User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Air pollution contribution to lung cancer may be underestimated
There is a growing body of evidence to show that air pollution is a major risk factor for lung cancer among never-smokers, although there is less certainty about the duration of exposure to fine particulate matter in ambient air as it relates to risk for lung cancer.
But as Canadian researchers now report, even 20 years of data on cumulative exposure to air pollution may underestimate the magnitude of the effect, especially among people diagnosed with lung cancer who have migrated from regions where heavy air pollution is the norm.
In a study of Canadian women with newly diagnosed lung cancer who never smoked, Renelle Myers, MD, FRCPC, from the University of British Columbia in Vancouver and colleagues found that shorter-term assessment of cumulative exposure to ambient air particles smaller than 2.5 microns (PM2.5) may underestimate the health effects of chronic exposure to pollution, especially among those patients who had migrated to Canada after living in areas of high PM2.5 exposure for long periods of time.
“Our study points to the importance of incorporating this long-term cumulative exposure to air pollutants in the assessment of individual lung cancer risk, of course in combination with traditional risk factors, and depending on the country of residence, I think that even a 20-year cumulative exposure may underestimate the effects of PM2.5, as we’re not capturing childhood or adolescent exposure when the lung is developing, and what effect that will have,” she said in an oral abstract presented at the World Conference on Lung Cancer.
Satellite data on local pollution
With the objective of comparing cumulative 3-year vs. 20-year exposure to PM2.5 in women who had never smoked and had a new diagnosis of lung cancer, Dr. Myers and colleagues conducted a cross-sectional study.
They recruited a total of 236 women and had them fill out a detailed residential history questionnaire, and demographic details including age, race, country of birth, arrival in Canada for those born out of the country, occupations, family history of lung cancer, and exposure to second-hand smoke.
The investigators linked local addresses or postal to satellite-derived data on local PM2.5 levels, which first became available in 1996.
The median age of participants was 66.1 years. Of the 236 participants, 190 (80.5%) were born outside of Canada, and came to the country at the median age of 45. About half of all participants came from mainland China or Hong Kong, and another one-third came from elsewhere in Asia.
Tumor histologies included adenocarcinomas in 219 patients, squamous cell carcinoma in 1, and other types in 16 patients. Slightly more than half of the patients (55.%) had stage III or IV disease at diagnosis. In all, 106 of 227 evaluable patients had EGFR mutations.
3 years not enough
Among the foreign-born patients, only 4 (2%) had 3-year cumulative PM2.5 exposure greater than 10 mcg/m3, but 38 (20%) had 20-year cumulative exposure greater than 10 mcg/m3 (P < .0001).
All of the patients had cumulative PM2.5 exposures greater than 5 mcg/m3.
Comparing patients with and without EGFR mutations, the investigators found that higher 3-year cumulative PM2.5 exposure was significantly associated with EGFR mutations compared with nonmutated cancers (P = .049), but there was no significant association with higher 20-year cumulative exposures.
“The significance of this study really captures that short term or at least less than 3-year cumulative exposure risk for PM2.5 will probably underestimate the adverse effects that chronic exposure to air pollution has, especially among patients who lived elsewhere that may have had higher exposure throughout their lifetime than where you actually meet them,” Dr. Myers said in a media briefing held prior to her presentation.
Lung cancer in female nonsmokers
During the oral abstract session, invited discussant Chang-Chuan Chan, ScD, National Taiwan University, Taipei, said that the study’s focus on female patients with lung cancer is important. He pointed to a 2019 study examining the relationship between air pollution and lung cancer among nonsmokers in Taiwan, in which the authors found that, although smoking levels among women remained low over time (about 5%), the incidence of lung adenocarcinomas among women increased from 7.05 per 100,000 in 1995, to 24.22 per 100,000 in 2015.
The authors of that study also found that changes in PM2.5 levels in Taiwan were predictive of fluctuations in lung cancer prevalence in never-smokers.
“We’re moving from 50-year studies of smoking to these new issues of air pollution, asbestos, and radon, and I think it’s better that these three factors can be combined together,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was supported by the BC Cancer Foundation, Terry Fox Research Institute, and VGH-UBC Hospital Foundation. Dr. Myers and Dr. Chan reported having no financial conflicts of interest to disclose.
There is a growing body of evidence to show that air pollution is a major risk factor for lung cancer among never-smokers, although there is less certainty about the duration of exposure to fine particulate matter in ambient air as it relates to risk for lung cancer.
But as Canadian researchers now report, even 20 years of data on cumulative exposure to air pollution may underestimate the magnitude of the effect, especially among people diagnosed with lung cancer who have migrated from regions where heavy air pollution is the norm.
In a study of Canadian women with newly diagnosed lung cancer who never smoked, Renelle Myers, MD, FRCPC, from the University of British Columbia in Vancouver and colleagues found that shorter-term assessment of cumulative exposure to ambient air particles smaller than 2.5 microns (PM2.5) may underestimate the health effects of chronic exposure to pollution, especially among those patients who had migrated to Canada after living in areas of high PM2.5 exposure for long periods of time.
“Our study points to the importance of incorporating this long-term cumulative exposure to air pollutants in the assessment of individual lung cancer risk, of course in combination with traditional risk factors, and depending on the country of residence, I think that even a 20-year cumulative exposure may underestimate the effects of PM2.5, as we’re not capturing childhood or adolescent exposure when the lung is developing, and what effect that will have,” she said in an oral abstract presented at the World Conference on Lung Cancer.
Satellite data on local pollution
With the objective of comparing cumulative 3-year vs. 20-year exposure to PM2.5 in women who had never smoked and had a new diagnosis of lung cancer, Dr. Myers and colleagues conducted a cross-sectional study.
They recruited a total of 236 women and had them fill out a detailed residential history questionnaire, and demographic details including age, race, country of birth, arrival in Canada for those born out of the country, occupations, family history of lung cancer, and exposure to second-hand smoke.
The investigators linked local addresses or postal to satellite-derived data on local PM2.5 levels, which first became available in 1996.
The median age of participants was 66.1 years. Of the 236 participants, 190 (80.5%) were born outside of Canada, and came to the country at the median age of 45. About half of all participants came from mainland China or Hong Kong, and another one-third came from elsewhere in Asia.
Tumor histologies included adenocarcinomas in 219 patients, squamous cell carcinoma in 1, and other types in 16 patients. Slightly more than half of the patients (55.%) had stage III or IV disease at diagnosis. In all, 106 of 227 evaluable patients had EGFR mutations.
3 years not enough
Among the foreign-born patients, only 4 (2%) had 3-year cumulative PM2.5 exposure greater than 10 mcg/m3, but 38 (20%) had 20-year cumulative exposure greater than 10 mcg/m3 (P < .0001).
All of the patients had cumulative PM2.5 exposures greater than 5 mcg/m3.
Comparing patients with and without EGFR mutations, the investigators found that higher 3-year cumulative PM2.5 exposure was significantly associated with EGFR mutations compared with nonmutated cancers (P = .049), but there was no significant association with higher 20-year cumulative exposures.
“The significance of this study really captures that short term or at least less than 3-year cumulative exposure risk for PM2.5 will probably underestimate the adverse effects that chronic exposure to air pollution has, especially among patients who lived elsewhere that may have had higher exposure throughout their lifetime than where you actually meet them,” Dr. Myers said in a media briefing held prior to her presentation.
Lung cancer in female nonsmokers
During the oral abstract session, invited discussant Chang-Chuan Chan, ScD, National Taiwan University, Taipei, said that the study’s focus on female patients with lung cancer is important. He pointed to a 2019 study examining the relationship between air pollution and lung cancer among nonsmokers in Taiwan, in which the authors found that, although smoking levels among women remained low over time (about 5%), the incidence of lung adenocarcinomas among women increased from 7.05 per 100,000 in 1995, to 24.22 per 100,000 in 2015.
The authors of that study also found that changes in PM2.5 levels in Taiwan were predictive of fluctuations in lung cancer prevalence in never-smokers.
“We’re moving from 50-year studies of smoking to these new issues of air pollution, asbestos, and radon, and I think it’s better that these three factors can be combined together,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was supported by the BC Cancer Foundation, Terry Fox Research Institute, and VGH-UBC Hospital Foundation. Dr. Myers and Dr. Chan reported having no financial conflicts of interest to disclose.
There is a growing body of evidence to show that air pollution is a major risk factor for lung cancer among never-smokers, although there is less certainty about the duration of exposure to fine particulate matter in ambient air as it relates to risk for lung cancer.
But as Canadian researchers now report, even 20 years of data on cumulative exposure to air pollution may underestimate the magnitude of the effect, especially among people diagnosed with lung cancer who have migrated from regions where heavy air pollution is the norm.
In a study of Canadian women with newly diagnosed lung cancer who never smoked, Renelle Myers, MD, FRCPC, from the University of British Columbia in Vancouver and colleagues found that shorter-term assessment of cumulative exposure to ambient air particles smaller than 2.5 microns (PM2.5) may underestimate the health effects of chronic exposure to pollution, especially among those patients who had migrated to Canada after living in areas of high PM2.5 exposure for long periods of time.
“Our study points to the importance of incorporating this long-term cumulative exposure to air pollutants in the assessment of individual lung cancer risk, of course in combination with traditional risk factors, and depending on the country of residence, I think that even a 20-year cumulative exposure may underestimate the effects of PM2.5, as we’re not capturing childhood or adolescent exposure when the lung is developing, and what effect that will have,” she said in an oral abstract presented at the World Conference on Lung Cancer.
Satellite data on local pollution
With the objective of comparing cumulative 3-year vs. 20-year exposure to PM2.5 in women who had never smoked and had a new diagnosis of lung cancer, Dr. Myers and colleagues conducted a cross-sectional study.
They recruited a total of 236 women and had them fill out a detailed residential history questionnaire, and demographic details including age, race, country of birth, arrival in Canada for those born out of the country, occupations, family history of lung cancer, and exposure to second-hand smoke.
The investigators linked local addresses or postal to satellite-derived data on local PM2.5 levels, which first became available in 1996.
The median age of participants was 66.1 years. Of the 236 participants, 190 (80.5%) were born outside of Canada, and came to the country at the median age of 45. About half of all participants came from mainland China or Hong Kong, and another one-third came from elsewhere in Asia.
Tumor histologies included adenocarcinomas in 219 patients, squamous cell carcinoma in 1, and other types in 16 patients. Slightly more than half of the patients (55.%) had stage III or IV disease at diagnosis. In all, 106 of 227 evaluable patients had EGFR mutations.
3 years not enough
Among the foreign-born patients, only 4 (2%) had 3-year cumulative PM2.5 exposure greater than 10 mcg/m3, but 38 (20%) had 20-year cumulative exposure greater than 10 mcg/m3 (P < .0001).
All of the patients had cumulative PM2.5 exposures greater than 5 mcg/m3.
Comparing patients with and without EGFR mutations, the investigators found that higher 3-year cumulative PM2.5 exposure was significantly associated with EGFR mutations compared with nonmutated cancers (P = .049), but there was no significant association with higher 20-year cumulative exposures.
“The significance of this study really captures that short term or at least less than 3-year cumulative exposure risk for PM2.5 will probably underestimate the adverse effects that chronic exposure to air pollution has, especially among patients who lived elsewhere that may have had higher exposure throughout their lifetime than where you actually meet them,” Dr. Myers said in a media briefing held prior to her presentation.
Lung cancer in female nonsmokers
During the oral abstract session, invited discussant Chang-Chuan Chan, ScD, National Taiwan University, Taipei, said that the study’s focus on female patients with lung cancer is important. He pointed to a 2019 study examining the relationship between air pollution and lung cancer among nonsmokers in Taiwan, in which the authors found that, although smoking levels among women remained low over time (about 5%), the incidence of lung adenocarcinomas among women increased from 7.05 per 100,000 in 1995, to 24.22 per 100,000 in 2015.
The authors of that study also found that changes in PM2.5 levels in Taiwan were predictive of fluctuations in lung cancer prevalence in never-smokers.
“We’re moving from 50-year studies of smoking to these new issues of air pollution, asbestos, and radon, and I think it’s better that these three factors can be combined together,” he said at the meeting sponsored by the International Association for the Study of Lung Cancer.
The study was supported by the BC Cancer Foundation, Terry Fox Research Institute, and VGH-UBC Hospital Foundation. Dr. Myers and Dr. Chan reported having no financial conflicts of interest to disclose.
FROM WCLC
Smoking cessation with lung screening ups quit rates
Nearly one-third of smokers who were offered smoking cessation support on the spot when they showed up for lung cancer screening remained off cigarettes 1 year later, a quit-smoking rate considerably higher than that reported in clinical studies, investigators from the United Kingdom found.
When they added a stop-smoking component to the Yorkshire Lung Screening Trial, Rachael Murray, PhD, and colleagues at the University of Nottingham (England), found that immediately offering a combination of behavioral support and pharmacotherapy to help smokers kick the habit resulted in a 7-day validated point prevalent abstinence rate at 3 months of 30% among smokers randomized to a standard smoking cessation program, and 33.6% among patients randomized to also receive a personalized intervention that included images of their heart and lungs to demonstrate the harmful effects of tobacco.
In contrast, smoking cessation rates reported in trials of lung cancer screening have ranged from approximately 10% to 20%.
Although there was no overall statistical difference in quit-smoking rates between the standard and enhanced intervention arms of the study, the investigators found that women, but not men, were significantly more likely to quit when shown the heart and lung images, compared with those who received the standard smoking cessation support, Dr. Murray said at the World Conference on Lung Cancer held this week in Vienna.
“I think having smoking cessation as an integrated part of the lung cancer track was really positively received by our participants, particularly through having a physical presence and being conveniently located within the setting,” she said in a presidential symposium highlighting the best abstracts presented at the meeting.
“We’ve offered a high-intensity intervention, which is not going to be cheap to offer but I think is really important for these individuals with complex smoking histories and multiple comorbidities,” she added.
No judgment
In an interview, Dr. Murray noted that colocating stop-smoking services with lung screening is important for capturing smokers who may have the will but not the means to quit, and that participants especially appreciated the offer of help without the usual condescending attitude.
“We’re not an add-on: We’re there and physically present at the time of the lung health check,” she said. “It’s a standard of care that our smoking cessation advisers are able to provide. It’s very nonjudgmental and very holistic, providing social support that these people need. They’ve got long smoking histories, and they’re often made to feel guilty for that, and just being able to approach them in a nonjudgmental way makes a big difference.”
Smoking cessation is known to be the most effective way to reduce lung cancer deaths, Dr. Murray said in her presentation, pointing to a 2020 study by University of Michigan researchers showing that adding tobacco treatment to lung cancer screening can reduce deaths by 14% and increase the overall number of life-years gained by 81%.
Reduce smoking?
To see whether adding a personalized on-site smoking cessation program to lung cancer screening could improve quit-smoking rates, Dr. Murray and colleagues enrolled 1,003 smokers who attended the lung cancer screening program and randomly assigned them to either the intervention arm with personalized feedback, supportive communications, ongoing behavioral support and pharmacotherapy, or to a control arm consisting of ongoing behavioral support and pharmacotherapy.
Participants in the intervention arm were shown CT scans of the heart and lungs plus drawings highlighting coronary artery calcification and areas of their lungs damaged by smoking, and information on how quitting smoking can help to improve their health. The smoking cessation advisers followed a tightly controlled script to ensure that the messages were delivered in a uniform fashion to all participants.
As noted before, rates of 7-day validated point prevalent abstinence, measured by exhaled carbon dioxide, were 33.8% in the intervention arm, and 30% in the control arm. The respective costs per quitter were £521.30 ($630.77) and £412.80 ($499.48).
The validated 12-month smoking-free rates were 29.% in the intervention arm, and 28.6% in the control arm. None of the differences were statistically significant.
However, when they looked at between-arm differences by sex, the investigators found that significantly more women assigned to the intervention arm remained abstinent at 3 months, with rates of 33.9% compared with 23.1% of controls, a difference that translated into an unadjusted odds ratio of 1.70 favoring the intervention among women (P = .008).
Effective and durable
“My interpretation of this study is that the abstinence rates were very high, and this in fact was durable because this effect was maintained after 12 months,” commented invited discussant and smoking cessation expert Jacek Jassem, MD, from the University of Gdansk (Poland).
He said that the lack of a difference between the intervention and control arms might be attributable to lower levels of concern about heart disease or emphysema among participants, or possibly to the efficacy of the on-site support program itself.
The differences in efficacy of the intervention between men and women suggest that there may be a need for a sex- or gender-adapted approach, he said at the conference sponsored by the International Association for the Study of Lung Cancer.
“Lung cancer screening is a unique opportunity to motivate smoking cessation. All cancer screening programs should included best available and ongoing cessation support, and please, don’t blame smoking persons: Be compassionate, and helpful, and smile like our British colleagues did,” he concluded.
The study was supported by Yorkshire Cancer Research. Dr. Murray and Dr. Jassem reported no financial conflicts of interest.
Nearly one-third of smokers who were offered smoking cessation support on the spot when they showed up for lung cancer screening remained off cigarettes 1 year later, a quit-smoking rate considerably higher than that reported in clinical studies, investigators from the United Kingdom found.
When they added a stop-smoking component to the Yorkshire Lung Screening Trial, Rachael Murray, PhD, and colleagues at the University of Nottingham (England), found that immediately offering a combination of behavioral support and pharmacotherapy to help smokers kick the habit resulted in a 7-day validated point prevalent abstinence rate at 3 months of 30% among smokers randomized to a standard smoking cessation program, and 33.6% among patients randomized to also receive a personalized intervention that included images of their heart and lungs to demonstrate the harmful effects of tobacco.
In contrast, smoking cessation rates reported in trials of lung cancer screening have ranged from approximately 10% to 20%.
Although there was no overall statistical difference in quit-smoking rates between the standard and enhanced intervention arms of the study, the investigators found that women, but not men, were significantly more likely to quit when shown the heart and lung images, compared with those who received the standard smoking cessation support, Dr. Murray said at the World Conference on Lung Cancer held this week in Vienna.
“I think having smoking cessation as an integrated part of the lung cancer track was really positively received by our participants, particularly through having a physical presence and being conveniently located within the setting,” she said in a presidential symposium highlighting the best abstracts presented at the meeting.
“We’ve offered a high-intensity intervention, which is not going to be cheap to offer but I think is really important for these individuals with complex smoking histories and multiple comorbidities,” she added.
No judgment
In an interview, Dr. Murray noted that colocating stop-smoking services with lung screening is important for capturing smokers who may have the will but not the means to quit, and that participants especially appreciated the offer of help without the usual condescending attitude.
“We’re not an add-on: We’re there and physically present at the time of the lung health check,” she said. “It’s a standard of care that our smoking cessation advisers are able to provide. It’s very nonjudgmental and very holistic, providing social support that these people need. They’ve got long smoking histories, and they’re often made to feel guilty for that, and just being able to approach them in a nonjudgmental way makes a big difference.”
Smoking cessation is known to be the most effective way to reduce lung cancer deaths, Dr. Murray said in her presentation, pointing to a 2020 study by University of Michigan researchers showing that adding tobacco treatment to lung cancer screening can reduce deaths by 14% and increase the overall number of life-years gained by 81%.
Reduce smoking?
To see whether adding a personalized on-site smoking cessation program to lung cancer screening could improve quit-smoking rates, Dr. Murray and colleagues enrolled 1,003 smokers who attended the lung cancer screening program and randomly assigned them to either the intervention arm with personalized feedback, supportive communications, ongoing behavioral support and pharmacotherapy, or to a control arm consisting of ongoing behavioral support and pharmacotherapy.
Participants in the intervention arm were shown CT scans of the heart and lungs plus drawings highlighting coronary artery calcification and areas of their lungs damaged by smoking, and information on how quitting smoking can help to improve their health. The smoking cessation advisers followed a tightly controlled script to ensure that the messages were delivered in a uniform fashion to all participants.
As noted before, rates of 7-day validated point prevalent abstinence, measured by exhaled carbon dioxide, were 33.8% in the intervention arm, and 30% in the control arm. The respective costs per quitter were £521.30 ($630.77) and £412.80 ($499.48).
The validated 12-month smoking-free rates were 29.% in the intervention arm, and 28.6% in the control arm. None of the differences were statistically significant.
However, when they looked at between-arm differences by sex, the investigators found that significantly more women assigned to the intervention arm remained abstinent at 3 months, with rates of 33.9% compared with 23.1% of controls, a difference that translated into an unadjusted odds ratio of 1.70 favoring the intervention among women (P = .008).
Effective and durable
“My interpretation of this study is that the abstinence rates were very high, and this in fact was durable because this effect was maintained after 12 months,” commented invited discussant and smoking cessation expert Jacek Jassem, MD, from the University of Gdansk (Poland).
He said that the lack of a difference between the intervention and control arms might be attributable to lower levels of concern about heart disease or emphysema among participants, or possibly to the efficacy of the on-site support program itself.
The differences in efficacy of the intervention between men and women suggest that there may be a need for a sex- or gender-adapted approach, he said at the conference sponsored by the International Association for the Study of Lung Cancer.
“Lung cancer screening is a unique opportunity to motivate smoking cessation. All cancer screening programs should included best available and ongoing cessation support, and please, don’t blame smoking persons: Be compassionate, and helpful, and smile like our British colleagues did,” he concluded.
The study was supported by Yorkshire Cancer Research. Dr. Murray and Dr. Jassem reported no financial conflicts of interest.
Nearly one-third of smokers who were offered smoking cessation support on the spot when they showed up for lung cancer screening remained off cigarettes 1 year later, a quit-smoking rate considerably higher than that reported in clinical studies, investigators from the United Kingdom found.
When they added a stop-smoking component to the Yorkshire Lung Screening Trial, Rachael Murray, PhD, and colleagues at the University of Nottingham (England), found that immediately offering a combination of behavioral support and pharmacotherapy to help smokers kick the habit resulted in a 7-day validated point prevalent abstinence rate at 3 months of 30% among smokers randomized to a standard smoking cessation program, and 33.6% among patients randomized to also receive a personalized intervention that included images of their heart and lungs to demonstrate the harmful effects of tobacco.
In contrast, smoking cessation rates reported in trials of lung cancer screening have ranged from approximately 10% to 20%.
Although there was no overall statistical difference in quit-smoking rates between the standard and enhanced intervention arms of the study, the investigators found that women, but not men, were significantly more likely to quit when shown the heart and lung images, compared with those who received the standard smoking cessation support, Dr. Murray said at the World Conference on Lung Cancer held this week in Vienna.
“I think having smoking cessation as an integrated part of the lung cancer track was really positively received by our participants, particularly through having a physical presence and being conveniently located within the setting,” she said in a presidential symposium highlighting the best abstracts presented at the meeting.
“We’ve offered a high-intensity intervention, which is not going to be cheap to offer but I think is really important for these individuals with complex smoking histories and multiple comorbidities,” she added.
No judgment
In an interview, Dr. Murray noted that colocating stop-smoking services with lung screening is important for capturing smokers who may have the will but not the means to quit, and that participants especially appreciated the offer of help without the usual condescending attitude.
“We’re not an add-on: We’re there and physically present at the time of the lung health check,” she said. “It’s a standard of care that our smoking cessation advisers are able to provide. It’s very nonjudgmental and very holistic, providing social support that these people need. They’ve got long smoking histories, and they’re often made to feel guilty for that, and just being able to approach them in a nonjudgmental way makes a big difference.”
Smoking cessation is known to be the most effective way to reduce lung cancer deaths, Dr. Murray said in her presentation, pointing to a 2020 study by University of Michigan researchers showing that adding tobacco treatment to lung cancer screening can reduce deaths by 14% and increase the overall number of life-years gained by 81%.
Reduce smoking?
To see whether adding a personalized on-site smoking cessation program to lung cancer screening could improve quit-smoking rates, Dr. Murray and colleagues enrolled 1,003 smokers who attended the lung cancer screening program and randomly assigned them to either the intervention arm with personalized feedback, supportive communications, ongoing behavioral support and pharmacotherapy, or to a control arm consisting of ongoing behavioral support and pharmacotherapy.
Participants in the intervention arm were shown CT scans of the heart and lungs plus drawings highlighting coronary artery calcification and areas of their lungs damaged by smoking, and information on how quitting smoking can help to improve their health. The smoking cessation advisers followed a tightly controlled script to ensure that the messages were delivered in a uniform fashion to all participants.
As noted before, rates of 7-day validated point prevalent abstinence, measured by exhaled carbon dioxide, were 33.8% in the intervention arm, and 30% in the control arm. The respective costs per quitter were £521.30 ($630.77) and £412.80 ($499.48).
The validated 12-month smoking-free rates were 29.% in the intervention arm, and 28.6% in the control arm. None of the differences were statistically significant.
However, when they looked at between-arm differences by sex, the investigators found that significantly more women assigned to the intervention arm remained abstinent at 3 months, with rates of 33.9% compared with 23.1% of controls, a difference that translated into an unadjusted odds ratio of 1.70 favoring the intervention among women (P = .008).
Effective and durable
“My interpretation of this study is that the abstinence rates were very high, and this in fact was durable because this effect was maintained after 12 months,” commented invited discussant and smoking cessation expert Jacek Jassem, MD, from the University of Gdansk (Poland).
He said that the lack of a difference between the intervention and control arms might be attributable to lower levels of concern about heart disease or emphysema among participants, or possibly to the efficacy of the on-site support program itself.
The differences in efficacy of the intervention between men and women suggest that there may be a need for a sex- or gender-adapted approach, he said at the conference sponsored by the International Association for the Study of Lung Cancer.
“Lung cancer screening is a unique opportunity to motivate smoking cessation. All cancer screening programs should included best available and ongoing cessation support, and please, don’t blame smoking persons: Be compassionate, and helpful, and smile like our British colleagues did,” he concluded.
The study was supported by Yorkshire Cancer Research. Dr. Murray and Dr. Jassem reported no financial conflicts of interest.
FROM WCLC
Long COVID’s grip will likely tighten as infections continue
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
COVID-19 is far from done in the United States, with more than 111,000 new cases being recorded a day in the second week of August, according to Johns Hopkins University, and 625 deaths being reported every day. , a condition that already has affected between 7.7 million and 23 million Americans, according to U.S. government estimates.
“It is evident that long COVID is real, that it already impacts a substantial number of people, and that this number may continue to grow as new infections occur,” the U.S. Department of Health and Human Services (HHS) said in a research action plan released Aug. 4.
“We are heading towards a big problem on our hands,” says Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs Hospital in St. Louis. “It’s like if we are falling in a plane, hurtling towards the ground. It doesn’t matter at what speed we are falling; what matters is that we are all falling, and falling fast. It’s a real problem. We needed to bring attention to this, yesterday,” he said.
Bryan Lau, PhD, professor of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, and co-lead of a long COVID study there, says whether it’s 5% of the 92 million officially recorded U.S. COVID-19 cases, or 30% – on the higher end of estimates – that means anywhere between 4.5 million and 27 million Americans will have the effects of long COVID.
Other experts put the estimates even higher.
“If we conservatively assume 100 million working-age adults have been infected, that implies 10 to 33 million may have long COVID,” Alice Burns, PhD, associate director for the Kaiser Family Foundation’s Program on Medicaid and the Uninsured, wrote in an analysis.
And even the Centers for Disease Control and Prevention says only a fraction of cases have been recorded.
That, in turn, means tens of millions of people who struggle to work, to get to school, and to take care of their families – and who will be making demands on an already stressed U.S. health care system.
The HHS said in its Aug. 4 report that long COVID could keep 1 million people a day out of work, with a loss of $50 billion in annual pay.
Dr. Lau said health workers and policymakers are woefully unprepared.
“If you have a family unit, and the mom or dad can’t work, or has trouble taking their child to activities, where does the question of support come into play? Where is there potential for food issues, or housing issues?” he asked. “I see the potential for the burden to be extremely large in that capacity.”
Dr. Lau said he has yet to see any strong estimates of how many cases of long COVID might develop. Because a person has to get COVID-19 to ultimately get long COVID, the two are linked. In other words, as COVID-19 cases rise, so will cases of long COVID, and vice versa.
Evidence from the Kaiser Family Foundation analysis suggests a significant impact on employment: Surveys showed more than half of adults with long COVID who worked before becoming infected are either out of work or working fewer hours. Conditions associated with long COVID – such as fatigue, malaise, or problems concentrating – limit people’s ability to work, even if they have jobs that allow for accommodations.
Two surveys of people with long COVID who had worked before becoming infected showed that between 22% and 27% of them were out of work after getting long COVID. In comparison, among all working-age adults in 2019, only 7% were out of work. Given the sheer number of working-age adults with long COVID, the effects on employment may be profound and are likely to involve more people over time. One study estimates that long COVID already accounts for 15% of unfilled jobs.
The most severe symptoms of long COVID include brain fog and heart complications, known to persist for weeks for months after a COVID-19 infection.
A study from the University of Norway published in Open Forum Infectious Diseases found 53% of people tested had at least one symptom of thinking problems 13 months after infection with COVID-19. According to the HHS’ latest report on long COVID, people with thinking problems, heart conditions, mobility issues, and other symptoms are going to need a considerable amount of care. Many will need lengthy periods of rehabilitation.
Dr. Al-Aly worries that long COVID has already severely affected the labor force and the job market, all while burdening the country’s health care system.
“While there are variations in how individuals respond and cope with long COVID, the unifying thread is that with the level of disability it causes, more people will be struggling to keep up with the demands of the workforce and more people will be out on disability than ever before,” he said.
Studies from Johns Hopkins and the University of Washington estimate that 5%-30% of people could get long COVID in the future. Projections beyond that are hazy.
“So far, all the studies we have done on long COVID have been reactionary. Much of the activism around long COVID has been patient led. We are seeing more and more people with lasting symptoms. We need our research to catch up,” Dr. Lau said.
Theo Vos, MD, PhD, professor of health sciences at University of Washington, Seattle, said the main reasons for the huge range of predictions are the variety of methods used, as well as differences in sample size. Also, much long COVID data is self-reported, making it difficult for epidemiologists to track.
“With self-reported data, you can’t plug people into a machine and say this is what they have or this is what they don’t have. At the population level, the only thing you can do is ask questions. There is no systematic way to define long COVID,” he said.
Dr. Vos’s most recent study, which is being peer-reviewed and revised, found that most people with long COVID have symptoms similar to those seen in other autoimmune diseases. But sometimes the immune system can overreact, causing the more severe symptoms, such as brain fog and heart problems, associated with long COVID.
One reason that researchers struggle to come up with numbers, said Dr. Al-Aly, is the rapid rise of new variants. These variants appear to sometimes cause less severe disease than previous ones, but it’s not clear whether that means different risks for long COVID.
“There’s a wide diversity in severity. Someone can have long COVID and be fully functional, while others are not functional at all. We still have a long way to go before we figure out why,” Dr. Lau said.
A version of this article first appeared on WebMD.com.
Stressed about weight gain? Well, stress causes weight gain
Stress, meet weight gain. Weight gain, meet stress
You’re not eating differently and you’re keeping active, but your waistline is expanding. How is that happening? Since eating healthy and exercising shouldn’t make you gain weight, there may be a hidden factor getting in your way. Stress. The one thing that can have a grip on your circadian rhythm stronger than any bodybuilder.

Investigators at Weill Cornell Medicine published two mouse studies that suggest stress and other factors that throw the body’s circadian clocks out of rhythm may contribute to weight gain.
In the first study, the researchers imitated disruptive condition effects like high cortisol exposure and chronic stress by implanting pellets under the skin that released glucocorticoid at a constant rate for 21 days. Mice that received the pellets had twice as much white and brown fat, as well as much higher insulin levels, regardless of their unchanged and still-healthy diet.
In the second study, they used tagged proteins as markers to monitor the daily fluctuations of a protein that regulates fat cell production and circadian gene expression in mouse fat cell precursors. The results showed “that fat cell precursors commit to becoming fat cells only during the circadian cycle phase corresponding to evening in humans,” they said in a written statement.
“Every cell in our body has an intrinsic cell clock, just like the fat cells, and we have a master clock in our brain, which controls hormone secretion,” said senior author Mary Teruel of Cornell University. “A lot of forces are working against a healthy metabolism when we are out of circadian rhythm. The more we understand, the more likely we will be able to do something about it.”
So if you’re stressing out that the scale is or isn’t moving in the direction you want, you could be standing in your own way. Take a chill pill.
Who can smell cancer? The locust nose
If you need to smell some gas, there’s nothing better than a nose. Just ask a scientist: “Noses are still state of the art,” said Debajit Saha, PhD, of Michigan State University. “There’s really nothing like them when it comes to gas sensing.”

And when it comes to noses, dogs are best, right? After all, there’s a reason we don’t have bomb-sniffing wombats and drug-sniffing ostriches. Dogs are better. Better, but not perfect. And if they’re not perfect, then human technology can do better.
Enter the electronic nose. Which is better than dogs … except that it isn’t. “People have been working on ‘electronic noses’ for more than 15 years, but they’re still not close to achieving what biology can do seamlessly,” Dr. Saha explained in a statement from the university.
Which brings us back to dogs. If you want to detect early-stage cancer using smell, you go to the dogs, right? Nope.
Here’s Christopher Contag, PhD, also of Michigan State, who recruited Dr. Saha to the university: “I told him, ‘When you come here, we’ll detect cancer. I’m sure your locusts can do it.’ ”
Yes, locusts. Dr. Contag and his research team were looking at mouth cancers and noticed that different cell lines had different appearances. Then they discovered that those different-looking cell lines produced different metabolites, some of which were volatile.
Enter Dr. Saha’s locusts. They were able to tell the difference between normal cells and cancer cells and could even distinguish between the different cell lines. And how they were able to share this information? Not voluntarily, that’s for sure. The researchers attached electrodes to the insects’ brains and recorded their responses to gas samples from both healthy and cancer cells. Those brain signals were then used to create chemical profiles of the different cells. Piece of cake.
The whole getting-electrodes-attached-to-their-brains thing seemed at least a bit ethically ambiguous, so we contacted the locusts’ PR office, which offered some positive spin: “Humans get their early cancer detection and we get that whole swarms-that-devour-entire-countrysides thing off our backs. Win win.”
Bad news for vampires everywhere
Pop culture has been extraordinarily kind to the vampire. A few hundred years ago, vampires were demon-possessed, often-inhuman monsters. Now? They’re suave, sophisticated, beautiful, and oh-so dramatic and angst-filled about their “curse.” Drink a little human blood, live and look young forever. Such monsters they are.

It does make sense in a morbid sort of way. An old person receiving the blood of the young does seem like a good idea for rejuvenation, right? A team of Ukrainian researchers sought to find out, conducting a study in which older mice were linked with young mice via heterochronic parabiosis. For 3 months, old-young mice pairs were surgically connected and shared blood. After 3 months, the mice were disconnected from each other and the effects of the blood link were studied.
For all the vampire enthusiasts out there, we have bad news and worse news. The bad news first: The older mice received absolutely no benefit from heterochronic parabiosis. No youthfulness, no increased lifespan, nothing. The worse news is that the younger mice were adversely affected by the older blood. They aged more and experienced a shortened lifespan, even after the connection was severed. The old blood, according to the investigators, contains factors capable of inducing aging in younger mice, but the opposite is not true. Further research into aging, they added, should focus on suppressing the aging factors in older blood.
Of note, the paper was written by doctors who are currently refugees, fleeing the war in Ukraine. We don’t want to speculate on the true cause of the war, but we’re onto you, Putin. We know you wanted the vampire research for yourself, but it won’t work. Your dream of becoming Vlad “Dracula” Putin will never come to pass.
Hearing is not always believing
Have you ever heard yourself on a voice mail, or from a recording you did at work? No matter how good you sound, you still might feel like the recording sounds nothing like you. It may even cause low self-esteem for those who don’t like how their voice sounds or don’t recognize it when it’s played back to them.

Since one possible symptom of schizophrenia is not recognizing one’s own speech and having a false sense of control over actions, and those with schizophrenia may hallucinate or hear voices, not being able to recognize their own voices may be alarming.
A recent study on the sense of agency, or sense of control, involved having volunteers speak with different pitches in their voices and then having it played back to them to gauge their reactions.
“Our results demonstrate that hearing one’s own voice is a critical factor to increased self-agency over speech. In other words, we do not strongly feel that ‘I’ am generating the speech if we hear someone else’s voice as an outcome of the speech. Our study provides empirical evidence of the tight link between the sense of agency and self-voice identity,” lead author Ryu Ohata, PhD, of the University of Tokyo, said in a written statement.
As social interaction becomes more digital through platforms such as FaceTime, Zoom, and voicemail, especially since the pandemic has promoted social distancing, it makes sense that people may be more aware and more surprised by how they sound on recordings.
So, if you ever promised someone something that you don’t want to do, and they play it back to you from the recording you made, maybe you can just say you don’t recognize the voice. And if it’s not you, then you don’t have to do it.
Stress, meet weight gain. Weight gain, meet stress
You’re not eating differently and you’re keeping active, but your waistline is expanding. How is that happening? Since eating healthy and exercising shouldn’t make you gain weight, there may be a hidden factor getting in your way. Stress. The one thing that can have a grip on your circadian rhythm stronger than any bodybuilder.
Investigators at Weill Cornell Medicine published two mouse studies that suggest stress and other factors that throw the body’s circadian clocks out of rhythm may contribute to weight gain.
In the first study, the researchers imitated disruptive condition effects like high cortisol exposure and chronic stress by implanting pellets under the skin that released glucocorticoid at a constant rate for 21 days. Mice that received the pellets had twice as much white and brown fat, as well as much higher insulin levels, regardless of their unchanged and still-healthy diet.
In the second study, they used tagged proteins as markers to monitor the daily fluctuations of a protein that regulates fat cell production and circadian gene expression in mouse fat cell precursors. The results showed “that fat cell precursors commit to becoming fat cells only during the circadian cycle phase corresponding to evening in humans,” they said in a written statement.
“Every cell in our body has an intrinsic cell clock, just like the fat cells, and we have a master clock in our brain, which controls hormone secretion,” said senior author Mary Teruel of Cornell University. “A lot of forces are working against a healthy metabolism when we are out of circadian rhythm. The more we understand, the more likely we will be able to do something about it.”
So if you’re stressing out that the scale is or isn’t moving in the direction you want, you could be standing in your own way. Take a chill pill.
Who can smell cancer? The locust nose
If you need to smell some gas, there’s nothing better than a nose. Just ask a scientist: “Noses are still state of the art,” said Debajit Saha, PhD, of Michigan State University. “There’s really nothing like them when it comes to gas sensing.”
And when it comes to noses, dogs are best, right? After all, there’s a reason we don’t have bomb-sniffing wombats and drug-sniffing ostriches. Dogs are better. Better, but not perfect. And if they’re not perfect, then human technology can do better.
Enter the electronic nose. Which is better than dogs … except that it isn’t. “People have been working on ‘electronic noses’ for more than 15 years, but they’re still not close to achieving what biology can do seamlessly,” Dr. Saha explained in a statement from the university.
Which brings us back to dogs. If you want to detect early-stage cancer using smell, you go to the dogs, right? Nope.
Here’s Christopher Contag, PhD, also of Michigan State, who recruited Dr. Saha to the university: “I told him, ‘When you come here, we’ll detect cancer. I’m sure your locusts can do it.’ ”
Yes, locusts. Dr. Contag and his research team were looking at mouth cancers and noticed that different cell lines had different appearances. Then they discovered that those different-looking cell lines produced different metabolites, some of which were volatile.
Enter Dr. Saha’s locusts. They were able to tell the difference between normal cells and cancer cells and could even distinguish between the different cell lines. And how they were able to share this information? Not voluntarily, that’s for sure. The researchers attached electrodes to the insects’ brains and recorded their responses to gas samples from both healthy and cancer cells. Those brain signals were then used to create chemical profiles of the different cells. Piece of cake.
The whole getting-electrodes-attached-to-their-brains thing seemed at least a bit ethically ambiguous, so we contacted the locusts’ PR office, which offered some positive spin: “Humans get their early cancer detection and we get that whole swarms-that-devour-entire-countrysides thing off our backs. Win win.”
Bad news for vampires everywhere
Pop culture has been extraordinarily kind to the vampire. A few hundred years ago, vampires were demon-possessed, often-inhuman monsters. Now? They’re suave, sophisticated, beautiful, and oh-so dramatic and angst-filled about their “curse.” Drink a little human blood, live and look young forever. Such monsters they are.
It does make sense in a morbid sort of way. An old person receiving the blood of the young does seem like a good idea for rejuvenation, right? A team of Ukrainian researchers sought to find out, conducting a study in which older mice were linked with young mice via heterochronic parabiosis. For 3 months, old-young mice pairs were surgically connected and shared blood. After 3 months, the mice were disconnected from each other and the effects of the blood link were studied.
For all the vampire enthusiasts out there, we have bad news and worse news. The bad news first: The older mice received absolutely no benefit from heterochronic parabiosis. No youthfulness, no increased lifespan, nothing. The worse news is that the younger mice were adversely affected by the older blood. They aged more and experienced a shortened lifespan, even after the connection was severed. The old blood, according to the investigators, contains factors capable of inducing aging in younger mice, but the opposite is not true. Further research into aging, they added, should focus on suppressing the aging factors in older blood.
Of note, the paper was written by doctors who are currently refugees, fleeing the war in Ukraine. We don’t want to speculate on the true cause of the war, but we’re onto you, Putin. We know you wanted the vampire research for yourself, but it won’t work. Your dream of becoming Vlad “Dracula” Putin will never come to pass.
Hearing is not always believing
Have you ever heard yourself on a voice mail, or from a recording you did at work? No matter how good you sound, you still might feel like the recording sounds nothing like you. It may even cause low self-esteem for those who don’t like how their voice sounds or don’t recognize it when it’s played back to them.
Since one possible symptom of schizophrenia is not recognizing one’s own speech and having a false sense of control over actions, and those with schizophrenia may hallucinate or hear voices, not being able to recognize their own voices may be alarming.
A recent study on the sense of agency, or sense of control, involved having volunteers speak with different pitches in their voices and then having it played back to them to gauge their reactions.
“Our results demonstrate that hearing one’s own voice is a critical factor to increased self-agency over speech. In other words, we do not strongly feel that ‘I’ am generating the speech if we hear someone else’s voice as an outcome of the speech. Our study provides empirical evidence of the tight link between the sense of agency and self-voice identity,” lead author Ryu Ohata, PhD, of the University of Tokyo, said in a written statement.
As social interaction becomes more digital through platforms such as FaceTime, Zoom, and voicemail, especially since the pandemic has promoted social distancing, it makes sense that people may be more aware and more surprised by how they sound on recordings.
So, if you ever promised someone something that you don’t want to do, and they play it back to you from the recording you made, maybe you can just say you don’t recognize the voice. And if it’s not you, then you don’t have to do it.
Stress, meet weight gain. Weight gain, meet stress
You’re not eating differently and you’re keeping active, but your waistline is expanding. How is that happening? Since eating healthy and exercising shouldn’t make you gain weight, there may be a hidden factor getting in your way. Stress. The one thing that can have a grip on your circadian rhythm stronger than any bodybuilder.
Investigators at Weill Cornell Medicine published two mouse studies that suggest stress and other factors that throw the body’s circadian clocks out of rhythm may contribute to weight gain.
In the first study, the researchers imitated disruptive condition effects like high cortisol exposure and chronic stress by implanting pellets under the skin that released glucocorticoid at a constant rate for 21 days. Mice that received the pellets had twice as much white and brown fat, as well as much higher insulin levels, regardless of their unchanged and still-healthy diet.
In the second study, they used tagged proteins as markers to monitor the daily fluctuations of a protein that regulates fat cell production and circadian gene expression in mouse fat cell precursors. The results showed “that fat cell precursors commit to becoming fat cells only during the circadian cycle phase corresponding to evening in humans,” they said in a written statement.
“Every cell in our body has an intrinsic cell clock, just like the fat cells, and we have a master clock in our brain, which controls hormone secretion,” said senior author Mary Teruel of Cornell University. “A lot of forces are working against a healthy metabolism when we are out of circadian rhythm. The more we understand, the more likely we will be able to do something about it.”
So if you’re stressing out that the scale is or isn’t moving in the direction you want, you could be standing in your own way. Take a chill pill.
Who can smell cancer? The locust nose
If you need to smell some gas, there’s nothing better than a nose. Just ask a scientist: “Noses are still state of the art,” said Debajit Saha, PhD, of Michigan State University. “There’s really nothing like them when it comes to gas sensing.”
And when it comes to noses, dogs are best, right? After all, there’s a reason we don’t have bomb-sniffing wombats and drug-sniffing ostriches. Dogs are better. Better, but not perfect. And if they’re not perfect, then human technology can do better.
Enter the electronic nose. Which is better than dogs … except that it isn’t. “People have been working on ‘electronic noses’ for more than 15 years, but they’re still not close to achieving what biology can do seamlessly,” Dr. Saha explained in a statement from the university.
Which brings us back to dogs. If you want to detect early-stage cancer using smell, you go to the dogs, right? Nope.
Here’s Christopher Contag, PhD, also of Michigan State, who recruited Dr. Saha to the university: “I told him, ‘When you come here, we’ll detect cancer. I’m sure your locusts can do it.’ ”
Yes, locusts. Dr. Contag and his research team were looking at mouth cancers and noticed that different cell lines had different appearances. Then they discovered that those different-looking cell lines produced different metabolites, some of which were volatile.
Enter Dr. Saha’s locusts. They were able to tell the difference between normal cells and cancer cells and could even distinguish between the different cell lines. And how they were able to share this information? Not voluntarily, that’s for sure. The researchers attached electrodes to the insects’ brains and recorded their responses to gas samples from both healthy and cancer cells. Those brain signals were then used to create chemical profiles of the different cells. Piece of cake.
The whole getting-electrodes-attached-to-their-brains thing seemed at least a bit ethically ambiguous, so we contacted the locusts’ PR office, which offered some positive spin: “Humans get their early cancer detection and we get that whole swarms-that-devour-entire-countrysides thing off our backs. Win win.”
Bad news for vampires everywhere
Pop culture has been extraordinarily kind to the vampire. A few hundred years ago, vampires were demon-possessed, often-inhuman monsters. Now? They’re suave, sophisticated, beautiful, and oh-so dramatic and angst-filled about their “curse.” Drink a little human blood, live and look young forever. Such monsters they are.
It does make sense in a morbid sort of way. An old person receiving the blood of the young does seem like a good idea for rejuvenation, right? A team of Ukrainian researchers sought to find out, conducting a study in which older mice were linked with young mice via heterochronic parabiosis. For 3 months, old-young mice pairs were surgically connected and shared blood. After 3 months, the mice were disconnected from each other and the effects of the blood link were studied.
For all the vampire enthusiasts out there, we have bad news and worse news. The bad news first: The older mice received absolutely no benefit from heterochronic parabiosis. No youthfulness, no increased lifespan, nothing. The worse news is that the younger mice were adversely affected by the older blood. They aged more and experienced a shortened lifespan, even after the connection was severed. The old blood, according to the investigators, contains factors capable of inducing aging in younger mice, but the opposite is not true. Further research into aging, they added, should focus on suppressing the aging factors in older blood.
Of note, the paper was written by doctors who are currently refugees, fleeing the war in Ukraine. We don’t want to speculate on the true cause of the war, but we’re onto you, Putin. We know you wanted the vampire research for yourself, but it won’t work. Your dream of becoming Vlad “Dracula” Putin will never come to pass.
Hearing is not always believing
Have you ever heard yourself on a voice mail, or from a recording you did at work? No matter how good you sound, you still might feel like the recording sounds nothing like you. It may even cause low self-esteem for those who don’t like how their voice sounds or don’t recognize it when it’s played back to them.
Since one possible symptom of schizophrenia is not recognizing one’s own speech and having a false sense of control over actions, and those with schizophrenia may hallucinate or hear voices, not being able to recognize their own voices may be alarming.
A recent study on the sense of agency, or sense of control, involved having volunteers speak with different pitches in their voices and then having it played back to them to gauge their reactions.
“Our results demonstrate that hearing one’s own voice is a critical factor to increased self-agency over speech. In other words, we do not strongly feel that ‘I’ am generating the speech if we hear someone else’s voice as an outcome of the speech. Our study provides empirical evidence of the tight link between the sense of agency and self-voice identity,” lead author Ryu Ohata, PhD, of the University of Tokyo, said in a written statement.
As social interaction becomes more digital through platforms such as FaceTime, Zoom, and voicemail, especially since the pandemic has promoted social distancing, it makes sense that people may be more aware and more surprised by how they sound on recordings.
So, if you ever promised someone something that you don’t want to do, and they play it back to you from the recording you made, maybe you can just say you don’t recognize the voice. And if it’s not you, then you don’t have to do it.
Cardiorespiratory fitness key to longevity for all?
Cardiorespiratory fitness emerged as a stronger predictor of all-cause mortality than did any traditional risk factor across the spectrum of age, sex, and race in a modeling study that included more than 750,000 U.S. veterans.
In addition, mortality risk was cut in half if individuals achieved a moderate cardiorespiratory fitness (CRF) level – that is, by meeting the current U.S. physical activity recommendations of 150 minutes per week, the authors note.
Furthermore, contrary to some previous research, “extremely high” fitness was not associated with an increased risk for mortality in the study, published online in the Journal of the American College of Cardiology.
“This study has been 15 years in the making,” lead author Peter Kokkinos, PhD, Rutgers University, New Brunswick, N.J., and the VA Medical Center, Washington, told this news organization. “We waited until we had the computer power and the right people to really assess this. We wanted to be very liberal in excluding patients we thought might contaminate the results, such as those with cardiovascular disease in the 6 months prior to a stress test.”
Figuring the time was right, the team analyzed data from the VA’s Exercise Testing and Health Outcomes Study (ETHOS) on individuals aged 30-95 years who underwent exercise treadmill tests between 1999 and 2020.
After exclusions, 750,302 individuals (from among 822,995) were included: 6.5% were women; 73.7% were White individuals; 19% were African American individuals; 4.7% were Hispanic individuals; and 2.1% were Native American, Asian, or Hawaiian individuals. Septuagenarians made up 14.7% of the cohort, and octogenarians made up 3.6%.
CRF categories for age and sex were determined by the peak metabolic equivalent of task (MET) achieved during the treadmill test. One MET is the energy spent at rest – that is the basal metabolic rate.
Although some physicians may resist putting patients through a stress test, “the amount of information we get from it is incredible,” Dr. Kokkinos noted. “We get blood pressure, we get heart rate, we get a response if you’re not doing exercise. This tells us a lot more than having you sit around so we can measure resting heart rate and blood pressure.”
Lowest mortality at 14.0 METs
During a median follow-up of 10.2 years (7,803,861 person-years), 23% of participants died, for an average of 22.4 events per 1,000 person-years.
Higher exercise capacity was inversely related to mortality risk across the cohort and within each age category. Specifically, every 1 MET increase in exercise capacity yielded an adjusted hazard ratio for mortality of 0.86 (95% confidence interval, 0.85-0.87; P < .001) for the entire cohort and similar HRs by sex and race.
The mortality risk for the least-fit individuals (20th percentile) was fourfold higher than for extremely fit individuals (HR, 4.09; 95% CI, 3.90-4.20), with the lowest mortality risk at about 14.0 METs for both men (HR, 0.24; 95% CI, 0.23-0.25) and women (HR, 0.23; 95% CI, 0.17-0.29). Extremely high CRF did not increase the risk.
In addition, at 20 years of follow-up, about 80% of men and 95% of women in the highest CRF category (98th percentile) were alive vs. less than 40% of men and approximately 75% of women in the least fit CRF category.
“We know CRF declines by 1% per year after age 30,” Dr. Kokkinos said. “But the age-related decline is cut in half if you are fit, meaning that an expected 10% decline over a decade will be only a 5% decline if you stay active. We cannot stop or reverse the decline, but we can kind of put the brakes on, and that’s a reason for clinicians to continue to encourage fitness.”
Indeed, “improving CRF should be considered a target in CVD prevention, similar to improving lipids, blood sugar, blood pressure, and weight,” Carl J. Lavie, MD, Ochsner Health, New Orleans, and colleagues affirm in a related editorial.
‘A difficult battle’
But that may not happen any time soon. “Unfortunately, despite having been recognized in an American Heart Association scientific statement as a clinical vital sign, aerobic fitness is undervalued and underutilized,” Claudio Gil Araújo, MD, PhD, research director of the Exercise Medicine Clinic-CLINIMEX, Rio de Janeiro, told this news organization.
Dr. Araújo led a recent study showing that the ability to stand on one leg for at least 10 seconds is strongly linked to the risk for death over the next 7 years.
Although physicians should be encouraging fitness, he said that “a substantial part of health professionals are physically unfit and feel uncomfortable talking about and prescribing exercise for their patients. Also, physicians tend to be better trained in treating diseases (using medications and/or prescribing procedures) than in preventing diseases by stimulating adoption of healthy habits. So, this a long road and a difficult battle.”
Nonetheless, he added, “Darwin said a long time ago that only the fittest will survive. If Darwin could read this study, he would surely smile.”
No commercial funding or conflicts of interest related to the study were reported. Dr. Lavie previously served as a speaker and consultant for PAI Health on their PAI (Personalized Activity Intelligence) applications.
A version of this article first appeared on Medscape.com.
Cardiorespiratory fitness emerged as a stronger predictor of all-cause mortality than did any traditional risk factor across the spectrum of age, sex, and race in a modeling study that included more than 750,000 U.S. veterans.
In addition, mortality risk was cut in half if individuals achieved a moderate cardiorespiratory fitness (CRF) level – that is, by meeting the current U.S. physical activity recommendations of 150 minutes per week, the authors note.
Furthermore, contrary to some previous research, “extremely high” fitness was not associated with an increased risk for mortality in the study, published online in the Journal of the American College of Cardiology.
“This study has been 15 years in the making,” lead author Peter Kokkinos, PhD, Rutgers University, New Brunswick, N.J., and the VA Medical Center, Washington, told this news organization. “We waited until we had the computer power and the right people to really assess this. We wanted to be very liberal in excluding patients we thought might contaminate the results, such as those with cardiovascular disease in the 6 months prior to a stress test.”
Figuring the time was right, the team analyzed data from the VA’s Exercise Testing and Health Outcomes Study (ETHOS) on individuals aged 30-95 years who underwent exercise treadmill tests between 1999 and 2020.
After exclusions, 750,302 individuals (from among 822,995) were included: 6.5% were women; 73.7% were White individuals; 19% were African American individuals; 4.7% were Hispanic individuals; and 2.1% were Native American, Asian, or Hawaiian individuals. Septuagenarians made up 14.7% of the cohort, and octogenarians made up 3.6%.
CRF categories for age and sex were determined by the peak metabolic equivalent of task (MET) achieved during the treadmill test. One MET is the energy spent at rest – that is the basal metabolic rate.
Although some physicians may resist putting patients through a stress test, “the amount of information we get from it is incredible,” Dr. Kokkinos noted. “We get blood pressure, we get heart rate, we get a response if you’re not doing exercise. This tells us a lot more than having you sit around so we can measure resting heart rate and blood pressure.”
Lowest mortality at 14.0 METs
During a median follow-up of 10.2 years (7,803,861 person-years), 23% of participants died, for an average of 22.4 events per 1,000 person-years.
Higher exercise capacity was inversely related to mortality risk across the cohort and within each age category. Specifically, every 1 MET increase in exercise capacity yielded an adjusted hazard ratio for mortality of 0.86 (95% confidence interval, 0.85-0.87; P < .001) for the entire cohort and similar HRs by sex and race.
The mortality risk for the least-fit individuals (20th percentile) was fourfold higher than for extremely fit individuals (HR, 4.09; 95% CI, 3.90-4.20), with the lowest mortality risk at about 14.0 METs for both men (HR, 0.24; 95% CI, 0.23-0.25) and women (HR, 0.23; 95% CI, 0.17-0.29). Extremely high CRF did not increase the risk.
In addition, at 20 years of follow-up, about 80% of men and 95% of women in the highest CRF category (98th percentile) were alive vs. less than 40% of men and approximately 75% of women in the least fit CRF category.
“We know CRF declines by 1% per year after age 30,” Dr. Kokkinos said. “But the age-related decline is cut in half if you are fit, meaning that an expected 10% decline over a decade will be only a 5% decline if you stay active. We cannot stop or reverse the decline, but we can kind of put the brakes on, and that’s a reason for clinicians to continue to encourage fitness.”
Indeed, “improving CRF should be considered a target in CVD prevention, similar to improving lipids, blood sugar, blood pressure, and weight,” Carl J. Lavie, MD, Ochsner Health, New Orleans, and colleagues affirm in a related editorial.
‘A difficult battle’
But that may not happen any time soon. “Unfortunately, despite having been recognized in an American Heart Association scientific statement as a clinical vital sign, aerobic fitness is undervalued and underutilized,” Claudio Gil Araújo, MD, PhD, research director of the Exercise Medicine Clinic-CLINIMEX, Rio de Janeiro, told this news organization.
Dr. Araújo led a recent study showing that the ability to stand on one leg for at least 10 seconds is strongly linked to the risk for death over the next 7 years.
Although physicians should be encouraging fitness, he said that “a substantial part of health professionals are physically unfit and feel uncomfortable talking about and prescribing exercise for their patients. Also, physicians tend to be better trained in treating diseases (using medications and/or prescribing procedures) than in preventing diseases by stimulating adoption of healthy habits. So, this a long road and a difficult battle.”
Nonetheless, he added, “Darwin said a long time ago that only the fittest will survive. If Darwin could read this study, he would surely smile.”
No commercial funding or conflicts of interest related to the study were reported. Dr. Lavie previously served as a speaker and consultant for PAI Health on their PAI (Personalized Activity Intelligence) applications.
A version of this article first appeared on Medscape.com.
Cardiorespiratory fitness emerged as a stronger predictor of all-cause mortality than did any traditional risk factor across the spectrum of age, sex, and race in a modeling study that included more than 750,000 U.S. veterans.
In addition, mortality risk was cut in half if individuals achieved a moderate cardiorespiratory fitness (CRF) level – that is, by meeting the current U.S. physical activity recommendations of 150 minutes per week, the authors note.
Furthermore, contrary to some previous research, “extremely high” fitness was not associated with an increased risk for mortality in the study, published online in the Journal of the American College of Cardiology.
“This study has been 15 years in the making,” lead author Peter Kokkinos, PhD, Rutgers University, New Brunswick, N.J., and the VA Medical Center, Washington, told this news organization. “We waited until we had the computer power and the right people to really assess this. We wanted to be very liberal in excluding patients we thought might contaminate the results, such as those with cardiovascular disease in the 6 months prior to a stress test.”
Figuring the time was right, the team analyzed data from the VA’s Exercise Testing and Health Outcomes Study (ETHOS) on individuals aged 30-95 years who underwent exercise treadmill tests between 1999 and 2020.
After exclusions, 750,302 individuals (from among 822,995) were included: 6.5% were women; 73.7% were White individuals; 19% were African American individuals; 4.7% were Hispanic individuals; and 2.1% were Native American, Asian, or Hawaiian individuals. Septuagenarians made up 14.7% of the cohort, and octogenarians made up 3.6%.
CRF categories for age and sex were determined by the peak metabolic equivalent of task (MET) achieved during the treadmill test. One MET is the energy spent at rest – that is the basal metabolic rate.
Although some physicians may resist putting patients through a stress test, “the amount of information we get from it is incredible,” Dr. Kokkinos noted. “We get blood pressure, we get heart rate, we get a response if you’re not doing exercise. This tells us a lot more than having you sit around so we can measure resting heart rate and blood pressure.”
Lowest mortality at 14.0 METs
During a median follow-up of 10.2 years (7,803,861 person-years), 23% of participants died, for an average of 22.4 events per 1,000 person-years.
Higher exercise capacity was inversely related to mortality risk across the cohort and within each age category. Specifically, every 1 MET increase in exercise capacity yielded an adjusted hazard ratio for mortality of 0.86 (95% confidence interval, 0.85-0.87; P < .001) for the entire cohort and similar HRs by sex and race.
The mortality risk for the least-fit individuals (20th percentile) was fourfold higher than for extremely fit individuals (HR, 4.09; 95% CI, 3.90-4.20), with the lowest mortality risk at about 14.0 METs for both men (HR, 0.24; 95% CI, 0.23-0.25) and women (HR, 0.23; 95% CI, 0.17-0.29). Extremely high CRF did not increase the risk.
In addition, at 20 years of follow-up, about 80% of men and 95% of women in the highest CRF category (98th percentile) were alive vs. less than 40% of men and approximately 75% of women in the least fit CRF category.
“We know CRF declines by 1% per year after age 30,” Dr. Kokkinos said. “But the age-related decline is cut in half if you are fit, meaning that an expected 10% decline over a decade will be only a 5% decline if you stay active. We cannot stop or reverse the decline, but we can kind of put the brakes on, and that’s a reason for clinicians to continue to encourage fitness.”
Indeed, “improving CRF should be considered a target in CVD prevention, similar to improving lipids, blood sugar, blood pressure, and weight,” Carl J. Lavie, MD, Ochsner Health, New Orleans, and colleagues affirm in a related editorial.
‘A difficult battle’
But that may not happen any time soon. “Unfortunately, despite having been recognized in an American Heart Association scientific statement as a clinical vital sign, aerobic fitness is undervalued and underutilized,” Claudio Gil Araújo, MD, PhD, research director of the Exercise Medicine Clinic-CLINIMEX, Rio de Janeiro, told this news organization.
Dr. Araújo led a recent study showing that the ability to stand on one leg for at least 10 seconds is strongly linked to the risk for death over the next 7 years.
Although physicians should be encouraging fitness, he said that “a substantial part of health professionals are physically unfit and feel uncomfortable talking about and prescribing exercise for their patients. Also, physicians tend to be better trained in treating diseases (using medications and/or prescribing procedures) than in preventing diseases by stimulating adoption of healthy habits. So, this a long road and a difficult battle.”
Nonetheless, he added, “Darwin said a long time ago that only the fittest will survive. If Darwin could read this study, he would surely smile.”
No commercial funding or conflicts of interest related to the study were reported. Dr. Lavie previously served as a speaker and consultant for PAI Health on their PAI (Personalized Activity Intelligence) applications.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Partnering for pulmonary fibrosis
The CHEST Foundation raises awareness for the most common interstitial lung disease.
On August 27, the CHEST Foundation and the Feldman Family Foundation will be hosting the 9th annual Irv Feldman Texas Hold ‘Em Tournament & Casino Night fundraiser supporting patient access and the provision of better quality of life for patients battling the interstitial lung disease – pulmonary fibrosis.
“My dad, Irv, had pulmonary fibrosis and deeply loved to play poker. It was always a family activity, and it continued through when he got sick. We played at his kitchen table when he couldn’t leave the house, and we even brought cards and chips to his hospital and rehab rooms,” said Mitch Feldman, President of the Feldman Family Foundation and member of the CHEST Foundation Board of Trustees. “During these few hours of poker play, he all but forgot about his illness and showed virtually no symptoms of the disease. In his honor, we created an event where people would come together to have fun playing poker while raising money for the disease [that] so deeply impacted our family.”
Through years of hosting the event, the Feldman family and the CHEST Foundation secured funding to develop a pulmonary fibrosis patient education resource hub that serves as a resource for those newly diagnosed and living with this disease. The Feldman Family and the CHEST Foundation continue to raise funds to support both early diagnosis and closing the gap between diagnosis and beginning treatment.
Partnering to address gaps
Affecting around 400,000 people in the United States, ILDs are frequently misdiagnosed as more common lung diseases. Some studies show that reaching an appropriate diagnosis for rarer lung diseases can take upwards of several years.
To begin addressing the issue of delays in diagnosis, the American College of Chest Physicians (CHEST) and Three Lakes Foundation are collaborating on a multiphase educational initiative aiming to reduce the time it takes to identify interstitial lung diseases like pulmonary fibrosis.
The initiative is called “Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients” to highlight the collaboration of pulmonary and primary care medicine. A steering committee of medical experts – including pulmonologists, primary care physicians, and a nursing professional – will work to create materials that will aid in identifying and diagnosing complex lung diseases quicker.
“By having experts from both pulmonary and primary care medicine as members of the steering committee, we are bringing together the pieces of the puzzle that is a complex diagnosis,” said Bridging Specialties steering committee member and family medicine physician, Dr. William Lago. “Patients first see their family medicine or primary care clinicians and, all too often, the most complex lung diseases present in ways that are indistinguishable from more common conditions like asthma and COPD. Bringing together experts in both fields will yield the best results in creating a path to diagnosis.”
To learn more about the Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients initiative and to sign up for updates, visit https://tinyurl.com/2p92ha6r.
For ticket and donation information to the Irv Feldman Texas Hold ‘Em Tournament & Casino Night, visit the CHEST Foundation website at foundation.chestnet.org.
The CHEST Foundation raises awareness for the most common interstitial lung disease.
On August 27, the CHEST Foundation and the Feldman Family Foundation will be hosting the 9th annual Irv Feldman Texas Hold ‘Em Tournament & Casino Night fundraiser supporting patient access and the provision of better quality of life for patients battling the interstitial lung disease – pulmonary fibrosis.
“My dad, Irv, had pulmonary fibrosis and deeply loved to play poker. It was always a family activity, and it continued through when he got sick. We played at his kitchen table when he couldn’t leave the house, and we even brought cards and chips to his hospital and rehab rooms,” said Mitch Feldman, President of the Feldman Family Foundation and member of the CHEST Foundation Board of Trustees. “During these few hours of poker play, he all but forgot about his illness and showed virtually no symptoms of the disease. In his honor, we created an event where people would come together to have fun playing poker while raising money for the disease [that] so deeply impacted our family.”
Through years of hosting the event, the Feldman family and the CHEST Foundation secured funding to develop a pulmonary fibrosis patient education resource hub that serves as a resource for those newly diagnosed and living with this disease. The Feldman Family and the CHEST Foundation continue to raise funds to support both early diagnosis and closing the gap between diagnosis and beginning treatment.
Partnering to address gaps
Affecting around 400,000 people in the United States, ILDs are frequently misdiagnosed as more common lung diseases. Some studies show that reaching an appropriate diagnosis for rarer lung diseases can take upwards of several years.
To begin addressing the issue of delays in diagnosis, the American College of Chest Physicians (CHEST) and Three Lakes Foundation are collaborating on a multiphase educational initiative aiming to reduce the time it takes to identify interstitial lung diseases like pulmonary fibrosis.
The initiative is called “Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients” to highlight the collaboration of pulmonary and primary care medicine. A steering committee of medical experts – including pulmonologists, primary care physicians, and a nursing professional – will work to create materials that will aid in identifying and diagnosing complex lung diseases quicker.
“By having experts from both pulmonary and primary care medicine as members of the steering committee, we are bringing together the pieces of the puzzle that is a complex diagnosis,” said Bridging Specialties steering committee member and family medicine physician, Dr. William Lago. “Patients first see their family medicine or primary care clinicians and, all too often, the most complex lung diseases present in ways that are indistinguishable from more common conditions like asthma and COPD. Bringing together experts in both fields will yield the best results in creating a path to diagnosis.”
To learn more about the Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients initiative and to sign up for updates, visit https://tinyurl.com/2p92ha6r.
For ticket and donation information to the Irv Feldman Texas Hold ‘Em Tournament & Casino Night, visit the CHEST Foundation website at foundation.chestnet.org.
The CHEST Foundation raises awareness for the most common interstitial lung disease.
On August 27, the CHEST Foundation and the Feldman Family Foundation will be hosting the 9th annual Irv Feldman Texas Hold ‘Em Tournament & Casino Night fundraiser supporting patient access and the provision of better quality of life for patients battling the interstitial lung disease – pulmonary fibrosis.
“My dad, Irv, had pulmonary fibrosis and deeply loved to play poker. It was always a family activity, and it continued through when he got sick. We played at his kitchen table when he couldn’t leave the house, and we even brought cards and chips to his hospital and rehab rooms,” said Mitch Feldman, President of the Feldman Family Foundation and member of the CHEST Foundation Board of Trustees. “During these few hours of poker play, he all but forgot about his illness and showed virtually no symptoms of the disease. In his honor, we created an event where people would come together to have fun playing poker while raising money for the disease [that] so deeply impacted our family.”
Through years of hosting the event, the Feldman family and the CHEST Foundation secured funding to develop a pulmonary fibrosis patient education resource hub that serves as a resource for those newly diagnosed and living with this disease. The Feldman Family and the CHEST Foundation continue to raise funds to support both early diagnosis and closing the gap between diagnosis and beginning treatment.
Partnering to address gaps
Affecting around 400,000 people in the United States, ILDs are frequently misdiagnosed as more common lung diseases. Some studies show that reaching an appropriate diagnosis for rarer lung diseases can take upwards of several years.
To begin addressing the issue of delays in diagnosis, the American College of Chest Physicians (CHEST) and Three Lakes Foundation are collaborating on a multiphase educational initiative aiming to reduce the time it takes to identify interstitial lung diseases like pulmonary fibrosis.
The initiative is called “Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients” to highlight the collaboration of pulmonary and primary care medicine. A steering committee of medical experts – including pulmonologists, primary care physicians, and a nursing professional – will work to create materials that will aid in identifying and diagnosing complex lung diseases quicker.
“By having experts from both pulmonary and primary care medicine as members of the steering committee, we are bringing together the pieces of the puzzle that is a complex diagnosis,” said Bridging Specialties steering committee member and family medicine physician, Dr. William Lago. “Patients first see their family medicine or primary care clinicians and, all too often, the most complex lung diseases present in ways that are indistinguishable from more common conditions like asthma and COPD. Bringing together experts in both fields will yield the best results in creating a path to diagnosis.”
To learn more about the Bridging SpecialtiesTM: Timely Diagnosis for ILD Patients initiative and to sign up for updates, visit https://tinyurl.com/2p92ha6r.
For ticket and donation information to the Irv Feldman Texas Hold ‘Em Tournament & Casino Night, visit the CHEST Foundation website at foundation.chestnet.org.
Tobramycin tames infection in bronchiectasis
Nebulized tobramycin significantly reduced the density of Pseudomonas aeruginosa in sputum and improved quality of life for adults with bronchiectasis in a study with more than 300 individuals.
Chronic P. aeruginosa infection remains a challenge for bronchiectasis patients, and treatment options are limited, wrote Wei-jie Guan, MD, of the First Affiliated Hospital of Guangzhou Medical University, Guangdong, China, and colleagues. Tobramycin has demonstrated antipseudomonal effects, but previous studies have been small, results have been inconclusive, and there are safety concerns with the currently approved method of intravenous injection.
In a study published in the journal Chest, the researchers randomly assigned 167 patients to receive nebulized tobramycin inhalation solution (TIS) and 172 patients to receive placebo. Patients in the active-treatment group received 300 mg/5 mL of TIS twice daily in two cycles of 28 days on- and off-treatment alternating periods. The primary endpoints were changes in P. aeruginosa density from baseline and scores on the Quality of Life–Bronchiectasis questionnaire at day 29. Follow-up data were collected every 4 weeks for 16 weeks. Secondary endpoints included rate of negative P. aeruginosa culture at day 29; change in P. aeruginosa density from baseline; quality of life at day 85; and 24-hour sputum volume and purulence at day 29, 57, and 85.
The study population included adults aged 18-75 years with symptomatic bronchiectasis. The participants’ conditions had been clinically stable for 4 weeks. Sputum cultures tested positive for P. aeruginosa at two consecutive screening visits prior to randomization. The study was conducted at 33 sites within mainland China.
Overall, with an adjusted mean difference of 1.74 Log10 colony-forming units/g (P < .001). TIS patients also showed significantly greater improvement in Quality of Life–Bronchiectasis respiratory symptom scores, with an adjusted mean difference of 7.91 (P < .001) at day 29.
In addition, more TIS patients became culture negative for P. aeruginosa by day 29, compared with placebo patients (29.3% vs. 10.6%), and 24-hour sputum volume and sputum purulence scores were significantly lower for TIS patients at day 29, day 57, and day 85, compared with placebo patients.
Adverse events were similar and occurred in 81.5% of TIS patients and 81.6% of placebo patients. The most common were hemoptysis, chest discomfort, and acute upper respiratory tract infections. A total of 10 patients in the TIS group experienced transient wheezing that resolved within 30 minutes. A total of 11 TIS patients and 5 placebo patients experienced an adverse event that caused them to discontinue participation in the study. These events included blurred vision and dizziness, which occurred in two TIS patients and was deemed related to the study drug. One TIS patient died as a result of acute myocardial infarction, but this was deemed to be unrelated to the study drug.
The findings were limited by several factors, including the short duration of treatment and relatively young population, which might affect generalizability, the researchers noted. Other limitations include a lack of data on the effects of TIS on microorganisms other than P. aeruginosa, as well as limited outpatient visits, owing to COVID-19 restrictions.
However, the results confirm the ability of TIS nebulization to reduce P. aeruginosa and improve quality of life for adult patients with bronchiectasis, the authors concluded.
The study was funded by grants to multiple researchers from the National Science and Technology Major Project of the Ministry of Science and Technology of China and other government sources. The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nebulized tobramycin significantly reduced the density of Pseudomonas aeruginosa in sputum and improved quality of life for adults with bronchiectasis in a study with more than 300 individuals.
Chronic P. aeruginosa infection remains a challenge for bronchiectasis patients, and treatment options are limited, wrote Wei-jie Guan, MD, of the First Affiliated Hospital of Guangzhou Medical University, Guangdong, China, and colleagues. Tobramycin has demonstrated antipseudomonal effects, but previous studies have been small, results have been inconclusive, and there are safety concerns with the currently approved method of intravenous injection.
In a study published in the journal Chest, the researchers randomly assigned 167 patients to receive nebulized tobramycin inhalation solution (TIS) and 172 patients to receive placebo. Patients in the active-treatment group received 300 mg/5 mL of TIS twice daily in two cycles of 28 days on- and off-treatment alternating periods. The primary endpoints were changes in P. aeruginosa density from baseline and scores on the Quality of Life–Bronchiectasis questionnaire at day 29. Follow-up data were collected every 4 weeks for 16 weeks. Secondary endpoints included rate of negative P. aeruginosa culture at day 29; change in P. aeruginosa density from baseline; quality of life at day 85; and 24-hour sputum volume and purulence at day 29, 57, and 85.
The study population included adults aged 18-75 years with symptomatic bronchiectasis. The participants’ conditions had been clinically stable for 4 weeks. Sputum cultures tested positive for P. aeruginosa at two consecutive screening visits prior to randomization. The study was conducted at 33 sites within mainland China.
Overall, with an adjusted mean difference of 1.74 Log10 colony-forming units/g (P < .001). TIS patients also showed significantly greater improvement in Quality of Life–Bronchiectasis respiratory symptom scores, with an adjusted mean difference of 7.91 (P < .001) at day 29.
In addition, more TIS patients became culture negative for P. aeruginosa by day 29, compared with placebo patients (29.3% vs. 10.6%), and 24-hour sputum volume and sputum purulence scores were significantly lower for TIS patients at day 29, day 57, and day 85, compared with placebo patients.
Adverse events were similar and occurred in 81.5% of TIS patients and 81.6% of placebo patients. The most common were hemoptysis, chest discomfort, and acute upper respiratory tract infections. A total of 10 patients in the TIS group experienced transient wheezing that resolved within 30 minutes. A total of 11 TIS patients and 5 placebo patients experienced an adverse event that caused them to discontinue participation in the study. These events included blurred vision and dizziness, which occurred in two TIS patients and was deemed related to the study drug. One TIS patient died as a result of acute myocardial infarction, but this was deemed to be unrelated to the study drug.
The findings were limited by several factors, including the short duration of treatment and relatively young population, which might affect generalizability, the researchers noted. Other limitations include a lack of data on the effects of TIS on microorganisms other than P. aeruginosa, as well as limited outpatient visits, owing to COVID-19 restrictions.
However, the results confirm the ability of TIS nebulization to reduce P. aeruginosa and improve quality of life for adult patients with bronchiectasis, the authors concluded.
The study was funded by grants to multiple researchers from the National Science and Technology Major Project of the Ministry of Science and Technology of China and other government sources. The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Nebulized tobramycin significantly reduced the density of Pseudomonas aeruginosa in sputum and improved quality of life for adults with bronchiectasis in a study with more than 300 individuals.
Chronic P. aeruginosa infection remains a challenge for bronchiectasis patients, and treatment options are limited, wrote Wei-jie Guan, MD, of the First Affiliated Hospital of Guangzhou Medical University, Guangdong, China, and colleagues. Tobramycin has demonstrated antipseudomonal effects, but previous studies have been small, results have been inconclusive, and there are safety concerns with the currently approved method of intravenous injection.
In a study published in the journal Chest, the researchers randomly assigned 167 patients to receive nebulized tobramycin inhalation solution (TIS) and 172 patients to receive placebo. Patients in the active-treatment group received 300 mg/5 mL of TIS twice daily in two cycles of 28 days on- and off-treatment alternating periods. The primary endpoints were changes in P. aeruginosa density from baseline and scores on the Quality of Life–Bronchiectasis questionnaire at day 29. Follow-up data were collected every 4 weeks for 16 weeks. Secondary endpoints included rate of negative P. aeruginosa culture at day 29; change in P. aeruginosa density from baseline; quality of life at day 85; and 24-hour sputum volume and purulence at day 29, 57, and 85.
The study population included adults aged 18-75 years with symptomatic bronchiectasis. The participants’ conditions had been clinically stable for 4 weeks. Sputum cultures tested positive for P. aeruginosa at two consecutive screening visits prior to randomization. The study was conducted at 33 sites within mainland China.
Overall, with an adjusted mean difference of 1.74 Log10 colony-forming units/g (P < .001). TIS patients also showed significantly greater improvement in Quality of Life–Bronchiectasis respiratory symptom scores, with an adjusted mean difference of 7.91 (P < .001) at day 29.
In addition, more TIS patients became culture negative for P. aeruginosa by day 29, compared with placebo patients (29.3% vs. 10.6%), and 24-hour sputum volume and sputum purulence scores were significantly lower for TIS patients at day 29, day 57, and day 85, compared with placebo patients.
Adverse events were similar and occurred in 81.5% of TIS patients and 81.6% of placebo patients. The most common were hemoptysis, chest discomfort, and acute upper respiratory tract infections. A total of 10 patients in the TIS group experienced transient wheezing that resolved within 30 minutes. A total of 11 TIS patients and 5 placebo patients experienced an adverse event that caused them to discontinue participation in the study. These events included blurred vision and dizziness, which occurred in two TIS patients and was deemed related to the study drug. One TIS patient died as a result of acute myocardial infarction, but this was deemed to be unrelated to the study drug.
The findings were limited by several factors, including the short duration of treatment and relatively young population, which might affect generalizability, the researchers noted. Other limitations include a lack of data on the effects of TIS on microorganisms other than P. aeruginosa, as well as limited outpatient visits, owing to COVID-19 restrictions.
However, the results confirm the ability of TIS nebulization to reduce P. aeruginosa and improve quality of life for adult patients with bronchiectasis, the authors concluded.
The study was funded by grants to multiple researchers from the National Science and Technology Major Project of the Ministry of Science and Technology of China and other government sources. The researchers disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CHEST
CT scan changes indicate increased mortality risk in ever-smokers
Longitudinal progression of parenchymal changes on CT images — also referred to as quantitative interstitial abnormalities (QIA) – is independently associated with decreased lung function and an increased all-cause mortality risk, an analysis of two cohorts of ever-smokers indicates. And among the main risk factors for QIA progression is smoking.
“These abnormalities have gone by a few different names but fundamentally, they are high density findings of chest CT that in some cases represent early or subtle evidence of pulmonary fibrosis,” Samuel Ash, MD, MPH, assistant professor of medicine, Brigham and Women’s Hospital, Boston, told this news organization.
So when I see someone with visual evidence of this type of change on their chest CT, I make sure to emphasize that while they don’t have interstitial lung disease [ILD] yet, these findings suggest they may be susceptible to lung injury from tobacco smoke and that if they don’t stop smoking now, they are at risk for a disease like interstitial pulmonary fibrosis [IPF] which is a highly morbid disease with a high mortality risk,” he added.
The study was published online in the journal CHEST.
Ever-smoking cohorts
Analysis of QIA progression on CT chest scans was carried out on participants from the Genetic Epidemiology of COPD (COPDGene) study as well as those from the Pittsburgh Lung Screening Study (PLuSS). COPDGene was a prospective cohort of over 10,300 ever-smokers with at least a 10–pack-year smoking history between the ages of 45 and 80. Participants underwent a series of tests including chest CT scans at baseline between 2006 and 2011 and again approximately 5 years later.
Patients with a postbronchodilator forced expiratory volume in 1 second (FEV1) of 80% or more of predicted and a FEV1-to-FVC (forced vital capacity) ratio of at least 0.7 were defined to have GOLD stage 0 disease while those with a postbronchodilator FEV1 of 80% or less than predicted and a FEV1-to-FVC ratio of at least 0.7 were defined to have preserved ratio impaired spirometry (PRISm) disease.
PLuSS involved 3,642 ever-smokers between the ages of 50 years and 79 years with at least a 12.5–pack-year history with no prior history of lung cancer. Participants again underwent a series of tests including a CT scan on visit 1 between 2002 and 2005 and then a second CT scan at a second visit almost 9 years later. “In the COPDGene cohort, 4,635 participants had complete clinical data, CT scans and spirometry from visits 1 and 2 for analysis,” the authors reported.
At visit 1 almost 48% of participants were current smokers and the mean pack-year history of the cohort was 41.9 years. The mean time between visits 1 and 2 was 5.6 years. Both the mean prebronchodilator FEV1 as well as the mean FVC decreased between visits 1 and 2. For example, the mean prebronchodilator FEV1 dropped from 2.2 liters to 2.0 liters between visits 1 and 2 while the mean prebronchodilator FVC decreased from 3.2 liters to 3.0 liters between the first and second visits.
In the PLuSS cohort, 1,307 participants had complete imaging and spirometry data available for visits 1 and 2 for analysis. The mean time between visits 1 and 2 was 8.6 years. Over 59% of the cohort were current smokers with a mean pack-year history of 65. Again, the mean prebronchodilator FEV1 and FVC both dropped between visit 1 and 2, as the authors note.
The mean prebronchodilator FEV1, for example, decreased from 2.5 liters to 2.1 liters between visits 1 and 2 while the mean prebronchodilator FVC dropped from 3.6 liters to 3.2 liters during the same interval. Looking at risk factors associated with QIA progression, investigators note that each additional year of baseline age was associated with a higher annual increase in QIA by 0.01% per year (95% confidence interval, 0.01%-0.02%; P < .001) in the COPDGene cohort and a 0.02% increase (95% CI, 0.01%-0.02%; P < .001) in the PLuSS cohort.
Female sex in turn was associated with a 0.07% per year (95% CI, 0.02%-0.12%; P = .003) higher increase in the QIA, compared with men in the COPDGene cohort and a 0.14% (95% CI, 0.02%-0.26%; P = .025) per year higher increase in the QIA in the PLuSS cohort. Current smoking status was only associated with a higher rate of QIA progression in the COPDGene cohort at a rate of 0.10% per year (95% CI, 0.06%-0.15%; P < .001).
Lastly, every copy of the minor allele of the MUIC5B promoter polymorphism was associated with a 0.12% per year (95% CI, 0.07%-0.16%; P < .0001) increase in QIA in the COPDGene cohort as well.
Smoking cessation
Smoking cessation is the obvious first step for patients with evidence of QIA progression but physicians can probably do more for these patients sooner, Dr. Ash said. “If we use heart disease as an analogy, we don’t want to start treating someone until they have a heart attack or are in heart failure, we start by checking their cholesterol and blood pressure and treating them with medications to prevent progression.”
Similarly, physicians need to start thinking about IPF and other lung diseases in the same way. For IPF, medications such as pirfenidone (Esbriet) and nintedanib (Ofev) do not reverse prior lung damage but they do slow disease progression and physicians need to initiate treatment before patients are short of breath, not after. Meantime, Dr. Ash advised physicians that, if they have a patient who is getting a CT scan for whatever reason, they should keep a close eye on whether or not patients have any of these interstitial changes and, if they do, then if the changes are getting worse.
“These patients are likely to be the ones who are going to develop IPF and who may benefit from ongoing imaging surveillance,” he said. And while clinicians may not yet be ready to use a quantitative tool at the bedside, “this tool – or one like it – is coming and we have to start thinking about how to incorporate these types of devices into our clinical practice.”
Temporal changes
Asked to comment on the findings, Surya Bhatt, MD, associate professor of medicine at the University of Alabama at Birmingham, said that the study advances the community’s understanding of the relationship between temporal changes in objectively measured interstitial lung abnormalities and several important clinical outcomes, including lung function decline and mortality. “Several risk factors for progression were also identified,” he noted.
“And these results make a case for initiating clinical trials to determine whether early treatment with existing antifibrotic medications in these high risk individuals can decrease the perpetuation of these permanent lung changes,” Dr. Bhatt said.
The COPDGene study was supported in part by contributions made by an industry advisory board. Dr. Ash was supported in part by Quantitative Imaging Solutions. Dr. Bhatt declared that he has receiving consulting fees or has service on advisory boards for Boehringer Ingelheim and Sanofi/Regeneron. He ha also received fee for CME from IntegrityCE.
Longitudinal progression of parenchymal changes on CT images — also referred to as quantitative interstitial abnormalities (QIA) – is independently associated with decreased lung function and an increased all-cause mortality risk, an analysis of two cohorts of ever-smokers indicates. And among the main risk factors for QIA progression is smoking.
“These abnormalities have gone by a few different names but fundamentally, they are high density findings of chest CT that in some cases represent early or subtle evidence of pulmonary fibrosis,” Samuel Ash, MD, MPH, assistant professor of medicine, Brigham and Women’s Hospital, Boston, told this news organization.
So when I see someone with visual evidence of this type of change on their chest CT, I make sure to emphasize that while they don’t have interstitial lung disease [ILD] yet, these findings suggest they may be susceptible to lung injury from tobacco smoke and that if they don’t stop smoking now, they are at risk for a disease like interstitial pulmonary fibrosis [IPF] which is a highly morbid disease with a high mortality risk,” he added.
The study was published online in the journal CHEST.
Ever-smoking cohorts
Analysis of QIA progression on CT chest scans was carried out on participants from the Genetic Epidemiology of COPD (COPDGene) study as well as those from the Pittsburgh Lung Screening Study (PLuSS). COPDGene was a prospective cohort of over 10,300 ever-smokers with at least a 10–pack-year smoking history between the ages of 45 and 80. Participants underwent a series of tests including chest CT scans at baseline between 2006 and 2011 and again approximately 5 years later.
Patients with a postbronchodilator forced expiratory volume in 1 second (FEV1) of 80% or more of predicted and a FEV1-to-FVC (forced vital capacity) ratio of at least 0.7 were defined to have GOLD stage 0 disease while those with a postbronchodilator FEV1 of 80% or less than predicted and a FEV1-to-FVC ratio of at least 0.7 were defined to have preserved ratio impaired spirometry (PRISm) disease.
PLuSS involved 3,642 ever-smokers between the ages of 50 years and 79 years with at least a 12.5–pack-year history with no prior history of lung cancer. Participants again underwent a series of tests including a CT scan on visit 1 between 2002 and 2005 and then a second CT scan at a second visit almost 9 years later. “In the COPDGene cohort, 4,635 participants had complete clinical data, CT scans and spirometry from visits 1 and 2 for analysis,” the authors reported.
At visit 1 almost 48% of participants were current smokers and the mean pack-year history of the cohort was 41.9 years. The mean time between visits 1 and 2 was 5.6 years. Both the mean prebronchodilator FEV1 as well as the mean FVC decreased between visits 1 and 2. For example, the mean prebronchodilator FEV1 dropped from 2.2 liters to 2.0 liters between visits 1 and 2 while the mean prebronchodilator FVC decreased from 3.2 liters to 3.0 liters between the first and second visits.
In the PLuSS cohort, 1,307 participants had complete imaging and spirometry data available for visits 1 and 2 for analysis. The mean time between visits 1 and 2 was 8.6 years. Over 59% of the cohort were current smokers with a mean pack-year history of 65. Again, the mean prebronchodilator FEV1 and FVC both dropped between visit 1 and 2, as the authors note.
The mean prebronchodilator FEV1, for example, decreased from 2.5 liters to 2.1 liters between visits 1 and 2 while the mean prebronchodilator FVC dropped from 3.6 liters to 3.2 liters during the same interval. Looking at risk factors associated with QIA progression, investigators note that each additional year of baseline age was associated with a higher annual increase in QIA by 0.01% per year (95% confidence interval, 0.01%-0.02%; P < .001) in the COPDGene cohort and a 0.02% increase (95% CI, 0.01%-0.02%; P < .001) in the PLuSS cohort.
Female sex in turn was associated with a 0.07% per year (95% CI, 0.02%-0.12%; P = .003) higher increase in the QIA, compared with men in the COPDGene cohort and a 0.14% (95% CI, 0.02%-0.26%; P = .025) per year higher increase in the QIA in the PLuSS cohort. Current smoking status was only associated with a higher rate of QIA progression in the COPDGene cohort at a rate of 0.10% per year (95% CI, 0.06%-0.15%; P < .001).
Lastly, every copy of the minor allele of the MUIC5B promoter polymorphism was associated with a 0.12% per year (95% CI, 0.07%-0.16%; P < .0001) increase in QIA in the COPDGene cohort as well.
Smoking cessation
Smoking cessation is the obvious first step for patients with evidence of QIA progression but physicians can probably do more for these patients sooner, Dr. Ash said. “If we use heart disease as an analogy, we don’t want to start treating someone until they have a heart attack or are in heart failure, we start by checking their cholesterol and blood pressure and treating them with medications to prevent progression.”
Similarly, physicians need to start thinking about IPF and other lung diseases in the same way. For IPF, medications such as pirfenidone (Esbriet) and nintedanib (Ofev) do not reverse prior lung damage but they do slow disease progression and physicians need to initiate treatment before patients are short of breath, not after. Meantime, Dr. Ash advised physicians that, if they have a patient who is getting a CT scan for whatever reason, they should keep a close eye on whether or not patients have any of these interstitial changes and, if they do, then if the changes are getting worse.
“These patients are likely to be the ones who are going to develop IPF and who may benefit from ongoing imaging surveillance,” he said. And while clinicians may not yet be ready to use a quantitative tool at the bedside, “this tool – or one like it – is coming and we have to start thinking about how to incorporate these types of devices into our clinical practice.”
Temporal changes
Asked to comment on the findings, Surya Bhatt, MD, associate professor of medicine at the University of Alabama at Birmingham, said that the study advances the community’s understanding of the relationship between temporal changes in objectively measured interstitial lung abnormalities and several important clinical outcomes, including lung function decline and mortality. “Several risk factors for progression were also identified,” he noted.
“And these results make a case for initiating clinical trials to determine whether early treatment with existing antifibrotic medications in these high risk individuals can decrease the perpetuation of these permanent lung changes,” Dr. Bhatt said.
The COPDGene study was supported in part by contributions made by an industry advisory board. Dr. Ash was supported in part by Quantitative Imaging Solutions. Dr. Bhatt declared that he has receiving consulting fees or has service on advisory boards for Boehringer Ingelheim and Sanofi/Regeneron. He ha also received fee for CME from IntegrityCE.
Longitudinal progression of parenchymal changes on CT images — also referred to as quantitative interstitial abnormalities (QIA) – is independently associated with decreased lung function and an increased all-cause mortality risk, an analysis of two cohorts of ever-smokers indicates. And among the main risk factors for QIA progression is smoking.
“These abnormalities have gone by a few different names but fundamentally, they are high density findings of chest CT that in some cases represent early or subtle evidence of pulmonary fibrosis,” Samuel Ash, MD, MPH, assistant professor of medicine, Brigham and Women’s Hospital, Boston, told this news organization.
So when I see someone with visual evidence of this type of change on their chest CT, I make sure to emphasize that while they don’t have interstitial lung disease [ILD] yet, these findings suggest they may be susceptible to lung injury from tobacco smoke and that if they don’t stop smoking now, they are at risk for a disease like interstitial pulmonary fibrosis [IPF] which is a highly morbid disease with a high mortality risk,” he added.
The study was published online in the journal CHEST.
Ever-smoking cohorts
Analysis of QIA progression on CT chest scans was carried out on participants from the Genetic Epidemiology of COPD (COPDGene) study as well as those from the Pittsburgh Lung Screening Study (PLuSS). COPDGene was a prospective cohort of over 10,300 ever-smokers with at least a 10–pack-year smoking history between the ages of 45 and 80. Participants underwent a series of tests including chest CT scans at baseline between 2006 and 2011 and again approximately 5 years later.
Patients with a postbronchodilator forced expiratory volume in 1 second (FEV1) of 80% or more of predicted and a FEV1-to-FVC (forced vital capacity) ratio of at least 0.7 were defined to have GOLD stage 0 disease while those with a postbronchodilator FEV1 of 80% or less than predicted and a FEV1-to-FVC ratio of at least 0.7 were defined to have preserved ratio impaired spirometry (PRISm) disease.
PLuSS involved 3,642 ever-smokers between the ages of 50 years and 79 years with at least a 12.5–pack-year history with no prior history of lung cancer. Participants again underwent a series of tests including a CT scan on visit 1 between 2002 and 2005 and then a second CT scan at a second visit almost 9 years later. “In the COPDGene cohort, 4,635 participants had complete clinical data, CT scans and spirometry from visits 1 and 2 for analysis,” the authors reported.
At visit 1 almost 48% of participants were current smokers and the mean pack-year history of the cohort was 41.9 years. The mean time between visits 1 and 2 was 5.6 years. Both the mean prebronchodilator FEV1 as well as the mean FVC decreased between visits 1 and 2. For example, the mean prebronchodilator FEV1 dropped from 2.2 liters to 2.0 liters between visits 1 and 2 while the mean prebronchodilator FVC decreased from 3.2 liters to 3.0 liters between the first and second visits.
In the PLuSS cohort, 1,307 participants had complete imaging and spirometry data available for visits 1 and 2 for analysis. The mean time between visits 1 and 2 was 8.6 years. Over 59% of the cohort were current smokers with a mean pack-year history of 65. Again, the mean prebronchodilator FEV1 and FVC both dropped between visit 1 and 2, as the authors note.
The mean prebronchodilator FEV1, for example, decreased from 2.5 liters to 2.1 liters between visits 1 and 2 while the mean prebronchodilator FVC dropped from 3.6 liters to 3.2 liters during the same interval. Looking at risk factors associated with QIA progression, investigators note that each additional year of baseline age was associated with a higher annual increase in QIA by 0.01% per year (95% confidence interval, 0.01%-0.02%; P < .001) in the COPDGene cohort and a 0.02% increase (95% CI, 0.01%-0.02%; P < .001) in the PLuSS cohort.
Female sex in turn was associated with a 0.07% per year (95% CI, 0.02%-0.12%; P = .003) higher increase in the QIA, compared with men in the COPDGene cohort and a 0.14% (95% CI, 0.02%-0.26%; P = .025) per year higher increase in the QIA in the PLuSS cohort. Current smoking status was only associated with a higher rate of QIA progression in the COPDGene cohort at a rate of 0.10% per year (95% CI, 0.06%-0.15%; P < .001).
Lastly, every copy of the minor allele of the MUIC5B promoter polymorphism was associated with a 0.12% per year (95% CI, 0.07%-0.16%; P < .0001) increase in QIA in the COPDGene cohort as well.
Smoking cessation
Smoking cessation is the obvious first step for patients with evidence of QIA progression but physicians can probably do more for these patients sooner, Dr. Ash said. “If we use heart disease as an analogy, we don’t want to start treating someone until they have a heart attack or are in heart failure, we start by checking their cholesterol and blood pressure and treating them with medications to prevent progression.”
Similarly, physicians need to start thinking about IPF and other lung diseases in the same way. For IPF, medications such as pirfenidone (Esbriet) and nintedanib (Ofev) do not reverse prior lung damage but they do slow disease progression and physicians need to initiate treatment before patients are short of breath, not after. Meantime, Dr. Ash advised physicians that, if they have a patient who is getting a CT scan for whatever reason, they should keep a close eye on whether or not patients have any of these interstitial changes and, if they do, then if the changes are getting worse.
“These patients are likely to be the ones who are going to develop IPF and who may benefit from ongoing imaging surveillance,” he said. And while clinicians may not yet be ready to use a quantitative tool at the bedside, “this tool – or one like it – is coming and we have to start thinking about how to incorporate these types of devices into our clinical practice.”
Temporal changes
Asked to comment on the findings, Surya Bhatt, MD, associate professor of medicine at the University of Alabama at Birmingham, said that the study advances the community’s understanding of the relationship between temporal changes in objectively measured interstitial lung abnormalities and several important clinical outcomes, including lung function decline and mortality. “Several risk factors for progression were also identified,” he noted.
“And these results make a case for initiating clinical trials to determine whether early treatment with existing antifibrotic medications in these high risk individuals can decrease the perpetuation of these permanent lung changes,” Dr. Bhatt said.
The COPDGene study was supported in part by contributions made by an industry advisory board. Dr. Ash was supported in part by Quantitative Imaging Solutions. Dr. Bhatt declared that he has receiving consulting fees or has service on advisory boards for Boehringer Ingelheim and Sanofi/Regeneron. He ha also received fee for CME from IntegrityCE.
FROM CHEST
Climate change can worsen more than half of infectious diseases
An extensive new study shows that climate change can aggravate over half of known human pathogenic diseases. This comprehensive systematic review of the literature narrowed down 3,213 cases, linking 286 infectious diseases to specific climate change hazards. Of these, 58% were worsened, and only 9 conditions showed any benefit associated with environmental change.
The study was published online in Nature Climate Change. The complete list of cases, transmission pathways, and associated papers can be explored in detail – a remarkable, interactive data visualization.
To compile the data, investigators searched 10 keywords on the Global Infectious Disease and Epidemiology Network (GIDEON) and Center for Disease Control and Prevention databases. They then filled gaps by examining alternative names of the diseases, pathogens, and hazards.
Coauthor Tristan McKenzie, PhD, a postdoctoral researcher at the University of Gothenburg, Sweden, told this news organization: “If someone is interested in a certain pathway, it’s a beautiful starting point.” Or if someone wants to “do a modeling study and they want to focus on a specific area, the specific examples in the literature are already there” in the extensive database.
An early key finding is that warming and increased precipitation broadened the range of many pathogens through expansion of their habitat. This shift brings many pathogens closer to people. Examples are viruses (dengue, Chikungunya), bacteria (Lyme), protozoans (trypanosomes), and more. Warming has affected aquatic systems (for example, Vibrio) and higher altitudes and latitudes (malaria, dengue).
Pathogenic hazards are not just moving closer to people. People are also moving closer to the pathogenic hazards, with heat waves causing people to seek refuge with water activities, for example. This increases their exposure to pathogens, such as Vibrio, hepatitis, and water-borne gastroenteritis.
Some hazards, such as warming, can even make pathogens more virulent. Heat can upregulate Vibrio’s gene expression of proteins affecting transmission, adhesion, penetration, and host injury.
Heat and rainfall can increase stagnant water, enhancing mosquitoes’ breeding and growing grounds and enabling them to transmit many more infections.
People’s capacity to respond to climate hazards can also be impaired. For example, there is a reduced concentration of nutrients in crops under high CO2 levels, which can result in malnutrition. Lower crop yields can further fuel outbreaks of measles, cholera, or Cryptosporidium. Drought also likely forces people to drink contaminated water.
Among all this bad news, the authors found a small number of cases where climate hazards reduced the risk of infection. For example, droughts reduced the breeding grounds of mosquitoes, reducing the prevalence of malaria and chikungunya. But in other cases, the density of mosquitoes increased in some pools, causing an increased local risk of infection.
Naomi Hauser, MD, MPH, assistant clinical professor at UC Davis, Sacramento, told this news organization she was particularly impressed with the data visualization. “It really emphasizes the magnitude of what we’re dealing with. It makes you feel the weight of what they’re trying to represent,” she said.
On the other hand, Dr. Hauser said she would have liked “more emphasis on how the climate hazards interact with each other. It sort of made it sound like each of these climate hazards is in a vacuum – like when there’s floods, and that’s the problem. But there are a lot of other things ... like when we have warming and surface water temperature changes, it can also change the pH of the water and the salinity of the water, and those can also impact what we see with pathogens in the water.”
Dr. McKenzie explained one limitation: The study looked only at 10 keywords. So an example of a dust storm in Africa causing an increase in Vibrio in the United States could not be identified by this approach. “This also goes back to the scale of the problem, because we have something going on in the Sahara that’s impacting the East Coast of the United States,” he said. “And finding that link is not necessarily obvious – or at least not as obvious as [if] there [were] a hurricane and a bunch of people got sick from waterborne disease. So I think that really highlights the scale of this problem.”
Instead of looking at only one individual or group of pathogens, the study provided a much broader review of infections caused by an array of climate hazards. As Dr. McKenzie said, “no one’s actually done the work previously to really just try and get a comprehensive picture of what we might be dealing with. And so that was the goal for us.” The 58% estimate of diseases worsened by climate change is conservative, and, he says, “arguably, this is an even bigger problem than what we present.”
Dr. McKenzie concluded: “If we’re looking at the spread of some more serious or rare diseases in areas, to me then the answer is ... we need to be aggressively mitigating greenhouse gas emissions. Let’s start with the source.”
Dr. McKenzie and Dr. Hauser report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An extensive new study shows that climate change can aggravate over half of known human pathogenic diseases. This comprehensive systematic review of the literature narrowed down 3,213 cases, linking 286 infectious diseases to specific climate change hazards. Of these, 58% were worsened, and only 9 conditions showed any benefit associated with environmental change.
The study was published online in Nature Climate Change. The complete list of cases, transmission pathways, and associated papers can be explored in detail – a remarkable, interactive data visualization.
To compile the data, investigators searched 10 keywords on the Global Infectious Disease and Epidemiology Network (GIDEON) and Center for Disease Control and Prevention databases. They then filled gaps by examining alternative names of the diseases, pathogens, and hazards.
Coauthor Tristan McKenzie, PhD, a postdoctoral researcher at the University of Gothenburg, Sweden, told this news organization: “If someone is interested in a certain pathway, it’s a beautiful starting point.” Or if someone wants to “do a modeling study and they want to focus on a specific area, the specific examples in the literature are already there” in the extensive database.
An early key finding is that warming and increased precipitation broadened the range of many pathogens through expansion of their habitat. This shift brings many pathogens closer to people. Examples are viruses (dengue, Chikungunya), bacteria (Lyme), protozoans (trypanosomes), and more. Warming has affected aquatic systems (for example, Vibrio) and higher altitudes and latitudes (malaria, dengue).
Pathogenic hazards are not just moving closer to people. People are also moving closer to the pathogenic hazards, with heat waves causing people to seek refuge with water activities, for example. This increases their exposure to pathogens, such as Vibrio, hepatitis, and water-borne gastroenteritis.
Some hazards, such as warming, can even make pathogens more virulent. Heat can upregulate Vibrio’s gene expression of proteins affecting transmission, adhesion, penetration, and host injury.
Heat and rainfall can increase stagnant water, enhancing mosquitoes’ breeding and growing grounds and enabling them to transmit many more infections.
People’s capacity to respond to climate hazards can also be impaired. For example, there is a reduced concentration of nutrients in crops under high CO2 levels, which can result in malnutrition. Lower crop yields can further fuel outbreaks of measles, cholera, or Cryptosporidium. Drought also likely forces people to drink contaminated water.
Among all this bad news, the authors found a small number of cases where climate hazards reduced the risk of infection. For example, droughts reduced the breeding grounds of mosquitoes, reducing the prevalence of malaria and chikungunya. But in other cases, the density of mosquitoes increased in some pools, causing an increased local risk of infection.
Naomi Hauser, MD, MPH, assistant clinical professor at UC Davis, Sacramento, told this news organization she was particularly impressed with the data visualization. “It really emphasizes the magnitude of what we’re dealing with. It makes you feel the weight of what they’re trying to represent,” she said.
On the other hand, Dr. Hauser said she would have liked “more emphasis on how the climate hazards interact with each other. It sort of made it sound like each of these climate hazards is in a vacuum – like when there’s floods, and that’s the problem. But there are a lot of other things ... like when we have warming and surface water temperature changes, it can also change the pH of the water and the salinity of the water, and those can also impact what we see with pathogens in the water.”
Dr. McKenzie explained one limitation: The study looked only at 10 keywords. So an example of a dust storm in Africa causing an increase in Vibrio in the United States could not be identified by this approach. “This also goes back to the scale of the problem, because we have something going on in the Sahara that’s impacting the East Coast of the United States,” he said. “And finding that link is not necessarily obvious – or at least not as obvious as [if] there [were] a hurricane and a bunch of people got sick from waterborne disease. So I think that really highlights the scale of this problem.”
Instead of looking at only one individual or group of pathogens, the study provided a much broader review of infections caused by an array of climate hazards. As Dr. McKenzie said, “no one’s actually done the work previously to really just try and get a comprehensive picture of what we might be dealing with. And so that was the goal for us.” The 58% estimate of diseases worsened by climate change is conservative, and, he says, “arguably, this is an even bigger problem than what we present.”
Dr. McKenzie concluded: “If we’re looking at the spread of some more serious or rare diseases in areas, to me then the answer is ... we need to be aggressively mitigating greenhouse gas emissions. Let’s start with the source.”
Dr. McKenzie and Dr. Hauser report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An extensive new study shows that climate change can aggravate over half of known human pathogenic diseases. This comprehensive systematic review of the literature narrowed down 3,213 cases, linking 286 infectious diseases to specific climate change hazards. Of these, 58% were worsened, and only 9 conditions showed any benefit associated with environmental change.
The study was published online in Nature Climate Change. The complete list of cases, transmission pathways, and associated papers can be explored in detail – a remarkable, interactive data visualization.
To compile the data, investigators searched 10 keywords on the Global Infectious Disease and Epidemiology Network (GIDEON) and Center for Disease Control and Prevention databases. They then filled gaps by examining alternative names of the diseases, pathogens, and hazards.
Coauthor Tristan McKenzie, PhD, a postdoctoral researcher at the University of Gothenburg, Sweden, told this news organization: “If someone is interested in a certain pathway, it’s a beautiful starting point.” Or if someone wants to “do a modeling study and they want to focus on a specific area, the specific examples in the literature are already there” in the extensive database.
An early key finding is that warming and increased precipitation broadened the range of many pathogens through expansion of their habitat. This shift brings many pathogens closer to people. Examples are viruses (dengue, Chikungunya), bacteria (Lyme), protozoans (trypanosomes), and more. Warming has affected aquatic systems (for example, Vibrio) and higher altitudes and latitudes (malaria, dengue).
Pathogenic hazards are not just moving closer to people. People are also moving closer to the pathogenic hazards, with heat waves causing people to seek refuge with water activities, for example. This increases their exposure to pathogens, such as Vibrio, hepatitis, and water-borne gastroenteritis.
Some hazards, such as warming, can even make pathogens more virulent. Heat can upregulate Vibrio’s gene expression of proteins affecting transmission, adhesion, penetration, and host injury.
Heat and rainfall can increase stagnant water, enhancing mosquitoes’ breeding and growing grounds and enabling them to transmit many more infections.
People’s capacity to respond to climate hazards can also be impaired. For example, there is a reduced concentration of nutrients in crops under high CO2 levels, which can result in malnutrition. Lower crop yields can further fuel outbreaks of measles, cholera, or Cryptosporidium. Drought also likely forces people to drink contaminated water.
Among all this bad news, the authors found a small number of cases where climate hazards reduced the risk of infection. For example, droughts reduced the breeding grounds of mosquitoes, reducing the prevalence of malaria and chikungunya. But in other cases, the density of mosquitoes increased in some pools, causing an increased local risk of infection.
Naomi Hauser, MD, MPH, assistant clinical professor at UC Davis, Sacramento, told this news organization she was particularly impressed with the data visualization. “It really emphasizes the magnitude of what we’re dealing with. It makes you feel the weight of what they’re trying to represent,” she said.
On the other hand, Dr. Hauser said she would have liked “more emphasis on how the climate hazards interact with each other. It sort of made it sound like each of these climate hazards is in a vacuum – like when there’s floods, and that’s the problem. But there are a lot of other things ... like when we have warming and surface water temperature changes, it can also change the pH of the water and the salinity of the water, and those can also impact what we see with pathogens in the water.”
Dr. McKenzie explained one limitation: The study looked only at 10 keywords. So an example of a dust storm in Africa causing an increase in Vibrio in the United States could not be identified by this approach. “This also goes back to the scale of the problem, because we have something going on in the Sahara that’s impacting the East Coast of the United States,” he said. “And finding that link is not necessarily obvious – or at least not as obvious as [if] there [were] a hurricane and a bunch of people got sick from waterborne disease. So I think that really highlights the scale of this problem.”
Instead of looking at only one individual or group of pathogens, the study provided a much broader review of infections caused by an array of climate hazards. As Dr. McKenzie said, “no one’s actually done the work previously to really just try and get a comprehensive picture of what we might be dealing with. And so that was the goal for us.” The 58% estimate of diseases worsened by climate change is conservative, and, he says, “arguably, this is an even bigger problem than what we present.”
Dr. McKenzie concluded: “If we’re looking at the spread of some more serious or rare diseases in areas, to me then the answer is ... we need to be aggressively mitigating greenhouse gas emissions. Let’s start with the source.”
Dr. McKenzie and Dr. Hauser report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and COVID: Severe illness rising as vaccination effort stalls
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.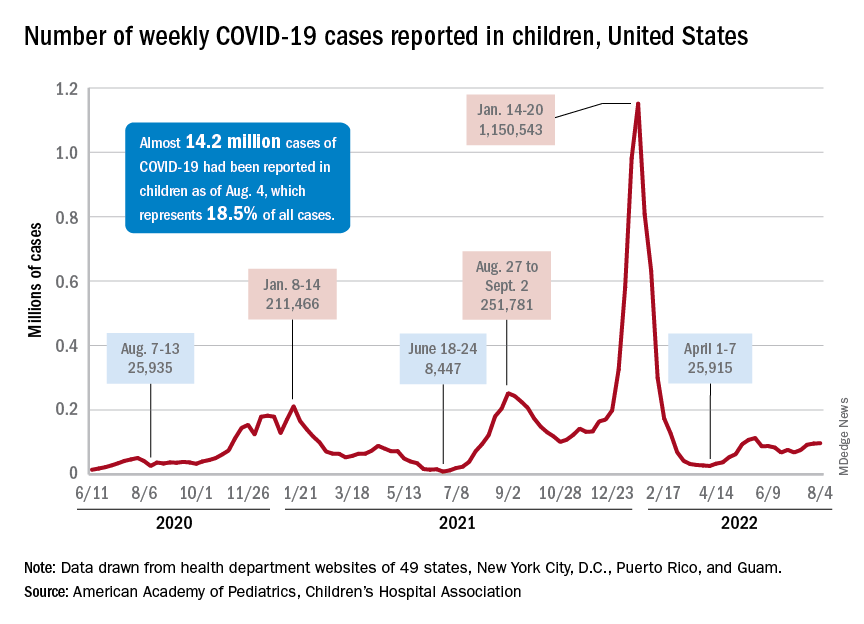
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.