User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Score predicts risk for ventilation in COVID-19 patients
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.

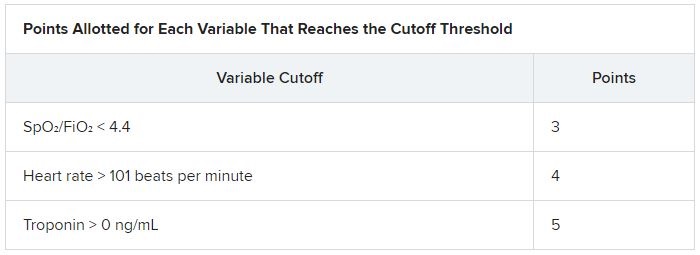
The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.

Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.
The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.
Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
A new scoring system can predict whether COVID-19 patients will require invasive mechanical ventilation, researchers report.
The score uses three variables to predict future risk: heart rate; the ratio of oxygen saturation (SpO2) to fraction of inspired oxygen (FiO2); and a positive troponin I level.
“What excites us is it’s a really benign tool,” said Muhtadi Alnababteh, MD, from the Medstar Washington (D.C.) Hospital Center. “For the first two variables you only need to look at vital signs, no labs or invasive diagnostics.”
“The third part is a simple lab, which is performed universally and can be done in any hospital,” he told this news organization. “We know that even rural hospitals can do this.”
For their retrospective analysis, Dr. Alnababteh and his colleagues assessed 265 adults with confirmed COVID-19 infection who were admitted to a single tertiary care center in March and April. They looked at demographic characteristics, lab results, and clinical and outcome information.
Ultimately, 54 of these patients required invasive mechanical ventilation.
On multiple-regression analysis, the researchers determined that three variables independently predicted the need for invasive mechanical ventilation.
Calibration of the model was good (Hosmer–Lemeshow score, 6.3; P = .39), as was predictive ability (area under the curve, 0.80).
The risk for invasive mechanical ventilation increased as the number of positive variables increased (P < .001), from 15.4% for those with one positive variable, to 29.0% for those with two, to 60.5% for those with three positive variables.
The team established cutoff points for each variable and developed a points-based scoring system to predict risk.
It was an initial surprise that troponin – a cardiac marker – would be a risk factor. “Originally, we thought COVID-19 only affects the lung,” Dr. Alnababteh explained during his presentation at CHEST 2020. Later studies, however, showed it can cause myocarditis symptoms.
The case for looking at cardiac markers was made when a study of young athletes who recovered from COVID-19 after experiencing mild or no symptoms showed that 15% had signs of myocarditis on cardiac MRI.
“If mild COVID disease in young patients caused cardiac injury, you can imagine what it can do to older patients with severe disease,” Alnababteh said.
This tool will help triage patients who are not sick enough for the ICU but are known to be at high risk for ventilation. “It’s one of the biggest decisions you have to make: Where do you send your patient? This score helps determine that,” he said.
The researchers are now working to validate the score and evaluate how it performs, he reported.
Existing scores evaluated for COVID-19 outcome prediction
The MuLBSTA score can also be used to predict outcomes in patients with COVID-19.
A retrospective evaluation of 163 patients was presented at CHEST 2020 by Jurgena Tusha, MD, from Wayne State University in Detroit.
Patients who survived their illness had a mean MuLBSTA score of 8.67, whereas patients who died had a mean score of 13.60.
The score “correlated significantly with mortality, ventilator support, and length of stay, which may be used to provide guidance to screen patients and make further clinical decisions,” Dr. Tusha said in a press release.
“Further studies are required to validate this study in larger patient cohorts,” she added.
The three-variable scoring system is easier to use than the MuLBSTA, and more specific, said Dr. Alnababteh.
“The main difference between our study and the MuLBSTA study is that we came up with a novel score for COVID-19 patients,” he said. “Our study score doesn’t require chest x-rays or blood cultures, and the outcome is need for invasive mechanical ventilation, not mortality.”
A version of this article originally appeared on Medscape.com.
Trump and Biden face off over COVID-19, ACA in final debate
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
The COVID-19 pandemic figured prominently in the final debate between President Donald Trump and former Vice President Joe Biden when they met on stage for a 90-minute debate in Nashville, Tennessee, Thursday evening.
The adequacy of the COVID-19 response to date, the likely timeline for vaccine availability, and how to reopen businesses while keeping Americans safe were among the points on which the two candidates disagreed. The two candidates also sparred over the value of the Affordable Care Act (ACA) and the future of healthcare in the United States.
Trump and Biden also differed on whether or not the country is facing a “dark winter” because of the pandemic.
Moderator Kristen Welker, NBC News White House correspondent, asked Trump to comment on the fact that 40,000 people are in the hospital on debate night with COVID-19 and that 16,000 have died since the last presidential debate.
Trump said, “2.2 million people modeled out were expected to die.” He said COVID-19 is a worldwide disease that does not only affect the United States.
“The mortality rate is down 85%, and the excess mortality is also down,” he added. He pointed out that previous spikes in Florida, Texas, and Arizona are now gone, and “spikes and surges in other places will soon be gone.
“It will go away, we are rounding the corner,” Trump said. “From personal experience, I was in the hospital, I had it, and they gave me a therapeutic, some would call it a cure...and now they say I’m immune. Whether it’s for a month or lifetime, nobody has been able to say that, but I’m immune.”
Biden countered by saying that “220,000 people are dead. If you hear nothing else I say tonight, hear this: Anyone who’s responsible for that many deaths should not remain president of the United States of America.”
Biden said there are a thousand deaths a day now and that there are over 70K new cases per day. “The expectation is we will have another 200,000 people down before the end of this year. If we just all wore these masks, we could save 100,000.”
“The New England Journal of Medicine said the way the president has handled this is absolutely tragic,” Biden added.
Vaccine timeline
Welker asked Trump if he could guarantee that there will be a COVID-19 vaccine within weeks.
“I can’t guarantee that, but it will be by end of the year. It will be distributed very quickly,” Trump said. He added that three leading vaccine developers, Johnson & Johnson, Moderna, and Pfizer, “are doing very well.”
“We’re about to go into a dark winter and he has no clear plan,” Biden said. “There is no prospect there will be a vaccine for most Americans by middle of next year.”
“It will not be a dark winter,” Trump responded.
Reopening the economy
Trump and Biden disagreed on how aggressively the economy should be reopened in light of the pandemic.
“I want to open the schools. We can’t keep this country closed,” Trump said. “This is a massive country with a massive economy.” He pointed out that rates of depression and suicide have risen because of the economic shutdown. “The cure cannot be worse than the problem.
“His Democrat governors...shut down so tight, and they’re dying,” the president added, gesturing toward Biden. “We are not going to shut down. We are going to open the schools.” As an example of the resiliency of young people, he mentioned that his son Barron tested positive for COVID-19 and recovered.
“I would shut down the virus, not the country,” Biden said. “It’s his ineptitude that caused so many schools and businesses to close in large part. Instead of being in a sand trap playing golf, he should have been negotiating with Nancy Pelosi.”
“He says we’re learning to live with it,” the former vice president said, but instead, “people are learning to die with it.”
Biden added that reopening the economy and minimizing transmission of COVID-19 are not mutually exclusive. “We can walk and chew gum at the same time.”
Divergence over the ACA
The fate of the ACA also garnered considerable attention. The discussion underlined a vast difference of opinion between the two candidates on the US healthcare system.
The moderator asked Trump what he would do for the 20 million Americans who get their healthcare through the ACA if it’s taken away.
“Through the legislature, I terminated the individual mandate, the worst part of Obamacare,” Trump said. “And now it’s in court because Obamacare is no good.
“Preexisting conditions will stay,” Trump added.
“I want to terminate Obamacare, and I want to come up with a beautiful healthcare [plan],” Trump added, turning the discussion toward private health insurance. “One thing that is very important is we have 180 million out there who have great private healthcare. Joe Biden will terminate all of their healthcare.”
Trump described Biden’s plan as “socialized medicine.” He also emphasized that protections for people with preexisting conditions “will stay.”
The Trump administration is supporting a lawsuit to overturn the ACA. The suit was filed by 18 Republican-led states. Arguments before the US Supreme Court on the constitutionality of the ACA are scheduled for November 10.
The moderator asked what Biden plans to do if the ACA is struck down. “I will pass Obamacare with a public option ― that will be ‘Bidencare.’ “ He said his plan will reduce premiums and drug prices. “I support private insurance. No one lost their private insurance under Obamacare.
“There is no way he can protect preexisting conditions,” Biden said. He added that 10 million people have already lost their private healthcare through unemployment during the pandemic.
Muting the mic
Following what many described as a chaotic first debate at the Cleveland Clinic in Ohio on September 29, the Commission on Presidential Debate opted to allow the muting of the microphone during the first 2 minutes of remarks made by each candidate during each debate segment.
The muting of the microphones appeared to prevent crosstalk during the beginning of each segment of the debate. The candidates did manage to talk over and interrupt each other, as well as the moderator, during portions of the debate.
This article first appeared on Medscape.com.
COVID-19 a new opportunity for suicide prevention
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.
The ongoing COVID-19 pandemic poses clear threats to mental well-being, but an increase in suicide is not inevitable if appropriate action is taken, one expert says.
“Increases in suicide rates should not be a foregone conclusion, even with the negative effects of the pandemic. If the lessons of suicide prevention research are heeded during and after the pandemic, this potential for increased risk could be substantially mitigated,” writes Christine Moutier, MD, chief medical officer of the American Foundation for Suicide Prevention, in an invited communication in JAMA Psychiatry.
“This is a moment in history when suicide prevention must be prioritized as a serious public health concern,” she writes.
Mitigating suicide risk
Although evidence from the first 6 months of the pandemic reveal specific effects on suicide risk, real-time data on suicide deaths are not available in most regions of the world. From emerging data from several countries, there is no evidence of increased suicide rates during the pandemic thus far, Moutier notes.
Still, a number of pandemic-related risk factors could increase individual and population suicide risk.
They include deterioration or recurrence of serious mental illness; increased isolation, loneliness, and bereavement; increased use of drugs and alcohol; job loss and other financial stressors; and increases in domestic violence.
There are mitigating strategies for each of these “threats to suicide risk.” The science is “very clear,” Moutier told Medscape Medical News.
“Suicide risk is never a situation of inevitability. It’s dynamic, with multiple forces at play in each individual and in the population. Lives can be saved simply by making people feel more connected to each other, that they are part of a larger community,” she added.
The political will
Moutier notes that prior to the pandemic, four countries ― Finland, Norway, Sweden, and Australia ― had fully implemented national suicide prevention plans and had achieved reductions in their national suicide rates. However, in the United States, the suicide rate has been steadily increasing since 1999.
A Centers for Disease Control and Prevention survey released in August 2020 found that 40% of US adults reported symptoms of depression, anxiety, or increased substance use during COVID-19 and that about 11% reported suicidal ideation in the past month, all increases from prior surveys.
COVID-19 presents a “new and urgent opportunity” to focus political will, federal investments, and the global community on suicide prevention, Moutier writes.
“The political will to address suicide has actually moved in the right direction during COVID, as evidenced by a number of pieces of legislation that have suddenly found their way to passing that we’ve been working on for years,” she said in an interview.
One example, she said, is the National Suicide Hotline Designation Act, signed into law earlier this month by President Donald Trump.
As previously reported, under the law, beginning in July 2022, Americans experiencing a mental health crisis will be able to dial 9-8-8 and be connected to the services and counselors at the National Suicide Prevention Lifeline.
Moutier reports no relevant financial relationships.
This article first appeared on Medscape.com.
Florida will investigate all COVID-19 deaths
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
The Florida Department of Health will investigate the state’s 16,000 coronavirus deaths due to questions about the integrity of the data, according to an announcement issued Wednesday.
State health department officials said the “fatality data reported to the state consistently presents confusion and warrants a rigorous review.” The review is meant to “ensure data integrity.”
“During a pandemic, the public must be able to rely on accurate public health data to make informed decisions,” Scott Rivkees, the surgeon general for Florida, said in the statement.
Among the 95 deaths reported Wednesday for instance, 16 had more than a 2-month separation between the time of testing positive for COVID-19 and passing away, and 5 cases had a 3-month gap. In addition, 11 of the deaths occurred more than a month ago.
The health department then listed data for all 95 cases, including the age, gender, county and the dates of test positivity and death. Palm Beach County had 50 of the COVID-19 deaths.
“To ensure the accuracy of COVID-19 related deaths, the department will be performing additional reviews of all deaths,” Rivkees said. “Timely and accurate data remains a top priority of the Department of Health.”
Last week, Jose Oliva, speaker of the Florida House of Representatives, said medical examiner reports were “often lacking in rigor.” House Democrats then said Republicans were trying to “downplay the death toll,” according to the South Florida Sun Sentinel .
Fred Piccolo Jr., a spokesman for Florida Gov. Ron DeSantis, told the newspaper Wednesday that officials have struggled to obtain timely data. Labs sometimes report test results from weeks before, he added.
“It’s really one of those things that you gotta know if someone is dying of COVID or if they’re not,” Piccolo said. “Then you can legitimately say, here are the numbers.”
Sources
Florida Department of Health, “Florida Surgeon General Implements Additional Review Process for Fatalities Attributed to COVID-19 to Ensure Data Integrity.”
South Florida Sun Sentinel, “Florida to investigate all COVID-19 deaths after questions about ‘integrity’ of data.”
WebMD Health News © 2020
This article first appeared on Medscape.com.
When should students resume sports after a COVID-19 diagnosis?
Many student athletes who test positive for COVID-19 likely can have an uneventful return to their sports after they have rested for 2 weeks in quarantine, doctors suggest.

There are reasons for caution, however, especially when a patient has symptoms that indicate possible cardiac involvement. In these cases, patients should undergo cardiac testing before a physician clears them to return to play, according to guidance from professional associations. Reports of myocarditis in college athletes who tested positive for SARS-CoV-2 but were asymptomatic are among the reasons for concern. Myocarditis may increase the risk of sudden death during exercise.
“The thing that you need to keep in mind is that this is not just a respiratory illness,” David T. Bernhardt, MD, professor of pediatrics, orthopedics, and rehabilitation at the University of Wisconsin in Madison, said in a presentation at the annual meeting of the American Academy of Pediatrics, held virtually this year. High school and college athletes have had cardiac, neurologic, hematologic, and renal problems that “can complicate their recovery and their return to sport.”
Still, children who test positive for COVID-19 tend to have mild illness and often are asymptomatic. “It is more than likely going to be safe for the majority of the student athletes who are in the elementary and middle school age to return to sport,” said Dr. Bernhardt. Given that 18-year-old college freshmen have had cardiac complications, there may be reason for more caution with high school students.
Limited data

The AAP has released interim guidance on returning to sports and recommends that primary care physicians clear all patients with COVID-19 before they resume training. Physicians should screen for cardiac symptoms such as chest pain, shortness of breath, fatigue, palpitations, or syncope.
Those with severe illness should be restricted from exercise and participation for 3-6 months. Primary care physicians, preferably in consultation with pediatric cardiologists, should clear athletes who experience severe illness.
“Most of the recommendations come from the fact that we simply do not know what we do not know with COVID-19,” Susannah Briskin, MD, a coauthor of the interim guidance, said in an interview. “We have to be cautious in returning individuals to play and closely monitor them as we learn more about the disease process and its effect on kids.”
Patients with severe illness could include those who were hospitalized and experienced hypotension or arrhythmias, required intubation or extracorporeal membrane oxygenation (ECMO) support, had kidney or cardiac failure, or developed multisystem inflammatory syndrome in children (MIS-C), said Dr. Briskin, a specialist in pediatric sports medicine at Case Western Reserve University, Cleveland.
“The majority of COVID-19 cases will not present like this in kids. We have no idea how common myocarditis is in kids post infection. We do know that, if anyone has chest pain, shortness of breath, excessive fatigue, syncope [passing out], or arrhythmia [feeling of their heart skipping beats], they should undergo further evaluation for myocarditis,” Dr. Briskin said.
Patients who are asymptomatic or have mild symptoms should rest for 14 days after their positive test. After their infectious period has passed, a doctor should assess for any concerning cardiac symptoms. “Anyone with prolonged fever or moderate symptoms should see their pediatrician and have an EKG performed, at a minimum, prior to return to sports,” Dr. Briskin said. “Anyone with an abnormal EKG or concerning signs or symptoms should be referred on to pediatric cardiology for a further assessment.”
Most patients who Dr. Briskin has seen have been asymptomatic or mildly symptomatic. “They have done well with a gradual return to physical activity,” she said. “We recommend a gradual return so individuals can be monitored for any signs or symptoms concerning for myocarditis. The far majority of individuals likely have an uneventful return to play.”
Mitigating risk

COVID-19 adds elements of uncertainty and complexity to the usual process of mitigating risk in sports, Dr. Bernhardt noted in his lecture. “You are dealing with an infection that we do not know a lot about,” he said. “And we are trying to mitigate risk not only for the individual who may or may not have underlying health problems, but you are also trying to mitigate risk for anybody else involved with the sport, including athletic trainers and team physicians, coaches, spectators, custodial staff, people working at a snack shack, and all the other people that can be involved in a typical sporting type of atmosphere.”
When patients do return to play after an illness, they should gradually increase the training load to avoid injury. In addition, clinicians should screen for depression and anxiety using tools such as the Four-Item Patient Health Questionnaire (PHQ-4) when they see patients. “The pandemic has been quite stressful for everybody, including our high school student athletes,” Dr. Bernhardt said. “Giving everybody a PHQ-4 when they come into clinic right now probably makes sense in terms of the stress levels that all of us are experiencing.”
If a patient screens positive, take additional history and refer for more in-depth mental health evaluation and treatment if warranted. Sharing breathing and relaxation exercises, promoting healthy behaviors, and paying attention to unhealthy strategies also may help, Dr. Bernhardt suggested.
Ultimately, determining when an athlete with COVID-19 can be medically cleared to return to play may be a challenge. There are limited data on epidemiology and clinical presentations that could help identify cardiac injury related to the disease, Dr. Bernhardt said. Guidance from the American College of Cardiology provides a framework for evaluating athletes for return to play, and pediatric cardiologists have discussed how the guidance relates to a pediatric population. Cardiac assessments may include measures of biomarkers such as troponin, B-type natriuretic peptide, and sedimentation rate, along with electrocardiograms, echocardiograms, and cardiac MRI.
Beyond return-to-play decisions, encourage the use of cloth face coverings on the sidelines and away from the playing field, and stress proper quarantining, Dr. Briskin added. Too often, she hears about children not quarantining properly. “Individuals with a known exposure should be quarantined in their house – ideally in a separate room from everyone else. ... When they come out of their room, they should wash their hands well and wear a cloth face covering. They should not be eating with other people.”
Dr. Bernhardt had no relevant disclosures.
Many student athletes who test positive for COVID-19 likely can have an uneventful return to their sports after they have rested for 2 weeks in quarantine, doctors suggest.
There are reasons for caution, however, especially when a patient has symptoms that indicate possible cardiac involvement. In these cases, patients should undergo cardiac testing before a physician clears them to return to play, according to guidance from professional associations. Reports of myocarditis in college athletes who tested positive for SARS-CoV-2 but were asymptomatic are among the reasons for concern. Myocarditis may increase the risk of sudden death during exercise.
“The thing that you need to keep in mind is that this is not just a respiratory illness,” David T. Bernhardt, MD, professor of pediatrics, orthopedics, and rehabilitation at the University of Wisconsin in Madison, said in a presentation at the annual meeting of the American Academy of Pediatrics, held virtually this year. High school and college athletes have had cardiac, neurologic, hematologic, and renal problems that “can complicate their recovery and their return to sport.”
Still, children who test positive for COVID-19 tend to have mild illness and often are asymptomatic. “It is more than likely going to be safe for the majority of the student athletes who are in the elementary and middle school age to return to sport,” said Dr. Bernhardt. Given that 18-year-old college freshmen have had cardiac complications, there may be reason for more caution with high school students.
Limited data
The AAP has released interim guidance on returning to sports and recommends that primary care physicians clear all patients with COVID-19 before they resume training. Physicians should screen for cardiac symptoms such as chest pain, shortness of breath, fatigue, palpitations, or syncope.
Those with severe illness should be restricted from exercise and participation for 3-6 months. Primary care physicians, preferably in consultation with pediatric cardiologists, should clear athletes who experience severe illness.
“Most of the recommendations come from the fact that we simply do not know what we do not know with COVID-19,” Susannah Briskin, MD, a coauthor of the interim guidance, said in an interview. “We have to be cautious in returning individuals to play and closely monitor them as we learn more about the disease process and its effect on kids.”
Patients with severe illness could include those who were hospitalized and experienced hypotension or arrhythmias, required intubation or extracorporeal membrane oxygenation (ECMO) support, had kidney or cardiac failure, or developed multisystem inflammatory syndrome in children (MIS-C), said Dr. Briskin, a specialist in pediatric sports medicine at Case Western Reserve University, Cleveland.
“The majority of COVID-19 cases will not present like this in kids. We have no idea how common myocarditis is in kids post infection. We do know that, if anyone has chest pain, shortness of breath, excessive fatigue, syncope [passing out], or arrhythmia [feeling of their heart skipping beats], they should undergo further evaluation for myocarditis,” Dr. Briskin said.
Patients who are asymptomatic or have mild symptoms should rest for 14 days after their positive test. After their infectious period has passed, a doctor should assess for any concerning cardiac symptoms. “Anyone with prolonged fever or moderate symptoms should see their pediatrician and have an EKG performed, at a minimum, prior to return to sports,” Dr. Briskin said. “Anyone with an abnormal EKG or concerning signs or symptoms should be referred on to pediatric cardiology for a further assessment.”
Most patients who Dr. Briskin has seen have been asymptomatic or mildly symptomatic. “They have done well with a gradual return to physical activity,” she said. “We recommend a gradual return so individuals can be monitored for any signs or symptoms concerning for myocarditis. The far majority of individuals likely have an uneventful return to play.”
Mitigating risk
COVID-19 adds elements of uncertainty and complexity to the usual process of mitigating risk in sports, Dr. Bernhardt noted in his lecture. “You are dealing with an infection that we do not know a lot about,” he said. “And we are trying to mitigate risk not only for the individual who may or may not have underlying health problems, but you are also trying to mitigate risk for anybody else involved with the sport, including athletic trainers and team physicians, coaches, spectators, custodial staff, people working at a snack shack, and all the other people that can be involved in a typical sporting type of atmosphere.”
When patients do return to play after an illness, they should gradually increase the training load to avoid injury. In addition, clinicians should screen for depression and anxiety using tools such as the Four-Item Patient Health Questionnaire (PHQ-4) when they see patients. “The pandemic has been quite stressful for everybody, including our high school student athletes,” Dr. Bernhardt said. “Giving everybody a PHQ-4 when they come into clinic right now probably makes sense in terms of the stress levels that all of us are experiencing.”
If a patient screens positive, take additional history and refer for more in-depth mental health evaluation and treatment if warranted. Sharing breathing and relaxation exercises, promoting healthy behaviors, and paying attention to unhealthy strategies also may help, Dr. Bernhardt suggested.
Ultimately, determining when an athlete with COVID-19 can be medically cleared to return to play may be a challenge. There are limited data on epidemiology and clinical presentations that could help identify cardiac injury related to the disease, Dr. Bernhardt said. Guidance from the American College of Cardiology provides a framework for evaluating athletes for return to play, and pediatric cardiologists have discussed how the guidance relates to a pediatric population. Cardiac assessments may include measures of biomarkers such as troponin, B-type natriuretic peptide, and sedimentation rate, along with electrocardiograms, echocardiograms, and cardiac MRI.
Beyond return-to-play decisions, encourage the use of cloth face coverings on the sidelines and away from the playing field, and stress proper quarantining, Dr. Briskin added. Too often, she hears about children not quarantining properly. “Individuals with a known exposure should be quarantined in their house – ideally in a separate room from everyone else. ... When they come out of their room, they should wash their hands well and wear a cloth face covering. They should not be eating with other people.”
Dr. Bernhardt had no relevant disclosures.
Many student athletes who test positive for COVID-19 likely can have an uneventful return to their sports after they have rested for 2 weeks in quarantine, doctors suggest.
There are reasons for caution, however, especially when a patient has symptoms that indicate possible cardiac involvement. In these cases, patients should undergo cardiac testing before a physician clears them to return to play, according to guidance from professional associations. Reports of myocarditis in college athletes who tested positive for SARS-CoV-2 but were asymptomatic are among the reasons for concern. Myocarditis may increase the risk of sudden death during exercise.
“The thing that you need to keep in mind is that this is not just a respiratory illness,” David T. Bernhardt, MD, professor of pediatrics, orthopedics, and rehabilitation at the University of Wisconsin in Madison, said in a presentation at the annual meeting of the American Academy of Pediatrics, held virtually this year. High school and college athletes have had cardiac, neurologic, hematologic, and renal problems that “can complicate their recovery and their return to sport.”
Still, children who test positive for COVID-19 tend to have mild illness and often are asymptomatic. “It is more than likely going to be safe for the majority of the student athletes who are in the elementary and middle school age to return to sport,” said Dr. Bernhardt. Given that 18-year-old college freshmen have had cardiac complications, there may be reason for more caution with high school students.
Limited data
The AAP has released interim guidance on returning to sports and recommends that primary care physicians clear all patients with COVID-19 before they resume training. Physicians should screen for cardiac symptoms such as chest pain, shortness of breath, fatigue, palpitations, or syncope.
Those with severe illness should be restricted from exercise and participation for 3-6 months. Primary care physicians, preferably in consultation with pediatric cardiologists, should clear athletes who experience severe illness.
“Most of the recommendations come from the fact that we simply do not know what we do not know with COVID-19,” Susannah Briskin, MD, a coauthor of the interim guidance, said in an interview. “We have to be cautious in returning individuals to play and closely monitor them as we learn more about the disease process and its effect on kids.”
Patients with severe illness could include those who were hospitalized and experienced hypotension or arrhythmias, required intubation or extracorporeal membrane oxygenation (ECMO) support, had kidney or cardiac failure, or developed multisystem inflammatory syndrome in children (MIS-C), said Dr. Briskin, a specialist in pediatric sports medicine at Case Western Reserve University, Cleveland.
“The majority of COVID-19 cases will not present like this in kids. We have no idea how common myocarditis is in kids post infection. We do know that, if anyone has chest pain, shortness of breath, excessive fatigue, syncope [passing out], or arrhythmia [feeling of their heart skipping beats], they should undergo further evaluation for myocarditis,” Dr. Briskin said.
Patients who are asymptomatic or have mild symptoms should rest for 14 days after their positive test. After their infectious period has passed, a doctor should assess for any concerning cardiac symptoms. “Anyone with prolonged fever or moderate symptoms should see their pediatrician and have an EKG performed, at a minimum, prior to return to sports,” Dr. Briskin said. “Anyone with an abnormal EKG or concerning signs or symptoms should be referred on to pediatric cardiology for a further assessment.”
Most patients who Dr. Briskin has seen have been asymptomatic or mildly symptomatic. “They have done well with a gradual return to physical activity,” she said. “We recommend a gradual return so individuals can be monitored for any signs or symptoms concerning for myocarditis. The far majority of individuals likely have an uneventful return to play.”
Mitigating risk
COVID-19 adds elements of uncertainty and complexity to the usual process of mitigating risk in sports, Dr. Bernhardt noted in his lecture. “You are dealing with an infection that we do not know a lot about,” he said. “And we are trying to mitigate risk not only for the individual who may or may not have underlying health problems, but you are also trying to mitigate risk for anybody else involved with the sport, including athletic trainers and team physicians, coaches, spectators, custodial staff, people working at a snack shack, and all the other people that can be involved in a typical sporting type of atmosphere.”
When patients do return to play after an illness, they should gradually increase the training load to avoid injury. In addition, clinicians should screen for depression and anxiety using tools such as the Four-Item Patient Health Questionnaire (PHQ-4) when they see patients. “The pandemic has been quite stressful for everybody, including our high school student athletes,” Dr. Bernhardt said. “Giving everybody a PHQ-4 when they come into clinic right now probably makes sense in terms of the stress levels that all of us are experiencing.”
If a patient screens positive, take additional history and refer for more in-depth mental health evaluation and treatment if warranted. Sharing breathing and relaxation exercises, promoting healthy behaviors, and paying attention to unhealthy strategies also may help, Dr. Bernhardt suggested.
Ultimately, determining when an athlete with COVID-19 can be medically cleared to return to play may be a challenge. There are limited data on epidemiology and clinical presentations that could help identify cardiac injury related to the disease, Dr. Bernhardt said. Guidance from the American College of Cardiology provides a framework for evaluating athletes for return to play, and pediatric cardiologists have discussed how the guidance relates to a pediatric population. Cardiac assessments may include measures of biomarkers such as troponin, B-type natriuretic peptide, and sedimentation rate, along with electrocardiograms, echocardiograms, and cardiac MRI.
Beyond return-to-play decisions, encourage the use of cloth face coverings on the sidelines and away from the playing field, and stress proper quarantining, Dr. Briskin added. Too often, she hears about children not quarantining properly. “Individuals with a known exposure should be quarantined in their house – ideally in a separate room from everyone else. ... When they come out of their room, they should wash their hands well and wear a cloth face covering. They should not be eating with other people.”
Dr. Bernhardt had no relevant disclosures.
FROM AAP 2020

Add-on psychotherapy a win in bipolar disorder
Adding psychotherapy to pharmacotherapy benefits patients with bipolar disorder (BD), particularly when delivered in family or group settings, results of a new meta-analysis confirms.
Outpatients with BD receiving drug therapy “should also be offered psychosocial treatments that emphasize illness management strategies and enhance coping skills; delivering these components in family or group format may be especially advantageous,” wrote the investigators, led by David Miklowitz, PhD, University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior.
The study was published online Oct. 14 in JAMA Psychiatry.
Drugs alone not enough
It’s increasingly recognized that drug therapy alone can’t prevent recurrences of BD or fully alleviate postepisode symptoms or functional impairment, the researchers noted in their article. Several psychotherapy protocols have been shown to benefit patients with BD when used in conjunction with drug therapy, but little is known about their comparative effectiveness.
To investigate, the researchers conducted a systematic review and component network meta-analysis of 39 randomized clinical trials (36 involving adults and three involving adolescents).
The trials involved 3,863 patients with BD and compared pharmacotherapy used in conjunction with manualized psychotherapy (cognitive-behavioral therapy [CBT], family or conjoint therapy, interpersonal therapy, and/or psychoeducational therapy) with pharmacotherapy delivered in conjunction with a control intervention (supportive therapy or treatment as usual).
Across 20 two-group trials that provided usable information, manualized psychotherapies were associated with a lower probability of illness recurrence (the primary outcome), compared with control interventions (odds ratio, 0.56; 95% CI, 0.43-0.74).
Psychoeducation with guided practice of illness management skills in a family or group format was superior to these strategies delivered in an individual format (OR, 0.12; 95% CI, 0.02-0.94).
Family or conjoint therapy and brief psychoeducation were associated with lower attrition rates than standard psychoeducation.
For the secondary outcome of stabilization of depressive or manic symptoms over 12 months, CBT and, with less certainty, family or conjoint therapy and interpersonal therapy were more effective than treatment as usual.
The investigators note that the findings are in line with a network meta-analysis published earlier this year that found that combining psychotherapy with pharmacotherapy is the best option for stabilizing episodes and preventing recurrences of major depression.
“[T]here is enough evidence from this analysis and others to conclude that health care systems should offer combinations of evidence-based pharmacotherapy and psychotherapy” to outpatients with BD, the researchers note.
and active tasks to enhance coping skills (e.g., monitoring and managing prodromal symptoms) rather than being passive recipients of didactic education,” they wrote.
“When the immediate goal is recovery from moderately severe depressive or manic symptoms, cognitive restructuring, regulating daily rhythms, and communication training may be associated with stabilization,” they added.
A call to action
The coauthors of an editorial in JAMA Psychiatry noted that the findings “further reinforce extant treatment guidelines recommending medication management and adjunctive evidence-based psychosocial treatments for individuals with BD.”
The findings also “identify specific treatment components and formats most strongly associated with preventing relapse and addressing mood symptoms,” write Tina Goldstein, PhD, and Danella Hafeman, MD, PhD, from Western Psychiatric Hospital, University of Pittsburgh.
The study “may further serve as a call to action to enhance availability and uptake of these treatments in the community. Unfortunately, data suggest substantially lower rates of psychotherapy receipt (26%-50%), compared with medication management (46%-90%) among adults with BD,” they wrote.
Dr. Goldstein and Dr. Hafeman noted future steps for the field include “demonstrating effectiveness of evidence-based treatment approaches for BD in the community, maximizing accessibility, and furthering knowledge that informs individualized treatment selection with substantial promise to optimize outcomes for individuals with BD.”
The study was supported in part by a grant from the National Institute for Health Research Oxford Health Biomedical Research Centre. Dr. Miklowitz has received research support from the NIHR, the Danny Alberts Foundation, the Attias Family Foundation, the Carl and Roberta Deutsch Foundation, the Kayne Family Foundation, AIM for Mental Health, and the Max Gray Fund; book royalties from Guilford Press and John Wiley and Sons; and served as principal investigator on four of the trials included in this meta-analysis. Dr. Goldstein has received grants from the National Institute of Mental Health, the American Foundation for Suicide Prevention, the University of Pittsburgh Clinical and Translational Science Institute, and the Brain and Behavior Research Foundation and royalties from Guilford Press outside the submitted work. Dr. Hafeman has received grants from the National Institute of Mental Health, the Brain and Behavior Research Foundation, and the Klingenstein Third Generation Foundation.
This article first appeared on Medscape.com.
Adding psychotherapy to pharmacotherapy benefits patients with bipolar disorder (BD), particularly when delivered in family or group settings, results of a new meta-analysis confirms.
Outpatients with BD receiving drug therapy “should also be offered psychosocial treatments that emphasize illness management strategies and enhance coping skills; delivering these components in family or group format may be especially advantageous,” wrote the investigators, led by David Miklowitz, PhD, University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior.
The study was published online Oct. 14 in JAMA Psychiatry.
Drugs alone not enough
It’s increasingly recognized that drug therapy alone can’t prevent recurrences of BD or fully alleviate postepisode symptoms or functional impairment, the researchers noted in their article. Several psychotherapy protocols have been shown to benefit patients with BD when used in conjunction with drug therapy, but little is known about their comparative effectiveness.
To investigate, the researchers conducted a systematic review and component network meta-analysis of 39 randomized clinical trials (36 involving adults and three involving adolescents).
The trials involved 3,863 patients with BD and compared pharmacotherapy used in conjunction with manualized psychotherapy (cognitive-behavioral therapy [CBT], family or conjoint therapy, interpersonal therapy, and/or psychoeducational therapy) with pharmacotherapy delivered in conjunction with a control intervention (supportive therapy or treatment as usual).
Across 20 two-group trials that provided usable information, manualized psychotherapies were associated with a lower probability of illness recurrence (the primary outcome), compared with control interventions (odds ratio, 0.56; 95% CI, 0.43-0.74).
Psychoeducation with guided practice of illness management skills in a family or group format was superior to these strategies delivered in an individual format (OR, 0.12; 95% CI, 0.02-0.94).
Family or conjoint therapy and brief psychoeducation were associated with lower attrition rates than standard psychoeducation.
For the secondary outcome of stabilization of depressive or manic symptoms over 12 months, CBT and, with less certainty, family or conjoint therapy and interpersonal therapy were more effective than treatment as usual.
The investigators note that the findings are in line with a network meta-analysis published earlier this year that found that combining psychotherapy with pharmacotherapy is the best option for stabilizing episodes and preventing recurrences of major depression.
“[T]here is enough evidence from this analysis and others to conclude that health care systems should offer combinations of evidence-based pharmacotherapy and psychotherapy” to outpatients with BD, the researchers note.
and active tasks to enhance coping skills (e.g., monitoring and managing prodromal symptoms) rather than being passive recipients of didactic education,” they wrote.
“When the immediate goal is recovery from moderately severe depressive or manic symptoms, cognitive restructuring, regulating daily rhythms, and communication training may be associated with stabilization,” they added.
A call to action
The coauthors of an editorial in JAMA Psychiatry noted that the findings “further reinforce extant treatment guidelines recommending medication management and adjunctive evidence-based psychosocial treatments for individuals with BD.”
The findings also “identify specific treatment components and formats most strongly associated with preventing relapse and addressing mood symptoms,” write Tina Goldstein, PhD, and Danella Hafeman, MD, PhD, from Western Psychiatric Hospital, University of Pittsburgh.
The study “may further serve as a call to action to enhance availability and uptake of these treatments in the community. Unfortunately, data suggest substantially lower rates of psychotherapy receipt (26%-50%), compared with medication management (46%-90%) among adults with BD,” they wrote.
Dr. Goldstein and Dr. Hafeman noted future steps for the field include “demonstrating effectiveness of evidence-based treatment approaches for BD in the community, maximizing accessibility, and furthering knowledge that informs individualized treatment selection with substantial promise to optimize outcomes for individuals with BD.”
The study was supported in part by a grant from the National Institute for Health Research Oxford Health Biomedical Research Centre. Dr. Miklowitz has received research support from the NIHR, the Danny Alberts Foundation, the Attias Family Foundation, the Carl and Roberta Deutsch Foundation, the Kayne Family Foundation, AIM for Mental Health, and the Max Gray Fund; book royalties from Guilford Press and John Wiley and Sons; and served as principal investigator on four of the trials included in this meta-analysis. Dr. Goldstein has received grants from the National Institute of Mental Health, the American Foundation for Suicide Prevention, the University of Pittsburgh Clinical and Translational Science Institute, and the Brain and Behavior Research Foundation and royalties from Guilford Press outside the submitted work. Dr. Hafeman has received grants from the National Institute of Mental Health, the Brain and Behavior Research Foundation, and the Klingenstein Third Generation Foundation.
This article first appeared on Medscape.com.
Adding psychotherapy to pharmacotherapy benefits patients with bipolar disorder (BD), particularly when delivered in family or group settings, results of a new meta-analysis confirms.
Outpatients with BD receiving drug therapy “should also be offered psychosocial treatments that emphasize illness management strategies and enhance coping skills; delivering these components in family or group format may be especially advantageous,” wrote the investigators, led by David Miklowitz, PhD, University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior.
The study was published online Oct. 14 in JAMA Psychiatry.
Drugs alone not enough
It’s increasingly recognized that drug therapy alone can’t prevent recurrences of BD or fully alleviate postepisode symptoms or functional impairment, the researchers noted in their article. Several psychotherapy protocols have been shown to benefit patients with BD when used in conjunction with drug therapy, but little is known about their comparative effectiveness.
To investigate, the researchers conducted a systematic review and component network meta-analysis of 39 randomized clinical trials (36 involving adults and three involving adolescents).
The trials involved 3,863 patients with BD and compared pharmacotherapy used in conjunction with manualized psychotherapy (cognitive-behavioral therapy [CBT], family or conjoint therapy, interpersonal therapy, and/or psychoeducational therapy) with pharmacotherapy delivered in conjunction with a control intervention (supportive therapy or treatment as usual).
Across 20 two-group trials that provided usable information, manualized psychotherapies were associated with a lower probability of illness recurrence (the primary outcome), compared with control interventions (odds ratio, 0.56; 95% CI, 0.43-0.74).
Psychoeducation with guided practice of illness management skills in a family or group format was superior to these strategies delivered in an individual format (OR, 0.12; 95% CI, 0.02-0.94).
Family or conjoint therapy and brief psychoeducation were associated with lower attrition rates than standard psychoeducation.
For the secondary outcome of stabilization of depressive or manic symptoms over 12 months, CBT and, with less certainty, family or conjoint therapy and interpersonal therapy were more effective than treatment as usual.
The investigators note that the findings are in line with a network meta-analysis published earlier this year that found that combining psychotherapy with pharmacotherapy is the best option for stabilizing episodes and preventing recurrences of major depression.
“[T]here is enough evidence from this analysis and others to conclude that health care systems should offer combinations of evidence-based pharmacotherapy and psychotherapy” to outpatients with BD, the researchers note.
and active tasks to enhance coping skills (e.g., monitoring and managing prodromal symptoms) rather than being passive recipients of didactic education,” they wrote.
“When the immediate goal is recovery from moderately severe depressive or manic symptoms, cognitive restructuring, regulating daily rhythms, and communication training may be associated with stabilization,” they added.
A call to action
The coauthors of an editorial in JAMA Psychiatry noted that the findings “further reinforce extant treatment guidelines recommending medication management and adjunctive evidence-based psychosocial treatments for individuals with BD.”
The findings also “identify specific treatment components and formats most strongly associated with preventing relapse and addressing mood symptoms,” write Tina Goldstein, PhD, and Danella Hafeman, MD, PhD, from Western Psychiatric Hospital, University of Pittsburgh.
The study “may further serve as a call to action to enhance availability and uptake of these treatments in the community. Unfortunately, data suggest substantially lower rates of psychotherapy receipt (26%-50%), compared with medication management (46%-90%) among adults with BD,” they wrote.
Dr. Goldstein and Dr. Hafeman noted future steps for the field include “demonstrating effectiveness of evidence-based treatment approaches for BD in the community, maximizing accessibility, and furthering knowledge that informs individualized treatment selection with substantial promise to optimize outcomes for individuals with BD.”
The study was supported in part by a grant from the National Institute for Health Research Oxford Health Biomedical Research Centre. Dr. Miklowitz has received research support from the NIHR, the Danny Alberts Foundation, the Attias Family Foundation, the Carl and Roberta Deutsch Foundation, the Kayne Family Foundation, AIM for Mental Health, and the Max Gray Fund; book royalties from Guilford Press and John Wiley and Sons; and served as principal investigator on four of the trials included in this meta-analysis. Dr. Goldstein has received grants from the National Institute of Mental Health, the American Foundation for Suicide Prevention, the University of Pittsburgh Clinical and Translational Science Institute, and the Brain and Behavior Research Foundation and royalties from Guilford Press outside the submitted work. Dr. Hafeman has received grants from the National Institute of Mental Health, the Brain and Behavior Research Foundation, and the Klingenstein Third Generation Foundation.
This article first appeared on Medscape.com.
COVID-19 vaccine standards questioned at FDA advisory meeting

The FDA’s Vaccines and Related Biological Products Advisory Committee met for a wide-ranging discussion beginning around 10 am. The FDA did not ask the panel to weigh in on any particular vaccine. Instead, the FDA asked for the panel’s feedback on a series of questions, including considerations for continuing phase 3 trials if a product were to get an interim clearance known as an emergency use authorization (EUA).
Speakers at the hearing made a variety of requests, including asking for data showing COVID-19 vaccines can prevent serious illness and urging transparency about the agency’s deliberations for each product to be considered.
FDA staff are closely tracking the crop of experimental vaccines that have made it into advanced stages of testing, including products from Pfizer Inc, AstraZeneca, Johnson & Johnson, and Moderna.
‘Time for a reset’
Among the speakers at the public hearing was Peter Lurie, MD, who served as an FDA associate commissioner from 2014 to 2017. Now the president of the Center for Science in the Public Interest, Lurie was among the speakers who asked the agency to make its independence clear.
President Donald Trump has for months been making predictions about COVID-19 vaccine approvals that have been overly optimistic. In one example, the president, who is seeking re-election on November 3, last month spoke about being able to begin distributing a vaccine in October.
“Until now the process of developing candidate vaccines has been inappropriately politicized with an eye on the election calendar, rather than the deliberate timeframe science requires,” Lurie told the FDA advisory panel. “Now is the time for a reset. This committee has a unique opportunity to set a new tone for vaccine deliberations going forward.”
Lurie asked the panel to press the FDA to commit to hold an advisory committee meeting on requests by drugmakers for EUAs. He also asked the panel to demand that informed consent forms and minutes from institutional review board (IRB) discussions of COVID-19 vaccines trials be made public.
Also among the speakers at the public hearing was Peter Doshi, PhD, an associate professor at the University of Maryland School of Pharmacy, who argued that the current trials won’t answer the right questions about the COVID-19 vaccines.
“We could end up with approved vaccines that reduce the risk of mild infection, but do not decrease the risk of hospitalization, ICU use, or death — either at all or by a clinically relevant amount,” Doshi told the panel.
In his presentation, he reiterated points he had made previously, including in an October 21 article in the BMJ, for which he is an associate editor. Doshi also raised these concerns in a September opinion article in The New York Times, co-authored with Eric Topol, MD, director of the Scripps Research Translational Institute and editor-in-chief of Medscape.
Risks of a ‘rushed vaccine’
Other complaints about the FDA’s approach included criticism of a 2-month follow-up time after vaccination, which was seen as too short. ECRI, a nonprofit organization that seeks to improve the safety, quality, and cost-effectiveness of medicines, has argued that approving a weak COVID-19 vaccine might worsen the pandemic.
In an October 21 statement, ECRI noted the risk of a partially effective vaccine, which could be welcomed as a means of slowing transmission of the virus. But public response and attitudes over the past 9 months in the United States suggest that people would relax their precautions as soon as a vaccine is available.
“Resulting infections may offset the vaccine’s impact and end up increasing the mortality and morbidity burden,” ECRI said in the brief.
“The risks and consequences of a rushed vaccine could be very severe if the review is anything shy of thorough,” ECRI Chief Executive Officer Marcus Schabacker, MD, PhD, said in a statement prepared for the hearing.
This article first appeared on Medscape.com.
The FDA’s Vaccines and Related Biological Products Advisory Committee met for a wide-ranging discussion beginning around 10 am. The FDA did not ask the panel to weigh in on any particular vaccine. Instead, the FDA asked for the panel’s feedback on a series of questions, including considerations for continuing phase 3 trials if a product were to get an interim clearance known as an emergency use authorization (EUA).
Speakers at the hearing made a variety of requests, including asking for data showing COVID-19 vaccines can prevent serious illness and urging transparency about the agency’s deliberations for each product to be considered.
FDA staff are closely tracking the crop of experimental vaccines that have made it into advanced stages of testing, including products from Pfizer Inc, AstraZeneca, Johnson & Johnson, and Moderna.
‘Time for a reset’
Among the speakers at the public hearing was Peter Lurie, MD, who served as an FDA associate commissioner from 2014 to 2017. Now the president of the Center for Science in the Public Interest, Lurie was among the speakers who asked the agency to make its independence clear.
President Donald Trump has for months been making predictions about COVID-19 vaccine approvals that have been overly optimistic. In one example, the president, who is seeking re-election on November 3, last month spoke about being able to begin distributing a vaccine in October.
“Until now the process of developing candidate vaccines has been inappropriately politicized with an eye on the election calendar, rather than the deliberate timeframe science requires,” Lurie told the FDA advisory panel. “Now is the time for a reset. This committee has a unique opportunity to set a new tone for vaccine deliberations going forward.”
Lurie asked the panel to press the FDA to commit to hold an advisory committee meeting on requests by drugmakers for EUAs. He also asked the panel to demand that informed consent forms and minutes from institutional review board (IRB) discussions of COVID-19 vaccines trials be made public.
Also among the speakers at the public hearing was Peter Doshi, PhD, an associate professor at the University of Maryland School of Pharmacy, who argued that the current trials won’t answer the right questions about the COVID-19 vaccines.
“We could end up with approved vaccines that reduce the risk of mild infection, but do not decrease the risk of hospitalization, ICU use, or death — either at all or by a clinically relevant amount,” Doshi told the panel.
In his presentation, he reiterated points he had made previously, including in an October 21 article in the BMJ, for which he is an associate editor. Doshi also raised these concerns in a September opinion article in The New York Times, co-authored with Eric Topol, MD, director of the Scripps Research Translational Institute and editor-in-chief of Medscape.
Risks of a ‘rushed vaccine’
Other complaints about the FDA’s approach included criticism of a 2-month follow-up time after vaccination, which was seen as too short. ECRI, a nonprofit organization that seeks to improve the safety, quality, and cost-effectiveness of medicines, has argued that approving a weak COVID-19 vaccine might worsen the pandemic.
In an October 21 statement, ECRI noted the risk of a partially effective vaccine, which could be welcomed as a means of slowing transmission of the virus. But public response and attitudes over the past 9 months in the United States suggest that people would relax their precautions as soon as a vaccine is available.
“Resulting infections may offset the vaccine’s impact and end up increasing the mortality and morbidity burden,” ECRI said in the brief.
“The risks and consequences of a rushed vaccine could be very severe if the review is anything shy of thorough,” ECRI Chief Executive Officer Marcus Schabacker, MD, PhD, said in a statement prepared for the hearing.
This article first appeared on Medscape.com.
The FDA’s Vaccines and Related Biological Products Advisory Committee met for a wide-ranging discussion beginning around 10 am. The FDA did not ask the panel to weigh in on any particular vaccine. Instead, the FDA asked for the panel’s feedback on a series of questions, including considerations for continuing phase 3 trials if a product were to get an interim clearance known as an emergency use authorization (EUA).
Speakers at the hearing made a variety of requests, including asking for data showing COVID-19 vaccines can prevent serious illness and urging transparency about the agency’s deliberations for each product to be considered.
FDA staff are closely tracking the crop of experimental vaccines that have made it into advanced stages of testing, including products from Pfizer Inc, AstraZeneca, Johnson & Johnson, and Moderna.
‘Time for a reset’
Among the speakers at the public hearing was Peter Lurie, MD, who served as an FDA associate commissioner from 2014 to 2017. Now the president of the Center for Science in the Public Interest, Lurie was among the speakers who asked the agency to make its independence clear.
President Donald Trump has for months been making predictions about COVID-19 vaccine approvals that have been overly optimistic. In one example, the president, who is seeking re-election on November 3, last month spoke about being able to begin distributing a vaccine in October.
“Until now the process of developing candidate vaccines has been inappropriately politicized with an eye on the election calendar, rather than the deliberate timeframe science requires,” Lurie told the FDA advisory panel. “Now is the time for a reset. This committee has a unique opportunity to set a new tone for vaccine deliberations going forward.”
Lurie asked the panel to press the FDA to commit to hold an advisory committee meeting on requests by drugmakers for EUAs. He also asked the panel to demand that informed consent forms and minutes from institutional review board (IRB) discussions of COVID-19 vaccines trials be made public.
Also among the speakers at the public hearing was Peter Doshi, PhD, an associate professor at the University of Maryland School of Pharmacy, who argued that the current trials won’t answer the right questions about the COVID-19 vaccines.
“We could end up with approved vaccines that reduce the risk of mild infection, but do not decrease the risk of hospitalization, ICU use, or death — either at all or by a clinically relevant amount,” Doshi told the panel.
In his presentation, he reiterated points he had made previously, including in an October 21 article in the BMJ, for which he is an associate editor. Doshi also raised these concerns in a September opinion article in The New York Times, co-authored with Eric Topol, MD, director of the Scripps Research Translational Institute and editor-in-chief of Medscape.
Risks of a ‘rushed vaccine’
Other complaints about the FDA’s approach included criticism of a 2-month follow-up time after vaccination, which was seen as too short. ECRI, a nonprofit organization that seeks to improve the safety, quality, and cost-effectiveness of medicines, has argued that approving a weak COVID-19 vaccine might worsen the pandemic.
In an October 21 statement, ECRI noted the risk of a partially effective vaccine, which could be welcomed as a means of slowing transmission of the virus. But public response and attitudes over the past 9 months in the United States suggest that people would relax their precautions as soon as a vaccine is available.
“Resulting infections may offset the vaccine’s impact and end up increasing the mortality and morbidity burden,” ECRI said in the brief.
“The risks and consequences of a rushed vaccine could be very severe if the review is anything shy of thorough,” ECRI Chief Executive Officer Marcus Schabacker, MD, PhD, said in a statement prepared for the hearing.
This article first appeared on Medscape.com.
Data on potential risks of COVID-19 in psoriasis patients limited, but reassuring
The available according to a summary of published studies and expert opinions summarized at the annual Coastal Dermatology Symposium, held virtually.

For patients with psoriasis concerned about their outcome if infected with COVID-19, “there is no evidence to support stopping biologics or systemic agents, so I am asking my patients to continue,” Kristina C. Duffin, MD, professor and chair of dermatology at the University of Utah, Salt Lake City, said at the meeting.
The National Psoriasis Foundation, which created a COVID-19 task force and maintains a COVID-19 Resource Center on its website, has provided similar advice. Many statements are phrased cautiously and clinicians are encouraged to practice shared decision-making, but the NPF guidance supports continuing effective therapy – or, in newly diagnosed patients, starting effective therapy – among those who are not infected with SARS-CoV2.
Patients with a new diagnosis of psoriasis “should be aware that untreated psoriatic disease is associated with serious impact on physical and emotional health, and in the case of psoriatic arthritis, can lead to permanent joint damage and disability,” according to the NPF guidance.
Overall, the “existing data generally suggest” that most treatments for psoriasis and psoriatic arthritis “do not meaningfully alter the risks of contracting SARS-CoV2 or having a worse course of COVID-19 illness,” the current guidance states. Yet, because of limited data this “is not known with certainty.”
Chronic systemic steroids are an exception. In a review of recently published studies evaluating whether psoriasis or its therapies increase risk of adverse outcomes in patients with COVID-19 infection, Dr. Duffin pointed to several that associated systemic steroids with hospitalization or other markers of severe disease.
The NPF guidance also recommends avoiding chronic systemic steroids in patients with psoriasis during the current COVID-19 era “if possible.” In patients with psoriatic arthritis who require systemic steroids, the guidance recommends “the lowest dose necessary to achieve the desired therapeutic effect.”
This is not necessarily true in patients with psoriasis and COVID-19 infection. Based on the potential for systemic steroids to improve outcomes in hospitalized COVID-19 patients requiring oxygen, steroids “should not be withheld” even when the justification is concern about the potential risk of flares with withdrawal, according to the NPF guidance statement.
The NPF guidance specifically cautions against use of hydroxychloroquine or chloroquine for prevention or treatment of COVID-19. In addition to an uncertain benefit, these antimalarial drugs have been associated previously with flares of psoriasis.
Dr. Duffin agreed and went on to warn that COVID-19 infection itself is a potential trigger for flares. She cited two published case reports of flares associated with psoriasis. Although one patient had also been exposed to hydroxychloroquine, she said the risk of psoriasis-induced flare “makes sense” based on previous associations made between flares and other viral infections and stress.
In patients with psoriasis who contract COVID-19 infection, Dr. Duffin concurred with the NPF guidance that management decisions should be made on a “case-by-case basis.” Although the NPF guidance states that “most patients can restart psoriasis and/or psoriatic arthritis treatments after complete resolution of COVID-19 symptoms,” no specific advice was offered on the decision to stop treatments.
For protecting psoriasis patients from infection and managing COVID-19 in those who become infected, much of the NPF advice is consistent with that offered to patients without psoriasis. This involves practicing infection control that reduces risk of transmission. Both the NPF guidance and Dr. Duffin suggested telemedicine is appropriate for limiting in-patient visits under pandemic conditions.
Although patients with psoriasis are more likely than the general population to have the comorbidities associated with bad COVID-19 infection outcomes, according to the NPF guidance, Dr. Duffin called the overall data evaluating susceptibility among psoriasis patients “reassuring.” She cautioned that the data are still limited, but the evidence so far suggests that neither psoriasis nor biologics are independent risk factors for acquiring COVID-19 or having a worse outcome if infected.
Yet, more definitive data are needed, and Dr. Duffin advised clinicians and patients to consult the NPF website for updates. “More up-to-date information will certainly be added as we go forward,” she said at the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education.

This NPF task force on COVID-19 is meeting every 2 weeks, according to Joel M. Gelfand, MD, professor of dermatology, University of Pennsylvania, Philadelphia, and cochair of the task force. Dr. Gelfand reported that updates are based on a discussion of the available data.
“We will be releasing additional recommendations as necessary based on the developments,” he said in an interview. Updates are not necessarily required at this frequency but can be if appropriate. The goal is to keep recommendations current and evidence-based.
Dr. Duffin reported financial relationships with Amgen, AbbVie, Bristol-Myers Squibb, Boehringer-Ingelheim, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Siena, and UCB. Dr. Gelfand reported financial relationships with AbbVie, Bristol-Myers Squibb, GlaxoSmithKline, Lilly, Pfizer, Roche, and UCB.
This publication and Global Academy for Medical Education are owned by the same parent company.
The available according to a summary of published studies and expert opinions summarized at the annual Coastal Dermatology Symposium, held virtually.
For patients with psoriasis concerned about their outcome if infected with COVID-19, “there is no evidence to support stopping biologics or systemic agents, so I am asking my patients to continue,” Kristina C. Duffin, MD, professor and chair of dermatology at the University of Utah, Salt Lake City, said at the meeting.
The National Psoriasis Foundation, which created a COVID-19 task force and maintains a COVID-19 Resource Center on its website, has provided similar advice. Many statements are phrased cautiously and clinicians are encouraged to practice shared decision-making, but the NPF guidance supports continuing effective therapy – or, in newly diagnosed patients, starting effective therapy – among those who are not infected with SARS-CoV2.
Patients with a new diagnosis of psoriasis “should be aware that untreated psoriatic disease is associated with serious impact on physical and emotional health, and in the case of psoriatic arthritis, can lead to permanent joint damage and disability,” according to the NPF guidance.
Overall, the “existing data generally suggest” that most treatments for psoriasis and psoriatic arthritis “do not meaningfully alter the risks of contracting SARS-CoV2 or having a worse course of COVID-19 illness,” the current guidance states. Yet, because of limited data this “is not known with certainty.”
Chronic systemic steroids are an exception. In a review of recently published studies evaluating whether psoriasis or its therapies increase risk of adverse outcomes in patients with COVID-19 infection, Dr. Duffin pointed to several that associated systemic steroids with hospitalization or other markers of severe disease.
The NPF guidance also recommends avoiding chronic systemic steroids in patients with psoriasis during the current COVID-19 era “if possible.” In patients with psoriatic arthritis who require systemic steroids, the guidance recommends “the lowest dose necessary to achieve the desired therapeutic effect.”
This is not necessarily true in patients with psoriasis and COVID-19 infection. Based on the potential for systemic steroids to improve outcomes in hospitalized COVID-19 patients requiring oxygen, steroids “should not be withheld” even when the justification is concern about the potential risk of flares with withdrawal, according to the NPF guidance statement.
The NPF guidance specifically cautions against use of hydroxychloroquine or chloroquine for prevention or treatment of COVID-19. In addition to an uncertain benefit, these antimalarial drugs have been associated previously with flares of psoriasis.
Dr. Duffin agreed and went on to warn that COVID-19 infection itself is a potential trigger for flares. She cited two published case reports of flares associated with psoriasis. Although one patient had also been exposed to hydroxychloroquine, she said the risk of psoriasis-induced flare “makes sense” based on previous associations made between flares and other viral infections and stress.
In patients with psoriasis who contract COVID-19 infection, Dr. Duffin concurred with the NPF guidance that management decisions should be made on a “case-by-case basis.” Although the NPF guidance states that “most patients can restart psoriasis and/or psoriatic arthritis treatments after complete resolution of COVID-19 symptoms,” no specific advice was offered on the decision to stop treatments.
For protecting psoriasis patients from infection and managing COVID-19 in those who become infected, much of the NPF advice is consistent with that offered to patients without psoriasis. This involves practicing infection control that reduces risk of transmission. Both the NPF guidance and Dr. Duffin suggested telemedicine is appropriate for limiting in-patient visits under pandemic conditions.
Although patients with psoriasis are more likely than the general population to have the comorbidities associated with bad COVID-19 infection outcomes, according to the NPF guidance, Dr. Duffin called the overall data evaluating susceptibility among psoriasis patients “reassuring.” She cautioned that the data are still limited, but the evidence so far suggests that neither psoriasis nor biologics are independent risk factors for acquiring COVID-19 or having a worse outcome if infected.
Yet, more definitive data are needed, and Dr. Duffin advised clinicians and patients to consult the NPF website for updates. “More up-to-date information will certainly be added as we go forward,” she said at the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education.
This NPF task force on COVID-19 is meeting every 2 weeks, according to Joel M. Gelfand, MD, professor of dermatology, University of Pennsylvania, Philadelphia, and cochair of the task force. Dr. Gelfand reported that updates are based on a discussion of the available data.
“We will be releasing additional recommendations as necessary based on the developments,” he said in an interview. Updates are not necessarily required at this frequency but can be if appropriate. The goal is to keep recommendations current and evidence-based.
Dr. Duffin reported financial relationships with Amgen, AbbVie, Bristol-Myers Squibb, Boehringer-Ingelheim, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Siena, and UCB. Dr. Gelfand reported financial relationships with AbbVie, Bristol-Myers Squibb, GlaxoSmithKline, Lilly, Pfizer, Roche, and UCB.
This publication and Global Academy for Medical Education are owned by the same parent company.
The available according to a summary of published studies and expert opinions summarized at the annual Coastal Dermatology Symposium, held virtually.
For patients with psoriasis concerned about their outcome if infected with COVID-19, “there is no evidence to support stopping biologics or systemic agents, so I am asking my patients to continue,” Kristina C. Duffin, MD, professor and chair of dermatology at the University of Utah, Salt Lake City, said at the meeting.
The National Psoriasis Foundation, which created a COVID-19 task force and maintains a COVID-19 Resource Center on its website, has provided similar advice. Many statements are phrased cautiously and clinicians are encouraged to practice shared decision-making, but the NPF guidance supports continuing effective therapy – or, in newly diagnosed patients, starting effective therapy – among those who are not infected with SARS-CoV2.
Patients with a new diagnosis of psoriasis “should be aware that untreated psoriatic disease is associated with serious impact on physical and emotional health, and in the case of psoriatic arthritis, can lead to permanent joint damage and disability,” according to the NPF guidance.
Overall, the “existing data generally suggest” that most treatments for psoriasis and psoriatic arthritis “do not meaningfully alter the risks of contracting SARS-CoV2 or having a worse course of COVID-19 illness,” the current guidance states. Yet, because of limited data this “is not known with certainty.”
Chronic systemic steroids are an exception. In a review of recently published studies evaluating whether psoriasis or its therapies increase risk of adverse outcomes in patients with COVID-19 infection, Dr. Duffin pointed to several that associated systemic steroids with hospitalization or other markers of severe disease.
The NPF guidance also recommends avoiding chronic systemic steroids in patients with psoriasis during the current COVID-19 era “if possible.” In patients with psoriatic arthritis who require systemic steroids, the guidance recommends “the lowest dose necessary to achieve the desired therapeutic effect.”
This is not necessarily true in patients with psoriasis and COVID-19 infection. Based on the potential for systemic steroids to improve outcomes in hospitalized COVID-19 patients requiring oxygen, steroids “should not be withheld” even when the justification is concern about the potential risk of flares with withdrawal, according to the NPF guidance statement.
The NPF guidance specifically cautions against use of hydroxychloroquine or chloroquine for prevention or treatment of COVID-19. In addition to an uncertain benefit, these antimalarial drugs have been associated previously with flares of psoriasis.
Dr. Duffin agreed and went on to warn that COVID-19 infection itself is a potential trigger for flares. She cited two published case reports of flares associated with psoriasis. Although one patient had also been exposed to hydroxychloroquine, she said the risk of psoriasis-induced flare “makes sense” based on previous associations made between flares and other viral infections and stress.
In patients with psoriasis who contract COVID-19 infection, Dr. Duffin concurred with the NPF guidance that management decisions should be made on a “case-by-case basis.” Although the NPF guidance states that “most patients can restart psoriasis and/or psoriatic arthritis treatments after complete resolution of COVID-19 symptoms,” no specific advice was offered on the decision to stop treatments.
For protecting psoriasis patients from infection and managing COVID-19 in those who become infected, much of the NPF advice is consistent with that offered to patients without psoriasis. This involves practicing infection control that reduces risk of transmission. Both the NPF guidance and Dr. Duffin suggested telemedicine is appropriate for limiting in-patient visits under pandemic conditions.
Although patients with psoriasis are more likely than the general population to have the comorbidities associated with bad COVID-19 infection outcomes, according to the NPF guidance, Dr. Duffin called the overall data evaluating susceptibility among psoriasis patients “reassuring.” She cautioned that the data are still limited, but the evidence so far suggests that neither psoriasis nor biologics are independent risk factors for acquiring COVID-19 or having a worse outcome if infected.
Yet, more definitive data are needed, and Dr. Duffin advised clinicians and patients to consult the NPF website for updates. “More up-to-date information will certainly be added as we go forward,” she said at the meeting, jointly presented by the University of Louisville and Global Academy for Medical Education.
This NPF task force on COVID-19 is meeting every 2 weeks, according to Joel M. Gelfand, MD, professor of dermatology, University of Pennsylvania, Philadelphia, and cochair of the task force. Dr. Gelfand reported that updates are based on a discussion of the available data.
“We will be releasing additional recommendations as necessary based on the developments,” he said in an interview. Updates are not necessarily required at this frequency but can be if appropriate. The goal is to keep recommendations current and evidence-based.
Dr. Duffin reported financial relationships with Amgen, AbbVie, Bristol-Myers Squibb, Boehringer-Ingelheim, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Siena, and UCB. Dr. Gelfand reported financial relationships with AbbVie, Bristol-Myers Squibb, GlaxoSmithKline, Lilly, Pfizer, Roche, and UCB.
This publication and Global Academy for Medical Education are owned by the same parent company.
FROM COASTAL DERM
Dr. Anique K. Forrester joins editorial advisory board of Clinical Psychiatry News
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.

Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
Clinical Psychiatry News is pleased to announce that Anique K. Forrester, MD, has joined its editorial advisory board.
Dr. Forrester, who is board certified in the subspecialty of psychosomatic medicine (consultation-liaison psychiatry), holds numerous leadership positions at the University of Maryland, Baltimore. She is director of the consultation-liaison psychiatry fellowship at the university and serves as director of education for the C-L psychiatry PGY-2 rotation. Dr. Forrester, an assistant professor, also serves as chair of the department of psychiatry’s diversity committee and is the coordinator of the cultural psychiatry resident course.
Dr. Forrester completed her psychiatry residency training as well as psychosomatic medicine fellowship training at Sidney Kimmel Medical College, Philadelphia. She is a diplomate of the American Board of Psychiatry and Neurology. In addition, Dr. Forrester is a member of the Academy of Consultation-Liaison Psychiatry. She is a graduate of Howard University, Washington.
Her research interests include perinatal psychiatry, psycho-oncology, and cultural competence in medicine.
Welcome aboard, Dr. Forrester!
CDC expands definition of COVID-19 exposure from ‘close contact’
![]()
New data suggest each close encounter – coming within 6 feet of an infected person – can increase the risk for transmission, CDC director Robert Redfield, MD, said during a media briefing.
“As we get more data and understand the science of COVID, we’re going to continue to incorporate that in our recommendations,” Dr. Redfield said in response to a reporter’s question about a recent study.
Previously, the CDC cautioned against spending 15 minutes or longer in close proximity to an infected person, particularly in enclosed indoor spaces.
In a new report published online Oct. 21 in Morbidity and Mortality Weekly Report, however, investigators “determined that an individual who had a series of shorter contacts that over time added up to more than 15 minutes became infected.”
Beware of brief encounters?
On July 28, a 20-year-old male correctional officer in Vermont had multiple brief encounters with six transferred incarcerated or detained people while their SARS-CoV-2 test results were pending. The six were asymptomatic at the time and were housed in a quarantine unit, reported CDC researcher Julia Pringle, PhD, and colleagues.
The following day, all six inmates tested polymerase chain reaction (PCR) positive for COVID-19. The correctional officer did not spend 15 minutes or more within 6 feet of any of the inmates, according to video surveillance footage, and he continued to work.
On Aug. 4, however, he developed symptoms that included loss of smell and taste, myalgia, runny nose, cough, shortness of breath, headache, loss of appetite, and gastrointestinal symptoms. He stayed home starting the next day and tested PCR positive for COVID-19 on Aug. 11.
Further review of the surveillance video showed that the officer had numerous brief encounters of approximately 1 minute each that cumulatively exceeded 15 minutes over a 24-hour period, the researchers reported.
During all the interactions with inmates, the correctional officer wore a cloth mask, gown, and eye protection. The inmates wore masks while in their cells but did not have them on during brief cell doorway interactions or in the recreation room, according to the report.
No interaction is 100% safe
“We know that every activity that involves interacting with others has some degree of risk right now,” said Jay Butler, MD, CDC deputy director for infectious diseases.
“Unfortunately, we’re seeing a distressing trend here in the United States with COVID-19 cases increasing in nearly 75% of the country,” he said. “We’ve confirmed 8.1 million cases and, sadly, over 220,000 deaths since January.
“I know these are numbers, but these are also people,” Dr. Butler added.
“The pandemic is not over,” Dr. Redfield said. “Earlier this week, COVID virus cases reached over 40 million globally. Here in the United States we are approaching a critical phase.”
Four factors associated with higher risk for transmission are the proximity of each encounter, its duration, whether an interaction takes place indoors or outdoors, and the number of people encountered, Dr. Butler said.
Dr. Butler acknowledged widespread fatigue with adherence to personal protection measures, but added that social distancing, mask-wearing, and other measures are more important now than ever. He noted that more Americans will be spending time indoors with the onset of cooler weather and the upcoming holidays.
A note of optimism
Dr. Redfield remains optimistic about the limited availability of a vaccine or vaccines by year’s end but added that “it’s important for all of us to remain diligent in our efforts to defeat this virus.”
“There is hope on the way, in the form of safe and effective vaccines in a matter of weeks or months. To bridge to that next phase, we have to take steps to keep ourselves, our families, and our communities safe,” said Alex Azar, secretary of the Department of Health & Human Services.
“I know it’s been a difficult year for Americans, but we are going to come through this on the other side,” Dr. Redfield said.
![]()
New data suggest each close encounter – coming within 6 feet of an infected person – can increase the risk for transmission, CDC director Robert Redfield, MD, said during a media briefing.
“As we get more data and understand the science of COVID, we’re going to continue to incorporate that in our recommendations,” Dr. Redfield said in response to a reporter’s question about a recent study.
Previously, the CDC cautioned against spending 15 minutes or longer in close proximity to an infected person, particularly in enclosed indoor spaces.
In a new report published online Oct. 21 in Morbidity and Mortality Weekly Report, however, investigators “determined that an individual who had a series of shorter contacts that over time added up to more than 15 minutes became infected.”
Beware of brief encounters?
On July 28, a 20-year-old male correctional officer in Vermont had multiple brief encounters with six transferred incarcerated or detained people while their SARS-CoV-2 test results were pending. The six were asymptomatic at the time and were housed in a quarantine unit, reported CDC researcher Julia Pringle, PhD, and colleagues.
The following day, all six inmates tested polymerase chain reaction (PCR) positive for COVID-19. The correctional officer did not spend 15 minutes or more within 6 feet of any of the inmates, according to video surveillance footage, and he continued to work.
On Aug. 4, however, he developed symptoms that included loss of smell and taste, myalgia, runny nose, cough, shortness of breath, headache, loss of appetite, and gastrointestinal symptoms. He stayed home starting the next day and tested PCR positive for COVID-19 on Aug. 11.
Further review of the surveillance video showed that the officer had numerous brief encounters of approximately 1 minute each that cumulatively exceeded 15 minutes over a 24-hour period, the researchers reported.
During all the interactions with inmates, the correctional officer wore a cloth mask, gown, and eye protection. The inmates wore masks while in their cells but did not have them on during brief cell doorway interactions or in the recreation room, according to the report.
No interaction is 100% safe
“We know that every activity that involves interacting with others has some degree of risk right now,” said Jay Butler, MD, CDC deputy director for infectious diseases.
“Unfortunately, we’re seeing a distressing trend here in the United States with COVID-19 cases increasing in nearly 75% of the country,” he said. “We’ve confirmed 8.1 million cases and, sadly, over 220,000 deaths since January.
“I know these are numbers, but these are also people,” Dr. Butler added.
“The pandemic is not over,” Dr. Redfield said. “Earlier this week, COVID virus cases reached over 40 million globally. Here in the United States we are approaching a critical phase.”
Four factors associated with higher risk for transmission are the proximity of each encounter, its duration, whether an interaction takes place indoors or outdoors, and the number of people encountered, Dr. Butler said.
Dr. Butler acknowledged widespread fatigue with adherence to personal protection measures, but added that social distancing, mask-wearing, and other measures are more important now than ever. He noted that more Americans will be spending time indoors with the onset of cooler weather and the upcoming holidays.
A note of optimism
Dr. Redfield remains optimistic about the limited availability of a vaccine or vaccines by year’s end but added that “it’s important for all of us to remain diligent in our efforts to defeat this virus.”
“There is hope on the way, in the form of safe and effective vaccines in a matter of weeks or months. To bridge to that next phase, we have to take steps to keep ourselves, our families, and our communities safe,” said Alex Azar, secretary of the Department of Health & Human Services.
“I know it’s been a difficult year for Americans, but we are going to come through this on the other side,” Dr. Redfield said.
![]()
New data suggest each close encounter – coming within 6 feet of an infected person – can increase the risk for transmission, CDC director Robert Redfield, MD, said during a media briefing.
“As we get more data and understand the science of COVID, we’re going to continue to incorporate that in our recommendations,” Dr. Redfield said in response to a reporter’s question about a recent study.
Previously, the CDC cautioned against spending 15 minutes or longer in close proximity to an infected person, particularly in enclosed indoor spaces.
In a new report published online Oct. 21 in Morbidity and Mortality Weekly Report, however, investigators “determined that an individual who had a series of shorter contacts that over time added up to more than 15 minutes became infected.”
Beware of brief encounters?
On July 28, a 20-year-old male correctional officer in Vermont had multiple brief encounters with six transferred incarcerated or detained people while their SARS-CoV-2 test results were pending. The six were asymptomatic at the time and were housed in a quarantine unit, reported CDC researcher Julia Pringle, PhD, and colleagues.
The following day, all six inmates tested polymerase chain reaction (PCR) positive for COVID-19. The correctional officer did not spend 15 minutes or more within 6 feet of any of the inmates, according to video surveillance footage, and he continued to work.
On Aug. 4, however, he developed symptoms that included loss of smell and taste, myalgia, runny nose, cough, shortness of breath, headache, loss of appetite, and gastrointestinal symptoms. He stayed home starting the next day and tested PCR positive for COVID-19 on Aug. 11.
Further review of the surveillance video showed that the officer had numerous brief encounters of approximately 1 minute each that cumulatively exceeded 15 minutes over a 24-hour period, the researchers reported.
During all the interactions with inmates, the correctional officer wore a cloth mask, gown, and eye protection. The inmates wore masks while in their cells but did not have them on during brief cell doorway interactions or in the recreation room, according to the report.
No interaction is 100% safe
“We know that every activity that involves interacting with others has some degree of risk right now,” said Jay Butler, MD, CDC deputy director for infectious diseases.
“Unfortunately, we’re seeing a distressing trend here in the United States with COVID-19 cases increasing in nearly 75% of the country,” he said. “We’ve confirmed 8.1 million cases and, sadly, over 220,000 deaths since January.
“I know these are numbers, but these are also people,” Dr. Butler added.
“The pandemic is not over,” Dr. Redfield said. “Earlier this week, COVID virus cases reached over 40 million globally. Here in the United States we are approaching a critical phase.”
Four factors associated with higher risk for transmission are the proximity of each encounter, its duration, whether an interaction takes place indoors or outdoors, and the number of people encountered, Dr. Butler said.
Dr. Butler acknowledged widespread fatigue with adherence to personal protection measures, but added that social distancing, mask-wearing, and other measures are more important now than ever. He noted that more Americans will be spending time indoors with the onset of cooler weather and the upcoming holidays.
A note of optimism
Dr. Redfield remains optimistic about the limited availability of a vaccine or vaccines by year’s end but added that “it’s important for all of us to remain diligent in our efforts to defeat this virus.”
“There is hope on the way, in the form of safe and effective vaccines in a matter of weeks or months. To bridge to that next phase, we have to take steps to keep ourselves, our families, and our communities safe,” said Alex Azar, secretary of the Department of Health & Human Services.
“I know it’s been a difficult year for Americans, but we are going to come through this on the other side,” Dr. Redfield said.