User login
New ESC ACS guideline combines STEMI and NSTE-ACS
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AMSTERDAM –
The new guideline was released at the annual congress of the European Society of Cardiology, and was published online in the European Heart Journal.
“We found that it was realized by the cardiology community that patients with STEMI, NSTEMI, or unstable angina represent a spectrum,” the chair of the guideline task force, Robert Byrne, MD, chair of cardiovascular research at the RCSI University of Medicine and Health Sciences, Dublin, explained to this news organization. “After the initial triage and management decisions, then most of the rest of the care follows a common pathway so it would make sense to consider everything in one guideline.”
Dr. Byrne noted that for all patients with a suspected ACS, the guideline recommendation is to administer an ECG within 10 minutes of presentation. The time is critical particularly for those with an occluded epicardial vessel. If there are features on the ECG that suggest an acutely occluded epicardial vessel, then the patient needs immediate angiography or primary angioplasty.
“The 10-minute guidance has been maintained from previous guidelines, but the nuance in the new guideline is that typically when we think of an occluded epicardial vessel we think of ST-elevation on the ECG,” Byrne said. “While this captures most occluded epicardial vessels, it doesn’t capture all of them. So, we have provided some guidance on alternative ECG patterns which might be indicative of an acute occlusion of the epicardial vessel and should be dealt with in the same way as an ST-elevation MI. This is a new concept.”
This situation could arise when a patient has an occluded circumflex artery and the regular ECG may not show ST elevation but the patient has ongoing pain, he noted. “There are additional ECG leads that can be looked at that might identify patients who need an immediate invasive strategy.
“This is one more reason why all ACS patients should be considered as part of one spectrum, and while the ECG gives us important information, it is not the only thing to consider. Dividing the conditions up as to whether a patient has ST elevation or not does not always make pathophysiological sense,” he added.
Dr. Byrne noted that the new guidelines have tried to reach a wider stakeholder group that includes emergency doctors, internal medicine physicians, general practitioners, and surgeons, as well as cardiologists. The document includes animations in an effort to increase the reach of the guidelines to noncardiology stakeholders, and for the first time, the task force included a patient representative.
“As part of this strategy, we have put more structure in to emphasize the importance that at first contact, we already want to be thinking of antithrombotic therapy and whether the patient needs urgent transfer to the nearest cath lab. We also want to be thinking straight away about preventing the next heart attack by implementing strong secondary prevention measures,” he commented.
Dr. Byrne highlighted a few changes to individual recommendations in the new guidelines.
Invasive management in NSTE-ACS
He pointed out that a small change has been made in the advice on invasive management for patients with non–ST-elevation ACS.
Dr. Byrne explained that patients with ST elevation should be sent immediately to a cath lab for PCI. If this is not possible within 120 minutes, then the patient should receive thrombolysis. This recommendation is the same as in previous guidelines.
He added, however, that there is some novelty in recommendations for patients who don’t have ST elevation but do have a positive troponin. For this group, previous guidelines gave a Class I recommendation that all such patients undergo an angiogram within the first 24 hours. However, an additional meta-analysis that was published in 2022 showed that the evidence for triaging all patients to the cath lab within 24 hours is somewhat limited, Dr. Byrne noted.
“At the end of the day, the task force felt that a Class I recommendation to get all patients to the cath lab within 24 hours was too strong and couldn’t be sustained, so it has been downgraded to a Class IIa recommendation, which we thought was more appropriate,” he said.
“So, while all patients should still have an angiogram during the hospital admission, if they are high-risk ACS, the imperative to get everyone to the cath lab within 24 hours – which many of our colleagues were finding difficult to achieve – does not seem to be backed up by the evidence,” he added.
Antithrombotic therapy
Addressing administration of antithrombotics, the guidelines emphasize that at the time of initial diagnosis, all patients should receive antithrombotic therapy, usually aspirin and a parenteral antithrombotic, such as heparin, enoxaparin, bivalirudin, or fondaparinux. Dr. Byrne noted that the guidelines have a new algorithm as to which of these antithrombotics to give, depending on the clinical presentation of the patient.
On the use of upfront P2Y12 inhibitors, Dr. Byrne said the new guidelines only give a weak recommendation for this.
“Giving a P2Y12 inhibitor up front does not have a strong evidence base, and it’s not unreasonable to wait, do the angiogram, see where you are, and then start the P2Y12 inhibitor. This is something that’s not widely done in clinical practice,” he commented.
“The last 2020 guideline gave a Class III recommendation for upfront P2Y12 inhibitor therapy for ACS patients who do not have STEMI. We’ve generally maintained that with the introduction of the exception that if you are in a health care system where there is a long wait to get to the cath lab – 5 ,6 or 7 days – then it’s reasonable to make an exception and give a P2Y12 inhibitor, but otherwise we’ve sustained the Class III recommendation,” he noted.
Also, for patients who have STEMI, there is a new Class IIb recommendation that upfront P2Y12 inhibitors may be considered.
“This is also rather a weak recommendation. There isn’t a strong rationale to give a P2Y12 inhibitor it in ST elevation either. It’s also reasonable to wait,” he added.
Don’t rush cardiac arrest patients to the cath lab
Another update in the guidelines involves the management of patients with cardiac arrest who have been resuscitated. Dr. Byrne explained that these patients would all receive an immediate ECG, and if it is found that they have ST elevation, they would be sent immediately to the cath lab. But a series of randomized trials has suggested that for patients who don’t have ST elevation, it is not necessary to rush these patients to the cath lab.
“We’ve given a Class III recommendation for this, saying it may be better to stabilize the patients first in the ICU. This is in recognition that a large proportion of these patients turn out not to have an MI. They have had a cardiac arrest for another reason,” Dr. Byrne noted. “Moving them to the cath lab when they are still unstable could be harming these patients rather than helping them.”
Revascularization for multivessel disease
Dr. Byrne notes that revascularization remains a critical element in the care for patients with STEMI, and there is a new recommendation in this area for patients with multivessel disease.
“Up to half of patients presenting with STEMI have multivessel disease, and we now have five randomized trials to say that these patients should have complete revascularization rather than just the culprit vessel. There is a new Class I recommendation for this,” he said.
However, the optimal timing of revascularization (immediate vs. staged) has still not been investigated in adequately sized randomized trials, and no recommendation has been made on this, the task force notes.
Dr. Byrne commented: “If you want to do everything in one go, that’s fine, but it’s also okay to do the culprit lesion first and then the other vessels at a later date within 45 days. This might depend on individual circumstances. For example, if there are complex lesions or the vessels are heavily calcified, then it may be best to get the culprit lesion fixed first and let the patient recover, then bring them back in for the rest.”
He pointed out that the results of the MULTISTARS trial, which were not available when the task force was formulating the guidelines, were reported at the ESC Congress and confirmed their recommendation.
DAPT after PCI
On the duration of dual antiplatelet therapy (DAPT) after PCI, the new guidelines have largely retained prior recommendations for a default strategy of 12 months for the combination of aspirin and a P2Y12 inhibitor.
“This was the subject of some discussion, as there have been several trials now looking at shorter durations of DAPT and deescalating after a few months to just one of these treatments. And while there is a rationale to do this, we think it’s best to be kept as an alternative strategy rather than the default strategy,” Dr. Byrne said.
He explained that the trials of DAPT deescalation tended to enroll lower-risk patients, which reduced the generalizability of the results.
Most of the trials only randomly assigned patients to shorter durations of DAPT when they were event-free for some period, she said.
“This is a dynamic decision-making process and reflects the real world to some extent. We think it is best to recommend the standard aspirin and a P2Y12 inhibitor for the 12-month duration, but at 3 months, if the patient is doing well but you may be worried about bleeding risk, then you could decide to deescalate to single antiplatelet therapy,” she noted. “So, there is Class IIa recommendation that this can be considered, but it is not recommended as the default position.”
Polypill for secondary prevention
Another innovation in the new guidelines is a new Class IIa recommendation for prescription of a polypill containing secondary prevention medications for patients on discharge from hospital.
This recommendation follows a trial that showed that the use of such a polypill helps patients be more adherent to the therapies prescribed.
Byrne explains that such a polypill may contain aspirin, an ACE inhibitor, and a statin. Several varieties are available in most European countries, but they are not widely used.
On secondary prevention, he stressed, “Prevention of the next heart attack starts before the patient leaves hospital. It is important to make sure the patient has the right medication on board, including a high-dose, high-intensity statin, and has been referred to a cardiac rehabilitation program. These are largely maintained recommendations from previous guidelines, but they are very important.”
A version of this article appeared on Medscape.com.
AT ESC CONGRESS 2023
No benefit of anti-inflammatory strategy in acute myocarditis
AMSTERDAM – A short course of the interleukin-1 receptor antagonist, anakinra, appeared safe but did not reduce complications of acute myocarditis in the ARAMIS trial.
The trial was presented at the annual congress of the European Society of Cardiology.
Lead investigator, Mathieu Kerneis, MD, Pitie Salpetriere APHP University Hospital, Paris, said this was the largest randomized controlled trial of patients with acute myocarditis and probably the first ever study in the acute setting of myocarditis patients diagnosed with cardiac magnetic resonance (CMR) imaging, not on biopsy, who are mostly at low risk for events.
He suggested that one of the reasons for the neutral result could have been the low-risk population involved and the low complication rate. “We enrolled an all-comer acute myocarditis population diagnosed with CMR, who were mostly at a low risk of complications,” he noted.
“I don’t think the story of anti-inflammatory drugs in acute myocarditis is over. This is just the beginning. This was the first trial, and it was just a phase 2 trial. We need further randomized trials to explore the potential benefit of an anti-inflammatory strategy in acute myocarditis patients at higher risk of complications. In addition, larger studies are needed to evaluate prolonged anti-inflammatory strategies in acute myocarditis patients at low-to-moderate risk of complications,” Dr. Kerneis concluded.
“It is very challenging to do a trial in high-risk patients with myocarditis as these patients are quite rare,” he added.
Inflammation of the myocardium
Dr. Kerneis explained that acute myocarditis is an inflammation of the myocardium that can cause permanent damage to the heart muscle and lead to myocardial infarction, stroke, heart failure, arrhythmias, and death. The condition can occur in individuals of all ages but is most frequent in young people. There is no specific treatment, but patients are generally treated with beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and sometimes steroids.
Anakinra is an interleukin-1 receptor antagonist that works by targeting the interleukin-1β innate immune pathway. Anakinra is used for the treatment of rheumatoid arthritis and has shown efficacy in pericarditis. Dr. Kerneis noted that there have been several case reports of successful treatment with anakinra in acute myocarditis.
The ARAMIS trial – conducted at six academic centers in France – was the first randomized study to evaluate inhibition of the interleukin-1β innate immune pathway in myocarditis patients. The trial enrolled 120 hospitalized, symptomatic patients with chest pain, increased cardiac troponin, and acute myocarditis diagnosed using CMR. More than half had had a recent bacterial or viral infection.
Patients were randomized within 72 hours of hospital admission to a daily subcutaneous dose of anakinra 100 mg or placebo until hospital discharge. Patients in both groups received standard-of-care treatments, including an ACE inhibitor, for at least 1 month. Consistent with prior data, the median age of participants was 28 years and 90% were men.
The primary endpoint was the number of days free of myocarditis complications (heart failure requiring hospitalization, chest pain requiring medication, left ventricular ejection fraction less than 50%, and ventricular arrhythmias) within 28 days postdischarge.
There was no significant difference in this endpoint between the two arms, with a median of 30 days for anakinra versus 31 days for placebo.
Overall, the rate of the composite endpoint of myocarditis complications occurred in 13.7% of patients, and there was a numerical reduction in the number of patients with these myocarditis complications with anakinra – 6 patients (10.5%) in the anakinra group versus 10 patients (16.5%) in the placebo group (odds ratio, 0.59; 95% confidence interval, 0.19-1.78). This was driven by fewer patients with chest pain requiring new medication (two patients versus six patients).
The safety endpoint was the number of serious adverse events within 28 days postdischarge. This endpoint occurred in seven patients (12.1%) in the anakinra arm and six patients (10.2%) in the placebo arm, with no significant difference between groups. Cases of severe infection within 28 days postdischarge were reported in both arms.
Low-risk population
Designated discussant of the study at the ESC Hotline session, Enrico Ammirati, MD, PhD, University of Milano-Bicocca, Monza, Italy, said that patients involved in ARAMIS fit the profile of acute myocarditis and that the CMR diagnosis was positive in all the patients enrolled.
Dr. Ammirati agreed with Dr. Kerneis that the neutral results of the study were probably caused by the low-risk population. “If we look at retrospective registries, at 30 days there are zero cardiac deaths or heart transplants at 30 days in patients with a low-risk presentation.
“The ARAMIS trial has shown the feasibility of conducting studies in the setting of acute myocarditis, and even if the primary endpoint was neutral, some important data are still missing, such as change in ejection fraction and troponin levels,” he noted.
“In terms of future perspective, we are moving to assessing efficacy of anakinra or other immunosuppressive drugs from acute low risk patients to higher risk patients with heart failure and severe dysfunction,” he said.
Dr. Ammirati is the lead investigator of another ongoing study in such a higher-risk population; the MYTHS trial is investigating the use of intravenous steroids in patients with suspected acute myocarditis complicated by acute heart failure or cardiogenic shock, and an ejection fraction below 41%.
“So, we will have more results on the best treatment in this higher risk group of patients,” he concluded.
The ARAMIS trial was an academic study funded by the French Health Ministry and coordinated by the ACTION Group. Dr. Kerneis reports having received consulting fees from Kiniksa, Sanofi, and Bayer, and holds a patent for use of abatacept in immune checkpoint inhibitor (ICI)–induced myocarditis.
A version of this article first appeared on Medscape.com.
AMSTERDAM – A short course of the interleukin-1 receptor antagonist, anakinra, appeared safe but did not reduce complications of acute myocarditis in the ARAMIS trial.
The trial was presented at the annual congress of the European Society of Cardiology.
Lead investigator, Mathieu Kerneis, MD, Pitie Salpetriere APHP University Hospital, Paris, said this was the largest randomized controlled trial of patients with acute myocarditis and probably the first ever study in the acute setting of myocarditis patients diagnosed with cardiac magnetic resonance (CMR) imaging, not on biopsy, who are mostly at low risk for events.
He suggested that one of the reasons for the neutral result could have been the low-risk population involved and the low complication rate. “We enrolled an all-comer acute myocarditis population diagnosed with CMR, who were mostly at a low risk of complications,” he noted.
“I don’t think the story of anti-inflammatory drugs in acute myocarditis is over. This is just the beginning. This was the first trial, and it was just a phase 2 trial. We need further randomized trials to explore the potential benefit of an anti-inflammatory strategy in acute myocarditis patients at higher risk of complications. In addition, larger studies are needed to evaluate prolonged anti-inflammatory strategies in acute myocarditis patients at low-to-moderate risk of complications,” Dr. Kerneis concluded.
“It is very challenging to do a trial in high-risk patients with myocarditis as these patients are quite rare,” he added.
Inflammation of the myocardium
Dr. Kerneis explained that acute myocarditis is an inflammation of the myocardium that can cause permanent damage to the heart muscle and lead to myocardial infarction, stroke, heart failure, arrhythmias, and death. The condition can occur in individuals of all ages but is most frequent in young people. There is no specific treatment, but patients are generally treated with beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and sometimes steroids.
Anakinra is an interleukin-1 receptor antagonist that works by targeting the interleukin-1β innate immune pathway. Anakinra is used for the treatment of rheumatoid arthritis and has shown efficacy in pericarditis. Dr. Kerneis noted that there have been several case reports of successful treatment with anakinra in acute myocarditis.
The ARAMIS trial – conducted at six academic centers in France – was the first randomized study to evaluate inhibition of the interleukin-1β innate immune pathway in myocarditis patients. The trial enrolled 120 hospitalized, symptomatic patients with chest pain, increased cardiac troponin, and acute myocarditis diagnosed using CMR. More than half had had a recent bacterial or viral infection.
Patients were randomized within 72 hours of hospital admission to a daily subcutaneous dose of anakinra 100 mg or placebo until hospital discharge. Patients in both groups received standard-of-care treatments, including an ACE inhibitor, for at least 1 month. Consistent with prior data, the median age of participants was 28 years and 90% were men.
The primary endpoint was the number of days free of myocarditis complications (heart failure requiring hospitalization, chest pain requiring medication, left ventricular ejection fraction less than 50%, and ventricular arrhythmias) within 28 days postdischarge.
There was no significant difference in this endpoint between the two arms, with a median of 30 days for anakinra versus 31 days for placebo.
Overall, the rate of the composite endpoint of myocarditis complications occurred in 13.7% of patients, and there was a numerical reduction in the number of patients with these myocarditis complications with anakinra – 6 patients (10.5%) in the anakinra group versus 10 patients (16.5%) in the placebo group (odds ratio, 0.59; 95% confidence interval, 0.19-1.78). This was driven by fewer patients with chest pain requiring new medication (two patients versus six patients).
The safety endpoint was the number of serious adverse events within 28 days postdischarge. This endpoint occurred in seven patients (12.1%) in the anakinra arm and six patients (10.2%) in the placebo arm, with no significant difference between groups. Cases of severe infection within 28 days postdischarge were reported in both arms.
Low-risk population
Designated discussant of the study at the ESC Hotline session, Enrico Ammirati, MD, PhD, University of Milano-Bicocca, Monza, Italy, said that patients involved in ARAMIS fit the profile of acute myocarditis and that the CMR diagnosis was positive in all the patients enrolled.
Dr. Ammirati agreed with Dr. Kerneis that the neutral results of the study were probably caused by the low-risk population. “If we look at retrospective registries, at 30 days there are zero cardiac deaths or heart transplants at 30 days in patients with a low-risk presentation.
“The ARAMIS trial has shown the feasibility of conducting studies in the setting of acute myocarditis, and even if the primary endpoint was neutral, some important data are still missing, such as change in ejection fraction and troponin levels,” he noted.
“In terms of future perspective, we are moving to assessing efficacy of anakinra or other immunosuppressive drugs from acute low risk patients to higher risk patients with heart failure and severe dysfunction,” he said.
Dr. Ammirati is the lead investigator of another ongoing study in such a higher-risk population; the MYTHS trial is investigating the use of intravenous steroids in patients with suspected acute myocarditis complicated by acute heart failure or cardiogenic shock, and an ejection fraction below 41%.
“So, we will have more results on the best treatment in this higher risk group of patients,” he concluded.
The ARAMIS trial was an academic study funded by the French Health Ministry and coordinated by the ACTION Group. Dr. Kerneis reports having received consulting fees from Kiniksa, Sanofi, and Bayer, and holds a patent for use of abatacept in immune checkpoint inhibitor (ICI)–induced myocarditis.
A version of this article first appeared on Medscape.com.
AMSTERDAM – A short course of the interleukin-1 receptor antagonist, anakinra, appeared safe but did not reduce complications of acute myocarditis in the ARAMIS trial.
The trial was presented at the annual congress of the European Society of Cardiology.
Lead investigator, Mathieu Kerneis, MD, Pitie Salpetriere APHP University Hospital, Paris, said this was the largest randomized controlled trial of patients with acute myocarditis and probably the first ever study in the acute setting of myocarditis patients diagnosed with cardiac magnetic resonance (CMR) imaging, not on biopsy, who are mostly at low risk for events.
He suggested that one of the reasons for the neutral result could have been the low-risk population involved and the low complication rate. “We enrolled an all-comer acute myocarditis population diagnosed with CMR, who were mostly at a low risk of complications,” he noted.
“I don’t think the story of anti-inflammatory drugs in acute myocarditis is over. This is just the beginning. This was the first trial, and it was just a phase 2 trial. We need further randomized trials to explore the potential benefit of an anti-inflammatory strategy in acute myocarditis patients at higher risk of complications. In addition, larger studies are needed to evaluate prolonged anti-inflammatory strategies in acute myocarditis patients at low-to-moderate risk of complications,” Dr. Kerneis concluded.
“It is very challenging to do a trial in high-risk patients with myocarditis as these patients are quite rare,” he added.
Inflammation of the myocardium
Dr. Kerneis explained that acute myocarditis is an inflammation of the myocardium that can cause permanent damage to the heart muscle and lead to myocardial infarction, stroke, heart failure, arrhythmias, and death. The condition can occur in individuals of all ages but is most frequent in young people. There is no specific treatment, but patients are generally treated with beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and sometimes steroids.
Anakinra is an interleukin-1 receptor antagonist that works by targeting the interleukin-1β innate immune pathway. Anakinra is used for the treatment of rheumatoid arthritis and has shown efficacy in pericarditis. Dr. Kerneis noted that there have been several case reports of successful treatment with anakinra in acute myocarditis.
The ARAMIS trial – conducted at six academic centers in France – was the first randomized study to evaluate inhibition of the interleukin-1β innate immune pathway in myocarditis patients. The trial enrolled 120 hospitalized, symptomatic patients with chest pain, increased cardiac troponin, and acute myocarditis diagnosed using CMR. More than half had had a recent bacterial or viral infection.
Patients were randomized within 72 hours of hospital admission to a daily subcutaneous dose of anakinra 100 mg or placebo until hospital discharge. Patients in both groups received standard-of-care treatments, including an ACE inhibitor, for at least 1 month. Consistent with prior data, the median age of participants was 28 years and 90% were men.
The primary endpoint was the number of days free of myocarditis complications (heart failure requiring hospitalization, chest pain requiring medication, left ventricular ejection fraction less than 50%, and ventricular arrhythmias) within 28 days postdischarge.
There was no significant difference in this endpoint between the two arms, with a median of 30 days for anakinra versus 31 days for placebo.
Overall, the rate of the composite endpoint of myocarditis complications occurred in 13.7% of patients, and there was a numerical reduction in the number of patients with these myocarditis complications with anakinra – 6 patients (10.5%) in the anakinra group versus 10 patients (16.5%) in the placebo group (odds ratio, 0.59; 95% confidence interval, 0.19-1.78). This was driven by fewer patients with chest pain requiring new medication (two patients versus six patients).
The safety endpoint was the number of serious adverse events within 28 days postdischarge. This endpoint occurred in seven patients (12.1%) in the anakinra arm and six patients (10.2%) in the placebo arm, with no significant difference between groups. Cases of severe infection within 28 days postdischarge were reported in both arms.
Low-risk population
Designated discussant of the study at the ESC Hotline session, Enrico Ammirati, MD, PhD, University of Milano-Bicocca, Monza, Italy, said that patients involved in ARAMIS fit the profile of acute myocarditis and that the CMR diagnosis was positive in all the patients enrolled.
Dr. Ammirati agreed with Dr. Kerneis that the neutral results of the study were probably caused by the low-risk population. “If we look at retrospective registries, at 30 days there are zero cardiac deaths or heart transplants at 30 days in patients with a low-risk presentation.
“The ARAMIS trial has shown the feasibility of conducting studies in the setting of acute myocarditis, and even if the primary endpoint was neutral, some important data are still missing, such as change in ejection fraction and troponin levels,” he noted.
“In terms of future perspective, we are moving to assessing efficacy of anakinra or other immunosuppressive drugs from acute low risk patients to higher risk patients with heart failure and severe dysfunction,” he said.
Dr. Ammirati is the lead investigator of another ongoing study in such a higher-risk population; the MYTHS trial is investigating the use of intravenous steroids in patients with suspected acute myocarditis complicated by acute heart failure or cardiogenic shock, and an ejection fraction below 41%.
“So, we will have more results on the best treatment in this higher risk group of patients,” he concluded.
The ARAMIS trial was an academic study funded by the French Health Ministry and coordinated by the ACTION Group. Dr. Kerneis reports having received consulting fees from Kiniksa, Sanofi, and Bayer, and holds a patent for use of abatacept in immune checkpoint inhibitor (ICI)–induced myocarditis.
A version of this article first appeared on Medscape.com.
AT ESC CONGRESS 2023
Aspirin still needed in first month after PCI: STOPDAPT-3
AMSTERDAM – Dropping aspirin and using low-dose prasugrel (Effient) alone in the initial month of treatment after percutaneous coronary intervention (PCI) failed to lower bleeding risk, compared with dual antiplatelet therapy (DAPT), and there was a signal of possible harm in terms of increased subacute stent thrombosis, in the STOPDAPT-3 trial.
“Therefore, dual antiplatelet therapy with aspirin and a P2Y12 inhibitor should still remain the standard strategy at least for 1 month after PCI,” said the trial’s lead investigator Masahiro Natsuaki, MD, Saga (Japan) University.
The STOPDAPT-3 trial was presented at the recent annual congress of the European Society of Cardiology.
Designated discussant Marco Valgimigli, MD, Cardiocentro Ticino Foundation, Lugano, Switzerland, explained that the current wisdom before this study was that aspirin withdrawal in the postacute phase after PCI (after 1 month of DAPT onwards) is associated with lower bleeding risk without affecting ischemic risk, but this STOPDAPT-3 trial is the first to look at the idea of not giving aspirin at all.
“This study is a well-designed, well-conducted trial, and the results are very clear: Dr. Valgimigli said.
He pointed out that the possible harm was not related to the coprimary cardiovascular composite endpoint, which did fulfill noninferiority, although he acknowledged the “generous” noninferiority margin.
Rather, the possible harm was related to an increase in subacute stent thrombosis, which was three times higher in the nonaspirin group (0.58% vs. 0.17%).
“While these absolute event rates are extremely low, they are unquestionably higher in the nonaspirin group,” he added.
In his presentation, Dr. Natsuaki explained that very short durations (1-3 months) of DAPT followed by P2Y12 inhibitor monotherapy has been shown to reduce bleeding events without increasing cardiovascular events, compared with longer durations of DAPT after PCI using drug-eluting stents.
However, the incidence of major bleeding events within the 1-month mandatory DAPT period after PCI remains high in clinical practice, particularly in patients with ACS or high bleeding risk.
In single-arm studies, use of prasugrel or ticagrelor (Brilinta) alone following new-generation drug-eluting stent implantation was not associated with any stent thrombosis in selected low-risk patients with or without ACS, and it is thought that removing aspirin from the DAPT regimen might reduce bleeding events early after PCI without compromising the risk of cardiovascular events. However, the efficacy and safety of this strategy has not been proven in randomized trials.
STOPDAPT-3 trial
STOPDAPT-3 investigated the efficacy and safety of prasugrel monotherapy compared with 1-month DAPT with aspirin and prasugrel in Japanese patients with ACS or high bleeding risk undergoing PCI with cobalt-chromium everolimus-eluting stents.
The study enrolled 6,002 patients with ACS or high bleeding risk who were randomly assigned to prasugrel monotherapy (3.75 mg/day; the licensed dose in Japan) or to DAPT with aspirin (81-100 mg/day) and prasugrel after a loading dose of prasugrel 20 mg in both groups.
There were two primary endpoints: major bleeding events (defined as BARC type 3 or 5) at 1 month for superiority and cardiovascular events (a composite of cardiovascular death, myocardial infarction, definite stent thrombosis, or stroke) at 1 month for noninferiority.
The major secondary endpoint was a composite of the coprimary bleeding and cardiovascular endpoints (cardiovascular death, myocardial infarction, definite stent thrombosis, stroke, or major bleeding) at 1 month representing net clinical benefit.
Results showed that, at 1 month, the no-aspirin strategy was not superior to DAPT for the coprimary bleeding endpoint, with major bleeding events occurring in 4.47% of the prasugrel monotherapy group versus 4.71% of those on DAPT (hazard ratio, 0.95; 95% confidence interval, 0.75-1.20).
The prasugrel monotherapy strategy was noninferior to DAPT, although there was a relative 50% margin for the coprimary cardiovascular endpoint. Cardiovascular endpoints occurred in 4.12% of prasugrel monotherapy group versus 3.69% of the DAPT patients (HR, 1.12; 95% CI, 0.87-1.45; P for noninferiority = .01).
The major secondary net clinical benefit endpoint occurred in 7.14% patients in the prasugrel monotherapy group and 7.38% patients in the DAPT group, with no between-group difference, indicating a similar effect on net clinical benefit for both groups.
However, there was an excess of any coronary revascularization (1.15% vs. 0.57%) and definite or probable stent thrombosis (0.71% vs. 0.44%) in the prasugrel monotherapy group compared with the DAPT group, while definite stent thrombosis was not different between the two groups (0.47% vs. 0.37%).
In a subgroup analysis stratified by ACS and non-ACS, the excess risk for cardiovascular events in the no-aspirin group, compared with the DAPT group, was seen in patients with ACS, but not in those without ACS.
Future: Focus on dose and timing
In his discussion, Dr. Valgimigli said the implications of this trial for clinical practice were very clear: “Aspirin remains a cornerstone treatment in the periprocedural and acute phase of PCI in patients without indications for oral anticoagulation.”
However, he added that the study opens several important points for subsequent discussion.
These include the role of type and dose of P2Y12 inhibitor therapy used; specifically, he questioned whether the 3.75-mg dose of prasugrel was enough.
Dr. Valgimigli also pointed out that this study did not include a purely high bleeding risk population, and he said there was still potential to investigate periprocedure versus postprocedure aspirin administration.
The STOPDAPT-3 trial was funded by Abbott Medical Japan. Dr. Natsuaki reported receiving honoraria from Abbott Medical Japan, Daiichi Sankyo, and Bayer.
A version of this article first appeared on Medscape.com.
AMSTERDAM – Dropping aspirin and using low-dose prasugrel (Effient) alone in the initial month of treatment after percutaneous coronary intervention (PCI) failed to lower bleeding risk, compared with dual antiplatelet therapy (DAPT), and there was a signal of possible harm in terms of increased subacute stent thrombosis, in the STOPDAPT-3 trial.
“Therefore, dual antiplatelet therapy with aspirin and a P2Y12 inhibitor should still remain the standard strategy at least for 1 month after PCI,” said the trial’s lead investigator Masahiro Natsuaki, MD, Saga (Japan) University.
The STOPDAPT-3 trial was presented at the recent annual congress of the European Society of Cardiology.
Designated discussant Marco Valgimigli, MD, Cardiocentro Ticino Foundation, Lugano, Switzerland, explained that the current wisdom before this study was that aspirin withdrawal in the postacute phase after PCI (after 1 month of DAPT onwards) is associated with lower bleeding risk without affecting ischemic risk, but this STOPDAPT-3 trial is the first to look at the idea of not giving aspirin at all.
“This study is a well-designed, well-conducted trial, and the results are very clear: Dr. Valgimigli said.
He pointed out that the possible harm was not related to the coprimary cardiovascular composite endpoint, which did fulfill noninferiority, although he acknowledged the “generous” noninferiority margin.
Rather, the possible harm was related to an increase in subacute stent thrombosis, which was three times higher in the nonaspirin group (0.58% vs. 0.17%).
“While these absolute event rates are extremely low, they are unquestionably higher in the nonaspirin group,” he added.
In his presentation, Dr. Natsuaki explained that very short durations (1-3 months) of DAPT followed by P2Y12 inhibitor monotherapy has been shown to reduce bleeding events without increasing cardiovascular events, compared with longer durations of DAPT after PCI using drug-eluting stents.
However, the incidence of major bleeding events within the 1-month mandatory DAPT period after PCI remains high in clinical practice, particularly in patients with ACS or high bleeding risk.
In single-arm studies, use of prasugrel or ticagrelor (Brilinta) alone following new-generation drug-eluting stent implantation was not associated with any stent thrombosis in selected low-risk patients with or without ACS, and it is thought that removing aspirin from the DAPT regimen might reduce bleeding events early after PCI without compromising the risk of cardiovascular events. However, the efficacy and safety of this strategy has not been proven in randomized trials.
STOPDAPT-3 trial
STOPDAPT-3 investigated the efficacy and safety of prasugrel monotherapy compared with 1-month DAPT with aspirin and prasugrel in Japanese patients with ACS or high bleeding risk undergoing PCI with cobalt-chromium everolimus-eluting stents.
The study enrolled 6,002 patients with ACS or high bleeding risk who were randomly assigned to prasugrel monotherapy (3.75 mg/day; the licensed dose in Japan) or to DAPT with aspirin (81-100 mg/day) and prasugrel after a loading dose of prasugrel 20 mg in both groups.
There were two primary endpoints: major bleeding events (defined as BARC type 3 or 5) at 1 month for superiority and cardiovascular events (a composite of cardiovascular death, myocardial infarction, definite stent thrombosis, or stroke) at 1 month for noninferiority.
The major secondary endpoint was a composite of the coprimary bleeding and cardiovascular endpoints (cardiovascular death, myocardial infarction, definite stent thrombosis, stroke, or major bleeding) at 1 month representing net clinical benefit.
Results showed that, at 1 month, the no-aspirin strategy was not superior to DAPT for the coprimary bleeding endpoint, with major bleeding events occurring in 4.47% of the prasugrel monotherapy group versus 4.71% of those on DAPT (hazard ratio, 0.95; 95% confidence interval, 0.75-1.20).
The prasugrel monotherapy strategy was noninferior to DAPT, although there was a relative 50% margin for the coprimary cardiovascular endpoint. Cardiovascular endpoints occurred in 4.12% of prasugrel monotherapy group versus 3.69% of the DAPT patients (HR, 1.12; 95% CI, 0.87-1.45; P for noninferiority = .01).
The major secondary net clinical benefit endpoint occurred in 7.14% patients in the prasugrel monotherapy group and 7.38% patients in the DAPT group, with no between-group difference, indicating a similar effect on net clinical benefit for both groups.
However, there was an excess of any coronary revascularization (1.15% vs. 0.57%) and definite or probable stent thrombosis (0.71% vs. 0.44%) in the prasugrel monotherapy group compared with the DAPT group, while definite stent thrombosis was not different between the two groups (0.47% vs. 0.37%).
In a subgroup analysis stratified by ACS and non-ACS, the excess risk for cardiovascular events in the no-aspirin group, compared with the DAPT group, was seen in patients with ACS, but not in those without ACS.
Future: Focus on dose and timing
In his discussion, Dr. Valgimigli said the implications of this trial for clinical practice were very clear: “Aspirin remains a cornerstone treatment in the periprocedural and acute phase of PCI in patients without indications for oral anticoagulation.”
However, he added that the study opens several important points for subsequent discussion.
These include the role of type and dose of P2Y12 inhibitor therapy used; specifically, he questioned whether the 3.75-mg dose of prasugrel was enough.
Dr. Valgimigli also pointed out that this study did not include a purely high bleeding risk population, and he said there was still potential to investigate periprocedure versus postprocedure aspirin administration.
The STOPDAPT-3 trial was funded by Abbott Medical Japan. Dr. Natsuaki reported receiving honoraria from Abbott Medical Japan, Daiichi Sankyo, and Bayer.
A version of this article first appeared on Medscape.com.
AMSTERDAM – Dropping aspirin and using low-dose prasugrel (Effient) alone in the initial month of treatment after percutaneous coronary intervention (PCI) failed to lower bleeding risk, compared with dual antiplatelet therapy (DAPT), and there was a signal of possible harm in terms of increased subacute stent thrombosis, in the STOPDAPT-3 trial.
“Therefore, dual antiplatelet therapy with aspirin and a P2Y12 inhibitor should still remain the standard strategy at least for 1 month after PCI,” said the trial’s lead investigator Masahiro Natsuaki, MD, Saga (Japan) University.
The STOPDAPT-3 trial was presented at the recent annual congress of the European Society of Cardiology.
Designated discussant Marco Valgimigli, MD, Cardiocentro Ticino Foundation, Lugano, Switzerland, explained that the current wisdom before this study was that aspirin withdrawal in the postacute phase after PCI (after 1 month of DAPT onwards) is associated with lower bleeding risk without affecting ischemic risk, but this STOPDAPT-3 trial is the first to look at the idea of not giving aspirin at all.
“This study is a well-designed, well-conducted trial, and the results are very clear: Dr. Valgimigli said.
He pointed out that the possible harm was not related to the coprimary cardiovascular composite endpoint, which did fulfill noninferiority, although he acknowledged the “generous” noninferiority margin.
Rather, the possible harm was related to an increase in subacute stent thrombosis, which was three times higher in the nonaspirin group (0.58% vs. 0.17%).
“While these absolute event rates are extremely low, they are unquestionably higher in the nonaspirin group,” he added.
In his presentation, Dr. Natsuaki explained that very short durations (1-3 months) of DAPT followed by P2Y12 inhibitor monotherapy has been shown to reduce bleeding events without increasing cardiovascular events, compared with longer durations of DAPT after PCI using drug-eluting stents.
However, the incidence of major bleeding events within the 1-month mandatory DAPT period after PCI remains high in clinical practice, particularly in patients with ACS or high bleeding risk.
In single-arm studies, use of prasugrel or ticagrelor (Brilinta) alone following new-generation drug-eluting stent implantation was not associated with any stent thrombosis in selected low-risk patients with or without ACS, and it is thought that removing aspirin from the DAPT regimen might reduce bleeding events early after PCI without compromising the risk of cardiovascular events. However, the efficacy and safety of this strategy has not been proven in randomized trials.
STOPDAPT-3 trial
STOPDAPT-3 investigated the efficacy and safety of prasugrel monotherapy compared with 1-month DAPT with aspirin and prasugrel in Japanese patients with ACS or high bleeding risk undergoing PCI with cobalt-chromium everolimus-eluting stents.
The study enrolled 6,002 patients with ACS or high bleeding risk who were randomly assigned to prasugrel monotherapy (3.75 mg/day; the licensed dose in Japan) or to DAPT with aspirin (81-100 mg/day) and prasugrel after a loading dose of prasugrel 20 mg in both groups.
There were two primary endpoints: major bleeding events (defined as BARC type 3 or 5) at 1 month for superiority and cardiovascular events (a composite of cardiovascular death, myocardial infarction, definite stent thrombosis, or stroke) at 1 month for noninferiority.
The major secondary endpoint was a composite of the coprimary bleeding and cardiovascular endpoints (cardiovascular death, myocardial infarction, definite stent thrombosis, stroke, or major bleeding) at 1 month representing net clinical benefit.
Results showed that, at 1 month, the no-aspirin strategy was not superior to DAPT for the coprimary bleeding endpoint, with major bleeding events occurring in 4.47% of the prasugrel monotherapy group versus 4.71% of those on DAPT (hazard ratio, 0.95; 95% confidence interval, 0.75-1.20).
The prasugrel monotherapy strategy was noninferior to DAPT, although there was a relative 50% margin for the coprimary cardiovascular endpoint. Cardiovascular endpoints occurred in 4.12% of prasugrel monotherapy group versus 3.69% of the DAPT patients (HR, 1.12; 95% CI, 0.87-1.45; P for noninferiority = .01).
The major secondary net clinical benefit endpoint occurred in 7.14% patients in the prasugrel monotherapy group and 7.38% patients in the DAPT group, with no between-group difference, indicating a similar effect on net clinical benefit for both groups.
However, there was an excess of any coronary revascularization (1.15% vs. 0.57%) and definite or probable stent thrombosis (0.71% vs. 0.44%) in the prasugrel monotherapy group compared with the DAPT group, while definite stent thrombosis was not different between the two groups (0.47% vs. 0.37%).
In a subgroup analysis stratified by ACS and non-ACS, the excess risk for cardiovascular events in the no-aspirin group, compared with the DAPT group, was seen in patients with ACS, but not in those without ACS.
Future: Focus on dose and timing
In his discussion, Dr. Valgimigli said the implications of this trial for clinical practice were very clear: “Aspirin remains a cornerstone treatment in the periprocedural and acute phase of PCI in patients without indications for oral anticoagulation.”
However, he added that the study opens several important points for subsequent discussion.
These include the role of type and dose of P2Y12 inhibitor therapy used; specifically, he questioned whether the 3.75-mg dose of prasugrel was enough.
Dr. Valgimigli also pointed out that this study did not include a purely high bleeding risk population, and he said there was still potential to investigate periprocedure versus postprocedure aspirin administration.
The STOPDAPT-3 trial was funded by Abbott Medical Japan. Dr. Natsuaki reported receiving honoraria from Abbott Medical Japan, Daiichi Sankyo, and Bayer.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
Dietary nitrates reduce contrast-induced nephropathy in ACS
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
IV iron shows only modest benefit in HF: HEART-FID
AMSTERDAM – , but the study failed to meet the specified more rigorous definition of significance (P = .01) on the primary hierarchical composite of death, hospitalizations for heart failure, or 6-minute walk distance.
The trial, which investigated intravenous ferric carboxymaltose treatment vs. placebo, also showed no statistical difference in the main secondary endpoint: time to cardiovascular death or first heart failure hospitalization.
It was hoped that HEART-FID, the largest study to date to look at intravenous iron supplementation in heart failure, would confirm benefits suggested in previous smaller studies, but its modest results seem to have, if anything, caused more uncertainly on whether supplementing iron is actually worthwhile.
The HEART-FID trial was presented at the annual congress of the European Society of Cardiology and simultaneously published online in the New England Journal of Medicine.
Another presentation at the ESC Congress reported a pooled meta-analysis of all the intravenous iron supplementation studies, including HEART-FID. This showed a significant reduction in one coprimary endpoint (cardiovascular hospitalization/CV death) but not in the other (heart failure hospitalization/CV death), which is the more traditional and well-recognized endpoint in heart failure trials.
The meta-analysis was also published online in the European Heart Journal.
HEART-FID lead investigator, Robert J. Mentz, MD, Duke University, Durham, N.C., said the totality of the evidence showed clinical benefits of intravenous iron supplementation with intravenous ferric carboxymaltose.
“I worry that people will focus on a P value rather than the actual clinical benefits seen across all the studies,” Dr. Mentz said in an interview. “Technically, this study was neutral in respect to the primary endpoint, but when we look at all the evidence with respect to ferric carboxymaltose, including this new pooled analysis, this does support clinical benefits.”
Comoderator of the ESC Hotline session at which the trial was presented, John McMurray, MD, University of Glasgow (Scotland), thought the trial had “muddied the waters a bit” on the issue of iron supplementation in heart failure.
“I would say we are in a less clear position on iron supplementation now than we were a few months ago. Those clinicians who have believed that checking iron levels and supplementing iron in those who are low is the right thing to do may now be wondering about that,” he told this news organization.
Dr. McMurray noted that initial impressions of the data from both HEART-FID and the meta-analysis suggested some benefit of intravenous iron on CV death/heart failure hospitalization in the first year, but on longer term follow-up, that benefit was less evident.
“We need to look further into why there is that discrepancy,” he said. “This could be a statistical phenomenon or could be something to do with the frequency of redosing over the longer term.”
He explained that several previous studies of intravenous iron supplementation in heart failure have reported apparent convincing benefits on quality of life and functional capacity, but there has been some uncertainty on this because of the difficulty in producing a placebo for intravenous iron.
“So, it would have been great to have some additional confirmation of these benefits and on harder endpoints,” he said, “but even in HEART-FID, there was only a small nonsignificant benefit in walking distance.”
HEART-FID
The HEART-FID trial randomly assigned 3,065 ambulatory patients with heart failure, a left ventricular ejection fraction of 40% or less, and iron deficiency to intravenous ferric carboxymaltose or placebo, given every 6 months as needed on the basis of iron indexes and hemoglobin levels, in addition to standard therapy for heart failure.
The primary outcome was a hierarchical composite of death within 12 months after randomization, hospitalizations for heart failure within 12 months after randomization, or change from baseline to 6 months in the 6-minute walk distance. The significance level was set at .01.
Results showed that death by month 12 occurred in 8.6% of the ferric carboxymaltose group and 10.3% of the placebo group; a total of 297 and 332 hospitalizations for heart failure, respectively, occurred by month 12; and the mean change from baseline to 6 months in the 6-minute walk distance was 8 meters in the ferric carboxymaltose group and 4 meters with placebo. The P value for the primary composite was .02.
The trial also used another method (unmatched win ratio) to analyze the hierarchical composite outcome in the ferric carboxymaltose group as compared with the placebo group that gave a result of 1.10 (99% confidence interval, 0.99-1.23).
During the follow-up period, CV death or hospitalization for heart failure (the main secondary outcome) occurred in 31.0% of the ferric carboxymaltose group and in 32.2% of the placebo group (hazard ratio, 0.93; 96% CI, 0.81-1.06).
Repeated dosing of ferric carboxymaltose appeared to be safe, with an acceptable adverse-event profile in most patients. The number of patients with serious adverse events occurring during the treatment period was similar in the two groups (27.0% in the ferric carboxymaltose group and 26.2% in the placebo group).
‘It’s hard to argue that we are not disappointed’
Designated discussant of the HEART-FID study at the ESC HOTLINE session, Scott Solomon, MD, Brigham and Women’s Hospital, Boston, described HEART-FID as “an extremely important and well-conducted trial.”
He noted that iron deficiency is extremely common in patients with heart failure, affecting at least about a third of patients, and is associated with reduced New York Heart Association class and reduced survival. Previous smaller studies have suggested benefit but have narrowly missed their primary endpoints. HEART-FID was a larger and sufficiently well-powered trial to test the hypothesis that iron supplementation can improve harder clinical endpoints.
Dr. Solomon said that the primary endpoint could be difficult to interpret, with a hierarchical composite, and a win ratio. “But I think it’s fair to say that the results are modest at best,” he added.
“When we look at the traditional cardiovascular death/heart failure hospitalization endpoint, one of the hard endpoints that we care about most in heart failure, it’s hard to argue that we are not disappointed,” he commented.
Referring to the P value of .01 threshold set for significance, which is based on new U.S. Food and Drug Administration regulatory standards, Dr. Solomon noted, “If they had used a standard P = .05 threshold, then they would be able to claim that this trial had met its primary endpoint. But, nevertheless, whatever threshold for significance we look at, the benefit was clearly modest.”
“As with all trials that show modest results, it will be useful to look at subgroups that are most likely to respond to the greatest extent to this therapy, and I look forward to learning more on this from further analyses,” Dr. Solomon concluded.
In an accompanying editorial in the New England Journal of Medicine, Pieter Martens, MD, and Wilfried Mullens, MD, PhD, Ziekenhuis Oost-Limburg, Genk, Belgium, and Hasselt (Belgium) University, point out that analyses from previous trials have suggested that intravenous iron did not have a treatment effect in patients with a transferrin saturation of more than 20%.
They note that, in the ferric carboxymaltose group in the HEART-FID trial, the mean transferrin saturation was 23.9% at baseline, higher than in previous studies.
Future analyses should assess the importance of the transferrin saturation value at baseline, which “could help redefine the definition of iron deficiency in patients with heart failure and, we hope, help clinicians determine which patients might benefit from intravenous iron supplementation,” they write.
Meta-analysis of trials
The meta-analysis of intravenous iron supplementation trials in heart failure was presented by Piotr Ponikowski, MD, Medical University Wroclaw (Poland).
The analysis pooled individual patient data from three double-blind, placebo-controlled trials – CONFIRM-HF 2, AFFIRM-AHF 3, and HEART-FID – giving a total of 4,475 patients, with 2,241 receiving ferric carboxymaltose and 2,234 receiving placebo.
The two prespecified composite primary endpoints were CV hospitalizations/CV death and heart failure hospitalizations/CV death.
These showed similar 13%-14% relative risk reductions with ferric carboxymaltose, but only the former was statistically significant.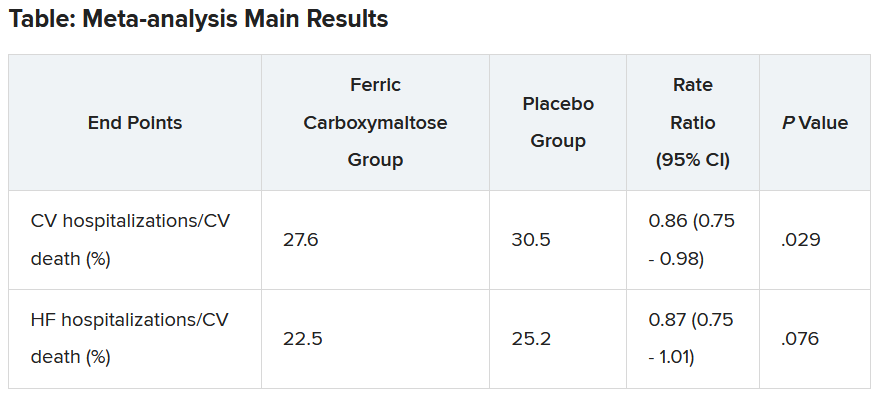
Similar results were seen when a fourth trial – IRONMAN (an open-label trial) – was included. In this case, the heart failure hospitalization/CV death endpoint was also nonsignificantly reduced with ferric carboxymaltose (rate ratio, 0.82; 95% CI, 0.58-1.07).
Subgroup analysis suggested that patients with higher transferrin saturation levels appeared to have a lack of treatment effect, whereas those with lower transferrin saturation (< 15%) showed significant treatment benefits.
A higher 6-month cumulative dose of ferric carboxymaltose – likely the result of redosing – may be associated with a slightly greater treatment effect after 6 months, Dr. Ponikowski reported.
He concluded: “These data support the use of intravenous ferric carboxymaltose to treat iron deficiency among patients with heart failure with reduced/mildly reduced LVEF [left ventricular ejection fraction] to reduce the risk of future hospitalization.”
“Our findings support additional research to challenge the current definition of iron deficiency in heart failure as an indication for IV iron therapy and to identify eligibility criteria for optimal redosing strategy,” Dr. Ponikowski added.
Discussant of the meta-analysis presentation at the ESC Hotline session, Pardeep Jhund, MD, University of Glasgow, suggested that the endpoint of most interest would be heart failure hospitalization/CV death in the analysis that included the IRONMAN trial, “which unfortunately did not meet statistical significance.”
In answer to the question “Where does this leave clinicians when treating patients?”Dr. Jhund said, “After yet another meta-analysis, I think the role of IV iron in reducing morbidity and mortality outcomes in heart failure remains questionable.”
“While the absence of evidence is not evidence of absence, the wide confidence intervals of the treatment effect on heart failure hospitalization/CV death leaves a lot of room for doubt about the efficacy of IV iron for reducing HF hospitalizations,” he concluded.
The HEART-FID trial was funded by American Regent, a Daiichi Sankyo Group company. Dr. Mentz reports receiving research support from American Regent and honoraria from American Regent, Vifor, and Pharmacosmos. Dr. Ponikowski reports consultancy fees/honoraria from Vifor Pharma, Boehringer Ingelheim, AstraZeneca, Servier, Novartis, Bayer, MSD, Pfizer, Moderna, Sanofi, and Radcliffe Group.
A version of this article first appeared on Medscape.com.
AMSTERDAM – , but the study failed to meet the specified more rigorous definition of significance (P = .01) on the primary hierarchical composite of death, hospitalizations for heart failure, or 6-minute walk distance.
The trial, which investigated intravenous ferric carboxymaltose treatment vs. placebo, also showed no statistical difference in the main secondary endpoint: time to cardiovascular death or first heart failure hospitalization.
It was hoped that HEART-FID, the largest study to date to look at intravenous iron supplementation in heart failure, would confirm benefits suggested in previous smaller studies, but its modest results seem to have, if anything, caused more uncertainly on whether supplementing iron is actually worthwhile.
The HEART-FID trial was presented at the annual congress of the European Society of Cardiology and simultaneously published online in the New England Journal of Medicine.
Another presentation at the ESC Congress reported a pooled meta-analysis of all the intravenous iron supplementation studies, including HEART-FID. This showed a significant reduction in one coprimary endpoint (cardiovascular hospitalization/CV death) but not in the other (heart failure hospitalization/CV death), which is the more traditional and well-recognized endpoint in heart failure trials.
The meta-analysis was also published online in the European Heart Journal.
HEART-FID lead investigator, Robert J. Mentz, MD, Duke University, Durham, N.C., said the totality of the evidence showed clinical benefits of intravenous iron supplementation with intravenous ferric carboxymaltose.
“I worry that people will focus on a P value rather than the actual clinical benefits seen across all the studies,” Dr. Mentz said in an interview. “Technically, this study was neutral in respect to the primary endpoint, but when we look at all the evidence with respect to ferric carboxymaltose, including this new pooled analysis, this does support clinical benefits.”
Comoderator of the ESC Hotline session at which the trial was presented, John McMurray, MD, University of Glasgow (Scotland), thought the trial had “muddied the waters a bit” on the issue of iron supplementation in heart failure.
“I would say we are in a less clear position on iron supplementation now than we were a few months ago. Those clinicians who have believed that checking iron levels and supplementing iron in those who are low is the right thing to do may now be wondering about that,” he told this news organization.
Dr. McMurray noted that initial impressions of the data from both HEART-FID and the meta-analysis suggested some benefit of intravenous iron on CV death/heart failure hospitalization in the first year, but on longer term follow-up, that benefit was less evident.
“We need to look further into why there is that discrepancy,” he said. “This could be a statistical phenomenon or could be something to do with the frequency of redosing over the longer term.”
He explained that several previous studies of intravenous iron supplementation in heart failure have reported apparent convincing benefits on quality of life and functional capacity, but there has been some uncertainty on this because of the difficulty in producing a placebo for intravenous iron.
“So, it would have been great to have some additional confirmation of these benefits and on harder endpoints,” he said, “but even in HEART-FID, there was only a small nonsignificant benefit in walking distance.”
HEART-FID
The HEART-FID trial randomly assigned 3,065 ambulatory patients with heart failure, a left ventricular ejection fraction of 40% or less, and iron deficiency to intravenous ferric carboxymaltose or placebo, given every 6 months as needed on the basis of iron indexes and hemoglobin levels, in addition to standard therapy for heart failure.
The primary outcome was a hierarchical composite of death within 12 months after randomization, hospitalizations for heart failure within 12 months after randomization, or change from baseline to 6 months in the 6-minute walk distance. The significance level was set at .01.
Results showed that death by month 12 occurred in 8.6% of the ferric carboxymaltose group and 10.3% of the placebo group; a total of 297 and 332 hospitalizations for heart failure, respectively, occurred by month 12; and the mean change from baseline to 6 months in the 6-minute walk distance was 8 meters in the ferric carboxymaltose group and 4 meters with placebo. The P value for the primary composite was .02.
The trial also used another method (unmatched win ratio) to analyze the hierarchical composite outcome in the ferric carboxymaltose group as compared with the placebo group that gave a result of 1.10 (99% confidence interval, 0.99-1.23).
During the follow-up period, CV death or hospitalization for heart failure (the main secondary outcome) occurred in 31.0% of the ferric carboxymaltose group and in 32.2% of the placebo group (hazard ratio, 0.93; 96% CI, 0.81-1.06).
Repeated dosing of ferric carboxymaltose appeared to be safe, with an acceptable adverse-event profile in most patients. The number of patients with serious adverse events occurring during the treatment period was similar in the two groups (27.0% in the ferric carboxymaltose group and 26.2% in the placebo group).
‘It’s hard to argue that we are not disappointed’
Designated discussant of the HEART-FID study at the ESC HOTLINE session, Scott Solomon, MD, Brigham and Women’s Hospital, Boston, described HEART-FID as “an extremely important and well-conducted trial.”
He noted that iron deficiency is extremely common in patients with heart failure, affecting at least about a third of patients, and is associated with reduced New York Heart Association class and reduced survival. Previous smaller studies have suggested benefit but have narrowly missed their primary endpoints. HEART-FID was a larger and sufficiently well-powered trial to test the hypothesis that iron supplementation can improve harder clinical endpoints.
Dr. Solomon said that the primary endpoint could be difficult to interpret, with a hierarchical composite, and a win ratio. “But I think it’s fair to say that the results are modest at best,” he added.
“When we look at the traditional cardiovascular death/heart failure hospitalization endpoint, one of the hard endpoints that we care about most in heart failure, it’s hard to argue that we are not disappointed,” he commented.
Referring to the P value of .01 threshold set for significance, which is based on new U.S. Food and Drug Administration regulatory standards, Dr. Solomon noted, “If they had used a standard P = .05 threshold, then they would be able to claim that this trial had met its primary endpoint. But, nevertheless, whatever threshold for significance we look at, the benefit was clearly modest.”
“As with all trials that show modest results, it will be useful to look at subgroups that are most likely to respond to the greatest extent to this therapy, and I look forward to learning more on this from further analyses,” Dr. Solomon concluded.
In an accompanying editorial in the New England Journal of Medicine, Pieter Martens, MD, and Wilfried Mullens, MD, PhD, Ziekenhuis Oost-Limburg, Genk, Belgium, and Hasselt (Belgium) University, point out that analyses from previous trials have suggested that intravenous iron did not have a treatment effect in patients with a transferrin saturation of more than 20%.
They note that, in the ferric carboxymaltose group in the HEART-FID trial, the mean transferrin saturation was 23.9% at baseline, higher than in previous studies.
Future analyses should assess the importance of the transferrin saturation value at baseline, which “could help redefine the definition of iron deficiency in patients with heart failure and, we hope, help clinicians determine which patients might benefit from intravenous iron supplementation,” they write.
Meta-analysis of trials
The meta-analysis of intravenous iron supplementation trials in heart failure was presented by Piotr Ponikowski, MD, Medical University Wroclaw (Poland).
The analysis pooled individual patient data from three double-blind, placebo-controlled trials – CONFIRM-HF 2, AFFIRM-AHF 3, and HEART-FID – giving a total of 4,475 patients, with 2,241 receiving ferric carboxymaltose and 2,234 receiving placebo.
The two prespecified composite primary endpoints were CV hospitalizations/CV death and heart failure hospitalizations/CV death.
These showed similar 13%-14% relative risk reductions with ferric carboxymaltose, but only the former was statistically significant.
Similar results were seen when a fourth trial – IRONMAN (an open-label trial) – was included. In this case, the heart failure hospitalization/CV death endpoint was also nonsignificantly reduced with ferric carboxymaltose (rate ratio, 0.82; 95% CI, 0.58-1.07).
Subgroup analysis suggested that patients with higher transferrin saturation levels appeared to have a lack of treatment effect, whereas those with lower transferrin saturation (< 15%) showed significant treatment benefits.
A higher 6-month cumulative dose of ferric carboxymaltose – likely the result of redosing – may be associated with a slightly greater treatment effect after 6 months, Dr. Ponikowski reported.
He concluded: “These data support the use of intravenous ferric carboxymaltose to treat iron deficiency among patients with heart failure with reduced/mildly reduced LVEF [left ventricular ejection fraction] to reduce the risk of future hospitalization.”
“Our findings support additional research to challenge the current definition of iron deficiency in heart failure as an indication for IV iron therapy and to identify eligibility criteria for optimal redosing strategy,” Dr. Ponikowski added.
Discussant of the meta-analysis presentation at the ESC Hotline session, Pardeep Jhund, MD, University of Glasgow, suggested that the endpoint of most interest would be heart failure hospitalization/CV death in the analysis that included the IRONMAN trial, “which unfortunately did not meet statistical significance.”
In answer to the question “Where does this leave clinicians when treating patients?”Dr. Jhund said, “After yet another meta-analysis, I think the role of IV iron in reducing morbidity and mortality outcomes in heart failure remains questionable.”
“While the absence of evidence is not evidence of absence, the wide confidence intervals of the treatment effect on heart failure hospitalization/CV death leaves a lot of room for doubt about the efficacy of IV iron for reducing HF hospitalizations,” he concluded.
The HEART-FID trial was funded by American Regent, a Daiichi Sankyo Group company. Dr. Mentz reports receiving research support from American Regent and honoraria from American Regent, Vifor, and Pharmacosmos. Dr. Ponikowski reports consultancy fees/honoraria from Vifor Pharma, Boehringer Ingelheim, AstraZeneca, Servier, Novartis, Bayer, MSD, Pfizer, Moderna, Sanofi, and Radcliffe Group.
A version of this article first appeared on Medscape.com.
AMSTERDAM – , but the study failed to meet the specified more rigorous definition of significance (P = .01) on the primary hierarchical composite of death, hospitalizations for heart failure, or 6-minute walk distance.
The trial, which investigated intravenous ferric carboxymaltose treatment vs. placebo, also showed no statistical difference in the main secondary endpoint: time to cardiovascular death or first heart failure hospitalization.
It was hoped that HEART-FID, the largest study to date to look at intravenous iron supplementation in heart failure, would confirm benefits suggested in previous smaller studies, but its modest results seem to have, if anything, caused more uncertainly on whether supplementing iron is actually worthwhile.
The HEART-FID trial was presented at the annual congress of the European Society of Cardiology and simultaneously published online in the New England Journal of Medicine.
Another presentation at the ESC Congress reported a pooled meta-analysis of all the intravenous iron supplementation studies, including HEART-FID. This showed a significant reduction in one coprimary endpoint (cardiovascular hospitalization/CV death) but not in the other (heart failure hospitalization/CV death), which is the more traditional and well-recognized endpoint in heart failure trials.
The meta-analysis was also published online in the European Heart Journal.
HEART-FID lead investigator, Robert J. Mentz, MD, Duke University, Durham, N.C., said the totality of the evidence showed clinical benefits of intravenous iron supplementation with intravenous ferric carboxymaltose.
“I worry that people will focus on a P value rather than the actual clinical benefits seen across all the studies,” Dr. Mentz said in an interview. “Technically, this study was neutral in respect to the primary endpoint, but when we look at all the evidence with respect to ferric carboxymaltose, including this new pooled analysis, this does support clinical benefits.”
Comoderator of the ESC Hotline session at which the trial was presented, John McMurray, MD, University of Glasgow (Scotland), thought the trial had “muddied the waters a bit” on the issue of iron supplementation in heart failure.
“I would say we are in a less clear position on iron supplementation now than we were a few months ago. Those clinicians who have believed that checking iron levels and supplementing iron in those who are low is the right thing to do may now be wondering about that,” he told this news organization.
Dr. McMurray noted that initial impressions of the data from both HEART-FID and the meta-analysis suggested some benefit of intravenous iron on CV death/heart failure hospitalization in the first year, but on longer term follow-up, that benefit was less evident.
“We need to look further into why there is that discrepancy,” he said. “This could be a statistical phenomenon or could be something to do with the frequency of redosing over the longer term.”
He explained that several previous studies of intravenous iron supplementation in heart failure have reported apparent convincing benefits on quality of life and functional capacity, but there has been some uncertainty on this because of the difficulty in producing a placebo for intravenous iron.
“So, it would have been great to have some additional confirmation of these benefits and on harder endpoints,” he said, “but even in HEART-FID, there was only a small nonsignificant benefit in walking distance.”
HEART-FID
The HEART-FID trial randomly assigned 3,065 ambulatory patients with heart failure, a left ventricular ejection fraction of 40% or less, and iron deficiency to intravenous ferric carboxymaltose or placebo, given every 6 months as needed on the basis of iron indexes and hemoglobin levels, in addition to standard therapy for heart failure.
The primary outcome was a hierarchical composite of death within 12 months after randomization, hospitalizations for heart failure within 12 months after randomization, or change from baseline to 6 months in the 6-minute walk distance. The significance level was set at .01.
Results showed that death by month 12 occurred in 8.6% of the ferric carboxymaltose group and 10.3% of the placebo group; a total of 297 and 332 hospitalizations for heart failure, respectively, occurred by month 12; and the mean change from baseline to 6 months in the 6-minute walk distance was 8 meters in the ferric carboxymaltose group and 4 meters with placebo. The P value for the primary composite was .02.
The trial also used another method (unmatched win ratio) to analyze the hierarchical composite outcome in the ferric carboxymaltose group as compared with the placebo group that gave a result of 1.10 (99% confidence interval, 0.99-1.23).
During the follow-up period, CV death or hospitalization for heart failure (the main secondary outcome) occurred in 31.0% of the ferric carboxymaltose group and in 32.2% of the placebo group (hazard ratio, 0.93; 96% CI, 0.81-1.06).
Repeated dosing of ferric carboxymaltose appeared to be safe, with an acceptable adverse-event profile in most patients. The number of patients with serious adverse events occurring during the treatment period was similar in the two groups (27.0% in the ferric carboxymaltose group and 26.2% in the placebo group).
‘It’s hard to argue that we are not disappointed’
Designated discussant of the HEART-FID study at the ESC HOTLINE session, Scott Solomon, MD, Brigham and Women’s Hospital, Boston, described HEART-FID as “an extremely important and well-conducted trial.”
He noted that iron deficiency is extremely common in patients with heart failure, affecting at least about a third of patients, and is associated with reduced New York Heart Association class and reduced survival. Previous smaller studies have suggested benefit but have narrowly missed their primary endpoints. HEART-FID was a larger and sufficiently well-powered trial to test the hypothesis that iron supplementation can improve harder clinical endpoints.
Dr. Solomon said that the primary endpoint could be difficult to interpret, with a hierarchical composite, and a win ratio. “But I think it’s fair to say that the results are modest at best,” he added.
“When we look at the traditional cardiovascular death/heart failure hospitalization endpoint, one of the hard endpoints that we care about most in heart failure, it’s hard to argue that we are not disappointed,” he commented.
Referring to the P value of .01 threshold set for significance, which is based on new U.S. Food and Drug Administration regulatory standards, Dr. Solomon noted, “If they had used a standard P = .05 threshold, then they would be able to claim that this trial had met its primary endpoint. But, nevertheless, whatever threshold for significance we look at, the benefit was clearly modest.”
“As with all trials that show modest results, it will be useful to look at subgroups that are most likely to respond to the greatest extent to this therapy, and I look forward to learning more on this from further analyses,” Dr. Solomon concluded.
In an accompanying editorial in the New England Journal of Medicine, Pieter Martens, MD, and Wilfried Mullens, MD, PhD, Ziekenhuis Oost-Limburg, Genk, Belgium, and Hasselt (Belgium) University, point out that analyses from previous trials have suggested that intravenous iron did not have a treatment effect in patients with a transferrin saturation of more than 20%.
They note that, in the ferric carboxymaltose group in the HEART-FID trial, the mean transferrin saturation was 23.9% at baseline, higher than in previous studies.
Future analyses should assess the importance of the transferrin saturation value at baseline, which “could help redefine the definition of iron deficiency in patients with heart failure and, we hope, help clinicians determine which patients might benefit from intravenous iron supplementation,” they write.
Meta-analysis of trials
The meta-analysis of intravenous iron supplementation trials in heart failure was presented by Piotr Ponikowski, MD, Medical University Wroclaw (Poland).
The analysis pooled individual patient data from three double-blind, placebo-controlled trials – CONFIRM-HF 2, AFFIRM-AHF 3, and HEART-FID – giving a total of 4,475 patients, with 2,241 receiving ferric carboxymaltose and 2,234 receiving placebo.
The two prespecified composite primary endpoints were CV hospitalizations/CV death and heart failure hospitalizations/CV death.
These showed similar 13%-14% relative risk reductions with ferric carboxymaltose, but only the former was statistically significant.
Similar results were seen when a fourth trial – IRONMAN (an open-label trial) – was included. In this case, the heart failure hospitalization/CV death endpoint was also nonsignificantly reduced with ferric carboxymaltose (rate ratio, 0.82; 95% CI, 0.58-1.07).
Subgroup analysis suggested that patients with higher transferrin saturation levels appeared to have a lack of treatment effect, whereas those with lower transferrin saturation (< 15%) showed significant treatment benefits.
A higher 6-month cumulative dose of ferric carboxymaltose – likely the result of redosing – may be associated with a slightly greater treatment effect after 6 months, Dr. Ponikowski reported.
He concluded: “These data support the use of intravenous ferric carboxymaltose to treat iron deficiency among patients with heart failure with reduced/mildly reduced LVEF [left ventricular ejection fraction] to reduce the risk of future hospitalization.”
“Our findings support additional research to challenge the current definition of iron deficiency in heart failure as an indication for IV iron therapy and to identify eligibility criteria for optimal redosing strategy,” Dr. Ponikowski added.
Discussant of the meta-analysis presentation at the ESC Hotline session, Pardeep Jhund, MD, University of Glasgow, suggested that the endpoint of most interest would be heart failure hospitalization/CV death in the analysis that included the IRONMAN trial, “which unfortunately did not meet statistical significance.”
In answer to the question “Where does this leave clinicians when treating patients?”Dr. Jhund said, “After yet another meta-analysis, I think the role of IV iron in reducing morbidity and mortality outcomes in heart failure remains questionable.”
“While the absence of evidence is not evidence of absence, the wide confidence intervals of the treatment effect on heart failure hospitalization/CV death leaves a lot of room for doubt about the efficacy of IV iron for reducing HF hospitalizations,” he concluded.
The HEART-FID trial was funded by American Regent, a Daiichi Sankyo Group company. Dr. Mentz reports receiving research support from American Regent and honoraria from American Regent, Vifor, and Pharmacosmos. Dr. Ponikowski reports consultancy fees/honoraria from Vifor Pharma, Boehringer Ingelheim, AstraZeneca, Servier, Novartis, Bayer, MSD, Pfizer, Moderna, Sanofi, and Radcliffe Group.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
Anticoagulation no benefit in presumed AFib detected by cardiac devices
AMSTERDAM – Among patients with atrial high-rate episodes detected by implantable devices, anticoagulation with edoxaban did not significantly reduce the incidence of a composite outcome of cardiovascular death, stroke, or systemic embolism in comparison with placebo but was associated with a higher bleeding risk in the NOAH-AFNET 6 trial.
“ They do not need to be anticoagulated. That is a relief,” the lead investigator of the trial, Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), said in an interview.
Dr. Kirchhof pointed out that this result was unexpected. “Many of us thought that because atrial high-rate episodes look like AF[ib] when they occur, then they are an indication for anticoagulation. But based on these results from the first-ever randomized trial on this population, there is no need for anticoagulation in these patients.”
Dr. Kirchhof presented the NOAH-AFNET 6 trial at the annual congress of the European Society of Cardiology. The study was also simultaneously published in the New England Journal of Medicine.
The trial recruited patients with implanted devices that enable continuous monitoring of atrial rhythm, such as pacemakers and defibrillators. “Because we can record the rhythm day and night with these devices, they pick up small abnormalities. About 20% of these patients experience these occasional atrial high-rate episodes – short episodes that look like AF[ib], but they are rare and brief,” Dr. Kirchhof noted.
He explained that whether the occurrence of these atrial high-rate episodes in patients without AFib, as documented on a conventional electrocardiogram, justifies the initiation of anticoagulants has been unclear. “But this trial tells us that these episodes are different to AF[ib] that is diagnosed on ECG,” he added.
Another finding in the trial was that among these patients, there was an unexpectedly low rate of stroke, despite the patients’ having a CHADSVASC score of 4.
“Based on the result of this trial, these occasional atrial high-rate episodes do not appear to be associated with stroke. It appears quite benign,” Dr. Kirchhof said.
Implications for wearable technology?
He said the results may also have implications for wearable devices that pick up abnormal heart rhythm, such as smartwatches.
“We don’t know exactly what these wearable technologies are picking up, but most likely it is these atrial high-rate episodes. But we need more research on the value of these wearable technologies; we need randomized trials in this particular patient population before we consider anticoagulation in these patients,” Dr. Kirchhof stated.
The NOAH-AFNET 6 study was an event-driven, double-blind, double-dummy, randomized trial involving 2,536 patients aged 65 years or older who had atrial high-rate episodes that lasted for at least 6 minutes and who had at least one additional risk factor for stroke.
Patients were randomly assigned in a 1:1 ratio to receive edoxaban or placebo. The primary efficacy outcome was a composite of cardiovascular death, stroke, or systemic embolism, evaluated in a time-to-event analysis. The safety outcome was a composite of death from any cause or major bleeding.
The mean age of the patients was 78 years, 37.4% were women, and the median duration of atrial high-rate episodes was 2.8 hours. The trial was terminated early, at a median follow-up of 21 months, on the basis of safety concerns and the results of an independent, informal assessment of futility for the efficacy of edoxaban; at termination, the planned enrollment had been completed.
Results showed that a primary efficacy outcome event occurred in 83 patients (3.2% per patient-year) in the edoxaban group and in 101 patients (4.0% per patient-year) in the placebo group (hazard ratio, 0.81; 95% confidence interval, 0.60-1.08; P = .15). The incidence of stroke was approximately 1% per patient-year in both groups.
A safety outcome event occurred in 149 patients (5.9% per patient-year) in the edoxaban group and in 114 patients (4.5% per patient-year) in the placebo group (HR, 1.31; 95% CI, 1.02-1.67; P = .03).
ECG-diagnosed AFib developed in 462 of 2,536 patients (18.2% total, 8.7% per patient-year).
In the NEJM article, the authors wrote that the findings of this trial – the low incidence of stroke that was not further reduced by treatment with edoxaban – may make it appropriate to withhold anticoagulant therapy for patients with atrial high-rate episodes.
The main difference between the population studied in this trial and patients with AFib, as documented on an ECG, appears to be the paucity and brevity of atrial arrhythmias in patients with atrial high-rate episodes (termed low arrhythmia burden). Published reports show that a low arrhythmia burden contributes to a low incidence of stroke among patients with AFib, the study authors wrote.
They added that the low rate of stroke in this trial suggests that in addition to clinical risk prediction formulas for stroke, methods to improve the estimation of stroke risk among patients with infrequent atrial arrhythmias detected by long-term monitoring are needed to guide decision-making on the use of anticoagulation.
Commenting on the NOAH-AFNET 6 results, the comoderator of the ESC HOTLINE session at which they were presented, Barbara Casadei, MD, John Radcliffe Hospital, Oxford, England, said: “Finally we know what to with these patients. Before we just had a variety of opinions with no evidence. I think that the trial really highlights that patients who come to the doctor with symptoms of AF[ib] or who have ECG-documented AF[ib] have a much higher risk of cardioembolic stroke than patients in whom this presumed AF[ib] is picked up incidentally from implanted devices.”
She added: “The stroke rates are very low in this trial, so anticoagulation was never going to work. But this is an important finding. We know that anticoagulants are not a free lunch. There is a significant bleeding risk. These results suggest that unless a patient has clinical AF[ib] that shows up on an ECG then we need to more cautious in prescribing anticoagulation.”
Also commenting on the study, immediate past president of the American College of Cardiology Ed Fry, MD, Ascension Indiana St. Vincent Heart Center, Indianapolis, said the management of patients with implanted cardiac devices or personal wearable technology that has picked up an abnormal rhythm suggestive of AFib was a big question in clinical practice.
“These episodes could be AF[ib], which comes with an increased stroke risk, but it could also be something else like atrial tachycardia or supraventricular tachycardia, which do not confer an increased stroke risk,” he explained.
“This study shows that without a firm diagnosis of AF[ib] on an ECG or some sort of continuous AF[ib] monitoring device, we are going to be anticoagulating people who don’t need it. They were exposed to the risk of bleeding without getting the benefit of a reduction in stroke risk,” Dr. Fry noted.
“The important outcome from this trial is that it gives comfort in we can be more confident in withholding anticoagulation until we get a firm diagnosis of AF[ib]. If we have a high index of suspicion that this could be AF[ib], then we can arrange for a further testing,” he added.
Second trial reporting soon
A trial similar to NOAH-AFNET 6 is currently underway – the ARTESIA trial, which is expected to be reported later in 2023.
“We are in close contact with the leadership of that trial, and we hope to do some meta-analysis,” Dr. Kirchhof said. “But I think today we’ve gone from no evidence to one outcome-based trial which shows there is no reason to use anticoagulation in these patients with atrial high-rate episodes. I think this is reason to change practice now, but yes, of course we need to look at the data in totality once the second trial has reported.”
But the lead investigator of the ARTESIA trial, Stuart Connolly, MD, McMaster University, Hamilton, Ont., does not believe the NOAH-AFNET 6 trial should change practice at this time.
“This trial fails to adequately address the critical issue that drives clinical decision-making in these patients because it is underpowered for the most important endpoint of stroke,” he said in an interview.
“The key question is whether anticoagulation reduces stroke in these patients,” he added. “To answer that, a clinical trial needs to have a lot of strokes, and this trial had very few. The trial was stopped early and had way too few strokes to properly answer this key question.”
The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
AMSTERDAM – Among patients with atrial high-rate episodes detected by implantable devices, anticoagulation with edoxaban did not significantly reduce the incidence of a composite outcome of cardiovascular death, stroke, or systemic embolism in comparison with placebo but was associated with a higher bleeding risk in the NOAH-AFNET 6 trial.
“ They do not need to be anticoagulated. That is a relief,” the lead investigator of the trial, Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), said in an interview.
Dr. Kirchhof pointed out that this result was unexpected. “Many of us thought that because atrial high-rate episodes look like AF[ib] when they occur, then they are an indication for anticoagulation. But based on these results from the first-ever randomized trial on this population, there is no need for anticoagulation in these patients.”
Dr. Kirchhof presented the NOAH-AFNET 6 trial at the annual congress of the European Society of Cardiology. The study was also simultaneously published in the New England Journal of Medicine.
The trial recruited patients with implanted devices that enable continuous monitoring of atrial rhythm, such as pacemakers and defibrillators. “Because we can record the rhythm day and night with these devices, they pick up small abnormalities. About 20% of these patients experience these occasional atrial high-rate episodes – short episodes that look like AF[ib], but they are rare and brief,” Dr. Kirchhof noted.
He explained that whether the occurrence of these atrial high-rate episodes in patients without AFib, as documented on a conventional electrocardiogram, justifies the initiation of anticoagulants has been unclear. “But this trial tells us that these episodes are different to AF[ib] that is diagnosed on ECG,” he added.
Another finding in the trial was that among these patients, there was an unexpectedly low rate of stroke, despite the patients’ having a CHADSVASC score of 4.
“Based on the result of this trial, these occasional atrial high-rate episodes do not appear to be associated with stroke. It appears quite benign,” Dr. Kirchhof said.
Implications for wearable technology?
He said the results may also have implications for wearable devices that pick up abnormal heart rhythm, such as smartwatches.
“We don’t know exactly what these wearable technologies are picking up, but most likely it is these atrial high-rate episodes. But we need more research on the value of these wearable technologies; we need randomized trials in this particular patient population before we consider anticoagulation in these patients,” Dr. Kirchhof stated.
The NOAH-AFNET 6 study was an event-driven, double-blind, double-dummy, randomized trial involving 2,536 patients aged 65 years or older who had atrial high-rate episodes that lasted for at least 6 minutes and who had at least one additional risk factor for stroke.
Patients were randomly assigned in a 1:1 ratio to receive edoxaban or placebo. The primary efficacy outcome was a composite of cardiovascular death, stroke, or systemic embolism, evaluated in a time-to-event analysis. The safety outcome was a composite of death from any cause or major bleeding.
The mean age of the patients was 78 years, 37.4% were women, and the median duration of atrial high-rate episodes was 2.8 hours. The trial was terminated early, at a median follow-up of 21 months, on the basis of safety concerns and the results of an independent, informal assessment of futility for the efficacy of edoxaban; at termination, the planned enrollment had been completed.
Results showed that a primary efficacy outcome event occurred in 83 patients (3.2% per patient-year) in the edoxaban group and in 101 patients (4.0% per patient-year) in the placebo group (hazard ratio, 0.81; 95% confidence interval, 0.60-1.08; P = .15). The incidence of stroke was approximately 1% per patient-year in both groups.
A safety outcome event occurred in 149 patients (5.9% per patient-year) in the edoxaban group and in 114 patients (4.5% per patient-year) in the placebo group (HR, 1.31; 95% CI, 1.02-1.67; P = .03).
ECG-diagnosed AFib developed in 462 of 2,536 patients (18.2% total, 8.7% per patient-year).
In the NEJM article, the authors wrote that the findings of this trial – the low incidence of stroke that was not further reduced by treatment with edoxaban – may make it appropriate to withhold anticoagulant therapy for patients with atrial high-rate episodes.
The main difference between the population studied in this trial and patients with AFib, as documented on an ECG, appears to be the paucity and brevity of atrial arrhythmias in patients with atrial high-rate episodes (termed low arrhythmia burden). Published reports show that a low arrhythmia burden contributes to a low incidence of stroke among patients with AFib, the study authors wrote.
They added that the low rate of stroke in this trial suggests that in addition to clinical risk prediction formulas for stroke, methods to improve the estimation of stroke risk among patients with infrequent atrial arrhythmias detected by long-term monitoring are needed to guide decision-making on the use of anticoagulation.
Commenting on the NOAH-AFNET 6 results, the comoderator of the ESC HOTLINE session at which they were presented, Barbara Casadei, MD, John Radcliffe Hospital, Oxford, England, said: “Finally we know what to with these patients. Before we just had a variety of opinions with no evidence. I think that the trial really highlights that patients who come to the doctor with symptoms of AF[ib] or who have ECG-documented AF[ib] have a much higher risk of cardioembolic stroke than patients in whom this presumed AF[ib] is picked up incidentally from implanted devices.”
She added: “The stroke rates are very low in this trial, so anticoagulation was never going to work. But this is an important finding. We know that anticoagulants are not a free lunch. There is a significant bleeding risk. These results suggest that unless a patient has clinical AF[ib] that shows up on an ECG then we need to more cautious in prescribing anticoagulation.”
Also commenting on the study, immediate past president of the American College of Cardiology Ed Fry, MD, Ascension Indiana St. Vincent Heart Center, Indianapolis, said the management of patients with implanted cardiac devices or personal wearable technology that has picked up an abnormal rhythm suggestive of AFib was a big question in clinical practice.
“These episodes could be AF[ib], which comes with an increased stroke risk, but it could also be something else like atrial tachycardia or supraventricular tachycardia, which do not confer an increased stroke risk,” he explained.
“This study shows that without a firm diagnosis of AF[ib] on an ECG or some sort of continuous AF[ib] monitoring device, we are going to be anticoagulating people who don’t need it. They were exposed to the risk of bleeding without getting the benefit of a reduction in stroke risk,” Dr. Fry noted.
“The important outcome from this trial is that it gives comfort in we can be more confident in withholding anticoagulation until we get a firm diagnosis of AF[ib]. If we have a high index of suspicion that this could be AF[ib], then we can arrange for a further testing,” he added.
Second trial reporting soon
A trial similar to NOAH-AFNET 6 is currently underway – the ARTESIA trial, which is expected to be reported later in 2023.
“We are in close contact with the leadership of that trial, and we hope to do some meta-analysis,” Dr. Kirchhof said. “But I think today we’ve gone from no evidence to one outcome-based trial which shows there is no reason to use anticoagulation in these patients with atrial high-rate episodes. I think this is reason to change practice now, but yes, of course we need to look at the data in totality once the second trial has reported.”
But the lead investigator of the ARTESIA trial, Stuart Connolly, MD, McMaster University, Hamilton, Ont., does not believe the NOAH-AFNET 6 trial should change practice at this time.
“This trial fails to adequately address the critical issue that drives clinical decision-making in these patients because it is underpowered for the most important endpoint of stroke,” he said in an interview.
“The key question is whether anticoagulation reduces stroke in these patients,” he added. “To answer that, a clinical trial needs to have a lot of strokes, and this trial had very few. The trial was stopped early and had way too few strokes to properly answer this key question.”
The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
AMSTERDAM – Among patients with atrial high-rate episodes detected by implantable devices, anticoagulation with edoxaban did not significantly reduce the incidence of a composite outcome of cardiovascular death, stroke, or systemic embolism in comparison with placebo but was associated with a higher bleeding risk in the NOAH-AFNET 6 trial.
“ They do not need to be anticoagulated. That is a relief,” the lead investigator of the trial, Paulus Kirchhof, MD, University Heart and Vascular Center Hamburg (Germany), said in an interview.
Dr. Kirchhof pointed out that this result was unexpected. “Many of us thought that because atrial high-rate episodes look like AF[ib] when they occur, then they are an indication for anticoagulation. But based on these results from the first-ever randomized trial on this population, there is no need for anticoagulation in these patients.”
Dr. Kirchhof presented the NOAH-AFNET 6 trial at the annual congress of the European Society of Cardiology. The study was also simultaneously published in the New England Journal of Medicine.
The trial recruited patients with implanted devices that enable continuous monitoring of atrial rhythm, such as pacemakers and defibrillators. “Because we can record the rhythm day and night with these devices, they pick up small abnormalities. About 20% of these patients experience these occasional atrial high-rate episodes – short episodes that look like AF[ib], but they are rare and brief,” Dr. Kirchhof noted.
He explained that whether the occurrence of these atrial high-rate episodes in patients without AFib, as documented on a conventional electrocardiogram, justifies the initiation of anticoagulants has been unclear. “But this trial tells us that these episodes are different to AF[ib] that is diagnosed on ECG,” he added.
Another finding in the trial was that among these patients, there was an unexpectedly low rate of stroke, despite the patients’ having a CHADSVASC score of 4.
“Based on the result of this trial, these occasional atrial high-rate episodes do not appear to be associated with stroke. It appears quite benign,” Dr. Kirchhof said.
Implications for wearable technology?
He said the results may also have implications for wearable devices that pick up abnormal heart rhythm, such as smartwatches.
“We don’t know exactly what these wearable technologies are picking up, but most likely it is these atrial high-rate episodes. But we need more research on the value of these wearable technologies; we need randomized trials in this particular patient population before we consider anticoagulation in these patients,” Dr. Kirchhof stated.
The NOAH-AFNET 6 study was an event-driven, double-blind, double-dummy, randomized trial involving 2,536 patients aged 65 years or older who had atrial high-rate episodes that lasted for at least 6 minutes and who had at least one additional risk factor for stroke.
Patients were randomly assigned in a 1:1 ratio to receive edoxaban or placebo. The primary efficacy outcome was a composite of cardiovascular death, stroke, or systemic embolism, evaluated in a time-to-event analysis. The safety outcome was a composite of death from any cause or major bleeding.
The mean age of the patients was 78 years, 37.4% were women, and the median duration of atrial high-rate episodes was 2.8 hours. The trial was terminated early, at a median follow-up of 21 months, on the basis of safety concerns and the results of an independent, informal assessment of futility for the efficacy of edoxaban; at termination, the planned enrollment had been completed.
Results showed that a primary efficacy outcome event occurred in 83 patients (3.2% per patient-year) in the edoxaban group and in 101 patients (4.0% per patient-year) in the placebo group (hazard ratio, 0.81; 95% confidence interval, 0.60-1.08; P = .15). The incidence of stroke was approximately 1% per patient-year in both groups.
A safety outcome event occurred in 149 patients (5.9% per patient-year) in the edoxaban group and in 114 patients (4.5% per patient-year) in the placebo group (HR, 1.31; 95% CI, 1.02-1.67; P = .03).
ECG-diagnosed AFib developed in 462 of 2,536 patients (18.2% total, 8.7% per patient-year).
In the NEJM article, the authors wrote that the findings of this trial – the low incidence of stroke that was not further reduced by treatment with edoxaban – may make it appropriate to withhold anticoagulant therapy for patients with atrial high-rate episodes.
The main difference between the population studied in this trial and patients with AFib, as documented on an ECG, appears to be the paucity and brevity of atrial arrhythmias in patients with atrial high-rate episodes (termed low arrhythmia burden). Published reports show that a low arrhythmia burden contributes to a low incidence of stroke among patients with AFib, the study authors wrote.
They added that the low rate of stroke in this trial suggests that in addition to clinical risk prediction formulas for stroke, methods to improve the estimation of stroke risk among patients with infrequent atrial arrhythmias detected by long-term monitoring are needed to guide decision-making on the use of anticoagulation.
Commenting on the NOAH-AFNET 6 results, the comoderator of the ESC HOTLINE session at which they were presented, Barbara Casadei, MD, John Radcliffe Hospital, Oxford, England, said: “Finally we know what to with these patients. Before we just had a variety of opinions with no evidence. I think that the trial really highlights that patients who come to the doctor with symptoms of AF[ib] or who have ECG-documented AF[ib] have a much higher risk of cardioembolic stroke than patients in whom this presumed AF[ib] is picked up incidentally from implanted devices.”
She added: “The stroke rates are very low in this trial, so anticoagulation was never going to work. But this is an important finding. We know that anticoagulants are not a free lunch. There is a significant bleeding risk. These results suggest that unless a patient has clinical AF[ib] that shows up on an ECG then we need to more cautious in prescribing anticoagulation.”
Also commenting on the study, immediate past president of the American College of Cardiology Ed Fry, MD, Ascension Indiana St. Vincent Heart Center, Indianapolis, said the management of patients with implanted cardiac devices or personal wearable technology that has picked up an abnormal rhythm suggestive of AFib was a big question in clinical practice.
“These episodes could be AF[ib], which comes with an increased stroke risk, but it could also be something else like atrial tachycardia or supraventricular tachycardia, which do not confer an increased stroke risk,” he explained.
“This study shows that without a firm diagnosis of AF[ib] on an ECG or some sort of continuous AF[ib] monitoring device, we are going to be anticoagulating people who don’t need it. They were exposed to the risk of bleeding without getting the benefit of a reduction in stroke risk,” Dr. Fry noted.
“The important outcome from this trial is that it gives comfort in we can be more confident in withholding anticoagulation until we get a firm diagnosis of AF[ib]. If we have a high index of suspicion that this could be AF[ib], then we can arrange for a further testing,” he added.
Second trial reporting soon
A trial similar to NOAH-AFNET 6 is currently underway – the ARTESIA trial, which is expected to be reported later in 2023.
“We are in close contact with the leadership of that trial, and we hope to do some meta-analysis,” Dr. Kirchhof said. “But I think today we’ve gone from no evidence to one outcome-based trial which shows there is no reason to use anticoagulation in these patients with atrial high-rate episodes. I think this is reason to change practice now, but yes, of course we need to look at the data in totality once the second trial has reported.”
But the lead investigator of the ARTESIA trial, Stuart Connolly, MD, McMaster University, Hamilton, Ont., does not believe the NOAH-AFNET 6 trial should change practice at this time.
“This trial fails to adequately address the critical issue that drives clinical decision-making in these patients because it is underpowered for the most important endpoint of stroke,” he said in an interview.
“The key question is whether anticoagulation reduces stroke in these patients,” he added. “To answer that, a clinical trial needs to have a lot of strokes, and this trial had very few. The trial was stopped early and had way too few strokes to properly answer this key question.”
The NOAH-AFNET 6 trial was an investigator-initiated trial funded by the German Center for Cardiovascular Research and Daiichi Sankyo Europe. Dr. Kirchhof reported research support from several drug and device companies active in AFib. He is also listed as an inventor on two patents held by the University of Hamburg on AFib therapy and AFib markers.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
Acoramidis shows encouraging results in ATTR cardiomyopathy
AMSTERDAM –
The drug, acoramidis (BridgeBio Pharma), showed a significant reduction, compared with placebo, in the primary endpoint, a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) and 6-minute walking distance, in the ATTRibute-CM trial.
The combination of all-cause mortality/cardiovascular hospitalization was also significantly reduced.
The trial was presented at the annual congress of the European Society of Cardiology by Julian Gillmore, MD, head of the University College London Centre for Amyloidosis.
“ATTRibute-CM was a robustly positive trial, showing benefits across the board for acoramidis, and suggest the tantalizing possibility of genuine clinical improvements,” Dr. Gillmore concluded.
ATTR-CM is a debilitating and progressive condition that increases mortality and reduces quality of life. Although this form of cardiomyopathy was considered to be very rare not long ago, improvements in imaging techniques and treatment developments have resulted in an upsurge in diagnosis throughout the world, and the disease is being diagnosed at an earlier stage, Dr. Gillmore noted.
ATTR-CM results from aggregation and deposition of transthyretin amyloid fibrils in the heart and various tissues. Acoramidis stabilizes the TTR tetramer and avoids the production of the fibrils.
Another similar drug, tafamidis (Vyndaqel, Vyndamax, Pfizer), was approved by the Food and Drug Administration in 2019 for ATTR-CM and is now available in several counties, including Japan and Europe.
BridgeBio Pharma is planning to file for FDA approval for acoramidis toward the end of 2023 and in other countries in 2024, Dr. Gillmore reported.
“It will be a huge benefit to patients to have another effective drug available,” he said.
Tafamidis also showed impressive results with its pivotal trial – ATTR-ACT – including a significant reduction in all-cause mortality, which was not seen in the ATTRibute-CM trial with acoramidis.
Asked about this, Dr. Gillmore replied: “It is difficult to comment on comparison with tafamidis as there isn’t a head-to-head trial. All I can say is that these results with acoramidis are fantastically encouraging, and I think we are going to have two effective drugs to treat this progressive and fatal condition.”
He elaborated that the difference in all-cause mortality results between the trials was “entirely consistent” with differences in the trial populations, with the ATTRibute-CM trial recruiting much lower-risk patients, in line with the earlier diagnosis of the condition that is now occurring.
“The survival in the placebo group in the ATTRibute study was greater than that in the treatment group in the ATTR-ACT study. So, it’s not all that surprising, given the reduced number of events, that mortality alone was not statistically significant in ATTRibute. What is important is that the trend in mortality was in the right direction, with an impressive risk reduction,” Dr. Gillmore noted.
“Incredibly, survival at 30 months and hospitalization rates among patients receiving acoramidis approached that of age-matched individuals who do not have ATTR,” he added.
Noting that more patients in the placebo group started taking tafamidis during the trial, Dr. Gillmore suggested that this would be expected to dilute the treatment effect of acoramidis.
“To have such a strongly positive study despite the change in the patient population and drop-in use of tafamidis is incredibly powerful,” he concluded.
ATTRibute trial
The randomized double-blind ATTRibute-CM trial included 632 patients with ATTR-CM and New York Heart Association class I-III heart failure.
They were randomly assigned 2:1 to acoramidis (800 mg twice daily) or placebo, with a follow-up of 30 months. After the first 12 months, tafamidis was permitted if available. This was more prevalent in the placebo arm (22% vs. 14%).
The trial met the primary endpoint – a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in NT-proBNP and 6-minute walking distance – with a win ratio of 1.8, which was highly statistically significant (P < .0001).
Results were consistent across all components of the primary endpoint and across all subgroups, Dr. Gillmore reported.
“Importantly, 58% of the win ratio ties were broken by the first two components of the hierarchical analysis – all-cause mortality and cardiovascular hospitalizations – and a separate analysis of these two components alone was also statistically significant,” he noted.
A trend was seen toward a treatment effect on all-cause mortality favoring acoramidis, with an 81% survival rate in the treated group, representing an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 25%.
Of the deaths reported in the study, 78% were cardiovascular in nature. Cardiovascular death also showed a trend favoring treatment with the study drug (14.9% in the acoramidis group vs. 21.3% in the placebo group), giving an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 30%.
Acoramidis was also associated with 50% reduction in cardiovascular hospitalizations, which was highly significant (P < .0001).
A treatment effect was also seen in terms of functional status; at 30 months, the difference in 6-minute walk distance between the groups was 40 meters, a “highly statistically significant improvement and clinically important difference, Dr. Gillmore said. Improvement from baseline occurred in 40% of the acoramidis group versus 22% of the placebo group.
Acoramidis recipients showed a blunting of the progressive rise of NT-proBNP, which Dr. Gillmore noted has been shown to be strongly associated with outcomes, with 45% of the acoramidis treated patients showing an improvement in NT-proBNP levels, compared with 9% of placebo group.
There was also a relative preservation of quality of life in the acoramidis group consistent with the separation of NT-proBNP curves, he added.
“Consistent with the mechanism of action and preclinical data showing near-complete stabilization of TTR at therapeutic drug concentrations, serum TTR (an in vivo reflection of TTR stabilization) was promptly and persistently elevated in patients receiving acoramidis,” Dr. Gillmore said.
Safety data showed that treatment-related adverse events were equal between the two groups, and there were fewer treatment emergent serious adverse events in the acoramidis group. The drug was said to be “generally well tolerated, with no findings of potential clinical concern.”
Second primary endpoint not significant
Discussant of the study at the ESC Hotline session, Thibaud Damy, MD, Hospital Henri Mondor, Paris East Creteil University, pointed out that a second primary endpoint of the study, change from baseline to month 12 in the 6-minute walking test, did not significantly differ between acoramidis and placebo.
Dr. Damy also highlighted the significant all-cause mortality reduction seen with tafamidis in ATTR-ACT but not achieved with acoramidis in ATTRibute.
He agreed with Dr. Gillmore’s interpretation that this was probably stemmed from the ATTRibute trial recruiting lower-risk patients, pointing out that patients in this trial had lower levels of NT-proBNP and less severe heart failure.
“It is clear that there is a place for acoramidis in patients with ATTR-CM,” Dr. Damy concluded, adding that many other treatments are in development.
The ATTribute trial was supported by BridgeBio Pharma. Dr. Gillmore reported advisory/consultant roles with BridgeBio, Alnylam, Ionis, AstraZeneca, Intellia, Pfizer, ATTRalus, and Lycia.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
The drug, acoramidis (BridgeBio Pharma), showed a significant reduction, compared with placebo, in the primary endpoint, a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) and 6-minute walking distance, in the ATTRibute-CM trial.
The combination of all-cause mortality/cardiovascular hospitalization was also significantly reduced.
The trial was presented at the annual congress of the European Society of Cardiology by Julian Gillmore, MD, head of the University College London Centre for Amyloidosis.
“ATTRibute-CM was a robustly positive trial, showing benefits across the board for acoramidis, and suggest the tantalizing possibility of genuine clinical improvements,” Dr. Gillmore concluded.
ATTR-CM is a debilitating and progressive condition that increases mortality and reduces quality of life. Although this form of cardiomyopathy was considered to be very rare not long ago, improvements in imaging techniques and treatment developments have resulted in an upsurge in diagnosis throughout the world, and the disease is being diagnosed at an earlier stage, Dr. Gillmore noted.
ATTR-CM results from aggregation and deposition of transthyretin amyloid fibrils in the heart and various tissues. Acoramidis stabilizes the TTR tetramer and avoids the production of the fibrils.
Another similar drug, tafamidis (Vyndaqel, Vyndamax, Pfizer), was approved by the Food and Drug Administration in 2019 for ATTR-CM and is now available in several counties, including Japan and Europe.
BridgeBio Pharma is planning to file for FDA approval for acoramidis toward the end of 2023 and in other countries in 2024, Dr. Gillmore reported.
“It will be a huge benefit to patients to have another effective drug available,” he said.
Tafamidis also showed impressive results with its pivotal trial – ATTR-ACT – including a significant reduction in all-cause mortality, which was not seen in the ATTRibute-CM trial with acoramidis.
Asked about this, Dr. Gillmore replied: “It is difficult to comment on comparison with tafamidis as there isn’t a head-to-head trial. All I can say is that these results with acoramidis are fantastically encouraging, and I think we are going to have two effective drugs to treat this progressive and fatal condition.”
He elaborated that the difference in all-cause mortality results between the trials was “entirely consistent” with differences in the trial populations, with the ATTRibute-CM trial recruiting much lower-risk patients, in line with the earlier diagnosis of the condition that is now occurring.
“The survival in the placebo group in the ATTRibute study was greater than that in the treatment group in the ATTR-ACT study. So, it’s not all that surprising, given the reduced number of events, that mortality alone was not statistically significant in ATTRibute. What is important is that the trend in mortality was in the right direction, with an impressive risk reduction,” Dr. Gillmore noted.
“Incredibly, survival at 30 months and hospitalization rates among patients receiving acoramidis approached that of age-matched individuals who do not have ATTR,” he added.
Noting that more patients in the placebo group started taking tafamidis during the trial, Dr. Gillmore suggested that this would be expected to dilute the treatment effect of acoramidis.
“To have such a strongly positive study despite the change in the patient population and drop-in use of tafamidis is incredibly powerful,” he concluded.
ATTRibute trial
The randomized double-blind ATTRibute-CM trial included 632 patients with ATTR-CM and New York Heart Association class I-III heart failure.
They were randomly assigned 2:1 to acoramidis (800 mg twice daily) or placebo, with a follow-up of 30 months. After the first 12 months, tafamidis was permitted if available. This was more prevalent in the placebo arm (22% vs. 14%).
The trial met the primary endpoint – a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in NT-proBNP and 6-minute walking distance – with a win ratio of 1.8, which was highly statistically significant (P < .0001).
Results were consistent across all components of the primary endpoint and across all subgroups, Dr. Gillmore reported.
“Importantly, 58% of the win ratio ties were broken by the first two components of the hierarchical analysis – all-cause mortality and cardiovascular hospitalizations – and a separate analysis of these two components alone was also statistically significant,” he noted.
A trend was seen toward a treatment effect on all-cause mortality favoring acoramidis, with an 81% survival rate in the treated group, representing an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 25%.
Of the deaths reported in the study, 78% were cardiovascular in nature. Cardiovascular death also showed a trend favoring treatment with the study drug (14.9% in the acoramidis group vs. 21.3% in the placebo group), giving an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 30%.
Acoramidis was also associated with 50% reduction in cardiovascular hospitalizations, which was highly significant (P < .0001).
A treatment effect was also seen in terms of functional status; at 30 months, the difference in 6-minute walk distance between the groups was 40 meters, a “highly statistically significant improvement and clinically important difference, Dr. Gillmore said. Improvement from baseline occurred in 40% of the acoramidis group versus 22% of the placebo group.
Acoramidis recipients showed a blunting of the progressive rise of NT-proBNP, which Dr. Gillmore noted has been shown to be strongly associated with outcomes, with 45% of the acoramidis treated patients showing an improvement in NT-proBNP levels, compared with 9% of placebo group.
There was also a relative preservation of quality of life in the acoramidis group consistent with the separation of NT-proBNP curves, he added.
“Consistent with the mechanism of action and preclinical data showing near-complete stabilization of TTR at therapeutic drug concentrations, serum TTR (an in vivo reflection of TTR stabilization) was promptly and persistently elevated in patients receiving acoramidis,” Dr. Gillmore said.
Safety data showed that treatment-related adverse events were equal between the two groups, and there were fewer treatment emergent serious adverse events in the acoramidis group. The drug was said to be “generally well tolerated, with no findings of potential clinical concern.”
Second primary endpoint not significant
Discussant of the study at the ESC Hotline session, Thibaud Damy, MD, Hospital Henri Mondor, Paris East Creteil University, pointed out that a second primary endpoint of the study, change from baseline to month 12 in the 6-minute walking test, did not significantly differ between acoramidis and placebo.
Dr. Damy also highlighted the significant all-cause mortality reduction seen with tafamidis in ATTR-ACT but not achieved with acoramidis in ATTRibute.
He agreed with Dr. Gillmore’s interpretation that this was probably stemmed from the ATTRibute trial recruiting lower-risk patients, pointing out that patients in this trial had lower levels of NT-proBNP and less severe heart failure.
“It is clear that there is a place for acoramidis in patients with ATTR-CM,” Dr. Damy concluded, adding that many other treatments are in development.
The ATTribute trial was supported by BridgeBio Pharma. Dr. Gillmore reported advisory/consultant roles with BridgeBio, Alnylam, Ionis, AstraZeneca, Intellia, Pfizer, ATTRalus, and Lycia.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
The drug, acoramidis (BridgeBio Pharma), showed a significant reduction, compared with placebo, in the primary endpoint, a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in N-terminal of the prohormone brain natriuretic peptide (NT-proBNP) and 6-minute walking distance, in the ATTRibute-CM trial.
The combination of all-cause mortality/cardiovascular hospitalization was also significantly reduced.
The trial was presented at the annual congress of the European Society of Cardiology by Julian Gillmore, MD, head of the University College London Centre for Amyloidosis.
“ATTRibute-CM was a robustly positive trial, showing benefits across the board for acoramidis, and suggest the tantalizing possibility of genuine clinical improvements,” Dr. Gillmore concluded.
ATTR-CM is a debilitating and progressive condition that increases mortality and reduces quality of life. Although this form of cardiomyopathy was considered to be very rare not long ago, improvements in imaging techniques and treatment developments have resulted in an upsurge in diagnosis throughout the world, and the disease is being diagnosed at an earlier stage, Dr. Gillmore noted.
ATTR-CM results from aggregation and deposition of transthyretin amyloid fibrils in the heart and various tissues. Acoramidis stabilizes the TTR tetramer and avoids the production of the fibrils.
Another similar drug, tafamidis (Vyndaqel, Vyndamax, Pfizer), was approved by the Food and Drug Administration in 2019 for ATTR-CM and is now available in several counties, including Japan and Europe.
BridgeBio Pharma is planning to file for FDA approval for acoramidis toward the end of 2023 and in other countries in 2024, Dr. Gillmore reported.
“It will be a huge benefit to patients to have another effective drug available,” he said.
Tafamidis also showed impressive results with its pivotal trial – ATTR-ACT – including a significant reduction in all-cause mortality, which was not seen in the ATTRibute-CM trial with acoramidis.
Asked about this, Dr. Gillmore replied: “It is difficult to comment on comparison with tafamidis as there isn’t a head-to-head trial. All I can say is that these results with acoramidis are fantastically encouraging, and I think we are going to have two effective drugs to treat this progressive and fatal condition.”
He elaborated that the difference in all-cause mortality results between the trials was “entirely consistent” with differences in the trial populations, with the ATTRibute-CM trial recruiting much lower-risk patients, in line with the earlier diagnosis of the condition that is now occurring.
“The survival in the placebo group in the ATTRibute study was greater than that in the treatment group in the ATTR-ACT study. So, it’s not all that surprising, given the reduced number of events, that mortality alone was not statistically significant in ATTRibute. What is important is that the trend in mortality was in the right direction, with an impressive risk reduction,” Dr. Gillmore noted.
“Incredibly, survival at 30 months and hospitalization rates among patients receiving acoramidis approached that of age-matched individuals who do not have ATTR,” he added.
Noting that more patients in the placebo group started taking tafamidis during the trial, Dr. Gillmore suggested that this would be expected to dilute the treatment effect of acoramidis.
“To have such a strongly positive study despite the change in the patient population and drop-in use of tafamidis is incredibly powerful,” he concluded.
ATTRibute trial
The randomized double-blind ATTRibute-CM trial included 632 patients with ATTR-CM and New York Heart Association class I-III heart failure.
They were randomly assigned 2:1 to acoramidis (800 mg twice daily) or placebo, with a follow-up of 30 months. After the first 12 months, tafamidis was permitted if available. This was more prevalent in the placebo arm (22% vs. 14%).
The trial met the primary endpoint – a hierarchical analysis of all-cause mortality, cumulative frequency of cardiovascular hospitalizations, and change from baseline in NT-proBNP and 6-minute walking distance – with a win ratio of 1.8, which was highly statistically significant (P < .0001).
Results were consistent across all components of the primary endpoint and across all subgroups, Dr. Gillmore reported.
“Importantly, 58% of the win ratio ties were broken by the first two components of the hierarchical analysis – all-cause mortality and cardiovascular hospitalizations – and a separate analysis of these two components alone was also statistically significant,” he noted.
A trend was seen toward a treatment effect on all-cause mortality favoring acoramidis, with an 81% survival rate in the treated group, representing an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 25%.
Of the deaths reported in the study, 78% were cardiovascular in nature. Cardiovascular death also showed a trend favoring treatment with the study drug (14.9% in the acoramidis group vs. 21.3% in the placebo group), giving an absolute risk reduction of 6.4 percentage points and a relative risk reduction of 30%.
Acoramidis was also associated with 50% reduction in cardiovascular hospitalizations, which was highly significant (P < .0001).
A treatment effect was also seen in terms of functional status; at 30 months, the difference in 6-minute walk distance between the groups was 40 meters, a “highly statistically significant improvement and clinically important difference, Dr. Gillmore said. Improvement from baseline occurred in 40% of the acoramidis group versus 22% of the placebo group.
Acoramidis recipients showed a blunting of the progressive rise of NT-proBNP, which Dr. Gillmore noted has been shown to be strongly associated with outcomes, with 45% of the acoramidis treated patients showing an improvement in NT-proBNP levels, compared with 9% of placebo group.
There was also a relative preservation of quality of life in the acoramidis group consistent with the separation of NT-proBNP curves, he added.
“Consistent with the mechanism of action and preclinical data showing near-complete stabilization of TTR at therapeutic drug concentrations, serum TTR (an in vivo reflection of TTR stabilization) was promptly and persistently elevated in patients receiving acoramidis,” Dr. Gillmore said.
Safety data showed that treatment-related adverse events were equal between the two groups, and there were fewer treatment emergent serious adverse events in the acoramidis group. The drug was said to be “generally well tolerated, with no findings of potential clinical concern.”
Second primary endpoint not significant
Discussant of the study at the ESC Hotline session, Thibaud Damy, MD, Hospital Henri Mondor, Paris East Creteil University, pointed out that a second primary endpoint of the study, change from baseline to month 12 in the 6-minute walking test, did not significantly differ between acoramidis and placebo.
Dr. Damy also highlighted the significant all-cause mortality reduction seen with tafamidis in ATTR-ACT but not achieved with acoramidis in ATTRibute.
He agreed with Dr. Gillmore’s interpretation that this was probably stemmed from the ATTRibute trial recruiting lower-risk patients, pointing out that patients in this trial had lower levels of NT-proBNP and less severe heart failure.
“It is clear that there is a place for acoramidis in patients with ATTR-CM,” Dr. Damy concluded, adding that many other treatments are in development.
The ATTribute trial was supported by BridgeBio Pharma. Dr. Gillmore reported advisory/consultant roles with BridgeBio, Alnylam, Ionis, AstraZeneca, Intellia, Pfizer, ATTRalus, and Lycia.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
New ESH hypertension guidelines aim for simplified message
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
‘Striking’ benefit of lipid lowering in primary prevention
SAN DIEGO – two-thirds of whom also had type 2 diabetes, leading to calls for more attention to be paid to this group of patients.
The main results of the CLEAR Outcomes trial of bempedoic acid (Nexletol, Esperion) in a mixed secondary and primary prevention population intolerant to statins, presented in March at the 2023 joint scientific sessions of the American College of Cardiology and the World Heart Federation, showed a 13% relative risk reduction in the main primary endpoint, a composite of cardiovascular death, myocardial infarction, stroke, or coronary revascularization.
This new analysis of the 4,206 high-risk primary prevention patients in the study – 67% of whom also had type 2 diabetes – has shown a 30% relative risk reduction in the same endpoint.
Other key endpoints were reduced to a similar or even greater extent, with the composite of cardiovascular death/stroke/MI showing a 36% relative risk reduction, and a 39% relative risk reduction for cardiovascular death and MI individually.

“These results are frankly striking,” lead investigator Steve Nissen, MD, said in an interview.
“These are really large reductions. These results are telling us that high-risk primary prevention patients, although their absolute event rate is lower than secondary prevention patients, can have very impressive relative risk reductions in major cardiovascular events with lipid-lowering therapy,” he said.
But Dr. Nissen, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, pointed out that this population of patients is not well treated.
“This is the problem: Less than half of high-risk primary prevention patients in the U.S., and in virtually every other developed country, are receiving cholesterol-lowering medication. These patients tend to get ignored,” he stressed.
Asked what advice he would give to clinicians based on the current findings, Dr. Nissen said: “If a patient is at high risk of developing cardiovascular disease, particularly those with [type 2] diabetes, they need to go on a lipid-lowering drug.”
“If patients can tolerate a statin then that should be the first choice. We know statins work, and they are now inexpensive. They are likely to give the exact same benefit as we have shown in this study with bempedoic acid, as the two drug classes work by very similar mechanisms. But if patients can’t tolerate a statin, then treat them with bempedoic acid. The bottom line is that these patients just need to be treated,” he said.
‘Wake-up call’
He said these new results are a “wake-up call for the medical community that we need to pay far more attention to high-risk primary prevention patients.”
Dr. Nissen does not believe the effect is specific to bempedoic acid; rather, it is more likely an effect of lowering LDL cholesterol (LDL-C) levels.
“This message is not about bempedoic acid, in particular. We have seen similar findings in historical studies with the statins, but that seems to have been forgotten. The message is about lowering LDL in patients who are at high risk of having a first cardiovascular event. We need to identify patients at high risk for a first cardiac event and get them on a cholesterol-lowering drug – and in most cases that will be a statin.”
Dr. Nissen presented the new analysis from the CLEAR OUTCOMES trial at the annual scientific sessions of the American Diabetes Association. It was simultaneously published online in JAMA.
He pointed out that large trials of lipid-lowering therapy in the primary prevention population have not been done for many years.
“All the contemporary trials with lipid-lowering therapy have only included secondary prevention patients and they often enroll patients after an acute coronary syndrome event.
“But for the CLEAR OUTCOMES trial, we included a significant amount of primary prevention patients – those with risk factors such as [type 2] diabetes and hypertension who are considered to be at high risk of developing cardiovascular disease,” he explained.
CLEAR OUTCOMES was a masked, randomized, trial that enrolled 13,970 statin-intolerant patients. The new analysis included 4,206 of those patients with risk factors for heart disease but without a prior cardiovascular event – the primary prevention group. The mean age of these participants was 68 years, 67% had diabetes, and 59% were women.
Treatment with bempedoic acid showed a 22% reduction in LDL-C, compared with placebo, with a reduction of 30.2 mg/dL from a mean baseline of 142.5 mg/dL. High-sensitivity C-reactive protein (CRP) levels were also reduced by 0.56 mg/L (21.5%), from a median baseline of 2.4 mg/L.
Dr. Nissen told a press briefing at the ADA meeting that he believes “it’s the combination of LDL lowering and reduction in CRP that might have been the driver [for the effects we saw in the trial]. Certainly, bempedoic acid lowers both.”
And he noted the recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco, Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD), which represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
Bempedoic acid is a prodrug that works along the same pathways as statins but does not cause muscle pain, which makes many people intolerant to statins. Bempedoic acid was first approved by the Food and Drug Administration in 2020 for the treatment of adults with heterozygous familial hypercholesterolemia or established ASCVD who require additional LDL-C lowering.
Greater benefit in primary prevention?
In this primary prevention group, treatment with bempedoic acid for 40 months was associated with a significant risk reduction for the primary endpoint – a composite of cardiovascular death, nonfatal MI, nonfatal stroke, or coronary revascularization – which occurred in 5.3% of the treatment group versus 7.6% in the placebo group (adjusted hazard ratio, 0.70; P = .002). This represents a 30% relative risk reduction in major cardiovascular events.
Other key secondary endpoints also showed impressive reductions.
The rate of the composite endpoint of cardiovascular death, MI, or stroke was 6.4% in the placebo group and 4.0% with bempedoic acid (HR, 0.64; P < .001); MI occurred in 2.2% versus 1.4% (HR, 0.61), cardiovascular death in 3.1% versus 1.8% (HR, 0.61), and all-cause mortality in 5.2% versus 3.6% (HR, 0.73), respectively.
Adverse effects with bempedoic acid included a higher incidence of gout (2.6% vs 2.0%), cholelithiasis (2.5% vs. 1.1%), and increases in serum creatinine, uric acid, and hepatic enzyme levels.
Dr. Nissen believed these results suggest that there may be a greater benefit of lipid lowering in high-risk primary prevention patients than in the secondary prevention population.
“It may seem paradoxical, but there is actually some history that this may be the case,” he said.
He pointed out that the JUPITER trial of rosuvastatin in 2008 was the last major primary prevention trial of a lipid-lowering agent, which was stopped early with a 44% reduction of the primary endpoint.
He noted that one of the arguments against the use of statins in primary prevention is the belief that absolute risk reductions are quite modest.
“But in this analysis, we found an absolute risk reduction of 2.3% for the primary endpoint. That’s a number needed to treat to prevent 1 event of 43. That’s pretty good,” he said.
Trying to explain why there may be more benefit in the primary prevention population, Dr. Nissen suggested that these patients may have more vulnerable plaques.
“I think high-risk primary prevention patients probably have a lot of lipid-laden plaque – some people call it ‘vulnerable’ plaque. These are softer, cholesterol-laden plaque. We know that treatment with cholesterol-lowering medication causes these plaques to shrink. The lipid core is delipidated and the plaque stabilizes,” he explained. “It may be that in secondary prevention patients to some extent the horse is already out of the barn – they have advanced disease. But primary prevention patients may have plaques that are more amenable to modification by cholesterol lowering.”
He admitted that the idea is only speculation. “But that is a potential explanation for our observations.”
Editorial cautious
In an accompanying editorial, also published in JAMA, Dhruv S. Kazi, MD, Beth Israel Deaconess Medical Center, Boston, said the findings need to be interpreted with caution as they come from one of many subgroup analyses of a larger trial.
Dr. Kazi pointed out that the intervention and control survival curves separate right away, on the first day of follow-up, whereas the true effect of lipid-lowering therapy for primary prevention would be expected to have a somewhat delayed onset, an observation he says supports the argument that this is a chance finding.
Dr. Kazi also reminded clinicians that bempedoic acid should not be regarded as a substitute for statins, which should remain the first-line therapy for primary prevention.
“For now, available evidence suggests that, although bempedoic acid is not a perfect substitute for a statin, it is a reasonable therapeutic choice for primary prevention of ASCVD events in high-risk, statin-intolerant patients,” he concluded.
A version of this article first appeared on Medscape.com.
SAN DIEGO – two-thirds of whom also had type 2 diabetes, leading to calls for more attention to be paid to this group of patients.
The main results of the CLEAR Outcomes trial of bempedoic acid (Nexletol, Esperion) in a mixed secondary and primary prevention population intolerant to statins, presented in March at the 2023 joint scientific sessions of the American College of Cardiology and the World Heart Federation, showed a 13% relative risk reduction in the main primary endpoint, a composite of cardiovascular death, myocardial infarction, stroke, or coronary revascularization.
This new analysis of the 4,206 high-risk primary prevention patients in the study – 67% of whom also had type 2 diabetes – has shown a 30% relative risk reduction in the same endpoint.
Other key endpoints were reduced to a similar or even greater extent, with the composite of cardiovascular death/stroke/MI showing a 36% relative risk reduction, and a 39% relative risk reduction for cardiovascular death and MI individually.
“These results are frankly striking,” lead investigator Steve Nissen, MD, said in an interview.
“These are really large reductions. These results are telling us that high-risk primary prevention patients, although their absolute event rate is lower than secondary prevention patients, can have very impressive relative risk reductions in major cardiovascular events with lipid-lowering therapy,” he said.
But Dr. Nissen, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, pointed out that this population of patients is not well treated.
“This is the problem: Less than half of high-risk primary prevention patients in the U.S., and in virtually every other developed country, are receiving cholesterol-lowering medication. These patients tend to get ignored,” he stressed.
Asked what advice he would give to clinicians based on the current findings, Dr. Nissen said: “If a patient is at high risk of developing cardiovascular disease, particularly those with [type 2] diabetes, they need to go on a lipid-lowering drug.”
“If patients can tolerate a statin then that should be the first choice. We know statins work, and they are now inexpensive. They are likely to give the exact same benefit as we have shown in this study with bempedoic acid, as the two drug classes work by very similar mechanisms. But if patients can’t tolerate a statin, then treat them with bempedoic acid. The bottom line is that these patients just need to be treated,” he said.
‘Wake-up call’
He said these new results are a “wake-up call for the medical community that we need to pay far more attention to high-risk primary prevention patients.”
Dr. Nissen does not believe the effect is specific to bempedoic acid; rather, it is more likely an effect of lowering LDL cholesterol (LDL-C) levels.
“This message is not about bempedoic acid, in particular. We have seen similar findings in historical studies with the statins, but that seems to have been forgotten. The message is about lowering LDL in patients who are at high risk of having a first cardiovascular event. We need to identify patients at high risk for a first cardiac event and get them on a cholesterol-lowering drug – and in most cases that will be a statin.”
Dr. Nissen presented the new analysis from the CLEAR OUTCOMES trial at the annual scientific sessions of the American Diabetes Association. It was simultaneously published online in JAMA.
He pointed out that large trials of lipid-lowering therapy in the primary prevention population have not been done for many years.
“All the contemporary trials with lipid-lowering therapy have only included secondary prevention patients and they often enroll patients after an acute coronary syndrome event.
“But for the CLEAR OUTCOMES trial, we included a significant amount of primary prevention patients – those with risk factors such as [type 2] diabetes and hypertension who are considered to be at high risk of developing cardiovascular disease,” he explained.
CLEAR OUTCOMES was a masked, randomized, trial that enrolled 13,970 statin-intolerant patients. The new analysis included 4,206 of those patients with risk factors for heart disease but without a prior cardiovascular event – the primary prevention group. The mean age of these participants was 68 years, 67% had diabetes, and 59% were women.
Treatment with bempedoic acid showed a 22% reduction in LDL-C, compared with placebo, with a reduction of 30.2 mg/dL from a mean baseline of 142.5 mg/dL. High-sensitivity C-reactive protein (CRP) levels were also reduced by 0.56 mg/L (21.5%), from a median baseline of 2.4 mg/L.
Dr. Nissen told a press briefing at the ADA meeting that he believes “it’s the combination of LDL lowering and reduction in CRP that might have been the driver [for the effects we saw in the trial]. Certainly, bempedoic acid lowers both.”
And he noted the recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco, Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD), which represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
Bempedoic acid is a prodrug that works along the same pathways as statins but does not cause muscle pain, which makes many people intolerant to statins. Bempedoic acid was first approved by the Food and Drug Administration in 2020 for the treatment of adults with heterozygous familial hypercholesterolemia or established ASCVD who require additional LDL-C lowering.
Greater benefit in primary prevention?
In this primary prevention group, treatment with bempedoic acid for 40 months was associated with a significant risk reduction for the primary endpoint – a composite of cardiovascular death, nonfatal MI, nonfatal stroke, or coronary revascularization – which occurred in 5.3% of the treatment group versus 7.6% in the placebo group (adjusted hazard ratio, 0.70; P = .002). This represents a 30% relative risk reduction in major cardiovascular events.
Other key secondary endpoints also showed impressive reductions.
The rate of the composite endpoint of cardiovascular death, MI, or stroke was 6.4% in the placebo group and 4.0% with bempedoic acid (HR, 0.64; P < .001); MI occurred in 2.2% versus 1.4% (HR, 0.61), cardiovascular death in 3.1% versus 1.8% (HR, 0.61), and all-cause mortality in 5.2% versus 3.6% (HR, 0.73), respectively.
Adverse effects with bempedoic acid included a higher incidence of gout (2.6% vs 2.0%), cholelithiasis (2.5% vs. 1.1%), and increases in serum creatinine, uric acid, and hepatic enzyme levels.
Dr. Nissen believed these results suggest that there may be a greater benefit of lipid lowering in high-risk primary prevention patients than in the secondary prevention population.
“It may seem paradoxical, but there is actually some history that this may be the case,” he said.
He pointed out that the JUPITER trial of rosuvastatin in 2008 was the last major primary prevention trial of a lipid-lowering agent, which was stopped early with a 44% reduction of the primary endpoint.
He noted that one of the arguments against the use of statins in primary prevention is the belief that absolute risk reductions are quite modest.
“But in this analysis, we found an absolute risk reduction of 2.3% for the primary endpoint. That’s a number needed to treat to prevent 1 event of 43. That’s pretty good,” he said.
Trying to explain why there may be more benefit in the primary prevention population, Dr. Nissen suggested that these patients may have more vulnerable plaques.
“I think high-risk primary prevention patients probably have a lot of lipid-laden plaque – some people call it ‘vulnerable’ plaque. These are softer, cholesterol-laden plaque. We know that treatment with cholesterol-lowering medication causes these plaques to shrink. The lipid core is delipidated and the plaque stabilizes,” he explained. “It may be that in secondary prevention patients to some extent the horse is already out of the barn – they have advanced disease. But primary prevention patients may have plaques that are more amenable to modification by cholesterol lowering.”
He admitted that the idea is only speculation. “But that is a potential explanation for our observations.”
Editorial cautious
In an accompanying editorial, also published in JAMA, Dhruv S. Kazi, MD, Beth Israel Deaconess Medical Center, Boston, said the findings need to be interpreted with caution as they come from one of many subgroup analyses of a larger trial.
Dr. Kazi pointed out that the intervention and control survival curves separate right away, on the first day of follow-up, whereas the true effect of lipid-lowering therapy for primary prevention would be expected to have a somewhat delayed onset, an observation he says supports the argument that this is a chance finding.
Dr. Kazi also reminded clinicians that bempedoic acid should not be regarded as a substitute for statins, which should remain the first-line therapy for primary prevention.
“For now, available evidence suggests that, although bempedoic acid is not a perfect substitute for a statin, it is a reasonable therapeutic choice for primary prevention of ASCVD events in high-risk, statin-intolerant patients,” he concluded.
A version of this article first appeared on Medscape.com.
SAN DIEGO – two-thirds of whom also had type 2 diabetes, leading to calls for more attention to be paid to this group of patients.
The main results of the CLEAR Outcomes trial of bempedoic acid (Nexletol, Esperion) in a mixed secondary and primary prevention population intolerant to statins, presented in March at the 2023 joint scientific sessions of the American College of Cardiology and the World Heart Federation, showed a 13% relative risk reduction in the main primary endpoint, a composite of cardiovascular death, myocardial infarction, stroke, or coronary revascularization.
This new analysis of the 4,206 high-risk primary prevention patients in the study – 67% of whom also had type 2 diabetes – has shown a 30% relative risk reduction in the same endpoint.
Other key endpoints were reduced to a similar or even greater extent, with the composite of cardiovascular death/stroke/MI showing a 36% relative risk reduction, and a 39% relative risk reduction for cardiovascular death and MI individually.
“These results are frankly striking,” lead investigator Steve Nissen, MD, said in an interview.
“These are really large reductions. These results are telling us that high-risk primary prevention patients, although their absolute event rate is lower than secondary prevention patients, can have very impressive relative risk reductions in major cardiovascular events with lipid-lowering therapy,” he said.
But Dr. Nissen, chief academic officer at the Heart Vascular & Thoracic Institute at the Cleveland Clinic, pointed out that this population of patients is not well treated.
“This is the problem: Less than half of high-risk primary prevention patients in the U.S., and in virtually every other developed country, are receiving cholesterol-lowering medication. These patients tend to get ignored,” he stressed.
Asked what advice he would give to clinicians based on the current findings, Dr. Nissen said: “If a patient is at high risk of developing cardiovascular disease, particularly those with [type 2] diabetes, they need to go on a lipid-lowering drug.”
“If patients can tolerate a statin then that should be the first choice. We know statins work, and they are now inexpensive. They are likely to give the exact same benefit as we have shown in this study with bempedoic acid, as the two drug classes work by very similar mechanisms. But if patients can’t tolerate a statin, then treat them with bempedoic acid. The bottom line is that these patients just need to be treated,” he said.
‘Wake-up call’
He said these new results are a “wake-up call for the medical community that we need to pay far more attention to high-risk primary prevention patients.”
Dr. Nissen does not believe the effect is specific to bempedoic acid; rather, it is more likely an effect of lowering LDL cholesterol (LDL-C) levels.
“This message is not about bempedoic acid, in particular. We have seen similar findings in historical studies with the statins, but that seems to have been forgotten. The message is about lowering LDL in patients who are at high risk of having a first cardiovascular event. We need to identify patients at high risk for a first cardiac event and get them on a cholesterol-lowering drug – and in most cases that will be a statin.”
Dr. Nissen presented the new analysis from the CLEAR OUTCOMES trial at the annual scientific sessions of the American Diabetes Association. It was simultaneously published online in JAMA.
He pointed out that large trials of lipid-lowering therapy in the primary prevention population have not been done for many years.
“All the contemporary trials with lipid-lowering therapy have only included secondary prevention patients and they often enroll patients after an acute coronary syndrome event.
“But for the CLEAR OUTCOMES trial, we included a significant amount of primary prevention patients – those with risk factors such as [type 2] diabetes and hypertension who are considered to be at high risk of developing cardiovascular disease,” he explained.
CLEAR OUTCOMES was a masked, randomized, trial that enrolled 13,970 statin-intolerant patients. The new analysis included 4,206 of those patients with risk factors for heart disease but without a prior cardiovascular event – the primary prevention group. The mean age of these participants was 68 years, 67% had diabetes, and 59% were women.
Treatment with bempedoic acid showed a 22% reduction in LDL-C, compared with placebo, with a reduction of 30.2 mg/dL from a mean baseline of 142.5 mg/dL. High-sensitivity C-reactive protein (CRP) levels were also reduced by 0.56 mg/L (21.5%), from a median baseline of 2.4 mg/L.
Dr. Nissen told a press briefing at the ADA meeting that he believes “it’s the combination of LDL lowering and reduction in CRP that might have been the driver [for the effects we saw in the trial]. Certainly, bempedoic acid lowers both.”
And he noted the recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco, Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD), which represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
Bempedoic acid is a prodrug that works along the same pathways as statins but does not cause muscle pain, which makes many people intolerant to statins. Bempedoic acid was first approved by the Food and Drug Administration in 2020 for the treatment of adults with heterozygous familial hypercholesterolemia or established ASCVD who require additional LDL-C lowering.
Greater benefit in primary prevention?
In this primary prevention group, treatment with bempedoic acid for 40 months was associated with a significant risk reduction for the primary endpoint – a composite of cardiovascular death, nonfatal MI, nonfatal stroke, or coronary revascularization – which occurred in 5.3% of the treatment group versus 7.6% in the placebo group (adjusted hazard ratio, 0.70; P = .002). This represents a 30% relative risk reduction in major cardiovascular events.
Other key secondary endpoints also showed impressive reductions.
The rate of the composite endpoint of cardiovascular death, MI, or stroke was 6.4% in the placebo group and 4.0% with bempedoic acid (HR, 0.64; P < .001); MI occurred in 2.2% versus 1.4% (HR, 0.61), cardiovascular death in 3.1% versus 1.8% (HR, 0.61), and all-cause mortality in 5.2% versus 3.6% (HR, 0.73), respectively.
Adverse effects with bempedoic acid included a higher incidence of gout (2.6% vs 2.0%), cholelithiasis (2.5% vs. 1.1%), and increases in serum creatinine, uric acid, and hepatic enzyme levels.
Dr. Nissen believed these results suggest that there may be a greater benefit of lipid lowering in high-risk primary prevention patients than in the secondary prevention population.
“It may seem paradoxical, but there is actually some history that this may be the case,” he said.
He pointed out that the JUPITER trial of rosuvastatin in 2008 was the last major primary prevention trial of a lipid-lowering agent, which was stopped early with a 44% reduction of the primary endpoint.
He noted that one of the arguments against the use of statins in primary prevention is the belief that absolute risk reductions are quite modest.
“But in this analysis, we found an absolute risk reduction of 2.3% for the primary endpoint. That’s a number needed to treat to prevent 1 event of 43. That’s pretty good,” he said.
Trying to explain why there may be more benefit in the primary prevention population, Dr. Nissen suggested that these patients may have more vulnerable plaques.
“I think high-risk primary prevention patients probably have a lot of lipid-laden plaque – some people call it ‘vulnerable’ plaque. These are softer, cholesterol-laden plaque. We know that treatment with cholesterol-lowering medication causes these plaques to shrink. The lipid core is delipidated and the plaque stabilizes,” he explained. “It may be that in secondary prevention patients to some extent the horse is already out of the barn – they have advanced disease. But primary prevention patients may have plaques that are more amenable to modification by cholesterol lowering.”
He admitted that the idea is only speculation. “But that is a potential explanation for our observations.”
Editorial cautious
In an accompanying editorial, also published in JAMA, Dhruv S. Kazi, MD, Beth Israel Deaconess Medical Center, Boston, said the findings need to be interpreted with caution as they come from one of many subgroup analyses of a larger trial.
Dr. Kazi pointed out that the intervention and control survival curves separate right away, on the first day of follow-up, whereas the true effect of lipid-lowering therapy for primary prevention would be expected to have a somewhat delayed onset, an observation he says supports the argument that this is a chance finding.
Dr. Kazi also reminded clinicians that bempedoic acid should not be regarded as a substitute for statins, which should remain the first-line therapy for primary prevention.
“For now, available evidence suggests that, although bempedoic acid is not a perfect substitute for a statin, it is a reasonable therapeutic choice for primary prevention of ASCVD events in high-risk, statin-intolerant patients,” he concluded.
A version of this article first appeared on Medscape.com.
AT ADA 2023
Low-dose colchicine approved for CVD: Now what?
The recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco; Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD) represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
The Food and Drug Administration granted colchicine a very broad label: to reduce the risk for cardiovascular events in adult patients with established ASCVD or with multiple risk factors for cardiovascular disease. But how will the drug be used in clinical practice?
“The idea of inflammation as a driver of atherosclerosis and cardiovascular risk has been around for decades, and it is very well known that atherosclerosis is an inflammatory process. However, treating inflammation is new as we haven’t had a specific agent targeting inflammation before, noted Michael Joseph Blaha, MD, director of clinical research, Ciccarone Center for the Prevention of Cardiovascular Disease at Johns Hopkins Hospital, Baltimore.
Dr. Blaha, who has been an unpaid scientific adviser to Agepha, added that the approval of low-dose colchicine “will open the door toward having a routine conversation about residual inflammatory risk in our patients; and we need to work out exactly how we do that.”
Dr. Blaha is not surprised by the FDA-approved indication for colchicine, pointing out that the main large-scale trial supporting its use in ASCVD, the LoDoCo-2 trial, included a similar broad population.
“I think the approval was appropriate as the indication should always follow the data. But I think how the drug will actually be used will depend on the context for different individual patients,” he said.
“The paradigm coming forward is the idea of residual risk that patients have after they been treated with the standard of care – which in most cases is a statin and blood pressure control – and what is driving that residual risk,” he noted. “If we think patients are still at high risk of recurrent cardiovascular events, we have to think what we will do next. This is where this drug will come in.”
Dr. Blaha pointed out that there are now multiple options for reducing residual risk; he believes that it will depend on the profile of the patient as to which of those options is chosen first.
“If after high-dose statin treatment they still have raised LDL, then we can add another LDL lowering drug; or it might be diabetes and obesity that we want to address first; or elevated triglycerides. But now, we can also consider residual inflammatory risk if we think the patient has residual plaque inflammation,” he said. “So, colchicine will be one of several choices beyond a statin that we can think about as the next step for treating residual risk.”
Is CRP measurement necessary?
Though elevated levels of high-sensitivity C-reactive protein (hsCRP) is a marker of inflammation in ASCVD, the two main trials of colchicine in ASCVD, both of which showed large benefits of the drug, did not measure hsCRP, leading to questions as to whether measurement of this biomarker is necessary to select patients for colchicine treatment.
“Some clinicians will favor testing hsCRP and treating those with levels above 2 mg/L. I think that’s very reasonable,” Dr. Blaha said. “However, because hsCRP was not measured in the trials, I don’t think testing for this biomarker is mandatory to establish that there is inflammation,” he added.
“The label does not stipulate that CRP has to be measured. It is giving physicians latitude; they can measure CRP, or they don’t have to.”
Dr. Blaha added that clinicians need to think about what is driving residual risk in each individual patient: “If you think their other risk factors are well controlled but they are still having recurrent events, then we can consider colchicine as a way of reducing their residual risk which is likely being caused by inflammation.
“We are at a great place in cardiovascular medicine as we have several different options to use after a statin, and now we have this new therapy targeted at inflammation as well. While we can use all these options together, I think most clinicians will want to prioritize therapies by using the ones that they believe will reduce the residual risk the most in each individual patient,” Dr. Blaha explained.
‘An entire other axis driving atherosclerosis’
Paul Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, is one of the major players in the cardiovascular inflammation field and has helped develop hsCRP testing. He has similar views.
“This FDA approval is extremely important, as it will draw attention to the role of inflammation in atherosclerosis and the need to treat it,” he said.
“Physicians need to be aware that, yes, we need to lower cholesterol aggressively, but they also need to know that there is an entire other axis driving atherosclerosis – and that is inflammation. And until now, we haven’t had an FDA-approved drug to treat inflammation.”
Dr. Ridker stressed that he doesn’t want to undermine lowering lipids: “Therapies aimed at inflammation are not in competition with those aimed at lipid lowering. We know lipid lowering works. But now we have another approach as well. The challenge here is educating physicians on this new approach.”
Dr. Ridker said he already uses low-dose colchicine for patients whom he refers to as “frequent flyers”; those who keep coming back despite aggressive lipid lowering. “They have multiple angioplasties, bypass surgery, etc.”
Like Dr. Blaha, Dr. Ridker thinks that doctors should start using this drug in high-risk patients who are already on a statin and who have residual inflammatory risk: “[The] patient whose underlying biologic problem is inflammation [is whom] we really want to treat with this drug. That is where it is most likely to be highly effective and where the comfort level will be the greatest.”
He said that measurement of hsCRP is an appropriate way to select these patients.
“I think this is a great impetus to start having much wider CRP measurement so we can actually target this anti-inflammatory drug to the patients with residual inflammatory risk – those with hsCRP level above 2 mg/L,” he said, estimating that this could apply to around 30%-40% of patients with ASCVD who are already taking a statin.
A second pillar of ASCVD treatment?
A somewhat different view is held by Jean-Claude Tardif, MD, director of the Research Centre at the Montréal Heart Institute, Canada, who was the lead investigator of the other randomized controlled trial of colchicine in heart disease, the COLCOT trial.
He said that colchicine should become the “second pillar” of ASCVD treatment, along with statins, for almost all patients.
Tardif referred to the recent study (led by Dr. Ridker) in The Lancet, which showed that among patients who are already on a statin, those with high inflammation levels had the highest risk for future events.
“So, the next step after a statin has to be to consider inflammation reduction,” he said.
“Despite all the drugs we have, ASCVD remains the leading cause of death in the Western world. What drives these events is largely inflammation, so it makes sense to directly tackle reduction of inflammation in the vessel, with a drug like colchicine,” he noted.
“I would say all patients with coronary atherosclerosis are potential candidates for low-dose colchicine as long as they do not have severe kidney disease, which is a contraindication,” Dr. Tardif said.
“If you want to fine tune this a bit more, those that are at particular risk are those that have recurrent events, those with multiple risk factors, and those with a recent [myocardial infarction]. In these patients, it would make a lot of sense to add low-dose colchicine to high-dose statins,” he added.
Dr. Tardif said he is not going to use CRP measurements to select patients for colchicine treatment: “Although measuring CRP may make sense intuitively, both large, randomized trials of colchicine did not select patients based on raised CRP, and they showed a benefit across the board.
If I consider a patient with ASCVD to be at high risk of future events and they are already on a statin I’m going to consider colchicine in all these patients, as long as they don’t have severe kidney disease.”
Dr. Tardif said that ASCVD needs to follow the model of heart failure which has several pillars of treatment directed at different targets that are all used together.
“I think we should apply the same approach to patients with ASCVD,” he added. “Yes, we need to hit the cholesterol with a statin, but we can now also hit the inflammation with colchicine.”
Polypharmacy concerns
Steve Nissen, MD, professor of medicine at the Cleveland Clinic, who was not involved in the colchicine trials, is also enthusiastic about use of colchicine. But like Dr. Ridker and Dr. Blaha, he favors selecting patients who are likely to benefit the most.
“I have been an advocate of the inflammatory hypothesis for many years, and we have been on a quest for a pure anti-inflammatory therapy that we can add to the standard treatment of patients with coronary disease. And colchicine has the safety and efficacy to do this,” Dr. Nissen said.
“What colchicine offers here is an inexpensive drug with pretty good data on reduction in morbidity from coronary disease. It has a completely different mechanism, so its benefit is likely to be additive to statins. I think we could probably do a lot of good at very little expense by just using these two therapies,” he said.
“But at present my preference will be to use colchicine selectively in those with raised CRP. I think that’s logical. I’m just worried about polypharmacy. Some of my patients are already on five, six, or seven meds. I need to have a reason to add an additional drug, and I’m not sure if we really analyze this carefully that patients with a low CRP would derive the same benefit. They might do, but I doubt it,” he noted.
“There may be further research and analyses that help us understand the relationship between CRP and efficacy of colchicine, and that may help us figure this out,” he added.
Safety is reassuring
In terms of safety and tolerability of the 0.5-mg colchicine dose, the experts seem to think that this is very manageable.
“When used for gout or pericarditis, colchicine is generally given at a dose of 0.6 mg twice a day and this can cause a lot of gastrointestinal [GI] side effects,” Dr. Nissen said. “But the low dose approved for ASCVD – 0.5 mg once a day – appears to be much better tolerated. There are some GI side effects, but these are not intolerable, and they generally go away with time.”
Dr. Ridker added that in the randomized trials, the adverse effects were “quite minimal,” but, “that being said, this drug is not to be used in severe kidney or liver disease, and there are some drug interactions that we need to be aware of. But in general, side effects are rare with the low dose. There may be some GI effects but they are mainly mild and you can generally treat through them.”
Dr. Blaha agreed that this is not a drug for patients with advanced kidney disease, “and there are some drug interactions that we have to be mindful of, but the list is not so long. There is a signal of modest gastrointestinal and muscle side effects, but most patients will be able to take it without issues. Because it’s already used in gout, physicians are already quite comfortable with its use.”
Part of the backbone of CV treatment?
Concluding, Dr. Blaha said he believes that prescribing of colchicine will start with cardiologists who will use it in their highest-risk patients first.
“But as we become comfortable with it, I think we will start using it in a broader range of patients and eventually primary care doctors will start prescribing it – much like what has happened with the statins,” he suggested.
“Where it sits along with statins in the future will be very interesting to see, but I think some people can envision it being up there with statins as part of the backbone of cardiovascular treatment in future.”
Dr. Tardif holds patents on methods for using low-dose colchicine after myocardial infarction, licensed to Montreal Heart Institute. Dr. Ridker is a consultant to Agepha and has research grants from Novo Nordisk related to the development of alternative anti-inflammatory therapies for atherosclerotic disease. Dr. Blaha reports being an unpaid scientific adviser to Agepha Pharma.
A version of this article first appeared on Medscape.com.
The recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco; Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD) represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
The Food and Drug Administration granted colchicine a very broad label: to reduce the risk for cardiovascular events in adult patients with established ASCVD or with multiple risk factors for cardiovascular disease. But how will the drug be used in clinical practice?
“The idea of inflammation as a driver of atherosclerosis and cardiovascular risk has been around for decades, and it is very well known that atherosclerosis is an inflammatory process. However, treating inflammation is new as we haven’t had a specific agent targeting inflammation before, noted Michael Joseph Blaha, MD, director of clinical research, Ciccarone Center for the Prevention of Cardiovascular Disease at Johns Hopkins Hospital, Baltimore.
Dr. Blaha, who has been an unpaid scientific adviser to Agepha, added that the approval of low-dose colchicine “will open the door toward having a routine conversation about residual inflammatory risk in our patients; and we need to work out exactly how we do that.”
Dr. Blaha is not surprised by the FDA-approved indication for colchicine, pointing out that the main large-scale trial supporting its use in ASCVD, the LoDoCo-2 trial, included a similar broad population.
“I think the approval was appropriate as the indication should always follow the data. But I think how the drug will actually be used will depend on the context for different individual patients,” he said.
“The paradigm coming forward is the idea of residual risk that patients have after they been treated with the standard of care – which in most cases is a statin and blood pressure control – and what is driving that residual risk,” he noted. “If we think patients are still at high risk of recurrent cardiovascular events, we have to think what we will do next. This is where this drug will come in.”
Dr. Blaha pointed out that there are now multiple options for reducing residual risk; he believes that it will depend on the profile of the patient as to which of those options is chosen first.
“If after high-dose statin treatment they still have raised LDL, then we can add another LDL lowering drug; or it might be diabetes and obesity that we want to address first; or elevated triglycerides. But now, we can also consider residual inflammatory risk if we think the patient has residual plaque inflammation,” he said. “So, colchicine will be one of several choices beyond a statin that we can think about as the next step for treating residual risk.”
Is CRP measurement necessary?
Though elevated levels of high-sensitivity C-reactive protein (hsCRP) is a marker of inflammation in ASCVD, the two main trials of colchicine in ASCVD, both of which showed large benefits of the drug, did not measure hsCRP, leading to questions as to whether measurement of this biomarker is necessary to select patients for colchicine treatment.
“Some clinicians will favor testing hsCRP and treating those with levels above 2 mg/L. I think that’s very reasonable,” Dr. Blaha said. “However, because hsCRP was not measured in the trials, I don’t think testing for this biomarker is mandatory to establish that there is inflammation,” he added.
“The label does not stipulate that CRP has to be measured. It is giving physicians latitude; they can measure CRP, or they don’t have to.”
Dr. Blaha added that clinicians need to think about what is driving residual risk in each individual patient: “If you think their other risk factors are well controlled but they are still having recurrent events, then we can consider colchicine as a way of reducing their residual risk which is likely being caused by inflammation.
“We are at a great place in cardiovascular medicine as we have several different options to use after a statin, and now we have this new therapy targeted at inflammation as well. While we can use all these options together, I think most clinicians will want to prioritize therapies by using the ones that they believe will reduce the residual risk the most in each individual patient,” Dr. Blaha explained.
‘An entire other axis driving atherosclerosis’
Paul Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, is one of the major players in the cardiovascular inflammation field and has helped develop hsCRP testing. He has similar views.
“This FDA approval is extremely important, as it will draw attention to the role of inflammation in atherosclerosis and the need to treat it,” he said.
“Physicians need to be aware that, yes, we need to lower cholesterol aggressively, but they also need to know that there is an entire other axis driving atherosclerosis – and that is inflammation. And until now, we haven’t had an FDA-approved drug to treat inflammation.”
Dr. Ridker stressed that he doesn’t want to undermine lowering lipids: “Therapies aimed at inflammation are not in competition with those aimed at lipid lowering. We know lipid lowering works. But now we have another approach as well. The challenge here is educating physicians on this new approach.”
Dr. Ridker said he already uses low-dose colchicine for patients whom he refers to as “frequent flyers”; those who keep coming back despite aggressive lipid lowering. “They have multiple angioplasties, bypass surgery, etc.”
Like Dr. Blaha, Dr. Ridker thinks that doctors should start using this drug in high-risk patients who are already on a statin and who have residual inflammatory risk: “[The] patient whose underlying biologic problem is inflammation [is whom] we really want to treat with this drug. That is where it is most likely to be highly effective and where the comfort level will be the greatest.”
He said that measurement of hsCRP is an appropriate way to select these patients.
“I think this is a great impetus to start having much wider CRP measurement so we can actually target this anti-inflammatory drug to the patients with residual inflammatory risk – those with hsCRP level above 2 mg/L,” he said, estimating that this could apply to around 30%-40% of patients with ASCVD who are already taking a statin.
A second pillar of ASCVD treatment?
A somewhat different view is held by Jean-Claude Tardif, MD, director of the Research Centre at the Montréal Heart Institute, Canada, who was the lead investigator of the other randomized controlled trial of colchicine in heart disease, the COLCOT trial.
He said that colchicine should become the “second pillar” of ASCVD treatment, along with statins, for almost all patients.
Tardif referred to the recent study (led by Dr. Ridker) in The Lancet, which showed that among patients who are already on a statin, those with high inflammation levels had the highest risk for future events.
“So, the next step after a statin has to be to consider inflammation reduction,” he said.
“Despite all the drugs we have, ASCVD remains the leading cause of death in the Western world. What drives these events is largely inflammation, so it makes sense to directly tackle reduction of inflammation in the vessel, with a drug like colchicine,” he noted.
“I would say all patients with coronary atherosclerosis are potential candidates for low-dose colchicine as long as they do not have severe kidney disease, which is a contraindication,” Dr. Tardif said.
“If you want to fine tune this a bit more, those that are at particular risk are those that have recurrent events, those with multiple risk factors, and those with a recent [myocardial infarction]. In these patients, it would make a lot of sense to add low-dose colchicine to high-dose statins,” he added.
Dr. Tardif said he is not going to use CRP measurements to select patients for colchicine treatment: “Although measuring CRP may make sense intuitively, both large, randomized trials of colchicine did not select patients based on raised CRP, and they showed a benefit across the board.
If I consider a patient with ASCVD to be at high risk of future events and they are already on a statin I’m going to consider colchicine in all these patients, as long as they don’t have severe kidney disease.”
Dr. Tardif said that ASCVD needs to follow the model of heart failure which has several pillars of treatment directed at different targets that are all used together.
“I think we should apply the same approach to patients with ASCVD,” he added. “Yes, we need to hit the cholesterol with a statin, but we can now also hit the inflammation with colchicine.”
Polypharmacy concerns
Steve Nissen, MD, professor of medicine at the Cleveland Clinic, who was not involved in the colchicine trials, is also enthusiastic about use of colchicine. But like Dr. Ridker and Dr. Blaha, he favors selecting patients who are likely to benefit the most.
“I have been an advocate of the inflammatory hypothesis for many years, and we have been on a quest for a pure anti-inflammatory therapy that we can add to the standard treatment of patients with coronary disease. And colchicine has the safety and efficacy to do this,” Dr. Nissen said.
“What colchicine offers here is an inexpensive drug with pretty good data on reduction in morbidity from coronary disease. It has a completely different mechanism, so its benefit is likely to be additive to statins. I think we could probably do a lot of good at very little expense by just using these two therapies,” he said.
“But at present my preference will be to use colchicine selectively in those with raised CRP. I think that’s logical. I’m just worried about polypharmacy. Some of my patients are already on five, six, or seven meds. I need to have a reason to add an additional drug, and I’m not sure if we really analyze this carefully that patients with a low CRP would derive the same benefit. They might do, but I doubt it,” he noted.
“There may be further research and analyses that help us understand the relationship between CRP and efficacy of colchicine, and that may help us figure this out,” he added.
Safety is reassuring
In terms of safety and tolerability of the 0.5-mg colchicine dose, the experts seem to think that this is very manageable.
“When used for gout or pericarditis, colchicine is generally given at a dose of 0.6 mg twice a day and this can cause a lot of gastrointestinal [GI] side effects,” Dr. Nissen said. “But the low dose approved for ASCVD – 0.5 mg once a day – appears to be much better tolerated. There are some GI side effects, but these are not intolerable, and they generally go away with time.”
Dr. Ridker added that in the randomized trials, the adverse effects were “quite minimal,” but, “that being said, this drug is not to be used in severe kidney or liver disease, and there are some drug interactions that we need to be aware of. But in general, side effects are rare with the low dose. There may be some GI effects but they are mainly mild and you can generally treat through them.”
Dr. Blaha agreed that this is not a drug for patients with advanced kidney disease, “and there are some drug interactions that we have to be mindful of, but the list is not so long. There is a signal of modest gastrointestinal and muscle side effects, but most patients will be able to take it without issues. Because it’s already used in gout, physicians are already quite comfortable with its use.”
Part of the backbone of CV treatment?
Concluding, Dr. Blaha said he believes that prescribing of colchicine will start with cardiologists who will use it in their highest-risk patients first.
“But as we become comfortable with it, I think we will start using it in a broader range of patients and eventually primary care doctors will start prescribing it – much like what has happened with the statins,” he suggested.
“Where it sits along with statins in the future will be very interesting to see, but I think some people can envision it being up there with statins as part of the backbone of cardiovascular treatment in future.”
Dr. Tardif holds patents on methods for using low-dose colchicine after myocardial infarction, licensed to Montreal Heart Institute. Dr. Ridker is a consultant to Agepha and has research grants from Novo Nordisk related to the development of alternative anti-inflammatory therapies for atherosclerotic disease. Dr. Blaha reports being an unpaid scientific adviser to Agepha Pharma.
A version of this article first appeared on Medscape.com.
The recent U.S. approval of a new low dose of colchicine 0.5 mg (Lodoco; Agepha Pharma) with a broad indication for use in atherosclerotic cardiovascular disease (ASCVD) represents a completely new approach to treatment, specifically targeting inflammation as a driver of atherosclerosis.
The Food and Drug Administration granted colchicine a very broad label: to reduce the risk for cardiovascular events in adult patients with established ASCVD or with multiple risk factors for cardiovascular disease. But how will the drug be used in clinical practice?
“The idea of inflammation as a driver of atherosclerosis and cardiovascular risk has been around for decades, and it is very well known that atherosclerosis is an inflammatory process. However, treating inflammation is new as we haven’t had a specific agent targeting inflammation before, noted Michael Joseph Blaha, MD, director of clinical research, Ciccarone Center for the Prevention of Cardiovascular Disease at Johns Hopkins Hospital, Baltimore.
Dr. Blaha, who has been an unpaid scientific adviser to Agepha, added that the approval of low-dose colchicine “will open the door toward having a routine conversation about residual inflammatory risk in our patients; and we need to work out exactly how we do that.”
Dr. Blaha is not surprised by the FDA-approved indication for colchicine, pointing out that the main large-scale trial supporting its use in ASCVD, the LoDoCo-2 trial, included a similar broad population.
“I think the approval was appropriate as the indication should always follow the data. But I think how the drug will actually be used will depend on the context for different individual patients,” he said.
“The paradigm coming forward is the idea of residual risk that patients have after they been treated with the standard of care – which in most cases is a statin and blood pressure control – and what is driving that residual risk,” he noted. “If we think patients are still at high risk of recurrent cardiovascular events, we have to think what we will do next. This is where this drug will come in.”
Dr. Blaha pointed out that there are now multiple options for reducing residual risk; he believes that it will depend on the profile of the patient as to which of those options is chosen first.
“If after high-dose statin treatment they still have raised LDL, then we can add another LDL lowering drug; or it might be diabetes and obesity that we want to address first; or elevated triglycerides. But now, we can also consider residual inflammatory risk if we think the patient has residual plaque inflammation,” he said. “So, colchicine will be one of several choices beyond a statin that we can think about as the next step for treating residual risk.”
Is CRP measurement necessary?
Though elevated levels of high-sensitivity C-reactive protein (hsCRP) is a marker of inflammation in ASCVD, the two main trials of colchicine in ASCVD, both of which showed large benefits of the drug, did not measure hsCRP, leading to questions as to whether measurement of this biomarker is necessary to select patients for colchicine treatment.
“Some clinicians will favor testing hsCRP and treating those with levels above 2 mg/L. I think that’s very reasonable,” Dr. Blaha said. “However, because hsCRP was not measured in the trials, I don’t think testing for this biomarker is mandatory to establish that there is inflammation,” he added.
“The label does not stipulate that CRP has to be measured. It is giving physicians latitude; they can measure CRP, or they don’t have to.”
Dr. Blaha added that clinicians need to think about what is driving residual risk in each individual patient: “If you think their other risk factors are well controlled but they are still having recurrent events, then we can consider colchicine as a way of reducing their residual risk which is likely being caused by inflammation.
“We are at a great place in cardiovascular medicine as we have several different options to use after a statin, and now we have this new therapy targeted at inflammation as well. While we can use all these options together, I think most clinicians will want to prioritize therapies by using the ones that they believe will reduce the residual risk the most in each individual patient,” Dr. Blaha explained.
‘An entire other axis driving atherosclerosis’
Paul Ridker, MD, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, is one of the major players in the cardiovascular inflammation field and has helped develop hsCRP testing. He has similar views.
“This FDA approval is extremely important, as it will draw attention to the role of inflammation in atherosclerosis and the need to treat it,” he said.
“Physicians need to be aware that, yes, we need to lower cholesterol aggressively, but they also need to know that there is an entire other axis driving atherosclerosis – and that is inflammation. And until now, we haven’t had an FDA-approved drug to treat inflammation.”
Dr. Ridker stressed that he doesn’t want to undermine lowering lipids: “Therapies aimed at inflammation are not in competition with those aimed at lipid lowering. We know lipid lowering works. But now we have another approach as well. The challenge here is educating physicians on this new approach.”
Dr. Ridker said he already uses low-dose colchicine for patients whom he refers to as “frequent flyers”; those who keep coming back despite aggressive lipid lowering. “They have multiple angioplasties, bypass surgery, etc.”
Like Dr. Blaha, Dr. Ridker thinks that doctors should start using this drug in high-risk patients who are already on a statin and who have residual inflammatory risk: “[The] patient whose underlying biologic problem is inflammation [is whom] we really want to treat with this drug. That is where it is most likely to be highly effective and where the comfort level will be the greatest.”
He said that measurement of hsCRP is an appropriate way to select these patients.
“I think this is a great impetus to start having much wider CRP measurement so we can actually target this anti-inflammatory drug to the patients with residual inflammatory risk – those with hsCRP level above 2 mg/L,” he said, estimating that this could apply to around 30%-40% of patients with ASCVD who are already taking a statin.
A second pillar of ASCVD treatment?
A somewhat different view is held by Jean-Claude Tardif, MD, director of the Research Centre at the Montréal Heart Institute, Canada, who was the lead investigator of the other randomized controlled trial of colchicine in heart disease, the COLCOT trial.
He said that colchicine should become the “second pillar” of ASCVD treatment, along with statins, for almost all patients.
Tardif referred to the recent study (led by Dr. Ridker) in The Lancet, which showed that among patients who are already on a statin, those with high inflammation levels had the highest risk for future events.
“So, the next step after a statin has to be to consider inflammation reduction,” he said.
“Despite all the drugs we have, ASCVD remains the leading cause of death in the Western world. What drives these events is largely inflammation, so it makes sense to directly tackle reduction of inflammation in the vessel, with a drug like colchicine,” he noted.
“I would say all patients with coronary atherosclerosis are potential candidates for low-dose colchicine as long as they do not have severe kidney disease, which is a contraindication,” Dr. Tardif said.
“If you want to fine tune this a bit more, those that are at particular risk are those that have recurrent events, those with multiple risk factors, and those with a recent [myocardial infarction]. In these patients, it would make a lot of sense to add low-dose colchicine to high-dose statins,” he added.
Dr. Tardif said he is not going to use CRP measurements to select patients for colchicine treatment: “Although measuring CRP may make sense intuitively, both large, randomized trials of colchicine did not select patients based on raised CRP, and they showed a benefit across the board.
If I consider a patient with ASCVD to be at high risk of future events and they are already on a statin I’m going to consider colchicine in all these patients, as long as they don’t have severe kidney disease.”
Dr. Tardif said that ASCVD needs to follow the model of heart failure which has several pillars of treatment directed at different targets that are all used together.
“I think we should apply the same approach to patients with ASCVD,” he added. “Yes, we need to hit the cholesterol with a statin, but we can now also hit the inflammation with colchicine.”
Polypharmacy concerns
Steve Nissen, MD, professor of medicine at the Cleveland Clinic, who was not involved in the colchicine trials, is also enthusiastic about use of colchicine. But like Dr. Ridker and Dr. Blaha, he favors selecting patients who are likely to benefit the most.
“I have been an advocate of the inflammatory hypothesis for many years, and we have been on a quest for a pure anti-inflammatory therapy that we can add to the standard treatment of patients with coronary disease. And colchicine has the safety and efficacy to do this,” Dr. Nissen said.
“What colchicine offers here is an inexpensive drug with pretty good data on reduction in morbidity from coronary disease. It has a completely different mechanism, so its benefit is likely to be additive to statins. I think we could probably do a lot of good at very little expense by just using these two therapies,” he said.
“But at present my preference will be to use colchicine selectively in those with raised CRP. I think that’s logical. I’m just worried about polypharmacy. Some of my patients are already on five, six, or seven meds. I need to have a reason to add an additional drug, and I’m not sure if we really analyze this carefully that patients with a low CRP would derive the same benefit. They might do, but I doubt it,” he noted.
“There may be further research and analyses that help us understand the relationship between CRP and efficacy of colchicine, and that may help us figure this out,” he added.
Safety is reassuring
In terms of safety and tolerability of the 0.5-mg colchicine dose, the experts seem to think that this is very manageable.
“When used for gout or pericarditis, colchicine is generally given at a dose of 0.6 mg twice a day and this can cause a lot of gastrointestinal [GI] side effects,” Dr. Nissen said. “But the low dose approved for ASCVD – 0.5 mg once a day – appears to be much better tolerated. There are some GI side effects, but these are not intolerable, and they generally go away with time.”
Dr. Ridker added that in the randomized trials, the adverse effects were “quite minimal,” but, “that being said, this drug is not to be used in severe kidney or liver disease, and there are some drug interactions that we need to be aware of. But in general, side effects are rare with the low dose. There may be some GI effects but they are mainly mild and you can generally treat through them.”
Dr. Blaha agreed that this is not a drug for patients with advanced kidney disease, “and there are some drug interactions that we have to be mindful of, but the list is not so long. There is a signal of modest gastrointestinal and muscle side effects, but most patients will be able to take it without issues. Because it’s already used in gout, physicians are already quite comfortable with its use.”
Part of the backbone of CV treatment?
Concluding, Dr. Blaha said he believes that prescribing of colchicine will start with cardiologists who will use it in their highest-risk patients first.
“But as we become comfortable with it, I think we will start using it in a broader range of patients and eventually primary care doctors will start prescribing it – much like what has happened with the statins,” he suggested.
“Where it sits along with statins in the future will be very interesting to see, but I think some people can envision it being up there with statins as part of the backbone of cardiovascular treatment in future.”
Dr. Tardif holds patents on methods for using low-dose colchicine after myocardial infarction, licensed to Montreal Heart Institute. Dr. Ridker is a consultant to Agepha and has research grants from Novo Nordisk related to the development of alternative anti-inflammatory therapies for atherosclerotic disease. Dr. Blaha reports being an unpaid scientific adviser to Agepha Pharma.
A version of this article first appeared on Medscape.com.