User login
Capecitabine maintenance improved DFS, not OS, in TNBC patients
according to results of a phase 3 trial.
Patients who received metronomic capecitabine maintenance had significantly higher rates of 5-year DFS and distant DFS, but not OS, when compared with patients who did not receive capecitabine, reported Xi Wang, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
“TNBC has the worst outcomes among all subtypes of breast cancer,” Dr. Wang said. “Effective strategies to reduce risk of relapse are a critical clinical need.”
He went on to describe capecitabine as a “potential ideal drug for metronomic administration,” particularly among patients with high risk of distant metastasis.
With that in mind, Dr. Wang and colleagues tested metronomic capecitabine maintenance in the phase 3 SYSUCC-001 trial. The trial included 434 patients with invasive ductal carcinoma. They had undergone standard therapy, which included surgery, neoadjuvant/adjuvant chemotherapy, and radiation therapy.
Patients were randomized to receive capecitabine at 650 mg/m2 twice daily for 1 year (n = 221) or undergo observation (n = 213). The primary endpoint was DFS, while secondary endpoints included safety, distant DFS, and OS.
According to Dr. Wang, the two patient groups were “well balanced,” with similar baseline characteristics. Most patients underwent adjuvant chemotherapy (93%), had histological grade 3 tumors (71%-74%), had a Ki-67 index of at least 30% (73%-80%), had negative lymph node status (61%-62%), had a tumor size of 2.1-5 cm (55%-58%), and/or pathologic stage II disease (54%-55%).
Survival and safety
At a median follow-up of 56.5 months, the median 5-year DFS rate was 83% in the capecitabine group, compared with 73% in the observation group (P = .027). Similarly, capecitabine use correlated with a significantly better rate of distant DFS (85% vs. 76%; P = .016).
Although the capecitabine group demonstrated a slight trend toward improved OS at 5 years, this finding was not statistically significant (86% vs. 81%; P = .203).
Capecitabine was generally well tolerated, with 91% of patients completing 1 year of therapy, and 75% completing therapy at the full dose.
Almost half of patients in the capecitabine group experienced hand-foot syndrome (45%), and one in four developed leukopenia (24%). Less common adverse events included hyperbilirubinemia (13%), gastrointestinal pain (7%), and elevated serum transaminases (5%). No unexpected serious adverse events occurred.
Effects on practice
Amy Tiersten, MD, of the Icahn School of Medicine at Mount Sinai in New York, suggested these findings may lead to broader use of capecitabine among patients with TNBC.
“[This is a] very exciting study showing an impressive disease-free survival benefit in the adjuvant setting for capecitabine in patients with early stage TNBC,” Dr. Tiersten said. “Presently, we only have positive data for capecitabine in patients with residual disease after neoadjuvant therapy, but this current study now suggests that this benefit could extend to all comers.”
Dr. Tiersten advised that the medical community stay tuned, since longer-term data may provide a clearer picture of survival benefit.
“It will be interesting to see if there is an impact on overall survival with further follow-up,” she said.
According to invited discussant Naamit Kurshan Gerber, MD, of New York University, the results support previous findings from the CREATE-X trial, along with meta-analyses that have shown a “preferential benefit” of capecitabine when used to treat TNBC, compared with estrogen receptor–positive disease.
Still, Dr. Gerber noted that, for most patients, the findings from the SYSUCC-001 trial are unlikely to influence clinical decision-making since most patients with TNBC receive neoadjuvant chemotherapy followed by treatment based on pathologic response. However, she also suggested that, after peer review, the findings could influence treatment for a select few.
“For the small population of patients who receive adjuvant chemotherapy for higher-stage TNBC and who would have met eligibility criteria, this approach may be considered,” Dr. Gerber said.
The study was funded by the Sun Yat-sen University Clinical Research 5010 Program. The investigators disclosed no conflicts of interest. Dr. Gerber reported a relationship with OncLive. Dr. Tiersten reported no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 507.
according to results of a phase 3 trial.
Patients who received metronomic capecitabine maintenance had significantly higher rates of 5-year DFS and distant DFS, but not OS, when compared with patients who did not receive capecitabine, reported Xi Wang, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
“TNBC has the worst outcomes among all subtypes of breast cancer,” Dr. Wang said. “Effective strategies to reduce risk of relapse are a critical clinical need.”
He went on to describe capecitabine as a “potential ideal drug for metronomic administration,” particularly among patients with high risk of distant metastasis.
With that in mind, Dr. Wang and colleagues tested metronomic capecitabine maintenance in the phase 3 SYSUCC-001 trial. The trial included 434 patients with invasive ductal carcinoma. They had undergone standard therapy, which included surgery, neoadjuvant/adjuvant chemotherapy, and radiation therapy.
Patients were randomized to receive capecitabine at 650 mg/m2 twice daily for 1 year (n = 221) or undergo observation (n = 213). The primary endpoint was DFS, while secondary endpoints included safety, distant DFS, and OS.
According to Dr. Wang, the two patient groups were “well balanced,” with similar baseline characteristics. Most patients underwent adjuvant chemotherapy (93%), had histological grade 3 tumors (71%-74%), had a Ki-67 index of at least 30% (73%-80%), had negative lymph node status (61%-62%), had a tumor size of 2.1-5 cm (55%-58%), and/or pathologic stage II disease (54%-55%).
Survival and safety
At a median follow-up of 56.5 months, the median 5-year DFS rate was 83% in the capecitabine group, compared with 73% in the observation group (P = .027). Similarly, capecitabine use correlated with a significantly better rate of distant DFS (85% vs. 76%; P = .016).
Although the capecitabine group demonstrated a slight trend toward improved OS at 5 years, this finding was not statistically significant (86% vs. 81%; P = .203).
Capecitabine was generally well tolerated, with 91% of patients completing 1 year of therapy, and 75% completing therapy at the full dose.
Almost half of patients in the capecitabine group experienced hand-foot syndrome (45%), and one in four developed leukopenia (24%). Less common adverse events included hyperbilirubinemia (13%), gastrointestinal pain (7%), and elevated serum transaminases (5%). No unexpected serious adverse events occurred.
Effects on practice
Amy Tiersten, MD, of the Icahn School of Medicine at Mount Sinai in New York, suggested these findings may lead to broader use of capecitabine among patients with TNBC.
“[This is a] very exciting study showing an impressive disease-free survival benefit in the adjuvant setting for capecitabine in patients with early stage TNBC,” Dr. Tiersten said. “Presently, we only have positive data for capecitabine in patients with residual disease after neoadjuvant therapy, but this current study now suggests that this benefit could extend to all comers.”
Dr. Tiersten advised that the medical community stay tuned, since longer-term data may provide a clearer picture of survival benefit.
“It will be interesting to see if there is an impact on overall survival with further follow-up,” she said.
According to invited discussant Naamit Kurshan Gerber, MD, of New York University, the results support previous findings from the CREATE-X trial, along with meta-analyses that have shown a “preferential benefit” of capecitabine when used to treat TNBC, compared with estrogen receptor–positive disease.
Still, Dr. Gerber noted that, for most patients, the findings from the SYSUCC-001 trial are unlikely to influence clinical decision-making since most patients with TNBC receive neoadjuvant chemotherapy followed by treatment based on pathologic response. However, she also suggested that, after peer review, the findings could influence treatment for a select few.
“For the small population of patients who receive adjuvant chemotherapy for higher-stage TNBC and who would have met eligibility criteria, this approach may be considered,” Dr. Gerber said.
The study was funded by the Sun Yat-sen University Clinical Research 5010 Program. The investigators disclosed no conflicts of interest. Dr. Gerber reported a relationship with OncLive. Dr. Tiersten reported no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 507.
according to results of a phase 3 trial.
Patients who received metronomic capecitabine maintenance had significantly higher rates of 5-year DFS and distant DFS, but not OS, when compared with patients who did not receive capecitabine, reported Xi Wang, PhD, of Sun Yat-sen University Cancer Center in Guangzhou, China, who presented the findings as part of the American Society of Clinical Oncology virtual scientific program.
“TNBC has the worst outcomes among all subtypes of breast cancer,” Dr. Wang said. “Effective strategies to reduce risk of relapse are a critical clinical need.”
He went on to describe capecitabine as a “potential ideal drug for metronomic administration,” particularly among patients with high risk of distant metastasis.
With that in mind, Dr. Wang and colleagues tested metronomic capecitabine maintenance in the phase 3 SYSUCC-001 trial. The trial included 434 patients with invasive ductal carcinoma. They had undergone standard therapy, which included surgery, neoadjuvant/adjuvant chemotherapy, and radiation therapy.
Patients were randomized to receive capecitabine at 650 mg/m2 twice daily for 1 year (n = 221) or undergo observation (n = 213). The primary endpoint was DFS, while secondary endpoints included safety, distant DFS, and OS.
According to Dr. Wang, the two patient groups were “well balanced,” with similar baseline characteristics. Most patients underwent adjuvant chemotherapy (93%), had histological grade 3 tumors (71%-74%), had a Ki-67 index of at least 30% (73%-80%), had negative lymph node status (61%-62%), had a tumor size of 2.1-5 cm (55%-58%), and/or pathologic stage II disease (54%-55%).
Survival and safety
At a median follow-up of 56.5 months, the median 5-year DFS rate was 83% in the capecitabine group, compared with 73% in the observation group (P = .027). Similarly, capecitabine use correlated with a significantly better rate of distant DFS (85% vs. 76%; P = .016).
Although the capecitabine group demonstrated a slight trend toward improved OS at 5 years, this finding was not statistically significant (86% vs. 81%; P = .203).
Capecitabine was generally well tolerated, with 91% of patients completing 1 year of therapy, and 75% completing therapy at the full dose.
Almost half of patients in the capecitabine group experienced hand-foot syndrome (45%), and one in four developed leukopenia (24%). Less common adverse events included hyperbilirubinemia (13%), gastrointestinal pain (7%), and elevated serum transaminases (5%). No unexpected serious adverse events occurred.
Effects on practice
Amy Tiersten, MD, of the Icahn School of Medicine at Mount Sinai in New York, suggested these findings may lead to broader use of capecitabine among patients with TNBC.
“[This is a] very exciting study showing an impressive disease-free survival benefit in the adjuvant setting for capecitabine in patients with early stage TNBC,” Dr. Tiersten said. “Presently, we only have positive data for capecitabine in patients with residual disease after neoadjuvant therapy, but this current study now suggests that this benefit could extend to all comers.”
Dr. Tiersten advised that the medical community stay tuned, since longer-term data may provide a clearer picture of survival benefit.
“It will be interesting to see if there is an impact on overall survival with further follow-up,” she said.
According to invited discussant Naamit Kurshan Gerber, MD, of New York University, the results support previous findings from the CREATE-X trial, along with meta-analyses that have shown a “preferential benefit” of capecitabine when used to treat TNBC, compared with estrogen receptor–positive disease.
Still, Dr. Gerber noted that, for most patients, the findings from the SYSUCC-001 trial are unlikely to influence clinical decision-making since most patients with TNBC receive neoadjuvant chemotherapy followed by treatment based on pathologic response. However, she also suggested that, after peer review, the findings could influence treatment for a select few.
“For the small population of patients who receive adjuvant chemotherapy for higher-stage TNBC and who would have met eligibility criteria, this approach may be considered,” Dr. Gerber said.
The study was funded by the Sun Yat-sen University Clinical Research 5010 Program. The investigators disclosed no conflicts of interest. Dr. Gerber reported a relationship with OncLive. Dr. Tiersten reported no relevant disclosures.
SOURCE: Wang X et al. ASCO 2020, Abstract 507.
FROM ASCO 2020
PPI added to chemo improves breast tumor response rate
The proton pump inhibitor (PPI) omeprazole may be a useful addition to treatment for triple-negative breast cancer, as it boosted the expected rate of tumor disappearance among women with early-stage disease, according to the results of a phase 2 trial.
The trial results are presented online at the 2020 virtual annual meeting of the American Society of Clinical Oncology.
The rationale behind the approach includes the fact that PPIs inhibit fatty acid synthase (FASN), an enzyme overexpressed in 70% of newly diagnosed triple-negative breast cancers (TNBC) and associated with poor prognosis.
In the study, omeprazole, a generic drug for gastroesophageal reflux, was added to standard chemotherapy. Both were given to 42 women as neoadjuvant treatment in the weeks before breast surgery at five US centers in the single-arm study.
The pathologic complete response (pCR) rate was 71% in the study population, which is higher than the typical 40% seen in patients treated with standard AC-T (adriamycin and cyclophosphamide plus a taxane), said lead author Sagar D. Sardesai, MBBS, a medical oncologist at Ohio State Comprehensive Cancer Center in Columbus.
“It’s exciting,” said Dr. Sardesai in an interview. “Overall, triple-negative patients who achieve a pCR have a very good outcome.”
That complete disappearance of the tumor is a surrogate for overall survival in TNBC, and patients who achieve it have a greatly reduced risk of recurrence or death, he explained.
Natalie Berger, MD, medical oncologist, Icahn School of Medicine at Mount Sinai, New York City, said the study’s pCR rates were “much higher” than expected and “intriguing and hypothesis generating.”
But Dr. Berger, who was not involved in the study, wanted to see more data.
“Having a non-chemotherapeutic agent to offer our patients with TNBC that improves pCR rates without added toxicity would be an exciting finding, but we need a larger randomized study,” she said in an email.
The researchers, who include high-profile breast cancer specialist Kathy Miller, MD, of Indiana University, are seeking a National Cancer Institute or Department of Defense grant to mount a 100-plus patient randomized trial.
Potential Drug Target for Some Years
Dr. Sardesai explained that FASN, which is an enzyme, helps generate fatty acids that are a key to cancer cell survival. FASN is primarily found in hormone-dominated tissue such as those of the endometrium, prostate, and breast.
PPIs “selectively inhibit FASN activity and induce apoptosis in breast cancer cell lines with minimal effect on non-malignant cells,” wrote the study authors in their meeting abstract.
The only other known agent known to inhibit FASN is the weight loss drug orlistat, which is poorly absorbed by the body and unlikely to impact cancer cells, Dr. Sardesai said.
FASN has been a potential drug target in TNBC for 10 to 15 years, but the first clinical evidence of efficacy in solid tumors was only seen in the last 5 years, he commented.
In 2015, Chinese investigators reported that the PPI esomeprazole in combination with chemotherapy produced a 5-month improvement in progression-free survival (vs. chemo alone) among a subset of 15 TNBC patients in a randomized trial of 94 patients with a variety of breast cancer types.
No Added Toxicity, But Some Unexpected Findings
The study was conducted in patients with early-stage, operable TNBC (with and without baseline FASN expression) and no prior PPI use within 12 months.
All patients started daily high-dose omeprazole 4 to 7 days prior to start of AC-T neoadjuvant chemotherapy (the addition of carboplatin was allowed per physician discretion) and continued until surgery.
The primary endpoint was pCR, defined as no residual invasive disease in breast or axilla, in patients with baseline FASN expression (FASN+). The pCR rate was 71.4% in the 28 FASN+ patients and 71.8% in all 42 enrolled patients. The researchers had targeted a pCR rate of 60% in the FASN+ patients. Also, among the subset of 15 patients who received carboplatin with AC-T, the pCR was 73%.
These two findings both have limitations, commented Dr. Berger. She pointed out that it is “unexplained” as to why the pCR rates were similar among the FASN+ patients and the total population (including 14 FASN– patients); the pCR rate would be expected to be lower in the total population, she suggested.
Further, it was also unexplained as to why there were similar pCR rates with or without carboplatin; other research has demonstrated improved pCR rates in patients receiving additional carboplatin (compared to AC-T alone) but at the cost of increased toxicity, she said.
Dr. Sardesai said that omeprazole was well tolerated with no known grade 3 or 4 toxicities and that the chemotherapy toxicity was similar to prior studies of AC-T. PPIs have side effects if taken for longer than a year, including a higher risk of infections, osteoporosis, and low magnesium, he also commented.
“Omeprazole can be safely administered in doses that inhibit FASN. The addition of high-dose omeprazole to neoadjuvant AC-T yields a promising pCR rate without adding toxicity,” the authors concluded in their abstract.
Dr. Sardesai also highlighted the fact that using a PPI for breast cancer is an example of drug repurposing. The approach offers a way of rapid drug development because PPIs have complete safety and pharmacokinetics data available, he said. “If we can prove the efficacy, the treatment can move forward quickly and be available in clinical practice much sooner than with traditional drug development.”
The study was funded by the Breast Cancer Research Foundation. Dr. Sardesai disclosed financial ties to Novartis and Immunomedics. Other study authors have ties to industry. Dr. Berger disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The proton pump inhibitor (PPI) omeprazole may be a useful addition to treatment for triple-negative breast cancer, as it boosted the expected rate of tumor disappearance among women with early-stage disease, according to the results of a phase 2 trial.
The trial results are presented online at the 2020 virtual annual meeting of the American Society of Clinical Oncology.
The rationale behind the approach includes the fact that PPIs inhibit fatty acid synthase (FASN), an enzyme overexpressed in 70% of newly diagnosed triple-negative breast cancers (TNBC) and associated with poor prognosis.
In the study, omeprazole, a generic drug for gastroesophageal reflux, was added to standard chemotherapy. Both were given to 42 women as neoadjuvant treatment in the weeks before breast surgery at five US centers in the single-arm study.
The pathologic complete response (pCR) rate was 71% in the study population, which is higher than the typical 40% seen in patients treated with standard AC-T (adriamycin and cyclophosphamide plus a taxane), said lead author Sagar D. Sardesai, MBBS, a medical oncologist at Ohio State Comprehensive Cancer Center in Columbus.
“It’s exciting,” said Dr. Sardesai in an interview. “Overall, triple-negative patients who achieve a pCR have a very good outcome.”
That complete disappearance of the tumor is a surrogate for overall survival in TNBC, and patients who achieve it have a greatly reduced risk of recurrence or death, he explained.
Natalie Berger, MD, medical oncologist, Icahn School of Medicine at Mount Sinai, New York City, said the study’s pCR rates were “much higher” than expected and “intriguing and hypothesis generating.”
But Dr. Berger, who was not involved in the study, wanted to see more data.
“Having a non-chemotherapeutic agent to offer our patients with TNBC that improves pCR rates without added toxicity would be an exciting finding, but we need a larger randomized study,” she said in an email.
The researchers, who include high-profile breast cancer specialist Kathy Miller, MD, of Indiana University, are seeking a National Cancer Institute or Department of Defense grant to mount a 100-plus patient randomized trial.
Potential Drug Target for Some Years
Dr. Sardesai explained that FASN, which is an enzyme, helps generate fatty acids that are a key to cancer cell survival. FASN is primarily found in hormone-dominated tissue such as those of the endometrium, prostate, and breast.
PPIs “selectively inhibit FASN activity and induce apoptosis in breast cancer cell lines with minimal effect on non-malignant cells,” wrote the study authors in their meeting abstract.
The only other known agent known to inhibit FASN is the weight loss drug orlistat, which is poorly absorbed by the body and unlikely to impact cancer cells, Dr. Sardesai said.
FASN has been a potential drug target in TNBC for 10 to 15 years, but the first clinical evidence of efficacy in solid tumors was only seen in the last 5 years, he commented.
In 2015, Chinese investigators reported that the PPI esomeprazole in combination with chemotherapy produced a 5-month improvement in progression-free survival (vs. chemo alone) among a subset of 15 TNBC patients in a randomized trial of 94 patients with a variety of breast cancer types.
No Added Toxicity, But Some Unexpected Findings
The study was conducted in patients with early-stage, operable TNBC (with and without baseline FASN expression) and no prior PPI use within 12 months.
All patients started daily high-dose omeprazole 4 to 7 days prior to start of AC-T neoadjuvant chemotherapy (the addition of carboplatin was allowed per physician discretion) and continued until surgery.
The primary endpoint was pCR, defined as no residual invasive disease in breast or axilla, in patients with baseline FASN expression (FASN+). The pCR rate was 71.4% in the 28 FASN+ patients and 71.8% in all 42 enrolled patients. The researchers had targeted a pCR rate of 60% in the FASN+ patients. Also, among the subset of 15 patients who received carboplatin with AC-T, the pCR was 73%.
These two findings both have limitations, commented Dr. Berger. She pointed out that it is “unexplained” as to why the pCR rates were similar among the FASN+ patients and the total population (including 14 FASN– patients); the pCR rate would be expected to be lower in the total population, she suggested.
Further, it was also unexplained as to why there were similar pCR rates with or without carboplatin; other research has demonstrated improved pCR rates in patients receiving additional carboplatin (compared to AC-T alone) but at the cost of increased toxicity, she said.
Dr. Sardesai said that omeprazole was well tolerated with no known grade 3 or 4 toxicities and that the chemotherapy toxicity was similar to prior studies of AC-T. PPIs have side effects if taken for longer than a year, including a higher risk of infections, osteoporosis, and low magnesium, he also commented.
“Omeprazole can be safely administered in doses that inhibit FASN. The addition of high-dose omeprazole to neoadjuvant AC-T yields a promising pCR rate without adding toxicity,” the authors concluded in their abstract.
Dr. Sardesai also highlighted the fact that using a PPI for breast cancer is an example of drug repurposing. The approach offers a way of rapid drug development because PPIs have complete safety and pharmacokinetics data available, he said. “If we can prove the efficacy, the treatment can move forward quickly and be available in clinical practice much sooner than with traditional drug development.”
The study was funded by the Breast Cancer Research Foundation. Dr. Sardesai disclosed financial ties to Novartis and Immunomedics. Other study authors have ties to industry. Dr. Berger disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
The proton pump inhibitor (PPI) omeprazole may be a useful addition to treatment for triple-negative breast cancer, as it boosted the expected rate of tumor disappearance among women with early-stage disease, according to the results of a phase 2 trial.
The trial results are presented online at the 2020 virtual annual meeting of the American Society of Clinical Oncology.
The rationale behind the approach includes the fact that PPIs inhibit fatty acid synthase (FASN), an enzyme overexpressed in 70% of newly diagnosed triple-negative breast cancers (TNBC) and associated with poor prognosis.
In the study, omeprazole, a generic drug for gastroesophageal reflux, was added to standard chemotherapy. Both were given to 42 women as neoadjuvant treatment in the weeks before breast surgery at five US centers in the single-arm study.
The pathologic complete response (pCR) rate was 71% in the study population, which is higher than the typical 40% seen in patients treated with standard AC-T (adriamycin and cyclophosphamide plus a taxane), said lead author Sagar D. Sardesai, MBBS, a medical oncologist at Ohio State Comprehensive Cancer Center in Columbus.
“It’s exciting,” said Dr. Sardesai in an interview. “Overall, triple-negative patients who achieve a pCR have a very good outcome.”
That complete disappearance of the tumor is a surrogate for overall survival in TNBC, and patients who achieve it have a greatly reduced risk of recurrence or death, he explained.
Natalie Berger, MD, medical oncologist, Icahn School of Medicine at Mount Sinai, New York City, said the study’s pCR rates were “much higher” than expected and “intriguing and hypothesis generating.”
But Dr. Berger, who was not involved in the study, wanted to see more data.
“Having a non-chemotherapeutic agent to offer our patients with TNBC that improves pCR rates without added toxicity would be an exciting finding, but we need a larger randomized study,” she said in an email.
The researchers, who include high-profile breast cancer specialist Kathy Miller, MD, of Indiana University, are seeking a National Cancer Institute or Department of Defense grant to mount a 100-plus patient randomized trial.
Potential Drug Target for Some Years
Dr. Sardesai explained that FASN, which is an enzyme, helps generate fatty acids that are a key to cancer cell survival. FASN is primarily found in hormone-dominated tissue such as those of the endometrium, prostate, and breast.
PPIs “selectively inhibit FASN activity and induce apoptosis in breast cancer cell lines with minimal effect on non-malignant cells,” wrote the study authors in their meeting abstract.
The only other known agent known to inhibit FASN is the weight loss drug orlistat, which is poorly absorbed by the body and unlikely to impact cancer cells, Dr. Sardesai said.
FASN has been a potential drug target in TNBC for 10 to 15 years, but the first clinical evidence of efficacy in solid tumors was only seen in the last 5 years, he commented.
In 2015, Chinese investigators reported that the PPI esomeprazole in combination with chemotherapy produced a 5-month improvement in progression-free survival (vs. chemo alone) among a subset of 15 TNBC patients in a randomized trial of 94 patients with a variety of breast cancer types.
No Added Toxicity, But Some Unexpected Findings
The study was conducted in patients with early-stage, operable TNBC (with and without baseline FASN expression) and no prior PPI use within 12 months.
All patients started daily high-dose omeprazole 4 to 7 days prior to start of AC-T neoadjuvant chemotherapy (the addition of carboplatin was allowed per physician discretion) and continued until surgery.
The primary endpoint was pCR, defined as no residual invasive disease in breast or axilla, in patients with baseline FASN expression (FASN+). The pCR rate was 71.4% in the 28 FASN+ patients and 71.8% in all 42 enrolled patients. The researchers had targeted a pCR rate of 60% in the FASN+ patients. Also, among the subset of 15 patients who received carboplatin with AC-T, the pCR was 73%.
These two findings both have limitations, commented Dr. Berger. She pointed out that it is “unexplained” as to why the pCR rates were similar among the FASN+ patients and the total population (including 14 FASN– patients); the pCR rate would be expected to be lower in the total population, she suggested.
Further, it was also unexplained as to why there were similar pCR rates with or without carboplatin; other research has demonstrated improved pCR rates in patients receiving additional carboplatin (compared to AC-T alone) but at the cost of increased toxicity, she said.
Dr. Sardesai said that omeprazole was well tolerated with no known grade 3 or 4 toxicities and that the chemotherapy toxicity was similar to prior studies of AC-T. PPIs have side effects if taken for longer than a year, including a higher risk of infections, osteoporosis, and low magnesium, he also commented.
“Omeprazole can be safely administered in doses that inhibit FASN. The addition of high-dose omeprazole to neoadjuvant AC-T yields a promising pCR rate without adding toxicity,” the authors concluded in their abstract.
Dr. Sardesai also highlighted the fact that using a PPI for breast cancer is an example of drug repurposing. The approach offers a way of rapid drug development because PPIs have complete safety and pharmacokinetics data available, he said. “If we can prove the efficacy, the treatment can move forward quickly and be available in clinical practice much sooner than with traditional drug development.”
The study was funded by the Breast Cancer Research Foundation. Dr. Sardesai disclosed financial ties to Novartis and Immunomedics. Other study authors have ties to industry. Dr. Berger disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
FROM ASCO 2020
Pembrolizumab plus chemo shows benefits for PD-L1–rich triple-negative breast cancer
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
Adding pembrolizumab to standard chemotherapy significantly improved progression-free survival for patients with metastatic triple-negative breast cancer, but only if their tumors were enriched with comparatively high levels of the target programmed death ligand-1 (PD-L1), results of the KEYNOTE 355 trial showed.
Among 843 patients with triple-negative breast cancer (TNBC) randomized to receive either investigator’s choice of chemotherapy plus pembrolizumab (Keytruda) or placebo, patients whose tumors had a PD-L1 combined positive score (CPS) of 10 or higher had a median progression-free survival (PFS) of 9.7 months when treated with pembrolizumab and chemotherapy, compared with 5.6 months among patients treated with chemotherapy and placebo, reported Javier Cortes, MD, PhD, from the Vall d´Hebron Institute of Oncology in Madrid and Barcelona.
However, among patients with CPS between 1 and 10, there was no significant difference in PFS between the treatment arms, he said in a presentation made as a part of the 2020 American Society of Clinical Oncology virtual scientific program.
“The inclusion of taxanes and a known taxane/platinum–based regimen permits assessment of the clinical benefit of pembro in combination with several routinely used chemo partners. A trend toward improved efficacy with PD-L1 enrichment was observed in patients treated with pembro plus chemo. The improvement in progression-free survival with chemotherapy and pembrolizumab was observed across patient subgroups,” said Dr. Cortes.
In the KEYNOTE-522 study, adding pembrolizumab to chemotherapy in the neoadjuvant setting increased the likelihood that women with stage III or early node-positive TNBC would have a pathologic complete response and sustained clinical benefit.
KEYNOTE-355 examined whether pembrolizumab in combination with chemotherapy could provide additional benefit over chemotherapy alone in patients with previously untreated locally recurrent inoperable or metastatic TNBC.
Patients with previously untreated metastatic triple-negative breast cancer who had at least 6 months between definite surgery or last dose of adjuvant chemotherapy (whichever came last) and first disease recurrence were stratified by study chemotherapy received, tumor PD-L1 expression at baseline, and prior treatment with the same class of chemotherapy in the neoadjuvant and/or adjuvant setting.
The patients were then randomized in a 2:1 ratio to pembrolizumab plus chemotherapy based on the investigator’s choice of nab-paclitaxel, paclitaxel, or carboplatin-gemcitabine (562 patients) or to chemotherapy alone (281).
Pembrolizumab and placebo were administered in a double-blind fashion for up to 35 doses. Chemotherapy was given at the investigator’s discretion according to local guidelines. This trial was not powered or designed to compare differential efficacy of the various chemotherapy regimens, Dr. Cortes noted.
The trial had dual primary endpoints of PFS in patients with PD-L1–positive tumors (CPS > 10 and > 1) and in the intention-to-treat population, and overall survival both in PD-L1-positive patients and the ITT population. Overall survival results will be reported at a later date.
As noted before, the primary endpoint was met in the population of patients with CPS higher than 10, with median PFS of 9.7 among those receiving pembrolizumab versus 5.6 months among those receiving placebo, and an estimated 1 year PFS of 39.1% versus 23% for controls, translating into a hazard ratio for progression on pembrolizumab of 0.65 (P = .0012).
In the patients with CPS higher than 1, however, the median PFS was 7.6 months with pembrolizumab compared with 5.6 months with placebo, translating into a hazard ratio of 0.74. However, the results did not meet the prespecified boundary for significance. Because of this, the statistical significance in the ITT population was not tested.
“In patients with PD-L1 CPS 10 or higher tumors, the benefit of pembro/chemo on progression-free survival was generally consistent across most predefined subgroups, including eight geographic regions, ECOG performance status, on-study chemo, and prior treatment with the same class of chemo,” Dr. Cortes said.
Treatment-related adverse events occurred in 96.3% of the patients on pembrolizumab and 95% of patients on placebo. Grade 3 or greater adverse events occurred in 68.1% versus 66.9%, respectively. Two patients in the pembrolizumab arm died from a treatment-related event. There were no treatment-related deaths in the placebo arm.
The most common events were those typically associated with chemotherapy, including anemia, neutropenia, nausea, alopecia, fatigue, decreased neutrophil counts, and elevated liver transaminases. Immune-mediated adverse events of any grade occurred in 25.6% of patients in the pembrolizumab arm versus 6% of controls; none of these events were fatal.
“What is clear in this study is that again we’re seeing efficacy of pembrolizumab in combination with chemotherapy increases with increases in CPS,” according to the invited discussant Catherine M. Kelly, MB, BCh, from University College Dublin and Mater Misericordiae University Hospital in Dublin.
“The results from today’s KEYNOTE-355 appear consistent in terms of progression-free survival. However, it is ‘watch this space’ until we get overall survival data before we can make any further comparisons,” she added.
Questions that still need to be answered include which is the best test for measuring PD-L1, whether patients with CPS of 1 or more but less than 10 benefit from the treatment, which of the available chemotherapy regimens is the best partner for pembrolizumab, how to treat patients who don’t respond to the combination, and what are the implications for PD-1/PD-L1 inhibitors in late-stage disease if they are approved in the neoadjuvant or adjuvant setting, Dr. Kelly said.
The study was funded by Merck. Dr. Cortes disclosed honoraria from, a consulting/advisory role for, and institutional research funding from Merck and others. Dr. Kelly disclosed honoraria from MSD Oncology and others, and travel expenses from Pfizer and Roche.
SOURCE: Cortes J et al. ASCO 2020, Abstract 1000.
FROM ASCO 2020
Active cancer increases death risk in patients with COVID-19
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.

Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.
Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
Patients with COVID-19 and progressing cancer had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients who were in remission or had no evidence of cancer, according to data from the COVID-19 and Cancer Consortium (CCC19) registry.
Other independent risk factors for death in patients with COVID-19 and cancer were older age, male sex, former smoking, number of comorbidities, Eastern Cooperative Oncology Group (ECOG) performance status of 2 or greater, and treatment with hydroxychloroquine plus azithromycin.
In fact, patients who received hydroxychloroquine and azithromycin had a nearly threefold higher risk of death than did patients who had not received the combination. However, this finding was of “uncertain validity due to a high risk of residual confounding; for example, patients receiving this combination were more likely to have severe disease or more likely to be hospitalized,” said Jeremy L. Warner, MD, of Vanderbilt University Medical Center in Nashville, Tennessee.
Dr. Warner presented these findings in an online press briefing. Additional findings from the CCC19 registry are set to be presented as part of the American Society of Clinical Oncology (ASCO) virtual scientific program. The findings were also published in The Lancet.
‘Severe impact’ in cancer patients
“For people with cancer, the impact of COVID-19 is especially severe, whether they have been exposed to the virus or not. Patients with cancer are typically older adults, often with other underlying conditions, and their immune systems may be suppressed by the cancer, or due to chemotherapy, radiation, or other treatment,” commented ASCO President Howard A. Burris III, MD, who moderated the press briefing but was not involved in the study of CCC19 registry data.
“ASCO members tell us that they have had to delay or modify treatment plans to reduce patients’ risk of infection, and we’re unclear what the impact of these changes will be. Delays in cancer screening and diagnosis are also a major concern,” Dr. Burris continued.
“This does confirm reports that have come out from other centers, including other parts of the world, where they have found that people who have cancer and COVID-19 have a worse outcome,” said Andrew T. Chan, MD, MPH, of Massachusetts General Hospital in Boston, who was not involved in the research.
Dr. Chan’s group has developed a COVID-19 symptom study app with the aim of defining whether people living with cancer are at increased risk for infections, in addition to whether cancer is an independent risk factor for COVID-19 severity or mortality.
“Using data from our app, we were able to show that people who reported living with cancer did have a higher risk of developing COVID and were more likely to be hospitalized related to COVID,” Dr. Chan said in an interview.
Study details
The CCC19 registry collects information from 104 participating institutions in the United States and Canada, as well as anonymous data from individuals in the United States, Argentina, Canada, the European Union, and the United Kingdom.
The sample of 928 patients Dr. Warner presented was evenly balanced by sex. The median age was 66 years, and 30% of patients were aged 75 years or older.
In all, 39% of patients were on active anticancer therapy, and 43% had measurable disease. Breast cancer was the most common diagnosis, followed by prostate cancer, gastrointestinal cancers, lymphomas, and thoracic cancers.
Two-thirds of the patients (68%) had an ECOG performance status of 0 or 1, 8% had a performance status of 2, and 5% a status of 3 or 4. The remaining patients had unknown performance status.
Slightly more than half of patients (52%) were never smokers, 37% were former smokers, and 5% were current smokers. The remaining 6% of patients had unknown smoking status.
At a median follow-up of 21 days, 121 patients (13%) had died. All deaths occurred within 30 days of COVID-19 diagnosis. Among patients who died, 78 were male, 64 were former smokers, 70 were aged 75 years or older, 41 had active stable or responding cancer, 25 had progressing cancer, and 42 had an ECOG performance status of 2 or higher.
In all, 466 patients were hospitalized, and 106 in this group (23%) died. Among the 132 patients admitted to an ICU, 50 (38%) died, including 27 patients aged 75 years or older, and 15 with an ECOG performance status of 2 or greater. Of the 116 patients who required intubation, 50 (43%) died, including 26 who were 75 years or older, and 11 who had a performance status of 2 or greater.
It’s early days yet, and a larger sample size with longer follow-up will be needed to get a more complete picture of how COVID-19 affects specific patient subsets over time, Dr. Warner said.
ASCO has established its own COVID-19 registry to collect both near-term and longitudinal data during the pandemic.
“We’ll be able to learn about both how the pandemic has impacted delivery of cancer care, as well as the longer-term effects of COVID-19 on cancer patients and understand what care approaches are working best,” said Richard L. Schilsky, MD, chief medical officer and executive vice president of ASCO, during the briefing.
The study of CCC19 registry data was supported in part by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed stock/ownership in HemOnc.org, consulting for IBM and Westat, and travel expenses from IBM. Dr. Burris, Dr. Schilsky, and Dr. Chan reported no disclosures relevant to the study.
SOURCE: Warner J L et al. ASCO 2020, Abstract LBA110.
FROM ASCO 2020
Key clinical point: Patients with progressing cancer and COVID-19 are at an especially high risk of 30-day mortality.
Major finding: Patients with COVID-19 whose cancers were progressing had a fivefold increase in the risk of 30-day mortality, compared with COVID-19–positive cancer patients in remission or with no evidence of cancer.
Study details: Analysis of data on 928 patients enrolled in the COVID-19 and Cancer Consortium (CCC19) registry.
Disclosures: The research was supported, in part, by the National Institutes of Health and the American Cancer Society. Dr. Warner disclosed relationships with HemOnc.org, IBM, and Westat.
Source: Warner J L et al. ASCO 2020, Abstract LBA110.

LOTUS: Ipatasertib plus paclitaxel may prolong OS in TNBC
according to final results of the phase 2 LOTUS trial.
The median OS was 25.8 months in patients who received ipatasertib plus paclitaxel and 16.9 months in patients who received paclitaxel plus placebo. Although this difference was not statistically significant, it was “clinically meaningful,” according to Rebecca Dent, MD, of the National Cancer Center Singapore. Dr. Dent presented OS data from the LOTUS trial at the European Society of Medical Oncology: Breast Cancer virtual meeting.
Previously reported data showed a progression-free survival benefit in the ipatasertib arm, compared with the placebo arm – 6.2 months and 4.9 months, respectively (Lancet Oncol. 2017 Oct;18[10]:1360-72). An enhanced effect was noted in patients with PIK3CA/AKT1/PTEN–altered tumors, but the OS data were not mature at the time of that primary analysis.
Patients, treatment, and safety
LOTUS participants had measurable locally advanced/metastatic TNBC that was previously untreated with systemic therapy, and they were stratified by prior adjuvant therapy, chemotherapy-free interval, and tumor immunohistochemistry PTEN status.
Patients were randomized 1:1 to receive paclitaxel at a dose of 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle plus either placebo (n = 62) or ipatasertib at a dose of 400 mg on days 1-21 (n = 62).
The safety results didn’t differ between the primary and updated results, Dr. Dent noted.
“What we can say is that the combination is extremely well tolerated, especially when we compare it to other targeted agents targeting this pathway,” she said. “What we do see is noticeable diarrhea ... [and] an increase in sensory neuropathy, which is not entirely unexpected.”
Subsequent systemic anticancer therapy was required in 77% of patients in the ipatasertib arm and 90% of patients in the placebo arm.
OS results
The final OS data show a numerical advantage for patients in the ipatasertib arm compared with the placebo arm. The 1-year OS was 83% in the ipatasertib arm and 68% in the placebo arm. The median OS was 25.8 months and 16.9 months, respectively (stratified hazard ratio, 0.80).
“This is a clinically meaningful improvement of 9 months in overall survival, which is indeed not too dissimilar to what we have seen in patients with PD-L1-positive TNBC who are receiving immune checkpoint inhibition in combination with chemotherapy,” Dr. Dent said.
However, the 95% confidence interval for the stratified OS hazard ratio crossed 1 (0.50-1.28). Therefore, the findings require confirmatory phase 3 trial results, Dr. Dent said.
The OS improvements with ipatasertib were seen “in all biomarker-defined subgroups – PTEN normal or low, PIK3CA/AKT1/PTEN altered or non-altered,” she said. OS benefits were more pronounced in patients with altered PIK3C/AKT1/PTEN status, but the numbers are too small to make definitive conclusions, according to Dr. Dent.
‘Promising’ results, confirmation needed
Invited discussant Suzette Delaloge, MD, head of the breast cancer department at Gustave Roussy, Paris, said the OS findings from LOTUS are “quite promising,” and the safety data are “reassuring.”
The findings are comparable to those of the recently published PAKT trial (J Clin Oncol. 2020 Feb 10;38[5]:423-33), she said, noting that “AKT inhibition in combination with paclitaxel deserves phase 3 development, and this is ongoing in major phase 3 trials.”
Dr. Delaloge also noted that the efficacy may not be limited to PIK3CA/AKT–altered tumors, and given the heterogeneity of TNBC – which may explain the differences seen among various studies – “it is very important that such phase 3 trials ideally involve extensive genomical definitions of tumors so that we understand what it is we are talking about and what is the real effect of the drug.”
“The adequate positioning of AKT inhibition in competition/complementation with other ongoing strategies remains to be defined,” she said. “I think these drugs are ready for translation to early phases.”
Dr. Dent said the results of LOTUS warrant confirmation in the ongoing, randomized phase 3 IPATunity130 trial , in which researchers are evaluating first-line ipatasertib plus paclitaxel for metastatic TNBC. She noted that the small sample sizes and heterogeneity of TNBC among LOTUS participants limited the interpretation of the findings.
In another trial, IPATunity170, researchers are evaluating the first-line role of ipatasertib plus paclitaxel and atezolizumab in locally advanced or metastatic TNBC.
“This is an exciting triplet combination that’s been evaluated already in the phase 1 setting, and now we have a phase 3 study evaluating the triplet,” Dr. Dent said.
The LOTUS trial was funded by Roche/Genentech. Dr. Dent reported receiving honoraria from Roche, Novartis, Lilly, Pfizer, Eisai, Merck, and AstraZeneca. Dr. Delaloge reported personal financial interests in AstraZeneca until 2018 and travel and accommodation support from AstraZeneca, Pfizer, Roche, and Pierre Fabre.
SOURCE: Dent R et al. ESMO Breast Cancer 2020, Abstract 139O
according to final results of the phase 2 LOTUS trial.
The median OS was 25.8 months in patients who received ipatasertib plus paclitaxel and 16.9 months in patients who received paclitaxel plus placebo. Although this difference was not statistically significant, it was “clinically meaningful,” according to Rebecca Dent, MD, of the National Cancer Center Singapore. Dr. Dent presented OS data from the LOTUS trial at the European Society of Medical Oncology: Breast Cancer virtual meeting.
Previously reported data showed a progression-free survival benefit in the ipatasertib arm, compared with the placebo arm – 6.2 months and 4.9 months, respectively (Lancet Oncol. 2017 Oct;18[10]:1360-72). An enhanced effect was noted in patients with PIK3CA/AKT1/PTEN–altered tumors, but the OS data were not mature at the time of that primary analysis.
Patients, treatment, and safety
LOTUS participants had measurable locally advanced/metastatic TNBC that was previously untreated with systemic therapy, and they were stratified by prior adjuvant therapy, chemotherapy-free interval, and tumor immunohistochemistry PTEN status.
Patients were randomized 1:1 to receive paclitaxel at a dose of 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle plus either placebo (n = 62) or ipatasertib at a dose of 400 mg on days 1-21 (n = 62).
The safety results didn’t differ between the primary and updated results, Dr. Dent noted.
“What we can say is that the combination is extremely well tolerated, especially when we compare it to other targeted agents targeting this pathway,” she said. “What we do see is noticeable diarrhea ... [and] an increase in sensory neuropathy, which is not entirely unexpected.”
Subsequent systemic anticancer therapy was required in 77% of patients in the ipatasertib arm and 90% of patients in the placebo arm.
OS results
The final OS data show a numerical advantage for patients in the ipatasertib arm compared with the placebo arm. The 1-year OS was 83% in the ipatasertib arm and 68% in the placebo arm. The median OS was 25.8 months and 16.9 months, respectively (stratified hazard ratio, 0.80).
“This is a clinically meaningful improvement of 9 months in overall survival, which is indeed not too dissimilar to what we have seen in patients with PD-L1-positive TNBC who are receiving immune checkpoint inhibition in combination with chemotherapy,” Dr. Dent said.
However, the 95% confidence interval for the stratified OS hazard ratio crossed 1 (0.50-1.28). Therefore, the findings require confirmatory phase 3 trial results, Dr. Dent said.
The OS improvements with ipatasertib were seen “in all biomarker-defined subgroups – PTEN normal or low, PIK3CA/AKT1/PTEN altered or non-altered,” she said. OS benefits were more pronounced in patients with altered PIK3C/AKT1/PTEN status, but the numbers are too small to make definitive conclusions, according to Dr. Dent.
‘Promising’ results, confirmation needed
Invited discussant Suzette Delaloge, MD, head of the breast cancer department at Gustave Roussy, Paris, said the OS findings from LOTUS are “quite promising,” and the safety data are “reassuring.”
The findings are comparable to those of the recently published PAKT trial (J Clin Oncol. 2020 Feb 10;38[5]:423-33), she said, noting that “AKT inhibition in combination with paclitaxel deserves phase 3 development, and this is ongoing in major phase 3 trials.”
Dr. Delaloge also noted that the efficacy may not be limited to PIK3CA/AKT–altered tumors, and given the heterogeneity of TNBC – which may explain the differences seen among various studies – “it is very important that such phase 3 trials ideally involve extensive genomical definitions of tumors so that we understand what it is we are talking about and what is the real effect of the drug.”
“The adequate positioning of AKT inhibition in competition/complementation with other ongoing strategies remains to be defined,” she said. “I think these drugs are ready for translation to early phases.”
Dr. Dent said the results of LOTUS warrant confirmation in the ongoing, randomized phase 3 IPATunity130 trial , in which researchers are evaluating first-line ipatasertib plus paclitaxel for metastatic TNBC. She noted that the small sample sizes and heterogeneity of TNBC among LOTUS participants limited the interpretation of the findings.
In another trial, IPATunity170, researchers are evaluating the first-line role of ipatasertib plus paclitaxel and atezolizumab in locally advanced or metastatic TNBC.
“This is an exciting triplet combination that’s been evaluated already in the phase 1 setting, and now we have a phase 3 study evaluating the triplet,” Dr. Dent said.
The LOTUS trial was funded by Roche/Genentech. Dr. Dent reported receiving honoraria from Roche, Novartis, Lilly, Pfizer, Eisai, Merck, and AstraZeneca. Dr. Delaloge reported personal financial interests in AstraZeneca until 2018 and travel and accommodation support from AstraZeneca, Pfizer, Roche, and Pierre Fabre.
SOURCE: Dent R et al. ESMO Breast Cancer 2020, Abstract 139O
according to final results of the phase 2 LOTUS trial.
The median OS was 25.8 months in patients who received ipatasertib plus paclitaxel and 16.9 months in patients who received paclitaxel plus placebo. Although this difference was not statistically significant, it was “clinically meaningful,” according to Rebecca Dent, MD, of the National Cancer Center Singapore. Dr. Dent presented OS data from the LOTUS trial at the European Society of Medical Oncology: Breast Cancer virtual meeting.
Previously reported data showed a progression-free survival benefit in the ipatasertib arm, compared with the placebo arm – 6.2 months and 4.9 months, respectively (Lancet Oncol. 2017 Oct;18[10]:1360-72). An enhanced effect was noted in patients with PIK3CA/AKT1/PTEN–altered tumors, but the OS data were not mature at the time of that primary analysis.
Patients, treatment, and safety
LOTUS participants had measurable locally advanced/metastatic TNBC that was previously untreated with systemic therapy, and they were stratified by prior adjuvant therapy, chemotherapy-free interval, and tumor immunohistochemistry PTEN status.
Patients were randomized 1:1 to receive paclitaxel at a dose of 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle plus either placebo (n = 62) or ipatasertib at a dose of 400 mg on days 1-21 (n = 62).
The safety results didn’t differ between the primary and updated results, Dr. Dent noted.
“What we can say is that the combination is extremely well tolerated, especially when we compare it to other targeted agents targeting this pathway,” she said. “What we do see is noticeable diarrhea ... [and] an increase in sensory neuropathy, which is not entirely unexpected.”
Subsequent systemic anticancer therapy was required in 77% of patients in the ipatasertib arm and 90% of patients in the placebo arm.
OS results
The final OS data show a numerical advantage for patients in the ipatasertib arm compared with the placebo arm. The 1-year OS was 83% in the ipatasertib arm and 68% in the placebo arm. The median OS was 25.8 months and 16.9 months, respectively (stratified hazard ratio, 0.80).
“This is a clinically meaningful improvement of 9 months in overall survival, which is indeed not too dissimilar to what we have seen in patients with PD-L1-positive TNBC who are receiving immune checkpoint inhibition in combination with chemotherapy,” Dr. Dent said.
However, the 95% confidence interval for the stratified OS hazard ratio crossed 1 (0.50-1.28). Therefore, the findings require confirmatory phase 3 trial results, Dr. Dent said.
The OS improvements with ipatasertib were seen “in all biomarker-defined subgroups – PTEN normal or low, PIK3CA/AKT1/PTEN altered or non-altered,” she said. OS benefits were more pronounced in patients with altered PIK3C/AKT1/PTEN status, but the numbers are too small to make definitive conclusions, according to Dr. Dent.
‘Promising’ results, confirmation needed
Invited discussant Suzette Delaloge, MD, head of the breast cancer department at Gustave Roussy, Paris, said the OS findings from LOTUS are “quite promising,” and the safety data are “reassuring.”
The findings are comparable to those of the recently published PAKT trial (J Clin Oncol. 2020 Feb 10;38[5]:423-33), she said, noting that “AKT inhibition in combination with paclitaxel deserves phase 3 development, and this is ongoing in major phase 3 trials.”
Dr. Delaloge also noted that the efficacy may not be limited to PIK3CA/AKT–altered tumors, and given the heterogeneity of TNBC – which may explain the differences seen among various studies – “it is very important that such phase 3 trials ideally involve extensive genomical definitions of tumors so that we understand what it is we are talking about and what is the real effect of the drug.”
“The adequate positioning of AKT inhibition in competition/complementation with other ongoing strategies remains to be defined,” she said. “I think these drugs are ready for translation to early phases.”
Dr. Dent said the results of LOTUS warrant confirmation in the ongoing, randomized phase 3 IPATunity130 trial , in which researchers are evaluating first-line ipatasertib plus paclitaxel for metastatic TNBC. She noted that the small sample sizes and heterogeneity of TNBC among LOTUS participants limited the interpretation of the findings.
In another trial, IPATunity170, researchers are evaluating the first-line role of ipatasertib plus paclitaxel and atezolizumab in locally advanced or metastatic TNBC.
“This is an exciting triplet combination that’s been evaluated already in the phase 1 setting, and now we have a phase 3 study evaluating the triplet,” Dr. Dent said.
The LOTUS trial was funded by Roche/Genentech. Dr. Dent reported receiving honoraria from Roche, Novartis, Lilly, Pfizer, Eisai, Merck, and AstraZeneca. Dr. Delaloge reported personal financial interests in AstraZeneca until 2018 and travel and accommodation support from AstraZeneca, Pfizer, Roche, and Pierre Fabre.
SOURCE: Dent R et al. ESMO Breast Cancer 2020, Abstract 139O
FROM ESMO BREAST CANCER 2020
Patient-focused precautions, testing help blunt pandemic effects on heme-onc unit
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.

That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.
That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Keeping hematologic oncology patients on their treatment regimens and caring for inpatients with hematologic malignancies remained “manageable” during the first 2 months of the COVID-19 pandemic at Levine Cancer Institute in Charlotte, N.C.
That level of manageability has partly been because a surge in cases so far hasn’t arrived at Levine or in most of the surrounding North Carolina and South Carolina communities it serves. As of May 15, 2020, the total number of confirmed and reported COVID-19 cases had reached about 19,000 in North Carolina, and just under 9,000 in South Carolina, out of a total population in the two states of close to 16 million. What’s happened instead at Levine Cancer Institute (LCI) has been a steady but low drumbeat of cases that, by mid-May 2020, totaled fewer than 10 patients with hematologic malignancies diagnosed with COVID-19.
“For a large system with multiple sites throughout North and South Carolina that saw 17,200 new patients in 2019 – including solid tumor, benign hematology, and malignant hematology patients – with 198,000 total patient visits, it is safe to say that we are off to a good start. However, we remain in the early throes of the pandemic and we will need to remain vigilant going forward,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in LCI’s Department of Hematologic Oncology and Blood Disorders.
The limited effects to date of COVID-19 at LCI has been thanks to a regimen of great caution for preventing infections that’s been consistently conveyed to LCI patients from before the pandemic’s onset, liberal testing that started early, a proactive plan to defer and temporarily replace infusion care when medically appropriate, a novel staffing approach designed to minimize and contain potential staff outbreaks, and an early pivot to virtual patient contact when feasible.
COVID-19 has had limited penetration into the LCI case load because patients have, in general, “been very careful,” said Dr. Voorhees.
“My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious even before the coronavirus using distancing, masking, and meticulous hand hygiene,” he said in an interview that reviewed the steps LCI took starting in March to confront and manage the effects of the then-nascent pandemic. “Since we started screening asymptomatic patients in the inpatient and outpatient settings we have identified only one patient with COVID-19 infection, which supports the low rate of infection in our patient population thus far.”
Another key step was the launch of “robust” testing for the COVID-19 virus starting on March 9, using an in-house assay from LCI’s parent health system, Atrium Health, that delivered results within 24 hours. Testing became available at LCI “earlier than at many other health systems.” At first, testing was limited to patients or staff presenting with symptoms, but in the following weeks, it expanded to more patients, including those without symptoms who were scheduled for treatment at the apheresis center, cell donors and cell recipients, patients arriving for inpatient chemotherapy or cellular therapy, patients arriving from a skilled nursing facility or similar environments, and more recently, outpatient chemotherapy patients. “We’re now doing a lot of screening,” Dr. Voorhees said. “In general, screening has been well received because patients recognize that it’s for their own safety.”
Another piece of COVID-19 preparedness was a move toward technology as an alternative to face-to-face encounters between patients and staff. “We adopted virtual technology early.” When medically appropriate, they provided either video consultations with more tech-savvy patients or telephone-based virtual visits for patients who preferred a more familiar interface. As LCI starts the process of reentry for patients whose face-to-face encounters were deferred, virtual visits will remain an important facet of maintaining care while limiting exposure for appropriate patients and facilitating adequate space for social distancing in the clinics and infusion centers.
Atrium Health also launched a “virtual hospital” geared to intensified remote management of COVID-19 patients who aren’t sick enough for hospitalization. “People who test positive automatically enter the virtual hospital and have regular interactions with their team of providers,” with LCI providing additional support for their patients who get infected. Patients receive an equipment kit that lets them monitor and transmit their vital signs. The virtual hospital program also helps expedite personal needs like delivery of prescriptions and food. “It helps patients manage at home, and has been incredibly useful,” said Dr. Voorhees.
Perhaps the most challenging step LCI clinicians took to preclude a potential COVID-19 case surge was to review all patients receiving infusional therapy or planned cellular therapy and triage those who could potentially tolerate a temporary change to either an oral, at-home regimen or to a brief hold on their treatment. Some patients on maintenance, outpatient infusion-therapy regimens “expressed concern about coming to the clinic. We looked at the patients scheduled to come for infusions and decided which visits were essential and which were deferrable without disrupting care by briefly using a noninfusional approach,” said Dr. Voorhees. The number of patients who had their regimens modified or held was “relatively small,” and with the recent recognition that a surge of infections has not occurred, “we’re now rolling out cautious reentry of those patients back to their originally prescribed chemotherapy.”
In addition to concerns of exposure at infusion clinics, there are concerns about the heightened susceptibility of immunosuppressed hematologic oncology patients to COVID-19 and their risk for more severe infection. “Our view is that, if patients tested positive, continuing immunosuppressive treatment would likely be detrimental,” so when possible treatment is temporarily suspended and then resumed when the infection has cleared. “When patients test positive for a prolonged period, a decision to resume treatment must be in the best interests of the patient and weigh the benefits of resuming therapy against the risks of incurring a more severe infection by restarting potentially immunosuppressive therapy,” Dr. Voorhees said.
The enhanced risk that cancer patients face if they develop COVID-19 was documented in a recent review of 218 cancer patients hospitalized for COVID-19 during parts of March and April in a large New York health system. The results showed an overall mortality rate of 28%, including a 37% rate among 54 patients with hematologic malignancies and a 25% rate among 164 patients with solid tumors. The mortality rate “may not be quite as high as they reported because that depends on how many patients you test, but there is no question that patients with more comorbidities are at higher risk. Patients with active cancer on chemotherapy are a particularly vulnerable population, and many have expressed concerns about their vulnerability,” he observed.
For the few LCI patients who developed COVID-19 infection, the medical staff has had several therapeutic options they could match to each patient’s needs, with help from the Atrium Health infectious disease team. LCI and Atrium Health are participating in several COVID-19 clinical treatment trials, including an investigational convalescent plasma protocol spearheaded by the Mayo Clinic. They have also opened a randomized, phase 2 trial evaluating the safety and efficacy of selinexor (Xpovio), an oral drug that’s Food and Drug Administration approved for patients with multiple myeloma, for treatment of moderate or severe COVID-19 infection. Additional studies evaluating blockade of granulocyte-macrophage colony-stimulating factor, as well as inhaled antiviral therapy, have recently launched, and several additional studies are poised to open in the coming weeks.
The LCI and Atrium Health team also has a supply of the antiviral agent remdesivir as part of the FDA’s expanded access protocol and emergency use authorization. They also have a supply of and experience administering the interleukin-6 receptor inhibitor tocilizumab (Actemra), which showed some suggestion of efficacy in limited experience treating patients with severe or critical COVID-19 infections. Clinicians at LCI have not used the investigational and unproven agents hydroxychloroquine, chloroquine, and azithromycin to either prevent or treat COVID-19.
LCI also instituted measures to try to minimize the risk that staff members could become infected and transmit the virus while asymptomatic. Following conversations held early on with COVID-19–experienced health authorities in China and Italy, the patient-facing LCI staff split into two teams starting on March 23 that alternated responsibility for direct patient interactions every 2 weeks. When one of these teams was off from direct patient contact they continued to care for patients remotely through virtual technologies. The concept was that, if a staffer became infected while remaining asymptomatic during their contact with patients, their status would either become diagnosable or resolve during their 2 weeks away from seeing any patients. Perhaps in part because of this approach infections among staff members “have not been a big issue. We’ve had an incredibly low infection rate among the LCI staff,” Dr. Voorhees noted.
By mid-May, with the imminent threat of a sudden CODIV-19 surge moderated, heme-onc operations at LCI began to cautiously revert to more normal operations. “We’re continuing patient screening for signs and symptoms of COVID-19 infection, testing for asymptomatic infections, and requiring masking and social distancing in the clinics and hospitals, but we’re starting to slowly restore the number of patients at our clinics [virtual and face to face[ and infusion centers,” and the staff’s division into two teams ended. “The idea was to get past a surge and make sure our system was not overwhelmed. We anticipated a local surge in late April, but then it kept getting pushed back. Current projections are for the infection rate among LCI patients to remain low provided that community spread remains stable or, ideally, decreases.” The LCI infectious disease staff is closely monitoring infection rates for early recognition of an outbreak, with plans to follow any new cases with contact tracing. So far, the COVID-19 pandemic at LCI “has been very manageable,” Dr. Voorhees concluded.
“We’re now better positioned to deal with a case surge if it were to happen. We could resume the two-team approach, hospital-wide plans are now in place for a future surge, and we are now up and running with robust testing and inpatient and outpatient virtual technology. The first time, we were all learning on the fly.”
The LCI biostatistics team has been prospectively collecting the Institutes’s COVID-19 patient data, with plans to report their findings.
Dr. Voorhees has had financial relationships with Bristol-Myers Squibb/Celgene, Janssen, Novartis, and Oncopeptides, none of which are relevant to this article.
Neurologists’ pay gets a boost, most happy with career choice
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
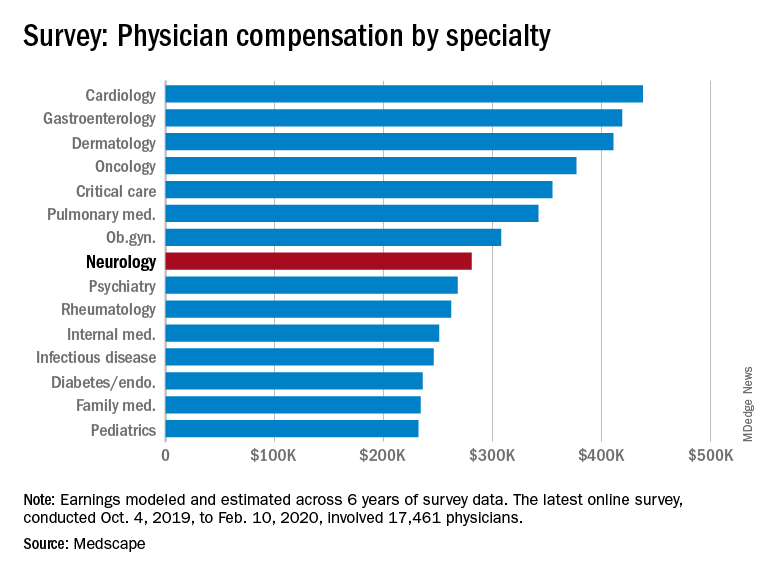
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
Framingham risk score may also predict cognitive decline
“In the absence of effective treatments for dementia, we need to monitor and control cardiovascular risk burden as a way to maintain patient’s cognitive health as they age,” said Weili Xu, PhD, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China, in a press release.
“Given the progressive increase in the number of dementia cases worldwide, our findings have both clinical and public health relevance.”
Dr. Xu and first author Ruixue Song, MSc, also from Tianjin Medical University, published their findings online ahead of print May 18 in the Journal of the American College of Cardiology.
The World Health Organization projects that up to 82 million people will have dementia by 2050. Given the lack of effective treatments for dementia, identifying modifiable risk factors for cognitive decline and aggressively managing them is an increasingly appealing strategy.
Assessing cardiovascular risk and cognition
The researchers followed 1,588 dementia-free participants from the Rush Memory and Aging Project for 21 years (median, 5.8 years). FGCRS was assessed at baseline and categorized into tertiles (lowest, middle, and highest). Mean age of the studied population was 79.5 years, 75.8% of participants were female, and mean Framingham score was 15.6 (range, 4 to 28).
Annual evaluations included assessment of episodic memory (memory of everyday events), semantic memory (long-term memory), working memory (short-term memory), visuospatial ability (capacity to identify visual and spatial relationships among objects), and perceptual speed (ability to accurately and completely compare letters, numbers, objects, pictures, or patterns) using 19 tests to derive a composite score.
A subsample (n = 378) of participants underwent MRI, and structural total and regional brain volumes were estimated.
Linear regression was used to estimate beta-coefficients for the relationship between cardiovascular risk burden at baseline and longitudinally. If the beta-coefficient is negative, the interpretation is that for every 1-unit increase in the predictor variable (FGCRS), the outcome variable (cognitive function) will decrease by the beta-coefficient value.
At baseline, higher FGCRS was related to small but consistent (although not usually statistically significant) decreases in hippocampal volume, gray matter, and total brain volume.
Considered longitudinally, participants in the highest-risk tertile of FGCRS experienced faster decline in global cognition (beta = −0.019), episodic memory (beta = −0.023), working memory (beta = −0.021), and perceptual speed (beta = −0.027) during follow-up (P < .05 for all) than those in the lowest-risk tertile.
The declines in semantic memory (beta = –0.012) and visuospatial ability (beta = –0.010) did not reach statistical significance.
Bringing dementia prevention into the exam room early
Commenting on the research, Costantino Iadecola, MD, director of the Feil Family Brain and Mind Research Institute at Weill Cornell Medicine in New York City, said the study has immediate clinical usefulness.
“The link between the cardiovascular risk factors and dementia is well known, but in your doctor’s office, that link is not seen. If your GP or cardiologist sees you with high blood pressure, he’s not immediately going to think about the risk of dementia 20 years later,” said Dr. Iadecola.
“What this study does is it directly links a simple score that’s commonly used to assess cardiovascular risk to dementia risk, which can be used to counsel patients and, hopefully, reduce the risk of both cardiovascular disease and cognitive disorders.”
Dr. Iadecola wrote an editorial together with Neal S. Parikh, MD, MS, also from Weill Cornell Medicine, that accompanied the findings of the trial.
Even neurologists sometimes fail to make the connection between vascular risk and dementia, he said. “They think that by making a stroke patient move their hand better, they’re treating them, but 30% of stroke patients get dementia 6 or 8 months later and they’re missing this link between cerebrovascular pathology and dementia.
Dr. Iadecola is one of 26 experts who authored the recent Berlin Manifesto, an effort led by Vladimir Hachinski, MD, professor of neurology and epidemiology at Western University in Ontario, Canada, to raise awareness of the link between cardiovascular and brain health.
Dr. Hachinski coined the term “brain attack” and devised the Hachinski Ischemic Score that remains the standard for identifying a vascular component of cognitive impairment.
The current study has some strengths and limitations, noted Dr. Iadecola. The average age of participants was 80 years, which is appropriate given the high risk for cognitive decline at this age, but the generalizability of the study may be limited given that most participants were white women.
Going forward, he said, rigorous studies are needed to confirm these findings and to determine how to best prevent dementia through treatment of individual cardiovascular risk factors.
Dr. Xu has received grants from nonindustry entities, including the Swedish Research Council and the National Natural Science Foundation of China. The study was funded by the European Union’s Horizon 320230 research and innovation program. Dr. Iadecola is a member of the scientific advisory board for Broadview Ventures.
This article appeared on Medscape.com.
“In the absence of effective treatments for dementia, we need to monitor and control cardiovascular risk burden as a way to maintain patient’s cognitive health as they age,” said Weili Xu, PhD, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China, in a press release.
“Given the progressive increase in the number of dementia cases worldwide, our findings have both clinical and public health relevance.”
Dr. Xu and first author Ruixue Song, MSc, also from Tianjin Medical University, published their findings online ahead of print May 18 in the Journal of the American College of Cardiology.
The World Health Organization projects that up to 82 million people will have dementia by 2050. Given the lack of effective treatments for dementia, identifying modifiable risk factors for cognitive decline and aggressively managing them is an increasingly appealing strategy.
Assessing cardiovascular risk and cognition
The researchers followed 1,588 dementia-free participants from the Rush Memory and Aging Project for 21 years (median, 5.8 years). FGCRS was assessed at baseline and categorized into tertiles (lowest, middle, and highest). Mean age of the studied population was 79.5 years, 75.8% of participants were female, and mean Framingham score was 15.6 (range, 4 to 28).
Annual evaluations included assessment of episodic memory (memory of everyday events), semantic memory (long-term memory), working memory (short-term memory), visuospatial ability (capacity to identify visual and spatial relationships among objects), and perceptual speed (ability to accurately and completely compare letters, numbers, objects, pictures, or patterns) using 19 tests to derive a composite score.
A subsample (n = 378) of participants underwent MRI, and structural total and regional brain volumes were estimated.
Linear regression was used to estimate beta-coefficients for the relationship between cardiovascular risk burden at baseline and longitudinally. If the beta-coefficient is negative, the interpretation is that for every 1-unit increase in the predictor variable (FGCRS), the outcome variable (cognitive function) will decrease by the beta-coefficient value.
At baseline, higher FGCRS was related to small but consistent (although not usually statistically significant) decreases in hippocampal volume, gray matter, and total brain volume.
Considered longitudinally, participants in the highest-risk tertile of FGCRS experienced faster decline in global cognition (beta = −0.019), episodic memory (beta = −0.023), working memory (beta = −0.021), and perceptual speed (beta = −0.027) during follow-up (P < .05 for all) than those in the lowest-risk tertile.
The declines in semantic memory (beta = –0.012) and visuospatial ability (beta = –0.010) did not reach statistical significance.
Bringing dementia prevention into the exam room early
Commenting on the research, Costantino Iadecola, MD, director of the Feil Family Brain and Mind Research Institute at Weill Cornell Medicine in New York City, said the study has immediate clinical usefulness.
“The link between the cardiovascular risk factors and dementia is well known, but in your doctor’s office, that link is not seen. If your GP or cardiologist sees you with high blood pressure, he’s not immediately going to think about the risk of dementia 20 years later,” said Dr. Iadecola.
“What this study does is it directly links a simple score that’s commonly used to assess cardiovascular risk to dementia risk, which can be used to counsel patients and, hopefully, reduce the risk of both cardiovascular disease and cognitive disorders.”
Dr. Iadecola wrote an editorial together with Neal S. Parikh, MD, MS, also from Weill Cornell Medicine, that accompanied the findings of the trial.
Even neurologists sometimes fail to make the connection between vascular risk and dementia, he said. “They think that by making a stroke patient move their hand better, they’re treating them, but 30% of stroke patients get dementia 6 or 8 months later and they’re missing this link between cerebrovascular pathology and dementia.
Dr. Iadecola is one of 26 experts who authored the recent Berlin Manifesto, an effort led by Vladimir Hachinski, MD, professor of neurology and epidemiology at Western University in Ontario, Canada, to raise awareness of the link between cardiovascular and brain health.
Dr. Hachinski coined the term “brain attack” and devised the Hachinski Ischemic Score that remains the standard for identifying a vascular component of cognitive impairment.
The current study has some strengths and limitations, noted Dr. Iadecola. The average age of participants was 80 years, which is appropriate given the high risk for cognitive decline at this age, but the generalizability of the study may be limited given that most participants were white women.
Going forward, he said, rigorous studies are needed to confirm these findings and to determine how to best prevent dementia through treatment of individual cardiovascular risk factors.
Dr. Xu has received grants from nonindustry entities, including the Swedish Research Council and the National Natural Science Foundation of China. The study was funded by the European Union’s Horizon 320230 research and innovation program. Dr. Iadecola is a member of the scientific advisory board for Broadview Ventures.
This article appeared on Medscape.com.
“In the absence of effective treatments for dementia, we need to monitor and control cardiovascular risk burden as a way to maintain patient’s cognitive health as they age,” said Weili Xu, PhD, Department of Epidemiology and Biostatistics, School of Public Health, Tianjin Medical University, Tianjin, China, in a press release.
“Given the progressive increase in the number of dementia cases worldwide, our findings have both clinical and public health relevance.”
Dr. Xu and first author Ruixue Song, MSc, also from Tianjin Medical University, published their findings online ahead of print May 18 in the Journal of the American College of Cardiology.
The World Health Organization projects that up to 82 million people will have dementia by 2050. Given the lack of effective treatments for dementia, identifying modifiable risk factors for cognitive decline and aggressively managing them is an increasingly appealing strategy.
Assessing cardiovascular risk and cognition
The researchers followed 1,588 dementia-free participants from the Rush Memory and Aging Project for 21 years (median, 5.8 years). FGCRS was assessed at baseline and categorized into tertiles (lowest, middle, and highest). Mean age of the studied population was 79.5 years, 75.8% of participants were female, and mean Framingham score was 15.6 (range, 4 to 28).
Annual evaluations included assessment of episodic memory (memory of everyday events), semantic memory (long-term memory), working memory (short-term memory), visuospatial ability (capacity to identify visual and spatial relationships among objects), and perceptual speed (ability to accurately and completely compare letters, numbers, objects, pictures, or patterns) using 19 tests to derive a composite score.
A subsample (n = 378) of participants underwent MRI, and structural total and regional brain volumes were estimated.
Linear regression was used to estimate beta-coefficients for the relationship between cardiovascular risk burden at baseline and longitudinally. If the beta-coefficient is negative, the interpretation is that for every 1-unit increase in the predictor variable (FGCRS), the outcome variable (cognitive function) will decrease by the beta-coefficient value.
At baseline, higher FGCRS was related to small but consistent (although not usually statistically significant) decreases in hippocampal volume, gray matter, and total brain volume.
Considered longitudinally, participants in the highest-risk tertile of FGCRS experienced faster decline in global cognition (beta = −0.019), episodic memory (beta = −0.023), working memory (beta = −0.021), and perceptual speed (beta = −0.027) during follow-up (P < .05 for all) than those in the lowest-risk tertile.
The declines in semantic memory (beta = –0.012) and visuospatial ability (beta = –0.010) did not reach statistical significance.
Bringing dementia prevention into the exam room early
Commenting on the research, Costantino Iadecola, MD, director of the Feil Family Brain and Mind Research Institute at Weill Cornell Medicine in New York City, said the study has immediate clinical usefulness.
“The link between the cardiovascular risk factors and dementia is well known, but in your doctor’s office, that link is not seen. If your GP or cardiologist sees you with high blood pressure, he’s not immediately going to think about the risk of dementia 20 years later,” said Dr. Iadecola.
“What this study does is it directly links a simple score that’s commonly used to assess cardiovascular risk to dementia risk, which can be used to counsel patients and, hopefully, reduce the risk of both cardiovascular disease and cognitive disorders.”
Dr. Iadecola wrote an editorial together with Neal S. Parikh, MD, MS, also from Weill Cornell Medicine, that accompanied the findings of the trial.
Even neurologists sometimes fail to make the connection between vascular risk and dementia, he said. “They think that by making a stroke patient move their hand better, they’re treating them, but 30% of stroke patients get dementia 6 or 8 months later and they’re missing this link between cerebrovascular pathology and dementia.
Dr. Iadecola is one of 26 experts who authored the recent Berlin Manifesto, an effort led by Vladimir Hachinski, MD, professor of neurology and epidemiology at Western University in Ontario, Canada, to raise awareness of the link between cardiovascular and brain health.
Dr. Hachinski coined the term “brain attack” and devised the Hachinski Ischemic Score that remains the standard for identifying a vascular component of cognitive impairment.
The current study has some strengths and limitations, noted Dr. Iadecola. The average age of participants was 80 years, which is appropriate given the high risk for cognitive decline at this age, but the generalizability of the study may be limited given that most participants were white women.
Going forward, he said, rigorous studies are needed to confirm these findings and to determine how to best prevent dementia through treatment of individual cardiovascular risk factors.
Dr. Xu has received grants from nonindustry entities, including the Swedish Research Council and the National Natural Science Foundation of China. The study was funded by the European Union’s Horizon 320230 research and innovation program. Dr. Iadecola is a member of the scientific advisory board for Broadview Ventures.
This article appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Oncologists’ income and satisfaction are up
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
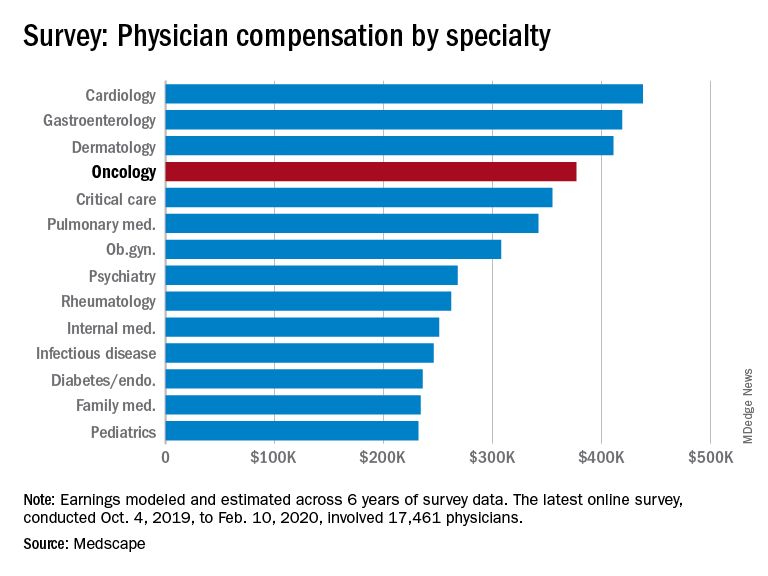
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
Oncologists continue to rank above the middle range for all specialties in annual compensation for physicians, according to findings from the newly released Medscape Oncologist Compensation Report 2020.
The average earnings for oncologists who participated in the survey was $377,000, which was a 5% increase from the $359,000 reported for 2018.
Just over two-thirds (67%) of oncologists reported that they felt that they were fairly compensated, which is quite a jump from 53% last year.
In addition, oncologists appear to be very satisfied with their profession. Similar to last year’s findings, 84% said they would choose medicine again, and 96% said they would choose the specialty of oncology again.
Earning in top third of all specialties
The average annual earnings reported by oncologists put this specialty in eleventh place among 29 specialties. Orthopedic specialists remain at the head of the list, with estimated earnings of $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according to Medscape’s compensation report, which included responses from 17,461 physicians in over 30 specialties.
At the bottom of the estimated earnings list were public health and preventive medicine doctors and pediatricians. For both specialties, the reported annual earnings was $232,000. Family medicine specialists were only marginally higher at $234,000.
Radiologists ($427,000), gastroenterologists ($419,000), and urologists ($417,000) all reported higher earnings than oncologists, whereas neurologists, at $280,000, rheumatologists, at $262,000, and internal medicine physicians, at $251,000, earned less.
The report also found that gender disparities in income persist, with male oncologists earning 17% more than their female colleagues. The gender gap in oncology is somewhat less than that seen for all specialties combined, in which men earned 31% more than women, similar to last year’s figure of 33%.
Male oncologists reported spending 38.8 hours per week seeing patients, compared with 34.9 hours reported by female oncologists. This could be a factor contributing to the gender pay disparity. Overall, the average amount of time seeing patients was 37.9 hours per week.
Frustrations with paperwork and denied claims
Surveyed oncologists cited some of the frustrations they are facing, such as spending nearly 17 hours a week on paperwork and administrative tasks. They reported that 16% of claims are denied or have to be resubmitted. As for the most challenging part of the job, oncologists (22%), similar to physicians overall (26%), found that having so many rules and regulations takes first place, followed by working with electronic health record systems (20%), difficulties getting fair reimbursement (19%), having to work long hours (12%), and dealing with difficult patients (8%). Few oncologists were concerned about lawsuits (4%), and 4% reported that there were no challenges.
Oncologists reported that the most rewarding part of their job was gratitude/relationships with patients (31%), followed by knowing that they are making the world a better place (27%). After that, oncologists agreed with statements about being very good at what they do/finding answers/diagnoses (22%), having pride in being a doctor (9%), and making good money at a job they like (8%).
Other key findings
Other key findings from the Medscape Oncologist Compensation Report 2020 included the following:
- Regarding payment models, 80% take insurance, 41% are in fee-for-service arrangements, and 18% are in accountable care organizations (21%). Only 3% are in direct primary care, and 1% are cash-only practices or have a concierge practice.
- 65% of oncologists state that they will continue taking new and current Medicare/Medicaid patients. None said that they would not take on new Medicare/Medicaid patients, and 35% remain undecided. These numbers differed from physicians overall; 73% of all physicians surveyed said they would continue taking new/current Medicare/Medicaid patients, 6% said that will not take on new Medicare patients, and 4% said they will not take new Medicaid patients. In addition, 3% and 2% said that they would stop treating some or all of their Medicare and Medicaid patients, respectively.
- About half (51%) of oncologists use nurse practitioners, about a third (34%) use physician assistants, and 37% use neither. This was about the same as physicians overall.
- A larger percentage of oncologists (38%) expect to participate in MIPS (merit-based incentive payment system), and only 8% expect to participate in APMs (alternative payment models). This was similar to the findings for physicians overall, with more than one-third (37%) expecting to participate in MIPS and 9% planning to take part in APMs.
Impact of COVID-19 pandemic
The Medscape compensation reports also gives a glimpse of the impact the COVID-19 pandemic is having on physician compensation.
Since the beginning of the pandemic, practices have reported a 55% decrease in revenue and a 60% drop in patient volume. Physician practices and hospitals have laid off or furloughed personnel and have cut pay, and 9% of practices have closed their doors, at least for the time being.
A total of 43,000 health care workers were laid off in March, the report notes.
The findings tie in with those reported elsewhere. For example, a survey conducted by the Medical Group Management Association, which was reported by Medscape Medical News, found that 97% of physician practices have experienced negative financial effects directly or indirectly related to COVID-19.
Specialties were hard hit, especially those that rely on elective procedures, such as dermatology and cardiology. Oncology care has also been disrupted. For example, a survey conducted by the American Cancer Society Cancer Action Network found that half of the cancer patients and survivors who responded reported changes, delays, or disruptions to the care they were receiving.
This article first appeared on Medscape.com.
Tumor molecular profiling may help identify ‘exceptional responders’
Virtually all oncologists, at one time or another, have treated a patient who defied the odds and achieved an unexpectedly long-lasting response. These “exceptional responders” are patients who experience a unique response to therapies that have largely failed to be effective for others with similar cancers.
Genetic and molecular mechanisms may partly account for these responses and may offer clues about why the treatment works for only a few and not for others. To delve more deeply into that area of research, the National Cancer Institute (NCI) began the Exceptional Responders Initiative (ERI) with the goal of identifying potential biological processes that may be responsible, at least in part, for these unusual responses.
NCI researchers have now successfully completed a pilot study that analyzed tumor specimens from more than 100 cases, and the study has affirmed the feasibility of this approach.
Of these cases, six were identified as involving potentially clinically actionable germline mutations.
The findings were published online ahead of print in the Journal of the National Cancer Institute.
“Clearly, the analysis and validation of these results will prove critical to determining the success of this approach,” write James M. Ford, MD, and Beverly S. Mitchell, MD, both of Stanford University School of Medicine, California, in an accompanying editorial. “Ultimately, prospective studies of tumors from exceptional responders, particularly to novel, genomically-targeted agents, may provide a powerful approach to cancer treatment discoveries.”
A special case
Molecular profiling technology, including next-generation sequencing, has significantly changed the landscape of the development of cancer therapies, and clinical trials in early drug development are increasingly selecting patients on the basis of molecular alterations.
The ERI grew out of several meetings held by the NCI in 2013 and 2014. It was built on the ability to profile archived tumor material, explained study author S. Percy Ivy, PhD, associate chief of the Investigational Drug Branch in the Division of Cancer Treatment and Diagnosis of the NCI. “This made it possible to collect cases from participating clinicians from all over the country.
“Published cases included patients treated with a targeted therapy but not treated with knowledge of their tumor’s genomics, who then later turned out to have genomic changes that made their tumor exquisitely sensitive to inhibition of a driving pathway,” she said. “There have been published cases as well as cases in the experience of practicing oncologists that seem to do much better than expected.
“We wondered if we could find molecular reasons why tumors respond not only to targeted therapies but also to standard chemotherapy,” said Percy. “If so, we could refine our choice of therapy to patients who are most likely to respond to it.”’
On its website, the NCI writes that there was a particular case that triggered the interest in going ahead with this initiative. Mutations in the TSC1 and NF2 genes, which result in a loss of gene function, were detected in a patient with metastatic bladder cancer. In a clinical trial, the patient was treated with everolimus (Afinitor, Novartis), an inhibitor of the mammalian target of rapamycin (mTORC1), and achieved a complete response with a duration of more than 2 years.
In a separate analysis, researchers sequenced tumors from 96 other individuals with high-grade bladder cancer and identified five TSC1 gene mutations. Tumors were sequenced from 13 patients with bladder cancer who had received everolimus. Results showed that 3 of 4 patients with TSC1 gene mutations experienced some degree of tumor shrinkage after treatment; 8 of 9 patients who did not have the mutation experienced disease progression.
The NCI notes that in “subsequent workshops and discussions, it became obvious that all clinicians have seen a few exceptional responders.”
Testing for feasibility
The aim of the current study was to assess the feasibility and potential usefulness of sequencing DNA and RNA from clinical tumor specimens from patients who had experienced unusually profound or durable responses to systemic therapy.
Its main feasibility goal was to identify at least 100 cases involving exceptional responders whose cases could be analyzed in less than 3 years.
An exceptional patient was defined as one who had experienced a complete response to one or more drugs in which complete responses were seen in fewer than 10% of patients who received similar treatment; or a partial response lasting at least 6 months in which such a response is seen in fewer than 10% of patients who receive similar treatment; or a complete or partial response of a duration that is three times the median response duration represented in the literature for the treatment.
Studying exceptional responders presents many challenges, the first being to define what an exceptional response is and what it is not, explained Ivy. “This definition relies on the existence of data that a particular therapy will produce particular responses in groups of patients with similar tumors, as defined by organ of origin,” she said.
Other challenges include obtaining tumor tissue and all the relevant clinical data, such as the number of prior treatments and the patient’s response, as well as any known molecular characteristics (eg, HER2/NEU amplification, estrogen-receptor expression, germline mutations). “We also do not have data on other exposures, such as smoking or chemical exposure,” she said. “In addition, when patients are not on clinical trial, the data are not uniformly obtained ― such as that scans may not be performed at particular intervals.”
Importantly, the molecular tools used to analyze tumors were not available in the past, so many trials did not collect tumor tissue for subsequent research. “Even now, we are learning that there are characteristics beyond DNA and RNA that are potentially important to the ability of a tumor to respond, such as the immune system or epigenetic changes,” she said.
From August 2014 to July 2017, a total of 520 cases were proposed by clinicians as possibly involving exceptional responders, and 222 cases met the criteria.
Analyzable tissue was available for 117 patients. Most of the responders (n = 80, 68.4%) had been treated with combination chemotherapy regimens; 34 patients (29.0%) had received one or more antiangiogenesis agents. In addition, six patients had an exceptional response following treatment with immune checkpoint inhibitors. The final analysis included 109 cases.
One exceptional responder was a woman with metastatic squamous lung cancer that was treated with paclitaxel and carboplatin. The patient achieved a 41-month complete response (expected rate, <10%). Another patient with esophageal adenocarcinoma who was treated with docetaxel and cisplatin experienced a partial response that lasted 128 months (reported median response duration, 24 months). After the patient’s tumor recurred, he experienced for the second time a response to concurrent chemoradiation with the same drug regimen.
Overall, potentially clinically relevant germline mutations were identified in six tumors. Pathogenic BRCA1 or BRCA2 mutations were found in two breast cancer patients, one patient with non–small cell lung cancer, and one patient with rectal cancer. A breast cancer patient had a pathogenic BRCA1 germline mutation, and another had a likely germline mutation in CHEK2. A patient with poorly differentiated lung cancer and a history of breast cancer had a PALB2 mutation.
Future steps
Molecular mechanisms are important, but other factors could also play a role in eliciting a response. One is the presence of comorbidities, which was not assessed in the study. Ivy noted that comorbidities could be very important to responses, along with medications that the patient is using for different types of ailments. In addition, the use of complementary and alternative medicines may also have an impact.
“As the field matures, we hope that others will collect these and other characteristics, so that all the data could be used to develop hypotheses about molecular and other factors that can better predict response or resistance,” she said.
The results from this pilot study demonstrated feasibility. Ivy noted that “additional collaboration in similar studies would be welcome, as would methods to use data from various sources to improve our ability to correlate patient characteristics, tumor characteristics and response.
“We envision a larger national and international effort to collect more exceptional responder cases, including more from patients treated with targeted therapies,” she added. “The NCI has been meeting with an interest group that focuses on ER cases in the UK, France, Italy, Canada, and Australia, and this collaborative effort is maturing, albeit slowly.”
The project has been funded in whole or in part with federal funds from the NCI and NIH. Ivy has disclosed no relevant financial relationships. Several coauthors report relationships with industry. The editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Virtually all oncologists, at one time or another, have treated a patient who defied the odds and achieved an unexpectedly long-lasting response. These “exceptional responders” are patients who experience a unique response to therapies that have largely failed to be effective for others with similar cancers.
Genetic and molecular mechanisms may partly account for these responses and may offer clues about why the treatment works for only a few and not for others. To delve more deeply into that area of research, the National Cancer Institute (NCI) began the Exceptional Responders Initiative (ERI) with the goal of identifying potential biological processes that may be responsible, at least in part, for these unusual responses.
NCI researchers have now successfully completed a pilot study that analyzed tumor specimens from more than 100 cases, and the study has affirmed the feasibility of this approach.
Of these cases, six were identified as involving potentially clinically actionable germline mutations.
The findings were published online ahead of print in the Journal of the National Cancer Institute.
“Clearly, the analysis and validation of these results will prove critical to determining the success of this approach,” write James M. Ford, MD, and Beverly S. Mitchell, MD, both of Stanford University School of Medicine, California, in an accompanying editorial. “Ultimately, prospective studies of tumors from exceptional responders, particularly to novel, genomically-targeted agents, may provide a powerful approach to cancer treatment discoveries.”
A special case
Molecular profiling technology, including next-generation sequencing, has significantly changed the landscape of the development of cancer therapies, and clinical trials in early drug development are increasingly selecting patients on the basis of molecular alterations.
The ERI grew out of several meetings held by the NCI in 2013 and 2014. It was built on the ability to profile archived tumor material, explained study author S. Percy Ivy, PhD, associate chief of the Investigational Drug Branch in the Division of Cancer Treatment and Diagnosis of the NCI. “This made it possible to collect cases from participating clinicians from all over the country.
“Published cases included patients treated with a targeted therapy but not treated with knowledge of their tumor’s genomics, who then later turned out to have genomic changes that made their tumor exquisitely sensitive to inhibition of a driving pathway,” she said. “There have been published cases as well as cases in the experience of practicing oncologists that seem to do much better than expected.
“We wondered if we could find molecular reasons why tumors respond not only to targeted therapies but also to standard chemotherapy,” said Percy. “If so, we could refine our choice of therapy to patients who are most likely to respond to it.”’
On its website, the NCI writes that there was a particular case that triggered the interest in going ahead with this initiative. Mutations in the TSC1 and NF2 genes, which result in a loss of gene function, were detected in a patient with metastatic bladder cancer. In a clinical trial, the patient was treated with everolimus (Afinitor, Novartis), an inhibitor of the mammalian target of rapamycin (mTORC1), and achieved a complete response with a duration of more than 2 years.
In a separate analysis, researchers sequenced tumors from 96 other individuals with high-grade bladder cancer and identified five TSC1 gene mutations. Tumors were sequenced from 13 patients with bladder cancer who had received everolimus. Results showed that 3 of 4 patients with TSC1 gene mutations experienced some degree of tumor shrinkage after treatment; 8 of 9 patients who did not have the mutation experienced disease progression.
The NCI notes that in “subsequent workshops and discussions, it became obvious that all clinicians have seen a few exceptional responders.”
Testing for feasibility
The aim of the current study was to assess the feasibility and potential usefulness of sequencing DNA and RNA from clinical tumor specimens from patients who had experienced unusually profound or durable responses to systemic therapy.
Its main feasibility goal was to identify at least 100 cases involving exceptional responders whose cases could be analyzed in less than 3 years.
An exceptional patient was defined as one who had experienced a complete response to one or more drugs in which complete responses were seen in fewer than 10% of patients who received similar treatment; or a partial response lasting at least 6 months in which such a response is seen in fewer than 10% of patients who receive similar treatment; or a complete or partial response of a duration that is three times the median response duration represented in the literature for the treatment.
Studying exceptional responders presents many challenges, the first being to define what an exceptional response is and what it is not, explained Ivy. “This definition relies on the existence of data that a particular therapy will produce particular responses in groups of patients with similar tumors, as defined by organ of origin,” she said.
Other challenges include obtaining tumor tissue and all the relevant clinical data, such as the number of prior treatments and the patient’s response, as well as any known molecular characteristics (eg, HER2/NEU amplification, estrogen-receptor expression, germline mutations). “We also do not have data on other exposures, such as smoking or chemical exposure,” she said. “In addition, when patients are not on clinical trial, the data are not uniformly obtained ― such as that scans may not be performed at particular intervals.”
Importantly, the molecular tools used to analyze tumors were not available in the past, so many trials did not collect tumor tissue for subsequent research. “Even now, we are learning that there are characteristics beyond DNA and RNA that are potentially important to the ability of a tumor to respond, such as the immune system or epigenetic changes,” she said.
From August 2014 to July 2017, a total of 520 cases were proposed by clinicians as possibly involving exceptional responders, and 222 cases met the criteria.
Analyzable tissue was available for 117 patients. Most of the responders (n = 80, 68.4%) had been treated with combination chemotherapy regimens; 34 patients (29.0%) had received one or more antiangiogenesis agents. In addition, six patients had an exceptional response following treatment with immune checkpoint inhibitors. The final analysis included 109 cases.
One exceptional responder was a woman with metastatic squamous lung cancer that was treated with paclitaxel and carboplatin. The patient achieved a 41-month complete response (expected rate, <10%). Another patient with esophageal adenocarcinoma who was treated with docetaxel and cisplatin experienced a partial response that lasted 128 months (reported median response duration, 24 months). After the patient’s tumor recurred, he experienced for the second time a response to concurrent chemoradiation with the same drug regimen.
Overall, potentially clinically relevant germline mutations were identified in six tumors. Pathogenic BRCA1 or BRCA2 mutations were found in two breast cancer patients, one patient with non–small cell lung cancer, and one patient with rectal cancer. A breast cancer patient had a pathogenic BRCA1 germline mutation, and another had a likely germline mutation in CHEK2. A patient with poorly differentiated lung cancer and a history of breast cancer had a PALB2 mutation.
Future steps
Molecular mechanisms are important, but other factors could also play a role in eliciting a response. One is the presence of comorbidities, which was not assessed in the study. Ivy noted that comorbidities could be very important to responses, along with medications that the patient is using for different types of ailments. In addition, the use of complementary and alternative medicines may also have an impact.
“As the field matures, we hope that others will collect these and other characteristics, so that all the data could be used to develop hypotheses about molecular and other factors that can better predict response or resistance,” she said.
The results from this pilot study demonstrated feasibility. Ivy noted that “additional collaboration in similar studies would be welcome, as would methods to use data from various sources to improve our ability to correlate patient characteristics, tumor characteristics and response.
“We envision a larger national and international effort to collect more exceptional responder cases, including more from patients treated with targeted therapies,” she added. “The NCI has been meeting with an interest group that focuses on ER cases in the UK, France, Italy, Canada, and Australia, and this collaborative effort is maturing, albeit slowly.”
The project has been funded in whole or in part with federal funds from the NCI and NIH. Ivy has disclosed no relevant financial relationships. Several coauthors report relationships with industry. The editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Virtually all oncologists, at one time or another, have treated a patient who defied the odds and achieved an unexpectedly long-lasting response. These “exceptional responders” are patients who experience a unique response to therapies that have largely failed to be effective for others with similar cancers.
Genetic and molecular mechanisms may partly account for these responses and may offer clues about why the treatment works for only a few and not for others. To delve more deeply into that area of research, the National Cancer Institute (NCI) began the Exceptional Responders Initiative (ERI) with the goal of identifying potential biological processes that may be responsible, at least in part, for these unusual responses.
NCI researchers have now successfully completed a pilot study that analyzed tumor specimens from more than 100 cases, and the study has affirmed the feasibility of this approach.
Of these cases, six were identified as involving potentially clinically actionable germline mutations.
The findings were published online ahead of print in the Journal of the National Cancer Institute.
“Clearly, the analysis and validation of these results will prove critical to determining the success of this approach,” write James M. Ford, MD, and Beverly S. Mitchell, MD, both of Stanford University School of Medicine, California, in an accompanying editorial. “Ultimately, prospective studies of tumors from exceptional responders, particularly to novel, genomically-targeted agents, may provide a powerful approach to cancer treatment discoveries.”
A special case
Molecular profiling technology, including next-generation sequencing, has significantly changed the landscape of the development of cancer therapies, and clinical trials in early drug development are increasingly selecting patients on the basis of molecular alterations.
The ERI grew out of several meetings held by the NCI in 2013 and 2014. It was built on the ability to profile archived tumor material, explained study author S. Percy Ivy, PhD, associate chief of the Investigational Drug Branch in the Division of Cancer Treatment and Diagnosis of the NCI. “This made it possible to collect cases from participating clinicians from all over the country.
“Published cases included patients treated with a targeted therapy but not treated with knowledge of their tumor’s genomics, who then later turned out to have genomic changes that made their tumor exquisitely sensitive to inhibition of a driving pathway,” she said. “There have been published cases as well as cases in the experience of practicing oncologists that seem to do much better than expected.
“We wondered if we could find molecular reasons why tumors respond not only to targeted therapies but also to standard chemotherapy,” said Percy. “If so, we could refine our choice of therapy to patients who are most likely to respond to it.”’
On its website, the NCI writes that there was a particular case that triggered the interest in going ahead with this initiative. Mutations in the TSC1 and NF2 genes, which result in a loss of gene function, were detected in a patient with metastatic bladder cancer. In a clinical trial, the patient was treated with everolimus (Afinitor, Novartis), an inhibitor of the mammalian target of rapamycin (mTORC1), and achieved a complete response with a duration of more than 2 years.
In a separate analysis, researchers sequenced tumors from 96 other individuals with high-grade bladder cancer and identified five TSC1 gene mutations. Tumors were sequenced from 13 patients with bladder cancer who had received everolimus. Results showed that 3 of 4 patients with TSC1 gene mutations experienced some degree of tumor shrinkage after treatment; 8 of 9 patients who did not have the mutation experienced disease progression.
The NCI notes that in “subsequent workshops and discussions, it became obvious that all clinicians have seen a few exceptional responders.”
Testing for feasibility
The aim of the current study was to assess the feasibility and potential usefulness of sequencing DNA and RNA from clinical tumor specimens from patients who had experienced unusually profound or durable responses to systemic therapy.
Its main feasibility goal was to identify at least 100 cases involving exceptional responders whose cases could be analyzed in less than 3 years.
An exceptional patient was defined as one who had experienced a complete response to one or more drugs in which complete responses were seen in fewer than 10% of patients who received similar treatment; or a partial response lasting at least 6 months in which such a response is seen in fewer than 10% of patients who receive similar treatment; or a complete or partial response of a duration that is three times the median response duration represented in the literature for the treatment.
Studying exceptional responders presents many challenges, the first being to define what an exceptional response is and what it is not, explained Ivy. “This definition relies on the existence of data that a particular therapy will produce particular responses in groups of patients with similar tumors, as defined by organ of origin,” she said.
Other challenges include obtaining tumor tissue and all the relevant clinical data, such as the number of prior treatments and the patient’s response, as well as any known molecular characteristics (eg, HER2/NEU amplification, estrogen-receptor expression, germline mutations). “We also do not have data on other exposures, such as smoking or chemical exposure,” she said. “In addition, when patients are not on clinical trial, the data are not uniformly obtained ― such as that scans may not be performed at particular intervals.”
Importantly, the molecular tools used to analyze tumors were not available in the past, so many trials did not collect tumor tissue for subsequent research. “Even now, we are learning that there are characteristics beyond DNA and RNA that are potentially important to the ability of a tumor to respond, such as the immune system or epigenetic changes,” she said.
From August 2014 to July 2017, a total of 520 cases were proposed by clinicians as possibly involving exceptional responders, and 222 cases met the criteria.
Analyzable tissue was available for 117 patients. Most of the responders (n = 80, 68.4%) had been treated with combination chemotherapy regimens; 34 patients (29.0%) had received one or more antiangiogenesis agents. In addition, six patients had an exceptional response following treatment with immune checkpoint inhibitors. The final analysis included 109 cases.
One exceptional responder was a woman with metastatic squamous lung cancer that was treated with paclitaxel and carboplatin. The patient achieved a 41-month complete response (expected rate, <10%). Another patient with esophageal adenocarcinoma who was treated with docetaxel and cisplatin experienced a partial response that lasted 128 months (reported median response duration, 24 months). After the patient’s tumor recurred, he experienced for the second time a response to concurrent chemoradiation with the same drug regimen.
Overall, potentially clinically relevant germline mutations were identified in six tumors. Pathogenic BRCA1 or BRCA2 mutations were found in two breast cancer patients, one patient with non–small cell lung cancer, and one patient with rectal cancer. A breast cancer patient had a pathogenic BRCA1 germline mutation, and another had a likely germline mutation in CHEK2. A patient with poorly differentiated lung cancer and a history of breast cancer had a PALB2 mutation.
Future steps
Molecular mechanisms are important, but other factors could also play a role in eliciting a response. One is the presence of comorbidities, which was not assessed in the study. Ivy noted that comorbidities could be very important to responses, along with medications that the patient is using for different types of ailments. In addition, the use of complementary and alternative medicines may also have an impact.
“As the field matures, we hope that others will collect these and other characteristics, so that all the data could be used to develop hypotheses about molecular and other factors that can better predict response or resistance,” she said.
The results from this pilot study demonstrated feasibility. Ivy noted that “additional collaboration in similar studies would be welcome, as would methods to use data from various sources to improve our ability to correlate patient characteristics, tumor characteristics and response.
“We envision a larger national and international effort to collect more exceptional responder cases, including more from patients treated with targeted therapies,” she added. “The NCI has been meeting with an interest group that focuses on ER cases in the UK, France, Italy, Canada, and Australia, and this collaborative effort is maturing, albeit slowly.”
The project has been funded in whole or in part with federal funds from the NCI and NIH. Ivy has disclosed no relevant financial relationships. Several coauthors report relationships with industry. The editorialists have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.