User login
Is Skip N2 metastasis its own category?
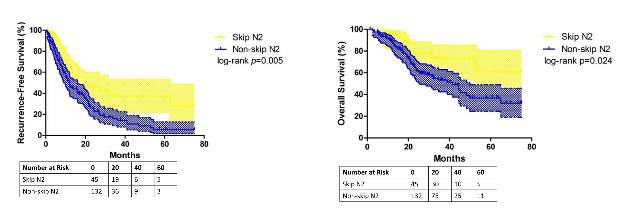
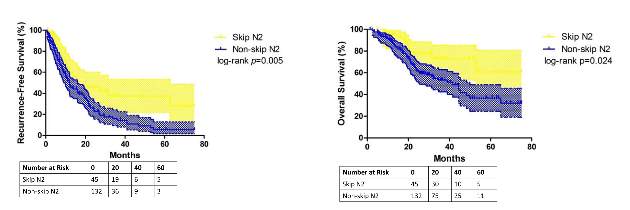
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
Key clinical point: Skip N2 metastases in resectable lung cancer have distinct histological characteristics from non-skip N2 disease.
Major finding: A subset of patients with skip N2 metastasis had higher rates of acinar adenocarcinoma subtype and right-lung disease.
Data source: Retrospective analysis of 177 patients with lung adenocarcinoma and N2 metastasis
Disclosures: The study received funding from the government of China and Shanghai Municipality as well as Shanghai Hospital Development Center. The authors have no relationships to disclose.
Combined percutaneous procedures emerging in Europe
NEW YORK – Combined transcatheter mitral valve interventions with the potential to have results as good as cardiac surgery are beginning to emerge in Europe, where cardiac surgeons are also getting early experience with newer transcatheter systems that offer alternatives to existing mitral valve treatments, said Dr. Francesco Maisano.
Surgeons in Europe are investigating for mitral valve repair, as alternatives to the MitraClip (Abbott Vascular) percutaneous mitral valve system, and developers of these devices have met their share of challenges, Dr. Maisano of the University Hospital Zurich (Switzerland) said at the 2015 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
“This list was much longer in the past, but some of the companies have lost their way in the past few years,” he said. “This is because it is difficult to pursue such a tremendous effort of doing a transcatheter repair that is competing with a device that has been commercially available.”
The NeoChord system (NeoChord) has been approved in Europe and has been implanted in about 200 patients so far. It is implanted through a small (2-3–inch) left thoracotomy and deploys implantation of multiple neochordae. “This is slowly getting into practice,” Dr. Maisano said. “The main problem with this technology is that it still is a hybrid procedure; it requires general anesthesia. It’s still doubtful what the role will be for this procedure in the spectrum of mitral interventions.”
The Carillon Mitral Contour System (Cardiac Dimension Inc.) is “the only coronary sinus annuloplasty technology that survived in these years,” he said. The device is in clinical trials in Europe and Australia. However, he noted, efficacy with the device “doesn’t happen at the implant, but it happens over time.” Group outcomes data is pending. “Enthusiasm around coronary sinus annuloplasty never took, so a lot of physicians are still reluctant to embrace this technology,” he said. Nonetheless, in some patients the device has show results ”as good as other procedures.”
Meanwhile, three other percutaneous systems that aim to reproduce surgical annuloplasty are in development: the Mitralign (Mitralign), a percutaneous system that selectively plicates the annulus using pledget sutures; the Accucinch (Guided Delivery Systems) which completes a full-seal annuloplasty using suture-connected mitral anchors; and Cardioband (ValtechCardio), which can perform surgery-like annuloplasty without sutures. Dr. Maisano said Mitralign is hopeful to get CE-mark approval possibly as early as this year, and the Cardioband has been implanted in 42 patients in Europe with an average 22% reduction in septal dimensions – “good outcomes in terms of reduction of mitral regurgitation and improvement of symptoms,” he said.
Helping to advance the development of percutaneous procedures and the promise of combining those procedures to replicate surgery is the integration of multimodal imaging in the cardiac suite, Dr. Maisano said.
“There are many problems to be solved” in pursuing combined percutaneous procedures to replicate surgical results, he said. “It’s not easy from a regulatory standpoint or from an economical standpoint, but there is the potential to simulate what is done today in surgery-associated procedures. This is something that is happening in Europe, which is land of freedom in terms of utilizing devices.”
He related the story of a patient in whom he implanted two mitral valve clips and then, to stop leakage, used a vascular plug to fill the gap in the subcommissure. European cardiac surgeons have pondered or attempted transcatheter aortic implantation (TAVI) in combination with other procedures, including left atrial appendage closure (LAAC) and mitral clip insertion in varied combinations. “This is still feasible and something that is getting done more in Europe in experienced centers,” Dr. Maisano said. Although feasibility, safety, and efficacy of such approaches need to be proved in larger series, combination therapy will evolve in the future, in an attempt to reproduce surgical standards, he said.
Findings were presented on behalf of the European Society of Cardiology. Dr. Maisano is a consultant for Abbott Vascular and ValtechCardio, among other companies. He receives royalties from Edwards Lifesciences.
NEW YORK – Combined transcatheter mitral valve interventions with the potential to have results as good as cardiac surgery are beginning to emerge in Europe, where cardiac surgeons are also getting early experience with newer transcatheter systems that offer alternatives to existing mitral valve treatments, said Dr. Francesco Maisano.
Surgeons in Europe are investigating for mitral valve repair, as alternatives to the MitraClip (Abbott Vascular) percutaneous mitral valve system, and developers of these devices have met their share of challenges, Dr. Maisano of the University Hospital Zurich (Switzerland) said at the 2015 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
“This list was much longer in the past, but some of the companies have lost their way in the past few years,” he said. “This is because it is difficult to pursue such a tremendous effort of doing a transcatheter repair that is competing with a device that has been commercially available.”
The NeoChord system (NeoChord) has been approved in Europe and has been implanted in about 200 patients so far. It is implanted through a small (2-3–inch) left thoracotomy and deploys implantation of multiple neochordae. “This is slowly getting into practice,” Dr. Maisano said. “The main problem with this technology is that it still is a hybrid procedure; it requires general anesthesia. It’s still doubtful what the role will be for this procedure in the spectrum of mitral interventions.”
The Carillon Mitral Contour System (Cardiac Dimension Inc.) is “the only coronary sinus annuloplasty technology that survived in these years,” he said. The device is in clinical trials in Europe and Australia. However, he noted, efficacy with the device “doesn’t happen at the implant, but it happens over time.” Group outcomes data is pending. “Enthusiasm around coronary sinus annuloplasty never took, so a lot of physicians are still reluctant to embrace this technology,” he said. Nonetheless, in some patients the device has show results ”as good as other procedures.”
Meanwhile, three other percutaneous systems that aim to reproduce surgical annuloplasty are in development: the Mitralign (Mitralign), a percutaneous system that selectively plicates the annulus using pledget sutures; the Accucinch (Guided Delivery Systems) which completes a full-seal annuloplasty using suture-connected mitral anchors; and Cardioband (ValtechCardio), which can perform surgery-like annuloplasty without sutures. Dr. Maisano said Mitralign is hopeful to get CE-mark approval possibly as early as this year, and the Cardioband has been implanted in 42 patients in Europe with an average 22% reduction in septal dimensions – “good outcomes in terms of reduction of mitral regurgitation and improvement of symptoms,” he said.
Helping to advance the development of percutaneous procedures and the promise of combining those procedures to replicate surgery is the integration of multimodal imaging in the cardiac suite, Dr. Maisano said.
“There are many problems to be solved” in pursuing combined percutaneous procedures to replicate surgical results, he said. “It’s not easy from a regulatory standpoint or from an economical standpoint, but there is the potential to simulate what is done today in surgery-associated procedures. This is something that is happening in Europe, which is land of freedom in terms of utilizing devices.”
He related the story of a patient in whom he implanted two mitral valve clips and then, to stop leakage, used a vascular plug to fill the gap in the subcommissure. European cardiac surgeons have pondered or attempted transcatheter aortic implantation (TAVI) in combination with other procedures, including left atrial appendage closure (LAAC) and mitral clip insertion in varied combinations. “This is still feasible and something that is getting done more in Europe in experienced centers,” Dr. Maisano said. Although feasibility, safety, and efficacy of such approaches need to be proved in larger series, combination therapy will evolve in the future, in an attempt to reproduce surgical standards, he said.
Findings were presented on behalf of the European Society of Cardiology. Dr. Maisano is a consultant for Abbott Vascular and ValtechCardio, among other companies. He receives royalties from Edwards Lifesciences.
NEW YORK – Combined transcatheter mitral valve interventions with the potential to have results as good as cardiac surgery are beginning to emerge in Europe, where cardiac surgeons are also getting early experience with newer transcatheter systems that offer alternatives to existing mitral valve treatments, said Dr. Francesco Maisano.
Surgeons in Europe are investigating for mitral valve repair, as alternatives to the MitraClip (Abbott Vascular) percutaneous mitral valve system, and developers of these devices have met their share of challenges, Dr. Maisano of the University Hospital Zurich (Switzerland) said at the 2015 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
“This list was much longer in the past, but some of the companies have lost their way in the past few years,” he said. “This is because it is difficult to pursue such a tremendous effort of doing a transcatheter repair that is competing with a device that has been commercially available.”
The NeoChord system (NeoChord) has been approved in Europe and has been implanted in about 200 patients so far. It is implanted through a small (2-3–inch) left thoracotomy and deploys implantation of multiple neochordae. “This is slowly getting into practice,” Dr. Maisano said. “The main problem with this technology is that it still is a hybrid procedure; it requires general anesthesia. It’s still doubtful what the role will be for this procedure in the spectrum of mitral interventions.”
The Carillon Mitral Contour System (Cardiac Dimension Inc.) is “the only coronary sinus annuloplasty technology that survived in these years,” he said. The device is in clinical trials in Europe and Australia. However, he noted, efficacy with the device “doesn’t happen at the implant, but it happens over time.” Group outcomes data is pending. “Enthusiasm around coronary sinus annuloplasty never took, so a lot of physicians are still reluctant to embrace this technology,” he said. Nonetheless, in some patients the device has show results ”as good as other procedures.”
Meanwhile, three other percutaneous systems that aim to reproduce surgical annuloplasty are in development: the Mitralign (Mitralign), a percutaneous system that selectively plicates the annulus using pledget sutures; the Accucinch (Guided Delivery Systems) which completes a full-seal annuloplasty using suture-connected mitral anchors; and Cardioband (ValtechCardio), which can perform surgery-like annuloplasty without sutures. Dr. Maisano said Mitralign is hopeful to get CE-mark approval possibly as early as this year, and the Cardioband has been implanted in 42 patients in Europe with an average 22% reduction in septal dimensions – “good outcomes in terms of reduction of mitral regurgitation and improvement of symptoms,” he said.
Helping to advance the development of percutaneous procedures and the promise of combining those procedures to replicate surgery is the integration of multimodal imaging in the cardiac suite, Dr. Maisano said.
“There are many problems to be solved” in pursuing combined percutaneous procedures to replicate surgical results, he said. “It’s not easy from a regulatory standpoint or from an economical standpoint, but there is the potential to simulate what is done today in surgery-associated procedures. This is something that is happening in Europe, which is land of freedom in terms of utilizing devices.”
He related the story of a patient in whom he implanted two mitral valve clips and then, to stop leakage, used a vascular plug to fill the gap in the subcommissure. European cardiac surgeons have pondered or attempted transcatheter aortic implantation (TAVI) in combination with other procedures, including left atrial appendage closure (LAAC) and mitral clip insertion in varied combinations. “This is still feasible and something that is getting done more in Europe in experienced centers,” Dr. Maisano said. Although feasibility, safety, and efficacy of such approaches need to be proved in larger series, combination therapy will evolve in the future, in an attempt to reproduce surgical standards, he said.
Findings were presented on behalf of the European Society of Cardiology. Dr. Maisano is a consultant for Abbott Vascular and ValtechCardio, among other companies. He receives royalties from Edwards Lifesciences.
EXPERT ANALYSIS FROM THE 2015 MITRAL VALVE CONCLAVE
Right-side mini-AVR an option for frail patients
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.

|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
“Have we found the end of the road, and the future for isolated AVR is made up of RAMT with sutureless AVR?” asks Dr. Patrick M. McCarthy, chief of cardiac surgery at Northwestern University Feinberg School of Medicine in Chicago, in his invited commentary (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.007). “The cardiology literature serves as a reality check.”
He noted that results from the NOTION Trial of transaortic valve replacement (TAVR) vs. surgical AVR (J Am Coll Cardiol. 2015;65:2184-94) had 30-day results similar to the G. Pasquinucci Heart Hospital results. However, 34% in the TAVR group in NOTION needed pacemakers, and 16% had moderate or greater valvular regurgitation and higher rates of dyspnea.
|
|
Dr. Patrick M. McCarthy |
Right anterior minithoracotomy is different from other minimally invasive approaches, Dr. McCarthy said. “It’s more of a tunnel down to the aortic valve which is why patient selection based on anatomic factors determined by preoperative CT scan (which is an unnecessary expense for hemisternotomy) is so important,” he said.
The evolution of TAVR is still in the early stage, so the “flaws” involved in the approach can yet be eliminated, “but the message that TAVR outcomes today are still very different than [surgical] AVR in low-risk patients, the type that have a minimally invasive AVR, may be lost on many readers,” Dr. McCarthy said.
For isolated aortic stenosis, the era of minimally invasive procedures that involve bypass, cross-clamping and a difficult surgical approach may be fading, he said. “The handwriting is on the wall, or in the journals in this case.”
Dr. McCarthy disclosed relationships with Edwards Lifesciences and Abbott Vascular. He is the inventor of the Edwards MC3 Ring and dETlogix Ring and coinventor of the IMR ETlogix Ring.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
Many patients with aortic valve disease still undergo conventional aortic valve replacement (AVR) with standard full sternotomy or seek out alternative treatments like transcatheter aortic valve insertion (TAVI). But a minimally invasive approach that uses a sutureless prostheses may reduce operation times and put AVR within reach of more frail patients.
Investigators from G. Pasquinucci Heart Hospital in Massa, Italy, reported on 593 patients who had AVR through right anterior minithoracotomy (RAMT) over 10 years at their institution (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.06.045). In 302 of the patients, the researchers used a sutureless or rapidly implantable biological prosthesis.
“More surgeons should enrich their armamentarium by RAMT AVR,” lead author Dr. Mattia Glauber and his coauthors said. “Sutureless prostheses can increase adoption of RAMT AVR.”
The authors acknowledged that minimally invasive approaches to AVR, including partial sternotomy, require longer operation times than open surgery despite reduced aortic cross-clamping and cardiopulmonary bypass times, but have resulted in better outcomes and lower death rates.
A new generation of aortic valve prostheses, including sutureless devices, have emerged in an attempt to further reduce operative times and improve outcomes, so the Italian investigators designed their study to compare early and midterm outcomes after minimally invasive AVR using sutured and sutureless repair at their institution between 2004 and 2014.
In 302 (50.9%) patients, sutureless or rapidly implantable biological prosthesis was used, 23 (3.9%) had a mechanical prosthesis, and the remainder received a conventional biological prosthesis.
The investigators determined patients were suitable for RAMT if CT scan showed specific anatomic features, including rightward positioning of the ascending aorta at the level of the main pulmonary artery. Once the sutureless prostheses became available in 2011, every patient undergoing AVR via RAMT was considered a potential candidate, although the investigators decided that patients with type 1 and 2 bicuspid aortic valves without raphe and asymmetric aortic root were not suitable for the sutureless approach.
The subgroup that underwent sutureless repair tended to be older and sicker than the overall study population and had a higher prevalence of tricuspid aortic valve and aortic stenosis, a slightly higher body mass index, and a higher propensity to be obese. The sutureless subgroup also had fewer smokers.
Cardiopulmonary bypass time averaged 88 minutes and aortic cross-clamping times 55 minutes in the sutureless subgroup vs. 107 and 74 minutes, respectively, in the overall RAMT study subgroup.
The death before discharge rate of patients who had RAMT repair was 1%, and the 30-day in-hospital death rate was 1.5%. Overall, 97% of patients who had RAMT did not require reoperation at 5 years.
Between the sutured and sutureless subgroups, hospital and intensive care unit lengths of stay were similar, as were bleeding rates and in-hospital mortality. One measure in which the two subgroups deviated was prolonged ICU stay – a rate of 11.3% in the sutureless subgroup and 6.6% in the sutured subgroup.
“To the best of our knowledge, this is the largest up-to-date single-center experience on minimally invasive AVR through RAMT,” Dr. Glauber and coauthors said. “Our data along with earlier reports confirm that minimally invasive AVR through RAMT is safe and reproducible. It is associated with low perioperative mortality and morbidity.”
Dr. Glauber and coauthor Dr. Marco Solinas disclosed a commercial/financial relationship with Sorin Group.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Aortic valve replacement through right anterior minithoracotomy provides excellent outcomes. Sutureless prostheses facilitate mini-AVR.
Major finding: Study subjects had a survival rate of 95% at 31.5 months follow-up on average, and operative times were significantly shorter with sutureless prostheses, compared with sutured prostheses.
Data source: A retrospective, observational cohort study with prospective data collection on 593 patients who had right anterior minithoracotomy for AVR at a single institution over a 10-yar period.
Disclosures: Study coauthors Mattia Glauber and Marco Solinas disclosed a commercial/financial relationship with Sorin Group.

SYNTAX: Early CABG results with arterial grafts similar to venous in matched groups
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
That arterial grafts are a better long-term match in coronary bypass surgery has been a tenet in cardiac surgery, but multiple factors have prevented their more widespread acceptance, Dr. Davis C. Drinkwater Jr. said in his invited commentary (J Thorac Cardiovasc Surg. 2015.doi:10.1016/j.jtcvs.2015.06.014). Concerns about sternal wound healing, particularly in diabetic or obese patients, as well as the alternative generally good early and mid-term results in multivessel coronary artery disease using the left internal thoracic artery to LAD accompanied by saphenous vein grafts, have made surgeons hesitant to take up the approach more readily, said Dr. Drinkwater of Frist Cardiology, Tristar Centennial Medical Center, Nashville, Tenn.
The SYNTAX investigators’ main finding of no survival advantage among the matched groups at 5 years is in line with most reports comparing patency between arterial and venous grafts, “requiring between 5- and 10-year follow-up to show a divergence,” Dr. Drinkwater said.
He pointed out that the patients who had second arterial grafts in the unmatched group were younger and healthier – the average age was 62 years, and 27% of them had previous heart attacks, compared with 66 years of age and a heart attack rate of 35.6% in the venous graft group – and that may explain the higher reintervention rate in the former group. Another factor may be the younger and healthier patients had longer cardiopulmonary bypass and aortic cross clamp times despite a greater percentage having undergone the off-pump technique.
“This counterintuitive information underscores an inherent weakness of this multicenter trial that is without surgical randomization into the two arterial groups, and with potentially varied surgical experience using nonstandardized technical and management protocols,” Dr. Drinkwater said. “This is in stark contrast to the previous and well accepted single high-volume-center reports of the benefits of using multiple arterial bypass grafts.”
Because the report points out the technical challenges of achieving complete revascularization with multiple arterial grafting at “the early” interval of up to 5 years, the authors may be inappropriately discouraging centers that do not currently offer multiarterial grafting from embracing it, Dr. Drinkwater concluded.
He had no disclosures to report.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
While single-center studies have supported the advantages of multiple arterial grafts over venous grafts in coronary artery bypass surgery, an analysis of patients in the international and multicenter SYNTAX trial has shown that, on propensity matching, rates of cardiac events and death are actually similar between the two groups.
These findings of the SYNTAX investigators, led by Dr. Catalina Parasca of Erasmus University in Rotterdam, the Netherlands, were published online in the Journal of Thoracic and Cardiovascular Surgery (doi:10.1016/j.jtcvs.2015.05.010).
The SYNTAX trial compared percutaneous coronary intervention (PCI) with coronary artery bypass grafting (CABG) in patients with left main or three-vessel coronary artery disease (Lancet. 2013;381[9867]:629-38).
In the latest report, the SYNTAX investigators found that patients in unmatched groups who received arterial grafts in addition to an arterial graft of the left anterior descending artery (LAD) had noticeably lower rates of death and a composite endpoint of death-stroke-MI than did those who received a second venous graft. However, when the researchers applied propensity matching, the outcomes between the two groups were similar.
Because large randomized trials have yet to prove the superiority of multiarterial grafts, the adoption rate has been low, Dr. Parasca and colleagues said. “The objective of this study was to assess the effect of using a second arterial graft on 5-year outcomes in patients who underwent CABG in the SYNTAX trial and registry,” they said.
They looked at 1,322 SYNTAX trial patients who had CABG with 5-year follow-up. In unmatched groups, the safety endpoint of the death-stroke-MI composite was 13.3% in the multiarterial group vs. 18.7% in the vein graft group. Although the incidence of stroke, MI, and graft occlusion was similar between the unmatched groups, the second-graft arterial group had a higher revascularization rate at 5 years, 12.6% vs. 9.6%, mainly due to repeat PCI. The element of the composite where the two unmatched groups deviated was the all-cause death rate at 5 years: 8.9% in the second-graft arterial group and 13.1% in the venous group.
However, when the investigators applied propensity matching, the differences between the two groups were insignificant.
“The results of the present study must be seen in the light of a multicenter CABG cohort with complex coronary disease, where revascularization was performed according to surgeon’s personal experience and local practices,” Dr. Parasca and coauthors noted. “The result was a high heterogeneity of CABG techniques, which shows different understanding of the best ‘graft-target match’ across centers.”
While the SYNTAX analysis demonstrates the variation in patient selection and operator technique with regard to arterial revascularization typical of a multicenter study, “extended follow-up beyond 5 years is required to estimate its impact on long-term outcomes,” Dr. Parasca and colleagues said.
Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgeons should choose arterial grafts for multigraft coronary artery bypass surgery when feasible.
Major finding: Patients who received multiple arterial graft had significantly lower rates of death and other problems than did those who received venous grafts in unmatched groups, but results were similar between propensity matched groups.
Data source: Registry of 1,322 patients who had 5-year follow-up after coronary artery bypass surgery within the SYNTAX trial.
Disclosures: Boston Scientific supported the trial. Coauthor Keith Dawkins is employed by Boston Scientific and coauthor Ted Feldman has received consulting fees from the company. The other authors reported no disclosures.
Surgeon volume may affect choice of surgery type for NSCLC
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
Because the McMaster University study derived the reported outcomes from registry data, determining the reasons that influenced surgeons’ choices of lung resection is impossible, Dr. Eric Lim of the Imperial College of Medicine, London, said in his invited commentary (J Thorac Cardiovasc Surg. 2015 May 21 [doi:10.1016/j.jtcvs.2015.05.048]).
The study authors noted that lower-volume surgeons were more inclined to perform pneumonectomy, and, Dr. Lim noted, previous studies have found that higher-volume centers tended to see more patients with advanced-stage cancers and increased morbidities. “An alternative explanation is that higher-volume surgeons have better skill sets to undertake procedures such as sleeve lobectomies that would lower the pneumonectomy rates and possibly more segmentectomies to lower the wedge-resection rate,” Dr. Lim said.
Until better evidence exists on what procedure is best for central and peripheral tumors, “surgeons can argue either way,” Dr. Lim said. The questions that follow from the study should concentrate on the relative harm of each procedure and the level of practice variation that’s unacceptable.
“As a surgical community, it is incumbent on us to continue to evaluate surgical treatments generating the highest levels of evidence possible (randomized trials) and have sufficient humility to cross refer to colleagues when appropriate to ensure the best care for our patients,” Dr. Lim concluded.
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
A surgeon’s comfort level with a favored operation for non–small cell lung cancer can strongly influence whether the patient will have that operation, which, in turn, can affect the patient’s outcome and long-term survival, according to an analysis of a population-linked database. For patients whose surgeons have lower levels of experience, that could mean a greater chance they will have more invasive total lung removal rather than more difficult operations that spare part of the affected lung, according to investigators at McMaster University in Hamilton, Ontario.
“If a surgeon with high surgical volumes is less likely to perform higher-risk pneumonectomy procedures than one with lower volumes, this may translate to a significant reduction in adverse events,” said lead author Dr. Christian Finley and coauthors online in the Journal of Thoracic and Cardiovascular Surgery (2015 Jun 30 [doi: 10.1016/j.jtcvs.2015.04.060]). “Surgeon volume should be considered an important component in how care is delivered in this population.”
The McMaster investigators evaluated 8,070 patients in an Ontario population-based linked database who underwent surgical resection for non–small cell lung cancer during 2004-2011, including pneumonectomy, or total lung removal (842 patients), lobectomy (6,212 patients), and wedge resection (1,002 patients). Over the years of the study, the proportion of patients who underwent pneumonectomy fell by more than half, from 14.8% in 2004 to 7.6% in 2011.
Of the three procedures, pneumonectomy carries a threefold greater mortality and while the procedure is often avoidable, there may be cases where it’s necessary because of the location of the tumor, Dr. Finley and his colleagues said. Lobectomy is desirable because it spares the parenchyma and has lower recurrence rates than laser resections.
The study investigators aimed to explore the hypothesis that surgeons with less expertise are more inclined to perform the higher-risk pneumonectomy or sublobar resections such as a segmentectomy or a wedge resection than a lobectomy, the rationale being that these procedures can be less challenging than a standard or sleeve lobectomy. The study analyzed results from 124 different physicians at 45 institutions in Ontario.
Data analysis showed that physician volume, age, year of procedure, sex, and comorbidities were predictive of the surgeon performing a pneumonectomy. “Adjusting for these variables, the results indicated that for each 10-unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%,” Dr. Finley and his colleagues wrote. They also found no significant difference in stage distribution among low-, medium-, and high-volume surgeons.
“This is meaningful as pneumonectomy is known to have the highest mortality rate of lung cancer resection, found in this study to be 12.6%, demonstrating a potentially large impact on patient survival,” Dr. Finley and his colleagues said.
This analysis cites an earlier study that surgeon volume for many procedures was a key determinant in the link between hospital volume and operative mortality (N Engl J Med. 2003 Nov 27;349[2]:2117-27.). “This study suggests that a patient may improve their chance of survival substantially, even at high-volume institutions, by selecting surgeons who perform operations more frequently,” Dr. Finley and his colleagues said.
They said that despite their study’s limitations, the findings on how surgeon experience can influence the choice of lung resection for cancer warrant further study.
McMaster University, Division of Thoracic Surgery, provided funding for the study. The study authors had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgeon volume is a predictor of procedure selection for lung cancer surgery and has implications on outcomes.
Major finding: For each 10 unit increase in physician volume, the relative risk of performing a pneumonectomy decreased by 9.1%.
Data source: Dataset of 8,070 patients constructed from Ontario population-based linked databases accessed via the Institute for Clinical Evaluate Sciences.
Disclosures: McMaster University, Division of Thoracic Surgery, provided study funding. The authors had no disclosures.
How patient-reported outcomes may alter care
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
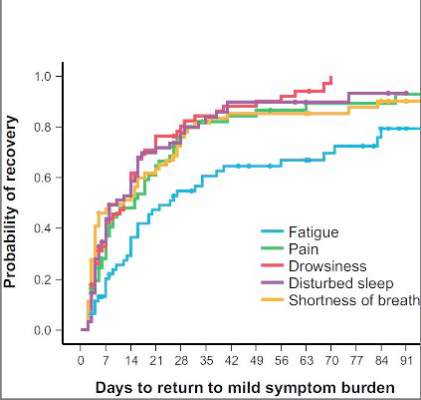
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
“Whether ‘subjective’ or not, the measurements of five common postoperative symptoms appear to reflect the real world experience of many,” Dr. Robert B. Cameron of the University of California, Los Angeles, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.06.017]).
What’s more, because the study investigators collected patient data after discharge, they eliminated opportunities to “game the system,” in Dr. Cameron’s words. One example of gaming the outcome measures would be to discharge patients early after surgery with a Heimlich chest tube, subjecting them to problems at home and requiring physicians visits and even emergency department care that can go unrecorded.
“Subjective” patient experiences are “real issues,” Dr. Cameron said. “After all, patients are the customers that the health care system serves.”
Patient-reported outcome measures could dramatically influence how physicians and health systems report patient outcomes. “While length of stay (LOS) and hospital complication rates appear to be valid outcome measures to report, in reality, they are outcomes only in a world when hospitals are the ‘customers,’ ” Dr. Cameron said. “In a patient-centric system, when patient outcomes matter, [patient-reported outcomes], such as those proposed by the MD Anderson investigators, are what truly matter.”
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
As Medicare and commercial payers rely increasingly on quality outcomes to determine reimbursement levels, clinicians focused on traditional clinical outcomes like length of hospital stay and readmission may be missing the point if they don’t take into consideration more patient-centric outcome. A team of investigators at MD Anderson Cancer Center in Houston recently evaluated that institution’s tool for measuring patient-reported outcomes in tracking results after thoracic surgery for lung cancer.
Christopher P. Fagundes, Ph.D., led the research team that reported their findings in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.057]).
“We used the MD Anderson Symptom Inventory (MDASI) to elicit patient reports of the worst symptoms experienced after thoracic surgery,” Dr. Fagundes and his colleagues said in what may be the first study to use patient-reported outcomes to chart a recovery course after surgery. “This study demonstrates that the MDASI is a sensitive tool for detecting symptomatic recovery with an expected relationship among surgery type, preoperative performance status, and comorbid conditions,” the authors stated.
The MDASI measures the severity of 13 common cancer-related symptoms over the previous 24 hours and rates each on a scale from 0-10, with 10 as most severe. Patients in the study completed a written MDASI questionnaire, 60 upon enrollment, and 77 patients 3 and 5 days after surgery in the hospital. After discharge and for 3 months after surgery, patients received weekly calls from a computer/telephone interactive voice-response system that asked them to rate their symptoms.
All patients were newly diagnosed and treatment naive with early-stage non–small cell lung cancer (NSCLC) who had either standard open thoracotomy or video-assisted thoracoscopic surgery (VATS) lobectomy.
The investigators used a two-pronged approach to define recovery after surgery: symptoms returning to their baseline levels or to a mild level of severity. In the first week after surgery, pain, fatigue, and shortness of breath were “highly prevalent,” perhaps a combined effect from surgical insult and care during and after surgery. After a month, ratings for most symptoms returned to baseline, but fatigue remained the most-persistent symptom during the 3-month study.
NSCLC patients typically have a host of symptoms after major surgery, including inflammation, organ stress, and reaction to medications. In addition, up to a quarter have postsurgical complications that can amplify their symptoms and even delay their course of cancer treatment. The five most-severe postoperative symptoms patients in the study reported were fatigue, pain, shortness of breath, disturbed sleep, and drowsiness.
The median time to return to mild symptom severity for these five symptoms was shorter than return to baseline severity, with fatigue taking longer. Pain recovered significantly faster for patients who underwent VATS lobectomy vs. standard open thoracotomy (8 vs. 18 days, respectively; P = .022), according to the researchers. In addition, the researchers found that patients who had poor preoperative performance status or comorbidities reported significantly higher postoperative pain (P less than .05).
Having the ability to measure patient-reported outcomes allows physicians to identify patients at greatest risk for symptoms after surgery and to help caregivers develop pathways to speed up recovery and get patients to chemotherapy or other cancer treatments on schedule, Dr. Fagundes and his coauthors said.
“Using a straightforward, concise tool like the MDASI to obtain the patient’s perspective on how well he or she is recovering is a clinically relevant and user-friendly method for optimizing perioperative care,” the authors added.
Minimally invasive surgical techniques along with opioid-sparing analgesia have been incorporated into enhanced recovery programs to aim for better objective postoperative outcomes like fewer complications and shorter hospital stays. “Missing from these metrics is the voice of the patient, who is arguably the best source of information about what ‘recovery’ from surgery means,” Dr. Fagundes and colleagues said. “Lack of research on how to define and measure symptomatic and functional recovery after major cancer surgery from the patent’s perspective is an important gap in comprehensive postoperative care; it also compromises any comparison of ERP [enhanced recovery program] innovations against standard care.”
Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Using the MD Anderson Symptom Inventory to elicit patient-reported symptom burden is a simple, clinically relevant way to optimize care after thoracic surgery for lung cancer.
Major finding: Assessing symptoms from the patient’s perspective throughout the postoperative recovery period is an effective strategy for evaluating perioperative care.
Data source: Sixty newly diagnosed patients with early-stage non–small cell lung cancer scheduled for thoracic surgery prospectively were recruited for evaluation.
Disclosures: Study coauthors received funding from the National Cancer Institute of the National Institutes of Health, the MD Anderson Cancer Center Support Grant program, and the American Cancer Society Research Scholar Grant program. The coauthors reported no conflicts of interest in this work.
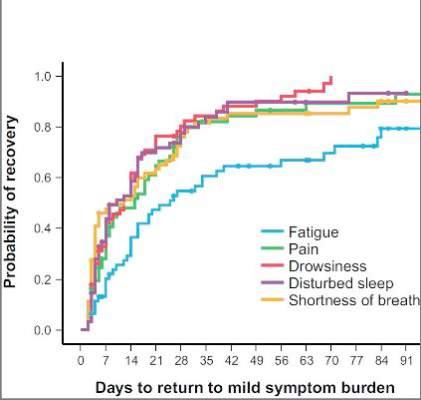
‘David technique’ may enhance aortic repair
Many techniques for repair of aortic dissection have evolved, but no trials have compared those techniques to determine which is the best. However, a study team has attempted to evaluate a surgical approach (the “David technique”) that includes three specific steps – no aortic cross clamp, the use of deep hypothermic circulatory arrest (DHCA), and the antegrade resumption of cardiopulmonary bypass. They found that this approach yielded significantly better long-term outcomes than did other approaches tried.
The study investigators, led by Dr. Jennifer S. Lawton of Washington University in St. Louis, reported their findings in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.023]). “We hypothesized that a surgical strategy to prevent cross-clamp injury or false lumen pressurization would be associated with reduced morbidity, mortality, persistent false lumen patency, and improved survival,” Dr. Lawton and her coauthors wrote. “This study was designed to determine the differences in outcomes between operative techniques.”
The study evaluated 196 patients who had surgery for acute type A aortic dissection over 17 years. Group 1, which comprised 49 patients, had the operation according to the protocol that involved the three specific steps, as Dr. Tirone David of the University of Toronto first reported in 1999 (Ann. Thorac. Surg. 1999;67:1999-2001) — the “David technique,” as the study authors called it. Group 2 consisted of patients whose repair involved a variety of techniques, including one or two steps of the David technique but not all three.
Study endpoints were 30-day mortality rate, postoperative adverse events, presence of a false aortic lumen, and overall survival, the latter defined as the time from the date of surgery to the date or death or last follow-up. The evaluation included examination of patients’ latest CT scan or MRI that was at least 6 months after the operation for false lumen, but only 78 patients had imaging at that interval.
Patients in Group 1 had a higher rate of persistent false lumen – 74% vs. 68% in Group 2. Thirty-day mortality was 6.1% in Group 1 and 15.7% in Group 2, but Dr. Lawton and her coauthors said this difference was not statistically significant.
Survival rates at 1, 5 and 10 years among both groups were “consistent with published ranges,” the authors said. At 5 years, the predicted survival was 86% for Group 1 and 56% for Group 2; and at 10 years, 72% and 37% respectively.
The study authors acknowledged the controversy that surrounds the use of retrograde resumption of cardiopulmonary bypass after replacement of the ascending aorta and that there’s no consensus on which method is best for resuming cardiopulmonary bypass after repair of a type A aortic dissection.
The study also found no difference in the incidence of false lumen between the two groups, but again, this is a source of controversy. “Persistence of a false lumen following repair for type A aortic dissection has been reported to be associated with poor prognosis and reduced long-term survival,” Dr. Lawton and her colleagues said.
“Others have reported a patent false lumen was not an independent predictor of late reoperation, but was a predictor of aortic growth following repair of type A aortic dissection.”
The study authors said one limit of their findings is its retrospective nature, but they also said that a prospective, randomized trial would be difficult to conduct.
None of the study coauthors had any relationships to disclose. They presented their original data at the American Association for Thoracic Surgery Aortic Symposium, April 24-25, 2014, in New York.
Whether or not to use a cross-clamp in type A aortic dissection repair is a critical question, but a major concern of this study was the wide variability of techniques used in the comparison group, Dr. Richard J. Shemin said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.038]). “The variety of approaches attests to the lack of institutional agreement on the surgical principles tested in the study,” he said. “The large variety of techniques in the control group makes the comparison and interpretation of this study difficult.”
“There are more questions to consider from this study than answers derived from the data about the clamp strategy,” he said
But, Dr. Shemin said, using the cross-clamp with axillary antegrade perfusion is “not a major issue.” And the use of clamping during the cooling period can save overall cardiac arrest time during the operation.
“If one does use femoral cannulation, then not applying the cross-clamp until achieving circulatory arrest is prudent,” he said. “With axillary cannulation, one achieves antegrade perfusion so early cross-clamping can be safely performed with the advantages of saving operative time.”
The clamp site must be inspected during circulatory arrest. Antegrade cerebral perfusion is proven to be an excellent technique and is facilitated by right axillary cannulation, Dr. Shemin said. “Most importantly, establishing antegrade CPB [cardiopulmonary bypass] perfusion after circulatory arrest is mandatory in all cases to minimize distal aorta trauma,” he said.
Dr. Richard J. Shemin is a cardiothoracic surgeon at UCLA Medical Center, Santa Monica, Calif.
Whether or not to use a cross-clamp in type A aortic dissection repair is a critical question, but a major concern of this study was the wide variability of techniques used in the comparison group, Dr. Richard J. Shemin said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.038]). “The variety of approaches attests to the lack of institutional agreement on the surgical principles tested in the study,” he said. “The large variety of techniques in the control group makes the comparison and interpretation of this study difficult.”
“There are more questions to consider from this study than answers derived from the data about the clamp strategy,” he said
But, Dr. Shemin said, using the cross-clamp with axillary antegrade perfusion is “not a major issue.” And the use of clamping during the cooling period can save overall cardiac arrest time during the operation.
“If one does use femoral cannulation, then not applying the cross-clamp until achieving circulatory arrest is prudent,” he said. “With axillary cannulation, one achieves antegrade perfusion so early cross-clamping can be safely performed with the advantages of saving operative time.”
The clamp site must be inspected during circulatory arrest. Antegrade cerebral perfusion is proven to be an excellent technique and is facilitated by right axillary cannulation, Dr. Shemin said. “Most importantly, establishing antegrade CPB [cardiopulmonary bypass] perfusion after circulatory arrest is mandatory in all cases to minimize distal aorta trauma,” he said.
Dr. Richard J. Shemin is a cardiothoracic surgeon at UCLA Medical Center, Santa Monica, Calif.
Whether or not to use a cross-clamp in type A aortic dissection repair is a critical question, but a major concern of this study was the wide variability of techniques used in the comparison group, Dr. Richard J. Shemin said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.038]). “The variety of approaches attests to the lack of institutional agreement on the surgical principles tested in the study,” he said. “The large variety of techniques in the control group makes the comparison and interpretation of this study difficult.”
“There are more questions to consider from this study than answers derived from the data about the clamp strategy,” he said
But, Dr. Shemin said, using the cross-clamp with axillary antegrade perfusion is “not a major issue.” And the use of clamping during the cooling period can save overall cardiac arrest time during the operation.
“If one does use femoral cannulation, then not applying the cross-clamp until achieving circulatory arrest is prudent,” he said. “With axillary cannulation, one achieves antegrade perfusion so early cross-clamping can be safely performed with the advantages of saving operative time.”
The clamp site must be inspected during circulatory arrest. Antegrade cerebral perfusion is proven to be an excellent technique and is facilitated by right axillary cannulation, Dr. Shemin said. “Most importantly, establishing antegrade CPB [cardiopulmonary bypass] perfusion after circulatory arrest is mandatory in all cases to minimize distal aorta trauma,” he said.
Dr. Richard J. Shemin is a cardiothoracic surgeon at UCLA Medical Center, Santa Monica, Calif.
Many techniques for repair of aortic dissection have evolved, but no trials have compared those techniques to determine which is the best. However, a study team has attempted to evaluate a surgical approach (the “David technique”) that includes three specific steps – no aortic cross clamp, the use of deep hypothermic circulatory arrest (DHCA), and the antegrade resumption of cardiopulmonary bypass. They found that this approach yielded significantly better long-term outcomes than did other approaches tried.
The study investigators, led by Dr. Jennifer S. Lawton of Washington University in St. Louis, reported their findings in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.023]). “We hypothesized that a surgical strategy to prevent cross-clamp injury or false lumen pressurization would be associated with reduced morbidity, mortality, persistent false lumen patency, and improved survival,” Dr. Lawton and her coauthors wrote. “This study was designed to determine the differences in outcomes between operative techniques.”
The study evaluated 196 patients who had surgery for acute type A aortic dissection over 17 years. Group 1, which comprised 49 patients, had the operation according to the protocol that involved the three specific steps, as Dr. Tirone David of the University of Toronto first reported in 1999 (Ann. Thorac. Surg. 1999;67:1999-2001) — the “David technique,” as the study authors called it. Group 2 consisted of patients whose repair involved a variety of techniques, including one or two steps of the David technique but not all three.
Study endpoints were 30-day mortality rate, postoperative adverse events, presence of a false aortic lumen, and overall survival, the latter defined as the time from the date of surgery to the date or death or last follow-up. The evaluation included examination of patients’ latest CT scan or MRI that was at least 6 months after the operation for false lumen, but only 78 patients had imaging at that interval.
Patients in Group 1 had a higher rate of persistent false lumen – 74% vs. 68% in Group 2. Thirty-day mortality was 6.1% in Group 1 and 15.7% in Group 2, but Dr. Lawton and her coauthors said this difference was not statistically significant.
Survival rates at 1, 5 and 10 years among both groups were “consistent with published ranges,” the authors said. At 5 years, the predicted survival was 86% for Group 1 and 56% for Group 2; and at 10 years, 72% and 37% respectively.
The study authors acknowledged the controversy that surrounds the use of retrograde resumption of cardiopulmonary bypass after replacement of the ascending aorta and that there’s no consensus on which method is best for resuming cardiopulmonary bypass after repair of a type A aortic dissection.
The study also found no difference in the incidence of false lumen between the two groups, but again, this is a source of controversy. “Persistence of a false lumen following repair for type A aortic dissection has been reported to be associated with poor prognosis and reduced long-term survival,” Dr. Lawton and her colleagues said.
“Others have reported a patent false lumen was not an independent predictor of late reoperation, but was a predictor of aortic growth following repair of type A aortic dissection.”
The study authors said one limit of their findings is its retrospective nature, but they also said that a prospective, randomized trial would be difficult to conduct.
None of the study coauthors had any relationships to disclose. They presented their original data at the American Association for Thoracic Surgery Aortic Symposium, April 24-25, 2014, in New York.
Many techniques for repair of aortic dissection have evolved, but no trials have compared those techniques to determine which is the best. However, a study team has attempted to evaluate a surgical approach (the “David technique”) that includes three specific steps – no aortic cross clamp, the use of deep hypothermic circulatory arrest (DHCA), and the antegrade resumption of cardiopulmonary bypass. They found that this approach yielded significantly better long-term outcomes than did other approaches tried.
The study investigators, led by Dr. Jennifer S. Lawton of Washington University in St. Louis, reported their findings in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.023]). “We hypothesized that a surgical strategy to prevent cross-clamp injury or false lumen pressurization would be associated with reduced morbidity, mortality, persistent false lumen patency, and improved survival,” Dr. Lawton and her coauthors wrote. “This study was designed to determine the differences in outcomes between operative techniques.”
The study evaluated 196 patients who had surgery for acute type A aortic dissection over 17 years. Group 1, which comprised 49 patients, had the operation according to the protocol that involved the three specific steps, as Dr. Tirone David of the University of Toronto first reported in 1999 (Ann. Thorac. Surg. 1999;67:1999-2001) — the “David technique,” as the study authors called it. Group 2 consisted of patients whose repair involved a variety of techniques, including one or two steps of the David technique but not all three.
Study endpoints were 30-day mortality rate, postoperative adverse events, presence of a false aortic lumen, and overall survival, the latter defined as the time from the date of surgery to the date or death or last follow-up. The evaluation included examination of patients’ latest CT scan or MRI that was at least 6 months after the operation for false lumen, but only 78 patients had imaging at that interval.
Patients in Group 1 had a higher rate of persistent false lumen – 74% vs. 68% in Group 2. Thirty-day mortality was 6.1% in Group 1 and 15.7% in Group 2, but Dr. Lawton and her coauthors said this difference was not statistically significant.
Survival rates at 1, 5 and 10 years among both groups were “consistent with published ranges,” the authors said. At 5 years, the predicted survival was 86% for Group 1 and 56% for Group 2; and at 10 years, 72% and 37% respectively.
The study authors acknowledged the controversy that surrounds the use of retrograde resumption of cardiopulmonary bypass after replacement of the ascending aorta and that there’s no consensus on which method is best for resuming cardiopulmonary bypass after repair of a type A aortic dissection.
The study also found no difference in the incidence of false lumen between the two groups, but again, this is a source of controversy. “Persistence of a false lumen following repair for type A aortic dissection has been reported to be associated with poor prognosis and reduced long-term survival,” Dr. Lawton and her colleagues said.
“Others have reported a patent false lumen was not an independent predictor of late reoperation, but was a predictor of aortic growth following repair of type A aortic dissection.”
The study authors said one limit of their findings is its retrospective nature, but they also said that a prospective, randomized trial would be difficult to conduct.
None of the study coauthors had any relationships to disclose. They presented their original data at the American Association for Thoracic Surgery Aortic Symposium, April 24-25, 2014, in New York.
Key clinical point: An operation to repair type A aortic dissection that involves three specific steps achieves better outcomes than do other surgical approaches.
Major finding: Survival rates at 5 years were 86% for the group that had operations in which the surgeons used the three specific steps vs. 56% for the other group.
Data source: Retrospective analysis of single-center population of 146 patients who had repairs for type A aortic dissection.
Disclosures: None of the study coauthors had any relationships to disclose.
Combined ablation–mitral surgery safe for atrial fib
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.

The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.
The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
NEW YORK – Patients with both mitral valve regurgitation and atrial fibrillation who undergo concurrent mitral valve surgery and surgical ablation are more than twice as likely to be free of AF a year after surgery than are their counterparts who have mitral valve surgery alone, according to results of a randomized trial.
“About a quarter to a half of our your patients coming for mitral valve surgery also have AF,” Dr. A. Marc Gillinov said at the 2015 Mitral Valve Conclave sponsored by the American Association for Thoracic Surgery. “A great mitral valve repair is your first priority, but you also want to treat the AF.” Currently, cardiac surgeons perform concurrent mitral valve surgery and surgical ablation about 60% of the time in patients eligible for both procedures, he said.
The American College of Cardiology/American Health Association Guidelines state that surgical ablation in patients with AF having cardiac surgery for other indications is “reasonable” – “not very strong language,” he noted, and the level of evidence for concurrent procedures is C.
That led the Cardiothoracic Surgical Trials Network to pursue the clinical trial. The investigators randomized 260 patients with persistent or long-standing persistent atrial fibrillation who needed mitral valve surgery to also undergo either surgical ablation (133) or no ablation (127). The primary endpoint was freedom from AF at both 6 months and 12 months as assessed by 3-day Holter monitoring.
Almost two-thirds (63%) of patients in the ablation group were free from atrial fibrillation at both 6 and 12 months, compared with 29% of those who had mitral valve surgery only, a highly significant difference. Dr. Gillinov described the trial population as “tougher patients” with persistent AF whose average age was around 70 years, and most had organic mitral valve regurgitation.
Results were similar whether the patients underwent pulmonary vein isolation or biatrial maze procedure (61% and 66%, respectively). One-year mortality was 6.8% in the ablation group and 8.7% in the control group, reported Dr. Gillinov, who is surgical director of the Center for Atrial Fibrillation at Cleveland Clinic.
The trial found no significant differences between the ablation and nonablation groups in major cardiac or cerebrovascular adverse events, overall serious adverse events, or hospital readmissions. The results were published prior to the Dr. Gillinov’s presentation (N. Engl. J. Med. 2015;372:1399-409).
These results debunk findings from a survey a few years ago that found cardiac surgeons avoided doing surgical ablation during mitral valve surgery because it makes the operation too complex, requires longer pump times, and raises the risk of surgery, said Dr. Gillinov. “Does ablation improve rhythm control? Yes. Does ablation increase risk? No. Does ablation improve clinical outcomes? It probably does,” he said.
The trial had some limitations, Dr. Gillinov said. Its endpoint was not a clinical outcome, although looking at stroke risk or mortality would have required thousands of patients. Also, 20% of patients did not have follow-up with the 3-day Holter test. However, previous studies have shown a strong association between surgical ablation and a reduced risk of stroke. When Dr. Jolanda Kluin of Utrecht (the Netherlands) University asked if a patient would be better off with AF or a pacemaker, Dr. Gillinov replied, “I think it’s better to have an AV sequential rhythm, but the truth is no one can answer that question without clinical data.”
The bottom line is, “if you have a patient who’s having mitral valve surgery who also has AF, do an ablation,” he said.
The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
AT THE 2015 MITRAL VALVE CONCLAVE
Key clinical point: Patients with atrial fibrillation who have mitral valve surgery would benefit from surgical ablation at the same time.
Major finding: People with AF who had surgical ablation along with mitral valve surgery were more than twice as likely to be free of AF afterwards than were those who had mitral valve surgery only (63.2% vs. 29.4%).
Data source: A clinical trial in 260 patients with AF undergoing mitral valve surgery that randomized 127 to mitral valve surgery alone and 133 to mitral valve surgery with surgical ablation.
Disclosures: The study was supported by the National Institutes of Health and the Canadian Institutes of Health Research. Dr. Gillinov disclosed relationships with AtriCure, Medtronic, Edwards Lifesciences, On-X Life Technologies, Abbott, Tendyne, and Clear Catheter.
Contrast imaging detects some lung tumors in surgery
Injecting patients with a molecular contrast agent before lung cancer surgery and then using fluorescent imaging during the operation proved safe and somewhat effective at finding lung adenocarcinomas and discovering tumor metastases in a pilot clinical trial of 50 patients.
Investigators from the University of Pennsylvania, Philadelphia, and Emory (Atlanta) and Purdue (West Lafayette, Ind.) universities reported their findings online in the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.014]).
“We believe the most important finding in this study was the ability to systemically inject our contrast agent into patients prior to surgery and have 92% of the lung adenocarcinomas fluoresce in the operating room,” Dr. Olugbenga Okusanya of the University of Pennsylvania, Philadelphia, and his colleagues said. Their approach overcomes some of the limitations of other contrast agents for imaging of lung cancer.
The approach involves intravenous administration of 0.1 mg/kg of a fluorescent folate receptor-alpha (FR-alpha)–targeted molecule contrast agent 4 hours before surgery. The specific agent they used is a synthetic conjugate between folate and fluorescein isothiocyanate that binds to serum proteins.
They set out to determine if an optical-targeted molecular contrast agent to FR-alpha could bind lung adenocarcinoma and then if real-time optical imaging, either in situ or ex vivo during surgery, would show the lesions. The 50 study subjects all had biopsy-confirmed lung adenocarcinoma. In the OR, the researchers used a gantry-mounted fluorescent imaging system to capture images of the tumors.
With the operating room lights switched off, imaging of the cancer was captured by fluorescence and white light in situ. The lung was deflated during imaging to expose as much of the lung surface to the imaging as possible. The in situ optical imaging required on average eight minutes to perform. Only seven tumors (14%) appeared fluorescent in situ before they were excised. Computed tomography (CT) before surgery showed that all seven of these tumors were below the pleural surface and within 1.2 cm of the lung surface.
Among the other 43 tumors, 39 exhibited uniform fluorescence once the surgical team exposed their surfaces while 4 – all invasive adenocarcinomas – did not. Final pathology confirmed that all 50 tumors were cancerous.
“With further refinements, this tool may prove useful in locating adenocarcinomas deeper in the lung parenchyma, lymph nodes and at pleural and resection margins,” Dr. Okusanya and his coauthors said.
The investigators noted that one advantage of this imaging strategy is that it can locate tumors of varying sizes, subtypes and metabolic activity with tumor-to-background ratios “not markedly different” among them. “This finding demonstrates that intraoperative molecular imaging may be potentially broadly applicable to all FR-alpha lung tumors,” they said.
Other advantages is that wavelength fluorophore poses no radiation exposure and that surgeons readily understand optical imaging “with no need for special training to interpret or process the data.” They did acknowledge that a significant drawback of the molecular contrast agent was its lack of penetration into the lung parenchyma.
“New molecular tools are emerging to identify lung adenocarcinomas during pulmonary resection,” Dr. Okusanya and colleagues said. “This technology will permit precise visualization of tumor margins, localization of small malignant ground-glass opacities, and accurate selection of lymph nodes with metastatic cancer cells. With miniaturization of imaging devices, this method will be particularly useful in minimally invasive surgery.”
The pilot clinical trial was partially supported by grant from the Biomedical Laboratory Research & Development Service of the Veterans Affairs Office of Research and Development and by the CHEST Foundation One Breath Clinical Research Award (SS).
Dr. Shuming Nie is a coauthor and a consultant for Spectropath, a start-up company that is developing advanced instrumentation and nanoparticle contrast agents. Dr. Philip S. Low is a coauthor and a consultant and stakeholder in OnTarget Laboratories. None of the other coauthors had any relationships to disclose.
“Not unexpectedly, the Achilles’ heel of the technique is tumor depth beneath the pleural surface,” Dr. Michael I. Ebright of Columbia University, New York, said in his commentary of the results of the pilot study. He noted that only 7 of the 50 tumors were visible before resection – and those were all large and close to the pleural surface.
“As we move toward the detection of smaller lesions through lung cancer screening, as well as toward the use of minimally invasive surgical techniques challenging direct palpation, more practical techniques for intraoperative localization are sorely needed,” Dr. Ebright said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.029]). But the techniques that have emerged are “time consuming, unreliable, or resource intensive.”
He likened the study results to a half-full glass of water: Those who see it half-empty will identify the weaknesses of the study because, among other findings, the technique does not image tumors more than 1 cm below the pleural surface; the half-full cohort will take the position that “new technology has to start somewhere, usually at proof of principle.”
But the in situ optical imaging approach is faster than the current localization options surgeons have, and the possibilities of the approach “are certainly exciting,” Dr. Ebright said.
“Imagination is an essential component of any technological progress,” Dr. Ebright said. “This study should be viewed as a launching pad rather than be judged solely on practicality in its current form.
Dr. Ebright is with the section of thoracic surgery, Columbia University Medical Center, New York.
“Not unexpectedly, the Achilles’ heel of the technique is tumor depth beneath the pleural surface,” Dr. Michael I. Ebright of Columbia University, New York, said in his commentary of the results of the pilot study. He noted that only 7 of the 50 tumors were visible before resection – and those were all large and close to the pleural surface.
“As we move toward the detection of smaller lesions through lung cancer screening, as well as toward the use of minimally invasive surgical techniques challenging direct palpation, more practical techniques for intraoperative localization are sorely needed,” Dr. Ebright said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.029]). But the techniques that have emerged are “time consuming, unreliable, or resource intensive.”
He likened the study results to a half-full glass of water: Those who see it half-empty will identify the weaknesses of the study because, among other findings, the technique does not image tumors more than 1 cm below the pleural surface; the half-full cohort will take the position that “new technology has to start somewhere, usually at proof of principle.”
But the in situ optical imaging approach is faster than the current localization options surgeons have, and the possibilities of the approach “are certainly exciting,” Dr. Ebright said.
“Imagination is an essential component of any technological progress,” Dr. Ebright said. “This study should be viewed as a launching pad rather than be judged solely on practicality in its current form.
Dr. Ebright is with the section of thoracic surgery, Columbia University Medical Center, New York.
“Not unexpectedly, the Achilles’ heel of the technique is tumor depth beneath the pleural surface,” Dr. Michael I. Ebright of Columbia University, New York, said in his commentary of the results of the pilot study. He noted that only 7 of the 50 tumors were visible before resection – and those were all large and close to the pleural surface.
“As we move toward the detection of smaller lesions through lung cancer screening, as well as toward the use of minimally invasive surgical techniques challenging direct palpation, more practical techniques for intraoperative localization are sorely needed,” Dr. Ebright said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.029]). But the techniques that have emerged are “time consuming, unreliable, or resource intensive.”
He likened the study results to a half-full glass of water: Those who see it half-empty will identify the weaknesses of the study because, among other findings, the technique does not image tumors more than 1 cm below the pleural surface; the half-full cohort will take the position that “new technology has to start somewhere, usually at proof of principle.”
But the in situ optical imaging approach is faster than the current localization options surgeons have, and the possibilities of the approach “are certainly exciting,” Dr. Ebright said.
“Imagination is an essential component of any technological progress,” Dr. Ebright said. “This study should be viewed as a launching pad rather than be judged solely on practicality in its current form.
Dr. Ebright is with the section of thoracic surgery, Columbia University Medical Center, New York.
Injecting patients with a molecular contrast agent before lung cancer surgery and then using fluorescent imaging during the operation proved safe and somewhat effective at finding lung adenocarcinomas and discovering tumor metastases in a pilot clinical trial of 50 patients.
Investigators from the University of Pennsylvania, Philadelphia, and Emory (Atlanta) and Purdue (West Lafayette, Ind.) universities reported their findings online in the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.014]).
“We believe the most important finding in this study was the ability to systemically inject our contrast agent into patients prior to surgery and have 92% of the lung adenocarcinomas fluoresce in the operating room,” Dr. Olugbenga Okusanya of the University of Pennsylvania, Philadelphia, and his colleagues said. Their approach overcomes some of the limitations of other contrast agents for imaging of lung cancer.
The approach involves intravenous administration of 0.1 mg/kg of a fluorescent folate receptor-alpha (FR-alpha)–targeted molecule contrast agent 4 hours before surgery. The specific agent they used is a synthetic conjugate between folate and fluorescein isothiocyanate that binds to serum proteins.
They set out to determine if an optical-targeted molecular contrast agent to FR-alpha could bind lung adenocarcinoma and then if real-time optical imaging, either in situ or ex vivo during surgery, would show the lesions. The 50 study subjects all had biopsy-confirmed lung adenocarcinoma. In the OR, the researchers used a gantry-mounted fluorescent imaging system to capture images of the tumors.
With the operating room lights switched off, imaging of the cancer was captured by fluorescence and white light in situ. The lung was deflated during imaging to expose as much of the lung surface to the imaging as possible. The in situ optical imaging required on average eight minutes to perform. Only seven tumors (14%) appeared fluorescent in situ before they were excised. Computed tomography (CT) before surgery showed that all seven of these tumors were below the pleural surface and within 1.2 cm of the lung surface.
Among the other 43 tumors, 39 exhibited uniform fluorescence once the surgical team exposed their surfaces while 4 – all invasive adenocarcinomas – did not. Final pathology confirmed that all 50 tumors were cancerous.
“With further refinements, this tool may prove useful in locating adenocarcinomas deeper in the lung parenchyma, lymph nodes and at pleural and resection margins,” Dr. Okusanya and his coauthors said.
The investigators noted that one advantage of this imaging strategy is that it can locate tumors of varying sizes, subtypes and metabolic activity with tumor-to-background ratios “not markedly different” among them. “This finding demonstrates that intraoperative molecular imaging may be potentially broadly applicable to all FR-alpha lung tumors,” they said.
Other advantages is that wavelength fluorophore poses no radiation exposure and that surgeons readily understand optical imaging “with no need for special training to interpret or process the data.” They did acknowledge that a significant drawback of the molecular contrast agent was its lack of penetration into the lung parenchyma.
“New molecular tools are emerging to identify lung adenocarcinomas during pulmonary resection,” Dr. Okusanya and colleagues said. “This technology will permit precise visualization of tumor margins, localization of small malignant ground-glass opacities, and accurate selection of lymph nodes with metastatic cancer cells. With miniaturization of imaging devices, this method will be particularly useful in minimally invasive surgery.”
The pilot clinical trial was partially supported by grant from the Biomedical Laboratory Research & Development Service of the Veterans Affairs Office of Research and Development and by the CHEST Foundation One Breath Clinical Research Award (SS).
Dr. Shuming Nie is a coauthor and a consultant for Spectropath, a start-up company that is developing advanced instrumentation and nanoparticle contrast agents. Dr. Philip S. Low is a coauthor and a consultant and stakeholder in OnTarget Laboratories. None of the other coauthors had any relationships to disclose.
Injecting patients with a molecular contrast agent before lung cancer surgery and then using fluorescent imaging during the operation proved safe and somewhat effective at finding lung adenocarcinomas and discovering tumor metastases in a pilot clinical trial of 50 patients.
Investigators from the University of Pennsylvania, Philadelphia, and Emory (Atlanta) and Purdue (West Lafayette, Ind.) universities reported their findings online in the Journal of Thoracic and Cardiovascular Surgery (2015 [doi:10.1016/j.jtcvs.2015.05.014]).
“We believe the most important finding in this study was the ability to systemically inject our contrast agent into patients prior to surgery and have 92% of the lung adenocarcinomas fluoresce in the operating room,” Dr. Olugbenga Okusanya of the University of Pennsylvania, Philadelphia, and his colleagues said. Their approach overcomes some of the limitations of other contrast agents for imaging of lung cancer.
The approach involves intravenous administration of 0.1 mg/kg of a fluorescent folate receptor-alpha (FR-alpha)–targeted molecule contrast agent 4 hours before surgery. The specific agent they used is a synthetic conjugate between folate and fluorescein isothiocyanate that binds to serum proteins.
They set out to determine if an optical-targeted molecular contrast agent to FR-alpha could bind lung adenocarcinoma and then if real-time optical imaging, either in situ or ex vivo during surgery, would show the lesions. The 50 study subjects all had biopsy-confirmed lung adenocarcinoma. In the OR, the researchers used a gantry-mounted fluorescent imaging system to capture images of the tumors.
With the operating room lights switched off, imaging of the cancer was captured by fluorescence and white light in situ. The lung was deflated during imaging to expose as much of the lung surface to the imaging as possible. The in situ optical imaging required on average eight minutes to perform. Only seven tumors (14%) appeared fluorescent in situ before they were excised. Computed tomography (CT) before surgery showed that all seven of these tumors were below the pleural surface and within 1.2 cm of the lung surface.
Among the other 43 tumors, 39 exhibited uniform fluorescence once the surgical team exposed their surfaces while 4 – all invasive adenocarcinomas – did not. Final pathology confirmed that all 50 tumors were cancerous.
“With further refinements, this tool may prove useful in locating adenocarcinomas deeper in the lung parenchyma, lymph nodes and at pleural and resection margins,” Dr. Okusanya and his coauthors said.
The investigators noted that one advantage of this imaging strategy is that it can locate tumors of varying sizes, subtypes and metabolic activity with tumor-to-background ratios “not markedly different” among them. “This finding demonstrates that intraoperative molecular imaging may be potentially broadly applicable to all FR-alpha lung tumors,” they said.
Other advantages is that wavelength fluorophore poses no radiation exposure and that surgeons readily understand optical imaging “with no need for special training to interpret or process the data.” They did acknowledge that a significant drawback of the molecular contrast agent was its lack of penetration into the lung parenchyma.
“New molecular tools are emerging to identify lung adenocarcinomas during pulmonary resection,” Dr. Okusanya and colleagues said. “This technology will permit precise visualization of tumor margins, localization of small malignant ground-glass opacities, and accurate selection of lymph nodes with metastatic cancer cells. With miniaturization of imaging devices, this method will be particularly useful in minimally invasive surgery.”
The pilot clinical trial was partially supported by grant from the Biomedical Laboratory Research & Development Service of the Veterans Affairs Office of Research and Development and by the CHEST Foundation One Breath Clinical Research Award (SS).
Dr. Shuming Nie is a coauthor and a consultant for Spectropath, a start-up company that is developing advanced instrumentation and nanoparticle contrast agents. Dr. Philip S. Low is a coauthor and a consultant and stakeholder in OnTarget Laboratories. None of the other coauthors had any relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: A pilot clinical trial reported that molecular contrast imaging during lung cancer surgery is safe and somewhat effective at isolating malignancies.
Major finding: Among 50 patients, the imaging technique detected seven tumors close to the lung surface while 39 others showed fluorescence in the operating room once they were removed.
Data source: Single-center population of 50 patients with biopsy-proven lung adenocarcinoma.
Disclosures: The pilot clinical trial was partially supported by grant from the Biomedical Laboratory Research & Development Service of the Veterans Affairs Office of Research and Development and by the CHEST Foundation One Breath Clinical Research Award (SS). Dr. Nie is a coauthor and a consultant for Spectropath, a start-up company that is developing advanced instrumentation and nanoparticle contrast agents. Dr. Low is a coauthor and a consultant and stakeholder in OnTarget Laboratories. None of the other coauthors had any relationships to disclose.
Post-CABG stroke risk same with one or two clamps
When performing on-pump coronary artery bypass grafting (CABG), cardiac surgeons can control very few factors to reduce the risk of stroke – with the exception of which method of aortic manipulation they use. Debate and controversy, however, have surrounded which aortic manipulation technique is best: single- or double-clamp occlusion.
A large retrospective study of almost 8,500 patients who had CABG at the Mayo Clinic in Rochester, Minn., over a 17-year period showed that, while use of the single-aortic cross-clamp (SC) technique steadily increased, the risk of stroke is virtually the same as it is with the partial aortic cross-clamp (PC), or double cross-clamp, technique. The study authors, led by Dr. Juan C. Araque, published their results online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.010]).
“It is intuitive that less aortic manipulation would result in less risk of stroke,” Dr. Araque and colleagues said, but even off-pump CABG, which requires no aortic manipulation, is not without stroke risk.
“It is conceivable that there is some inherent risk of stroke associated with any cardiac operation, and that risk may increase with manipulation of the ascending aortic with the aortic cross clamp,” they wrote. “Our data would suggest, however, that the risk does not increase further with the additional aortic manipulation of the partial occlusion clamp.”
The study comes on the heels of a 2008 meta-analysis that found no benefit of SC in comparison to PC (Interact. Cardiovasc. Thorac. Surg. 2008;7:500-3), while another study in 2011 suggested that less aortic manipulation carried a significantly lower stroke risk (Heart Lung Circ. 2011;20:318-24).
The Mayo study evaluated the SC technique in 2,051 patients and PC in 6,446 patients who had isolated on-pump CABG between 1993 and 2010. The rate of stroke was 1.2% in the SC group and 1.5% among those who had PC. In two propensity-matched cohorts of 1,333 patients each, the stroke rate was 1.2% in each group. The investigators used the Society of Thoracic Surgeons’ risk calculator variables to create the propensity-matched cohorts.
The study group excluded high-risk patients, including those who had off-pump operations or previous cardiac surgeries or required replacement of a cross clamp during an unplanned operation.
The goal of the study was not to compare outcomes with the off-pump technique. “It is only to bring attention to the associated non-zero stroke rate with both techniques,” Dr. Araque and colleagues said.
Their findings are significant because on-pump CABG is the preferred operation of cardiac surgeons, accounting for more than 80% of the CABG operations in the SYNTAX study (N. Engl. J. Med. 2009;360:961-72). “The ‘anaortic’ off-pump technique may be a more specialized technique, representing less than 15% of operations in one large series,” Dr. Araque and coauthors said.
They acknowledged a few limitations resulting from the observational nature of the study, including that surgeons may have missed some strokes because they did not use a routine, standardized procedure for evaluating stroke signs along with the lack of documented assessment of the descending aorta. But they also stated that the large number of patients in the study, along with the use of propensity matching, addresses some of the bias inherent in an observational study.
The study authors disclosed no relationships.
“A randomized trial is needed to answer the question, ‘Can CABG [coronary artery bypass grafting] be safely performed with either one or two aortic clamps in all patients?’ ” Dr. Jennifer S. Lawton said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.05.002]).
Dr. Lawton acknowledged the positions that advocates of both techniques have staked out: advocates of the single-clamp (SC) technique prefer the ability to perform the proximal anastomoses without the added space constraints and reduced visibility of the partial clamp and moving heart; proponents of the partial-clamp (PC) method cite advantages in the ability to determine graft length with the full heart and the likelihood to reanimate the heart earlier to reduce the risk of a heart attack.
The PC technique required longer cardiopulmonary bypass time, 88.2 minutes vs. 73.7 minutes, but the SC group had longer cross-clamp times, 54.5. vs. 50.7 minutes. “The longer clamp time did not alter the outcomes reported (stroke and mortality) – although specific outcomes of myocardial injury including need for inotropes, troponin levels, myocardial infarction, etc. were not reported,” Dr. Lawton said. “Thus, the question for the surgeon is, ‘What is more important, the brain or the heart?’ ”
The results from Dr. Araque’s study “are valuable” because of the large patient cohort and the suggestion that “the use of a second clamp is not likely to significantly alter outcomes of stroke and mortality,” she wrote.
But their study leaves a few questions remaining, Dr. Lawton said. “What is the best treatment of high-risk patients who may benefit from limited aortic manipulation the most? Can two clamps be safely applied to all types of aortas? And does the risk of dissection go up with the use of two clamps?”
Although a randomized trial would be difficult because of the low risk of stroke in on-pump CABG, such a trial could answer those questions if it involved routine epiaortic ultrasound, Dr. Lawton said.
Dr. Lawton is professor of surgery in the division of cardiothoracic surgery at Washington University, St. Louis.
“A randomized trial is needed to answer the question, ‘Can CABG [coronary artery bypass grafting] be safely performed with either one or two aortic clamps in all patients?’ ” Dr. Jennifer S. Lawton said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.05.002]).
Dr. Lawton acknowledged the positions that advocates of both techniques have staked out: advocates of the single-clamp (SC) technique prefer the ability to perform the proximal anastomoses without the added space constraints and reduced visibility of the partial clamp and moving heart; proponents of the partial-clamp (PC) method cite advantages in the ability to determine graft length with the full heart and the likelihood to reanimate the heart earlier to reduce the risk of a heart attack.
The PC technique required longer cardiopulmonary bypass time, 88.2 minutes vs. 73.7 minutes, but the SC group had longer cross-clamp times, 54.5. vs. 50.7 minutes. “The longer clamp time did not alter the outcomes reported (stroke and mortality) – although specific outcomes of myocardial injury including need for inotropes, troponin levels, myocardial infarction, etc. were not reported,” Dr. Lawton said. “Thus, the question for the surgeon is, ‘What is more important, the brain or the heart?’ ”
The results from Dr. Araque’s study “are valuable” because of the large patient cohort and the suggestion that “the use of a second clamp is not likely to significantly alter outcomes of stroke and mortality,” she wrote.
But their study leaves a few questions remaining, Dr. Lawton said. “What is the best treatment of high-risk patients who may benefit from limited aortic manipulation the most? Can two clamps be safely applied to all types of aortas? And does the risk of dissection go up with the use of two clamps?”
Although a randomized trial would be difficult because of the low risk of stroke in on-pump CABG, such a trial could answer those questions if it involved routine epiaortic ultrasound, Dr. Lawton said.
Dr. Lawton is professor of surgery in the division of cardiothoracic surgery at Washington University, St. Louis.
“A randomized trial is needed to answer the question, ‘Can CABG [coronary artery bypass grafting] be safely performed with either one or two aortic clamps in all patients?’ ” Dr. Jennifer S. Lawton said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.05.002]).
Dr. Lawton acknowledged the positions that advocates of both techniques have staked out: advocates of the single-clamp (SC) technique prefer the ability to perform the proximal anastomoses without the added space constraints and reduced visibility of the partial clamp and moving heart; proponents of the partial-clamp (PC) method cite advantages in the ability to determine graft length with the full heart and the likelihood to reanimate the heart earlier to reduce the risk of a heart attack.
The PC technique required longer cardiopulmonary bypass time, 88.2 minutes vs. 73.7 minutes, but the SC group had longer cross-clamp times, 54.5. vs. 50.7 minutes. “The longer clamp time did not alter the outcomes reported (stroke and mortality) – although specific outcomes of myocardial injury including need for inotropes, troponin levels, myocardial infarction, etc. were not reported,” Dr. Lawton said. “Thus, the question for the surgeon is, ‘What is more important, the brain or the heart?’ ”
The results from Dr. Araque’s study “are valuable” because of the large patient cohort and the suggestion that “the use of a second clamp is not likely to significantly alter outcomes of stroke and mortality,” she wrote.
But their study leaves a few questions remaining, Dr. Lawton said. “What is the best treatment of high-risk patients who may benefit from limited aortic manipulation the most? Can two clamps be safely applied to all types of aortas? And does the risk of dissection go up with the use of two clamps?”
Although a randomized trial would be difficult because of the low risk of stroke in on-pump CABG, such a trial could answer those questions if it involved routine epiaortic ultrasound, Dr. Lawton said.
Dr. Lawton is professor of surgery in the division of cardiothoracic surgery at Washington University, St. Louis.
When performing on-pump coronary artery bypass grafting (CABG), cardiac surgeons can control very few factors to reduce the risk of stroke – with the exception of which method of aortic manipulation they use. Debate and controversy, however, have surrounded which aortic manipulation technique is best: single- or double-clamp occlusion.
A large retrospective study of almost 8,500 patients who had CABG at the Mayo Clinic in Rochester, Minn., over a 17-year period showed that, while use of the single-aortic cross-clamp (SC) technique steadily increased, the risk of stroke is virtually the same as it is with the partial aortic cross-clamp (PC), or double cross-clamp, technique. The study authors, led by Dr. Juan C. Araque, published their results online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.010]).
“It is intuitive that less aortic manipulation would result in less risk of stroke,” Dr. Araque and colleagues said, but even off-pump CABG, which requires no aortic manipulation, is not without stroke risk.
“It is conceivable that there is some inherent risk of stroke associated with any cardiac operation, and that risk may increase with manipulation of the ascending aortic with the aortic cross clamp,” they wrote. “Our data would suggest, however, that the risk does not increase further with the additional aortic manipulation of the partial occlusion clamp.”
The study comes on the heels of a 2008 meta-analysis that found no benefit of SC in comparison to PC (Interact. Cardiovasc. Thorac. Surg. 2008;7:500-3), while another study in 2011 suggested that less aortic manipulation carried a significantly lower stroke risk (Heart Lung Circ. 2011;20:318-24).
The Mayo study evaluated the SC technique in 2,051 patients and PC in 6,446 patients who had isolated on-pump CABG between 1993 and 2010. The rate of stroke was 1.2% in the SC group and 1.5% among those who had PC. In two propensity-matched cohorts of 1,333 patients each, the stroke rate was 1.2% in each group. The investigators used the Society of Thoracic Surgeons’ risk calculator variables to create the propensity-matched cohorts.
The study group excluded high-risk patients, including those who had off-pump operations or previous cardiac surgeries or required replacement of a cross clamp during an unplanned operation.
The goal of the study was not to compare outcomes with the off-pump technique. “It is only to bring attention to the associated non-zero stroke rate with both techniques,” Dr. Araque and colleagues said.
Their findings are significant because on-pump CABG is the preferred operation of cardiac surgeons, accounting for more than 80% of the CABG operations in the SYNTAX study (N. Engl. J. Med. 2009;360:961-72). “The ‘anaortic’ off-pump technique may be a more specialized technique, representing less than 15% of operations in one large series,” Dr. Araque and coauthors said.
They acknowledged a few limitations resulting from the observational nature of the study, including that surgeons may have missed some strokes because they did not use a routine, standardized procedure for evaluating stroke signs along with the lack of documented assessment of the descending aorta. But they also stated that the large number of patients in the study, along with the use of propensity matching, addresses some of the bias inherent in an observational study.
The study authors disclosed no relationships.
When performing on-pump coronary artery bypass grafting (CABG), cardiac surgeons can control very few factors to reduce the risk of stroke – with the exception of which method of aortic manipulation they use. Debate and controversy, however, have surrounded which aortic manipulation technique is best: single- or double-clamp occlusion.
A large retrospective study of almost 8,500 patients who had CABG at the Mayo Clinic in Rochester, Minn., over a 17-year period showed that, while use of the single-aortic cross-clamp (SC) technique steadily increased, the risk of stroke is virtually the same as it is with the partial aortic cross-clamp (PC), or double cross-clamp, technique. The study authors, led by Dr. Juan C. Araque, published their results online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.010]).
“It is intuitive that less aortic manipulation would result in less risk of stroke,” Dr. Araque and colleagues said, but even off-pump CABG, which requires no aortic manipulation, is not without stroke risk.
“It is conceivable that there is some inherent risk of stroke associated with any cardiac operation, and that risk may increase with manipulation of the ascending aortic with the aortic cross clamp,” they wrote. “Our data would suggest, however, that the risk does not increase further with the additional aortic manipulation of the partial occlusion clamp.”
The study comes on the heels of a 2008 meta-analysis that found no benefit of SC in comparison to PC (Interact. Cardiovasc. Thorac. Surg. 2008;7:500-3), while another study in 2011 suggested that less aortic manipulation carried a significantly lower stroke risk (Heart Lung Circ. 2011;20:318-24).
The Mayo study evaluated the SC technique in 2,051 patients and PC in 6,446 patients who had isolated on-pump CABG between 1993 and 2010. The rate of stroke was 1.2% in the SC group and 1.5% among those who had PC. In two propensity-matched cohorts of 1,333 patients each, the stroke rate was 1.2% in each group. The investigators used the Society of Thoracic Surgeons’ risk calculator variables to create the propensity-matched cohorts.
The study group excluded high-risk patients, including those who had off-pump operations or previous cardiac surgeries or required replacement of a cross clamp during an unplanned operation.
The goal of the study was not to compare outcomes with the off-pump technique. “It is only to bring attention to the associated non-zero stroke rate with both techniques,” Dr. Araque and colleagues said.
Their findings are significant because on-pump CABG is the preferred operation of cardiac surgeons, accounting for more than 80% of the CABG operations in the SYNTAX study (N. Engl. J. Med. 2009;360:961-72). “The ‘anaortic’ off-pump technique may be a more specialized technique, representing less than 15% of operations in one large series,” Dr. Araque and coauthors said.
They acknowledged a few limitations resulting from the observational nature of the study, including that surgeons may have missed some strokes because they did not use a routine, standardized procedure for evaluating stroke signs along with the lack of documented assessment of the descending aorta. But they also stated that the large number of patients in the study, along with the use of propensity matching, addresses some of the bias inherent in an observational study.
The study authors disclosed no relationships.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Two different approaches to aortic manipulation that surgeons use during on-pump coronary artery bypass graft surgery – single and double cross-clamp techniques – had similar rates of postoperative stroke.
Major finding: The single cross-clamp group had a stroke rate of 1.2% within 30 days of the operation, compared with 1.5% in the double cross-clamp group in unmatched cohorts.
Data source: Retrospective analysis of 8,497 patients treated with isolated on-pump coronary artery bypass grafting from 1993 to 2010.
Disclosures: The study authors reported having no financial disclosures.