User login
Psoriasis associated with an increased risk of COVID-19 in real-world study
in patients, compared with those on topical therapy, a new study finds.
“Our study results suggest that psoriasis is an independent risk factor for COVID-19 illness,” study coauthor Jeffrey Liu, a medical student at the University of Southern California, Los Angeles, said in an interview after he presented the findings at the American Academy of Dermatology Virtual Meeting Experience. “And our findings are consistent with the hypothesis that certain systemic agents may confer a protective effect against COVID-19 illness.”
Mr. Liu and coinvestigators used a Symphony Health dataset to analyze the health records of 167,027 U.S. patients diagnosed with psoriasis and a control group of 1,002,162 patients. The participants, all at least 20 years old, had been treated for psoriasis or psoriatic arthritis from May 2019 through Jan. 1, 2020, and were tracked until Nov. 11, 2020.
The ages and races of peoples in the two groups were roughly similar. Overall, 55% were women and 75% were White, and their average age was 58 years. Type 2 diabetes was more common in the psoriasis group than the control group (23% vs. 16%), as was obesity (27% vs. 15%). Of the patients with psoriasis, 60% were on topical treatments, 19% were on oral therapies, and 22% were on biologic therapy, with only a few taking both oral and biologic therapies.
After adjustment for age and gender, patients with psoriasis were 33% more likely than the control group to develop COVID-19 (adjusted incidence rate ratio, 1.33; 95% confidence interval, 1.23-1.38; P < .0001).
In a separate analysis, the gap persisted after adjustment for demographics and comorbidities: Patients with psoriasis had a higher rate of COVID-19 infection vs. controls (adjusted odds ratio, 1.18; 95% CI, 1.13-1.23; P < .0001). Among all patients, non-White race, older age, and comorbidities were all linked to higher risk of COVID-19 (all P < .0001).
Psoriasis might make patients more vulnerable to COVID-19 because the presence of up-regulated genes in psoriatic skin “may lead to systemic hyperinflammation and sensitization of patients with psoriasis to proinflammatory cytokine storm,” Mr. Liu said. This, in turn, may trigger more severe symptomatic disease that requires medical treatment, he said.
Reduced risk, compared with topical therapies
After adjustment for age and gender, those treated with TNF-alpha inhibitors, methotrexate, and apremilast (Otezla) all had statistically lower risks of COVID-19 vs. those on topical therapy (aIRR, 0.82; 95% CI, 0.69-0.95; P < .0029 for TNF-alpha inhibitors; aIRR, 0.75; 95% CI, 0.67-0.86; P < .0001 for methotrexate; and aIRR, 0.69; 95% CI, 0.55-0.85; P < .0006 for apremilast).
Reduced risk held true for those in the separate analysis after adjustment for comorbidities and demographics (respectively, aOR, 0.87; 95% CI, 0.77-1.00; P < .0469; aOR, 0.81; 95% CI, 0.71-0.92; P < .0011; and aOR, 0.70; 95% CI, 0.57-0.87; P < .0014).
Apremilast and methotrexate may boost protection against COVID-19 by inhibiting the body’s production of cytokines, Mr. Liu said.
One message of the study is that “dermatologists should not be scared of prescribing biologics or oral therapies for psoriasis,” the study’s lead author Jashin J. Wu, MD, of the Dermatology Research and Education Foundation in Irvine, Calif., said in an interview.
However, the results on the effects of systemic therapies were not all positive. Interleukin (IL)–17 inhibitors were an outlier: After adjustment for age and gender, patients treated with this class of drugs were 36% more likely to develop COVID-19 than those on oral agents (aIRR, 1.36; 95% CI, 1.13-1.63; P < .0009).
Among patients on biologics, those taking IL-17 inhibitors had the highest risk of COVID-19, Mr. Liu said. “The risk was higher in this class regardless of reference group – general population, the topical cohort, and the oral cohort,” he said. “This may relate to the observation that this biologic class exerts more broad immunosuppressive effects on antiviral host immunity. Notably, large meta-estimates of pivotal trials have observed increased risk of respiratory tract infections for patients on IL-17 inhibitors.”
In an interview, Erica Dommasch, MD, MPH, of the department of dermatology at Beth Israel Deaconess Medical Center, Boston, cautioned that “the data from this study is very hard to interpret.”
It’s likely that some patients with psoriasis on systemic medications “may have been the most careful about limiting exposures,” she said. “Thus, it’s hard to account for behavioral changes in individuals that may have led to the decreased incidence in psoriasis in patients on systemic agents versus topical therapy alone.”
Patients with psoriasis may also be tested more often for COVID-19, and unmeasured comorbidities like chronic kidney disease may play a role too, she said. Still, she added, “it’s reassuring that the authors did not find an increased rate of COVID among psoriasis patients on systemic agents versus topicals alone.” And she agreed with Dr. Wu about the importance of treating psoriasis with therapy beyond topical treatments during the pandemic: “Providers should feel comfortable prescribing systemic medications to psoriasis patients when otherwise appropriate.”
As for the next steps, Dr. Wu said, “we will be exploring more about the prognosis of COVID-19 infection in psoriasis patients. In addition, we will be exploring the relationship of COVID-19 infection with other inflammatory skin diseases, such as atopic dermatitis.”
No study funding is reported. Dr. Wu discloses investigator, consultant, or speaker relationships with AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, Dr. Reddy’s Laboratories, Eli Lilly, Galderma, Janssen, LEO Pharma, Mindera, Novartis, Regeneron, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, Valeant Pharmaceuticals North America, and Zerigo Health. Mr. Liu and Dr. Dommasch have no disclosures.
in patients, compared with those on topical therapy, a new study finds.
“Our study results suggest that psoriasis is an independent risk factor for COVID-19 illness,” study coauthor Jeffrey Liu, a medical student at the University of Southern California, Los Angeles, said in an interview after he presented the findings at the American Academy of Dermatology Virtual Meeting Experience. “And our findings are consistent with the hypothesis that certain systemic agents may confer a protective effect against COVID-19 illness.”
Mr. Liu and coinvestigators used a Symphony Health dataset to analyze the health records of 167,027 U.S. patients diagnosed with psoriasis and a control group of 1,002,162 patients. The participants, all at least 20 years old, had been treated for psoriasis or psoriatic arthritis from May 2019 through Jan. 1, 2020, and were tracked until Nov. 11, 2020.
The ages and races of peoples in the two groups were roughly similar. Overall, 55% were women and 75% were White, and their average age was 58 years. Type 2 diabetes was more common in the psoriasis group than the control group (23% vs. 16%), as was obesity (27% vs. 15%). Of the patients with psoriasis, 60% were on topical treatments, 19% were on oral therapies, and 22% were on biologic therapy, with only a few taking both oral and biologic therapies.
After adjustment for age and gender, patients with psoriasis were 33% more likely than the control group to develop COVID-19 (adjusted incidence rate ratio, 1.33; 95% confidence interval, 1.23-1.38; P < .0001).
In a separate analysis, the gap persisted after adjustment for demographics and comorbidities: Patients with psoriasis had a higher rate of COVID-19 infection vs. controls (adjusted odds ratio, 1.18; 95% CI, 1.13-1.23; P < .0001). Among all patients, non-White race, older age, and comorbidities were all linked to higher risk of COVID-19 (all P < .0001).
Psoriasis might make patients more vulnerable to COVID-19 because the presence of up-regulated genes in psoriatic skin “may lead to systemic hyperinflammation and sensitization of patients with psoriasis to proinflammatory cytokine storm,” Mr. Liu said. This, in turn, may trigger more severe symptomatic disease that requires medical treatment, he said.
Reduced risk, compared with topical therapies
After adjustment for age and gender, those treated with TNF-alpha inhibitors, methotrexate, and apremilast (Otezla) all had statistically lower risks of COVID-19 vs. those on topical therapy (aIRR, 0.82; 95% CI, 0.69-0.95; P < .0029 for TNF-alpha inhibitors; aIRR, 0.75; 95% CI, 0.67-0.86; P < .0001 for methotrexate; and aIRR, 0.69; 95% CI, 0.55-0.85; P < .0006 for apremilast).
Reduced risk held true for those in the separate analysis after adjustment for comorbidities and demographics (respectively, aOR, 0.87; 95% CI, 0.77-1.00; P < .0469; aOR, 0.81; 95% CI, 0.71-0.92; P < .0011; and aOR, 0.70; 95% CI, 0.57-0.87; P < .0014).
Apremilast and methotrexate may boost protection against COVID-19 by inhibiting the body’s production of cytokines, Mr. Liu said.
One message of the study is that “dermatologists should not be scared of prescribing biologics or oral therapies for psoriasis,” the study’s lead author Jashin J. Wu, MD, of the Dermatology Research and Education Foundation in Irvine, Calif., said in an interview.
However, the results on the effects of systemic therapies were not all positive. Interleukin (IL)–17 inhibitors were an outlier: After adjustment for age and gender, patients treated with this class of drugs were 36% more likely to develop COVID-19 than those on oral agents (aIRR, 1.36; 95% CI, 1.13-1.63; P < .0009).
Among patients on biologics, those taking IL-17 inhibitors had the highest risk of COVID-19, Mr. Liu said. “The risk was higher in this class regardless of reference group – general population, the topical cohort, and the oral cohort,” he said. “This may relate to the observation that this biologic class exerts more broad immunosuppressive effects on antiviral host immunity. Notably, large meta-estimates of pivotal trials have observed increased risk of respiratory tract infections for patients on IL-17 inhibitors.”
In an interview, Erica Dommasch, MD, MPH, of the department of dermatology at Beth Israel Deaconess Medical Center, Boston, cautioned that “the data from this study is very hard to interpret.”
It’s likely that some patients with psoriasis on systemic medications “may have been the most careful about limiting exposures,” she said. “Thus, it’s hard to account for behavioral changes in individuals that may have led to the decreased incidence in psoriasis in patients on systemic agents versus topical therapy alone.”
Patients with psoriasis may also be tested more often for COVID-19, and unmeasured comorbidities like chronic kidney disease may play a role too, she said. Still, she added, “it’s reassuring that the authors did not find an increased rate of COVID among psoriasis patients on systemic agents versus topicals alone.” And she agreed with Dr. Wu about the importance of treating psoriasis with therapy beyond topical treatments during the pandemic: “Providers should feel comfortable prescribing systemic medications to psoriasis patients when otherwise appropriate.”
As for the next steps, Dr. Wu said, “we will be exploring more about the prognosis of COVID-19 infection in psoriasis patients. In addition, we will be exploring the relationship of COVID-19 infection with other inflammatory skin diseases, such as atopic dermatitis.”
No study funding is reported. Dr. Wu discloses investigator, consultant, or speaker relationships with AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, Dr. Reddy’s Laboratories, Eli Lilly, Galderma, Janssen, LEO Pharma, Mindera, Novartis, Regeneron, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, Valeant Pharmaceuticals North America, and Zerigo Health. Mr. Liu and Dr. Dommasch have no disclosures.
in patients, compared with those on topical therapy, a new study finds.
“Our study results suggest that psoriasis is an independent risk factor for COVID-19 illness,” study coauthor Jeffrey Liu, a medical student at the University of Southern California, Los Angeles, said in an interview after he presented the findings at the American Academy of Dermatology Virtual Meeting Experience. “And our findings are consistent with the hypothesis that certain systemic agents may confer a protective effect against COVID-19 illness.”
Mr. Liu and coinvestigators used a Symphony Health dataset to analyze the health records of 167,027 U.S. patients diagnosed with psoriasis and a control group of 1,002,162 patients. The participants, all at least 20 years old, had been treated for psoriasis or psoriatic arthritis from May 2019 through Jan. 1, 2020, and were tracked until Nov. 11, 2020.
The ages and races of peoples in the two groups were roughly similar. Overall, 55% were women and 75% were White, and their average age was 58 years. Type 2 diabetes was more common in the psoriasis group than the control group (23% vs. 16%), as was obesity (27% vs. 15%). Of the patients with psoriasis, 60% were on topical treatments, 19% were on oral therapies, and 22% were on biologic therapy, with only a few taking both oral and biologic therapies.
After adjustment for age and gender, patients with psoriasis were 33% more likely than the control group to develop COVID-19 (adjusted incidence rate ratio, 1.33; 95% confidence interval, 1.23-1.38; P < .0001).
In a separate analysis, the gap persisted after adjustment for demographics and comorbidities: Patients with psoriasis had a higher rate of COVID-19 infection vs. controls (adjusted odds ratio, 1.18; 95% CI, 1.13-1.23; P < .0001). Among all patients, non-White race, older age, and comorbidities were all linked to higher risk of COVID-19 (all P < .0001).
Psoriasis might make patients more vulnerable to COVID-19 because the presence of up-regulated genes in psoriatic skin “may lead to systemic hyperinflammation and sensitization of patients with psoriasis to proinflammatory cytokine storm,” Mr. Liu said. This, in turn, may trigger more severe symptomatic disease that requires medical treatment, he said.
Reduced risk, compared with topical therapies
After adjustment for age and gender, those treated with TNF-alpha inhibitors, methotrexate, and apremilast (Otezla) all had statistically lower risks of COVID-19 vs. those on topical therapy (aIRR, 0.82; 95% CI, 0.69-0.95; P < .0029 for TNF-alpha inhibitors; aIRR, 0.75; 95% CI, 0.67-0.86; P < .0001 for methotrexate; and aIRR, 0.69; 95% CI, 0.55-0.85; P < .0006 for apremilast).
Reduced risk held true for those in the separate analysis after adjustment for comorbidities and demographics (respectively, aOR, 0.87; 95% CI, 0.77-1.00; P < .0469; aOR, 0.81; 95% CI, 0.71-0.92; P < .0011; and aOR, 0.70; 95% CI, 0.57-0.87; P < .0014).
Apremilast and methotrexate may boost protection against COVID-19 by inhibiting the body’s production of cytokines, Mr. Liu said.
One message of the study is that “dermatologists should not be scared of prescribing biologics or oral therapies for psoriasis,” the study’s lead author Jashin J. Wu, MD, of the Dermatology Research and Education Foundation in Irvine, Calif., said in an interview.
However, the results on the effects of systemic therapies were not all positive. Interleukin (IL)–17 inhibitors were an outlier: After adjustment for age and gender, patients treated with this class of drugs were 36% more likely to develop COVID-19 than those on oral agents (aIRR, 1.36; 95% CI, 1.13-1.63; P < .0009).
Among patients on biologics, those taking IL-17 inhibitors had the highest risk of COVID-19, Mr. Liu said. “The risk was higher in this class regardless of reference group – general population, the topical cohort, and the oral cohort,” he said. “This may relate to the observation that this biologic class exerts more broad immunosuppressive effects on antiviral host immunity. Notably, large meta-estimates of pivotal trials have observed increased risk of respiratory tract infections for patients on IL-17 inhibitors.”
In an interview, Erica Dommasch, MD, MPH, of the department of dermatology at Beth Israel Deaconess Medical Center, Boston, cautioned that “the data from this study is very hard to interpret.”
It’s likely that some patients with psoriasis on systemic medications “may have been the most careful about limiting exposures,” she said. “Thus, it’s hard to account for behavioral changes in individuals that may have led to the decreased incidence in psoriasis in patients on systemic agents versus topical therapy alone.”
Patients with psoriasis may also be tested more often for COVID-19, and unmeasured comorbidities like chronic kidney disease may play a role too, she said. Still, she added, “it’s reassuring that the authors did not find an increased rate of COVID among psoriasis patients on systemic agents versus topicals alone.” And she agreed with Dr. Wu about the importance of treating psoriasis with therapy beyond topical treatments during the pandemic: “Providers should feel comfortable prescribing systemic medications to psoriasis patients when otherwise appropriate.”
As for the next steps, Dr. Wu said, “we will be exploring more about the prognosis of COVID-19 infection in psoriasis patients. In addition, we will be exploring the relationship of COVID-19 infection with other inflammatory skin diseases, such as atopic dermatitis.”
No study funding is reported. Dr. Wu discloses investigator, consultant, or speaker relationships with AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, Dermavant, Dr. Reddy’s Laboratories, Eli Lilly, Galderma, Janssen, LEO Pharma, Mindera, Novartis, Regeneron, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, Valeant Pharmaceuticals North America, and Zerigo Health. Mr. Liu and Dr. Dommasch have no disclosures.
FROM AAD VMX 2021
Tofacitinib: Small study shows big cutaneous sarcoidosis response
Researchers are reporting impressive results in a small, , and all patients improved by an average of 83% via a scoring system.

“Not only did patients get better, but they were in many cases able to come off their baseline immunosuppressive regimen, including prednisone and methotrexate. They’d get off prednisone entirely or, in some cases, decrease it substantially,” study investigator William Damsky, MD, PhD, reported at the American Academy of Dermatology Virtual Meeting Experience.
Sarcoidosis is a common disease that affects an estimated 1 in 25 Black women and is believed to contribute to the deaths of about 4,000 people in the United States each year, noted Dr. Damsky of the department of dermatology, Yale University, New Haven, Conn. One famous patient is comedian Bernie Mac, who died from the condition in 2008.
“Approximately one third of patients have cutaneous involvement,” Dr. Damsky said, and skin may be the only manifestation of the disease. There is no Food and Drug Administration-approved therapy for cutaneous sarcoidosis, he added. Prednisone, the first-line therapy in skin manifestations, is approved only for pulmonary sarcoidosis.
“Oftentimes, there’s an attempt to transition either partially or fully to other therapies, including methotrexate and TNF-alpha blockers. But there’s been mixed success in doing that,” he said. This is not always possible, “so a lot of patients end up on prednisone.”
Earlier, a team at Yale prescribed 5 mg tofacitinib (Xeljanz) for several patients with severe cutaneous sarcoidosis and saw impressive results, Dr. Damsky said, including a patient with pulmonary sarcoidosis that also improved. He noted that there are case reports in the medical literature with similar findings.
Those positive results inspired the new study. Researchers recruited 10 patients with cutaneous sarcoidosis (9 with internal organ involvement) with a Cutaneous Sarcoidosis Activity and Morphology Instrument ( CSAMI ) score of 10 or higher. Nine patients were in their 50s, one was aged 63 years, and five were men. Skin colors of the patients ranged from Fitzpatrick skin types I to VI, and all had been taking at least two medications, typically methotrexate and prednisone.
The patients received 5 mg of tofacitinib twice a day for 6 months. “Everyone got better during the study, and six patients had a complete response, which we defined as a CSAMI score of zero activity,” Dr. Damsky said. “It’s really quite remarkable to see that.” Overall, the patients saw an 83% improvement in CSAMI scores.
In regard to safety, “all patients completed the study,” he said. “Tofacitinib was well tolerated, and there were no serious adverse effects or events.”
Tofacitinib is approved for treating rheumatoid arthritis, psoriatic arthritis, ulcerative colitis, and polyarticular course juvenile idiopathic arthritis.
A month’s supply of twice-daily 5 mg tofacitinib pills would cost $4,900-$5,100 with free coupons, according to information accessed on April 24, 2021, on GoodRx.com. Generics are not available.
In an interview, Sotonye Imadojemu, MD, of the department of dermatology, Brigham and Women’s Hospital, Boston, praised the study, and said “tofacitinib is a reasonable treatment for treatment-refractory or extensive cutaneous sarcoidosis,” although it will be helpful to get results from randomized-controlled trials.
She cautioned that the drug “is a powerful immunosuppressant, so the risk of infection must be discussed with patients before prescribing. Screening for chronic infections such as viral hepatitis, tuberculosis, and HIV should be completed prior to treatment initiation. Blood counts, liver function, and lipid panels should be regularly monitored. The vaccines necessary for those who are immunosuppressed should be administered as able, and age-appropriate cancer screening must be kept up to date.”
The study was funded by Pfizer, the Dermatology Foundation, and the Yale Department of Dermatology. Dr. Damsky disclosed research support (Pfizer), consulting fees (Eli Lilly, Pfizer, TWi Biotechnology), and licensing fees (EMD Millipore/MillporeSigma). Dr. Imadojemu has no disclosures.
This article was updated 5/5/21.
Researchers are reporting impressive results in a small, , and all patients improved by an average of 83% via a scoring system.
“Not only did patients get better, but they were in many cases able to come off their baseline immunosuppressive regimen, including prednisone and methotrexate. They’d get off prednisone entirely or, in some cases, decrease it substantially,” study investigator William Damsky, MD, PhD, reported at the American Academy of Dermatology Virtual Meeting Experience.
Sarcoidosis is a common disease that affects an estimated 1 in 25 Black women and is believed to contribute to the deaths of about 4,000 people in the United States each year, noted Dr. Damsky of the department of dermatology, Yale University, New Haven, Conn. One famous patient is comedian Bernie Mac, who died from the condition in 2008.
“Approximately one third of patients have cutaneous involvement,” Dr. Damsky said, and skin may be the only manifestation of the disease. There is no Food and Drug Administration-approved therapy for cutaneous sarcoidosis, he added. Prednisone, the first-line therapy in skin manifestations, is approved only for pulmonary sarcoidosis.
“Oftentimes, there’s an attempt to transition either partially or fully to other therapies, including methotrexate and TNF-alpha blockers. But there’s been mixed success in doing that,” he said. This is not always possible, “so a lot of patients end up on prednisone.”
Earlier, a team at Yale prescribed 5 mg tofacitinib (Xeljanz) for several patients with severe cutaneous sarcoidosis and saw impressive results, Dr. Damsky said, including a patient with pulmonary sarcoidosis that also improved. He noted that there are case reports in the medical literature with similar findings.
Those positive results inspired the new study. Researchers recruited 10 patients with cutaneous sarcoidosis (9 with internal organ involvement) with a Cutaneous Sarcoidosis Activity and Morphology Instrument ( CSAMI ) score of 10 or higher. Nine patients were in their 50s, one was aged 63 years, and five were men. Skin colors of the patients ranged from Fitzpatrick skin types I to VI, and all had been taking at least two medications, typically methotrexate and prednisone.
The patients received 5 mg of tofacitinib twice a day for 6 months. “Everyone got better during the study, and six patients had a complete response, which we defined as a CSAMI score of zero activity,” Dr. Damsky said. “It’s really quite remarkable to see that.” Overall, the patients saw an 83% improvement in CSAMI scores.
In regard to safety, “all patients completed the study,” he said. “Tofacitinib was well tolerated, and there were no serious adverse effects or events.”
Tofacitinib is approved for treating rheumatoid arthritis, psoriatic arthritis, ulcerative colitis, and polyarticular course juvenile idiopathic arthritis.
A month’s supply of twice-daily 5 mg tofacitinib pills would cost $4,900-$5,100 with free coupons, according to information accessed on April 24, 2021, on GoodRx.com. Generics are not available.
In an interview, Sotonye Imadojemu, MD, of the department of dermatology, Brigham and Women’s Hospital, Boston, praised the study, and said “tofacitinib is a reasonable treatment for treatment-refractory or extensive cutaneous sarcoidosis,” although it will be helpful to get results from randomized-controlled trials.
She cautioned that the drug “is a powerful immunosuppressant, so the risk of infection must be discussed with patients before prescribing. Screening for chronic infections such as viral hepatitis, tuberculosis, and HIV should be completed prior to treatment initiation. Blood counts, liver function, and lipid panels should be regularly monitored. The vaccines necessary for those who are immunosuppressed should be administered as able, and age-appropriate cancer screening must be kept up to date.”
The study was funded by Pfizer, the Dermatology Foundation, and the Yale Department of Dermatology. Dr. Damsky disclosed research support (Pfizer), consulting fees (Eli Lilly, Pfizer, TWi Biotechnology), and licensing fees (EMD Millipore/MillporeSigma). Dr. Imadojemu has no disclosures.
This article was updated 5/5/21.
Researchers are reporting impressive results in a small, , and all patients improved by an average of 83% via a scoring system.
“Not only did patients get better, but they were in many cases able to come off their baseline immunosuppressive regimen, including prednisone and methotrexate. They’d get off prednisone entirely or, in some cases, decrease it substantially,” study investigator William Damsky, MD, PhD, reported at the American Academy of Dermatology Virtual Meeting Experience.
Sarcoidosis is a common disease that affects an estimated 1 in 25 Black women and is believed to contribute to the deaths of about 4,000 people in the United States each year, noted Dr. Damsky of the department of dermatology, Yale University, New Haven, Conn. One famous patient is comedian Bernie Mac, who died from the condition in 2008.
“Approximately one third of patients have cutaneous involvement,” Dr. Damsky said, and skin may be the only manifestation of the disease. There is no Food and Drug Administration-approved therapy for cutaneous sarcoidosis, he added. Prednisone, the first-line therapy in skin manifestations, is approved only for pulmonary sarcoidosis.
“Oftentimes, there’s an attempt to transition either partially or fully to other therapies, including methotrexate and TNF-alpha blockers. But there’s been mixed success in doing that,” he said. This is not always possible, “so a lot of patients end up on prednisone.”
Earlier, a team at Yale prescribed 5 mg tofacitinib (Xeljanz) for several patients with severe cutaneous sarcoidosis and saw impressive results, Dr. Damsky said, including a patient with pulmonary sarcoidosis that also improved. He noted that there are case reports in the medical literature with similar findings.
Those positive results inspired the new study. Researchers recruited 10 patients with cutaneous sarcoidosis (9 with internal organ involvement) with a Cutaneous Sarcoidosis Activity and Morphology Instrument ( CSAMI ) score of 10 or higher. Nine patients were in their 50s, one was aged 63 years, and five were men. Skin colors of the patients ranged from Fitzpatrick skin types I to VI, and all had been taking at least two medications, typically methotrexate and prednisone.
The patients received 5 mg of tofacitinib twice a day for 6 months. “Everyone got better during the study, and six patients had a complete response, which we defined as a CSAMI score of zero activity,” Dr. Damsky said. “It’s really quite remarkable to see that.” Overall, the patients saw an 83% improvement in CSAMI scores.
In regard to safety, “all patients completed the study,” he said. “Tofacitinib was well tolerated, and there were no serious adverse effects or events.”
Tofacitinib is approved for treating rheumatoid arthritis, psoriatic arthritis, ulcerative colitis, and polyarticular course juvenile idiopathic arthritis.
A month’s supply of twice-daily 5 mg tofacitinib pills would cost $4,900-$5,100 with free coupons, according to information accessed on April 24, 2021, on GoodRx.com. Generics are not available.
In an interview, Sotonye Imadojemu, MD, of the department of dermatology, Brigham and Women’s Hospital, Boston, praised the study, and said “tofacitinib is a reasonable treatment for treatment-refractory or extensive cutaneous sarcoidosis,” although it will be helpful to get results from randomized-controlled trials.
She cautioned that the drug “is a powerful immunosuppressant, so the risk of infection must be discussed with patients before prescribing. Screening for chronic infections such as viral hepatitis, tuberculosis, and HIV should be completed prior to treatment initiation. Blood counts, liver function, and lipid panels should be regularly monitored. The vaccines necessary for those who are immunosuppressed should be administered as able, and age-appropriate cancer screening must be kept up to date.”
The study was funded by Pfizer, the Dermatology Foundation, and the Yale Department of Dermatology. Dr. Damsky disclosed research support (Pfizer), consulting fees (Eli Lilly, Pfizer, TWi Biotechnology), and licensing fees (EMD Millipore/MillporeSigma). Dr. Imadojemu has no disclosures.
This article was updated 5/5/21.
REPORTING FROM AAD VMX 2021
S1P-receptor modulator shows promise in phase 2b AD trial
, according to researchers who released their findings at the American Academy of Dermatology Virtual Meeting Experience.

The drug, called etrasimod, did not meet the primary endpoint for improvement in the Eczema Area and Severity Index. However, nearly a third (29.8%) of those treated with a 2-mg dose daily reached “clear” or “almost clear” skin at 12 weeks vs. 13% for placebo as measured with clinician-reported Validated Investigator Global Assessment (vIGA) scores of 0 or 1 (P = .0450), study presenter Emma Guttman-Yassky, MD, PhD, professor and chair, department of dermatology, Icahn School of Medicine at Mount Sinai, New York, noted in an interview.
“This was a short proof-of-concept study to show this mechanism is valid. The results are promising,” Dr. Guttman-Yassky said. “They tell us that this can be a valid treatment for atopic dermatitis, a completely new mechanism of action that has potential in improving and even modifying the disease.”
Arena Pharmaceuticals, which developed the drug, hopes to launch a phase 3 study of the medication.
The ADVISE study enrolled 140 people in the United States, Australia, and Canada with chronic, moderate to severe eczema lasting for at least a year. (Their average age was 43, 61% were female, and 60% were White). They were randomly assigned to cohorts who took 1 mg or 2 mg daily of etrasimod or placebo for 12 weeks.
Those in the 2-mg cohort saw their scores on the peak pruritus numeric rating scale (PP-NRS) fall by 15.3% at week 4, compared with 1% for placebo (P = .0380); at week 12, the scores fell by 34.1% among those on 2 mg vs. 23.9% for placebo (P = .15 49). At 12 weeks, patients on the 2-mg dose also had more improvement in the Dermatology Life Quality Index or DLQI (a 7.6-point decline in degree of impairment vs. 4.2 points for placebo, P = .0122) and in the Patient-Oriented Eczema Measure or POEM (8.4-point reduction versus 4 points for placebo, P = .0045).
“Basically, there was a dose response. It doesn’t show a plateau,” Dr. Guttman-Yassky said. “ I think the data will be even better in a longer study.”
In regards to adverse events, participants who took etrasimod reported nausea, constipation, back pain, and dizziness at levels above 5% and above the levels for the placebo.
The drug appears to work by preventing immune cells from entering the skin, Dr. Guttman-Yassky said, and may be able to treat existing lesions and prevent new ones from appearing. Etrasimod is also being explored as a treatment for ulcerative colitis, alopecia areata, and multiple sclerosis, she said.
Dr. Guttman-Yassky noted that 12 weeks is a short time in AD, and she said some participants left the study because it took place during the coronavirus pandemic.
“There’s a huge unmet need in atopic dermatitis,” she said. “We need more drugs and different classes of drugs to treat the disease in all patients.” While biologics are often helpful, she said, they don’t work in many cases. And “some patients just don’t want a biologic, no matter how much we tell them it’s safe, and they may want an oral medication,” she said.
Dr. Guttman-Yassky is a paid consultant and researcher for Arena.
, according to researchers who released their findings at the American Academy of Dermatology Virtual Meeting Experience.
The drug, called etrasimod, did not meet the primary endpoint for improvement in the Eczema Area and Severity Index. However, nearly a third (29.8%) of those treated with a 2-mg dose daily reached “clear” or “almost clear” skin at 12 weeks vs. 13% for placebo as measured with clinician-reported Validated Investigator Global Assessment (vIGA) scores of 0 or 1 (P = .0450), study presenter Emma Guttman-Yassky, MD, PhD, professor and chair, department of dermatology, Icahn School of Medicine at Mount Sinai, New York, noted in an interview.
“This was a short proof-of-concept study to show this mechanism is valid. The results are promising,” Dr. Guttman-Yassky said. “They tell us that this can be a valid treatment for atopic dermatitis, a completely new mechanism of action that has potential in improving and even modifying the disease.”
Arena Pharmaceuticals, which developed the drug, hopes to launch a phase 3 study of the medication.
The ADVISE study enrolled 140 people in the United States, Australia, and Canada with chronic, moderate to severe eczema lasting for at least a year. (Their average age was 43, 61% were female, and 60% were White). They were randomly assigned to cohorts who took 1 mg or 2 mg daily of etrasimod or placebo for 12 weeks.
Those in the 2-mg cohort saw their scores on the peak pruritus numeric rating scale (PP-NRS) fall by 15.3% at week 4, compared with 1% for placebo (P = .0380); at week 12, the scores fell by 34.1% among those on 2 mg vs. 23.9% for placebo (P = .15 49). At 12 weeks, patients on the 2-mg dose also had more improvement in the Dermatology Life Quality Index or DLQI (a 7.6-point decline in degree of impairment vs. 4.2 points for placebo, P = .0122) and in the Patient-Oriented Eczema Measure or POEM (8.4-point reduction versus 4 points for placebo, P = .0045).
“Basically, there was a dose response. It doesn’t show a plateau,” Dr. Guttman-Yassky said. “ I think the data will be even better in a longer study.”
In regards to adverse events, participants who took etrasimod reported nausea, constipation, back pain, and dizziness at levels above 5% and above the levels for the placebo.
The drug appears to work by preventing immune cells from entering the skin, Dr. Guttman-Yassky said, and may be able to treat existing lesions and prevent new ones from appearing. Etrasimod is also being explored as a treatment for ulcerative colitis, alopecia areata, and multiple sclerosis, she said.
Dr. Guttman-Yassky noted that 12 weeks is a short time in AD, and she said some participants left the study because it took place during the coronavirus pandemic.
“There’s a huge unmet need in atopic dermatitis,” she said. “We need more drugs and different classes of drugs to treat the disease in all patients.” While biologics are often helpful, she said, they don’t work in many cases. And “some patients just don’t want a biologic, no matter how much we tell them it’s safe, and they may want an oral medication,” she said.
Dr. Guttman-Yassky is a paid consultant and researcher for Arena.
, according to researchers who released their findings at the American Academy of Dermatology Virtual Meeting Experience.
The drug, called etrasimod, did not meet the primary endpoint for improvement in the Eczema Area and Severity Index. However, nearly a third (29.8%) of those treated with a 2-mg dose daily reached “clear” or “almost clear” skin at 12 weeks vs. 13% for placebo as measured with clinician-reported Validated Investigator Global Assessment (vIGA) scores of 0 or 1 (P = .0450), study presenter Emma Guttman-Yassky, MD, PhD, professor and chair, department of dermatology, Icahn School of Medicine at Mount Sinai, New York, noted in an interview.
“This was a short proof-of-concept study to show this mechanism is valid. The results are promising,” Dr. Guttman-Yassky said. “They tell us that this can be a valid treatment for atopic dermatitis, a completely new mechanism of action that has potential in improving and even modifying the disease.”
Arena Pharmaceuticals, which developed the drug, hopes to launch a phase 3 study of the medication.
The ADVISE study enrolled 140 people in the United States, Australia, and Canada with chronic, moderate to severe eczema lasting for at least a year. (Their average age was 43, 61% were female, and 60% were White). They were randomly assigned to cohorts who took 1 mg or 2 mg daily of etrasimod or placebo for 12 weeks.
Those in the 2-mg cohort saw their scores on the peak pruritus numeric rating scale (PP-NRS) fall by 15.3% at week 4, compared with 1% for placebo (P = .0380); at week 12, the scores fell by 34.1% among those on 2 mg vs. 23.9% for placebo (P = .15 49). At 12 weeks, patients on the 2-mg dose also had more improvement in the Dermatology Life Quality Index or DLQI (a 7.6-point decline in degree of impairment vs. 4.2 points for placebo, P = .0122) and in the Patient-Oriented Eczema Measure or POEM (8.4-point reduction versus 4 points for placebo, P = .0045).
“Basically, there was a dose response. It doesn’t show a plateau,” Dr. Guttman-Yassky said. “ I think the data will be even better in a longer study.”
In regards to adverse events, participants who took etrasimod reported nausea, constipation, back pain, and dizziness at levels above 5% and above the levels for the placebo.
The drug appears to work by preventing immune cells from entering the skin, Dr. Guttman-Yassky said, and may be able to treat existing lesions and prevent new ones from appearing. Etrasimod is also being explored as a treatment for ulcerative colitis, alopecia areata, and multiple sclerosis, she said.
Dr. Guttman-Yassky noted that 12 weeks is a short time in AD, and she said some participants left the study because it took place during the coronavirus pandemic.
“There’s a huge unmet need in atopic dermatitis,” she said. “We need more drugs and different classes of drugs to treat the disease in all patients.” While biologics are often helpful, she said, they don’t work in many cases. And “some patients just don’t want a biologic, no matter how much we tell them it’s safe, and they may want an oral medication,” she said.
Dr. Guttman-Yassky is a paid consultant and researcher for Arena.
REPORTING FROM AAD VMX 2021
CDC: STI rates rise for sixth year in a row
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
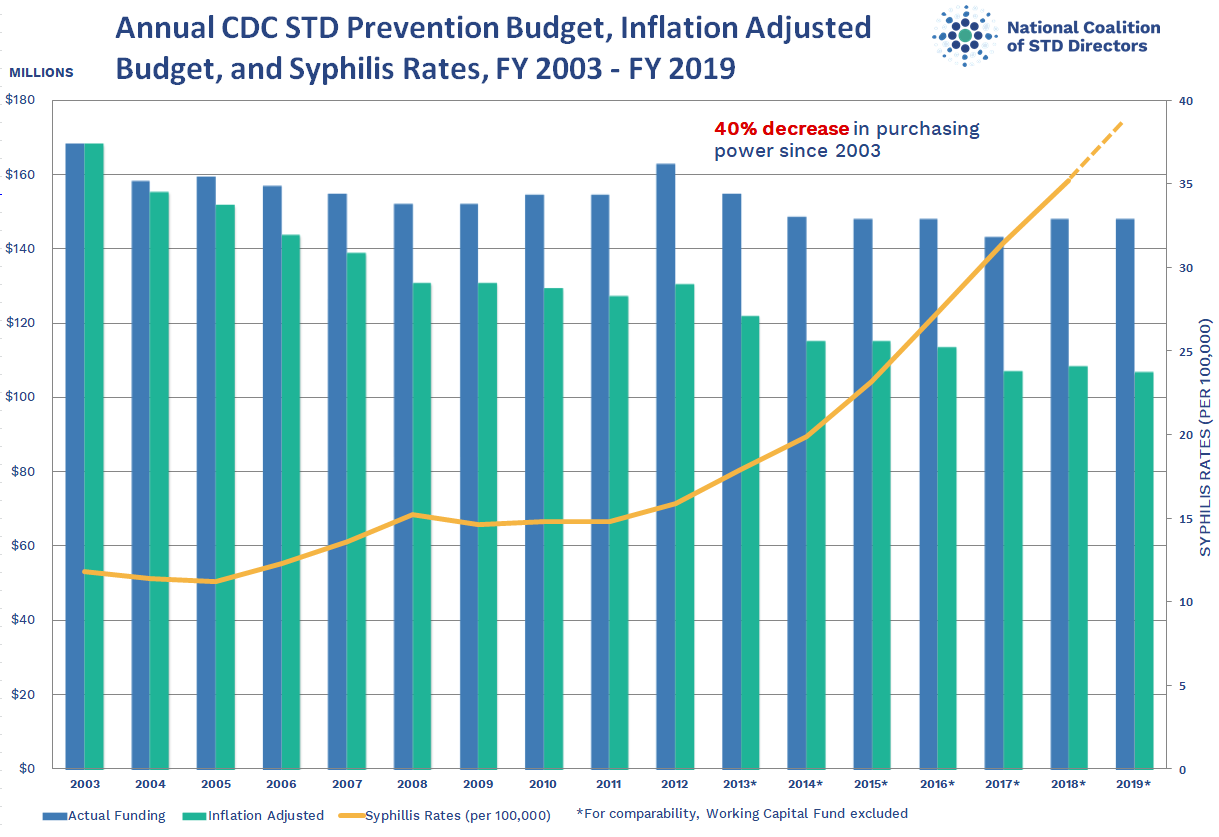
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
{kind=link}
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
Annual cases of sexually transmitted infections in the United States jumped for the sixth year in a row in 2019, according to a new Centers for Disease Control and Prevention report that highlights an increase in congenital syphilis and rising rates of syphilis, chlamydia, and gonorrhea in men, especially men who have sex with men (MSM).
The report says nothing about STI rates during the COVID-19 pandemic, when both casual sex and disease screening and surveillance declined significantly, at least in the early months. But epidemiologist Patricia Kissinger, PhD, MPH, from Tulane University School, New Orleans, said in an interview that the findings reflect how “a confluence of factors” drove up rates before the age of COVID. Those factors include online dating, the opioid epidemic, the decline in condom use in the MSM community as HIV became more preventable, and indifference among policy makers and the community at large.
The CDC report, based on data from local health departments, says there were 129,813 cases of syphilis in 2019, up 74% since 2015. Almost 2,000 cases of congenital syphilis were reported, up 279% since 2015, and 128 infants died.
“There’s no reason for us to have congenital syphilis,” said Dr. Kissinger, who noted that the disease can cause birth defects and meningitis in addition to death. “Women should be screened, and it’s relatively easy to treat via penicillin injections.”
Indeed, medical guidelines suggest that pregnant women be routinely tested for syphilis. But that doesn’t always happen because “it falls through the cracks,” Dr. Kissinger said. Or, she added, women might not be tested enough times during their pregnancies: “You have to screen women in the third trimester. You can’t just do it in the first trimester because people do have sex when they’re pregnant.”
Rising congenital syphilis numbers have convinced at least one health system to take action. As of June 1, the University of California, San Diego, will routinely test pregnant women in the emergency department for syphilis in addition to HIV and hepatitis C, Martin Hoenigl, MD, a UCSF infectious disease specialist, said in an interview.
The CDC report also notes 1.8 million cases of chlamydia in 2019, a jump of 19% in 4 years, and a 56% increase in gonorrhea in that time period, to a total of 616,392 cases.
The report says increasing gonorrhea and chlamydia cases in men, especially MSM, could be caused by increased testing/screening, increased transmission, or both. Although women are generally diagnosed with chlamydia more often than men, the report says, numbers among men grew by 32% from 2015 to 2019. And since 2013, rates of gonorrhea among men have risen at a much faster clip than among women.
MSM accounted for most male cases of primary and secondary syphilis in 2019, although the report said the apparent long-term rise in these cases might be slowing.
Many MSM no longer use condoms because they’re using pre-exposure prophylaxis (PrEP) or have undetectable levels of HIV because of treatment, said Jeffrey Klausner, MD, MPH, an STI specialist at the University of Southern California in Los Angeles, said in an interview.
Many MSM might be getting screened much more often for STIs than in the past because frequent screening is required for those on PrEP. However, Dr. Kissinger said some clinics weren’t able to test at times during the pandemic because of a swab shortage. In addition, patients of all types avoided routine medical care during the pandemic, and some medical professionals in the infectious disease field were redirected to COVID care.
Clinical trials have been investigating a possible preventive STI strategy in MSM who don’t wear condoms – prophylaxis, either before or after exposure, with the antibiotic doxycycline. “That’s a very good solution,” Dr. Klausner said, but he believes bigger challenges remain. According to him, the existence of the report itself – which offers statistics from 2 years ago instead of more relevant recent numbers – is evidence of how the federal government isn’t doing enough to fight STIs. “If we’re taking the STD epidemic seriously, there should be timely and regular reporting.” Dr. Klausner said he likes the idea of monthly reports, as well as more funding for prevention.
Instead, he noted, the federal government cut STI prevention funding by 40% in inflation-adjusted dollars from 2002-2003 to 2018-2019, according to the National Coalition of STD Directors. “Burying your head in the sand and hoping the problem goes away is not an effective strategy,” he said.
It’s not clear whether STI rates are on the decline because of pandemic restrictions and stay-at-home orders. Surveys suggest that a dip in casual sex early in pandemic – when much of society shut down – was only temporary, Dr. Klausner said.
Dr. Kissinger disclosed no relevant financial relationships. Dr. Hoenigl reported receiving research funding via his university from Gilead. Dr. Klausner has recently provided consulting services to Danaher, Cepheid, Roche, GlaxoSmithKline, Talis Bio, SpeeDx, and Visby Medical, all manufacturers of diagnostic assays for STIs.
A version of this article first appeared on Medscape.com.
What will neurology look like post pandemic?
Jose Angel Soria-Lopez, MD, has an unusually wide perspective on how neurology patients are responding to the coronavirus pandemic. He treats patients at two San Diego–area clinics, one in a poor neighborhood near the Mexican border and another in an upscale city about 65 miles to the north. While the patient populations are quite different, he’s noticed they’ve share one thing in common lately: An unusually intense focus on their personal health.

“All of a sudden people are really thinking about their health,” Dr. Soria-Lopez said. “There’s a sense that their health is even more important than it used to be.”
But patients are divided on how exactly they want their health care delivered. Some are embracing the convenience of telemedicine, while others want to be seen in person no matter what. Moving forward beyond the pandemic, Dr. Soria-Lopez expects the upswing of interest in health will persist. And he predicts two kinds of neurological care will emerge: “One based on ongoing relationships that rely on physical encounters as a culture, and a second kind of neurology service where other patients – perhaps the younger ones – will switch to convenient, online follow-ups.”
Telemedicine will endure post pandemic
While some don’t foresee such a big divide between in-person and online visits, several of Dr. Soria-Lopez’s colleagues from around the country agreed in interviews that . One neurologist, however, cautioned that telemedicine can worsen disparities in care. And he raised the alarm about another aspect of the pandemic that isn’t going to lift when it’s over: The rise in neurological disorders linked to infection with COVID-19.
Before the pandemic, neurologists said, they rarely if ever treated patients via telemedicine outside of specific settings such as remote stroke care. Over the past year, the use of telemedicine has dramatically increased in neurology as in medicine as a whole. But the levels of adoption differ markedly. Neurologist Andrew N. Wilner, MD, of University of Tennessee Health Science Center, said he has used telemedicine to see a single patient so far. But Johns Hopkins Center for Sleep neurologist Charlene Gamaldo, MD, said her clinic converted to 100% remote visits in March 2020 and remains at that level.
“Where [the rate of telemedicine use] will land will be based on insurance reimbursement and license reciprocation, so it is difficult to predict,” she said. “I imagine that sleep will likely remain a hybrid model if current allowances remain.”
Some patients, especially the older ones, resisted the telemedicine visits at first, Dr. Gamaldo said, and family members had to step in to help. Now, she said, patients prefer them because of their convenience.
Some neurological conditions, of course, can’t be easily evaluated via online video. Dr. Soria-Lopez, who has offices in Chula Vista and Temecula, Calif., prefers that a patient appear in person at first. “It really takes 1-2 physical encounters for there to be some level of trust,” he said, adding that “it’s hard to do the first few visits online unless it’s a very straightforward case with one or two symptoms.”
Neurologists have found that telemedicine is especially useful for med-check visits. Mitzi Joi Williams, MD, an Atlanta-area neurologist and multiple sclerosis specialist, said some patients previously drove 2-3 hours for these visits, which can easily be conducted online. Dr. Williams added that online software can allow her to show MRIs to patients remotely. She simply shares her screen and talks about what the images show.

Physical exams are more difficult online, of course, she said: “You can’t see nuances.” And it can be difficult to not have family members in the room to assist with the patient’s history. But some have joined via conference call and that’s been helpful, she said.
Neurologist Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles, whose clinic has gone to all-telemedicine visits, said telemedicine will make a huge difference for patients who live in remote areas or have mobility problems. In some cases, patients will actually be able to see their doctors more often, she said.

But she cautioned that it can be challenging to evaluate patients who are having difficulties with walking and sensation, although neurologists could try workarounds such as asking a patient to touch something cold. “We can do some things with coordination like watch patients walk, but walking motor strength is hard to check [via video],” she said. “The best thing to evaluate is cognition. You can talk to them and get a lot of it by asking questions.”
Carlos A. Pérez, MD, a neurologist at the University of Texas Health Science Center at Houston, noted that virtual visits can make it difficult to conduct comprehensive eye evaluations and examine vestibular and neuromuscular components such as weakness. “In multiple sclerosis patients, for example, diagnosing an MS relapse can be particularly difficult, especially when the patients present with mostly visual or sensory problems,” he said.
While he’s a fan of telemedicine overall, Dr. Pérez cautioned that low-income patients may lack computers and access to the Internet. “Access to resources in general seems to vary quite significantly,” he said. “Some patients use their cellphones for virtual visits, and that makes it extremely hard to examine them.”
Neurologist Amit Bar-Or, MD, of the University of Pennsylvania, Philadelphia, noted that in some cases, creativity can make a big difference in helping telemedicine visits to run smoothly. “In examining the cranial nerves, for example, you can get a lot of information. You need to have the person position the camera properly and get close to the camera so you can look at eye movements and facial symmetry.”
Still, he said, “if a patient wants to be seen in person, we should never deny them.”
As for other changes that will linger after the pandemic, San Diego–area neurologist Dr. Soria-Lopez said he expects that waiting rooms will continue to be less populated as patients wait elsewhere to avoid the spread of germs. He predicts there will be more use of “virtual waiting rooms” that allow patients to fill out paperwork remotely and get alerts when medical professionals are ready to see them.
Neurological sequelae from COVID-19
Dr. Pérez, the Houston neurologist, said his colleagues should expect another aspect of the pandemic to persist: an influx of patients with neurological sequelae from COVID-19. As he noted in a 2020 report in Neurology Clinical Practice, coronaviruses have been linked to numerous neurological complications during and after the infectious period. “I have seen a few cases of Guillain-Barré and even postinfectious encephalitis in the clinic [linked to COVID-19],” he said. “Neurologists in general should be aware of the risk for chronic, postinfectious neurologic complications from prior COVID-19 infection.”
And, he said, it’s reasonable for neurologists to add a question to patient histories. It’s a simple yet powerful query: Have you had COVID-19?
Jose Angel Soria-Lopez, MD, has an unusually wide perspective on how neurology patients are responding to the coronavirus pandemic. He treats patients at two San Diego–area clinics, one in a poor neighborhood near the Mexican border and another in an upscale city about 65 miles to the north. While the patient populations are quite different, he’s noticed they’ve share one thing in common lately: An unusually intense focus on their personal health.
“All of a sudden people are really thinking about their health,” Dr. Soria-Lopez said. “There’s a sense that their health is even more important than it used to be.”
But patients are divided on how exactly they want their health care delivered. Some are embracing the convenience of telemedicine, while others want to be seen in person no matter what. Moving forward beyond the pandemic, Dr. Soria-Lopez expects the upswing of interest in health will persist. And he predicts two kinds of neurological care will emerge: “One based on ongoing relationships that rely on physical encounters as a culture, and a second kind of neurology service where other patients – perhaps the younger ones – will switch to convenient, online follow-ups.”
Telemedicine will endure post pandemic
While some don’t foresee such a big divide between in-person and online visits, several of Dr. Soria-Lopez’s colleagues from around the country agreed in interviews that . One neurologist, however, cautioned that telemedicine can worsen disparities in care. And he raised the alarm about another aspect of the pandemic that isn’t going to lift when it’s over: The rise in neurological disorders linked to infection with COVID-19.
Before the pandemic, neurologists said, they rarely if ever treated patients via telemedicine outside of specific settings such as remote stroke care. Over the past year, the use of telemedicine has dramatically increased in neurology as in medicine as a whole. But the levels of adoption differ markedly. Neurologist Andrew N. Wilner, MD, of University of Tennessee Health Science Center, said he has used telemedicine to see a single patient so far. But Johns Hopkins Center for Sleep neurologist Charlene Gamaldo, MD, said her clinic converted to 100% remote visits in March 2020 and remains at that level.
“Where [the rate of telemedicine use] will land will be based on insurance reimbursement and license reciprocation, so it is difficult to predict,” she said. “I imagine that sleep will likely remain a hybrid model if current allowances remain.”
Some patients, especially the older ones, resisted the telemedicine visits at first, Dr. Gamaldo said, and family members had to step in to help. Now, she said, patients prefer them because of their convenience.
Some neurological conditions, of course, can’t be easily evaluated via online video. Dr. Soria-Lopez, who has offices in Chula Vista and Temecula, Calif., prefers that a patient appear in person at first. “It really takes 1-2 physical encounters for there to be some level of trust,” he said, adding that “it’s hard to do the first few visits online unless it’s a very straightforward case with one or two symptoms.”
Neurologists have found that telemedicine is especially useful for med-check visits. Mitzi Joi Williams, MD, an Atlanta-area neurologist and multiple sclerosis specialist, said some patients previously drove 2-3 hours for these visits, which can easily be conducted online. Dr. Williams added that online software can allow her to show MRIs to patients remotely. She simply shares her screen and talks about what the images show.
Physical exams are more difficult online, of course, she said: “You can’t see nuances.” And it can be difficult to not have family members in the room to assist with the patient’s history. But some have joined via conference call and that’s been helpful, she said.
Neurologist Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles, whose clinic has gone to all-telemedicine visits, said telemedicine will make a huge difference for patients who live in remote areas or have mobility problems. In some cases, patients will actually be able to see their doctors more often, she said.
But she cautioned that it can be challenging to evaluate patients who are having difficulties with walking and sensation, although neurologists could try workarounds such as asking a patient to touch something cold. “We can do some things with coordination like watch patients walk, but walking motor strength is hard to check [via video],” she said. “The best thing to evaluate is cognition. You can talk to them and get a lot of it by asking questions.”
Carlos A. Pérez, MD, a neurologist at the University of Texas Health Science Center at Houston, noted that virtual visits can make it difficult to conduct comprehensive eye evaluations and examine vestibular and neuromuscular components such as weakness. “In multiple sclerosis patients, for example, diagnosing an MS relapse can be particularly difficult, especially when the patients present with mostly visual or sensory problems,” he said.
While he’s a fan of telemedicine overall, Dr. Pérez cautioned that low-income patients may lack computers and access to the Internet. “Access to resources in general seems to vary quite significantly,” he said. “Some patients use their cellphones for virtual visits, and that makes it extremely hard to examine them.”
Neurologist Amit Bar-Or, MD, of the University of Pennsylvania, Philadelphia, noted that in some cases, creativity can make a big difference in helping telemedicine visits to run smoothly. “In examining the cranial nerves, for example, you can get a lot of information. You need to have the person position the camera properly and get close to the camera so you can look at eye movements and facial symmetry.”
Still, he said, “if a patient wants to be seen in person, we should never deny them.”
As for other changes that will linger after the pandemic, San Diego–area neurologist Dr. Soria-Lopez said he expects that waiting rooms will continue to be less populated as patients wait elsewhere to avoid the spread of germs. He predicts there will be more use of “virtual waiting rooms” that allow patients to fill out paperwork remotely and get alerts when medical professionals are ready to see them.
Neurological sequelae from COVID-19
Dr. Pérez, the Houston neurologist, said his colleagues should expect another aspect of the pandemic to persist: an influx of patients with neurological sequelae from COVID-19. As he noted in a 2020 report in Neurology Clinical Practice, coronaviruses have been linked to numerous neurological complications during and after the infectious period. “I have seen a few cases of Guillain-Barré and even postinfectious encephalitis in the clinic [linked to COVID-19],” he said. “Neurologists in general should be aware of the risk for chronic, postinfectious neurologic complications from prior COVID-19 infection.”
And, he said, it’s reasonable for neurologists to add a question to patient histories. It’s a simple yet powerful query: Have you had COVID-19?
Jose Angel Soria-Lopez, MD, has an unusually wide perspective on how neurology patients are responding to the coronavirus pandemic. He treats patients at two San Diego–area clinics, one in a poor neighborhood near the Mexican border and another in an upscale city about 65 miles to the north. While the patient populations are quite different, he’s noticed they’ve share one thing in common lately: An unusually intense focus on their personal health.
“All of a sudden people are really thinking about their health,” Dr. Soria-Lopez said. “There’s a sense that their health is even more important than it used to be.”
But patients are divided on how exactly they want their health care delivered. Some are embracing the convenience of telemedicine, while others want to be seen in person no matter what. Moving forward beyond the pandemic, Dr. Soria-Lopez expects the upswing of interest in health will persist. And he predicts two kinds of neurological care will emerge: “One based on ongoing relationships that rely on physical encounters as a culture, and a second kind of neurology service where other patients – perhaps the younger ones – will switch to convenient, online follow-ups.”
Telemedicine will endure post pandemic
While some don’t foresee such a big divide between in-person and online visits, several of Dr. Soria-Lopez’s colleagues from around the country agreed in interviews that . One neurologist, however, cautioned that telemedicine can worsen disparities in care. And he raised the alarm about another aspect of the pandemic that isn’t going to lift when it’s over: The rise in neurological disorders linked to infection with COVID-19.
Before the pandemic, neurologists said, they rarely if ever treated patients via telemedicine outside of specific settings such as remote stroke care. Over the past year, the use of telemedicine has dramatically increased in neurology as in medicine as a whole. But the levels of adoption differ markedly. Neurologist Andrew N. Wilner, MD, of University of Tennessee Health Science Center, said he has used telemedicine to see a single patient so far. But Johns Hopkins Center for Sleep neurologist Charlene Gamaldo, MD, said her clinic converted to 100% remote visits in March 2020 and remains at that level.
“Where [the rate of telemedicine use] will land will be based on insurance reimbursement and license reciprocation, so it is difficult to predict,” she said. “I imagine that sleep will likely remain a hybrid model if current allowances remain.”
Some patients, especially the older ones, resisted the telemedicine visits at first, Dr. Gamaldo said, and family members had to step in to help. Now, she said, patients prefer them because of their convenience.
Some neurological conditions, of course, can’t be easily evaluated via online video. Dr. Soria-Lopez, who has offices in Chula Vista and Temecula, Calif., prefers that a patient appear in person at first. “It really takes 1-2 physical encounters for there to be some level of trust,” he said, adding that “it’s hard to do the first few visits online unless it’s a very straightforward case with one or two symptoms.”
Neurologists have found that telemedicine is especially useful for med-check visits. Mitzi Joi Williams, MD, an Atlanta-area neurologist and multiple sclerosis specialist, said some patients previously drove 2-3 hours for these visits, which can easily be conducted online. Dr. Williams added that online software can allow her to show MRIs to patients remotely. She simply shares her screen and talks about what the images show.
Physical exams are more difficult online, of course, she said: “You can’t see nuances.” And it can be difficult to not have family members in the room to assist with the patient’s history. But some have joined via conference call and that’s been helpful, she said.
Neurologist Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles, whose clinic has gone to all-telemedicine visits, said telemedicine will make a huge difference for patients who live in remote areas or have mobility problems. In some cases, patients will actually be able to see their doctors more often, she said.
But she cautioned that it can be challenging to evaluate patients who are having difficulties with walking and sensation, although neurologists could try workarounds such as asking a patient to touch something cold. “We can do some things with coordination like watch patients walk, but walking motor strength is hard to check [via video],” she said. “The best thing to evaluate is cognition. You can talk to them and get a lot of it by asking questions.”
Carlos A. Pérez, MD, a neurologist at the University of Texas Health Science Center at Houston, noted that virtual visits can make it difficult to conduct comprehensive eye evaluations and examine vestibular and neuromuscular components such as weakness. “In multiple sclerosis patients, for example, diagnosing an MS relapse can be particularly difficult, especially when the patients present with mostly visual or sensory problems,” he said.
While he’s a fan of telemedicine overall, Dr. Pérez cautioned that low-income patients may lack computers and access to the Internet. “Access to resources in general seems to vary quite significantly,” he said. “Some patients use their cellphones for virtual visits, and that makes it extremely hard to examine them.”
Neurologist Amit Bar-Or, MD, of the University of Pennsylvania, Philadelphia, noted that in some cases, creativity can make a big difference in helping telemedicine visits to run smoothly. “In examining the cranial nerves, for example, you can get a lot of information. You need to have the person position the camera properly and get close to the camera so you can look at eye movements and facial symmetry.”
Still, he said, “if a patient wants to be seen in person, we should never deny them.”
As for other changes that will linger after the pandemic, San Diego–area neurologist Dr. Soria-Lopez said he expects that waiting rooms will continue to be less populated as patients wait elsewhere to avoid the spread of germs. He predicts there will be more use of “virtual waiting rooms” that allow patients to fill out paperwork remotely and get alerts when medical professionals are ready to see them.
Neurological sequelae from COVID-19
Dr. Pérez, the Houston neurologist, said his colleagues should expect another aspect of the pandemic to persist: an influx of patients with neurological sequelae from COVID-19. As he noted in a 2020 report in Neurology Clinical Practice, coronaviruses have been linked to numerous neurological complications during and after the infectious period. “I have seen a few cases of Guillain-Barré and even postinfectious encephalitis in the clinic [linked to COVID-19],” he said. “Neurologists in general should be aware of the risk for chronic, postinfectious neurologic complications from prior COVID-19 infection.”
And, he said, it’s reasonable for neurologists to add a question to patient histories. It’s a simple yet powerful query: Have you had COVID-19?
Can supplementary estrogen relieve MS symptoms in menopausal women?
, a neurologist told colleagues at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
This kind of research should explore the effects of aging, including in the brain, and “focus on what is preventable – this dramatic and abrupt loss of estrogen in women with MS,” said Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles.
“This is a call to action. There’s a huge gap that needs to be filled,” she added in an interview. “Not enough attention has been paid to menopause and cognitive issues in MS and even in healthy women.”
Research has found that many women with MS experience a decline in function during menopause, she said. “They’re having a worsening of their preexisting disabilities,” she noted, due to neurodegeneration.
Dr. Voskuhl highlighted a 2016 study, for instance, that found postmenopausal women with MS on hormone replacement therapy reported better physical function and quality of life than did their counterparts after adjustment for covariates. She also pointed to a 2019 study that concluded that “natural menopause seems to be a turning point to a more progressive phase of MS.”
Estrogen appears to play a significant role. “It’s involved in synaptic plasticity,” she said. “That’s why the disabilities are worsening.”
Dr. Voskuhl supports a year-long, randomized and controlled study of estrogen supplementation in 150-200 participants. The goal, she said, is “not just to prevent loss and bad things from happening but also make improvements.”
In healthy patients, she said, outcomes should include cognitive decline in menopause, cognitive domain outcomes, and region-specific biomarkers in the frontal cortex and hippocampus instead of global cognition and global brain volume. In patients with MS, she said, the focus should be on worsening of disability with emphasis on specific disabilities such as walking and region-specific biomarkers for the motor cortex and spinal cord.
“We need to be looking at cortical gray matter, which we know is responsive to estrogen,” Dr. Voskuhl said. She led a 2018 placebo-controlled study that found women with MS who took estrogen supplements appeared to experience localized sparing of progressive gray matter, which the researchers linked to improved results in cognitive testing. The findings, the study authors wrote, suggest “a clinically relevant, disability-specific biomarker for clinical trials of candidate neuroprotective treatments in MS.”
What about men? Does hormone loss worsen their MS? Dr. Voskuhl said there seems to be a connection between lower levels of testosterone and more disability in men with MS. But their situation is different. Loss of testosterone in men is gradual and happens over decades instead of over the short period of menopause in women, she said.
Jennifer Graves, MD, a neurologist at the University of California, San Diego, agreed that it’s time for further research into estrogen supplementation in MS. As she noted, “we don’t know the exact biological mechanism that might link perimenopause with developing a more progressive type of MS.”
She added: “An overall decrease in estrogen may be at play but there are other biological changes around menopause. We must also take care in studies to try to separate out what might be due to ovarian aging versus other types of aging processes that might be happening at the same time.”
Dr. Voskuhl disclosed that she is an inventor on university patents for use of estriol and estrogen receptor–beta ligands as treatments. Dr. Graves reports no relevant disclosures.
, a neurologist told colleagues at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
This kind of research should explore the effects of aging, including in the brain, and “focus on what is preventable – this dramatic and abrupt loss of estrogen in women with MS,” said Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles.
“This is a call to action. There’s a huge gap that needs to be filled,” she added in an interview. “Not enough attention has been paid to menopause and cognitive issues in MS and even in healthy women.”
Research has found that many women with MS experience a decline in function during menopause, she said. “They’re having a worsening of their preexisting disabilities,” she noted, due to neurodegeneration.
Dr. Voskuhl highlighted a 2016 study, for instance, that found postmenopausal women with MS on hormone replacement therapy reported better physical function and quality of life than did their counterparts after adjustment for covariates. She also pointed to a 2019 study that concluded that “natural menopause seems to be a turning point to a more progressive phase of MS.”
Estrogen appears to play a significant role. “It’s involved in synaptic plasticity,” she said. “That’s why the disabilities are worsening.”
Dr. Voskuhl supports a year-long, randomized and controlled study of estrogen supplementation in 150-200 participants. The goal, she said, is “not just to prevent loss and bad things from happening but also make improvements.”
In healthy patients, she said, outcomes should include cognitive decline in menopause, cognitive domain outcomes, and region-specific biomarkers in the frontal cortex and hippocampus instead of global cognition and global brain volume. In patients with MS, she said, the focus should be on worsening of disability with emphasis on specific disabilities such as walking and region-specific biomarkers for the motor cortex and spinal cord.
“We need to be looking at cortical gray matter, which we know is responsive to estrogen,” Dr. Voskuhl said. She led a 2018 placebo-controlled study that found women with MS who took estrogen supplements appeared to experience localized sparing of progressive gray matter, which the researchers linked to improved results in cognitive testing. The findings, the study authors wrote, suggest “a clinically relevant, disability-specific biomarker for clinical trials of candidate neuroprotective treatments in MS.”
What about men? Does hormone loss worsen their MS? Dr. Voskuhl said there seems to be a connection between lower levels of testosterone and more disability in men with MS. But their situation is different. Loss of testosterone in men is gradual and happens over decades instead of over the short period of menopause in women, she said.
Jennifer Graves, MD, a neurologist at the University of California, San Diego, agreed that it’s time for further research into estrogen supplementation in MS. As she noted, “we don’t know the exact biological mechanism that might link perimenopause with developing a more progressive type of MS.”
She added: “An overall decrease in estrogen may be at play but there are other biological changes around menopause. We must also take care in studies to try to separate out what might be due to ovarian aging versus other types of aging processes that might be happening at the same time.”
Dr. Voskuhl disclosed that she is an inventor on university patents for use of estriol and estrogen receptor–beta ligands as treatments. Dr. Graves reports no relevant disclosures.
, a neurologist told colleagues at the meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis.
This kind of research should explore the effects of aging, including in the brain, and “focus on what is preventable – this dramatic and abrupt loss of estrogen in women with MS,” said Rhonda Voskuhl, MD, of the Brain Research Institute at the University of California, Los Angeles.
“This is a call to action. There’s a huge gap that needs to be filled,” she added in an interview. “Not enough attention has been paid to menopause and cognitive issues in MS and even in healthy women.”
Research has found that many women with MS experience a decline in function during menopause, she said. “They’re having a worsening of their preexisting disabilities,” she noted, due to neurodegeneration.
Dr. Voskuhl highlighted a 2016 study, for instance, that found postmenopausal women with MS on hormone replacement therapy reported better physical function and quality of life than did their counterparts after adjustment for covariates. She also pointed to a 2019 study that concluded that “natural menopause seems to be a turning point to a more progressive phase of MS.”
Estrogen appears to play a significant role. “It’s involved in synaptic plasticity,” she said. “That’s why the disabilities are worsening.”
Dr. Voskuhl supports a year-long, randomized and controlled study of estrogen supplementation in 150-200 participants. The goal, she said, is “not just to prevent loss and bad things from happening but also make improvements.”
In healthy patients, she said, outcomes should include cognitive decline in menopause, cognitive domain outcomes, and region-specific biomarkers in the frontal cortex and hippocampus instead of global cognition and global brain volume. In patients with MS, she said, the focus should be on worsening of disability with emphasis on specific disabilities such as walking and region-specific biomarkers for the motor cortex and spinal cord.
“We need to be looking at cortical gray matter, which we know is responsive to estrogen,” Dr. Voskuhl said. She led a 2018 placebo-controlled study that found women with MS who took estrogen supplements appeared to experience localized sparing of progressive gray matter, which the researchers linked to improved results in cognitive testing. The findings, the study authors wrote, suggest “a clinically relevant, disability-specific biomarker for clinical trials of candidate neuroprotective treatments in MS.”
What about men? Does hormone loss worsen their MS? Dr. Voskuhl said there seems to be a connection between lower levels of testosterone and more disability in men with MS. But their situation is different. Loss of testosterone in men is gradual and happens over decades instead of over the short period of menopause in women, she said.
Jennifer Graves, MD, a neurologist at the University of California, San Diego, agreed that it’s time for further research into estrogen supplementation in MS. As she noted, “we don’t know the exact biological mechanism that might link perimenopause with developing a more progressive type of MS.”
She added: “An overall decrease in estrogen may be at play but there are other biological changes around menopause. We must also take care in studies to try to separate out what might be due to ovarian aging versus other types of aging processes that might be happening at the same time.”
Dr. Voskuhl disclosed that she is an inventor on university patents for use of estriol and estrogen receptor–beta ligands as treatments. Dr. Graves reports no relevant disclosures.
FROM ACTRIMS FORUM 2021
Infantile hemangiomas: Accurate diagnosis is crucial
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
The first rule about infantile hemangiomas: Make sure they’re actually infantile hemangiomas, a pediatric dermatologist urged colleagues. Then watch patients closely, refer to specialists when appropriate, and consider propranolol in complicated or high-risk cases, Andrea L. Zaenglein, MD, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
“In my career as a pediatric dermatologist, propranolol has been a life changer for us more than any other medicine,” said Dr. Zaenglein, professor of dermatology and pediatric dermatology, Penn State University, Hershey.
Before the point where propranolol is prescribed, confirm the diagnosis and use the correct terminology, she advised. It’s still appropriate to use the International Society for the Study of Vascular Anomalies (ISSVA) vascular lesion classification system released in 1982. “For most people, it serves the purpose well,” she said. Another option is an updated and more complex classification system from 2015.
Dr. Zaenglein highlighted two studies – one published in 2011 and the other published in 2020 – that revealed high levels of misclassification of vascular malformations in research reports. The earlier study found that 21% of patients with misclassified lesions were mistreated, compared with none of those who were classified using ISSVA terminology.
“I cannot stress [proper classification] enough when you’re dealing with babies and children with vascular lesions. If not sure, be vague. Say ‘a vascular tumor’ or a ‘vascular malformation.’ But only reserve ‘infantile hemangioma’ for that very diagnosis,” she said.
As Dr. Zaenglein noted, infantile hemangiomas affect 5%-10% of 1-year-olds, of whom 20% have multiple lesions. They’re more common in females by a 3-to-1 margin, and also seen more in premature infants, and in cases of multiple births, higher maternal age, and low birth weight.
The pathogenesis of these lesions is unclear, she said, although there are hints about genetic components and tissue hypoxia, among other possible causes. “Importantly, you get 80% of the growth by 3-4 months of age. Then it’ll slow in its growth and kind of slowly go away over time, but it’s not linear regression. It’s more that you get more improvement up front, usually until about 5, and then you can get some continued gradual evolution up until about 7 or 10 years of age.”
Complications can include ulceration, infection and – in rare cases – hemorrhage and high-output cardiac failure, she said. “Knowing which ones are at high risk for complications is important, and also there are systemic associations that we have to be mindful of. We also want to think about aesthetic outcomes as well when we talk about management of infantile hemangiomas.”
High-risk infantile hemangiomas include those with the following features:
- Extensive facial involvement. Dr. Zaenglein highlighted a case of a 2-year-old baby with a large, bulky hemangioma that distorted facial features around the eye. “This would be a medical emergency” requiring immediate evaluation and treatment, she said.
- Periocular involvement. Refer to ophthalmology, she recommended. “Even smaller hemangiomas can cause refractive errors or amblyopia, and oftentimes need to be treated with either systemic or topical therapy depending on the size and extent,” she said.
- PHACE syndrome (Posterior fossa malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, eye abnormalities). “Propranolol has been safely used in PHACE, but every patient is different,” she said. “You need to make sure to do a good risk assessment before starting because if they have narrowed blood flow or limited blood flow, there is a question of whether there is potential risk for stroke if you drop a baby’s blood pressure. Make sure that the vasculature is evaluated before started on propranolol. Also, there are recent reports of risk of long-term risk of stroke with PHACE syndrome as patients are getting into their adulthood.”
- Beard distribution. Be aware of possible airway involvement that can be revealed by biphasic stridor. In those cases, immediate treatment – perhaps even with tracheostomy – is needed to avoid mortality, she said.
- Multiple sites: Patients with five or more hemangiomas may have liver involvement, she said, and should undergo hepatic evaluation. Consider evaluating if this is suspected, even if the number of hemangiomas is under five, she said.
- Perineal/lumbosacral involvement: A third of these cases are associated with spinal dysraphism. Refer to neurosurgery, she recommended.
Dr. Zaenglein highlighted a report on the use of propranolol published in 2008 and noted that clinical practice guidelines for managing infantile hemangiomas published in 2019 are also helpful.
Flat hemangiomas, meanwhile, can benefit from timolol maleate 0.5% solution or gel-forming solution – 1 drop twice daily or 2 drops once daily, she said. This treatment should be avoided in thick hemangiomas, she said.
MedscapeLive and this news organization are owned by the same parent company. Dr. Zaenglein disclosed consulting fees (Dermata, Cassiopea, and Regeneron), and fees for contracted research support (Incyte).
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Managing hyperhidrosis, HS: Ask questions first
A wide variety of medications exists for treating hyperhidrosis, a dermatologist told colleagues, but before prescribing anything to a pediatric patient, he recommended, ask the patient a simple question: “What bothers you the most?”
The answer will provide guidance for developing a step-by-step treatment strategy and help provide the patient “a set of realistic expectations in terms of what the response will look like,” George Hightower, MD, PhD, a pediatric dermatologist at Rady Children’s Hospital and the University of California, San Diego, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
A similar question-based approach will help guide therapy for patients with hidradenitis suppurativa (HS), he said.
With regards to hyperhidrosis, Dr. Hightower said that patients most commonly complain that their underarms are too smelly, too sweaty, and red, itchy, or painful. Causes, he said, can include irritation/contact dermatitis, folliculitis, and seborrheic dermatitis, as well as hyperhidrosis or HS.
Primary focal axillary hyperhidrosis is defined as focal, visible, excessive sweating for at least 6 months without an apparent cause plus at least two of the following characteristics: Sweating is bilateral and relatively symmetric, it impairs daily activities, it starts before the age of 25 with at least one episode per week (many patients have it daily), a family history of idiopathic hyperhidrosis is present, and focal sweating does not occur during sleep.
Secondary hyperhidrosis can be linked to other conditions, such as a spinal column injury, Dr. Hightower noted.
The first step on the treatment ladder is topical 20% aluminum chloride, which is available over the counter. This should be applied nightly for 1 week then every 1-2 weeks, Dr. Hightower recommended. All of his patients with hyperhidrosis have had at least one trial of this treatment.
The next option is daily topical treatment with 2.4% glycopyrronium tosylate (Qbrexza) cloths, approved by the Food and Drug Administration in 2018 for primary axillary hyperhidrosis in patients aged 9 and older. According to the prescribing information, dry mouth was by far the most common treatment-associated adverse effect in clinical trials (24% versus almost 6% among those on vehicle). As for skin reactions, erythema occurred in about 17% of both the intervention and vehicle groups, and burning/stinging occurred in 14% of those on treatment and almost 17% of those on vehicle.
“If they’re not able to get access to the cloths due to [insurance] coverage issues, or they don’t allow them to reach the clinical endpoint desired, then I use an oral daily glycopyrrolate pill,” Dr. Hightower said.
He recommends 1 mg to 6 mg daily of the anticholinergic drug, which has been used off-label for hyperhidrosis for several years. A 2012 study of 31 children with hyperhidrosis, he noted, supported the use of the drug. The retrospective study found that 90% of the patients, at a mean daily dose of 2 mg, experienced improvements, reported as major in 71%. In addition, patients experienced improvement within hours of taking the medication, and benefits disappeared within a day of stopping the medication. In the study, patients were on the treatment for an average of 2.1 years, and 29% experienced side effects, which were dose related; the most common were dry mouth in 26% and dry eyes in 10%.
According to goodrx.com, a month’s supply of 2 mg of the drug costs as little as $13 with a discount or coupon.
The next steps in treatment are procedural interventions such as microwave-based therapies.
Dr. Hightower said that patients should be advised that treatment may take years, and to encourage them to return for follow-up. He suggested this helpful message: “We’re still trying to find the best treatment for you, and we’ll need to see you back in the office.”
Hidradenitis suppurativa
Dr. Hightower said that too often, HS goes undiagnosed for a significant period of time, preventing patients from seeing a dermatologist for treatment. Hallmarks of HS include inflammatory nodules, abscesses, and scarring, he said. “It can be disfiguring, painful, embarrassing, and associated with significantly decreased quality of life. Early recognition in terms of making and solidifying the diagnosis is important so we can prevent further worsening of the disease.”
The goal of treatment include preventing scars and unnecessary emergency department visits, and stopping flares from worsening, Dr. Hightower said. For specifics, he pointed to clinical management guidelines released by the United States and Canadian hidradenitis suppurativa foundations in 2019.
Make sure to set individualized treatment goals and understand the impact of treatment on the patient’s interactions with family, school, and peers, he said. And keep in mind that “parent-defined goals may be different from patient-defined goals.”
Dr. Hightower reported no relevant disclosures. MedscapeLive and this news organization are owned by the same parent company
A wide variety of medications exists for treating hyperhidrosis, a dermatologist told colleagues, but before prescribing anything to a pediatric patient, he recommended, ask the patient a simple question: “What bothers you the most?”
The answer will provide guidance for developing a step-by-step treatment strategy and help provide the patient “a set of realistic expectations in terms of what the response will look like,” George Hightower, MD, PhD, a pediatric dermatologist at Rady Children’s Hospital and the University of California, San Diego, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
A similar question-based approach will help guide therapy for patients with hidradenitis suppurativa (HS), he said.
With regards to hyperhidrosis, Dr. Hightower said that patients most commonly complain that their underarms are too smelly, too sweaty, and red, itchy, or painful. Causes, he said, can include irritation/contact dermatitis, folliculitis, and seborrheic dermatitis, as well as hyperhidrosis or HS.
Primary focal axillary hyperhidrosis is defined as focal, visible, excessive sweating for at least 6 months without an apparent cause plus at least two of the following characteristics: Sweating is bilateral and relatively symmetric, it impairs daily activities, it starts before the age of 25 with at least one episode per week (many patients have it daily), a family history of idiopathic hyperhidrosis is present, and focal sweating does not occur during sleep.
Secondary hyperhidrosis can be linked to other conditions, such as a spinal column injury, Dr. Hightower noted.
The first step on the treatment ladder is topical 20% aluminum chloride, which is available over the counter. This should be applied nightly for 1 week then every 1-2 weeks, Dr. Hightower recommended. All of his patients with hyperhidrosis have had at least one trial of this treatment.
The next option is daily topical treatment with 2.4% glycopyrronium tosylate (Qbrexza) cloths, approved by the Food and Drug Administration in 2018 for primary axillary hyperhidrosis in patients aged 9 and older. According to the prescribing information, dry mouth was by far the most common treatment-associated adverse effect in clinical trials (24% versus almost 6% among those on vehicle). As for skin reactions, erythema occurred in about 17% of both the intervention and vehicle groups, and burning/stinging occurred in 14% of those on treatment and almost 17% of those on vehicle.
“If they’re not able to get access to the cloths due to [insurance] coverage issues, or they don’t allow them to reach the clinical endpoint desired, then I use an oral daily glycopyrrolate pill,” Dr. Hightower said.
He recommends 1 mg to 6 mg daily of the anticholinergic drug, which has been used off-label for hyperhidrosis for several years. A 2012 study of 31 children with hyperhidrosis, he noted, supported the use of the drug. The retrospective study found that 90% of the patients, at a mean daily dose of 2 mg, experienced improvements, reported as major in 71%. In addition, patients experienced improvement within hours of taking the medication, and benefits disappeared within a day of stopping the medication. In the study, patients were on the treatment for an average of 2.1 years, and 29% experienced side effects, which were dose related; the most common were dry mouth in 26% and dry eyes in 10%.
According to goodrx.com, a month’s supply of 2 mg of the drug costs as little as $13 with a discount or coupon.
The next steps in treatment are procedural interventions such as microwave-based therapies.
Dr. Hightower said that patients should be advised that treatment may take years, and to encourage them to return for follow-up. He suggested this helpful message: “We’re still trying to find the best treatment for you, and we’ll need to see you back in the office.”
Hidradenitis suppurativa
Dr. Hightower said that too often, HS goes undiagnosed for a significant period of time, preventing patients from seeing a dermatologist for treatment. Hallmarks of HS include inflammatory nodules, abscesses, and scarring, he said. “It can be disfiguring, painful, embarrassing, and associated with significantly decreased quality of life. Early recognition in terms of making and solidifying the diagnosis is important so we can prevent further worsening of the disease.”
The goal of treatment include preventing scars and unnecessary emergency department visits, and stopping flares from worsening, Dr. Hightower said. For specifics, he pointed to clinical management guidelines released by the United States and Canadian hidradenitis suppurativa foundations in 2019.
Make sure to set individualized treatment goals and understand the impact of treatment on the patient’s interactions with family, school, and peers, he said. And keep in mind that “parent-defined goals may be different from patient-defined goals.”
Dr. Hightower reported no relevant disclosures. MedscapeLive and this news organization are owned by the same parent company
A wide variety of medications exists for treating hyperhidrosis, a dermatologist told colleagues, but before prescribing anything to a pediatric patient, he recommended, ask the patient a simple question: “What bothers you the most?”
The answer will provide guidance for developing a step-by-step treatment strategy and help provide the patient “a set of realistic expectations in terms of what the response will look like,” George Hightower, MD, PhD, a pediatric dermatologist at Rady Children’s Hospital and the University of California, San Diego, said at MedscapeLive’s Women’s & Pediatric Dermatology Seminar.
A similar question-based approach will help guide therapy for patients with hidradenitis suppurativa (HS), he said.
With regards to hyperhidrosis, Dr. Hightower said that patients most commonly complain that their underarms are too smelly, too sweaty, and red, itchy, or painful. Causes, he said, can include irritation/contact dermatitis, folliculitis, and seborrheic dermatitis, as well as hyperhidrosis or HS.
Primary focal axillary hyperhidrosis is defined as focal, visible, excessive sweating for at least 6 months without an apparent cause plus at least two of the following characteristics: Sweating is bilateral and relatively symmetric, it impairs daily activities, it starts before the age of 25 with at least one episode per week (many patients have it daily), a family history of idiopathic hyperhidrosis is present, and focal sweating does not occur during sleep.
Secondary hyperhidrosis can be linked to other conditions, such as a spinal column injury, Dr. Hightower noted.
The first step on the treatment ladder is topical 20% aluminum chloride, which is available over the counter. This should be applied nightly for 1 week then every 1-2 weeks, Dr. Hightower recommended. All of his patients with hyperhidrosis have had at least one trial of this treatment.
The next option is daily topical treatment with 2.4% glycopyrronium tosylate (Qbrexza) cloths, approved by the Food and Drug Administration in 2018 for primary axillary hyperhidrosis in patients aged 9 and older. According to the prescribing information, dry mouth was by far the most common treatment-associated adverse effect in clinical trials (24% versus almost 6% among those on vehicle). As for skin reactions, erythema occurred in about 17% of both the intervention and vehicle groups, and burning/stinging occurred in 14% of those on treatment and almost 17% of those on vehicle.
“If they’re not able to get access to the cloths due to [insurance] coverage issues, or they don’t allow them to reach the clinical endpoint desired, then I use an oral daily glycopyrrolate pill,” Dr. Hightower said.
He recommends 1 mg to 6 mg daily of the anticholinergic drug, which has been used off-label for hyperhidrosis for several years. A 2012 study of 31 children with hyperhidrosis, he noted, supported the use of the drug. The retrospective study found that 90% of the patients, at a mean daily dose of 2 mg, experienced improvements, reported as major in 71%. In addition, patients experienced improvement within hours of taking the medication, and benefits disappeared within a day of stopping the medication. In the study, patients were on the treatment for an average of 2.1 years, and 29% experienced side effects, which were dose related; the most common were dry mouth in 26% and dry eyes in 10%.
According to goodrx.com, a month’s supply of 2 mg of the drug costs as little as $13 with a discount or coupon.
The next steps in treatment are procedural interventions such as microwave-based therapies.
Dr. Hightower said that patients should be advised that treatment may take years, and to encourage them to return for follow-up. He suggested this helpful message: “We’re still trying to find the best treatment for you, and we’ll need to see you back in the office.”
Hidradenitis suppurativa
Dr. Hightower said that too often, HS goes undiagnosed for a significant period of time, preventing patients from seeing a dermatologist for treatment. Hallmarks of HS include inflammatory nodules, abscesses, and scarring, he said. “It can be disfiguring, painful, embarrassing, and associated with significantly decreased quality of life. Early recognition in terms of making and solidifying the diagnosis is important so we can prevent further worsening of the disease.”
The goal of treatment include preventing scars and unnecessary emergency department visits, and stopping flares from worsening, Dr. Hightower said. For specifics, he pointed to clinical management guidelines released by the United States and Canadian hidradenitis suppurativa foundations in 2019.
Make sure to set individualized treatment goals and understand the impact of treatment on the patient’s interactions with family, school, and peers, he said. And keep in mind that “parent-defined goals may be different from patient-defined goals.”
Dr. Hightower reported no relevant disclosures. MedscapeLive and this news organization are owned by the same parent company
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Disease progression and therapy response vary in MS by ethnicity
a new study finds, and there are big gaps in how they respond to disease-modifying therapies (DMTs).
“Hispanics and African Americans develop a more severe disease course and accumulate more MS-related disability over time despite similar sociodemographic backgrounds and similar patterns of DMT use throughout their disease, suggesting that socioeconomic status and access to health care may not be the main determinants of health,” said neurologist Carlos Pérez, MD, of the University of Texas Health Science Center, Houston. He spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and in a follow-up interview.
“In addition,” Dr. Pérez said, “therapeutic responses to individual DMTs, as well as tolerance and side-effect profiles, are also variable among racial/ethnic groups.”
The researchers tracked 150 patients with MS at the University of Texas Health Science Center – 50 Whites, 50 African American, and 50 Hispanic – who were age and gender matched. The average age of the subjects was 45, and 74% of those in each group were women.
While educational levels between the groups were similar, African Americans had a much higher rate of lost employment because of disability (38%) than Hispanics (19%) and Whites (15%, P = .02). Fifty-seven patients (38%) needed escalation of therapy, and 63% were African American.
About 30% of subjects switched DMTs because of intolerance/adverse events, and 47% of those were African American. Interferons most commonly caused adverse effects in African Americans (61%), and Whites were the most likely to not tolerate glatiramer acetate (39%) than Hispanics (8%) and African Americans (13%).
What might be behind the disparities? “It is possible that genetic factors may play a greater role than previously thought. A recent study reported that Hispanic and African American patients with MS have higher levels of peripheral blood plasmablasts, which may provide indirect evidence for potential biological mechanisms underlying racial and clinical disparities in MS,” Dr. Pérez said. “These mechanisms appear to involve higher degrees of inflammation in the central nervous system. This may explain why African Americans may respond better to higher-efficacy therapies initially, when inflammatory processes predominate MS-related pathology, rather than at later stages of the disease when inflammation plays a less prominent role. Neurologists should consider higher-efficacy DMT as first line. We have begun to do this in our practice.”
Dr. Pérez said the findings offer other lessons. “Neurologists should consider that Caucasian patients tolerate glatiramer acetate less frequently, compared with other racial groups, and potentially consider using alternative DMTs unless the benefits outweigh the risks, such as during pregnancy.”
He also noted that African Americans treated with oral DMTs at baseline were more likely to develop worsening disability over time. “This argues in favor of infusion therapies as first-line treatment,” he said, adding that more Hispanics with MS were not on treatment – or discontinued treatment – compared with Whites and African Americans.
Close patient monitoring is key
Atlanta-area neurologist Mitzi Joi Williams, MD, who was asked to comment on the study findings, said in an interview that it “adds to the body of real-world evidence to assist understanding of MS in minority populations.”
She noted that African American patients who started on infusions appeared to be more stable. “There are a great deal of questions surrounding starting patients on injectables versus higher-efficacy therapy initially to prevent disability and this may lend credence to the need for closer examination of initial therapy for these patients. It is important to closely monitor patients and consider a switch in DMT if there is any clinical or radiologic progression, especially for African American and Hispanic patients since there is a great deal of data to suggest they may have more aggressive disease.”
Moving forward, more research like this is needed, she said. “Patients did all have insurance and were largely educated, but there could be other social determinants of health – i.e., transportation, lapses in insurance, or technology barriers – that may have led to worse outcomes.”
No study funding was reported, and Dr. Pérez reported no disclosures. Dr. Williams disclosed research support from EMD Serono, Genentech, and Novartis and advisory committee/consultant relationships with AbbVie, Biogen Idec, Bristol-Myers Squibb, EMD Serono, Genentech, Novartis, and Sanofi Genzyme.
a new study finds, and there are big gaps in how they respond to disease-modifying therapies (DMTs).
“Hispanics and African Americans develop a more severe disease course and accumulate more MS-related disability over time despite similar sociodemographic backgrounds and similar patterns of DMT use throughout their disease, suggesting that socioeconomic status and access to health care may not be the main determinants of health,” said neurologist Carlos Pérez, MD, of the University of Texas Health Science Center, Houston. He spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and in a follow-up interview.
“In addition,” Dr. Pérez said, “therapeutic responses to individual DMTs, as well as tolerance and side-effect profiles, are also variable among racial/ethnic groups.”
The researchers tracked 150 patients with MS at the University of Texas Health Science Center – 50 Whites, 50 African American, and 50 Hispanic – who were age and gender matched. The average age of the subjects was 45, and 74% of those in each group were women.
While educational levels between the groups were similar, African Americans had a much higher rate of lost employment because of disability (38%) than Hispanics (19%) and Whites (15%, P = .02). Fifty-seven patients (38%) needed escalation of therapy, and 63% were African American.
About 30% of subjects switched DMTs because of intolerance/adverse events, and 47% of those were African American. Interferons most commonly caused adverse effects in African Americans (61%), and Whites were the most likely to not tolerate glatiramer acetate (39%) than Hispanics (8%) and African Americans (13%).
What might be behind the disparities? “It is possible that genetic factors may play a greater role than previously thought. A recent study reported that Hispanic and African American patients with MS have higher levels of peripheral blood plasmablasts, which may provide indirect evidence for potential biological mechanisms underlying racial and clinical disparities in MS,” Dr. Pérez said. “These mechanisms appear to involve higher degrees of inflammation in the central nervous system. This may explain why African Americans may respond better to higher-efficacy therapies initially, when inflammatory processes predominate MS-related pathology, rather than at later stages of the disease when inflammation plays a less prominent role. Neurologists should consider higher-efficacy DMT as first line. We have begun to do this in our practice.”
Dr. Pérez said the findings offer other lessons. “Neurologists should consider that Caucasian patients tolerate glatiramer acetate less frequently, compared with other racial groups, and potentially consider using alternative DMTs unless the benefits outweigh the risks, such as during pregnancy.”
He also noted that African Americans treated with oral DMTs at baseline were more likely to develop worsening disability over time. “This argues in favor of infusion therapies as first-line treatment,” he said, adding that more Hispanics with MS were not on treatment – or discontinued treatment – compared with Whites and African Americans.
Close patient monitoring is key
Atlanta-area neurologist Mitzi Joi Williams, MD, who was asked to comment on the study findings, said in an interview that it “adds to the body of real-world evidence to assist understanding of MS in minority populations.”
She noted that African American patients who started on infusions appeared to be more stable. “There are a great deal of questions surrounding starting patients on injectables versus higher-efficacy therapy initially to prevent disability and this may lend credence to the need for closer examination of initial therapy for these patients. It is important to closely monitor patients and consider a switch in DMT if there is any clinical or radiologic progression, especially for African American and Hispanic patients since there is a great deal of data to suggest they may have more aggressive disease.”
Moving forward, more research like this is needed, she said. “Patients did all have insurance and were largely educated, but there could be other social determinants of health – i.e., transportation, lapses in insurance, or technology barriers – that may have led to worse outcomes.”
No study funding was reported, and Dr. Pérez reported no disclosures. Dr. Williams disclosed research support from EMD Serono, Genentech, and Novartis and advisory committee/consultant relationships with AbbVie, Biogen Idec, Bristol-Myers Squibb, EMD Serono, Genentech, Novartis, and Sanofi Genzyme.
a new study finds, and there are big gaps in how they respond to disease-modifying therapies (DMTs).
“Hispanics and African Americans develop a more severe disease course and accumulate more MS-related disability over time despite similar sociodemographic backgrounds and similar patterns of DMT use throughout their disease, suggesting that socioeconomic status and access to health care may not be the main determinants of health,” said neurologist Carlos Pérez, MD, of the University of Texas Health Science Center, Houston. He spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and in a follow-up interview.
“In addition,” Dr. Pérez said, “therapeutic responses to individual DMTs, as well as tolerance and side-effect profiles, are also variable among racial/ethnic groups.”
The researchers tracked 150 patients with MS at the University of Texas Health Science Center – 50 Whites, 50 African American, and 50 Hispanic – who were age and gender matched. The average age of the subjects was 45, and 74% of those in each group were women.
While educational levels between the groups were similar, African Americans had a much higher rate of lost employment because of disability (38%) than Hispanics (19%) and Whites (15%, P = .02). Fifty-seven patients (38%) needed escalation of therapy, and 63% were African American.
About 30% of subjects switched DMTs because of intolerance/adverse events, and 47% of those were African American. Interferons most commonly caused adverse effects in African Americans (61%), and Whites were the most likely to not tolerate glatiramer acetate (39%) than Hispanics (8%) and African Americans (13%).
What might be behind the disparities? “It is possible that genetic factors may play a greater role than previously thought. A recent study reported that Hispanic and African American patients with MS have higher levels of peripheral blood plasmablasts, which may provide indirect evidence for potential biological mechanisms underlying racial and clinical disparities in MS,” Dr. Pérez said. “These mechanisms appear to involve higher degrees of inflammation in the central nervous system. This may explain why African Americans may respond better to higher-efficacy therapies initially, when inflammatory processes predominate MS-related pathology, rather than at later stages of the disease when inflammation plays a less prominent role. Neurologists should consider higher-efficacy DMT as first line. We have begun to do this in our practice.”
Dr. Pérez said the findings offer other lessons. “Neurologists should consider that Caucasian patients tolerate glatiramer acetate less frequently, compared with other racial groups, and potentially consider using alternative DMTs unless the benefits outweigh the risks, such as during pregnancy.”
He also noted that African Americans treated with oral DMTs at baseline were more likely to develop worsening disability over time. “This argues in favor of infusion therapies as first-line treatment,” he said, adding that more Hispanics with MS were not on treatment – or discontinued treatment – compared with Whites and African Americans.
Close patient monitoring is key
Atlanta-area neurologist Mitzi Joi Williams, MD, who was asked to comment on the study findings, said in an interview that it “adds to the body of real-world evidence to assist understanding of MS in minority populations.”
She noted that African American patients who started on infusions appeared to be more stable. “There are a great deal of questions surrounding starting patients on injectables versus higher-efficacy therapy initially to prevent disability and this may lend credence to the need for closer examination of initial therapy for these patients. It is important to closely monitor patients and consider a switch in DMT if there is any clinical or radiologic progression, especially for African American and Hispanic patients since there is a great deal of data to suggest they may have more aggressive disease.”
Moving forward, more research like this is needed, she said. “Patients did all have insurance and were largely educated, but there could be other social determinants of health – i.e., transportation, lapses in insurance, or technology barriers – that may have led to worse outcomes.”
No study funding was reported, and Dr. Pérez reported no disclosures. Dr. Williams disclosed research support from EMD Serono, Genentech, and Novartis and advisory committee/consultant relationships with AbbVie, Biogen Idec, Bristol-Myers Squibb, EMD Serono, Genentech, Novartis, and Sanofi Genzyme.
FROM ACTRIMS FORUM 2021
Newly approved drugs offer new hope in NMOSD
a neurologist told colleagues.

“Patients have a choice of different options with different types of action. It’s good news,” said Sean J. Pittock, MD, of the Mayo Clinic in Rochester, Minn. “If you don’t stop the clinical attacks, patients can become very disabled very quickly. These medications have a significant impact in reducing the likelihood of having a clinical relapse. If you can stop the relapses, you certainly can eventually stop most – if not all – of the disability accrual.”
Dr. Pittock spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and answered follow-up questions in an interview.
Treatment advances for NMOSD
NMOSD, also known as NMO, is a relapsing autoimmune inflammatory disorder that causes recurrent optic neuritis and myelitis. It’s a rare disease, affecting 0.5-10 people per 100,000, mostly women.
Several recent trials have supported the use of the drugs eculizumab (Soliris), satralizumab (Enspryng) and inebilizumab (Uplizna) in NMOSD, Dr. Pittock said, and all have received Food and Drug Administration approval to treat the condition over the past 2 years. Dr. Pittock led the PREVENT trial of eculizumab, which showed a 94% reduction of relapse risk versus placebo.
The newly approved drugs are stunningly expensive. According to Dr. Pittock, eculizumab costs $710,000 a year, while inebilizumab runs $393,000 the first year, then $262,000 a year. Satralizumab is $219,000 the first year, then $190,000 a year. Assistance programs are available, Dr. Pittock said, “and we’ve not had any major problems in terms of initiation.”
The cost of rituximab (Rituxan), which has a history of use as an off-label treatment option, is $18,000 a year and dropping, according to Dr. Pittock. There’s also new research on rituximab: In 2020, a small Japanese trial (n = 38) reported prevention of relapses compared with placebo, but Dr. Pittock cautioned that “the placebo patients seem to have a more benign course or more benign phenotypes” than the intervention group.
“There’s no doubt that rituximab works, but does it work as well as the other medications that have been through more of a robust trial process?” he asked. Keep in mind, he added, that perhaps 20%-50% of patients will relapse on rituximab.
Dr. Pittock advised colleagues to consider factors like patient schedules and compliance when choosing a drug. Satralizumab is self-administered monthly, while inebilizumab and rituximab are infused every 6 months.
Progress in anti-MOG disease
The trials in NMOSD should spur studies of the drugs in anti–myelin oligodendrocyte glycoprotein (MOG) disease, he said. “I think we’ll see a more rapid move toward phase 3 trials because of the experience with NMO. We will just have to wait and see which medications enter trial.”
Anti-MOG disease, also known as MOG antibody disease (MOGAD) and anti-MOG–associated encephalomyelitis, is caused by anti-MOG antibodies. Optic neuritis is very common, and transverse myelitis can occur.
The condition “actually responds to different drugs than MS and has a different immune pathophysiology,” Dr. Pittock said.
He cautioned colleagues to be aware that “the ability of the antibody to tell you whether or not the patient has the disease is less clear for MOGAD than it is for other diseases. If your patient has a low titer of MOG antibody, and their phenotype really doesn’t look like [MOGAD], you really need to interpret that with significant caution.”
He also highlighted a 2018 report that offers guidance about diagnosis and when MOG-IgC antibody tests are appropriate in CNS demyelinating disease.
Dr. Pittock reported numerous disclosures plus patents issued or pending.
a neurologist told colleagues.
“Patients have a choice of different options with different types of action. It’s good news,” said Sean J. Pittock, MD, of the Mayo Clinic in Rochester, Minn. “If you don’t stop the clinical attacks, patients can become very disabled very quickly. These medications have a significant impact in reducing the likelihood of having a clinical relapse. If you can stop the relapses, you certainly can eventually stop most – if not all – of the disability accrual.”
Dr. Pittock spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and answered follow-up questions in an interview.
Treatment advances for NMOSD
NMOSD, also known as NMO, is a relapsing autoimmune inflammatory disorder that causes recurrent optic neuritis and myelitis. It’s a rare disease, affecting 0.5-10 people per 100,000, mostly women.
Several recent trials have supported the use of the drugs eculizumab (Soliris), satralizumab (Enspryng) and inebilizumab (Uplizna) in NMOSD, Dr. Pittock said, and all have received Food and Drug Administration approval to treat the condition over the past 2 years. Dr. Pittock led the PREVENT trial of eculizumab, which showed a 94% reduction of relapse risk versus placebo.
The newly approved drugs are stunningly expensive. According to Dr. Pittock, eculizumab costs $710,000 a year, while inebilizumab runs $393,000 the first year, then $262,000 a year. Satralizumab is $219,000 the first year, then $190,000 a year. Assistance programs are available, Dr. Pittock said, “and we’ve not had any major problems in terms of initiation.”
The cost of rituximab (Rituxan), which has a history of use as an off-label treatment option, is $18,000 a year and dropping, according to Dr. Pittock. There’s also new research on rituximab: In 2020, a small Japanese trial (n = 38) reported prevention of relapses compared with placebo, but Dr. Pittock cautioned that “the placebo patients seem to have a more benign course or more benign phenotypes” than the intervention group.
“There’s no doubt that rituximab works, but does it work as well as the other medications that have been through more of a robust trial process?” he asked. Keep in mind, he added, that perhaps 20%-50% of patients will relapse on rituximab.
Dr. Pittock advised colleagues to consider factors like patient schedules and compliance when choosing a drug. Satralizumab is self-administered monthly, while inebilizumab and rituximab are infused every 6 months.
Progress in anti-MOG disease
The trials in NMOSD should spur studies of the drugs in anti–myelin oligodendrocyte glycoprotein (MOG) disease, he said. “I think we’ll see a more rapid move toward phase 3 trials because of the experience with NMO. We will just have to wait and see which medications enter trial.”
Anti-MOG disease, also known as MOG antibody disease (MOGAD) and anti-MOG–associated encephalomyelitis, is caused by anti-MOG antibodies. Optic neuritis is very common, and transverse myelitis can occur.
The condition “actually responds to different drugs than MS and has a different immune pathophysiology,” Dr. Pittock said.
He cautioned colleagues to be aware that “the ability of the antibody to tell you whether or not the patient has the disease is less clear for MOGAD than it is for other diseases. If your patient has a low titer of MOG antibody, and their phenotype really doesn’t look like [MOGAD], you really need to interpret that with significant caution.”
He also highlighted a 2018 report that offers guidance about diagnosis and when MOG-IgC antibody tests are appropriate in CNS demyelinating disease.
Dr. Pittock reported numerous disclosures plus patents issued or pending.
a neurologist told colleagues.
“Patients have a choice of different options with different types of action. It’s good news,” said Sean J. Pittock, MD, of the Mayo Clinic in Rochester, Minn. “If you don’t stop the clinical attacks, patients can become very disabled very quickly. These medications have a significant impact in reducing the likelihood of having a clinical relapse. If you can stop the relapses, you certainly can eventually stop most – if not all – of the disability accrual.”
Dr. Pittock spoke at the annual meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis and answered follow-up questions in an interview.
Treatment advances for NMOSD
NMOSD, also known as NMO, is a relapsing autoimmune inflammatory disorder that causes recurrent optic neuritis and myelitis. It’s a rare disease, affecting 0.5-10 people per 100,000, mostly women.
Several recent trials have supported the use of the drugs eculizumab (Soliris), satralizumab (Enspryng) and inebilizumab (Uplizna) in NMOSD, Dr. Pittock said, and all have received Food and Drug Administration approval to treat the condition over the past 2 years. Dr. Pittock led the PREVENT trial of eculizumab, which showed a 94% reduction of relapse risk versus placebo.
The newly approved drugs are stunningly expensive. According to Dr. Pittock, eculizumab costs $710,000 a year, while inebilizumab runs $393,000 the first year, then $262,000 a year. Satralizumab is $219,000 the first year, then $190,000 a year. Assistance programs are available, Dr. Pittock said, “and we’ve not had any major problems in terms of initiation.”
The cost of rituximab (Rituxan), which has a history of use as an off-label treatment option, is $18,000 a year and dropping, according to Dr. Pittock. There’s also new research on rituximab: In 2020, a small Japanese trial (n = 38) reported prevention of relapses compared with placebo, but Dr. Pittock cautioned that “the placebo patients seem to have a more benign course or more benign phenotypes” than the intervention group.
“There’s no doubt that rituximab works, but does it work as well as the other medications that have been through more of a robust trial process?” he asked. Keep in mind, he added, that perhaps 20%-50% of patients will relapse on rituximab.
Dr. Pittock advised colleagues to consider factors like patient schedules and compliance when choosing a drug. Satralizumab is self-administered monthly, while inebilizumab and rituximab are infused every 6 months.
Progress in anti-MOG disease
The trials in NMOSD should spur studies of the drugs in anti–myelin oligodendrocyte glycoprotein (MOG) disease, he said. “I think we’ll see a more rapid move toward phase 3 trials because of the experience with NMO. We will just have to wait and see which medications enter trial.”
Anti-MOG disease, also known as MOG antibody disease (MOGAD) and anti-MOG–associated encephalomyelitis, is caused by anti-MOG antibodies. Optic neuritis is very common, and transverse myelitis can occur.
The condition “actually responds to different drugs than MS and has a different immune pathophysiology,” Dr. Pittock said.
He cautioned colleagues to be aware that “the ability of the antibody to tell you whether or not the patient has the disease is less clear for MOGAD than it is for other diseases. If your patient has a low titer of MOG antibody, and their phenotype really doesn’t look like [MOGAD], you really need to interpret that with significant caution.”
He also highlighted a 2018 report that offers guidance about diagnosis and when MOG-IgC antibody tests are appropriate in CNS demyelinating disease.
Dr. Pittock reported numerous disclosures plus patents issued or pending.
FROM ACTRIMS FORUM 2021