User login
Monitoring effectively identifies seizures in postbypass neonates
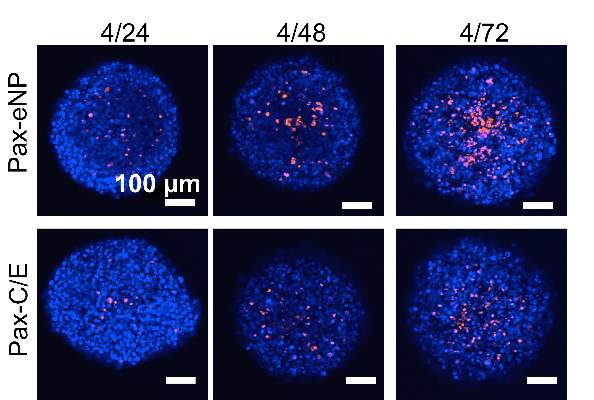
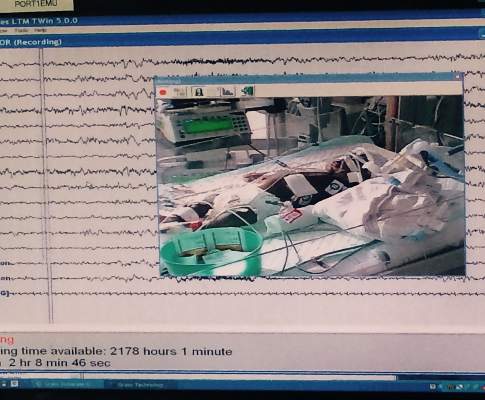
In the first report evaluating the impact of a clinical guideline that calls for the use of postoperative continuous electroencephalography (CEEG) on infants after they’ve had cardiopulmonary bypass surgery, investigators at Children’s Hospital of Philadelphia and the University of Pennsylvania validated the clinical utility of routine CEEG monitoring and found that clinical assessment for seizures without CEEG is not a reliable marker for diagnosis and treatment.
In a report online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.045]), Dr. Maryam Naim and colleagues said that CEEG identified electroencephalographic seizures in 8% of newborns after cardiopulmonary bypass surgery. The study, conducted over 18 months, evaluated 172 newborns, none older than 1 month, with 161 (94%) having undergone postoperative CEEG. They had CEEG within 6 hours of their return to the cardiac intensive care unit.
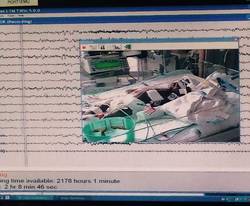
The study classified electroencephalographic seizures as EEG-only (also termed nonconvulsive seizures, with no observable clinical signs either at bedside or via video) or electroclinical seizures. Dr. Naim and colleagues said the majority of seizures they identified with CEEG would not have been noticed otherwise as they had no clinically obvious signs or symptoms.
The American Clinical Neurophysiology Society (ACNS) recommends that cardiac surgeons consider continuous CEEG monitoring in high-risk neonates with congenital heart disease (CHD) after bypass surgery, but Dr. Naim and coauthors raised the question of whether seizure incidence would justify routine CEEG for all neonates with CHD who’ve had bypass surgery, especially as health systems place greater emphasis on quality improvement programs and cost-effective strategies. The authors said that neonates with all types of congenital heart disease had seizures.
“In adult populations, CEEG has not been shown to significantly increase hospital costs, but cost-effectiveness analyses have not been performed in neonates with CHD,” the authors said.
So they attempted to identify at-risk populations of newborns who would benefit most from routine CEEG monitoring. In a multivariable model that the investigators used, both delayed sternal closure and longer deep hypothermic circulatory arrest (DHCA) during surgery seemed predictive of seizures, but the odds ratios for both were low, “suggesting the statistically significant findings may not be very useful in focusing CEEG implementation on a high-risk group.”
Previous studies have reported that identifying and treating seizures in newborns who have had bypass surgery may reduce secondary brain injury and improve outcomes (Pediatrics 2008;121:e759-67), and the Boston Circulatory Arrest Study showed an association between postoperative seizures and lower reading and math scores and lower cognitive and functional skills later in life (Circulation 2011;124:1361-1369). The authors cited other studies that showed older, critically ill children with “high seizure burdens” have had worse outcomes. (Critical Care Medicine 2013;31:215-23; Neurology 2014;82:396-404; Brain 2014;137:1429-38). They also pointed out increased risk if the seizure is not treated. “While occurrence of a seizure is a marker of brain injury, there may also be secondary injury if the seizure activity is not terminated,” Dr. Naim and coauthors said.
The investigators concluded that postoperative CEEG to identify seizures “is warranted,” and while they found some newborns may be at greater risk of postbypass seizures than others, they advocated for “widespread” monitoring strategies.
Their work also questioned the effectiveness of non-CEEG assessment. In the study, clinicians identified bedside events indicative of seizures – what the study termed “push-button events” – in 32 newborns, or about 18% of patients, but none of the events had an EEG correlate, so they were considered nonepileptic. When the authors looked more closely at those “push-button” events, they found they ranged from abnormal body movement in 14 and hypertension in 7 to tachycardia and abnormal face movements, among other characterizations, in lesser numbers.
“Furthermore, push-button events by bedside clinicians, including abnormal movements and hypertensive episodes concerning for possible seizures, did not have any EEG correlate, indicating that bedside clinical assessment for seizures without CEEG monitoring is unreliable,” Dr. Naim and colleagues said.
As to whether identifying and treating postbypass seizures in young newborns with CHD will improve long-term neurodevelopment in these children, the authors acknowledged that further study is needed.
They reported having no financial disclosures.
The findings of Dr. Maryam Naim and coauthors show that relying on physical examination alone is no longer adequate to rule out postoperative neurologic complications, Dr. Carl L. Backer and Dr. Bradley S. Marino said in their invited commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.028]).
However, they noted that the level of “sophisticated monitoring” the investigators had at their disposal – 24-hour availability of EEG technologists, comprehensive 12-scalp electrode monitoring – is not available at all institutions. “What we need is a screening tool that is not as labor intensive,” Dr. Backer and Dr. Marino said – a screening CEEG monitor that would allow care teams to identify seizure activity at a minimal expense and serve as a basis for a full EEG for evaluation and avoid the expense and manpower for the vast majority of patients who do not have seizures.
Nonetheless, prevention of seizures in this newborn population is “critically important,” but that can only be achieved if the care team monitors for seizures and then assesses strategies, both during and after surgery, to eliminate development of seizures, the commentary authors said.
But the recent study points to the need for a multicenter, observational cross-sectional study using CEEG monitoring, Dr. Backer and Dr. Marino said.
Dr. Backer is a cardiovascular-thoracic surgeon and Dr. Marino is a cardiac surgeon at the Ann and Robert H. Lurie Children’s Hospital of Chicago.
The findings of Dr. Maryam Naim and coauthors show that relying on physical examination alone is no longer adequate to rule out postoperative neurologic complications, Dr. Carl L. Backer and Dr. Bradley S. Marino said in their invited commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.028]).
However, they noted that the level of “sophisticated monitoring” the investigators had at their disposal – 24-hour availability of EEG technologists, comprehensive 12-scalp electrode monitoring – is not available at all institutions. “What we need is a screening tool that is not as labor intensive,” Dr. Backer and Dr. Marino said – a screening CEEG monitor that would allow care teams to identify seizure activity at a minimal expense and serve as a basis for a full EEG for evaluation and avoid the expense and manpower for the vast majority of patients who do not have seizures.
Nonetheless, prevention of seizures in this newborn population is “critically important,” but that can only be achieved if the care team monitors for seizures and then assesses strategies, both during and after surgery, to eliminate development of seizures, the commentary authors said.
But the recent study points to the need for a multicenter, observational cross-sectional study using CEEG monitoring, Dr. Backer and Dr. Marino said.
Dr. Backer is a cardiovascular-thoracic surgeon and Dr. Marino is a cardiac surgeon at the Ann and Robert H. Lurie Children’s Hospital of Chicago.
The findings of Dr. Maryam Naim and coauthors show that relying on physical examination alone is no longer adequate to rule out postoperative neurologic complications, Dr. Carl L. Backer and Dr. Bradley S. Marino said in their invited commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.04.028]).
However, they noted that the level of “sophisticated monitoring” the investigators had at their disposal – 24-hour availability of EEG technologists, comprehensive 12-scalp electrode monitoring – is not available at all institutions. “What we need is a screening tool that is not as labor intensive,” Dr. Backer and Dr. Marino said – a screening CEEG monitor that would allow care teams to identify seizure activity at a minimal expense and serve as a basis for a full EEG for evaluation and avoid the expense and manpower for the vast majority of patients who do not have seizures.
Nonetheless, prevention of seizures in this newborn population is “critically important,” but that can only be achieved if the care team monitors for seizures and then assesses strategies, both during and after surgery, to eliminate development of seizures, the commentary authors said.
But the recent study points to the need for a multicenter, observational cross-sectional study using CEEG monitoring, Dr. Backer and Dr. Marino said.
Dr. Backer is a cardiovascular-thoracic surgeon and Dr. Marino is a cardiac surgeon at the Ann and Robert H. Lurie Children’s Hospital of Chicago.
In the first report evaluating the impact of a clinical guideline that calls for the use of postoperative continuous electroencephalography (CEEG) on infants after they’ve had cardiopulmonary bypass surgery, investigators at Children’s Hospital of Philadelphia and the University of Pennsylvania validated the clinical utility of routine CEEG monitoring and found that clinical assessment for seizures without CEEG is not a reliable marker for diagnosis and treatment.
In a report online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.045]), Dr. Maryam Naim and colleagues said that CEEG identified electroencephalographic seizures in 8% of newborns after cardiopulmonary bypass surgery. The study, conducted over 18 months, evaluated 172 newborns, none older than 1 month, with 161 (94%) having undergone postoperative CEEG. They had CEEG within 6 hours of their return to the cardiac intensive care unit.
The study classified electroencephalographic seizures as EEG-only (also termed nonconvulsive seizures, with no observable clinical signs either at bedside or via video) or electroclinical seizures. Dr. Naim and colleagues said the majority of seizures they identified with CEEG would not have been noticed otherwise as they had no clinically obvious signs or symptoms.
The American Clinical Neurophysiology Society (ACNS) recommends that cardiac surgeons consider continuous CEEG monitoring in high-risk neonates with congenital heart disease (CHD) after bypass surgery, but Dr. Naim and coauthors raised the question of whether seizure incidence would justify routine CEEG for all neonates with CHD who’ve had bypass surgery, especially as health systems place greater emphasis on quality improvement programs and cost-effective strategies. The authors said that neonates with all types of congenital heart disease had seizures.
“In adult populations, CEEG has not been shown to significantly increase hospital costs, but cost-effectiveness analyses have not been performed in neonates with CHD,” the authors said.
So they attempted to identify at-risk populations of newborns who would benefit most from routine CEEG monitoring. In a multivariable model that the investigators used, both delayed sternal closure and longer deep hypothermic circulatory arrest (DHCA) during surgery seemed predictive of seizures, but the odds ratios for both were low, “suggesting the statistically significant findings may not be very useful in focusing CEEG implementation on a high-risk group.”
Previous studies have reported that identifying and treating seizures in newborns who have had bypass surgery may reduce secondary brain injury and improve outcomes (Pediatrics 2008;121:e759-67), and the Boston Circulatory Arrest Study showed an association between postoperative seizures and lower reading and math scores and lower cognitive and functional skills later in life (Circulation 2011;124:1361-1369). The authors cited other studies that showed older, critically ill children with “high seizure burdens” have had worse outcomes. (Critical Care Medicine 2013;31:215-23; Neurology 2014;82:396-404; Brain 2014;137:1429-38). They also pointed out increased risk if the seizure is not treated. “While occurrence of a seizure is a marker of brain injury, there may also be secondary injury if the seizure activity is not terminated,” Dr. Naim and coauthors said.
The investigators concluded that postoperative CEEG to identify seizures “is warranted,” and while they found some newborns may be at greater risk of postbypass seizures than others, they advocated for “widespread” monitoring strategies.
Their work also questioned the effectiveness of non-CEEG assessment. In the study, clinicians identified bedside events indicative of seizures – what the study termed “push-button events” – in 32 newborns, or about 18% of patients, but none of the events had an EEG correlate, so they were considered nonepileptic. When the authors looked more closely at those “push-button” events, they found they ranged from abnormal body movement in 14 and hypertension in 7 to tachycardia and abnormal face movements, among other characterizations, in lesser numbers.
“Furthermore, push-button events by bedside clinicians, including abnormal movements and hypertensive episodes concerning for possible seizures, did not have any EEG correlate, indicating that bedside clinical assessment for seizures without CEEG monitoring is unreliable,” Dr. Naim and colleagues said.
As to whether identifying and treating postbypass seizures in young newborns with CHD will improve long-term neurodevelopment in these children, the authors acknowledged that further study is needed.
They reported having no financial disclosures.
In the first report evaluating the impact of a clinical guideline that calls for the use of postoperative continuous electroencephalography (CEEG) on infants after they’ve had cardiopulmonary bypass surgery, investigators at Children’s Hospital of Philadelphia and the University of Pennsylvania validated the clinical utility of routine CEEG monitoring and found that clinical assessment for seizures without CEEG is not a reliable marker for diagnosis and treatment.
In a report online in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.045]), Dr. Maryam Naim and colleagues said that CEEG identified electroencephalographic seizures in 8% of newborns after cardiopulmonary bypass surgery. The study, conducted over 18 months, evaluated 172 newborns, none older than 1 month, with 161 (94%) having undergone postoperative CEEG. They had CEEG within 6 hours of their return to the cardiac intensive care unit.
The study classified electroencephalographic seizures as EEG-only (also termed nonconvulsive seizures, with no observable clinical signs either at bedside or via video) or electroclinical seizures. Dr. Naim and colleagues said the majority of seizures they identified with CEEG would not have been noticed otherwise as they had no clinically obvious signs or symptoms.
The American Clinical Neurophysiology Society (ACNS) recommends that cardiac surgeons consider continuous CEEG monitoring in high-risk neonates with congenital heart disease (CHD) after bypass surgery, but Dr. Naim and coauthors raised the question of whether seizure incidence would justify routine CEEG for all neonates with CHD who’ve had bypass surgery, especially as health systems place greater emphasis on quality improvement programs and cost-effective strategies. The authors said that neonates with all types of congenital heart disease had seizures.
“In adult populations, CEEG has not been shown to significantly increase hospital costs, but cost-effectiveness analyses have not been performed in neonates with CHD,” the authors said.
So they attempted to identify at-risk populations of newborns who would benefit most from routine CEEG monitoring. In a multivariable model that the investigators used, both delayed sternal closure and longer deep hypothermic circulatory arrest (DHCA) during surgery seemed predictive of seizures, but the odds ratios for both were low, “suggesting the statistically significant findings may not be very useful in focusing CEEG implementation on a high-risk group.”
Previous studies have reported that identifying and treating seizures in newborns who have had bypass surgery may reduce secondary brain injury and improve outcomes (Pediatrics 2008;121:e759-67), and the Boston Circulatory Arrest Study showed an association between postoperative seizures and lower reading and math scores and lower cognitive and functional skills later in life (Circulation 2011;124:1361-1369). The authors cited other studies that showed older, critically ill children with “high seizure burdens” have had worse outcomes. (Critical Care Medicine 2013;31:215-23; Neurology 2014;82:396-404; Brain 2014;137:1429-38). They also pointed out increased risk if the seizure is not treated. “While occurrence of a seizure is a marker of brain injury, there may also be secondary injury if the seizure activity is not terminated,” Dr. Naim and coauthors said.
The investigators concluded that postoperative CEEG to identify seizures “is warranted,” and while they found some newborns may be at greater risk of postbypass seizures than others, they advocated for “widespread” monitoring strategies.
Their work also questioned the effectiveness of non-CEEG assessment. In the study, clinicians identified bedside events indicative of seizures – what the study termed “push-button events” – in 32 newborns, or about 18% of patients, but none of the events had an EEG correlate, so they were considered nonepileptic. When the authors looked more closely at those “push-button” events, they found they ranged from abnormal body movement in 14 and hypertension in 7 to tachycardia and abnormal face movements, among other characterizations, in lesser numbers.
“Furthermore, push-button events by bedside clinicians, including abnormal movements and hypertensive episodes concerning for possible seizures, did not have any EEG correlate, indicating that bedside clinical assessment for seizures without CEEG monitoring is unreliable,” Dr. Naim and colleagues said.
As to whether identifying and treating postbypass seizures in young newborns with CHD will improve long-term neurodevelopment in these children, the authors acknowledged that further study is needed.
They reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Electroencephalography is more effective than clinical observation in identifying seizures in infants immediately after they’ve had cardiopulmonary bypass surgery.
Major finding: Postoperative CEEG identified seizures in 8% of newborns with congenital heart disease after coronary bypass surgery.
Data source: Chart review involved 172 neonates from a single center. Multiple logistic regression analysis assessed seizures and clinical and predictive factors.
Disclosures: The authors reported having no financial disclosures.
Elephant stent aorta repair – good outcomes, but is it too complex?
An acute aortic tear can be lethal, and more cardiac surgeons are favoring extended aortic arch replacement in these cases. Cardiac surgeons have tried many different arch replacement techniques, but en bloc repair and double- or triple-branch stent grafting carry significant risks, so a team of cardiac surgeons in Beijing has reported good 2-year results with a novel technique that combines stented elephant-trunk implantation with preservation of key vessels.
The technique accomplishes total arch replacement with the stent while preserving the autologous brachiocephalic vessels.
“This technique simplified hemostasis and anastomosis, reduced the size of the residual aortic patch wall, and preserved the autologous brachiocephalic vessels, yielding satisfactory surgical results,” wrote Dr. Li-Zhong Sun and colleagues at Beijing’s Capital Medical University (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.002]).
There are four keys to the procedure:
• The use of forceps to grasp the stent-free sewing edge of the stented elephant trunk and straightening of the spiral shaped Dacron graft to approximately 3 cm.
• Preservation of the native brachiocephalic vessels.
• Creating a residual aortic wall containing the innominate artery and LCCA that’s as small as possible.
• An end-to-side anastomosis between the left subclavian artery (LSCA) and the left common carotid artery (LCCA), a key junction in their technique.
The 20 study subjects had surgery within 2 weeks of the onset of pain. All 20 were discharged after the procedure, and in a mean follow-up period of 26 months, 18 had good outcomes while 1 patient had thoracoabdominal aortic replacement 9 months after the initial surgery (1 patient was lost to follow-up).
The researchers used computed tomography to confirm patency of the anastomosis between the LSCA and LCCA.
In 2 of the 20 patients, the aorta was normal with aortic dissection limited to the descending aorta. In the remaining patients, the investigators observed thrombus obliteration of the false lumen around the surgical graft in 16, partial thrombosis in 1 and patency in 1.
The surgical technique exposes the right axillary artery through a right subclavicular incision and a median sternotomy, then dissects and exposes the brachiocephalic vessels and the transverse arch. Dissection of the LSCA and LCCA is the key step in making the end-to-end anastomosis between the two vessels. The researchers accomplished this by partially transecting the sternocleidomastoid muscle and other cervical muscles.
Dr. Sun and coauthors said that a separated graft technique offers a number of advantages over other techniques for aortic arch reconstruction. While en bloc repair preserves the native brachiocephalic vessels and, thus, results in long-term patency, the technique carries risk for postoperative rupture of the aortic patch containing the brachiocephalic vessels. Double- or triple-branched stent grafting has resulted in shifting or kinking of the graft and eventually graft occlusion or aortic disruption.
The authors acknowledged the study’s small sample size, and that the outcomes are “preliminary.” They said long-term follow-up would be required to confirm the outcomes.
They had no disclosures to report.
The Beijing study authors’ excellent postoperative outcomes show that alternative surgical techniques for elephant-trunk implantation can be employed safely, but their technique also raises questions about the use of advanced technology, Dr. Prashanth Vallabhajosyula and Dr. Wilson Y. Szeto of the University of Pennsylvania said in their commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.04.003]).
“But does this mean we should be doing [elephant-trunk] operation on every type A dissection patient?” wrote Dr. Vallabhajosyula and Dr. Szeto. If no primary tear appears in the aortic arch or the proximal descending thoracic aorta (DTA), “then should we empirically dissect the arch vessels and perform total arch replacement in an emergent situation?” They also questioned extensive dissection of the left subclavian artery (LSCA) by cutting into the muscles around the surgical site.
Elephant-trunk implantation is more complex than other aortic repair procedures, they noted. “So, if a total arch replacement is not required, then why do it?”
While they acknowledged advantages of total arch replacement, and elephant-trunk implantation in particular, most operations for type A dissection occur in smaller, community hospitals that are ill equipped to perform the procedure. “This raises the issue of wide clinical application of the [elephant-trunk] technique for acute type A dissection,” they said. The real issue may not be what type of anastomosis for the elephant-trunk technique surgeons should use, but rather what surgical technique – the elephant-trunk technique vs. transverse hemiarch reconstruction, they said. (Dr. Vallabhajosyula and Dr. Szeto mentioned that their institution has advocated for the latter.)
“To address this, a more comprehensive and meticulous approach is warranted based on parameters such as patient clinical picture, acuity, malperfusion, arch and DTA anatomy, and primary tear site location,” they said. But for now, Dr. Vallabhajosyula and Dr. Szeto said, the medical literature does not support total arch replacement over transverse hemiarch reconstruction.
Dr. Vallabhajosyula is assistant professor of surgery at the Hospital of the University of Pennsylvania; Dr. Szeto is associate professor of surgery in the division of cardiovascular surgery at the University of Pennsylvania Medical Center–Penn Presbyterian Medical Center.
The Beijing study authors’ excellent postoperative outcomes show that alternative surgical techniques for elephant-trunk implantation can be employed safely, but their technique also raises questions about the use of advanced technology, Dr. Prashanth Vallabhajosyula and Dr. Wilson Y. Szeto of the University of Pennsylvania said in their commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.04.003]).
“But does this mean we should be doing [elephant-trunk] operation on every type A dissection patient?” wrote Dr. Vallabhajosyula and Dr. Szeto. If no primary tear appears in the aortic arch or the proximal descending thoracic aorta (DTA), “then should we empirically dissect the arch vessels and perform total arch replacement in an emergent situation?” They also questioned extensive dissection of the left subclavian artery (LSCA) by cutting into the muscles around the surgical site.
Elephant-trunk implantation is more complex than other aortic repair procedures, they noted. “So, if a total arch replacement is not required, then why do it?”
While they acknowledged advantages of total arch replacement, and elephant-trunk implantation in particular, most operations for type A dissection occur in smaller, community hospitals that are ill equipped to perform the procedure. “This raises the issue of wide clinical application of the [elephant-trunk] technique for acute type A dissection,” they said. The real issue may not be what type of anastomosis for the elephant-trunk technique surgeons should use, but rather what surgical technique – the elephant-trunk technique vs. transverse hemiarch reconstruction, they said. (Dr. Vallabhajosyula and Dr. Szeto mentioned that their institution has advocated for the latter.)
“To address this, a more comprehensive and meticulous approach is warranted based on parameters such as patient clinical picture, acuity, malperfusion, arch and DTA anatomy, and primary tear site location,” they said. But for now, Dr. Vallabhajosyula and Dr. Szeto said, the medical literature does not support total arch replacement over transverse hemiarch reconstruction.
Dr. Vallabhajosyula is assistant professor of surgery at the Hospital of the University of Pennsylvania; Dr. Szeto is associate professor of surgery in the division of cardiovascular surgery at the University of Pennsylvania Medical Center–Penn Presbyterian Medical Center.
The Beijing study authors’ excellent postoperative outcomes show that alternative surgical techniques for elephant-trunk implantation can be employed safely, but their technique also raises questions about the use of advanced technology, Dr. Prashanth Vallabhajosyula and Dr. Wilson Y. Szeto of the University of Pennsylvania said in their commentary on the study (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.04.003]).
“But does this mean we should be doing [elephant-trunk] operation on every type A dissection patient?” wrote Dr. Vallabhajosyula and Dr. Szeto. If no primary tear appears in the aortic arch or the proximal descending thoracic aorta (DTA), “then should we empirically dissect the arch vessels and perform total arch replacement in an emergent situation?” They also questioned extensive dissection of the left subclavian artery (LSCA) by cutting into the muscles around the surgical site.
Elephant-trunk implantation is more complex than other aortic repair procedures, they noted. “So, if a total arch replacement is not required, then why do it?”
While they acknowledged advantages of total arch replacement, and elephant-trunk implantation in particular, most operations for type A dissection occur in smaller, community hospitals that are ill equipped to perform the procedure. “This raises the issue of wide clinical application of the [elephant-trunk] technique for acute type A dissection,” they said. The real issue may not be what type of anastomosis for the elephant-trunk technique surgeons should use, but rather what surgical technique – the elephant-trunk technique vs. transverse hemiarch reconstruction, they said. (Dr. Vallabhajosyula and Dr. Szeto mentioned that their institution has advocated for the latter.)
“To address this, a more comprehensive and meticulous approach is warranted based on parameters such as patient clinical picture, acuity, malperfusion, arch and DTA anatomy, and primary tear site location,” they said. But for now, Dr. Vallabhajosyula and Dr. Szeto said, the medical literature does not support total arch replacement over transverse hemiarch reconstruction.
Dr. Vallabhajosyula is assistant professor of surgery at the Hospital of the University of Pennsylvania; Dr. Szeto is associate professor of surgery in the division of cardiovascular surgery at the University of Pennsylvania Medical Center–Penn Presbyterian Medical Center.
An acute aortic tear can be lethal, and more cardiac surgeons are favoring extended aortic arch replacement in these cases. Cardiac surgeons have tried many different arch replacement techniques, but en bloc repair and double- or triple-branch stent grafting carry significant risks, so a team of cardiac surgeons in Beijing has reported good 2-year results with a novel technique that combines stented elephant-trunk implantation with preservation of key vessels.
The technique accomplishes total arch replacement with the stent while preserving the autologous brachiocephalic vessels.
“This technique simplified hemostasis and anastomosis, reduced the size of the residual aortic patch wall, and preserved the autologous brachiocephalic vessels, yielding satisfactory surgical results,” wrote Dr. Li-Zhong Sun and colleagues at Beijing’s Capital Medical University (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.002]).
There are four keys to the procedure:
• The use of forceps to grasp the stent-free sewing edge of the stented elephant trunk and straightening of the spiral shaped Dacron graft to approximately 3 cm.
• Preservation of the native brachiocephalic vessels.
• Creating a residual aortic wall containing the innominate artery and LCCA that’s as small as possible.
• An end-to-side anastomosis between the left subclavian artery (LSCA) and the left common carotid artery (LCCA), a key junction in their technique.
The 20 study subjects had surgery within 2 weeks of the onset of pain. All 20 were discharged after the procedure, and in a mean follow-up period of 26 months, 18 had good outcomes while 1 patient had thoracoabdominal aortic replacement 9 months after the initial surgery (1 patient was lost to follow-up).
The researchers used computed tomography to confirm patency of the anastomosis between the LSCA and LCCA.
In 2 of the 20 patients, the aorta was normal with aortic dissection limited to the descending aorta. In the remaining patients, the investigators observed thrombus obliteration of the false lumen around the surgical graft in 16, partial thrombosis in 1 and patency in 1.
The surgical technique exposes the right axillary artery through a right subclavicular incision and a median sternotomy, then dissects and exposes the brachiocephalic vessels and the transverse arch. Dissection of the LSCA and LCCA is the key step in making the end-to-end anastomosis between the two vessels. The researchers accomplished this by partially transecting the sternocleidomastoid muscle and other cervical muscles.
Dr. Sun and coauthors said that a separated graft technique offers a number of advantages over other techniques for aortic arch reconstruction. While en bloc repair preserves the native brachiocephalic vessels and, thus, results in long-term patency, the technique carries risk for postoperative rupture of the aortic patch containing the brachiocephalic vessels. Double- or triple-branched stent grafting has resulted in shifting or kinking of the graft and eventually graft occlusion or aortic disruption.
The authors acknowledged the study’s small sample size, and that the outcomes are “preliminary.” They said long-term follow-up would be required to confirm the outcomes.
They had no disclosures to report.
An acute aortic tear can be lethal, and more cardiac surgeons are favoring extended aortic arch replacement in these cases. Cardiac surgeons have tried many different arch replacement techniques, but en bloc repair and double- or triple-branch stent grafting carry significant risks, so a team of cardiac surgeons in Beijing has reported good 2-year results with a novel technique that combines stented elephant-trunk implantation with preservation of key vessels.
The technique accomplishes total arch replacement with the stent while preserving the autologous brachiocephalic vessels.
“This technique simplified hemostasis and anastomosis, reduced the size of the residual aortic patch wall, and preserved the autologous brachiocephalic vessels, yielding satisfactory surgical results,” wrote Dr. Li-Zhong Sun and colleagues at Beijing’s Capital Medical University (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.002]).
There are four keys to the procedure:
• The use of forceps to grasp the stent-free sewing edge of the stented elephant trunk and straightening of the spiral shaped Dacron graft to approximately 3 cm.
• Preservation of the native brachiocephalic vessels.
• Creating a residual aortic wall containing the innominate artery and LCCA that’s as small as possible.
• An end-to-side anastomosis between the left subclavian artery (LSCA) and the left common carotid artery (LCCA), a key junction in their technique.
The 20 study subjects had surgery within 2 weeks of the onset of pain. All 20 were discharged after the procedure, and in a mean follow-up period of 26 months, 18 had good outcomes while 1 patient had thoracoabdominal aortic replacement 9 months after the initial surgery (1 patient was lost to follow-up).
The researchers used computed tomography to confirm patency of the anastomosis between the LSCA and LCCA.
In 2 of the 20 patients, the aorta was normal with aortic dissection limited to the descending aorta. In the remaining patients, the investigators observed thrombus obliteration of the false lumen around the surgical graft in 16, partial thrombosis in 1 and patency in 1.
The surgical technique exposes the right axillary artery through a right subclavicular incision and a median sternotomy, then dissects and exposes the brachiocephalic vessels and the transverse arch. Dissection of the LSCA and LCCA is the key step in making the end-to-end anastomosis between the two vessels. The researchers accomplished this by partially transecting the sternocleidomastoid muscle and other cervical muscles.
Dr. Sun and coauthors said that a separated graft technique offers a number of advantages over other techniques for aortic arch reconstruction. While en bloc repair preserves the native brachiocephalic vessels and, thus, results in long-term patency, the technique carries risk for postoperative rupture of the aortic patch containing the brachiocephalic vessels. Double- or triple-branched stent grafting has resulted in shifting or kinking of the graft and eventually graft occlusion or aortic disruption.
The authors acknowledged the study’s small sample size, and that the outcomes are “preliminary.” They said long-term follow-up would be required to confirm the outcomes.
They had no disclosures to report.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Total aortic arch replacement with implantation of an elephant-trunk stent avoids risks of other more conventional approaches.
Major finding: Among 20 patients who had the elephant-trunk procedure, 18 had good results at a mean of 26 months after the operation (one had thoracoabdominal aortic arch replacement at 9 months and one was lost to follow-up).
Data source: Retrospective review of 20 patients with acute type A dissection who had total arch replacement at a single center.
Disclosures: The study authors reported having no financial disclosures.
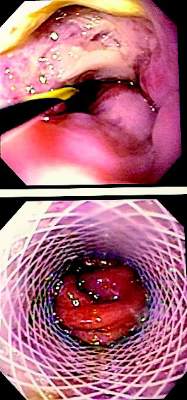
Stents better than surgery for esophagus tears?
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
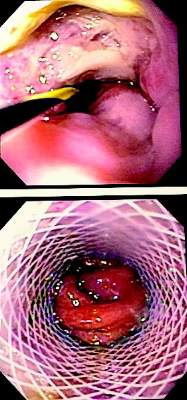
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
“This paper addresses an important question for thoracic surgeons and the findings are promising,” Dr. Katie S. Nason of the University of Pittsburgh said in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.02.028]). She also commended the study authors for using propensity matching to create comparable groups.
Document
|
Dr. Katie S. Nason |
However, the study did not address several patient factors that can influence a surgeon’s selection of an operation or stent placement, Dr. Nason said: injury size and location, other esophageal disorders patients might have, and the degree of contamination around the operative site. “It is premature to definitively interpret the higher rate of mortality, morbidity, cost, and length of stay with surgery as a direct result of treatment choice, when unmeasured differences in the patient’s perforation-associated condition are not accounted for in propensity-matching or outcomes analysis,” she said.
Nonetheless, she called the data “compelling” and that examination of other studies was warranted. Dr. Nason cited four other reports that arrived at similar conclusions (Ann. Surg. 2014;259:852-60; World J. Surg. 2013;37:1051-9; J. Am. Coll. Surg. 2014;218:768-74; World J. Surg. 2014;38:902-9). “Taken together with these prior studies, the data for management of iatrogenic perforation increasingly favor early intervention with esophageal stenting,” Dr. Nason said.
Dr. Nason is an assistant professor of cardiothoracic surgery at the University of Pittsburgh.
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
While stent placement has proved to be safe and effective for acute esophageal perforation, a head-to-head comparison with surgical repair has never been reported, so a team of investigators performed a small, single-system analysis that compared stenting and surgery and found that while both are equally effective, esophageal stent placement resulted in lower costs and lower morbidity rates.
Investigators led by Dr. Richard Freeman of St. Vincent Hospital in Indianapolis published their results in the June issue of the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.01.066]). Their study evaluated only 60 patients who had either stent placement or an operation for acute intrathoracic esophageal perforation between 2009 and 2012 within Ascension Health, a national Catholic-based network of 36 regional health systems; but the authors noted that they had extracted their data from the national Premier Inc. database, which covers 20% of U.S. hospital discharges, and used propensity matching to generate similar stent and surgical groups. Dr. Freeman presented the results at the annual meeting of the American Association of Thoracic Surgery in Toronto, April 28-30.
Patients who received stents had intensive care unit stays about half that of the surgery group – an average of 2 vs. 4 days. Likewise, their total hospital stays were about half: 6 days vs. 11 days for the surgery group. Complication rates were comparable: postrepair leaks were reported in 17% of the stent group and 20% who had surgery. While reoperation rates were significantly lower in the stent group (3% vs. 13%), four patients (13%) of the stent group did have stent migration. Morbidity was significantly higher in the surgery group (43% vs. 17%). While postprocedure leak rates were similar, those who had surgery were more likely to have reoperation for persistent leaks, the authors said.
Further, stent recipients were able to take nutrition by mouth earlier after surgery and had lower rates of needing enteral feeding at discharge – 17% vs. 60% for the surgery group. Dr. Freeman and his team also analyzed costs between the two procedures and found that total costs, including inpatient and outpatient costs, averaged $142,000 for surgery vs. $91,000 for stenting.
Because the incidence of esophageal perforation is so low, Dr. Freeman and his coauthors reported that performing a randomized trial comparing esophageal stenting and surgery has been difficult. The off-label nature of stenting for esophageal perforation has also complicated funding of a prospective trial. The study authors said a prospective, randomized design would have been preferable to the propensity-matched approach.
Surgery for esophageal tear has been around for almost 70 years with many improvements in technique, anesthesia, and antimicrobial therapy, but with a need for prolonged inpatient and outpatient care along with a postoperative leak rate as high as 39% (Ann. Thorac. Surg. 2010;90:1669-73). “A persistent leak following operative repair may also result in the need for esophageal diversion and subsequent reconstruction with its associated significant morbidity and patient dissatisfaction,” Dr. Freeman and his coauthors said.
The authors acknowledged shortcomings of their study included not accounting for how different stents used in the stenting group and individual surgeons and facilities may have influenced outcomes. Other shortcomings were that cost calculations may not have accounted for inflation or costs outside the Ascension Health system and the uniqueness of the procedure itself. “Lastly, the fact that both treatment strategies employed for iatrogenic esophageal perforation are likely uncommon procedures at most treatment facilities implies that standardization, even at the local level, may be lacking,” the authors stated.
The authors reported having no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Esophageal stent placement for the treatment of an acute esophageal tear seems to be as effective as surgery in propensity-matched patients.
Major finding: Morbidity scores were 43% for patients who had surgical repair vs. 17% for those who underwent stent placement for esophageal tear.
Data source: Retrospective analysis of 60 propensity-matched patients over a 4-year period at a single health system’s hospitals, as drawn from the Premiere national database.
Disclosures: The authors reported having no financial disclosures.
Ablation may raise risk for later myectomy
How patients with hypertrophic obstructive cardiomyopathy who have already undergone alcohol septal ablation fare after going on to have surgical septal myectomy has been a matter of speculation and conjecture among cardiac surgeons for years, so a team of investigators set out to evaluate the outcomes among those patients.
What they found was that patients with a history of alcohol septal ablation may have an increased risk of cardiac death and complications after they have transaortic septal myectomy later on instead of just having septal myectomy as the primary procedure. In the Journal of Thoracic and Cardiovascular Surgery, Dr. Eduard Quintana of the University of Barcelona and the Mayo Clinic in Rochester, Minn., and coauthors reported that their findings support the use of surgical septal myectomy as the preferred treatment for septal reduction therapy for hypertrophic obstructive cardiomyopathy (HOCM) (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.03.044]).
This small study evaluated 31 patients who had a failed alcohol septal ablation and then underwent septal myectomy and compared them to a group of 62 patients who had a septal myectomy only for HOCM. A total of 28 of the failed septal ablation patients had one such previous procedure and three had two or more percutaneous procedures before undergoing surgical septal myectomy. Study outcomes were cardiac death, advanced heart failure, and placement of an implantable cardioverter defibrillator (ICD). The study was conducted at the Mayo Clinic.
Percutaneous alcohol septal ablation utilizes injection of ethanol to correct left ventricular outflow tract obstruction (LVOT) in hypertrophic cardiomyopathy. Dr. Quintana and his coauthors reported that despite the percutaneous nature of alcohol septal ablation, its incidence of death and morbidity are not lower than surgical myectomy. They also reported that some countries are using alcohol ablation exclusively for septal reduction in HOCM. The rate of recurrence of severe symptoms after septal ablation is 20%, Dr. Quintana and his colleagues pointed out. “Thus, a sizeable proportion of patients having alcohol septal ablation may require transaortic septal myectomy for relief of LVOT, and outcome of such patients may be impaired,” they reported.
The 31 prior-ablation patients had a three times higher rate of implanted ICDs (32% vs. 11%), more arrhythmias (43% vs. 13% based on preoperative Holter monitoring), and a 12 times higher rate of postoperative complete heart block (19.4% vs. 1.6%). The prior–septal ablation group progressed to advanced heart failure at twice the rate, 22.5% at an average follow-up of 3.2 years, compared with about 10% in the primary septal myectomy group.
The authors also reported the 31 prior-ablation patients had significantly higher rates of interstitial and endocardial fibrosis – 70% vs. 26% and 87% vs. 67%, respectively.
“Our data contributes to accumulating evidence that the infarction induced by alcohol septal ablation may have adverse and unexpected consequences,” Dr. Quintana and his colleagues said.
However, the authors also acknowledged that one limit of their study was that it could not identify the overall failure rate of alcohol septal ablation among the larger patient population that underwent the procedure – “the inability to clearly define the denominator.” Nineteen of the 31 prior-ablation subjects had been referred from other institutions.
Coauthor Dr. Anna Sabata-Rotes received funding from Fundacia La Caxia, Barcelona. The other authors had no relationships to disclose.
Surgeons have a bias toward always seeing surgery as the better alternative, and that may explain the conclusion Dr. Eduard Quintana and his colleagues stated in this study – that the accumulating evidence suggests that the myocardial infarction induced during percutaneous alcohol septal ablation may have harmful effects, Dr. Richard Lee said in his commentary. (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.05.019]) “I am not sure this is true,” he wrote.
He noted that the authors’ acknowledged limitation that the denominator is not known is a “critical shortcoming.” Dr. Lee asked, “What happens to the ablations that DON’T fail? And, more importantly, how many succeed? Without that information, the merits or limitations of alcohol ablation are unknown as well.” As for study participants from outside institutions, the study did not quantify if those institutions perform a large number of alcohol ablations and their success rates.
Dr. Lee also noted that the study included “only” 31 patients who failed alcohol ablation. “If the number of surgical procedures is 1,500, this is very low, even if many surgeries occurred before the development of ablation,” he said.
A larger, head-to-head, randomized comparison that evaluates quality of life and recovery time would answer questions about the risks facing patients who had previous alcohol septal ablation, Dr. Lee said. In the meantime, in an institution with less surgical experience, percutaneous alcohol septal ablation may be the wise choice, he said. And patients will always gravitate to the least invasive option. “The fact is,” Dr. Lee concluded, “they might be right.”
Dr. Lee is a professor of surgery at St. Louis University, Center for Comprehensive Cardiovascular Care.
Surgeons have a bias toward always seeing surgery as the better alternative, and that may explain the conclusion Dr. Eduard Quintana and his colleagues stated in this study – that the accumulating evidence suggests that the myocardial infarction induced during percutaneous alcohol septal ablation may have harmful effects, Dr. Richard Lee said in his commentary. (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.05.019]) “I am not sure this is true,” he wrote.
He noted that the authors’ acknowledged limitation that the denominator is not known is a “critical shortcoming.” Dr. Lee asked, “What happens to the ablations that DON’T fail? And, more importantly, how many succeed? Without that information, the merits or limitations of alcohol ablation are unknown as well.” As for study participants from outside institutions, the study did not quantify if those institutions perform a large number of alcohol ablations and their success rates.
Dr. Lee also noted that the study included “only” 31 patients who failed alcohol ablation. “If the number of surgical procedures is 1,500, this is very low, even if many surgeries occurred before the development of ablation,” he said.
A larger, head-to-head, randomized comparison that evaluates quality of life and recovery time would answer questions about the risks facing patients who had previous alcohol septal ablation, Dr. Lee said. In the meantime, in an institution with less surgical experience, percutaneous alcohol septal ablation may be the wise choice, he said. And patients will always gravitate to the least invasive option. “The fact is,” Dr. Lee concluded, “they might be right.”
Dr. Lee is a professor of surgery at St. Louis University, Center for Comprehensive Cardiovascular Care.
Surgeons have a bias toward always seeing surgery as the better alternative, and that may explain the conclusion Dr. Eduard Quintana and his colleagues stated in this study – that the accumulating evidence suggests that the myocardial infarction induced during percutaneous alcohol septal ablation may have harmful effects, Dr. Richard Lee said in his commentary. (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.05.019]) “I am not sure this is true,” he wrote.
He noted that the authors’ acknowledged limitation that the denominator is not known is a “critical shortcoming.” Dr. Lee asked, “What happens to the ablations that DON’T fail? And, more importantly, how many succeed? Without that information, the merits or limitations of alcohol ablation are unknown as well.” As for study participants from outside institutions, the study did not quantify if those institutions perform a large number of alcohol ablations and their success rates.
Dr. Lee also noted that the study included “only” 31 patients who failed alcohol ablation. “If the number of surgical procedures is 1,500, this is very low, even if many surgeries occurred before the development of ablation,” he said.
A larger, head-to-head, randomized comparison that evaluates quality of life and recovery time would answer questions about the risks facing patients who had previous alcohol septal ablation, Dr. Lee said. In the meantime, in an institution with less surgical experience, percutaneous alcohol septal ablation may be the wise choice, he said. And patients will always gravitate to the least invasive option. “The fact is,” Dr. Lee concluded, “they might be right.”
Dr. Lee is a professor of surgery at St. Louis University, Center for Comprehensive Cardiovascular Care.
How patients with hypertrophic obstructive cardiomyopathy who have already undergone alcohol septal ablation fare after going on to have surgical septal myectomy has been a matter of speculation and conjecture among cardiac surgeons for years, so a team of investigators set out to evaluate the outcomes among those patients.
What they found was that patients with a history of alcohol septal ablation may have an increased risk of cardiac death and complications after they have transaortic septal myectomy later on instead of just having septal myectomy as the primary procedure. In the Journal of Thoracic and Cardiovascular Surgery, Dr. Eduard Quintana of the University of Barcelona and the Mayo Clinic in Rochester, Minn., and coauthors reported that their findings support the use of surgical septal myectomy as the preferred treatment for septal reduction therapy for hypertrophic obstructive cardiomyopathy (HOCM) (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.03.044]).
This small study evaluated 31 patients who had a failed alcohol septal ablation and then underwent septal myectomy and compared them to a group of 62 patients who had a septal myectomy only for HOCM. A total of 28 of the failed septal ablation patients had one such previous procedure and three had two or more percutaneous procedures before undergoing surgical septal myectomy. Study outcomes were cardiac death, advanced heart failure, and placement of an implantable cardioverter defibrillator (ICD). The study was conducted at the Mayo Clinic.
Percutaneous alcohol septal ablation utilizes injection of ethanol to correct left ventricular outflow tract obstruction (LVOT) in hypertrophic cardiomyopathy. Dr. Quintana and his coauthors reported that despite the percutaneous nature of alcohol septal ablation, its incidence of death and morbidity are not lower than surgical myectomy. They also reported that some countries are using alcohol ablation exclusively for septal reduction in HOCM. The rate of recurrence of severe symptoms after septal ablation is 20%, Dr. Quintana and his colleagues pointed out. “Thus, a sizeable proportion of patients having alcohol septal ablation may require transaortic septal myectomy for relief of LVOT, and outcome of such patients may be impaired,” they reported.
The 31 prior-ablation patients had a three times higher rate of implanted ICDs (32% vs. 11%), more arrhythmias (43% vs. 13% based on preoperative Holter monitoring), and a 12 times higher rate of postoperative complete heart block (19.4% vs. 1.6%). The prior–septal ablation group progressed to advanced heart failure at twice the rate, 22.5% at an average follow-up of 3.2 years, compared with about 10% in the primary septal myectomy group.
The authors also reported the 31 prior-ablation patients had significantly higher rates of interstitial and endocardial fibrosis – 70% vs. 26% and 87% vs. 67%, respectively.
“Our data contributes to accumulating evidence that the infarction induced by alcohol septal ablation may have adverse and unexpected consequences,” Dr. Quintana and his colleagues said.
However, the authors also acknowledged that one limit of their study was that it could not identify the overall failure rate of alcohol septal ablation among the larger patient population that underwent the procedure – “the inability to clearly define the denominator.” Nineteen of the 31 prior-ablation subjects had been referred from other institutions.
Coauthor Dr. Anna Sabata-Rotes received funding from Fundacia La Caxia, Barcelona. The other authors had no relationships to disclose.
How patients with hypertrophic obstructive cardiomyopathy who have already undergone alcohol septal ablation fare after going on to have surgical septal myectomy has been a matter of speculation and conjecture among cardiac surgeons for years, so a team of investigators set out to evaluate the outcomes among those patients.
What they found was that patients with a history of alcohol septal ablation may have an increased risk of cardiac death and complications after they have transaortic septal myectomy later on instead of just having septal myectomy as the primary procedure. In the Journal of Thoracic and Cardiovascular Surgery, Dr. Eduard Quintana of the University of Barcelona and the Mayo Clinic in Rochester, Minn., and coauthors reported that their findings support the use of surgical septal myectomy as the preferred treatment for septal reduction therapy for hypertrophic obstructive cardiomyopathy (HOCM) (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.03.044]).
This small study evaluated 31 patients who had a failed alcohol septal ablation and then underwent septal myectomy and compared them to a group of 62 patients who had a septal myectomy only for HOCM. A total of 28 of the failed septal ablation patients had one such previous procedure and three had two or more percutaneous procedures before undergoing surgical septal myectomy. Study outcomes were cardiac death, advanced heart failure, and placement of an implantable cardioverter defibrillator (ICD). The study was conducted at the Mayo Clinic.
Percutaneous alcohol septal ablation utilizes injection of ethanol to correct left ventricular outflow tract obstruction (LVOT) in hypertrophic cardiomyopathy. Dr. Quintana and his coauthors reported that despite the percutaneous nature of alcohol septal ablation, its incidence of death and morbidity are not lower than surgical myectomy. They also reported that some countries are using alcohol ablation exclusively for septal reduction in HOCM. The rate of recurrence of severe symptoms after septal ablation is 20%, Dr. Quintana and his colleagues pointed out. “Thus, a sizeable proportion of patients having alcohol septal ablation may require transaortic septal myectomy for relief of LVOT, and outcome of such patients may be impaired,” they reported.
The 31 prior-ablation patients had a three times higher rate of implanted ICDs (32% vs. 11%), more arrhythmias (43% vs. 13% based on preoperative Holter monitoring), and a 12 times higher rate of postoperative complete heart block (19.4% vs. 1.6%). The prior–septal ablation group progressed to advanced heart failure at twice the rate, 22.5% at an average follow-up of 3.2 years, compared with about 10% in the primary septal myectomy group.
The authors also reported the 31 prior-ablation patients had significantly higher rates of interstitial and endocardial fibrosis – 70% vs. 26% and 87% vs. 67%, respectively.
“Our data contributes to accumulating evidence that the infarction induced by alcohol septal ablation may have adverse and unexpected consequences,” Dr. Quintana and his colleagues said.
However, the authors also acknowledged that one limit of their study was that it could not identify the overall failure rate of alcohol septal ablation among the larger patient population that underwent the procedure – “the inability to clearly define the denominator.” Nineteen of the 31 prior-ablation subjects had been referred from other institutions.
Coauthor Dr. Anna Sabata-Rotes received funding from Fundacia La Caxia, Barcelona. The other authors had no relationships to disclose.
Key clinical point: Patients who had a failed alcohol septal ablation for hypertrophic obstructive cardiomyopathy may be at greater risk for cardiac events if they need surgical septal myectomy later on.
Major finding: Prior-ablation patients had higher rates of ICD implantation, more arrhythmias, and a 12 times higher rate of postoperative complete heart block after having a subsequent surgical septal myectomy.
Data source: A single-center study of 31 patients who had prior alcohol septal ablation and later surgical septal myectomy, compared with 62 subjects who had surgical septal myectomy as the primary procedure for hypertrophic obstructive cardiomyopathy.
Disclosures: The authors had no relevant relationships with industry to disclose, although coauthor Dr. Anna Sabata-Rotes received funding from Fundacia La Caxia, Barcelona.
Hemodynamics after MVR better than annuloplasty's
Individuals with chronic ischemic mitral regurgitation who undergo mitral valve replacement show significantly superior exercise performance up to almost 3½ years after the operation when compared with those who have restrictive mitral valve annuloplasty, according to a study in the June issue of the Journal of Cardiovascular Surgery. (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.003]).
Doctors at three institutions in France, Italy, and the United Kingdom set out to predict what factors determined long-term functional capacity in patients with chronic ischemic mitral regurgitation (CIMR) who had either mitral valve replacement (MVR) or annuloplasty. They performed a retrospective analysis of 121 patients with significant chronic mitral regurgitation, 62 of whom had restrictive mitral valve annuloplasty and 59 of whom underwent MVR between 2005 and 2011. All the subjects had a resting echocardiography and a 6-minute treadmill test before their procedures and again at an average of 41 months afterwards. The MVR group walked an average of 37 meters farther at the postoperative stress test, whereas the annuloplasty patients walked on average 24 meters less than their preoperative test.
“The most important finding of this study is that, in patients with CIMR who underwent mitral valve surgery, the improvement in functional capacity at long-term follow-up is mainly related to the type of treatment and to the mitral valve hemodynamic performance, as expressed by changes in IEOA [indexed effective orifice area] during exercise,” reported lead author Dr. Carlo Fino of the Bristol (England) Heart Institute and Pope John XXIII Hospital in Bergamo, Italy, and his colleagues. Investigators from Hospital Dupuytren in Limoges, France, also participated.
The study noted inconclusive results of previous reports of patients treated for mitral regurgitation: the Cardiothoracic Surgical Trials Network study that showed similar 1-year outcomes among patients who had either MVR or annuloplasty (N. Engl. J. Med. 2014;370:23-32) ; an earlier study that showed annuloplasty patients may develop functional mitral stenosis with decreasing functional capacity (J. Am. Coll. Cardiol. 2008;51:1692-1701); and Dr. Fino and colleagues’ previous work that showed worse hemodynamics in annuloplasty patients, compared with MVR counterparts (J. Thorac. Cardiovasc. Surg. 2014;148:447-53).
Other comparative measures the latest study evaluated were: change in exercise indexed effective orifice area, increasing from 1.3 to 1.5 cm2/m2 in the MVR group vs. 1.1 to 1.2 cm2/m2 in the annuloplasty group; change in mean mitral gradients from rest to exercise, which increased significantly in both groups – from 4.3 to 9 mm Hg in the replacement group and 4.4 to 11 mm Hg in the annuloplasty group; postoperative cardiovascular events – 8% in the MVR group and 21% in the annuloplasty population; and follow-up survival – 88% for MVR vs. 83% for annuloplasty.
The annuloplasty patients received either a Carpentier-Edwards Physio ring (71%) or Carpentier-Edwards Classic ring (29%); Edwards Lifesciences. The MVR group received either a biological or mechanical prosthesis, although the study did not report how many of each. All patients had associated coronary bypass grafting surgery and all achieved complete revascularization. The MVR and annuloplasty groups were similar in terms of demographics and cardiac function, although a higher percentage of patients in the annuloplasty group had severe mitral regurgitation preoperatively – 41% vs. 32% in the MVR group.
Procedures like annuloplasty that aim to restore ventricular geometry or target the subvalvular mechanism “seem to be promising but they require further scientific evidence,” Dr. Fino and his coauthors said. They suggested that until 24-month results from the Cardiothoracic Surgical Trials Network are available, MVR with chordal sparing might be a “reliable option” for patients with chronic ischemic mitral regurgitation.
The authors had no disclosures.
Although mitral valve annuloplasty is the most common procedure for treatment of ischemic mitral regurgitation, surgeons had only been concerned that this procedure resulted in significant rates of recurrence of mitral regurgitation (MR), Dr. Ehud Raanani said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.038) . He noted that the study by Dr. Carlo Fino and colleagues elaborates on a body of evidence that suggests concerns about restrictive annuloplasty are going beyond MR recurrence.
The idea that annuloplasty is always superior to mitral valve replacement (MVR) “was no more than conjecture based on weak evidence from several retrospective, nonrandomized studies that reported lower early and late mortality in patients who had undergone [annuloplasty] rather than MVR,” Dr. Raanani said. In those nonrandomized studies, the MVR patients were older with and sicker – “factors that are difficult to adjust or control.”
Dr. Fino and colleagues’ findings are “in accord” with other recent studies that question the universal superiority of annuloplasty over MVR in terms of hemodynamics and outcome, Dr. Raanani noted. Their study and the recent report on the Cardiothoracic Surgical Trials Network study (N. Engl. J. Med. 2014 Jan. 2 370:23-32) raise questions about the belief that annuloplasty is the optimal treatment for all types of patients with ischemic mitral regurgitation.
“The answer is probably no,” Dr. Raanani said. “For now, there is no one single procedure that is suitable for all.” Not all patients with ischemic mitral regurgitation are the same, and each must be treated individually. “We are close to the point where there is sufficient accumulated data to provide comprehensive imaging, stratify patients, and cater to individual surgical treatment,” Dr. Raanani said.
Dr. Raanani is a surgeon in the department of cardiac surgery at the Sheba Medical Center, Ramat-Gan, Israel.
Although mitral valve annuloplasty is the most common procedure for treatment of ischemic mitral regurgitation, surgeons had only been concerned that this procedure resulted in significant rates of recurrence of mitral regurgitation (MR), Dr. Ehud Raanani said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.038) . He noted that the study by Dr. Carlo Fino and colleagues elaborates on a body of evidence that suggests concerns about restrictive annuloplasty are going beyond MR recurrence.
The idea that annuloplasty is always superior to mitral valve replacement (MVR) “was no more than conjecture based on weak evidence from several retrospective, nonrandomized studies that reported lower early and late mortality in patients who had undergone [annuloplasty] rather than MVR,” Dr. Raanani said. In those nonrandomized studies, the MVR patients were older with and sicker – “factors that are difficult to adjust or control.”
Dr. Fino and colleagues’ findings are “in accord” with other recent studies that question the universal superiority of annuloplasty over MVR in terms of hemodynamics and outcome, Dr. Raanani noted. Their study and the recent report on the Cardiothoracic Surgical Trials Network study (N. Engl. J. Med. 2014 Jan. 2 370:23-32) raise questions about the belief that annuloplasty is the optimal treatment for all types of patients with ischemic mitral regurgitation.
“The answer is probably no,” Dr. Raanani said. “For now, there is no one single procedure that is suitable for all.” Not all patients with ischemic mitral regurgitation are the same, and each must be treated individually. “We are close to the point where there is sufficient accumulated data to provide comprehensive imaging, stratify patients, and cater to individual surgical treatment,” Dr. Raanani said.
Dr. Raanani is a surgeon in the department of cardiac surgery at the Sheba Medical Center, Ramat-Gan, Israel.
Although mitral valve annuloplasty is the most common procedure for treatment of ischemic mitral regurgitation, surgeons had only been concerned that this procedure resulted in significant rates of recurrence of mitral regurgitation (MR), Dr. Ehud Raanani said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.038) . He noted that the study by Dr. Carlo Fino and colleagues elaborates on a body of evidence that suggests concerns about restrictive annuloplasty are going beyond MR recurrence.
The idea that annuloplasty is always superior to mitral valve replacement (MVR) “was no more than conjecture based on weak evidence from several retrospective, nonrandomized studies that reported lower early and late mortality in patients who had undergone [annuloplasty] rather than MVR,” Dr. Raanani said. In those nonrandomized studies, the MVR patients were older with and sicker – “factors that are difficult to adjust or control.”
Dr. Fino and colleagues’ findings are “in accord” with other recent studies that question the universal superiority of annuloplasty over MVR in terms of hemodynamics and outcome, Dr. Raanani noted. Their study and the recent report on the Cardiothoracic Surgical Trials Network study (N. Engl. J. Med. 2014 Jan. 2 370:23-32) raise questions about the belief that annuloplasty is the optimal treatment for all types of patients with ischemic mitral regurgitation.
“The answer is probably no,” Dr. Raanani said. “For now, there is no one single procedure that is suitable for all.” Not all patients with ischemic mitral regurgitation are the same, and each must be treated individually. “We are close to the point where there is sufficient accumulated data to provide comprehensive imaging, stratify patients, and cater to individual surgical treatment,” Dr. Raanani said.
Dr. Raanani is a surgeon in the department of cardiac surgery at the Sheba Medical Center, Ramat-Gan, Israel.
Individuals with chronic ischemic mitral regurgitation who undergo mitral valve replacement show significantly superior exercise performance up to almost 3½ years after the operation when compared with those who have restrictive mitral valve annuloplasty, according to a study in the June issue of the Journal of Cardiovascular Surgery. (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.003]).
Doctors at three institutions in France, Italy, and the United Kingdom set out to predict what factors determined long-term functional capacity in patients with chronic ischemic mitral regurgitation (CIMR) who had either mitral valve replacement (MVR) or annuloplasty. They performed a retrospective analysis of 121 patients with significant chronic mitral regurgitation, 62 of whom had restrictive mitral valve annuloplasty and 59 of whom underwent MVR between 2005 and 2011. All the subjects had a resting echocardiography and a 6-minute treadmill test before their procedures and again at an average of 41 months afterwards. The MVR group walked an average of 37 meters farther at the postoperative stress test, whereas the annuloplasty patients walked on average 24 meters less than their preoperative test.
“The most important finding of this study is that, in patients with CIMR who underwent mitral valve surgery, the improvement in functional capacity at long-term follow-up is mainly related to the type of treatment and to the mitral valve hemodynamic performance, as expressed by changes in IEOA [indexed effective orifice area] during exercise,” reported lead author Dr. Carlo Fino of the Bristol (England) Heart Institute and Pope John XXIII Hospital in Bergamo, Italy, and his colleagues. Investigators from Hospital Dupuytren in Limoges, France, also participated.
The study noted inconclusive results of previous reports of patients treated for mitral regurgitation: the Cardiothoracic Surgical Trials Network study that showed similar 1-year outcomes among patients who had either MVR or annuloplasty (N. Engl. J. Med. 2014;370:23-32) ; an earlier study that showed annuloplasty patients may develop functional mitral stenosis with decreasing functional capacity (J. Am. Coll. Cardiol. 2008;51:1692-1701); and Dr. Fino and colleagues’ previous work that showed worse hemodynamics in annuloplasty patients, compared with MVR counterparts (J. Thorac. Cardiovasc. Surg. 2014;148:447-53).
Other comparative measures the latest study evaluated were: change in exercise indexed effective orifice area, increasing from 1.3 to 1.5 cm2/m2 in the MVR group vs. 1.1 to 1.2 cm2/m2 in the annuloplasty group; change in mean mitral gradients from rest to exercise, which increased significantly in both groups – from 4.3 to 9 mm Hg in the replacement group and 4.4 to 11 mm Hg in the annuloplasty group; postoperative cardiovascular events – 8% in the MVR group and 21% in the annuloplasty population; and follow-up survival – 88% for MVR vs. 83% for annuloplasty.
The annuloplasty patients received either a Carpentier-Edwards Physio ring (71%) or Carpentier-Edwards Classic ring (29%); Edwards Lifesciences. The MVR group received either a biological or mechanical prosthesis, although the study did not report how many of each. All patients had associated coronary bypass grafting surgery and all achieved complete revascularization. The MVR and annuloplasty groups were similar in terms of demographics and cardiac function, although a higher percentage of patients in the annuloplasty group had severe mitral regurgitation preoperatively – 41% vs. 32% in the MVR group.
Procedures like annuloplasty that aim to restore ventricular geometry or target the subvalvular mechanism “seem to be promising but they require further scientific evidence,” Dr. Fino and his coauthors said. They suggested that until 24-month results from the Cardiothoracic Surgical Trials Network are available, MVR with chordal sparing might be a “reliable option” for patients with chronic ischemic mitral regurgitation.
The authors had no disclosures.
Individuals with chronic ischemic mitral regurgitation who undergo mitral valve replacement show significantly superior exercise performance up to almost 3½ years after the operation when compared with those who have restrictive mitral valve annuloplasty, according to a study in the June issue of the Journal of Cardiovascular Surgery. (J. Thorac. Cardiovasc. Surg. 2015 [doi:10.1016/j.jtcvs.2015.03.003]).
Doctors at three institutions in France, Italy, and the United Kingdom set out to predict what factors determined long-term functional capacity in patients with chronic ischemic mitral regurgitation (CIMR) who had either mitral valve replacement (MVR) or annuloplasty. They performed a retrospective analysis of 121 patients with significant chronic mitral regurgitation, 62 of whom had restrictive mitral valve annuloplasty and 59 of whom underwent MVR between 2005 and 2011. All the subjects had a resting echocardiography and a 6-minute treadmill test before their procedures and again at an average of 41 months afterwards. The MVR group walked an average of 37 meters farther at the postoperative stress test, whereas the annuloplasty patients walked on average 24 meters less than their preoperative test.
“The most important finding of this study is that, in patients with CIMR who underwent mitral valve surgery, the improvement in functional capacity at long-term follow-up is mainly related to the type of treatment and to the mitral valve hemodynamic performance, as expressed by changes in IEOA [indexed effective orifice area] during exercise,” reported lead author Dr. Carlo Fino of the Bristol (England) Heart Institute and Pope John XXIII Hospital in Bergamo, Italy, and his colleagues. Investigators from Hospital Dupuytren in Limoges, France, also participated.
The study noted inconclusive results of previous reports of patients treated for mitral regurgitation: the Cardiothoracic Surgical Trials Network study that showed similar 1-year outcomes among patients who had either MVR or annuloplasty (N. Engl. J. Med. 2014;370:23-32) ; an earlier study that showed annuloplasty patients may develop functional mitral stenosis with decreasing functional capacity (J. Am. Coll. Cardiol. 2008;51:1692-1701); and Dr. Fino and colleagues’ previous work that showed worse hemodynamics in annuloplasty patients, compared with MVR counterparts (J. Thorac. Cardiovasc. Surg. 2014;148:447-53).
Other comparative measures the latest study evaluated were: change in exercise indexed effective orifice area, increasing from 1.3 to 1.5 cm2/m2 in the MVR group vs. 1.1 to 1.2 cm2/m2 in the annuloplasty group; change in mean mitral gradients from rest to exercise, which increased significantly in both groups – from 4.3 to 9 mm Hg in the replacement group and 4.4 to 11 mm Hg in the annuloplasty group; postoperative cardiovascular events – 8% in the MVR group and 21% in the annuloplasty population; and follow-up survival – 88% for MVR vs. 83% for annuloplasty.
The annuloplasty patients received either a Carpentier-Edwards Physio ring (71%) or Carpentier-Edwards Classic ring (29%); Edwards Lifesciences. The MVR group received either a biological or mechanical prosthesis, although the study did not report how many of each. All patients had associated coronary bypass grafting surgery and all achieved complete revascularization. The MVR and annuloplasty groups were similar in terms of demographics and cardiac function, although a higher percentage of patients in the annuloplasty group had severe mitral regurgitation preoperatively – 41% vs. 32% in the MVR group.
Procedures like annuloplasty that aim to restore ventricular geometry or target the subvalvular mechanism “seem to be promising but they require further scientific evidence,” Dr. Fino and his coauthors said. They suggested that until 24-month results from the Cardiothoracic Surgical Trials Network are available, MVR with chordal sparing might be a “reliable option” for patients with chronic ischemic mitral regurgitation.
The authors had no disclosures.
Key clinical point: Mitral valve replacement seems to be associated with better exercise hemodynamics than restrictive annuloplasty in patients with preoperative chronic ischemic mitral regurgitation.
Major finding: Individuals who underwent mitral valve replacement improved their performance on the walking stress test 3 years after surgery while those in the annuloplasty group actually did worse.
Data source: Retrospective analysis of 121 patients with significant chronic ischemic mitral regurgitation who underwent either mitral valve replacement (n=59) or restrictive mitral valve annuloplasty (n=62).
Disclosures: The study authors had no conflicts to disclose.
The ‘threats and obstacles’ facing TMVR
NEW YORK – What if correcting secondary mitral regurgitation doesn’t improve patients’ lives or helps them live longer? What if results of the COAPT trial of the MitraClip (Abbott Vascular) repair for mitral regurgitation are negative or inconclusive? What if transcatheter mitral valve repair works too well?
The answers to these questions could determine the future landscape of transcatheter mitral valve replacement (TMVR) for mitral regurgitation (MR) and the prosthetics in various stages of clinical and preclinical investigation, Dr. Michael Mack of Baylor University said at the 2015 Mitral Valve Conclave, which was sponsored by the American Association for Thoracic Surgery.

Dr. Mack reviewed the first four transcatheter mitral valve replacement devices approved for early feasibility studies in the United States, noting that “it has become a very crowded field very quickly,” especially when one considers that only between 20 and 50 TMVR procedures have been done worldwide up until now.
For the makers of the devices, it is becoming a potentially perilous field as well. Replacement, Dr. Mack said, does meet a “large clinical unmet need” in that it can completely correct mitral regurgitation better than valve repair.
“But what are the challenges for transcatheter mitral valve replacement and why isn’t this going to be the same as TAVR (transcatheter aortic valve replacement) all over again?” he said. “Unlike aortic stenosis, there is not a single cause of mitral regurgitation. In addition, it has never even been definitively proven that correcting MR helps prolong survival and improve quality of life.”
Another obstacle for TMVR is that delivery of the device into the mitral valve is more complex than doing so in the aortic valve. “The seating and the anchoring of the valve is more complex,” Dr. Mack said. “Based on the profile of the device, left ventricular outflow tract obstruction can be an issue, and perivalvular leak may carry more import here because mitral perivalvular leaks have the potential to cause hemololysis.”
He reviewed the four systems cleared for early feasibility studies.
CardiAQ (CardiAQ Valve Technologies), a porcine pericardial valve, has been implanted in eight patients worldwide and last month received Food and Drug Administration (FDA) approval for early feasibility study in 20 U.S. patients: 10 by a transfemoral approach and 10 by a transapical approach.
Tendyne Bioprosthetic Mitral Valve (Tendyne Holdings), a trileaflet porcine pericardium, also has been implanted in eight patients worldwide and was used for the first time in the United States last month by Dr. Wes Pederson and colleagues at the Minneapolis Heart Institute.
FORTIS (Edwards Lifesciences), a bovine pericardium valve, has been implanted in early feasibility trials in Europe and has been approved for an early feasibility trial of 15 patients in the United States.
Tiara (Neovasc), a D-shaped bovine pericardium valve, received FDA approval last year for the TIARA-I early feasibility trial in the United States (NCT02276547). The trial will enroll up to 30 patients worldwide.
At least five other TMVR devices are in preclinical studies, Dr. Mack said. These emerging devices face “threats and obstacles” as they move through the pipeline – a number of “what ifs,” Dr. Mack said.
“What if you can’t prove that correcting secondary mitral regurgitation makes a difference? What are the repercussions of the COAPT Trial (NCT01626079) of the MitraClip if it is positive and shows that correcting mitral regurgitation does make a difference? Does completely correcting mitral regurgitation then really make a difference? What if transcatheter mitral valve repair works too well?” (COAPT stands for Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation). “With the excellent safety profile of MitraClip, it may be hard to justify TMVR,” he said.
Dr. Mack noted that MitraClip for mitral valve repair has “a superb safety profile.” He added, “How do you choose what patients should be treated by a mitral valve replacement vs. a MitraClip by a transfemoral venous approach that enables them to go home the next day?”
The early feasibility trials of TMVR devices may point a way to answers.
Dr. Mack has received research grants from Edwards Lifesciences. He is a principal investigator in the ongoing COAPT Trial, which is sponsored by EVALVE with the collaboration of Abbott Vascular.
NEW YORK – What if correcting secondary mitral regurgitation doesn’t improve patients’ lives or helps them live longer? What if results of the COAPT trial of the MitraClip (Abbott Vascular) repair for mitral regurgitation are negative or inconclusive? What if transcatheter mitral valve repair works too well?
The answers to these questions could determine the future landscape of transcatheter mitral valve replacement (TMVR) for mitral regurgitation (MR) and the prosthetics in various stages of clinical and preclinical investigation, Dr. Michael Mack of Baylor University said at the 2015 Mitral Valve Conclave, which was sponsored by the American Association for Thoracic Surgery.
Dr. Mack reviewed the first four transcatheter mitral valve replacement devices approved for early feasibility studies in the United States, noting that “it has become a very crowded field very quickly,” especially when one considers that only between 20 and 50 TMVR procedures have been done worldwide up until now.
For the makers of the devices, it is becoming a potentially perilous field as well. Replacement, Dr. Mack said, does meet a “large clinical unmet need” in that it can completely correct mitral regurgitation better than valve repair.
“But what are the challenges for transcatheter mitral valve replacement and why isn’t this going to be the same as TAVR (transcatheter aortic valve replacement) all over again?” he said. “Unlike aortic stenosis, there is not a single cause of mitral regurgitation. In addition, it has never even been definitively proven that correcting MR helps prolong survival and improve quality of life.”
Another obstacle for TMVR is that delivery of the device into the mitral valve is more complex than doing so in the aortic valve. “The seating and the anchoring of the valve is more complex,” Dr. Mack said. “Based on the profile of the device, left ventricular outflow tract obstruction can be an issue, and perivalvular leak may carry more import here because mitral perivalvular leaks have the potential to cause hemololysis.”
He reviewed the four systems cleared for early feasibility studies.
CardiAQ (CardiAQ Valve Technologies), a porcine pericardial valve, has been implanted in eight patients worldwide and last month received Food and Drug Administration (FDA) approval for early feasibility study in 20 U.S. patients: 10 by a transfemoral approach and 10 by a transapical approach.
Tendyne Bioprosthetic Mitral Valve (Tendyne Holdings), a trileaflet porcine pericardium, also has been implanted in eight patients worldwide and was used for the first time in the United States last month by Dr. Wes Pederson and colleagues at the Minneapolis Heart Institute.
FORTIS (Edwards Lifesciences), a bovine pericardium valve, has been implanted in early feasibility trials in Europe and has been approved for an early feasibility trial of 15 patients in the United States.
Tiara (Neovasc), a D-shaped bovine pericardium valve, received FDA approval last year for the TIARA-I early feasibility trial in the United States (NCT02276547). The trial will enroll up to 30 patients worldwide.
At least five other TMVR devices are in preclinical studies, Dr. Mack said. These emerging devices face “threats and obstacles” as they move through the pipeline – a number of “what ifs,” Dr. Mack said.
“What if you can’t prove that correcting secondary mitral regurgitation makes a difference? What are the repercussions of the COAPT Trial (NCT01626079) of the MitraClip if it is positive and shows that correcting mitral regurgitation does make a difference? Does completely correcting mitral regurgitation then really make a difference? What if transcatheter mitral valve repair works too well?” (COAPT stands for Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation). “With the excellent safety profile of MitraClip, it may be hard to justify TMVR,” he said.
Dr. Mack noted that MitraClip for mitral valve repair has “a superb safety profile.” He added, “How do you choose what patients should be treated by a mitral valve replacement vs. a MitraClip by a transfemoral venous approach that enables them to go home the next day?”
The early feasibility trials of TMVR devices may point a way to answers.
Dr. Mack has received research grants from Edwards Lifesciences. He is a principal investigator in the ongoing COAPT Trial, which is sponsored by EVALVE with the collaboration of Abbott Vascular.
NEW YORK – What if correcting secondary mitral regurgitation doesn’t improve patients’ lives or helps them live longer? What if results of the COAPT trial of the MitraClip (Abbott Vascular) repair for mitral regurgitation are negative or inconclusive? What if transcatheter mitral valve repair works too well?
The answers to these questions could determine the future landscape of transcatheter mitral valve replacement (TMVR) for mitral regurgitation (MR) and the prosthetics in various stages of clinical and preclinical investigation, Dr. Michael Mack of Baylor University said at the 2015 Mitral Valve Conclave, which was sponsored by the American Association for Thoracic Surgery.
Dr. Mack reviewed the first four transcatheter mitral valve replacement devices approved for early feasibility studies in the United States, noting that “it has become a very crowded field very quickly,” especially when one considers that only between 20 and 50 TMVR procedures have been done worldwide up until now.
For the makers of the devices, it is becoming a potentially perilous field as well. Replacement, Dr. Mack said, does meet a “large clinical unmet need” in that it can completely correct mitral regurgitation better than valve repair.
“But what are the challenges for transcatheter mitral valve replacement and why isn’t this going to be the same as TAVR (transcatheter aortic valve replacement) all over again?” he said. “Unlike aortic stenosis, there is not a single cause of mitral regurgitation. In addition, it has never even been definitively proven that correcting MR helps prolong survival and improve quality of life.”
Another obstacle for TMVR is that delivery of the device into the mitral valve is more complex than doing so in the aortic valve. “The seating and the anchoring of the valve is more complex,” Dr. Mack said. “Based on the profile of the device, left ventricular outflow tract obstruction can be an issue, and perivalvular leak may carry more import here because mitral perivalvular leaks have the potential to cause hemololysis.”
He reviewed the four systems cleared for early feasibility studies.
CardiAQ (CardiAQ Valve Technologies), a porcine pericardial valve, has been implanted in eight patients worldwide and last month received Food and Drug Administration (FDA) approval for early feasibility study in 20 U.S. patients: 10 by a transfemoral approach and 10 by a transapical approach.
Tendyne Bioprosthetic Mitral Valve (Tendyne Holdings), a trileaflet porcine pericardium, also has been implanted in eight patients worldwide and was used for the first time in the United States last month by Dr. Wes Pederson and colleagues at the Minneapolis Heart Institute.
FORTIS (Edwards Lifesciences), a bovine pericardium valve, has been implanted in early feasibility trials in Europe and has been approved for an early feasibility trial of 15 patients in the United States.
Tiara (Neovasc), a D-shaped bovine pericardium valve, received FDA approval last year for the TIARA-I early feasibility trial in the United States (NCT02276547). The trial will enroll up to 30 patients worldwide.
At least five other TMVR devices are in preclinical studies, Dr. Mack said. These emerging devices face “threats and obstacles” as they move through the pipeline – a number of “what ifs,” Dr. Mack said.
“What if you can’t prove that correcting secondary mitral regurgitation makes a difference? What are the repercussions of the COAPT Trial (NCT01626079) of the MitraClip if it is positive and shows that correcting mitral regurgitation does make a difference? Does completely correcting mitral regurgitation then really make a difference? What if transcatheter mitral valve repair works too well?” (COAPT stands for Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation). “With the excellent safety profile of MitraClip, it may be hard to justify TMVR,” he said.
Dr. Mack noted that MitraClip for mitral valve repair has “a superb safety profile.” He added, “How do you choose what patients should be treated by a mitral valve replacement vs. a MitraClip by a transfemoral venous approach that enables them to go home the next day?”
The early feasibility trials of TMVR devices may point a way to answers.
Dr. Mack has received research grants from Edwards Lifesciences. He is a principal investigator in the ongoing COAPT Trial, which is sponsored by EVALVE with the collaboration of Abbott Vascular.
EXPERT ANALYSIS FROM THE 2015 MITRAL VALVE CONCLAVE

Cardiac surgeons defy guidelines for severe disease
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).

|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).
|
|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Gathering evidence over recent years has shown that multidisciplinary teams can improve overall outcomes in many clinical scenarios, Dr. M. Sertac Cicek said in his commentary (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.12.008]). He cited a 2012 study that showed an 18% lower mortality at 5 years when multidisciplinary teams got involved in the treatment of breast cancer, compared with cases that did not involve team consultation (BMJ 2012;344:e2718).
|
|
Dr. M. Sertac Cicek |
Cardiovascular disease is a specialty that demands teamwork, but controversy still surrounds the role of surgery vs. PCI for patients with severe coronary disease, despite the evidence supporting CABG as the “gold standard,” Dr. Cicek said. The data presented by Dr. Yates and his colleagues, Dr. Cicek said, “simply confirm once again how far we are away from providing the optimal care to our patients, raising the question: ‘Are guidelines there to be disrespected?’ ”
A key factor in implementing the multidisciplinary approach involves educating patients and accepting them as members of the heart team during decision-making, Dr. Cicek noted. “It seems increasingly evident that multidisciplinary teams clearly strengthen our ability to provide higher quality and more efficient care; so much so that it may not come as surprise to anyone in the practice if in the very near future practicing ‘medicine without teamwork’ were declared and added to the Seven [Social] Sins of Mahatma Gandhi as the eighth [social] sin,” Dr. Cicek wrote.
Dr. Cicek is professor of cardiovascular surgery at the Anadolu Medical Center in Kocaeli, Turkey.
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
Although expert committees spend hours developing guidelines for best practices, clinicians on the front line of care can be somewhat hesitant to adopt them, as a recent study evaluating the use of guidelines for treatment of heart attack patients at three major cardiothoracic centers in London revealed.
The study, published in the Journal of Thoracic and Cardiovascular Surgery (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2014.10.110]) , found that surgeons more often than not flaunted the Joint European Society of Cardiology and European Association for Cardiothoracic Surgery (ESC/EACTS) guidelines that call for a multidisciplinary “Heart Team” to discuss each case of severe coronary artery disease before treatment.
The investigators looked at January-to-June periods in 2010 (before the guidelines) and 2012 (after the guidelines had been in place for 18 months) and found identical 17% rates of multidisciplinary team discussions before treatment. Both samples involved patients who had percutaneous coronary interventions (PCI). The 621 cases in the 2010 sample and 686 cases in the 2012 group comprise “a significant proportion of the coronary revascularization workload” of the National Health Service (NHS) hospitals in London, Dr. Martin T. Yates of St. George’s Hospital, University of London, and coauthors reported. The other participating centers were Barts Health NHS Trust and King College Hospital.
The ESC/EACTS guidelines (Eur. Heart J. 2010;31:2501-55) determined that PCI at the same catheterization session as the diagnostic angiogram and elective PCI are inappropriate for patients with severe coronary artery disease, defined as proximal left-anterior descending, left-main stem or three-vessel disease. The guidelines state that these patients should be considered for surgery first.
In a previous single-center study a year after the guidelines were adopted, Dr. Yates and his colleagues reported that almost a third of all elective PCI (29%) were carried out on patients who may have benefited more from coronary artery bypass grafting (CABG) (J. Thorac. Cardiovasc. Surg. 2014;147:606-10). Of those cases, the multidisciplinary team again discussed only 17% of cases before PCI.
Dr. Yates and his colleagues intimated that the rush to PCI might be circumventing in-depth discussions about more appropriate CABG for patients with severe coronary artery disease. “Furthermore, despite the guidelines suggesting that ad hoc PCI is inappropriate in the elective setting, this practice continues,” they said. “Although this is convenient for the patient and more cost effective, it does not allow time for Heart Team discussions prior to intervention.”
In the current study, the 2010 group included 187 patients with severe coronary artery disease who had treatment without a multidisciplinary team consultation, and less than half (44%) achieved complete revascularization. The 2012 group included 225 patients with severe heart disease, and precisely half achieved complete revascularization.
In both groups, a considerable majority of patients with three-vessel disease had PCI without the multidisciplinary team discussion: 76% in 2010 and 64% in 2012.
Dr. Yates and his associates noted that this is not a problem specific to London cardiac centers. They cited variations in the use of PCI and CABG in a large study of the New York State Registry, which showed that only 53% of patients suitable for CABG, according to the American College of Cardiology/American Heart Association guidelines, actually had the procedure (Circulation 2010;121:267-75). They cited similar results in a Canadian study (CMAJ 2012;184;179-86).
One way to get cardiac surgeons to adhere to guidelines is to tie payment to treatment – an approach that may work better in the United States than in Canada or the United Kingdom. “This may be easier to implement in countries with payment linked to insurance systems as opposed to those with a nationalized service,” Dr. Yates and his associates wrote.
The authors reported no financial disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Cardiac surgeons at three London hospitals complied poorly with clinical guidelines for managing patients with severe coronary artery disease.
Major finding: Only 17% of patients with severe coronary artery disease were subjects of multidisciplinary discussions before treatment in periods before and after treatment guidelines, and most were likely to have percutaneous coronary intervention rather than the recommended surgical revascularization.
Data source: Surgical patients were from the Central Cardiac Audit Database; PCI patients were from the British Cardiovascular Intervention Society database.
Disclosures: The authors reported no financial disclosures.

AATS: Simplified mitral valve repair effective in children with Marfan’s
NEW YORK – A simplified surgical approach that uses an adult-sized, basic ring annuloplasty with a complete edge-to-edge leaflet repair has been found to yield good outcomes in a group of children with connective tissue disorders like Marfan syndrome and Loeys-Dietz syndrome and mitral regurgitation, based on an evaluation of the technique at four centers.
Cardiac surgeons employed the simplified operation in 18 patients under age 18 (median age 8.2 years) and found that after 2.4 years of follow-up, no patients required another operation for mitral regurgitation, reported Dr. Luca Vricella, pediatrics director, pediatric cardiac surgery and heart transplantation, John Hopkins University, Baltimore.
The patients underwent the simplified mitral valve repair at Johns Hopkins Pediatric Cardiac Surgery in Baltimore and Orlando; Duke University School of Medicine in Durham, N.C.; and University of Pavia Medical School in Italy.
These young patients can be challenging to operate on because of skeletal abnormalities and marginal pulmonary reserve, Dr. Vricella said at the meeting sponsored by the American Association for Thoracic Surgery. Of the 18 children in the study, 15 had Marfan syndrome, a genetic disorder that commonly affects the heart valves and aorta. “The most common mode of early presentation of mitral valve pathology, from a morphological standpoint, is that mitral regurgitation is often characterized as severe bileaflet prolapse and annular and left ventricular dilation,” Dr. Vricella said.
The simplified technique involves an approach through an atriotomy and placing an adult-sized annuloplasty ring in the valve. The next step is to place an Alfieri stitch, named for the Italian cardiac surgeon Dr. Ottavio Alfieri, with a braided suture in the middle of the valve, which opposes the leaflet “very effectively,” Dr. Vricella said.
In the study group, all 18 patients had severe bileaflet prolapse and severe mitral regurgitation of grade 4 or higher, but all patients also had normal ejection fraction, Dr. Vricella said. One infant was being considered for a heart transplant.
The operation was achieved in isolation in less than an hour. Five patients underwent simultaneous valve-sparing aortic root replacement, one of whom died (one of two deaths in a larger 300-plus group of both adults and children who had valve-sparing aortic root repair). No other complications were reported among the 18-patient group. Median length of stay in the hospital was 9 days.
After the operation, all patients had significant reductions in mitral regurgitation. After 2.4 years, 94% of survivors maintained mild regurgitation or better without stenosis. Entering the study, the median left ventricular end-diastolic diameter (LVEDD) score of all patients was 4.9 (range 2.1-11.9), but at 2.4 years after the operation the median LVEDD score had regressed to 1.3 (range –0.51-4.3).
“In pediatric patients with severe mitral regurgitation and connective tissue disorders, a simplified repair can result in intermediate-term competency without systolic anterior motion and with no mitral stenosis,” Dr. Vricella said. “We’ve been pleasantly surprised in seeing this reduction in left ventricular enlargement, and particularly in this group of patients in which you may need to have a longer plant time, simplifying things so you don’t have to intervene on the subvalvular annuloplasty.”
NEW YORK – A simplified surgical approach that uses an adult-sized, basic ring annuloplasty with a complete edge-to-edge leaflet repair has been found to yield good outcomes in a group of children with connective tissue disorders like Marfan syndrome and Loeys-Dietz syndrome and mitral regurgitation, based on an evaluation of the technique at four centers.
Cardiac surgeons employed the simplified operation in 18 patients under age 18 (median age 8.2 years) and found that after 2.4 years of follow-up, no patients required another operation for mitral regurgitation, reported Dr. Luca Vricella, pediatrics director, pediatric cardiac surgery and heart transplantation, John Hopkins University, Baltimore.
The patients underwent the simplified mitral valve repair at Johns Hopkins Pediatric Cardiac Surgery in Baltimore and Orlando; Duke University School of Medicine in Durham, N.C.; and University of Pavia Medical School in Italy.
These young patients can be challenging to operate on because of skeletal abnormalities and marginal pulmonary reserve, Dr. Vricella said at the meeting sponsored by the American Association for Thoracic Surgery. Of the 18 children in the study, 15 had Marfan syndrome, a genetic disorder that commonly affects the heart valves and aorta. “The most common mode of early presentation of mitral valve pathology, from a morphological standpoint, is that mitral regurgitation is often characterized as severe bileaflet prolapse and annular and left ventricular dilation,” Dr. Vricella said.
The simplified technique involves an approach through an atriotomy and placing an adult-sized annuloplasty ring in the valve. The next step is to place an Alfieri stitch, named for the Italian cardiac surgeon Dr. Ottavio Alfieri, with a braided suture in the middle of the valve, which opposes the leaflet “very effectively,” Dr. Vricella said.
In the study group, all 18 patients had severe bileaflet prolapse and severe mitral regurgitation of grade 4 or higher, but all patients also had normal ejection fraction, Dr. Vricella said. One infant was being considered for a heart transplant.
The operation was achieved in isolation in less than an hour. Five patients underwent simultaneous valve-sparing aortic root replacement, one of whom died (one of two deaths in a larger 300-plus group of both adults and children who had valve-sparing aortic root repair). No other complications were reported among the 18-patient group. Median length of stay in the hospital was 9 days.
After the operation, all patients had significant reductions in mitral regurgitation. After 2.4 years, 94% of survivors maintained mild regurgitation or better without stenosis. Entering the study, the median left ventricular end-diastolic diameter (LVEDD) score of all patients was 4.9 (range 2.1-11.9), but at 2.4 years after the operation the median LVEDD score had regressed to 1.3 (range –0.51-4.3).
“In pediatric patients with severe mitral regurgitation and connective tissue disorders, a simplified repair can result in intermediate-term competency without systolic anterior motion and with no mitral stenosis,” Dr. Vricella said. “We’ve been pleasantly surprised in seeing this reduction in left ventricular enlargement, and particularly in this group of patients in which you may need to have a longer plant time, simplifying things so you don’t have to intervene on the subvalvular annuloplasty.”
NEW YORK – A simplified surgical approach that uses an adult-sized, basic ring annuloplasty with a complete edge-to-edge leaflet repair has been found to yield good outcomes in a group of children with connective tissue disorders like Marfan syndrome and Loeys-Dietz syndrome and mitral regurgitation, based on an evaluation of the technique at four centers.
Cardiac surgeons employed the simplified operation in 18 patients under age 18 (median age 8.2 years) and found that after 2.4 years of follow-up, no patients required another operation for mitral regurgitation, reported Dr. Luca Vricella, pediatrics director, pediatric cardiac surgery and heart transplantation, John Hopkins University, Baltimore.
The patients underwent the simplified mitral valve repair at Johns Hopkins Pediatric Cardiac Surgery in Baltimore and Orlando; Duke University School of Medicine in Durham, N.C.; and University of Pavia Medical School in Italy.
These young patients can be challenging to operate on because of skeletal abnormalities and marginal pulmonary reserve, Dr. Vricella said at the meeting sponsored by the American Association for Thoracic Surgery. Of the 18 children in the study, 15 had Marfan syndrome, a genetic disorder that commonly affects the heart valves and aorta. “The most common mode of early presentation of mitral valve pathology, from a morphological standpoint, is that mitral regurgitation is often characterized as severe bileaflet prolapse and annular and left ventricular dilation,” Dr. Vricella said.
The simplified technique involves an approach through an atriotomy and placing an adult-sized annuloplasty ring in the valve. The next step is to place an Alfieri stitch, named for the Italian cardiac surgeon Dr. Ottavio Alfieri, with a braided suture in the middle of the valve, which opposes the leaflet “very effectively,” Dr. Vricella said.
In the study group, all 18 patients had severe bileaflet prolapse and severe mitral regurgitation of grade 4 or higher, but all patients also had normal ejection fraction, Dr. Vricella said. One infant was being considered for a heart transplant.
The operation was achieved in isolation in less than an hour. Five patients underwent simultaneous valve-sparing aortic root replacement, one of whom died (one of two deaths in a larger 300-plus group of both adults and children who had valve-sparing aortic root repair). No other complications were reported among the 18-patient group. Median length of stay in the hospital was 9 days.
After the operation, all patients had significant reductions in mitral regurgitation. After 2.4 years, 94% of survivors maintained mild regurgitation or better without stenosis. Entering the study, the median left ventricular end-diastolic diameter (LVEDD) score of all patients was 4.9 (range 2.1-11.9), but at 2.4 years after the operation the median LVEDD score had regressed to 1.3 (range –0.51-4.3).
“In pediatric patients with severe mitral regurgitation and connective tissue disorders, a simplified repair can result in intermediate-term competency without systolic anterior motion and with no mitral stenosis,” Dr. Vricella said. “We’ve been pleasantly surprised in seeing this reduction in left ventricular enlargement, and particularly in this group of patients in which you may need to have a longer plant time, simplifying things so you don’t have to intervene on the subvalvular annuloplasty.”
AT THE 2015 MITRAL VALVE CONCLAVE
Key clinical point: A simplified approach for mitral valve repair resulted in good outcomes in a group of children with connective tissue disorders.
Major finding: All 18 children in the study avoided reoperation after mitral valve repair.
Data source: A small trial involving 18 patients at four hospitals.
Disclosures: Dr. Vricella had no relevant relationships to disclose.
Three-dimensional models show superiority of nanoparticles in mesothelioma
Malignant mesothelioma poses a significant challenge for clinicians because of its ability to resist chemotherapy, but the use of three-dimensional tumor spheroid models has shown that local administration of paclitaxel in a nanoparticle platform achieved better tumor penetration than conventional paclitaxel therapy, investigators reported. The study is in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Hongyi Lei of Brigham and Women’s Hospital, Boston, and his colleagues used the in vitro mesothelioma spheroid model because two-dimensional in vitro monolayer cell culture experiments do not replicate the superior efficacy of paclitaxel-loaded expansile nanoparticles (Pax-eNPs), suggesting that Pax-eNPs utilize a unique drug delivery mechanism.

The study observed that spheroids treated with Pax-eNP showed increased drug penetration and a 38-fold higher intraspheroidal drug concentration at 24 hours than that of paclitaxel dissolved in Cremophor EL/ethanol (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.02.020]).
The researchers said their findings showed that three-dimensional spheroid models “are valuable tools for investigating cytotoxic mechanisms and nanoparticle-tumor interactions, particularly given the costs and limitations of in vivo animal studies.” Their findings were first presented at the 94th Annual Meeting of the American Association of Thoracic Surgery last year in Toronto.
Despite advances of nanoparticle-based drug delivery systems, difficulties in evaluating the effectiveness of these drugs in local chemotherapy have hindered their adoption in the clinic. Studies of the same agent utilizing in vitro vs. in vivo methods have shown conflicting results.
The observation that Pax-eNP treatment of intraperitoneal mesothelioma significantly improved survival in lab animals in vivo compared to conventional paclitaxel led to the use of the three-dimensional spheroid model. Dr. Lei and colleagues called this revelation “striking” because Pax-eNP exposure of the identical mesothelioma tumor cells plated as a two-dimensional monolayer in vitro demonstrated equal or worse results. “This suggested that eNP may be more effective at penetration and/or persistence within multicellular tumors and led to the use of a 3-D tumor spheroid mode,” they said.
“Given the high cost and limitations of in vivo animal studies, spheroid models may present a clinically relevant platform for screening novel pharmaceuticals and unique drug-delivery systems during the preclinical phase,” the researchers indicated.
They also investigated spheroid cytotoxicity in a clinic-like setting following a 4-hour, high-dose (1,000 ng/mL) paclitaxel exposure via conventional and eNP vehicles. They found that Pax-eNP exposure led to greater tumor cytotoxicity at 72 hours, and that cytotoxicity continued seven days later because Pax-eNPs rapidly enter the tumor spheroid and remain intracellular, slowly releasing the drug.
“The prolonged drug release mechanism that pH-triggered Pax-eNP uses appears to be unique, leading to markedly higher intraspheroidal drug delivery, prolonged intratumoral drug release and superior antitumor efficacy,” the investigators concluded. The authors had no disclosures.
“While this study contributes greatly to the body of knowledge available regarding potential treatment strategies for malignant mesothelioma, one might argue that the more important impact of this paper relates to the successful implementation of an unconventional tumor model,” Dr. Mara B. Antonoff wrote in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.02.015].
The investigators’ earlier studies noted the limitations of the two-dimensional cell monolayer for in vitro experiments, but Dr. Antonoff acknowledged their quest for a solution that was more cost-effective than animal models and better approximated in vivo biological actions of the drug.

|
Dr. Mara B. Antonoff |
However, she noted the three-dimensional models “are not without limits, either.” Widespread adoption is limited because of the time and expertise involved in spheroid formation. “Nonetheless, it is clear that such models are a huge improvement over our current in vitro models,” she wrote.
Among the limits of the three-dimensional spheroid model she pointed out are that it lacks the multiple cell types typical in an actual tumor and quantitative assessment of the results can be difficult.
But the spheroid model does enhance the ability to screen novel drugs and drug-delivery systems, she wrote. “This timely and well-constructed study provides a foundation upon which we may build our knowledge of chemotherapeutic delivery mechanisms, while setting an outstanding example, and perhaps a new standard, for in vitro methodology,” she wrote.
Dr. Antonoff is a clinical instructor at University of Texas M.D. Anderson Cancer Center in Houston.
“While this study contributes greatly to the body of knowledge available regarding potential treatment strategies for malignant mesothelioma, one might argue that the more important impact of this paper relates to the successful implementation of an unconventional tumor model,” Dr. Mara B. Antonoff wrote in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.02.015].
The investigators’ earlier studies noted the limitations of the two-dimensional cell monolayer for in vitro experiments, but Dr. Antonoff acknowledged their quest for a solution that was more cost-effective than animal models and better approximated in vivo biological actions of the drug.
|
|
Dr. Mara B. Antonoff |
However, she noted the three-dimensional models “are not without limits, either.” Widespread adoption is limited because of the time and expertise involved in spheroid formation. “Nonetheless, it is clear that such models are a huge improvement over our current in vitro models,” she wrote.
Among the limits of the three-dimensional spheroid model she pointed out are that it lacks the multiple cell types typical in an actual tumor and quantitative assessment of the results can be difficult.
But the spheroid model does enhance the ability to screen novel drugs and drug-delivery systems, she wrote. “This timely and well-constructed study provides a foundation upon which we may build our knowledge of chemotherapeutic delivery mechanisms, while setting an outstanding example, and perhaps a new standard, for in vitro methodology,” she wrote.
Dr. Antonoff is a clinical instructor at University of Texas M.D. Anderson Cancer Center in Houston.
“While this study contributes greatly to the body of knowledge available regarding potential treatment strategies for malignant mesothelioma, one might argue that the more important impact of this paper relates to the successful implementation of an unconventional tumor model,” Dr. Mara B. Antonoff wrote in her invited commentary (J. Thorac. Cardiovasc. Surg. 2015 [doi: 10.1016/j.jtcvs.2015.02.015].
The investigators’ earlier studies noted the limitations of the two-dimensional cell monolayer for in vitro experiments, but Dr. Antonoff acknowledged their quest for a solution that was more cost-effective than animal models and better approximated in vivo biological actions of the drug.
|
|
Dr. Mara B. Antonoff |
However, she noted the three-dimensional models “are not without limits, either.” Widespread adoption is limited because of the time and expertise involved in spheroid formation. “Nonetheless, it is clear that such models are a huge improvement over our current in vitro models,” she wrote.
Among the limits of the three-dimensional spheroid model she pointed out are that it lacks the multiple cell types typical in an actual tumor and quantitative assessment of the results can be difficult.
But the spheroid model does enhance the ability to screen novel drugs and drug-delivery systems, she wrote. “This timely and well-constructed study provides a foundation upon which we may build our knowledge of chemotherapeutic delivery mechanisms, while setting an outstanding example, and perhaps a new standard, for in vitro methodology,” she wrote.
Dr. Antonoff is a clinical instructor at University of Texas M.D. Anderson Cancer Center in Houston.
Malignant mesothelioma poses a significant challenge for clinicians because of its ability to resist chemotherapy, but the use of three-dimensional tumor spheroid models has shown that local administration of paclitaxel in a nanoparticle platform achieved better tumor penetration than conventional paclitaxel therapy, investigators reported. The study is in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Hongyi Lei of Brigham and Women’s Hospital, Boston, and his colleagues used the in vitro mesothelioma spheroid model because two-dimensional in vitro monolayer cell culture experiments do not replicate the superior efficacy of paclitaxel-loaded expansile nanoparticles (Pax-eNPs), suggesting that Pax-eNPs utilize a unique drug delivery mechanism.
The study observed that spheroids treated with Pax-eNP showed increased drug penetration and a 38-fold higher intraspheroidal drug concentration at 24 hours than that of paclitaxel dissolved in Cremophor EL/ethanol (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.02.020]).
The researchers said their findings showed that three-dimensional spheroid models “are valuable tools for investigating cytotoxic mechanisms and nanoparticle-tumor interactions, particularly given the costs and limitations of in vivo animal studies.” Their findings were first presented at the 94th Annual Meeting of the American Association of Thoracic Surgery last year in Toronto.
Despite advances of nanoparticle-based drug delivery systems, difficulties in evaluating the effectiveness of these drugs in local chemotherapy have hindered their adoption in the clinic. Studies of the same agent utilizing in vitro vs. in vivo methods have shown conflicting results.
The observation that Pax-eNP treatment of intraperitoneal mesothelioma significantly improved survival in lab animals in vivo compared to conventional paclitaxel led to the use of the three-dimensional spheroid model. Dr. Lei and colleagues called this revelation “striking” because Pax-eNP exposure of the identical mesothelioma tumor cells plated as a two-dimensional monolayer in vitro demonstrated equal or worse results. “This suggested that eNP may be more effective at penetration and/or persistence within multicellular tumors and led to the use of a 3-D tumor spheroid mode,” they said.
“Given the high cost and limitations of in vivo animal studies, spheroid models may present a clinically relevant platform for screening novel pharmaceuticals and unique drug-delivery systems during the preclinical phase,” the researchers indicated.
They also investigated spheroid cytotoxicity in a clinic-like setting following a 4-hour, high-dose (1,000 ng/mL) paclitaxel exposure via conventional and eNP vehicles. They found that Pax-eNP exposure led to greater tumor cytotoxicity at 72 hours, and that cytotoxicity continued seven days later because Pax-eNPs rapidly enter the tumor spheroid and remain intracellular, slowly releasing the drug.
“The prolonged drug release mechanism that pH-triggered Pax-eNP uses appears to be unique, leading to markedly higher intraspheroidal drug delivery, prolonged intratumoral drug release and superior antitumor efficacy,” the investigators concluded. The authors had no disclosures.
Malignant mesothelioma poses a significant challenge for clinicians because of its ability to resist chemotherapy, but the use of three-dimensional tumor spheroid models has shown that local administration of paclitaxel in a nanoparticle platform achieved better tumor penetration than conventional paclitaxel therapy, investigators reported. The study is in the May issue of the Journal of Thoracic and Cardiovascular Surgery.
Dr. Hongyi Lei of Brigham and Women’s Hospital, Boston, and his colleagues used the in vitro mesothelioma spheroid model because two-dimensional in vitro monolayer cell culture experiments do not replicate the superior efficacy of paclitaxel-loaded expansile nanoparticles (Pax-eNPs), suggesting that Pax-eNPs utilize a unique drug delivery mechanism.
The study observed that spheroids treated with Pax-eNP showed increased drug penetration and a 38-fold higher intraspheroidal drug concentration at 24 hours than that of paclitaxel dissolved in Cremophor EL/ethanol (J. Thorac. Cardiovasc. Surg. 2014 [doi:10.1016/j.jtcvs.2015.02.020]).
The researchers said their findings showed that three-dimensional spheroid models “are valuable tools for investigating cytotoxic mechanisms and nanoparticle-tumor interactions, particularly given the costs and limitations of in vivo animal studies.” Their findings were first presented at the 94th Annual Meeting of the American Association of Thoracic Surgery last year in Toronto.
Despite advances of nanoparticle-based drug delivery systems, difficulties in evaluating the effectiveness of these drugs in local chemotherapy have hindered their adoption in the clinic. Studies of the same agent utilizing in vitro vs. in vivo methods have shown conflicting results.
The observation that Pax-eNP treatment of intraperitoneal mesothelioma significantly improved survival in lab animals in vivo compared to conventional paclitaxel led to the use of the three-dimensional spheroid model. Dr. Lei and colleagues called this revelation “striking” because Pax-eNP exposure of the identical mesothelioma tumor cells plated as a two-dimensional monolayer in vitro demonstrated equal or worse results. “This suggested that eNP may be more effective at penetration and/or persistence within multicellular tumors and led to the use of a 3-D tumor spheroid mode,” they said.
“Given the high cost and limitations of in vivo animal studies, spheroid models may present a clinically relevant platform for screening novel pharmaceuticals and unique drug-delivery systems during the preclinical phase,” the researchers indicated.
They also investigated spheroid cytotoxicity in a clinic-like setting following a 4-hour, high-dose (1,000 ng/mL) paclitaxel exposure via conventional and eNP vehicles. They found that Pax-eNP exposure led to greater tumor cytotoxicity at 72 hours, and that cytotoxicity continued seven days later because Pax-eNPs rapidly enter the tumor spheroid and remain intracellular, slowly releasing the drug.
“The prolonged drug release mechanism that pH-triggered Pax-eNP uses appears to be unique, leading to markedly higher intraspheroidal drug delivery, prolonged intratumoral drug release and superior antitumor efficacy,” the investigators concluded. The authors had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Three-dimensional spheroid models, as opposed to monolayer cell cultures, are valuable tools for predicting the efficacy of nanoparticle-tumor interactions in malignant mesothelioma.
Major finding: There was increased drug penetration and a 38-fold higher drug concentration 24 hours after human malignant mesothelioma spheroids were treated with paclitaxel-loaded expansile nanoparticles, compared to conventional drug delivery.
Data source: A study of a mesothelioma spheroid model comparing treatment with Pax-eNP and paclitaxel dissolved in Cremophor EL/ethanol.
Disclosures: This work was supported by the Brigham and Women’s Hospital International Mesothelioma Program, National Science Foundation and Boston University’s Nanomedicine Program and Cross-Disciplinary Training in Nanotechnology for Cancer, and the Zhujiang Hospital (Guangzhou, China) Scholarship Program. The authors had no relevant disclosures.