User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Real-world study extends benralizumab asthma benefit
The real-world Zephyr 2 study, which assessed benralizumab for effectiveness in treating severe eosinophilic asthma, was extended with an analysis of a larger population stratified into three cohorts of participants who were aged 12 years or older.
Immunotherapy with monoclonal antibodies designed to block specific inflammatory pathways is a recommended add-on treatment option for adults to manage severe, uncontrolled eosinophilic-dependent (> 150 cells/µl) and corticosteroid-dependent asthma. One such biologic, benralizumab, targets the interleukin-5 receptor alpha chain (IL-5Rα).
For asthma patients who had previously been treated with benralizumab, there were significant reductions in exacerbation rates in the ZEPHYR 1 study. However, information regarding benefit associated with specific profiles was limited, warranting a larger study to address effectiveness when considering various blood eosinophil counts, prior treatments with other biologics, or benralizumab use for up to 24 months, Donna Carstens, MD, of AstraZeneca, Wilmington, Del., and colleagues write.
Study details
In the retrospective cohort Zephyr 2 study, which was published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers retrieved deidentified patient information from medical, laboratory, and pharmacy U.S. insurance claims records from the PatientSource and DiagnosticSource databases and compared asthma exacerbation rates before and after treatment with benralizumab.
Age, asthma diagnosis, number of exacerbations, and number of benralizumab treatment records within specified periods were used to identify a total of 1,795 participants for inclusion in the study. The index date for establishing before-treatment and after-treatment index time intervals of 12 months each was defined as the day after the initial benralizumab treatment occurring between November 2017 and June 2019.
The cohort was stratified into three nonmutually exclusive groups consisting of 349 patients who had switched primarily from either omalizumab or mepolizumab biologics to benralizumab; 429 patients subdivided by closest to the index date blood eosinophil counts of less than 150, greater than or equal to 150, 150-299, less than 300, and greater than or equal to 300, and 419 patients with post data collection extended beyond 12 months to 18 or 24 months.
Similarities in baseline patient characteristics that were were observed across the three cohorts included a mean age range of 51-53 years, preponderance of women (67%-69%), obesity diagnosis (31.5%-32.9%), and a mean Charlson Comorbidity Index of 1.47-1.52. Allergic rhinitis was the most frequently reported (60%-67%) comorbidity, followed by hypertension and gastroesophageal reflex.
Effectiveness
Benralizumab was found to be a significantly effective treatment for managing severe eosinophilic asthma for all three evaluated cohorts, as evidenced by reductions in asthma exacerbations post-index, compared with pre-index. Specifically, the exacerbation rate for all five subgroups of the blood eosinophil cohort significantly decreased from the pre-index 3.10-3.55 person per year (PPY) rate to a 1.11-1.72 PPY post-index rate, equivalent to a 52%-64% decrease in exacerbations (P < .001 for all pre-index vs. post-index comparisons).
Comparable reductions also occurred with the cohort in which the biologic treatment was changed to benralizumab. A greater effect was observed when the switch was made from omalizumab to benralizumab with a pre-post PPY rate reduction of 3.25-1.25 (62%) than when the switch was made from mepolizumab (pre-post PPY rate reduction was 3.81-1.78 [53%], but both resulted in significant post-treatment improvements (P < .001).
Results from the extended follow-up analysis cohort showed consistency for significant exacerbation rate decline going from a pre-index rate of 3.38 PPY down to 1.34 PPY (60% rate reduction vs. pre-index) in the first 12 post-index months, continuing to decline to 1.18 PPY (65% reduction) over the following six months (both significant at P < .001).
Likewise, the results from the extended follow-up 24-month subgroup presented significant down trending exacerbation rates from pre-index 3.38 PPY to 1.38 (comparative 59% reduction) for the first 12 months continuing down to 1.08 PPY (68% reduction) over the 12-24 month post-index period (both P < .001). In the first and second 12 post-index months for the 24-month subgroup, 39% and 49% of the patients, respectively, experienced no exacerbations.
Following treatment with benralizumab, in addition to the observed decline in asthma exacerbation rates, the need for concomitant asthma medications was also significantly reduced for all three cohorts.
This retrospective ZEPHYR 2 study contributes evidence supporting the significant effectiveness of benralizumab in improving disease management for “specific subsets of severe asthma patients that are frequently seen in real-world practice and may be excluded from clinical trials,” according to the authors. The treatment resulted in reduced rates of asthma exacerbations with defined standards for hospitalizations, visits to emergency department or urgent care, or outpatient visits with separate exacerbations occurring at greater than or equal to 14 days, as reported in database records. Reduction in the rate of asthma exacerbations when benralizumab is switched for another biologic increases the disease management options for achieving optimal patient care, the authors add.
The authors have financial relationships with AstraZeneca, the source of funding for the study.
A version of this article first appeared on Medscape.com.
The real-world Zephyr 2 study, which assessed benralizumab for effectiveness in treating severe eosinophilic asthma, was extended with an analysis of a larger population stratified into three cohorts of participants who were aged 12 years or older.
Immunotherapy with monoclonal antibodies designed to block specific inflammatory pathways is a recommended add-on treatment option for adults to manage severe, uncontrolled eosinophilic-dependent (> 150 cells/µl) and corticosteroid-dependent asthma. One such biologic, benralizumab, targets the interleukin-5 receptor alpha chain (IL-5Rα).
For asthma patients who had previously been treated with benralizumab, there were significant reductions in exacerbation rates in the ZEPHYR 1 study. However, information regarding benefit associated with specific profiles was limited, warranting a larger study to address effectiveness when considering various blood eosinophil counts, prior treatments with other biologics, or benralizumab use for up to 24 months, Donna Carstens, MD, of AstraZeneca, Wilmington, Del., and colleagues write.
Study details
In the retrospective cohort Zephyr 2 study, which was published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers retrieved deidentified patient information from medical, laboratory, and pharmacy U.S. insurance claims records from the PatientSource and DiagnosticSource databases and compared asthma exacerbation rates before and after treatment with benralizumab.
Age, asthma diagnosis, number of exacerbations, and number of benralizumab treatment records within specified periods were used to identify a total of 1,795 participants for inclusion in the study. The index date for establishing before-treatment and after-treatment index time intervals of 12 months each was defined as the day after the initial benralizumab treatment occurring between November 2017 and June 2019.
The cohort was stratified into three nonmutually exclusive groups consisting of 349 patients who had switched primarily from either omalizumab or mepolizumab biologics to benralizumab; 429 patients subdivided by closest to the index date blood eosinophil counts of less than 150, greater than or equal to 150, 150-299, less than 300, and greater than or equal to 300, and 419 patients with post data collection extended beyond 12 months to 18 or 24 months.
Similarities in baseline patient characteristics that were were observed across the three cohorts included a mean age range of 51-53 years, preponderance of women (67%-69%), obesity diagnosis (31.5%-32.9%), and a mean Charlson Comorbidity Index of 1.47-1.52. Allergic rhinitis was the most frequently reported (60%-67%) comorbidity, followed by hypertension and gastroesophageal reflex.
Effectiveness
Benralizumab was found to be a significantly effective treatment for managing severe eosinophilic asthma for all three evaluated cohorts, as evidenced by reductions in asthma exacerbations post-index, compared with pre-index. Specifically, the exacerbation rate for all five subgroups of the blood eosinophil cohort significantly decreased from the pre-index 3.10-3.55 person per year (PPY) rate to a 1.11-1.72 PPY post-index rate, equivalent to a 52%-64% decrease in exacerbations (P < .001 for all pre-index vs. post-index comparisons).
Comparable reductions also occurred with the cohort in which the biologic treatment was changed to benralizumab. A greater effect was observed when the switch was made from omalizumab to benralizumab with a pre-post PPY rate reduction of 3.25-1.25 (62%) than when the switch was made from mepolizumab (pre-post PPY rate reduction was 3.81-1.78 [53%], but both resulted in significant post-treatment improvements (P < .001).
Results from the extended follow-up analysis cohort showed consistency for significant exacerbation rate decline going from a pre-index rate of 3.38 PPY down to 1.34 PPY (60% rate reduction vs. pre-index) in the first 12 post-index months, continuing to decline to 1.18 PPY (65% reduction) over the following six months (both significant at P < .001).
Likewise, the results from the extended follow-up 24-month subgroup presented significant down trending exacerbation rates from pre-index 3.38 PPY to 1.38 (comparative 59% reduction) for the first 12 months continuing down to 1.08 PPY (68% reduction) over the 12-24 month post-index period (both P < .001). In the first and second 12 post-index months for the 24-month subgroup, 39% and 49% of the patients, respectively, experienced no exacerbations.
Following treatment with benralizumab, in addition to the observed decline in asthma exacerbation rates, the need for concomitant asthma medications was also significantly reduced for all three cohorts.
This retrospective ZEPHYR 2 study contributes evidence supporting the significant effectiveness of benralizumab in improving disease management for “specific subsets of severe asthma patients that are frequently seen in real-world practice and may be excluded from clinical trials,” according to the authors. The treatment resulted in reduced rates of asthma exacerbations with defined standards for hospitalizations, visits to emergency department or urgent care, or outpatient visits with separate exacerbations occurring at greater than or equal to 14 days, as reported in database records. Reduction in the rate of asthma exacerbations when benralizumab is switched for another biologic increases the disease management options for achieving optimal patient care, the authors add.
The authors have financial relationships with AstraZeneca, the source of funding for the study.
A version of this article first appeared on Medscape.com.
The real-world Zephyr 2 study, which assessed benralizumab for effectiveness in treating severe eosinophilic asthma, was extended with an analysis of a larger population stratified into three cohorts of participants who were aged 12 years or older.
Immunotherapy with monoclonal antibodies designed to block specific inflammatory pathways is a recommended add-on treatment option for adults to manage severe, uncontrolled eosinophilic-dependent (> 150 cells/µl) and corticosteroid-dependent asthma. One such biologic, benralizumab, targets the interleukin-5 receptor alpha chain (IL-5Rα).
For asthma patients who had previously been treated with benralizumab, there were significant reductions in exacerbation rates in the ZEPHYR 1 study. However, information regarding benefit associated with specific profiles was limited, warranting a larger study to address effectiveness when considering various blood eosinophil counts, prior treatments with other biologics, or benralizumab use for up to 24 months, Donna Carstens, MD, of AstraZeneca, Wilmington, Del., and colleagues write.
Study details
In the retrospective cohort Zephyr 2 study, which was published in the Journal of Allergy and Clinical Immunology: In Practice, the researchers retrieved deidentified patient information from medical, laboratory, and pharmacy U.S. insurance claims records from the PatientSource and DiagnosticSource databases and compared asthma exacerbation rates before and after treatment with benralizumab.
Age, asthma diagnosis, number of exacerbations, and number of benralizumab treatment records within specified periods were used to identify a total of 1,795 participants for inclusion in the study. The index date for establishing before-treatment and after-treatment index time intervals of 12 months each was defined as the day after the initial benralizumab treatment occurring between November 2017 and June 2019.
The cohort was stratified into three nonmutually exclusive groups consisting of 349 patients who had switched primarily from either omalizumab or mepolizumab biologics to benralizumab; 429 patients subdivided by closest to the index date blood eosinophil counts of less than 150, greater than or equal to 150, 150-299, less than 300, and greater than or equal to 300, and 419 patients with post data collection extended beyond 12 months to 18 or 24 months.
Similarities in baseline patient characteristics that were were observed across the three cohorts included a mean age range of 51-53 years, preponderance of women (67%-69%), obesity diagnosis (31.5%-32.9%), and a mean Charlson Comorbidity Index of 1.47-1.52. Allergic rhinitis was the most frequently reported (60%-67%) comorbidity, followed by hypertension and gastroesophageal reflex.
Effectiveness
Benralizumab was found to be a significantly effective treatment for managing severe eosinophilic asthma for all three evaluated cohorts, as evidenced by reductions in asthma exacerbations post-index, compared with pre-index. Specifically, the exacerbation rate for all five subgroups of the blood eosinophil cohort significantly decreased from the pre-index 3.10-3.55 person per year (PPY) rate to a 1.11-1.72 PPY post-index rate, equivalent to a 52%-64% decrease in exacerbations (P < .001 for all pre-index vs. post-index comparisons).
Comparable reductions also occurred with the cohort in which the biologic treatment was changed to benralizumab. A greater effect was observed when the switch was made from omalizumab to benralizumab with a pre-post PPY rate reduction of 3.25-1.25 (62%) than when the switch was made from mepolizumab (pre-post PPY rate reduction was 3.81-1.78 [53%], but both resulted in significant post-treatment improvements (P < .001).
Results from the extended follow-up analysis cohort showed consistency for significant exacerbation rate decline going from a pre-index rate of 3.38 PPY down to 1.34 PPY (60% rate reduction vs. pre-index) in the first 12 post-index months, continuing to decline to 1.18 PPY (65% reduction) over the following six months (both significant at P < .001).
Likewise, the results from the extended follow-up 24-month subgroup presented significant down trending exacerbation rates from pre-index 3.38 PPY to 1.38 (comparative 59% reduction) for the first 12 months continuing down to 1.08 PPY (68% reduction) over the 12-24 month post-index period (both P < .001). In the first and second 12 post-index months for the 24-month subgroup, 39% and 49% of the patients, respectively, experienced no exacerbations.
Following treatment with benralizumab, in addition to the observed decline in asthma exacerbation rates, the need for concomitant asthma medications was also significantly reduced for all three cohorts.
This retrospective ZEPHYR 2 study contributes evidence supporting the significant effectiveness of benralizumab in improving disease management for “specific subsets of severe asthma patients that are frequently seen in real-world practice and may be excluded from clinical trials,” according to the authors. The treatment resulted in reduced rates of asthma exacerbations with defined standards for hospitalizations, visits to emergency department or urgent care, or outpatient visits with separate exacerbations occurring at greater than or equal to 14 days, as reported in database records. Reduction in the rate of asthma exacerbations when benralizumab is switched for another biologic increases the disease management options for achieving optimal patient care, the authors add.
The authors have financial relationships with AstraZeneca, the source of funding for the study.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
The enemy of carcinogenic fumes is my friendly begonia
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.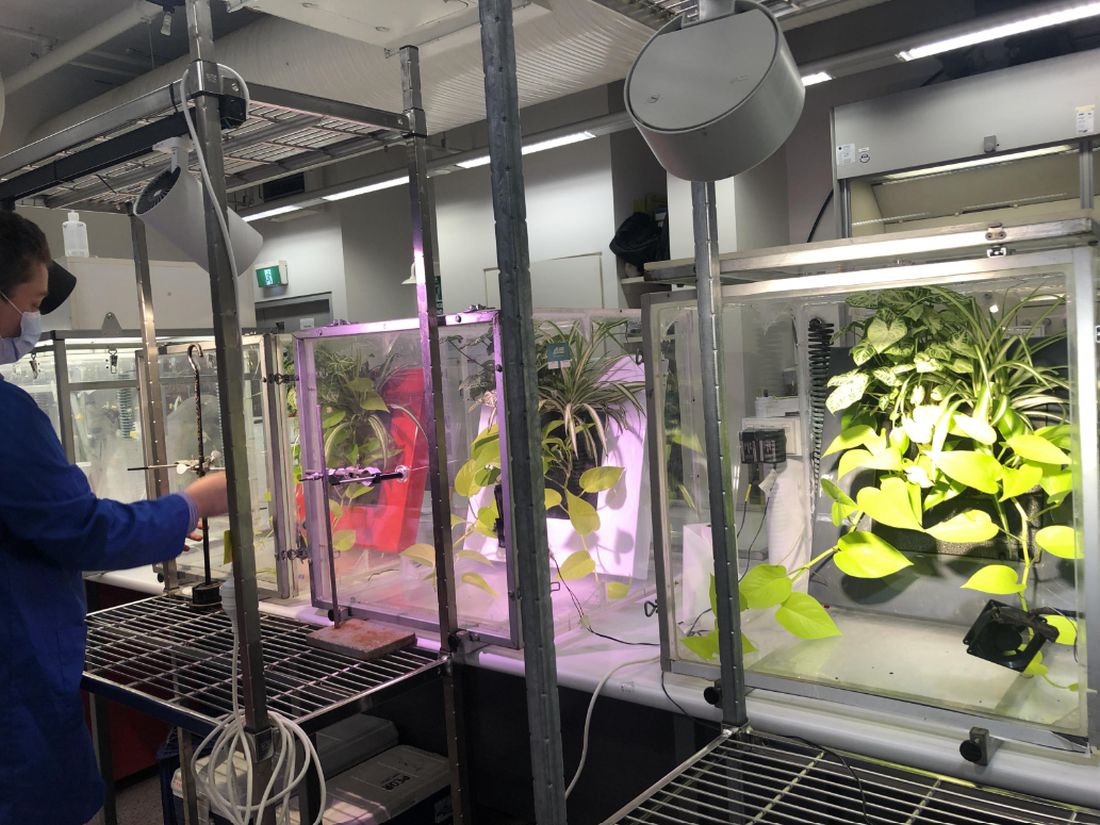
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.

In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.
In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Sowing the seeds of cancer prevention
Are you looking to add to your quality of life, even though pets are not your speed? Might we suggest something with lower maintenance? Something a little greener?
Indoor plants can purify the air that comes from outside. Researchers at the University of Technology Sydney, in partnership with the plantscaping company Ambius, showed that a “green wall” made up of mixed indoor plants was able to suck up 97% of “the most toxic compounds” from the air in just 8 hours. We’re talking about lung-irritating, headache-inducing, cancer risk–boosting compounds from gasoline fumes, including benzene.
Public health initiatives often strive to reduce cardiovascular and obesity risks, but breathing seems pretty important too. According to the World Health Organization, household air pollution is responsible for about 2.5 million global premature deaths each year. And since 2020 we’ve become accustomed to spending more time inside and at home.
“This new research proves that plants should not just be seen as ‘nice to have,’ but rather a crucial part of every workplace wellness plan,” Ambius General Manager Johan Hodgson said in statement released by the university.
So don’t spend hundreds of dollars on a fancy air filtration system when a wall of plants can do that for next to nothing. Find what works for you and your space and become a plant parent today! Your lungs will thank you.
But officer, I had to swerve to miss the duodenal ampulla
Tiny video capsule endoscopes have been around for many years, but they have one big weakness: The ingestible cameras’ journey through the GI tract is passively driven by gravity and the natural movement of the body, so they often miss potential problem areas.
Not anymore. That flaw has been addressed by medical technology company AnX Robotica, which has taken endoscopy to the next level by adding that wondrous directional control device of the modern electronic age, a joystick.
The new system “uses an external magnet and hand-held video game style joysticks to move the capsule in three dimensions,” which allows physicians to “remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas,” according to Andrew C. Meltzer, MD, of George Washington University and associates, who conducted a pilot study funded by AnX Robotica.
The video capsule provided a 95% rate of visualization in the stomachs of 40 patients who were examined at a medical office building by an emergency medicine physician who had no previous specialty training in endoscopy. “Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off site,” the investigators said in a written statement.
The capsule operator did receive some additional training, and development of artificial intelligence to self-drive the capsule is in the works, but for now, we’re talking about a device controlled by a human using a joystick. And we all know that 50-year-olds are not especially known for their joystick skills. For that we need real experts. Yup, we need to put those joystick-controlled capsule endoscopes in the hands of teenage gamers. Who wants to go first?
Maybe AI isn’t ready for the big time after all
“How long before some intrepid stockholder says: ‘Hey, instead of paying doctors, why don’t we just use the free robot instead?’ ” Those words appeared on LOTME but a month ago. After all, the AI is supposed to be smarter and more empathetic than a doctor. And did we mention it’s free? Or at least extremely cheap. Cheaper than, say, a group of recently unionized health care workers.
In early May, the paid employees manning the National Eating Disorders Association emergency hotline voted to unionize, as they felt overwhelmed and underpaid. Apparently, paying six people an extra few thousand a year was too much for NEDA’s leadership, as they decided a few weeks later to fire those workers, fully closing down the hotline. Instead of talking to a real person, people “calling in” for support would be met with Tessa, a wellness chatbot that would hopefully guide them through their crisis. Key word, hopefully.
In perhaps the least surprising twist of the year, NEDA was forced to walk back its decision about a week after its initial announcement. It all started with a viral Instagram post from a woman who called in and received the following advice from Tessa: Lose 1-2 pounds a week, count calories and work for a 500- to 1,000-calorie deficit, weigh herself weekly, and restrict her diet. Unfortunately, all of these suggestions were things that led to the development of the woman’s eating disorder.
Naturally, NEDA responded in good grace, accusing the woman of lying. A NEDA vice president even left some nasty comments on the post, but hastily deleted them a day later when NEDA announced it was shutting down Tessa “until further notice for a complete investigation.” NEDA’s CEO insisted they hadn’t seen that behavior from Tessa before, calling it a “bug” and insisting the bot would only be down temporarily until the triggers causing the bug were fixed.
In the aftermath, several doctors and psychologists chimed in, terming the rush to automate human roles dangerous and risky. After all, much of what makes these hotlines effective is the volunteers speaking from their own experience. An unsupervised bot doesn’t seem to have what it takes to deal with a mental health crisis, but we’re betting that Tessa will be back. As a wise cephalopod once said: Nobody gives a care about the fate of labor as long as they can get their instant gratification.
You can’t spell existential without s-t-e-n-t
This week, we’re including a special “bonus” item that, to be honest, has nothing to do with stents. That’s why our editor is making us call this a “bonus” (and making us use quote marks, too): It doesn’t really have anything to do with stents or health care or those who practice health care. Actually, his exact words were, “You can’t just give the readers someone else’s ****ing list and expect to get paid for it.” Did we mention that he looks like Jack Nicklaus but acts like BoJack Horseman?
Anywaaay, we’re pretty sure that the list in question – “America’s Top 10 Most Googled Existential Questions” – says something about the human condition, just not about stents:
1. Why is the sky blue?
2. What do dreams mean?
3. What is the meaning of life?
4. Why am I so tired?
5. Who am I?
6. What is love?
7. Is a hot dog a sandwich?
8. What came first, the chicken or the egg?
9. What should I do?
10. Do animals have souls?
Safe to stop immunotherapy at 2 years in stable lung cancer
A new review of clinical trial data suggests that it is safe to stop immunotherapy after 2 years if the patient is progression free. There was no difference in overall survival between such patients and those who carried on with immunotherapy for another 2 years, so for 4 years in total.
“For patients who are progression free on immunotherapy for NSCLC, it is reasonable to stop therapy at 2 years, rather than continuing indefinitely,” said the investigators, led by medical oncologist Lova Sun, MD, a lung and head and neck cancer specialist at the University of Pennsylvania, Philadelphia.
“The lack of statistically significant overall survival advantage for” indefinite treatment “on adjusted analysis provides reassurance to patients and clinicians who wish to discontinue immunotherapy at 2 years,” they added.
The study was published online in JAMA Oncology to coincide with a presentation at the annual meeting of the American Society of Clinical Oncology.
Dr. Sun and colleagues commented that there have been a number of trials that have shown durable benefits persisting long after immunotherapy was stopped at 2 years, but clinicians seem to have been spooked into preferring indefinite treatment by a trial that showed worse survival with nivolumab when it was stopped at 1 year in responders versus ongoing treatment.
In an accompanying editorial, Jack West, MD, a medical oncologist and lung cancer specialist at City of Hope, Duarte, Calif., noted that given the “clear limitations in retrospective clinical data, we may want to wait for prospective randomized clinical trial data, but this will be a difficult study to complete, and results will take many years to become available.
“In the meantime, the perfect should not be the enemy of the good. These data may provide reassurance to us and patients that discontinuing treatment at 2 years can confer the same overall survival as extended treatment with lower risk of toxic effects, less time in treatment for patients, and considerably lower costs for our health care system,” he said.
Study details
For their review, Dr. Sun and colleagues included patients with advanced NSCLC called from 280 cancer clinics from across the United States.
The investigators compared overall survival in 113 advanced NSCLC patients treated with up-front immune checkpoint inhibitors (ICIs) for 700-760 days (that is, stopping within 2 years) with survival in 593 patients treated beyond 760 days (the indefinite therapy group).
Patients were diagnosed from 2016 to 2020 at a median age of 69 years and were about evenly split between the sexes. The team noted that although all the patients were progression free at 2 years, only about one in five discontinued ICIs, highlighting “a strong bias toward potential overtreatment [vs.] possible undertreatment,” as Dr. West put it in the editorial.
Approximately half of the patients in both groups were treated initially with immunotherapy alone and the rest in combination with chemotherapy.
The 2-year overall survival from the 760-day mark was 79% in the fixed-duration group versus 81% with indefinite treatment, with no difference on either univariate (hazard ratio, 1.26; P = .36) or multivariable (HR, 1.33; P = .29) analysis adjusting for smoking history, PD-L1 status, histology, and other covariates.
Eleven patients in the fixed-duration cohort (10%) subsequently had progression and were rechallenged with an ICI; all but one with the same ICI used frontline.
Median progression-free survival after rechallenge was 8.1 months, demonstrating that patients can still benefit from ICIs even after discontinuation, the investigators said.
The groups were well balanced except that patients in the fixed-duration group were more likely to be treated at an academic center and have a history of smoking, with a trend toward being more likely to have squamous cell carcinoma. “Even after adjusting for these covariates, there was no overall survival benefit for indefinite-duration therapy,” the team said.
There was no funding for the work. The investigators have numerous pharmaceutical industry ties, including Dr. Sun, who is a consultant for Regeneron, Genmab, Seagen, and Bayer, and disclosed funding from BluePrint Research, Seagen Research, and IO Biotech Research. Dr. West reported receiving personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article first appeared on Medscape.com.
A new review of clinical trial data suggests that it is safe to stop immunotherapy after 2 years if the patient is progression free. There was no difference in overall survival between such patients and those who carried on with immunotherapy for another 2 years, so for 4 years in total.
“For patients who are progression free on immunotherapy for NSCLC, it is reasonable to stop therapy at 2 years, rather than continuing indefinitely,” said the investigators, led by medical oncologist Lova Sun, MD, a lung and head and neck cancer specialist at the University of Pennsylvania, Philadelphia.
“The lack of statistically significant overall survival advantage for” indefinite treatment “on adjusted analysis provides reassurance to patients and clinicians who wish to discontinue immunotherapy at 2 years,” they added.
The study was published online in JAMA Oncology to coincide with a presentation at the annual meeting of the American Society of Clinical Oncology.
Dr. Sun and colleagues commented that there have been a number of trials that have shown durable benefits persisting long after immunotherapy was stopped at 2 years, but clinicians seem to have been spooked into preferring indefinite treatment by a trial that showed worse survival with nivolumab when it was stopped at 1 year in responders versus ongoing treatment.
In an accompanying editorial, Jack West, MD, a medical oncologist and lung cancer specialist at City of Hope, Duarte, Calif., noted that given the “clear limitations in retrospective clinical data, we may want to wait for prospective randomized clinical trial data, but this will be a difficult study to complete, and results will take many years to become available.
“In the meantime, the perfect should not be the enemy of the good. These data may provide reassurance to us and patients that discontinuing treatment at 2 years can confer the same overall survival as extended treatment with lower risk of toxic effects, less time in treatment for patients, and considerably lower costs for our health care system,” he said.
Study details
For their review, Dr. Sun and colleagues included patients with advanced NSCLC called from 280 cancer clinics from across the United States.
The investigators compared overall survival in 113 advanced NSCLC patients treated with up-front immune checkpoint inhibitors (ICIs) for 700-760 days (that is, stopping within 2 years) with survival in 593 patients treated beyond 760 days (the indefinite therapy group).
Patients were diagnosed from 2016 to 2020 at a median age of 69 years and were about evenly split between the sexes. The team noted that although all the patients were progression free at 2 years, only about one in five discontinued ICIs, highlighting “a strong bias toward potential overtreatment [vs.] possible undertreatment,” as Dr. West put it in the editorial.
Approximately half of the patients in both groups were treated initially with immunotherapy alone and the rest in combination with chemotherapy.
The 2-year overall survival from the 760-day mark was 79% in the fixed-duration group versus 81% with indefinite treatment, with no difference on either univariate (hazard ratio, 1.26; P = .36) or multivariable (HR, 1.33; P = .29) analysis adjusting for smoking history, PD-L1 status, histology, and other covariates.
Eleven patients in the fixed-duration cohort (10%) subsequently had progression and were rechallenged with an ICI; all but one with the same ICI used frontline.
Median progression-free survival after rechallenge was 8.1 months, demonstrating that patients can still benefit from ICIs even after discontinuation, the investigators said.
The groups were well balanced except that patients in the fixed-duration group were more likely to be treated at an academic center and have a history of smoking, with a trend toward being more likely to have squamous cell carcinoma. “Even after adjusting for these covariates, there was no overall survival benefit for indefinite-duration therapy,” the team said.
There was no funding for the work. The investigators have numerous pharmaceutical industry ties, including Dr. Sun, who is a consultant for Regeneron, Genmab, Seagen, and Bayer, and disclosed funding from BluePrint Research, Seagen Research, and IO Biotech Research. Dr. West reported receiving personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article first appeared on Medscape.com.
A new review of clinical trial data suggests that it is safe to stop immunotherapy after 2 years if the patient is progression free. There was no difference in overall survival between such patients and those who carried on with immunotherapy for another 2 years, so for 4 years in total.
“For patients who are progression free on immunotherapy for NSCLC, it is reasonable to stop therapy at 2 years, rather than continuing indefinitely,” said the investigators, led by medical oncologist Lova Sun, MD, a lung and head and neck cancer specialist at the University of Pennsylvania, Philadelphia.
“The lack of statistically significant overall survival advantage for” indefinite treatment “on adjusted analysis provides reassurance to patients and clinicians who wish to discontinue immunotherapy at 2 years,” they added.
The study was published online in JAMA Oncology to coincide with a presentation at the annual meeting of the American Society of Clinical Oncology.
Dr. Sun and colleagues commented that there have been a number of trials that have shown durable benefits persisting long after immunotherapy was stopped at 2 years, but clinicians seem to have been spooked into preferring indefinite treatment by a trial that showed worse survival with nivolumab when it was stopped at 1 year in responders versus ongoing treatment.
In an accompanying editorial, Jack West, MD, a medical oncologist and lung cancer specialist at City of Hope, Duarte, Calif., noted that given the “clear limitations in retrospective clinical data, we may want to wait for prospective randomized clinical trial data, but this will be a difficult study to complete, and results will take many years to become available.
“In the meantime, the perfect should not be the enemy of the good. These data may provide reassurance to us and patients that discontinuing treatment at 2 years can confer the same overall survival as extended treatment with lower risk of toxic effects, less time in treatment for patients, and considerably lower costs for our health care system,” he said.
Study details
For their review, Dr. Sun and colleagues included patients with advanced NSCLC called from 280 cancer clinics from across the United States.
The investigators compared overall survival in 113 advanced NSCLC patients treated with up-front immune checkpoint inhibitors (ICIs) for 700-760 days (that is, stopping within 2 years) with survival in 593 patients treated beyond 760 days (the indefinite therapy group).
Patients were diagnosed from 2016 to 2020 at a median age of 69 years and were about evenly split between the sexes. The team noted that although all the patients were progression free at 2 years, only about one in five discontinued ICIs, highlighting “a strong bias toward potential overtreatment [vs.] possible undertreatment,” as Dr. West put it in the editorial.
Approximately half of the patients in both groups were treated initially with immunotherapy alone and the rest in combination with chemotherapy.
The 2-year overall survival from the 760-day mark was 79% in the fixed-duration group versus 81% with indefinite treatment, with no difference on either univariate (hazard ratio, 1.26; P = .36) or multivariable (HR, 1.33; P = .29) analysis adjusting for smoking history, PD-L1 status, histology, and other covariates.
Eleven patients in the fixed-duration cohort (10%) subsequently had progression and were rechallenged with an ICI; all but one with the same ICI used frontline.
Median progression-free survival after rechallenge was 8.1 months, demonstrating that patients can still benefit from ICIs even after discontinuation, the investigators said.
The groups were well balanced except that patients in the fixed-duration group were more likely to be treated at an academic center and have a history of smoking, with a trend toward being more likely to have squamous cell carcinoma. “Even after adjusting for these covariates, there was no overall survival benefit for indefinite-duration therapy,” the team said.
There was no funding for the work. The investigators have numerous pharmaceutical industry ties, including Dr. Sun, who is a consultant for Regeneron, Genmab, Seagen, and Bayer, and disclosed funding from BluePrint Research, Seagen Research, and IO Biotech Research. Dr. West reported receiving personal fees from AstraZeneca, Genentech/Roche, Merck, and Regeneron.
A version of this article first appeared on Medscape.com.
FROM JAMA ONCOLOGY
We may need a new defense against new COVID variants
At the end of 2022, the European Medicines Agency’s Emergency Task Force warned European regulatory bodies, governments, and doctors that Antiviral drugs remain available but have many limitations. And, of course, there are still vaccines, which can significantly reduce (but not remove) the risk of severe cases and decrease the number of deaths, although they have lost the efficacy that they once had in countering the original virus.
Research therefore continues. Immunologists continue to search for new targets to synthesize broadly neutralizing monoclonal antibodies for treating or preventing the infection. These results could also lead to new vaccines that induce longer-lasting immunity not only against the thousands of subvariants and recombinant versions of SARS-CoV-2 being identified around the world, but also possibly against other coronaviruses that could emerge in the coming years. A study conducted at Stanford (Calif.) University and published in the journal Science Translational Medicine has afforded a glimmer of hope by discovering the broadly neutralizing efficacy of some antibodies produced by macaque monkeys in response to vaccination with AS03 (squalene) adjuvanted monovalent subunit vaccines.
The speed with which the virus continues to evolve has rendered the plan for annual vaccine updates, which initially was envisioned early in the pandemic, unfeasible for the time being. In 2020, scientists were considering updating vaccines annually based on the prevalent variants of the disease, similar to the approach to the flu. Perhaps that day will come, but in the meantime, laboratories are pursuing other routes: finding spike epitopes that are preserved more than others each time the virus evolves or focusing on other virus proteins that still manage to induce a neutralizing antibody response.
Eventually, artificial intelligence might be able to custom design monoclonal antibodies that are even more effective than natural ones. Or researchers could completely change tack and shift their attention to the host, rather than the virus itself.
This is the approach taken by one study published in Nature Microbiology, which starts from a simple assumption: SARS-CoV-2 continues to modify its spike protein because of the evolutionary pressure of the antibodies produced by millions of infected people, but all these variants and subvariants, both present and future, enter cells by binding – not solely, but mostly – to the ACE2 receptor. Instead of neutralizing the virus, why not try to block its access to the cells occupying its route in? In this way, we could also be ready for future emerging sarbecoviruses that will have a spike sequence that cannot yet be predicted.
Researchers at Rockefeller University, New York, have generated six human monoclonal antibodies that bind to the ACE2 receptor, rather than to the spike, preventing infection by all sarbecoviruses tested, even at low concentrations, including the virus that originated in Wuhan, China; the aggressive Delta variant; and various forms of Omicron.
The monoclonal antibodies bind to the ACE2 receptor at a part of the protein that is distal to the active enzyme portion that converts angiotensin and does not modify its expression on the cell surface. Therefore, no adverse effects are expected at this level. In animal models, these monoclonal antibodies succeed in stopping the infection. Moving into the clinical phase will be needed to find out if it will be possible to create products adapted to preventing and treating all SARS-CoV-2 variants, and perhaps also the next coronavirus large enough to spill over into a new epidemic that threatens the human race.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
At the end of 2022, the European Medicines Agency’s Emergency Task Force warned European regulatory bodies, governments, and doctors that Antiviral drugs remain available but have many limitations. And, of course, there are still vaccines, which can significantly reduce (but not remove) the risk of severe cases and decrease the number of deaths, although they have lost the efficacy that they once had in countering the original virus.
Research therefore continues. Immunologists continue to search for new targets to synthesize broadly neutralizing monoclonal antibodies for treating or preventing the infection. These results could also lead to new vaccines that induce longer-lasting immunity not only against the thousands of subvariants and recombinant versions of SARS-CoV-2 being identified around the world, but also possibly against other coronaviruses that could emerge in the coming years. A study conducted at Stanford (Calif.) University and published in the journal Science Translational Medicine has afforded a glimmer of hope by discovering the broadly neutralizing efficacy of some antibodies produced by macaque monkeys in response to vaccination with AS03 (squalene) adjuvanted monovalent subunit vaccines.
The speed with which the virus continues to evolve has rendered the plan for annual vaccine updates, which initially was envisioned early in the pandemic, unfeasible for the time being. In 2020, scientists were considering updating vaccines annually based on the prevalent variants of the disease, similar to the approach to the flu. Perhaps that day will come, but in the meantime, laboratories are pursuing other routes: finding spike epitopes that are preserved more than others each time the virus evolves or focusing on other virus proteins that still manage to induce a neutralizing antibody response.
Eventually, artificial intelligence might be able to custom design monoclonal antibodies that are even more effective than natural ones. Or researchers could completely change tack and shift their attention to the host, rather than the virus itself.
This is the approach taken by one study published in Nature Microbiology, which starts from a simple assumption: SARS-CoV-2 continues to modify its spike protein because of the evolutionary pressure of the antibodies produced by millions of infected people, but all these variants and subvariants, both present and future, enter cells by binding – not solely, but mostly – to the ACE2 receptor. Instead of neutralizing the virus, why not try to block its access to the cells occupying its route in? In this way, we could also be ready for future emerging sarbecoviruses that will have a spike sequence that cannot yet be predicted.
Researchers at Rockefeller University, New York, have generated six human monoclonal antibodies that bind to the ACE2 receptor, rather than to the spike, preventing infection by all sarbecoviruses tested, even at low concentrations, including the virus that originated in Wuhan, China; the aggressive Delta variant; and various forms of Omicron.
The monoclonal antibodies bind to the ACE2 receptor at a part of the protein that is distal to the active enzyme portion that converts angiotensin and does not modify its expression on the cell surface. Therefore, no adverse effects are expected at this level. In animal models, these monoclonal antibodies succeed in stopping the infection. Moving into the clinical phase will be needed to find out if it will be possible to create products adapted to preventing and treating all SARS-CoV-2 variants, and perhaps also the next coronavirus large enough to spill over into a new epidemic that threatens the human race.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
At the end of 2022, the European Medicines Agency’s Emergency Task Force warned European regulatory bodies, governments, and doctors that Antiviral drugs remain available but have many limitations. And, of course, there are still vaccines, which can significantly reduce (but not remove) the risk of severe cases and decrease the number of deaths, although they have lost the efficacy that they once had in countering the original virus.
Research therefore continues. Immunologists continue to search for new targets to synthesize broadly neutralizing monoclonal antibodies for treating or preventing the infection. These results could also lead to new vaccines that induce longer-lasting immunity not only against the thousands of subvariants and recombinant versions of SARS-CoV-2 being identified around the world, but also possibly against other coronaviruses that could emerge in the coming years. A study conducted at Stanford (Calif.) University and published in the journal Science Translational Medicine has afforded a glimmer of hope by discovering the broadly neutralizing efficacy of some antibodies produced by macaque monkeys in response to vaccination with AS03 (squalene) adjuvanted monovalent subunit vaccines.
The speed with which the virus continues to evolve has rendered the plan for annual vaccine updates, which initially was envisioned early in the pandemic, unfeasible for the time being. In 2020, scientists were considering updating vaccines annually based on the prevalent variants of the disease, similar to the approach to the flu. Perhaps that day will come, but in the meantime, laboratories are pursuing other routes: finding spike epitopes that are preserved more than others each time the virus evolves or focusing on other virus proteins that still manage to induce a neutralizing antibody response.
Eventually, artificial intelligence might be able to custom design monoclonal antibodies that are even more effective than natural ones. Or researchers could completely change tack and shift their attention to the host, rather than the virus itself.
This is the approach taken by one study published in Nature Microbiology, which starts from a simple assumption: SARS-CoV-2 continues to modify its spike protein because of the evolutionary pressure of the antibodies produced by millions of infected people, but all these variants and subvariants, both present and future, enter cells by binding – not solely, but mostly – to the ACE2 receptor. Instead of neutralizing the virus, why not try to block its access to the cells occupying its route in? In this way, we could also be ready for future emerging sarbecoviruses that will have a spike sequence that cannot yet be predicted.
Researchers at Rockefeller University, New York, have generated six human monoclonal antibodies that bind to the ACE2 receptor, rather than to the spike, preventing infection by all sarbecoviruses tested, even at low concentrations, including the virus that originated in Wuhan, China; the aggressive Delta variant; and various forms of Omicron.
The monoclonal antibodies bind to the ACE2 receptor at a part of the protein that is distal to the active enzyme portion that converts angiotensin and does not modify its expression on the cell surface. Therefore, no adverse effects are expected at this level. In animal models, these monoclonal antibodies succeed in stopping the infection. Moving into the clinical phase will be needed to find out if it will be possible to create products adapted to preventing and treating all SARS-CoV-2 variants, and perhaps also the next coronavirus large enough to spill over into a new epidemic that threatens the human race.
This article was translated from Univadis Italy. A version appeared on Medscape.com.
COVID nonvaccination linked with avoidable hospitalizations
A retrospective, population-based cohort study in Alberta, Edmonton, found that between late September 2021 and late January 2022, eligible unvaccinated patients with COVID-19 had a nearly 10-fold higher risk for hospitalization than did patients who were fully vaccinated with two doses. Unvaccinated patients had a nearly 21-fold higher risk than did patients who were boosted with three doses.
“We have shown that eligible nonvaccinated persons, especially in the age strata 50-79 years, accounted for 3,000-4,000 potentially avoidable hospitalizations, 35,000-40,000 avoidable bed-days, and $100–$110 million [Canadian dollars] in avoidable health care costs during a 120-day period coinciding with the fourth (Delta) and fifth (Omicron) COVID-19 waves, respectively,” wrote Sean M. Bagshaw, MD, chair of critical care medicine at the University of Alberta, Edmonton, and colleagues.
The findings were published in the Canadian Journal of Public Health.
‘Unsatisfactory’ vaccine uptake
While a previous study by Dr. Bagshaw and colleagues recently showed that higher vaccine uptake could have avoided significant intensive care unit admissions and costs, the researchers sought to expand their analysis to include non-ICU use.
The current study examined data from the government of Alberta and the Discharge Abstract Database to assess vaccination status and hospitalization with confirmed SARS-CoV-2. Secondary outcomes included avoidable hospitalizations, avoidable hospital bed-days, and the potential cost avoidance related to COVID-19.
During the study period, “societal factors contributed to an unsatisfactory voluntary vaccine uptake, particularly in the province of Alberta,” wrote the authors, adding that “only 63.7% and 2.7% of the eligible population in Alberta [had] received two (full) and three (boosted) COVID-19 vaccine doses as of September 27, 2021.”
The analysis found the highest number of hospitalizations among unvaccinated patients (n = 3,835), compared with vaccinated (n = 1,907) and boosted patients (n = 481). This finding yielded a risk ratio (RR) of hospitalization of 9.7 for unvaccinated patients, compared with fully vaccinated patients, and an RR of 20.6, compared with patients who were boosted. Unvaccinated patients aged 60-69 years had the highest RR for hospitalization, compared with vaccinated (RR, 16.4) and boosted patients (RR, 151.9).
The estimated number of avoidable hospitalizations for unvaccinated patients was 3,439 (total of 36,331 bed-days), compared with vaccinated patients, and 3,764 (total of 40,185 bed-days), compared with boosted patients.
The avoidable hospitalization-related costs for unvaccinated patients totaled $101.4 million (Canadian dollars) if they had been vaccinated and $110.24 million if they had been boosted.
“Moreover, strained hospital systems and the widespread adoption of crisis standards of care in response to surges in COVID-19 hospitalizations have contributed to unnecessary excess deaths,” wrote the authors. “These are preventable and missed public health opportunities that provoked massive health system disruptions and resource diversions, including deferral of routine health services (e.g., cancer and chronic disease screening and monitoring and scheduled vaccinations), postponement of scheduled procedures and surgeries, and redeployment of health care professionals.”
Dr. Bagshaw said in an interview that he was not surprised by the findings. “However, I wonder whether the public and those who direct policy and make decisions about the health system would be interested in better understanding the scope and sheer disruption the health system suffered due to COVID-19,” he said.
The current study suggests that “at least some of this could have been avoided,” said Dr. Bagshaw. “I hope we – that is the public, users of the health system, decision-makers and health care professionals – can learn from our experiences.” Studies such as the current analysis “will reinforce the importance of timely and clearly articulated public health promotion, education, and policy,” he added.
Economic benefit underestimated
Commenting on the study, David Fisman, MD, MPH, an epidemiologist and professor at the University of Toronto, said: “The approach these investigators have taken is clear and straightforward. It is easy to reproduce. It is also entirely consistent with what other scientific groups have been demonstrating for a couple of years now.” Dr. Fisman was not involved with the study.
A group led by Dr. Fisman as senior author has just completed a study examining the effectiveness of the Canadian pandemic response, compared with responses in four peer countries. In the as-yet unpublished paper, the researchers concluded that “relative to the United States, United Kingdom, and France, the Canadian pandemic response was estimated to have averted 94,492, 64,306, and 13,641 deaths, respectively, with more than 480,000 hospitalizations averted and 1 million QALY [quality-adjusted life-years] saved, relative to the United States. A United States pandemic response applied to Canada would have resulted in more than $40 billion in economic losses due to healthcare expenditures and lost QALY; losses relative to the United Kingdom and France would have been $21 billion and $5 billion, respectively. By contrast, an Australian pandemic response would have averted over 28,000 additional deaths and averted nearly $9 billion in costs in Canada.”
Dr. Fisman added that while the current researchers focused their study on the direct protective effects of vaccines, “we know that, even with initial waves of Omicron, vaccinated individuals continued to be protected against infection as well as disease, and even if they were infected, we know from household contact studies that they were less infectious to others. That means that even though the implicit estimate of cost savings that could have been achieved through better coverage are pretty high in this paper, the economic benefit of vaccination is underestimated in this analysis, because we can’t quantify the infections that never happened because of vaccination.”
The study was supported by the Strategic Clinical Networks, Alberta Health Services. Dr. Bagshaw declared no relevant financial relationships. Dr. Fisman has taken part in advisory boards for Seqirus, Pfizer, AstraZeneca, Sanofi, and Merck vaccines during the past 3 years.
A version of this article first appeared on Medscape.com.
A retrospective, population-based cohort study in Alberta, Edmonton, found that between late September 2021 and late January 2022, eligible unvaccinated patients with COVID-19 had a nearly 10-fold higher risk for hospitalization than did patients who were fully vaccinated with two doses. Unvaccinated patients had a nearly 21-fold higher risk than did patients who were boosted with three doses.
“We have shown that eligible nonvaccinated persons, especially in the age strata 50-79 years, accounted for 3,000-4,000 potentially avoidable hospitalizations, 35,000-40,000 avoidable bed-days, and $100–$110 million [Canadian dollars] in avoidable health care costs during a 120-day period coinciding with the fourth (Delta) and fifth (Omicron) COVID-19 waves, respectively,” wrote Sean M. Bagshaw, MD, chair of critical care medicine at the University of Alberta, Edmonton, and colleagues.
The findings were published in the Canadian Journal of Public Health.
‘Unsatisfactory’ vaccine uptake
While a previous study by Dr. Bagshaw and colleagues recently showed that higher vaccine uptake could have avoided significant intensive care unit admissions and costs, the researchers sought to expand their analysis to include non-ICU use.
The current study examined data from the government of Alberta and the Discharge Abstract Database to assess vaccination status and hospitalization with confirmed SARS-CoV-2. Secondary outcomes included avoidable hospitalizations, avoidable hospital bed-days, and the potential cost avoidance related to COVID-19.
During the study period, “societal factors contributed to an unsatisfactory voluntary vaccine uptake, particularly in the province of Alberta,” wrote the authors, adding that “only 63.7% and 2.7% of the eligible population in Alberta [had] received two (full) and three (boosted) COVID-19 vaccine doses as of September 27, 2021.”
The analysis found the highest number of hospitalizations among unvaccinated patients (n = 3,835), compared with vaccinated (n = 1,907) and boosted patients (n = 481). This finding yielded a risk ratio (RR) of hospitalization of 9.7 for unvaccinated patients, compared with fully vaccinated patients, and an RR of 20.6, compared with patients who were boosted. Unvaccinated patients aged 60-69 years had the highest RR for hospitalization, compared with vaccinated (RR, 16.4) and boosted patients (RR, 151.9).
The estimated number of avoidable hospitalizations for unvaccinated patients was 3,439 (total of 36,331 bed-days), compared with vaccinated patients, and 3,764 (total of 40,185 bed-days), compared with boosted patients.
The avoidable hospitalization-related costs for unvaccinated patients totaled $101.4 million (Canadian dollars) if they had been vaccinated and $110.24 million if they had been boosted.
“Moreover, strained hospital systems and the widespread adoption of crisis standards of care in response to surges in COVID-19 hospitalizations have contributed to unnecessary excess deaths,” wrote the authors. “These are preventable and missed public health opportunities that provoked massive health system disruptions and resource diversions, including deferral of routine health services (e.g., cancer and chronic disease screening and monitoring and scheduled vaccinations), postponement of scheduled procedures and surgeries, and redeployment of health care professionals.”
Dr. Bagshaw said in an interview that he was not surprised by the findings. “However, I wonder whether the public and those who direct policy and make decisions about the health system would be interested in better understanding the scope and sheer disruption the health system suffered due to COVID-19,” he said.
The current study suggests that “at least some of this could have been avoided,” said Dr. Bagshaw. “I hope we – that is the public, users of the health system, decision-makers and health care professionals – can learn from our experiences.” Studies such as the current analysis “will reinforce the importance of timely and clearly articulated public health promotion, education, and policy,” he added.
Economic benefit underestimated
Commenting on the study, David Fisman, MD, MPH, an epidemiologist and professor at the University of Toronto, said: “The approach these investigators have taken is clear and straightforward. It is easy to reproduce. It is also entirely consistent with what other scientific groups have been demonstrating for a couple of years now.” Dr. Fisman was not involved with the study.
A group led by Dr. Fisman as senior author has just completed a study examining the effectiveness of the Canadian pandemic response, compared with responses in four peer countries. In the as-yet unpublished paper, the researchers concluded that “relative to the United States, United Kingdom, and France, the Canadian pandemic response was estimated to have averted 94,492, 64,306, and 13,641 deaths, respectively, with more than 480,000 hospitalizations averted and 1 million QALY [quality-adjusted life-years] saved, relative to the United States. A United States pandemic response applied to Canada would have resulted in more than $40 billion in economic losses due to healthcare expenditures and lost QALY; losses relative to the United Kingdom and France would have been $21 billion and $5 billion, respectively. By contrast, an Australian pandemic response would have averted over 28,000 additional deaths and averted nearly $9 billion in costs in Canada.”
Dr. Fisman added that while the current researchers focused their study on the direct protective effects of vaccines, “we know that, even with initial waves of Omicron, vaccinated individuals continued to be protected against infection as well as disease, and even if they were infected, we know from household contact studies that they were less infectious to others. That means that even though the implicit estimate of cost savings that could have been achieved through better coverage are pretty high in this paper, the economic benefit of vaccination is underestimated in this analysis, because we can’t quantify the infections that never happened because of vaccination.”
The study was supported by the Strategic Clinical Networks, Alberta Health Services. Dr. Bagshaw declared no relevant financial relationships. Dr. Fisman has taken part in advisory boards for Seqirus, Pfizer, AstraZeneca, Sanofi, and Merck vaccines during the past 3 years.
A version of this article first appeared on Medscape.com.
A retrospective, population-based cohort study in Alberta, Edmonton, found that between late September 2021 and late January 2022, eligible unvaccinated patients with COVID-19 had a nearly 10-fold higher risk for hospitalization than did patients who were fully vaccinated with two doses. Unvaccinated patients had a nearly 21-fold higher risk than did patients who were boosted with three doses.
“We have shown that eligible nonvaccinated persons, especially in the age strata 50-79 years, accounted for 3,000-4,000 potentially avoidable hospitalizations, 35,000-40,000 avoidable bed-days, and $100–$110 million [Canadian dollars] in avoidable health care costs during a 120-day period coinciding with the fourth (Delta) and fifth (Omicron) COVID-19 waves, respectively,” wrote Sean M. Bagshaw, MD, chair of critical care medicine at the University of Alberta, Edmonton, and colleagues.
The findings were published in the Canadian Journal of Public Health.
‘Unsatisfactory’ vaccine uptake
While a previous study by Dr. Bagshaw and colleagues recently showed that higher vaccine uptake could have avoided significant intensive care unit admissions and costs, the researchers sought to expand their analysis to include non-ICU use.
The current study examined data from the government of Alberta and the Discharge Abstract Database to assess vaccination status and hospitalization with confirmed SARS-CoV-2. Secondary outcomes included avoidable hospitalizations, avoidable hospital bed-days, and the potential cost avoidance related to COVID-19.
During the study period, “societal factors contributed to an unsatisfactory voluntary vaccine uptake, particularly in the province of Alberta,” wrote the authors, adding that “only 63.7% and 2.7% of the eligible population in Alberta [had] received two (full) and three (boosted) COVID-19 vaccine doses as of September 27, 2021.”
The analysis found the highest number of hospitalizations among unvaccinated patients (n = 3,835), compared with vaccinated (n = 1,907) and boosted patients (n = 481). This finding yielded a risk ratio (RR) of hospitalization of 9.7 for unvaccinated patients, compared with fully vaccinated patients, and an RR of 20.6, compared with patients who were boosted. Unvaccinated patients aged 60-69 years had the highest RR for hospitalization, compared with vaccinated (RR, 16.4) and boosted patients (RR, 151.9).
The estimated number of avoidable hospitalizations for unvaccinated patients was 3,439 (total of 36,331 bed-days), compared with vaccinated patients, and 3,764 (total of 40,185 bed-days), compared with boosted patients.
The avoidable hospitalization-related costs for unvaccinated patients totaled $101.4 million (Canadian dollars) if they had been vaccinated and $110.24 million if they had been boosted.
“Moreover, strained hospital systems and the widespread adoption of crisis standards of care in response to surges in COVID-19 hospitalizations have contributed to unnecessary excess deaths,” wrote the authors. “These are preventable and missed public health opportunities that provoked massive health system disruptions and resource diversions, including deferral of routine health services (e.g., cancer and chronic disease screening and monitoring and scheduled vaccinations), postponement of scheduled procedures and surgeries, and redeployment of health care professionals.”
Dr. Bagshaw said in an interview that he was not surprised by the findings. “However, I wonder whether the public and those who direct policy and make decisions about the health system would be interested in better understanding the scope and sheer disruption the health system suffered due to COVID-19,” he said.
The current study suggests that “at least some of this could have been avoided,” said Dr. Bagshaw. “I hope we – that is the public, users of the health system, decision-makers and health care professionals – can learn from our experiences.” Studies such as the current analysis “will reinforce the importance of timely and clearly articulated public health promotion, education, and policy,” he added.
Economic benefit underestimated
Commenting on the study, David Fisman, MD, MPH, an epidemiologist and professor at the University of Toronto, said: “The approach these investigators have taken is clear and straightforward. It is easy to reproduce. It is also entirely consistent with what other scientific groups have been demonstrating for a couple of years now.” Dr. Fisman was not involved with the study.
A group led by Dr. Fisman as senior author has just completed a study examining the effectiveness of the Canadian pandemic response, compared with responses in four peer countries. In the as-yet unpublished paper, the researchers concluded that “relative to the United States, United Kingdom, and France, the Canadian pandemic response was estimated to have averted 94,492, 64,306, and 13,641 deaths, respectively, with more than 480,000 hospitalizations averted and 1 million QALY [quality-adjusted life-years] saved, relative to the United States. A United States pandemic response applied to Canada would have resulted in more than $40 billion in economic losses due to healthcare expenditures and lost QALY; losses relative to the United Kingdom and France would have been $21 billion and $5 billion, respectively. By contrast, an Australian pandemic response would have averted over 28,000 additional deaths and averted nearly $9 billion in costs in Canada.”
Dr. Fisman added that while the current researchers focused their study on the direct protective effects of vaccines, “we know that, even with initial waves of Omicron, vaccinated individuals continued to be protected against infection as well as disease, and even if they were infected, we know from household contact studies that they were less infectious to others. That means that even though the implicit estimate of cost savings that could have been achieved through better coverage are pretty high in this paper, the economic benefit of vaccination is underestimated in this analysis, because we can’t quantify the infections that never happened because of vaccination.”
The study was supported by the Strategic Clinical Networks, Alberta Health Services. Dr. Bagshaw declared no relevant financial relationships. Dr. Fisman has taken part in advisory boards for Seqirus, Pfizer, AstraZeneca, Sanofi, and Merck vaccines during the past 3 years.
A version of this article first appeared on Medscape.com.
FROM CANADIAN JOURNAL OF PUBLIC HEALTH
SCLC: Bispecific antibody shows phase 1 promise
CHICAGO –
The antibody promotes the destruction of tumor cells by T cells by acting as a bridge between T cells and tumors.
SCLC has largely resisted efforts to identify unique surface markers. DLL3 is an exception: It is rarely expressed in normal cells, and it seems to be important to tumor biology, according to Martin Wermke, MD, who presented the study at the annual meeting of the American Society of Clinical Oncology.
A rare SCLC biomarker
“The problem, I think, is that small cell [lung cancer] with its high mutational burden is a bunch of many different subentities and you will probably not find a single driver mutation as you do in non–small cell lung cancer. So in that [way] it’s different in its biology,” said Dr. Wermke, professor of experimental tumor therapy at the National Center for Tumor Diseases in Dresden, Germany.
Nevertheless, DLL3 is a sensitive biomarker, with over 90% of SCLC tumors positive for the surface marker, according to Dr. Wermke. “It’s one of the first which proved to be a reliable [SCLC] biomarker for therapeutic approaches,” said Dr. Wermke.
This isn’t the first clinical experience with DLL3. An anti-DLL3 antibody was used as part of an antibody-drug conjugate called Rova-T, which failed a phase 3 trial in SCLC in 2021 and was subsequently canceled by AbbVie, but Dr. Wermke believes that the issue was with the drug and linker (a chemical tag that links the cytotoxic drug to the antibody, which is designed to release the drug in an appropriate environment such as the interior of a tumor cell after an antibody-drug conjugate has been internalized by the tumor cell), not DLL3. DLL3 is also being investigated as a component of chimeric antigen receptor T-cell therapy, though no clinical results have been reported, Dr. Wermke said.
Study methods and results
The study included 107 patients. The median age was 60.0 years, and 57% were male. To be included, patients had to have advanced SCLC, large cell neuroendocrine carcinoma, or extrapulmonary neuroendocrine carcinoma, as well as test positive for DLL3 expression.
The drug was well tolerated: 86% of patients experienced at least one treatment-related adverse event: 59% with a grade 1-2 TRAE and 27% with a grade 3-5 TRAE. Cytokine release syndrome (CRS) occurred in 59% of patients, but just 2% were grade 3-5. TRAEs led to discontinuation in 4% of patients. Physicians were able to manage CRS with supportive care, steroids, and anti–interleukin-6 receptor antibodies.
The treatment showed signs of efficacy, with partial responses occurring in 18% of patients, stable disease in 23%, progressive disease in 45%, while 13% were not evaluable.
At doses of 90 mg/kg or above, partial response occurred in 25% of patients, stable disease in 27%, and progressive disease in 31%, while 13% were not evaluable. Similar patterns were seen across three tumor types.
Of 18 responders, 14 continued to be responders at the time of the presentation. The longest response lengths were 13.1 months, 10.7 months, and 9.4 months.
Dr. Wermke said that the responses were encouraging, particularly the duration of some responses.
“Having a small cell [lung cancer] patient responding to something for more than a year is extraordinary. It comes with side effects, which are usually seen during the first [doses]. After that, the drug is pretty well tolerable, and that is also something which distinguishes it from alternative second-line approaches,” he said.
Well tolerated, but take efficacy data with a grain of salt
The study was encouraging but should be treated with caution, according to Vamsidhar Velcheti, MD, who moderated the session where the research was presented.
“The toxicity profile is actually very promising and it’s still very early, but there’s certainly a lot of interest in DLL3-targeted [therapies]. We’ve seen some very exciting data with other assets in this category as well,” said Dr. Velcheti, director of thoracic oncology at NYU Langone Health, New York.
Phase 1 efficacy data can be tantalizing but often fails to hold up to further testing, according to Dr. Velcheti. “We’ve seen signals in phase 1 data before, and we’ve been burned. We saw really promising data with Rova-T, and the confirmatory trials were negative, – so we want to be cautiously optimistic,” said Dr. Velcheti.
He also pointed out that patient selection will be important for such studies, considering that SCLC patients often have a lot of comorbidities and the therapy’s potential for causing CRS.
Both Dr. Wermke and Dr. Velcheti have received funding from numerous pharmaceutical companies. Dr. Wermke has consulted with or advised with Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, ImCheck Therapeutics, Immatics, ISA Pharmaceuticals, Lilly, and Novartis.
CHICAGO –
The antibody promotes the destruction of tumor cells by T cells by acting as a bridge between T cells and tumors.
SCLC has largely resisted efforts to identify unique surface markers. DLL3 is an exception: It is rarely expressed in normal cells, and it seems to be important to tumor biology, according to Martin Wermke, MD, who presented the study at the annual meeting of the American Society of Clinical Oncology.
A rare SCLC biomarker
“The problem, I think, is that small cell [lung cancer] with its high mutational burden is a bunch of many different subentities and you will probably not find a single driver mutation as you do in non–small cell lung cancer. So in that [way] it’s different in its biology,” said Dr. Wermke, professor of experimental tumor therapy at the National Center for Tumor Diseases in Dresden, Germany.
Nevertheless, DLL3 is a sensitive biomarker, with over 90% of SCLC tumors positive for the surface marker, according to Dr. Wermke. “It’s one of the first which proved to be a reliable [SCLC] biomarker for therapeutic approaches,” said Dr. Wermke.
This isn’t the first clinical experience with DLL3. An anti-DLL3 antibody was used as part of an antibody-drug conjugate called Rova-T, which failed a phase 3 trial in SCLC in 2021 and was subsequently canceled by AbbVie, but Dr. Wermke believes that the issue was with the drug and linker (a chemical tag that links the cytotoxic drug to the antibody, which is designed to release the drug in an appropriate environment such as the interior of a tumor cell after an antibody-drug conjugate has been internalized by the tumor cell), not DLL3. DLL3 is also being investigated as a component of chimeric antigen receptor T-cell therapy, though no clinical results have been reported, Dr. Wermke said.
Study methods and results
The study included 107 patients. The median age was 60.0 years, and 57% were male. To be included, patients had to have advanced SCLC, large cell neuroendocrine carcinoma, or extrapulmonary neuroendocrine carcinoma, as well as test positive for DLL3 expression.
The drug was well tolerated: 86% of patients experienced at least one treatment-related adverse event: 59% with a grade 1-2 TRAE and 27% with a grade 3-5 TRAE. Cytokine release syndrome (CRS) occurred in 59% of patients, but just 2% were grade 3-5. TRAEs led to discontinuation in 4% of patients. Physicians were able to manage CRS with supportive care, steroids, and anti–interleukin-6 receptor antibodies.
The treatment showed signs of efficacy, with partial responses occurring in 18% of patients, stable disease in 23%, progressive disease in 45%, while 13% were not evaluable.
At doses of 90 mg/kg or above, partial response occurred in 25% of patients, stable disease in 27%, and progressive disease in 31%, while 13% were not evaluable. Similar patterns were seen across three tumor types.
Of 18 responders, 14 continued to be responders at the time of the presentation. The longest response lengths were 13.1 months, 10.7 months, and 9.4 months.
Dr. Wermke said that the responses were encouraging, particularly the duration of some responses.
“Having a small cell [lung cancer] patient responding to something for more than a year is extraordinary. It comes with side effects, which are usually seen during the first [doses]. After that, the drug is pretty well tolerable, and that is also something which distinguishes it from alternative second-line approaches,” he said.
Well tolerated, but take efficacy data with a grain of salt
The study was encouraging but should be treated with caution, according to Vamsidhar Velcheti, MD, who moderated the session where the research was presented.
“The toxicity profile is actually very promising and it’s still very early, but there’s certainly a lot of interest in DLL3-targeted [therapies]. We’ve seen some very exciting data with other assets in this category as well,” said Dr. Velcheti, director of thoracic oncology at NYU Langone Health, New York.
Phase 1 efficacy data can be tantalizing but often fails to hold up to further testing, according to Dr. Velcheti. “We’ve seen signals in phase 1 data before, and we’ve been burned. We saw really promising data with Rova-T, and the confirmatory trials were negative, – so we want to be cautiously optimistic,” said Dr. Velcheti.
He also pointed out that patient selection will be important for such studies, considering that SCLC patients often have a lot of comorbidities and the therapy’s potential for causing CRS.
Both Dr. Wermke and Dr. Velcheti have received funding from numerous pharmaceutical companies. Dr. Wermke has consulted with or advised with Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, ImCheck Therapeutics, Immatics, ISA Pharmaceuticals, Lilly, and Novartis.
CHICAGO –
The antibody promotes the destruction of tumor cells by T cells by acting as a bridge between T cells and tumors.
SCLC has largely resisted efforts to identify unique surface markers. DLL3 is an exception: It is rarely expressed in normal cells, and it seems to be important to tumor biology, according to Martin Wermke, MD, who presented the study at the annual meeting of the American Society of Clinical Oncology.
A rare SCLC biomarker
“The problem, I think, is that small cell [lung cancer] with its high mutational burden is a bunch of many different subentities and you will probably not find a single driver mutation as you do in non–small cell lung cancer. So in that [way] it’s different in its biology,” said Dr. Wermke, professor of experimental tumor therapy at the National Center for Tumor Diseases in Dresden, Germany.
Nevertheless, DLL3 is a sensitive biomarker, with over 90% of SCLC tumors positive for the surface marker, according to Dr. Wermke. “It’s one of the first which proved to be a reliable [SCLC] biomarker for therapeutic approaches,” said Dr. Wermke.
This isn’t the first clinical experience with DLL3. An anti-DLL3 antibody was used as part of an antibody-drug conjugate called Rova-T, which failed a phase 3 trial in SCLC in 2021 and was subsequently canceled by AbbVie, but Dr. Wermke believes that the issue was with the drug and linker (a chemical tag that links the cytotoxic drug to the antibody, which is designed to release the drug in an appropriate environment such as the interior of a tumor cell after an antibody-drug conjugate has been internalized by the tumor cell), not DLL3. DLL3 is also being investigated as a component of chimeric antigen receptor T-cell therapy, though no clinical results have been reported, Dr. Wermke said.
Study methods and results
The study included 107 patients. The median age was 60.0 years, and 57% were male. To be included, patients had to have advanced SCLC, large cell neuroendocrine carcinoma, or extrapulmonary neuroendocrine carcinoma, as well as test positive for DLL3 expression.
The drug was well tolerated: 86% of patients experienced at least one treatment-related adverse event: 59% with a grade 1-2 TRAE and 27% with a grade 3-5 TRAE. Cytokine release syndrome (CRS) occurred in 59% of patients, but just 2% were grade 3-5. TRAEs led to discontinuation in 4% of patients. Physicians were able to manage CRS with supportive care, steroids, and anti–interleukin-6 receptor antibodies.
The treatment showed signs of efficacy, with partial responses occurring in 18% of patients, stable disease in 23%, progressive disease in 45%, while 13% were not evaluable.
At doses of 90 mg/kg or above, partial response occurred in 25% of patients, stable disease in 27%, and progressive disease in 31%, while 13% were not evaluable. Similar patterns were seen across three tumor types.
Of 18 responders, 14 continued to be responders at the time of the presentation. The longest response lengths were 13.1 months, 10.7 months, and 9.4 months.
Dr. Wermke said that the responses were encouraging, particularly the duration of some responses.
“Having a small cell [lung cancer] patient responding to something for more than a year is extraordinary. It comes with side effects, which are usually seen during the first [doses]. After that, the drug is pretty well tolerable, and that is also something which distinguishes it from alternative second-line approaches,” he said.
Well tolerated, but take efficacy data with a grain of salt
The study was encouraging but should be treated with caution, according to Vamsidhar Velcheti, MD, who moderated the session where the research was presented.
“The toxicity profile is actually very promising and it’s still very early, but there’s certainly a lot of interest in DLL3-targeted [therapies]. We’ve seen some very exciting data with other assets in this category as well,” said Dr. Velcheti, director of thoracic oncology at NYU Langone Health, New York.
Phase 1 efficacy data can be tantalizing but often fails to hold up to further testing, according to Dr. Velcheti. “We’ve seen signals in phase 1 data before, and we’ve been burned. We saw really promising data with Rova-T, and the confirmatory trials were negative, – so we want to be cautiously optimistic,” said Dr. Velcheti.
He also pointed out that patient selection will be important for such studies, considering that SCLC patients often have a lot of comorbidities and the therapy’s potential for causing CRS.
Both Dr. Wermke and Dr. Velcheti have received funding from numerous pharmaceutical companies. Dr. Wermke has consulted with or advised with Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, ImCheck Therapeutics, Immatics, ISA Pharmaceuticals, Lilly, and Novartis.
AT ASCO 2023
One in 10 people who had Omicron got long COVID: Study
About 10% of people infected with Omicron reported having long COVID, a lower percentage than estimated for people infected with earlier strains of the coronavirus, according to a study published in JAMA.
The research team looked at data from 8,646 adults infected with COVID-19 at different times of the pandemic and 1,118 who did not have COVID.
“Based on a subset of 2,231 patients in this analysis who had a first COVID-19 infection the National Institutes of Health said in a news release.
People who were unvaccinated or got COVID before Omicron were more likely to have long COVID and had more severe cases, the NIH said.
Previous studies have come up with higher figures than 10% for people who have long COVID.
For instance, in June 2022 the CDC said one in five Americans who had COVID reported having long COVID. And a University of Oxford study published in September 2021 found more than a third of patients had long COVID symptoms.
The scientists in the most recent study identified 12 symptoms that distinguished people who did and didn’t have COVID. The scientists developed a scoring system for the symptoms to set a threshold to identify people who had long COVID, the NIH said.
The symptoms were fatigue, brain fog, dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements. Another symptom was postexertional malaise, or worse symptoms after mental or physical exertion.
Scientists still have many questions about long COVID, such as how many people get it and why some people get it and others don’t.
The study was coordinated through the NIH’s RECOVER (Researching COVID to Enhance Recovery) initiative, which aims to find out how to define, detect, and treat long COVID.
“The researchers hope this study is the next step toward potential treatments for long COVID, which affects the health and wellbeing of millions of Americans,” the NIH said.
A version of this article first appeared on WebMD.com.
About 10% of people infected with Omicron reported having long COVID, a lower percentage than estimated for people infected with earlier strains of the coronavirus, according to a study published in JAMA.
The research team looked at data from 8,646 adults infected with COVID-19 at different times of the pandemic and 1,118 who did not have COVID.
“Based on a subset of 2,231 patients in this analysis who had a first COVID-19 infection the National Institutes of Health said in a news release.
People who were unvaccinated or got COVID before Omicron were more likely to have long COVID and had more severe cases, the NIH said.
Previous studies have come up with higher figures than 10% for people who have long COVID.
For instance, in June 2022 the CDC said one in five Americans who had COVID reported having long COVID. And a University of Oxford study published in September 2021 found more than a third of patients had long COVID symptoms.
The scientists in the most recent study identified 12 symptoms that distinguished people who did and didn’t have COVID. The scientists developed a scoring system for the symptoms to set a threshold to identify people who had long COVID, the NIH said.
The symptoms were fatigue, brain fog, dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements. Another symptom was postexertional malaise, or worse symptoms after mental or physical exertion.
Scientists still have many questions about long COVID, such as how many people get it and why some people get it and others don’t.
The study was coordinated through the NIH’s RECOVER (Researching COVID to Enhance Recovery) initiative, which aims to find out how to define, detect, and treat long COVID.
“The researchers hope this study is the next step toward potential treatments for long COVID, which affects the health and wellbeing of millions of Americans,” the NIH said.
A version of this article first appeared on WebMD.com.
About 10% of people infected with Omicron reported having long COVID, a lower percentage than estimated for people infected with earlier strains of the coronavirus, according to a study published in JAMA.
The research team looked at data from 8,646 adults infected with COVID-19 at different times of the pandemic and 1,118 who did not have COVID.
“Based on a subset of 2,231 patients in this analysis who had a first COVID-19 infection the National Institutes of Health said in a news release.
People who were unvaccinated or got COVID before Omicron were more likely to have long COVID and had more severe cases, the NIH said.
Previous studies have come up with higher figures than 10% for people who have long COVID.
For instance, in June 2022 the CDC said one in five Americans who had COVID reported having long COVID. And a University of Oxford study published in September 2021 found more than a third of patients had long COVID symptoms.
The scientists in the most recent study identified 12 symptoms that distinguished people who did and didn’t have COVID. The scientists developed a scoring system for the symptoms to set a threshold to identify people who had long COVID, the NIH said.
The symptoms were fatigue, brain fog, dizziness, stomach upset, heart palpitations, issues with sexual desire or capacity, loss of smell or taste, thirst, chronic coughing, chest pain, and abnormal movements. Another symptom was postexertional malaise, or worse symptoms after mental or physical exertion.
Scientists still have many questions about long COVID, such as how many people get it and why some people get it and others don’t.
The study was coordinated through the NIH’s RECOVER (Researching COVID to Enhance Recovery) initiative, which aims to find out how to define, detect, and treat long COVID.
“The researchers hope this study is the next step toward potential treatments for long COVID, which affects the health and wellbeing of millions of Americans,” the NIH said.
A version of this article first appeared on WebMD.com.
FROM JAMA
Study finds COVID-19 boosters don’t increase miscarriage risk
COVID-19 boosters are not linked to an increased chance of miscarriage, according to a new study in JAMA Network Open.
Researchers were seeking to learn whether a booster in early pregnancy, before 20 weeks, was associated with greater likelihood of spontaneous abortion.
They examined more than 100,000 pregnancies at 6-19 weeks from eight health systems in the Vaccine Safety Datalink (VSD). They found that receiving a COVID-19 booster shot in a 28-day or 42-day exposure window did not increase the chances of miscarriage.
The VSD is a collaboration between the Centers for Disease Control and Prevention’s Immunization Safety Office and large health care systems. The “observational, case-control, surveillance study” was conducted from Nov. 1, 2021, to June 12, 2022.
“COVID infection during pregnancy increases risk of poor outcomes, yet many people who are pregnant or thinking about getting pregnant are hesitant to get a booster dose because of questions about safety,” said Elyse Kharbanda, MD, senior investigator at HealthPartners Institute and lead author of the study in a press release.
The University of Minnesota reported that “previous studies have shown COIVD-19 primary vaccination is safe in pregnancy and not associated with an increased risk for miscarriage. Several studies have also shown COVID-19 can be more severe in pregnancy and lead to worse outcomes for the mother.”
The study was funded by the CDC. Five study authors reported conflicts of interest with Pfizer, Merck, GlaxoSmithKline, AbbVie, and Sanofi Pasteur.
A version of this article first appeared on Medscape.com.
COVID-19 boosters are not linked to an increased chance of miscarriage, according to a new study in JAMA Network Open.
Researchers were seeking to learn whether a booster in early pregnancy, before 20 weeks, was associated with greater likelihood of spontaneous abortion.
They examined more than 100,000 pregnancies at 6-19 weeks from eight health systems in the Vaccine Safety Datalink (VSD). They found that receiving a COVID-19 booster shot in a 28-day or 42-day exposure window did not increase the chances of miscarriage.
The VSD is a collaboration between the Centers for Disease Control and Prevention’s Immunization Safety Office and large health care systems. The “observational, case-control, surveillance study” was conducted from Nov. 1, 2021, to June 12, 2022.
“COVID infection during pregnancy increases risk of poor outcomes, yet many people who are pregnant or thinking about getting pregnant are hesitant to get a booster dose because of questions about safety,” said Elyse Kharbanda, MD, senior investigator at HealthPartners Institute and lead author of the study in a press release.
The University of Minnesota reported that “previous studies have shown COIVD-19 primary vaccination is safe in pregnancy and not associated with an increased risk for miscarriage. Several studies have also shown COVID-19 can be more severe in pregnancy and lead to worse outcomes for the mother.”
The study was funded by the CDC. Five study authors reported conflicts of interest with Pfizer, Merck, GlaxoSmithKline, AbbVie, and Sanofi Pasteur.
A version of this article first appeared on Medscape.com.
COVID-19 boosters are not linked to an increased chance of miscarriage, according to a new study in JAMA Network Open.
Researchers were seeking to learn whether a booster in early pregnancy, before 20 weeks, was associated with greater likelihood of spontaneous abortion.
They examined more than 100,000 pregnancies at 6-19 weeks from eight health systems in the Vaccine Safety Datalink (VSD). They found that receiving a COVID-19 booster shot in a 28-day or 42-day exposure window did not increase the chances of miscarriage.
The VSD is a collaboration between the Centers for Disease Control and Prevention’s Immunization Safety Office and large health care systems. The “observational, case-control, surveillance study” was conducted from Nov. 1, 2021, to June 12, 2022.
“COVID infection during pregnancy increases risk of poor outcomes, yet many people who are pregnant or thinking about getting pregnant are hesitant to get a booster dose because of questions about safety,” said Elyse Kharbanda, MD, senior investigator at HealthPartners Institute and lead author of the study in a press release.
The University of Minnesota reported that “previous studies have shown COIVD-19 primary vaccination is safe in pregnancy and not associated with an increased risk for miscarriage. Several studies have also shown COVID-19 can be more severe in pregnancy and lead to worse outcomes for the mother.”
The study was funded by the CDC. Five study authors reported conflicts of interest with Pfizer, Merck, GlaxoSmithKline, AbbVie, and Sanofi Pasteur.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Potential new treatment for REM sleep behavior disorder
Dual orexin receptor antagonists (DORAs), a class of drugs approved to treat insomnia, may also be effective for rapid eye movement sleep behavior disorder (RBD), a study suggests.
About 3 million people in the United States have RBD, which is often a precursor to Parkinson’s disease. People with the disorder act out their dreams by talking, flailing their arms and legs, punching, kicking, and exhibiting other behaviors while asleep.
Researchers used an animal model for the study, which they say is the first to identify a new form of treatment for RBD.
“REM behavior disorder is difficult to treat, and the treatments are mostly limited to clonazepam and melatonin,” which may have side effects, senior investigator Andrew Varga, MD, PhD, associate professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai, New York, told this news organization. “We’re using something completely different, which raises the possibility this might be something useful for REM behavior disorders.”
The findings, with Mount Sinai assistant professor Korey Kam, PhD, as lead author, were published online in the Journal of Neuroscience.
A new model for RBD?
RBD can signal risk for synucleinopathies, a group of neurological conditions such as Parkinson’s disease that involve the formation of clumps of alpha-synuclein protein in the brain.
Prior research on RBD was done in synucleinopathy mouse models. For this study, however, researchers used a tauopathy mouse model to investigate how the abnormal accumulation of tau protein might affect RBD.
Researchers collected data on biophysical properties when the mice were awake and in REM and non-REM sleep. They examined length of sleep, transitions from waking to sleep, and how some factors are related to age.
Nearly a third of the older animals showed behaviors similar to REM sleep behavior disorder in humans, including chewing and limb extension.
But after researchers administered a DORA medication twice during a 24-hour period, they noted that the medication not only helped the animals fall asleep faster and for longer, it also reduced levels of dream enactment that are a hallmark of RBD.
The ‘bigger highlight’
Finding RBD behaviors in a tauopathy animal model was surprising, Dr. Varga said, because RBD has been previously linked to synucleinopathies. There was no known correlation between RBD and abnormal accumulation of tau.
Another unexpected finding was the detection of RBD in some of the younger animals, who had not yet shown evidence of tau accumulation.
“It appears to be a biomarker or a signature of something that’s going on that predicts the impending tauopathy at a time where there is very little, or no, tau pathology going on in the brain,” Dr. Varga said.
If RBD is an early predictor of future tau accumulation, the model could guide future prevention and treatment. However, the more important finding is the potential new treatment for the condition.
“The bigger highlight here is less about what’s causing the RBD [than about] what you can do to make it better,” he said.
The next step in the work is to study whether the effect of DORAs on RBD seen in this tauopathy mouse model is evidenced in other animals and whether it is effective in humans with RBD, Dr. Varga said.
The study was funded by the Alzheimer’s Association and Merck Investigator Studies Program. Dr. Kam, Dr. Varga, and coauthors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dual orexin receptor antagonists (DORAs), a class of drugs approved to treat insomnia, may also be effective for rapid eye movement sleep behavior disorder (RBD), a study suggests.
About 3 million people in the United States have RBD, which is often a precursor to Parkinson’s disease. People with the disorder act out their dreams by talking, flailing their arms and legs, punching, kicking, and exhibiting other behaviors while asleep.
Researchers used an animal model for the study, which they say is the first to identify a new form of treatment for RBD.
“REM behavior disorder is difficult to treat, and the treatments are mostly limited to clonazepam and melatonin,” which may have side effects, senior investigator Andrew Varga, MD, PhD, associate professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai, New York, told this news organization. “We’re using something completely different, which raises the possibility this might be something useful for REM behavior disorders.”
The findings, with Mount Sinai assistant professor Korey Kam, PhD, as lead author, were published online in the Journal of Neuroscience.
A new model for RBD?
RBD can signal risk for synucleinopathies, a group of neurological conditions such as Parkinson’s disease that involve the formation of clumps of alpha-synuclein protein in the brain.
Prior research on RBD was done in synucleinopathy mouse models. For this study, however, researchers used a tauopathy mouse model to investigate how the abnormal accumulation of tau protein might affect RBD.
Researchers collected data on biophysical properties when the mice were awake and in REM and non-REM sleep. They examined length of sleep, transitions from waking to sleep, and how some factors are related to age.
Nearly a third of the older animals showed behaviors similar to REM sleep behavior disorder in humans, including chewing and limb extension.
But after researchers administered a DORA medication twice during a 24-hour period, they noted that the medication not only helped the animals fall asleep faster and for longer, it also reduced levels of dream enactment that are a hallmark of RBD.
The ‘bigger highlight’
Finding RBD behaviors in a tauopathy animal model was surprising, Dr. Varga said, because RBD has been previously linked to synucleinopathies. There was no known correlation between RBD and abnormal accumulation of tau.
Another unexpected finding was the detection of RBD in some of the younger animals, who had not yet shown evidence of tau accumulation.
“It appears to be a biomarker or a signature of something that’s going on that predicts the impending tauopathy at a time where there is very little, or no, tau pathology going on in the brain,” Dr. Varga said.
If RBD is an early predictor of future tau accumulation, the model could guide future prevention and treatment. However, the more important finding is the potential new treatment for the condition.
“The bigger highlight here is less about what’s causing the RBD [than about] what you can do to make it better,” he said.
The next step in the work is to study whether the effect of DORAs on RBD seen in this tauopathy mouse model is evidenced in other animals and whether it is effective in humans with RBD, Dr. Varga said.
The study was funded by the Alzheimer’s Association and Merck Investigator Studies Program. Dr. Kam, Dr. Varga, and coauthors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dual orexin receptor antagonists (DORAs), a class of drugs approved to treat insomnia, may also be effective for rapid eye movement sleep behavior disorder (RBD), a study suggests.
About 3 million people in the United States have RBD, which is often a precursor to Parkinson’s disease. People with the disorder act out their dreams by talking, flailing their arms and legs, punching, kicking, and exhibiting other behaviors while asleep.
Researchers used an animal model for the study, which they say is the first to identify a new form of treatment for RBD.
“REM behavior disorder is difficult to treat, and the treatments are mostly limited to clonazepam and melatonin,” which may have side effects, senior investigator Andrew Varga, MD, PhD, associate professor of pulmonary, critical care, and sleep medicine at the Icahn School of Medicine at Mount Sinai, New York, told this news organization. “We’re using something completely different, which raises the possibility this might be something useful for REM behavior disorders.”
The findings, with Mount Sinai assistant professor Korey Kam, PhD, as lead author, were published online in the Journal of Neuroscience.
A new model for RBD?
RBD can signal risk for synucleinopathies, a group of neurological conditions such as Parkinson’s disease that involve the formation of clumps of alpha-synuclein protein in the brain.
Prior research on RBD was done in synucleinopathy mouse models. For this study, however, researchers used a tauopathy mouse model to investigate how the abnormal accumulation of tau protein might affect RBD.
Researchers collected data on biophysical properties when the mice were awake and in REM and non-REM sleep. They examined length of sleep, transitions from waking to sleep, and how some factors are related to age.
Nearly a third of the older animals showed behaviors similar to REM sleep behavior disorder in humans, including chewing and limb extension.
But after researchers administered a DORA medication twice during a 24-hour period, they noted that the medication not only helped the animals fall asleep faster and for longer, it also reduced levels of dream enactment that are a hallmark of RBD.
The ‘bigger highlight’
Finding RBD behaviors in a tauopathy animal model was surprising, Dr. Varga said, because RBD has been previously linked to synucleinopathies. There was no known correlation between RBD and abnormal accumulation of tau.
Another unexpected finding was the detection of RBD in some of the younger animals, who had not yet shown evidence of tau accumulation.
“It appears to be a biomarker or a signature of something that’s going on that predicts the impending tauopathy at a time where there is very little, or no, tau pathology going on in the brain,” Dr. Varga said.
If RBD is an early predictor of future tau accumulation, the model could guide future prevention and treatment. However, the more important finding is the potential new treatment for the condition.
“The bigger highlight here is less about what’s causing the RBD [than about] what you can do to make it better,” he said.
The next step in the work is to study whether the effect of DORAs on RBD seen in this tauopathy mouse model is evidenced in other animals and whether it is effective in humans with RBD, Dr. Varga said.
The study was funded by the Alzheimer’s Association and Merck Investigator Studies Program. Dr. Kam, Dr. Varga, and coauthors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF NEUROSCIENCE
Enthesitis, arthritis, tenosynovitis linked to dupilumab use for atopic dermatitis
Around 5% of patients treated with dupilumab (Dupixent) for moderate-to-severe atopic dermatitis experience musculoskeletal (MSK) symptoms, according to the results of a descriptive study.
The main MSK symptom seen in the observational cohort was enthesitis, but some patients also experienced arthritis and tenosynovitis a median of 17 weeks after starting dupilumab treatment. Together these symptoms represent a new MSK syndrome, say researchers from the United Kingdom.
“The pattern of MSK symptoms and signs is characteristic of psoriatic arthritis/peripheral spondyloarthritis,” Bruce Kirkham, MD, and collaborators report in Arthritis & Rheumatology.
“We started a few years ago and have been following the patients for quite a long time,” Dr. Kirkham, a consultant rheumatologist at Guy’s and St. Thomas’ NHS Foundation Trust, London, told this news organization.
“We’re still seeing patients with the same type of syndrome presenting occasionally. It’s not a very common adverse event, but we think it continues,” he observed.
“Most of them don’t have very severe problems, and a lot of them can be treated with quite simple drugs or, alternatively, reducing the frequency of the injection,” Dr. Kirkham added.
Characterizing the MSK symptoms
Of 470 patients with atopic dermatitis who started treatment with dupilumab at Guy’s and St. Thomas’ NHS Foundation Trust between October 2018 and February 2021, 36 (7.65%) developed rheumatic symptoms and were referred to the rheumatology department. These individuals had their family history assessed and thorough MSK evaluations, which included antibody and inflammatory markers, ultrasound of the peripheral small joints, and MRI of the large joints and spine.
A total of 26 (5.5%) patients – 14 of whom were male – had inflammatory enthesitis, arthritis, and/or tenosynovitis. Of the others, seven had osteoarthritis and three had degenerative spine disease.
Enthesitis was the most common finding in those with rheumatic symptoms, occurring on its own in 11 patients, with arthritis in three patients, and tenosynovitis in two patients.
These symptoms appeared 2-48 weeks after starting dupilumab treatment and were categorized as mild in 16 (61%) cases, moderate in six cases, and severe in four cases.
No specific predictors of the MSK symptoms seen were noted. Patient age, sex, duration of their atopic dermatitis, or how their skin condition had been previously treated did not help identify those who might develop rheumatic problems.
Conservative management approach
All patients had “outstanding” responses to treatment, Dr. Kirkham noted: The mean Eczema Area and Severity Index score before dupilumab treatment was 21, falling to 4.2 with treatment, indicating a mean 80% improvement.
Co-author Joseph Nathan, MBChB, of London North West Healthcare NHS Trust, who collaborated on the research while working within Dr. Kirkham’s group, said separately: “The concern that patients have is that when they start a medication and develop a side effect is that the medication is going to be stopped.”
Clinicians treating the patients took a conservative approach, prescribing NSAIDs such as cyclooxygenase-2 inhibitors or altering the frequency with which dupilumab was given.
With this approach, MSK symptoms resolved in 15 patients who remained on treatment and in seven who had to stop dupilumab. There were four patients, however, who had unresolved symptoms even once dupilumab treatment had been stopped.
Altering the local cytokine balance
Dupilumab is a monoclonal antibody that binds to the alpha subunit of the interleukin-4 receptor. This results in blocking the function of not only IL-4 but also IL-13.
Dr. Kirkham and colleagues think this might not only alter the balance of cytokines in the skin but also in the joints and entheses with IL-17, IL-23, or even tumor necrosis factor playing a possible role. Another thought is that many circulating T-cells in the skin move to the joints and entheses to trigger symptoms.
IL-13 inhibition does seem to be important, as another British research team, from the Centre for Epidemiology Versus Arthritis at the University of Manchester (England), has found.
At the recent annual meeting of the British Society for Rheumatology, Sizheng Steven Zhao, MBChB, PhD, and colleagues reported that among people who carried a genetic variant predisposing them to having low IL-13 function, there was a higher risk for inflammatory diseases such as psoriatic arthritis and other spondyloarthropathy-related diseases.

Indeed, when the single nucleotide polymorphism rs20541 was present, the odds for having psoriatic arthritis and psoriasis were higher than when it was not.
The findings are consistent with the idea that IL-4 and IL-13 may be acting as a restraint towards MSK diseases in some patients, Dr. Zhao and co-authors suggest.
“The genetic data supports what [Dr. Kirkham and team] have said from a mechanistic point of view,” Dr. Zhao said in an interview. “What you’re observing has a genetic basis.”
Dermatology perspective
Approved by the U.S. Food and Drug Administration in 2017, dupilumab has since been hailed as a “breakthrough” in atopic dermatitis treatment. Given as a subcutaneous injection every 2 weeks, it provides a much-needed option for people who have moderate-to-severe disease and have tried other available treatments, including corticosteroids.
Dupilumab has since also been approved for asthma, chronic sinusitis with nasal polyposis, eosinophilic esophagitis, and prurigo nodularis and is used off-label for other skin conditions such as contact dermatitis, chronic spontaneous urticaria, and alopecia areata.
“Dupilumab, like a lot of medications for atopic dermatitis, is a relatively new drug, and we are still learning about its safety,” Joel M. Gelfand, MD, MSCE, of the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
“Inflammatory arthritis has been reported in patients treated with dupilumab, and this new study provides some useful estimates,” added Dr. Gelfand, who is a professor of dermatology and epidemiology and directs the Psoriasis and Phototherapy Treatment Center, Philadelphia.
“There was no control group,” Dr. Gelfand said, so “a causal relationship cannot be well established based on these data alone. The mechanism is not known but may result from a shifting of the immune system.”
Dr. Zhao observed: “We don’t know what the natural history of these adverse events is. We don’t know if stopping the drug early will prevent long-term adverse events. So, we don’t know if people will ultimately develop permanent psoriatic arthritis if we don’t intervene quick enough when we observe an adverse event.”
Being aware of the possibility of rheumatic side effects occurring with dupilumab and similar agents is key, Dr. Gelfand and Dr. Kirkham both said independently.
“I have personally seen this entity in my practice,” Dr. Gelfand said. “It is important to clinicians prescribing dupilumab to alert patients about this potential side effect and ask about joint symptoms in follow-up.”
Dr. Kirkham said: “Prescribers need to be aware of it, because up until now it’s been just very vaguely discussed as sort of aches and pains, arthralgias, and it’s a much more specific of a kind of syndrome of enthesitis, arthritis, tenosynovitis – a little like psoriatic arthritis.”
Not everyone has come across these side effects, however, as Steven Daveluy, MD, associate professor and dermatology program director at Wayne State University, Detroit, said in an interview.
“This article and the other case series both noted the musculoskeletal symptoms occurred in about 5% of patients, which surprised me since I haven’t seen it in my practice and have enough patients being treated with dupilumab that I would expect to see a case at that rate,” Dr. Daveluy said.
“The majority of cases are mild and respond to treatment with anti-inflammatories like naproxen, which is available over the counter. It’s likely that patients with a mild case could simply treat their pain with naproxen that’s already in their medicine cabinet until it resolves, never bringing it to the doctor’s attention,” he suggested.
“Dupilumab is still a safe and effective medication that can change the lives of patients suffering from atopic dermatitis,” he said.
“Awareness of this potential side effect can help dermatologists recognize it early and work together with patients to determine the best course of action.”
All research mentioned in this article was independently supported. Dr. Kirkham, Mr. Nathan, Dr. Zhao, and Dr. Daveluy report no relevant financial relationships. Dr. Gelfand has served as a consultant for numerous pharmaceutical companies and receives research grants from Amgen, Boehringer Ingelheim, and Pfizer. He is a co-patent holder of resiquimod for treatment of cutaneous T-cell lymphoma.
A version of this article first appeared on Medscape.com.
Around 5% of patients treated with dupilumab (Dupixent) for moderate-to-severe atopic dermatitis experience musculoskeletal (MSK) symptoms, according to the results of a descriptive study.
The main MSK symptom seen in the observational cohort was enthesitis, but some patients also experienced arthritis and tenosynovitis a median of 17 weeks after starting dupilumab treatment. Together these symptoms represent a new MSK syndrome, say researchers from the United Kingdom.
“The pattern of MSK symptoms and signs is characteristic of psoriatic arthritis/peripheral spondyloarthritis,” Bruce Kirkham, MD, and collaborators report in Arthritis & Rheumatology.
“We started a few years ago and have been following the patients for quite a long time,” Dr. Kirkham, a consultant rheumatologist at Guy’s and St. Thomas’ NHS Foundation Trust, London, told this news organization.
“We’re still seeing patients with the same type of syndrome presenting occasionally. It’s not a very common adverse event, but we think it continues,” he observed.
“Most of them don’t have very severe problems, and a lot of them can be treated with quite simple drugs or, alternatively, reducing the frequency of the injection,” Dr. Kirkham added.
Characterizing the MSK symptoms
Of 470 patients with atopic dermatitis who started treatment with dupilumab at Guy’s and St. Thomas’ NHS Foundation Trust between October 2018 and February 2021, 36 (7.65%) developed rheumatic symptoms and were referred to the rheumatology department. These individuals had their family history assessed and thorough MSK evaluations, which included antibody and inflammatory markers, ultrasound of the peripheral small joints, and MRI of the large joints and spine.
A total of 26 (5.5%) patients – 14 of whom were male – had inflammatory enthesitis, arthritis, and/or tenosynovitis. Of the others, seven had osteoarthritis and three had degenerative spine disease.
Enthesitis was the most common finding in those with rheumatic symptoms, occurring on its own in 11 patients, with arthritis in three patients, and tenosynovitis in two patients.
These symptoms appeared 2-48 weeks after starting dupilumab treatment and were categorized as mild in 16 (61%) cases, moderate in six cases, and severe in four cases.
No specific predictors of the MSK symptoms seen were noted. Patient age, sex, duration of their atopic dermatitis, or how their skin condition had been previously treated did not help identify those who might develop rheumatic problems.
Conservative management approach
All patients had “outstanding” responses to treatment, Dr. Kirkham noted: The mean Eczema Area and Severity Index score before dupilumab treatment was 21, falling to 4.2 with treatment, indicating a mean 80% improvement.
Co-author Joseph Nathan, MBChB, of London North West Healthcare NHS Trust, who collaborated on the research while working within Dr. Kirkham’s group, said separately: “The concern that patients have is that when they start a medication and develop a side effect is that the medication is going to be stopped.”
Clinicians treating the patients took a conservative approach, prescribing NSAIDs such as cyclooxygenase-2 inhibitors or altering the frequency with which dupilumab was given.
With this approach, MSK symptoms resolved in 15 patients who remained on treatment and in seven who had to stop dupilumab. There were four patients, however, who had unresolved symptoms even once dupilumab treatment had been stopped.
Altering the local cytokine balance
Dupilumab is a monoclonal antibody that binds to the alpha subunit of the interleukin-4 receptor. This results in blocking the function of not only IL-4 but also IL-13.
Dr. Kirkham and colleagues think this might not only alter the balance of cytokines in the skin but also in the joints and entheses with IL-17, IL-23, or even tumor necrosis factor playing a possible role. Another thought is that many circulating T-cells in the skin move to the joints and entheses to trigger symptoms.
IL-13 inhibition does seem to be important, as another British research team, from the Centre for Epidemiology Versus Arthritis at the University of Manchester (England), has found.
At the recent annual meeting of the British Society for Rheumatology, Sizheng Steven Zhao, MBChB, PhD, and colleagues reported that among people who carried a genetic variant predisposing them to having low IL-13 function, there was a higher risk for inflammatory diseases such as psoriatic arthritis and other spondyloarthropathy-related diseases.
Indeed, when the single nucleotide polymorphism rs20541 was present, the odds for having psoriatic arthritis and psoriasis were higher than when it was not.
The findings are consistent with the idea that IL-4 and IL-13 may be acting as a restraint towards MSK diseases in some patients, Dr. Zhao and co-authors suggest.
“The genetic data supports what [Dr. Kirkham and team] have said from a mechanistic point of view,” Dr. Zhao said in an interview. “What you’re observing has a genetic basis.”
Dermatology perspective
Approved by the U.S. Food and Drug Administration in 2017, dupilumab has since been hailed as a “breakthrough” in atopic dermatitis treatment. Given as a subcutaneous injection every 2 weeks, it provides a much-needed option for people who have moderate-to-severe disease and have tried other available treatments, including corticosteroids.
Dupilumab has since also been approved for asthma, chronic sinusitis with nasal polyposis, eosinophilic esophagitis, and prurigo nodularis and is used off-label for other skin conditions such as contact dermatitis, chronic spontaneous urticaria, and alopecia areata.
“Dupilumab, like a lot of medications for atopic dermatitis, is a relatively new drug, and we are still learning about its safety,” Joel M. Gelfand, MD, MSCE, of the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
“Inflammatory arthritis has been reported in patients treated with dupilumab, and this new study provides some useful estimates,” added Dr. Gelfand, who is a professor of dermatology and epidemiology and directs the Psoriasis and Phototherapy Treatment Center, Philadelphia.
“There was no control group,” Dr. Gelfand said, so “a causal relationship cannot be well established based on these data alone. The mechanism is not known but may result from a shifting of the immune system.”
Dr. Zhao observed: “We don’t know what the natural history of these adverse events is. We don’t know if stopping the drug early will prevent long-term adverse events. So, we don’t know if people will ultimately develop permanent psoriatic arthritis if we don’t intervene quick enough when we observe an adverse event.”
Being aware of the possibility of rheumatic side effects occurring with dupilumab and similar agents is key, Dr. Gelfand and Dr. Kirkham both said independently.
“I have personally seen this entity in my practice,” Dr. Gelfand said. “It is important to clinicians prescribing dupilumab to alert patients about this potential side effect and ask about joint symptoms in follow-up.”
Dr. Kirkham said: “Prescribers need to be aware of it, because up until now it’s been just very vaguely discussed as sort of aches and pains, arthralgias, and it’s a much more specific of a kind of syndrome of enthesitis, arthritis, tenosynovitis – a little like psoriatic arthritis.”
Not everyone has come across these side effects, however, as Steven Daveluy, MD, associate professor and dermatology program director at Wayne State University, Detroit, said in an interview.
“This article and the other case series both noted the musculoskeletal symptoms occurred in about 5% of patients, which surprised me since I haven’t seen it in my practice and have enough patients being treated with dupilumab that I would expect to see a case at that rate,” Dr. Daveluy said.
“The majority of cases are mild and respond to treatment with anti-inflammatories like naproxen, which is available over the counter. It’s likely that patients with a mild case could simply treat their pain with naproxen that’s already in their medicine cabinet until it resolves, never bringing it to the doctor’s attention,” he suggested.
“Dupilumab is still a safe and effective medication that can change the lives of patients suffering from atopic dermatitis,” he said.
“Awareness of this potential side effect can help dermatologists recognize it early and work together with patients to determine the best course of action.”
All research mentioned in this article was independently supported. Dr. Kirkham, Mr. Nathan, Dr. Zhao, and Dr. Daveluy report no relevant financial relationships. Dr. Gelfand has served as a consultant for numerous pharmaceutical companies and receives research grants from Amgen, Boehringer Ingelheim, and Pfizer. He is a co-patent holder of resiquimod for treatment of cutaneous T-cell lymphoma.
A version of this article first appeared on Medscape.com.
Around 5% of patients treated with dupilumab (Dupixent) for moderate-to-severe atopic dermatitis experience musculoskeletal (MSK) symptoms, according to the results of a descriptive study.
The main MSK symptom seen in the observational cohort was enthesitis, but some patients also experienced arthritis and tenosynovitis a median of 17 weeks after starting dupilumab treatment. Together these symptoms represent a new MSK syndrome, say researchers from the United Kingdom.
“The pattern of MSK symptoms and signs is characteristic of psoriatic arthritis/peripheral spondyloarthritis,” Bruce Kirkham, MD, and collaborators report in Arthritis & Rheumatology.
“We started a few years ago and have been following the patients for quite a long time,” Dr. Kirkham, a consultant rheumatologist at Guy’s and St. Thomas’ NHS Foundation Trust, London, told this news organization.
“We’re still seeing patients with the same type of syndrome presenting occasionally. It’s not a very common adverse event, but we think it continues,” he observed.
“Most of them don’t have very severe problems, and a lot of them can be treated with quite simple drugs or, alternatively, reducing the frequency of the injection,” Dr. Kirkham added.
Characterizing the MSK symptoms
Of 470 patients with atopic dermatitis who started treatment with dupilumab at Guy’s and St. Thomas’ NHS Foundation Trust between October 2018 and February 2021, 36 (7.65%) developed rheumatic symptoms and were referred to the rheumatology department. These individuals had their family history assessed and thorough MSK evaluations, which included antibody and inflammatory markers, ultrasound of the peripheral small joints, and MRI of the large joints and spine.
A total of 26 (5.5%) patients – 14 of whom were male – had inflammatory enthesitis, arthritis, and/or tenosynovitis. Of the others, seven had osteoarthritis and three had degenerative spine disease.
Enthesitis was the most common finding in those with rheumatic symptoms, occurring on its own in 11 patients, with arthritis in three patients, and tenosynovitis in two patients.
These symptoms appeared 2-48 weeks after starting dupilumab treatment and were categorized as mild in 16 (61%) cases, moderate in six cases, and severe in four cases.
No specific predictors of the MSK symptoms seen were noted. Patient age, sex, duration of their atopic dermatitis, or how their skin condition had been previously treated did not help identify those who might develop rheumatic problems.
Conservative management approach
All patients had “outstanding” responses to treatment, Dr. Kirkham noted: The mean Eczema Area and Severity Index score before dupilumab treatment was 21, falling to 4.2 with treatment, indicating a mean 80% improvement.
Co-author Joseph Nathan, MBChB, of London North West Healthcare NHS Trust, who collaborated on the research while working within Dr. Kirkham’s group, said separately: “The concern that patients have is that when they start a medication and develop a side effect is that the medication is going to be stopped.”
Clinicians treating the patients took a conservative approach, prescribing NSAIDs such as cyclooxygenase-2 inhibitors or altering the frequency with which dupilumab was given.
With this approach, MSK symptoms resolved in 15 patients who remained on treatment and in seven who had to stop dupilumab. There were four patients, however, who had unresolved symptoms even once dupilumab treatment had been stopped.
Altering the local cytokine balance
Dupilumab is a monoclonal antibody that binds to the alpha subunit of the interleukin-4 receptor. This results in blocking the function of not only IL-4 but also IL-13.
Dr. Kirkham and colleagues think this might not only alter the balance of cytokines in the skin but also in the joints and entheses with IL-17, IL-23, or even tumor necrosis factor playing a possible role. Another thought is that many circulating T-cells in the skin move to the joints and entheses to trigger symptoms.
IL-13 inhibition does seem to be important, as another British research team, from the Centre for Epidemiology Versus Arthritis at the University of Manchester (England), has found.
At the recent annual meeting of the British Society for Rheumatology, Sizheng Steven Zhao, MBChB, PhD, and colleagues reported that among people who carried a genetic variant predisposing them to having low IL-13 function, there was a higher risk for inflammatory diseases such as psoriatic arthritis and other spondyloarthropathy-related diseases.
Indeed, when the single nucleotide polymorphism rs20541 was present, the odds for having psoriatic arthritis and psoriasis were higher than when it was not.
The findings are consistent with the idea that IL-4 and IL-13 may be acting as a restraint towards MSK diseases in some patients, Dr. Zhao and co-authors suggest.
“The genetic data supports what [Dr. Kirkham and team] have said from a mechanistic point of view,” Dr. Zhao said in an interview. “What you’re observing has a genetic basis.”
Dermatology perspective
Approved by the U.S. Food and Drug Administration in 2017, dupilumab has since been hailed as a “breakthrough” in atopic dermatitis treatment. Given as a subcutaneous injection every 2 weeks, it provides a much-needed option for people who have moderate-to-severe disease and have tried other available treatments, including corticosteroids.
Dupilumab has since also been approved for asthma, chronic sinusitis with nasal polyposis, eosinophilic esophagitis, and prurigo nodularis and is used off-label for other skin conditions such as contact dermatitis, chronic spontaneous urticaria, and alopecia areata.
“Dupilumab, like a lot of medications for atopic dermatitis, is a relatively new drug, and we are still learning about its safety,” Joel M. Gelfand, MD, MSCE, of the University of Pennsylvania Perelman School of Medicine, Philadelphia, told this news organization.
“Inflammatory arthritis has been reported in patients treated with dupilumab, and this new study provides some useful estimates,” added Dr. Gelfand, who is a professor of dermatology and epidemiology and directs the Psoriasis and Phototherapy Treatment Center, Philadelphia.
“There was no control group,” Dr. Gelfand said, so “a causal relationship cannot be well established based on these data alone. The mechanism is not known but may result from a shifting of the immune system.”
Dr. Zhao observed: “We don’t know what the natural history of these adverse events is. We don’t know if stopping the drug early will prevent long-term adverse events. So, we don’t know if people will ultimately develop permanent psoriatic arthritis if we don’t intervene quick enough when we observe an adverse event.”
Being aware of the possibility of rheumatic side effects occurring with dupilumab and similar agents is key, Dr. Gelfand and Dr. Kirkham both said independently.
“I have personally seen this entity in my practice,” Dr. Gelfand said. “It is important to clinicians prescribing dupilumab to alert patients about this potential side effect and ask about joint symptoms in follow-up.”
Dr. Kirkham said: “Prescribers need to be aware of it, because up until now it’s been just very vaguely discussed as sort of aches and pains, arthralgias, and it’s a much more specific of a kind of syndrome of enthesitis, arthritis, tenosynovitis – a little like psoriatic arthritis.”
Not everyone has come across these side effects, however, as Steven Daveluy, MD, associate professor and dermatology program director at Wayne State University, Detroit, said in an interview.
“This article and the other case series both noted the musculoskeletal symptoms occurred in about 5% of patients, which surprised me since I haven’t seen it in my practice and have enough patients being treated with dupilumab that I would expect to see a case at that rate,” Dr. Daveluy said.
“The majority of cases are mild and respond to treatment with anti-inflammatories like naproxen, which is available over the counter. It’s likely that patients with a mild case could simply treat their pain with naproxen that’s already in their medicine cabinet until it resolves, never bringing it to the doctor’s attention,” he suggested.
“Dupilumab is still a safe and effective medication that can change the lives of patients suffering from atopic dermatitis,” he said.
“Awareness of this potential side effect can help dermatologists recognize it early and work together with patients to determine the best course of action.”
All research mentioned in this article was independently supported. Dr. Kirkham, Mr. Nathan, Dr. Zhao, and Dr. Daveluy report no relevant financial relationships. Dr. Gelfand has served as a consultant for numerous pharmaceutical companies and receives research grants from Amgen, Boehringer Ingelheim, and Pfizer. He is a co-patent holder of resiquimod for treatment of cutaneous T-cell lymphoma.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS & RHEUMATOLOGY