User login
2020 presidential election tied to spike in cardiac events
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Cancer hospitals often mark up drug prices, ignore price transparency rules
Among those that do provide this information, new research shows that hospitals substantially mark up prices for top-selling cancer therapies relative to acquisition costs. Median drug price markups across NCI centers and payers ranged from nearly 120% to more than 600%.
As a result, “the total price for an entire treatment course could vary on the order of hundreds of thousands of dollars,” Roy Xiao, MD, department of otolaryngology–head and neck surgery, Massachusetts Eye and Ear Infirmary, Boston, said in an interview.
The study was published online in JAMA Internal Medicine.
Manufacturers often price novel anticancer therapies at more than $100,000 per year, but less is known about how much hospitals mark up these prices for patients with private health insurance and how much negotiated prices vary across centers and payers.
Dr. Xiao and colleagues analyzed private payer-specific negotiated prices for the top 25 parenteral cancer therapies by Medicare Part B spending in 2019 using publicly available hospital price transparency files for 61 NCI-designated cancer centers.
Fewer than half of the centers (44.3%) disclosed payer-specific negotiated prices for at least one top-selling cancer drug. Disclosure rates for different drugs ranged from 21.3% (13 centers) for rituximab with hyaluronidase to 42.6% (26 centers) for rituximab, bevacizumab, or leuprolide.
The researchers also found a wide variation in negotiated prices for cancer therapies across hospitals. Across-center price ratios – defined as the ratio between the 90th and 10th percentile median price per unit – ranged from 2.2 ($16 vs. $36 for pembrolizumab 1 mg) and 15.8 ($247 vs. $3,914 for leuprolide 7.5 mg).
Payer-specific prices also varied considerably between payers at the same center. Among all centers, the median within-center price ratios for cancer therapies ranged from 1.8 (brentuximab) to 2.5 (bevacizumab).
As for the extent of cancer therapy markups, median price markups across centers and payers ranged from 118% (sipuleucel-T) to 634% (leuprolide) more than the estimated cost paid by hospitals.
Conservative estimates of acquisition costs and payer-specific prices yielded markups ranging from 42.1% (sipuleucel-T) to 234.1% (leuprolide).
The authors also provided examples of how these variations might affect the total cost of treatment. For instance, the median total price variation across centers to treat metastatic non–small cell lung cancer with pembrolizumab was $168,405. At one institution, the within-center median price variation for daratumumab as third-line therapy for multiple myeloma was $174,225.
To reduce the financial burden of cancer treatment for patients, the authors suggested implementing public policies “to discourage or prevent excessive hospital price markups on parenteral chemotherapeutics.”
To promote hospital compliance with transparency regulations, in January 2022, the Centers for Medicare & Medicare Services increased penalties for nondisclosure from a fixed maximum of $300 per day to up to $5,500 per day, based on hospital bed size, which would total over $2 million per year, Dr. Xiao said in an interview.
“We would expect that this significant financial penalty would encourage more consistent reporting,” he said.
The study had no specific funding. Dr. Xiao has disclosed no relevant disclosures.
A version of this article first appeared on Medscape.com.
Among those that do provide this information, new research shows that hospitals substantially mark up prices for top-selling cancer therapies relative to acquisition costs. Median drug price markups across NCI centers and payers ranged from nearly 120% to more than 600%.
As a result, “the total price for an entire treatment course could vary on the order of hundreds of thousands of dollars,” Roy Xiao, MD, department of otolaryngology–head and neck surgery, Massachusetts Eye and Ear Infirmary, Boston, said in an interview.
The study was published online in JAMA Internal Medicine.
Manufacturers often price novel anticancer therapies at more than $100,000 per year, but less is known about how much hospitals mark up these prices for patients with private health insurance and how much negotiated prices vary across centers and payers.
Dr. Xiao and colleagues analyzed private payer-specific negotiated prices for the top 25 parenteral cancer therapies by Medicare Part B spending in 2019 using publicly available hospital price transparency files for 61 NCI-designated cancer centers.
Fewer than half of the centers (44.3%) disclosed payer-specific negotiated prices for at least one top-selling cancer drug. Disclosure rates for different drugs ranged from 21.3% (13 centers) for rituximab with hyaluronidase to 42.6% (26 centers) for rituximab, bevacizumab, or leuprolide.
The researchers also found a wide variation in negotiated prices for cancer therapies across hospitals. Across-center price ratios – defined as the ratio between the 90th and 10th percentile median price per unit – ranged from 2.2 ($16 vs. $36 for pembrolizumab 1 mg) and 15.8 ($247 vs. $3,914 for leuprolide 7.5 mg).
Payer-specific prices also varied considerably between payers at the same center. Among all centers, the median within-center price ratios for cancer therapies ranged from 1.8 (brentuximab) to 2.5 (bevacizumab).
As for the extent of cancer therapy markups, median price markups across centers and payers ranged from 118% (sipuleucel-T) to 634% (leuprolide) more than the estimated cost paid by hospitals.
Conservative estimates of acquisition costs and payer-specific prices yielded markups ranging from 42.1% (sipuleucel-T) to 234.1% (leuprolide).
The authors also provided examples of how these variations might affect the total cost of treatment. For instance, the median total price variation across centers to treat metastatic non–small cell lung cancer with pembrolizumab was $168,405. At one institution, the within-center median price variation for daratumumab as third-line therapy for multiple myeloma was $174,225.
To reduce the financial burden of cancer treatment for patients, the authors suggested implementing public policies “to discourage or prevent excessive hospital price markups on parenteral chemotherapeutics.”
To promote hospital compliance with transparency regulations, in January 2022, the Centers for Medicare & Medicare Services increased penalties for nondisclosure from a fixed maximum of $300 per day to up to $5,500 per day, based on hospital bed size, which would total over $2 million per year, Dr. Xiao said in an interview.
“We would expect that this significant financial penalty would encourage more consistent reporting,” he said.
The study had no specific funding. Dr. Xiao has disclosed no relevant disclosures.
A version of this article first appeared on Medscape.com.
Among those that do provide this information, new research shows that hospitals substantially mark up prices for top-selling cancer therapies relative to acquisition costs. Median drug price markups across NCI centers and payers ranged from nearly 120% to more than 600%.
As a result, “the total price for an entire treatment course could vary on the order of hundreds of thousands of dollars,” Roy Xiao, MD, department of otolaryngology–head and neck surgery, Massachusetts Eye and Ear Infirmary, Boston, said in an interview.
The study was published online in JAMA Internal Medicine.
Manufacturers often price novel anticancer therapies at more than $100,000 per year, but less is known about how much hospitals mark up these prices for patients with private health insurance and how much negotiated prices vary across centers and payers.
Dr. Xiao and colleagues analyzed private payer-specific negotiated prices for the top 25 parenteral cancer therapies by Medicare Part B spending in 2019 using publicly available hospital price transparency files for 61 NCI-designated cancer centers.
Fewer than half of the centers (44.3%) disclosed payer-specific negotiated prices for at least one top-selling cancer drug. Disclosure rates for different drugs ranged from 21.3% (13 centers) for rituximab with hyaluronidase to 42.6% (26 centers) for rituximab, bevacizumab, or leuprolide.
The researchers also found a wide variation in negotiated prices for cancer therapies across hospitals. Across-center price ratios – defined as the ratio between the 90th and 10th percentile median price per unit – ranged from 2.2 ($16 vs. $36 for pembrolizumab 1 mg) and 15.8 ($247 vs. $3,914 for leuprolide 7.5 mg).
Payer-specific prices also varied considerably between payers at the same center. Among all centers, the median within-center price ratios for cancer therapies ranged from 1.8 (brentuximab) to 2.5 (bevacizumab).
As for the extent of cancer therapy markups, median price markups across centers and payers ranged from 118% (sipuleucel-T) to 634% (leuprolide) more than the estimated cost paid by hospitals.
Conservative estimates of acquisition costs and payer-specific prices yielded markups ranging from 42.1% (sipuleucel-T) to 234.1% (leuprolide).
The authors also provided examples of how these variations might affect the total cost of treatment. For instance, the median total price variation across centers to treat metastatic non–small cell lung cancer with pembrolizumab was $168,405. At one institution, the within-center median price variation for daratumumab as third-line therapy for multiple myeloma was $174,225.
To reduce the financial burden of cancer treatment for patients, the authors suggested implementing public policies “to discourage or prevent excessive hospital price markups on parenteral chemotherapeutics.”
To promote hospital compliance with transparency regulations, in January 2022, the Centers for Medicare & Medicare Services increased penalties for nondisclosure from a fixed maximum of $300 per day to up to $5,500 per day, based on hospital bed size, which would total over $2 million per year, Dr. Xiao said in an interview.
“We would expect that this significant financial penalty would encourage more consistent reporting,” he said.
The study had no specific funding. Dr. Xiao has disclosed no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA INTERNAL MEDICINE
Mental illness tied to COVID-19 breakthrough infection
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
“Psychiatric disorders remained significantly associated with incident breakthrough infections above and beyond sociodemographic and medical factors, suggesting that mental health is important to consider in conjunction with other risk factors,” wrote the investigators, led by Aoife O’Donovan, PhD, University of California, San Francisco.
Individuals with psychiatric disorders “should be prioritized for booster vaccinations and other critical preventive efforts, including increased SARS-CoV-2 screening, public health campaigns, or COVID-19 discussions during clinical care,” they added.
The study was published online in JAMA Network Open.
Elderly most vulnerable
The researchers reviewed the records of 263,697 veterans who were fully vaccinated against COVID-19.
Just over a half (51.4%) had one or more psychiatric diagnoses within the last 5 years and 14.8% developed breakthrough COVID-19 infections, confirmed by a positive SARS-CoV-2 test.
Psychiatric diagnoses among the veterans included depression, posttraumatic stress, anxiety, adjustment disorder, substance use disorder, bipolar disorder, psychosis, ADHD, dissociation, and eating disorders.
In the overall sample, a history of any psychiatric disorder was associated with a 7% higher incidence of breakthrough COVID-19 infection in models adjusted for potential confounders (adjusted relative risk, 1.07; 95% confidence interval, 1.05-1.09) and a 3% higher incidence in models additionally adjusted for underlying medical comorbidities and smoking (aRR, 1.03; 95% CI, 1.01-1.05).
Most psychiatric disorders were associated with a higher incidence of breakthrough infection, with the highest relative risk observed for substance use disorders (aRR, 1.16; 95% CI, 1.12 -1.21) and adjustment disorder (aRR, 1.13; 95% CI, 1.10-1.16) in fully adjusted models.
Older vaccinated veterans with psychiatric illnesses appear to be most vulnerable to COVID-19 reinfection.
In veterans aged 65 and older, all psychiatric disorders were associated with an increased incidence of breakthrough infection, with increases in the incidence rate ranging from 3% to 24% in fully adjusted models.
In the younger veterans, in contrast, only anxiety, adjustment, and substance use disorders were associated with an increased incidence of breakthrough infection in fully adjusted models.
Psychotic disorders were associated with a 10% lower incidence of breakthrough infection among younger veterans, perhaps because of greater social isolation, the researchers said.
Risky behavior or impaired immunity?
“Although some of the larger observed effect sizes are compelling at an individual level, even the relatively modest effect sizes may have a large effect at the population level when considering the high prevalence of psychiatric disorders and the global reach and scale of the pandemic,” Dr. O’Donovan and colleagues wrote.
They noted that psychiatric disorders, including depression, schizophrenia, and bipolar disorders, have been associated with impaired cellular immunity and blunted response to vaccines. Therefore, it’s possible that those with psychiatric disorders have poorer responses to COVID-19 vaccination.
It’s also possible that immunity following vaccination wanes more quickly or more strongly in people with psychiatric disorders and they could have less protection against new variants, they added.
Patients with psychiatric disorders could be more apt to engage in risky behaviors for contracting COVID-19, which could also increase the risk for breakthrough infection, they said.
The study was supported by a UCSF Department of Psychiatry Rapid Award and UCSF Faculty Resource Fund Award. Dr. O’Donovan reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Can pickle juice help ease cirrhotic cramps?
In the trial, patients with cirrhotic cramps who sipped pickle brine at the onset of a muscle cramp saw a significant decrease in cramp severity relative to peers who sipped tap water when the cramp hit.
“The acid (vinegar) in the brine triggers a nerve reflex to stop the cramp when it hits the throat. This is why only a sip is needed,” lead investigator Elliot Tapper, MD, division of gastroenterology and hepatology, University of Michigan, Ann Arbor, told this news organization. The study was published online April 13 in American Journal of Gastroenterology.
Common and bothersome
Cramps are common in adults with cirrhosis, irrespective of disease severity. They can sometimes last for hours, and treatment options are limited.
In a prior study, 1 tablespoon of pickle juice rapidly stopped experimentally induced cramps.
“This is something that athletes use, and kidney doctors often recommend to their patients, so it is nothing unique to cirrhosis,” Dr. Tapper said.
The PICCLES trial involved 74 adults (mean age, 56.6 years) with at least 4 muscle cramps in the prior month. In the cohort, 54% were men, and 41% had ascites.
The median cramp frequency was 11-12 per month, with an average cramp severity of more than 4 out of 10 on the Visual Analog Scale (VAS) for cramps.
Some patients were receiving medications for their cramps at baseline, such as magnesium, potassium, baclofen, vitamin E, taurine, and gabapentin/pregabalin.
Thirty-eight patients were randomly allocated to sip pickle juice and 36 to sip tap water at the onset of a muscle cramp.
The proportion of cramps treated was similar in the pickle juice and tap water groups (77% and 72%). More patients in the pickle juice group said their cramps were aborted by the intervention (69% vs. 40%).
The primary outcome was the change in cramp severity at 28-days VAS for cramps. Cramps were assessed 10 times over 28 days using interactive text messages.
Pickle juice was associated with a larger average reduction in cramp severity than tap water (–2.25 points vs. –0.36 on the VAS-cramps), a difference that was statistically significant (P = .03).
There were no significant changes in the proportion of days with cramp severity of more than 5 on the VAS, or on sleep quality or health-related quality of life.
Because pickle juice contains sodium, the researchers also assessed weight change as a safety outcome. They found no significant differences in weight change between the two groups overall or in the subset with ascites.
Pickle juice is a “safe option that can stop painful cramps,” Dr. Tapper said in an interview, but was “disheartened” that it did not improve quality of life.
Dr. Tapper encourages patients with cramps to ask their doctor about pickle juice and doctors to ask their patients about muscle cramps.
“Awareness of a patient’s cramps is often lacking. Asking about cramps is not routine but could be the most important advance relating to this study,” he said.
While sips of pickle juice are “unlikely to cause harm,” Dr. Tapper said, he is “a little nervous about advising patients to address their complex needs alone. [Doctors] are there to think through the root causes and help make adjustments that could prevent the cramps in the first place,” he said.
Outside experts weigh in
This news organization reached out to several outside experts for their perspective on the study.
Nancy Reau, MD, professor of internal medicine, associate director of solid organ transplantation, and section chief of hepatology. Rush University Medical Center, Chicago, noted that interventions to manage and prevent muscle cramps are “important, as cramping is common in cirrhosis and strongly affects quality of life.”
Dr. Reau cautioned that while pickle juice “sounds benign, it does have a lot of salt. Despite the salt content, this study didn’t show any difference between patients with and without ascites.
“However, cramping is more common in our patients with sarcopenia and those on diuretics for fluid management and it would be easy to see how this might impact fluid management,” Dr. Reau noted.
“Given that it is the acid (not the salt) in the pickle juice, there might be low salt alternatives,” Dr. Reau said.
Echoing Dr. Reau, Ankur Shah, MD, division of kidney disease and hypertension, Brown University, Providence, R.I., noted that “overuse of pickle juice could place patients at risk of developing high blood pressure and fluid overload, and pickle juice should be included in the sodium restriction guidance given to patients with high blood pressure and heart failure.”
In this study, however, the individual dose consumed was low, Dr. Shah noted.
He said the study “elegantly provides evidence to support the practice of sipping pickle juice for cramping.”
The authors should be “applauded for studying a simple solution with the most rigorous of methodologies, a randomized controlled trial,” Dr. Shah added.
“This simple treatment may be helpful to patients far beyond those with just cirrhosis, and expect future studies to explore this treatment in other populations,” Dr. Shah said in an interview.
Paul Martin, MD, chief of the division of digestive health and liver diseases and Mandel Chair in Gastroenterology, University of Miami, noted that, while muscle cramps can have a major impact on quality of life, “in terms of some of the other complications of cirrhosis that health care providers are dealing with, they may seem relatively innocuous, but obviously patients have a slightly different interpretation because of the effect cramps can have on sleep and so on.
“There have been a variety of home remedies to treat muscle cramps, but this study is intriguing as it suggests that pickle juice, which is freely available, helps mitigate the severity of the cramps. However, it’s unclear whether it prevents cramps,” Dr. Martin said in an interview.
Given that the study is getting traction on Twitter, Dr. Martin encouraged health care providers to be aware of the study and prepared to answer questions from patients.
The study had no specific funding. Dr. Tapper has served as a consultant to Novartis, Axcella, and Allergan, has served on advisory boards for Mallinckrodt, Bausch Health, Kaleido, and Novo Nordisk, and has received unrestricted research grants from Gilead and Valeant. Dr. Reau, Dr. Shah, and Dr. Martin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the trial, patients with cirrhotic cramps who sipped pickle brine at the onset of a muscle cramp saw a significant decrease in cramp severity relative to peers who sipped tap water when the cramp hit.
“The acid (vinegar) in the brine triggers a nerve reflex to stop the cramp when it hits the throat. This is why only a sip is needed,” lead investigator Elliot Tapper, MD, division of gastroenterology and hepatology, University of Michigan, Ann Arbor, told this news organization. The study was published online April 13 in American Journal of Gastroenterology.
Common and bothersome
Cramps are common in adults with cirrhosis, irrespective of disease severity. They can sometimes last for hours, and treatment options are limited.
In a prior study, 1 tablespoon of pickle juice rapidly stopped experimentally induced cramps.
“This is something that athletes use, and kidney doctors often recommend to their patients, so it is nothing unique to cirrhosis,” Dr. Tapper said.
The PICCLES trial involved 74 adults (mean age, 56.6 years) with at least 4 muscle cramps in the prior month. In the cohort, 54% were men, and 41% had ascites.
The median cramp frequency was 11-12 per month, with an average cramp severity of more than 4 out of 10 on the Visual Analog Scale (VAS) for cramps.
Some patients were receiving medications for their cramps at baseline, such as magnesium, potassium, baclofen, vitamin E, taurine, and gabapentin/pregabalin.
Thirty-eight patients were randomly allocated to sip pickle juice and 36 to sip tap water at the onset of a muscle cramp.
The proportion of cramps treated was similar in the pickle juice and tap water groups (77% and 72%). More patients in the pickle juice group said their cramps were aborted by the intervention (69% vs. 40%).
The primary outcome was the change in cramp severity at 28-days VAS for cramps. Cramps were assessed 10 times over 28 days using interactive text messages.
Pickle juice was associated with a larger average reduction in cramp severity than tap water (–2.25 points vs. –0.36 on the VAS-cramps), a difference that was statistically significant (P = .03).
There were no significant changes in the proportion of days with cramp severity of more than 5 on the VAS, or on sleep quality or health-related quality of life.
Because pickle juice contains sodium, the researchers also assessed weight change as a safety outcome. They found no significant differences in weight change between the two groups overall or in the subset with ascites.
Pickle juice is a “safe option that can stop painful cramps,” Dr. Tapper said in an interview, but was “disheartened” that it did not improve quality of life.
Dr. Tapper encourages patients with cramps to ask their doctor about pickle juice and doctors to ask their patients about muscle cramps.
“Awareness of a patient’s cramps is often lacking. Asking about cramps is not routine but could be the most important advance relating to this study,” he said.
While sips of pickle juice are “unlikely to cause harm,” Dr. Tapper said, he is “a little nervous about advising patients to address their complex needs alone. [Doctors] are there to think through the root causes and help make adjustments that could prevent the cramps in the first place,” he said.
Outside experts weigh in
This news organization reached out to several outside experts for their perspective on the study.
Nancy Reau, MD, professor of internal medicine, associate director of solid organ transplantation, and section chief of hepatology. Rush University Medical Center, Chicago, noted that interventions to manage and prevent muscle cramps are “important, as cramping is common in cirrhosis and strongly affects quality of life.”
Dr. Reau cautioned that while pickle juice “sounds benign, it does have a lot of salt. Despite the salt content, this study didn’t show any difference between patients with and without ascites.
“However, cramping is more common in our patients with sarcopenia and those on diuretics for fluid management and it would be easy to see how this might impact fluid management,” Dr. Reau noted.
“Given that it is the acid (not the salt) in the pickle juice, there might be low salt alternatives,” Dr. Reau said.
Echoing Dr. Reau, Ankur Shah, MD, division of kidney disease and hypertension, Brown University, Providence, R.I., noted that “overuse of pickle juice could place patients at risk of developing high blood pressure and fluid overload, and pickle juice should be included in the sodium restriction guidance given to patients with high blood pressure and heart failure.”
In this study, however, the individual dose consumed was low, Dr. Shah noted.
He said the study “elegantly provides evidence to support the practice of sipping pickle juice for cramping.”
The authors should be “applauded for studying a simple solution with the most rigorous of methodologies, a randomized controlled trial,” Dr. Shah added.
“This simple treatment may be helpful to patients far beyond those with just cirrhosis, and expect future studies to explore this treatment in other populations,” Dr. Shah said in an interview.
Paul Martin, MD, chief of the division of digestive health and liver diseases and Mandel Chair in Gastroenterology, University of Miami, noted that, while muscle cramps can have a major impact on quality of life, “in terms of some of the other complications of cirrhosis that health care providers are dealing with, they may seem relatively innocuous, but obviously patients have a slightly different interpretation because of the effect cramps can have on sleep and so on.
“There have been a variety of home remedies to treat muscle cramps, but this study is intriguing as it suggests that pickle juice, which is freely available, helps mitigate the severity of the cramps. However, it’s unclear whether it prevents cramps,” Dr. Martin said in an interview.
Given that the study is getting traction on Twitter, Dr. Martin encouraged health care providers to be aware of the study and prepared to answer questions from patients.
The study had no specific funding. Dr. Tapper has served as a consultant to Novartis, Axcella, and Allergan, has served on advisory boards for Mallinckrodt, Bausch Health, Kaleido, and Novo Nordisk, and has received unrestricted research grants from Gilead and Valeant. Dr. Reau, Dr. Shah, and Dr. Martin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In the trial, patients with cirrhotic cramps who sipped pickle brine at the onset of a muscle cramp saw a significant decrease in cramp severity relative to peers who sipped tap water when the cramp hit.
“The acid (vinegar) in the brine triggers a nerve reflex to stop the cramp when it hits the throat. This is why only a sip is needed,” lead investigator Elliot Tapper, MD, division of gastroenterology and hepatology, University of Michigan, Ann Arbor, told this news organization. The study was published online April 13 in American Journal of Gastroenterology.
Common and bothersome
Cramps are common in adults with cirrhosis, irrespective of disease severity. They can sometimes last for hours, and treatment options are limited.
In a prior study, 1 tablespoon of pickle juice rapidly stopped experimentally induced cramps.
“This is something that athletes use, and kidney doctors often recommend to their patients, so it is nothing unique to cirrhosis,” Dr. Tapper said.
The PICCLES trial involved 74 adults (mean age, 56.6 years) with at least 4 muscle cramps in the prior month. In the cohort, 54% were men, and 41% had ascites.
The median cramp frequency was 11-12 per month, with an average cramp severity of more than 4 out of 10 on the Visual Analog Scale (VAS) for cramps.
Some patients were receiving medications for their cramps at baseline, such as magnesium, potassium, baclofen, vitamin E, taurine, and gabapentin/pregabalin.
Thirty-eight patients were randomly allocated to sip pickle juice and 36 to sip tap water at the onset of a muscle cramp.
The proportion of cramps treated was similar in the pickle juice and tap water groups (77% and 72%). More patients in the pickle juice group said their cramps were aborted by the intervention (69% vs. 40%).
The primary outcome was the change in cramp severity at 28-days VAS for cramps. Cramps were assessed 10 times over 28 days using interactive text messages.
Pickle juice was associated with a larger average reduction in cramp severity than tap water (–2.25 points vs. –0.36 on the VAS-cramps), a difference that was statistically significant (P = .03).
There were no significant changes in the proportion of days with cramp severity of more than 5 on the VAS, or on sleep quality or health-related quality of life.
Because pickle juice contains sodium, the researchers also assessed weight change as a safety outcome. They found no significant differences in weight change between the two groups overall or in the subset with ascites.
Pickle juice is a “safe option that can stop painful cramps,” Dr. Tapper said in an interview, but was “disheartened” that it did not improve quality of life.
Dr. Tapper encourages patients with cramps to ask their doctor about pickle juice and doctors to ask their patients about muscle cramps.
“Awareness of a patient’s cramps is often lacking. Asking about cramps is not routine but could be the most important advance relating to this study,” he said.
While sips of pickle juice are “unlikely to cause harm,” Dr. Tapper said, he is “a little nervous about advising patients to address their complex needs alone. [Doctors] are there to think through the root causes and help make adjustments that could prevent the cramps in the first place,” he said.
Outside experts weigh in
This news organization reached out to several outside experts for their perspective on the study.
Nancy Reau, MD, professor of internal medicine, associate director of solid organ transplantation, and section chief of hepatology. Rush University Medical Center, Chicago, noted that interventions to manage and prevent muscle cramps are “important, as cramping is common in cirrhosis and strongly affects quality of life.”
Dr. Reau cautioned that while pickle juice “sounds benign, it does have a lot of salt. Despite the salt content, this study didn’t show any difference between patients with and without ascites.
“However, cramping is more common in our patients with sarcopenia and those on diuretics for fluid management and it would be easy to see how this might impact fluid management,” Dr. Reau noted.
“Given that it is the acid (not the salt) in the pickle juice, there might be low salt alternatives,” Dr. Reau said.
Echoing Dr. Reau, Ankur Shah, MD, division of kidney disease and hypertension, Brown University, Providence, R.I., noted that “overuse of pickle juice could place patients at risk of developing high blood pressure and fluid overload, and pickle juice should be included in the sodium restriction guidance given to patients with high blood pressure and heart failure.”
In this study, however, the individual dose consumed was low, Dr. Shah noted.
He said the study “elegantly provides evidence to support the practice of sipping pickle juice for cramping.”
The authors should be “applauded for studying a simple solution with the most rigorous of methodologies, a randomized controlled trial,” Dr. Shah added.
“This simple treatment may be helpful to patients far beyond those with just cirrhosis, and expect future studies to explore this treatment in other populations,” Dr. Shah said in an interview.
Paul Martin, MD, chief of the division of digestive health and liver diseases and Mandel Chair in Gastroenterology, University of Miami, noted that, while muscle cramps can have a major impact on quality of life, “in terms of some of the other complications of cirrhosis that health care providers are dealing with, they may seem relatively innocuous, but obviously patients have a slightly different interpretation because of the effect cramps can have on sleep and so on.
“There have been a variety of home remedies to treat muscle cramps, but this study is intriguing as it suggests that pickle juice, which is freely available, helps mitigate the severity of the cramps. However, it’s unclear whether it prevents cramps,” Dr. Martin said in an interview.
Given that the study is getting traction on Twitter, Dr. Martin encouraged health care providers to be aware of the study and prepared to answer questions from patients.
The study had no specific funding. Dr. Tapper has served as a consultant to Novartis, Axcella, and Allergan, has served on advisory boards for Mallinckrodt, Bausch Health, Kaleido, and Novo Nordisk, and has received unrestricted research grants from Gilead and Valeant. Dr. Reau, Dr. Shah, and Dr. Martin have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To engage injection drug users in HCV care, go to where they are
For injection drug users with hepatitis C virus (HCV) infection, providing treatment opportunities within a local needle exchange program can provide care to more patients and eventually cure more patients, a new study suggests.
The study’s findings help “counteract the implicit belief within the medical community that people who inject drugs can’t or don’t want to engage in health care,” lead author Benjamin Eckhardt, MD, with NYU Grossman School of Medicine, told this news organization.
“By simply focusing on patient accompaniment, limiting stigma, and removing the punitive response for missed appointments, we can effectively engage people who inject drugs in health care and more specifically cure their infection, making significant inroads to HCV elimination,” Dr. Eckhardt said.
The study was published online in JAMA Internal Medicine.
Nonjudgmental, patient-centered approach
Researchers included 165 injection drug users with HCV (mean age, 42 years; 78% men); 82 were randomly allocated to the accessible care intervention and 83 to a usual care control group.
The accessible care model provides HCV treatment within a community-based needle exchange program in a comfortable, nonjudgmental atmosphere, “without fear of shame or stigma that people who inject drugs often experience in mainstream institutions,” the investigators explain.
Control participants were connected to a patient navigator who facilitated referrals to community direct antigen antiviral therapy programs that were not at a syringe service program.
In an intent-to-treat analysis, those enrolled in the accessible care group achieved sustained viral eradication at 12 months at significantly higher rates than those in the control group (67% vs. 23%; P < .001).
Once patients initiated treatment, cure rates were the same in both groups (86%), indicating that the major benefit of the accessible care program was in facilitating treatment, rather than increasing adherence to or response to treatment, the researchers noted.
This is reflected in the fact that the percentage of participants who advanced along the care cascade was significantly higher at each step for the accessible care group than the control group, from referral to an HCV clinician (93% vs. 45%), attendance of the initial HCV clinical visit (87% vs. 37%), completion of baseline laboratory testing (87% vs. 31%), and treatment initiation (78% vs. 27%).
Getting to the population in need
“The most surprising aspect of the study was how successful we were at recruiting, engaging, and treating people who inject drugs who lived outside the immediate community where the syringe exchange program was located and had no prior connection to the program,” Dr. Eckhardt said.
“We had numerous individuals travel 45-plus minutes on the subway from the South Bronx, passing four major medical centers with robust hepatitis C treatment programs, to seek care for hepatitis C in a small, dark office – but also an office they’d heard can be trusted – without fear of stigma or preconditions,” Dr. Eckhardt said.
Commenting on the study’s findings, Nancy Reau, MD, section chief of hepatology at Rush Medical College, Chicago, said, “This is another successful example of making therapy accessible to the population who is in need versus trying to move them into a tertiary care model.”
Dr. Reau noted that similar care models exist in the United States but are not always accessible to the population in need.
“The safety and efficacy of current therapy and the simplified care cascade make HCV an appropriate disease for this delivery,” she said, adding that this study “highlights not just the importance of these programs but also the necessity of engaging the medical community, changing policy, and using patient navigators and monetary support/prioritization to provide appropriate HCV management to those who are at high risk for the disease and for transmission.”
Accessible care beyond HCV
The coauthors of an accompanying editor’s note point out that the treatment for HCV has improved substantially, but it can be a real challenge to provide treatment to injection drug users because the U.S. health care system is not oriented toward the needs of this population.
“It is not surprising that the accessible care arm achieved a higher rate of viral eradication, as it created a patient-focused experience,” write Asha Choudhury, MD, MPH, with the University of California, San Francisco, and Mitchell Katz, MD, with NYC Health and Hospitals. “Creating inviting and engaging environments is particularly important when caring for patients from stigmatized groups. Having more sites that are accessible and inclusive like this for treating patients will likely increase treatment of hepatitis C.”
In their view, the study raises “two dueling questions: Is this model replicable across the U.S.? And, conversely, why isn’t all medical care offered in friendly, nonjudgmental settings with the intention of meeting patient goals?”
They conclude that the study’s lessons extend beyond this particular population and have implications for the field at large.
“The model is replicable to the extent that health care systems are prepared to provide nonjudgmental supportive care for persons who inject drugs,” they write. “However, all patients would benefit from a health care system that provided more patient-centered environments.”
The study was funded by the National Institute on Drug Abuse. Dr. Eckhardt reports receiving grants from the National Institutes of Health and Gilead during the conduct of the study. Dr. Choudhury, Dr. Katz, and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For injection drug users with hepatitis C virus (HCV) infection, providing treatment opportunities within a local needle exchange program can provide care to more patients and eventually cure more patients, a new study suggests.
The study’s findings help “counteract the implicit belief within the medical community that people who inject drugs can’t or don’t want to engage in health care,” lead author Benjamin Eckhardt, MD, with NYU Grossman School of Medicine, told this news organization.
“By simply focusing on patient accompaniment, limiting stigma, and removing the punitive response for missed appointments, we can effectively engage people who inject drugs in health care and more specifically cure their infection, making significant inroads to HCV elimination,” Dr. Eckhardt said.
The study was published online in JAMA Internal Medicine.
Nonjudgmental, patient-centered approach
Researchers included 165 injection drug users with HCV (mean age, 42 years; 78% men); 82 were randomly allocated to the accessible care intervention and 83 to a usual care control group.
The accessible care model provides HCV treatment within a community-based needle exchange program in a comfortable, nonjudgmental atmosphere, “without fear of shame or stigma that people who inject drugs often experience in mainstream institutions,” the investigators explain.
Control participants were connected to a patient navigator who facilitated referrals to community direct antigen antiviral therapy programs that were not at a syringe service program.
In an intent-to-treat analysis, those enrolled in the accessible care group achieved sustained viral eradication at 12 months at significantly higher rates than those in the control group (67% vs. 23%; P < .001).
Once patients initiated treatment, cure rates were the same in both groups (86%), indicating that the major benefit of the accessible care program was in facilitating treatment, rather than increasing adherence to or response to treatment, the researchers noted.
This is reflected in the fact that the percentage of participants who advanced along the care cascade was significantly higher at each step for the accessible care group than the control group, from referral to an HCV clinician (93% vs. 45%), attendance of the initial HCV clinical visit (87% vs. 37%), completion of baseline laboratory testing (87% vs. 31%), and treatment initiation (78% vs. 27%).
Getting to the population in need
“The most surprising aspect of the study was how successful we were at recruiting, engaging, and treating people who inject drugs who lived outside the immediate community where the syringe exchange program was located and had no prior connection to the program,” Dr. Eckhardt said.
“We had numerous individuals travel 45-plus minutes on the subway from the South Bronx, passing four major medical centers with robust hepatitis C treatment programs, to seek care for hepatitis C in a small, dark office – but also an office they’d heard can be trusted – without fear of stigma or preconditions,” Dr. Eckhardt said.
Commenting on the study’s findings, Nancy Reau, MD, section chief of hepatology at Rush Medical College, Chicago, said, “This is another successful example of making therapy accessible to the population who is in need versus trying to move them into a tertiary care model.”
Dr. Reau noted that similar care models exist in the United States but are not always accessible to the population in need.
“The safety and efficacy of current therapy and the simplified care cascade make HCV an appropriate disease for this delivery,” she said, adding that this study “highlights not just the importance of these programs but also the necessity of engaging the medical community, changing policy, and using patient navigators and monetary support/prioritization to provide appropriate HCV management to those who are at high risk for the disease and for transmission.”
Accessible care beyond HCV
The coauthors of an accompanying editor’s note point out that the treatment for HCV has improved substantially, but it can be a real challenge to provide treatment to injection drug users because the U.S. health care system is not oriented toward the needs of this population.
“It is not surprising that the accessible care arm achieved a higher rate of viral eradication, as it created a patient-focused experience,” write Asha Choudhury, MD, MPH, with the University of California, San Francisco, and Mitchell Katz, MD, with NYC Health and Hospitals. “Creating inviting and engaging environments is particularly important when caring for patients from stigmatized groups. Having more sites that are accessible and inclusive like this for treating patients will likely increase treatment of hepatitis C.”
In their view, the study raises “two dueling questions: Is this model replicable across the U.S.? And, conversely, why isn’t all medical care offered in friendly, nonjudgmental settings with the intention of meeting patient goals?”
They conclude that the study’s lessons extend beyond this particular population and have implications for the field at large.
“The model is replicable to the extent that health care systems are prepared to provide nonjudgmental supportive care for persons who inject drugs,” they write. “However, all patients would benefit from a health care system that provided more patient-centered environments.”
The study was funded by the National Institute on Drug Abuse. Dr. Eckhardt reports receiving grants from the National Institutes of Health and Gilead during the conduct of the study. Dr. Choudhury, Dr. Katz, and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For injection drug users with hepatitis C virus (HCV) infection, providing treatment opportunities within a local needle exchange program can provide care to more patients and eventually cure more patients, a new study suggests.
The study’s findings help “counteract the implicit belief within the medical community that people who inject drugs can’t or don’t want to engage in health care,” lead author Benjamin Eckhardt, MD, with NYU Grossman School of Medicine, told this news organization.
“By simply focusing on patient accompaniment, limiting stigma, and removing the punitive response for missed appointments, we can effectively engage people who inject drugs in health care and more specifically cure their infection, making significant inroads to HCV elimination,” Dr. Eckhardt said.
The study was published online in JAMA Internal Medicine.
Nonjudgmental, patient-centered approach
Researchers included 165 injection drug users with HCV (mean age, 42 years; 78% men); 82 were randomly allocated to the accessible care intervention and 83 to a usual care control group.
The accessible care model provides HCV treatment within a community-based needle exchange program in a comfortable, nonjudgmental atmosphere, “without fear of shame or stigma that people who inject drugs often experience in mainstream institutions,” the investigators explain.
Control participants were connected to a patient navigator who facilitated referrals to community direct antigen antiviral therapy programs that were not at a syringe service program.
In an intent-to-treat analysis, those enrolled in the accessible care group achieved sustained viral eradication at 12 months at significantly higher rates than those in the control group (67% vs. 23%; P < .001).
Once patients initiated treatment, cure rates were the same in both groups (86%), indicating that the major benefit of the accessible care program was in facilitating treatment, rather than increasing adherence to or response to treatment, the researchers noted.
This is reflected in the fact that the percentage of participants who advanced along the care cascade was significantly higher at each step for the accessible care group than the control group, from referral to an HCV clinician (93% vs. 45%), attendance of the initial HCV clinical visit (87% vs. 37%), completion of baseline laboratory testing (87% vs. 31%), and treatment initiation (78% vs. 27%).
Getting to the population in need
“The most surprising aspect of the study was how successful we were at recruiting, engaging, and treating people who inject drugs who lived outside the immediate community where the syringe exchange program was located and had no prior connection to the program,” Dr. Eckhardt said.
“We had numerous individuals travel 45-plus minutes on the subway from the South Bronx, passing four major medical centers with robust hepatitis C treatment programs, to seek care for hepatitis C in a small, dark office – but also an office they’d heard can be trusted – without fear of stigma or preconditions,” Dr. Eckhardt said.
Commenting on the study’s findings, Nancy Reau, MD, section chief of hepatology at Rush Medical College, Chicago, said, “This is another successful example of making therapy accessible to the population who is in need versus trying to move them into a tertiary care model.”
Dr. Reau noted that similar care models exist in the United States but are not always accessible to the population in need.
“The safety and efficacy of current therapy and the simplified care cascade make HCV an appropriate disease for this delivery,” she said, adding that this study “highlights not just the importance of these programs but also the necessity of engaging the medical community, changing policy, and using patient navigators and monetary support/prioritization to provide appropriate HCV management to those who are at high risk for the disease and for transmission.”
Accessible care beyond HCV
The coauthors of an accompanying editor’s note point out that the treatment for HCV has improved substantially, but it can be a real challenge to provide treatment to injection drug users because the U.S. health care system is not oriented toward the needs of this population.
“It is not surprising that the accessible care arm achieved a higher rate of viral eradication, as it created a patient-focused experience,” write Asha Choudhury, MD, MPH, with the University of California, San Francisco, and Mitchell Katz, MD, with NYC Health and Hospitals. “Creating inviting and engaging environments is particularly important when caring for patients from stigmatized groups. Having more sites that are accessible and inclusive like this for treating patients will likely increase treatment of hepatitis C.”
In their view, the study raises “two dueling questions: Is this model replicable across the U.S.? And, conversely, why isn’t all medical care offered in friendly, nonjudgmental settings with the intention of meeting patient goals?”
They conclude that the study’s lessons extend beyond this particular population and have implications for the field at large.
“The model is replicable to the extent that health care systems are prepared to provide nonjudgmental supportive care for persons who inject drugs,” they write. “However, all patients would benefit from a health care system that provided more patient-centered environments.”
The study was funded by the National Institute on Drug Abuse. Dr. Eckhardt reports receiving grants from the National Institutes of Health and Gilead during the conduct of the study. Dr. Choudhury, Dr. Katz, and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Statins tied to lower risk for parkinsonism
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests. An observational study showed older adults taking statins had a lower risk for parkinsonism than their counterparts not taking statins – an effect that may be partially mediated by less severe intracranial atherosclerosis in statin users.
“These findings further support the idea that cerebrovascular disease pathologies accumulating in older brains may be an unrecognized contributor to the common occurrence of parkinsonism in old age,” the investigators wrote. “More importantly, these findings suggest that statins may have a potential therapeutic role in decreasing the magnitude of parkinsonism in older adults,” they added.
The study was published online in Neurology.
No clinical recommendations ... yet
The findings are based on 2,841 older adults enrolled in one of three ongoing clinical pathological studies at Rush Alzheimer’s Disease Center, Chicago.
Participants’ average age at baseline was 76 years, and 75% were women. None had parkinsonism at the start of the study. One-third of participants (n = 936) were taking statins. During an average follow-up of 6 years, 1,432 (50%) participants developed parkinsonism.
After controlling for demographics, vascular risk factors, and diseases, use of a statin at baseline was associated with a 16% lower risk for parkinsonism (hazard ratio, 0.84; 95% confidence interval, 0.74-0.96; P = .008). Compared with low-intensity statin therapy, moderate- or high-intensity statin therapy was associated with a 7% lower risk for parkinsonism (HR, 0.93; 95% CI, 0.87-1.00; P = .043).
The researchers also examined the brains of 1,044 people who died during the study at a mean age of 89 years. They found statin use prior to death was associated with a 37% lower odds of cerebral atherosclerosis, compared with no statin use prior to death (odds ratio, 0.63; 95% CI, 0.50-0.79; P < .001).
In a mediation analysis, both a direct (OR, 0.73; 95% CI, 0.54-0.93; P = .008) and an indirect (OR, 0.92; 95% CI, 0.88-0.97; P = .002) pathway via less severe cerebrovascular disease linked statins to parkinsonism, indicating that cerebral atherosclerosis mediated 17% of the association between statins and parkinsonism.
In line with other studies, there was no association between statins and other neurodegenerative pathologies, including Parkinson’s disease pathology. However, even older adults with a clinical diagnosis of Parkinson’s disease often show mixed brain pathologies, including cerebrovascular disease pathologies.
“Therefore, we think that statins may be beneficial against parkinsonism in patients with Parkinson’s disease, dependent on how much cerebrovascular disease pathologies they have, including atherosclerosis,” said study investigator Shahram Oveisgharan, MD, with Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago.
However, since the results stem from an observational study, “we do not yet recommend using statins in large scale for older adults at risk for parkinsonism,” Dr. Oveisgharan said.
A mixed picture
Reached for comment, Shaheen Lakhan, MD, neurologist in Newton, Massachusetts, noted that since statins were first discovered in the fermented broth of a common soil fungus in the late 1970s, they have proven to reduce cholesterol, heart disease, and stroke.
“The jury is out, however, on [their] effects on diseases such as dementia, autoimmune/inflammatory conditions, bacterial/viral infections, cancer, and parkinsonism,” he said.
“Also, the question often remains whether any benefit gained from statins is from cholesterol-lowering or through another mechanism. When there is such a mixed picture, it generally means that the drug has an effect, but not for everyone,” Dr. Lakhan said. “Much work must now be done to stratify for which patients are statins effective, ineffective, or even harmful in these conditions,” he added.
The study was supported by the National Institutes of Health. Dr. Oveisgharan and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Abnormal growth of the amygdala in infants tied to autism
A new study suggests that overgrowth of the amygdala in infants during the first 6-12 months of life is tied to a later diagnosis of autism spectrum disorder (ASD).
“The faster the amygdala grew in infancy, the more social difficulties the child showed when diagnosed with autism a year later,” first author Mark Shen, PhD, assistant professor of psychiatry and neuroscience, University of North Carolina, Chapel Hill, told this news organization.
The study was published online in the American Journal of Psychiatry.
Unique to autism
The amygdala plays a key role in processing memory, emotional responses, and decisionmaking.
It’s long been known that the amygdala is abnormally large in school-aged children with ASD, but until now, it was not known precisely when aberrant amygdala growth happens, what the clinical consequences may be, and whether amygdala overgrowth is unique to autism.
To investigate, Dr. Shen and colleagues evaluated 1,099 longitudinal MRI scans obtained during natural sleep at 6, 12, and 24 months of age in 408 infants in the Infant Brain Imaging Study (IBIS) Network.
The cohort included 58 infants at high likelihood of developing ASD who were later diagnosed with the disorder, 212 infants at high likelihood of ASD who did not develop ASD, 109 typically-developing control infants, and 29 infants with fragile X syndrome.
At 6 months, infants who developed ASD had typically sized amygdala volumes but showed significantly faster amygdala growth between 6 and 24 months, such that by 12 months the ASD group had significantly larger amygdala volume (Cohen’s d = 0.56), compared with all other groups.
Amygdala growth rate between 6 and 12 months was significantly associated with greater social deficits at 24 months when the children were diagnosed with ASD.
“We found that the amygdala grows too rapidly between 6 and 12 months of age, during a presymptomatic period in autism, prior to when the diagnostic symptoms of autism (social difficulties and repetitive behaviors) are evident and lead to the later diagnosis of autism,” Dr. Shen said in an interview.
This brain growth pattern appears to be unique to autism, as babies with the genetic disorder fragile X syndrome – another neurodevelopmental condition – showed a markedly different brain growth pattern: no differences in amygdala growth but enlargement of a different brain structure, the caudate, which was linked to increased repetitive behaviors, the investigators found.
Earlier intervention
Prior research has shown that children who are later diagnosed with ASD often display problems in infancy with how they attend to visual stimuli in their surroundings.
These early problems with processing visual and sensory information may put increased stress on the amygdala, potentially leading to amygdala hyperactivity, deficits in pruning dendritic connections, and overgrowth, Dr. Shen and colleagues hypothesize.
Amygdala overgrowth has also been linked to chronic stress in studies of other psychiatric conditions, such as depression and anxiety, and may provide a clue to understanding this observation in infants who later develop autism.
“This research suggests that an optimal time to begin supports for children who are at the highest likelihood of developing autism may be during the first year of life: to improve early precursors to social development, such as sensory processing, in babies even before social difficulties arise,” Dr. Shen said.
Cyrus A. Raji, MD, PhD, assistant professor of radiology and neurology, Washington University, St. Louis, said, “What makes this study important is the finding of abnormally increased amygdala growth rate in autism using a longitudinal design that focuses on earlier development.”
“While we are typically used to understanding brain structure as abnormally decreasing over time in certain disorders like Alzheimer’s disease, this study challenges us to understand that too much brain volume growth can also be abnormal in specific conditions,” Dr. Raji added.
This research was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, and National Institute of Mental Health, along with Autism Speaks and the Simons Foundation. Dr. Shen and Dr. Raji have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that overgrowth of the amygdala in infants during the first 6-12 months of life is tied to a later diagnosis of autism spectrum disorder (ASD).
“The faster the amygdala grew in infancy, the more social difficulties the child showed when diagnosed with autism a year later,” first author Mark Shen, PhD, assistant professor of psychiatry and neuroscience, University of North Carolina, Chapel Hill, told this news organization.
The study was published online in the American Journal of Psychiatry.
Unique to autism
The amygdala plays a key role in processing memory, emotional responses, and decisionmaking.
It’s long been known that the amygdala is abnormally large in school-aged children with ASD, but until now, it was not known precisely when aberrant amygdala growth happens, what the clinical consequences may be, and whether amygdala overgrowth is unique to autism.
To investigate, Dr. Shen and colleagues evaluated 1,099 longitudinal MRI scans obtained during natural sleep at 6, 12, and 24 months of age in 408 infants in the Infant Brain Imaging Study (IBIS) Network.
The cohort included 58 infants at high likelihood of developing ASD who were later diagnosed with the disorder, 212 infants at high likelihood of ASD who did not develop ASD, 109 typically-developing control infants, and 29 infants with fragile X syndrome.
At 6 months, infants who developed ASD had typically sized amygdala volumes but showed significantly faster amygdala growth between 6 and 24 months, such that by 12 months the ASD group had significantly larger amygdala volume (Cohen’s d = 0.56), compared with all other groups.
Amygdala growth rate between 6 and 12 months was significantly associated with greater social deficits at 24 months when the children were diagnosed with ASD.
“We found that the amygdala grows too rapidly between 6 and 12 months of age, during a presymptomatic period in autism, prior to when the diagnostic symptoms of autism (social difficulties and repetitive behaviors) are evident and lead to the later diagnosis of autism,” Dr. Shen said in an interview.
This brain growth pattern appears to be unique to autism, as babies with the genetic disorder fragile X syndrome – another neurodevelopmental condition – showed a markedly different brain growth pattern: no differences in amygdala growth but enlargement of a different brain structure, the caudate, which was linked to increased repetitive behaviors, the investigators found.
Earlier intervention
Prior research has shown that children who are later diagnosed with ASD often display problems in infancy with how they attend to visual stimuli in their surroundings.
These early problems with processing visual and sensory information may put increased stress on the amygdala, potentially leading to amygdala hyperactivity, deficits in pruning dendritic connections, and overgrowth, Dr. Shen and colleagues hypothesize.
Amygdala overgrowth has also been linked to chronic stress in studies of other psychiatric conditions, such as depression and anxiety, and may provide a clue to understanding this observation in infants who later develop autism.
“This research suggests that an optimal time to begin supports for children who are at the highest likelihood of developing autism may be during the first year of life: to improve early precursors to social development, such as sensory processing, in babies even before social difficulties arise,” Dr. Shen said.
Cyrus A. Raji, MD, PhD, assistant professor of radiology and neurology, Washington University, St. Louis, said, “What makes this study important is the finding of abnormally increased amygdala growth rate in autism using a longitudinal design that focuses on earlier development.”
“While we are typically used to understanding brain structure as abnormally decreasing over time in certain disorders like Alzheimer’s disease, this study challenges us to understand that too much brain volume growth can also be abnormal in specific conditions,” Dr. Raji added.
This research was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, and National Institute of Mental Health, along with Autism Speaks and the Simons Foundation. Dr. Shen and Dr. Raji have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that overgrowth of the amygdala in infants during the first 6-12 months of life is tied to a later diagnosis of autism spectrum disorder (ASD).
“The faster the amygdala grew in infancy, the more social difficulties the child showed when diagnosed with autism a year later,” first author Mark Shen, PhD, assistant professor of psychiatry and neuroscience, University of North Carolina, Chapel Hill, told this news organization.
The study was published online in the American Journal of Psychiatry.
Unique to autism
The amygdala plays a key role in processing memory, emotional responses, and decisionmaking.
It’s long been known that the amygdala is abnormally large in school-aged children with ASD, but until now, it was not known precisely when aberrant amygdala growth happens, what the clinical consequences may be, and whether amygdala overgrowth is unique to autism.
To investigate, Dr. Shen and colleagues evaluated 1,099 longitudinal MRI scans obtained during natural sleep at 6, 12, and 24 months of age in 408 infants in the Infant Brain Imaging Study (IBIS) Network.
The cohort included 58 infants at high likelihood of developing ASD who were later diagnosed with the disorder, 212 infants at high likelihood of ASD who did not develop ASD, 109 typically-developing control infants, and 29 infants with fragile X syndrome.
At 6 months, infants who developed ASD had typically sized amygdala volumes but showed significantly faster amygdala growth between 6 and 24 months, such that by 12 months the ASD group had significantly larger amygdala volume (Cohen’s d = 0.56), compared with all other groups.
Amygdala growth rate between 6 and 12 months was significantly associated with greater social deficits at 24 months when the children were diagnosed with ASD.
“We found that the amygdala grows too rapidly between 6 and 12 months of age, during a presymptomatic period in autism, prior to when the diagnostic symptoms of autism (social difficulties and repetitive behaviors) are evident and lead to the later diagnosis of autism,” Dr. Shen said in an interview.
This brain growth pattern appears to be unique to autism, as babies with the genetic disorder fragile X syndrome – another neurodevelopmental condition – showed a markedly different brain growth pattern: no differences in amygdala growth but enlargement of a different brain structure, the caudate, which was linked to increased repetitive behaviors, the investigators found.
Earlier intervention
Prior research has shown that children who are later diagnosed with ASD often display problems in infancy with how they attend to visual stimuli in their surroundings.
These early problems with processing visual and sensory information may put increased stress on the amygdala, potentially leading to amygdala hyperactivity, deficits in pruning dendritic connections, and overgrowth, Dr. Shen and colleagues hypothesize.
Amygdala overgrowth has also been linked to chronic stress in studies of other psychiatric conditions, such as depression and anxiety, and may provide a clue to understanding this observation in infants who later develop autism.
“This research suggests that an optimal time to begin supports for children who are at the highest likelihood of developing autism may be during the first year of life: to improve early precursors to social development, such as sensory processing, in babies even before social difficulties arise,” Dr. Shen said.
Cyrus A. Raji, MD, PhD, assistant professor of radiology and neurology, Washington University, St. Louis, said, “What makes this study important is the finding of abnormally increased amygdala growth rate in autism using a longitudinal design that focuses on earlier development.”
“While we are typically used to understanding brain structure as abnormally decreasing over time in certain disorders like Alzheimer’s disease, this study challenges us to understand that too much brain volume growth can also be abnormal in specific conditions,” Dr. Raji added.
This research was supported by grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, and National Institute of Mental Health, along with Autism Speaks and the Simons Foundation. Dr. Shen and Dr. Raji have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physical fitness tied to lower risk of Alzheimer’s disease
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
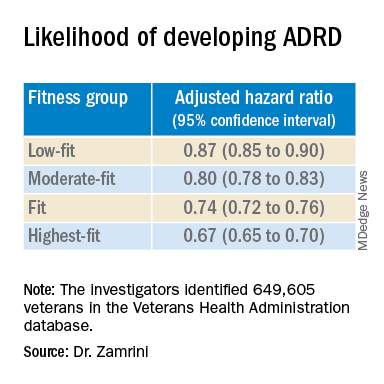
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new findings suggest. “One exciting finding of this study is that as people’s fitness improved, their risk of Alzheimer’s disease decreased – it was not an all-or-nothing proposition,” study investigator Edward Zamrini, MD, of the Washington DC VA Medical Center, said in a news release.
The findings suggest that people can work toward making incremental changes and improvements in their physical fitness, which may help decrease their risk of dementia, Dr. Zamrini added.
The findings were presented at the 2022 annual meeting of the American Academy of Neurology.
Effective prevention strategy
Using the Veterans Health Administration database, Dr. Zamrini and colleagues identified 649,605 veterans (mean age, 61 years) free of Alzheimer’s disease and related disorders (ADRD) when they completed standardized exercise treadmill tests between 2000 and 2017.
They divided participants into five age-specific fitness groups, from least fit to most fit, based on peak metabolic equivalents (METs) achieved during the treadmill test: lowest-fit (METs, ±3.8), low-fit (METs, ±5.8), moderate-fit (METs, ±7.5), fit (METs, ±9.2), and highest-fit (METs, ±11.7).
In unadjusted analysis, veterans with the lowest cardiorespiratory fitness developed ADRD at a rate of 9.5 cases per 1,000 person-years, compared with a rate of 6.4 cases per 1,000 person-years for the most fit group (P < .001).
After adjusting for factors that could affect risk of ADRD, compared with the lowest-fit group, the highest-fit and fit groups were 33% and 26% less likely to develop ADRD, respectively, while the moderate-fit and low-fit groups were 20% and 13% less likely to develop the disease, respectively.
The findings suggest that the association between cardiorespiratory fitness and ADRD risk is “inverse, independent, and graded,” the researchers said in their conference abstract.
“The idea that you can reduce your risk for Alzheimer’s disease by simply increasing your activity is very promising, especially since there are no adequate treatments to prevent or stop the progression of the disease,” Dr. Zamrini added in the news release.
“We hope to develop a simple scale that can be individualized so people can see the benefits that even incremental improvements in fitness can deliver,” he said.
The next vital sign?
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “for decades and with increasing body of support from studies like this, we have known that preventing dementia is based on healthy behaviors for the brain including a proper diet (NASH and/or Mediterranean), exercise regimen (aerobic/cardio more than anaerobic/weight-lifting), sleep hygiene, and social and intellectual engagements.”
“Frankly, what’s good for the body is good for the brain,” said Dr. Lakhan.
“It should be noted that the measure studied here is cardiorespiratory fitness, which has been associated with heart disease and resulting death, death from any cause, and now brain health,” Dr. Lakhan said.
“This powerful predictor may in fact be the next vital sign, after your heart rate and blood pressure, from which your primary care provider can make a personalized treatment plan,” he added.
“Accelerating this process, the ability to measure cardiorespiratory fitness traditionally from huge stationary machines down to wearables like a watch or ring, or even your iPhone or Android, is just on the horizon,” Dr. Lakhan said.
“Instead of tracking just your weight, shape, and BMI, personal fitness may be tailored to optimizing this indicator and further empowering individuals to take charge of their health,” he said.
The study was supported by the National Institute on Aging, the National Institutes of Health, the U.S. Department of Veterans Affairs, the Washington DC VA Medical Center, and George Washington University. Dr. Zamrini and Dr. Lakhan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022
First comprehensive guidelines for managing anorexia in pregnancy
The first comprehensive guidelines to manage pregnant women with anorexia nervosa (AN) have been released.
Pregnant women with AN are at greater risk of poor outcomes, including stillbirth, underweight infant, or pre-term birth, yet there are no clear guidelines on the management of the condition.
“Anorexia in pregnancy has been an overlooked area of clinical care, as many believed only women in remission become pregnant, and it is clear that is not the case,” lead author Megan Galbally, MBBS, PhD, professor and director, Centre of Women’s and Children’s Mental Health at Monash University School of Clinical Sciences, Melbourne, told this news organization.
“There are great opportunities to support women in their mental health and give them and their babies a healthier start to parenthood and life,” said Dr. Galbally.
“For instance, reducing the likelihood of prematurity or low birth weight at birth that can be associated with anorexia in pregnancy has extraordinary benefits for that child for lifelong health and well-being,” she added.
The guidelines were published online in Lancet Psychiatry.
Spike in cases
Dr. Galbally noted that during her 20 years of working in perinatal mental health within tertiary maternity services, she only ever saw an occasional pregnant woman with current AN.
In contrast, over the last 3 to 4 years, there has been a “steep increase in women presenting in pregnancy with very low body mass index (BMI) and current anorexia nervosa requiring treatment in pregnancy,” Dr. Galbally said.
Despite the complexity of managing AN in pregnancy, few studies are available to guide care. In a systematic literature review, the researchers identified only eight studies that addressed the management of AN in pregnancy. These studies were case studies or case reports examining narrow aspects of management.
Digging deeper, the researchers conducted a state-of-the-art research review in relevant disciplines and areas of expertise for managing anorexia nervosa in pregnancy. They synthesized their findings into “recommendations and principles” for multidisciplinary care of pregnant women with AN.
The researchers note that AN in pregnancy is associated with increased risks of pregnancy complications and poorer outcomes for infants, and measures such as BMI are less accurate in pregnancy for assessing severity or change in anorexia nervosa.
Anorexia affects pregnancy and neonatal outcomes through low calorie intake, nutritional and vitamin deficiencies, stress, fasting, low body mass, and poor placentation and uteroplacental function.
The authors note that managing AN in pregnancy requires multidisciplinary care that considers the substantial physiological changes for women and requirements for monitoring fetal growth and development.
At a minimum, they recommend monitoring the following:
- Sodium, potassium, magnesium, phosphate, and chloride concentration
- Iron status, vitamin D and bone mineral density, blood sugar concentration (fasting or random), and A1c
- Liver function (including bilirubin, aspartate transaminase, alanine aminotransferase, and gamma-glutamyl transferase) and bone marrow function (including full blood examination, white cell count, neutrophil count, platelets, and hemoglobin)
- Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate)
- Cardiac function (electrocardiogram and echocardiogram)
- Blood pressure and heart rate (lying and standing) and body temperature
“There are considerable risks for women and their unborn child in managing moderate to severe AN in pregnancy,” said Dr. Galbally.
“While we have provided some recommendations, it still requires considerable adaptation to individual presentations and circumstances, and this is best done with a maternity service that manages other high-risk pregnancies such as through maternal-fetal medicine teams,” she said.
“While this area of clinical care can be new to high-risk pregnancy teams, it is clearly important that high-risk pregnancy services and mental health work together to improve care for women with anorexia in pregnancy,” Dr. Galbally added.
A nightmare, a dream come true
Reached for comment, Kamryn T. Eddy, PhD, co-director, Eating Disorders Clinical and Research Program, Massachusetts General Hospital, said, “for many with anorexia nervosa, pregnancy realizes their greatest nightmare and dream come true, both at once.”
“The physical demands of pregnancy can be taxing, and for those with anorexia nervosa, closer clinical management makes sense and may help to support patients who are at risk for return to or worsening of symptoms with the increased nutritional needs and weight gain that occur in pregnancy,” Dr. Eddy, associate professor, department of psychiatry, Harvard Medical School, Boston, told this news organization.
“At the same time, the desire to have a child can be a strong motivator for patients to make the changes needed to recover, and for some, the transition to mother can also help in recovery by broadening the range of things that influence their self-worth,” Dr. Eddy added.
This research had no specific funding. Dr. Galbally and Dr. Eddy report no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The first comprehensive guidelines to manage pregnant women with anorexia nervosa (AN) have been released.
Pregnant women with AN are at greater risk of poor outcomes, including stillbirth, underweight infant, or pre-term birth, yet there are no clear guidelines on the management of the condition.
“Anorexia in pregnancy has been an overlooked area of clinical care, as many believed only women in remission become pregnant, and it is clear that is not the case,” lead author Megan Galbally, MBBS, PhD, professor and director, Centre of Women’s and Children’s Mental Health at Monash University School of Clinical Sciences, Melbourne, told this news organization.
“There are great opportunities to support women in their mental health and give them and their babies a healthier start to parenthood and life,” said Dr. Galbally.
“For instance, reducing the likelihood of prematurity or low birth weight at birth that can be associated with anorexia in pregnancy has extraordinary benefits for that child for lifelong health and well-being,” she added.
The guidelines were published online in Lancet Psychiatry.
Spike in cases
Dr. Galbally noted that during her 20 years of working in perinatal mental health within tertiary maternity services, she only ever saw an occasional pregnant woman with current AN.
In contrast, over the last 3 to 4 years, there has been a “steep increase in women presenting in pregnancy with very low body mass index (BMI) and current anorexia nervosa requiring treatment in pregnancy,” Dr. Galbally said.
Despite the complexity of managing AN in pregnancy, few studies are available to guide care. In a systematic literature review, the researchers identified only eight studies that addressed the management of AN in pregnancy. These studies were case studies or case reports examining narrow aspects of management.
Digging deeper, the researchers conducted a state-of-the-art research review in relevant disciplines and areas of expertise for managing anorexia nervosa in pregnancy. They synthesized their findings into “recommendations and principles” for multidisciplinary care of pregnant women with AN.
The researchers note that AN in pregnancy is associated with increased risks of pregnancy complications and poorer outcomes for infants, and measures such as BMI are less accurate in pregnancy for assessing severity or change in anorexia nervosa.
Anorexia affects pregnancy and neonatal outcomes through low calorie intake, nutritional and vitamin deficiencies, stress, fasting, low body mass, and poor placentation and uteroplacental function.
The authors note that managing AN in pregnancy requires multidisciplinary care that considers the substantial physiological changes for women and requirements for monitoring fetal growth and development.
At a minimum, they recommend monitoring the following:
- Sodium, potassium, magnesium, phosphate, and chloride concentration
- Iron status, vitamin D and bone mineral density, blood sugar concentration (fasting or random), and A1c
- Liver function (including bilirubin, aspartate transaminase, alanine aminotransferase, and gamma-glutamyl transferase) and bone marrow function (including full blood examination, white cell count, neutrophil count, platelets, and hemoglobin)
- Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate)
- Cardiac function (electrocardiogram and echocardiogram)
- Blood pressure and heart rate (lying and standing) and body temperature
“There are considerable risks for women and their unborn child in managing moderate to severe AN in pregnancy,” said Dr. Galbally.
“While we have provided some recommendations, it still requires considerable adaptation to individual presentations and circumstances, and this is best done with a maternity service that manages other high-risk pregnancies such as through maternal-fetal medicine teams,” she said.
“While this area of clinical care can be new to high-risk pregnancy teams, it is clearly important that high-risk pregnancy services and mental health work together to improve care for women with anorexia in pregnancy,” Dr. Galbally added.
A nightmare, a dream come true
Reached for comment, Kamryn T. Eddy, PhD, co-director, Eating Disorders Clinical and Research Program, Massachusetts General Hospital, said, “for many with anorexia nervosa, pregnancy realizes their greatest nightmare and dream come true, both at once.”
“The physical demands of pregnancy can be taxing, and for those with anorexia nervosa, closer clinical management makes sense and may help to support patients who are at risk for return to or worsening of symptoms with the increased nutritional needs and weight gain that occur in pregnancy,” Dr. Eddy, associate professor, department of psychiatry, Harvard Medical School, Boston, told this news organization.
“At the same time, the desire to have a child can be a strong motivator for patients to make the changes needed to recover, and for some, the transition to mother can also help in recovery by broadening the range of things that influence their self-worth,” Dr. Eddy added.
This research had no specific funding. Dr. Galbally and Dr. Eddy report no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The first comprehensive guidelines to manage pregnant women with anorexia nervosa (AN) have been released.
Pregnant women with AN are at greater risk of poor outcomes, including stillbirth, underweight infant, or pre-term birth, yet there are no clear guidelines on the management of the condition.
“Anorexia in pregnancy has been an overlooked area of clinical care, as many believed only women in remission become pregnant, and it is clear that is not the case,” lead author Megan Galbally, MBBS, PhD, professor and director, Centre of Women’s and Children’s Mental Health at Monash University School of Clinical Sciences, Melbourne, told this news organization.
“There are great opportunities to support women in their mental health and give them and their babies a healthier start to parenthood and life,” said Dr. Galbally.
“For instance, reducing the likelihood of prematurity or low birth weight at birth that can be associated with anorexia in pregnancy has extraordinary benefits for that child for lifelong health and well-being,” she added.
The guidelines were published online in Lancet Psychiatry.
Spike in cases
Dr. Galbally noted that during her 20 years of working in perinatal mental health within tertiary maternity services, she only ever saw an occasional pregnant woman with current AN.
In contrast, over the last 3 to 4 years, there has been a “steep increase in women presenting in pregnancy with very low body mass index (BMI) and current anorexia nervosa requiring treatment in pregnancy,” Dr. Galbally said.
Despite the complexity of managing AN in pregnancy, few studies are available to guide care. In a systematic literature review, the researchers identified only eight studies that addressed the management of AN in pregnancy. These studies were case studies or case reports examining narrow aspects of management.
Digging deeper, the researchers conducted a state-of-the-art research review in relevant disciplines and areas of expertise for managing anorexia nervosa in pregnancy. They synthesized their findings into “recommendations and principles” for multidisciplinary care of pregnant women with AN.
The researchers note that AN in pregnancy is associated with increased risks of pregnancy complications and poorer outcomes for infants, and measures such as BMI are less accurate in pregnancy for assessing severity or change in anorexia nervosa.
Anorexia affects pregnancy and neonatal outcomes through low calorie intake, nutritional and vitamin deficiencies, stress, fasting, low body mass, and poor placentation and uteroplacental function.
The authors note that managing AN in pregnancy requires multidisciplinary care that considers the substantial physiological changes for women and requirements for monitoring fetal growth and development.
At a minimum, they recommend monitoring the following:
- Sodium, potassium, magnesium, phosphate, and chloride concentration
- Iron status, vitamin D and bone mineral density, blood sugar concentration (fasting or random), and A1c
- Liver function (including bilirubin, aspartate transaminase, alanine aminotransferase, and gamma-glutamyl transferase) and bone marrow function (including full blood examination, white cell count, neutrophil count, platelets, and hemoglobin)
- Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate)
- Cardiac function (electrocardiogram and echocardiogram)
- Blood pressure and heart rate (lying and standing) and body temperature
“There are considerable risks for women and their unborn child in managing moderate to severe AN in pregnancy,” said Dr. Galbally.
“While we have provided some recommendations, it still requires considerable adaptation to individual presentations and circumstances, and this is best done with a maternity service that manages other high-risk pregnancies such as through maternal-fetal medicine teams,” she said.
“While this area of clinical care can be new to high-risk pregnancy teams, it is clearly important that high-risk pregnancy services and mental health work together to improve care for women with anorexia in pregnancy,” Dr. Galbally added.
A nightmare, a dream come true
Reached for comment, Kamryn T. Eddy, PhD, co-director, Eating Disorders Clinical and Research Program, Massachusetts General Hospital, said, “for many with anorexia nervosa, pregnancy realizes their greatest nightmare and dream come true, both at once.”
“The physical demands of pregnancy can be taxing, and for those with anorexia nervosa, closer clinical management makes sense and may help to support patients who are at risk for return to or worsening of symptoms with the increased nutritional needs and weight gain that occur in pregnancy,” Dr. Eddy, associate professor, department of psychiatry, Harvard Medical School, Boston, told this news organization.
“At the same time, the desire to have a child can be a strong motivator for patients to make the changes needed to recover, and for some, the transition to mother can also help in recovery by broadening the range of things that influence their self-worth,” Dr. Eddy added.
This research had no specific funding. Dr. Galbally and Dr. Eddy report no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Keto diet in MS tied to less disability, better quality of life
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research suggests.
High-fat, low-carbohydrate ketogenic diets mimic a fasting state and promote a more efficient use of energy – and have previously been shown to affect immune regulation. The diet helps lower blood sugar in individuals with type 2 diabetes and has been used for years to improve seizure control in patients with epilepsy, researchers note.
However, “there is a paucity of literature on the ketogenic diet in MS currently,” said principal investigator J. Nicholas Brenton, MD, University of Virginia, Charlottesville.
“The current study demonstrates the safety, tolerability, and potential clinical benefits of a ketogenic diet over 6 months in patients with relapsing MS,” Dr. Brenton said.
The were presented at the 2022 annual meeting of the American Academy of Neurology.
Palatable, beneficial
The open-label, uncontrolled study included 65 patients with relapsing MS who followed a ketogenic diet for 6 months. Investigators monitored adherence by daily urine ketone testing.
Patient-reported fatigue, depression, and quality-of-life scores were obtained at baseline, in addition to fasting adipokines and pertinent MS-related clinical outcome metrics. Baseline study metrics were repeated at 3 and/or 6 months while on the ketogenic diet.
Of the patient group, 83% adhered to the ketogenic diet for the full 6-month study period.
The ketogenic diet was associated with reductions in fat mass from baseline to 6 months (41.3 vs. 32.0 kg; P < .001) and a significant decline in fatigue and depression scores, the investigators reported.
MS quality-of-life physical and mental composite scores also improved while on the ketogenic diet (P < .001 for both).
A significant decrease from baseline to 6 months in Expanded Disability Status Scale scores, signifying improvement, was observed (2.3 vs. 1.9; P < .001).
Improvements were also shown on the 6-minute walk (1,631 vs. 1,733 feet; P < .001) and the nine-hole peg test (21.5 vs. 20.3 seconds; P < .001).
At 6 months on the diet, fasting serum leptin was significantly lower (25.5 vs. 14 ng/mL; P <.001), and adiponectin was higher (11.4 vs. 13.5 μg/mL, P = .002).
Justifies further research
The current study builds on an earlier one that Dr. Brenton and colleagues conducted in 2019 that showed that the ketogenic diet was feasible in patients with MS. “Our data justify the need for future studies of ketogenic diets as a complementary therapeutic approach to the treatment of MS,” Dr. Brenton said.
He noted that there may be multiple mechanisms of benefit when considering the ketogenic diet. “One avenue is via reduction in total body fat. This is an important aspect as we continue to learn more about the role of obesity and fat-derived inflammation in MS,” Dr. Brenton said.
“Ketogenic diets also have immunomodulatory properties,” such as the capacity to reduce oxidative damage from metabolic stress, increase mitochondrial biogenesis, and reduce systemic inflammation, he added. “These intrinsic properties of the ketogenic diet make it appealing to study in immune-mediated diseases, such as MS.”
Dr. Brenton cautioned that the data demonstrate the diet’s safety over 6 months but that the study was not designed to assess its long-term implications in MS. “Thus, while our results support the rationale for a larger-scale study of ketogenic diets as a complementary treatment for MS, our data does not support its widespread adoption outside of a clinical trial,” he said.
Remarkable adherence
Commenting on the study, Shaheen E. Lakhan, MD, PhD, a neurologist in Boston, noted that “variations of the ketogenic diet have been popularized in the general population for weight loss and further studied for other medical conditions [that are] largely immune-related, including MS.”
He noted that it was “remarkable” that the vast majority of study participants with MS adhered to the very regimented ketogenic diet for 6 months.
Seeing this translate into the real world “will be the next milestone, in addition to its impact on relapses and brain lesions as seen on MRI,” which are the classic markers of MS, said Dr. Lakhan, who was not involved with the research.
He cautioned that “even if one can follow the ketogenic diet, certain conditions can be made worse. This includes kidney stones, liver disease, reflux, constipation, and other metabolic disorders.”
The study was funded by the National Center for Advancing Translational Sciences of the National Institutes of Health and by the ZiMS Foundation. Dr. Brenton and Dr. Lakhan have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2022