User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Unlocking the riddle of REM sleep
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.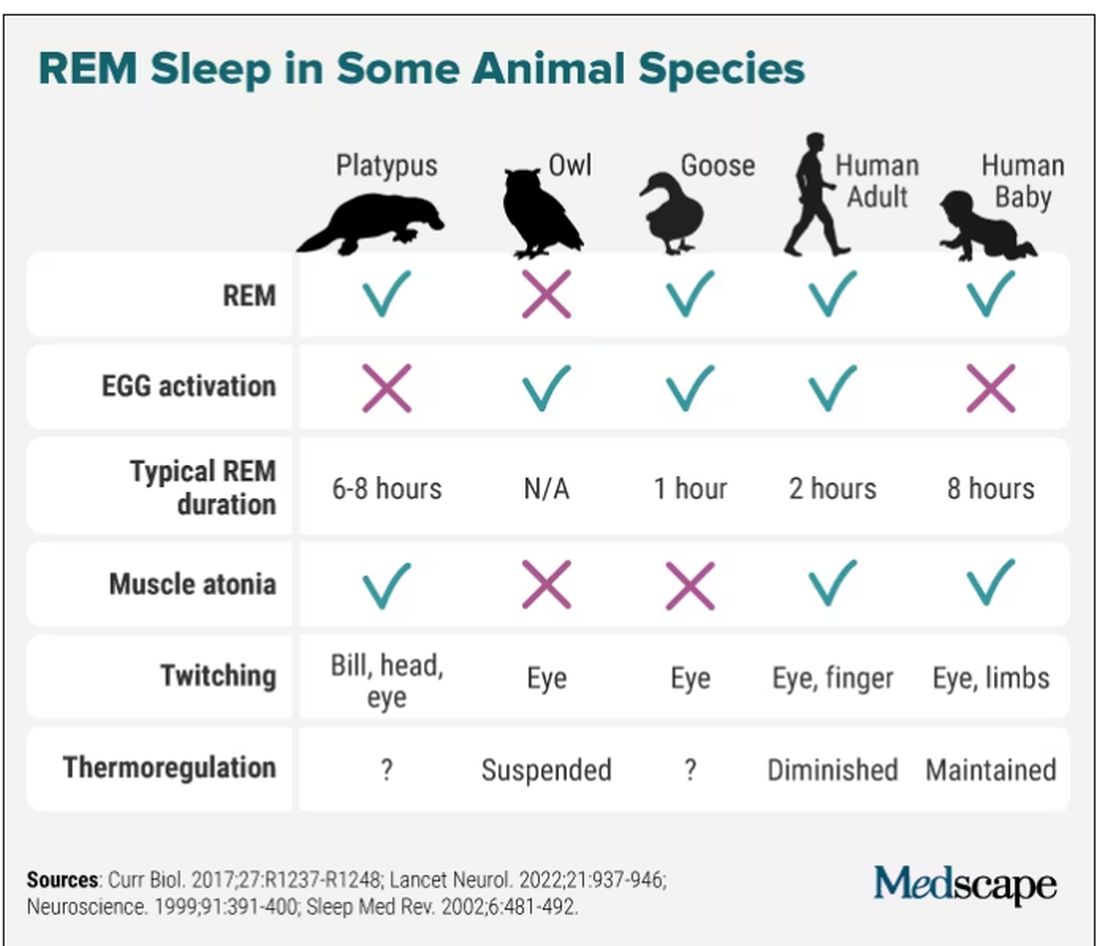
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Eugene Aserinsky, PhD, never wanted to study sleep. He tried being a social worker, a dental student, and even did a stint in the army as an explosives handler. He enrolled at the University of Chicago to pursue organ physiology, but all potential supervisors were too busy to take him on. His only choice was Nathaniel Kleitman, PhD, a middle-aged professor whom Dr. Aserinsky described as “always serious.” Dr. Kleitman was doing research on sleep and so, grudgingly, Dr. Aserinsky had followed suit.
Two years later, in 1953, the duo published a paper that shattered the way we saw sleep. They described a weird phenomenon Dr. Aserinsky later called REM sleep: periods of rapid eye movements paired with wakefulness-like activity in the brain. “We are still at the very beginning of understanding this phenomenon,” Mark Blumberg, PhD, professor of psychological and brain sciences at University of Iowa, Iowa City, said in an interview.
Before Dr. Aserinsky had walked into Dr. Kleitman’s lab, the widespread belief held that sleep was “the antithesis of wakefulness,” as Dr. Kleitman wrote in his seminal 1939 book, “Sleep and Wakefulness.” Others saw it as a kind of a coma, a passive state. Another theory, developed in the early 20th century by French psychologist Henri Piéron, PhD, held that sleepiness is caused by an accumulation of ‘hypnotoxins’ in the brain.
In his 1913 study that would likely fail a contemporary ethics review, Dr. Piéron drew fluid from the brains of sleep-deprived dogs and injected it into other dogs to induce sleep. As he explained in an interview with The Washington Times in 1933, he said he believed that fatigue toxins accumulate in the brain throughout the wakeful hours, then slowly seep into the spinal column, promoting drowsiness. Once we fall asleep, Dr. Piéron claimed, the hypnotoxins burn away.
From blinking to rapid eye movement
In 1925 when Dr. Kleitman established the world’s first sleep laboratory at the University of Chicago, sleep was a fringe science that most researchers avoided with a wide berth. Yet Dr. Kleitman was obsessed. The Moldova-born scientist famously worked 24/7 – literally. He not only stayed long hours in his lab, but also slept attached to a plethora of instruments to measure his brain waves, breathing, and heartbeat. At one point, Dr. Kleitman stayed awake for 180 hours (more than a week), to check how forced sleeplessness would affect his body (he later compared it to torture). He also lived 2 weeks aboard a submarine, moved his family north of the Arctic Circle, and spent over a month 119 feet below the surface in a cave in Kentucky, fighting rats, cold, and humidity to study circadian rhythms.
Dr. Kleitman was intrigued by an article in Nature in which the author asserted that he could detect the approach of slumber in train passengers by observing their blink frequencies. He instructed Dr. Aserinsky to observe sleeping infants (being monitored for a different study), to see how their blinking related to sleep. Yet Dr. Aserinsky was not amused. The project, he later wrote, “seemed about as exciting as warm milk.”
Dr. Aserinsky was uncertain whether eyelid movement with the eyes closed constituted a blink, then he noticed a 20-minute span in each hour when eye movement ceased entirely. Still short of getting his degree, Dr. Aserinsky decided to observe sleeping adults. He hauled a dusty clanker of a brain-wave machine out of the university’s basement, and started registering the electrical activity of the brain of his dozing subjects. Soon, he noticed something weird.
As he kept staring at the sleeping adults, he noticed that at times they’d have saccadic-like eye movements, just as the EEG machine would register a wake-like state of the brain. At first, he thought the machine was broken (it was ancient, after all). Then, that the subjects were awake and just keeping their eyes shut. Yet after conducting several sessions and tinkering with the EEG machine, Dr. Aserinsky finally concluded that the recordings and observations were correct: Something was indeed happening during sleep that kept the cortex activated and made the subjects’ eyes move in a jerky manner.
Dreams, memory, and thermoregulation
After studying dozens of subjects, including his son and Dr. Kleitman’s daughter, and using miles of polygraph paper, the two scientists published their findings in September 1953 in the journal Science. Dr. Kleitman didn’t expect the discovery to be particularly earth-shattering. When asked in a later interview how much research and excitement he thought the paper would generate, he replied: “none whatsoever.” That’s not how things went, though. “They completely changed the way people think,” Dr. Blumberg said. Once and for all, the REM discovery put to rest the idea that sleep was a passive state where nothing interesting happens.
Dr. Aserinsky soon left the University of Chicago, while Dr. Kleitman continued research on rapid eye movements in sleep with his new student, William Dement, MD. Together, they published studies suggesting that REM periods were when dreaming occurred – they reported that people who were awakened during REM sleep were far more likely to recall dreams than were those awakened outside of that period. “REM sleep = dreams” became established dogma for decades, even though first reports of dreams during non-REM sleep came as early as Dr. Kleitman’s and Dr. Dement’s original research (they assumed these were recollections from the preceding REM episodes).
“It turns out that you can have a perfectly good dream when you haven’t had a previous REM sleep period,” said Jerome Siegel, PhD, professor of psychiatry and biobehavioral sciences at UCLA’s Center for Sleep Research, pointing out that equating REM sleep with dreams is still “a common misconception.”
By the 1960s, REM sleep seemed to be well defined as the combination of rapid eye movement with EEG showing brain activation, first noted by Dr. Aserinsky, as well as muscle atonia – a state of near-total muscle relaxation or paralysis. Today, however, Dr. Blumberg said, things are considerably less clear cut. In one recent paper, Dr. Blumberg and his colleagues went as far as to question whether REM sleep is even “a thing.” REM sleep is prevalent across terrestrial vertebrates, but they found that it is also highly nuanced, messing up old definitions.
Take the platypus, for example, the animal with the most REM sleep (as far as we know): They have rapid eye movements and their bills twitch during REM (stillness punctuated by sudden twitches is typical of that period of sleep), but they don’t have the classic brain activation on EEG. Owls have EEG activation and twitching, but no rapid eye movements, since their eyes are largely immobile. Geese, meanwhile, are missing muscle atonia – that’s why they can sleep standing. And new studies are still coming in, showing, for instance, that even jumping spiders may have REM sleep, complete with jerky eye movements and limb twitching.
For Dr. Siegel, the findings on REM sleep in animals point to the potential explanation of what that bizarre stage of sleep may be all about: thermoregulation. “When you look at differences in sleep among the groups of warm-blooded animals, the correlation is almost perfect, and inverse. The colder they are, the more REM sleep they get,” Dr. Siegel said. During REM sleep, body thermoregulation is basically suspended, and so, as Dr. Siegel argued in The Lancet Neurology last fall, REM sleep could be a vital player in managing our brain’s temperature and metabolic activity during sleep.
Wallace B. Mendelson, MD, professor emeritus of psychiatry at the University of Chicago, said it’s likely, however, that REM sleep has more than one function. “There is no reason why one single theory has to be an answer. Most important physiological functions have multiple functions,” he said. The ideas are many, including that REM sleep helps consolidate our memories and plays an important role in emotion regulation But it’s not that simple. A Swiss study of nearly 1,000 healthy participants did not show any correlation between sleep stage and memory consolidation. Sleep disruption of any stage can prevent memory consolidation and quiet wakefulness with closed eyes can be as effective as sleep for memory recall.
In 1971, researchers from the National Institute of Mental Health published results of their study on total suppression of REM sleep. For as long as 40 days, they administered the monoamine oxidase inhibitor (MAOI) phenelzine, a type of drug that can completely eliminate REM sleep, to six patients with anxiety and depression. They showed that suppression of REM sleep could improve symptoms of depression, seemingly without impairing the patients’ cognitive function. Modern antidepressants, too, can greatly diminish REM sleep, Dr. Siegel said. “I’m not aware that there is any dramatic downside in having REM sleep reduced,” he said.
So do we even need REM sleep for optimal performance? Dr. Siegel said that there is a lot of exaggeration about how great REM sleep is for our health. “People just indulge their imaginations,” he said.
Dr. Blumberg pointed out that, in general, as long as you get enough sleep in the first place, you will get enough REM. “You can’t control the amount of REM sleep you have,” he explained.
REM sleep behavior disorder
Even though we may not need REM sleep to function well, REM sleep behavior disorder (RBD) is a sign that our health may be in trouble. In 1986, scientists from the University of Minnesota reported a bizarre REM sleep pathology in four men and one woman who would act out their dreams. One 67-year-old man, for example, reportedly punched and kicked his wife at night for years. One time he found himself kneeling alongside the bed with his arms extended as if he were holding a rifle (he dreamt he was in a shootout). His overall health, however, seemed unaffected apart from self-injury during some episodes.
However, in 1996 the same group of researchers reported that 11 of 29 men originally diagnosed with RBD went on to develop a parkinsonian disorder. Combined data from 24 centers of the International RBD Study Group puts that number as high as 74% at 12-year follow-up. These patients get diagnosed with Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy. Scientists believe that the protein alpha-synuclein forms toxic clumps in the brain, which are responsible both for malfunctioning of muscle atonia during REM sleep and subsequent neurodegenerative disorders.
While some researchers say that RBD may offer a unique window into better understanding REM sleep, we’re still a long way off from fully figuring out this biological phenomenon. According to Dr. Blumberg, the story of REM sleep has arguably become more muddled in the 7 decades since Dr. Aserinsky and Dr. Kleitman published their original findings, dispelling myths about ‘fatigue toxins’ and sleep as a passive, coma-like state. Dr. Mendelson concurred: “It truly remains a mystery.”
Dr. Blumberg, Dr. Mendelson, and Dr. Siegel reported no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Music therapy helps motivate patients with schizophrenia
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”

She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.

The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”
She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.
The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
SAN FRANCISCO –
Although the study had conflicting results regarding the effects of music therapy on positive symptoms of schizophrenia, such as hallucinations, delusions, and disordered thoughts, it consistently shows that music therapy improves negative symptoms, poster presenter Amy Agrawal, MD, VA Boston Healthcare System and instructor of psychiatry at Harvard Medical School, Boston, said in an interview.
Current antipsychotic drugs aren’t very effective in addressing negative symptoms of schizophrenia, and many patients are noncompliant with these drug regimens because of side effects.
“We need to target the negative symptoms of schizophrenia better,” said Dr. Agrawal. “The antipsychotic medications we have are not enough, so why don’t we start incorporating music therapy groups into the inpatient psychiatry setting as a standard of care?”
The findings were presented at the annual meeting of the American Psychiatric Association.
Dr. Agrawal has long been interested in music. As a child, she was a member of a state choir, but she hadn’t sung for years. After receiving several medals for her clarinet playing during her youth, she stopped playing while in medical school.
Instant boost
During the pandemic, though, she turned back to music and started singing regularly. “I noticed an instant boost in my mood and wondered why I stopped making music for so long, as it made me feel so much happier and calmer.”
She also noticed how music affected her sister, who has paranoid schizophrenia. She described an incident in which her sibling became so loud and paranoid at a restaurant that Dr. Agrawal thought they would be asked to leave.
Then her sister started singing a song she’d sung during a beauty contest years before. “With the music, she calmed right down; she was smiling; she was happy,” said Dr. Agrawal.
That incident made Dr. Agrawal feel, “I had my sister back.” She decided to bring music therapy to her inpatient psychiatry unit and soon noted the benefits for individual patients.
For this new study, Dr. Agrawal and her mentor carried out a literature search. “I was surprised at how many articles popped up, because the field of psychiatry can be very heavily medication based, but people are now getting very interested in this topic,” said Dr. Agrawal.
The review included seven articles, most of which were published within the past 3 years. Some articles specified that the therapy was conducted on an inpatient psychiatric unit, but others didn’t indicate the setting. Studies also didn’t specify whether the therapy was delivered by a trained music therapist.
There was an overall lack of clear measures, graphs, or statistics quantifying the benefits of music therapy on schizophrenia, noted Dr. Agrawal. “But from general statements in the articles, music therapy helped treat sleep disturbances and improved negative symptoms.”
Gets patients socializing
The music, she said, led patients to start socializing, talking about their emotions, and opening up to their clinicians about their mental health symptoms. “Some patients just did not engage at all, and then when the music came on, they would actively participate with the clinician.”
Dancing to music also tended to motivate patients to participate in their treatment, she added. Different forms of movement, such as rhythmic movements and creative exercises, can be added during music therapy.
In addition to improving negative schizophrenia symptoms, music therapy helps with sleep disturbances, depression, and regulating emotional behavior, the research shows. “When patients were agitated or upset, certain music would help them regulate their own affect,” said Dr. Agrawal.
However, it’s not clear from these studies what type of music – classical, rock, country, etc. – was most effective for people.
One article discussed the positive impact of music on patients with schizophrenia while at work. “They seem to have improved work performance,” Dr. Agrawal said.
The length of exposure to music therapy did not seem to make a difference in terms of whether the therapy had a positive effect, she added.
Key research wave
A “key next wave” of research should be to determine whether music therapy decreases the hospital readmission rate, said Dr. Agrawal.
There are several barriers to implementing music therapy programs in hospitals, including cost, the availability of trained therapists, and time constraints, she said.
“Regardless of the barriers, hospital administrators and psychiatrists need to know about this research so they will invest more efforts in recruiting music therapists and incorporating music group therapy into standard clinical practice for psychiatric patients so there are better clinical outcomes.”
Commenting on the research, Michelle B. Riba, MD, professor, department of psychiatry, University of Michigan, Ann Arbor, said the study adds to the literature “and helps us think about adjunctive treatments in a very difficult population.”
She added, “It’s good to see physicians get interested in this topic.”
Difficult topic to study
Although she found the review “very limited,” she recognizes the difficulty of studying music therapy on in-patient psychiatry units.
“Patients are there for short stays, most are getting other treatments, and it’s hard to segment people into negative vs. positive. Also, the ages and genders are different, and their previous treatments are different.”
While it’s sometimes difficult to conduct major research on a topic, “that doesn’t mean we can’t help people,” said Dr. Riba.
She noted that music therapy is beneficial not only for patients with schizophrenia but also is “soothing and relaxing” for those with other conditions. She runs a psychiatric oncology program at her institution’s cancer center, which offers music therapy along with art therapy.
Kevin M. Malone, MD, of University College Dublin, also has firsthand experience with music therapy. “We had a terrific music therapist as part of our clinical psychosis team,” he said in an interview.
The music therapist is no longer there, but, he said, “as far as I’m concerned, every clinical psychosis team should have a music therapist as an essential team member.”
Dr. Agrawal, Dr. Riba, and Dr. Malone had no reported disclosures.
A version of this article was first published on Medscape.com.
AT APA 2023
Community workers may address psychiatrist shortage
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.

A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.

“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.
A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.
“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – promises to bring timely, evidence-based health services to those with little to no access to effective care.
The current shortage of mental health clinicians is driven by increased demand from a population more willing to seek psychiatric help and clinicians leaving the workforce. Both factors were exacerbated by the COVID-19 pandemic.
“It would be costly to address the problem through additional specialist training, and doing so would take decades to see any changes,” project director Milton L. Wainberg, MD, professor of clinical psychiatry at Columbia University, New York, and New York State Psychiatric Institute, said in an interview.
A better solution is to train members of the community to be the entry point to the mental health care system, a strategy that has been proven effective.
Details of the project were discussed at the annual meeting of the American Psychiatric Association.
Half of the United States population will be diagnosed with a mental or substance use disorder in their lifetime, but only about half of those will receive proper treatment. That percentage is even greater among lower-income groups and minorities, said Dr. Wainberg.
Despite the availability of multiple evidence-based therapies, there has been no reduction in the global prevalence of psychiatric illness since 1990 – the first time this burden was determined, he said.
Unfeasible model
“The historic paradigm of ongoing long-term care is costly and not a feasible public mental health model. There is no evidence that it works, and there is increasing demand for brief interventions,” said Dr. Wainberg.
The new initiative – called ENGAGE – has its origins in parts of Africa, where nurses had to be trained during the AIDS crisis as there weren’t enough doctors to roll out antiretroviral therapy.
In the United States, the program trains and certifies community workers who are passionate about their community. “Members of the community want to learn how to help their neighbors,” said Dr. Wainberg. “When we give them the opportunity to learn skills that can actually change community members’ symptoms, they are excited.”
The training involves a didactic component and an experiential component, in which trainees work with at least three cases under supervision to demonstrate competency. Technical assistance and other supports, such as refresher training, are offered for a year after training.
Workers ask three initial questions to quickly determine if a person has a mental health disorder. Asking 10 additional questions tells the worker if the person has a common mental health disorder like depression, anxiety, or posttraumatic stress disorder (PTSD), a substance use disorder involving alcohol or drugs, suicide risk, or a severe disorder requiring referral to a mental health specialist.
Those who do not require a referral are offered an intervention personalized to their need.
The training costs $5,000 per person. “We calculated for New York State it would cost only $18 million to train everybody we need,” said Dr. Wainberg.
Cost effective
He stressed the program, which is funded by the New York Office of Mental Health, is cost effective. Just like patients don’t need to see a plastic surgeon to have a small mole removed, they don’t always need to see a psychiatrist for run-of-the-mill mild depression, he said.
To date, 20 workers have been trained and have started to meet with clients in clinics in four New York City neighborhoods/boroughs (Harlem, Brooklyn, the Bronx, and Washington Heights). Additional clinics in West Harlem and Staten Island are expected to begin training soon.
Dr. Wainberg has been inundated with interest in the initiative. “Over the last 3 months I have been having 15 meetings a day” with parties interested in getting more information or wanting to know how to start such a program.
He plans to examine the program’s effectiveness in a number of areas, including patient symptoms, timeliness of services, access, sustainability, and cost. And he aims to expand the project beyond New York.
Mental health specialists shouldn’t worry about becoming irrelevant with the addition of community workers, as the demand is so great, said Dr. Wainberg. “There will always be a need for the kind of care mental health specialists are trained for. This initiative aims to expand capacity for those with less severe symptoms, who might not need an intensive level of intervention.”
Unique program
In a comment, Jonathan E. Alpert, MD, PhD, chair of the department of psychiatry and behavioral sciences, Montefiore Medical Center and Albert Einstein College of Medicine, New York, said the project is “unique” and an “excellent” idea.
“This is one of the first pilots that I know of in this country to train lay-members of the community to screen for mental illness and substance use disorders and even to provide evidence-based treatment for people who may have more mild symptoms and might not yet need to see a professional but otherwise would not have access to care.”
Dr. Alpert noted the current challenges of accessing care for a mental health or substance abuse disorder. “Many clinics have wait lists of 3-6 months.”
Another issue is the “stigma and lack of trust” among minority communities when it comes to formal mental health treatments. “Having lay-members who know the community, who look like the community, who understand the community, and who are available for screening and treatment is exceptionally important.”
Although this pilot program will have to be assessed for effectiveness, “the concept behind it is very important,” said Dr. Alpert. “If you’re relying on MDs and PhDs to provide mental health services, there just aren’t enough of us to go around.”
Dr. Wainberg and Dr. Alpert report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM APA 2023
U.S. psychiatrist shortage causing months-long wait times
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.

“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.

“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.
“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.
“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO –
“Long wait times for mental health care were a huge problem even before the pandemic but especially during the pandemic,” study investigator Erin McDaid, BS, Virginia Tech Carilion School of Medicine, Roanoke, said in an interview.
“It’s not like you have a cold or a virus and maybe you wait a little bit and it goes away. Mental health problems can completely impact your life; you can’t do anything, you can’t go to work, you can’t build relationships, you can’t take care of your kids. It’s a really big issue,” Ms. McDaid said.
The study was presented at the annual meeting of the American Psychiatric Association.
Few psychiatrists taking new patients
To find out just how big an issue wait times are, the researchers examined general psychiatry outpatient availability during the COVID-19 pandemic in five states – New York, California, North Dakota, Virginia, and Wyoming.
Altogether, 948 psychiatrists were sampled. Simulated adult patients made 864 calls seeking an initial psychiatric evaluation for general mental health care. The calls were made late in the pandemic, between May and July 2022.
Only 18.5% of psychiatrists were available to see new patients. The median wait time was 67 days for in-person appointments and 43 days for telepsychiatry appointments (P < .001).
More than half of psychiatrists who were contacted said they were not taking new patients, which was the most common reason given for unavailability.
“This is happening at the worst time, when we are seeing mental health issues spike,” Ms. McDaid said.
Telepsychiatry helpful but no panacea
The fact that wait times were a bit shorter for telepsychiatry is encouraging, Ms. McDaid said.
Telepsychiatry is a potential solution to provider shortages and geographic barriers, but it does not resolve the concerning shortage of psychiatric outpatient care, she noted.
“Psychiatrists adapted very well to telepsychiatry during COVID,” Saul Levin, MD, MPA, chief executive officer and medical director of the APA, noted during a preconference briefing with reporters.
“Before COVID, we always thought that the psychiatrist had to be with the patient in the room,” said Dr. Levin. But now we see that either “sitting inside the room with your psychiatrist or mental health specialist or [being there virtually] has the same effect. The patient is concentrating and working out their problems with you. I think that’s one of the positives – if anything coming out of COVID is positive.”
In an interview, Robert Trestman, MD, chair of the APA Council on Healthcare Systems and Financing, said telepsychiatry “will help, but there is not one simple solution that will fix the problem” regarding access to mental health care.
One promising approach is the collaborative care model, which enlists primary care physicians to provide mental health care in consultation with psychiatry and case management, Dr. Trestman said.
“There’s no question that there aren’t enough providers. There aren’t enough primary care doctors, and there certainly aren’t enough psychiatrists,” Dr. Trestman noted.
Encouragingly, however, the past few years have seen a steady increase in medical students choosing psychiatry.
“Psychiatry is now being thought of as a branch of neuroscience. We are understanding so much more about the field and about the brain. So that’s intriguing and intellectually challenging to many,” Dr. Trestman said.
He also noted that the pandemic has helped to “break down stigma. More people acknowledge and talk about mental health, and when an area is destigmatized, it’s so much easier for people to consider.”
Jack Resneck, Jr., MD, president of the American Medical Association, acknowledged that there is a “severe workforce shortage in health care right now.”
“I’m a physician and the president of the AMA, and it took me way too long to be able to find a primary care physician for myself,” he said.
“I also am a physician who refers patients to rheumatology and endocrinology, psychiatry, and other areas of medicine, and it is, in many geographic areas both rural and urban, a huge struggle right now,” said Dr. Resneck.
The study had no specific funding. Ms. McDaid, Dr. Levin, and Dr. Trestman have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT APA 2023
Psychiatrists: Don’t fear clozapine in treatment-resistant schizophrenia
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.

T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.
T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
SAN FRANCISCO – A trio of psychiatrists urged colleagues at the annual meeting of the American Psychiatric Association to embrace the venerable antipsychotic clozapine in patients with treatment-resistant schizophrenia. They cautioned that clinicians may overestimate the true risk of the adverse effect of neutropenia in minority populations.
“Although clozapine is known to be a life-improving and even potentially lifesaving treatment, it remains underutilized in the U.S.,” said Claire C. Holderness, MD, a psychiatrist at Columbia University Irving Medical Center, New York. “It’s been estimated that between 35% and 40% of all patients with schizophrenia should be considered for a clozapine trial. However, only 4%-5% of patients with schizophrenia in the U.S. have ever received clozapine. This is in sharp contrast to other industrialized countries where approximately 20% or more of patients with schizophrenia are treated with clozapine.”
According to Dr. Holderness, research has shown that clozapine is even less likely to be prescribed to racial and ethnic minorities. A 2022 systematic review, for example, found that Black patients in the United States had between one-third and two-thirds the odds of being treated with the drug, compared with White patients after adjustment for potential confounders such as demographics. Hispanic/Latino patients were also less likely than Whites to be prescribed the drug.
As Dr. Holderness put it, the drug “been shown to be more effective in treatment-resistant schizophrenia than any other antipsychotic medication. Clozapine is also the most cost-effective treatment for treatment-resistant schizophrenia.” So why does this disparity exist despite clozapine’s benefits?
A 2018 systematic review of barriers to the drug’s usage identified several factors: “mandatory blood testing, fear of serious side-effects and lack of adherence by the patients, difficulty in identifying suitable patients, service fragmentation, and inadequate training in or exposure to using clozapine.” A 2016 British study, meanwhile, looked at the reasons that 45% of 316 patients stopped clozapine before 2 years. More than half of these patients stopped because of adverse effects.
Risk of neutropenia
At the APA presentation, psychiatrist Laura Clarke, MD, also of Columbia University Irving Medical Center, noted that there’s concern about one adverse effect in particular: neutropenia, or an abnormally low white blood cell count. Clozapine, she said, has a boxed warning about severe neutropenia that can lead to death.
However, she cautioned that white blood cell counts can be misleading. Some people in non-White ethnic groups have a condition known as benign ethnic neutropenia: their white blood cell counts are abnormal by the standards of people of European heritage, but they’re otherwise healthy. “These individuals do not show an increased risk of infections, and their response to infection is similar to those without them,” she said.
As many as 25%-50% of people of African ancestry may have benign ethnic neutropenia, making their blood levels appear abnormally low. Others with higher levels of the condition include certain Middle Eastern ethnicities and other ethnic groups with darker skin.
In these patents, “clinicians may avoid prescribing clozapine out of the mistaken concern that it can worsen neutropenia,” Dr. Clarke said. In fact, benign ethnic neutropenia “does not increase the risk of clozapine-induced severe neutropenia.”
Dr. Clarke highlighted drug use guidelines from the Clozapine Risk Evaluation and Mitigation Strategy, a Food and Drug Administration–mandated safety program designed to prevent severe neutropenia in patients taking clozapine. The guidelines note that the recommended absolute neutrophil count monitoring algorithm differs when patients are diagnosed with benign ethnic neutropenia.
T. Scott Stroup, MD, MPH, a psychiatrist at Columbia University, New York, urged his colleagues to consider clozapine early on in treatment-resistant schizophrenia. “Don’t go through three, four, or five antipsychotics. Even after trying two, I’d encourage people to [try clozapine].”
However, he acknowledged that “not everyone believes that. Many of my colleagues think that, before you try clozapine, you should have a trial of long-acting injectable medications to rule out pseudo–treatment resistance. I don’t totally agree with that, but I’ve more or less lost that battle,” he added.
In the big picture, Dr. Stroup said, clozapine “is good when other things aren’t working efficacy wise.”
Dr. Holderness and Dr. Clarke have no disclosures. Dr. Stroup discloses grants from the National Institutes of Health and royalties from APA Publishing and UpToDate.
AT APA 2023
Higher buprenorphine doses help OUD patients stay in treatment
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
SAN FRANCISCO – . Eighty-five percent of patients who were titrated up to 32 mg remained in treatment for 1 year vs. 22% of those who never went higher than 16 mg, and those on higher doses stayed in treatment 3.83 times longer than those who didn’t.
“Simply put, we demonstrated better retention in treatment if patients were given higher buprenorphine doses when they complained of opioid craving,” said Andrew Gilbert, a medical student at California Northstate University, Elk Grove, Calif. He is lead author of a poster presented at the 2023 annual meeting of the American Psychiatric Association.
There’s an ongoing debate over ideal doses of buprenorphine (Suboxone), an opioid that’s used to help treat withdrawal symptoms in users of drugs such as heroin and fentanyl. Some sources recommend lower doses. The Substance Abuse and Mental Health Administration, for example, says “ideally, average dosing does not exceed 16 mg” in a guide to the drug’s usage, referring to the sublingual form. (A long-lasting injectable is also available.) Drugs.com says 24 mg is the maximum, and “higher doses have not shown a clinical advantage.
However, some emergency departments have begun providing doses up to 28 mg or higher amid the increased use of the powerful opioid fentanyl. “There are mountains of evidence demonstrating the safety of higher doses at 32 mg, and even several-fold higher than that,” study coauthor Phillip Summers MD, MPH, medical director of the harm-reduction organization Safer Alternatives Thru Networking and Education, Sacramento, Calif., said in an interview. “The question is: Is there clinical benefit to these higher doses?”
‘Significantly higher’ retention
For the new study, researchers tracked 328 patients who were treated for opioid use disorder at the Transitions Buprenorphine Clinic of Sacramento from 2010 to 2017. They were followed until 2022. Their average age was 36, 37.2% were female, 75.0% were White, and 24.1% had a history of overdose.
Clinicians titrated up the doses of buprenorphine to address withdrawal and craving. Five patients never went past 4 mg, and two of them stayed in treatment for a year. Nine of 19 who went up to 8 mg stayed in treatment for 1 year, and 4 of 21 did among those who reached 12 mg.
“Our data suggest that the highest rate of patient dropout is at the beginning of treatment, and that there is significantly higher treatment retention in patients on greater than 24 mg or higher of buprenorphine,” the researchers wrote.
Mr. Gilbert said clinicians start at 8 mg the first day in patients who haven’t taken buprenorphine before, then they go to 16 mg the second day. “We then reevaluate in at least 1 week, oftentimes sooner if the patient’s opioid craving is uncontrolled, and determine if 16 mg is too low, too high, or the correct dosage for the patient.”
If a dose of over 32 mg is needed, clinicians turn to the long-lasting injectable form of the drug, study coauthor Neil Flynn MD, MPH, former medical director of the Transitions Buprenorphine Clinic of Sacramento, said in an interview. “We controlled craving with this form for every patient that did not have opioid craving relief with 32 mg. We believe this form achieved opioid craving cessation due to increased buprenorphine blood levels and increased ratio of unmetabolized buprenorphine to metabolized buprenorphine in our patients.”
According to Dr. Summers, it’s clear that too-low doses hurt the recovery process. “If we prescribe subtherapeutic doses of buprenorphine, our patients will experience opioid craving, which leads to treatment dropout and most likely to relapse. Higher doses of buprenorphine are more likely to cease opioid cravings, leading patients to remain in treatment for longer periods of time.”
Mr. Gilbert said buprenorphine has few side effects, which include decreased libido and hot flashes in both men and women. Testosterone therapy can relieve these symptoms in men, he said, but “unfortunately, we do not have any good medications for reversing this side effect in women. Further research should investigate eliminating this side effect in women.”
Mr. Gilbert declined to comment on the extra cost of higher doses since that is outside the scope of the study.
Medication is the ‘star’
In an interview, addiction specialist Dave Cundiff, MD, MPH, of Ilwaco, Wash., praised the study and agreed with its conclusions about the value of high doses of buprenorphine.
“They’re confirming what the science has already shown, but the world does not accept,” he said, adding that “for opioid use disorder, the medication is the star of the show, although counseling is a necessary adjunct for some patients.”
Dr. Cundiff said he’s coauthored a pending review article that finds that studies support higher doses of buprenorphine.
MaryAnne Murray, DNP, EdD, MBA, a psychiatric mental health nurse practitioner who’s married to Dr. Cundiff, said in an interview that the evolution of the opioid epidemic supports the use of higher doses. “The old way we used to do with heroin users was to wait until they’re in moderate withdrawal, and then start up buprenorphine, usually slowly. With fentanyl, it takes longer, and the wait is often less bearable – unbearable for many people.”
Transitions Buprenorphine Clinic of Sacramento funded the study. The authors, Dr. Cundiff, and Dr. Murray have no disclosures.
AT APA 2023
Peak seasons, times for suicidal thoughts, attempts identified
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
In addition, the results from Harvard University’s Project Implicit Health also show that people are most likely to make an attempt at suicide between 4 and 6 a.m.
“No research has demonstrated a peak in suicidal ideation in winter until our paper,” study investigator Brian O’Shea, PhD, assistant professor of social psychology at the University of Nottingham, England, told this news organization.
“Most people incorrectly assume that suicide behaviours peak in winter and are surprised, as I was, when learning about this phenomenon, that suicide actually peaks in spring/early summer,” he added.
However, at least one expert cautioned that the database, which comprises mostly responses from younger women, doesn’t capture responses from those who are most likely to attempt suicide: older men with substance abuse.
The findings were published online in Translational Psychiatry.
New insight into suicide risk
Previous studies examining the seasonality of suicides and suicide attempts have reported a peak in spring and early summer, but there has been very little information about why this may be, the investigators noted.
Dr. O’Shea and his colleague from the University of Amsterdam, René Freichel, mined one of the databases from Project Implicit Health, which contains self-report measures on suicidal ideation, self-harm, and past suicide attempts, as well as respondents’ implicit biases on these topics.
The analysis included data from 10,000 respondents living in the United States, United Kingdom, and Canada provided between April 2012 and November 2018.
The sample was predominantly young and female, with 38% (3,247) of the sample reporting that they had made at least one suicide attempt.
The researchers found a peak in negative mood and desire to die occurring in December, especially among those who reported attempting suicide (P ≤ .001)
Suicidal ideation peaked approximately 3-4 months before the annual seasonal crest of suicide attempts in early spring and summer.
“Affected individuals may become severely depressed and experience a lack of energy throughout the winter months. Essentially, this period may put them below a threshold of severe suicide risk as the high level of suicidal ideation coincides with a low level of energy,” said Dr. O’Shea.
When the days get longer, brighter, and warmer, these changes likely improve an individuals’ mood, he explained. “Hence, the most at-risk individuals become slightly less depressed and may gain more energy to contemplate and plan their method to attempt suicide,” Dr. O’Shea noted.
A major limitation of the study is that all responses included in analysis were based on self-report.
To confirm the findings, future research should include ecological momentary assessment, which involves using a large community sample to question participants about suicidal intent at various time points, along with real-time monitoring of vital signs, said Dr. O’Shea.
Ideally, the investigators noted, the study’s findings will inform clinician assessments of patients who are at risk for suicide.
A research gap?
Commenting on the findings, Justin Shuster, MD, MPH, assistant professor of psychiatry at the University of Pittsburgh and medical director of two psychiatric units at Western Psychiatric Hospital, noted that the database used in the study did not include responses from those who were most likely to attempt or commit suicide: older men with a history of substance abuse, who require social supports, and who have a family history of suicide.
Though Dr. Shuster agreed with Dr. O’Shea about the possibility that spring brought energy to a desire to take one’s life, he had another theory.
“When people are depressed in the winter, they expect to feel better with the advent of the warmer weather in spring. When they don’t feel better, they may think to themselves, ‘If I’m going to feel like this forever, I may as well follow through with these plans,’ ” he said.
As for the early morning attempts, he noted that 4-6 a.m. is often when people are alone, and there are fewer distractions.
“The other thing I see a great deal of clinically is intoxication,” said Dr. Shuster. “Either intoxication with substances or alcohol, or the fact that intoxication is waning at those early morning hours, and people are becoming desperate as they face a new day,” he said.
The study was funded by a German Academic Exchange Service Scholarship and an EU Horizon 2020 Fellowship. Dr. O’Shea reports being an unpaid member of Project Implicit’s scientific advisory board and is on the executive committee of Project Implicit Health.
A version of this article first appeared on Medscape.com.
FROM TRANSLATIONAL PSYCHIATRY
Finding a home in psychiatry: A medical student’s story
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.

My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.
My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.
My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
Prenatal sleep problems, depression linked to poorer outcomes
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
BALTIMORE – , according to research presented at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
Together, the two studies suggest that commonly overlooked experiences in the prenatal period can have negative effects down the line if clinicians aren’t asking patients about them and addressing the issue.
”I think the national conversation around mental health in general will hopefully carry us forward to better supporting the patients who are coming in with preexisting conditions,” lead author Minnie Jang, a 4th-year medical student at Johns Hopkins University, Baltimore, said in an interview.
Most of the attention on mood disorders of pregnancy focus on the postpartum period, but preexisting or new-onset depression during pregnancy deserves more attention, Ms. Jang told attendees. ACOG recommends that clinicians screen all patients at least once during the perinatal period, but that could be anywhere from early pregnancy to the postpartum period. Ms. Jang would like to see recommendations addressing both early pregnancy and the postpartum period.
“I think there’s this framing that postpartum depression is a distinct entity from other mental health conditions whereas it’s really part of a continuum,” Ms. Jang said in an interview.
She retrospectively analyzed the medical records of all pregnant women who completed the Edinburgh Postnatal Depression Scale (EPDS) during their first or second trimesters between 2002 and 2021 at Johns Hopkins Hospital. Among the 718 women who were screened in early pregnancy, 44.6% were Black or African American, 39.7% were white, and 15.7% were of a different race. Nearly all (94%) were not Hispanic/Latino.
Most (59%) were partnered, employed (68%), and had private insurance (58%). Only 7% used tobacco while 11% used alcohol and 6% used illicit drugs.
Twelve percent of the patients scored positive for depression, with a score of at least 10 or an affirmative answer to question 10 regarding self-harm. These women tended to be younger (P = .034), with an median age of 28 at their first visit versus 31 for those who screened negative, and were more likely to be publicly insured (P = .013) and without a partner (P = .005).
Patients who screened positive were more likely to have a history of substance use or history of a previous psychiatric diagnosis (P < .0001 for both). In addition, more patients who screened positive (49%) than those who screened negative (26%) had fetal complications (P < .001).
”There are some interesting subgroups of patients who are screening positive for depressive symptoms early on in pregnancy,” Ms. Jang said. Some come into pregnancy with preexisting mental health conditions while others have situational depressive symptoms, such as the subgroup referred to social work who had diagnosed fetal complications, she said. “Then there’s a whole other group of patients who are developing new symptoms during pregnancy.”
Patients who screened positive tended to start prenatal care later, at a median 12.3 weeks gestational age, than patients who screened negative, at a median 10.7 weeks gestational age (P = .002), the analysis found.
The number of routine prenatal care visits did not significantly differ between those who screened positive and those who screened negative, but patients with positive depression screens were almost half as likely to complete glucose tolerance testing (odds ratio, 0.6) or group B streptococcus testing (OR, 0.56) after adjusting for insurance status, gravidity, and gestational age at the patient’s first visit.
The researchers also identified a significant positive association between higher EPDS scores and the number of labor and delivery triage visits (P = .006). There were no significant differences in the rates of Tdap vaccination or screening for sexually transmitted infections between the two groups.
Poor sleep linked to later depression
The other study was prospective, using data from the PATCH Prenatal Care and Maternal and Child Health Outcomes study, which initially “compared health outcomes and satisfaction with prenatal care between patients receiving Centering Pregnancy group prenatal care and patients receiving traditional prenatal care,” the authors explained. This secondary analysis looked at sleep problems and postpartum depression.
“We don’t routinely ask patients about sleep or screen patients for sleeping issues,” lead author Carolyn Sinow, MD, a 4th-year resident at Kaiser Permanente Santa Clara (Calif.) Medical Center, said in an interview. “I think that we need to take sleep complaints more seriously overall, especially in early pregnancy.” While sleep problems in the third trimester often have more to do with discomforts from pregnancy itself, better sleep “in the first and second trimester is something we can really target with good sleep hygiene,” she added.
The 336 pregnant participants were recruited from Health Connect as long as they had a singleton pregnancy, were receiving prenatal care from Kaiser Permanente Northern California, and completed baseline questionnaires about their sleep and depression and anxiety symptoms during their first trimester between August 2020 and April 2021. Those with clinical depression or a high-risk pregnancy were excluded. The participants then completed the questionnaires again between 4 and 8 weeks post partum.
After adjusting for baseline depression and potential confounders, patients with poor sleep quality, indicated by a score greater than 5 on the Pittsburgh Sleep Quality Index (PSQI), were 12% more likely to develop postpartum depression, indicated by a score on the Patient Health Questionnaire depression scale (PHQ-8) of 10 or greater (relative risk, 1.12; 95% confidence interval, 1.01-1.25).
The two aspects of sleep that specifically correlated with postpartum depression were sleep quality and sleep latency, or taking a long time to fall asleep. Those reporting poor sleep quality were twice as likely to develop postpartum depression (relative risk, 2.18; 95% CI, 1.22-3.91), and those who took a while to fall asleep were 52% more likely to develop postpartum depression (RR, 1.52; 95% CI, 1.06-2.17).
Though the study also found prenatal sleep problems correlated with higher postpartum anxiety scores on the General Anxiety Disorder scale (GAD-7), the results were not statistically significant.
Kathleen Morrell, MD, MPH, an ob.gyn. in New York, was not involved in the study and said she was surprised it wasn’t something that had been studied much before because it makes sense.
“I always like it when studies confirm what we think should make sense, so it’s nice to see it,” Dr. Morrell said in an interview. “I think anytime you put something out, research it, and define it with numbers for doctors, that sometimes allows us to [realize], ‘Oh, that’s probably something we should be paying more attention to, especially if we have available treatments for it,’” she added.
“The clinical takeaway is that we really need to be screening for sleep pattern disruptions early in pregnancy, because even though it makes logical sense, it might not be something on our radar to think about,” Dr. Morrell said. “If people aren’t sleeping, well, their mental health is negatively affected.”
The most promising therapy for sleep issues currently is cognitive-behavioral therapy, which can accessed through various apps, Dr. Sinow said in an interview. “There are also safe interventions, such as melatonin and Unisom, that are totally safe in pregnancy that we can use to target sleep in early pregnancy.”
Dr. Morrell added that vitamin B6, often taken for nausea and vomiting during pregnancy, can also sometimes help people sleep and is safe during pregnancy.
“We know that postpartum depression does not necessarily only have a negative effect on the mother, but also has a negative effect on the infant and the family dynamic as well,” Dr. Morrell said. “So, we should be looking and screening for it so that we can offer people potential treatment because we know it can have long-term effects.”
Ms. Jang and Dr. Sinow did not have any disclosures. Dr. Morrell has done training for Nexplanon. Neither study noted external funding.
AT ACOG 2023
As Medicaid purge begins, ‘staggering numbers’ of Americans lose coverage
More than 600,000 Americans have lost Medicaid coverage since pandemic protections ended on April 1. And a KFF Health News analysis of state data shows the vast majority were removed from state rolls for not completing paperwork.
Under normal circumstances, states review their Medicaid enrollment lists regularly to ensure every recipient qualifies for coverage. But because of a nationwide pause in those reviews during the pandemic, the health insurance program for low-income and disabled Americans kept people covered even if they no longer qualified.
Now, in what’s known as the Medicaid unwinding, states are combing through rolls and deciding who stays and who goes. People who are no longer eligible or don’t complete paperwork in time will be dropped.
The overwhelming majority of people who have lost coverage in most states were dropped because of technicalities, not because state officials determined they no longer meet Medicaid income limits. Four out of every five people dropped so far either never returned the paperwork or omitted required documents, according to a KFF Health News analysis of data from 11 states that provided details on recent cancellations. Now, lawmakers and advocates are expressing alarm over the volume of people losing coverage and, in some states, calling to pause the process.
KFF Health News sought data from the 19 states that started cancellations by May 1. Based on records from 14 states that provided detailed numbers, either in response to a public records request or by posting online, 36% of people whose eligibility was reviewed have been disenrolled.
In Indiana, 53,000 residents lost coverage in the first month of the unwinding, 89% for procedural reasons like not returning renewal forms. State Rep. Ed Clere, a Republican, expressed dismay at those “staggering numbers” in a May 24 Medicaid advisory group meeting, repeatedly questioning state officials about forms mailed to out-of-date addresses and urging them to give people more than 2 weeks’ notice before canceling their coverage.
Rep. Clere warned that the cancellations set in motion an avoidable revolving door. Some people dropped from Medicaid will have to forgo filling prescriptions and cancel doctor visits because they can’t afford care. Months down the line, after untreated chronic illnesses spiral out of control, they’ll end up in the emergency room where social workers will need to again help them join the program, he said.
Before the unwinding, more than one in four Americans – 93 million – were covered by Medicaid or CHIP, the Children’s Health Insurance Program, according to KFF Health News’ analysis of the latest enrollment data. Half of all kids are covered by the programs.
About 15 million people will be dropped over the next year as states review participants’ eligibility in monthly tranches.
Most people will find health coverage through new jobs or qualify for subsidized plans through the Affordable Care Act. But millions of others, including many children, will become uninsured and unable to afford basic prescriptions or preventive care. The uninsured rate among those under 65 is projected to rise from a historical low of 8.3% today to 9.3% next year, according to the Congressional Budget Office.
Because each state is handling the unwinding differently, the share of enrollees dropped in the first weeks varies widely.
Several states are first reviewing people officials believe are no longer eligible or who haven’t recently used their insurance. High cancellation rates in those states should level out as the agencies move on to people who likely still qualify.
In Utah, nearly 56% of people included in early reviews were dropped. In New Hampshire, 44% received cancellation letters within the first 2 months – almost all for procedural reasons, like not returning paperwork.
But New Hampshire officials found that thousands of people who didn’t fill out the forms indeed earn too much to qualify, according to Henry Lipman, the state’s Medicaid director. They would have been denied anyway. Even so, more people than he expected are not returning renewal forms. “That tells us that we need to change up our strategy,” said Mr. Lipman.
In other states, like Virginia and Nebraska, which aren’t prioritizing renewals by likely eligibility, about 90% have been renewed.
Because of the 3-year pause in renewals, many people on Medicaid have never been through the process or aren’t aware they may need to fill out long verification forms, as a recent KFF poll found. Some people moved and didn’t update their contact information.
And while agencies are required to assist enrollees who don’t speak English well, many are sending the forms in only a few common languages.
Tens of thousands of children are losing coverage, as researchers have warned, even though some may still qualify for Medicaid or CHIP. In its first month of reviews, South Dakota ended coverage for 10% of all Medicaid and CHIP enrollees in the state. More than half of them were children. In Arkansas, about 40% were kids.
Many parents don’t know that limits on household income are significantly higher for children than adults. Parents should fill out renewal forms even if they don’t qualify themselves, said Joan Alker, executive director of the Georgetown University Center for Children and Families, Washington.
New Hampshire has moved most families with children to the end of the review process. Mr. Lipman said his biggest worry is that a child will end up uninsured. Florida also planned to push kids with serious health conditions and other vulnerable groups to the end of the review line.
But according to Miriam Harmatz, advocacy director and founder of the Florida Health Justice Project, state officials sent cancellation letters to several clients with disabled children who probably still qualify. She’s helping those families appeal.
Nearly 250,000 Floridians reviewed in the first month of the unwinding lost coverage, 82% of them for reasons like incomplete paperwork, the state reported to federal authorities. House Democrats from the state petitioned Republican Gov. Ron DeSantis to pause the unwinding.
Advocacy coalitions in both Florida and Arkansas also have called for investigations into the review process and a pause on cancellations.
The state is contacting enrollees by phone, email, and text, and continues to process late applications, said Tori Cuddy, a spokesperson for the Florida Department of Children and Families. Ms. Cuddy did not respond to questions about issues raised in the petitions.
Federal officials are investigating those complaints and any other problems that emerge, said Dan Tsai, director of the Center for Medicaid & CHIP Services. “If we find that the rules are not being followed, we will take action.”
His agency has directed states to automatically reenroll residents using data from other government programs like unemployment and food assistance when possible. Anyone who can’t be approved through that process must act quickly.
“For the past 3 years, people have been told to ignore the mail around this, that the renewal was not going to lead to a termination.” Suddenly that mail matters, he said.
Federal law requires states to tell people why they’re losing Medicaid coverage and how to appeal the decision.
Ms. Harmatz said some cancellation notices in Florida are vague and could violate due process rules. Letters that she’s seen say “your Medicaid for this period is ending” rather than providing a specific reason for disenrollment, like having too high an income or incomplete paperwork.
If a person requests a hearing before their cancellation takes effect, they can stay covered during the appeals process. Even after being disenrolled, many still have a 90-day window to restore coverage.
In New Hampshire, 13% of people deemed ineligible in the first month have asked for extra time to provide the necessary records. “If you’re eligible for Medicaid, we don’t want you to lose it,” said Mr. Lipman.
Rep. Clere pushed Indiana’s Medicaid officials during the May meeting to immediately make changes to avoid people unnecessarily becoming uninsured. One official responded that they’ll learn and improve over time.
“I’m just concerned that we’re going to be ‘learning’ as a result of people losing coverage,” Rep. Clere replied. “So I don’t want to learn at their expense.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
More than 600,000 Americans have lost Medicaid coverage since pandemic protections ended on April 1. And a KFF Health News analysis of state data shows the vast majority were removed from state rolls for not completing paperwork.
Under normal circumstances, states review their Medicaid enrollment lists regularly to ensure every recipient qualifies for coverage. But because of a nationwide pause in those reviews during the pandemic, the health insurance program for low-income and disabled Americans kept people covered even if they no longer qualified.
Now, in what’s known as the Medicaid unwinding, states are combing through rolls and deciding who stays and who goes. People who are no longer eligible or don’t complete paperwork in time will be dropped.
The overwhelming majority of people who have lost coverage in most states were dropped because of technicalities, not because state officials determined they no longer meet Medicaid income limits. Four out of every five people dropped so far either never returned the paperwork or omitted required documents, according to a KFF Health News analysis of data from 11 states that provided details on recent cancellations. Now, lawmakers and advocates are expressing alarm over the volume of people losing coverage and, in some states, calling to pause the process.
KFF Health News sought data from the 19 states that started cancellations by May 1. Based on records from 14 states that provided detailed numbers, either in response to a public records request or by posting online, 36% of people whose eligibility was reviewed have been disenrolled.
In Indiana, 53,000 residents lost coverage in the first month of the unwinding, 89% for procedural reasons like not returning renewal forms. State Rep. Ed Clere, a Republican, expressed dismay at those “staggering numbers” in a May 24 Medicaid advisory group meeting, repeatedly questioning state officials about forms mailed to out-of-date addresses and urging them to give people more than 2 weeks’ notice before canceling their coverage.
Rep. Clere warned that the cancellations set in motion an avoidable revolving door. Some people dropped from Medicaid will have to forgo filling prescriptions and cancel doctor visits because they can’t afford care. Months down the line, after untreated chronic illnesses spiral out of control, they’ll end up in the emergency room where social workers will need to again help them join the program, he said.
Before the unwinding, more than one in four Americans – 93 million – were covered by Medicaid or CHIP, the Children’s Health Insurance Program, according to KFF Health News’ analysis of the latest enrollment data. Half of all kids are covered by the programs.
About 15 million people will be dropped over the next year as states review participants’ eligibility in monthly tranches.
Most people will find health coverage through new jobs or qualify for subsidized plans through the Affordable Care Act. But millions of others, including many children, will become uninsured and unable to afford basic prescriptions or preventive care. The uninsured rate among those under 65 is projected to rise from a historical low of 8.3% today to 9.3% next year, according to the Congressional Budget Office.
Because each state is handling the unwinding differently, the share of enrollees dropped in the first weeks varies widely.
Several states are first reviewing people officials believe are no longer eligible or who haven’t recently used their insurance. High cancellation rates in those states should level out as the agencies move on to people who likely still qualify.
In Utah, nearly 56% of people included in early reviews were dropped. In New Hampshire, 44% received cancellation letters within the first 2 months – almost all for procedural reasons, like not returning paperwork.
But New Hampshire officials found that thousands of people who didn’t fill out the forms indeed earn too much to qualify, according to Henry Lipman, the state’s Medicaid director. They would have been denied anyway. Even so, more people than he expected are not returning renewal forms. “That tells us that we need to change up our strategy,” said Mr. Lipman.
In other states, like Virginia and Nebraska, which aren’t prioritizing renewals by likely eligibility, about 90% have been renewed.
Because of the 3-year pause in renewals, many people on Medicaid have never been through the process or aren’t aware they may need to fill out long verification forms, as a recent KFF poll found. Some people moved and didn’t update their contact information.
And while agencies are required to assist enrollees who don’t speak English well, many are sending the forms in only a few common languages.
Tens of thousands of children are losing coverage, as researchers have warned, even though some may still qualify for Medicaid or CHIP. In its first month of reviews, South Dakota ended coverage for 10% of all Medicaid and CHIP enrollees in the state. More than half of them were children. In Arkansas, about 40% were kids.
Many parents don’t know that limits on household income are significantly higher for children than adults. Parents should fill out renewal forms even if they don’t qualify themselves, said Joan Alker, executive director of the Georgetown University Center for Children and Families, Washington.
New Hampshire has moved most families with children to the end of the review process. Mr. Lipman said his biggest worry is that a child will end up uninsured. Florida also planned to push kids with serious health conditions and other vulnerable groups to the end of the review line.
But according to Miriam Harmatz, advocacy director and founder of the Florida Health Justice Project, state officials sent cancellation letters to several clients with disabled children who probably still qualify. She’s helping those families appeal.
Nearly 250,000 Floridians reviewed in the first month of the unwinding lost coverage, 82% of them for reasons like incomplete paperwork, the state reported to federal authorities. House Democrats from the state petitioned Republican Gov. Ron DeSantis to pause the unwinding.
Advocacy coalitions in both Florida and Arkansas also have called for investigations into the review process and a pause on cancellations.
The state is contacting enrollees by phone, email, and text, and continues to process late applications, said Tori Cuddy, a spokesperson for the Florida Department of Children and Families. Ms. Cuddy did not respond to questions about issues raised in the petitions.
Federal officials are investigating those complaints and any other problems that emerge, said Dan Tsai, director of the Center for Medicaid & CHIP Services. “If we find that the rules are not being followed, we will take action.”
His agency has directed states to automatically reenroll residents using data from other government programs like unemployment and food assistance when possible. Anyone who can’t be approved through that process must act quickly.
“For the past 3 years, people have been told to ignore the mail around this, that the renewal was not going to lead to a termination.” Suddenly that mail matters, he said.
Federal law requires states to tell people why they’re losing Medicaid coverage and how to appeal the decision.
Ms. Harmatz said some cancellation notices in Florida are vague and could violate due process rules. Letters that she’s seen say “your Medicaid for this period is ending” rather than providing a specific reason for disenrollment, like having too high an income or incomplete paperwork.
If a person requests a hearing before their cancellation takes effect, they can stay covered during the appeals process. Even after being disenrolled, many still have a 90-day window to restore coverage.
In New Hampshire, 13% of people deemed ineligible in the first month have asked for extra time to provide the necessary records. “If you’re eligible for Medicaid, we don’t want you to lose it,” said Mr. Lipman.
Rep. Clere pushed Indiana’s Medicaid officials during the May meeting to immediately make changes to avoid people unnecessarily becoming uninsured. One official responded that they’ll learn and improve over time.
“I’m just concerned that we’re going to be ‘learning’ as a result of people losing coverage,” Rep. Clere replied. “So I don’t want to learn at their expense.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
More than 600,000 Americans have lost Medicaid coverage since pandemic protections ended on April 1. And a KFF Health News analysis of state data shows the vast majority were removed from state rolls for not completing paperwork.
Under normal circumstances, states review their Medicaid enrollment lists regularly to ensure every recipient qualifies for coverage. But because of a nationwide pause in those reviews during the pandemic, the health insurance program for low-income and disabled Americans kept people covered even if they no longer qualified.
Now, in what’s known as the Medicaid unwinding, states are combing through rolls and deciding who stays and who goes. People who are no longer eligible or don’t complete paperwork in time will be dropped.
The overwhelming majority of people who have lost coverage in most states were dropped because of technicalities, not because state officials determined they no longer meet Medicaid income limits. Four out of every five people dropped so far either never returned the paperwork or omitted required documents, according to a KFF Health News analysis of data from 11 states that provided details on recent cancellations. Now, lawmakers and advocates are expressing alarm over the volume of people losing coverage and, in some states, calling to pause the process.
KFF Health News sought data from the 19 states that started cancellations by May 1. Based on records from 14 states that provided detailed numbers, either in response to a public records request or by posting online, 36% of people whose eligibility was reviewed have been disenrolled.
In Indiana, 53,000 residents lost coverage in the first month of the unwinding, 89% for procedural reasons like not returning renewal forms. State Rep. Ed Clere, a Republican, expressed dismay at those “staggering numbers” in a May 24 Medicaid advisory group meeting, repeatedly questioning state officials about forms mailed to out-of-date addresses and urging them to give people more than 2 weeks’ notice before canceling their coverage.
Rep. Clere warned that the cancellations set in motion an avoidable revolving door. Some people dropped from Medicaid will have to forgo filling prescriptions and cancel doctor visits because they can’t afford care. Months down the line, after untreated chronic illnesses spiral out of control, they’ll end up in the emergency room where social workers will need to again help them join the program, he said.
Before the unwinding, more than one in four Americans – 93 million – were covered by Medicaid or CHIP, the Children’s Health Insurance Program, according to KFF Health News’ analysis of the latest enrollment data. Half of all kids are covered by the programs.
About 15 million people will be dropped over the next year as states review participants’ eligibility in monthly tranches.
Most people will find health coverage through new jobs or qualify for subsidized plans through the Affordable Care Act. But millions of others, including many children, will become uninsured and unable to afford basic prescriptions or preventive care. The uninsured rate among those under 65 is projected to rise from a historical low of 8.3% today to 9.3% next year, according to the Congressional Budget Office.
Because each state is handling the unwinding differently, the share of enrollees dropped in the first weeks varies widely.
Several states are first reviewing people officials believe are no longer eligible or who haven’t recently used their insurance. High cancellation rates in those states should level out as the agencies move on to people who likely still qualify.
In Utah, nearly 56% of people included in early reviews were dropped. In New Hampshire, 44% received cancellation letters within the first 2 months – almost all for procedural reasons, like not returning paperwork.
But New Hampshire officials found that thousands of people who didn’t fill out the forms indeed earn too much to qualify, according to Henry Lipman, the state’s Medicaid director. They would have been denied anyway. Even so, more people than he expected are not returning renewal forms. “That tells us that we need to change up our strategy,” said Mr. Lipman.
In other states, like Virginia and Nebraska, which aren’t prioritizing renewals by likely eligibility, about 90% have been renewed.
Because of the 3-year pause in renewals, many people on Medicaid have never been through the process or aren’t aware they may need to fill out long verification forms, as a recent KFF poll found. Some people moved and didn’t update their contact information.
And while agencies are required to assist enrollees who don’t speak English well, many are sending the forms in only a few common languages.
Tens of thousands of children are losing coverage, as researchers have warned, even though some may still qualify for Medicaid or CHIP. In its first month of reviews, South Dakota ended coverage for 10% of all Medicaid and CHIP enrollees in the state. More than half of them were children. In Arkansas, about 40% were kids.
Many parents don’t know that limits on household income are significantly higher for children than adults. Parents should fill out renewal forms even if they don’t qualify themselves, said Joan Alker, executive director of the Georgetown University Center for Children and Families, Washington.
New Hampshire has moved most families with children to the end of the review process. Mr. Lipman said his biggest worry is that a child will end up uninsured. Florida also planned to push kids with serious health conditions and other vulnerable groups to the end of the review line.
But according to Miriam Harmatz, advocacy director and founder of the Florida Health Justice Project, state officials sent cancellation letters to several clients with disabled children who probably still qualify. She’s helping those families appeal.
Nearly 250,000 Floridians reviewed in the first month of the unwinding lost coverage, 82% of them for reasons like incomplete paperwork, the state reported to federal authorities. House Democrats from the state petitioned Republican Gov. Ron DeSantis to pause the unwinding.
Advocacy coalitions in both Florida and Arkansas also have called for investigations into the review process and a pause on cancellations.
The state is contacting enrollees by phone, email, and text, and continues to process late applications, said Tori Cuddy, a spokesperson for the Florida Department of Children and Families. Ms. Cuddy did not respond to questions about issues raised in the petitions.
Federal officials are investigating those complaints and any other problems that emerge, said Dan Tsai, director of the Center for Medicaid & CHIP Services. “If we find that the rules are not being followed, we will take action.”
His agency has directed states to automatically reenroll residents using data from other government programs like unemployment and food assistance when possible. Anyone who can’t be approved through that process must act quickly.
“For the past 3 years, people have been told to ignore the mail around this, that the renewal was not going to lead to a termination.” Suddenly that mail matters, he said.
Federal law requires states to tell people why they’re losing Medicaid coverage and how to appeal the decision.
Ms. Harmatz said some cancellation notices in Florida are vague and could violate due process rules. Letters that she’s seen say “your Medicaid for this period is ending” rather than providing a specific reason for disenrollment, like having too high an income or incomplete paperwork.
If a person requests a hearing before their cancellation takes effect, they can stay covered during the appeals process. Even after being disenrolled, many still have a 90-day window to restore coverage.
In New Hampshire, 13% of people deemed ineligible in the first month have asked for extra time to provide the necessary records. “If you’re eligible for Medicaid, we don’t want you to lose it,” said Mr. Lipman.
Rep. Clere pushed Indiana’s Medicaid officials during the May meeting to immediately make changes to avoid people unnecessarily becoming uninsured. One official responded that they’ll learn and improve over time.
“I’m just concerned that we’re going to be ‘learning’ as a result of people losing coverage,” Rep. Clere replied. “So I don’t want to learn at their expense.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.