and other drugs that he knew or should have known were potentially lethal. “You don’t need 2,000 micrograms of fentanyl plus other drugs for comfort care, and repeat that again and again for patient after patient,” said Mr. Cohen, of the Institute for Safe Medication Practices. “No one gives that to patients. You’ll knock them off.”
During the trial, prosecutors said repeatedly that no one except Dr. Husel knows what he was thinking when he ordered those huge drug dosages for his ICU patients. Judge Holbrook told the jury the state did not have to prove motive, only intent. But many observers still have wondered what his motives were.
Dr. Husel’s own view of his care in these cases soon will become public. Immediately after the April 20 verdict, Mr. Leeseberg filed a notice requesting a May 9 deposition of Dr. Husel, who will no longer be able to claim the Fifth Amendment right against self-incrimination. He predicted the deposition will last about a week, and then the transcript will be publicly available.
A version of this article first appeared on Medscape.com.
In an unprecedented murder case about end-of-life care, a physician accused of killing 14 critically ill patients with opioid overdoses in a Columbus, Ohio, hospital ICU over a period of 4 years was found not guilty by a jury April 20.
The jury, after a 7-week trial featuring more than 50 witnesses in the Franklin County Court of Common Pleas, declared William Husel, DO, not guilty on 14 counts of murder and attempted murder.
In a news conference after the verdict was announced, lead defense attorney Jose Baez said Dr. Husel, whom he called a “great doctor,” hopes to practice medicine again in the future. “They don’t need to be looking over their shoulders worrying about whether they’ll get charged with crimes,” he said.
The prosecutors in the case declined to comment, other than to say they “accept” the verdict.
Legal experts said it’s highly unlikely that Ohio or any other state would restore Dr. Husel’s suspended medical license. “I doubt he could ever work in medicine again,” said Mark Schumacher, a Columbus medical malpractice defense attorney who retired in 2020 after practicing for 39 years. Mr. Schumacher followed the trial closely.
The trial raised the specific issue of what constitutes a medically justifiable dose of opioid painkillers during the end-of-life procedure known as palliative extubation, in which critically ill patients are withdrawn from the ventilator when they are expected to die. Under medicine’s so-called double-effect principle, physicians must weigh the benefits and risks of ordering potentially lethal doses of painkillers and sedatives to provide comfort care for critically ill patients.
To many observers, however, the case really centered on the largely hidden debate over whether it’s acceptable to hasten the deaths of dying patients who haven’t chosen that path. That’s called euthanasia, which is illegal in the United States. In contrast, 10 states plus the District of Columbia allow physicians to prescribe lethal drugs to terminally ill, mentally competent adults who can self-administer them. That’s called medical aid in dying, or physician-assisted dying or suicide.
“Maybe this is a wake-up call that people believe this is the right thing to do,” said Lewis Nelson, MD, chair of emergency medicine at New Jersey Medical School in Newark. “The medical community has a sense that we often prolong life unnecessarily. But a physician cannot unilaterally decide it’s time for someone to die. It sounds like [Dr. Husel] took that decision into his own hands.”
The case also exposed major gaps in the patient safety culture at Mount Carmel West Hospital in Columbus, which is owned by the Catholic chain Trinity Health. Experts say failures by hospital staff to question physicians’ orders and raise patient safety concerns, as happened at Mount Carmel, occur at many hospitals around the country. Experts say the Husel case offers vital lessons for health care professionals about improving safety procedures.
“This is an extreme example, that everyone should learn from, about what not to do,” said Michael Cohen, RPh, founder and president emeritus of the Institute for Safe Medication Practices. “Husel was giving massive overdoses of drugs, people knew it was problematic, and someone didn’t put their foot down. You’ve got to have a process in place to address these situations where there is disagreement over the safety of a medication order.”
Dr. Husel was charged with killing the 14 patients from 2015 through 2018 by ordering single large doses of the painkiller fentanyl – from 500 to 2,000 micrograms – often in combination with other opioids and sedatives, while working as the solo physician on the overnight shift in the ICU at Mount Carmel West Hospital and at Mount Carmel St. Ann’s Hospital in Westerville, Ohio.
Dr. Husel ordered administration of the drugs while his patients were having an endotracheal tube removed as part of palliative extubation. There was conflicting testimony during the trial about whether the patients were showing signs of pain or were even capable of feeling pain.
Prosecutors argued that Dr. Husel, who did a residency and fellowship in critical care medicine at Cleveland Clinic and started working at Mount Carmel in 2013 in his first job as a full-fledged physician, intended to kill the patients or hasten their deaths. They contended that the inexperienced nurses in the ICU went along with his large drug doses because they were “in thrall” to him because of his prestigious background at the Cleveland Clinic and his willingness to take the time to teach them.
“With his training in anesthesiology, he knew what those drugs do,” assistant prosecutor David Zeyen said in closing arguments. “This isn’t negligence. This is on purpose ... Euthanizing animals with the intent to kill is fine in veterinary medicine. It’s not fine in the ICU at Mount Carmel or anywhere.”
The defense team argued that Dr. Husel was a caring and compassionate physician who ordered the drugs to relieve the patients’ pain and discomfort during the extubation process. He did not testify.
“Common sense says Dr Husel had no motive to harm patients,” defense attorney Baez said in his closing. “He dedicated his life to taking care of patients and saving lives, not taking them. ... Why would this man risk his family, career, and 17 years of trying to be a doctor to hasten someone’s death or kill them?”
There were 35 Mount Carmel patients who died in the ICU under Dr. Husel’s care after receiving large fentanyl doses during palliative extubation. The state originally charged him with murder in 25 of those cases, then reduced that to 14.
Many of Dr. Husel’s drug orders were given verbally instead of through the regular process of being entered into the electronic health record. He and the nurses on duty also skipped the standard nonemergency process of getting approval from the pharmacist on duty, instead using the override function on Mount Carmel’s automated Pyxis drug dispensing system.
Dr. Husel’s unusual dosing patterns were first reported to Mount Carmel officials by pharmacists in October 2018, spurring an investigation. The hospital system let him go in December 2018, after concluding that the opioid dosages he used were “significantly excessive and potentially fatal” and “went beyond providing comfort.”
Nearly two dozen RNs and two pharmacists involved in these cases have faced state disciplinary action, mostly license suspension. Federal and state agencies have cited the Mount Carmel system for faults in its patient safety processes and culture that were exposed by the Husel cases.
The Mount Carmel CEO; the chief clinical officer; other physician, nursing, and pharmacy leaders; and dozens of nurses and pharmacists were forced out following the Husel investigation.
In 2019, the Centers for Medicare & Medicaid Services, after threatening to cut off federal reimbursements to Mount Carmel, accepted the hospital system’s correction plan restricting the use of verbal drug orders and prohibiting Pyxis system overrides for opioids except in life-threatening emergencies. The Ohio Board of Pharmacy hit Mount Carmel with $477,000 in fines and costs for pharmacy rules violations.
Mount Carmel and Trinity have settled a number of civil wrongful death lawsuits filed by the families of Dr. Husel’s patients for nearly $20 million, with many more suits pending. Gerry Leeseberg, a Columbus medical malpractice plaintiff attorney who is representing 17 of the families, said a number of the cases are set for trial starting in June.
During the trial, family members of many of the 14 patients whom Dr. Husel allegedly murdered testified that Dr. Husel told them their loved ones were dying. Some said they felt rushed into making a decision to extubate the person.
Before performing a palliative extubation, physicians commonly administer opioids and/or sedatives to ease pain and discomfort, and spare family members from witnessing their loved ones gasping for breath. But most medical experts – including the state’s two physician expert witnesses – say the fentanyl doses Dr. Husel ordered were 5-20 times larger than doses normally used in palliative extubation. Such doses, they say, will quickly kill most patients – except those with high opioid tolerance – by stopping their breathing.
Physicians say they typically give much smaller doses of fentanyl or morphine, then administer more as needed if they observe the patient experiencing pain or distress. Mount Carmel’s 2016 guidelines for IV administration of fentanyl specified a dosage range of 50-100 micrograms for relieving pain, and its 2018 guidelines reduced that to 25-50 micrograms.
The doses Dr. Husel ordered are lethal, even for most patients with some tolerance to opioids, said Rutgers EM chair Dr. Nelson, who practices medical toxicology and addiction medicine. “Those are doses to provide euthanasia, not to relieve pain.”
At trial, the prosecutors had to overcome two big challenges to win murder convictions against Dr. Husel: They had to prove beyond a reasonable doubt that the drugs Dr. Husel ordered are what directly caused these critically ill patients to die, and that he intended to kill them.
Late in the trial, at the state’s request, the judge ruled to allow the jury to also consider attempted murder charges, which require proof of intent but not that the defendant’s actions directly caused the deaths.
Another challenge was that physicians have certain legal protections for administering drugs to patients for the purpose of relieving pain and suffering, even if the drugs hasten the patients’ deaths – as long the intent was not to cause death and the drugs were properly used. This is known as the double-effect principle. In contrast, intentional killing to relieve pain and suffering is called euthanasia. That’s what prosecutors accused Dr. Husel of doing.
“If you hasten a person’s death, even if their death is as sure as the sun is going to rise in the morning ... you have caused their death in the eyes of the law,” assistant prosecutor Mr. Zeyen said in his closing. “You don’t get a pass for killing a dying man ...”
Mr. Leeseberg said it was always going to be extremely hard to convince a jury to convict a physician of murder, with the potential of life in prison, in a case where the physician’s acts occurred openly over 4 years in a hospital setting where no one did anything to stop him. It would have been much easier to convince a jury to convict him of reckless homicide, a lesser offense with a shorter prison term. That would have required proving that he acted in reckless disregard for his patients’ health and safety.
In post-verdict comments to the news media, Judge Michael Holbrook said jurors told him that the procedures for the dispensing of fentanyl and other drugs at Mount Carmel weren’t properly explained to them during the trial, and that they were confused by the large number of prosecution witnesses. He also said they were confused that no one had stated a maximum dosage for fentanyl.
Mr. Schumacher, the retired malpractice defense lawyer who followed the trial, disagreed with defense attorney Baez’s takeaway about the impact of the case on pain-relief practices. In his view, the case likely will heighten rather than reduce the anxiety of physicians and nurses about administering opioids, even when the dosages are clearly needed and appropriate. He doesn’t think Dr. Husel’s dosages can be justified, however.
“Physicians have a naive overreaction to any legal development, and overgeneralize from a particular case to everyday practice,” he said.
There is only one known prior case that’s somewhat comparable of a physician tried for murder or attempted murder for giving a critically ill patient opioids for pain relief. In 1996, a Kansas jury convicted Lloyd Stanley Naramore, DO, of attempted murder in the death of a patient to whom he gave an opioid, and of second-degree murder for removing a patient from a ventilator. After Dr. Naramore served 6 months in prison, an appellate court reversed the convictions for lack of evidence.
In March, RaDonda Vaught, a nurse who worked at Vanderbilt University Medical Center in Nashville, Tenn., was convicted of criminal neglect and negligent homicide for mistakenly administering a fatal dose of the paralyzing drug vecuronium, instead of the prescribed drug Versed (midazolam), to a patient. Providers around the country were alarmed by her criminal prosecution for what was clearly an unintentional error.
But legal and medical experts said Dr. Husel’s case was sharply different from Vaught’s and Dr. Naramore’s because he deliberately and repeatedly ordered large doses of fentanyl and other drugs that he knew or should have known were potentially lethal. “You don’t need 2,000 micrograms of fentanyl plus other drugs for comfort care, and repeat that again and again for patient after patient,” said Mr. Cohen, of the Institute for Safe Medication Practices. “No one gives that to patients. You’ll knock them off.”
During the trial, prosecutors said repeatedly that no one except Dr. Husel knows what he was thinking when he ordered those huge drug dosages for his ICU patients. Judge Holbrook told the jury the state did not have to prove motive, only intent. But many observers still have wondered what his motives were.
Dr. Husel’s own view of his care in these cases soon will become public. Immediately after the April 20 verdict, Mr. Leeseberg filed a notice requesting a May 9 deposition of Dr. Husel, who will no longer be able to claim the Fifth Amendment right against self-incrimination. He predicted the deposition will last about a week, and then the transcript will be publicly available.
A version of this article first appeared on Medscape.com.
In an unprecedented murder case about end-of-life care, a physician accused of killing 14 critically ill patients with opioid overdoses in a Columbus, Ohio, hospital ICU over a period of 4 years was found not guilty by a jury April 20.
The jury, after a 7-week trial featuring more than 50 witnesses in the Franklin County Court of Common Pleas, declared William Husel, DO, not guilty on 14 counts of murder and attempted murder.
In a news conference after the verdict was announced, lead defense attorney Jose Baez said Dr. Husel, whom he called a “great doctor,” hopes to practice medicine again in the future. “They don’t need to be looking over their shoulders worrying about whether they’ll get charged with crimes,” he said.
The prosecutors in the case declined to comment, other than to say they “accept” the verdict.
Legal experts said it’s highly unlikely that Ohio or any other state would restore Dr. Husel’s suspended medical license. “I doubt he could ever work in medicine again,” said Mark Schumacher, a Columbus medical malpractice defense attorney who retired in 2020 after practicing for 39 years. Mr. Schumacher followed the trial closely.
The trial raised the specific issue of what constitutes a medically justifiable dose of opioid painkillers during the end-of-life procedure known as palliative extubation, in which critically ill patients are withdrawn from the ventilator when they are expected to die. Under medicine’s so-called double-effect principle, physicians must weigh the benefits and risks of ordering potentially lethal doses of painkillers and sedatives to provide comfort care for critically ill patients.
To many observers, however, the case really centered on the largely hidden debate over whether it’s acceptable to hasten the deaths of dying patients who haven’t chosen that path. That’s called euthanasia, which is illegal in the United States. In contrast, 10 states plus the District of Columbia allow physicians to prescribe lethal drugs to terminally ill, mentally competent adults who can self-administer them. That’s called medical aid in dying, or physician-assisted dying or suicide.
“Maybe this is a wake-up call that people believe this is the right thing to do,” said Lewis Nelson, MD, chair of emergency medicine at New Jersey Medical School in Newark. “The medical community has a sense that we often prolong life unnecessarily. But a physician cannot unilaterally decide it’s time for someone to die. It sounds like [Dr. Husel] took that decision into his own hands.”
The case also exposed major gaps in the patient safety culture at Mount Carmel West Hospital in Columbus, which is owned by the Catholic chain Trinity Health. Experts say failures by hospital staff to question physicians’ orders and raise patient safety concerns, as happened at Mount Carmel, occur at many hospitals around the country. Experts say the Husel case offers vital lessons for health care professionals about improving safety procedures.
“This is an extreme example, that everyone should learn from, about what not to do,” said Michael Cohen, RPh, founder and president emeritus of the Institute for Safe Medication Practices. “Husel was giving massive overdoses of drugs, people knew it was problematic, and someone didn’t put their foot down. You’ve got to have a process in place to address these situations where there is disagreement over the safety of a medication order.”
Dr. Husel was charged with killing the 14 patients from 2015 through 2018 by ordering single large doses of the painkiller fentanyl – from 500 to 2,000 micrograms – often in combination with other opioids and sedatives, while working as the solo physician on the overnight shift in the ICU at Mount Carmel West Hospital and at Mount Carmel St. Ann’s Hospital in Westerville, Ohio.
Dr. Husel ordered administration of the drugs while his patients were having an endotracheal tube removed as part of palliative extubation. There was conflicting testimony during the trial about whether the patients were showing signs of pain or were even capable of feeling pain.
Prosecutors argued that Dr. Husel, who did a residency and fellowship in critical care medicine at Cleveland Clinic and started working at Mount Carmel in 2013 in his first job as a full-fledged physician, intended to kill the patients or hasten their deaths. They contended that the inexperienced nurses in the ICU went along with his large drug doses because they were “in thrall” to him because of his prestigious background at the Cleveland Clinic and his willingness to take the time to teach them.
“With his training in anesthesiology, he knew what those drugs do,” assistant prosecutor David Zeyen said in closing arguments. “This isn’t negligence. This is on purpose ... Euthanizing animals with the intent to kill is fine in veterinary medicine. It’s not fine in the ICU at Mount Carmel or anywhere.”
The defense team argued that Dr. Husel was a caring and compassionate physician who ordered the drugs to relieve the patients’ pain and discomfort during the extubation process. He did not testify.
“Common sense says Dr Husel had no motive to harm patients,” defense attorney Baez said in his closing. “He dedicated his life to taking care of patients and saving lives, not taking them. ... Why would this man risk his family, career, and 17 years of trying to be a doctor to hasten someone’s death or kill them?”
There were 35 Mount Carmel patients who died in the ICU under Dr. Husel’s care after receiving large fentanyl doses during palliative extubation. The state originally charged him with murder in 25 of those cases, then reduced that to 14.
Many of Dr. Husel’s drug orders were given verbally instead of through the regular process of being entered into the electronic health record. He and the nurses on duty also skipped the standard nonemergency process of getting approval from the pharmacist on duty, instead using the override function on Mount Carmel’s automated Pyxis drug dispensing system.
Dr. Husel’s unusual dosing patterns were first reported to Mount Carmel officials by pharmacists in October 2018, spurring an investigation. The hospital system let him go in December 2018, after concluding that the opioid dosages he used were “significantly excessive and potentially fatal” and “went beyond providing comfort.”
Nearly two dozen RNs and two pharmacists involved in these cases have faced state disciplinary action, mostly license suspension. Federal and state agencies have cited the Mount Carmel system for faults in its patient safety processes and culture that were exposed by the Husel cases.
The Mount Carmel CEO; the chief clinical officer; other physician, nursing, and pharmacy leaders; and dozens of nurses and pharmacists were forced out following the Husel investigation.
In 2019, the Centers for Medicare & Medicaid Services, after threatening to cut off federal reimbursements to Mount Carmel, accepted the hospital system’s correction plan restricting the use of verbal drug orders and prohibiting Pyxis system overrides for opioids except in life-threatening emergencies. The Ohio Board of Pharmacy hit Mount Carmel with $477,000 in fines and costs for pharmacy rules violations.
Mount Carmel and Trinity have settled a number of civil wrongful death lawsuits filed by the families of Dr. Husel’s patients for nearly $20 million, with many more suits pending. Gerry Leeseberg, a Columbus medical malpractice plaintiff attorney who is representing 17 of the families, said a number of the cases are set for trial starting in June.
During the trial, family members of many of the 14 patients whom Dr. Husel allegedly murdered testified that Dr. Husel told them their loved ones were dying. Some said they felt rushed into making a decision to extubate the person.
Before performing a palliative extubation, physicians commonly administer opioids and/or sedatives to ease pain and discomfort, and spare family members from witnessing their loved ones gasping for breath. But most medical experts – including the state’s two physician expert witnesses – say the fentanyl doses Dr. Husel ordered were 5-20 times larger than doses normally used in palliative extubation. Such doses, they say, will quickly kill most patients – except those with high opioid tolerance – by stopping their breathing.
Physicians say they typically give much smaller doses of fentanyl or morphine, then administer more as needed if they observe the patient experiencing pain or distress. Mount Carmel’s 2016 guidelines for IV administration of fentanyl specified a dosage range of 50-100 micrograms for relieving pain, and its 2018 guidelines reduced that to 25-50 micrograms.
The doses Dr. Husel ordered are lethal, even for most patients with some tolerance to opioids, said Rutgers EM chair Dr. Nelson, who practices medical toxicology and addiction medicine. “Those are doses to provide euthanasia, not to relieve pain.”
At trial, the prosecutors had to overcome two big challenges to win murder convictions against Dr. Husel: They had to prove beyond a reasonable doubt that the drugs Dr. Husel ordered are what directly caused these critically ill patients to die, and that he intended to kill them.
Late in the trial, at the state’s request, the judge ruled to allow the jury to also consider attempted murder charges, which require proof of intent but not that the defendant’s actions directly caused the deaths.
Another challenge was that physicians have certain legal protections for administering drugs to patients for the purpose of relieving pain and suffering, even if the drugs hasten the patients’ deaths – as long the intent was not to cause death and the drugs were properly used. This is known as the double-effect principle. In contrast, intentional killing to relieve pain and suffering is called euthanasia. That’s what prosecutors accused Dr. Husel of doing.
“If you hasten a person’s death, even if their death is as sure as the sun is going to rise in the morning ... you have caused their death in the eyes of the law,” assistant prosecutor Mr. Zeyen said in his closing. “You don’t get a pass for killing a dying man ...”
Mr. Leeseberg said it was always going to be extremely hard to convince a jury to convict a physician of murder, with the potential of life in prison, in a case where the physician’s acts occurred openly over 4 years in a hospital setting where no one did anything to stop him. It would have been much easier to convince a jury to convict him of reckless homicide, a lesser offense with a shorter prison term. That would have required proving that he acted in reckless disregard for his patients’ health and safety.
In post-verdict comments to the news media, Judge Michael Holbrook said jurors told him that the procedures for the dispensing of fentanyl and other drugs at Mount Carmel weren’t properly explained to them during the trial, and that they were confused by the large number of prosecution witnesses. He also said they were confused that no one had stated a maximum dosage for fentanyl.
Mr. Schumacher, the retired malpractice defense lawyer who followed the trial, disagreed with defense attorney Baez’s takeaway about the impact of the case on pain-relief practices. In his view, the case likely will heighten rather than reduce the anxiety of physicians and nurses about administering opioids, even when the dosages are clearly needed and appropriate. He doesn’t think Dr. Husel’s dosages can be justified, however.
“Physicians have a naive overreaction to any legal development, and overgeneralize from a particular case to everyday practice,” he said.
There is only one known prior case that’s somewhat comparable of a physician tried for murder or attempted murder for giving a critically ill patient opioids for pain relief. In 1996, a Kansas jury convicted Lloyd Stanley Naramore, DO, of attempted murder in the death of a patient to whom he gave an opioid, and of second-degree murder for removing a patient from a ventilator. After Dr. Naramore served 6 months in prison, an appellate court reversed the convictions for lack of evidence.
In March, RaDonda Vaught, a nurse who worked at Vanderbilt University Medical Center in Nashville, Tenn., was convicted of criminal neglect and negligent homicide for mistakenly administering a fatal dose of the paralyzing drug vecuronium, instead of the prescribed drug Versed (midazolam), to a patient. Providers around the country were alarmed by her criminal prosecution for what was clearly an unintentional error.
But legal and medical experts said Dr. Husel’s case was sharply different from Vaught’s and Dr. Naramore’s because he deliberately and repeatedly ordered large doses of fentanyl and other drugs that he knew or should have known were potentially lethal. “You don’t need 2,000 micrograms of fentanyl plus other drugs for comfort care, and repeat that again and again for patient after patient,” said Mr. Cohen, of the Institute for Safe Medication Practices. “No one gives that to patients. You’ll knock them off.”
During the trial, prosecutors said repeatedly that no one except Dr. Husel knows what he was thinking when he ordered those huge drug dosages for his ICU patients. Judge Holbrook told the jury the state did not have to prove motive, only intent. But many observers still have wondered what his motives were.
Dr. Husel’s own view of his care in these cases soon will become public. Immediately after the April 20 verdict, Mr. Leeseberg filed a notice requesting a May 9 deposition of Dr. Husel, who will no longer be able to claim the Fifth Amendment right against self-incrimination. He predicted the deposition will last about a week, and then the transcript will be publicly available.
A version of this article first appeared on Medscape.com.