User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Switching gears at high speed
Michigan hospitalists prepare for COVID-19 care
When March began, Valerie Vaughn, MD, split her time between caring for general inpatients at the University of Michigan’s hospitals in Ann Arbor and doing research on how to reduce overuse of antibiotics in hospitals nationwide.

By the time the month was over, she had helped create a new kind of hospital team focused on caring for patients with COVID-19, learned how to provide an intensive level of care for the sickest among them, trained hundreds of physicians in how to do the same, and created free online learning tools for physicians nationwide.
Call it switching gears while driving a race car. Changing horses in the middle of a raging river. Or going to medical boot camp. Whatever the metaphor, Dr. Vaughn and her colleagues did it.
And now they’re hoping that sharing what they learned will help others if their hospitals go through the same thing.
Near the epicenter
Michigan Medicine, the University of Michigan’s academic medical center, is a few dozen miles west of the Detroit hospitals that have become a national epicenter for COVID-19 cases. It’s gotten plenty of direct and transferred COVID-19 patients since mid-March.

When Dr. Vaughn’s boss, division of hospital medicine chief Vineet Chopra, MD, was tapped to lead the creation of an all-COVID unit, he asked Dr. Vaughn to work with him and the team of hospitalists, nurse practitioners, physician assistants, nurses, respiratory therapists, and other staff that had volunteered for the team.
They had 3 days to prepare.
The “SWAT team”, as Dr. Vaughn calls it, opened the RICU, or Regional Infectious Containment Unit, on March 16. They doubled the number of beds 2 weeks later.
By the end of March, the team had handed over the reins to a team of experienced intensive care professionals so the unit could focus on the sickest patients. And the RICU team had moved on to transforming other areas of the hospital, and training their staff, in the same way.
By early April, more than 200 beds across the University of Michigan’s hospitals were devoted to COVID-19 care. General medicine physicians who hadn’t practiced inside a hospital since their residency days – thanks to the ability to hand off to hospitalists – were being pulled into inpatient duty. Hospitalists were being pulled into caring for patients who would normally have been in the care of an intensive care team.
“What’s amazed me most is how much people have stepped up to the challenge,” says Dr. Vaughn. “As hard and uncomfortable as it is to do something you’re not typically doing, it can also be therapeutic to say how can I help, let me do something. Yes, they’re anxious, but they want to know how they can be as prepared as they can be, to be as helpful as possible to these patients.”
Dr. Chopra agrees. “The silver lining in all of this is that I have personally seen the best in us come to the surface. Nurses, physicians, pharmacists, and therapists have come together and have shown selflessness, kindness, empathy and resilience in profound ways.”
Making the leap
Even though they didn’t choose hospital medicine, or ICU medicine, as their specialty, physicians may greatly underestimate how useful they can be with a little just-in-time training and the help of residents, fellows, advanced practice providers, and experienced nurses and respiratory therapists.
That training is now available for free through Michigan Medicine’s new online COVID-19 CME portal. The session in “Inpatient Management of COVID-19 patients” provides an important overview for those who have never cared for a case, especially if they haven’t been on inpatient duty in a while. The ICU Bootcamp is for those who will be caring for sicker COVID-19 patients but haven’t practiced in an ICU for a while.
One of the most important roles of a COVID-19 inpatient physician, Dr. Vaughn notes, doesn’t involve new skills. Rather, it draws on the doctoring skills that general medicine and hospital medicine physicians have already honed: the ability to assess and treat the entire patient, to talk with families who can’t be with their loved ones, to humanize the experience for patients and their loved ones as much as possible, and to bring messages of love from the family back to the bedside.
By pairing a general medicine physician newly placed on inpatient duty with a resident, nurse practitioner, or physician assistant who can handle inpatient charting duties, the team can make the most of each kind of provider’s time. Administrators, too, can reduce the burden on the entire team by simplifying processes for what must be charted and recorded in the EMR.
“Hospitals facing a COVID-19 crunch need to make it easier for teams to focus on the medicine and the human connection” and to shorten the learning curve for those shifting into unfamiliar duties, she advises.
Other lessons learned
Placing COVID-19 patients on the same unit, and keeping non–COVID-19 patients in another area of the hospital, isn’t just a good idea for protecting uninfected patients, Dr. Vaughn notes. It’s also good for providers who are getting used to treating COVID-19 because they don’t have to shift between the needs of different types of patients as they go from room to room.
“The learning curve is steep, but after a couple of days taking care of these patients, you have a good feeling about how to care for them and a great sense of camaraderie with the rest of the team involved in caring for them,” she says. “Everyone jumps in to help because they know we’re in this as a team and that it’s OK for respiratory therapists to step up to help a physician who doesn’t know as much about ventilator care or for nurses to suggest medications based on what other physicians have used.”
The flattening of professional hierarchies long ingrained in hospitals may be a side effect of the tremendous and urgent sense of mission that has developed around responding to COVID-19, Dr. Vaughn notes.
Those stepping into new roles should invite their colleagues to alert them when they see them about to slip up on protective practices that might be new to them. Similarly, they should help each other resist the urge to rush into a COVID-19 patient’s room unprotected in order to help with an urgent situation. The safety of providers – to preserve their ability to care for the many more patients who will need them – must be paramount.
“To handle this pandemic, we need to all be all-in and working toward a common goal, without competing priorities,” she says. “We need to use everyone’s skill sets to the fullest, without creating burnout. We’re going to be different when all this is done.”
Avoiding provider burnout is harder than ever because team members caring for COVID-19 must stay apart from family at home and avoid in-person visits with loved ones and friends. Those who are switching to inpatient or ICU-level care should make a point of focusing on exercise, sleep, virtual connections with loved ones, and healthy eating in between shifts.
“You’re no good to anyone else if you’re not healthy,” Dr. Vaughn says. “Your mental and physical health have to come first because they enable you to help others.”
Paying attention to the appreciation that the community is showing health care workers can also brighten the day of a stressed COVID-19 inpatient clinician, she notes.
“All the little signs of love from the community – the thank you signs, sidewalk chalk drawings, hearts in people’s windows – really do help.”
This article is published courtesy of the University of Michigan Health Lab, where it appeared originally.
Michigan hospitalists prepare for COVID-19 care
Michigan hospitalists prepare for COVID-19 care
When March began, Valerie Vaughn, MD, split her time between caring for general inpatients at the University of Michigan’s hospitals in Ann Arbor and doing research on how to reduce overuse of antibiotics in hospitals nationwide.
By the time the month was over, she had helped create a new kind of hospital team focused on caring for patients with COVID-19, learned how to provide an intensive level of care for the sickest among them, trained hundreds of physicians in how to do the same, and created free online learning tools for physicians nationwide.
Call it switching gears while driving a race car. Changing horses in the middle of a raging river. Or going to medical boot camp. Whatever the metaphor, Dr. Vaughn and her colleagues did it.
And now they’re hoping that sharing what they learned will help others if their hospitals go through the same thing.
Near the epicenter
Michigan Medicine, the University of Michigan’s academic medical center, is a few dozen miles west of the Detroit hospitals that have become a national epicenter for COVID-19 cases. It’s gotten plenty of direct and transferred COVID-19 patients since mid-March.
When Dr. Vaughn’s boss, division of hospital medicine chief Vineet Chopra, MD, was tapped to lead the creation of an all-COVID unit, he asked Dr. Vaughn to work with him and the team of hospitalists, nurse practitioners, physician assistants, nurses, respiratory therapists, and other staff that had volunteered for the team.
They had 3 days to prepare.
The “SWAT team”, as Dr. Vaughn calls it, opened the RICU, or Regional Infectious Containment Unit, on March 16. They doubled the number of beds 2 weeks later.
By the end of March, the team had handed over the reins to a team of experienced intensive care professionals so the unit could focus on the sickest patients. And the RICU team had moved on to transforming other areas of the hospital, and training their staff, in the same way.
By early April, more than 200 beds across the University of Michigan’s hospitals were devoted to COVID-19 care. General medicine physicians who hadn’t practiced inside a hospital since their residency days – thanks to the ability to hand off to hospitalists – were being pulled into inpatient duty. Hospitalists were being pulled into caring for patients who would normally have been in the care of an intensive care team.
“What’s amazed me most is how much people have stepped up to the challenge,” says Dr. Vaughn. “As hard and uncomfortable as it is to do something you’re not typically doing, it can also be therapeutic to say how can I help, let me do something. Yes, they’re anxious, but they want to know how they can be as prepared as they can be, to be as helpful as possible to these patients.”
Dr. Chopra agrees. “The silver lining in all of this is that I have personally seen the best in us come to the surface. Nurses, physicians, pharmacists, and therapists have come together and have shown selflessness, kindness, empathy and resilience in profound ways.”
Making the leap
Even though they didn’t choose hospital medicine, or ICU medicine, as their specialty, physicians may greatly underestimate how useful they can be with a little just-in-time training and the help of residents, fellows, advanced practice providers, and experienced nurses and respiratory therapists.
That training is now available for free through Michigan Medicine’s new online COVID-19 CME portal. The session in “Inpatient Management of COVID-19 patients” provides an important overview for those who have never cared for a case, especially if they haven’t been on inpatient duty in a while. The ICU Bootcamp is for those who will be caring for sicker COVID-19 patients but haven’t practiced in an ICU for a while.
One of the most important roles of a COVID-19 inpatient physician, Dr. Vaughn notes, doesn’t involve new skills. Rather, it draws on the doctoring skills that general medicine and hospital medicine physicians have already honed: the ability to assess and treat the entire patient, to talk with families who can’t be with their loved ones, to humanize the experience for patients and their loved ones as much as possible, and to bring messages of love from the family back to the bedside.
By pairing a general medicine physician newly placed on inpatient duty with a resident, nurse practitioner, or physician assistant who can handle inpatient charting duties, the team can make the most of each kind of provider’s time. Administrators, too, can reduce the burden on the entire team by simplifying processes for what must be charted and recorded in the EMR.
“Hospitals facing a COVID-19 crunch need to make it easier for teams to focus on the medicine and the human connection” and to shorten the learning curve for those shifting into unfamiliar duties, she advises.
Other lessons learned
Placing COVID-19 patients on the same unit, and keeping non–COVID-19 patients in another area of the hospital, isn’t just a good idea for protecting uninfected patients, Dr. Vaughn notes. It’s also good for providers who are getting used to treating COVID-19 because they don’t have to shift between the needs of different types of patients as they go from room to room.
“The learning curve is steep, but after a couple of days taking care of these patients, you have a good feeling about how to care for them and a great sense of camaraderie with the rest of the team involved in caring for them,” she says. “Everyone jumps in to help because they know we’re in this as a team and that it’s OK for respiratory therapists to step up to help a physician who doesn’t know as much about ventilator care or for nurses to suggest medications based on what other physicians have used.”
The flattening of professional hierarchies long ingrained in hospitals may be a side effect of the tremendous and urgent sense of mission that has developed around responding to COVID-19, Dr. Vaughn notes.
Those stepping into new roles should invite their colleagues to alert them when they see them about to slip up on protective practices that might be new to them. Similarly, they should help each other resist the urge to rush into a COVID-19 patient’s room unprotected in order to help with an urgent situation. The safety of providers – to preserve their ability to care for the many more patients who will need them – must be paramount.
“To handle this pandemic, we need to all be all-in and working toward a common goal, without competing priorities,” she says. “We need to use everyone’s skill sets to the fullest, without creating burnout. We’re going to be different when all this is done.”
Avoiding provider burnout is harder than ever because team members caring for COVID-19 must stay apart from family at home and avoid in-person visits with loved ones and friends. Those who are switching to inpatient or ICU-level care should make a point of focusing on exercise, sleep, virtual connections with loved ones, and healthy eating in between shifts.
“You’re no good to anyone else if you’re not healthy,” Dr. Vaughn says. “Your mental and physical health have to come first because they enable you to help others.”
Paying attention to the appreciation that the community is showing health care workers can also brighten the day of a stressed COVID-19 inpatient clinician, she notes.
“All the little signs of love from the community – the thank you signs, sidewalk chalk drawings, hearts in people’s windows – really do help.”
This article is published courtesy of the University of Michigan Health Lab, where it appeared originally.
When March began, Valerie Vaughn, MD, split her time between caring for general inpatients at the University of Michigan’s hospitals in Ann Arbor and doing research on how to reduce overuse of antibiotics in hospitals nationwide.
By the time the month was over, she had helped create a new kind of hospital team focused on caring for patients with COVID-19, learned how to provide an intensive level of care for the sickest among them, trained hundreds of physicians in how to do the same, and created free online learning tools for physicians nationwide.
Call it switching gears while driving a race car. Changing horses in the middle of a raging river. Or going to medical boot camp. Whatever the metaphor, Dr. Vaughn and her colleagues did it.
And now they’re hoping that sharing what they learned will help others if their hospitals go through the same thing.
Near the epicenter
Michigan Medicine, the University of Michigan’s academic medical center, is a few dozen miles west of the Detroit hospitals that have become a national epicenter for COVID-19 cases. It’s gotten plenty of direct and transferred COVID-19 patients since mid-March.
When Dr. Vaughn’s boss, division of hospital medicine chief Vineet Chopra, MD, was tapped to lead the creation of an all-COVID unit, he asked Dr. Vaughn to work with him and the team of hospitalists, nurse practitioners, physician assistants, nurses, respiratory therapists, and other staff that had volunteered for the team.
They had 3 days to prepare.
The “SWAT team”, as Dr. Vaughn calls it, opened the RICU, or Regional Infectious Containment Unit, on March 16. They doubled the number of beds 2 weeks later.
By the end of March, the team had handed over the reins to a team of experienced intensive care professionals so the unit could focus on the sickest patients. And the RICU team had moved on to transforming other areas of the hospital, and training their staff, in the same way.
By early April, more than 200 beds across the University of Michigan’s hospitals were devoted to COVID-19 care. General medicine physicians who hadn’t practiced inside a hospital since their residency days – thanks to the ability to hand off to hospitalists – were being pulled into inpatient duty. Hospitalists were being pulled into caring for patients who would normally have been in the care of an intensive care team.
“What’s amazed me most is how much people have stepped up to the challenge,” says Dr. Vaughn. “As hard and uncomfortable as it is to do something you’re not typically doing, it can also be therapeutic to say how can I help, let me do something. Yes, they’re anxious, but they want to know how they can be as prepared as they can be, to be as helpful as possible to these patients.”
Dr. Chopra agrees. “The silver lining in all of this is that I have personally seen the best in us come to the surface. Nurses, physicians, pharmacists, and therapists have come together and have shown selflessness, kindness, empathy and resilience in profound ways.”
Making the leap
Even though they didn’t choose hospital medicine, or ICU medicine, as their specialty, physicians may greatly underestimate how useful they can be with a little just-in-time training and the help of residents, fellows, advanced practice providers, and experienced nurses and respiratory therapists.
That training is now available for free through Michigan Medicine’s new online COVID-19 CME portal. The session in “Inpatient Management of COVID-19 patients” provides an important overview for those who have never cared for a case, especially if they haven’t been on inpatient duty in a while. The ICU Bootcamp is for those who will be caring for sicker COVID-19 patients but haven’t practiced in an ICU for a while.
One of the most important roles of a COVID-19 inpatient physician, Dr. Vaughn notes, doesn’t involve new skills. Rather, it draws on the doctoring skills that general medicine and hospital medicine physicians have already honed: the ability to assess and treat the entire patient, to talk with families who can’t be with their loved ones, to humanize the experience for patients and their loved ones as much as possible, and to bring messages of love from the family back to the bedside.
By pairing a general medicine physician newly placed on inpatient duty with a resident, nurse practitioner, or physician assistant who can handle inpatient charting duties, the team can make the most of each kind of provider’s time. Administrators, too, can reduce the burden on the entire team by simplifying processes for what must be charted and recorded in the EMR.
“Hospitals facing a COVID-19 crunch need to make it easier for teams to focus on the medicine and the human connection” and to shorten the learning curve for those shifting into unfamiliar duties, she advises.
Other lessons learned
Placing COVID-19 patients on the same unit, and keeping non–COVID-19 patients in another area of the hospital, isn’t just a good idea for protecting uninfected patients, Dr. Vaughn notes. It’s also good for providers who are getting used to treating COVID-19 because they don’t have to shift between the needs of different types of patients as they go from room to room.
“The learning curve is steep, but after a couple of days taking care of these patients, you have a good feeling about how to care for them and a great sense of camaraderie with the rest of the team involved in caring for them,” she says. “Everyone jumps in to help because they know we’re in this as a team and that it’s OK for respiratory therapists to step up to help a physician who doesn’t know as much about ventilator care or for nurses to suggest medications based on what other physicians have used.”
The flattening of professional hierarchies long ingrained in hospitals may be a side effect of the tremendous and urgent sense of mission that has developed around responding to COVID-19, Dr. Vaughn notes.
Those stepping into new roles should invite their colleagues to alert them when they see them about to slip up on protective practices that might be new to them. Similarly, they should help each other resist the urge to rush into a COVID-19 patient’s room unprotected in order to help with an urgent situation. The safety of providers – to preserve their ability to care for the many more patients who will need them – must be paramount.
“To handle this pandemic, we need to all be all-in and working toward a common goal, without competing priorities,” she says. “We need to use everyone’s skill sets to the fullest, without creating burnout. We’re going to be different when all this is done.”
Avoiding provider burnout is harder than ever because team members caring for COVID-19 must stay apart from family at home and avoid in-person visits with loved ones and friends. Those who are switching to inpatient or ICU-level care should make a point of focusing on exercise, sleep, virtual connections with loved ones, and healthy eating in between shifts.
“You’re no good to anyone else if you’re not healthy,” Dr. Vaughn says. “Your mental and physical health have to come first because they enable you to help others.”
Paying attention to the appreciation that the community is showing health care workers can also brighten the day of a stressed COVID-19 inpatient clinician, she notes.
“All the little signs of love from the community – the thank you signs, sidewalk chalk drawings, hearts in people’s windows – really do help.”
This article is published courtesy of the University of Michigan Health Lab, where it appeared originally.
President’s report
As I write, I must admit this message is different than the one I’d envisioned sharing with you weeks ago. I anticipated updating you on meetings and collaborations with sister societies, new educational offerings, and how the Bologna World Congress and Annual Meeting plans were progressing, but activities at CHEST – and our sense of priority – have evolved along with those of our global community.

Pulmonary and critical care providers are now at the forefront of health care. Our patients, and now the greater public, are relying on our efforts and those of our teams. Amid this crisis, there is a renewed appreciation for the work all of you do; and with it, an opportunity for CHEST to lead and help ensure that the profession and our systems emerge stronger.
Back in February, we held the program committee meeting for the Annual Meeting with over 1000 submissions. It is astounding how the program came together over just a few days thanks to the preemptive work done by Chair, Dr. Victor Test, and, Co-Chair, Dr. Christopher Carroll, and all of the curricular groups, program committee members, and staff putting in so much work prior to the face-to-face meeting. Also during February, CHEST leadership held the Forum of International Respiratory Societies’ (FIRS) strategic planning meeting. The main outcome is a plan to engage a lobbyist to represent the worldwide respiratory societies in the WHO in Geneva on universal topics such as air pollution and now, unfortunately, COVID-19. CHEST was represented at the Society of Critical Care Medicine (SCCM) Congress where we heard late-breaking information as the pandemic was beginning to unfold. We met with the Critical Care Societies Collaborative (CCSC), which is composed of representatives from CHEST, SCCM, the American Thoracic Society (ATS), and the American Association of Critical-Care Nurses (AACN). We had an opportunity to meet with the European Society of Intensive Care Medicine (ESICM) and initiate discussions toward future collaboration.
In early March, as COVID-19 began to interfere with in-person meetings, we participated virtually in the NAMDRC meeting, and finalized our commitment to formally joining forces under the umbrella of CHEST to better serve our members in the area of advocacy. To this end, a new standing CHEST committee was founded, consisting of members from the former NAMRDC Board and members from the CHEST Board of Regents and Board of Trustees and chaired by Dr. Neil Freedman and Dr. Jim Lamberti. We look forward to hosting advocacy sessions during our October meeting, and going forward, our Spring Leadership Meeting will be combined with the former NAMDRC meeting to allow our leaders to participate in advocacy efforts. We will continue to publish the Washington Watchline, bringing important news on efforts to enhance access to care and our ability to deliver it effectively. Our spring leadership meetings, board meetings, and committee meetings in early April were held virtually in light of the pandemic.
Since March, CHEST has been heavily immersed in COVID-19 preparation with new plans for alternate methods of educational delivery, new business models, and curtailment of travel on both our home fronts and on the CHEST front. Zoom and like platforms are now my best friend! Our daily vocabulary now includes an abundance of caution, surge, sheltering in place, quarantine, social distancing, flattening the curve, tele-medicine, and don and doff, and we close e-mails, texts, and phone calls with Stay Safe! I established a COVID task force led by Dr. Steve Simpson (CHEST President-Elect) and with representation from the Critical Care, Chest Infections, and Disaster Response and Global Health NetWorks. They have been meeting weekly with the goals of disseminating and distilling COVID-related materials for the busy practitioner with links to the specific article or statement along with the BLUF (Bottom Line Up Front). I’m sure you were able to see and hear some of the reports by Dr. Mangala Narasimhan and others on the front lines in New York, on the CHEST website, 60 Minutes, and CNN. CHEST held a two-part webinar with our Chinese colleagues who shared their COVID experiences with us. These relationships were in part built from the PCCM Fellowship Training program we conducted with Chinese physicians, led by Dr. Darcy Marciniuk and Dr. Chen Wang under the guidance of Dr. Renli Qiao, and with the help of the late Dr. Mark Rosen, Dr. Jack Buckley, and myself. CHEST has posted a webinar on point of care ultrasound testing in the setting of COVID since many units are now using more POCUS instead of standard imaging for the critically ill. We have also posted some of our board review lectures on demand for those who want to brush up on their critical care skills and knowledge.
CHEST, unfortunately, had to reschedule the Bologna meeting due to the tragic situation in Italy and plans to reconvene the meeting June 24-26 of 2021. As of now, CHEST 2020 in Chicago is a go, but, of course, we will monitor that situation carefully. We have extended the deadline for abstracts and case reports to June 1, 2020, given the ongoing crisis. The team is busy planning for standalone and complementary online offerings to ensure seamless delivery of critical education in formats that cater easily to our newly formed habits.
CHEST staff have been working from home due to the Illinois shelter in place order but continue to work tremendously hard. They are implementing new areas to the website in an effort to improve the user experience by making information easier to find and more timely. In the publishing space, Dr. Peter Mazzone and the journal team have been receiving hundreds of COVID-related publications, which they have been reviewing and expediting for publication where appropriate. There will also be additional podcasts coming from our journal. The guidelines group has been working on shorter expert panel statements in the setting of rapidly changing evidence. And, to keep us all well, there are opportunities to share our personal feelings and experiences with treating those with COVID in video format on the website and across CHEST social media channels. The CHEST and the CHEST Foundation have initiated a new microgrants program and have reached out to over 150 ILD and COPD support groups across the country to offer them the opportunity to apply for a max $2,500 grant. So far, 7seven groups have requested support. These grants go directly to patients and caregivers and provide needed relief through provision of:
1. Groceries
2. Gift cards
3. Medical supplies (including PPE for patients)
4. Technology needed to communicate with their community and HCPs
5. Household supplies, cleaning supplies
In an attempt to assist our colleagues in New York City, a call went out for volunteers at the end of March and has resulted in over 200 volunteers and more than 400 inquiries from our members. Bravo!!! We want to thank our sister societies for joining our efforts during this time to help all of our respective members and, ultimately, those patients stricken with this terrible illness. As I don and doff my COVID gear, I hope you are all safe and well in this time of unprecedented change in our lives. I look forward to my next report in a few months, hopefully on a happier note.
Stay safe!
Stephanie
As I write, I must admit this message is different than the one I’d envisioned sharing with you weeks ago. I anticipated updating you on meetings and collaborations with sister societies, new educational offerings, and how the Bologna World Congress and Annual Meeting plans were progressing, but activities at CHEST – and our sense of priority – have evolved along with those of our global community.
Pulmonary and critical care providers are now at the forefront of health care. Our patients, and now the greater public, are relying on our efforts and those of our teams. Amid this crisis, there is a renewed appreciation for the work all of you do; and with it, an opportunity for CHEST to lead and help ensure that the profession and our systems emerge stronger.
Back in February, we held the program committee meeting for the Annual Meeting with over 1000 submissions. It is astounding how the program came together over just a few days thanks to the preemptive work done by Chair, Dr. Victor Test, and, Co-Chair, Dr. Christopher Carroll, and all of the curricular groups, program committee members, and staff putting in so much work prior to the face-to-face meeting. Also during February, CHEST leadership held the Forum of International Respiratory Societies’ (FIRS) strategic planning meeting. The main outcome is a plan to engage a lobbyist to represent the worldwide respiratory societies in the WHO in Geneva on universal topics such as air pollution and now, unfortunately, COVID-19. CHEST was represented at the Society of Critical Care Medicine (SCCM) Congress where we heard late-breaking information as the pandemic was beginning to unfold. We met with the Critical Care Societies Collaborative (CCSC), which is composed of representatives from CHEST, SCCM, the American Thoracic Society (ATS), and the American Association of Critical-Care Nurses (AACN). We had an opportunity to meet with the European Society of Intensive Care Medicine (ESICM) and initiate discussions toward future collaboration.
In early March, as COVID-19 began to interfere with in-person meetings, we participated virtually in the NAMDRC meeting, and finalized our commitment to formally joining forces under the umbrella of CHEST to better serve our members in the area of advocacy. To this end, a new standing CHEST committee was founded, consisting of members from the former NAMRDC Board and members from the CHEST Board of Regents and Board of Trustees and chaired by Dr. Neil Freedman and Dr. Jim Lamberti. We look forward to hosting advocacy sessions during our October meeting, and going forward, our Spring Leadership Meeting will be combined with the former NAMDRC meeting to allow our leaders to participate in advocacy efforts. We will continue to publish the Washington Watchline, bringing important news on efforts to enhance access to care and our ability to deliver it effectively. Our spring leadership meetings, board meetings, and committee meetings in early April were held virtually in light of the pandemic.
Since March, CHEST has been heavily immersed in COVID-19 preparation with new plans for alternate methods of educational delivery, new business models, and curtailment of travel on both our home fronts and on the CHEST front. Zoom and like platforms are now my best friend! Our daily vocabulary now includes an abundance of caution, surge, sheltering in place, quarantine, social distancing, flattening the curve, tele-medicine, and don and doff, and we close e-mails, texts, and phone calls with Stay Safe! I established a COVID task force led by Dr. Steve Simpson (CHEST President-Elect) and with representation from the Critical Care, Chest Infections, and Disaster Response and Global Health NetWorks. They have been meeting weekly with the goals of disseminating and distilling COVID-related materials for the busy practitioner with links to the specific article or statement along with the BLUF (Bottom Line Up Front). I’m sure you were able to see and hear some of the reports by Dr. Mangala Narasimhan and others on the front lines in New York, on the CHEST website, 60 Minutes, and CNN. CHEST held a two-part webinar with our Chinese colleagues who shared their COVID experiences with us. These relationships were in part built from the PCCM Fellowship Training program we conducted with Chinese physicians, led by Dr. Darcy Marciniuk and Dr. Chen Wang under the guidance of Dr. Renli Qiao, and with the help of the late Dr. Mark Rosen, Dr. Jack Buckley, and myself. CHEST has posted a webinar on point of care ultrasound testing in the setting of COVID since many units are now using more POCUS instead of standard imaging for the critically ill. We have also posted some of our board review lectures on demand for those who want to brush up on their critical care skills and knowledge.
CHEST, unfortunately, had to reschedule the Bologna meeting due to the tragic situation in Italy and plans to reconvene the meeting June 24-26 of 2021. As of now, CHEST 2020 in Chicago is a go, but, of course, we will monitor that situation carefully. We have extended the deadline for abstracts and case reports to June 1, 2020, given the ongoing crisis. The team is busy planning for standalone and complementary online offerings to ensure seamless delivery of critical education in formats that cater easily to our newly formed habits.
CHEST staff have been working from home due to the Illinois shelter in place order but continue to work tremendously hard. They are implementing new areas to the website in an effort to improve the user experience by making information easier to find and more timely. In the publishing space, Dr. Peter Mazzone and the journal team have been receiving hundreds of COVID-related publications, which they have been reviewing and expediting for publication where appropriate. There will also be additional podcasts coming from our journal. The guidelines group has been working on shorter expert panel statements in the setting of rapidly changing evidence. And, to keep us all well, there are opportunities to share our personal feelings and experiences with treating those with COVID in video format on the website and across CHEST social media channels. The CHEST and the CHEST Foundation have initiated a new microgrants program and have reached out to over 150 ILD and COPD support groups across the country to offer them the opportunity to apply for a max $2,500 grant. So far, 7seven groups have requested support. These grants go directly to patients and caregivers and provide needed relief through provision of:
1. Groceries
2. Gift cards
3. Medical supplies (including PPE for patients)
4. Technology needed to communicate with their community and HCPs
5. Household supplies, cleaning supplies
In an attempt to assist our colleagues in New York City, a call went out for volunteers at the end of March and has resulted in over 200 volunteers and more than 400 inquiries from our members. Bravo!!! We want to thank our sister societies for joining our efforts during this time to help all of our respective members and, ultimately, those patients stricken with this terrible illness. As I don and doff my COVID gear, I hope you are all safe and well in this time of unprecedented change in our lives. I look forward to my next report in a few months, hopefully on a happier note.
Stay safe!
Stephanie
As I write, I must admit this message is different than the one I’d envisioned sharing with you weeks ago. I anticipated updating you on meetings and collaborations with sister societies, new educational offerings, and how the Bologna World Congress and Annual Meeting plans were progressing, but activities at CHEST – and our sense of priority – have evolved along with those of our global community.
Pulmonary and critical care providers are now at the forefront of health care. Our patients, and now the greater public, are relying on our efforts and those of our teams. Amid this crisis, there is a renewed appreciation for the work all of you do; and with it, an opportunity for CHEST to lead and help ensure that the profession and our systems emerge stronger.
Back in February, we held the program committee meeting for the Annual Meeting with over 1000 submissions. It is astounding how the program came together over just a few days thanks to the preemptive work done by Chair, Dr. Victor Test, and, Co-Chair, Dr. Christopher Carroll, and all of the curricular groups, program committee members, and staff putting in so much work prior to the face-to-face meeting. Also during February, CHEST leadership held the Forum of International Respiratory Societies’ (FIRS) strategic planning meeting. The main outcome is a plan to engage a lobbyist to represent the worldwide respiratory societies in the WHO in Geneva on universal topics such as air pollution and now, unfortunately, COVID-19. CHEST was represented at the Society of Critical Care Medicine (SCCM) Congress where we heard late-breaking information as the pandemic was beginning to unfold. We met with the Critical Care Societies Collaborative (CCSC), which is composed of representatives from CHEST, SCCM, the American Thoracic Society (ATS), and the American Association of Critical-Care Nurses (AACN). We had an opportunity to meet with the European Society of Intensive Care Medicine (ESICM) and initiate discussions toward future collaboration.
In early March, as COVID-19 began to interfere with in-person meetings, we participated virtually in the NAMDRC meeting, and finalized our commitment to formally joining forces under the umbrella of CHEST to better serve our members in the area of advocacy. To this end, a new standing CHEST committee was founded, consisting of members from the former NAMRDC Board and members from the CHEST Board of Regents and Board of Trustees and chaired by Dr. Neil Freedman and Dr. Jim Lamberti. We look forward to hosting advocacy sessions during our October meeting, and going forward, our Spring Leadership Meeting will be combined with the former NAMDRC meeting to allow our leaders to participate in advocacy efforts. We will continue to publish the Washington Watchline, bringing important news on efforts to enhance access to care and our ability to deliver it effectively. Our spring leadership meetings, board meetings, and committee meetings in early April were held virtually in light of the pandemic.
Since March, CHEST has been heavily immersed in COVID-19 preparation with new plans for alternate methods of educational delivery, new business models, and curtailment of travel on both our home fronts and on the CHEST front. Zoom and like platforms are now my best friend! Our daily vocabulary now includes an abundance of caution, surge, sheltering in place, quarantine, social distancing, flattening the curve, tele-medicine, and don and doff, and we close e-mails, texts, and phone calls with Stay Safe! I established a COVID task force led by Dr. Steve Simpson (CHEST President-Elect) and with representation from the Critical Care, Chest Infections, and Disaster Response and Global Health NetWorks. They have been meeting weekly with the goals of disseminating and distilling COVID-related materials for the busy practitioner with links to the specific article or statement along with the BLUF (Bottom Line Up Front). I’m sure you were able to see and hear some of the reports by Dr. Mangala Narasimhan and others on the front lines in New York, on the CHEST website, 60 Minutes, and CNN. CHEST held a two-part webinar with our Chinese colleagues who shared their COVID experiences with us. These relationships were in part built from the PCCM Fellowship Training program we conducted with Chinese physicians, led by Dr. Darcy Marciniuk and Dr. Chen Wang under the guidance of Dr. Renli Qiao, and with the help of the late Dr. Mark Rosen, Dr. Jack Buckley, and myself. CHEST has posted a webinar on point of care ultrasound testing in the setting of COVID since many units are now using more POCUS instead of standard imaging for the critically ill. We have also posted some of our board review lectures on demand for those who want to brush up on their critical care skills and knowledge.
CHEST, unfortunately, had to reschedule the Bologna meeting due to the tragic situation in Italy and plans to reconvene the meeting June 24-26 of 2021. As of now, CHEST 2020 in Chicago is a go, but, of course, we will monitor that situation carefully. We have extended the deadline for abstracts and case reports to June 1, 2020, given the ongoing crisis. The team is busy planning for standalone and complementary online offerings to ensure seamless delivery of critical education in formats that cater easily to our newly formed habits.
CHEST staff have been working from home due to the Illinois shelter in place order but continue to work tremendously hard. They are implementing new areas to the website in an effort to improve the user experience by making information easier to find and more timely. In the publishing space, Dr. Peter Mazzone and the journal team have been receiving hundreds of COVID-related publications, which they have been reviewing and expediting for publication where appropriate. There will also be additional podcasts coming from our journal. The guidelines group has been working on shorter expert panel statements in the setting of rapidly changing evidence. And, to keep us all well, there are opportunities to share our personal feelings and experiences with treating those with COVID in video format on the website and across CHEST social media channels. The CHEST and the CHEST Foundation have initiated a new microgrants program and have reached out to over 150 ILD and COPD support groups across the country to offer them the opportunity to apply for a max $2,500 grant. So far, 7seven groups have requested support. These grants go directly to patients and caregivers and provide needed relief through provision of:
1. Groceries
2. Gift cards
3. Medical supplies (including PPE for patients)
4. Technology needed to communicate with their community and HCPs
5. Household supplies, cleaning supplies
In an attempt to assist our colleagues in New York City, a call went out for volunteers at the end of March and has resulted in over 200 volunteers and more than 400 inquiries from our members. Bravo!!! We want to thank our sister societies for joining our efforts during this time to help all of our respective members and, ultimately, those patients stricken with this terrible illness. As I don and doff my COVID gear, I hope you are all safe and well in this time of unprecedented change in our lives. I look forward to my next report in a few months, hopefully on a happier note.
Stay safe!
Stephanie
From the EVP/CEO: How CHEST is helping to flatten the curve
As you know, the COVID-19 pandemic has caused immense strain on global health systems. With our membership at the epicenter, many of you have experienced firsthand the shortages that result from a surging patient population – lack of personal protective equipment (PPE), access to ventilators, and increasing demand for more qualified health-care workers needed on the front lines to treat and care for patients. As the staff leader of your organization, I feel an immense responsibility to support our community through this crisis.

In recent weeks, CHEST petitioned the federal and local governments on several issues, advocating for tax relief for COVID responders, expansion of liability protections, and the development of a provider relief fund. We will continue to collaborate with other societies and push such efforts. However, we also recognize an obligation to make a more tangible, real-time difference in the circumstances of our membership and the lives of the patients you are working to save.
An opportunity arose when we received a call from Dr. Doreen Addrizzo-Harris, Immediate Past President of the CHEST Foundation and Professor of Medicine at NYU Langone Health. In late March, New York City was seeing an uptick in patients with confirmed COVID infection in critical condition that was escalating by the day. The situation was beginning to resemble the trajectory of hotspots in Wuhan, China and Italy, and it was already taking a toll on health-care teams. Dr. Adrizzo-Harris asked whether there was any way to leverage the strength of the CHEST community to provide help. Already, our headquarters team had received unsolicited offers to travel to areas in need from our members. The question was how could we more proactively identify such willing and able clinicians.
We quickly drew upon our existing CHEST Analytics platform to target physicians outside New York City who might be well-positioned to travel. We harnessed our communication channels to get the word out. The response was immediate, with more than 100 people completing applications to join forces with their colleagues in New York. In the first 10 days of recruitment efforts, we added an additional 250 interested volunteers to the system. The positive response from members showed both the willingness of qualified medical staff to assist on the front lines but also highlighted deficiencies in other registration systems overwhelmed with requests in the face of this pandemic. Finding certified pulmonary and critical care physicians who are willing to step in where they are needed is time- and labor-intensive and detracts from health systems’ ability to focus on care. Watching the projections in other regions, we recognized other areas may soon need this same help.
With this in mind, CHEST approached ATS and our long-time partner PA Consulting to help us address the problem on a national scale. We felt we had the resources to leverage our databases and our analytic tools to create a more efficient process that would put physicians in hospitals where they could do the most good more efficiently. We knew that if we could apply our knowledge and deploy our heroic members, we could develop a solution that could save lives and relieve frontline clinicians. By leveraging the existing CHEST Analytics platform, the team created a solution that can be used by provider institutions, government agencies, and willing clinicians to quickly and effectively provide care where it is needed most. The team has engineered the solution to be scalable nationally and expandable to other critical care specialties (eg, anesthesia, emergency, nursing, respiratory therapy).
The Clinician Matching Network formally launched on April 14, 2020. It provides a two-way input that accepts sign up from individual clinicians and gathers needs and requirements from hospital systems, connecting health-care providers with the systems most in need of the specific support they are equipped to provide. We believe this has the potential to enable us to move ahead of the curve of the crisis.
I am very proud of the teams that lead this effort and have gained a greater appreciation of how CHEST, in partnership with other medical societies, can fully utilize data and analytics toward implementing public health solutions. The design and development of the Clinician Matching Network was accomplished in less than a week, leveraging a methodology that will enable the team to continuously improve and iterate through weekly releases, adding functionality quickly as the pandemic evolves.
In the weeks ahead, communications will be distributed to hospitals and hospital systems to help identify their staffing needs, encourage them to input their needs into the Clinician Matching Network, and expand the clinician-to-hospital matching effort. We aim to increase the number of collaborationg associations to grow the pool of clinicians who can be deployed to areas in need.
Please visit www.chestnet.org/clinician-matching to learn more, sign up to serve, tell us about the needs of your institution, or collaborate toward this cause.
As you know, the COVID-19 pandemic has caused immense strain on global health systems. With our membership at the epicenter, many of you have experienced firsthand the shortages that result from a surging patient population – lack of personal protective equipment (PPE), access to ventilators, and increasing demand for more qualified health-care workers needed on the front lines to treat and care for patients. As the staff leader of your organization, I feel an immense responsibility to support our community through this crisis.
In recent weeks, CHEST petitioned the federal and local governments on several issues, advocating for tax relief for COVID responders, expansion of liability protections, and the development of a provider relief fund. We will continue to collaborate with other societies and push such efforts. However, we also recognize an obligation to make a more tangible, real-time difference in the circumstances of our membership and the lives of the patients you are working to save.
An opportunity arose when we received a call from Dr. Doreen Addrizzo-Harris, Immediate Past President of the CHEST Foundation and Professor of Medicine at NYU Langone Health. In late March, New York City was seeing an uptick in patients with confirmed COVID infection in critical condition that was escalating by the day. The situation was beginning to resemble the trajectory of hotspots in Wuhan, China and Italy, and it was already taking a toll on health-care teams. Dr. Adrizzo-Harris asked whether there was any way to leverage the strength of the CHEST community to provide help. Already, our headquarters team had received unsolicited offers to travel to areas in need from our members. The question was how could we more proactively identify such willing and able clinicians.
We quickly drew upon our existing CHEST Analytics platform to target physicians outside New York City who might be well-positioned to travel. We harnessed our communication channels to get the word out. The response was immediate, with more than 100 people completing applications to join forces with their colleagues in New York. In the first 10 days of recruitment efforts, we added an additional 250 interested volunteers to the system. The positive response from members showed both the willingness of qualified medical staff to assist on the front lines but also highlighted deficiencies in other registration systems overwhelmed with requests in the face of this pandemic. Finding certified pulmonary and critical care physicians who are willing to step in where they are needed is time- and labor-intensive and detracts from health systems’ ability to focus on care. Watching the projections in other regions, we recognized other areas may soon need this same help.
With this in mind, CHEST approached ATS and our long-time partner PA Consulting to help us address the problem on a national scale. We felt we had the resources to leverage our databases and our analytic tools to create a more efficient process that would put physicians in hospitals where they could do the most good more efficiently. We knew that if we could apply our knowledge and deploy our heroic members, we could develop a solution that could save lives and relieve frontline clinicians. By leveraging the existing CHEST Analytics platform, the team created a solution that can be used by provider institutions, government agencies, and willing clinicians to quickly and effectively provide care where it is needed most. The team has engineered the solution to be scalable nationally and expandable to other critical care specialties (eg, anesthesia, emergency, nursing, respiratory therapy).
The Clinician Matching Network formally launched on April 14, 2020. It provides a two-way input that accepts sign up from individual clinicians and gathers needs and requirements from hospital systems, connecting health-care providers with the systems most in need of the specific support they are equipped to provide. We believe this has the potential to enable us to move ahead of the curve of the crisis.
I am very proud of the teams that lead this effort and have gained a greater appreciation of how CHEST, in partnership with other medical societies, can fully utilize data and analytics toward implementing public health solutions. The design and development of the Clinician Matching Network was accomplished in less than a week, leveraging a methodology that will enable the team to continuously improve and iterate through weekly releases, adding functionality quickly as the pandemic evolves.
In the weeks ahead, communications will be distributed to hospitals and hospital systems to help identify their staffing needs, encourage them to input their needs into the Clinician Matching Network, and expand the clinician-to-hospital matching effort. We aim to increase the number of collaborationg associations to grow the pool of clinicians who can be deployed to areas in need.
Please visit www.chestnet.org/clinician-matching to learn more, sign up to serve, tell us about the needs of your institution, or collaborate toward this cause.
As you know, the COVID-19 pandemic has caused immense strain on global health systems. With our membership at the epicenter, many of you have experienced firsthand the shortages that result from a surging patient population – lack of personal protective equipment (PPE), access to ventilators, and increasing demand for more qualified health-care workers needed on the front lines to treat and care for patients. As the staff leader of your organization, I feel an immense responsibility to support our community through this crisis.
In recent weeks, CHEST petitioned the federal and local governments on several issues, advocating for tax relief for COVID responders, expansion of liability protections, and the development of a provider relief fund. We will continue to collaborate with other societies and push such efforts. However, we also recognize an obligation to make a more tangible, real-time difference in the circumstances of our membership and the lives of the patients you are working to save.
An opportunity arose when we received a call from Dr. Doreen Addrizzo-Harris, Immediate Past President of the CHEST Foundation and Professor of Medicine at NYU Langone Health. In late March, New York City was seeing an uptick in patients with confirmed COVID infection in critical condition that was escalating by the day. The situation was beginning to resemble the trajectory of hotspots in Wuhan, China and Italy, and it was already taking a toll on health-care teams. Dr. Adrizzo-Harris asked whether there was any way to leverage the strength of the CHEST community to provide help. Already, our headquarters team had received unsolicited offers to travel to areas in need from our members. The question was how could we more proactively identify such willing and able clinicians.
We quickly drew upon our existing CHEST Analytics platform to target physicians outside New York City who might be well-positioned to travel. We harnessed our communication channels to get the word out. The response was immediate, with more than 100 people completing applications to join forces with their colleagues in New York. In the first 10 days of recruitment efforts, we added an additional 250 interested volunteers to the system. The positive response from members showed both the willingness of qualified medical staff to assist on the front lines but also highlighted deficiencies in other registration systems overwhelmed with requests in the face of this pandemic. Finding certified pulmonary and critical care physicians who are willing to step in where they are needed is time- and labor-intensive and detracts from health systems’ ability to focus on care. Watching the projections in other regions, we recognized other areas may soon need this same help.
With this in mind, CHEST approached ATS and our long-time partner PA Consulting to help us address the problem on a national scale. We felt we had the resources to leverage our databases and our analytic tools to create a more efficient process that would put physicians in hospitals where they could do the most good more efficiently. We knew that if we could apply our knowledge and deploy our heroic members, we could develop a solution that could save lives and relieve frontline clinicians. By leveraging the existing CHEST Analytics platform, the team created a solution that can be used by provider institutions, government agencies, and willing clinicians to quickly and effectively provide care where it is needed most. The team has engineered the solution to be scalable nationally and expandable to other critical care specialties (eg, anesthesia, emergency, nursing, respiratory therapy).
The Clinician Matching Network formally launched on April 14, 2020. It provides a two-way input that accepts sign up from individual clinicians and gathers needs and requirements from hospital systems, connecting health-care providers with the systems most in need of the specific support they are equipped to provide. We believe this has the potential to enable us to move ahead of the curve of the crisis.
I am very proud of the teams that lead this effort and have gained a greater appreciation of how CHEST, in partnership with other medical societies, can fully utilize data and analytics toward implementing public health solutions. The design and development of the Clinician Matching Network was accomplished in less than a week, leveraging a methodology that will enable the team to continuously improve and iterate through weekly releases, adding functionality quickly as the pandemic evolves.
In the weeks ahead, communications will be distributed to hospitals and hospital systems to help identify their staffing needs, encourage them to input their needs into the Clinician Matching Network, and expand the clinician-to-hospital matching effort. We aim to increase the number of collaborationg associations to grow the pool of clinicians who can be deployed to areas in need.
Please visit www.chestnet.org/clinician-matching to learn more, sign up to serve, tell us about the needs of your institution, or collaborate toward this cause.
Almost half of med practices furloughing staff, one-fifth have layoffs
Clinicians all over the country already likely know this, but a survey by the Medical Group Management Association (MGMA) made it official: 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
The survey, which was conducted April 7-8, also shows that 55% of practices have seen a decrease in revenue and 60% have experienced a decline in patient volume since the beginning of the COVID-19 crisis.
A significant number of medical practices have also been forced to lay off or furlough staff in response to the COVID-19 crisis, the MGMA said. Many practices that have not yet laid off or furloughed employees will consider doing so if the conditions persist over the next 30 days.
Through April 8, 22% of survey respondents reported they had laid off staff. In the same period, 48% had furloughed employees. The survey projects that, by May 8, if the COVID-19 situation hasn’t improved, 36% of practices will have laid off staff members and 60% will have furloughed them.
The survey received 724 applicable responses, the MGMA said. Approximately 75% of respondents are part of independent medical practices and employ fewer than 50 full-time-equivalent physicians. But the respondents belong to practices of all sizes and specialties.
The bare numbers only scratch the surface of the pain that many groups and owners of physician practices are feeling.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day, exposing themselves to risks, taking care of patients, and taking care of their employees by continuing to pay them while they have taken over a 50% pay cut,” said a representative of an independent anesthesiology practice in Alabama in the MGMA press release.
“All doctors and administrative staff have deferred their salaries during this period,” a representative from a small independent practice in Mississippi that specializes in pain management said in the press release. “We have laid off most of our staff except five people.”
Employed groups tend to be in better financial shape than independent practices because they have the resources of large health care systems behind them. Some hospitals have laid off employees, however, and some of the cuts are starting to hit outpatient clinics.
Elective procedures down
In an interview conducted before the survey was released, Halee Fischer-Wright, MD, president and CEO of MGMA, said in an interview that single-specialty groups that perform elective procedures have seen “dramatic decreases in volume.” The Trump administration and at least two dozen states have asked hospitals to halt those procedures during this phase of the crisis, according to multiple media reports.
Some groups with multiple offices, Dr. Fischer-Wright noted, are deciding whether to staff them all because of their decreased volume and their concern about staff exposure to the coronavirus.
“We see them condensing down and delegating sick and well offices,” she said. “The benefit is that it allows them to be efficient with their staff use and also to place their limited PPE [personal protective equipment] supplies in the right office.”
Noting that there are costs involved in laying off staff and that practices want to retain good people if possible, Dr. Fischer-Wright advised practices to furlough employees rather than lay them off if they can.
A version of this article originally appeared on Medscape.com.
Clinicians all over the country already likely know this, but a survey by the Medical Group Management Association (MGMA) made it official: 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
The survey, which was conducted April 7-8, also shows that 55% of practices have seen a decrease in revenue and 60% have experienced a decline in patient volume since the beginning of the COVID-19 crisis.
A significant number of medical practices have also been forced to lay off or furlough staff in response to the COVID-19 crisis, the MGMA said. Many practices that have not yet laid off or furloughed employees will consider doing so if the conditions persist over the next 30 days.
Through April 8, 22% of survey respondents reported they had laid off staff. In the same period, 48% had furloughed employees. The survey projects that, by May 8, if the COVID-19 situation hasn’t improved, 36% of practices will have laid off staff members and 60% will have furloughed them.
The survey received 724 applicable responses, the MGMA said. Approximately 75% of respondents are part of independent medical practices and employ fewer than 50 full-time-equivalent physicians. But the respondents belong to practices of all sizes and specialties.
The bare numbers only scratch the surface of the pain that many groups and owners of physician practices are feeling.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day, exposing themselves to risks, taking care of patients, and taking care of their employees by continuing to pay them while they have taken over a 50% pay cut,” said a representative of an independent anesthesiology practice in Alabama in the MGMA press release.
“All doctors and administrative staff have deferred their salaries during this period,” a representative from a small independent practice in Mississippi that specializes in pain management said in the press release. “We have laid off most of our staff except five people.”
Employed groups tend to be in better financial shape than independent practices because they have the resources of large health care systems behind them. Some hospitals have laid off employees, however, and some of the cuts are starting to hit outpatient clinics.
Elective procedures down
In an interview conducted before the survey was released, Halee Fischer-Wright, MD, president and CEO of MGMA, said in an interview that single-specialty groups that perform elective procedures have seen “dramatic decreases in volume.” The Trump administration and at least two dozen states have asked hospitals to halt those procedures during this phase of the crisis, according to multiple media reports.
Some groups with multiple offices, Dr. Fischer-Wright noted, are deciding whether to staff them all because of their decreased volume and their concern about staff exposure to the coronavirus.
“We see them condensing down and delegating sick and well offices,” she said. “The benefit is that it allows them to be efficient with their staff use and also to place their limited PPE [personal protective equipment] supplies in the right office.”
Noting that there are costs involved in laying off staff and that practices want to retain good people if possible, Dr. Fischer-Wright advised practices to furlough employees rather than lay them off if they can.
A version of this article originally appeared on Medscape.com.
Clinicians all over the country already likely know this, but a survey by the Medical Group Management Association (MGMA) made it official: 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
The survey, which was conducted April 7-8, also shows that 55% of practices have seen a decrease in revenue and 60% have experienced a decline in patient volume since the beginning of the COVID-19 crisis.
A significant number of medical practices have also been forced to lay off or furlough staff in response to the COVID-19 crisis, the MGMA said. Many practices that have not yet laid off or furloughed employees will consider doing so if the conditions persist over the next 30 days.
Through April 8, 22% of survey respondents reported they had laid off staff. In the same period, 48% had furloughed employees. The survey projects that, by May 8, if the COVID-19 situation hasn’t improved, 36% of practices will have laid off staff members and 60% will have furloughed them.
The survey received 724 applicable responses, the MGMA said. Approximately 75% of respondents are part of independent medical practices and employ fewer than 50 full-time-equivalent physicians. But the respondents belong to practices of all sizes and specialties.
The bare numbers only scratch the surface of the pain that many groups and owners of physician practices are feeling.
“Not only has 70% of our revenue disappeared, but our physicians are still working every day, exposing themselves to risks, taking care of patients, and taking care of their employees by continuing to pay them while they have taken over a 50% pay cut,” said a representative of an independent anesthesiology practice in Alabama in the MGMA press release.
“All doctors and administrative staff have deferred their salaries during this period,” a representative from a small independent practice in Mississippi that specializes in pain management said in the press release. “We have laid off most of our staff except five people.”
Employed groups tend to be in better financial shape than independent practices because they have the resources of large health care systems behind them. Some hospitals have laid off employees, however, and some of the cuts are starting to hit outpatient clinics.
Elective procedures down
In an interview conducted before the survey was released, Halee Fischer-Wright, MD, president and CEO of MGMA, said in an interview that single-specialty groups that perform elective procedures have seen “dramatic decreases in volume.” The Trump administration and at least two dozen states have asked hospitals to halt those procedures during this phase of the crisis, according to multiple media reports.
Some groups with multiple offices, Dr. Fischer-Wright noted, are deciding whether to staff them all because of their decreased volume and their concern about staff exposure to the coronavirus.
“We see them condensing down and delegating sick and well offices,” she said. “The benefit is that it allows them to be efficient with their staff use and also to place their limited PPE [personal protective equipment] supplies in the right office.”
Noting that there are costs involved in laying off staff and that practices want to retain good people if possible, Dr. Fischer-Wright advised practices to furlough employees rather than lay them off if they can.
A version of this article originally appeared on Medscape.com.
In praise of parents and children
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.

Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”

This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
2019-2020 flu season ends with ‘very high’ activity in New Jersey
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
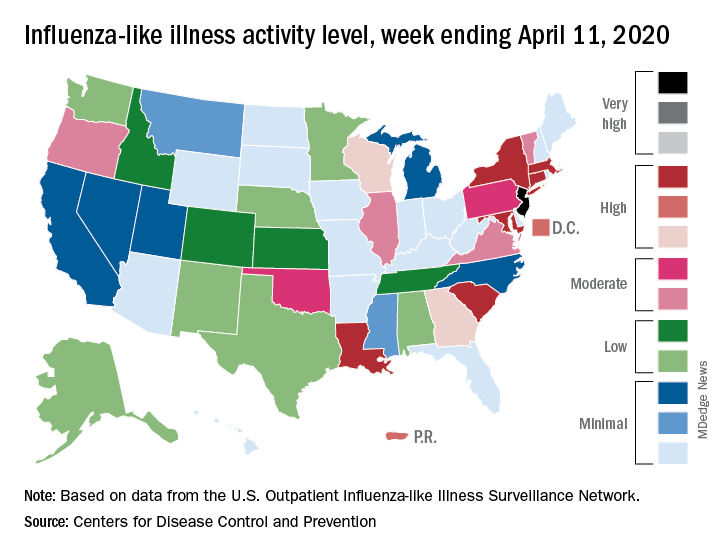
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
N.Y. universal testing: Many COVID-19+ pregnant women are asymptomatic
based on data from 215 pregnant women in New York City.

“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.

However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.

“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Universal COVID-19 testing for pregnant women entering hospitals for delivery could better protect patients and staff.
Major finding: Approximately 88% of 33 pregnant women who tested positive for COVID-19 infection at hospital admission were asymptomatic; about 14% of the 215 women overall tested positive for the novel coronavirus.
Study details: The data come from a review of 215 pregnant women who delivered infants between March 22 and April 4, 2020, in New York City.
Disclosures: The authors had no financial conflicts to disclose.
Source: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
Infectious disease experts say testing is key to reopening
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
The key to opening up the American economy rests on the ability to conduct mass testing, according to the Infectious Diseases Society of America (IDSA).
As policymakers weigh how to safely reopen parts of the United States, the IDSA, along with its HIV Medicine Association, issued a set of recommendations outlining the steps that would be necessary in order to begin easing physical distancing measures.
“A stepwise approach to reopening should reflect early diagnosis and enhanced surveillance for COVID-19 cases, linkage of cases to appropriate levels of care, isolation and/or quarantine, contact tracing, and data processing capabilities for state and local public health departments,” according to the recommendation document.
Some of the recommended steps include the following:
- Widespread testing and surveillance, including use of validated nucleic acid amplification assays and anti–SARS-CoV-2 antibody detection.
- The ability to diagnose, treat, and isolate individuals with COVID-19.
- Scaling up of health care capacity and supplies to manage recurrent episodic outbreaks.
- Maintaining a degree of physical distancing to prevent recurrent outbreaks, including use of masks, limiting gatherings, and continued distancing for susceptible adults.
“The recommendations stress that physical distancing policy changes must be based on relevant data and adequate public health resources and capacities and calls for a rolling and incremental approach to lifting these restrictions, ” Thomas File Jr., MD, IDSA president and a professor at Northeastern Ohio Universities, Rootstown, said during an April 17 press briefing.
The rolling approach “must reflect state and regional capacities for diagnosing, isolating, and treating people with the virus, tracing their contacts, protecting health care workers, and addressing the needs of populations disproportionately affected by COVID-19,” he continued.
In order to fully lift physical distancing restrictions, there would need to be effective treatments for COVID-19 and a protective vaccine that can be deployed to key at-risk populations, according to the recommendations.
During the call, Tina Q. Tan, MD, professor of pediatrics at Northwestern University, Chicago, and a member of the IDSA board of directors, said that easing social distancing requirements requires comprehensive data and that “one of the major missing data points” is the number of people who are currently infected or have been infected. She warned that easing restrictions too soon could have “disastrous consequences,” including an increase in spread of infection, hospitalization, and death rates, as well as overwhelming health care facilities.
“In order to reopen, we have to have the ability to safely, successfully, and rapidly diagnose and treat, as well as isolate, individuals with COVID-19, as well as track their contacts,” she said.
The implementation of more widespread, comprehensive testing would better enable targeting of resources, such as personal protective equipment, ICU beds, and ventilators, Dr. Tan said. “This is needed in order to ensure that, if there is an outbreak and it does occur again, the health care system and the first responders are ready for this,” she said.
How to sanitize N95 masks for reuse: NIH study
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Exposing contaminated N95 respirators to vaporized hydrogen peroxide (VHP) or ultraviolet (UV) light appears to eliminate the SARS-CoV-2 virus from the material and preserve the integrity of the masks fit for up to three uses, a National Institutes of Health (NIH) study shows.
Dry heat (70° C) was also found to eliminate the virus on masks but was effective for two uses instead of three.
Robert Fischer, PhD, with the National Institute of Allergy and Infectious Diseases in Hamilton, Montana, and colleagues posted the findings on a preprint server on April 15. The paper has not yet been peer reviewed.
Four methods tested
Fischer and colleagues compared four methods for decontaminating the masks, which are designed for one-time use: UV radiation (260-285 nm); 70° C dry heat; 70% ethanol spray; and VHP.
For each method, the researchers compared the rate at which SARS-CoV-2 is inactivated on N95 filter fabric to that on stainless steel.
All four methods eliminated detectable SARS-CoV-2 virus from the fabric test samples, though the time needed for decontamination varied. VHP was the quickest, requiring 10 minutes. Dry heat and UV light each required approximately 60 minutes. Ethanol required an intermediate amount of time.
To test durability over three uses, the researchers treated intact, clean masks with the same decontamination method and assessed function via quantitative fit testing.
Volunteers from the Rocky Mountain laboratory wore the masks for 2 hours to test fit and seal.
The researchers found that masks that had been decontaminated with ethanol spray did not function effectively after decontamination, and they did not recommend use of that method.
By contrast, masks decontaminated with UV and VHP could be used up to three times and function properly. Masks decontaminated with dry heat could be used two times before function declined.
“Our results indicate that N95 respirators can be decontaminated and reused in times of shortage for up to three times for UV and HPV, and up to two times for dry heat,” the authors write. “However, utmost care should be given to ensure the proper functioning of the N95 respirator after each decontamination using readily available qualitative fit testing tools and to ensure that treatments are carried out for sufficient time to achieve desired risk-reduction.”
Reassurance for clinicians
The results will reassure clinicians, many of whom are already using these decontamination methods, Ravina Kullar, PharmD, MPH, an infectious disease expert with the Infectious Diseases Society of America, told Medscape Medical News.
Kullar, who is also an adjunct faculty member at the David Geffen School of Medicine of the University of California, Los Angeles, said the most widely used methods have been UV light and VPH.
UV light has been used for years to decontaminate rooms, she said. She also said that so far, supplies of hydrogen peroxide are adequate.
A shortcoming of the study, Kullar said, is that it tested the masks for only 2 hours, whereas in clinical practice, they are being worn for much longer periods.
After the study is peer reviewed, the Centers for Disease Control and Prevention (CDC) may update its recommendations, she said.
So far, she noted, the CDC has not approved any method for decontaminating masks, “but it has said that it does not object to using these sterilizers, disinfectants, devices, and air purifiers for effectively killing this virus.”
Safe, multiple use of the masks is critical in the COVID-19 crisis, she said.
“We have to look at other mechanisms to keep these N95 respirators in use when there’s such a shortage,” she said.
Integrity of the fit was an important factor in the study.
“All health care workers have to go through a fitting to have that mask fitted appropriately. That’s why these N95s are only approved for health care professionals, not the lay public,” she said.
The study was supported by the National Institutes of Health; the Defense Advanced Research Projects Agency; the University of California, Los Angeles; the US National Science Foundation; and the US Department of Defense.
This article first appeared on Medscape.com.
Cautionary tale spurs ‘world’s first’ COVID-19 psychiatric ward
There was no hand sanitizer on the hospital’s psychiatric ward for fear patients would drink it; they slept together on futons in communal rooms and the windows were sealed shut to prevent suicide attempts — all conditions that created the perfect environment for the rapid spread of a potentially deadly virus.

This scenario may sound like a something out of a horror film, but as reported last month by the UK newspaper The Independent, it was the reality in the psychiatric ward of South Korea’s Daenam Hospital after COVID-19 struck. Eventually health officials put the ward on lockdown, but it wasn’t long before all but two of the unit’s 103 patients were positive for the virus.
To avoid a similar catastrophe, staff at an Israeli hospital have created what they describe as the “world’s first” dedicated COVID-19 unit for psychiatric inpatients.
Clinicians at Israel’s national hospital, Sheba Medical Center Tel HaShomer in Tel Aviv, believe the 16-bed unit, which officially opened on March 26, will stop psychiatric inpatients with the virus — who may have trouble with social distancing — from spreading it to others on the ward.
“Psychiatric patients are going to get sick from coronavirus just like anybody else,” Mark Weiser, MD, head of the psychiatric division at the institution told Medscape Medical News. “But we’re concerned that, on a psychiatric ward, a patient who is COVID-19 positive can also be psychotic, manic, cognitively impaired, or have poor judgment … making it difficult for that patient to keep social distancing, and very quickly you’ll have an entire ward of patients infected.
“So the basic public health issue is how to prevent a single psychiatric patient who is hospitalized and COVID-19-positive from making everybody else sick,” he added.
Unique Challenges, Rapid Response
Adapting an existing psychiatric ward to one exclusively used by inpatients with COVID-19 required significant planning, coordination, and modifications to ensure the well-being of patients and staff.
A dedicated entrance for the exclusive use of infected psychiatric inpatients was also created.
In addition, two-way television cameras in patients’ rooms were installed to facilitate a constant flow of communication and enable therapeutic sessions and family visits. All of these modifications were completed in under a week.
“Under normal circumstances, we have cameras in the public areas of our wards, but in order to respect people’s privacy, we do not have cameras in their rooms.
“In this specific ward, on the other hand, we did put cameras in the rooms, so if a patient needs to be watched more closely, it could be done remotely without exposing staff to the virus. We have a person who’s watching the screens at all times, just to see what’s going on and see what patients are doing,” said Weiser.
Protective personal equipment (PPE) and clothing for staff was tailored to the unique challenges posed by the ward’s patient population.
“Of course, you need to wear clothes that are protective against the virus,” said Weiser. “But sometimes our patients can get agitated or even violent, so you’ve got protect against that as well.”
With this in mind, all personnel working on the ward must put on an extra layer of PPE as well as a tear-proof robe. The institution has also implemented a strict protocol that dictates the order in which PPE is donned and doffed.
“It’s got to be done in a very careful and very specific way,” said Weiser. “We have all of it organized with a poster that explains what should be taken off or put on, and in what order.”
For institutions considering setting up a similar unit, Weiser said close proximity to an active care hospital with the capacity to provide urgent care is key.
“We’re psychiatrists; we’re not great at treating acute respiratory problems. So patients with significant respiratory problems need a place to get appropriate care quickly,” he said.
In setting up the unit, there were still a few obstacles, Weiser noted. For instance, despite the many protective and safety measures undertaken by the institution, some of the hospital staff were concerned about their risk of contracting the virus.
To address these concerns, the hospital’s leadership brought in infectious disease experts to educate hospital personnel about the virus and transmission risk.
“They told our staff that given all the precautions we had taken, there was very little risk anyone else could become infected,” Weiser said.
Despite the many challenges, Weiser said he and his colleagues are thrilled with the dedicated ward and the positive reception it has received.
“My colleagues and the directors of psychiatric hospitals all around the country are very happy with this because now they’re not hospitalizing infected patients. They’re very happy for us to take care of this,” he said.
“No Easy Solutions”
Commenting on the initiative for Medscape Medical News, John M. Oldham, MD, chief of staff at Baylor College of Medicine’s Menninger Clinic in Houston, Texas, raised some questions.
“Is it really going to be the treatment unit or a quarantine unit? Because if you don’t have a comparable level of established, effective treatment for these patients, then you’re simply herding them off to a different place where they’re going to suffer both illnesses,” he cautioned.
Nevertheless, Oldham recognized that the issue of how to treat psychiatric patients who test positive for COVID-19 is complex.
“We’re still wrestling with that question here at Menninger. We have created an enclosed section of the inpatient area reserved for this possibility.
“If we have a patient who tests positive, we will immediately put that patient in one of these rooms in the quarantine section. Then we will use protective equipment for our staff to go and provide care for the patient,” he said.
However, he acknowledged that a psychiatric hospital is in no position to treat patients who develop severe illness from COVID-19.
“We’re certainly worried about it,” he said, “because how many inpatient general medical units are going to want to take a significantly symptomatic COVID-19 patient who was in the hospital for being acutely suicidal? There are no easy solutions.”
This article first appeared on Medscape.com.
There was no hand sanitizer on the hospital’s psychiatric ward for fear patients would drink it; they slept together on futons in communal rooms and the windows were sealed shut to prevent suicide attempts — all conditions that created the perfect environment for the rapid spread of a potentially deadly virus.
This scenario may sound like a something out of a horror film, but as reported last month by the UK newspaper The Independent, it was the reality in the psychiatric ward of South Korea’s Daenam Hospital after COVID-19 struck. Eventually health officials put the ward on lockdown, but it wasn’t long before all but two of the unit’s 103 patients were positive for the virus.
To avoid a similar catastrophe, staff at an Israeli hospital have created what they describe as the “world’s first” dedicated COVID-19 unit for psychiatric inpatients.
Clinicians at Israel’s national hospital, Sheba Medical Center Tel HaShomer in Tel Aviv, believe the 16-bed unit, which officially opened on March 26, will stop psychiatric inpatients with the virus — who may have trouble with social distancing — from spreading it to others on the ward.
“Psychiatric patients are going to get sick from coronavirus just like anybody else,” Mark Weiser, MD, head of the psychiatric division at the institution told Medscape Medical News. “But we’re concerned that, on a psychiatric ward, a patient who is COVID-19 positive can also be psychotic, manic, cognitively impaired, or have poor judgment … making it difficult for that patient to keep social distancing, and very quickly you’ll have an entire ward of patients infected.
“So the basic public health issue is how to prevent a single psychiatric patient who is hospitalized and COVID-19-positive from making everybody else sick,” he added.
Unique Challenges, Rapid Response
Adapting an existing psychiatric ward to one exclusively used by inpatients with COVID-19 required significant planning, coordination, and modifications to ensure the well-being of patients and staff.
A dedicated entrance for the exclusive use of infected psychiatric inpatients was also created.
In addition, two-way television cameras in patients’ rooms were installed to facilitate a constant flow of communication and enable therapeutic sessions and family visits. All of these modifications were completed in under a week.
“Under normal circumstances, we have cameras in the public areas of our wards, but in order to respect people’s privacy, we do not have cameras in their rooms.
“In this specific ward, on the other hand, we did put cameras in the rooms, so if a patient needs to be watched more closely, it could be done remotely without exposing staff to the virus. We have a person who’s watching the screens at all times, just to see what’s going on and see what patients are doing,” said Weiser.
Protective personal equipment (PPE) and clothing for staff was tailored to the unique challenges posed by the ward’s patient population.
“Of course, you need to wear clothes that are protective against the virus,” said Weiser. “But sometimes our patients can get agitated or even violent, so you’ve got protect against that as well.”
With this in mind, all personnel working on the ward must put on an extra layer of PPE as well as a tear-proof robe. The institution has also implemented a strict protocol that dictates the order in which PPE is donned and doffed.
“It’s got to be done in a very careful and very specific way,” said Weiser. “We have all of it organized with a poster that explains what should be taken off or put on, and in what order.”
For institutions considering setting up a similar unit, Weiser said close proximity to an active care hospital with the capacity to provide urgent care is key.
“We’re psychiatrists; we’re not great at treating acute respiratory problems. So patients with significant respiratory problems need a place to get appropriate care quickly,” he said.
In setting up the unit, there were still a few obstacles, Weiser noted. For instance, despite the many protective and safety measures undertaken by the institution, some of the hospital staff were concerned about their risk of contracting the virus.
To address these concerns, the hospital’s leadership brought in infectious disease experts to educate hospital personnel about the virus and transmission risk.
“They told our staff that given all the precautions we had taken, there was very little risk anyone else could become infected,” Weiser said.
Despite the many challenges, Weiser said he and his colleagues are thrilled with the dedicated ward and the positive reception it has received.
“My colleagues and the directors of psychiatric hospitals all around the country are very happy with this because now they’re not hospitalizing infected patients. They’re very happy for us to take care of this,” he said.
“No Easy Solutions”
Commenting on the initiative for Medscape Medical News, John M. Oldham, MD, chief of staff at Baylor College of Medicine’s Menninger Clinic in Houston, Texas, raised some questions.
“Is it really going to be the treatment unit or a quarantine unit? Because if you don’t have a comparable level of established, effective treatment for these patients, then you’re simply herding them off to a different place where they’re going to suffer both illnesses,” he cautioned.
Nevertheless, Oldham recognized that the issue of how to treat psychiatric patients who test positive for COVID-19 is complex.
“We’re still wrestling with that question here at Menninger. We have created an enclosed section of the inpatient area reserved for this possibility.
“If we have a patient who tests positive, we will immediately put that patient in one of these rooms in the quarantine section. Then we will use protective equipment for our staff to go and provide care for the patient,” he said.
However, he acknowledged that a psychiatric hospital is in no position to treat patients who develop severe illness from COVID-19.
“We’re certainly worried about it,” he said, “because how many inpatient general medical units are going to want to take a significantly symptomatic COVID-19 patient who was in the hospital for being acutely suicidal? There are no easy solutions.”
This article first appeared on Medscape.com.
There was no hand sanitizer on the hospital’s psychiatric ward for fear patients would drink it; they slept together on futons in communal rooms and the windows were sealed shut to prevent suicide attempts — all conditions that created the perfect environment for the rapid spread of a potentially deadly virus.
This scenario may sound like a something out of a horror film, but as reported last month by the UK newspaper The Independent, it was the reality in the psychiatric ward of South Korea’s Daenam Hospital after COVID-19 struck. Eventually health officials put the ward on lockdown, but it wasn’t long before all but two of the unit’s 103 patients were positive for the virus.
To avoid a similar catastrophe, staff at an Israeli hospital have created what they describe as the “world’s first” dedicated COVID-19 unit for psychiatric inpatients.
Clinicians at Israel’s national hospital, Sheba Medical Center Tel HaShomer in Tel Aviv, believe the 16-bed unit, which officially opened on March 26, will stop psychiatric inpatients with the virus — who may have trouble with social distancing — from spreading it to others on the ward.
“Psychiatric patients are going to get sick from coronavirus just like anybody else,” Mark Weiser, MD, head of the psychiatric division at the institution told Medscape Medical News. “But we’re concerned that, on a psychiatric ward, a patient who is COVID-19 positive can also be psychotic, manic, cognitively impaired, or have poor judgment … making it difficult for that patient to keep social distancing, and very quickly you’ll have an entire ward of patients infected.
“So the basic public health issue is how to prevent a single psychiatric patient who is hospitalized and COVID-19-positive from making everybody else sick,” he added.
Unique Challenges, Rapid Response
Adapting an existing psychiatric ward to one exclusively used by inpatients with COVID-19 required significant planning, coordination, and modifications to ensure the well-being of patients and staff.
A dedicated entrance for the exclusive use of infected psychiatric inpatients was also created.
In addition, two-way television cameras in patients’ rooms were installed to facilitate a constant flow of communication and enable therapeutic sessions and family visits. All of these modifications were completed in under a week.
“Under normal circumstances, we have cameras in the public areas of our wards, but in order to respect people’s privacy, we do not have cameras in their rooms.
“In this specific ward, on the other hand, we did put cameras in the rooms, so if a patient needs to be watched more closely, it could be done remotely without exposing staff to the virus. We have a person who’s watching the screens at all times, just to see what’s going on and see what patients are doing,” said Weiser.
Protective personal equipment (PPE) and clothing for staff was tailored to the unique challenges posed by the ward’s patient population.
“Of course, you need to wear clothes that are protective against the virus,” said Weiser. “But sometimes our patients can get agitated or even violent, so you’ve got protect against that as well.”
With this in mind, all personnel working on the ward must put on an extra layer of PPE as well as a tear-proof robe. The institution has also implemented a strict protocol that dictates the order in which PPE is donned and doffed.
“It’s got to be done in a very careful and very specific way,” said Weiser. “We have all of it organized with a poster that explains what should be taken off or put on, and in what order.”
For institutions considering setting up a similar unit, Weiser said close proximity to an active care hospital with the capacity to provide urgent care is key.
“We’re psychiatrists; we’re not great at treating acute respiratory problems. So patients with significant respiratory problems need a place to get appropriate care quickly,” he said.
In setting up the unit, there were still a few obstacles, Weiser noted. For instance, despite the many protective and safety measures undertaken by the institution, some of the hospital staff were concerned about their risk of contracting the virus.
To address these concerns, the hospital’s leadership brought in infectious disease experts to educate hospital personnel about the virus and transmission risk.
“They told our staff that given all the precautions we had taken, there was very little risk anyone else could become infected,” Weiser said.
Despite the many challenges, Weiser said he and his colleagues are thrilled with the dedicated ward and the positive reception it has received.
“My colleagues and the directors of psychiatric hospitals all around the country are very happy with this because now they’re not hospitalizing infected patients. They’re very happy for us to take care of this,” he said.
“No Easy Solutions”
Commenting on the initiative for Medscape Medical News, John M. Oldham, MD, chief of staff at Baylor College of Medicine’s Menninger Clinic in Houston, Texas, raised some questions.
“Is it really going to be the treatment unit or a quarantine unit? Because if you don’t have a comparable level of established, effective treatment for these patients, then you’re simply herding them off to a different place where they’re going to suffer both illnesses,” he cautioned.
Nevertheless, Oldham recognized that the issue of how to treat psychiatric patients who test positive for COVID-19 is complex.
“We’re still wrestling with that question here at Menninger. We have created an enclosed section of the inpatient area reserved for this possibility.
“If we have a patient who tests positive, we will immediately put that patient in one of these rooms in the quarantine section. Then we will use protective equipment for our staff to go and provide care for the patient,” he said.
However, he acknowledged that a psychiatric hospital is in no position to treat patients who develop severe illness from COVID-19.
“We’re certainly worried about it,” he said, “because how many inpatient general medical units are going to want to take a significantly symptomatic COVID-19 patient who was in the hospital for being acutely suicidal? There are no easy solutions.”
This article first appeared on Medscape.com.