User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Study: Pubic Bone Stabilization Slings Don't Cause Osteomyelitis
ST. LOUIS – Treatment of urinary incontinence by means of a pubic bone stabilization sling – a suburethral sling that is anchored to the pubic bone using titanium screws – is highly effective and is not associated with an increased risk of osteomyelitis, according to findings from the largest prospective observational study to date.
Although concerns that the procedure could cause osseous complications have been circulating for years and have discouraged some surgeons from using the pubic bone stabilization sling, only 1 case occurred in the 2,331 patients in the study, for an incidence of 0.000043%, Dr. S. Robert Kovac reported at the 19th International Pelvic Reconstructive and Vaginal Surgery Conference, which was sponsored by the Society of Pelvic Reconstructive Surgeons.
Patients were treated for intrinsic sphincter dysfunction (ISD) and/or stress urinary incontinence (SUI), and were followed for a mean of 13 years, and up to 17 years at four different institutions, said Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the center for pelvic reconstructive surgery and urogynecology at Emory University, Atlanta. His associates are Dr. P.D. Dietz, Dr. M. Muniz, and Dr. S.H. Cruikshank.
Follow-up was done by exams, questionnaires, and telephone conversations.
The cure rate for those with ISD and/or SUI who had total dryness was 92%.
In a prospective study published in 2004, the incidence of osteomyelitis was 0.08% in 1,228 patients who underwent transvaginal bone anchor fixation in female pelvic reconstructive surgery, Dr. Kovac noted (Urology 2004; 64:669-74).
By comparison, abdominal sacrocolpopexy is associated with an osteomyelitis incidence of 11%, according to reports in the literature, Dr. Kovac said.
“I think we got off on the wrong track,” he said of the unfounded fears regarding osteomyelitis in patients undergoing pubic bone stabilization (PBS) sling procedures.
Dr. Kovac, who developed the PBS sling procedure more than 20 years ago, said that more than 350,000 have been performed worldwide, and that in all that time he hasn’t seen a single case of osteomyelitis or osteitis pubis in any of his patients who underwent the procedure.
Furthermore, the PBS sling has the lowest complication rate and the best long-term outcomes of the various suburethral slings currently used for urinary incontinence, he said.
Currently, the procedure is performed transvaginally by placing a suburethral sling of Biodesign Surgisis over the midurethra, and securing it with titanium bone screws to the posterior-inferior pubis to restore proper anatomy for continence.
In addition to the high cure rate and low complication rate, the approach has several other advantages, Dr. Kovac said, including the following:
• It is a totally vaginal, unified approach; all defects can be treated during one procedure.
• There is efficacy for both urethral hypermobility and ISD-related SUI.
• It functions as a retropubic procedure, a vaginal Marshall-Marchetti-Krantz (MMK) operation without the need for an abdominal incision.
• It is easy to learn and teach.
• There is low or no pain.
• There is rapid return to normal voiding postoperatively.
• There is no need for blindly placed trocars.
• Surgical time is less than 30 minutes.
• There is no need for mesh, so there are no mesh-related complications.
• There is no voiding dysfunction; it is truly tension free.
The procedure also has little reliance on cystoscopy, although Dr. Kovac said that he recommends cystoscoping all patients to avoid potential bladder-related hazards.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon-Endo Surgery Inc., but he sold his patent on the PBS sling to American Medical Systems and has no financial interest in the procedure.
ST. LOUIS – Treatment of urinary incontinence by means of a pubic bone stabilization sling – a suburethral sling that is anchored to the pubic bone using titanium screws – is highly effective and is not associated with an increased risk of osteomyelitis, according to findings from the largest prospective observational study to date.
Although concerns that the procedure could cause osseous complications have been circulating for years and have discouraged some surgeons from using the pubic bone stabilization sling, only 1 case occurred in the 2,331 patients in the study, for an incidence of 0.000043%, Dr. S. Robert Kovac reported at the 19th International Pelvic Reconstructive and Vaginal Surgery Conference, which was sponsored by the Society of Pelvic Reconstructive Surgeons.
Patients were treated for intrinsic sphincter dysfunction (ISD) and/or stress urinary incontinence (SUI), and were followed for a mean of 13 years, and up to 17 years at four different institutions, said Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the center for pelvic reconstructive surgery and urogynecology at Emory University, Atlanta. His associates are Dr. P.D. Dietz, Dr. M. Muniz, and Dr. S.H. Cruikshank.
Follow-up was done by exams, questionnaires, and telephone conversations.
The cure rate for those with ISD and/or SUI who had total dryness was 92%.
In a prospective study published in 2004, the incidence of osteomyelitis was 0.08% in 1,228 patients who underwent transvaginal bone anchor fixation in female pelvic reconstructive surgery, Dr. Kovac noted (Urology 2004; 64:669-74).
By comparison, abdominal sacrocolpopexy is associated with an osteomyelitis incidence of 11%, according to reports in the literature, Dr. Kovac said.
“I think we got off on the wrong track,” he said of the unfounded fears regarding osteomyelitis in patients undergoing pubic bone stabilization (PBS) sling procedures.
Dr. Kovac, who developed the PBS sling procedure more than 20 years ago, said that more than 350,000 have been performed worldwide, and that in all that time he hasn’t seen a single case of osteomyelitis or osteitis pubis in any of his patients who underwent the procedure.
Furthermore, the PBS sling has the lowest complication rate and the best long-term outcomes of the various suburethral slings currently used for urinary incontinence, he said.
Currently, the procedure is performed transvaginally by placing a suburethral sling of Biodesign Surgisis over the midurethra, and securing it with titanium bone screws to the posterior-inferior pubis to restore proper anatomy for continence.
In addition to the high cure rate and low complication rate, the approach has several other advantages, Dr. Kovac said, including the following:
• It is a totally vaginal, unified approach; all defects can be treated during one procedure.
• There is efficacy for both urethral hypermobility and ISD-related SUI.
• It functions as a retropubic procedure, a vaginal Marshall-Marchetti-Krantz (MMK) operation without the need for an abdominal incision.
• It is easy to learn and teach.
• There is low or no pain.
• There is rapid return to normal voiding postoperatively.
• There is no need for blindly placed trocars.
• Surgical time is less than 30 minutes.
• There is no need for mesh, so there are no mesh-related complications.
• There is no voiding dysfunction; it is truly tension free.
The procedure also has little reliance on cystoscopy, although Dr. Kovac said that he recommends cystoscoping all patients to avoid potential bladder-related hazards.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon-Endo Surgery Inc., but he sold his patent on the PBS sling to American Medical Systems and has no financial interest in the procedure.
ST. LOUIS – Treatment of urinary incontinence by means of a pubic bone stabilization sling – a suburethral sling that is anchored to the pubic bone using titanium screws – is highly effective and is not associated with an increased risk of osteomyelitis, according to findings from the largest prospective observational study to date.
Although concerns that the procedure could cause osseous complications have been circulating for years and have discouraged some surgeons from using the pubic bone stabilization sling, only 1 case occurred in the 2,331 patients in the study, for an incidence of 0.000043%, Dr. S. Robert Kovac reported at the 19th International Pelvic Reconstructive and Vaginal Surgery Conference, which was sponsored by the Society of Pelvic Reconstructive Surgeons.
Patients were treated for intrinsic sphincter dysfunction (ISD) and/or stress urinary incontinence (SUI), and were followed for a mean of 13 years, and up to 17 years at four different institutions, said Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the center for pelvic reconstructive surgery and urogynecology at Emory University, Atlanta. His associates are Dr. P.D. Dietz, Dr. M. Muniz, and Dr. S.H. Cruikshank.
Follow-up was done by exams, questionnaires, and telephone conversations.
The cure rate for those with ISD and/or SUI who had total dryness was 92%.
In a prospective study published in 2004, the incidence of osteomyelitis was 0.08% in 1,228 patients who underwent transvaginal bone anchor fixation in female pelvic reconstructive surgery, Dr. Kovac noted (Urology 2004; 64:669-74).
By comparison, abdominal sacrocolpopexy is associated with an osteomyelitis incidence of 11%, according to reports in the literature, Dr. Kovac said.
“I think we got off on the wrong track,” he said of the unfounded fears regarding osteomyelitis in patients undergoing pubic bone stabilization (PBS) sling procedures.
Dr. Kovac, who developed the PBS sling procedure more than 20 years ago, said that more than 350,000 have been performed worldwide, and that in all that time he hasn’t seen a single case of osteomyelitis or osteitis pubis in any of his patients who underwent the procedure.
Furthermore, the PBS sling has the lowest complication rate and the best long-term outcomes of the various suburethral slings currently used for urinary incontinence, he said.
Currently, the procedure is performed transvaginally by placing a suburethral sling of Biodesign Surgisis over the midurethra, and securing it with titanium bone screws to the posterior-inferior pubis to restore proper anatomy for continence.
In addition to the high cure rate and low complication rate, the approach has several other advantages, Dr. Kovac said, including the following:
• It is a totally vaginal, unified approach; all defects can be treated during one procedure.
• There is efficacy for both urethral hypermobility and ISD-related SUI.
• It functions as a retropubic procedure, a vaginal Marshall-Marchetti-Krantz (MMK) operation without the need for an abdominal incision.
• It is easy to learn and teach.
• There is low or no pain.
• There is rapid return to normal voiding postoperatively.
• There is no need for blindly placed trocars.
• Surgical time is less than 30 minutes.
• There is no need for mesh, so there are no mesh-related complications.
• There is no voiding dysfunction; it is truly tension free.
The procedure also has little reliance on cystoscopy, although Dr. Kovac said that he recommends cystoscoping all patients to avoid potential bladder-related hazards.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon-Endo Surgery Inc., but he sold his patent on the PBS sling to American Medical Systems and has no financial interest in the procedure.
Major Finding: Although concerns that the procedure could cause osseous complications have been circulating for years and have discouraged some surgeons from using the procedure, only 1 case occurred in the 2,331 patients in the study, for an incidence of 0.000043%.
Data Source: A prospective observational study of 2,331 patients.
Disclosures: Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon-Endo Surgery Inc. He developed the PBS sling, but sold the procedure’s patent to American Medical Systems and has no financial interest in it.
Vitamin B Didn't Cut Poststroke Vascular Events
Daily B vitamin supplementation is no more effective than is placebo for reducing the incidence of major vascular events in patients who have had a recent stroke or transient ischemic attack, according to findings from the Vitamins to Prevent Stroke (VITATOPS) trial.
Among 8,164 patients enrolled in the multicenter, parallel, double-blind trial, major vascular events (nonfatal stroke, nonfatal myocardial infarction, or death from any vascular cause) occurred in 15% of patients randomized to B vitamin supplementation and in 17% randomized to placebo after a median follow-up period of 3.4 years. This translated into a nonsignificant relative risk of 0.91, Dr. Graeme J. Hankey of Royal Perth (Australia) Hospital and his colleagues from the VITATOPS Trial Study Group reported.
When each type of vascular event was analyzed separately, B vitamin supplementation was not associated with a significant reduction in the relative risk for nonfatal or fatal stroke, nonfatal or fatal MI, or death from any cause. However, there was a slight, but statistically significant, reduction in the risk of death from vascular causes (relative risk, 0.86).
Dr. Hankey and his associates wrote that the findings suggest that B vitamins, while safe in poststroke and post-TIA patients, should not be recommended to prevent recurrent stroke (Lancet Neurology 2010 Aug. 4 [doi:10.1016/S1474-4422(10)70187-3]).
Study participants were enrolled between Nov. 19, 1998, and Dec. 31, 2008, within 7 months of experiencing stroke or TIA and were randomized to receive placebo or 2 mg of folic acid, 25 mg of vitamin B6, and 0.5 mg of vitamin B12 daily in addition to usual medical care.
No unexpected adverse events occurred during follow-up, and no significant differences were seen between the treatment and placebo groups in regard to common adverse events, the investigators noted.
Although prior cross-sectional and observational epidemiological studies have suggested that raised plasma concentrations of total homocysteine are associated with increased risk for major vascular events, and that B vitamin supplementation can lower total homocysteine—as it did in this study—this did not translate to a reduced incidence of subsequent vascular events in the study, they said.
Fasting blood tests performed at the end of follow-up in 1,164 patients showed that the B vitamin group had 3.8 micromol/L lower homocysteine than in the placebo group (10.5 vs. 14.3 micromol/L). An analysis of a subset of 925 patients with fasting blood levels of homocysteine available from baseline and follow-up indicated that each 1.0-micromol/L decrease in total homocysteine was associated with only a nonstatistically significant 2% reduction in risk of the primary outcome.
The study is limited by incomplete adherence to trial drugs and by incomplete follow-up, as well as by a relatively short duration of follow-up, the investigators said.
To control for random error, the researchers added their data to those from other randomized controlled trials of homocysteine-lowering therapy in patients with or without preexisting cardiovascular disease. This “updated meta-analysis” also showed that B vitamins are not significantly more effective than placebo for reducing the risk of the composite outcome of stroke, myocardial infarction, or vascular death (RR, 0.99).
In a subgroup analysis, B vitamins were shown to possibly reduce the risk of stroke, myocardial infarction, or vascular death in patients with symptomatic small vessel disease of the brain causing lacunar infarction or intracerebral hemorrhage—a reduction that has also been suggested by other investigators who have reported that homocysteine is a risk factor for cerebral small vessel disease, they noted.
Dr. Hankey and some other authors of the study reported receiving payments and honoraria for various duties from companies that manufacture stroke therapies, including Johnson and Johnson, Sanofi-Aventis, and Schering Plough, Boehringer Ingelheim, and Pfizer.
The study was funded by the Australia National Health and Medical Research Council, the U.K. Medical Research Council, the Singapore Biomedical Research Council, the Singapore National Medical Research Council, the Australia National Heart Foundation, the Royal Perth Hospital Medical Research Foundation, and the Health Department of Western Australia.
My Take
Don't Give Up on B Vitamins Yet
The VITATOPS trial indicated that there is still weak evidence for a small relative risk reduction in fatal or nonfatal stroke with B vitamin supplementation. This is one reason why B vitamins might still be potentially worthwhile in stroke and TIA patients. A much larger global trial would be needed to confirm or refute such moderate effects.
Indeed, there are numerous examples of treatments that required an accumulation of data from large, sufficiently powered trials along with meta-analyses of the data from those trials before the benefits of the treatments were appreciated. Examples include antiplatelet treatment with aspirin, cholesterol reduction with drugs, and tamoxifen for breast cancer.
While the VITATOPS trial does not provide sufficiently robust evidence in support of B vitamin supplementation for secondary prevention of vascular events after stroke or TIA, there is still a place for further trials of homocysteine-lowering treatment.
PETER SANDERCOCK, M.D., is with the department of clinical neurosciences, Western General Hospital, Edinburgh. His comments are paraphrased from an editorial (Lancet Neurology 2010 Aug 4 [doi:10.1016/S1474-4422(10)70188-5]). He reported that he has no conflicts of interest.
Daily B vitamin supplementation is no more effective than is placebo for reducing the incidence of major vascular events in patients who have had a recent stroke or transient ischemic attack, according to findings from the Vitamins to Prevent Stroke (VITATOPS) trial.
Among 8,164 patients enrolled in the multicenter, parallel, double-blind trial, major vascular events (nonfatal stroke, nonfatal myocardial infarction, or death from any vascular cause) occurred in 15% of patients randomized to B vitamin supplementation and in 17% randomized to placebo after a median follow-up period of 3.4 years. This translated into a nonsignificant relative risk of 0.91, Dr. Graeme J. Hankey of Royal Perth (Australia) Hospital and his colleagues from the VITATOPS Trial Study Group reported.
When each type of vascular event was analyzed separately, B vitamin supplementation was not associated with a significant reduction in the relative risk for nonfatal or fatal stroke, nonfatal or fatal MI, or death from any cause. However, there was a slight, but statistically significant, reduction in the risk of death from vascular causes (relative risk, 0.86).
Dr. Hankey and his associates wrote that the findings suggest that B vitamins, while safe in poststroke and post-TIA patients, should not be recommended to prevent recurrent stroke (Lancet Neurology 2010 Aug. 4 [doi:10.1016/S1474-4422(10)70187-3]).
Study participants were enrolled between Nov. 19, 1998, and Dec. 31, 2008, within 7 months of experiencing stroke or TIA and were randomized to receive placebo or 2 mg of folic acid, 25 mg of vitamin B6, and 0.5 mg of vitamin B12 daily in addition to usual medical care.
No unexpected adverse events occurred during follow-up, and no significant differences were seen between the treatment and placebo groups in regard to common adverse events, the investigators noted.
Although prior cross-sectional and observational epidemiological studies have suggested that raised plasma concentrations of total homocysteine are associated with increased risk for major vascular events, and that B vitamin supplementation can lower total homocysteine—as it did in this study—this did not translate to a reduced incidence of subsequent vascular events in the study, they said.
Fasting blood tests performed at the end of follow-up in 1,164 patients showed that the B vitamin group had 3.8 micromol/L lower homocysteine than in the placebo group (10.5 vs. 14.3 micromol/L). An analysis of a subset of 925 patients with fasting blood levels of homocysteine available from baseline and follow-up indicated that each 1.0-micromol/L decrease in total homocysteine was associated with only a nonstatistically significant 2% reduction in risk of the primary outcome.
The study is limited by incomplete adherence to trial drugs and by incomplete follow-up, as well as by a relatively short duration of follow-up, the investigators said.
To control for random error, the researchers added their data to those from other randomized controlled trials of homocysteine-lowering therapy in patients with or without preexisting cardiovascular disease. This “updated meta-analysis” also showed that B vitamins are not significantly more effective than placebo for reducing the risk of the composite outcome of stroke, myocardial infarction, or vascular death (RR, 0.99).
In a subgroup analysis, B vitamins were shown to possibly reduce the risk of stroke, myocardial infarction, or vascular death in patients with symptomatic small vessel disease of the brain causing lacunar infarction or intracerebral hemorrhage—a reduction that has also been suggested by other investigators who have reported that homocysteine is a risk factor for cerebral small vessel disease, they noted.
Dr. Hankey and some other authors of the study reported receiving payments and honoraria for various duties from companies that manufacture stroke therapies, including Johnson and Johnson, Sanofi-Aventis, and Schering Plough, Boehringer Ingelheim, and Pfizer.
The study was funded by the Australia National Health and Medical Research Council, the U.K. Medical Research Council, the Singapore Biomedical Research Council, the Singapore National Medical Research Council, the Australia National Heart Foundation, the Royal Perth Hospital Medical Research Foundation, and the Health Department of Western Australia.
My Take
Don't Give Up on B Vitamins Yet
The VITATOPS trial indicated that there is still weak evidence for a small relative risk reduction in fatal or nonfatal stroke with B vitamin supplementation. This is one reason why B vitamins might still be potentially worthwhile in stroke and TIA patients. A much larger global trial would be needed to confirm or refute such moderate effects.
Indeed, there are numerous examples of treatments that required an accumulation of data from large, sufficiently powered trials along with meta-analyses of the data from those trials before the benefits of the treatments were appreciated. Examples include antiplatelet treatment with aspirin, cholesterol reduction with drugs, and tamoxifen for breast cancer.
While the VITATOPS trial does not provide sufficiently robust evidence in support of B vitamin supplementation for secondary prevention of vascular events after stroke or TIA, there is still a place for further trials of homocysteine-lowering treatment.
PETER SANDERCOCK, M.D., is with the department of clinical neurosciences, Western General Hospital, Edinburgh. His comments are paraphrased from an editorial (Lancet Neurology 2010 Aug 4 [doi:10.1016/S1474-4422(10)70188-5]). He reported that he has no conflicts of interest.
Daily B vitamin supplementation is no more effective than is placebo for reducing the incidence of major vascular events in patients who have had a recent stroke or transient ischemic attack, according to findings from the Vitamins to Prevent Stroke (VITATOPS) trial.
Among 8,164 patients enrolled in the multicenter, parallel, double-blind trial, major vascular events (nonfatal stroke, nonfatal myocardial infarction, or death from any vascular cause) occurred in 15% of patients randomized to B vitamin supplementation and in 17% randomized to placebo after a median follow-up period of 3.4 years. This translated into a nonsignificant relative risk of 0.91, Dr. Graeme J. Hankey of Royal Perth (Australia) Hospital and his colleagues from the VITATOPS Trial Study Group reported.
When each type of vascular event was analyzed separately, B vitamin supplementation was not associated with a significant reduction in the relative risk for nonfatal or fatal stroke, nonfatal or fatal MI, or death from any cause. However, there was a slight, but statistically significant, reduction in the risk of death from vascular causes (relative risk, 0.86).
Dr. Hankey and his associates wrote that the findings suggest that B vitamins, while safe in poststroke and post-TIA patients, should not be recommended to prevent recurrent stroke (Lancet Neurology 2010 Aug. 4 [doi:10.1016/S1474-4422(10)70187-3]).
Study participants were enrolled between Nov. 19, 1998, and Dec. 31, 2008, within 7 months of experiencing stroke or TIA and were randomized to receive placebo or 2 mg of folic acid, 25 mg of vitamin B6, and 0.5 mg of vitamin B12 daily in addition to usual medical care.
No unexpected adverse events occurred during follow-up, and no significant differences were seen between the treatment and placebo groups in regard to common adverse events, the investigators noted.
Although prior cross-sectional and observational epidemiological studies have suggested that raised plasma concentrations of total homocysteine are associated with increased risk for major vascular events, and that B vitamin supplementation can lower total homocysteine—as it did in this study—this did not translate to a reduced incidence of subsequent vascular events in the study, they said.
Fasting blood tests performed at the end of follow-up in 1,164 patients showed that the B vitamin group had 3.8 micromol/L lower homocysteine than in the placebo group (10.5 vs. 14.3 micromol/L). An analysis of a subset of 925 patients with fasting blood levels of homocysteine available from baseline and follow-up indicated that each 1.0-micromol/L decrease in total homocysteine was associated with only a nonstatistically significant 2% reduction in risk of the primary outcome.
The study is limited by incomplete adherence to trial drugs and by incomplete follow-up, as well as by a relatively short duration of follow-up, the investigators said.
To control for random error, the researchers added their data to those from other randomized controlled trials of homocysteine-lowering therapy in patients with or without preexisting cardiovascular disease. This “updated meta-analysis” also showed that B vitamins are not significantly more effective than placebo for reducing the risk of the composite outcome of stroke, myocardial infarction, or vascular death (RR, 0.99).
In a subgroup analysis, B vitamins were shown to possibly reduce the risk of stroke, myocardial infarction, or vascular death in patients with symptomatic small vessel disease of the brain causing lacunar infarction or intracerebral hemorrhage—a reduction that has also been suggested by other investigators who have reported that homocysteine is a risk factor for cerebral small vessel disease, they noted.
Dr. Hankey and some other authors of the study reported receiving payments and honoraria for various duties from companies that manufacture stroke therapies, including Johnson and Johnson, Sanofi-Aventis, and Schering Plough, Boehringer Ingelheim, and Pfizer.
The study was funded by the Australia National Health and Medical Research Council, the U.K. Medical Research Council, the Singapore Biomedical Research Council, the Singapore National Medical Research Council, the Australia National Heart Foundation, the Royal Perth Hospital Medical Research Foundation, and the Health Department of Western Australia.
My Take
Don't Give Up on B Vitamins Yet
The VITATOPS trial indicated that there is still weak evidence for a small relative risk reduction in fatal or nonfatal stroke with B vitamin supplementation. This is one reason why B vitamins might still be potentially worthwhile in stroke and TIA patients. A much larger global trial would be needed to confirm or refute such moderate effects.
Indeed, there are numerous examples of treatments that required an accumulation of data from large, sufficiently powered trials along with meta-analyses of the data from those trials before the benefits of the treatments were appreciated. Examples include antiplatelet treatment with aspirin, cholesterol reduction with drugs, and tamoxifen for breast cancer.
While the VITATOPS trial does not provide sufficiently robust evidence in support of B vitamin supplementation for secondary prevention of vascular events after stroke or TIA, there is still a place for further trials of homocysteine-lowering treatment.
PETER SANDERCOCK, M.D., is with the department of clinical neurosciences, Western General Hospital, Edinburgh. His comments are paraphrased from an editorial (Lancet Neurology 2010 Aug 4 [doi:10.1016/S1474-4422(10)70188-5]). He reported that he has no conflicts of interest.
Biologics for Diabetic Foot Ulcers Often Delayed
Major Finding: First use of an advanced biologic therapy in a cohort of patients with diabetic foot ulcers occurred at a mean of 28 days, and healing occurred at a median of 100 days.
Data Source: A retrospective cohort study of 2,517 patients.
Disclosures: This study was supported in part by Organogenesis, makers of Apligraf. Coauthor Laure Stasik reported that she was employed by Diversified Clinical Services during the study and is now employed by Organogenesis.
The earlier an advanced biologic therapy is initiated in a patient with a diabetic foot ulcer, the sooner the wound is likely to heal, with first use of engineered skin resulting in the fastest healing, findings from a large retrospective cohort study suggest.
First use of an advanced biologic therapy occurred at a mean of 28 days in 2,517 patients who presented with a diabetic neuropathic foot ulcer between Jan. 1, 2001, and Dec. 31, 2004, and who were treated with at least one such therapy. Healing occurred at a median of 100 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported.
The advanced biologic therapies reviewed included bilayered living skin substitute (Apligraf), recombinant human platelet–derived growth factor (becaplermin [Regranex]), and platelet releasate (Procuren). Human fibroblast–derived dermal substitute (Dermagraft) was not commercially available at the start of the study and so was not included.
A total of 1,892 patients (75%) were treated with recombinant growth factor, 446 (18%) with bilayered living cell therapy, 125 (5%) with platelet releasate, and 54 (2%) with platelet releasate or recombinant growth factor followed by bilayered living cell therapy.
Healing was faster in those who received engineered skin as the first advanced biologic therapy used (median of 84 days vs. 101 days for recombinant growth factor therapy and 108 days for platelet releasate, after adjustment for confounding factors). In addition, healing was 31.2% more likely than when topical recombinant growth factor was used first, and 40% more likely than when platelet releasate was used first, the researchers found. The differences were statistically significant (Arch. Dermatol. 2010;146:857-62).
However, the median time to use of engineered skin was 6 weeks, compared with 4 weeks for platelet releasate and 3 weeks for recombinant growth factor, and 25% of wounds treated with engineered skin were not treated until after 24 weeks.
The delay in using engineered skin vs. the other biologic treatments might be related to cost concerns, they suggested, but they also cited studies that have found that use of advanced biologic therapies reduced costs.
Longer time to healing after the first advanced biologic therapy was used was significantly associated with larger wound area, more severe wound grade, longer duration prior to first visit, and longer time from first visit to use of advanced biologic therapy. These associations were present across all treatment groups, the researchers said.
Foot ulcers are a major complication of diabetes, affecting up to 15% of diabetic patients and accounting for 20% of all diabetes-related hospital admissions in the United States. Faster foot healing can reduce the incidence of amputation in diabetic patients, the investigators said.
Although the findings underscore the importance of appropriate treatment for the management of chronic diabetic foot ulcers, this study focused on usage patterns with advanced biologic therapies and did not compare outcomes with these therapies and with standard therapy. Because of this and other limitations of the study—including its retrospective nature and the lack of detail on wound history and therapy for some patients—the results “should not be used in isolation when making decisions regarding when to use adjuvant therapy in combination with standard care,” the investigators wrote.
Nonetheless, proper treatment is critical, and delays in providing that treatment will lengthen time to healing, they concluded.
Major Finding: First use of an advanced biologic therapy in a cohort of patients with diabetic foot ulcers occurred at a mean of 28 days, and healing occurred at a median of 100 days.
Data Source: A retrospective cohort study of 2,517 patients.
Disclosures: This study was supported in part by Organogenesis, makers of Apligraf. Coauthor Laure Stasik reported that she was employed by Diversified Clinical Services during the study and is now employed by Organogenesis.
The earlier an advanced biologic therapy is initiated in a patient with a diabetic foot ulcer, the sooner the wound is likely to heal, with first use of engineered skin resulting in the fastest healing, findings from a large retrospective cohort study suggest.
First use of an advanced biologic therapy occurred at a mean of 28 days in 2,517 patients who presented with a diabetic neuropathic foot ulcer between Jan. 1, 2001, and Dec. 31, 2004, and who were treated with at least one such therapy. Healing occurred at a median of 100 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported.
The advanced biologic therapies reviewed included bilayered living skin substitute (Apligraf), recombinant human platelet–derived growth factor (becaplermin [Regranex]), and platelet releasate (Procuren). Human fibroblast–derived dermal substitute (Dermagraft) was not commercially available at the start of the study and so was not included.
A total of 1,892 patients (75%) were treated with recombinant growth factor, 446 (18%) with bilayered living cell therapy, 125 (5%) with platelet releasate, and 54 (2%) with platelet releasate or recombinant growth factor followed by bilayered living cell therapy.
Healing was faster in those who received engineered skin as the first advanced biologic therapy used (median of 84 days vs. 101 days for recombinant growth factor therapy and 108 days for platelet releasate, after adjustment for confounding factors). In addition, healing was 31.2% more likely than when topical recombinant growth factor was used first, and 40% more likely than when platelet releasate was used first, the researchers found. The differences were statistically significant (Arch. Dermatol. 2010;146:857-62).
However, the median time to use of engineered skin was 6 weeks, compared with 4 weeks for platelet releasate and 3 weeks for recombinant growth factor, and 25% of wounds treated with engineered skin were not treated until after 24 weeks.
The delay in using engineered skin vs. the other biologic treatments might be related to cost concerns, they suggested, but they also cited studies that have found that use of advanced biologic therapies reduced costs.
Longer time to healing after the first advanced biologic therapy was used was significantly associated with larger wound area, more severe wound grade, longer duration prior to first visit, and longer time from first visit to use of advanced biologic therapy. These associations were present across all treatment groups, the researchers said.
Foot ulcers are a major complication of diabetes, affecting up to 15% of diabetic patients and accounting for 20% of all diabetes-related hospital admissions in the United States. Faster foot healing can reduce the incidence of amputation in diabetic patients, the investigators said.
Although the findings underscore the importance of appropriate treatment for the management of chronic diabetic foot ulcers, this study focused on usage patterns with advanced biologic therapies and did not compare outcomes with these therapies and with standard therapy. Because of this and other limitations of the study—including its retrospective nature and the lack of detail on wound history and therapy for some patients—the results “should not be used in isolation when making decisions regarding when to use adjuvant therapy in combination with standard care,” the investigators wrote.
Nonetheless, proper treatment is critical, and delays in providing that treatment will lengthen time to healing, they concluded.
Major Finding: First use of an advanced biologic therapy in a cohort of patients with diabetic foot ulcers occurred at a mean of 28 days, and healing occurred at a median of 100 days.
Data Source: A retrospective cohort study of 2,517 patients.
Disclosures: This study was supported in part by Organogenesis, makers of Apligraf. Coauthor Laure Stasik reported that she was employed by Diversified Clinical Services during the study and is now employed by Organogenesis.
The earlier an advanced biologic therapy is initiated in a patient with a diabetic foot ulcer, the sooner the wound is likely to heal, with first use of engineered skin resulting in the fastest healing, findings from a large retrospective cohort study suggest.
First use of an advanced biologic therapy occurred at a mean of 28 days in 2,517 patients who presented with a diabetic neuropathic foot ulcer between Jan. 1, 2001, and Dec. 31, 2004, and who were treated with at least one such therapy. Healing occurred at a median of 100 days, Dr. Robert S. Kirsner of the University of Miami and his colleagues reported.
The advanced biologic therapies reviewed included bilayered living skin substitute (Apligraf), recombinant human platelet–derived growth factor (becaplermin [Regranex]), and platelet releasate (Procuren). Human fibroblast–derived dermal substitute (Dermagraft) was not commercially available at the start of the study and so was not included.
A total of 1,892 patients (75%) were treated with recombinant growth factor, 446 (18%) with bilayered living cell therapy, 125 (5%) with platelet releasate, and 54 (2%) with platelet releasate or recombinant growth factor followed by bilayered living cell therapy.
Healing was faster in those who received engineered skin as the first advanced biologic therapy used (median of 84 days vs. 101 days for recombinant growth factor therapy and 108 days for platelet releasate, after adjustment for confounding factors). In addition, healing was 31.2% more likely than when topical recombinant growth factor was used first, and 40% more likely than when platelet releasate was used first, the researchers found. The differences were statistically significant (Arch. Dermatol. 2010;146:857-62).
However, the median time to use of engineered skin was 6 weeks, compared with 4 weeks for platelet releasate and 3 weeks for recombinant growth factor, and 25% of wounds treated with engineered skin were not treated until after 24 weeks.
The delay in using engineered skin vs. the other biologic treatments might be related to cost concerns, they suggested, but they also cited studies that have found that use of advanced biologic therapies reduced costs.
Longer time to healing after the first advanced biologic therapy was used was significantly associated with larger wound area, more severe wound grade, longer duration prior to first visit, and longer time from first visit to use of advanced biologic therapy. These associations were present across all treatment groups, the researchers said.
Foot ulcers are a major complication of diabetes, affecting up to 15% of diabetic patients and accounting for 20% of all diabetes-related hospital admissions in the United States. Faster foot healing can reduce the incidence of amputation in diabetic patients, the investigators said.
Although the findings underscore the importance of appropriate treatment for the management of chronic diabetic foot ulcers, this study focused on usage patterns with advanced biologic therapies and did not compare outcomes with these therapies and with standard therapy. Because of this and other limitations of the study—including its retrospective nature and the lack of detail on wound history and therapy for some patients—the results “should not be used in isolation when making decisions regarding when to use adjuvant therapy in combination with standard care,” the investigators wrote.
Nonetheless, proper treatment is critical, and delays in providing that treatment will lengthen time to healing, they concluded.
Larger Uteri Can Be Removed Using Vaginal Hysterectomy Technique
ST. LOUIS – The vast majority of benign hysterectomies can – and should – be performed vaginally, according to Dr. Carl W. Zimmerman.
In fact, more than 90% of uteri weighing less than 250 g are accessible and can safely be removed vaginally by using guidelines endorsed by the board of directors of the Society of Pelvic Reconstructive Surgeons. Considerable evidence exists that many larger uteri also can be removed safely via the vaginal route, he said at the conference, which was sponsored by the society.
Despite this evidence, however, the minimally invasive vaginal approach remains underused in the United States, said Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University, Nashville, Tenn.
A lack of experience, familiarity with technique, and confidence is the main reasons why surgeons avoid the vaginal approach in favor of more invasive abdominal, laparoscopic, and robotic techniques. While the choice for vaginal hysterectomy should be made based – to a certain extent – on guidelines, it is important to consider skill acquisition, experience and competency, he said.
He encouraged those who are “on a learning curve” in terms of performing vaginal hysterectomy in patients with large uteri to obtain more experience by using this technique for uteri of 14-16 week size.
“That may sound big, but you’ll be amazed, you’ll be empowered, and your patients will do well,” he said, strongly recommending consideration of the concept of removing larger uteri by this method.
He outlined five main steps that must be completed to successfully remove an enlarged uterus vaginally, and provided tips on surgical instrumentation that can facilitate vaginal hysterectomy in cases involving a large uterus.
The first step is entry into the peritoneal cavity. This can be accomplished anteriorly or posteriorly, but experienced operators will delay entry into the anterior segment until the uterosacral and cardinal ligaments have been detached, and therefore they typically enter posteriorly.
“It’s often available to you, and it’s the easiest entry into the peritoneal cavity,” he said of the posterior approach.
The next two steps are to detach the uterosacral and cardinal ligaments, and to ligate the uterine artery.
Keep in mind that fibroids are the most common cause of uterine enlargement, and that most of the anatomical distortions in the fibroid uterus are limited to the area superior to the uterine artery. This “concept of uterine anatomic distortion” means that once steps 1-3 are completed, you “can be innovative about the way you debulk and remove the uterus. Once you have secured the support system, and you have divided the blood supply, then it becomes a mechanical exercise in converting a roughly globular structure into either various components that will come out, or a shape that will change and come out,” he explained.
Once the fourth step of debulking and removing the uterus is completed, the final step – vaginal adnexectomy – can be performed as needed based on the same indications that would be used if a scope was in place, or if the procedure was done abdominally, he said.
As for the best approaches to debulking the uterus, Dr. Zimmerman said morcellation is his primary technique, followed by coring, which is very useful for the adenomyotic uterus – and is particularly valuable for managing uteri up to 17 weeks in size.
The typical tools used in gynecologic surgery, such as Haney clamps, straight needle holders, and short instruments may be inadequate for performing vaginal hysterectomy involving large uteri. Instruments Dr. Zimmerman recommends for improving surgical skill and outcome include:
• Retractors. The correct retractors are one of the keys to success in vaginal hysterectomy; shop around and find the type that fits best into your system, Dr. Zimmerman advised. He listed Heaney, Harrington, malleable ribbon, Breisky-Navratil, and Steiner-Auvard among good options. Deaver retractors should be avoided because they increase risk of bladder injury, he said.
• Scissors. The right scissors can help with debulking when difficult angles are encountered. Jorgenson scissors, which Dr. Zimmerman learned to use in abdominal hysterectomy, are also useful in vaginal hysterectomy, because they create a right angle very valuable for debulking the uterus. Martin cartilage scissors, which have sharp points at the tips that can allow for insertion into a myoma and allow wedges to be cut, are very helpful, he said. Even a very dense or calcified myoma can be transected and debulked using these scissors.
• Lights. Whatever you choose to use to gain extra light is a good idea, he added. The Vital Vue surgical light, and a newer version – the Versalight, which is a multifunctional surgical light that provides irrigation, suction, and retraction, are good options. Dr. Zimmerman disclosed that he helped design the Versalight.
• Vulsellum forceps. These are useful for grasping myoma. Lahey, Gordon, and Segond forceps are all good options.
• Myotomes. Cobb and Langenbeck periosteal elevators that have been modified into both chisel tip and spoon tip myotomes can be helpful for enucleation.
With the proper equipment and surgical skills, vaginal hysterectomy is feasible in most cases, and the reduced morbidity, costs, and hospital length of stay associated with this approach should be enough incentive to encourage gynecologists to increase proficiency in the vaginal approach, Dr. Zimmerman said.
Keep in mind, he added, that in appropriately informed patients who have given consent to surgery, conversion to a more invasive approach is not a complication.
Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – The vast majority of benign hysterectomies can – and should – be performed vaginally, according to Dr. Carl W. Zimmerman.
In fact, more than 90% of uteri weighing less than 250 g are accessible and can safely be removed vaginally by using guidelines endorsed by the board of directors of the Society of Pelvic Reconstructive Surgeons. Considerable evidence exists that many larger uteri also can be removed safely via the vaginal route, he said at the conference, which was sponsored by the society.
Despite this evidence, however, the minimally invasive vaginal approach remains underused in the United States, said Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University, Nashville, Tenn.
A lack of experience, familiarity with technique, and confidence is the main reasons why surgeons avoid the vaginal approach in favor of more invasive abdominal, laparoscopic, and robotic techniques. While the choice for vaginal hysterectomy should be made based – to a certain extent – on guidelines, it is important to consider skill acquisition, experience and competency, he said.
He encouraged those who are “on a learning curve” in terms of performing vaginal hysterectomy in patients with large uteri to obtain more experience by using this technique for uteri of 14-16 week size.
“That may sound big, but you’ll be amazed, you’ll be empowered, and your patients will do well,” he said, strongly recommending consideration of the concept of removing larger uteri by this method.
He outlined five main steps that must be completed to successfully remove an enlarged uterus vaginally, and provided tips on surgical instrumentation that can facilitate vaginal hysterectomy in cases involving a large uterus.
The first step is entry into the peritoneal cavity. This can be accomplished anteriorly or posteriorly, but experienced operators will delay entry into the anterior segment until the uterosacral and cardinal ligaments have been detached, and therefore they typically enter posteriorly.
“It’s often available to you, and it’s the easiest entry into the peritoneal cavity,” he said of the posterior approach.
The next two steps are to detach the uterosacral and cardinal ligaments, and to ligate the uterine artery.
Keep in mind that fibroids are the most common cause of uterine enlargement, and that most of the anatomical distortions in the fibroid uterus are limited to the area superior to the uterine artery. This “concept of uterine anatomic distortion” means that once steps 1-3 are completed, you “can be innovative about the way you debulk and remove the uterus. Once you have secured the support system, and you have divided the blood supply, then it becomes a mechanical exercise in converting a roughly globular structure into either various components that will come out, or a shape that will change and come out,” he explained.
Once the fourth step of debulking and removing the uterus is completed, the final step – vaginal adnexectomy – can be performed as needed based on the same indications that would be used if a scope was in place, or if the procedure was done abdominally, he said.
As for the best approaches to debulking the uterus, Dr. Zimmerman said morcellation is his primary technique, followed by coring, which is very useful for the adenomyotic uterus – and is particularly valuable for managing uteri up to 17 weeks in size.
The typical tools used in gynecologic surgery, such as Haney clamps, straight needle holders, and short instruments may be inadequate for performing vaginal hysterectomy involving large uteri. Instruments Dr. Zimmerman recommends for improving surgical skill and outcome include:
• Retractors. The correct retractors are one of the keys to success in vaginal hysterectomy; shop around and find the type that fits best into your system, Dr. Zimmerman advised. He listed Heaney, Harrington, malleable ribbon, Breisky-Navratil, and Steiner-Auvard among good options. Deaver retractors should be avoided because they increase risk of bladder injury, he said.
• Scissors. The right scissors can help with debulking when difficult angles are encountered. Jorgenson scissors, which Dr. Zimmerman learned to use in abdominal hysterectomy, are also useful in vaginal hysterectomy, because they create a right angle very valuable for debulking the uterus. Martin cartilage scissors, which have sharp points at the tips that can allow for insertion into a myoma and allow wedges to be cut, are very helpful, he said. Even a very dense or calcified myoma can be transected and debulked using these scissors.
• Lights. Whatever you choose to use to gain extra light is a good idea, he added. The Vital Vue surgical light, and a newer version – the Versalight, which is a multifunctional surgical light that provides irrigation, suction, and retraction, are good options. Dr. Zimmerman disclosed that he helped design the Versalight.
• Vulsellum forceps. These are useful for grasping myoma. Lahey, Gordon, and Segond forceps are all good options.
• Myotomes. Cobb and Langenbeck periosteal elevators that have been modified into both chisel tip and spoon tip myotomes can be helpful for enucleation.
With the proper equipment and surgical skills, vaginal hysterectomy is feasible in most cases, and the reduced morbidity, costs, and hospital length of stay associated with this approach should be enough incentive to encourage gynecologists to increase proficiency in the vaginal approach, Dr. Zimmerman said.
Keep in mind, he added, that in appropriately informed patients who have given consent to surgery, conversion to a more invasive approach is not a complication.
Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – The vast majority of benign hysterectomies can – and should – be performed vaginally, according to Dr. Carl W. Zimmerman.
In fact, more than 90% of uteri weighing less than 250 g are accessible and can safely be removed vaginally by using guidelines endorsed by the board of directors of the Society of Pelvic Reconstructive Surgeons. Considerable evidence exists that many larger uteri also can be removed safely via the vaginal route, he said at the conference, which was sponsored by the society.
Despite this evidence, however, the minimally invasive vaginal approach remains underused in the United States, said Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University, Nashville, Tenn.
A lack of experience, familiarity with technique, and confidence is the main reasons why surgeons avoid the vaginal approach in favor of more invasive abdominal, laparoscopic, and robotic techniques. While the choice for vaginal hysterectomy should be made based – to a certain extent – on guidelines, it is important to consider skill acquisition, experience and competency, he said.
He encouraged those who are “on a learning curve” in terms of performing vaginal hysterectomy in patients with large uteri to obtain more experience by using this technique for uteri of 14-16 week size.
“That may sound big, but you’ll be amazed, you’ll be empowered, and your patients will do well,” he said, strongly recommending consideration of the concept of removing larger uteri by this method.
He outlined five main steps that must be completed to successfully remove an enlarged uterus vaginally, and provided tips on surgical instrumentation that can facilitate vaginal hysterectomy in cases involving a large uterus.
The first step is entry into the peritoneal cavity. This can be accomplished anteriorly or posteriorly, but experienced operators will delay entry into the anterior segment until the uterosacral and cardinal ligaments have been detached, and therefore they typically enter posteriorly.
“It’s often available to you, and it’s the easiest entry into the peritoneal cavity,” he said of the posterior approach.
The next two steps are to detach the uterosacral and cardinal ligaments, and to ligate the uterine artery.
Keep in mind that fibroids are the most common cause of uterine enlargement, and that most of the anatomical distortions in the fibroid uterus are limited to the area superior to the uterine artery. This “concept of uterine anatomic distortion” means that once steps 1-3 are completed, you “can be innovative about the way you debulk and remove the uterus. Once you have secured the support system, and you have divided the blood supply, then it becomes a mechanical exercise in converting a roughly globular structure into either various components that will come out, or a shape that will change and come out,” he explained.
Once the fourth step of debulking and removing the uterus is completed, the final step – vaginal adnexectomy – can be performed as needed based on the same indications that would be used if a scope was in place, or if the procedure was done abdominally, he said.
As for the best approaches to debulking the uterus, Dr. Zimmerman said morcellation is his primary technique, followed by coring, which is very useful for the adenomyotic uterus – and is particularly valuable for managing uteri up to 17 weeks in size.
The typical tools used in gynecologic surgery, such as Haney clamps, straight needle holders, and short instruments may be inadequate for performing vaginal hysterectomy involving large uteri. Instruments Dr. Zimmerman recommends for improving surgical skill and outcome include:
• Retractors. The correct retractors are one of the keys to success in vaginal hysterectomy; shop around and find the type that fits best into your system, Dr. Zimmerman advised. He listed Heaney, Harrington, malleable ribbon, Breisky-Navratil, and Steiner-Auvard among good options. Deaver retractors should be avoided because they increase risk of bladder injury, he said.
• Scissors. The right scissors can help with debulking when difficult angles are encountered. Jorgenson scissors, which Dr. Zimmerman learned to use in abdominal hysterectomy, are also useful in vaginal hysterectomy, because they create a right angle very valuable for debulking the uterus. Martin cartilage scissors, which have sharp points at the tips that can allow for insertion into a myoma and allow wedges to be cut, are very helpful, he said. Even a very dense or calcified myoma can be transected and debulked using these scissors.
• Lights. Whatever you choose to use to gain extra light is a good idea, he added. The Vital Vue surgical light, and a newer version – the Versalight, which is a multifunctional surgical light that provides irrigation, suction, and retraction, are good options. Dr. Zimmerman disclosed that he helped design the Versalight.
• Vulsellum forceps. These are useful for grasping myoma. Lahey, Gordon, and Segond forceps are all good options.
• Myotomes. Cobb and Langenbeck periosteal elevators that have been modified into both chisel tip and spoon tip myotomes can be helpful for enucleation.
With the proper equipment and surgical skills, vaginal hysterectomy is feasible in most cases, and the reduced morbidity, costs, and hospital length of stay associated with this approach should be enough incentive to encourage gynecologists to increase proficiency in the vaginal approach, Dr. Zimmerman said.
Keep in mind, he added, that in appropriately informed patients who have given consent to surgery, conversion to a more invasive approach is not a complication.
Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
Expert analysis from an international pelvic reconstructive and vaginal surgery conference
Cilostazol Matches Aspirin’s Effectiveness in Preventing Secondary Stroke
The antiplatelet drug cilostazol works at least as well as aspirin for preventing stroke in patients who have had an ischemic stroke, according to the results of a randomized trial published online in the Sept. 11 issue of The Lancet.
At a mean follow-up of 29 months in the aspirin-controlled, double-blind, noninferiority trial, first-time secondary strokes occurred at a yearly rate of 2.76% among patients who received 100 mg cilostazol twice daily and 3.71% in patients who received 81 mg aspirin once daily. This difference resulted in a hazard ratio of 0.743, or a 25.7% relative reduction of the risk of stroke with the use of cilostazol in comparison with aspirin.
The findings are important because few regimens have proven significantly more effective for stroke prevention than aspirin alone, according to Dr. Yukito Shinahara of Tachikawa Hospital, Tokyo, and colleagues from the Japanese Cilostazol for Prevention of Secondary Stroke (CSPS 2) trial group.
Since cilostazol was shown in the original CSPS trial in 2000 to be more effective than placebo for prevention of secondary cerebral infarction, it has been used in Japan for this purpose and is listed in Japanese guidelines for the management of stroke.
The 2,757 patients in the CSPS 2 trial were adults aged 20-79 years who had experienced a noncardioembolic cerebral infarction within the previous 26 weeks. They were enrolled at 278 sites in Japan between December 2003 and October 2006, and underwent treatment for 1-5 years. (Lancet 2010 Sept. 11 [doi:10.1016/S1474-4422(10)70198-8]).
Dr. Yukito Shinahara and colleagues said that they considered cilostazol to be noninferior to aspirin for the prevention of stroke because the upper limit of the 95% confidence interval was lower than the prespecified inferiority margin of 1.33.
In addition to reducing stroke risk, cilostazol significantly reduced the risk of a composite secondary endpoint (cerebral infarction, ischemic cerebrovascular disease, or death from any cause) by 20.1%, compared with aspirin. Cilostazol also was associated with a reduced risk of hemorrhagic events, which occurred at a rate of 0.77% per person-year in cilostazol-treated patients and 1.78% per person-year in aspirin-treated patients.
Dr. Shinahara and associates noted that “because significantly fewer hemorrhagic events were recorded in the cilostazol group than in the aspirin group, cilostazol might be particularly useful in patients with increased risk of hemorrhage.”
Other adverse events, however, occurred significantly more often in cilostazol-treated patients. These included headache, diarrhea, palpitations, dizziness, and tachycardia. None of these were serious, and all resolved after treatment discontinuation or dose tapering, the investigators said.
“The results of CSPS 2 suggest that cilostazol can be recommended as an option for the prevention of stroke in Asian patients with noncardioembolic stroke who can tolerate long-term treatment with this drug,” wrote the authors, noting that previous studies have suggested that cilostazol is effective for patients of other ethnic origins as well.
In a U.S. study, patients with peripheral artery disease who took cilostazol experienced significantly fewer cerebrovascular events, compared with placebo (J. Stroke. Cerebrovasc. Dis. 2008; 17:129-33).
In addition to its antiplatelet effects, cilostazol also has beneficial effects on other factors associated with thrombus formation, including endothelial function and dilation of blood vessels by increased production of nitric oxide, and reduction of intracellular calcium ion concentrations. The drug also inhibits smooth muscle proliferation and inflammation in various vascular beds, according to the researchers.
Otsuka Pharmaceutical funded the study. Dr. Shinohara disclosed providing consultancy for Schering-Plough and Pfizer Japan, and receiving grants from the Japan Ministry of Health, Labour and Welfare, and receiving lecture fees from Otsuka and other companies. Other authors on the study reported various financial relationships with Otsuka and other companies.
The findings of the CSPS 2 trial suggest that there might be another promising approach to secondary stroke prevention other than aspirin, but the study has several limiting factors.
Because ethnic differences in the pharmacokinetics and pharmacodynamics of antiplatelet agents have been observed in some studies, the results of the trial have limited generalizability. Positive results noted in one ethnic group might not be as impressive, or might even be negative, in other ethnic groups.
The trial was powered to detect noninferiority between the drugs, and although the results seemed to indicate that cilostazol is superior to aspirin, its apparent superiority must be confirmed in trials powered to make such an assessment.
CSPS 2 enrolled only patients with non-severe strokes, possibly limiting applicability of the findings to patients with more severe strokes. Other factors to consider include the high incidence of side effects in the cilostazol patients, the high cost of the drug, compared with aspirin, and the low concomitant use of other secondary prevention therapies, such as statins and antihypertensive drugs.
Dr. Dharam J. Kumbhani and Dr. Deepak L. Bhatt are with Brigham and Women’s Hospital and Harvard Medical School, Boston. Their comments are paraphrased from an editorial (Lancet 2010 Sept. 11 [doi: 10.1016/S1474-4422(10)70217-9]). Dr. Kumbhani reported having no disclosures. Dr. Bhatt reported receiving institutional research support from AstraZeneca, Bristol-Myers Squibb, Eisai, Sanofi-Aventis, and The Medicine Company, and he has received honoraria from Duke Clinical Research Institute.
The findings of the CSPS 2 trial suggest that there might be another promising approach to secondary stroke prevention other than aspirin, but the study has several limiting factors.
Because ethnic differences in the pharmacokinetics and pharmacodynamics of antiplatelet agents have been observed in some studies, the results of the trial have limited generalizability. Positive results noted in one ethnic group might not be as impressive, or might even be negative, in other ethnic groups.
The trial was powered to detect noninferiority between the drugs, and although the results seemed to indicate that cilostazol is superior to aspirin, its apparent superiority must be confirmed in trials powered to make such an assessment.
CSPS 2 enrolled only patients with non-severe strokes, possibly limiting applicability of the findings to patients with more severe strokes. Other factors to consider include the high incidence of side effects in the cilostazol patients, the high cost of the drug, compared with aspirin, and the low concomitant use of other secondary prevention therapies, such as statins and antihypertensive drugs.
Dr. Dharam J. Kumbhani and Dr. Deepak L. Bhatt are with Brigham and Women’s Hospital and Harvard Medical School, Boston. Their comments are paraphrased from an editorial (Lancet 2010 Sept. 11 [doi: 10.1016/S1474-4422(10)70217-9]). Dr. Kumbhani reported having no disclosures. Dr. Bhatt reported receiving institutional research support from AstraZeneca, Bristol-Myers Squibb, Eisai, Sanofi-Aventis, and The Medicine Company, and he has received honoraria from Duke Clinical Research Institute.
The findings of the CSPS 2 trial suggest that there might be another promising approach to secondary stroke prevention other than aspirin, but the study has several limiting factors.
Because ethnic differences in the pharmacokinetics and pharmacodynamics of antiplatelet agents have been observed in some studies, the results of the trial have limited generalizability. Positive results noted in one ethnic group might not be as impressive, or might even be negative, in other ethnic groups.
The trial was powered to detect noninferiority between the drugs, and although the results seemed to indicate that cilostazol is superior to aspirin, its apparent superiority must be confirmed in trials powered to make such an assessment.
CSPS 2 enrolled only patients with non-severe strokes, possibly limiting applicability of the findings to patients with more severe strokes. Other factors to consider include the high incidence of side effects in the cilostazol patients, the high cost of the drug, compared with aspirin, and the low concomitant use of other secondary prevention therapies, such as statins and antihypertensive drugs.
Dr. Dharam J. Kumbhani and Dr. Deepak L. Bhatt are with Brigham and Women’s Hospital and Harvard Medical School, Boston. Their comments are paraphrased from an editorial (Lancet 2010 Sept. 11 [doi: 10.1016/S1474-4422(10)70217-9]). Dr. Kumbhani reported having no disclosures. Dr. Bhatt reported receiving institutional research support from AstraZeneca, Bristol-Myers Squibb, Eisai, Sanofi-Aventis, and The Medicine Company, and he has received honoraria from Duke Clinical Research Institute.
The antiplatelet drug cilostazol works at least as well as aspirin for preventing stroke in patients who have had an ischemic stroke, according to the results of a randomized trial published online in the Sept. 11 issue of The Lancet.
At a mean follow-up of 29 months in the aspirin-controlled, double-blind, noninferiority trial, first-time secondary strokes occurred at a yearly rate of 2.76% among patients who received 100 mg cilostazol twice daily and 3.71% in patients who received 81 mg aspirin once daily. This difference resulted in a hazard ratio of 0.743, or a 25.7% relative reduction of the risk of stroke with the use of cilostazol in comparison with aspirin.
The findings are important because few regimens have proven significantly more effective for stroke prevention than aspirin alone, according to Dr. Yukito Shinahara of Tachikawa Hospital, Tokyo, and colleagues from the Japanese Cilostazol for Prevention of Secondary Stroke (CSPS 2) trial group.
Since cilostazol was shown in the original CSPS trial in 2000 to be more effective than placebo for prevention of secondary cerebral infarction, it has been used in Japan for this purpose and is listed in Japanese guidelines for the management of stroke.
The 2,757 patients in the CSPS 2 trial were adults aged 20-79 years who had experienced a noncardioembolic cerebral infarction within the previous 26 weeks. They were enrolled at 278 sites in Japan between December 2003 and October 2006, and underwent treatment for 1-5 years. (Lancet 2010 Sept. 11 [doi:10.1016/S1474-4422(10)70198-8]).
Dr. Yukito Shinahara and colleagues said that they considered cilostazol to be noninferior to aspirin for the prevention of stroke because the upper limit of the 95% confidence interval was lower than the prespecified inferiority margin of 1.33.
In addition to reducing stroke risk, cilostazol significantly reduced the risk of a composite secondary endpoint (cerebral infarction, ischemic cerebrovascular disease, or death from any cause) by 20.1%, compared with aspirin. Cilostazol also was associated with a reduced risk of hemorrhagic events, which occurred at a rate of 0.77% per person-year in cilostazol-treated patients and 1.78% per person-year in aspirin-treated patients.
Dr. Shinahara and associates noted that “because significantly fewer hemorrhagic events were recorded in the cilostazol group than in the aspirin group, cilostazol might be particularly useful in patients with increased risk of hemorrhage.”
Other adverse events, however, occurred significantly more often in cilostazol-treated patients. These included headache, diarrhea, palpitations, dizziness, and tachycardia. None of these were serious, and all resolved after treatment discontinuation or dose tapering, the investigators said.
“The results of CSPS 2 suggest that cilostazol can be recommended as an option for the prevention of stroke in Asian patients with noncardioembolic stroke who can tolerate long-term treatment with this drug,” wrote the authors, noting that previous studies have suggested that cilostazol is effective for patients of other ethnic origins as well.
In a U.S. study, patients with peripheral artery disease who took cilostazol experienced significantly fewer cerebrovascular events, compared with placebo (J. Stroke. Cerebrovasc. Dis. 2008; 17:129-33).
In addition to its antiplatelet effects, cilostazol also has beneficial effects on other factors associated with thrombus formation, including endothelial function and dilation of blood vessels by increased production of nitric oxide, and reduction of intracellular calcium ion concentrations. The drug also inhibits smooth muscle proliferation and inflammation in various vascular beds, according to the researchers.
Otsuka Pharmaceutical funded the study. Dr. Shinohara disclosed providing consultancy for Schering-Plough and Pfizer Japan, and receiving grants from the Japan Ministry of Health, Labour and Welfare, and receiving lecture fees from Otsuka and other companies. Other authors on the study reported various financial relationships with Otsuka and other companies.
The antiplatelet drug cilostazol works at least as well as aspirin for preventing stroke in patients who have had an ischemic stroke, according to the results of a randomized trial published online in the Sept. 11 issue of The Lancet.
At a mean follow-up of 29 months in the aspirin-controlled, double-blind, noninferiority trial, first-time secondary strokes occurred at a yearly rate of 2.76% among patients who received 100 mg cilostazol twice daily and 3.71% in patients who received 81 mg aspirin once daily. This difference resulted in a hazard ratio of 0.743, or a 25.7% relative reduction of the risk of stroke with the use of cilostazol in comparison with aspirin.
The findings are important because few regimens have proven significantly more effective for stroke prevention than aspirin alone, according to Dr. Yukito Shinahara of Tachikawa Hospital, Tokyo, and colleagues from the Japanese Cilostazol for Prevention of Secondary Stroke (CSPS 2) trial group.
Since cilostazol was shown in the original CSPS trial in 2000 to be more effective than placebo for prevention of secondary cerebral infarction, it has been used in Japan for this purpose and is listed in Japanese guidelines for the management of stroke.
The 2,757 patients in the CSPS 2 trial were adults aged 20-79 years who had experienced a noncardioembolic cerebral infarction within the previous 26 weeks. They were enrolled at 278 sites in Japan between December 2003 and October 2006, and underwent treatment for 1-5 years. (Lancet 2010 Sept. 11 [doi:10.1016/S1474-4422(10)70198-8]).
Dr. Yukito Shinahara and colleagues said that they considered cilostazol to be noninferior to aspirin for the prevention of stroke because the upper limit of the 95% confidence interval was lower than the prespecified inferiority margin of 1.33.
In addition to reducing stroke risk, cilostazol significantly reduced the risk of a composite secondary endpoint (cerebral infarction, ischemic cerebrovascular disease, or death from any cause) by 20.1%, compared with aspirin. Cilostazol also was associated with a reduced risk of hemorrhagic events, which occurred at a rate of 0.77% per person-year in cilostazol-treated patients and 1.78% per person-year in aspirin-treated patients.
Dr. Shinahara and associates noted that “because significantly fewer hemorrhagic events were recorded in the cilostazol group than in the aspirin group, cilostazol might be particularly useful in patients with increased risk of hemorrhage.”
Other adverse events, however, occurred significantly more often in cilostazol-treated patients. These included headache, diarrhea, palpitations, dizziness, and tachycardia. None of these were serious, and all resolved after treatment discontinuation or dose tapering, the investigators said.
“The results of CSPS 2 suggest that cilostazol can be recommended as an option for the prevention of stroke in Asian patients with noncardioembolic stroke who can tolerate long-term treatment with this drug,” wrote the authors, noting that previous studies have suggested that cilostazol is effective for patients of other ethnic origins as well.
In a U.S. study, patients with peripheral artery disease who took cilostazol experienced significantly fewer cerebrovascular events, compared with placebo (J. Stroke. Cerebrovasc. Dis. 2008; 17:129-33).
In addition to its antiplatelet effects, cilostazol also has beneficial effects on other factors associated with thrombus formation, including endothelial function and dilation of blood vessels by increased production of nitric oxide, and reduction of intracellular calcium ion concentrations. The drug also inhibits smooth muscle proliferation and inflammation in various vascular beds, according to the researchers.
Otsuka Pharmaceutical funded the study. Dr. Shinohara disclosed providing consultancy for Schering-Plough and Pfizer Japan, and receiving grants from the Japan Ministry of Health, Labour and Welfare, and receiving lecture fees from Otsuka and other companies. Other authors on the study reported various financial relationships with Otsuka and other companies.
From The Lancet
Major Finding: At a mean follow-up of 29 months, the primary end point of a first occurrence of stroke occurred at a yearly rate of 2.76% in the cilostazol group, and 3.71% in the aspirin group (hazard ratio 0.743).
Data Source: An aspirin-controlled, double-blind, randomized, noninferiority trial involving 2,757 patients.
Disclosures: Otsuka Pharmaceutical funded the study. Dr. Shinohara disclosed providing consultancy for Schering-Plough and Pfizer Japan, and receiving grants from the Japan Ministry of Health, Labour and Welfare, and receiving lecture fees from Otsuka and other companies. Other authors on the study reported various financial relationships with Otsuka and other companies.
Carotid Stenting Less Safe Than Surgery After Age 70
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
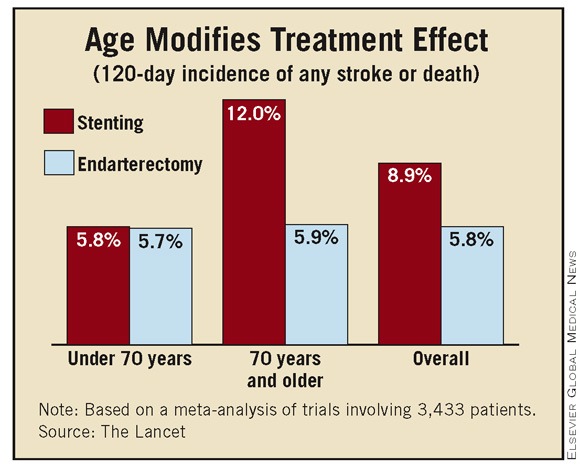
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Carotid Stenting Less Safe Than Surgery After Age 70
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Carotid stenting may be a safe alternative to endarterectomy in patients under age 70 years with symptomatic carotid stenosis, but stenting should be avoided in those aged 70 years or older, according to findings from a meta-analysis of data from three randomized controlled trials published online Sept. 10 in the Lancet.
While current recommendations restrict the use of stenting to symptomatic patients with contraindications to endarterectomy, carotid stenosis at surgically inaccessible sites, recurrent stenosis after previous endarterectomy, and stenosis after irradiation, the findings of this meta-analysis suggest stenting is also a viable alternative in younger patients in whom surgery could otherwise be undertaken without increased risk, said Dr. Leo H. Bonati of University Hospital Basel, Switzerland, and of the Institute of Neurology at University College, London, and his colleagues from the Carotid Stenting Trialists’ Collaboration.
They advised, however, that some uncertainty remains about whether recurrent stenosis rates are high after stenting vs. endarterectomy and recommended an approach of offering stenting when “technically feasible as an alternative option to endarterectomy to patients younger than 65-70 years with symptomatic carotid stenosis, in centers in which acceptable periprocedural outcomes have been independently verified ... as long as patients are made aware of a possible increase in the risk of restenosis.”
Among the 3,433 patients in the trials, the overall incidence of any stroke or death in the 120 days following randomization in the three trials was significantly greater in the patients who underwent carotid stenting vs. carotid endarterectomy (8.9% vs. 5.8%, respectively; risk ratio 1.53).
However, assessment of multiple subgroup variables showed that age modified the treatment effect; no difference was seen in the estimated 120-day risk of stroke or death in those under age 70 years who underwent stenting vs. endarterectomy (5.8% and 5.7%, respectively; risk ratio 1.00), but the risk of stroke or death was doubled in those aged 70 years or older who underwent stenting vs. endarterectomy (12.0% vs. 5.9%; risk ratio 2.04).
Similarly, the relative risk estimates for stroke or death at 30 days after treatment were comparable in those under age 70 years who underwent stenting vs. endarterectomy (5.1% and 4.5%, respectively; risk ratio 1.11), but were more than double in those aged 70 years or older for stenting vs. endarterectomy (10.5% and 4.4%, respectively; risk ratio 2.41).
The findings provide “strong evidence that, in the short term, the harm of stenting compared with endarterectomy decreases with younger age,” the investigators wrote.
For their meta-analysis, which was funded by the Stroke Association, the investigators analyzed pooled data from the Endarterectomy vs. Angioplasty in Patients With Symptomatic Severe Carotid Stenosis (EVA-3S) trial, the Stent-Protected Angioplasty vs. Carotid Endarterectomy (SPACE) trial, and the International Carotid Stenting Study (ICSS).
These and other trials have suggested there is a higher periprocedural risk of stroke with stenting vs. endarterectomy, but none of the trials on their own were sufficiently powered to show whether stenting might be a safe alternative in specific subgroups of patients, the investigators noted (Lancet 2010 Sept. 10 [doi:10.1016/S0140-6736(10)61009-4]).
Indeed, the risk of stenting remained strongly dependent on age even after additional assessment based on sex, type of recent symptoms, degree of treated carotid stenosis, systolic blood pressure at randomization, whether treatment occurred within 14 days of the most recent event, the number of patients recruited per center, the center recruitment rate, and history of diabetes, hypertension, hypercholesterolemia, smoking, coronary heart disease, peripheral artery disease, and prior stroke, the investigators noted.
“Age might represent a marker of the general burden of atherosclerosis of the aortic arch, or might be associated with increased plaque instability, altered configuration of the aortic arch, or vessel tortuosity. Hence, elderly patients might be at increased risk of dislodgement of plaque debris or thrombi during the stent procedures,” Dr. Bonati and his associates wrote.
In an update of an earlier systematic summary-data meta-analysis of randomized trials that compared endovascular treatment with endarterectomy for symptomatic carotid stenosis, the authors included recently released results from the Carotid Revascularization Endarterectomy vs. Stent Trial (CREST), among others, and found a short-term risk ratio of any stroke or death that was very similar to that seen in the current meta-analysis. This indicated that “the current findings are not biased by exclusion of previous trials and CREST,” noted the authors, who stated that they have no conflicts of interest.
Vaginal Cerclage: New Option for Select Women With Pelvic Organ Prolapse
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
Vaginal Cerclage: New Option for Select Women With Pelvic Organ Prolapse
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
ST. LOUIS – Vaginal cerclage, a novel surgical procedure for pelvic organ prolapse, is proving effective as a treatment option for severe and refractory prolapse in select patients.
Also known as introital cerclage, the procedure involves permanent suturing of the introitus, and is often performed in conjunction with vaginectomy. This obliterative approach is suitable only in those who are certain they no longer desire coital function, but on its own, vaginal cerclage also can serve as a bridge to nonobliterative repair, Dr. S. Robert Kovac and Dr. Carl W. Zimmerman said at an international pelvic reconstructive and vaginal surgery conference sponsored by the Society of Pelvic Reconstructive Surgeons.
Dr. Kovac, the John D. Thompson Distinguished Professor of Gynecologic Surgery and director of the Emory Center for Reconstructive Pelvic Surgery at Emory University, Atlanta, used a video demonstration to show the surgical technique in an 82-year-old woman who had undergone two prior procedures for the treatment of prolapse, including a total abdominal hysterectomy followed by transvaginal repair with graft augmentation.
She presented with recurrent prolapse and complaints of vaginal bulge and discomfort, difficulty with voiding, and recurrent urinary tract infections.
A decision was made to perform vaginectomy augmented by the placement of a simple introital cerclage.
Dr. Kovac adequately infiltrated the introitus with 0.5% Marcaine with epinephrine, then used nonabsorbable braided sterile polyester suture beginning at the 12 o’clock position. The suture was placed away from the midurethra and closer to the bladder neck to decrease the risk of de novo stress urinary incontinence.
Suture placement continued in a circumferential manner toward the 6 o’clock position in several steps, ending at the 7 o’clock position to minimize discomfort. The suture ends were cut and tied down to obliterate the vagina and reduce the prolapse, and the ends were buried under the skin to decrease discomfort.
The same approach was used in a 77-year-old patient who had undergone total abdominal hysterectomy and bilateral salpingo-oophorectomy, as well as multiple prior prolapse repairs, including transvaginal repair with graft augmentation, a pubic bone sling, and transvaginal enterocele repair with graft augmentation and repeat enterocele repair with colpocleisis.
The patient presented with vaginal bulge, pressure, discharge, defecation dysfunction, and abdominal pain; she was diagnosed with stage IV vaginal vault prolapse. As in the first patient, vaginectomy was performed and augmented by vaginal cerclage. The patient’s vagina was obliterated, and her prolapse reduced with no change in urethral angle.
Both patients were doing well at 8 months’ follow-up, Dr. Kovac said.
Dr. Kovac, who argued that vaginal cerclage is superior to the “very outdated” LeFort colpocleisis procedure that’s used in patients with severe prolapse who still have their uterus, noted that the new technique also can be used as an intermediate procedure in certain patients awaiting nonobliterative prolapse repair.
For example, he described a patient with a significant prolapse who was unable to undergo surgery because of elevated creatinine. Vaginal cerclage allowed for temporary relief over the 8-9 days required for her creatinine levels to normalize.
“This approach provided improved comfort and quality of life, and reduced her hydronephrosis, which was causing the elevated creatinine, thus enabling her to undergo the full repair,” he said.
Similarly, Dr. Zimmerman, professor of obstetrics and gynecology at Vanderbilt University in Nashville, Tenn., described a patient who was preparing to undergo liver transplant and was found to have severe prolapse during a pelvic exam prior to surgery. Vaginal cerclage was used as a rescue procedure so that she could undergo the transplant surgery. The prolapse was reduced, the cerclage was placed, and the transplant was successful, he said.
Vaginal cerclage is a simple and “clever” procedure that can be accomplished in about 5 minutes, is reimbursed as a colpocleisis, and vastly improves patient comfort, Dr. Kovac said.
“It has great advantages, and we’re doing it routinely today on select patients who come in with recurrent prolapse after multiple attempts at correctional surgery – with excellent results.”
The availability of such a technique is important because, typically, the repair used for a failed colpocleisis is a repeat colpocleisis. Also, an increase in patients who seek treatment is anticipated, given that U.S. Census data indicate that the number of adults older than age 65 is expected to reach 90 million by 2050, and that 30%-50% of women experience prolapse in their lifetime, 11% undergo surgery for prolapse, and a third of prolapse and incontinence surgeries are for recurrent prolapse.
Improved techniques are needed, particularly in light of the high rate of repeat repairs, Dr. Kovac said.
Dr. Kovac disclosed that he is a consultant for Cook Medical Inc. and Ethicon Endo-Surgery Inc. Dr. Zimmerman is a speaker/proctor for Cook Medical, proctor for Boston Scientific Corp. and Covidien, and receives Royalties from Lumitex Inc. and Marina Medical Instruments Inc.
CDC Group on RSV Immunoprophylaxis Still Working
ATLANTA — In the wake of a Food and Drug Administration advisory panel vote against recommending licensure of a new drug for the prevention of respiratory syncytial virus, a Centers for Disease Control and Prevention working group on RSV immunoprophylaxis will continue to develop recommendations for the use of currently available products, the group's chair said.
The new drug currently under FDA review is motavizumab (MedImmune/AstraZeneca), a humanized monoclonal antibody. The FDA advisory panel expressed concern that the drug has additional safety issues but no clear benefit over existing products on the market, Dr. Lance Chilton reported at the meeting.
Efforts will continue to develop recommendations for prophylaxis, based on available information on disease burden, safety, efficacy, and economics, said Dr. Chilton, chair of the RSV immunoprophylaxis working group and a pediatrician with the Young Children's Health Center at the University of New Mexico, Albuquerque.
RSV is the leading cause of lower respiratory tract illness in infants and young children, and currently there is no vaccine available, Dr. Chilton said, noting that efforts to develop a vaccine are ongoing, and “when it comes, it will change the face of pediatrics.”
Until then, preventive treatment is available in the form of palivizumab—a safe and effective product for immunoprophylaxis, according to Dr. Chilton. However, the drug is expensive, with an estimated cost of nearly $6,700 per patient per year, and guidelines for appropriate use are needed, he said.
Dr. Chilton said the working group's efforts to develop such guidelines will include:
▸ A review of the epidemiology of RSV infection, including seasonality and host and environmental risk factors for severe disease.
▸ A review of the safety and efficacy of prophylaxis.
▸ An assessment of the costs and benefits of prophylaxis.
▸ Identification of the areas requiring further research for informing recommendations.
▸ Drafting of recommendations for ACIP consideration.
Up to 125,000 hospitalizations for RSV occur in the United States each year, with the highest incidence in young infants, and with a disproportionate burden among those with lung disease, heart disease, and prematurity. The FDA is currently scheduled to review the biologics licensing application for motavizumab in August.
Disclosures: Dr. Chilton reported no conflicts of interest.
ATLANTA — In the wake of a Food and Drug Administration advisory panel vote against recommending licensure of a new drug for the prevention of respiratory syncytial virus, a Centers for Disease Control and Prevention working group on RSV immunoprophylaxis will continue to develop recommendations for the use of currently available products, the group's chair said.
The new drug currently under FDA review is motavizumab (MedImmune/AstraZeneca), a humanized monoclonal antibody. The FDA advisory panel expressed concern that the drug has additional safety issues but no clear benefit over existing products on the market, Dr. Lance Chilton reported at the meeting.
Efforts will continue to develop recommendations for prophylaxis, based on available information on disease burden, safety, efficacy, and economics, said Dr. Chilton, chair of the RSV immunoprophylaxis working group and a pediatrician with the Young Children's Health Center at the University of New Mexico, Albuquerque.
RSV is the leading cause of lower respiratory tract illness in infants and young children, and currently there is no vaccine available, Dr. Chilton said, noting that efforts to develop a vaccine are ongoing, and “when it comes, it will change the face of pediatrics.”
Until then, preventive treatment is available in the form of palivizumab—a safe and effective product for immunoprophylaxis, according to Dr. Chilton. However, the drug is expensive, with an estimated cost of nearly $6,700 per patient per year, and guidelines for appropriate use are needed, he said.
Dr. Chilton said the working group's efforts to develop such guidelines will include:
▸ A review of the epidemiology of RSV infection, including seasonality and host and environmental risk factors for severe disease.
▸ A review of the safety and efficacy of prophylaxis.
▸ An assessment of the costs and benefits of prophylaxis.
▸ Identification of the areas requiring further research for informing recommendations.
▸ Drafting of recommendations for ACIP consideration.
Up to 125,000 hospitalizations for RSV occur in the United States each year, with the highest incidence in young infants, and with a disproportionate burden among those with lung disease, heart disease, and prematurity. The FDA is currently scheduled to review the biologics licensing application for motavizumab in August.
Disclosures: Dr. Chilton reported no conflicts of interest.
ATLANTA — In the wake of a Food and Drug Administration advisory panel vote against recommending licensure of a new drug for the prevention of respiratory syncytial virus, a Centers for Disease Control and Prevention working group on RSV immunoprophylaxis will continue to develop recommendations for the use of currently available products, the group's chair said.
The new drug currently under FDA review is motavizumab (MedImmune/AstraZeneca), a humanized monoclonal antibody. The FDA advisory panel expressed concern that the drug has additional safety issues but no clear benefit over existing products on the market, Dr. Lance Chilton reported at the meeting.
Efforts will continue to develop recommendations for prophylaxis, based on available information on disease burden, safety, efficacy, and economics, said Dr. Chilton, chair of the RSV immunoprophylaxis working group and a pediatrician with the Young Children's Health Center at the University of New Mexico, Albuquerque.
RSV is the leading cause of lower respiratory tract illness in infants and young children, and currently there is no vaccine available, Dr. Chilton said, noting that efforts to develop a vaccine are ongoing, and “when it comes, it will change the face of pediatrics.”
Until then, preventive treatment is available in the form of palivizumab—a safe and effective product for immunoprophylaxis, according to Dr. Chilton. However, the drug is expensive, with an estimated cost of nearly $6,700 per patient per year, and guidelines for appropriate use are needed, he said.
Dr. Chilton said the working group's efforts to develop such guidelines will include:
▸ A review of the epidemiology of RSV infection, including seasonality and host and environmental risk factors for severe disease.
▸ A review of the safety and efficacy of prophylaxis.
▸ An assessment of the costs and benefits of prophylaxis.
▸ Identification of the areas requiring further research for informing recommendations.
▸ Drafting of recommendations for ACIP consideration.
Up to 125,000 hospitalizations for RSV occur in the United States each year, with the highest incidence in young infants, and with a disproportionate burden among those with lung disease, heart disease, and prematurity. The FDA is currently scheduled to review the biologics licensing application for motavizumab in August.
Disclosures: Dr. Chilton reported no conflicts of interest.